User login
Abortion laws link to state-level mortality
States that have moderate state abortion laws had lower rates of maternal, fetal, and infant mortality, but not lower all-cause mortality, in reproductive-aged females compared with states that have restrictive laws, new research using 2000-2019 data indicates.
Additionally, having a higher number of laws that restrict abortion in a state was linked with higher maternal and infant mortality in the state, the study states.
Mortality increases with number of laws
“Each additional abortion regulation was associated with an increase in maternal mortality (1.09/100,000 live births; 95% confidence interval, 0.36-1.82) and infant mortality (0.20/1,000 live births; 95% CI, 0.12-0.26),” the authors write.
Lorie M. Harper, MD, MSCI, with the department of women’s health, University of Texas at Austin, led a team that simultaneously studied four categories of mortality: all-cause mortality in females ages 15-49 years; maternal mortality; infant mortality; and fetal mortality.
Her team did a retrospective cohort study using the Centers for Disease Control and Prevention’s WONDER (Wide-ranging ONline Data for Epidemiologic Research) database. WONDER collects publicly available data with information on mortality by state.
Data were available from 2000 to 2019 for all-cause, maternal, and infant mortality. Fetal mortality data were available from 2005 to 2019.
Findings were published ahead of print in February’s Obstetrics & Gynecology.
Though the study was done before the Supreme Court decision overturning Roe v. Wade in June 2022, its findings may shed light on potential trends depending on states’ decisions.
In the wake of the Dobbs v. Jackson Women’s Health Organization, an estimated 33 million U.S. women will live in states without available abortion services, the authors note.
State abortion laws changed dramatically in the study period
The authors chose the 2-decade time frame because data could be accessed for both maternal and infant mortality for all the years and because state level abortion laws changed dramatically in that time.
The Guttmacher Institute has analyzed each state’s abortion policy landscape and scored states as restrictive, moderate, or supportive. Certain types of abortion laws were associated with higher rates of all-cause mortality in reproductive-age females.
Those laws included trigger laws (the laws that automatically outlaw abortion in a state when federal law is overturned), laws that limit access to medication abortion, and parental consent laws, according to the paper.
Additionally, states that restrict access to abortion have higher rates of maternal and infant death, even after accounting for the general health of the population.
Trigger-law states have strong mortality association
Blair G. Darney, PhD, MPH, with the department of obstetrics and gynecology, Oregon Health & Science University and the OHSU-PSU School of Public Health in Portland, and two OHSU coauthors note in an accompanying editorial that having a trigger law in place was associated with elevations in all four mortality measures. However, trigger laws had not yet been enacted during the study.
The existence of trigger laws is likely a proxy for other factors, they write.
“[T]he relationship between trigger laws and increased mortality may more likely be explained by other factors that were not considered in the analysis than by laws that were not enacted at the time of the study,” the editorialists write.
Those factors may include lack of Medicaid expansion, socioeconomic inequities, and other policies.
The editorialists also caution that just because some types of abortion restrictions don’t appear to increase mortality, it doesn’t mean they aren’t harmful.
“For example, laws prohibiting private or Medicaid insurance coverage for abortions were not associated with maternal mortality, but these laws may simply shift the burden of payment to the individual seeking an abortion or be mitigated by funds that support an individual’s out-of-pocket cost for care. The lack of an association may therefore reflect women’s resilience and their ability to obtain needed health care in the face of financial challenges,” they write.
They point out that, conversely, Targeted Regulation of Abortion Providers (TRAP) laws, which supporters say protect women, have been associated instead with increases in maternal mortality.
Dr. Harper and study coauthors, noting that the relationship between abortion laws and mortality is complex, urge states with restrictive abortion laws to consider proven countermeasures to offset the rates, including Medicaid expansion.
One coauthor served on a medical advisory board, was a site primary investigator for several clinical trials, and received royalties from UpToDate for two topics related to trial of labor after cesarean. The other authors did not report any potential conflicts of interest. Dr. Darney’s institution receives research funding from Organon and the Office of Population Affairs on which she is the primary investigator, and she is a member of the board of directors of the Society of Family Planning and a deputy editor at Contraception. She has received an honorarium from ACOG for committee work. The other editorialists did not report any potential conflicts of interest.
States that have moderate state abortion laws had lower rates of maternal, fetal, and infant mortality, but not lower all-cause mortality, in reproductive-aged females compared with states that have restrictive laws, new research using 2000-2019 data indicates.
Additionally, having a higher number of laws that restrict abortion in a state was linked with higher maternal and infant mortality in the state, the study states.
Mortality increases with number of laws
“Each additional abortion regulation was associated with an increase in maternal mortality (1.09/100,000 live births; 95% confidence interval, 0.36-1.82) and infant mortality (0.20/1,000 live births; 95% CI, 0.12-0.26),” the authors write.
Lorie M. Harper, MD, MSCI, with the department of women’s health, University of Texas at Austin, led a team that simultaneously studied four categories of mortality: all-cause mortality in females ages 15-49 years; maternal mortality; infant mortality; and fetal mortality.
Her team did a retrospective cohort study using the Centers for Disease Control and Prevention’s WONDER (Wide-ranging ONline Data for Epidemiologic Research) database. WONDER collects publicly available data with information on mortality by state.
Data were available from 2000 to 2019 for all-cause, maternal, and infant mortality. Fetal mortality data were available from 2005 to 2019.
Findings were published ahead of print in February’s Obstetrics & Gynecology.
Though the study was done before the Supreme Court decision overturning Roe v. Wade in June 2022, its findings may shed light on potential trends depending on states’ decisions.
In the wake of the Dobbs v. Jackson Women’s Health Organization, an estimated 33 million U.S. women will live in states without available abortion services, the authors note.
State abortion laws changed dramatically in the study period
The authors chose the 2-decade time frame because data could be accessed for both maternal and infant mortality for all the years and because state level abortion laws changed dramatically in that time.
The Guttmacher Institute has analyzed each state’s abortion policy landscape and scored states as restrictive, moderate, or supportive. Certain types of abortion laws were associated with higher rates of all-cause mortality in reproductive-age females.
Those laws included trigger laws (the laws that automatically outlaw abortion in a state when federal law is overturned), laws that limit access to medication abortion, and parental consent laws, according to the paper.
Additionally, states that restrict access to abortion have higher rates of maternal and infant death, even after accounting for the general health of the population.
Trigger-law states have strong mortality association
Blair G. Darney, PhD, MPH, with the department of obstetrics and gynecology, Oregon Health & Science University and the OHSU-PSU School of Public Health in Portland, and two OHSU coauthors note in an accompanying editorial that having a trigger law in place was associated with elevations in all four mortality measures. However, trigger laws had not yet been enacted during the study.
The existence of trigger laws is likely a proxy for other factors, they write.
“[T]he relationship between trigger laws and increased mortality may more likely be explained by other factors that were not considered in the analysis than by laws that were not enacted at the time of the study,” the editorialists write.
Those factors may include lack of Medicaid expansion, socioeconomic inequities, and other policies.
The editorialists also caution that just because some types of abortion restrictions don’t appear to increase mortality, it doesn’t mean they aren’t harmful.
“For example, laws prohibiting private or Medicaid insurance coverage for abortions were not associated with maternal mortality, but these laws may simply shift the burden of payment to the individual seeking an abortion or be mitigated by funds that support an individual’s out-of-pocket cost for care. The lack of an association may therefore reflect women’s resilience and their ability to obtain needed health care in the face of financial challenges,” they write.
They point out that, conversely, Targeted Regulation of Abortion Providers (TRAP) laws, which supporters say protect women, have been associated instead with increases in maternal mortality.
Dr. Harper and study coauthors, noting that the relationship between abortion laws and mortality is complex, urge states with restrictive abortion laws to consider proven countermeasures to offset the rates, including Medicaid expansion.
One coauthor served on a medical advisory board, was a site primary investigator for several clinical trials, and received royalties from UpToDate for two topics related to trial of labor after cesarean. The other authors did not report any potential conflicts of interest. Dr. Darney’s institution receives research funding from Organon and the Office of Population Affairs on which she is the primary investigator, and she is a member of the board of directors of the Society of Family Planning and a deputy editor at Contraception. She has received an honorarium from ACOG for committee work. The other editorialists did not report any potential conflicts of interest.
States that have moderate state abortion laws had lower rates of maternal, fetal, and infant mortality, but not lower all-cause mortality, in reproductive-aged females compared with states that have restrictive laws, new research using 2000-2019 data indicates.
Additionally, having a higher number of laws that restrict abortion in a state was linked with higher maternal and infant mortality in the state, the study states.
Mortality increases with number of laws
“Each additional abortion regulation was associated with an increase in maternal mortality (1.09/100,000 live births; 95% confidence interval, 0.36-1.82) and infant mortality (0.20/1,000 live births; 95% CI, 0.12-0.26),” the authors write.
Lorie M. Harper, MD, MSCI, with the department of women’s health, University of Texas at Austin, led a team that simultaneously studied four categories of mortality: all-cause mortality in females ages 15-49 years; maternal mortality; infant mortality; and fetal mortality.
Her team did a retrospective cohort study using the Centers for Disease Control and Prevention’s WONDER (Wide-ranging ONline Data for Epidemiologic Research) database. WONDER collects publicly available data with information on mortality by state.
Data were available from 2000 to 2019 for all-cause, maternal, and infant mortality. Fetal mortality data were available from 2005 to 2019.
Findings were published ahead of print in February’s Obstetrics & Gynecology.
Though the study was done before the Supreme Court decision overturning Roe v. Wade in June 2022, its findings may shed light on potential trends depending on states’ decisions.
In the wake of the Dobbs v. Jackson Women’s Health Organization, an estimated 33 million U.S. women will live in states without available abortion services, the authors note.
State abortion laws changed dramatically in the study period
The authors chose the 2-decade time frame because data could be accessed for both maternal and infant mortality for all the years and because state level abortion laws changed dramatically in that time.
The Guttmacher Institute has analyzed each state’s abortion policy landscape and scored states as restrictive, moderate, or supportive. Certain types of abortion laws were associated with higher rates of all-cause mortality in reproductive-age females.
Those laws included trigger laws (the laws that automatically outlaw abortion in a state when federal law is overturned), laws that limit access to medication abortion, and parental consent laws, according to the paper.
Additionally, states that restrict access to abortion have higher rates of maternal and infant death, even after accounting for the general health of the population.
Trigger-law states have strong mortality association
Blair G. Darney, PhD, MPH, with the department of obstetrics and gynecology, Oregon Health & Science University and the OHSU-PSU School of Public Health in Portland, and two OHSU coauthors note in an accompanying editorial that having a trigger law in place was associated with elevations in all four mortality measures. However, trigger laws had not yet been enacted during the study.
The existence of trigger laws is likely a proxy for other factors, they write.
“[T]he relationship between trigger laws and increased mortality may more likely be explained by other factors that were not considered in the analysis than by laws that were not enacted at the time of the study,” the editorialists write.
Those factors may include lack of Medicaid expansion, socioeconomic inequities, and other policies.
The editorialists also caution that just because some types of abortion restrictions don’t appear to increase mortality, it doesn’t mean they aren’t harmful.
