User login
Love hormone plein air, posh preused Kleenex, and dieting plague vectors
Paint me like one of your French girls
If you’re trying to think of a fun Valentine’s activity, look no further than paint night! Normally associated with a ladies night out (and heavy on the wine), a recent study found that painting releases high levels of the “love hormone”, a.k.a. oxytocin, in men.

Researchers compared the levels of oxytocin with partners painting and partners playing board games, and were surprised by the results: While all the couples released oxytocin during these activities, men in paint class had the highest levels – twice as much as any other group.
Feel free to cite this study next time your man complains about being dragged to a paint-and-sip. Painting partners also experienced more touching than the gaming group (unless you count throwing Monopoly pieces at your significant other as touching).
You won’t get me sick, I’ll get me sick!
There are certain items that, after being used once, you really wouldn’t want to reuse. A snotty, mucus-filled tissue is pretty high up on that list ... or so you would hope. But that’s not thinking with real American entrepreneurial spirit! Welcome to Vaev Tissue, a startup based in Los Angeles that sells used tissues containing germs from a sick person for the bargain price of $79.99.

Yes, you read that correctly. They sell an $80 used tissue. The purpose, according to Vaev’s mission statement, is “to get sick on your own terms,” as “using a tissue that carries a human sneeze is safer than needles or pills.”
As you might expect, the tissues are popular with young parents and adults who are “critical” of vaccines. Who else could hear advice from actual doctors who told Time magazine that “there is nothing positive that can come from this, only things that are adverse,” or that the tissues are an “incredible liability,” and continue on, regardless?
And if you’re thinking, “If these people want to get sick, why not just have someone sneeze on them?” Don’t be ridiculous. Focus testers responded highly negatively to simply being handed a dirty tissue. The premium packaging and high price tag are a necessity.
Our advice? Well, as tempting as all this sounds, we think we’ll stick with washing our hands and not sticking used tissues in our faces. You know, like reasonable people.
Why Bullwinkle thinks pink
Flying squirrels are secretly doing their best flamingo impression – who knew? A forestry professor discovered, by happy accident, that flying squirrels are fluorescent – they glow hot pink under ultraviolet light.

Turns out, almost all species of gliders – even blue-helmeted Rocket “Rocky” J. Squirrel – are members of the Pink Ladies. They are one of the very few glowing mammals; the only other known mammalian species to have fluorescent fur are certain opossums.
But why do these airborne rodents glow pink? Is it because of an overintake of bubblegum? Are flying squirrels just really flamboyant but also shy? Are they huge fans of the singer Pink?
A biologist involved in studying these colorful critters hypothesized that the reason is slightly more related to environment than musical preference. Flying squirrels are nocturnal, making them most active when UV light is most prominent. The garish glow might have something to do with nighttime perception.
However, we don’t know the answer for sure. And in the meantime, we can choose to believe flying squirrels eat way too much cotton candy.
Buzz, feed, diet. Repeat
Guns don’t hurt this mass murderer. Police can’t arrest it. Background checks are pointless. A border wall won’t keep it out. So, how do you stop a mosquito?
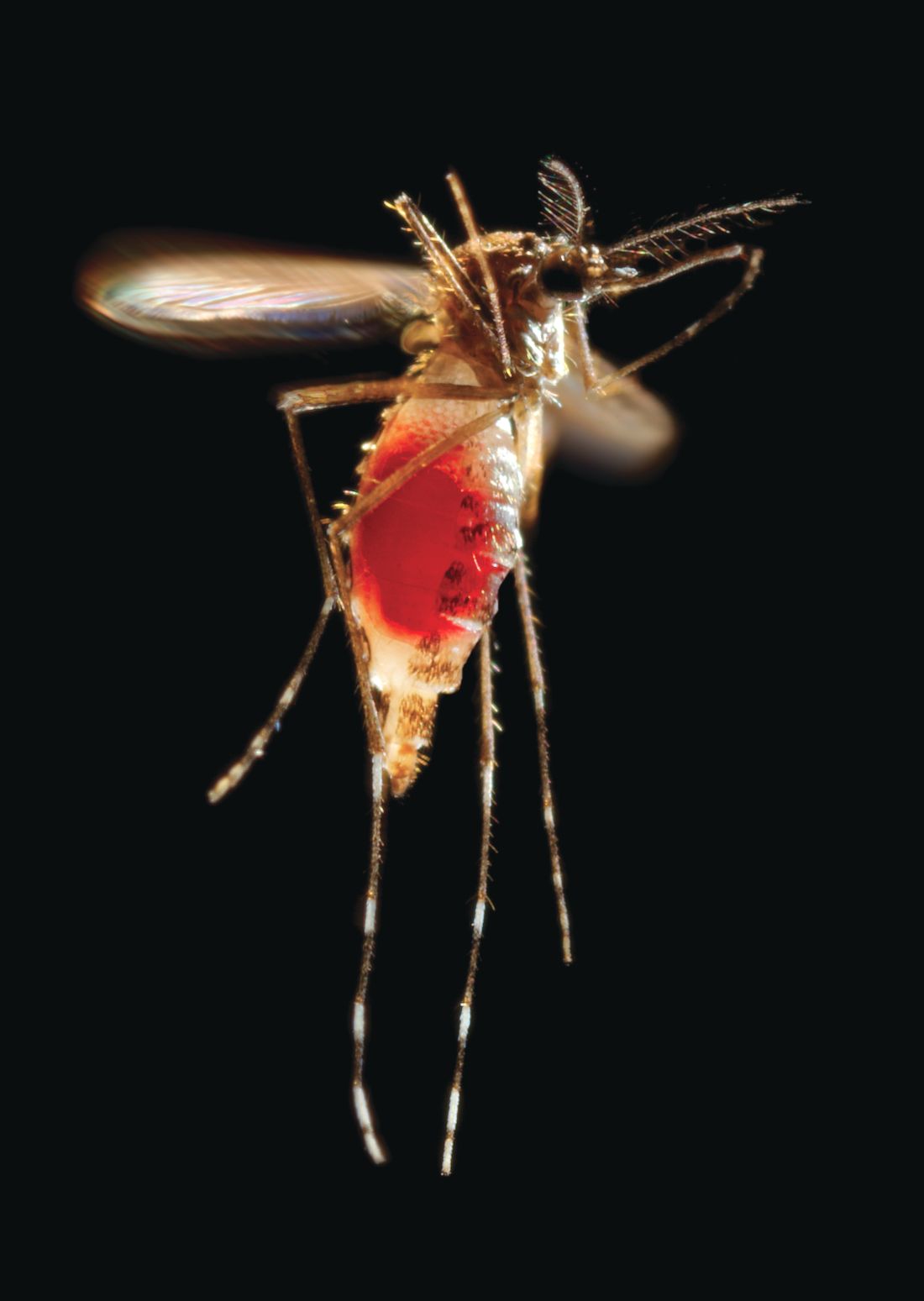
Diet drugs.
Because female mosquitoes transmit malaria, Zika, and other diseases when they move from person to person feeding on human blood, investigators sought to curb that appetite by chemically re-creating the feeling of fullness they get after a big meal.
The lady killers in their study – Aedes aegypti, to be exact – when given an antiobesity drug that suppresses human appetite by activating neuropeptide receptors that regulate food intake, turned away from a tempting piece of nylon stocking that had been worn by one of the researchers. Further work showed that treated mosquitoes were as disinterested in feeding on a live mouse as mosquitoes that had already enjoyed a full blood meal.
The LOTME research staff (What? Of course, we have a research staff. You don’t?) is working on the mosquito problem too, although we’ve taken a somewhat different approach: The “volunteers” who walk into the mosquito-filled room wear a sign that says, “My blood will make your butt look bigger.”
Paint me like one of your French girls
If you’re trying to think of a fun Valentine’s activity, look no further than paint night! Normally associated with a ladies night out (and heavy on the wine), a recent study found that painting releases high levels of the “love hormone”, a.k.a. oxytocin, in men.
Researchers compared the levels of oxytocin with partners painting and partners playing board games, and were surprised by the results: While all the couples released oxytocin during these activities, men in paint class had the highest levels – twice as much as any other group.
Feel free to cite this study next time your man complains about being dragged to a paint-and-sip. Painting partners also experienced more touching than the gaming group (unless you count throwing Monopoly pieces at your significant other as touching).
You won’t get me sick, I’ll get me sick!
There are certain items that, after being used once, you really wouldn’t want to reuse. A snotty, mucus-filled tissue is pretty high up on that list ... or so you would hope. But that’s not thinking with real American entrepreneurial spirit! Welcome to Vaev Tissue, a startup based in Los Angeles that sells used tissues containing germs from a sick person for the bargain price of $79.99.
Yes, you read that correctly. They sell an $80 used tissue. The purpose, according to Vaev’s mission statement, is “to get sick on your own terms,” as “using a tissue that carries a human sneeze is safer than needles or pills.”
As you might expect, the tissues are popular with young parents and adults who are “critical” of vaccines. Who else could hear advice from actual doctors who told Time magazine that “there is nothing positive that can come from this, only things that are adverse,” or that the tissues are an “incredible liability,” and continue on, regardless?
And if you’re thinking, “If these people want to get sick, why not just have someone sneeze on them?” Don’t be ridiculous. Focus testers responded highly negatively to simply being handed a dirty tissue. The premium packaging and high price tag are a necessity.
Our advice? Well, as tempting as all this sounds, we think we’ll stick with washing our hands and not sticking used tissues in our faces. You know, like reasonable people.
Why Bullwinkle thinks pink
Flying squirrels are secretly doing their best flamingo impression – who knew? A forestry professor discovered, by happy accident, that flying squirrels are fluorescent – they glow hot pink under ultraviolet light.
Turns out, almost all species of gliders – even blue-helmeted Rocket “Rocky” J. Squirrel – are members of the Pink Ladies. They are one of the very few glowing mammals; the only other known mammalian species to have fluorescent fur are certain opossums.
But why do these airborne rodents glow pink? Is it because of an overintake of bubblegum? Are flying squirrels just really flamboyant but also shy? Are they huge fans of the singer Pink?
A biologist involved in studying these colorful critters hypothesized that the reason is slightly more related to environment than musical preference. Flying squirrels are nocturnal, making them most active when UV light is most prominent. The garish glow might have something to do with nighttime perception.
However, we don’t know the answer for sure. And in the meantime, we can choose to believe flying squirrels eat way too much cotton candy.
Buzz, feed, diet. Repeat
Guns don’t hurt this mass murderer. Police can’t arrest it. Background checks are pointless. A border wall won’t keep it out. So, how do you stop a mosquito?
Diet drugs.
Because female mosquitoes transmit malaria, Zika, and other diseases when they move from person to person feeding on human blood, investigators sought to curb that appetite by chemically re-creating the feeling of fullness they get after a big meal.
The lady killers in their study – Aedes aegypti, to be exact – when given an antiobesity drug that suppresses human appetite by activating neuropeptide receptors that regulate food intake, turned away from a tempting piece of nylon stocking that had been worn by one of the researchers. Further work showed that treated mosquitoes were as disinterested in feeding on a live mouse as mosquitoes that had already enjoyed a full blood meal.
The LOTME research staff (What? Of course, we have a research staff. You don’t?) is working on the mosquito problem too, although we’ve taken a somewhat different approach: The “volunteers” who walk into the mosquito-filled room wear a sign that says, “My blood will make your butt look bigger.”
Paint me like one of your French girls
If you’re trying to think of a fun Valentine’s activity, look no further than paint night! Normally associated with a ladies night out (and heavy on the wine), a recent study found that painting releases high levels of the “love hormone”, a.k.a. oxytocin, in men.
Researchers compared the levels of oxytocin with partners painting and partners playing board games, and were surprised by the results: While all the couples released oxytocin during these activities, men in paint class had the highest levels – twice as much as any other group.
Feel free to cite this study next time your man complains about being dragged to a paint-and-sip. Painting partners also experienced more touching than the gaming group (unless you count throwing Monopoly pieces at your significant other as touching).
You won’t get me sick, I’ll get me sick!
There are certain items that, after being used once, you really wouldn’t want to reuse. A snotty, mucus-filled tissue is pretty high up on that list ... or so you would hope. But that’s not thinking with real American entrepreneurial spirit! Welcome to Vaev Tissue, a startup based in Los Angeles that sells used tissues containing germs from a sick person for the bargain price of $79.99.
Yes, you read that correctly. They sell an $80 used tissue. The purpose, according to Vaev’s mission statement, is “to get sick on your own terms,” as “using a tissue that carries a human sneeze is safer than needles or pills.”
As you might expect, the tissues are popular with young parents and adults who are “critical” of vaccines. Who else could hear advice from actual doctors who told Time magazine that “there is nothing positive that can come from this, only things that are adverse,” or that the tissues are an “incredible liability,” and continue on, regardless?
And if you’re thinking, “If these people want to get sick, why not just have someone sneeze on them?” Don’t be ridiculous. Focus testers responded highly negatively to simply being handed a dirty tissue. The premium packaging and high price tag are a necessity.
Our advice? Well, as tempting as all this sounds, we think we’ll stick with washing our hands and not sticking used tissues in our faces. You know, like reasonable people.
Why Bullwinkle thinks pink
Flying squirrels are secretly doing their best flamingo impression – who knew? A forestry professor discovered, by happy accident, that flying squirrels are fluorescent – they glow hot pink under ultraviolet light.
Turns out, almost all species of gliders – even blue-helmeted Rocket “Rocky” J. Squirrel – are members of the Pink Ladies. They are one of the very few glowing mammals; the only other known mammalian species to have fluorescent fur are certain opossums.
But why do these airborne rodents glow pink? Is it because of an overintake of bubblegum? Are flying squirrels just really flamboyant but also shy? Are they huge fans of the singer Pink?
A biologist involved in studying these colorful critters hypothesized that the reason is slightly more related to environment than musical preference. Flying squirrels are nocturnal, making them most active when UV light is most prominent. The garish glow might have something to do with nighttime perception.
However, we don’t know the answer for sure. And in the meantime, we can choose to believe flying squirrels eat way too much cotton candy.
Buzz, feed, diet. Repeat
Guns don’t hurt this mass murderer. Police can’t arrest it. Background checks are pointless. A border wall won’t keep it out. So, how do you stop a mosquito?
Diet drugs.
Because female mosquitoes transmit malaria, Zika, and other diseases when they move from person to person feeding on human blood, investigators sought to curb that appetite by chemically re-creating the feeling of fullness they get after a big meal.
The lady killers in their study – Aedes aegypti, to be exact – when given an antiobesity drug that suppresses human appetite by activating neuropeptide receptors that regulate food intake, turned away from a tempting piece of nylon stocking that had been worn by one of the researchers. Further work showed that treated mosquitoes were as disinterested in feeding on a live mouse as mosquitoes that had already enjoyed a full blood meal.
The LOTME research staff (What? Of course, we have a research staff. You don’t?) is working on the mosquito problem too, although we’ve taken a somewhat different approach: The “volunteers” who walk into the mosquito-filled room wear a sign that says, “My blood will make your butt look bigger.”
Getting a good night’s sleep
For most things, the harder you work at it, the more successful you’ll be. Except when it comes to sleep. Nothing frightens sleep away faster than an all-out effort to find it. And yet, it should be the easiest of all health habits to cultivate. Sleep should be a hardwired, physiologic, default condition (sort of like eating and sex, all are which are evolutionary imperatives). And yet, lack of sleep is a common and grave problem even in our safe and comfortable modern environment.

Lack of sleep depletes your willpower, making it less likely you’ll actually go to the gym or be able to resist that bear claw pastry calling you back to the break room. Poor sleep impairs your ability to lose and keep off weight. It can lead to mistakes of inattention – a problem if you’re flying a plane or screening for melanoma.
As a recovering insomniac, I’ve scouted out the territory for you and have taken a few notes as a Baedeker on your journey to better sleep. Tracking sleep is easy; most any fitness tracker or smart watch outfitted with the right app will do the work for you. I’ve used my Apple Watch and Pillow for years. (I’ve no conflict of interest). I’ve found that the quality score it provides each night is interesting, but not all that important. Using pad and paper you could just as easily quantify your sleep: How many hours were you in bed, asleep, and how did you feel the next day.
Here is something important I learned about myself: I don’t need 8 hours. You might not either. Most articles say that we adults need 7-8 hours of sleep. I wasted a lot of effort trying to keep it above the 7-hour mark. Then I realized that even on nights when I got 6-7, I felt fine the next day! Don’t assume you need 8 hours. It could be 6 or it could be 9. It might in fact change depending on how you slept recently, what is happening in your life, or which season it is. If you feel alert and well rested, then you’ve likely found all the sleep you need.
Let’s assume you aren’t well rested. Now what? Like most of good health, a behavioral approach is needed to get you on the right path. You’ve likely heard that bright, particularly blue, light is harmful to falling asleep. Good news! Most devices will let you filter blue light out if you must continue that “Better Call Saul” binge. Better options: Leave your tablet in the living room and plug in your phone on the opposite side of the room (with a short cord). Invest instead in a book light and actual books. There is something about the patina of paper that can encourage sleep to come find you.
Keep the room comfortably cool. What’s important here is the temperature drop. That is, going from warm to cool. This is why a warm shower or bath before getting into bed can help you. Your temperature will drop, a signal for sleep.

