User login
Muscle-related AEs reported in statin trial suggest ‘nocebo’ effect
Patients are more likely to report muscle-related adverse events (AEs) with statin therapy if a trial is unblinded, according to an analysis of a large clinical trial.
In the lipid-lowering arm of the Anglo-Scandinavian Cardiac Outcomes trial (ASCOT-LLA), 10,180 patients were randomized 1:1 to atorvastatin 10 mg daily or matching placebo for a median for 3.3 years. After the trial was terminated for efficacy, all patients were offered open-label atorvastatin, with 6,409 users and 3,490 nonusers then followed for a median of 2.3 years.
However, during the nonblinded, nonrandomized phase, the rate of muscle-related adverse events was 41% higher in individuals taking atorvastatin, compared with nonusers (1.26% vs. 1% per annum, P = .006). This was despite the fact that patients who reported muscle-related adverse events during the blinded phase were less likely to remain on a statin during the nonblinded phase, compared with those who had not reported this adverse event (Lancet. 2017 May 2. doi: 10.1016/S0140-6736[17]31075-9).
“This observation is consistent with a nocebo effect, whereby subjective AEs (e.g., symptoms reported by patients) can be more likely to be attributed to a treatment thought to cause some particular side effect,” wrote Ajay Gupta, MD, of the National Heart and Lung Institute at Imperial College London and his coauthors.
Musculoskeletal and connective tissue disorders and blood and lymphatic system disorders were also reported more commonly among those taking statins, compared with those not in the nonblinded phase. Apart from these, there were no other significant differences in the rate of other adverse events.
In the blinded phase, patients taking atorvastatin reported significantly lower rates of sleep disturbance, compared with those on placebo, but there was a significant 23% higher rate of renal and urinary adverse events in the atorvastatin arm, compared with the placebo arm. Researchers were not able to draw any conclusions about the incidence of cognitive impairment because there were too few cases.
“We hope that the demonstration in the ASCOT-LLA, of not only the absence of adverse effects of statin therapy on muscle-related and other AEs but also the effect of ascertainment bias in nonblinding studies (which have been the basis of many of the misleading claims), will help to counter the adverse effect on public health of exaggerated claims about statin side effects,” the authors wrote.
The study was funded by Pfizer, Servier Research Group, and Leo Laboratories. Four authors declared personal fees, funding, or speakers honoraria from pharmaceutical companies, including Pfizer. One author was also noted for having sought retraction of papers published about the side-effects of statin therapy. No other conflicts of interest were declared.
Patients are more likely to report muscle-related adverse events (AEs) with statin therapy if a trial is unblinded, according to an analysis of a large clinical trial.
In the lipid-lowering arm of the Anglo-Scandinavian Cardiac Outcomes trial (ASCOT-LLA), 10,180 patients were randomized 1:1 to atorvastatin 10 mg daily or matching placebo for a median for 3.3 years. After the trial was terminated for efficacy, all patients were offered open-label atorvastatin, with 6,409 users and 3,490 nonusers then followed for a median of 2.3 years.
However, during the nonblinded, nonrandomized phase, the rate of muscle-related adverse events was 41% higher in individuals taking atorvastatin, compared with nonusers (1.26% vs. 1% per annum, P = .006). This was despite the fact that patients who reported muscle-related adverse events during the blinded phase were less likely to remain on a statin during the nonblinded phase, compared with those who had not reported this adverse event (Lancet. 2017 May 2. doi: 10.1016/S0140-6736[17]31075-9).
“This observation is consistent with a nocebo effect, whereby subjective AEs (e.g., symptoms reported by patients) can be more likely to be attributed to a treatment thought to cause some particular side effect,” wrote Ajay Gupta, MD, of the National Heart and Lung Institute at Imperial College London and his coauthors.
Musculoskeletal and connective tissue disorders and blood and lymphatic system disorders were also reported more commonly among those taking statins, compared with those not in the nonblinded phase. Apart from these, there were no other significant differences in the rate of other adverse events.
In the blinded phase, patients taking atorvastatin reported significantly lower rates of sleep disturbance, compared with those on placebo, but there was a significant 23% higher rate of renal and urinary adverse events in the atorvastatin arm, compared with the placebo arm. Researchers were not able to draw any conclusions about the incidence of cognitive impairment because there were too few cases.
“We hope that the demonstration in the ASCOT-LLA, of not only the absence of adverse effects of statin therapy on muscle-related and other AEs but also the effect of ascertainment bias in nonblinding studies (which have been the basis of many of the misleading claims), will help to counter the adverse effect on public health of exaggerated claims about statin side effects,” the authors wrote.
The study was funded by Pfizer, Servier Research Group, and Leo Laboratories. Four authors declared personal fees, funding, or speakers honoraria from pharmaceutical companies, including Pfizer. One author was also noted for having sought retraction of papers published about the side-effects of statin therapy. No other conflicts of interest were declared.
Patients are more likely to report muscle-related adverse events (AEs) with statin therapy if a trial is unblinded, according to an analysis of a large clinical trial.
In the lipid-lowering arm of the Anglo-Scandinavian Cardiac Outcomes trial (ASCOT-LLA), 10,180 patients were randomized 1:1 to atorvastatin 10 mg daily or matching placebo for a median for 3.3 years. After the trial was terminated for efficacy, all patients were offered open-label atorvastatin, with 6,409 users and 3,490 nonusers then followed for a median of 2.3 years.
However, during the nonblinded, nonrandomized phase, the rate of muscle-related adverse events was 41% higher in individuals taking atorvastatin, compared with nonusers (1.26% vs. 1% per annum, P = .006). This was despite the fact that patients who reported muscle-related adverse events during the blinded phase were less likely to remain on a statin during the nonblinded phase, compared with those who had not reported this adverse event (Lancet. 2017 May 2. doi: 10.1016/S0140-6736[17]31075-9).
“This observation is consistent with a nocebo effect, whereby subjective AEs (e.g., symptoms reported by patients) can be more likely to be attributed to a treatment thought to cause some particular side effect,” wrote Ajay Gupta, MD, of the National Heart and Lung Institute at Imperial College London and his coauthors.
Musculoskeletal and connective tissue disorders and blood and lymphatic system disorders were also reported more commonly among those taking statins, compared with those not in the nonblinded phase. Apart from these, there were no other significant differences in the rate of other adverse events.
In the blinded phase, patients taking atorvastatin reported significantly lower rates of sleep disturbance, compared with those on placebo, but there was a significant 23% higher rate of renal and urinary adverse events in the atorvastatin arm, compared with the placebo arm. Researchers were not able to draw any conclusions about the incidence of cognitive impairment because there were too few cases.
“We hope that the demonstration in the ASCOT-LLA, of not only the absence of adverse effects of statin therapy on muscle-related and other AEs but also the effect of ascertainment bias in nonblinding studies (which have been the basis of many of the misleading claims), will help to counter the adverse effect on public health of exaggerated claims about statin side effects,” the authors wrote.
The study was funded by Pfizer, Servier Research Group, and Leo Laboratories. Four authors declared personal fees, funding, or speakers honoraria from pharmaceutical companies, including Pfizer. One author was also noted for having sought retraction of papers published about the side-effects of statin therapy. No other conflicts of interest were declared.
FROM THE LANCET
Key clinical point: Patient reports of muscle-related adverse events related to statin use increases significantly after unblinding.
Major finding: The rate of muscle-related adverse events was 41% higher in individuals taking atorvastatin than in nonusers in the nonblinded phase of a trial, compared with no significant difference between arms in the blinded phase.
Data source: The lipid-lowering arm of the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT-LLA) involving 10,180 patients.
Disclosures: The study was funded by Pfizer, Servier Research Group, and Leo Laboratories. Four authors declared personal fees, funding, or speakers honoraria from pharmaceutical companies, including Pfizer. One author was also noted for having sought retraction of papers published about the side effects of statin therapy. No other conflicts of interest were declared.
Vascular surgeons underutilize palliative care planning
Investment in advanced palliative care planning has the potential to improve the quality of care for vascular surgery patients, according to investigators from Oregon Health and Science University, Portland.
Dale G. Wilson, MD, and his colleagues performed a retrospective review of electronic medical records for 111 patients, who died while on the vascular surgery service at the OHSU Hospital during 2005-2014.
Almost three-quarters (73%) of patients were transitioned to palliative care; of those, 14% presented with an advanced directive, and 28% received a palliative care consultation (JAMA Surg. 2017;152[2]:183-90. doi: 10.1001/jamasurg.2016.3970).
While palliative care services are increasing in hospitals, accounting for 4% of annual hospital admissions in 2012 according to the study, they are not implemented consistently. “Many teams from various specialties care for patients at end of life; however, we still do not know what prompts end-of-life discussions,” Dr. Wilson said. “There is still no consensus on when to involve palliative services in the care of critically ill patients.”
While the decision to advise a consultation is “variable and physician dependent,” the type of treatment required may help identify when consultations are appropriate.
Of the 14 patients who did not choose comfort care, 11 (79%) required CPR. Additionally, all had to be taken to the operating room and required mechanical ventilation.
Of 81 patients who chose palliative care, 31 did so despite potential medical options. These patients were older – average age, 77 years, as compared with 68 years for patients who did not choose comfort care – with 8 of the 31 (26%) presenting an advanced directive, compared with only 7 of 83 patients (8%) for those who did not receive palliative care.
Dr. Wilson and his colleagues found that patients who chose palliative care were more likely to have received a palliative care consultation, as well: 10 of 31 patients who chose comfort care received a consultation, as opposed to 1 of 83 who chose comfort care but did not receive a consultation.
The nature of the vascular surgery service calls for early efforts to gather information regarding patients’ views on end-of-life care, Dr. Wilson said, noting that 73% of patients studied were admitted emergently and 87% underwent surgery, leaving little time for patients to express their wishes.
“Because the events associated with withdrawal of care are often not anticipated, we argue that all vascular surgical patients should have an advance directive, and perhaps, those at particular high risk should have a preoperative palliative care consultation,” Dr. Wilson wrote.
Limitations to the study included the data abstraction, which was performed by a single unblinded physician. Researchers also gathered patients’ reasons for transitioning to comfort care retrospectively.
The low rate of palliative care consultations found in this study mirrors my own experience, as does the feeling of urgency to shed more light on the issue. The biggest hurdle surgeons face when it comes to palliative care consultations is that, in their minds, seeking these meetings is associated with immediate death care. Many surgeons are shy about bringing palliative care specialists on board because approaching families can be daunting.
Family members who do not know enough about comfort care can be upset by the idea. Addressing this misunderstanding is crucial. Consultations are not just conversations about hospice care but can be emotional and spiritual experiences that prepare both the family and the patient for alternative options when surgical intervention cannot guarantee a good quality of life. I would encourage surgeons to be more proactive and less defensive about comfort care . Luckily, understanding the importance of this issue among professionals is growing.
When I approach these situations, it’s important for me to have a full understanding of what families and patients usually expect. Decisions should not be based on how bad things are now but on the future. What was the patient’s last year like? What is the best-case scenario for moving forward on a proposed intervention? What will the patient’s quality of life be? Answering these questions helps the patient understand his or her situation, without diminishing a surgeon’s ability. If you are honest, the family will usually come to the conclusion that they do not want to subject the patient to ultimately unnecessary treatment.
Palliative care services help patients and their families deal with pain beyond the physical symptoms. Dealing with pain, depression, or delirium is only a part of comfort care – coping with a sense of hopelessness, family disruption, or feelings of guilt also can be a part and, significantly, a part that surgeons are not trained to diagnose or treat.
With more than 70 surgeons certified in hospice care and a growing number of fellowships in palliative care, I am extremely optimistic in the progress we have made and will continue to make.
Geoffrey Dunn, MD, FACS, is the medical director of the Palliative Care Consultation Service at UPMC Hamot Medical Center, Erie, Penn. He currently is Community Editor for the Pain and Palliative Care Community for the ACS’s web portal.
The low rate of palliative care consultations found in this study mirrors my own experience, as does the feeling of urgency to shed more light on the issue. The biggest hurdle surgeons face when it comes to palliative care consultations is that, in their minds, seeking these meetings is associated with immediate death care. Many surgeons are shy about bringing palliative care specialists on board because approaching families can be daunting.
Family members who do not know enough about comfort care can be upset by the idea. Addressing this misunderstanding is crucial. Consultations are not just conversations about hospice care but can be emotional and spiritual experiences that prepare both the family and the patient for alternative options when surgical intervention cannot guarantee a good quality of life. I would encourage surgeons to be more proactive and less defensive about comfort care . Luckily, understanding the importance of this issue among professionals is growing.
When I approach these situations, it’s important for me to have a full understanding of what families and patients usually expect. Decisions should not be based on how bad things are now but on the future. What was the patient’s last year like? What is the best-case scenario for moving forward on a proposed intervention? What will the patient’s quality of life be? Answering these questions helps the patient understand his or her situation, without diminishing a surgeon’s ability. If you are honest, the family will usually come to the conclusion that they do not want to subject the patient to ultimately unnecessary treatment.
Palliative care services help patients and their families deal with pain beyond the physical symptoms. Dealing with pain, depression, or delirium is only a part of comfort care – coping with a sense of hopelessness, family disruption, or feelings of guilt also can be a part and, significantly, a part that surgeons are not trained to diagnose or treat.
With more than 70 surgeons certified in hospice care and a growing number of fellowships in palliative care, I am extremely optimistic in the progress we have made and will continue to make.
Geoffrey Dunn, MD, FACS, is the medical director of the Palliative Care Consultation Service at UPMC Hamot Medical Center, Erie, Penn. He currently is Community Editor for the Pain and Palliative Care Community for the ACS’s web portal.
The low rate of palliative care consultations found in this study mirrors my own experience, as does the feeling of urgency to shed more light on the issue. The biggest hurdle surgeons face when it comes to palliative care consultations is that, in their minds, seeking these meetings is associated with immediate death care. Many surgeons are shy about bringing palliative care specialists on board because approaching families can be daunting.
Family members who do not know enough about comfort care can be upset by the idea. Addressing this misunderstanding is crucial. Consultations are not just conversations about hospice care but can be emotional and spiritual experiences that prepare both the family and the patient for alternative options when surgical intervention cannot guarantee a good quality of life. I would encourage surgeons to be more proactive and less defensive about comfort care . Luckily, understanding the importance of this issue among professionals is growing.
