User login
Post–Roe v. Wade: What’s next?
The U.S. Supreme Court’s decision to overturn Roe v. Wade, the landmark ruling in 1973 establishing a constitutional right to abortion, has spurred abortion rights supporters and opponents into action, speeding up their efforts to protect or remove access to abortion.
For now, the fight moves to the states, where so-called trigger laws have already banned nearly all abortions in a handful of states. More will likely take effect soon.
“Half of [the states] are going to have quite restrictive abortion laws, and about half will pretty much maintain the status quo,” said Ron Allen, JD, a constitutional law expert and professor of law at Northwestern University, Chicago. “My guess is, the largest population will be in those states that maintain the status quo, [though] that’s not terribly consoling to somebody in Arkansas, [which has a trigger law.]”
Federal and state officials spoke out quickly about what protections are still in place for access to abortion, and some governors have taken new actions to expand that protection.
While abortion rights advocates called on Congress to pass legislation legalizing abortion access nationwide, others, including former Vice President Mike Pence, said a national ban on abortions should be the next step.
Federal, state protections
President Joe Biden quickly addressed the issue of women needing to travel out of state to access abortion. In his statement on June 24, he said: “So if a woman lives in a state that restricts abortion, the Supreme Court’s decision does not prevent her from traveling from her home state to the state that allows it. It does not prevent a doctor in that state from treating her.”
In a statement also issued June 24, Attorney General Merrick Garland expressed strong disagreement with the court’s decision and also pointed out it does not mean that states can’t keep abortion legal within their borders. Nor can states ban reproductive services provided to their residents outside their own borders.
Women living in states banning access to abortion, “must be free to seek care in states where it is legal.” Others are free to inform and counsel each other about reproductive care available in other states, he said, citing the First Amendment.
Doctors who provide abortion services in states where the services remain legal, as well as patients who receive the services, will be protected under the Freedom of Access to Clinic Entrances Act, Mr. Garland said in a statement from the Department of Justice.
States reiterated protection for health care providers. For instance, California Gov. Gavin Newsom signed a law June 24 protecting California abortion providers from civil liability when they provide care for women traveling from states where abortion is banned or access to it is narrowed.
Officials from other states with abortion access began publicizing their status as “safe havens.” New York Attorney General Letitia James tweeted: “While other states strip away the fundamental right to choose, New York will always be a safe haven for anyone seeking an abortion.”
Gov. Newsom, too, among other state officials, has promised his state would be a sanctuary for women in need.
After the ruling, New York Gov. Kathy Hochul and the New York State Department of Health launched a new website and campaign, Abortion Access Always, providing a single destination for information about rights, providers, support, and other details.
Abortion pill
Mr. Garland and President Biden strongly warned states not to try to interfere with access to the so-called abortion pill. Approved 20 years ago by the FDA to safely end early pregnancies, the medication, mifepristone (formerly called RU-486) is taken along with misoprostol, a drug also used to prevent stomach ulcers. Medication abortion now accounts for more than half of all abortions, according to the Guttmacher Institute.
In his statement, Mr. Garland noted that the “FDA has approved the use of the medication mifepristone. States may not ban mifepristone based on disagreement with the FDA’s expert judgment about its safety and efficacy.”
Plan C, an information campaign for abortion services, has a state-by-state directory of ways to find the pills, even in states restricting access to abortion, said Elisa Wells, Plan C’s cofounder and codirector.
Calls for national access
On June 24, President Biden called on Congress to restore the protections of Roe v. Wade as federal law. “No executive action from the president can do that,” he said. If Congress lacks the vote to do that now, voters need to make their voices heard, he said.
“The Supreme Court is but one of many government bodies that can protect the right to abortion,” Nancy Northup, JD, president and CEO of the Center for Reproductive Rights, New York, said June 24. “We will be looking to the Congress to pass the Women’s Health Protection Act. Congress can solve this as a national problem. We’ll be looking to the Biden administration to use the extent of its powers.”
The Women’s Health Protection Act would prohibit government restrictions on access to abortion services.
Sen. Bernie Sanders (I-Vt.) tweeted: “Democrats must now end the filibuster in the Senate, codify Roe v. Wade, and once again make abortion legal and safe.”
“The federal government can do a lot of things,” said Mr. Allen. “It’s interesting that we focus on the administrative agencies. The fight over Roe is a fight in large measure over who should be deciding and whether these are issues that should be decided by agencies or a court or legislators.”
Anger, he said, “should be directed at legislators, and that’s who should be acting here, and that means people have to get out and vote.”
Calls for a national ban
Former Vice President Pence told far-right publication Breitbart News that the court’s decision should lead to a national ban on abortion.
He also took to Twitter. Among other posts, he said: “Having been given this second chance for Life, we must not rest and must not relent until the sanctity of life is restored to the center of American law in every state in the land!”
Organizations’ actions
Organizations on both sides of the issue have mobilization and expansion plans.
NRLC: The National Right to Life Committee will now focus on state legislatures, said Laura Echevarria, the group’s communications director.
“We will continue to work on these [antiabortion] laws in the states we can get these passed,” she said. There’s no one size fits all. “New York is not going to pass a law that Alabama is going to pass. Every state is going to be doing something different.”
“The next big thing is to build that safety net” for women who decide to avoid abortion, she said. More than 2,700 “pregnancy help” centers operate in the United States. “We don’t run them, they are independent.” But the NRLC supports them. The centers provide pregnancy support and financial help, “two big reasons why women get abortions.”
She added: “The prolife movement often gets a bad rap, like we don’t care about women, and we do.” In an open letter issued May 12 to state lawmakers, the NRLC said: “We state unequivocally that we do not support any measure seeking to criminalize or punish women and we stand firmly opposed to include such penalties in legislation.”
ACLU: Anthony D. Romero, JD, executive director of the American Civil Liberties Union, issued a statement on Jun 24 that read in part: “Second-class status for women has once again become the law because of today’s decisions.”
As the fight plays out in the court, the ACLU urges voters to head to the polls, noting that state constitutional amendments to preserve reproductive freedom are on the ballot in Kansas in August and in Vermont and Kentucky in November.
Planned Parenthood
“A majority of justices ruled to throw away nearly 50 years of precedent and take away the right to control our bodies and personal health care decisions,” the Planned Parenthood site posted.
On June 25, the Planned Parenthood Association of Utah filed suit in Utah state court, planning to request a temporary restraining order against the state’s ban on abortion at any point in pregnancy. The law took effect June 24.
Abortion rights offers of help
As legislators and public officials focused on what the next steps should be, social media lit up over the weekend with offers of help for women in states without access to abortion.
One meme posted on social media focused on “camping.” Reportedly created by a woman who needed abortions before the 1973 Roe v. Wade decision, it reads: “If you are a person who suddenly finds yourself with a need to go camping in another state friendly towards camping, just know that I will happily drive you, support you, and not talk about the camping trip to anyone ever.”
While the camping code word quickly picked up steam, one Twitter user who favored the court’s decision called the trend of using camping as a code word to help people access abortions “horrible.”
TikTok users also offered their homes and help to women from other states who might need either. And one Airbnb host posted this invitation on Facebook: “My Airbnb is free for any American woman coming to Los Angeles for an abortion. Hugs and cute kittens, too.”
A version of this article first appeared on Medscape.com.
The U.S. Supreme Court’s decision to overturn Roe v. Wade, the landmark ruling in 1973 establishing a constitutional right to abortion, has spurred abortion rights supporters and opponents into action, speeding up their efforts to protect or remove access to abortion.
For now, the fight moves to the states, where so-called trigger laws have already banned nearly all abortions in a handful of states. More will likely take effect soon.
“Half of [the states] are going to have quite restrictive abortion laws, and about half will pretty much maintain the status quo,” said Ron Allen, JD, a constitutional law expert and professor of law at Northwestern University, Chicago. “My guess is, the largest population will be in those states that maintain the status quo, [though] that’s not terribly consoling to somebody in Arkansas, [which has a trigger law.]”
Federal and state officials spoke out quickly about what protections are still in place for access to abortion, and some governors have taken new actions to expand that protection.
While abortion rights advocates called on Congress to pass legislation legalizing abortion access nationwide, others, including former Vice President Mike Pence, said a national ban on abortions should be the next step.
Federal, state protections
President Joe Biden quickly addressed the issue of women needing to travel out of state to access abortion. In his statement on June 24, he said: “So if a woman lives in a state that restricts abortion, the Supreme Court’s decision does not prevent her from traveling from her home state to the state that allows it. It does not prevent a doctor in that state from treating her.”
In a statement also issued June 24, Attorney General Merrick Garland expressed strong disagreement with the court’s decision and also pointed out it does not mean that states can’t keep abortion legal within their borders. Nor can states ban reproductive services provided to their residents outside their own borders.
Women living in states banning access to abortion, “must be free to seek care in states where it is legal.” Others are free to inform and counsel each other about reproductive care available in other states, he said, citing the First Amendment.
Doctors who provide abortion services in states where the services remain legal, as well as patients who receive the services, will be protected under the Freedom of Access to Clinic Entrances Act, Mr. Garland said in a statement from the Department of Justice.
States reiterated protection for health care providers. For instance, California Gov. Gavin Newsom signed a law June 24 protecting California abortion providers from civil liability when they provide care for women traveling from states where abortion is banned or access to it is narrowed.
Officials from other states with abortion access began publicizing their status as “safe havens.” New York Attorney General Letitia James tweeted: “While other states strip away the fundamental right to choose, New York will always be a safe haven for anyone seeking an abortion.”
Gov. Newsom, too, among other state officials, has promised his state would be a sanctuary for women in need.
After the ruling, New York Gov. Kathy Hochul and the New York State Department of Health launched a new website and campaign, Abortion Access Always, providing a single destination for information about rights, providers, support, and other details.
Abortion pill
Mr. Garland and President Biden strongly warned states not to try to interfere with access to the so-called abortion pill. Approved 20 years ago by the FDA to safely end early pregnancies, the medication, mifepristone (formerly called RU-486) is taken along with misoprostol, a drug also used to prevent stomach ulcers. Medication abortion now accounts for more than half of all abortions, according to the Guttmacher Institute.
In his statement, Mr. Garland noted that the “FDA has approved the use of the medication mifepristone. States may not ban mifepristone based on disagreement with the FDA’s expert judgment about its safety and efficacy.”
Plan C, an information campaign for abortion services, has a state-by-state directory of ways to find the pills, even in states restricting access to abortion, said Elisa Wells, Plan C’s cofounder and codirector.
Calls for national access
On June 24, President Biden called on Congress to restore the protections of Roe v. Wade as federal law. “No executive action from the president can do that,” he said. If Congress lacks the vote to do that now, voters need to make their voices heard, he said.
“The Supreme Court is but one of many government bodies that can protect the right to abortion,” Nancy Northup, JD, president and CEO of the Center for Reproductive Rights, New York, said June 24. “We will be looking to the Congress to pass the Women’s Health Protection Act. Congress can solve this as a national problem. We’ll be looking to the Biden administration to use the extent of its powers.”
The Women’s Health Protection Act would prohibit government restrictions on access to abortion services.
Sen. Bernie Sanders (I-Vt.) tweeted: “Democrats must now end the filibuster in the Senate, codify Roe v. Wade, and once again make abortion legal and safe.”
“The federal government can do a lot of things,” said Mr. Allen. “It’s interesting that we focus on the administrative agencies. The fight over Roe is a fight in large measure over who should be deciding and whether these are issues that should be decided by agencies or a court or legislators.”
Anger, he said, “should be directed at legislators, and that’s who should be acting here, and that means people have to get out and vote.”
Calls for a national ban
Former Vice President Pence told far-right publication Breitbart News that the court’s decision should lead to a national ban on abortion.
He also took to Twitter. Among other posts, he said: “Having been given this second chance for Life, we must not rest and must not relent until the sanctity of life is restored to the center of American law in every state in the land!”
Organizations’ actions
Organizations on both sides of the issue have mobilization and expansion plans.
NRLC: The National Right to Life Committee will now focus on state legislatures, said Laura Echevarria, the group’s communications director.
“We will continue to work on these [antiabortion] laws in the states we can get these passed,” she said. There’s no one size fits all. “New York is not going to pass a law that Alabama is going to pass. Every state is going to be doing something different.”
“The next big thing is to build that safety net” for women who decide to avoid abortion, she said. More than 2,700 “pregnancy help” centers operate in the United States. “We don’t run them, they are independent.” But the NRLC supports them. The centers provide pregnancy support and financial help, “two big reasons why women get abortions.”
She added: “The prolife movement often gets a bad rap, like we don’t care about women, and we do.” In an open letter issued May 12 to state lawmakers, the NRLC said: “We state unequivocally that we do not support any measure seeking to criminalize or punish women and we stand firmly opposed to include such penalties in legislation.”