So now you’re asleep. But wait, you say you’re awake again and it’s 3:00 a.m.? This is sleep maintenance insomnia. You lie there, patiently waiting, like anticipating your waiter’s return when you’re eating in Rome – ah, you could be there all night. Nothing you do seems to bring sleep back around. The best advice is to try to retrain yourself that when you are up, you’re up, and when in bed, you’re asleep. You can try getting up, moving to a different room. Try meditation or reading. Wait until you feel the urge to sleep sneak back on you, then head back to bed. Although sometimes difficult, you might consider riding it out. If you can’t fall back, then get on with your day (although I don’t recommend sending emails at 3:45 a.m., it freaks people out, I’ve learned). The following night, you will likely be sleep deprived and might find you can fall asleep easier and for longer.
Be forgiving. Unlike your diet or exercise, sleep isn’t as much in your control. You can work a little harder in spin, or double your effort to keep to your plant/keto diet. But for sleep, you must just be patient. It will come. When it is good and ready.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
For most things, the harder you work at it, the more successful you’ll be. Except when it comes to sleep. Nothing frightens sleep away faster than an all-out effort to find it. And yet, it should be the easiest of all health habits to cultivate. Sleep should be a hardwired, physiologic, default condition (sort of like eating and sex, all are which are evolutionary imperatives). And yet, lack of sleep is a common and grave problem even in our safe and comfortable modern environment.
Lack of sleep depletes your willpower, making it less likely you’ll actually go to the gym or be able to resist that bear claw pastry calling you back to the break room. Poor sleep impairs your ability to lose and keep off weight. It can lead to mistakes of inattention – a problem if you’re flying a plane or screening for melanoma.
As a recovering insomniac, I’ve scouted out the territory for you and have taken a few notes as a Baedeker on your journey to better sleep. Tracking sleep is easy; most any fitness tracker or smart watch outfitted with the right app will do the work for you. I’ve used my Apple Watch and Pillow for years. (I’ve no conflict of interest). I’ve found that the quality score it provides each night is interesting, but not all that important. Using pad and paper you could just as easily quantify your sleep: How many hours were you in bed, asleep, and how did you feel the next day.
Here is something important I learned about myself: I don’t need 8 hours. You might not either. Most articles say that we adults need 7-8 hours of sleep. I wasted a lot of effort trying to keep it above the 7-hour mark. Then I realized that even on nights when I got 6-7, I felt fine the next day! Don’t assume you need 8 hours. It could be 6 or it could be 9. It might in fact change depending on how you slept recently, what is happening in your life, or which season it is. If you feel alert and well rested, then you’ve likely found all the sleep you need.
Let’s assume you aren’t well rested. Now what? Like most of good health, a behavioral approach is needed to get you on the right path. You’ve likely heard that bright, particularly blue, light is harmful to falling asleep. Good news! Most devices will let you filter blue light out if you must continue that “Better Call Saul” binge. Better options: Leave your tablet in the living room and plug in your phone on the opposite side of the room (with a short cord). Invest instead in a book light and actual books. There is something about the patina of paper that can encourage sleep to come find you.
Keep the room comfortably cool. What’s important here is the temperature drop. That is, going from warm to cool. This is why a warm shower or bath before getting into bed can help you. Your temperature will drop, a signal for sleep.
So now you’re asleep. But wait, you say you’re awake again and it’s 3:00 a.m.? This is sleep maintenance insomnia. You lie there, patiently waiting, like anticipating your waiter’s return when you’re eating in Rome – ah, you could be there all night. Nothing you do seems to bring sleep back around. The best advice is to try to retrain yourself that when you are up, you’re up, and when in bed, you’re asleep. You can try getting up, moving to a different room. Try meditation or reading. Wait until you feel the urge to sleep sneak back on you, then head back to bed. Although sometimes difficult, you might consider riding it out. If you can’t fall back, then get on with your day (although I don’t recommend sending emails at 3:45 a.m., it freaks people out, I’ve learned). The following night, you will likely be sleep deprived and might find you can fall asleep easier and for longer.
Be forgiving. Unlike your diet or exercise, sleep isn’t as much in your control. You can work a little harder in spin, or double your effort to keep to your plant/keto diet. But for sleep, you must just be patient. It will come. When it is good and ready.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
For most things, the harder you work at it, the more successful you’ll be. Except when it comes to sleep. Nothing frightens sleep away faster than an all-out effort to find it. And yet, it should be the easiest of all health habits to cultivate. Sleep should be a hardwired, physiologic, default condition (sort of like eating and sex, all are which are evolutionary imperatives). And yet, lack of sleep is a common and grave problem even in our safe and comfortable modern environment.
Lack of sleep depletes your willpower, making it less likely you’ll actually go to the gym or be able to resist that bear claw pastry calling you back to the break room. Poor sleep impairs your ability to lose and keep off weight. It can lead to mistakes of inattention – a problem if you’re flying a plane or screening for melanoma.
As a recovering insomniac, I’ve scouted out the territory for you and have taken a few notes as a Baedeker on your journey to better sleep. Tracking sleep is easy; most any fitness tracker or smart watch outfitted with the right app will do the work for you. I’ve used my Apple Watch and Pillow for years. (I’ve no conflict of interest). I’ve found that the quality score it provides each night is interesting, but not all that important. Using pad and paper you could just as easily quantify your sleep: How many hours were you in bed, asleep, and how did you feel the next day.
Here is something important I learned about myself: I don’t need 8 hours. You might not either. Most articles say that we adults need 7-8 hours of sleep. I wasted a lot of effort trying to keep it above the 7-hour mark. Then I realized that even on nights when I got 6-7, I felt fine the next day! Don’t assume you need 8 hours. It could be 6 or it could be 9. It might in fact change depending on how you slept recently, what is happening in your life, or which season it is. If you feel alert and well rested, then you’ve likely found all the sleep you need.
Let’s assume you aren’t well rested. Now what? Like most of good health, a behavioral approach is needed to get you on the right path. You’ve likely heard that bright, particularly blue, light is harmful to falling asleep. Good news! Most devices will let you filter blue light out if you must continue that “Better Call Saul” binge. Better options: Leave your tablet in the living room and plug in your phone on the opposite side of the room (with a short cord). Invest instead in a book light and actual books. There is something about the patina of paper that can encourage sleep to come find you.
Keep the room comfortably cool. What’s important here is the temperature drop. That is, going from warm to cool. This is why a warm shower or bath before getting into bed can help you. Your temperature will drop, a signal for sleep.
So now you’re asleep. But wait, you say you’re awake again and it’s 3:00 a.m.? This is sleep maintenance insomnia. You lie there, patiently waiting, like anticipating your waiter’s return when you’re eating in Rome – ah, you could be there all night. Nothing you do seems to bring sleep back around. The best advice is to try to retrain yourself that when you are up, you’re up, and when in bed, you’re asleep. You can try getting up, moving to a different room. Try meditation or reading. Wait until you feel the urge to sleep sneak back on you, then head back to bed. Although sometimes difficult, you might consider riding it out. If you can’t fall back, then get on with your day (although I don’t recommend sending emails at 3:45 a.m., it freaks people out, I’ve learned). The following night, you will likely be sleep deprived and might find you can fall asleep easier and for longer.
Be forgiving. Unlike your diet or exercise, sleep isn’t as much in your control. You can work a little harder in spin, or double your effort to keep to your plant/keto diet. But for sleep, you must just be patient. It will come. When it is good and ready.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.

Medical students and psychiatry
I have the unfortunate task of trying to teach medical students about psychiatry. I say “unfortunate,” as most of them find psychiatry a difficult art to understand, and they seem reluctant to classify psychiatry as a branch of medicine.

In my efforts to keep things simple, I tell that them psychiatry is one of the most difficult branches of medicine as there are very few objective measures we can rely on to make sense of people’s behavior. Regrettably, the American Psychiatric Association’s Diagnostic and Statistical Manual only seems to confuse them more. So, I remind them that, in medicine, 90%-95% of diagnoses can be obtained from doing a good history, and, if we are lucky a drug level will show drugs in the system, a CT scan without contrast will show cerebral atrophy, or there will be a lab result that will be abnormal and point to a diagnosis. But mostly what they will be seeing is unusual behavior they are unable to classify.
So I identifiable brain damage, psychosis, affective disorders, anxiety disorders, and personality disorders. Under the brain damage category, I include the short- and long-term effects of drugs, major neurocognitive disorders (called dementia before DSM-5), cerebrovascular infarcts, traumatic brain injury, and neurodevelopmental disorders. For their exams and, if they are interested in psychiatry, I tell them to study the DSM. I explain to them that when I was in medical school my dermatology professor told us that if we could recognize the 10 most common dermatologic disorders, we would be able to recognize 90% of the skin disorders we would see. It is similar in psychiatry – thus, my five categories.
However, because I do not want them thinking that only schizophrenia causes psychosis, I let them know that at least 40 different factors cause people to be psychotic indicated by auditory hallucinations. Those 40 factors are: 1) acute alcohol intoxication, 2) alcohol withdrawal, 3) alcoholism, 4) Alzheimer’s disease, 5) benzodiazepine withdrawal, 6) cocaine abuse and addiction, 7) chemical poisoning, 8) dehydration, 9) delirium, 10) dissociative disorders, 11) electrolyte imbalances, 12) encephalopathy of various forms, 13) ecstasy, 14) extreme fatigue, 15) falling asleep, 16) fetal alcohol exposure, 17) grief, 18) hallucinogen use, 19) heroin abuse and dependence, 20) high fever, 21) hyperglycemia, 22) hypoglycemia, 23) intellectual disability, 24) lupus, 25) major depression, 26) mania, 27) methamphetamine use, 28) Parkinson’s disease, 29) phencyclidine, 30) postictal states, 31) posttraumatic stress disorder, 32) schizoid or schizotypal personality disorder, 33) schizophrenia, 34) sleep deprivation, 35) sleep paralysis, 36) solvent abuse, 37) traumatic brain injury, 38) temporal lobe epilepsy, 39) uremia. Lastly, I ask them about No. 40 – “normal” (For example, have you ever been walking down the street and thought you heard someone calling your name, but when you turned around no one was there?). Of course, there are many more causes of psychosis, but keeping it simple makes the principle easier to remember.

Regarding affective disorders, I point out to them, as I did in a previous column, that there is a huge difference between major depressive disorders, unhappiness, or sadness, grief, and demoralization. Regarding anxiety disorders, I let the medical students know that, like personality disorders, there is a lot of comorbidity. Yet, if they can distinguish brain damage, psychosis, and affective disorders from anxiety and personality disorders, that will be good enough.
In keeping with trying to help medical students not make assumptions, I always ask them what’s wrong with people who wash their hands 30 times a day. Invariably, the answer is obsessive-compulsive disorder. So, next I ask: Isn’t it possible that the person who washes his hands 30 times a day is a surgeon – or perhaps a patient with schizophrenia who thinks that Martians are beaming germs to his hands?
I guess I raise this issue because I am concerned with the future of psychiatry, and I think that my approach to medical school education provides a framework that can help students learn how to think about and provide care for psychiatric patients.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital’s Medical/Surgical-Psychiatry Inpatient Unit in Chicago, clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago, former president/CEO of the Community Mental Health Council, and former director of the Institute for Juvenile Research (birthplace of child psychiatry), also in Chicago. If you have tricks of the medical school teaching trade that you would like to share, email Dr. Bell at cpnews@mededge.com.
I have the unfortunate task of trying to teach medical students about psychiatry. I say “unfortunate,” as most of them find psychiatry a difficult art to understand, and they seem reluctant to classify psychiatry as a branch of medicine.
In my efforts to keep things simple, I tell that them psychiatry is one of the most difficult branches of medicine as there are very few objective measures we can rely on to make sense of people’s behavior. Regrettably, the American Psychiatric Association’s Diagnostic and Statistical Manual only seems to confuse them more. So, I remind them that, in medicine, 90%-95% of diagnoses can be obtained from doing a good history, and, if we are lucky a drug level will show drugs in the system, a CT scan without contrast will show cerebral atrophy, or there will be a lab result that will be abnormal and point to a diagnosis. But mostly what they will be seeing is unusual behavior they are unable to classify.
So I identifiable brain damage, psychosis, affective disorders, anxiety disorders, and personality disorders. Under the brain damage category, I include the short- and long-term effects of drugs, major neurocognitive disorders (called dementia before DSM-5), cerebrovascular infarcts, traumatic brain injury, and neurodevelopmental disorders. For their exams and, if they are interested in psychiatry, I tell them to study the DSM. I explain to them that when I was in medical school my dermatology professor told us that if we could recognize the 10 most common dermatologic disorders, we would be able to recognize 90% of the skin disorders we would see. It is similar in psychiatry – thus, my five categories.
However, because I do not want them thinking that only schizophrenia causes psychosis, I let them know that at least 40 different factors cause people to be psychotic indicated by auditory hallucinations. Those 40 factors are: 1) acute alcohol intoxication, 2) alcohol withdrawal, 3) alcoholism, 4) Alzheimer’s disease, 5) benzodiazepine withdrawal, 6) cocaine abuse and addiction, 7) chemical poisoning, 8) dehydration, 9) delirium, 10) dissociative disorders, 11) electrolyte imbalances, 12) encephalopathy of various forms, 13) ecstasy, 14) extreme fatigue, 15) falling asleep, 16) fetal alcohol exposure, 17) grief, 18) hallucinogen use, 19) heroin abuse and dependence, 20) high fever, 21) hyperglycemia, 22) hypoglycemia, 23) intellectual disability, 24) lupus, 25) major depression, 26) mania, 27) methamphetamine use, 28) Parkinson’s disease, 29) phencyclidine, 30) postictal states, 31) posttraumatic stress disorder, 32) schizoid or schizotypal personality disorder, 33) schizophrenia, 34) sleep deprivation, 35) sleep paralysis, 36) solvent abuse, 37) traumatic brain injury, 38) temporal lobe epilepsy, 39) uremia. Lastly, I ask them about No. 40 – “normal” (For example, have you ever been walking down the street and thought you heard someone calling your name, but when you turned around no one was there?). Of course, there are many more causes of psychosis, but keeping it simple makes the principle easier to remember.
Regarding affective disorders, I point out to them, as I did in a previous column, that there is a huge difference between major depressive disorders, unhappiness, or sadness, grief, and demoralization. Regarding anxiety disorders, I let the medical students know that, like personality disorders, there is a lot of comorbidity. Yet, if they can distinguish brain damage, psychosis, and affective disorders from anxiety and personality disorders, that will be good enough.
In keeping with trying to help medical students not make assumptions, I always ask them what’s wrong with people who wash their hands 30 times a day. Invariably, the answer is obsessive-compulsive disorder. So, next I ask: Isn’t it possible that the person who washes his hands 30 times a day is a surgeon – or perhaps a patient with schizophrenia who thinks that Martians are beaming germs to his hands?
I guess I raise this issue because I am concerned with the future of psychiatry, and I think that my approach to medical school education provides a framework that can help students learn how to think about and provide care for psychiatric patients.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital’s Medical/Surgical-Psychiatry Inpatient Unit in Chicago, clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago, former president/CEO of the Community Mental Health Council, and former director of the Institute for Juvenile Research (birthplace of child psychiatry), also in Chicago. If you have tricks of the medical school teaching trade that you would like to share, email Dr. Bell at cpnews@mededge.com.
I have the unfortunate task of trying to teach medical students about psychiatry. I say “unfortunate,” as most of them find psychiatry a difficult art to understand, and they seem reluctant to classify psychiatry as a branch of medicine.
In my efforts to keep things simple, I tell that them psychiatry is one of the most difficult branches of medicine as there are very few objective measures we can rely on to make sense of people’s behavior. Regrettably, the American Psychiatric Association’s Diagnostic and Statistical Manual only seems to confuse them more. So, I remind them that, in medicine, 90%-95% of diagnoses can be obtained from doing a good history, and, if we are lucky a drug level will show drugs in the system, a CT scan without contrast will show cerebral atrophy, or there will be a lab result that will be abnormal and point to a diagnosis. But mostly what they will be seeing is unusual behavior they are unable to classify.
So I identifiable brain damage, psychosis, affective disorders, anxiety disorders, and personality disorders. Under the brain damage category, I include the short- and long-term effects of drugs, major neurocognitive disorders (called dementia before DSM-5), cerebrovascular infarcts, traumatic brain injury, and neurodevelopmental disorders. For their exams and, if they are interested in psychiatry, I tell them to study the DSM. I explain to them that when I was in medical school my dermatology professor told us that if we could recognize the 10 most common dermatologic disorders, we would be able to recognize 90% of the skin disorders we would see. It is similar in psychiatry – thus, my five categories.
However, because I do not want them thinking that only schizophrenia causes psychosis, I let them know that at least 40 different factors cause people to be psychotic indicated by auditory hallucinations. Those 40 factors are: 1) acute alcohol intoxication, 2) alcohol withdrawal, 3) alcoholism, 4) Alzheimer’s disease, 5) benzodiazepine withdrawal, 6) cocaine abuse and addiction, 7) chemical poisoning, 8) dehydration, 9) delirium, 10) dissociative disorders, 11) electrolyte imbalances, 12) encephalopathy of various forms, 13) ecstasy, 14) extreme fatigue, 15) falling asleep, 16) fetal alcohol exposure, 17) grief, 18) hallucinogen use, 19) heroin abuse and dependence, 20) high fever, 21) hyperglycemia, 22) hypoglycemia, 23) intellectual disability, 24) lupus, 25) major depression, 26) mania, 27) methamphetamine use, 28) Parkinson’s disease, 29) phencyclidine, 30) postictal states, 31) posttraumatic stress disorder, 32) schizoid or schizotypal personality disorder, 33) schizophrenia, 34) sleep deprivation, 35) sleep paralysis, 36) solvent abuse, 37) traumatic brain injury, 38) temporal lobe epilepsy, 39) uremia. Lastly, I ask them about No. 40 – “normal” (For example, have you ever been walking down the street and thought you heard someone calling your name, but when you turned around no one was there?). Of course, there are many more causes of psychosis, but keeping it simple makes the principle easier to remember.
Regarding affective disorders, I point out to them, as I did in a previous column, that there is a huge difference between major depressive disorders, unhappiness, or sadness, grief, and demoralization. Regarding anxiety disorders, I let the medical students know that, like personality disorders, there is a lot of comorbidity. Yet, if they can distinguish brain damage, psychosis, and affective disorders from anxiety and personality disorders, that will be good enough.
In keeping with trying to help medical students not make assumptions, I always ask them what’s wrong with people who wash their hands 30 times a day. Invariably, the answer is obsessive-compulsive disorder. So, next I ask: Isn’t it possible that the person who washes his hands 30 times a day is a surgeon – or perhaps a patient with schizophrenia who thinks that Martians are beaming germs to his hands?
I guess I raise this issue because I am concerned with the future of psychiatry, and I think that my approach to medical school education provides a framework that can help students learn how to think about and provide care for psychiatric patients.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital’s Medical/Surgical-Psychiatry Inpatient Unit in Chicago, clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago, former president/CEO of the Community Mental Health Council, and former director of the Institute for Juvenile Research (birthplace of child psychiatry), also in Chicago. If you have tricks of the medical school teaching trade that you would like to share, email Dr. Bell at cpnews@mededge.com.

Failure to launch can happen to college students
March often is the time of year when college freshmen truly begin to feel comfortable in their new settings. Many students report feeling excited to get back to campus after the long winter break, and once into their second semester, they feel more comfortable with the independence from family and high school supports. It also is a time for some college freshmen to return home after failing to manage this major transition.

