User login
Unsung Heroes: ED Social Workers
When we think of essential nonphysician ED staff and the roles they play in the successful management of our patients, we tend to think of nurses, nurse practitioners, physician assistants, technicians, pharmacists, patient representatives, and even transporters, housekeepers, and clerks. But we typically overlook the ED social worker, without whose efforts the modern ED would come to a grinding halt. In the early years after emergency medicine (EM) became a specialty, few, if any, EDs were staffed around the clock by social workers. This was true even in the county and municipal acute care hospitals now referred to as “safety net” hospitals.
In those days, the role of the ED social worker frequently centered around contacting the appropriate agencies for cases of child abuse and sexual assault and arranging transportation or shelter for patients who were to be discharged from the ED.
But just as the roles of EM and EDs have evolved and expanded enormously in recent decades, so too has the role of and need for ED social workers. The presence of a skilled ED social worker will almost always make it possible to safely discharge several patients a day to their homes—with arrangements made for the services and medical equipment needed—instead of admitting them to inpatient beds. Such needed services include physical and occupational therapists, visiting nurses for wound care, medication management, blood work, intravenous infusions, and meal preparation and delivery (“Meals on Wheels,” etc). Durable medical equipment needs include bedside commodes, rails, grab bars, and hospital beds. Even preventive medicine is now initiated by the ED social worker, who arranges for age-appropriate home-safety assessments and equipment installations for the increasing number of elderly who have “aged in place” in the same dwelling over many years.
As the percentage of ED patients over the age of 65—currently 18%—continues to rise during the next 40 to 50 years, the need for skilled ED social workers is increasing exponentially. There is frequently a need to temporarily relocate older discharged ED patients with families or friends when they are alone, for assessing whether a spouse or family member is capable of caring for a discharged patient at home, and even for arranging care of a pet for patients who live alone and require admission. Another way of looking at the current situation is that EDs now serve two clients—our patients and the hospital and healthcare system. Many patients who were formerly admitted to hospitals are now expected to be sent home from the ED to avoid diminishing hospital reimbursement for short-stay “observation services,” or denials. At the same time, the complex range and degree of health insurance coverage that patients have, and the scarce availability of appropriate, timely physician follow-up, are beyond the ability of an EP to deal with while continuing to care for other patients.
As the number of ED patients eligible for Medicare and Medicaid continues to rise, and the benefits are linked to changing requirements for length and type of care (“two-midnight rule” and observation services, for example), the 24/7 ED social worker has become a truly essential member of the ED staff—and now is the time to start ramping up the coverage.
Acknowledgments
We wish to thank NewYork Presbyterian/Weill Cornell Medical Center ED Social Workers, George Haskell, LMSW, and Laura Kramer, LMSW, for providing details regarding the home services and equipment they arrange for patients discharged from our ED.
When we think of essential nonphysician ED staff and the roles they play in the successful management of our patients, we tend to think of nurses, nurse practitioners, physician assistants, technicians, pharmacists, patient representatives, and even transporters, housekeepers, and clerks. But we typically overlook the ED social worker, without whose efforts the modern ED would come to a grinding halt. In the early years after emergency medicine (EM) became a specialty, few, if any, EDs were staffed around the clock by social workers. This was true even in the county and municipal acute care hospitals now referred to as “safety net” hospitals.
In those days, the role of the ED social worker frequently centered around contacting the appropriate agencies for cases of child abuse and sexual assault and arranging transportation or shelter for patients who were to be discharged from the ED.
But just as the roles of EM and EDs have evolved and expanded enormously in recent decades, so too has the role of and need for ED social workers. The presence of a skilled ED social worker will almost always make it possible to safely discharge several patients a day to their homes—with arrangements made for the services and medical equipment needed—instead of admitting them to inpatient beds. Such needed services include physical and occupational therapists, visiting nurses for wound care, medication management, blood work, intravenous infusions, and meal preparation and delivery (“Meals on Wheels,” etc). Durable medical equipment needs include bedside commodes, rails, grab bars, and hospital beds. Even preventive medicine is now initiated by the ED social worker, who arranges for age-appropriate home-safety assessments and equipment installations for the increasing number of elderly who have “aged in place” in the same dwelling over many years.
As the percentage of ED patients over the age of 65—currently 18%—continues to rise during the next 40 to 50 years, the need for skilled ED social workers is increasing exponentially. There is frequently a need to temporarily relocate older discharged ED patients with families or friends when they are alone, for assessing whether a spouse or family member is capable of caring for a discharged patient at home, and even for arranging care of a pet for patients who live alone and require admission. Another way of looking at the current situation is that EDs now serve two clients—our patients and the hospital and healthcare system. Many patients who were formerly admitted to hospitals are now expected to be sent home from the ED to avoid diminishing hospital reimbursement for short-stay “observation services,” or denials. At the same time, the complex range and degree of health insurance coverage that patients have, and the scarce availability of appropriate, timely physician follow-up, are beyond the ability of an EP to deal with while continuing to care for other patients.
As the number of ED patients eligible for Medicare and Medicaid continues to rise, and the benefits are linked to changing requirements for length and type of care (“two-midnight rule” and observation services, for example), the 24/7 ED social worker has become a truly essential member of the ED staff—and now is the time to start ramping up the coverage.
Acknowledgments
We wish to thank NewYork Presbyterian/Weill Cornell Medical Center ED Social Workers, George Haskell, LMSW, and Laura Kramer, LMSW, for providing details regarding the home services and equipment they arrange for patients discharged from our ED.
When we think of essential nonphysician ED staff and the roles they play in the successful management of our patients, we tend to think of nurses, nurse practitioners, physician assistants, technicians, pharmacists, patient representatives, and even transporters, housekeepers, and clerks. But we typically overlook the ED social worker, without whose efforts the modern ED would come to a grinding halt. In the early years after emergency medicine (EM) became a specialty, few, if any, EDs were staffed around the clock by social workers. This was true even in the county and municipal acute care hospitals now referred to as “safety net” hospitals.
In those days, the role of the ED social worker frequently centered around contacting the appropriate agencies for cases of child abuse and sexual assault and arranging transportation or shelter for patients who were to be discharged from the ED.
But just as the roles of EM and EDs have evolved and expanded enormously in recent decades, so too has the role of and need for ED social workers. The presence of a skilled ED social worker will almost always make it possible to safely discharge several patients a day to their homes—with arrangements made for the services and medical equipment needed—instead of admitting them to inpatient beds. Such needed services include physical and occupational therapists, visiting nurses for wound care, medication management, blood work, intravenous infusions, and meal preparation and delivery (“Meals on Wheels,” etc). Durable medical equipment needs include bedside commodes, rails, grab bars, and hospital beds. Even preventive medicine is now initiated by the ED social worker, who arranges for age-appropriate home-safety assessments and equipment installations for the increasing number of elderly who have “aged in place” in the same dwelling over many years.
As the percentage of ED patients over the age of 65—currently 18%—continues to rise during the next 40 to 50 years, the need for skilled ED social workers is increasing exponentially. There is frequently a need to temporarily relocate older discharged ED patients with families or friends when they are alone, for assessing whether a spouse or family member is capable of caring for a discharged patient at home, and even for arranging care of a pet for patients who live alone and require admission. Another way of looking at the current situation is that EDs now serve two clients—our patients and the hospital and healthcare system. Many patients who were formerly admitted to hospitals are now expected to be sent home from the ED to avoid diminishing hospital reimbursement for short-stay “observation services,” or denials. At the same time, the complex range and degree of health insurance coverage that patients have, and the scarce availability of appropriate, timely physician follow-up, are beyond the ability of an EP to deal with while continuing to care for other patients.
As the number of ED patients eligible for Medicare and Medicaid continues to rise, and the benefits are linked to changing requirements for length and type of care (“two-midnight rule” and observation services, for example), the 24/7 ED social worker has become a truly essential member of the ED staff—and now is the time to start ramping up the coverage.
Acknowledgments
We wish to thank NewYork Presbyterian/Weill Cornell Medical Center ED Social Workers, George Haskell, LMSW, and Laura Kramer, LMSW, for providing details regarding the home services and equipment they arrange for patients discharged from our ED.
“Present”: Ebola’s Impact on PAs in Liberia
In November 2012 and January 2014, I traveled to Liberia to conduct a needs assessment of the health care system there on behalf of a company that was interested in supporting efforts to rebuild the country’s infrastructure. I discovered that the physician assistant profession has been in existence in Liberia since 1965—the same year that it started in the United States.
During my time in Liberia, I became close friends with Jerry Kollie, PA, President of the Liberia National Physician Assistants Association (LINPAA). I recently interviewed him to learn more about his organization and the PA profession in Liberia, where they have spent almost a year and a half dealing with the worst Ebola virus outbreak in history.
Editor’s note: The following excerpt focuses on the Ebola outbreak. Please visit our website (http://bit.ly/1NgHX2Q) to learn more about the PA profession in Liberia.
John Oliphant: What impact has the Ebola epidemic had on PAs’ clinical practice in Liberia?
Jerry Kollie: The Ebola epidemic has had a serious impact on us in many ways. It created fear among many PAs about continued clinical practice. Some of our students have lost interest in the profession for fear of contracting the virus and dying after graduation.
Workforce is also an issue. Training has been delayed, which means there are fewer PAs available in the various health facilities providing services to people. Many PAs died and others were ill with Ebola, which increased the workload in our health facilities.
The outbreak also created fear among patients; many of them stopped going to health facilities for care. As a result, PAs would go to work and not see any patients.
JO: Do you know how many PAs in Liberia lost their lives due to Ebola? And how many contracted the virus but survived?
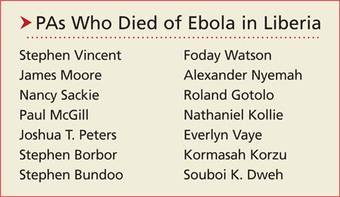
JK: A total of 26 PAs were affected by Ebola virus disease. Many contracted the virus at their workplaces and were taken to various Ebola Treatment Units (ETUs), where some died while others survived. Of the total number, 14 died (see box on page 42 for a list of their names), nine survived, and three were quarantined but did not contract the virus. Those three PAs spent 21 days in quarantine after unknowingly attending to patients who were later confirmed to have Ebola. As God would have it, they all went through the quarantine without experiencing or developing signs or symptoms.
JO: What has been your greatest leadership challenge as the President of LINPAA during the Ebola epidemic?
JK: My greatest challenge was the stress of responding to the demands of PAs who were in the various ETUs seeking medical care; responding to the numerous calls from family members, relatives, and friends wanting me to advocate for their well-being; creating awareness and informing other PAs of the status of their colleagues; and also informing the world at large of the situation we were in. I had many sleepless days and nights, with most of those happening in the months of August, September, and October 2014, when I could not sleep at my own house. I just kept moving from one ETU, radio station, or office to another, advocating and soliciting assistance for the well-being of the health care providers—especially for PAs.
Continue for the aftermath >>
AFTERMATH
On May 9, 2015, the World Health Organization declared Liberia free of Ebola after 42 consecutive days without a new case. That changed on June 29, when Liberia experienced its first new case of Ebola virus since March 20.