When I approach these situations, it’s important for me to have a full understanding of what families and patients usually expect. Decisions should not be based on how bad things are now but on the future. What was the patient’s last year like? What is the best-case scenario for moving forward on a proposed intervention? What will the patient’s quality of life be? Answering these questions helps the patient understand his or her situation, without diminishing a surgeon’s ability. If you are honest, the family will usually come to the conclusion that they do not want to subject the patient to ultimately unnecessary treatment.
Palliative care services help patients and their families deal with pain beyond the physical symptoms. Dealing with pain, depression, or delirium is only a part of comfort care – coping with a sense of hopelessness, family disruption, or feelings of guilt also can be a part and, significantly, a part that surgeons are not trained to diagnose or treat.
With more than 70 surgeons certified in hospice care and a growing number of fellowships in palliative care, I am extremely optimistic in the progress we have made and will continue to make.
Geoffrey Dunn, MD, FACS, is the medical director of the Palliative Care Consultation Service at UPMC Hamot Medical Center, Erie, Penn. He currently is Community Editor for the Pain and Palliative Care Community for the ACS’s web portal.
Investment in advanced palliative care planning has the potential to improve the quality of care for vascular surgery patients, according to investigators from Oregon Health and Science University, Portland.
Dale G. Wilson, MD, and his colleagues performed a retrospective review of electronic medical records for 111 patients, who died while on the vascular surgery service at the OHSU Hospital during 2005-2014.
Almost three-quarters (73%) of patients were transitioned to palliative care; of those, 14% presented with an advanced directive, and 28% received a palliative care consultation (JAMA Surg. 2017;152[2]:183-90. doi: 10.1001/jamasurg.2016.3970).
While palliative care services are increasing in hospitals, accounting for 4% of annual hospital admissions in 2012 according to the study, they are not implemented consistently. “Many teams from various specialties care for patients at end of life; however, we still do not know what prompts end-of-life discussions,” Dr. Wilson said. “There is still no consensus on when to involve palliative services in the care of critically ill patients.”
While the decision to advise a consultation is “variable and physician dependent,” the type of treatment required may help identify when consultations are appropriate.
Of the 14 patients who did not choose comfort care, 11 (79%) required CPR. Additionally, all had to be taken to the operating room and required mechanical ventilation.
Of 81 patients who chose palliative care, 31 did so despite potential medical options. These patients were older – average age, 77 years, as compared with 68 years for patients who did not choose comfort care – with 8 of the 31 (26%) presenting an advanced directive, compared with only 7 of 83 patients (8%) for those who did not receive palliative care.
Dr. Wilson and his colleagues found that patients who chose palliative care were more likely to have received a palliative care consultation, as well: 10 of 31 patients who chose comfort care received a consultation, as opposed to 1 of 83 who chose comfort care but did not receive a consultation.
The nature of the vascular surgery service calls for early efforts to gather information regarding patients’ views on end-of-life care, Dr. Wilson said, noting that 73% of patients studied were admitted emergently and 87% underwent surgery, leaving little time for patients to express their wishes.
“Because the events associated with withdrawal of care are often not anticipated, we argue that all vascular surgical patients should have an advance directive, and perhaps, those at particular high risk should have a preoperative palliative care consultation,” Dr. Wilson wrote.
Limitations to the study included the data abstraction, which was performed by a single unblinded physician. Researchers also gathered patients’ reasons for transitioning to comfort care retrospectively.
Investment in advanced palliative care planning has the potential to improve the quality of care for vascular surgery patients, according to investigators from Oregon Health and Science University, Portland.
Dale G. Wilson, MD, and his colleagues performed a retrospective review of electronic medical records for 111 patients, who died while on the vascular surgery service at the OHSU Hospital during 2005-2014.
Almost three-quarters (73%) of patients were transitioned to palliative care; of those, 14% presented with an advanced directive, and 28% received a palliative care consultation (JAMA Surg. 2017;152[2]:183-90. doi: 10.1001/jamasurg.2016.3970).
While palliative care services are increasing in hospitals, accounting for 4% of annual hospital admissions in 2012 according to the study, they are not implemented consistently. “Many teams from various specialties care for patients at end of life; however, we still do not know what prompts end-of-life discussions,” Dr. Wilson said. “There is still no consensus on when to involve palliative services in the care of critically ill patients.”
While the decision to advise a consultation is “variable and physician dependent,” the type of treatment required may help identify when consultations are appropriate.
Of the 14 patients who did not choose comfort care, 11 (79%) required CPR. Additionally, all had to be taken to the operating room and required mechanical ventilation.
Of 81 patients who chose palliative care, 31 did so despite potential medical options. These patients were older – average age, 77 years, as compared with 68 years for patients who did not choose comfort care – with 8 of the 31 (26%) presenting an advanced directive, compared with only 7 of 83 patients (8%) for those who did not receive palliative care.
Dr. Wilson and his colleagues found that patients who chose palliative care were more likely to have received a palliative care consultation, as well: 10 of 31 patients who chose comfort care received a consultation, as opposed to 1 of 83 who chose comfort care but did not receive a consultation.
The nature of the vascular surgery service calls for early efforts to gather information regarding patients’ views on end-of-life care, Dr. Wilson said, noting that 73% of patients studied were admitted emergently and 87% underwent surgery, leaving little time for patients to express their wishes.
“Because the events associated with withdrawal of care are often not anticipated, we argue that all vascular surgical patients should have an advance directive, and perhaps, those at particular high risk should have a preoperative palliative care consultation,” Dr. Wilson wrote.
Limitations to the study included the data abstraction, which was performed by a single unblinded physician. Researchers also gathered patients’ reasons for transitioning to comfort care retrospectively.
FROM JAMA SURGERY
Key clinical point:
Major finding: Of the 111 patients studied, 81 died on palliative care, but only 15 presented an advanced directive.
Data source: A retrospective cohort study of the records of patients aged 18-99 years who died in the vascular surgery service at Oregon Health and Science University Hospital from 2005-2014.
Disclosures: The authors reported no financial disclosures.
Mesh cylinder effective for small to medium wide-necked aneurysms
HOUSTON – An expandable mesh cylinder that is approved to treat large, wide-necked carotid aneurysms has now proved successful in treating small lesions of the internal carotid or vertebral artery up to 12 mm in diameter.
The Pipeline Embolization Device (PED, Medtronic) completely occluded 84% of such lesions without significant stenosis or retreatment within 1 year in the PREMIER trial, Ricardo Hanel, MD, PhD, said at the International Stroke Conference sponsored by the American Heart Association.
Overall morbidity and mortality in the year-long trial was very low (2.2%). However, within the first year, three patients had a major stroke in brain regions supplied by the treated artery; one of these was related to device deployment and was fatal, said Dr. Hanel, director of the Baptist Neurological Institute, Jacksonville, Fla.

Counseling patients with these lesions is not easy, Dr. Hanel said. Treatment decisions must take into account not only the patient’s current clinical status and comorbidities, but family history and personal preference. In fact, patient preference was the largest driver of treatment (63%) in the PREMIER study.
In an interview, Dr. Hanel illustrated the importance of individualized decision making. A middle-aged female had been monitored for a small aneurysm for 7 years. When the patient was 6 years old, her mother died during an open operation to treat an aneurysm.
“We had tried to treat this patient with coiling [when the lesion was first detected], but it was unsuccessful,” Dr. Hanel said. “And since her mother had died during surgery, she did not want to go for an open approach. Now, 6 years later, we have the technology to cure her with a single device, and the odds of [recurrence over 10 years] are virtually zero. It is a very personal decision, and we take a lot of factors under consideration before we decide to expose the patient to the risks of this treatment.”
The PED is a flexible 75% cobalt-chromium/25% platinum-tungsten mesh with a braided configuration. It is advanced slightly beyond the aneurysm neck and then deployed. As it opens, it partially occludes the lesion, immediately decreasing the amount of blood entering the sac. Within a month, vascular remodeling is well underway; as endothelium grows throughout the mesh, blood flow into the aneurysm is gradually cut off. Eventually the aneurysmal sac recedes, and the normal vascular architecture is restored.
“Within 4 weeks you can’t see the metal at all,” Dr. Hanel said. “It’s covered by a thin layer of endothelial cells. This device allows the patient’s body to heal and close the aneurysm, and we don’t have to deal with the reoccurrence problem we have with stent coils. The pipeline treats the entire circumference of the vessel.”
The PED is used in combination with dual-antiplatelet therapy (DAP, aspirin/clopidogrel). Dr. Hanel initiates DAP 7 days before the procedure and continues it for 3 months. At that time, clopidogrel may be discontinued. “I advise my patients to then take a baby aspirin every day for the rest of their lives,” and they are regularly monitored, he said. “Aspirin seems to protect against the formation and rupture of aneurysms.”
PREMIER followed 141 patients with unruptured, wide-necked small aneurysms of the internal carotid (up to the terminus) or the vertebral artery segment up to and including the posterior inferior cerebellar artery. The primary efficacy endpoint was complete aneurysm occlusion and absence of significant parent artery stenosis at 1 year. The secondary endpoint was successful device deployment.
The primary safety endpoint was major stroke in the territory supplied by the treated artery or neurologic death at 1 year. There were two secondary safety endpoints: major stroke or neurologic death within 30 days, attributable to procedural complications, and intracerebral hemorrhage more than 30 days later.
The patients were largely female (88%) with a mean age of 55 years. They were asymptomatic with a mean modified Rankin Scale score of 0.2 and National Institutes of Health Stroke Scale score of 0.1. Nearly half of the patients had hypertension, and 38% had hyperlipidemia. About 28% were current smokers, and another 16% had a history of smoking.
The patients’ mean maximal aneurysm diameter was 4.6 mm, with a mean neck width of 3.7 mm. The majority of lesions (84%) were less than 7 mm in diameter, but they ranged up to 12 mm.
Internal carotid artery aneurysms comprised 95% of all in the study; 5% were in the vertebral artery. Most involved the side wall (84%), while the remainder involved a side branch (12%) or were fusiform (4%).
There was only one unsuccessful initial deployment, resulting in a 99.3% deployment success rate. The mean procedure time was 78 minutes. While most patients received just one PED, 10 received multiple devices. The PED completely covered the entire neck of the lesion in 97%. There were no intraoperative aneurysm ruptures and no intraoperative deaths.
At 1 year after implantation, 84% of the aneurysms were completely occluded, with the aneurysmal sac eliminated in 92%. A residual aneurysm remained in 11 patients (8%), and a residual neck in 8 patients (6%). Two patients (1.4%) had arterial stenosis of more than 50%. Three patients (2.2%) required retreatment.
There were three major strokes in the region supplied by the target artery in three patients.
The fatal stroke occurred in a patient who had an aneurysm on the right ophthalmic carotid segment. The first device failed to deploy correctly and was removed. A second device was implanted. The next day the patient developed a facial droop, slurred speech, and a headache. She experienced a distal intraparenchymal hemorrhage and underwent hemicraniotomy, but did not survive.
The second stroke occurred in a patient who needed two devices to occlude a lesion in the left ophthalmic segment of the carotid. The patient developed an intraparenchymal hemorrhage on postoperative day 15. The stroke resolved with sequelae and the clopidogrel dose was increased.
The third stroke was associated with treatment of a right communicating segment aneurysm. The patient stopped taking the recommended DAP and experienced an acute ischemic stroke 169 days after the procedure. This stroke also resolved with sequelae.
Based on the results of PREMIER, Medtronic will pursue Food and Drug Administration approval of the PED for small to medium wide-necked aneurysms, Dr. Hanel noted.
Medtronic sponsored the study. Dr. Hanel is an adviser to the company and has received research funds from it.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
HOUSTON – An expandable mesh cylinder that is approved to treat large, wide-necked carotid aneurysms has now proved successful in treating small lesions of the internal carotid or vertebral artery up to 12 mm in diameter.
The Pipeline Embolization Device (PED, Medtronic) completely occluded 84% of such lesions without significant stenosis or retreatment within 1 year in the PREMIER trial, Ricardo Hanel, MD, PhD, said at the International Stroke Conference sponsored by the American Heart Association.
Overall morbidity and mortality in the year-long trial was very low (2.2%). However, within the first year, three patients had a major stroke in brain regions supplied by the treated artery; one of these was related to device deployment and was fatal, said Dr. Hanel, director of the Baptist Neurological Institute, Jacksonville, Fla.
Counseling patients with these lesions is not easy, Dr. Hanel said. Treatment decisions must take into account not only the patient’s current clinical status and comorbidities, but family history and personal preference. In fact, patient preference was the largest driver of treatment (63%) in the PREMIER study.
In an interview, Dr. Hanel illustrated the importance of individualized decision making. A middle-aged female had been monitored for a small aneurysm for 7 years. When the patient was 6 years old, her mother died during an open operation to treat an aneurysm.
“We had tried to treat this patient with coiling [when the lesion was first detected], but it was unsuccessful,” Dr. Hanel said. “And since her mother had died during surgery, she did not want to go for an open approach. Now, 6 years later, we have the technology to cure her with a single device, and the odds of [recurrence over 10 years] are virtually zero. It is a very personal decision, and we take a lot of factors under consideration before we decide to expose the patient to the risks of this treatment.”
The PED is a flexible 75% cobalt-chromium/25% platinum-tungsten mesh with a braided configuration. It is advanced slightly beyond the aneurysm neck and then deployed. As it opens, it partially occludes the lesion, immediately decreasing the amount of blood entering the sac. Within a month, vascular remodeling is well underway; as endothelium grows throughout the mesh, blood flow into the aneurysm is gradually cut off. Eventually the aneurysmal sac recedes, and the normal vascular architecture is restored.
“Within 4 weeks you can’t see the metal at all,” Dr. Hanel said. “It’s covered by a thin layer of endothelial cells. This device allows the patient’s body to heal and close the aneurysm, and we don’t have to deal with the reoccurrence problem we have with stent coils. The pipeline treats the entire circumference of the vessel.”
The PED is used in combination with dual-antiplatelet therapy (DAP, aspirin/clopidogrel). Dr. Hanel initiates DAP 7 days before the procedure and continues it for 3 months. At that time, clopidogrel may be discontinued. “I advise my patients to then take a baby aspirin every day for the rest of their lives,” and they are regularly monitored, he said. “Aspirin seems to protect against the formation and rupture of aneurysms.”
PREMIER followed 141 patients with unruptured, wide-necked small aneurysms of the internal carotid (up to the terminus) or the vertebral artery segment up to and including the posterior inferior cerebellar artery. The primary efficacy endpoint was complete aneurysm occlusion and absence of significant parent artery stenosis at 1 year. The secondary endpoint was successful device deployment.
The primary safety endpoint was major stroke in the territory supplied by the treated artery or neurologic death at 1 year. There were two secondary safety endpoints: major stroke or neurologic death within 30 days, attributable to procedural complications, and intracerebral hemorrhage more than 30 days later.
