User login
NK cell product receives orphan designation

The European Commission has granted orphan designation to a natural killer (NK) cell product for the treatment of multiple myeloma.
The product, called CellProtect, is manufactured from a patient’s own blood.
It consists of NK cells that have been activated and expanded so they can recognize and attack cancer cells.
CellProtect has been studied in a phase 1/2 trial of patients with multiple myeloma.
In this trial, the NK cell product was used as a supplement to autologous stem cell transplant.
CellProtect exhibited a good safety profile and signals of effect in the trial, according to CellProtect Nordic Pharmaceuticals AB, the company developing CellProtect.
Results from the trial are expected to be published in 2018.
“The decision from the commission is based on a recommendation from the European Medicines Agency’s Committee for Orphan Medicinal Products and confirms that a future product is considered to be of significant benefit to those suffering from multiple myeloma,” said Karin Mellström, chief executive officer of CellProtect Nordic Pharmaceuticals AB.
“We can now proceed and plan for additional clinical trials in order to receive approval to market CellProtect.”
Orphan designation from the European Commission provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if a therapy receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure.
The European Medicines Agency’s Committee for Orphan Medicinal Products adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision. ![]()
The European Commission has granted orphan designation to a natural killer (NK) cell product for the treatment of multiple myeloma.
The product, called CellProtect, is manufactured from a patient’s own blood.
It consists of NK cells that have been activated and expanded so they can recognize and attack cancer cells.
CellProtect has been studied in a phase 1/2 trial of patients with multiple myeloma.
In this trial, the NK cell product was used as a supplement to autologous stem cell transplant.
CellProtect exhibited a good safety profile and signals of effect in the trial, according to CellProtect Nordic Pharmaceuticals AB, the company developing CellProtect.
Results from the trial are expected to be published in 2018.
“The decision from the commission is based on a recommendation from the European Medicines Agency’s Committee for Orphan Medicinal Products and confirms that a future product is considered to be of significant benefit to those suffering from multiple myeloma,” said Karin Mellström, chief executive officer of CellProtect Nordic Pharmaceuticals AB.
“We can now proceed and plan for additional clinical trials in order to receive approval to market CellProtect.”
Orphan designation from the European Commission provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if a therapy receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure.
The European Medicines Agency’s Committee for Orphan Medicinal Products adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision. ![]()
The European Commission has granted orphan designation to a natural killer (NK) cell product for the treatment of multiple myeloma.
The product, called CellProtect, is manufactured from a patient’s own blood.
It consists of NK cells that have been activated and expanded so they can recognize and attack cancer cells.
CellProtect has been studied in a phase 1/2 trial of patients with multiple myeloma.
In this trial, the NK cell product was used as a supplement to autologous stem cell transplant.
CellProtect exhibited a good safety profile and signals of effect in the trial, according to CellProtect Nordic Pharmaceuticals AB, the company developing CellProtect.
Results from the trial are expected to be published in 2018.
“The decision from the commission is based on a recommendation from the European Medicines Agency’s Committee for Orphan Medicinal Products and confirms that a future product is considered to be of significant benefit to those suffering from multiple myeloma,” said Karin Mellström, chief executive officer of CellProtect Nordic Pharmaceuticals AB.
“We can now proceed and plan for additional clinical trials in order to receive approval to market CellProtect.”
Orphan designation from the European Commission provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if a therapy receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure.
The European Medicines Agency’s Committee for Orphan Medicinal Products adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision. ![]()
FDA approves topical antibiotic for impetigo infections
The Food and Drug Administration has approved in patients aged 2 months or older.
This is the first topical treatment for impetigo to be approved in more than 10 years, according to the press release from the manufacturer, Medimetriks Pharmaceuticals.
Ozenoxacin is a quinolone antimicrobial. The prescribing information is available on the FDA website.
The Food and Drug Administration has approved in patients aged 2 months or older.
This is the first topical treatment for impetigo to be approved in more than 10 years, according to the press release from the manufacturer, Medimetriks Pharmaceuticals.
Ozenoxacin is a quinolone antimicrobial. The prescribing information is available on the FDA website.
The Food and Drug Administration has approved in patients aged 2 months or older.
This is the first topical treatment for impetigo to be approved in more than 10 years, according to the press release from the manufacturer, Medimetriks Pharmaceuticals.
Ozenoxacin is a quinolone antimicrobial. The prescribing information is available on the FDA website.
Juvéderm Voluma for Cheek Rejuvenation


Rare neurological complication linked to Waldenstrom disease
Bilateral facial nerve palsy has been associated with underlying Waldenstrom disease in only one other known published case report, which was published in 2014. In a more recent case report published in the Journal of Clinical Neuroscience, Gabriel Torrealba-Acosta, MD, and colleagues in the department of neurology at Massachusetts General Hospital, Boston, described a second case involving a 67-year-old Hispanic man with a history of Waldenstrom disease who presented with subacute onset of bilateral facial weakness.
The patient, who had longstanding painful neuropathy, had presented to urgent care with a new-onset left facial nerve palsy, was then diagnosed with left Bell’s palsy, and began treatment with valacyclovir and prednisone.
The left-sided facial weakness gradually progressed to total paralysis of the left lower face and inability to close the left eye, and 2 weeks later, he developed right facial weakness that ran a similar course. The patient had a complicated clinical course that included symptomatic acute-on-chronic subdural hematoma, among other complications; eventually the patient’s symptoms stabilized and cranial neuropathies gradually improved, according to the report.
Bilateral facial nerve palsy is an extremely rare condition, occurring in just 0.3%-2% of all facial nerve palsy cases, according to the authors. By contrast, unilateral facial nerve palsy (or Bell’s palsy) is far more common, but it still occurs in only 25 patients per 100,000 population, they said.
Most cases of bilateral facial nerve palsy are caused by underlying Guillain-Barré syndrome, though some are congenital, related to trauma, or caused by etiologies that are metabolic, immunologic, or neoplastic in nature. While various types of neurological disturbances – from ischemic and hemorrhagic events to meningoencephalitis – have been documented to occur in up to a quarter of patients with Waldenstrom disease.
“Given the large differential that comprises the assessment of a bilateral facial nerve palsy, it warrants for an extensive work-up, and Waldenstrom’s macroglobulinemia should be sought as an additional possible etiology,” the authors wrote.
Dr. Torrealba-Acosta and coauthors reported having no financial disclosures.
SOURCE: Torrealba-Acosta G et al. J Clin Neurosci. 2017. doi: 10.1016/j.jocn.2017.10.081.
Bilateral facial nerve palsy has been associated with underlying Waldenstrom disease in only one other known published case report, which was published in 2014. In a more recent case report published in the Journal of Clinical Neuroscience, Gabriel Torrealba-Acosta, MD, and colleagues in the department of neurology at Massachusetts General Hospital, Boston, described a second case involving a 67-year-old Hispanic man with a history of Waldenstrom disease who presented with subacute onset of bilateral facial weakness.
The patient, who had longstanding painful neuropathy, had presented to urgent care with a new-onset left facial nerve palsy, was then diagnosed with left Bell’s palsy, and began treatment with valacyclovir and prednisone.
The left-sided facial weakness gradually progressed to total paralysis of the left lower face and inability to close the left eye, and 2 weeks later, he developed right facial weakness that ran a similar course. The patient had a complicated clinical course that included symptomatic acute-on-chronic subdural hematoma, among other complications; eventually the patient’s symptoms stabilized and cranial neuropathies gradually improved, according to the report.
Bilateral facial nerve palsy is an extremely rare condition, occurring in just 0.3%-2% of all facial nerve palsy cases, according to the authors. By contrast, unilateral facial nerve palsy (or Bell’s palsy) is far more common, but it still occurs in only 25 patients per 100,000 population, they said.
Most cases of bilateral facial nerve palsy are caused by underlying Guillain-Barré syndrome, though some are congenital, related to trauma, or caused by etiologies that are metabolic, immunologic, or neoplastic in nature. While various types of neurological disturbances – from ischemic and hemorrhagic events to meningoencephalitis – have been documented to occur in up to a quarter of patients with Waldenstrom disease.
“Given the large differential that comprises the assessment of a bilateral facial nerve palsy, it warrants for an extensive work-up, and Waldenstrom’s macroglobulinemia should be sought as an additional possible etiology,” the authors wrote.
Dr. Torrealba-Acosta and coauthors reported having no financial disclosures.
SOURCE: Torrealba-Acosta G et al. J Clin Neurosci. 2017. doi: 10.1016/j.jocn.2017.10.081.
Bilateral facial nerve palsy has been associated with underlying Waldenstrom disease in only one other known published case report, which was published in 2014. In a more recent case report published in the Journal of Clinical Neuroscience, Gabriel Torrealba-Acosta, MD, and colleagues in the department of neurology at Massachusetts General Hospital, Boston, described a second case involving a 67-year-old Hispanic man with a history of Waldenstrom disease who presented with subacute onset of bilateral facial weakness.