Of the latter group, many will have had difficult months of depression, anxiety, or substance use, and most will be suffering from a deep sense of shame after failing to navigate this long-anticipated transition. Asking detailed questions about their academic challenges, social lives, self-care, and sleep while they were on campus will help you make thoughtful recommendations to your patients and their parents about how they might best get back on track.
Some students will report a great social experience, but academic struggles. They will report some normal ups and downs emotionally, but most of their distress will have been focused on their academic performance. Many 18-year-olds have not had to organize their time and effort around homework without the attention and support of parents and teachers. College often has much bigger classes, with less personal attention. There is a lot of assigned reading, but no regular incremental homework, only a major midterm and final exam, or a substantial paper. For a student who gets anxious about performance, or one with organizational challenges, this can lead to procrastination and poor performance.
Find out details about how they did academically. Did they fail one class or many classes? Did they receive some incompletes in their first semester and then struggle to catch up with them while keeping up with their second semester work? Did they have tutoring or support? Were they unrealistic about their course load? Or did they have their first serious relationship and not spend enough time on homework? Did they spend too much time partying with their new friends and not enough time sleeping and getting their homework done?
It is important to dig deeper if patients report regular or binge drug and alcohol use that interfered with their academic performance, as they may need more substantial substance use disorder treatment. Most students, though, will not have a substance use disorder. Instead, their academic failure could represent something as simple as the need for more academic support and time management support. Many schools have such programs to help students learn how to better manage their time and effort as they take fuller responsibility than they had for it in high school.
For other students, you will learn that their emotional distress preceded their academic troubles. The stress of the transition to college may be enough to trigger an episode of depression or to exacerbate a mood or anxiety disorder that was subclinical or in remission before school started. These students usually will report that sadness, intense anxiety, or loss of interest came early in their semester; perhaps they were even doing well academically when these problems started.
Ask about how their sleep was. Often they had difficulty falling asleep or woke up often at night, unlike most college students, whose sleep is compromised because they stay up late with new friends or because they are hard at work, but could easily sleep at any time.
Find out about their eating habits. Did they lose their appetite? Lose weight? Did they become preoccupied with weight or body image issues and begin restricting their intake? Eating disorders can begin in college when vulnerable students are stressed and have more control over their diet. While weight gain is more common in freshman year, it often is connected to poor stress management skills, and is more often a marker of a student who was struggling academically and then managing stress by overeating.
In the case where the distress came first, it is critical that your patients have a thorough psychiatric evaluation and treatment. It may be possible for them to return to school quickly, but it is most important that they are engaged in effective treatment and in at last partial remission before adding to their stress by attempting to return to school. Often, ambitious students and their parents need to hear this message very clearly from a pediatrician. A rushed return to school may be a set-up for a more protracted and difficult course of illness. For these students, it may be better to have a fresh start in a new semester. Help them (and their parents) to understand that they should use their time off to focus on treatment and good self-care so they might benefit from the many opportunities of college.
For a small minority of college students who do not succeed at college, their social withdrawal, academic deterioration, anxiety, and loss of interest in previous passions may occur alongside more serious psychiatric symptoms such as auditory hallucinations, paranoia, or grandiosity. Any time there is a suggestion of psychotic symptoms in a previously healthy person in the late teens or early 20s, a prompt comprehensive psychiatric evaluation is critical. These years are when most chronic psychotic disorders, such as schizophrenia, are likely to emerge. These patients require a thorough evaluation to distinguish these disorders from other illnesses, especially when they occur with substance use. And these patients require specialized care.
If your patient appears to have any psychotic symptoms, it is critical that you help the family find an excellent psychiatrist, or even a clinic that specializes in thought disorders so that he or she may get the best possible care early.

There is another class of students who withdraw from college who will need more comprehensive remediation, but not connected to any psychiatric diagnosis. Some young people may not be developmentally ready for college. These are your patients who often were excellent performers in high school, perhaps academically and athletically, but whose performance was more connected to pleasing important adults than to genuine motivating passions or sense of purpose. These young adults may have been drawn into the intense, results-oriented forces that are powerful in many of our high schools. If they did not have enough time or space to explore a host of interests, and to then manage the routine failures, setbacks, and disappointments that are essential to healthy adolescent development, they are going to run out of fuel in college. Such students often are quite dependent on their parents, and struggle with the independence college offers.

If your patients report that they could not muster the same intense work ethic they previously had, without any evidence of a psychiatric illness interfering with motivation, they may need time to finish the developmental work of cultivating a deep and rich sense of their own identity. Some students can do this at college, provided they, their parents and their school offer them adequate time before they have to declare a major. Other students will need to get a job and explore interests with a few courses at a community college, cultivating independence while learning about their own strengths and weaknesses and their genuine interests. This way, when they return to school, they will be motivated by a genuine sense of purpose and self-knowledge.
“Failure to launch” is a critical symptom at a key transitional moment. Pediatric providers can be essential to their patients and families by clarifying the nature of the difficulty and coordinating a reasonable plan to get these young adults back on track to healthy adulthood.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
March often is the time of year when college freshmen truly begin to feel comfortable in their new settings. Many students report feeling excited to get back to campus after the long winter break, and once into their second semester, they feel more comfortable with the independence from family and high school supports. It also is a time for some college freshmen to return home after failing to manage this major transition.
Of the latter group, many will have had difficult months of depression, anxiety, or substance use, and most will be suffering from a deep sense of shame after failing to navigate this long-anticipated transition. Asking detailed questions about their academic challenges, social lives, self-care, and sleep while they were on campus will help you make thoughtful recommendations to your patients and their parents about how they might best get back on track.
Some students will report a great social experience, but academic struggles. They will report some normal ups and downs emotionally, but most of their distress will have been focused on their academic performance. Many 18-year-olds have not had to organize their time and effort around homework without the attention and support of parents and teachers. College often has much bigger classes, with less personal attention. There is a lot of assigned reading, but no regular incremental homework, only a major midterm and final exam, or a substantial paper. For a student who gets anxious about performance, or one with organizational challenges, this can lead to procrastination and poor performance.
Find out details about how they did academically. Did they fail one class or many classes? Did they receive some incompletes in their first semester and then struggle to catch up with them while keeping up with their second semester work? Did they have tutoring or support? Were they unrealistic about their course load? Or did they have their first serious relationship and not spend enough time on homework? Did they spend too much time partying with their new friends and not enough time sleeping and getting their homework done?
It is important to dig deeper if patients report regular or binge drug and alcohol use that interfered with their academic performance, as they may need more substantial substance use disorder treatment. Most students, though, will not have a substance use disorder. Instead, their academic failure could represent something as simple as the need for more academic support and time management support. Many schools have such programs to help students learn how to better manage their time and effort as they take fuller responsibility than they had for it in high school.
For other students, you will learn that their emotional distress preceded their academic troubles. The stress of the transition to college may be enough to trigger an episode of depression or to exacerbate a mood or anxiety disorder that was subclinical or in remission before school started. These students usually will report that sadness, intense anxiety, or loss of interest came early in their semester; perhaps they were even doing well academically when these problems started.
Ask about how their sleep was. Often they had difficulty falling asleep or woke up often at night, unlike most college students, whose sleep is compromised because they stay up late with new friends or because they are hard at work, but could easily sleep at any time.
Find out about their eating habits. Did they lose their appetite? Lose weight? Did they become preoccupied with weight or body image issues and begin restricting their intake? Eating disorders can begin in college when vulnerable students are stressed and have more control over their diet. While weight gain is more common in freshman year, it often is connected to poor stress management skills, and is more often a marker of a student who was struggling academically and then managing stress by overeating.
In the case where the distress came first, it is critical that your patients have a thorough psychiatric evaluation and treatment. It may be possible for them to return to school quickly, but it is most important that they are engaged in effective treatment and in at last partial remission before adding to their stress by attempting to return to school. Often, ambitious students and their parents need to hear this message very clearly from a pediatrician. A rushed return to school may be a set-up for a more protracted and difficult course of illness. For these students, it may be better to have a fresh start in a new semester. Help them (and their parents) to understand that they should use their time off to focus on treatment and good self-care so they might benefit from the many opportunities of college.
For a small minority of college students who do not succeed at college, their social withdrawal, academic deterioration, anxiety, and loss of interest in previous passions may occur alongside more serious psychiatric symptoms such as auditory hallucinations, paranoia, or grandiosity. Any time there is a suggestion of psychotic symptoms in a previously healthy person in the late teens or early 20s, a prompt comprehensive psychiatric evaluation is critical. These years are when most chronic psychotic disorders, such as schizophrenia, are likely to emerge. These patients require a thorough evaluation to distinguish these disorders from other illnesses, especially when they occur with substance use. And these patients require specialized care.
If your patient appears to have any psychotic symptoms, it is critical that you help the family find an excellent psychiatrist, or even a clinic that specializes in thought disorders so that he or she may get the best possible care early.
There is another class of students who withdraw from college who will need more comprehensive remediation, but not connected to any psychiatric diagnosis. Some young people may not be developmentally ready for college. These are your patients who often were excellent performers in high school, perhaps academically and athletically, but whose performance was more connected to pleasing important adults than to genuine motivating passions or sense of purpose. These young adults may have been drawn into the intense, results-oriented forces that are powerful in many of our high schools. If they did not have enough time or space to explore a host of interests, and to then manage the routine failures, setbacks, and disappointments that are essential to healthy adolescent development, they are going to run out of fuel in college. Such students often are quite dependent on their parents, and struggle with the independence college offers.
If your patients report that they could not muster the same intense work ethic they previously had, without any evidence of a psychiatric illness interfering with motivation, they may need time to finish the developmental work of cultivating a deep and rich sense of their own identity. Some students can do this at college, provided they, their parents and their school offer them adequate time before they have to declare a major. Other students will need to get a job and explore interests with a few courses at a community college, cultivating independence while learning about their own strengths and weaknesses and their genuine interests. This way, when they return to school, they will be motivated by a genuine sense of purpose and self-knowledge.
“Failure to launch” is a critical symptom at a key transitional moment. Pediatric providers can be essential to their patients and families by clarifying the nature of the difficulty and coordinating a reasonable plan to get these young adults back on track to healthy adulthood.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
March often is the time of year when college freshmen truly begin to feel comfortable in their new settings. Many students report feeling excited to get back to campus after the long winter break, and once into their second semester, they feel more comfortable with the independence from family and high school supports. It also is a time for some college freshmen to return home after failing to manage this major transition.
Of the latter group, many will have had difficult months of depression, anxiety, or substance use, and most will be suffering from a deep sense of shame after failing to navigate this long-anticipated transition. Asking detailed questions about their academic challenges, social lives, self-care, and sleep while they were on campus will help you make thoughtful recommendations to your patients and their parents about how they might best get back on track.
Some students will report a great social experience, but academic struggles. They will report some normal ups and downs emotionally, but most of their distress will have been focused on their academic performance. Many 18-year-olds have not had to organize their time and effort around homework without the attention and support of parents and teachers. College often has much bigger classes, with less personal attention. There is a lot of assigned reading, but no regular incremental homework, only a major midterm and final exam, or a substantial paper. For a student who gets anxious about performance, or one with organizational challenges, this can lead to procrastination and poor performance.
Find out details about how they did academically. Did they fail one class or many classes? Did they receive some incompletes in their first semester and then struggle to catch up with them while keeping up with their second semester work? Did they have tutoring or support? Were they unrealistic about their course load? Or did they have their first serious relationship and not spend enough time on homework? Did they spend too much time partying with their new friends and not enough time sleeping and getting their homework done?
It is important to dig deeper if patients report regular or binge drug and alcohol use that interfered with their academic performance, as they may need more substantial substance use disorder treatment. Most students, though, will not have a substance use disorder. Instead, their academic failure could represent something as simple as the need for more academic support and time management support. Many schools have such programs to help students learn how to better manage their time and effort as they take fuller responsibility than they had for it in high school.
For other students, you will learn that their emotional distress preceded their academic troubles. The stress of the transition to college may be enough to trigger an episode of depression or to exacerbate a mood or anxiety disorder that was subclinical or in remission before school started. These students usually will report that sadness, intense anxiety, or loss of interest came early in their semester; perhaps they were even doing well academically when these problems started.
Ask about how their sleep was. Often they had difficulty falling asleep or woke up often at night, unlike most college students, whose sleep is compromised because they stay up late with new friends or because they are hard at work, but could easily sleep at any time.
Find out about their eating habits. Did they lose their appetite? Lose weight? Did they become preoccupied with weight or body image issues and begin restricting their intake? Eating disorders can begin in college when vulnerable students are stressed and have more control over their diet. While weight gain is more common in freshman year, it often is connected to poor stress management skills, and is more often a marker of a student who was struggling academically and then managing stress by overeating.
In the case where the distress came first, it is critical that your patients have a thorough psychiatric evaluation and treatment. It may be possible for them to return to school quickly, but it is most important that they are engaged in effective treatment and in at last partial remission before adding to their stress by attempting to return to school. Often, ambitious students and their parents need to hear this message very clearly from a pediatrician. A rushed return to school may be a set-up for a more protracted and difficult course of illness. For these students, it may be better to have a fresh start in a new semester. Help them (and their parents) to understand that they should use their time off to focus on treatment and good self-care so they might benefit from the many opportunities of college.
For a small minority of college students who do not succeed at college, their social withdrawal, academic deterioration, anxiety, and loss of interest in previous passions may occur alongside more serious psychiatric symptoms such as auditory hallucinations, paranoia, or grandiosity. Any time there is a suggestion of psychotic symptoms in a previously healthy person in the late teens or early 20s, a prompt comprehensive psychiatric evaluation is critical. These years are when most chronic psychotic disorders, such as schizophrenia, are likely to emerge. These patients require a thorough evaluation to distinguish these disorders from other illnesses, especially when they occur with substance use. And these patients require specialized care.
If your patient appears to have any psychotic symptoms, it is critical that you help the family find an excellent psychiatrist, or even a clinic that specializes in thought disorders so that he or she may get the best possible care early.
There is another class of students who withdraw from college who will need more comprehensive remediation, but not connected to any psychiatric diagnosis. Some young people may not be developmentally ready for college. These are your patients who often were excellent performers in high school, perhaps academically and athletically, but whose performance was more connected to pleasing important adults than to genuine motivating passions or sense of purpose. These young adults may have been drawn into the intense, results-oriented forces that are powerful in many of our high schools. If they did not have enough time or space to explore a host of interests, and to then manage the routine failures, setbacks, and disappointments that are essential to healthy adolescent development, they are going to run out of fuel in college. Such students often are quite dependent on their parents, and struggle with the independence college offers.
If your patients report that they could not muster the same intense work ethic they previously had, without any evidence of a psychiatric illness interfering with motivation, they may need time to finish the developmental work of cultivating a deep and rich sense of their own identity. Some students can do this at college, provided they, their parents and their school offer them adequate time before they have to declare a major. Other students will need to get a job and explore interests with a few courses at a community college, cultivating independence while learning about their own strengths and weaknesses and their genuine interests. This way, when they return to school, they will be motivated by a genuine sense of purpose and self-knowledge.
“Failure to launch” is a critical symptom at a key transitional moment. Pediatric providers can be essential to their patients and families by clarifying the nature of the difficulty and coordinating a reasonable plan to get these young adults back on track to healthy adulthood.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
Adenovirus: More than just another viral illness
The mother of three looked tired and little worried. She wasn’t one to bring her kids to the pediatrician’s office with every minor illness, but her youngest had 3 days of fever, runny nose, cough, and little of her normal energy.

The pediatrician entered the room and smiled sympathetically.
“We ran tests for flu and RSV [respiratory syncytial virus] and it’s neither of those so. ...”
“So it’s just a virus that we don’t routinely test for and it’s going to need to run its course,” the mother finished his sentence. She knew the drill.
Before the doctor could leave the room though, the mother had one more question. “You don’t think it could be adenovirus do you?”
Most years, influenza and RSV command center stage, and adenovirus is relegated to the wings. It is not so much lack of disease or morbidity, but rather lack of recognition. Yes, we all learned in medical school that it is a cause of epidemic keratoconjunctivitis, but many adenoviral infections are clinically indistinguishable from infections caused by other viruses. Common symptoms – fever, cough, sore throat, and malaise – overlap with those caused by influenza. Like rhinovirus, adenovirus can cause common cold symptoms. Like RSV, it can cause bronchiolitis. Just like parainfluenza, it can cause croup. It can cause a pertussislike syndrome with prolonged cough, and enteric adenoviruses, especially types 40 and 41, cause gastroenteritis that mimics norovirus or rotavirus infection.
Testing for adenovirus is not readily available or routine in most pediatricians’ offices, and while many hospitals and reference labs offer adenovirus polymerase chain reaction testing as part of a comprehensive respiratory virus panel, the test can be expensive and unlikely to change management in most ambulatory patients. This makes it difficult to count the number of adenoviruses annually.
This winter though, adenovirus was in the news ... repeatedly. In November 2018, CBS News reported that a University of Maryland freshman had died of an adenovirus-related illness. The family of Olivia Paregol told reporters that she was being treated for Crohn’s disease. Immune suppression is one recognized risk factor for more severe adenoviral disease; underlying heart and lung disease are others. Testing at the Centers for Disease Control and Prevention revealed that the student and several others on campus were infected with adenovirus type 7, a strain that has been associated with outbreaks of acute, severe respiratory illness in military recruits. As of Jan. 24, 2019, university officials reported 42 confirmed cases of adenovirus in University of Maryland students, 13 of which were confirmed as adenovirus 7.
Adenovirus type 7 also caused an outbreak at a pediatric long-term care facility in New Jersey late last year. Between Sept. 26 and Nov. 11, 2018, 36 residents and 1 staff member became ill. Eleven individuals died. In an unrelated outbreak at a second pediatric long-term care facility, 17 residents were affected between Oct. 20 and Dec. 10, 2018. Adenovirus 3 was identified and all children recovered.
Between October 2013 and July 2014, public health officials in Oregon identified an increase in adenoviral infections in people with respiratory illness. Sixty-nine percent were hospitalized (136/198), 31% needed intensive care, and 18% were mechanically ventilated. Multiple types of adenovirus were recovered but the most common was adenovirus 7 (Emerg Infect Dis. 2016. doi: 10.3201/eid2206.151898).