“For example, laws prohibiting private or Medicaid insurance coverage for abortions were not associated with maternal mortality, but these laws may simply shift the burden of payment to the individual seeking an abortion or be mitigated by funds that support an individual’s out-of-pocket cost for care. The lack of an association may therefore reflect women’s resilience and their ability to obtain needed health care in the face of financial challenges,” they write.
They point out that, conversely, Targeted Regulation of Abortion Providers (TRAP) laws, which supporters say protect women, have been associated instead with increases in maternal mortality.
Dr. Harper and study coauthors, noting that the relationship between abortion laws and mortality is complex, urge states with restrictive abortion laws to consider proven countermeasures to offset the rates, including Medicaid expansion.
One coauthor served on a medical advisory board, was a site primary investigator for several clinical trials, and received royalties from UpToDate for two topics related to trial of labor after cesarean. The other authors did not report any potential conflicts of interest. Dr. Darney’s institution receives research funding from Organon and the Office of Population Affairs on which she is the primary investigator, and she is a member of the board of directors of the Society of Family Planning and a deputy editor at Contraception. She has received an honorarium from ACOG for committee work. The other editorialists did not report any potential conflicts of interest.
FROM OBSTETRICS & GYNECOLOGY
Year in Review: How Targeted Drug Therapies Have Expanded Breast Cancer Treatment Options in 2022

Breast cancer (BC) is the most diagnosed cancer and the second leading cause of cancer deaths in women. In 2022, more than 275,000 women were diagnosed with BC, and at least 43,000 of these cases resulted in death. With targeted drug therapy for treating BC now approved by the US Food and Drug Administration (FDA) and available (or in the late phases of clinical trials and pending availability and FDA approval), clinicians are beginning to be able to move away from a “one-size-fits-all” treatment approach that has been used in the past, enhancing prognosis and survival rates in their patients living with BC.
The new targeted drug therapies available are more precise and individualized. They treat patients more effectively because they are based on the patient’s own biology. These therapies open the possibility of having more valuable treatment options, which can be beneficial for the outcome of many patients diagnosed with BC—especially the highly aggressive forms that were previously difficult to treat.
In March 2022, the FDA approved the drug olaparib to treat HER2-, high-risk, early breast cancer (EBC). The approval was made after the conclusion of the phase 3 OlympiA trial. The clinical trial results showed a statistically significant improvement in overall survival rates (by 32%) with adjuvant olaparib compared with placebo for germline BRCA1/2-mutated EBC.
In August 2022, the FDA approved the antibody drug conjugate fam-trastuzumab deruxtecan-nxki (or T-DXd), which is the first FDA-approved therapy targeted to treat patients who have the HER2-low BC subtype. It is also approved for patients with unresectable or metastatic HER2+ breast cancer who have already been treated with 2 or more prior anti-HER2–based therapies in the metastatic setting. The approval of T-DXd was given on the basis of DESTINY-Breast04, a randomized, multicenter, open-label clinical trial that was published in June 2022. T-DXd had been previously approved in HER2+ metastatic breast cancer.
The results from the phase 3 CAPItello-291 clinical trial of capivasertib in combination with fulvestrant suggests the combination could become a new treatment option for patients with hormone receptor–positive, HER2-low, locally advanced or metastatic BC following recurrence or progression after treatment with endocrine therapy and a CDK4/6 inhibitor. Capivasertib is a novel, selective, ATP-competitive, pan-AKT kinase inhibitor. In clinical trials, the drug was shown to successfully block activity of the cancer-driving protein molecule AKT. This research was presented at the 2022 San Antonio Breast Cancer Symposium, and the findings demonstrated a significant improvement in the overall population, as well as the subgroup of patients with PI3K pathway–altered tumors.
The year 2022 was full of exciting discoveries in the field of targeted drug therapies for treating BC, expanding patients’ treatment options and giving hope to people who have been diagnosed with breast cancer and their loved ones. In addition, emerging technologies such as immunotherapy and new antibody-drug conjugates continue to be evaluated as potential treatment options for treating breast cancer in the near future.
Breast cancer (BC) is the most diagnosed cancer and the second leading cause of cancer deaths in women. In 2022, more than 275,000 women were diagnosed with BC, and at least 43,000 of these cases resulted in death. With targeted drug therapy for treating BC now approved by the US Food and Drug Administration (FDA) and available (or in the late phases of clinical trials and pending availability and FDA approval), clinicians are beginning to be able to move away from a “one-size-fits-all” treatment approach that has been used in the past, enhancing prognosis and survival rates in their patients living with BC.
The new targeted drug therapies available are more precise and individualized. They treat patients more effectively because they are based on the patient’s own biology. These therapies open the possibility of having more valuable treatment options, which can be beneficial for the outcome of many patients diagnosed with BC—especially the highly aggressive forms that were previously difficult to treat.
In March 2022, the FDA approved the drug olaparib to treat HER2-, high-risk, early breast cancer (EBC). The approval was made after the conclusion of the phase 3 OlympiA trial. The clinical trial results showed a statistically significant improvement in overall survival rates (by 32%) with adjuvant olaparib compared with placebo for germline BRCA1/2-mutated EBC.
In August 2022, the FDA approved the antibody drug conjugate fam-trastuzumab deruxtecan-nxki (or T-DXd), which is the first FDA-approved therapy targeted to treat patients who have the HER2-low BC subtype. It is also approved for patients with unresectable or metastatic HER2+ breast cancer who have already been treated with 2 or more prior anti-HER2–based therapies in the metastatic setting. The approval of T-DXd was given on the basis of DESTINY-Breast04, a randomized, multicenter, open-label clinical trial that was published in June 2022. T-DXd had been previously approved in HER2+ metastatic breast cancer.
The results from the phase 3 CAPItello-291 clinical trial of capivasertib in combination with fulvestrant suggests the combination could become a new treatment option for patients with hormone receptor–positive, HER2-low, locally advanced or metastatic BC following recurrence or progression after treatment with endocrine therapy and a CDK4/6 inhibitor. Capivasertib is a novel, selective, ATP-competitive, pan-AKT kinase inhibitor. In clinical trials, the drug was shown to successfully block activity of the cancer-driving protein molecule AKT. This research was presented at the 2022 San Antonio Breast Cancer Symposium, and the findings demonstrated a significant improvement in the overall population, as well as the subgroup of patients with PI3K pathway–altered tumors.
The year 2022 was full of exciting discoveries in the field of targeted drug therapies for treating BC, expanding patients’ treatment options and giving hope to people who have been diagnosed with breast cancer and their loved ones. In addition, emerging technologies such as immunotherapy and new antibody-drug conjugates continue to be evaluated as potential treatment options for treating breast cancer in the near future.
Breast cancer (BC) is the most diagnosed cancer and the second leading cause of cancer deaths in women. In 2022, more than 275,000 women were diagnosed with BC, and at least 43,000 of these cases resulted in death. With targeted drug therapy for treating BC now approved by the US Food and Drug Administration (FDA) and available (or in the late phases of clinical trials and pending availability and FDA approval), clinicians are beginning to be able to move away from a “one-size-fits-all” treatment approach that has been used in the past, enhancing prognosis and survival rates in their patients living with BC.
The new targeted drug therapies available are more precise and individualized. They treat patients more effectively because they are based on the patient’s own biology. These therapies open the possibility of having more valuable treatment options, which can be beneficial for the outcome of many patients diagnosed with BC—especially the highly aggressive forms that were previously difficult to treat.
In March 2022, the FDA approved the drug olaparib to treat HER2-, high-risk, early breast cancer (EBC). The approval was made after the conclusion of the phase 3 OlympiA trial. The clinical trial results showed a statistically significant improvement in overall survival rates (by 32%) with adjuvant olaparib compared with placebo for germline BRCA1/2-mutated EBC.
In August 2022, the FDA approved the antibody drug conjugate fam-trastuzumab deruxtecan-nxki (or T-DXd), which is the first FDA-approved therapy targeted to treat patients who have the HER2-low BC subtype. It is also approved for patients with unresectable or metastatic HER2+ breast cancer who have already been treated with 2 or more prior anti-HER2–based therapies in the metastatic setting. The approval of T-DXd was given on the basis of DESTINY-Breast04, a randomized, multicenter, open-label clinical trial that was published in June 2022. T-DXd had been previously approved in HER2+ metastatic breast cancer.
The results from the phase 3 CAPItello-291 clinical trial of capivasertib in combination with fulvestrant suggests the combination could become a new treatment option for patients with hormone receptor–positive, HER2-low, locally advanced or metastatic BC following recurrence or progression after treatment with endocrine therapy and a CDK4/6 inhibitor. Capivasertib is a novel, selective, ATP-competitive, pan-AKT kinase inhibitor. In clinical trials, the drug was shown to successfully block activity of the cancer-driving protein molecule AKT. This research was presented at the 2022 San Antonio Breast Cancer Symposium, and the findings demonstrated a significant improvement in the overall population, as well as the subgroup of patients with PI3K pathway–altered tumors.
The year 2022 was full of exciting discoveries in the field of targeted drug therapies for treating BC, expanding patients’ treatment options and giving hope to people who have been diagnosed with breast cancer and their loved ones. In addition, emerging technologies such as immunotherapy and new antibody-drug conjugates continue to be evaluated as potential treatment options for treating breast cancer in the near future.
We Have the Tools to Prevent Cervical Cancer— So Why Are Rates Increasing?
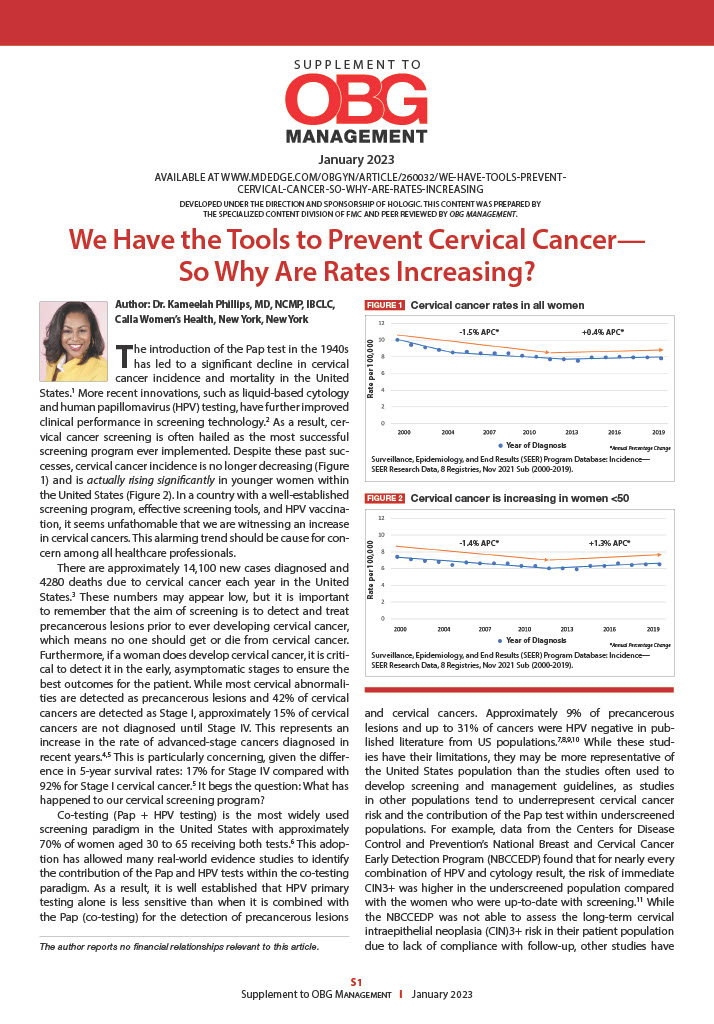
Cervical cancer screening is often hailed as the most successful screening program ever implemented. Despite these past successes, cervical cancer incidence is no longer decreasing and is actually rising significantly in younger women within the United States. In a country with a well-established screening program, effective screening tools, and HPV vaccination, it seems unfathomable that we are witnessing an increase in cervical cancers. This alarming trend should be cause for concern among all healthcare professionals.
