User login
Partial, whole breast irradiation 10-year outcomes similar
SAN FRANCISCO – Ten years of follow-up showed no significant difference in breast cancer locoregional recurrence, distant metastasis, or survival rates in 274 patients treated with accelerated partial breast irradiation compared with 274 matched patients treated with whole breast irradiation.
The data came from records on 3,009 patients with early-stage breast cancer who were treated with breast-conserving therapy at one institution between 1980 and 2012.
Four percent in each group developed local recurrence, 1% in each group had a regional recurrence, and 6% had distant metastases after partial breast irradiation and 3%, after whole breast irradiation. There was a nonsignificant statistical trend toward a higher rate of contralateral breast failure in the whole breast irradiation group (9%) compared with the partial breast irradiation group (3%, P = .06), Dr. Jessica Wobb reported in a poster presentation at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
Rates of disease-free survival were 91% in the partial breast irradiation group and 93% in the whole breast irradiation group. Cause-specific survival rates were 93% and 94%, respectively, and overall survival rates were 75% and 82%, reported Dr. Wobb of the Beaumont Cancer Institute, Royal Oak, Mich. None of these differences reached statistical significance.
This is one of the first reports on prolonged follow-up after accelerated partial breast irradiation, she noted. Mean follow-up was 7.8 years after partial breast irradiation and 8.1 years after whole breast irradiation, a difference that was statistically significant, but amounted to less than 4 months. All patients were followed for at least 1 year.
Patients in the cohorts were matched by age (within 3 years); T stage (Tis, T1, or T2); and estrogen receptor (ER) status. The mean age was 63 years of age in both groups. Eighty-eight percent in both groups had ER-positive tumors. The stage distribution in both groups consisted of 18% with stage Tis tumors, 71% with T1 tumors, and 11% with T2 tumors.
Significantly fewer patients in the partial breast irradiation group received adjuvant hormonal therapy (54%) compared with those in the whole breast irradiation group (68%). There was a trend toward smaller tumors in patients undergoing partial breast irradiation than in those receiving whole breast irradiation, with mean tumor sizes of 11.4 mm and 13 mm (P = .06).
Other characteristics were similar between the groups, including the proportion with negative lymph nodes (91% of patients undergoing partial breast irradiation and 86% of those who got whole breast irradiation), the proportion with negative final margins (94% and 95%, respectively), and the proportion who received adjuvant chemotherapy (15% and 18%).
Close tumor margins increased the risk for ipsilateral breast tumor recurrence in both groups, and positive margins increased the recurrence risk in the whole breast irradiation group, a univariate analysis found.
Dr. Wobb reported having no relevant financial disclosures.
On Twitter @sherryboschert
In the absence of prospective, randomized trial data on accelerated partial breast irradiation to guide us, we are left with the accumulation of institutional data. The institution that, in my opinion, has contributed most to our knowledge base is the group at William Beaumont Hospital. We’re fortunate to have an update of their experience in that they’ve performed an updated a matched-pair analysis looking at their partial breast irradiation patients (using interstitial catheter or balloon-based brachytherapy two different techniques), compared with their whole breast irradiation patients.
In this matched-pair comparison, the investigators saw no difference in local failure, regional failure, distant metastases, or overall survival.

|
|
Of course, we have to ask, in a matched pair, how good is the match? We do notice that in their group it’s a pretty good match, but we see that for whole breast irradiation, there are slightly larger tumors in that cohort and slightly more positive-node patients. Perhaps the most unsettling aspect is that there is more hormonal therapy in the whole breast irradiation group. This could reflect two things: One is an imbalance in prognostic factors between the two cohorts; the other is an impact of hormonal therapy on local and regional control outcomes.
When we look at their results related to clinical variables and outcome, not surprisingly we find that a negative margin is always better irrespective of whether the patient is getting whole breast irradiation or partial breast irradiation. Interestingly, in the partial breast irradiation group, younger age was associated with a higher risk of local failure.
What’s missing from this analysis? Again, this is not a fault of the investigators; just by virtue of this being a retrospective collection of data, it’s sometimes hard to get all this data. The questions that I think are pertinent in 2013 relate to grade, triple-negative phenotype versus other phenotypes, human epidermal growth factor receptor 2 status, and lymphatic vascular invasion. Unfortunately, none of that information is present in this analysis.
Dr. David E. Wazer is a professor of radiation oncology at Brown University, Providence, R.I. These are excerpts of his remarks as the discussant of Dr. Wobb’s study at the meeting. Dr. Wazer reported financial associations with the American Brachytherapy Society, Advanced Radiation Therapy, and American Journal of Clinical Oncology.
In the absence of prospective, randomized trial data on accelerated partial breast irradiation to guide us, we are left with the accumulation of institutional data. The institution that, in my opinion, has contributed most to our knowledge base is the group at William Beaumont Hospital. We’re fortunate to have an update of their experience in that they’ve performed an updated a matched-pair analysis looking at their partial breast irradiation patients (using interstitial catheter or balloon-based brachytherapy two different techniques), compared with their whole breast irradiation patients.
In this matched-pair comparison, the investigators saw no difference in local failure, regional failure, distant metastases, or overall survival.
|
|
|
Of course, we have to ask, in a matched pair, how good is the match? We do notice that in their group it’s a pretty good match, but we see that for whole breast irradiation, there are slightly larger tumors in that cohort and slightly more positive-node patients. Perhaps the most unsettling aspect is that there is more hormonal therapy in the whole breast irradiation group. This could reflect two things: One is an imbalance in prognostic factors between the two cohorts; the other is an impact of hormonal therapy on local and regional control outcomes.
When we look at their results related to clinical variables and outcome, not surprisingly we find that a negative margin is always better irrespective of whether the patient is getting whole breast irradiation or partial breast irradiation. Interestingly, in the partial breast irradiation group, younger age was associated with a higher risk of local failure.
What’s missing from this analysis? Again, this is not a fault of the investigators; just by virtue of this being a retrospective collection of data, it’s sometimes hard to get all this data. The questions that I think are pertinent in 2013 relate to grade, triple-negative phenotype versus other phenotypes, human epidermal growth factor receptor 2 status, and lymphatic vascular invasion. Unfortunately, none of that information is present in this analysis.
Dr. David E. Wazer is a professor of radiation oncology at Brown University, Providence, R.I. These are excerpts of his remarks as the discussant of Dr. Wobb’s study at the meeting. Dr. Wazer reported financial associations with the American Brachytherapy Society, Advanced Radiation Therapy, and American Journal of Clinical Oncology.
In the absence of prospective, randomized trial data on accelerated partial breast irradiation to guide us, we are left with the accumulation of institutional data. The institution that, in my opinion, has contributed most to our knowledge base is the group at William Beaumont Hospital. We’re fortunate to have an update of their experience in that they’ve performed an updated a matched-pair analysis looking at their partial breast irradiation patients (using interstitial catheter or balloon-based brachytherapy two different techniques), compared with their whole breast irradiation patients.
In this matched-pair comparison, the investigators saw no difference in local failure, regional failure, distant metastases, or overall survival.
|
|
|
Of course, we have to ask, in a matched pair, how good is the match? We do notice that in their group it’s a pretty good match, but we see that for whole breast irradiation, there are slightly larger tumors in that cohort and slightly more positive-node patients. Perhaps the most unsettling aspect is that there is more hormonal therapy in the whole breast irradiation group. This could reflect two things: One is an imbalance in prognostic factors between the two cohorts; the other is an impact of hormonal therapy on local and regional control outcomes.
When we look at their results related to clinical variables and outcome, not surprisingly we find that a negative margin is always better irrespective of whether the patient is getting whole breast irradiation or partial breast irradiation. Interestingly, in the partial breast irradiation group, younger age was associated with a higher risk of local failure.
What’s missing from this analysis? Again, this is not a fault of the investigators; just by virtue of this being a retrospective collection of data, it’s sometimes hard to get all this data. The questions that I think are pertinent in 2013 relate to grade, triple-negative phenotype versus other phenotypes, human epidermal growth factor receptor 2 status, and lymphatic vascular invasion. Unfortunately, none of that information is present in this analysis.
Dr. David E. Wazer is a professor of radiation oncology at Brown University, Providence, R.I. These are excerpts of his remarks as the discussant of Dr. Wobb’s study at the meeting. Dr. Wazer reported financial associations with the American Brachytherapy Society, Advanced Radiation Therapy, and American Journal of Clinical Oncology.
SAN FRANCISCO – Ten years of follow-up showed no significant difference in breast cancer locoregional recurrence, distant metastasis, or survival rates in 274 patients treated with accelerated partial breast irradiation compared with 274 matched patients treated with whole breast irradiation.
The data came from records on 3,009 patients with early-stage breast cancer who were treated with breast-conserving therapy at one institution between 1980 and 2012.
Four percent in each group developed local recurrence, 1% in each group had a regional recurrence, and 6% had distant metastases after partial breast irradiation and 3%, after whole breast irradiation. There was a nonsignificant statistical trend toward a higher rate of contralateral breast failure in the whole breast irradiation group (9%) compared with the partial breast irradiation group (3%, P = .06), Dr. Jessica Wobb reported in a poster presentation at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
Rates of disease-free survival were 91% in the partial breast irradiation group and 93% in the whole breast irradiation group. Cause-specific survival rates were 93% and 94%, respectively, and overall survival rates were 75% and 82%, reported Dr. Wobb of the Beaumont Cancer Institute, Royal Oak, Mich. None of these differences reached statistical significance.
This is one of the first reports on prolonged follow-up after accelerated partial breast irradiation, she noted. Mean follow-up was 7.8 years after partial breast irradiation and 8.1 years after whole breast irradiation, a difference that was statistically significant, but amounted to less than 4 months. All patients were followed for at least 1 year.
Patients in the cohorts were matched by age (within 3 years); T stage (Tis, T1, or T2); and estrogen receptor (ER) status. The mean age was 63 years of age in both groups. Eighty-eight percent in both groups had ER-positive tumors. The stage distribution in both groups consisted of 18% with stage Tis tumors, 71% with T1 tumors, and 11% with T2 tumors.
Significantly fewer patients in the partial breast irradiation group received adjuvant hormonal therapy (54%) compared with those in the whole breast irradiation group (68%). There was a trend toward smaller tumors in patients undergoing partial breast irradiation than in those receiving whole breast irradiation, with mean tumor sizes of 11.4 mm and 13 mm (P = .06).
Other characteristics were similar between the groups, including the proportion with negative lymph nodes (91% of patients undergoing partial breast irradiation and 86% of those who got whole breast irradiation), the proportion with negative final margins (94% and 95%, respectively), and the proportion who received adjuvant chemotherapy (15% and 18%).
Close tumor margins increased the risk for ipsilateral breast tumor recurrence in both groups, and positive margins increased the recurrence risk in the whole breast irradiation group, a univariate analysis found.
Dr. Wobb reported having no relevant financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – Ten years of follow-up showed no significant difference in breast cancer locoregional recurrence, distant metastasis, or survival rates in 274 patients treated with accelerated partial breast irradiation compared with 274 matched patients treated with whole breast irradiation.
The data came from records on 3,009 patients with early-stage breast cancer who were treated with breast-conserving therapy at one institution between 1980 and 2012.
Four percent in each group developed local recurrence, 1% in each group had a regional recurrence, and 6% had distant metastases after partial breast irradiation and 3%, after whole breast irradiation. There was a nonsignificant statistical trend toward a higher rate of contralateral breast failure in the whole breast irradiation group (9%) compared with the partial breast irradiation group (3%, P = .06), Dr. Jessica Wobb reported in a poster presentation at a breast cancer symposium sponsored by the American Society of Clinical Oncology.
Rates of disease-free survival were 91% in the partial breast irradiation group and 93% in the whole breast irradiation group. Cause-specific survival rates were 93% and 94%, respectively, and overall survival rates were 75% and 82%, reported Dr. Wobb of the Beaumont Cancer Institute, Royal Oak, Mich. None of these differences reached statistical significance.
This is one of the first reports on prolonged follow-up after accelerated partial breast irradiation, she noted. Mean follow-up was 7.8 years after partial breast irradiation and 8.1 years after whole breast irradiation, a difference that was statistically significant, but amounted to less than 4 months. All patients were followed for at least 1 year.
Patients in the cohorts were matched by age (within 3 years); T stage (Tis, T1, or T2); and estrogen receptor (ER) status. The mean age was 63 years of age in both groups. Eighty-eight percent in both groups had ER-positive tumors. The stage distribution in both groups consisted of 18% with stage Tis tumors, 71% with T1 tumors, and 11% with T2 tumors.
Significantly fewer patients in the partial breast irradiation group received adjuvant hormonal therapy (54%) compared with those in the whole breast irradiation group (68%). There was a trend toward smaller tumors in patients undergoing partial breast irradiation than in those receiving whole breast irradiation, with mean tumor sizes of 11.4 mm and 13 mm (P = .06).
Other characteristics were similar between the groups, including the proportion with negative lymph nodes (91% of patients undergoing partial breast irradiation and 86% of those who got whole breast irradiation), the proportion with negative final margins (94% and 95%, respectively), and the proportion who received adjuvant chemotherapy (15% and 18%).
Close tumor margins increased the risk for ipsilateral breast tumor recurrence in both groups, and positive margins increased the recurrence risk in the whole breast irradiation group, a univariate analysis found.
Dr. Wobb reported having no relevant financial disclosures.
On Twitter @sherryboschert
AT THE ASCO BREAST CANCER SYMPOSIUM
Major finding: Four percent developed local recurrence and 1% had regional recurrence in both partial and whole breast irradiation groups. For the partial vs. whole breast irradiation groups, distant metastases developed in 6% and 3%, disease-free survival rates were 91% and 93%, and overall survival rates were 75% and 82.
Data source: A retrospective study of 274 matched pairs of patients with early-stage breast cancer treated with breast-conserving therapy at one institution.
Disclosures: Dr. Wobb reported having no relevant financial disclosures.

Heart irradiation is lower with contemporary breast radiotherapy
SAN FRANCISCO – The hearts of 100 consecutive patients who underwent adjuvant radiotherapy for left-sided breast cancer in 2011 received an average of 2.9 Gray of radiation, considerably less than the mean cardiac exposure of 4.9-Gy reported in a recent review of 2,168 patients treated from 1958 to 2001 in Sweden and Denmark.
The findings confirm that three-dimensional conformal radiation therapy (3D-CRT) reduces cardiac exposure to radiation, Dr. Federico Lonardi and his associates reported at a breast cancer symposium sponsored by the American Society of Clinical Oncology. But certain areas of the heart still receive high doses when patients have adverse anatomic conditions that are not well suited to 3D-CRT. Because heart structures may differ in radiosensitivity, higher doses to small volumes of the heart, such as the coronary artery, might be associated with more risk, the researchers cautioned.
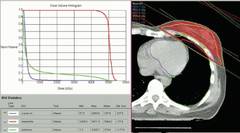
Most patients received a mean cardiac dose of 2-3 Gy (32%), 21% of patients were exposed to 1.15-1.99 Gy, and 1% got 0.8 Gy in a study of a consecutive series of breast cancer patients treated at Mater Salutis Hospital in Legnago, Italy. Only 17% of patients received a mean cardiac dose of more than 5 Gy, and 13% received 4.16-4.83 Gy.
The cardiac dose ranged from 0.8 to 13.05 Gy in Dr. Lonardi’s study, compared with a range of 0.03 to 27.72 Gy in the recently published Scandinavian study (N. Engl. J. Med. 2013;368:987-998). In the published study, the longitudinal risk for major cardiac events increased in a linear fashion, with a 7% increase for cardiac events with every 1 Gy increase in radiation to the heart.
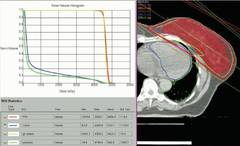
In the Italian study, the median volumes of heart exposed to higher doses of radiation were "consistently low" with 4% of heart volumes exposed to 5 Gy or more, 3% exposed to 10Gy or more, 2% exposed to 15 Gy or more, and 0.7% exposed to 25 Gy or more Dr. Lonardi reported.
