User login
Whole-genome sequencing not ready for prime time
Clinicians and the public have held great hope for years that genomic analysis would transform the prevention and treatment of disease, but although costs may be plummeting, challenges persist, investigators reported March 12th in JAMA.
Sequencing the genome of individuals has become much less expensive, but translating those results into clinically useful information is labor intensive, and fraught with inconsistencies and uncertainties, reported Dr. Frederick E. Dewey of the Stanford (Calif.) Center for Inherited Cardiovascular Disease and his associates (JAMA 2014;311:1035-44).
Three academic primary care physicians and two academic medical geneticists separately reviewed whole-genome sequencing (WGS) results from 12 adult participants, and each proposed clinical follow-up based on the findings. The DNA from whole-blood samples obtained from five men and seven women without any known inherited disease risk was sequenced by commonly used platforms (all 12 at Illumina, with confirmatory sequencing performed for 9 of the participants by Complete Genomics). Two of the primary care physicians had no previous experience with genomic medicine or genetics training, the investigators reported.
Up to one-fifth of gene variants known to be associated with disease risk were not covered at a minimum threshold for discovery, meaning there could be significant gaps in predicting individual risk. For those genetic variants that met the threshold, concordance between the two sequencing platforms was high for common variants (99%), but was substantially lower for genetic variants that were candidates for inherited disease risk (median, 33%; range, 10%-75%), Dr. Dewey and his associates said.
For each participant, the WGS identified between 90 and 127 novel or rare genetic variations, and between 12 and 20 commonly reported variations, all candidates for curation with respect to personal risk and carrier status for inherited disease. The geneticists’ review of the evidence for pathogenicity for each variant required a median time of 54 minutes (range, 5-223 minutes). Based on this finding, investigators estimated the median cost for sequencing and variant interpretation for each participant was $14,815.
Review of the medical genomics report by the three primary care physicians prompted consideration of a median one to three initial follow-up referrals and diagnostic tests per participant. The agreement between physicians about suitability for follow-up of findings was fair, the investigators reported.
In the end, 1 of the 12 participants went on to take action as a result of the findings. A BRCA1 mutation was found in a woman with no family history of breast or ovarian cancer, and she subsequently underwent prophylactic bilateral salpingo-oophorectomy.
Overall, the results illustrate several challenges to clinical adoption of whole-genome sequencing, the authors suggested. Although the analytical validity of WGS is improving, technical challenges to sensitive and accurate assessment of individual genetic variation remain. The finding of only one-third of insertion/deletion genetic variants in inherited disease genes confirmed by the second sequencing platform suggests that variants likely to be pathogenic are more often inconsistently identified, Dr. Dewey and his associates said.
"In this exploratory study of 12 volunteer adults, the use of WGS was associated with incomplete coverage of inherited disease genes, low reproducibility of genetic variation with the highest potential clinical effects, and uncertainty about clinically reportable findings," they wrote.
The research was supported by grants from the National Institutes of Health, the Breetwor Family Foundation, and the LeDucq Foundation. Dr. Dewey reported being a stockholder and member of the scientific advisory board of Personalis, a privately held genome interpretation company, and receiving royalties for patented technology related to genome sequencing. Some of his associates were scientific advisers for companies involved in genomics or received royalties for patented technologies related to genome sequencing.
lnikolaides@frontlinemedcom.com
On Twitter @nikolaideslaura
Clinicians and the public have held great hope for years that genomic analysis would transform the prevention and treatment of disease, but although costs may be plummeting, challenges persist, investigators reported March 12th in JAMA.
Sequencing the genome of individuals has become much less expensive, but translating those results into clinically useful information is labor intensive, and fraught with inconsistencies and uncertainties, reported Dr. Frederick E. Dewey of the Stanford (Calif.) Center for Inherited Cardiovascular Disease and his associates (JAMA 2014;311:1035-44).
Three academic primary care physicians and two academic medical geneticists separately reviewed whole-genome sequencing (WGS) results from 12 adult participants, and each proposed clinical follow-up based on the findings. The DNA from whole-blood samples obtained from five men and seven women without any known inherited disease risk was sequenced by commonly used platforms (all 12 at Illumina, with confirmatory sequencing performed for 9 of the participants by Complete Genomics). Two of the primary care physicians had no previous experience with genomic medicine or genetics training, the investigators reported.
Up to one-fifth of gene variants known to be associated with disease risk were not covered at a minimum threshold for discovery, meaning there could be significant gaps in predicting individual risk. For those genetic variants that met the threshold, concordance between the two sequencing platforms was high for common variants (99%), but was substantially lower for genetic variants that were candidates for inherited disease risk (median, 33%; range, 10%-75%), Dr. Dewey and his associates said.
For each participant, the WGS identified between 90 and 127 novel or rare genetic variations, and between 12 and 20 commonly reported variations, all candidates for curation with respect to personal risk and carrier status for inherited disease. The geneticists’ review of the evidence for pathogenicity for each variant required a median time of 54 minutes (range, 5-223 minutes). Based on this finding, investigators estimated the median cost for sequencing and variant interpretation for each participant was $14,815.
Review of the medical genomics report by the three primary care physicians prompted consideration of a median one to three initial follow-up referrals and diagnostic tests per participant. The agreement between physicians about suitability for follow-up of findings was fair, the investigators reported.
In the end, 1 of the 12 participants went on to take action as a result of the findings. A BRCA1 mutation was found in a woman with no family history of breast or ovarian cancer, and she subsequently underwent prophylactic bilateral salpingo-oophorectomy.
Overall, the results illustrate several challenges to clinical adoption of whole-genome sequencing, the authors suggested. Although the analytical validity of WGS is improving, technical challenges to sensitive and accurate assessment of individual genetic variation remain. The finding of only one-third of insertion/deletion genetic variants in inherited disease genes confirmed by the second sequencing platform suggests that variants likely to be pathogenic are more often inconsistently identified, Dr. Dewey and his associates said.
"In this exploratory study of 12 volunteer adults, the use of WGS was associated with incomplete coverage of inherited disease genes, low reproducibility of genetic variation with the highest potential clinical effects, and uncertainty about clinically reportable findings," they wrote.
The research was supported by grants from the National Institutes of Health, the Breetwor Family Foundation, and the LeDucq Foundation. Dr. Dewey reported being a stockholder and member of the scientific advisory board of Personalis, a privately held genome interpretation company, and receiving royalties for patented technology related to genome sequencing. Some of his associates were scientific advisers for companies involved in genomics or received royalties for patented technologies related to genome sequencing.
lnikolaides@frontlinemedcom.com
On Twitter @nikolaideslaura
Clinicians and the public have held great hope for years that genomic analysis would transform the prevention and treatment of disease, but although costs may be plummeting, challenges persist, investigators reported March 12th in JAMA.
Sequencing the genome of individuals has become much less expensive, but translating those results into clinically useful information is labor intensive, and fraught with inconsistencies and uncertainties, reported Dr. Frederick E. Dewey of the Stanford (Calif.) Center for Inherited Cardiovascular Disease and his associates (JAMA 2014;311:1035-44).
Three academic primary care physicians and two academic medical geneticists separately reviewed whole-genome sequencing (WGS) results from 12 adult participants, and each proposed clinical follow-up based on the findings. The DNA from whole-blood samples obtained from five men and seven women without any known inherited disease risk was sequenced by commonly used platforms (all 12 at Illumina, with confirmatory sequencing performed for 9 of the participants by Complete Genomics). Two of the primary care physicians had no previous experience with genomic medicine or genetics training, the investigators reported.
Up to one-fifth of gene variants known to be associated with disease risk were not covered at a minimum threshold for discovery, meaning there could be significant gaps in predicting individual risk. For those genetic variants that met the threshold, concordance between the two sequencing platforms was high for common variants (99%), but was substantially lower for genetic variants that were candidates for inherited disease risk (median, 33%; range, 10%-75%), Dr. Dewey and his associates said.
For each participant, the WGS identified between 90 and 127 novel or rare genetic variations, and between 12 and 20 commonly reported variations, all candidates for curation with respect to personal risk and carrier status for inherited disease. The geneticists’ review of the evidence for pathogenicity for each variant required a median time of 54 minutes (range, 5-223 minutes). Based on this finding, investigators estimated the median cost for sequencing and variant interpretation for each participant was $14,815.
Review of the medical genomics report by the three primary care physicians prompted consideration of a median one to three initial follow-up referrals and diagnostic tests per participant. The agreement between physicians about suitability for follow-up of findings was fair, the investigators reported.
In the end, 1 of the 12 participants went on to take action as a result of the findings. A BRCA1 mutation was found in a woman with no family history of breast or ovarian cancer, and she subsequently underwent prophylactic bilateral salpingo-oophorectomy.
Overall, the results illustrate several challenges to clinical adoption of whole-genome sequencing, the authors suggested. Although the analytical validity of WGS is improving, technical challenges to sensitive and accurate assessment of individual genetic variation remain. The finding of only one-third of insertion/deletion genetic variants in inherited disease genes confirmed by the second sequencing platform suggests that variants likely to be pathogenic are more often inconsistently identified, Dr. Dewey and his associates said.
"In this exploratory study of 12 volunteer adults, the use of WGS was associated with incomplete coverage of inherited disease genes, low reproducibility of genetic variation with the highest potential clinical effects, and uncertainty about clinically reportable findings," they wrote.
The research was supported by grants from the National Institutes of Health, the Breetwor Family Foundation, and the LeDucq Foundation. Dr. Dewey reported being a stockholder and member of the scientific advisory board of Personalis, a privately held genome interpretation company, and receiving royalties for patented technology related to genome sequencing. Some of his associates were scientific advisers for companies involved in genomics or received royalties for patented technologies related to genome sequencing.
lnikolaides@frontlinemedcom.com
On Twitter @nikolaideslaura
FROM JAMA
Major finding: For each participant, whole-genome sequencing identified between 90 and 127 novel or rare genetic variations, and between 12 and 20 commonly reported variations.
Data source: Whole-genome sequencing was performed from whole-blood samples of 12 adult volunteers, and reports were analyzed by geneticists and primary care physicians for follow-up.
Disclosures: The research was supported by grants from the National Institutes of Health, the Breetwor Family Foundation, and the LeDucq Foundation. Dr. Dewey reported being a stockholder and member of the scientific advisory board of Personalis, a privately held genome interpretation company, and receiving royalties for patented technology related to genome sequencing. Some of his associates were scientific advisers for companies involved in genomics or received royalties for patented technologies related to genome sequencing.
Genomic analyses led to targeted treatment for metastatic breast cancer, though response rate disappointing
Genomic abnormalities can be identified in individual patients with metastatic breast cancer, which can then lead to targeted therapy, investigators reported in the March issue of Lancet Oncology.
In a prospective study of 423 patients who had breast cancer with a metastasis accessible for biopsy, comparative genomic hybridization array was feasible in 283 patients and Sanger sequencing was feasible in 297 patients. A targetable genomic alteration was found in 195 patients (46%), most often PIK3CA mutation (25%), CCND1 amplification (18%), and FGFR1 amplification (12%), reported Dr. Fabrice André of Institut Gustave Roussy, Villejuif, France, and his associates.

The primary endpoint – the ability to offer targeted therapy based on genomic sequencing – was achieved for 55 patients (13%). Of the 43 patients who ultimately received targeted therapy as a result of the genomic analyses, four (9%) had an objective response, and nine others (21%) had stable disease for more than 16 weeks. Grade 3 or higher adverse events related to biopsy were reported in four patients (Lancet Oncol. 2014;15:267-74).
The response rate was "disappointing," but the patient population had been heavily pretreated, the researchers noted.
The result "justifies the development of multiple strategies to improve efficacy of screening" for targeted therapy, the investigators said. They recommended improving algorithms for analyzing genomic data, using highly bioactive agents for targeted therapy, and combining therapies to delay drug resistance.
The study was sponsored by the French National Cancer Institute, Breast Cancer Research Foundation, Odyssea, and Operation Parrains Chercheurs. The authors reported no relevant financial conflicts of interest.