The patient, who had longstanding painful neuropathy, had presented to urgent care with a new-onset left facial nerve palsy, was then diagnosed with left Bell’s palsy, and began treatment with valacyclovir and prednisone.
The left-sided facial weakness gradually progressed to total paralysis of the left lower face and inability to close the left eye, and 2 weeks later, he developed right facial weakness that ran a similar course. The patient had a complicated clinical course that included symptomatic acute-on-chronic subdural hematoma, among other complications; eventually the patient’s symptoms stabilized and cranial neuropathies gradually improved, according to the report.
Bilateral facial nerve palsy is an extremely rare condition, occurring in just 0.3%-2% of all facial nerve palsy cases, according to the authors. By contrast, unilateral facial nerve palsy (or Bell’s palsy) is far more common, but it still occurs in only 25 patients per 100,000 population, they said.
Most cases of bilateral facial nerve palsy are caused by underlying Guillain-Barré syndrome, though some are congenital, related to trauma, or caused by etiologies that are metabolic, immunologic, or neoplastic in nature. While various types of neurological disturbances – from ischemic and hemorrhagic events to meningoencephalitis – have been documented to occur in up to a quarter of patients with Waldenstrom disease.
“Given the large differential that comprises the assessment of a bilateral facial nerve palsy, it warrants for an extensive work-up, and Waldenstrom’s macroglobulinemia should be sought as an additional possible etiology,” the authors wrote.
Dr. Torrealba-Acosta and coauthors reported having no financial disclosures.
SOURCE: Torrealba-Acosta G et al. J Clin Neurosci. 2017. doi: 10.1016/j.jocn.2017.10.081.
FROM THE JOURNAL OF CLINICAL NEUROSCIENCE
Postmenopausal women who shed pounds see lower breast cancer risk
SAN ANTONIO – Postmenopausal women may be able to lower their risk of invasive breast cancer by simply losing some weight, according to an analysis of the large prospective Women’s Health Initiative Observational Study.
“While obesity is an established risk factor for postmenopausal breast cancer, studies of weight loss and breast cancer provide inconsistent results. It’s been very, very difficult to show that losing weight changes breast cancer incidence,” said lead investigator Rowan T. Chlebowski, MD, PhD, research professor in the department of medical oncology and therapeutics research at City of Hope in Duarte, Calif. “Consequently, the current public health message is limited to ‘avoid body fatness’ [N Engl J Med. 2016;375:794-8]. That’s not a very strong public health message.”

Results showed that compared with peers whose weight remained stable, women who lost at least 5% of their body weight (an average of about 17-20 pounds) had a significant 12% reduction in breast cancer risk, Dr. Chlebowski reported in a session and press briefing at the San Antonio Breast Cancer Symposium. Benefit was similar whether the weight loss was intentional or not, and whether women were normal weight, overweight, or obese at baseline.
“These findings suggest that interventions in postmenopausal women designed to generate weight loss may reduce breast cancer risk. I feel these are very optimistic findings in that they provide a lesson to postmenopausal women that even a moderate degree of weight loss may be associated with health benefits,” he said. “This is a relatively new finding, and I think it should have public health implications.”
Parsing the findings
“I hope that you can present this to general doctors rather than oncologists because those are the ones seeing healthy women, by and large,” said press briefing moderator C. Kent Osborne, MD, codirector of SABCS and director of the Dan L. Duncan Cancer Center at Baylor College of Medicine in Houston. “But in my patients, I’ve always suggested that they lose weight. Most of them with breast cancer are overweight, it seems. And I always had to do it because of diabetes and other factors. Now we can do it because we have a breast cancer endpoint that also suggests that losing weight will help with that as well.”

Additional results from the study showed that women who experienced a weight gain of at least 5% did not have a significantly elevated risk of breast cancer overall.
“Do you think that the women who gained a little bit of weight didn’t have an increase in incidence because they were already overweight?” Dr. Osborne asked.
“When we go over all these very complex mechanisms and the different drivers, there’s probably a threshold. So obesity’s association with inflammatory factors, I think that’s a driver to a certain degree. But then something else takes over, or maybe the main driver takes over,” Dr. Chlebowski replied. “We don’t have enough data to decide exactly what that threshold is, but that’s the ongoing hypothesis.”
In the session, attendee Daniel McGrail, PhD, of the MD Anderson Cancer Center, Houston, asked, “Since this [risk reduction with weight loss] occurred regardless of initial [body mass index], and you have all these covariates accounted for, does that imply that actually caloric deficits or decreasing caloric intake could be preventing breast cancer risk regardless of initial weight or any other parameters?”
“In all these western diseases, what we take for normal is probably less normal than it might have been 250 years ago or thousands of years ago when we were eating berries and being chased by animals,” Dr. Chlebowski replied. “So this raises a question as to whether the normal weight cutoff should be an ideal weight for western cancer prevention.”
Study details
The Women’s Health Initiative Observational Study recruited 93,676 postmenopausal women aged 50-79 years from 40 U.S. clinical centers during 1993-1998. The women had measurements taken of height and weight at baseline and at year 3 for calculation of BMI, and were asked about intentionality of any weight loss during that period.
Analyses were based on 61,335 women who had normal or higher body weight and were cancer free at baseline, survived at least 3 years, and had adequate data.
Overall, about 13.3% of women lost at least 5% of their body weight between baseline and year 3; 7.9% did so intentionally, losing an average of 19.6 pounds, and 5.5% did so unintentionally, losing an average of 16.9 pounds.
“We used the 5% decrease because this level has been shown to change some biochemical markers potentially associated with cancer. And it has been shown in a different study population, a randomized trial, to reduce the frequency of diabetes,” Dr. Chlebowski noted.
“There was nothing that the study did to induce the weight loss. And based on a partial look at the data, it doesn’t look like many of the women went to some kind of program to lose weight. So it was probably self-directed weight loss,” he noted. “Interestingly, the body mass index of this group was 29.9, so they were on the verge of going into obesity. We wondered in retrospect whether that was a motivating factor for them.”
In multivariate analysis, relative to peers having a stable weight over time, the women losing at least 5% of their weight had a lower risk of breast cancer (hazard ratio, 0.88; 95% confidence interval, 0.78-0.98; P = .02).
Findings were unchanged after further adjustment for mammography frequency. In addition, risk reduction was statistically indistinguishable whether the weight loss was intentional or not (P = .2 for interaction), and whether women were normal weight, overweight, or obese at baseline (P = .4 for interaction).
The 19.6% of women who had a weight gain of at least 5% did not have a significantly elevated risk of breast cancer overall, but they did have a significantly elevated risk of triple-negative breast cancer (HR, 1.54; 95% CI, 1.16-2.05). “We really don’t have a good explanation for this,” Dr. Chlebowski said.
Tackling the global obesity epidemic by conventional means to reduce cancer risk is an uphill battle, he concluded. “We are going to be looking for possible mediating factors. If you can find the mediating factors, pharmacologic intervention would have a much greater chance of success.”
Dr. Chlebowski disclosed that he had no relevant conflicts of interest. Research was supported by the National Heart, Lung and Blood Institute; National Institutes of Health; Department of Health and Human Services; and American Institute for Cancer Research.
SOURCE: Chlebowski et al., SABCS 2017 Abstract GS5-07
SAN ANTONIO – Postmenopausal women may be able to lower their risk of invasive breast cancer by simply losing some weight, according to an analysis of the large prospective Women’s Health Initiative Observational Study.
“While obesity is an established risk factor for postmenopausal breast cancer, studies of weight loss and breast cancer provide inconsistent results. It’s been very, very difficult to show that losing weight changes breast cancer incidence,” said lead investigator Rowan T. Chlebowski, MD, PhD, research professor in the department of medical oncology and therapeutics research at City of Hope in Duarte, Calif. “Consequently, the current public health message is limited to ‘avoid body fatness’ [N Engl J Med. 2016;375:794-8]. That’s not a very strong public health message.”
Results showed that compared with peers whose weight remained stable, women who lost at least 5% of their body weight (an average of about 17-20 pounds) had a significant 12% reduction in breast cancer risk, Dr. Chlebowski reported in a session and press briefing at the San Antonio Breast Cancer Symposium. Benefit was similar whether the weight loss was intentional or not, and whether women were normal weight, overweight, or obese at baseline.
“These findings suggest that interventions in postmenopausal women designed to generate weight loss may reduce breast cancer risk. I feel these are very optimistic findings in that they provide a lesson to postmenopausal women that even a moderate degree of weight loss may be associated with health benefits,” he said. “This is a relatively new finding, and I think it should have public health implications.”