Cervical cancer screening is often hailed as the most successful screening program ever implemented. Despite these past successes, cervical cancer incidence is no longer decreasing and is actually rising significantly in younger women within the United States. In a country with a well-established screening program, effective screening tools, and HPV vaccination, it seems unfathomable that we are witnessing an increase in cervical cancers. This alarming trend should be cause for concern among all healthcare professionals.
Cervical cancer screening is often hailed as the most successful screening program ever implemented. Despite these past successes, cervical cancer incidence is no longer decreasing and is actually rising significantly in younger women within the United States. In a country with a well-established screening program, effective screening tools, and HPV vaccination, it seems unfathomable that we are witnessing an increase in cervical cancers. This alarming trend should be cause for concern among all healthcare professionals.
The anecdote as antidote: Psychiatric paradigms in Disney films
A common refrain in psychiatry is that the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision, (DSM-5-TR), published in 2022, is the best we can do.

Since the DSM-III was released in 1980, the American Psychiatric Association, which publishes the manual, has espoused the position that we should list symptoms, in a manner that is reminiscent of a checklist. For example, having a depressed mood on most days for a 2-week period, or a loss of interest in pleasurable things, as well as 4 additional symptoms – among them changes in appetite, changes in sleep, changes in psychomotor activity, fatigue, worthlessness, poor concentration, or thoughts of death – can lead to a diagnosis of a major depressive episode as part of a major depressive disorder.
Criticisms of this approach can be apparent. Patients subjected to such checklists, including being repeatedly asked to complete the Patient Health Questionnaire 9 (PHQ-9), which closely follows those criteria, can feel lost and even alienated by their providers. After all, one can ask all those questions and make a diagnosis of depression without even knowing about the patient’s stressors, their history, or their social context.

The DSM permits the diagnosis of psychiatric disorders without an understanding of the narrative of the patient. In its defense, the DSM is not a textbook of psychiatry, it is a guide on how to diagnose individuals. The DSM does not demand that psychiatrists only ask about the symptoms on the checklists; it is the providers who can choose to dismiss asking about the important facets of one’s life.
Yet every time we attend a lecture that starts by enumerating the DSM symptoms of the disorder being discussed, we are left with the dissatisfying impression that a specialist of this disorder should have a more nuanced and interesting description of their disorder of study. This feeling of discontent is compounded when we see a movie that encompasses so much of what is missing in today’s psychiatric parlance, and even more so if that movie is ostensibly made for children. Movies, by design, are particularly adept at encapsulating the narrative of someone’s life in a way that psychiatry can learn from.
Other than the embarrassment of not knowing a patient outside the checklist, the importance of narrative cannot be understated. Dr. Erik Erikson rightfully suggested that the point of life is “the acceptance of one’s one and only life cycle”1 or rather to know it was okay to have been oneself without additions or substitutions. Therefore, one must know what it has meant to be themselves to reconcile this question and achieve Ego Integrity rather than disgust and despair. Narrative is the way in which we understand who we are and what it has meant to be ourselves. An understanding of our personal narrative presents a unique opportunity in expressing what is missing in the DSM. Below, we provide two of our favorite examples in Disney films, among many.
‘Ratatouille’ (2007)
One of the missing features of the DSM is its inability to explain to patients the intrapsychic processes that guide us. One of these processes is how our values can lead us to a deep sense of guilt, shame, and the resulting feelings of alienation. It is extremely common for patients to enter our clinical practice feeling shackled by beliefs that they should accomplish more and be more than they are.
The animated film “Ratatouille” does an excellent job at addressing this feeling. The film follows Remy, the protagonist rat, and his adventures as he explores his passion for cooking. Remy teams up with the inept but good-natured human Alfredo Linguini and guides him through cooking while hiding under his chef’s hat. The primary antagonist, Anton Ego, is a particularly harsh food critic. His presence and appearance are somber. He exudes disdain. His trim physique and scarf suggest a man that will break and react to anything, and his skull-shaped typewriter in his coffin-shaped office informs the viewer that he is out to kill with his cruel words. Anton Ego serves as our projected super-ego. He is not an external judge but the judgment deep inside ourselves, goading us to be better with such severity that we are ultimately left feeling condemned.
Remy is the younger of two siblings. He is less physically adept but more intellectual than his older brother, who does not understand why Remy isn’t content eating scraps from the garbage like the rest of their rat clan. Remy is the creative part within us that wants to challenge the status quo and try something new. Remy also represents our shame and guilt for leaving our home. On one hand, we want to dare greatly, in this case at being an extraordinary chef, but on the other we are shy and cook in secret, hiding within the hat of another person. Remy struggles with the deep feeling that we do not deserve our success, that our family will leave us for being who we are, and that we are better off isolating and segregating from our challenges.
The movie concludes that through talent and hard work, our critics will accept us. Furthermore, once accepted for what we do, we can be further accepted for who we are. The movie ends with Remy cooking the eponymous dish ratatouille. He prepares it so remarkably well, the dish transports Anton Ego back to a sublime experience of eating ratatouille as a child, a touching moment which not only underscores food’s evocative link to memory but gives a glimpse at Anton Ego’s own narrative.
Ego is first won over by the dish, and only afterward learns of Remy’s true identity. Remy’s talent is undeniable though, and even the stuffy Ego must accept the film’s theme that “Anyone can cook,” even a rat – the rat that we all sometimes feel we are deep inside, rotten to the core but trying so hard to be accepted by others, and ultimately by ourselves. In the end, we overcome the disgust inherent in the imagery of a rat in a kitchen and instead embrace our hero’s achievement of ego integrity as he combines his identities as a member of a clan of rats, and one of Paris’s finest chefs.
While modern psychiatry can favor looking at people through the lens of biology rather than narrative, “Ratatouille” can serve as a reminder of the powerful unconscious forces that guide our lives. “Ratatouille” is not a successful movie only because of the compelling narrative, but also because the narrative matches the important psychic paradigms that psychiatry once embraced.
‘Inside Out’ (2015)
Another missing feature of the DSM is its inability to explain how symptoms feel and manifest psychologically. One such feeling is that of control – whether one is in control of one’s life, feelings, and action or rather a victim of external forces. It is extremely common for patients to enter our clinical practice feeling traumatized by the life they’ve lived and powerless to produce any change. Part of our role is to guide them through this journey from the object of their lives to the subject of their lives.
In the animated feature “Inside Out,” Riley, a preteen girl, goes through the tribulation of growing up and learning about herself. This seemingly happy child, content playing hockey with her best friend, Meg, on the picturesque frozen lakes of Minnesota, reaches her inevitable conflict. Her parents uproot her life, moving the family to San Francisco. By doing so, they disconnect her from her school, her friends, and her hobbies. While all this is happening, we spend time inside Riley’s psyche with the personified characters of Riley’s emotions as they affect her decisions and daily actions amidst the backdrop of her core memories and islands of personality.
During the move, her parents seemingly change and ultimately destroy every facet of Riley’s sense of self, which is animated as the collapse of her personality islands. Her best friend engages Riley in a video call just to inform her that she has a new friend who plays hockey equally well. Her parents do not hear Riley’s concerns and are portrayed as distracted by their adult problems. Riley feels ridiculed in her new school and unable to share her feelings with her parents, who ask her to still be their “happy girl” and indirectly ask her to fake pleasure to alleviate their own anxiety.
The climax of the movie is when Riley decides to run away from San Francisco and her parents, to return to her perceived true home, Minnesota. The climax is resolved when Riley realizes that her parents’ love, representing the connection we have to others, transcends her need for control. To some degree, we are all powerless in the face of the tremendous forces of life and share the difficult task of accepting the cards we were dealt, thus making the story of Riley so compelling.
Additionally, the climax is further resolved by another argument that psychiatry (and the DSM) should consider embracing. Emotions are not all symptoms and living without negative emotion is not the goal of life. Riley grows from preteen to teenager, and from object to subject of her life, by realizing that her symptoms/feelings are not just nuisances to avoid and hide, but the key to meaning. Our anger drives us to try hard. Our fear protects us from harm. Our sadness attracts the warmth and care of others. Our disgust protects us physically from noxious material (symbolized as a dreaded broccoli floret for preteen Riley) and socially by encouraging us to share societal norms. Similarly, patients and people in general would benefit by being taught that, while symptoms may permit the better assessment of psychiatric conditions using the DSM, life is much more than that.
It is unfair to blame the DSM for things it was not designed to do. The DSM doesn’t advertise itself as a guidebook of all behaviors, at all times. However, for a variety of reasons, it has become the main way psychiatry describes people. While we commend the APA for its effort and do not know that we could make it any better, we are frequently happily reminded that in about 90 minutes, filmmakers are able to display an empathic understanding of personal narratives that biologic psychiatry can miss.
Dr. Pulido is a psychiatry resident at the University of California, San Diego. She is interested in women’s mental health, medical education, and outpatient psychiatry. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. Erikson, EH. Childhood and society (New York: WW Norton, 1950).
A common refrain in psychiatry is that the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision, (DSM-5-TR), published in 2022, is the best we can do.
Since the DSM-III was released in 1980, the American Psychiatric Association, which publishes the manual, has espoused the position that we should list symptoms, in a manner that is reminiscent of a checklist. For example, having a depressed mood on most days for a 2-week period, or a loss of interest in pleasurable things, as well as 4 additional symptoms – among them changes in appetite, changes in sleep, changes in psychomotor activity, fatigue, worthlessness, poor concentration, or thoughts of death – can lead to a diagnosis of a major depressive episode as part of a major depressive disorder.
Criticisms of this approach can be apparent. Patients subjected to such checklists, including being repeatedly asked to complete the Patient Health Questionnaire 9 (PHQ-9), which closely follows those criteria, can feel lost and even alienated by their providers. After all, one can ask all those questions and make a diagnosis of depression without even knowing about the patient’s stressors, their history, or their social context.
The DSM permits the diagnosis of psychiatric disorders without an understanding of the narrative of the patient. In its defense, the DSM is not a textbook of psychiatry, it is a guide on how to diagnose individuals. The DSM does not demand that psychiatrists only ask about the symptoms on the checklists; it is the providers who can choose to dismiss asking about the important facets of one’s life.