In the neighboring countries of Guinea and Sierra Leone, Ebola cases are still regularly occurring (although fewer than at the peak of the outbreak).
As of August 19, 2015, 880 health care workers have become infected with the Ebola virus in Liberia, Guinea, and Sierra Leone; 512 have reportedly died. In Liberia alone, 192 health care worker deaths have been attributed to Ebola.1
REFERENCES
1. World Health Organization. Ebola Situation Report, 19 August, 2015. http://apps.who.int/ebola/current-situation/ebola-situation-report-19-august-2015. Accessed August 24, 2015.
In November 2012 and January 2014, I traveled to Liberia to conduct a needs assessment of the health care system there on behalf of a company that was interested in supporting efforts to rebuild the country’s infrastructure. I discovered that the physician assistant profession has been in existence in Liberia since 1965—the same year that it started in the United States.
During my time in Liberia, I became close friends with Jerry Kollie, PA, President of the Liberia National Physician Assistants Association (LINPAA). I recently interviewed him to learn more about his organization and the PA profession in Liberia, where they have spent almost a year and a half dealing with the worst Ebola virus outbreak in history.
Editor’s note: The following excerpt focuses on the Ebola outbreak. Please visit our website (http://bit.ly/1NgHX2Q) to learn more about the PA profession in Liberia.
John Oliphant: What impact has the Ebola epidemic had on PAs’ clinical practice in Liberia?
Jerry Kollie: The Ebola epidemic has had a serious impact on us in many ways. It created fear among many PAs about continued clinical practice. Some of our students have lost interest in the profession for fear of contracting the virus and dying after graduation.
Workforce is also an issue. Training has been delayed, which means there are fewer PAs available in the various health facilities providing services to people. Many PAs died and others were ill with Ebola, which increased the workload in our health facilities.
The outbreak also created fear among patients; many of them stopped going to health facilities for care. As a result, PAs would go to work and not see any patients.
JO: Do you know how many PAs in Liberia lost their lives due to Ebola? And how many contracted the virus but survived?
JK: A total of 26 PAs were affected by Ebola virus disease. Many contracted the virus at their workplaces and were taken to various Ebola Treatment Units (ETUs), where some died while others survived. Of the total number, 14 died (see box on page 42 for a list of their names), nine survived, and three were quarantined but did not contract the virus. Those three PAs spent 21 days in quarantine after unknowingly attending to patients who were later confirmed to have Ebola. As God would have it, they all went through the quarantine without experiencing or developing signs or symptoms.
JO: What has been your greatest leadership challenge as the President of LINPAA during the Ebola epidemic?
JK: My greatest challenge was the stress of responding to the demands of PAs who were in the various ETUs seeking medical care; responding to the numerous calls from family members, relatives, and friends wanting me to advocate for their well-being; creating awareness and informing other PAs of the status of their colleagues; and also informing the world at large of the situation we were in. I had many sleepless days and nights, with most of those happening in the months of August, September, and October 2014, when I could not sleep at my own house. I just kept moving from one ETU, radio station, or office to another, advocating and soliciting assistance for the well-being of the health care providers—especially for PAs.
Continue for the aftermath >>
AFTERMATH
On May 9, 2015, the World Health Organization declared Liberia free of Ebola after 42 consecutive days without a new case. That changed on June 29, when Liberia experienced its first new case of Ebola virus since March 20.
In the neighboring countries of Guinea and Sierra Leone, Ebola cases are still regularly occurring (although fewer than at the peak of the outbreak).
As of August 19, 2015, 880 health care workers have become infected with the Ebola virus in Liberia, Guinea, and Sierra Leone; 512 have reportedly died. In Liberia alone, 192 health care worker deaths have been attributed to Ebola.1
REFERENCES
1. World Health Organization. Ebola Situation Report, 19 August, 2015. http://apps.who.int/ebola/current-situation/ebola-situation-report-19-august-2015. Accessed August 24, 2015.
In November 2012 and January 2014, I traveled to Liberia to conduct a needs assessment of the health care system there on behalf of a company that was interested in supporting efforts to rebuild the country’s infrastructure. I discovered that the physician assistant profession has been in existence in Liberia since 1965—the same year that it started in the United States.
During my time in Liberia, I became close friends with Jerry Kollie, PA, President of the Liberia National Physician Assistants Association (LINPAA). I recently interviewed him to learn more about his organization and the PA profession in Liberia, where they have spent almost a year and a half dealing with the worst Ebola virus outbreak in history.
Editor’s note: The following excerpt focuses on the Ebola outbreak. Please visit our website (http://bit.ly/1NgHX2Q) to learn more about the PA profession in Liberia.
John Oliphant: What impact has the Ebola epidemic had on PAs’ clinical practice in Liberia?
Jerry Kollie: The Ebola epidemic has had a serious impact on us in many ways. It created fear among many PAs about continued clinical practice. Some of our students have lost interest in the profession for fear of contracting the virus and dying after graduation.
Workforce is also an issue. Training has been delayed, which means there are fewer PAs available in the various health facilities providing services to people. Many PAs died and others were ill with Ebola, which increased the workload in our health facilities.
The outbreak also created fear among patients; many of them stopped going to health facilities for care. As a result, PAs would go to work and not see any patients.
JO: Do you know how many PAs in Liberia lost their lives due to Ebola? And how many contracted the virus but survived?
JK: A total of 26 PAs were affected by Ebola virus disease. Many contracted the virus at their workplaces and were taken to various Ebola Treatment Units (ETUs), where some died while others survived. Of the total number, 14 died (see box on page 42 for a list of their names), nine survived, and three were quarantined but did not contract the virus. Those three PAs spent 21 days in quarantine after unknowingly attending to patients who were later confirmed to have Ebola. As God would have it, they all went through the quarantine without experiencing or developing signs or symptoms.
JO: What has been your greatest leadership challenge as the President of LINPAA during the Ebola epidemic?
JK: My greatest challenge was the stress of responding to the demands of PAs who were in the various ETUs seeking medical care; responding to the numerous calls from family members, relatives, and friends wanting me to advocate for their well-being; creating awareness and informing other PAs of the status of their colleagues; and also informing the world at large of the situation we were in. I had many sleepless days and nights, with most of those happening in the months of August, September, and October 2014, when I could not sleep at my own house. I just kept moving from one ETU, radio station, or office to another, advocating and soliciting assistance for the well-being of the health care providers—especially for PAs.
Continue for the aftermath >>
AFTERMATH
On May 9, 2015, the World Health Organization declared Liberia free of Ebola after 42 consecutive days without a new case. That changed on June 29, when Liberia experienced its first new case of Ebola virus since March 20.
In the neighboring countries of Guinea and Sierra Leone, Ebola cases are still regularly occurring (although fewer than at the peak of the outbreak).
As of August 19, 2015, 880 health care workers have become infected with the Ebola virus in Liberia, Guinea, and Sierra Leone; 512 have reportedly died. In Liberia alone, 192 health care worker deaths have been attributed to Ebola.1
REFERENCES
1. World Health Organization. Ebola Situation Report, 19 August, 2015. http://apps.who.int/ebola/current-situation/ebola-situation-report-19-august-2015. Accessed August 24, 2015.
Cases of liver failure linked to “fat-burning” supplement
In late 2013, there were 45 cases of acute liver failure (ALF) in Hawaii, and 29 of those people reported taking OxyELITE Pro (an herbal dietary supplement marketed for weight reduction and “fat-burning”) 60 days before illness onset. Of 8 initial cases, 2 patients needed urgent liver transplants, one died, and 5 eventually recovered.1 The manufacturer of OxyELITE Pro voluntarily recalled the product after receiving a warning letter from the US Food and Drug Administration (FDA).
One way to prevent situations like this from occurring might be to ban the sale of weight loss or sports enhancement supplements unless they are rigorously tested and approved by the FDA. Voluntary reporting to the FDA is time-consuming and it takes time for the FDA to follow up on these reports.
As primary care physicians, we need to consistently ask patients about their use of supplements, educate them about the potential dangers, and identify those who are experiencing adverse reactions. While we can’t put a stop to the harm that some herbal dietary supplements might inflict on a public eager to embrace quick fixes for weight loss and improved strength, we can be the best first responders.
Linda L. Wong, MD
Honolulu, Hawaii
Reference
1. Centers for Disease Control and Prevention (CDC). Notes from the field: acute hepatitis and liver failure following the use of a dietary supplement intended for weight loss or muscle building—May-October 2013. MMWR Morb Mortal Wkly Rep. 2013;62:817-819.
In late 2013, there were 45 cases of acute liver failure (ALF) in Hawaii, and 29 of those people reported taking OxyELITE Pro (an herbal dietary supplement marketed for weight reduction and “fat-burning”) 60 days before illness onset. Of 8 initial cases, 2 patients needed urgent liver transplants, one died, and 5 eventually recovered.1 The manufacturer of OxyELITE Pro voluntarily recalled the product after receiving a warning letter from the US Food and Drug Administration (FDA).
One way to prevent situations like this from occurring might be to ban the sale of weight loss or sports enhancement supplements unless they are rigorously tested and approved by the FDA. Voluntary reporting to the FDA is time-consuming and it takes time for the FDA to follow up on these reports.
As primary care physicians, we need to consistently ask patients about their use of supplements, educate them about the potential dangers, and identify those who are experiencing adverse reactions. While we can’t put a stop to the harm that some herbal dietary supplements might inflict on a public eager to embrace quick fixes for weight loss and improved strength, we can be the best first responders.
Linda L. Wong, MD
Honolulu, Hawaii
In late 2013, there were 45 cases of acute liver failure (ALF) in Hawaii, and 29 of those people reported taking OxyELITE Pro (an herbal dietary supplement marketed for weight reduction and “fat-burning”) 60 days before illness onset. Of 8 initial cases, 2 patients needed urgent liver transplants, one died, and 5 eventually recovered.1 The manufacturer of OxyELITE Pro voluntarily recalled the product after receiving a warning letter from the US Food and Drug Administration (FDA).
One way to prevent situations like this from occurring might be to ban the sale of weight loss or sports enhancement supplements unless they are rigorously tested and approved by the FDA. Voluntary reporting to the FDA is time-consuming and it takes time for the FDA to follow up on these reports.
As primary care physicians, we need to consistently ask patients about their use of supplements, educate them about the potential dangers, and identify those who are experiencing adverse reactions. While we can’t put a stop to the harm that some herbal dietary supplements might inflict on a public eager to embrace quick fixes for weight loss and improved strength, we can be the best first responders.
Linda L. Wong, MD
Honolulu, Hawaii
Reference
1. Centers for Disease Control and Prevention (CDC). Notes from the field: acute hepatitis and liver failure following the use of a dietary supplement intended for weight loss or muscle building—May-October 2013. MMWR Morb Mortal Wkly Rep. 2013;62:817-819.
