User login
Elderly patients with psoriasis can benefit from biologics with low rates of adverse events
according to a new retrospective study.
Among 266 older patients, 65% achieved a 75% improvement in Psoriasis Area Severity Index score (PASI 75) after 1 year of therapy; 50% reached a PASI 90, and 40% a PASI 100, Francesca Prignano MD, PhD, and her colleagues reported in the Journal of the European Academy of Dermatology and Venereology. The rate of serious adverse events was less than 10%.
Elderly patients – those aged 65 years and older – are commonly excluded from studies on biologic treatments because they have more medical comorbidities and are thought to be more at risk for serious adverse events, like infections and malignancy, wrote Dr. Prignano of the dermatology unit, University of Florence, Italy, and her colleagues.
As a result, they noted, there is a “lack of information concerning safety and effectiveness of available treatments for psoriasis in the elderly, particularly about new biologic agents. Disease remission should be an objective for both younger patients and older patients, and biologic therapy should be considered a treatment option for all patients.”
To examine both the benefit and risk of biologics in this population, the team reviewed the records of 266 elderly psoriasis patients; everyone had been on a biologic treatment for at least 1 year.
The primary outcome was PASI score at weeks 8, 16, 28, and 52. The secondary outcomes were the rate and types of biologic-associated adverse events.
The study comprised 266 patients (mean age 72 years). Their mean psoriasis duration was 25.7 years. Comorbidities included psoriatic arthritis; hypertension and dyslipidemia; diabetes mellitus; cardiovascular, gastrointestinal and respiratory diseases; osteoporosis; thyroid dysfunction; depression; and cancer.
Adalimumab was the most commonly prescribed biologic (31%), followed by ustekinumab (28.9%), etanercept (20%), and secukinumab (15%). A smaller proportion of patients were taking infliximab, golimumab, or certolizumab pegol.
The mean baseline PASI was 16.5, although the range was wide (4-54). At the time of review, the average biologic treatment duration was 44 months. Almost half of the cohort (128) were on their second biologic, and 20 more had been on three biologics. A few patients were taking concomitant medications, including steroids, cyclosporine, and acitretin.
The mean PASI scores decreased to 3.7 at week 16, 1.6 at week 28, and 1.2 at week 52. The group exhibited a rapid response to biologic treatment. By 16 weeks, about 55% had achieved a PASI 75, about 28% a PASI 90, and about 20% a PASI 100. By 28 weeks, these numbers were about 64%, 45%, and 35%, respectively. At 1 year, they were about 65%, 50%, and 40%, respectively.
The rate of adverse events was 9.4%. There were 25 events in the cohort, the majority of which (48%) were infections; these included four respiratory infections, three urinary tract infections, two cases of mucocutaneous candidiasis, two cases of herpes zoster infection, and one case of erysipelas.
There were four malignancies: three nonmelanoma skin cancers and one vocal cord cancer.
Noting that, to date, their study represented “the broadest experience on the use of biological drugs” for elderly patients with psoriasis, they wrote that while “comorbidities should be taken into consideration when a long-term treatment is proposed, for the higher risk of side effects and drug interactions,” they wrote, noting that none of the 266 patients had a serious infection and the malignancy rate was low (1.5%).
None of the authors had financial disclosures, and the study had no funding source.
SOURCE: Ricceri F et al. J Eur Acad Dermatol Venereol. 2018 Jun 15. doi: 10.1111/jdv.15139.
according to a new retrospective study.
Among 266 older patients, 65% achieved a 75% improvement in Psoriasis Area Severity Index score (PASI 75) after 1 year of therapy; 50% reached a PASI 90, and 40% a PASI 100, Francesca Prignano MD, PhD, and her colleagues reported in the Journal of the European Academy of Dermatology and Venereology. The rate of serious adverse events was less than 10%.
Elderly patients – those aged 65 years and older – are commonly excluded from studies on biologic treatments because they have more medical comorbidities and are thought to be more at risk for serious adverse events, like infections and malignancy, wrote Dr. Prignano of the dermatology unit, University of Florence, Italy, and her colleagues.
As a result, they noted, there is a “lack of information concerning safety and effectiveness of available treatments for psoriasis in the elderly, particularly about new biologic agents. Disease remission should be an objective for both younger patients and older patients, and biologic therapy should be considered a treatment option for all patients.”
To examine both the benefit and risk of biologics in this population, the team reviewed the records of 266 elderly psoriasis patients; everyone had been on a biologic treatment for at least 1 year.
The primary outcome was PASI score at weeks 8, 16, 28, and 52. The secondary outcomes were the rate and types of biologic-associated adverse events.
The study comprised 266 patients (mean age 72 years). Their mean psoriasis duration was 25.7 years. Comorbidities included psoriatic arthritis; hypertension and dyslipidemia; diabetes mellitus; cardiovascular, gastrointestinal and respiratory diseases; osteoporosis; thyroid dysfunction; depression; and cancer.
Adalimumab was the most commonly prescribed biologic (31%), followed by ustekinumab (28.9%), etanercept (20%), and secukinumab (15%). A smaller proportion of patients were taking infliximab, golimumab, or certolizumab pegol.
The mean baseline PASI was 16.5, although the range was wide (4-54). At the time of review, the average biologic treatment duration was 44 months. Almost half of the cohort (128) were on their second biologic, and 20 more had been on three biologics. A few patients were taking concomitant medications, including steroids, cyclosporine, and acitretin.
The mean PASI scores decreased to 3.7 at week 16, 1.6 at week 28, and 1.2 at week 52. The group exhibited a rapid response to biologic treatment. By 16 weeks, about 55% had achieved a PASI 75, about 28% a PASI 90, and about 20% a PASI 100. By 28 weeks, these numbers were about 64%, 45%, and 35%, respectively. At 1 year, they were about 65%, 50%, and 40%, respectively.
The rate of adverse events was 9.4%. There were 25 events in the cohort, the majority of which (48%) were infections; these included four respiratory infections, three urinary tract infections, two cases of mucocutaneous candidiasis, two cases of herpes zoster infection, and one case of erysipelas.
There were four malignancies: three nonmelanoma skin cancers and one vocal cord cancer.
Noting that, to date, their study represented “the broadest experience on the use of biological drugs” for elderly patients with psoriasis, they wrote that while “comorbidities should be taken into consideration when a long-term treatment is proposed, for the higher risk of side effects and drug interactions,” they wrote, noting that none of the 266 patients had a serious infection and the malignancy rate was low (1.5%).
None of the authors had financial disclosures, and the study had no funding source.
SOURCE: Ricceri F et al. J Eur Acad Dermatol Venereol. 2018 Jun 15. doi: 10.1111/jdv.15139.
according to a new retrospective study.
Among 266 older patients, 65% achieved a 75% improvement in Psoriasis Area Severity Index score (PASI 75) after 1 year of therapy; 50% reached a PASI 90, and 40% a PASI 100, Francesca Prignano MD, PhD, and her colleagues reported in the Journal of the European Academy of Dermatology and Venereology. The rate of serious adverse events was less than 10%.
Elderly patients – those aged 65 years and older – are commonly excluded from studies on biologic treatments because they have more medical comorbidities and are thought to be more at risk for serious adverse events, like infections and malignancy, wrote Dr. Prignano of the dermatology unit, University of Florence, Italy, and her colleagues.
As a result, they noted, there is a “lack of information concerning safety and effectiveness of available treatments for psoriasis in the elderly, particularly about new biologic agents. Disease remission should be an objective for both younger patients and older patients, and biologic therapy should be considered a treatment option for all patients.”
To examine both the benefit and risk of biologics in this population, the team reviewed the records of 266 elderly psoriasis patients; everyone had been on a biologic treatment for at least 1 year.
The primary outcome was PASI score at weeks 8, 16, 28, and 52. The secondary outcomes were the rate and types of biologic-associated adverse events.
The study comprised 266 patients (mean age 72 years). Their mean psoriasis duration was 25.7 years. Comorbidities included psoriatic arthritis; hypertension and dyslipidemia; diabetes mellitus; cardiovascular, gastrointestinal and respiratory diseases; osteoporosis; thyroid dysfunction; depression; and cancer.
Adalimumab was the most commonly prescribed biologic (31%), followed by ustekinumab (28.9%), etanercept (20%), and secukinumab (15%). A smaller proportion of patients were taking infliximab, golimumab, or certolizumab pegol.
The mean baseline PASI was 16.5, although the range was wide (4-54). At the time of review, the average biologic treatment duration was 44 months. Almost half of the cohort (128) were on their second biologic, and 20 more had been on three biologics. A few patients were taking concomitant medications, including steroids, cyclosporine, and acitretin.
The mean PASI scores decreased to 3.7 at week 16, 1.6 at week 28, and 1.2 at week 52. The group exhibited a rapid response to biologic treatment. By 16 weeks, about 55% had achieved a PASI 75, about 28% a PASI 90, and about 20% a PASI 100. By 28 weeks, these numbers were about 64%, 45%, and 35%, respectively. At 1 year, they were about 65%, 50%, and 40%, respectively.
The rate of adverse events was 9.4%. There were 25 events in the cohort, the majority of which (48%) were infections; these included four respiratory infections, three urinary tract infections, two cases of mucocutaneous candidiasis, two cases of herpes zoster infection, and one case of erysipelas.
There were four malignancies: three nonmelanoma skin cancers and one vocal cord cancer.
Noting that, to date, their study represented “the broadest experience on the use of biological drugs” for elderly patients with psoriasis, they wrote that while “comorbidities should be taken into consideration when a long-term treatment is proposed, for the higher risk of side effects and drug interactions,” they wrote, noting that none of the 266 patients had a serious infection and the malignancy rate was low (1.5%).
None of the authors had financial disclosures, and the study had no funding source.
SOURCE: Ricceri F et al. J Eur Acad Dermatol Venereol. 2018 Jun 15. doi: 10.1111/jdv.15139.
FROM THE JOURNAL OF THE EUROPEAN ACADEMY OF DERMATOLOGY AND VENEREOLOGY
Key clinical point: Patients aged 65 years and older responded well to biologics and had a low rate of serious adverse events.
Major finding: At 1 year, 65% achieved a PASI 75, 50% achieved a reached PASI 90, and 40% achieved a PASI 100, with a 9.4% rate of serious adverse events.
Study details: The retrospective study comprised 266 patients aged 65 years and older treated with biologics for psoriasis.
Disclosures: None of the authors had financial disclosures, and the study had no funding source.
Source: Ricceri F et al. J Eur Acad Dermatol Venereol. 2018. doi: 10.1111/jdv.15139.
Low risk of complications from sedation-associated GI endoscopies
Background: Most GI endoscopies use sedation to keep patients comfortable during procedures, but sedation puts patients at increased risk of complications. Most of the available studies reporting sedation-related complications are retrospective and dated. There is a lack of prospective studies investigating sedation-related complications and their associated risk factors.
Study design: Prospective study.
Setting: Thirty-nine hospitals in Germany.
Synopsis: Using data collected from 314,190 adult endoscopies in which sedation was used, this study identified that there was only a 0.01% rate of major complications. Major complications for this study included intubation, ICU admission, resuscitation, or death. Propofol was the most commonly used sedative (61.7% of cases) and had the lowest risk of complications (odds ratio, 0.7509; P = .028). The top risk factors for complications were an American Society of Anesthesiologists class greater than 2 (OR, 2.2998; P less than .001), emergent need for the endoscopy (9 of the 13 fatal cases), and longer procedure length (P less than .001).
Bottom line: GI endoscopic procedures with sedation are tolerated well in the general population and have low risk of complications.
Citation: Behrens A et al. Acute sedation-associated complications in GI endoscopy (ProSed 2 Study): Results from the prospective multicentre electronic registry of sedation-associated complications. Gut. 2018 Jan 3. doi: 10.1136/gutjnl-2015-311037.

Dr. Ally is a hospitalist at UC San Diego Health and an assistant clinical professor at the University of California, San Diego.
Background: Most GI endoscopies use sedation to keep patients comfortable during procedures, but sedation puts patients at increased risk of complications. Most of the available studies reporting sedation-related complications are retrospective and dated. There is a lack of prospective studies investigating sedation-related complications and their associated risk factors.