The patients were largely female (88%) with a mean age of 55 years. They were asymptomatic with a mean modified Rankin Scale score of 0.2 and National Institutes of Health Stroke Scale score of 0.1. Nearly half of the patients had hypertension, and 38% had hyperlipidemia. About 28% were current smokers, and another 16% had a history of smoking.
The patients’ mean maximal aneurysm diameter was 4.6 mm, with a mean neck width of 3.7 mm. The majority of lesions (84%) were less than 7 mm in diameter, but they ranged up to 12 mm.
Internal carotid artery aneurysms comprised 95% of all in the study; 5% were in the vertebral artery. Most involved the side wall (84%), while the remainder involved a side branch (12%) or were fusiform (4%).
There was only one unsuccessful initial deployment, resulting in a 99.3% deployment success rate. The mean procedure time was 78 minutes. While most patients received just one PED, 10 received multiple devices. The PED completely covered the entire neck of the lesion in 97%. There were no intraoperative aneurysm ruptures and no intraoperative deaths.
At 1 year after implantation, 84% of the aneurysms were completely occluded, with the aneurysmal sac eliminated in 92%. A residual aneurysm remained in 11 patients (8%), and a residual neck in 8 patients (6%). Two patients (1.4%) had arterial stenosis of more than 50%. Three patients (2.2%) required retreatment.
There were three major strokes in the region supplied by the target artery in three patients.
The fatal stroke occurred in a patient who had an aneurysm on the right ophthalmic carotid segment. The first device failed to deploy correctly and was removed. A second device was implanted. The next day the patient developed a facial droop, slurred speech, and a headache. She experienced a distal intraparenchymal hemorrhage and underwent hemicraniotomy, but did not survive.
The second stroke occurred in a patient who needed two devices to occlude a lesion in the left ophthalmic segment of the carotid. The patient developed an intraparenchymal hemorrhage on postoperative day 15. The stroke resolved with sequelae and the clopidogrel dose was increased.
The third stroke was associated with treatment of a right communicating segment aneurysm. The patient stopped taking the recommended DAP and experienced an acute ischemic stroke 169 days after the procedure. This stroke also resolved with sequelae.
Based on the results of PREMIER, Medtronic will pursue Food and Drug Administration approval of the PED for small to medium wide-necked aneurysms, Dr. Hanel noted.
Medtronic sponsored the study. Dr. Hanel is an adviser to the company and has received research funds from it.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
HOUSTON – An expandable mesh cylinder that is approved to treat large, wide-necked carotid aneurysms has now proved successful in treating small lesions of the internal carotid or vertebral artery up to 12 mm in diameter.
The Pipeline Embolization Device (PED, Medtronic) completely occluded 84% of such lesions without significant stenosis or retreatment within 1 year in the PREMIER trial, Ricardo Hanel, MD, PhD, said at the International Stroke Conference sponsored by the American Heart Association.
Overall morbidity and mortality in the year-long trial was very low (2.2%). However, within the first year, three patients had a major stroke in brain regions supplied by the treated artery; one of these was related to device deployment and was fatal, said Dr. Hanel, director of the Baptist Neurological Institute, Jacksonville, Fla.
Counseling patients with these lesions is not easy, Dr. Hanel said. Treatment decisions must take into account not only the patient’s current clinical status and comorbidities, but family history and personal preference. In fact, patient preference was the largest driver of treatment (63%) in the PREMIER study.
In an interview, Dr. Hanel illustrated the importance of individualized decision making. A middle-aged female had been monitored for a small aneurysm for 7 years. When the patient was 6 years old, her mother died during an open operation to treat an aneurysm.
“We had tried to treat this patient with coiling [when the lesion was first detected], but it was unsuccessful,” Dr. Hanel said. “And since her mother had died during surgery, she did not want to go for an open approach. Now, 6 years later, we have the technology to cure her with a single device, and the odds of [recurrence over 10 years] are virtually zero. It is a very personal decision, and we take a lot of factors under consideration before we decide to expose the patient to the risks of this treatment.”
The PED is a flexible 75% cobalt-chromium/25% platinum-tungsten mesh with a braided configuration. It is advanced slightly beyond the aneurysm neck and then deployed. As it opens, it partially occludes the lesion, immediately decreasing the amount of blood entering the sac. Within a month, vascular remodeling is well underway; as endothelium grows throughout the mesh, blood flow into the aneurysm is gradually cut off. Eventually the aneurysmal sac recedes, and the normal vascular architecture is restored.
“Within 4 weeks you can’t see the metal at all,” Dr. Hanel said. “It’s covered by a thin layer of endothelial cells. This device allows the patient’s body to heal and close the aneurysm, and we don’t have to deal with the reoccurrence problem we have with stent coils. The pipeline treats the entire circumference of the vessel.”
The PED is used in combination with dual-antiplatelet therapy (DAP, aspirin/clopidogrel). Dr. Hanel initiates DAP 7 days before the procedure and continues it for 3 months. At that time, clopidogrel may be discontinued. “I advise my patients to then take a baby aspirin every day for the rest of their lives,” and they are regularly monitored, he said. “Aspirin seems to protect against the formation and rupture of aneurysms.”
PREMIER followed 141 patients with unruptured, wide-necked small aneurysms of the internal carotid (up to the terminus) or the vertebral artery segment up to and including the posterior inferior cerebellar artery. The primary efficacy endpoint was complete aneurysm occlusion and absence of significant parent artery stenosis at 1 year. The secondary endpoint was successful device deployment.
The primary safety endpoint was major stroke in the territory supplied by the treated artery or neurologic death at 1 year. There were two secondary safety endpoints: major stroke or neurologic death within 30 days, attributable to procedural complications, and intracerebral hemorrhage more than 30 days later.
The patients were largely female (88%) with a mean age of 55 years. They were asymptomatic with a mean modified Rankin Scale score of 0.2 and National Institutes of Health Stroke Scale score of 0.1. Nearly half of the patients had hypertension, and 38% had hyperlipidemia. About 28% were current smokers, and another 16% had a history of smoking.
The patients’ mean maximal aneurysm diameter was 4.6 mm, with a mean neck width of 3.7 mm. The majority of lesions (84%) were less than 7 mm in diameter, but they ranged up to 12 mm.
Internal carotid artery aneurysms comprised 95% of all in the study; 5% were in the vertebral artery. Most involved the side wall (84%), while the remainder involved a side branch (12%) or were fusiform (4%).
There was only one unsuccessful initial deployment, resulting in a 99.3% deployment success rate. The mean procedure time was 78 minutes. While most patients received just one PED, 10 received multiple devices. The PED completely covered the entire neck of the lesion in 97%. There were no intraoperative aneurysm ruptures and no intraoperative deaths.
At 1 year after implantation, 84% of the aneurysms were completely occluded, with the aneurysmal sac eliminated in 92%. A residual aneurysm remained in 11 patients (8%), and a residual neck in 8 patients (6%). Two patients (1.4%) had arterial stenosis of more than 50%. Three patients (2.2%) required retreatment.
There were three major strokes in the region supplied by the target artery in three patients.
The fatal stroke occurred in a patient who had an aneurysm on the right ophthalmic carotid segment. The first device failed to deploy correctly and was removed. A second device was implanted. The next day the patient developed a facial droop, slurred speech, and a headache. She experienced a distal intraparenchymal hemorrhage and underwent hemicraniotomy, but did not survive.
The second stroke occurred in a patient who needed two devices to occlude a lesion in the left ophthalmic segment of the carotid. The patient developed an intraparenchymal hemorrhage on postoperative day 15. The stroke resolved with sequelae and the clopidogrel dose was increased.
The third stroke was associated with treatment of a right communicating segment aneurysm. The patient stopped taking the recommended DAP and experienced an acute ischemic stroke 169 days after the procedure. This stroke also resolved with sequelae.
Based on the results of PREMIER, Medtronic will pursue Food and Drug Administration approval of the PED for small to medium wide-necked aneurysms, Dr. Hanel noted.
Medtronic sponsored the study. Dr. Hanel is an adviser to the company and has received research funds from it.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
AT THE INTERNATIONAL STROKE CONFERENCE
Key clinical point:
Major finding: The PED completely occluded 84% of aneurysms of the internal carotid or vertebral artery up to 12 mm in diameter at 1 year.
Data source: PREMIER investigators prospectively evaluated the PED in 141 patients.
Disclosures: Medtronic sponsored the study. Dr. Hanel is an adviser to the company and has received research funds from it.
Abatacept efficacy differs in trials of giant cell and Takayasu’s arteritis
A pair of new studies offer mixed results regarding the use of the rheumatoid arthritis drug abatacept to treat two forms of large-vessel vasculitis: It appears to help patients with giant cell arteritis but not those with the rarer Takayasu’s arteritis.
“The results from the GCA [giant cell arteritis] study found that treatment with abatacept [Orencia] combined with prednisone resulted in a lower rate of relapse than treatment with prednisone alone,” said Carol A. Langford, MD, lead author of both studies, which were conducted by the Vasculitis Clinical Research Consortium. She is chair in rheumatic and immunologic diseases and director of the Center for Vasculitis Care and Research at the Cleveland Clinic.

Both studies appear online Jan. 30 in Arthritis & Rheumatology.
“GCA is the most common form of vasculitis with an estimated incidence of 19.8 per 100,000,” she said. “It occurs in people over the age of 50 with the average age of onset in the 70s.” Women are most affected by a 2:1 ratio.
She said the disease affects the cranium (causing headaches, scalp tenderness, and a risk of blindness) and causes signs of systemic inflammation.
“Almost one-third of patients with GCA can have large vessel involvement that specifically include thoracic aortic aneurysms and stenosis of the cervical and subclavian arteries,” she said. Fatal thoracic aneurysms are possible, she said, but “studies have shown that in GCA overall, while short-term mortality may be increased, long-term survival is similar to the age-matched general population.”
TAK is much rarer, she said, affecting 3-9 people per 1,000,000. “TAK has an average age of onset in the 20s with an even stronger female predisposition of up to 9:1.”
The condition affects the aorta, its main branches, and pulmonary arteries, she said, “Some of the more frequent vascular symptoms/signs can include extremity claudication, hypertension, chest pain, and features associated with cerebral hypoperfusion. TAK is associated with substantial morbidity which is influenced by a low rate of sustained remission in 28%-50% of patients. Up to 47% of patients experience permanent disability, which has a significant impact on this young population.”
The mortality from TAK is unclear, she said.
Glucocorticoids are the main treatment for both GCA and TAK, Dr. Langford said, but “while glucocorticoids effectively control disease, they do not prevent relapse and they are associated with significant toxicity.”
For GCA, methotrexate has shown a mild benefit at best, she said, while two studies show promise for tocilizumab (Actemra). As for TAK, she said doctors often turn to the use of immunosuppressants and tumor necrosis factor inhibitors, although their use is based on retrospective studies and small, open-label trials.
Dr. Langford and her colleagues launched the two randomized, double-blind, placebo-controlled, multicenter studies in parallel with the same protocols.
In the GCA trial (doi: 10.1002/art.40044), researchers enrolled 49 patients with newly diagnosed GCA or disease that had relapsed within the 2 prior months to prednisone 40-60 mg/day followed by a standardized tapering schedule plus abatacept 10 mg/kg IV on days 1, 15, 29, and week 8. At 12 weeks, 8 patients had withdrawn, relapsed, or were not in remission, and so 41 were randomized to receive placebo or monthly abatacept until they met criteria for early termination or 12 months had passed after the last patient was enrolled. At the time of the randomization at 12 weeks, all patients were taking prednisone 20 mg/day, which was tapered until discontinuation at week 28.
At 12 months, 48% of those who took abatacept survived without relapse, compared with 31% of those who took placebo (P = .049), and the median remission period was longer for abatacept (9.9 months) than placebo (3.9 months; P = .023).
“This difference between groups is clinically meaningful to patients with GCA, corresponding to a prolonged duration of remission during which time they are not exposed to glucocorticoids and their potential toxicities that can impact quality of life,” Dr. Langford said.
No patients died during the trial, and 23 serious adverse events were reported in 15 patients. The frequency and severity of adverse events and infections didn’t differ between the treatment and placebo groups.
The drug may work in GCA patients by blocking T-cell activation, Dr. Langford said. Physicians could consider the drug in clinical practice, she said, although more research is needed to understand the long-term effects of using the medication.
In the other study (doi: 10.1002/art.40037), researchers used the same protocol to treat 34 patients with TAK; 26 reached the 12-week midpoint and were randomized to placebo or continuing abatacept on a monthly basis.
At 12 months, the relapse-free rate was 22% for the abatacept group and 40% for the placebo group (P = .853). The median duration of remission was similar for the groups at 5.5 months for abatacept and 5.7 months for placebo (P = .125).
The researchers reported no difference in frequency or severity of adverse events such as infection.
Based on the study results, Dr. Langford said abatacept is not appropriate in clinical practice to treat TAK.
The National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the studies, and Bristol-Myers Squibb, which markets abatacept, provided the drug. Dr. Langford disclosed receiving research grants from Bristol-Myers Squibb, Genentech, and GlaxoSmithKline.
A pair of new studies offer mixed results regarding the use of the rheumatoid arthritis drug abatacept to treat two forms of large-vessel vasculitis: It appears to help patients with giant cell arteritis but not those with the rarer Takayasu’s arteritis.
“The results from the GCA [giant cell arteritis] study found that treatment with abatacept [Orencia] combined with prednisone resulted in a lower rate of relapse than treatment with prednisone alone,” said Carol A. Langford, MD, lead author of both studies, which were conducted by the Vasculitis Clinical Research Consortium. She is chair in rheumatic and immunologic diseases and director of the Center for Vasculitis Care and Research at the Cleveland Clinic.
Both studies appear online Jan. 30 in Arthritis & Rheumatology.
“GCA is the most common form of vasculitis with an estimated incidence of 19.8 per 100,000,” she said. “It occurs in people over the age of 50 with the average age of onset in the 70s.” Women are most affected by a 2:1 ratio.
She said the disease affects the cranium (causing headaches, scalp tenderness, and a risk of blindness) and causes signs of systemic inflammation.
“Almost one-third of patients with GCA can have large vessel involvement that specifically include thoracic aortic aneurysms and stenosis of the cervical and subclavian arteries,” she said. Fatal thoracic aneurysms are possible, she said, but “studies have shown that in GCA overall, while short-term mortality may be increased, long-term survival is similar to the age-matched general population.”
