User login
Moral distress in the COVID era weighs on hospitalists
Focus on effort, not just outcomes
Moral distress can result when health professionals like doctors and nurses feel prevented from doing what they know is right and ethically correct – reflecting the values of their profession and their own sense of professional integrity – because of unmanageable caseload demands, lack of resources, coverage limitations, or institutional policies.

Hospitalists are not exempt from moral distress, which is associated with soul-searching, burnout, and even PTSD. It is also associated with a higher likelihood for professionals to report an intention to leave their jobs. But the COVID-19 pandemic has superimposed a whole new layer of challenges, constraints, and frustrations, creating a potent mix of trauma and exhaustion, cumulative unease, depleted job satisfaction, and difficult ethical choices.
These challenges include seeing so many patients die and working with short supplies of personal protective equipment (PPE) – with resulting fears that they could catch the virus or pass it on to others, including loved ones. Also, not having enough ventilators or even beds for patients in hospitals hit hard by COVID surges raises fears that decisions for rationing medical care might become necessary.
In a commentary published in the Journal of General Internal Medicine in October 2019 – shortly before the COVID pandemic burst onto the scene – hospitalist and medical sociologist Elizabeth Dzeng, MD, PhD, MPH, and hospital medicine pioneer Robert Wachter, MD, MHM, both from the University of California, San Francisco, described “moral distress and professional ethical dissonance as root causes of burnout.”1 They characterized moral distress by its emotional exhaustion, depersonalization, reduced sense of accomplishment, and moral apathy, and they called for renewed attention to social and ethical dimensions of practice and threats to physician professionalism.

Prevailing explanations for documented high rates of burnout in doctors have tended to focus on work hours and struggles with electronic medical records and the like, Dr. Dzeng and Dr. Wachter wrote. “We see evidence of an insidious moral distress resulting from physicians’ inability to act in accord with their individual and professional ethical values due to institutional and social constraints.”
COVID has intensified these issues surrounding moral distress. “In a short period of time it created more situations that raise issues of moral distress than I have seen since the early days of HIV,” Dr. Wachter said. “Those of us who work in hospitals often find ourselves in complex circumstances with limited resources. What was so striking about COVID was finding ourselves caring for large volumes of patients who had a condition that was new to us.”
And the fact that constraints imposed by COVID, such as having to don unwieldy PPE and not allowing families to be present with hospitalized loved ones, are explainable and rational only helps a little with the clinician’s distress.
People talk about the need for doctors to be more resilient, Dr. Dzeng added, but that’s too narrow of an approach to these very real challenges. There are huge issues of workforce retention and costs, major mental health issues, suicide – and implications for patient care, because burned-out doctors can be bad doctors.
What is moral distress?
Moral distress is a term from the nursing ethics literature, attributed to philosopher Andrew Jameton in 1984.2 Contributors to moral distress imposed by COVID include having to make difficult medical decisions under stressful circumstances – especially early on, when effective treatment options were few. Doctors felt the demands of the pandemic were putting care quality and patient safety at risk. Poor working conditions overall, being pushed to work beyond their normal physical limits for days at a time, and feelings of not being valued added to this stress. But some say the pandemic has only highlighted and amplified existing inequities and disparities in the health care system.
Experts say moral distress is about feeling powerless, especially in a system driven by market values, and feeling let down by a society that has put them in harm’s way. They work all day under physically and emotionally exhausting conditions and then go home to hear specious conspiracy theories about the pandemic and see other people unwilling to wear masks.

Moral distress is complicated, said Lucia Wocial, PhD, RN, a nurse ethicist and cochair of the ethics consultation subcommittee at Indiana University Health in Indianapolis. “If you say you have moral distress, my first response is: tell me more. It helps to peel back the layers of this complexity. Emotion is only part of moral distress. It’s about the professional’s sense of responsibility and obligation – and the inability to honor that.”
Dr. Wocial, whose research specialty is moral distress, is corresponding author of a study published in the Journal of General Internal Medicine in February 2020, which identified moral distress in 4 out of 10 surveyed physicians who cared for older hospitalized adults and found themselves needing to work with their surrogate decision-makers.3 “We know physician moral distress is higher when people haven’t had the chance to hold conversations about their end-of-life care preferences,” she said, such as whether to continue life support.
“We have also learned that communication is key to diminishing physician moral distress. Our responsibility as clinicians is to guide patients and families through these decisions. If the family feels a high level of support from me, then my moral distress is lower,” she added. “If you think about how COVID has evolved, at first people were dying so quickly. Some patients were going to the ICU on ventilators without ever having a goals-of-care conversation.”
COVID has shifted the usual standard of care in U.S. hospitals in the face of patient surges. “How can you feel okay in accepting a level of care that in the prepandemic world would not have been acceptable?” Dr. Wocial posed. “What if you know the standard of care has shifted, of necessity, but you haven’t had time to prepare for it and nobody’s talking about what that means? Who is going to help you accept that good enough under these circumstances is enough – at least for today?”
What to call it
Michael J. Asken, PhD, director of provider well-being at UPMC Pinnacle Harrisburg (Pa.), has questioned in print the use of the military and wartime term “moral injury” when applied to a variety of less serious physician stressors.4 More recently, however, he observed, “The pandemic has muted or erased many of the distinctions between medical care and military conflict. ... The onslaught and volume of critical patients and resulting deaths is beyond what most providers have ever contemplated as part of care.”5

In a recent interview with the Hospitalist, he said: “While I initially resisted using the term moral injury, especially pre-COVID, because it was not equivalent to the moral injury created by war, I have relented a bit.” The volume of deaths and the apparent dangers to providers themselves reflect some of the critical aspects of war, and repetitive, intense, and/or incessant ethical challenges may have longer term negative psychological or emotional effects.
“Feeling emotional pain in situations of multiple deaths is to be expected and, perhaps, should even be welcomed as a sign of retained humanity and a buffer against burnout and cynicism in these times of unabating stress,” Dr. Asken said. “This is only true, however, if the emotional impact is tolerable and not experienced in repetitive extremes.”

“These things are real,” said Clarissa Barnes, MD, a physician adviser, hospitalist at Avera McKennan Hospital in Sioux Falls, S.D., and former medical director of Avera’s LIGHT Program, a wellness-oriented service for clinicians. Dr. Barnes herself caught the virus on the job but has since recovered.
“Physicians don’t see their work as an occupation. It’s their core identity: I am a doctor; I practice medicine. If things are being done in ways I don’t think are right, that’s fundamentally a breach,” she said. “As internists, we have an opportunity to forestall death whenever we can and, if not, promote a peaceful death. That’s what made me choose this specialty. I think there’s value in allowing a person to end well. But when that doesn’t happen because of social or administrative reasons, that’s hard.”
Where is the leadership?
“A lot of moral injury comes down to the individual health system and its leaders. Some have done well; others you hear saying things that make you question whether these are the people you want leading the organization. Hospitalists need to have a clear value framework and an idea of how to negotiate things when decisions don’t match that framework,” Dr. Barnes said.
“Sometimes administrators have additional information that they’re not sharing,” she added. “They’re caught between a rock and a hard place regarding the decisions they have to make, but they need to be more transparent and not hold things so close to their vest while thinking they are helping clinicians [by doing so]. Physicians need to understand why they are being asked to do things counter to what they believe is appropriate.”
David Oliver, MD, a geriatrics and internal medicine consultant at Royal Berkshire Hospital in Reading, England, also practices as a hospital physician, a role similar to the hospitalist in the United States. “In any system, in any environment, the job of being a doctor, nurse, or other health professional carries a lot of responsibility. That is a timeless, inherent stress of medical practice. With COVID, we’ve seen a lot of emotional burdens – a whole separate set of problems outside of your control, where you are responsible for care but don’t have accountability,” he said.
“People like me, hospital doctors, are used to chronic workforce issues in the National Health Service. But we didn’t sign up to come and get COVID and be hospitalized ourselves.” More than 850 frontline health care providers in the U.K. have so far died from the virus, Dr. Oliver said. “I saw five patients die in 90 minutes one day in April. That’s above and beyond normal human capacity.”
In England specifically, he said, it has exposed underlying structural issues and serious workforce gaps, unfilled vacancies, and a much lower number of ICU beds per 100,000 population than the United States or Europe. And there is consistent pressure to send patients home in order to empty beds for new patients.
But a range of supportive services is offered in U.K. hospitals, such as making senior clinicians available to speak to frontline clinicians, providing mentorship and a sounding board. The Point of Care Foundation has helped to disseminate the practice of Schwartz Rounds, a group reflective practice forum for health care teams developed by the Schwartz Center for Compassionate Healthcare in Boston.
“We don’t need this clap-for-the-NHS heroes stuff,” Dr. Oliver said. “We need an adequate workforce and [better] working conditions. What happened on the front lines of the pandemic was heroic – all done by local clinical teams. But where was the government – the centralized NHS? A lot of frontline clinicians aren’t feeling valued, supported, or listened to.”
What can be done?
What are some things that hospitalists can do, individually and collectively, to try to prevent moral distress from turning into full-scale burnout? Dr. Wocial emphasized the importance of unit-based ethics conversations. “At IU Health we have someone who is available to sit down with frontline clinicians and help unpack what they are experiencing,” she said. Clinicians need to be able to process this terrible experience in order to sort out the feelings of sadness from questions of whether they are doing something wrong.
Hospital chaplains are exquisitely skilled at supporting people and debriefing hospital teams, Dr. Wocial added. Palliative care professionals are also skilled at facilitating goals of care conversations with patients and families and can support hospitalists through coaching and joint family meetings.
“It’s about raising your sense of agency in your job – what in your practice you can control. People need to be able to talk frankly about it. Some managers say to clinicians: ‘Just buck up,’ while others are doing a fabulous job of offering support to their staff,” Dr. Wocial said. Hospitalists have to be willing to say when they’ve had too much. “You may not get help when you first ask for it. Be persistent. Asking for help doesn’t make you weak.”
Most doctors have their own strategies for managing stress on the job, Dr. Wachter noted. “What makes it a little easier is not having to do it alone. Many find solace in community, but community has been constrained by this pandemic. You can’t just go out for a beer after work anymore. So what are other ways to let off steam?”
The people leading hospitalist programs need to work harder at creating community and empathy when the tools allowing people to get together are somewhat limited. “Everybody is tired of Zoom,” he said. “One thing I learned as a manager was to just send messages to people acknowledging that I know this is hard. Try to think from the lens of other people and what they would find useful.”
The pandemic has been terribly unpredictable, Dr. Wachter added, but it won’t go on forever. For some doctors, yoga or mindfulness meditation may be very comforting. “For me, that’s not what I do. Golf or a good Seinfeld episode works for me.”

SHM’s Wellbeing Taskforce has created a “Hospital Medicine COVID Check-in Guide for Self & Peers” to promote both sharing and support for one another. It can be found at SHM’s Wellbeing webpage [www.hospitalmedicine.org/practice-management/wellbeing/]. The Taskforce believes that sharing common stressors as hospitalists can be healing, said its chair, Sarah Richards, MD, assistant professor of medicine at the University of Nebraska, Omaha. “This is especially true in situations where we feel we can’t provide the type of care we know our patients deserve.”
Respect, advocacy, self-care
Dr. Asken encouraged clinicians to focus on the efforts they are making on the job, not just the outcomes. “If someone has done their absolute best in a given circumstance, satisfaction and solace needs to be taken from that,” he said.
“Ongoing support group meetings, which we have called frontline support groups, should occur on a regular basis. Designated for physicians on the medical floors and in critical care units who are directly involved with COVID patients, these provide a brief respite but also engagement, sharing, and strengthening of mutual support.”
A lot of these issues have a fundamental thread, which comes down to respect, Dr. Barnes said. “Hospitalists need to hear their hospital administrators say: ‘I hear what you’re saying [about a problem]. Let’s think together about how to solve it.’ We need to work on being clear, and we need to speak up for what’s right. If you aren’t comfortable doing things you are being asked to do in the hospital, maybe you’re not working in the right place.”
Some efforts in the area of wellness and self-care really are helpful, Dr. Barnes said. “But you can’t exercise you way through a health system that doesn’t respect you. You need to get out of the mindset that you have no ability to make things different. We are not powerless as doctors. We can do a lot, actually. Physicians need to take ownership. If you are a hospitalist and you’re not part of any local or state or national organization that advocates for physicians, you should be.”
References
1. Dzeng L and Wachter RM. Ethics in conflict: Moral distress as a root cause of burnout. J Gen Intern Med. 2020 Feb;35(2):409-11. doi: 10.1007/s11606-019-05505-6.
2. Jameton A, Nursing Practice: The ethical issues. Prentice Hall Series in the Philosophy of Medicine. 1984, Englewood Cliffs, N.J.: Prentice Hall.
3. Wocial LD et al. Factors associated with physician moral distress caring for hospitalized elderly patients needing a surrogate decision-maker: A prospective study. J Gen Intern Med. 2020 May;35(5):1405-12. doi: 10.1007/s11606-020-05652-1.
4. Asken MJ. It’s not moral injury: It’s burnout (or something else). Medical Economics; June 7, 2019.
5. Asken MJ. Now it is moral injury: The COVID-19 pandemic and moral distress. Medical Economics; April 29, 2020.
Focus on effort, not just outcomes
Focus on effort, not just outcomes
Moral distress can result when health professionals like doctors and nurses feel prevented from doing what they know is right and ethically correct – reflecting the values of their profession and their own sense of professional integrity – because of unmanageable caseload demands, lack of resources, coverage limitations, or institutional policies.
Hospitalists are not exempt from moral distress, which is associated with soul-searching, burnout, and even PTSD. It is also associated with a higher likelihood for professionals to report an intention to leave their jobs. But the COVID-19 pandemic has superimposed a whole new layer of challenges, constraints, and frustrations, creating a potent mix of trauma and exhaustion, cumulative unease, depleted job satisfaction, and difficult ethical choices.
These challenges include seeing so many patients die and working with short supplies of personal protective equipment (PPE) – with resulting fears that they could catch the virus or pass it on to others, including loved ones. Also, not having enough ventilators or even beds for patients in hospitals hit hard by COVID surges raises fears that decisions for rationing medical care might become necessary.
In a commentary published in the Journal of General Internal Medicine in October 2019 – shortly before the COVID pandemic burst onto the scene – hospitalist and medical sociologist Elizabeth Dzeng, MD, PhD, MPH, and hospital medicine pioneer Robert Wachter, MD, MHM, both from the University of California, San Francisco, described “moral distress and professional ethical dissonance as root causes of burnout.”1 They characterized moral distress by its emotional exhaustion, depersonalization, reduced sense of accomplishment, and moral apathy, and they called for renewed attention to social and ethical dimensions of practice and threats to physician professionalism.
Prevailing explanations for documented high rates of burnout in doctors have tended to focus on work hours and struggles with electronic medical records and the like, Dr. Dzeng and Dr. Wachter wrote. “We see evidence of an insidious moral distress resulting from physicians’ inability to act in accord with their individual and professional ethical values due to institutional and social constraints.”
COVID has intensified these issues surrounding moral distress. “In a short period of time it created more situations that raise issues of moral distress than I have seen since the early days of HIV,” Dr. Wachter said. “Those of us who work in hospitals often find ourselves in complex circumstances with limited resources. What was so striking about COVID was finding ourselves caring for large volumes of patients who had a condition that was new to us.”
And the fact that constraints imposed by COVID, such as having to don unwieldy PPE and not allowing families to be present with hospitalized loved ones, are explainable and rational only helps a little with the clinician’s distress.
People talk about the need for doctors to be more resilient, Dr. Dzeng added, but that’s too narrow of an approach to these very real challenges. There are huge issues of workforce retention and costs, major mental health issues, suicide – and implications for patient care, because burned-out doctors can be bad doctors.
What is moral distress?
Moral distress is a term from the nursing ethics literature, attributed to philosopher Andrew Jameton in 1984.2 Contributors to moral distress imposed by COVID include having to make difficult medical decisions under stressful circumstances – especially early on, when effective treatment options were few. Doctors felt the demands of the pandemic were putting care quality and patient safety at risk. Poor working conditions overall, being pushed to work beyond their normal physical limits for days at a time, and feelings of not being valued added to this stress. But some say the pandemic has only highlighted and amplified existing inequities and disparities in the health care system.
Experts say moral distress is about feeling powerless, especially in a system driven by market values, and feeling let down by a society that has put them in harm’s way. They work all day under physically and emotionally exhausting conditions and then go home to hear specious conspiracy theories about the pandemic and see other people unwilling to wear masks.
Moral distress is complicated, said Lucia Wocial, PhD, RN, a nurse ethicist and cochair of the ethics consultation subcommittee at Indiana University Health in Indianapolis. “If you say you have moral distress, my first response is: tell me more. It helps to peel back the layers of this complexity. Emotion is only part of moral distress. It’s about the professional’s sense of responsibility and obligation – and the inability to honor that.”
Dr. Wocial, whose research specialty is moral distress, is corresponding author of a study published in the Journal of General Internal Medicine in February 2020, which identified moral distress in 4 out of 10 surveyed physicians who cared for older hospitalized adults and found themselves needing to work with their surrogate decision-makers.3 “We know physician moral distress is higher when people haven’t had the chance to hold conversations about their end-of-life care preferences,” she said, such as whether to continue life support.
“We have also learned that communication is key to diminishing physician moral distress. Our responsibility as clinicians is to guide patients and families through these decisions. If the family feels a high level of support from me, then my moral distress is lower,” she added. “If you think about how COVID has evolved, at first people were dying so quickly. Some patients were going to the ICU on ventilators without ever having a goals-of-care conversation.”
COVID has shifted the usual standard of care in U.S. hospitals in the face of patient surges. “How can you feel okay in accepting a level of care that in the prepandemic world would not have been acceptable?” Dr. Wocial posed. “What if you know the standard of care has shifted, of necessity, but you haven’t had time to prepare for it and nobody’s talking about what that means? Who is going to help you accept that good enough under these circumstances is enough – at least for today?”
What to call it
Michael J. Asken, PhD, director of provider well-being at UPMC Pinnacle Harrisburg (Pa.), has questioned in print the use of the military and wartime term “moral injury” when applied to a variety of less serious physician stressors.4 More recently, however, he observed, “The pandemic has muted or erased many of the distinctions between medical care and military conflict. ... The onslaught and volume of critical patients and resulting deaths is beyond what most providers have ever contemplated as part of care.”5
In a recent interview with the Hospitalist, he said: “While I initially resisted using the term moral injury, especially pre-COVID, because it was not equivalent to the moral injury created by war, I have relented a bit.” The volume of deaths and the apparent dangers to providers themselves reflect some of the critical aspects of war, and repetitive, intense, and/or incessant ethical challenges may have longer term negative psychological or emotional effects.
“Feeling emotional pain in situations of multiple deaths is to be expected and, perhaps, should even be welcomed as a sign of retained humanity and a buffer against burnout and cynicism in these times of unabating stress,” Dr. Asken said. “This is only true, however, if the emotional impact is tolerable and not experienced in repetitive extremes.”
“These things are real,” said Clarissa Barnes, MD, a physician adviser, hospitalist at Avera McKennan Hospital in Sioux Falls, S.D., and former medical director of Avera’s LIGHT Program, a wellness-oriented service for clinicians. Dr. Barnes herself caught the virus on the job but has since recovered.
“Physicians don’t see their work as an occupation. It’s their core identity: I am a doctor; I practice medicine. If things are being done in ways I don’t think are right, that’s fundamentally a breach,” she said. “As internists, we have an opportunity to forestall death whenever we can and, if not, promote a peaceful death. That’s what made me choose this specialty. I think there’s value in allowing a person to end well. But when that doesn’t happen because of social or administrative reasons, that’s hard.”
Where is the leadership?
“A lot of moral injury comes down to the individual health system and its leaders. Some have done well; others you hear saying things that make you question whether these are the people you want leading the organization. Hospitalists need to have a clear value framework and an idea of how to negotiate things when decisions don’t match that framework,” Dr. Barnes said.
