User login
Impatient patients
Patients are often impatient. They want answers.
To some extent, I can’t blame them. When it’s your disease, you want to know what’s going on and what you can do about it. So I try to keep on top of results as they come in and have my staff contact people to relay the news.
The problem is that medicine (like life) does not provide immediate gratification. It takes time to get routine labs back, and some (such as send-outs) can even take a few weeks.
Radiology reports usually have a 24-hour turnaround, and radiologists will call me if they find something urgent. Yet, it’s amazing how many people will call for results before they even leave that facility.
Did it always used to be like this? Were people always this demanding of immediate answers and test results from their doctors?
We live in a world that gets faster and faster, and people get used to things happening quickly. It’s an age of instant gratification, and having to wait for test results seems silly to laypeople. After all, don’t TV medical shows have results coming back quickly, gleaming advanced scanners, and the machine that goes “ping”? So why doesn’t that happen when you visit a doctor in real life?
Of course, I could get the results faster. I could order everything STAT and abuse the privilege ... but crying wolf only works a few times, and then you can’t do it when you really need it. I could call the radiologists for verbal MRI reads ... but then I’m taking their time away from more urgent cases, and other patients with more concerning issues are affected. So I don’t do that routinely, either.
Even people in slow-moving lines of work can have trouble grasping that medicine is the same way. I tell them we’ll call them when we get results, and try to stay on top of things. I admit sometimes things may slip through, and they’re right to call and ask.
Most patients understand this, and are, well, patient. I just wish more were. It would save a lot of time, effort, and frustration for all involved, including them.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Patients are often impatient. They want answers.
To some extent, I can’t blame them. When it’s your disease, you want to know what’s going on and what you can do about it. So I try to keep on top of results as they come in and have my staff contact people to relay the news.
The problem is that medicine (like life) does not provide immediate gratification. It takes time to get routine labs back, and some (such as send-outs) can even take a few weeks.
Radiology reports usually have a 24-hour turnaround, and radiologists will call me if they find something urgent. Yet, it’s amazing how many people will call for results before they even leave that facility.
Did it always used to be like this? Were people always this demanding of immediate answers and test results from their doctors?
We live in a world that gets faster and faster, and people get used to things happening quickly. It’s an age of instant gratification, and having to wait for test results seems silly to laypeople. After all, don’t TV medical shows have results coming back quickly, gleaming advanced scanners, and the machine that goes “ping”? So why doesn’t that happen when you visit a doctor in real life?
Of course, I could get the results faster. I could order everything STAT and abuse the privilege ... but crying wolf only works a few times, and then you can’t do it when you really need it. I could call the radiologists for verbal MRI reads ... but then I’m taking their time away from more urgent cases, and other patients with more concerning issues are affected. So I don’t do that routinely, either.
Even people in slow-moving lines of work can have trouble grasping that medicine is the same way. I tell them we’ll call them when we get results, and try to stay on top of things. I admit sometimes things may slip through, and they’re right to call and ask.
Most patients understand this, and are, well, patient. I just wish more were. It would save a lot of time, effort, and frustration for all involved, including them.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Patients are often impatient. They want answers.
To some extent, I can’t blame them. When it’s your disease, you want to know what’s going on and what you can do about it. So I try to keep on top of results as they come in and have my staff contact people to relay the news.
The problem is that medicine (like life) does not provide immediate gratification. It takes time to get routine labs back, and some (such as send-outs) can even take a few weeks.
Radiology reports usually have a 24-hour turnaround, and radiologists will call me if they find something urgent. Yet, it’s amazing how many people will call for results before they even leave that facility.
Did it always used to be like this? Were people always this demanding of immediate answers and test results from their doctors?
We live in a world that gets faster and faster, and people get used to things happening quickly. It’s an age of instant gratification, and having to wait for test results seems silly to laypeople. After all, don’t TV medical shows have results coming back quickly, gleaming advanced scanners, and the machine that goes “ping”? So why doesn’t that happen when you visit a doctor in real life?
Of course, I could get the results faster. I could order everything STAT and abuse the privilege ... but crying wolf only works a few times, and then you can’t do it when you really need it. I could call the radiologists for verbal MRI reads ... but then I’m taking their time away from more urgent cases, and other patients with more concerning issues are affected. So I don’t do that routinely, either.
Even people in slow-moving lines of work can have trouble grasping that medicine is the same way. I tell them we’ll call them when we get results, and try to stay on top of things. I admit sometimes things may slip through, and they’re right to call and ask.
Most patients understand this, and are, well, patient. I just wish more were. It would save a lot of time, effort, and frustration for all involved, including them.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.

Resorbable coronary scaffolds require ‘leap of faith’
Results reported earlier this month at the Transcatheter Cardiovascular Therapeutics annual meeting for the Absorb bioresorbable vascular scaffold made by Abbott Vascular showed the device was statistically noninferior for treating selected coronary stenoses, compared with Xience, a standard of care drug-eluting metallic stent, in the ABSORB III trial, designed as the study to get Absorb onto the U.S. market.
Given the way such trials develop now, after consultation with the Food and Drug Administration, it seems very likely that proving noninferiority against the best metallic-stent competitor will mean that, sometime in 2016, the Absorb bioresorbable scaffold will become the first U.S. routinely available coronary device built to dissolve away after a period of time, about 3 years in this case.

That means that sometime in the next year, U.S. interventional cardiologists, patients, other collaborating physicians, and payers will have to start deciding whether the potential advantages of using a stentlike device that eventually disappears is worth a probable uptick in price as well as certain other limitations. One of the key variables is that for the moment the advantages remain mostly hypothetical.
Dr. Gregg W. Stone, chairman of the ABSORB III trial and one of the leading advocates for U.S. development of bioresorbable vascular scaffolds (BVS) told me about some of the hoped-for benefits that BVS could provide by leaving the coronaries. Imaging data have already suggested that it improves vasomotion, and other possible benefits include restored vascular adaptability, stimulated plaque regression, and reduced late polymer reactions and neoatherosclerosis. “This is all hypothetical, and we won’t know whether the promise is a reality until we have the 5-year results from ABSORB IV, which won’t be until 6-7 years from now,” Dr. Stone said.
Of course, he added, other, more modest benefits are already real: It’s been proven that the BVS really goes away after about 3 years, which makes noninvasive imaging of coronaries where a BVS was placed easier; and it also frees side-branch arteries, as well as the treated segment itself, from the metal jacket of a stent. And some patients like the idea of a disappearing stent for “personal, religious, or cultural reasons,” he said.
Balancing this are the device’s very real limitations. Because a BVS is stiffer and less maneuverable than is a metallic stent, it isn’t appropriate for heavily calcified lesions, tortuous arteries, chronic total occlusions, true bifurcations, or bypass grafts. Also, the width of the struts on the Absorb BVS make it unsuitable for use in coronary arteries less than 2.5 mm in diameter, a limitation borne out by the ABSORB III results, which showed a much higher rate of target-lesion failure and stent thrombosis, compared with the Xience stent in the 19% of lesions that sneaked into the study in coronaries narrower than 2.5 mm. Also, for the time being, BVS is targeted only for patients with stable coronary disease or patients who have stabilized following an acute coronary syndrome event and not for patients with an acute MI or unstable acute coronary syndrome.
Dr. Stone estimated that, collectively, these clinical and anatomic limitations exclude roughly half the patients who undergo percutaneous interventions today. “The sweet spot may be young patients with relatively noncomplex lesions.”
There are more restrictions, based on what using a BVS means for the operator. Not only is the device harder to deliver to a specific coronary site, but it requires “more lesion preparation, more accurate sizing, and more frequent postdilitation.” Operators “need to realize that if they use a BVS, they can’t get away with as much as they can with state-of-the-art metallic stents,” Dr. Stone said. In fact, he felt that the ABSORB III results showed “we could do better with more training and more attention to detail.” In the future, operators “will need to work harder and pay attention to procedural factors.”
The increased technical demands posed by a BVS and the possibility that not all of the devices were placed optimally in the trial may have led to another source of doubt about Absorb: its performance relative to Xience.
At the meeting, Dr. Stone reported results from a meta-analysis of the four randomized controlled trials that have now reported 1-year outcomes data for the Absorb BVS compared with Xience: ABSORB III (with 2,008 patients), ABSORB II (502 patients), ABSORB Japan (400 patients), and ABSORB China (480 patients).
The meta-analysis confirmed two concerning trends also seen in the results from ABSORB III by itself: a strong trend toward an increased risk of 1-year stent thrombosis with Absorb, at 1.3%, compared with a 0.6% risk with Xience (P = .08); and a statistically significant excess of target-vessel MI with Absorb, at 5.1%, compared with 3.3% with Xience (P = .04). Results from both the meta-analysis and from ABSORB III by itself also showed numerically higher rates of target-lesion failure – the primary efficacy endpoint – with Absorb, although not enough of a difference to undermine fulfilling the prespecified definition of noninferiority in ABSORB III.
“I think we can do better if people pay better attention to their technique.” Dr. Stone said. But it remains to be seen whether the inferior performance of Absorb relative to a metallic stent can be overcome with better training and technique, and if so, whether operators will be willing to take the extra steps required to overcome the challenges of the device. Some physicians “will focus on the fact that target-lesion failure was higher with Absorb, and they will want to wait to see whether Absorb actually improves hard outcomes,” he acknowledged. “Some will focus on the promise; other will say ‘show me the data.’ ”
One of his collaborators on ABSORB III, Dr. Dean J. Kereiakes, said that opting for Absorb will require a “leap of faith.”
“Absorb has limitations,” Dr. Stone concluded. “Physician and patient opinions will vary, and the device is not for every patient and every lesion.”
Physicians will soon need to start deciding exactly which patients in their practice, if any, are good candidates for a BVS.
On Twitter @mitchelzoler
Results reported earlier this month at the Transcatheter Cardiovascular Therapeutics annual meeting for the Absorb bioresorbable vascular scaffold made by Abbott Vascular showed the device was statistically noninferior for treating selected coronary stenoses, compared with Xience, a standard of care drug-eluting metallic stent, in the ABSORB III trial, designed as the study to get Absorb onto the U.S. market.
Given the way such trials develop now, after consultation with the Food and Drug Administration, it seems very likely that proving noninferiority against the best metallic-stent competitor will mean that, sometime in 2016, the Absorb bioresorbable scaffold will become the first U.S. routinely available coronary device built to dissolve away after a period of time, about 3 years in this case.
That means that sometime in the next year, U.S. interventional cardiologists, patients, other collaborating physicians, and payers will have to start deciding whether the potential advantages of using a stentlike device that eventually disappears is worth a probable uptick in price as well as certain other limitations. One of the key variables is that for the moment the advantages remain mostly hypothetical.
Dr. Gregg W. Stone, chairman of the ABSORB III trial and one of the leading advocates for U.S. development of bioresorbable vascular scaffolds (BVS) told me about some of the hoped-for benefits that BVS could provide by leaving the coronaries. Imaging data have already suggested that it improves vasomotion, and other possible benefits include restored vascular adaptability, stimulated plaque regression, and reduced late polymer reactions and neoatherosclerosis. “This is all hypothetical, and we won’t know whether the promise is a reality until we have the 5-year results from ABSORB IV, which won’t be until 6-7 years from now,” Dr. Stone said.
Of course, he added, other, more modest benefits are already real: It’s been proven that the BVS really goes away after about 3 years, which makes noninvasive imaging of coronaries where a BVS was placed easier; and it also frees side-branch arteries, as well as the treated segment itself, from the metal jacket of a stent. And some patients like the idea of a disappearing stent for “personal, religious, or cultural reasons,” he said.
Balancing this are the device’s very real limitations. Because a BVS is stiffer and less maneuverable than is a metallic stent, it isn’t appropriate for heavily calcified lesions, tortuous arteries, chronic total occlusions, true bifurcations, or bypass grafts. Also, the width of the struts on the Absorb BVS make it unsuitable for use in coronary arteries less than 2.5 mm in diameter, a limitation borne out by the ABSORB III results, which showed a much higher rate of target-lesion failure and stent thrombosis, compared with the Xience stent in the 19% of lesions that sneaked into the study in coronaries narrower than 2.5 mm. Also, for the time being, BVS is targeted only for patients with stable coronary disease or patients who have stabilized following an acute coronary syndrome event and not for patients with an acute MI or unstable acute coronary syndrome.
Dr. Stone estimated that, collectively, these clinical and anatomic limitations exclude roughly half the patients who undergo percutaneous interventions today. “The sweet spot may be young patients with relatively noncomplex lesions.”
There are more restrictions, based on what using a BVS means for the operator. Not only is the device harder to deliver to a specific coronary site, but it requires “more lesion preparation, more accurate sizing, and more frequent postdilitation.” Operators “need to realize that if they use a BVS, they can’t get away with as much as they can with state-of-the-art metallic stents,” Dr. Stone said. In fact, he felt that the ABSORB III results showed “we could do better with more training and more attention to detail.” In the future, operators “will need to work harder and pay attention to procedural factors.”
The increased technical demands posed by a BVS and the possibility that not all of the devices were placed optimally in the trial may have led to another source of doubt about Absorb: its performance relative to Xience.
At the meeting, Dr. Stone reported results from a meta-analysis of the four randomized controlled trials that have now reported 1-year outcomes data for the Absorb BVS compared with Xience: ABSORB III (with 2,008 patients), ABSORB II (502 patients), ABSORB Japan (400 patients), and ABSORB China (480 patients).
The meta-analysis confirmed two concerning trends also seen in the results from ABSORB III by itself: a strong trend toward an increased risk of 1-year stent thrombosis with Absorb, at 1.3%, compared with a 0.6% risk with Xience (P = .08); and a statistically significant excess of target-vessel MI with Absorb, at 5.1%, compared with 3.3% with Xience (P = .04). Results from both the meta-analysis and from ABSORB III by itself also showed numerically higher rates of target-lesion failure – the primary efficacy endpoint – with Absorb, although not enough of a difference to undermine fulfilling the prespecified definition of noninferiority in ABSORB III.
“I think we can do better if people pay better attention to their technique.” Dr. Stone said. But it remains to be seen whether the inferior performance of Absorb relative to a metallic stent can be overcome with better training and technique, and if so, whether operators will be willing to take the extra steps required to overcome the challenges of the device. Some physicians “will focus on the fact that target-lesion failure was higher with Absorb, and they will want to wait to see whether Absorb actually improves hard outcomes,” he acknowledged. “Some will focus on the promise; other will say ‘show me the data.’ ”
One of his collaborators on ABSORB III, Dr. Dean J. Kereiakes, said that opting for Absorb will require a “leap of faith.”
“Absorb has limitations,” Dr. Stone concluded. “Physician and patient opinions will vary, and the device is not for every patient and every lesion.”
Physicians will soon need to start deciding exactly which patients in their practice, if any, are good candidates for a BVS.
On Twitter @mitchelzoler
Results reported earlier this month at the Transcatheter Cardiovascular Therapeutics annual meeting for the Absorb bioresorbable vascular scaffold made by Abbott Vascular showed the device was statistically noninferior for treating selected coronary stenoses, compared with Xience, a standard of care drug-eluting metallic stent, in the ABSORB III trial, designed as the study to get Absorb onto the U.S. market.
Given the way such trials develop now, after consultation with the Food and Drug Administration, it seems very likely that proving noninferiority against the best metallic-stent competitor will mean that, sometime in 2016, the Absorb bioresorbable scaffold will become the first U.S. routinely available coronary device built to dissolve away after a period of time, about 3 years in this case.
That means that sometime in the next year, U.S. interventional cardiologists, patients, other collaborating physicians, and payers will have to start deciding whether the potential advantages of using a stentlike device that eventually disappears is worth a probable uptick in price as well as certain other limitations. One of the key variables is that for the moment the advantages remain mostly hypothetical.
Dr. Gregg W. Stone, chairman of the ABSORB III trial and one of the leading advocates for U.S. development of bioresorbable vascular scaffolds (BVS) told me about some of the hoped-for benefits that BVS could provide by leaving the coronaries. Imaging data have already suggested that it improves vasomotion, and other possible benefits include restored vascular adaptability, stimulated plaque regression, and reduced late polymer reactions and neoatherosclerosis. “This is all hypothetical, and we won’t know whether the promise is a reality until we have the 5-year results from ABSORB IV, which won’t be until 6-7 years from now,” Dr. Stone said.
Of course, he added, other, more modest benefits are already real: It’s been proven that the BVS really goes away after about 3 years, which makes noninvasive imaging of coronaries where a BVS was placed easier; and it also frees side-branch arteries, as well as the treated segment itself, from the metal jacket of a stent. And some patients like the idea of a disappearing stent for “personal, religious, or cultural reasons,” he said.
Balancing this are the device’s very real limitations. Because a BVS is stiffer and less maneuverable than is a metallic stent, it isn’t appropriate for heavily calcified lesions, tortuous arteries, chronic total occlusions, true bifurcations, or bypass grafts. Also, the width of the struts on the Absorb BVS make it unsuitable for use in coronary arteries less than 2.5 mm in diameter, a limitation borne out by the ABSORB III results, which showed a much higher rate of target-lesion failure and stent thrombosis, compared with the Xience stent in the 19% of lesions that sneaked into the study in coronaries narrower than 2.5 mm. Also, for the time being, BVS is targeted only for patients with stable coronary disease or patients who have stabilized following an acute coronary syndrome event and not for patients with an acute MI or unstable acute coronary syndrome.
Dr. Stone estimated that, collectively, these clinical and anatomic limitations exclude roughly half the patients who undergo percutaneous interventions today. “The sweet spot may be young patients with relatively noncomplex lesions.”
There are more restrictions, based on what using a BVS means for the operator. Not only is the device harder to deliver to a specific coronary site, but it requires “more lesion preparation, more accurate sizing, and more frequent postdilitation.” Operators “need to realize that if they use a BVS, they can’t get away with as much as they can with state-of-the-art metallic stents,” Dr. Stone said. In fact, he felt that the ABSORB III results showed “we could do better with more training and more attention to detail.” In the future, operators “will need to work harder and pay attention to procedural factors.”
The increased technical demands posed by a BVS and the possibility that not all of the devices were placed optimally in the trial may have led to another source of doubt about Absorb: its performance relative to Xience.
At the meeting, Dr. Stone reported results from a meta-analysis of the four randomized controlled trials that have now reported 1-year outcomes data for the Absorb BVS compared with Xience: ABSORB III (with 2,008 patients), ABSORB II (502 patients), ABSORB Japan (400 patients), and ABSORB China (480 patients).
The meta-analysis confirmed two concerning trends also seen in the results from ABSORB III by itself: a strong trend toward an increased risk of 1-year stent thrombosis with Absorb, at 1.3%, compared with a 0.6% risk with Xience (P = .08); and a statistically significant excess of target-vessel MI with Absorb, at 5.1%, compared with 3.3% with Xience (P = .04). Results from both the meta-analysis and from ABSORB III by itself also showed numerically higher rates of target-lesion failure – the primary efficacy endpoint – with Absorb, although not enough of a difference to undermine fulfilling the prespecified definition of noninferiority in ABSORB III.
“I think we can do better if people pay better attention to their technique.” Dr. Stone said. But it remains to be seen whether the inferior performance of Absorb relative to a metallic stent can be overcome with better training and technique, and if so, whether operators will be willing to take the extra steps required to overcome the challenges of the device. Some physicians “will focus on the fact that target-lesion failure was higher with Absorb, and they will want to wait to see whether Absorb actually improves hard outcomes,” he acknowledged. “Some will focus on the promise; other will say ‘show me the data.’ ”
One of his collaborators on ABSORB III, Dr. Dean J. Kereiakes, said that opting for Absorb will require a “leap of faith.”
“Absorb has limitations,” Dr. Stone concluded. “Physician and patient opinions will vary, and the device is not for every patient and every lesion.”
Physicians will soon need to start deciding exactly which patients in their practice, if any, are good candidates for a BVS.
On Twitter @mitchelzoler
The fellowship of motherhood
I expected that having a baby as a pediatric subspecialty fellow was going to be a challenge. But I could never have anticipated how scary it would feel to step into the world on the other side of the clinic door. My friends invited me to join a breastfeeding support group on social media “so that I knew I wasn’t the only one up with my baby at 3 a.m.” I learned a lot more than that.
I learned that some mothers trust anecdotes from strangers more than advice from their pediatricians. They recount unsatisfying visits with their pediatricians and then ask other mothers to comment on the advice. As I sifted through a lot of nonscientific and sometimes medically dangerous advice, I also was offered a new perspective. Many mothers will lie to their pediatricians about sleeping and feeding habits because they don’t want to be judged or don’t want another canned answer. Instead of engaging in discussion, they nod, smile, and return to their online support groups.