These patients received full-breast 3D-CRT with two to four customized tangential fields after mastectomy (10% of patients) or quadrantectomy (90%). The whole breast (or chest wall) received 50 Gy/25 fractions in 66 patients and 45 Gy/18 fractions in 34 patients. Boost to surgical bed (10 Gy/4-5 fractions) was delivered by photons in 10 patients. Median number of tangential fields was two (range, two to four). Patients were treated while supine on a breast board, without immobilization devices or instructions to hold their breath. They were freely breathing but were asked to minimize respiratory motion during the CT scan used to plan radiation delivery and the treatment itself. No dose constraints were specified for heart structures; a mean heart dose lower than 5 Gy was recommended at the time of treatment.
A preliminary assessment of radiation delivered to the left anterior descending coronary arteries in this series suggests that they received 9-25 Gy, Dr. Lonardi reported.
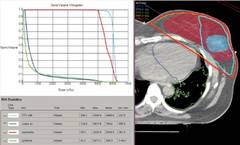
Based on estimates using previous models, the probability of death from cardiac causes within 15 years after standard fractionated radiotherapy may be less than 1% if less than 10% of the heart is exposed to 25Gy or more, he noted. "In this perspective, our results appear very favorable, though they confirm that the heart may receive high doses to limited volumes despite the use of standard 3D techniques. In such cases, high-conformal, intensity-modulated techniques are helpful" to further reduce the exposure of critical heart structures to radiation.
The symposium was cosponsored by the American Society of Breast Disease, the American Society of Breast Surgeons, the National Consortium of Breast Centers, the Society of Surgical Oncology, and the American Society for Radiation Oncology.
Dr. Lonardi reported having no financial disclosures.
On Twitter @sherryboschert
This was an interesting study. I really give the authors a lot of credit. They basically looked at 100 consecutive cases of patients treated with adjuvant radiotherapy for left-sided breast cancer and brought forward what they were doing without trying to optimize or minimize the presentation or cardiac dose in the patients they were treating.

|
| Dr. Julia White |
Their mean doses were lower than those reported by Darby et al. in a study that looked at 2,168 patients treated during 1958-2001 in both Sweden and Denmark. The researchers reviewed individual radiotherapy charts, and then did 20 consecutive individual CT-based three-dimensional planning scans to model what the type of radiotherapy looked like many years ago (N. Engl. J. Med. 2013;368:987-98).
This was an interesting study. I really give the authors a lot of credit. They basically looked at 100 consecutive cases of patients treated with adjuvant radiotherapy for left-sided breast cancer and brought forward what they were doing without trying to optimize or minimize the presentation or cardiac dose in the patients they were treating.
|
|
| Dr. Julia White |
Their mean doses were lower than those reported by Darby et al. in a study that looked at 2,168 patients treated during 1958-2001 in both Sweden and Denmark. The researchers reviewed individual radiotherapy charts, and then did 20 consecutive individual CT-based three-dimensional planning scans to model what the type of radiotherapy looked like many years ago (N. Engl. J. Med. 2013;368:987-98).
This was an interesting study. I really give the authors a lot of credit. They basically looked at 100 consecutive cases of patients treated with adjuvant radiotherapy for left-sided breast cancer and brought forward what they were doing without trying to optimize or minimize the presentation or cardiac dose in the patients they were treating.
|
|
| Dr. Julia White |
Their mean doses were lower than those reported by Darby et al. in a study that looked at 2,168 patients treated during 1958-2001 in both Sweden and Denmark. The researchers reviewed individual radiotherapy charts, and then did 20 consecutive individual CT-based three-dimensional planning scans to model what the type of radiotherapy looked like many years ago (N. Engl. J. Med. 2013;368:987-98).
SAN FRANCISCO – The hearts of 100 consecutive patients who underwent adjuvant radiotherapy for left-sided breast cancer in 2011 received an average of 2.9 Gray of radiation, considerably less than the mean cardiac exposure of 4.9-Gy reported in a recent review of 2,168 patients treated from 1958 to 2001 in Sweden and Denmark.
The findings confirm that three-dimensional conformal radiation therapy (3D-CRT) reduces cardiac exposure to radiation, Dr. Federico Lonardi and his associates reported at a breast cancer symposium sponsored by the American Society of Clinical Oncology. But certain areas of the heart still receive high doses when patients have adverse anatomic conditions that are not well suited to 3D-CRT. Because heart structures may differ in radiosensitivity, higher doses to small volumes of the heart, such as the coronary artery, might be associated with more risk, the researchers cautioned.
Most patients received a mean cardiac dose of 2-3 Gy (32%), 21% of patients were exposed to 1.15-1.99 Gy, and 1% got 0.8 Gy in a study of a consecutive series of breast cancer patients treated at Mater Salutis Hospital in Legnago, Italy. Only 17% of patients received a mean cardiac dose of more than 5 Gy, and 13% received 4.16-4.83 Gy.
The cardiac dose ranged from 0.8 to 13.05 Gy in Dr. Lonardi’s study, compared with a range of 0.03 to 27.72 Gy in the recently published Scandinavian study (N. Engl. J. Med. 2013;368:987-998). In the published study, the longitudinal risk for major cardiac events increased in a linear fashion, with a 7% increase for cardiac events with every 1 Gy increase in radiation to the heart.
In the Italian study, the median volumes of heart exposed to higher doses of radiation were "consistently low" with 4% of heart volumes exposed to 5 Gy or more, 3% exposed to 10Gy or more, 2% exposed to 15 Gy or more, and 0.7% exposed to 25 Gy or more Dr. Lonardi reported.
These patients received full-breast 3D-CRT with two to four customized tangential fields after mastectomy (10% of patients) or quadrantectomy (90%). The whole breast (or chest wall) received 50 Gy/25 fractions in 66 patients and 45 Gy/18 fractions in 34 patients. Boost to surgical bed (10 Gy/4-5 fractions) was delivered by photons in 10 patients. Median number of tangential fields was two (range, two to four). Patients were treated while supine on a breast board, without immobilization devices or instructions to hold their breath. They were freely breathing but were asked to minimize respiratory motion during the CT scan used to plan radiation delivery and the treatment itself. No dose constraints were specified for heart structures; a mean heart dose lower than 5 Gy was recommended at the time of treatment.
A preliminary assessment of radiation delivered to the left anterior descending coronary arteries in this series suggests that they received 9-25 Gy, Dr. Lonardi reported.
Based on estimates using previous models, the probability of death from cardiac causes within 15 years after standard fractionated radiotherapy may be less than 1% if less than 10% of the heart is exposed to 25Gy or more, he noted. "In this perspective, our results appear very favorable, though they confirm that the heart may receive high doses to limited volumes despite the use of standard 3D techniques. In such cases, high-conformal, intensity-modulated techniques are helpful" to further reduce the exposure of critical heart structures to radiation.
The symposium was cosponsored by the American Society of Breast Disease, the American Society of Breast Surgeons, the National Consortium of Breast Centers, the Society of Surgical Oncology, and the American Society for Radiation Oncology.
Dr. Lonardi reported having no financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – The hearts of 100 consecutive patients who underwent adjuvant radiotherapy for left-sided breast cancer in 2011 received an average of 2.9 Gray of radiation, considerably less than the mean cardiac exposure of 4.9-Gy reported in a recent review of 2,168 patients treated from 1958 to 2001 in Sweden and Denmark.
The findings confirm that three-dimensional conformal radiation therapy (3D-CRT) reduces cardiac exposure to radiation, Dr. Federico Lonardi and his associates reported at a breast cancer symposium sponsored by the American Society of Clinical Oncology. But certain areas of the heart still receive high doses when patients have adverse anatomic conditions that are not well suited to 3D-CRT. Because heart structures may differ in radiosensitivity, higher doses to small volumes of the heart, such as the coronary artery, might be associated with more risk, the researchers cautioned.
Most patients received a mean cardiac dose of 2-3 Gy (32%), 21% of patients were exposed to 1.15-1.99 Gy, and 1% got 0.8 Gy in a study of a consecutive series of breast cancer patients treated at Mater Salutis Hospital in Legnago, Italy. Only 17% of patients received a mean cardiac dose of more than 5 Gy, and 13% received 4.16-4.83 Gy.
The cardiac dose ranged from 0.8 to 13.05 Gy in Dr. Lonardi’s study, compared with a range of 0.03 to 27.72 Gy in the recently published Scandinavian study (N. Engl. J. Med. 2013;368:987-998). In the published study, the longitudinal risk for major cardiac events increased in a linear fashion, with a 7% increase for cardiac events with every 1 Gy increase in radiation to the heart.
In the Italian study, the median volumes of heart exposed to higher doses of radiation were "consistently low" with 4% of heart volumes exposed to 5 Gy or more, 3% exposed to 10Gy or more, 2% exposed to 15 Gy or more, and 0.7% exposed to 25 Gy or more Dr. Lonardi reported.
These patients received full-breast 3D-CRT with two to four customized tangential fields after mastectomy (10% of patients) or quadrantectomy (90%). The whole breast (or chest wall) received 50 Gy/25 fractions in 66 patients and 45 Gy/18 fractions in 34 patients. Boost to surgical bed (10 Gy/4-5 fractions) was delivered by photons in 10 patients. Median number of tangential fields was two (range, two to four). Patients were treated while supine on a breast board, without immobilization devices or instructions to hold their breath. They were freely breathing but were asked to minimize respiratory motion during the CT scan used to plan radiation delivery and the treatment itself. No dose constraints were specified for heart structures; a mean heart dose lower than 5 Gy was recommended at the time of treatment.
A preliminary assessment of radiation delivered to the left anterior descending coronary arteries in this series suggests that they received 9-25 Gy, Dr. Lonardi reported.
Based on estimates using previous models, the probability of death from cardiac causes within 15 years after standard fractionated radiotherapy may be less than 1% if less than 10% of the heart is exposed to 25Gy or more, he noted. "In this perspective, our results appear very favorable, though they confirm that the heart may receive high doses to limited volumes despite the use of standard 3D techniques. In such cases, high-conformal, intensity-modulated techniques are helpful" to further reduce the exposure of critical heart structures to radiation.
The symposium was cosponsored by the American Society of Breast Disease, the American Society of Breast Surgeons, the National Consortium of Breast Centers, the Society of Surgical Oncology, and the American Society for Radiation Oncology.
Dr. Lonardi reported having no financial disclosures.
On Twitter @sherryboschert
AT THE ASCO BREAST CANCER SYMPOSIUM
Major finding: In an Italian study, the median volumes of heart exposed to higher doses of radiation were "consistently low" with 4% of heart volumes exposed to 5 Gy or more, 3% exposed to 10Gy or more, 2% exposed to 15 Gy or more, and 0.7% exposed to 25 Gy or more.
Data source: Retrospective review of 100 consecutive patients treated with radiotherapy for left-sided breast cancer at one institution in 2011.
Disclosures: Dr. Lonardi reported having no financial disclosures.
Radiation of early breast cancer does not increase cardiac death risk
ATLANTA – A decade after treatment for early-stage breast cancer, women who underwent surgery and radiation had higher survival rates than women who had surgery alone, with no increase in radiation-related cardiac or secondary cancer deaths, investigators reported at the annual meeting of the American Society for Radiation Oncology.
An analysis of Surveillance, Epidemiology and End Results (SEER) data on women treated for stage TIA N0 breast cancer in their mid to late 50s showed that after a median follow-up of 14 years, 10-year overall survival among the 2,397 women who received lumpectomy or mastectomy and radiation was 91.6%, compared with 87% for 2,988 women who had lumpectomy or mastectomy only (P less than .001).
Ten-year cardiac cause–specific survival was 96.7% vs. 92.7% (P less than .001), respectively. Breast cancer–specific survival was also higher among women who had undergone radiation, at 97% vs. 95.7% (P = .01), reported Dr. Jason C. Ye, a resident in radiation oncology at Weill Cornell Medical College, New York.

The data also suggest that breast irradiation does not increase the risk of lung cancer death, which occurred in 6 patients (1.9%) who underwent lumpectomy and radiation, and in 48 (1.6%) of those who had lumpectomies only, a difference that was not significant.
Dr. Ye noted, however, that between-group differences may begin to show up with longer follow-up.
"Although 14 years is a long time, studies have found increases in cardiac mortality and secondary cancers at 20 and 30 years after radiation. Also, there might have been a selection bias by physicians treating at the time, based on patients’ comorbidities and the patient’s health status. This might explain why the overall survival and the cardiac cause–specific survival were different between the two groups, with the no-radiation arm doing worse," he said at a media briefing.
In addition, changes in techniques introduced since the 1990s, such as three-dimensional conformal radiation, prone irradiation, hypofractionation, and intensity-modulated radiation therapy, may have effects on cardiac-specific and overall survival rates in the future, Dr. Ye said.
Dr. Ye and his colleagues reviewed SEER records on 5,385 women treated for early breast cancer during 1990-1997, and stratified them according to treatment with external-beam radiation or no radiation.
They included only patients with stage TIA N0 breast cancer identified as their first malignancy.
The authors used cause-of-death codes to identify cardiac deaths (either from cardiac disease or from atherosclerosis, breast cancer mortality, and deaths from second cancers in the chest area).
Radiation was associated with significantly lower overall mortality (relative risk, 0.69; P less than .001), breast cancer mortality (RR, 0.75; P = .02), and cardiac mortality (RR, 0.53; P less than .001).
Women with tumors in the left breast, whose hearts would presumably receive a larger dose of radiation than women with right breast tumors, were not at increased risk for cardiac-specific death. Deaths from second cancers included lung cancer in 2%; lymphomas and leukemias, each in 0.4%; soft-tissue malignancies (including the heart) in 0.06%; and cancer of the esophagus in 0.04%.
There were no significant differences between the radiation and no-radiation groups in incidence of death from second cancers.
The study was supported by the National Cancer Institute. Dr. Ye reported having no relevant disclosures.

|
|
We’ve heard some reassuring news for our early breast cancer patients, that perhaps they will not have to endure cardiac mortality or death from other cancers because they received radiation to their breast, were thereby able to keep their breast, and were able to be cured without the need for mastectomy. I think that’s great news.
Dr. Beth Erickson is a professor of radiation oncology at the Medical College of Wisconsin in Milwaukee.
|
|
|
We’ve heard some reassuring news for our early breast cancer patients, that perhaps they will not have to endure cardiac mortality or death from other cancers because they received radiation to their breast, were thereby able to keep their breast, and were able to be cured without the need for mastectomy. I think that’s great news.
Dr. Beth Erickson is a professor of radiation oncology at the Medical College of Wisconsin in Milwaukee.
|
|
|
We’ve heard some reassuring news for our early breast cancer patients, that perhaps they will not have to endure cardiac mortality or death from other cancers because they received radiation to their breast, were thereby able to keep their breast, and were able to be cured without the need for mastectomy. I think that’s great news.
Dr. Beth Erickson is a professor of radiation oncology at the Medical College of Wisconsin in Milwaukee.
ATLANTA – A decade after treatment for early-stage breast cancer, women who underwent surgery and radiation had higher survival rates than women who had surgery alone, with no increase in radiation-related cardiac or secondary cancer deaths, investigators reported at the annual meeting of the American Society for Radiation Oncology.
An analysis of Surveillance, Epidemiology and End Results (SEER) data on women treated for stage TIA N0 breast cancer in their mid to late 50s showed that after a median follow-up of 14 years, 10-year overall survival among the 2,397 women who received lumpectomy or mastectomy and radiation was 91.6%, compared with 87% for 2,988 women who had lumpectomy or mastectomy only (P less than .001).
Ten-year cardiac cause–specific survival was 96.7% vs. 92.7% (P less than .001), respectively. Breast cancer–specific survival was also higher among women who had undergone radiation, at 97% vs. 95.7% (P = .01), reported Dr. Jason C. Ye, a resident in radiation oncology at Weill Cornell Medical College, New York.