“Sometimes administrators have additional information that they’re not sharing,” she added. “They’re caught between a rock and a hard place regarding the decisions they have to make, but they need to be more transparent and not hold things so close to their vest while thinking they are helping clinicians [by doing so]. Physicians need to understand why they are being asked to do things counter to what they believe is appropriate.”
David Oliver, MD, a geriatrics and internal medicine consultant at Royal Berkshire Hospital in Reading, England, also practices as a hospital physician, a role similar to the hospitalist in the United States. “In any system, in any environment, the job of being a doctor, nurse, or other health professional carries a lot of responsibility. That is a timeless, inherent stress of medical practice. With COVID, we’ve seen a lot of emotional burdens – a whole separate set of problems outside of your control, where you are responsible for care but don’t have accountability,” he said.
“People like me, hospital doctors, are used to chronic workforce issues in the National Health Service. But we didn’t sign up to come and get COVID and be hospitalized ourselves.” More than 850 frontline health care providers in the U.K. have so far died from the virus, Dr. Oliver said. “I saw five patients die in 90 minutes one day in April. That’s above and beyond normal human capacity.”
In England specifically, he said, it has exposed underlying structural issues and serious workforce gaps, unfilled vacancies, and a much lower number of ICU beds per 100,000 population than the United States or Europe. And there is consistent pressure to send patients home in order to empty beds for new patients.
But a range of supportive services is offered in U.K. hospitals, such as making senior clinicians available to speak to frontline clinicians, providing mentorship and a sounding board. The Point of Care Foundation has helped to disseminate the practice of Schwartz Rounds, a group reflective practice forum for health care teams developed by the Schwartz Center for Compassionate Healthcare in Boston.
“We don’t need this clap-for-the-NHS heroes stuff,” Dr. Oliver said. “We need an adequate workforce and [better] working conditions. What happened on the front lines of the pandemic was heroic – all done by local clinical teams. But where was the government – the centralized NHS? A lot of frontline clinicians aren’t feeling valued, supported, or listened to.”
What can be done?
What are some things that hospitalists can do, individually and collectively, to try to prevent moral distress from turning into full-scale burnout? Dr. Wocial emphasized the importance of unit-based ethics conversations. “At IU Health we have someone who is available to sit down with frontline clinicians and help unpack what they are experiencing,” she said. Clinicians need to be able to process this terrible experience in order to sort out the feelings of sadness from questions of whether they are doing something wrong.
Hospital chaplains are exquisitely skilled at supporting people and debriefing hospital teams, Dr. Wocial added. Palliative care professionals are also skilled at facilitating goals of care conversations with patients and families and can support hospitalists through coaching and joint family meetings.
“It’s about raising your sense of agency in your job – what in your practice you can control. People need to be able to talk frankly about it. Some managers say to clinicians: ‘Just buck up,’ while others are doing a fabulous job of offering support to their staff,” Dr. Wocial said. Hospitalists have to be willing to say when they’ve had too much. “You may not get help when you first ask for it. Be persistent. Asking for help doesn’t make you weak.”
Most doctors have their own strategies for managing stress on the job, Dr. Wachter noted. “What makes it a little easier is not having to do it alone. Many find solace in community, but community has been constrained by this pandemic. You can’t just go out for a beer after work anymore. So what are other ways to let off steam?”
The people leading hospitalist programs need to work harder at creating community and empathy when the tools allowing people to get together are somewhat limited. “Everybody is tired of Zoom,” he said. “One thing I learned as a manager was to just send messages to people acknowledging that I know this is hard. Try to think from the lens of other people and what they would find useful.”
The pandemic has been terribly unpredictable, Dr. Wachter added, but it won’t go on forever. For some doctors, yoga or mindfulness meditation may be very comforting. “For me, that’s not what I do. Golf or a good Seinfeld episode works for me.”
SHM’s Wellbeing Taskforce has created a “Hospital Medicine COVID Check-in Guide for Self & Peers” to promote both sharing and support for one another. It can be found at SHM’s Wellbeing webpage [www.hospitalmedicine.org/practice-management/wellbeing/]. The Taskforce believes that sharing common stressors as hospitalists can be healing, said its chair, Sarah Richards, MD, assistant professor of medicine at the University of Nebraska, Omaha. “This is especially true in situations where we feel we can’t provide the type of care we know our patients deserve.”
Respect, advocacy, self-care
Dr. Asken encouraged clinicians to focus on the efforts they are making on the job, not just the outcomes. “If someone has done their absolute best in a given circumstance, satisfaction and solace needs to be taken from that,” he said.
“Ongoing support group meetings, which we have called frontline support groups, should occur on a regular basis. Designated for physicians on the medical floors and in critical care units who are directly involved with COVID patients, these provide a brief respite but also engagement, sharing, and strengthening of mutual support.”
A lot of these issues have a fundamental thread, which comes down to respect, Dr. Barnes said. “Hospitalists need to hear their hospital administrators say: ‘I hear what you’re saying [about a problem]. Let’s think together about how to solve it.’ We need to work on being clear, and we need to speak up for what’s right. If you aren’t comfortable doing things you are being asked to do in the hospital, maybe you’re not working in the right place.”
Some efforts in the area of wellness and self-care really are helpful, Dr. Barnes said. “But you can’t exercise you way through a health system that doesn’t respect you. You need to get out of the mindset that you have no ability to make things different. We are not powerless as doctors. We can do a lot, actually. Physicians need to take ownership. If you are a hospitalist and you’re not part of any local or state or national organization that advocates for physicians, you should be.”
References
1. Dzeng L and Wachter RM. Ethics in conflict: Moral distress as a root cause of burnout. J Gen Intern Med. 2020 Feb;35(2):409-11. doi: 10.1007/s11606-019-05505-6.
2. Jameton A, Nursing Practice: The ethical issues. Prentice Hall Series in the Philosophy of Medicine. 1984, Englewood Cliffs, N.J.: Prentice Hall.
3. Wocial LD et al. Factors associated with physician moral distress caring for hospitalized elderly patients needing a surrogate decision-maker: A prospective study. J Gen Intern Med. 2020 May;35(5):1405-12. doi: 10.1007/s11606-020-05652-1.
4. Asken MJ. It’s not moral injury: It’s burnout (or something else). Medical Economics; June 7, 2019.
5. Asken MJ. Now it is moral injury: The COVID-19 pandemic and moral distress. Medical Economics; April 29, 2020.
Moral distress can result when health professionals like doctors and nurses feel prevented from doing what they know is right and ethically correct – reflecting the values of their profession and their own sense of professional integrity – because of unmanageable caseload demands, lack of resources, coverage limitations, or institutional policies.
Hospitalists are not exempt from moral distress, which is associated with soul-searching, burnout, and even PTSD. It is also associated with a higher likelihood for professionals to report an intention to leave their jobs. But the COVID-19 pandemic has superimposed a whole new layer of challenges, constraints, and frustrations, creating a potent mix of trauma and exhaustion, cumulative unease, depleted job satisfaction, and difficult ethical choices.
These challenges include seeing so many patients die and working with short supplies of personal protective equipment (PPE) – with resulting fears that they could catch the virus or pass it on to others, including loved ones. Also, not having enough ventilators or even beds for patients in hospitals hit hard by COVID surges raises fears that decisions for rationing medical care might become necessary.
In a commentary published in the Journal of General Internal Medicine in October 2019 – shortly before the COVID pandemic burst onto the scene – hospitalist and medical sociologist Elizabeth Dzeng, MD, PhD, MPH, and hospital medicine pioneer Robert Wachter, MD, MHM, both from the University of California, San Francisco, described “moral distress and professional ethical dissonance as root causes of burnout.”1 They characterized moral distress by its emotional exhaustion, depersonalization, reduced sense of accomplishment, and moral apathy, and they called for renewed attention to social and ethical dimensions of practice and threats to physician professionalism.
Prevailing explanations for documented high rates of burnout in doctors have tended to focus on work hours and struggles with electronic medical records and the like, Dr. Dzeng and Dr. Wachter wrote. “We see evidence of an insidious moral distress resulting from physicians’ inability to act in accord with their individual and professional ethical values due to institutional and social constraints.”
COVID has intensified these issues surrounding moral distress. “In a short period of time it created more situations that raise issues of moral distress than I have seen since the early days of HIV,” Dr. Wachter said. “Those of us who work in hospitals often find ourselves in complex circumstances with limited resources. What was so striking about COVID was finding ourselves caring for large volumes of patients who had a condition that was new to us.”
And the fact that constraints imposed by COVID, such as having to don unwieldy PPE and not allowing families to be present with hospitalized loved ones, are explainable and rational only helps a little with the clinician’s distress.
People talk about the need for doctors to be more resilient, Dr. Dzeng added, but that’s too narrow of an approach to these very real challenges. There are huge issues of workforce retention and costs, major mental health issues, suicide – and implications for patient care, because burned-out doctors can be bad doctors.
What is moral distress?
Moral distress is a term from the nursing ethics literature, attributed to philosopher Andrew Jameton in 1984.2 Contributors to moral distress imposed by COVID include having to make difficult medical decisions under stressful circumstances – especially early on, when effective treatment options were few. Doctors felt the demands of the pandemic were putting care quality and patient safety at risk. Poor working conditions overall, being pushed to work beyond their normal physical limits for days at a time, and feelings of not being valued added to this stress. But some say the pandemic has only highlighted and amplified existing inequities and disparities in the health care system.
Experts say moral distress is about feeling powerless, especially in a system driven by market values, and feeling let down by a society that has put them in harm’s way. They work all day under physically and emotionally exhausting conditions and then go home to hear specious conspiracy theories about the pandemic and see other people unwilling to wear masks.
Moral distress is complicated, said Lucia Wocial, PhD, RN, a nurse ethicist and cochair of the ethics consultation subcommittee at Indiana University Health in Indianapolis. “If you say you have moral distress, my first response is: tell me more. It helps to peel back the layers of this complexity. Emotion is only part of moral distress. It’s about the professional’s sense of responsibility and obligation – and the inability to honor that.”
Dr. Wocial, whose research specialty is moral distress, is corresponding author of a study published in the Journal of General Internal Medicine in February 2020, which identified moral distress in 4 out of 10 surveyed physicians who cared for older hospitalized adults and found themselves needing to work with their surrogate decision-makers.3 “We know physician moral distress is higher when people haven’t had the chance to hold conversations about their end-of-life care preferences,” she said, such as whether to continue life support.
“We have also learned that communication is key to diminishing physician moral distress. Our responsibility as clinicians is to guide patients and families through these decisions. If the family feels a high level of support from me, then my moral distress is lower,” she added. “If you think about how COVID has evolved, at first people were dying so quickly. Some patients were going to the ICU on ventilators without ever having a goals-of-care conversation.”
COVID has shifted the usual standard of care in U.S. hospitals in the face of patient surges. “How can you feel okay in accepting a level of care that in the prepandemic world would not have been acceptable?” Dr. Wocial posed. “What if you know the standard of care has shifted, of necessity, but you haven’t had time to prepare for it and nobody’s talking about what that means? Who is going to help you accept that good enough under these circumstances is enough – at least for today?”
What to call it
Michael J. Asken, PhD, director of provider well-being at UPMC Pinnacle Harrisburg (Pa.), has questioned in print the use of the military and wartime term “moral injury” when applied to a variety of less serious physician stressors.4 More recently, however, he observed, “The pandemic has muted or erased many of the distinctions between medical care and military conflict. ... The onslaught and volume of critical patients and resulting deaths is beyond what most providers have ever contemplated as part of care.”5
In a recent interview with the Hospitalist, he said: “While I initially resisted using the term moral injury, especially pre-COVID, because it was not equivalent to the moral injury created by war, I have relented a bit.” The volume of deaths and the apparent dangers to providers themselves reflect some of the critical aspects of war, and repetitive, intense, and/or incessant ethical challenges may have longer term negative psychological or emotional effects.
“Feeling emotional pain in situations of multiple deaths is to be expected and, perhaps, should even be welcomed as a sign of retained humanity and a buffer against burnout and cynicism in these times of unabating stress,” Dr. Asken said. “This is only true, however, if the emotional impact is tolerable and not experienced in repetitive extremes.”
“These things are real,” said Clarissa Barnes, MD, a physician adviser, hospitalist at Avera McKennan Hospital in Sioux Falls, S.D., and former medical director of Avera’s LIGHT Program, a wellness-oriented service for clinicians. Dr. Barnes herself caught the virus on the job but has since recovered.
“Physicians don’t see their work as an occupation. It’s their core identity: I am a doctor; I practice medicine. If things are being done in ways I don’t think are right, that’s fundamentally a breach,” she said. “As internists, we have an opportunity to forestall death whenever we can and, if not, promote a peaceful death. That’s what made me choose this specialty. I think there’s value in allowing a person to end well. But when that doesn’t happen because of social or administrative reasons, that’s hard.”
Where is the leadership?
“A lot of moral injury comes down to the individual health system and its leaders. Some have done well; others you hear saying things that make you question whether these are the people you want leading the organization. Hospitalists need to have a clear value framework and an idea of how to negotiate things when decisions don’t match that framework,” Dr. Barnes said.
“Sometimes administrators have additional information that they’re not sharing,” she added. “They’re caught between a rock and a hard place regarding the decisions they have to make, but they need to be more transparent and not hold things so close to their vest while thinking they are helping clinicians [by doing so]. Physicians need to understand why they are being asked to do things counter to what they believe is appropriate.”
David Oliver, MD, a geriatrics and internal medicine consultant at Royal Berkshire Hospital in Reading, England, also practices as a hospital physician, a role similar to the hospitalist in the United States. “In any system, in any environment, the job of being a doctor, nurse, or other health professional carries a lot of responsibility. That is a timeless, inherent stress of medical practice. With COVID, we’ve seen a lot of emotional burdens – a whole separate set of problems outside of your control, where you are responsible for care but don’t have accountability,” he said.
“People like me, hospital doctors, are used to chronic workforce issues in the National Health Service. But we didn’t sign up to come and get COVID and be hospitalized ourselves.” More than 850 frontline health care providers in the U.K. have so far died from the virus, Dr. Oliver said. “I saw five patients die in 90 minutes one day in April. That’s above and beyond normal human capacity.”
In England specifically, he said, it has exposed underlying structural issues and serious workforce gaps, unfilled vacancies, and a much lower number of ICU beds per 100,000 population than the United States or Europe. And there is consistent pressure to send patients home in order to empty beds for new patients.
But a range of supportive services is offered in U.K. hospitals, such as making senior clinicians available to speak to frontline clinicians, providing mentorship and a sounding board. The Point of Care Foundation has helped to disseminate the practice of Schwartz Rounds, a group reflective practice forum for health care teams developed by the Schwartz Center for Compassionate Healthcare in Boston.
“We don’t need this clap-for-the-NHS heroes stuff,” Dr. Oliver said. “We need an adequate workforce and [better] working conditions. What happened on the front lines of the pandemic was heroic – all done by local clinical teams. But where was the government – the centralized NHS? A lot of frontline clinicians aren’t feeling valued, supported, or listened to.”
What can be done?
What are some things that hospitalists can do, individually and collectively, to try to prevent moral distress from turning into full-scale burnout? Dr. Wocial emphasized the importance of unit-based ethics conversations. “At IU Health we have someone who is available to sit down with frontline clinicians and help unpack what they are experiencing,” she said. Clinicians need to be able to process this terrible experience in order to sort out the feelings of sadness from questions of whether they are doing something wrong.
Hospital chaplains are exquisitely skilled at supporting people and debriefing hospital teams, Dr. Wocial added. Palliative care professionals are also skilled at facilitating goals of care conversations with patients and families and can support hospitalists through coaching and joint family meetings.
“It’s about raising your sense of agency in your job – what in your practice you can control. People need to be able to talk frankly about it. Some managers say to clinicians: ‘Just buck up,’ while others are doing a fabulous job of offering support to their staff,” Dr. Wocial said. Hospitalists have to be willing to say when they’ve had too much. “You may not get help when you first ask for it. Be persistent. Asking for help doesn’t make you weak.”
Most doctors have their own strategies for managing stress on the job, Dr. Wachter noted. “What makes it a little easier is not having to do it alone. Many find solace in community, but community has been constrained by this pandemic. You can’t just go out for a beer after work anymore. So what are other ways to let off steam?”
The people leading hospitalist programs need to work harder at creating community and empathy when the tools allowing people to get together are somewhat limited. “Everybody is tired of Zoom,” he said. “One thing I learned as a manager was to just send messages to people acknowledging that I know this is hard. Try to think from the lens of other people and what they would find useful.”
The pandemic has been terribly unpredictable, Dr. Wachter added, but it won’t go on forever. For some doctors, yoga or mindfulness meditation may be very comforting. “For me, that’s not what I do. Golf or a good Seinfeld episode works for me.”
SHM’s Wellbeing Taskforce has created a “Hospital Medicine COVID Check-in Guide for Self & Peers” to promote both sharing and support for one another. It can be found at SHM’s Wellbeing webpage [www.hospitalmedicine.org/practice-management/wellbeing/]. The Taskforce believes that sharing common stressors as hospitalists can be healing, said its chair, Sarah Richards, MD, assistant professor of medicine at the University of Nebraska, Omaha. “This is especially true in situations where we feel we can’t provide the type of care we know our patients deserve.”
Respect, advocacy, self-care
Dr. Asken encouraged clinicians to focus on the efforts they are making on the job, not just the outcomes. “If someone has done their absolute best in a given circumstance, satisfaction and solace needs to be taken from that,” he said.
“Ongoing support group meetings, which we have called frontline support groups, should occur on a regular basis. Designated for physicians on the medical floors and in critical care units who are directly involved with COVID patients, these provide a brief respite but also engagement, sharing, and strengthening of mutual support.”
A lot of these issues have a fundamental thread, which comes down to respect, Dr. Barnes said. “Hospitalists need to hear their hospital administrators say: ‘I hear what you’re saying [about a problem]. Let’s think together about how to solve it.’ We need to work on being clear, and we need to speak up for what’s right. If you aren’t comfortable doing things you are being asked to do in the hospital, maybe you’re not working in the right place.”
Some efforts in the area of wellness and self-care really are helpful, Dr. Barnes said. “But you can’t exercise you way through a health system that doesn’t respect you. You need to get out of the mindset that you have no ability to make things different. We are not powerless as doctors. We can do a lot, actually. Physicians need to take ownership. If you are a hospitalist and you’re not part of any local or state or national organization that advocates for physicians, you should be.”
References
1. Dzeng L and Wachter RM. Ethics in conflict: Moral distress as a root cause of burnout. J Gen Intern Med. 2020 Feb;35(2):409-11. doi: 10.1007/s11606-019-05505-6.
2. Jameton A, Nursing Practice: The ethical issues. Prentice Hall Series in the Philosophy of Medicine. 1984, Englewood Cliffs, N.J.: Prentice Hall.
3. Wocial LD et al. Factors associated with physician moral distress caring for hospitalized elderly patients needing a surrogate decision-maker: A prospective study. J Gen Intern Med. 2020 May;35(5):1405-12. doi: 10.1007/s11606-020-05652-1.
4. Asken MJ. It’s not moral injury: It’s burnout (or something else). Medical Economics; June 7, 2019.
5. Asken MJ. Now it is moral injury: The COVID-19 pandemic and moral distress. Medical Economics; April 29, 2020.
Most kids with type 1 diabetes and COVID-19 in U.S. fared well
The majority of children with type 1 diabetes who tested positive for SARS-CoV-2 were cared for at home and did well, according to the first report of outcomes of pediatric patients with type 1 diabetes and COVID-19 from the United States.
Most children who were hospitalized had diabetic ketoacidosis (DKA) and high hemoglobin A1c levels, the new report from the T1D Exchange Quality Improvement Collaborative indicates. Fewer than 2% required respiratory support, and no deaths were recorded.
The greatest risk for adverse COVID-19 outcomes was among children with A1c levels >9%. In addition, children of certain ethnic minority groups and those with public health insurance were more likely to be hospitalized.