TAK is much rarer, she said, affecting 3-9 people per 1,000,000. “TAK has an average age of onset in the 20s with an even stronger female predisposition of up to 9:1.”
The condition affects the aorta, its main branches, and pulmonary arteries, she said, “Some of the more frequent vascular symptoms/signs can include extremity claudication, hypertension, chest pain, and features associated with cerebral hypoperfusion. TAK is associated with substantial morbidity which is influenced by a low rate of sustained remission in 28%-50% of patients. Up to 47% of patients experience permanent disability, which has a significant impact on this young population.”
The mortality from TAK is unclear, she said.
Glucocorticoids are the main treatment for both GCA and TAK, Dr. Langford said, but “while glucocorticoids effectively control disease, they do not prevent relapse and they are associated with significant toxicity.”
For GCA, methotrexate has shown a mild benefit at best, she said, while two studies show promise for tocilizumab (Actemra). As for TAK, she said doctors often turn to the use of immunosuppressants and tumor necrosis factor inhibitors, although their use is based on retrospective studies and small, open-label trials.
Dr. Langford and her colleagues launched the two randomized, double-blind, placebo-controlled, multicenter studies in parallel with the same protocols.
In the GCA trial (doi: 10.1002/art.40044), researchers enrolled 49 patients with newly diagnosed GCA or disease that had relapsed within the 2 prior months to prednisone 40-60 mg/day followed by a standardized tapering schedule plus abatacept 10 mg/kg IV on days 1, 15, 29, and week 8. At 12 weeks, 8 patients had withdrawn, relapsed, or were not in remission, and so 41 were randomized to receive placebo or monthly abatacept until they met criteria for early termination or 12 months had passed after the last patient was enrolled. At the time of the randomization at 12 weeks, all patients were taking prednisone 20 mg/day, which was tapered until discontinuation at week 28.
At 12 months, 48% of those who took abatacept survived without relapse, compared with 31% of those who took placebo (P = .049), and the median remission period was longer for abatacept (9.9 months) than placebo (3.9 months; P = .023).
“This difference between groups is clinically meaningful to patients with GCA, corresponding to a prolonged duration of remission during which time they are not exposed to glucocorticoids and their potential toxicities that can impact quality of life,” Dr. Langford said.
No patients died during the trial, and 23 serious adverse events were reported in 15 patients. The frequency and severity of adverse events and infections didn’t differ between the treatment and placebo groups.
The drug may work in GCA patients by blocking T-cell activation, Dr. Langford said. Physicians could consider the drug in clinical practice, she said, although more research is needed to understand the long-term effects of using the medication.
In the other study (doi: 10.1002/art.40037), researchers used the same protocol to treat 34 patients with TAK; 26 reached the 12-week midpoint and were randomized to placebo or continuing abatacept on a monthly basis.
At 12 months, the relapse-free rate was 22% for the abatacept group and 40% for the placebo group (P = .853). The median duration of remission was similar for the groups at 5.5 months for abatacept and 5.7 months for placebo (P = .125).
The researchers reported no difference in frequency or severity of adverse events such as infection.
Based on the study results, Dr. Langford said abatacept is not appropriate in clinical practice to treat TAK.
The National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the studies, and Bristol-Myers Squibb, which markets abatacept, provided the drug. Dr. Langford disclosed receiving research grants from Bristol-Myers Squibb, Genentech, and GlaxoSmithKline.
A pair of new studies offer mixed results regarding the use of the rheumatoid arthritis drug abatacept to treat two forms of large-vessel vasculitis: It appears to help patients with giant cell arteritis but not those with the rarer Takayasu’s arteritis.
“The results from the GCA [giant cell arteritis] study found that treatment with abatacept [Orencia] combined with prednisone resulted in a lower rate of relapse than treatment with prednisone alone,” said Carol A. Langford, MD, lead author of both studies, which were conducted by the Vasculitis Clinical Research Consortium. She is chair in rheumatic and immunologic diseases and director of the Center for Vasculitis Care and Research at the Cleveland Clinic.
Both studies appear online Jan. 30 in Arthritis & Rheumatology.
“GCA is the most common form of vasculitis with an estimated incidence of 19.8 per 100,000,” she said. “It occurs in people over the age of 50 with the average age of onset in the 70s.” Women are most affected by a 2:1 ratio.
She said the disease affects the cranium (causing headaches, scalp tenderness, and a risk of blindness) and causes signs of systemic inflammation.
“Almost one-third of patients with GCA can have large vessel involvement that specifically include thoracic aortic aneurysms and stenosis of the cervical and subclavian arteries,” she said. Fatal thoracic aneurysms are possible, she said, but “studies have shown that in GCA overall, while short-term mortality may be increased, long-term survival is similar to the age-matched general population.”
TAK is much rarer, she said, affecting 3-9 people per 1,000,000. “TAK has an average age of onset in the 20s with an even stronger female predisposition of up to 9:1.”
The condition affects the aorta, its main branches, and pulmonary arteries, she said, “Some of the more frequent vascular symptoms/signs can include extremity claudication, hypertension, chest pain, and features associated with cerebral hypoperfusion. TAK is associated with substantial morbidity which is influenced by a low rate of sustained remission in 28%-50% of patients. Up to 47% of patients experience permanent disability, which has a significant impact on this young population.”
The mortality from TAK is unclear, she said.
Glucocorticoids are the main treatment for both GCA and TAK, Dr. Langford said, but “while glucocorticoids effectively control disease, they do not prevent relapse and they are associated with significant toxicity.”
For GCA, methotrexate has shown a mild benefit at best, she said, while two studies show promise for tocilizumab (Actemra). As for TAK, she said doctors often turn to the use of immunosuppressants and tumor necrosis factor inhibitors, although their use is based on retrospective studies and small, open-label trials.
Dr. Langford and her colleagues launched the two randomized, double-blind, placebo-controlled, multicenter studies in parallel with the same protocols.
In the GCA trial (doi: 10.1002/art.40044), researchers enrolled 49 patients with newly diagnosed GCA or disease that had relapsed within the 2 prior months to prednisone 40-60 mg/day followed by a standardized tapering schedule plus abatacept 10 mg/kg IV on days 1, 15, 29, and week 8. At 12 weeks, 8 patients had withdrawn, relapsed, or were not in remission, and so 41 were randomized to receive placebo or monthly abatacept until they met criteria for early termination or 12 months had passed after the last patient was enrolled. At the time of the randomization at 12 weeks, all patients were taking prednisone 20 mg/day, which was tapered until discontinuation at week 28.
At 12 months, 48% of those who took abatacept survived without relapse, compared with 31% of those who took placebo (P = .049), and the median remission period was longer for abatacept (9.9 months) than placebo (3.9 months; P = .023).
“This difference between groups is clinically meaningful to patients with GCA, corresponding to a prolonged duration of remission during which time they are not exposed to glucocorticoids and their potential toxicities that can impact quality of life,” Dr. Langford said.
No patients died during the trial, and 23 serious adverse events were reported in 15 patients. The frequency and severity of adverse events and infections didn’t differ between the treatment and placebo groups.
The drug may work in GCA patients by blocking T-cell activation, Dr. Langford said. Physicians could consider the drug in clinical practice, she said, although more research is needed to understand the long-term effects of using the medication.
In the other study (doi: 10.1002/art.40037), researchers used the same protocol to treat 34 patients with TAK; 26 reached the 12-week midpoint and were randomized to placebo or continuing abatacept on a monthly basis.
At 12 months, the relapse-free rate was 22% for the abatacept group and 40% for the placebo group (P = .853). The median duration of remission was similar for the groups at 5.5 months for abatacept and 5.7 months for placebo (P = .125).
The researchers reported no difference in frequency or severity of adverse events such as infection.
Based on the study results, Dr. Langford said abatacept is not appropriate in clinical practice to treat TAK.
The National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the studies, and Bristol-Myers Squibb, which markets abatacept, provided the drug. Dr. Langford disclosed receiving research grants from Bristol-Myers Squibb, Genentech, and GlaxoSmithKline.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point:
Major finding: At 12 months, 48% of GCA patients who took abatacept survived without relapse, compared with 31% of those who took placebo (P = .049), and the median remission period was longer for abatacept (9.9 months) than placebo (3.9 months; P = .023) For TAK patients, the relapse-free rates were 22% for the abatacept group and 40% for the placebo group (P = .853). The median duration of remission was similar for the groups at 5.5 months for abatacept and 5.7 months for placebo (P = .125).
Data source: Two randomized, double-blinded, placebo-controlled, multicenter trials with identical protocols of prednisone plus abatacept 10 mg/kg IV on days 1, 15, 29, and week 8, then randomization to placebo or monthly abatacept until patients met criteria for early termination or 12 months passed after the last patient was enrolled.
Disclosures: The National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the studies, and Bristol-Myers Squibb, which markets abatacept, provided the drug. Dr. Langford disclosed receiving research grants from Bristol-Myers Squibb, Genentech, and GlaxoSmithKline.
PPIs may boost ischemic stroke risk
NEW ORLEANS – The use of proton pump inhibitors (PPIs) was associated with significantly increased risk of having a first ischemic stroke in a large nationwide Danish cohort study, Thomas S. Sehested, MD, reported at the American Heart Association scientific sessions.
The relationship was dose dependent. At the lowest available dose of each of the four PPIs studied there was no significantly increased risk. At the intermediate doses of three of the four PPIs studied, the increased risk of ischemic stroke became statistically significant. And the highest dose of each drug was associated with the greatest ischemic stroke risk.

In Denmark, for instance, where most PPIs are prescription only and use is easily trackable, it’s estimated that, at any given time, 7% of the adult population is taking a PPI, often not as directed in the labeling.
The impetus for this study, Dr. Sehested explained, was the mounting evidence that PPIs may constitute an independent risk factor for acute MI and other cardiovascular events. For example, a recent meta-analysis of 17 randomized controlled trials totaling 7,540 participants published through mid-2015 concluded that the use of PPIs was associated with a 70% increase in cardiovascular risk (Neurogastroenterol Motil. 2016 Aug 30. doi: 10.1111/nmo.12926).
He reported on 245,676 Danes above age 30 who were free of prior MI or stroke when they underwent elective GI endoscopy during 1997-2012. After a 30-day postendoscopy grace period during which 1,476 patients had a first MI, stroke, or died of any cause, the final study population was 244,200, of whom 43.7% were PPI users during the grace period and beyond.
During a median 5.8 years of follow-up, 9,489 subjects (3.9%) had a first ischemic stroke. Because of the comprehensive nature of Denmark’s interlocking birth to death registries, there was virtually no loss to follow-up in this study.
The unadjusted incidence of ischemic stroke in PPI nonusers was 55.7 per 10,000 person-years, compared with 88.9 per 10,000 in PPI users.
The PPI users were slightly older than nonusers by roughly 3 years. They were also an absolute 5% more likely to be hypertensive and an absolute 1.7% more likely to be regular users of NSAIDs. All of these differences, while modest, were statistically significant because of the large patient numbers involved.
In a multivariate analysis adjusted for age, sex, calendar year, comorbid diabetes, hypertension, alcohol use disorder, heart failure, peptic ulcer, peripheral artery disease, kidney disease, aspirin, oral anticoagulants and other medications, and socioeconomic status, current users of PPIs were 19% more likely to have a first ischemic stroke than nonusers. That difference is statistically significant and clinically meaningful, Dr. Sehested said.
In contrast, when the same sort of nationwide analysis was repeated, comparing current users of histamine-2 receptor antagonists to nonusers of those drugs or PPIs, there was no difference in ischemic stroke risk between the two groups.
The message, according to Dr. Sehested, is that physicians should encourage more cautious use of PPIs. And especially in the United States, where most PPIs are available over the counter, it’s prudent during office visits to ask what nonprescription drugs a patient is taking.
Dr. Sehested presented his study findings in a session devoted to original research in cardiovascular epidemiology. Many top American epidemiologists were present in the audience, and several rose to congratulate him on his presentation of the latest elegant epidemiologic study to come out of Denmark, the only place in the world where this sort of nationwide comprehensive research is possible.
“Wow! I just love the work you do in Denmark. It’s really inspiring,” commented David Siscovick, MD, senior vice president for research at the New York Academy of Medicine and professor emeritus of medicine and epidemiology at the University of Washington in Seattle.
He had a question: “Did you deal with PPI starters and stoppers and compliance in any way?”
Dr. Sehested replied that he and his coinvestigators were able to see who was on a PPI at any given point in the study, and they accounted for that. One issue the researchers plan to examine but haven’t yet had a chance to, however, is the relationship between duration of PPI therapy and ischemic stroke risk. It’s likely that some patients had already been on a PPI for a lengthy time at elective endoscopy, which is when the study in its current form began.
“I think that would strengthen the study,” he said.
Comoderator Jorge Kizer, MD, of Albert Einstein College of Medicine in New York, commented, “Confounding by indication is clearly the elephant in the room. The guidelines actually recommend adding a PPI if a patient is on dual-antiplatelet therapy and has an NSAID added. Did you adjust for that? It would boost confidence that the results are actually due to the PPI.”
Dr. Sehested answered that the great majority of individuals with cardiovascular disease at baseline were excluded from the analysis.
“I don’t think we had that many on dual-antiplatelet therapy,” he added.
Preclinical studies suggest a possible mechanism by which PPIs may harm cardiovascular health. The drugs reduce nitric oxide synthase levels, with resultant endothelial dysfunction, he said.
Dr. Sehested is employed at the Danish Heart Foundation, which funded the study.
A growing number of retrospective studies have associated proton pump inhibitors with a host of serious adverse effects. These include chronic kidney disease, dementia, osteoporosis, cardiovascular events, pneumonia, enteric infections, and others. The authors of this large, retrospective Danish study have now added ischemic stroke to the list.
Nonetheless, this study should serve as wake-up call to closely examine the risks and benefits of ongoing PPI use for each individual patient. For example, guidelines clearly advocate the use of PPIs in patients at high risk for peptic ulcer disease (for example, use of aspirin and warfarin together), and these patients should continue PPIs unless more convincing evidence of serious side effects emerge. On the other hand, several studies have shown that many patients with uncomplicated gastroesophageal reflux disease symptoms can achieve symptom control with substitution of histamine2 blockers, p.r.n. dosing of PPIs, or without acid-reducing medications entirely. Still, many patients with confirmed pathologic acid reflux are likely to require ongoing PPIs. For patients who continue PPIs, they should use the lowest effective dose.
Surely, physicians will be discussing PPI adverse effects with increasing numbers of patients. Until higher-quality evidence in the form of a randomized controlled trial emerges, physicians should get used to explaining the principles of epidemiology.
