User login
Asian American teens have highest rate of suicidal ideation
NEW ORLEANS – In an unexpected finding, researchers discovered that According to a weighted analysis, 24% of Asian Americans reported thinking about or planning suicide vs. 22% of Whites and Blacks and 20% of Hispanics (P < .01).
“We were shocked,” said study lead author Esha Hansoti, MD, who conducted the research at UT Southwestern Medical Center, Dallas, and is now a psychiatry resident at Zucker Hillside Hospital Northwell/Hofstra in Glen Oaks, NY. The findings were released at the annual meeting of the American Psychiatric Association.

Dr. Hansoti and colleagues launched the analysis in light of sparse research into Asian American mental health, she said. Even within this population, she said, mental illness “tends to be overlooked” and discussion of the topic may be considered taboo.
For the new study, researchers analyzed the 2019 Youth Risk Behavior Survey, conducted biennially by the Centers for Disease Control and Prevention, which had more than 13,000 participants in grades 9-12.
A weighted bivariate analysis of 618 Asian American adolescents – adjusted for age, sex, and depressive symptoms – found no statistically significant impact on suicidal ideation by gender, age, substance use, sexual/physical dating violence, or fluency in English.
However, several groups had a statistically significant higher risk, including victims of forced sexual intercourse and those who were threatened or bullied at school.
Those who didn’t get mostly A grades were also at high risk: Adolescents with mostly Ds and Fs were more likely to have acknowledged suicidal ideation than those with mostly As (adjusted odds ratio [AOR] = 3.2).
Gays and lesbians (AOR = 7.9 vs. heterosexuals), and bisexuals (AOR = 5.2 vs. heterosexuals) also showed sharply higher rates of suicidal ideation.
It’s not clear why Asian American adolescents may be at higher risk of suicidal ideation. The survey was completed prior to the COVID-19 pandemic, which spawned bigotry against people of Asian descent and an ongoing outbreak of high-profile violence against Asian Americans across the country.
Dr. Hansoti noted that Asian Americans face the pressures to live up to the standards of being a “model minority.” In addition, “very few Asian American adolescents are taken to a therapist, and few mental health providers are Asian Americans.”
She urged fellow psychiatrists “to remember that our perceptions of Asian Americans might hinder some of the diagnoses we could be making. Be thoughtful about how their ethnicity and race affects their presentation and their own perception of their illness.”
She added that Asian Americans may experience mental illness and anxiety “more somatically and physically than emotionally.”
In an interview, Anne Saw, PhD, associate professor of clinical-community psychology at DePaul University, Chicago, said the findings are “helpful for corroborating other studies identifying risk factors of suicidal ideation among Asian American adolescents. Since this research utilizes the Youth Risk Behavior Survey, these findings can be compared with risk factors of suicidal ideation among adolescents from other racial/ethnic backgrounds to pinpoint general as well as specific risk factors, thus informing how we can tailor interventions for specific groups.”
According to Dr. Saw, while it’s clear that suicide is a leading cause of death among Asian American adolescents, it’s still unknown which specific subgroups other than girls and LGBTIA+ individuals are especially vulnerable and which culturally tailored interventions are most effective for decreasing suicide risk.
“Psychiatrists should understand that risk and protective factors for suicidal behavior in Asian American adolescents are multifaceted and require careful attention and intervention across different environments,” she said.
No funding and no disclosures were reported.
NEW ORLEANS – In an unexpected finding, researchers discovered that According to a weighted analysis, 24% of Asian Americans reported thinking about or planning suicide vs. 22% of Whites and Blacks and 20% of Hispanics (P < .01).
“We were shocked,” said study lead author Esha Hansoti, MD, who conducted the research at UT Southwestern Medical Center, Dallas, and is now a psychiatry resident at Zucker Hillside Hospital Northwell/Hofstra in Glen Oaks, NY. The findings were released at the annual meeting of the American Psychiatric Association.
Dr. Hansoti and colleagues launched the analysis in light of sparse research into Asian American mental health, she said. Even within this population, she said, mental illness “tends to be overlooked” and discussion of the topic may be considered taboo.
For the new study, researchers analyzed the 2019 Youth Risk Behavior Survey, conducted biennially by the Centers for Disease Control and Prevention, which had more than 13,000 participants in grades 9-12.
A weighted bivariate analysis of 618 Asian American adolescents – adjusted for age, sex, and depressive symptoms – found no statistically significant impact on suicidal ideation by gender, age, substance use, sexual/physical dating violence, or fluency in English.
However, several groups had a statistically significant higher risk, including victims of forced sexual intercourse and those who were threatened or bullied at school.
Those who didn’t get mostly A grades were also at high risk: Adolescents with mostly Ds and Fs were more likely to have acknowledged suicidal ideation than those with mostly As (adjusted odds ratio [AOR] = 3.2).
Gays and lesbians (AOR = 7.9 vs. heterosexuals), and bisexuals (AOR = 5.2 vs. heterosexuals) also showed sharply higher rates of suicidal ideation.
It’s not clear why Asian American adolescents may be at higher risk of suicidal ideation. The survey was completed prior to the COVID-19 pandemic, which spawned bigotry against people of Asian descent and an ongoing outbreak of high-profile violence against Asian Americans across the country.
Dr. Hansoti noted that Asian Americans face the pressures to live up to the standards of being a “model minority.” In addition, “very few Asian American adolescents are taken to a therapist, and few mental health providers are Asian Americans.”
She urged fellow psychiatrists “to remember that our perceptions of Asian Americans might hinder some of the diagnoses we could be making. Be thoughtful about how their ethnicity and race affects their presentation and their own perception of their illness.”
She added that Asian Americans may experience mental illness and anxiety “more somatically and physically than emotionally.”
In an interview, Anne Saw, PhD, associate professor of clinical-community psychology at DePaul University, Chicago, said the findings are “helpful for corroborating other studies identifying risk factors of suicidal ideation among Asian American adolescents. Since this research utilizes the Youth Risk Behavior Survey, these findings can be compared with risk factors of suicidal ideation among adolescents from other racial/ethnic backgrounds to pinpoint general as well as specific risk factors, thus informing how we can tailor interventions for specific groups.”
According to Dr. Saw, while it’s clear that suicide is a leading cause of death among Asian American adolescents, it’s still unknown which specific subgroups other than girls and LGBTIA+ individuals are especially vulnerable and which culturally tailored interventions are most effective for decreasing suicide risk.
“Psychiatrists should understand that risk and protective factors for suicidal behavior in Asian American adolescents are multifaceted and require careful attention and intervention across different environments,” she said.
No funding and no disclosures were reported.
NEW ORLEANS – In an unexpected finding, researchers discovered that According to a weighted analysis, 24% of Asian Americans reported thinking about or planning suicide vs. 22% of Whites and Blacks and 20% of Hispanics (P < .01).
“We were shocked,” said study lead author Esha Hansoti, MD, who conducted the research at UT Southwestern Medical Center, Dallas, and is now a psychiatry resident at Zucker Hillside Hospital Northwell/Hofstra in Glen Oaks, NY. The findings were released at the annual meeting of the American Psychiatric Association.
Dr. Hansoti and colleagues launched the analysis in light of sparse research into Asian American mental health, she said. Even within this population, she said, mental illness “tends to be overlooked” and discussion of the topic may be considered taboo.
For the new study, researchers analyzed the 2019 Youth Risk Behavior Survey, conducted biennially by the Centers for Disease Control and Prevention, which had more than 13,000 participants in grades 9-12.
A weighted bivariate analysis of 618 Asian American adolescents – adjusted for age, sex, and depressive symptoms – found no statistically significant impact on suicidal ideation by gender, age, substance use, sexual/physical dating violence, or fluency in English.
However, several groups had a statistically significant higher risk, including victims of forced sexual intercourse and those who were threatened or bullied at school.
Those who didn’t get mostly A grades were also at high risk: Adolescents with mostly Ds and Fs were more likely to have acknowledged suicidal ideation than those with mostly As (adjusted odds ratio [AOR] = 3.2).
Gays and lesbians (AOR = 7.9 vs. heterosexuals), and bisexuals (AOR = 5.2 vs. heterosexuals) also showed sharply higher rates of suicidal ideation.
It’s not clear why Asian American adolescents may be at higher risk of suicidal ideation. The survey was completed prior to the COVID-19 pandemic, which spawned bigotry against people of Asian descent and an ongoing outbreak of high-profile violence against Asian Americans across the country.
Dr. Hansoti noted that Asian Americans face the pressures to live up to the standards of being a “model minority.” In addition, “very few Asian American adolescents are taken to a therapist, and few mental health providers are Asian Americans.”
She urged fellow psychiatrists “to remember that our perceptions of Asian Americans might hinder some of the diagnoses we could be making. Be thoughtful about how their ethnicity and race affects their presentation and their own perception of their illness.”
She added that Asian Americans may experience mental illness and anxiety “more somatically and physically than emotionally.”
In an interview, Anne Saw, PhD, associate professor of clinical-community psychology at DePaul University, Chicago, said the findings are “helpful for corroborating other studies identifying risk factors of suicidal ideation among Asian American adolescents. Since this research utilizes the Youth Risk Behavior Survey, these findings can be compared with risk factors of suicidal ideation among adolescents from other racial/ethnic backgrounds to pinpoint general as well as specific risk factors, thus informing how we can tailor interventions for specific groups.”
According to Dr. Saw, while it’s clear that suicide is a leading cause of death among Asian American adolescents, it’s still unknown which specific subgroups other than girls and LGBTIA+ individuals are especially vulnerable and which culturally tailored interventions are most effective for decreasing suicide risk.
“Psychiatrists should understand that risk and protective factors for suicidal behavior in Asian American adolescents are multifaceted and require careful attention and intervention across different environments,” she said.
No funding and no disclosures were reported.
AT APA 2022
Collagen ‘tile’ delivers postsurgical radiation in glioblastoma
and spares healthy tissue, new research suggests.
The results showed inserting a collagen matrix containing radioactive seeds into the brain postsurgery did not impede wound healing. It also showed a favorable safety profile, researchers note.
Benefits for patients undergoing this GammaTile (GT) intervention include not having to wait weeks to receive radiation treatment, which in turn improves their quality of life, said study investigator Clark C. Chen, MD, PhD, chair, department of neurosurgery, University of Minnesota Medical School, Minneapolis.
“These initial results are highly promising and offer hope for patients afflicted with an otherwise devastating disease,” Dr. Chen said in an interview.
If replicated in larger trials, GT therapy “could define a new standard of care, and there would really be no reason why patients shouldn’t get this therapy,” he added.
This is the first clinical series describing GT use since its approval by the U.S. Food and Drug Administration (FDA) for recurrent brain cancer.
The findings were presented at the annual meeting of the American Association of Neurological Surgeons (AANS) and were published recently in Neuro-Oncology Advances.
Radioactive seeds
GT therapy is a version of brachytherapy where radioactive sources are placed adjacent to cancerous tissue. It consists of radioactive seeds embedded with a collagen tile.
The neurosurgeon inserts these “tiles” immediately after tumor removal to cover the entire resection cavity, Dr. Chen said. The tiles maintain the cavity architecture to prevent radiation “hot spots” associated with cavity collapse.
Dr. Chen noted the therapy is “short range,” with most of the radiation delivered within 8 millimeters of the radioactive seeds.
The radiation lasts for about a month and the collagen tiles are eventually absorbed within the body. “You put in the tiles and you don’t need to do anything more,” Dr. Chen said.
GT has a number of advantages. Unlike with traditional brachytherapy, the collagen tile provides a buffer around the radiation sources, allowing delivery of the optimal radiation dose while preserving healthy tissue.
It also avoids the up-to-6-weeks patients have to wait postsurgery to get external beam radiation therapy. “If you start radiation too early, it actually compromises wound healing, and in the meantime the tumor is growing,” said Dr. Chen.
“I have several patients where I removed a large tumor and within that 6-week period, the tumor came back entirely,” he added.
With the gamma-tile, however, radiation from the seeds kills the tumor while the body heals.
Safety profile
The study included 22 patients (mean age, 57.7 years; 15 men, 7 women) with wild-type isocitrate dehydrogenase glioblastoma. They were all having surgery for recurrent tumors.
“One of the most challenging aspects of glioblastomas is that not only do the tumors come back, they come back immediately adjacent to where you have done the surgery, and for many patients this is demoralizing,” Dr. Chen said.
Six participants had 0 6 -Methylguanine-DNA methyltranferase (MGMT) methylated glioblastoma, while the others had unmethylated MGMT.
The mean follow-up from initial diagnosis was 733 days (2 years).
Results showed one patient had to be readmitted to the hospital for hydrocephalus, but there were no re-admissions within 30 days attributable to GT.
Despite participants having undergone a second and third resection through the same surgical incision, there were no wound infections. “One of the concerns of giving radiation right after surgery is it can compromise wound healing, and this is why you wait 6 weeks,” Dr. Chen noted.