The study, conducted by G. Todd Alonso, MD, of the University of Colorado, Barbara Davis Center, Aurora, and colleagues, was published online April 14 in the Journal of Diabetes..
“As early reports identified diabetes as a risk factor for increased morbidity and mortality with COVID-19, the findings from this surveillance study should provide measured reassurance for families of children with type 1 diabetes as well as pediatric endocrinologists and their care teams,” say Dr. Alonso and colleagues.
Disproportionate rate of hospitalization, DKA among Black patients
Initiated in April 2020, the T1D Exchange Quality Improvement Collaborative comprises 56 diabetes centers, of which 52 submitted a total of 266 cases involving patients younger than 19 years who had type 1 diabetes and who tested positive for SARS-CoV-2 infection. Those with new-onset type 1 diabetes were excluded from this analysis and were reported separately. The data were collected between April 9, 2020, and Jan. 15, 2021.
Of the 266 patients, 23% (61) were hospitalized, and 205 were not. There were no differences by age, gender, or diabetes duration.
However, those hospitalized were more likely to be Black (34% vs. 13% among White patients; P < .001) and to have public health insurance (64% vs. 41%; P < .001). They also had higher A1c levels than patients who were not hospitalized (11% vs. 8.2%; P < .001), and fewer used insulin pumps (26% vs. 54%; P < .001) and continuous glucose monitors (39% vs. 75%; P < .001).
Those hospitalized were also more likely to have hyperglycemia (48% vs. 28%; P = .007), nausea (33% vs. 6%; P < .001), and vomiting (49% vs. 3%; P < .001). Rates of dry cough, excess fatigue, and body aches/headaches did not differ between those hospitalized and those who remained at home.
The most common adverse outcome was DKA, which occurred in 72% (44) of those hospitalized.
The most recent A1c level was less than 9% in 82% of those hospitalized vs. 31% of those who weren’t (P < .001) and in 38 of the 44 (86%) who had DKA.
“Our data reveal a disproportionate rate of hospitalization and DKA among racial and ethnic minority groups, children who were publicly insured, and those with higher A1c. It is essential to find pathways for the most vulnerable patients to have adequate, equitable access to medical care via in person and telehealth services, to obtain and successfully use diabetes technology, and to optimize sick day management,” say Dr. Alonso and colleagues.
One child, a 15-year-old White boy, underwent intubation and was placed on a ventilator. His most recent A1c was 8.9%. Another child, a 13-year-old boy whose most recent A1c level was 11.1%, developed multisystem inflammatory syndrome of childhood.
The registry remains open.
The T1D Exchange QI Collaborative is funded by the Helmsley Charitable Trust. The T1D Exchange received partial financial support for this study from Abbott Diabetes, Dexcom, Medtronic, Insulet Corporation, JDRF, Eli Lilly, and Tandem Diabetes Care. None of the sponsors were involved in initiating, designing, or preparing the manuscript for this study.
A version of this article first appeared on Medscape.com.
The majority of children with type 1 diabetes who tested positive for SARS-CoV-2 were cared for at home and did well, according to the first report of outcomes of pediatric patients with type 1 diabetes and COVID-19 from the United States.
Most children who were hospitalized had diabetic ketoacidosis (DKA) and high hemoglobin A1c levels, the new report from the T1D Exchange Quality Improvement Collaborative indicates. Fewer than 2% required respiratory support, and no deaths were recorded.
The greatest risk for adverse COVID-19 outcomes was among children with A1c levels >9%. In addition, children of certain ethnic minority groups and those with public health insurance were more likely to be hospitalized.
The study, conducted by G. Todd Alonso, MD, of the University of Colorado, Barbara Davis Center, Aurora, and colleagues, was published online April 14 in the Journal of Diabetes..
“As early reports identified diabetes as a risk factor for increased morbidity and mortality with COVID-19, the findings from this surveillance study should provide measured reassurance for families of children with type 1 diabetes as well as pediatric endocrinologists and their care teams,” say Dr. Alonso and colleagues.
Disproportionate rate of hospitalization, DKA among Black patients
Initiated in April 2020, the T1D Exchange Quality Improvement Collaborative comprises 56 diabetes centers, of which 52 submitted a total of 266 cases involving patients younger than 19 years who had type 1 diabetes and who tested positive for SARS-CoV-2 infection. Those with new-onset type 1 diabetes were excluded from this analysis and were reported separately. The data were collected between April 9, 2020, and Jan. 15, 2021.
Of the 266 patients, 23% (61) were hospitalized, and 205 were not. There were no differences by age, gender, or diabetes duration.
However, those hospitalized were more likely to be Black (34% vs. 13% among White patients; P < .001) and to have public health insurance (64% vs. 41%; P < .001). They also had higher A1c levels than patients who were not hospitalized (11% vs. 8.2%; P < .001), and fewer used insulin pumps (26% vs. 54%; P < .001) and continuous glucose monitors (39% vs. 75%; P < .001).
Those hospitalized were also more likely to have hyperglycemia (48% vs. 28%; P = .007), nausea (33% vs. 6%; P < .001), and vomiting (49% vs. 3%; P < .001). Rates of dry cough, excess fatigue, and body aches/headaches did not differ between those hospitalized and those who remained at home.
The most common adverse outcome was DKA, which occurred in 72% (44) of those hospitalized.
The most recent A1c level was less than 9% in 82% of those hospitalized vs. 31% of those who weren’t (P < .001) and in 38 of the 44 (86%) who had DKA.
“Our data reveal a disproportionate rate of hospitalization and DKA among racial and ethnic minority groups, children who were publicly insured, and those with higher A1c. It is essential to find pathways for the most vulnerable patients to have adequate, equitable access to medical care via in person and telehealth services, to obtain and successfully use diabetes technology, and to optimize sick day management,” say Dr. Alonso and colleagues.
One child, a 15-year-old White boy, underwent intubation and was placed on a ventilator. His most recent A1c was 8.9%. Another child, a 13-year-old boy whose most recent A1c level was 11.1%, developed multisystem inflammatory syndrome of childhood.
The registry remains open.
The T1D Exchange QI Collaborative is funded by the Helmsley Charitable Trust. The T1D Exchange received partial financial support for this study from Abbott Diabetes, Dexcom, Medtronic, Insulet Corporation, JDRF, Eli Lilly, and Tandem Diabetes Care. None of the sponsors were involved in initiating, designing, or preparing the manuscript for this study.
A version of this article first appeared on Medscape.com.
The majority of children with type 1 diabetes who tested positive for SARS-CoV-2 were cared for at home and did well, according to the first report of outcomes of pediatric patients with type 1 diabetes and COVID-19 from the United States.
Most children who were hospitalized had diabetic ketoacidosis (DKA) and high hemoglobin A1c levels, the new report from the T1D Exchange Quality Improvement Collaborative indicates. Fewer than 2% required respiratory support, and no deaths were recorded.
The greatest risk for adverse COVID-19 outcomes was among children with A1c levels >9%. In addition, children of certain ethnic minority groups and those with public health insurance were more likely to be hospitalized.
The study, conducted by G. Todd Alonso, MD, of the University of Colorado, Barbara Davis Center, Aurora, and colleagues, was published online April 14 in the Journal of Diabetes..
“As early reports identified diabetes as a risk factor for increased morbidity and mortality with COVID-19, the findings from this surveillance study should provide measured reassurance for families of children with type 1 diabetes as well as pediatric endocrinologists and their care teams,” say Dr. Alonso and colleagues.
Disproportionate rate of hospitalization, DKA among Black patients
Initiated in April 2020, the T1D Exchange Quality Improvement Collaborative comprises 56 diabetes centers, of which 52 submitted a total of 266 cases involving patients younger than 19 years who had type 1 diabetes and who tested positive for SARS-CoV-2 infection. Those with new-onset type 1 diabetes were excluded from this analysis and were reported separately. The data were collected between April 9, 2020, and Jan. 15, 2021.
Of the 266 patients, 23% (61) were hospitalized, and 205 were not. There were no differences by age, gender, or diabetes duration.
However, those hospitalized were more likely to be Black (34% vs. 13% among White patients; P < .001) and to have public health insurance (64% vs. 41%; P < .001). They also had higher A1c levels than patients who were not hospitalized (11% vs. 8.2%; P < .001), and fewer used insulin pumps (26% vs. 54%; P < .001) and continuous glucose monitors (39% vs. 75%; P < .001).
Those hospitalized were also more likely to have hyperglycemia (48% vs. 28%; P = .007), nausea (33% vs. 6%; P < .001), and vomiting (49% vs. 3%; P < .001). Rates of dry cough, excess fatigue, and body aches/headaches did not differ between those hospitalized and those who remained at home.
The most common adverse outcome was DKA, which occurred in 72% (44) of those hospitalized.
The most recent A1c level was less than 9% in 82% of those hospitalized vs. 31% of those who weren’t (P < .001) and in 38 of the 44 (86%) who had DKA.
“Our data reveal a disproportionate rate of hospitalization and DKA among racial and ethnic minority groups, children who were publicly insured, and those with higher A1c. It is essential to find pathways for the most vulnerable patients to have adequate, equitable access to medical care via in person and telehealth services, to obtain and successfully use diabetes technology, and to optimize sick day management,” say Dr. Alonso and colleagues.
One child, a 15-year-old White boy, underwent intubation and was placed on a ventilator. His most recent A1c was 8.9%. Another child, a 13-year-old boy whose most recent A1c level was 11.1%, developed multisystem inflammatory syndrome of childhood.
The registry remains open.
The T1D Exchange QI Collaborative is funded by the Helmsley Charitable Trust. The T1D Exchange received partial financial support for this study from Abbott Diabetes, Dexcom, Medtronic, Insulet Corporation, JDRF, Eli Lilly, and Tandem Diabetes Care. None of the sponsors were involved in initiating, designing, or preparing the manuscript for this study.
A version of this article first appeared on Medscape.com.
COVID lockdowns linked to PTSD in patients with eating disorders
COVID-19 and its resulting lockdowns are linked to posttraumatic stress disorder symptoms and other adverse outcomes among patients with eating disorders (EDs), two new studies show.

Results of the first study show that patients with EDs had more stress, anxiety, depression, and PTSD-related symptoms during the lockdowns than their mentally healthy peers.
In the second study, treatment-related symptom improvement among patients with bulimia nervosa (BN) slowed following lockdown. In addition, patients with BN or anorexia nervosa (AN) experienced significant worsening of disorder-specific behaviors, including binge eating and overexercising.
Because of the strict lockdown measures introduced by the Italian government to contain the COVID-19 pandemic, “everyday life of all citizens was disrupted,” Veronica Nisticò, MS, Università Degli Studi Di Milano, who led the first study, told delegates attending the virtual European Psychiatric Association 2021 Congress.

In addition to difficulties in accessing health care, “it became difficult to go to the supermarket, to the gym, and to have the social support we were all used to,” all of which had a well-documented impact on mental health, added Ms. Nisticò, who is also affiliated with Aldo Ravelli Research Center for Neurotechnology and Experimental Brain Therapeutics.
Loss of control
Previous research suggests that individuals with EDs experience high levels of anxiety and an increase in binge eating, exercise, and purging behaviors, said Ms. Nisticò.
To investigate further, the researchers conducted a longitudinal study of the changes in prevalence of adverse outcomes. In the study, two assessments were conducted.
The second group served as the control group.
Participants completed an online survey that included several standardized depression and anxiety scales, as well as an ad hoc survey adapted from the Eating Disorder Examination Questionnaire. This assessed changes in restrictive dieting, control over food, body image, and psychological well-being in comparison with prepandemic levels.
The results, which were also recently published online in Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity, showed that patients with EDs experienced significantly more stress, anxiety, depression, and PTSD-related symptoms in comparison with control persons (P < .05 for all).
In addition, the investigators found that those with EDs were more fearful of losing control over their eating behavior, spent more time thinking about food and their body, and became more uncomfortable seeing their body than before the lockdown in comparison with those without EDs (P < .05).
Clinical implications
A second assessment, which occurred in June 2020, after lockdown restrictions were lifted, included 40 patients with EDs who had taken part in the first assessment. This time, participants were asked to compare their current eating behavior with their eating behavior during the lockdown.
Although the lifting of lockdown restrictions was associated with significant improvement in PTSD-related symptoms, the impact on stress, anxiety, and depression persisted.
These findings, said Ms. Nisticó, support the hypothesis that specific conditions that occurred during the lockdown had a direct effect on specific ED symptoms.
These findings, she added, should be considered when developing interventions for EDs in the context of individual psychotherapy and when designing large, preventive interventions.
In the second study, Eleonora Rossi, MD, psychiatric unit, department of health sciences, University of Florence (Italy), and colleagues examined the longitudinal impact of the pandemic on individuals with EDs.
They examined 74 patients with AN or BN who had undergone baseline assessments and had completed a number of questionnaires in the first months of 2019 in conjunction with being enrolled in another study.
Participants were treated with enhanced cognitive-behavioral therapy and were reevaluated between November 2019 and January 2020. They were then compared with 97 healthy individuals.
Bulimia patients more vulnerable
After the outbreak of the pandemic, most treatment was administered online, so patients were able to continue therapy, Dr. Rossi said during her presentation.
All participants were assessed again in April 2020, 6 weeks after the start of Italy’s lockdown.
The results, which were published in the International Journal of Eating Disorders, show that the patients with EDs “underwent a significant improvement in terms of general and eating disorder specific psychopathology” during the first treatment period, Dr. Rossi reported. In addition, among those with AN, body mass index increased significantly (P < .05 for all).
Patients with AN continued to improve during the lockdown when therapy was administered online. However, improvements that had occurred among those with BN slowed, Dr. Rossi noted.
In addition, both groups of patients with EDs experienced a worsening of their pathological eating behaviors during the lockdown, in particular, objective binge eating and compensatory physical exercise (P < .05).
“Indeed, the positive trajectory of improvement observed before lockdown was clearly interrupted during the pandemic period,” Dr. Rossi said. This could “represent a possible hint of an imminent exacerbation of the disease.”
The results also suggest that the occurrence of arguments within the household and fear regarding the safety of loved ones predicted an increase in symptoms during the lockdown, she added.
In addition, patients with BN reported more severe COVID-related PTSD symptoms than did those with AN and the control group. This increase in severity of symptoms was more prevalent among patients who had a history of childhood trauma and among those with insecure attachment, suggesting that such patients may be more vulnerable.
Evidence of recovery
Commenting on the studies, David Spiegel, MD, associate chair of psychiatry, Stanford (Calif.) University, noted that EDs commonly occur after physical or sexual trauma earlier in life.

“It’s a standard thing with trauma-related disorders that any other, even relatively minor, traumatic experience can exacerbate PTSD symptoms,” said Dr. Spiegel, who was not involved in the studies. In addition, the trauma of the COVID pandemic “was not minor.
“The relative isolation and the lack of outside contact may focus many people with eating disorders even more on their struggles with how they are taking care of their bodies,” said Dr. Spiegel.
“It struck me that the anorexia nervosa group were more impervious than the bulimia nervosa group, but I think that’s the case with the disorder. In some ways it’s more severe, obviously a more life-threatening disorder,” he added.
The “hopeful thing is that there seemed to be some evidence of recovery and improvement, particularly with the posttraumatic stress exacerbation, as time went on,” Dr. Spiegel said, “and that’s a good thing.”
The study authors and Dr. Spiegel reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID-19 and its resulting lockdowns are linked to posttraumatic stress disorder symptoms and other adverse outcomes among patients with eating disorders (EDs), two new studies show.
Results of the first study show that patients with EDs had more stress, anxiety, depression, and PTSD-related symptoms during the lockdowns than their mentally healthy peers.
In the second study, treatment-related symptom improvement among patients with bulimia nervosa (BN) slowed following lockdown. In addition, patients with BN or anorexia nervosa (AN) experienced significant worsening of disorder-specific behaviors, including binge eating and overexercising.
Because of the strict lockdown measures introduced by the Italian government to contain the COVID-19 pandemic, “everyday life of all citizens was disrupted,” Veronica Nisticò, MS, Università Degli Studi Di Milano, who led the first study, told delegates attending the virtual European Psychiatric Association 2021 Congress.
In addition to difficulties in accessing health care, “it became difficult to go to the supermarket, to the gym, and to have the social support we were all used to,” all of which had a well-documented impact on mental health, added Ms. Nisticò, who is also affiliated with Aldo Ravelli Research Center for Neurotechnology and Experimental Brain Therapeutics.
Loss of control
Previous research suggests that individuals with EDs experience high levels of anxiety and an increase in binge eating, exercise, and purging behaviors, said Ms. Nisticò.
To investigate further, the researchers conducted a longitudinal study of the changes in prevalence of adverse outcomes. In the study, two assessments were conducted.
The second group served as the control group.
Participants completed an online survey that included several standardized depression and anxiety scales, as well as an ad hoc survey adapted from the Eating Disorder Examination Questionnaire. This assessed changes in restrictive dieting, control over food, body image, and psychological well-being in comparison with prepandemic levels.
The results, which were also recently published online in Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity, showed that patients with EDs experienced significantly more stress, anxiety, depression, and PTSD-related symptoms in comparison with control persons (P < .05 for all).
In addition, the investigators found that those with EDs were more fearful of losing control over their eating behavior, spent more time thinking about food and their body, and became more uncomfortable seeing their body than before the lockdown in comparison with those without EDs (P < .05).
Clinical implications
A second assessment, which occurred in June 2020, after lockdown restrictions were lifted, included 40 patients with EDs who had taken part in the first assessment. This time, participants were asked to compare their current eating behavior with their eating behavior during the lockdown.
Although the lifting of lockdown restrictions was associated with significant improvement in PTSD-related symptoms, the impact on stress, anxiety, and depression persisted.
These findings, said Ms. Nisticó, support the hypothesis that specific conditions that occurred during the lockdown had a direct effect on specific ED symptoms.
These findings, she added, should be considered when developing interventions for EDs in the context of individual psychotherapy and when designing large, preventive interventions.
In the second study, Eleonora Rossi, MD, psychiatric unit, department of health sciences, University of Florence (Italy), and colleagues examined the longitudinal impact of the pandemic on individuals with EDs.
They examined 74 patients with AN or BN who had undergone baseline assessments and had completed a number of questionnaires in the first months of 2019 in conjunction with being enrolled in another study.
Participants were treated with enhanced cognitive-behavioral therapy and were reevaluated between November 2019 and January 2020. They were then compared with 97 healthy individuals.
Bulimia patients more vulnerable
After the outbreak of the pandemic, most treatment was administered online, so patients were able to continue therapy, Dr. Rossi said during her presentation.
All participants were assessed again in April 2020, 6 weeks after the start of Italy’s lockdown.
The results, which were published in the International Journal of Eating Disorders, show that the patients with EDs “underwent a significant improvement in terms of general and eating disorder specific psychopathology” during the first treatment period, Dr. Rossi reported. In addition, among those with AN, body mass index increased significantly (P < .05 for all).
Patients with AN continued to improve during the lockdown when therapy was administered online. However, improvements that had occurred among those with BN slowed, Dr. Rossi noted.
In addition, both groups of patients with EDs experienced a worsening of their pathological eating behaviors during the lockdown, in particular, objective binge eating and compensatory physical exercise (P < .05).
“Indeed, the positive trajectory of improvement observed before lockdown was clearly interrupted during the pandemic period,” Dr. Rossi said. This could “represent a possible hint of an imminent exacerbation of the disease.”
The results also suggest that the occurrence of arguments within the household and fear regarding the safety of loved ones predicted an increase in symptoms during the lockdown, she added.
In addition, patients with BN reported more severe COVID-related PTSD symptoms than did those with AN and the control group. This increase in severity of symptoms was more prevalent among patients who had a history of childhood trauma and among those with insecure attachment, suggesting that such patients may be more vulnerable.
Evidence of recovery
Commenting on the studies, David Spiegel, MD, associate chair of psychiatry, Stanford (Calif.) University, noted that EDs commonly occur after physical or sexual trauma earlier in life.