Yet every time we attend a lecture that starts by enumerating the DSM symptoms of the disorder being discussed, we are left with the dissatisfying impression that a specialist of this disorder should have a more nuanced and interesting description of their disorder of study. This feeling of discontent is compounded when we see a movie that encompasses so much of what is missing in today’s psychiatric parlance, and even more so if that movie is ostensibly made for children. Movies, by design, are particularly adept at encapsulating the narrative of someone’s life in a way that psychiatry can learn from.
Other than the embarrassment of not knowing a patient outside the checklist, the importance of narrative cannot be understated. Dr. Erik Erikson rightfully suggested that the point of life is “the acceptance of one’s one and only life cycle”1 or rather to know it was okay to have been oneself without additions or substitutions. Therefore, one must know what it has meant to be themselves to reconcile this question and achieve Ego Integrity rather than disgust and despair. Narrative is the way in which we understand who we are and what it has meant to be ourselves. An understanding of our personal narrative presents a unique opportunity in expressing what is missing in the DSM. Below, we provide two of our favorite examples in Disney films, among many.
‘Ratatouille’ (2007)
One of the missing features of the DSM is its inability to explain to patients the intrapsychic processes that guide us. One of these processes is how our values can lead us to a deep sense of guilt, shame, and the resulting feelings of alienation. It is extremely common for patients to enter our clinical practice feeling shackled by beliefs that they should accomplish more and be more than they are.
The animated film “Ratatouille” does an excellent job at addressing this feeling. The film follows Remy, the protagonist rat, and his adventures as he explores his passion for cooking. Remy teams up with the inept but good-natured human Alfredo Linguini and guides him through cooking while hiding under his chef’s hat. The primary antagonist, Anton Ego, is a particularly harsh food critic. His presence and appearance are somber. He exudes disdain. His trim physique and scarf suggest a man that will break and react to anything, and his skull-shaped typewriter in his coffin-shaped office informs the viewer that he is out to kill with his cruel words. Anton Ego serves as our projected super-ego. He is not an external judge but the judgment deep inside ourselves, goading us to be better with such severity that we are ultimately left feeling condemned.
Remy is the younger of two siblings. He is less physically adept but more intellectual than his older brother, who does not understand why Remy isn’t content eating scraps from the garbage like the rest of their rat clan. Remy is the creative part within us that wants to challenge the status quo and try something new. Remy also represents our shame and guilt for leaving our home. On one hand, we want to dare greatly, in this case at being an extraordinary chef, but on the other we are shy and cook in secret, hiding within the hat of another person. Remy struggles with the deep feeling that we do not deserve our success, that our family will leave us for being who we are, and that we are better off isolating and segregating from our challenges.
The movie concludes that through talent and hard work, our critics will accept us. Furthermore, once accepted for what we do, we can be further accepted for who we are. The movie ends with Remy cooking the eponymous dish ratatouille. He prepares it so remarkably well, the dish transports Anton Ego back to a sublime experience of eating ratatouille as a child, a touching moment which not only underscores food’s evocative link to memory but gives a glimpse at Anton Ego’s own narrative.
Ego is first won over by the dish, and only afterward learns of Remy’s true identity. Remy’s talent is undeniable though, and even the stuffy Ego must accept the film’s theme that “Anyone can cook,” even a rat – the rat that we all sometimes feel we are deep inside, rotten to the core but trying so hard to be accepted by others, and ultimately by ourselves. In the end, we overcome the disgust inherent in the imagery of a rat in a kitchen and instead embrace our hero’s achievement of ego integrity as he combines his identities as a member of a clan of rats, and one of Paris’s finest chefs.
While modern psychiatry can favor looking at people through the lens of biology rather than narrative, “Ratatouille” can serve as a reminder of the powerful unconscious forces that guide our lives. “Ratatouille” is not a successful movie only because of the compelling narrative, but also because the narrative matches the important psychic paradigms that psychiatry once embraced.
‘Inside Out’ (2015)
Another missing feature of the DSM is its inability to explain how symptoms feel and manifest psychologically. One such feeling is that of control – whether one is in control of one’s life, feelings, and action or rather a victim of external forces. It is extremely common for patients to enter our clinical practice feeling traumatized by the life they’ve lived and powerless to produce any change. Part of our role is to guide them through this journey from the object of their lives to the subject of their lives.
In the animated feature “Inside Out,” Riley, a preteen girl, goes through the tribulation of growing up and learning about herself. This seemingly happy child, content playing hockey with her best friend, Meg, on the picturesque frozen lakes of Minnesota, reaches her inevitable conflict. Her parents uproot her life, moving the family to San Francisco. By doing so, they disconnect her from her school, her friends, and her hobbies. While all this is happening, we spend time inside Riley’s psyche with the personified characters of Riley’s emotions as they affect her decisions and daily actions amidst the backdrop of her core memories and islands of personality.
During the move, her parents seemingly change and ultimately destroy every facet of Riley’s sense of self, which is animated as the collapse of her personality islands. Her best friend engages Riley in a video call just to inform her that she has a new friend who plays hockey equally well. Her parents do not hear Riley’s concerns and are portrayed as distracted by their adult problems. Riley feels ridiculed in her new school and unable to share her feelings with her parents, who ask her to still be their “happy girl” and indirectly ask her to fake pleasure to alleviate their own anxiety.
The climax of the movie is when Riley decides to run away from San Francisco and her parents, to return to her perceived true home, Minnesota. The climax is resolved when Riley realizes that her parents’ love, representing the connection we have to others, transcends her need for control. To some degree, we are all powerless in the face of the tremendous forces of life and share the difficult task of accepting the cards we were dealt, thus making the story of Riley so compelling.
Additionally, the climax is further resolved by another argument that psychiatry (and the DSM) should consider embracing. Emotions are not all symptoms and living without negative emotion is not the goal of life. Riley grows from preteen to teenager, and from object to subject of her life, by realizing that her symptoms/feelings are not just nuisances to avoid and hide, but the key to meaning. Our anger drives us to try hard. Our fear protects us from harm. Our sadness attracts the warmth and care of others. Our disgust protects us physically from noxious material (symbolized as a dreaded broccoli floret for preteen Riley) and socially by encouraging us to share societal norms. Similarly, patients and people in general would benefit by being taught that, while symptoms may permit the better assessment of psychiatric conditions using the DSM, life is much more than that.
It is unfair to blame the DSM for things it was not designed to do. The DSM doesn’t advertise itself as a guidebook of all behaviors, at all times. However, for a variety of reasons, it has become the main way psychiatry describes people. While we commend the APA for its effort and do not know that we could make it any better, we are frequently happily reminded that in about 90 minutes, filmmakers are able to display an empathic understanding of personal narratives that biologic psychiatry can miss.
Dr. Pulido is a psychiatry resident at the University of California, San Diego. She is interested in women’s mental health, medical education, and outpatient psychiatry. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. Erikson, EH. Childhood and society (New York: WW Norton, 1950).
A common refrain in psychiatry is that the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision, (DSM-5-TR), published in 2022, is the best we can do.
Since the DSM-III was released in 1980, the American Psychiatric Association, which publishes the manual, has espoused the position that we should list symptoms, in a manner that is reminiscent of a checklist. For example, having a depressed mood on most days for a 2-week period, or a loss of interest in pleasurable things, as well as 4 additional symptoms – among them changes in appetite, changes in sleep, changes in psychomotor activity, fatigue, worthlessness, poor concentration, or thoughts of death – can lead to a diagnosis of a major depressive episode as part of a major depressive disorder.
Criticisms of this approach can be apparent. Patients subjected to such checklists, including being repeatedly asked to complete the Patient Health Questionnaire 9 (PHQ-9), which closely follows those criteria, can feel lost and even alienated by their providers. After all, one can ask all those questions and make a diagnosis of depression without even knowing about the patient’s stressors, their history, or their social context.
The DSM permits the diagnosis of psychiatric disorders without an understanding of the narrative of the patient. In its defense, the DSM is not a textbook of psychiatry, it is a guide on how to diagnose individuals. The DSM does not demand that psychiatrists only ask about the symptoms on the checklists; it is the providers who can choose to dismiss asking about the important facets of one’s life.
Yet every time we attend a lecture that starts by enumerating the DSM symptoms of the disorder being discussed, we are left with the dissatisfying impression that a specialist of this disorder should have a more nuanced and interesting description of their disorder of study. This feeling of discontent is compounded when we see a movie that encompasses so much of what is missing in today’s psychiatric parlance, and even more so if that movie is ostensibly made for children. Movies, by design, are particularly adept at encapsulating the narrative of someone’s life in a way that psychiatry can learn from.
Other than the embarrassment of not knowing a patient outside the checklist, the importance of narrative cannot be understated. Dr. Erik Erikson rightfully suggested that the point of life is “the acceptance of one’s one and only life cycle”1 or rather to know it was okay to have been oneself without additions or substitutions. Therefore, one must know what it has meant to be themselves to reconcile this question and achieve Ego Integrity rather than disgust and despair. Narrative is the way in which we understand who we are and what it has meant to be ourselves. An understanding of our personal narrative presents a unique opportunity in expressing what is missing in the DSM. Below, we provide two of our favorite examples in Disney films, among many.
‘Ratatouille’ (2007)
One of the missing features of the DSM is its inability to explain to patients the intrapsychic processes that guide us. One of these processes is how our values can lead us to a deep sense of guilt, shame, and the resulting feelings of alienation. It is extremely common for patients to enter our clinical practice feeling shackled by beliefs that they should accomplish more and be more than they are.
The animated film “Ratatouille” does an excellent job at addressing this feeling. The film follows Remy, the protagonist rat, and his adventures as he explores his passion for cooking. Remy teams up with the inept but good-natured human Alfredo Linguini and guides him through cooking while hiding under his chef’s hat. The primary antagonist, Anton Ego, is a particularly harsh food critic. His presence and appearance are somber. He exudes disdain. His trim physique and scarf suggest a man that will break and react to anything, and his skull-shaped typewriter in his coffin-shaped office informs the viewer that he is out to kill with his cruel words. Anton Ego serves as our projected super-ego. He is not an external judge but the judgment deep inside ourselves, goading us to be better with such severity that we are ultimately left feeling condemned.
Remy is the younger of two siblings. He is less physically adept but more intellectual than his older brother, who does not understand why Remy isn’t content eating scraps from the garbage like the rest of their rat clan. Remy is the creative part within us that wants to challenge the status quo and try something new. Remy also represents our shame and guilt for leaving our home. On one hand, we want to dare greatly, in this case at being an extraordinary chef, but on the other we are shy and cook in secret, hiding within the hat of another person. Remy struggles with the deep feeling that we do not deserve our success, that our family will leave us for being who we are, and that we are better off isolating and segregating from our challenges.
The movie concludes that through talent and hard work, our critics will accept us. Furthermore, once accepted for what we do, we can be further accepted for who we are. The movie ends with Remy cooking the eponymous dish ratatouille. He prepares it so remarkably well, the dish transports Anton Ego back to a sublime experience of eating ratatouille as a child, a touching moment which not only underscores food’s evocative link to memory but gives a glimpse at Anton Ego’s own narrative.