Study design: Prospective study.
Setting: Thirty-nine hospitals in Germany.
Synopsis: Using data collected from 314,190 adult endoscopies in which sedation was used, this study identified that there was only a 0.01% rate of major complications. Major complications for this study included intubation, ICU admission, resuscitation, or death. Propofol was the most commonly used sedative (61.7% of cases) and had the lowest risk of complications (odds ratio, 0.7509; P = .028). The top risk factors for complications were an American Society of Anesthesiologists class greater than 2 (OR, 2.2998; P less than .001), emergent need for the endoscopy (9 of the 13 fatal cases), and longer procedure length (P less than .001).
Bottom line: GI endoscopic procedures with sedation are tolerated well in the general population and have low risk of complications.
Citation: Behrens A et al. Acute sedation-associated complications in GI endoscopy (ProSed 2 Study): Results from the prospective multicentre electronic registry of sedation-associated complications. Gut. 2018 Jan 3. doi: 10.1136/gutjnl-2015-311037.
Dr. Ally is a hospitalist at UC San Diego Health and an assistant clinical professor at the University of California, San Diego.
Background: Most GI endoscopies use sedation to keep patients comfortable during procedures, but sedation puts patients at increased risk of complications. Most of the available studies reporting sedation-related complications are retrospective and dated. There is a lack of prospective studies investigating sedation-related complications and their associated risk factors.
Study design: Prospective study.
Setting: Thirty-nine hospitals in Germany.
Synopsis: Using data collected from 314,190 adult endoscopies in which sedation was used, this study identified that there was only a 0.01% rate of major complications. Major complications for this study included intubation, ICU admission, resuscitation, or death. Propofol was the most commonly used sedative (61.7% of cases) and had the lowest risk of complications (odds ratio, 0.7509; P = .028). The top risk factors for complications were an American Society of Anesthesiologists class greater than 2 (OR, 2.2998; P less than .001), emergent need for the endoscopy (9 of the 13 fatal cases), and longer procedure length (P less than .001).
Bottom line: GI endoscopic procedures with sedation are tolerated well in the general population and have low risk of complications.
Citation: Behrens A et al. Acute sedation-associated complications in GI endoscopy (ProSed 2 Study): Results from the prospective multicentre electronic registry of sedation-associated complications. Gut. 2018 Jan 3. doi: 10.1136/gutjnl-2015-311037.
Dr. Ally is a hospitalist at UC San Diego Health and an assistant clinical professor at the University of California, San Diego.
What's your diagnosis? - July 2018
Polycystic pancreas
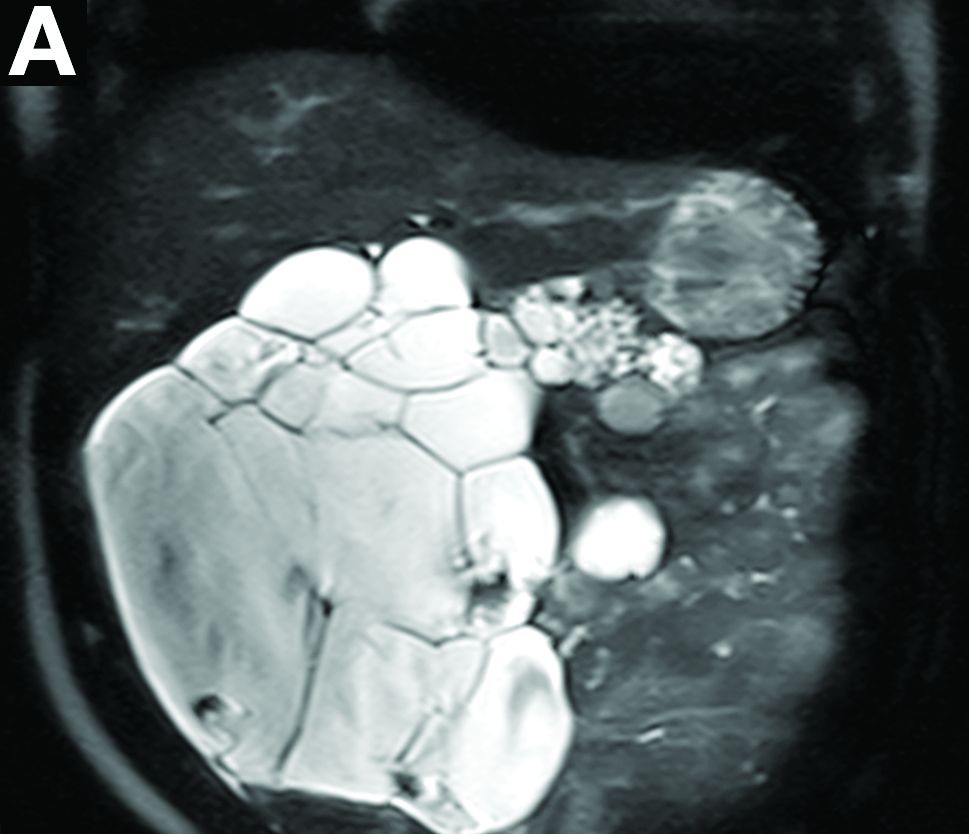
Cross-sectional imaging revealed the diagnosis of polycystic pancreas (diffuse cystic degeneration of the whole organ) with giant cysts in the head and multiple cysts across the whole organ in the absence of concomitant kidney or liver cysts (Figure A, B).
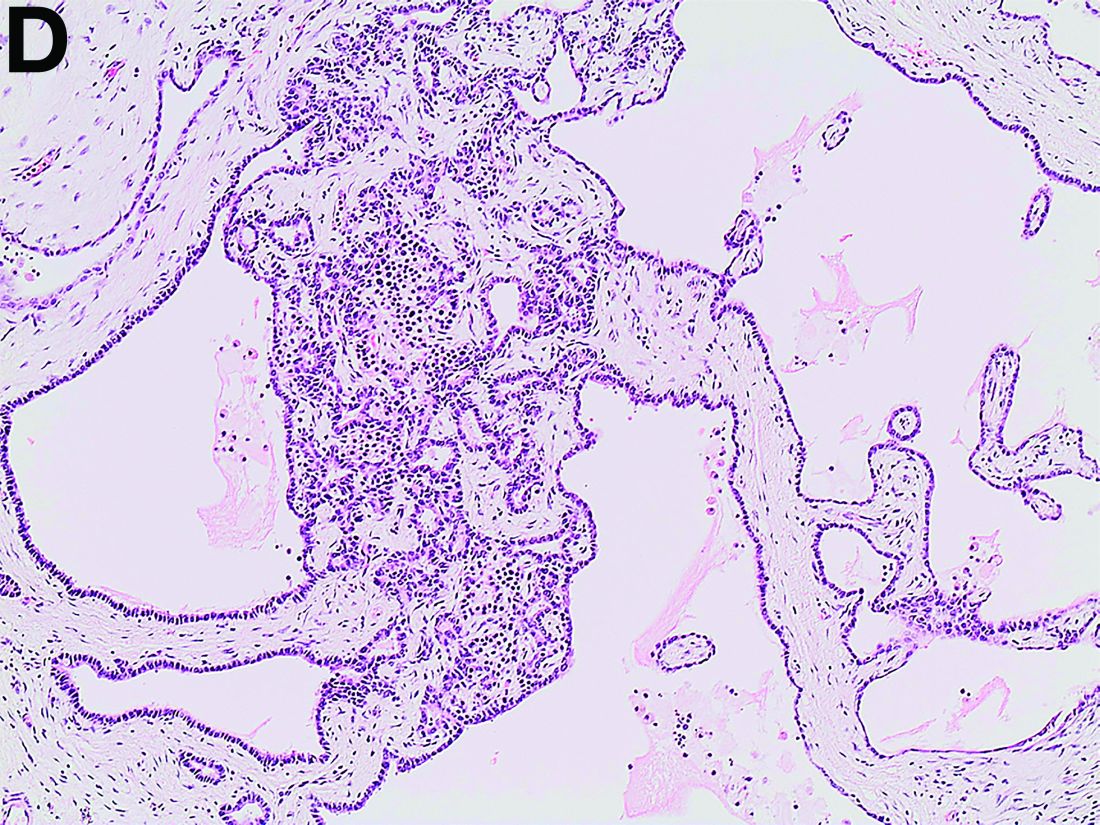
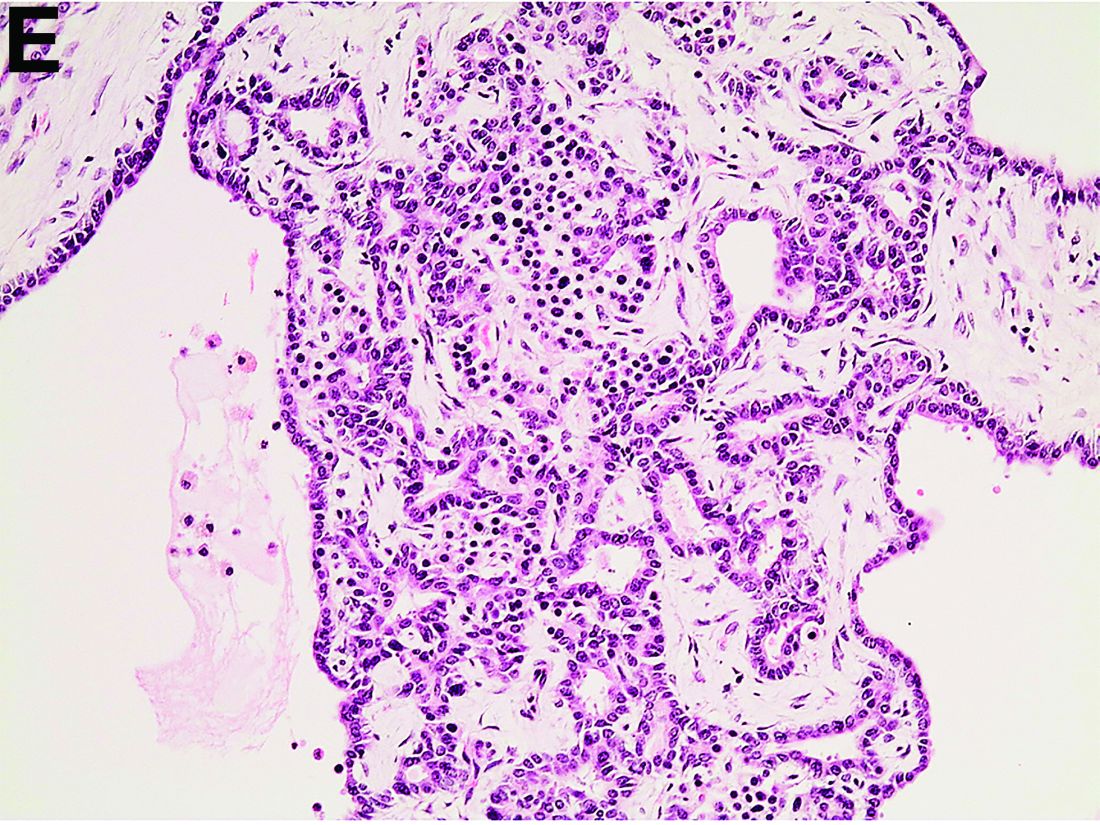
The patient underwent an endoscopic ultrasound-guided fine-needle aspiration before the operation, and a mucinous cystic neoplasm was documented. A total duodenopancreatosplenectomy followed. The postoperative course was uneventful. Histology showed multiple cysts of variable diameter lined by monolayer flattened or cuboidal epithelium without atypia and confirmed the diagnosis of polycystic pancreas (Figures D, E; stain: hematoxylin and eosin; original magnifications: ×100 and ×200, respectively).
Genetic testing was negative for von Hippel-Lindau (VHL) disease. The patient remains in good general condition under diabetes management and oral administration of pancreatic enzymes 45 months 4 years after pancreatectomy. Magnetic resonance imaging of the central nervous system and abdomen were without pathologic findings.