“It’s a standard thing with trauma-related disorders that any other, even relatively minor, traumatic experience can exacerbate PTSD symptoms,” said Dr. Spiegel, who was not involved in the studies. In addition, the trauma of the COVID pandemic “was not minor.
“The relative isolation and the lack of outside contact may focus many people with eating disorders even more on their struggles with how they are taking care of their bodies,” said Dr. Spiegel.
“It struck me that the anorexia nervosa group were more impervious than the bulimia nervosa group, but I think that’s the case with the disorder. In some ways it’s more severe, obviously a more life-threatening disorder,” he added.
The “hopeful thing is that there seemed to be some evidence of recovery and improvement, particularly with the posttraumatic stress exacerbation, as time went on,” Dr. Spiegel said, “and that’s a good thing.”
The study authors and Dr. Spiegel reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID-19 and its resulting lockdowns are linked to posttraumatic stress disorder symptoms and other adverse outcomes among patients with eating disorders (EDs), two new studies show.
Results of the first study show that patients with EDs had more stress, anxiety, depression, and PTSD-related symptoms during the lockdowns than their mentally healthy peers.
In the second study, treatment-related symptom improvement among patients with bulimia nervosa (BN) slowed following lockdown. In addition, patients with BN or anorexia nervosa (AN) experienced significant worsening of disorder-specific behaviors, including binge eating and overexercising.
Because of the strict lockdown measures introduced by the Italian government to contain the COVID-19 pandemic, “everyday life of all citizens was disrupted,” Veronica Nisticò, MS, Università Degli Studi Di Milano, who led the first study, told delegates attending the virtual European Psychiatric Association 2021 Congress.
In addition to difficulties in accessing health care, “it became difficult to go to the supermarket, to the gym, and to have the social support we were all used to,” all of which had a well-documented impact on mental health, added Ms. Nisticò, who is also affiliated with Aldo Ravelli Research Center for Neurotechnology and Experimental Brain Therapeutics.
Loss of control
Previous research suggests that individuals with EDs experience high levels of anxiety and an increase in binge eating, exercise, and purging behaviors, said Ms. Nisticò.
To investigate further, the researchers conducted a longitudinal study of the changes in prevalence of adverse outcomes. In the study, two assessments were conducted.
The second group served as the control group.
Participants completed an online survey that included several standardized depression and anxiety scales, as well as an ad hoc survey adapted from the Eating Disorder Examination Questionnaire. This assessed changes in restrictive dieting, control over food, body image, and psychological well-being in comparison with prepandemic levels.
The results, which were also recently published online in Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity, showed that patients with EDs experienced significantly more stress, anxiety, depression, and PTSD-related symptoms in comparison with control persons (P < .05 for all).
In addition, the investigators found that those with EDs were more fearful of losing control over their eating behavior, spent more time thinking about food and their body, and became more uncomfortable seeing their body than before the lockdown in comparison with those without EDs (P < .05).
Clinical implications
A second assessment, which occurred in June 2020, after lockdown restrictions were lifted, included 40 patients with EDs who had taken part in the first assessment. This time, participants were asked to compare their current eating behavior with their eating behavior during the lockdown.
Although the lifting of lockdown restrictions was associated with significant improvement in PTSD-related symptoms, the impact on stress, anxiety, and depression persisted.
These findings, said Ms. Nisticó, support the hypothesis that specific conditions that occurred during the lockdown had a direct effect on specific ED symptoms.
These findings, she added, should be considered when developing interventions for EDs in the context of individual psychotherapy and when designing large, preventive interventions.
In the second study, Eleonora Rossi, MD, psychiatric unit, department of health sciences, University of Florence (Italy), and colleagues examined the longitudinal impact of the pandemic on individuals with EDs.
They examined 74 patients with AN or BN who had undergone baseline assessments and had completed a number of questionnaires in the first months of 2019 in conjunction with being enrolled in another study.
Participants were treated with enhanced cognitive-behavioral therapy and were reevaluated between November 2019 and January 2020. They were then compared with 97 healthy individuals.
Bulimia patients more vulnerable
After the outbreak of the pandemic, most treatment was administered online, so patients were able to continue therapy, Dr. Rossi said during her presentation.
All participants were assessed again in April 2020, 6 weeks after the start of Italy’s lockdown.
The results, which were published in the International Journal of Eating Disorders, show that the patients with EDs “underwent a significant improvement in terms of general and eating disorder specific psychopathology” during the first treatment period, Dr. Rossi reported. In addition, among those with AN, body mass index increased significantly (P < .05 for all).
Patients with AN continued to improve during the lockdown when therapy was administered online. However, improvements that had occurred among those with BN slowed, Dr. Rossi noted.
In addition, both groups of patients with EDs experienced a worsening of their pathological eating behaviors during the lockdown, in particular, objective binge eating and compensatory physical exercise (P < .05).
“Indeed, the positive trajectory of improvement observed before lockdown was clearly interrupted during the pandemic period,” Dr. Rossi said. This could “represent a possible hint of an imminent exacerbation of the disease.”
The results also suggest that the occurrence of arguments within the household and fear regarding the safety of loved ones predicted an increase in symptoms during the lockdown, she added.
In addition, patients with BN reported more severe COVID-related PTSD symptoms than did those with AN and the control group. This increase in severity of symptoms was more prevalent among patients who had a history of childhood trauma and among those with insecure attachment, suggesting that such patients may be more vulnerable.
Evidence of recovery
Commenting on the studies, David Spiegel, MD, associate chair of psychiatry, Stanford (Calif.) University, noted that EDs commonly occur after physical or sexual trauma earlier in life.
“It’s a standard thing with trauma-related disorders that any other, even relatively minor, traumatic experience can exacerbate PTSD symptoms,” said Dr. Spiegel, who was not involved in the studies. In addition, the trauma of the COVID pandemic “was not minor.
“The relative isolation and the lack of outside contact may focus many people with eating disorders even more on their struggles with how they are taking care of their bodies,” said Dr. Spiegel.
“It struck me that the anorexia nervosa group were more impervious than the bulimia nervosa group, but I think that’s the case with the disorder. In some ways it’s more severe, obviously a more life-threatening disorder,” he added.
The “hopeful thing is that there seemed to be some evidence of recovery and improvement, particularly with the posttraumatic stress exacerbation, as time went on,” Dr. Spiegel said, “and that’s a good thing.”
The study authors and Dr. Spiegel reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AHA guidance on blood clots linked to COVID-19 vaccine
A newly released report is offering guidance concerning rare conditions associated with COVID-19 as well as vaccines against the virus.
The report was released April 29, 2021, by the American Heart Association/American Stroke Association Stroke Council Leadership in answer to the decision April 23 by the Centers for Disease Control and Prevention and the Food and Drug Administration to lift an earlier “pause” in administration of the Johnson & Johnson (Janssen) vaccine.
That pause had been put in place after reports were received of a possible association between the J&J vaccine and cerebral venous sinus thrombosis (CVST) and thrombosis-thrombocytopenia syndrome (TTS, blood clots plus low blood platelets). CVST and TTS were also linked to patients in Europe and Canada who received the AstraZeneca COVID-19 vaccine.
However, the new report noted that these conditions are very rare.
“The risk of CVST due to infection with COVID-19 is 8-10 times higher than the risk of CVST after receiving a COVID-19 vaccine,” lead author Karen L. Furie, MD, chair of the department of neurology at Brown University, Providence, R.I., said in a press release.
“The public can be reassured by the CDC’s and FDA’s investigation and these statistics – the likelihood of developing CVST after a COVID-19 vaccine is extremely low,” said Dr. Furie, adding that the authors “urge all adults to receive any of the approved COVID-19 vaccines.”
The new guidance, which was published online April 29, 2021, in Stroke, discusses signs and symptoms of CVST and TTS, as well as vaccine-induced immune thrombotic thrombocytopenia (VITT). It also recommends best options for treating these conditions.
Assessing 81 million patients
In their analysis, the investigators assessed a database of 59 health care organizations and 81 million patients, 98% of whom were in the United States.
Of almost 514,000 patients diagnosed with COVID-19 between January 2020 and March 2021, 20 also received a diagnosis of CVST.
Among about 490,000 adults who received either the Pfizer or Moderna vaccines, there were no diagnosed cases of thrombocytopenia.
Dr. Furie reiterated that CVST blood clots “are very rare adverse events,” but recommended that any patient in the ED with a suspected clot should be screened immediately to determine if they received a COVID vaccine during the previous few weeks.
For those who have recently received the COVID-19 vaccine, a suspected clot should be treated with nonheparin anticoagulants, Dr. Furie said.
“No heparin products in any dose should be given for suspected CVST, TTS, or VITT. With the right treatment, most patients can have a full recovery,” she added. The report includes additional, detailed treatment recommendations if one of these conditions are suspected.
Rare events
The authors noted that cases of TTS/VITT occurred up to 2.5 weeks after receiving the J&J vaccine in the United States and up to 3.5 weeks after receiving the AstraZeneca vaccine in Europe.
An April 23 report from the CDC and FDA noted that, out of almost 7 million adults who received the J&J vaccine, the agencies investigated only 15 reported cases of TTS.
An April 7 report from the European Medicines Agency noted that, out of more than 25 million people who received the AstraZeneca vaccine in the European Union, it found 62 cases of CVST.
A statement put out by the American Heart Association/American Stroke Association urges “everyone to receive a COVID-19 vaccine” as soon as possible.
“We are confident the benefits of vaccination far exceed the very small, rare risks,” the organizations said. “The risks of vaccination are also far smaller than the risk of COVID-19 and its potentially fatal consequences.”
A version of this article first appeared on Medscape.com.
A newly released report is offering guidance concerning rare conditions associated with COVID-19 as well as vaccines against the virus.
The report was released April 29, 2021, by the American Heart Association/American Stroke Association Stroke Council Leadership in answer to the decision April 23 by the Centers for Disease Control and Prevention and the Food and Drug Administration to lift an earlier “pause” in administration of the Johnson & Johnson (Janssen) vaccine.
That pause had been put in place after reports were received of a possible association between the J&J vaccine and cerebral venous sinus thrombosis (CVST) and thrombosis-thrombocytopenia syndrome (TTS, blood clots plus low blood platelets). CVST and TTS were also linked to patients in Europe and Canada who received the AstraZeneca COVID-19 vaccine.
However, the new report noted that these conditions are very rare.
“The risk of CVST due to infection with COVID-19 is 8-10 times higher than the risk of CVST after receiving a COVID-19 vaccine,” lead author Karen L. Furie, MD, chair of the department of neurology at Brown University, Providence, R.I., said in a press release.
“The public can be reassured by the CDC’s and FDA’s investigation and these statistics – the likelihood of developing CVST after a COVID-19 vaccine is extremely low,” said Dr. Furie, adding that the authors “urge all adults to receive any of the approved COVID-19 vaccines.”
The new guidance, which was published online April 29, 2021, in Stroke, discusses signs and symptoms of CVST and TTS, as well as vaccine-induced immune thrombotic thrombocytopenia (VITT). It also recommends best options for treating these conditions.
Assessing 81 million patients
In their analysis, the investigators assessed a database of 59 health care organizations and 81 million patients, 98% of whom were in the United States.
Of almost 514,000 patients diagnosed with COVID-19 between January 2020 and March 2021, 20 also received a diagnosis of CVST.
Among about 490,000 adults who received either the Pfizer or Moderna vaccines, there were no diagnosed cases of thrombocytopenia.
Dr. Furie reiterated that CVST blood clots “are very rare adverse events,” but recommended that any patient in the ED with a suspected clot should be screened immediately to determine if they received a COVID vaccine during the previous few weeks.
For those who have recently received the COVID-19 vaccine, a suspected clot should be treated with nonheparin anticoagulants, Dr. Furie said.
“No heparin products in any dose should be given for suspected CVST, TTS, or VITT. With the right treatment, most patients can have a full recovery,” she added. The report includes additional, detailed treatment recommendations if one of these conditions are suspected.
Rare events
The authors noted that cases of TTS/VITT occurred up to 2.5 weeks after receiving the J&J vaccine in the United States and up to 3.5 weeks after receiving the AstraZeneca vaccine in Europe.
An April 23 report from the CDC and FDA noted that, out of almost 7 million adults who received the J&J vaccine, the agencies investigated only 15 reported cases of TTS.
An April 7 report from the European Medicines Agency noted that, out of more than 25 million people who received the AstraZeneca vaccine in the European Union, it found 62 cases of CVST.
A statement put out by the American Heart Association/American Stroke Association urges “everyone to receive a COVID-19 vaccine” as soon as possible.
“We are confident the benefits of vaccination far exceed the very small, rare risks,” the organizations said. “The risks of vaccination are also far smaller than the risk of COVID-19 and its potentially fatal consequences.”
A version of this article first appeared on Medscape.com.
A newly released report is offering guidance concerning rare conditions associated with COVID-19 as well as vaccines against the virus.
The report was released April 29, 2021, by the American Heart Association/American Stroke Association Stroke Council Leadership in answer to the decision April 23 by the Centers for Disease Control and Prevention and the Food and Drug Administration to lift an earlier “pause” in administration of the Johnson & Johnson (Janssen) vaccine.
That pause had been put in place after reports were received of a possible association between the J&J vaccine and cerebral venous sinus thrombosis (CVST) and thrombosis-thrombocytopenia syndrome (TTS, blood clots plus low blood platelets). CVST and TTS were also linked to patients in Europe and Canada who received the AstraZeneca COVID-19 vaccine.
However, the new report noted that these conditions are very rare.
“The risk of CVST due to infection with COVID-19 is 8-10 times higher than the risk of CVST after receiving a COVID-19 vaccine,” lead author Karen L. Furie, MD, chair of the department of neurology at Brown University, Providence, R.I., said in a press release.
“The public can be reassured by the CDC’s and FDA’s investigation and these statistics – the likelihood of developing CVST after a COVID-19 vaccine is extremely low,” said Dr. Furie, adding that the authors “urge all adults to receive any of the approved COVID-19 vaccines.”
The new guidance, which was published online April 29, 2021, in Stroke, discusses signs and symptoms of CVST and TTS, as well as vaccine-induced immune thrombotic thrombocytopenia (VITT). It also recommends best options for treating these conditions.
Assessing 81 million patients
In their analysis, the investigators assessed a database of 59 health care organizations and 81 million patients, 98% of whom were in the United States.
Of almost 514,000 patients diagnosed with COVID-19 between January 2020 and March 2021, 20 also received a diagnosis of CVST.
Among about 490,000 adults who received either the Pfizer or Moderna vaccines, there were no diagnosed cases of thrombocytopenia.
Dr. Furie reiterated that CVST blood clots “are very rare adverse events,” but recommended that any patient in the ED with a suspected clot should be screened immediately to determine if they received a COVID vaccine during the previous few weeks.
For those who have recently received the COVID-19 vaccine, a suspected clot should be treated with nonheparin anticoagulants, Dr. Furie said.
“No heparin products in any dose should be given for suspected CVST, TTS, or VITT. With the right treatment, most patients can have a full recovery,” she added. The report includes additional, detailed treatment recommendations if one of these conditions are suspected.
Rare events
The authors noted that cases of TTS/VITT occurred up to 2.5 weeks after receiving the J&J vaccine in the United States and up to 3.5 weeks after receiving the AstraZeneca vaccine in Europe.
An April 23 report from the CDC and FDA noted that, out of almost 7 million adults who received the J&J vaccine, the agencies investigated only 15 reported cases of TTS.
An April 7 report from the European Medicines Agency noted that, out of more than 25 million people who received the AstraZeneca vaccine in the European Union, it found 62 cases of CVST.
A statement put out by the American Heart Association/American Stroke Association urges “everyone to receive a COVID-19 vaccine” as soon as possible.
“We are confident the benefits of vaccination far exceed the very small, rare risks,” the organizations said. “The risks of vaccination are also far smaller than the risk of COVID-19 and its potentially fatal consequences.”
A version of this article first appeared on Medscape.com.
Doctors more likely to prescribe opioids to COVID ‘long-haulers,’ raising addiction fears
COVID-19 survivors are at risk from a possible second pandemic, this time of opioid addiction, given the high rate of painkillers being prescribed to these patients, health experts say.

A new study in Nature found alarmingly high rates of opioid use among COVID survivors with lingering symptoms at Veterans Affairs facilities. About 10% of COVID survivors develop “long COVID,” struggling with often disabling health problems even 6 months or longer after a diagnosis.
For every 1,000 long-COVID patients, known as “long-haulers,” who were treated at a VA facility, doctors wrote nine more prescriptions for opioids than they otherwise would have, along with 22 additional prescriptions for benzodiazepines, which include Xanax and other addictive pills used to treat anxiety.
Although previous studies have found many COVID survivors experience persistent health problems, the new article is the first to show they’re using more addictive medications, said Ziyad Al-Aly, MD, the paper’s lead author.

He’s concerned that even an apparently small increase in the inappropriate use of addictive pain pills will lead to a resurgence of the prescription opioid crisis, given the large number of COVID survivors. More than 3 million of the 31 million Americans infected with COVID develop long-term symptoms, which can include fatigue, shortness of breath, depression, anxiety, and memory problems known as “brain fog.”
The new study also found many patients have significant muscle and bone pain.
The frequent use of opioids was surprising, given concerns about their potential for addiction, said Dr. Al-Aly, chief of research and education service at the VA St. Louis Health Care System.
“Physicians now are supposed to shy away from prescribing opioids,” said Dr. Al-Aly, who studied more than 73,000 patients in the VA system. When Dr. Al-Aly saw the number of opioids prescriptions, he said, he thought to himself: “Is this really happening all over again?”
Doctors need to act now, before “it’s too late to do something,” Dr. Al-Aly said. “We must act now and ensure that people are getting the care they need. We do not want this to balloon into a suicide crisis or another opioid epidemic.”
As more doctors became aware of their addictive potential, new opioid prescriptions fell, by more than half since 2012. But said Andrew Kolodny, MD, medical director of opioid policy research at Brandeis University, Waltham, Mass.
Some patients who became addicted to prescription painkillers switched to heroin, either because it was cheaper or because they could no longer obtain opioids from their doctors. Overdose deaths surged in recent years as drug dealers began spiking heroin with a powerful synthetic opioid called fentanyl.
More than 88,000 Americans died from overdoses during the 12 months ending in August 2020, according to the Centers for Disease Control and Prevention. Health experts now advise doctors to avoid prescribing opioids for long periods.

The new study “suggests to me that many clinicians still don’t get it,” Dr. Kolodny said. “Many clinicians are under the false impression that opioids are appropriate for chronic pain patients.”
Hospitalized COVID patients often receive a lot of medication to control pain and anxiety, especially in ICUs, said Greg Martin, MD, president of the Society of Critical Care Medicine. Patients placed on ventilators, for example, are often sedated to make them more comfortable.
Martin said he’s concerned by the study’s findings, which suggest patients are unnecessarily continuing medications after leaving the hospital.
“I worry that COVID-19 patients, especially those who are severely and critically ill, receive a lot of medications during the hospitalization, and because they have persistent symptoms, the medications are continued after hospital discharge,” Dr. Martin said.
While some COVID patients are experiencing muscle and bone pain for the first time, others say the illness has intensified their preexisting pain.
Rachael Sunshine Burnett has suffered from chronic pain in her back and feet for 20 years, ever since an accident at a warehouse where she once worked. But Ms. Burnett, who first was diagnosed with COVID in April 2020, said the pain soon became 10 times worse and spread to the area between her shoulders and spine. Although she was already taking long-acting OxyContin twice a day, her doctor prescribed an additional opioid called oxycodone, which relieves pain immediately. She was reinfected with COVID in December.
“It’s been a horrible, horrible year,” said Ms. Burnett, 43, of Coxsackie, N.Y.
Doctors should recognize that pain can be a part of long COVID, Dr. Martin said. “We need to find the proper nonnarcotic treatment for it, just like we do with other forms of chronic pain,” he said.
The CDC recommends a number of alternatives to opioids – from physical therapy to biofeedback, over-the-counter anti-inflammatories, antidepressants, and antiseizure drugs that also relieve nerve pain.
