User login
Mental illness and the criminal justice system: Reducing the risks
NEW YORK – The overrepresentation of people with serious mental illness (SMI) in the criminal justice system has led to creation of a resource from the Judges’ and Psychiatrists’ Leadership Initiative (JPLI) aimed at helping psychiatry and law enforcement address the problem.

The resource, “Supporting People with Serious Mental Illnesses and Reducing Their Risk of Contact with the Criminal Justice System: A Primer for Psychiatrists,” released last year, was designed to provide psychiatrists with specific knowledge and tools, according to Michael Champion, MD, forensic chief at the Hawaii State Department of Health, Adult Mental Health Division, Honolulu, and a member of the JPLI executive leadership team.
In developing the primer, the JPLI, which was created about 10 years ago by the American Psychiatric Association Foundation in partnership with the Council of State Governments Justice Center in response to the growing problem of such overrepresentation, sought to teach psychiatrists about what the criminal justice literature has dubbed “criminogenic risk” and to explore strategies to address those risks in community treatment settings, Dr. Champion said at the annual meeting of the American Psychiatric Association.
“The fact is that one in three Americans has a criminal record, and people with serious mental illness and criminal justice involvement are frequently part of our patient population – particularly in the public mental health sector,” Dr. Champion said. “Part of the challenge is that psychiatrists ... aren’t typically trained in these principles ... so the JPLI saw that this as an area that we could try to make some traction in and try to make a difference.”
The JPLI’s goals in publishing this resource are to reduce the risk of patient involvement in the criminal justice system, and to improve clinical and recovery outcomes by educating community psychiatrists about Risk-Need-Responsivity (RNR) principles. The JPLI also seeks to provide strategies for collaborating with criminal justice partners, incorporating criminal justice history into screening and assessment, and integrating criminogenic risk needs of patients into comprehensive treatment plans, Dr. Champion said.
Criminogenic risk and RNR
Many factors contribute to the involvement of people with serious mental illnesses in the criminal justice system, including higher rates of arrest, longer stays, recidivism, and limited access to health care, said Fred C. Osher, MD, former director of health systems and services policy for the Council of State Governments Justice Center.
“We used to think that ... if we could just get folks the health care that they need, they wouldn’t get involved with the criminal justice system. It turns out that that’s a gross oversimplification, in that their needs are terribly complex, and while treatment is a necessary component, it isn’t often sufficient for a large number of individuals,” said Dr. Osher, now a member of the JPLI executive leadership team.
Criminogenic risk – the likelihood that a person who has been arrested and jailed will commit a new crime after release or return to custody – helps explain why that is the case, he said, adding: “We have ways in which we can understand those risks.”
The risks are measured via static factors (unchanging conditions such as criminal history, age at first arrest, current age, and gender) and dynamic factors, he explained.
he said, noting that the research has shown there are eight specific criminogenic risk factors: substance abuse, history of antisocial behavior, antisocial personality pattern, antisocial cognition, antisocial associates, family and/or marital discord, poor school and/or work output, and having few leisure/recreation outlets.
Notably, mental illness is not a part of that list, he said.
“The reason for that is it’s not explanatory in and of itself,” he added.
However, research shows that people with mental illness have more of these dynamic risk factors, and research by Jennifer L. Skeem, PhD, and others shows that those with mental illness were coming back to jail not for new criminal activity, but for failing to comply with their conditions of release.
“These risks, then, have been brought into a paradigm that is central to our criminal justice operations, and it’s called the Risk-Need-Responsivity model,” Dr. Osher said. “This paradigm is what allows a criminal justice system to think about how to prioritize the resources – to think about who really needs to be wrapped tight, who needs to have close supervision, frequent reporting, lots of contact.”
The risk principle in the RNR model says that resources should be focused on high-risk cases, with limited supervision in lower-risk cases. This is based on experience demonstrating that recidivism is lower in high-risk individuals with close supervision but higher in low-risk individuals with close supervision.
The needs principle suggests that dynamic needs are “the issues that get folks in trouble,” he said.
“So, if we’re going to intervene, if we’re going to provide programming, if we’re going to try and help that individual stay out of jail or prison, we need to address these criminogenic needs,” he said, adding that the “big four” are related to their antisocial thinking and personality and friends.
Targeted interventions can help those individuals make better choices going forward, he noted.
The responsivity principle is an acknowledgment that individuals have different ways of learning, different cultural factors and backgrounds that influence them, and social determinants that are important to understand if they predict the ability to stay out of trouble.
“This is where mental illness fits in,” Dr. Osher said. “It’s absolutely important that we understand that.”
Examples would be patients with severe major depressive disorder who need their depression treated before they can participate in a group treatment setting designed to address criminogenic risks.
Dynamic risk factors are best treated with cognitive-behavioral interventions, Dr. Osher said, noting that the most effective interventions provide opportunities for participants to practice new behavior patterns and skills with feedback from program staff.
In many states, those interventions are being provided by criminal justice personnel, including probation officers, partly because of “an absence of [psychiatrists’] understanding, willingness, or ability to step forward.” The JPLI primer is designed to “really amp up our own excitement about, and willingness to learn how to develop interventions to help that individual stay out of trouble,” and it includes detailed descriptions of numerous well-researched, standardized, manualized interventions that people can access that make it less likely for them to have criminal justice access going forward, he said.
Those include programs such as “Thinking for a Change,” “Reasoning and Rehabilitation,” “Moral Reconation Therapy,” and “Interactive Journaling.”
A focus on the Sequential Intercept Model, which describes how individuals move through the criminal justice system, illustrates multiple points where psychiatrists can “do things better and differently to intervene,” he said, noting that the primer includes a framework for prioritizing the target population, and validated screening and assessment tools, including tools to help corrections officers identify mental health/substance abuse/criminogenic issues at the time individuals are booked into jail so they can be referred for appropriate interventions.
Achieving positive public health and safety outcomes requires changes to policy and practice, Dr. Osher said.
The JPLI primer is a step toward making such changes, and with it comes a set of four principles:
1. Conduct universal risk, substance use, and mental health screening at booking, and full assessments as appropriate, he said, noting that “13 million times this year (9 million unduplicated count), 2 million folks with serious mental illness are going to be arrested and brought to jail. Let’s make sure they get assessed, identified, and then a plan can be made.”
2. Get relevant information into the hands of decision makers in time to inform pretrial release decisions. For example, knowing if someone is eligible for a mental health court could lead to that person’s receiving necessary support and supervision, he said.
3. Use assessment information to connect people to appropriate jail-based services and post-release services and supervision, and ensure that there is communication between the two.
4. Ensure services and supervision are evidence based and hold systems accountable by measuring outcomes.
In addition, the goal is to partner with the criminal justice system through information-sharing agreements and integrating dynamic criminogenic risk factors into treatment plans, he said.
The intercepts
To demonstrate ways in which psychiatrists can intervene over the course of a patients’ journey toward involvement in the criminal justice system, Stephanie Le Melle, MD, provided a case example involving a 30-year-old African American man diagnosed with schizophrenia at age 18 years.

As a child, “Joe” was neglected and abused; both parents had a history of mental illness and substance use. He experienced homelessness, never finished high school, and was hospitalized or visited the emergency department more than 15 times after going off medications or because of intoxication.
His history with the legal system involved a first arrest at age 14 years for gang-related fighting and assault (after being bullied as a child and seeking safety in a gang), followed by 3 years in juvenile detention. He was released with supervision at age 17 years, was arrested several times after that for public intoxication and loitering, and was held for several days or weeks each time – then released with time served or summons paid. His first hospitalization occurred at age 18, when he was diagnosed with psychosis.
Subsequent experiences included treatment in a community mental health program at age 25 for heroin use and drinking. However, he was denied admission to a substance abuse program because of his history of psychosis and violence. After stopping his medications because of side effects, he tried to buy heroin, got into a fight, and was arrested for assault with a pocket knife. He resisted arrest and was tasered, handcuffed, and taken to prison, where he was held because he could not afford bail. Involvement in gang activity while in prison led to sanctions, including time in solitary confinement.
During all of his time in the criminal justice system, Joe refused treatment, because he was afraid he’d be considered “crazy” and would be preyed upon even more by other inmates. After about 3 years, he was released to a Forensic Assertive Community Treatment team for 2 years and completed that program, and is now receiving treatment in the community. He lives alone in supported housing and has Supplemental Security Income. He does not engage in clinic-related activities and has a lack of trust in the clinical team. He often is agitated and disruptive in the clinic. Staff members have concerns about his history of violence and drug use, and were reluctant to bring him into the program.
“Going back to ... the sequential intercept model, we can think about things, as psychiatrists, that we could have done for Joe all along the way to help him not get into the criminal justice system in the first place,” said Dr. Le Melle, director of public psychiatry education at Columbia University/New York State Psychiatric Institute, New York.
This is a framework for thinking through treatment for a patient like Joe:
Intercept 0 (community services). At this early stage, Joe would have been screened for adverse childhood experiences, and that could have led to trauma treatment, substance abuse treatment, and educational and vocational services. Awareness of his family illness, discord, and poverty would have led to parenting interventions, early school involvement, and promotion of meaningful activities, she said.
“These are things, again, that we can address as clinicians ... to intervene with families and with schools and communities to try to give young people an opportunity to not get into the criminal justice system,” she said, adding that providing early co-occurring treatment for mental health and substance use is particularly important.
Intercept 1 (law enforcement) also is a stage during which a psychiatrist can intervene by giving pertinent information when 911 is called by providing police or corrections with contact information for follow-up. For Joe, psychiatrist involvement at this intercept could have allowed for treatment recommendations or assessment for diversion programs, and in fact, at some point during his care, did allow for communication about his treatment needs, Dr. Le Melle said.
In general, psychiatrists also can participate at this stage through provision of crisis intervention team training for first responders or by being part of a co-response team, she said.
Intercept 2 (initial detention/initial court hearings). Attending court on behalf of a patient can make a real difference in outcomes, she noted.
“Judges want to know that someone is out there who can help, and they want to know that there’s a team of people who can intervene and try to get someone out of the criminal justice system,” she said.
At this stage, psychiatrists can help by recommending a treatment plan for a diversion program, and – within HIPAA guidelines – can share pertinent information about treatment needs and preferences.
Intercept 3 (jails/courts). At this in-the-system stage, information shared between corrections and community behavioral health would have led to Joe’s transfer to a mental health/observation unit; he would have been offered mental health treatment and been started on substance use treatment; and he would have participated in motivational treatment and cognitive-behavioral therapy targeting his criminogenic needs, she said.
Meeting with individuals while they are incarcerated can be helpful for “keeping them grounded.”
This also is a stage where psychiatrists could help individuals prepare for release by getting them into a GED program or other training.
Intercept 4 (reentry). With appropriate intervention at this stage, Joe would have his benefits, such as Medicaid and Supplemental Security Income, reinstated prior to reentry to the community. Also, his psychiatrist and treatment program would be contacted. He would be welcomed back into treatment, and he would have assistance finding a permanent place to live with services provided in the community.
Intercept 5 (community corrections). At this stage, community behavioral health clinicians would maintain awareness of their biases and fears about people involved in the criminal justice system and avoid making assumptions about Joe. His risks, needs, and priorities would be assessed and addressed, and he would be asked about his experiences with the system and about what could be done to help him avoid incarceration in the future.
He would receive help in incorporating alternative behaviors and thinking to address dynamic criminogenic risk, and evidence-based practices would be used in treatment.
The sequential intercept model reflects the fact that the criminal justice system and the people it serves are part of the community, Dr. Le Melle said.
“The community and the behavioral health system and the criminal justice system are partners in our shared mission of public safety and public health, so we are one and we can’t expect that our responsibility for providing people with the best care and services ends if someone is in the criminal justice system,” she said.
Dr. Champion, Dr. Osher, and Dr. Le Melle reported having no disclosures.
NEW YORK – The overrepresentation of people with serious mental illness (SMI) in the criminal justice system has led to creation of a resource from the Judges’ and Psychiatrists’ Leadership Initiative (JPLI) aimed at helping psychiatry and law enforcement address the problem.
The resource, “Supporting People with Serious Mental Illnesses and Reducing Their Risk of Contact with the Criminal Justice System: A Primer for Psychiatrists,” released last year, was designed to provide psychiatrists with specific knowledge and tools, according to Michael Champion, MD, forensic chief at the Hawaii State Department of Health, Adult Mental Health Division, Honolulu, and a member of the JPLI executive leadership team.
In developing the primer, the JPLI, which was created about 10 years ago by the American Psychiatric Association Foundation in partnership with the Council of State Governments Justice Center in response to the growing problem of such overrepresentation, sought to teach psychiatrists about what the criminal justice literature has dubbed “criminogenic risk” and to explore strategies to address those risks in community treatment settings, Dr. Champion said at the annual meeting of the American Psychiatric Association.
“The fact is that one in three Americans has a criminal record, and people with serious mental illness and criminal justice involvement are frequently part of our patient population – particularly in the public mental health sector,” Dr. Champion said. “Part of the challenge is that psychiatrists ... aren’t typically trained in these principles ... so the JPLI saw that this as an area that we could try to make some traction in and try to make a difference.”
The JPLI’s goals in publishing this resource are to reduce the risk of patient involvement in the criminal justice system, and to improve clinical and recovery outcomes by educating community psychiatrists about Risk-Need-Responsivity (RNR) principles. The JPLI also seeks to provide strategies for collaborating with criminal justice partners, incorporating criminal justice history into screening and assessment, and integrating criminogenic risk needs of patients into comprehensive treatment plans, Dr. Champion said.
Criminogenic risk and RNR
Many factors contribute to the involvement of people with serious mental illnesses in the criminal justice system, including higher rates of arrest, longer stays, recidivism, and limited access to health care, said Fred C. Osher, MD, former director of health systems and services policy for the Council of State Governments Justice Center.
“We used to think that ... if we could just get folks the health care that they need, they wouldn’t get involved with the criminal justice system. It turns out that that’s a gross oversimplification, in that their needs are terribly complex, and while treatment is a necessary component, it isn’t often sufficient for a large number of individuals,” said Dr. Osher, now a member of the JPLI executive leadership team.
Criminogenic risk – the likelihood that a person who has been arrested and jailed will commit a new crime after release or return to custody – helps explain why that is the case, he said, adding: “We have ways in which we can understand those risks.”
The risks are measured via static factors (unchanging conditions such as criminal history, age at first arrest, current age, and gender) and dynamic factors, he explained.
he said, noting that the research has shown there are eight specific criminogenic risk factors: substance abuse, history of antisocial behavior, antisocial personality pattern, antisocial cognition, antisocial associates, family and/or marital discord, poor school and/or work output, and having few leisure/recreation outlets.
Notably, mental illness is not a part of that list, he said.
“The reason for that is it’s not explanatory in and of itself,” he added.
However, research shows that people with mental illness have more of these dynamic risk factors, and research by Jennifer L. Skeem, PhD, and others shows that those with mental illness were coming back to jail not for new criminal activity, but for failing to comply with their conditions of release.
“These risks, then, have been brought into a paradigm that is central to our criminal justice operations, and it’s called the Risk-Need-Responsivity model,” Dr. Osher said. “This paradigm is what allows a criminal justice system to think about how to prioritize the resources – to think about who really needs to be wrapped tight, who needs to have close supervision, frequent reporting, lots of contact.”
The risk principle in the RNR model says that resources should be focused on high-risk cases, with limited supervision in lower-risk cases. This is based on experience demonstrating that recidivism is lower in high-risk individuals with close supervision but higher in low-risk individuals with close supervision.
The needs principle suggests that dynamic needs are “the issues that get folks in trouble,” he said.
“So, if we’re going to intervene, if we’re going to provide programming, if we’re going to try and help that individual stay out of jail or prison, we need to address these criminogenic needs,” he said, adding that the “big four” are related to their antisocial thinking and personality and friends.
Targeted interventions can help those individuals make better choices going forward, he noted.
The responsivity principle is an acknowledgment that individuals have different ways of learning, different cultural factors and backgrounds that influence them, and social determinants that are important to understand if they predict the ability to stay out of trouble.
“This is where mental illness fits in,” Dr. Osher said. “It’s absolutely important that we understand that.”
Examples would be patients with severe major depressive disorder who need their depression treated before they can participate in a group treatment setting designed to address criminogenic risks.
Dynamic risk factors are best treated with cognitive-behavioral interventions, Dr. Osher said, noting that the most effective interventions provide opportunities for participants to practice new behavior patterns and skills with feedback from program staff.
In many states, those interventions are being provided by criminal justice personnel, including probation officers, partly because of “an absence of [psychiatrists’] understanding, willingness, or ability to step forward.” The JPLI primer is designed to “really amp up our own excitement about, and willingness to learn how to develop interventions to help that individual stay out of trouble,” and it includes detailed descriptions of numerous well-researched, standardized, manualized interventions that people can access that make it less likely for them to have criminal justice access going forward, he said.
Those include programs such as “Thinking for a Change,” “Reasoning and Rehabilitation,” “Moral Reconation Therapy,” and “Interactive Journaling.”
A focus on the Sequential Intercept Model, which describes how individuals move through the criminal justice system, illustrates multiple points where psychiatrists can “do things better and differently to intervene,” he said, noting that the primer includes a framework for prioritizing the target population, and validated screening and assessment tools, including tools to help corrections officers identify mental health/substance abuse/criminogenic issues at the time individuals are booked into jail so they can be referred for appropriate interventions.
Achieving positive public health and safety outcomes requires changes to policy and practice, Dr. Osher said.
The JPLI primer is a step toward making such changes, and with it comes a set of four principles:
1. Conduct universal risk, substance use, and mental health screening at booking, and full assessments as appropriate, he said, noting that “13 million times this year (9 million unduplicated count), 2 million folks with serious mental illness are going to be arrested and brought to jail. Let’s make sure they get assessed, identified, and then a plan can be made.”
2. Get relevant information into the hands of decision makers in time to inform pretrial release decisions. For example, knowing if someone is eligible for a mental health court could lead to that person’s receiving necessary support and supervision, he said.
3. Use assessment information to connect people to appropriate jail-based services and post-release services and supervision, and ensure that there is communication between the two.
4. Ensure services and supervision are evidence based and hold systems accountable by measuring outcomes.
In addition, the goal is to partner with the criminal justice system through information-sharing agreements and integrating dynamic criminogenic risk factors into treatment plans, he said.
The intercepts
To demonstrate ways in which psychiatrists can intervene over the course of a patients’ journey toward involvement in the criminal justice system, Stephanie Le Melle, MD, provided a case example involving a 30-year-old African American man diagnosed with schizophrenia at age 18 years.
As a child, “Joe” was neglected and abused; both parents had a history of mental illness and substance use. He experienced homelessness, never finished high school, and was hospitalized or visited the emergency department more than 15 times after going off medications or because of intoxication.
His history with the legal system involved a first arrest at age 14 years for gang-related fighting and assault (after being bullied as a child and seeking safety in a gang), followed by 3 years in juvenile detention. He was released with supervision at age 17 years, was arrested several times after that for public intoxication and loitering, and was held for several days or weeks each time – then released with time served or summons paid. His first hospitalization occurred at age 18, when he was diagnosed with psychosis.
Subsequent experiences included treatment in a community mental health program at age 25 for heroin use and drinking. However, he was denied admission to a substance abuse program because of his history of psychosis and violence. After stopping his medications because of side effects, he tried to buy heroin, got into a fight, and was arrested for assault with a pocket knife. He resisted arrest and was tasered, handcuffed, and taken to prison, where he was held because he could not afford bail. Involvement in gang activity while in prison led to sanctions, including time in solitary confinement.
During all of his time in the criminal justice system, Joe refused treatment, because he was afraid he’d be considered “crazy” and would be preyed upon even more by other inmates. After about 3 years, he was released to a Forensic Assertive Community Treatment team for 2 years and completed that program, and is now receiving treatment in the community. He lives alone in supported housing and has Supplemental Security Income. He does not engage in clinic-related activities and has a lack of trust in the clinical team. He often is agitated and disruptive in the clinic. Staff members have concerns about his history of violence and drug use, and were reluctant to bring him into the program.
“Going back to ... the sequential intercept model, we can think about things, as psychiatrists, that we could have done for Joe all along the way to help him not get into the criminal justice system in the first place,” said Dr. Le Melle, director of public psychiatry education at Columbia University/New York State Psychiatric Institute, New York.
This is a framework for thinking through treatment for a patient like Joe:
Intercept 0 (community services). At this early stage, Joe would have been screened for adverse childhood experiences, and that could have led to trauma treatment, substance abuse treatment, and educational and vocational services. Awareness of his family illness, discord, and poverty would have led to parenting interventions, early school involvement, and promotion of meaningful activities, she said.
“These are things, again, that we can address as clinicians ... to intervene with families and with schools and communities to try to give young people an opportunity to not get into the criminal justice system,” she said, adding that providing early co-occurring treatment for mental health and substance use is particularly important.
Intercept 1 (law enforcement) also is a stage during which a psychiatrist can intervene by giving pertinent information when 911 is called by providing police or corrections with contact information for follow-up. For Joe, psychiatrist involvement at this intercept could have allowed for treatment recommendations or assessment for diversion programs, and in fact, at some point during his care, did allow for communication about his treatment needs, Dr. Le Melle said.