ACLU: Anthony D. Romero, JD, executive director of the American Civil Liberties Union, issued a statement on Jun 24 that read in part: “Second-class status for women has once again become the law because of today’s decisions.”
As the fight plays out in the court, the ACLU urges voters to head to the polls, noting that state constitutional amendments to preserve reproductive freedom are on the ballot in Kansas in August and in Vermont and Kentucky in November.
Planned Parenthood
“A majority of justices ruled to throw away nearly 50 years of precedent and take away the right to control our bodies and personal health care decisions,” the Planned Parenthood site posted.
On June 25, the Planned Parenthood Association of Utah filed suit in Utah state court, planning to request a temporary restraining order against the state’s ban on abortion at any point in pregnancy. The law took effect June 24.
Abortion rights offers of help
As legislators and public officials focused on what the next steps should be, social media lit up over the weekend with offers of help for women in states without access to abortion.
One meme posted on social media focused on “camping.” Reportedly created by a woman who needed abortions before the 1973 Roe v. Wade decision, it reads: “If you are a person who suddenly finds yourself with a need to go camping in another state friendly towards camping, just know that I will happily drive you, support you, and not talk about the camping trip to anyone ever.”
While the camping code word quickly picked up steam, one Twitter user who favored the court’s decision called the trend of using camping as a code word to help people access abortions “horrible.”
TikTok users also offered their homes and help to women from other states who might need either. And one Airbnb host posted this invitation on Facebook: “My Airbnb is free for any American woman coming to Los Angeles for an abortion. Hugs and cute kittens, too.”
A version of this article first appeared on Medscape.com.
The U.S. Supreme Court’s decision to overturn Roe v. Wade, the landmark ruling in 1973 establishing a constitutional right to abortion, has spurred abortion rights supporters and opponents into action, speeding up their efforts to protect or remove access to abortion.
For now, the fight moves to the states, where so-called trigger laws have already banned nearly all abortions in a handful of states. More will likely take effect soon.
“Half of [the states] are going to have quite restrictive abortion laws, and about half will pretty much maintain the status quo,” said Ron Allen, JD, a constitutional law expert and professor of law at Northwestern University, Chicago. “My guess is, the largest population will be in those states that maintain the status quo, [though] that’s not terribly consoling to somebody in Arkansas, [which has a trigger law.]”
Federal and state officials spoke out quickly about what protections are still in place for access to abortion, and some governors have taken new actions to expand that protection.
While abortion rights advocates called on Congress to pass legislation legalizing abortion access nationwide, others, including former Vice President Mike Pence, said a national ban on abortions should be the next step.
Federal, state protections
President Joe Biden quickly addressed the issue of women needing to travel out of state to access abortion. In his statement on June 24, he said: “So if a woman lives in a state that restricts abortion, the Supreme Court’s decision does not prevent her from traveling from her home state to the state that allows it. It does not prevent a doctor in that state from treating her.”
In a statement also issued June 24, Attorney General Merrick Garland expressed strong disagreement with the court’s decision and also pointed out it does not mean that states can’t keep abortion legal within their borders. Nor can states ban reproductive services provided to their residents outside their own borders.
Women living in states banning access to abortion, “must be free to seek care in states where it is legal.” Others are free to inform and counsel each other about reproductive care available in other states, he said, citing the First Amendment.
Doctors who provide abortion services in states where the services remain legal, as well as patients who receive the services, will be protected under the Freedom of Access to Clinic Entrances Act, Mr. Garland said in a statement from the Department of Justice.
States reiterated protection for health care providers. For instance, California Gov. Gavin Newsom signed a law June 24 protecting California abortion providers from civil liability when they provide care for women traveling from states where abortion is banned or access to it is narrowed.
Officials from other states with abortion access began publicizing their status as “safe havens.” New York Attorney General Letitia James tweeted: “While other states strip away the fundamental right to choose, New York will always be a safe haven for anyone seeking an abortion.”
Gov. Newsom, too, among other state officials, has promised his state would be a sanctuary for women in need.
After the ruling, New York Gov. Kathy Hochul and the New York State Department of Health launched a new website and campaign, Abortion Access Always, providing a single destination for information about rights, providers, support, and other details.
Abortion pill
Mr. Garland and President Biden strongly warned states not to try to interfere with access to the so-called abortion pill. Approved 20 years ago by the FDA to safely end early pregnancies, the medication, mifepristone (formerly called RU-486) is taken along with misoprostol, a drug also used to prevent stomach ulcers. Medication abortion now accounts for more than half of all abortions, according to the Guttmacher Institute.
In his statement, Mr. Garland noted that the “FDA has approved the use of the medication mifepristone. States may not ban mifepristone based on disagreement with the FDA’s expert judgment about its safety and efficacy.”
Plan C, an information campaign for abortion services, has a state-by-state directory of ways to find the pills, even in states restricting access to abortion, said Elisa Wells, Plan C’s cofounder and codirector.
Calls for national access
On June 24, President Biden called on Congress to restore the protections of Roe v. Wade as federal law. “No executive action from the president can do that,” he said. If Congress lacks the vote to do that now, voters need to make their voices heard, he said.
“The Supreme Court is but one of many government bodies that can protect the right to abortion,” Nancy Northup, JD, president and CEO of the Center for Reproductive Rights, New York, said June 24. “We will be looking to the Congress to pass the Women’s Health Protection Act. Congress can solve this as a national problem. We’ll be looking to the Biden administration to use the extent of its powers.”
The Women’s Health Protection Act would prohibit government restrictions on access to abortion services.
Sen. Bernie Sanders (I-Vt.) tweeted: “Democrats must now end the filibuster in the Senate, codify Roe v. Wade, and once again make abortion legal and safe.”
“The federal government can do a lot of things,” said Mr. Allen. “It’s interesting that we focus on the administrative agencies. The fight over Roe is a fight in large measure over who should be deciding and whether these are issues that should be decided by agencies or a court or legislators.”
Anger, he said, “should be directed at legislators, and that’s who should be acting here, and that means people have to get out and vote.”
Calls for a national ban
Former Vice President Pence told far-right publication Breitbart News that the court’s decision should lead to a national ban on abortion.
He also took to Twitter. Among other posts, he said: “Having been given this second chance for Life, we must not rest and must not relent until the sanctity of life is restored to the center of American law in every state in the land!”
Organizations’ actions
Organizations on both sides of the issue have mobilization and expansion plans.
NRLC: The National Right to Life Committee will now focus on state legislatures, said Laura Echevarria, the group’s communications director.
“We will continue to work on these [antiabortion] laws in the states we can get these passed,” she said. There’s no one size fits all. “New York is not going to pass a law that Alabama is going to pass. Every state is going to be doing something different.”
“The next big thing is to build that safety net” for women who decide to avoid abortion, she said. More than 2,700 “pregnancy help” centers operate in the United States. “We don’t run them, they are independent.” But the NRLC supports them. The centers provide pregnancy support and financial help, “two big reasons why women get abortions.”
She added: “The prolife movement often gets a bad rap, like we don’t care about women, and we do.” In an open letter issued May 12 to state lawmakers, the NRLC said: “We state unequivocally that we do not support any measure seeking to criminalize or punish women and we stand firmly opposed to include such penalties in legislation.”
ACLU: Anthony D. Romero, JD, executive director of the American Civil Liberties Union, issued a statement on Jun 24 that read in part: “Second-class status for women has once again become the law because of today’s decisions.”
As the fight plays out in the court, the ACLU urges voters to head to the polls, noting that state constitutional amendments to preserve reproductive freedom are on the ballot in Kansas in August and in Vermont and Kentucky in November.
Planned Parenthood
“A majority of justices ruled to throw away nearly 50 years of precedent and take away the right to control our bodies and personal health care decisions,” the Planned Parenthood site posted.
On June 25, the Planned Parenthood Association of Utah filed suit in Utah state court, planning to request a temporary restraining order against the state’s ban on abortion at any point in pregnancy. The law took effect June 24.
Abortion rights offers of help
As legislators and public officials focused on what the next steps should be, social media lit up over the weekend with offers of help for women in states without access to abortion.
One meme posted on social media focused on “camping.” Reportedly created by a woman who needed abortions before the 1973 Roe v. Wade decision, it reads: “If you are a person who suddenly finds yourself with a need to go camping in another state friendly towards camping, just know that I will happily drive you, support you, and not talk about the camping trip to anyone ever.”
While the camping code word quickly picked up steam, one Twitter user who favored the court’s decision called the trend of using camping as a code word to help people access abortions “horrible.”
TikTok users also offered their homes and help to women from other states who might need either. And one Airbnb host posted this invitation on Facebook: “My Airbnb is free for any American woman coming to Los Angeles for an abortion. Hugs and cute kittens, too.”
A version of this article first appeared on Medscape.com.
Highlights in Early Breast Cancer From the 2022 American Society of Clinical Oncology Annual Meeting
Dr Ann Partridge from the Dana-Farber Cancer Institute in Boston, Massachusetts, highlights important new data in early breast cancer presented at American Society of Clinical Oncology (ASCO) 2022.
Dr Partridge begins with promising results from the NeoSTAR study, which looked at the use of the novel antibody-drug conjugate (ADC) sacituzumab govitecan in the neoadjuvant setting. This is the first trial of an ADC in patients with triple-negative breast cancer (TNBC) and demonstrated single-agent efficacy in localized TNBC.
Next, Dr Partridge discusses the 8-year post-trial follow-up of the ASTRRA study, which randomly assigned patients to 5 years of tamoxifen or 5 years of tamoxifen plus 2 years of ovarian suppression. The findings demonstrated consistent survival advantage and suggest that adding ovarian function suppression to tamoxifen should be considered for those who remain in a premenopausal state or resume ovarian function after chemotherapy.
Looking to potential new biomarkers for risk recurrence, Dr Partridge reports on provocative data from the CHiRP study. The investigators looked at the use of circulating tumor DNA to identify minimal residual disease and predict clinical outcomes in high-risk, early-stage HR+ breast cancer. Although additional research is needed, Dr Partridge is encouraged that in the near future, the use of circulating DNA technology will help guide therapeutic decisions in early breast cancer.
--
Ann H. Partridge, MD, MPH, Professor of Medicine; Vice Chair of Medical Oncology, Department of Breast Oncology, Dana-Farber Cancer Institute, Boston, Massachusetts
Ann H. Partridge, MD, MPH, has disclosed no relevant financial relationships.
Dr Ann Partridge from the Dana-Farber Cancer Institute in Boston, Massachusetts, highlights important new data in early breast cancer presented at American Society of Clinical Oncology (ASCO) 2022.
Dr Partridge begins with promising results from the NeoSTAR study, which looked at the use of the novel antibody-drug conjugate (ADC) sacituzumab govitecan in the neoadjuvant setting. This is the first trial of an ADC in patients with triple-negative breast cancer (TNBC) and demonstrated single-agent efficacy in localized TNBC.
Next, Dr Partridge discusses the 8-year post-trial follow-up of the ASTRRA study, which randomly assigned patients to 5 years of tamoxifen or 5 years of tamoxifen plus 2 years of ovarian suppression. The findings demonstrated consistent survival advantage and suggest that adding ovarian function suppression to tamoxifen should be considered for those who remain in a premenopausal state or resume ovarian function after chemotherapy.
Looking to potential new biomarkers for risk recurrence, Dr Partridge reports on provocative data from the CHiRP study. The investigators looked at the use of circulating tumor DNA to identify minimal residual disease and predict clinical outcomes in high-risk, early-stage HR+ breast cancer. Although additional research is needed, Dr Partridge is encouraged that in the near future, the use of circulating DNA technology will help guide therapeutic decisions in early breast cancer.
--
Ann H. Partridge, MD, MPH, Professor of Medicine; Vice Chair of Medical Oncology, Department of Breast Oncology, Dana-Farber Cancer Institute, Boston, Massachusetts
Ann H. Partridge, MD, MPH, has disclosed no relevant financial relationships.
Dr Ann Partridge from the Dana-Farber Cancer Institute in Boston, Massachusetts, highlights important new data in early breast cancer presented at American Society of Clinical Oncology (ASCO) 2022.
Dr Partridge begins with promising results from the NeoSTAR study, which looked at the use of the novel antibody-drug conjugate (ADC) sacituzumab govitecan in the neoadjuvant setting. This is the first trial of an ADC in patients with triple-negative breast cancer (TNBC) and demonstrated single-agent efficacy in localized TNBC.
Next, Dr Partridge discusses the 8-year post-trial follow-up of the ASTRRA study, which randomly assigned patients to 5 years of tamoxifen or 5 years of tamoxifen plus 2 years of ovarian suppression. The findings demonstrated consistent survival advantage and suggest that adding ovarian function suppression to tamoxifen should be considered for those who remain in a premenopausal state or resume ovarian function after chemotherapy.