The country also needs an overall strategy to cope with the wave of post-COVID complications, Dr. Al-Aly said.
“It’s better to be prepared than to be caught off guard years from now, when doctors realize: ‘Oh, we have a resurgence in opioids,’ ” Dr. Al-Aly said.
Dr. Al-Aly noted that his study may not capture the full complexity of post-COVID patient needs. Although women make up the majority of long-COVID patients in most studies, most patients in the VA system are men.
The study of VA patients makes it “abundantly clear that we are not prepared to meet the needs of 3 million Americans with long COVID,” said Eric Topol, MD, founder and director of the Scripps Research Translational Institute in San Diego. “We desperately need an intervention that will effectively treat these individuals.”
Dr. Al-Aly said COVID survivors may need care for years.
“That’s going to be a huge, significant burden on the health care system,” Dr. Al-Aly said. “Long COVID will reverberate in the health system for years or even decades to come.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
COVID-19 survivors are at risk from a possible second pandemic, this time of opioid addiction, given the high rate of painkillers being prescribed to these patients, health experts say.
A new study in Nature found alarmingly high rates of opioid use among COVID survivors with lingering symptoms at Veterans Affairs facilities. About 10% of COVID survivors develop “long COVID,” struggling with often disabling health problems even 6 months or longer after a diagnosis.
For every 1,000 long-COVID patients, known as “long-haulers,” who were treated at a VA facility, doctors wrote nine more prescriptions for opioids than they otherwise would have, along with 22 additional prescriptions for benzodiazepines, which include Xanax and other addictive pills used to treat anxiety.
Although previous studies have found many COVID survivors experience persistent health problems, the new article is the first to show they’re using more addictive medications, said Ziyad Al-Aly, MD, the paper’s lead author.
He’s concerned that even an apparently small increase in the inappropriate use of addictive pain pills will lead to a resurgence of the prescription opioid crisis, given the large number of COVID survivors. More than 3 million of the 31 million Americans infected with COVID develop long-term symptoms, which can include fatigue, shortness of breath, depression, anxiety, and memory problems known as “brain fog.”
The new study also found many patients have significant muscle and bone pain.
The frequent use of opioids was surprising, given concerns about their potential for addiction, said Dr. Al-Aly, chief of research and education service at the VA St. Louis Health Care System.
“Physicians now are supposed to shy away from prescribing opioids,” said Dr. Al-Aly, who studied more than 73,000 patients in the VA system. When Dr. Al-Aly saw the number of opioids prescriptions, he said, he thought to himself: “Is this really happening all over again?”
Doctors need to act now, before “it’s too late to do something,” Dr. Al-Aly said. “We must act now and ensure that people are getting the care they need. We do not want this to balloon into a suicide crisis or another opioid epidemic.”
As more doctors became aware of their addictive potential, new opioid prescriptions fell, by more than half since 2012. But said Andrew Kolodny, MD, medical director of opioid policy research at Brandeis University, Waltham, Mass.
Some patients who became addicted to prescription painkillers switched to heroin, either because it was cheaper or because they could no longer obtain opioids from their doctors. Overdose deaths surged in recent years as drug dealers began spiking heroin with a powerful synthetic opioid called fentanyl.
More than 88,000 Americans died from overdoses during the 12 months ending in August 2020, according to the Centers for Disease Control and Prevention. Health experts now advise doctors to avoid prescribing opioids for long periods.
The new study “suggests to me that many clinicians still don’t get it,” Dr. Kolodny said. “Many clinicians are under the false impression that opioids are appropriate for chronic pain patients.”
Hospitalized COVID patients often receive a lot of medication to control pain and anxiety, especially in ICUs, said Greg Martin, MD, president of the Society of Critical Care Medicine. Patients placed on ventilators, for example, are often sedated to make them more comfortable.
Martin said he’s concerned by the study’s findings, which suggest patients are unnecessarily continuing medications after leaving the hospital.
“I worry that COVID-19 patients, especially those who are severely and critically ill, receive a lot of medications during the hospitalization, and because they have persistent symptoms, the medications are continued after hospital discharge,” Dr. Martin said.
While some COVID patients are experiencing muscle and bone pain for the first time, others say the illness has intensified their preexisting pain.
Rachael Sunshine Burnett has suffered from chronic pain in her back and feet for 20 years, ever since an accident at a warehouse where she once worked. But Ms. Burnett, who first was diagnosed with COVID in April 2020, said the pain soon became 10 times worse and spread to the area between her shoulders and spine. Although she was already taking long-acting OxyContin twice a day, her doctor prescribed an additional opioid called oxycodone, which relieves pain immediately. She was reinfected with COVID in December.
“It’s been a horrible, horrible year,” said Ms. Burnett, 43, of Coxsackie, N.Y.
Doctors should recognize that pain can be a part of long COVID, Dr. Martin said. “We need to find the proper nonnarcotic treatment for it, just like we do with other forms of chronic pain,” he said.
The CDC recommends a number of alternatives to opioids – from physical therapy to biofeedback, over-the-counter anti-inflammatories, antidepressants, and antiseizure drugs that also relieve nerve pain.
The country also needs an overall strategy to cope with the wave of post-COVID complications, Dr. Al-Aly said.
“It’s better to be prepared than to be caught off guard years from now, when doctors realize: ‘Oh, we have a resurgence in opioids,’ ” Dr. Al-Aly said.
Dr. Al-Aly noted that his study may not capture the full complexity of post-COVID patient needs. Although women make up the majority of long-COVID patients in most studies, most patients in the VA system are men.
The study of VA patients makes it “abundantly clear that we are not prepared to meet the needs of 3 million Americans with long COVID,” said Eric Topol, MD, founder and director of the Scripps Research Translational Institute in San Diego. “We desperately need an intervention that will effectively treat these individuals.”
Dr. Al-Aly said COVID survivors may need care for years.
“That’s going to be a huge, significant burden on the health care system,” Dr. Al-Aly said. “Long COVID will reverberate in the health system for years or even decades to come.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
COVID-19 survivors are at risk from a possible second pandemic, this time of opioid addiction, given the high rate of painkillers being prescribed to these patients, health experts say.
A new study in Nature found alarmingly high rates of opioid use among COVID survivors with lingering symptoms at Veterans Affairs facilities. About 10% of COVID survivors develop “long COVID,” struggling with often disabling health problems even 6 months or longer after a diagnosis.
For every 1,000 long-COVID patients, known as “long-haulers,” who were treated at a VA facility, doctors wrote nine more prescriptions for opioids than they otherwise would have, along with 22 additional prescriptions for benzodiazepines, which include Xanax and other addictive pills used to treat anxiety.
Although previous studies have found many COVID survivors experience persistent health problems, the new article is the first to show they’re using more addictive medications, said Ziyad Al-Aly, MD, the paper’s lead author.
He’s concerned that even an apparently small increase in the inappropriate use of addictive pain pills will lead to a resurgence of the prescription opioid crisis, given the large number of COVID survivors. More than 3 million of the 31 million Americans infected with COVID develop long-term symptoms, which can include fatigue, shortness of breath, depression, anxiety, and memory problems known as “brain fog.”
The new study also found many patients have significant muscle and bone pain.
The frequent use of opioids was surprising, given concerns about their potential for addiction, said Dr. Al-Aly, chief of research and education service at the VA St. Louis Health Care System.
“Physicians now are supposed to shy away from prescribing opioids,” said Dr. Al-Aly, who studied more than 73,000 patients in the VA system. When Dr. Al-Aly saw the number of opioids prescriptions, he said, he thought to himself: “Is this really happening all over again?”
Doctors need to act now, before “it’s too late to do something,” Dr. Al-Aly said. “We must act now and ensure that people are getting the care they need. We do not want this to balloon into a suicide crisis or another opioid epidemic.”
As more doctors became aware of their addictive potential, new opioid prescriptions fell, by more than half since 2012. But said Andrew Kolodny, MD, medical director of opioid policy research at Brandeis University, Waltham, Mass.
Some patients who became addicted to prescription painkillers switched to heroin, either because it was cheaper or because they could no longer obtain opioids from their doctors. Overdose deaths surged in recent years as drug dealers began spiking heroin with a powerful synthetic opioid called fentanyl.
More than 88,000 Americans died from overdoses during the 12 months ending in August 2020, according to the Centers for Disease Control and Prevention. Health experts now advise doctors to avoid prescribing opioids for long periods.
The new study “suggests to me that many clinicians still don’t get it,” Dr. Kolodny said. “Many clinicians are under the false impression that opioids are appropriate for chronic pain patients.”
Hospitalized COVID patients often receive a lot of medication to control pain and anxiety, especially in ICUs, said Greg Martin, MD, president of the Society of Critical Care Medicine. Patients placed on ventilators, for example, are often sedated to make them more comfortable.
Martin said he’s concerned by the study’s findings, which suggest patients are unnecessarily continuing medications after leaving the hospital.
“I worry that COVID-19 patients, especially those who are severely and critically ill, receive a lot of medications during the hospitalization, and because they have persistent symptoms, the medications are continued after hospital discharge,” Dr. Martin said.
While some COVID patients are experiencing muscle and bone pain for the first time, others say the illness has intensified their preexisting pain.
Rachael Sunshine Burnett has suffered from chronic pain in her back and feet for 20 years, ever since an accident at a warehouse where she once worked. But Ms. Burnett, who first was diagnosed with COVID in April 2020, said the pain soon became 10 times worse and spread to the area between her shoulders and spine. Although she was already taking long-acting OxyContin twice a day, her doctor prescribed an additional opioid called oxycodone, which relieves pain immediately. She was reinfected with COVID in December.
“It’s been a horrible, horrible year,” said Ms. Burnett, 43, of Coxsackie, N.Y.
Doctors should recognize that pain can be a part of long COVID, Dr. Martin said. “We need to find the proper nonnarcotic treatment for it, just like we do with other forms of chronic pain,” he said.
The CDC recommends a number of alternatives to opioids – from physical therapy to biofeedback, over-the-counter anti-inflammatories, antidepressants, and antiseizure drugs that also relieve nerve pain.
The country also needs an overall strategy to cope with the wave of post-COVID complications, Dr. Al-Aly said.
“It’s better to be prepared than to be caught off guard years from now, when doctors realize: ‘Oh, we have a resurgence in opioids,’ ” Dr. Al-Aly said.
Dr. Al-Aly noted that his study may not capture the full complexity of post-COVID patient needs. Although women make up the majority of long-COVID patients in most studies, most patients in the VA system are men.
The study of VA patients makes it “abundantly clear that we are not prepared to meet the needs of 3 million Americans with long COVID,” said Eric Topol, MD, founder and director of the Scripps Research Translational Institute in San Diego. “We desperately need an intervention that will effectively treat these individuals.”
Dr. Al-Aly said COVID survivors may need care for years.
“That’s going to be a huge, significant burden on the health care system,” Dr. Al-Aly said. “Long COVID will reverberate in the health system for years or even decades to come.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
CDC guidelines coming on long COVID
The Centers for Disease Control and Prevention is finalizing new guidelines to help clinicians diagnose and manage long COVID, or postacute sequelae of SARS-CoV-2 infection.
In a day-long congressional hearing on April 28, John Brooks, MD, a medical epidemiologist at the CDC’s division of HIV/AIDS prevention, testified that the guidelines were going through the clearance process at the agency, but would be forthcoming.
“They should be coming out very shortly,” Dr. Brooks said.
The guidelines, which were developed in collaboration with newly established long-COVID clinics and patient advocacy groups, will “illustrate how to diagnose and begin to pull together what we know about management,” of the complex condition, he said.
For many doctors and patients who are struggling to understand symptoms that persist for months after the initial viral infection, the guidelines can’t come soon enough.
National Institutes of Health Director Francis Collins, MD, PhD, who also testified at the hearing, estimated that as many as 3 million people could be left with chronic health problems after even mild COVID infections.
“I can’t overstate how serious this issue is for the health of our nation,” he said.
Dr. Collins said his estimate was based on studies showing that roughly 10% of people who get COVID could be affected by this and whose “long-term course is uncertain,” he said. So far, more than 32 million Americans are known to have been infected with the new coronavirus.
“We need to make sure we put our arms around them and bring answers and care to them,” said Rep. Anna Eshoo (D-Calif.), chairwoman of the Subcommittee on Health.
Jennifer Possick, MD, who directs the post-COVID recovery program at Yale New Haven (Conn.) Hospital, testified that the tidal wave of patients she and her colleagues were seeing was overwhelming.
“We are a well-resourced program at an academic medical center, but we are swamped by the need in our community. This year, we have seen more patients with post COVID-19 conditions in our clinic alone than we have new cases of asthma and COPD combined,” she said. “The magnitude of the challenge is daunting.”
Dr. Possick estimated that there are “over 60” clinics in the United States that have started to treat long-COVID patients, but said they are grassroots efforts and all very different from each other.
“Whoever had the resources, had the time, [and] was able to take the initiative and forge to the relationships because most of them are multidisciplinary, did so,” she said.
Patients testify
Several representatives shared moving personal stories of loved ones or staffers who remained ill months after a COVID diagnosis.
Rep. Ann Kuster, from New Hampshire, talked about her 34-year-old niece, a member of the U.S. Ski Team, who had COVID just over a year ago and “continues to struggle with everything, even the simplest activities of daily living” she said. “She has to choose between taking a shower or making dinner. I’m so proud of her for hanging in there.”
Long-COVID patients invited to testify by the subcommittee described months of disability that left them with soaring medical bills and no ability to work to pay them.
“I am now a poor, Black, disabled woman, living with long COVID,” said Chimere Smith, who said she had been a school teacher in Baltimore. “Saying it aloud makes it no more easy to accept.”
She said COVID had affected her ability to think clearly and caused debilitating fatigue, which prevented her from working. She said she lost her vision for almost 5 months because doctors misdiagnosed a cataract caused by long COVID as dry eye.
“If I did not have a loving family, I [would] be speaking to you today [from] my car, the only property I now own.”
Ms. Smith said that long-COVID clinics, which are mostly housed within academic medical centers, were not going to be accessible for all long-haulers, who are disproportionately women of color. She has started a clinic, based out of her church, to help other patients from her community.
“No one wants to hear that long COVID has decimated my life or the lives of other black women in less than a year,” Ms. Smith said. “We’ve just been waiting and hoping for compassionate doctors and politicians who would acknowledge us.”
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention is finalizing new guidelines to help clinicians diagnose and manage long COVID, or postacute sequelae of SARS-CoV-2 infection.
In a day-long congressional hearing on April 28, John Brooks, MD, a medical epidemiologist at the CDC’s division of HIV/AIDS prevention, testified that the guidelines were going through the clearance process at the agency, but would be forthcoming.
“They should be coming out very shortly,” Dr. Brooks said.
The guidelines, which were developed in collaboration with newly established long-COVID clinics and patient advocacy groups, will “illustrate how to diagnose and begin to pull together what we know about management,” of the complex condition, he said.
For many doctors and patients who are struggling to understand symptoms that persist for months after the initial viral infection, the guidelines can’t come soon enough.
National Institutes of Health Director Francis Collins, MD, PhD, who also testified at the hearing, estimated that as many as 3 million people could be left with chronic health problems after even mild COVID infections.
“I can’t overstate how serious this issue is for the health of our nation,” he said.
Dr. Collins said his estimate was based on studies showing that roughly 10% of people who get COVID could be affected by this and whose “long-term course is uncertain,” he said. So far, more than 32 million Americans are known to have been infected with the new coronavirus.
“We need to make sure we put our arms around them and bring answers and care to them,” said Rep. Anna Eshoo (D-Calif.), chairwoman of the Subcommittee on Health.
Jennifer Possick, MD, who directs the post-COVID recovery program at Yale New Haven (Conn.) Hospital, testified that the tidal wave of patients she and her colleagues were seeing was overwhelming.
“We are a well-resourced program at an academic medical center, but we are swamped by the need in our community. This year, we have seen more patients with post COVID-19 conditions in our clinic alone than we have new cases of asthma and COPD combined,” she said. “The magnitude of the challenge is daunting.”
Dr. Possick estimated that there are “over 60” clinics in the United States that have started to treat long-COVID patients, but said they are grassroots efforts and all very different from each other.
“Whoever had the resources, had the time, [and] was able to take the initiative and forge to the relationships because most of them are multidisciplinary, did so,” she said.
Patients testify
Several representatives shared moving personal stories of loved ones or staffers who remained ill months after a COVID diagnosis.
Rep. Ann Kuster, from New Hampshire, talked about her 34-year-old niece, a member of the U.S. Ski Team, who had COVID just over a year ago and “continues to struggle with everything, even the simplest activities of daily living” she said. “She has to choose between taking a shower or making dinner. I’m so proud of her for hanging in there.”
Long-COVID patients invited to testify by the subcommittee described months of disability that left them with soaring medical bills and no ability to work to pay them.
“I am now a poor, Black, disabled woman, living with long COVID,” said Chimere Smith, who said she had been a school teacher in Baltimore. “Saying it aloud makes it no more easy to accept.”
She said COVID had affected her ability to think clearly and caused debilitating fatigue, which prevented her from working. She said she lost her vision for almost 5 months because doctors misdiagnosed a cataract caused by long COVID as dry eye.
“If I did not have a loving family, I [would] be speaking to you today [from] my car, the only property I now own.”
Ms. Smith said that long-COVID clinics, which are mostly housed within academic medical centers, were not going to be accessible for all long-haulers, who are disproportionately women of color. She has started a clinic, based out of her church, to help other patients from her community.
“No one wants to hear that long COVID has decimated my life or the lives of other black women in less than a year,” Ms. Smith said. “We’ve just been waiting and hoping for compassionate doctors and politicians who would acknowledge us.”
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention is finalizing new guidelines to help clinicians diagnose and manage long COVID, or postacute sequelae of SARS-CoV-2 infection.
In a day-long congressional hearing on April 28, John Brooks, MD, a medical epidemiologist at the CDC’s division of HIV/AIDS prevention, testified that the guidelines were going through the clearance process at the agency, but would be forthcoming.
“They should be coming out very shortly,” Dr. Brooks said.
The guidelines, which were developed in collaboration with newly established long-COVID clinics and patient advocacy groups, will “illustrate how to diagnose and begin to pull together what we know about management,” of the complex condition, he said.
For many doctors and patients who are struggling to understand symptoms that persist for months after the initial viral infection, the guidelines can’t come soon enough.
National Institutes of Health Director Francis Collins, MD, PhD, who also testified at the hearing, estimated that as many as 3 million people could be left with chronic health problems after even mild COVID infections.
“I can’t overstate how serious this issue is for the health of our nation,” he said.
Dr. Collins said his estimate was based on studies showing that roughly 10% of people who get COVID could be affected by this and whose “long-term course is uncertain,” he said. So far, more than 32 million Americans are known to have been infected with the new coronavirus.
“We need to make sure we put our arms around them and bring answers and care to them,” said Rep. Anna Eshoo (D-Calif.), chairwoman of the Subcommittee on Health.
Jennifer Possick, MD, who directs the post-COVID recovery program at Yale New Haven (Conn.) Hospital, testified that the tidal wave of patients she and her colleagues were seeing was overwhelming.
“We are a well-resourced program at an academic medical center, but we are swamped by the need in our community. This year, we have seen more patients with post COVID-19 conditions in our clinic alone than we have new cases of asthma and COPD combined,” she said. “The magnitude of the challenge is daunting.”
Dr. Possick estimated that there are “over 60” clinics in the United States that have started to treat long-COVID patients, but said they are grassroots efforts and all very different from each other.
“Whoever had the resources, had the time, [and] was able to take the initiative and forge to the relationships because most of them are multidisciplinary, did so,” she said.
Patients testify
Several representatives shared moving personal stories of loved ones or staffers who remained ill months after a COVID diagnosis.
Rep. Ann Kuster, from New Hampshire, talked about her 34-year-old niece, a member of the U.S. Ski Team, who had COVID just over a year ago and “continues to struggle with everything, even the simplest activities of daily living” she said. “She has to choose between taking a shower or making dinner. I’m so proud of her for hanging in there.”