He stressed that no patient in the study suffered from adverse radiation effects that required medical or surgical intervention.
As the radiation is so short-range, hair loss and skin irritation are not side effects of GT, he added.
“The radiation is inside the brain and highly targeted, so it doesn’t hit hair follicles,” said Dr. Chen. “As best as I can observe in these patients, I did not see toxicity associated with radiation.”
One and done
Among the 22 participants, 18 had neurologic symptoms at baseline. There were no new neurologic deficits that developed after GT placement.
In addition, GT therapy improved “local control” — preventing the tumor from growing back at the site of the surgery. The local control was 86% at 6 months and 81% at 12 months.
The median progression-free survival was about 8 months. The median overall survival was 20 months (about 600 days) for the unmethylated MGMT group and 37.4 months (about 1120 days) for the methylated group.
Outcomes compared favorably to an independent glioblastoma cohort of similar patients who did not receive GT treatment during the study period, Dr. Chen noted.
“This therapy can potentially redefine how we treat glioblastoma patients whose cancer came back,” he said.
A study limitation was that it did not include quality-of-life data, which makes it challenging to assess the therapy’s overall impact, Dr. Chen said. However, he added that from his experience, patients very much appreciate not having to repeatedly take time off work for clinic or hospital visits to receive radiation treatments.
“One of the beauties of this therapy is it’s a one-and-done deal,” he said.
Interesting, timely
Commenting for this news organization, William T. Curry Jr, MD, co-director at MassGeneral Neuroscience and director of neurosurgical oncology at Mass General Cancer Center, Boston, called the study “interesting and timely.”
These new data “underscore that GT is safe in patients that have undergone gross total resection of recurrent glioblastoma and that rates of progression free survival may exceed those treated with resection alone,” said Dr. Curry, who was not involved with the research.
“Surgeons are excited about anything that has the potential to improve outcomes for patients with this very challenging disease, and it is wonderful to be able to offer hope and survival tools to patients,” he added.
However, Dr. Curry noted there are challenges and potential biases when studying survival in cancer patients without conducting a randomization process. The investigators “admit to methodological flaws inherent in the single-arm design in a patient population with recurrent glioblastoma not treated uniformly,” he said.
In addition, he noted overall survival may not have been related to the GT intervention. “Multicenter randomization is probably required to get to the bottom of the survival advantage in different subsets of glioblastoma patients,” Dr. Curry said.
Further research is needed to confirm the efficacy, appropriate indications, and timing of the intervention, but “I would support a randomized multicenter study in patients undergoing near gross total resection of recurrent glioblastoma,” he concluded.
The study received no outside funding. Dr. Chen and Dr. Curry have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
and spares healthy tissue, new research suggests.
The results showed inserting a collagen matrix containing radioactive seeds into the brain postsurgery did not impede wound healing. It also showed a favorable safety profile, researchers note.
Benefits for patients undergoing this GammaTile (GT) intervention include not having to wait weeks to receive radiation treatment, which in turn improves their quality of life, said study investigator Clark C. Chen, MD, PhD, chair, department of neurosurgery, University of Minnesota Medical School, Minneapolis.
“These initial results are highly promising and offer hope for patients afflicted with an otherwise devastating disease,” Dr. Chen said in an interview.
If replicated in larger trials, GT therapy “could define a new standard of care, and there would really be no reason why patients shouldn’t get this therapy,” he added.
This is the first clinical series describing GT use since its approval by the U.S. Food and Drug Administration (FDA) for recurrent brain cancer.
The findings were presented at the annual meeting of the American Association of Neurological Surgeons (AANS) and were published recently in Neuro-Oncology Advances.
Radioactive seeds
GT therapy is a version of brachytherapy where radioactive sources are placed adjacent to cancerous tissue. It consists of radioactive seeds embedded with a collagen tile.
The neurosurgeon inserts these “tiles” immediately after tumor removal to cover the entire resection cavity, Dr. Chen said. The tiles maintain the cavity architecture to prevent radiation “hot spots” associated with cavity collapse.
Dr. Chen noted the therapy is “short range,” with most of the radiation delivered within 8 millimeters of the radioactive seeds.
The radiation lasts for about a month and the collagen tiles are eventually absorbed within the body. “You put in the tiles and you don’t need to do anything more,” Dr. Chen said.
GT has a number of advantages. Unlike with traditional brachytherapy, the collagen tile provides a buffer around the radiation sources, allowing delivery of the optimal radiation dose while preserving healthy tissue.
It also avoids the up-to-6-weeks patients have to wait postsurgery to get external beam radiation therapy. “If you start radiation too early, it actually compromises wound healing, and in the meantime the tumor is growing,” said Dr. Chen.
“I have several patients where I removed a large tumor and within that 6-week period, the tumor came back entirely,” he added.
With the gamma-tile, however, radiation from the seeds kills the tumor while the body heals.
Safety profile
The study included 22 patients (mean age, 57.7 years; 15 men, 7 women) with wild-type isocitrate dehydrogenase glioblastoma. They were all having surgery for recurrent tumors.
“One of the most challenging aspects of glioblastomas is that not only do the tumors come back, they come back immediately adjacent to where you have done the surgery, and for many patients this is demoralizing,” Dr. Chen said.
Six participants had 0 6 -Methylguanine-DNA methyltranferase (MGMT) methylated glioblastoma, while the others had unmethylated MGMT.
The mean follow-up from initial diagnosis was 733 days (2 years).
Results showed one patient had to be readmitted to the hospital for hydrocephalus, but there were no re-admissions within 30 days attributable to GT.
Despite participants having undergone a second and third resection through the same surgical incision, there were no wound infections. “One of the concerns of giving radiation right after surgery is it can compromise wound healing, and this is why you wait 6 weeks,” Dr. Chen noted.
He stressed that no patient in the study suffered from adverse radiation effects that required medical or surgical intervention.
As the radiation is so short-range, hair loss and skin irritation are not side effects of GT, he added.
“The radiation is inside the brain and highly targeted, so it doesn’t hit hair follicles,” said Dr. Chen. “As best as I can observe in these patients, I did not see toxicity associated with radiation.”
One and done
Among the 22 participants, 18 had neurologic symptoms at baseline. There were no new neurologic deficits that developed after GT placement.
In addition, GT therapy improved “local control” — preventing the tumor from growing back at the site of the surgery. The local control was 86% at 6 months and 81% at 12 months.
The median progression-free survival was about 8 months. The median overall survival was 20 months (about 600 days) for the unmethylated MGMT group and 37.4 months (about 1120 days) for the methylated group.
Outcomes compared favorably to an independent glioblastoma cohort of similar patients who did not receive GT treatment during the study period, Dr. Chen noted.
“This therapy can potentially redefine how we treat glioblastoma patients whose cancer came back,” he said.
A study limitation was that it did not include quality-of-life data, which makes it challenging to assess the therapy’s overall impact, Dr. Chen said. However, he added that from his experience, patients very much appreciate not having to repeatedly take time off work for clinic or hospital visits to receive radiation treatments.
“One of the beauties of this therapy is it’s a one-and-done deal,” he said.
Interesting, timely
Commenting for this news organization, William T. Curry Jr, MD, co-director at MassGeneral Neuroscience and director of neurosurgical oncology at Mass General Cancer Center, Boston, called the study “interesting and timely.”
These new data “underscore that GT is safe in patients that have undergone gross total resection of recurrent glioblastoma and that rates of progression free survival may exceed those treated with resection alone,” said Dr. Curry, who was not involved with the research.
“Surgeons are excited about anything that has the potential to improve outcomes for patients with this very challenging disease, and it is wonderful to be able to offer hope and survival tools to patients,” he added.
However, Dr. Curry noted there are challenges and potential biases when studying survival in cancer patients without conducting a randomization process. The investigators “admit to methodological flaws inherent in the single-arm design in a patient population with recurrent glioblastoma not treated uniformly,” he said.
In addition, he noted overall survival may not have been related to the GT intervention. “Multicenter randomization is probably required to get to the bottom of the survival advantage in different subsets of glioblastoma patients,” Dr. Curry said.
Further research is needed to confirm the efficacy, appropriate indications, and timing of the intervention, but “I would support a randomized multicenter study in patients undergoing near gross total resection of recurrent glioblastoma,” he concluded.
The study received no outside funding. Dr. Chen and Dr. Curry have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
and spares healthy tissue, new research suggests.
The results showed inserting a collagen matrix containing radioactive seeds into the brain postsurgery did not impede wound healing. It also showed a favorable safety profile, researchers note.
Benefits for patients undergoing this GammaTile (GT) intervention include not having to wait weeks to receive radiation treatment, which in turn improves their quality of life, said study investigator Clark C. Chen, MD, PhD, chair, department of neurosurgery, University of Minnesota Medical School, Minneapolis.
“These initial results are highly promising and offer hope for patients afflicted with an otherwise devastating disease,” Dr. Chen said in an interview.
If replicated in larger trials, GT therapy “could define a new standard of care, and there would really be no reason why patients shouldn’t get this therapy,” he added.
This is the first clinical series describing GT use since its approval by the U.S. Food and Drug Administration (FDA) for recurrent brain cancer.
The findings were presented at the annual meeting of the American Association of Neurological Surgeons (AANS) and were published recently in Neuro-Oncology Advances.
Radioactive seeds
GT therapy is a version of brachytherapy where radioactive sources are placed adjacent to cancerous tissue. It consists of radioactive seeds embedded with a collagen tile.
The neurosurgeon inserts these “tiles” immediately after tumor removal to cover the entire resection cavity, Dr. Chen said. The tiles maintain the cavity architecture to prevent radiation “hot spots” associated with cavity collapse.
Dr. Chen noted the therapy is “short range,” with most of the radiation delivered within 8 millimeters of the radioactive seeds.
The radiation lasts for about a month and the collagen tiles are eventually absorbed within the body. “You put in the tiles and you don’t need to do anything more,” Dr. Chen said.
GT has a number of advantages. Unlike with traditional brachytherapy, the collagen tile provides a buffer around the radiation sources, allowing delivery of the optimal radiation dose while preserving healthy tissue.
It also avoids the up-to-6-weeks patients have to wait postsurgery to get external beam radiation therapy. “If you start radiation too early, it actually compromises wound healing, and in the meantime the tumor is growing,” said Dr. Chen.
“I have several patients where I removed a large tumor and within that 6-week period, the tumor came back entirely,” he added.
With the gamma-tile, however, radiation from the seeds kills the tumor while the body heals.
Safety profile
The study included 22 patients (mean age, 57.7 years; 15 men, 7 women) with wild-type isocitrate dehydrogenase glioblastoma. They were all having surgery for recurrent tumors.
“One of the most challenging aspects of glioblastomas is that not only do the tumors come back, they come back immediately adjacent to where you have done the surgery, and for many patients this is demoralizing,” Dr. Chen said.
Six participants had 0 6 -Methylguanine-DNA methyltranferase (MGMT) methylated glioblastoma, while the others had unmethylated MGMT.
The mean follow-up from initial diagnosis was 733 days (2 years).
Results showed one patient had to be readmitted to the hospital for hydrocephalus, but there were no re-admissions within 30 days attributable to GT.
Despite participants having undergone a second and third resection through the same surgical incision, there were no wound infections. “One of the concerns of giving radiation right after surgery is it can compromise wound healing, and this is why you wait 6 weeks,” Dr. Chen noted.
He stressed that no patient in the study suffered from adverse radiation effects that required medical or surgical intervention.
As the radiation is so short-range, hair loss and skin irritation are not side effects of GT, he added.
“The radiation is inside the brain and highly targeted, so it doesn’t hit hair follicles,” said Dr. Chen. “As best as I can observe in these patients, I did not see toxicity associated with radiation.”
One and done
Among the 22 participants, 18 had neurologic symptoms at baseline. There were no new neurologic deficits that developed after GT placement.
In addition, GT therapy improved “local control” — preventing the tumor from growing back at the site of the surgery. The local control was 86% at 6 months and 81% at 12 months.
The median progression-free survival was about 8 months. The median overall survival was 20 months (about 600 days) for the unmethylated MGMT group and 37.4 months (about 1120 days) for the methylated group.
Outcomes compared favorably to an independent glioblastoma cohort of similar patients who did not receive GT treatment during the study period, Dr. Chen noted.
“This therapy can potentially redefine how we treat glioblastoma patients whose cancer came back,” he said.
A study limitation was that it did not include quality-of-life data, which makes it challenging to assess the therapy’s overall impact, Dr. Chen said. However, he added that from his experience, patients very much appreciate not having to repeatedly take time off work for clinic or hospital visits to receive radiation treatments.
“One of the beauties of this therapy is it’s a one-and-done deal,” he said.
Interesting, timely
Commenting for this news organization, William T. Curry Jr, MD, co-director at MassGeneral Neuroscience and director of neurosurgical oncology at Mass General Cancer Center, Boston, called the study “interesting and timely.”