Jacob Kurlander, MD, is a clinical lecturer in the division of gastroenterology, University of Michigan, Ann Arbor. He has received research funding from Ironwood Pharmaceuticals.
A growing number of retrospective studies have associated proton pump inhibitors with a host of serious adverse effects. These include chronic kidney disease, dementia, osteoporosis, cardiovascular events, pneumonia, enteric infections, and others. The authors of this large, retrospective Danish study have now added ischemic stroke to the list.
Nonetheless, this study should serve as wake-up call to closely examine the risks and benefits of ongoing PPI use for each individual patient. For example, guidelines clearly advocate the use of PPIs in patients at high risk for peptic ulcer disease (for example, use of aspirin and warfarin together), and these patients should continue PPIs unless more convincing evidence of serious side effects emerge. On the other hand, several studies have shown that many patients with uncomplicated gastroesophageal reflux disease symptoms can achieve symptom control with substitution of histamine2 blockers, p.r.n. dosing of PPIs, or without acid-reducing medications entirely. Still, many patients with confirmed pathologic acid reflux are likely to require ongoing PPIs. For patients who continue PPIs, they should use the lowest effective dose.
Surely, physicians will be discussing PPI adverse effects with increasing numbers of patients. Until higher-quality evidence in the form of a randomized controlled trial emerges, physicians should get used to explaining the principles of epidemiology.
Jacob Kurlander, MD, is a clinical lecturer in the division of gastroenterology, University of Michigan, Ann Arbor. He has received research funding from Ironwood Pharmaceuticals.
A growing number of retrospective studies have associated proton pump inhibitors with a host of serious adverse effects. These include chronic kidney disease, dementia, osteoporosis, cardiovascular events, pneumonia, enteric infections, and others. The authors of this large, retrospective Danish study have now added ischemic stroke to the list.
Nonetheless, this study should serve as wake-up call to closely examine the risks and benefits of ongoing PPI use for each individual patient. For example, guidelines clearly advocate the use of PPIs in patients at high risk for peptic ulcer disease (for example, use of aspirin and warfarin together), and these patients should continue PPIs unless more convincing evidence of serious side effects emerge. On the other hand, several studies have shown that many patients with uncomplicated gastroesophageal reflux disease symptoms can achieve symptom control with substitution of histamine2 blockers, p.r.n. dosing of PPIs, or without acid-reducing medications entirely. Still, many patients with confirmed pathologic acid reflux are likely to require ongoing PPIs. For patients who continue PPIs, they should use the lowest effective dose.
Surely, physicians will be discussing PPI adverse effects with increasing numbers of patients. Until higher-quality evidence in the form of a randomized controlled trial emerges, physicians should get used to explaining the principles of epidemiology.
Jacob Kurlander, MD, is a clinical lecturer in the division of gastroenterology, University of Michigan, Ann Arbor. He has received research funding from Ironwood Pharmaceuticals.
NEW ORLEANS – The use of proton pump inhibitors (PPIs) was associated with significantly increased risk of having a first ischemic stroke in a large nationwide Danish cohort study, Thomas S. Sehested, MD, reported at the American Heart Association scientific sessions.
The relationship was dose dependent. At the lowest available dose of each of the four PPIs studied there was no significantly increased risk. At the intermediate doses of three of the four PPIs studied, the increased risk of ischemic stroke became statistically significant. And the highest dose of each drug was associated with the greatest ischemic stroke risk.
In Denmark, for instance, where most PPIs are prescription only and use is easily trackable, it’s estimated that, at any given time, 7% of the adult population is taking a PPI, often not as directed in the labeling.
The impetus for this study, Dr. Sehested explained, was the mounting evidence that PPIs may constitute an independent risk factor for acute MI and other cardiovascular events. For example, a recent meta-analysis of 17 randomized controlled trials totaling 7,540 participants published through mid-2015 concluded that the use of PPIs was associated with a 70% increase in cardiovascular risk (Neurogastroenterol Motil. 2016 Aug 30. doi: 10.1111/nmo.12926).
He reported on 245,676 Danes above age 30 who were free of prior MI or stroke when they underwent elective GI endoscopy during 1997-2012. After a 30-day postendoscopy grace period during which 1,476 patients had a first MI, stroke, or died of any cause, the final study population was 244,200, of whom 43.7% were PPI users during the grace period and beyond.
During a median 5.8 years of follow-up, 9,489 subjects (3.9%) had a first ischemic stroke. Because of the comprehensive nature of Denmark’s interlocking birth to death registries, there was virtually no loss to follow-up in this study.
The unadjusted incidence of ischemic stroke in PPI nonusers was 55.7 per 10,000 person-years, compared with 88.9 per 10,000 in PPI users.
The PPI users were slightly older than nonusers by roughly 3 years. They were also an absolute 5% more likely to be hypertensive and an absolute 1.7% more likely to be regular users of NSAIDs. All of these differences, while modest, were statistically significant because of the large patient numbers involved.
In a multivariate analysis adjusted for age, sex, calendar year, comorbid diabetes, hypertension, alcohol use disorder, heart failure, peptic ulcer, peripheral artery disease, kidney disease, aspirin, oral anticoagulants and other medications, and socioeconomic status, current users of PPIs were 19% more likely to have a first ischemic stroke than nonusers. That difference is statistically significant and clinically meaningful, Dr. Sehested said.
In contrast, when the same sort of nationwide analysis was repeated, comparing current users of histamine-2 receptor antagonists to nonusers of those drugs or PPIs, there was no difference in ischemic stroke risk between the two groups.
The message, according to Dr. Sehested, is that physicians should encourage more cautious use of PPIs. And especially in the United States, where most PPIs are available over the counter, it’s prudent during office visits to ask what nonprescription drugs a patient is taking.
Dr. Sehested presented his study findings in a session devoted to original research in cardiovascular epidemiology. Many top American epidemiologists were present in the audience, and several rose to congratulate him on his presentation of the latest elegant epidemiologic study to come out of Denmark, the only place in the world where this sort of nationwide comprehensive research is possible.
“Wow! I just love the work you do in Denmark. It’s really inspiring,” commented David Siscovick, MD, senior vice president for research at the New York Academy of Medicine and professor emeritus of medicine and epidemiology at the University of Washington in Seattle.
He had a question: “Did you deal with PPI starters and stoppers and compliance in any way?”
Dr. Sehested replied that he and his coinvestigators were able to see who was on a PPI at any given point in the study, and they accounted for that. One issue the researchers plan to examine but haven’t yet had a chance to, however, is the relationship between duration of PPI therapy and ischemic stroke risk. It’s likely that some patients had already been on a PPI for a lengthy time at elective endoscopy, which is when the study in its current form began.
“I think that would strengthen the study,” he said.
Comoderator Jorge Kizer, MD, of Albert Einstein College of Medicine in New York, commented, “Confounding by indication is clearly the elephant in the room. The guidelines actually recommend adding a PPI if a patient is on dual-antiplatelet therapy and has an NSAID added. Did you adjust for that? It would boost confidence that the results are actually due to the PPI.”
Dr. Sehested answered that the great majority of individuals with cardiovascular disease at baseline were excluded from the analysis.
“I don’t think we had that many on dual-antiplatelet therapy,” he added.
Preclinical studies suggest a possible mechanism by which PPIs may harm cardiovascular health. The drugs reduce nitric oxide synthase levels, with resultant endothelial dysfunction, he said.
Dr. Sehested is employed at the Danish Heart Foundation, which funded the study.
NEW ORLEANS – The use of proton pump inhibitors (PPIs) was associated with significantly increased risk of having a first ischemic stroke in a large nationwide Danish cohort study, Thomas S. Sehested, MD, reported at the American Heart Association scientific sessions.
The relationship was dose dependent. At the lowest available dose of each of the four PPIs studied there was no significantly increased risk. At the intermediate doses of three of the four PPIs studied, the increased risk of ischemic stroke became statistically significant. And the highest dose of each drug was associated with the greatest ischemic stroke risk.
In Denmark, for instance, where most PPIs are prescription only and use is easily trackable, it’s estimated that, at any given time, 7% of the adult population is taking a PPI, often not as directed in the labeling.
The impetus for this study, Dr. Sehested explained, was the mounting evidence that PPIs may constitute an independent risk factor for acute MI and other cardiovascular events. For example, a recent meta-analysis of 17 randomized controlled trials totaling 7,540 participants published through mid-2015 concluded that the use of PPIs was associated with a 70% increase in cardiovascular risk (Neurogastroenterol Motil. 2016 Aug 30. doi: 10.1111/nmo.12926).
He reported on 245,676 Danes above age 30 who were free of prior MI or stroke when they underwent elective GI endoscopy during 1997-2012. After a 30-day postendoscopy grace period during which 1,476 patients had a first MI, stroke, or died of any cause, the final study population was 244,200, of whom 43.7% were PPI users during the grace period and beyond.
During a median 5.8 years of follow-up, 9,489 subjects (3.9%) had a first ischemic stroke. Because of the comprehensive nature of Denmark’s interlocking birth to death registries, there was virtually no loss to follow-up in this study.
The unadjusted incidence of ischemic stroke in PPI nonusers was 55.7 per 10,000 person-years, compared with 88.9 per 10,000 in PPI users.
The PPI users were slightly older than nonusers by roughly 3 years. They were also an absolute 5% more likely to be hypertensive and an absolute 1.7% more likely to be regular users of NSAIDs. All of these differences, while modest, were statistically significant because of the large patient numbers involved.
In a multivariate analysis adjusted for age, sex, calendar year, comorbid diabetes, hypertension, alcohol use disorder, heart failure, peptic ulcer, peripheral artery disease, kidney disease, aspirin, oral anticoagulants and other medications, and socioeconomic status, current users of PPIs were 19% more likely to have a first ischemic stroke than nonusers. That difference is statistically significant and clinically meaningful, Dr. Sehested said.
In contrast, when the same sort of nationwide analysis was repeated, comparing current users of histamine-2 receptor antagonists to nonusers of those drugs or PPIs, there was no difference in ischemic stroke risk between the two groups.
The message, according to Dr. Sehested, is that physicians should encourage more cautious use of PPIs. And especially in the United States, where most PPIs are available over the counter, it’s prudent during office visits to ask what nonprescription drugs a patient is taking.
Dr. Sehested presented his study findings in a session devoted to original research in cardiovascular epidemiology. Many top American epidemiologists were present in the audience, and several rose to congratulate him on his presentation of the latest elegant epidemiologic study to come out of Denmark, the only place in the world where this sort of nationwide comprehensive research is possible.
“Wow! I just love the work you do in Denmark. It’s really inspiring,” commented David Siscovick, MD, senior vice president for research at the New York Academy of Medicine and professor emeritus of medicine and epidemiology at the University of Washington in Seattle.
He had a question: “Did you deal with PPI starters and stoppers and compliance in any way?”
Dr. Sehested replied that he and his coinvestigators were able to see who was on a PPI at any given point in the study, and they accounted for that. One issue the researchers plan to examine but haven’t yet had a chance to, however, is the relationship between duration of PPI therapy and ischemic stroke risk. It’s likely that some patients had already been on a PPI for a lengthy time at elective endoscopy, which is when the study in its current form began.
“I think that would strengthen the study,” he said.
Comoderator Jorge Kizer, MD, of Albert Einstein College of Medicine in New York, commented, “Confounding by indication is clearly the elephant in the room. The guidelines actually recommend adding a PPI if a patient is on dual-antiplatelet therapy and has an NSAID added. Did you adjust for that? It would boost confidence that the results are actually due to the PPI.”
Dr. Sehested answered that the great majority of individuals with cardiovascular disease at baseline were excluded from the analysis.
“I don’t think we had that many on dual-antiplatelet therapy,” he added.
Preclinical studies suggest a possible mechanism by which PPIs may harm cardiovascular health. The drugs reduce nitric oxide synthase levels, with resultant endothelial dysfunction, he said.
Dr. Sehested is employed at the Danish Heart Foundation, which funded the study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Current use of a proton pump inhibitor was independently associated with a 19% increased risk of a first ischemic stroke, and the risk was greater at the top approved doses.
Data source: This retrospective nationwide Danish study involved 244,200 adults age 30 or older followed for a median of nearly 6 years following elective GI endoscopy.
Disclosures: The presenter is employed at the Danish Heart Foundation, which funded the study.
Is regional anesthesia safer in CEA?
COLUMBUS, OHIO – General anesthesia during carotid endarterectomy carries almost twice the risk of complications and unplanned intubation as regional anesthesia, but the latter approach, which is not available in all hospitals, has its own issues, an analysis of procedures from a statewide database in Michigan found.
“This study is timely because of CMS [Center for Medicare & Medicaid Services] initiatives tying reimbursement to specific quality measures,” Ahmad S Hussain, MD, of Wayne State University in Detroit said in reporting the study results at the annual meeting of the Midwestern Vascular Surgery Society.

Regional anesthesia in CEA emerged in the 1990s, Dr. Hussain said, and allows for more reliable neurologic monitoring and more direct evaluation of the need for stenting during CEA than general anesthesia, which requires continuous monitoring of cerebral perfusion with carotid stump pressures, electroencephalogram, and transcranial doppler.
The researchers retrospectively analyzed 4,558 patients who had CEA at hospitals participating in the Michigan Surgical Quality Cooperative from 2012 to 2014 – 4,008 of whom had general anesthesia and 550 regional anesthesia.
“Advocates for carotid endarterectomy with regional anesthesia cite a reduction in hemodynamic instability and the ability for neurological monitoring, but many still prefer general anesthesia because the benefits of regional anesthesia have not been clearly demonstrated, allowing that regional anesthesia may not be available in all centers and allowing that a certain amount of patient movement during the procedure may not be uniformly tolerated,” Dr. Hussain said.
General anesthesia patients in the study had more than twice the rate of any morbidity at 30 days than those who had regional, 8.7% vs. 4.2%, and significantly higher rates of unplanned intervention, 2.1% vs. 0.6%. Dr. Hussain said. However, the study could not determine differences in 30-day mortality or other key outcomes, such as rates of pneumonia, sepsis, deep vein thrombosis, or pulmonary embolism, becauseof insufficient sample sizes, Dr. Hussain said
The study found less significant differences between general and regional anesthesia techniques, respectively, in rates of extended length of stay, 12.1% vs. 9.5%; readmissions, 9.2% vs. 6.1%; and reoperation, 4.5% vs. 3%.
The retrospective study used two models to analyze odds ratios: Model 1 adjusted for case mix; and model 2 adjusted for case mix as fixed effects and site as a random effect. While the retrospective nature of the study may be a limitation, the findings support the use of regional anesthesia for CEA when available, Dr. Hussain said.