Reference
1. Centers for Disease Control and Prevention (CDC). Notes from the field: acute hepatitis and liver failure following the use of a dietary supplement intended for weight loss or muscle building—May-October 2013. MMWR Morb Mortal Wkly Rep. 2013;62:817-819.
Public misperception about doctors’ wealth
I’m rich. Aren’t you?
In reality, you’re probably not (depending on what your definition of rich is), and I’m not either.
The problem, unfortunately, is the public perception that all doctors are rich. They see raw numbers, hear about well-publicized cases of criminal medical fraud, read about some world-famous brain surgeon and his 5-million-square-foot house, and immediately figure we’re all rolling in dough.
For most of us, though, that’s far from the norm. We struggle with declining reimbursements and increasing overheads: rent, staff salaries, office supplies, etc. By the time you take the myriad expenses out, there often isn’t much left for us. And, like everyone else, we have mortgages, families to take care of, student loans, and grocery bills. While most of us can still support families and a moderate lifestyle, we sure aren’t rich. When you take time into account (60-70 hours per week), my hourly salary isn’t that high.
Yet, the majority of people don’t see it that way. Granted, we may be in a better financial position than some of our patients, but it still amazes me when they ask me to waive copays or other visit costs. I always say no, and some argue, “But you’re a doctor! You can afford it.” Whether I can or can’t is immaterial. I pay my family’s medical bills in full and on time and would never dream of asking for a discount or freebie for any reason. You let one person skip, then another, then another ... and it starts to add up quickly.
I have several patients who are quite wealthy. I wouldn’t ask them to pay an extra copay “because you can afford it,” but that’s no different from others asking me to waive theirs for the same reason.
I just wish patients would see, or the lay press would show, the reality of finances for a modern-day average doctor. I, personally, am sick of people who still affiliate us with Porsches, two homes, and Wednesday-afternoon golfing. A few of those docs may still be around, but they are a rare exception, not the rule. And I don’t see that changing any time soon.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m rich. Aren’t you?
In reality, you’re probably not (depending on what your definition of rich is), and I’m not either.
The problem, unfortunately, is the public perception that all doctors are rich. They see raw numbers, hear about well-publicized cases of criminal medical fraud, read about some world-famous brain surgeon and his 5-million-square-foot house, and immediately figure we’re all rolling in dough.
For most of us, though, that’s far from the norm. We struggle with declining reimbursements and increasing overheads: rent, staff salaries, office supplies, etc. By the time you take the myriad expenses out, there often isn’t much left for us. And, like everyone else, we have mortgages, families to take care of, student loans, and grocery bills. While most of us can still support families and a moderate lifestyle, we sure aren’t rich. When you take time into account (60-70 hours per week), my hourly salary isn’t that high.
Yet, the majority of people don’t see it that way. Granted, we may be in a better financial position than some of our patients, but it still amazes me when they ask me to waive copays or other visit costs. I always say no, and some argue, “But you’re a doctor! You can afford it.” Whether I can or can’t is immaterial. I pay my family’s medical bills in full and on time and would never dream of asking for a discount or freebie for any reason. You let one person skip, then another, then another ... and it starts to add up quickly.
I have several patients who are quite wealthy. I wouldn’t ask them to pay an extra copay “because you can afford it,” but that’s no different from others asking me to waive theirs for the same reason.
I just wish patients would see, or the lay press would show, the reality of finances for a modern-day average doctor. I, personally, am sick of people who still affiliate us with Porsches, two homes, and Wednesday-afternoon golfing. A few of those docs may still be around, but they are a rare exception, not the rule. And I don’t see that changing any time soon.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m rich. Aren’t you?
In reality, you’re probably not (depending on what your definition of rich is), and I’m not either.
The problem, unfortunately, is the public perception that all doctors are rich. They see raw numbers, hear about well-publicized cases of criminal medical fraud, read about some world-famous brain surgeon and his 5-million-square-foot house, and immediately figure we’re all rolling in dough.
For most of us, though, that’s far from the norm. We struggle with declining reimbursements and increasing overheads: rent, staff salaries, office supplies, etc. By the time you take the myriad expenses out, there often isn’t much left for us. And, like everyone else, we have mortgages, families to take care of, student loans, and grocery bills. While most of us can still support families and a moderate lifestyle, we sure aren’t rich. When you take time into account (60-70 hours per week), my hourly salary isn’t that high.
Yet, the majority of people don’t see it that way. Granted, we may be in a better financial position than some of our patients, but it still amazes me when they ask me to waive copays or other visit costs. I always say no, and some argue, “But you’re a doctor! You can afford it.” Whether I can or can’t is immaterial. I pay my family’s medical bills in full and on time and would never dream of asking for a discount or freebie for any reason. You let one person skip, then another, then another ... and it starts to add up quickly.
I have several patients who are quite wealthy. I wouldn’t ask them to pay an extra copay “because you can afford it,” but that’s no different from others asking me to waive theirs for the same reason.
I just wish patients would see, or the lay press would show, the reality of finances for a modern-day average doctor. I, personally, am sick of people who still affiliate us with Porsches, two homes, and Wednesday-afternoon golfing. A few of those docs may still be around, but they are a rare exception, not the rule. And I don’t see that changing any time soon.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.

Is the risk of EPT substantially higher?

Is the risk of EPT
substantially higher?
I found this article interesting, and I agree that women who have atypical hyperplasia should be counseled to consider the possible additional risk of hormone use. I didn’t see a reference, however, that supported this assertion: “Accordingly, the absolute risk of invasive breast cancer associated with use of
estrogen-progestin menopausal hormone therapy (EPT) is also likely substantially higher than in average-risk women.”
Are there any high-quality studies that support this?
Brad Logan, MD
Tampa, Florida
Adverse effects from agents that suppress estrogen levels
Are any studies being done to look at bazedoxifene in these patients alone or especially in combination with an estrogen? Encouraging the use of agents long term that profoundly suppress actual or effective estrogen levels, especially in young women, ignores the very profound adverse effects these agents can have both in the immediate and long term. I would be curious to know if there are any studies or recommendations regarding the use of gonadotropin agonists or antiandrogens in men older than age 35 to prevent prostate cancer.
Jewell E. Malick, DO
Rockwall, Texas
Drs. Kaunitz and Samiian respond
We appreciate the thoughtful letters from Drs. Logan and Malick concerning our article on atypical
hyperplasia (AH) of the breast. Regarding Dr. Logan’s question, we are not aware of any randomized controlled trials that have assessed the impact of EPT on the risk of being diagnosed with invasive breast
cancer in women with a history of AH. An observational study looking
at this issue did not distinguish between estrogen hormone therapy (ET) and EPT.1
However, we do know that in women at average risk for breast cancer, EPT increases the absolute risk of an invasive breast cancer by 1 additional case per 1,000 person- years of use.2 Accordingly, since women with a prior biopsy diagnosis of AH have a 4-fold elevated risk of being diagnosed with invasive breast cancer, it is reasonable to speculate that EPT would elevate this risk to some 4 additional cases per 1,000 person- years of use. This is why we recommend that women with a history of AH considering use of EPT be counseled regarding this potential elevated risk of being diagnosed with invasive breast cancer.
Regarding Dr. Malick’s questions, we are not aware of trials assessing the impact that bazedoxifene (with or without estrogen) has in women with a prior biopsy demonstrating AH. With respect to trials assessing androgen blockers in men to prevent prostate cancer, the Prostate Cancer Prevention Trial is assessing the use of finasteride in men aged 55 years and older.3
Do forceps have a place in your obstetric toolbox?
“UPDATE ON OPERATIVE VAGINAL DELIVERY”
WILLIAM H. BARTH JR, MD (July 2015)
With the US cesarean delivery rate hovering at 31%, it may be time to revisit forceps
(Keilland forceps in particular), says William H. Barth Jr, MD, in the July “Update on operative vaginal delivery.” More than
130 readers weighed in when asked if they agree if forceps have a place in their obstetric toolbox:
- 88 readers (64.7%) agreed
- 48 readers (35.3%) disagreed
To participate in the latest Quick Poll, visit obgmanagement.com
READERS WEIGH IN:
Patients’ unrealistic expectations influence
clinicians’ decisions
We all have been trained in the use of forceps at delivery. Perhaps the fact that more than one-third of the Quick Poll votes registered “no” reflects the reluctance of providers to use forceps because of our patients’ tendencies to have unrealistic expectations about childbirth and risk. Given the marginally better outcomes, I will continue to use vacuum extraction when faced with an outlet delivery dilemma.
William White, MD
Mammoth Lakes, California
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Byrne C, Connolly JL, Colditz GA, Schnitt SJ. Biopsy confirmed benign breast disease, postmenopausal use of exogenous female hormones, and breast carcinoma risk. Cancer. 2000;89(10):2046–2052.
- Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353–1368.
- Hoque A, Yao S, Till C, et al. Effect of finasteride on serum androstenedione and risk of prostate cancer within the Prostate Cancer Prevention Trial: differential effect on high- and low-grade disease. Urology. 2015;85(3):616–620.
Is the risk of EPT
substantially higher?
I found this article interesting, and I agree that women who have atypical hyperplasia should be counseled to consider the possible additional risk of hormone use. I didn’t see a reference, however, that supported this assertion: “Accordingly, the absolute risk of invasive breast cancer associated with use of
estrogen-progestin menopausal hormone therapy (EPT) is also likely substantially higher than in average-risk women.”
Are there any high-quality studies that support this?
Brad Logan, MD
Tampa, Florida
Adverse effects from agents that suppress estrogen levels
Are any studies being done to look at bazedoxifene in these patients alone or especially in combination with an estrogen? Encouraging the use of agents long term that profoundly suppress actual or effective estrogen levels, especially in young women, ignores the very profound adverse effects these agents can have both in the immediate and long term. I would be curious to know if there are any studies or recommendations regarding the use of gonadotropin agonists or antiandrogens in men older than age 35 to prevent prostate cancer.
Jewell E. Malick, DO
Rockwall, Texas
Drs. Kaunitz and Samiian respond
We appreciate the thoughtful letters from Drs. Logan and Malick concerning our article on atypical
hyperplasia (AH) of the breast. Regarding Dr. Logan’s question, we are not aware of any randomized controlled trials that have assessed the impact of EPT on the risk of being diagnosed with invasive breast
cancer in women with a history of AH. An observational study looking
at this issue did not distinguish between estrogen hormone therapy (ET) and EPT.1
However, we do know that in women at average risk for breast cancer, EPT increases the absolute risk of an invasive breast cancer by 1 additional case per 1,000 person- years of use.2 Accordingly, since women with a prior biopsy diagnosis of AH have a 4-fold elevated risk of being diagnosed with invasive breast cancer, it is reasonable to speculate that EPT would elevate this risk to some 4 additional cases per 1,000 person- years of use. This is why we recommend that women with a history of AH considering use of EPT be counseled regarding this potential elevated risk of being diagnosed with invasive breast cancer.
Regarding Dr. Malick’s questions, we are not aware of trials assessing the impact that bazedoxifene (with or without estrogen) has in women with a prior biopsy demonstrating AH. With respect to trials assessing androgen blockers in men to prevent prostate cancer, the Prostate Cancer Prevention Trial is assessing the use of finasteride in men aged 55 years and older.3
Do forceps have a place in your obstetric toolbox?