Looking to potential new biomarkers for risk recurrence, Dr Partridge reports on provocative data from the CHiRP study. The investigators looked at the use of circulating tumor DNA to identify minimal residual disease and predict clinical outcomes in high-risk, early-stage HR+ breast cancer. Although additional research is needed, Dr Partridge is encouraged that in the near future, the use of circulating DNA technology will help guide therapeutic decisions in early breast cancer.
--
Ann H. Partridge, MD, MPH, Professor of Medicine; Vice Chair of Medical Oncology, Department of Breast Oncology, Dana-Farber Cancer Institute, Boston, Massachusetts
Ann H. Partridge, MD, MPH, has disclosed no relevant financial relationships.
Key Abstracts in Metastatic Breast Cancer From the 2022 American Society of Clinical Oncology Annual Meeting
Dr Harold J. Burstein, from the Dana-Farber Cancer Institute in Boston, Massachusetts, reports on important abstracts in the management of metastatic breast cancer from the 2022 American Society of Clinical Oncology (ASCO) annual meeting.
Dr Burstein first highlights results from the NRG-BR002 trial, a randomized phase 2 study comparing standard therapy vs standard therapy in combination with focal stereotactic radiation treatment for oligometastatic disease in up to four sites. Investigators reported no impact on progression-free or overall survival.
Exciting results from the DESTINY-Breast04 trial were a "showstopper," according to Dr Burstein. Investigators reported prolonged progression-free survival and overall survival in patients with HER2-low unresectable and/or metastatic disease with the use of the antibody-drug conjugate trastuzumab deruxtecan compared with physicians' choice of standard single-agent chemotherapy, advancing a new treatment option for the large subset of patients with HER2-low disease.
Next, Dr Burstein discusses results from the TROPiCS-02 trial, which compared another antibody-drug conjugate, sacituzumab govitecan, with standard chemotherapy in patients with ER+/HER- breast cancer. A statistically significant benefit was reported, although the progression-free survival at just 6 weeks was relatively modest.
Finally, Dr Burstein reports on interesting data from the MAINTAIN study, a phase 2 randomized trial looking at maintenance CDK4/6 inhibition after progression on initial treatment. Results suggest that switching endocrine therapy and continuing treatment with CDK4/6 inhibitor ribociclib beyond progression may be of clinical value to patients.
--
Harold J. Burstein, MD, PhD, Professor, Department of Medicine, Harvard Medical School; Medical Oncologist, Dana-Farber Cancer Institute, Brigham & Women's Hospital, Boston, Massachusetts
Harold J. Burstein, MD, PhD, has disclosed no relevant financial relationships.
Dr Harold J. Burstein, from the Dana-Farber Cancer Institute in Boston, Massachusetts, reports on important abstracts in the management of metastatic breast cancer from the 2022 American Society of Clinical Oncology (ASCO) annual meeting.
Dr Burstein first highlights results from the NRG-BR002 trial, a randomized phase 2 study comparing standard therapy vs standard therapy in combination with focal stereotactic radiation treatment for oligometastatic disease in up to four sites. Investigators reported no impact on progression-free or overall survival.
Exciting results from the DESTINY-Breast04 trial were a "showstopper," according to Dr Burstein. Investigators reported prolonged progression-free survival and overall survival in patients with HER2-low unresectable and/or metastatic disease with the use of the antibody-drug conjugate trastuzumab deruxtecan compared with physicians' choice of standard single-agent chemotherapy, advancing a new treatment option for the large subset of patients with HER2-low disease.
Next, Dr Burstein discusses results from the TROPiCS-02 trial, which compared another antibody-drug conjugate, sacituzumab govitecan, with standard chemotherapy in patients with ER+/HER- breast cancer. A statistically significant benefit was reported, although the progression-free survival at just 6 weeks was relatively modest.
Finally, Dr Burstein reports on interesting data from the MAINTAIN study, a phase 2 randomized trial looking at maintenance CDK4/6 inhibition after progression on initial treatment. Results suggest that switching endocrine therapy and continuing treatment with CDK4/6 inhibitor ribociclib beyond progression may be of clinical value to patients.
--
Harold J. Burstein, MD, PhD, Professor, Department of Medicine, Harvard Medical School; Medical Oncologist, Dana-Farber Cancer Institute, Brigham & Women's Hospital, Boston, Massachusetts
Harold J. Burstein, MD, PhD, has disclosed no relevant financial relationships.
Dr Harold J. Burstein, from the Dana-Farber Cancer Institute in Boston, Massachusetts, reports on important abstracts in the management of metastatic breast cancer from the 2022 American Society of Clinical Oncology (ASCO) annual meeting.
Dr Burstein first highlights results from the NRG-BR002 trial, a randomized phase 2 study comparing standard therapy vs standard therapy in combination with focal stereotactic radiation treatment for oligometastatic disease in up to four sites. Investigators reported no impact on progression-free or overall survival.
Exciting results from the DESTINY-Breast04 trial were a "showstopper," according to Dr Burstein. Investigators reported prolonged progression-free survival and overall survival in patients with HER2-low unresectable and/or metastatic disease with the use of the antibody-drug conjugate trastuzumab deruxtecan compared with physicians' choice of standard single-agent chemotherapy, advancing a new treatment option for the large subset of patients with HER2-low disease.
Next, Dr Burstein discusses results from the TROPiCS-02 trial, which compared another antibody-drug conjugate, sacituzumab govitecan, with standard chemotherapy in patients with ER+/HER- breast cancer. A statistically significant benefit was reported, although the progression-free survival at just 6 weeks was relatively modest.
Finally, Dr Burstein reports on interesting data from the MAINTAIN study, a phase 2 randomized trial looking at maintenance CDK4/6 inhibition after progression on initial treatment. Results suggest that switching endocrine therapy and continuing treatment with CDK4/6 inhibitor ribociclib beyond progression may be of clinical value to patients.
--
Harold J. Burstein, MD, PhD, Professor, Department of Medicine, Harvard Medical School; Medical Oncologist, Dana-Farber Cancer Institute, Brigham & Women's Hospital, Boston, Massachusetts
Harold J. Burstein, MD, PhD, has disclosed no relevant financial relationships.

Study finds higher risk of skin cancer after childhood organ transplant
A large study showing an increased risk of keratinocyte carcinoma (KC) in children who receive a solid-organ transplant highlights the need for early education about risk reduction and more research to determine optimal timing for screening, say an investigator and two dermatologists with expertise in transplant-related skin issues.
The increased incidence of KC in pediatric transplant recipients is “really high, so we definitely know there’s risk there,” just as there is for adult recipients of solid-organ transplants, said Cathryn Sibbald, MD, MSc, a dermatologist at the Hospital for Sick Children in Toronto and coauthor of a research letter published in June in JAMA Dermatology.

For their study, Dr. Sibbald and her coinvestigators turned to the Ontario Health Insurance plan database, which covers health care for Canadian citizens and qualified residents in the province. They identified 951 patients younger than the age of 18 who received a solid-organ transplant between 1991 and 2004 at an Ontario hospital
They then used a validated health insurance claims–based algorithm to identify diagnoses of KC for the transplant recipients and for more than 5 million age-matched controls. KC, including squamous and basal cell carcinoma, is the most prevalent skin cancer for people who have had a solid-organ transplant.
Fifteen posttransplant KCs (10 patients, 1.1%) were reported a mean of 13.1 years after transplant, with none reported in the first 4 years. The mean age at transplant was 7.8 years, and the mean age at KC diagnosis was 25.2 years. Kidney transplants were the most common (42.1% of transplantations). Most of the transplants recipients (eight patients) who developed KC had kidney transplantation, and most of them had functional graft at the time of KC diagnosis.
Researchers found an increased incidence of KC compared with that of the general population (standardized incidence ratio, 9.09; 95% confidence interval, 5.48-15.08). And the risk for KC increased with time since transplant, with adjusted hazard ratios for KC of 3.63 (95% CI, 0.51-25.77) for 1-5 years, 5.14 (95% CI, 1.28-20.55) for 5-10 years, and 4.80 (95% CI, 2.29-10.08) for 10 years or more, compared with the control population.
Several years ago, another research team performed a similar population-based cohort study of adult transplant recipients in Ontario and found a 6.6-times increased risk of KC in transplant recipients compared with the general population.
Sun protection and skin cancer screening
In commenting on the study, Sarah Arron, MD, PhD, a San Francisco Bay area dermatologist and immediate past president of the International Immunosuppression and Transplant Skin Cancer Collaborative (www.itscc.org), said she feels “reassured” that young transplant patients tend not to develop the skin cancer until young adulthood.

A ”large study like this is important because the overall rate of KC is low in this age group,” she noted.
The findings “suggest that we can focus our efforts on prevention during childhood, with sun protection and skin cancer education,” she said. “Then, as these children move into adulthood, we can begin screening with skin examinations. Of course, [any child] with a skin lesion or mole that concerns their parents or transplant team should be referred to dermatology for evaluation.”
Pediatric transplant recipients and their parents are most interested in learning about skin cancer prevention either before or immediately after transplantation, according to a survey by other researchers.
Intervention studies needed
The increased risk of KC probably stems largely from immunosuppression, said Dr. Sibbald in an interview. “We know [this is the case] in the older population, and it’s likely true in the younger population as well that it’s one of the primary drivers,” she said.
More research to extensively analyze risk factors should come next, she said. This includes “the granularity of what [immunosuppressants and other] medications are received, and at what dose and for what periods of time, so we can calculate cumulative exposure and its relation to risk,” she said.

Kristin Bibee, MD, PhD, assistant professor of dermatology at Johns Hopkins University in Baltimore, said she’d like to see further studies “evaluate appropriate interventions, like sun-protective behavior in childhood and adolescence or immunosuppression modulation, to prevent malignancy development.”
The optimal time and intensity of screening for young transplant recipients must still be determined, both Dr. Bibee and Dr. Arron said. Patients deemed through further research to be at higher risk may need earlier and/or more intensive surveillance.
The role of race in skin cancer risk in this population is “one question the study leaves open,” said Dr. Arron. U.S. studies have shown that among adult transplant recipients White patients are “at highest risk for the ultraviolet-associated melanoma and squamous cell carcinoma, followed by Asian and Latino patients. African Americans have had the lowest risk, but some still developed skin cancer after transplant,” she said.
Prior studies of cancer in pediatric transplant recipients have reported primarily on internal malignant neoplasms, with limited data on KC, Dr. Sibbald and coauthors wrote. It is possible the incidence of KS is underestimated in the new study because of “undiagnosed or unreported KCs,” they noted.
The new study was funded by a grant from the Pediatric Dermatology Research Alliance and a Hospital for Sick Children grant. In disclosures, Dr. Sibbald reported to JAMA Dermatology receiving grants from the alliance and from Paediatric Consultants Partnership during the conduct of the study. Dr. Arron and Dr. Bibee both said they have no disclosures relevant to the study and its content.
A large study showing an increased risk of keratinocyte carcinoma (KC) in children who receive a solid-organ transplant highlights the need for early education about risk reduction and more research to determine optimal timing for screening, say an investigator and two dermatologists with expertise in transplant-related skin issues.
The increased incidence of KC in pediatric transplant recipients is “really high, so we definitely know there’s risk there,” just as there is for adult recipients of solid-organ transplants, said Cathryn Sibbald, MD, MSc, a dermatologist at the Hospital for Sick Children in Toronto and coauthor of a research letter published in June in JAMA Dermatology.
For their study, Dr. Sibbald and her coinvestigators turned to the Ontario Health Insurance plan database, which covers health care for Canadian citizens and qualified residents in the province. They identified 951 patients younger than the age of 18 who received a solid-organ transplant between 1991 and 2004 at an Ontario hospital
They then used a validated health insurance claims–based algorithm to identify diagnoses of KC for the transplant recipients and for more than 5 million age-matched controls. KC, including squamous and basal cell carcinoma, is the most prevalent skin cancer for people who have had a solid-organ transplant.
Fifteen posttransplant KCs (10 patients, 1.1%) were reported a mean of 13.1 years after transplant, with none reported in the first 4 years. The mean age at transplant was 7.8 years, and the mean age at KC diagnosis was 25.2 years. Kidney transplants were the most common (42.1% of transplantations). Most of the transplants recipients (eight patients) who developed KC had kidney transplantation, and most of them had functional graft at the time of KC diagnosis.
Researchers found an increased incidence of KC compared with that of the general population (standardized incidence ratio, 9.09; 95% confidence interval, 5.48-15.08). And the risk for KC increased with time since transplant, with adjusted hazard ratios for KC of 3.63 (95% CI, 0.51-25.77) for 1-5 years, 5.14 (95% CI, 1.28-20.55) for 5-10 years, and 4.80 (95% CI, 2.29-10.08) for 10 years or more, compared with the control population.
Several years ago, another research team performed a similar population-based cohort study of adult transplant recipients in Ontario and found a 6.6-times increased risk of KC in transplant recipients compared with the general population.