Very little literature exists on how to partner with mothers to guide them through the breastfeeding journey. These are intimate and individual journeys for each mother and often for each new child. For most mothers who choose to breastfeed, their infant is asking them to learn a new endurance sport, and the body and mind have to start running a marathon on day 1. Breastfeeding consumes nearly every waking moment of at least the first 6 weeks of the infant’s life. It is the most important, stressful, and wonderful part of their young child’s life to date. Pediatricians need to understand and offer advice that reflects this struggle.
So how do we expect pediatricians to help new mothers when our pediatrics residencies lack a basic breastfeeding curriculum? We need to fix it soon because breastfeeding mothers expect evidence-based breastfeeding advice, and as I learned online, they may even fire you if they don’t like what they hear. Although many pediatricians may feel uncomfortable with counseling an adult woman about her body or even treating her, the American Academy of Pediatrics recommends that we do so (Pediatrics 2012 Mar;129[3]:e827-41). There are even resources available to guide billing of extended breastfeeding visits.
The basic science of breastfeeding and how to counsel on common concerns need to be represented in our residency curriculums, as a lack of training early on can perpetuate itself in practice, leading to pediatricians who give outdated advice, reassure when they should counsel further, or give the mother the impression her concerns are irrelevant. Mothers expect more of us when it comes to breastfeeding, and we should expect it of ourselves.
In the meantime, some resources I found helpful were:
• “The Nursing Mother’s Companion,” by Kathleen Huggins (Boston: Harvard Common Press, 2010). This is a great book to help those in training really understand the stresses and common concerns of breastfeeding moms.
• newborns.stanford.edu/Breastfeeding. This is a good online source for those who want a quick tutorial about the early days of breastfeeding.
• AAP Breastfeeding Residency Curriculum (www2.aap.org/breastfeeding/curriculum/medical_knowledge.html). These are learning modules to build knowledge of lactation pathophysiology and how to address mothers’ common concerns.
• www.drmilk.org. This is a support group for breastfeeding moms who are doctors.
Dr. Fricchione is a pediatric infectious diseases fellow at McGaw Medical Center of Northwestern University and the Ann and Robert H. Lurie Children’s Hospital of Chicago.
I expected that having a baby as a pediatric subspecialty fellow was going to be a challenge. But I could never have anticipated how scary it would feel to step into the world on the other side of the clinic door. My friends invited me to join a breastfeeding support group on social media “so that I knew I wasn’t the only one up with my baby at 3 a.m.” I learned a lot more than that.
I learned that some mothers trust anecdotes from strangers more than advice from their pediatricians. They recount unsatisfying visits with their pediatricians and then ask other mothers to comment on the advice. As I sifted through a lot of nonscientific and sometimes medically dangerous advice, I also was offered a new perspective. Many mothers will lie to their pediatricians about sleeping and feeding habits because they don’t want to be judged or don’t want another canned answer. Instead of engaging in discussion, they nod, smile, and return to their online support groups.
Very little literature exists on how to partner with mothers to guide them through the breastfeeding journey. These are intimate and individual journeys for each mother and often for each new child. For most mothers who choose to breastfeed, their infant is asking them to learn a new endurance sport, and the body and mind have to start running a marathon on day 1. Breastfeeding consumes nearly every waking moment of at least the first 6 weeks of the infant’s life. It is the most important, stressful, and wonderful part of their young child’s life to date. Pediatricians need to understand and offer advice that reflects this struggle.
So how do we expect pediatricians to help new mothers when our pediatrics residencies lack a basic breastfeeding curriculum? We need to fix it soon because breastfeeding mothers expect evidence-based breastfeeding advice, and as I learned online, they may even fire you if they don’t like what they hear. Although many pediatricians may feel uncomfortable with counseling an adult woman about her body or even treating her, the American Academy of Pediatrics recommends that we do so (Pediatrics 2012 Mar;129[3]:e827-41). There are even resources available to guide billing of extended breastfeeding visits.
The basic science of breastfeeding and how to counsel on common concerns need to be represented in our residency curriculums, as a lack of training early on can perpetuate itself in practice, leading to pediatricians who give outdated advice, reassure when they should counsel further, or give the mother the impression her concerns are irrelevant. Mothers expect more of us when it comes to breastfeeding, and we should expect it of ourselves.
In the meantime, some resources I found helpful were:
• “The Nursing Mother’s Companion,” by Kathleen Huggins (Boston: Harvard Common Press, 2010). This is a great book to help those in training really understand the stresses and common concerns of breastfeeding moms.
• newborns.stanford.edu/Breastfeeding. This is a good online source for those who want a quick tutorial about the early days of breastfeeding.
• AAP Breastfeeding Residency Curriculum (www2.aap.org/breastfeeding/curriculum/medical_knowledge.html). These are learning modules to build knowledge of lactation pathophysiology and how to address mothers’ common concerns.
• www.drmilk.org. This is a support group for breastfeeding moms who are doctors.
Dr. Fricchione is a pediatric infectious diseases fellow at McGaw Medical Center of Northwestern University and the Ann and Robert H. Lurie Children’s Hospital of Chicago.
I expected that having a baby as a pediatric subspecialty fellow was going to be a challenge. But I could never have anticipated how scary it would feel to step into the world on the other side of the clinic door. My friends invited me to join a breastfeeding support group on social media “so that I knew I wasn’t the only one up with my baby at 3 a.m.” I learned a lot more than that.
I learned that some mothers trust anecdotes from strangers more than advice from their pediatricians. They recount unsatisfying visits with their pediatricians and then ask other mothers to comment on the advice. As I sifted through a lot of nonscientific and sometimes medically dangerous advice, I also was offered a new perspective. Many mothers will lie to their pediatricians about sleeping and feeding habits because they don’t want to be judged or don’t want another canned answer. Instead of engaging in discussion, they nod, smile, and return to their online support groups.
Very little literature exists on how to partner with mothers to guide them through the breastfeeding journey. These are intimate and individual journeys for each mother and often for each new child. For most mothers who choose to breastfeed, their infant is asking them to learn a new endurance sport, and the body and mind have to start running a marathon on day 1. Breastfeeding consumes nearly every waking moment of at least the first 6 weeks of the infant’s life. It is the most important, stressful, and wonderful part of their young child’s life to date. Pediatricians need to understand and offer advice that reflects this struggle.
So how do we expect pediatricians to help new mothers when our pediatrics residencies lack a basic breastfeeding curriculum? We need to fix it soon because breastfeeding mothers expect evidence-based breastfeeding advice, and as I learned online, they may even fire you if they don’t like what they hear. Although many pediatricians may feel uncomfortable with counseling an adult woman about her body or even treating her, the American Academy of Pediatrics recommends that we do so (Pediatrics 2012 Mar;129[3]:e827-41). There are even resources available to guide billing of extended breastfeeding visits.
The basic science of breastfeeding and how to counsel on common concerns need to be represented in our residency curriculums, as a lack of training early on can perpetuate itself in practice, leading to pediatricians who give outdated advice, reassure when they should counsel further, or give the mother the impression her concerns are irrelevant. Mothers expect more of us when it comes to breastfeeding, and we should expect it of ourselves.
In the meantime, some resources I found helpful were:
• “The Nursing Mother’s Companion,” by Kathleen Huggins (Boston: Harvard Common Press, 2010). This is a great book to help those in training really understand the stresses and common concerns of breastfeeding moms.
• newborns.stanford.edu/Breastfeeding. This is a good online source for those who want a quick tutorial about the early days of breastfeeding.
• AAP Breastfeeding Residency Curriculum (www2.aap.org/breastfeeding/curriculum/medical_knowledge.html). These are learning modules to build knowledge of lactation pathophysiology and how to address mothers’ common concerns.
• www.drmilk.org. This is a support group for breastfeeding moms who are doctors.
Dr. Fricchione is a pediatric infectious diseases fellow at McGaw Medical Center of Northwestern University and the Ann and Robert H. Lurie Children’s Hospital of Chicago.