“UPDATE ON OPERATIVE VAGINAL DELIVERY”
WILLIAM H. BARTH JR, MD (July 2015)
With the US cesarean delivery rate hovering at 31%, it may be time to revisit forceps
(Keilland forceps in particular), says William H. Barth Jr, MD, in the July “Update on operative vaginal delivery.” More than
130 readers weighed in when asked if they agree if forceps have a place in their obstetric toolbox:
- 88 readers (64.7%) agreed
- 48 readers (35.3%) disagreed
To participate in the latest Quick Poll, visit obgmanagement.com
READERS WEIGH IN:
Patients’ unrealistic expectations influence
clinicians’ decisions
We all have been trained in the use of forceps at delivery. Perhaps the fact that more than one-third of the Quick Poll votes registered “no” reflects the reluctance of providers to use forceps because of our patients’ tendencies to have unrealistic expectations about childbirth and risk. Given the marginally better outcomes, I will continue to use vacuum extraction when faced with an outlet delivery dilemma.
William White, MD
Mammoth Lakes, California
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Is the risk of EPT
substantially higher?
I found this article interesting, and I agree that women who have atypical hyperplasia should be counseled to consider the possible additional risk of hormone use. I didn’t see a reference, however, that supported this assertion: “Accordingly, the absolute risk of invasive breast cancer associated with use of
estrogen-progestin menopausal hormone therapy (EPT) is also likely substantially higher than in average-risk women.”
Are there any high-quality studies that support this?
Brad Logan, MD
Tampa, Florida
Adverse effects from agents that suppress estrogen levels
Are any studies being done to look at bazedoxifene in these patients alone or especially in combination with an estrogen? Encouraging the use of agents long term that profoundly suppress actual or effective estrogen levels, especially in young women, ignores the very profound adverse effects these agents can have both in the immediate and long term. I would be curious to know if there are any studies or recommendations regarding the use of gonadotropin agonists or antiandrogens in men older than age 35 to prevent prostate cancer.
Jewell E. Malick, DO
Rockwall, Texas
Drs. Kaunitz and Samiian respond
We appreciate the thoughtful letters from Drs. Logan and Malick concerning our article on atypical
hyperplasia (AH) of the breast. Regarding Dr. Logan’s question, we are not aware of any randomized controlled trials that have assessed the impact of EPT on the risk of being diagnosed with invasive breast
cancer in women with a history of AH. An observational study looking
at this issue did not distinguish between estrogen hormone therapy (ET) and EPT.1
However, we do know that in women at average risk for breast cancer, EPT increases the absolute risk of an invasive breast cancer by 1 additional case per 1,000 person- years of use.2 Accordingly, since women with a prior biopsy diagnosis of AH have a 4-fold elevated risk of being diagnosed with invasive breast cancer, it is reasonable to speculate that EPT would elevate this risk to some 4 additional cases per 1,000 person- years of use. This is why we recommend that women with a history of AH considering use of EPT be counseled regarding this potential elevated risk of being diagnosed with invasive breast cancer.
Regarding Dr. Malick’s questions, we are not aware of trials assessing the impact that bazedoxifene (with or without estrogen) has in women with a prior biopsy demonstrating AH. With respect to trials assessing androgen blockers in men to prevent prostate cancer, the Prostate Cancer Prevention Trial is assessing the use of finasteride in men aged 55 years and older.3
Do forceps have a place in your obstetric toolbox?
“UPDATE ON OPERATIVE VAGINAL DELIVERY”
WILLIAM H. BARTH JR, MD (July 2015)
With the US cesarean delivery rate hovering at 31%, it may be time to revisit forceps
(Keilland forceps in particular), says William H. Barth Jr, MD, in the July “Update on operative vaginal delivery.” More than
130 readers weighed in when asked if they agree if forceps have a place in their obstetric toolbox:
- 88 readers (64.7%) agreed
- 48 readers (35.3%) disagreed
To participate in the latest Quick Poll, visit obgmanagement.com
READERS WEIGH IN:
Patients’ unrealistic expectations influence
clinicians’ decisions
We all have been trained in the use of forceps at delivery. Perhaps the fact that more than one-third of the Quick Poll votes registered “no” reflects the reluctance of providers to use forceps because of our patients’ tendencies to have unrealistic expectations about childbirth and risk. Given the marginally better outcomes, I will continue to use vacuum extraction when faced with an outlet delivery dilemma.
William White, MD
Mammoth Lakes, California
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Byrne C, Connolly JL, Colditz GA, Schnitt SJ. Biopsy confirmed benign breast disease, postmenopausal use of exogenous female hormones, and breast carcinoma risk. Cancer. 2000;89(10):2046–2052.
- Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353–1368.
- Hoque A, Yao S, Till C, et al. Effect of finasteride on serum androstenedione and risk of prostate cancer within the Prostate Cancer Prevention Trial: differential effect on high- and low-grade disease. Urology. 2015;85(3):616–620.
- Byrne C, Connolly JL, Colditz GA, Schnitt SJ. Biopsy confirmed benign breast disease, postmenopausal use of exogenous female hormones, and breast carcinoma risk. Cancer. 2000;89(10):2046–2052.
- Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353–1368.
- Hoque A, Yao S, Till C, et al. Effect of finasteride on serum androstenedione and risk of prostate cancer within the Prostate Cancer Prevention Trial: differential effect on high- and low-grade disease. Urology. 2015;85(3):616–620.
CDC Will Soon Issue Guidelines for the Prevention of Surgical Site Infection
Surgical site infections (SSIs) and hospital-acquired infections (HAIs) have become two of the most feared complications associated with the delivery of medical care. The issue of infection has become so important that the American Academy of Orthopaedic Surgeons (AAOS), the Infectious Diseases Society of America (IDSA), the Musculoskeletal Infection Society (MSIS), and numerous other organizations have issued guidelines for the prevention and diagnosis of infection after orthopedic procedures. Similar efforts have taken place in other surgical disciplines.
It is fair to state that the issue of infection after surgical procedures has come to the forefront of all complications and strikes fear in the minds of patients and surgeons who enter the operating room on a daily basis. The immense financial and psychological burden associated with SSIs and HAIs has also prompted regulatory bodies and governmental agencies in the United States and other parts of the world to seek strategies to counter the rising incidence of infection. It is anticipated that “striving for lower incidence of surgical site infection” will be part of the “quality metric” that most payers in the United States, including the Centers for Medicare and Medicaid Services (CMS), will implement in the future. In fact, the incidence of infection after most surgical procedures is tracked carefully by the surveillance arm of the Centers for Disease Control and Prevention (CDC), the National Healthcare Safety Network (NHSN). Most hospitals in the United States are required to report infections occurring after surgical procedures and patient admissions. The CDC has issued specific definitions and reporting instructions for this purpose.
As part of the important mission of reducing the burden of SSIs and HAIs, the CDC has had an active role in producing guidelines for the prevention of SSI. Their latest guidelines, issued in 1999, had relevant and important expert-based recommendations that have certainly served the medical community. The CDC will soon issue their updated guidelines for the prevention of SSI. This time, the CDC has decided to issue evidence-based recommendations. To accomplish this, the CDC convened a large workgroup consisting of experts and representatives of numerous societies, including the AAOS and the MSIS, to evaluate the available literature in issuing these guidelines. The guidelines are divided into 2 sections: the “Core” addresses recommendations applicable across a broad spectrum of surgical procedures, and the new procedure-specific component sections each focus on a single high-volume, high-burden surgical procedure. The first of these component sections focuses on arthroplasty procedures.
One of the sobering discoveries of the workgroup is the fact that there is little evidence to support many of our daily practices applicable to the prevention of infection. Thus, the guidelines, when issued, will reflect the lack of evidence for some of our established and common practices. There will be, however, many other recommendations that are based on available evidence, such as the importance of administration of perioperative antibiotics, to name one. Huge effort has been invested by the CDC and the numerous experts who served in the workgroup to produce these guidelines. The literature has been evaluated extensively. Many conference calls have taken place to discuss the issues, when necessary. In addition, these recommendations have been carefully evaluated by the Healthcare Infection Control Practices Advisory Committee (HICPAC). The guidelines, when issued, will no doubt play a critical role in helping us make strides in reducing the burden of this dreaded complication. The guidelines will also provide a great impetus for the medical community to generate and seek evidence for practices that lack such evidence currently. ◾
Click here to read the commentary on this editorial by Scott R. Nodzo, MD
Surgical site infections (SSIs) and hospital-acquired infections (HAIs) have become two of the most feared complications associated with the delivery of medical care. The issue of infection has become so important that the American Academy of Orthopaedic Surgeons (AAOS), the Infectious Diseases Society of America (IDSA), the Musculoskeletal Infection Society (MSIS), and numerous other organizations have issued guidelines for the prevention and diagnosis of infection after orthopedic procedures. Similar efforts have taken place in other surgical disciplines.
It is fair to state that the issue of infection after surgical procedures has come to the forefront of all complications and strikes fear in the minds of patients and surgeons who enter the operating room on a daily basis. The immense financial and psychological burden associated with SSIs and HAIs has also prompted regulatory bodies and governmental agencies in the United States and other parts of the world to seek strategies to counter the rising incidence of infection. It is anticipated that “striving for lower incidence of surgical site infection” will be part of the “quality metric” that most payers in the United States, including the Centers for Medicare and Medicaid Services (CMS), will implement in the future. In fact, the incidence of infection after most surgical procedures is tracked carefully by the surveillance arm of the Centers for Disease Control and Prevention (CDC), the National Healthcare Safety Network (NHSN). Most hospitals in the United States are required to report infections occurring after surgical procedures and patient admissions. The CDC has issued specific definitions and reporting instructions for this purpose.
As part of the important mission of reducing the burden of SSIs and HAIs, the CDC has had an active role in producing guidelines for the prevention of SSI. Their latest guidelines, issued in 1999, had relevant and important expert-based recommendations that have certainly served the medical community. The CDC will soon issue their updated guidelines for the prevention of SSI. This time, the CDC has decided to issue evidence-based recommendations. To accomplish this, the CDC convened a large workgroup consisting of experts and representatives of numerous societies, including the AAOS and the MSIS, to evaluate the available literature in issuing these guidelines. The guidelines are divided into 2 sections: the “Core” addresses recommendations applicable across a broad spectrum of surgical procedures, and the new procedure-specific component sections each focus on a single high-volume, high-burden surgical procedure. The first of these component sections focuses on arthroplasty procedures.