Sun protection and skin cancer screening
In commenting on the study, Sarah Arron, MD, PhD, a San Francisco Bay area dermatologist and immediate past president of the International Immunosuppression and Transplant Skin Cancer Collaborative (www.itscc.org), said she feels “reassured” that young transplant patients tend not to develop the skin cancer until young adulthood.
A ”large study like this is important because the overall rate of KC is low in this age group,” she noted.
The findings “suggest that we can focus our efforts on prevention during childhood, with sun protection and skin cancer education,” she said. “Then, as these children move into adulthood, we can begin screening with skin examinations. Of course, [any child] with a skin lesion or mole that concerns their parents or transplant team should be referred to dermatology for evaluation.”
Pediatric transplant recipients and their parents are most interested in learning about skin cancer prevention either before or immediately after transplantation, according to a survey by other researchers.
Intervention studies needed
The increased risk of KC probably stems largely from immunosuppression, said Dr. Sibbald in an interview. “We know [this is the case] in the older population, and it’s likely true in the younger population as well that it’s one of the primary drivers,” she said.
More research to extensively analyze risk factors should come next, she said. This includes “the granularity of what [immunosuppressants and other] medications are received, and at what dose and for what periods of time, so we can calculate cumulative exposure and its relation to risk,” she said.
Kristin Bibee, MD, PhD, assistant professor of dermatology at Johns Hopkins University in Baltimore, said she’d like to see further studies “evaluate appropriate interventions, like sun-protective behavior in childhood and adolescence or immunosuppression modulation, to prevent malignancy development.”
The optimal time and intensity of screening for young transplant recipients must still be determined, both Dr. Bibee and Dr. Arron said. Patients deemed through further research to be at higher risk may need earlier and/or more intensive surveillance.
The role of race in skin cancer risk in this population is “one question the study leaves open,” said Dr. Arron. U.S. studies have shown that among adult transplant recipients White patients are “at highest risk for the ultraviolet-associated melanoma and squamous cell carcinoma, followed by Asian and Latino patients. African Americans have had the lowest risk, but some still developed skin cancer after transplant,” she said.
Prior studies of cancer in pediatric transplant recipients have reported primarily on internal malignant neoplasms, with limited data on KC, Dr. Sibbald and coauthors wrote. It is possible the incidence of KS is underestimated in the new study because of “undiagnosed or unreported KCs,” they noted.
The new study was funded by a grant from the Pediatric Dermatology Research Alliance and a Hospital for Sick Children grant. In disclosures, Dr. Sibbald reported to JAMA Dermatology receiving grants from the alliance and from Paediatric Consultants Partnership during the conduct of the study. Dr. Arron and Dr. Bibee both said they have no disclosures relevant to the study and its content.
A large study showing an increased risk of keratinocyte carcinoma (KC) in children who receive a solid-organ transplant highlights the need for early education about risk reduction and more research to determine optimal timing for screening, say an investigator and two dermatologists with expertise in transplant-related skin issues.
The increased incidence of KC in pediatric transplant recipients is “really high, so we definitely know there’s risk there,” just as there is for adult recipients of solid-organ transplants, said Cathryn Sibbald, MD, MSc, a dermatologist at the Hospital for Sick Children in Toronto and coauthor of a research letter published in June in JAMA Dermatology.
For their study, Dr. Sibbald and her coinvestigators turned to the Ontario Health Insurance plan database, which covers health care for Canadian citizens and qualified residents in the province. They identified 951 patients younger than the age of 18 who received a solid-organ transplant between 1991 and 2004 at an Ontario hospital
They then used a validated health insurance claims–based algorithm to identify diagnoses of KC for the transplant recipients and for more than 5 million age-matched controls. KC, including squamous and basal cell carcinoma, is the most prevalent skin cancer for people who have had a solid-organ transplant.
Fifteen posttransplant KCs (10 patients, 1.1%) were reported a mean of 13.1 years after transplant, with none reported in the first 4 years. The mean age at transplant was 7.8 years, and the mean age at KC diagnosis was 25.2 years. Kidney transplants were the most common (42.1% of transplantations). Most of the transplants recipients (eight patients) who developed KC had kidney transplantation, and most of them had functional graft at the time of KC diagnosis.
Researchers found an increased incidence of KC compared with that of the general population (standardized incidence ratio, 9.09; 95% confidence interval, 5.48-15.08). And the risk for KC increased with time since transplant, with adjusted hazard ratios for KC of 3.63 (95% CI, 0.51-25.77) for 1-5 years, 5.14 (95% CI, 1.28-20.55) for 5-10 years, and 4.80 (95% CI, 2.29-10.08) for 10 years or more, compared with the control population.
Several years ago, another research team performed a similar population-based cohort study of adult transplant recipients in Ontario and found a 6.6-times increased risk of KC in transplant recipients compared with the general population.
Sun protection and skin cancer screening
In commenting on the study, Sarah Arron, MD, PhD, a San Francisco Bay area dermatologist and immediate past president of the International Immunosuppression and Transplant Skin Cancer Collaborative (www.itscc.org), said she feels “reassured” that young transplant patients tend not to develop the skin cancer until young adulthood.
A ”large study like this is important because the overall rate of KC is low in this age group,” she noted.
The findings “suggest that we can focus our efforts on prevention during childhood, with sun protection and skin cancer education,” she said. “Then, as these children move into adulthood, we can begin screening with skin examinations. Of course, [any child] with a skin lesion or mole that concerns their parents or transplant team should be referred to dermatology for evaluation.”
Pediatric transplant recipients and their parents are most interested in learning about skin cancer prevention either before or immediately after transplantation, according to a survey by other researchers.
Intervention studies needed
The increased risk of KC probably stems largely from immunosuppression, said Dr. Sibbald in an interview. “We know [this is the case] in the older population, and it’s likely true in the younger population as well that it’s one of the primary drivers,” she said.
More research to extensively analyze risk factors should come next, she said. This includes “the granularity of what [immunosuppressants and other] medications are received, and at what dose and for what periods of time, so we can calculate cumulative exposure and its relation to risk,” she said.
Kristin Bibee, MD, PhD, assistant professor of dermatology at Johns Hopkins University in Baltimore, said she’d like to see further studies “evaluate appropriate interventions, like sun-protective behavior in childhood and adolescence or immunosuppression modulation, to prevent malignancy development.”
The optimal time and intensity of screening for young transplant recipients must still be determined, both Dr. Bibee and Dr. Arron said. Patients deemed through further research to be at higher risk may need earlier and/or more intensive surveillance.
The role of race in skin cancer risk in this population is “one question the study leaves open,” said Dr. Arron. U.S. studies have shown that among adult transplant recipients White patients are “at highest risk for the ultraviolet-associated melanoma and squamous cell carcinoma, followed by Asian and Latino patients. African Americans have had the lowest risk, but some still developed skin cancer after transplant,” she said.
Prior studies of cancer in pediatric transplant recipients have reported primarily on internal malignant neoplasms, with limited data on KC, Dr. Sibbald and coauthors wrote. It is possible the incidence of KS is underestimated in the new study because of “undiagnosed or unreported KCs,” they noted.
The new study was funded by a grant from the Pediatric Dermatology Research Alliance and a Hospital for Sick Children grant. In disclosures, Dr. Sibbald reported to JAMA Dermatology receiving grants from the alliance and from Paediatric Consultants Partnership during the conduct of the study. Dr. Arron and Dr. Bibee both said they have no disclosures relevant to the study and its content.
FROM JAMA DERMATOLOGY
Diabetes and Heart Disease Highlights From ACC 2022
Cardiologist Martha Gulati, from the American Society for Preventive Cardiology, offers insight on the key findings in diabetes and heart disease presented at the 2022 annual meeting of the American College of Cardiology.
First, Dr Gulati shares updates from the SCORED trial, which looked at SGLT2 inhibitors and cardiovascular and renal event reduction in patients with type 2 diabetes and chronic kidney disease.
Next, she shares insight on CHAP, an important study about chronic hypertension in pregnancy. Researchers found that more aggressive blood pressure control reduced adverse pregnancy outcomes.
She then discusses the SuperWIN trial, which looked at various types of educational interventions regarding heart-healthy diet provided in supermarkets. The goal of this study was to assess adherence to the DASH diet.
Dr Gulati closes her report with the PROMPT-HF trial, which aimed at improving the use of guideline-directed medical therapy in outpatients with heart failure.
--
President, American Society for Preventive Cardiology, Jacksonville, Florida
Martha Gulati, MD, has disclosed no relevant financial relationships.
Cardiologist Martha Gulati, from the American Society for Preventive Cardiology, offers insight on the key findings in diabetes and heart disease presented at the 2022 annual meeting of the American College of Cardiology.
First, Dr Gulati shares updates from the SCORED trial, which looked at SGLT2 inhibitors and cardiovascular and renal event reduction in patients with type 2 diabetes and chronic kidney disease.
Next, she shares insight on CHAP, an important study about chronic hypertension in pregnancy. Researchers found that more aggressive blood pressure control reduced adverse pregnancy outcomes.
She then discusses the SuperWIN trial, which looked at various types of educational interventions regarding heart-healthy diet provided in supermarkets. The goal of this study was to assess adherence to the DASH diet.
Dr Gulati closes her report with the PROMPT-HF trial, which aimed at improving the use of guideline-directed medical therapy in outpatients with heart failure.
--
President, American Society for Preventive Cardiology, Jacksonville, Florida
Martha Gulati, MD, has disclosed no relevant financial relationships.
Cardiologist Martha Gulati, from the American Society for Preventive Cardiology, offers insight on the key findings in diabetes and heart disease presented at the 2022 annual meeting of the American College of Cardiology.
First, Dr Gulati shares updates from the SCORED trial, which looked at SGLT2 inhibitors and cardiovascular and renal event reduction in patients with type 2 diabetes and chronic kidney disease.
Next, she shares insight on CHAP, an important study about chronic hypertension in pregnancy. Researchers found that more aggressive blood pressure control reduced adverse pregnancy outcomes.
She then discusses the SuperWIN trial, which looked at various types of educational interventions regarding heart-healthy diet provided in supermarkets. The goal of this study was to assess adherence to the DASH diet.
Dr Gulati closes her report with the PROMPT-HF trial, which aimed at improving the use of guideline-directed medical therapy in outpatients with heart failure.
--
President, American Society for Preventive Cardiology, Jacksonville, Florida
Martha Gulati, MD, has disclosed no relevant financial relationships.

Cardiologists concerned for patient safety after abortion ruling
Pregnancy termination for medical reasons had been part of the fabric of everyday health care in the United States since the Supreme Court’s 1973 Roe v. Wade decision, which the current high court overturned in a ruling announced on June 24.
That means many clinicians across specialties are entering uncharted territory with the country’s new patchwork of abortion legality. Some specialties, cardiology among them, may feel the impact more than others.

“We know that the rising maternal mortality rate is predominantly driven by cardiovascular disease, women having children at older ages, and ... risk factors like hypertension, diabetes, and obesity,” Jennifer H. Haythe, MD, told this news organization.
So the high court’s decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade and leaves the legality of abortion up to the 50 separate state legislatures, “is very relevant to cardiologists specifically,” said Dr. Haythe, who is director of cardiology in the cardio-obstetrics program at New York-Presbyterian/Columbia University Irving Medical Center, New York.
The ruling “is going to have a huge effect on women who may not be able to tolerate pregnancy,” she said. Whether to terminate a pregnancy “is a relatively common discussion I have with women with bad heart failure about their risk of further decompensation, death, or needing a heart transplant or heart pump after delivery, or the risk of death in women with pulmonary hypertension.”
The high court’s decision “is a direct attack on the practice of medicine and really the sanctity of the patient-clinician relationship,” Rachel M. Bond, MD, director of Women’s Heart Health Systems Dignity Health of Arizona, told this news organization.
Physicians take an oath “that we should do no harm to our patients, and once the law or governance impacts that, it places us in a very vulnerable situation,” Dr. Bond said. “As a cardiologist who focuses a lot on high-risk pregnancies, I am worried and hesitant to give guidance to many of these patients in the states that may not have access to something that is a medical right, which at times is an abortion.”
She has colleagues in obstetrics in states where abortion is newly illegal who “don’t know what to do,” Dr. Bond said. Many have sought guidance from their legal teams, she said, “and many of them are now trying to figure out what is the best path.”
Pregnancy is “a very significant cardiovascular stress test, and women who may tolerate certain conditions reasonably well outside of the setting of pregnancy may have severe issues, not just for the mother, but for the baby as well,” Ki Park, MD, University of Florida Health, Gainesville, said in an interview.
“As clinicians, none of us like recommending a medically indicated abortion. But it is health care, just like any other medication or treatment that we advise to our patients in cases where the risk of the mother is excessively high and mortality risk is elevated,” said Dr. Park, who is cochair of the American College of Cardiology Cardio-Obstetrics Work Group.