The data also suggest that breast irradiation does not increase the risk of lung cancer death, which occurred in 6 patients (1.9%) who underwent lumpectomy and radiation, and in 48 (1.6%) of those who had lumpectomies only, a difference that was not significant.
Dr. Ye noted, however, that between-group differences may begin to show up with longer follow-up.
"Although 14 years is a long time, studies have found increases in cardiac mortality and secondary cancers at 20 and 30 years after radiation. Also, there might have been a selection bias by physicians treating at the time, based on patients’ comorbidities and the patient’s health status. This might explain why the overall survival and the cardiac cause–specific survival were different between the two groups, with the no-radiation arm doing worse," he said at a media briefing.
In addition, changes in techniques introduced since the 1990s, such as three-dimensional conformal radiation, prone irradiation, hypofractionation, and intensity-modulated radiation therapy, may have effects on cardiac-specific and overall survival rates in the future, Dr. Ye said.
Dr. Ye and his colleagues reviewed SEER records on 5,385 women treated for early breast cancer during 1990-1997, and stratified them according to treatment with external-beam radiation or no radiation.
They included only patients with stage TIA N0 breast cancer identified as their first malignancy.
The authors used cause-of-death codes to identify cardiac deaths (either from cardiac disease or from atherosclerosis, breast cancer mortality, and deaths from second cancers in the chest area).
Radiation was associated with significantly lower overall mortality (relative risk, 0.69; P less than .001), breast cancer mortality (RR, 0.75; P = .02), and cardiac mortality (RR, 0.53; P less than .001).
Women with tumors in the left breast, whose hearts would presumably receive a larger dose of radiation than women with right breast tumors, were not at increased risk for cardiac-specific death. Deaths from second cancers included lung cancer in 2%; lymphomas and leukemias, each in 0.4%; soft-tissue malignancies (including the heart) in 0.06%; and cancer of the esophagus in 0.04%.
There were no significant differences between the radiation and no-radiation groups in incidence of death from second cancers.
The study was supported by the National Cancer Institute. Dr. Ye reported having no relevant disclosures.
ATLANTA – A decade after treatment for early-stage breast cancer, women who underwent surgery and radiation had higher survival rates than women who had surgery alone, with no increase in radiation-related cardiac or secondary cancer deaths, investigators reported at the annual meeting of the American Society for Radiation Oncology.
An analysis of Surveillance, Epidemiology and End Results (SEER) data on women treated for stage TIA N0 breast cancer in their mid to late 50s showed that after a median follow-up of 14 years, 10-year overall survival among the 2,397 women who received lumpectomy or mastectomy and radiation was 91.6%, compared with 87% for 2,988 women who had lumpectomy or mastectomy only (P less than .001).
Ten-year cardiac cause–specific survival was 96.7% vs. 92.7% (P less than .001), respectively. Breast cancer–specific survival was also higher among women who had undergone radiation, at 97% vs. 95.7% (P = .01), reported Dr. Jason C. Ye, a resident in radiation oncology at Weill Cornell Medical College, New York.
The data also suggest that breast irradiation does not increase the risk of lung cancer death, which occurred in 6 patients (1.9%) who underwent lumpectomy and radiation, and in 48 (1.6%) of those who had lumpectomies only, a difference that was not significant.
Dr. Ye noted, however, that between-group differences may begin to show up with longer follow-up.
"Although 14 years is a long time, studies have found increases in cardiac mortality and secondary cancers at 20 and 30 years after radiation. Also, there might have been a selection bias by physicians treating at the time, based on patients’ comorbidities and the patient’s health status. This might explain why the overall survival and the cardiac cause–specific survival were different between the two groups, with the no-radiation arm doing worse," he said at a media briefing.
In addition, changes in techniques introduced since the 1990s, such as three-dimensional conformal radiation, prone irradiation, hypofractionation, and intensity-modulated radiation therapy, may have effects on cardiac-specific and overall survival rates in the future, Dr. Ye said.
Dr. Ye and his colleagues reviewed SEER records on 5,385 women treated for early breast cancer during 1990-1997, and stratified them according to treatment with external-beam radiation or no radiation.
They included only patients with stage TIA N0 breast cancer identified as their first malignancy.
The authors used cause-of-death codes to identify cardiac deaths (either from cardiac disease or from atherosclerosis, breast cancer mortality, and deaths from second cancers in the chest area).
Radiation was associated with significantly lower overall mortality (relative risk, 0.69; P less than .001), breast cancer mortality (RR, 0.75; P = .02), and cardiac mortality (RR, 0.53; P less than .001).
Women with tumors in the left breast, whose hearts would presumably receive a larger dose of radiation than women with right breast tumors, were not at increased risk for cardiac-specific death. Deaths from second cancers included lung cancer in 2%; lymphomas and leukemias, each in 0.4%; soft-tissue malignancies (including the heart) in 0.06%; and cancer of the esophagus in 0.04%.
There were no significant differences between the radiation and no-radiation groups in incidence of death from second cancers.
The study was supported by the National Cancer Institute. Dr. Ye reported having no relevant disclosures.
AT THE ASTRO ANNUAL MEETING
Major finding: Ten-year cardiac cause–specific survival was 96.7% for women who had surgery and radiation, compared with 92.7% for women who had surgery alone (P less than .001).
Data source: Retrospective study of SEER data on 5,385 women treated for early breast cancer from 1990 through 1997.
Disclosures: The study was supported by the National Cancer Institute. Dr. Ye and Dr. Erickson reported having no relevant disclosures.

PIK3CA breast cancer mutations blunt dual HER2 blockade
AMSTERDAM – PIK3CA mutations were associated with lower pathologic complete responses in women with human epidermal growth factor receptor 2 breast cancer treated with neoadjuvant anti-HER2 therapy in the phase III NeoALTTO trial.
"The lower pCR rate in PIK3CA-mutant tumors is observed in all treatment arms, irrespective of estrogen receptor status," Dr. José Baselga said at the European multidisciplinary European cancer congresses.

Earlier results from NeoALTTO (Neoadjuvant Lapatinib and/or Trastuzumab Treatment Optimization) showed that dual HER2 blockade with trastuzumab (Herceptin) and lapatinib (Tykerb) nearly doubled the pCR rate compared with single-agent trastuzumab or lapatinib (51.3% vs. 29.5% vs. 24.7%; P = .0001).
For the analysis, the investigators performed mutational analyses on tumor samples from 355 (78%) of the 455 study participants. Of these, 23% had a PIK3CA mutation, which is highly consistent with other published analyses, said Dr. Baselga, physician-in-chief at Memorial Sloan-Kettering Cancer Center, in New York City.
No BRAF mutations were found, and one patient had a KRAS mutation.
Overall, pCRs occurred in 21% of PIK3CA mutant tumors and 34% of PIK3CA wildtype tumors (P = .03), he said.
The pCR rate was 28.6% in women with a PIK3CA mutation and 55.8% in those without it in the combination trastuzumab/lapatinib arm, 14.8% vs. 20.4% in the lapatinib arm, and 20% vs. 28.4% in the trastuzumab arm. The difference was statistically significant only for the combination arm (P = .012), but Dr. Baselga urged caution in interpreting this because of the small patient numbers.
PIK3CA mutations were also associated with lower pCR rates in both estrogen receptor (ER)–positive (5% vs. 31%) and ER-negative (11% vs. 61%) patients.
In all, PIK3CA mutations were found in 23% of 124 women in the lapatinib arm, 19% of 112 in the trastuzumab arm, 25% of 119 in the combination arm, 23% of 169 ER-positive patients, and 22% of 186 ER-negative patients.
In a logistic regression model that adjusted for treatment arm and ER status, a significant difference was observed in pCR between PIK3CA mutant and wildtype tumors (odds ratio, 0.45; P = .015), by treatment arm (lapatinib vs. trastuzumab: OR, 0.67; P less than .0001 and combination vs. trastuzumab: OR, 2.97; P less than .0001), and by ER status (negative vs. positive: OR, 2.44; P = .0005).
The findings are concordant with two metastatic breast cancer studies, Dr. Baselga said. In the CLEOPATRA trial, women with PIK3CA-mutant tumors had less benefit from first-line trastuzumab with or without pertuzumab (Perjeta), as did those treated with lapatinib plus capecitabine (Xeloda) in the EMILIA trial.
In the FinHER trial, however, PIK3CA mutations were not predictive of resistance to trastuzumab, he said.
"These findings will lead us to analyze carefully PIK3CA mutation status in adjuvant HER2-positive studies. In this setting, PIK3CA status might be both prognostic and predictive," Dr. Baselga concluded.
Invited discussant Prof. Sibylle Loibl, leader of the medicine and research department, University of Frankfurt (Germany)and member of the German Breast Group, observed that ER-positive PIK3CA-mutant tumors achieved the lowest pCR rate of any group in the current analysis and in the NeoSphere trial of pertuzumab/trastuzumab in treatment-naive HER2-positive breast cancer. "This suggests an interaction of the different pathways and a need to better select the HER2-positive patients," she said.
GlaxoSmithKline sponsored the trial. Dr. Baselga reported no relevant financial disclosures.
AMSTERDAM – PIK3CA mutations were associated with lower pathologic complete responses in women with human epidermal growth factor receptor 2 breast cancer treated with neoadjuvant anti-HER2 therapy in the phase III NeoALTTO trial.
"The lower pCR rate in PIK3CA-mutant tumors is observed in all treatment arms, irrespective of estrogen receptor status," Dr. José Baselga said at the European multidisciplinary European cancer congresses.
Earlier results from NeoALTTO (Neoadjuvant Lapatinib and/or Trastuzumab Treatment Optimization) showed that dual HER2 blockade with trastuzumab (Herceptin) and lapatinib (Tykerb) nearly doubled the pCR rate compared with single-agent trastuzumab or lapatinib (51.3% vs. 29.5% vs. 24.7%; P = .0001).
For the analysis, the investigators performed mutational analyses on tumor samples from 355 (78%) of the 455 study participants. Of these, 23% had a PIK3CA mutation, which is highly consistent with other published analyses, said Dr. Baselga, physician-in-chief at Memorial Sloan-Kettering Cancer Center, in New York City.
No BRAF mutations were found, and one patient had a KRAS mutation.
Overall, pCRs occurred in 21% of PIK3CA mutant tumors and 34% of PIK3CA wildtype tumors (P = .03), he said.
The pCR rate was 28.6% in women with a PIK3CA mutation and 55.8% in those without it in the combination trastuzumab/lapatinib arm, 14.8% vs. 20.4% in the lapatinib arm, and 20% vs. 28.4% in the trastuzumab arm. The difference was statistically significant only for the combination arm (P = .012), but Dr. Baselga urged caution in interpreting this because of the small patient numbers.
PIK3CA mutations were also associated with lower pCR rates in both estrogen receptor (ER)–positive (5% vs. 31%) and ER-negative (11% vs. 61%) patients.
In all, PIK3CA mutations were found in 23% of 124 women in the lapatinib arm, 19% of 112 in the trastuzumab arm, 25% of 119 in the combination arm, 23% of 169 ER-positive patients, and 22% of 186 ER-negative patients.
In a logistic regression model that adjusted for treatment arm and ER status, a significant difference was observed in pCR between PIK3CA mutant and wildtype tumors (odds ratio, 0.45; P = .015), by treatment arm (lapatinib vs. trastuzumab: OR, 0.67; P less than .0001 and combination vs. trastuzumab: OR, 2.97; P less than .0001), and by ER status (negative vs. positive: OR, 2.44; P = .0005).
The findings are concordant with two metastatic breast cancer studies, Dr. Baselga said. In the CLEOPATRA trial, women with PIK3CA-mutant tumors had less benefit from first-line trastuzumab with or without pertuzumab (Perjeta), as did those treated with lapatinib plus capecitabine (Xeloda) in the EMILIA trial.
In the FinHER trial, however, PIK3CA mutations were not predictive of resistance to trastuzumab, he said.
"These findings will lead us to analyze carefully PIK3CA mutation status in adjuvant HER2-positive studies. In this setting, PIK3CA status might be both prognostic and predictive," Dr. Baselga concluded.
Invited discussant Prof. Sibylle Loibl, leader of the medicine and research department, University of Frankfurt (Germany)and member of the German Breast Group, observed that ER-positive PIK3CA-mutant tumors achieved the lowest pCR rate of any group in the current analysis and in the NeoSphere trial of pertuzumab/trastuzumab in treatment-naive HER2-positive breast cancer. "This suggests an interaction of the different pathways and a need to better select the HER2-positive patients," she said.
GlaxoSmithKline sponsored the trial. Dr. Baselga reported no relevant financial disclosures.
AMSTERDAM – PIK3CA mutations were associated with lower pathologic complete responses in women with human epidermal growth factor receptor 2 breast cancer treated with neoadjuvant anti-HER2 therapy in the phase III NeoALTTO trial.
"The lower pCR rate in PIK3CA-mutant tumors is observed in all treatment arms, irrespective of estrogen receptor status," Dr. José Baselga said at the European multidisciplinary European cancer congresses.
Earlier results from NeoALTTO (Neoadjuvant Lapatinib and/or Trastuzumab Treatment Optimization) showed that dual HER2 blockade with trastuzumab (Herceptin) and lapatinib (Tykerb) nearly doubled the pCR rate compared with single-agent trastuzumab or lapatinib (51.3% vs. 29.5% vs. 24.7%; P = .0001).
For the analysis, the investigators performed mutational analyses on tumor samples from 355 (78%) of the 455 study participants. Of these, 23% had a PIK3CA mutation, which is highly consistent with other published analyses, said Dr. Baselga, physician-in-chief at Memorial Sloan-Kettering Cancer Center, in New York City.
No BRAF mutations were found, and one patient had a KRAS mutation.
Overall, pCRs occurred in 21% of PIK3CA mutant tumors and 34% of PIK3CA wildtype tumors (P = .03), he said.
The pCR rate was 28.6% in women with a PIK3CA mutation and 55.8% in those without it in the combination trastuzumab/lapatinib arm, 14.8% vs. 20.4% in the lapatinib arm, and 20% vs. 28.4% in the trastuzumab arm. The difference was statistically significant only for the combination arm (P = .012), but Dr. Baselga urged caution in interpreting this because of the small patient numbers.
PIK3CA mutations were also associated with lower pCR rates in both estrogen receptor (ER)–positive (5% vs. 31%) and ER-negative (11% vs. 61%) patients.
In all, PIK3CA mutations were found in 23% of 124 women in the lapatinib arm, 19% of 112 in the trastuzumab arm, 25% of 119 in the combination arm, 23% of 169 ER-positive patients, and 22% of 186 ER-negative patients.
In a logistic regression model that adjusted for treatment arm and ER status, a significant difference was observed in pCR between PIK3CA mutant and wildtype tumors (odds ratio, 0.45; P = .015), by treatment arm (lapatinib vs. trastuzumab: OR, 0.67; P less than .0001 and combination vs. trastuzumab: OR, 2.97; P less than .0001), and by ER status (negative vs. positive: OR, 2.44; P = .0005).
The findings are concordant with two metastatic breast cancer studies, Dr. Baselga said. In the CLEOPATRA trial, women with PIK3CA-mutant tumors had less benefit from first-line trastuzumab with or without pertuzumab (Perjeta), as did those treated with lapatinib plus capecitabine (Xeloda) in the EMILIA trial.
In the FinHER trial, however, PIK3CA mutations were not predictive of resistance to trastuzumab, he said.
"These findings will lead us to analyze carefully PIK3CA mutation status in adjuvant HER2-positive studies. In this setting, PIK3CA status might be both prognostic and predictive," Dr. Baselga concluded.
Invited discussant Prof. Sibylle Loibl, leader of the medicine and research department, University of Frankfurt (Germany)and member of the German Breast Group, observed that ER-positive PIK3CA-mutant tumors achieved the lowest pCR rate of any group in the current analysis and in the NeoSphere trial of pertuzumab/trastuzumab in treatment-naive HER2-positive breast cancer. "This suggests an interaction of the different pathways and a need to better select the HER2-positive patients," she said.