One of the sobering discoveries of the workgroup is the fact that there is little evidence to support many of our daily practices applicable to the prevention of infection. Thus, the guidelines, when issued, will reflect the lack of evidence for some of our established and common practices. There will be, however, many other recommendations that are based on available evidence, such as the importance of administration of perioperative antibiotics, to name one. Huge effort has been invested by the CDC and the numerous experts who served in the workgroup to produce these guidelines. The literature has been evaluated extensively. Many conference calls have taken place to discuss the issues, when necessary. In addition, these recommendations have been carefully evaluated by the Healthcare Infection Control Practices Advisory Committee (HICPAC). The guidelines, when issued, will no doubt play a critical role in helping us make strides in reducing the burden of this dreaded complication. The guidelines will also provide a great impetus for the medical community to generate and seek evidence for practices that lack such evidence currently. ◾
Click here to read the commentary on this editorial by Scott R. Nodzo, MD
Surgical site infections (SSIs) and hospital-acquired infections (HAIs) have become two of the most feared complications associated with the delivery of medical care. The issue of infection has become so important that the American Academy of Orthopaedic Surgeons (AAOS), the Infectious Diseases Society of America (IDSA), the Musculoskeletal Infection Society (MSIS), and numerous other organizations have issued guidelines for the prevention and diagnosis of infection after orthopedic procedures. Similar efforts have taken place in other surgical disciplines.
It is fair to state that the issue of infection after surgical procedures has come to the forefront of all complications and strikes fear in the minds of patients and surgeons who enter the operating room on a daily basis. The immense financial and psychological burden associated with SSIs and HAIs has also prompted regulatory bodies and governmental agencies in the United States and other parts of the world to seek strategies to counter the rising incidence of infection. It is anticipated that “striving for lower incidence of surgical site infection” will be part of the “quality metric” that most payers in the United States, including the Centers for Medicare and Medicaid Services (CMS), will implement in the future. In fact, the incidence of infection after most surgical procedures is tracked carefully by the surveillance arm of the Centers for Disease Control and Prevention (CDC), the National Healthcare Safety Network (NHSN). Most hospitals in the United States are required to report infections occurring after surgical procedures and patient admissions. The CDC has issued specific definitions and reporting instructions for this purpose.
As part of the important mission of reducing the burden of SSIs and HAIs, the CDC has had an active role in producing guidelines for the prevention of SSI. Their latest guidelines, issued in 1999, had relevant and important expert-based recommendations that have certainly served the medical community. The CDC will soon issue their updated guidelines for the prevention of SSI. This time, the CDC has decided to issue evidence-based recommendations. To accomplish this, the CDC convened a large workgroup consisting of experts and representatives of numerous societies, including the AAOS and the MSIS, to evaluate the available literature in issuing these guidelines. The guidelines are divided into 2 sections: the “Core” addresses recommendations applicable across a broad spectrum of surgical procedures, and the new procedure-specific component sections each focus on a single high-volume, high-burden surgical procedure. The first of these component sections focuses on arthroplasty procedures.
One of the sobering discoveries of the workgroup is the fact that there is little evidence to support many of our daily practices applicable to the prevention of infection. Thus, the guidelines, when issued, will reflect the lack of evidence for some of our established and common practices. There will be, however, many other recommendations that are based on available evidence, such as the importance of administration of perioperative antibiotics, to name one. Huge effort has been invested by the CDC and the numerous experts who served in the workgroup to produce these guidelines. The literature has been evaluated extensively. Many conference calls have taken place to discuss the issues, when necessary. In addition, these recommendations have been carefully evaluated by the Healthcare Infection Control Practices Advisory Committee (HICPAC). The guidelines, when issued, will no doubt play a critical role in helping us make strides in reducing the burden of this dreaded complication. The guidelines will also provide a great impetus for the medical community to generate and seek evidence for practices that lack such evidence currently. ◾
Click here to read the commentary on this editorial by Scott R. Nodzo, MD

Legal matters – not just child’s play
Social media platforms are by far the most common form of communication among our teens. A 2015 study by the Pew Research Center stated that 71% of teens between the ages of 12 and 18 years use more than one form of social media. But little education and awareness of the legal implications of the information exchanged is provided to these teens, which has landed some of them in significant legal trouble.
Gone are the days when rivals could just pass mean comments to each other in the hallway or leave obnoxious comments on a bathroom wall. Today, within minutes malicious comments are quickly posted on social media to be shared by all. This makes the impact of the impulsive, mindless, and usually immature sentiments much more damaging, and unfortunately can result in severe, sometimes unforeseen consequences.
Cyberbullying is bullying or intimidating through electronic technology. This has become all too commonplace among teenagers because it takes so little to post unflattering pictures, or quotes, or threating messages from the privacy of your home. Much of what would never be spoken face to face is posted without regard. Two teen girls in Florida were charged with a felony for the suicide of a classmate they unrelentingly bullied. This was just one of many stories of a child being brought to despair by immature and cowardly teens misusing social media. Surely they never realized that their immature act would land them in jail. It is a crime to threaten to kill or seriously harm, menace, or harass a person for any reason, regardless of one’s age.
Defamation is a social tort that protects the reputation of a person from untrue comments or innuendos. In the past this was considered to be gossip or rumor-mongering, but now, given the advent of new technology, publishing these same comments makes one the author and, therefore, may be liable for defamation of character. This may not mean jail time for a person, but can certainly land that person in court, requiring his or her parents to incur significant legal fees.
Probably the most important legal issue that teens – as well as adults – should know about are the laws regarding sexual texting or “sexting.” For those of us born in the era before social media, sexting is the distribution of nude pictures of themselves or anyone else. When the image is that of a person under the age of 18 years, it is considered child pornography and subject to punishment by law. Because child pornography is taken very seriously, dosomething.org is a website for young people that promotes social awareness in hopes of changing behavior. This site presents the alarming percentages of teens who send and or receive nude or sexually explicit photos. Many have no idea they are committing a felony.
The unfortunate reality is that many photos or videos that were exchanged between trusted friends end up in the hands of ill-intended teens and get widely disseminated on social media. Anyone caught having or disseminating child pornography, regardless of who started it, is at risk of criminal repercussions. There have been several so-called “THOT” pages (That Ho Over There) started at high schools where students published nude pictures of classmates. These pages go viral within minutes, and although they are taken down quickly, the damage usually is already done. These actions can result in expulsion and suspension of students and significant emotional distress to the victim.
Another legal concern is the issue of privacy. Many users don’t realize that personal information displayed on social media can be easily obtained and misused. Identity theft is on the rise, not just because criminals are more savvy, but because so many people are careless with their information. Disclosure of email, birth date, and cell phone number are all desirable pieces of information that drive marketing, but more importantly, allows information to be used and misconstrued by anyone to create a phony identity, gain access to accounts, stalk, harass, or even resort to blackmail. The unauthorized use of personal information is illegal and punishable by law.
Another legal issue associated with social media are copyright laws. Many teens, as well as adults, have no idea of the laws that protect the music, videos, pictures, and images thoughtlessly placed on social media. Most don’t realize that just because it is commonly done doesn’t mean that it’s legal. Once a picture is posted, it can be shared, altered, and downloaded all over the world by anyone.
There have been reports of lawsuits brought by parents who found pictures of their children were used in advertisements by major companies without their knowledge or permission. Companies, likewise, have brought suit against individuals who have unknowingly misused their product in a post to entertain their friends. In fact, many of the apps that people download have a check box to acknowledge that the owners are free to use material posted at their discretion, which most folks check without reading the fine print. Because the laws on the books lag behind the changing times, there is often a lot of room for interpretation that puts everyone at risk. So teenagers must understand that just because material is published doesn’t mean it is free to be used for personal distribution.
Primary care physicians play a critical role in educating families. Dosomething.org and stopbullying.gov are two great resources for parents and children alike. Educating teens to the legal and social repercussions is key in protecting them. Schools and parents have to be aware themselves and continually stress the importance of Internet safety and appropriate use of social media.
Dr. Pearce is a pediatrician in Frankfort, Ill. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Email her at pdnews@frontlinemedcom.com
Social media platforms are by far the most common form of communication among our teens. A 2015 study by the Pew Research Center stated that 71% of teens between the ages of 12 and 18 years use more than one form of social media. But little education and awareness of the legal implications of the information exchanged is provided to these teens, which has landed some of them in significant legal trouble.
Gone are the days when rivals could just pass mean comments to each other in the hallway or leave obnoxious comments on a bathroom wall. Today, within minutes malicious comments are quickly posted on social media to be shared by all. This makes the impact of the impulsive, mindless, and usually immature sentiments much more damaging, and unfortunately can result in severe, sometimes unforeseen consequences.
Cyberbullying is bullying or intimidating through electronic technology. This has become all too commonplace among teenagers because it takes so little to post unflattering pictures, or quotes, or threating messages from the privacy of your home. Much of what would never be spoken face to face is posted without regard. Two teen girls in Florida were charged with a felony for the suicide of a classmate they unrelentingly bullied. This was just one of many stories of a child being brought to despair by immature and cowardly teens misusing social media. Surely they never realized that their immature act would land them in jail. It is a crime to threaten to kill or seriously harm, menace, or harass a person for any reason, regardless of one’s age.
Defamation is a social tort that protects the reputation of a person from untrue comments or innuendos. In the past this was considered to be gossip or rumor-mongering, but now, given the advent of new technology, publishing these same comments makes one the author and, therefore, may be liable for defamation of character. This may not mean jail time for a person, but can certainly land that person in court, requiring his or her parents to incur significant legal fees.
Probably the most important legal issue that teens – as well as adults – should know about are the laws regarding sexual texting or “sexting.” For those of us born in the era before social media, sexting is the distribution of nude pictures of themselves or anyone else. When the image is that of a person under the age of 18 years, it is considered child pornography and subject to punishment by law. Because child pornography is taken very seriously, dosomething.org is a website for young people that promotes social awareness in hopes of changing behavior. This site presents the alarming percentages of teens who send and or receive nude or sexually explicit photos. Many have no idea they are committing a felony.
The unfortunate reality is that many photos or videos that were exchanged between trusted friends end up in the hands of ill-intended teens and get widely disseminated on social media. Anyone caught having or disseminating child pornography, regardless of who started it, is at risk of criminal repercussions. There have been several so-called “THOT” pages (That Ho Over There) started at high schools where students published nude pictures of classmates. These pages go viral within minutes, and although they are taken down quickly, the damage usually is already done. These actions can result in expulsion and suspension of students and significant emotional distress to the victim.
Another legal concern is the issue of privacy. Many users don’t realize that personal information displayed on social media can be easily obtained and misused. Identity theft is on the rise, not just because criminals are more savvy, but because so many people are careless with their information. Disclosure of email, birth date, and cell phone number are all desirable pieces of information that drive marketing, but more importantly, allows information to be used and misconstrued by anyone to create a phony identity, gain access to accounts, stalk, harass, or even resort to blackmail. The unauthorized use of personal information is illegal and punishable by law.
Another legal issue associated with social media are copyright laws. Many teens, as well as adults, have no idea of the laws that protect the music, videos, pictures, and images thoughtlessly placed on social media. Most don’t realize that just because it is commonly done doesn’t mean that it’s legal. Once a picture is posted, it can be shared, altered, and downloaded all over the world by anyone.