Is monitoring of plasma antipsychotic levels useful?
Although there has been success in defining the minimum therapeutic response threshold for certain antipsychotics—for example, clozapine (350 to 450 ng/mL), haloperidol (3 to 5 ng/mL), and fluphenazine (0.8 ng/mL)—one aspect of antipsychotic plasma levels not widely discussed is their value as a marker of adherence.
Many schizophrenia patients achieve an optimal response to agents for which there is no depot formulation. For them, maintenance of symptom control depends wholly on oral medication adherence.1 Regrettably, nonadherence with oral antipsychotic treatment is prevalent among patients with schizophrenia; yet, in routine clinical practice, the extent of nonadherence rarely is measured.
Studies have been able to quantify oral medication nonadherence using monitoring devices, such as the Medication Event Monitoring System (MEMS) that electronically records opening of the medication container and strongly correlates with pill count. Although patients knew they were participating in a trial using MEMS technology, only 48% were able to take their medication at least 80% of the time in a 4-week study,2 and only 43% met the 70% adherence threshold in a 6-month trial.3
Clinicians, patients: Unreliable indicators of adherence
Neither clinician rating nor patient self-reporting is a reliable predictor of adherence with an oral medication regimen. In the 6-month adherence trial,3 clinicians estimated that 95% of their patients met the 70% adherence threshold (the actual percentage was 43%); in a 12-week study, clinician ratings correlated weakly with adherence (r = 0.32; P = .001), but patient self-reporting showed no significant correlation (r = 0.18; P = .08) with pill count.4
Clinicians underestimate not only the extent of nonadherence but also the impact that even a brief period of modest nonadherence has on the risk of relapse. In an 18-month prospective study of patients who recently had been given a diagnosis of schizophrenia, and in whom clinician and patient reports were supplemented with a pill count every 1 to 2 weeks and plasma antipsychotic levels every 4 weeks, any period of at least mild nonadherence was significantly predictive of symptom exacerbation or relapse (hazard ratio [HR], 3.4; 95% CI, 1.4–8.4; P < .002).1 Moreover, 50% to 75% adherence for ≥ 2 consecutive weeks increased the HR to 5.8, and moderate nonadherence (<50% for 2.0 to 3.9 weeks) to an HR of 28.5.
There might be a better method already available
Given the poor correlation between a clinician’s judgment and a patient’s actual pill-taking, it is clear that more accurate methods of tracking adherence must be devised. Because MEMS technology is not widely available, and because pill counts require a home visit or a cooperative patient who brings medications to office visits, plasma antipsychotic monitoring potentially is an appealing method of tracking adherence.
Correlation between the plasma antipsychotic level and relapse is not consistently seen in the literature,4 but plasma levels obtained during periods of clinical stability offer the opportunity to define, for the individual patient, a range of drug exposure that is associated with clinical response. The ideal plasma level baseline is obtained at steady state during a presumed period of observed adherence, such as during a hospital stay. Although patients can be nonadherent in the hospital, this setting offers the best proxy for an acute clinical response to a given plasma level. The alternative is to obtain several plasma levels during a period of outpatient clinical stability.
Clinicians must be mindful that changes in the plasma antipsychotic level after hospital discharge might not reflect poor adherence; environmental factors (eg, exposure to cytochrome P450 or P-glycoprotein inducers) can have a significant impact on results. Resumption of smoking is a classic example, and routinely is associated with a 50% reduction in plasma clozapine levels.5
There also is expected variability in plasma antipsychotic levels based on (1) the timing of prior doses with regard to trough levels, and (2) the effects of an occasional missed dose. Nevertheless, in a sample of adherent clozapine-treated patients, investigators found that 98% of patients had a coefficient of variability (CV) of 30% for sequential plasma concentrations (mean CV, 14%).6
Clinicians should inform patients that the plasma antipsychotic level is a tool for helping track treatment engagement before relapse—the same way metabolic monitoring helps track abnormalities that can be associated with future cardiovascular events. (Clinicians also must be charitable with their patients when discussing a significant drop in the plasma antipsychotic level [eg, >30%], acknowledging that many patients often miss doses.)
Using the patient’s input about specific difficulties with a medication regimen, clinicians should strive to find ways to improve oral medication adherence. In many cases, the clinician can assist through medication simplification, consolidation of multiple daily doses, provision of pill boxes, and discussions about long-acting injectable (LAI) antipsychotics.
In short, plasma antipsychotic levels offer an opportunity to have a richer, evidence-based discussion about adherence, beyond the trite, ineffective question “Did you take your medication?” Use of an objective measure can (1) serve as a benchmark for the patient (eg, “You seemed to do better when your clozapine level was above 400 ng/mL”), and (2) remind clinicians of the variable adherence inherent with oral medication regimens.
A note about long-acting injectable antipsychotics
Because nonadherence is seen throughout the course of schizophrenia, discussion of LAI therapy should not be limited to patients with chronic illness. Results of recent naturalistic7 and randomized studies8 show significant reduction in the rate of psychotic relapse and improved symptom control8 among first-episode patients who are taking an LAI. Moreover, compelling data show that most first-episode patients who are taking an oral antipsychotic will accept a recommendation for treatment with an LAI.9
Summing up: 2 Tools for achieving therapeutic success
Monitoring plasma levels of antipsychotics offers a method for quantifying the problem of nonadherence. For many patients, an LAI antipsychotic provides a solution to nonadherence, and the increasing variety of LAI preparations means more options with which to match individual patients.
Clinicians have a limited amount of time to spend with patients in the office, but time spent discussing LAIs is an investment in the patient’s stability and functional outcome. Minutes once spent managing nonadherence can be devoted to understanding the patient’s aspirations and to developing strategies to achieve those goals.
In the end, isn’t that what we’d rather be talking about with our patients?
1. Subotnik KL, Nuechterlein KH, Ventura J, et al. Risperidone nonadherence and return of positive symptoms in the early course of schizophrenia. Am J Psychiatry. 2011;168(3):286-292.
2. Remington G, Teo C, Mann S, et al. Examining levels of antipsychotic adherence to better understand nonadherence. J Clin Psychopharmacol. 2013;33(2):261-263.
3. Byerly MJ, Thompson A, Carmody T, et al. Validity of electronically monitored medication adherence and conventional adherence measures in schizophrenia. Psychiatr Serv. 2007;58(6):844-847.
4. Velligan DI, Wang M, Diamond P, et al. Relationships among subjective and objective measures of adherence to oral antipsychotic medications. Psychiatr Serv. 2007;58(9):1187-1192.
5. Meyer JM. Individual changes in clozapine levels after smoking cessation: results and a predictive model. J Clin Psychopharmacol. 2001;21(6):569-574.
6. Dugan DJ, Ereshefsky L, Toney GB, et al. Dose and interval adherence among stabilized clozapine-treated patients measured by medication event monitoring. Presented at: Meeting of the New Clinical Drug Evaluation Unit; May 30-June 2, 2000; Boca Raton, FL.
7. Tiihonen J, Haukka J, Taylor M, et al. A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia. [Erratum in Am J Psychiatry. 2012;169(2):223]. Am J Psychiatry. 2011;168(6):603-609.
8. Subotnik KL, Casaus LR, Ventura J, et al. Long-acting injectable risperidone for relapse prevention and control of breakthrough symptoms after a recent first episode of schizophrenia: a randomized clinical trial. JAMA Psychiatry. 2015;72(8):822-829.
9. Weiden PJ, Schooler NR, Weedon JC, et al. A randomized controlled trial of long-acting injectable risperidone vs continuation on oral atypical antipsychotics for first-episode schizophrenia patients: initial adherence outcome. J Clin Psychiatry. 2009;70(10):1397-1406.
Although there has been success in defining the minimum therapeutic response threshold for certain antipsychotics—for example, clozapine (350 to 450 ng/mL), haloperidol (3 to 5 ng/mL), and fluphenazine (0.8 ng/mL)—one aspect of antipsychotic plasma levels not widely discussed is their value as a marker of adherence.
Many schizophrenia patients achieve an optimal response to agents for which there is no depot formulation. For them, maintenance of symptom control depends wholly on oral medication adherence.1 Regrettably, nonadherence with oral antipsychotic treatment is prevalent among patients with schizophrenia; yet, in routine clinical practice, the extent of nonadherence rarely is measured.
Studies have been able to quantify oral medication nonadherence using monitoring devices, such as the Medication Event Monitoring System (MEMS) that electronically records opening of the medication container and strongly correlates with pill count. Although patients knew they were participating in a trial using MEMS technology, only 48% were able to take their medication at least 80% of the time in a 4-week study,2 and only 43% met the 70% adherence threshold in a 6-month trial.3
Clinicians, patients: Unreliable indicators of adherence
Neither clinician rating nor patient self-reporting is a reliable predictor of adherence with an oral medication regimen. In the 6-month adherence trial,3 clinicians estimated that 95% of their patients met the 70% adherence threshold (the actual percentage was 43%); in a 12-week study, clinician ratings correlated weakly with adherence (r = 0.32; P = .001), but patient self-reporting showed no significant correlation (r = 0.18; P = .08) with pill count.4
Clinicians underestimate not only the extent of nonadherence but also the impact that even a brief period of modest nonadherence has on the risk of relapse. In an 18-month prospective study of patients who recently had been given a diagnosis of schizophrenia, and in whom clinician and patient reports were supplemented with a pill count every 1 to 2 weeks and plasma antipsychotic levels every 4 weeks, any period of at least mild nonadherence was significantly predictive of symptom exacerbation or relapse (hazard ratio [HR], 3.4; 95% CI, 1.4–8.4; P < .002).1 Moreover, 50% to 75% adherence for ≥ 2 consecutive weeks increased the HR to 5.8, and moderate nonadherence (<50% for 2.0 to 3.9 weeks) to an HR of 28.5.
There might be a better method already available
Given the poor correlation between a clinician’s judgment and a patient’s actual pill-taking, it is clear that more accurate methods of tracking adherence must be devised. Because MEMS technology is not widely available, and because pill counts require a home visit or a cooperative patient who brings medications to office visits, plasma antipsychotic monitoring potentially is an appealing method of tracking adherence.
Correlation between the plasma antipsychotic level and relapse is not consistently seen in the literature,4 but plasma levels obtained during periods of clinical stability offer the opportunity to define, for the individual patient, a range of drug exposure that is associated with clinical response. The ideal plasma level baseline is obtained at steady state during a presumed period of observed adherence, such as during a hospital stay. Although patients can be nonadherent in the hospital, this setting offers the best proxy for an acute clinical response to a given plasma level. The alternative is to obtain several plasma levels during a period of outpatient clinical stability.
Clinicians must be mindful that changes in the plasma antipsychotic level after hospital discharge might not reflect poor adherence; environmental factors (eg, exposure to cytochrome P450 or P-glycoprotein inducers) can have a significant impact on results. Resumption of smoking is a classic example, and routinely is associated with a 50% reduction in plasma clozapine levels.5
There also is expected variability in plasma antipsychotic levels based on (1) the timing of prior doses with regard to trough levels, and (2) the effects of an occasional missed dose. Nevertheless, in a sample of adherent clozapine-treated patients, investigators found that 98% of patients had a coefficient of variability (CV) of 30% for sequential plasma concentrations (mean CV, 14%).6
Clinicians should inform patients that the plasma antipsychotic level is a tool for helping track treatment engagement before relapse—the same way metabolic monitoring helps track abnormalities that can be associated with future cardiovascular events. (Clinicians also must be charitable with their patients when discussing a significant drop in the plasma antipsychotic level [eg, >30%], acknowledging that many patients often miss doses.)
Using the patient’s input about specific difficulties with a medication regimen, clinicians should strive to find ways to improve oral medication adherence. In many cases, the clinician can assist through medication simplification, consolidation of multiple daily doses, provision of pill boxes, and discussions about long-acting injectable (LAI) antipsychotics.
In short, plasma antipsychotic levels offer an opportunity to have a richer, evidence-based discussion about adherence, beyond the trite, ineffective question “Did you take your medication?” Use of an objective measure can (1) serve as a benchmark for the patient (eg, “You seemed to do better when your clozapine level was above 400 ng/mL”), and (2) remind clinicians of the variable adherence inherent with oral medication regimens.
A note about long-acting injectable antipsychotics
Because nonadherence is seen throughout the course of schizophrenia, discussion of LAI therapy should not be limited to patients with chronic illness. Results of recent naturalistic7 and randomized studies8 show significant reduction in the rate of psychotic relapse and improved symptom control8 among first-episode patients who are taking an LAI. Moreover, compelling data show that most first-episode patients who are taking an oral antipsychotic will accept a recommendation for treatment with an LAI.9
Summing up: 2 Tools for achieving therapeutic success
Monitoring plasma levels of antipsychotics offers a method for quantifying the problem of nonadherence. For many patients, an LAI antipsychotic provides a solution to nonadherence, and the increasing variety of LAI preparations means more options with which to match individual patients.
Clinicians have a limited amount of time to spend with patients in the office, but time spent discussing LAIs is an investment in the patient’s stability and functional outcome. Minutes once spent managing nonadherence can be devoted to understanding the patient’s aspirations and to developing strategies to achieve those goals.
In the end, isn’t that what we’d rather be talking about with our patients?
Although there has been success in defining the minimum therapeutic response threshold for certain antipsychotics—for example, clozapine (350 to 450 ng/mL), haloperidol (3 to 5 ng/mL), and fluphenazine (0.8 ng/mL)—one aspect of antipsychotic plasma levels not widely discussed is their value as a marker of adherence.
Many schizophrenia patients achieve an optimal response to agents for which there is no depot formulation. For them, maintenance of symptom control depends wholly on oral medication adherence.1 Regrettably, nonadherence with oral antipsychotic treatment is prevalent among patients with schizophrenia; yet, in routine clinical practice, the extent of nonadherence rarely is measured.
Studies have been able to quantify oral medication nonadherence using monitoring devices, such as the Medication Event Monitoring System (MEMS) that electronically records opening of the medication container and strongly correlates with pill count. Although patients knew they were participating in a trial using MEMS technology, only 48% were able to take their medication at least 80% of the time in a 4-week study,2 and only 43% met the 70% adherence threshold in a 6-month trial.3
Clinicians, patients: Unreliable indicators of adherence
Neither clinician rating nor patient self-reporting is a reliable predictor of adherence with an oral medication regimen. In the 6-month adherence trial,3 clinicians estimated that 95% of their patients met the 70% adherence threshold (the actual percentage was 43%); in a 12-week study, clinician ratings correlated weakly with adherence (r = 0.32; P = .001), but patient self-reporting showed no significant correlation (r = 0.18; P = .08) with pill count.4
Clinicians underestimate not only the extent of nonadherence but also the impact that even a brief period of modest nonadherence has on the risk of relapse. In an 18-month prospective study of patients who recently had been given a diagnosis of schizophrenia, and in whom clinician and patient reports were supplemented with a pill count every 1 to 2 weeks and plasma antipsychotic levels every 4 weeks, any period of at least mild nonadherence was significantly predictive of symptom exacerbation or relapse (hazard ratio [HR], 3.4; 95% CI, 1.4–8.4; P < .002).1 Moreover, 50% to 75% adherence for ≥ 2 consecutive weeks increased the HR to 5.8, and moderate nonadherence (<50% for 2.0 to 3.9 weeks) to an HR of 28.5.
There might be a better method already available
Given the poor correlation between a clinician’s judgment and a patient’s actual pill-taking, it is clear that more accurate methods of tracking adherence must be devised. Because MEMS technology is not widely available, and because pill counts require a home visit or a cooperative patient who brings medications to office visits, plasma antipsychotic monitoring potentially is an appealing method of tracking adherence.
Correlation between the plasma antipsychotic level and relapse is not consistently seen in the literature,4 but plasma levels obtained during periods of clinical stability offer the opportunity to define, for the individual patient, a range of drug exposure that is associated with clinical response. The ideal plasma level baseline is obtained at steady state during a presumed period of observed adherence, such as during a hospital stay. Although patients can be nonadherent in the hospital, this setting offers the best proxy for an acute clinical response to a given plasma level. The alternative is to obtain several plasma levels during a period of outpatient clinical stability.
Clinicians must be mindful that changes in the plasma antipsychotic level after hospital discharge might not reflect poor adherence; environmental factors (eg, exposure to cytochrome P450 or P-glycoprotein inducers) can have a significant impact on results. Resumption of smoking is a classic example, and routinely is associated with a 50% reduction in plasma clozapine levels.5
There also is expected variability in plasma antipsychotic levels based on (1) the timing of prior doses with regard to trough levels, and (2) the effects of an occasional missed dose. Nevertheless, in a sample of adherent clozapine-treated patients, investigators found that 98% of patients had a coefficient of variability (CV) of 30% for sequential plasma concentrations (mean CV, 14%).6
Clinicians should inform patients that the plasma antipsychotic level is a tool for helping track treatment engagement before relapse—the same way metabolic monitoring helps track abnormalities that can be associated with future cardiovascular events. (Clinicians also must be charitable with their patients when discussing a significant drop in the plasma antipsychotic level [eg, >30%], acknowledging that many patients often miss doses.)
Using the patient’s input about specific difficulties with a medication regimen, clinicians should strive to find ways to improve oral medication adherence. In many cases, the clinician can assist through medication simplification, consolidation of multiple daily doses, provision of pill boxes, and discussions about long-acting injectable (LAI) antipsychotics.
In short, plasma antipsychotic levels offer an opportunity to have a richer, evidence-based discussion about adherence, beyond the trite, ineffective question “Did you take your medication?” Use of an objective measure can (1) serve as a benchmark for the patient (eg, “You seemed to do better when your clozapine level was above 400 ng/mL”), and (2) remind clinicians of the variable adherence inherent with oral medication regimens.
A note about long-acting injectable antipsychotics
Because nonadherence is seen throughout the course of schizophrenia, discussion of LAI therapy should not be limited to patients with chronic illness. Results of recent naturalistic7 and randomized studies8 show significant reduction in the rate of psychotic relapse and improved symptom control8 among first-episode patients who are taking an LAI. Moreover, compelling data show that most first-episode patients who are taking an oral antipsychotic will accept a recommendation for treatment with an LAI.9
Summing up: 2 Tools for achieving therapeutic success
Monitoring plasma levels of antipsychotics offers a method for quantifying the problem of nonadherence. For many patients, an LAI antipsychotic provides a solution to nonadherence, and the increasing variety of LAI preparations means more options with which to match individual patients.
Clinicians have a limited amount of time to spend with patients in the office, but time spent discussing LAIs is an investment in the patient’s stability and functional outcome. Minutes once spent managing nonadherence can be devoted to understanding the patient’s aspirations and to developing strategies to achieve those goals.
In the end, isn’t that what we’d rather be talking about with our patients?
1. Subotnik KL, Nuechterlein KH, Ventura J, et al. Risperidone nonadherence and return of positive symptoms in the early course of schizophrenia. Am J Psychiatry. 2011;168(3):286-292.
2. Remington G, Teo C, Mann S, et al. Examining levels of antipsychotic adherence to better understand nonadherence. J Clin Psychopharmacol. 2013;33(2):261-263.
3. Byerly MJ, Thompson A, Carmody T, et al. Validity of electronically monitored medication adherence and conventional adherence measures in schizophrenia. Psychiatr Serv. 2007;58(6):844-847.
4. Velligan DI, Wang M, Diamond P, et al. Relationships among subjective and objective measures of adherence to oral antipsychotic medications. Psychiatr Serv. 2007;58(9):1187-1192.
5. Meyer JM. Individual changes in clozapine levels after smoking cessation: results and a predictive model. J Clin Psychopharmacol. 2001;21(6):569-574.
6. Dugan DJ, Ereshefsky L, Toney GB, et al. Dose and interval adherence among stabilized clozapine-treated patients measured by medication event monitoring. Presented at: Meeting of the New Clinical Drug Evaluation Unit; May 30-June 2, 2000; Boca Raton, FL.
7. Tiihonen J, Haukka J, Taylor M, et al. A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia. [Erratum in Am J Psychiatry. 2012;169(2):223]. Am J Psychiatry. 2011;168(6):603-609.
8. Subotnik KL, Casaus LR, Ventura J, et al. Long-acting injectable risperidone for relapse prevention and control of breakthrough symptoms after a recent first episode of schizophrenia: a randomized clinical trial. JAMA Psychiatry. 2015;72(8):822-829.
9. Weiden PJ, Schooler NR, Weedon JC, et al. A randomized controlled trial of long-acting injectable risperidone vs continuation on oral atypical antipsychotics for first-episode schizophrenia patients: initial adherence outcome. J Clin Psychiatry. 2009;70(10):1397-1406.
1. Subotnik KL, Nuechterlein KH, Ventura J, et al. Risperidone nonadherence and return of positive symptoms in the early course of schizophrenia. Am J Psychiatry. 2011;168(3):286-292.
2. Remington G, Teo C, Mann S, et al. Examining levels of antipsychotic adherence to better understand nonadherence. J Clin Psychopharmacol. 2013;33(2):261-263.
3. Byerly MJ, Thompson A, Carmody T, et al. Validity of electronically monitored medication adherence and conventional adherence measures in schizophrenia. Psychiatr Serv. 2007;58(6):844-847.
4. Velligan DI, Wang M, Diamond P, et al. Relationships among subjective and objective measures of adherence to oral antipsychotic medications. Psychiatr Serv. 2007;58(9):1187-1192.
5. Meyer JM. Individual changes in clozapine levels after smoking cessation: results and a predictive model. J Clin Psychopharmacol. 2001;21(6):569-574.
6. Dugan DJ, Ereshefsky L, Toney GB, et al. Dose and interval adherence among stabilized clozapine-treated patients measured by medication event monitoring. Presented at: Meeting of the New Clinical Drug Evaluation Unit; May 30-June 2, 2000; Boca Raton, FL.
7. Tiihonen J, Haukka J, Taylor M, et al. A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia. [Erratum in Am J Psychiatry. 2012;169(2):223]. Am J Psychiatry. 2011;168(6):603-609.
8. Subotnik KL, Casaus LR, Ventura J, et al. Long-acting injectable risperidone for relapse prevention and control of breakthrough symptoms after a recent first episode of schizophrenia: a randomized clinical trial. JAMA Psychiatry. 2015;72(8):822-829.
9. Weiden PJ, Schooler NR, Weedon JC, et al. A randomized controlled trial of long-acting injectable risperidone vs continuation on oral atypical antipsychotics for first-episode schizophrenia patients: initial adherence outcome. J Clin Psychiatry. 2009;70(10):1397-1406.

Approaches to smoking cessation before and during pregnancy
Data consistently support the negative impact of tobacco use in pregnancy with respect to pregnancy outcome, and the benefits of discontinuation or reduction as early as possible.
Recent analyses by investigators at the National Center on Birth Defects and Developmental Disabilities at the Centers for Disease Control and Prevention suggest that more than 6% of oral clefts, or 430 affected infants per year in the United States, could be prevented annually if women can discontinue tobacco use prior to conception (Birth Defects Res A Clin Mol Teratol. 2014 Nov;100[11]:822-5). Similarly, preconception smoking cessation could prevent the 1.4% of nonsyndromic congenital heart defects that are attributable to maternal smoking in the first trimester (J Pediatr. 2015 Apr;166[4]:978-984.e2).
With respect to the risk for adverse outcomes beyond the first trimester, recent data also show clearly that the trimester of discontinuation is related to intrauterine growth restriction in a dose-response fashion (Obstet Gynecol. 2015 Jun;125[6]:1452-9).

In a recent population-based retrospective cohort study of 927,424 singleton births 2006-2012 in Ohio, the adjusted relative risk of infant birth weight less than the 5th percentile for those women who discontinued smoking after the first trimester compared with nonsmokers was 1.25 (95% confidence interval, 1.17-1.33); for those who discontinued after the second trimester the relative risk was 1.83 (95% CI, 1.68-1.99); and for those who smoked throughout pregnancy the relative risk was 2.44 (95% CI, 2.37-2.51).
Given the compelling reasons to encourage women to stop smoking or at least to reduce harm during pregnancy, options for assistance with smoking cessation are of high interest. Beyond simple screening and advice to quit, cognitive behavioral therapy has been shown to provide some benefit. The addition of pharmacologic treatment with nicotine replacement therapy (NRT) has been studied in six randomized clinical trials (RCTs) conducted in pregnant women, four of which compared NRT plus advice/behavioral support to placebo plus advice/behavioral support, and two of which compared NRT plus advice/behavioral support to advice/behavioral support alone.
In a recent Cochrane systematic review of these studies, no statistically significant evidence of effectiveness was demonstrated for NRT versus placebo/control in a pooled sample of 1,745 pregnant patients (risk ratio, 1.33, 95% CI, 0.93-1.91). However, there was high heterogeneity in the dose of NRT and the delivery method (e.g., gum, patch) across studies, and poor adherence to the NRT treatment in all trials (Cochrane Database Syst Rev. 2012 Sep 12;9:CD010078).
With respect to safety, in the same Cochrane review there were no statistically significant differences in rates of miscarriage, stillbirth, premature birth, birth weight, low birth weight, admissions to neonatal intensive care, or neonatal death between NRT and control groups. However, small sample sizes and adherence issues across these trials hampered the interpretability of these data.
One relatively large claims database study from the United Kingdom, which was published recently, examined major congenital anomalies following prescription of NRT. The investigators found no increased risks for most major defects following NRT prescription; the only significant association was with respiratory defects (Pediatrics. 2015 May;135[5]:859-67).
The general thinking has been that for a woman who is unable to quit smoking without pharmacological assistance, NRT that delivers nicotine alone to the developing fetus may be a better option than exposure to the multiple toxins that are contained in tobacco smoke. However, there is considerable controversy over the potential adverse neurotoxic effects of nicotine itself and long-term neurodevelopmental studies on children prenatally exposed to NRT are lacking.