GlaxoSmithKline sponsored the trial. Dr. Baselga reported no relevant financial disclosures.
AT THE EUROPEAN CANCER CONGRESS 2013
Major finding: In women treated with trastuzumab plus lapatinib, the pathologic complete response rate was 28.6% with a PIK3CA mutation and 55.8% without (P = .012).
Data source: Molecular profiling of 355 women with HER2-positive breast cancer in the NEOALTTO trial.
Disclosures: GlaxoSmithKline sponsored the trial. Dr. Baselga reported no relevant financial disclosures.

Single-drug chemo for breast cancer makes ASCO’s Choosing Wisely list
A recommendation to consider the use of single-drug chemotherapy in most women with metastatic breast cancer is one of five newly recommended changes issued in the second round of the Choosing Wisely campaign.
The recommendations advise reconsidering tests and treatments that are often seen as routine, yet add costs without necessarily benefitting patients.
The action items are meant as a guide, not a demand, Dr. Lowell Schnipper said during a press briefing announcing the recommendations in advance of their release at a symposium on quality care sponsored by the American Society of Clinical Oncology.
"This is an attempt to encourage physicians and patients to curb the use of certain tests and procedures that are not supported by clinical research," said Dr. Schnipper, clinical director of Beth Israel Deaconess Medical Center Cancer Center in New York. "They are not meant to be legislative dictums. They are evidence-based suggestions presented as a foundation for discussion between doctor and patient – but there may be individual circumstances when they may decide to do otherwise."
The goal of the Choosing Wisely campaign – led by the American Board of Internal Medicine Foundation and joined by much of organized medicine – is to promote conversations that help patients and physicians choose care that is evidence driven, does not replicate care already provided, is free from harm, and is truly necessary.
ASCO’s second list of recommendations as part of the Choosing Wisely campaign includes the following:
• Restrict the use of antiemetic drugs to patients who are on chemotherapy regimens with a high risk of inducing nausea.
"One of the most important and unpleasant side effects of cancer drugs is nausea and vomiting," Dr. Schnipper said. "Over the years there has been an enormous degree of progress in medications to reduce and sometimes completely negate this."
But some of these drugs are "phenomenally expensive," he said. They should be saved for use in regimens that have a high potential to produce severe or persistent nausea and vomiting.
• Consider the use of single-drug chemotherapy in metastatic breast cancer.
"How much treatment is the optimal amount for metastatic breast cancer?" Dr. Schnipper said. "The concept is that more is better, but if we look at the outcomes for the majority of women, multiple drugs don’t add to survival and sometimes, because of the toxicities, actually detract from quality of life."
ASCO suggests that single drugs be used consecutively – a regimen that that may improve quality of life, even if it does not extend life. Multiple-drug regimens "should only be used in exceptional circumstances when a very rapid response to severe symptoms or life-threatening complications is at hand," according to the recommendation. "In a patient with advanced breast cancer who is not heavily pretreated and in whom symptomatic visceral crisis is apparent and rapid tumor response necessary, short courses of multiple agent
chemotherapy may be useful. However, as a general rule,
administration of sequential single agents lowers the risk of adverse
effects, may improve a patient’s quality of life, and does not typically
compromise overall survival.
• Avoid PET or PET-CT scans as part of routine follow-up care to monitor for recurrence in asymptomatic patients.
For patients who have completed treatment and show no clinical signs of relapse or new disease, routine imaging may not be necessary, Dr. Schnipper said.
"When we look too hard we almost always find some abnormality that, because of the patient’s medical history, we feel compelled to pursue. We don’t believe there’s any evidence showing that routine surveillance with CT or PET imaging provides anything that helps us keep patients alive longer. We think we can care for patients better with fewer risks, avoiding the cost of expensive imaging, and not compromising the cancer care they have received."
The report noted that "the utility of PET or PET-CT scanning for surveillance of both solid tumors and lymphomas remains unproven. In addition to clinical and economic considerations, the specter of unnecessary interventions and associated morbidity is a concern in the routine use of this technology for post-treatment surveillance."
• Avoid PSA testing in men who have a life expectancy of 10 years or less.
Again, the issue is whether any benefit of treatment would be worth the risk. "It’s not uncommon for these men to have comorbid illnesses that are more threatening than a low-grade prostate cancer. Most studies don’t show that treating affects mortality at all," although it can confer problems that really detract from quality of life.
Reserve targeted therapies intended for use against tumors with a specific genetic blueprint unless the patient’s tumor cells are expected to respond.
"These drugs are incredibly expensive," and there is no evidence that they are helpful in any but the rare cancers with specific biomarkers, Dr. Schnipper said.
"We can use biomarkers to identify patients who might have a good response – and also to identify patients who are not appropriate for these drugs," he said. "This is a good example of doing less while still maintaining a high quality of care."
Dr. Schnipper had no financial disclosures.
A recommendation to consider the use of single-drug chemotherapy in most women with metastatic breast cancer is one of five newly recommended changes issued in the second round of the Choosing Wisely campaign.
The recommendations advise reconsidering tests and treatments that are often seen as routine, yet add costs without necessarily benefitting patients.
The action items are meant as a guide, not a demand, Dr. Lowell Schnipper said during a press briefing announcing the recommendations in advance of their release at a symposium on quality care sponsored by the American Society of Clinical Oncology.
"This is an attempt to encourage physicians and patients to curb the use of certain tests and procedures that are not supported by clinical research," said Dr. Schnipper, clinical director of Beth Israel Deaconess Medical Center Cancer Center in New York. "They are not meant to be legislative dictums. They are evidence-based suggestions presented as a foundation for discussion between doctor and patient – but there may be individual circumstances when they may decide to do otherwise."
The goal of the Choosing Wisely campaign – led by the American Board of Internal Medicine Foundation and joined by much of organized medicine – is to promote conversations that help patients and physicians choose care that is evidence driven, does not replicate care already provided, is free from harm, and is truly necessary.
ASCO’s second list of recommendations as part of the Choosing Wisely campaign includes the following:
• Restrict the use of antiemetic drugs to patients who are on chemotherapy regimens with a high risk of inducing nausea.
"One of the most important and unpleasant side effects of cancer drugs is nausea and vomiting," Dr. Schnipper said. "Over the years there has been an enormous degree of progress in medications to reduce and sometimes completely negate this."
But some of these drugs are "phenomenally expensive," he said. They should be saved for use in regimens that have a high potential to produce severe or persistent nausea and vomiting.
• Consider the use of single-drug chemotherapy in metastatic breast cancer.
"How much treatment is the optimal amount for metastatic breast cancer?" Dr. Schnipper said. "The concept is that more is better, but if we look at the outcomes for the majority of women, multiple drugs don’t add to survival and sometimes, because of the toxicities, actually detract from quality of life."
ASCO suggests that single drugs be used consecutively – a regimen that that may improve quality of life, even if it does not extend life. Multiple-drug regimens "should only be used in exceptional circumstances when a very rapid response to severe symptoms or life-threatening complications is at hand," according to the recommendation. "In a patient with advanced breast cancer who is not heavily pretreated and in whom symptomatic visceral crisis is apparent and rapid tumor response necessary, short courses of multiple agent
chemotherapy may be useful. However, as a general rule,
administration of sequential single agents lowers the risk of adverse
effects, may improve a patient’s quality of life, and does not typically
compromise overall survival.
• Avoid PET or PET-CT scans as part of routine follow-up care to monitor for recurrence in asymptomatic patients.
For patients who have completed treatment and show no clinical signs of relapse or new disease, routine imaging may not be necessary, Dr. Schnipper said.
"When we look too hard we almost always find some abnormality that, because of the patient’s medical history, we feel compelled to pursue. We don’t believe there’s any evidence showing that routine surveillance with CT or PET imaging provides anything that helps us keep patients alive longer. We think we can care for patients better with fewer risks, avoiding the cost of expensive imaging, and not compromising the cancer care they have received."
The report noted that "the utility of PET or PET-CT scanning for surveillance of both solid tumors and lymphomas remains unproven. In addition to clinical and economic considerations, the specter of unnecessary interventions and associated morbidity is a concern in the routine use of this technology for post-treatment surveillance."
• Avoid PSA testing in men who have a life expectancy of 10 years or less.
Again, the issue is whether any benefit of treatment would be worth the risk. "It’s not uncommon for these men to have comorbid illnesses that are more threatening than a low-grade prostate cancer. Most studies don’t show that treating affects mortality at all," although it can confer problems that really detract from quality of life.
Reserve targeted therapies intended for use against tumors with a specific genetic blueprint unless the patient’s tumor cells are expected to respond.
"These drugs are incredibly expensive," and there is no evidence that they are helpful in any but the rare cancers with specific biomarkers, Dr. Schnipper said.
"We can use biomarkers to identify patients who might have a good response – and also to identify patients who are not appropriate for these drugs," he said. "This is a good example of doing less while still maintaining a high quality of care."
Dr. Schnipper had no financial disclosures.
A recommendation to consider the use of single-drug chemotherapy in most women with metastatic breast cancer is one of five newly recommended changes issued in the second round of the Choosing Wisely campaign.
The recommendations advise reconsidering tests and treatments that are often seen as routine, yet add costs without necessarily benefitting patients.
The action items are meant as a guide, not a demand, Dr. Lowell Schnipper said during a press briefing announcing the recommendations in advance of their release at a symposium on quality care sponsored by the American Society of Clinical Oncology.
"This is an attempt to encourage physicians and patients to curb the use of certain tests and procedures that are not supported by clinical research," said Dr. Schnipper, clinical director of Beth Israel Deaconess Medical Center Cancer Center in New York. "They are not meant to be legislative dictums. They are evidence-based suggestions presented as a foundation for discussion between doctor and patient – but there may be individual circumstances when they may decide to do otherwise."
The goal of the Choosing Wisely campaign – led by the American Board of Internal Medicine Foundation and joined by much of organized medicine – is to promote conversations that help patients and physicians choose care that is evidence driven, does not replicate care already provided, is free from harm, and is truly necessary.
ASCO’s second list of recommendations as part of the Choosing Wisely campaign includes the following:
• Restrict the use of antiemetic drugs to patients who are on chemotherapy regimens with a high risk of inducing nausea.
"One of the most important and unpleasant side effects of cancer drugs is nausea and vomiting," Dr. Schnipper said. "Over the years there has been an enormous degree of progress in medications to reduce and sometimes completely negate this."
But some of these drugs are "phenomenally expensive," he said. They should be saved for use in regimens that have a high potential to produce severe or persistent nausea and vomiting.
• Consider the use of single-drug chemotherapy in metastatic breast cancer.
"How much treatment is the optimal amount for metastatic breast cancer?" Dr. Schnipper said. "The concept is that more is better, but if we look at the outcomes for the majority of women, multiple drugs don’t add to survival and sometimes, because of the toxicities, actually detract from quality of life."
ASCO suggests that single drugs be used consecutively – a regimen that that may improve quality of life, even if it does not extend life. Multiple-drug regimens "should only be used in exceptional circumstances when a very rapid response to severe symptoms or life-threatening complications is at hand," according to the recommendation. "In a patient with advanced breast cancer who is not heavily pretreated and in whom symptomatic visceral crisis is apparent and rapid tumor response necessary, short courses of multiple agent
chemotherapy may be useful. However, as a general rule,
administration of sequential single agents lowers the risk of adverse
effects, may improve a patient’s quality of life, and does not typically
compromise overall survival.
• Avoid PET or PET-CT scans as part of routine follow-up care to monitor for recurrence in asymptomatic patients.
For patients who have completed treatment and show no clinical signs of relapse or new disease, routine imaging may not be necessary, Dr. Schnipper said.
"When we look too hard we almost always find some abnormality that, because of the patient’s medical history, we feel compelled to pursue. We don’t believe there’s any evidence showing that routine surveillance with CT or PET imaging provides anything that helps us keep patients alive longer. We think we can care for patients better with fewer risks, avoiding the cost of expensive imaging, and not compromising the cancer care they have received."
The report noted that "the utility of PET or PET-CT scanning for surveillance of both solid tumors and lymphomas remains unproven. In addition to clinical and economic considerations, the specter of unnecessary interventions and associated morbidity is a concern in the routine use of this technology for post-treatment surveillance."
• Avoid PSA testing in men who have a life expectancy of 10 years or less.
Again, the issue is whether any benefit of treatment would be worth the risk. "It’s not uncommon for these men to have comorbid illnesses that are more threatening than a low-grade prostate cancer. Most studies don’t show that treating affects mortality at all," although it can confer problems that really detract from quality of life.
Reserve targeted therapies intended for use against tumors with a specific genetic blueprint unless the patient’s tumor cells are expected to respond.
"These drugs are incredibly expensive," and there is no evidence that they are helpful in any but the rare cancers with specific biomarkers, Dr. Schnipper said.
"We can use biomarkers to identify patients who might have a good response – and also to identify patients who are not appropriate for these drugs," he said. "This is a good example of doing less while still maintaining a high quality of care."
Dr. Schnipper had no financial disclosures.
FROM AN ASCO PRESS BRIEFING
Osteoporosis treatment and breast cancer prevention: Two goals, one treatment?
CASE: ACTIVE, HEALTHY, OSTEOPOROTIC, AND AT-RISK FOR BREAST CANCER
Your patient, a 58-year-old, G0 healthy and active woman underwent early menopause at 44 years. She recently had a bone mineral density test, results of which showed a T-score of –2.8 at the spine and –2.5 at the hip. She is taking vitamin D and calcium. She is an exceptionally active woman who plays tennis and walks more than 5 miles daily. Two years earlier, at age 56, she had abnormal mammography results, and a breast biopsy revealed atypical hyperplasia. Her mother has a history of Paget disease of the breast.
Prior to selecting a bone medicine to treat this woman’s osteoporosis, should you assess her risk of breast cancer?
In this editorial, I make the argument that, yes, you should assess this patient’s risk of breast cancer prior to selecting treatment for her osteoporosis, as her level of breast cancer risk can help determine the optimal osteoporosis therapy.
An expert panel convened by the American Society of Clinical Oncology noted that far too few American women are being assessed for their risk of breast cancer, and too few American women at increased risk for breast cancer are being offered pharmacologic preventive therapy.1 One small step to increase the frequency of risk assessment and counseling regarding preventive therapy is to assess breast cancer risk in women with osteoporosis to help guide the selection of a bone medicine.
Options for osteoporosis treatment
Most experts recommend that menopausal women with osteoporosis (T-score ≤–2.5) should be offered a bone medicine in addition to the standard prescription therapy of vitamin D and calcium, exercise, and smoking cessation.
The most commonly prescribed bone medicines are bisphosphonates, estrogen, and raloxifene. Following the publication of the Women’s Health Initiative (WHI) in 2002, the use of estrogen and raloxifene for the treatment of osteoporosis decreased significantly. Both the bisphosphonates and estrogen are believed to be slightly more effective at increasing bone density than raloxifene, but there are no direct head-to-head, large-scale fracture-reduction studies comparing these agents.2 In one large retrospective database study, women taking alendronate or raloxifene were reported to have similar vertebral and nonvertebral fracture rates.3
Unlike the bisphosphonates and estrogen, raloxifene has been demonstrated to reduce the risk of breast cancer by about 50%. For women with newly diagnosed osteoporosis and an above-average risk of developing breast cancer, raloxifene may represent an optimal pharmacologic intervention. But, how would you know if your patient with newly diagnosed osteoporosis is at increased risk for breast cancer?
Assessing breast cancer risk
The Gail breast cancer risk assessment tool is often used in clinical practice to identify women who are at above-average risk for breast cancer (defined as a 5-year risk of developing breast cancer ≥1.66%).4 For the patient described in the opening case, the Gail tool predicts that her 5-year risk of breast cancer is 6%, compared with 1.7% for a woman of the same age who is at average risk. In addition, the Gail tool predicts that for the woman in this case, her lifetime risk of breast cancer, to age 90, is 30.1%, compared with 9.5% for a woman of the same age who is at average risk.