Genomic abnormalities can be identified in individual patients with metastatic breast cancer, which can then lead to targeted therapy, investigators reported in the March issue of Lancet Oncology.
In a prospective study of 423 patients who had breast cancer with a metastasis accessible for biopsy, comparative genomic hybridization array was feasible in 283 patients and Sanger sequencing was feasible in 297 patients. A targetable genomic alteration was found in 195 patients (46%), most often PIK3CA mutation (25%), CCND1 amplification (18%), and FGFR1 amplification (12%), reported Dr. Fabrice André of Institut Gustave Roussy, Villejuif, France, and his associates.
The primary endpoint – the ability to offer targeted therapy based on genomic sequencing – was achieved for 55 patients (13%). Of the 43 patients who ultimately received targeted therapy as a result of the genomic analyses, four (9%) had an objective response, and nine others (21%) had stable disease for more than 16 weeks. Grade 3 or higher adverse events related to biopsy were reported in four patients (Lancet Oncol. 2014;15:267-74).
The response rate was "disappointing," but the patient population had been heavily pretreated, the researchers noted.
The result "justifies the development of multiple strategies to improve efficacy of screening" for targeted therapy, the investigators said. They recommended improving algorithms for analyzing genomic data, using highly bioactive agents for targeted therapy, and combining therapies to delay drug resistance.
The study was sponsored by the French National Cancer Institute, Breast Cancer Research Foundation, Odyssea, and Operation Parrains Chercheurs. The authors reported no relevant financial conflicts of interest.
Genomic abnormalities can be identified in individual patients with metastatic breast cancer, which can then lead to targeted therapy, investigators reported in the March issue of Lancet Oncology.
In a prospective study of 423 patients who had breast cancer with a metastasis accessible for biopsy, comparative genomic hybridization array was feasible in 283 patients and Sanger sequencing was feasible in 297 patients. A targetable genomic alteration was found in 195 patients (46%), most often PIK3CA mutation (25%), CCND1 amplification (18%), and FGFR1 amplification (12%), reported Dr. Fabrice André of Institut Gustave Roussy, Villejuif, France, and his associates.
The primary endpoint – the ability to offer targeted therapy based on genomic sequencing – was achieved for 55 patients (13%). Of the 43 patients who ultimately received targeted therapy as a result of the genomic analyses, four (9%) had an objective response, and nine others (21%) had stable disease for more than 16 weeks. Grade 3 or higher adverse events related to biopsy were reported in four patients (Lancet Oncol. 2014;15:267-74).
The response rate was "disappointing," but the patient population had been heavily pretreated, the researchers noted.
The result "justifies the development of multiple strategies to improve efficacy of screening" for targeted therapy, the investigators said. They recommended improving algorithms for analyzing genomic data, using highly bioactive agents for targeted therapy, and combining therapies to delay drug resistance.
The study was sponsored by the French National Cancer Institute, Breast Cancer Research Foundation, Odyssea, and Operation Parrains Chercheurs. The authors reported no relevant financial conflicts of interest.
FROM LANCET ONCOLOGY
Major finding: Targeted therapy was possible for 13% of patients screened with genomic analyses. A total of 9% of patients treated with targeted therapy had an objective response, and 21% had stable disease for more than 16 weeks.
Data source: Multicenter, prospective trial of 423 patients with metastatic breast cancer.
Disclosures: The study was funded by the French National Cancer Institute, Breast Cancer Research Foundation, Odyssea, and Operation Parrains Chercheurs. The authors reported no relevant conflicts of interest.

Prophylactic oophorectomy cuts all-cause mortality 77% in BRCA mutation carriers
Undergoing prophylactic oophorectomy reduces all-cause mortality by 77% among women who carry a deleterious BRCA1 or BRCA2 genetic mutation, according to a report published online Feb. 24 in the Journal of Clinical Oncology.
The surgery’s protective effect stems largely from a reduction in the incidence of ovarian, tubal, and peritoneal cancers, "but there is an important component from reducing breast cancer incidence and mortality as well," reported Dr. Amy P.M. Finch of the University of Toronto and her associates in the Hereditary Ovarian Cancer Clinical Study Group.

In addition, the results of this prospective cohort study support the recommendation that these women should undergo prophylactic oophorectomy by age 35, because their risk of developing cancer rises markedly after that, the investigators said.
Noting that the effect of oophorectomy on mortality has not been well studied and that the optimal age for undergoing the procedure hasn’t yet been determined, Dr. Finch and her colleagues analyzed data in an international registry of carriers of deleterious BRCA1 and BRCA2 mutations. Their study cohort included 5,783 women followed at 43 medical centers in Canada, the United States, Austria, France, Italy, Norway, and Poland, who were enrolled in 1995-2011.
Just under half of these women had a history of breast cancer, and the mean age at enrollment was 46 years (range, 30-88 years). They were followed for an average of 5.6 years for the development of cancer.
A total of 2,270 women did not undergo prophylactic oophorectomy, while 2,123 had already undergone the surgery at baseline and another 1,390 had it during the study period.
A total of 186 new ovarian, fallopian, and peritoneal cancers were diagnosed during follow-up. These included cases in 108 women with intact ovaries who were diagnosed clinically, 46 cases of occult cancer diagnosed at oophorectomy, and 32 cases of peritoneal cancer that developed after oophorectomy.
Of the 507 women who died during follow-up, 329 died from breast cancer; 67 died from ovarian, fallopian, or peritoneal cancer; 49 died from other cancers; 44 died of noncancer causes; and 18 died from unknown causes.
Oophorectomy had a profound protective effect on all-cause mortality and cancer-specific mortality, both for BRCA1 carriers and for BRCA2 carriers. Those who were cancer free at baseline and underwent the surgery showed a 77% reduction in all-cause mortality to age 70. Women who had a history of breast cancer at enrollment – including those whose mutation-carrier status was discovered when their breast cancer was diagnosed – showed a similar reduction in all-cause mortality after undergoing oophorectomy, the investigators reported (J. Clin. Oncol. 2014 Feb. 24 [doi: 10.1200/jco.2013.53.2820]).
The findings also support the current recommendation to undergo oophorectomy at age 35. "If a woman with a BRCA1 mutation chooses to delay salpingo-oophorectomy until age 40 years, we estimate that she will have a 4.0% chance of being diagnosed with ovarian cancer, either clinically before or at the time of salpingo-oophorectomy. If she chooses to wait until age 50 years, the probability rises to 14.2%," Dr. Finch and her associates said.
In view of this recommendation, "it is important that we ascertain the long-term effects of salpingo-oophorectomy and design effective treatments and preventive strategies for these," they added.
The researchers noted that their study began in 1995, before it was recommended that removal and detailed pathological evaluation of the fallopian tubes be included at oophorectomy. Eighteen of the 46 occult cancers discovered at surgery in this cohort were classified as primary fallopian tube cancers, which reinforces that the standard of care should now include removal of the tubes, they said.
This study was supported by the Canadian Breast Cancer Research Alliance, the National Institutes of Health, and the Ontario Ministry of Research and Innovation. Dr. Finch and her associates reported no financial conflicts of interest.
Undergoing prophylactic oophorectomy reduces all-cause mortality by 77% among women who carry a deleterious BRCA1 or BRCA2 genetic mutation, according to a report published online Feb. 24 in the Journal of Clinical Oncology.
The surgery’s protective effect stems largely from a reduction in the incidence of ovarian, tubal, and peritoneal cancers, "but there is an important component from reducing breast cancer incidence and mortality as well," reported Dr. Amy P.M. Finch of the University of Toronto and her associates in the Hereditary Ovarian Cancer Clinical Study Group.
In addition, the results of this prospective cohort study support the recommendation that these women should undergo prophylactic oophorectomy by age 35, because their risk of developing cancer rises markedly after that, the investigators said.
Noting that the effect of oophorectomy on mortality has not been well studied and that the optimal age for undergoing the procedure hasn’t yet been determined, Dr. Finch and her colleagues analyzed data in an international registry of carriers of deleterious BRCA1 and BRCA2 mutations. Their study cohort included 5,783 women followed at 43 medical centers in Canada, the United States, Austria, France, Italy, Norway, and Poland, who were enrolled in 1995-2011.
Just under half of these women had a history of breast cancer, and the mean age at enrollment was 46 years (range, 30-88 years). They were followed for an average of 5.6 years for the development of cancer.
A total of 2,270 women did not undergo prophylactic oophorectomy, while 2,123 had already undergone the surgery at baseline and another 1,390 had it during the study period.
A total of 186 new ovarian, fallopian, and peritoneal cancers were diagnosed during follow-up. These included cases in 108 women with intact ovaries who were diagnosed clinically, 46 cases of occult cancer diagnosed at oophorectomy, and 32 cases of peritoneal cancer that developed after oophorectomy.
Of the 507 women who died during follow-up, 329 died from breast cancer; 67 died from ovarian, fallopian, or peritoneal cancer; 49 died from other cancers; 44 died of noncancer causes; and 18 died from unknown causes.
Oophorectomy had a profound protective effect on all-cause mortality and cancer-specific mortality, both for BRCA1 carriers and for BRCA2 carriers. Those who were cancer free at baseline and underwent the surgery showed a 77% reduction in all-cause mortality to age 70. Women who had a history of breast cancer at enrollment – including those whose mutation-carrier status was discovered when their breast cancer was diagnosed – showed a similar reduction in all-cause mortality after undergoing oophorectomy, the investigators reported (J. Clin. Oncol. 2014 Feb. 24 [doi: 10.1200/jco.2013.53.2820]).
The findings also support the current recommendation to undergo oophorectomy at age 35. "If a woman with a BRCA1 mutation chooses to delay salpingo-oophorectomy until age 40 years, we estimate that she will have a 4.0% chance of being diagnosed with ovarian cancer, either clinically before or at the time of salpingo-oophorectomy. If she chooses to wait until age 50 years, the probability rises to 14.2%," Dr. Finch and her associates said.
In view of this recommendation, "it is important that we ascertain the long-term effects of salpingo-oophorectomy and design effective treatments and preventive strategies for these," they added.
The researchers noted that their study began in 1995, before it was recommended that removal and detailed pathological evaluation of the fallopian tubes be included at oophorectomy. Eighteen of the 46 occult cancers discovered at surgery in this cohort were classified as primary fallopian tube cancers, which reinforces that the standard of care should now include removal of the tubes, they said.
This study was supported by the Canadian Breast Cancer Research Alliance, the National Institutes of Health, and the Ontario Ministry of Research and Innovation. Dr. Finch and her associates reported no financial conflicts of interest.
Undergoing prophylactic oophorectomy reduces all-cause mortality by 77% among women who carry a deleterious BRCA1 or BRCA2 genetic mutation, according to a report published online Feb. 24 in the Journal of Clinical Oncology.
The surgery’s protective effect stems largely from a reduction in the incidence of ovarian, tubal, and peritoneal cancers, "but there is an important component from reducing breast cancer incidence and mortality as well," reported Dr. Amy P.M. Finch of the University of Toronto and her associates in the Hereditary Ovarian Cancer Clinical Study Group.
In addition, the results of this prospective cohort study support the recommendation that these women should undergo prophylactic oophorectomy by age 35, because their risk of developing cancer rises markedly after that, the investigators said.
Noting that the effect of oophorectomy on mortality has not been well studied and that the optimal age for undergoing the procedure hasn’t yet been determined, Dr. Finch and her colleagues analyzed data in an international registry of carriers of deleterious BRCA1 and BRCA2 mutations. Their study cohort included 5,783 women followed at 43 medical centers in Canada, the United States, Austria, France, Italy, Norway, and Poland, who were enrolled in 1995-2011.
Just under half of these women had a history of breast cancer, and the mean age at enrollment was 46 years (range, 30-88 years). They were followed for an average of 5.6 years for the development of cancer.
A total of 2,270 women did not undergo prophylactic oophorectomy, while 2,123 had already undergone the surgery at baseline and another 1,390 had it during the study period.