Depending on your perspective, measures to prevent the spread of adenovirus are elegantly simple, evidence-based, public health intervention or maddeningly little more than common sense. Wash your hands often with soap and water. Avoid touching your eyes, mouth, and nose with unwashed hands. Avoid close contact with people who are sick. The latter is easier if those who are sick stay home. Prior to the start of the most recent academic semester at the University of Maryland, university officials urged students who were sick not to return to campus but to stay at home to rest and recover. Those who fell ill on campus were urged to return home via nonpublic transportation if possible. Those who stayed on campus were advised to stay in their living spaces and clean high-touch surfaces with bleach. Like other nonenveloped viruses, adenovirus is not easily destroyed by many commonly used disinfectants. Under ideal conditions, it can survive on surfaces – remaining infectious – for up to 3 months.
Back at the pediatrician’s office, “We need an adenovirus vaccine,” the mother said as she picked up her child and headed for the door.
There is, in fact, a live oral vaccine that protects against adenovirus types 4 and 7. It is only approved for use in United States military personnel aged 17-50 years and it is given to all recruits as soon as they enter basic training. It works too. Before vaccine was available, up to 80% of recruits became infected during their initial training, half of those developing significant illness and a quarter being hospitalized. When the current vaccine was introduced in 2011, there was a 100-fold decrease in adenovirus-related disease burden (from 5.8 to 0.02 cases per 1,000 person-weeks, P less than .0001). That translates to 1 death, 1,100-2,700 hospitalizations and 13,000 febrile illnesses prevented each year (Clin Infect Dis. 2014 Oct 1. doi: 10.1093/cid/ciu507).
Some experts have suggested that adenovirus vaccine could be useful in civilian populations, too, but I question what the public reception would be. We have safe influenza vaccines that reduce the need for hospitalization and reduce mortality from influenza, but we still can’t convince some people to immunize themselves and their children. In the last 4 years, flu vaccination rates among children have remained just shy of 60% and adult rates are even lower. Collectively, we don’t seem to be ready to relinquish – or at least diminish – the annual suffering that goes with flu. I have to wonder if the same would be true for adenovirus.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
The mother of three looked tired and little worried. She wasn’t one to bring her kids to the pediatrician’s office with every minor illness, but her youngest had 3 days of fever, runny nose, cough, and little of her normal energy.
The pediatrician entered the room and smiled sympathetically.
“We ran tests for flu and RSV [respiratory syncytial virus] and it’s neither of those so. ...”
“So it’s just a virus that we don’t routinely test for and it’s going to need to run its course,” the mother finished his sentence. She knew the drill.
Before the doctor could leave the room though, the mother had one more question. “You don’t think it could be adenovirus do you?”
Most years, influenza and RSV command center stage, and adenovirus is relegated to the wings. It is not so much lack of disease or morbidity, but rather lack of recognition. Yes, we all learned in medical school that it is a cause of epidemic keratoconjunctivitis, but many adenoviral infections are clinically indistinguishable from infections caused by other viruses. Common symptoms – fever, cough, sore throat, and malaise – overlap with those caused by influenza. Like rhinovirus, adenovirus can cause common cold symptoms. Like RSV, it can cause bronchiolitis. Just like parainfluenza, it can cause croup. It can cause a pertussislike syndrome with prolonged cough, and enteric adenoviruses, especially types 40 and 41, cause gastroenteritis that mimics norovirus or rotavirus infection.
Testing for adenovirus is not readily available or routine in most pediatricians’ offices, and while many hospitals and reference labs offer adenovirus polymerase chain reaction testing as part of a comprehensive respiratory virus panel, the test can be expensive and unlikely to change management in most ambulatory patients. This makes it difficult to count the number of adenoviruses annually.
This winter though, adenovirus was in the news ... repeatedly. In November 2018, CBS News reported that a University of Maryland freshman had died of an adenovirus-related illness. The family of Olivia Paregol told reporters that she was being treated for Crohn’s disease. Immune suppression is one recognized risk factor for more severe adenoviral disease; underlying heart and lung disease are others. Testing at the Centers for Disease Control and Prevention revealed that the student and several others on campus were infected with adenovirus type 7, a strain that has been associated with outbreaks of acute, severe respiratory illness in military recruits. As of Jan. 24, 2019, university officials reported 42 confirmed cases of adenovirus in University of Maryland students, 13 of which were confirmed as adenovirus 7.
Adenovirus type 7 also caused an outbreak at a pediatric long-term care facility in New Jersey late last year. Between Sept. 26 and Nov. 11, 2018, 36 residents and 1 staff member became ill. Eleven individuals died. In an unrelated outbreak at a second pediatric long-term care facility, 17 residents were affected between Oct. 20 and Dec. 10, 2018. Adenovirus 3 was identified and all children recovered.
Between October 2013 and July 2014, public health officials in Oregon identified an increase in adenoviral infections in people with respiratory illness. Sixty-nine percent were hospitalized (136/198), 31% needed intensive care, and 18% were mechanically ventilated. Multiple types of adenovirus were recovered but the most common was adenovirus 7 (Emerg Infect Dis. 2016. doi: 10.3201/eid2206.151898).
Depending on your perspective, measures to prevent the spread of adenovirus are elegantly simple, evidence-based, public health intervention or maddeningly little more than common sense. Wash your hands often with soap and water. Avoid touching your eyes, mouth, and nose with unwashed hands. Avoid close contact with people who are sick. The latter is easier if those who are sick stay home. Prior to the start of the most recent academic semester at the University of Maryland, university officials urged students who were sick not to return to campus but to stay at home to rest and recover. Those who fell ill on campus were urged to return home via nonpublic transportation if possible. Those who stayed on campus were advised to stay in their living spaces and clean high-touch surfaces with bleach. Like other nonenveloped viruses, adenovirus is not easily destroyed by many commonly used disinfectants. Under ideal conditions, it can survive on surfaces – remaining infectious – for up to 3 months.
Back at the pediatrician’s office, “We need an adenovirus vaccine,” the mother said as she picked up her child and headed for the door.
There is, in fact, a live oral vaccine that protects against adenovirus types 4 and 7. It is only approved for use in United States military personnel aged 17-50 years and it is given to all recruits as soon as they enter basic training. It works too. Before vaccine was available, up to 80% of recruits became infected during their initial training, half of those developing significant illness and a quarter being hospitalized. When the current vaccine was introduced in 2011, there was a 100-fold decrease in adenovirus-related disease burden (from 5.8 to 0.02 cases per 1,000 person-weeks, P less than .0001). That translates to 1 death, 1,100-2,700 hospitalizations and 13,000 febrile illnesses prevented each year (Clin Infect Dis. 2014 Oct 1. doi: 10.1093/cid/ciu507).
Some experts have suggested that adenovirus vaccine could be useful in civilian populations, too, but I question what the public reception would be. We have safe influenza vaccines that reduce the need for hospitalization and reduce mortality from influenza, but we still can’t convince some people to immunize themselves and their children. In the last 4 years, flu vaccination rates among children have remained just shy of 60% and adult rates are even lower. Collectively, we don’t seem to be ready to relinquish – or at least diminish – the annual suffering that goes with flu. I have to wonder if the same would be true for adenovirus.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
The mother of three looked tired and little worried. She wasn’t one to bring her kids to the pediatrician’s office with every minor illness, but her youngest had 3 days of fever, runny nose, cough, and little of her normal energy.
The pediatrician entered the room and smiled sympathetically.
“We ran tests for flu and RSV [respiratory syncytial virus] and it’s neither of those so. ...”
“So it’s just a virus that we don’t routinely test for and it’s going to need to run its course,” the mother finished his sentence. She knew the drill.
Before the doctor could leave the room though, the mother had one more question. “You don’t think it could be adenovirus do you?”
Most years, influenza and RSV command center stage, and adenovirus is relegated to the wings. It is not so much lack of disease or morbidity, but rather lack of recognition. Yes, we all learned in medical school that it is a cause of epidemic keratoconjunctivitis, but many adenoviral infections are clinically indistinguishable from infections caused by other viruses. Common symptoms – fever, cough, sore throat, and malaise – overlap with those caused by influenza. Like rhinovirus, adenovirus can cause common cold symptoms. Like RSV, it can cause bronchiolitis. Just like parainfluenza, it can cause croup. It can cause a pertussislike syndrome with prolonged cough, and enteric adenoviruses, especially types 40 and 41, cause gastroenteritis that mimics norovirus or rotavirus infection.
Testing for adenovirus is not readily available or routine in most pediatricians’ offices, and while many hospitals and reference labs offer adenovirus polymerase chain reaction testing as part of a comprehensive respiratory virus panel, the test can be expensive and unlikely to change management in most ambulatory patients. This makes it difficult to count the number of adenoviruses annually.
This winter though, adenovirus was in the news ... repeatedly. In November 2018, CBS News reported that a University of Maryland freshman had died of an adenovirus-related illness. The family of Olivia Paregol told reporters that she was being treated for Crohn’s disease. Immune suppression is one recognized risk factor for more severe adenoviral disease; underlying heart and lung disease are others. Testing at the Centers for Disease Control and Prevention revealed that the student and several others on campus were infected with adenovirus type 7, a strain that has been associated with outbreaks of acute, severe respiratory illness in military recruits. As of Jan. 24, 2019, university officials reported 42 confirmed cases of adenovirus in University of Maryland students, 13 of which were confirmed as adenovirus 7.
Adenovirus type 7 also caused an outbreak at a pediatric long-term care facility in New Jersey late last year. Between Sept. 26 and Nov. 11, 2018, 36 residents and 1 staff member became ill. Eleven individuals died. In an unrelated outbreak at a second pediatric long-term care facility, 17 residents were affected between Oct. 20 and Dec. 10, 2018. Adenovirus 3 was identified and all children recovered.
Between October 2013 and July 2014, public health officials in Oregon identified an increase in adenoviral infections in people with respiratory illness. Sixty-nine percent were hospitalized (136/198), 31% needed intensive care, and 18% were mechanically ventilated. Multiple types of adenovirus were recovered but the most common was adenovirus 7 (Emerg Infect Dis. 2016. doi: 10.3201/eid2206.151898).
Depending on your perspective, measures to prevent the spread of adenovirus are elegantly simple, evidence-based, public health intervention or maddeningly little more than common sense. Wash your hands often with soap and water. Avoid touching your eyes, mouth, and nose with unwashed hands. Avoid close contact with people who are sick. The latter is easier if those who are sick stay home. Prior to the start of the most recent academic semester at the University of Maryland, university officials urged students who were sick not to return to campus but to stay at home to rest and recover. Those who fell ill on campus were urged to return home via nonpublic transportation if possible. Those who stayed on campus were advised to stay in their living spaces and clean high-touch surfaces with bleach. Like other nonenveloped viruses, adenovirus is not easily destroyed by many commonly used disinfectants. Under ideal conditions, it can survive on surfaces – remaining infectious – for up to 3 months.
Back at the pediatrician’s office, “We need an adenovirus vaccine,” the mother said as she picked up her child and headed for the door.
There is, in fact, a live oral vaccine that protects against adenovirus types 4 and 7. It is only approved for use in United States military personnel aged 17-50 years and it is given to all recruits as soon as they enter basic training. It works too. Before vaccine was available, up to 80% of recruits became infected during their initial training, half of those developing significant illness and a quarter being hospitalized. When the current vaccine was introduced in 2011, there was a 100-fold decrease in adenovirus-related disease burden (from 5.8 to 0.02 cases per 1,000 person-weeks, P less than .0001). That translates to 1 death, 1,100-2,700 hospitalizations and 13,000 febrile illnesses prevented each year (Clin Infect Dis. 2014 Oct 1. doi: 10.1093/cid/ciu507).
Some experts have suggested that adenovirus vaccine could be useful in civilian populations, too, but I question what the public reception would be. We have safe influenza vaccines that reduce the need for hospitalization and reduce mortality from influenza, but we still can’t convince some people to immunize themselves and their children. In the last 4 years, flu vaccination rates among children have remained just shy of 60% and adult rates are even lower. Collectively, we don’t seem to be ready to relinquish – or at least diminish – the annual suffering that goes with flu. I have to wonder if the same would be true for adenovirus.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
The Best of 2018 Is Also the Worst
I am a doctor, not an engineer.Dr. McCoy, Star Trek “Mirror, Mirror” episode
Last year in my annual wrap-up, I wrote back-to-back editorials (December 2017 and January 2018) on the worst and best of 2017 from a federal health care perspective, emphasizing ethics or the lack thereof. I featured the altruism of federal health care providers (HCPs) responding to natural disasters and the terrible outcome of seemingly banal moral lapses.
This year the best and worst are one and the same, and I am not sure how it could be otherwise: the Department of Veterans Affairs (VA) and Department of Defense (DoD) electronic health record (EHR) contract with Cerner (North Kansas City, MO). Former VA Secretary David Shulkin, MD, announced the deal in 2017 shortly before his departure, and it was signed under then Acting VA Secretary Robert Wilkie in May of 2018.1 But the reason the Cerner contract is the most impactful and momentous ethical event of the year is perhaps not what readers expect. Search engines will efficiently unearth plentiful drama with ethical import about the contract. There were conspiracy charges that the shadow regime improperly engineered the selection.2 The usual Congressional hearings on the VA leadership mismanagement of the EHR culminated in Sen Jon Tester’s (D-MO) martial declaration in a letter to the newly sworn-in VA Chief Information Officer James Paul Gfrerer that “EHR modernization cannot fail.”3
While all this is obviously important, it is not why the annual awards for ethical and unethical behaviors are bestowed on what is essentially an information technology acquisition. The Cerner contract is chosen because of its enormous potential to change the human practice of health care for good or ill; hence, the dual nomination. This column is not about Cerner qua Cerner but about how the EHR has transformed—or deformed—the humanistic aspects of medical practice.
I am old enough to remember the original transition from paper charts to VistA EHR. As an intern with illegible handwriting, I can remember breathing a sigh of relief when the blue screen appeared for the first time. The commands were cumbersome and the code laborious, but it was a technologic marvel to see the clean, organized progress notes and be able to print your medication list or discharge summary. However, it also was the first stuttering waves of a tsunami that would alter medical practice forever. The human cost of the revolution could be seen almost immediately as older clinicians or those who could not type struggled to complete work that with paper and pen would have been easily accomplished.
For many years there was a steady stream of updates to VistA, including the Computerized Patient Record System (CPRS). For a relatively long time in technology terms, VistA and CPRS were the envy of the medical world, which rushed to catch up. Gradually though, VA fell behind; the wizard IT guys could not patch and fix new versions fast enough, and eventually, like all things created, VistA and CPRS became obsolete.4 Attitudes toward this microcosm of the modernization of an aging organization were intense and diverse. Some of us held onto CPRS as though it was a transitional object that we had personalized and became attached to with all its quirks and problems. Others could not wait to get rid of it, believing anything new and streamlined had to be better.
Yet the opposite also is true. EHRs have been, and could be again, incredible time-savers, enabling HCPs to deliver more evidence-based, patient-centered care in a more accurate, integrated, timely, and comprehensive manner. For example, Cerner finally could discover the Holy Grail of VA-DoD interoperability and even—dare we dream—integrate with the community. Yet as science fiction aficionados know, the machine designed to free humankind of drudgery may also end up controlling us.
The other commonplace year-end practice is for ersatz prophets to predict the future. I have no idea whether the Cerner EHR will be good or bad for VA and DoD. According to the insightful critic of medical culture, Atul Gawande, MD, who has examined the practitioner-computer interface, what we must guard against is that it does not replace the practitioner-patient relationship.5 The most common complaint I hear from patients in VA mental health care is: “They never listen to me, they just sit there typing.” Similarly, clinicians complain: “I spend all my time looking at a screen not at a patient.” As an ethicist, I cannot tell you how many times the blight of copy and paste has thwarted or damaged a patient’s care. And the direct correlation between medical computing and burnout has been well documented as all health care systems struggle with a doctor shortage particularly in primary care—arguably where computer fatigue hits hardest.6
What will decide whether EHR modernization will be a positive or negative development for VA and DoD patients? And is there anything we as federal HCPs can do to tip the scales in favor of the what is best for patients and clinicians? The most encouraging step has already been taken: VA and Cerner have set up EHR Councils composed of 60% practicing VA HCPs to provide the clinical perspective and 40% from VA Central Office to encourage synchronization of the top-down and bottom-up processes.7
Many experts have pointed out the inherent tension between how computers and human beings work, which I will simplify as the battle between the 3 S’s and the 3 F’s.5 The optimal operation of EHRs requires systems, structure, stability; to function successfully human beings need flexibility, freedom, and fragmentation. VistA had more than 100 versions according to a report from the Federal News Network (FNN), which is a striking example of the challenge EHR modernization faces in bridging the 2 orientations. As former VA Chief Information Officer Roger Baker told FNN, replacing this approach of EHR tinkering with a locked-down commercial system will require “a culture change that is orders of magnitude bigger than expected.”8
Think of the 2 domains as a Venn diagram. Where the circles overlap is all the things we and patients want and need in health care: empathic listening, strong enduring relationships, accurate diagnosis, accessibility, personalized treatment, continuity of care, mutual respect, patient safety, room to exercise professional judgment, and the data needed to promote shared decision making. Our contribution and duty are to make that inner circle where we all dwell together as wide and full as possible and the overlap between the 2 outer circles as seamless as human imperfection and artificial intelligence permit.
The Gawande article is titled “Why Doctors Hate Their Computers.” Of course, his piece shows that we also love them. None of the proposed liberations from our EHR domination—be they medical scribes or dictation programs—has solved the problem, probably because they are all technologic and just move the slavery downstream. We have come too far, and medicine is too complex, to go back to the age of paper. If we can no longer do the good work of healing and caring without computers, then we have to learn to live with them as our allies not our enemies. After all, even Dr. McCoy had a tricorder.
1. VA Office of Public and Intergovernmental Affairs. Statement by Acting Secretary Robert Wilkie—VA signs contract with Cerner for an electronic health record system. https://www.va.gov/opa/pressrel/pressrelease.cfm?id=4061. Published May 17, 2018. Accessed January 15, 2019.
2. Arnsdorf I. The VA shadow ruler’s signature program is “trending towards red.” https://www.propublica.org/article/va-shadow-rulers-program-is-trending-towards-red. Published November 1, 2018. Accessed January 15, 2019.
3. Murphy K. Senate committee says EHR modernization cannot be allowed to fail. https://ehrintelligence.com/news/senate-committee-says-ehr-modernization-cannot-be-allowed-to-fail. Published January 14, 2019. Accessed January 15, 2019.
4. US Department of Veterans Affairs. A history of the electronic health record. https://www.ehrm.va.gov/about/history. Updated September 28, 2018. Accessed January 16, 2019.
5. Gawande A. Why doctors hate their computers. https://www.newyorker.com/magazine/2018/11/12/why-doctors-hate-their-computers. Published November 12, 2018. Accessed January 16, 2019.
6. Babbott S, Manwell LB, Brown R, et al. Electronic medical records and physician stress in primary care results from the MEMO study. J Am Med Inform Assoc. 2014;21(e1):100-106.
7. US Department of Veterans Affairs. EHRM councils. https://www.ehrm.va.gov/deployment/councils. Updated July 17, 2018. Accessed January 15, 2019.
8. Ogrysko N. In abandoning VistA, VA faces culture change that’s ‘orders of magnitude bigger’ than expected. https://federalnewsnetwork.com/veterans-affairs/2017/06/in-abandoning-vista-va-faces-culture-change-thats-orders-of-magnitude-bigger-than-expected. Published June 26, 2017. Accessed January 16, 2018.
I am a doctor, not an engineer.Dr. McCoy, Star Trek “Mirror, Mirror” episode
Last year in my annual wrap-up, I wrote back-to-back editorials (December 2017 and January 2018) on the worst and best of 2017 from a federal health care perspective, emphasizing ethics or the lack thereof. I featured the altruism of federal health care providers (HCPs) responding to natural disasters and the terrible outcome of seemingly banal moral lapses.
This year the best and worst are one and the same, and I am not sure how it could be otherwise: the Department of Veterans Affairs (VA) and Department of Defense (DoD) electronic health record (EHR) contract with Cerner (North Kansas City, MO). Former VA Secretary David Shulkin, MD, announced the deal in 2017 shortly before his departure, and it was signed under then Acting VA Secretary Robert Wilkie in May of 2018.1 But the reason the Cerner contract is the most impactful and momentous ethical event of the year is perhaps not what readers expect. Search engines will efficiently unearth plentiful drama with ethical import about the contract. There were conspiracy charges that the shadow regime improperly engineered the selection.2 The usual Congressional hearings on the VA leadership mismanagement of the EHR culminated in Sen Jon Tester’s (D-MO) martial declaration in a letter to the newly sworn-in VA Chief Information Officer James Paul Gfrerer that “EHR modernization cannot fail.”3
While all this is obviously important, it is not why the annual awards for ethical and unethical behaviors are bestowed on what is essentially an information technology acquisition. The Cerner contract is chosen because of its enormous potential to change the human practice of health care for good or ill; hence, the dual nomination. This column is not about Cerner qua Cerner but about how the EHR has transformed—or deformed—the humanistic aspects of medical practice.
I am old enough to remember the original transition from paper charts to VistA EHR. As an intern with illegible handwriting, I can remember breathing a sigh of relief when the blue screen appeared for the first time. The commands were cumbersome and the code laborious, but it was a technologic marvel to see the clean, organized progress notes and be able to print your medication list or discharge summary. However, it also was the first stuttering waves of a tsunami that would alter medical practice forever. The human cost of the revolution could be seen almost immediately as older clinicians or those who could not type struggled to complete work that with paper and pen would have been easily accomplished.
For many years there was a steady stream of updates to VistA, including the Computerized Patient Record System (CPRS). For a relatively long time in technology terms, VistA and CPRS were the envy of the medical world, which rushed to catch up. Gradually though, VA fell behind; the wizard IT guys could not patch and fix new versions fast enough, and eventually, like all things created, VistA and CPRS became obsolete.4 Attitudes toward this microcosm of the modernization of an aging organization were intense and diverse. Some of us held onto CPRS as though it was a transitional object that we had personalized and became attached to with all its quirks and problems. Others could not wait to get rid of it, believing anything new and streamlined had to be better.
Yet the opposite also is true. EHRs have been, and could be again, incredible time-savers, enabling HCPs to deliver more evidence-based, patient-centered care in a more accurate, integrated, timely, and comprehensive manner. For example, Cerner finally could discover the Holy Grail of VA-DoD interoperability and even—dare we dream—integrate with the community. Yet as science fiction aficionados know, the machine designed to free humankind of drudgery may also end up controlling us.
The other commonplace year-end practice is for ersatz prophets to predict the future. I have no idea whether the Cerner EHR will be good or bad for VA and DoD. According to the insightful critic of medical culture, Atul Gawande, MD, who has examined the practitioner-computer interface, what we must guard against is that it does not replace the practitioner-patient relationship.5 The most common complaint I hear from patients in VA mental health care is: “They never listen to me, they just sit there typing.” Similarly, clinicians complain: “I spend all my time looking at a screen not at a patient.” As an ethicist, I cannot tell you how many times the blight of copy and paste has thwarted or damaged a patient’s care. And the direct correlation between medical computing and burnout has been well documented as all health care systems struggle with a doctor shortage particularly in primary care—arguably where computer fatigue hits hardest.6
What will decide whether EHR modernization will be a positive or negative development for VA and DoD patients? And is there anything we as federal HCPs can do to tip the scales in favor of the what is best for patients and clinicians? The most encouraging step has already been taken: VA and Cerner have set up EHR Councils composed of 60% practicing VA HCPs to provide the clinical perspective and 40% from VA Central Office to encourage synchronization of the top-down and bottom-up processes.7
Many experts have pointed out the inherent tension between how computers and human beings work, which I will simplify as the battle between the 3 S’s and the 3 F’s.5 The optimal operation of EHRs requires systems, structure, stability; to function successfully human beings need flexibility, freedom, and fragmentation. VistA had more than 100 versions according to a report from the Federal News Network (FNN), which is a striking example of the challenge EHR modernization faces in bridging the 2 orientations. As former VA Chief Information Officer Roger Baker told FNN, replacing this approach of EHR tinkering with a locked-down commercial system will require “a culture change that is orders of magnitude bigger than expected.”8
Think of the 2 domains as a Venn diagram. Where the circles overlap is all the things we and patients want and need in health care: empathic listening, strong enduring relationships, accurate diagnosis, accessibility, personalized treatment, continuity of care, mutual respect, patient safety, room to exercise professional judgment, and the data needed to promote shared decision making. Our contribution and duty are to make that inner circle where we all dwell together as wide and full as possible and the overlap between the 2 outer circles as seamless as human imperfection and artificial intelligence permit.
The Gawande article is titled “Why Doctors Hate Their Computers.” Of course, his piece shows that we also love them. None of the proposed liberations from our EHR domination—be they medical scribes or dictation programs—has solved the problem, probably because they are all technologic and just move the slavery downstream. We have come too far, and medicine is too complex, to go back to the age of paper. If we can no longer do the good work of healing and caring without computers, then we have to learn to live with them as our allies not our enemies. After all, even Dr. McCoy had a tricorder.
I am a doctor, not an engineer.Dr. McCoy, Star Trek “Mirror, Mirror” episode
Last year in my annual wrap-up, I wrote back-to-back editorials (December 2017 and January 2018) on the worst and best of 2017 from a federal health care perspective, emphasizing ethics or the lack thereof. I featured the altruism of federal health care providers (HCPs) responding to natural disasters and the terrible outcome of seemingly banal moral lapses.
This year the best and worst are one and the same, and I am not sure how it could be otherwise: the Department of Veterans Affairs (VA) and Department of Defense (DoD) electronic health record (EHR) contract with Cerner (North Kansas City, MO). Former VA Secretary David Shulkin, MD, announced the deal in 2017 shortly before his departure, and it was signed under then Acting VA Secretary Robert Wilkie in May of 2018.1 But the reason the Cerner contract is the most impactful and momentous ethical event of the year is perhaps not what readers expect. Search engines will efficiently unearth plentiful drama with ethical import about the contract. There were conspiracy charges that the shadow regime improperly engineered the selection.2 The usual Congressional hearings on the VA leadership mismanagement of the EHR culminated in Sen Jon Tester’s (D-MO) martial declaration in a letter to the newly sworn-in VA Chief Information Officer James Paul Gfrerer that “EHR modernization cannot fail.”3
While all this is obviously important, it is not why the annual awards for ethical and unethical behaviors are bestowed on what is essentially an information technology acquisition. The Cerner contract is chosen because of its enormous potential to change the human practice of health care for good or ill; hence, the dual nomination. This column is not about Cerner qua Cerner but about how the EHR has transformed—or deformed—the humanistic aspects of medical practice.
I am old enough to remember the original transition from paper charts to VistA EHR. As an intern with illegible handwriting, I can remember breathing a sigh of relief when the blue screen appeared for the first time. The commands were cumbersome and the code laborious, but it was a technologic marvel to see the clean, organized progress notes and be able to print your medication list or discharge summary. However, it also was the first stuttering waves of a tsunami that would alter medical practice forever. The human cost of the revolution could be seen almost immediately as older clinicians or those who could not type struggled to complete work that with paper and pen would have been easily accomplished.
For many years there was a steady stream of updates to VistA, including the Computerized Patient Record System (CPRS). For a relatively long time in technology terms, VistA and CPRS were the envy of the medical world, which rushed to catch up. Gradually though, VA fell behind; the wizard IT guys could not patch and fix new versions fast enough, and eventually, like all things created, VistA and CPRS became obsolete.4 Attitudes toward this microcosm of the modernization of an aging organization were intense and diverse. Some of us held onto CPRS as though it was a transitional object that we had personalized and became attached to with all its quirks and problems. Others could not wait to get rid of it, believing anything new and streamlined had to be better.
Yet the opposite also is true. EHRs have been, and could be again, incredible time-savers, enabling HCPs to deliver more evidence-based, patient-centered care in a more accurate, integrated, timely, and comprehensive manner. For example, Cerner finally could discover the Holy Grail of VA-DoD interoperability and even—dare we dream—integrate with the community. Yet as science fiction aficionados know, the machine designed to free humankind of drudgery may also end up controlling us.
The other commonplace year-end practice is for ersatz prophets to predict the future. I have no idea whether the Cerner EHR will be good or bad for VA and DoD. According to the insightful critic of medical culture, Atul Gawande, MD, who has examined the practitioner-computer interface, what we must guard against is that it does not replace the practitioner-patient relationship.5 The most common complaint I hear from patients in VA mental health care is: “They never listen to me, they just sit there typing.” Similarly, clinicians complain: “I spend all my time looking at a screen not at a patient.” As an ethicist, I cannot tell you how many times the blight of copy and paste has thwarted or damaged a patient’s care. And the direct correlation between medical computing and burnout has been well documented as all health care systems struggle with a doctor shortage particularly in primary care—arguably where computer fatigue hits hardest.6
What will decide whether EHR modernization will be a positive or negative development for VA and DoD patients? And is there anything we as federal HCPs can do to tip the scales in favor of the what is best for patients and clinicians? The most encouraging step has already been taken: VA and Cerner have set up EHR Councils composed of 60% practicing VA HCPs to provide the clinical perspective and 40% from VA Central Office to encourage synchronization of the top-down and bottom-up processes.7
Many experts have pointed out the inherent tension between how computers and human beings work, which I will simplify as the battle between the 3 S’s and the 3 F’s.5 The optimal operation of EHRs requires systems, structure, stability; to function successfully human beings need flexibility, freedom, and fragmentation. VistA had more than 100 versions according to a report from the Federal News Network (FNN), which is a striking example of the challenge EHR modernization faces in bridging the 2 orientations. As former VA Chief Information Officer Roger Baker told FNN, replacing this approach of EHR tinkering with a locked-down commercial system will require “a culture change that is orders of magnitude bigger than expected.”8
Think of the 2 domains as a Venn diagram. Where the circles overlap is all the things we and patients want and need in health care: empathic listening, strong enduring relationships, accurate diagnosis, accessibility, personalized treatment, continuity of care, mutual respect, patient safety, room to exercise professional judgment, and the data needed to promote shared decision making. Our contribution and duty are to make that inner circle where we all dwell together as wide and full as possible and the overlap between the 2 outer circles as seamless as human imperfection and artificial intelligence permit.
The Gawande article is titled “Why Doctors Hate Their Computers.” Of course, his piece shows that we also love them. None of the proposed liberations from our EHR domination—be they medical scribes or dictation programs—has solved the problem, probably because they are all technologic and just move the slavery downstream. We have come too far, and medicine is too complex, to go back to the age of paper. If we can no longer do the good work of healing and caring without computers, then we have to learn to live with them as our allies not our enemies. After all, even Dr. McCoy had a tricorder.
1. VA Office of Public and Intergovernmental Affairs. Statement by Acting Secretary Robert Wilkie—VA signs contract with Cerner for an electronic health record system. https://www.va.gov/opa/pressrel/pressrelease.cfm?id=4061. Published May 17, 2018. Accessed January 15, 2019.
2. Arnsdorf I. The VA shadow ruler’s signature program is “trending towards red.” https://www.propublica.org/article/va-shadow-rulers-program-is-trending-towards-red. Published November 1, 2018. Accessed January 15, 2019.
3. Murphy K. Senate committee says EHR modernization cannot be allowed to fail. https://ehrintelligence.com/news/senate-committee-says-ehr-modernization-cannot-be-allowed-to-fail. Published January 14, 2019. Accessed January 15, 2019.
4. US Department of Veterans Affairs. A history of the electronic health record. https://www.ehrm.va.gov/about/history. Updated September 28, 2018. Accessed January 16, 2019.
5. Gawande A. Why doctors hate their computers. https://www.newyorker.com/magazine/2018/11/12/why-doctors-hate-their-computers. Published November 12, 2018. Accessed January 16, 2019.
6. Babbott S, Manwell LB, Brown R, et al. Electronic medical records and physician stress in primary care results from the MEMO study. J Am Med Inform Assoc. 2014;21(e1):100-106.
7. US Department of Veterans Affairs. EHRM councils. https://www.ehrm.va.gov/deployment/councils. Updated July 17, 2018. Accessed January 15, 2019.
8. Ogrysko N. In abandoning VistA, VA faces culture change that’s ‘orders of magnitude bigger’ than expected. https://federalnewsnetwork.com/veterans-affairs/2017/06/in-abandoning-vista-va-faces-culture-change-thats-orders-of-magnitude-bigger-than-expected. Published June 26, 2017. Accessed January 16, 2018.
1. VA Office of Public and Intergovernmental Affairs. Statement by Acting Secretary Robert Wilkie—VA signs contract with Cerner for an electronic health record system. https://www.va.gov/opa/pressrel/pressrelease.cfm?id=4061. Published May 17, 2018. Accessed January 15, 2019.
2. Arnsdorf I. The VA shadow ruler’s signature program is “trending towards red.” https://www.propublica.org/article/va-shadow-rulers-program-is-trending-towards-red. Published November 1, 2018. Accessed January 15, 2019.
3. Murphy K. Senate committee says EHR modernization cannot be allowed to fail. https://ehrintelligence.com/news/senate-committee-says-ehr-modernization-cannot-be-allowed-to-fail. Published January 14, 2019. Accessed January 15, 2019.
4. US Department of Veterans Affairs. A history of the electronic health record. https://www.ehrm.va.gov/about/history. Updated September 28, 2018. Accessed January 16, 2019.
5. Gawande A. Why doctors hate their computers. https://www.newyorker.com/magazine/2018/11/12/why-doctors-hate-their-computers. Published November 12, 2018. Accessed January 16, 2019.
6. Babbott S, Manwell LB, Brown R, et al. Electronic medical records and physician stress in primary care results from the MEMO study. J Am Med Inform Assoc. 2014;21(e1):100-106.
7. US Department of Veterans Affairs. EHRM councils. https://www.ehrm.va.gov/deployment/councils. Updated July 17, 2018. Accessed January 15, 2019.
8. Ogrysko N. In abandoning VistA, VA faces culture change that’s ‘orders of magnitude bigger’ than expected. https://federalnewsnetwork.com/veterans-affairs/2017/06/in-abandoning-vista-va-faces-culture-change-thats-orders-of-magnitude-bigger-than-expected. Published June 26, 2017. Accessed January 16, 2018.

