User login
AGA News – August 2022
Huge win for patients: CRC screening coverage continuum is complete
In a huge win for patients, Medicare will begin covering colonoscopies after a positive noninvasive stool test starting next year. Medicare was previously the only insurer who did not cover this critical prevention procedure.
This change comes after a year of advocacy led by AGA – including multiple meetings with senior officials at Health & Human Services and legislative pressure by members across the country.
“Cost-sharing is a well-recognized barrier to screening and has resulted in disparities. Patients can now engage in CRC screening programs and be confident that they will not face unexpected cost-sharing for colonoscopy after a positive noninvasive screening test,” says David Lieberman, MD, AGAF, who met with Centers for Medicare & Medicaid Services officials multiple times to push this policy forward. “AGA knows that increased participation in screening will further reduce the burden of colorectal cancer.”
“This is a win for all patients and should elevate our nation’s screening rates while lowering the overall cancer burden, saving lives. Importantly, the CMS proposed rule changes will lessen colorectal cancer disparities eliminating a financial burden for many patients,” says AGA president John Carethers, MD, AGAF, who met with CMS earlier this month to advocate for this change.
Thank you to everyone in the GI community who advocated for this important change!
CMS announced the coverage change as part of the 2023 Medicare proposed rule, which was released July 7, 2022. The rule must be finalized this Fall before taking effect Jan. 2, 2023.
What you need to know about proposed changes to Medicare payment policies
On July 7, CMS released the calendar year (CY) 2023 Medicare Physician Fee Schedule (MPFS) Proposed Rule. The rule will be posted in the Federal Register no later than July 11.
Good news!
In a win for patients and thanks to collective advocacy efforts from AGA and partner societies, CMS is proposing to expand the regulatory definition of “colorectal cancer screening tests” and waive cost sharing for a necessary follow-up colonoscopy after a positive stool-based screening test.
Looming cuts
The rule proposes 4% cuts to Medicare physician reimbursement through required decreases in the conversion factor and expiration of temporary fixes passed by Congress. AGA will continue to work with a coalition of national and state medical societies in urging Congress to prevent these cuts before Jan. 1, 2023.
What to know
CMS expands CRC screening in a proposal to waive cost-sharing for a follow-up colonoscopy to a positive stool-based colorectal cancer screening test and to cover the service for individuals 45 years of age and above.
Medicare payment cuts are looming with cuts to the proposed CY 2023 conversion factor.
Split/shared visits policy delayed until CY 2024.
Payment rates for new bariatric device codes proposed.
Don’t let insurance policies burden GI practices
Join us at AGA Advocacy Day on Thursday, Sept. 22, 2022, to virtually meet with your members of Congress to urge them to rein in insurance policies like prior authorization and step therapy.
If GI providers don’t have a seat at the table and engage with lawmakers, these decisions will be influenced by payers and other parties that do not have you or your patients’ best interests at heart.
AGA Advocacy Day is held shortly before the end of the fiscal year – prime time to educate policymakers and their staff about your everyday challenges and the reality of GI patient care in your state. We will also discuss the need for robust federal funding for GI research and the devastating impact that Medicare cuts could have on your practice.
Register today and AGA will take care of the rest, including scheduling your meetings and providing comprehensive advocacy training. Now more than ever, your voice needs to be heard on Capitol Hill.
Huge win for patients: CRC screening coverage continuum is complete
In a huge win for patients, Medicare will begin covering colonoscopies after a positive noninvasive stool test starting next year. Medicare was previously the only insurer who did not cover this critical prevention procedure.
This change comes after a year of advocacy led by AGA – including multiple meetings with senior officials at Health & Human Services and legislative pressure by members across the country.
“Cost-sharing is a well-recognized barrier to screening and has resulted in disparities. Patients can now engage in CRC screening programs and be confident that they will not face unexpected cost-sharing for colonoscopy after a positive noninvasive screening test,” says David Lieberman, MD, AGAF, who met with Centers for Medicare & Medicaid Services officials multiple times to push this policy forward. “AGA knows that increased participation in screening will further reduce the burden of colorectal cancer.”
“This is a win for all patients and should elevate our nation’s screening rates while lowering the overall cancer burden, saving lives. Importantly, the CMS proposed rule changes will lessen colorectal cancer disparities eliminating a financial burden for many patients,” says AGA president John Carethers, MD, AGAF, who met with CMS earlier this month to advocate for this change.
Thank you to everyone in the GI community who advocated for this important change!
CMS announced the coverage change as part of the 2023 Medicare proposed rule, which was released July 7, 2022. The rule must be finalized this Fall before taking effect Jan. 2, 2023.
What you need to know about proposed changes to Medicare payment policies
On July 7, CMS released the calendar year (CY) 2023 Medicare Physician Fee Schedule (MPFS) Proposed Rule. The rule will be posted in the Federal Register no later than July 11.
Good news!
In a win for patients and thanks to collective advocacy efforts from AGA and partner societies, CMS is proposing to expand the regulatory definition of “colorectal cancer screening tests” and waive cost sharing for a necessary follow-up colonoscopy after a positive stool-based screening test.
Looming cuts
The rule proposes 4% cuts to Medicare physician reimbursement through required decreases in the conversion factor and expiration of temporary fixes passed by Congress. AGA will continue to work with a coalition of national and state medical societies in urging Congress to prevent these cuts before Jan. 1, 2023.
What to know
CMS expands CRC screening in a proposal to waive cost-sharing for a follow-up colonoscopy to a positive stool-based colorectal cancer screening test and to cover the service for individuals 45 years of age and above.
Medicare payment cuts are looming with cuts to the proposed CY 2023 conversion factor.
Split/shared visits policy delayed until CY 2024.
Payment rates for new bariatric device codes proposed.
Don’t let insurance policies burden GI practices
Join us at AGA Advocacy Day on Thursday, Sept. 22, 2022, to virtually meet with your members of Congress to urge them to rein in insurance policies like prior authorization and step therapy.
If GI providers don’t have a seat at the table and engage with lawmakers, these decisions will be influenced by payers and other parties that do not have you or your patients’ best interests at heart.
AGA Advocacy Day is held shortly before the end of the fiscal year – prime time to educate policymakers and their staff about your everyday challenges and the reality of GI patient care in your state. We will also discuss the need for robust federal funding for GI research and the devastating impact that Medicare cuts could have on your practice.
Register today and AGA will take care of the rest, including scheduling your meetings and providing comprehensive advocacy training. Now more than ever, your voice needs to be heard on Capitol Hill.
Huge win for patients: CRC screening coverage continuum is complete
In a huge win for patients, Medicare will begin covering colonoscopies after a positive noninvasive stool test starting next year. Medicare was previously the only insurer who did not cover this critical prevention procedure.
This change comes after a year of advocacy led by AGA – including multiple meetings with senior officials at Health & Human Services and legislative pressure by members across the country.
“Cost-sharing is a well-recognized barrier to screening and has resulted in disparities. Patients can now engage in CRC screening programs and be confident that they will not face unexpected cost-sharing for colonoscopy after a positive noninvasive screening test,” says David Lieberman, MD, AGAF, who met with Centers for Medicare & Medicaid Services officials multiple times to push this policy forward. “AGA knows that increased participation in screening will further reduce the burden of colorectal cancer.”
“This is a win for all patients and should elevate our nation’s screening rates while lowering the overall cancer burden, saving lives. Importantly, the CMS proposed rule changes will lessen colorectal cancer disparities eliminating a financial burden for many patients,” says AGA president John Carethers, MD, AGAF, who met with CMS earlier this month to advocate for this change.
Thank you to everyone in the GI community who advocated for this important change!
CMS announced the coverage change as part of the 2023 Medicare proposed rule, which was released July 7, 2022. The rule must be finalized this Fall before taking effect Jan. 2, 2023.
What you need to know about proposed changes to Medicare payment policies
On July 7, CMS released the calendar year (CY) 2023 Medicare Physician Fee Schedule (MPFS) Proposed Rule. The rule will be posted in the Federal Register no later than July 11.
Good news!
In a win for patients and thanks to collective advocacy efforts from AGA and partner societies, CMS is proposing to expand the regulatory definition of “colorectal cancer screening tests” and waive cost sharing for a necessary follow-up colonoscopy after a positive stool-based screening test.
Looming cuts
The rule proposes 4% cuts to Medicare physician reimbursement through required decreases in the conversion factor and expiration of temporary fixes passed by Congress. AGA will continue to work with a coalition of national and state medical societies in urging Congress to prevent these cuts before Jan. 1, 2023.
What to know
CMS expands CRC screening in a proposal to waive cost-sharing for a follow-up colonoscopy to a positive stool-based colorectal cancer screening test and to cover the service for individuals 45 years of age and above.
Medicare payment cuts are looming with cuts to the proposed CY 2023 conversion factor.
Split/shared visits policy delayed until CY 2024.
Payment rates for new bariatric device codes proposed.
Don’t let insurance policies burden GI practices
Join us at AGA Advocacy Day on Thursday, Sept. 22, 2022, to virtually meet with your members of Congress to urge them to rein in insurance policies like prior authorization and step therapy.
If GI providers don’t have a seat at the table and engage with lawmakers, these decisions will be influenced by payers and other parties that do not have you or your patients’ best interests at heart.
AGA Advocacy Day is held shortly before the end of the fiscal year – prime time to educate policymakers and their staff about your everyday challenges and the reality of GI patient care in your state. We will also discuss the need for robust federal funding for GI research and the devastating impact that Medicare cuts could have on your practice.
Register today and AGA will take care of the rest, including scheduling your meetings and providing comprehensive advocacy training. Now more than ever, your voice needs to be heard on Capitol Hill.
Injectable HIV prevention better than pills in two trials
MONTREAL – , according to new data from two HIV Prevention Trials Network (HPTN) studies reported at the International AIDS Society Conference.
Follow-up data from the HPTN 084 trial, which compared the two regimens in 3,224 sub-Saharan persons who were assigned female sex at birth, show that three new HIV infections occurred in the CAB LA group in the 12 months since the study was unblinded, versus 20 new infections among the TDF-FTC group. That translates to an 89% lower risk of infection in the CAB LA arm across both the blinded and unblinded phases of the trial, said lead investigator Sinead Delany-Moretlwe, MD, PhD, director of research, Wits Reproductive Health and HIV Institute, the University of the Witwatersrand, Johannesburg, South Africa, during a press conference.
“The trial was designed with the assumption that both drugs were highly effective in preventing HIV infection but that, given the challenges with taking a pill a day, that injectable cabotegravir may offer an adherence advantage,” she said in an interview. “Our data appear to confirm this, as most of the participants in the TDF-FTC arm who became infected with HIV had evidence of poor or inconsistent use of PrEP.”
The study also found that pregnancy incidence increased “two- to threefold” between the blinded and the unblinded period, “and this emphasizes to us the desire of women to conceive safely, without the threat of HIV, and the importance of us continuing to evaluate the safety and pharmacology of cabotegravir in pregnant and breastfeeding women during open-label extension phase of HPTN 084, so that [they] are not excluded from access to this highly effective PrEP agent,” she said. To date, no congenital anomalies have been reported in babies born during the study.
In an update report from HPTN 083, which also showed superiority of CAB LA over TDF-FTC in cisgender men and transgender women (TGW), researchers reported the safety and efficacy of CAB LA use in TGW using gender-affirming hormone therapy (GAHT).
Among the 4,566 participants in HPTN 083, 570 were TGW, and of those, 58% used GAHT at baseline, reported Beatriz Grinsztejn, MD, PhD, head of the STD/AIDS Clinical Research Laboratory at the Instituto Nacional de Infectologicia/Fundação Oswaldo Cruz.
CAB LA drug concentrations measured in a subset of 53 TGW who received on-time CAB injections were comparable between those taking (n = 30) and those not taking GAHT (n = 23), “suggesting the lack of a gender-affirming hormone effect on CAB pharmacokinetics,” she said. “These are very promising results, as we all know that the use of gender-affirming hormone therapy is a major priority for our transgender women community, ... so the lack of drug-drug interaction is really a very important result.”
“Cabotegravir long-acting PrEP is now approved for all at-risk populations, including men who have sex with men, transgender women, and cisgender women, after the results of HPTN 083 and 084,” commented Monica Gandhi, MD, MPH, an infectious disease physician, professor of medicine, and associate chief in the division of HIV, infectious diseases, and global medicine at the University of California, San Francisco (UCSF).
Dr. Gandhi, who was not involved in either study, is also director of the UCSF Center for AIDS Research and medical director of the HIV Clinic (“Ward 86”) at San Francisco General Hospital. “The incredible efficacy of long-acting PrEP for cisgender women shown by HPTN 084 is game-changing for our practice, and we have already instituted CAB LA across a range of populations at Ward 86,” she said in an interview. “The durability of the 89% additional efficacy of CAB LA over oral TDF/FTC is thrilling and will lead to a greater use of long-acting options.”
She acknowledged that information on potential interactions of GAHT was needed from the HPTN 083 trial. “That cabotegravir levels did not change with the use of estradiol or spironolactone for gender-affirming therapy is important news for our practice and to reassure our TGW that they can safely and effectively use CAB LA for HIV prevention.”
The HPTN 084 and 083 trials were funded by the National Institutes for Allergy and Infectious Diseases. Dr. Delany-Moretlwe, Dr. Grinsztejn, and Dr. Gandhi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MONTREAL – , according to new data from two HIV Prevention Trials Network (HPTN) studies reported at the International AIDS Society Conference.
Follow-up data from the HPTN 084 trial, which compared the two regimens in 3,224 sub-Saharan persons who were assigned female sex at birth, show that three new HIV infections occurred in the CAB LA group in the 12 months since the study was unblinded, versus 20 new infections among the TDF-FTC group. That translates to an 89% lower risk of infection in the CAB LA arm across both the blinded and unblinded phases of the trial, said lead investigator Sinead Delany-Moretlwe, MD, PhD, director of research, Wits Reproductive Health and HIV Institute, the University of the Witwatersrand, Johannesburg, South Africa, during a press conference.
“The trial was designed with the assumption that both drugs were highly effective in preventing HIV infection but that, given the challenges with taking a pill a day, that injectable cabotegravir may offer an adherence advantage,” she said in an interview. “Our data appear to confirm this, as most of the participants in the TDF-FTC arm who became infected with HIV had evidence of poor or inconsistent use of PrEP.”
The study also found that pregnancy incidence increased “two- to threefold” between the blinded and the unblinded period, “and this emphasizes to us the desire of women to conceive safely, without the threat of HIV, and the importance of us continuing to evaluate the safety and pharmacology of cabotegravir in pregnant and breastfeeding women during open-label extension phase of HPTN 084, so that [they] are not excluded from access to this highly effective PrEP agent,” she said. To date, no congenital anomalies have been reported in babies born during the study.
In an update report from HPTN 083, which also showed superiority of CAB LA over TDF-FTC in cisgender men and transgender women (TGW), researchers reported the safety and efficacy of CAB LA use in TGW using gender-affirming hormone therapy (GAHT).
Among the 4,566 participants in HPTN 083, 570 were TGW, and of those, 58% used GAHT at baseline, reported Beatriz Grinsztejn, MD, PhD, head of the STD/AIDS Clinical Research Laboratory at the Instituto Nacional de Infectologicia/Fundação Oswaldo Cruz.
CAB LA drug concentrations measured in a subset of 53 TGW who received on-time CAB injections were comparable between those taking (n = 30) and those not taking GAHT (n = 23), “suggesting the lack of a gender-affirming hormone effect on CAB pharmacokinetics,” she said. “These are very promising results, as we all know that the use of gender-affirming hormone therapy is a major priority for our transgender women community, ... so the lack of drug-drug interaction is really a very important result.”
“Cabotegravir long-acting PrEP is now approved for all at-risk populations, including men who have sex with men, transgender women, and cisgender women, after the results of HPTN 083 and 084,” commented Monica Gandhi, MD, MPH, an infectious disease physician, professor of medicine, and associate chief in the division of HIV, infectious diseases, and global medicine at the University of California, San Francisco (UCSF).
Dr. Gandhi, who was not involved in either study, is also director of the UCSF Center for AIDS Research and medical director of the HIV Clinic (“Ward 86”) at San Francisco General Hospital. “The incredible efficacy of long-acting PrEP for cisgender women shown by HPTN 084 is game-changing for our practice, and we have already instituted CAB LA across a range of populations at Ward 86,” she said in an interview. “The durability of the 89% additional efficacy of CAB LA over oral TDF/FTC is thrilling and will lead to a greater use of long-acting options.”
She acknowledged that information on potential interactions of GAHT was needed from the HPTN 083 trial. “That cabotegravir levels did not change with the use of estradiol or spironolactone for gender-affirming therapy is important news for our practice and to reassure our TGW that they can safely and effectively use CAB LA for HIV prevention.”
The HPTN 084 and 083 trials were funded by the National Institutes for Allergy and Infectious Diseases. Dr. Delany-Moretlwe, Dr. Grinsztejn, and Dr. Gandhi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MONTREAL – , according to new data from two HIV Prevention Trials Network (HPTN) studies reported at the International AIDS Society Conference.