A total of 186 new ovarian, fallopian, and peritoneal cancers were diagnosed during follow-up. These included cases in 108 women with intact ovaries who were diagnosed clinically, 46 cases of occult cancer diagnosed at oophorectomy, and 32 cases of peritoneal cancer that developed after oophorectomy.
Of the 507 women who died during follow-up, 329 died from breast cancer; 67 died from ovarian, fallopian, or peritoneal cancer; 49 died from other cancers; 44 died of noncancer causes; and 18 died from unknown causes.
Oophorectomy had a profound protective effect on all-cause mortality and cancer-specific mortality, both for BRCA1 carriers and for BRCA2 carriers. Those who were cancer free at baseline and underwent the surgery showed a 77% reduction in all-cause mortality to age 70. Women who had a history of breast cancer at enrollment – including those whose mutation-carrier status was discovered when their breast cancer was diagnosed – showed a similar reduction in all-cause mortality after undergoing oophorectomy, the investigators reported (J. Clin. Oncol. 2014 Feb. 24 [doi: 10.1200/jco.2013.53.2820]).
The findings also support the current recommendation to undergo oophorectomy at age 35. "If a woman with a BRCA1 mutation chooses to delay salpingo-oophorectomy until age 40 years, we estimate that she will have a 4.0% chance of being diagnosed with ovarian cancer, either clinically before or at the time of salpingo-oophorectomy. If she chooses to wait until age 50 years, the probability rises to 14.2%," Dr. Finch and her associates said.
In view of this recommendation, "it is important that we ascertain the long-term effects of salpingo-oophorectomy and design effective treatments and preventive strategies for these," they added.
The researchers noted that their study began in 1995, before it was recommended that removal and detailed pathological evaluation of the fallopian tubes be included at oophorectomy. Eighteen of the 46 occult cancers discovered at surgery in this cohort were classified as primary fallopian tube cancers, which reinforces that the standard of care should now include removal of the tubes, they said.
This study was supported by the Canadian Breast Cancer Research Alliance, the National Institutes of Health, and the Ontario Ministry of Research and Innovation. Dr. Finch and her associates reported no financial conflicts of interest.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Major finding: Oophorectomy had a profound protective effect on all-cause mortality and cancer-specific mortality both for BRCA1 carriers and for BRCA2 carriers, reducing all-cause mortality by 77% overall.
Data source: A prospective cohort study involving 5,783 women in an international registry who carried BRCA1 or BRCA2 mutations and were followed for an average of 5.6 years for the development of ovarian, fallopian tube, peritoneal, or breast cancer.
Disclosures: This study was supported by the Canadian Breast Cancer Research Alliance, the National Institutes of Health, and the Ontario Ministry of Research and Innovation. Dr. Finch and her associates reported no financial conflicts of interest.

Randomized trial of vitamin B6 for preventing hand-foot syndrome from capecitabine chemotherapy
Background Capecitabine is an oral fluoropyrimidine that is used to treat various malignancies. Hand-foot syndrome (HFS) is a dose-limiting toxicity of capecitabine that can limit the use of this agent in some patients. Some investigators have observed that pyridoxine (vitamin B6) can ameliorate HFS that is caused by capecitabine. We designed a prospective trial to determine if pyridoxine can prevent HFS in patients who receive capecitabine.
Methods In our double-blind, placebo-controlled trial, we randomly assigned eligible patients who were treated with capecitabine to receive either daily pyridoxine 100 mg or placebo along with their capecitabine-containing chemotherapy regimen. Patients were observed during the first 4 cycles of capecitabine treatment. The primary endpoint was the incidence and grade of HFS that occurred in both study arms.
Results Between 2008 and 2011, 77 patients were randomly assigned to receive either pyridoxine (n = 38) or placebo (n = 39). Dosages of capecitabine were equally matched between both arms of the study. HFS occurred after a median of 2 chemotherapy cycles in both groups. HFS developed in 10 of 38 (26%) patients in the pyridoxine group and in 8 of 39 (21%) patients in the placebo group (P = .547). Therefore, the risk of HFS was 5 percentage points higher in pyridoxine group (95% confdence interval [CI] for difference, –13 percentage points to +25 percentage points). Given our study results, a true beneft from pyridoxine can be excluded. No difference in HFS grades was observed.
Limitations Single-institution study.
Conclusion Prophylactic pyridoxine (vitamin B6), given concomitantly with capecitabine-containing chemotherapy, was not effective for the prevention of HFS.
*To read the full article, click on the PDF icon at the top of this introduction.
Background Capecitabine is an oral fluoropyrimidine that is used to treat various malignancies. Hand-foot syndrome (HFS) is a dose-limiting toxicity of capecitabine that can limit the use of this agent in some patients. Some investigators have observed that pyridoxine (vitamin B6) can ameliorate HFS that is caused by capecitabine. We designed a prospective trial to determine if pyridoxine can prevent HFS in patients who receive capecitabine.
Methods In our double-blind, placebo-controlled trial, we randomly assigned eligible patients who were treated with capecitabine to receive either daily pyridoxine 100 mg or placebo along with their capecitabine-containing chemotherapy regimen. Patients were observed during the first 4 cycles of capecitabine treatment. The primary endpoint was the incidence and grade of HFS that occurred in both study arms.
Results Between 2008 and 2011, 77 patients were randomly assigned to receive either pyridoxine (n = 38) or placebo (n = 39). Dosages of capecitabine were equally matched between both arms of the study. HFS occurred after a median of 2 chemotherapy cycles in both groups. HFS developed in 10 of 38 (26%) patients in the pyridoxine group and in 8 of 39 (21%) patients in the placebo group (P = .547). Therefore, the risk of HFS was 5 percentage points higher in pyridoxine group (95% confdence interval [CI] for difference, –13 percentage points to +25 percentage points). Given our study results, a true beneft from pyridoxine can be excluded. No difference in HFS grades was observed.
Limitations Single-institution study.
Conclusion Prophylactic pyridoxine (vitamin B6), given concomitantly with capecitabine-containing chemotherapy, was not effective for the prevention of HFS.
*To read the full article, click on the PDF icon at the top of this introduction.
Background Capecitabine is an oral fluoropyrimidine that is used to treat various malignancies. Hand-foot syndrome (HFS) is a dose-limiting toxicity of capecitabine that can limit the use of this agent in some patients. Some investigators have observed that pyridoxine (vitamin B6) can ameliorate HFS that is caused by capecitabine. We designed a prospective trial to determine if pyridoxine can prevent HFS in patients who receive capecitabine.
Methods In our double-blind, placebo-controlled trial, we randomly assigned eligible patients who were treated with capecitabine to receive either daily pyridoxine 100 mg or placebo along with their capecitabine-containing chemotherapy regimen. Patients were observed during the first 4 cycles of capecitabine treatment. The primary endpoint was the incidence and grade of HFS that occurred in both study arms.
Results Between 2008 and 2011, 77 patients were randomly assigned to receive either pyridoxine (n = 38) or placebo (n = 39). Dosages of capecitabine were equally matched between both arms of the study. HFS occurred after a median of 2 chemotherapy cycles in both groups. HFS developed in 10 of 38 (26%) patients in the pyridoxine group and in 8 of 39 (21%) patients in the placebo group (P = .547). Therefore, the risk of HFS was 5 percentage points higher in pyridoxine group (95% confdence interval [CI] for difference, –13 percentage points to +25 percentage points). Given our study results, a true beneft from pyridoxine can be excluded. No difference in HFS grades was observed.
Limitations Single-institution study.
Conclusion Prophylactic pyridoxine (vitamin B6), given concomitantly with capecitabine-containing chemotherapy, was not effective for the prevention of HFS.
*To read the full article, click on the PDF icon at the top of this introduction.
Annual mammography at age 40-59 provides no survival benefit
Annual mammography in women aged 40 to 59 years was no more effective than was physical examination or usual care for reducing breast cancer mortality when adjuvant therapy for breast cancer is readily available, according to 25-year findings from the Canadian National Breast Screening Study.
During a 5-year screening period beginning in 1980, 666 invasive breast cancers were detected in 44,925 women randomized to receive annual mammography and annual physical breast examinations, and 524 were detected in 44,910 women randomized to receive a single physical breast examination followed by usual care in the community. Of these, 180 and 171 in the mammography and control arms, respectively, died of breast cancer during up to 25 years of follow-up (mean of 22 years), Dr. Anthony B. Miller of the University of Toronto, and his colleagues reported.
The 25-year cumulative mortality from breast cancer detected during the screening period was similar between the women in the mammography arm and the control arm (hazard ratio, 1.05), the investigators reported Feb. 11 in BMJ.
After the screening period, an additional 2,584 breast cancers were detected in the mammography arm and 2,609 in the control arm during the follow-up period. Overall, 1,005 women died from breast cancer during follow-up, including 351 who were diagnosed during the screening period.
Of the breast cancers detected in the mammography arm during the initial screening period, 484 were screen detected, 176 were interval cancers, and 6 were lacking data. The mean size of cancers diagnosed in the mammography arm was 1.91 cm vs. 2.10 cm in the control arm, they said.
"In the mammography arm, 30.6% of cancers were node positive and 68.2% were palpable. In the control arm, 32.4% of the cancers were node positive and all were palpable ...on average, palpable cancer were larger than cancers that were detected only by mammography (2.1 cm v 1.4 cm) and were more likely to be node positive (34.7% vs. 16.5%)," the investigators wrote (BMJ 2014 Feb.11;348 [doi:10.1136/bmj.g366]).
Although 25-year survival was better for those with tumors less than 2 cm vs. greater than 2 cm, those with breast cancer detected in the mammography vs. the control arm, and for those in the mammography arm with nonpalpable vs. palpable tumors (HR, 0.46, 0.79, and 0.58, respectively), the overall 25-year cumulative mortality from breast cancer was similar between women in the mammography arm and control arm, (HR, 0.99), the investigators wrote.
The findings were nearly identical for those aged 40-49 years, and those aged 50-59 years, the investigators noted.
Notably, at the end of the screening period, an excess of 142 breast cancers were detected in the mammography group, compared with the control group, and at 15 years, that excess remained at 106, implying that 22% of the screen-detected invasive cancers in the mammography arm were overdiagnosed, meaning that the cancer might not otherwise have become clinically apparent during the patient’s lifetime.
"This represents one overdiagnosed breast cancer for every 424 women who received mammography screening in the trial. Assuming that nearly all overdiagnosed cancers in the Canadian National Breast Screening Study were nonpalpable, 50% of mammogram detected, nonpalpable cancers were overdiagnosed," they said.
The Canadian National Breast Screening Study was supported by the various Canadian health agencies and advocacy groups. Dr. Miller was supported in part by a national health scientist award from Health and Welfare Canada.
Annual mammography in women aged 40 to 59 years was no more effective than was physical examination or usual care for reducing breast cancer mortality when adjuvant therapy for breast cancer is readily available, according to 25-year findings from the Canadian National Breast Screening Study.
During a 5-year screening period beginning in 1980, 666 invasive breast cancers were detected in 44,925 women randomized to receive annual mammography and annual physical breast examinations, and 524 were detected in 44,910 women randomized to receive a single physical breast examination followed by usual care in the community. Of these, 180 and 171 in the mammography and control arms, respectively, died of breast cancer during up to 25 years of follow-up (mean of 22 years), Dr. Anthony B. Miller of the University of Toronto, and his colleagues reported.
The 25-year cumulative mortality from breast cancer detected during the screening period was similar between the women in the mammography arm and the control arm (hazard ratio, 1.05), the investigators reported Feb. 11 in BMJ.
After the screening period, an additional 2,584 breast cancers were detected in the mammography arm and 2,609 in the control arm during the follow-up period. Overall, 1,005 women died from breast cancer during follow-up, including 351 who were diagnosed during the screening period.
Of the breast cancers detected in the mammography arm during the initial screening period, 484 were screen detected, 176 were interval cancers, and 6 were lacking data. The mean size of cancers diagnosed in the mammography arm was 1.91 cm vs. 2.10 cm in the control arm, they said.