These new data “underscore that GT is safe in patients that have undergone gross total resection of recurrent glioblastoma and that rates of progression free survival may exceed those treated with resection alone,” said Dr. Curry, who was not involved with the research.
“Surgeons are excited about anything that has the potential to improve outcomes for patients with this very challenging disease, and it is wonderful to be able to offer hope and survival tools to patients,” he added.
However, Dr. Curry noted there are challenges and potential biases when studying survival in cancer patients without conducting a randomization process. The investigators “admit to methodological flaws inherent in the single-arm design in a patient population with recurrent glioblastoma not treated uniformly,” he said.
In addition, he noted overall survival may not have been related to the GT intervention. “Multicenter randomization is probably required to get to the bottom of the survival advantage in different subsets of glioblastoma patients,” Dr. Curry said.
Further research is needed to confirm the efficacy, appropriate indications, and timing of the intervention, but “I would support a randomized multicenter study in patients undergoing near gross total resection of recurrent glioblastoma,” he concluded.
The study received no outside funding. Dr. Chen and Dr. Curry have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AANS 2022
Radiotherapy for brain metastases: ASTRO updates guidelines
“In the decade since the previous ASTRO brain metastases guideline, there has been a tremendous evolution in the way we manage patients’ disease,” said Paul D. Brown, MD, chair of the guideline task force and a professor of radiation oncology at the Mayo Clinic in Rochester, Minn.
“The development of stereotactic radiosurgery (SRS) has allowed treatment of limited brain metastases alone, often in a single fraction, while largely sparing the surrounding brain,” he elaborated in a statement. Also, novel techniques such as hippocampal avoidance with whole-brain radiation can greatly improve quality of life, he added.
The guideline was published May 6 in Practical Radiation Oncology.
“With the emergence of novel radiotherapy techniques and technologies, brain-penetrating drug therapies and neurosurgical interventions, modern management of brain metastases has become increasingly personalized, complex and multidisciplinary,” Vinai Gondi, MD, vice chair of the guideline task force and director of research and education at the Northwestern Medicine Cancer Center and Proton Center in Chicago, said in a statement.
“We developed this guideline to help inform and guide clinicians in patient-centered, multidisciplinary care for their patients with brain metastases,” he added.
Key recommendations
Overall, the recommendations address a wide range of topics related to radiation therapy in patients with cancer that has spread to the brain, including delivery techniques for radiation therapy to manage both unresected and resected brain metastases. The guideline also includes treatment algorithms for limited brain metastases and extensive brain metastases.
Key recommendations are as follows:
For patients with intact/unresected brain metastases:
- SRS is recommended for patients with 1-4 brain metastases and reasonable performance status (ECOG performance status 0-2); SRS is conditionally recommended for those with 5-10 brain metastases and reasonable performance status; for patients with tumors exerting mass effect and/or larger size, multidisciplinary discussion with neurosurgery to consider surgical resection is suggested.
- Upfront local therapy (radiation and/or surgery) is strongly recommended for patients with symptomatic brain metastases.
- For patients with asymptomatic brain metastases who are eligible for central nervous system-directed systemic therapy, multidisciplinary and patient-centered decision-making to determine whether local therapy may be safely deferred is conditionally recommended.
- Whole brain radiation therapy (WBRT) is recommended as a primary treatment for patients with favorable prognosis who have brain metastases that are ineligible for surgery and/or SRS. Hippocampal avoidance (HA) is recommended when appropriate to preserve memory function, as is the addition of memantine to delay neurocognitive decline. Adjuvant WBRT added to SRS routinely is not recommended.
- Supportive care only, without WBRT, should be considered for patients with poor prognosis and brain metastases. Reasonable options for this population include palliative care or hospice, or short-course WBRT for symptomatic brain metastases
- Recommendations also include guidance for SRS and WBRT dosing as well as the use of single-fraction vs hypofractionated SRS. Although SRS use is driven by the number of brain metastases, it is critical that other important factors (eg, total tumor volume and location, patient age, and extracranial disease status) should be taken into consideration during patient-centered decision-making by the multidisciplinary team.
For patients with resected brain metastases:
- Radiation therapy is recommended for all patients after resection in order to improve intracranial control.
- For patients with limited brain metastases after resection, postoperative SRS is recommended over WBRT to preserve the patient’s neurocognitive function and quality of life.
- As a potential alternative to SRS postresection, SRS prior to brain metastasis resection is conditionally recommended.
Updating the guidelines
ASTRO emphasizes that the scope of this paper is limited to the radiotherapeutic management of intact and resected brain metastases resulting from nonhematologic solid tumors. It provides guidance on the reasonable use of modern radiation therapy strategies, including single-fraction and fractionated (ie, hypofractionated SRS) SRS and HA-WBRT, and also discusses clinical considerations in selecting the optimal radiation therapy strategy or in deferring it in favor of best supportive care or close neuro-oncologic surveillance.
The authors note, however, that beyond the scope of this guideline, there are many other important questions that may be the subject of other guidance, such as the appropriate role for CNS-active systemic therapies and/or surgical intervention.
A version of this article was first published on Medscape.com.
“In the decade since the previous ASTRO brain metastases guideline, there has been a tremendous evolution in the way we manage patients’ disease,” said Paul D. Brown, MD, chair of the guideline task force and a professor of radiation oncology at the Mayo Clinic in Rochester, Minn.
“The development of stereotactic radiosurgery (SRS) has allowed treatment of limited brain metastases alone, often in a single fraction, while largely sparing the surrounding brain,” he elaborated in a statement. Also, novel techniques such as hippocampal avoidance with whole-brain radiation can greatly improve quality of life, he added.
The guideline was published May 6 in Practical Radiation Oncology.
“With the emergence of novel radiotherapy techniques and technologies, brain-penetrating drug therapies and neurosurgical interventions, modern management of brain metastases has become increasingly personalized, complex and multidisciplinary,” Vinai Gondi, MD, vice chair of the guideline task force and director of research and education at the Northwestern Medicine Cancer Center and Proton Center in Chicago, said in a statement.
“We developed this guideline to help inform and guide clinicians in patient-centered, multidisciplinary care for their patients with brain metastases,” he added.
Key recommendations
Overall, the recommendations address a wide range of topics related to radiation therapy in patients with cancer that has spread to the brain, including delivery techniques for radiation therapy to manage both unresected and resected brain metastases. The guideline also includes treatment algorithms for limited brain metastases and extensive brain metastases.
Key recommendations are as follows:
For patients with intact/unresected brain metastases:
- SRS is recommended for patients with 1-4 brain metastases and reasonable performance status (ECOG performance status 0-2); SRS is conditionally recommended for those with 5-10 brain metastases and reasonable performance status; for patients with tumors exerting mass effect and/or larger size, multidisciplinary discussion with neurosurgery to consider surgical resection is suggested.
- Upfront local therapy (radiation and/or surgery) is strongly recommended for patients with symptomatic brain metastases.
- For patients with asymptomatic brain metastases who are eligible for central nervous system-directed systemic therapy, multidisciplinary and patient-centered decision-making to determine whether local therapy may be safely deferred is conditionally recommended.
- Whole brain radiation therapy (WBRT) is recommended as a primary treatment for patients with favorable prognosis who have brain metastases that are ineligible for surgery and/or SRS. Hippocampal avoidance (HA) is recommended when appropriate to preserve memory function, as is the addition of memantine to delay neurocognitive decline. Adjuvant WBRT added to SRS routinely is not recommended.
- Supportive care only, without WBRT, should be considered for patients with poor prognosis and brain metastases. Reasonable options for this population include palliative care or hospice, or short-course WBRT for symptomatic brain metastases
- Recommendations also include guidance for SRS and WBRT dosing as well as the use of single-fraction vs hypofractionated SRS. Although SRS use is driven by the number of brain metastases, it is critical that other important factors (eg, total tumor volume and location, patient age, and extracranial disease status) should be taken into consideration during patient-centered decision-making by the multidisciplinary team.
For patients with resected brain metastases:
- Radiation therapy is recommended for all patients after resection in order to improve intracranial control.
- For patients with limited brain metastases after resection, postoperative SRS is recommended over WBRT to preserve the patient’s neurocognitive function and quality of life.
- As a potential alternative to SRS postresection, SRS prior to brain metastasis resection is conditionally recommended.
Updating the guidelines
ASTRO emphasizes that the scope of this paper is limited to the radiotherapeutic management of intact and resected brain metastases resulting from nonhematologic solid tumors. It provides guidance on the reasonable use of modern radiation therapy strategies, including single-fraction and fractionated (ie, hypofractionated SRS) SRS and HA-WBRT, and also discusses clinical considerations in selecting the optimal radiation therapy strategy or in deferring it in favor of best supportive care or close neuro-oncologic surveillance.
The authors note, however, that beyond the scope of this guideline, there are many other important questions that may be the subject of other guidance, such as the appropriate role for CNS-active systemic therapies and/or surgical intervention.
A version of this article was first published on Medscape.com.
“In the decade since the previous ASTRO brain metastases guideline, there has been a tremendous evolution in the way we manage patients’ disease,” said Paul D. Brown, MD, chair of the guideline task force and a professor of radiation oncology at the Mayo Clinic in Rochester, Minn.
“The development of stereotactic radiosurgery (SRS) has allowed treatment of limited brain metastases alone, often in a single fraction, while largely sparing the surrounding brain,” he elaborated in a statement. Also, novel techniques such as hippocampal avoidance with whole-brain radiation can greatly improve quality of life, he added.
The guideline was published May 6 in Practical Radiation Oncology.
“With the emergence of novel radiotherapy techniques and technologies, brain-penetrating drug therapies and neurosurgical interventions, modern management of brain metastases has become increasingly personalized, complex and multidisciplinary,” Vinai Gondi, MD, vice chair of the guideline task force and director of research and education at the Northwestern Medicine Cancer Center and Proton Center in Chicago, said in a statement.
“We developed this guideline to help inform and guide clinicians in patient-centered, multidisciplinary care for their patients with brain metastases,” he added.
Key recommendations
Overall, the recommendations address a wide range of topics related to radiation therapy in patients with cancer that has spread to the brain, including delivery techniques for radiation therapy to manage both unresected and resected brain metastases. The guideline also includes treatment algorithms for limited brain metastases and extensive brain metastases.
Key recommendations are as follows:
For patients with intact/unresected brain metastases:
- SRS is recommended for patients with 1-4 brain metastases and reasonable performance status (ECOG performance status 0-2); SRS is conditionally recommended for those with 5-10 brain metastases and reasonable performance status; for patients with tumors exerting mass effect and/or larger size, multidisciplinary discussion with neurosurgery to consider surgical resection is suggested.
- Upfront local therapy (radiation and/or surgery) is strongly recommended for patients with symptomatic brain metastases.
- For patients with asymptomatic brain metastases who are eligible for central nervous system-directed systemic therapy, multidisciplinary and patient-centered decision-making to determine whether local therapy may be safely deferred is conditionally recommended.
- Whole brain radiation therapy (WBRT) is recommended as a primary treatment for patients with favorable prognosis who have brain metastases that are ineligible for surgery and/or SRS. Hippocampal avoidance (HA) is recommended when appropriate to preserve memory function, as is the addition of memantine to delay neurocognitive decline. Adjuvant WBRT added to SRS routinely is not recommended.
- Supportive care only, without WBRT, should be considered for patients with poor prognosis and brain metastases. Reasonable options for this population include palliative care or hospice, or short-course WBRT for symptomatic brain metastases
- Recommendations also include guidance for SRS and WBRT dosing as well as the use of single-fraction vs hypofractionated SRS. Although SRS use is driven by the number of brain metastases, it is critical that other important factors (eg, total tumor volume and location, patient age, and extracranial disease status) should be taken into consideration during patient-centered decision-making by the multidisciplinary team.
For patients with resected brain metastases:
- Radiation therapy is recommended for all patients after resection in order to improve intracranial control.
- For patients with limited brain metastases after resection, postoperative SRS is recommended over WBRT to preserve the patient’s neurocognitive function and quality of life.
- As a potential alternative to SRS postresection, SRS prior to brain metastasis resection is conditionally recommended.
Updating the guidelines
ASTRO emphasizes that the scope of this paper is limited to the radiotherapeutic management of intact and resected brain metastases resulting from nonhematologic solid tumors. It provides guidance on the reasonable use of modern radiation therapy strategies, including single-fraction and fractionated (ie, hypofractionated SRS) SRS and HA-WBRT, and also discusses clinical considerations in selecting the optimal radiation therapy strategy or in deferring it in favor of best supportive care or close neuro-oncologic surveillance.
The authors note, however, that beyond the scope of this guideline, there are many other important questions that may be the subject of other guidance, such as the appropriate role for CNS-active systemic therapies and/or surgical intervention.
A version of this article was first published on Medscape.com.