The woman in this case is clearly at increased risk for breast cancer. What are her choices for reducing her risk of developing breast cancer?
Options for preventing breast cancer
There are many strategies to prevent breast cancer, including lifestyle interventions, pharmacotherapy, and mastectomy. Lifestyle interventions that may reduce the risk of breast cancer in postmenopausal women include: maintain a body weight in the normal range,5 reduce or eliminate the consumption of alcoholic beverages,6 exercise daily,7 and quit smoking.8
Mastectomy has been demonstrated to reduce the risk of breast cancer in women at very high risk (BRCA positive), but it is seldom used in women at moderate risk for breast cancer.
Pharmacologic interventions for the prevention of breast cancer include tamoxifen, raloxifene, and exemestane.1 All three agents reduce the risk of breast cancer by about 50%. In fact, the US Preventive Services Task Force (USPSTF) recently recommended the use of tamoxifen or raloxifene to reduce breast cancer risk in patients at high risk. (See “USPSTF recommends tamoxifen or raloxifene to reduce breast cancer risk in high-risk patients”.)
Exemestane is an aromatase inhibitor that causes bone loss. Consequently, this agent would not be an optimal choice for use in a woman with osteoporosis. Like raloxifene, tamoxifen is thought to increase bone density and decrease the risk of osteoporotic fracture.9,10 Consequently, for a woman with osteoporosis, with an elevated risk of breast cancer, raloxifene or tamoxifen could be prescribed with the dual goals of reducing the risk of osteoporoticfracture and reducing the risk of breast cancer.
Two good options: Raloxifene and tamoxifen
Raloxifene and tamoxifen are both good choices for treating osteoporosis in women at high risk for breast cancer. For women with a uterus, raloxifene is the preferred agent because tamoxifen can cause endometrial cancer. For women without a uterus, either raloxifene or tamoxifen could be utilized.
What is the benefit-to-risk ratio for these agents?
Dr. Gabriel Hortobagyi and Dr. Powel Brown have provided a snapshot of the pros and cons of using raloxifene and tamoxifen for breast cancer prophylaxis by estimating benefits and risks in 1,000 women treated for 5 years with an additional 2 years of follow-up (7 years of observation).11 In their analysis it was assumed that the women had a 5-year risk of developing breast cancer of 4% (the mean risk for “high risk” subjects entered into the STAR P-2 Trial).
They calculated that after 7 years of observation, treating 1,000 women with tamoxifen 20 mg daily for 5 years will prevent 20 invasive and 20 noninvasive breast cancers and cause 2.25 endometrial cancers and 3.3 thromboembolic events. Treating 1,000 women with raloxifene 60 mg daily for 5 years will prevent15 invasive and 16 noninvasive breast cancers and cause no cases of endometrial cancer and 2.47 thromboembolic events. They concluded that for these major events, tamoxifen caused 40 beneficial events and 5.55 adverse events for a benefit-to-risk ratio of approximately 7. Raloxifene caused 31 beneficial events and 2.47 adverse events for a benefit-to-risk ratio of approximately 13.
Be aware of treatment-specific adverse effects
Raloxifene and tamoxifen treatment cause different patterns of symptom side effects and gynecologic problems. Tamoxifen treatment results in more vasomotor symptoms, leg cramps, and bladder control problems than treatment with raloxifene. Raloxifene is associated with more dyspareunia, lower libido, and more vaginal dryness, weight gain, and musculoskeletal problems than tamoxifen.12
Tamoxifen treatment results in more problems with leiomyomata, endometriosis, endometrial polyps, and endometrial cancer than treatment with raloxifene.13 In turn, this results in more gynecologic surgical procedures, such as endometrial biopsy, oophorectomy, laparoscopy, and hysteroscopy being performed on women taking tamoxifen than on women taking raloxifene. In the largest clinical trial, adherence to treatment was greater for raloxifene than tamoxifen.12 For women with an intact uterus, raloxifene is likely the better choice for breast cancer prevention.
CASE: I WOULD RECOMMEND RALOXIFENE TO THE CASE PATIENT
For the woman presented in this case—who has osteoporosis and a 5-year risk for breast cancer of 6%, as well as an intact uterus—a 5-year course of raloxifene would be an appropriate treatment both to reduce her risk of breast cancer and to treat her osteoporosis.
To achieve the goal of the American Society of Clinical Oncology to increase the use of chemoprevention in women at increased risk of breast cancer, ObGyns will need to take a lead role in assessing our patients for breast cancer risk and counseling them about chemopreventive options.
We want to hear from you! Tell us what you think.
- Visvanathan K, Hurley P, Bantug E, et al. Use of pharmacologic interventions for breast cancer risk reduction: American Society for Clinical Oncology clinical practice guideline. J Clin Oncol. 2013;31(23):2942–2962.
- Luckey M, Kagan R, Greenspan S, et al. Once-weekly alendronate 70 mg and raloxifene 60 mg daily in the treatment of postmenopausal osteoporosis. Menopause. 2004;11(4):405–415.
- Foster SA, Shi N, Curkendall S, et al. Fractures in women treated with raloxifene or alendronate: A retrospective database analysis. BMC Women’s Health. 2013;13:15–24.
- National Cancer Institute. Breast Cancer Risk Assessment Tool. http://www.cancer.gov/bcrisktool/. Updated May 16, 2011. Accessed October 21, 2013.
- van den Brandt PA, Spiegelman D, Yaun SS, et al. Pooled analysis of prospective cohort studies on height, weight, and breast cancer risk. Am J Epidemiol. 2000;152(6):514–527.
- Bagnardi V, Rota M, Botteri E, et al. Light alcohol drinking and cancer: A meta-analysis. Ann Oncol. 2013;24(5):301–308.
- Lynch BM, Neilson HK, Friedenreich CM. Physical activity and breast cancer prevention. Recent Results Cancer Res. 2011;186:13–42.
- Gaudet MM, Gapstur SM, Sun J, Diver WR, Hannan LM, Thun MJ. Active smoking and breast cancer risk: Original cohort data and meta-analysis. J Natl Cancer Inst. 2013;105(8):515–525.
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: Current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J Natl Cancer Inst. 2005;97(22):1652–1662.
- Cooke AL, Metge C, Lix L, Prior HJ, Leslie WD. Tamoxifen use and osteoporotic fracture risk: A population-based analysis. J Clin Oncol. 2008;26(32):5227–5232.
- Hortobagyi GN, Brown PH. Two good choices to prevent breast cancer: great taste, less filling. Cancer Prev Res (Phila). 2010;3(6):681–685.
- Land SR, Wickerham DL, Costantino JP, et al. Patient-reported symptoms and quality of life during treatment with tamoxifen or raloxifene for breast cancer prevention. JAMA. 2006;295(23):2742–2751.
- Runowicz CD, Costantino JP, Wickerham L, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205(6):535.e1–e5.

Robert L. Barbieri, MD
Editor in Chief
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief
Dr. Barbieri reports no financial relationships relevant to this article.
CASE: ACTIVE, HEALTHY, OSTEOPOROTIC, AND AT-RISK FOR BREAST CANCER
Your patient, a 58-year-old, G0 healthy and active woman underwent early menopause at 44 years. She recently had a bone mineral density test, results of which showed a T-score of –2.8 at the spine and –2.5 at the hip. She is taking vitamin D and calcium. She is an exceptionally active woman who plays tennis and walks more than 5 miles daily. Two years earlier, at age 56, she had abnormal mammography results, and a breast biopsy revealed atypical hyperplasia. Her mother has a history of Paget disease of the breast.
Prior to selecting a bone medicine to treat this woman’s osteoporosis, should you assess her risk of breast cancer?
In this editorial, I make the argument that, yes, you should assess this patient’s risk of breast cancer prior to selecting treatment for her osteoporosis, as her level of breast cancer risk can help determine the optimal osteoporosis therapy.
An expert panel convened by the American Society of Clinical Oncology noted that far too few American women are being assessed for their risk of breast cancer, and too few American women at increased risk for breast cancer are being offered pharmacologic preventive therapy.1 One small step to increase the frequency of risk assessment and counseling regarding preventive therapy is to assess breast cancer risk in women with osteoporosis to help guide the selection of a bone medicine.
Options for osteoporosis treatment
Most experts recommend that menopausal women with osteoporosis (T-score ≤–2.5) should be offered a bone medicine in addition to the standard prescription therapy of vitamin D and calcium, exercise, and smoking cessation.
The most commonly prescribed bone medicines are bisphosphonates, estrogen, and raloxifene. Following the publication of the Women’s Health Initiative (WHI) in 2002, the use of estrogen and raloxifene for the treatment of osteoporosis decreased significantly. Both the bisphosphonates and estrogen are believed to be slightly more effective at increasing bone density than raloxifene, but there are no direct head-to-head, large-scale fracture-reduction studies comparing these agents.2 In one large retrospective database study, women taking alendronate or raloxifene were reported to have similar vertebral and nonvertebral fracture rates.3
Unlike the bisphosphonates and estrogen, raloxifene has been demonstrated to reduce the risk of breast cancer by about 50%. For women with newly diagnosed osteoporosis and an above-average risk of developing breast cancer, raloxifene may represent an optimal pharmacologic intervention. But, how would you know if your patient with newly diagnosed osteoporosis is at increased risk for breast cancer?
Assessing breast cancer risk
The Gail breast cancer risk assessment tool is often used in clinical practice to identify women who are at above-average risk for breast cancer (defined as a 5-year risk of developing breast cancer ≥1.66%).4 For the patient described in the opening case, the Gail tool predicts that her 5-year risk of breast cancer is 6%, compared with 1.7% for a woman of the same age who is at average risk. In addition, the Gail tool predicts that for the woman in this case, her lifetime risk of breast cancer, to age 90, is 30.1%, compared with 9.5% for a woman of the same age who is at average risk.
The woman in this case is clearly at increased risk for breast cancer. What are her choices for reducing her risk of developing breast cancer?
Options for preventing breast cancer
There are many strategies to prevent breast cancer, including lifestyle interventions, pharmacotherapy, and mastectomy. Lifestyle interventions that may reduce the risk of breast cancer in postmenopausal women include: maintain a body weight in the normal range,5 reduce or eliminate the consumption of alcoholic beverages,6 exercise daily,7 and quit smoking.8
Mastectomy has been demonstrated to reduce the risk of breast cancer in women at very high risk (BRCA positive), but it is seldom used in women at moderate risk for breast cancer.
Pharmacologic interventions for the prevention of breast cancer include tamoxifen, raloxifene, and exemestane.1 All three agents reduce the risk of breast cancer by about 50%. In fact, the US Preventive Services Task Force (USPSTF) recently recommended the use of tamoxifen or raloxifene to reduce breast cancer risk in patients at high risk. (See “USPSTF recommends tamoxifen or raloxifene to reduce breast cancer risk in high-risk patients”.)
Exemestane is an aromatase inhibitor that causes bone loss. Consequently, this agent would not be an optimal choice for use in a woman with osteoporosis. Like raloxifene, tamoxifen is thought to increase bone density and decrease the risk of osteoporotic fracture.9,10 Consequently, for a woman with osteoporosis, with an elevated risk of breast cancer, raloxifene or tamoxifen could be prescribed with the dual goals of reducing the risk of osteoporoticfracture and reducing the risk of breast cancer.
Two good options: Raloxifene and tamoxifen
Raloxifene and tamoxifen are both good choices for treating osteoporosis in women at high risk for breast cancer. For women with a uterus, raloxifene is the preferred agent because tamoxifen can cause endometrial cancer. For women without a uterus, either raloxifene or tamoxifen could be utilized.
What is the benefit-to-risk ratio for these agents?
Dr. Gabriel Hortobagyi and Dr. Powel Brown have provided a snapshot of the pros and cons of using raloxifene and tamoxifen for breast cancer prophylaxis by estimating benefits and risks in 1,000 women treated for 5 years with an additional 2 years of follow-up (7 years of observation).11 In their analysis it was assumed that the women had a 5-year risk of developing breast cancer of 4% (the mean risk for “high risk” subjects entered into the STAR P-2 Trial).
They calculated that after 7 years of observation, treating 1,000 women with tamoxifen 20 mg daily for 5 years will prevent 20 invasive and 20 noninvasive breast cancers and cause 2.25 endometrial cancers and 3.3 thromboembolic events. Treating 1,000 women with raloxifene 60 mg daily for 5 years will prevent15 invasive and 16 noninvasive breast cancers and cause no cases of endometrial cancer and 2.47 thromboembolic events. They concluded that for these major events, tamoxifen caused 40 beneficial events and 5.55 adverse events for a benefit-to-risk ratio of approximately 7. Raloxifene caused 31 beneficial events and 2.47 adverse events for a benefit-to-risk ratio of approximately 13.
Be aware of treatment-specific adverse effects
Raloxifene and tamoxifen treatment cause different patterns of symptom side effects and gynecologic problems. Tamoxifen treatment results in more vasomotor symptoms, leg cramps, and bladder control problems than treatment with raloxifene. Raloxifene is associated with more dyspareunia, lower libido, and more vaginal dryness, weight gain, and musculoskeletal problems than tamoxifen.12
Tamoxifen treatment results in more problems with leiomyomata, endometriosis, endometrial polyps, and endometrial cancer than treatment with raloxifene.13 In turn, this results in more gynecologic surgical procedures, such as endometrial biopsy, oophorectomy, laparoscopy, and hysteroscopy being performed on women taking tamoxifen than on women taking raloxifene. In the largest clinical trial, adherence to treatment was greater for raloxifene than tamoxifen.12 For women with an intact uterus, raloxifene is likely the better choice for breast cancer prevention.
CASE: I WOULD RECOMMEND RALOXIFENE TO THE CASE PATIENT
For the woman presented in this case—who has osteoporosis and a 5-year risk for breast cancer of 6%, as well as an intact uterus—a 5-year course of raloxifene would be an appropriate treatment both to reduce her risk of breast cancer and to treat her osteoporosis.
To achieve the goal of the American Society of Clinical Oncology to increase the use of chemoprevention in women at increased risk of breast cancer, ObGyns will need to take a lead role in assessing our patients for breast cancer risk and counseling them about chemopreventive options.
We want to hear from you! Tell us what you think.
CASE: ACTIVE, HEALTHY, OSTEOPOROTIC, AND AT-RISK FOR BREAST CANCER
Your patient, a 58-year-old, G0 healthy and active woman underwent early menopause at 44 years. She recently had a bone mineral density test, results of which showed a T-score of –2.8 at the spine and –2.5 at the hip. She is taking vitamin D and calcium. She is an exceptionally active woman who plays tennis and walks more than 5 miles daily. Two years earlier, at age 56, she had abnormal mammography results, and a breast biopsy revealed atypical hyperplasia. Her mother has a history of Paget disease of the breast.
Prior to selecting a bone medicine to treat this woman’s osteoporosis, should you assess her risk of breast cancer?
In this editorial, I make the argument that, yes, you should assess this patient’s risk of breast cancer prior to selecting treatment for her osteoporosis, as her level of breast cancer risk can help determine the optimal osteoporosis therapy.
An expert panel convened by the American Society of Clinical Oncology noted that far too few American women are being assessed for their risk of breast cancer, and too few American women at increased risk for breast cancer are being offered pharmacologic preventive therapy.1 One small step to increase the frequency of risk assessment and counseling regarding preventive therapy is to assess breast cancer risk in women with osteoporosis to help guide the selection of a bone medicine.
Options for osteoporosis treatment
Most experts recommend that menopausal women with osteoporosis (T-score ≤–2.5) should be offered a bone medicine in addition to the standard prescription therapy of vitamin D and calcium, exercise, and smoking cessation.