"In the mammography arm, 30.6% of cancers were node positive and 68.2% were palpable. In the control arm, 32.4% of the cancers were node positive and all were palpable ...on average, palpable cancer were larger than cancers that were detected only by mammography (2.1 cm v 1.4 cm) and were more likely to be node positive (34.7% vs. 16.5%)," the investigators wrote (BMJ 2014 Feb.11;348 [doi:10.1136/bmj.g366]).
Although 25-year survival was better for those with tumors less than 2 cm vs. greater than 2 cm, those with breast cancer detected in the mammography vs. the control arm, and for those in the mammography arm with nonpalpable vs. palpable tumors (HR, 0.46, 0.79, and 0.58, respectively), the overall 25-year cumulative mortality from breast cancer was similar between women in the mammography arm and control arm, (HR, 0.99), the investigators wrote.
The findings were nearly identical for those aged 40-49 years, and those aged 50-59 years, the investigators noted.
Notably, at the end of the screening period, an excess of 142 breast cancers were detected in the mammography group, compared with the control group, and at 15 years, that excess remained at 106, implying that 22% of the screen-detected invasive cancers in the mammography arm were overdiagnosed, meaning that the cancer might not otherwise have become clinically apparent during the patient’s lifetime.
"This represents one overdiagnosed breast cancer for every 424 women who received mammography screening in the trial. Assuming that nearly all overdiagnosed cancers in the Canadian National Breast Screening Study were nonpalpable, 50% of mammogram detected, nonpalpable cancers were overdiagnosed," they said.
The Canadian National Breast Screening Study was supported by the various Canadian health agencies and advocacy groups. Dr. Miller was supported in part by a national health scientist award from Health and Welfare Canada.
Annual mammography in women aged 40 to 59 years was no more effective than was physical examination or usual care for reducing breast cancer mortality when adjuvant therapy for breast cancer is readily available, according to 25-year findings from the Canadian National Breast Screening Study.
During a 5-year screening period beginning in 1980, 666 invasive breast cancers were detected in 44,925 women randomized to receive annual mammography and annual physical breast examinations, and 524 were detected in 44,910 women randomized to receive a single physical breast examination followed by usual care in the community. Of these, 180 and 171 in the mammography and control arms, respectively, died of breast cancer during up to 25 years of follow-up (mean of 22 years), Dr. Anthony B. Miller of the University of Toronto, and his colleagues reported.
The 25-year cumulative mortality from breast cancer detected during the screening period was similar between the women in the mammography arm and the control arm (hazard ratio, 1.05), the investigators reported Feb. 11 in BMJ.
After the screening period, an additional 2,584 breast cancers were detected in the mammography arm and 2,609 in the control arm during the follow-up period. Overall, 1,005 women died from breast cancer during follow-up, including 351 who were diagnosed during the screening period.
Of the breast cancers detected in the mammography arm during the initial screening period, 484 were screen detected, 176 were interval cancers, and 6 were lacking data. The mean size of cancers diagnosed in the mammography arm was 1.91 cm vs. 2.10 cm in the control arm, they said.
"In the mammography arm, 30.6% of cancers were node positive and 68.2% were palpable. In the control arm, 32.4% of the cancers were node positive and all were palpable ...on average, palpable cancer were larger than cancers that were detected only by mammography (2.1 cm v 1.4 cm) and were more likely to be node positive (34.7% vs. 16.5%)," the investigators wrote (BMJ 2014 Feb.11;348 [doi:10.1136/bmj.g366]).
Although 25-year survival was better for those with tumors less than 2 cm vs. greater than 2 cm, those with breast cancer detected in the mammography vs. the control arm, and for those in the mammography arm with nonpalpable vs. palpable tumors (HR, 0.46, 0.79, and 0.58, respectively), the overall 25-year cumulative mortality from breast cancer was similar between women in the mammography arm and control arm, (HR, 0.99), the investigators wrote.
The findings were nearly identical for those aged 40-49 years, and those aged 50-59 years, the investigators noted.
Notably, at the end of the screening period, an excess of 142 breast cancers were detected in the mammography group, compared with the control group, and at 15 years, that excess remained at 106, implying that 22% of the screen-detected invasive cancers in the mammography arm were overdiagnosed, meaning that the cancer might not otherwise have become clinically apparent during the patient’s lifetime.
"This represents one overdiagnosed breast cancer for every 424 women who received mammography screening in the trial. Assuming that nearly all overdiagnosed cancers in the Canadian National Breast Screening Study were nonpalpable, 50% of mammogram detected, nonpalpable cancers were overdiagnosed," they said.
The Canadian National Breast Screening Study was supported by the various Canadian health agencies and advocacy groups. Dr. Miller was supported in part by a national health scientist award from Health and Welfare Canada.
FROM BMJ
Major finding: Overall 25-year cumulative mortality from breast cancer was similar between women in the mammography arm and control arm, (HR, 0.99).
Data source: The randomized Canadian National Breast Screening Study of nearly 90,000 women.
Disclosures: This study was supported by various Canadian health agencies and advocacy groups. Dr. Miller was supported in part by a national health scientist award from Health and Welfare Canada.
Guidelines: No ink on tumor is adequate surgical margin for early-stage breast cancer
Negative surgical margins defined by the absence of any ink on the excised tumor are adequate in most cases of early-stage breast cancer treated with breast-conserving therapy, suggest new consensus guidelines from the Society of Surgical Oncology and American Society for Radiation Oncology.
"The use of no ink on tumor as the standard for an adequate margin in invasive cancer in the era of multidisciplinary therapy is associated with low rates of ipsilateral breast tumor recurrence and has the potential to decrease re-excision rates, improve cosmetic outcomes, and decrease health care costs," concludes the 12-member multidisciplinary panel. "The routine practice to obtain negative margin widths wider than no ink on tumor is not indicated" (J. Clin. Oncol. 2014 Feb. 10 [doi:10.1200/JCO.2013.53.3935]).

The panel used as their evidence a systematic review and a meta-analysis based on 33 studies having a total of 28,162 patients with stage I or II breast cancer who were treated with breast-conserving surgery plus whole-breast radiation therapy.
Results showed that, compared with peers having negative margins, patients having positive margins were twice as likely to experience an ipsilateral recurrence, regardless of whether they had favorable tumor biology, were given a radiation boost, or received endocrine therapy (Int. J. Radiation Oncol. Biol. Phys. 2014;88:553-64).
But taking wider margins beyond the point of no ink on tumor did not further reduce the risk of ipsilateral recurrence in the patients overall or in a variety of subsets having unfavorable features (young age, aggressive biology, lobular cancers, or tumors with an extensive intraductal component).
"Our hope is that this guideline will ultimately lead to significant reductions in the high re-excision rate for women with early-stage breast cancer undergoing breast-conserving surgery. Based on the consensus panel’s extensive review of the literature, the vast majority of re-excisions are unnecessary because disease control in the breast is excellent for women with early-stage disease when radiation and hormonal therapy and/or chemotherapy are added to a women’s treatment plan," panel cochair Dr. Meena S. Moran of Yale University, New Haven, Conn., commented in a prepared statement.
In an accompanying editorial, Dr. Reshma Jagsi, University of Michigan, Ann Arbor, and her colleagues write, "We agree with the general idea that routine reexcision of close margins (beyond no ink on tumor) is not necessary, and we expect that these guidelines will have a substantial impact on the community of practicing surgeons. Therefore, radiation oncologists should be prepared to encounter an increasing number of patients with microscopically close margins who might have undergone re-excision in previous years" (Int. J. Radiation Oncol. Biol. Phys. 2014;88:535-36).
At the same time, they note that the wording of the new guidelines gives physicians and patients latitude in individualizing decisions about whether re-excision is warranted.
"Physicians applying these guidelines must have an appreciation of the rationale for the recommendations, as well as the limitations of the evidence available, so that they can interpret and apply the guidelines appropriately. Only with a sophisticated understanding of these issues can we, as a profession, continue to deliver individualized care of consistently high quality, avoiding the sort of ‘cookbook medicine’ that serves well neither physicians nor patients," the editorialists conclude.
The studies included in the meta-analysis were published between 1965 and early 2013 and had a median or mean follow-up of at least 4 years. Patients were excluded if they received neoadjuvant chemotherapy or had only ductal carcinoma in situ.

Overall, 78% of the patients studied had negative margins, defined as no ink on the invasive tumor or any ductal carcinoma in situ component. After a median follow-up of 6.6 years, the median prevalence of ipsilateral recurrence was 5.3% overall.
Patients with positive or close margins were twice as likely to have an ipsilateral recurrence (odds ratio, 1.96). In the subset of studies that were able to separate out close margins, risk was elevated with both positive margins (OR, 2.44) and close margins (OR, 1.74).
The adverse impact of positive margins was still evident in analyses taking into account use of a radiation boost (OR, 2.45) and receipt of endocrine therapy (OR, 2.53), and among patients with favorable biology in the form of estrogen receptor–positive tumors (OR, 2.66).
When the impact of the width of the negative margin was evaluated, the risks of ipsilateral recurrence with 2-mm and 5-mm margins were statistically indistinguishable from those with 1-mm margins.
The analysis confirmed that giving systemic therapy (endocrine therapy, chemotherapy, and/or biologic therapy) reduces the risk of ipsilateral recurrence. But the evidence also suggested that in the small number of patients who do not receive this therapy, wider margins beyond no ink on tumor do not further reduce that risk.
In additional findings, there was no evidence that wider margins beyond no ink on tumor are indicated in patients having more aggressive biological subtypes of breast cancer, invasive lobular carcinoma, or tumors with an extensive intraductal component, or in patients aged 40 years or younger.
The panel also concluded that margin width should not dictate the choice of whole-breast radiation therapy delivery technique, fractionation, and boost dose.
Negative surgical margins defined by the absence of any ink on the excised tumor are adequate in most cases of early-stage breast cancer treated with breast-conserving therapy, suggest new consensus guidelines from the Society of Surgical Oncology and American Society for Radiation Oncology.
"The use of no ink on tumor as the standard for an adequate margin in invasive cancer in the era of multidisciplinary therapy is associated with low rates of ipsilateral breast tumor recurrence and has the potential to decrease re-excision rates, improve cosmetic outcomes, and decrease health care costs," concludes the 12-member multidisciplinary panel. "The routine practice to obtain negative margin widths wider than no ink on tumor is not indicated" (J. Clin. Oncol. 2014 Feb. 10 [doi:10.1200/JCO.2013.53.3935]).
The panel used as their evidence a systematic review and a meta-analysis based on 33 studies having a total of 28,162 patients with stage I or II breast cancer who were treated with breast-conserving surgery plus whole-breast radiation therapy.
Results showed that, compared with peers having negative margins, patients having positive margins were twice as likely to experience an ipsilateral recurrence, regardless of whether they had favorable tumor biology, were given a radiation boost, or received endocrine therapy (Int. J. Radiation Oncol. Biol. Phys. 2014;88:553-64).
But taking wider margins beyond the point of no ink on tumor did not further reduce the risk of ipsilateral recurrence in the patients overall or in a variety of subsets having unfavorable features (young age, aggressive biology, lobular cancers, or tumors with an extensive intraductal component).
"Our hope is that this guideline will ultimately lead to significant reductions in the high re-excision rate for women with early-stage breast cancer undergoing breast-conserving surgery. Based on the consensus panel’s extensive review of the literature, the vast majority of re-excisions are unnecessary because disease control in the breast is excellent for women with early-stage disease when radiation and hormonal therapy and/or chemotherapy are added to a women’s treatment plan," panel cochair Dr. Meena S. Moran of Yale University, New Haven, Conn., commented in a prepared statement.
In an accompanying editorial, Dr. Reshma Jagsi, University of Michigan, Ann Arbor, and her colleagues write, "We agree with the general idea that routine reexcision of close margins (beyond no ink on tumor) is not necessary, and we expect that these guidelines will have a substantial impact on the community of practicing surgeons. Therefore, radiation oncologists should be prepared to encounter an increasing number of patients with microscopically close margins who might have undergone re-excision in previous years" (Int. J. Radiation Oncol. Biol. Phys. 2014;88:535-36).