Other options include bupropion and varenicline, neither of which have been studied in RCTs in pregnancy. Bupropion has been evaluated in a small controlled cohort study, a claims database study (n = 1,236 first-trimester exposed), and two case-control studies. None of these studies was focused on use of bupropion exclusively for smoking cessation, but rather for the more common indication of maternal depression. The first two studies suggested no increased risks for adverse pregnancy outcomes compared to women the same underlying conditions; the case control studies suggested small increased risks for heart defects but not the same ones in both studies (Expert Opin Drug Saf. 2014 Dec;13[12]:1721-31). The limited data on varenicline are too sparse to make any inferences.
Another possible alternative that has been gaining in popularity are e-cigarettes or related vapor products, which are touted to have advantages with respect to harm reduction, primarily because of possible improved adherence due to their similarity to conventional smoking. However, there is large variability in the amount of nicotine in the vapor of various e-cigarette brands, and some have suggested that e-cigarette users engage in longer puff duration than do those who smoke conventional cigarettes. To my knowledge, there are no controlled studies of e-cigarette use in pregnancy, but the concerns previously raised regarding nicotine exposure in any form likely apply to this delivery method (Birth Defects Res A Clin Mol Teratol. 2015 Mar;103[3]:186-95).
What is the role of the obstetrician in identifying nicotine and tobacco exposure in their patients and encouraging cessation or reduction prior to and during pregnancy?
The first responsibility is to screen pregnant women. A recent survey study suggests that 40% of the responding ob.gyns. never screened pregnant patients for use of noncombustible tobacco products such as e-cigarettes (Am J Obstet Gynecol. 2014 Dec;211[6]:695.e1-7). In the United States, an analysis of the Pregnancy Risk Assessment Monitoring System data collected across several states from 2009 to 2010 suggests that about a quarter of 3,559 pregnant women who reported smoking in the 3 months before pregnancy did not receive any interventions to stop smoking (Prev Med. 2015 Sep;78:92-100). In addition, four out of five ob.gyns. surveyed in 2012 were unaware of the Affordable Care Act provision that requires states to provide tobacco cessation coverage for pregnant Medicaid beneficiaries (Prev Med Rep. 2015;2:686-88).
Dr. Chambers is professor of pediatrics and director of clinical research at Rady Children’s Hospital, and associate director of the Clinical and Translational Research Institute at the University of California, San Diego. She is director of MotherToBaby California, past president of the Organization of Teratology Information Specialists, and past president of the Teratology Society. She reported having no financial disclosures relevant to this column, but has received research funding from GlaxoSmithKline and Pfizer for unrelated products.
Data consistently support the negative impact of tobacco use in pregnancy with respect to pregnancy outcome, and the benefits of discontinuation or reduction as early as possible.
Recent analyses by investigators at the National Center on Birth Defects and Developmental Disabilities at the Centers for Disease Control and Prevention suggest that more than 6% of oral clefts, or 430 affected infants per year in the United States, could be prevented annually if women can discontinue tobacco use prior to conception (Birth Defects Res A Clin Mol Teratol. 2014 Nov;100[11]:822-5). Similarly, preconception smoking cessation could prevent the 1.4% of nonsyndromic congenital heart defects that are attributable to maternal smoking in the first trimester (J Pediatr. 2015 Apr;166[4]:978-984.e2).
With respect to the risk for adverse outcomes beyond the first trimester, recent data also show clearly that the trimester of discontinuation is related to intrauterine growth restriction in a dose-response fashion (Obstet Gynecol. 2015 Jun;125[6]:1452-9).
In a recent population-based retrospective cohort study of 927,424 singleton births 2006-2012 in Ohio, the adjusted relative risk of infant birth weight less than the 5th percentile for those women who discontinued smoking after the first trimester compared with nonsmokers was 1.25 (95% confidence interval, 1.17-1.33); for those who discontinued after the second trimester the relative risk was 1.83 (95% CI, 1.68-1.99); and for those who smoked throughout pregnancy the relative risk was 2.44 (95% CI, 2.37-2.51).
Given the compelling reasons to encourage women to stop smoking or at least to reduce harm during pregnancy, options for assistance with smoking cessation are of high interest. Beyond simple screening and advice to quit, cognitive behavioral therapy has been shown to provide some benefit. The addition of pharmacologic treatment with nicotine replacement therapy (NRT) has been studied in six randomized clinical trials (RCTs) conducted in pregnant women, four of which compared NRT plus advice/behavioral support to placebo plus advice/behavioral support, and two of which compared NRT plus advice/behavioral support to advice/behavioral support alone.
In a recent Cochrane systematic review of these studies, no statistically significant evidence of effectiveness was demonstrated for NRT versus placebo/control in a pooled sample of 1,745 pregnant patients (risk ratio, 1.33, 95% CI, 0.93-1.91). However, there was high heterogeneity in the dose of NRT and the delivery method (e.g., gum, patch) across studies, and poor adherence to the NRT treatment in all trials (Cochrane Database Syst Rev. 2012 Sep 12;9:CD010078).
With respect to safety, in the same Cochrane review there were no statistically significant differences in rates of miscarriage, stillbirth, premature birth, birth weight, low birth weight, admissions to neonatal intensive care, or neonatal death between NRT and control groups. However, small sample sizes and adherence issues across these trials hampered the interpretability of these data.
One relatively large claims database study from the United Kingdom, which was published recently, examined major congenital anomalies following prescription of NRT. The investigators found no increased risks for most major defects following NRT prescription; the only significant association was with respiratory defects (Pediatrics. 2015 May;135[5]:859-67).
The general thinking has been that for a woman who is unable to quit smoking without pharmacological assistance, NRT that delivers nicotine alone to the developing fetus may be a better option than exposure to the multiple toxins that are contained in tobacco smoke. However, there is considerable controversy over the potential adverse neurotoxic effects of nicotine itself and long-term neurodevelopmental studies on children prenatally exposed to NRT are lacking.
Other options include bupropion and varenicline, neither of which have been studied in RCTs in pregnancy. Bupropion has been evaluated in a small controlled cohort study, a claims database study (n = 1,236 first-trimester exposed), and two case-control studies. None of these studies was focused on use of bupropion exclusively for smoking cessation, but rather for the more common indication of maternal depression. The first two studies suggested no increased risks for adverse pregnancy outcomes compared to women the same underlying conditions; the case control studies suggested small increased risks for heart defects but not the same ones in both studies (Expert Opin Drug Saf. 2014 Dec;13[12]:1721-31). The limited data on varenicline are too sparse to make any inferences.
Another possible alternative that has been gaining in popularity are e-cigarettes or related vapor products, which are touted to have advantages with respect to harm reduction, primarily because of possible improved adherence due to their similarity to conventional smoking. However, there is large variability in the amount of nicotine in the vapor of various e-cigarette brands, and some have suggested that e-cigarette users engage in longer puff duration than do those who smoke conventional cigarettes. To my knowledge, there are no controlled studies of e-cigarette use in pregnancy, but the concerns previously raised regarding nicotine exposure in any form likely apply to this delivery method (Birth Defects Res A Clin Mol Teratol. 2015 Mar;103[3]:186-95).
What is the role of the obstetrician in identifying nicotine and tobacco exposure in their patients and encouraging cessation or reduction prior to and during pregnancy?
The first responsibility is to screen pregnant women. A recent survey study suggests that 40% of the responding ob.gyns. never screened pregnant patients for use of noncombustible tobacco products such as e-cigarettes (Am J Obstet Gynecol. 2014 Dec;211[6]:695.e1-7). In the United States, an analysis of the Pregnancy Risk Assessment Monitoring System data collected across several states from 2009 to 2010 suggests that about a quarter of 3,559 pregnant women who reported smoking in the 3 months before pregnancy did not receive any interventions to stop smoking (Prev Med. 2015 Sep;78:92-100). In addition, four out of five ob.gyns. surveyed in 2012 were unaware of the Affordable Care Act provision that requires states to provide tobacco cessation coverage for pregnant Medicaid beneficiaries (Prev Med Rep. 2015;2:686-88).
Dr. Chambers is professor of pediatrics and director of clinical research at Rady Children’s Hospital, and associate director of the Clinical and Translational Research Institute at the University of California, San Diego. She is director of MotherToBaby California, past president of the Organization of Teratology Information Specialists, and past president of the Teratology Society. She reported having no financial disclosures relevant to this column, but has received research funding from GlaxoSmithKline and Pfizer for unrelated products.
Data consistently support the negative impact of tobacco use in pregnancy with respect to pregnancy outcome, and the benefits of discontinuation or reduction as early as possible.
Recent analyses by investigators at the National Center on Birth Defects and Developmental Disabilities at the Centers for Disease Control and Prevention suggest that more than 6% of oral clefts, or 430 affected infants per year in the United States, could be prevented annually if women can discontinue tobacco use prior to conception (Birth Defects Res A Clin Mol Teratol. 2014 Nov;100[11]:822-5). Similarly, preconception smoking cessation could prevent the 1.4% of nonsyndromic congenital heart defects that are attributable to maternal smoking in the first trimester (J Pediatr. 2015 Apr;166[4]:978-984.e2).
With respect to the risk for adverse outcomes beyond the first trimester, recent data also show clearly that the trimester of discontinuation is related to intrauterine growth restriction in a dose-response fashion (Obstet Gynecol. 2015 Jun;125[6]:1452-9).
In a recent population-based retrospective cohort study of 927,424 singleton births 2006-2012 in Ohio, the adjusted relative risk of infant birth weight less than the 5th percentile for those women who discontinued smoking after the first trimester compared with nonsmokers was 1.25 (95% confidence interval, 1.17-1.33); for those who discontinued after the second trimester the relative risk was 1.83 (95% CI, 1.68-1.99); and for those who smoked throughout pregnancy the relative risk was 2.44 (95% CI, 2.37-2.51).
Given the compelling reasons to encourage women to stop smoking or at least to reduce harm during pregnancy, options for assistance with smoking cessation are of high interest. Beyond simple screening and advice to quit, cognitive behavioral therapy has been shown to provide some benefit. The addition of pharmacologic treatment with nicotine replacement therapy (NRT) has been studied in six randomized clinical trials (RCTs) conducted in pregnant women, four of which compared NRT plus advice/behavioral support to placebo plus advice/behavioral support, and two of which compared NRT plus advice/behavioral support to advice/behavioral support alone.
In a recent Cochrane systematic review of these studies, no statistically significant evidence of effectiveness was demonstrated for NRT versus placebo/control in a pooled sample of 1,745 pregnant patients (risk ratio, 1.33, 95% CI, 0.93-1.91). However, there was high heterogeneity in the dose of NRT and the delivery method (e.g., gum, patch) across studies, and poor adherence to the NRT treatment in all trials (Cochrane Database Syst Rev. 2012 Sep 12;9:CD010078).
With respect to safety, in the same Cochrane review there were no statistically significant differences in rates of miscarriage, stillbirth, premature birth, birth weight, low birth weight, admissions to neonatal intensive care, or neonatal death between NRT and control groups. However, small sample sizes and adherence issues across these trials hampered the interpretability of these data.
One relatively large claims database study from the United Kingdom, which was published recently, examined major congenital anomalies following prescription of NRT. The investigators found no increased risks for most major defects following NRT prescription; the only significant association was with respiratory defects (Pediatrics. 2015 May;135[5]:859-67).
The general thinking has been that for a woman who is unable to quit smoking without pharmacological assistance, NRT that delivers nicotine alone to the developing fetus may be a better option than exposure to the multiple toxins that are contained in tobacco smoke. However, there is considerable controversy over the potential adverse neurotoxic effects of nicotine itself and long-term neurodevelopmental studies on children prenatally exposed to NRT are lacking.
Other options include bupropion and varenicline, neither of which have been studied in RCTs in pregnancy. Bupropion has been evaluated in a small controlled cohort study, a claims database study (n = 1,236 first-trimester exposed), and two case-control studies. None of these studies was focused on use of bupropion exclusively for smoking cessation, but rather for the more common indication of maternal depression. The first two studies suggested no increased risks for adverse pregnancy outcomes compared to women the same underlying conditions; the case control studies suggested small increased risks for heart defects but not the same ones in both studies (Expert Opin Drug Saf. 2014 Dec;13[12]:1721-31). The limited data on varenicline are too sparse to make any inferences.
Another possible alternative that has been gaining in popularity are e-cigarettes or related vapor products, which are touted to have advantages with respect to harm reduction, primarily because of possible improved adherence due to their similarity to conventional smoking. However, there is large variability in the amount of nicotine in the vapor of various e-cigarette brands, and some have suggested that e-cigarette users engage in longer puff duration than do those who smoke conventional cigarettes. To my knowledge, there are no controlled studies of e-cigarette use in pregnancy, but the concerns previously raised regarding nicotine exposure in any form likely apply to this delivery method (Birth Defects Res A Clin Mol Teratol. 2015 Mar;103[3]:186-95).
What is the role of the obstetrician in identifying nicotine and tobacco exposure in their patients and encouraging cessation or reduction prior to and during pregnancy?
The first responsibility is to screen pregnant women. A recent survey study suggests that 40% of the responding ob.gyns. never screened pregnant patients for use of noncombustible tobacco products such as e-cigarettes (Am J Obstet Gynecol. 2014 Dec;211[6]:695.e1-7). In the United States, an analysis of the Pregnancy Risk Assessment Monitoring System data collected across several states from 2009 to 2010 suggests that about a quarter of 3,559 pregnant women who reported smoking in the 3 months before pregnancy did not receive any interventions to stop smoking (Prev Med. 2015 Sep;78:92-100). In addition, four out of five ob.gyns. surveyed in 2012 were unaware of the Affordable Care Act provision that requires states to provide tobacco cessation coverage for pregnant Medicaid beneficiaries (Prev Med Rep. 2015;2:686-88).
Dr. Chambers is professor of pediatrics and director of clinical research at Rady Children’s Hospital, and associate director of the Clinical and Translational Research Institute at the University of California, San Diego. She is director of MotherToBaby California, past president of the Organization of Teratology Information Specialists, and past president of the Teratology Society. She reported having no financial disclosures relevant to this column, but has received research funding from GlaxoSmithKline and Pfizer for unrelated products.

Mental health care is ‘Code Black’
The initial explanation for why the teenager needed to be admitted seemed very flimsy to me. Finally, the office pediatrician came clean. The girl is an honor roll student, high achieving but currently overwhelmed by events in her life. She cannot handle being at home, but there is nowhere else for her to go for the weekend. Come Monday morning, the primary care physician (PCP) has arranged for her acceptance into a local mental health facility where she could get the care she needs. The prognosis was excellent. Her entire future could be markedly improved with just a little help getting through these current troubles. I thought about the patient down the hall. My partner had admitted her 2 days ago for acute-on-chronic abdominal pain, shortly after her third normal CT scan in 6 months. I strongly doubted that that patient had any more business being in a hospital than this latest admission – except, of course, for all the profit the hospital was making on the imaging. On reflection, I decided the PCP’s request no longer seemed so out of place.
The latest emergency department drama on TV has a tagline, “In the ER when there are more patients than resources, it’s called Code Black.” It contains scenes of mopping up bloody floors in the trauma bay. I’ve worked in an ED that was a major portal into a nearby pediatric mental health facility. The major traumas I cared for didn’t bleed from their life-threatening emotional wounds. Multiple times per week, children from across the city were brought in for evaluation. A few needed a toxicology work-up for ingestions. A few more needed some glue or sutures for very superficial self-inflicted forearm lacerations. Mostly I provided a medical screening before getting those teenagers moved as quickly as possible to a team of specialists who could help them. In some parts of this country that can take days.

On Oct. 5, 2015, California’s governor signed a state law permitting physician-assisted suicide. It is now the fifth state allowing that option. The pros and cons have been endlessly debated by ethicists. A brief Google search can find the philosophical arguments. I recommend a June 22, 2015, New Yorker article entitled, “The Death Treatment” by Rachel Aviv to provide a broad narrative perspective. Oregon’s Death With Dignity Act was passed 20 years ago, so it provides some scientific data. There are now 100 deaths per year under that Oregon act. The state also has 700 suicides yearly. So the leading method of suicide in Oregon, by a wide margin, continues to be used by people who are not terminally ill. That was the method of choice recently for my cousin. There was nothing dignified about it. My favorite actor, Robin Williams, in the movie “World’s Greatest Dad,” had the line, “If you’re that depressed, reach out to someone, and remember suicide is a permanent solution to temporary problems.” Five years later he took his own life.
I do enjoy debating the nuances of physician-assisted suicide with other ethicists, but I don’t confuse those academic exercises with addressing the real world problem of endemic suicide. Nationwide, there are 41,000 suicides each year, with about 5,000 in the 15- to 24-year age group. In comparison, 10,000 children annually will get cancer, but only 1,250 children will die of it. There will be about 900 pediatric recipients of lifesaving heart or liver transplants. With all this wealth, knowledge, and technology, the United States should be able to provide better treatment of mental illness. Parity of mental health services became law under President Clinton in 1996, repeated as law under President Bush in 2008, and affirmed again under President Obama. But those political promises have yet to bear fruit in real life. The system remains overloaded. For the sake of the children and young adults, pediatricians must promote expansion of mental health services.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures or conflicts of interest.
The initial explanation for why the teenager needed to be admitted seemed very flimsy to me. Finally, the office pediatrician came clean. The girl is an honor roll student, high achieving but currently overwhelmed by events in her life. She cannot handle being at home, but there is nowhere else for her to go for the weekend. Come Monday morning, the primary care physician (PCP) has arranged for her acceptance into a local mental health facility where she could get the care she needs. The prognosis was excellent. Her entire future could be markedly improved with just a little help getting through these current troubles. I thought about the patient down the hall. My partner had admitted her 2 days ago for acute-on-chronic abdominal pain, shortly after her third normal CT scan in 6 months. I strongly doubted that that patient had any more business being in a hospital than this latest admission – except, of course, for all the profit the hospital was making on the imaging. On reflection, I decided the PCP’s request no longer seemed so out of place.
The latest emergency department drama on TV has a tagline, “In the ER when there are more patients than resources, it’s called Code Black.” It contains scenes of mopping up bloody floors in the trauma bay. I’ve worked in an ED that was a major portal into a nearby pediatric mental health facility. The major traumas I cared for didn’t bleed from their life-threatening emotional wounds. Multiple times per week, children from across the city were brought in for evaluation. A few needed a toxicology work-up for ingestions. A few more needed some glue or sutures for very superficial self-inflicted forearm lacerations. Mostly I provided a medical screening before getting those teenagers moved as quickly as possible to a team of specialists who could help them. In some parts of this country that can take days.
On Oct. 5, 2015, California’s governor signed a state law permitting physician-assisted suicide. It is now the fifth state allowing that option. The pros and cons have been endlessly debated by ethicists. A brief Google search can find the philosophical arguments. I recommend a June 22, 2015, New Yorker article entitled, “The Death Treatment” by Rachel Aviv to provide a broad narrative perspective. Oregon’s Death With Dignity Act was passed 20 years ago, so it provides some scientific data. There are now 100 deaths per year under that Oregon act. The state also has 700 suicides yearly. So the leading method of suicide in Oregon, by a wide margin, continues to be used by people who are not terminally ill. That was the method of choice recently for my cousin. There was nothing dignified about it. My favorite actor, Robin Williams, in the movie “World’s Greatest Dad,” had the line, “If you’re that depressed, reach out to someone, and remember suicide is a permanent solution to temporary problems.” Five years later he took his own life.
I do enjoy debating the nuances of physician-assisted suicide with other ethicists, but I don’t confuse those academic exercises with addressing the real world problem of endemic suicide. Nationwide, there are 41,000 suicides each year, with about 5,000 in the 15- to 24-year age group. In comparison, 10,000 children annually will get cancer, but only 1,250 children will die of it. There will be about 900 pediatric recipients of lifesaving heart or liver transplants. With all this wealth, knowledge, and technology, the United States should be able to provide better treatment of mental illness. Parity of mental health services became law under President Clinton in 1996, repeated as law under President Bush in 2008, and affirmed again under President Obama. But those political promises have yet to bear fruit in real life. The system remains overloaded. For the sake of the children and young adults, pediatricians must promote expansion of mental health services.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures or conflicts of interest.
The initial explanation for why the teenager needed to be admitted seemed very flimsy to me. Finally, the office pediatrician came clean. The girl is an honor roll student, high achieving but currently overwhelmed by events in her life. She cannot handle being at home, but there is nowhere else for her to go for the weekend. Come Monday morning, the primary care physician (PCP) has arranged for her acceptance into a local mental health facility where she could get the care she needs. The prognosis was excellent. Her entire future could be markedly improved with just a little help getting through these current troubles. I thought about the patient down the hall. My partner had admitted her 2 days ago for acute-on-chronic abdominal pain, shortly after her third normal CT scan in 6 months. I strongly doubted that that patient had any more business being in a hospital than this latest admission – except, of course, for all the profit the hospital was making on the imaging. On reflection, I decided the PCP’s request no longer seemed so out of place.
The latest emergency department drama on TV has a tagline, “In the ER when there are more patients than resources, it’s called Code Black.” It contains scenes of mopping up bloody floors in the trauma bay. I’ve worked in an ED that was a major portal into a nearby pediatric mental health facility. The major traumas I cared for didn’t bleed from their life-threatening emotional wounds. Multiple times per week, children from across the city were brought in for evaluation. A few needed a toxicology work-up for ingestions. A few more needed some glue or sutures for very superficial self-inflicted forearm lacerations. Mostly I provided a medical screening before getting those teenagers moved as quickly as possible to a team of specialists who could help them. In some parts of this country that can take days.
On Oct. 5, 2015, California’s governor signed a state law permitting physician-assisted suicide. It is now the fifth state allowing that option. The pros and cons have been endlessly debated by ethicists. A brief Google search can find the philosophical arguments. I recommend a June 22, 2015, New Yorker article entitled, “The Death Treatment” by Rachel Aviv to provide a broad narrative perspective. Oregon’s Death With Dignity Act was passed 20 years ago, so it provides some scientific data. There are now 100 deaths per year under that Oregon act. The state also has 700 suicides yearly. So the leading method of suicide in Oregon, by a wide margin, continues to be used by people who are not terminally ill. That was the method of choice recently for my cousin. There was nothing dignified about it. My favorite actor, Robin Williams, in the movie “World’s Greatest Dad,” had the line, “If you’re that depressed, reach out to someone, and remember suicide is a permanent solution to temporary problems.” Five years later he took his own life.
I do enjoy debating the nuances of physician-assisted suicide with other ethicists, but I don’t confuse those academic exercises with addressing the real world problem of endemic suicide. Nationwide, there are 41,000 suicides each year, with about 5,000 in the 15- to 24-year age group. In comparison, 10,000 children annually will get cancer, but only 1,250 children will die of it. There will be about 900 pediatric recipients of lifesaving heart or liver transplants. With all this wealth, knowledge, and technology, the United States should be able to provide better treatment of mental illness. Parity of mental health services became law under President Clinton in 1996, repeated as law under President Bush in 2008, and affirmed again under President Obama. But those political promises have yet to bear fruit in real life. The system remains overloaded. For the sake of the children and young adults, pediatricians must promote expansion of mental health services.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures or conflicts of interest.