Follow-up data from the HPTN 084 trial, which compared the two regimens in 3,224 sub-Saharan persons who were assigned female sex at birth, show that three new HIV infections occurred in the CAB LA group in the 12 months since the study was unblinded, versus 20 new infections among the TDF-FTC group. That translates to an 89% lower risk of infection in the CAB LA arm across both the blinded and unblinded phases of the trial, said lead investigator Sinead Delany-Moretlwe, MD, PhD, director of research, Wits Reproductive Health and HIV Institute, the University of the Witwatersrand, Johannesburg, South Africa, during a press conference.
“The trial was designed with the assumption that both drugs were highly effective in preventing HIV infection but that, given the challenges with taking a pill a day, that injectable cabotegravir may offer an adherence advantage,” she said in an interview. “Our data appear to confirm this, as most of the participants in the TDF-FTC arm who became infected with HIV had evidence of poor or inconsistent use of PrEP.”
The study also found that pregnancy incidence increased “two- to threefold” between the blinded and the unblinded period, “and this emphasizes to us the desire of women to conceive safely, without the threat of HIV, and the importance of us continuing to evaluate the safety and pharmacology of cabotegravir in pregnant and breastfeeding women during open-label extension phase of HPTN 084, so that [they] are not excluded from access to this highly effective PrEP agent,” she said. To date, no congenital anomalies have been reported in babies born during the study.
In an update report from HPTN 083, which also showed superiority of CAB LA over TDF-FTC in cisgender men and transgender women (TGW), researchers reported the safety and efficacy of CAB LA use in TGW using gender-affirming hormone therapy (GAHT).
Among the 4,566 participants in HPTN 083, 570 were TGW, and of those, 58% used GAHT at baseline, reported Beatriz Grinsztejn, MD, PhD, head of the STD/AIDS Clinical Research Laboratory at the Instituto Nacional de Infectologicia/Fundação Oswaldo Cruz.
CAB LA drug concentrations measured in a subset of 53 TGW who received on-time CAB injections were comparable between those taking (n = 30) and those not taking GAHT (n = 23), “suggesting the lack of a gender-affirming hormone effect on CAB pharmacokinetics,” she said. “These are very promising results, as we all know that the use of gender-affirming hormone therapy is a major priority for our transgender women community, ... so the lack of drug-drug interaction is really a very important result.”
“Cabotegravir long-acting PrEP is now approved for all at-risk populations, including men who have sex with men, transgender women, and cisgender women, after the results of HPTN 083 and 084,” commented Monica Gandhi, MD, MPH, an infectious disease physician, professor of medicine, and associate chief in the division of HIV, infectious diseases, and global medicine at the University of California, San Francisco (UCSF).
Dr. Gandhi, who was not involved in either study, is also director of the UCSF Center for AIDS Research and medical director of the HIV Clinic (“Ward 86”) at San Francisco General Hospital. “The incredible efficacy of long-acting PrEP for cisgender women shown by HPTN 084 is game-changing for our practice, and we have already instituted CAB LA across a range of populations at Ward 86,” she said in an interview. “The durability of the 89% additional efficacy of CAB LA over oral TDF/FTC is thrilling and will lead to a greater use of long-acting options.”
She acknowledged that information on potential interactions of GAHT was needed from the HPTN 083 trial. “That cabotegravir levels did not change with the use of estradiol or spironolactone for gender-affirming therapy is important news for our practice and to reassure our TGW that they can safely and effectively use CAB LA for HIV prevention.”
The HPTN 084 and 083 trials were funded by the National Institutes for Allergy and Infectious Diseases. Dr. Delany-Moretlwe, Dr. Grinsztejn, and Dr. Gandhi have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AIDS 2022
University to train ‘trip facilitators’ for psychedelic therapy
The UC Berkeley Center for the Science of Psychedelics (BCSP) training program aims to create a cadre of facilitators who will be ready to help if, and when, substances such as psilocybin, MDMA, and LSD are approved in the United States, Tina Trujillo, PhD, an associate professor at UC Berkeley’s School of Education, told reporters at a press briefing.
Hallucinogenic drugs are on the Drug Enforcement Administration’s (DEA) Schedule I list because they are considered to have no currently accepted medical use and high abuse potential. But there has been an explosion of research into psychedelics – combined with therapy – as treatment for severe depression, posttraumatic stress disorder, substance-use disorder, and other mental health conditions. Some 100 clinical trials are underway.
“The estimates are that we’re going to need 100,000 trained psychedelic facilitators once psilocybin and MDMA are approved by the [U.S. Food and Drug Administration] FDA, which is expected to happen within the next 5 years or so,” said Michael Pollan, co-founder of the BCSP. He is author of “How to Change Your Mind,” a 2018 book about psychedelics, which has been adapted into a four-part docuseries currently streaming on Netflix.

Nine-month program
The first 24 trainees – a mix of physicians, nurses, psychotherapists, and social workers – will undergo 9 months of education and preparation in “the technical, the cultural, the mystical, and the ethical dimensions of psychedelic facilitation,” said Dr. Trujillo.
The BCSP’s Certificate Program in Psychedelic Facilitation will have “an emphasis on both western science and spiritual care traditions,” she said.
Trainees will receive 150 instructional hours and a 25-hour practicum and will take part in a final 5-day retreat. The program will initially focus only on psilocybin, in part because the BCSP is involved in several FDA-approved trials testing the drug.
In one study – which aims to enroll participants in the fall – researchers will use functional MRI to examine the neural correlates of the psychedelic experience in individuals receiving low-dose psilocybin.
Eligible trainees will have an opportunity to participate in the Berkeley psilocybin trials and “increase their first-hand knowledge,” Dr. Trujillo said.
At the conclusion of the training, students will receive a certificate, “not a license or sanction to go off and practice,” she said. She noted that eventually, when facilitation is legal, certificate holders will be able to practice in clinical research settings or in health care settings.
Growing acceptance in psychiatry
Mr. Pollan said there has been a radical change in acceptance of psychedelics as potential therapies.
“The shift from destroyer of young minds in the ‘60s to effective medicine in the 2020s is as sudden as it is confusing for many people,” he said. He noted that the Berkeley center hopes to provide evidence-based information for journalists, the public, and clinicians.
He said that after his book was released, he expected pushback from “mainstream psychiatry.” Instead, he was invited to give grand rounds talks. Psychiatrists are “very open to the potential of psychedelics,” Mr. Pollan said.
“The reason for that, quite frankly, is because they are desperate,” he said. “The tools of conventional psychiatry to deal with things like depression and anxiety and addiction are not very good, and some of them are failing,” he said.
Mr. Pollan cited some other indicators of acceptance. In Oregon, beginning in 2023, psilocybin will be available to anyone older than 21 years but only for use in licensed facilities with licensed facilitators, and the substance must be produced by a licensed manufacturer.
In November, Colorado will ask voters whether they want to follow the Oregon model and legalize psilocybin. If approved, another Colorado ballot initiative would decriminalize possession.
Mr. Pollan noted that Cory Booker, the Democratic Senator from New Jersey, and Rand Paul, a conservative Republican Senator from Kentucky, have found a common cause, introducing legislation to let select terminally ill patients have access to psychedelics and other Schedule I drugs.
Some 400 companies are conducting research on psychedelics. Researchers must have a license from the DEA to obtain and study the substances, Andrea Gomez, assistant professor of neurobiology at UC Berkeley, told reporters.
She said growing interest in the potential of these drugs might lead more researchers to “jump through the hoops” to get the licenses. The floodgates would truly open if the National Institutes of Health started funding studies, she said.
A version of this article first appeared on Medscape.com.
The UC Berkeley Center for the Science of Psychedelics (BCSP) training program aims to create a cadre of facilitators who will be ready to help if, and when, substances such as psilocybin, MDMA, and LSD are approved in the United States, Tina Trujillo, PhD, an associate professor at UC Berkeley’s School of Education, told reporters at a press briefing.
Hallucinogenic drugs are on the Drug Enforcement Administration’s (DEA) Schedule I list because they are considered to have no currently accepted medical use and high abuse potential. But there has been an explosion of research into psychedelics – combined with therapy – as treatment for severe depression, posttraumatic stress disorder, substance-use disorder, and other mental health conditions. Some 100 clinical trials are underway.
“The estimates are that we’re going to need 100,000 trained psychedelic facilitators once psilocybin and MDMA are approved by the [U.S. Food and Drug Administration] FDA, which is expected to happen within the next 5 years or so,” said Michael Pollan, co-founder of the BCSP. He is author of “How to Change Your Mind,” a 2018 book about psychedelics, which has been adapted into a four-part docuseries currently streaming on Netflix.
Nine-month program
The first 24 trainees – a mix of physicians, nurses, psychotherapists, and social workers – will undergo 9 months of education and preparation in “the technical, the cultural, the mystical, and the ethical dimensions of psychedelic facilitation,” said Dr. Trujillo.
The BCSP’s Certificate Program in Psychedelic Facilitation will have “an emphasis on both western science and spiritual care traditions,” she said.
Trainees will receive 150 instructional hours and a 25-hour practicum and will take part in a final 5-day retreat. The program will initially focus only on psilocybin, in part because the BCSP is involved in several FDA-approved trials testing the drug.
In one study – which aims to enroll participants in the fall – researchers will use functional MRI to examine the neural correlates of the psychedelic experience in individuals receiving low-dose psilocybin.
Eligible trainees will have an opportunity to participate in the Berkeley psilocybin trials and “increase their first-hand knowledge,” Dr. Trujillo said.
At the conclusion of the training, students will receive a certificate, “not a license or sanction to go off and practice,” she said. She noted that eventually, when facilitation is legal, certificate holders will be able to practice in clinical research settings or in health care settings.
Growing acceptance in psychiatry
Mr. Pollan said there has been a radical change in acceptance of psychedelics as potential therapies.
“The shift from destroyer of young minds in the ‘60s to effective medicine in the 2020s is as sudden as it is confusing for many people,” he said. He noted that the Berkeley center hopes to provide evidence-based information for journalists, the public, and clinicians.
He said that after his book was released, he expected pushback from “mainstream psychiatry.” Instead, he was invited to give grand rounds talks. Psychiatrists are “very open to the potential of psychedelics,” Mr. Pollan said.
“The reason for that, quite frankly, is because they are desperate,” he said. “The tools of conventional psychiatry to deal with things like depression and anxiety and addiction are not very good, and some of them are failing,” he said.
Mr. Pollan cited some other indicators of acceptance. In Oregon, beginning in 2023, psilocybin will be available to anyone older than 21 years but only for use in licensed facilities with licensed facilitators, and the substance must be produced by a licensed manufacturer.
In November, Colorado will ask voters whether they want to follow the Oregon model and legalize psilocybin. If approved, another Colorado ballot initiative would decriminalize possession.
Mr. Pollan noted that Cory Booker, the Democratic Senator from New Jersey, and Rand Paul, a conservative Republican Senator from Kentucky, have found a common cause, introducing legislation to let select terminally ill patients have access to psychedelics and other Schedule I drugs.
Some 400 companies are conducting research on psychedelics. Researchers must have a license from the DEA to obtain and study the substances, Andrea Gomez, assistant professor of neurobiology at UC Berkeley, told reporters.
She said growing interest in the potential of these drugs might lead more researchers to “jump through the hoops” to get the licenses. The floodgates would truly open if the National Institutes of Health started funding studies, she said.
A version of this article first appeared on Medscape.com.
The UC Berkeley Center for the Science of Psychedelics (BCSP) training program aims to create a cadre of facilitators who will be ready to help if, and when, substances such as psilocybin, MDMA, and LSD are approved in the United States, Tina Trujillo, PhD, an associate professor at UC Berkeley’s School of Education, told reporters at a press briefing.
Hallucinogenic drugs are on the Drug Enforcement Administration’s (DEA) Schedule I list because they are considered to have no currently accepted medical use and high abuse potential. But there has been an explosion of research into psychedelics – combined with therapy – as treatment for severe depression, posttraumatic stress disorder, substance-use disorder, and other mental health conditions. Some 100 clinical trials are underway.
“The estimates are that we’re going to need 100,000 trained psychedelic facilitators once psilocybin and MDMA are approved by the [U.S. Food and Drug Administration] FDA, which is expected to happen within the next 5 years or so,” said Michael Pollan, co-founder of the BCSP. He is author of “How to Change Your Mind,” a 2018 book about psychedelics, which has been adapted into a four-part docuseries currently streaming on Netflix.
Nine-month program
The first 24 trainees – a mix of physicians, nurses, psychotherapists, and social workers – will undergo 9 months of education and preparation in “the technical, the cultural, the mystical, and the ethical dimensions of psychedelic facilitation,” said Dr. Trujillo.
The BCSP’s Certificate Program in Psychedelic Facilitation will have “an emphasis on both western science and spiritual care traditions,” she said.
Trainees will receive 150 instructional hours and a 25-hour practicum and will take part in a final 5-day retreat. The program will initially focus only on psilocybin, in part because the BCSP is involved in several FDA-approved trials testing the drug.
In one study – which aims to enroll participants in the fall – researchers will use functional MRI to examine the neural correlates of the psychedelic experience in individuals receiving low-dose psilocybin.
Eligible trainees will have an opportunity to participate in the Berkeley psilocybin trials and “increase their first-hand knowledge,” Dr. Trujillo said.
At the conclusion of the training, students will receive a certificate, “not a license or sanction to go off and practice,” she said. She noted that eventually, when facilitation is legal, certificate holders will be able to practice in clinical research settings or in health care settings.
Growing acceptance in psychiatry
Mr. Pollan said there has been a radical change in acceptance of psychedelics as potential therapies.
“The shift from destroyer of young minds in the ‘60s to effective medicine in the 2020s is as sudden as it is confusing for many people,” he said. He noted that the Berkeley center hopes to provide evidence-based information for journalists, the public, and clinicians.
He said that after his book was released, he expected pushback from “mainstream psychiatry.” Instead, he was invited to give grand rounds talks. Psychiatrists are “very open to the potential of psychedelics,” Mr. Pollan said.
“The reason for that, quite frankly, is because they are desperate,” he said. “The tools of conventional psychiatry to deal with things like depression and anxiety and addiction are not very good, and some of them are failing,” he said.
Mr. Pollan cited some other indicators of acceptance. In Oregon, beginning in 2023, psilocybin will be available to anyone older than 21 years but only for use in licensed facilities with licensed facilitators, and the substance must be produced by a licensed manufacturer.
In November, Colorado will ask voters whether they want to follow the Oregon model and legalize psilocybin. If approved, another Colorado ballot initiative would decriminalize possession.
Mr. Pollan noted that Cory Booker, the Democratic Senator from New Jersey, and Rand Paul, a conservative Republican Senator from Kentucky, have found a common cause, introducing legislation to let select terminally ill patients have access to psychedelics and other Schedule I drugs.
Some 400 companies are conducting research on psychedelics. Researchers must have a license from the DEA to obtain and study the substances, Andrea Gomez, assistant professor of neurobiology at UC Berkeley, told reporters.
She said growing interest in the potential of these drugs might lead more researchers to “jump through the hoops” to get the licenses. The floodgates would truly open if the National Institutes of Health started funding studies, she said.
A version of this article first appeared on Medscape.com.
Children and COVID: Weekly cases top 95,000, admissions continue to rise
New pediatric COVID-19 cases increased for the third straight week as a substantial number of children under age 5 years started to receive their second doses of the vaccine.
Despite the 3-week trend, however, there are some positive signs. The new-case count for the latest reporting week (July 22-28) was over 95,000, but the 3.9% increase over the previous week’s 92,000 cases is much smaller than that week’s (July 15-21) corresponding jump of almost 22% over the July 8-14 total (75,000), according to the American Academy of Pediatrics and the Children’s Hospital Association.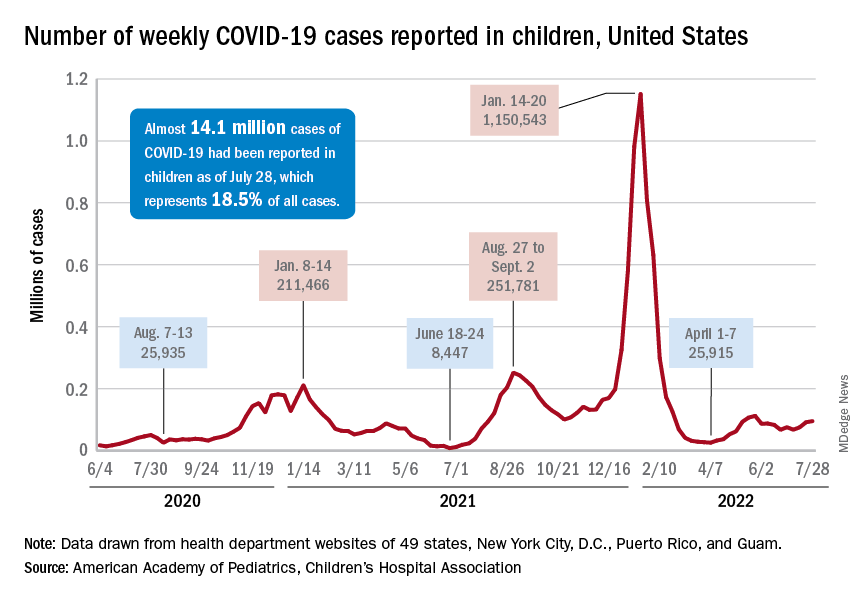
On the not-so-positive side is the trend in admissions among children aged 0-17 years, which continue to climb steadily and have nearly equaled the highest rate seen during the Delta surge in 2021. The rate on July 29 was 0.46 admissions per 100,000 population, and the highest rate over the course of the Delta surge was 0.47 per 100,000, but the all-time high from the Omicron surge – 1.25 per 100,000 in mid-January – is still a long way off, based on data from the Centers for Disease Control and Prevention.