Although pancreatic cysts are very common, a diffuse cystic degeneration of the pancreas in the form of polycystic pancreas is very infrequent and has been described in patients with VHL disease.1 It is almost always associated with multiple renal cysts.1 Genetic testing for VHL disease is suggested in all cases presenting with multiple pancreatic cysts by some investigators.2 It has an accuracy greater than 80%, which reaches 95%-100% in patients who fulfill the clinical criteria for VHL disease.3
The novelty of this case is double; to the best of our knowledge, polycystic pancreas with such a volume (cysts up to 25 cm) has not yet been documented in the literature and has not been at all described in the absence of VHL disease up to now.
References
1. Leung R., Biswas S., Duncan M. et al. Imaging features of Von Hippel-Lindau disease. Radiographics. 2008;28:65-79.
2. Kapur V. Brower S.T. Cystic replacement of pancreas in patient with von Hippel-Lindau syndrome. Gastrointest Cancer Res. 2013;6:25-6.
3. Nielsen S.M., Rhodes L., Blanco I. et al. Von Hippel-Lindau disease: genetics and role of genetic counseling in a multiple neoplasia syndrome. J Clin Oncol. 2016;34:2172-81.
Polycystic pancreas
Cross-sectional imaging revealed the diagnosis of polycystic pancreas (diffuse cystic degeneration of the whole organ) with giant cysts in the head and multiple cysts across the whole organ in the absence of concomitant kidney or liver cysts (Figure A, B).
The patient underwent an endoscopic ultrasound-guided fine-needle aspiration before the operation, and a mucinous cystic neoplasm was documented. A total duodenopancreatosplenectomy followed. The postoperative course was uneventful. Histology showed multiple cysts of variable diameter lined by monolayer flattened or cuboidal epithelium without atypia and confirmed the diagnosis of polycystic pancreas (Figures D, E; stain: hematoxylin and eosin; original magnifications: ×100 and ×200, respectively).
Genetic testing was negative for von Hippel-Lindau (VHL) disease. The patient remains in good general condition under diabetes management and oral administration of pancreatic enzymes 45 months 4 years after pancreatectomy. Magnetic resonance imaging of the central nervous system and abdomen were without pathologic findings.
Although pancreatic cysts are very common, a diffuse cystic degeneration of the pancreas in the form of polycystic pancreas is very infrequent and has been described in patients with VHL disease.1 It is almost always associated with multiple renal cysts.1 Genetic testing for VHL disease is suggested in all cases presenting with multiple pancreatic cysts by some investigators.2 It has an accuracy greater than 80%, which reaches 95%-100% in patients who fulfill the clinical criteria for VHL disease.3
The novelty of this case is double; to the best of our knowledge, polycystic pancreas with such a volume (cysts up to 25 cm) has not yet been documented in the literature and has not been at all described in the absence of VHL disease up to now.
References
1. Leung R., Biswas S., Duncan M. et al. Imaging features of Von Hippel-Lindau disease. Radiographics. 2008;28:65-79.
2. Kapur V. Brower S.T. Cystic replacement of pancreas in patient with von Hippel-Lindau syndrome. Gastrointest Cancer Res. 2013;6:25-6.
3. Nielsen S.M., Rhodes L., Blanco I. et al. Von Hippel-Lindau disease: genetics and role of genetic counseling in a multiple neoplasia syndrome. J Clin Oncol. 2016;34:2172-81.
Polycystic pancreas
Cross-sectional imaging revealed the diagnosis of polycystic pancreas (diffuse cystic degeneration of the whole organ) with giant cysts in the head and multiple cysts across the whole organ in the absence of concomitant kidney or liver cysts (Figure A, B).
The patient underwent an endoscopic ultrasound-guided fine-needle aspiration before the operation, and a mucinous cystic neoplasm was documented. A total duodenopancreatosplenectomy followed. The postoperative course was uneventful. Histology showed multiple cysts of variable diameter lined by monolayer flattened or cuboidal epithelium without atypia and confirmed the diagnosis of polycystic pancreas (Figures D, E; stain: hematoxylin and eosin; original magnifications: ×100 and ×200, respectively).
Genetic testing was negative for von Hippel-Lindau (VHL) disease. The patient remains in good general condition under diabetes management and oral administration of pancreatic enzymes 45 months 4 years after pancreatectomy. Magnetic resonance imaging of the central nervous system and abdomen were without pathologic findings.
Although pancreatic cysts are very common, a diffuse cystic degeneration of the pancreas in the form of polycystic pancreas is very infrequent and has been described in patients with VHL disease.1 It is almost always associated with multiple renal cysts.1 Genetic testing for VHL disease is suggested in all cases presenting with multiple pancreatic cysts by some investigators.2 It has an accuracy greater than 80%, which reaches 95%-100% in patients who fulfill the clinical criteria for VHL disease.3
The novelty of this case is double; to the best of our knowledge, polycystic pancreas with such a volume (cysts up to 25 cm) has not yet been documented in the literature and has not been at all described in the absence of VHL disease up to now.
References
1. Leung R., Biswas S., Duncan M. et al. Imaging features of Von Hippel-Lindau disease. Radiographics. 2008;28:65-79.
2. Kapur V. Brower S.T. Cystic replacement of pancreas in patient with von Hippel-Lindau syndrome. Gastrointest Cancer Res. 2013;6:25-6.
3. Nielsen S.M., Rhodes L., Blanco I. et al. Von Hippel-Lindau disease: genetics and role of genetic counseling in a multiple neoplasia syndrome. J Clin Oncol. 2016;34:2172-81.

Doc reports favorable results from trial on hold

STOCKHOLM—Interim trial results suggest the EZH2 inhibitor tazemetostat can produce durable responses in patients with relapsed or refractory follicular lymphoma (FL).
In patients with EZH2 mutations, the overall response rate (ORR) was 71%, and the median duration of response (DOR) was 32 weeks.
For patients with wild-type (WT) EZH2, the ORR was 33%, and the median DOR was 76 weeks.
Tazemetostat was considered generally well tolerated in this phase 2 trial, which is currently on partial clinical hold.
Gilles Salles, MD, PhD, of the University Hospital of Lyon France, presented results from the trial at the 23rd Congress of the European Hematology Association (EHA) as abstract S100.
The trial is sponsored by Epizyme, Inc.
In April, Epizyme announced that all US-based trials of tazemetostat had been placed on partial hold after a pediatric patient on a phase 1 trial developed secondary T-cell lymphoma.
Enrollment was stopped in all the trials, but patients could continue receiving tazemetostat if they had not progressed on the drug.
The phase 2 trial of tazemetostat in non-Hodgkin lymphoma has enrolled 89 adults with relapsed/refractory FL.
At EHA, Dr Salles presented results in 82 of these patients. There were 28 patients with EZH2-mutated FL and 54 with EZH2-WT FL.
The median age was 61 in both cohorts. Forty-three percent of EZH2-mutated and 63% of WT patients were male.
EZH2-mutated patients had a median of 3 prior therapies, and WT patients had a median of 4. Thirty-eight percent and 42%, respectively, were refractory to their last therapy. Eleven percent and 39%, respectively, had received prior transplant.
The median time from diagnosis was 5.1 years for EZH2-mutated patients and 6.4 years for WT patients. The median time from last prior therapy was 18.4 weeks and 28.1 weeks, respectively.
The patients received tazemetostat at 800 mg twice daily until disease progression or withdrawal.
Safety
In all 82 patients, the rate of treatment-emergent adverse events (AEs) was 95%, and the rate of treatment-related AEs was 78%. The rate of grade 3 or higher treatment-related AEs was 17%, and the rate of serious treatment-related AEs was 4%.
Six percent of patients discontinued treatment due to a related AE, 18% had a dose interruption, and 5% had a dose reduction due to a related AE.
Treatment-related AEs included nausea (20%), fatigue (13%), anemia (13%), diarrhea (11%), alopecia (11%), asthenia (10%), thrombocytopenia (10%), muscle spasms (6%), bronchitis (5%), vomiting (5%), headache (5%), abdominal pain (2%), pyrexia (1%), and cough (1%).
Grade 3 or higher treatment-related AEs included thrombocytopenia (4%), anemia (4%), fatigue (1%), and asthenia (1%).
Efficacy
In the EZH2-mutated cohort, the ORR was 71% (n=20). Eleven percent of patients (n=3) achieved a complete response, and 61% (n=17) had a partial response.
Twenty-nine percent (n=8) had stable disease as their best response. And 21% (n=6) of patients are still on study with stable disease.
All patients in this cohort experienced a reduction in tumor burden. None of the patients had progressive disease as their best response.
At the time of analysis (May 1, 2018), the median DOR was 32.3 weeks, and 55% of responders (n=11) had an ongoing response.
The median progression-free survival was 48.6 weeks.
In patients with WT EZH2 (n=54), the ORR was 33% (n=18). Six percent of patients (n=3) achieved a complete response, and 28% (n=15) had a partial response.
Thirty-one percent of patients (n=17) had stable disease as their best response, including 1 patient who is still receiving treatment.
Thirty-one percent of patients (n=17) progressed. For 4% (n=2), their response status was unknown.
At the time of analysis, the median DOR was 76 weeks, and 56% of responders (n=10) had an ongoing response.
The median progression-free survival was 29.9 weeks.
“I am impressed by the sustained clinical activity and the good tolerability of tazemetostat in this heavily pretreated patient population,” Dr Salles said. “This is important for patients with relapsed or refractory follicular lymphoma, as both the response rates and durations of response usually tend to decrease with each successive line of treatment.”
“I believe tazemetostat has the potential to fill a significant unmet need for these patients, and continued investigation of tazemetostat as a single agent or in combination with other agents is warranted.”
Epizyme’s president and chief executive officer, Robert Bazemore, said the company is still working to resolve the partial clinical hold on tazemetostat trials and is “making good progress.”
STOCKHOLM—Interim trial results suggest the EZH2 inhibitor tazemetostat can produce durable responses in patients with relapsed or refractory follicular lymphoma (FL).
In patients with EZH2 mutations, the overall response rate (ORR) was 71%, and the median duration of response (DOR) was 32 weeks.
For patients with wild-type (WT) EZH2, the ORR was 33%, and the median DOR was 76 weeks.
Tazemetostat was considered generally well tolerated in this phase 2 trial, which is currently on partial clinical hold.
Gilles Salles, MD, PhD, of the University Hospital of Lyon France, presented results from the trial at the 23rd Congress of the European Hematology Association (EHA) as abstract S100.
The trial is sponsored by Epizyme, Inc.
In April, Epizyme announced that all US-based trials of tazemetostat had been placed on partial hold after a pediatric patient on a phase 1 trial developed secondary T-cell lymphoma.
Enrollment was stopped in all the trials, but patients could continue receiving tazemetostat if they had not progressed on the drug.
The phase 2 trial of tazemetostat in non-Hodgkin lymphoma has enrolled 89 adults with relapsed/refractory FL.
At EHA, Dr Salles presented results in 82 of these patients. There were 28 patients with EZH2-mutated FL and 54 with EZH2-WT FL.
The median age was 61 in both cohorts. Forty-three percent of EZH2-mutated and 63% of WT patients were male.
EZH2-mutated patients had a median of 3 prior therapies, and WT patients had a median of 4. Thirty-eight percent and 42%, respectively, were refractory to their last therapy. Eleven percent and 39%, respectively, had received prior transplant.
The median time from diagnosis was 5.1 years for EZH2-mutated patients and 6.4 years for WT patients. The median time from last prior therapy was 18.4 weeks and 28.1 weeks, respectively.
The patients received tazemetostat at 800 mg twice daily until disease progression or withdrawal.
Safety
In all 82 patients, the rate of treatment-emergent adverse events (AEs) was 95%, and the rate of treatment-related AEs was 78%. The rate of grade 3 or higher treatment-related AEs was 17%, and the rate of serious treatment-related AEs was 4%.
Six percent of patients discontinued treatment due to a related AE, 18% had a dose interruption, and 5% had a dose reduction due to a related AE.