Parsing the findings
“I hope that you can present this to general doctors rather than oncologists because those are the ones seeing healthy women, by and large,” said press briefing moderator C. Kent Osborne, MD, codirector of SABCS and director of the Dan L. Duncan Cancer Center at Baylor College of Medicine in Houston. “But in my patients, I’ve always suggested that they lose weight. Most of them with breast cancer are overweight, it seems. And I always had to do it because of diabetes and other factors. Now we can do it because we have a breast cancer endpoint that also suggests that losing weight will help with that as well.”
Additional results from the study showed that women who experienced a weight gain of at least 5% did not have a significantly elevated risk of breast cancer overall.
“Do you think that the women who gained a little bit of weight didn’t have an increase in incidence because they were already overweight?” Dr. Osborne asked.
“When we go over all these very complex mechanisms and the different drivers, there’s probably a threshold. So obesity’s association with inflammatory factors, I think that’s a driver to a certain degree. But then something else takes over, or maybe the main driver takes over,” Dr. Chlebowski replied. “We don’t have enough data to decide exactly what that threshold is, but that’s the ongoing hypothesis.”
In the session, attendee Daniel McGrail, PhD, of the MD Anderson Cancer Center, Houston, asked, “Since this [risk reduction with weight loss] occurred regardless of initial [body mass index], and you have all these covariates accounted for, does that imply that actually caloric deficits or decreasing caloric intake could be preventing breast cancer risk regardless of initial weight or any other parameters?”
“In all these western diseases, what we take for normal is probably less normal than it might have been 250 years ago or thousands of years ago when we were eating berries and being chased by animals,” Dr. Chlebowski replied. “So this raises a question as to whether the normal weight cutoff should be an ideal weight for western cancer prevention.”
Study details
The Women’s Health Initiative Observational Study recruited 93,676 postmenopausal women aged 50-79 years from 40 U.S. clinical centers during 1993-1998. The women had measurements taken of height and weight at baseline and at year 3 for calculation of BMI, and were asked about intentionality of any weight loss during that period.
Analyses were based on 61,335 women who had normal or higher body weight and were cancer free at baseline, survived at least 3 years, and had adequate data.
Overall, about 13.3% of women lost at least 5% of their body weight between baseline and year 3; 7.9% did so intentionally, losing an average of 19.6 pounds, and 5.5% did so unintentionally, losing an average of 16.9 pounds.
“We used the 5% decrease because this level has been shown to change some biochemical markers potentially associated with cancer. And it has been shown in a different study population, a randomized trial, to reduce the frequency of diabetes,” Dr. Chlebowski noted.
“There was nothing that the study did to induce the weight loss. And based on a partial look at the data, it doesn’t look like many of the women went to some kind of program to lose weight. So it was probably self-directed weight loss,” he noted. “Interestingly, the body mass index of this group was 29.9, so they were on the verge of going into obesity. We wondered in retrospect whether that was a motivating factor for them.”
In multivariate analysis, relative to peers having a stable weight over time, the women losing at least 5% of their weight had a lower risk of breast cancer (hazard ratio, 0.88; 95% confidence interval, 0.78-0.98; P = .02).
Findings were unchanged after further adjustment for mammography frequency. In addition, risk reduction was statistically indistinguishable whether the weight loss was intentional or not (P = .2 for interaction), and whether women were normal weight, overweight, or obese at baseline (P = .4 for interaction).
The 19.6% of women who had a weight gain of at least 5% did not have a significantly elevated risk of breast cancer overall, but they did have a significantly elevated risk of triple-negative breast cancer (HR, 1.54; 95% CI, 1.16-2.05). “We really don’t have a good explanation for this,” Dr. Chlebowski said.
Tackling the global obesity epidemic by conventional means to reduce cancer risk is an uphill battle, he concluded. “We are going to be looking for possible mediating factors. If you can find the mediating factors, pharmacologic intervention would have a much greater chance of success.”
Dr. Chlebowski disclosed that he had no relevant conflicts of interest. Research was supported by the National Heart, Lung and Blood Institute; National Institutes of Health; Department of Health and Human Services; and American Institute for Cancer Research.
SOURCE: Chlebowski et al., SABCS 2017 Abstract GS5-07
SAN ANTONIO – Postmenopausal women may be able to lower their risk of invasive breast cancer by simply losing some weight, according to an analysis of the large prospective Women’s Health Initiative Observational Study.
“While obesity is an established risk factor for postmenopausal breast cancer, studies of weight loss and breast cancer provide inconsistent results. It’s been very, very difficult to show that losing weight changes breast cancer incidence,” said lead investigator Rowan T. Chlebowski, MD, PhD, research professor in the department of medical oncology and therapeutics research at City of Hope in Duarte, Calif. “Consequently, the current public health message is limited to ‘avoid body fatness’ [N Engl J Med. 2016;375:794-8]. That’s not a very strong public health message.”
Results showed that compared with peers whose weight remained stable, women who lost at least 5% of their body weight (an average of about 17-20 pounds) had a significant 12% reduction in breast cancer risk, Dr. Chlebowski reported in a session and press briefing at the San Antonio Breast Cancer Symposium. Benefit was similar whether the weight loss was intentional or not, and whether women were normal weight, overweight, or obese at baseline.
“These findings suggest that interventions in postmenopausal women designed to generate weight loss may reduce breast cancer risk. I feel these are very optimistic findings in that they provide a lesson to postmenopausal women that even a moderate degree of weight loss may be associated with health benefits,” he said. “This is a relatively new finding, and I think it should have public health implications.”
Parsing the findings
“I hope that you can present this to general doctors rather than oncologists because those are the ones seeing healthy women, by and large,” said press briefing moderator C. Kent Osborne, MD, codirector of SABCS and director of the Dan L. Duncan Cancer Center at Baylor College of Medicine in Houston. “But in my patients, I’ve always suggested that they lose weight. Most of them with breast cancer are overweight, it seems. And I always had to do it because of diabetes and other factors. Now we can do it because we have a breast cancer endpoint that also suggests that losing weight will help with that as well.”
Additional results from the study showed that women who experienced a weight gain of at least 5% did not have a significantly elevated risk of breast cancer overall.
“Do you think that the women who gained a little bit of weight didn’t have an increase in incidence because they were already overweight?” Dr. Osborne asked.
“When we go over all these very complex mechanisms and the different drivers, there’s probably a threshold. So obesity’s association with inflammatory factors, I think that’s a driver to a certain degree. But then something else takes over, or maybe the main driver takes over,” Dr. Chlebowski replied. “We don’t have enough data to decide exactly what that threshold is, but that’s the ongoing hypothesis.”
In the session, attendee Daniel McGrail, PhD, of the MD Anderson Cancer Center, Houston, asked, “Since this [risk reduction with weight loss] occurred regardless of initial [body mass index], and you have all these covariates accounted for, does that imply that actually caloric deficits or decreasing caloric intake could be preventing breast cancer risk regardless of initial weight or any other parameters?”
“In all these western diseases, what we take for normal is probably less normal than it might have been 250 years ago or thousands of years ago when we were eating berries and being chased by animals,” Dr. Chlebowski replied. “So this raises a question as to whether the normal weight cutoff should be an ideal weight for western cancer prevention.”
Study details
The Women’s Health Initiative Observational Study recruited 93,676 postmenopausal women aged 50-79 years from 40 U.S. clinical centers during 1993-1998. The women had measurements taken of height and weight at baseline and at year 3 for calculation of BMI, and were asked about intentionality of any weight loss during that period.
Analyses were based on 61,335 women who had normal or higher body weight and were cancer free at baseline, survived at least 3 years, and had adequate data.
Overall, about 13.3% of women lost at least 5% of their body weight between baseline and year 3; 7.9% did so intentionally, losing an average of 19.6 pounds, and 5.5% did so unintentionally, losing an average of 16.9 pounds.
“We used the 5% decrease because this level has been shown to change some biochemical markers potentially associated with cancer. And it has been shown in a different study population, a randomized trial, to reduce the frequency of diabetes,” Dr. Chlebowski noted.
“There was nothing that the study did to induce the weight loss. And based on a partial look at the data, it doesn’t look like many of the women went to some kind of program to lose weight. So it was probably self-directed weight loss,” he noted. “Interestingly, the body mass index of this group was 29.9, so they were on the verge of going into obesity. We wondered in retrospect whether that was a motivating factor for them.”
In multivariate analysis, relative to peers having a stable weight over time, the women losing at least 5% of their weight had a lower risk of breast cancer (hazard ratio, 0.88; 95% confidence interval, 0.78-0.98; P = .02).
Findings were unchanged after further adjustment for mammography frequency. In addition, risk reduction was statistically indistinguishable whether the weight loss was intentional or not (P = .2 for interaction), and whether women were normal weight, overweight, or obese at baseline (P = .4 for interaction).
The 19.6% of women who had a weight gain of at least 5% did not have a significantly elevated risk of breast cancer overall, but they did have a significantly elevated risk of triple-negative breast cancer (HR, 1.54; 95% CI, 1.16-2.05). “We really don’t have a good explanation for this,” Dr. Chlebowski said.