In general, psychiatrists also can participate at this stage through provision of crisis intervention team training for first responders or by being part of a co-response team, she said.
Intercept 2 (initial detention/initial court hearings). Attending court on behalf of a patient can make a real difference in outcomes, she noted.
“Judges want to know that someone is out there who can help, and they want to know that there’s a team of people who can intervene and try to get someone out of the criminal justice system,” she said.
At this stage, psychiatrists can help by recommending a treatment plan for a diversion program, and – within HIPAA guidelines – can share pertinent information about treatment needs and preferences.
Intercept 3 (jails/courts). At this in-the-system stage, information shared between corrections and community behavioral health would have led to Joe’s transfer to a mental health/observation unit; he would have been offered mental health treatment and been started on substance use treatment; and he would have participated in motivational treatment and cognitive-behavioral therapy targeting his criminogenic needs, she said.
Meeting with individuals while they are incarcerated can be helpful for “keeping them grounded.”
This also is a stage where psychiatrists could help individuals prepare for release by getting them into a GED program or other training.
Intercept 4 (reentry). With appropriate intervention at this stage, Joe would have his benefits, such as Medicaid and Supplemental Security Income, reinstated prior to reentry to the community. Also, his psychiatrist and treatment program would be contacted. He would be welcomed back into treatment, and he would have assistance finding a permanent place to live with services provided in the community.
Intercept 5 (community corrections). At this stage, community behavioral health clinicians would maintain awareness of their biases and fears about people involved in the criminal justice system and avoid making assumptions about Joe. His risks, needs, and priorities would be assessed and addressed, and he would be asked about his experiences with the system and about what could be done to help him avoid incarceration in the future.
He would receive help in incorporating alternative behaviors and thinking to address dynamic criminogenic risk, and evidence-based practices would be used in treatment.
The sequential intercept model reflects the fact that the criminal justice system and the people it serves are part of the community, Dr. Le Melle said.
“The community and the behavioral health system and the criminal justice system are partners in our shared mission of public safety and public health, so we are one and we can’t expect that our responsibility for providing people with the best care and services ends if someone is in the criminal justice system,” she said.
Dr. Champion, Dr. Osher, and Dr. Le Melle reported having no disclosures.
NEW YORK – The overrepresentation of people with serious mental illness (SMI) in the criminal justice system has led to creation of a resource from the Judges’ and Psychiatrists’ Leadership Initiative (JPLI) aimed at helping psychiatry and law enforcement address the problem.
The resource, “Supporting People with Serious Mental Illnesses and Reducing Their Risk of Contact with the Criminal Justice System: A Primer for Psychiatrists,” released last year, was designed to provide psychiatrists with specific knowledge and tools, according to Michael Champion, MD, forensic chief at the Hawaii State Department of Health, Adult Mental Health Division, Honolulu, and a member of the JPLI executive leadership team.
In developing the primer, the JPLI, which was created about 10 years ago by the American Psychiatric Association Foundation in partnership with the Council of State Governments Justice Center in response to the growing problem of such overrepresentation, sought to teach psychiatrists about what the criminal justice literature has dubbed “criminogenic risk” and to explore strategies to address those risks in community treatment settings, Dr. Champion said at the annual meeting of the American Psychiatric Association.
“The fact is that one in three Americans has a criminal record, and people with serious mental illness and criminal justice involvement are frequently part of our patient population – particularly in the public mental health sector,” Dr. Champion said. “Part of the challenge is that psychiatrists ... aren’t typically trained in these principles ... so the JPLI saw that this as an area that we could try to make some traction in and try to make a difference.”
The JPLI’s goals in publishing this resource are to reduce the risk of patient involvement in the criminal justice system, and to improve clinical and recovery outcomes by educating community psychiatrists about Risk-Need-Responsivity (RNR) principles. The JPLI also seeks to provide strategies for collaborating with criminal justice partners, incorporating criminal justice history into screening and assessment, and integrating criminogenic risk needs of patients into comprehensive treatment plans, Dr. Champion said.
Criminogenic risk and RNR
Many factors contribute to the involvement of people with serious mental illnesses in the criminal justice system, including higher rates of arrest, longer stays, recidivism, and limited access to health care, said Fred C. Osher, MD, former director of health systems and services policy for the Council of State Governments Justice Center.
“We used to think that ... if we could just get folks the health care that they need, they wouldn’t get involved with the criminal justice system. It turns out that that’s a gross oversimplification, in that their needs are terribly complex, and while treatment is a necessary component, it isn’t often sufficient for a large number of individuals,” said Dr. Osher, now a member of the JPLI executive leadership team.
Criminogenic risk – the likelihood that a person who has been arrested and jailed will commit a new crime after release or return to custody – helps explain why that is the case, he said, adding: “We have ways in which we can understand those risks.”
The risks are measured via static factors (unchanging conditions such as criminal history, age at first arrest, current age, and gender) and dynamic factors, he explained.
he said, noting that the research has shown there are eight specific criminogenic risk factors: substance abuse, history of antisocial behavior, antisocial personality pattern, antisocial cognition, antisocial associates, family and/or marital discord, poor school and/or work output, and having few leisure/recreation outlets.
Notably, mental illness is not a part of that list, he said.
“The reason for that is it’s not explanatory in and of itself,” he added.
However, research shows that people with mental illness have more of these dynamic risk factors, and research by Jennifer L. Skeem, PhD, and others shows that those with mental illness were coming back to jail not for new criminal activity, but for failing to comply with their conditions of release.
“These risks, then, have been brought into a paradigm that is central to our criminal justice operations, and it’s called the Risk-Need-Responsivity model,” Dr. Osher said. “This paradigm is what allows a criminal justice system to think about how to prioritize the resources – to think about who really needs to be wrapped tight, who needs to have close supervision, frequent reporting, lots of contact.”
The risk principle in the RNR model says that resources should be focused on high-risk cases, with limited supervision in lower-risk cases. This is based on experience demonstrating that recidivism is lower in high-risk individuals with close supervision but higher in low-risk individuals with close supervision.
The needs principle suggests that dynamic needs are “the issues that get folks in trouble,” he said.
“So, if we’re going to intervene, if we’re going to provide programming, if we’re going to try and help that individual stay out of jail or prison, we need to address these criminogenic needs,” he said, adding that the “big four” are related to their antisocial thinking and personality and friends.
Targeted interventions can help those individuals make better choices going forward, he noted.
The responsivity principle is an acknowledgment that individuals have different ways of learning, different cultural factors and backgrounds that influence them, and social determinants that are important to understand if they predict the ability to stay out of trouble.
“This is where mental illness fits in,” Dr. Osher said. “It’s absolutely important that we understand that.”
Examples would be patients with severe major depressive disorder who need their depression treated before they can participate in a group treatment setting designed to address criminogenic risks.
Dynamic risk factors are best treated with cognitive-behavioral interventions, Dr. Osher said, noting that the most effective interventions provide opportunities for participants to practice new behavior patterns and skills with feedback from program staff.
In many states, those interventions are being provided by criminal justice personnel, including probation officers, partly because of “an absence of [psychiatrists’] understanding, willingness, or ability to step forward.” The JPLI primer is designed to “really amp up our own excitement about, and willingness to learn how to develop interventions to help that individual stay out of trouble,” and it includes detailed descriptions of numerous well-researched, standardized, manualized interventions that people can access that make it less likely for them to have criminal justice access going forward, he said.
Those include programs such as “Thinking for a Change,” “Reasoning and Rehabilitation,” “Moral Reconation Therapy,” and “Interactive Journaling.”
A focus on the Sequential Intercept Model, which describes how individuals move through the criminal justice system, illustrates multiple points where psychiatrists can “do things better and differently to intervene,” he said, noting that the primer includes a framework for prioritizing the target population, and validated screening and assessment tools, including tools to help corrections officers identify mental health/substance abuse/criminogenic issues at the time individuals are booked into jail so they can be referred for appropriate interventions.
Achieving positive public health and safety outcomes requires changes to policy and practice, Dr. Osher said.
The JPLI primer is a step toward making such changes, and with it comes a set of four principles:
1. Conduct universal risk, substance use, and mental health screening at booking, and full assessments as appropriate, he said, noting that “13 million times this year (9 million unduplicated count), 2 million folks with serious mental illness are going to be arrested and brought to jail. Let’s make sure they get assessed, identified, and then a plan can be made.”
2. Get relevant information into the hands of decision makers in time to inform pretrial release decisions. For example, knowing if someone is eligible for a mental health court could lead to that person’s receiving necessary support and supervision, he said.
3. Use assessment information to connect people to appropriate jail-based services and post-release services and supervision, and ensure that there is communication between the two.
4. Ensure services and supervision are evidence based and hold systems accountable by measuring outcomes.
In addition, the goal is to partner with the criminal justice system through information-sharing agreements and integrating dynamic criminogenic risk factors into treatment plans, he said.
The intercepts
To demonstrate ways in which psychiatrists can intervene over the course of a patients’ journey toward involvement in the criminal justice system, Stephanie Le Melle, MD, provided a case example involving a 30-year-old African American man diagnosed with schizophrenia at age 18 years.
As a child, “Joe” was neglected and abused; both parents had a history of mental illness and substance use. He experienced homelessness, never finished high school, and was hospitalized or visited the emergency department more than 15 times after going off medications or because of intoxication.
His history with the legal system involved a first arrest at age 14 years for gang-related fighting and assault (after being bullied as a child and seeking safety in a gang), followed by 3 years in juvenile detention. He was released with supervision at age 17 years, was arrested several times after that for public intoxication and loitering, and was held for several days or weeks each time – then released with time served or summons paid. His first hospitalization occurred at age 18, when he was diagnosed with psychosis.
Subsequent experiences included treatment in a community mental health program at age 25 for heroin use and drinking. However, he was denied admission to a substance abuse program because of his history of psychosis and violence. After stopping his medications because of side effects, he tried to buy heroin, got into a fight, and was arrested for assault with a pocket knife. He resisted arrest and was tasered, handcuffed, and taken to prison, where he was held because he could not afford bail. Involvement in gang activity while in prison led to sanctions, including time in solitary confinement.
During all of his time in the criminal justice system, Joe refused treatment, because he was afraid he’d be considered “crazy” and would be preyed upon even more by other inmates. After about 3 years, he was released to a Forensic Assertive Community Treatment team for 2 years and completed that program, and is now receiving treatment in the community. He lives alone in supported housing and has Supplemental Security Income. He does not engage in clinic-related activities and has a lack of trust in the clinical team. He often is agitated and disruptive in the clinic. Staff members have concerns about his history of violence and drug use, and were reluctant to bring him into the program.
“Going back to ... the sequential intercept model, we can think about things, as psychiatrists, that we could have done for Joe all along the way to help him not get into the criminal justice system in the first place,” said Dr. Le Melle, director of public psychiatry education at Columbia University/New York State Psychiatric Institute, New York.
This is a framework for thinking through treatment for a patient like Joe:
Intercept 0 (community services). At this early stage, Joe would have been screened for adverse childhood experiences, and that could have led to trauma treatment, substance abuse treatment, and educational and vocational services. Awareness of his family illness, discord, and poverty would have led to parenting interventions, early school involvement, and promotion of meaningful activities, she said.
“These are things, again, that we can address as clinicians ... to intervene with families and with schools and communities to try to give young people an opportunity to not get into the criminal justice system,” she said, adding that providing early co-occurring treatment for mental health and substance use is particularly important.
Intercept 1 (law enforcement) also is a stage during which a psychiatrist can intervene by giving pertinent information when 911 is called by providing police or corrections with contact information for follow-up. For Joe, psychiatrist involvement at this intercept could have allowed for treatment recommendations or assessment for diversion programs, and in fact, at some point during his care, did allow for communication about his treatment needs, Dr. Le Melle said.
In general, psychiatrists also can participate at this stage through provision of crisis intervention team training for first responders or by being part of a co-response team, she said.
Intercept 2 (initial detention/initial court hearings). Attending court on behalf of a patient can make a real difference in outcomes, she noted.
“Judges want to know that someone is out there who can help, and they want to know that there’s a team of people who can intervene and try to get someone out of the criminal justice system,” she said.
At this stage, psychiatrists can help by recommending a treatment plan for a diversion program, and – within HIPAA guidelines – can share pertinent information about treatment needs and preferences.
Intercept 3 (jails/courts). At this in-the-system stage, information shared between corrections and community behavioral health would have led to Joe’s transfer to a mental health/observation unit; he would have been offered mental health treatment and been started on substance use treatment; and he would have participated in motivational treatment and cognitive-behavioral therapy targeting his criminogenic needs, she said.
Meeting with individuals while they are incarcerated can be helpful for “keeping them grounded.”
This also is a stage where psychiatrists could help individuals prepare for release by getting them into a GED program or other training.
Intercept 4 (reentry). With appropriate intervention at this stage, Joe would have his benefits, such as Medicaid and Supplemental Security Income, reinstated prior to reentry to the community. Also, his psychiatrist and treatment program would be contacted. He would be welcomed back into treatment, and he would have assistance finding a permanent place to live with services provided in the community.
Intercept 5 (community corrections). At this stage, community behavioral health clinicians would maintain awareness of their biases and fears about people involved in the criminal justice system and avoid making assumptions about Joe. His risks, needs, and priorities would be assessed and addressed, and he would be asked about his experiences with the system and about what could be done to help him avoid incarceration in the future.
He would receive help in incorporating alternative behaviors and thinking to address dynamic criminogenic risk, and evidence-based practices would be used in treatment.
The sequential intercept model reflects the fact that the criminal justice system and the people it serves are part of the community, Dr. Le Melle said.
“The community and the behavioral health system and the criminal justice system are partners in our shared mission of public safety and public health, so we are one and we can’t expect that our responsibility for providing people with the best care and services ends if someone is in the criminal justice system,” she said.
Dr. Champion, Dr. Osher, and Dr. Le Melle reported having no disclosures.
REPORTING FROM APA 2018
ADA/EASD: Draft consensus statement on managing hyperglycemia in T2DM
ORLANDO – according to a draft consensus report on the management of hyperglycemia in patients with type 2 diabetes mellitus (T2DM).
The report, a project of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD), is currently under review and will be presented in final form Oct. 5 at the EASD annual meeting in Berlin.
The current draft calls, generally, for the initial use of metformin followed by the addition of antihyperglycemic medications based on patient comorbidities and concerns “as we await answers to the many questions that remain,” John Buse, MD, PhD, cochair of the consensus statement writing group, said during a summary of the draft recommendations at the annual scientific sessions of the ADA.
The first step, however, is to assess key patient characteristics; these can include comorbidities, clinical characteristics, issues such as motivation and depression, and cultural and socio-economic context, Deborah J. Wexler, MD, 1 of 10 writing group members, said during the same presentation.
Patients with ASCVD or heart failure
Given new evidence from trials such as EMPA-REG and LEADER showing outcomes benefits with the use of specific antihyperglycemic medications in patients with established atherosclerotic cardiovascular disease (ASCVD), an important early step in the proposed approach is to consider the presence or absence of ASCVD and heart failure, said Dr. Wexler of Massachusetts General Hospital, Boston.
“The presence of cardiovascular disease is a compelling indication for the selection of certain glucose-lowering drugs,” she said.
The draft consensus recommendation in this regard – a new recommendation since the last consensus report in 2015 – differentiates between T2DM patients in whom ASCVD predominates and those in whom heart failure predominates.
“What’s new since 2015 is that we recommend that these comorbidities be considered first and foremost because they do influence the choice of a particular glucose-lowering medication, and the recommendation is that, among patients with type 2 diabetes with established ASCVD, sodium-glucose cotransporter 2 [SGLT2] inhibitors or glucagonlike peptide 1 [GLP-1] receptor agonists with proven cardiovascular benefit are recommended as part of glycemic management,” she said.
However, it is important to note that ASCVD is defined differently across trials, and patients considered in the development of these recommendations are those with much higher cardiovascular risk than the average patient with T2DM, she added.
“It’s also important to keep in mind that each cardiovascular outcomes trial, while large, is but a single experiment ... and we don’t have the benefit of replication,” she said, noting that it is not always clear whether differences in trial findings within a drug class are related to trial design or true differences in individual medications.
“So we try to read into them and interpret these data, but it’s just important to consider that ... and when evidence suggests a hierarchy, we noted that,” she said.
That said, if ASCVD predominates, the recommendation is for treatment with either a GLP-1 receptor agonist with proven cardiovascular benefit (favoring liraglutide over semaglutide and over long-acting exenatide) or an SGLT2 inhibitor with proven cardiovascular benefit if estimated glomerular filtration (eGFR) is adequate (favoring empagliflozin over canagliflozin).
These recommendations are based on the LEADER trial finding of significant improvement in the primary outcome of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke with liraglutide vs. placebo (hazard ratio, 0.87; number needed to treat [NNT], 52 over 3.8 years) and on the EMPA-REG trial finding of significant improvement in the same primary outcome with empagliflozin vs. placebo (HR, 0.86; NNT, 62 over 3.1 years).
Keep in mind that there is no evidence of cardiovascular benefit from these treatments in patients at lower risk and also that the “expensive and complicated” combination of an SGLT2 inhibitor and a GLP-1 receptor agonist has not been tested in cardiovascular outcomes trials and there is no evidence of additional benefit from a cardiovascular perspective with this combination, Dr. Wexler said.
If heart failure predominates, the recommendations call for consideration of an SGLT2 inhibitor as part of the treatment strategy because patients with T2DM are at increased risk for heart failure with reduced or preserved ejection fraction and because significant, consistent reduction in hospitalizations for heart failure were seen in SGLT2 inhibitor trials, writing group member Peter Rossing, MD, explained during the session; he noted, however, that the trials were not designed to adjudicate heart failure and that most patients did not have clinical heart failure at baseline.
In those in whom SGLT2 inhibitors are contraindicated – because of impaired renal function, for example – a GLP-1 receptor agonist with proven cardiovascular benefit is recommended.
“Then we suggest that if you are still not at [hemoglobin A1c] target, you should avoid thiazolidinediones [TZD] because of the risk of fluid overload, and you could then consider, if needed, combining an SGLT2-inhibitor and a GLP-1 receptor agonist ... or you could use a [dipeptidyl peptidase–4 (DPP-4) inhibitor] if you are not on an GLP-1 receptor agonist. And we point out that saxagliptin has unfavorable data on heart failure,” Dr. Rossing of Steno Diabetes Center, Copenhagen, said, noting that basal insulin or sulfonylurea are other alternative options.
In EMPA-REG, hospitalization for heart failure was reduced by 35% with empagliflozin vs. placebo (HR, 0.65; NNT, 71 over 3 years), and similar findings were seen in the CANVAS trial. In LEADER, a nonsignificant 13% reduction was seen in hospitalization for heart failure with liraglutide vs. placebo (HR, 0.87). However, this was a secondary outcome; ongoing studies are addressing heart failure as a primary outcome, Dr. Rossing said.
The report also includes a recommendation that, for patients with chronic kidney disease and high cardiovascular risk, GLP-1 receptor agonists and SGLT2 inhibitors can be used but with dose reductions for some medications – several of which have demonstrated renal benefit and cardiovascular benefits in those populations and can be considered as part of treatment.
Lifestyle management and medication
With respect to lifestyle management and pharmacologic treatment, the proposed recommendations, which are based on several large trials, state that an individualized program of medical nutritional therapy should be offered to all patients and that all overweight and obese patients with diabetes should be advised of the health benefits of weight loss. They also should be encouraged to engage in a program of intensive lifestyle management, which may include food substitution, writing group member Walter Kernan, MD, said at the meeting.
In the DiRECT Trial, the average weight loss was about 10 kg in an intervention group that had complete food replacement for 3 months followed by gradual food reintroduction and ongoing counseling versus about 1 kg in controls, and the diabetes remission rate at 1 year was 46% versus 4%, respectively, said Dr. Kernan of Yale University, New Haven, Conn.
In addition, intentional physical activity is known to improve glycemic control and should be encouraged in all patients with T2DM, he said.
“The foundation of hyperglycemia treatment in type 2 diabetes is, for sure, lifestyle modification,” said group member Geltrude Mingrone, MD, of Catholic University of the Sacred Heart in Rome. “Those patients who are very well motivated and adherent to the [recommendations] can achieve very good results,” she added.
In those in whom lifestyle modification fails to lead to adequate improvement, “a pretty large medication portfolio is available,” she said, adding that the choice of treatment should be based on safety, efficacy, cost, and convenience, factors which are described in the statement.
The hope is that the final consensus statement will make it easier to navigate them, she said.
Finally, bariatric surgery can be considered a very effective salvage therapy, Dr. Mingrone said, noting that only lifestyle modification or bariatric surgery will lead to diabetes remission.
The draft consensus recommendation for bariatric surgery is to consider it in patients with T2DM and a body mass index of 40 kg/m2 or greater (37.5 or greater in those of Asian ancestry), regardless of the level of glycemic control, and in those with BMI of 35-39.9 (32.5-37.4 in those of Asian ancestry) when hyperglycemia is inadequately controlled despite lifestyle and optimal medical therapy.