Terminating an employee
I’ve written more than once about the private practitioner’s least favorite task. Now, new federal worker protection laws are making terminations even more difficult, even when they’re justified; however, that’s still no excuse for keeping an employee that should be replaced.

Once you make the decision to replace an employee, be sure that you have legitimate grounds and assemble as much documentation as you can. Record all terminable transgressions in the employee’s permanent record and document all verbal and written warnings. This is essential; you must be prepared to prove that your reasons for termination were legal.
Former employees will sometimes charge that any of a number of their civil rights were violated. For example, federal law prohibits you from firing anyone because of race, gender, national origin, disability, religion, or age – if the employee is over 40. You cannot fire a woman because she is pregnant or recently gave birth. Other illegal reasons include assertion of antidiscrimination rights, refusing to take a lie detector test, and reporting Occupational Safety and Health Administration violations.
You also can’t terminate someone for refusing to commit an illegal act – such as filing false insurance claims – or for exercising a legal right – such as voting or participating in a political demonstration.
While you cannot fire an alcohol abuser unless he or she is caught drinking at work, many forms of illegal drug use are legitimate causes for termination. Other laws may apply, depending on where you live. When in doubt, contact your attorney, state labor department, or fair employment office.
If a fired employee alleges that he or she was fired for any of these illegal reasons and you do not have convincing documentation to counter the charge, you may find yourself defending your actions in court. If you anticipate such problems, you can ask the employee to sign a waiver of future litigation in exchange for a concession from you – such as extra severance pay or a promise not to contest an unemployment application. Also, consider adding employment practices liability insurance – which I covered in detail a few months ago – to your umbrella policy, since lawsuits are always a possibility, despite all efforts to prevent them.
Once you have all your legal ducks in a row, don’t procrastinate. Get it over with first thing on Monday morning. If you wait until Friday afternoon, you will worry about the dreaded task all week long, and the fired employee will stew about it all weekend. Ask your manager or another trusted employee to be present to reduce the risk of subsequent disputes over what was discussed.
I’ve been asked to share exactly what I say; so for what it’s worth, here it is: “We have called you in to discuss a difficult issue. You know that we have not been happy with your performance. We are still not happy with it, despite all the discussions we have had, and we feel that you can do better elsewhere. So today we will part company, and I wish you the best of luck in your future endeavors. Here is your severance check. I hope there are no hard feelings.”

There will, of course, be hard feelings, despite all your “hopes,” but that cannot be helped. The point is to be quick, firm, and decisive. Get it over with and allow everyone to move on. Make it clear, when necessary, that the decision has already been made, so arguing or pleading will change nothing.
Be sure to get all your office keys back – or change the locks if you cannot. Back up all important computer files and change all your passwords. Most employees know more of them than you would ever suspect.
Finally, call the staff together and explain everything. They should hear it from you, not some distorted version via the rumor mill. You don’t have to divulge every detail, but do explain how the termination will affect everyone else. Responsibilities will need to be shifted until a replacement can be hired, and all employees should understand that.
If you are asked in the future to give a reference or write a letter of recommendation for the terminated employee, be sure that everything you say is truthful and well documented.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
I’ve written more than once about the private practitioner’s least favorite task. Now, new federal worker protection laws are making terminations even more difficult, even when they’re justified; however, that’s still no excuse for keeping an employee that should be replaced.
Once you make the decision to replace an employee, be sure that you have legitimate grounds and assemble as much documentation as you can. Record all terminable transgressions in the employee’s permanent record and document all verbal and written warnings. This is essential; you must be prepared to prove that your reasons for termination were legal.
Former employees will sometimes charge that any of a number of their civil rights were violated. For example, federal law prohibits you from firing anyone because of race, gender, national origin, disability, religion, or age – if the employee is over 40. You cannot fire a woman because she is pregnant or recently gave birth. Other illegal reasons include assertion of antidiscrimination rights, refusing to take a lie detector test, and reporting Occupational Safety and Health Administration violations.
You also can’t terminate someone for refusing to commit an illegal act – such as filing false insurance claims – or for exercising a legal right – such as voting or participating in a political demonstration.
While you cannot fire an alcohol abuser unless he or she is caught drinking at work, many forms of illegal drug use are legitimate causes for termination. Other laws may apply, depending on where you live. When in doubt, contact your attorney, state labor department, or fair employment office.
If a fired employee alleges that he or she was fired for any of these illegal reasons and you do not have convincing documentation to counter the charge, you may find yourself defending your actions in court. If you anticipate such problems, you can ask the employee to sign a waiver of future litigation in exchange for a concession from you – such as extra severance pay or a promise not to contest an unemployment application. Also, consider adding employment practices liability insurance – which I covered in detail a few months ago – to your umbrella policy, since lawsuits are always a possibility, despite all efforts to prevent them.
Once you have all your legal ducks in a row, don’t procrastinate. Get it over with first thing on Monday morning. If you wait until Friday afternoon, you will worry about the dreaded task all week long, and the fired employee will stew about it all weekend. Ask your manager or another trusted employee to be present to reduce the risk of subsequent disputes over what was discussed.
I’ve been asked to share exactly what I say; so for what it’s worth, here it is: “We have called you in to discuss a difficult issue. You know that we have not been happy with your performance. We are still not happy with it, despite all the discussions we have had, and we feel that you can do better elsewhere. So today we will part company, and I wish you the best of luck in your future endeavors. Here is your severance check. I hope there are no hard feelings.”
There will, of course, be hard feelings, despite all your “hopes,” but that cannot be helped. The point is to be quick, firm, and decisive. Get it over with and allow everyone to move on. Make it clear, when necessary, that the decision has already been made, so arguing or pleading will change nothing.
Be sure to get all your office keys back – or change the locks if you cannot. Back up all important computer files and change all your passwords. Most employees know more of them than you would ever suspect.
Finally, call the staff together and explain everything. They should hear it from you, not some distorted version via the rumor mill. You don’t have to divulge every detail, but do explain how the termination will affect everyone else. Responsibilities will need to be shifted until a replacement can be hired, and all employees should understand that.
If you are asked in the future to give a reference or write a letter of recommendation for the terminated employee, be sure that everything you say is truthful and well documented.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
I’ve written more than once about the private practitioner’s least favorite task. Now, new federal worker protection laws are making terminations even more difficult, even when they’re justified; however, that’s still no excuse for keeping an employee that should be replaced.
Once you make the decision to replace an employee, be sure that you have legitimate grounds and assemble as much documentation as you can. Record all terminable transgressions in the employee’s permanent record and document all verbal and written warnings. This is essential; you must be prepared to prove that your reasons for termination were legal.
Former employees will sometimes charge that any of a number of their civil rights were violated. For example, federal law prohibits you from firing anyone because of race, gender, national origin, disability, religion, or age – if the employee is over 40. You cannot fire a woman because she is pregnant or recently gave birth. Other illegal reasons include assertion of antidiscrimination rights, refusing to take a lie detector test, and reporting Occupational Safety and Health Administration violations.
You also can’t terminate someone for refusing to commit an illegal act – such as filing false insurance claims – or for exercising a legal right – such as voting or participating in a political demonstration.
While you cannot fire an alcohol abuser unless he or she is caught drinking at work, many forms of illegal drug use are legitimate causes for termination. Other laws may apply, depending on where you live. When in doubt, contact your attorney, state labor department, or fair employment office.
If a fired employee alleges that he or she was fired for any of these illegal reasons and you do not have convincing documentation to counter the charge, you may find yourself defending your actions in court. If you anticipate such problems, you can ask the employee to sign a waiver of future litigation in exchange for a concession from you – such as extra severance pay or a promise not to contest an unemployment application. Also, consider adding employment practices liability insurance – which I covered in detail a few months ago – to your umbrella policy, since lawsuits are always a possibility, despite all efforts to prevent them.
Once you have all your legal ducks in a row, don’t procrastinate. Get it over with first thing on Monday morning. If you wait until Friday afternoon, you will worry about the dreaded task all week long, and the fired employee will stew about it all weekend. Ask your manager or another trusted employee to be present to reduce the risk of subsequent disputes over what was discussed.
I’ve been asked to share exactly what I say; so for what it’s worth, here it is: “We have called you in to discuss a difficult issue. You know that we have not been happy with your performance. We are still not happy with it, despite all the discussions we have had, and we feel that you can do better elsewhere. So today we will part company, and I wish you the best of luck in your future endeavors. Here is your severance check. I hope there are no hard feelings.”
There will, of course, be hard feelings, despite all your “hopes,” but that cannot be helped. The point is to be quick, firm, and decisive. Get it over with and allow everyone to move on. Make it clear, when necessary, that the decision has already been made, so arguing or pleading will change nothing.
Be sure to get all your office keys back – or change the locks if you cannot. Back up all important computer files and change all your passwords. Most employees know more of them than you would ever suspect.
Finally, call the staff together and explain everything. They should hear it from you, not some distorted version via the rumor mill. You don’t have to divulge every detail, but do explain how the termination will affect everyone else. Responsibilities will need to be shifted until a replacement can be hired, and all employees should understand that.
If you are asked in the future to give a reference or write a letter of recommendation for the terminated employee, be sure that everything you say is truthful and well documented.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
In search of an ear
On our way up north to go backcountry skiing with another couple, we stopped at a roadside restaurant/tavern for lunch. We seated ourselves and, after a long 10 minutes, our waitperson arrived like a tornado, looking frazzled. She offered an apology and the first installment of her tale of woe. Before taking our order, she explained it all began when her car wouldn’t start, and then her day care provider called to say that she was sick and our server would have to find some other arrangement for the day. When our meal finally arrived, it looked appetizing but didn’t quite match our order. Again, our waitperson apologized, adding that it has been a particularly hard week because her husband was out of town and not around to help with her three children.