Tackling the global obesity epidemic by conventional means to reduce cancer risk is an uphill battle, he concluded. “We are going to be looking for possible mediating factors. If you can find the mediating factors, pharmacologic intervention would have a much greater chance of success.”
Dr. Chlebowski disclosed that he had no relevant conflicts of interest. Research was supported by the National Heart, Lung and Blood Institute; National Institutes of Health; Department of Health and Human Services; and American Institute for Cancer Research.
SOURCE: Chlebowski et al., SABCS 2017 Abstract GS5-07
REPORTING FROM SABCS 2017
Key clinical point:
Major finding: Compared with peers who had stable weight, women who lost at least 5% of their body weight had a lower risk of invasive breast cancer (hazard ratio, 0.88; P = .02).
Data source: A prospective cohort study of 93,676 postmenopausal women from the Women’s Health Initiative Observational Study.
Disclosures: Dr. Chlebowski disclosed that he had no relevant conflicts of interest. Research was supported by the National Heart, Lung, and Blood Institute; National Institutes of Health; Department of Health and Human Services; and American Institute for Cancer Research.
Source: Chlebowski et al. SABCS 2017 Abstract GS5-07.
New DBS device gains approval for Parkinson’s disease
The approval is based on as-yet unpublished results of the INTREPID trial, which successfully met its primary endpoint of mean change in waking hours with good symptom control, according to an announcement from the device’s manufacturer, Boston Scientific. The INTREPID study is the first multicenter, prospective, double-blind, randomized, sham-controlled study of DBS for Parkinson’s disease in the United States and enrolled in 292 patients at 23 sites.
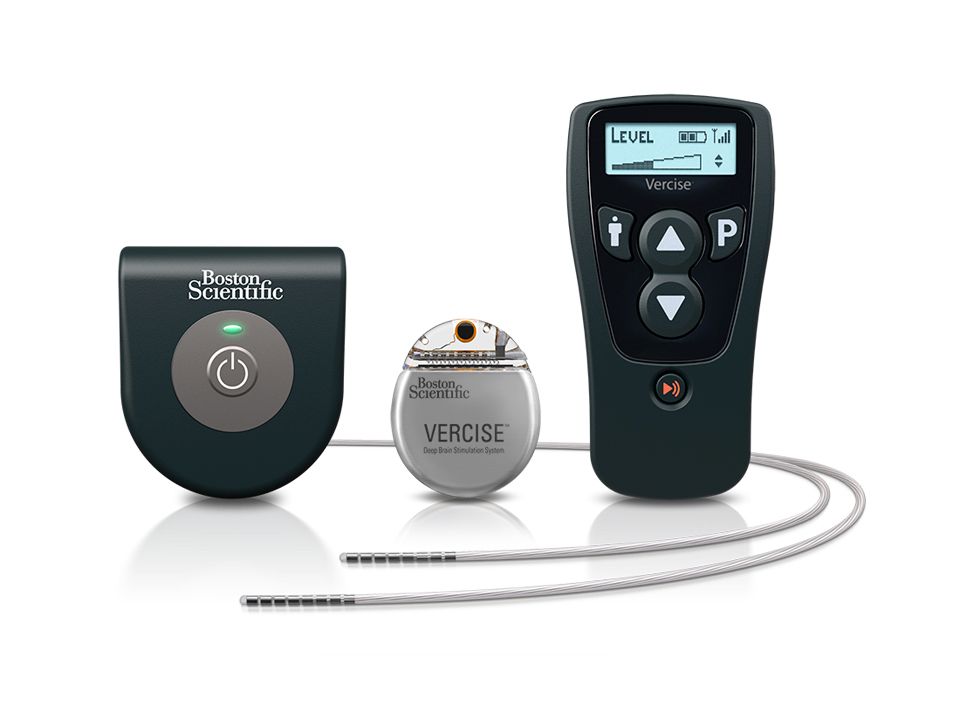
The implantable pulse generator of the device is “the smallest, rechargeable DBS device available in the U.S.,” according to Boston Scientific, and can independently control the amount of current delivered by each of the electrodes on the implanted leads, allowing them “to work together to address common challenges in DBS therapy such as fluctuations in symptoms and the progressive nature of the condition by offering more adaptable delivery of stimulation.”
“The Vercise DBS System changes the landscape of what physicians can do to help improve the quality of life for people living with Parkinson’s disease,” Jerry Vitek, MD, PhD, professor and chair of the department of neurology at the University of Minnesota, Minneapolis, and coordinating principal investigator for the INTREPID study said in the Boston Scientific announcement. “This system provides an ability to sculpt the current field in the DBS target using novel technology that offers flexibility in programming. This flexibility allows us to target different regions of the subthalamic nucleus, which we believe will improve outcomes while reducing side effects.”
The approval is based on as-yet unpublished results of the INTREPID trial, which successfully met its primary endpoint of mean change in waking hours with good symptom control, according to an announcement from the device’s manufacturer, Boston Scientific. The INTREPID study is the first multicenter, prospective, double-blind, randomized, sham-controlled study of DBS for Parkinson’s disease in the United States and enrolled in 292 patients at 23 sites.
The implantable pulse generator of the device is “the smallest, rechargeable DBS device available in the U.S.,” according to Boston Scientific, and can independently control the amount of current delivered by each of the electrodes on the implanted leads, allowing them “to work together to address common challenges in DBS therapy such as fluctuations in symptoms and the progressive nature of the condition by offering more adaptable delivery of stimulation.”
“The Vercise DBS System changes the landscape of what physicians can do to help improve the quality of life for people living with Parkinson’s disease,” Jerry Vitek, MD, PhD, professor and chair of the department of neurology at the University of Minnesota, Minneapolis, and coordinating principal investigator for the INTREPID study said in the Boston Scientific announcement. “This system provides an ability to sculpt the current field in the DBS target using novel technology that offers flexibility in programming. This flexibility allows us to target different regions of the subthalamic nucleus, which we believe will improve outcomes while reducing side effects.”
The approval is based on as-yet unpublished results of the INTREPID trial, which successfully met its primary endpoint of mean change in waking hours with good symptom control, according to an announcement from the device’s manufacturer, Boston Scientific. The INTREPID study is the first multicenter, prospective, double-blind, randomized, sham-controlled study of DBS for Parkinson’s disease in the United States and enrolled in 292 patients at 23 sites.
The implantable pulse generator of the device is “the smallest, rechargeable DBS device available in the U.S.,” according to Boston Scientific, and can independently control the amount of current delivered by each of the electrodes on the implanted leads, allowing them “to work together to address common challenges in DBS therapy such as fluctuations in symptoms and the progressive nature of the condition by offering more adaptable delivery of stimulation.”
“The Vercise DBS System changes the landscape of what physicians can do to help improve the quality of life for people living with Parkinson’s disease,” Jerry Vitek, MD, PhD, professor and chair of the department of neurology at the University of Minnesota, Minneapolis, and coordinating principal investigator for the INTREPID study said in the Boston Scientific announcement. “This system provides an ability to sculpt the current field in the DBS target using novel technology that offers flexibility in programming. This flexibility allows us to target different regions of the subthalamic nucleus, which we believe will improve outcomes while reducing side effects.”
Hospitals will feel the squeeze of DSH payment changes
Earlier this year, the Centers for Medicare and Medicaid Services finalized fundamental changes to how it reimburses hospitals for uncompensated care costs. When first proposed, the move raised alarm among physicians, hospitals, health systems, state health departments, and others around the country, and even prompted a lawsuit in New Hampshire.
In the months since the official adoption by the CMS, it remains unclear how the change will affect hospitals around the country, particularly the safety net hospitals that rely on these payments most.

In its final rule issued in April 2017 and finalized on August 2, 2017, the federal agency said the intent of the change is to more fairly distribute a fixed amount of DSH funds to the hospitals most in need. It also argued the change is a more consistent interpretation of the existing statute [Section 1923(g)], provides clarification around language that has been the subject of inquiry over the last decade, and promotes what it calls “fiscal integrity.”
“These allotments essentially establish a finite pool of available federal DSH funds that states use to pay the federal portion of payments to all qualifying hospitals in each state,” the final rule reads. “As states often use most or all of their federal DSH allotment, in practice, if one hospital gets more DSH funding, other DSH-eligible hospitals in the state may get less.”
This is not, however, the way all parties see it. For instance, in a comment submitted to the CMS in September 2016, the National Association of Urban Hospitals expressed its concern that DSH payments already are inadequate to cover the financial burden associated with providing care in low-income communities, such as translation services and the costs of employing physicians to practice in more challenged settings.2
In a letter to the CMS, the Minnesota Department of Human Services said it agrees with the agency that DSH payments should not be used to “subsidize costs that have been paid by Medicare and other insurers” but disagrees with the agency’s approach. Its argument includes a challenge to the CMS’ statutory authority to change the formula based on existing language.3
“I think the reason it’s contentious is because when you’re dealing with a fixed dollar amount and you’re talking about redistributing dollars, someone is going to lose,” said John McHugh, PhD, professor of health management at the Mailman School of Public Health at Columbia University. “A facility receiving DSH payments is already dealing with high levels of uncompensated care; the hospitals are operating on very thin margins. They are very often getting by because of these payments.”