Decision making and injectable therapies
The statement includes decision-making strategies and algorithms for treatment and addresses issues such as choosing antihyperglycemic medications when weight is a concern (consider an SGLT2 inhibitor or a GLP-1 receptor agonist with good efficacy for weight loss to start – or a combination of both if HbA1c is not on target), when minimizing hypoglycemia is the priority (consider adding an SGLT2 inhibitors, GLP-1 receptor agonist, a TZD, or a DPP-4 inhibitor to metformin therapy to start, followed by reintensification of lifestyle modifications and combination therapies if HbA1c is above target), and when drug costs need to be minimized, as well as when and how to initiate injectable therapies, according to writing group members David D’Alessio, MD, of Duke University, Durham, N.C, and Chantal Mathieu, MD, of Katholieke Universteit Leuven (Belgium).
The draft consensus recommendation regarding the latter is that, in patients who need the greater glucose-lowering effect of an injectable medication, GLP-1 receptor agonists should be considered as the first choice and that, when insulin is the medication of choice on the basis of clinical characteristics, basal insulin is preferred. Additionally, in patients who are unable to maintain glycemic targets on basal insulin in combination with oral medication, intensification with a GLP-1 receptor agonist, SGLT2 inhibitor, or prandial insulin can be considered.
This recommendation is based on “overwhelming evidence that GLP-1 receptor agonists give you HbA1c lowering in the same range as basal insulin but can do so without hypoglycemia and with weight loss, in contrast to weight gain with most insulin preparations,” Dr. Mathieu noted.
The bottom line, however, is that “the patient is at the center of everything and ... should become an integral part of the team treating this patient,” Dr. Mathieu said.
Knowledge gaps
In a review of remaining knowledge gaps regarding glycemic control in T2DM, Dr. Buse said that, while the tools available to treat and prevent diabetes are vastly improved, implementation of effective innovation has lagged behind and “requires fundamental changes in health care policy and societal approaches to wellness.”
Additionally, the management of overweight and obesity is clearly inadequate and requires much greater emphasis on lifestyle techniques, behavioral approaches, medication, and surgery, said Dr. Buse, who is the Verne S. Caviness distinguished professor and chief of the division of endocrinology, as well as director of the Diabetes Center, at the University of North Carolina, Chapel Hill.
These and numerous other knowledge gaps (with respect to preserving and enhancing beta-cell function, incorporating personalized medicine, the value of combinations for additive benefit, the identification of biomarkers, the use of early intensive therapy, metabolic surgery decision making, the value of self-monitoring of blood glucose, and the need for better drugs – including those for the primary prevention of cardiovascular disease) need to be addressed and “require additional investment in basic, translational, clinical, and implementation research,” he said.
“More time- and cost-efficient research paradigms to address patient-centered endpoints are needed through regulatory reform and leveraging informatics and coordinated learning health care systems. Additionally, the increasing burden of cardiometabolic disease is an existential threat to society,” he said, stressing that “urgent attention to improve prevention and treatment is of the essence.”
Consensus statement development
The draft consensus statement is the work of group members selected by the ADA and EASD to ensure regional representation (five each from the United States and Europe). The group had two face-to-face meetings, as well as regular teleconferences; the members also conducted a “robust evidence review, which informed the content,” said group cochair Melanie J. Davies, MD, of the University of Leicester (U.K.).
The group reviewed randomized controlled trials, systematic reviews, and meta-analyses published from Jan. 1, 2014, (to capture research that may have been missed during development of the 2015 statement) through Feb. 28, 2018.
The process was based on consensus among members; areas of disagreement were voted on and the group proceeded according to 60% supermajority votes.
The updates were mainly based on research generated over the past 2 years, Dr. Davies said.
The final draft will be submitted for publication to Diabetes Care and Diabetologia.
Dr. Buse reported relationships (research support, stock ownership, and/or advisory roles) with Adocia, AstraZeneca, Boehringer Ingelheim, Dexcom, Elcelyx Therapeutics, Eli Lilly, Intarcia Therapeutics, Johnson & Johnson, Lexicon Pharmaceuticals, Mellitus Health, Metavention, NovaTarg Therapeutics, Novo Nordisk, PhaseBio Pharmaceuticals, Sanofi, Senseonics, Theracos, and vTv Therapeutics; Dr. Wexler reported having no disclosures; Dr. Rossing reported relationships (consultancy and/or speaking fees, research grants, stock ownership) with AbbVie, Astellas Pharma, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, MDS Medical, Novo Nordisk, and Sanofi; Dr. Kernan reported having no disclosures; Dr. Mingrone is a consultant for Novo Nordisk, Fractyl, and Johnson & Johnson; Dr. D’Alessio reported advisory board membership with and/or research support from Eli Lilly, Intarcia Therapeutics, Merck, and Novo Nordisk; Dr. Mathieu reported relationships (advisory board membership, speaker’s bureau, and/or research support) with Abbott, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Hanmi Pharmaceuticals, Intrexon, Janssen Pharmaceuticals, MannKind, Medtronic, Merck Sharp & Dohme (MSD), Novartis, Novo Nordisk, Pfizer, Roche Diagnostics, Sanofi, and UCB; Dr. Davies reported relationships (advisory panel, consulting, research support, and/or speaker’s bureau) with AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, Intarcia Therapeutics, Janssen Pharmaceuticals, MSD, Mitsubishi Tanabi Pharma, Novo Nordisk, Sanofi, and Servier.
ORLANDO – according to a draft consensus report on the management of hyperglycemia in patients with type 2 diabetes mellitus (T2DM).
The report, a project of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD), is currently under review and will be presented in final form Oct. 5 at the EASD annual meeting in Berlin.
The current draft calls, generally, for the initial use of metformin followed by the addition of antihyperglycemic medications based on patient comorbidities and concerns “as we await answers to the many questions that remain,” John Buse, MD, PhD, cochair of the consensus statement writing group, said during a summary of the draft recommendations at the annual scientific sessions of the ADA.
The first step, however, is to assess key patient characteristics; these can include comorbidities, clinical characteristics, issues such as motivation and depression, and cultural and socio-economic context, Deborah J. Wexler, MD, 1 of 10 writing group members, said during the same presentation.
Patients with ASCVD or heart failure
Given new evidence from trials such as EMPA-REG and LEADER showing outcomes benefits with the use of specific antihyperglycemic medications in patients with established atherosclerotic cardiovascular disease (ASCVD), an important early step in the proposed approach is to consider the presence or absence of ASCVD and heart failure, said Dr. Wexler of Massachusetts General Hospital, Boston.
“The presence of cardiovascular disease is a compelling indication for the selection of certain glucose-lowering drugs,” she said.
The draft consensus recommendation in this regard – a new recommendation since the last consensus report in 2015 – differentiates between T2DM patients in whom ASCVD predominates and those in whom heart failure predominates.
“What’s new since 2015 is that we recommend that these comorbidities be considered first and foremost because they do influence the choice of a particular glucose-lowering medication, and the recommendation is that, among patients with type 2 diabetes with established ASCVD, sodium-glucose cotransporter 2 [SGLT2] inhibitors or glucagonlike peptide 1 [GLP-1] receptor agonists with proven cardiovascular benefit are recommended as part of glycemic management,” she said.
However, it is important to note that ASCVD is defined differently across trials, and patients considered in the development of these recommendations are those with much higher cardiovascular risk than the average patient with T2DM, she added.
“It’s also important to keep in mind that each cardiovascular outcomes trial, while large, is but a single experiment ... and we don’t have the benefit of replication,” she said, noting that it is not always clear whether differences in trial findings within a drug class are related to trial design or true differences in individual medications.
“So we try to read into them and interpret these data, but it’s just important to consider that ... and when evidence suggests a hierarchy, we noted that,” she said.
That said, if ASCVD predominates, the recommendation is for treatment with either a GLP-1 receptor agonist with proven cardiovascular benefit (favoring liraglutide over semaglutide and over long-acting exenatide) or an SGLT2 inhibitor with proven cardiovascular benefit if estimated glomerular filtration (eGFR) is adequate (favoring empagliflozin over canagliflozin).
These recommendations are based on the LEADER trial finding of significant improvement in the primary outcome of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke with liraglutide vs. placebo (hazard ratio, 0.87; number needed to treat [NNT], 52 over 3.8 years) and on the EMPA-REG trial finding of significant improvement in the same primary outcome with empagliflozin vs. placebo (HR, 0.86; NNT, 62 over 3.1 years).
Keep in mind that there is no evidence of cardiovascular benefit from these treatments in patients at lower risk and also that the “expensive and complicated” combination of an SGLT2 inhibitor and a GLP-1 receptor agonist has not been tested in cardiovascular outcomes trials and there is no evidence of additional benefit from a cardiovascular perspective with this combination, Dr. Wexler said.
If heart failure predominates, the recommendations call for consideration of an SGLT2 inhibitor as part of the treatment strategy because patients with T2DM are at increased risk for heart failure with reduced or preserved ejection fraction and because significant, consistent reduction in hospitalizations for heart failure were seen in SGLT2 inhibitor trials, writing group member Peter Rossing, MD, explained during the session; he noted, however, that the trials were not designed to adjudicate heart failure and that most patients did not have clinical heart failure at baseline.
In those in whom SGLT2 inhibitors are contraindicated – because of impaired renal function, for example – a GLP-1 receptor agonist with proven cardiovascular benefit is recommended.
“Then we suggest that if you are still not at [hemoglobin A1c] target, you should avoid thiazolidinediones [TZD] because of the risk of fluid overload, and you could then consider, if needed, combining an SGLT2-inhibitor and a GLP-1 receptor agonist ... or you could use a [dipeptidyl peptidase–4 (DPP-4) inhibitor] if you are not on an GLP-1 receptor agonist. And we point out that saxagliptin has unfavorable data on heart failure,” Dr. Rossing of Steno Diabetes Center, Copenhagen, said, noting that basal insulin or sulfonylurea are other alternative options.
In EMPA-REG, hospitalization for heart failure was reduced by 35% with empagliflozin vs. placebo (HR, 0.65; NNT, 71 over 3 years), and similar findings were seen in the CANVAS trial. In LEADER, a nonsignificant 13% reduction was seen in hospitalization for heart failure with liraglutide vs. placebo (HR, 0.87). However, this was a secondary outcome; ongoing studies are addressing heart failure as a primary outcome, Dr. Rossing said.
The report also includes a recommendation that, for patients with chronic kidney disease and high cardiovascular risk, GLP-1 receptor agonists and SGLT2 inhibitors can be used but with dose reductions for some medications – several of which have demonstrated renal benefit and cardiovascular benefits in those populations and can be considered as part of treatment.
Lifestyle management and medication
With respect to lifestyle management and pharmacologic treatment, the proposed recommendations, which are based on several large trials, state that an individualized program of medical nutritional therapy should be offered to all patients and that all overweight and obese patients with diabetes should be advised of the health benefits of weight loss. They also should be encouraged to engage in a program of intensive lifestyle management, which may include food substitution, writing group member Walter Kernan, MD, said at the meeting.
In the DiRECT Trial, the average weight loss was about 10 kg in an intervention group that had complete food replacement for 3 months followed by gradual food reintroduction and ongoing counseling versus about 1 kg in controls, and the diabetes remission rate at 1 year was 46% versus 4%, respectively, said Dr. Kernan of Yale University, New Haven, Conn.
In addition, intentional physical activity is known to improve glycemic control and should be encouraged in all patients with T2DM, he said.
“The foundation of hyperglycemia treatment in type 2 diabetes is, for sure, lifestyle modification,” said group member Geltrude Mingrone, MD, of Catholic University of the Sacred Heart in Rome. “Those patients who are very well motivated and adherent to the [recommendations] can achieve very good results,” she added.
In those in whom lifestyle modification fails to lead to adequate improvement, “a pretty large medication portfolio is available,” she said, adding that the choice of treatment should be based on safety, efficacy, cost, and convenience, factors which are described in the statement.
The hope is that the final consensus statement will make it easier to navigate them, she said.
Finally, bariatric surgery can be considered a very effective salvage therapy, Dr. Mingrone said, noting that only lifestyle modification or bariatric surgery will lead to diabetes remission.
The draft consensus recommendation for bariatric surgery is to consider it in patients with T2DM and a body mass index of 40 kg/m2 or greater (37.5 or greater in those of Asian ancestry), regardless of the level of glycemic control, and in those with BMI of 35-39.9 (32.5-37.4 in those of Asian ancestry) when hyperglycemia is inadequately controlled despite lifestyle and optimal medical therapy.
Decision making and injectable therapies
The statement includes decision-making strategies and algorithms for treatment and addresses issues such as choosing antihyperglycemic medications when weight is a concern (consider an SGLT2 inhibitor or a GLP-1 receptor agonist with good efficacy for weight loss to start – or a combination of both if HbA1c is not on target), when minimizing hypoglycemia is the priority (consider adding an SGLT2 inhibitors, GLP-1 receptor agonist, a TZD, or a DPP-4 inhibitor to metformin therapy to start, followed by reintensification of lifestyle modifications and combination therapies if HbA1c is above target), and when drug costs need to be minimized, as well as when and how to initiate injectable therapies, according to writing group members David D’Alessio, MD, of Duke University, Durham, N.C, and Chantal Mathieu, MD, of Katholieke Universteit Leuven (Belgium).
The draft consensus recommendation regarding the latter is that, in patients who need the greater glucose-lowering effect of an injectable medication, GLP-1 receptor agonists should be considered as the first choice and that, when insulin is the medication of choice on the basis of clinical characteristics, basal insulin is preferred. Additionally, in patients who are unable to maintain glycemic targets on basal insulin in combination with oral medication, intensification with a GLP-1 receptor agonist, SGLT2 inhibitor, or prandial insulin can be considered.
This recommendation is based on “overwhelming evidence that GLP-1 receptor agonists give you HbA1c lowering in the same range as basal insulin but can do so without hypoglycemia and with weight loss, in contrast to weight gain with most insulin preparations,” Dr. Mathieu noted.
The bottom line, however, is that “the patient is at the center of everything and ... should become an integral part of the team treating this patient,” Dr. Mathieu said.
Knowledge gaps
In a review of remaining knowledge gaps regarding glycemic control in T2DM, Dr. Buse said that, while the tools available to treat and prevent diabetes are vastly improved, implementation of effective innovation has lagged behind and “requires fundamental changes in health care policy and societal approaches to wellness.”
Additionally, the management of overweight and obesity is clearly inadequate and requires much greater emphasis on lifestyle techniques, behavioral approaches, medication, and surgery, said Dr. Buse, who is the Verne S. Caviness distinguished professor and chief of the division of endocrinology, as well as director of the Diabetes Center, at the University of North Carolina, Chapel Hill.
These and numerous other knowledge gaps (with respect to preserving and enhancing beta-cell function, incorporating personalized medicine, the value of combinations for additive benefit, the identification of biomarkers, the use of early intensive therapy, metabolic surgery decision making, the value of self-monitoring of blood glucose, and the need for better drugs – including those for the primary prevention of cardiovascular disease) need to be addressed and “require additional investment in basic, translational, clinical, and implementation research,” he said.
“More time- and cost-efficient research paradigms to address patient-centered endpoints are needed through regulatory reform and leveraging informatics and coordinated learning health care systems. Additionally, the increasing burden of cardiometabolic disease is an existential threat to society,” he said, stressing that “urgent attention to improve prevention and treatment is of the essence.”
Consensus statement development
The draft consensus statement is the work of group members selected by the ADA and EASD to ensure regional representation (five each from the United States and Europe). The group had two face-to-face meetings, as well as regular teleconferences; the members also conducted a “robust evidence review, which informed the content,” said group cochair Melanie J. Davies, MD, of the University of Leicester (U.K.).
The group reviewed randomized controlled trials, systematic reviews, and meta-analyses published from Jan. 1, 2014, (to capture research that may have been missed during development of the 2015 statement) through Feb. 28, 2018.
The process was based on consensus among members; areas of disagreement were voted on and the group proceeded according to 60% supermajority votes.
The updates were mainly based on research generated over the past 2 years, Dr. Davies said.
The final draft will be submitted for publication to Diabetes Care and Diabetologia.
Dr. Buse reported relationships (research support, stock ownership, and/or advisory roles) with Adocia, AstraZeneca, Boehringer Ingelheim, Dexcom, Elcelyx Therapeutics, Eli Lilly, Intarcia Therapeutics, Johnson & Johnson, Lexicon Pharmaceuticals, Mellitus Health, Metavention, NovaTarg Therapeutics, Novo Nordisk, PhaseBio Pharmaceuticals, Sanofi, Senseonics, Theracos, and vTv Therapeutics; Dr. Wexler reported having no disclosures; Dr. Rossing reported relationships (consultancy and/or speaking fees, research grants, stock ownership) with AbbVie, Astellas Pharma, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, MDS Medical, Novo Nordisk, and Sanofi; Dr. Kernan reported having no disclosures; Dr. Mingrone is a consultant for Novo Nordisk, Fractyl, and Johnson & Johnson; Dr. D’Alessio reported advisory board membership with and/or research support from Eli Lilly, Intarcia Therapeutics, Merck, and Novo Nordisk; Dr. Mathieu reported relationships (advisory board membership, speaker’s bureau, and/or research support) with Abbott, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Hanmi Pharmaceuticals, Intrexon, Janssen Pharmaceuticals, MannKind, Medtronic, Merck Sharp & Dohme (MSD), Novartis, Novo Nordisk, Pfizer, Roche Diagnostics, Sanofi, and UCB; Dr. Davies reported relationships (advisory panel, consulting, research support, and/or speaker’s bureau) with AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, Intarcia Therapeutics, Janssen Pharmaceuticals, MSD, Mitsubishi Tanabi Pharma, Novo Nordisk, Sanofi, and Servier.
ORLANDO – according to a draft consensus report on the management of hyperglycemia in patients with type 2 diabetes mellitus (T2DM).
The report, a project of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD), is currently under review and will be presented in final form Oct. 5 at the EASD annual meeting in Berlin.
The current draft calls, generally, for the initial use of metformin followed by the addition of antihyperglycemic medications based on patient comorbidities and concerns “as we await answers to the many questions that remain,” John Buse, MD, PhD, cochair of the consensus statement writing group, said during a summary of the draft recommendations at the annual scientific sessions of the ADA.
The first step, however, is to assess key patient characteristics; these can include comorbidities, clinical characteristics, issues such as motivation and depression, and cultural and socio-economic context, Deborah J. Wexler, MD, 1 of 10 writing group members, said during the same presentation.
Patients with ASCVD or heart failure
Given new evidence from trials such as EMPA-REG and LEADER showing outcomes benefits with the use of specific antihyperglycemic medications in patients with established atherosclerotic cardiovascular disease (ASCVD), an important early step in the proposed approach is to consider the presence or absence of ASCVD and heart failure, said Dr. Wexler of Massachusetts General Hospital, Boston.
“The presence of cardiovascular disease is a compelling indication for the selection of certain glucose-lowering drugs,” she said.
The draft consensus recommendation in this regard – a new recommendation since the last consensus report in 2015 – differentiates between T2DM patients in whom ASCVD predominates and those in whom heart failure predominates.
“What’s new since 2015 is that we recommend that these comorbidities be considered first and foremost because they do influence the choice of a particular glucose-lowering medication, and the recommendation is that, among patients with type 2 diabetes with established ASCVD, sodium-glucose cotransporter 2 [SGLT2] inhibitors or glucagonlike peptide 1 [GLP-1] receptor agonists with proven cardiovascular benefit are recommended as part of glycemic management,” she said.
However, it is important to note that ASCVD is defined differently across trials, and patients considered in the development of these recommendations are those with much higher cardiovascular risk than the average patient with T2DM, she added.
“It’s also important to keep in mind that each cardiovascular outcomes trial, while large, is but a single experiment ... and we don’t have the benefit of replication,” she said, noting that it is not always clear whether differences in trial findings within a drug class are related to trial design or true differences in individual medications.
“So we try to read into them and interpret these data, but it’s just important to consider that ... and when evidence suggests a hierarchy, we noted that,” she said.
That said, if ASCVD predominates, the recommendation is for treatment with either a GLP-1 receptor agonist with proven cardiovascular benefit (favoring liraglutide over semaglutide and over long-acting exenatide) or an SGLT2 inhibitor with proven cardiovascular benefit if estimated glomerular filtration (eGFR) is adequate (favoring empagliflozin over canagliflozin).
These recommendations are based on the LEADER trial finding of significant improvement in the primary outcome of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke with liraglutide vs. placebo (hazard ratio, 0.87; number needed to treat [NNT], 52 over 3.8 years) and on the EMPA-REG trial finding of significant improvement in the same primary outcome with empagliflozin vs. placebo (HR, 0.86; NNT, 62 over 3.1 years).
Keep in mind that there is no evidence of cardiovascular benefit from these treatments in patients at lower risk and also that the “expensive and complicated” combination of an SGLT2 inhibitor and a GLP-1 receptor agonist has not been tested in cardiovascular outcomes trials and there is no evidence of additional benefit from a cardiovascular perspective with this combination, Dr. Wexler said.
If heart failure predominates, the recommendations call for consideration of an SGLT2 inhibitor as part of the treatment strategy because patients with T2DM are at increased risk for heart failure with reduced or preserved ejection fraction and because significant, consistent reduction in hospitalizations for heart failure were seen in SGLT2 inhibitor trials, writing group member Peter Rossing, MD, explained during the session; he noted, however, that the trials were not designed to adjudicate heart failure and that most patients did not have clinical heart failure at baseline.