Some conditions, such as pulmonary hypertension and severe aortic valve stenosis, during pregnancy are well recognized as very high risk, and there are various scoring systems to help clinicians with risk stratification, she observed. “But there are also a lot of gray areas where patients don’t necessarily fit into these risk scores that we use.”
So physician-patient discussions in high-risk pregnancies “are already complicated,” Dr. Park said. “Patients want to have options, and they look to us as physicians for guidance with regard to their risks. And if abortion is not available as an option, then part of our toolbox is no longer available to help us care for the mother.”
In the new legal climate, clinicians in states where abortion is illegal may well want to put more emphasis on preconception counseling, so more of their patients with high-risk conditions are aware of the new barriers to pregnancy termination.
“Unfortunately,” Dr. Haythe said, “many of the states that are going to make or have made abortion illegal are not providing that kind of preconception counseling or good prenatal care to women.”
Cardiologists can provide such counseling to their female patients of childbearing age who have high-risk cardiac conditions, “but not everybody knows that they have a heart problem when they get pregnant, and not everybody is getting screened for heart problems when they’re of childbearing age,” Dr. Haythe said.
“Sometimes it’s not clear whether the problems could have been picked up until a woman is pregnant and has started to have symptoms.” For example, “a lot of women with poor access to health care have rheumatic heart disease. They may have no idea that they have severe aortic stenosis, and it’s not until their second trimester that they start to feel really short of breath.” Often that can be treated in the cath lab, “but again, that’s putting the woman and the baby at risk.”
Cardiologists in states where abortion is illegal will still present the option to their patients with high-risk pregnancies, noted Dr. Haythe. But the conversation may sound something like, “you are at very high risk, termination of the pregnancy takes that risk away, but you’ll have to find a state where it’s legal to do that.”
Dr. Park said such a situation, when abortion is recommended but locally unavailable, is much like any other in cardiology for which the patient may want a second opinion. If a center “doesn’t have the capability or the technology to offer a certain treatment, the patient can opt to seek another opinion at another center,” she said. “Patients will often travel out of state to get the care they need.”
A requirement for out-of-state travel to obtain abortions is likely to worsen socioeconomic disparities in health care, Dr. Bond observed, “because we know that those who are low-income won’t be able to afford that travel.”
Dr. Bond is cosignatory on a statement from the Association of Black Cardiologists (ABC) responding to the high court’s ruling in Dobbs v. Jackson. “This decision will isolate the poor, socioeconomically disadvantaged, and minority populations specifically, widening the already large gaps in health care for our most vulnerable communities,” it states.
“The loss of broad protections supporting the medical and often lifesaving procedure of abortions is likely to have a real impact on the maternal mortality rate, especially in those with congenital and/or acquired cardiovascular conditions where evidence-based guidelines advise at times on termination of such high-risk pregnancies.”
The ABC, it states, “believes that every woman, and every person, should be afforded the right to safe, accessible, legal, timely, patient-centered, equitable, and affordable health care.”
The American College of Cardiology (ACC) released a statement on the matter June 24, signed by its president, Edward T.A. Fry, MD, along with five former ACC presidents. “While the ACC has no official policy on abortion, clinical practice guidelines and other clinical guidance tools address the dangers of pregnancy in certain patient populations at higher risk of death or serious cardiac events.”
The college, it states, is “deeply concerned about the potential implications of the Supreme Court decision regarding Roe vs. Wade on the ability of patients and clinicians to engage in important shared discussions about maternal health, or to remove previously available health care options.”
Dr. Bond proposed that a “vocal stance” from medical societies involved in women’s health, “perhaps even a collective stance from our cardiovascular societies and our obstetrics societies,” would also perhaps reach “the masses of doctors in private practice who are dealing with these patients.”
A version of this article first appeared on Medscape.com.
Pregnancy termination for medical reasons had been part of the fabric of everyday health care in the United States since the Supreme Court’s 1973 Roe v. Wade decision, which the current high court overturned in a ruling announced on June 24.
That means many clinicians across specialties are entering uncharted territory with the country’s new patchwork of abortion legality. Some specialties, cardiology among them, may feel the impact more than others.
“We know that the rising maternal mortality rate is predominantly driven by cardiovascular disease, women having children at older ages, and ... risk factors like hypertension, diabetes, and obesity,” Jennifer H. Haythe, MD, told this news organization.
So the high court’s decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade and leaves the legality of abortion up to the 50 separate state legislatures, “is very relevant to cardiologists specifically,” said Dr. Haythe, who is director of cardiology in the cardio-obstetrics program at New York-Presbyterian/Columbia University Irving Medical Center, New York.
The ruling “is going to have a huge effect on women who may not be able to tolerate pregnancy,” she said. Whether to terminate a pregnancy “is a relatively common discussion I have with women with bad heart failure about their risk of further decompensation, death, or needing a heart transplant or heart pump after delivery, or the risk of death in women with pulmonary hypertension.”
The high court’s decision “is a direct attack on the practice of medicine and really the sanctity of the patient-clinician relationship,” Rachel M. Bond, MD, director of Women’s Heart Health Systems Dignity Health of Arizona, told this news organization.
Physicians take an oath “that we should do no harm to our patients, and once the law or governance impacts that, it places us in a very vulnerable situation,” Dr. Bond said. “As a cardiologist who focuses a lot on high-risk pregnancies, I am worried and hesitant to give guidance to many of these patients in the states that may not have access to something that is a medical right, which at times is an abortion.”
She has colleagues in obstetrics in states where abortion is newly illegal who “don’t know what to do,” Dr. Bond said. Many have sought guidance from their legal teams, she said, “and many of them are now trying to figure out what is the best path.”
Pregnancy is “a very significant cardiovascular stress test, and women who may tolerate certain conditions reasonably well outside of the setting of pregnancy may have severe issues, not just for the mother, but for the baby as well,” Ki Park, MD, University of Florida Health, Gainesville, said in an interview.
“As clinicians, none of us like recommending a medically indicated abortion. But it is health care, just like any other medication or treatment that we advise to our patients in cases where the risk of the mother is excessively high and mortality risk is elevated,” said Dr. Park, who is cochair of the American College of Cardiology Cardio-Obstetrics Work Group.
Some conditions, such as pulmonary hypertension and severe aortic valve stenosis, during pregnancy are well recognized as very high risk, and there are various scoring systems to help clinicians with risk stratification, she observed. “But there are also a lot of gray areas where patients don’t necessarily fit into these risk scores that we use.”
So physician-patient discussions in high-risk pregnancies “are already complicated,” Dr. Park said. “Patients want to have options, and they look to us as physicians for guidance with regard to their risks. And if abortion is not available as an option, then part of our toolbox is no longer available to help us care for the mother.”
In the new legal climate, clinicians in states where abortion is illegal may well want to put more emphasis on preconception counseling, so more of their patients with high-risk conditions are aware of the new barriers to pregnancy termination.
“Unfortunately,” Dr. Haythe said, “many of the states that are going to make or have made abortion illegal are not providing that kind of preconception counseling or good prenatal care to women.”
Cardiologists can provide such counseling to their female patients of childbearing age who have high-risk cardiac conditions, “but not everybody knows that they have a heart problem when they get pregnant, and not everybody is getting screened for heart problems when they’re of childbearing age,” Dr. Haythe said.
“Sometimes it’s not clear whether the problems could have been picked up until a woman is pregnant and has started to have symptoms.” For example, “a lot of women with poor access to health care have rheumatic heart disease. They may have no idea that they have severe aortic stenosis, and it’s not until their second trimester that they start to feel really short of breath.” Often that can be treated in the cath lab, “but again, that’s putting the woman and the baby at risk.”
Cardiologists in states where abortion is illegal will still present the option to their patients with high-risk pregnancies, noted Dr. Haythe. But the conversation may sound something like, “you are at very high risk, termination of the pregnancy takes that risk away, but you’ll have to find a state where it’s legal to do that.”
Dr. Park said such a situation, when abortion is recommended but locally unavailable, is much like any other in cardiology for which the patient may want a second opinion. If a center “doesn’t have the capability or the technology to offer a certain treatment, the patient can opt to seek another opinion at another center,” she said. “Patients will often travel out of state to get the care they need.”
A requirement for out-of-state travel to obtain abortions is likely to worsen socioeconomic disparities in health care, Dr. Bond observed, “because we know that those who are low-income won’t be able to afford that travel.”
Dr. Bond is cosignatory on a statement from the Association of Black Cardiologists (ABC) responding to the high court’s ruling in Dobbs v. Jackson. “This decision will isolate the poor, socioeconomically disadvantaged, and minority populations specifically, widening the already large gaps in health care for our most vulnerable communities,” it states.
“The loss of broad protections supporting the medical and often lifesaving procedure of abortions is likely to have a real impact on the maternal mortality rate, especially in those with congenital and/or acquired cardiovascular conditions where evidence-based guidelines advise at times on termination of such high-risk pregnancies.”
The ABC, it states, “believes that every woman, and every person, should be afforded the right to safe, accessible, legal, timely, patient-centered, equitable, and affordable health care.”
The American College of Cardiology (ACC) released a statement on the matter June 24, signed by its president, Edward T.A. Fry, MD, along with five former ACC presidents. “While the ACC has no official policy on abortion, clinical practice guidelines and other clinical guidance tools address the dangers of pregnancy in certain patient populations at higher risk of death or serious cardiac events.”
The college, it states, is “deeply concerned about the potential implications of the Supreme Court decision regarding Roe vs. Wade on the ability of patients and clinicians to engage in important shared discussions about maternal health, or to remove previously available health care options.”
Dr. Bond proposed that a “vocal stance” from medical societies involved in women’s health, “perhaps even a collective stance from our cardiovascular societies and our obstetrics societies,” would also perhaps reach “the masses of doctors in private practice who are dealing with these patients.”
A version of this article first appeared on Medscape.com.
Pregnancy termination for medical reasons had been part of the fabric of everyday health care in the United States since the Supreme Court’s 1973 Roe v. Wade decision, which the current high court overturned in a ruling announced on June 24.
That means many clinicians across specialties are entering uncharted territory with the country’s new patchwork of abortion legality. Some specialties, cardiology among them, may feel the impact more than others.
“We know that the rising maternal mortality rate is predominantly driven by cardiovascular disease, women having children at older ages, and ... risk factors like hypertension, diabetes, and obesity,” Jennifer H. Haythe, MD, told this news organization.
So the high court’s decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade and leaves the legality of abortion up to the 50 separate state legislatures, “is very relevant to cardiologists specifically,” said Dr. Haythe, who is director of cardiology in the cardio-obstetrics program at New York-Presbyterian/Columbia University Irving Medical Center, New York.
The ruling “is going to have a huge effect on women who may not be able to tolerate pregnancy,” she said. Whether to terminate a pregnancy “is a relatively common discussion I have with women with bad heart failure about their risk of further decompensation, death, or needing a heart transplant or heart pump after delivery, or the risk of death in women with pulmonary hypertension.”
The high court’s decision “is a direct attack on the practice of medicine and really the sanctity of the patient-clinician relationship,” Rachel M. Bond, MD, director of Women’s Heart Health Systems Dignity Health of Arizona, told this news organization.
Physicians take an oath “that we should do no harm to our patients, and once the law or governance impacts that, it places us in a very vulnerable situation,” Dr. Bond said. “As a cardiologist who focuses a lot on high-risk pregnancies, I am worried and hesitant to give guidance to many of these patients in the states that may not have access to something that is a medical right, which at times is an abortion.”
She has colleagues in obstetrics in states where abortion is newly illegal who “don’t know what to do,” Dr. Bond said. Many have sought guidance from their legal teams, she said, “and many of them are now trying to figure out what is the best path.”
Pregnancy is “a very significant cardiovascular stress test, and women who may tolerate certain conditions reasonably well outside of the setting of pregnancy may have severe issues, not just for the mother, but for the baby as well,” Ki Park, MD, University of Florida Health, Gainesville, said in an interview.
“As clinicians, none of us like recommending a medically indicated abortion. But it is health care, just like any other medication or treatment that we advise to our patients in cases where the risk of the mother is excessively high and mortality risk is elevated,” said Dr. Park, who is cochair of the American College of Cardiology Cardio-Obstetrics Work Group.
Some conditions, such as pulmonary hypertension and severe aortic valve stenosis, during pregnancy are well recognized as very high risk, and there are various scoring systems to help clinicians with risk stratification, she observed. “But there are also a lot of gray areas where patients don’t necessarily fit into these risk scores that we use.”
So physician-patient discussions in high-risk pregnancies “are already complicated,” Dr. Park said. “Patients want to have options, and they look to us as physicians for guidance with regard to their risks. And if abortion is not available as an option, then part of our toolbox is no longer available to help us care for the mother.”