At the same time, they note that the wording of the new guidelines gives physicians and patients latitude in individualizing decisions about whether re-excision is warranted.
"Physicians applying these guidelines must have an appreciation of the rationale for the recommendations, as well as the limitations of the evidence available, so that they can interpret and apply the guidelines appropriately. Only with a sophisticated understanding of these issues can we, as a profession, continue to deliver individualized care of consistently high quality, avoiding the sort of ‘cookbook medicine’ that serves well neither physicians nor patients," the editorialists conclude.
The studies included in the meta-analysis were published between 1965 and early 2013 and had a median or mean follow-up of at least 4 years. Patients were excluded if they received neoadjuvant chemotherapy or had only ductal carcinoma in situ.
Overall, 78% of the patients studied had negative margins, defined as no ink on the invasive tumor or any ductal carcinoma in situ component. After a median follow-up of 6.6 years, the median prevalence of ipsilateral recurrence was 5.3% overall.
Patients with positive or close margins were twice as likely to have an ipsilateral recurrence (odds ratio, 1.96). In the subset of studies that were able to separate out close margins, risk was elevated with both positive margins (OR, 2.44) and close margins (OR, 1.74).
The adverse impact of positive margins was still evident in analyses taking into account use of a radiation boost (OR, 2.45) and receipt of endocrine therapy (OR, 2.53), and among patients with favorable biology in the form of estrogen receptor–positive tumors (OR, 2.66).
When the impact of the width of the negative margin was evaluated, the risks of ipsilateral recurrence with 2-mm and 5-mm margins were statistically indistinguishable from those with 1-mm margins.
The analysis confirmed that giving systemic therapy (endocrine therapy, chemotherapy, and/or biologic therapy) reduces the risk of ipsilateral recurrence. But the evidence also suggested that in the small number of patients who do not receive this therapy, wider margins beyond no ink on tumor do not further reduce that risk.
In additional findings, there was no evidence that wider margins beyond no ink on tumor are indicated in patients having more aggressive biological subtypes of breast cancer, invasive lobular carcinoma, or tumors with an extensive intraductal component, or in patients aged 40 years or younger.
The panel also concluded that margin width should not dictate the choice of whole-breast radiation therapy delivery technique, fractionation, and boost dose.
Negative surgical margins defined by the absence of any ink on the excised tumor are adequate in most cases of early-stage breast cancer treated with breast-conserving therapy, suggest new consensus guidelines from the Society of Surgical Oncology and American Society for Radiation Oncology.
"The use of no ink on tumor as the standard for an adequate margin in invasive cancer in the era of multidisciplinary therapy is associated with low rates of ipsilateral breast tumor recurrence and has the potential to decrease re-excision rates, improve cosmetic outcomes, and decrease health care costs," concludes the 12-member multidisciplinary panel. "The routine practice to obtain negative margin widths wider than no ink on tumor is not indicated" (J. Clin. Oncol. 2014 Feb. 10 [doi:10.1200/JCO.2013.53.3935]).
The panel used as their evidence a systematic review and a meta-analysis based on 33 studies having a total of 28,162 patients with stage I or II breast cancer who were treated with breast-conserving surgery plus whole-breast radiation therapy.
Results showed that, compared with peers having negative margins, patients having positive margins were twice as likely to experience an ipsilateral recurrence, regardless of whether they had favorable tumor biology, were given a radiation boost, or received endocrine therapy (Int. J. Radiation Oncol. Biol. Phys. 2014;88:553-64).
But taking wider margins beyond the point of no ink on tumor did not further reduce the risk of ipsilateral recurrence in the patients overall or in a variety of subsets having unfavorable features (young age, aggressive biology, lobular cancers, or tumors with an extensive intraductal component).
"Our hope is that this guideline will ultimately lead to significant reductions in the high re-excision rate for women with early-stage breast cancer undergoing breast-conserving surgery. Based on the consensus panel’s extensive review of the literature, the vast majority of re-excisions are unnecessary because disease control in the breast is excellent for women with early-stage disease when radiation and hormonal therapy and/or chemotherapy are added to a women’s treatment plan," panel cochair Dr. Meena S. Moran of Yale University, New Haven, Conn., commented in a prepared statement.
In an accompanying editorial, Dr. Reshma Jagsi, University of Michigan, Ann Arbor, and her colleagues write, "We agree with the general idea that routine reexcision of close margins (beyond no ink on tumor) is not necessary, and we expect that these guidelines will have a substantial impact on the community of practicing surgeons. Therefore, radiation oncologists should be prepared to encounter an increasing number of patients with microscopically close margins who might have undergone re-excision in previous years" (Int. J. Radiation Oncol. Biol. Phys. 2014;88:535-36).
At the same time, they note that the wording of the new guidelines gives physicians and patients latitude in individualizing decisions about whether re-excision is warranted.
"Physicians applying these guidelines must have an appreciation of the rationale for the recommendations, as well as the limitations of the evidence available, so that they can interpret and apply the guidelines appropriately. Only with a sophisticated understanding of these issues can we, as a profession, continue to deliver individualized care of consistently high quality, avoiding the sort of ‘cookbook medicine’ that serves well neither physicians nor patients," the editorialists conclude.
The studies included in the meta-analysis were published between 1965 and early 2013 and had a median or mean follow-up of at least 4 years. Patients were excluded if they received neoadjuvant chemotherapy or had only ductal carcinoma in situ.
Overall, 78% of the patients studied had negative margins, defined as no ink on the invasive tumor or any ductal carcinoma in situ component. After a median follow-up of 6.6 years, the median prevalence of ipsilateral recurrence was 5.3% overall.
Patients with positive or close margins were twice as likely to have an ipsilateral recurrence (odds ratio, 1.96). In the subset of studies that were able to separate out close margins, risk was elevated with both positive margins (OR, 2.44) and close margins (OR, 1.74).
The adverse impact of positive margins was still evident in analyses taking into account use of a radiation boost (OR, 2.45) and receipt of endocrine therapy (OR, 2.53), and among patients with favorable biology in the form of estrogen receptor–positive tumors (OR, 2.66).
When the impact of the width of the negative margin was evaluated, the risks of ipsilateral recurrence with 2-mm and 5-mm margins were statistically indistinguishable from those with 1-mm margins.
The analysis confirmed that giving systemic therapy (endocrine therapy, chemotherapy, and/or biologic therapy) reduces the risk of ipsilateral recurrence. But the evidence also suggested that in the small number of patients who do not receive this therapy, wider margins beyond no ink on tumor do not further reduce that risk.
In additional findings, there was no evidence that wider margins beyond no ink on tumor are indicated in patients having more aggressive biological subtypes of breast cancer, invasive lobular carcinoma, or tumors with an extensive intraductal component, or in patients aged 40 years or younger.
The panel also concluded that margin width should not dictate the choice of whole-breast radiation therapy delivery technique, fractionation, and boost dose.
Removing opposite breast cuts 20-year mortality 48% in BRCA mutation carriers
Among early-stage breast cancer patients who carry BRCA mutations, prophylactic mastectomy of the contralateral breast appears to reduce the risk of dying from breast cancer within 20 years by 48%, according to a report published online Feb. 11 in the British Medical Journal.
This significant mortality benefit is most pronounced during the second decade after the initial breast cancer diagnosis, said Dr. Kelly Metcalfe of the University of Toronto, and her associates.
"We conclude that it is reasonable to propose bilateral mastectomy as the initial treatment option for women with early-stage breast cancer who are carriers of a BRCA1 or BRCA2 mutation. For those who have been treated in the past with unilateral mastectomy or breast-conserving surgery, the possibility of a second surgery should be discussed," they said.
Until now, the data regarding long-term survival after prophylactic mastectomy have been sparse, and no study has examined mortality specifically related to mastectomy of the contralateral breast. "Traditionally, breast cancer trialists and clinical epidemiologists focus their attention on the 10-year period after diagnosis, because this is when the majority of cancer-related deaths occur. However, a mortality benefit from preventing a second primary breast cancer is unlikely to be apparent within this narrow interval, given that second primary cancers accumulate slowly and for an extended period," Dr. Metcalfe and her colleagues said.
They reviewed the medical records and pathology reports of 390 women who had been diagnosed as having stage I or II breast cancer in 1975-2009 when they were aged 65 or younger, were known or likely carriers of a deleterious mutation in the BRCA1 or BRCA2 gene, and were treated with unilateral or bilateral mastectomy. These study participants were identified from the histories of 290 different families in which one member had received genetic counseling at any of 12 specialty clinics.
A total of 44 of the women were initially treated with bilateral mastectomy. The remaining 346 initially underwent unilateral mastectomy, but 137 of them went on to have mastectomy of the contralateral breast at a later time. Thus, in the final analysis 181 women had prophylactic mastectomy of the contralateral breast and 209 did not.
The mean follow-up was 13 years (range, 0.1-20.0 years).
Overall, 79 women (20% of the entire study population) died from breast cancer during follow-up: 18 of the 181 women who had prophylactic mastectomy of the contralateral breast (9.9%), compared with 61 of 209 who did not have prophylactic mastectomy (29.1%).
At 20 years, the survival rate for women who underwent prophylactic mastectomy was 88%, compared with a 66% survival rate among those who did not have prophylactic mastectomy of the contralateral breast.
In a multivariable analysis that controlled for age at diagnosis, tumor size, nodal status, treatment, and other prognostic factors, 20-year breast-cancer-specific mortality was 48% lower for those who underwent contralateral mastectomy than for those who did not (hazard ratio 0.52, 95% confidence interval 0.29 to 0.93; P = .03), the investigators wrote (Br. Med. J. 2014 Feb. 11 [doi:10.1136/bmj.g226]).
The reduction in mortality was much greater during the second decade of follow-up (80% reduction) than during the first decade (35% reduction). "On average, the time from first breast cancer to ... cancer of the contralateral breast is 5.7 years. Therefore, a delay in the observed benefit of contralateral mastectomy is to be expected – that is, the reduction in mortality results from a reduction in deaths from cancer of the contralateral breast," Dr. Metcalfe and her associates said.
They noted that it is critical that these findings be confirmed in other study populations, especially in view of their relatively small study population.
This study was funded by the Canadian Breast Cancer Foundation. Dr. Metcalfe is supported by the Canadian Institutes of Health Research and the Ontario Women’s Health Council. No financial conflicts of interest were reported.
The main limitation of the study by Metcalfe and colleagues is the relatively small number of endpoints (breast cancer deaths), "which provide unstable estimates and make statistical inferences more challenging," wrote Dr. Karin B. Michels, Sc.D., Ph.D. As the authors noted, larger studies of this issue are needed, she said.
Breasts are not statistics; they are essential parts of women’s identity, sexuality, and self-perception, and the decision to undergo a bilateral mastectomy is highly individual. "A woman needs to weigh up alternative options, including regular close monitoring and the use of tamoxifen or raloxifene, while considering the opportunities but also possible complications of reconstructive surgery. No statistics and no statistician can make this decision for her," Dr. Michels said.
Dr. Michels is at the Obstetrics and Gynecology Epidemiology Center at Brigham and Women’s Hospital and at Harvard Medical School, both in Boston. She reported no financial conflicts of interest. These remarks were taken from her editorial accompanying Dr. Metcalfe’s report (Br. Med. J. 2014 Feb. 11 [doi:10.1136/bmj.g1379]).
The main limitation of the study by Metcalfe and colleagues is the relatively small number of endpoints (breast cancer deaths), "which provide unstable estimates and make statistical inferences more challenging," wrote Dr. Karin B. Michels, Sc.D., Ph.D. As the authors noted, larger studies of this issue are needed, she said.
Breasts are not statistics; they are essential parts of women’s identity, sexuality, and self-perception, and the decision to undergo a bilateral mastectomy is highly individual. "A woman needs to weigh up alternative options, including regular close monitoring and the use of tamoxifen or raloxifene, while considering the opportunities but also possible complications of reconstructive surgery. No statistics and no statistician can make this decision for her," Dr. Michels said.