FROM PRACTICAL RADIATION ONCOLOGY
Novel gene therapy offers hope for some lymphomas
Not all patients with relapsed or refractory large B cell lymphoma (r/r LBCL) are candidates for high-dose chemotherapy or hematopoietic stem cell transplantation (HSCT), and options for second-line therapies for this population are limited, said Dr. Alison Sehgal of the University of Pittsburgh Medical Center in her presentation of the findings.
Lisocabtagene maraleucel (liso-cel) is a CD19-directed CAR T-cell product. In a previous phase 3 randomized trial (the TRANSFORM study), lisocabtagene showed superiority over salvage chemotherapy for LBCL patients who were fit candidates for stem cell transplant, but its use in older, frail patients who are not transplant candidates remains uncertain, wrote Dr. Sehgal and colleagues in their poster at the meeting.
In the study, the researchers identified 74 patients with r/r LBCL. Of these, 61 were treated with liso-cel. The patients ranged in age from 53 to 84 years, with a median age of 74 years, 61% were male, and 89% were white. Approximately half were refractory and half were relapsed.
For the therapy, patients underwent lymphodepletion with cyclophosphamide and fludarabine, followed 2-7 days later by an infusion of liso-cel at a target dose of 100 x 106 CAR+ T cells; all patients had at least 6 months of follow-up from their first response.
The primary endpoint of overall response rate occurred in 80% of the patients, and clinically meaningful complete response occurred in 54% over a median follow-up of 12.3 months.
“Clinically meaningful CRs were observed across all subgroups,” Dr. Sehgal said in her presentation.
The response lasted a median of 21.7 months, and the median follow-up for duration of response was 15.5 months. The median overall survival was not reached, but the median progression-free survival was 9.0 months, with a median follow-up period of 13.0 months.
Responses occurred across all prespecified subgroups, with no significant differences in either safety or efficacy based on hematopoietic cell transplantation–specific comorbidity index (HCT-CI) scores.
“Despite the advanced age and comorbidities of the population, the safety profile was consistent with previous reports,” and no new or increased safety signals appeared, Dr. Sehgal said.
The most common treatment-emergent adverse events of grade 3 or higher were neutropenia (48%), leukopenia (21%), thrombocytopenia (20%), and anemia (11%). Cytokine-release syndrome (CRS) occurred in 23 patients (38%); of these, 1 patient was grade 3 and none were grades 4 or 5.
Approximately one-third of the patients (31%) experienced neurological events during the study; three cases were grade 3, none were grades 4 or 5. Patients with CRS or NE were treated with tocilizumab (10%), corticosteroids (3%), or both (20%). Treatment-emergent adverse events of grade 3 or higher occurred in 79% of patients overall, including grade 5 events in two patients because of COVID-19.
The study findings were limited by the small sample size and lack of controls. However, the results support the potential use of liso-cel as a second-line therapy for r/r LBCL patients who are not candidates for HSCT, Dr. Sehgal concluded.
Addressing an ongoing unmet need
In an interview, study coauthor Dr. Leo I. Gordon of Northwestern University, Chicago, observed, “Patients with relapsed or refractory large B-cell lymphoma who are not considered candidates for stem cell transplant following first-line treatment, based on age, comorbidities, health status, or other prognostic factors, have more difficult-to-treat disease, poor prognosis, and more limited treatment options.”
Dr. Gordon noted that the PILOT study is the only trial to evaluate a CAR T-cell therapy as a second-line treatment for r/r LBCL patients who are not considered candidates for stem cell transplant.
“Data from the primary analysis of the PILOT study further demonstrate the potential value of using CAR T-cell therapies earlier in the treatment paradigm for relapsed or refractory LBCL to help improve clinical outcomes and address ongoing unmet need,” he said.
CAR T-cell therapies have shown benefits in later lines for r/r LBCL and as a second-line treatment for r/r LBCL patients who are deemed candidates for stem cell transplant, “so we were encouraged and not surprised by these data.”
However, Dr. Gordon noted, “There may be some patients with similar presentations that might have a transplant, so one limitation of the trial is how one defines patients where transplant is the intended therapy, and that assessment varies among institutions and clinicians.”
An application for liso-cel as a treatment for patients with r/r LBCL who have failed front-line therapy is currently under Priority Review with the FDA, with a Prescription Drug User Fee Act (PDUFA) goal date of June 24, 2022, he added.
Liso-cel may fill treatment gap as second-line therapy
The current study is important because “the long-term outcomes of patients with relapsed or refractory large B-cell lymphoma who are not candidates for stem cell transplantation is very poor,” said Dr. Brian Till of Fred Hutchinson Cancer Research Center, Seattle, in an interview.
“CAR T therapy leads to about a 40% cure rate, but is currently only available in this population after the failure of second-line therapy,” said Dr. Till, who was not involved in the study.
“Given that liso-cel was shown to improve outcomes in the second-line setting among transplant candidates, it is logical to consider it as second-line therapy in nontransplant candidates as well, who are otherwise fit enough to receive CAR T therapy,” Dr. Till explained.
“This study showed a rate of long-term progression-free survival similar to what has been observed in the third-line setting and was reasonably well tolerated in these older patients,” said Dr. Till. The results suggest “that second-line liso-cel may be an attractive treatment strategy for patients who are not candidates for stem cell transplantation due to advanced age or comorbidities,” he noted.
Dr. Till had no relevant financial conflicts to disclose.
The study was funded by Bristol Myers Squibb.
Not all patients with relapsed or refractory large B cell lymphoma (r/r LBCL) are candidates for high-dose chemotherapy or hematopoietic stem cell transplantation (HSCT), and options for second-line therapies for this population are limited, said Dr. Alison Sehgal of the University of Pittsburgh Medical Center in her presentation of the findings.
Lisocabtagene maraleucel (liso-cel) is a CD19-directed CAR T-cell product. In a previous phase 3 randomized trial (the TRANSFORM study), lisocabtagene showed superiority over salvage chemotherapy for LBCL patients who were fit candidates for stem cell transplant, but its use in older, frail patients who are not transplant candidates remains uncertain, wrote Dr. Sehgal and colleagues in their poster at the meeting.
In the study, the researchers identified 74 patients with r/r LBCL. Of these, 61 were treated with liso-cel. The patients ranged in age from 53 to 84 years, with a median age of 74 years, 61% were male, and 89% were white. Approximately half were refractory and half were relapsed.
For the therapy, patients underwent lymphodepletion with cyclophosphamide and fludarabine, followed 2-7 days later by an infusion of liso-cel at a target dose of 100 x 106 CAR+ T cells; all patients had at least 6 months of follow-up from their first response.
The primary endpoint of overall response rate occurred in 80% of the patients, and clinically meaningful complete response occurred in 54% over a median follow-up of 12.3 months.
“Clinically meaningful CRs were observed across all subgroups,” Dr. Sehgal said in her presentation.
The response lasted a median of 21.7 months, and the median follow-up for duration of response was 15.5 months. The median overall survival was not reached, but the median progression-free survival was 9.0 months, with a median follow-up period of 13.0 months.
Responses occurred across all prespecified subgroups, with no significant differences in either safety or efficacy based on hematopoietic cell transplantation–specific comorbidity index (HCT-CI) scores.
“Despite the advanced age and comorbidities of the population, the safety profile was consistent with previous reports,” and no new or increased safety signals appeared, Dr. Sehgal said.
The most common treatment-emergent adverse events of grade 3 or higher were neutropenia (48%), leukopenia (21%), thrombocytopenia (20%), and anemia (11%). Cytokine-release syndrome (CRS) occurred in 23 patients (38%); of these, 1 patient was grade 3 and none were grades 4 or 5.
Approximately one-third of the patients (31%) experienced neurological events during the study; three cases were grade 3, none were grades 4 or 5. Patients with CRS or NE were treated with tocilizumab (10%), corticosteroids (3%), or both (20%). Treatment-emergent adverse events of grade 3 or higher occurred in 79% of patients overall, including grade 5 events in two patients because of COVID-19.
The study findings were limited by the small sample size and lack of controls. However, the results support the potential use of liso-cel as a second-line therapy for r/r LBCL patients who are not candidates for HSCT, Dr. Sehgal concluded.
Addressing an ongoing unmet need
In an interview, study coauthor Dr. Leo I. Gordon of Northwestern University, Chicago, observed, “Patients with relapsed or refractory large B-cell lymphoma who are not considered candidates for stem cell transplant following first-line treatment, based on age, comorbidities, health status, or other prognostic factors, have more difficult-to-treat disease, poor prognosis, and more limited treatment options.”
Dr. Gordon noted that the PILOT study is the only trial to evaluate a CAR T-cell therapy as a second-line treatment for r/r LBCL patients who are not considered candidates for stem cell transplant.
“Data from the primary analysis of the PILOT study further demonstrate the potential value of using CAR T-cell therapies earlier in the treatment paradigm for relapsed or refractory LBCL to help improve clinical outcomes and address ongoing unmet need,” he said.
CAR T-cell therapies have shown benefits in later lines for r/r LBCL and as a second-line treatment for r/r LBCL patients who are deemed candidates for stem cell transplant, “so we were encouraged and not surprised by these data.”
However, Dr. Gordon noted, “There may be some patients with similar presentations that might have a transplant, so one limitation of the trial is how one defines patients where transplant is the intended therapy, and that assessment varies among institutions and clinicians.”
An application for liso-cel as a treatment for patients with r/r LBCL who have failed front-line therapy is currently under Priority Review with the FDA, with a Prescription Drug User Fee Act (PDUFA) goal date of June 24, 2022, he added.
Liso-cel may fill treatment gap as second-line therapy
The current study is important because “the long-term outcomes of patients with relapsed or refractory large B-cell lymphoma who are not candidates for stem cell transplantation is very poor,” said Dr. Brian Till of Fred Hutchinson Cancer Research Center, Seattle, in an interview.
“CAR T therapy leads to about a 40% cure rate, but is currently only available in this population after the failure of second-line therapy,” said Dr. Till, who was not involved in the study.
“Given that liso-cel was shown to improve outcomes in the second-line setting among transplant candidates, it is logical to consider it as second-line therapy in nontransplant candidates as well, who are otherwise fit enough to receive CAR T therapy,” Dr. Till explained.
“This study showed a rate of long-term progression-free survival similar to what has been observed in the third-line setting and was reasonably well tolerated in these older patients,” said Dr. Till. The results suggest “that second-line liso-cel may be an attractive treatment strategy for patients who are not candidates for stem cell transplantation due to advanced age or comorbidities,” he noted.
Dr. Till had no relevant financial conflicts to disclose.
The study was funded by Bristol Myers Squibb.
Not all patients with relapsed or refractory large B cell lymphoma (r/r LBCL) are candidates for high-dose chemotherapy or hematopoietic stem cell transplantation (HSCT), and options for second-line therapies for this population are limited, said Dr. Alison Sehgal of the University of Pittsburgh Medical Center in her presentation of the findings.
Lisocabtagene maraleucel (liso-cel) is a CD19-directed CAR T-cell product. In a previous phase 3 randomized trial (the TRANSFORM study), lisocabtagene showed superiority over salvage chemotherapy for LBCL patients who were fit candidates for stem cell transplant, but its use in older, frail patients who are not transplant candidates remains uncertain, wrote Dr. Sehgal and colleagues in their poster at the meeting.
In the study, the researchers identified 74 patients with r/r LBCL. Of these, 61 were treated with liso-cel. The patients ranged in age from 53 to 84 years, with a median age of 74 years, 61% were male, and 89% were white. Approximately half were refractory and half were relapsed.
For the therapy, patients underwent lymphodepletion with cyclophosphamide and fludarabine, followed 2-7 days later by an infusion of liso-cel at a target dose of 100 x 106 CAR+ T cells; all patients had at least 6 months of follow-up from their first response.
The primary endpoint of overall response rate occurred in 80% of the patients, and clinically meaningful complete response occurred in 54% over a median follow-up of 12.3 months.
“Clinically meaningful CRs were observed across all subgroups,” Dr. Sehgal said in her presentation.
The response lasted a median of 21.7 months, and the median follow-up for duration of response was 15.5 months. The median overall survival was not reached, but the median progression-free survival was 9.0 months, with a median follow-up period of 13.0 months.
Responses occurred across all prespecified subgroups, with no significant differences in either safety or efficacy based on hematopoietic cell transplantation–specific comorbidity index (HCT-CI) scores.
“Despite the advanced age and comorbidities of the population, the safety profile was consistent with previous reports,” and no new or increased safety signals appeared, Dr. Sehgal said.
The most common treatment-emergent adverse events of grade 3 or higher were neutropenia (48%), leukopenia (21%), thrombocytopenia (20%), and anemia (11%). Cytokine-release syndrome (CRS) occurred in 23 patients (38%); of these, 1 patient was grade 3 and none were grades 4 or 5.
Approximately one-third of the patients (31%) experienced neurological events during the study; three cases were grade 3, none were grades 4 or 5. Patients with CRS or NE were treated with tocilizumab (10%), corticosteroids (3%), or both (20%). Treatment-emergent adverse events of grade 3 or higher occurred in 79% of patients overall, including grade 5 events in two patients because of COVID-19.