Despite the CMS’ seemingly good intentions, Bradley Flansbaum, DO, MPH, MHM, a hospitalist at Geisinger Health System and member of the SHM Public Policy Committee, remains skeptical that the hospitals that need and deserve DSH payments will actually see more redistributed in their favor.

If hospitals in need see fewer DSH dollars, Dr. McHugh noted, they will feel the squeeze.
“It’s not easy to operate safety net hospitals,” he said. “And on top of that, hospitals have been operating under a certain assumption and it’s changing, and it takes time to incorporate those changes. There will probably be some fallout for the first couple of years as hospitals are adapting their practices. It could mean loss of services. It could mean the loss of quality physicians and quality staffing, and that can impact patient care.”
How will hospitals adapt?
The CMS did not give hospitals transition time. The reinterpretation became effective in June 2017, just 60 days after the agency issued the final rule. Dr. McHugh said he is not sure why the agency did not build in time for hospitals to adapt, particularly given the uncertainty around the national uninsured rate going forward, with so many potential changes to the American health care system under a new administration.
How any of these changes trickle down to hospitalists remains to be seen, said Dr. Flansbaum. Dr. McHugh believes it could lead to increased patient loads, higher turnover and churn, and fewer experienced physicians in safety net hospitals as younger doctors are hired and burn out. “At the end of the day, that feeds into patient care and patient satisfaction and quality,” he said.
However, hospitals across the country have been living with this “slow burn” for a long time, said Dr. Flansbaum, though not necessarily due to inadequate DSH payments. At least in some areas, reimbursements have gone down, hospital occupancy rates have declined, rural hospitals have closed, hospitals have consolidated, and people have been laid off.
It’s important to ensure the hospitals providing care for high levels of uninsured or underinsured patients receive the help they need, he said, and it’s also important to examine the role hospitals play as a whole in the American health care system.
“It’s an expensive system,” he said. “We have we created a system where, unlike other countries that have developed more vigorous primary or outpatient care, we have created an inpatient health system.”
With the CMS’ change, the government is the only entity that seems to win across the board, Dr. McHugh said. He said he would not be surprised if analysts looked to see how hospitals were affected by it in coming months.
But, he remains optimistic. In fact, the final rule also came with an $800 million increase in the amount of uncompensated care payments for acute care hospitals in fiscal year 2018, the CMS says.4
“Hospitals are adaptable,” Dr. McHugh said. “I think what you’ll see is this will spur some innovation in terms of patient care maybe a few years down the road. It may hit some stumbling blocks in the early going but there may be some positive changes in the future.”
References
1. Medicaid Program; Disproportionate Share Hospital Payments –Treatment of Third Party Payers in Calculating Uncompensated Care Costs. Centers for Medicare and Medicaid Services final rule. Citation 82 FR 16114. Published April 3, 2017. Last accessed August 14, 2017. https://www.federalregister.gov/documents/2017/04/03/2017-06538/medicaid-program-disproportionate-share-hospital-payments-treatment-of-third-party-payers-in
2. Kugler E. 2016-09-14 NAUH Medicaid Program DSH Payments – Treatment of Third Party Payer in Calculating Uncompensated Care Costs. September 14, 2016. Last accessed August 14, 2017. https://www.regulations.gov/document?D=CMS-2016-0144-0020
3. Berg A. Proposed Rule on Disproportionate Share Hospital Payments – Treatment of Third Party Payers in Calculating Uncompensated Care Costs, CMS-2399-P. September 14, 2016. Last accessed August 14, 2017. https://www.regulations.gov/document?D=CMS-2016-0144-0046
4. CMS finalizes 2018 payment and policy updates for Medicare hospital admissions. Published August 2, 2017. Last accessed August 14, 2017. https://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2017-Press-releases-items/2017-08-02.html
Earlier this year, the Centers for Medicare and Medicaid Services finalized fundamental changes to how it reimburses hospitals for uncompensated care costs. When first proposed, the move raised alarm among physicians, hospitals, health systems, state health departments, and others around the country, and even prompted a lawsuit in New Hampshire.
In the months since the official adoption by the CMS, it remains unclear how the change will affect hospitals around the country, particularly the safety net hospitals that rely on these payments most.
In its final rule issued in April 2017 and finalized on August 2, 2017, the federal agency said the intent of the change is to more fairly distribute a fixed amount of DSH funds to the hospitals most in need. It also argued the change is a more consistent interpretation of the existing statute [Section 1923(g)], provides clarification around language that has been the subject of inquiry over the last decade, and promotes what it calls “fiscal integrity.”
“These allotments essentially establish a finite pool of available federal DSH funds that states use to pay the federal portion of payments to all qualifying hospitals in each state,” the final rule reads. “As states often use most or all of their federal DSH allotment, in practice, if one hospital gets more DSH funding, other DSH-eligible hospitals in the state may get less.”
This is not, however, the way all parties see it. For instance, in a comment submitted to the CMS in September 2016, the National Association of Urban Hospitals expressed its concern that DSH payments already are inadequate to cover the financial burden associated with providing care in low-income communities, such as translation services and the costs of employing physicians to practice in more challenged settings.2
In a letter to the CMS, the Minnesota Department of Human Services said it agrees with the agency that DSH payments should not be used to “subsidize costs that have been paid by Medicare and other insurers” but disagrees with the agency’s approach. Its argument includes a challenge to the CMS’ statutory authority to change the formula based on existing language.3
“I think the reason it’s contentious is because when you’re dealing with a fixed dollar amount and you’re talking about redistributing dollars, someone is going to lose,” said John McHugh, PhD, professor of health management at the Mailman School of Public Health at Columbia University. “A facility receiving DSH payments is already dealing with high levels of uncompensated care; the hospitals are operating on very thin margins. They are very often getting by because of these payments.”
Despite the CMS’ seemingly good intentions, Bradley Flansbaum, DO, MPH, MHM, a hospitalist at Geisinger Health System and member of the SHM Public Policy Committee, remains skeptical that the hospitals that need and deserve DSH payments will actually see more redistributed in their favor.
If hospitals in need see fewer DSH dollars, Dr. McHugh noted, they will feel the squeeze.
“It’s not easy to operate safety net hospitals,” he said. “And on top of that, hospitals have been operating under a certain assumption and it’s changing, and it takes time to incorporate those changes. There will probably be some fallout for the first couple of years as hospitals are adapting their practices. It could mean loss of services. It could mean the loss of quality physicians and quality staffing, and that can impact patient care.”
How will hospitals adapt?
The CMS did not give hospitals transition time. The reinterpretation became effective in June 2017, just 60 days after the agency issued the final rule. Dr. McHugh said he is not sure why the agency did not build in time for hospitals to adapt, particularly given the uncertainty around the national uninsured rate going forward, with so many potential changes to the American health care system under a new administration.
How any of these changes trickle down to hospitalists remains to be seen, said Dr. Flansbaum. Dr. McHugh believes it could lead to increased patient loads, higher turnover and churn, and fewer experienced physicians in safety net hospitals as younger doctors are hired and burn out. “At the end of the day, that feeds into patient care and patient satisfaction and quality,” he said.
However, hospitals across the country have been living with this “slow burn” for a long time, said Dr. Flansbaum, though not necessarily due to inadequate DSH payments. At least in some areas, reimbursements have gone down, hospital occupancy rates have declined, rural hospitals have closed, hospitals have consolidated, and people have been laid off.
It’s important to ensure the hospitals providing care for high levels of uninsured or underinsured patients receive the help they need, he said, and it’s also important to examine the role hospitals play as a whole in the American health care system.
“It’s an expensive system,” he said. “We have we created a system where, unlike other countries that have developed more vigorous primary or outpatient care, we have created an inpatient health system.”
With the CMS’ change, the government is the only entity that seems to win across the board, Dr. McHugh said. He said he would not be surprised if analysts looked to see how hospitals were affected by it in coming months.
But, he remains optimistic. In fact, the final rule also came with an $800 million increase in the amount of uncompensated care payments for acute care hospitals in fiscal year 2018, the CMS says.4
“Hospitals are adaptable,” Dr. McHugh said. “I think what you’ll see is this will spur some innovation in terms of patient care maybe a few years down the road. It may hit some stumbling blocks in the early going but there may be some positive changes in the future.”