Dr. Michels is at the Obstetrics and Gynecology Epidemiology Center at Brigham and Women’s Hospital and at Harvard Medical School, both in Boston. She reported no financial conflicts of interest. These remarks were taken from her editorial accompanying Dr. Metcalfe’s report (Br. Med. J. 2014 Feb. 11 [doi:10.1136/bmj.g1379]).
The main limitation of the study by Metcalfe and colleagues is the relatively small number of endpoints (breast cancer deaths), "which provide unstable estimates and make statistical inferences more challenging," wrote Dr. Karin B. Michels, Sc.D., Ph.D. As the authors noted, larger studies of this issue are needed, she said.
Breasts are not statistics; they are essential parts of women’s identity, sexuality, and self-perception, and the decision to undergo a bilateral mastectomy is highly individual. "A woman needs to weigh up alternative options, including regular close monitoring and the use of tamoxifen or raloxifene, while considering the opportunities but also possible complications of reconstructive surgery. No statistics and no statistician can make this decision for her," Dr. Michels said.
Dr. Michels is at the Obstetrics and Gynecology Epidemiology Center at Brigham and Women’s Hospital and at Harvard Medical School, both in Boston. She reported no financial conflicts of interest. These remarks were taken from her editorial accompanying Dr. Metcalfe’s report (Br. Med. J. 2014 Feb. 11 [doi:10.1136/bmj.g1379]).
Among early-stage breast cancer patients who carry BRCA mutations, prophylactic mastectomy of the contralateral breast appears to reduce the risk of dying from breast cancer within 20 years by 48%, according to a report published online Feb. 11 in the British Medical Journal.
This significant mortality benefit is most pronounced during the second decade after the initial breast cancer diagnosis, said Dr. Kelly Metcalfe of the University of Toronto, and her associates.
"We conclude that it is reasonable to propose bilateral mastectomy as the initial treatment option for women with early-stage breast cancer who are carriers of a BRCA1 or BRCA2 mutation. For those who have been treated in the past with unilateral mastectomy or breast-conserving surgery, the possibility of a second surgery should be discussed," they said.
Until now, the data regarding long-term survival after prophylactic mastectomy have been sparse, and no study has examined mortality specifically related to mastectomy of the contralateral breast. "Traditionally, breast cancer trialists and clinical epidemiologists focus their attention on the 10-year period after diagnosis, because this is when the majority of cancer-related deaths occur. However, a mortality benefit from preventing a second primary breast cancer is unlikely to be apparent within this narrow interval, given that second primary cancers accumulate slowly and for an extended period," Dr. Metcalfe and her colleagues said.
They reviewed the medical records and pathology reports of 390 women who had been diagnosed as having stage I or II breast cancer in 1975-2009 when they were aged 65 or younger, were known or likely carriers of a deleterious mutation in the BRCA1 or BRCA2 gene, and were treated with unilateral or bilateral mastectomy. These study participants were identified from the histories of 290 different families in which one member had received genetic counseling at any of 12 specialty clinics.
A total of 44 of the women were initially treated with bilateral mastectomy. The remaining 346 initially underwent unilateral mastectomy, but 137 of them went on to have mastectomy of the contralateral breast at a later time. Thus, in the final analysis 181 women had prophylactic mastectomy of the contralateral breast and 209 did not.
The mean follow-up was 13 years (range, 0.1-20.0 years).
Overall, 79 women (20% of the entire study population) died from breast cancer during follow-up: 18 of the 181 women who had prophylactic mastectomy of the contralateral breast (9.9%), compared with 61 of 209 who did not have prophylactic mastectomy (29.1%).
At 20 years, the survival rate for women who underwent prophylactic mastectomy was 88%, compared with a 66% survival rate among those who did not have prophylactic mastectomy of the contralateral breast.
In a multivariable analysis that controlled for age at diagnosis, tumor size, nodal status, treatment, and other prognostic factors, 20-year breast-cancer-specific mortality was 48% lower for those who underwent contralateral mastectomy than for those who did not (hazard ratio 0.52, 95% confidence interval 0.29 to 0.93; P = .03), the investigators wrote (Br. Med. J. 2014 Feb. 11 [doi:10.1136/bmj.g226]).
The reduction in mortality was much greater during the second decade of follow-up (80% reduction) than during the first decade (35% reduction). "On average, the time from first breast cancer to ... cancer of the contralateral breast is 5.7 years. Therefore, a delay in the observed benefit of contralateral mastectomy is to be expected – that is, the reduction in mortality results from a reduction in deaths from cancer of the contralateral breast," Dr. Metcalfe and her associates said.
They noted that it is critical that these findings be confirmed in other study populations, especially in view of their relatively small study population.
This study was funded by the Canadian Breast Cancer Foundation. Dr. Metcalfe is supported by the Canadian Institutes of Health Research and the Ontario Women’s Health Council. No financial conflicts of interest were reported.
Among early-stage breast cancer patients who carry BRCA mutations, prophylactic mastectomy of the contralateral breast appears to reduce the risk of dying from breast cancer within 20 years by 48%, according to a report published online Feb. 11 in the British Medical Journal.
This significant mortality benefit is most pronounced during the second decade after the initial breast cancer diagnosis, said Dr. Kelly Metcalfe of the University of Toronto, and her associates.
"We conclude that it is reasonable to propose bilateral mastectomy as the initial treatment option for women with early-stage breast cancer who are carriers of a BRCA1 or BRCA2 mutation. For those who have been treated in the past with unilateral mastectomy or breast-conserving surgery, the possibility of a second surgery should be discussed," they said.
Until now, the data regarding long-term survival after prophylactic mastectomy have been sparse, and no study has examined mortality specifically related to mastectomy of the contralateral breast. "Traditionally, breast cancer trialists and clinical epidemiologists focus their attention on the 10-year period after diagnosis, because this is when the majority of cancer-related deaths occur. However, a mortality benefit from preventing a second primary breast cancer is unlikely to be apparent within this narrow interval, given that second primary cancers accumulate slowly and for an extended period," Dr. Metcalfe and her colleagues said.
They reviewed the medical records and pathology reports of 390 women who had been diagnosed as having stage I or II breast cancer in 1975-2009 when they were aged 65 or younger, were known or likely carriers of a deleterious mutation in the BRCA1 or BRCA2 gene, and were treated with unilateral or bilateral mastectomy. These study participants were identified from the histories of 290 different families in which one member had received genetic counseling at any of 12 specialty clinics.
A total of 44 of the women were initially treated with bilateral mastectomy. The remaining 346 initially underwent unilateral mastectomy, but 137 of them went on to have mastectomy of the contralateral breast at a later time. Thus, in the final analysis 181 women had prophylactic mastectomy of the contralateral breast and 209 did not.
The mean follow-up was 13 years (range, 0.1-20.0 years).
Overall, 79 women (20% of the entire study population) died from breast cancer during follow-up: 18 of the 181 women who had prophylactic mastectomy of the contralateral breast (9.9%), compared with 61 of 209 who did not have prophylactic mastectomy (29.1%).
At 20 years, the survival rate for women who underwent prophylactic mastectomy was 88%, compared with a 66% survival rate among those who did not have prophylactic mastectomy of the contralateral breast.
In a multivariable analysis that controlled for age at diagnosis, tumor size, nodal status, treatment, and other prognostic factors, 20-year breast-cancer-specific mortality was 48% lower for those who underwent contralateral mastectomy than for those who did not (hazard ratio 0.52, 95% confidence interval 0.29 to 0.93; P = .03), the investigators wrote (Br. Med. J. 2014 Feb. 11 [doi:10.1136/bmj.g226]).
The reduction in mortality was much greater during the second decade of follow-up (80% reduction) than during the first decade (35% reduction). "On average, the time from first breast cancer to ... cancer of the contralateral breast is 5.7 years. Therefore, a delay in the observed benefit of contralateral mastectomy is to be expected – that is, the reduction in mortality results from a reduction in deaths from cancer of the contralateral breast," Dr. Metcalfe and her associates said.
They noted that it is critical that these findings be confirmed in other study populations, especially in view of their relatively small study population.
This study was funded by the Canadian Breast Cancer Foundation. Dr. Metcalfe is supported by the Canadian Institutes of Health Research and the Ontario Women’s Health Council. No financial conflicts of interest were reported.
FROM THE BRITISH MEDICAL JOURNAL
Major finding: Twenty-year breast-cancer-specific mortality was 48% lower for women with BRCA mutations who underwent prophylactic contralateral mastectomy than for those who did not (hazard ratio 0.52, 95% confidence interval 0.29 to 0.93; P = .03).
Data source: A retrospective analysis of breast-cancer-specific mortality in 390 women with BRCA1 or BRCA2 mutations who underwent mastectomy for stage I or II breast cancer, then either underwent or did not undergo prophylactic mastectomy of the contralateral breast, and were followed for up to 20 years.
Disclosures: This study was funded by the Canadian Breast Cancer Foundation. Dr. Metcalfe is supported by the Canadian Institutes of Health Research and the Ontario Women’s Health Council. No financial conflicts of interest were reported.
Synthetic lethality: beating cancer at its own game
The primary focus for targeted cancer agents has typically been to counteract the oncogenic signaling that results from genetic defects. A new strategy is emerging that actually seeks to exploit the oncogenic features of tumor cells rather than overcome them. Synthetic lethality (SL) is a situation in which 2 nonlethal mutations become lethal to a cell when they are present simultaneously. If SL were to be exploited for anticancer therapy, it could lead to the development of highly selective, less toxic drugs, while expanding therapeutic targets to include those that have, until now, proven pharmaceutically intractable. Here, we discuss the idea of SL and how it can be applied to cancer therapy.
Click on the PDF icon at the top of this introduction to read the full article.
The primary focus for targeted cancer agents has typically been to counteract the oncogenic signaling that results from genetic defects. A new strategy is emerging that actually seeks to exploit the oncogenic features of tumor cells rather than overcome them. Synthetic lethality (SL) is a situation in which 2 nonlethal mutations become lethal to a cell when they are present simultaneously. If SL were to be exploited for anticancer therapy, it could lead to the development of highly selective, less toxic drugs, while expanding therapeutic targets to include those that have, until now, proven pharmaceutically intractable. Here, we discuss the idea of SL and how it can be applied to cancer therapy.
Click on the PDF icon at the top of this introduction to read the full article.
The primary focus for targeted cancer agents has typically been to counteract the oncogenic signaling that results from genetic defects. A new strategy is emerging that actually seeks to exploit the oncogenic features of tumor cells rather than overcome them. Synthetic lethality (SL) is a situation in which 2 nonlethal mutations become lethal to a cell when they are present simultaneously. If SL were to be exploited for anticancer therapy, it could lead to the development of highly selective, less toxic drugs, while expanding therapeutic targets to include those that have, until now, proven pharmaceutically intractable. Here, we discuss the idea of SL and how it can be applied to cancer therapy.
Click on the PDF icon at the top of this introduction to read the full article.
Biennial mammography keeps women safe and saves billions of dollars
Following United States Preventive Services Task Force mammography screening guidelines would save about $4.4 billion annually, without sacrificing quality of care, according to a study published online Feb. 3 in the Annals of Internal Medicine.
Taking the costs of mammography, computer-aided detection, recalls, biopsies, and other variables into account, the investigators estimated that it would have cost $3.5 billion to screen 85% of women in 2010 who met the USPSTF criteria: Screen women aged 50-74 years every other year, plus high-risk women aged 40-49 years and women aged 75-85 years with few comorbidities biennially (Ann. Intern. Med. 2014 Feb. 3;160:145-53 [doi:10.7326/M13-1217]).

Instead, $7.8 billion was actually spent in 2010 to screen just 70% of women using the mélange of screening practices in place today in the United States, a byproduct of the country’s uncertainty about the right way to proceed, the researchers noted.
Meanwhile, following the advice of the American Cancer Society and other groups for annual screenings of women aged 40-84 years would have cost $10.1 billion if 85% had come into the clinic. Screening 85% of women aged 50-69 years biennially – in keeping with the European approach – would have cost $2.6 billion.