Dr. Hussain had no relationships to disclose.
COLUMBUS, OHIO – General anesthesia during carotid endarterectomy carries almost twice the risk of complications and unplanned intubation as regional anesthesia, but the latter approach, which is not available in all hospitals, has its own issues, an analysis of procedures from a statewide database in Michigan found.
“This study is timely because of CMS [Center for Medicare & Medicaid Services] initiatives tying reimbursement to specific quality measures,” Ahmad S Hussain, MD, of Wayne State University in Detroit said in reporting the study results at the annual meeting of the Midwestern Vascular Surgery Society.
Regional anesthesia in CEA emerged in the 1990s, Dr. Hussain said, and allows for more reliable neurologic monitoring and more direct evaluation of the need for stenting during CEA than general anesthesia, which requires continuous monitoring of cerebral perfusion with carotid stump pressures, electroencephalogram, and transcranial doppler.
The researchers retrospectively analyzed 4,558 patients who had CEA at hospitals participating in the Michigan Surgical Quality Cooperative from 2012 to 2014 – 4,008 of whom had general anesthesia and 550 regional anesthesia.
“Advocates for carotid endarterectomy with regional anesthesia cite a reduction in hemodynamic instability and the ability for neurological monitoring, but many still prefer general anesthesia because the benefits of regional anesthesia have not been clearly demonstrated, allowing that regional anesthesia may not be available in all centers and allowing that a certain amount of patient movement during the procedure may not be uniformly tolerated,” Dr. Hussain said.
General anesthesia patients in the study had more than twice the rate of any morbidity at 30 days than those who had regional, 8.7% vs. 4.2%, and significantly higher rates of unplanned intervention, 2.1% vs. 0.6%. Dr. Hussain said. However, the study could not determine differences in 30-day mortality or other key outcomes, such as rates of pneumonia, sepsis, deep vein thrombosis, or pulmonary embolism, becauseof insufficient sample sizes, Dr. Hussain said
The study found less significant differences between general and regional anesthesia techniques, respectively, in rates of extended length of stay, 12.1% vs. 9.5%; readmissions, 9.2% vs. 6.1%; and reoperation, 4.5% vs. 3%.
The retrospective study used two models to analyze odds ratios: Model 1 adjusted for case mix; and model 2 adjusted for case mix as fixed effects and site as a random effect. While the retrospective nature of the study may be a limitation, the findings support the use of regional anesthesia for CEA when available, Dr. Hussain said.
Dr. Hussain had no relationships to disclose.
COLUMBUS, OHIO – General anesthesia during carotid endarterectomy carries almost twice the risk of complications and unplanned intubation as regional anesthesia, but the latter approach, which is not available in all hospitals, has its own issues, an analysis of procedures from a statewide database in Michigan found.
“This study is timely because of CMS [Center for Medicare & Medicaid Services] initiatives tying reimbursement to specific quality measures,” Ahmad S Hussain, MD, of Wayne State University in Detroit said in reporting the study results at the annual meeting of the Midwestern Vascular Surgery Society.
Regional anesthesia in CEA emerged in the 1990s, Dr. Hussain said, and allows for more reliable neurologic monitoring and more direct evaluation of the need for stenting during CEA than general anesthesia, which requires continuous monitoring of cerebral perfusion with carotid stump pressures, electroencephalogram, and transcranial doppler.
The researchers retrospectively analyzed 4,558 patients who had CEA at hospitals participating in the Michigan Surgical Quality Cooperative from 2012 to 2014 – 4,008 of whom had general anesthesia and 550 regional anesthesia.
“Advocates for carotid endarterectomy with regional anesthesia cite a reduction in hemodynamic instability and the ability for neurological monitoring, but many still prefer general anesthesia because the benefits of regional anesthesia have not been clearly demonstrated, allowing that regional anesthesia may not be available in all centers and allowing that a certain amount of patient movement during the procedure may not be uniformly tolerated,” Dr. Hussain said.
General anesthesia patients in the study had more than twice the rate of any morbidity at 30 days than those who had regional, 8.7% vs. 4.2%, and significantly higher rates of unplanned intervention, 2.1% vs. 0.6%. Dr. Hussain said. However, the study could not determine differences in 30-day mortality or other key outcomes, such as rates of pneumonia, sepsis, deep vein thrombosis, or pulmonary embolism, becauseof insufficient sample sizes, Dr. Hussain said
The study found less significant differences between general and regional anesthesia techniques, respectively, in rates of extended length of stay, 12.1% vs. 9.5%; readmissions, 9.2% vs. 6.1%; and reoperation, 4.5% vs. 3%.
The retrospective study used two models to analyze odds ratios: Model 1 adjusted for case mix; and model 2 adjusted for case mix as fixed effects and site as a random effect. While the retrospective nature of the study may be a limitation, the findings support the use of regional anesthesia for CEA when available, Dr. Hussain said.
Dr. Hussain had no relationships to disclose.
AT MIDWESTERN VASCULAR 2016
Key clinical point: General anesthesia for carotid endarterectomy carries a higher risk of complications and readmissions than regional anesthesia.
Major finding: Any morbidity after CEA with general anesthesia was 8.7% vs. 4.2% for regional anesthesia, and readmissions rates were 9.2% vs. 6.1%.
Data source: Retrospective analysis of 4,558 patients who had CEA between 2012 and 2014 at hospitals participating in the Michigan Surgical Quality Collaborative database.
Disclosures: Dr. Hussain reported having no financial disclosures.
Carotid stenting tied to cardiovascular events in real-world study
ROME – Carotid stenting was associated with a roughly 30% higher risk of cardiovascular events than that of carotid endarterectomy during 12 years of follow-up in a large, real-world, population-based cohort study, Mohamad A. Hussain, MD, reported at the annual congress of the European Society of Cardiology.
“Our data raise concerns about the external validity of randomized controlled trials of carotid endarterectomy versus stenting and question the potential interchangeability of carotid endarterectomy and stenting as stated in clinical practice guidelines,” said Dr. Hussain of the University of Toronto.

Major practice guidelines cite randomized trial evidence in suggesting that CEA and stenting can be used interchangeably in treating low- or average-risk patients with significant carotid artery disease. Dr. Hussain and his coinvestigators, suspicious that the generalizability of the randomized trial findings may be limited because of operator and institutional selection bias, decided to conduct a retrospective cohort study of all patients over age 40 years who underwent CEA or carotid stenting in the province of Ontario from April 2002 through March 2013.
Using validated chart abstraction software, they identified 12,529 patients who had CEA and 1,935 with carotid stenting. The two groups were similar in terms of most baseline characteristics. Notably, however, stent recipients were significantly more likely to have symptomatic carotid disease and also had more comorbid conditions as reflected in a higher Charlson Comorbidity Index score.
The primary outcome in the study was the 12-year rate of a composite comprising ischemic stroke, transient ischemic attack (TIA), MI, or death. The rate was 35.4% in the CEA group and 44.5% in the stent group. After adjustment for the baseline differences, the stent group still had a statistically significant 28% greater risk of the primary outcome.
“We found the difference remained significant in all of our subgroup analyses, regardless of age, sex, year of procedure, symptomatic or asymptomatic carotid artery disease, CAD [coronary artery disease] or no CAD, diabetes (type 1 or 2) or no diabetes. Outcomes with endarterectomy were always significantly better,” said Dr. Hussain.
“I think our study shows that in clinical practice we’re not quite seeing the outcomes reported in the clinical trials,” he added.
As for the individual components of the composite endpoint, the 12-year rate of ischemic stroke or TIA was 9% in the CEA group and 14% with stenting, for an adjusted 40% increased risk in the stent group. The 12-year all-cause mortality rate was 26% in the CEA group and 34% with stenting, for an adjusted 28% increased risk. The incidence of MI was 8% in both groups.
The investigators next conducted a confirmatory propensity-matched analysis in which 1,927 of the stented patients were closely matched to 3,844 surgical patients, eliminating baseline differences in the prevalence of symptomatic carotid artery disease and other disparities. In this matched cohort, the primary outcome occurred in 37.4% of the CEA group and 44.3% of stent patients, for an adjusted 32% increase in risk in the stented group.
The differences in outcome were driven by sharply higher periprocedural risk in the stented group. After the periprocedural period, the outcome curves remained parallel in the two treatment groups.
In that first 30 days post procedure, the primary composite outcome occurred in 5.4% of the CEA group and 10% of stented patients, for an adjusted 40% increase in relative risk in percutaneously treated patients. The 30-day rate of ischemic stroke or TIA was 3.4% in the surgical group compared with 6.4% in stented patients. Thirty-day mortality was 0.9% with CEA versus 3.3% with stenting.
Asked by the award panel for his thoughts on the disparity between the results of his real-world study and the major randomized trials of CEA versus stenting, Dr. Hussain replied, “It may be because the trials had high-volume operators at high-volume centers who are really experts in carotid stenting, while in the real world many physicians may not be selecting the right people for carotid stenting.”
Differences in sample size may also figure in the disparity, he continued. He noted that in the recent 10-year report from the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST), the composite endpoint of stroke, MI, or death occurred in 9.9% of the CEA group compared with 11.8% of the stenting group (N Engl J Med. 2016 Mar 17;374[11]:1021-31), but this difference in favor of CEA didn’t achieve statistical significance because of the wide confidence intervals resulting from a smaller sample size than in the Ontario study.
Looking to the future, Dr. Hussain said he thinks the ongoing CREST-2 trial is “very important.” It is randomizing patients with asymptomatic high-grade carotid stenosis to uniform intensive medical management either alone or in combination with CEA or stenting with embolic protection.
“That study might end up showing us that medical therapy is as good as or even better than stenting or CEA, especially in asymptomatic patients,” he said.
Dr. Hussain reported having no financial conflicts regarding his academically funded study.
ROME – Carotid stenting was associated with a roughly 30% higher risk of cardiovascular events than that of carotid endarterectomy during 12 years of follow-up in a large, real-world, population-based cohort study, Mohamad A. Hussain, MD, reported at the annual congress of the European Society of Cardiology.
“Our data raise concerns about the external validity of randomized controlled trials of carotid endarterectomy versus stenting and question the potential interchangeability of carotid endarterectomy and stenting as stated in clinical practice guidelines,” said Dr. Hussain of the University of Toronto.
Major practice guidelines cite randomized trial evidence in suggesting that CEA and stenting can be used interchangeably in treating low- or average-risk patients with significant carotid artery disease. Dr. Hussain and his coinvestigators, suspicious that the generalizability of the randomized trial findings may be limited because of operator and institutional selection bias, decided to conduct a retrospective cohort study of all patients over age 40 years who underwent CEA or carotid stenting in the province of Ontario from April 2002 through March 2013.
Using validated chart abstraction software, they identified 12,529 patients who had CEA and 1,935 with carotid stenting. The two groups were similar in terms of most baseline characteristics. Notably, however, stent recipients were significantly more likely to have symptomatic carotid disease and also had more comorbid conditions as reflected in a higher Charlson Comorbidity Index score.
The primary outcome in the study was the 12-year rate of a composite comprising ischemic stroke, transient ischemic attack (TIA), MI, or death. The rate was 35.4% in the CEA group and 44.5% in the stent group. After adjustment for the baseline differences, the stent group still had a statistically significant 28% greater risk of the primary outcome.
“We found the difference remained significant in all of our subgroup analyses, regardless of age, sex, year of procedure, symptomatic or asymptomatic carotid artery disease, CAD [coronary artery disease] or no CAD, diabetes (type 1 or 2) or no diabetes. Outcomes with endarterectomy were always significantly better,” said Dr. Hussain.
“I think our study shows that in clinical practice we’re not quite seeing the outcomes reported in the clinical trials,” he added.
As for the individual components of the composite endpoint, the 12-year rate of ischemic stroke or TIA was 9% in the CEA group and 14% with stenting, for an adjusted 40% increased risk in the stent group. The 12-year all-cause mortality rate was 26% in the CEA group and 34% with stenting, for an adjusted 28% increased risk. The incidence of MI was 8% in both groups.
The investigators next conducted a confirmatory propensity-matched analysis in which 1,927 of the stented patients were closely matched to 3,844 surgical patients, eliminating baseline differences in the prevalence of symptomatic carotid artery disease and other disparities. In this matched cohort, the primary outcome occurred in 37.4% of the CEA group and 44.3% of stent patients, for an adjusted 32% increase in risk in the stented group.
The differences in outcome were driven by sharply higher periprocedural risk in the stented group. After the periprocedural period, the outcome curves remained parallel in the two treatment groups.
In that first 30 days post procedure, the primary composite outcome occurred in 5.4% of the CEA group and 10% of stented patients, for an adjusted 40% increase in relative risk in percutaneously treated patients. The 30-day rate of ischemic stroke or TIA was 3.4% in the surgical group compared with 6.4% in stented patients. Thirty-day mortality was 0.9% with CEA versus 3.3% with stenting.
Asked by the award panel for his thoughts on the disparity between the results of his real-world study and the major randomized trials of CEA versus stenting, Dr. Hussain replied, “It may be because the trials had high-volume operators at high-volume centers who are really experts in carotid stenting, while in the real world many physicians may not be selecting the right people for carotid stenting.”
Differences in sample size may also figure in the disparity, he continued. He noted that in the recent 10-year report from the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST), the composite endpoint of stroke, MI, or death occurred in 9.9% of the CEA group compared with 11.8% of the stenting group (N Engl J Med. 2016 Mar 17;374[11]:1021-31), but this difference in favor of CEA didn’t achieve statistical significance because of the wide confidence intervals resulting from a smaller sample size than in the Ontario study.
Looking to the future, Dr. Hussain said he thinks the ongoing CREST-2 trial is “very important.” It is randomizing patients with asymptomatic high-grade carotid stenosis to uniform intensive medical management either alone or in combination with CEA or stenting with embolic protection.
“That study might end up showing us that medical therapy is as good as or even better than stenting or CEA, especially in asymptomatic patients,” he said.
Dr. Hussain reported having no financial conflicts regarding his academically funded study.
ROME – Carotid stenting was associated with a roughly 30% higher risk of cardiovascular events than that of carotid endarterectomy during 12 years of follow-up in a large, real-world, population-based cohort study, Mohamad A. Hussain, MD, reported at the annual congress of the European Society of Cardiology.
“Our data raise concerns about the external validity of randomized controlled trials of carotid endarterectomy versus stenting and question the potential interchangeability of carotid endarterectomy and stenting as stated in clinical practice guidelines,” said Dr. Hussain of the University of Toronto.