A similar situation is occurring with emergency department visits, but there is differentiation by age group. Among those aged 0-11 years, visits with diagnosed COVID made up 6.5% of all their ED visits on July 25, which was well above the high (4.0%) during the Delta surge, the CDC said.
That is not the case, however, for the older children, for whom rates are rising more slowly. Those aged 12-15 have reached 3.4% so far this summer, as have the 16- to 17-years-olds, versus Delta highs last year of around 7%, the CDC said on its COVID Data Tracker. As with admissions, though, current rates are well below the all-time Omicron high points, the CDC data show.
Joining the ranks of the fully vaccinated
Over the last 2 weeks, the first children to receive the COVID vaccine after its approval for those under age 5 years have been coming back for their second doses. Almost 50,000, about 0.3% of all those in that age group, had done so by July 27. Just over 662,000, about 3.4% of the total under-5 population, have received at least one dose, the CDC said.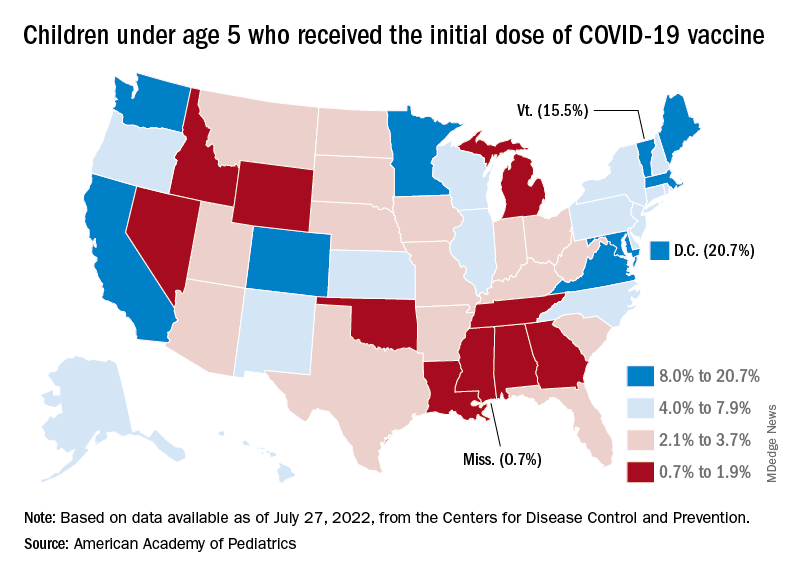
Meanwhile, analysis of “data from the first several weeks following availability of the vaccine in this age group indicate high variability across states,” the AAP said in its weekly vaccination report. In the District of Columbia, 20.7% of all children under age 5 have received an initial dose as of July 27, as have 15.5% of those in Vermont and 12.5% in Massachusetts. No other state was above 10%, but Mississippi, at 0.7%, was the only one below 1%.
The older children, obviously, have a head start, so their numbers are much higher. At the state level, Vermont has the highest initial dose rate, 69%, for those aged 5-11 years, while Alabama, Mississippi, and Wyoming, at 17%, are looking up at everyone else in the country. Among children aged 12-17 years, D.C. is the highest with 100% vaccination – Massachusetts and Rhode Island are at 98% – and Wyoming is the lowest with 40%, the AAP said.
New pediatric COVID-19 cases increased for the third straight week as a substantial number of children under age 5 years started to receive their second doses of the vaccine.
Despite the 3-week trend, however, there are some positive signs. The new-case count for the latest reporting week (July 22-28) was over 95,000, but the 3.9% increase over the previous week’s 92,000 cases is much smaller than that week’s (July 15-21) corresponding jump of almost 22% over the July 8-14 total (75,000), according to the American Academy of Pediatrics and the Children’s Hospital Association.
On the not-so-positive side is the trend in admissions among children aged 0-17 years, which continue to climb steadily and have nearly equaled the highest rate seen during the Delta surge in 2021. The rate on July 29 was 0.46 admissions per 100,000 population, and the highest rate over the course of the Delta surge was 0.47 per 100,000, but the all-time high from the Omicron surge – 1.25 per 100,000 in mid-January – is still a long way off, based on data from the Centers for Disease Control and Prevention.
A similar situation is occurring with emergency department visits, but there is differentiation by age group. Among those aged 0-11 years, visits with diagnosed COVID made up 6.5% of all their ED visits on July 25, which was well above the high (4.0%) during the Delta surge, the CDC said.
That is not the case, however, for the older children, for whom rates are rising more slowly. Those aged 12-15 have reached 3.4% so far this summer, as have the 16- to 17-years-olds, versus Delta highs last year of around 7%, the CDC said on its COVID Data Tracker. As with admissions, though, current rates are well below the all-time Omicron high points, the CDC data show.
Joining the ranks of the fully vaccinated
Over the last 2 weeks, the first children to receive the COVID vaccine after its approval for those under age 5 years have been coming back for their second doses. Almost 50,000, about 0.3% of all those in that age group, had done so by July 27. Just over 662,000, about 3.4% of the total under-5 population, have received at least one dose, the CDC said.
Meanwhile, analysis of “data from the first several weeks following availability of the vaccine in this age group indicate high variability across states,” the AAP said in its weekly vaccination report. In the District of Columbia, 20.7% of all children under age 5 have received an initial dose as of July 27, as have 15.5% of those in Vermont and 12.5% in Massachusetts. No other state was above 10%, but Mississippi, at 0.7%, was the only one below 1%.
The older children, obviously, have a head start, so their numbers are much higher. At the state level, Vermont has the highest initial dose rate, 69%, for those aged 5-11 years, while Alabama, Mississippi, and Wyoming, at 17%, are looking up at everyone else in the country. Among children aged 12-17 years, D.C. is the highest with 100% vaccination – Massachusetts and Rhode Island are at 98% – and Wyoming is the lowest with 40%, the AAP said.
New pediatric COVID-19 cases increased for the third straight week as a substantial number of children under age 5 years started to receive their second doses of the vaccine.
Despite the 3-week trend, however, there are some positive signs. The new-case count for the latest reporting week (July 22-28) was over 95,000, but the 3.9% increase over the previous week’s 92,000 cases is much smaller than that week’s (July 15-21) corresponding jump of almost 22% over the July 8-14 total (75,000), according to the American Academy of Pediatrics and the Children’s Hospital Association.
On the not-so-positive side is the trend in admissions among children aged 0-17 years, which continue to climb steadily and have nearly equaled the highest rate seen during the Delta surge in 2021. The rate on July 29 was 0.46 admissions per 100,000 population, and the highest rate over the course of the Delta surge was 0.47 per 100,000, but the all-time high from the Omicron surge – 1.25 per 100,000 in mid-January – is still a long way off, based on data from the Centers for Disease Control and Prevention.
A similar situation is occurring with emergency department visits, but there is differentiation by age group. Among those aged 0-11 years, visits with diagnosed COVID made up 6.5% of all their ED visits on July 25, which was well above the high (4.0%) during the Delta surge, the CDC said.
That is not the case, however, for the older children, for whom rates are rising more slowly. Those aged 12-15 have reached 3.4% so far this summer, as have the 16- to 17-years-olds, versus Delta highs last year of around 7%, the CDC said on its COVID Data Tracker. As with admissions, though, current rates are well below the all-time Omicron high points, the CDC data show.
Joining the ranks of the fully vaccinated
Over the last 2 weeks, the first children to receive the COVID vaccine after its approval for those under age 5 years have been coming back for their second doses. Almost 50,000, about 0.3% of all those in that age group, had done so by July 27. Just over 662,000, about 3.4% of the total under-5 population, have received at least one dose, the CDC said.
Meanwhile, analysis of “data from the first several weeks following availability of the vaccine in this age group indicate high variability across states,” the AAP said in its weekly vaccination report. In the District of Columbia, 20.7% of all children under age 5 have received an initial dose as of July 27, as have 15.5% of those in Vermont and 12.5% in Massachusetts. No other state was above 10%, but Mississippi, at 0.7%, was the only one below 1%.
The older children, obviously, have a head start, so their numbers are much higher. At the state level, Vermont has the highest initial dose rate, 69%, for those aged 5-11 years, while Alabama, Mississippi, and Wyoming, at 17%, are looking up at everyone else in the country. Among children aged 12-17 years, D.C. is the highest with 100% vaccination – Massachusetts and Rhode Island are at 98% – and Wyoming is the lowest with 40%, the AAP said.
Six specialties attracting the highest private equity acquisitions
While tracking the extent of physician practice acquisition by private equity firms may be difficult, new research highlights what specialties and U.S. regions are most affected by such purchases.
The study, supported by the National Institute for Health Care Management (NIHCM), examined 97,094 physicians practicing in six specialties, 4,738 of whom worked in private equity–acquired practices. Of these specialties, 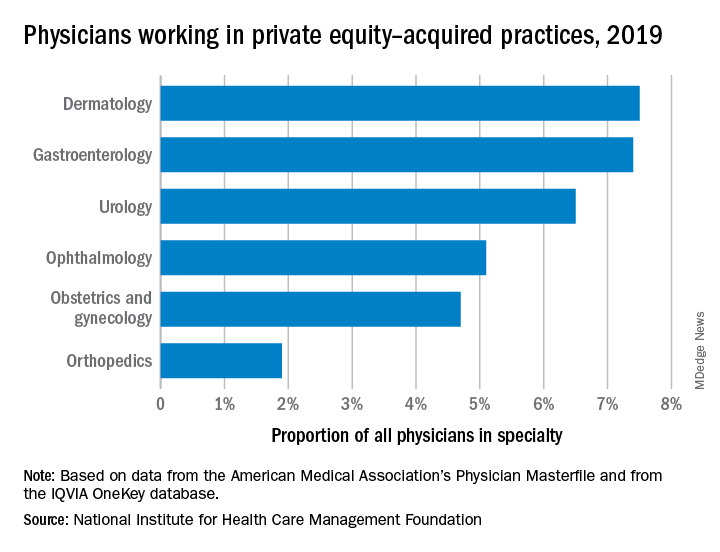
“These specialties offer private equity firms diverse revenue streams. You have a mix of commercially insured individuals with Medicare insurance and self-pay,” said Yashaswini Singh, MPA, a doctoral student at the Johns Hopkins Bloomberg School of Public Health, Baltimore, and coauthor of the study, which was published in JAMA Health Forum as a research letter.
“In dermatology, you have a mix of surgical procedures that are covered under insurance, but also a lot of cosmetic procedures that are most likely to be self-pay procedures. This offers private equity several mechanisms to which they can increase their revenues.”
Ms. Singh’s coauthors were part of a previous study looking at private practice penetration by private equity firms. That research found such deals surged from 59 deals in 2013 representing 843 physicians, to 136 private equity acquisition deals representing 1,882 physicians in 2016.
The most recent study notes limited data and use of nondisclosure agreements during early negotiations as part of the difficulty in truly pinpointing private equity’s presence in health care. Monitoring private equity activity has become necessary across all industries, noted the authors of the study. If continued at this rate, long-term private equity acquisition has a multitude of potential pros and cons.
Ms. Singh explained that such specialties are highly fragmented and they allow for economies of scale and scope. In particular, an aging population increases demand for dermatology, ophthalmology, and gastroenterology services such as skin biopsies, cataracts, and colonoscopies. This makes these specialties very attractive to private equity firms. The same can be said for obstetrics and gynecology, as fertility clinics have attracted many private equity investments.
“This is another area where understanding changes to physician practice patterns and patient outcomes is critical as women continue to delay motherhood,” said Ms. Singh.
Reducing competition, increasing focus on patient care
Researchers found significant geographical trends for private equity penetration, as it varies across the country. It is highest in the Northeast, Florida, and Arizona in hospital referral regions. Researchers are still analyzing the cause of this occurrence.
Geographic concentration of private equity penetration likely reflects strategic selection of investment opportunities by private equity funds as the decision to invest in a practice does not happen at random, Ms. Singh noted.
Ms. Singh said she hopes that by documenting a variation and geographic concentration that the NIHCM is providing the first foundational step to tackle questions related to incentives and regulations that facilitate investment.
“Understanding the regulatory and economic environments that facilitate private equity activity is an interesting and important question to explore further,” she said in an interview. “This can include supply-side factors that can shape the business environment, e.g., taxation environment, regulatory burden to complete acquisitions, as well as demand-side factors that facilitate growth.”
Researchers found that continued growth of private equity penetration may lead to consolidation among independent practices facing financial pressures, as well as reduced competition and increased prices within each local health care market.
“Localized consolidation in certain markets has the potential for competition to reduce, [and] reduced competition has been shown in a variety of settings to be associated with increases in prices and reduced access for patients,” said Ms. Singh.
Conversely, Ms. Singh addressed several benefits of growing private equity presence. Companies can exploit their full potential through the addition of private equity expertise and contacts. Specifically, health care development of technological infrastructure is likely, along with reduced patient wait times and the expansion of business hours. It could also be a way for practices to offload administrative responsibilities and for physicians to focus more on the care delivery process.
A version of this article first appeared on Medscape.com.
While tracking the extent of physician practice acquisition by private equity firms may be difficult, new research highlights what specialties and U.S. regions are most affected by such purchases.
The study, supported by the National Institute for Health Care Management (NIHCM), examined 97,094 physicians practicing in six specialties, 4,738 of whom worked in private equity–acquired practices. Of these specialties,
“These specialties offer private equity firms diverse revenue streams. You have a mix of commercially insured individuals with Medicare insurance and self-pay,” said Yashaswini Singh, MPA, a doctoral student at the Johns Hopkins Bloomberg School of Public Health, Baltimore, and coauthor of the study, which was published in JAMA Health Forum as a research letter.
“In dermatology, you have a mix of surgical procedures that are covered under insurance, but also a lot of cosmetic procedures that are most likely to be self-pay procedures. This offers private equity several mechanisms to which they can increase their revenues.”
Ms. Singh’s coauthors were part of a previous study looking at private practice penetration by private equity firms. That research found such deals surged from 59 deals in 2013 representing 843 physicians, to 136 private equity acquisition deals representing 1,882 physicians in 2016.
The most recent study notes limited data and use of nondisclosure agreements during early negotiations as part of the difficulty in truly pinpointing private equity’s presence in health care. Monitoring private equity activity has become necessary across all industries, noted the authors of the study. If continued at this rate, long-term private equity acquisition has a multitude of potential pros and cons.
Ms. Singh explained that such specialties are highly fragmented and they allow for economies of scale and scope. In particular, an aging population increases demand for dermatology, ophthalmology, and gastroenterology services such as skin biopsies, cataracts, and colonoscopies. This makes these specialties very attractive to private equity firms. The same can be said for obstetrics and gynecology, as fertility clinics have attracted many private equity investments.
“This is another area where understanding changes to physician practice patterns and patient outcomes is critical as women continue to delay motherhood,” said Ms. Singh.
Reducing competition, increasing focus on patient care
Researchers found significant geographical trends for private equity penetration, as it varies across the country. It is highest in the Northeast, Florida, and Arizona in hospital referral regions. Researchers are still analyzing the cause of this occurrence.
Geographic concentration of private equity penetration likely reflects strategic selection of investment opportunities by private equity funds as the decision to invest in a practice does not happen at random, Ms. Singh noted.
Ms. Singh said she hopes that by documenting a variation and geographic concentration that the NIHCM is providing the first foundational step to tackle questions related to incentives and regulations that facilitate investment.
“Understanding the regulatory and economic environments that facilitate private equity activity is an interesting and important question to explore further,” she said in an interview. “This can include supply-side factors that can shape the business environment, e.g., taxation environment, regulatory burden to complete acquisitions, as well as demand-side factors that facilitate growth.”
Researchers found that continued growth of private equity penetration may lead to consolidation among independent practices facing financial pressures, as well as reduced competition and increased prices within each local health care market.
“Localized consolidation in certain markets has the potential for competition to reduce, [and] reduced competition has been shown in a variety of settings to be associated with increases in prices and reduced access for patients,” said Ms. Singh.
Conversely, Ms. Singh addressed several benefits of growing private equity presence. Companies can exploit their full potential through the addition of private equity expertise and contacts. Specifically, health care development of technological infrastructure is likely, along with reduced patient wait times and the expansion of business hours. It could also be a way for practices to offload administrative responsibilities and for physicians to focus more on the care delivery process.