The study findings were limited by the small sample size and lack of controls. However, the results support the potential use of liso-cel as a second-line therapy for r/r LBCL patients who are not candidates for HSCT, Dr. Sehgal concluded.
Addressing an ongoing unmet need
In an interview, study coauthor Dr. Leo I. Gordon of Northwestern University, Chicago, observed, “Patients with relapsed or refractory large B-cell lymphoma who are not considered candidates for stem cell transplant following first-line treatment, based on age, comorbidities, health status, or other prognostic factors, have more difficult-to-treat disease, poor prognosis, and more limited treatment options.”
Dr. Gordon noted that the PILOT study is the only trial to evaluate a CAR T-cell therapy as a second-line treatment for r/r LBCL patients who are not considered candidates for stem cell transplant.
“Data from the primary analysis of the PILOT study further demonstrate the potential value of using CAR T-cell therapies earlier in the treatment paradigm for relapsed or refractory LBCL to help improve clinical outcomes and address ongoing unmet need,” he said.
CAR T-cell therapies have shown benefits in later lines for r/r LBCL and as a second-line treatment for r/r LBCL patients who are deemed candidates for stem cell transplant, “so we were encouraged and not surprised by these data.”
However, Dr. Gordon noted, “There may be some patients with similar presentations that might have a transplant, so one limitation of the trial is how one defines patients where transplant is the intended therapy, and that assessment varies among institutions and clinicians.”
An application for liso-cel as a treatment for patients with r/r LBCL who have failed front-line therapy is currently under Priority Review with the FDA, with a Prescription Drug User Fee Act (PDUFA) goal date of June 24, 2022, he added.
Liso-cel may fill treatment gap as second-line therapy
The current study is important because “the long-term outcomes of patients with relapsed or refractory large B-cell lymphoma who are not candidates for stem cell transplantation is very poor,” said Dr. Brian Till of Fred Hutchinson Cancer Research Center, Seattle, in an interview.
“CAR T therapy leads to about a 40% cure rate, but is currently only available in this population after the failure of second-line therapy,” said Dr. Till, who was not involved in the study.
“Given that liso-cel was shown to improve outcomes in the second-line setting among transplant candidates, it is logical to consider it as second-line therapy in nontransplant candidates as well, who are otherwise fit enough to receive CAR T therapy,” Dr. Till explained.
“This study showed a rate of long-term progression-free survival similar to what has been observed in the third-line setting and was reasonably well tolerated in these older patients,” said Dr. Till. The results suggest “that second-line liso-cel may be an attractive treatment strategy for patients who are not candidates for stem cell transplantation due to advanced age or comorbidities,” he noted.
Dr. Till had no relevant financial conflicts to disclose.
The study was funded by Bristol Myers Squibb.
FROM ASCO 2022
Double morning-after pill dose for women with obesity not effective
Emergency contraception is more likely to fail in women with obesity, but simply doubling the dose of levonorgestrel (LNG)-based contraception does not appear to be effective according to the results of a randomized, controlled trial.
Alison B. Edelman, MD, MPH, of the department of obstetrics & gynecology at Oregon Health & Science University, Portland, led the study published online in Obstetrics & Gynecology.
The researchers included healthy women ages 18-35 with regular menstrual cycles, body mass index (BMI) higher than 30 kg/m2, and weight at least 176 pounds in a randomized study.
After confirming ovulation, researchers monitored participants with transvaginal ultrasonography and blood sampling for progesterone, luteinizing hormone, and estradiol every other day until a dominant follicle 15 mm or greater was seen.
At that point the women received either LNG 1.5 mg or 3 mg and returned for daily monitoring up to 7 days.
Emergency contraception with LNG works by preventing the luteinizing hormone surge, blocking follicle rupture. The researchers had hypothesized that women with obesity might not be getting enough LNG to block the surge after oral dosing.
Previous trials had shown women with obesity had a fourfold higher risk of pregnancy, compared with women with normal BMI taking emergency contraception.
The primary outcome in this trial was whether women had follicle rupture 5 days after dosing.
The authors wrote: “The study had 80% power to detect a 30% difference in the proportion of cycles with at least a 5-day delay in follicle rupture (50% decrease).”
A total of 70 women completed study procedures. The two groups (35 women in each) had similar demographics (mean age, 28 years; BMI, 38).
No differences found between groups
“We found no difference between groups in the proportion of participants without follicle rupture,” the researchers wrote.
More than 5 days after dosing, 51.4% in the lower-dose group did not experience follicle rupture. In the double-dose group 68.6% did not experience rupture but the difference was not significant (P = .14).
Among participants with follicle rupture before 5 days, the time to rupture – the secondary endpoint – also did not differ between groups.
The researchers concluded that more research on the failures of hormonal emergency contraception in women with obesity is needed.

Eve Espey, MD, MPH, distinguished professor and chair of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, said in an interview that the study was well designed and the results “form a strong basis for clinical recommendations.”
“Providers should not recommend a higher dose of LNG emergency contraception for patients who are overweight or obese, but rather should counsel patients on the superior effectiveness of ulipristal acetate for those seeking oral emergency contraception as well as the longer time period after unprotected sex – 5 days – that ulipristal maintains its effectiveness.”
“Providers should also counsel patients on the most effective emergency contraception methods, the copper or LNG intrauterine device,” she said.
She said the unique study design of a pharmacodynamic randomized controlled trial adds weight to the findings.
She and the authors noted a limitation is the use of a surrogate outcome, ovulation delay, for ethical and feasibility reasons, instead of the outcome of interest, pregnancy.
The trial was conducted at Oregon Health & Science University and Eastern Virginia Medical School, Norfolk, from June 2017 to February 2021.
Study enrollees were compensated for their time. They were required not to be at risk for pregnancy (abstinent or using a nonhormonal method of contraception).
Dr. Edelman reported receiving honoraria and travel reimbursement from the American College of Obstetricians and Gynecologists, the World Health Organization, and Gynuity for committee activities and honoraria for peer review from the Karolinska Institute. She receives royalties from UpToDate. Several coauthors have received payments for consulting from multiple pharmaceutical companies. These companies and organizations may have a commercial or financial interest in the results of this research and technology. Another was involved in this study as a private consultant and is employed by Gilead Sciences, which was not involved in this research.
Emergency contraception is more likely to fail in women with obesity, but simply doubling the dose of levonorgestrel (LNG)-based contraception does not appear to be effective according to the results of a randomized, controlled trial.
Alison B. Edelman, MD, MPH, of the department of obstetrics & gynecology at Oregon Health & Science University, Portland, led the study published online in Obstetrics & Gynecology.
The researchers included healthy women ages 18-35 with regular menstrual cycles, body mass index (BMI) higher than 30 kg/m2, and weight at least 176 pounds in a randomized study.
After confirming ovulation, researchers monitored participants with transvaginal ultrasonography and blood sampling for progesterone, luteinizing hormone, and estradiol every other day until a dominant follicle 15 mm or greater was seen.
At that point the women received either LNG 1.5 mg or 3 mg and returned for daily monitoring up to 7 days.
Emergency contraception with LNG works by preventing the luteinizing hormone surge, blocking follicle rupture. The researchers had hypothesized that women with obesity might not be getting enough LNG to block the surge after oral dosing.
Previous trials had shown women with obesity had a fourfold higher risk of pregnancy, compared with women with normal BMI taking emergency contraception.
The primary outcome in this trial was whether women had follicle rupture 5 days after dosing.
The authors wrote: “The study had 80% power to detect a 30% difference in the proportion of cycles with at least a 5-day delay in follicle rupture (50% decrease).”
A total of 70 women completed study procedures. The two groups (35 women in each) had similar demographics (mean age, 28 years; BMI, 38).
No differences found between groups
“We found no difference between groups in the proportion of participants without follicle rupture,” the researchers wrote.
More than 5 days after dosing, 51.4% in the lower-dose group did not experience follicle rupture. In the double-dose group 68.6% did not experience rupture but the difference was not significant (P = .14).
Among participants with follicle rupture before 5 days, the time to rupture – the secondary endpoint – also did not differ between groups.
The researchers concluded that more research on the failures of hormonal emergency contraception in women with obesity is needed.
Eve Espey, MD, MPH, distinguished professor and chair of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, said in an interview that the study was well designed and the results “form a strong basis for clinical recommendations.”
“Providers should not recommend a higher dose of LNG emergency contraception for patients who are overweight or obese, but rather should counsel patients on the superior effectiveness of ulipristal acetate for those seeking oral emergency contraception as well as the longer time period after unprotected sex – 5 days – that ulipristal maintains its effectiveness.”
“Providers should also counsel patients on the most effective emergency contraception methods, the copper or LNG intrauterine device,” she said.
She said the unique study design of a pharmacodynamic randomized controlled trial adds weight to the findings.
She and the authors noted a limitation is the use of a surrogate outcome, ovulation delay, for ethical and feasibility reasons, instead of the outcome of interest, pregnancy.
The trial was conducted at Oregon Health & Science University and Eastern Virginia Medical School, Norfolk, from June 2017 to February 2021.
Study enrollees were compensated for their time. They were required not to be at risk for pregnancy (abstinent or using a nonhormonal method of contraception).
Dr. Edelman reported receiving honoraria and travel reimbursement from the American College of Obstetricians and Gynecologists, the World Health Organization, and Gynuity for committee activities and honoraria for peer review from the Karolinska Institute. She receives royalties from UpToDate. Several coauthors have received payments for consulting from multiple pharmaceutical companies. These companies and organizations may have a commercial or financial interest in the results of this research and technology. Another was involved in this study as a private consultant and is employed by Gilead Sciences, which was not involved in this research.
Emergency contraception is more likely to fail in women with obesity, but simply doubling the dose of levonorgestrel (LNG)-based contraception does not appear to be effective according to the results of a randomized, controlled trial.
Alison B. Edelman, MD, MPH, of the department of obstetrics & gynecology at Oregon Health & Science University, Portland, led the study published online in Obstetrics & Gynecology.
The researchers included healthy women ages 18-35 with regular menstrual cycles, body mass index (BMI) higher than 30 kg/m2, and weight at least 176 pounds in a randomized study.
After confirming ovulation, researchers monitored participants with transvaginal ultrasonography and blood sampling for progesterone, luteinizing hormone, and estradiol every other day until a dominant follicle 15 mm or greater was seen.
At that point the women received either LNG 1.5 mg or 3 mg and returned for daily monitoring up to 7 days.
Emergency contraception with LNG works by preventing the luteinizing hormone surge, blocking follicle rupture. The researchers had hypothesized that women with obesity might not be getting enough LNG to block the surge after oral dosing.
Previous trials had shown women with obesity had a fourfold higher risk of pregnancy, compared with women with normal BMI taking emergency contraception.
The primary outcome in this trial was whether women had follicle rupture 5 days after dosing.
The authors wrote: “The study had 80% power to detect a 30% difference in the proportion of cycles with at least a 5-day delay in follicle rupture (50% decrease).”
A total of 70 women completed study procedures. The two groups (35 women in each) had similar demographics (mean age, 28 years; BMI, 38).
No differences found between groups
“We found no difference between groups in the proportion of participants without follicle rupture,” the researchers wrote.
More than 5 days after dosing, 51.4% in the lower-dose group did not experience follicle rupture. In the double-dose group 68.6% did not experience rupture but the difference was not significant (P = .14).
Among participants with follicle rupture before 5 days, the time to rupture – the secondary endpoint – also did not differ between groups.
The researchers concluded that more research on the failures of hormonal emergency contraception in women with obesity is needed.
Eve Espey, MD, MPH, distinguished professor and chair of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, said in an interview that the study was well designed and the results “form a strong basis for clinical recommendations.”
“Providers should not recommend a higher dose of LNG emergency contraception for patients who are overweight or obese, but rather should counsel patients on the superior effectiveness of ulipristal acetate for those seeking oral emergency contraception as well as the longer time period after unprotected sex – 5 days – that ulipristal maintains its effectiveness.”
“Providers should also counsel patients on the most effective emergency contraception methods, the copper or LNG intrauterine device,” she said.
She said the unique study design of a pharmacodynamic randomized controlled trial adds weight to the findings.
She and the authors noted a limitation is the use of a surrogate outcome, ovulation delay, for ethical and feasibility reasons, instead of the outcome of interest, pregnancy.
The trial was conducted at Oregon Health & Science University and Eastern Virginia Medical School, Norfolk, from June 2017 to February 2021.
Study enrollees were compensated for their time. They were required not to be at risk for pregnancy (abstinent or using a nonhormonal method of contraception).
Dr. Edelman reported receiving honoraria and travel reimbursement from the American College of Obstetricians and Gynecologists, the World Health Organization, and Gynuity for committee activities and honoraria for peer review from the Karolinska Institute. She receives royalties from UpToDate. Several coauthors have received payments for consulting from multiple pharmaceutical companies. These companies and organizations may have a commercial or financial interest in the results of this research and technology. Another was involved in this study as a private consultant and is employed by Gilead Sciences, which was not involved in this research.