Treatment-related AEs included nausea (20%), fatigue (13%), anemia (13%), diarrhea (11%), alopecia (11%), asthenia (10%), thrombocytopenia (10%), muscle spasms (6%), bronchitis (5%), vomiting (5%), headache (5%), abdominal pain (2%), pyrexia (1%), and cough (1%).
Grade 3 or higher treatment-related AEs included thrombocytopenia (4%), anemia (4%), fatigue (1%), and asthenia (1%).
Efficacy
In the EZH2-mutated cohort, the ORR was 71% (n=20). Eleven percent of patients (n=3) achieved a complete response, and 61% (n=17) had a partial response.
Twenty-nine percent (n=8) had stable disease as their best response. And 21% (n=6) of patients are still on study with stable disease.
All patients in this cohort experienced a reduction in tumor burden. None of the patients had progressive disease as their best response.
At the time of analysis (May 1, 2018), the median DOR was 32.3 weeks, and 55% of responders (n=11) had an ongoing response.
The median progression-free survival was 48.6 weeks.
In patients with WT EZH2 (n=54), the ORR was 33% (n=18). Six percent of patients (n=3) achieved a complete response, and 28% (n=15) had a partial response.
Thirty-one percent of patients (n=17) had stable disease as their best response, including 1 patient who is still receiving treatment.
Thirty-one percent of patients (n=17) progressed. For 4% (n=2), their response status was unknown.
At the time of analysis, the median DOR was 76 weeks, and 56% of responders (n=10) had an ongoing response.
The median progression-free survival was 29.9 weeks.
“I am impressed by the sustained clinical activity and the good tolerability of tazemetostat in this heavily pretreated patient population,” Dr Salles said. “This is important for patients with relapsed or refractory follicular lymphoma, as both the response rates and durations of response usually tend to decrease with each successive line of treatment.”
“I believe tazemetostat has the potential to fill a significant unmet need for these patients, and continued investigation of tazemetostat as a single agent or in combination with other agents is warranted.”
Epizyme’s president and chief executive officer, Robert Bazemore, said the company is still working to resolve the partial clinical hold on tazemetostat trials and is “making good progress.”
STOCKHOLM—Interim trial results suggest the EZH2 inhibitor tazemetostat can produce durable responses in patients with relapsed or refractory follicular lymphoma (FL).
In patients with EZH2 mutations, the overall response rate (ORR) was 71%, and the median duration of response (DOR) was 32 weeks.
For patients with wild-type (WT) EZH2, the ORR was 33%, and the median DOR was 76 weeks.
Tazemetostat was considered generally well tolerated in this phase 2 trial, which is currently on partial clinical hold.
Gilles Salles, MD, PhD, of the University Hospital of Lyon France, presented results from the trial at the 23rd Congress of the European Hematology Association (EHA) as abstract S100.
The trial is sponsored by Epizyme, Inc.
In April, Epizyme announced that all US-based trials of tazemetostat had been placed on partial hold after a pediatric patient on a phase 1 trial developed secondary T-cell lymphoma.
Enrollment was stopped in all the trials, but patients could continue receiving tazemetostat if they had not progressed on the drug.
The phase 2 trial of tazemetostat in non-Hodgkin lymphoma has enrolled 89 adults with relapsed/refractory FL.
At EHA, Dr Salles presented results in 82 of these patients. There were 28 patients with EZH2-mutated FL and 54 with EZH2-WT FL.
The median age was 61 in both cohorts. Forty-three percent of EZH2-mutated and 63% of WT patients were male.
EZH2-mutated patients had a median of 3 prior therapies, and WT patients had a median of 4. Thirty-eight percent and 42%, respectively, were refractory to their last therapy. Eleven percent and 39%, respectively, had received prior transplant.
The median time from diagnosis was 5.1 years for EZH2-mutated patients and 6.4 years for WT patients. The median time from last prior therapy was 18.4 weeks and 28.1 weeks, respectively.
The patients received tazemetostat at 800 mg twice daily until disease progression or withdrawal.
Safety
In all 82 patients, the rate of treatment-emergent adverse events (AEs) was 95%, and the rate of treatment-related AEs was 78%. The rate of grade 3 or higher treatment-related AEs was 17%, and the rate of serious treatment-related AEs was 4%.
Six percent of patients discontinued treatment due to a related AE, 18% had a dose interruption, and 5% had a dose reduction due to a related AE.
Treatment-related AEs included nausea (20%), fatigue (13%), anemia (13%), diarrhea (11%), alopecia (11%), asthenia (10%), thrombocytopenia (10%), muscle spasms (6%), bronchitis (5%), vomiting (5%), headache (5%), abdominal pain (2%), pyrexia (1%), and cough (1%).
Grade 3 or higher treatment-related AEs included thrombocytopenia (4%), anemia (4%), fatigue (1%), and asthenia (1%).
Efficacy
In the EZH2-mutated cohort, the ORR was 71% (n=20). Eleven percent of patients (n=3) achieved a complete response, and 61% (n=17) had a partial response.
Twenty-nine percent (n=8) had stable disease as their best response. And 21% (n=6) of patients are still on study with stable disease.
All patients in this cohort experienced a reduction in tumor burden. None of the patients had progressive disease as their best response.
At the time of analysis (May 1, 2018), the median DOR was 32.3 weeks, and 55% of responders (n=11) had an ongoing response.
The median progression-free survival was 48.6 weeks.
In patients with WT EZH2 (n=54), the ORR was 33% (n=18). Six percent of patients (n=3) achieved a complete response, and 28% (n=15) had a partial response.
Thirty-one percent of patients (n=17) had stable disease as their best response, including 1 patient who is still receiving treatment.
Thirty-one percent of patients (n=17) progressed. For 4% (n=2), their response status was unknown.
At the time of analysis, the median DOR was 76 weeks, and 56% of responders (n=10) had an ongoing response.
The median progression-free survival was 29.9 weeks.
“I am impressed by the sustained clinical activity and the good tolerability of tazemetostat in this heavily pretreated patient population,” Dr Salles said. “This is important for patients with relapsed or refractory follicular lymphoma, as both the response rates and durations of response usually tend to decrease with each successive line of treatment.”
“I believe tazemetostat has the potential to fill a significant unmet need for these patients, and continued investigation of tazemetostat as a single agent or in combination with other agents is warranted.”
Epizyme’s president and chief executive officer, Robert Bazemore, said the company is still working to resolve the partial clinical hold on tazemetostat trials and is “making good progress.”
Group updates guidelines on CLL

Recent advances in chronic lymphocytic leukemia (CLL) have prompted an update to the 2008 International Workshop in Chronic Lymphocytic Leukemia (iwCLL) consensus guidelines.
The updated iwCLL guidelines include new information on genomic alterations, the use of clinical staging and prognostic markers/scores, response assessment, minimal residual disease (MRD), and viral diseases in CLL patients.
The update was recently published in Blood.
Diagnosis, prognosis, and staging
To verify CLL diagnosis, the iwCLL guidelines recommend obtaining complete blood counts and differential counts as well as immunophenotyping of peripheral blood lymphocytes. A panel of CD19, CD5, CD20, CD23, κ, and λ typically suffices to establish a diagnosis.
Other tests that may help in prognosis or assessing tumor burden include molecular cytogenetics for del(13q), del(11q), del(17p), and add(12) in peripheral blood lymphocytes and determining TP53 and IGHV mutational status.
These tests can help identify poor-prognosis patients who are not likely to benefit from standard chemotherapy but are likely to benefit from small-molecule inhibitors of BTK, PI3K, or BCL2.
In addition, serum markers such as β2-microglogulin provide insight into overall survival and progression-free survival.
With regard to clinical staging, the guidelines highlight the Binet and Rai systems, which are routinely used in clinical practice and clinical trials.
However, the guidelines also note that “there are a large number of biomarkers that can provide additional prognostic information,” and, recently, “several prognostic scores and stratification systems have been proposed based on multivariate analyses.”
For example, the CLL international prognostic index (CLL-IPI) provides a weighted score that uses clinical stage, age, IGHV mutational status, β2-microglogulin, and the presence of del(17p) and/or TP53 mutations.
Indications for treatment
The guidelines note that active disease must be documented to initiate therapy. At least 1 of the following criteria must be met:
- Evidence of progressive marrow failure
- Massive, progressive, or symptomatic splenomegaly
- Progressive/symptomatic lymphadenopathy or massive nodes
- Progressive lymphocytosis
- Autoimmune complications
- Extranodal involvement
- Disease-related symptoms (unintentional weight loss, significant fatigue, fevers, night sweats for over a month without evidence of infection).
Following relapse, subsequent lines of treatment should follow the same principles as those used for initial treatment decisions.
Response, MRD, and more
The guidelines say 2 groups of parameters must be assessed to determine response to therapy:
- Group A: lymphoid tumor load and constitutional symptoms, including liver and/or spleen size, lymph node evaluation, and circulating lymphocyte count
- Group B: the hematopoietic system (platelet count, hemoglobin, and marrow).
For therapies with a defined treatment duration, response should be assessed at least 2 months after treatment is completed. For continued therapies or maintenance, response should be assessed at a predefined time point or at least 2 months after patients achieve their maximum response.
The guidelines also say MRD should be assessed in clinical trials aimed at maximizing the depth of remission. Furthermore, it “may be important” to confirm MRD negativity in the blood and marrow, as there are therapies that preferentially clear the blood but not the marrow (such as monoclonal antibodies).
In addition to the aforementioned recommendations, the updated iwCLL guidelines also include information on patient eligibility for clinical trials, guidance regarding treatment-related toxicities, and recommendations for supportive care and managing complications.
Recent advances in chronic lymphocytic leukemia (CLL) have prompted an update to the 2008 International Workshop in Chronic Lymphocytic Leukemia (iwCLL) consensus guidelines.
The updated iwCLL guidelines include new information on genomic alterations, the use of clinical staging and prognostic markers/scores, response assessment, minimal residual disease (MRD), and viral diseases in CLL patients.
The update was recently published in Blood.
Diagnosis, prognosis, and staging
To verify CLL diagnosis, the iwCLL guidelines recommend obtaining complete blood counts and differential counts as well as immunophenotyping of peripheral blood lymphocytes. A panel of CD19, CD5, CD20, CD23, κ, and λ typically suffices to establish a diagnosis.
Other tests that may help in prognosis or assessing tumor burden include molecular cytogenetics for del(13q), del(11q), del(17p), and add(12) in peripheral blood lymphocytes and determining TP53 and IGHV mutational status.
These tests can help identify poor-prognosis patients who are not likely to benefit from standard chemotherapy but are likely to benefit from small-molecule inhibitors of BTK, PI3K, or BCL2.
In addition, serum markers such as β2-microglogulin provide insight into overall survival and progression-free survival.
With regard to clinical staging, the guidelines highlight the Binet and Rai systems, which are routinely used in clinical practice and clinical trials.
However, the guidelines also note that “there are a large number of biomarkers that can provide additional prognostic information,” and, recently, “several prognostic scores and stratification systems have been proposed based on multivariate analyses.”
For example, the CLL international prognostic index (CLL-IPI) provides a weighted score that uses clinical stage, age, IGHV mutational status, β2-microglogulin, and the presence of del(17p) and/or TP53 mutations.
Indications for treatment
The guidelines note that active disease must be documented to initiate therapy. At least 1 of the following criteria must be met:
- Evidence of progressive marrow failure
- Massive, progressive, or symptomatic splenomegaly
- Progressive/symptomatic lymphadenopathy or massive nodes
- Progressive lymphocytosis
- Autoimmune complications
- Extranodal involvement
- Disease-related symptoms (unintentional weight loss, significant fatigue, fevers, night sweats for over a month without evidence of infection).
Following relapse, subsequent lines of treatment should follow the same principles as those used for initial treatment decisions.
Response, MRD, and more
The guidelines say 2 groups of parameters must be assessed to determine response to therapy:
- Group A: lymphoid tumor load and constitutional symptoms, including liver and/or spleen size, lymph node evaluation, and circulating lymphocyte count
- Group B: the hematopoietic system (platelet count, hemoglobin, and marrow).
For therapies with a defined treatment duration, response should be assessed at least 2 months after treatment is completed. For continued therapies or maintenance, response should be assessed at a predefined time point or at least 2 months after patients achieve their maximum response.