The most commonly prescribed bone medicines are bisphosphonates, estrogen, and raloxifene. Following the publication of the Women’s Health Initiative (WHI) in 2002, the use of estrogen and raloxifene for the treatment of osteoporosis decreased significantly. Both the bisphosphonates and estrogen are believed to be slightly more effective at increasing bone density than raloxifene, but there are no direct head-to-head, large-scale fracture-reduction studies comparing these agents.2 In one large retrospective database study, women taking alendronate or raloxifene were reported to have similar vertebral and nonvertebral fracture rates.3
Unlike the bisphosphonates and estrogen, raloxifene has been demonstrated to reduce the risk of breast cancer by about 50%. For women with newly diagnosed osteoporosis and an above-average risk of developing breast cancer, raloxifene may represent an optimal pharmacologic intervention. But, how would you know if your patient with newly diagnosed osteoporosis is at increased risk for breast cancer?
Assessing breast cancer risk
The Gail breast cancer risk assessment tool is often used in clinical practice to identify women who are at above-average risk for breast cancer (defined as a 5-year risk of developing breast cancer ≥1.66%).4 For the patient described in the opening case, the Gail tool predicts that her 5-year risk of breast cancer is 6%, compared with 1.7% for a woman of the same age who is at average risk. In addition, the Gail tool predicts that for the woman in this case, her lifetime risk of breast cancer, to age 90, is 30.1%, compared with 9.5% for a woman of the same age who is at average risk.
The woman in this case is clearly at increased risk for breast cancer. What are her choices for reducing her risk of developing breast cancer?
Options for preventing breast cancer
There are many strategies to prevent breast cancer, including lifestyle interventions, pharmacotherapy, and mastectomy. Lifestyle interventions that may reduce the risk of breast cancer in postmenopausal women include: maintain a body weight in the normal range,5 reduce or eliminate the consumption of alcoholic beverages,6 exercise daily,7 and quit smoking.8
Mastectomy has been demonstrated to reduce the risk of breast cancer in women at very high risk (BRCA positive), but it is seldom used in women at moderate risk for breast cancer.
Pharmacologic interventions for the prevention of breast cancer include tamoxifen, raloxifene, and exemestane.1 All three agents reduce the risk of breast cancer by about 50%. In fact, the US Preventive Services Task Force (USPSTF) recently recommended the use of tamoxifen or raloxifene to reduce breast cancer risk in patients at high risk. (See “USPSTF recommends tamoxifen or raloxifene to reduce breast cancer risk in high-risk patients”.)
Exemestane is an aromatase inhibitor that causes bone loss. Consequently, this agent would not be an optimal choice for use in a woman with osteoporosis. Like raloxifene, tamoxifen is thought to increase bone density and decrease the risk of osteoporotic fracture.9,10 Consequently, for a woman with osteoporosis, with an elevated risk of breast cancer, raloxifene or tamoxifen could be prescribed with the dual goals of reducing the risk of osteoporoticfracture and reducing the risk of breast cancer.
Two good options: Raloxifene and tamoxifen
Raloxifene and tamoxifen are both good choices for treating osteoporosis in women at high risk for breast cancer. For women with a uterus, raloxifene is the preferred agent because tamoxifen can cause endometrial cancer. For women without a uterus, either raloxifene or tamoxifen could be utilized.
What is the benefit-to-risk ratio for these agents?
Dr. Gabriel Hortobagyi and Dr. Powel Brown have provided a snapshot of the pros and cons of using raloxifene and tamoxifen for breast cancer prophylaxis by estimating benefits and risks in 1,000 women treated for 5 years with an additional 2 years of follow-up (7 years of observation).11 In their analysis it was assumed that the women had a 5-year risk of developing breast cancer of 4% (the mean risk for “high risk” subjects entered into the STAR P-2 Trial).
They calculated that after 7 years of observation, treating 1,000 women with tamoxifen 20 mg daily for 5 years will prevent 20 invasive and 20 noninvasive breast cancers and cause 2.25 endometrial cancers and 3.3 thromboembolic events. Treating 1,000 women with raloxifene 60 mg daily for 5 years will prevent15 invasive and 16 noninvasive breast cancers and cause no cases of endometrial cancer and 2.47 thromboembolic events. They concluded that for these major events, tamoxifen caused 40 beneficial events and 5.55 adverse events for a benefit-to-risk ratio of approximately 7. Raloxifene caused 31 beneficial events and 2.47 adverse events for a benefit-to-risk ratio of approximately 13.
Be aware of treatment-specific adverse effects
Raloxifene and tamoxifen treatment cause different patterns of symptom side effects and gynecologic problems. Tamoxifen treatment results in more vasomotor symptoms, leg cramps, and bladder control problems than treatment with raloxifene. Raloxifene is associated with more dyspareunia, lower libido, and more vaginal dryness, weight gain, and musculoskeletal problems than tamoxifen.12
Tamoxifen treatment results in more problems with leiomyomata, endometriosis, endometrial polyps, and endometrial cancer than treatment with raloxifene.13 In turn, this results in more gynecologic surgical procedures, such as endometrial biopsy, oophorectomy, laparoscopy, and hysteroscopy being performed on women taking tamoxifen than on women taking raloxifene. In the largest clinical trial, adherence to treatment was greater for raloxifene than tamoxifen.12 For women with an intact uterus, raloxifene is likely the better choice for breast cancer prevention.
CASE: I WOULD RECOMMEND RALOXIFENE TO THE CASE PATIENT
For the woman presented in this case—who has osteoporosis and a 5-year risk for breast cancer of 6%, as well as an intact uterus—a 5-year course of raloxifene would be an appropriate treatment both to reduce her risk of breast cancer and to treat her osteoporosis.
To achieve the goal of the American Society of Clinical Oncology to increase the use of chemoprevention in women at increased risk of breast cancer, ObGyns will need to take a lead role in assessing our patients for breast cancer risk and counseling them about chemopreventive options.
We want to hear from you! Tell us what you think.
- Visvanathan K, Hurley P, Bantug E, et al. Use of pharmacologic interventions for breast cancer risk reduction: American Society for Clinical Oncology clinical practice guideline. J Clin Oncol. 2013;31(23):2942–2962.
- Luckey M, Kagan R, Greenspan S, et al. Once-weekly alendronate 70 mg and raloxifene 60 mg daily in the treatment of postmenopausal osteoporosis. Menopause. 2004;11(4):405–415.
- Foster SA, Shi N, Curkendall S, et al. Fractures in women treated with raloxifene or alendronate: A retrospective database analysis. BMC Women’s Health. 2013;13:15–24.
- National Cancer Institute. Breast Cancer Risk Assessment Tool. http://www.cancer.gov/bcrisktool/. Updated May 16, 2011. Accessed October 21, 2013.
- van den Brandt PA, Spiegelman D, Yaun SS, et al. Pooled analysis of prospective cohort studies on height, weight, and breast cancer risk. Am J Epidemiol. 2000;152(6):514–527.
- Bagnardi V, Rota M, Botteri E, et al. Light alcohol drinking and cancer: A meta-analysis. Ann Oncol. 2013;24(5):301–308.
- Lynch BM, Neilson HK, Friedenreich CM. Physical activity and breast cancer prevention. Recent Results Cancer Res. 2011;186:13–42.
- Gaudet MM, Gapstur SM, Sun J, Diver WR, Hannan LM, Thun MJ. Active smoking and breast cancer risk: Original cohort data and meta-analysis. J Natl Cancer Inst. 2013;105(8):515–525.
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: Current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J Natl Cancer Inst. 2005;97(22):1652–1662.
- Cooke AL, Metge C, Lix L, Prior HJ, Leslie WD. Tamoxifen use and osteoporotic fracture risk: A population-based analysis. J Clin Oncol. 2008;26(32):5227–5232.
- Hortobagyi GN, Brown PH. Two good choices to prevent breast cancer: great taste, less filling. Cancer Prev Res (Phila). 2010;3(6):681–685.
- Land SR, Wickerham DL, Costantino JP, et al. Patient-reported symptoms and quality of life during treatment with tamoxifen or raloxifene for breast cancer prevention. JAMA. 2006;295(23):2742–2751.
- Runowicz CD, Costantino JP, Wickerham L, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205(6):535.e1–e5.
- Visvanathan K, Hurley P, Bantug E, et al. Use of pharmacologic interventions for breast cancer risk reduction: American Society for Clinical Oncology clinical practice guideline. J Clin Oncol. 2013;31(23):2942–2962.
- Luckey M, Kagan R, Greenspan S, et al. Once-weekly alendronate 70 mg and raloxifene 60 mg daily in the treatment of postmenopausal osteoporosis. Menopause. 2004;11(4):405–415.
- Foster SA, Shi N, Curkendall S, et al. Fractures in women treated with raloxifene or alendronate: A retrospective database analysis. BMC Women’s Health. 2013;13:15–24.
- National Cancer Institute. Breast Cancer Risk Assessment Tool. http://www.cancer.gov/bcrisktool/. Updated May 16, 2011. Accessed October 21, 2013.
- van den Brandt PA, Spiegelman D, Yaun SS, et al. Pooled analysis of prospective cohort studies on height, weight, and breast cancer risk. Am J Epidemiol. 2000;152(6):514–527.
- Bagnardi V, Rota M, Botteri E, et al. Light alcohol drinking and cancer: A meta-analysis. Ann Oncol. 2013;24(5):301–308.
- Lynch BM, Neilson HK, Friedenreich CM. Physical activity and breast cancer prevention. Recent Results Cancer Res. 2011;186:13–42.
- Gaudet MM, Gapstur SM, Sun J, Diver WR, Hannan LM, Thun MJ. Active smoking and breast cancer risk: Original cohort data and meta-analysis. J Natl Cancer Inst. 2013;105(8):515–525.
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: Current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J Natl Cancer Inst. 2005;97(22):1652–1662.
- Cooke AL, Metge C, Lix L, Prior HJ, Leslie WD. Tamoxifen use and osteoporotic fracture risk: A population-based analysis. J Clin Oncol. 2008;26(32):5227–5232.
- Hortobagyi GN, Brown PH. Two good choices to prevent breast cancer: great taste, less filling. Cancer Prev Res (Phila). 2010;3(6):681–685.
- Land SR, Wickerham DL, Costantino JP, et al. Patient-reported symptoms and quality of life during treatment with tamoxifen or raloxifene for breast cancer prevention. JAMA. 2006;295(23):2742–2751.
- Runowicz CD, Costantino JP, Wickerham L, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205(6):535.e1–e5.

Molecular profiling leads to improved targeted treatment
AMSTERDAM – Two-fifths of patients with refractory recurrent or metastatic cancers were successfully matched to an appropriate targeted treatment using molecular profiling, according to research presented at the multidisciplinary European cancer congresses.
Feasibility findings from the phase II, proof-of-concept SHIVA study showed that a molecular abnormality leading to targeted treatment was present in 40% patients.

This is the first randomized trial to consider treating patients purely on the basis of their molecular profile rather than the type of tumor that they have. It is also the first trial designed to determine what the outcome of such an approach will be, with the primary endpoint being progression-free survival.
Currently, the prescription of approved molecularly targeted agents relies on the primary tumor location and histological subtype. For example, a woman with breast cancer overexpressing HER2 may be treated with a HER2-targeting agent such as trastuzumab or lapatinib, or with endocrine therapies such as tamoxifen and letrozole, if there is overexpression of the estrogen or progestogen receptor (ER/PR).
However, it is not clear if this is the best means of using these therapies, as their molecular targets may not be specific to a single tumor type. Indeed, HER2 is overexpressed in several tumor types other than breast cancer, including ovarian, gastric, colorectal, pancreatic, and endometrial cancers.
The idea of giving patients treatment based on their molecular profiles rather than their tumor types represents a new paradigm and requires prospective validation before being implemented in clinical practice, Dr. Christophe Le Tourneau of Institut Curie, Paris, said in an interview.
The SHIVA trial was therefore initiated to compare molecularly targeted therapy based on tumor molecular profiling versus conventional therapy in patients with refractory cancer (Target Oncol. 2012;7:253-65). Although two previous studies have suggested that this approach is possible and could improve patient outcomes (J. Clin. Oncol. 2010;4877-83; Clin. Cancer Res. 2012;18:6373-83), these studies were not randomized against the standard of care and so the conclusions that can be drawn from their results are not robust.
Patients are eligible for inclusion in the ongoing SHIVA trial if they have recurrent or metastatic disease despite standard treatment, an ECOG performance status of 0 or 1, adequate organ function, and measurable disease that can be biopsied not involving the bone or brain.
After recruitment, all patients will have a biopsy taken of one metastasis that is then assessed for gene mutations and amplifications, and for the expression of hormone (estrogen, progestogen and androgen) receptors. If a molecular abnormality is identified for which an approved targeted agent is available, then patients are randomized to receive either the matching targeted therapy or the conventional therapy that they would have received had they not be identified as having a possible molecular target. At progression, patients in the conventional treatment arm may crossover to targeted therapy.
Patients are only randomized if they have a molecular target that is not already known for their disease. So a patient with breast cancer found to have amplified HER2 or a patient with non–small-cell lung cancer and overexpression of EGFR would not be included, Dr. Le Tourneau said.
The SHIVA investigators have developed an algorithm or Molecular Biology Board (MBB) to help guide treatment in the experimental arm. The following targeted agents may be used if an appropriate molecular target is found: KIT or ABL for imatinib; PTEN or mTOR, among others, for everolimus; BRAF for vemurafenib; PDGFRA/B or FLT-3 for sorafenib; EGFR for erlotinib; HER2 for lapatinib in combination with trastuzumab; SRC, and others, for dasatinib; ER and PR for tamoxifen or letrozole; and the androgen receptor for abiraterone.
The trial is using high throughput sequencing, so processing the biopsies involves only two assays – one for gene mutation analysis and one for gene copy number alterations – "so we look at everything at the same time," Dr. Le Tourneau said.
As of September 2013, 350 patients had been included in the study and feasibility of the molecular profiling approach was tested in the first 95 patients. Of these, a complete molecular profile could be obtained in 61%. The median time to obtaining the biopsy sample and performing the MBB was 26 days, ranging from 2 weeks to 42 days. Mutations could be assessed in two-thirds of samples, with gene copy alterations analyzed in 68%, and immunohistochemistry for hormone receptors possible in 92%.
In the experimental arm, 14 patients (15%) with a variety of tumor types are now being treated with abiraterone, 13 (14%) with everolimus, nine (9%) with endocrine treatment, and two (2%) with anti-HER2 treatment or sorafenib.
The primary efficacy analysis for progression-free survival will be performed once 100 patients have been randomized into each study arm. Other analyses will determine the overall response rate (ORR) and overall survival, among other key endpoints.
The SHIVA trial is planned to run for 3 years, and as it is already a year in, "within 2 years the study will be finished," Dr. Le Tourneau said.
The SHIVA trial is funded by Institut Curie. Dr. Le Tourneau had no conflicts of interest.
AMSTERDAM – Two-fifths of patients with refractory recurrent or metastatic cancers were successfully matched to an appropriate targeted treatment using molecular profiling, according to research presented at the multidisciplinary European cancer congresses.
Feasibility findings from the phase II, proof-of-concept SHIVA study showed that a molecular abnormality leading to targeted treatment was present in 40% patients.
This is the first randomized trial to consider treating patients purely on the basis of their molecular profile rather than the type of tumor that they have. It is also the first trial designed to determine what the outcome of such an approach will be, with the primary endpoint being progression-free survival.
Currently, the prescription of approved molecularly targeted agents relies on the primary tumor location and histological subtype. For example, a woman with breast cancer overexpressing HER2 may be treated with a HER2-targeting agent such as trastuzumab or lapatinib, or with endocrine therapies such as tamoxifen and letrozole, if there is overexpression of the estrogen or progestogen receptor (ER/PR).
However, it is not clear if this is the best means of using these therapies, as their molecular targets may not be specific to a single tumor type. Indeed, HER2 is overexpressed in several tumor types other than breast cancer, including ovarian, gastric, colorectal, pancreatic, and endometrial cancers.
The idea of giving patients treatment based on their molecular profiles rather than their tumor types represents a new paradigm and requires prospective validation before being implemented in clinical practice, Dr. Christophe Le Tourneau of Institut Curie, Paris, said in an interview.