A version of this article first appeared on Medscape.com.
While tracking the extent of physician practice acquisition by private equity firms may be difficult, new research highlights what specialties and U.S. regions are most affected by such purchases.
The study, supported by the National Institute for Health Care Management (NIHCM), examined 97,094 physicians practicing in six specialties, 4,738 of whom worked in private equity–acquired practices. Of these specialties,
“These specialties offer private equity firms diverse revenue streams. You have a mix of commercially insured individuals with Medicare insurance and self-pay,” said Yashaswini Singh, MPA, a doctoral student at the Johns Hopkins Bloomberg School of Public Health, Baltimore, and coauthor of the study, which was published in JAMA Health Forum as a research letter.
“In dermatology, you have a mix of surgical procedures that are covered under insurance, but also a lot of cosmetic procedures that are most likely to be self-pay procedures. This offers private equity several mechanisms to which they can increase their revenues.”
Ms. Singh’s coauthors were part of a previous study looking at private practice penetration by private equity firms. That research found such deals surged from 59 deals in 2013 representing 843 physicians, to 136 private equity acquisition deals representing 1,882 physicians in 2016.
The most recent study notes limited data and use of nondisclosure agreements during early negotiations as part of the difficulty in truly pinpointing private equity’s presence in health care. Monitoring private equity activity has become necessary across all industries, noted the authors of the study. If continued at this rate, long-term private equity acquisition has a multitude of potential pros and cons.
Ms. Singh explained that such specialties are highly fragmented and they allow for economies of scale and scope. In particular, an aging population increases demand for dermatology, ophthalmology, and gastroenterology services such as skin biopsies, cataracts, and colonoscopies. This makes these specialties very attractive to private equity firms. The same can be said for obstetrics and gynecology, as fertility clinics have attracted many private equity investments.
“This is another area where understanding changes to physician practice patterns and patient outcomes is critical as women continue to delay motherhood,” said Ms. Singh.
Reducing competition, increasing focus on patient care
Researchers found significant geographical trends for private equity penetration, as it varies across the country. It is highest in the Northeast, Florida, and Arizona in hospital referral regions. Researchers are still analyzing the cause of this occurrence.
Geographic concentration of private equity penetration likely reflects strategic selection of investment opportunities by private equity funds as the decision to invest in a practice does not happen at random, Ms. Singh noted.
Ms. Singh said she hopes that by documenting a variation and geographic concentration that the NIHCM is providing the first foundational step to tackle questions related to incentives and regulations that facilitate investment.
“Understanding the regulatory and economic environments that facilitate private equity activity is an interesting and important question to explore further,” she said in an interview. “This can include supply-side factors that can shape the business environment, e.g., taxation environment, regulatory burden to complete acquisitions, as well as demand-side factors that facilitate growth.”
Researchers found that continued growth of private equity penetration may lead to consolidation among independent practices facing financial pressures, as well as reduced competition and increased prices within each local health care market.
“Localized consolidation in certain markets has the potential for competition to reduce, [and] reduced competition has been shown in a variety of settings to be associated with increases in prices and reduced access for patients,” said Ms. Singh.
Conversely, Ms. Singh addressed several benefits of growing private equity presence. Companies can exploit their full potential through the addition of private equity expertise and contacts. Specifically, health care development of technological infrastructure is likely, along with reduced patient wait times and the expansion of business hours. It could also be a way for practices to offload administrative responsibilities and for physicians to focus more on the care delivery process.
A version of this article first appeared on Medscape.com.
FROM JAMA HEALTH FORUM
Low calcium, potassium key risk factors for kidney stones
as well as their symptomatic recurrence, a population-based study of dietary factors shows.
“Our research is of particular importance as recommendations for preventing symptomatic recurrence of kidney stones has largely been based on dietary factors associated with the incidence rather than the recurrence of stone formation,” Api Chewcharat, MD, Mayo Clinic, Rochester, Minn., said in a video discussing the study.
“We recommend a daily intake of calcium of approximately 1,200 mg and a diet that is high in potassium, especially high in fruits and vegetables, in order to prevent both incident and recurrent symptomatic kidney stone formation,” he stressed.
The study was published online in Mayo Clinic Proceedings.
Lower dietary calcium, potassium, and fluid associated with increased incidence
Some 411 patients with incident symptomatic kidney stone formation were recruited. Diets were compared between them and 384 controls. Patients were seen at the Mayo Clinic in either Minnesota or Florida between Jan. 1, 2009, and Aug. 31, 2018. “Dietary factors were based on a Viocare food frequency questionnaire administered during a baseline in-person study visit,” Dr. Chewcharat and colleagues observed.
During a median follow-up of 4.1 years, 73 patients experienced a symptomatic recurrence. In a fully adjusted analysis, a dietary calcium intake less than 1,200 mg/d was associated with incident stone formation. Similarly, among participants with a fluid intake less than 3,400 mL/d – about nine 12-oz glasses of fluid – was also associated with incident stone formation, as was a lower intake of dietary potassium, caffeine, and phytate. Phytate is an antioxidant found in whole grains, nuts, and other foods that can increase calcium absorption and urinary calcium excretion.
After excluding patients who were taking either a thiazide diuretic or a calcium supplement, lower dietary calcium and potassium, fluid, and phytate intake remained significantly associated with incident stone formation.
However, only lower dietary calcium intake was associated with a higher risk for symptomatic recurrence, although a lower dietary potassium intake was also associated with a higher risk for symptomatic recurrence in an analysis that adjusted for body mass index, fluid, and energy intake.
As the authors suggested, patients may be less keen to adjust their diet to prevent the development of incident kidney stones. On the other hand, they may be much more willing to adjust their diet to prevent their symptomatic recurrence. The Department of Agriculture currently recommends that individuals get approximately 1,200 mg/d of dietary calcium which, given the study results, appears to be justified for the prevention of symptomatic stone recurrence.
A higher-calcium diet is associated with a higher urinary pH, and citrate confers an alkali load which helps protect against the formation of calcium oxalate stones. Foods that are high in potassium also contain more fluid, citrate, and phytate, which, again, have been reported to be protective against kidney stones. “Changing your diet to prevent kidney stones can be very difficult,” Andrew Rule, MD, a nephrologist at the Mayo Clinic said in a statement.
“Thus, knowing the dietary factors that are most important for preventing kidney stone recurrence can help patients and providers know what to prioritize,” he added.
The authors have no conflicts of interest to declare.
A version of this article first appeared on Medscape.com.
as well as their symptomatic recurrence, a population-based study of dietary factors shows.
“Our research is of particular importance as recommendations for preventing symptomatic recurrence of kidney stones has largely been based on dietary factors associated with the incidence rather than the recurrence of stone formation,” Api Chewcharat, MD, Mayo Clinic, Rochester, Minn., said in a video discussing the study.
“We recommend a daily intake of calcium of approximately 1,200 mg and a diet that is high in potassium, especially high in fruits and vegetables, in order to prevent both incident and recurrent symptomatic kidney stone formation,” he stressed.
The study was published online in Mayo Clinic Proceedings.
Lower dietary calcium, potassium, and fluid associated with increased incidence
Some 411 patients with incident symptomatic kidney stone formation were recruited. Diets were compared between them and 384 controls. Patients were seen at the Mayo Clinic in either Minnesota or Florida between Jan. 1, 2009, and Aug. 31, 2018. “Dietary factors were based on a Viocare food frequency questionnaire administered during a baseline in-person study visit,” Dr. Chewcharat and colleagues observed.
During a median follow-up of 4.1 years, 73 patients experienced a symptomatic recurrence. In a fully adjusted analysis, a dietary calcium intake less than 1,200 mg/d was associated with incident stone formation. Similarly, among participants with a fluid intake less than 3,400 mL/d – about nine 12-oz glasses of fluid – was also associated with incident stone formation, as was a lower intake of dietary potassium, caffeine, and phytate. Phytate is an antioxidant found in whole grains, nuts, and other foods that can increase calcium absorption and urinary calcium excretion.
After excluding patients who were taking either a thiazide diuretic or a calcium supplement, lower dietary calcium and potassium, fluid, and phytate intake remained significantly associated with incident stone formation.
However, only lower dietary calcium intake was associated with a higher risk for symptomatic recurrence, although a lower dietary potassium intake was also associated with a higher risk for symptomatic recurrence in an analysis that adjusted for body mass index, fluid, and energy intake.
As the authors suggested, patients may be less keen to adjust their diet to prevent the development of incident kidney stones. On the other hand, they may be much more willing to adjust their diet to prevent their symptomatic recurrence. The Department of Agriculture currently recommends that individuals get approximately 1,200 mg/d of dietary calcium which, given the study results, appears to be justified for the prevention of symptomatic stone recurrence.
A higher-calcium diet is associated with a higher urinary pH, and citrate confers an alkali load which helps protect against the formation of calcium oxalate stones. Foods that are high in potassium also contain more fluid, citrate, and phytate, which, again, have been reported to be protective against kidney stones. “Changing your diet to prevent kidney stones can be very difficult,” Andrew Rule, MD, a nephrologist at the Mayo Clinic said in a statement.
“Thus, knowing the dietary factors that are most important for preventing kidney stone recurrence can help patients and providers know what to prioritize,” he added.
The authors have no conflicts of interest to declare.
A version of this article first appeared on Medscape.com.
as well as their symptomatic recurrence, a population-based study of dietary factors shows.
“Our research is of particular importance as recommendations for preventing symptomatic recurrence of kidney stones has largely been based on dietary factors associated with the incidence rather than the recurrence of stone formation,” Api Chewcharat, MD, Mayo Clinic, Rochester, Minn., said in a video discussing the study.
“We recommend a daily intake of calcium of approximately 1,200 mg and a diet that is high in potassium, especially high in fruits and vegetables, in order to prevent both incident and recurrent symptomatic kidney stone formation,” he stressed.
The study was published online in Mayo Clinic Proceedings.
Lower dietary calcium, potassium, and fluid associated with increased incidence
Some 411 patients with incident symptomatic kidney stone formation were recruited. Diets were compared between them and 384 controls. Patients were seen at the Mayo Clinic in either Minnesota or Florida between Jan. 1, 2009, and Aug. 31, 2018. “Dietary factors were based on a Viocare food frequency questionnaire administered during a baseline in-person study visit,” Dr. Chewcharat and colleagues observed.
During a median follow-up of 4.1 years, 73 patients experienced a symptomatic recurrence. In a fully adjusted analysis, a dietary calcium intake less than 1,200 mg/d was associated with incident stone formation. Similarly, among participants with a fluid intake less than 3,400 mL/d – about nine 12-oz glasses of fluid – was also associated with incident stone formation, as was a lower intake of dietary potassium, caffeine, and phytate. Phytate is an antioxidant found in whole grains, nuts, and other foods that can increase calcium absorption and urinary calcium excretion.
After excluding patients who were taking either a thiazide diuretic or a calcium supplement, lower dietary calcium and potassium, fluid, and phytate intake remained significantly associated with incident stone formation.
However, only lower dietary calcium intake was associated with a higher risk for symptomatic recurrence, although a lower dietary potassium intake was also associated with a higher risk for symptomatic recurrence in an analysis that adjusted for body mass index, fluid, and energy intake.
As the authors suggested, patients may be less keen to adjust their diet to prevent the development of incident kidney stones. On the other hand, they may be much more willing to adjust their diet to prevent their symptomatic recurrence. The Department of Agriculture currently recommends that individuals get approximately 1,200 mg/d of dietary calcium which, given the study results, appears to be justified for the prevention of symptomatic stone recurrence.
A higher-calcium diet is associated with a higher urinary pH, and citrate confers an alkali load which helps protect against the formation of calcium oxalate stones. Foods that are high in potassium also contain more fluid, citrate, and phytate, which, again, have been reported to be protective against kidney stones. “Changing your diet to prevent kidney stones can be very difficult,” Andrew Rule, MD, a nephrologist at the Mayo Clinic said in a statement.
“Thus, knowing the dietary factors that are most important for preventing kidney stone recurrence can help patients and providers know what to prioritize,” he added.
The authors have no conflicts of interest to declare.
A version of this article first appeared on Medscape.com.
FROM MAYO CLINIC PRECEEDINGS
COVID skin manifestations vary by type of variant, U.K. study finds
during the Omicron and Delta waves.
Among the key findings, the study shows that skin involvement during the Omicron wave was less frequent than during the Delta wave (11.4% vs. 17.6%), skin symptoms generally resolved more quickly, and that the risk for skin symptoms was similar whether patients had or had not been vaccinated, according to a team led by Alessia Visconti, PhD, a research fellow in the department of twin research and genetic epidemiology, King’s College, London.
These data are consistent with the experience of those dermatologists who have been following this area closely, according to Esther Freeman, MD, PhD, associate professor of dermatology at Harvard Medical School and director of MGH Global Health Dermatology at Massachusetts General Hospital, both in Boston.
“Anecdotally, we thought we were seeing fewer skin symptoms with Omicron versus Delta and the ancestral strains, and now this study shows it is true,” said Dr. Freeman, who is also principal investigator of the American Academy of Dermatology’s International Dermatology COVID-19 Registry.
The data also confirm that the skin is less likely to be involved than in past waves of COVID-19 infections.
“Up to this point, it was hard to know if we were seeing fewer referrals for COVID-related skin rashes or if clinicians had just become more comfortable with these rashes and were not referring them as often,” added Dr. Freeman, who was among the study coauthors.
Data captured from 348,691 patients
The data from the study was generated by 348,691 users in the United Kingdom of the ZOE COVID study app, a smartphone-based tool introduced relatively early in the pandemic. It asked users to provide demographic data, information on COVID-19 symptoms, including those involving the skin, and treatments. Of 33 COVID-related symptoms included in the app, five related to the skin (acral rash, burning rash, erythematopapular rash, urticarial rash, and unusual hair loss).
While the focus of this study was to compare skin manifestations during the Omicron wave with the Delta wave of COVID-19, the investigators also had data on the experience in 2020 with wild-type COVID-19 that preceded both variants. Overall, this showed a stepwise decline in skin symptoms overall, as well in as skin symptoms that occurred in the absence of systemic symptoms.
“The shift in the skin manifestations makes sense when you think about the change that is also being seen in the systemic symptoms,” said Dr. Freeman, referring to lower rates of cough and loss of smell but higher rates of sore throat and fatigue. “Omicron is achieving immune escape, which is why there is a shift in involved tissues,” she said in an interview.
Previous data collected during the wild-type COVID-19 stage of the pandemic by the same group of investigators showed that 17% of patients reported skin rash as the first symptom of COVID-19 infection, and 21% reported skin rash as the only clinical sign of infection.
In the Delta and Omicron waves, skin rash was an isolated initial symptom in only 0.8% and 0.5% of patients, respectively. (The authors noted that, in the United Kingdom, the first documented samples of the Delta variant were detected in October 2020, and the first documented samples of the Omicron variant were detected in November 2021.)
During the early stages of wild-type COVID, an acral rash was characteristic, occurring in 3.1% of patients, according to the U.K. data. In the Delta wave, acral rashes, at an incidence of 1.1% remained positively correlated with a diagnosis of COVID-19 infection. In the Omicron wave, acral rashes were observed in only 0.7% of patients and were no longer statistically correlated with a positive COVID diagnosis.
Characteristic cutaneous symptoms are evolving
Early in the course of the COVID-19 epidemic, more than 30 types of rashes were observed in patients with COVID-19 infection. Cutaneous symptoms continue to be diverse, but some, such as acral rash, are being seen less frequently. For example, the odds ratio of a positive COVID-19 diagnosis among those with an erythematopapular rash fell from 1.76 to 1.08 between the Delta and Omicron waves.
While specific cutaneous symptoms are less predictive of a diagnosis of COVID-19, clinicians should not discount cutaneous symptoms as a sign of disease, according to Veronique Bataille, MD, PhD, a consultant dermatologist at King’s College.
“You need to keep an open mind” regarding cutaneous signs and a diagnosis of COVID-19, Dr. Bataille, one of the coauthors of the U.K. report, said in an interview. In general, she considers a low threshold of suspicion appropriate. “If the patient has no past history of skin disease and no other triggers for a rash, then, in a high prevalence area, COVID must be suspected.”
In most cases, the rash resolves on its own, but Dr. Bataille emphasized the need for individualized care. Even as the risk of life-threatening COVID-19 infections appears to be diminishing with current variants, cutaneous manifestations can be severe.
“There are cases of long COVID affecting the skin, such as urticaria or a lichenoid erythematopapular rash, both of which can be very pruritic and difficult to control,” she said.
Dr. Freeman echoed the importance of an individualized approach. She agreed that most cutaneous symptoms are self-limited, but there are exceptions and treatments vary for the different types of skin involvement. “I think another point to consider when examining skin lesions is monkey pox. The fact that these are overlapping outbreaks should not be ignored. You need to be alert for both.”
Dr. Visconti, Dr. Freeman, and Dr. Bataille reported no potential conflicts of interest.
during the Omicron and Delta waves.