Ego is first won over by the dish, and only afterward learns of Remy’s true identity. Remy’s talent is undeniable though, and even the stuffy Ego must accept the film’s theme that “Anyone can cook,” even a rat – the rat that we all sometimes feel we are deep inside, rotten to the core but trying so hard to be accepted by others, and ultimately by ourselves. In the end, we overcome the disgust inherent in the imagery of a rat in a kitchen and instead embrace our hero’s achievement of ego integrity as he combines his identities as a member of a clan of rats, and one of Paris’s finest chefs.
While modern psychiatry can favor looking at people through the lens of biology rather than narrative, “Ratatouille” can serve as a reminder of the powerful unconscious forces that guide our lives. “Ratatouille” is not a successful movie only because of the compelling narrative, but also because the narrative matches the important psychic paradigms that psychiatry once embraced.
‘Inside Out’ (2015)
Another missing feature of the DSM is its inability to explain how symptoms feel and manifest psychologically. One such feeling is that of control – whether one is in control of one’s life, feelings, and action or rather a victim of external forces. It is extremely common for patients to enter our clinical practice feeling traumatized by the life they’ve lived and powerless to produce any change. Part of our role is to guide them through this journey from the object of their lives to the subject of their lives.
In the animated feature “Inside Out,” Riley, a preteen girl, goes through the tribulation of growing up and learning about herself. This seemingly happy child, content playing hockey with her best friend, Meg, on the picturesque frozen lakes of Minnesota, reaches her inevitable conflict. Her parents uproot her life, moving the family to San Francisco. By doing so, they disconnect her from her school, her friends, and her hobbies. While all this is happening, we spend time inside Riley’s psyche with the personified characters of Riley’s emotions as they affect her decisions and daily actions amidst the backdrop of her core memories and islands of personality.
During the move, her parents seemingly change and ultimately destroy every facet of Riley’s sense of self, which is animated as the collapse of her personality islands. Her best friend engages Riley in a video call just to inform her that she has a new friend who plays hockey equally well. Her parents do not hear Riley’s concerns and are portrayed as distracted by their adult problems. Riley feels ridiculed in her new school and unable to share her feelings with her parents, who ask her to still be their “happy girl” and indirectly ask her to fake pleasure to alleviate their own anxiety.
The climax of the movie is when Riley decides to run away from San Francisco and her parents, to return to her perceived true home, Minnesota. The climax is resolved when Riley realizes that her parents’ love, representing the connection we have to others, transcends her need for control. To some degree, we are all powerless in the face of the tremendous forces of life and share the difficult task of accepting the cards we were dealt, thus making the story of Riley so compelling.
Additionally, the climax is further resolved by another argument that psychiatry (and the DSM) should consider embracing. Emotions are not all symptoms and living without negative emotion is not the goal of life. Riley grows from preteen to teenager, and from object to subject of her life, by realizing that her symptoms/feelings are not just nuisances to avoid and hide, but the key to meaning. Our anger drives us to try hard. Our fear protects us from harm. Our sadness attracts the warmth and care of others. Our disgust protects us physically from noxious material (symbolized as a dreaded broccoli floret for preteen Riley) and socially by encouraging us to share societal norms. Similarly, patients and people in general would benefit by being taught that, while symptoms may permit the better assessment of psychiatric conditions using the DSM, life is much more than that.
It is unfair to blame the DSM for things it was not designed to do. The DSM doesn’t advertise itself as a guidebook of all behaviors, at all times. However, for a variety of reasons, it has become the main way psychiatry describes people. While we commend the APA for its effort and do not know that we could make it any better, we are frequently happily reminded that in about 90 minutes, filmmakers are able to display an empathic understanding of personal narratives that biologic psychiatry can miss.
Dr. Pulido is a psychiatry resident at the University of California, San Diego. She is interested in women’s mental health, medical education, and outpatient psychiatry. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. He has no conflicts of interest.
References
1. Erikson, EH. Childhood and society (New York: WW Norton, 1950).
IBD patients have limited protection against Omicron with third vaccine dose
For people with inflammatory bowel disease (IBD) taking immunosuppressive medication, a third dose of a COVID-19 mRNA vaccine significantly increases neutralizing antibodies against the original SARS-CoV-2 strain, but the picture is more complicated for protection against the Omicron variant, according to a research letter published in Gastroenterology.
“As further mutations in the viral genome accumulate over time, with the attendant risk of immune evasion, it remains important to continue to reappraise vaccination strategy, including the implementation of personalized approaches for some patients, such as those treated with anti-TNF drugs and JAK inhibitors,” wrote Zhigang Liu, PhD, a research associate in the department of metabolism, digestion, and reproduction at Imperial College London, and his colleagues. “Preferential use of bivalent vaccines may be especially valuable in IBD patients taking anti-TNF agents or JAK inhibitors,” they wrote. Their study did not assess neutralizing antibodies resulting from use of the bivalent vaccine, however.
The researchers tracked 268 participants, including 49 healthy participants serving as controls, from May 2021 through March 2022. The other participants had IBD and included 51 patients taking thiopurines, 36 patients taking infliximab, 39 taking both infliximab and thiopurines, 39 taking ustekinumab, 38 taking vedolizumab, and 16 taking tofacitinib. The IBD patients were all enrolled in the SARS-CoV-2 Vaccination Immunogenicity in Immunosuppressed Inflammatory Bowel Disease Patients (VIP) cohort.
None of the participants had evidence of a SARS-CoV-2 infection at baseline. All had received two doses of an mRNA COVID-19 vaccine (all received Pfizer, except two controls who received Moderna) or two doses of the AstraZeneca vaccine as their primary vaccination. All received an mRNA vaccine for their third dose. Among the IBD patients, 137 received the AstraZeneca in their primary two-dose series, and 82 received Pfizer.
First the researchers assessed the participants’ humoral response to the vaccine against the original SARS-CoV-2 strain and against the Omicron BA.1 variant. Neutralizing antibody titers rose significantly against both strains after the third vaccine dose for all participants.
“However, 50% neutralization titer (NT50) values were significantly lower against Omicron than against the ancestral strain in all study groups, irrespective of the immunosuppressive treatment regimen,” the authors reported. NT50 values are a measure that reflect a vaccine-induced humoral immunity against SARS-CoV-2 after vaccination.
Compared to the healthy controls, individuals receiving infliximab, tofacitinib, or infliximab/thiopurine combination therapy showed significantly lower responses after the second and third vaccine doses. Thirteen patients did not generate NT50 against Omicron after the second vaccine dose, and 7 of them were on infliximab monotherapy. They represented nearly 20% of all infliximab monotherapy participants.
Next the researchers assessed the risk of a breakthrough infection according to neutralizing titer thresholds. Individuals with an NT50 less than 500 had 1.6 times greater odds of a breakthrough infection than those with an NT50 above 500, they noted. After two vaccine doses, 46% of participants with IBD had an NT50 above 500 for the ancestral strain, which rose to 85% of those with IBD after a third dose.
In the healthy control group, 35% had an NT50 under 500 after two doses, and 14% of them had a breakthrough infection, all of which were mild and none of which required hospitalization. The NT50 in healthy controls, however, was not significantly associated with risk of breakthrough infection.
“In this study, neutralizing titers elicited against the omicron variant were generally poor for all individuals and were substantially lower in recipients of infliximab, infliximab/thiopurine combination, or tofacitinib therapy,” the authors concluded. “This raises concerns about whether currently available vaccines will be sufficient to protect against continually evolving SARS-CoV-2 variants, especially in patients established on certain immunosuppressive drugs.”
The small population sizes for each subgroup based on medication was one of the study’s limitations. Another was the fact that it was underpowered to conclusively determine whether an increased risk of breakthrough infection exists in IBD patients who have lower titers of neutralizing antibodies. A limitation for generalization to U.S. patients is that just 64% of the IBD patients received the AstraZeneca vaccine, which is not offered in the United States, for their first two doses before receiving the third mRNA (Pfizer) dose.
The study was funded by Pfizer in an independent research grant and by the NIHR Biomedical Research Centres in Imperial College London and Imperial College Healthcare NHS Trust and Cambridge, and the NIHR Clinical Research Facility Cambridge.
Dr. Liu and one other author had no disclosures. The other 18 authors have a range of disclosures related to various pharmaceutical companies, including Pfizer.
Understanding how inflammatory bowel disease (IBD) impacts COVID-19 infection risk and how IBD medications influence this risk remains an ever-evolving discussion, particularly with the emergence of new SARS-CoV-2 variants and booster vaccines. In this study, Liu et al. further shape this conversation: They show that a third mRNA COVID-19 vaccine dose increases neutralizing antibody levels against the Omicron variant in IBD patients compared to the level following a second vaccine dose, but that infliximab and tofacitinib significantly attenuate this response. They additionally suggest that IBD patients achieve lower neutralizing antibody levels after a third COVID-19 vaccine and may have a higher breakthrough infection risk compared to healthy controls without IBD.

Whether to change booster vaccination recommendations specifically for IBD patients on tofacitinib or infliximab, however, remains an unanswered question. The small sample of patients on tofacitinib precludes definitive conclusions regarding tofacitinib’s impact on vaccine response. Moreover, this humoral antibody-based study tells only half the story: We need analyses of the cell-mediated booster vaccine response to truly understand vaccine efficacy during immunosuppressant use. Lastly, future studies including the bivalent booster will provide the most up-to-date information on protecting our IBD patients from the Omicron variant.
Dr. Erica J. Brenner MD, MSCR is an Assistant Professor, Department of Pediatrics, Division of Pediatric Gastroenterology, University of North Carolina School of Medicine; and a cofounder of the Surveillance Epidemiology of Coronavirus Under Research Exclusion for Inflammatory Bowel Disease (SECURE-IBD) Registry. She has no relevant financial conflicts of interest.
Understanding how inflammatory bowel disease (IBD) impacts COVID-19 infection risk and how IBD medications influence this risk remains an ever-evolving discussion, particularly with the emergence of new SARS-CoV-2 variants and booster vaccines. In this study, Liu et al. further shape this conversation: They show that a third mRNA COVID-19 vaccine dose increases neutralizing antibody levels against the Omicron variant in IBD patients compared to the level following a second vaccine dose, but that infliximab and tofacitinib significantly attenuate this response. They additionally suggest that IBD patients achieve lower neutralizing antibody levels after a third COVID-19 vaccine and may have a higher breakthrough infection risk compared to healthy controls without IBD.
Whether to change booster vaccination recommendations specifically for IBD patients on tofacitinib or infliximab, however, remains an unanswered question. The small sample of patients on tofacitinib precludes definitive conclusions regarding tofacitinib’s impact on vaccine response. Moreover, this humoral antibody-based study tells only half the story: We need analyses of the cell-mediated booster vaccine response to truly understand vaccine efficacy during immunosuppressant use. Lastly, future studies including the bivalent booster will provide the most up-to-date information on protecting our IBD patients from the Omicron variant.
Dr. Erica J. Brenner MD, MSCR is an Assistant Professor, Department of Pediatrics, Division of Pediatric Gastroenterology, University of North Carolina School of Medicine; and a cofounder of the Surveillance Epidemiology of Coronavirus Under Research Exclusion for Inflammatory Bowel Disease (SECURE-IBD) Registry. She has no relevant financial conflicts of interest.