Long-COVID patients invited to testify by the subcommittee described months of disability that left them with soaring medical bills and no ability to work to pay them.
“I am now a poor, Black, disabled woman, living with long COVID,” said Chimere Smith, who said she had been a school teacher in Baltimore. “Saying it aloud makes it no more easy to accept.”
She said COVID had affected her ability to think clearly and caused debilitating fatigue, which prevented her from working. She said she lost her vision for almost 5 months because doctors misdiagnosed a cataract caused by long COVID as dry eye.
“If I did not have a loving family, I [would] be speaking to you today [from] my car, the only property I now own.”
Ms. Smith said that long-COVID clinics, which are mostly housed within academic medical centers, were not going to be accessible for all long-haulers, who are disproportionately women of color. She has started a clinic, based out of her church, to help other patients from her community.
“No one wants to hear that long COVID has decimated my life or the lives of other black women in less than a year,” Ms. Smith said. “We’ve just been waiting and hoping for compassionate doctors and politicians who would acknowledge us.”
A version of this article first appeared on Medscape.com.
Being overweight ups risk of severe COVID-19 in hospital
In a global meta-analysis of more than 7,000 patients who were hospitalized with COVID-19, individuals with overweight or obesity were more likely to need respiratory support but were not more likely to die in the hospital, compared to individuals of normal weight.
Compared to patients without diabetes, those with diabetes had higher odds of needing invasive respiratory support (with intubation) but not for needing noninvasive respiratory support or of dying in the hospital.
“Surprisingly,” among patients with diabetes, being overweight or having obesity did not further increase the odds of any of these outcomes, the researchers wrote. The finding needs to be confirmed in larger studies, they said, because the sample sizes in these subanalyses were small and the confidence intervals were large.
The study by Danielle K. Longmore, PhD, of Murdoch Children’s Research Institute (MCRI), Melbourne, and colleagues from the International BMI-COVID consortium, was published online April 15 in Diabetes Care.
This new research “adds to the known data on the associations between obesity and severe COVID-19 disease and extends these findings” to patients who are overweight and/or have diabetes, Dr. Longmore, a pediatric endocrinologist with a clinical and research interest in childhood and youth obesity, said in an interview.
Immunologist Siroon Bekkering, PhD, of Radboud University Medical Center, Nijmegen, the Netherlands, explained that never before have so much data of different types regarding obesity been combined in one large study. Dr. Bekkering is a coauthor of the article and was a principal investigator.
“Several national and international observations already showed the important role of overweight and obesity in a more severe COVID-19 course. This study adds to those observations by combining data from several countries with the possibility to look at the risk factors separately,” she said in a statement from her institution.
“Regardless of other risk factors (such as heart disease or diabetes), we now see that too high a BMI [body mass index] can actually lead to a more severe course in [coronavirus] infection,” she said.
Study implications: Data show that overweight, obesity add to risk
These latest findings highlight the urgent need to develop public health policies to address socioeconomic and psychological drivers of obesity, Dr. Longmore said.
“Although taking steps to address obesity in the short term is unlikely to have an immediate impact in the COVID-19 pandemic, it will likely reduce the disease burden in future viral pandemics and reduce risks of complications like heart disease and stroke,” she observed in a statement issued by MCRI.
Coauthor Kirsty R. Short, PhD, a research fellow at the University of Queensland, Brisbane, Australia, noted that “obesity is associated with numerous poor health outcomes, including increased risk of cardiometabolic and respiratory disease and more severe viral disease including influenza, dengue, and SARS-CoV-1.
“Given the large scale of this study,” she said, “we have conclusively shown that being overweight or obese are independent risk factors for worse outcomes in adults hospitalized with COVID-19.”
“At the moment, the World Health Organization has not had enough high-quality data to include being overweight or obese as a risk factor for severe COVID-19 disease,” added another author, David P. Burgner, PhD, a pediatric infectious diseases clinician scientist from MCRI.

“Our study should help inform decisions about which higher-risk groups should be vaccinated as a priority,” he observed.
Does being overweight up risk of worse COVID-19 outcomes?
About 13% of the world’s population are overweight, and 40% have obesity. There are wide between-country variations in these data, and about 90% of patients with type 2 diabetes are overweight or obese, the researchers noted.
The Organisation for Economic Co-operation and Development reported that the prevalence of obesity in 2016-2017 was 5.7% to 8.9% in Asia, 9.8% to 16.8% in Europe, 26.5% in South Africa, and 40.0% in the United States, they added.
Obesity is common and has emerged as an important risk factor for severe COVID-19. However, most previous studies of COVID-19 and elevated BMI were conducted in single centers and did not focus on patients with overweight.
To investigate, the researchers identified 7,244 patients (two-thirds were overweight or obese) who were hospitalized with COVID-19 in 69 hospitals (18 sites) in 11 countries from Jan. 17, 2020, to June 2, 2020.
Most patients were hospitalized with COVID-19 in the Netherlands (2,260), followed by New York City (1,682), Switzerland (920), St. Louis (805), Norway, Italy, China, South Africa, Indonesia, Denmark, Los Angeles, Austria, and Singapore.
Just over half (60%) of the individuals were male, and 52% were older than 65.
Overall, 34.8% were overweight, and 30.8% had obesity, but the average weight varied considerably between countries and sites.
Increased need for respiratory support, same mortality risk
Compared with patients with normal weight, patients who were overweight had a 44% increased risk of needing supplemental oxygen/noninvasive ventilation, and those with obesity had a 75% increased risk of this, after adjustment for age (< 65, ≥ 65), sex, hypertension, diabetes, or preexisting cardiovascular disease or respiratory conditions.
Patients who were overweight had a 22% increased risk of needing invasive (mechanical) ventilation, and those with obesity had a 73% increased risk of this, after multivariable adjustment.
Being overweight or having obesity was not associated with a significantly increased risk of dying in the hospital, however.
“In other viral respiratory infections, such as influenza, there is a similar pattern of increased requirement for ventilatory support but lower in-hospital mortality among individuals with obesity, when compared to those with normal range BMI,” Dr. Longmore noted. She said that larger studies are needed to further explore this finding regarding COVID-19.
Compared to patients without diabetes, those with diabetes had a 21% increased risk of requiring invasive ventilation, but they did not have an increased risk of needing noninvasive ventilation or of dying in the hospital.
As in previous studies, individuals who had cardiovascular and preexisting respiratory diseases were not at greater risk of needing oxygen or mechanical ventilation but were at increased risk for in-hospital death. Men had a greater risk of needing invasive mechanical ventilation, and individuals who were older than 65 had an increased risk of requiring oxygen or of dying in the hospital.
A living meta-analysis, call for more collaborators
“We consider this a ‘living meta-analysis’ and invite other centers to join us,” Dr. Longmore said. “We hope to update the analyses as more data are contributed.”
No specific project funded the study. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a global meta-analysis of more than 7,000 patients who were hospitalized with COVID-19, individuals with overweight or obesity were more likely to need respiratory support but were not more likely to die in the hospital, compared to individuals of normal weight.
Compared to patients without diabetes, those with diabetes had higher odds of needing invasive respiratory support (with intubation) but not for needing noninvasive respiratory support or of dying in the hospital.
“Surprisingly,” among patients with diabetes, being overweight or having obesity did not further increase the odds of any of these outcomes, the researchers wrote. The finding needs to be confirmed in larger studies, they said, because the sample sizes in these subanalyses were small and the confidence intervals were large.
The study by Danielle K. Longmore, PhD, of Murdoch Children’s Research Institute (MCRI), Melbourne, and colleagues from the International BMI-COVID consortium, was published online April 15 in Diabetes Care.
This new research “adds to the known data on the associations between obesity and severe COVID-19 disease and extends these findings” to patients who are overweight and/or have diabetes, Dr. Longmore, a pediatric endocrinologist with a clinical and research interest in childhood and youth obesity, said in an interview.
Immunologist Siroon Bekkering, PhD, of Radboud University Medical Center, Nijmegen, the Netherlands, explained that never before have so much data of different types regarding obesity been combined in one large study. Dr. Bekkering is a coauthor of the article and was a principal investigator.
“Several national and international observations already showed the important role of overweight and obesity in a more severe COVID-19 course. This study adds to those observations by combining data from several countries with the possibility to look at the risk factors separately,” she said in a statement from her institution.
“Regardless of other risk factors (such as heart disease or diabetes), we now see that too high a BMI [body mass index] can actually lead to a more severe course in [coronavirus] infection,” she said.
Study implications: Data show that overweight, obesity add to risk
These latest findings highlight the urgent need to develop public health policies to address socioeconomic and psychological drivers of obesity, Dr. Longmore said.
“Although taking steps to address obesity in the short term is unlikely to have an immediate impact in the COVID-19 pandemic, it will likely reduce the disease burden in future viral pandemics and reduce risks of complications like heart disease and stroke,” she observed in a statement issued by MCRI.
Coauthor Kirsty R. Short, PhD, a research fellow at the University of Queensland, Brisbane, Australia, noted that “obesity is associated with numerous poor health outcomes, including increased risk of cardiometabolic and respiratory disease and more severe viral disease including influenza, dengue, and SARS-CoV-1.
“Given the large scale of this study,” she said, “we have conclusively shown that being overweight or obese are independent risk factors for worse outcomes in adults hospitalized with COVID-19.”
“At the moment, the World Health Organization has not had enough high-quality data to include being overweight or obese as a risk factor for severe COVID-19 disease,” added another author, David P. Burgner, PhD, a pediatric infectious diseases clinician scientist from MCRI.
“Our study should help inform decisions about which higher-risk groups should be vaccinated as a priority,” he observed.
Does being overweight up risk of worse COVID-19 outcomes?
About 13% of the world’s population are overweight, and 40% have obesity. There are wide between-country variations in these data, and about 90% of patients with type 2 diabetes are overweight or obese, the researchers noted.
The Organisation for Economic Co-operation and Development reported that the prevalence of obesity in 2016-2017 was 5.7% to 8.9% in Asia, 9.8% to 16.8% in Europe, 26.5% in South Africa, and 40.0% in the United States, they added.
Obesity is common and has emerged as an important risk factor for severe COVID-19. However, most previous studies of COVID-19 and elevated BMI were conducted in single centers and did not focus on patients with overweight.
To investigate, the researchers identified 7,244 patients (two-thirds were overweight or obese) who were hospitalized with COVID-19 in 69 hospitals (18 sites) in 11 countries from Jan. 17, 2020, to June 2, 2020.
Most patients were hospitalized with COVID-19 in the Netherlands (2,260), followed by New York City (1,682), Switzerland (920), St. Louis (805), Norway, Italy, China, South Africa, Indonesia, Denmark, Los Angeles, Austria, and Singapore.
Just over half (60%) of the individuals were male, and 52% were older than 65.
Overall, 34.8% were overweight, and 30.8% had obesity, but the average weight varied considerably between countries and sites.
Increased need for respiratory support, same mortality risk
Compared with patients with normal weight, patients who were overweight had a 44% increased risk of needing supplemental oxygen/noninvasive ventilation, and those with obesity had a 75% increased risk of this, after adjustment for age (< 65, ≥ 65), sex, hypertension, diabetes, or preexisting cardiovascular disease or respiratory conditions.
Patients who were overweight had a 22% increased risk of needing invasive (mechanical) ventilation, and those with obesity had a 73% increased risk of this, after multivariable adjustment.
Being overweight or having obesity was not associated with a significantly increased risk of dying in the hospital, however.
“In other viral respiratory infections, such as influenza, there is a similar pattern of increased requirement for ventilatory support but lower in-hospital mortality among individuals with obesity, when compared to those with normal range BMI,” Dr. Longmore noted. She said that larger studies are needed to further explore this finding regarding COVID-19.
Compared to patients without diabetes, those with diabetes had a 21% increased risk of requiring invasive ventilation, but they did not have an increased risk of needing noninvasive ventilation or of dying in the hospital.
As in previous studies, individuals who had cardiovascular and preexisting respiratory diseases were not at greater risk of needing oxygen or mechanical ventilation but were at increased risk for in-hospital death. Men had a greater risk of needing invasive mechanical ventilation, and individuals who were older than 65 had an increased risk of requiring oxygen or of dying in the hospital.
A living meta-analysis, call for more collaborators
“We consider this a ‘living meta-analysis’ and invite other centers to join us,” Dr. Longmore said. “We hope to update the analyses as more data are contributed.”
No specific project funded the study. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a global meta-analysis of more than 7,000 patients who were hospitalized with COVID-19, individuals with overweight or obesity were more likely to need respiratory support but were not more likely to die in the hospital, compared to individuals of normal weight.
Compared to patients without diabetes, those with diabetes had higher odds of needing invasive respiratory support (with intubation) but not for needing noninvasive respiratory support or of dying in the hospital.
“Surprisingly,” among patients with diabetes, being overweight or having obesity did not further increase the odds of any of these outcomes, the researchers wrote. The finding needs to be confirmed in larger studies, they said, because the sample sizes in these subanalyses were small and the confidence intervals were large.
The study by Danielle K. Longmore, PhD, of Murdoch Children’s Research Institute (MCRI), Melbourne, and colleagues from the International BMI-COVID consortium, was published online April 15 in Diabetes Care.
This new research “adds to the known data on the associations between obesity and severe COVID-19 disease and extends these findings” to patients who are overweight and/or have diabetes, Dr. Longmore, a pediatric endocrinologist with a clinical and research interest in childhood and youth obesity, said in an interview.
Immunologist Siroon Bekkering, PhD, of Radboud University Medical Center, Nijmegen, the Netherlands, explained that never before have so much data of different types regarding obesity been combined in one large study. Dr. Bekkering is a coauthor of the article and was a principal investigator.
“Several national and international observations already showed the important role of overweight and obesity in a more severe COVID-19 course. This study adds to those observations by combining data from several countries with the possibility to look at the risk factors separately,” she said in a statement from her institution.
“Regardless of other risk factors (such as heart disease or diabetes), we now see that too high a BMI [body mass index] can actually lead to a more severe course in [coronavirus] infection,” she said.
Study implications: Data show that overweight, obesity add to risk
These latest findings highlight the urgent need to develop public health policies to address socioeconomic and psychological drivers of obesity, Dr. Longmore said.
“Although taking steps to address obesity in the short term is unlikely to have an immediate impact in the COVID-19 pandemic, it will likely reduce the disease burden in future viral pandemics and reduce risks of complications like heart disease and stroke,” she observed in a statement issued by MCRI.
Coauthor Kirsty R. Short, PhD, a research fellow at the University of Queensland, Brisbane, Australia, noted that “obesity is associated with numerous poor health outcomes, including increased risk of cardiometabolic and respiratory disease and more severe viral disease including influenza, dengue, and SARS-CoV-1.
“Given the large scale of this study,” she said, “we have conclusively shown that being overweight or obese are independent risk factors for worse outcomes in adults hospitalized with COVID-19.”
“At the moment, the World Health Organization has not had enough high-quality data to include being overweight or obese as a risk factor for severe COVID-19 disease,” added another author, David P. Burgner, PhD, a pediatric infectious diseases clinician scientist from MCRI.
“Our study should help inform decisions about which higher-risk groups should be vaccinated as a priority,” he observed.
Does being overweight up risk of worse COVID-19 outcomes?
About 13% of the world’s population are overweight, and 40% have obesity. There are wide between-country variations in these data, and about 90% of patients with type 2 diabetes are overweight or obese, the researchers noted.
The Organisation for Economic Co-operation and Development reported that the prevalence of obesity in 2016-2017 was 5.7% to 8.9% in Asia, 9.8% to 16.8% in Europe, 26.5% in South Africa, and 40.0% in the United States, they added.
Obesity is common and has emerged as an important risk factor for severe COVID-19. However, most previous studies of COVID-19 and elevated BMI were conducted in single centers and did not focus on patients with overweight.
To investigate, the researchers identified 7,244 patients (two-thirds were overweight or obese) who were hospitalized with COVID-19 in 69 hospitals (18 sites) in 11 countries from Jan. 17, 2020, to June 2, 2020.
Most patients were hospitalized with COVID-19 in the Netherlands (2,260), followed by New York City (1,682), Switzerland (920), St. Louis (805), Norway, Italy, China, South Africa, Indonesia, Denmark, Los Angeles, Austria, and Singapore.
Just over half (60%) of the individuals were male, and 52% were older than 65.
Overall, 34.8% were overweight, and 30.8% had obesity, but the average weight varied considerably between countries and sites.
Increased need for respiratory support, same mortality risk
Compared with patients with normal weight, patients who were overweight had a 44% increased risk of needing supplemental oxygen/noninvasive ventilation, and those with obesity had a 75% increased risk of this, after adjustment for age (< 65, ≥ 65), sex, hypertension, diabetes, or preexisting cardiovascular disease or respiratory conditions.
Patients who were overweight had a 22% increased risk of needing invasive (mechanical) ventilation, and those with obesity had a 73% increased risk of this, after multivariable adjustment.
Being overweight or having obesity was not associated with a significantly increased risk of dying in the hospital, however.
“In other viral respiratory infections, such as influenza, there is a similar pattern of increased requirement for ventilatory support but lower in-hospital mortality among individuals with obesity, when compared to those with normal range BMI,” Dr. Longmore noted. She said that larger studies are needed to further explore this finding regarding COVID-19.
Compared to patients without diabetes, those with diabetes had a 21% increased risk of requiring invasive ventilation, but they did not have an increased risk of needing noninvasive ventilation or of dying in the hospital.
As in previous studies, individuals who had cardiovascular and preexisting respiratory diseases were not at greater risk of needing oxygen or mechanical ventilation but were at increased risk for in-hospital death. Men had a greater risk of needing invasive mechanical ventilation, and individuals who were older than 65 had an increased risk of requiring oxygen or of dying in the hospital.
A living meta-analysis, call for more collaborators
“We consider this a ‘living meta-analysis’ and invite other centers to join us,” Dr. Longmore said. “We hope to update the analyses as more data are contributed.”
No specific project funded the study. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Suicide in the early months of the pandemic: Unexpected trends
Every psychiatrist knows that this past year has been a challenge. The COVID-19 pandemic altered our lives, practically overnight, in ways that most of us had never anticipated.

There were months of lockdown. A new work-from-home transition. Recommendations to distance and mask. The destruction and recreation of our social lives. And the end of some industries as we have known them.
Over a year later, many children are still in virtual school. This lifestyle and economic toll do not even begin to include the horror experienced by exhausted and distressed health care workers or by the many who have lost a loved one or survived a hospitalization. National and international anxiety are running high. More people are seeking mental health care, and many of the patients we were caring for prior to the pandemic have been distressed.
Rates of both depression and anxiety are up, and the fear has been that the isolation of lockdowns, with their emotional and economic toll, would also increase suicide rates. Despite the increase in psychiatric symptoms and general distress, initial studies in the United States have shown that overall suicide rates in the early months of the pandemic were lower than in prior years.
A study published in The Lancet looked at suicide data from around the world and compared expected suicides, based on data from past years, with observed suicides. The researchers restricted their analysis to the countries, and regions of countries, where real-time suicide data were available through internet searches. Their paper is based on findings from 21 countries, including 16 high-income countries and five upper-middle–income countries (from regions where data were available). The overall analysis showed a drop in suicides by 5% when looking at the first 4 months of the pandemic, defined as April 1, 2020, to July 31, 2020. There were statistically significant increases in suicide only in Vienna, Puerto Rico, and Japan.
Igor Galynker, MD, PhD, directs the Suicide Research and Prevention Lab and the Zirinsky Center for Bipolar Disorder at the Icahn School of Medicine at Mount Sinai. He was not surprised by these findings.
“This is an important study,” Dr. Galynker said. “When it was discovered that U.S. rates went down, it was ‘U.S. specific’ and it was confounded by the fact that there was a dramatic increase in opiate overdose deaths in the U.S., which are not reported as suicides. This study shows that the decrease is international and that the finding in the United States is not related to the spike in overdose deaths.”