FROM OBSTETRICS & GYNECOLOGY
Youth with bipolar disorder at high risk of eating disorders
Investigators studied close to 200 youth with BD and found that more than 25% had a lifetime ED, which included anorexia nervosa (AN), bulimia nervosa (BN), and an ED not otherwise specified (NOS).
Those with comorbid EDs were more likely to be female and to have BD-II subtype. Their presentations were also more complicated and included a history of suicidality, additional psychiatric conditions, smoking, and a history of sexual abuse, as well as more severe depression and emotional instability.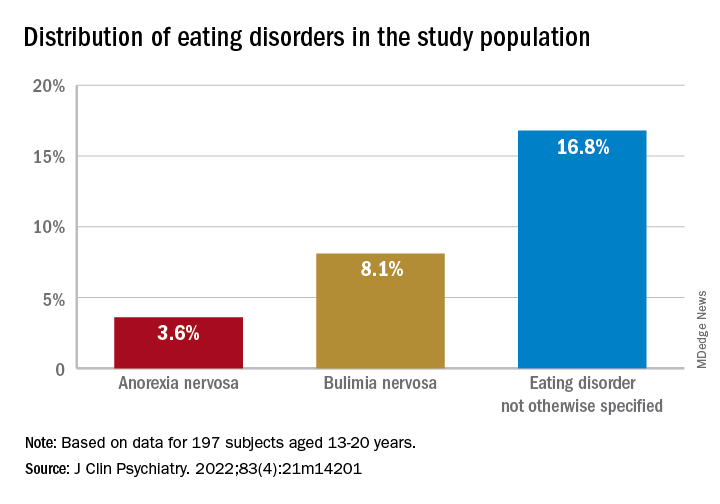
“We think the take-home message is that, in addition to other more recognized psychiatric comorbidities, youth with BD are also vulnerable to developing EDs. Thus, clinicians should be routinely monitoring for eating, appetite, and body image disturbances when working with this population,” lead author Diana Khoubaeva, research analyst at the Centre for Youth Bipolar Disorder, Centre for Addiction and Mental Health, Toronto, and senior author Benjamin Goldstein, MD, PhD, director of the Centre for Youth Bipolar Disorder, wrote in an e-mail to this news organization.
“Given the more complicated clinical picture of youth with co-occurring BD and EDs, this combination warrants careful attention,” the investigators note.
The study was published online May 11 in the Journal of Clinical Psychiatry.
Lack of research
“From the existing literature, we learned that EDs are not uncommon in individuals with BD, and that they are often associated with a more severe clinical profile,” say the researchers. “However, the majority of these studies have been limited to adult samples, and there was a real scarcity of studies that examined this co-occurrence in youth.”
This is “surprising” because EDs often have their onset in adolescence, so the researchers decided to explore the issue in their “fairly large sample of youth with BD.”
To investigate the issue, the researchers studied 197 youth (aged 13-20 years) with a diagnosis of BD (BD-I, BD-II, or BD-NOS) who were recruited between 2009 and 2017 (mean [standard deviation] age, 16.69 [1.50] years; 67.5% female).
ED diagnoses included both current and lifetime AN, BN, and ED-NOS. The researchers used the Kiddie Schedule for Affective Disorders and Schizophrenia for School Age Children, Present and Lifetime Version (K-SADS-PL) to determine the diagnosis of BD.
They also collected information about comorbid psychiatric disorders, as well as substance use disorders and cigarette smoking. The Life Problems Inventory (LPI) was used to identify dimensional borderline personality traits.
Information about physical and sexual abuse, suicidal ideation, nonsuicidal self-injury (NSSI), and affect regulation were obtained from other measurement tools. Participants’ height and weight were measured to calculate body mass index.
Neurobiological and environmental factors
Of the total sample, 24.84% had received a diagnosis of ED in their lifetime.
Moreover, 28.9% had a lifetime history of binge eating. Of these, 17.7% also had been diagnosed with an ED.
Participants with BD-II were significantly more likely than those with BD-I to report both current and lifetime BN. There were no significant differences by BD subtype in AN, ED-NOS, or binge eating.
Higher correlates of clinical characteristics, psychiatric morbidity, treatment history, and dimensional traits in those with vs. those without an ED are detailed in the accompanying table.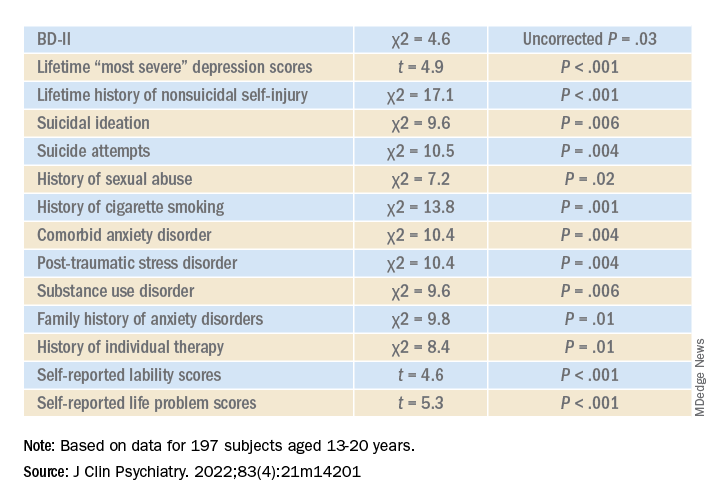
The ED group scored significantly higher on all LPI scores, including impulsivity, emotional dysregulation, identity confusion, and interpersonal problems, compared to those without an ED. They also were less likely to report lifetime lithium use (chi2 = 7.9, P = .01).
Multivariate analysis revealed that lifetime EDs were significantly associated with female sex, history of cigarette smoking, history of individual therapy, family history of anxiety, and LPI total score and were negatively associated with BD-I subtype.
“The comorbidity [between EDs and BD] could be driven by both neurobiological and environmental factors,” Dr. Khoubaeva and Dr. Goldstein noted. EDs and BD “are both illnesses that are fundamentally linked with dysfunction in reward systems – that is, there are imbalances in terms of too much or too little reward seeking.”
They added that individuals affected by these conditions have “ongoing challenges with instability of emotions and ability to manage emotions; and eating too much or too little can be a manifestation of coping with emotions.”
In addition, medications commonly used to treat BD “are known to have side effects such as weight/appetite/metabolic changes, which may make it harder to regulate eating, and which may exacerbate preexisting body image challenges.”
The researchers recommend implementing trauma-informed care, assessing and addressing suicidality and self-injury, and prioritizing therapies that target emotional dysregulation, such as dialectical behavioral therapy.
‘Clarion call’
Commenting on the study, Roger McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the Mood Disorders Psychopharmacology Unit, said the study is “the first of its kind to comprehensively characterize the prevalence of ED in youth living with BD.
“It could be hypothesized that EDs have overlapping domain disturbances of cognitive dysfunction, such as executive function and impulse control, as well as cognitive reward processes,” said Dr. McIntyre, who is the chairman and executive director of the Brain and Cognitive Discover Foundation, Toronto, and was not involved with the study.
“The data are a clarion call for clinicians to routinely screen for EDs in youth with BD and, when present, to be aware of the greater complexity, severity, and risk in this patient subpopulation. The higher prevalence of ED in youth with BD-II is an additional reminder of the severity, morbidity, and complexity of BD-II,” Dr. McIntyre said.
The study received no direct funding. It was supported by philanthropic donations to the Centre for Youth Bipolar Disorder and the CAMH Discovery Fund. Dr. Goldstein reports grant support from Brain Canada, Canadian Institutes of Health Research, Heart and Stroke Foundation, National Institute of Mental Health, and the departments of psychiatry at the University of Toronto and Sunnybrook Health Sciences Centre. He also acknowledges his position as RBC investments chair in Children›s Mental Health and Developmental Psychopathology at CAMH, a joint Hospital-University chair among the University of Toronto, CAMH, and the CAMH Foundation. Ms. Khoubaeva reports no relevant financial relationships. The other authors’ disclosures are listed in the original article. Dr. McIntyre has received research grant support from CIHR/GACD/National Natural Science Foundation of China (NSFC); speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Abbvie, and Atai Life Sciences. Dr. McIntyre is a CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
Investigators studied close to 200 youth with BD and found that more than 25% had a lifetime ED, which included anorexia nervosa (AN), bulimia nervosa (BN), and an ED not otherwise specified (NOS).
Those with comorbid EDs were more likely to be female and to have BD-II subtype. Their presentations were also more complicated and included a history of suicidality, additional psychiatric conditions, smoking, and a history of sexual abuse, as well as more severe depression and emotional instability.
“We think the take-home message is that, in addition to other more recognized psychiatric comorbidities, youth with BD are also vulnerable to developing EDs. Thus, clinicians should be routinely monitoring for eating, appetite, and body image disturbances when working with this population,” lead author Diana Khoubaeva, research analyst at the Centre for Youth Bipolar Disorder, Centre for Addiction and Mental Health, Toronto, and senior author Benjamin Goldstein, MD, PhD, director of the Centre for Youth Bipolar Disorder, wrote in an e-mail to this news organization.
“Given the more complicated clinical picture of youth with co-occurring BD and EDs, this combination warrants careful attention,” the investigators note.
The study was published online May 11 in the Journal of Clinical Psychiatry.
Lack of research
“From the existing literature, we learned that EDs are not uncommon in individuals with BD, and that they are often associated with a more severe clinical profile,” say the researchers. “However, the majority of these studies have been limited to adult samples, and there was a real scarcity of studies that examined this co-occurrence in youth.”
This is “surprising” because EDs often have their onset in adolescence, so the researchers decided to explore the issue in their “fairly large sample of youth with BD.”
To investigate the issue, the researchers studied 197 youth (aged 13-20 years) with a diagnosis of BD (BD-I, BD-II, or BD-NOS) who were recruited between 2009 and 2017 (mean [standard deviation] age, 16.69 [1.50] years; 67.5% female).
ED diagnoses included both current and lifetime AN, BN, and ED-NOS. The researchers used the Kiddie Schedule for Affective Disorders and Schizophrenia for School Age Children, Present and Lifetime Version (K-SADS-PL) to determine the diagnosis of BD.
They also collected information about comorbid psychiatric disorders, as well as substance use disorders and cigarette smoking. The Life Problems Inventory (LPI) was used to identify dimensional borderline personality traits.
Information about physical and sexual abuse, suicidal ideation, nonsuicidal self-injury (NSSI), and affect regulation were obtained from other measurement tools. Participants’ height and weight were measured to calculate body mass index.
Neurobiological and environmental factors
Of the total sample, 24.84% had received a diagnosis of ED in their lifetime.
Moreover, 28.9% had a lifetime history of binge eating. Of these, 17.7% also had been diagnosed with an ED.
Participants with BD-II were significantly more likely than those with BD-I to report both current and lifetime BN. There were no significant differences by BD subtype in AN, ED-NOS, or binge eating.
Higher correlates of clinical characteristics, psychiatric morbidity, treatment history, and dimensional traits in those with vs. those without an ED are detailed in the accompanying table.
The ED group scored significantly higher on all LPI scores, including impulsivity, emotional dysregulation, identity confusion, and interpersonal problems, compared to those without an ED. They also were less likely to report lifetime lithium use (chi2 = 7.9, P = .01).
Multivariate analysis revealed that lifetime EDs were significantly associated with female sex, history of cigarette smoking, history of individual therapy, family history of anxiety, and LPI total score and were negatively associated with BD-I subtype.
“The comorbidity [between EDs and BD] could be driven by both neurobiological and environmental factors,” Dr. Khoubaeva and Dr. Goldstein noted. EDs and BD “are both illnesses that are fundamentally linked with dysfunction in reward systems – that is, there are imbalances in terms of too much or too little reward seeking.”
They added that individuals affected by these conditions have “ongoing challenges with instability of emotions and ability to manage emotions; and eating too much or too little can be a manifestation of coping with emotions.”
In addition, medications commonly used to treat BD “are known to have side effects such as weight/appetite/metabolic changes, which may make it harder to regulate eating, and which may exacerbate preexisting body image challenges.”
The researchers recommend implementing trauma-informed care, assessing and addressing suicidality and self-injury, and prioritizing therapies that target emotional dysregulation, such as dialectical behavioral therapy.
‘Clarion call’
Commenting on the study, Roger McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the Mood Disorders Psychopharmacology Unit, said the study is “the first of its kind to comprehensively characterize the prevalence of ED in youth living with BD.
“It could be hypothesized that EDs have overlapping domain disturbances of cognitive dysfunction, such as executive function and impulse control, as well as cognitive reward processes,” said Dr. McIntyre, who is the chairman and executive director of the Brain and Cognitive Discover Foundation, Toronto, and was not involved with the study.