The guidelines also say MRD should be assessed in clinical trials aimed at maximizing the depth of remission. Furthermore, it “may be important” to confirm MRD negativity in the blood and marrow, as there are therapies that preferentially clear the blood but not the marrow (such as monoclonal antibodies).
In addition to the aforementioned recommendations, the updated iwCLL guidelines also include information on patient eligibility for clinical trials, guidance regarding treatment-related toxicities, and recommendations for supportive care and managing complications.
Recent advances in chronic lymphocytic leukemia (CLL) have prompted an update to the 2008 International Workshop in Chronic Lymphocytic Leukemia (iwCLL) consensus guidelines.
The updated iwCLL guidelines include new information on genomic alterations, the use of clinical staging and prognostic markers/scores, response assessment, minimal residual disease (MRD), and viral diseases in CLL patients.
The update was recently published in Blood.
Diagnosis, prognosis, and staging
To verify CLL diagnosis, the iwCLL guidelines recommend obtaining complete blood counts and differential counts as well as immunophenotyping of peripheral blood lymphocytes. A panel of CD19, CD5, CD20, CD23, κ, and λ typically suffices to establish a diagnosis.
Other tests that may help in prognosis or assessing tumor burden include molecular cytogenetics for del(13q), del(11q), del(17p), and add(12) in peripheral blood lymphocytes and determining TP53 and IGHV mutational status.
These tests can help identify poor-prognosis patients who are not likely to benefit from standard chemotherapy but are likely to benefit from small-molecule inhibitors of BTK, PI3K, or BCL2.
In addition, serum markers such as β2-microglogulin provide insight into overall survival and progression-free survival.
With regard to clinical staging, the guidelines highlight the Binet and Rai systems, which are routinely used in clinical practice and clinical trials.
However, the guidelines also note that “there are a large number of biomarkers that can provide additional prognostic information,” and, recently, “several prognostic scores and stratification systems have been proposed based on multivariate analyses.”
For example, the CLL international prognostic index (CLL-IPI) provides a weighted score that uses clinical stage, age, IGHV mutational status, β2-microglogulin, and the presence of del(17p) and/or TP53 mutations.
Indications for treatment
The guidelines note that active disease must be documented to initiate therapy. At least 1 of the following criteria must be met:
- Evidence of progressive marrow failure
- Massive, progressive, or symptomatic splenomegaly
- Progressive/symptomatic lymphadenopathy or massive nodes
- Progressive lymphocytosis
- Autoimmune complications
- Extranodal involvement
- Disease-related symptoms (unintentional weight loss, significant fatigue, fevers, night sweats for over a month without evidence of infection).
Following relapse, subsequent lines of treatment should follow the same principles as those used for initial treatment decisions.
Response, MRD, and more
The guidelines say 2 groups of parameters must be assessed to determine response to therapy:
- Group A: lymphoid tumor load and constitutional symptoms, including liver and/or spleen size, lymph node evaluation, and circulating lymphocyte count
- Group B: the hematopoietic system (platelet count, hemoglobin, and marrow).
For therapies with a defined treatment duration, response should be assessed at least 2 months after treatment is completed. For continued therapies or maintenance, response should be assessed at a predefined time point or at least 2 months after patients achieve their maximum response.
The guidelines also say MRD should be assessed in clinical trials aimed at maximizing the depth of remission. Furthermore, it “may be important” to confirm MRD negativity in the blood and marrow, as there are therapies that preferentially clear the blood but not the marrow (such as monoclonal antibodies).
In addition to the aforementioned recommendations, the updated iwCLL guidelines also include information on patient eligibility for clinical trials, guidance regarding treatment-related toxicities, and recommendations for supportive care and managing complications.
CPI-613 receives orphan designation for BL

The US Food and Drug Administration (FDA) has granted orphan drug designation to CPI-613 for the treatment of Burkitt lymphoma (BL).
CPI-613 is a novel lipoic acid analogue that inhibits multiple enzyme targets within the tricarboxylic acid cycle.
The drug is in development as a treatment for hematologic malignancies and solid tumors.
In a phase 1 trial of patients with advanced hematologic malignancies, CPI-613 produced a response in a patient with relapsed BL.
Now, Rafael Pharmaceuticals, Inc., the company developing CPI-613, is launching a phase 2 trial of the drug in patients with relapsed or refractory BL and high-grade B-cell lymphoma with rearrangements of MYC and BCL2 and/or BCL6.
In the phase 1 trial, the patient with relapsed BL achieved a partial response to CPI-613 monotherapy and was ultimately cleared of disease after surgery.
The patient, a 19-year-old female, began taking CPI-613 (2940 mg/m2) after her second relapse. She achieved a radiographic partial response after the third cycle of CPI-613.
The patient completed 17 cycles of CPI-613 over 51 weeks. She decided to stop treatment after the 17th cycle to pursue a surgical resection of residual tumor. The pathology of the surgical specimen revealed BL with extensive necrosis.
Clinical follow-up on the patient showed no evidence of disease more than 36 months later. And CPI-613 was considered well tolerated in this patient.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
The US Food and Drug Administration (FDA) has granted orphan drug designation to CPI-613 for the treatment of Burkitt lymphoma (BL).
CPI-613 is a novel lipoic acid analogue that inhibits multiple enzyme targets within the tricarboxylic acid cycle.
The drug is in development as a treatment for hematologic malignancies and solid tumors.
In a phase 1 trial of patients with advanced hematologic malignancies, CPI-613 produced a response in a patient with relapsed BL.
Now, Rafael Pharmaceuticals, Inc., the company developing CPI-613, is launching a phase 2 trial of the drug in patients with relapsed or refractory BL and high-grade B-cell lymphoma with rearrangements of MYC and BCL2 and/or BCL6.
In the phase 1 trial, the patient with relapsed BL achieved a partial response to CPI-613 monotherapy and was ultimately cleared of disease after surgery.
The patient, a 19-year-old female, began taking CPI-613 (2940 mg/m2) after her second relapse. She achieved a radiographic partial response after the third cycle of CPI-613.
The patient completed 17 cycles of CPI-613 over 51 weeks. She decided to stop treatment after the 17th cycle to pursue a surgical resection of residual tumor. The pathology of the surgical specimen revealed BL with extensive necrosis.
Clinical follow-up on the patient showed no evidence of disease more than 36 months later. And CPI-613 was considered well tolerated in this patient.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
The US Food and Drug Administration (FDA) has granted orphan drug designation to CPI-613 for the treatment of Burkitt lymphoma (BL).
CPI-613 is a novel lipoic acid analogue that inhibits multiple enzyme targets within the tricarboxylic acid cycle.
The drug is in development as a treatment for hematologic malignancies and solid tumors.
In a phase 1 trial of patients with advanced hematologic malignancies, CPI-613 produced a response in a patient with relapsed BL.
Now, Rafael Pharmaceuticals, Inc., the company developing CPI-613, is launching a phase 2 trial of the drug in patients with relapsed or refractory BL and high-grade B-cell lymphoma with rearrangements of MYC and BCL2 and/or BCL6.
In the phase 1 trial, the patient with relapsed BL achieved a partial response to CPI-613 monotherapy and was ultimately cleared of disease after surgery.
The patient, a 19-year-old female, began taking CPI-613 (2940 mg/m2) after her second relapse. She achieved a radiographic partial response after the third cycle of CPI-613.
The patient completed 17 cycles of CPI-613 over 51 weeks. She decided to stop treatment after the 17th cycle to pursue a surgical resection of residual tumor. The pathology of the surgical specimen revealed BL with extensive necrosis.
Clinical follow-up on the patient showed no evidence of disease more than 36 months later. And CPI-613 was considered well tolerated in this patient.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
PVd improved survival in lenalidomide-exposed myeloma
CHICAGO – For patients with relapsed/refractory multiple myeloma previously exposed to lenalidomide, the combination of pomalidomide plus bortezomib and low‐dose dexamethasone (PVd) improved response and progression-free survival, results of the phase 3 OPTIMISMM trial showed.
Risk of disease progression or death was reduced by 39%, compared with bortezomib and low-dose dexamethasone alone (Vd), among patients in the trial, of whom approximately 70% were lenalidomide refractory, reported investigator Paul G. Richardson, MD, of the Dana-Farber Cancer Institute in Boston.
The improvements in efficacy seen with the PVd regimen were more pronounced in patients with only one prior line of therapy, and overall, the safety profile of the triplet regimen was consistent with known toxicities of each individual agent, Dr. Richardson reported.
Together, those results “would seem to support the use of this triplet [therapy] in first relapse in patients with relapsed/refractory myeloma and prior exposure to lenalidomide,” he said at the annual meeting of the American Society of Clinical Oncology.
“This study, importantly, evaluated a clinically relevant patient population and a growing patient population who receive upfront lenalidomide and maintenance in that setting and for whom lenalidomide is no longer a viable treatment option,” Dr. Richardson added.
Lenalidomide has become a mainstay of upfront myeloma treatment, and the Food and Drug Administration recently gave approval to lenalidomide as maintenance after autologous hematopoietic stem cell transplantation. Accordingly, it’s important to understand the benefits of triplet therapies in patients progressing on lenalidomide therapy and in whom lenalidomide is no longer a treatment option, Dr. Richardson said.
Pomalidomide, a potent oral immunomodulatory agent, is already approved for relapsed/refractory myeloma after two or more previous therapies that include lenalidomide and a proteasome inhibitor in patients who progress on or within 60 days of treatment.
In the OPTIMISMM trial, 559 patients who had received prior therapy, including at least two cycles of lenalidomide, were randomized to receive either PVd or Vd until disease progression or unacceptable toxicity.
Median progression-free survival was 11.20 months for PVd versus 7.10 months for Vd (hazard ratio, 0.61; 95% confidence interval, 0.49-0.77; P less than .0001).
Progression-free survival results were “even more encouraging” in the subset of patients with only one prior line of therapy, Dr. Richardson said, reporting a median of 20.73 months for PVd versus 11.63 for Vd (HR, 0.54; 95% CI, 0.36-0.82; P = .0027).
The overall response rate was 82.2% for PVd versus 50.0% for Vd (P less than .001). In patients with only one prior line of therapy, the overall response rate was 90.1% and 54.8% for PVd and Vd, respectively (P less than .001).
The progression-free survival advantage occurred regardless of whether patients were refractory to lenalidomide, Dr. Richardson added. Median progression-free survival for PVd versus Vd was 9.53 and 5.59 months, respectively, in the lenalidomide-refractory patients (P less than .001) and 22.01 versus 11.63 months in non–lenalidomide refractory patients (P less than .001).
The side effect profile of PVd was “very much as expected,” with more neutropenia seen with the PVd than with Vd, though rates of febrile neutropenia were low, Dr. Richardson said. Likewise, the rate of infection was higher in the triplet arm, but it was generally manageable, he added.
Deep vein thrombosis and pulmonary embolism rates were low in both arms, as were the rates of secondary primary malignancies. Analysis of minimal residual disease and quality of life are ongoing.
PVd could “arguably be now an important treatment platform for future directions in combination with other strategies,” Dr. Richardson said.
The study was supported by Celgene. Dr. Richardson reported advisory board work for Celgene, Novartis, Oncopeptides, Janssen, Amgen, and Takeda, and research funding from Bristol-Myers Squibb, Celgene, and Takeda.
SOURCE: Richardson PG et al. ASCO 2018, Abstract 8001.
CHICAGO – For patients with relapsed/refractory multiple myeloma previously exposed to lenalidomide, the combination of pomalidomide plus bortezomib and low‐dose dexamethasone (PVd) improved response and progression-free survival, results of the phase 3 OPTIMISMM trial showed.
Risk of disease progression or death was reduced by 39%, compared with bortezomib and low-dose dexamethasone alone (Vd), among patients in the trial, of whom approximately 70% were lenalidomide refractory, reported investigator Paul G. Richardson, MD, of the Dana-Farber Cancer Institute in Boston.
The improvements in efficacy seen with the PVd regimen were more pronounced in patients with only one prior line of therapy, and overall, the safety profile of the triplet regimen was consistent with known toxicities of each individual agent, Dr. Richardson reported.