The study authors postulated that the drop in suicide may be due to proactive protective measures that societies have put in place, such as improved mental health services and fiscal support to mitigate financial consequences of the pandemic. They explained that “communities might have actively tried to support at-risk individuals, people might have connected in new ways, and some relationships might have been strengthened by households spending more time with each other. For some people, everyday stresses might have been reduced during stay-at-home periods, and for others the collective feeling of ‘we’re all in this together’ might have been beneficial”.
Dr. Galynker noted that, in times of calamity, suicide rates historically go down. “Short-term disasters invoke a fight-or-flight response that mobilizes us and improves our functioning under stress. Those acute responses last 2-3 months and then chronic stress sets in.” He is concerned that there will be increases in suicide rates down the road.
It is possible that individuals who consider social gatherings to be stressful, or who are bullied at school, may have found some relief from social interactions and expectations during the lockdown. “Some people have discovered that they like their families!” Dr. Galynker said.
While suicide rates have gone down, that is not true for all population subsets, and the authors of the Lancet paper noted that they were unable to give breakdowns of rates for different demographics.
Paul Nestadt, MD, is codirector of the Johns Hopkins Anxiety Disorders Clinic and studies suicide, firearms, and opiates. He looked at suicides in Maryland during the first 2 months of the lockdown (March 5, 2020 to May 7, 2020) and found that, Studies in Connecticut and Chicago yielded similar findings. These findings indicate that the overall trends may not reflect the impact on a specific subpopulation.
Dr. Nestadt talked about the disparities of suicide trends. “Communities hit harder by this pandemic in terms of sickness and death may experience more distress in ways that may come out as suicide in the context of other comorbid mood disorders. Also, in line with the idea of suicide as a marker of community- or population-level distress, there’s a general idea that having less of an economic cushion makes the pandemic more of a problem for some than for others. We know that suicide has been correlated to economic distress in general, and it makes sense that it would be community-specific where there is more economic duress.”
It has been a difficult year – not just for the United States, but for the entire world. One thing that may come of it is a unique opportunity to look at how stress and loss affect suicide rates, with the hope that preventive measures will follow.
A version of this article first appeared on Medscape.com.
Every psychiatrist knows that this past year has been a challenge. The COVID-19 pandemic altered our lives, practically overnight, in ways that most of us had never anticipated.
There were months of lockdown. A new work-from-home transition. Recommendations to distance and mask. The destruction and recreation of our social lives. And the end of some industries as we have known them.
Over a year later, many children are still in virtual school. This lifestyle and economic toll do not even begin to include the horror experienced by exhausted and distressed health care workers or by the many who have lost a loved one or survived a hospitalization. National and international anxiety are running high. More people are seeking mental health care, and many of the patients we were caring for prior to the pandemic have been distressed.
Rates of both depression and anxiety are up, and the fear has been that the isolation of lockdowns, with their emotional and economic toll, would also increase suicide rates. Despite the increase in psychiatric symptoms and general distress, initial studies in the United States have shown that overall suicide rates in the early months of the pandemic were lower than in prior years.
A study published in The Lancet looked at suicide data from around the world and compared expected suicides, based on data from past years, with observed suicides. The researchers restricted their analysis to the countries, and regions of countries, where real-time suicide data were available through internet searches. Their paper is based on findings from 21 countries, including 16 high-income countries and five upper-middle–income countries (from regions where data were available). The overall analysis showed a drop in suicides by 5% when looking at the first 4 months of the pandemic, defined as April 1, 2020, to July 31, 2020. There were statistically significant increases in suicide only in Vienna, Puerto Rico, and Japan.
Igor Galynker, MD, PhD, directs the Suicide Research and Prevention Lab and the Zirinsky Center for Bipolar Disorder at the Icahn School of Medicine at Mount Sinai. He was not surprised by these findings.
“This is an important study,” Dr. Galynker said. “When it was discovered that U.S. rates went down, it was ‘U.S. specific’ and it was confounded by the fact that there was a dramatic increase in opiate overdose deaths in the U.S., which are not reported as suicides. This study shows that the decrease is international and that the finding in the United States is not related to the spike in overdose deaths.”
The study authors postulated that the drop in suicide may be due to proactive protective measures that societies have put in place, such as improved mental health services and fiscal support to mitigate financial consequences of the pandemic. They explained that “communities might have actively tried to support at-risk individuals, people might have connected in new ways, and some relationships might have been strengthened by households spending more time with each other. For some people, everyday stresses might have been reduced during stay-at-home periods, and for others the collective feeling of ‘we’re all in this together’ might have been beneficial”.
Dr. Galynker noted that, in times of calamity, suicide rates historically go down. “Short-term disasters invoke a fight-or-flight response that mobilizes us and improves our functioning under stress. Those acute responses last 2-3 months and then chronic stress sets in.” He is concerned that there will be increases in suicide rates down the road.
It is possible that individuals who consider social gatherings to be stressful, or who are bullied at school, may have found some relief from social interactions and expectations during the lockdown. “Some people have discovered that they like their families!” Dr. Galynker said.
While suicide rates have gone down, that is not true for all population subsets, and the authors of the Lancet paper noted that they were unable to give breakdowns of rates for different demographics.
Paul Nestadt, MD, is codirector of the Johns Hopkins Anxiety Disorders Clinic and studies suicide, firearms, and opiates. He looked at suicides in Maryland during the first 2 months of the lockdown (March 5, 2020 to May 7, 2020) and found that, Studies in Connecticut and Chicago yielded similar findings. These findings indicate that the overall trends may not reflect the impact on a specific subpopulation.
Dr. Nestadt talked about the disparities of suicide trends. “Communities hit harder by this pandemic in terms of sickness and death may experience more distress in ways that may come out as suicide in the context of other comorbid mood disorders. Also, in line with the idea of suicide as a marker of community- or population-level distress, there’s a general idea that having less of an economic cushion makes the pandemic more of a problem for some than for others. We know that suicide has been correlated to economic distress in general, and it makes sense that it would be community-specific where there is more economic duress.”
It has been a difficult year – not just for the United States, but for the entire world. One thing that may come of it is a unique opportunity to look at how stress and loss affect suicide rates, with the hope that preventive measures will follow.
A version of this article first appeared on Medscape.com.
Every psychiatrist knows that this past year has been a challenge. The COVID-19 pandemic altered our lives, practically overnight, in ways that most of us had never anticipated.
There were months of lockdown. A new work-from-home transition. Recommendations to distance and mask. The destruction and recreation of our social lives. And the end of some industries as we have known them.
Over a year later, many children are still in virtual school. This lifestyle and economic toll do not even begin to include the horror experienced by exhausted and distressed health care workers or by the many who have lost a loved one or survived a hospitalization. National and international anxiety are running high. More people are seeking mental health care, and many of the patients we were caring for prior to the pandemic have been distressed.
Rates of both depression and anxiety are up, and the fear has been that the isolation of lockdowns, with their emotional and economic toll, would also increase suicide rates. Despite the increase in psychiatric symptoms and general distress, initial studies in the United States have shown that overall suicide rates in the early months of the pandemic were lower than in prior years.
A study published in The Lancet looked at suicide data from around the world and compared expected suicides, based on data from past years, with observed suicides. The researchers restricted their analysis to the countries, and regions of countries, where real-time suicide data were available through internet searches. Their paper is based on findings from 21 countries, including 16 high-income countries and five upper-middle–income countries (from regions where data were available). The overall analysis showed a drop in suicides by 5% when looking at the first 4 months of the pandemic, defined as April 1, 2020, to July 31, 2020. There were statistically significant increases in suicide only in Vienna, Puerto Rico, and Japan.
Igor Galynker, MD, PhD, directs the Suicide Research and Prevention Lab and the Zirinsky Center for Bipolar Disorder at the Icahn School of Medicine at Mount Sinai. He was not surprised by these findings.
“This is an important study,” Dr. Galynker said. “When it was discovered that U.S. rates went down, it was ‘U.S. specific’ and it was confounded by the fact that there was a dramatic increase in opiate overdose deaths in the U.S., which are not reported as suicides. This study shows that the decrease is international and that the finding in the United States is not related to the spike in overdose deaths.”
The study authors postulated that the drop in suicide may be due to proactive protective measures that societies have put in place, such as improved mental health services and fiscal support to mitigate financial consequences of the pandemic. They explained that “communities might have actively tried to support at-risk individuals, people might have connected in new ways, and some relationships might have been strengthened by households spending more time with each other. For some people, everyday stresses might have been reduced during stay-at-home periods, and for others the collective feeling of ‘we’re all in this together’ might have been beneficial”.
Dr. Galynker noted that, in times of calamity, suicide rates historically go down. “Short-term disasters invoke a fight-or-flight response that mobilizes us and improves our functioning under stress. Those acute responses last 2-3 months and then chronic stress sets in.” He is concerned that there will be increases in suicide rates down the road.
It is possible that individuals who consider social gatherings to be stressful, or who are bullied at school, may have found some relief from social interactions and expectations during the lockdown. “Some people have discovered that they like their families!” Dr. Galynker said.
While suicide rates have gone down, that is not true for all population subsets, and the authors of the Lancet paper noted that they were unable to give breakdowns of rates for different demographics.
Paul Nestadt, MD, is codirector of the Johns Hopkins Anxiety Disorders Clinic and studies suicide, firearms, and opiates. He looked at suicides in Maryland during the first 2 months of the lockdown (March 5, 2020 to May 7, 2020) and found that, Studies in Connecticut and Chicago yielded similar findings. These findings indicate that the overall trends may not reflect the impact on a specific subpopulation.
Dr. Nestadt talked about the disparities of suicide trends. “Communities hit harder by this pandemic in terms of sickness and death may experience more distress in ways that may come out as suicide in the context of other comorbid mood disorders. Also, in line with the idea of suicide as a marker of community- or population-level distress, there’s a general idea that having less of an economic cushion makes the pandemic more of a problem for some than for others. We know that suicide has been correlated to economic distress in general, and it makes sense that it would be community-specific where there is more economic duress.”
It has been a difficult year – not just for the United States, but for the entire world. One thing that may come of it is a unique opportunity to look at how stress and loss affect suicide rates, with the hope that preventive measures will follow.
A version of this article first appeared on Medscape.com.
Pfizer developing pill to treat COVID-19 symptoms
“If all goes well, and we implement the same speed that we are, and if regulators do the same, and they are, I hope that (it will be available) by the end of the year,” Dr. Bourla said on CNBC’s Squawk Box.
So far, the only antiviral drug authorized for use with COVID-19 is remdesivir, which is produced by Gilead Sciences and must be administered by injection in a health care setting.
An oral drug like the one Pfizer is developing could be taken at home and might keep people out of the hospital.
“Particular attention is on the oral because it provides several advantages,” Dr. Bourla said. “One of them is that you don’t need to go to the hospital to get the treatment, which is the case with all the injectables so far. You could get it at home, and that could be a game-changer.”
The drug might be effective against the emerging variants, he said. Pfizer is also working on an injectable antiviral drug.
Pfizer, with its European partner BioNTech, developed the first coronavirus vaccine authorized for use in the United States and Europe. The Pfizer pill under development would not be a vaccine to protect people from the virus but a drug to treat people who catch the virus.
The company announced in late March that it was starting clinical trials on the oral drug.
In a news release, the company said the oral drug would work by blocking protease, a critical enzyme that the virus needs to replicate. Protease inhibitors are used in medicines to treat HIV and hepatitis C.
A coronavirus vaccine that could be taken as a pill may enter clinical trials in the second quarter of 2021. The oral vaccine is being developed by Oravax Medical, a new joint venture of the Israeli-American company Oramed and the Indian company Premas Biotech. So far, all coronavirus vaccines are injectable.
A version of this article first appeared on WebMD.com.
“If all goes well, and we implement the same speed that we are, and if regulators do the same, and they are, I hope that (it will be available) by the end of the year,” Dr. Bourla said on CNBC’s Squawk Box.
So far, the only antiviral drug authorized for use with COVID-19 is remdesivir, which is produced by Gilead Sciences and must be administered by injection in a health care setting.
An oral drug like the one Pfizer is developing could be taken at home and might keep people out of the hospital.
“Particular attention is on the oral because it provides several advantages,” Dr. Bourla said. “One of them is that you don’t need to go to the hospital to get the treatment, which is the case with all the injectables so far. You could get it at home, and that could be a game-changer.”
The drug might be effective against the emerging variants, he said. Pfizer is also working on an injectable antiviral drug.
Pfizer, with its European partner BioNTech, developed the first coronavirus vaccine authorized for use in the United States and Europe. The Pfizer pill under development would not be a vaccine to protect people from the virus but a drug to treat people who catch the virus.
The company announced in late March that it was starting clinical trials on the oral drug.
In a news release, the company said the oral drug would work by blocking protease, a critical enzyme that the virus needs to replicate. Protease inhibitors are used in medicines to treat HIV and hepatitis C.
A coronavirus vaccine that could be taken as a pill may enter clinical trials in the second quarter of 2021. The oral vaccine is being developed by Oravax Medical, a new joint venture of the Israeli-American company Oramed and the Indian company Premas Biotech. So far, all coronavirus vaccines are injectable.
A version of this article first appeared on WebMD.com.
“If all goes well, and we implement the same speed that we are, and if regulators do the same, and they are, I hope that (it will be available) by the end of the year,” Dr. Bourla said on CNBC’s Squawk Box.
So far, the only antiviral drug authorized for use with COVID-19 is remdesivir, which is produced by Gilead Sciences and must be administered by injection in a health care setting.
An oral drug like the one Pfizer is developing could be taken at home and might keep people out of the hospital.
“Particular attention is on the oral because it provides several advantages,” Dr. Bourla said. “One of them is that you don’t need to go to the hospital to get the treatment, which is the case with all the injectables so far. You could get it at home, and that could be a game-changer.”
The drug might be effective against the emerging variants, he said. Pfizer is also working on an injectable antiviral drug.
Pfizer, with its European partner BioNTech, developed the first coronavirus vaccine authorized for use in the United States and Europe. The Pfizer pill under development would not be a vaccine to protect people from the virus but a drug to treat people who catch the virus.
The company announced in late March that it was starting clinical trials on the oral drug.
In a news release, the company said the oral drug would work by blocking protease, a critical enzyme that the virus needs to replicate. Protease inhibitors are used in medicines to treat HIV and hepatitis C.
A coronavirus vaccine that could be taken as a pill may enter clinical trials in the second quarter of 2021. The oral vaccine is being developed by Oravax Medical, a new joint venture of the Israeli-American company Oramed and the Indian company Premas Biotech. So far, all coronavirus vaccines are injectable.
A version of this article first appeared on WebMD.com.
Head to Toe: Recommendations for Physician Head and Shoe Coverings to Limit COVID-19 Transmission
Personal protective equipment (PPE) is an important component in limiting transmission of SARS-CoV-2. The World Health Organization and Centers for Disease Control and Prevention issued guidelines for appropriate PPE use, but recommendations for head and shoe coverings are lacking. In this article, we analyze the literature on pathogen transmission via hair and shoes and make evidence-based recommendations for PPE selection during the COVID-19 pandemic.
Pathogens on Shoes and Hair
Hair and shoes may act as vehicles for pathogen transmission. In a study that simulated contamination of uncovered skin in health care workers after intubating manikins in respiratory distress, 8 (100%) had fluorescent markers on the hair, 6 (75%) on the neck, and 4 (50%) on the shoes.1 In another study of postsurgical operating room (OR) surfaces (517 cultures), uncovered shoe tops and reusable hair coverings had 10-times more bacterial colony–forming units compared to other surfaces. On average, disposable shoe covers/head coverings had less than one-third bacterial colony–forming units compared with uncovered shoes/reusable hair coverings.2
Hair characteristics and coverings may affect pathogen transmission. Exposed hair may collect bacteria, as Staphylococcus aureus and Staphylococcus epidermidis attach to both scalp and facial hair. In one case, β-hemolytic streptococci cultured from the scalp of a perioperative nurse was linked to postsurgical infections in 20 patients.3 Hair coverings include bouffant caps and skullcaps. The bouffant cap is similar to a shower cap; it is relatively loose and secured around the head with elastic. The skullcap, or scrub cap, is tighter but leaves the neck nape and sideburns exposed. In a study comparing disposable bouffant caps, disposable skullcaps, and home-laundered cloth skullcaps worn by 2 teams of 5 surgeons, the disposable bouffant caps had the highest permeability, penetration, and microbial shed of airborne particles.4
Physicians’ shoes may act as fomites for transmission of pathogens to patients. In a study of 41 physicians and nurses in an acute care hospital, shoe soles were positive for at least one pathogen in 12 (29.3%) participants; methicillin-resistant Staphylococcus aureus was most common. Additionally, 98% (49/50) of shoes worn outdoors showed positive bacterial cultures compared to 56% (28/50) of shoes reserved for the OR only.5 In a study examining ventilation effects on airborne pathogens in the OR, 15% of OR airborne bacteria originated from OR floors, and higher bacterial counts correlated with a higher number of steps in the OR.2 In another study designed to evaluate SARS-CoV-2 distribution on hospital floors, 70% (7/10) of quantitative polymerase chain reaction assays performed on floor samples from intensive care units were positive. In addition, 100% (3/3) of swabs taken from hospital pharmacy floors with no COVID-19 patients were positive for SARS-CoV-2, meaning contaminated shoes likely served as vectors.6 Middle East respiratory syndrome, SARS-CoV-2, and influenza viruses may survive on porous and nonporous materials for hours to days.7Enterococcus, Candida, and Aspergillus may survive on textiles for up to 90 days.3
Recommendations for Hair and Shoe Coverings
We recommend that physicians utilize disposable skullcaps to cover the hair and consider a hooded gown or coverall for neck/ear coverage. We also recommend that physicians designate shoes that remain in the workplace and can be easily washed or disinfected at least weekly; physicians may choose to wash or disinfect shoes more often if they frequently are performing procedures that generate aerosols. Additionally, physicians should always wear shoe coverings when caring for patients (Table 1).