In the new legal climate, clinicians in states where abortion is illegal may well want to put more emphasis on preconception counseling, so more of their patients with high-risk conditions are aware of the new barriers to pregnancy termination.
“Unfortunately,” Dr. Haythe said, “many of the states that are going to make or have made abortion illegal are not providing that kind of preconception counseling or good prenatal care to women.”
Cardiologists can provide such counseling to their female patients of childbearing age who have high-risk cardiac conditions, “but not everybody knows that they have a heart problem when they get pregnant, and not everybody is getting screened for heart problems when they’re of childbearing age,” Dr. Haythe said.
“Sometimes it’s not clear whether the problems could have been picked up until a woman is pregnant and has started to have symptoms.” For example, “a lot of women with poor access to health care have rheumatic heart disease. They may have no idea that they have severe aortic stenosis, and it’s not until their second trimester that they start to feel really short of breath.” Often that can be treated in the cath lab, “but again, that’s putting the woman and the baby at risk.”
Cardiologists in states where abortion is illegal will still present the option to their patients with high-risk pregnancies, noted Dr. Haythe. But the conversation may sound something like, “you are at very high risk, termination of the pregnancy takes that risk away, but you’ll have to find a state where it’s legal to do that.”
Dr. Park said such a situation, when abortion is recommended but locally unavailable, is much like any other in cardiology for which the patient may want a second opinion. If a center “doesn’t have the capability or the technology to offer a certain treatment, the patient can opt to seek another opinion at another center,” she said. “Patients will often travel out of state to get the care they need.”
A requirement for out-of-state travel to obtain abortions is likely to worsen socioeconomic disparities in health care, Dr. Bond observed, “because we know that those who are low-income won’t be able to afford that travel.”
Dr. Bond is cosignatory on a statement from the Association of Black Cardiologists (ABC) responding to the high court’s ruling in Dobbs v. Jackson. “This decision will isolate the poor, socioeconomically disadvantaged, and minority populations specifically, widening the already large gaps in health care for our most vulnerable communities,” it states.
“The loss of broad protections supporting the medical and often lifesaving procedure of abortions is likely to have a real impact on the maternal mortality rate, especially in those with congenital and/or acquired cardiovascular conditions where evidence-based guidelines advise at times on termination of such high-risk pregnancies.”
The ABC, it states, “believes that every woman, and every person, should be afforded the right to safe, accessible, legal, timely, patient-centered, equitable, and affordable health care.”
The American College of Cardiology (ACC) released a statement on the matter June 24, signed by its president, Edward T.A. Fry, MD, along with five former ACC presidents. “While the ACC has no official policy on abortion, clinical practice guidelines and other clinical guidance tools address the dangers of pregnancy in certain patient populations at higher risk of death or serious cardiac events.”
The college, it states, is “deeply concerned about the potential implications of the Supreme Court decision regarding Roe vs. Wade on the ability of patients and clinicians to engage in important shared discussions about maternal health, or to remove previously available health care options.”
Dr. Bond proposed that a “vocal stance” from medical societies involved in women’s health, “perhaps even a collective stance from our cardiovascular societies and our obstetrics societies,” would also perhaps reach “the masses of doctors in private practice who are dealing with these patients.”
A version of this article first appeared on Medscape.com.
‘Superior’ CLL regimen cuts chemo in half
“Overall, our data suggests that [the chemoimmunotherapy] regimen is very effective and appears superior to published six cycles of chemotherapy regimen for the same favorable risk features,” first author Dr. Nitin Jain, an associate professor in the department of leukemia at the University of Texas MD Anderson Cancer Center, Houston, told MDedge.
Chemoimmunotherapy with fludarabine, cyclophosphamide and rituximab (FCR) has been a standard frontline treatment for young, fit patients with CLL, resulting in 10-year PFS rates above 55% in patients with mutated IGHV status, said coauthor Dr. Alessandra Ferrajoli, also of the MD Anderson Cancer Center, in presenting the findings at the European Hematology Association annual congress.
The authors sought to investigate the efficacy of a targeted therapy combination of ibrutinib and obinutuzumab with fludarabine and cyclophosphamide (iFCG). They also sought to determine whether a three-cycle regimen of the chemotherapy, as compared to six cycles, could reduce the risk of myelodysplastic syndrome (MDS), which increases with chemotherapy in CLL patients who have mutated IGHV status.
For the phase 2 study, 45 previously untreated patients with CLL, who had mutated IGHV and an absence of del(17p)/TP53 mutation (both of which are associated with more favorable outcomes in CLL) were enrolled between March 2016 and August 2018. The patients were deemed fit for chemotherapy and had a median age of 60.
All patients were initially treated with three cycles of the iFCG regimen, and among them, 39 (87%) achieved undetectable measurable residual disease (MRD) in their bone marrow.
After the three cycles, an MRD-driven strategy was then used to determine subsequent treatment: All patients received nine courses of ibrutinib, and for those achieving complete remission (CR) or CR with incomplete count recovery (CRi) and undetectable MRD, three cycles of obinutuzumab were administered, while all others received nine additional cycles of obinutuzumab.
At completion of the 12 courses, those who still had MRD positivity continued on ibrutinib, while those with undetectable MRD discontinued ibrutinib.
By cycle six of iFCG, 40 (89%) of the patients achieved undetectable MRD. Overall, 44 of the 45 patients (98%) achieved undetectable MRD as their best response at any time during the study, with 69% of patients achieving CR/CRi. Four patients came off the study prior to cycle 12, including one death, one infection, and one patient who opted to pursue treatment locally. With a median follow-up of 59.6 months, there were no cases of CLL progression or Richter transformation and the lone death was from heart failure.
One patient developed treatment-related myelodysplastic syndrome (MDS), and that patient has maintained normal blood counts over 38 months of monitoring and has not required MDS therapy, Dr. Ferrajoli reported.
Over the follow-up, the six patients who were MRD positive after the completion of three cycles experienced a recurrence of MRD, defined as two consecutive values of 0.01% or higher in peripheral blood by flow cytometry, at a median of 27.2 months after stopping all therapy.
“Not unexpectedly, MRD recurrence during follow-up correlated with MRD positivity during therapy,” Dr. Ferrajoli said.
She noted that all six of the patients were being monitored, with no clinical progression or active therapy. However, with a median follow-up of 5 years, the progression-free survival (PFS) rate among the 45 patients was 97.7%, and the overall survival (OS) rate was 97.8%. Dr. Ferrajoli noted that, while the study population was clearly different, the results compare favorably with CLL clinical trial results that have previously shown a 5-year PFS of approximately 65% with FCR alone; approximately 70% with ibrutinib; and 81% with ibrutinib among patients with mutated IGHV status.
Furthermore, the rate of undetectable MRD status in mutated IGHV patients being 95% in evaluable patients in the current study is notably higher than rates of 51% through 67% reported in five other trials of CLL treatment with six cycles of FCR and with a rate of 79% in the DFCI trial of six-cycle chemotherapy plus ibrutinib.
And the current study’s undetectable MRD rate of 89% in the intention-to-treat population compares with just 13% though 40% in the five other chemotherapy trials and 79% in the DFCI trial, the authors note.
The current trial was the only one of any of their comparisons to utilize the three-cycle regimen.
Asked at the meeting about concerns of toxicities reported with obinutuzumab and chemotherapy, Dr. Ferrajoli said “the treatment was very well tolerated.”
“Myelosuppression is a concern with this combination, but we did make the use of prophylactic growth-factor mandatory in the study, so we were able to control that,” she said.
Dr. Jain noted that, while treatment trends have moved largely to chemo-free regimens, particularly in the United States because of concerns about the MDS, the current study’s results importantly shed light on a potentially beneficial approach of just three cycles of chemotherapy.
“In Europe and the rest of the world where chemo use is still common, this regimen could be considered,” he told MDedge. “The findings show that if you still use chemo in your practice, this regimen uses 50% less chemotherapy, yet seems to give higher response rates.”
“While MDS and acute myeloid leukemia (AML) remain a concern with any chemotherapy regimen, it is possible that 50% less chemo will lead to less risk of MDS AML, but longer-term follow-up [is needed],” he said.
Dr. Ferrajoli reported that she has received research support from Astra-Zeneca and Beigene. Dr. Jain has received research funding and honoraria from Genentech and Pharmacyclics.
“Overall, our data suggests that [the chemoimmunotherapy] regimen is very effective and appears superior to published six cycles of chemotherapy regimen for the same favorable risk features,” first author Dr. Nitin Jain, an associate professor in the department of leukemia at the University of Texas MD Anderson Cancer Center, Houston, told MDedge.
Chemoimmunotherapy with fludarabine, cyclophosphamide and rituximab (FCR) has been a standard frontline treatment for young, fit patients with CLL, resulting in 10-year PFS rates above 55% in patients with mutated IGHV status, said coauthor Dr. Alessandra Ferrajoli, also of the MD Anderson Cancer Center, in presenting the findings at the European Hematology Association annual congress.
The authors sought to investigate the efficacy of a targeted therapy combination of ibrutinib and obinutuzumab with fludarabine and cyclophosphamide (iFCG). They also sought to determine whether a three-cycle regimen of the chemotherapy, as compared to six cycles, could reduce the risk of myelodysplastic syndrome (MDS), which increases with chemotherapy in CLL patients who have mutated IGHV status.
For the phase 2 study, 45 previously untreated patients with CLL, who had mutated IGHV and an absence of del(17p)/TP53 mutation (both of which are associated with more favorable outcomes in CLL) were enrolled between March 2016 and August 2018. The patients were deemed fit for chemotherapy and had a median age of 60.
All patients were initially treated with three cycles of the iFCG regimen, and among them, 39 (87%) achieved undetectable measurable residual disease (MRD) in their bone marrow.
After the three cycles, an MRD-driven strategy was then used to determine subsequent treatment: All patients received nine courses of ibrutinib, and for those achieving complete remission (CR) or CR with incomplete count recovery (CRi) and undetectable MRD, three cycles of obinutuzumab were administered, while all others received nine additional cycles of obinutuzumab.
At completion of the 12 courses, those who still had MRD positivity continued on ibrutinib, while those with undetectable MRD discontinued ibrutinib.
By cycle six of iFCG, 40 (89%) of the patients achieved undetectable MRD. Overall, 44 of the 45 patients (98%) achieved undetectable MRD as their best response at any time during the study, with 69% of patients achieving CR/CRi. Four patients came off the study prior to cycle 12, including one death, one infection, and one patient who opted to pursue treatment locally. With a median follow-up of 59.6 months, there were no cases of CLL progression or Richter transformation and the lone death was from heart failure.
One patient developed treatment-related myelodysplastic syndrome (MDS), and that patient has maintained normal blood counts over 38 months of monitoring and has not required MDS therapy, Dr. Ferrajoli reported.
Over the follow-up, the six patients who were MRD positive after the completion of three cycles experienced a recurrence of MRD, defined as two consecutive values of 0.01% or higher in peripheral blood by flow cytometry, at a median of 27.2 months after stopping all therapy.
“Not unexpectedly, MRD recurrence during follow-up correlated with MRD positivity during therapy,” Dr. Ferrajoli said.
She noted that all six of the patients were being monitored, with no clinical progression or active therapy. However, with a median follow-up of 5 years, the progression-free survival (PFS) rate among the 45 patients was 97.7%, and the overall survival (OS) rate was 97.8%. Dr. Ferrajoli noted that, while the study population was clearly different, the results compare favorably with CLL clinical trial results that have previously shown a 5-year PFS of approximately 65% with FCR alone; approximately 70% with ibrutinib; and 81% with ibrutinib among patients with mutated IGHV status.
Furthermore, the rate of undetectable MRD status in mutated IGHV patients being 95% in evaluable patients in the current study is notably higher than rates of 51% through 67% reported in five other trials of CLL treatment with six cycles of FCR and with a rate of 79% in the DFCI trial of six-cycle chemotherapy plus ibrutinib.
And the current study’s undetectable MRD rate of 89% in the intention-to-treat population compares with just 13% though 40% in the five other chemotherapy trials and 79% in the DFCI trial, the authors note.
The current trial was the only one of any of their comparisons to utilize the three-cycle regimen.
Asked at the meeting about concerns of toxicities reported with obinutuzumab and chemotherapy, Dr. Ferrajoli said “the treatment was very well tolerated.”
“Myelosuppression is a concern with this combination, but we did make the use of prophylactic growth-factor mandatory in the study, so we were able to control that,” she said.
Dr. Jain noted that, while treatment trends have moved largely to chemo-free regimens, particularly in the United States because of concerns about the MDS, the current study’s results importantly shed light on a potentially beneficial approach of just three cycles of chemotherapy.
“In Europe and the rest of the world where chemo use is still common, this regimen could be considered,” he told MDedge. “The findings show that if you still use chemo in your practice, this regimen uses 50% less chemotherapy, yet seems to give higher response rates.”