Had we been dining at a high-end restaurant with a white tablecloth and a candle, we would have considered our server’s behavior unprofessional and off-putting. However, we were in no hurry as the light snow had turned to a ski-unfriendly drizzle. While our original intent had been to simply have lunch, we accepted our role as a sympathetic audience for this unfortunate woman. In fact, we asked a few open-ended questions to help the cathartic process along.
The need to share one’s troubles seems to be a universal human trait. Our server had no illusions that we were going to provide any solutions to her problems. Nor was she seeking any expression of sympathy beyond our patience. However, I’m sure that unburdening herself by telling the story made her feel better, at least temporarily. Hopefully, there would be additional understanding diners to help her through the day.
For many people, the workplace serves as a therapeutic outlet where they can share their troubles and concerns. At times, the whining can be annoying to coworkers but in general, woe sharing is a harmless and valuable perk of having a job. Unless, of course, one’s job is primarily serving the public.
As physicians we are accustomed listening to our patients’ troubles. However, our job is not one of those that affords much opportunity to unburden ourselves of our own concerns. The patients assume that we are the problem solvers and don’t have any of our own. Or, if we do have some troubles, their office visit is not the time for us to share them.

The occasional sharing, such as that we are running late because we’ve had a flat on the way to the office, is harmless and can remind patients that we are human. But one must be careful stay off the slippery slope that leads to unprofessional oversharing.
Without that luxury of a workplace that allows for occasional catharsis, physicians have an additional risk for burnout. There are no easy solutions. Sharing with patients is unprofessional. Our peers are as busy as we are and probably don’t have the time to listen. Or at least they don’t seem to have the time. And then there is that ego-vulnerability issue where we are hesitant to reveal to anyone, be they staff or peers, that we have a soft underbelly.
I don’t have any easy answers to the problem beyond the usual suggestion that, Personally, I have to admit that, when my bad day was the result of an accumulation of minor bumps, I would follow our waitperson’s example and share them selectively with patients whom I deluded myself into believing had the time and concern to listen. It probably was unprofessional, but it made me feel better.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
On our way up north to go backcountry skiing with another couple, we stopped at a roadside restaurant/tavern for lunch. We seated ourselves and, after a long 10 minutes, our waitperson arrived like a tornado, looking frazzled. She offered an apology and the first installment of her tale of woe. Before taking our order, she explained it all began when her car wouldn’t start, and then her day care provider called to say that she was sick and our server would have to find some other arrangement for the day. When our meal finally arrived, it looked appetizing but didn’t quite match our order. Again, our waitperson apologized, adding that it has been a particularly hard week because her husband was out of town and not around to help with her three children.
Had we been dining at a high-end restaurant with a white tablecloth and a candle, we would have considered our server’s behavior unprofessional and off-putting. However, we were in no hurry as the light snow had turned to a ski-unfriendly drizzle. While our original intent had been to simply have lunch, we accepted our role as a sympathetic audience for this unfortunate woman. In fact, we asked a few open-ended questions to help the cathartic process along.
The need to share one’s troubles seems to be a universal human trait. Our server had no illusions that we were going to provide any solutions to her problems. Nor was she seeking any expression of sympathy beyond our patience. However, I’m sure that unburdening herself by telling the story made her feel better, at least temporarily. Hopefully, there would be additional understanding diners to help her through the day.
For many people, the workplace serves as a therapeutic outlet where they can share their troubles and concerns. At times, the whining can be annoying to coworkers but in general, woe sharing is a harmless and valuable perk of having a job. Unless, of course, one’s job is primarily serving the public.
As physicians we are accustomed listening to our patients’ troubles. However, our job is not one of those that affords much opportunity to unburden ourselves of our own concerns. The patients assume that we are the problem solvers and don’t have any of our own. Or, if we do have some troubles, their office visit is not the time for us to share them.
The occasional sharing, such as that we are running late because we’ve had a flat on the way to the office, is harmless and can remind patients that we are human. But one must be careful stay off the slippery slope that leads to unprofessional oversharing.
Without that luxury of a workplace that allows for occasional catharsis, physicians have an additional risk for burnout. There are no easy solutions. Sharing with patients is unprofessional. Our peers are as busy as we are and probably don’t have the time to listen. Or at least they don’t seem to have the time. And then there is that ego-vulnerability issue where we are hesitant to reveal to anyone, be they staff or peers, that we have a soft underbelly.
I don’t have any easy answers to the problem beyond the usual suggestion that, Personally, I have to admit that, when my bad day was the result of an accumulation of minor bumps, I would follow our waitperson’s example and share them selectively with patients whom I deluded myself into believing had the time and concern to listen. It probably was unprofessional, but it made me feel better.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
On our way up north to go backcountry skiing with another couple, we stopped at a roadside restaurant/tavern for lunch. We seated ourselves and, after a long 10 minutes, our waitperson arrived like a tornado, looking frazzled. She offered an apology and the first installment of her tale of woe. Before taking our order, she explained it all began when her car wouldn’t start, and then her day care provider called to say that she was sick and our server would have to find some other arrangement for the day. When our meal finally arrived, it looked appetizing but didn’t quite match our order. Again, our waitperson apologized, adding that it has been a particularly hard week because her husband was out of town and not around to help with her three children.
Had we been dining at a high-end restaurant with a white tablecloth and a candle, we would have considered our server’s behavior unprofessional and off-putting. However, we were in no hurry as the light snow had turned to a ski-unfriendly drizzle. While our original intent had been to simply have lunch, we accepted our role as a sympathetic audience for this unfortunate woman. In fact, we asked a few open-ended questions to help the cathartic process along.
The need to share one’s troubles seems to be a universal human trait. Our server had no illusions that we were going to provide any solutions to her problems. Nor was she seeking any expression of sympathy beyond our patience. However, I’m sure that unburdening herself by telling the story made her feel better, at least temporarily. Hopefully, there would be additional understanding diners to help her through the day.
For many people, the workplace serves as a therapeutic outlet where they can share their troubles and concerns. At times, the whining can be annoying to coworkers but in general, woe sharing is a harmless and valuable perk of having a job. Unless, of course, one’s job is primarily serving the public.
As physicians we are accustomed listening to our patients’ troubles. However, our job is not one of those that affords much opportunity to unburden ourselves of our own concerns. The patients assume that we are the problem solvers and don’t have any of our own. Or, if we do have some troubles, their office visit is not the time for us to share them.
The occasional sharing, such as that we are running late because we’ve had a flat on the way to the office, is harmless and can remind patients that we are human. But one must be careful stay off the slippery slope that leads to unprofessional oversharing.
Without that luxury of a workplace that allows for occasional catharsis, physicians have an additional risk for burnout. There are no easy solutions. Sharing with patients is unprofessional. Our peers are as busy as we are and probably don’t have the time to listen. Or at least they don’t seem to have the time. And then there is that ego-vulnerability issue where we are hesitant to reveal to anyone, be they staff or peers, that we have a soft underbelly.
I don’t have any easy answers to the problem beyond the usual suggestion that, Personally, I have to admit that, when my bad day was the result of an accumulation of minor bumps, I would follow our waitperson’s example and share them selectively with patients whom I deluded myself into believing had the time and concern to listen. It probably was unprofessional, but it made me feel better.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Obstetric hospitalists can screen for postpartum depression
Postpartum depression (PPD) is the most common complication of pregnancy, and onset can occur at any time from pregnancy until up to 1 year post partum.1,2 The immediate postpartum period is a time during which care is shared among multiple providers for both mother and child, and the transition from inpatient to outpatient postpartum care can impede communication between those caring for the patient in each setting. In 2018, the American College of Obstetricians and Gynecologists published a committee opinion emphasizing the importance of the “fourth trimester” and calling for health care providers to assist women in navigating the transition from pre- to postpartum care.3 An important consideration of perinatal care is mental health care for the mother, including screening and care for postpartum depression; however, the optimal role for the obstetric hospitalist in providing such services has been unclear.

Estimates of the prevalence of PPD in new mothers in the United States varied by state from 8% to 20% in 2012, with an overall average of 12%.2 Left untreated, PPD may result in significant negative outcomes for women, their children, and families. The depressive symptoms of PPD may persist for months or years afterward,4 with one study finding elevated depressive symptoms in women up to 11 years post partum.5 Suicide is also a leading cause of pregnancy-related mortality associated with depressive symptoms.6-9 In addition, maternal postpartum depression symptoms have been associated with impaired mother-infant bonding at 6 months of age10 and decreased cognitive and fine motor development of children at 18 months.11
Importance of screening
Evidence from the literature shows that, without proper screening, approximately 50% of cases of PPD go undiagnosed, and that increasing the number of women being screened by perinatal providers is an important first step to improving outcomes.12-18 Current recommendations for the timing and frequency of screening for PPD vary among the published guidelines. ACOG recommends screening at least once during the perinatal period for depression and anxiety using a standardized, validated tool; an update of the ACOG committee opinion in 2018 also states: “It is recommended that all obstetrician-gynecologists and other obstetric care providers complete a full assessment of mood and emotional well-being (including screening for PPD and anxiety with a validated instrument) during the comprehensive postpartum visit for each patient.”19 The American Medical Association adopted new policies in 2017 promoting the implementation of a routine protocol for depression screening of perinatal women.20 The American Academy of Pediatrics recommends more frequent screening, with assessments at the 1-, 2-, 4-, and 6-month visits.21 Finally, the U.S. Preventive Services Task Force recommends screening for depression in the general population including pregnant and postpartum women.22
Multiple standardized, validated screening instruments are available for detecting possible symptoms of PPD, including the most widely used tools: the Edinburgh Postnatal Depression Scale (EPDS)19,23 and the Patient Health Questionnaire (PHQ-9).24 Two recent studies have shown that screening women for symptoms of PPD with a validated tool may reduce the duration or severity of depressive symptoms,25,26 further reinforcing the need to ensure that women experiencing symptoms of PPD are identified and treated early.
The inpatient hospitalization for labor, delivery, and birth of a child has not traditionally been viewed as an opportunity for PPD screening. While private practitioners and obstetric medical group practices typically have inquired about and documented the individual patient’s mental health history and risk factors for PPD, the obstetric hospitalist is most commonly meeting a patient in labor or in a postpartum encounter for the first time. As obstetric practices grow ever more consolidated, and as obstetric hospitalist care is implemented for a variety of reasons including, but not limited to, preventing burnout among private practitioners, serving as a safety net for all inpatient obstetric services, and increasing standardization in obstetric triage and obstetric emergency departments,
Barriers remain
Despite the need for early detection of PPD, screening practices remain inconsistent. A literature review of health care provider practices showed only one in four physicians reported using screening tools; obstetrician-gynecologists were most likely (36%) to use screening tools, followed by family practitioners (31%), with pediatricians the least likely (7%).27 This low rate is at least partially the result of perceived barriers to screening among health care providers, which contributes to underdiagnosis. A survey of more than 200 physicians who were members of ACOG showed that the top three barriers restricting screening practices were time constraints, inadequate training, and a lack of knowledge of the diagnostic criteria.28
Since 2017, Dignity Health has instituted routine screening of all inpatient postpartum patients at its 29 birth centers in Arizona, California, and Nevada. In this program, of which I am a physician participant, more than 30,000 women have been screened with the EPDS. In addition to providing screening, Dignity Health staff (physicians, certified nurse midwives, nurse practitioners, registered nurses, social workers, mental health therapists, lactation consultants, health educators, and others) have received in-person Perinatal Mental Health training. In this way, the entire care team coordinates inpatient screening and referral to outpatient care providers – thus bridging the gap in postpartum mental health care. For those patients who screen positive while an inpatient, a psychiatric telemedicine appointment is provided and, if necessary, short-course medications can be prescribed until the patient has outpatient follow-up and continuity of care. While we as obstetric hospitalists and community obstetrician-gynecologists recognize that inpatient postpartum screening may be limited in its sensitivity for capturing all women who will go on to develop PPD, there is definitely a benefit to having a discussion about PPD and maternal mental health early and often throughout the postpartum period. For many women suffering in silence, a 6-week postpartum outpatient visit is too late, especially given that approximately one-third of women are lost to postpartum follow-up.29,30