In those in whom SGLT2 inhibitors are contraindicated – because of impaired renal function, for example – a GLP-1 receptor agonist with proven cardiovascular benefit is recommended.
“Then we suggest that if you are still not at [hemoglobin A1c] target, you should avoid thiazolidinediones [TZD] because of the risk of fluid overload, and you could then consider, if needed, combining an SGLT2-inhibitor and a GLP-1 receptor agonist ... or you could use a [dipeptidyl peptidase–4 (DPP-4) inhibitor] if you are not on an GLP-1 receptor agonist. And we point out that saxagliptin has unfavorable data on heart failure,” Dr. Rossing of Steno Diabetes Center, Copenhagen, said, noting that basal insulin or sulfonylurea are other alternative options.
In EMPA-REG, hospitalization for heart failure was reduced by 35% with empagliflozin vs. placebo (HR, 0.65; NNT, 71 over 3 years), and similar findings were seen in the CANVAS trial. In LEADER, a nonsignificant 13% reduction was seen in hospitalization for heart failure with liraglutide vs. placebo (HR, 0.87). However, this was a secondary outcome; ongoing studies are addressing heart failure as a primary outcome, Dr. Rossing said.
The report also includes a recommendation that, for patients with chronic kidney disease and high cardiovascular risk, GLP-1 receptor agonists and SGLT2 inhibitors can be used but with dose reductions for some medications – several of which have demonstrated renal benefit and cardiovascular benefits in those populations and can be considered as part of treatment.
Lifestyle management and medication
With respect to lifestyle management and pharmacologic treatment, the proposed recommendations, which are based on several large trials, state that an individualized program of medical nutritional therapy should be offered to all patients and that all overweight and obese patients with diabetes should be advised of the health benefits of weight loss. They also should be encouraged to engage in a program of intensive lifestyle management, which may include food substitution, writing group member Walter Kernan, MD, said at the meeting.
In the DiRECT Trial, the average weight loss was about 10 kg in an intervention group that had complete food replacement for 3 months followed by gradual food reintroduction and ongoing counseling versus about 1 kg in controls, and the diabetes remission rate at 1 year was 46% versus 4%, respectively, said Dr. Kernan of Yale University, New Haven, Conn.
In addition, intentional physical activity is known to improve glycemic control and should be encouraged in all patients with T2DM, he said.
“The foundation of hyperglycemia treatment in type 2 diabetes is, for sure, lifestyle modification,” said group member Geltrude Mingrone, MD, of Catholic University of the Sacred Heart in Rome. “Those patients who are very well motivated and adherent to the [recommendations] can achieve very good results,” she added.
In those in whom lifestyle modification fails to lead to adequate improvement, “a pretty large medication portfolio is available,” she said, adding that the choice of treatment should be based on safety, efficacy, cost, and convenience, factors which are described in the statement.
The hope is that the final consensus statement will make it easier to navigate them, she said.
Finally, bariatric surgery can be considered a very effective salvage therapy, Dr. Mingrone said, noting that only lifestyle modification or bariatric surgery will lead to diabetes remission.
The draft consensus recommendation for bariatric surgery is to consider it in patients with T2DM and a body mass index of 40 kg/m2 or greater (37.5 or greater in those of Asian ancestry), regardless of the level of glycemic control, and in those with BMI of 35-39.9 (32.5-37.4 in those of Asian ancestry) when hyperglycemia is inadequately controlled despite lifestyle and optimal medical therapy.
Decision making and injectable therapies
The statement includes decision-making strategies and algorithms for treatment and addresses issues such as choosing antihyperglycemic medications when weight is a concern (consider an SGLT2 inhibitor or a GLP-1 receptor agonist with good efficacy for weight loss to start – or a combination of both if HbA1c is not on target), when minimizing hypoglycemia is the priority (consider adding an SGLT2 inhibitors, GLP-1 receptor agonist, a TZD, or a DPP-4 inhibitor to metformin therapy to start, followed by reintensification of lifestyle modifications and combination therapies if HbA1c is above target), and when drug costs need to be minimized, as well as when and how to initiate injectable therapies, according to writing group members David D’Alessio, MD, of Duke University, Durham, N.C, and Chantal Mathieu, MD, of Katholieke Universteit Leuven (Belgium).
The draft consensus recommendation regarding the latter is that, in patients who need the greater glucose-lowering effect of an injectable medication, GLP-1 receptor agonists should be considered as the first choice and that, when insulin is the medication of choice on the basis of clinical characteristics, basal insulin is preferred. Additionally, in patients who are unable to maintain glycemic targets on basal insulin in combination with oral medication, intensification with a GLP-1 receptor agonist, SGLT2 inhibitor, or prandial insulin can be considered.
This recommendation is based on “overwhelming evidence that GLP-1 receptor agonists give you HbA1c lowering in the same range as basal insulin but can do so without hypoglycemia and with weight loss, in contrast to weight gain with most insulin preparations,” Dr. Mathieu noted.
The bottom line, however, is that “the patient is at the center of everything and ... should become an integral part of the team treating this patient,” Dr. Mathieu said.
Knowledge gaps
In a review of remaining knowledge gaps regarding glycemic control in T2DM, Dr. Buse said that, while the tools available to treat and prevent diabetes are vastly improved, implementation of effective innovation has lagged behind and “requires fundamental changes in health care policy and societal approaches to wellness.”
Additionally, the management of overweight and obesity is clearly inadequate and requires much greater emphasis on lifestyle techniques, behavioral approaches, medication, and surgery, said Dr. Buse, who is the Verne S. Caviness distinguished professor and chief of the division of endocrinology, as well as director of the Diabetes Center, at the University of North Carolina, Chapel Hill.
These and numerous other knowledge gaps (with respect to preserving and enhancing beta-cell function, incorporating personalized medicine, the value of combinations for additive benefit, the identification of biomarkers, the use of early intensive therapy, metabolic surgery decision making, the value of self-monitoring of blood glucose, and the need for better drugs – including those for the primary prevention of cardiovascular disease) need to be addressed and “require additional investment in basic, translational, clinical, and implementation research,” he said.
“More time- and cost-efficient research paradigms to address patient-centered endpoints are needed through regulatory reform and leveraging informatics and coordinated learning health care systems. Additionally, the increasing burden of cardiometabolic disease is an existential threat to society,” he said, stressing that “urgent attention to improve prevention and treatment is of the essence.”
Consensus statement development
The draft consensus statement is the work of group members selected by the ADA and EASD to ensure regional representation (five each from the United States and Europe). The group had two face-to-face meetings, as well as regular teleconferences; the members also conducted a “robust evidence review, which informed the content,” said group cochair Melanie J. Davies, MD, of the University of Leicester (U.K.).
The group reviewed randomized controlled trials, systematic reviews, and meta-analyses published from Jan. 1, 2014, (to capture research that may have been missed during development of the 2015 statement) through Feb. 28, 2018.
The process was based on consensus among members; areas of disagreement were voted on and the group proceeded according to 60% supermajority votes.
The updates were mainly based on research generated over the past 2 years, Dr. Davies said.
The final draft will be submitted for publication to Diabetes Care and Diabetologia.
Dr. Buse reported relationships (research support, stock ownership, and/or advisory roles) with Adocia, AstraZeneca, Boehringer Ingelheim, Dexcom, Elcelyx Therapeutics, Eli Lilly, Intarcia Therapeutics, Johnson & Johnson, Lexicon Pharmaceuticals, Mellitus Health, Metavention, NovaTarg Therapeutics, Novo Nordisk, PhaseBio Pharmaceuticals, Sanofi, Senseonics, Theracos, and vTv Therapeutics; Dr. Wexler reported having no disclosures; Dr. Rossing reported relationships (consultancy and/or speaking fees, research grants, stock ownership) with AbbVie, Astellas Pharma, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, MDS Medical, Novo Nordisk, and Sanofi; Dr. Kernan reported having no disclosures; Dr. Mingrone is a consultant for Novo Nordisk, Fractyl, and Johnson & Johnson; Dr. D’Alessio reported advisory board membership with and/or research support from Eli Lilly, Intarcia Therapeutics, Merck, and Novo Nordisk; Dr. Mathieu reported relationships (advisory board membership, speaker’s bureau, and/or research support) with Abbott, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Hanmi Pharmaceuticals, Intrexon, Janssen Pharmaceuticals, MannKind, Medtronic, Merck Sharp & Dohme (MSD), Novartis, Novo Nordisk, Pfizer, Roche Diagnostics, Sanofi, and UCB; Dr. Davies reported relationships (advisory panel, consulting, research support, and/or speaker’s bureau) with AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, Intarcia Therapeutics, Janssen Pharmaceuticals, MSD, Mitsubishi Tanabi Pharma, Novo Nordisk, Sanofi, and Servier.
EXPERT ANALYSIS FROM ADA 2018

The evolving role of expert testimony
Question: Which of the following statements regarding the law on evidence is incorrect?
A. Expert testimony is always needed to establish the applicable standard of care in a negligence lawsuit.
B. According to the Federal Rules of Evidence, a witness may be qualified as an expert based on knowledge, skill, experience, training, or education.
C. It is the judge, not the jury, who determines whether a witness is admissible as an expert.
D. Expert testimony is a requirement in medical malpractice lawsuits, unless a plaintiff can successfully invoke the res ipsa loquitur doctrine.
E. Only a few states have enacted statutes specifying that an expert must be in the same specialty as the defendant, and in some cases, a nonphysician such as a nurse or pharmacist may be allowed to testify.
Answer: A. Under the tort of negligence, a defendant’s conduct is measured by what is expected of the reasonable person – the man on the street. The jury can usually decide on its own, without the aid of an expert, what that level of care ought to be. However, in medical malpractice lawsuits, the law requires an expert to testify to the requisite standard of care, as this determination is believed to be beyond the scope of the layperson.
An exception, rarely invoked, is the res ipsa loquitur doctrine, where “the thing speaks for itself.” There, an expert is not necessary because of common knowledge, e.g., when a surgeon inadvertently leaves a sponge or instrument inside a body cavity.
Whether one is admitted as an expert is within the sole discretion of the judge, who is guided by the Federal Rules of Evidence. Typically, an expert is in the same medical specialty, but there are instances of professionals of unlike specialties qualifying as experts. Examples include a nephrologist testifying against a urologist, an infectious disease specialist offering an expert opinion in a stroke case, a pharmacist testifying on the issue of a medication side effect, and a nurse on bedsores.
We had previously reviewed the law governing expert medical testimony in these columns.1 However, three recent cases awaiting final adjudication caught our attention, as they raise important and serious legal issues.
The first frontally suggests that jury members may rely on their own notion of what constitutes an appropriate standard of care. Although it is established law in Maryland that expert testimony is required to set that standard in medical malpractice litigation, the recent Maryland case of Armacost v. Davis appeared to modify this principle, leading to a plaintiff verdict.2
The facts involved a neurosurgeon’s anterior cervical discectomy and fusion surgery, which was complicated by a pinpoint opening at the end of the incision. This eventually developed into a MRSA abscess. In his lawsuit, the plaintiff alleged that surgery was neither medically necessary nor appropriate, that there was no proper informed consent, and that the diagnosis of his postoperative infection was delayed.
A pivotal part of the trial centered on a Baltimore county judge’s instructions to the jury that it could consider what a layperson would deem reasonable standard of care. Moreover, the judge refused to modify the jury instructions when the doctor-defendant objected and asked that the standard of care be measured by the expectations for a neurosurgeon. The jury returned a verdict in favor of the plaintiff in the amount of $329,000.
Upon appeal, the Court of Special Appeals of Maryland ruled that the jury instructions were improper and therefore ordered a new trial. It held: “Medical malpractice claims are not general negligence claims, and so jury instructions on general negligence, although correct statements of Maryland law, are not supported by the facts of a case centered on the allegedly negligent conduct of a physician. Accordingly, we hold that the trial court erred in giving general negligence instructions in a medical malpractice case.”
The case is now before Maryland’s highest court, the Court of Appeals of Maryland, which is expected to uphold this decision and reject the reasonable person (instead of reasonable doctor) standard used by the lower court.
The second case deals with whether a jury in a medical liability trial may be prejudiced if they hear four medical experts testify for the physician and just one expert testify for the plaintiff. In Shallow v. Follwell, the defendant doctor performed a laparoscopic hernia repair, which was complicated by bowel perforation, atrial fibrillation, sepsis, and death.3
At trial, plaintiffs produced one expert witness, whereas Dr. Follwell had four, with expertise in cardiology, critical care, vascular surgery, and colorectal surgery. The trial court judge instructed the jury not to give weight to the number of experts on either side, and based on the testimony, the jury found that Dr. Follwell did not cause the perforated bowel or the patient’s death.
However, on appeal, the Missouri Court of Appeals overturned the verdict after finding that the trial court erred in allowing “unfairly cumulative and prejudicial repetition of certain expert opinions.” The Missouri Supreme Court is currently being asked to render a final opinion on the matter. In its supporting brief, the American Medical Association’s Litigation Center is urging the high court to “ensure that Missouri trial judges are empowered to safeguard the use of sound science in their courtrooms,” and that “given the highly specialized nature of medicine today, multiple experts may be required to ensure a jury has a proper understanding of the relevant medical science.”4
The third case addresses whether trial judges can suppress expert witness testimony attesting that a known complication of a medical procedure can occur absent any negligence.
The case involved a laparoscopic hysterectomy performed by a gynecologist. The patient’s bowel was perforated during the procedure.5 Expert witnesses from both sides testified about bowel perforation and professional standards, and the trial court allowed the defendant’s expert to state that such an injury was a commonplace risk even if surgery was performed properly.
The plaintiff objected to this testimony; but the trial judge overruled the plaintiff’s objection, and the jury found in favor of the gynecologist. Upon appeal, the Pennsylvania Superior Court reversed, concluding that the defendant’s expert testimony was irrelevant and misleading, and immaterial to the issue of whether the defendant’s treatment met the standard of care. It held that the evidence was inadmissible and ordered a new trial. The case is now before the Pennsylvania Supreme Court.

The foregoing three cases are yet to be finally adjudicated, but controversies in these and similar issues can be expected to continue. Expert testimony is dispositive at trial, and both sides rely heavily on it. Little wonder malpractice litigation is frequently framed as a “battle of the experts.”
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. Internal Medicine News, “Expert medical testimony,” Sept. 9, 2010; “Qualifying as an expert,” Jan. 2, 2015; “Dispensing with expert testimony,” April 19, 2016.
2. Armacost v. Davis, 175 A.3d 150 (Ct. App. Md, 2017).
3. Shallow v. Follwell, (No. ED103811, Mo. App., Eastern Dist., Div. 4, 2017).
4. Henry TA, “Is it OK to have 4-to-1 expert ratio in medical liability case?” AMA Wire, June 22, 2018.
5. Mitchell v. Shikora, 161 A.3d 970 (Pa. Super. 2017).
Question: Which of the following statements regarding the law on evidence is incorrect?
A. Expert testimony is always needed to establish the applicable standard of care in a negligence lawsuit.
B. According to the Federal Rules of Evidence, a witness may be qualified as an expert based on knowledge, skill, experience, training, or education.
C. It is the judge, not the jury, who determines whether a witness is admissible as an expert.
D. Expert testimony is a requirement in medical malpractice lawsuits, unless a plaintiff can successfully invoke the res ipsa loquitur doctrine.
E. Only a few states have enacted statutes specifying that an expert must be in the same specialty as the defendant, and in some cases, a nonphysician such as a nurse or pharmacist may be allowed to testify.
Answer: A. Under the tort of negligence, a defendant’s conduct is measured by what is expected of the reasonable person – the man on the street. The jury can usually decide on its own, without the aid of an expert, what that level of care ought to be. However, in medical malpractice lawsuits, the law requires an expert to testify to the requisite standard of care, as this determination is believed to be beyond the scope of the layperson.
An exception, rarely invoked, is the res ipsa loquitur doctrine, where “the thing speaks for itself.” There, an expert is not necessary because of common knowledge, e.g., when a surgeon inadvertently leaves a sponge or instrument inside a body cavity.
Whether one is admitted as an expert is within the sole discretion of the judge, who is guided by the Federal Rules of Evidence. Typically, an expert is in the same medical specialty, but there are instances of professionals of unlike specialties qualifying as experts. Examples include a nephrologist testifying against a urologist, an infectious disease specialist offering an expert opinion in a stroke case, a pharmacist testifying on the issue of a medication side effect, and a nurse on bedsores.
We had previously reviewed the law governing expert medical testimony in these columns.1 However, three recent cases awaiting final adjudication caught our attention, as they raise important and serious legal issues.
The first frontally suggests that jury members may rely on their own notion of what constitutes an appropriate standard of care. Although it is established law in Maryland that expert testimony is required to set that standard in medical malpractice litigation, the recent Maryland case of Armacost v. Davis appeared to modify this principle, leading to a plaintiff verdict.2
The facts involved a neurosurgeon’s anterior cervical discectomy and fusion surgery, which was complicated by a pinpoint opening at the end of the incision. This eventually developed into a MRSA abscess. In his lawsuit, the plaintiff alleged that surgery was neither medically necessary nor appropriate, that there was no proper informed consent, and that the diagnosis of his postoperative infection was delayed.
A pivotal part of the trial centered on a Baltimore county judge’s instructions to the jury that it could consider what a layperson would deem reasonable standard of care. Moreover, the judge refused to modify the jury instructions when the doctor-defendant objected and asked that the standard of care be measured by the expectations for a neurosurgeon. The jury returned a verdict in favor of the plaintiff in the amount of $329,000.
Upon appeal, the Court of Special Appeals of Maryland ruled that the jury instructions were improper and therefore ordered a new trial. It held: “Medical malpractice claims are not general negligence claims, and so jury instructions on general negligence, although correct statements of Maryland law, are not supported by the facts of a case centered on the allegedly negligent conduct of a physician. Accordingly, we hold that the trial court erred in giving general negligence instructions in a medical malpractice case.”
The case is now before Maryland’s highest court, the Court of Appeals of Maryland, which is expected to uphold this decision and reject the reasonable person (instead of reasonable doctor) standard used by the lower court.
The second case deals with whether a jury in a medical liability trial may be prejudiced if they hear four medical experts testify for the physician and just one expert testify for the plaintiff. In Shallow v. Follwell, the defendant doctor performed a laparoscopic hernia repair, which was complicated by bowel perforation, atrial fibrillation, sepsis, and death.3
At trial, plaintiffs produced one expert witness, whereas Dr. Follwell had four, with expertise in cardiology, critical care, vascular surgery, and colorectal surgery. The trial court judge instructed the jury not to give weight to the number of experts on either side, and based on the testimony, the jury found that Dr. Follwell did not cause the perforated bowel or the patient’s death.
However, on appeal, the Missouri Court of Appeals overturned the verdict after finding that the trial court erred in allowing “unfairly cumulative and prejudicial repetition of certain expert opinions.” The Missouri Supreme Court is currently being asked to render a final opinion on the matter. In its supporting brief, the American Medical Association’s Litigation Center is urging the high court to “ensure that Missouri trial judges are empowered to safeguard the use of sound science in their courtrooms,” and that “given the highly specialized nature of medicine today, multiple experts may be required to ensure a jury has a proper understanding of the relevant medical science.”4
The third case addresses whether trial judges can suppress expert witness testimony attesting that a known complication of a medical procedure can occur absent any negligence.
The case involved a laparoscopic hysterectomy performed by a gynecologist. The patient’s bowel was perforated during the procedure.5 Expert witnesses from both sides testified about bowel perforation and professional standards, and the trial court allowed the defendant’s expert to state that such an injury was a commonplace risk even if surgery was performed properly.
The plaintiff objected to this testimony; but the trial judge overruled the plaintiff’s objection, and the jury found in favor of the gynecologist. Upon appeal, the Pennsylvania Superior Court reversed, concluding that the defendant’s expert testimony was irrelevant and misleading, and immaterial to the issue of whether the defendant’s treatment met the standard of care. It held that the evidence was inadmissible and ordered a new trial. The case is now before the Pennsylvania Supreme Court.
The foregoing three cases are yet to be finally adjudicated, but controversies in these and similar issues can be expected to continue. Expert testimony is dispositive at trial, and both sides rely heavily on it. Little wonder malpractice litigation is frequently framed as a “battle of the experts.”
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. Internal Medicine News, “Expert medical testimony,” Sept. 9, 2010; “Qualifying as an expert,” Jan. 2, 2015; “Dispensing with expert testimony,” April 19, 2016.
2. Armacost v. Davis, 175 A.3d 150 (Ct. App. Md, 2017).
3. Shallow v. Follwell, (No. ED103811, Mo. App., Eastern Dist., Div. 4, 2017).
4. Henry TA, “Is it OK to have 4-to-1 expert ratio in medical liability case?” AMA Wire, June 22, 2018.
5. Mitchell v. Shikora, 161 A.3d 970 (Pa. Super. 2017).
Question: Which of the following statements regarding the law on evidence is incorrect?
A. Expert testimony is always needed to establish the applicable standard of care in a negligence lawsuit.
B. According to the Federal Rules of Evidence, a witness may be qualified as an expert based on knowledge, skill, experience, training, or education.
C. It is the judge, not the jury, who determines whether a witness is admissible as an expert.
D. Expert testimony is a requirement in medical malpractice lawsuits, unless a plaintiff can successfully invoke the res ipsa loquitur doctrine.