Together, those results “would seem to support the use of this triplet [therapy] in first relapse in patients with relapsed/refractory myeloma and prior exposure to lenalidomide,” he said at the annual meeting of the American Society of Clinical Oncology.
“This study, importantly, evaluated a clinically relevant patient population and a growing patient population who receive upfront lenalidomide and maintenance in that setting and for whom lenalidomide is no longer a viable treatment option,” Dr. Richardson added.
Lenalidomide has become a mainstay of upfront myeloma treatment, and the Food and Drug Administration recently gave approval to lenalidomide as maintenance after autologous hematopoietic stem cell transplantation. Accordingly, it’s important to understand the benefits of triplet therapies in patients progressing on lenalidomide therapy and in whom lenalidomide is no longer a treatment option, Dr. Richardson said.
Pomalidomide, a potent oral immunomodulatory agent, is already approved for relapsed/refractory myeloma after two or more previous therapies that include lenalidomide and a proteasome inhibitor in patients who progress on or within 60 days of treatment.
In the OPTIMISMM trial, 559 patients who had received prior therapy, including at least two cycles of lenalidomide, were randomized to receive either PVd or Vd until disease progression or unacceptable toxicity.
Median progression-free survival was 11.20 months for PVd versus 7.10 months for Vd (hazard ratio, 0.61; 95% confidence interval, 0.49-0.77; P less than .0001).
Progression-free survival results were “even more encouraging” in the subset of patients with only one prior line of therapy, Dr. Richardson said, reporting a median of 20.73 months for PVd versus 11.63 for Vd (HR, 0.54; 95% CI, 0.36-0.82; P = .0027).
The overall response rate was 82.2% for PVd versus 50.0% for Vd (P less than .001). In patients with only one prior line of therapy, the overall response rate was 90.1% and 54.8% for PVd and Vd, respectively (P less than .001).
The progression-free survival advantage occurred regardless of whether patients were refractory to lenalidomide, Dr. Richardson added. Median progression-free survival for PVd versus Vd was 9.53 and 5.59 months, respectively, in the lenalidomide-refractory patients (P less than .001) and 22.01 versus 11.63 months in non–lenalidomide refractory patients (P less than .001).
The side effect profile of PVd was “very much as expected,” with more neutropenia seen with the PVd than with Vd, though rates of febrile neutropenia were low, Dr. Richardson said. Likewise, the rate of infection was higher in the triplet arm, but it was generally manageable, he added.
Deep vein thrombosis and pulmonary embolism rates were low in both arms, as were the rates of secondary primary malignancies. Analysis of minimal residual disease and quality of life are ongoing.
PVd could “arguably be now an important treatment platform for future directions in combination with other strategies,” Dr. Richardson said.
The study was supported by Celgene. Dr. Richardson reported advisory board work for Celgene, Novartis, Oncopeptides, Janssen, Amgen, and Takeda, and research funding from Bristol-Myers Squibb, Celgene, and Takeda.
SOURCE: Richardson PG et al. ASCO 2018, Abstract 8001.
CHICAGO – For patients with relapsed/refractory multiple myeloma previously exposed to lenalidomide, the combination of pomalidomide plus bortezomib and low‐dose dexamethasone (PVd) improved response and progression-free survival, results of the phase 3 OPTIMISMM trial showed.
Risk of disease progression or death was reduced by 39%, compared with bortezomib and low-dose dexamethasone alone (Vd), among patients in the trial, of whom approximately 70% were lenalidomide refractory, reported investigator Paul G. Richardson, MD, of the Dana-Farber Cancer Institute in Boston.
The improvements in efficacy seen with the PVd regimen were more pronounced in patients with only one prior line of therapy, and overall, the safety profile of the triplet regimen was consistent with known toxicities of each individual agent, Dr. Richardson reported.
Together, those results “would seem to support the use of this triplet [therapy] in first relapse in patients with relapsed/refractory myeloma and prior exposure to lenalidomide,” he said at the annual meeting of the American Society of Clinical Oncology.
“This study, importantly, evaluated a clinically relevant patient population and a growing patient population who receive upfront lenalidomide and maintenance in that setting and for whom lenalidomide is no longer a viable treatment option,” Dr. Richardson added.
Lenalidomide has become a mainstay of upfront myeloma treatment, and the Food and Drug Administration recently gave approval to lenalidomide as maintenance after autologous hematopoietic stem cell transplantation. Accordingly, it’s important to understand the benefits of triplet therapies in patients progressing on lenalidomide therapy and in whom lenalidomide is no longer a treatment option, Dr. Richardson said.
Pomalidomide, a potent oral immunomodulatory agent, is already approved for relapsed/refractory myeloma after two or more previous therapies that include lenalidomide and a proteasome inhibitor in patients who progress on or within 60 days of treatment.
In the OPTIMISMM trial, 559 patients who had received prior therapy, including at least two cycles of lenalidomide, were randomized to receive either PVd or Vd until disease progression or unacceptable toxicity.
Median progression-free survival was 11.20 months for PVd versus 7.10 months for Vd (hazard ratio, 0.61; 95% confidence interval, 0.49-0.77; P less than .0001).
Progression-free survival results were “even more encouraging” in the subset of patients with only one prior line of therapy, Dr. Richardson said, reporting a median of 20.73 months for PVd versus 11.63 for Vd (HR, 0.54; 95% CI, 0.36-0.82; P = .0027).
The overall response rate was 82.2% for PVd versus 50.0% for Vd (P less than .001). In patients with only one prior line of therapy, the overall response rate was 90.1% and 54.8% for PVd and Vd, respectively (P less than .001).
The progression-free survival advantage occurred regardless of whether patients were refractory to lenalidomide, Dr. Richardson added. Median progression-free survival for PVd versus Vd was 9.53 and 5.59 months, respectively, in the lenalidomide-refractory patients (P less than .001) and 22.01 versus 11.63 months in non–lenalidomide refractory patients (P less than .001).
The side effect profile of PVd was “very much as expected,” with more neutropenia seen with the PVd than with Vd, though rates of febrile neutropenia were low, Dr. Richardson said. Likewise, the rate of infection was higher in the triplet arm, but it was generally manageable, he added.
Deep vein thrombosis and pulmonary embolism rates were low in both arms, as were the rates of secondary primary malignancies. Analysis of minimal residual disease and quality of life are ongoing.
PVd could “arguably be now an important treatment platform for future directions in combination with other strategies,” Dr. Richardson said.
The study was supported by Celgene. Dr. Richardson reported advisory board work for Celgene, Novartis, Oncopeptides, Janssen, Amgen, and Takeda, and research funding from Bristol-Myers Squibb, Celgene, and Takeda.
SOURCE: Richardson PG et al. ASCO 2018, Abstract 8001.
REPORTING FROM ASCO 2018
Key clinical point:
Major finding: Risk of disease progression or death was reduced by 39% with pomalidomide plus bortezomib and low‐dose dexamethasone (PVd), compared with use of bortezomib and low-dose dexamethasone alone (Vd).
Study details: The phase 3 OPTIMISMM trial including 559 patients who had received prior therapy with at least two cycles of lenalidomide.
Disclosures: The study was supported by Celgene. Dr. Richardson reported advisory board work for Celgene, Novartis, Oncopeptides, Janssen, Amgen, and Takeda and research funding from Bristol-Myers Squibb, Celgene, and Takeda.
Source: Richardson PG et al. ASCO 2018, Abstract 8001.
Screen sooner and more often for those with family history of CRC
WASHINGTON – The number of first- and second-degree relatives with colorectal cancer can increase an individual’s risk for CRC, which could require screening to be done more frequently.
“There have been multiple guidelines reported as to what should be done for these individuals,” Harminder Singh, MD, of the University of Manitoba and his associates stated. “However, for the most part, they have not systematically analyzed the data.” He went on to say that, “more importantly, there’s been no recent AGA [American Gastroenterological Association] or Canadian Association of Gastroenterology statement, which led the development of this guideline.”
To address this issue, Dr. Singh and his colleagues conducted a systematic review of 10 literature searches to answer the following five questions concerning colorectal risk and screening practices: What is the effect of a family history of CRC on an individual’s risk of CRC? What is the effect of a family history of adenoma on an individual’s risk of CRC? At what age should CRC screening begin? Which screening tests are optimal? What are the optimal testing intervals for people with a family history of CRC or adenoma?
These questions were developed via an iterative online platform and then further developed and voted on by a team of specialists. GRADE (Grading of Recommendation Assessment, Development and Evaluation) was used to assess the quality of evidence to support these questions.
Similarly, individuals with two or more first-degree relatives with CRC had a two- to fourfold increased risk of developing CRC, compared with the general population. The review also found that, of the 20 recommendation statements from the review panel, there was consensus about 19 of them.
Colorectal cancer screening is recommended for all individuals with a family history of CRC or documented adenoma. Similarly, colonoscopy is recommended as the preferred test for individuals at the highest risk– those with one or more affected first-degree relatives. Fecal immunochemistry tests are considered a viable alternative except in patients with two or more first-degree relatives.
If a patient is considered to have an elevated risk of CRC because of family history, then screening should begin when they are aged 10 years younger than when that first-degree relative was diagnosed, and a 5-year screening interval should be followed after that.
Dr. Singh pointed out that the age of the affected first-degree relative should be considered when weighing an individual’s related risk of developing CRC. For example, having an first-degree relative who is diagnosed after the age of 75 is not likely to elevate an individual’s risk of developing CRC. Individuals with one or more second-degree relatives with CRC or nonadvanced adenoma do not appear to have an elevated risk of developing CRC and should be screened according to average-risk guidelines.
Dr. Singh reported receiving funding for from Merck Canada.
SOURCE: Leddin D. Gastroenterology. 2018 Jun. doi: 10.1016/S0016-5085(18)31083-7.
WASHINGTON – The number of first- and second-degree relatives with colorectal cancer can increase an individual’s risk for CRC, which could require screening to be done more frequently.
“There have been multiple guidelines reported as to what should be done for these individuals,” Harminder Singh, MD, of the University of Manitoba and his associates stated. “However, for the most part, they have not systematically analyzed the data.” He went on to say that, “more importantly, there’s been no recent AGA [American Gastroenterological Association] or Canadian Association of Gastroenterology statement, which led the development of this guideline.”
To address this issue, Dr. Singh and his colleagues conducted a systematic review of 10 literature searches to answer the following five questions concerning colorectal risk and screening practices: What is the effect of a family history of CRC on an individual’s risk of CRC? What is the effect of a family history of adenoma on an individual’s risk of CRC? At what age should CRC screening begin? Which screening tests are optimal? What are the optimal testing intervals for people with a family history of CRC or adenoma?
These questions were developed via an iterative online platform and then further developed and voted on by a team of specialists. GRADE (Grading of Recommendation Assessment, Development and Evaluation) was used to assess the quality of evidence to support these questions.
Similarly, individuals with two or more first-degree relatives with CRC had a two- to fourfold increased risk of developing CRC, compared with the general population. The review also found that, of the 20 recommendation statements from the review panel, there was consensus about 19 of them.
Colorectal cancer screening is recommended for all individuals with a family history of CRC or documented adenoma. Similarly, colonoscopy is recommended as the preferred test for individuals at the highest risk– those with one or more affected first-degree relatives. Fecal immunochemistry tests are considered a viable alternative except in patients with two or more first-degree relatives.
If a patient is considered to have an elevated risk of CRC because of family history, then screening should begin when they are aged 10 years younger than when that first-degree relative was diagnosed, and a 5-year screening interval should be followed after that.
Dr. Singh pointed out that the age of the affected first-degree relative should be considered when weighing an individual’s related risk of developing CRC. For example, having an first-degree relative who is diagnosed after the age of 75 is not likely to elevate an individual’s risk of developing CRC. Individuals with one or more second-degree relatives with CRC or nonadvanced adenoma do not appear to have an elevated risk of developing CRC and should be screened according to average-risk guidelines.
Dr. Singh reported receiving funding for from Merck Canada.
SOURCE: Leddin D. Gastroenterology. 2018 Jun. doi: 10.1016/S0016-5085(18)31083-7.