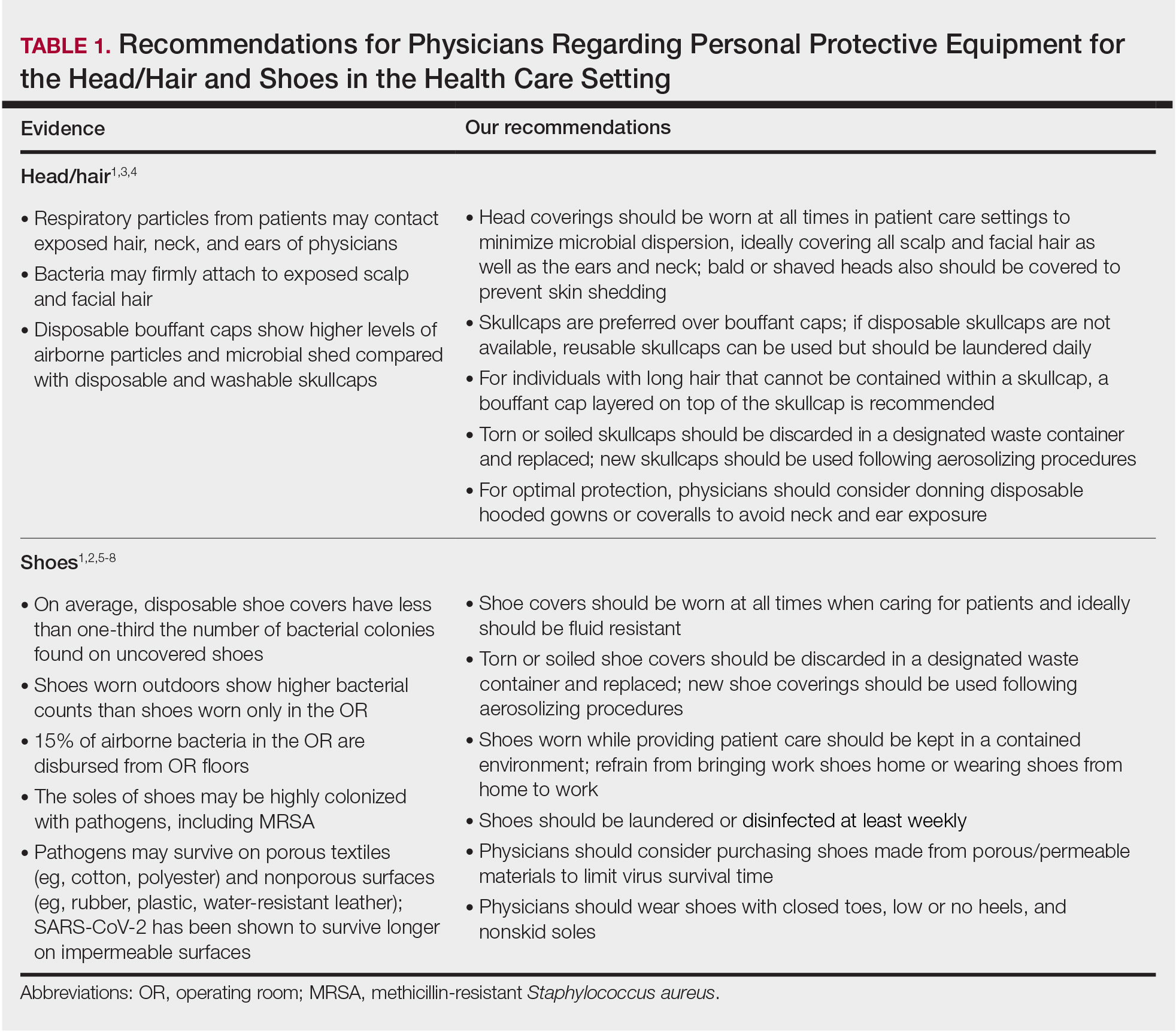
Our hair and shoe covering recommendations may serve to protect dermatologists when caring for patients. These protocols may be particularly important for dermatologists performing high-risk procedures, including facial surgery, intraoral/intranasal procedures, and treatment with ablative lasers and facial injectables, especially when the patient is unmasked. These recommendations may limit viral transmission to dermatologists and also protect individuals living in their households. Additional established guidelines by the American Academy of Dermatology, American Society for Dermatologic Surgery, and World Health Organization are listed in Table 2.8-10
Current PPE recommendations that do not include hair and shoe coverings may be inadequate for limiting SARS-CoV-2 exposure between and among physicians and patients. Adherence to head covering and shoe recommendations may aid in reducing unwanted SARS-CoV-2 transmission in the health care setting, even as the pandemic continues.
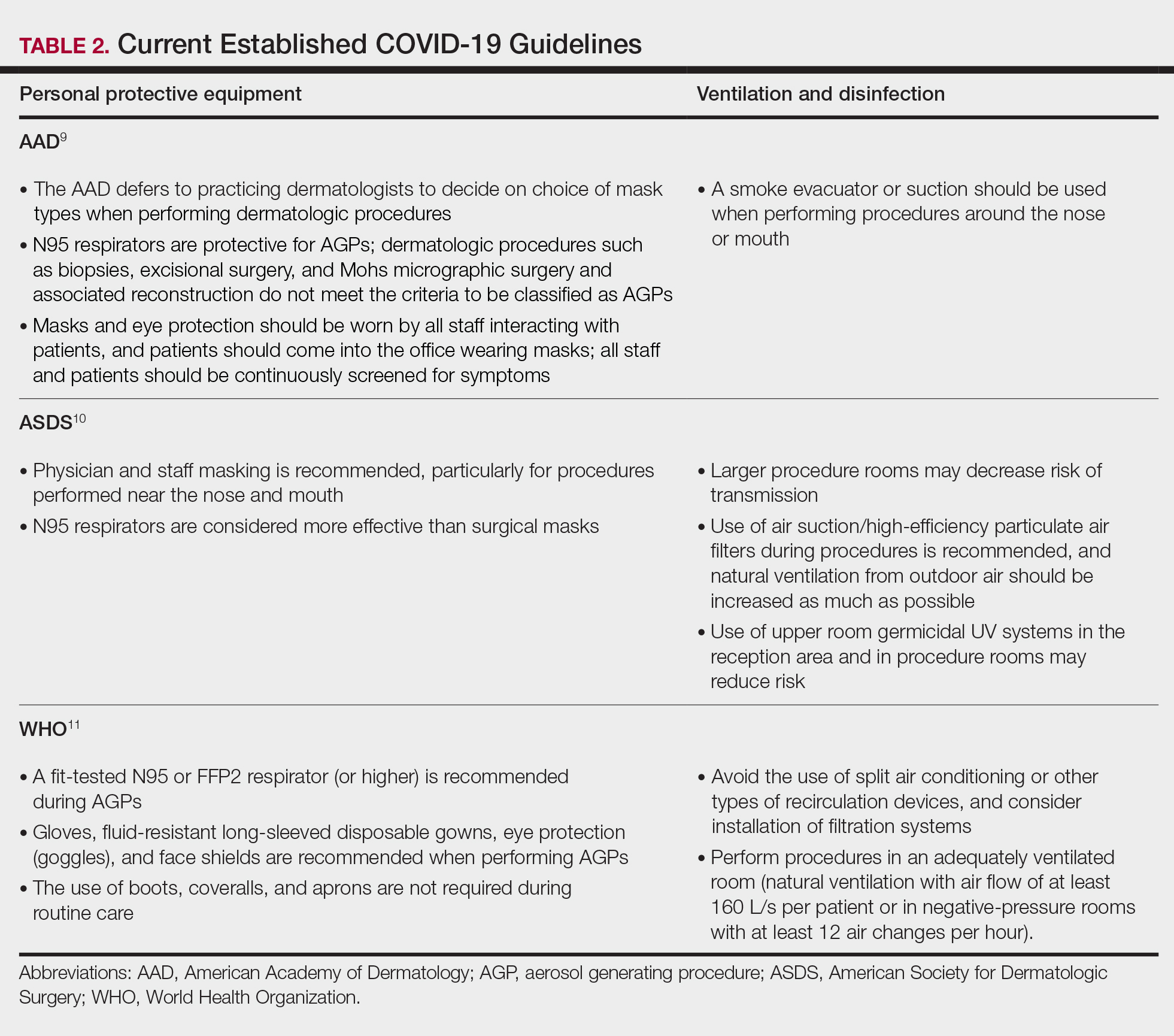
- Feldman O, Meir M, Shavit D, et al. Exposure to a surrogate measure of contamination from simulated patients by emergency department personnel wearing personal protective equipment. JAMA. 2020;323:2091-2093. doi:10.1001/jama.2020.6633
- Alexander JW, Van Sweringen H, Vanoss K, et al. Surveillance of bacterial colonization in operating rooms. Surg Infect (Larchmt). 2013;14:345-351. doi:10.1089/sur.2012.134
- Blanchard J. Clinical issues—August 2010. AORN Journal. 2010;92:228-232. doi:10.1016/j.aorn.2010.06.001
- Markel TA, Gormley T, Greeley D, et al. Hats off: a study of different operating room headgear assessed by environmental quality indicators. J Am Coll Surg. 2017;225:573-581. doi:10.1016/j.jamcollsurg.2017.08.014
- Kanwar A, Thakur M, Wazzan M, et al. Clothing and shoes of personnel as potential vectors for transfer of health care-associated pathogens to the community. Am J Infect Control. 2019;47:577-579. doi:10.1016/j.ajic.2019.01.028
- Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26:1583-1591. doi:10.3201/eid2607.200885
- Otter JA, Donskey C, Yezli S, et al. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect. 2016;92:235-250. doi:10.1016/j.jhin.2015.08.027
- Centers for Disease Control and Prevention. Science Brief: SARS-CoV-2 and Surface (Fomite) Transmission for Indoor Community Environments. https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html#ref10
- American Academy of Dermatology. Clinical guidance for COVID-19. Accessed March 15, 2021. https://www.aad.org/member/practice/coronavirus/clinical-guidance
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed March 15, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- World Health Organization. Country & technical guidance—coronavirus disease (COVID-19). Accessed March 15, 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance-publications
Personal protective equipment (PPE) is an important component in limiting transmission of SARS-CoV-2. The World Health Organization and Centers for Disease Control and Prevention issued guidelines for appropriate PPE use, but recommendations for head and shoe coverings are lacking. In this article, we analyze the literature on pathogen transmission via hair and shoes and make evidence-based recommendations for PPE selection during the COVID-19 pandemic.
Pathogens on Shoes and Hair
Hair and shoes may act as vehicles for pathogen transmission. In a study that simulated contamination of uncovered skin in health care workers after intubating manikins in respiratory distress, 8 (100%) had fluorescent markers on the hair, 6 (75%) on the neck, and 4 (50%) on the shoes.1 In another study of postsurgical operating room (OR) surfaces (517 cultures), uncovered shoe tops and reusable hair coverings had 10-times more bacterial colony–forming units compared to other surfaces. On average, disposable shoe covers/head coverings had less than one-third bacterial colony–forming units compared with uncovered shoes/reusable hair coverings.2
Hair characteristics and coverings may affect pathogen transmission. Exposed hair may collect bacteria, as Staphylococcus aureus and Staphylococcus epidermidis attach to both scalp and facial hair. In one case, β-hemolytic streptococci cultured from the scalp of a perioperative nurse was linked to postsurgical infections in 20 patients.3 Hair coverings include bouffant caps and skullcaps. The bouffant cap is similar to a shower cap; it is relatively loose and secured around the head with elastic. The skullcap, or scrub cap, is tighter but leaves the neck nape and sideburns exposed. In a study comparing disposable bouffant caps, disposable skullcaps, and home-laundered cloth skullcaps worn by 2 teams of 5 surgeons, the disposable bouffant caps had the highest permeability, penetration, and microbial shed of airborne particles.4
Physicians’ shoes may act as fomites for transmission of pathogens to patients. In a study of 41 physicians and nurses in an acute care hospital, shoe soles were positive for at least one pathogen in 12 (29.3%) participants; methicillin-resistant Staphylococcus aureus was most common. Additionally, 98% (49/50) of shoes worn outdoors showed positive bacterial cultures compared to 56% (28/50) of shoes reserved for the OR only.5 In a study examining ventilation effects on airborne pathogens in the OR, 15% of OR airborne bacteria originated from OR floors, and higher bacterial counts correlated with a higher number of steps in the OR.2 In another study designed to evaluate SARS-CoV-2 distribution on hospital floors, 70% (7/10) of quantitative polymerase chain reaction assays performed on floor samples from intensive care units were positive. In addition, 100% (3/3) of swabs taken from hospital pharmacy floors with no COVID-19 patients were positive for SARS-CoV-2, meaning contaminated shoes likely served as vectors.6 Middle East respiratory syndrome, SARS-CoV-2, and influenza viruses may survive on porous and nonporous materials for hours to days.7Enterococcus, Candida, and Aspergillus may survive on textiles for up to 90 days.3
Recommendations for Hair and Shoe Coverings
We recommend that physicians utilize disposable skullcaps to cover the hair and consider a hooded gown or coverall for neck/ear coverage. We also recommend that physicians designate shoes that remain in the workplace and can be easily washed or disinfected at least weekly; physicians may choose to wash or disinfect shoes more often if they frequently are performing procedures that generate aerosols. Additionally, physicians should always wear shoe coverings when caring for patients (Table 1).
Our hair and shoe covering recommendations may serve to protect dermatologists when caring for patients. These protocols may be particularly important for dermatologists performing high-risk procedures, including facial surgery, intraoral/intranasal procedures, and treatment with ablative lasers and facial injectables, especially when the patient is unmasked. These recommendations may limit viral transmission to dermatologists and also protect individuals living in their households. Additional established guidelines by the American Academy of Dermatology, American Society for Dermatologic Surgery, and World Health Organization are listed in Table 2.8-10
Current PPE recommendations that do not include hair and shoe coverings may be inadequate for limiting SARS-CoV-2 exposure between and among physicians and patients. Adherence to head covering and shoe recommendations may aid in reducing unwanted SARS-CoV-2 transmission in the health care setting, even as the pandemic continues.
Personal protective equipment (PPE) is an important component in limiting transmission of SARS-CoV-2. The World Health Organization and Centers for Disease Control and Prevention issued guidelines for appropriate PPE use, but recommendations for head and shoe coverings are lacking. In this article, we analyze the literature on pathogen transmission via hair and shoes and make evidence-based recommendations for PPE selection during the COVID-19 pandemic.
Pathogens on Shoes and Hair
Hair and shoes may act as vehicles for pathogen transmission. In a study that simulated contamination of uncovered skin in health care workers after intubating manikins in respiratory distress, 8 (100%) had fluorescent markers on the hair, 6 (75%) on the neck, and 4 (50%) on the shoes.1 In another study of postsurgical operating room (OR) surfaces (517 cultures), uncovered shoe tops and reusable hair coverings had 10-times more bacterial colony–forming units compared to other surfaces. On average, disposable shoe covers/head coverings had less than one-third bacterial colony–forming units compared with uncovered shoes/reusable hair coverings.2
Hair characteristics and coverings may affect pathogen transmission. Exposed hair may collect bacteria, as Staphylococcus aureus and Staphylococcus epidermidis attach to both scalp and facial hair. In one case, β-hemolytic streptococci cultured from the scalp of a perioperative nurse was linked to postsurgical infections in 20 patients.3 Hair coverings include bouffant caps and skullcaps. The bouffant cap is similar to a shower cap; it is relatively loose and secured around the head with elastic. The skullcap, or scrub cap, is tighter but leaves the neck nape and sideburns exposed. In a study comparing disposable bouffant caps, disposable skullcaps, and home-laundered cloth skullcaps worn by 2 teams of 5 surgeons, the disposable bouffant caps had the highest permeability, penetration, and microbial shed of airborne particles.4
Physicians’ shoes may act as fomites for transmission of pathogens to patients. In a study of 41 physicians and nurses in an acute care hospital, shoe soles were positive for at least one pathogen in 12 (29.3%) participants; methicillin-resistant Staphylococcus aureus was most common. Additionally, 98% (49/50) of shoes worn outdoors showed positive bacterial cultures compared to 56% (28/50) of shoes reserved for the OR only.5 In a study examining ventilation effects on airborne pathogens in the OR, 15% of OR airborne bacteria originated from OR floors, and higher bacterial counts correlated with a higher number of steps in the OR.2 In another study designed to evaluate SARS-CoV-2 distribution on hospital floors, 70% (7/10) of quantitative polymerase chain reaction assays performed on floor samples from intensive care units were positive. In addition, 100% (3/3) of swabs taken from hospital pharmacy floors with no COVID-19 patients were positive for SARS-CoV-2, meaning contaminated shoes likely served as vectors.6 Middle East respiratory syndrome, SARS-CoV-2, and influenza viruses may survive on porous and nonporous materials for hours to days.7Enterococcus, Candida, and Aspergillus may survive on textiles for up to 90 days.3
Recommendations for Hair and Shoe Coverings
We recommend that physicians utilize disposable skullcaps to cover the hair and consider a hooded gown or coverall for neck/ear coverage. We also recommend that physicians designate shoes that remain in the workplace and can be easily washed or disinfected at least weekly; physicians may choose to wash or disinfect shoes more often if they frequently are performing procedures that generate aerosols. Additionally, physicians should always wear shoe coverings when caring for patients (Table 1).
Our hair and shoe covering recommendations may serve to protect dermatologists when caring for patients. These protocols may be particularly important for dermatologists performing high-risk procedures, including facial surgery, intraoral/intranasal procedures, and treatment with ablative lasers and facial injectables, especially when the patient is unmasked. These recommendations may limit viral transmission to dermatologists and also protect individuals living in their households. Additional established guidelines by the American Academy of Dermatology, American Society for Dermatologic Surgery, and World Health Organization are listed in Table 2.8-10
Current PPE recommendations that do not include hair and shoe coverings may be inadequate for limiting SARS-CoV-2 exposure between and among physicians and patients. Adherence to head covering and shoe recommendations may aid in reducing unwanted SARS-CoV-2 transmission in the health care setting, even as the pandemic continues.
- Feldman O, Meir M, Shavit D, et al. Exposure to a surrogate measure of contamination from simulated patients by emergency department personnel wearing personal protective equipment. JAMA. 2020;323:2091-2093. doi:10.1001/jama.2020.6633
- Alexander JW, Van Sweringen H, Vanoss K, et al. Surveillance of bacterial colonization in operating rooms. Surg Infect (Larchmt). 2013;14:345-351. doi:10.1089/sur.2012.134
- Blanchard J. Clinical issues—August 2010. AORN Journal. 2010;92:228-232. doi:10.1016/j.aorn.2010.06.001
- Markel TA, Gormley T, Greeley D, et al. Hats off: a study of different operating room headgear assessed by environmental quality indicators. J Am Coll Surg. 2017;225:573-581. doi:10.1016/j.jamcollsurg.2017.08.014
- Kanwar A, Thakur M, Wazzan M, et al. Clothing and shoes of personnel as potential vectors for transfer of health care-associated pathogens to the community. Am J Infect Control. 2019;47:577-579. doi:10.1016/j.ajic.2019.01.028
- Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26:1583-1591. doi:10.3201/eid2607.200885
- Otter JA, Donskey C, Yezli S, et al. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect. 2016;92:235-250. doi:10.1016/j.jhin.2015.08.027
- Centers for Disease Control and Prevention. Science Brief: SARS-CoV-2 and Surface (Fomite) Transmission for Indoor Community Environments. https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html#ref10
- American Academy of Dermatology. Clinical guidance for COVID-19. Accessed March 15, 2021. https://www.aad.org/member/practice/coronavirus/clinical-guidance
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed March 15, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- World Health Organization. Country & technical guidance—coronavirus disease (COVID-19). Accessed March 15, 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance-publications
- Feldman O, Meir M, Shavit D, et al. Exposure to a surrogate measure of contamination from simulated patients by emergency department personnel wearing personal protective equipment. JAMA. 2020;323:2091-2093. doi:10.1001/jama.2020.6633
- Alexander JW, Van Sweringen H, Vanoss K, et al. Surveillance of bacterial colonization in operating rooms. Surg Infect (Larchmt). 2013;14:345-351. doi:10.1089/sur.2012.134
- Blanchard J. Clinical issues—August 2010. AORN Journal. 2010;92:228-232. doi:10.1016/j.aorn.2010.06.001
- Markel TA, Gormley T, Greeley D, et al. Hats off: a study of different operating room headgear assessed by environmental quality indicators. J Am Coll Surg. 2017;225:573-581. doi:10.1016/j.jamcollsurg.2017.08.014
- Kanwar A, Thakur M, Wazzan M, et al. Clothing and shoes of personnel as potential vectors for transfer of health care-associated pathogens to the community. Am J Infect Control. 2019;47:577-579. doi:10.1016/j.ajic.2019.01.028
- Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26:1583-1591. doi:10.3201/eid2607.200885
- Otter JA, Donskey C, Yezli S, et al. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect. 2016;92:235-250. doi:10.1016/j.jhin.2015.08.027
- Centers for Disease Control and Prevention. Science Brief: SARS-CoV-2 and Surface (Fomite) Transmission for Indoor Community Environments. https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html#ref10
- American Academy of Dermatology. Clinical guidance for COVID-19. Accessed March 15, 2021. https://www.aad.org/member/practice/coronavirus/clinical-guidance
- Narla S, Alam M, Ozog DM, et al. American Society of Dermatologic Surgery Association (ASDSA) and American Society for Laser Medicine & Surgery (ASLMS) guidance for cosmetic dermatology practices during COVID-19. Updated January 11, 2021. Accessed March 15, 2021. https://www.asds.net/Portals/0/PDF/asdsa/asdsa-aslms-cosmetic-reopening-guidance.pdf
- World Health Organization. Country & technical guidance—coronavirus disease (COVID-19). Accessed March 15, 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance-publications
Practice Points
- Consistent use of personal protective equipment, including masks, face shields, goggles, and gloves, may limit transmission of SARS-CoV-2.
- Hair and shoes also may transmit SARS-CoV-2, but recommendations for hair and shoe coverings to prevent SARS-CoV-2 are lacking.