References
1. Medicaid Program; Disproportionate Share Hospital Payments –Treatment of Third Party Payers in Calculating Uncompensated Care Costs. Centers for Medicare and Medicaid Services final rule. Citation 82 FR 16114. Published April 3, 2017. Last accessed August 14, 2017. https://www.federalregister.gov/documents/2017/04/03/2017-06538/medicaid-program-disproportionate-share-hospital-payments-treatment-of-third-party-payers-in
2. Kugler E. 2016-09-14 NAUH Medicaid Program DSH Payments – Treatment of Third Party Payer in Calculating Uncompensated Care Costs. September 14, 2016. Last accessed August 14, 2017. https://www.regulations.gov/document?D=CMS-2016-0144-0020
3. Berg A. Proposed Rule on Disproportionate Share Hospital Payments – Treatment of Third Party Payers in Calculating Uncompensated Care Costs, CMS-2399-P. September 14, 2016. Last accessed August 14, 2017. https://www.regulations.gov/document?D=CMS-2016-0144-0046
4. CMS finalizes 2018 payment and policy updates for Medicare hospital admissions. Published August 2, 2017. Last accessed August 14, 2017. https://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2017-Press-releases-items/2017-08-02.html
Earlier this year, the Centers for Medicare and Medicaid Services finalized fundamental changes to how it reimburses hospitals for uncompensated care costs. When first proposed, the move raised alarm among physicians, hospitals, health systems, state health departments, and others around the country, and even prompted a lawsuit in New Hampshire.
In the months since the official adoption by the CMS, it remains unclear how the change will affect hospitals around the country, particularly the safety net hospitals that rely on these payments most.
In its final rule issued in April 2017 and finalized on August 2, 2017, the federal agency said the intent of the change is to more fairly distribute a fixed amount of DSH funds to the hospitals most in need. It also argued the change is a more consistent interpretation of the existing statute [Section 1923(g)], provides clarification around language that has been the subject of inquiry over the last decade, and promotes what it calls “fiscal integrity.”
“These allotments essentially establish a finite pool of available federal DSH funds that states use to pay the federal portion of payments to all qualifying hospitals in each state,” the final rule reads. “As states often use most or all of their federal DSH allotment, in practice, if one hospital gets more DSH funding, other DSH-eligible hospitals in the state may get less.”
This is not, however, the way all parties see it. For instance, in a comment submitted to the CMS in September 2016, the National Association of Urban Hospitals expressed its concern that DSH payments already are inadequate to cover the financial burden associated with providing care in low-income communities, such as translation services and the costs of employing physicians to practice in more challenged settings.2
In a letter to the CMS, the Minnesota Department of Human Services said it agrees with the agency that DSH payments should not be used to “subsidize costs that have been paid by Medicare and other insurers” but disagrees with the agency’s approach. Its argument includes a challenge to the CMS’ statutory authority to change the formula based on existing language.3
“I think the reason it’s contentious is because when you’re dealing with a fixed dollar amount and you’re talking about redistributing dollars, someone is going to lose,” said John McHugh, PhD, professor of health management at the Mailman School of Public Health at Columbia University. “A facility receiving DSH payments is already dealing with high levels of uncompensated care; the hospitals are operating on very thin margins. They are very often getting by because of these payments.”
Despite the CMS’ seemingly good intentions, Bradley Flansbaum, DO, MPH, MHM, a hospitalist at Geisinger Health System and member of the SHM Public Policy Committee, remains skeptical that the hospitals that need and deserve DSH payments will actually see more redistributed in their favor.
If hospitals in need see fewer DSH dollars, Dr. McHugh noted, they will feel the squeeze.
“It’s not easy to operate safety net hospitals,” he said. “And on top of that, hospitals have been operating under a certain assumption and it’s changing, and it takes time to incorporate those changes. There will probably be some fallout for the first couple of years as hospitals are adapting their practices. It could mean loss of services. It could mean the loss of quality physicians and quality staffing, and that can impact patient care.”
How will hospitals adapt?
The CMS did not give hospitals transition time. The reinterpretation became effective in June 2017, just 60 days after the agency issued the final rule. Dr. McHugh said he is not sure why the agency did not build in time for hospitals to adapt, particularly given the uncertainty around the national uninsured rate going forward, with so many potential changes to the American health care system under a new administration.
How any of these changes trickle down to hospitalists remains to be seen, said Dr. Flansbaum. Dr. McHugh believes it could lead to increased patient loads, higher turnover and churn, and fewer experienced physicians in safety net hospitals as younger doctors are hired and burn out. “At the end of the day, that feeds into patient care and patient satisfaction and quality,” he said.
However, hospitals across the country have been living with this “slow burn” for a long time, said Dr. Flansbaum, though not necessarily due to inadequate DSH payments. At least in some areas, reimbursements have gone down, hospital occupancy rates have declined, rural hospitals have closed, hospitals have consolidated, and people have been laid off.
It’s important to ensure the hospitals providing care for high levels of uninsured or underinsured patients receive the help they need, he said, and it’s also important to examine the role hospitals play as a whole in the American health care system.
“It’s an expensive system,” he said. “We have we created a system where, unlike other countries that have developed more vigorous primary or outpatient care, we have created an inpatient health system.”
With the CMS’ change, the government is the only entity that seems to win across the board, Dr. McHugh said. He said he would not be surprised if analysts looked to see how hospitals were affected by it in coming months.
But, he remains optimistic. In fact, the final rule also came with an $800 million increase in the amount of uncompensated care payments for acute care hospitals in fiscal year 2018, the CMS says.4
“Hospitals are adaptable,” Dr. McHugh said. “I think what you’ll see is this will spur some innovation in terms of patient care maybe a few years down the road. It may hit some stumbling blocks in the early going but there may be some positive changes in the future.”
References
1. Medicaid Program; Disproportionate Share Hospital Payments –Treatment of Third Party Payers in Calculating Uncompensated Care Costs. Centers for Medicare and Medicaid Services final rule. Citation 82 FR 16114. Published April 3, 2017. Last accessed August 14, 2017. https://www.federalregister.gov/documents/2017/04/03/2017-06538/medicaid-program-disproportionate-share-hospital-payments-treatment-of-third-party-payers-in
2. Kugler E. 2016-09-14 NAUH Medicaid Program DSH Payments – Treatment of Third Party Payer in Calculating Uncompensated Care Costs. September 14, 2016. Last accessed August 14, 2017. https://www.regulations.gov/document?D=CMS-2016-0144-0020
3. Berg A. Proposed Rule on Disproportionate Share Hospital Payments – Treatment of Third Party Payers in Calculating Uncompensated Care Costs, CMS-2399-P. September 14, 2016. Last accessed August 14, 2017. https://www.regulations.gov/document?D=CMS-2016-0144-0046
4. CMS finalizes 2018 payment and policy updates for Medicare hospital admissions. Published August 2, 2017. Last accessed August 14, 2017. https://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2017-Press-releases-items/2017-08-02.html
Leflunomide use in pregnancy shows little impact on newborns
Leflunomide, prescribed in Canada to treat active rheumatoid arthritis, was previously classified as a category X pregnancy medication because it is embryotoxic and teratogenic in rats and rabbits in doses similar to those used in humans, wrote Anick Bérard, MD, of CHU Sainte Justine, Montreal, and her colleagues, in a study published in Annals of the Rheumatic Diseases.
However, data on the impact of leflunomide on a developing human embryo are limited, so the researchers analyzed the Quebec Pregnancy Cohort, an ongoing study of all pregnancies in Quebec, Canada, between Jan. 1, 1998, and Dec. 31, 2015.
The findings are consistent with those from previous studies and suggest that continued caution is warranted for women of childbearing age who are taking or considering leflunomide, the researchers concluded.
They also examined the potential impact of several categories of other antirheumatic drugs to account for indication bias: other conventional disease-modifying antirheumatic drugs, biologic agents, nonsteroidal anti-inflammatory drugs, oral corticosteroids, and gold salts. Oral corticosteroid use in the first trimester was associated with an increased risk of major congenital malformations (aOR 1.31; 95% CI, 1.06-1.61), and the risk of prematurity also was significant with their use in the second or third trimester (aOR 1.32; 95% CI, 1.09 to 1.60). The risk of major congenital malformations was significantly higher with the use of NSAIDs in the first trimester (aOR 1.15; 95% CI, 1.03-1.29). Any use of disease-modifying antirheumatic drugs overall between the first day of gestation and the index date increased the odds for spontaneous abortion (aOR, 1.54; 95% CI, 1.06-2.22).
Cholestyramine may lower the blood level of the active metabolite of leflunomide to a safe level, the researchers noted, but the study population showed no evidence of cholestyramine or charcoal use for leflunomide washout, and any cholestyramine exposures during pregnancy were not concurrent with leflunomide exposure. “In three first-trimester leflunomide-exposed pregnancies, cholestyramine was introduced in monotherapy in the third trimester,” they wrote.
The results were limited by the small number of women exposed to leflunomide, despite the population-based study being the largest of its kind published to date, the researchers said.