E. Only a few states have enacted statutes specifying that an expert must be in the same specialty as the defendant, and in some cases, a nonphysician such as a nurse or pharmacist may be allowed to testify.
Answer: A. Under the tort of negligence, a defendant’s conduct is measured by what is expected of the reasonable person – the man on the street. The jury can usually decide on its own, without the aid of an expert, what that level of care ought to be. However, in medical malpractice lawsuits, the law requires an expert to testify to the requisite standard of care, as this determination is believed to be beyond the scope of the layperson.
An exception, rarely invoked, is the res ipsa loquitur doctrine, where “the thing speaks for itself.” There, an expert is not necessary because of common knowledge, e.g., when a surgeon inadvertently leaves a sponge or instrument inside a body cavity.
Whether one is admitted as an expert is within the sole discretion of the judge, who is guided by the Federal Rules of Evidence. Typically, an expert is in the same medical specialty, but there are instances of professionals of unlike specialties qualifying as experts. Examples include a nephrologist testifying against a urologist, an infectious disease specialist offering an expert opinion in a stroke case, a pharmacist testifying on the issue of a medication side effect, and a nurse on bedsores.
We had previously reviewed the law governing expert medical testimony in these columns.1 However, three recent cases awaiting final adjudication caught our attention, as they raise important and serious legal issues.
The first frontally suggests that jury members may rely on their own notion of what constitutes an appropriate standard of care. Although it is established law in Maryland that expert testimony is required to set that standard in medical malpractice litigation, the recent Maryland case of Armacost v. Davis appeared to modify this principle, leading to a plaintiff verdict.2
The facts involved a neurosurgeon’s anterior cervical discectomy and fusion surgery, which was complicated by a pinpoint opening at the end of the incision. This eventually developed into a MRSA abscess. In his lawsuit, the plaintiff alleged that surgery was neither medically necessary nor appropriate, that there was no proper informed consent, and that the diagnosis of his postoperative infection was delayed.
A pivotal part of the trial centered on a Baltimore county judge’s instructions to the jury that it could consider what a layperson would deem reasonable standard of care. Moreover, the judge refused to modify the jury instructions when the doctor-defendant objected and asked that the standard of care be measured by the expectations for a neurosurgeon. The jury returned a verdict in favor of the plaintiff in the amount of $329,000.
Upon appeal, the Court of Special Appeals of Maryland ruled that the jury instructions were improper and therefore ordered a new trial. It held: “Medical malpractice claims are not general negligence claims, and so jury instructions on general negligence, although correct statements of Maryland law, are not supported by the facts of a case centered on the allegedly negligent conduct of a physician. Accordingly, we hold that the trial court erred in giving general negligence instructions in a medical malpractice case.”
The case is now before Maryland’s highest court, the Court of Appeals of Maryland, which is expected to uphold this decision and reject the reasonable person (instead of reasonable doctor) standard used by the lower court.
The second case deals with whether a jury in a medical liability trial may be prejudiced if they hear four medical experts testify for the physician and just one expert testify for the plaintiff. In Shallow v. Follwell, the defendant doctor performed a laparoscopic hernia repair, which was complicated by bowel perforation, atrial fibrillation, sepsis, and death.3
At trial, plaintiffs produced one expert witness, whereas Dr. Follwell had four, with expertise in cardiology, critical care, vascular surgery, and colorectal surgery. The trial court judge instructed the jury not to give weight to the number of experts on either side, and based on the testimony, the jury found that Dr. Follwell did not cause the perforated bowel or the patient’s death.
However, on appeal, the Missouri Court of Appeals overturned the verdict after finding that the trial court erred in allowing “unfairly cumulative and prejudicial repetition of certain expert opinions.” The Missouri Supreme Court is currently being asked to render a final opinion on the matter. In its supporting brief, the American Medical Association’s Litigation Center is urging the high court to “ensure that Missouri trial judges are empowered to safeguard the use of sound science in their courtrooms,” and that “given the highly specialized nature of medicine today, multiple experts may be required to ensure a jury has a proper understanding of the relevant medical science.”4
The third case addresses whether trial judges can suppress expert witness testimony attesting that a known complication of a medical procedure can occur absent any negligence.
The case involved a laparoscopic hysterectomy performed by a gynecologist. The patient’s bowel was perforated during the procedure.5 Expert witnesses from both sides testified about bowel perforation and professional standards, and the trial court allowed the defendant’s expert to state that such an injury was a commonplace risk even if surgery was performed properly.
The plaintiff objected to this testimony; but the trial judge overruled the plaintiff’s objection, and the jury found in favor of the gynecologist. Upon appeal, the Pennsylvania Superior Court reversed, concluding that the defendant’s expert testimony was irrelevant and misleading, and immaterial to the issue of whether the defendant’s treatment met the standard of care. It held that the evidence was inadmissible and ordered a new trial. The case is now before the Pennsylvania Supreme Court.
The foregoing three cases are yet to be finally adjudicated, but controversies in these and similar issues can be expected to continue. Expert testimony is dispositive at trial, and both sides rely heavily on it. Little wonder malpractice litigation is frequently framed as a “battle of the experts.”
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. Internal Medicine News, “Expert medical testimony,” Sept. 9, 2010; “Qualifying as an expert,” Jan. 2, 2015; “Dispensing with expert testimony,” April 19, 2016.
2. Armacost v. Davis, 175 A.3d 150 (Ct. App. Md, 2017).
3. Shallow v. Follwell, (No. ED103811, Mo. App., Eastern Dist., Div. 4, 2017).
4. Henry TA, “Is it OK to have 4-to-1 expert ratio in medical liability case?” AMA Wire, June 22, 2018.
5. Mitchell v. Shikora, 161 A.3d 970 (Pa. Super. 2017).
Fewer groin infections with closed incision negative pressure therapy after vascular surgery
Closed incision negative pressure therapy (ciNPT) was found to reduce surgical site infections (SSI) in vascular surgery, according to the results of a prospective, randomized, industry-sponsored trial of patients who underwent vascular surgery for peripheral artery disease (PAD) published online in the European Journal of Vascular and Endovascular Surgery.
The investigator-initiated Reduction of Groin Wound Infections After Vascular Surgery by Using an Incision Management System trial (NCT02395159) included 204 patients who underwent vascular surgery involving longitudinal groin incision to treat the lower extremity or the iliac arteries between July 2015 and May 2017 at two study centers.
The primary endpoint was the occurrence of SSI assessed by the Szilagyi classification (grades I-III). The mean patient age was nearly 67 years and 70% were men. In terms of PAD staging, 52% were stage 2B, 28% were stage 3, and 19% were stage 4. Among the patients, 45% had a previous groin incision and 42% had diabetes.
All patients underwent similar preoperative treatment: hair shaving and preparation with Poly Alcohol (Antiseptica, Pulheim, Germany) and Braunoderm (Braun, Melsungen, Germany). At 30 minutes preincision, patients received intravenous antibiotic treatment (1.5 g cefuroxime or 600 mg clindamycin, if allergic to penicillin). After closure, the incision and surrounding skin area was cleaned and dried using sterile gauze. In the control group, a sterile adhesive wound dressing was applied to the wound, which was changed daily. In the treatment group, ciNPT was applied under sterile conditions in the operating room using the Prevena device, which exerts a continuous negative pressure of 125 mm Hg on the closed incision during the time of application. The device was removed at 5-7 days postoperatively, and no further wound dressings were used in the treatment group unless an SSI occurred.
The control group experienced more frequent SSIs (33.3%) than the intervention group (13.2%) (P =.0015). This difference was based on an increased rate of Szilagyi grade I SSI in the control group (24.6% vs. 8.1%, P = .0012), according to Alexander Gombert, MD, of the University Hospital Aachen (Germany), and his colleagues. The absolute risk difference based on the Szilagyi classification was –20.1 per 100 (95% confidence interval, –31.9 to –8.2).
In addition, there was a statistically significantly lower rate of SSI when using ciNPT within the subgroups at greater risk of infection, compared with controls: PAD stage greater than or equal to 3 (P less than .001), body mass index greater than 25 kg/m2 (P less than .001), and previous groin incision (P = .016).
There were no statistical differences between the two groups in Szilagyi grade II and III SSIs (which occurred in 5.8% of all procedures).
No potentially device-related complications were observed in the trial and there were no failures of the device seen.
“The use of ciNPT rather than standard wound dressing after groin incision as access for vascular surgery was associated with a reduced rate of superficial SSI classified by Szilagyi, suggesting that ciNPT may be useful for reducing the SSI rate among high-risk patients,” the researchers concluded.
The trial was funded by Acelity. Dr. Gombert received travel grants from Acelity.
SOURCE: Gombert A et al. Eur J Vasc Surg. 2018 Jul 2. doi: 10.1016/j.ejvs.2018.05.018.
Closed incision negative pressure therapy (ciNPT) was found to reduce surgical site infections (SSI) in vascular surgery, according to the results of a prospective, randomized, industry-sponsored trial of patients who underwent vascular surgery for peripheral artery disease (PAD) published online in the European Journal of Vascular and Endovascular Surgery.
The investigator-initiated Reduction of Groin Wound Infections After Vascular Surgery by Using an Incision Management System trial (NCT02395159) included 204 patients who underwent vascular surgery involving longitudinal groin incision to treat the lower extremity or the iliac arteries between July 2015 and May 2017 at two study centers.
The primary endpoint was the occurrence of SSI assessed by the Szilagyi classification (grades I-III). The mean patient age was nearly 67 years and 70% were men. In terms of PAD staging, 52% were stage 2B, 28% were stage 3, and 19% were stage 4. Among the patients, 45% had a previous groin incision and 42% had diabetes.
All patients underwent similar preoperative treatment: hair shaving and preparation with Poly Alcohol (Antiseptica, Pulheim, Germany) and Braunoderm (Braun, Melsungen, Germany). At 30 minutes preincision, patients received intravenous antibiotic treatment (1.5 g cefuroxime or 600 mg clindamycin, if allergic to penicillin). After closure, the incision and surrounding skin area was cleaned and dried using sterile gauze. In the control group, a sterile adhesive wound dressing was applied to the wound, which was changed daily. In the treatment group, ciNPT was applied under sterile conditions in the operating room using the Prevena device, which exerts a continuous negative pressure of 125 mm Hg on the closed incision during the time of application. The device was removed at 5-7 days postoperatively, and no further wound dressings were used in the treatment group unless an SSI occurred.
The control group experienced more frequent SSIs (33.3%) than the intervention group (13.2%) (P =.0015). This difference was based on an increased rate of Szilagyi grade I SSI in the control group (24.6% vs. 8.1%, P = .0012), according to Alexander Gombert, MD, of the University Hospital Aachen (Germany), and his colleagues. The absolute risk difference based on the Szilagyi classification was –20.1 per 100 (95% confidence interval, –31.9 to –8.2).
In addition, there was a statistically significantly lower rate of SSI when using ciNPT within the subgroups at greater risk of infection, compared with controls: PAD stage greater than or equal to 3 (P less than .001), body mass index greater than 25 kg/m2 (P less than .001), and previous groin incision (P = .016).
There were no statistical differences between the two groups in Szilagyi grade II and III SSIs (which occurred in 5.8% of all procedures).
No potentially device-related complications were observed in the trial and there were no failures of the device seen.
“The use of ciNPT rather than standard wound dressing after groin incision as access for vascular surgery was associated with a reduced rate of superficial SSI classified by Szilagyi, suggesting that ciNPT may be useful for reducing the SSI rate among high-risk patients,” the researchers concluded.
The trial was funded by Acelity. Dr. Gombert received travel grants from Acelity.
SOURCE: Gombert A et al. Eur J Vasc Surg. 2018 Jul 2. doi: 10.1016/j.ejvs.2018.05.018.
Closed incision negative pressure therapy (ciNPT) was found to reduce surgical site infections (SSI) in vascular surgery, according to the results of a prospective, randomized, industry-sponsored trial of patients who underwent vascular surgery for peripheral artery disease (PAD) published online in the European Journal of Vascular and Endovascular Surgery.
The investigator-initiated Reduction of Groin Wound Infections After Vascular Surgery by Using an Incision Management System trial (NCT02395159) included 204 patients who underwent vascular surgery involving longitudinal groin incision to treat the lower extremity or the iliac arteries between July 2015 and May 2017 at two study centers.
The primary endpoint was the occurrence of SSI assessed by the Szilagyi classification (grades I-III). The mean patient age was nearly 67 years and 70% were men. In terms of PAD staging, 52% were stage 2B, 28% were stage 3, and 19% were stage 4. Among the patients, 45% had a previous groin incision and 42% had diabetes.
All patients underwent similar preoperative treatment: hair shaving and preparation with Poly Alcohol (Antiseptica, Pulheim, Germany) and Braunoderm (Braun, Melsungen, Germany). At 30 minutes preincision, patients received intravenous antibiotic treatment (1.5 g cefuroxime or 600 mg clindamycin, if allergic to penicillin). After closure, the incision and surrounding skin area was cleaned and dried using sterile gauze. In the control group, a sterile adhesive wound dressing was applied to the wound, which was changed daily. In the treatment group, ciNPT was applied under sterile conditions in the operating room using the Prevena device, which exerts a continuous negative pressure of 125 mm Hg on the closed incision during the time of application. The device was removed at 5-7 days postoperatively, and no further wound dressings were used in the treatment group unless an SSI occurred.
The control group experienced more frequent SSIs (33.3%) than the intervention group (13.2%) (P =.0015). This difference was based on an increased rate of Szilagyi grade I SSI in the control group (24.6% vs. 8.1%, P = .0012), according to Alexander Gombert, MD, of the University Hospital Aachen (Germany), and his colleagues. The absolute risk difference based on the Szilagyi classification was –20.1 per 100 (95% confidence interval, –31.9 to –8.2).
In addition, there was a statistically significantly lower rate of SSI when using ciNPT within the subgroups at greater risk of infection, compared with controls: PAD stage greater than or equal to 3 (P less than .001), body mass index greater than 25 kg/m2 (P less than .001), and previous groin incision (P = .016).
There were no statistical differences between the two groups in Szilagyi grade II and III SSIs (which occurred in 5.8% of all procedures).
No potentially device-related complications were observed in the trial and there were no failures of the device seen.
“The use of ciNPT rather than standard wound dressing after groin incision as access for vascular surgery was associated with a reduced rate of superficial SSI classified by Szilagyi, suggesting that ciNPT may be useful for reducing the SSI rate among high-risk patients,” the researchers concluded.
The trial was funded by Acelity. Dr. Gombert received travel grants from Acelity.
SOURCE: Gombert A et al. Eur J Vasc Surg. 2018 Jul 2. doi: 10.1016/j.ejvs.2018.05.018.
FROM THE EUROPEAN JOURNAL OF VASCULAR AND ENDOVASCULAR SURGERY
Key clinical point: Closed incision negative pressure therapy lessened the incidence of groin infection after vascular surgery.
Major finding: The control group experienced more frequent surgical site infections (33.3%) than the intervention group (13.2%) (P =.0015).
Study details: A randomized, controlled trial of 204 patients with peripheral artery disease who underwent vascular surgery.
Disclosures: The trial was funded by Acelity. Dr. Gombert received travel grants from Acelity.
Source: Gombert A et al. Eur J Vasc Surg. 2018 Jul 2. doi: 10.1016/j.ejvs.2018.05.018.
Nivolumab plus ipilimumab boosts response rate in refractory esophagogastric cancer
Nivolumab alone or in combination with ipilimumab met multiple endpoints against metastatic or locally advanced chemotherapy-refractory esophagogastric cancer in the recent phase 1/2 CheckMate-032 trial, thereby opening doors to a future phase 3 trial.
The agents demonstrated “clinically meaningful antitumor activity,” reported Yelena Y. Janjigian, MD, of Memorial Sloan Kettering Cancer Center, New York, and her coauthors.
After the 2017 ATTRACTION-2 trial demonstrated improved survival rates, “nivolumab was approved in Japan for the treatment of patients with chemotherapy-refractory gastric and gastroesophageal junction [GEJ] cancers regardless of programmed death-ligand 1 [PD-L1] status,” the authors wrote in the Journal of Clinical Oncology.
Nivolumab is a checkpoint inhibitor, like pembrolizumab, which “was approved for the treatment of patients with chemotherapy-refractory PD-L1–positive gastric/GEJ cancer on the basis of the promising clinical activity observed in the KEYNOTE-059 trial,” the authors noted. Testing nivolumab in a Western population would therefore build on these previous trials. Combining nivolumab, a PD-l inhibitor, with ipilimumab, a monoclonal antibody targeting cytotoxic T-lymphocyte antigen 4, was based on “synergistic activity” reported in preclinical models, the authors wrote.
Results from the ongoing CheckMate-032 trial included 160 patients with metastatic or locally advanced chemotherapy-refractory esophageal, gastric, or gastroesophageal junction cancer treated at centers in Europe and the United States. Just under 80% of patients had received two or more prior therapies.
In the present trial, patients were given one of three treatment regimens: nivolumab 3 mg/kg every 2 weeks, nivolumab 1 mg/kg plus ipilimumab 3 mg/kg every 3 weeks for four cycles (NIVO1 + IPI3), or nivolumab 3 mg/kg plus ipilimumab 1 mg/kg every 3 weeks for four cycles (NIVO3 + IPI1). The primary endpoint was objective response rate (ORR). Secondary endpoints included 12-month progression-free survival and 12-month overall survival (OS).
Patients in the NIVO1 + IPI3 group achieved the best ORR (24%) and 12-month progression-free survival (17%) and also showed a promising 12-month OS (35%), second only to nivolumab monotherapy (39%). PD-L1 status was not predictive of treatment response.
Although NIVO1 + IPI3 was the most clinically effective, almost half (47%) of these patients also had grade 3 or higher adverse events, compared with more favorable rates of 17% and 27% for nivolumab monotherapy and NIVO3 + IPI1, respectively.
Still, the authors concluded, “on the basis of the numerically higher overall response and landmark OS rates in the NIVO1 + IPI3 arm, this combination was considered more likely to offer clinical benefit relative to currently available treatment regimens for first-line metastatic esophagogastric cancer and was selected for further evaluation in the phase 3 CheckMate-649 study (NCT02872116).” This trial, along with another to investigate nivolumab in the adjuvant setting (NCT02743494), are ongoing.
CheckMate-032 was supported by Bristol-Myers Squibb. The authors also reported funding from Merck, Incyte, Gilead Sciences, and others.
SOURCE: Janjigian YY et al. J Clin Oncol. 2018 Aug 15. doi: 10.1200/JCO.2017.76.6212.
Nivolumab alone or in combination with ipilimumab met multiple endpoints against metastatic or locally advanced chemotherapy-refractory esophagogastric cancer in the recent phase 1/2 CheckMate-032 trial, thereby opening doors to a future phase 3 trial.
The agents demonstrated “clinically meaningful antitumor activity,” reported Yelena Y. Janjigian, MD, of Memorial Sloan Kettering Cancer Center, New York, and her coauthors.
After the 2017 ATTRACTION-2 trial demonstrated improved survival rates, “nivolumab was approved in Japan for the treatment of patients with chemotherapy-refractory gastric and gastroesophageal junction [GEJ] cancers regardless of programmed death-ligand 1 [PD-L1] status,” the authors wrote in the Journal of Clinical Oncology.
Nivolumab is a checkpoint inhibitor, like pembrolizumab, which “was approved for the treatment of patients with chemotherapy-refractory PD-L1–positive gastric/GEJ cancer on the basis of the promising clinical activity observed in the KEYNOTE-059 trial,” the authors noted. Testing nivolumab in a Western population would therefore build on these previous trials. Combining nivolumab, a PD-l inhibitor, with ipilimumab, a monoclonal antibody targeting cytotoxic T-lymphocyte antigen 4, was based on “synergistic activity” reported in preclinical models, the authors wrote.
Results from the ongoing CheckMate-032 trial included 160 patients with metastatic or locally advanced chemotherapy-refractory esophageal, gastric, or gastroesophageal junction cancer treated at centers in Europe and the United States. Just under 80% of patients had received two or more prior therapies.
In the present trial, patients were given one of three treatment regimens: nivolumab 3 mg/kg every 2 weeks, nivolumab 1 mg/kg plus ipilimumab 3 mg/kg every 3 weeks for four cycles (NIVO1 + IPI3), or nivolumab 3 mg/kg plus ipilimumab 1 mg/kg every 3 weeks for four cycles (NIVO3 + IPI1). The primary endpoint was objective response rate (ORR). Secondary endpoints included 12-month progression-free survival and 12-month overall survival (OS).
Patients in the NIVO1 + IPI3 group achieved the best ORR (24%) and 12-month progression-free survival (17%) and also showed a promising 12-month OS (35%), second only to nivolumab monotherapy (39%). PD-L1 status was not predictive of treatment response.
Although NIVO1 + IPI3 was the most clinically effective, almost half (47%) of these patients also had grade 3 or higher adverse events, compared with more favorable rates of 17% and 27% for nivolumab monotherapy and NIVO3 + IPI1, respectively.
Still, the authors concluded, “on the basis of the numerically higher overall response and landmark OS rates in the NIVO1 + IPI3 arm, this combination was considered more likely to offer clinical benefit relative to currently available treatment regimens for first-line metastatic esophagogastric cancer and was selected for further evaluation in the phase 3 CheckMate-649 study (NCT02872116).” This trial, along with another to investigate nivolumab in the adjuvant setting (NCT02743494), are ongoing.