“While MDS and acute myeloid leukemia (AML) remain a concern with any chemotherapy regimen, it is possible that 50% less chemo will lead to less risk of MDS AML, but longer-term follow-up [is needed],” he said.
Dr. Ferrajoli reported that she has received research support from Astra-Zeneca and Beigene. Dr. Jain has received research funding and honoraria from Genentech and Pharmacyclics.
“Overall, our data suggests that [the chemoimmunotherapy] regimen is very effective and appears superior to published six cycles of chemotherapy regimen for the same favorable risk features,” first author Dr. Nitin Jain, an associate professor in the department of leukemia at the University of Texas MD Anderson Cancer Center, Houston, told MDedge.
Chemoimmunotherapy with fludarabine, cyclophosphamide and rituximab (FCR) has been a standard frontline treatment for young, fit patients with CLL, resulting in 10-year PFS rates above 55% in patients with mutated IGHV status, said coauthor Dr. Alessandra Ferrajoli, also of the MD Anderson Cancer Center, in presenting the findings at the European Hematology Association annual congress.
The authors sought to investigate the efficacy of a targeted therapy combination of ibrutinib and obinutuzumab with fludarabine and cyclophosphamide (iFCG). They also sought to determine whether a three-cycle regimen of the chemotherapy, as compared to six cycles, could reduce the risk of myelodysplastic syndrome (MDS), which increases with chemotherapy in CLL patients who have mutated IGHV status.
For the phase 2 study, 45 previously untreated patients with CLL, who had mutated IGHV and an absence of del(17p)/TP53 mutation (both of which are associated with more favorable outcomes in CLL) were enrolled between March 2016 and August 2018. The patients were deemed fit for chemotherapy and had a median age of 60.
All patients were initially treated with three cycles of the iFCG regimen, and among them, 39 (87%) achieved undetectable measurable residual disease (MRD) in their bone marrow.
After the three cycles, an MRD-driven strategy was then used to determine subsequent treatment: All patients received nine courses of ibrutinib, and for those achieving complete remission (CR) or CR with incomplete count recovery (CRi) and undetectable MRD, three cycles of obinutuzumab were administered, while all others received nine additional cycles of obinutuzumab.
At completion of the 12 courses, those who still had MRD positivity continued on ibrutinib, while those with undetectable MRD discontinued ibrutinib.
By cycle six of iFCG, 40 (89%) of the patients achieved undetectable MRD. Overall, 44 of the 45 patients (98%) achieved undetectable MRD as their best response at any time during the study, with 69% of patients achieving CR/CRi. Four patients came off the study prior to cycle 12, including one death, one infection, and one patient who opted to pursue treatment locally. With a median follow-up of 59.6 months, there were no cases of CLL progression or Richter transformation and the lone death was from heart failure.
One patient developed treatment-related myelodysplastic syndrome (MDS), and that patient has maintained normal blood counts over 38 months of monitoring and has not required MDS therapy, Dr. Ferrajoli reported.
Over the follow-up, the six patients who were MRD positive after the completion of three cycles experienced a recurrence of MRD, defined as two consecutive values of 0.01% or higher in peripheral blood by flow cytometry, at a median of 27.2 months after stopping all therapy.
“Not unexpectedly, MRD recurrence during follow-up correlated with MRD positivity during therapy,” Dr. Ferrajoli said.
She noted that all six of the patients were being monitored, with no clinical progression or active therapy. However, with a median follow-up of 5 years, the progression-free survival (PFS) rate among the 45 patients was 97.7%, and the overall survival (OS) rate was 97.8%. Dr. Ferrajoli noted that, while the study population was clearly different, the results compare favorably with CLL clinical trial results that have previously shown a 5-year PFS of approximately 65% with FCR alone; approximately 70% with ibrutinib; and 81% with ibrutinib among patients with mutated IGHV status.
Furthermore, the rate of undetectable MRD status in mutated IGHV patients being 95% in evaluable patients in the current study is notably higher than rates of 51% through 67% reported in five other trials of CLL treatment with six cycles of FCR and with a rate of 79% in the DFCI trial of six-cycle chemotherapy plus ibrutinib.
And the current study’s undetectable MRD rate of 89% in the intention-to-treat population compares with just 13% though 40% in the five other chemotherapy trials and 79% in the DFCI trial, the authors note.
The current trial was the only one of any of their comparisons to utilize the three-cycle regimen.
Asked at the meeting about concerns of toxicities reported with obinutuzumab and chemotherapy, Dr. Ferrajoli said “the treatment was very well tolerated.”
“Myelosuppression is a concern with this combination, but we did make the use of prophylactic growth-factor mandatory in the study, so we were able to control that,” she said.
Dr. Jain noted that, while treatment trends have moved largely to chemo-free regimens, particularly in the United States because of concerns about the MDS, the current study’s results importantly shed light on a potentially beneficial approach of just three cycles of chemotherapy.
“In Europe and the rest of the world where chemo use is still common, this regimen could be considered,” he told MDedge. “The findings show that if you still use chemo in your practice, this regimen uses 50% less chemotherapy, yet seems to give higher response rates.”
“While MDS and acute myeloid leukemia (AML) remain a concern with any chemotherapy regimen, it is possible that 50% less chemo will lead to less risk of MDS AML, but longer-term follow-up [is needed],” he said.
Dr. Ferrajoli reported that she has received research support from Astra-Zeneca and Beigene. Dr. Jain has received research funding and honoraria from Genentech and Pharmacyclics.
FROM EHA 2022
Upadacitinib recommended for nonradiographic axSpA in Europe
Upadacitinib may soon be used for the treatment of nonradiographic axial spondyloarthritis (nr-axSpA) after the European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) gave it its stamp of approval.
AbbVie, the drug’s manufacturer, announced on June 27 that the committee approved the use on June 23. The recommendation to approve market authorization for upadacitinib for nr-axSpA now goes to the European Commission, which is expected to make a decision by the third quarter of 2022.
“The CHMP’s recommendation to approve upadacitinib for patients with nr-axSpA is an important milestone in providing a new treatment option to patients in need,” said Neil Gallagher, MD, vice president of development and chief medical officer of AbbVie. He noted that currently, there are few options to treat symptoms such as inflammation, back pain, and stiffness for these patients.
Officially, the new indication for upadacitinib (Rinvoq) 15 mg once daily is for the treatment of active nr-axSpA in adult patients with objective signs of inflammation, as indicated by elevated C-reactive protein and/or MRI, whose condition has responded inadequately to NSAIDs.
Upadacitinib is a selective Janus kinase (JAK) inhibitor that in human cellular assays preferentially inhibits signaling by JAK1 or JAK1/3.
In the European Union, upadacitinib is currently approved for use in patients with moderate to severe active rheumatoid arthritis, active psoriatic arthritis, active ankylosing spondylitis, and moderate to severe atopic dermatitis. In addition to these indications, it is approved in the United States for ulcerative colitis but not for nr-axSpA.
The committee based its decision on the results of the nr-axSpA study within the SELECT-AXIS-2 trial, recently reported at the European Alliance of Associations for Rheumatology (EULAR) 2022 annual meeting.
The nr-axSpA study met the primary endpoint of a 40% improvement in Assessment of SpondyloArthritis International Society response criteria (ASAS40) and the first 12 of 14 ranked secondary endpoints, according to AbbVie.
The most commonly reported adverse reactions with upadacitinib 15 mg were upper respiratory tract infections, elevated blood creatine phosphokinase levels, elevated alanine transaminase levels, bronchitis, nausea, cough, elevated aspartate transaminase levels, and hypercholesterolemia. These occurred in 2% or more of patients with rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis in clinical trials.
The safety profile of upadacitinib with long-term treatment was generally similar to the safety profile during the placebo-controlled period across indications, AbbVie said.
A version of this article first appeared on Medscape.com.
Upadacitinib may soon be used for the treatment of nonradiographic axial spondyloarthritis (nr-axSpA) after the European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) gave it its stamp of approval.
AbbVie, the drug’s manufacturer, announced on June 27 that the committee approved the use on June 23. The recommendation to approve market authorization for upadacitinib for nr-axSpA now goes to the European Commission, which is expected to make a decision by the third quarter of 2022.
“The CHMP’s recommendation to approve upadacitinib for patients with nr-axSpA is an important milestone in providing a new treatment option to patients in need,” said Neil Gallagher, MD, vice president of development and chief medical officer of AbbVie. He noted that currently, there are few options to treat symptoms such as inflammation, back pain, and stiffness for these patients.
Officially, the new indication for upadacitinib (Rinvoq) 15 mg once daily is for the treatment of active nr-axSpA in adult patients with objective signs of inflammation, as indicated by elevated C-reactive protein and/or MRI, whose condition has responded inadequately to NSAIDs.
Upadacitinib is a selective Janus kinase (JAK) inhibitor that in human cellular assays preferentially inhibits signaling by JAK1 or JAK1/3.
In the European Union, upadacitinib is currently approved for use in patients with moderate to severe active rheumatoid arthritis, active psoriatic arthritis, active ankylosing spondylitis, and moderate to severe atopic dermatitis. In addition to these indications, it is approved in the United States for ulcerative colitis but not for nr-axSpA.
The committee based its decision on the results of the nr-axSpA study within the SELECT-AXIS-2 trial, recently reported at the European Alliance of Associations for Rheumatology (EULAR) 2022 annual meeting.
The nr-axSpA study met the primary endpoint of a 40% improvement in Assessment of SpondyloArthritis International Society response criteria (ASAS40) and the first 12 of 14 ranked secondary endpoints, according to AbbVie.
The most commonly reported adverse reactions with upadacitinib 15 mg were upper respiratory tract infections, elevated blood creatine phosphokinase levels, elevated alanine transaminase levels, bronchitis, nausea, cough, elevated aspartate transaminase levels, and hypercholesterolemia. These occurred in 2% or more of patients with rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis in clinical trials.
The safety profile of upadacitinib with long-term treatment was generally similar to the safety profile during the placebo-controlled period across indications, AbbVie said.
A version of this article first appeared on Medscape.com.
Upadacitinib may soon be used for the treatment of nonradiographic axial spondyloarthritis (nr-axSpA) after the European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) gave it its stamp of approval.
AbbVie, the drug’s manufacturer, announced on June 27 that the committee approved the use on June 23. The recommendation to approve market authorization for upadacitinib for nr-axSpA now goes to the European Commission, which is expected to make a decision by the third quarter of 2022.
“The CHMP’s recommendation to approve upadacitinib for patients with nr-axSpA is an important milestone in providing a new treatment option to patients in need,” said Neil Gallagher, MD, vice president of development and chief medical officer of AbbVie. He noted that currently, there are few options to treat symptoms such as inflammation, back pain, and stiffness for these patients.
Officially, the new indication for upadacitinib (Rinvoq) 15 mg once daily is for the treatment of active nr-axSpA in adult patients with objective signs of inflammation, as indicated by elevated C-reactive protein and/or MRI, whose condition has responded inadequately to NSAIDs.
Upadacitinib is a selective Janus kinase (JAK) inhibitor that in human cellular assays preferentially inhibits signaling by JAK1 or JAK1/3.
In the European Union, upadacitinib is currently approved for use in patients with moderate to severe active rheumatoid arthritis, active psoriatic arthritis, active ankylosing spondylitis, and moderate to severe atopic dermatitis. In addition to these indications, it is approved in the United States for ulcerative colitis but not for nr-axSpA.
The committee based its decision on the results of the nr-axSpA study within the SELECT-AXIS-2 trial, recently reported at the European Alliance of Associations for Rheumatology (EULAR) 2022 annual meeting.
The nr-axSpA study met the primary endpoint of a 40% improvement in Assessment of SpondyloArthritis International Society response criteria (ASAS40) and the first 12 of 14 ranked secondary endpoints, according to AbbVie.
The most commonly reported adverse reactions with upadacitinib 15 mg were upper respiratory tract infections, elevated blood creatine phosphokinase levels, elevated alanine transaminase levels, bronchitis, nausea, cough, elevated aspartate transaminase levels, and hypercholesterolemia. These occurred in 2% or more of patients with rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis in clinical trials.
The safety profile of upadacitinib with long-term treatment was generally similar to the safety profile during the placebo-controlled period across indications, AbbVie said.
A version of this article first appeared on Medscape.com.
Children and COVID: Vaccination off to slow start for the newly eligible
New cases of COVID-19 continue to drop among children, but the vaccination effort in those under age 5 years began with something less than a bang.