ADHD treatment – beyond medications
While it is well established that medications can be an important aspect of treatment for youth who meet the criteria for attention-deficit/hyperactivity disorder (ADHD), too often clinicians neglect to address important nonpharmacologic interventions that have increasingly been shown to be effective. This column is devoted to reviewing some of the many components of a treatment plan other than medications that could be utilized to provide a more comprehensive and wellness-informed approach to children who struggle with ADHD symptoms.
Case summary
Ethan is a 7-year-old boy who presents with his parents for an ADHD evaluation. The pediatrician conducts the evaluation according to American Academy of Pediatrics guidelines, which include the use of rating scales from multiple sources. The outcome of the assessment is that Ethan does indeed meet criteria for ADHD and his symptoms are causing impairment in his school work, home environment, and interactions with his peers. Treatment is recommended.
Discussion

It is easy to rely exclusively on medications when the focus of the evaluation is solely about symptoms. When clinicians expand their view to assess various domains of wellness and health promotion, however, several other potential avenues for intervention often become apparent. Asking about sleep routines, nutrition, participation in the arts and music, physical activity, reading, and screen time – among other things – can reveal the following specific areas that require guidance and support:
• Exercise. Children today are increasingly sedentary, and there is increasing evidence that physical activity is inversely related to several ADHD behaviors (J Am Acad Child Adolesc Psychiatry. 2015 Jul;54:565-70). Counsel families about the importance of exercise and try to help the family develop a plan that includes the provision for regular physical activity. Joining sports teams may be particularly useful as it ensures that regular exercise takes place and offers some additional benefits inherent in playing with a team.
• Screen time. Although there has been active discussion lately about what constitutes “too much” screen time, it is clear that many children well exceed even the most liberal thresholds. Furthermore, there is increasing evidence that excessive screen time can lead to worsening attention problems over time (Pediatrics. 2004;113:708-13). One technique that can be effective, especially for younger children, is to have them “earn” their screen time by engaging in other activities such as reading or exercise.
• Nutrition. Apart from any specific deficiency states, research shows that a healthier diet in general is associated with lower levels of behavioral problems. With regard to ADHD, one aspect that is often worth investigating specifically is whether the child gets a nutritious breakfast each morning that can help keep attentional skills optimal.
• Musical training. Some intriguing new research is showing links between brain maturation and musical training, and in some of the very regions of the brain that have been implicated in ADHD (J Am Acad Child Adolesc Psychiatry. 2014;53:1153-61).
• Omega-3s. A meta-analysis demonstrated that omega-3 supplementation can improve ADHD symptoms (J Am Acad Child Adolesc Psychiatry. 2011 Oct;50:991-1000). While the optimal dose remains under investigation, there is some evidence that improved response was related to higher eicosapentaenoic acid doses.
• Skills training. To some degree, many skills associated with ADHD (disorganization, forgetfulness, distractibility) can be specifically taught with techniques such as mindfulness (J Atten Disord. 2015 Feb;19[2]:147-57). Having families work with counselors who have specific training in ADHD can be a very useful part of treatment and can help teach important lifelong skills. Parent behavioral therapy also can be effective around many behaviors such as defiance and aggression that accompany ADHD.
Case follow-up
The pediatrician decides to enhance her assessment by inquiring about many domains of wellness, and she discovers that Ethan has chronic problems getting to sleep, and he spends many hours each day playing video games to the exclusion of physical activity. She offers some strategies to improve these areas while the family investigates working with a counselor who has specific expertise in enhancing cognitive skills. Initial improvements are encouraging, and the family decides to pursue these avenues further while delaying medication treatment, at least for now.
By keeping in mind these important other treatment domains, pediatricians can avoid the trap of overrelying on medications as the sole method of treatment while encouraging techniques that will provide long-term benefits in overall health and wellness.
Dr. Rettew is an associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Dr. Rettew said he has no relevant financial disclosures. Follow him on Twitter @pedipsych. E-mail him at pdnews@frontlinemedcom.com.
While it is well established that medications can be an important aspect of treatment for youth who meet the criteria for attention-deficit/hyperactivity disorder (ADHD), too often clinicians neglect to address important nonpharmacologic interventions that have increasingly been shown to be effective. This column is devoted to reviewing some of the many components of a treatment plan other than medications that could be utilized to provide a more comprehensive and wellness-informed approach to children who struggle with ADHD symptoms.
Case summary
Ethan is a 7-year-old boy who presents with his parents for an ADHD evaluation. The pediatrician conducts the evaluation according to American Academy of Pediatrics guidelines, which include the use of rating scales from multiple sources. The outcome of the assessment is that Ethan does indeed meet criteria for ADHD and his symptoms are causing impairment in his school work, home environment, and interactions with his peers. Treatment is recommended.
Discussion
It is easy to rely exclusively on medications when the focus of the evaluation is solely about symptoms. When clinicians expand their view to assess various domains of wellness and health promotion, however, several other potential avenues for intervention often become apparent. Asking about sleep routines, nutrition, participation in the arts and music, physical activity, reading, and screen time – among other things – can reveal the following specific areas that require guidance and support:
• Exercise. Children today are increasingly sedentary, and there is increasing evidence that physical activity is inversely related to several ADHD behaviors (J Am Acad Child Adolesc Psychiatry. 2015 Jul;54:565-70). Counsel families about the importance of exercise and try to help the family develop a plan that includes the provision for regular physical activity. Joining sports teams may be particularly useful as it ensures that regular exercise takes place and offers some additional benefits inherent in playing with a team.
• Screen time. Although there has been active discussion lately about what constitutes “too much” screen time, it is clear that many children well exceed even the most liberal thresholds. Furthermore, there is increasing evidence that excessive screen time can lead to worsening attention problems over time (Pediatrics. 2004;113:708-13). One technique that can be effective, especially for younger children, is to have them “earn” their screen time by engaging in other activities such as reading or exercise.
• Nutrition. Apart from any specific deficiency states, research shows that a healthier diet in general is associated with lower levels of behavioral problems. With regard to ADHD, one aspect that is often worth investigating specifically is whether the child gets a nutritious breakfast each morning that can help keep attentional skills optimal.
• Musical training. Some intriguing new research is showing links between brain maturation and musical training, and in some of the very regions of the brain that have been implicated in ADHD (J Am Acad Child Adolesc Psychiatry. 2014;53:1153-61).
• Omega-3s. A meta-analysis demonstrated that omega-3 supplementation can improve ADHD symptoms (J Am Acad Child Adolesc Psychiatry. 2011 Oct;50:991-1000). While the optimal dose remains under investigation, there is some evidence that improved response was related to higher eicosapentaenoic acid doses.
• Skills training. To some degree, many skills associated with ADHD (disorganization, forgetfulness, distractibility) can be specifically taught with techniques such as mindfulness (J Atten Disord. 2015 Feb;19[2]:147-57). Having families work with counselors who have specific training in ADHD can be a very useful part of treatment and can help teach important lifelong skills. Parent behavioral therapy also can be effective around many behaviors such as defiance and aggression that accompany ADHD.
Case follow-up
The pediatrician decides to enhance her assessment by inquiring about many domains of wellness, and she discovers that Ethan has chronic problems getting to sleep, and he spends many hours each day playing video games to the exclusion of physical activity. She offers some strategies to improve these areas while the family investigates working with a counselor who has specific expertise in enhancing cognitive skills. Initial improvements are encouraging, and the family decides to pursue these avenues further while delaying medication treatment, at least for now.
By keeping in mind these important other treatment domains, pediatricians can avoid the trap of overrelying on medications as the sole method of treatment while encouraging techniques that will provide long-term benefits in overall health and wellness.
Dr. Rettew is an associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Dr. Rettew said he has no relevant financial disclosures. Follow him on Twitter @pedipsych. E-mail him at pdnews@frontlinemedcom.com.
While it is well established that medications can be an important aspect of treatment for youth who meet the criteria for attention-deficit/hyperactivity disorder (ADHD), too often clinicians neglect to address important nonpharmacologic interventions that have increasingly been shown to be effective. This column is devoted to reviewing some of the many components of a treatment plan other than medications that could be utilized to provide a more comprehensive and wellness-informed approach to children who struggle with ADHD symptoms.
Case summary
Ethan is a 7-year-old boy who presents with his parents for an ADHD evaluation. The pediatrician conducts the evaluation according to American Academy of Pediatrics guidelines, which include the use of rating scales from multiple sources. The outcome of the assessment is that Ethan does indeed meet criteria for ADHD and his symptoms are causing impairment in his school work, home environment, and interactions with his peers. Treatment is recommended.
Discussion
It is easy to rely exclusively on medications when the focus of the evaluation is solely about symptoms. When clinicians expand their view to assess various domains of wellness and health promotion, however, several other potential avenues for intervention often become apparent. Asking about sleep routines, nutrition, participation in the arts and music, physical activity, reading, and screen time – among other things – can reveal the following specific areas that require guidance and support:
• Exercise. Children today are increasingly sedentary, and there is increasing evidence that physical activity is inversely related to several ADHD behaviors (J Am Acad Child Adolesc Psychiatry. 2015 Jul;54:565-70). Counsel families about the importance of exercise and try to help the family develop a plan that includes the provision for regular physical activity. Joining sports teams may be particularly useful as it ensures that regular exercise takes place and offers some additional benefits inherent in playing with a team.
• Screen time. Although there has been active discussion lately about what constitutes “too much” screen time, it is clear that many children well exceed even the most liberal thresholds. Furthermore, there is increasing evidence that excessive screen time can lead to worsening attention problems over time (Pediatrics. 2004;113:708-13). One technique that can be effective, especially for younger children, is to have them “earn” their screen time by engaging in other activities such as reading or exercise.
• Nutrition. Apart from any specific deficiency states, research shows that a healthier diet in general is associated with lower levels of behavioral problems. With regard to ADHD, one aspect that is often worth investigating specifically is whether the child gets a nutritious breakfast each morning that can help keep attentional skills optimal.
• Musical training. Some intriguing new research is showing links between brain maturation and musical training, and in some of the very regions of the brain that have been implicated in ADHD (J Am Acad Child Adolesc Psychiatry. 2014;53:1153-61).
• Omega-3s. A meta-analysis demonstrated that omega-3 supplementation can improve ADHD symptoms (J Am Acad Child Adolesc Psychiatry. 2011 Oct;50:991-1000). While the optimal dose remains under investigation, there is some evidence that improved response was related to higher eicosapentaenoic acid doses.
• Skills training. To some degree, many skills associated with ADHD (disorganization, forgetfulness, distractibility) can be specifically taught with techniques such as mindfulness (J Atten Disord. 2015 Feb;19[2]:147-57). Having families work with counselors who have specific training in ADHD can be a very useful part of treatment and can help teach important lifelong skills. Parent behavioral therapy also can be effective around many behaviors such as defiance and aggression that accompany ADHD.
Case follow-up
The pediatrician decides to enhance her assessment by inquiring about many domains of wellness, and she discovers that Ethan has chronic problems getting to sleep, and he spends many hours each day playing video games to the exclusion of physical activity. She offers some strategies to improve these areas while the family investigates working with a counselor who has specific expertise in enhancing cognitive skills. Initial improvements are encouraging, and the family decides to pursue these avenues further while delaying medication treatment, at least for now.
By keeping in mind these important other treatment domains, pediatricians can avoid the trap of overrelying on medications as the sole method of treatment while encouraging techniques that will provide long-term benefits in overall health and wellness.
Dr. Rettew is an associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Dr. Rettew said he has no relevant financial disclosures. Follow him on Twitter @pedipsych. E-mail him at pdnews@frontlinemedcom.com.

Lessons learned from the history of VBAC
In December 2014, The Wall Street Journal ran an article about a young mother who wanted a vaginal birth after C-section (VBAC) for her second child. After her hospital stopped offering VBACs, the woman had to find another place to deliver. She did have a successful VBAC, but her story is not unique – many women may not receive adequate consultations about or provider support for VBAC as a delivery option.
According to the article, a lack of clinical support was the reason the hospital discontinued VBACs. Although the hospital’s decision may have frustrated the mother, this ensured that she would not be promised a birthing option that the hospital could not deliver – in all senses of this word. Successful VBAC requires proper patient selection, appropriate consent and adequate provisions in case of emergencies.

Not every hospital has made such a choice. Based on studies of a trial of labor after cesarean, conducted after the 1960s, the rate of VBACs increased. As VBACs became more common, the approach to the procedure became more relaxed. VBACs went from only being performed in tertiary care hospitals with appropriate support for emergencies, to community hospitals with no backup. Patient selection became less rigorous, and the rate of complications went up, which, in turn, caused the number of associated legal claims to rise. Hospitals started discouraging VBACs, and ob.gyns. no longer counseled their patients about this option. The VBAC rate decreased, and the C-section rate increased.
Today, many women want to pursue a trial of labor after cesarean. Data from large clinical studies have demonstrated the safety and success of VBAC with proper care. Because of the storied history and a revival of interest in VBACs, we have invited Dr. Mark Landon, the Richard L. Meiling Professor and chairman of the department of obstetrics and gynecology at the Ohio State University, and the lead on one of the recent seminal VBAC studies, to address this topic.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece reported having no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
In December 2014, The Wall Street Journal ran an article about a young mother who wanted a vaginal birth after C-section (VBAC) for her second child. After her hospital stopped offering VBACs, the woman had to find another place to deliver. She did have a successful VBAC, but her story is not unique – many women may not receive adequate consultations about or provider support for VBAC as a delivery option.
According to the article, a lack of clinical support was the reason the hospital discontinued VBACs. Although the hospital’s decision may have frustrated the mother, this ensured that she would not be promised a birthing option that the hospital could not deliver – in all senses of this word. Successful VBAC requires proper patient selection, appropriate consent and adequate provisions in case of emergencies.
Not every hospital has made such a choice. Based on studies of a trial of labor after cesarean, conducted after the 1960s, the rate of VBACs increased. As VBACs became more common, the approach to the procedure became more relaxed. VBACs went from only being performed in tertiary care hospitals with appropriate support for emergencies, to community hospitals with no backup. Patient selection became less rigorous, and the rate of complications went up, which, in turn, caused the number of associated legal claims to rise. Hospitals started discouraging VBACs, and ob.gyns. no longer counseled their patients about this option. The VBAC rate decreased, and the C-section rate increased.
Today, many women want to pursue a trial of labor after cesarean. Data from large clinical studies have demonstrated the safety and success of VBAC with proper care. Because of the storied history and a revival of interest in VBACs, we have invited Dr. Mark Landon, the Richard L. Meiling Professor and chairman of the department of obstetrics and gynecology at the Ohio State University, and the lead on one of the recent seminal VBAC studies, to address this topic.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece reported having no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
In December 2014, The Wall Street Journal ran an article about a young mother who wanted a vaginal birth after C-section (VBAC) for her second child. After her hospital stopped offering VBACs, the woman had to find another place to deliver. She did have a successful VBAC, but her story is not unique – many women may not receive adequate consultations about or provider support for VBAC as a delivery option.
According to the article, a lack of clinical support was the reason the hospital discontinued VBACs. Although the hospital’s decision may have frustrated the mother, this ensured that she would not be promised a birthing option that the hospital could not deliver – in all senses of this word. Successful VBAC requires proper patient selection, appropriate consent and adequate provisions in case of emergencies.
Not every hospital has made such a choice. Based on studies of a trial of labor after cesarean, conducted after the 1960s, the rate of VBACs increased. As VBACs became more common, the approach to the procedure became more relaxed. VBACs went from only being performed in tertiary care hospitals with appropriate support for emergencies, to community hospitals with no backup. Patient selection became less rigorous, and the rate of complications went up, which, in turn, caused the number of associated legal claims to rise. Hospitals started discouraging VBACs, and ob.gyns. no longer counseled their patients about this option. The VBAC rate decreased, and the C-section rate increased.
Today, many women want to pursue a trial of labor after cesarean. Data from large clinical studies have demonstrated the safety and success of VBAC with proper care. Because of the storied history and a revival of interest in VBACs, we have invited Dr. Mark Landon, the Richard L. Meiling Professor and chairman of the department of obstetrics and gynecology at the Ohio State University, and the lead on one of the recent seminal VBAC studies, to address this topic.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece reported having no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.