CheckMate-032 was supported by Bristol-Myers Squibb. The authors also reported funding from Merck, Incyte, Gilead Sciences, and others.
SOURCE: Janjigian YY et al. J Clin Oncol. 2018 Aug 15. doi: 10.1200/JCO.2017.76.6212.
Nivolumab alone or in combination with ipilimumab met multiple endpoints against metastatic or locally advanced chemotherapy-refractory esophagogastric cancer in the recent phase 1/2 CheckMate-032 trial, thereby opening doors to a future phase 3 trial.
The agents demonstrated “clinically meaningful antitumor activity,” reported Yelena Y. Janjigian, MD, of Memorial Sloan Kettering Cancer Center, New York, and her coauthors.
After the 2017 ATTRACTION-2 trial demonstrated improved survival rates, “nivolumab was approved in Japan for the treatment of patients with chemotherapy-refractory gastric and gastroesophageal junction [GEJ] cancers regardless of programmed death-ligand 1 [PD-L1] status,” the authors wrote in the Journal of Clinical Oncology.
Nivolumab is a checkpoint inhibitor, like pembrolizumab, which “was approved for the treatment of patients with chemotherapy-refractory PD-L1–positive gastric/GEJ cancer on the basis of the promising clinical activity observed in the KEYNOTE-059 trial,” the authors noted. Testing nivolumab in a Western population would therefore build on these previous trials. Combining nivolumab, a PD-l inhibitor, with ipilimumab, a monoclonal antibody targeting cytotoxic T-lymphocyte antigen 4, was based on “synergistic activity” reported in preclinical models, the authors wrote.
Results from the ongoing CheckMate-032 trial included 160 patients with metastatic or locally advanced chemotherapy-refractory esophageal, gastric, or gastroesophageal junction cancer treated at centers in Europe and the United States. Just under 80% of patients had received two or more prior therapies.
In the present trial, patients were given one of three treatment regimens: nivolumab 3 mg/kg every 2 weeks, nivolumab 1 mg/kg plus ipilimumab 3 mg/kg every 3 weeks for four cycles (NIVO1 + IPI3), or nivolumab 3 mg/kg plus ipilimumab 1 mg/kg every 3 weeks for four cycles (NIVO3 + IPI1). The primary endpoint was objective response rate (ORR). Secondary endpoints included 12-month progression-free survival and 12-month overall survival (OS).
Patients in the NIVO1 + IPI3 group achieved the best ORR (24%) and 12-month progression-free survival (17%) and also showed a promising 12-month OS (35%), second only to nivolumab monotherapy (39%). PD-L1 status was not predictive of treatment response.
Although NIVO1 + IPI3 was the most clinically effective, almost half (47%) of these patients also had grade 3 or higher adverse events, compared with more favorable rates of 17% and 27% for nivolumab monotherapy and NIVO3 + IPI1, respectively.
Still, the authors concluded, “on the basis of the numerically higher overall response and landmark OS rates in the NIVO1 + IPI3 arm, this combination was considered more likely to offer clinical benefit relative to currently available treatment regimens for first-line metastatic esophagogastric cancer and was selected for further evaluation in the phase 3 CheckMate-649 study (NCT02872116).” This trial, along with another to investigate nivolumab in the adjuvant setting (NCT02743494), are ongoing.
CheckMate-032 was supported by Bristol-Myers Squibb. The authors also reported funding from Merck, Incyte, Gilead Sciences, and others.
SOURCE: Janjigian YY et al. J Clin Oncol. 2018 Aug 15. doi: 10.1200/JCO.2017.76.6212.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Both nivolumab and nivolumab plus ipilimumab were effective in patients with chemotherapy-refractory esophagogastric cancer.
Major finding: Treatment with nivolumab plus ipilimumab was associated with an objective response rate of 24%.
Study details: CheckMate-032 is an ongoing phase 1/2 trial involving 160 patients with metastatic or locally advanced chemotherapy-refractory esophageal, gastric, or gastroesophageal junction cancer from centers in Europe and the United States.
Disclosures: The study was supported by Bristol-Myers Squibb. The authors also reported funding from Merck, Incyte, Gilead Sciences, and others.
Source: Janjigian YY et al. J Clin Oncol. 2018 Aug 15. doi: 10.1200/JCO.2017.76.6212.
Replacing warfarin with a NOAC in patients on chronic anticoagulation therapy
Hospitalists must consider clinical factors and patient preferences
Case
A 70-year old woman with hypertension, diabetes, nonischemic stroke, moderate renal insufficiency (creatinine clearance [CrCl] 45 mL/min), heart failure, and nonvalvular atrial fibrillation (AF) on warfarin is admitted because of a very supratherapeutic INR. She reports labile INR values despite strict adherence to her medication regimen. Her cancer screening tests had previously been unremarkable. She inquires about the risks and benefits of switching to a novel oral anticoagulant (NOAC) as advertised on television. Should you consider it while she is still in the hospital?
Brief overview of the issue
Lifelong anticoagulation therapy is common among patients with AF or recurrent venous thromboembolism (VTE). Until the advent of NOACs, a great majority of patients were prescribed warfarin, the oral vitamin K antagonist that requires regular blood tests for monitoring of the INR. In contrast to warfarin, NOACs are direct-acting agents (hence also known as “direct oral anticoagulants” or DOACs) that are selective for one specific coagulation factor, either thrombin (e.g., dabigatran) or factor Xa (e.g., rivaroxaban, apixaban, and edoxaban, all with an “X” in their names).

NOACS have been studied and approved by the Food and Drug Administration for nonvalvular AF, i.e., patients without rheumatic mitral stenosis, mechanical or bioprosthetic heart valve, or prior mitral valve repair. Compared to warfarin, NOACS have fewer drug or food interactions, have more predictable pharmacokinetics, and may be associated with reduced risk of major bleeding depending on the agent. The latter is a particularly attractive feature of NOAC therapy, especially when its use is considered among older patients at risk of intracranial hemorrhage (ICH), such as those with previous strokes, ICH, or reduced renal function. Unfortunately, data on the efficacy and safety of the use of NOACs in certain patient populations (e.g., those with severe renal insufficiency, active malignancy, the elderly, patients with suboptimal medication adherence) are generally lacking.
Overview of the data
There are no randomized controlled trials (RCTs) addressing the clinical benefits of switching from warfarin to NOAC therapy. However, based on a number of RCTs comparing warfarin to individual NOACs and their related meta-analyses, the following conclusions may be made about their attributes:
1. Noninferiority to warfarin in reducing the risk of ischemic stroke in AF.
2. Association with a lower rate of major bleeds (statistically significant or trend) and a lower rate of ICH and hemorrhagic strokes compared to warfarin.
3. Association with a higher rate of gastrointestinal bleeding compared to warfarin (except for apixaban, low-dose dabigatran, and edoxaban1).
4. Association with a decreased rate of all stroke and thromboembolism events compared to warfarin.
5. Association with a slightly decreased all-cause mortality in AF compared to warfarin in many studies,2-8 but not all.1,9
6. Noninferiority to warfarin in all-cause mortality in patients with VTE and for its secondary prevention.1,4
NOACS should be used with caution or avoided altogether in patients with severe liver disease or renal insufficiency (see Table 1). 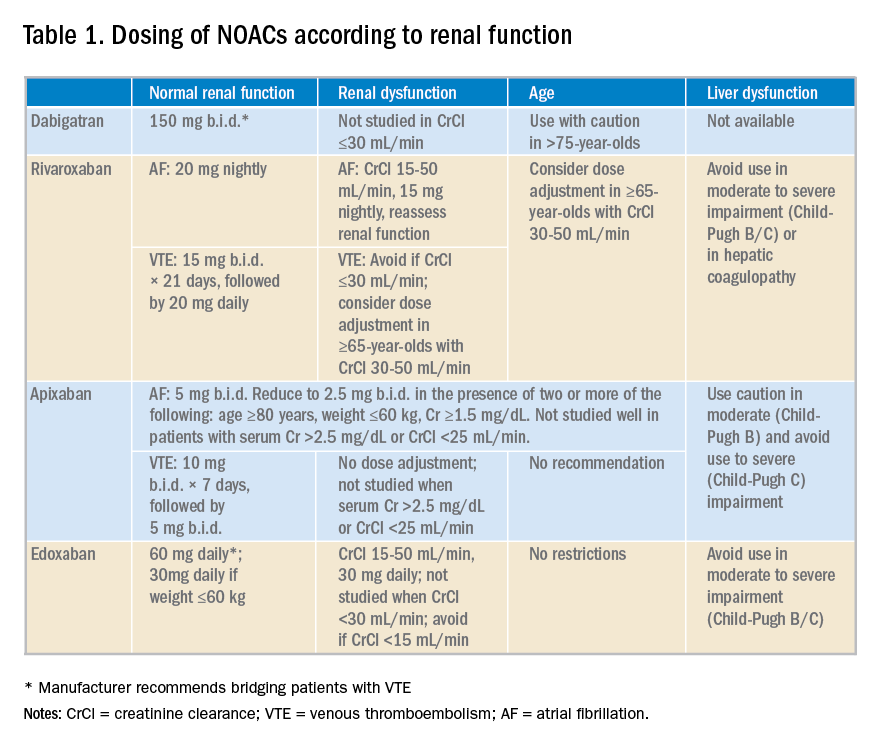
Potential advantages and disadvantages of NOAC therapy are listed in Table 2.
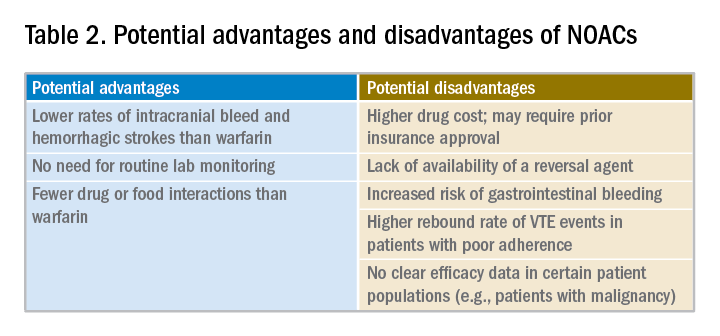
It should be emphasized that in patients with cancer or hypercoagulable state, no clear efficacy or safety data are currently available for the use of NOACs.

The 2016 CHEST guideline on antithrombotic therapy for VTE recommends NOACs over warfarin.10 The 2012 European Society of Cardiology AF guidelines also recommend NOACs over warfarin.11 However, the 2014 American College of Cardiology/American Heart Association/Heart Rhythm Society guidelines on AF state that it is not necessary to change to a NOAC when patients are “stable, easily controlled, and satisfied with warfarin therapy.”12
Data from a relatively small, short-term study examining the safety of switching patients from warfarin to a NOAC suggest that although bleeding events are relatively common (12%) following such a switch, major bleeding and cardiac or cerebrovascular events are rare.10
Application of the data to our original case
Given a high calculated CHADS2VASC score of 8 in our patient, she has a clear indication for anticoagulation for AF. Her history of labile INRs, ischemic stroke, and moderate renal insufficiency place her at high risk for ICH.
A NOAC may reduce this risk but possibly at the expense of an increased risk for a gastrointestinal bleed. More importantly, however, she may be a good candidate for a switch to a NOAC because of her labile INRs despite good medication adherence. Her warfarin can be held while hospitalized and a NOAC may be initiated when the INR falls below 2.

Prior to discharge, potential cost of the drug to the patient should be explored and discussed. It is also important to involve the primary care physician in the decision-making process. Ultimately, selection of an appropriate NOAC should be based on a careful review of its risks and benefits, clinical factors, patient preference, and shared decision making.
Bottom line
Hospitalists are in a great position to discuss a switch to a NOAC in selected patients with history of good medication adherence and labile INRs or ICH risk factors.
Dr. Geisler, Dr. Liao, and Dr. Manian are hospitalists at Massachusetts General Hospital in Boston.
References
1. Sharma M et al. Efficacy and harms of direct oral anticoagulants in the elderly for stroke prevention in atrial fibrillation and secondary prevention of venous thromboembolism: Systematic review and meta-analysis. Circulation. 2015;132(3):194-204.
2. Ruff CT et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet. 2014;383(9921):955-62.
3. Dentali F et al. Efficacy and safety of the novel oral anticoagulants in atrial fibrillation: A systematic review and meta-analysis of the literature. Circulation. 2012;126(20):2381-91.
4. Adam SS et al. Comparative effectiveness of warfarin and new oral anticoagulants for the management of atrial fibrillation and venous thromboembolism: A systematic review. Ann Intern Med. 2012;157(11):796-807.
5. Bruins Slot KM and Berge E. Factor Xa inhibitors versus vitamin K antagonists for preventing cerebral or systemic embolism in patients with atrial fibrillation. Cochrane Database Syst Rev. 2013(8):CD008980.
6. Gomez-Outes A et al. Dabigatran, rivaroxaban, or apixaban versus warfarin in patients with nonvalvular atrial fibrillation: A systematic review and meta-analysis of subgroups. Thrombosis. 2013;2013:640723.
7. Miller CS et al. Meta-analysis of efficacy and safety of new oral anticoagulants (dabigatran, rivaroxaban, apixaban) versus warfarin in patients with atrial fibrillation. Am J Cardiol. 2012;110(3):453-60.
8. Baker WL and Phung OJ. Systematic review and adjusted indirect comparison meta-analysis of oral anticoagulants in atrial fibrillation. Circ Cardiovasc Qual Outcomes. 2012;5(5):711-19.
9. Ntaios G et al. Nonvitamin-K-antagonist oral anticoagulants in patients with atrial fibrillation and previous stroke or transient ischemic attack: A systematic review and meta-analysis of randomized controlled trials. Stroke. 2012;43(12):3298-304.
10. Kearon C et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149(2):315-52.
11. Camm AJ et al. 2012 focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation – developed with the special contribution of the European Heart Rhythm Association. Europace. 2012;14(10):1385-413.
12. January CT et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association task force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):e199-267.
Quiz
When considering a switch from warfarin to a NOAC, all the following factors should be considered a potential advantage, except:
A. No need for routing lab monitoring.
B. Lower risk of gastrointestinal bleeding.
C. Fewer drug interactions.
D. Lower rates of intracranial bleed and hemorrhagic stroke.
The correct answer is B. NOACs have been associated with lower risk of intracranial bleed and hemorrhagic stroke but not gastrointestinal bleed. Routine lab monitoring is not necessary during their use and they are associated with fewer drug interactions compared to warfarin.
Key Points
- NOACs represent a clear advancement in our anticoagulation armamentarium.
- Potential advantages of their use include lower rates of intracranial bleed and hemorrhagic strokes, fewer drug or food interactions, and lack of need for routing lab monitoring.
- Potential disadvantages of their use include increased rates of gastrointestinal bleed with some agents, general lack of availability of reversal agents, higher drug cost, unsuitability in patients with poor medication compliance, and lack of efficacy data in certain patient populations.
- Decision to switch from warfarin to a NOAC should thoroughly consider its pros and cons, clinical factors, and patient preferences.
Hospitalists must consider clinical factors and patient preferences
Hospitalists must consider clinical factors and patient preferences
Case
A 70-year old woman with hypertension, diabetes, nonischemic stroke, moderate renal insufficiency (creatinine clearance [CrCl] 45 mL/min), heart failure, and nonvalvular atrial fibrillation (AF) on warfarin is admitted because of a very supratherapeutic INR. She reports labile INR values despite strict adherence to her medication regimen. Her cancer screening tests had previously been unremarkable. She inquires about the risks and benefits of switching to a novel oral anticoagulant (NOAC) as advertised on television. Should you consider it while she is still in the hospital?
Brief overview of the issue
Lifelong anticoagulation therapy is common among patients with AF or recurrent venous thromboembolism (VTE). Until the advent of NOACs, a great majority of patients were prescribed warfarin, the oral vitamin K antagonist that requires regular blood tests for monitoring of the INR. In contrast to warfarin, NOACs are direct-acting agents (hence also known as “direct oral anticoagulants” or DOACs) that are selective for one specific coagulation factor, either thrombin (e.g., dabigatran) or factor Xa (e.g., rivaroxaban, apixaban, and edoxaban, all with an “X” in their names).
NOACS have been studied and approved by the Food and Drug Administration for nonvalvular AF, i.e., patients without rheumatic mitral stenosis, mechanical or bioprosthetic heart valve, or prior mitral valve repair. Compared to warfarin, NOACS have fewer drug or food interactions, have more predictable pharmacokinetics, and may be associated with reduced risk of major bleeding depending on the agent. The latter is a particularly attractive feature of NOAC therapy, especially when its use is considered among older patients at risk of intracranial hemorrhage (ICH), such as those with previous strokes, ICH, or reduced renal function. Unfortunately, data on the efficacy and safety of the use of NOACs in certain patient populations (e.g., those with severe renal insufficiency, active malignancy, the elderly, patients with suboptimal medication adherence) are generally lacking.
Overview of the data
There are no randomized controlled trials (RCTs) addressing the clinical benefits of switching from warfarin to NOAC therapy. However, based on a number of RCTs comparing warfarin to individual NOACs and their related meta-analyses, the following conclusions may be made about their attributes:
1. Noninferiority to warfarin in reducing the risk of ischemic stroke in AF.
2. Association with a lower rate of major bleeds (statistically significant or trend) and a lower rate of ICH and hemorrhagic strokes compared to warfarin.
3. Association with a higher rate of gastrointestinal bleeding compared to warfarin (except for apixaban, low-dose dabigatran, and edoxaban1).
4. Association with a decreased rate of all stroke and thromboembolism events compared to warfarin.
5. Association with a slightly decreased all-cause mortality in AF compared to warfarin in many studies,2-8 but not all.1,9
6. Noninferiority to warfarin in all-cause mortality in patients with VTE and for its secondary prevention.1,4
NOACS should be used with caution or avoided altogether in patients with severe liver disease or renal insufficiency (see Table 1).
Potential advantages and disadvantages of NOAC therapy are listed in Table 2.
It should be emphasized that in patients with cancer or hypercoagulable state, no clear efficacy or safety data are currently available for the use of NOACs.
The 2016 CHEST guideline on antithrombotic therapy for VTE recommends NOACs over warfarin.10 The 2012 European Society of Cardiology AF guidelines also recommend NOACs over warfarin.11 However, the 2014 American College of Cardiology/American Heart Association/Heart Rhythm Society guidelines on AF state that it is not necessary to change to a NOAC when patients are “stable, easily controlled, and satisfied with warfarin therapy.”12
Data from a relatively small, short-term study examining the safety of switching patients from warfarin to a NOAC suggest that although bleeding events are relatively common (12%) following such a switch, major bleeding and cardiac or cerebrovascular events are rare.10
Application of the data to our original case
Given a high calculated CHADS2VASC score of 8 in our patient, she has a clear indication for anticoagulation for AF. Her history of labile INRs, ischemic stroke, and moderate renal insufficiency place her at high risk for ICH.
A NOAC may reduce this risk but possibly at the expense of an increased risk for a gastrointestinal bleed. More importantly, however, she may be a good candidate for a switch to a NOAC because of her labile INRs despite good medication adherence. Her warfarin can be held while hospitalized and a NOAC may be initiated when the INR falls below 2.
Prior to discharge, potential cost of the drug to the patient should be explored and discussed. It is also important to involve the primary care physician in the decision-making process. Ultimately, selection of an appropriate NOAC should be based on a careful review of its risks and benefits, clinical factors, patient preference, and shared decision making.
Bottom line
Hospitalists are in a great position to discuss a switch to a NOAC in selected patients with history of good medication adherence and labile INRs or ICH risk factors.
Dr. Geisler, Dr. Liao, and Dr. Manian are hospitalists at Massachusetts General Hospital in Boston.
References
1. Sharma M et al. Efficacy and harms of direct oral anticoagulants in the elderly for stroke prevention in atrial fibrillation and secondary prevention of venous thromboembolism: Systematic review and meta-analysis. Circulation. 2015;132(3):194-204.
2. Ruff CT et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet. 2014;383(9921):955-62.
3. Dentali F et al. Efficacy and safety of the novel oral anticoagulants in atrial fibrillation: A systematic review and meta-analysis of the literature. Circulation. 2012;126(20):2381-91.
4. Adam SS et al. Comparative effectiveness of warfarin and new oral anticoagulants for the management of atrial fibrillation and venous thromboembolism: A systematic review. Ann Intern Med. 2012;157(11):796-807.
5. Bruins Slot KM and Berge E. Factor Xa inhibitors versus vitamin K antagonists for preventing cerebral or systemic embolism in patients with atrial fibrillation. Cochrane Database Syst Rev. 2013(8):CD008980.
6. Gomez-Outes A et al. Dabigatran, rivaroxaban, or apixaban versus warfarin in patients with nonvalvular atrial fibrillation: A systematic review and meta-analysis of subgroups. Thrombosis. 2013;2013:640723.
7. Miller CS et al. Meta-analysis of efficacy and safety of new oral anticoagulants (dabigatran, rivaroxaban, apixaban) versus warfarin in patients with atrial fibrillation. Am J Cardiol. 2012;110(3):453-60.