The study was supported in part by the Fonds de la Recherche du Québec-Santé and by Sanofi. Two authors are employees of Sanofi.
SOURCE: Bérard A et al., Ann Rheum Dis. 2017 Dec 8. doi: 10.1136/annrheumdis-2017-212078
Leflunomide, prescribed in Canada to treat active rheumatoid arthritis, was previously classified as a category X pregnancy medication because it is embryotoxic and teratogenic in rats and rabbits in doses similar to those used in humans, wrote Anick Bérard, MD, of CHU Sainte Justine, Montreal, and her colleagues, in a study published in Annals of the Rheumatic Diseases.
However, data on the impact of leflunomide on a developing human embryo are limited, so the researchers analyzed the Quebec Pregnancy Cohort, an ongoing study of all pregnancies in Quebec, Canada, between Jan. 1, 1998, and Dec. 31, 2015.
The findings are consistent with those from previous studies and suggest that continued caution is warranted for women of childbearing age who are taking or considering leflunomide, the researchers concluded.
They also examined the potential impact of several categories of other antirheumatic drugs to account for indication bias: other conventional disease-modifying antirheumatic drugs, biologic agents, nonsteroidal anti-inflammatory drugs, oral corticosteroids, and gold salts. Oral corticosteroid use in the first trimester was associated with an increased risk of major congenital malformations (aOR 1.31; 95% CI, 1.06-1.61), and the risk of prematurity also was significant with their use in the second or third trimester (aOR 1.32; 95% CI, 1.09 to 1.60). The risk of major congenital malformations was significantly higher with the use of NSAIDs in the first trimester (aOR 1.15; 95% CI, 1.03-1.29). Any use of disease-modifying antirheumatic drugs overall between the first day of gestation and the index date increased the odds for spontaneous abortion (aOR, 1.54; 95% CI, 1.06-2.22).
Cholestyramine may lower the blood level of the active metabolite of leflunomide to a safe level, the researchers noted, but the study population showed no evidence of cholestyramine or charcoal use for leflunomide washout, and any cholestyramine exposures during pregnancy were not concurrent with leflunomide exposure. “In three first-trimester leflunomide-exposed pregnancies, cholestyramine was introduced in monotherapy in the third trimester,” they wrote.
The results were limited by the small number of women exposed to leflunomide, despite the population-based study being the largest of its kind published to date, the researchers said.
The study was supported in part by the Fonds de la Recherche du Québec-Santé and by Sanofi. Two authors are employees of Sanofi.
SOURCE: Bérard A et al., Ann Rheum Dis. 2017 Dec 8. doi: 10.1136/annrheumdis-2017-212078
Leflunomide, prescribed in Canada to treat active rheumatoid arthritis, was previously classified as a category X pregnancy medication because it is embryotoxic and teratogenic in rats and rabbits in doses similar to those used in humans, wrote Anick Bérard, MD, of CHU Sainte Justine, Montreal, and her colleagues, in a study published in Annals of the Rheumatic Diseases.
However, data on the impact of leflunomide on a developing human embryo are limited, so the researchers analyzed the Quebec Pregnancy Cohort, an ongoing study of all pregnancies in Quebec, Canada, between Jan. 1, 1998, and Dec. 31, 2015.
The findings are consistent with those from previous studies and suggest that continued caution is warranted for women of childbearing age who are taking or considering leflunomide, the researchers concluded.
They also examined the potential impact of several categories of other antirheumatic drugs to account for indication bias: other conventional disease-modifying antirheumatic drugs, biologic agents, nonsteroidal anti-inflammatory drugs, oral corticosteroids, and gold salts. Oral corticosteroid use in the first trimester was associated with an increased risk of major congenital malformations (aOR 1.31; 95% CI, 1.06-1.61), and the risk of prematurity also was significant with their use in the second or third trimester (aOR 1.32; 95% CI, 1.09 to 1.60). The risk of major congenital malformations was significantly higher with the use of NSAIDs in the first trimester (aOR 1.15; 95% CI, 1.03-1.29). Any use of disease-modifying antirheumatic drugs overall between the first day of gestation and the index date increased the odds for spontaneous abortion (aOR, 1.54; 95% CI, 1.06-2.22).
Cholestyramine may lower the blood level of the active metabolite of leflunomide to a safe level, the researchers noted, but the study population showed no evidence of cholestyramine or charcoal use for leflunomide washout, and any cholestyramine exposures during pregnancy were not concurrent with leflunomide exposure. “In three first-trimester leflunomide-exposed pregnancies, cholestyramine was introduced in monotherapy in the third trimester,” they wrote.
The results were limited by the small number of women exposed to leflunomide, despite the population-based study being the largest of its kind published to date, the researchers said.
The study was supported in part by the Fonds de la Recherche du Québec-Santé and by Sanofi. Two authors are employees of Sanofi.
SOURCE: Bérard A et al., Ann Rheum Dis. 2017 Dec 8. doi: 10.1136/annrheumdis-2017-212078
FROM ANNALS OF THE RHEUMATIC DISEASES
Key clinical point: Exposure to leflunomide during pregnancy was not associated with significantly increased risk of major congenital malformations, low birth weight, premature birth, or spontaneous abortions.
Major finding: No significant association was seen between leflunomide use in the first trimester and an increased risk of major congenital malformations based on five cases (adjusted odds ratio, 0.97).
Data source: A population-based cohort study of 289,688 pregnancies in Canada between 1998 and 2015.
Disclosures: The study was supported in part by the Fonds de la Recherche du Québec-Santé and by Sanofi. Two authors are employees of Sanofi.
Source: Bérard A et al., Ann Rheum Dis. 2017 Dec 8. doi: 10.1136/annrheumdis-2017-212078
MRI-guided focused ultrasound shows promise for subcortical epilepsy
WASHINGTON – MRI-guided focused ultrasound (FUS) is now being employed on an experimental basis to treat deep subcortical lesions, such as hypothalamic hamartoma, to control intractable epilepsy, according to an expert summary of a “hot topic” presented at the American Epilepsy Society annual meeting.
“If the risk of FUS is as low as we expect, it could change our paradigm,” reported Nathan B. Fountain, MD, director of the F.E. Dreifuss Comprehensive Epilepsy Program at the University of Virginia, Charlottesville.

FUS has been used clinically for the treatment of uterine fibroids since 2004, according to an overview provided by Dr. Fountain. Clinical studies of MRI-guided FUS for lesions in the brain began in 2009. The approval of MRI-guided FUS thalamotomy for essential tumor in 2016 was based on a pivotal trial led by Jeffrey Elias, MD, a colleague of Dr. Fountain’s at the University of Virginia (N Engl J Med. 2016;375:730-9). Many of the principles for treating subcortical lesions causing epilepsy are the same as those for treating essential tremor.
Under MRI guidance, FUS is delivered via a helmet with 1,024 transducers. These focus sound waves to a highly targeted area of the brain, resulting in thermal ablation. The treatment is noninvasive in the sense that no craniotomy is involved. It can be delivered without anesthesia. When used to treat essential tremor in awake patients, MRI-guided FUS confirms the target when the tremor resolves.
“There is no injury to the brain as far as we can tell,” reported Dr. Fountain, referring to the tremor studies.
Because the thermal ablation is delivered by sound waves, this approach appears to be safer to structures surrounding the lesion than would be anticipated with energy delivered by radiation. For treatment of lesions in the hypothalamus, where surrounding tissue is responsible for important brain functions, the apparent low risk of collateral damage is a major potential advantage, according to Dr. Fountain.
Although Dr. Fountain conceded that the term “subcortical” is not commonly used to describe epilepsy lesions, he considers it appropriate to explain the role of MRI-guided FUS. Without technical advancements, this tool is not appropriate for the cortical lesions that are responsible for the majority of epileptic seizures. Rather, lesions must be positioned deep in the skull to be in the “envelope” where energy can be concentrated. Lesions in the temporal or hippocampal areas of the brain, for example, will not be suitable without technical advances.
Due to its position in the brain, “hypothalamic hamartoma is the prototype lesion,” Dr. Fountain reported. Importantly, these and other lesions within the envelope where energy can be targeted are the most difficult to treat with other options. Due to the need to transverse much of the brain to reach these areas, open surgery is often not practical. Even though Dr. Fountain acknowledged that MRI-guided stereotactic laser has been proposed for these types of lesions, the laser must also transverse vulnerable structures of the brain that can be avoided with MR-guided FUS.
Results on the first patient in a planned pediatric treatment series with MRI-guided FUS were presented at the AES annual meeting by Travis Tierney, MD, PhD, a neurosurgeon associated with Nicklaus Children’s Hospital in Miami. According to the data presented by Dr. Tierney, the 21-year-old patient was treated for a hypothalamic hamartoma. She was rendered seizure free and had no complications.