The SHIVA trial was therefore initiated to compare molecularly targeted therapy based on tumor molecular profiling versus conventional therapy in patients with refractory cancer (Target Oncol. 2012;7:253-65). Although two previous studies have suggested that this approach is possible and could improve patient outcomes (J. Clin. Oncol. 2010;4877-83; Clin. Cancer Res. 2012;18:6373-83), these studies were not randomized against the standard of care and so the conclusions that can be drawn from their results are not robust.
Patients are eligible for inclusion in the ongoing SHIVA trial if they have recurrent or metastatic disease despite standard treatment, an ECOG performance status of 0 or 1, adequate organ function, and measurable disease that can be biopsied not involving the bone or brain.
After recruitment, all patients will have a biopsy taken of one metastasis that is then assessed for gene mutations and amplifications, and for the expression of hormone (estrogen, progestogen and androgen) receptors. If a molecular abnormality is identified for which an approved targeted agent is available, then patients are randomized to receive either the matching targeted therapy or the conventional therapy that they would have received had they not be identified as having a possible molecular target. At progression, patients in the conventional treatment arm may crossover to targeted therapy.
Patients are only randomized if they have a molecular target that is not already known for their disease. So a patient with breast cancer found to have amplified HER2 or a patient with non–small-cell lung cancer and overexpression of EGFR would not be included, Dr. Le Tourneau said.
The SHIVA investigators have developed an algorithm or Molecular Biology Board (MBB) to help guide treatment in the experimental arm. The following targeted agents may be used if an appropriate molecular target is found: KIT or ABL for imatinib; PTEN or mTOR, among others, for everolimus; BRAF for vemurafenib; PDGFRA/B or FLT-3 for sorafenib; EGFR for erlotinib; HER2 for lapatinib in combination with trastuzumab; SRC, and others, for dasatinib; ER and PR for tamoxifen or letrozole; and the androgen receptor for abiraterone.
The trial is using high throughput sequencing, so processing the biopsies involves only two assays – one for gene mutation analysis and one for gene copy number alterations – "so we look at everything at the same time," Dr. Le Tourneau said.
As of September 2013, 350 patients had been included in the study and feasibility of the molecular profiling approach was tested in the first 95 patients. Of these, a complete molecular profile could be obtained in 61%. The median time to obtaining the biopsy sample and performing the MBB was 26 days, ranging from 2 weeks to 42 days. Mutations could be assessed in two-thirds of samples, with gene copy alterations analyzed in 68%, and immunohistochemistry for hormone receptors possible in 92%.
In the experimental arm, 14 patients (15%) with a variety of tumor types are now being treated with abiraterone, 13 (14%) with everolimus, nine (9%) with endocrine treatment, and two (2%) with anti-HER2 treatment or sorafenib.
The primary efficacy analysis for progression-free survival will be performed once 100 patients have been randomized into each study arm. Other analyses will determine the overall response rate (ORR) and overall survival, among other key endpoints.
The SHIVA trial is planned to run for 3 years, and as it is already a year in, "within 2 years the study will be finished," Dr. Le Tourneau said.
The SHIVA trial is funded by Institut Curie. Dr. Le Tourneau had no conflicts of interest.
AMSTERDAM – Two-fifths of patients with refractory recurrent or metastatic cancers were successfully matched to an appropriate targeted treatment using molecular profiling, according to research presented at the multidisciplinary European cancer congresses.
Feasibility findings from the phase II, proof-of-concept SHIVA study showed that a molecular abnormality leading to targeted treatment was present in 40% patients.
This is the first randomized trial to consider treating patients purely on the basis of their molecular profile rather than the type of tumor that they have. It is also the first trial designed to determine what the outcome of such an approach will be, with the primary endpoint being progression-free survival.
Currently, the prescription of approved molecularly targeted agents relies on the primary tumor location and histological subtype. For example, a woman with breast cancer overexpressing HER2 may be treated with a HER2-targeting agent such as trastuzumab or lapatinib, or with endocrine therapies such as tamoxifen and letrozole, if there is overexpression of the estrogen or progestogen receptor (ER/PR).
However, it is not clear if this is the best means of using these therapies, as their molecular targets may not be specific to a single tumor type. Indeed, HER2 is overexpressed in several tumor types other than breast cancer, including ovarian, gastric, colorectal, pancreatic, and endometrial cancers.
The idea of giving patients treatment based on their molecular profiles rather than their tumor types represents a new paradigm and requires prospective validation before being implemented in clinical practice, Dr. Christophe Le Tourneau of Institut Curie, Paris, said in an interview.
The SHIVA trial was therefore initiated to compare molecularly targeted therapy based on tumor molecular profiling versus conventional therapy in patients with refractory cancer (Target Oncol. 2012;7:253-65). Although two previous studies have suggested that this approach is possible and could improve patient outcomes (J. Clin. Oncol. 2010;4877-83; Clin. Cancer Res. 2012;18:6373-83), these studies were not randomized against the standard of care and so the conclusions that can be drawn from their results are not robust.
Patients are eligible for inclusion in the ongoing SHIVA trial if they have recurrent or metastatic disease despite standard treatment, an ECOG performance status of 0 or 1, adequate organ function, and measurable disease that can be biopsied not involving the bone or brain.
After recruitment, all patients will have a biopsy taken of one metastasis that is then assessed for gene mutations and amplifications, and for the expression of hormone (estrogen, progestogen and androgen) receptors. If a molecular abnormality is identified for which an approved targeted agent is available, then patients are randomized to receive either the matching targeted therapy or the conventional therapy that they would have received had they not be identified as having a possible molecular target. At progression, patients in the conventional treatment arm may crossover to targeted therapy.
Patients are only randomized if they have a molecular target that is not already known for their disease. So a patient with breast cancer found to have amplified HER2 or a patient with non–small-cell lung cancer and overexpression of EGFR would not be included, Dr. Le Tourneau said.
The SHIVA investigators have developed an algorithm or Molecular Biology Board (MBB) to help guide treatment in the experimental arm. The following targeted agents may be used if an appropriate molecular target is found: KIT or ABL for imatinib; PTEN or mTOR, among others, for everolimus; BRAF for vemurafenib; PDGFRA/B or FLT-3 for sorafenib; EGFR for erlotinib; HER2 for lapatinib in combination with trastuzumab; SRC, and others, for dasatinib; ER and PR for tamoxifen or letrozole; and the androgen receptor for abiraterone.
The trial is using high throughput sequencing, so processing the biopsies involves only two assays – one for gene mutation analysis and one for gene copy number alterations – "so we look at everything at the same time," Dr. Le Tourneau said.
As of September 2013, 350 patients had been included in the study and feasibility of the molecular profiling approach was tested in the first 95 patients. Of these, a complete molecular profile could be obtained in 61%. The median time to obtaining the biopsy sample and performing the MBB was 26 days, ranging from 2 weeks to 42 days. Mutations could be assessed in two-thirds of samples, with gene copy alterations analyzed in 68%, and immunohistochemistry for hormone receptors possible in 92%.
In the experimental arm, 14 patients (15%) with a variety of tumor types are now being treated with abiraterone, 13 (14%) with everolimus, nine (9%) with endocrine treatment, and two (2%) with anti-HER2 treatment or sorafenib.
The primary efficacy analysis for progression-free survival will be performed once 100 patients have been randomized into each study arm. Other analyses will determine the overall response rate (ORR) and overall survival, among other key endpoints.
The SHIVA trial is planned to run for 3 years, and as it is already a year in, "within 2 years the study will be finished," Dr. Le Tourneau said.
The SHIVA trial is funded by Institut Curie. Dr. Le Tourneau had no conflicts of interest.
AT THE EUROPEAN CANCER CONGRESS 2013
Major finding: Forty percent of patients were identified as having a molecular target for which an approved treatment could be given.
Data source: Multicenter, proof-of-concept, phase II SHIVA trial of 350 patients with any type of refractory cancer randomized to targeted treatment or to conventional therapy based on molecular profiling.
Disclosures: The SHIVA trial is funded by Institut Curie. Dr. Le Tourneau had no conflicts of interest.

Which women are most likely to die from breast cancer—those screened annually starting at age 40, biennially starting at age 50, or not at all?
In 2009, the United States Preventive Services Task Force (USPSTF) released a controversial recommendation that breast cancer screening should routinely start at age 50 and be performed biennially.1 The Task Force further stated that the determination to screen women before the age of 50 “should take patient context into account, including the patient’s values regarding specific benefits and harms.”1
Although some professional societies have adopted this recommendation, others, including the American College of Obstetricians and Gynecologists (ACOG), have recommended that annual screening begin at age 40 in average-risk women.2
Related article: Is "overdiagnosis" of breast cancer common among women screened by mammography? Andrew M. Kaunitz, MD (January 2013)
With different professional societies lined up on both sides of this debate, practitioners and women remain confused about why different breast cancer screening guidelines exist in the United States.
Putting the study in context
A review of the data that informed the USPSTF recommendation demonstrate that routine screening mammography has similar efficacy in women in their fifth and sixth decade of life—a reduction in mortality of 16% and 15%, respectively.3 However, more mammograms need to be performed in women in their 40s than in women in their 50s to achieve that benefit. Moreover, because the specificity of screening mammography is less than ideal, about 10% of women are called back for additional imaging, and 10% of that population will undergo a biopsy. Only 30% of these biopsies will result in a diagnosis of cancer.
There has been considerable debate about the mortality improvement with routine screening mammography, including a nationwide administrative data review published in late 2012.4 This data-mining study suggested that routine screening mammography was only a minor contributor to the significant improvement in breast cancer mortality over the past 25 years.
Related article: Update on breast health Mark D. Pearlman, MD, and Jennifer L. Griffin Miller, MD, MPH (March 2013)
Details of the study
In this failure analysis from Massachusetts General Hospital and Brigham and Women’s Hospital, Webb and colleagues reviewed breast cancer deaths over 17 years (new breast cancer cases from 1990 through 1997, with cases followed through 2007). They compared the likelihood of death according to whether screening mammography had been performed in the preceding 2 years.
Of the 609 confirmed deaths from breast cancer, 71% occurred among unscreened women (ie, never screened or screening not done in the preceding 2 years). The median age at diagnosis of fatal cancers was 49 years, whereas women with breast cancer who ultimately died of other causes had a median age at diagnosis of 72 years.
Related article: Biennial vs annual mammography: How I manage my patients Andrew M. Kaunitz, MD (June 2013)
Webb and colleagues concluded: “Most deaths from breast cancer occur in unscreened women. To maximize mortality reduction and life-years gained, initiation of regular screening before age 50 years should be encouraged.”
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The findings of Webb and colleagues are not surprising, given the already demonstrated reduction in breast cancer mortality with the use of routine screening mammography in women in their 40s. What is particularly interesting in this study is that the preponderance of breast cancer deaths occurred in younger women. Biologically, this may be explained by the more aggressive nature of breast cancer in younger women.5
This study provides additional support for the ACOG recommendation to routinely offer breast cancer screening with mammography for women aged 40 to 49 years.
--Mark D. Pearlman, MD
We want to hear from you. Tell us what you think.
- US Preventive Services Task Force. Screening for Breast Cancer. http://www.uspreventiveservicestaskforce.org
/uspstf/uspsbrca.htm. Accessed October 22, 2013. - American College of Obstetricians and Gynecologists. Practice Bulletin No. 122: Breast cancer screening. Obstet Gynecol. 2011;118(2 Pt 1):372–382.
- Nelson HD, Tyne K, Naik A, Bougatsos C, Chan BK, Humphrey L. Screening for breast cancer: An update for the US Preventive Services Task Force. Ann Intern Med. 2009;151(10):727–737.
- Bleyer A, Welch HG. Effect of three decades of screening mammography on breast cancer incidence. N Engl J Med. 2012;367(21):1998–2005.
- Klauber-DeMore N. Tumor biology of breast cancer in young women. Breast Dis. 2006;23:9–15.
In 2009, the United States Preventive Services Task Force (USPSTF) released a controversial recommendation that breast cancer screening should routinely start at age 50 and be performed biennially.1 The Task Force further stated that the determination to screen women before the age of 50 “should take patient context into account, including the patient’s values regarding specific benefits and harms.”1
Although some professional societies have adopted this recommendation, others, including the American College of Obstetricians and Gynecologists (ACOG), have recommended that annual screening begin at age 40 in average-risk women.2
Related article: Is "overdiagnosis" of breast cancer common among women screened by mammography? Andrew M. Kaunitz, MD (January 2013)
With different professional societies lined up on both sides of this debate, practitioners and women remain confused about why different breast cancer screening guidelines exist in the United States.
Putting the study in context
A review of the data that informed the USPSTF recommendation demonstrate that routine screening mammography has similar efficacy in women in their fifth and sixth decade of life—a reduction in mortality of 16% and 15%, respectively.3 However, more mammograms need to be performed in women in their 40s than in women in their 50s to achieve that benefit. Moreover, because the specificity of screening mammography is less than ideal, about 10% of women are called back for additional imaging, and 10% of that population will undergo a biopsy. Only 30% of these biopsies will result in a diagnosis of cancer.
There has been considerable debate about the mortality improvement with routine screening mammography, including a nationwide administrative data review published in late 2012.4 This data-mining study suggested that routine screening mammography was only a minor contributor to the significant improvement in breast cancer mortality over the past 25 years.
Related article: Update on breast health Mark D. Pearlman, MD, and Jennifer L. Griffin Miller, MD, MPH (March 2013)
Details of the study
In this failure analysis from Massachusetts General Hospital and Brigham and Women’s Hospital, Webb and colleagues reviewed breast cancer deaths over 17 years (new breast cancer cases from 1990 through 1997, with cases followed through 2007). They compared the likelihood of death according to whether screening mammography had been performed in the preceding 2 years.
Of the 609 confirmed deaths from breast cancer, 71% occurred among unscreened women (ie, never screened or screening not done in the preceding 2 years). The median age at diagnosis of fatal cancers was 49 years, whereas women with breast cancer who ultimately died of other causes had a median age at diagnosis of 72 years.
Related article: Biennial vs annual mammography: How I manage my patients Andrew M. Kaunitz, MD (June 2013)
Webb and colleagues concluded: “Most deaths from breast cancer occur in unscreened women. To maximize mortality reduction and life-years gained, initiation of regular screening before age 50 years should be encouraged.”
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The findings of Webb and colleagues are not surprising, given the already demonstrated reduction in breast cancer mortality with the use of routine screening mammography in women in their 40s. What is particularly interesting in this study is that the preponderance of breast cancer deaths occurred in younger women. Biologically, this may be explained by the more aggressive nature of breast cancer in younger women.5
This study provides additional support for the ACOG recommendation to routinely offer breast cancer screening with mammography for women aged 40 to 49 years.
--Mark D. Pearlman, MD
We want to hear from you. Tell us what you think.
In 2009, the United States Preventive Services Task Force (USPSTF) released a controversial recommendation that breast cancer screening should routinely start at age 50 and be performed biennially.1 The Task Force further stated that the determination to screen women before the age of 50 “should take patient context into account, including the patient’s values regarding specific benefits and harms.”1
Although some professional societies have adopted this recommendation, others, including the American College of Obstetricians and Gynecologists (ACOG), have recommended that annual screening begin at age 40 in average-risk women.2
Related article: Is "overdiagnosis" of breast cancer common among women screened by mammography? Andrew M. Kaunitz, MD (January 2013)
With different professional societies lined up on both sides of this debate, practitioners and women remain confused about why different breast cancer screening guidelines exist in the United States.
Putting the study in context
A review of the data that informed the USPSTF recommendation demonstrate that routine screening mammography has similar efficacy in women in their fifth and sixth decade of life—a reduction in mortality of 16% and 15%, respectively.3 However, more mammograms need to be performed in women in their 40s than in women in their 50s to achieve that benefit. Moreover, because the specificity of screening mammography is less than ideal, about 10% of women are called back for additional imaging, and 10% of that population will undergo a biopsy. Only 30% of these biopsies will result in a diagnosis of cancer.