8. Baker WL and Phung OJ. Systematic review and adjusted indirect comparison meta-analysis of oral anticoagulants in atrial fibrillation. Circ Cardiovasc Qual Outcomes. 2012;5(5):711-19.
9. Ntaios G et al. Nonvitamin-K-antagonist oral anticoagulants in patients with atrial fibrillation and previous stroke or transient ischemic attack: A systematic review and meta-analysis of randomized controlled trials. Stroke. 2012;43(12):3298-304.
10. Kearon C et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149(2):315-52.
11. Camm AJ et al. 2012 focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation – developed with the special contribution of the European Heart Rhythm Association. Europace. 2012;14(10):1385-413.
12. January CT et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association task force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):e199-267.
Quiz
When considering a switch from warfarin to a NOAC, all the following factors should be considered a potential advantage, except:
A. No need for routing lab monitoring.
B. Lower risk of gastrointestinal bleeding.
C. Fewer drug interactions.
D. Lower rates of intracranial bleed and hemorrhagic stroke.
The correct answer is B. NOACs have been associated with lower risk of intracranial bleed and hemorrhagic stroke but not gastrointestinal bleed. Routine lab monitoring is not necessary during their use and they are associated with fewer drug interactions compared to warfarin.
Key Points
- NOACs represent a clear advancement in our anticoagulation armamentarium.
- Potential advantages of their use include lower rates of intracranial bleed and hemorrhagic strokes, fewer drug or food interactions, and lack of need for routing lab monitoring.
- Potential disadvantages of their use include increased rates of gastrointestinal bleed with some agents, general lack of availability of reversal agents, higher drug cost, unsuitability in patients with poor medication compliance, and lack of efficacy data in certain patient populations.
- Decision to switch from warfarin to a NOAC should thoroughly consider its pros and cons, clinical factors, and patient preferences.
Case
A 70-year old woman with hypertension, diabetes, nonischemic stroke, moderate renal insufficiency (creatinine clearance [CrCl] 45 mL/min), heart failure, and nonvalvular atrial fibrillation (AF) on warfarin is admitted because of a very supratherapeutic INR. She reports labile INR values despite strict adherence to her medication regimen. Her cancer screening tests had previously been unremarkable. She inquires about the risks and benefits of switching to a novel oral anticoagulant (NOAC) as advertised on television. Should you consider it while she is still in the hospital?
Brief overview of the issue
Lifelong anticoagulation therapy is common among patients with AF or recurrent venous thromboembolism (VTE). Until the advent of NOACs, a great majority of patients were prescribed warfarin, the oral vitamin K antagonist that requires regular blood tests for monitoring of the INR. In contrast to warfarin, NOACs are direct-acting agents (hence also known as “direct oral anticoagulants” or DOACs) that are selective for one specific coagulation factor, either thrombin (e.g., dabigatran) or factor Xa (e.g., rivaroxaban, apixaban, and edoxaban, all with an “X” in their names).
NOACS have been studied and approved by the Food and Drug Administration for nonvalvular AF, i.e., patients without rheumatic mitral stenosis, mechanical or bioprosthetic heart valve, or prior mitral valve repair. Compared to warfarin, NOACS have fewer drug or food interactions, have more predictable pharmacokinetics, and may be associated with reduced risk of major bleeding depending on the agent. The latter is a particularly attractive feature of NOAC therapy, especially when its use is considered among older patients at risk of intracranial hemorrhage (ICH), such as those with previous strokes, ICH, or reduced renal function. Unfortunately, data on the efficacy and safety of the use of NOACs in certain patient populations (e.g., those with severe renal insufficiency, active malignancy, the elderly, patients with suboptimal medication adherence) are generally lacking.
Overview of the data
There are no randomized controlled trials (RCTs) addressing the clinical benefits of switching from warfarin to NOAC therapy. However, based on a number of RCTs comparing warfarin to individual NOACs and their related meta-analyses, the following conclusions may be made about their attributes:
1. Noninferiority to warfarin in reducing the risk of ischemic stroke in AF.
2. Association with a lower rate of major bleeds (statistically significant or trend) and a lower rate of ICH and hemorrhagic strokes compared to warfarin.
3. Association with a higher rate of gastrointestinal bleeding compared to warfarin (except for apixaban, low-dose dabigatran, and edoxaban1).
4. Association with a decreased rate of all stroke and thromboembolism events compared to warfarin.
5. Association with a slightly decreased all-cause mortality in AF compared to warfarin in many studies,2-8 but not all.1,9
6. Noninferiority to warfarin in all-cause mortality in patients with VTE and for its secondary prevention.1,4
NOACS should be used with caution or avoided altogether in patients with severe liver disease or renal insufficiency (see Table 1).
Potential advantages and disadvantages of NOAC therapy are listed in Table 2.
It should be emphasized that in patients with cancer or hypercoagulable state, no clear efficacy or safety data are currently available for the use of NOACs.
The 2016 CHEST guideline on antithrombotic therapy for VTE recommends NOACs over warfarin.10 The 2012 European Society of Cardiology AF guidelines also recommend NOACs over warfarin.11 However, the 2014 American College of Cardiology/American Heart Association/Heart Rhythm Society guidelines on AF state that it is not necessary to change to a NOAC when patients are “stable, easily controlled, and satisfied with warfarin therapy.”12
Data from a relatively small, short-term study examining the safety of switching patients from warfarin to a NOAC suggest that although bleeding events are relatively common (12%) following such a switch, major bleeding and cardiac or cerebrovascular events are rare.10
Application of the data to our original case
Given a high calculated CHADS2VASC score of 8 in our patient, she has a clear indication for anticoagulation for AF. Her history of labile INRs, ischemic stroke, and moderate renal insufficiency place her at high risk for ICH.
A NOAC may reduce this risk but possibly at the expense of an increased risk for a gastrointestinal bleed. More importantly, however, she may be a good candidate for a switch to a NOAC because of her labile INRs despite good medication adherence. Her warfarin can be held while hospitalized and a NOAC may be initiated when the INR falls below 2.
Prior to discharge, potential cost of the drug to the patient should be explored and discussed. It is also important to involve the primary care physician in the decision-making process. Ultimately, selection of an appropriate NOAC should be based on a careful review of its risks and benefits, clinical factors, patient preference, and shared decision making.
Bottom line
Hospitalists are in a great position to discuss a switch to a NOAC in selected patients with history of good medication adherence and labile INRs or ICH risk factors.
Dr. Geisler, Dr. Liao, and Dr. Manian are hospitalists at Massachusetts General Hospital in Boston.
References
1. Sharma M et al. Efficacy and harms of direct oral anticoagulants in the elderly for stroke prevention in atrial fibrillation and secondary prevention of venous thromboembolism: Systematic review and meta-analysis. Circulation. 2015;132(3):194-204.
2. Ruff CT et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet. 2014;383(9921):955-62.
3. Dentali F et al. Efficacy and safety of the novel oral anticoagulants in atrial fibrillation: A systematic review and meta-analysis of the literature. Circulation. 2012;126(20):2381-91.
4. Adam SS et al. Comparative effectiveness of warfarin and new oral anticoagulants for the management of atrial fibrillation and venous thromboembolism: A systematic review. Ann Intern Med. 2012;157(11):796-807.
5. Bruins Slot KM and Berge E. Factor Xa inhibitors versus vitamin K antagonists for preventing cerebral or systemic embolism in patients with atrial fibrillation. Cochrane Database Syst Rev. 2013(8):CD008980.
6. Gomez-Outes A et al. Dabigatran, rivaroxaban, or apixaban versus warfarin in patients with nonvalvular atrial fibrillation: A systematic review and meta-analysis of subgroups. Thrombosis. 2013;2013:640723.
7. Miller CS et al. Meta-analysis of efficacy and safety of new oral anticoagulants (dabigatran, rivaroxaban, apixaban) versus warfarin in patients with atrial fibrillation. Am J Cardiol. 2012;110(3):453-60.
8. Baker WL and Phung OJ. Systematic review and adjusted indirect comparison meta-analysis of oral anticoagulants in atrial fibrillation. Circ Cardiovasc Qual Outcomes. 2012;5(5):711-19.
9. Ntaios G et al. Nonvitamin-K-antagonist oral anticoagulants in patients with atrial fibrillation and previous stroke or transient ischemic attack: A systematic review and meta-analysis of randomized controlled trials. Stroke. 2012;43(12):3298-304.
10. Kearon C et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149(2):315-52.
11. Camm AJ et al. 2012 focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation – developed with the special contribution of the European Heart Rhythm Association. Europace. 2012;14(10):1385-413.
12. January CT et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association task force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130(23):e199-267.
Quiz
When considering a switch from warfarin to a NOAC, all the following factors should be considered a potential advantage, except:
A. No need for routing lab monitoring.
B. Lower risk of gastrointestinal bleeding.
C. Fewer drug interactions.
D. Lower rates of intracranial bleed and hemorrhagic stroke.
The correct answer is B. NOACs have been associated with lower risk of intracranial bleed and hemorrhagic stroke but not gastrointestinal bleed. Routine lab monitoring is not necessary during their use and they are associated with fewer drug interactions compared to warfarin.
Key Points
- NOACs represent a clear advancement in our anticoagulation armamentarium.
- Potential advantages of their use include lower rates of intracranial bleed and hemorrhagic strokes, fewer drug or food interactions, and lack of need for routing lab monitoring.
- Potential disadvantages of their use include increased rates of gastrointestinal bleed with some agents, general lack of availability of reversal agents, higher drug cost, unsuitability in patients with poor medication compliance, and lack of efficacy data in certain patient populations.
- Decision to switch from warfarin to a NOAC should thoroughly consider its pros and cons, clinical factors, and patient preferences.
Childhood change of residence raises psychoses risk in young adults
Children and adolescents who moved longer distances or more frequently before 16 years of age were significantly more likely to develop psychosis in early adulthood than were those with less residential mobility, according to data from about 1.4 million children and adolescents in Sweden.
Data from previous studies have supported a link between childhood residential mobility and subsequent nonaffective psychoses, but no research has addressed the effects in later adolescence and young adulthood until now, wrote Ceri Price of Cardiff (Wales) University and colleagues.
In a study published in JAMA Psychiatry, the researchers reviewed data from a population-based cohort of individuals who were born in Sweden between Jan. 1, 1982, and Dec. 31, 1995, and lived in Sweden at age 16 years. The participants were followed from their 16th birthdays until a diagnosis of a nonaffective psychotic disorder, death, censorship because of emigration, or Dec. 31, 2011 – whichever came first.
Overall, the most sensitive range for an association between moving and psychosis was ages 16-19 years; the adjusted hazard ratio for a nonaffective psychotic disorder was 1.99 for participants who moved each year between ages 16 and 19 years, compared with those who never moved. In addition, moving greater distances before 16 years of age was independently associated with an increased risk of nonaffective psychosis (HR, 1.11) and the data suggested a nonlinear threshold effect when the distance moved exceeded 30 km.
A total of 4,537 individuals had a nonaffective psychotic disorder at a median 21 years of age, and a dose-response relationship emerged between more frequent moves and increased risk of nonaffective psychosis after controlling for confounding variables.
By contrast, a single move in young adulthood was not associated with increased psychosis risk, but moving at least four times during young adulthood was associated with an increased risk (adjusted HR, 1.82).
The study findings were strengthened by the longitudinal design and large population, but they were limited by several factors, including an absence of data on other adverse childhood experiences, such as family discord; peer relationships, such as friendships and bullying; and information on school changes and the disruption of peer relationships, the researchers wrote.
However, the results support the theory that psychosis risk can be affected by the disruption of social networks, peer support, and identity formation that occurs when children and adolescents move, and these results have potential implications for child health services and social policy, they noted.
“It is important that health, social, and educational practitioners ensure that children and adolescents who are newly resident to their neighborhoods receive adequate support to minimize the risks of adverse outcomes during adulthood, and every effort should be made to ensure the effective transfer of care for highly mobile children who are already in contact with health and social services,” they said.
The researchers had no financial conflicts to disclose. The study was supported in part by the Wellcome Trust and the Royal Society.
SOURCE: Price C et al. JAMA Psychiatry. 2018 Aug 22. doi: 10.1001/jamapsychiatry.2018.2233.
Children and adolescents who moved longer distances or more frequently before 16 years of age were significantly more likely to develop psychosis in early adulthood than were those with less residential mobility, according to data from about 1.4 million children and adolescents in Sweden.
Data from previous studies have supported a link between childhood residential mobility and subsequent nonaffective psychoses, but no research has addressed the effects in later adolescence and young adulthood until now, wrote Ceri Price of Cardiff (Wales) University and colleagues.
In a study published in JAMA Psychiatry, the researchers reviewed data from a population-based cohort of individuals who were born in Sweden between Jan. 1, 1982, and Dec. 31, 1995, and lived in Sweden at age 16 years. The participants were followed from their 16th birthdays until a diagnosis of a nonaffective psychotic disorder, death, censorship because of emigration, or Dec. 31, 2011 – whichever came first.
Overall, the most sensitive range for an association between moving and psychosis was ages 16-19 years; the adjusted hazard ratio for a nonaffective psychotic disorder was 1.99 for participants who moved each year between ages 16 and 19 years, compared with those who never moved. In addition, moving greater distances before 16 years of age was independently associated with an increased risk of nonaffective psychosis (HR, 1.11) and the data suggested a nonlinear threshold effect when the distance moved exceeded 30 km.
A total of 4,537 individuals had a nonaffective psychotic disorder at a median 21 years of age, and a dose-response relationship emerged between more frequent moves and increased risk of nonaffective psychosis after controlling for confounding variables.
By contrast, a single move in young adulthood was not associated with increased psychosis risk, but moving at least four times during young adulthood was associated with an increased risk (adjusted HR, 1.82).
The study findings were strengthened by the longitudinal design and large population, but they were limited by several factors, including an absence of data on other adverse childhood experiences, such as family discord; peer relationships, such as friendships and bullying; and information on school changes and the disruption of peer relationships, the researchers wrote.
However, the results support the theory that psychosis risk can be affected by the disruption of social networks, peer support, and identity formation that occurs when children and adolescents move, and these results have potential implications for child health services and social policy, they noted.
“It is important that health, social, and educational practitioners ensure that children and adolescents who are newly resident to their neighborhoods receive adequate support to minimize the risks of adverse outcomes during adulthood, and every effort should be made to ensure the effective transfer of care for highly mobile children who are already in contact with health and social services,” they said.
The researchers had no financial conflicts to disclose. The study was supported in part by the Wellcome Trust and the Royal Society.
SOURCE: Price C et al. JAMA Psychiatry. 2018 Aug 22. doi: 10.1001/jamapsychiatry.2018.2233.
Children and adolescents who moved longer distances or more frequently before 16 years of age were significantly more likely to develop psychosis in early adulthood than were those with less residential mobility, according to data from about 1.4 million children and adolescents in Sweden.
Data from previous studies have supported a link between childhood residential mobility and subsequent nonaffective psychoses, but no research has addressed the effects in later adolescence and young adulthood until now, wrote Ceri Price of Cardiff (Wales) University and colleagues.
In a study published in JAMA Psychiatry, the researchers reviewed data from a population-based cohort of individuals who were born in Sweden between Jan. 1, 1982, and Dec. 31, 1995, and lived in Sweden at age 16 years. The participants were followed from their 16th birthdays until a diagnosis of a nonaffective psychotic disorder, death, censorship because of emigration, or Dec. 31, 2011 – whichever came first.
Overall, the most sensitive range for an association between moving and psychosis was ages 16-19 years; the adjusted hazard ratio for a nonaffective psychotic disorder was 1.99 for participants who moved each year between ages 16 and 19 years, compared with those who never moved. In addition, moving greater distances before 16 years of age was independently associated with an increased risk of nonaffective psychosis (HR, 1.11) and the data suggested a nonlinear threshold effect when the distance moved exceeded 30 km.
A total of 4,537 individuals had a nonaffective psychotic disorder at a median 21 years of age, and a dose-response relationship emerged between more frequent moves and increased risk of nonaffective psychosis after controlling for confounding variables.
By contrast, a single move in young adulthood was not associated with increased psychosis risk, but moving at least four times during young adulthood was associated with an increased risk (adjusted HR, 1.82).
The study findings were strengthened by the longitudinal design and large population, but they were limited by several factors, including an absence of data on other adverse childhood experiences, such as family discord; peer relationships, such as friendships and bullying; and information on school changes and the disruption of peer relationships, the researchers wrote.
However, the results support the theory that psychosis risk can be affected by the disruption of social networks, peer support, and identity formation that occurs when children and adolescents move, and these results have potential implications for child health services and social policy, they noted.
“It is important that health, social, and educational practitioners ensure that children and adolescents who are newly resident to their neighborhoods receive adequate support to minimize the risks of adverse outcomes during adulthood, and every effort should be made to ensure the effective transfer of care for highly mobile children who are already in contact with health and social services,” they said.
The researchers had no financial conflicts to disclose. The study was supported in part by the Wellcome Trust and the Royal Society.
SOURCE: Price C et al. JAMA Psychiatry. 2018 Aug 22. doi: 10.1001/jamapsychiatry.2018.2233.
FROM JAMA PSYCHIATRY
Key clinical point: Clinicians and teachers should ensure that children and adolescents who are new to communities receive support “to minimize the risks of adverse outcomes during adulthood.”
Major finding: Those who moved residentially each year between 16 and 19 years of age were significantly more likely to develop nonaffective psychoses, compared with those who never moved (hazard ratio, 1.99).
Study details: The data come from a prospective cohort study of 1,440,383 youth living in Sweden.
Disclosures: The researchers had no financial conflicts to disclose. The study was supported in part by the Wellcome Trust and the Royal Society.
Source: Price C et al. JAMA Psychiatry. 2018 Aug 22. doi: 10.1001/jamapsychiatry.2018.2233.
Mailing out fecal tests may improve CRC screening rates
Mailing fecal immunochemical tests (FITs) to overdue patients improved the rate of colorectal cancer screening in community health centers, results of a recent randomized trial show.
Outreach by mail led to a 3.4–percentage point increase in completion of FIT, compared with clinics who did not participate in the intervention, according to results of the randomized Strategies and Opportunities to STOP Colon Cancer in Priority Populations (STOP CRC) trial.
Although that difference was statistically significant, investigators said the improvement was less than expected based on previous experience, including a pilot study showing that the strategy of mailing fecal tests boosted completion rates by 38%.
Based on that discrepancy, additional strategies may be needed to support implementation of FIT mailing programs in low-resource health centers, reported Gloria D. Coronado, PhD, Kaiser Permanente Center for Health Research, Portland, Ore., and coinvestigators.
“This work demonstrates that mailed FIT outreach programs can have clinical impact when integrated into clinical work flows, but emphasizes the need to identify additional strategies to support program implementation in low-resource health centers,” Dr. Coronado and coauthors said in JAMA Internal Medicine.
The STOP CRC study included 26 federally qualified health center clinics serving low-income populations in Oregon and California. Investigators identified a total of 41,193 adults overdue for colorectal cancer screening between Feb. 4, 2014 and Feb. 3, 2015.
The core of the intervention was a set of electronic health record–embedded tools that identified adults due for screening and allowed staff to generate letters and mailing labels for a series of three mailings. The first mailing was an introductory letter, the second was a FIT kit packet that included wordless instructions, and the third was a reminder letter.
For clinics that participated in the intervention, the rate of FIT completion was 13.9%, versus 10.4%, a difference that was statistically significant (95% confidence interval, 0.1%-6.8%; P = .047), according to investigators. Likewise, the proportion of participants completing any CRC screening was significantly higher in the intervention clinics (18.3% versus 14.5%; 3.8 percentage points difference; 95% CI, 0.6%-7.0%; P = .024).
Somewhat larger effects were seen in an analysis that accounted for delays in implementation of the program. In that analysis, FIT completion rates were 17.6% for the intervention clinics and 12.8% for the usual care clinics (95% CI, 0.9-8.6%; P = .020), with similar increases seen in the proportion of patients receiving any CRC screening.
These increases in screening occurred despite “relatively low” implementation of the program, Dr. Coronado and colleagues said.
In the pilot study, a concerted effort was made to ensure all eligible adults got the intervention; in this study, 6,925 out of 21,134 intervention participants (33%) got an introductory letter, and of those, 91% received the FIT and 59% got the reminder letter.
Implementation varied widely by health center, ranging from 6.5% to 68.2%, investigators said in their report.
One reason for low implementation may be that the program competed with other priorities in the clinics. In interviews, health center leaders said challenges in the clinic included time burden, limited organizational capacity, and challenges with the EHR and associated reporting tools.
“For most participating health centers, STOP CRC represented the first time EHR tools were used to deliver cancer screening services outside the clinic,” Dr. Coronado said. “Implementation might have increased with experience.”
The research reported by Dr. Coronado and coinvestigators was supported by the National Institutes of Health. Dr. Coronado reported serving as a coinvestigator on a study of an experimental blood test for colorectal cancer funded by EpiGenomics and as principal investigator on a study of an experimental FIT funded by Quidel Corporation. No other disclosures were reported.
SOURCE: Coronado GD et al. JAMA Intern Med. 2018 Aug 6. doi: 10.1001/jamainternmed.2018.3629.
Mailing fecal immunochemical tests (FITs) to overdue patients improved the rate of colorectal cancer screening in community health centers, results of a recent randomized trial show.