Barriers to VBAC remain in spite of evidence
The relative safety of vaginal birth after cesarean (VBAC) has been documented in several large-scale studies in the past 15 years, and was affirmed in 2010 through a National Institutes of Health consensus development conference and a practice bulletin from the American College of Obstetricians and Gynecologists. Yet, despite all this research and review, rates of a trial of labor after cesarean (TOLAC) have increased only modestly in the last several years.
Approximately 20% of all births in 2013 in women with a history of one cesarean section involved a trial of labor, according to a recent report from the Centers for Disease Control and Prevention. This represents only a small increase from 2006, when the TOLAC rate had plummeted to approximately 15%.
The limited change is concerning because up to two-thirds of women with a prior cesarean delivery are candidates for a trial of labor, and many of them are excellent candidates. In total, 70% of the women who attempted labor in 2013 after a previous cesarean had successful VBACs, the CDC data shows.

Several European countries have TOLAC rates between 50% and 70%, but in the United States, as evidenced by the recent CDC data, there continues to be an underutilization of attempted VBAC. We must ask ourselves, are women truly able to choose TOLAC, or are they being dissuaded by the health care system?
I believe that the barriers are still pervasive. Too often, women who are TOLAC candidates are not receiving appropriate counseling – and too often, women are not even being presented the option of a trial of labor, even when staff are immediately available to provide emergency care if needed.
Rupture concerns in perspective
When the NIH consensus development panel reviewed VBAC in 2010, it concluded that TOLAC is a reasonable option for many women with a prior cesarean. The panel found that restricted access to VBAC/TOLAC stemmed from existing practice guidelines and the medical liability climate, and it called upon providers and others to “mitigate or even eliminate” the barriers that women face in finding clinicians and facilities able and willing to offer TOLAC.
ACOG’s 2010 practice bulletin also acknowledged the problem of limited access. ACOG recommended, as it had in an earlier bulletin, that TOLAC-VBAC be undertaken in facilities where staff are immediately available for emergency care. It added, however, that when such resources are not available, the best alternative may be to refer patients to a facility with available resources. Health care providers and insurance carriers “should do all they can to facilitate transfer of care or comanagement in support of a desired TOLAC,” ACOG’s document states.
Why, given such recommendations, are we still falling so short of where we should be?
A number of nonclinical factors are involved, but clearly, as both the NIH and ACOG have stated, the fear of litigation in cases of uterine rupture is a contributing factor. A ruptured uterus is indeed the principal risk associated with TOLAC, and it can have serious sequelae including perinatal death, hypoxic ischemic encephalopathy (HIE), and hysterectomy.
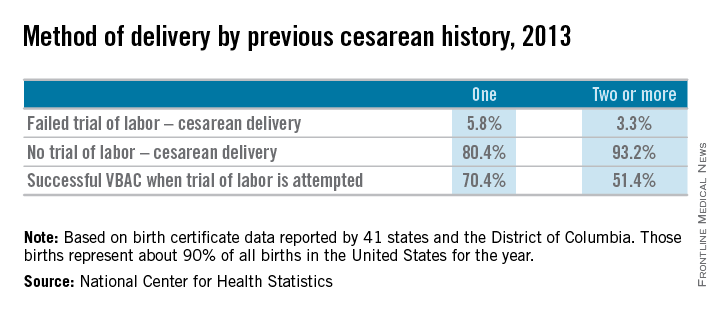
We must appreciate, however, that the absolute rates of uterine rupture and of serious adverse outcomes are quite low. The rupture rate in 2013 among women who underwent TOLAC but ultimately had a repeat cesarean section – the highest-risk group – was 495 per 100,000 live births, according to the CDC. This rate of approximately 0.5% is consistent with the level of risk reported in the literature for several decades.
In one of the two large observational studies done in the United States that have shed light on TOLAC outcomes, the rate of uterine rupture among women who underwent TOLAC was 0.7% for women with a prior low transverse incision, 2.0% for those with a prior low vertical incision, and 0.5% for those with an unknown type of prior incision. Overall, the rate of uterine rupture in this study’s cohort of 17,898 women who underwent TOLAC was 0.7% (N Engl J Med. 2004 Dec 16;351[25]:2581-9). The study was conducted at 19 medical centers belonging to the Eunice Kennedy Shriver National Institute of Child Health and Human Development’s Maternal-Fetal Medical Units (MFMU) Network.
The second large study conducted in the United States – a multicenter observational study in which records of approximately 25,000 women with a prior low-transverse cesarean section were reviewed – also showed rates of uterine rupture less than 1% (Am J Obstet Gynecol. 2005 Nov;193[5]:1656-62).
The attributable risk for perinatal death or HIE at term appears to be 1 per 2,000 TOLAC, according to the MFMU Network study.
Failed trials of labor resulting in repeat cesarean deliveries have consistently been associated with higher morbidity than scheduled repeat cesarean deliveries, with the greatest difference in rates for ruptured uterus. In the first MFMU Network study, there were no cases of uterine rupture among a cohort of 15,801 women who underwent elective repeat cesarean delivery, and in the second multicenter study of 25,000 women, this patient group had a rupture rate of 0.004%.
Yet, as ACOG points out, neither elective repeat cesarean deliveries nor TOLAC are without maternal or neonatal risk. Women who have successful VBAC delivery, on the other hand, have significantly lower morbidity and better outcomes than women who do not attempt labor. Women who undergo VBAC also avoid exposure to the significant risks of repeat cesarean deliveries in the long term.
Research unequivocally shows that the risk of placenta accreta, hysterectomy, hemorrhage, and other serious maternal morbidity increases progressively with each repeat cesarean delivery. Rates of placenta accreta have, in fact, been rising in the United States – a trend that should prompt us to think more about TOLAC.
Moreover, TOLAC is being shown to be a cost-effective strategy. In one analysis, TOLAC in a second pregnancy was cost-effective as long as the chance of VBAC exceeded approximately 74% (Obstet Gynecol. 2001 Jun;97[6]:932-41). More recently, TOLAC was found to be cost-effective across a wide variety of circumstances, including when a woman had a probability of VBAC as low as 43%. The model in this analysis, which used probability estimates from the MFMU Cesarean Registry, took a longer-term view by including probabilities of outcomes throughout a woman’s reproductive life that were contingent upon her initial choice regarding TOLAC (Am J Perinatol. 2013 Jan;30[1]:11-20).
Likelihood of success
Evaluating and discussing the likelihood of success with TOLAC is therefore key to the counseling process. The higher the likelihood of achieving VBAC, the more favorable the risk-benefit ratio will be and the more appealing it will be to consider.
According to one analysis, if a woman undergoing a TOLAC has at least a 60%-70% chance of VBAC, her chance of having major or minor morbidity is no greater than a woman undergoing a planned repeat cesarean delivery (Am J Obstet Gynecol 2009;200:56.e1-e6).
There are several prediction tools available that can be used at the first prenatal visit and in early labor to give a reasonably good estimate of success. One of these tools is available at the MFMU Network website (http://mfmu.bsc.gwu.edu). The tools take into account factors such as prior indication for cesarean delivery; history of vaginal delivery; demographic characteristics such as maternal age and body mass index; the occurrence of spontaneous labor; and cervical status at admission.
Prior vaginal delivery is one of the strongest predictors of a successful TOLAC. Research has consistently shown that women with a prior vaginal delivery – including a vaginal delivery predating an unsuccessful TOLAC – have significantly higher TOLAC success rates than women who did not have any prior vaginal delivery.
The indication for a prior cesarean delivery also clearly affects the likelihood of a successful TOLAC. Women whose first cesarean delivery was performed for a nonrecurring indication, such as breech presentation or low intolerance of labor, have TOLAC success rates that are similar to vaginal delivery rates for nulliparous women. Success rates for these women may exceed 85%. On the other hand, women who had a prior cesarean delivery for cephalopelvic disproportion or failure to progress have been shown to have lower TOLAC success rates ranging from 50%-67%.
Labor induction should be approached cautiously, as women who undergo induction of labor in TOLAC have an increased risk of repeat cesarean delivery. Still, success rates with induction are high. Data from the MFMU Cesarean Registry showed that about 66% of women undergoing induction after one prior cesarean delivery achieved VBAC versus 76% of women entering TOLAC spontaneously (Obstet Gynecol. 2007 Feb;109[2 Pt 1]:262-9). Another study of women undergoing induction after one prior cesarean reported an overall success rate of 78% (Obstet Gynecol. 2004 Mar;103[3]:534-8).
Whether induction specifically increases the risk for uterine rupture in TOLAC, compared with expectant management, is unclear. There also are conflicting data as to whether particular induction methods increase this risk.
Based on available data, ACOG considers induction of labor for either maternal or fetal indications to be an option for women undergoing TOLAC. Oxytocin may be used for induction as well as augmentation, but caution should be exercised at higher doses. While there is no clear dosing threshold for increased risk of rupture, research has suggested that higher doses of oxytocin are best avoided.
The use of prostaglandins is more controversial: Based on evidence from several small studies, ACOG concluded in its 2010 bulletin that misoprostol (prostaglandin E1) for cervical ripening is contraindicated in women undergoing TOLAC. It appears likely that rupture risk increases in patients who received both prostaglandins and oxytocin, so ACOG has advised avoiding their sequential use when prostaglandin E2 is used. This of course limits the options for the practitioner. Therefore, utilizing a Foley catheter followed by pitocin has been an approach advocated in some cases.
Uterine rupture is not predictable, and it is far more difficult to assess an individual’s risk of this complication than it is to assess the likelihood of VBAC. Still, there is value to discussing with the patient whether there are any other modifiers that could potentially influence the risk of rupture.
Since rates of uterine rupture are highest in women with previous classical or T-shaped incision, for example, it is important to try to ascertain what type of incision was previously used. It is widely appreciated that low-transverse uterine incisions are most favorable, but findings are mixed in regard to low-vertical incisions. Some research shows that women with a previous low-vertical incision do not have significantly lower VBAC success rates or higher risks of uterine rupture. TOLAC should therefore not be ruled out in these cases.
Additionally, TOLAC should not be ruled out for women who have had more than one cesarean delivery. Several studies have shown an increased risk of uterine rupture after two prior cesarean deliveries, compared with one, and one meta-analysis suggested a more than twofold increased risk (BJOG. 2010 Jan;117(1):5-19.).
In contrast, an analysis of the MFMU Cesarean Registry found no significant difference in rupture rates in women with one prior cesarean versus multiple prior cesareans (Obstet Gynecol. 2006 Jul;108[1]:12-20.).
It appears, therefore, that even if having more than one prior cesarean section is associated with an increased risk of rupture, the magnitude of this increase is small.
Just as women with a prior vaginal delivery have the highest chance of VBAC success, they also have the lowest rates of rupture among all women undergoing TOLAC.
Patient counseling
We must inform our patients who have had a cesarean section in the past of their options for childbirth in an unbiased manner.
The complications of both TOLAC and elective repeat cesarean section should be discussed, and every attempt should be made to individually assess both the likelihood of a successful VBAC and the comparative risk of maternal and perinatal morbidity. A shared decision-making process should be adopted, and whenever possible, the patient’s preference should be respected. In the end, a woman undergoing TOLAC should be truly motivated to pursue a trial of labor, because there are inherent risks.
One thing I’ve learned from my clinical practice and research on this issue is that the desire to undergo a vaginal delivery is powerful for some women. Many of my patients have self-referred for consultation about TOLAC after their ob.gyn. informed them that their hospital is not equipped, and they should therefore have a scheduled repeat operation. In many cases they discover that TOLAC is an option if they are willing to travel a half-hour or so.
We need to honor this desire and inform our patients of the option, and help facilitate delivery at another nearby hospital when our own facility is not equipped for TOLAC.
Dr. Landon is the Richard L. Meiling Professor and chairman of the department of obstetrics and gynecology at the Ohio State University, Columbus. He served for more than 25 years as Ohio State’s coinvestigator for the National Institutes of Child Health and Human Development Maternal Fetal Medicine Units Network. He reported having no relevant financial disclosures.
The relative safety of vaginal birth after cesarean (VBAC) has been documented in several large-scale studies in the past 15 years, and was affirmed in 2010 through a National Institutes of Health consensus development conference and a practice bulletin from the American College of Obstetricians and Gynecologists. Yet, despite all this research and review, rates of a trial of labor after cesarean (TOLAC) have increased only modestly in the last several years.
Approximately 20% of all births in 2013 in women with a history of one cesarean section involved a trial of labor, according to a recent report from the Centers for Disease Control and Prevention. This represents only a small increase from 2006, when the TOLAC rate had plummeted to approximately 15%.
The limited change is concerning because up to two-thirds of women with a prior cesarean delivery are candidates for a trial of labor, and many of them are excellent candidates. In total, 70% of the women who attempted labor in 2013 after a previous cesarean had successful VBACs, the CDC data shows.
Several European countries have TOLAC rates between 50% and 70%, but in the United States, as evidenced by the recent CDC data, there continues to be an underutilization of attempted VBAC. We must ask ourselves, are women truly able to choose TOLAC, or are they being dissuaded by the health care system?
I believe that the barriers are still pervasive. Too often, women who are TOLAC candidates are not receiving appropriate counseling – and too often, women are not even being presented the option of a trial of labor, even when staff are immediately available to provide emergency care if needed.
Rupture concerns in perspective
When the NIH consensus development panel reviewed VBAC in 2010, it concluded that TOLAC is a reasonable option for many women with a prior cesarean. The panel found that restricted access to VBAC/TOLAC stemmed from existing practice guidelines and the medical liability climate, and it called upon providers and others to “mitigate or even eliminate” the barriers that women face in finding clinicians and facilities able and willing to offer TOLAC.
ACOG’s 2010 practice bulletin also acknowledged the problem of limited access. ACOG recommended, as it had in an earlier bulletin, that TOLAC-VBAC be undertaken in facilities where staff are immediately available for emergency care. It added, however, that when such resources are not available, the best alternative may be to refer patients to a facility with available resources. Health care providers and insurance carriers “should do all they can to facilitate transfer of care or comanagement in support of a desired TOLAC,” ACOG’s document states.
Why, given such recommendations, are we still falling so short of where we should be?
A number of nonclinical factors are involved, but clearly, as both the NIH and ACOG have stated, the fear of litigation in cases of uterine rupture is a contributing factor. A ruptured uterus is indeed the principal risk associated with TOLAC, and it can have serious sequelae including perinatal death, hypoxic ischemic encephalopathy (HIE), and hysterectomy.
We must appreciate, however, that the absolute rates of uterine rupture and of serious adverse outcomes are quite low. The rupture rate in 2013 among women who underwent TOLAC but ultimately had a repeat cesarean section – the highest-risk group – was 495 per 100,000 live births, according to the CDC. This rate of approximately 0.5% is consistent with the level of risk reported in the literature for several decades.
In one of the two large observational studies done in the United States that have shed light on TOLAC outcomes, the rate of uterine rupture among women who underwent TOLAC was 0.7% for women with a prior low transverse incision, 2.0% for those with a prior low vertical incision, and 0.5% for those with an unknown type of prior incision. Overall, the rate of uterine rupture in this study’s cohort of 17,898 women who underwent TOLAC was 0.7% (N Engl J Med. 2004 Dec 16;351[25]:2581-9). The study was conducted at 19 medical centers belonging to the Eunice Kennedy Shriver National Institute of Child Health and Human Development’s Maternal-Fetal Medical Units (MFMU) Network.
The second large study conducted in the United States – a multicenter observational study in which records of approximately 25,000 women with a prior low-transverse cesarean section were reviewed – also showed rates of uterine rupture less than 1% (Am J Obstet Gynecol. 2005 Nov;193[5]:1656-62).
The attributable risk for perinatal death or HIE at term appears to be 1 per 2,000 TOLAC, according to the MFMU Network study.
Failed trials of labor resulting in repeat cesarean deliveries have consistently been associated with higher morbidity than scheduled repeat cesarean deliveries, with the greatest difference in rates for ruptured uterus. In the first MFMU Network study, there were no cases of uterine rupture among a cohort of 15,801 women who underwent elective repeat cesarean delivery, and in the second multicenter study of 25,000 women, this patient group had a rupture rate of 0.004%.
Yet, as ACOG points out, neither elective repeat cesarean deliveries nor TOLAC are without maternal or neonatal risk. Women who have successful VBAC delivery, on the other hand, have significantly lower morbidity and better outcomes than women who do not attempt labor. Women who undergo VBAC also avoid exposure to the significant risks of repeat cesarean deliveries in the long term.
Research unequivocally shows that the risk of placenta accreta, hysterectomy, hemorrhage, and other serious maternal morbidity increases progressively with each repeat cesarean delivery. Rates of placenta accreta have, in fact, been rising in the United States – a trend that should prompt us to think more about TOLAC.
Moreover, TOLAC is being shown to be a cost-effective strategy. In one analysis, TOLAC in a second pregnancy was cost-effective as long as the chance of VBAC exceeded approximately 74% (Obstet Gynecol. 2001 Jun;97[6]:932-41). More recently, TOLAC was found to be cost-effective across a wide variety of circumstances, including when a woman had a probability of VBAC as low as 43%. The model in this analysis, which used probability estimates from the MFMU Cesarean Registry, took a longer-term view by including probabilities of outcomes throughout a woman’s reproductive life that were contingent upon her initial choice regarding TOLAC (Am J Perinatol. 2013 Jan;30[1]:11-20).
Likelihood of success
Evaluating and discussing the likelihood of success with TOLAC is therefore key to the counseling process. The higher the likelihood of achieving VBAC, the more favorable the risk-benefit ratio will be and the more appealing it will be to consider.
According to one analysis, if a woman undergoing a TOLAC has at least a 60%-70% chance of VBAC, her chance of having major or minor morbidity is no greater than a woman undergoing a planned repeat cesarean delivery (Am J Obstet Gynecol 2009;200:56.e1-e6).
There are several prediction tools available that can be used at the first prenatal visit and in early labor to give a reasonably good estimate of success. One of these tools is available at the MFMU Network website (http://mfmu.bsc.gwu.edu). The tools take into account factors such as prior indication for cesarean delivery; history of vaginal delivery; demographic characteristics such as maternal age and body mass index; the occurrence of spontaneous labor; and cervical status at admission.