There have been reports of lawsuits brought by parents who found pictures of their children were used in advertisements by major companies without their knowledge or permission. Companies, likewise, have brought suit against individuals who have unknowingly misused their product in a post to entertain their friends. In fact, many of the apps that people download have a check box to acknowledge that the owners are free to use material posted at their discretion, which most folks check without reading the fine print. Because the laws on the books lag behind the changing times, there is often a lot of room for interpretation that puts everyone at risk. So teenagers must understand that just because material is published doesn’t mean it is free to be used for personal distribution.
Primary care physicians play a critical role in educating families. Dosomething.org and stopbullying.gov are two great resources for parents and children alike. Educating teens to the legal and social repercussions is key in protecting them. Schools and parents have to be aware themselves and continually stress the importance of Internet safety and appropriate use of social media.
Dr. Pearce is a pediatrician in Frankfort, Ill. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Email her at pdnews@frontlinemedcom.com
Social media platforms are by far the most common form of communication among our teens. A 2015 study by the Pew Research Center stated that 71% of teens between the ages of 12 and 18 years use more than one form of social media. But little education and awareness of the legal implications of the information exchanged is provided to these teens, which has landed some of them in significant legal trouble.
Gone are the days when rivals could just pass mean comments to each other in the hallway or leave obnoxious comments on a bathroom wall. Today, within minutes malicious comments are quickly posted on social media to be shared by all. This makes the impact of the impulsive, mindless, and usually immature sentiments much more damaging, and unfortunately can result in severe, sometimes unforeseen consequences.
Cyberbullying is bullying or intimidating through electronic technology. This has become all too commonplace among teenagers because it takes so little to post unflattering pictures, or quotes, or threating messages from the privacy of your home. Much of what would never be spoken face to face is posted without regard. Two teen girls in Florida were charged with a felony for the suicide of a classmate they unrelentingly bullied. This was just one of many stories of a child being brought to despair by immature and cowardly teens misusing social media. Surely they never realized that their immature act would land them in jail. It is a crime to threaten to kill or seriously harm, menace, or harass a person for any reason, regardless of one’s age.
Defamation is a social tort that protects the reputation of a person from untrue comments or innuendos. In the past this was considered to be gossip or rumor-mongering, but now, given the advent of new technology, publishing these same comments makes one the author and, therefore, may be liable for defamation of character. This may not mean jail time for a person, but can certainly land that person in court, requiring his or her parents to incur significant legal fees.
Probably the most important legal issue that teens – as well as adults – should know about are the laws regarding sexual texting or “sexting.” For those of us born in the era before social media, sexting is the distribution of nude pictures of themselves or anyone else. When the image is that of a person under the age of 18 years, it is considered child pornography and subject to punishment by law. Because child pornography is taken very seriously, dosomething.org is a website for young people that promotes social awareness in hopes of changing behavior. This site presents the alarming percentages of teens who send and or receive nude or sexually explicit photos. Many have no idea they are committing a felony.
The unfortunate reality is that many photos or videos that were exchanged between trusted friends end up in the hands of ill-intended teens and get widely disseminated on social media. Anyone caught having or disseminating child pornography, regardless of who started it, is at risk of criminal repercussions. There have been several so-called “THOT” pages (That Ho Over There) started at high schools where students published nude pictures of classmates. These pages go viral within minutes, and although they are taken down quickly, the damage usually is already done. These actions can result in expulsion and suspension of students and significant emotional distress to the victim.
Another legal concern is the issue of privacy. Many users don’t realize that personal information displayed on social media can be easily obtained and misused. Identity theft is on the rise, not just because criminals are more savvy, but because so many people are careless with their information. Disclosure of email, birth date, and cell phone number are all desirable pieces of information that drive marketing, but more importantly, allows information to be used and misconstrued by anyone to create a phony identity, gain access to accounts, stalk, harass, or even resort to blackmail. The unauthorized use of personal information is illegal and punishable by law.
Another legal issue associated with social media are copyright laws. Many teens, as well as adults, have no idea of the laws that protect the music, videos, pictures, and images thoughtlessly placed on social media. Most don’t realize that just because it is commonly done doesn’t mean that it’s legal. Once a picture is posted, it can be shared, altered, and downloaded all over the world by anyone.
There have been reports of lawsuits brought by parents who found pictures of their children were used in advertisements by major companies without their knowledge or permission. Companies, likewise, have brought suit against individuals who have unknowingly misused their product in a post to entertain their friends. In fact, many of the apps that people download have a check box to acknowledge that the owners are free to use material posted at their discretion, which most folks check without reading the fine print. Because the laws on the books lag behind the changing times, there is often a lot of room for interpretation that puts everyone at risk. So teenagers must understand that just because material is published doesn’t mean it is free to be used for personal distribution.
Primary care physicians play a critical role in educating families. Dosomething.org and stopbullying.gov are two great resources for parents and children alike. Educating teens to the legal and social repercussions is key in protecting them. Schools and parents have to be aware themselves and continually stress the importance of Internet safety and appropriate use of social media.
Dr. Pearce is a pediatrician in Frankfort, Ill. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Email her at pdnews@frontlinemedcom.com

From the Editor: The elephant in the operating room
Once again hospital administrators in their never-ending quest to reduce expenditures have placed vascular surgeons at a disadvantage. First they reduce the inventory of necessary items. Now they want to keep sales representatives out of the operating room. Their thought process is industry representatives will seduce us to use an expensive product which we otherwise would not consider using. Further, companies build support into the cost of their devices. Thus they would be expected to reduce prices if their personnel were no longer required in the OR.
Administrators as well as many lay public must also wonder why a nonphysician representative of a device company should be present in the operating room. This is certainly a valid question. The answer requires an understanding of how the complexity of vascular interventions has evolved in the era of endovascular procedures.
The vascular surgeon of yore learned basic vascular skills of dissection, excision, needles, and thread which could be applied with equal skill throughout the vascular system. Although they used multiple conduits as grafts, the technique of sewing an anastomosis was a general skill. Then, as surgeons still do now, they needed to know the benefits and drawbacks of the various graft materials and sutures. However, they certainly did not require a company representative to be in the room nor to instruct them on how to sew in the graft or how to deal with a broken suture.
But now vascular surgeons use wires, stents, catheters, balloons, lasers, and drills. When I last counted there were at least eight different companies selling aortic endografts and promoting never-ending variations or replacements for their ‘last year’s device.’ Often the advent of a new device produced an expanded repertoire of new procedures each with their own specific nuances many of which were device specific. Accordingly, it is essential that a surgeon become experienced with the new device in order to prevent or overcome glitches that otherwise might result in serious complications.
However, only the busiest vascular surgeons or those specifically involved in industry-supported trials may ever achieve sufficient experience to be able to use all these products. Certainly, a surgeon may elect to become familiar with just a few of the available choices. However, occasionally a specific indication may require them to use a device they seldom utilized. For example only certain endografts can be used in short or angulated aortic necks.
It must be stated emphatically that surgeons should be completely comfortable with the device and its instructions for use. It would be entirely inappropriate for a vascular surgeon to enter the operating room so ill-prepared as to require the company employee to walk him or her through the use of their device.
However, since some surgeons may have limited experience it would be beneficial to have someone else present who has more familiarity with its use. It is true that most companies have technical advisers who could come to the operating room but they are far and few between. Accordingly, sales representatives are well suited to be the other knowledgeable individual.
Most companies train their sales persons to have the core knowledge to function as advisers. They are well schooled in their device probably even more so than most surgeons. They know all its indications and the dangers in using the device outside of the instructions for use (IFU’s) published by the manufacturer. They also know the subtleties that make the device work more optimally. Many will have witnessed complications and so they will have learned how to overcome them. In some instances their accumulated knowledge may forestall an incorrect insertion or manipulation of the device. Of course salespersons will not have performed procedures themselves but most will have learned by attending many procedures, usually far more than performed by any one surgeon. Is it a coincidence that ‘rep,’ the diminutive word for representative, is the same word for the shortened form of ‘repetition?’
Once a trusting relationship develops between the surgeon and the sales rep, having both in the operating room can mean the difference between life and death for the patient. The security gained by knowing there will be another experienced person in the room is reassuring and should be reassuring to the patient and to the hospital administrators as well. After all, what is worse for the surgeon’s reputation, the hospital’s bottom line, or more importantly the patient, than an unnecessary complication that could have been easily avoided by a few cautionary words?Even when I use a device I have used many times, it has not been unusual for the sales rep in the operating room to help me work out a difficult portion of the procedure. How reassuring it is to have another educated adviser in there with you. Professional tennis players have their coach in the stands. Dr. O. William Brown, our associate editor, makes the point that even professional golfers have their caddy with them on the course. The caddy does not hit the ball nor play the course just like the rep does not touch the patient nor do the procedure. However the caddy (rep) knows the course, the player, ball and clubs and can read the greens and knows the distance to the hole. Advice from the supporting caddy can make the difference between winning and losing. Advice from the rep can save a life.
I used an automobile analogy in one of my last editorials and there is one which applies here as well.
Almost all of us by the time we are in our 30s or 40s can drive safely. However, when we buy a new car the sales person drives with us the first few times so we may become comfortable with the new features. When it comes to driving so-called exotics like a Ferrari or Lamborghini, potential buyers (such as hospital CEO’s) will go to a special track where they will drive with an accomplished company driver before they feel safe to drive the car on their own. The company drivers know the limits of their car and they know the limits of drivers unaccustomed to advanced automobiles. Press the gas pedal too soon or push too hard on the brake pedal and the car will spin out of control with fatal results. In the operating room, press the wrong button or push too hard and the device may deploy too soon and the procedure may spin out of control also with potentially fatal results.
It seems to me the whole controversy revolves around the phrase “sales-representative” since it implies at all times their sole goal is to increase sales. Perhaps if they were simply called “representatives” there would be no issue. Yes, it may be true that in some instances the selection of a device may be based on the relationship a surgeon has with a company’s sales representative rather than the quality of the company’s device.
However, administrators are misguided when they consider excluding the sales rep from the operating room or endovascular suite will achieve cost savings. Usually the decision to select a company’s device was made many days before the procedure. If the rep was going to influence the surgeon, it would have been done prior to the surgeon entering those sacrosanct spaces.
Thus, in their never-ending onslaught on cost, administrators who restrict sales reps from the operating room may be impeding quality care. Accordingly, ‘“the elephant in the room” may not be the sales representative but rather the administrator in the office down the corridor.
Dr. Samson is a clinical professor of surgery (vascular) at Florida State University Medical School, is president, Mote Vascular Foundation, Inc., and is an attending vascular surgeon, Sarasota Vascular Specialists. Dr. Samson also considers himself a member of his proposed American College of Vascular Surgery.
Once again hospital administrators in their never-ending quest to reduce expenditures have placed vascular surgeons at a disadvantage. First they reduce the inventory of necessary items. Now they want to keep sales representatives out of the operating room. Their thought process is industry representatives will seduce us to use an expensive product which we otherwise would not consider using. Further, companies build support into the cost of their devices. Thus they would be expected to reduce prices if their personnel were no longer required in the OR.
Administrators as well as many lay public must also wonder why a nonphysician representative of a device company should be present in the operating room. This is certainly a valid question. The answer requires an understanding of how the complexity of vascular interventions has evolved in the era of endovascular procedures.