Outreach by mail led to a 3.4–percentage point increase in completion of FIT, compared with clinics who did not participate in the intervention, according to results of the randomized Strategies and Opportunities to STOP Colon Cancer in Priority Populations (STOP CRC) trial.
Although that difference was statistically significant, investigators said the improvement was less than expected based on previous experience, including a pilot study showing that the strategy of mailing fecal tests boosted completion rates by 38%.
Based on that discrepancy, additional strategies may be needed to support implementation of FIT mailing programs in low-resource health centers, reported Gloria D. Coronado, PhD, Kaiser Permanente Center for Health Research, Portland, Ore., and coinvestigators.
“This work demonstrates that mailed FIT outreach programs can have clinical impact when integrated into clinical work flows, but emphasizes the need to identify additional strategies to support program implementation in low-resource health centers,” Dr. Coronado and coauthors said in JAMA Internal Medicine.
The STOP CRC study included 26 federally qualified health center clinics serving low-income populations in Oregon and California. Investigators identified a total of 41,193 adults overdue for colorectal cancer screening between Feb. 4, 2014 and Feb. 3, 2015.
The core of the intervention was a set of electronic health record–embedded tools that identified adults due for screening and allowed staff to generate letters and mailing labels for a series of three mailings. The first mailing was an introductory letter, the second was a FIT kit packet that included wordless instructions, and the third was a reminder letter.
For clinics that participated in the intervention, the rate of FIT completion was 13.9%, versus 10.4%, a difference that was statistically significant (95% confidence interval, 0.1%-6.8%; P = .047), according to investigators. Likewise, the proportion of participants completing any CRC screening was significantly higher in the intervention clinics (18.3% versus 14.5%; 3.8 percentage points difference; 95% CI, 0.6%-7.0%; P = .024).
Somewhat larger effects were seen in an analysis that accounted for delays in implementation of the program. In that analysis, FIT completion rates were 17.6% for the intervention clinics and 12.8% for the usual care clinics (95% CI, 0.9-8.6%; P = .020), with similar increases seen in the proportion of patients receiving any CRC screening.
These increases in screening occurred despite “relatively low” implementation of the program, Dr. Coronado and colleagues said.
In the pilot study, a concerted effort was made to ensure all eligible adults got the intervention; in this study, 6,925 out of 21,134 intervention participants (33%) got an introductory letter, and of those, 91% received the FIT and 59% got the reminder letter.
Implementation varied widely by health center, ranging from 6.5% to 68.2%, investigators said in their report.
One reason for low implementation may be that the program competed with other priorities in the clinics. In interviews, health center leaders said challenges in the clinic included time burden, limited organizational capacity, and challenges with the EHR and associated reporting tools.
“For most participating health centers, STOP CRC represented the first time EHR tools were used to deliver cancer screening services outside the clinic,” Dr. Coronado said. “Implementation might have increased with experience.”
The research reported by Dr. Coronado and coinvestigators was supported by the National Institutes of Health. Dr. Coronado reported serving as a coinvestigator on a study of an experimental blood test for colorectal cancer funded by EpiGenomics and as principal investigator on a study of an experimental FIT funded by Quidel Corporation. No other disclosures were reported.
SOURCE: Coronado GD et al. JAMA Intern Med. 2018 Aug 6. doi: 10.1001/jamainternmed.2018.3629.
Mailing fecal immunochemical tests (FITs) to overdue patients improved the rate of colorectal cancer screening in community health centers, results of a recent randomized trial show.
Outreach by mail led to a 3.4–percentage point increase in completion of FIT, compared with clinics who did not participate in the intervention, according to results of the randomized Strategies and Opportunities to STOP Colon Cancer in Priority Populations (STOP CRC) trial.
Although that difference was statistically significant, investigators said the improvement was less than expected based on previous experience, including a pilot study showing that the strategy of mailing fecal tests boosted completion rates by 38%.
Based on that discrepancy, additional strategies may be needed to support implementation of FIT mailing programs in low-resource health centers, reported Gloria D. Coronado, PhD, Kaiser Permanente Center for Health Research, Portland, Ore., and coinvestigators.
“This work demonstrates that mailed FIT outreach programs can have clinical impact when integrated into clinical work flows, but emphasizes the need to identify additional strategies to support program implementation in low-resource health centers,” Dr. Coronado and coauthors said in JAMA Internal Medicine.
The STOP CRC study included 26 federally qualified health center clinics serving low-income populations in Oregon and California. Investigators identified a total of 41,193 adults overdue for colorectal cancer screening between Feb. 4, 2014 and Feb. 3, 2015.
The core of the intervention was a set of electronic health record–embedded tools that identified adults due for screening and allowed staff to generate letters and mailing labels for a series of three mailings. The first mailing was an introductory letter, the second was a FIT kit packet that included wordless instructions, and the third was a reminder letter.
For clinics that participated in the intervention, the rate of FIT completion was 13.9%, versus 10.4%, a difference that was statistically significant (95% confidence interval, 0.1%-6.8%; P = .047), according to investigators. Likewise, the proportion of participants completing any CRC screening was significantly higher in the intervention clinics (18.3% versus 14.5%; 3.8 percentage points difference; 95% CI, 0.6%-7.0%; P = .024).
Somewhat larger effects were seen in an analysis that accounted for delays in implementation of the program. In that analysis, FIT completion rates were 17.6% for the intervention clinics and 12.8% for the usual care clinics (95% CI, 0.9-8.6%; P = .020), with similar increases seen in the proportion of patients receiving any CRC screening.
These increases in screening occurred despite “relatively low” implementation of the program, Dr. Coronado and colleagues said.
In the pilot study, a concerted effort was made to ensure all eligible adults got the intervention; in this study, 6,925 out of 21,134 intervention participants (33%) got an introductory letter, and of those, 91% received the FIT and 59% got the reminder letter.
Implementation varied widely by health center, ranging from 6.5% to 68.2%, investigators said in their report.
One reason for low implementation may be that the program competed with other priorities in the clinics. In interviews, health center leaders said challenges in the clinic included time burden, limited organizational capacity, and challenges with the EHR and associated reporting tools.
“For most participating health centers, STOP CRC represented the first time EHR tools were used to deliver cancer screening services outside the clinic,” Dr. Coronado said. “Implementation might have increased with experience.”
The research reported by Dr. Coronado and coinvestigators was supported by the National Institutes of Health. Dr. Coronado reported serving as a coinvestigator on a study of an experimental blood test for colorectal cancer funded by EpiGenomics and as principal investigator on a study of an experimental FIT funded by Quidel Corporation. No other disclosures were reported.
SOURCE: Coronado GD et al. JAMA Intern Med. 2018 Aug 6. doi: 10.1001/jamainternmed.2018.3629.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Mailing fecal immunochemical tests (FITs) to overdue patients improved the rate of colorectal cancer screening, though not to the extent that had been seen in a pilot study.
Major finding: Outreach by mail led to a 3.4–percentage point increase in FIT completion for participating clinics versus clinics that implemented usual care.
Study details: STOP CRC, a cluster-randomized pragmatic clinical trial including 26 federally qualified health center clinics and a total of 41,193 adults overdue for colorectal cancer screening.
Disclosures: The research was supported by the National Institutes of Health. One investigator reported disclosures related to EpiGenomics and Quidel Corporation.
Source: Coronado GD et al. JAMA Intern Med. 2018 Aug 6. doi: 10.1001/jamainternmed.2018.3629.
High autonomic dysfunction distinguishes persistent posttraumatic headache
SAN FRANCISCO – Symptoms of autonomic dysfunction are significantly greater in patients with persistent posttraumatic headache than in migraine, raising the welcome possibility that this characteristic might serve to reliably differentiate the two disorders, Levi Howard, MD, said at the annual meeting of the American Headache Society.

“Interestingly enough, in looking at other studies evaluating dysautonomia, the [autonomic dysfunction scores] in our persistent posttraumatic headache group were on a par with scores previously reported for patients with diseases such as small-fiber polyneuropathy and postural orthostatic tachycardia syndrome,” observed Dr. Howard, an active duty military physician assigned to obtain neurology training at the Mayo Clinic Arizona in Phoenix.
“This brings up two questions: Do autonomic symptoms contribute to accurate classification of persistent posttraumatic headache versus migraine? And if we treat this autonomic dysfunction, does the headache also improve? In our clinical observation, this appears to be the case,” he continued.
Right now, posttraumatic headache (PTH) is defined on the basis of its temporal relationship to head injury. At this time, PTH has no defining clinical characteristics, although most often it has a phenotype that meets diagnostic criteria for migraine.
However, Dr. Howard and his coinvestigators have observed anecdotally in clinical practice that persistent PTH – defined as PTH lasting longer than 3 months – is often accompanied by orthostatic intolerance. This observation, coupled with reports in multiple prior studies that dysautonomia is common in patients with mild traumatic brain injury (TBI) and postconcussion syndrome, prompted Dr. Howard and his coworkers to conduct a cross-sectional cohort study. It included 56 patients with persistent PTH due to mild TBI, 30 patients with migraine, and 36 healthy controls. Most of the persistent PTH group were military veterans with mild TBI due to blast injuries.
All subjects were assessed for autonomic dysfunction using the well-validated COMPASS-31 questionnaire. This instrument assesses six domains of autonomic function: orthostatic intolerance, bladder, gastrointestinal, vasomotor, secretomotor, and pupillomotor.
Scores in each of the six domains were numerically higher in the persistent PTH group, with the differences achieving statistical significance in the orthostatic intolerance and bladder domains.
Of note, the migraine group had a greater headache burden, with a mean 23-year headache history, compared with 10.56 years in the persistent PTH group. The migraine patients also averaged 21.1 headache days per month, versus 16.2 in the persistent PTH group. Yet the investigators found no strong association between autonomic dysfunction and headache burden as reflected in headache duration or headache days per month.
The study was funded by the Department of Defense. Dr. Howard reported having no financial conflicts of interest.
SOURCE: Howard L et al. AHS 2018, Abstract FHM03.
SAN FRANCISCO – Symptoms of autonomic dysfunction are significantly greater in patients with persistent posttraumatic headache than in migraine, raising the welcome possibility that this characteristic might serve to reliably differentiate the two disorders, Levi Howard, MD, said at the annual meeting of the American Headache Society.
“Interestingly enough, in looking at other studies evaluating dysautonomia, the [autonomic dysfunction scores] in our persistent posttraumatic headache group were on a par with scores previously reported for patients with diseases such as small-fiber polyneuropathy and postural orthostatic tachycardia syndrome,” observed Dr. Howard, an active duty military physician assigned to obtain neurology training at the Mayo Clinic Arizona in Phoenix.
“This brings up two questions: Do autonomic symptoms contribute to accurate classification of persistent posttraumatic headache versus migraine? And if we treat this autonomic dysfunction, does the headache also improve? In our clinical observation, this appears to be the case,” he continued.
Right now, posttraumatic headache (PTH) is defined on the basis of its temporal relationship to head injury. At this time, PTH has no defining clinical characteristics, although most often it has a phenotype that meets diagnostic criteria for migraine.
However, Dr. Howard and his coinvestigators have observed anecdotally in clinical practice that persistent PTH – defined as PTH lasting longer than 3 months – is often accompanied by orthostatic intolerance. This observation, coupled with reports in multiple prior studies that dysautonomia is common in patients with mild traumatic brain injury (TBI) and postconcussion syndrome, prompted Dr. Howard and his coworkers to conduct a cross-sectional cohort study. It included 56 patients with persistent PTH due to mild TBI, 30 patients with migraine, and 36 healthy controls. Most of the persistent PTH group were military veterans with mild TBI due to blast injuries.
All subjects were assessed for autonomic dysfunction using the well-validated COMPASS-31 questionnaire. This instrument assesses six domains of autonomic function: orthostatic intolerance, bladder, gastrointestinal, vasomotor, secretomotor, and pupillomotor.
Scores in each of the six domains were numerically higher in the persistent PTH group, with the differences achieving statistical significance in the orthostatic intolerance and bladder domains.
Of note, the migraine group had a greater headache burden, with a mean 23-year headache history, compared with 10.56 years in the persistent PTH group. The migraine patients also averaged 21.1 headache days per month, versus 16.2 in the persistent PTH group. Yet the investigators found no strong association between autonomic dysfunction and headache burden as reflected in headache duration or headache days per month.
The study was funded by the Department of Defense. Dr. Howard reported having no financial conflicts of interest.
SOURCE: Howard L et al. AHS 2018, Abstract FHM03.
SAN FRANCISCO – Symptoms of autonomic dysfunction are significantly greater in patients with persistent posttraumatic headache than in migraine, raising the welcome possibility that this characteristic might serve to reliably differentiate the two disorders, Levi Howard, MD, said at the annual meeting of the American Headache Society.
“Interestingly enough, in looking at other studies evaluating dysautonomia, the [autonomic dysfunction scores] in our persistent posttraumatic headache group were on a par with scores previously reported for patients with diseases such as small-fiber polyneuropathy and postural orthostatic tachycardia syndrome,” observed Dr. Howard, an active duty military physician assigned to obtain neurology training at the Mayo Clinic Arizona in Phoenix.
“This brings up two questions: Do autonomic symptoms contribute to accurate classification of persistent posttraumatic headache versus migraine? And if we treat this autonomic dysfunction, does the headache also improve? In our clinical observation, this appears to be the case,” he continued.
Right now, posttraumatic headache (PTH) is defined on the basis of its temporal relationship to head injury. At this time, PTH has no defining clinical characteristics, although most often it has a phenotype that meets diagnostic criteria for migraine.
However, Dr. Howard and his coinvestigators have observed anecdotally in clinical practice that persistent PTH – defined as PTH lasting longer than 3 months – is often accompanied by orthostatic intolerance. This observation, coupled with reports in multiple prior studies that dysautonomia is common in patients with mild traumatic brain injury (TBI) and postconcussion syndrome, prompted Dr. Howard and his coworkers to conduct a cross-sectional cohort study. It included 56 patients with persistent PTH due to mild TBI, 30 patients with migraine, and 36 healthy controls. Most of the persistent PTH group were military veterans with mild TBI due to blast injuries.
All subjects were assessed for autonomic dysfunction using the well-validated COMPASS-31 questionnaire. This instrument assesses six domains of autonomic function: orthostatic intolerance, bladder, gastrointestinal, vasomotor, secretomotor, and pupillomotor.
Scores in each of the six domains were numerically higher in the persistent PTH group, with the differences achieving statistical significance in the orthostatic intolerance and bladder domains.
Of note, the migraine group had a greater headache burden, with a mean 23-year headache history, compared with 10.56 years in the persistent PTH group. The migraine patients also averaged 21.1 headache days per month, versus 16.2 in the persistent PTH group. Yet the investigators found no strong association between autonomic dysfunction and headache burden as reflected in headache duration or headache days per month.
The study was funded by the Department of Defense. Dr. Howard reported having no financial conflicts of interest.
SOURCE: Howard L et al. AHS 2018, Abstract FHM03.
REPORTING FROM THE AHS ANNUAL MEETING
Key clinical point: New evidence that patients with persistent posttraumatic headache have high levels of autonomic dysfunction could open the door to novel treatments.
Major finding: Scores on the COMPASS-31 questionnaire, a measure of autonomic dysfunction, averaged 37.22 in patients with persistent posttraumatic headache, indicative of significantly greater impairment than the 27.15 in migraine patients and 11.67 in healthy controls.
Study details: This cross-sectional cohort study included 56 patients with persistent posttraumatic headache, 30 with migraine, and 36 healthy controls.
Disclosures: The study was sponsored by the Department of Defense and presented by an active duty military physician.
Source: Howard L et al. AHS 2018, Abstract FHM03
Earnings gap seen among Maryland physicians
Male physicians in Maryland reported higher earnings than did female physicians, even when they all worked 41 or more hours a week, according to a 2018 survey of physicians in the state.
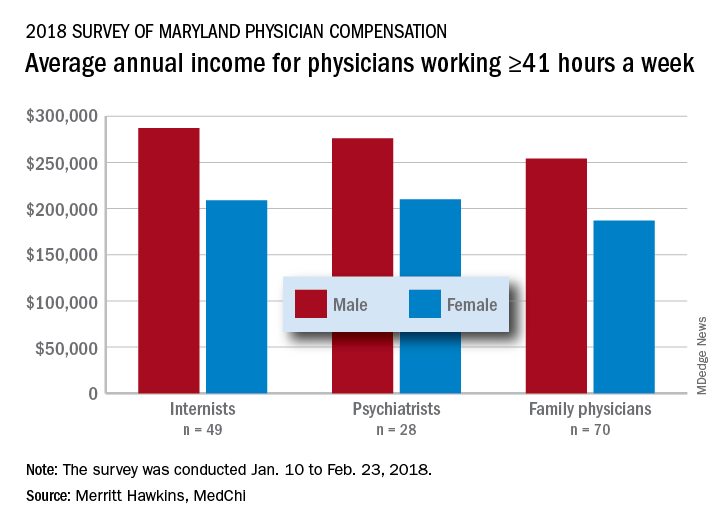
The average pretax income for all 508 respondents was $299,000 in 2016: Male physicians (66.6% of the sample) had an average of $335,000 and women averaged 33% lower at $224,000, MedChi (the Maryland State Medical Society) and Merritt Hawkins reported on July 31. Men did report working a longer week: Their average of 50.5 hours was 11% more than the 45.4-hour average for women.
“The biggest disparities we see in compensation are between male and female physicians in Maryland,” Gene Ransom, MedChi’s chief executive officer, said in a written statement. “Though such disparities have been noted in other research, it is still surprising to see the extent to which they persist.”
Of the respondents who worked an average of 41 or more hours per week – an analysis conducted only for the three largest specialties in the survey – female internists earned 27% less than their male counterparts, female psychiatrists earned 24% less, and female family physicians earned 26% less, the survey results showed.
Earnings were structured somewhat differently for Maryland’s male and female physicians. Women were more likely to be compensated in the form of a straight salary than men (35.0% vs. 30.3%), and men were more likely to paid based on production (22.7% vs. 16.9%) or in the form of an income guarantee (0.9% vs. 0.0%). Proportions receiving a salary with a production bonus were 42.7% for men and 42.5% for women, according to the survey.
The survey was commissioned by MedChi and conducted by Merritt Hawkins from Jan. 10 to Feb. 23, 2018. The margin of error was plus or minus 4.4%.
Male physicians in Maryland reported higher earnings than did female physicians, even when they all worked 41 or more hours a week, according to a 2018 survey of physicians in the state.
The average pretax income for all 508 respondents was $299,000 in 2016: Male physicians (66.6% of the sample) had an average of $335,000 and women averaged 33% lower at $224,000, MedChi (the Maryland State Medical Society) and Merritt Hawkins reported on July 31. Men did report working a longer week: Their average of 50.5 hours was 11% more than the 45.4-hour average for women.
“The biggest disparities we see in compensation are between male and female physicians in Maryland,” Gene Ransom, MedChi’s chief executive officer, said in a written statement. “Though such disparities have been noted in other research, it is still surprising to see the extent to which they persist.”
Of the respondents who worked an average of 41 or more hours per week – an analysis conducted only for the three largest specialties in the survey – female internists earned 27% less than their male counterparts, female psychiatrists earned 24% less, and female family physicians earned 26% less, the survey results showed.
Earnings were structured somewhat differently for Maryland’s male and female physicians. Women were more likely to be compensated in the form of a straight salary than men (35.0% vs. 30.3%), and men were more likely to paid based on production (22.7% vs. 16.9%) or in the form of an income guarantee (0.9% vs. 0.0%). Proportions receiving a salary with a production bonus were 42.7% for men and 42.5% for women, according to the survey.
The survey was commissioned by MedChi and conducted by Merritt Hawkins from Jan. 10 to Feb. 23, 2018. The margin of error was plus or minus 4.4%.
Male physicians in Maryland reported higher earnings than did female physicians, even when they all worked 41 or more hours a week, according to a 2018 survey of physicians in the state.
The average pretax income for all 508 respondents was $299,000 in 2016: Male physicians (66.6% of the sample) had an average of $335,000 and women averaged 33% lower at $224,000, MedChi (the Maryland State Medical Society) and Merritt Hawkins reported on July 31. Men did report working a longer week: Their average of 50.5 hours was 11% more than the 45.4-hour average for women.
“The biggest disparities we see in compensation are between male and female physicians in Maryland,” Gene Ransom, MedChi’s chief executive officer, said in a written statement. “Though such disparities have been noted in other research, it is still surprising to see the extent to which they persist.”
Of the respondents who worked an average of 41 or more hours per week – an analysis conducted only for the three largest specialties in the survey – female internists earned 27% less than their male counterparts, female psychiatrists earned 24% less, and female family physicians earned 26% less, the survey results showed.
Earnings were structured somewhat differently for Maryland’s male and female physicians. Women were more likely to be compensated in the form of a straight salary than men (35.0% vs. 30.3%), and men were more likely to paid based on production (22.7% vs. 16.9%) or in the form of an income guarantee (0.9% vs. 0.0%). Proportions receiving a salary with a production bonus were 42.7% for men and 42.5% for women, according to the survey.
The survey was commissioned by MedChi and conducted by Merritt Hawkins from Jan. 10 to Feb. 23, 2018. The margin of error was plus or minus 4.4%.