Prior vaginal delivery is one of the strongest predictors of a successful TOLAC. Research has consistently shown that women with a prior vaginal delivery – including a vaginal delivery predating an unsuccessful TOLAC – have significantly higher TOLAC success rates than women who did not have any prior vaginal delivery.
The indication for a prior cesarean delivery also clearly affects the likelihood of a successful TOLAC. Women whose first cesarean delivery was performed for a nonrecurring indication, such as breech presentation or low intolerance of labor, have TOLAC success rates that are similar to vaginal delivery rates for nulliparous women. Success rates for these women may exceed 85%. On the other hand, women who had a prior cesarean delivery for cephalopelvic disproportion or failure to progress have been shown to have lower TOLAC success rates ranging from 50%-67%.
Labor induction should be approached cautiously, as women who undergo induction of labor in TOLAC have an increased risk of repeat cesarean delivery. Still, success rates with induction are high. Data from the MFMU Cesarean Registry showed that about 66% of women undergoing induction after one prior cesarean delivery achieved VBAC versus 76% of women entering TOLAC spontaneously (Obstet Gynecol. 2007 Feb;109[2 Pt 1]:262-9). Another study of women undergoing induction after one prior cesarean reported an overall success rate of 78% (Obstet Gynecol. 2004 Mar;103[3]:534-8).
Whether induction specifically increases the risk for uterine rupture in TOLAC, compared with expectant management, is unclear. There also are conflicting data as to whether particular induction methods increase this risk.
Based on available data, ACOG considers induction of labor for either maternal or fetal indications to be an option for women undergoing TOLAC. Oxytocin may be used for induction as well as augmentation, but caution should be exercised at higher doses. While there is no clear dosing threshold for increased risk of rupture, research has suggested that higher doses of oxytocin are best avoided.
The use of prostaglandins is more controversial: Based on evidence from several small studies, ACOG concluded in its 2010 bulletin that misoprostol (prostaglandin E1) for cervical ripening is contraindicated in women undergoing TOLAC. It appears likely that rupture risk increases in patients who received both prostaglandins and oxytocin, so ACOG has advised avoiding their sequential use when prostaglandin E2 is used. This of course limits the options for the practitioner. Therefore, utilizing a Foley catheter followed by pitocin has been an approach advocated in some cases.
Uterine rupture is not predictable, and it is far more difficult to assess an individual’s risk of this complication than it is to assess the likelihood of VBAC. Still, there is value to discussing with the patient whether there are any other modifiers that could potentially influence the risk of rupture.
Since rates of uterine rupture are highest in women with previous classical or T-shaped incision, for example, it is important to try to ascertain what type of incision was previously used. It is widely appreciated that low-transverse uterine incisions are most favorable, but findings are mixed in regard to low-vertical incisions. Some research shows that women with a previous low-vertical incision do not have significantly lower VBAC success rates or higher risks of uterine rupture. TOLAC should therefore not be ruled out in these cases.
Additionally, TOLAC should not be ruled out for women who have had more than one cesarean delivery. Several studies have shown an increased risk of uterine rupture after two prior cesarean deliveries, compared with one, and one meta-analysis suggested a more than twofold increased risk (BJOG. 2010 Jan;117(1):5-19.).
In contrast, an analysis of the MFMU Cesarean Registry found no significant difference in rupture rates in women with one prior cesarean versus multiple prior cesareans (Obstet Gynecol. 2006 Jul;108[1]:12-20.).
It appears, therefore, that even if having more than one prior cesarean section is associated with an increased risk of rupture, the magnitude of this increase is small.
Just as women with a prior vaginal delivery have the highest chance of VBAC success, they also have the lowest rates of rupture among all women undergoing TOLAC.
Patient counseling
We must inform our patients who have had a cesarean section in the past of their options for childbirth in an unbiased manner.
The complications of both TOLAC and elective repeat cesarean section should be discussed, and every attempt should be made to individually assess both the likelihood of a successful VBAC and the comparative risk of maternal and perinatal morbidity. A shared decision-making process should be adopted, and whenever possible, the patient’s preference should be respected. In the end, a woman undergoing TOLAC should be truly motivated to pursue a trial of labor, because there are inherent risks.
One thing I’ve learned from my clinical practice and research on this issue is that the desire to undergo a vaginal delivery is powerful for some women. Many of my patients have self-referred for consultation about TOLAC after their ob.gyn. informed them that their hospital is not equipped, and they should therefore have a scheduled repeat operation. In many cases they discover that TOLAC is an option if they are willing to travel a half-hour or so.
We need to honor this desire and inform our patients of the option, and help facilitate delivery at another nearby hospital when our own facility is not equipped for TOLAC.
Dr. Landon is the Richard L. Meiling Professor and chairman of the department of obstetrics and gynecology at the Ohio State University, Columbus. He served for more than 25 years as Ohio State’s coinvestigator for the National Institutes of Child Health and Human Development Maternal Fetal Medicine Units Network. He reported having no relevant financial disclosures.
The relative safety of vaginal birth after cesarean (VBAC) has been documented in several large-scale studies in the past 15 years, and was affirmed in 2010 through a National Institutes of Health consensus development conference and a practice bulletin from the American College of Obstetricians and Gynecologists. Yet, despite all this research and review, rates of a trial of labor after cesarean (TOLAC) have increased only modestly in the last several years.
Approximately 20% of all births in 2013 in women with a history of one cesarean section involved a trial of labor, according to a recent report from the Centers for Disease Control and Prevention. This represents only a small increase from 2006, when the TOLAC rate had plummeted to approximately 15%.
The limited change is concerning because up to two-thirds of women with a prior cesarean delivery are candidates for a trial of labor, and many of them are excellent candidates. In total, 70% of the women who attempted labor in 2013 after a previous cesarean had successful VBACs, the CDC data shows.
Several European countries have TOLAC rates between 50% and 70%, but in the United States, as evidenced by the recent CDC data, there continues to be an underutilization of attempted VBAC. We must ask ourselves, are women truly able to choose TOLAC, or are they being dissuaded by the health care system?
I believe that the barriers are still pervasive. Too often, women who are TOLAC candidates are not receiving appropriate counseling – and too often, women are not even being presented the option of a trial of labor, even when staff are immediately available to provide emergency care if needed.
Rupture concerns in perspective
When the NIH consensus development panel reviewed VBAC in 2010, it concluded that TOLAC is a reasonable option for many women with a prior cesarean. The panel found that restricted access to VBAC/TOLAC stemmed from existing practice guidelines and the medical liability climate, and it called upon providers and others to “mitigate or even eliminate” the barriers that women face in finding clinicians and facilities able and willing to offer TOLAC.
ACOG’s 2010 practice bulletin also acknowledged the problem of limited access. ACOG recommended, as it had in an earlier bulletin, that TOLAC-VBAC be undertaken in facilities where staff are immediately available for emergency care. It added, however, that when such resources are not available, the best alternative may be to refer patients to a facility with available resources. Health care providers and insurance carriers “should do all they can to facilitate transfer of care or comanagement in support of a desired TOLAC,” ACOG’s document states.
Why, given such recommendations, are we still falling so short of where we should be?
A number of nonclinical factors are involved, but clearly, as both the NIH and ACOG have stated, the fear of litigation in cases of uterine rupture is a contributing factor. A ruptured uterus is indeed the principal risk associated with TOLAC, and it can have serious sequelae including perinatal death, hypoxic ischemic encephalopathy (HIE), and hysterectomy.
We must appreciate, however, that the absolute rates of uterine rupture and of serious adverse outcomes are quite low. The rupture rate in 2013 among women who underwent TOLAC but ultimately had a repeat cesarean section – the highest-risk group – was 495 per 100,000 live births, according to the CDC. This rate of approximately 0.5% is consistent with the level of risk reported in the literature for several decades.
In one of the two large observational studies done in the United States that have shed light on TOLAC outcomes, the rate of uterine rupture among women who underwent TOLAC was 0.7% for women with a prior low transverse incision, 2.0% for those with a prior low vertical incision, and 0.5% for those with an unknown type of prior incision. Overall, the rate of uterine rupture in this study’s cohort of 17,898 women who underwent TOLAC was 0.7% (N Engl J Med. 2004 Dec 16;351[25]:2581-9). The study was conducted at 19 medical centers belonging to the Eunice Kennedy Shriver National Institute of Child Health and Human Development’s Maternal-Fetal Medical Units (MFMU) Network.
The second large study conducted in the United States – a multicenter observational study in which records of approximately 25,000 women with a prior low-transverse cesarean section were reviewed – also showed rates of uterine rupture less than 1% (Am J Obstet Gynecol. 2005 Nov;193[5]:1656-62).
The attributable risk for perinatal death or HIE at term appears to be 1 per 2,000 TOLAC, according to the MFMU Network study.
Failed trials of labor resulting in repeat cesarean deliveries have consistently been associated with higher morbidity than scheduled repeat cesarean deliveries, with the greatest difference in rates for ruptured uterus. In the first MFMU Network study, there were no cases of uterine rupture among a cohort of 15,801 women who underwent elective repeat cesarean delivery, and in the second multicenter study of 25,000 women, this patient group had a rupture rate of 0.004%.
Yet, as ACOG points out, neither elective repeat cesarean deliveries nor TOLAC are without maternal or neonatal risk. Women who have successful VBAC delivery, on the other hand, have significantly lower morbidity and better outcomes than women who do not attempt labor. Women who undergo VBAC also avoid exposure to the significant risks of repeat cesarean deliveries in the long term.
Research unequivocally shows that the risk of placenta accreta, hysterectomy, hemorrhage, and other serious maternal morbidity increases progressively with each repeat cesarean delivery. Rates of placenta accreta have, in fact, been rising in the United States – a trend that should prompt us to think more about TOLAC.
Moreover, TOLAC is being shown to be a cost-effective strategy. In one analysis, TOLAC in a second pregnancy was cost-effective as long as the chance of VBAC exceeded approximately 74% (Obstet Gynecol. 2001 Jun;97[6]:932-41). More recently, TOLAC was found to be cost-effective across a wide variety of circumstances, including when a woman had a probability of VBAC as low as 43%. The model in this analysis, which used probability estimates from the MFMU Cesarean Registry, took a longer-term view by including probabilities of outcomes throughout a woman’s reproductive life that were contingent upon her initial choice regarding TOLAC (Am J Perinatol. 2013 Jan;30[1]:11-20).
Likelihood of success
Evaluating and discussing the likelihood of success with TOLAC is therefore key to the counseling process. The higher the likelihood of achieving VBAC, the more favorable the risk-benefit ratio will be and the more appealing it will be to consider.
According to one analysis, if a woman undergoing a TOLAC has at least a 60%-70% chance of VBAC, her chance of having major or minor morbidity is no greater than a woman undergoing a planned repeat cesarean delivery (Am J Obstet Gynecol 2009;200:56.e1-e6).
There are several prediction tools available that can be used at the first prenatal visit and in early labor to give a reasonably good estimate of success. One of these tools is available at the MFMU Network website (http://mfmu.bsc.gwu.edu). The tools take into account factors such as prior indication for cesarean delivery; history of vaginal delivery; demographic characteristics such as maternal age and body mass index; the occurrence of spontaneous labor; and cervical status at admission.
Prior vaginal delivery is one of the strongest predictors of a successful TOLAC. Research has consistently shown that women with a prior vaginal delivery – including a vaginal delivery predating an unsuccessful TOLAC – have significantly higher TOLAC success rates than women who did not have any prior vaginal delivery.
The indication for a prior cesarean delivery also clearly affects the likelihood of a successful TOLAC. Women whose first cesarean delivery was performed for a nonrecurring indication, such as breech presentation or low intolerance of labor, have TOLAC success rates that are similar to vaginal delivery rates for nulliparous women. Success rates for these women may exceed 85%. On the other hand, women who had a prior cesarean delivery for cephalopelvic disproportion or failure to progress have been shown to have lower TOLAC success rates ranging from 50%-67%.
Labor induction should be approached cautiously, as women who undergo induction of labor in TOLAC have an increased risk of repeat cesarean delivery. Still, success rates with induction are high. Data from the MFMU Cesarean Registry showed that about 66% of women undergoing induction after one prior cesarean delivery achieved VBAC versus 76% of women entering TOLAC spontaneously (Obstet Gynecol. 2007 Feb;109[2 Pt 1]:262-9). Another study of women undergoing induction after one prior cesarean reported an overall success rate of 78% (Obstet Gynecol. 2004 Mar;103[3]:534-8).
Whether induction specifically increases the risk for uterine rupture in TOLAC, compared with expectant management, is unclear. There also are conflicting data as to whether particular induction methods increase this risk.
Based on available data, ACOG considers induction of labor for either maternal or fetal indications to be an option for women undergoing TOLAC. Oxytocin may be used for induction as well as augmentation, but caution should be exercised at higher doses. While there is no clear dosing threshold for increased risk of rupture, research has suggested that higher doses of oxytocin are best avoided.
The use of prostaglandins is more controversial: Based on evidence from several small studies, ACOG concluded in its 2010 bulletin that misoprostol (prostaglandin E1) for cervical ripening is contraindicated in women undergoing TOLAC. It appears likely that rupture risk increases in patients who received both prostaglandins and oxytocin, so ACOG has advised avoiding their sequential use when prostaglandin E2 is used. This of course limits the options for the practitioner. Therefore, utilizing a Foley catheter followed by pitocin has been an approach advocated in some cases.
Uterine rupture is not predictable, and it is far more difficult to assess an individual’s risk of this complication than it is to assess the likelihood of VBAC. Still, there is value to discussing with the patient whether there are any other modifiers that could potentially influence the risk of rupture.
Since rates of uterine rupture are highest in women with previous classical or T-shaped incision, for example, it is important to try to ascertain what type of incision was previously used. It is widely appreciated that low-transverse uterine incisions are most favorable, but findings are mixed in regard to low-vertical incisions. Some research shows that women with a previous low-vertical incision do not have significantly lower VBAC success rates or higher risks of uterine rupture. TOLAC should therefore not be ruled out in these cases.
Additionally, TOLAC should not be ruled out for women who have had more than one cesarean delivery. Several studies have shown an increased risk of uterine rupture after two prior cesarean deliveries, compared with one, and one meta-analysis suggested a more than twofold increased risk (BJOG. 2010 Jan;117(1):5-19.).
In contrast, an analysis of the MFMU Cesarean Registry found no significant difference in rupture rates in women with one prior cesarean versus multiple prior cesareans (Obstet Gynecol. 2006 Jul;108[1]:12-20.).
It appears, therefore, that even if having more than one prior cesarean section is associated with an increased risk of rupture, the magnitude of this increase is small.
Just as women with a prior vaginal delivery have the highest chance of VBAC success, they also have the lowest rates of rupture among all women undergoing TOLAC.
Patient counseling
We must inform our patients who have had a cesarean section in the past of their options for childbirth in an unbiased manner.
The complications of both TOLAC and elective repeat cesarean section should be discussed, and every attempt should be made to individually assess both the likelihood of a successful VBAC and the comparative risk of maternal and perinatal morbidity. A shared decision-making process should be adopted, and whenever possible, the patient’s preference should be respected. In the end, a woman undergoing TOLAC should be truly motivated to pursue a trial of labor, because there are inherent risks.
One thing I’ve learned from my clinical practice and research on this issue is that the desire to undergo a vaginal delivery is powerful for some women. Many of my patients have self-referred for consultation about TOLAC after their ob.gyn. informed them that their hospital is not equipped, and they should therefore have a scheduled repeat operation. In many cases they discover that TOLAC is an option if they are willing to travel a half-hour or so.
We need to honor this desire and inform our patients of the option, and help facilitate delivery at another nearby hospital when our own facility is not equipped for TOLAC.
Dr. Landon is the Richard L. Meiling Professor and chairman of the department of obstetrics and gynecology at the Ohio State University, Columbus. He served for more than 25 years as Ohio State’s coinvestigator for the National Institutes of Child Health and Human Development Maternal Fetal Medicine Units Network. He reported having no relevant financial disclosures.
Discussions about sexual orientation
The biological transition to puberty has always marked a critical point in a primary care pediatrician’s relationship to a patient. Adolescents’ capacity for abstract reasoning, their movement to autonomy, their nuanced sense of identity, their need for privacy, and their emerging sexuality together give the pediatrician an opportunity and a responsibility to create a safe place to talk. Your office can be an oasis from parents, peers, and a society that seems saturated with sexuality. You can be trusted more than the Internet and offer discussions that are leavened by your long-standing relationship with the patient.
The growing public awareness, acceptance, and legal standing given to gay, lesbian, bisexual, and transgender individuals represents welcome societal progress, and we sense that amidst this richer public conversation, a growing number of children and adolescents are presenting with questions or worries about their own emerging sexual orientation or gender identity. We would like to start with our key takeaway: Discussions about sexual orientation and gender identity do not require that you give answers or predict the future. Focus instead on being a curious, compassionate, and nonjudgmental listener, and you will be effective at helping your patient to better manage new, uncertain, and possibly stressful feelings.