Previous studies have found fewer false-positives and recalls with biennial screening, and no significant increase in late-stage cancer detections, said Dr. Cristina O’Donoghue of the University of Illinois at Chicago and her associates.
"Following mammography screening guidelines, such as those from the USPSTF, [which] optimize frequency on the basis of best-available evidence will ... improve screening and save billions of dollars," money that’s better spent on expanding mammography access and increasing risk-based screening, breast-cancer prevention, and mammography reading by experts less likely to make mistakes, among other things, the researchers said.

Even so, "in the United States, there has been resistance to reducing frequency or modifying the age-range for mammography. Those who advocate annual screening should justify the increased costs of nearly $7 billion per year, compared with biennial policies," they said.
The project was a modeling exercise to price out various approaches to breast cancer screening using Medicare reimbursement rates; census figures; Breast Cancer Surveillance Consortium records; and other data sources. The researchers stated that they thought the cost information would help doctors, women, and policy makers find the right approach, especially as the Affordable Care Act improves mammography access and increases screening rates.
The U.S. task force’s biennial approach "is in line with our national goals of advancing health care delivery while improving cost-efficiency," the researchers said.
They concluded that screening frequency is the main driver of costs in mammography, followed by the percentage of women screened, cost per screen, percentage of women screened with digital mammography, and percentage of mammography recalls.
The researchers had no financial conflicts to disclose. The study was funded by the University of California and the Safeway Foundation.
We applaud [Dr.] O’Donoghue and [her] colleagues for meticulously assessing the total cost of breast cancer screening in the United States. Although there is often cause to be skeptical about simulation models because results are based on numerous assumptions, we find the article by O’Donoghue and colleagues to be reasonable and conservative.
Integrating cost into the cancer screening conversation is a challenge. Providers and patients are not only shielded from cost information, but some may raise concerns that the mere mention of costs is a step down the road to rationing. However, both advocates and skeptics should know the costs associated with different breast-cancer screening strategies, particularly when there is so much debate about which approach is most effective.
Costs, including out-of-pocket costs, should be part of the conversation because women with high-deductible health plans may find themselves facing a hefty bill for adjunctive imaging tests and procedures. At the societal level, costs should be integrated into our national dialogue about screening. It is unsustainable to remain ignorant of the costs associated with any health intervention, even breast-cancer screening.
The approximate $8 billion difference among breast-cancer screening strategies is roughly twice as large as the entire annual budget of the National Cancer Institute.
Dr. Joann Elmore and Dr. Cary Gross made the above comments in an editorial accompanying the study (Ann. Intern. Med. 2014 Feb. 3;160:203-4). Dr. Elmore is a professor of medicine at the University of Washington in Seattle. Dr. Gross is a professor of medicine at Yale University in New Haven, Conn., and director of the school’s Cancer Outcomes Public Policy and Effectiveness Research Center. Dr. Gross is a paid Fair Health Inc. board member and disclosed grants from Medtronic and 21st Century Oncology.
We applaud [Dr.] O’Donoghue and [her] colleagues for meticulously assessing the total cost of breast cancer screening in the United States. Although there is often cause to be skeptical about simulation models because results are based on numerous assumptions, we find the article by O’Donoghue and colleagues to be reasonable and conservative.
Integrating cost into the cancer screening conversation is a challenge. Providers and patients are not only shielded from cost information, but some may raise concerns that the mere mention of costs is a step down the road to rationing. However, both advocates and skeptics should know the costs associated with different breast-cancer screening strategies, particularly when there is so much debate about which approach is most effective.
Costs, including out-of-pocket costs, should be part of the conversation because women with high-deductible health plans may find themselves facing a hefty bill for adjunctive imaging tests and procedures. At the societal level, costs should be integrated into our national dialogue about screening. It is unsustainable to remain ignorant of the costs associated with any health intervention, even breast-cancer screening.
The approximate $8 billion difference among breast-cancer screening strategies is roughly twice as large as the entire annual budget of the National Cancer Institute.
Dr. Joann Elmore and Dr. Cary Gross made the above comments in an editorial accompanying the study (Ann. Intern. Med. 2014 Feb. 3;160:203-4). Dr. Elmore is a professor of medicine at the University of Washington in Seattle. Dr. Gross is a professor of medicine at Yale University in New Haven, Conn., and director of the school’s Cancer Outcomes Public Policy and Effectiveness Research Center. Dr. Gross is a paid Fair Health Inc. board member and disclosed grants from Medtronic and 21st Century Oncology.
We applaud [Dr.] O’Donoghue and [her] colleagues for meticulously assessing the total cost of breast cancer screening in the United States. Although there is often cause to be skeptical about simulation models because results are based on numerous assumptions, we find the article by O’Donoghue and colleagues to be reasonable and conservative.
Integrating cost into the cancer screening conversation is a challenge. Providers and patients are not only shielded from cost information, but some may raise concerns that the mere mention of costs is a step down the road to rationing. However, both advocates and skeptics should know the costs associated with different breast-cancer screening strategies, particularly when there is so much debate about which approach is most effective.
Costs, including out-of-pocket costs, should be part of the conversation because women with high-deductible health plans may find themselves facing a hefty bill for adjunctive imaging tests and procedures. At the societal level, costs should be integrated into our national dialogue about screening. It is unsustainable to remain ignorant of the costs associated with any health intervention, even breast-cancer screening.
The approximate $8 billion difference among breast-cancer screening strategies is roughly twice as large as the entire annual budget of the National Cancer Institute.
Dr. Joann Elmore and Dr. Cary Gross made the above comments in an editorial accompanying the study (Ann. Intern. Med. 2014 Feb. 3;160:203-4). Dr. Elmore is a professor of medicine at the University of Washington in Seattle. Dr. Gross is a professor of medicine at Yale University in New Haven, Conn., and director of the school’s Cancer Outcomes Public Policy and Effectiveness Research Center. Dr. Gross is a paid Fair Health Inc. board member and disclosed grants from Medtronic and 21st Century Oncology.
Following United States Preventive Services Task Force mammography screening guidelines would save about $4.4 billion annually, without sacrificing quality of care, according to a study published online Feb. 3 in the Annals of Internal Medicine.
Taking the costs of mammography, computer-aided detection, recalls, biopsies, and other variables into account, the investigators estimated that it would have cost $3.5 billion to screen 85% of women in 2010 who met the USPSTF criteria: Screen women aged 50-74 years every other year, plus high-risk women aged 40-49 years and women aged 75-85 years with few comorbidities biennially (Ann. Intern. Med. 2014 Feb. 3;160:145-53 [doi:10.7326/M13-1217]).
Instead, $7.8 billion was actually spent in 2010 to screen just 70% of women using the mélange of screening practices in place today in the United States, a byproduct of the country’s uncertainty about the right way to proceed, the researchers noted.
Meanwhile, following the advice of the American Cancer Society and other groups for annual screenings of women aged 40-84 years would have cost $10.1 billion if 85% had come into the clinic. Screening 85% of women aged 50-69 years biennially – in keeping with the European approach – would have cost $2.6 billion.
Previous studies have found fewer false-positives and recalls with biennial screening, and no significant increase in late-stage cancer detections, said Dr. Cristina O’Donoghue of the University of Illinois at Chicago and her associates.
"Following mammography screening guidelines, such as those from the USPSTF, [which] optimize frequency on the basis of best-available evidence will ... improve screening and save billions of dollars," money that’s better spent on expanding mammography access and increasing risk-based screening, breast-cancer prevention, and mammography reading by experts less likely to make mistakes, among other things, the researchers said.
Even so, "in the United States, there has been resistance to reducing frequency or modifying the age-range for mammography. Those who advocate annual screening should justify the increased costs of nearly $7 billion per year, compared with biennial policies," they said.
The project was a modeling exercise to price out various approaches to breast cancer screening using Medicare reimbursement rates; census figures; Breast Cancer Surveillance Consortium records; and other data sources. The researchers stated that they thought the cost information would help doctors, women, and policy makers find the right approach, especially as the Affordable Care Act improves mammography access and increases screening rates.
The U.S. task force’s biennial approach "is in line with our national goals of advancing health care delivery while improving cost-efficiency," the researchers said.
They concluded that screening frequency is the main driver of costs in mammography, followed by the percentage of women screened, cost per screen, percentage of women screened with digital mammography, and percentage of mammography recalls.
The researchers had no financial conflicts to disclose. The study was funded by the University of California and the Safeway Foundation.
Following United States Preventive Services Task Force mammography screening guidelines would save about $4.4 billion annually, without sacrificing quality of care, according to a study published online Feb. 3 in the Annals of Internal Medicine.
Taking the costs of mammography, computer-aided detection, recalls, biopsies, and other variables into account, the investigators estimated that it would have cost $3.5 billion to screen 85% of women in 2010 who met the USPSTF criteria: Screen women aged 50-74 years every other year, plus high-risk women aged 40-49 years and women aged 75-85 years with few comorbidities biennially (Ann. Intern. Med. 2014 Feb. 3;160:145-53 [doi:10.7326/M13-1217]).
Instead, $7.8 billion was actually spent in 2010 to screen just 70% of women using the mélange of screening practices in place today in the United States, a byproduct of the country’s uncertainty about the right way to proceed, the researchers noted.
Meanwhile, following the advice of the American Cancer Society and other groups for annual screenings of women aged 40-84 years would have cost $10.1 billion if 85% had come into the clinic. Screening 85% of women aged 50-69 years biennially – in keeping with the European approach – would have cost $2.6 billion.
Previous studies have found fewer false-positives and recalls with biennial screening, and no significant increase in late-stage cancer detections, said Dr. Cristina O’Donoghue of the University of Illinois at Chicago and her associates.
"Following mammography screening guidelines, such as those from the USPSTF, [which] optimize frequency on the basis of best-available evidence will ... improve screening and save billions of dollars," money that’s better spent on expanding mammography access and increasing risk-based screening, breast-cancer prevention, and mammography reading by experts less likely to make mistakes, among other things, the researchers said.
Even so, "in the United States, there has been resistance to reducing frequency or modifying the age-range for mammography. Those who advocate annual screening should justify the increased costs of nearly $7 billion per year, compared with biennial policies," they said.
The project was a modeling exercise to price out various approaches to breast cancer screening using Medicare reimbursement rates; census figures; Breast Cancer Surveillance Consortium records; and other data sources. The researchers stated that they thought the cost information would help doctors, women, and policy makers find the right approach, especially as the Affordable Care Act improves mammography access and increases screening rates.
The U.S. task force’s biennial approach "is in line with our national goals of advancing health care delivery while improving cost-efficiency," the researchers said.
They concluded that screening frequency is the main driver of costs in mammography, followed by the percentage of women screened, cost per screen, percentage of women screened with digital mammography, and percentage of mammography recalls.
The researchers had no financial conflicts to disclose. The study was funded by the University of California and the Safeway Foundation.
FROM THE ANNALS OF INTERNAL MEDICINE
Major finding: Following USPSTF mammography recommendations – which call for biennial screenings – would have saved the U.S. health care system approximately $4.4 billion in 2010.
Data source: Estimate of 2010 mammography costs based on modeling of Medicare and other expenses.
Disclosures: The authors had no disclosures. The study was funded by the University of California and the Safeway Foundation.

New insights into aromatase inhibitor therapy nonpersistence
SAN ANTONIO – Discontinuation of aromatase inhibitor therapy because of toxicity is significantly more likely to occur in breast cancer patients having a greater burden of specific symptoms even before starting on the endocrine agent.
The baseline predictive symptoms identified in the randomized prospective Exemestane and Letrozole Pharmacogenetics (ELPh) trial were self-reported depression, anxiety, poor sleep quality, difficulty concentrating, and a tired feeling. Patients with three to five of these symptoms before going on an aromatase inhibitor (AI) were 2.5-fold more likely to stop treatment because of toxicity within the first 12 months than were those with none of the symptoms, Dr. Norah L. Henry reported at the San Antonio Breast Cancer Symposium.