The vascular surgeon of yore learned basic vascular skills of dissection, excision, needles, and thread which could be applied with equal skill throughout the vascular system. Although they used multiple conduits as grafts, the technique of sewing an anastomosis was a general skill. Then, as surgeons still do now, they needed to know the benefits and drawbacks of the various graft materials and sutures. However, they certainly did not require a company representative to be in the room nor to instruct them on how to sew in the graft or how to deal with a broken suture.
But now vascular surgeons use wires, stents, catheters, balloons, lasers, and drills. When I last counted there were at least eight different companies selling aortic endografts and promoting never-ending variations or replacements for their ‘last year’s device.’ Often the advent of a new device produced an expanded repertoire of new procedures each with their own specific nuances many of which were device specific. Accordingly, it is essential that a surgeon become experienced with the new device in order to prevent or overcome glitches that otherwise might result in serious complications.
However, only the busiest vascular surgeons or those specifically involved in industry-supported trials may ever achieve sufficient experience to be able to use all these products. Certainly, a surgeon may elect to become familiar with just a few of the available choices. However, occasionally a specific indication may require them to use a device they seldom utilized. For example only certain endografts can be used in short or angulated aortic necks.
It must be stated emphatically that surgeons should be completely comfortable with the device and its instructions for use. It would be entirely inappropriate for a vascular surgeon to enter the operating room so ill-prepared as to require the company employee to walk him or her through the use of their device.
However, since some surgeons may have limited experience it would be beneficial to have someone else present who has more familiarity with its use. It is true that most companies have technical advisers who could come to the operating room but they are far and few between. Accordingly, sales representatives are well suited to be the other knowledgeable individual.
Most companies train their sales persons to have the core knowledge to function as advisers. They are well schooled in their device probably even more so than most surgeons. They know all its indications and the dangers in using the device outside of the instructions for use (IFU’s) published by the manufacturer. They also know the subtleties that make the device work more optimally. Many will have witnessed complications and so they will have learned how to overcome them. In some instances their accumulated knowledge may forestall an incorrect insertion or manipulation of the device. Of course salespersons will not have performed procedures themselves but most will have learned by attending many procedures, usually far more than performed by any one surgeon. Is it a coincidence that ‘rep,’ the diminutive word for representative, is the same word for the shortened form of ‘repetition?’
Once a trusting relationship develops between the surgeon and the sales rep, having both in the operating room can mean the difference between life and death for the patient. The security gained by knowing there will be another experienced person in the room is reassuring and should be reassuring to the patient and to the hospital administrators as well. After all, what is worse for the surgeon’s reputation, the hospital’s bottom line, or more importantly the patient, than an unnecessary complication that could have been easily avoided by a few cautionary words?Even when I use a device I have used many times, it has not been unusual for the sales rep in the operating room to help me work out a difficult portion of the procedure. How reassuring it is to have another educated adviser in there with you. Professional tennis players have their coach in the stands. Dr. O. William Brown, our associate editor, makes the point that even professional golfers have their caddy with them on the course. The caddy does not hit the ball nor play the course just like the rep does not touch the patient nor do the procedure. However the caddy (rep) knows the course, the player, ball and clubs and can read the greens and knows the distance to the hole. Advice from the supporting caddy can make the difference between winning and losing. Advice from the rep can save a life.
I used an automobile analogy in one of my last editorials and there is one which applies here as well.
Almost all of us by the time we are in our 30s or 40s can drive safely. However, when we buy a new car the sales person drives with us the first few times so we may become comfortable with the new features. When it comes to driving so-called exotics like a Ferrari or Lamborghini, potential buyers (such as hospital CEO’s) will go to a special track where they will drive with an accomplished company driver before they feel safe to drive the car on their own. The company drivers know the limits of their car and they know the limits of drivers unaccustomed to advanced automobiles. Press the gas pedal too soon or push too hard on the brake pedal and the car will spin out of control with fatal results. In the operating room, press the wrong button or push too hard and the device may deploy too soon and the procedure may spin out of control also with potentially fatal results.
It seems to me the whole controversy revolves around the phrase “sales-representative” since it implies at all times their sole goal is to increase sales. Perhaps if they were simply called “representatives” there would be no issue. Yes, it may be true that in some instances the selection of a device may be based on the relationship a surgeon has with a company’s sales representative rather than the quality of the company’s device.
However, administrators are misguided when they consider excluding the sales rep from the operating room or endovascular suite will achieve cost savings. Usually the decision to select a company’s device was made many days before the procedure. If the rep was going to influence the surgeon, it would have been done prior to the surgeon entering those sacrosanct spaces.
Thus, in their never-ending onslaught on cost, administrators who restrict sales reps from the operating room may be impeding quality care. Accordingly, ‘“the elephant in the room” may not be the sales representative but rather the administrator in the office down the corridor.
Dr. Samson is a clinical professor of surgery (vascular) at Florida State University Medical School, is president, Mote Vascular Foundation, Inc., and is an attending vascular surgeon, Sarasota Vascular Specialists. Dr. Samson also considers himself a member of his proposed American College of Vascular Surgery.
Once again hospital administrators in their never-ending quest to reduce expenditures have placed vascular surgeons at a disadvantage. First they reduce the inventory of necessary items. Now they want to keep sales representatives out of the operating room. Their thought process is industry representatives will seduce us to use an expensive product which we otherwise would not consider using. Further, companies build support into the cost of their devices. Thus they would be expected to reduce prices if their personnel were no longer required in the OR.
Administrators as well as many lay public must also wonder why a nonphysician representative of a device company should be present in the operating room. This is certainly a valid question. The answer requires an understanding of how the complexity of vascular interventions has evolved in the era of endovascular procedures.
The vascular surgeon of yore learned basic vascular skills of dissection, excision, needles, and thread which could be applied with equal skill throughout the vascular system. Although they used multiple conduits as grafts, the technique of sewing an anastomosis was a general skill. Then, as surgeons still do now, they needed to know the benefits and drawbacks of the various graft materials and sutures. However, they certainly did not require a company representative to be in the room nor to instruct them on how to sew in the graft or how to deal with a broken suture.
But now vascular surgeons use wires, stents, catheters, balloons, lasers, and drills. When I last counted there were at least eight different companies selling aortic endografts and promoting never-ending variations or replacements for their ‘last year’s device.’ Often the advent of a new device produced an expanded repertoire of new procedures each with their own specific nuances many of which were device specific. Accordingly, it is essential that a surgeon become experienced with the new device in order to prevent or overcome glitches that otherwise might result in serious complications.
However, only the busiest vascular surgeons or those specifically involved in industry-supported trials may ever achieve sufficient experience to be able to use all these products. Certainly, a surgeon may elect to become familiar with just a few of the available choices. However, occasionally a specific indication may require them to use a device they seldom utilized. For example only certain endografts can be used in short or angulated aortic necks.
It must be stated emphatically that surgeons should be completely comfortable with the device and its instructions for use. It would be entirely inappropriate for a vascular surgeon to enter the operating room so ill-prepared as to require the company employee to walk him or her through the use of their device.
However, since some surgeons may have limited experience it would be beneficial to have someone else present who has more familiarity with its use. It is true that most companies have technical advisers who could come to the operating room but they are far and few between. Accordingly, sales representatives are well suited to be the other knowledgeable individual.
Most companies train their sales persons to have the core knowledge to function as advisers. They are well schooled in their device probably even more so than most surgeons. They know all its indications and the dangers in using the device outside of the instructions for use (IFU’s) published by the manufacturer. They also know the subtleties that make the device work more optimally. Many will have witnessed complications and so they will have learned how to overcome them. In some instances their accumulated knowledge may forestall an incorrect insertion or manipulation of the device. Of course salespersons will not have performed procedures themselves but most will have learned by attending many procedures, usually far more than performed by any one surgeon. Is it a coincidence that ‘rep,’ the diminutive word for representative, is the same word for the shortened form of ‘repetition?’
Once a trusting relationship develops between the surgeon and the sales rep, having both in the operating room can mean the difference between life and death for the patient. The security gained by knowing there will be another experienced person in the room is reassuring and should be reassuring to the patient and to the hospital administrators as well. After all, what is worse for the surgeon’s reputation, the hospital’s bottom line, or more importantly the patient, than an unnecessary complication that could have been easily avoided by a few cautionary words?Even when I use a device I have used many times, it has not been unusual for the sales rep in the operating room to help me work out a difficult portion of the procedure. How reassuring it is to have another educated adviser in there with you. Professional tennis players have their coach in the stands. Dr. O. William Brown, our associate editor, makes the point that even professional golfers have their caddy with them on the course. The caddy does not hit the ball nor play the course just like the rep does not touch the patient nor do the procedure. However the caddy (rep) knows the course, the player, ball and clubs and can read the greens and knows the distance to the hole. Advice from the supporting caddy can make the difference between winning and losing. Advice from the rep can save a life.
I used an automobile analogy in one of my last editorials and there is one which applies here as well.
Almost all of us by the time we are in our 30s or 40s can drive safely. However, when we buy a new car the sales person drives with us the first few times so we may become comfortable with the new features. When it comes to driving so-called exotics like a Ferrari or Lamborghini, potential buyers (such as hospital CEO’s) will go to a special track where they will drive with an accomplished company driver before they feel safe to drive the car on their own. The company drivers know the limits of their car and they know the limits of drivers unaccustomed to advanced automobiles. Press the gas pedal too soon or push too hard on the brake pedal and the car will spin out of control with fatal results. In the operating room, press the wrong button or push too hard and the device may deploy too soon and the procedure may spin out of control also with potentially fatal results.
It seems to me the whole controversy revolves around the phrase “sales-representative” since it implies at all times their sole goal is to increase sales. Perhaps if they were simply called “representatives” there would be no issue. Yes, it may be true that in some instances the selection of a device may be based on the relationship a surgeon has with a company’s sales representative rather than the quality of the company’s device.
However, administrators are misguided when they consider excluding the sales rep from the operating room or endovascular suite will achieve cost savings. Usually the decision to select a company’s device was made many days before the procedure. If the rep was going to influence the surgeon, it would have been done prior to the surgeon entering those sacrosanct spaces.
Thus, in their never-ending onslaught on cost, administrators who restrict sales reps from the operating room may be impeding quality care. Accordingly, ‘“the elephant in the room” may not be the sales representative but rather the administrator in the office down the corridor.
Dr. Samson is a clinical professor of surgery (vascular) at Florida State University Medical School, is president, Mote Vascular Foundation, Inc., and is an attending vascular surgeon, Sarasota Vascular Specialists. Dr. Samson also considers himself a member of his proposed American College of Vascular Surgery.

Teaching residents can be more rewarding than you think
“Teach residents…really? You want to add yet another time-consuming responsibility to my already hectic schedule?” Residency. The mere mention of the word conjures up chilling memories of 3 am codes, 20-30 hour zombie shifts, and anxiety and stress levels that we never knew before and, fortunately, have not known since. That was a time in life many of us want to put in the deepest recesses of our minds, never to emerge again.