Our focus today is how to create a safe setting and specifically how to ask about and discuss sexual orientation. Most teenagers will wonder at some point about their orientation. Studies suggest that among adults, 5%-10% are attracted to the same sex and 3% describe themselves as gay or bisexual. Such surveys are very challenging, though, and in our experience, these percentages are higher. Sexual orientation is believed to exist on a continuum rather than in a simple binary state – some people identify as purely homosexual or heterosexual, and the rest exist somewhere in the middle. Sharing this fact alone can offer a very helpful perspective to young people who are feeling pressure to “figure out” if they are gay or straight.
While sexual orientation describes whom a person is attracted to, gender identity is a person’s internal sense of his or her own gender. It emerges in childhood and becomes more rich and nuanced in adolescence and adulthood, and, like sexual orientation, it is also believed to exist on a continuum rather than in a simple binary state. Less than 0.1% of youth will experience gender dysphoria, or the pressing feeling that their gender identity is not the same as their phenotypic sex. While questions about gender identity should be approached with the same curious, compassionate, and nonjudgmental style, we will not discuss the management of patients with gender dysphoria here. It is a very complex (and controversial) topic. And, as a practical matter, sexual orientation will likely be a more common issue with your patients, whereas questions about gender identity will come up much less frequently.

It is worth knowing that there is a range of mental health issues that are associated with the stress of feeling comfortable with one’s sexual identity. There is some evidence that young people who identify as gay or bisexual have elevated risk for mood disorders (depression), anxiety disorders, conduct disorder, and substance use disorders, but this finding has not been consistent (Am J Public Health. 2010:100[12]; 2426-32). However, there is unequivocal evidence that there is an elevated risk for suicide attempts in lesbian, gay, or bisexual (LGB) youth above their heterosexual peers. One survey found that 9th-12th grade students who identified as LGB were up to seven times as likely to have a suicide attempt as were their peers who identify as heterosexual. This risk is especially pronounced in male adolescents and continues into adulthood, when there is an elevated risk for suicide completion among adult males who identify as homosexual, although not in adult females (J Homosex. 2011 Jan;58[1]:10-51). Importantly, the risk for suicide attempt in LGB adolescents remains elevated even in those adolescents without any diagnosable mental illness, likely attributable to the stresses of isolation, family conflict, stigmatization, or bullying that LGB adolescents are likely to experience.
Asking your early-adolescent patients in a calm and comfortable manner about sexual feelings builds an environment in which thoughts, feelings, and questions about sex and sexuality are more easily shared. It is important to find language that feels like yours, which you can use with ease. Perhaps starting with, “At about your age, I ask every patient of mine whether they are beginning to have sexual feelings. This is when you really want to be around someone, in a way that’s more powerful and different from even your favorite friend. Some people call it getting butterflies in your stomach.” If your patient recognizes what you are talking about, you might continue, “Do you feel attracted to boys or girls or both? Do you have those feelings about kids in your class or people you know, like a teacher? Perhaps about a celebrity in a TV show or a band?” You should absolutely reassure them, “You don’t have to talk about anything you do not want to, but you should know that this is a normal part of becoming a teenager. I talk about this a lot with patients who are younger and older than you are. I keep what we talk about very private, and sometimes this is the only place a teenager feels safe to ask questions.” If you start this process early enough – by the start of middle school – the patient will probably be a bit embarrassed or giggle and not talk much. But, by the next annual physical or the one after that, the issue will be more familiar and less charged. A meaningful discussion may start.
With patients who do describe feeling attracted to people of the same sex, more specific questions may be appropriate. You should expect these feelings to exist on a continuum: You may encounter a school-age child with great clarity about exactly whom she is attracted to and what that means, or an older teenager who is far less certain, responding to a less intense interest or having been told by a peer that he is probably gay. It can be powerfully reassuring to remind your patient that adolescence is when we start to figure out to whom we are attracted. They don’t have to decide, but just be aware of these feelings as they emerge, essentially getting to know themselves without any feelings of urgency or pressure. You might ask, “Have you wondered if you were gay or bisexual? Have you spoken to any friends about your feelings or have you experimented with a boy or girl to try and figure this out?” It’s very helpful if you ask if they are worried or stressed by these feelings. Some young people will suffer from internalized homophobia, which may be helped by your accepting stance or may require a referral for more ongoing support. It can be valuable to find out if they are dating people of the same sex, or if their “relationships” have all been online. While this “virtual” dating may seem safer, it may not help them better understand themselves and may expose them to exploitation or predatory behavior. If your patient is sexually active, you should be comfortable talking with them about the risks of unprotected sex and same-sex safe-sex practices.
It is particularly important to ask your adolescent LGB patient about whom they have told, and what responses have they gotten. The presence of good friends and loving family members is critical to all adolescents’ emotional well-being. If they have talked about their sexual orientation with their peers, have their friends been supportive, or has it left them more isolated at school? You should find out if they have been teased or bullied, and ask specifically about online teasing or harassment. If they are being bullied, how have they handled that? Find out also if they feel free to ask or talk about this subject with their parents. If not, try to understand if they are simply embarrassed and unsure how to bring it up, or if there is a strong sense that they will be shamed or even rejected by their parents. If the parents are truly shaming or rejecting, it will be critical to consider what kind of support may be necessary. Teens who are facing isolation or bullying at school may benefit from resources such as a gay-straight student alliance or a community organization dedicated to issues facing LGB youth. For patients who are facing hostile or rejecting parents, it can be protective to connect them with a therapist as well, as you are mindful of their marked isolation and subsequently heightened risk for mood problems and even suicide attempts.
Along a similar vein, it is very important that you are aware of your own comfort level with these issues. While discussing sexual orientation may feel awkward if it is new for you, it is important to be realistic if you cannot be supportive of your patients who are gay. If for religious or other reasons you are not comfortable talking about sexual orientation in an accepting, nonjudgmental manner, you should seek guidance on how to thoughtfully care for your LGB patients or appropriately refer them to someone who can provide a more-supportive treatment setting.
When you create an office that makes sexuality a safe topic for discussion, you should expect that you will hear questions or concerns about which you yourself may not know the answers. Do not panic, just maintain your posture of being a curious, compassionate, and nonjudgmental listener, and then look for the answers. We are delighted this news organization has devoted a column to the optimal care of LGBT youth (LGBT Youth Consult) and encourage the primary care pediatrician to “never to worry alone,” and instead get some advice and expert teammates when dealing with these complex and important issues.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, in Newton, Mass. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston.
The biological transition to puberty has always marked a critical point in a primary care pediatrician’s relationship to a patient. Adolescents’ capacity for abstract reasoning, their movement to autonomy, their nuanced sense of identity, their need for privacy, and their emerging sexuality together give the pediatrician an opportunity and a responsibility to create a safe place to talk. Your office can be an oasis from parents, peers, and a society that seems saturated with sexuality. You can be trusted more than the Internet and offer discussions that are leavened by your long-standing relationship with the patient.
The growing public awareness, acceptance, and legal standing given to gay, lesbian, bisexual, and transgender individuals represents welcome societal progress, and we sense that amidst this richer public conversation, a growing number of children and adolescents are presenting with questions or worries about their own emerging sexual orientation or gender identity. We would like to start with our key takeaway: Discussions about sexual orientation and gender identity do not require that you give answers or predict the future. Focus instead on being a curious, compassionate, and nonjudgmental listener, and you will be effective at helping your patient to better manage new, uncertain, and possibly stressful feelings.
Our focus today is how to create a safe setting and specifically how to ask about and discuss sexual orientation. Most teenagers will wonder at some point about their orientation. Studies suggest that among adults, 5%-10% are attracted to the same sex and 3% describe themselves as gay or bisexual. Such surveys are very challenging, though, and in our experience, these percentages are higher. Sexual orientation is believed to exist on a continuum rather than in a simple binary state – some people identify as purely homosexual or heterosexual, and the rest exist somewhere in the middle. Sharing this fact alone can offer a very helpful perspective to young people who are feeling pressure to “figure out” if they are gay or straight.
While sexual orientation describes whom a person is attracted to, gender identity is a person’s internal sense of his or her own gender. It emerges in childhood and becomes more rich and nuanced in adolescence and adulthood, and, like sexual orientation, it is also believed to exist on a continuum rather than in a simple binary state. Less than 0.1% of youth will experience gender dysphoria, or the pressing feeling that their gender identity is not the same as their phenotypic sex. While questions about gender identity should be approached with the same curious, compassionate, and nonjudgmental style, we will not discuss the management of patients with gender dysphoria here. It is a very complex (and controversial) topic. And, as a practical matter, sexual orientation will likely be a more common issue with your patients, whereas questions about gender identity will come up much less frequently.
It is worth knowing that there is a range of mental health issues that are associated with the stress of feeling comfortable with one’s sexual identity. There is some evidence that young people who identify as gay or bisexual have elevated risk for mood disorders (depression), anxiety disorders, conduct disorder, and substance use disorders, but this finding has not been consistent (Am J Public Health. 2010:100[12]; 2426-32). However, there is unequivocal evidence that there is an elevated risk for suicide attempts in lesbian, gay, or bisexual (LGB) youth above their heterosexual peers. One survey found that 9th-12th grade students who identified as LGB were up to seven times as likely to have a suicide attempt as were their peers who identify as heterosexual. This risk is especially pronounced in male adolescents and continues into adulthood, when there is an elevated risk for suicide completion among adult males who identify as homosexual, although not in adult females (J Homosex. 2011 Jan;58[1]:10-51). Importantly, the risk for suicide attempt in LGB adolescents remains elevated even in those adolescents without any diagnosable mental illness, likely attributable to the stresses of isolation, family conflict, stigmatization, or bullying that LGB adolescents are likely to experience.
Asking your early-adolescent patients in a calm and comfortable manner about sexual feelings builds an environment in which thoughts, feelings, and questions about sex and sexuality are more easily shared. It is important to find language that feels like yours, which you can use with ease. Perhaps starting with, “At about your age, I ask every patient of mine whether they are beginning to have sexual feelings. This is when you really want to be around someone, in a way that’s more powerful and different from even your favorite friend. Some people call it getting butterflies in your stomach.” If your patient recognizes what you are talking about, you might continue, “Do you feel attracted to boys or girls or both? Do you have those feelings about kids in your class or people you know, like a teacher? Perhaps about a celebrity in a TV show or a band?” You should absolutely reassure them, “You don’t have to talk about anything you do not want to, but you should know that this is a normal part of becoming a teenager. I talk about this a lot with patients who are younger and older than you are. I keep what we talk about very private, and sometimes this is the only place a teenager feels safe to ask questions.” If you start this process early enough – by the start of middle school – the patient will probably be a bit embarrassed or giggle and not talk much. But, by the next annual physical or the one after that, the issue will be more familiar and less charged. A meaningful discussion may start.
With patients who do describe feeling attracted to people of the same sex, more specific questions may be appropriate. You should expect these feelings to exist on a continuum: You may encounter a school-age child with great clarity about exactly whom she is attracted to and what that means, or an older teenager who is far less certain, responding to a less intense interest or having been told by a peer that he is probably gay. It can be powerfully reassuring to remind your patient that adolescence is when we start to figure out to whom we are attracted. They don’t have to decide, but just be aware of these feelings as they emerge, essentially getting to know themselves without any feelings of urgency or pressure. You might ask, “Have you wondered if you were gay or bisexual? Have you spoken to any friends about your feelings or have you experimented with a boy or girl to try and figure this out?” It’s very helpful if you ask if they are worried or stressed by these feelings. Some young people will suffer from internalized homophobia, which may be helped by your accepting stance or may require a referral for more ongoing support. It can be valuable to find out if they are dating people of the same sex, or if their “relationships” have all been online. While this “virtual” dating may seem safer, it may not help them better understand themselves and may expose them to exploitation or predatory behavior. If your patient is sexually active, you should be comfortable talking with them about the risks of unprotected sex and same-sex safe-sex practices.
It is particularly important to ask your adolescent LGB patient about whom they have told, and what responses have they gotten. The presence of good friends and loving family members is critical to all adolescents’ emotional well-being. If they have talked about their sexual orientation with their peers, have their friends been supportive, or has it left them more isolated at school? You should find out if they have been teased or bullied, and ask specifically about online teasing or harassment. If they are being bullied, how have they handled that? Find out also if they feel free to ask or talk about this subject with their parents. If not, try to understand if they are simply embarrassed and unsure how to bring it up, or if there is a strong sense that they will be shamed or even rejected by their parents. If the parents are truly shaming or rejecting, it will be critical to consider what kind of support may be necessary. Teens who are facing isolation or bullying at school may benefit from resources such as a gay-straight student alliance or a community organization dedicated to issues facing LGB youth. For patients who are facing hostile or rejecting parents, it can be protective to connect them with a therapist as well, as you are mindful of their marked isolation and subsequently heightened risk for mood problems and even suicide attempts.
Along a similar vein, it is very important that you are aware of your own comfort level with these issues. While discussing sexual orientation may feel awkward if it is new for you, it is important to be realistic if you cannot be supportive of your patients who are gay. If for religious or other reasons you are not comfortable talking about sexual orientation in an accepting, nonjudgmental manner, you should seek guidance on how to thoughtfully care for your LGB patients or appropriately refer them to someone who can provide a more-supportive treatment setting.
When you create an office that makes sexuality a safe topic for discussion, you should expect that you will hear questions or concerns about which you yourself may not know the answers. Do not panic, just maintain your posture of being a curious, compassionate, and nonjudgmental listener, and then look for the answers. We are delighted this news organization has devoted a column to the optimal care of LGBT youth (LGBT Youth Consult) and encourage the primary care pediatrician to “never to worry alone,” and instead get some advice and expert teammates when dealing with these complex and important issues.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, in Newton, Mass. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston.
The biological transition to puberty has always marked a critical point in a primary care pediatrician’s relationship to a patient. Adolescents’ capacity for abstract reasoning, their movement to autonomy, their nuanced sense of identity, their need for privacy, and their emerging sexuality together give the pediatrician an opportunity and a responsibility to create a safe place to talk. Your office can be an oasis from parents, peers, and a society that seems saturated with sexuality. You can be trusted more than the Internet and offer discussions that are leavened by your long-standing relationship with the patient.
The growing public awareness, acceptance, and legal standing given to gay, lesbian, bisexual, and transgender individuals represents welcome societal progress, and we sense that amidst this richer public conversation, a growing number of children and adolescents are presenting with questions or worries about their own emerging sexual orientation or gender identity. We would like to start with our key takeaway: Discussions about sexual orientation and gender identity do not require that you give answers or predict the future. Focus instead on being a curious, compassionate, and nonjudgmental listener, and you will be effective at helping your patient to better manage new, uncertain, and possibly stressful feelings.
Our focus today is how to create a safe setting and specifically how to ask about and discuss sexual orientation. Most teenagers will wonder at some point about their orientation. Studies suggest that among adults, 5%-10% are attracted to the same sex and 3% describe themselves as gay or bisexual. Such surveys are very challenging, though, and in our experience, these percentages are higher. Sexual orientation is believed to exist on a continuum rather than in a simple binary state – some people identify as purely homosexual or heterosexual, and the rest exist somewhere in the middle. Sharing this fact alone can offer a very helpful perspective to young people who are feeling pressure to “figure out” if they are gay or straight.
While sexual orientation describes whom a person is attracted to, gender identity is a person’s internal sense of his or her own gender. It emerges in childhood and becomes more rich and nuanced in adolescence and adulthood, and, like sexual orientation, it is also believed to exist on a continuum rather than in a simple binary state. Less than 0.1% of youth will experience gender dysphoria, or the pressing feeling that their gender identity is not the same as their phenotypic sex. While questions about gender identity should be approached with the same curious, compassionate, and nonjudgmental style, we will not discuss the management of patients with gender dysphoria here. It is a very complex (and controversial) topic. And, as a practical matter, sexual orientation will likely be a more common issue with your patients, whereas questions about gender identity will come up much less frequently.
It is worth knowing that there is a range of mental health issues that are associated with the stress of feeling comfortable with one’s sexual identity. There is some evidence that young people who identify as gay or bisexual have elevated risk for mood disorders (depression), anxiety disorders, conduct disorder, and substance use disorders, but this finding has not been consistent (Am J Public Health. 2010:100[12]; 2426-32). However, there is unequivocal evidence that there is an elevated risk for suicide attempts in lesbian, gay, or bisexual (LGB) youth above their heterosexual peers. One survey found that 9th-12th grade students who identified as LGB were up to seven times as likely to have a suicide attempt as were their peers who identify as heterosexual. This risk is especially pronounced in male adolescents and continues into adulthood, when there is an elevated risk for suicide completion among adult males who identify as homosexual, although not in adult females (J Homosex. 2011 Jan;58[1]:10-51). Importantly, the risk for suicide attempt in LGB adolescents remains elevated even in those adolescents without any diagnosable mental illness, likely attributable to the stresses of isolation, family conflict, stigmatization, or bullying that LGB adolescents are likely to experience.
Asking your early-adolescent patients in a calm and comfortable manner about sexual feelings builds an environment in which thoughts, feelings, and questions about sex and sexuality are more easily shared. It is important to find language that feels like yours, which you can use with ease. Perhaps starting with, “At about your age, I ask every patient of mine whether they are beginning to have sexual feelings. This is when you really want to be around someone, in a way that’s more powerful and different from even your favorite friend. Some people call it getting butterflies in your stomach.” If your patient recognizes what you are talking about, you might continue, “Do you feel attracted to boys or girls or both? Do you have those feelings about kids in your class or people you know, like a teacher? Perhaps about a celebrity in a TV show or a band?” You should absolutely reassure them, “You don’t have to talk about anything you do not want to, but you should know that this is a normal part of becoming a teenager. I talk about this a lot with patients who are younger and older than you are. I keep what we talk about very private, and sometimes this is the only place a teenager feels safe to ask questions.” If you start this process early enough – by the start of middle school – the patient will probably be a bit embarrassed or giggle and not talk much. But, by the next annual physical or the one after that, the issue will be more familiar and less charged. A meaningful discussion may start.
With patients who do describe feeling attracted to people of the same sex, more specific questions may be appropriate. You should expect these feelings to exist on a continuum: You may encounter a school-age child with great clarity about exactly whom she is attracted to and what that means, or an older teenager who is far less certain, responding to a less intense interest or having been told by a peer that he is probably gay. It can be powerfully reassuring to remind your patient that adolescence is when we start to figure out to whom we are attracted. They don’t have to decide, but just be aware of these feelings as they emerge, essentially getting to know themselves without any feelings of urgency or pressure. You might ask, “Have you wondered if you were gay or bisexual? Have you spoken to any friends about your feelings or have you experimented with a boy or girl to try and figure this out?” It’s very helpful if you ask if they are worried or stressed by these feelings. Some young people will suffer from internalized homophobia, which may be helped by your accepting stance or may require a referral for more ongoing support. It can be valuable to find out if they are dating people of the same sex, or if their “relationships” have all been online. While this “virtual” dating may seem safer, it may not help them better understand themselves and may expose them to exploitation or predatory behavior. If your patient is sexually active, you should be comfortable talking with them about the risks of unprotected sex and same-sex safe-sex practices.
It is particularly important to ask your adolescent LGB patient about whom they have told, and what responses have they gotten. The presence of good friends and loving family members is critical to all adolescents’ emotional well-being. If they have talked about their sexual orientation with their peers, have their friends been supportive, or has it left them more isolated at school? You should find out if they have been teased or bullied, and ask specifically about online teasing or harassment. If they are being bullied, how have they handled that? Find out also if they feel free to ask or talk about this subject with their parents. If not, try to understand if they are simply embarrassed and unsure how to bring it up, or if there is a strong sense that they will be shamed or even rejected by their parents. If the parents are truly shaming or rejecting, it will be critical to consider what kind of support may be necessary. Teens who are facing isolation or bullying at school may benefit from resources such as a gay-straight student alliance or a community organization dedicated to issues facing LGB youth. For patients who are facing hostile or rejecting parents, it can be protective to connect them with a therapist as well, as you are mindful of their marked isolation and subsequently heightened risk for mood problems and even suicide attempts.
Along a similar vein, it is very important that you are aware of your own comfort level with these issues. While discussing sexual orientation may feel awkward if it is new for you, it is important to be realistic if you cannot be supportive of your patients who are gay. If for religious or other reasons you are not comfortable talking about sexual orientation in an accepting, nonjudgmental manner, you should seek guidance on how to thoughtfully care for your LGB patients or appropriately refer them to someone who can provide a more-supportive treatment setting.
When you create an office that makes sexuality a safe topic for discussion, you should expect that you will hear questions or concerns about which you yourself may not know the answers. Do not panic, just maintain your posture of being a curious, compassionate, and nonjudgmental listener, and then look for the answers. We are delighted this news organization has devoted a column to the optimal care of LGBT youth (LGBT Youth Consult) and encourage the primary care pediatrician to “never to worry alone,” and instead get some advice and expert teammates when dealing with these complex and important issues.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, in Newton, Mass. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston.