Among the key findings, the study shows that skin involvement during the Omicron wave was less frequent than during the Delta wave (11.4% vs. 17.6%), skin symptoms generally resolved more quickly, and that the risk for skin symptoms was similar whether patients had or had not been vaccinated, according to a team led by Alessia Visconti, PhD, a research fellow in the department of twin research and genetic epidemiology, King’s College, London.
These data are consistent with the experience of those dermatologists who have been following this area closely, according to Esther Freeman, MD, PhD, associate professor of dermatology at Harvard Medical School and director of MGH Global Health Dermatology at Massachusetts General Hospital, both in Boston.
“Anecdotally, we thought we were seeing fewer skin symptoms with Omicron versus Delta and the ancestral strains, and now this study shows it is true,” said Dr. Freeman, who is also principal investigator of the American Academy of Dermatology’s International Dermatology COVID-19 Registry.
The data also confirm that the skin is less likely to be involved than in past waves of COVID-19 infections.
“Up to this point, it was hard to know if we were seeing fewer referrals for COVID-related skin rashes or if clinicians had just become more comfortable with these rashes and were not referring them as often,” added Dr. Freeman, who was among the study coauthors.
Data captured from 348,691 patients
The data from the study was generated by 348,691 users in the United Kingdom of the ZOE COVID study app, a smartphone-based tool introduced relatively early in the pandemic. It asked users to provide demographic data, information on COVID-19 symptoms, including those involving the skin, and treatments. Of 33 COVID-related symptoms included in the app, five related to the skin (acral rash, burning rash, erythematopapular rash, urticarial rash, and unusual hair loss).
While the focus of this study was to compare skin manifestations during the Omicron wave with the Delta wave of COVID-19, the investigators also had data on the experience in 2020 with wild-type COVID-19 that preceded both variants. Overall, this showed a stepwise decline in skin symptoms overall, as well in as skin symptoms that occurred in the absence of systemic symptoms.
“The shift in the skin manifestations makes sense when you think about the change that is also being seen in the systemic symptoms,” said Dr. Freeman, referring to lower rates of cough and loss of smell but higher rates of sore throat and fatigue. “Omicron is achieving immune escape, which is why there is a shift in involved tissues,” she said in an interview.
Previous data collected during the wild-type COVID-19 stage of the pandemic by the same group of investigators showed that 17% of patients reported skin rash as the first symptom of COVID-19 infection, and 21% reported skin rash as the only clinical sign of infection.
In the Delta and Omicron waves, skin rash was an isolated initial symptom in only 0.8% and 0.5% of patients, respectively. (The authors noted that, in the United Kingdom, the first documented samples of the Delta variant were detected in October 2020, and the first documented samples of the Omicron variant were detected in November 2021.)
During the early stages of wild-type COVID, an acral rash was characteristic, occurring in 3.1% of patients, according to the U.K. data. In the Delta wave, acral rashes, at an incidence of 1.1% remained positively correlated with a diagnosis of COVID-19 infection. In the Omicron wave, acral rashes were observed in only 0.7% of patients and were no longer statistically correlated with a positive COVID diagnosis.
Characteristic cutaneous symptoms are evolving
Early in the course of the COVID-19 epidemic, more than 30 types of rashes were observed in patients with COVID-19 infection. Cutaneous symptoms continue to be diverse, but some, such as acral rash, are being seen less frequently. For example, the odds ratio of a positive COVID-19 diagnosis among those with an erythematopapular rash fell from 1.76 to 1.08 between the Delta and Omicron waves.
While specific cutaneous symptoms are less predictive of a diagnosis of COVID-19, clinicians should not discount cutaneous symptoms as a sign of disease, according to Veronique Bataille, MD, PhD, a consultant dermatologist at King’s College.
“You need to keep an open mind” regarding cutaneous signs and a diagnosis of COVID-19, Dr. Bataille, one of the coauthors of the U.K. report, said in an interview. In general, she considers a low threshold of suspicion appropriate. “If the patient has no past history of skin disease and no other triggers for a rash, then, in a high prevalence area, COVID must be suspected.”
In most cases, the rash resolves on its own, but Dr. Bataille emphasized the need for individualized care. Even as the risk of life-threatening COVID-19 infections appears to be diminishing with current variants, cutaneous manifestations can be severe.
“There are cases of long COVID affecting the skin, such as urticaria or a lichenoid erythematopapular rash, both of which can be very pruritic and difficult to control,” she said.
Dr. Freeman echoed the importance of an individualized approach. She agreed that most cutaneous symptoms are self-limited, but there are exceptions and treatments vary for the different types of skin involvement. “I think another point to consider when examining skin lesions is monkey pox. The fact that these are overlapping outbreaks should not be ignored. You need to be alert for both.”
Dr. Visconti, Dr. Freeman, and Dr. Bataille reported no potential conflicts of interest.
during the Omicron and Delta waves.
Among the key findings, the study shows that skin involvement during the Omicron wave was less frequent than during the Delta wave (11.4% vs. 17.6%), skin symptoms generally resolved more quickly, and that the risk for skin symptoms was similar whether patients had or had not been vaccinated, according to a team led by Alessia Visconti, PhD, a research fellow in the department of twin research and genetic epidemiology, King’s College, London.
These data are consistent with the experience of those dermatologists who have been following this area closely, according to Esther Freeman, MD, PhD, associate professor of dermatology at Harvard Medical School and director of MGH Global Health Dermatology at Massachusetts General Hospital, both in Boston.
“Anecdotally, we thought we were seeing fewer skin symptoms with Omicron versus Delta and the ancestral strains, and now this study shows it is true,” said Dr. Freeman, who is also principal investigator of the American Academy of Dermatology’s International Dermatology COVID-19 Registry.
The data also confirm that the skin is less likely to be involved than in past waves of COVID-19 infections.
“Up to this point, it was hard to know if we were seeing fewer referrals for COVID-related skin rashes or if clinicians had just become more comfortable with these rashes and were not referring them as often,” added Dr. Freeman, who was among the study coauthors.
Data captured from 348,691 patients
The data from the study was generated by 348,691 users in the United Kingdom of the ZOE COVID study app, a smartphone-based tool introduced relatively early in the pandemic. It asked users to provide demographic data, information on COVID-19 symptoms, including those involving the skin, and treatments. Of 33 COVID-related symptoms included in the app, five related to the skin (acral rash, burning rash, erythematopapular rash, urticarial rash, and unusual hair loss).
While the focus of this study was to compare skin manifestations during the Omicron wave with the Delta wave of COVID-19, the investigators also had data on the experience in 2020 with wild-type COVID-19 that preceded both variants. Overall, this showed a stepwise decline in skin symptoms overall, as well in as skin symptoms that occurred in the absence of systemic symptoms.
“The shift in the skin manifestations makes sense when you think about the change that is also being seen in the systemic symptoms,” said Dr. Freeman, referring to lower rates of cough and loss of smell but higher rates of sore throat and fatigue. “Omicron is achieving immune escape, which is why there is a shift in involved tissues,” she said in an interview.
Previous data collected during the wild-type COVID-19 stage of the pandemic by the same group of investigators showed that 17% of patients reported skin rash as the first symptom of COVID-19 infection, and 21% reported skin rash as the only clinical sign of infection.
In the Delta and Omicron waves, skin rash was an isolated initial symptom in only 0.8% and 0.5% of patients, respectively. (The authors noted that, in the United Kingdom, the first documented samples of the Delta variant were detected in October 2020, and the first documented samples of the Omicron variant were detected in November 2021.)
During the early stages of wild-type COVID, an acral rash was characteristic, occurring in 3.1% of patients, according to the U.K. data. In the Delta wave, acral rashes, at an incidence of 1.1% remained positively correlated with a diagnosis of COVID-19 infection. In the Omicron wave, acral rashes were observed in only 0.7% of patients and were no longer statistically correlated with a positive COVID diagnosis.
Characteristic cutaneous symptoms are evolving
Early in the course of the COVID-19 epidemic, more than 30 types of rashes were observed in patients with COVID-19 infection. Cutaneous symptoms continue to be diverse, but some, such as acral rash, are being seen less frequently. For example, the odds ratio of a positive COVID-19 diagnosis among those with an erythematopapular rash fell from 1.76 to 1.08 between the Delta and Omicron waves.
While specific cutaneous symptoms are less predictive of a diagnosis of COVID-19, clinicians should not discount cutaneous symptoms as a sign of disease, according to Veronique Bataille, MD, PhD, a consultant dermatologist at King’s College.
“You need to keep an open mind” regarding cutaneous signs and a diagnosis of COVID-19, Dr. Bataille, one of the coauthors of the U.K. report, said in an interview. In general, she considers a low threshold of suspicion appropriate. “If the patient has no past history of skin disease and no other triggers for a rash, then, in a high prevalence area, COVID must be suspected.”
In most cases, the rash resolves on its own, but Dr. Bataille emphasized the need for individualized care. Even as the risk of life-threatening COVID-19 infections appears to be diminishing with current variants, cutaneous manifestations can be severe.
“There are cases of long COVID affecting the skin, such as urticaria or a lichenoid erythematopapular rash, both of which can be very pruritic and difficult to control,” she said.
Dr. Freeman echoed the importance of an individualized approach. She agreed that most cutaneous symptoms are self-limited, but there are exceptions and treatments vary for the different types of skin involvement. “I think another point to consider when examining skin lesions is monkey pox. The fact that these are overlapping outbreaks should not be ignored. You need to be alert for both.”
Dr. Visconti, Dr. Freeman, and Dr. Bataille reported no potential conflicts of interest.
FROM THE BRITISH JOURNAL OF DERMATOLOGY
Devices to detect skin cancer: FDA advisers offer mixed views
.
So far, the U.S. Food and Drug Administration has cleared two devices. Both are computer-aided skin lesion classification devices meant to help clinicians assess cases of suspected melanoma.
Both were given a class III designation. That classification is intended for products that are considered to have a high risk of harm because of flawed design or implementation. Many such devices are under development, and there has been a proposal to include these devices in class II, which is less restrictive.
The FDA turned to one of its expert panels for advice. At a meeting held on Aug. 29, experts on the panel offered differing views and expressed concerns about the accuracy of these devices.
This was the second day of meetings of the general and plastic surgery devices panel of the FDA’s Medical Devices Advisory Committee. On the previous day, the panel held a wide-ranging discussion about expanding use of skin lesion analyzer devices.
The FDA sought the expert panel’s advice concerning a field that appears to be heating up quickly after relatively quiet times.
Two devices have been approved by the FDA so far, but only one is still being promoted – SciBase AB’s Nevisense. The Swedish company announced in May 2020 that it had received FDA approval for Nevisense 3.0, the third generation of their Nevisense system for early melanoma detection, an AI-based point-of-care system for the noninvasive evaluation of irregular moles.
The other device, known as MelaFind, was acquired by Strata Skin Sciences, but the company said in 2017 that it discontinued research and development, sales, and support activity related to the device, according to a filing with the Securities and Exchange Commission.
But there’s been a swell in recent years in the number of publications related to the use of AI and machine learning, which could give rise to new tools for aiding in the diagnosis of skin conditions, including cancer. Google is among the companies that are involved in these efforts.
So, the FDA asked the expert panel to discuss a series of questions related to how the agency should weigh the risks of computer-aided devices for melanoma diagnosis. The agency also asked the panel to provide feedback about how well risks associated with such devices and tools might be managed and to offer suggestions.
The discussion at the July 29 meeting spun beyond narrow questions about reclassification of the current class III devices to topics involving emerging technology, such as efforts to apply AI to dermatology.
“Innovation continues. Medical device developers are anxious to plan how they might be able to develop the level of evidence that would meet your expectations” for future products, Binita Ashar, MD, a senior official in FDA’s Center for Devices and Radiological Health, told the panel.
Company CEO backs tougher regulation
Simon Grant, the chief executive of SciBase, which markets Nevisense, the first and only skin cancer–detecting device currently on the U.S. market, sought to make a case for sticking with the tougher class III regulations.
Speaking during the public comment session, Mr. Grant said switching to class II designations would weaken the standards used in clearing products that analyze skin lesions so as to put patients at risk.
Under the FDA’s rules, the agency designates as class III devices that present potential unreasonable risk of illness or injury. Only about 10% of devices fall into this category. Such devices include implantable pacemakers and breast implants, as well as SciBase’s Nevisense.
About 43% of medical devices fall into the class II category, which includes powered wheelchairs and some pregnancy test kits, the FDA website says.
Class I medical devices pose minimal potential for harm and tend to be simpler in design. These include enema kits and elastic bandages, the FDA says.
Mr. Grant told the meeting that in his career he has worked on two class III products and about 20 class II products. (He had previously worked at medical startups Synectics Medical and Neoventa, as well as established multinationals such as Medtronic.)
“I can tell you that – practically – the FDA has many fewer sticks and much less control when it comes to class II devices,” he said. He offered an example of a manufacturer of a class II device having more latitude in making small changes to products without notifying the FDA.
In his hypothetical example, such a change could have unintended consequences, and “with AI systems, small changes can result in large and nonlinear or even random effects,” Mr. Grant said. “But it’s too late if the product is on the market and the harm has already occurred,” he said.
The American Society for Dermatologic Surgery Association also protested the reclassifying of approved computer-aided melanoma detection class III devices.
In a statement posted on the FDA website as part of the materials for the meeting, the ASDSA raised a series of concerns about the prospects of expanded U.S. use of tools for assisting in diagnosing melanoma, including ones that would be marketed to consumers.
“To the extent that algorithms and devices for patient self-diagnosis of skin lesions are already widely available, they should be required to include detailed disclaimers that include that they are for entertainment and educational purposes and not a diagnostic device, that they are not approved by dermatologists or a recognized medical regulatory authority for self-diagnosis,” the ASDSA said.
Devices and algorithms in screening tools “are not highly regulated and remain unproven. They may result in wrong diagnoses, missed diagnoses, or over- or underdiagnosis,” the ASDSA added. “Both patients at low risk and those at high risk are better served by scheduling an in-person examination with a board-certified dermatologist, who can also help them determine the appropriate future skin screening schedule that is most appropriate for them.”
‘Stepping stone’
However, there is strong consumer demand for better information about skin conditions, and many patients face hurdles in going to dermatologists.
Google research has shown that consumers are seeking “a stepping stone” between the information they can easily find online and what they could get from a medical professional, said Lily Peng, MD, PhD, a director of product management for the health AI team at Google. Dr. Peng was a scheduled presenter at the July 29 meeting.
Consumers often are looking for more information on common conditions such as acne and poison ivy, and they sometimes face challenges in getting access to clinicians, she said.
“There are many unmet needs for consumers experiencing skin issues, many of which are lower-acuity conditions. There’s a big opportunity to increase accessibility and relevance of health journeys for consumers,” Dr. Peng said. “We have heard from consumers that they would like to have a self-help tool for nonserious conditions so they can decide when to seek medical attention.”
Dr. Peng’s presentation was not directly related to the question of class II or class III designation for existing products. Instead, her talk served as a glimpse into the work already underway in creating apps and tools for consumers.
Google researchers have published a number of studies in recent years about the use of AI to improve dermatology diagnosis.
A 2020 article reported on Google’s test of a form of AI known as deep learning system (DLS) to provide a differential diagnosis of skin conditions. On 963 validation cases, where a rotating panel of three board-certified dermatologists defined the reference standard, the DLS was noninferior to six other dermatologists and was superior to six primary care physicians (PCPs) and six nurse practitioners (NPs), according to a summary of the article.
A 2021 report published in JAMA Network Open said that use of an AI tool was associated with a higher agreement rate with dermatologists’ reference diagnoses for both PCPs and NPs.
In a 2021 blog post, Google scientists wrote that their AI model that powers a tool for checking skin conditions had earned European clearance, known as a CE mark, as a class I medical device.
SkinVision has an app that the company says “is available worldwide (with the exception of the USA and Canada).” The firm’s website includes a link where people in the United States and Canada can sign up for notifications about when SkinVision will be available in these nations.
‘Not ready for prime time’
The FDA panel did not cast formal votes at the July 29 meeting. Rather, the members engaged in broad discussions about risks and potential benefits of new tools for aiding in the detection of skin cancer.
Among the key issues discussed was a question of whether the FDA could impose requirements and restrictions, known as special controls, to provide “reasonable assurance of safety and effectiveness” for computer-aided devices that provide adjunctive diagnostic information to dermatologists about lesions suspicious for melanoma.

Among the potential special controls would be clinical performance testing in regards to rates of the sensitivity (true-positive rate) and specificity (true-negative rate).
The FDA could also look at requirements on software validation and verification and cybersecurity testing, as well as directions on labeling so as to mitigate risk.
Dermatologists serving on the panel called for caution in proceeding with steps that would make it easier for companies to market tools for aiding in melanoma diagnosis than it would be within the class III framework used for MelaFind and Nevisense.
Many expressed concerns about the need to design studies that would answer questions about how well new tools could accurately identify concerning lesions.
The phrase “not ready for prime time” was used at least three times during the discussion.