WASHINGTON – The number of first- and second-degree relatives with colorectal cancer can increase an individual’s risk for CRC, which could require screening to be done more frequently.
“There have been multiple guidelines reported as to what should be done for these individuals,” Harminder Singh, MD, of the University of Manitoba and his associates stated. “However, for the most part, they have not systematically analyzed the data.” He went on to say that, “more importantly, there’s been no recent AGA [American Gastroenterological Association] or Canadian Association of Gastroenterology statement, which led the development of this guideline.”
To address this issue, Dr. Singh and his colleagues conducted a systematic review of 10 literature searches to answer the following five questions concerning colorectal risk and screening practices: What is the effect of a family history of CRC on an individual’s risk of CRC? What is the effect of a family history of adenoma on an individual’s risk of CRC? At what age should CRC screening begin? Which screening tests are optimal? What are the optimal testing intervals for people with a family history of CRC or adenoma?
These questions were developed via an iterative online platform and then further developed and voted on by a team of specialists. GRADE (Grading of Recommendation Assessment, Development and Evaluation) was used to assess the quality of evidence to support these questions.
Similarly, individuals with two or more first-degree relatives with CRC had a two- to fourfold increased risk of developing CRC, compared with the general population. The review also found that, of the 20 recommendation statements from the review panel, there was consensus about 19 of them.
Colorectal cancer screening is recommended for all individuals with a family history of CRC or documented adenoma. Similarly, colonoscopy is recommended as the preferred test for individuals at the highest risk– those with one or more affected first-degree relatives. Fecal immunochemistry tests are considered a viable alternative except in patients with two or more first-degree relatives.
If a patient is considered to have an elevated risk of CRC because of family history, then screening should begin when they are aged 10 years younger than when that first-degree relative was diagnosed, and a 5-year screening interval should be followed after that.
Dr. Singh pointed out that the age of the affected first-degree relative should be considered when weighing an individual’s related risk of developing CRC. For example, having an first-degree relative who is diagnosed after the age of 75 is not likely to elevate an individual’s risk of developing CRC. Individuals with one or more second-degree relatives with CRC or nonadvanced adenoma do not appear to have an elevated risk of developing CRC and should be screened according to average-risk guidelines.
Dr. Singh reported receiving funding for from Merck Canada.
SOURCE: Leddin D. Gastroenterology. 2018 Jun. doi: 10.1016/S0016-5085(18)31083-7.
REPORTING FROM DDW 2018
Key clinical point: Patients with 1 or more first-degree relative with CRC should be screened more often.
Major finding: Patients with one or more first-degree relatives with CRC or adenoma had a twofold greater risk of developing CRC, compared with those without a family history of these diseases.
Study details: A systematic review of 10 literature searches assessing risk of CRC in those with a family history of CRC.
Disclosures: Dr. Singh has received funding from Merck Canada.
Source: Leddin D. Gastroenterology. 2018 Jun. doi: 10.1016/S0016-5085(18)31083-7.
EULAR recommendations on steroids: ‘As necessary, but as little as possible’
AMSTERDAM – Glucocorticosteroids remain an important therapeutic option for many patients with rheumatic and nonrheumatic disease, but careful assessment of their relative benefits and risks needs to be considered when prescribing, according to an expert summary of currently available European League Against Rheumatism (EULAR) recommendations.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
From rheumatoid arthritis (RA) and polymyalgia rheumatica (PMR) to vasculitis, myositis, and even gout, steroids are widely used in the rheumatic diseases, said Frank Buttgereit, MD, during a final plenary session at the European Congress of Rheumatology.
“These are strong-acting, rapidly acting, efficacious drugs,” observed Dr. Buttgereit, who is a professor in the department of rheumatology at Charité–Universitätsmedizin Berlin. While effective at reducing inflammation and providing immunosuppression, they are, of course, not without their well-known risks. Some of the well-documented risks he pointed out were the development of osteoporosis, myopathy, and edema; the disruption of lipid and carbohydrate metabolism; and the risk of developing glaucoma and cataracts.
“This leads to the question on how to optimize the use of these drugs,” Dr. Buttgereit said. “EULAR is constantly working to improve its guidelines,” and updating these in line with the available evidence, he added. “The bottom line is always give as much as necessary but as little as possible.”
Over the past few years, EULAR’s Glucocorticoid Task Force has been reviewing and updating recommendations on the use of these drugs and it has published several important documents clarifying their use in RA and in PMR. The task force has also published a viewpoint article on the long-term use of steroids, defining the conditions where an “acceptably low level of harm” might exist to enable their continued use. There have also been separate recommendations, published in 2010, on how to monitor these drugs (Ann Rheum Dis. 2010;69[11]:1913-9).
Clarifying the role of steroids in rheumatoid arthritis
The latest (2016) EULAR recommendations on the use of glucocorticosteroids were published last year (Ann Rheum Dis. 2017;76[6]:960-77) and included an important adjustment on when they should be initially used in RA, Dr. Buttgereit explained. Previous recommendations had said that steroids could be combined with disease-modifying antirheumatic drugs (DMARDs) but had suggested that they be used at a low dose. Now the wording has changed to focus on short-term use rather than dosing.
“Glucocorticoids can be given initially at different dosages, and using different routes of administration,” he said in a video interview at the EULAR Congress. The practice on what dose to give varies from country to country, he noted, so the recommendations are now being less prescriptive.
“We have made it clear that glucocorticoids should really be used only when initiating conventional synthetic DMARDs, but not necessarily if you switch to biologics or targeted synthetics because usually the onset of their actions is pretty fast,” Dr. Buttgereit said.
One thing that hasn’t changed is that steroid should be tapered down as “rapidly as clinically feasible” until, ideally, their full withdrawal. Although there are cases when that might not be possible, and their long-term use might be warranted. This is when you get into discussion about the benefit-to-risk ratio, he said.
Steroids for polymyalgia rheumatica
Steroids may be used as monotherapy in patients with PMR, Dr. Buttgereit observed, which is in contrast to other conditions such as RA. Although the evidence for use of steroids in PMR is limited, the EULAR Glucocorticoid Task Force and American College of Rheumatology recommended (Ann Rheum Dis. 2015;74[10]:1799-807) using a starting dose of a prednisolone-equivalent dose between 12.5 and 25 mg/day, and if there is an improvement in few weeks, the dose can start to be reduced. Tapering should be rapid at first to bring the dose down to 10 mg/day and followed by a more gradual dose-reduction phase.
“So, you can see we are giving more or less precise recommendations on how to start, how to taper,” Dr. Buttgereit said.
Balancing long-term benefit vs. harm
Balancing the long-term benefits and risks of steroids in rheumatic disease was the focus of a EULAR viewpoint article published 3 years ago in 2015 (Ann Rheum Dis. 2015;75[6]:952-7).
Three main messages can be drawn out of this work, Dr. Buttgereit said.
First, treatment with steroids for 3-6 months is associated with more benefits than risks if doses of 5 mg/day or less are used. There is one important exception to this, however, and that is the use of steroids in patients with comorbid cardiovascular disease.
Second, using doses of 10 mg/day for long periods tips the balance toward more risks than benefits, and “this means you should avoid this.”
Third, doses of 5-10 mg/day may be appropriate, but there are certain patient factors that will influence the benefit-to-harm ratio that need to be considered. These include older age, smoking, high alcohol consumption, and poor nutrition. There are also factors that may help protect the patients from risk, such as early diagnosis, low disease activity, low cumulative dose of steroids, and a shorter duration of treatment.
“It’s not only the dose, it’s also the absence or presence of risk factors and/or preventive measures,” that’s important, Dr. Buttgereit said.
Dr. Buttgereit has received consultancy fees, honoraria, and/or travel expenses from Amgen, Horizon Pharma, Mundipharma, Roche, and Pfizer and grant or study support from Amgen, Mundipharma, and Pfizer.
SOURCE: Buttgereit F. EULAR 2018 Congress, Abstract SP160.
AMSTERDAM – Glucocorticosteroids remain an important therapeutic option for many patients with rheumatic and nonrheumatic disease, but careful assessment of their relative benefits and risks needs to be considered when prescribing, according to an expert summary of currently available European League Against Rheumatism (EULAR) recommendations.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
From rheumatoid arthritis (RA) and polymyalgia rheumatica (PMR) to vasculitis, myositis, and even gout, steroids are widely used in the rheumatic diseases, said Frank Buttgereit, MD, during a final plenary session at the European Congress of Rheumatology.
“These are strong-acting, rapidly acting, efficacious drugs,” observed Dr. Buttgereit, who is a professor in the department of rheumatology at Charité–Universitätsmedizin Berlin. While effective at reducing inflammation and providing immunosuppression, they are, of course, not without their well-known risks. Some of the well-documented risks he pointed out were the development of osteoporosis, myopathy, and edema; the disruption of lipid and carbohydrate metabolism; and the risk of developing glaucoma and cataracts.
“This leads to the question on how to optimize the use of these drugs,” Dr. Buttgereit said. “EULAR is constantly working to improve its guidelines,” and updating these in line with the available evidence, he added. “The bottom line is always give as much as necessary but as little as possible.”
Over the past few years, EULAR’s Glucocorticoid Task Force has been reviewing and updating recommendations on the use of these drugs and it has published several important documents clarifying their use in RA and in PMR. The task force has also published a viewpoint article on the long-term use of steroids, defining the conditions where an “acceptably low level of harm” might exist to enable their continued use. There have also been separate recommendations, published in 2010, on how to monitor these drugs (Ann Rheum Dis. 2010;69[11]:1913-9).
Clarifying the role of steroids in rheumatoid arthritis
The latest (2016) EULAR recommendations on the use of glucocorticosteroids were published last year (Ann Rheum Dis. 2017;76[6]:960-77) and included an important adjustment on when they should be initially used in RA, Dr. Buttgereit explained. Previous recommendations had said that steroids could be combined with disease-modifying antirheumatic drugs (DMARDs) but had suggested that they be used at a low dose. Now the wording has changed to focus on short-term use rather than dosing.
“Glucocorticoids can be given initially at different dosages, and using different routes of administration,” he said in a video interview at the EULAR Congress. The practice on what dose to give varies from country to country, he noted, so the recommendations are now being less prescriptive.
“We have made it clear that glucocorticoids should really be used only when initiating conventional synthetic DMARDs, but not necessarily if you switch to biologics or targeted synthetics because usually the onset of their actions is pretty fast,” Dr. Buttgereit said.
One thing that hasn’t changed is that steroid should be tapered down as “rapidly as clinically feasible” until, ideally, their full withdrawal. Although there are cases when that might not be possible, and their long-term use might be warranted. This is when you get into discussion about the benefit-to-risk ratio, he said.
Steroids for polymyalgia rheumatica
Steroids may be used as monotherapy in patients with PMR, Dr. Buttgereit observed, which is in contrast to other conditions such as RA. Although the evidence for use of steroids in PMR is limited, the EULAR Glucocorticoid Task Force and American College of Rheumatology recommended (Ann Rheum Dis. 2015;74[10]:1799-807) using a starting dose of a prednisolone-equivalent dose between 12.5 and 25 mg/day, and if there is an improvement in few weeks, the dose can start to be reduced. Tapering should be rapid at first to bring the dose down to 10 mg/day and followed by a more gradual dose-reduction phase.
“So, you can see we are giving more or less precise recommendations on how to start, how to taper,” Dr. Buttgereit said.
Balancing long-term benefit vs. harm
Balancing the long-term benefits and risks of steroids in rheumatic disease was the focus of a EULAR viewpoint article published 3 years ago in 2015 (Ann Rheum Dis. 2015;75[6]:952-7).
Three main messages can be drawn out of this work, Dr. Buttgereit said.
First, treatment with steroids for 3-6 months is associated with more benefits than risks if doses of 5 mg/day or less are used. There is one important exception to this, however, and that is the use of steroids in patients with comorbid cardiovascular disease.
Second, using doses of 10 mg/day for long periods tips the balance toward more risks than benefits, and “this means you should avoid this.”