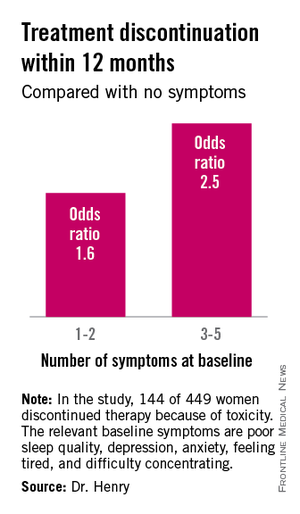
Early discontinuation of AI therapy because of toxicity is a big problem, occurring in 20%-30% of patients who start on treatment. In an earlier study by Dr. Henry and her colleagues, discontinuation was most often from arthralgias or other musculoskeletal complaints (J. Clin. Oncol. 2012;30:936-42).
The ELPh trial included 449 evaluable postmenopausal women with early-stage estrogen receptor–positive breast cancer who were randomized to open-label exemestane or letrozole for 2 years.
To test the study hypothesis that certain baseline patient-reported symptoms increased the likelihood of early treatment discontinuation, participants were evaluated at baseline and again 1, 3, 6, 12, and 24 months after starting on an AI. At each time point, depression was self-rated using the Center for Epidemiologic Studies Depression Scale, sleep disturbance by the Pittsburgh Sleep Quality Index, and anxiety by the Hospital Anxiety and Depression Scale. Other baseline self-reported symptoms included in the prospective evaluation were joint pain, vaginal dryness, forgetfulness, difficulty concentrating, and feeling tired, explained Dr. Henry, a medical oncologist at the University of Michigan, Ann Arbor.
One hundred forty-four of the 449 women (31.2%) discontinued AI therapy because of toxicity by 12 months. In a multivariate logistic regression analysis, two of the baseline symptoms turned out to be independently associated with a significantly increased rate of treatment discontinuation: poor sleep quality as defined by a PSQI score greater than 5, reported by 45% of subjects at baseline, was associated with a 1.8-fold increased risk; and moderate or severe difficulty in concentrating was associated with a 2.6-fold increased likelihood of treatment discontinuation.
While the other symptoms under study were not individually associated with an increased risk of treatment discontinuation, the collective burden imposed by having a greater number of baseline symptoms was associated with an increased risk.
Several earlier studies by other investigators had identified prior chemotherapy, older age, and greater body mass index as being predictive of nonpersistence with AI therapy. Interestingly, neither prior chemotherapy nor greater body mass index was associated with early treatment discontinuation in the ELPh study, Dr. Henry noted.
Patients assigned to exemestane were 63% more likely to halt treatment within 12 months than were those randomized to letrozole.
The clinical relevance of these ELPh study findings is that early identification of patients with a greater burden of baseline symptoms predictive of nonadherence might improve persistence on AI therapy.
"Up-front management of these symptoms rather than waiting until symptoms become particularly problematic may improve persistence with AI therapy," she said.
Possible interventions might include preferential use of letrozole or tamoxifen in such patients, adoption of an exercise program or behavioral intervention, or pharmacologic therapy with an SSRI or a serotonin–norepinephrine reuptake inhibitors, a strategy now under study in the ongoing SWOG S1202 trial, in which patients are randomized to duloxetine or placebo.
Audience member Steven E. Vogl called the ELPh results important information.
"It recalls the history of chemotherapy-induced cognitive impairment, which in the latest couple of analyses seems to exist before the chemotherapy," observed Dr. Vogl of Bronx, N.Y.
The ELPh study was conducted by the Consortium on Breast Cancer Pharmacogenomics and funded chiefly by the Damon Runyon Cancer Research Foundation. Dr. Henry reported having received research grants from Astra Zeneca, Eli Lilly, and Sanofi Aventis.
SAN ANTONIO – Discontinuation of aromatase inhibitor therapy because of toxicity is significantly more likely to occur in breast cancer patients having a greater burden of specific symptoms even before starting on the endocrine agent.
The baseline predictive symptoms identified in the randomized prospective Exemestane and Letrozole Pharmacogenetics (ELPh) trial were self-reported depression, anxiety, poor sleep quality, difficulty concentrating, and a tired feeling. Patients with three to five of these symptoms before going on an aromatase inhibitor (AI) were 2.5-fold more likely to stop treatment because of toxicity within the first 12 months than were those with none of the symptoms, Dr. Norah L. Henry reported at the San Antonio Breast Cancer Symposium.
Early discontinuation of AI therapy because of toxicity is a big problem, occurring in 20%-30% of patients who start on treatment. In an earlier study by Dr. Henry and her colleagues, discontinuation was most often from arthralgias or other musculoskeletal complaints (J. Clin. Oncol. 2012;30:936-42).
The ELPh trial included 449 evaluable postmenopausal women with early-stage estrogen receptor–positive breast cancer who were randomized to open-label exemestane or letrozole for 2 years.
To test the study hypothesis that certain baseline patient-reported symptoms increased the likelihood of early treatment discontinuation, participants were evaluated at baseline and again 1, 3, 6, 12, and 24 months after starting on an AI. At each time point, depression was self-rated using the Center for Epidemiologic Studies Depression Scale, sleep disturbance by the Pittsburgh Sleep Quality Index, and anxiety by the Hospital Anxiety and Depression Scale. Other baseline self-reported symptoms included in the prospective evaluation were joint pain, vaginal dryness, forgetfulness, difficulty concentrating, and feeling tired, explained Dr. Henry, a medical oncologist at the University of Michigan, Ann Arbor.
One hundred forty-four of the 449 women (31.2%) discontinued AI therapy because of toxicity by 12 months. In a multivariate logistic regression analysis, two of the baseline symptoms turned out to be independently associated with a significantly increased rate of treatment discontinuation: poor sleep quality as defined by a PSQI score greater than 5, reported by 45% of subjects at baseline, was associated with a 1.8-fold increased risk; and moderate or severe difficulty in concentrating was associated with a 2.6-fold increased likelihood of treatment discontinuation.
While the other symptoms under study were not individually associated with an increased risk of treatment discontinuation, the collective burden imposed by having a greater number of baseline symptoms was associated with an increased risk.
Several earlier studies by other investigators had identified prior chemotherapy, older age, and greater body mass index as being predictive of nonpersistence with AI therapy. Interestingly, neither prior chemotherapy nor greater body mass index was associated with early treatment discontinuation in the ELPh study, Dr. Henry noted.
Patients assigned to exemestane were 63% more likely to halt treatment within 12 months than were those randomized to letrozole.
The clinical relevance of these ELPh study findings is that early identification of patients with a greater burden of baseline symptoms predictive of nonadherence might improve persistence on AI therapy.
"Up-front management of these symptoms rather than waiting until symptoms become particularly problematic may improve persistence with AI therapy," she said.
Possible interventions might include preferential use of letrozole or tamoxifen in such patients, adoption of an exercise program or behavioral intervention, or pharmacologic therapy with an SSRI or a serotonin–norepinephrine reuptake inhibitors, a strategy now under study in the ongoing SWOG S1202 trial, in which patients are randomized to duloxetine or placebo.
Audience member Steven E. Vogl called the ELPh results important information.
"It recalls the history of chemotherapy-induced cognitive impairment, which in the latest couple of analyses seems to exist before the chemotherapy," observed Dr. Vogl of Bronx, N.Y.
The ELPh study was conducted by the Consortium on Breast Cancer Pharmacogenomics and funded chiefly by the Damon Runyon Cancer Research Foundation. Dr. Henry reported having received research grants from Astra Zeneca, Eli Lilly, and Sanofi Aventis.
SAN ANTONIO – Discontinuation of aromatase inhibitor therapy because of toxicity is significantly more likely to occur in breast cancer patients having a greater burden of specific symptoms even before starting on the endocrine agent.
The baseline predictive symptoms identified in the randomized prospective Exemestane and Letrozole Pharmacogenetics (ELPh) trial were self-reported depression, anxiety, poor sleep quality, difficulty concentrating, and a tired feeling. Patients with three to five of these symptoms before going on an aromatase inhibitor (AI) were 2.5-fold more likely to stop treatment because of toxicity within the first 12 months than were those with none of the symptoms, Dr. Norah L. Henry reported at the San Antonio Breast Cancer Symposium.
Early discontinuation of AI therapy because of toxicity is a big problem, occurring in 20%-30% of patients who start on treatment. In an earlier study by Dr. Henry and her colleagues, discontinuation was most often from arthralgias or other musculoskeletal complaints (J. Clin. Oncol. 2012;30:936-42).
The ELPh trial included 449 evaluable postmenopausal women with early-stage estrogen receptor–positive breast cancer who were randomized to open-label exemestane or letrozole for 2 years.
To test the study hypothesis that certain baseline patient-reported symptoms increased the likelihood of early treatment discontinuation, participants were evaluated at baseline and again 1, 3, 6, 12, and 24 months after starting on an AI. At each time point, depression was self-rated using the Center for Epidemiologic Studies Depression Scale, sleep disturbance by the Pittsburgh Sleep Quality Index, and anxiety by the Hospital Anxiety and Depression Scale. Other baseline self-reported symptoms included in the prospective evaluation were joint pain, vaginal dryness, forgetfulness, difficulty concentrating, and feeling tired, explained Dr. Henry, a medical oncologist at the University of Michigan, Ann Arbor.
One hundred forty-four of the 449 women (31.2%) discontinued AI therapy because of toxicity by 12 months. In a multivariate logistic regression analysis, two of the baseline symptoms turned out to be independently associated with a significantly increased rate of treatment discontinuation: poor sleep quality as defined by a PSQI score greater than 5, reported by 45% of subjects at baseline, was associated with a 1.8-fold increased risk; and moderate or severe difficulty in concentrating was associated with a 2.6-fold increased likelihood of treatment discontinuation.
While the other symptoms under study were not individually associated with an increased risk of treatment discontinuation, the collective burden imposed by having a greater number of baseline symptoms was associated with an increased risk.
Several earlier studies by other investigators had identified prior chemotherapy, older age, and greater body mass index as being predictive of nonpersistence with AI therapy. Interestingly, neither prior chemotherapy nor greater body mass index was associated with early treatment discontinuation in the ELPh study, Dr. Henry noted.
Patients assigned to exemestane were 63% more likely to halt treatment within 12 months than were those randomized to letrozole.
The clinical relevance of these ELPh study findings is that early identification of patients with a greater burden of baseline symptoms predictive of nonadherence might improve persistence on AI therapy.
"Up-front management of these symptoms rather than waiting until symptoms become particularly problematic may improve persistence with AI therapy," she said.
Possible interventions might include preferential use of letrozole or tamoxifen in such patients, adoption of an exercise program or behavioral intervention, or pharmacologic therapy with an SSRI or a serotonin–norepinephrine reuptake inhibitors, a strategy now under study in the ongoing SWOG S1202 trial, in which patients are randomized to duloxetine or placebo.
Audience member Steven E. Vogl called the ELPh results important information.
"It recalls the history of chemotherapy-induced cognitive impairment, which in the latest couple of analyses seems to exist before the chemotherapy," observed Dr. Vogl of Bronx, N.Y.
The ELPh study was conducted by the Consortium on Breast Cancer Pharmacogenomics and funded chiefly by the Damon Runyon Cancer Research Foundation. Dr. Henry reported having received research grants from Astra Zeneca, Eli Lilly, and Sanofi Aventis.
AT SABCS 2013
Major finding: Breast cancer patients with at least three of five self-reported symptoms prior to going on adjuvant aromatase inhibitor therapy were 2.5-fold more likely to discontinue treatment within the first 12 months because of toxicity.
Data source: The Exemestane and Letrozole Pharmacogenetics trial included 449 evaluable women with early-stage estrogen receptor–positive breast cancer who were prospectively evaluated for the relationship between a variety of baseline patient-reported symptoms and discontinuation of adjuvant aromatase inhibitor therapy.
Disclosures: The study was funded by the Damon Runyon Cancer Research Foundation. Dr. Norah L. Henry reported having received research grants from Astra Zeneca, Eli Lilly, and Sanofi Aventis.