FDA panelist Maral Skelsey, MD, a skin cancer specialist from Chevy Chase, Maryland, said that over the years, she had used both Nevisense and MelaFind.
She said she had found MelaFind “unusable,” owing in large part to the high number of false positives it generated. The device also was limited as to where on patients’ bodies it could be used.
However, she spoke with enthusiasm about the prospects for better devices to aid in diagnosis of skin lesions. “It’s an area where we’re on the verge, and we really need these devices. There’s a need for patients to be able to examine themselves, for nondermatologists to be able to assess lesions,” Dr. Skelsey said.
But this field is “just not ready for prime time” yet, even with special controls, Dr. Skelsey said. To loosen approval standards too quickly could be a “detriment to what’s coming down the pipeline,” she said.
“It’s harmful to things that are likely to be around the corner,” she said.
FDA panelist Renata Block, PA-C, who works in a Chicago dermatology practice, pressed for maintaining a class III designation. “We are not ready for prime time yet, though the data that is coming down the pipeline on what we have is quite exciting,” Ms. Block said.
FDA panelist Karla V. Ballman, PhD, a statistician from Weill Cornell Medicine, New York, said there would need to be a clear standard for clinical performance before proceeding toward reclassification of devices for aid in detecting melanoma. “I just don’t think it’s ready for prime time at this point and should remain in class III,” she said.
But there was support from some panelists for the idea of a lower bar for clearance, combined with special controls to ensure patient safety.
In expressing her view, FDA panelist Katalin Roth, MD, JD, professor of medicine, George Washington University, Washington, said she was an outlier in her support for the agency’s view that these risks could be managed and that future tools could allow more patients to take a step on the pathway toward critical diagnoses.
“I deal with a lot of people with cancer as a palliative care physician,” Dr. Roth said. “I think what we’re missing here is the issue of time. Melanoma is a terrible disease, and missing the diagnosis is a terrible thing, but I think special controls would be sufficient to counter the concerns of my colleagues on the committee.”
The FDA’s Dr. Ashar ended the meeting with questions posed to one panelist, Veronica Rotemberg, MD, PhD, a dermatologist at Memorial Sloan Kettering Cancer Center in New York.

Dr. Rotemberg has for years been working in the field of research on developing AI and other computer-based tools for detecting and diagnosing melanoma, the deadliest form of skin cancer.
She has been publicly skeptical of the performance of commercial apps that scan moles and other lesions and that claim to identify which are cancerous. A May blog post on the Memorial Sloan Kettering website highlighted a recent British Journal of Dermatology article in which Dr. Rotemberg and coauthors reported on their evaluations of commercial apps. They judged them to be on average only 59% accurate, the blog post said.
However, during an earlier discussion at the meeting, she had spoken more positively about the prospects for using special controls in the near term to mitigate risk, although she said she would have a “very long list” of these requirements.
In the closing exchange with Dr. Ashar, Dr. Rotemberg outlined steps that could potentially ensure the safe use of tools to aid in melanoma screening. These included a need for postmarketing surveillance, which would require evaluation over time of algorithms used in tools meant to detect skin cancer.
“We need to have a mechanism for sampling,” Dr. Rotemberg said. “Most of our data is electronic now anyway, so comparing an algorithm and performance with biopsy results should not be that challenging.”
A version of this article first appeared on Medscape.com.
.
So far, the U.S. Food and Drug Administration has cleared two devices. Both are computer-aided skin lesion classification devices meant to help clinicians assess cases of suspected melanoma.
Both were given a class III designation. That classification is intended for products that are considered to have a high risk of harm because of flawed design or implementation. Many such devices are under development, and there has been a proposal to include these devices in class II, which is less restrictive.
The FDA turned to one of its expert panels for advice. At a meeting held on Aug. 29, experts on the panel offered differing views and expressed concerns about the accuracy of these devices.
This was the second day of meetings of the general and plastic surgery devices panel of the FDA’s Medical Devices Advisory Committee. On the previous day, the panel held a wide-ranging discussion about expanding use of skin lesion analyzer devices.
The FDA sought the expert panel’s advice concerning a field that appears to be heating up quickly after relatively quiet times.
Two devices have been approved by the FDA so far, but only one is still being promoted – SciBase AB’s Nevisense. The Swedish company announced in May 2020 that it had received FDA approval for Nevisense 3.0, the third generation of their Nevisense system for early melanoma detection, an AI-based point-of-care system for the noninvasive evaluation of irregular moles.
The other device, known as MelaFind, was acquired by Strata Skin Sciences, but the company said in 2017 that it discontinued research and development, sales, and support activity related to the device, according to a filing with the Securities and Exchange Commission.
But there’s been a swell in recent years in the number of publications related to the use of AI and machine learning, which could give rise to new tools for aiding in the diagnosis of skin conditions, including cancer. Google is among the companies that are involved in these efforts.
So, the FDA asked the expert panel to discuss a series of questions related to how the agency should weigh the risks of computer-aided devices for melanoma diagnosis. The agency also asked the panel to provide feedback about how well risks associated with such devices and tools might be managed and to offer suggestions.
The discussion at the July 29 meeting spun beyond narrow questions about reclassification of the current class III devices to topics involving emerging technology, such as efforts to apply AI to dermatology.
“Innovation continues. Medical device developers are anxious to plan how they might be able to develop the level of evidence that would meet your expectations” for future products, Binita Ashar, MD, a senior official in FDA’s Center for Devices and Radiological Health, told the panel.
Company CEO backs tougher regulation
Simon Grant, the chief executive of SciBase, which markets Nevisense, the first and only skin cancer–detecting device currently on the U.S. market, sought to make a case for sticking with the tougher class III regulations.
Speaking during the public comment session, Mr. Grant said switching to class II designations would weaken the standards used in clearing products that analyze skin lesions so as to put patients at risk.
Under the FDA’s rules, the agency designates as class III devices that present potential unreasonable risk of illness or injury. Only about 10% of devices fall into this category. Such devices include implantable pacemakers and breast implants, as well as SciBase’s Nevisense.
About 43% of medical devices fall into the class II category, which includes powered wheelchairs and some pregnancy test kits, the FDA website says.
Class I medical devices pose minimal potential for harm and tend to be simpler in design. These include enema kits and elastic bandages, the FDA says.
Mr. Grant told the meeting that in his career he has worked on two class III products and about 20 class II products. (He had previously worked at medical startups Synectics Medical and Neoventa, as well as established multinationals such as Medtronic.)
“I can tell you that – practically – the FDA has many fewer sticks and much less control when it comes to class II devices,” he said. He offered an example of a manufacturer of a class II device having more latitude in making small changes to products without notifying the FDA.
In his hypothetical example, such a change could have unintended consequences, and “with AI systems, small changes can result in large and nonlinear or even random effects,” Mr. Grant said. “But it’s too late if the product is on the market and the harm has already occurred,” he said.
The American Society for Dermatologic Surgery Association also protested the reclassifying of approved computer-aided melanoma detection class III devices.
In a statement posted on the FDA website as part of the materials for the meeting, the ASDSA raised a series of concerns about the prospects of expanded U.S. use of tools for assisting in diagnosing melanoma, including ones that would be marketed to consumers.
“To the extent that algorithms and devices for patient self-diagnosis of skin lesions are already widely available, they should be required to include detailed disclaimers that include that they are for entertainment and educational purposes and not a diagnostic device, that they are not approved by dermatologists or a recognized medical regulatory authority for self-diagnosis,” the ASDSA said.
Devices and algorithms in screening tools “are not highly regulated and remain unproven. They may result in wrong diagnoses, missed diagnoses, or over- or underdiagnosis,” the ASDSA added. “Both patients at low risk and those at high risk are better served by scheduling an in-person examination with a board-certified dermatologist, who can also help them determine the appropriate future skin screening schedule that is most appropriate for them.”
‘Stepping stone’
However, there is strong consumer demand for better information about skin conditions, and many patients face hurdles in going to dermatologists.
Google research has shown that consumers are seeking “a stepping stone” between the information they can easily find online and what they could get from a medical professional, said Lily Peng, MD, PhD, a director of product management for the health AI team at Google. Dr. Peng was a scheduled presenter at the July 29 meeting.
Consumers often are looking for more information on common conditions such as acne and poison ivy, and they sometimes face challenges in getting access to clinicians, she said.
“There are many unmet needs for consumers experiencing skin issues, many of which are lower-acuity conditions. There’s a big opportunity to increase accessibility and relevance of health journeys for consumers,” Dr. Peng said. “We have heard from consumers that they would like to have a self-help tool for nonserious conditions so they can decide when to seek medical attention.”
Dr. Peng’s presentation was not directly related to the question of class II or class III designation for existing products. Instead, her talk served as a glimpse into the work already underway in creating apps and tools for consumers.
Google researchers have published a number of studies in recent years about the use of AI to improve dermatology diagnosis.
A 2020 article reported on Google’s test of a form of AI known as deep learning system (DLS) to provide a differential diagnosis of skin conditions. On 963 validation cases, where a rotating panel of three board-certified dermatologists defined the reference standard, the DLS was noninferior to six other dermatologists and was superior to six primary care physicians (PCPs) and six nurse practitioners (NPs), according to a summary of the article.
A 2021 report published in JAMA Network Open said that use of an AI tool was associated with a higher agreement rate with dermatologists’ reference diagnoses for both PCPs and NPs.
In a 2021 blog post, Google scientists wrote that their AI model that powers a tool for checking skin conditions had earned European clearance, known as a CE mark, as a class I medical device.
SkinVision has an app that the company says “is available worldwide (with the exception of the USA and Canada).” The firm’s website includes a link where people in the United States and Canada can sign up for notifications about when SkinVision will be available in these nations.
‘Not ready for prime time’
The FDA panel did not cast formal votes at the July 29 meeting. Rather, the members engaged in broad discussions about risks and potential benefits of new tools for aiding in the detection of skin cancer.
Among the key issues discussed was a question of whether the FDA could impose requirements and restrictions, known as special controls, to provide “reasonable assurance of safety and effectiveness” for computer-aided devices that provide adjunctive diagnostic information to dermatologists about lesions suspicious for melanoma.
Among the potential special controls would be clinical performance testing in regards to rates of the sensitivity (true-positive rate) and specificity (true-negative rate).
The FDA could also look at requirements on software validation and verification and cybersecurity testing, as well as directions on labeling so as to mitigate risk.
Dermatologists serving on the panel called for caution in proceeding with steps that would make it easier for companies to market tools for aiding in melanoma diagnosis than it would be within the class III framework used for MelaFind and Nevisense.
Many expressed concerns about the need to design studies that would answer questions about how well new tools could accurately identify concerning lesions.
The phrase “not ready for prime time” was used at least three times during the discussion.
FDA panelist Maral Skelsey, MD, a skin cancer specialist from Chevy Chase, Maryland, said that over the years, she had used both Nevisense and MelaFind.
She said she had found MelaFind “unusable,” owing in large part to the high number of false positives it generated. The device also was limited as to where on patients’ bodies it could be used.
However, she spoke with enthusiasm about the prospects for better devices to aid in diagnosis of skin lesions. “It’s an area where we’re on the verge, and we really need these devices. There’s a need for patients to be able to examine themselves, for nondermatologists to be able to assess lesions,” Dr. Skelsey said.
But this field is “just not ready for prime time” yet, even with special controls, Dr. Skelsey said. To loosen approval standards too quickly could be a “detriment to what’s coming down the pipeline,” she said.
“It’s harmful to things that are likely to be around the corner,” she said.
FDA panelist Renata Block, PA-C, who works in a Chicago dermatology practice, pressed for maintaining a class III designation. “We are not ready for prime time yet, though the data that is coming down the pipeline on what we have is quite exciting,” Ms. Block said.
FDA panelist Karla V. Ballman, PhD, a statistician from Weill Cornell Medicine, New York, said there would need to be a clear standard for clinical performance before proceeding toward reclassification of devices for aid in detecting melanoma. “I just don’t think it’s ready for prime time at this point and should remain in class III,” she said.
But there was support from some panelists for the idea of a lower bar for clearance, combined with special controls to ensure patient safety.
In expressing her view, FDA panelist Katalin Roth, MD, JD, professor of medicine, George Washington University, Washington, said she was an outlier in her support for the agency’s view that these risks could be managed and that future tools could allow more patients to take a step on the pathway toward critical diagnoses.
“I deal with a lot of people with cancer as a palliative care physician,” Dr. Roth said. “I think what we’re missing here is the issue of time. Melanoma is a terrible disease, and missing the diagnosis is a terrible thing, but I think special controls would be sufficient to counter the concerns of my colleagues on the committee.”
The FDA’s Dr. Ashar ended the meeting with questions posed to one panelist, Veronica Rotemberg, MD, PhD, a dermatologist at Memorial Sloan Kettering Cancer Center in New York.
Dr. Rotemberg has for years been working in the field of research on developing AI and other computer-based tools for detecting and diagnosing melanoma, the deadliest form of skin cancer.
She has been publicly skeptical of the performance of commercial apps that scan moles and other lesions and that claim to identify which are cancerous. A May blog post on the Memorial Sloan Kettering website highlighted a recent British Journal of Dermatology article in which Dr. Rotemberg and coauthors reported on their evaluations of commercial apps. They judged them to be on average only 59% accurate, the blog post said.
However, during an earlier discussion at the meeting, she had spoken more positively about the prospects for using special controls in the near term to mitigate risk, although she said she would have a “very long list” of these requirements.
In the closing exchange with Dr. Ashar, Dr. Rotemberg outlined steps that could potentially ensure the safe use of tools to aid in melanoma screening. These included a need for postmarketing surveillance, which would require evaluation over time of algorithms used in tools meant to detect skin cancer.
“We need to have a mechanism for sampling,” Dr. Rotemberg said. “Most of our data is electronic now anyway, so comparing an algorithm and performance with biopsy results should not be that challenging.”
A version of this article first appeared on Medscape.com.
.
So far, the U.S. Food and Drug Administration has cleared two devices. Both are computer-aided skin lesion classification devices meant to help clinicians assess cases of suspected melanoma.
Both were given a class III designation. That classification is intended for products that are considered to have a high risk of harm because of flawed design or implementation. Many such devices are under development, and there has been a proposal to include these devices in class II, which is less restrictive.
The FDA turned to one of its expert panels for advice. At a meeting held on Aug. 29, experts on the panel offered differing views and expressed concerns about the accuracy of these devices.
This was the second day of meetings of the general and plastic surgery devices panel of the FDA’s Medical Devices Advisory Committee. On the previous day, the panel held a wide-ranging discussion about expanding use of skin lesion analyzer devices.
The FDA sought the expert panel’s advice concerning a field that appears to be heating up quickly after relatively quiet times.
Two devices have been approved by the FDA so far, but only one is still being promoted – SciBase AB’s Nevisense. The Swedish company announced in May 2020 that it had received FDA approval for Nevisense 3.0, the third generation of their Nevisense system for early melanoma detection, an AI-based point-of-care system for the noninvasive evaluation of irregular moles.
The other device, known as MelaFind, was acquired by Strata Skin Sciences, but the company said in 2017 that it discontinued research and development, sales, and support activity related to the device, according to a filing with the Securities and Exchange Commission.
But there’s been a swell in recent years in the number of publications related to the use of AI and machine learning, which could give rise to new tools for aiding in the diagnosis of skin conditions, including cancer. Google is among the companies that are involved in these efforts.
So, the FDA asked the expert panel to discuss a series of questions related to how the agency should weigh the risks of computer-aided devices for melanoma diagnosis. The agency also asked the panel to provide feedback about how well risks associated with such devices and tools might be managed and to offer suggestions.
The discussion at the July 29 meeting spun beyond narrow questions about reclassification of the current class III devices to topics involving emerging technology, such as efforts to apply AI to dermatology.
“Innovation continues. Medical device developers are anxious to plan how they might be able to develop the level of evidence that would meet your expectations” for future products, Binita Ashar, MD, a senior official in FDA’s Center for Devices and Radiological Health, told the panel.
Company CEO backs tougher regulation
Simon Grant, the chief executive of SciBase, which markets Nevisense, the first and only skin cancer–detecting device currently on the U.S. market, sought to make a case for sticking with the tougher class III regulations.
Speaking during the public comment session, Mr. Grant said switching to class II designations would weaken the standards used in clearing products that analyze skin lesions so as to put patients at risk.
Under the FDA’s rules, the agency designates as class III devices that present potential unreasonable risk of illness or injury. Only about 10% of devices fall into this category. Such devices include implantable pacemakers and breast implants, as well as SciBase’s Nevisense.
About 43% of medical devices fall into the class II category, which includes powered wheelchairs and some pregnancy test kits, the FDA website says.
Class I medical devices pose minimal potential for harm and tend to be simpler in design. These include enema kits and elastic bandages, the FDA says.
Mr. Grant told the meeting that in his career he has worked on two class III products and about 20 class II products. (He had previously worked at medical startups Synectics Medical and Neoventa, as well as established multinationals such as Medtronic.)