But, on the other hand, there were a lot of good things about our residency training that we should probably never forget, such as the humility with which we approached patient care. At that time in our lives we gladly acknowledged we did not know everything and we were eager to research each and every condition to get a firm handle on what we could and should do to help our patients get better.
Fast forward a decade or two. Now many of us have spouses, children, aging parents, mortgages, and retirement accounts we are feverishly trying to fund. There never seems to be enough time to finish even the most fundamental responsibilities. Not to mention now there are national initiatives, mandatory rules, and sometimes frightening regulations in place that dramatically impact how we practice medicine and sometimes make us feel more like automatons than the physicians we dreamed of becoming when we first applied to medical school years ago.
With all of our current and future responsibilities, how can the average hospitalist embrace young physicians and pour himself into their lives? Or, perhaps the question is better asked, how can we not? None of us morphed from a green medical school graduate to a knowledgeable, well-respected physician without a great deal of hand holding (and sometimes hand wringing), encouragement and investment of time from our teaching attendings. But even if you are hesitant to invest the time and energy to teach resident physicians should you have the opportunity. Keep in mind, in 2015 we are not only teaching them, they are teaching us too!
Young physicians are overflowing with technological knowledge that many of us have never been exposed to, knowledge that can help escalate our own skill sets. They bring fresh ideas, novel approaches to patient care, and frequently, cutting edge medical innovations from the universities from which come.
So, if you are ever asked to teach our future colleagues, remember: you may very well find that the time you invest benefits you as much, if not more, than it does them.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.
“Teach residents…really? You want to add yet another time-consuming responsibility to my already hectic schedule?” Residency. The mere mention of the word conjures up chilling memories of 3 am codes, 20-30 hour zombie shifts, and anxiety and stress levels that we never knew before and, fortunately, have not known since. That was a time in life many of us want to put in the deepest recesses of our minds, never to emerge again.
But, on the other hand, there were a lot of good things about our residency training that we should probably never forget, such as the humility with which we approached patient care. At that time in our lives we gladly acknowledged we did not know everything and we were eager to research each and every condition to get a firm handle on what we could and should do to help our patients get better.
Fast forward a decade or two. Now many of us have spouses, children, aging parents, mortgages, and retirement accounts we are feverishly trying to fund. There never seems to be enough time to finish even the most fundamental responsibilities. Not to mention now there are national initiatives, mandatory rules, and sometimes frightening regulations in place that dramatically impact how we practice medicine and sometimes make us feel more like automatons than the physicians we dreamed of becoming when we first applied to medical school years ago.
With all of our current and future responsibilities, how can the average hospitalist embrace young physicians and pour himself into their lives? Or, perhaps the question is better asked, how can we not? None of us morphed from a green medical school graduate to a knowledgeable, well-respected physician without a great deal of hand holding (and sometimes hand wringing), encouragement and investment of time from our teaching attendings. But even if you are hesitant to invest the time and energy to teach resident physicians should you have the opportunity. Keep in mind, in 2015 we are not only teaching them, they are teaching us too!
Young physicians are overflowing with technological knowledge that many of us have never been exposed to, knowledge that can help escalate our own skill sets. They bring fresh ideas, novel approaches to patient care, and frequently, cutting edge medical innovations from the universities from which come.
So, if you are ever asked to teach our future colleagues, remember: you may very well find that the time you invest benefits you as much, if not more, than it does them.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.
“Teach residents…really? You want to add yet another time-consuming responsibility to my already hectic schedule?” Residency. The mere mention of the word conjures up chilling memories of 3 am codes, 20-30 hour zombie shifts, and anxiety and stress levels that we never knew before and, fortunately, have not known since. That was a time in life many of us want to put in the deepest recesses of our minds, never to emerge again.
But, on the other hand, there were a lot of good things about our residency training that we should probably never forget, such as the humility with which we approached patient care. At that time in our lives we gladly acknowledged we did not know everything and we were eager to research each and every condition to get a firm handle on what we could and should do to help our patients get better.
Fast forward a decade or two. Now many of us have spouses, children, aging parents, mortgages, and retirement accounts we are feverishly trying to fund. There never seems to be enough time to finish even the most fundamental responsibilities. Not to mention now there are national initiatives, mandatory rules, and sometimes frightening regulations in place that dramatically impact how we practice medicine and sometimes make us feel more like automatons than the physicians we dreamed of becoming when we first applied to medical school years ago.
With all of our current and future responsibilities, how can the average hospitalist embrace young physicians and pour himself into their lives? Or, perhaps the question is better asked, how can we not? None of us morphed from a green medical school graduate to a knowledgeable, well-respected physician without a great deal of hand holding (and sometimes hand wringing), encouragement and investment of time from our teaching attendings. But even if you are hesitant to invest the time and energy to teach resident physicians should you have the opportunity. Keep in mind, in 2015 we are not only teaching them, they are teaching us too!
Young physicians are overflowing with technological knowledge that many of us have never been exposed to, knowledge that can help escalate our own skill sets. They bring fresh ideas, novel approaches to patient care, and frequently, cutting edge medical innovations from the universities from which come.
So, if you are ever asked to teach our future colleagues, remember: you may very well find that the time you invest benefits you as much, if not more, than it does them.
Dr. Hester is a hospitalist at Baltimore-Washington Medical Center in Glen Burnie, Md. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at healthsavvy@aol.com.

Keeping laparoscopy safe for the obese patient
As I was writing my introduction to this current edition of the Master Class in Gynecologic Surgery, focusing on minimally invasive surgery for the obese female patient, I was listening to Chuck Todd, host of “Meet the Press.” Instantaneously, television and my thoughts became one; in the last segment of the program, Mr. Todd discussed what he was able to consume for $50 at the Iowa State Fair. I learned that his diet that day consisted of a pork chop on a stick, mac and cheese, a bacon-wrapped corn dog, cheese on a stick with jalapeños, a deep-fried Twinkie, and even fried apple pie with bacon. While Mr. Todd is thin and healthy, the array of foods at the fair reflects our nation’s penchant toward fast food that is fat laden and fried. Though our county is not alone in the world, obesity has reached epidemic proportion in the United States.

According to a May 2015 Department of Health & Human Services report on the health status of the nation, 69% of adults in the United States are overweight and 35% are obese. As a result, the minimally invasive gynecologic surgeon is dealing with an increasing population of women with comorbidities related to their obesity that can confound surgery outcomes. Moreover, anatomic landmarks that the young medical student learns in his or her first anatomy classes are modified due to the size of panniculus and the migration of the umbilicus relative to the bifurcation of the aorta.
I asked Dr. Amina Ahmed to join me in discussing the management of the obese patient undergoing minimally invasive gynecologic surgery. After completing her fellowship in gynecologic oncology, Dr. Ahmed has been on staff at both the University of Iowa Hospitals and Clinics, Iowa City, and Advocate Lutheran General Hospital, Park Ridge, Ill. She will soon join the gynecologic oncology faculty at Rush University Medical Center, Chicago. Given the increased rate of obesity in both Chicago and Iowa, Dr. Ahmed has become an expert in this area in a short period of time.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill; and the medical editor of this column, Master Class. Dr. Miller disclosed that he is a consultant and on the speakers bureau for Ethicon and Intuitive Surgical, and is a consultant for Covidien.
As I was writing my introduction to this current edition of the Master Class in Gynecologic Surgery, focusing on minimally invasive surgery for the obese female patient, I was listening to Chuck Todd, host of “Meet the Press.” Instantaneously, television and my thoughts became one; in the last segment of the program, Mr. Todd discussed what he was able to consume for $50 at the Iowa State Fair. I learned that his diet that day consisted of a pork chop on a stick, mac and cheese, a bacon-wrapped corn dog, cheese on a stick with jalapeños, a deep-fried Twinkie, and even fried apple pie with bacon. While Mr. Todd is thin and healthy, the array of foods at the fair reflects our nation’s penchant toward fast food that is fat laden and fried. Though our county is not alone in the world, obesity has reached epidemic proportion in the United States.
According to a May 2015 Department of Health & Human Services report on the health status of the nation, 69% of adults in the United States are overweight and 35% are obese. As a result, the minimally invasive gynecologic surgeon is dealing with an increasing population of women with comorbidities related to their obesity that can confound surgery outcomes. Moreover, anatomic landmarks that the young medical student learns in his or her first anatomy classes are modified due to the size of panniculus and the migration of the umbilicus relative to the bifurcation of the aorta.
I asked Dr. Amina Ahmed to join me in discussing the management of the obese patient undergoing minimally invasive gynecologic surgery. After completing her fellowship in gynecologic oncology, Dr. Ahmed has been on staff at both the University of Iowa Hospitals and Clinics, Iowa City, and Advocate Lutheran General Hospital, Park Ridge, Ill. She will soon join the gynecologic oncology faculty at Rush University Medical Center, Chicago. Given the increased rate of obesity in both Chicago and Iowa, Dr. Ahmed has become an expert in this area in a short period of time.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill; and the medical editor of this column, Master Class. Dr. Miller disclosed that he is a consultant and on the speakers bureau for Ethicon and Intuitive Surgical, and is a consultant for Covidien.
As I was writing my introduction to this current edition of the Master Class in Gynecologic Surgery, focusing on minimally invasive surgery for the obese female patient, I was listening to Chuck Todd, host of “Meet the Press.” Instantaneously, television and my thoughts became one; in the last segment of the program, Mr. Todd discussed what he was able to consume for $50 at the Iowa State Fair. I learned that his diet that day consisted of a pork chop on a stick, mac and cheese, a bacon-wrapped corn dog, cheese on a stick with jalapeños, a deep-fried Twinkie, and even fried apple pie with bacon. While Mr. Todd is thin and healthy, the array of foods at the fair reflects our nation’s penchant toward fast food that is fat laden and fried. Though our county is not alone in the world, obesity has reached epidemic proportion in the United States.
According to a May 2015 Department of Health & Human Services report on the health status of the nation, 69% of adults in the United States are overweight and 35% are obese. As a result, the minimally invasive gynecologic surgeon is dealing with an increasing population of women with comorbidities related to their obesity that can confound surgery outcomes. Moreover, anatomic landmarks that the young medical student learns in his or her first anatomy classes are modified due to the size of panniculus and the migration of the umbilicus relative to the bifurcation of the aorta.
I asked Dr. Amina Ahmed to join me in discussing the management of the obese patient undergoing minimally invasive gynecologic surgery. After completing her fellowship in gynecologic oncology, Dr. Ahmed has been on staff at both the University of Iowa Hospitals and Clinics, Iowa City, and Advocate Lutheran General Hospital, Park Ridge, Ill. She will soon join the gynecologic oncology faculty at Rush University Medical Center, Chicago. Given the increased rate of obesity in both Chicago and Iowa, Dr. Ahmed has become an expert in this area in a short period of time.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill; and the medical editor of this column, Master Class. Dr. Miller disclosed that he is a consultant and on the speakers bureau for Ethicon and Intuitive Surgical, and is a consultant for Covidien.