“The data are a clarion call for clinicians to routinely screen for EDs in youth with BD and, when present, to be aware of the greater complexity, severity, and risk in this patient subpopulation. The higher prevalence of ED in youth with BD-II is an additional reminder of the severity, morbidity, and complexity of BD-II,” Dr. McIntyre said.
The study received no direct funding. It was supported by philanthropic donations to the Centre for Youth Bipolar Disorder and the CAMH Discovery Fund. Dr. Goldstein reports grant support from Brain Canada, Canadian Institutes of Health Research, Heart and Stroke Foundation, National Institute of Mental Health, and the departments of psychiatry at the University of Toronto and Sunnybrook Health Sciences Centre. He also acknowledges his position as RBC investments chair in Children›s Mental Health and Developmental Psychopathology at CAMH, a joint Hospital-University chair among the University of Toronto, CAMH, and the CAMH Foundation. Ms. Khoubaeva reports no relevant financial relationships. The other authors’ disclosures are listed in the original article. Dr. McIntyre has received research grant support from CIHR/GACD/National Natural Science Foundation of China (NSFC); speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Abbvie, and Atai Life Sciences. Dr. McIntyre is a CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
Investigators studied close to 200 youth with BD and found that more than 25% had a lifetime ED, which included anorexia nervosa (AN), bulimia nervosa (BN), and an ED not otherwise specified (NOS).
Those with comorbid EDs were more likely to be female and to have BD-II subtype. Their presentations were also more complicated and included a history of suicidality, additional psychiatric conditions, smoking, and a history of sexual abuse, as well as more severe depression and emotional instability.
“We think the take-home message is that, in addition to other more recognized psychiatric comorbidities, youth with BD are also vulnerable to developing EDs. Thus, clinicians should be routinely monitoring for eating, appetite, and body image disturbances when working with this population,” lead author Diana Khoubaeva, research analyst at the Centre for Youth Bipolar Disorder, Centre for Addiction and Mental Health, Toronto, and senior author Benjamin Goldstein, MD, PhD, director of the Centre for Youth Bipolar Disorder, wrote in an e-mail to this news organization.
“Given the more complicated clinical picture of youth with co-occurring BD and EDs, this combination warrants careful attention,” the investigators note.
The study was published online May 11 in the Journal of Clinical Psychiatry.
Lack of research
“From the existing literature, we learned that EDs are not uncommon in individuals with BD, and that they are often associated with a more severe clinical profile,” say the researchers. “However, the majority of these studies have been limited to adult samples, and there was a real scarcity of studies that examined this co-occurrence in youth.”
This is “surprising” because EDs often have their onset in adolescence, so the researchers decided to explore the issue in their “fairly large sample of youth with BD.”
To investigate the issue, the researchers studied 197 youth (aged 13-20 years) with a diagnosis of BD (BD-I, BD-II, or BD-NOS) who were recruited between 2009 and 2017 (mean [standard deviation] age, 16.69 [1.50] years; 67.5% female).
ED diagnoses included both current and lifetime AN, BN, and ED-NOS. The researchers used the Kiddie Schedule for Affective Disorders and Schizophrenia for School Age Children, Present and Lifetime Version (K-SADS-PL) to determine the diagnosis of BD.
They also collected information about comorbid psychiatric disorders, as well as substance use disorders and cigarette smoking. The Life Problems Inventory (LPI) was used to identify dimensional borderline personality traits.
Information about physical and sexual abuse, suicidal ideation, nonsuicidal self-injury (NSSI), and affect regulation were obtained from other measurement tools. Participants’ height and weight were measured to calculate body mass index.
Neurobiological and environmental factors
Of the total sample, 24.84% had received a diagnosis of ED in their lifetime.
Moreover, 28.9% had a lifetime history of binge eating. Of these, 17.7% also had been diagnosed with an ED.
Participants with BD-II were significantly more likely than those with BD-I to report both current and lifetime BN. There were no significant differences by BD subtype in AN, ED-NOS, or binge eating.
Higher correlates of clinical characteristics, psychiatric morbidity, treatment history, and dimensional traits in those with vs. those without an ED are detailed in the accompanying table.
The ED group scored significantly higher on all LPI scores, including impulsivity, emotional dysregulation, identity confusion, and interpersonal problems, compared to those without an ED. They also were less likely to report lifetime lithium use (chi2 = 7.9, P = .01).
Multivariate analysis revealed that lifetime EDs were significantly associated with female sex, history of cigarette smoking, history of individual therapy, family history of anxiety, and LPI total score and were negatively associated with BD-I subtype.
“The comorbidity [between EDs and BD] could be driven by both neurobiological and environmental factors,” Dr. Khoubaeva and Dr. Goldstein noted. EDs and BD “are both illnesses that are fundamentally linked with dysfunction in reward systems – that is, there are imbalances in terms of too much or too little reward seeking.”
They added that individuals affected by these conditions have “ongoing challenges with instability of emotions and ability to manage emotions; and eating too much or too little can be a manifestation of coping with emotions.”
In addition, medications commonly used to treat BD “are known to have side effects such as weight/appetite/metabolic changes, which may make it harder to regulate eating, and which may exacerbate preexisting body image challenges.”
The researchers recommend implementing trauma-informed care, assessing and addressing suicidality and self-injury, and prioritizing therapies that target emotional dysregulation, such as dialectical behavioral therapy.
‘Clarion call’
Commenting on the study, Roger McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the Mood Disorders Psychopharmacology Unit, said the study is “the first of its kind to comprehensively characterize the prevalence of ED in youth living with BD.
“It could be hypothesized that EDs have overlapping domain disturbances of cognitive dysfunction, such as executive function and impulse control, as well as cognitive reward processes,” said Dr. McIntyre, who is the chairman and executive director of the Brain and Cognitive Discover Foundation, Toronto, and was not involved with the study.
“The data are a clarion call for clinicians to routinely screen for EDs in youth with BD and, when present, to be aware of the greater complexity, severity, and risk in this patient subpopulation. The higher prevalence of ED in youth with BD-II is an additional reminder of the severity, morbidity, and complexity of BD-II,” Dr. McIntyre said.
The study received no direct funding. It was supported by philanthropic donations to the Centre for Youth Bipolar Disorder and the CAMH Discovery Fund. Dr. Goldstein reports grant support from Brain Canada, Canadian Institutes of Health Research, Heart and Stroke Foundation, National Institute of Mental Health, and the departments of psychiatry at the University of Toronto and Sunnybrook Health Sciences Centre. He also acknowledges his position as RBC investments chair in Children›s Mental Health and Developmental Psychopathology at CAMH, a joint Hospital-University chair among the University of Toronto, CAMH, and the CAMH Foundation. Ms. Khoubaeva reports no relevant financial relationships. The other authors’ disclosures are listed in the original article. Dr. McIntyre has received research grant support from CIHR/GACD/National Natural Science Foundation of China (NSFC); speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Abbvie, and Atai Life Sciences. Dr. McIntyre is a CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
Genetic testing for best antidepressant accurate, cost effective
new research suggests.
CYP2D6 and CYP2C19, from the cytochrome P450 family, are involved in the metabolism and elimination of various molecules, including medications. Variants in the genes encoding these enzymes affect the speed at which drugs are metabolized, altering their pharmacokinetic profiles.
The researchers studied 125 patients with MDD and used CYP2D6 and CYP2C19 genotyping to determine the presence of actionable phenotypes in line with Food and Drug Administration labeling.
They found that, in many cases, pharmacogenetic testing could have predicted poor response to the initial treatment selection and could have helped guide subsequent choices to improve outcomes.
In addition, a pharmacoeconomic evaluation that combined direct and indirect costs resulting from MDD with the prevalence of CYP2D6 and CYP2C19 phenotypes showed that testing for functional variants in both genes would be cost effective at a national level.
Had psychiatrists who treated patients in the study known about their metabolizing profiles, it “might have contributed to switches in medication” and could have reduced “delays in response,” said lead researcher Alessio Squassina, PhD, associate professor of pharmacology at the University of Cagliari (Italy).
The findings were presented at the European Psychiatric Association 2022 Congress.
Highly variable response rates
Dr. Squassina noted that the response to antidepressants is a “highly variable trait,” and while it is known that genetics play a role, their contribution is “still not completely understood.”
He explained that the use of pharmacogenetics, which leverages genetic information to guide treatment decision-making, has increased significantly.
While regulatory bodies, including the FDA, have been “very active” in defining strict criteria for interpreting the information from pharmacogenetic tests, there remains some “discrepancy” in their clinical utility.
Dr. Squassina said the FDA provides guidance on use of genetic testing on the labels of 34 psychiatric medications. Of these, 79% relate to CYP2D6, 12% relate to CYP2C19, and 9% relate to other genes.
These labels provide guidance on when genetic testing is recommended or required, as well as potentially clinically actionable gene-drug associations in patients with certain functional alleles.
However, Dr. Squassina noted that the distribution of such alleles is not the same across Europe, so it’s possible that a psychiatrist in Italy may be less likely to treat a patient with a phenotype affecting response to treatment or risk of adverse events than one in Norway or Sweden.
For the study, the investigators examined the frequency of CYP2D6 and CYP2C19 phenotypes in psychiatric patients in Sardinia and their relationship with pharmacologic treatment and cost-effectiveness.
They set out to recruit 200 patients with MDD who had a documented 5-year medical and treatment history, including alterations in treatment, adverse events, hospitalizations, suicide, and symptom scores, as well as sociodemographic variables.
An interim analysis of the first 125 patients recruited to the study showed that the most common CYP2D6 phenotype was normal metabolizers (NM), at 60.5%, followed by intermediate metabolizers (IM), at 28.2%, ultrarapid metabolizers (UR), at 8.9%, and poor metabolizers (PM), at 2.4%.
For CYP2C19, the most common phenotype was NM (49%), followed by IM (29.0%), UR (25.0%), and PM (4.0%). While there were differences in the overall European averages, they were not significant.
To highlight the potential impact that pharmacogenetic testing could have had on patient care and outcome, Dr. Squassina highlighted two cases.
The first concerned a patient with a CYP2D6 IM and CYP2C19 UR phenotype, who did not respond to escitalopram. The FDA drug label indicates this phenotype is actionable and recommends an alternative drug.
The patient was subsequently switched to venlafaxine. The FDA drug label on venlafaxine notes that patients with this phenotype are likely to have a suboptimal response to this drug, and again, this patient did not respond to treatment.
Another patient with a CYP2D6 NM and CYP2C19 IM phenotype was also prescribed escitalopram. The FDA label on this drug notes that patients with this phenotype can try venlafaxine but may not respond. Indeed, this patient did not respond and was switched to venlafaxine and started responding.
“The psychiatrists [in these cases] may made have made different [drug] choices if they had known the genotypes in advance,” Dr. Squassina said.
Cost effective?
To determine the cost-effectiveness of screening for CYP2D6 and CYP2C19 phenotypes in patients with MDD, the researchers used real-world data to develop a Markov model with a hypothetical cohort of 2000 MDD patients, half of whom underwent pharmacogenetic testing, to determine the potential impact on outcomes over an 18-week period.
The model included the cost of medications and hospitalization, psychiatric counseling, loss of productivity, and the estimated probability of response and adverse events, adjusted for the patient’s likelihood of having a particular metabolizing phenotype.
Results showed that, for CYP2C19, compared to no testing, pharmacogenetic testing would be cost-effective at an incremental cost-effective ratio (ICER) of €60,000 ($64,000 USD) per quality-adjusted life-year (QALY).
This, Squassina said, is “below the willingness to pay threshold” for health authorities in developed countries.
For CYP2D6, pharmacogenetic testing would become cost-effective at an ICER of approximately €47,000 ($40,000 USD) per QALY.
The team plans to complete recruitment and perform a “detailed evaluation of all the variables, especially those relating to the medication history and changes in dosage, and adverse drug reactions.” The researchers would also like to study genetic phenotypes for other metabolizing enzymes and repeat the pharmacoeconomic analysis with the complete dataset.
A glimpse into the future
Approached for comment, Alessandro Serretti, MD, PhD, department of biomedical and neuromotor sciences, University of Bologna (Italy), who was not involved in the study, said the findings show there is a “small but evident benefit” from CYP profiling, “which makes sense.”
He added that in the Netherlands and other European countries, efforts are already underway to record the CYP status of patients at a national level. “Sooner or later, all Western countries will implement it as a routine,” he said in an interview.
He explained that, when such testing is widely available, electronic health record data will allow physicians to immediately select the optimal antidepressant for an individual patient. This will end the current trial-and-error process that leads to delayed treatment and will help avoid serious consequences, such as suicide.
While reducing a single patient’s treatment by a few weeks with the most appropriate antidepressant choice does not make a large difference in the cost per episode, at a population level, it has the potential to make a significant difference.
Dr. Serretti does not envisage genotyping all 333 million Europeans for the CYP phenotype at this point but imagines that in the future, individuals will undergo whole-genome sequencing to determine risks for cancer, dementia, and heart disease, at which point they will also undergo CYP functional allele profiling, and all these data will be recorded on individuals’ EHR.