Third, doses of 5-10 mg/day may be appropriate, but there are certain patient factors that will influence the benefit-to-harm ratio that need to be considered. These include older age, smoking, high alcohol consumption, and poor nutrition. There are also factors that may help protect the patients from risk, such as early diagnosis, low disease activity, low cumulative dose of steroids, and a shorter duration of treatment.
“It’s not only the dose, it’s also the absence or presence of risk factors and/or preventive measures,” that’s important, Dr. Buttgereit said.
Dr. Buttgereit has received consultancy fees, honoraria, and/or travel expenses from Amgen, Horizon Pharma, Mundipharma, Roche, and Pfizer and grant or study support from Amgen, Mundipharma, and Pfizer.
SOURCE: Buttgereit F. EULAR 2018 Congress, Abstract SP160.
AMSTERDAM – Glucocorticosteroids remain an important therapeutic option for many patients with rheumatic and nonrheumatic disease, but careful assessment of their relative benefits and risks needs to be considered when prescribing, according to an expert summary of currently available European League Against Rheumatism (EULAR) recommendations.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
From rheumatoid arthritis (RA) and polymyalgia rheumatica (PMR) to vasculitis, myositis, and even gout, steroids are widely used in the rheumatic diseases, said Frank Buttgereit, MD, during a final plenary session at the European Congress of Rheumatology.
“These are strong-acting, rapidly acting, efficacious drugs,” observed Dr. Buttgereit, who is a professor in the department of rheumatology at Charité–Universitätsmedizin Berlin. While effective at reducing inflammation and providing immunosuppression, they are, of course, not without their well-known risks. Some of the well-documented risks he pointed out were the development of osteoporosis, myopathy, and edema; the disruption of lipid and carbohydrate metabolism; and the risk of developing glaucoma and cataracts.
“This leads to the question on how to optimize the use of these drugs,” Dr. Buttgereit said. “EULAR is constantly working to improve its guidelines,” and updating these in line with the available evidence, he added. “The bottom line is always give as much as necessary but as little as possible.”
Over the past few years, EULAR’s Glucocorticoid Task Force has been reviewing and updating recommendations on the use of these drugs and it has published several important documents clarifying their use in RA and in PMR. The task force has also published a viewpoint article on the long-term use of steroids, defining the conditions where an “acceptably low level of harm” might exist to enable their continued use. There have also been separate recommendations, published in 2010, on how to monitor these drugs (Ann Rheum Dis. 2010;69[11]:1913-9).
Clarifying the role of steroids in rheumatoid arthritis
The latest (2016) EULAR recommendations on the use of glucocorticosteroids were published last year (Ann Rheum Dis. 2017;76[6]:960-77) and included an important adjustment on when they should be initially used in RA, Dr. Buttgereit explained. Previous recommendations had said that steroids could be combined with disease-modifying antirheumatic drugs (DMARDs) but had suggested that they be used at a low dose. Now the wording has changed to focus on short-term use rather than dosing.
“Glucocorticoids can be given initially at different dosages, and using different routes of administration,” he said in a video interview at the EULAR Congress. The practice on what dose to give varies from country to country, he noted, so the recommendations are now being less prescriptive.
“We have made it clear that glucocorticoids should really be used only when initiating conventional synthetic DMARDs, but not necessarily if you switch to biologics or targeted synthetics because usually the onset of their actions is pretty fast,” Dr. Buttgereit said.
One thing that hasn’t changed is that steroid should be tapered down as “rapidly as clinically feasible” until, ideally, their full withdrawal. Although there are cases when that might not be possible, and their long-term use might be warranted. This is when you get into discussion about the benefit-to-risk ratio, he said.
Steroids for polymyalgia rheumatica
Steroids may be used as monotherapy in patients with PMR, Dr. Buttgereit observed, which is in contrast to other conditions such as RA. Although the evidence for use of steroids in PMR is limited, the EULAR Glucocorticoid Task Force and American College of Rheumatology recommended (Ann Rheum Dis. 2015;74[10]:1799-807) using a starting dose of a prednisolone-equivalent dose between 12.5 and 25 mg/day, and if there is an improvement in few weeks, the dose can start to be reduced. Tapering should be rapid at first to bring the dose down to 10 mg/day and followed by a more gradual dose-reduction phase.
“So, you can see we are giving more or less precise recommendations on how to start, how to taper,” Dr. Buttgereit said.
Balancing long-term benefit vs. harm
Balancing the long-term benefits and risks of steroids in rheumatic disease was the focus of a EULAR viewpoint article published 3 years ago in 2015 (Ann Rheum Dis. 2015;75[6]:952-7).
Three main messages can be drawn out of this work, Dr. Buttgereit said.
First, treatment with steroids for 3-6 months is associated with more benefits than risks if doses of 5 mg/day or less are used. There is one important exception to this, however, and that is the use of steroids in patients with comorbid cardiovascular disease.
Second, using doses of 10 mg/day for long periods tips the balance toward more risks than benefits, and “this means you should avoid this.”
Third, doses of 5-10 mg/day may be appropriate, but there are certain patient factors that will influence the benefit-to-harm ratio that need to be considered. These include older age, smoking, high alcohol consumption, and poor nutrition. There are also factors that may help protect the patients from risk, such as early diagnosis, low disease activity, low cumulative dose of steroids, and a shorter duration of treatment.
“It’s not only the dose, it’s also the absence or presence of risk factors and/or preventive measures,” that’s important, Dr. Buttgereit said.
Dr. Buttgereit has received consultancy fees, honoraria, and/or travel expenses from Amgen, Horizon Pharma, Mundipharma, Roche, and Pfizer and grant or study support from Amgen, Mundipharma, and Pfizer.
SOURCE: Buttgereit F. EULAR 2018 Congress, Abstract SP160.
REPORTING FROM THE EULAR 2018 CONGRESS
Key clinical point: When dosing glucocorticoids, give as much as necessary but as little as possible.
Major finding:
Disclosures: Dr. Buttgereit has received consultancy fees, honoraria, and/or travel expenses from Amgen, Horizon Pharma, Mundipharma, Roche, and Pfizer and grant or study support from Amgen, Mundipharma, and Pfizer.
Source: Buttgereit F. EULAR 2018 Congress. Abstract SP160.

Anthrax vaccine recommendations updated in the event of a wide-area release
at their meeting.
The recommendations to the committee sought to optimize the use of Anthrax Vaccine Adsorbed (AVA) in post-exposure prophylaxis (PEP) in the event of a wide-area release of Bacillus anthracis spores. In this event, a mass vaccination effort would be undertaken, requiring expedited administration of AVA. ACIP now recommends that the intramuscular administration may be used over the traditional subcutaneous approach if there are any operational or logistical challenges that delay effective vaccination. Another recommendation from ACIP would allow two full doses or three half doses of AVA to be used to expand vaccine coverage for PEP in the event there is an inadequate vaccine supply. The committee also recommended that AbxPEP, an antimicrobial, be stopped 42 days after the first dose of AVA or 2 weeks after the last dose.
William A. Bower, MD, of the division of high-consequence pathogens and pathology at the Centers for Disease Control and Prevention, and the anthrax work group looked at three nonhuman primate studies and eight human immunogenicity and adverse event studies during the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE). All of the animal studies were used to predict human survival by vaccinating the nonhuman primates with AVA, then challenging them with B. anthracis. Using animal studies to predict human survival is common practice under the “animal rule.”
When Dr. Bower and the work group assessed the studies comparing intramuscular administration with subcutaneous administration of AVA, they rated the overall evidence as GRADE 2. However, they rated the adverse events data as GRADE 1.
Dr. Bower and his colleagues also reviewed dose-sparing studies to identify the feasibility of allowing two full doses or three half doses of AVA to be used to expand vaccine coverage for PEP in the event there is an inadequate vaccine supply. For these studies, the anthrax work group gave a GRADE score of 2.
The overall evidence score for microbial duration for PEP was judged to be GRADE 2.
“These forthcoming recommendations will be used by the CDC to inform state and local health departments to better prepare for an emergency response to a wide-area release of Bacillus anthracis spores,” said Dr. Bower.
The committee’s recommendations must be approved by the CDC’s director before they are considered official recommendations.
Dr. Bower did not report any relevant financial conflicts of interest.
at their meeting.
The recommendations to the committee sought to optimize the use of Anthrax Vaccine Adsorbed (AVA) in post-exposure prophylaxis (PEP) in the event of a wide-area release of Bacillus anthracis spores. In this event, a mass vaccination effort would be undertaken, requiring expedited administration of AVA. ACIP now recommends that the intramuscular administration may be used over the traditional subcutaneous approach if there are any operational or logistical challenges that delay effective vaccination. Another recommendation from ACIP would allow two full doses or three half doses of AVA to be used to expand vaccine coverage for PEP in the event there is an inadequate vaccine supply. The committee also recommended that AbxPEP, an antimicrobial, be stopped 42 days after the first dose of AVA or 2 weeks after the last dose.
William A. Bower, MD, of the division of high-consequence pathogens and pathology at the Centers for Disease Control and Prevention, and the anthrax work group looked at three nonhuman primate studies and eight human immunogenicity and adverse event studies during the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE). All of the animal studies were used to predict human survival by vaccinating the nonhuman primates with AVA, then challenging them with B. anthracis. Using animal studies to predict human survival is common practice under the “animal rule.”
When Dr. Bower and the work group assessed the studies comparing intramuscular administration with subcutaneous administration of AVA, they rated the overall evidence as GRADE 2. However, they rated the adverse events data as GRADE 1.
Dr. Bower and his colleagues also reviewed dose-sparing studies to identify the feasibility of allowing two full doses or three half doses of AVA to be used to expand vaccine coverage for PEP in the event there is an inadequate vaccine supply. For these studies, the anthrax work group gave a GRADE score of 2.
The overall evidence score for microbial duration for PEP was judged to be GRADE 2.
“These forthcoming recommendations will be used by the CDC to inform state and local health departments to better prepare for an emergency response to a wide-area release of Bacillus anthracis spores,” said Dr. Bower.
The committee’s recommendations must be approved by the CDC’s director before they are considered official recommendations.
Dr. Bower did not report any relevant financial conflicts of interest.
at their meeting.
The recommendations to the committee sought to optimize the use of Anthrax Vaccine Adsorbed (AVA) in post-exposure prophylaxis (PEP) in the event of a wide-area release of Bacillus anthracis spores. In this event, a mass vaccination effort would be undertaken, requiring expedited administration of AVA. ACIP now recommends that the intramuscular administration may be used over the traditional subcutaneous approach if there are any operational or logistical challenges that delay effective vaccination. Another recommendation from ACIP would allow two full doses or three half doses of AVA to be used to expand vaccine coverage for PEP in the event there is an inadequate vaccine supply. The committee also recommended that AbxPEP, an antimicrobial, be stopped 42 days after the first dose of AVA or 2 weeks after the last dose.
William A. Bower, MD, of the division of high-consequence pathogens and pathology at the Centers for Disease Control and Prevention, and the anthrax work group looked at three nonhuman primate studies and eight human immunogenicity and adverse event studies during the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE). All of the animal studies were used to predict human survival by vaccinating the nonhuman primates with AVA, then challenging them with B. anthracis. Using animal studies to predict human survival is common practice under the “animal rule.”
When Dr. Bower and the work group assessed the studies comparing intramuscular administration with subcutaneous administration of AVA, they rated the overall evidence as GRADE 2. However, they rated the adverse events data as GRADE 1.
Dr. Bower and his colleagues also reviewed dose-sparing studies to identify the feasibility of allowing two full doses or three half doses of AVA to be used to expand vaccine coverage for PEP in the event there is an inadequate vaccine supply. For these studies, the anthrax work group gave a GRADE score of 2.
The overall evidence score for microbial duration for PEP was judged to be GRADE 2.
“These forthcoming recommendations will be used by the CDC to inform state and local health departments to better prepare for an emergency response to a wide-area release of Bacillus anthracis spores,” said Dr. Bower.
The committee’s recommendations must be approved by the CDC’s director before they are considered official recommendations.
Dr. Bower did not report any relevant financial conflicts of interest.
REPORTING FROM AN ACIP MEETING