An adult series is now recruiting candidates, according to Dr. Fountain. He reported that adults of at least 18 years of age with intractable epilepsy due to subcortical lesions in the central envelope suitable for MRI-guided FUS are eligible if they have at least three seizures per month while taking at least two antiepileptic drugs. He encouraged referrals.
“The primary outcome will be just to demonstrate that a lesion can be created,” Dr. Fountain said. He reported that the planned enrollment of 15 subjects would not be sufficient to draw conclusions about efficacy “unless, of course, we eliminate everyone’s seizures – and that would be useful – but that is still a secondary outcome,”
There are a number of applications in neurology beyond treatment of tremors and epilepsy that are also being considered for MRI-guided FUS, Dr. Fountain reported. This could include, for example, clot lysis in stroke, but he indicated that there are a number of reasons to be particularly optimistic about its potential role in the treatment intractable epilepsy due to subcortical lesions. This strategy seems feasible in a condition with limited treatment options.
WASHINGTON – MRI-guided focused ultrasound (FUS) is now being employed on an experimental basis to treat deep subcortical lesions, such as hypothalamic hamartoma, to control intractable epilepsy, according to an expert summary of a “hot topic” presented at the American Epilepsy Society annual meeting.
“If the risk of FUS is as low as we expect, it could change our paradigm,” reported Nathan B. Fountain, MD, director of the F.E. Dreifuss Comprehensive Epilepsy Program at the University of Virginia, Charlottesville.
FUS has been used clinically for the treatment of uterine fibroids since 2004, according to an overview provided by Dr. Fountain. Clinical studies of MRI-guided FUS for lesions in the brain began in 2009. The approval of MRI-guided FUS thalamotomy for essential tumor in 2016 was based on a pivotal trial led by Jeffrey Elias, MD, a colleague of Dr. Fountain’s at the University of Virginia (N Engl J Med. 2016;375:730-9). Many of the principles for treating subcortical lesions causing epilepsy are the same as those for treating essential tremor.
Under MRI guidance, FUS is delivered via a helmet with 1,024 transducers. These focus sound waves to a highly targeted area of the brain, resulting in thermal ablation. The treatment is noninvasive in the sense that no craniotomy is involved. It can be delivered without anesthesia. When used to treat essential tremor in awake patients, MRI-guided FUS confirms the target when the tremor resolves.
“There is no injury to the brain as far as we can tell,” reported Dr. Fountain, referring to the tremor studies.
Because the thermal ablation is delivered by sound waves, this approach appears to be safer to structures surrounding the lesion than would be anticipated with energy delivered by radiation. For treatment of lesions in the hypothalamus, where surrounding tissue is responsible for important brain functions, the apparent low risk of collateral damage is a major potential advantage, according to Dr. Fountain.
Although Dr. Fountain conceded that the term “subcortical” is not commonly used to describe epilepsy lesions, he considers it appropriate to explain the role of MRI-guided FUS. Without technical advancements, this tool is not appropriate for the cortical lesions that are responsible for the majority of epileptic seizures. Rather, lesions must be positioned deep in the skull to be in the “envelope” where energy can be concentrated. Lesions in the temporal or hippocampal areas of the brain, for example, will not be suitable without technical advances.
Due to its position in the brain, “hypothalamic hamartoma is the prototype lesion,” Dr. Fountain reported. Importantly, these and other lesions within the envelope where energy can be targeted are the most difficult to treat with other options. Due to the need to transverse much of the brain to reach these areas, open surgery is often not practical. Even though Dr. Fountain acknowledged that MRI-guided stereotactic laser has been proposed for these types of lesions, the laser must also transverse vulnerable structures of the brain that can be avoided with MR-guided FUS.
Results on the first patient in a planned pediatric treatment series with MRI-guided FUS were presented at the AES annual meeting by Travis Tierney, MD, PhD, a neurosurgeon associated with Nicklaus Children’s Hospital in Miami. According to the data presented by Dr. Tierney, the 21-year-old patient was treated for a hypothalamic hamartoma. She was rendered seizure free and had no complications.
An adult series is now recruiting candidates, according to Dr. Fountain. He reported that adults of at least 18 years of age with intractable epilepsy due to subcortical lesions in the central envelope suitable for MRI-guided FUS are eligible if they have at least three seizures per month while taking at least two antiepileptic drugs. He encouraged referrals.
“The primary outcome will be just to demonstrate that a lesion can be created,” Dr. Fountain said. He reported that the planned enrollment of 15 subjects would not be sufficient to draw conclusions about efficacy “unless, of course, we eliminate everyone’s seizures – and that would be useful – but that is still a secondary outcome,”
There are a number of applications in neurology beyond treatment of tremors and epilepsy that are also being considered for MRI-guided FUS, Dr. Fountain reported. This could include, for example, clot lysis in stroke, but he indicated that there are a number of reasons to be particularly optimistic about its potential role in the treatment intractable epilepsy due to subcortical lesions. This strategy seems feasible in a condition with limited treatment options.
WASHINGTON – MRI-guided focused ultrasound (FUS) is now being employed on an experimental basis to treat deep subcortical lesions, such as hypothalamic hamartoma, to control intractable epilepsy, according to an expert summary of a “hot topic” presented at the American Epilepsy Society annual meeting.
“If the risk of FUS is as low as we expect, it could change our paradigm,” reported Nathan B. Fountain, MD, director of the F.E. Dreifuss Comprehensive Epilepsy Program at the University of Virginia, Charlottesville.
FUS has been used clinically for the treatment of uterine fibroids since 2004, according to an overview provided by Dr. Fountain. Clinical studies of MRI-guided FUS for lesions in the brain began in 2009. The approval of MRI-guided FUS thalamotomy for essential tumor in 2016 was based on a pivotal trial led by Jeffrey Elias, MD, a colleague of Dr. Fountain’s at the University of Virginia (N Engl J Med. 2016;375:730-9). Many of the principles for treating subcortical lesions causing epilepsy are the same as those for treating essential tremor.
Under MRI guidance, FUS is delivered via a helmet with 1,024 transducers. These focus sound waves to a highly targeted area of the brain, resulting in thermal ablation. The treatment is noninvasive in the sense that no craniotomy is involved. It can be delivered without anesthesia. When used to treat essential tremor in awake patients, MRI-guided FUS confirms the target when the tremor resolves.
“There is no injury to the brain as far as we can tell,” reported Dr. Fountain, referring to the tremor studies.
Because the thermal ablation is delivered by sound waves, this approach appears to be safer to structures surrounding the lesion than would be anticipated with energy delivered by radiation. For treatment of lesions in the hypothalamus, where surrounding tissue is responsible for important brain functions, the apparent low risk of collateral damage is a major potential advantage, according to Dr. Fountain.
Although Dr. Fountain conceded that the term “subcortical” is not commonly used to describe epilepsy lesions, he considers it appropriate to explain the role of MRI-guided FUS. Without technical advancements, this tool is not appropriate for the cortical lesions that are responsible for the majority of epileptic seizures. Rather, lesions must be positioned deep in the skull to be in the “envelope” where energy can be concentrated. Lesions in the temporal or hippocampal areas of the brain, for example, will not be suitable without technical advances.
Due to its position in the brain, “hypothalamic hamartoma is the prototype lesion,” Dr. Fountain reported. Importantly, these and other lesions within the envelope where energy can be targeted are the most difficult to treat with other options. Due to the need to transverse much of the brain to reach these areas, open surgery is often not practical. Even though Dr. Fountain acknowledged that MRI-guided stereotactic laser has been proposed for these types of lesions, the laser must also transverse vulnerable structures of the brain that can be avoided with MR-guided FUS.
Results on the first patient in a planned pediatric treatment series with MRI-guided FUS were presented at the AES annual meeting by Travis Tierney, MD, PhD, a neurosurgeon associated with Nicklaus Children’s Hospital in Miami. According to the data presented by Dr. Tierney, the 21-year-old patient was treated for a hypothalamic hamartoma. She was rendered seizure free and had no complications.
An adult series is now recruiting candidates, according to Dr. Fountain. He reported that adults of at least 18 years of age with intractable epilepsy due to subcortical lesions in the central envelope suitable for MRI-guided FUS are eligible if they have at least three seizures per month while taking at least two antiepileptic drugs. He encouraged referrals.
“The primary outcome will be just to demonstrate that a lesion can be created,” Dr. Fountain said. He reported that the planned enrollment of 15 subjects would not be sufficient to draw conclusions about efficacy “unless, of course, we eliminate everyone’s seizures – and that would be useful – but that is still a secondary outcome,”
There are a number of applications in neurology beyond treatment of tremors and epilepsy that are also being considered for MRI-guided FUS, Dr. Fountain reported. This could include, for example, clot lysis in stroke, but he indicated that there are a number of reasons to be particularly optimistic about its potential role in the treatment intractable epilepsy due to subcortical lesions. This strategy seems feasible in a condition with limited treatment options.
EXPERT ANALYSIS FROM AES 2017