Addressing barriers
A growing number of states have enacted policies to address the challenge of peripartum behavioral health needs, and several states – Illinois, Massachusetts, New Jersey, and West Virginia – now mandate routine PPD screening by health care providers.31 However, few of these laws or policies contain specific guidance, such as the optimal timing for screening, instead leaving the details to providers.32 The proper identification and management of PPD cannot be achieved by state-level policy mandates alone, but must include clinician buy-in and participation.
Obstetricians play an essential role in the identification and treatment of PPD. Among nonpsychiatric specialists, obstetrician-gynecologists are the most likely providers to see and screen during the perinatal period.33 In addition, women prefer to receive help for PPD from either their obstetric practitioners or a mental-health specialists located at the obstetric clinic, and are more likely to receive mental-health services if they are provided at the same location as that of the obstetric provider.34,35 According to ACOG’s new guidance on the fourth trimester, obstetricians are encouraged to take responsibility for women’s care immediately after birth, and this care would include contact with all mothers within the first 3 weeks post partum, at follow-up visits as needed, and for a comprehensive postpartum visit at 12 weeks.3
Our specialty has and will continue to evolve, and obstetric hospitalists will play an ever more essential role in the care of women during their inpatient obstetric admission. Whether we are a patient’s primary inpatient obstetric provider or a practice extender for single or multigroup practice, we are in a unique role to screen, begin treatment for, and offer anticipatory guidance for maternal mental health and postpartum depression disorders. Obstetric hospitalists can be a bridge between inpatient and outpatient follow-up and catalysts for implementing universal inpatient PPD screening. Our role presents an opportunity to start the discussion early and often in the fourth trimester and to make a significant difference in addressing this critical unmet need in postnatal care.
Dr. van Dis is the medical director of the Ob Hospitalist Group in Burbank, Calif. She disclosed she received editorial assistance from Erik MacLaren, PhD, of Boston Strategic Partners Inc., with funding support from Sage Therapeutics Inc. E-mail obnews@mdedge.com.
References
1. Centers for Disease Control and Prevention. Postpartum Depression. 2017.
2. Morb Mortal Wkly Rep. 2017;66(6):153-8.
3. Obstet Gynecol. 2018;131(5):e140-e150.
4. Harv Rev Psychiatry. 2014;22(1):1-22.
5. JAMA Psychiatry. 2018;75(3):247-53.
6. J Womens Health (Larchmt). 2016;25(12):1219-24.
7. J Psychiatr Res. 2017;84:284-91.
8. Br J Psychiatry. 2003;183:279-81.
9. Obstet Gynecol Surv. 2005;60(3):183-90.
10. Arch Womens Ment Health. 2016;19(1):87-94.
11. Soc Psychiatry Psychiatr Epidemiol. 2013;48(8):1335-45.
12. J Reprod Med. 1999;44(4):351-8.
13. J Behav Health Serv Res. 2004;31(2):117-33.
14. J Clin Psychiatry. 2016;77(9):1189-200.
15. Am J Obstet Gynecol. 2000;182(5):1080-2.
16. J Fam Pract. 2001;50(2):117-22.
17. Obstet Gynecol. 1999;93(5 Pt 1):653-7.
18. J Womens Health (Larchmt). 2010;19(3):477-90.
19. Obstet Gynecol. 2018;132:e208-12.
20. “Physicians back programs to address maternal mortality, depression,” AMA, Nov. 15, 2017
21. Pediatrics. 2019 Jan 1;143(1):e20183260.
22. JAMA. 2016;315(4):380-7.
23. Br J Psychiatry. 1987;150:782-6.
24. Ann Fam Med. 2009;7(1):63-70.
25. Obstet Gynecol. 2016;127(5):917-25.
26. Pediatrics. 2017 Oct;140(4). pii: e20170110.
27. Womens Health Issues. 2015;25(6):703-10.
28. J Psychosom Obstet Gynaecol. 2011;32(1):27-34.
29. Matern Child Health J. 2016;20(Suppl 1):22-7.
30. National Committee for Quality Assurance. Prenatal and Postpartum Care (PPC). 2018.
31. Psychiatr Serv. 2015;66(3):324-8.
32. Postpartum Support International. Legislation. 2018.
33. American Academy of Pediatrics, American College of Obstetricians and Gynecologists, eds. Guidelines for Perinatal Care. 7th ed. (Elk Grove Village, IL: Washington, DC: American Academy of Pediatrics; American College of Obstetricians and Gynecologists; Oct 2012.)
34. Birth. 2009;36(1):60-9.
35. Gen Hosp Psychiatry. 2009;31(2):155-62.
Postpartum depression (PPD) is the most common complication of pregnancy, and onset can occur at any time from pregnancy until up to 1 year post partum.1,2 The immediate postpartum period is a time during which care is shared among multiple providers for both mother and child, and the transition from inpatient to outpatient postpartum care can impede communication between those caring for the patient in each setting. In 2018, the American College of Obstetricians and Gynecologists published a committee opinion emphasizing the importance of the “fourth trimester” and calling for health care providers to assist women in navigating the transition from pre- to postpartum care.3 An important consideration of perinatal care is mental health care for the mother, including screening and care for postpartum depression; however, the optimal role for the obstetric hospitalist in providing such services has been unclear.
Estimates of the prevalence of PPD in new mothers in the United States varied by state from 8% to 20% in 2012, with an overall average of 12%.2 Left untreated, PPD may result in significant negative outcomes for women, their children, and families. The depressive symptoms of PPD may persist for months or years afterward,4 with one study finding elevated depressive symptoms in women up to 11 years post partum.5 Suicide is also a leading cause of pregnancy-related mortality associated with depressive symptoms.6-9 In addition, maternal postpartum depression symptoms have been associated with impaired mother-infant bonding at 6 months of age10 and decreased cognitive and fine motor development of children at 18 months.11
Importance of screening
Evidence from the literature shows that, without proper screening, approximately 50% of cases of PPD go undiagnosed, and that increasing the number of women being screened by perinatal providers is an important first step to improving outcomes.12-18 Current recommendations for the timing and frequency of screening for PPD vary among the published guidelines. ACOG recommends screening at least once during the perinatal period for depression and anxiety using a standardized, validated tool; an update of the ACOG committee opinion in 2018 also states: “It is recommended that all obstetrician-gynecologists and other obstetric care providers complete a full assessment of mood and emotional well-being (including screening for PPD and anxiety with a validated instrument) during the comprehensive postpartum visit for each patient.”19 The American Medical Association adopted new policies in 2017 promoting the implementation of a routine protocol for depression screening of perinatal women.20 The American Academy of Pediatrics recommends more frequent screening, with assessments at the 1-, 2-, 4-, and 6-month visits.21 Finally, the U.S. Preventive Services Task Force recommends screening for depression in the general population including pregnant and postpartum women.22
Multiple standardized, validated screening instruments are available for detecting possible symptoms of PPD, including the most widely used tools: the Edinburgh Postnatal Depression Scale (EPDS)19,23 and the Patient Health Questionnaire (PHQ-9).24 Two recent studies have shown that screening women for symptoms of PPD with a validated tool may reduce the duration or severity of depressive symptoms,25,26 further reinforcing the need to ensure that women experiencing symptoms of PPD are identified and treated early.
The inpatient hospitalization for labor, delivery, and birth of a child has not traditionally been viewed as an opportunity for PPD screening. While private practitioners and obstetric medical group practices typically have inquired about and documented the individual patient’s mental health history and risk factors for PPD, the obstetric hospitalist is most commonly meeting a patient in labor or in a postpartum encounter for the first time. As obstetric practices grow ever more consolidated, and as obstetric hospitalist care is implemented for a variety of reasons including, but not limited to, preventing burnout among private practitioners, serving as a safety net for all inpatient obstetric services, and increasing standardization in obstetric triage and obstetric emergency departments,
Barriers remain
Despite the need for early detection of PPD, screening practices remain inconsistent. A literature review of health care provider practices showed only one in four physicians reported using screening tools; obstetrician-gynecologists were most likely (36%) to use screening tools, followed by family practitioners (31%), with pediatricians the least likely (7%).27 This low rate is at least partially the result of perceived barriers to screening among health care providers, which contributes to underdiagnosis. A survey of more than 200 physicians who were members of ACOG showed that the top three barriers restricting screening practices were time constraints, inadequate training, and a lack of knowledge of the diagnostic criteria.28
Since 2017, Dignity Health has instituted routine screening of all inpatient postpartum patients at its 29 birth centers in Arizona, California, and Nevada. In this program, of which I am a physician participant, more than 30,000 women have been screened with the EPDS. In addition to providing screening, Dignity Health staff (physicians, certified nurse midwives, nurse practitioners, registered nurses, social workers, mental health therapists, lactation consultants, health educators, and others) have received in-person Perinatal Mental Health training. In this way, the entire care team coordinates inpatient screening and referral to outpatient care providers – thus bridging the gap in postpartum mental health care. For those patients who screen positive while an inpatient, a psychiatric telemedicine appointment is provided and, if necessary, short-course medications can be prescribed until the patient has outpatient follow-up and continuity of care. While we as obstetric hospitalists and community obstetrician-gynecologists recognize that inpatient postpartum screening may be limited in its sensitivity for capturing all women who will go on to develop PPD, there is definitely a benefit to having a discussion about PPD and maternal mental health early and often throughout the postpartum period. For many women suffering in silence, a 6-week postpartum outpatient visit is too late, especially given that approximately one-third of women are lost to postpartum follow-up.29,30
Addressing barriers
A growing number of states have enacted policies to address the challenge of peripartum behavioral health needs, and several states – Illinois, Massachusetts, New Jersey, and West Virginia – now mandate routine PPD screening by health care providers.31 However, few of these laws or policies contain specific guidance, such as the optimal timing for screening, instead leaving the details to providers.32 The proper identification and management of PPD cannot be achieved by state-level policy mandates alone, but must include clinician buy-in and participation.
Obstetricians play an essential role in the identification and treatment of PPD. Among nonpsychiatric specialists, obstetrician-gynecologists are the most likely providers to see and screen during the perinatal period.33 In addition, women prefer to receive help for PPD from either their obstetric practitioners or a mental-health specialists located at the obstetric clinic, and are more likely to receive mental-health services if they are provided at the same location as that of the obstetric provider.34,35 According to ACOG’s new guidance on the fourth trimester, obstetricians are encouraged to take responsibility for women’s care immediately after birth, and this care would include contact with all mothers within the first 3 weeks post partum, at follow-up visits as needed, and for a comprehensive postpartum visit at 12 weeks.3
Our specialty has and will continue to evolve, and obstetric hospitalists will play an ever more essential role in the care of women during their inpatient obstetric admission. Whether we are a patient’s primary inpatient obstetric provider or a practice extender for single or multigroup practice, we are in a unique role to screen, begin treatment for, and offer anticipatory guidance for maternal mental health and postpartum depression disorders. Obstetric hospitalists can be a bridge between inpatient and outpatient follow-up and catalysts for implementing universal inpatient PPD screening. Our role presents an opportunity to start the discussion early and often in the fourth trimester and to make a significant difference in addressing this critical unmet need in postnatal care.
Dr. van Dis is the medical director of the Ob Hospitalist Group in Burbank, Calif. She disclosed she received editorial assistance from Erik MacLaren, PhD, of Boston Strategic Partners Inc., with funding support from Sage Therapeutics Inc. E-mail obnews@mdedge.com.
References
1. Centers for Disease Control and Prevention. Postpartum Depression. 2017.
2. Morb Mortal Wkly Rep. 2017;66(6):153-8.
3. Obstet Gynecol. 2018;131(5):e140-e150.
4. Harv Rev Psychiatry. 2014;22(1):1-22.
5. JAMA Psychiatry. 2018;75(3):247-53.
6. J Womens Health (Larchmt). 2016;25(12):1219-24.
7. J Psychiatr Res. 2017;84:284-91.
8. Br J Psychiatry. 2003;183:279-81.
9. Obstet Gynecol Surv. 2005;60(3):183-90.
10. Arch Womens Ment Health. 2016;19(1):87-94.
11. Soc Psychiatry Psychiatr Epidemiol. 2013;48(8):1335-45.
12. J Reprod Med. 1999;44(4):351-8.
13. J Behav Health Serv Res. 2004;31(2):117-33.
14. J Clin Psychiatry. 2016;77(9):1189-200.
15. Am J Obstet Gynecol. 2000;182(5):1080-2.
16. J Fam Pract. 2001;50(2):117-22.
17. Obstet Gynecol. 1999;93(5 Pt 1):653-7.
18. J Womens Health (Larchmt). 2010;19(3):477-90.
19. Obstet Gynecol. 2018;132:e208-12.
20. “Physicians back programs to address maternal mortality, depression,” AMA, Nov. 15, 2017
21. Pediatrics. 2019 Jan 1;143(1):e20183260.
22. JAMA. 2016;315(4):380-7.
23. Br J Psychiatry. 1987;150:782-6.
24. Ann Fam Med. 2009;7(1):63-70.
25. Obstet Gynecol. 2016;127(5):917-25.
26. Pediatrics. 2017 Oct;140(4). pii: e20170110.
27. Womens Health Issues. 2015;25(6):703-10.
28. J Psychosom Obstet Gynaecol. 2011;32(1):27-34.
29. Matern Child Health J. 2016;20(Suppl 1):22-7.
30. National Committee for Quality Assurance. Prenatal and Postpartum Care (PPC). 2018.
31. Psychiatr Serv. 2015;66(3):324-8.
32. Postpartum Support International. Legislation. 2018.
33. American Academy of Pediatrics, American College of Obstetricians and Gynecologists, eds. Guidelines for Perinatal Care. 7th ed. (Elk Grove Village, IL: Washington, DC: American Academy of Pediatrics; American College of Obstetricians and Gynecologists; Oct 2012.)
34. Birth. 2009;36(1):60-9.
35. Gen Hosp Psychiatry. 2009;31(2):155-62.
Postpartum depression (PPD) is the most common complication of pregnancy, and onset can occur at any time from pregnancy until up to 1 year post partum.1,2 The immediate postpartum period is a time during which care is shared among multiple providers for both mother and child, and the transition from inpatient to outpatient postpartum care can impede communication between those caring for the patient in each setting. In 2018, the American College of Obstetricians and Gynecologists published a committee opinion emphasizing the importance of the “fourth trimester” and calling for health care providers to assist women in navigating the transition from pre- to postpartum care.3 An important consideration of perinatal care is mental health care for the mother, including screening and care for postpartum depression; however, the optimal role for the obstetric hospitalist in providing such services has been unclear.
Estimates of the prevalence of PPD in new mothers in the United States varied by state from 8% to 20% in 2012, with an overall average of 12%.2 Left untreated, PPD may result in significant negative outcomes for women, their children, and families. The depressive symptoms of PPD may persist for months or years afterward,4 with one study finding elevated depressive symptoms in women up to 11 years post partum.5 Suicide is also a leading cause of pregnancy-related mortality associated with depressive symptoms.6-9 In addition, maternal postpartum depression symptoms have been associated with impaired mother-infant bonding at 6 months of age10 and decreased cognitive and fine motor development of children at 18 months.11
Importance of screening
Evidence from the literature shows that, without proper screening, approximately 50% of cases of PPD go undiagnosed, and that increasing the number of women being screened by perinatal providers is an important first step to improving outcomes.12-18 Current recommendations for the timing and frequency of screening for PPD vary among the published guidelines. ACOG recommends screening at least once during the perinatal period for depression and anxiety using a standardized, validated tool; an update of the ACOG committee opinion in 2018 also states: “It is recommended that all obstetrician-gynecologists and other obstetric care providers complete a full assessment of mood and emotional well-being (including screening for PPD and anxiety with a validated instrument) during the comprehensive postpartum visit for each patient.”19 The American Medical Association adopted new policies in 2017 promoting the implementation of a routine protocol for depression screening of perinatal women.20 The American Academy of Pediatrics recommends more frequent screening, with assessments at the 1-, 2-, 4-, and 6-month visits.21 Finally, the U.S. Preventive Services Task Force recommends screening for depression in the general population including pregnant and postpartum women.22
Multiple standardized, validated screening instruments are available for detecting possible symptoms of PPD, including the most widely used tools: the Edinburgh Postnatal Depression Scale (EPDS)19,23 and the Patient Health Questionnaire (PHQ-9).24 Two recent studies have shown that screening women for symptoms of PPD with a validated tool may reduce the duration or severity of depressive symptoms,25,26 further reinforcing the need to ensure that women experiencing symptoms of PPD are identified and treated early.
The inpatient hospitalization for labor, delivery, and birth of a child has not traditionally been viewed as an opportunity for PPD screening. While private practitioners and obstetric medical group practices typically have inquired about and documented the individual patient’s mental health history and risk factors for PPD, the obstetric hospitalist is most commonly meeting a patient in labor or in a postpartum encounter for the first time. As obstetric practices grow ever more consolidated, and as obstetric hospitalist care is implemented for a variety of reasons including, but not limited to, preventing burnout among private practitioners, serving as a safety net for all inpatient obstetric services, and increasing standardization in obstetric triage and obstetric emergency departments,
Barriers remain
Despite the need for early detection of PPD, screening practices remain inconsistent. A literature review of health care provider practices showed only one in four physicians reported using screening tools; obstetrician-gynecologists were most likely (36%) to use screening tools, followed by family practitioners (31%), with pediatricians the least likely (7%).27 This low rate is at least partially the result of perceived barriers to screening among health care providers, which contributes to underdiagnosis. A survey of more than 200 physicians who were members of ACOG showed that the top three barriers restricting screening practices were time constraints, inadequate training, and a lack of knowledge of the diagnostic criteria.28
Since 2017, Dignity Health has instituted routine screening of all inpatient postpartum patients at its 29 birth centers in Arizona, California, and Nevada. In this program, of which I am a physician participant, more than 30,000 women have been screened with the EPDS. In addition to providing screening, Dignity Health staff (physicians, certified nurse midwives, nurse practitioners, registered nurses, social workers, mental health therapists, lactation consultants, health educators, and others) have received in-person Perinatal Mental Health training. In this way, the entire care team coordinates inpatient screening and referral to outpatient care providers – thus bridging the gap in postpartum mental health care. For those patients who screen positive while an inpatient, a psychiatric telemedicine appointment is provided and, if necessary, short-course medications can be prescribed until the patient has outpatient follow-up and continuity of care. While we as obstetric hospitalists and community obstetrician-gynecologists recognize that inpatient postpartum screening may be limited in its sensitivity for capturing all women who will go on to develop PPD, there is definitely a benefit to having a discussion about PPD and maternal mental health early and often throughout the postpartum period. For many women suffering in silence, a 6-week postpartum outpatient visit is too late, especially given that approximately one-third of women are lost to postpartum follow-up.29,30
Addressing barriers
A growing number of states have enacted policies to address the challenge of peripartum behavioral health needs, and several states – Illinois, Massachusetts, New Jersey, and West Virginia – now mandate routine PPD screening by health care providers.31 However, few of these laws or policies contain specific guidance, such as the optimal timing for screening, instead leaving the details to providers.32 The proper identification and management of PPD cannot be achieved by state-level policy mandates alone, but must include clinician buy-in and participation.
Obstetricians play an essential role in the identification and treatment of PPD. Among nonpsychiatric specialists, obstetrician-gynecologists are the most likely providers to see and screen during the perinatal period.33 In addition, women prefer to receive help for PPD from either their obstetric practitioners or a mental-health specialists located at the obstetric clinic, and are more likely to receive mental-health services if they are provided at the same location as that of the obstetric provider.34,35 According to ACOG’s new guidance on the fourth trimester, obstetricians are encouraged to take responsibility for women’s care immediately after birth, and this care would include contact with all mothers within the first 3 weeks post partum, at follow-up visits as needed, and for a comprehensive postpartum visit at 12 weeks.3
Our specialty has and will continue to evolve, and obstetric hospitalists will play an ever more essential role in the care of women during their inpatient obstetric admission. Whether we are a patient’s primary inpatient obstetric provider or a practice extender for single or multigroup practice, we are in a unique role to screen, begin treatment for, and offer anticipatory guidance for maternal mental health and postpartum depression disorders. Obstetric hospitalists can be a bridge between inpatient and outpatient follow-up and catalysts for implementing universal inpatient PPD screening. Our role presents an opportunity to start the discussion early and often in the fourth trimester and to make a significant difference in addressing this critical unmet need in postnatal care.
Dr. van Dis is the medical director of the Ob Hospitalist Group in Burbank, Calif. She disclosed she received editorial assistance from Erik MacLaren, PhD, of Boston Strategic Partners Inc., with funding support from Sage Therapeutics Inc. E-mail obnews@mdedge.com.
References
1. Centers for Disease Control and Prevention. Postpartum Depression. 2017.
2. Morb Mortal Wkly Rep. 2017;66(6):153-8.
3. Obstet Gynecol. 2018;131(5):e140-e150.
4. Harv Rev Psychiatry. 2014;22(1):1-22.
5. JAMA Psychiatry. 2018;75(3):247-53.
6. J Womens Health (Larchmt). 2016;25(12):1219-24.
7. J Psychiatr Res. 2017;84:284-91.
8. Br J Psychiatry. 2003;183:279-81.
9. Obstet Gynecol Surv. 2005;60(3):183-90.
10. Arch Womens Ment Health. 2016;19(1):87-94.
11. Soc Psychiatry Psychiatr Epidemiol. 2013;48(8):1335-45.
12. J Reprod Med. 1999;44(4):351-8.
13. J Behav Health Serv Res. 2004;31(2):117-33.
14. J Clin Psychiatry. 2016;77(9):1189-200.
15. Am J Obstet Gynecol. 2000;182(5):1080-2.
16. J Fam Pract. 2001;50(2):117-22.
17. Obstet Gynecol. 1999;93(5 Pt 1):653-7.
18. J Womens Health (Larchmt). 2010;19(3):477-90.
19. Obstet Gynecol. 2018;132:e208-12.
20. “Physicians back programs to address maternal mortality, depression,” AMA, Nov. 15, 2017
21. Pediatrics. 2019 Jan 1;143(1):e20183260.
22. JAMA. 2016;315(4):380-7.
23. Br J Psychiatry. 1987;150:782-6.
24. Ann Fam Med. 2009;7(1):63-70.
25. Obstet Gynecol. 2016;127(5):917-25.
26. Pediatrics. 2017 Oct;140(4). pii: e20170110.
27. Womens Health Issues. 2015;25(6):703-10.
28. J Psychosom Obstet Gynaecol. 2011;32(1):27-34.
29. Matern Child Health J. 2016;20(Suppl 1):22-7.
30. National Committee for Quality Assurance. Prenatal and Postpartum Care (PPC). 2018.
31. Psychiatr Serv. 2015;66(3):324-8.
32. Postpartum Support International. Legislation. 2018.
33. American Academy of Pediatrics, American College of Obstetricians and Gynecologists, eds. Guidelines for Perinatal Care. 7th ed. (Elk Grove Village, IL: Washington, DC: American Academy of Pediatrics; American College of Obstetricians and Gynecologists; Oct 2012.)
34. Birth. 2009;36(1):60-9.
35. Gen Hosp Psychiatry. 2009;31(2):155-62.