There has been considerable debate about the mortality improvement with routine screening mammography, including a nationwide administrative data review published in late 2012.4 This data-mining study suggested that routine screening mammography was only a minor contributor to the significant improvement in breast cancer mortality over the past 25 years.
Related article: Update on breast health Mark D. Pearlman, MD, and Jennifer L. Griffin Miller, MD, MPH (March 2013)
Details of the study
In this failure analysis from Massachusetts General Hospital and Brigham and Women’s Hospital, Webb and colleagues reviewed breast cancer deaths over 17 years (new breast cancer cases from 1990 through 1997, with cases followed through 2007). They compared the likelihood of death according to whether screening mammography had been performed in the preceding 2 years.
Of the 609 confirmed deaths from breast cancer, 71% occurred among unscreened women (ie, never screened or screening not done in the preceding 2 years). The median age at diagnosis of fatal cancers was 49 years, whereas women with breast cancer who ultimately died of other causes had a median age at diagnosis of 72 years.
Related article: Biennial vs annual mammography: How I manage my patients Andrew M. Kaunitz, MD (June 2013)
Webb and colleagues concluded: “Most deaths from breast cancer occur in unscreened women. To maximize mortality reduction and life-years gained, initiation of regular screening before age 50 years should be encouraged.”
WHAT THIS EVIDENCE MEANS FOR PRACTICE
The findings of Webb and colleagues are not surprising, given the already demonstrated reduction in breast cancer mortality with the use of routine screening mammography in women in their 40s. What is particularly interesting in this study is that the preponderance of breast cancer deaths occurred in younger women. Biologically, this may be explained by the more aggressive nature of breast cancer in younger women.5
This study provides additional support for the ACOG recommendation to routinely offer breast cancer screening with mammography for women aged 40 to 49 years.
--Mark D. Pearlman, MD
We want to hear from you. Tell us what you think.
- US Preventive Services Task Force. Screening for Breast Cancer. http://www.uspreventiveservicestaskforce.org
/uspstf/uspsbrca.htm. Accessed October 22, 2013. - American College of Obstetricians and Gynecologists. Practice Bulletin No. 122: Breast cancer screening. Obstet Gynecol. 2011;118(2 Pt 1):372–382.
- Nelson HD, Tyne K, Naik A, Bougatsos C, Chan BK, Humphrey L. Screening for breast cancer: An update for the US Preventive Services Task Force. Ann Intern Med. 2009;151(10):727–737.
- Bleyer A, Welch HG. Effect of three decades of screening mammography on breast cancer incidence. N Engl J Med. 2012;367(21):1998–2005.
- Klauber-DeMore N. Tumor biology of breast cancer in young women. Breast Dis. 2006;23:9–15.
- US Preventive Services Task Force. Screening for Breast Cancer. http://www.uspreventiveservicestaskforce.org
/uspstf/uspsbrca.htm. Accessed October 22, 2013. - American College of Obstetricians and Gynecologists. Practice Bulletin No. 122: Breast cancer screening. Obstet Gynecol. 2011;118(2 Pt 1):372–382.
- Nelson HD, Tyne K, Naik A, Bougatsos C, Chan BK, Humphrey L. Screening for breast cancer: An update for the US Preventive Services Task Force. Ann Intern Med. 2009;151(10):727–737.
- Bleyer A, Welch HG. Effect of three decades of screening mammography on breast cancer incidence. N Engl J Med. 2012;367(21):1998–2005.
- Klauber-DeMore N. Tumor biology of breast cancer in young women. Breast Dis. 2006;23:9–15.
USPSTF recommends tamoxifen or raloxifene to reduce breast cancer risk in high-risk patients
Clinicians should engage in shared, informed decision-making with women who are at increased risk for breast cancer about medications to reduce their risk. For women who are at increased risk for breast cancer and at low risk for adverse medication effects, clinicians should offer to prescribe risk-reducing medications, such as tamoxifen or raloxifene, recommends the US Preventive Services Task Force (USPSTF).
RELATED ARTICLE: Update on Breast Health Mark Pearlman, MD, and Jennifer Griffin Miller, MD, MPH (March 2013)
Tamoxifen and raloxifene
These agents are selective estrogen receptor (ER) modulators and have been shown to reduce the incidence of invasive, ER-positive breast cancer in several randomized, controlled trials. Tamoxifen has been approved by the US Food and Drug Administration (FDA) for this use in women aged 35 years or older, and raloxifene has been FDA-approved for this use in postmenopausal women.
RELATED ARTICLE: Osteoporosis treatment and breast cancer prevention: Two goals, one treatment? Robert L. Barbieri, MD (Editorial, November 2013)
A systematic review of clinical trials found that tamoxifen and raloxifene reduced the incidence of invasive breast cancer by 7 to 9 events per 1000 women over 5 years. Tamoxifen was found to reduce the incidence of breast cancer more than raloxifene. Tamoxifen also reduces the incidence of invasive breast cancer in premenopausal women who are at increased risk for the disease.
USPSTF-defined high risk
Women with an estimated 5-year risk for breast cancer of 3% or more are likely to benefit from treatment with tamoxifen or raloxifene. For women with no increased risk for breast cancer, the USPSTF found that the benefit of treatment with tamoxifen or raloxifene is limited (small). The USPSTF recommends against the routine use of medications, such as tamoxifen or raloxifene, for risk reduction of primary breast cancer in women who are not at increased risk for breast cancer.
The usual daily doses for tamoxifen and raloxifene are 20 mg and 60 mg, respectively, for 5 years. Tamoxifen is not recommended for use in combination with hormone therapy or hormonal contraception or in women who are pregnant, those who may become pregnant, or breastfeeding mothers.
RELATED ARTICLE: What is the gynecologist's role in the care of BRCA previvors? Robert L. Barbieri, MD (Editorial, September 2013)
Potential harms from tamoxifen and raloxifene
Tamoxifen and raloxifene increase risk for venous thromboembolic events (VTEs) by 4 to 7 events per 1000 women over 5 years; tamoxifen increases risk more than raloxifene. The USPSTF found that potential harms from thromboembolic events are small to moderate, with increased potential for harms in older women. Neither tamoxifen nor raloxifene should be used in women who have a history of thromboembolic events (deep venous thrombosis, pulmonary embolus, stroke, or transient ischemic attack).
Tamoxifen, but not raloxifene, has been found to increase risk for endometrial cancer (4 more cases per 1000 women). Potential harms from tamoxifen-related endometrial cancer are small to moderate and depend on hysterectomy status and age. The potential risks for tamoxifen-related harms are higher in women older than age 50 and in women with a uterus. Tamoxifen may also increase the incidence of cataracts.
Vasomotor symptoms are a common adverse effect of both tamoxifen and raloxifene. These symptoms may affect a patient's quality of life and willingness to use or adhere to the medications.
The final recommendation statement was published online in the Annals of Internal Medicine September 24, 2013, and is available on the USPSTF Web site.
Reference
- US Preventive Services Task Force. Medications for Risk Reduction of Primary Breast Cancer in Women: Final Recommendation Statement. AHRQ Publication No. 13-05189-EF-2. http://www.uspreventiveservicestaskforce.org/uspstf13/breastcanmeds/breastcanmedsrs.htm. Accessed October 21, 2013.
Clinicians should engage in shared, informed decision-making with women who are at increased risk for breast cancer about medications to reduce their risk. For women who are at increased risk for breast cancer and at low risk for adverse medication effects, clinicians should offer to prescribe risk-reducing medications, such as tamoxifen or raloxifene, recommends the US Preventive Services Task Force (USPSTF).
RELATED ARTICLE: Update on Breast Health Mark Pearlman, MD, and Jennifer Griffin Miller, MD, MPH (March 2013)
Tamoxifen and raloxifene
These agents are selective estrogen receptor (ER) modulators and have been shown to reduce the incidence of invasive, ER-positive breast cancer in several randomized, controlled trials. Tamoxifen has been approved by the US Food and Drug Administration (FDA) for this use in women aged 35 years or older, and raloxifene has been FDA-approved for this use in postmenopausal women.
RELATED ARTICLE: Osteoporosis treatment and breast cancer prevention: Two goals, one treatment? Robert L. Barbieri, MD (Editorial, November 2013)
A systematic review of clinical trials found that tamoxifen and raloxifene reduced the incidence of invasive breast cancer by 7 to 9 events per 1000 women over 5 years. Tamoxifen was found to reduce the incidence of breast cancer more than raloxifene. Tamoxifen also reduces the incidence of invasive breast cancer in premenopausal women who are at increased risk for the disease.
USPSTF-defined high risk
Women with an estimated 5-year risk for breast cancer of 3% or more are likely to benefit from treatment with tamoxifen or raloxifene. For women with no increased risk for breast cancer, the USPSTF found that the benefit of treatment with tamoxifen or raloxifene is limited (small). The USPSTF recommends against the routine use of medications, such as tamoxifen or raloxifene, for risk reduction of primary breast cancer in women who are not at increased risk for breast cancer.
The usual daily doses for tamoxifen and raloxifene are 20 mg and 60 mg, respectively, for 5 years. Tamoxifen is not recommended for use in combination with hormone therapy or hormonal contraception or in women who are pregnant, those who may become pregnant, or breastfeeding mothers.
RELATED ARTICLE: What is the gynecologist's role in the care of BRCA previvors? Robert L. Barbieri, MD (Editorial, September 2013)
Potential harms from tamoxifen and raloxifene
Tamoxifen and raloxifene increase risk for venous thromboembolic events (VTEs) by 4 to 7 events per 1000 women over 5 years; tamoxifen increases risk more than raloxifene. The USPSTF found that potential harms from thromboembolic events are small to moderate, with increased potential for harms in older women. Neither tamoxifen nor raloxifene should be used in women who have a history of thromboembolic events (deep venous thrombosis, pulmonary embolus, stroke, or transient ischemic attack).
Tamoxifen, but not raloxifene, has been found to increase risk for endometrial cancer (4 more cases per 1000 women). Potential harms from tamoxifen-related endometrial cancer are small to moderate and depend on hysterectomy status and age. The potential risks for tamoxifen-related harms are higher in women older than age 50 and in women with a uterus. Tamoxifen may also increase the incidence of cataracts.
Vasomotor symptoms are a common adverse effect of both tamoxifen and raloxifene. These symptoms may affect a patient's quality of life and willingness to use or adhere to the medications.
The final recommendation statement was published online in the Annals of Internal Medicine September 24, 2013, and is available on the USPSTF Web site.
Clinicians should engage in shared, informed decision-making with women who are at increased risk for breast cancer about medications to reduce their risk. For women who are at increased risk for breast cancer and at low risk for adverse medication effects, clinicians should offer to prescribe risk-reducing medications, such as tamoxifen or raloxifene, recommends the US Preventive Services Task Force (USPSTF).
RELATED ARTICLE: Update on Breast Health Mark Pearlman, MD, and Jennifer Griffin Miller, MD, MPH (March 2013)
Tamoxifen and raloxifene
These agents are selective estrogen receptor (ER) modulators and have been shown to reduce the incidence of invasive, ER-positive breast cancer in several randomized, controlled trials. Tamoxifen has been approved by the US Food and Drug Administration (FDA) for this use in women aged 35 years or older, and raloxifene has been FDA-approved for this use in postmenopausal women.
RELATED ARTICLE: Osteoporosis treatment and breast cancer prevention: Two goals, one treatment? Robert L. Barbieri, MD (Editorial, November 2013)
A systematic review of clinical trials found that tamoxifen and raloxifene reduced the incidence of invasive breast cancer by 7 to 9 events per 1000 women over 5 years. Tamoxifen was found to reduce the incidence of breast cancer more than raloxifene. Tamoxifen also reduces the incidence of invasive breast cancer in premenopausal women who are at increased risk for the disease.
USPSTF-defined high risk
Women with an estimated 5-year risk for breast cancer of 3% or more are likely to benefit from treatment with tamoxifen or raloxifene. For women with no increased risk for breast cancer, the USPSTF found that the benefit of treatment with tamoxifen or raloxifene is limited (small). The USPSTF recommends against the routine use of medications, such as tamoxifen or raloxifene, for risk reduction of primary breast cancer in women who are not at increased risk for breast cancer.
The usual daily doses for tamoxifen and raloxifene are 20 mg and 60 mg, respectively, for 5 years. Tamoxifen is not recommended for use in combination with hormone therapy or hormonal contraception or in women who are pregnant, those who may become pregnant, or breastfeeding mothers.
RELATED ARTICLE: What is the gynecologist's role in the care of BRCA previvors? Robert L. Barbieri, MD (Editorial, September 2013)
Potential harms from tamoxifen and raloxifene
Tamoxifen and raloxifene increase risk for venous thromboembolic events (VTEs) by 4 to 7 events per 1000 women over 5 years; tamoxifen increases risk more than raloxifene. The USPSTF found that potential harms from thromboembolic events are small to moderate, with increased potential for harms in older women. Neither tamoxifen nor raloxifene should be used in women who have a history of thromboembolic events (deep venous thrombosis, pulmonary embolus, stroke, or transient ischemic attack).
Tamoxifen, but not raloxifene, has been found to increase risk for endometrial cancer (4 more cases per 1000 women). Potential harms from tamoxifen-related endometrial cancer are small to moderate and depend on hysterectomy status and age. The potential risks for tamoxifen-related harms are higher in women older than age 50 and in women with a uterus. Tamoxifen may also increase the incidence of cataracts.
Vasomotor symptoms are a common adverse effect of both tamoxifen and raloxifene. These symptoms may affect a patient's quality of life and willingness to use or adhere to the medications.
The final recommendation statement was published online in the Annals of Internal Medicine September 24, 2013, and is available on the USPSTF Web site.
Reference
- US Preventive Services Task Force. Medications for Risk Reduction of Primary Breast Cancer in Women: Final Recommendation Statement. AHRQ Publication No. 13-05189-EF-2. http://www.uspreventiveservicestaskforce.org/uspstf13/breastcanmeds/breastcanmedsrs.htm. Accessed October 21, 2013.
Reference
- US Preventive Services Task Force. Medications for Risk Reduction of Primary Breast Cancer in Women: Final Recommendation Statement. AHRQ Publication No. 13-05189-EF-2. http://www.uspreventiveservicestaskforce.org/uspstf13/breastcanmeds/breastcanmedsrs.htm. Accessed October 21, 2013.
Lessons from the pink ribbon
“I am tired of your pink ribbons!” one of my leukemia doctors said half jokingly in a meeting. He is not alone. Some people think there is too much hype about October as the breast cancer awareness month. If there is one color, one disease, and one month that is clearly etched in public memory, is the pink ribbon and breast cancer awareness during the month of October. From grocery stores to National Football League teams, the message of breast cancer awareness during that month takes precedence. Is it too much to talk about one disease? Are we commercializing this message and perhaps detracting from the intended purpose?1
*Click on the link to the left for a PDF of the full article.
“I am tired of your pink ribbons!” one of my leukemia doctors said half jokingly in a meeting. He is not alone. Some people think there is too much hype about October as the breast cancer awareness month. If there is one color, one disease, and one month that is clearly etched in public memory, is the pink ribbon and breast cancer awareness during the month of October. From grocery stores to National Football League teams, the message of breast cancer awareness during that month takes precedence. Is it too much to talk about one disease? Are we commercializing this message and perhaps detracting from the intended purpose?1
*Click on the link to the left for a PDF of the full article.
“I am tired of your pink ribbons!” one of my leukemia doctors said half jokingly in a meeting. He is not alone. Some people think there is too much hype about October as the breast cancer awareness month. If there is one color, one disease, and one month that is clearly etched in public memory, is the pink ribbon and breast cancer awareness during the month of October. From grocery stores to National Football League teams, the message of breast cancer awareness during that month takes precedence. Is it too much to talk about one disease? Are we commercializing this message and perhaps detracting from the intended purpose?1
*Click on the link to the left for a PDF of the full article.