Major practice guidelines cite randomized trial evidence in suggesting that CEA and stenting can be used interchangeably in treating low- or average-risk patients with significant carotid artery disease. Dr. Hussain and his coinvestigators, suspicious that the generalizability of the randomized trial findings may be limited because of operator and institutional selection bias, decided to conduct a retrospective cohort study of all patients over age 40 years who underwent CEA or carotid stenting in the province of Ontario from April 2002 through March 2013.
Using validated chart abstraction software, they identified 12,529 patients who had CEA and 1,935 with carotid stenting. The two groups were similar in terms of most baseline characteristics. Notably, however, stent recipients were significantly more likely to have symptomatic carotid disease and also had more comorbid conditions as reflected in a higher Charlson Comorbidity Index score.
The primary outcome in the study was the 12-year rate of a composite comprising ischemic stroke, transient ischemic attack (TIA), MI, or death. The rate was 35.4% in the CEA group and 44.5% in the stent group. After adjustment for the baseline differences, the stent group still had a statistically significant 28% greater risk of the primary outcome.
“We found the difference remained significant in all of our subgroup analyses, regardless of age, sex, year of procedure, symptomatic or asymptomatic carotid artery disease, CAD [coronary artery disease] or no CAD, diabetes (type 1 or 2) or no diabetes. Outcomes with endarterectomy were always significantly better,” said Dr. Hussain.
“I think our study shows that in clinical practice we’re not quite seeing the outcomes reported in the clinical trials,” he added.
As for the individual components of the composite endpoint, the 12-year rate of ischemic stroke or TIA was 9% in the CEA group and 14% with stenting, for an adjusted 40% increased risk in the stent group. The 12-year all-cause mortality rate was 26% in the CEA group and 34% with stenting, for an adjusted 28% increased risk. The incidence of MI was 8% in both groups.
The investigators next conducted a confirmatory propensity-matched analysis in which 1,927 of the stented patients were closely matched to 3,844 surgical patients, eliminating baseline differences in the prevalence of symptomatic carotid artery disease and other disparities. In this matched cohort, the primary outcome occurred in 37.4% of the CEA group and 44.3% of stent patients, for an adjusted 32% increase in risk in the stented group.
The differences in outcome were driven by sharply higher periprocedural risk in the stented group. After the periprocedural period, the outcome curves remained parallel in the two treatment groups.
In that first 30 days post procedure, the primary composite outcome occurred in 5.4% of the CEA group and 10% of stented patients, for an adjusted 40% increase in relative risk in percutaneously treated patients. The 30-day rate of ischemic stroke or TIA was 3.4% in the surgical group compared with 6.4% in stented patients. Thirty-day mortality was 0.9% with CEA versus 3.3% with stenting.
Asked by the award panel for his thoughts on the disparity between the results of his real-world study and the major randomized trials of CEA versus stenting, Dr. Hussain replied, “It may be because the trials had high-volume operators at high-volume centers who are really experts in carotid stenting, while in the real world many physicians may not be selecting the right people for carotid stenting.”
Differences in sample size may also figure in the disparity, he continued. He noted that in the recent 10-year report from the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST), the composite endpoint of stroke, MI, or death occurred in 9.9% of the CEA group compared with 11.8% of the stenting group (N Engl J Med. 2016 Mar 17;374[11]:1021-31), but this difference in favor of CEA didn’t achieve statistical significance because of the wide confidence intervals resulting from a smaller sample size than in the Ontario study.
Looking to the future, Dr. Hussain said he thinks the ongoing CREST-2 trial is “very important.” It is randomizing patients with asymptomatic high-grade carotid stenosis to uniform intensive medical management either alone or in combination with CEA or stenting with embolic protection.
“That study might end up showing us that medical therapy is as good as or even better than stenting or CEA, especially in asymptomatic patients,” he said.
Dr. Hussain reported having no financial conflicts regarding his academically funded study.
AT THE ESC CONGRESS 2016
Key clinical point:
Major finding: The composite rate of ischemic stroke, TIA, MI, or death over 12 years of follow-up occurred in 35.4% of patients with carotid artery disease treated by carotid endarterectomy and 44.5% of those who underwent stenting.
Data source: A retrospective population-based cohort study comprising all 14,464 patients who underwent carotid endarterectomy or stenting for carotid artery disease in Ontario during 2002-2013.
Disclosures: The presenter reported having no financial conflicts of interest regarding his academically funded study.
CEA risk models fit for an app
COLUMBUS, OHIO – Carotid endarterectomy is an effective treatment for people with asymptomatic carotid artery disease when stroke rates are low and they survive long enough to benefit from the treatment. But determining who those patients are can be a challenge for vascular surgeons. A team of vascular specialists from around the country have developed risk prediction models to help surgeons better select asymptomatic patients for the procedure, Randall DeMartino, MD, said at the annual meeting of the Midwestern Vascular Surgical Society.
“These models will be used for mobile apps and web-based applications for point of care patient risk assessment,” said Dr. DeMartino of the Mayo Clinic in Rochester, Minn. He is the lead researcher for the study, which uses data from the Vascular Quality Initiative (VQI).

In developing the models, the researchers sampled asymptomatic patients in the VQI who had first-time elective CEA. There were 31,939 patients in the stroke analysis who had CEA from 2010-2015, and 24,086 patients in the mortality analysis who had procedures from 2010-2014. Dr. DeMartino and his colleagues evaluated all preoperative patient and surgeon characteristics, then used an algorithm to optimize the variables that were selected for the final logistic model.
The researchers also evaluated 30-day stroke rates and 1-year mortality at participating centers and found wide variability: an average of 0.9% for stroke, with a range of 0-8.3%; and 3.2% for mortality, with a range of 0-20%. “Actually, 22% of centers had a 1-year mortality rate that exceeded 5%,” Dr. DeMartino said.
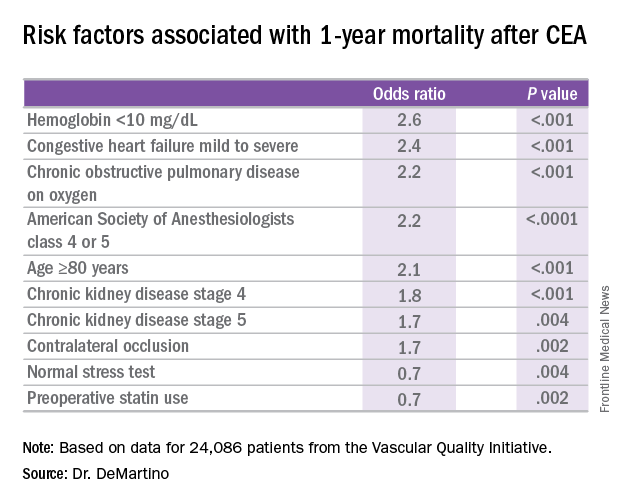
The model for 1-year mortality identified the following variables associated with the highest risk of death 1 year after CEA: age greater than or equal to 80 years; a preoperative hemoglobin less than 10 mg/dL; oxygen-dependent chronic obstructive pulmonary disease; mild to severe congestive heart failure; American Society of Anesthesiologists classification of IV or V; stage 4 or 5 chronic kidney disease; and a contralateral occlusion.
“Conversely, a normal stress test, when performed, and preoperative statin use were associated with reduced risk of death over a year,” Dr. DeMartino said.
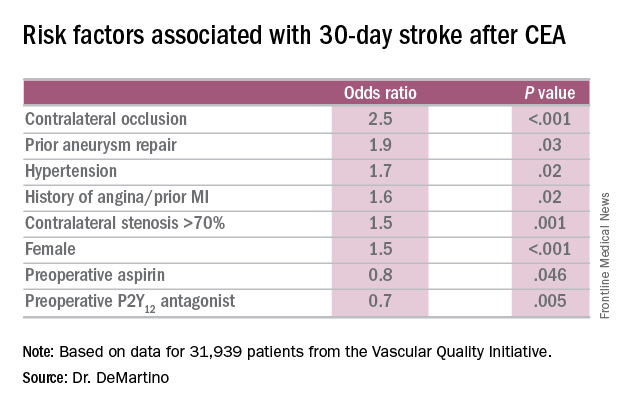
“These data have been used to provide Center Opportunity for Improvement reports through VQI where centers can identify if they are selecting patients with risk factors for stroke or mortality more often compared to other centers,” Dr. DeMartino said. “This allows centers to see where opportunities for improvement exist.”
Also, physicians can see the proportion of patients they select with a predicted mortality risk over 5% at one year – “a group of patients who may gain little benefit from prophylactic CEA,” he said. “Physicians can compare their patient selection to those in their region or nationally.”
Dr. DeMartino had no relationships to disclose.
COLUMBUS, OHIO – Carotid endarterectomy is an effective treatment for people with asymptomatic carotid artery disease when stroke rates are low and they survive long enough to benefit from the treatment. But determining who those patients are can be a challenge for vascular surgeons. A team of vascular specialists from around the country have developed risk prediction models to help surgeons better select asymptomatic patients for the procedure, Randall DeMartino, MD, said at the annual meeting of the Midwestern Vascular Surgical Society.
“These models will be used for mobile apps and web-based applications for point of care patient risk assessment,” said Dr. DeMartino of the Mayo Clinic in Rochester, Minn. He is the lead researcher for the study, which uses data from the Vascular Quality Initiative (VQI).
In developing the models, the researchers sampled asymptomatic patients in the VQI who had first-time elective CEA. There were 31,939 patients in the stroke analysis who had CEA from 2010-2015, and 24,086 patients in the mortality analysis who had procedures from 2010-2014. Dr. DeMartino and his colleagues evaluated all preoperative patient and surgeon characteristics, then used an algorithm to optimize the variables that were selected for the final logistic model.
The researchers also evaluated 30-day stroke rates and 1-year mortality at participating centers and found wide variability: an average of 0.9% for stroke, with a range of 0-8.3%; and 3.2% for mortality, with a range of 0-20%. “Actually, 22% of centers had a 1-year mortality rate that exceeded 5%,” Dr. DeMartino said.
The model for 1-year mortality identified the following variables associated with the highest risk of death 1 year after CEA: age greater than or equal to 80 years; a preoperative hemoglobin less than 10 mg/dL; oxygen-dependent chronic obstructive pulmonary disease; mild to severe congestive heart failure; American Society of Anesthesiologists classification of IV or V; stage 4 or 5 chronic kidney disease; and a contralateral occlusion.
“Conversely, a normal stress test, when performed, and preoperative statin use were associated with reduced risk of death over a year,” Dr. DeMartino said.
“These data have been used to provide Center Opportunity for Improvement reports through VQI where centers can identify if they are selecting patients with risk factors for stroke or mortality more often compared to other centers,” Dr. DeMartino said. “This allows centers to see where opportunities for improvement exist.”
Also, physicians can see the proportion of patients they select with a predicted mortality risk over 5% at one year – “a group of patients who may gain little benefit from prophylactic CEA,” he said. “Physicians can compare their patient selection to those in their region or nationally.”
Dr. DeMartino had no relationships to disclose.
COLUMBUS, OHIO – Carotid endarterectomy is an effective treatment for people with asymptomatic carotid artery disease when stroke rates are low and they survive long enough to benefit from the treatment. But determining who those patients are can be a challenge for vascular surgeons. A team of vascular specialists from around the country have developed risk prediction models to help surgeons better select asymptomatic patients for the procedure, Randall DeMartino, MD, said at the annual meeting of the Midwestern Vascular Surgical Society.
“These models will be used for mobile apps and web-based applications for point of care patient risk assessment,” said Dr. DeMartino of the Mayo Clinic in Rochester, Minn. He is the lead researcher for the study, which uses data from the Vascular Quality Initiative (VQI).
In developing the models, the researchers sampled asymptomatic patients in the VQI who had first-time elective CEA. There were 31,939 patients in the stroke analysis who had CEA from 2010-2015, and 24,086 patients in the mortality analysis who had procedures from 2010-2014. Dr. DeMartino and his colleagues evaluated all preoperative patient and surgeon characteristics, then used an algorithm to optimize the variables that were selected for the final logistic model.
The researchers also evaluated 30-day stroke rates and 1-year mortality at participating centers and found wide variability: an average of 0.9% for stroke, with a range of 0-8.3%; and 3.2% for mortality, with a range of 0-20%. “Actually, 22% of centers had a 1-year mortality rate that exceeded 5%,” Dr. DeMartino said.
The model for 1-year mortality identified the following variables associated with the highest risk of death 1 year after CEA: age greater than or equal to 80 years; a preoperative hemoglobin less than 10 mg/dL; oxygen-dependent chronic obstructive pulmonary disease; mild to severe congestive heart failure; American Society of Anesthesiologists classification of IV or V; stage 4 or 5 chronic kidney disease; and a contralateral occlusion.
“Conversely, a normal stress test, when performed, and preoperative statin use were associated with reduced risk of death over a year,” Dr. DeMartino said.
“These data have been used to provide Center Opportunity for Improvement reports through VQI where centers can identify if they are selecting patients with risk factors for stroke or mortality more often compared to other centers,” Dr. DeMartino said. “This allows centers to see where opportunities for improvement exist.”
Also, physicians can see the proportion of patients they select with a predicted mortality risk over 5% at one year – “a group of patients who may gain little benefit from prophylactic CEA,” he said. “Physicians can compare their patient selection to those in their region or nationally.”
Dr. DeMartino had no relationships to disclose.
AT MIDWESTERN VASCULAR 2016
Key clinical point: Risk-prediction models may identify patients at greatest risk of stroke and 1-year death after carotid endarterectomy (CEA).
Major finding: Contralateral occlusion has odds ratios of 2.5 for 30-day stroke after CEA and 1.7 for death at 1 year.
Data source: Sampling of patients from the Vascular Quality Initiative who had first-time CEA: 31,939 in the stroke analysis and 24,086 in the mortality analysis.
Disclosures: Dr. DeMartino reported having no financial disclosures.
Benefits of early endovascular thrombectomy outlined in five trials
For patients with large-vessel ischemic stroke, endovascular thrombectomy produces better functional outcomes at 90 days than does optimal medical therapy, as long as the procedure is started within 7.3 hours of symptom onset, according to a report published online Sept. 27 in JAMA.
The benefit of thrombectomy was greatest when the procedure was begun under 2 hours from symptom onset, and it became nonsignificant after 7 hours and 18 minutes elapsed. This emphasizes “the importance of programs to enhance patient awareness, out-of-hospital care, and in-hospital management to shorten symptom onset-to-treatment times,” wrote Jeffrey L. Saver, MD, of the University of California, Los Angeles, and his associates.