“I can tell you that – practically – the FDA has many fewer sticks and much less control when it comes to class II devices,” he said. He offered an example of a manufacturer of a class II device having more latitude in making small changes to products without notifying the FDA.
In his hypothetical example, such a change could have unintended consequences, and “with AI systems, small changes can result in large and nonlinear or even random effects,” Mr. Grant said. “But it’s too late if the product is on the market and the harm has already occurred,” he said.
The American Society for Dermatologic Surgery Association also protested the reclassifying of approved computer-aided melanoma detection class III devices.
In a statement posted on the FDA website as part of the materials for the meeting, the ASDSA raised a series of concerns about the prospects of expanded U.S. use of tools for assisting in diagnosing melanoma, including ones that would be marketed to consumers.
“To the extent that algorithms and devices for patient self-diagnosis of skin lesions are already widely available, they should be required to include detailed disclaimers that include that they are for entertainment and educational purposes and not a diagnostic device, that they are not approved by dermatologists or a recognized medical regulatory authority for self-diagnosis,” the ASDSA said.
Devices and algorithms in screening tools “are not highly regulated and remain unproven. They may result in wrong diagnoses, missed diagnoses, or over- or underdiagnosis,” the ASDSA added. “Both patients at low risk and those at high risk are better served by scheduling an in-person examination with a board-certified dermatologist, who can also help them determine the appropriate future skin screening schedule that is most appropriate for them.”
‘Stepping stone’
However, there is strong consumer demand for better information about skin conditions, and many patients face hurdles in going to dermatologists.
Google research has shown that consumers are seeking “a stepping stone” between the information they can easily find online and what they could get from a medical professional, said Lily Peng, MD, PhD, a director of product management for the health AI team at Google. Dr. Peng was a scheduled presenter at the July 29 meeting.
Consumers often are looking for more information on common conditions such as acne and poison ivy, and they sometimes face challenges in getting access to clinicians, she said.
“There are many unmet needs for consumers experiencing skin issues, many of which are lower-acuity conditions. There’s a big opportunity to increase accessibility and relevance of health journeys for consumers,” Dr. Peng said. “We have heard from consumers that they would like to have a self-help tool for nonserious conditions so they can decide when to seek medical attention.”
Dr. Peng’s presentation was not directly related to the question of class II or class III designation for existing products. Instead, her talk served as a glimpse into the work already underway in creating apps and tools for consumers.
Google researchers have published a number of studies in recent years about the use of AI to improve dermatology diagnosis.
A 2020 article reported on Google’s test of a form of AI known as deep learning system (DLS) to provide a differential diagnosis of skin conditions. On 963 validation cases, where a rotating panel of three board-certified dermatologists defined the reference standard, the DLS was noninferior to six other dermatologists and was superior to six primary care physicians (PCPs) and six nurse practitioners (NPs), according to a summary of the article.
A 2021 report published in JAMA Network Open said that use of an AI tool was associated with a higher agreement rate with dermatologists’ reference diagnoses for both PCPs and NPs.
In a 2021 blog post, Google scientists wrote that their AI model that powers a tool for checking skin conditions had earned European clearance, known as a CE mark, as a class I medical device.
SkinVision has an app that the company says “is available worldwide (with the exception of the USA and Canada).” The firm’s website includes a link where people in the United States and Canada can sign up for notifications about when SkinVision will be available in these nations.
‘Not ready for prime time’
The FDA panel did not cast formal votes at the July 29 meeting. Rather, the members engaged in broad discussions about risks and potential benefits of new tools for aiding in the detection of skin cancer.
Among the key issues discussed was a question of whether the FDA could impose requirements and restrictions, known as special controls, to provide “reasonable assurance of safety and effectiveness” for computer-aided devices that provide adjunctive diagnostic information to dermatologists about lesions suspicious for melanoma.
Among the potential special controls would be clinical performance testing in regards to rates of the sensitivity (true-positive rate) and specificity (true-negative rate).
The FDA could also look at requirements on software validation and verification and cybersecurity testing, as well as directions on labeling so as to mitigate risk.
Dermatologists serving on the panel called for caution in proceeding with steps that would make it easier for companies to market tools for aiding in melanoma diagnosis than it would be within the class III framework used for MelaFind and Nevisense.
Many expressed concerns about the need to design studies that would answer questions about how well new tools could accurately identify concerning lesions.
The phrase “not ready for prime time” was used at least three times during the discussion.
FDA panelist Maral Skelsey, MD, a skin cancer specialist from Chevy Chase, Maryland, said that over the years, she had used both Nevisense and MelaFind.
She said she had found MelaFind “unusable,” owing in large part to the high number of false positives it generated. The device also was limited as to where on patients’ bodies it could be used.
However, she spoke with enthusiasm about the prospects for better devices to aid in diagnosis of skin lesions. “It’s an area where we’re on the verge, and we really need these devices. There’s a need for patients to be able to examine themselves, for nondermatologists to be able to assess lesions,” Dr. Skelsey said.
But this field is “just not ready for prime time” yet, even with special controls, Dr. Skelsey said. To loosen approval standards too quickly could be a “detriment to what’s coming down the pipeline,” she said.
“It’s harmful to things that are likely to be around the corner,” she said.
FDA panelist Renata Block, PA-C, who works in a Chicago dermatology practice, pressed for maintaining a class III designation. “We are not ready for prime time yet, though the data that is coming down the pipeline on what we have is quite exciting,” Ms. Block said.
FDA panelist Karla V. Ballman, PhD, a statistician from Weill Cornell Medicine, New York, said there would need to be a clear standard for clinical performance before proceeding toward reclassification of devices for aid in detecting melanoma. “I just don’t think it’s ready for prime time at this point and should remain in class III,” she said.
But there was support from some panelists for the idea of a lower bar for clearance, combined with special controls to ensure patient safety.
In expressing her view, FDA panelist Katalin Roth, MD, JD, professor of medicine, George Washington University, Washington, said she was an outlier in her support for the agency’s view that these risks could be managed and that future tools could allow more patients to take a step on the pathway toward critical diagnoses.
“I deal with a lot of people with cancer as a palliative care physician,” Dr. Roth said. “I think what we’re missing here is the issue of time. Melanoma is a terrible disease, and missing the diagnosis is a terrible thing, but I think special controls would be sufficient to counter the concerns of my colleagues on the committee.”
The FDA’s Dr. Ashar ended the meeting with questions posed to one panelist, Veronica Rotemberg, MD, PhD, a dermatologist at Memorial Sloan Kettering Cancer Center in New York.
Dr. Rotemberg has for years been working in the field of research on developing AI and other computer-based tools for detecting and diagnosing melanoma, the deadliest form of skin cancer.
She has been publicly skeptical of the performance of commercial apps that scan moles and other lesions and that claim to identify which are cancerous. A May blog post on the Memorial Sloan Kettering website highlighted a recent British Journal of Dermatology article in which Dr. Rotemberg and coauthors reported on their evaluations of commercial apps. They judged them to be on average only 59% accurate, the blog post said.
However, during an earlier discussion at the meeting, she had spoken more positively about the prospects for using special controls in the near term to mitigate risk, although she said she would have a “very long list” of these requirements.
In the closing exchange with Dr. Ashar, Dr. Rotemberg outlined steps that could potentially ensure the safe use of tools to aid in melanoma screening. These included a need for postmarketing surveillance, which would require evaluation over time of algorithms used in tools meant to detect skin cancer.
“We need to have a mechanism for sampling,” Dr. Rotemberg said. “Most of our data is electronic now anyway, so comparing an algorithm and performance with biopsy results should not be that challenging.”
A version of this article first appeared on Medscape.com.
Landmark ALLIANCE results offer tenofovir guidance in HIV/HBV coinfection
MONTREAL – Interim results of ALLIANCE, the first head-to-head trial comparing two different tenofovir-containing antiretroviral regimens for the treatment of HIV and hepatitis B (HBV) coinfection, demonstrate the superiority of bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) over dolutegravir plus tenofovir disoproxil fumarate (DTG + F/TDF), researchers reported at a meeting of the International AIDS Society.
, with more HBV DNA suppression and significantly more seroconversion, reported lead investigator Anchalee Avihingsanon, MD, PhD, at a press conference during the meeting. Dr. Avihingsanon heads the medical department of the HIV Netherlands Australia Thailand Research Collaboration (HIV-NAT) at the Thai Red Cross AIDS Research Centre, Bangkok.
The ongoing phase 3, multicountry study has 48-week results for 243 participants, who were HIV/HBV coinfected and treatment naive. All subjects received three pills of ART per day, with blinded randomization to (active B/F/TAF + placebo DTG + placebo TDF/FTC or placebo B/F/TAF + active DTG + active TDF/FTC). The primary endpoints at 48 weeks were proportion of participants with HIV-1 RNA less than 50 copies/mL and plasma HBV DNA less than 29 IU/mL.
For the HIV endpoint, results showed both the B/F/TAF and DTG + F/TDF arms had high rates of suppression (95% and 91%, respectively, P = .21), but the B/F/TAF group had significantly higher rates of HBV DNA suppression (63% vs 43.4%, P = .0023) and HBeAg seroconversion (23.3% vs. 11.3%), with numerically higher, but not statistically significant differences in HBsAg loss/seroconversion (12.6% vs. 5.8% and 8.4% vs. 3.3%), HBeAg loss (25.6% vs 14.4%), and ALT normalization (73.3% vs 55.3%).
No participant developed treatment-emergent HIV-1 drug resistance while on B/F/TAF, and there were few study-drug–related AEs or discontinuations, she reported.
“There is hardly any good reason to give the two-pill DTG regimen over single-tablet BTG/TAF/FTC in HBV-coinfected people living with HIV [PLWH],” commented Babafemi Taiwo, MD, chief of infectious diseases and professor of medicine at Northwestern University in Evanston, Ill., who was not involved in the research. “This gives me confidence to prescribe bictegravir/TAF/FTC, which has the added advantage of being a single-tablet formulation, to HBV coinfected PLWH,” he said in an interview. However, he added, the results “call for some head-scratching since TAF is not known to be better than TDF for HBV treatment in persons without HIV.”
“The lower response rate of the TDF group is still poorly understood,” agreed Dr. Avihingsanon, emphasizing that “HBV and HIV/HBV are not the same, and TDF and TAF are also different. TAF has slightly more drug-drug interactions than TDF. I guess its end product in the liver might be higher. What is exciting to me is that there was such a high rate of HBsAg loss and HBs seroconversion in HIV/HBV coinfection, which is totally different from HBV monoinfection [< 1% at 48 weeks]. For me as an investigator, this important finding has additional benefit to further explore the immunologic outcome for possible HBV cure strategy.” She said the study remains blinded until week 96, at which time further data may shed light on this question.
“Perhaps a larger study would help clarify impact of TAF versus TDF on measures that did not achieve statistical significance in this study. Long-term follow up to better understand the clinical implications of these results could be helpful as well,” Dr. Taiwo added.
The study was funded by Gilead. Dr. Avihingsanon reported no relevant disclosures. Dr. Taiwo disclosed that he has served as consultant to ViiV/GlaxoSmithKline, Johnson & Johnson, and Merck, and consulted for Gilead on COVID.
A version of this article first appeared on Medscape.com.
MONTREAL – Interim results of ALLIANCE, the first head-to-head trial comparing two different tenofovir-containing antiretroviral regimens for the treatment of HIV and hepatitis B (HBV) coinfection, demonstrate the superiority of bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) over dolutegravir plus tenofovir disoproxil fumarate (DTG + F/TDF), researchers reported at a meeting of the International AIDS Society.
, with more HBV DNA suppression and significantly more seroconversion, reported lead investigator Anchalee Avihingsanon, MD, PhD, at a press conference during the meeting. Dr. Avihingsanon heads the medical department of the HIV Netherlands Australia Thailand Research Collaboration (HIV-NAT) at the Thai Red Cross AIDS Research Centre, Bangkok.
The ongoing phase 3, multicountry study has 48-week results for 243 participants, who were HIV/HBV coinfected and treatment naive. All subjects received three pills of ART per day, with blinded randomization to (active B/F/TAF + placebo DTG + placebo TDF/FTC or placebo B/F/TAF + active DTG + active TDF/FTC). The primary endpoints at 48 weeks were proportion of participants with HIV-1 RNA less than 50 copies/mL and plasma HBV DNA less than 29 IU/mL.
For the HIV endpoint, results showed both the B/F/TAF and DTG + F/TDF arms had high rates of suppression (95% and 91%, respectively, P = .21), but the B/F/TAF group had significantly higher rates of HBV DNA suppression (63% vs 43.4%, P = .0023) and HBeAg seroconversion (23.3% vs. 11.3%), with numerically higher, but not statistically significant differences in HBsAg loss/seroconversion (12.6% vs. 5.8% and 8.4% vs. 3.3%), HBeAg loss (25.6% vs 14.4%), and ALT normalization (73.3% vs 55.3%).
No participant developed treatment-emergent HIV-1 drug resistance while on B/F/TAF, and there were few study-drug–related AEs or discontinuations, she reported.
“There is hardly any good reason to give the two-pill DTG regimen over single-tablet BTG/TAF/FTC in HBV-coinfected people living with HIV [PLWH],” commented Babafemi Taiwo, MD, chief of infectious diseases and professor of medicine at Northwestern University in Evanston, Ill., who was not involved in the research. “This gives me confidence to prescribe bictegravir/TAF/FTC, which has the added advantage of being a single-tablet formulation, to HBV coinfected PLWH,” he said in an interview. However, he added, the results “call for some head-scratching since TAF is not known to be better than TDF for HBV treatment in persons without HIV.”
“The lower response rate of the TDF group is still poorly understood,” agreed Dr. Avihingsanon, emphasizing that “HBV and HIV/HBV are not the same, and TDF and TAF are also different. TAF has slightly more drug-drug interactions than TDF. I guess its end product in the liver might be higher. What is exciting to me is that there was such a high rate of HBsAg loss and HBs seroconversion in HIV/HBV coinfection, which is totally different from HBV monoinfection [< 1% at 48 weeks]. For me as an investigator, this important finding has additional benefit to further explore the immunologic outcome for possible HBV cure strategy.” She said the study remains blinded until week 96, at which time further data may shed light on this question.
“Perhaps a larger study would help clarify impact of TAF versus TDF on measures that did not achieve statistical significance in this study. Long-term follow up to better understand the clinical implications of these results could be helpful as well,” Dr. Taiwo added.
The study was funded by Gilead. Dr. Avihingsanon reported no relevant disclosures. Dr. Taiwo disclosed that he has served as consultant to ViiV/GlaxoSmithKline, Johnson & Johnson, and Merck, and consulted for Gilead on COVID.
A version of this article first appeared on Medscape.com.
MONTREAL – Interim results of ALLIANCE, the first head-to-head trial comparing two different tenofovir-containing antiretroviral regimens for the treatment of HIV and hepatitis B (HBV) coinfection, demonstrate the superiority of bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) over dolutegravir plus tenofovir disoproxil fumarate (DTG + F/TDF), researchers reported at a meeting of the International AIDS Society.
, with more HBV DNA suppression and significantly more seroconversion, reported lead investigator Anchalee Avihingsanon, MD, PhD, at a press conference during the meeting. Dr. Avihingsanon heads the medical department of the HIV Netherlands Australia Thailand Research Collaboration (HIV-NAT) at the Thai Red Cross AIDS Research Centre, Bangkok.
The ongoing phase 3, multicountry study has 48-week results for 243 participants, who were HIV/HBV coinfected and treatment naive. All subjects received three pills of ART per day, with blinded randomization to (active B/F/TAF + placebo DTG + placebo TDF/FTC or placebo B/F/TAF + active DTG + active TDF/FTC). The primary endpoints at 48 weeks were proportion of participants with HIV-1 RNA less than 50 copies/mL and plasma HBV DNA less than 29 IU/mL.
For the HIV endpoint, results showed both the B/F/TAF and DTG + F/TDF arms had high rates of suppression (95% and 91%, respectively, P = .21), but the B/F/TAF group had significantly higher rates of HBV DNA suppression (63% vs 43.4%, P = .0023) and HBeAg seroconversion (23.3% vs. 11.3%), with numerically higher, but not statistically significant differences in HBsAg loss/seroconversion (12.6% vs. 5.8% and 8.4% vs. 3.3%), HBeAg loss (25.6% vs 14.4%), and ALT normalization (73.3% vs 55.3%).
No participant developed treatment-emergent HIV-1 drug resistance while on B/F/TAF, and there were few study-drug–related AEs or discontinuations, she reported.
“There is hardly any good reason to give the two-pill DTG regimen over single-tablet BTG/TAF/FTC in HBV-coinfected people living with HIV [PLWH],” commented Babafemi Taiwo, MD, chief of infectious diseases and professor of medicine at Northwestern University in Evanston, Ill., who was not involved in the research. “This gives me confidence to prescribe bictegravir/TAF/FTC, which has the added advantage of being a single-tablet formulation, to HBV coinfected PLWH,” he said in an interview. However, he added, the results “call for some head-scratching since TAF is not known to be better than TDF for HBV treatment in persons without HIV.”