“So, every doctor, a psychiatrist or cardiologist, can see everything, whenever they need it,” he said.
The study was funded by Fondazione di Sardegna and Regione Autonoma della Sardegna. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
CYP2D6 and CYP2C19, from the cytochrome P450 family, are involved in the metabolism and elimination of various molecules, including medications. Variants in the genes encoding these enzymes affect the speed at which drugs are metabolized, altering their pharmacokinetic profiles.
The researchers studied 125 patients with MDD and used CYP2D6 and CYP2C19 genotyping to determine the presence of actionable phenotypes in line with Food and Drug Administration labeling.
They found that, in many cases, pharmacogenetic testing could have predicted poor response to the initial treatment selection and could have helped guide subsequent choices to improve outcomes.
In addition, a pharmacoeconomic evaluation that combined direct and indirect costs resulting from MDD with the prevalence of CYP2D6 and CYP2C19 phenotypes showed that testing for functional variants in both genes would be cost effective at a national level.
Had psychiatrists who treated patients in the study known about their metabolizing profiles, it “might have contributed to switches in medication” and could have reduced “delays in response,” said lead researcher Alessio Squassina, PhD, associate professor of pharmacology at the University of Cagliari (Italy).
The findings were presented at the European Psychiatric Association 2022 Congress.
Highly variable response rates
Dr. Squassina noted that the response to antidepressants is a “highly variable trait,” and while it is known that genetics play a role, their contribution is “still not completely understood.”
He explained that the use of pharmacogenetics, which leverages genetic information to guide treatment decision-making, has increased significantly.
While regulatory bodies, including the FDA, have been “very active” in defining strict criteria for interpreting the information from pharmacogenetic tests, there remains some “discrepancy” in their clinical utility.
Dr. Squassina said the FDA provides guidance on use of genetic testing on the labels of 34 psychiatric medications. Of these, 79% relate to CYP2D6, 12% relate to CYP2C19, and 9% relate to other genes.
These labels provide guidance on when genetic testing is recommended or required, as well as potentially clinically actionable gene-drug associations in patients with certain functional alleles.
However, Dr. Squassina noted that the distribution of such alleles is not the same across Europe, so it’s possible that a psychiatrist in Italy may be less likely to treat a patient with a phenotype affecting response to treatment or risk of adverse events than one in Norway or Sweden.
For the study, the investigators examined the frequency of CYP2D6 and CYP2C19 phenotypes in psychiatric patients in Sardinia and their relationship with pharmacologic treatment and cost-effectiveness.
They set out to recruit 200 patients with MDD who had a documented 5-year medical and treatment history, including alterations in treatment, adverse events, hospitalizations, suicide, and symptom scores, as well as sociodemographic variables.
An interim analysis of the first 125 patients recruited to the study showed that the most common CYP2D6 phenotype was normal metabolizers (NM), at 60.5%, followed by intermediate metabolizers (IM), at 28.2%, ultrarapid metabolizers (UR), at 8.9%, and poor metabolizers (PM), at 2.4%.
For CYP2C19, the most common phenotype was NM (49%), followed by IM (29.0%), UR (25.0%), and PM (4.0%). While there were differences in the overall European averages, they were not significant.
To highlight the potential impact that pharmacogenetic testing could have had on patient care and outcome, Dr. Squassina highlighted two cases.
The first concerned a patient with a CYP2D6 IM and CYP2C19 UR phenotype, who did not respond to escitalopram. The FDA drug label indicates this phenotype is actionable and recommends an alternative drug.
The patient was subsequently switched to venlafaxine. The FDA drug label on venlafaxine notes that patients with this phenotype are likely to have a suboptimal response to this drug, and again, this patient did not respond to treatment.
Another patient with a CYP2D6 NM and CYP2C19 IM phenotype was also prescribed escitalopram. The FDA label on this drug notes that patients with this phenotype can try venlafaxine but may not respond. Indeed, this patient did not respond and was switched to venlafaxine and started responding.
“The psychiatrists [in these cases] may made have made different [drug] choices if they had known the genotypes in advance,” Dr. Squassina said.
Cost effective?
To determine the cost-effectiveness of screening for CYP2D6 and CYP2C19 phenotypes in patients with MDD, the researchers used real-world data to develop a Markov model with a hypothetical cohort of 2000 MDD patients, half of whom underwent pharmacogenetic testing, to determine the potential impact on outcomes over an 18-week period.
The model included the cost of medications and hospitalization, psychiatric counseling, loss of productivity, and the estimated probability of response and adverse events, adjusted for the patient’s likelihood of having a particular metabolizing phenotype.
Results showed that, for CYP2C19, compared to no testing, pharmacogenetic testing would be cost-effective at an incremental cost-effective ratio (ICER) of €60,000 ($64,000 USD) per quality-adjusted life-year (QALY).
This, Squassina said, is “below the willingness to pay threshold” for health authorities in developed countries.
For CYP2D6, pharmacogenetic testing would become cost-effective at an ICER of approximately €47,000 ($40,000 USD) per QALY.
The team plans to complete recruitment and perform a “detailed evaluation of all the variables, especially those relating to the medication history and changes in dosage, and adverse drug reactions.” The researchers would also like to study genetic phenotypes for other metabolizing enzymes and repeat the pharmacoeconomic analysis with the complete dataset.
A glimpse into the future
Approached for comment, Alessandro Serretti, MD, PhD, department of biomedical and neuromotor sciences, University of Bologna (Italy), who was not involved in the study, said the findings show there is a “small but evident benefit” from CYP profiling, “which makes sense.”
He added that in the Netherlands and other European countries, efforts are already underway to record the CYP status of patients at a national level. “Sooner or later, all Western countries will implement it as a routine,” he said in an interview.
He explained that, when such testing is widely available, electronic health record data will allow physicians to immediately select the optimal antidepressant for an individual patient. This will end the current trial-and-error process that leads to delayed treatment and will help avoid serious consequences, such as suicide.
While reducing a single patient’s treatment by a few weeks with the most appropriate antidepressant choice does not make a large difference in the cost per episode, at a population level, it has the potential to make a significant difference.
Dr. Serretti does not envisage genotyping all 333 million Europeans for the CYP phenotype at this point but imagines that in the future, individuals will undergo whole-genome sequencing to determine risks for cancer, dementia, and heart disease, at which point they will also undergo CYP functional allele profiling, and all these data will be recorded on individuals’ EHR.
“So, every doctor, a psychiatrist or cardiologist, can see everything, whenever they need it,” he said.
The study was funded by Fondazione di Sardegna and Regione Autonoma della Sardegna. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
CYP2D6 and CYP2C19, from the cytochrome P450 family, are involved in the metabolism and elimination of various molecules, including medications. Variants in the genes encoding these enzymes affect the speed at which drugs are metabolized, altering their pharmacokinetic profiles.
The researchers studied 125 patients with MDD and used CYP2D6 and CYP2C19 genotyping to determine the presence of actionable phenotypes in line with Food and Drug Administration labeling.
They found that, in many cases, pharmacogenetic testing could have predicted poor response to the initial treatment selection and could have helped guide subsequent choices to improve outcomes.
In addition, a pharmacoeconomic evaluation that combined direct and indirect costs resulting from MDD with the prevalence of CYP2D6 and CYP2C19 phenotypes showed that testing for functional variants in both genes would be cost effective at a national level.
Had psychiatrists who treated patients in the study known about their metabolizing profiles, it “might have contributed to switches in medication” and could have reduced “delays in response,” said lead researcher Alessio Squassina, PhD, associate professor of pharmacology at the University of Cagliari (Italy).
The findings were presented at the European Psychiatric Association 2022 Congress.
Highly variable response rates
Dr. Squassina noted that the response to antidepressants is a “highly variable trait,” and while it is known that genetics play a role, their contribution is “still not completely understood.”
He explained that the use of pharmacogenetics, which leverages genetic information to guide treatment decision-making, has increased significantly.
While regulatory bodies, including the FDA, have been “very active” in defining strict criteria for interpreting the information from pharmacogenetic tests, there remains some “discrepancy” in their clinical utility.
Dr. Squassina said the FDA provides guidance on use of genetic testing on the labels of 34 psychiatric medications. Of these, 79% relate to CYP2D6, 12% relate to CYP2C19, and 9% relate to other genes.
These labels provide guidance on when genetic testing is recommended or required, as well as potentially clinically actionable gene-drug associations in patients with certain functional alleles.
However, Dr. Squassina noted that the distribution of such alleles is not the same across Europe, so it’s possible that a psychiatrist in Italy may be less likely to treat a patient with a phenotype affecting response to treatment or risk of adverse events than one in Norway or Sweden.
For the study, the investigators examined the frequency of CYP2D6 and CYP2C19 phenotypes in psychiatric patients in Sardinia and their relationship with pharmacologic treatment and cost-effectiveness.
They set out to recruit 200 patients with MDD who had a documented 5-year medical and treatment history, including alterations in treatment, adverse events, hospitalizations, suicide, and symptom scores, as well as sociodemographic variables.
An interim analysis of the first 125 patients recruited to the study showed that the most common CYP2D6 phenotype was normal metabolizers (NM), at 60.5%, followed by intermediate metabolizers (IM), at 28.2%, ultrarapid metabolizers (UR), at 8.9%, and poor metabolizers (PM), at 2.4%.
For CYP2C19, the most common phenotype was NM (49%), followed by IM (29.0%), UR (25.0%), and PM (4.0%). While there were differences in the overall European averages, they were not significant.
To highlight the potential impact that pharmacogenetic testing could have had on patient care and outcome, Dr. Squassina highlighted two cases.
The first concerned a patient with a CYP2D6 IM and CYP2C19 UR phenotype, who did not respond to escitalopram. The FDA drug label indicates this phenotype is actionable and recommends an alternative drug.
The patient was subsequently switched to venlafaxine. The FDA drug label on venlafaxine notes that patients with this phenotype are likely to have a suboptimal response to this drug, and again, this patient did not respond to treatment.
Another patient with a CYP2D6 NM and CYP2C19 IM phenotype was also prescribed escitalopram. The FDA label on this drug notes that patients with this phenotype can try venlafaxine but may not respond. Indeed, this patient did not respond and was switched to venlafaxine and started responding.
“The psychiatrists [in these cases] may made have made different [drug] choices if they had known the genotypes in advance,” Dr. Squassina said.
Cost effective?
To determine the cost-effectiveness of screening for CYP2D6 and CYP2C19 phenotypes in patients with MDD, the researchers used real-world data to develop a Markov model with a hypothetical cohort of 2000 MDD patients, half of whom underwent pharmacogenetic testing, to determine the potential impact on outcomes over an 18-week period.
The model included the cost of medications and hospitalization, psychiatric counseling, loss of productivity, and the estimated probability of response and adverse events, adjusted for the patient’s likelihood of having a particular metabolizing phenotype.
Results showed that, for CYP2C19, compared to no testing, pharmacogenetic testing would be cost-effective at an incremental cost-effective ratio (ICER) of €60,000 ($64,000 USD) per quality-adjusted life-year (QALY).
This, Squassina said, is “below the willingness to pay threshold” for health authorities in developed countries.
For CYP2D6, pharmacogenetic testing would become cost-effective at an ICER of approximately €47,000 ($40,000 USD) per QALY.
The team plans to complete recruitment and perform a “detailed evaluation of all the variables, especially those relating to the medication history and changes in dosage, and adverse drug reactions.” The researchers would also like to study genetic phenotypes for other metabolizing enzymes and repeat the pharmacoeconomic analysis with the complete dataset.
A glimpse into the future
Approached for comment, Alessandro Serretti, MD, PhD, department of biomedical and neuromotor sciences, University of Bologna (Italy), who was not involved in the study, said the findings show there is a “small but evident benefit” from CYP profiling, “which makes sense.”
He added that in the Netherlands and other European countries, efforts are already underway to record the CYP status of patients at a national level. “Sooner or later, all Western countries will implement it as a routine,” he said in an interview.
He explained that, when such testing is widely available, electronic health record data will allow physicians to immediately select the optimal antidepressant for an individual patient. This will end the current trial-and-error process that leads to delayed treatment and will help avoid serious consequences, such as suicide.
While reducing a single patient’s treatment by a few weeks with the most appropriate antidepressant choice does not make a large difference in the cost per episode, at a population level, it has the potential to make a significant difference.
Dr. Serretti does not envisage genotyping all 333 million Europeans for the CYP phenotype at this point but imagines that in the future, individuals will undergo whole-genome sequencing to determine risks for cancer, dementia, and heart disease, at which point they will also undergo CYP functional allele profiling, and all these data will be recorded on individuals’ EHR.
“So, every doctor, a psychiatrist or cardiologist, can see everything, whenever they need it,” he said.
The study was funded by Fondazione di Sardegna and Regione Autonoma della Sardegna. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EPA 2022