Understanding how inflammatory bowel disease (IBD) impacts COVID-19 infection risk and how IBD medications influence this risk remains an ever-evolving discussion, particularly with the emergence of new SARS-CoV-2 variants and booster vaccines. In this study, Liu et al. further shape this conversation: They show that a third mRNA COVID-19 vaccine dose increases neutralizing antibody levels against the Omicron variant in IBD patients compared to the level following a second vaccine dose, but that infliximab and tofacitinib significantly attenuate this response. They additionally suggest that IBD patients achieve lower neutralizing antibody levels after a third COVID-19 vaccine and may have a higher breakthrough infection risk compared to healthy controls without IBD.
Whether to change booster vaccination recommendations specifically for IBD patients on tofacitinib or infliximab, however, remains an unanswered question. The small sample of patients on tofacitinib precludes definitive conclusions regarding tofacitinib’s impact on vaccine response. Moreover, this humoral antibody-based study tells only half the story: We need analyses of the cell-mediated booster vaccine response to truly understand vaccine efficacy during immunosuppressant use. Lastly, future studies including the bivalent booster will provide the most up-to-date information on protecting our IBD patients from the Omicron variant.
Dr. Erica J. Brenner MD, MSCR is an Assistant Professor, Department of Pediatrics, Division of Pediatric Gastroenterology, University of North Carolina School of Medicine; and a cofounder of the Surveillance Epidemiology of Coronavirus Under Research Exclusion for Inflammatory Bowel Disease (SECURE-IBD) Registry. She has no relevant financial conflicts of interest.
For people with inflammatory bowel disease (IBD) taking immunosuppressive medication, a third dose of a COVID-19 mRNA vaccine significantly increases neutralizing antibodies against the original SARS-CoV-2 strain, but the picture is more complicated for protection against the Omicron variant, according to a research letter published in Gastroenterology.
“As further mutations in the viral genome accumulate over time, with the attendant risk of immune evasion, it remains important to continue to reappraise vaccination strategy, including the implementation of personalized approaches for some patients, such as those treated with anti-TNF drugs and JAK inhibitors,” wrote Zhigang Liu, PhD, a research associate in the department of metabolism, digestion, and reproduction at Imperial College London, and his colleagues. “Preferential use of bivalent vaccines may be especially valuable in IBD patients taking anti-TNF agents or JAK inhibitors,” they wrote. Their study did not assess neutralizing antibodies resulting from use of the bivalent vaccine, however.
The researchers tracked 268 participants, including 49 healthy participants serving as controls, from May 2021 through March 2022. The other participants had IBD and included 51 patients taking thiopurines, 36 patients taking infliximab, 39 taking both infliximab and thiopurines, 39 taking ustekinumab, 38 taking vedolizumab, and 16 taking tofacitinib. The IBD patients were all enrolled in the SARS-CoV-2 Vaccination Immunogenicity in Immunosuppressed Inflammatory Bowel Disease Patients (VIP) cohort.
None of the participants had evidence of a SARS-CoV-2 infection at baseline. All had received two doses of an mRNA COVID-19 vaccine (all received Pfizer, except two controls who received Moderna) or two doses of the AstraZeneca vaccine as their primary vaccination. All received an mRNA vaccine for their third dose. Among the IBD patients, 137 received the AstraZeneca in their primary two-dose series, and 82 received Pfizer.
First the researchers assessed the participants’ humoral response to the vaccine against the original SARS-CoV-2 strain and against the Omicron BA.1 variant. Neutralizing antibody titers rose significantly against both strains after the third vaccine dose for all participants.
“However, 50% neutralization titer (NT50) values were significantly lower against Omicron than against the ancestral strain in all study groups, irrespective of the immunosuppressive treatment regimen,” the authors reported. NT50 values are a measure that reflect a vaccine-induced humoral immunity against SARS-CoV-2 after vaccination.
Compared to the healthy controls, individuals receiving infliximab, tofacitinib, or infliximab/thiopurine combination therapy showed significantly lower responses after the second and third vaccine doses. Thirteen patients did not generate NT50 against Omicron after the second vaccine dose, and 7 of them were on infliximab monotherapy. They represented nearly 20% of all infliximab monotherapy participants.
Next the researchers assessed the risk of a breakthrough infection according to neutralizing titer thresholds. Individuals with an NT50 less than 500 had 1.6 times greater odds of a breakthrough infection than those with an NT50 above 500, they noted. After two vaccine doses, 46% of participants with IBD had an NT50 above 500 for the ancestral strain, which rose to 85% of those with IBD after a third dose.
In the healthy control group, 35% had an NT50 under 500 after two doses, and 14% of them had a breakthrough infection, all of which were mild and none of which required hospitalization. The NT50 in healthy controls, however, was not significantly associated with risk of breakthrough infection.
“In this study, neutralizing titers elicited against the omicron variant were generally poor for all individuals and were substantially lower in recipients of infliximab, infliximab/thiopurine combination, or tofacitinib therapy,” the authors concluded. “This raises concerns about whether currently available vaccines will be sufficient to protect against continually evolving SARS-CoV-2 variants, especially in patients established on certain immunosuppressive drugs.”
The small population sizes for each subgroup based on medication was one of the study’s limitations. Another was the fact that it was underpowered to conclusively determine whether an increased risk of breakthrough infection exists in IBD patients who have lower titers of neutralizing antibodies. A limitation for generalization to U.S. patients is that just 64% of the IBD patients received the AstraZeneca vaccine, which is not offered in the United States, for their first two doses before receiving the third mRNA (Pfizer) dose.
The study was funded by Pfizer in an independent research grant and by the NIHR Biomedical Research Centres in Imperial College London and Imperial College Healthcare NHS Trust and Cambridge, and the NIHR Clinical Research Facility Cambridge.
Dr. Liu and one other author had no disclosures. The other 18 authors have a range of disclosures related to various pharmaceutical companies, including Pfizer.
For people with inflammatory bowel disease (IBD) taking immunosuppressive medication, a third dose of a COVID-19 mRNA vaccine significantly increases neutralizing antibodies against the original SARS-CoV-2 strain, but the picture is more complicated for protection against the Omicron variant, according to a research letter published in Gastroenterology.
“As further mutations in the viral genome accumulate over time, with the attendant risk of immune evasion, it remains important to continue to reappraise vaccination strategy, including the implementation of personalized approaches for some patients, such as those treated with anti-TNF drugs and JAK inhibitors,” wrote Zhigang Liu, PhD, a research associate in the department of metabolism, digestion, and reproduction at Imperial College London, and his colleagues. “Preferential use of bivalent vaccines may be especially valuable in IBD patients taking anti-TNF agents or JAK inhibitors,” they wrote. Their study did not assess neutralizing antibodies resulting from use of the bivalent vaccine, however.
The researchers tracked 268 participants, including 49 healthy participants serving as controls, from May 2021 through March 2022. The other participants had IBD and included 51 patients taking thiopurines, 36 patients taking infliximab, 39 taking both infliximab and thiopurines, 39 taking ustekinumab, 38 taking vedolizumab, and 16 taking tofacitinib. The IBD patients were all enrolled in the SARS-CoV-2 Vaccination Immunogenicity in Immunosuppressed Inflammatory Bowel Disease Patients (VIP) cohort.
None of the participants had evidence of a SARS-CoV-2 infection at baseline. All had received two doses of an mRNA COVID-19 vaccine (all received Pfizer, except two controls who received Moderna) or two doses of the AstraZeneca vaccine as their primary vaccination. All received an mRNA vaccine for their third dose. Among the IBD patients, 137 received the AstraZeneca in their primary two-dose series, and 82 received Pfizer.
First the researchers assessed the participants’ humoral response to the vaccine against the original SARS-CoV-2 strain and against the Omicron BA.1 variant. Neutralizing antibody titers rose significantly against both strains after the third vaccine dose for all participants.
“However, 50% neutralization titer (NT50) values were significantly lower against Omicron than against the ancestral strain in all study groups, irrespective of the immunosuppressive treatment regimen,” the authors reported. NT50 values are a measure that reflect a vaccine-induced humoral immunity against SARS-CoV-2 after vaccination.
Compared to the healthy controls, individuals receiving infliximab, tofacitinib, or infliximab/thiopurine combination therapy showed significantly lower responses after the second and third vaccine doses. Thirteen patients did not generate NT50 against Omicron after the second vaccine dose, and 7 of them were on infliximab monotherapy. They represented nearly 20% of all infliximab monotherapy participants.
Next the researchers assessed the risk of a breakthrough infection according to neutralizing titer thresholds. Individuals with an NT50 less than 500 had 1.6 times greater odds of a breakthrough infection than those with an NT50 above 500, they noted. After two vaccine doses, 46% of participants with IBD had an NT50 above 500 for the ancestral strain, which rose to 85% of those with IBD after a third dose.
In the healthy control group, 35% had an NT50 under 500 after two doses, and 14% of them had a breakthrough infection, all of which were mild and none of which required hospitalization. The NT50 in healthy controls, however, was not significantly associated with risk of breakthrough infection.
“In this study, neutralizing titers elicited against the omicron variant were generally poor for all individuals and were substantially lower in recipients of infliximab, infliximab/thiopurine combination, or tofacitinib therapy,” the authors concluded. “This raises concerns about whether currently available vaccines will be sufficient to protect against continually evolving SARS-CoV-2 variants, especially in patients established on certain immunosuppressive drugs.”
The small population sizes for each subgroup based on medication was one of the study’s limitations. Another was the fact that it was underpowered to conclusively determine whether an increased risk of breakthrough infection exists in IBD patients who have lower titers of neutralizing antibodies. A limitation for generalization to U.S. patients is that just 64% of the IBD patients received the AstraZeneca vaccine, which is not offered in the United States, for their first two doses before receiving the third mRNA (Pfizer) dose.
The study was funded by Pfizer in an independent research grant and by the NIHR Biomedical Research Centres in Imperial College London and Imperial College Healthcare NHS Trust and Cambridge, and the NIHR Clinical Research Facility Cambridge.
Dr. Liu and one other author had no disclosures. The other 18 authors have a range of disclosures related to various pharmaceutical companies, including Pfizer.
FROM GASTROENTEROLOGY
CHEST simulation courses support learning for every career stage
One mark of an excellent clinician is their commitment to lifelong learning, and CHEST’s hands-on simulation courses offer the chance for practitioners of all experience levels to enhance their knowledge.
A variety of interactive courses are offered at CHEST’s state-of-the-art Innovation, Simulation, and Training Center in Glenview, Illinois, covering topics like ultrasonography, bronchoscopy, and mechanical ventilation. And this year, our simulation schedule will offer several new sessions on advances in invasive and noninvasive ventilation, critical care transesophageal echocardiography, master-level EBUS practice, and mechanical circulatory support.
Each course is led by expert instructors and includes attendees from a full range of career stages, from trainees and mid-career clinicians to long-time CHEST faculty members.
At a fall 2022 session of the Ultrasonography: Essentials in Critical Care course, Adil Ahmed, MD, an intern at the University of Texas Health Science Center at San Antonio, shared his perspective attending as a resident.
“CHEST has lots of specialized resources and renowned faculty members, and they’re doing an exceptional job,” he said. “A lot of the things I’ve learned in the first workshop alone are completely brand new to me. I think more programs should start sending residents to these courses.”