Five major randomized trials have demonstrated the benefit of second-generation endovascular recanalization therapies over medical therapy in this patient population, but uncertainties persist regarding the timing of the intervention. For example, practice guidelines in the United States recommend thrombectomy until 6 hours after symptom onset, but the Food and Drug Administration allows thrombectomy devices to be used up to 8 hours after symptom onset and Canadian guidelines recommend the procedure for selected patients up to 12 hours after symptom onset.
The investigators for the five trials formed the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials (HERMES) collaboration to pool their individual patient data and perform a meta-analysis to clarify the issue of timing. They assessed patients’ functional independence at 90 days using the modified Rankin Score (mRS). The study participants included 634 patients who had been randomly assigned to endovascular thrombectomy and 653 randomly assigned to medical therapy.
The intervention correlated with a substantially lower degree of patient disability at 90 days than did medical therapy: the mean mRS was 2.9 in the thrombectomy group and 3.6 in the medical therapy group. In addition, increasing delays in treatment were associated with higher levels of residual disability in the thrombectomy group but not in the medical therapy group, the investigators reported.
“Based on the current study, and assuming the findings are generalizable to the population of patients with acute ischemic stroke due to large-vessel occlusion, among every 1,000 patients achieving substantial endovascular reperfusion, for every 15-minute faster ED door-to-reperfusion time, an estimated 39 patients would have a less-disabled outcome at 3 months, including 25 more who would achieve functional independence (mRS 0-2),” Dr. Saver and his associates wrote (JAMA. 2016;316[12]:1279-88).
These findings reinforce current recommendations to attempt endovascular thrombectomy when the procedure can be initiated within 6 hours of symptom onset, and they also “provide evidence that potentially supports strengthening of the recommendation for treatment from 6 through 7.3 hours after symptom onset,” they added.
No specific sponsor of this study was cited. Dr. Saver reported ties to Medtronic, Stryker, Cognition Medical, Covidien, Neuravi, BrainsGate, Pfizer, Bristol-Myers Squibb, Boehringer Ingelheim, ZZ Biotech, St. Jude Medical, and Genentech. His associates reported ties to numerous industry sources.
Earlier thrombectomy has such a profound effect on stroke patients’ outcomes that substantial changes in the current medical system are warranted to shorten these times even further. In this study, median time from symptom onset to randomization was approximately 3 hours, median time to arterial puncture was approximately 4 hours, and median time to reperfusion was nearly 5 hours.
Reducing the number of patients who are transferred from community hospitals to facilities with stroke centers would shorten door-to-reperfusion time a great deal. It is estimated that direct transport to stroke centers would allow endovascular thrombectomy for an additional 13% of stroke patients. Telemedicine, mobile stroke units, and out-of-hospital administration of tissue plasminogen activator are other possibilities that should be investigated.
Steven Warach, MD, PhD, and S. Claiborne Johnston, MD, PhD, are with the University of Texas at Austin. They reported having no relevant financial disclosures. Dr. Warach and Dr. Johnston made these remarks in an editorial (JAMA. 2016;316[12]:1265-6) accompanying Dr. Saver’s report.
Earlier thrombectomy has such a profound effect on stroke patients’ outcomes that substantial changes in the current medical system are warranted to shorten these times even further. In this study, median time from symptom onset to randomization was approximately 3 hours, median time to arterial puncture was approximately 4 hours, and median time to reperfusion was nearly 5 hours.
Reducing the number of patients who are transferred from community hospitals to facilities with stroke centers would shorten door-to-reperfusion time a great deal. It is estimated that direct transport to stroke centers would allow endovascular thrombectomy for an additional 13% of stroke patients. Telemedicine, mobile stroke units, and out-of-hospital administration of tissue plasminogen activator are other possibilities that should be investigated.
Steven Warach, MD, PhD, and S. Claiborne Johnston, MD, PhD, are with the University of Texas at Austin. They reported having no relevant financial disclosures. Dr. Warach and Dr. Johnston made these remarks in an editorial (JAMA. 2016;316[12]:1265-6) accompanying Dr. Saver’s report.
Earlier thrombectomy has such a profound effect on stroke patients’ outcomes that substantial changes in the current medical system are warranted to shorten these times even further. In this study, median time from symptom onset to randomization was approximately 3 hours, median time to arterial puncture was approximately 4 hours, and median time to reperfusion was nearly 5 hours.
Reducing the number of patients who are transferred from community hospitals to facilities with stroke centers would shorten door-to-reperfusion time a great deal. It is estimated that direct transport to stroke centers would allow endovascular thrombectomy for an additional 13% of stroke patients. Telemedicine, mobile stroke units, and out-of-hospital administration of tissue plasminogen activator are other possibilities that should be investigated.
Steven Warach, MD, PhD, and S. Claiborne Johnston, MD, PhD, are with the University of Texas at Austin. They reported having no relevant financial disclosures. Dr. Warach and Dr. Johnston made these remarks in an editorial (JAMA. 2016;316[12]:1265-6) accompanying Dr. Saver’s report.
For patients with large-vessel ischemic stroke, endovascular thrombectomy produces better functional outcomes at 90 days than does optimal medical therapy, as long as the procedure is started within 7.3 hours of symptom onset, according to a report published online Sept. 27 in JAMA.
The benefit of thrombectomy was greatest when the procedure was begun under 2 hours from symptom onset, and it became nonsignificant after 7 hours and 18 minutes elapsed. This emphasizes “the importance of programs to enhance patient awareness, out-of-hospital care, and in-hospital management to shorten symptom onset-to-treatment times,” wrote Jeffrey L. Saver, MD, of the University of California, Los Angeles, and his associates.
Five major randomized trials have demonstrated the benefit of second-generation endovascular recanalization therapies over medical therapy in this patient population, but uncertainties persist regarding the timing of the intervention. For example, practice guidelines in the United States recommend thrombectomy until 6 hours after symptom onset, but the Food and Drug Administration allows thrombectomy devices to be used up to 8 hours after symptom onset and Canadian guidelines recommend the procedure for selected patients up to 12 hours after symptom onset.
The investigators for the five trials formed the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials (HERMES) collaboration to pool their individual patient data and perform a meta-analysis to clarify the issue of timing. They assessed patients’ functional independence at 90 days using the modified Rankin Score (mRS). The study participants included 634 patients who had been randomly assigned to endovascular thrombectomy and 653 randomly assigned to medical therapy.
The intervention correlated with a substantially lower degree of patient disability at 90 days than did medical therapy: the mean mRS was 2.9 in the thrombectomy group and 3.6 in the medical therapy group. In addition, increasing delays in treatment were associated with higher levels of residual disability in the thrombectomy group but not in the medical therapy group, the investigators reported.
“Based on the current study, and assuming the findings are generalizable to the population of patients with acute ischemic stroke due to large-vessel occlusion, among every 1,000 patients achieving substantial endovascular reperfusion, for every 15-minute faster ED door-to-reperfusion time, an estimated 39 patients would have a less-disabled outcome at 3 months, including 25 more who would achieve functional independence (mRS 0-2),” Dr. Saver and his associates wrote (JAMA. 2016;316[12]:1279-88).
These findings reinforce current recommendations to attempt endovascular thrombectomy when the procedure can be initiated within 6 hours of symptom onset, and they also “provide evidence that potentially supports strengthening of the recommendation for treatment from 6 through 7.3 hours after symptom onset,” they added.
No specific sponsor of this study was cited. Dr. Saver reported ties to Medtronic, Stryker, Cognition Medical, Covidien, Neuravi, BrainsGate, Pfizer, Bristol-Myers Squibb, Boehringer Ingelheim, ZZ Biotech, St. Jude Medical, and Genentech. His associates reported ties to numerous industry sources.
For patients with large-vessel ischemic stroke, endovascular thrombectomy produces better functional outcomes at 90 days than does optimal medical therapy, as long as the procedure is started within 7.3 hours of symptom onset, according to a report published online Sept. 27 in JAMA.
The benefit of thrombectomy was greatest when the procedure was begun under 2 hours from symptom onset, and it became nonsignificant after 7 hours and 18 minutes elapsed. This emphasizes “the importance of programs to enhance patient awareness, out-of-hospital care, and in-hospital management to shorten symptom onset-to-treatment times,” wrote Jeffrey L. Saver, MD, of the University of California, Los Angeles, and his associates.
Five major randomized trials have demonstrated the benefit of second-generation endovascular recanalization therapies over medical therapy in this patient population, but uncertainties persist regarding the timing of the intervention. For example, practice guidelines in the United States recommend thrombectomy until 6 hours after symptom onset, but the Food and Drug Administration allows thrombectomy devices to be used up to 8 hours after symptom onset and Canadian guidelines recommend the procedure for selected patients up to 12 hours after symptom onset.
The investigators for the five trials formed the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials (HERMES) collaboration to pool their individual patient data and perform a meta-analysis to clarify the issue of timing. They assessed patients’ functional independence at 90 days using the modified Rankin Score (mRS). The study participants included 634 patients who had been randomly assigned to endovascular thrombectomy and 653 randomly assigned to medical therapy.
The intervention correlated with a substantially lower degree of patient disability at 90 days than did medical therapy: the mean mRS was 2.9 in the thrombectomy group and 3.6 in the medical therapy group. In addition, increasing delays in treatment were associated with higher levels of residual disability in the thrombectomy group but not in the medical therapy group, the investigators reported.
“Based on the current study, and assuming the findings are generalizable to the population of patients with acute ischemic stroke due to large-vessel occlusion, among every 1,000 patients achieving substantial endovascular reperfusion, for every 15-minute faster ED door-to-reperfusion time, an estimated 39 patients would have a less-disabled outcome at 3 months, including 25 more who would achieve functional independence (mRS 0-2),” Dr. Saver and his associates wrote (JAMA. 2016;316[12]:1279-88).
These findings reinforce current recommendations to attempt endovascular thrombectomy when the procedure can be initiated within 6 hours of symptom onset, and they also “provide evidence that potentially supports strengthening of the recommendation for treatment from 6 through 7.3 hours after symptom onset,” they added.
No specific sponsor of this study was cited. Dr. Saver reported ties to Medtronic, Stryker, Cognition Medical, Covidien, Neuravi, BrainsGate, Pfizer, Bristol-Myers Squibb, Boehringer Ingelheim, ZZ Biotech, St. Jude Medical, and Genentech. His associates reported ties to numerous industry sources.
FROM JAMA
Key clinical point: Endovascular thrombectomy started within 7.3 hours of symptom onset for large-vessel ischemic stroke produces better outcomes than does optimal medical therapy.
Major finding: For every 15-minute shorter door-to-reperfusion time, an estimated 39 patients would have a less-disabled outcome at 3 months, including 25 more who would achieve functional independence.
Data source: A meta-analysis of pooled data from five randomized clinical trials involving 1,287 patients.
Disclosures: No specific sponsor of this study was cited. Dr. Saver reported ties to Medtronic, Stryker, Cognition Medical, Covidien, Neuravi, BrainsGate, Pfizer, Bristol Myers Squibb, Boehringer Ingelheim, ZZ Biotech, St. Jude Medical, and Genentech. His associates reported ties to numerous industry sources.

VIVA: Assessing aortic repair and more in the latest trials
Along with a strong focus on peripheral arterial disease, VIVA late-breaking clinical trial reports will also address other critical areas of the vascular domain, from the aorta to the carotids.
On Tuesday morning, the results of two trials will be presented, which are investigating endovascular aortic repair. Ali Azizzadeh, MD, Memorial Hermann Heart and Vascular Institute, Houston, will discuss the 3-year results from the Valiant IDE Study, examining endovascular repair in acute, complicated type B aortic dissection.
Then, Zvonimir Krajcer, MD, Texas Heart Institute, Houston, will present the final results from the Prospective LIFE Registry, looking at fast-track endovascular aortic repair.
Also on Tuesday morning, the issue of interventions after the creation of an arteriovenous fistula (AVF) will be addressed by Charmaine Lok, MD, Toronto General Hospital, comparing traditional surgical AVF creation with a new endovascular approach.
Wednesday morning, Ido Weinberg, MD, Massachusetts General Hospital, Boston, will address the issue of carotid stent fractures, demonstrating that they are not associated with restenosis, stroke, myocardial infarction, or death based on the results from the ACT 1 Multicenter Randomized Trial.
Along with a strong focus on peripheral arterial disease, VIVA late-breaking clinical trial reports will also address other critical areas of the vascular domain, from the aorta to the carotids.
On Tuesday morning, the results of two trials will be presented, which are investigating endovascular aortic repair. Ali Azizzadeh, MD, Memorial Hermann Heart and Vascular Institute, Houston, will discuss the 3-year results from the Valiant IDE Study, examining endovascular repair in acute, complicated type B aortic dissection.
Then, Zvonimir Krajcer, MD, Texas Heart Institute, Houston, will present the final results from the Prospective LIFE Registry, looking at fast-track endovascular aortic repair.
Also on Tuesday morning, the issue of interventions after the creation of an arteriovenous fistula (AVF) will be addressed by Charmaine Lok, MD, Toronto General Hospital, comparing traditional surgical AVF creation with a new endovascular approach.
Wednesday morning, Ido Weinberg, MD, Massachusetts General Hospital, Boston, will address the issue of carotid stent fractures, demonstrating that they are not associated with restenosis, stroke, myocardial infarction, or death based on the results from the ACT 1 Multicenter Randomized Trial.
Along with a strong focus on peripheral arterial disease, VIVA late-breaking clinical trial reports will also address other critical areas of the vascular domain, from the aorta to the carotids.
On Tuesday morning, the results of two trials will be presented, which are investigating endovascular aortic repair. Ali Azizzadeh, MD, Memorial Hermann Heart and Vascular Institute, Houston, will discuss the 3-year results from the Valiant IDE Study, examining endovascular repair in acute, complicated type B aortic dissection.
Then, Zvonimir Krajcer, MD, Texas Heart Institute, Houston, will present the final results from the Prospective LIFE Registry, looking at fast-track endovascular aortic repair.
Also on Tuesday morning, the issue of interventions after the creation of an arteriovenous fistula (AVF) will be addressed by Charmaine Lok, MD, Toronto General Hospital, comparing traditional surgical AVF creation with a new endovascular approach.
Wednesday morning, Ido Weinberg, MD, Massachusetts General Hospital, Boston, will address the issue of carotid stent fractures, demonstrating that they are not associated with restenosis, stroke, myocardial infarction, or death based on the results from the ACT 1 Multicenter Randomized Trial.