{kind=link}
ADHD: When and how do we choose to start medications?
- A 9-year-old boy has poor impulse control, throws things in class, and cannot sit still. Teachers ask: Is this ADHD and should we start a medication?
- A 9-year-old girl is an inattentive daydreamer with poor class performance and trouble turning in homework. Her parents and teachers ask: Is this ADHD and should we start a medication?
- A 17-year-old boy who is a high achiever is taking the upcoming SATs and does poorly on timed tests because of poor focus and is now wondering: Do I have ADHD and would a medication help me perform better?
- A 17-year-old boy had poor grades for much of his early school years, but his parents always thought he was just a “lazy kid” although he insists he is trying his best. His parents now ask: Is this ADHD and has it been all along?
The above cases may sound familiar to you. They are an oversimplification of the patients who may come to you with two questions: Do I or someone I care about have ADHD and should they have medication for it? What may matter even more is how they are doing with that inattentiveness and how much it impacts their lives.
Sigmund Freud was known to think about goals for treatment as “liebe und arbeit” translated into “to love and to work.” As in, can someone live, love, and work or are their psychiatric symptoms impairing those functionalities? For a child, to live, work, and play (well with others) is most apt here. It is often more helpful to think in terms of childhood daily life when choosing to begin a medication or not. With inattention, a child can range from having a parent hoping for performance enhancement to having a severe impairment in their day-to-day functioning in a classroom. In the above case examples, each child or adolescent has varying impairments in performance – one is a high academic performer with very few issues outside of testing and another is a young child who can’t even sit still in a classroom to learn. Who should be prescribed a stimulant? Any or all of the above? It’s not as easy an answer as you may suspect, and there may not be one “right” answer either.
We know that stimulants can help a great deal of patients. They have the highest effect size for ADHD in that about 80% of children can benefit from stimulant treatment for ADHD. Specifically, “a high response rate of 70%-85% has been noted with methylphenidate and amphetamine formulations. The response rate is lower for atomoxetine [60%-65%] and guanfacine [30%-40%]” (Venkat B, Hechtman L. Considerations in selecting pharmacological treatments for attention deficit hyperactivity disorder. Clinical Pharmacist. 2016 Feb 11). In thinking about when to prescribe, we want to balance offering nonpharmacologic means to address symptoms of inattention (like mindfulness, exercise, and school supports such as individualized learning plans where applicable). We also do not want to withhold helpful treatments such as stimulants or other nonstimulant medications or trend toward overprescribing potentially habit-forming and imperfect medications.
It is important to make that distinction between impairment and the desire for medications to “enhance” life and optimize performance rather than treating symptoms of a disorder. It is most helpful to gain skills to navigate those challenges simultaneously to ultimately help our patients live, learn, love, and play to the best of their abilities.
Where to begin
When I was in training, I had difficulty teasing out the various ADHD stimulant formations. There were and are so many Ritalin preparations! Mostly there is a variation in shorter-acting to longer-acting effects. If the diagnosis is highly suspected and uncomplicated ADHD, I usually choose to start with Concerta 18 mg daily (a long-acting methylphenidate) for children aged over 6 years. Many times I don’t see the need to titrate that upwards much further toward the maximum clinically used dose of 54 mg daily (despite guidelines saying otherwise up to 72 mg daily, which I have found unnecessary usually and poorly tolerated). Concerta has an immediate effect (20%) and then slowly peaks until 12 p.m. (80%) and then is out of system by about 3 p.m. (for a total of 7 hours duration of action). There also are shorter-acting preparations (Ritalin, Methylin) which are “on/off” in 4 hours and use of these is more consistent with an antiquated way of prescribing, often up to twice daily and three times daily dosing schedules with the risk of the harder to tolerate “drop-off” effects with stimulants. And, if there is not an effect, I often reconsider the diagnosis and any co-occurring anxiety disorder, stressful life events, or depression or other illness with the knowledge that these medications so often are effective.
Anxiety + ADHD
If there is prominent anxiety, anxiety disorder, or tics, I often consider Strattera 10-20 mg daily up to around 40 mg. I tend to dose this lower than as written for tolerability and in a “dose low and go slow” approach with kids, which often results in better experiences with the medication. This medication also is recommended to be dosed by weight; this should be taken into account as well. Atomoxetine is a selective serotonin and norepinephrine reuptake inhibitor which is likely similar to Cymbalta (duloxetine). It may have a lower effect size of around less than 60% but this also is around the reported effect sizes for selective serotonin reuptake inhibitors (SSRIs) for depression. If a patient has both ADHD and an anxiety disorder, I often consider an SSRI alternatively first to manage attention issues associated with anxiety and then would add on a stimulant if attention issues persist once anxiety is better treated.
Second/third line ADHD treatments
As a second-line approach to long-acting Ritalin and if there is not a response to it, I would consider extended-release Adderall preparations such as Vyvanse, which is an amphetamine preparation supposedly less abusable than Adderall (one can’t snort it), but I also caution that it releases dopamine, peaks faster, and does not reduce to zero stimulant in 24 hours because of a variable half-life.

In this way, I always have imagined that these amphetamines may be more theoretically concerning than Ritalin/methylphenidate because they increase dopamine dumping into the synapse (which is a different and extra mechanism than just reuptake). For a third line, I may consider guanfacine depending on weight daily, which is an Food and Drug Administration–approved, nonstimulant alpha-2 agonist, which also acts longer than clonidine and may be better for hyperactivity symptoms. I may begin with doses as low as 0.25-0.5 mg in the evening for concerns with sedation or groggy aftereffects in the morning.
Throughout all treatment with medication, I emphasize the importance of assertively managing ADHD symptoms which may be in the form of “behavioral treatment,” like cognitive behavioral therapy, organizational coaching available at some educational centers, or even finding ways to train one’s focus with athletics or practices such as yoga and mindfulness. In addition to this combined approach to treatment, stimulants are not perfect medications. All stimulants have a “drop-off effect” and were made to work during a school day lasting from 8 a.m. to 3 p.m. Some patients and families complain about the drop-off effect and may want to “dose” around a medication more frequently, in the late afternoon and in the evening, which can lead to poor appetite at dinner and insomnia.
My answers to the cases above would be that all the patients could have ADHD, but they also may have anxiety or stress-related disorders, depression, worries about performance, or poor skills to manage inattention. They may not yet have received school supports, coaching, or found ways to manage these symptoms either. Because stimulants can improve and enhance performance but also have their own drawbacks and risks not covered here, it’s important to consider each case as a whole with thoughtfulness about a child’s unique ability to “live and work” in this world.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and an assistant professor of psychiatry at UVM, both in Burlington. She reported no relevant financial disclosures. Email her at pdnews@mdedge.com.
- A 9-year-old boy has poor impulse control, throws things in class, and cannot sit still. Teachers ask: Is this ADHD and should we start a medication?
- A 9-year-old girl is an inattentive daydreamer with poor class performance and trouble turning in homework. Her parents and teachers ask: Is this ADHD and should we start a medication?
- A 17-year-old boy who is a high achiever is taking the upcoming SATs and does poorly on timed tests because of poor focus and is now wondering: Do I have ADHD and would a medication help me perform better?
- A 17-year-old boy had poor grades for much of his early school years, but his parents always thought he was just a “lazy kid” although he insists he is trying his best. His parents now ask: Is this ADHD and has it been all along?
The above cases may sound familiar to you. They are an oversimplification of the patients who may come to you with two questions: Do I or someone I care about have ADHD and should they have medication for it? What may matter even more is how they are doing with that inattentiveness and how much it impacts their lives.
Sigmund Freud was known to think about goals for treatment as “liebe und arbeit” translated into “to love and to work.” As in, can someone live, love, and work or are their psychiatric symptoms impairing those functionalities? For a child, to live, work, and play (well with others) is most apt here. It is often more helpful to think in terms of childhood daily life when choosing to begin a medication or not. With inattention, a child can range from having a parent hoping for performance enhancement to having a severe impairment in their day-to-day functioning in a classroom. In the above case examples, each child or adolescent has varying impairments in performance – one is a high academic performer with very few issues outside of testing and another is a young child who can’t even sit still in a classroom to learn. Who should be prescribed a stimulant? Any or all of the above? It’s not as easy an answer as you may suspect, and there may not be one “right” answer either.
We know that stimulants can help a great deal of patients. They have the highest effect size for ADHD in that about 80% of children can benefit from stimulant treatment for ADHD. Specifically, “a high response rate of 70%-85% has been noted with methylphenidate and amphetamine formulations. The response rate is lower for atomoxetine [60%-65%] and guanfacine [30%-40%]” (Venkat B, Hechtman L. Considerations in selecting pharmacological treatments for attention deficit hyperactivity disorder. Clinical Pharmacist. 2016 Feb 11). In thinking about when to prescribe, we want to balance offering nonpharmacologic means to address symptoms of inattention (like mindfulness, exercise, and school supports such as individualized learning plans where applicable). We also do not want to withhold helpful treatments such as stimulants or other nonstimulant medications or trend toward overprescribing potentially habit-forming and imperfect medications.
It is important to make that distinction between impairment and the desire for medications to “enhance” life and optimize performance rather than treating symptoms of a disorder. It is most helpful to gain skills to navigate those challenges simultaneously to ultimately help our patients live, learn, love, and play to the best of their abilities.
Where to begin
When I was in training, I had difficulty teasing out the various ADHD stimulant formations. There were and are so many Ritalin preparations! Mostly there is a variation in shorter-acting to longer-acting effects. If the diagnosis is highly suspected and uncomplicated ADHD, I usually choose to start with Concerta 18 mg daily (a long-acting methylphenidate) for children aged over 6 years. Many times I don’t see the need to titrate that upwards much further toward the maximum clinically used dose of 54 mg daily (despite guidelines saying otherwise up to 72 mg daily, which I have found unnecessary usually and poorly tolerated). Concerta has an immediate effect (20%) and then slowly peaks until 12 p.m. (80%) and then is out of system by about 3 p.m. (for a total of 7 hours duration of action). There also are shorter-acting preparations (Ritalin, Methylin) which are “on/off” in 4 hours and use of these is more consistent with an antiquated way of prescribing, often up to twice daily and three times daily dosing schedules with the risk of the harder to tolerate “drop-off” effects with stimulants. And, if there is not an effect, I often reconsider the diagnosis and any co-occurring anxiety disorder, stressful life events, or depression or other illness with the knowledge that these medications so often are effective.
Anxiety + ADHD
If there is prominent anxiety, anxiety disorder, or tics, I often consider Strattera 10-20 mg daily up to around 40 mg. I tend to dose this lower than as written for tolerability and in a “dose low and go slow” approach with kids, which often results in better experiences with the medication. This medication also is recommended to be dosed by weight; this should be taken into account as well. Atomoxetine is a selective serotonin and norepinephrine reuptake inhibitor which is likely similar to Cymbalta (duloxetine). It may have a lower effect size of around less than 60% but this also is around the reported effect sizes for selective serotonin reuptake inhibitors (SSRIs) for depression. If a patient has both ADHD and an anxiety disorder, I often consider an SSRI alternatively first to manage attention issues associated with anxiety and then would add on a stimulant if attention issues persist once anxiety is better treated.
Second/third line ADHD treatments
As a second-line approach to long-acting Ritalin and if there is not a response to it, I would consider extended-release Adderall preparations such as Vyvanse, which is an amphetamine preparation supposedly less abusable than Adderall (one can’t snort it), but I also caution that it releases dopamine, peaks faster, and does not reduce to zero stimulant in 24 hours because of a variable half-life.
In this way, I always have imagined that these amphetamines may be more theoretically concerning than Ritalin/methylphenidate because they increase dopamine dumping into the synapse (which is a different and extra mechanism than just reuptake). For a third line, I may consider guanfacine depending on weight daily, which is an Food and Drug Administration–approved, nonstimulant alpha-2 agonist, which also acts longer than clonidine and may be better for hyperactivity symptoms. I may begin with doses as low as 0.25-0.5 mg in the evening for concerns with sedation or groggy aftereffects in the morning.
Throughout all treatment with medication, I emphasize the importance of assertively managing ADHD symptoms which may be in the form of “behavioral treatment,” like cognitive behavioral therapy, organizational coaching available at some educational centers, or even finding ways to train one’s focus with athletics or practices such as yoga and mindfulness. In addition to this combined approach to treatment, stimulants are not perfect medications. All stimulants have a “drop-off effect” and were made to work during a school day lasting from 8 a.m. to 3 p.m. Some patients and families complain about the drop-off effect and may want to “dose” around a medication more frequently, in the late afternoon and in the evening, which can lead to poor appetite at dinner and insomnia.
My answers to the cases above would be that all the patients could have ADHD, but they also may have anxiety or stress-related disorders, depression, worries about performance, or poor skills to manage inattention. They may not yet have received school supports, coaching, or found ways to manage these symptoms either. Because stimulants can improve and enhance performance but also have their own drawbacks and risks not covered here, it’s important to consider each case as a whole with thoughtfulness about a child’s unique ability to “live and work” in this world.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and an assistant professor of psychiatry at UVM, both in Burlington. She reported no relevant financial disclosures. Email her at pdnews@mdedge.com.
- A 9-year-old boy has poor impulse control, throws things in class, and cannot sit still. Teachers ask: Is this ADHD and should we start a medication?
- A 9-year-old girl is an inattentive daydreamer with poor class performance and trouble turning in homework. Her parents and teachers ask: Is this ADHD and should we start a medication?
- A 17-year-old boy who is a high achiever is taking the upcoming SATs and does poorly on timed tests because of poor focus and is now wondering: Do I have ADHD and would a medication help me perform better?
- A 17-year-old boy had poor grades for much of his early school years, but his parents always thought he was just a “lazy kid” although he insists he is trying his best. His parents now ask: Is this ADHD and has it been all along?
The above cases may sound familiar to you. They are an oversimplification of the patients who may come to you with two questions: Do I or someone I care about have ADHD and should they have medication for it? What may matter even more is how they are doing with that inattentiveness and how much it impacts their lives.
Sigmund Freud was known to think about goals for treatment as “liebe und arbeit” translated into “to love and to work.” As in, can someone live, love, and work or are their psychiatric symptoms impairing those functionalities? For a child, to live, work, and play (well with others) is most apt here. It is often more helpful to think in terms of childhood daily life when choosing to begin a medication or not. With inattention, a child can range from having a parent hoping for performance enhancement to having a severe impairment in their day-to-day functioning in a classroom. In the above case examples, each child or adolescent has varying impairments in performance – one is a high academic performer with very few issues outside of testing and another is a young child who can’t even sit still in a classroom to learn. Who should be prescribed a stimulant? Any or all of the above? It’s not as easy an answer as you may suspect, and there may not be one “right” answer either.
We know that stimulants can help a great deal of patients. They have the highest effect size for ADHD in that about 80% of children can benefit from stimulant treatment for ADHD. Specifically, “a high response rate of 70%-85% has been noted with methylphenidate and amphetamine formulations. The response rate is lower for atomoxetine [60%-65%] and guanfacine [30%-40%]” (Venkat B, Hechtman L. Considerations in selecting pharmacological treatments for attention deficit hyperactivity disorder. Clinical Pharmacist. 2016 Feb 11). In thinking about when to prescribe, we want to balance offering nonpharmacologic means to address symptoms of inattention (like mindfulness, exercise, and school supports such as individualized learning plans where applicable). We also do not want to withhold helpful treatments such as stimulants or other nonstimulant medications or trend toward overprescribing potentially habit-forming and imperfect medications.
It is important to make that distinction between impairment and the desire for medications to “enhance” life and optimize performance rather than treating symptoms of a disorder. It is most helpful to gain skills to navigate those challenges simultaneously to ultimately help our patients live, learn, love, and play to the best of their abilities.
Where to begin
When I was in training, I had difficulty teasing out the various ADHD stimulant formations. There were and are so many Ritalin preparations! Mostly there is a variation in shorter-acting to longer-acting effects. If the diagnosis is highly suspected and uncomplicated ADHD, I usually choose to start with Concerta 18 mg daily (a long-acting methylphenidate) for children aged over 6 years. Many times I don’t see the need to titrate that upwards much further toward the maximum clinically used dose of 54 mg daily (despite guidelines saying otherwise up to 72 mg daily, which I have found unnecessary usually and poorly tolerated). Concerta has an immediate effect (20%) and then slowly peaks until 12 p.m. (80%) and then is out of system by about 3 p.m. (for a total of 7 hours duration of action). There also are shorter-acting preparations (Ritalin, Methylin) which are “on/off” in 4 hours and use of these is more consistent with an antiquated way of prescribing, often up to twice daily and three times daily dosing schedules with the risk of the harder to tolerate “drop-off” effects with stimulants. And, if there is not an effect, I often reconsider the diagnosis and any co-occurring anxiety disorder, stressful life events, or depression or other illness with the knowledge that these medications so often are effective.
Anxiety + ADHD
If there is prominent anxiety, anxiety disorder, or tics, I often consider Strattera 10-20 mg daily up to around 40 mg. I tend to dose this lower than as written for tolerability and in a “dose low and go slow” approach with kids, which often results in better experiences with the medication. This medication also is recommended to be dosed by weight; this should be taken into account as well. Atomoxetine is a selective serotonin and norepinephrine reuptake inhibitor which is likely similar to Cymbalta (duloxetine). It may have a lower effect size of around less than 60% but this also is around the reported effect sizes for selective serotonin reuptake inhibitors (SSRIs) for depression. If a patient has both ADHD and an anxiety disorder, I often consider an SSRI alternatively first to manage attention issues associated with anxiety and then would add on a stimulant if attention issues persist once anxiety is better treated.
Second/third line ADHD treatments
As a second-line approach to long-acting Ritalin and if there is not a response to it, I would consider extended-release Adderall preparations such as Vyvanse, which is an amphetamine preparation supposedly less abusable than Adderall (one can’t snort it), but I also caution that it releases dopamine, peaks faster, and does not reduce to zero stimulant in 24 hours because of a variable half-life.
In this way, I always have imagined that these amphetamines may be more theoretically concerning than Ritalin/methylphenidate because they increase dopamine dumping into the synapse (which is a different and extra mechanism than just reuptake). For a third line, I may consider guanfacine depending on weight daily, which is an Food and Drug Administration–approved, nonstimulant alpha-2 agonist, which also acts longer than clonidine and may be better for hyperactivity symptoms. I may begin with doses as low as 0.25-0.5 mg in the evening for concerns with sedation or groggy aftereffects in the morning.
Throughout all treatment with medication, I emphasize the importance of assertively managing ADHD symptoms which may be in the form of “behavioral treatment,” like cognitive behavioral therapy, organizational coaching available at some educational centers, or even finding ways to train one’s focus with athletics or practices such as yoga and mindfulness. In addition to this combined approach to treatment, stimulants are not perfect medications. All stimulants have a “drop-off effect” and were made to work during a school day lasting from 8 a.m. to 3 p.m. Some patients and families complain about the drop-off effect and may want to “dose” around a medication more frequently, in the late afternoon and in the evening, which can lead to poor appetite at dinner and insomnia.
My answers to the cases above would be that all the patients could have ADHD, but they also may have anxiety or stress-related disorders, depression, worries about performance, or poor skills to manage inattention. They may not yet have received school supports, coaching, or found ways to manage these symptoms either. Because stimulants can improve and enhance performance but also have their own drawbacks and risks not covered here, it’s important to consider each case as a whole with thoughtfulness about a child’s unique ability to “live and work” in this world.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and an assistant professor of psychiatry at UVM, both in Burlington. She reported no relevant financial disclosures. Email her at pdnews@mdedge.com.