Trainees don’t just attend simulation courses – they teach them, too. Carmen Mei, MD, a pulmonary and critical care fellow at Rutgers University, was a faculty member at the recent ultrasound course. She taught attendees representing a wide array of ages.
“It’s a learning environment. Everybody’s very engaged, no matter where they are in their career,” she said.
As a mid-career clinician, Yonatan Y. Greenstein, MD, FCCP – who serves as a co-chair of the ultrasonography course – appreciates the diversity of experiences among attendees.
“Over the years, we’ve found that the wide breadth enhances the course because learners appreciate the questions that are brought up from different angles,” he said.
For experienced clinicians like CHEST Immediate Past President David Schulman, MD, MPH, FCCP, the interactive courses provide an opportunity to continue expanding his expertise. At the ultrasound course, Dr. Schulman said he enjoyed the chance to extend and refine his skillset alongside clinicians with a broad range of experience levels.
“Ultrasound is one of those skills that many clinicians, even in their forties and older, have never trained in. It’s great to see how the more junior learners approach this with a very excited mindset, and they’re learning right beside mid-career faculty who didn’t have the exposure to ultrasound when they were young,” he said.
To find the simulation course that’s the best fit for your practice, visit chestnet.org/simulation.
One mark of an excellent clinician is their commitment to lifelong learning, and CHEST’s hands-on simulation courses offer the chance for practitioners of all experience levels to enhance their knowledge.
A variety of interactive courses are offered at CHEST’s state-of-the-art Innovation, Simulation, and Training Center in Glenview, Illinois, covering topics like ultrasonography, bronchoscopy, and mechanical ventilation. And this year, our simulation schedule will offer several new sessions on advances in invasive and noninvasive ventilation, critical care transesophageal echocardiography, master-level EBUS practice, and mechanical circulatory support.
Each course is led by expert instructors and includes attendees from a full range of career stages, from trainees and mid-career clinicians to long-time CHEST faculty members.
At a fall 2022 session of the Ultrasonography: Essentials in Critical Care course, Adil Ahmed, MD, an intern at the University of Texas Health Science Center at San Antonio, shared his perspective attending as a resident.
“CHEST has lots of specialized resources and renowned faculty members, and they’re doing an exceptional job,” he said. “A lot of the things I’ve learned in the first workshop alone are completely brand new to me. I think more programs should start sending residents to these courses.”
Trainees don’t just attend simulation courses – they teach them, too. Carmen Mei, MD, a pulmonary and critical care fellow at Rutgers University, was a faculty member at the recent ultrasound course. She taught attendees representing a wide array of ages.
“It’s a learning environment. Everybody’s very engaged, no matter where they are in their career,” she said.
As a mid-career clinician, Yonatan Y. Greenstein, MD, FCCP – who serves as a co-chair of the ultrasonography course – appreciates the diversity of experiences among attendees.
“Over the years, we’ve found that the wide breadth enhances the course because learners appreciate the questions that are brought up from different angles,” he said.
For experienced clinicians like CHEST Immediate Past President David Schulman, MD, MPH, FCCP, the interactive courses provide an opportunity to continue expanding his expertise. At the ultrasound course, Dr. Schulman said he enjoyed the chance to extend and refine his skillset alongside clinicians with a broad range of experience levels.
“Ultrasound is one of those skills that many clinicians, even in their forties and older, have never trained in. It’s great to see how the more junior learners approach this with a very excited mindset, and they’re learning right beside mid-career faculty who didn’t have the exposure to ultrasound when they were young,” he said.
To find the simulation course that’s the best fit for your practice, visit chestnet.org/simulation.
One mark of an excellent clinician is their commitment to lifelong learning, and CHEST’s hands-on simulation courses offer the chance for practitioners of all experience levels to enhance their knowledge.
A variety of interactive courses are offered at CHEST’s state-of-the-art Innovation, Simulation, and Training Center in Glenview, Illinois, covering topics like ultrasonography, bronchoscopy, and mechanical ventilation. And this year, our simulation schedule will offer several new sessions on advances in invasive and noninvasive ventilation, critical care transesophageal echocardiography, master-level EBUS practice, and mechanical circulatory support.
Each course is led by expert instructors and includes attendees from a full range of career stages, from trainees and mid-career clinicians to long-time CHEST faculty members.
At a fall 2022 session of the Ultrasonography: Essentials in Critical Care course, Adil Ahmed, MD, an intern at the University of Texas Health Science Center at San Antonio, shared his perspective attending as a resident.
“CHEST has lots of specialized resources and renowned faculty members, and they’re doing an exceptional job,” he said. “A lot of the things I’ve learned in the first workshop alone are completely brand new to me. I think more programs should start sending residents to these courses.”
Trainees don’t just attend simulation courses – they teach them, too. Carmen Mei, MD, a pulmonary and critical care fellow at Rutgers University, was a faculty member at the recent ultrasound course. She taught attendees representing a wide array of ages.
“It’s a learning environment. Everybody’s very engaged, no matter where they are in their career,” she said.
As a mid-career clinician, Yonatan Y. Greenstein, MD, FCCP – who serves as a co-chair of the ultrasonography course – appreciates the diversity of experiences among attendees.
“Over the years, we’ve found that the wide breadth enhances the course because learners appreciate the questions that are brought up from different angles,” he said.
For experienced clinicians like CHEST Immediate Past President David Schulman, MD, MPH, FCCP, the interactive courses provide an opportunity to continue expanding his expertise. At the ultrasound course, Dr. Schulman said he enjoyed the chance to extend and refine his skillset alongside clinicians with a broad range of experience levels.
“Ultrasound is one of those skills that many clinicians, even in their forties and older, have never trained in. It’s great to see how the more junior learners approach this with a very excited mindset, and they’re learning right beside mid-career faculty who didn’t have the exposure to ultrasound when they were young,” he said.
To find the simulation course that’s the best fit for your practice, visit chestnet.org/simulation.
Defining six asthma subtypes may promote personalized treatment
Six subtypes of asthma that may facilitate personalized treatment were identified and confirmed in a large database review of approximately 50,000 patients, according to a recent study.
Previous studies of asthma subtypes have involved age of disease onset, the presence of allergies, and level of eosinophilic inflammation, and have been limited by factors including small sample size and lack of formal validation, Elsie M.F. Horne, MD, of the Asthma UK Centre for Applied Research, Edinburgh, and colleagues wrote.
In a study published in the International Journal of Medical Informatics, the researchers used data from two databases in the United Kingdom: the Optimum Patient Care Research Database (OPCRD) and the Secure Anonymised Information Linkage Database (SAIL). Each dataset included 50,000 randomly selected nonoverlapping adult asthma patients.
The researchers identified 45 categorical features from primary care electronic health records. The features included those directly linked to asthma, such as medications; and features indirectly linked to asthma, such as comorbidities.
The subtypes were defined by the clinically applicable features of level of inhaled corticosteroid use, level of health care use, and the presence of comorbidities, using multiple correspondence analysis and k-means cluster analysis.
The six asthma subtypes were identified in the OPCRD study population as follows: low inhaled corticosteroid use and low health care utilization (30%); low to medium ICS use (36%); low to medium ICS use and comorbidities (12%); varied ICS use and comorbid chronic obstructive pulmonary disease (4%); high ICS use (10%); and very high ICS use (7%).
The researchers replicated the subtypes with 91%-92% accuracy in an internal dataset and 84%-86% accuracy in an external dataset. “These subtypes generalized well at two future time points, and in an additional EHR database from a different U.K. nation (the SAIL Databank),” they wrote in their discussion.
The findings were limited by several factors including the retrospective design, the possible inclusion of people without asthma because of the cohort selection criteria, and the possible biases associated with the use of EHRs; however, the results were strengthened by the large dataset and the additional validations, the researchers noted.
“Using these subtypes to summarize asthma populations could help with management and resource planning at the practice level, and could be useful for understanding regional differences in the asthma population,” they noted. For example, key clinical implications for individuals in a low health care utilization subtype could include being flagged for barriers to care and misdiagnoses, while those in a high health care utilization subtype could be considered for reassessment of medication and other options.
The study received no outside funding. Lead author Dr. Horne had no financial conflicts to disclose.
Six subtypes of asthma that may facilitate personalized treatment were identified and confirmed in a large database review of approximately 50,000 patients, according to a recent study.
Previous studies of asthma subtypes have involved age of disease onset, the presence of allergies, and level of eosinophilic inflammation, and have been limited by factors including small sample size and lack of formal validation, Elsie M.F. Horne, MD, of the Asthma UK Centre for Applied Research, Edinburgh, and colleagues wrote.
In a study published in the International Journal of Medical Informatics, the researchers used data from two databases in the United Kingdom: the Optimum Patient Care Research Database (OPCRD) and the Secure Anonymised Information Linkage Database (SAIL). Each dataset included 50,000 randomly selected nonoverlapping adult asthma patients.
The researchers identified 45 categorical features from primary care electronic health records. The features included those directly linked to asthma, such as medications; and features indirectly linked to asthma, such as comorbidities.
The subtypes were defined by the clinically applicable features of level of inhaled corticosteroid use, level of health care use, and the presence of comorbidities, using multiple correspondence analysis and k-means cluster analysis.
The six asthma subtypes were identified in the OPCRD study population as follows: low inhaled corticosteroid use and low health care utilization (30%); low to medium ICS use (36%); low to medium ICS use and comorbidities (12%); varied ICS use and comorbid chronic obstructive pulmonary disease (4%); high ICS use (10%); and very high ICS use (7%).
The researchers replicated the subtypes with 91%-92% accuracy in an internal dataset and 84%-86% accuracy in an external dataset. “These subtypes generalized well at two future time points, and in an additional EHR database from a different U.K. nation (the SAIL Databank),” they wrote in their discussion.
The findings were limited by several factors including the retrospective design, the possible inclusion of people without asthma because of the cohort selection criteria, and the possible biases associated with the use of EHRs; however, the results were strengthened by the large dataset and the additional validations, the researchers noted.
“Using these subtypes to summarize asthma populations could help with management and resource planning at the practice level, and could be useful for understanding regional differences in the asthma population,” they noted. For example, key clinical implications for individuals in a low health care utilization subtype could include being flagged for barriers to care and misdiagnoses, while those in a high health care utilization subtype could be considered for reassessment of medication and other options.
The study received no outside funding. Lead author Dr. Horne had no financial conflicts to disclose.
Six subtypes of asthma that may facilitate personalized treatment were identified and confirmed in a large database review of approximately 50,000 patients, according to a recent study.
Previous studies of asthma subtypes have involved age of disease onset, the presence of allergies, and level of eosinophilic inflammation, and have been limited by factors including small sample size and lack of formal validation, Elsie M.F. Horne, MD, of the Asthma UK Centre for Applied Research, Edinburgh, and colleagues wrote.
In a study published in the International Journal of Medical Informatics, the researchers used data from two databases in the United Kingdom: the Optimum Patient Care Research Database (OPCRD) and the Secure Anonymised Information Linkage Database (SAIL). Each dataset included 50,000 randomly selected nonoverlapping adult asthma patients.
The researchers identified 45 categorical features from primary care electronic health records. The features included those directly linked to asthma, such as medications; and features indirectly linked to asthma, such as comorbidities.