In the first 2 days after their respective approvals, almost 99,000 children aged 5-11 years and over 675,000 children aged 12-15 were vaccinated, according to data from the Centers for Disease Control and Prevention. Children aged 0-4 years represent almost 6% of the overall population, compared with 8.7% for the 5- to 11-year-olds and 5.1% for those aged 12-15.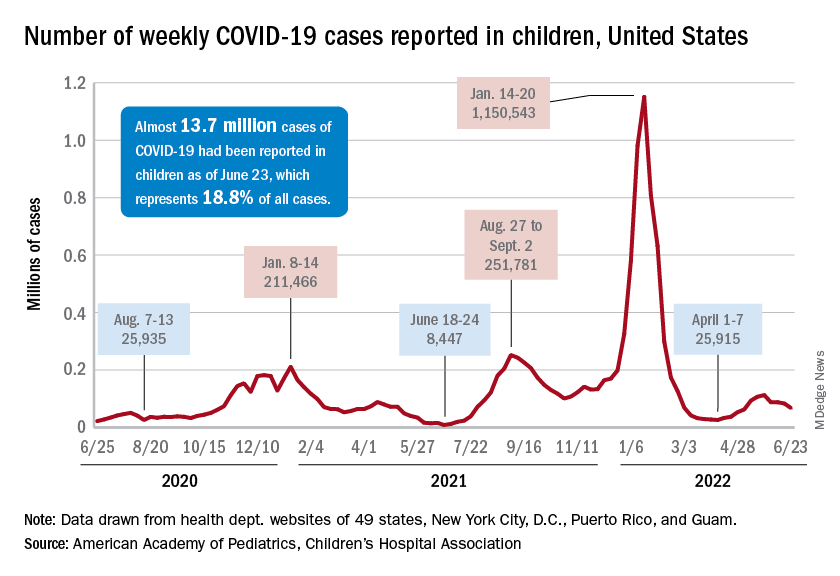
The recent decline in new cases over the past 4 weeks and the substantial decline since the Omicron surge could be a factor in the lack of response, but it is worth noting that the almost 68,000 new child cases reported in the past week, June 17-23, are “far higher than 1 year ago, June 24, 2021, when 8,400 child cases were reported,” the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
That total for June 17-23 was 19% lower than the previous week and down by 40% since new cases hit a spring peak of 112,000 in late May. Regionally, new cases were down in the Midwest, the South, and the West, the AAP/CHA report showed, but the Northeast saw a small increase, which could be a signal of things to come for the summer.
The decline in new cases, however, has not been accompanied by decreases in hospitalizations or emergency department visits. New admissions of children aged 0-17 with confirmed COVID were at 0.31 per 100,000 population on June 24 after reaching that level on June 15, so no drop-off has occurred yet but there are signs of leveling off, based on CDC data.
The ED visit rates have been fairly steady through June, although COVID-related visits were up to 3.4% of all ED visits on June 22 for children aged 0-11 years, after being below 3% for the first 2 weeks of the month. The rate for children aged 12-15 has been between 1.6% and 1.9% for the past 3 weeks and the rate for 16- and 17-year-olds has been hovering between 1.7% and 2.2% for most of June, after going as high as 2.7% in late May, the CDC said on its COVID Data Tracker.
New cases of COVID-19 continue to drop among children, but the vaccination effort in those under age 5 years began with something less than a bang.
In the first 2 days after their respective approvals, almost 99,000 children aged 5-11 years and over 675,000 children aged 12-15 were vaccinated, according to data from the Centers for Disease Control and Prevention. Children aged 0-4 years represent almost 6% of the overall population, compared with 8.7% for the 5- to 11-year-olds and 5.1% for those aged 12-15.
The recent decline in new cases over the past 4 weeks and the substantial decline since the Omicron surge could be a factor in the lack of response, but it is worth noting that the almost 68,000 new child cases reported in the past week, June 17-23, are “far higher than 1 year ago, June 24, 2021, when 8,400 child cases were reported,” the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
That total for June 17-23 was 19% lower than the previous week and down by 40% since new cases hit a spring peak of 112,000 in late May. Regionally, new cases were down in the Midwest, the South, and the West, the AAP/CHA report showed, but the Northeast saw a small increase, which could be a signal of things to come for the summer.
The decline in new cases, however, has not been accompanied by decreases in hospitalizations or emergency department visits. New admissions of children aged 0-17 with confirmed COVID were at 0.31 per 100,000 population on June 24 after reaching that level on June 15, so no drop-off has occurred yet but there are signs of leveling off, based on CDC data.
The ED visit rates have been fairly steady through June, although COVID-related visits were up to 3.4% of all ED visits on June 22 for children aged 0-11 years, after being below 3% for the first 2 weeks of the month. The rate for children aged 12-15 has been between 1.6% and 1.9% for the past 3 weeks and the rate for 16- and 17-year-olds has been hovering between 1.7% and 2.2% for most of June, after going as high as 2.7% in late May, the CDC said on its COVID Data Tracker.
New cases of COVID-19 continue to drop among children, but the vaccination effort in those under age 5 years began with something less than a bang.
In the first 2 days after their respective approvals, almost 99,000 children aged 5-11 years and over 675,000 children aged 12-15 were vaccinated, according to data from the Centers for Disease Control and Prevention. Children aged 0-4 years represent almost 6% of the overall population, compared with 8.7% for the 5- to 11-year-olds and 5.1% for those aged 12-15.
The recent decline in new cases over the past 4 weeks and the substantial decline since the Omicron surge could be a factor in the lack of response, but it is worth noting that the almost 68,000 new child cases reported in the past week, June 17-23, are “far higher than 1 year ago, June 24, 2021, when 8,400 child cases were reported,” the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID report.
That total for June 17-23 was 19% lower than the previous week and down by 40% since new cases hit a spring peak of 112,000 in late May. Regionally, new cases were down in the Midwest, the South, and the West, the AAP/CHA report showed, but the Northeast saw a small increase, which could be a signal of things to come for the summer.
The decline in new cases, however, has not been accompanied by decreases in hospitalizations or emergency department visits. New admissions of children aged 0-17 with confirmed COVID were at 0.31 per 100,000 population on June 24 after reaching that level on June 15, so no drop-off has occurred yet but there are signs of leveling off, based on CDC data.
The ED visit rates have been fairly steady through June, although COVID-related visits were up to 3.4% of all ED visits on June 22 for children aged 0-11 years, after being below 3% for the first 2 weeks of the month. The rate for children aged 12-15 has been between 1.6% and 1.9% for the past 3 weeks and the rate for 16- and 17-year-olds has been hovering between 1.7% and 2.2% for most of June, after going as high as 2.7% in late May, the CDC said on its COVID Data Tracker.
FDA approves Qsymia for treating teens with obesity
The indication is for use as additional therapy along with a reduced-calorie diet and increased physical activity in youth with obesity, defined as a body mass index of the 95th percentile or greater when standardized for age and sex.

Qsymia was first approved in July 2012 for chronic weight management in adults with an initial BMI of 30 kg/m2 or greater (obese) or 27 kg/m2 or greater (overweight) with one or more weight-related comorbidities, as an adjunct to lifestyle modification.
About 1 in 5 adolescents in the United States has obesity, according to the FDA.
The drug is the fourth to be approved for treating obesity in youth, along with liraglutide (Saxenda) and orlistat (Alli, Xenical), both approved down to age 12, and phentermine for those aged 16 and older.
The Qsymia approval was based on data from a phase 4 double-blind, placebo-controlled trial of 223 youth aged 12-16 with obesity who had not lost weight with lifestyle modifications. They were randomly assigned to Qsymia in doses of 7.5 mg phentermine/46 mg topiramate, 15 mg phentermine/92 mg topiramate, or placebo once daily, along with lifestyle counseling for all.
At 56 weeks, those taking the lower Qsymia dose lost an average of 4.8% of their BMI, and those on the higher dose lost 7.1%. In contrast, the placebo group gained about 3.3% of their BMI.
Because Qsymia increases the risk for oral clefts (lip and palate) in a fetus if taken during pregnancy, female patients should obtain negative pregnancy tests before starting the drug, take monthly pregnancy tests while on the drug, and use effective contraception throughout. Also because of the oral cleft risk, Qsymia is available only through an FDA program called a Risk Evaluation and Mitigation Strategy.
Additional potential adverse effects with Qsymia include increased heart rate and suicidal behavior/ideation. Patients should be advised to monitor for mood changes and discontinue the drug if depression or suicidal thoughts develop. The drug has also been linked to slowing of linear growth, so growth should be monitored in adolescents taking the drug, according to the FDA.
Qsymia is also associated with acute myopia, secondary angle closure glaucoma, visual problems, sleep disorders, cognitive impairment, metabolic acidosis, and decreased renal function.
The most common adverse reactions reported in the pediatric clinical trial included depression, dizziness, joint pain, fever, flu, and ankle sprain.
A version of this article first appeared on Medscape.com.
The indication is for use as additional therapy along with a reduced-calorie diet and increased physical activity in youth with obesity, defined as a body mass index of the 95th percentile or greater when standardized for age and sex.
Qsymia was first approved in July 2012 for chronic weight management in adults with an initial BMI of 30 kg/m2 or greater (obese) or 27 kg/m2 or greater (overweight) with one or more weight-related comorbidities, as an adjunct to lifestyle modification.
About 1 in 5 adolescents in the United States has obesity, according to the FDA.
The drug is the fourth to be approved for treating obesity in youth, along with liraglutide (Saxenda) and orlistat (Alli, Xenical), both approved down to age 12, and phentermine for those aged 16 and older.
The Qsymia approval was based on data from a phase 4 double-blind, placebo-controlled trial of 223 youth aged 12-16 with obesity who had not lost weight with lifestyle modifications. They were randomly assigned to Qsymia in doses of 7.5 mg phentermine/46 mg topiramate, 15 mg phentermine/92 mg topiramate, or placebo once daily, along with lifestyle counseling for all.
At 56 weeks, those taking the lower Qsymia dose lost an average of 4.8% of their BMI, and those on the higher dose lost 7.1%. In contrast, the placebo group gained about 3.3% of their BMI.
Because Qsymia increases the risk for oral clefts (lip and palate) in a fetus if taken during pregnancy, female patients should obtain negative pregnancy tests before starting the drug, take monthly pregnancy tests while on the drug, and use effective contraception throughout. Also because of the oral cleft risk, Qsymia is available only through an FDA program called a Risk Evaluation and Mitigation Strategy.
Additional potential adverse effects with Qsymia include increased heart rate and suicidal behavior/ideation. Patients should be advised to monitor for mood changes and discontinue the drug if depression or suicidal thoughts develop. The drug has also been linked to slowing of linear growth, so growth should be monitored in adolescents taking the drug, according to the FDA.
Qsymia is also associated with acute myopia, secondary angle closure glaucoma, visual problems, sleep disorders, cognitive impairment, metabolic acidosis, and decreased renal function.
The most common adverse reactions reported in the pediatric clinical trial included depression, dizziness, joint pain, fever, flu, and ankle sprain.
A version of this article first appeared on Medscape.com.
The indication is for use as additional therapy along with a reduced-calorie diet and increased physical activity in youth with obesity, defined as a body mass index of the 95th percentile or greater when standardized for age and sex.
Qsymia was first approved in July 2012 for chronic weight management in adults with an initial BMI of 30 kg/m2 or greater (obese) or 27 kg/m2 or greater (overweight) with one or more weight-related comorbidities, as an adjunct to lifestyle modification.
About 1 in 5 adolescents in the United States has obesity, according to the FDA.
The drug is the fourth to be approved for treating obesity in youth, along with liraglutide (Saxenda) and orlistat (Alli, Xenical), both approved down to age 12, and phentermine for those aged 16 and older.
The Qsymia approval was based on data from a phase 4 double-blind, placebo-controlled trial of 223 youth aged 12-16 with obesity who had not lost weight with lifestyle modifications. They were randomly assigned to Qsymia in doses of 7.5 mg phentermine/46 mg topiramate, 15 mg phentermine/92 mg topiramate, or placebo once daily, along with lifestyle counseling for all.
At 56 weeks, those taking the lower Qsymia dose lost an average of 4.8% of their BMI, and those on the higher dose lost 7.1%. In contrast, the placebo group gained about 3.3% of their BMI.
Because Qsymia increases the risk for oral clefts (lip and palate) in a fetus if taken during pregnancy, female patients should obtain negative pregnancy tests before starting the drug, take monthly pregnancy tests while on the drug, and use effective contraception throughout. Also because of the oral cleft risk, Qsymia is available only through an FDA program called a Risk Evaluation and Mitigation Strategy.
Additional potential adverse effects with Qsymia include increased heart rate and suicidal behavior/ideation. Patients should be advised to monitor for mood changes and discontinue the drug if depression or suicidal thoughts develop. The drug has also been linked to slowing of linear growth, so growth should be monitored in adolescents taking the drug, according to the FDA.
Qsymia is also associated with acute myopia, secondary angle closure glaucoma, visual problems, sleep disorders, cognitive impairment, metabolic acidosis, and decreased renal function.
The most common adverse reactions reported in the pediatric clinical trial included depression, dizziness, joint pain, fever, flu, and ankle sprain.
A version of this article first appeared on Medscape.com.