“The lower response rate of the TDF group is still poorly understood,” agreed Dr. Avihingsanon, emphasizing that “HBV and HIV/HBV are not the same, and TDF and TAF are also different. TAF has slightly more drug-drug interactions than TDF. I guess its end product in the liver might be higher. What is exciting to me is that there was such a high rate of HBsAg loss and HBs seroconversion in HIV/HBV coinfection, which is totally different from HBV monoinfection [< 1% at 48 weeks]. For me as an investigator, this important finding has additional benefit to further explore the immunologic outcome for possible HBV cure strategy.” She said the study remains blinded until week 96, at which time further data may shed light on this question.
“Perhaps a larger study would help clarify impact of TAF versus TDF on measures that did not achieve statistical significance in this study. Long-term follow up to better understand the clinical implications of these results could be helpful as well,” Dr. Taiwo added.
The study was funded by Gilead. Dr. Avihingsanon reported no relevant disclosures. Dr. Taiwo disclosed that he has served as consultant to ViiV/GlaxoSmithKline, Johnson & Johnson, and Merck, and consulted for Gilead on COVID.
A version of this article first appeared on Medscape.com.
AT AIDS 2022
Sexual assault flagged as a possible psychosis trigger
A new study sheds light on some of the risk factors for the development of psychosis, including the potentially causative role of sexual assault.
Investigators conducted an exposome-wide association analysis on more than 155,000 individuals. Of more than 140 correlates of psychotic experiences that they identified, they narrowed it down to 36 variables, which they further explored using Mendelian randomization analysis.
On the other hand, having experienced a physical violent crime, cannabis use, and prolonged worry after embarrassment showed a pleiotropic association and appeared to be an aftereffect of psychotic experience.

“From a public health perspective, we need more investment in comprehensive strategies to prevent traumatic experiences at the population level to decrease the burden of psychosis,” senior author Sinan Gülöksüz, MD, PhD, associate professor in the department of psychiatry and neuropsychiatry, Maastricht University Medical Center, the Netherlands, said in an interview.
“From a clinical perspective, clinicians should be aware of the harmful influence of traumatic experiences on mental health and address this through interventions such as trauma-informed care,” he said.
The study was published online in JAMA Psychiatry.
‘Disentangling’ cause and effect
“Previous research has shown associations between psychosis and a few environmental factors, such as substance use, urbanicity, pregnancy complications, and traumatic experiences, but research has so far investigated only a few specific environmental factors by singling them out in individual studies,” Dr. Gülöksüz said.
“Yet, environment is a much more complex and interactive network that includes many factors shaping our health – where we live, what we eat, our lifestyle preferences and habits such as exercise and smoking, and our social surrounding,” he continued. “Rarely has it been possible to understand whether these environmental factors have causal roles in developing psychosis.”
To investigate the question, the researchers turned to the UK Biobank, one of the largest population-based datasets in the world. The current study focused on individuals with completed data on mental questionnaires that assessed psychotic experiences (n = 155,247; mean [SD] age, 55.94 [7.74] years; 57% female).
They began by conducting an exposome-wide association study, using logistic regression analyses with psychotic experiences as the outcome and adjusting all analyses for age and sex.
“Initially, we identified many associations between environmental factors and psychotic experiences in this large cohort,” Dr. Gülöksüz reported.
In the final multivariable model, variables associated with psychotic experiences were further analyzed using “genetically informed approaches to probe potential associations.”
The researchers utilized Mendelian randomization (MR) methodology “to disentangle cause and effect in this observational study,” Dr. Gülöksüz said. “This method reduces confounding and reverse causation in observational studies by using genetic variants that have been passed on from generation to generation randomly as instruments.”
MR analysis “has allowed us to assess whether these associations reflect potentially causal influences of environmental factors on psychotic experiences,” he added.
Well-studied and unexplored risk factors
The researchers identified 162 variables associated with psychotic experiences in the discovery dataset and were able to replicate 148. When these 148 variables were subjected to multivariable analyses, 36 were found to be statistically significantly associated with psychotic experiences. Of these variables, 28 had “significant genetic overlap” with psychotic experiences.
When the researchers conducted one-sample MR analyses, they found forward associations with three variables and reverse associations with three variables.
Forward associations were found with ever having experienced sexual assault (odds ratio [OR], 1.32; 95% confidence interval [CI], 1.14-1.52; P = 2.67), and forward associations (with pleiotropy) were found with ever having experienced a physically violent crime and risk-taking behavior (OR, 1.25, 95% CI, 1.11-1.41; P = 3.28 and OR, 1.21, 95% CI, 1.08-1.35; P = 1.34, respectively).
“The allele scores for these 3 variables explained 0.03% to 0.23% variance of the corresponding variable” and the F statistics “ranged from 21.53 to 181.84, indicating that the results did not suffer from a weak-instrument bias,” the authors reported.
The researchers calculated an instrument based on increasing psychotic experiences risk allele scores and found that these scores explained 0.14% variance of psychotic experiences (F statistic, 19.26).
Using that calculation, they found a reverse association with having experienced a physically violent crime (OR, 1.08; 95% CI, 1.04-1.13; P = 3.92 × 10-4), cannabis use (OR, 1.11; 95% CI, 1.06-1.15; P = 2.64 × 10-6), and worrying too long after embarrassment (OR, 1.06; 95% CI, 1.03-1.10; P = 3.96 × 10-4). They then validated these associations.
The presence of all five correlates was associated with tenfold increased odds of psychotic experiences (OR, 10.63; 95% CI, 8.27-13.65, P = 1.2 × 10-114).
“Associations with psychotic experiences were found with both well-studied and unexplored multiple correlated variables,” the authors stated.
Era of ‘big data’
In a comment, Chirag Patel, PhD, associate professor of biomedical informatics at Harvard Medical School, Boston, who was not involved with the study, said he thought the study was “a nice example of a data-driven and comprehensive study of the environment coupled with attempts to triangulate evidence from genetics, made possible by biobank data.

“To guide public health policies and implementation of prevention strategies for psychosis, we need more systematic analyses and triangulate evidence with genetically informed methods to identify potentially modifiable risk factors in the era of ‘big data,’ ” he said.
“For instance, traumatic experiences contribute to poor mental and physical health, including psychosis,” Dr. Gülöksüz added.
The Kootstra Talent Fellowship, the Ophelia Research Project, and the Vidi Award from the Netherlands Scientific Organization provided funding to individual investigators. Dr. Gülöksüz and coauthors declared no relevant financial conflicts. Dr. Patel served as a reviewer on the study.
A version of this article first appeared on Medscape.com.
A new study sheds light on some of the risk factors for the development of psychosis, including the potentially causative role of sexual assault.
Investigators conducted an exposome-wide association analysis on more than 155,000 individuals. Of more than 140 correlates of psychotic experiences that they identified, they narrowed it down to 36 variables, which they further explored using Mendelian randomization analysis.
On the other hand, having experienced a physical violent crime, cannabis use, and prolonged worry after embarrassment showed a pleiotropic association and appeared to be an aftereffect of psychotic experience.
“From a public health perspective, we need more investment in comprehensive strategies to prevent traumatic experiences at the population level to decrease the burden of psychosis,” senior author Sinan Gülöksüz, MD, PhD, associate professor in the department of psychiatry and neuropsychiatry, Maastricht University Medical Center, the Netherlands, said in an interview.
“From a clinical perspective, clinicians should be aware of the harmful influence of traumatic experiences on mental health and address this through interventions such as trauma-informed care,” he said.
The study was published online in JAMA Psychiatry.
‘Disentangling’ cause and effect
“Previous research has shown associations between psychosis and a few environmental factors, such as substance use, urbanicity, pregnancy complications, and traumatic experiences, but research has so far investigated only a few specific environmental factors by singling them out in individual studies,” Dr. Gülöksüz said.
“Yet, environment is a much more complex and interactive network that includes many factors shaping our health – where we live, what we eat, our lifestyle preferences and habits such as exercise and smoking, and our social surrounding,” he continued. “Rarely has it been possible to understand whether these environmental factors have causal roles in developing psychosis.”
To investigate the question, the researchers turned to the UK Biobank, one of the largest population-based datasets in the world. The current study focused on individuals with completed data on mental questionnaires that assessed psychotic experiences (n = 155,247; mean [SD] age, 55.94 [7.74] years; 57% female).
They began by conducting an exposome-wide association study, using logistic regression analyses with psychotic experiences as the outcome and adjusting all analyses for age and sex.
“Initially, we identified many associations between environmental factors and psychotic experiences in this large cohort,” Dr. Gülöksüz reported.
In the final multivariable model, variables associated with psychotic experiences were further analyzed using “genetically informed approaches to probe potential associations.”
The researchers utilized Mendelian randomization (MR) methodology “to disentangle cause and effect in this observational study,” Dr. Gülöksüz said. “This method reduces confounding and reverse causation in observational studies by using genetic variants that have been passed on from generation to generation randomly as instruments.”
MR analysis “has allowed us to assess whether these associations reflect potentially causal influences of environmental factors on psychotic experiences,” he added.
Well-studied and unexplored risk factors
The researchers identified 162 variables associated with psychotic experiences in the discovery dataset and were able to replicate 148. When these 148 variables were subjected to multivariable analyses, 36 were found to be statistically significantly associated with psychotic experiences. Of these variables, 28 had “significant genetic overlap” with psychotic experiences.
When the researchers conducted one-sample MR analyses, they found forward associations with three variables and reverse associations with three variables.
Forward associations were found with ever having experienced sexual assault (odds ratio [OR], 1.32; 95% confidence interval [CI], 1.14-1.52; P = 2.67), and forward associations (with pleiotropy) were found with ever having experienced a physically violent crime and risk-taking behavior (OR, 1.25, 95% CI, 1.11-1.41; P = 3.28 and OR, 1.21, 95% CI, 1.08-1.35; P = 1.34, respectively).
“The allele scores for these 3 variables explained 0.03% to 0.23% variance of the corresponding variable” and the F statistics “ranged from 21.53 to 181.84, indicating that the results did not suffer from a weak-instrument bias,” the authors reported.
The researchers calculated an instrument based on increasing psychotic experiences risk allele scores and found that these scores explained 0.14% variance of psychotic experiences (F statistic, 19.26).
Using that calculation, they found a reverse association with having experienced a physically violent crime (OR, 1.08; 95% CI, 1.04-1.13; P = 3.92 × 10-4), cannabis use (OR, 1.11; 95% CI, 1.06-1.15; P = 2.64 × 10-6), and worrying too long after embarrassment (OR, 1.06; 95% CI, 1.03-1.10; P = 3.96 × 10-4). They then validated these associations.
The presence of all five correlates was associated with tenfold increased odds of psychotic experiences (OR, 10.63; 95% CI, 8.27-13.65, P = 1.2 × 10-114).
“Associations with psychotic experiences were found with both well-studied and unexplored multiple correlated variables,” the authors stated.
Era of ‘big data’
In a comment, Chirag Patel, PhD, associate professor of biomedical informatics at Harvard Medical School, Boston, who was not involved with the study, said he thought the study was “a nice example of a data-driven and comprehensive study of the environment coupled with attempts to triangulate evidence from genetics, made possible by biobank data.
“To guide public health policies and implementation of prevention strategies for psychosis, we need more systematic analyses and triangulate evidence with genetically informed methods to identify potentially modifiable risk factors in the era of ‘big data,’ ” he said.
“For instance, traumatic experiences contribute to poor mental and physical health, including psychosis,” Dr. Gülöksüz added.
The Kootstra Talent Fellowship, the Ophelia Research Project, and the Vidi Award from the Netherlands Scientific Organization provided funding to individual investigators. Dr. Gülöksüz and coauthors declared no relevant financial conflicts. Dr. Patel served as a reviewer on the study.
A version of this article first appeared on Medscape.com.
A new study sheds light on some of the risk factors for the development of psychosis, including the potentially causative role of sexual assault.
Investigators conducted an exposome-wide association analysis on more than 155,000 individuals. Of more than 140 correlates of psychotic experiences that they identified, they narrowed it down to 36 variables, which they further explored using Mendelian randomization analysis.
On the other hand, having experienced a physical violent crime, cannabis use, and prolonged worry after embarrassment showed a pleiotropic association and appeared to be an aftereffect of psychotic experience.
“From a public health perspective, we need more investment in comprehensive strategies to prevent traumatic experiences at the population level to decrease the burden of psychosis,” senior author Sinan Gülöksüz, MD, PhD, associate professor in the department of psychiatry and neuropsychiatry, Maastricht University Medical Center, the Netherlands, said in an interview.
“From a clinical perspective, clinicians should be aware of the harmful influence of traumatic experiences on mental health and address this through interventions such as trauma-informed care,” he said.
The study was published online in JAMA Psychiatry.
‘Disentangling’ cause and effect
“Previous research has shown associations between psychosis and a few environmental factors, such as substance use, urbanicity, pregnancy complications, and traumatic experiences, but research has so far investigated only a few specific environmental factors by singling them out in individual studies,” Dr. Gülöksüz said.
“Yet, environment is a much more complex and interactive network that includes many factors shaping our health – where we live, what we eat, our lifestyle preferences and habits such as exercise and smoking, and our social surrounding,” he continued. “Rarely has it been possible to understand whether these environmental factors have causal roles in developing psychosis.”
To investigate the question, the researchers turned to the UK Biobank, one of the largest population-based datasets in the world. The current study focused on individuals with completed data on mental questionnaires that assessed psychotic experiences (n = 155,247; mean [SD] age, 55.94 [7.74] years; 57% female).
They began by conducting an exposome-wide association study, using logistic regression analyses with psychotic experiences as the outcome and adjusting all analyses for age and sex.
“Initially, we identified many associations between environmental factors and psychotic experiences in this large cohort,” Dr. Gülöksüz reported.
In the final multivariable model, variables associated with psychotic experiences were further analyzed using “genetically informed approaches to probe potential associations.”
The researchers utilized Mendelian randomization (MR) methodology “to disentangle cause and effect in this observational study,” Dr. Gülöksüz said. “This method reduces confounding and reverse causation in observational studies by using genetic variants that have been passed on from generation to generation randomly as instruments.”
MR analysis “has allowed us to assess whether these associations reflect potentially causal influences of environmental factors on psychotic experiences,” he added.
Well-studied and unexplored risk factors
The researchers identified 162 variables associated with psychotic experiences in the discovery dataset and were able to replicate 148. When these 148 variables were subjected to multivariable analyses, 36 were found to be statistically significantly associated with psychotic experiences. Of these variables, 28 had “significant genetic overlap” with psychotic experiences.
When the researchers conducted one-sample MR analyses, they found forward associations with three variables and reverse associations with three variables.
Forward associations were found with ever having experienced sexual assault (odds ratio [OR], 1.32; 95% confidence interval [CI], 1.14-1.52; P = 2.67), and forward associations (with pleiotropy) were found with ever having experienced a physically violent crime and risk-taking behavior (OR, 1.25, 95% CI, 1.11-1.41; P = 3.28 and OR, 1.21, 95% CI, 1.08-1.35; P = 1.34, respectively).
“The allele scores for these 3 variables explained 0.03% to 0.23% variance of the corresponding variable” and the F statistics “ranged from 21.53 to 181.84, indicating that the results did not suffer from a weak-instrument bias,” the authors reported.
The researchers calculated an instrument based on increasing psychotic experiences risk allele scores and found that these scores explained 0.14% variance of psychotic experiences (F statistic, 19.26).
Using that calculation, they found a reverse association with having experienced a physically violent crime (OR, 1.08; 95% CI, 1.04-1.13; P = 3.92 × 10-4), cannabis use (OR, 1.11; 95% CI, 1.06-1.15; P = 2.64 × 10-6), and worrying too long after embarrassment (OR, 1.06; 95% CI, 1.03-1.10; P = 3.96 × 10-4). They then validated these associations.
The presence of all five correlates was associated with tenfold increased odds of psychotic experiences (OR, 10.63; 95% CI, 8.27-13.65, P = 1.2 × 10-114).
“Associations with psychotic experiences were found with both well-studied and unexplored multiple correlated variables,” the authors stated.
Era of ‘big data’
In a comment, Chirag Patel, PhD, associate professor of biomedical informatics at Harvard Medical School, Boston, who was not involved with the study, said he thought the study was “a nice example of a data-driven and comprehensive study of the environment coupled with attempts to triangulate evidence from genetics, made possible by biobank data.
“To guide public health policies and implementation of prevention strategies for psychosis, we need more systematic analyses and triangulate evidence with genetically informed methods to identify potentially modifiable risk factors in the era of ‘big data,’ ” he said.
“For instance, traumatic experiences contribute to poor mental and physical health, including psychosis,” Dr. Gülöksüz added.
The Kootstra Talent Fellowship, the Ophelia Research Project, and the Vidi Award from the Netherlands Scientific Organization provided funding to individual investigators. Dr. Gülöksüz and coauthors declared no relevant financial conflicts. Dr. Patel served as a reviewer on the study.
A version of this article first appeared on Medscape.com.
FROM JAMA PSYCHIATRY