The subtypes were defined by the clinically applicable features of level of inhaled corticosteroid use, level of health care use, and the presence of comorbidities, using multiple correspondence analysis and k-means cluster analysis.
The six asthma subtypes were identified in the OPCRD study population as follows: low inhaled corticosteroid use and low health care utilization (30%); low to medium ICS use (36%); low to medium ICS use and comorbidities (12%); varied ICS use and comorbid chronic obstructive pulmonary disease (4%); high ICS use (10%); and very high ICS use (7%).
The researchers replicated the subtypes with 91%-92% accuracy in an internal dataset and 84%-86% accuracy in an external dataset. “These subtypes generalized well at two future time points, and in an additional EHR database from a different U.K. nation (the SAIL Databank),” they wrote in their discussion.
The findings were limited by several factors including the retrospective design, the possible inclusion of people without asthma because of the cohort selection criteria, and the possible biases associated with the use of EHRs; however, the results were strengthened by the large dataset and the additional validations, the researchers noted.
“Using these subtypes to summarize asthma populations could help with management and resource planning at the practice level, and could be useful for understanding regional differences in the asthma population,” they noted. For example, key clinical implications for individuals in a low health care utilization subtype could include being flagged for barriers to care and misdiagnoses, while those in a high health care utilization subtype could be considered for reassessment of medication and other options.
The study received no outside funding. Lead author Dr. Horne had no financial conflicts to disclose.
FROM THE INTERNATIONAL JOURNAL OF MEDICAL INFORMATICS
CHEST President shares inside look at priorities, plans for 2023
Attendees at the CHEST 2022 Opening Session on October 16 got a sneak peek into plans and priorities for CHEST President Doreen J. Addrizzo-Harris, MD, FCCP, in 2023 – and some insights into her own path to the role.
A longtime leader at CHEST, she shared how members’ pandemic response reminded her of the great impact the organization can have. In March 2020, Dr. Addrizzo-Harris was overseeing ICU staffing at NYU Langone Health’s Bellevue Hospital Center and organizing dozens of volunteer physicians to help meet the pandemic care burden.

“I knew all too quickly that we wouldn’t have enough intensivists,” said Dr. Addrizzo-Harris. “It was a quick call very late one night, probably around 1 am, that I made to CHEST CEO, Bob Musacchio, that helped materialize a monumental effort ... many of these physicians were CHEST members themselves. They were fearless and unselfish, and they came to help us in our time of need.”
She saw this same spirit of dedication and drive in CHEST’s leadership and staff, she said – one she will continue and expand upon during her presidency.
“I’ve watched our last three presidents lead by great example ... with innovation and nimbleness, in a time when we were so isolated from each other and so tired from the long hours that we worked each day,” she said. “They, along with the Board of Regents, the CEO, and our phenomenal staff, were able to keep CHEST amazingly alive and vibrant and more connected than ever. They are truly inspiring. For 2023, I hope to take this incredible energy to the next level.”
As CHEST president, Dr. in the United States and advancing international outreach initiatives launched by CHEST Past President David Schulman, MD, MPH, FCCP. This also includes supporting and building upon CHEST’s ongoing commitment to diversity, equity, and inclusion initiatives to encourage greater representation in the field and improve patient care.
“Whether it’s through supporting our clinical research grants, expanding patient education and advocacy, or programs like the First 5 Minutes™ and the Harold Amos scholarship program, we want to train our leaders for the future,” she said.
Revisit the September issue of CHEST Physician, and watch future issues to learn more about Dr. Addrizzo-Harris and her plans for the presidency.
Attendees at the CHEST 2022 Opening Session on October 16 got a sneak peek into plans and priorities for CHEST President Doreen J. Addrizzo-Harris, MD, FCCP, in 2023 – and some insights into her own path to the role.
A longtime leader at CHEST, she shared how members’ pandemic response reminded her of the great impact the organization can have. In March 2020, Dr. Addrizzo-Harris was overseeing ICU staffing at NYU Langone Health’s Bellevue Hospital Center and organizing dozens of volunteer physicians to help meet the pandemic care burden.
“I knew all too quickly that we wouldn’t have enough intensivists,” said Dr. Addrizzo-Harris. “It was a quick call very late one night, probably around 1 am, that I made to CHEST CEO, Bob Musacchio, that helped materialize a monumental effort ... many of these physicians were CHEST members themselves. They were fearless and unselfish, and they came to help us in our time of need.”
She saw this same spirit of dedication and drive in CHEST’s leadership and staff, she said – one she will continue and expand upon during her presidency.
“I’ve watched our last three presidents lead by great example ... with innovation and nimbleness, in a time when we were so isolated from each other and so tired from the long hours that we worked each day,” she said. “They, along with the Board of Regents, the CEO, and our phenomenal staff, were able to keep CHEST amazingly alive and vibrant and more connected than ever. They are truly inspiring. For 2023, I hope to take this incredible energy to the next level.”
As CHEST president, Dr. in the United States and advancing international outreach initiatives launched by CHEST Past President David Schulman, MD, MPH, FCCP. This also includes supporting and building upon CHEST’s ongoing commitment to diversity, equity, and inclusion initiatives to encourage greater representation in the field and improve patient care.
“Whether it’s through supporting our clinical research grants, expanding patient education and advocacy, or programs like the First 5 Minutes™ and the Harold Amos scholarship program, we want to train our leaders for the future,” she said.
Revisit the September issue of CHEST Physician, and watch future issues to learn more about Dr. Addrizzo-Harris and her plans for the presidency.
Attendees at the CHEST 2022 Opening Session on October 16 got a sneak peek into plans and priorities for CHEST President Doreen J. Addrizzo-Harris, MD, FCCP, in 2023 – and some insights into her own path to the role.
A longtime leader at CHEST, she shared how members’ pandemic response reminded her of the great impact the organization can have. In March 2020, Dr. Addrizzo-Harris was overseeing ICU staffing at NYU Langone Health’s Bellevue Hospital Center and organizing dozens of volunteer physicians to help meet the pandemic care burden.
“I knew all too quickly that we wouldn’t have enough intensivists,” said Dr. Addrizzo-Harris. “It was a quick call very late one night, probably around 1 am, that I made to CHEST CEO, Bob Musacchio, that helped materialize a monumental effort ... many of these physicians were CHEST members themselves. They were fearless and unselfish, and they came to help us in our time of need.”
She saw this same spirit of dedication and drive in CHEST’s leadership and staff, she said – one she will continue and expand upon during her presidency.
“I’ve watched our last three presidents lead by great example ... with innovation and nimbleness, in a time when we were so isolated from each other and so tired from the long hours that we worked each day,” she said. “They, along with the Board of Regents, the CEO, and our phenomenal staff, were able to keep CHEST amazingly alive and vibrant and more connected than ever. They are truly inspiring. For 2023, I hope to take this incredible energy to the next level.”
As CHEST president, Dr. in the United States and advancing international outreach initiatives launched by CHEST Past President David Schulman, MD, MPH, FCCP. This also includes supporting and building upon CHEST’s ongoing commitment to diversity, equity, and inclusion initiatives to encourage greater representation in the field and improve patient care.
“Whether it’s through supporting our clinical research grants, expanding patient education and advocacy, or programs like the First 5 Minutes™ and the Harold Amos scholarship program, we want to train our leaders for the future,” she said.
Revisit the September issue of CHEST Physician, and watch future issues to learn more about Dr. Addrizzo-Harris and her plans for the presidency.
Genomics data reveal promising PSC therapeutic target
, according to a study published in Gastro Hep Advances.
PSC is very rare, with an incidence of 0-1.3 cases per 100,000 people per year. Because up to 80% of patients with PSC also have inflammatory bowel disease (IBD), a link along the gut-liver axis is suspected. So far, scientists have not understood the causes of PSC, the main complications of which include biliary cirrhosis, bacterial cholangitis, and cholangiocarcinoma.
No treatment is currently available for PSC, but the findings of this genomics study suggest several targets that may be worth pursuing, particularly the gene NR0B2.
“The therapeutic targeting of NR0B2 may potentiate that of FXR [farnesoid X receptor] and enable action on early events of the disease and prevent its progression,” wrote Christophe Desterke, PhD, of the Paul-Brousse Hospital, the French National Institute of Health and Medical Research, and the University of Paris-Saclay in Villejuif, France, and his associates.
The researchers used an algorithmic tool to mine the MEDLINE/PubMed/NCBI database using the three key symptoms of PSC – biliary fibrosis, biliary inflammation, and biliary stasis – as their keywords. This approach allowed them to discover the genes and potential pathways related to PSC in published research text or in clinical, animal, and cellular models.
The researchers initially found 525 genes linked to PSC and then compared them to RNA data from liver biopsies taken from patients with liver disease from various causes. This process led to a ranking of the 10 best markers of PSC, based on the data-mining method and the genes’ association with one or more of the three PSC symptoms.
At the top of the list is NR1H4, also called FXR, which ranks most highly with biliary fibrosis and biliary stasis. NR1H4 is already a clear target for cholestatic and fatty liver diseases, the authors noted. The other genes, in descending order of relevance, are: ABCB4, ABCB11, TGFB1, IFNL3, PNPLA3, IL6, TLR4, GPBAR1, and IL17A. In addition, complications of PSC were significantly associated with upregulation of TNFRS12A, SOX9, ANXA2, MMP7, and LCN2.
Separately, investigation of the 525 initially identified genes in mouse models of PSC revealed that NR0B2 is also a key player in the pathogenesis of PSC.
"NR0B2 was upregulated in PSC livers independent of gender, age, and body mass index,” the authors reported. “Importantly, it was not dependent on the severity of PSC in the prognostic cohort, suggesting that this may be an early event during the disease.”
The researchers also found a possible pathway explaining the autoimmunity of PSC – the involvement of CD274, also known as the PDL1 immune checkpoint. The authors noted that the PDL1 inhibitor pembrolizumab has previously been reported as a cause of sclerosing cholangitis.
Further, the researchers discovered overexpression of FOXP3 in the livers of patients with PSC. Because FOXP3 determines what T-cell subtypes look like, the finding suggests that an “imbalance between Foxp3þ regulatory T cells and Th17 cells may be involved in IBD and PSC,” they wrote.
Also of note was the overexpression of SOX9 in the livers of patients with PSC whose profiles suggested the worst clinical prognoses.
Finally, the researchers identified three genes as potentially involved in development of cholangiocarcinoma: GSTA3, ID2 (which is overexpressed in biliary tract cancer), and especially TMEM45A, a protein in cells’ Golgi apparatus that is already known to be involved in the development of several other cancers.
The research was funded by the French National Institute of Health and Medical Research. The authors reported no conflicts of interest.
Primary sclerosing cholangitis (PSC) is a bile duct disease with few therapeutic options other than liver transplant, and thus its prognosis remains grim. Additionally, the factors that cause the disease are not well understood. Identifying the pathways and genes involved in PSC pathogenesis could help in the development of potential therapeutic targets.

In this report Desterke et al. mined public data sets to identify and define a PSC-specific network. Of the top genes in this list, NR0B2 stood out as a potential player in pathogenesis because of its involvement in regulating bile acid metabolism. The authors showed that upregulation of NR0B2 occurs early in the disease process and in patient tissues is independent of variables such as gender and sex. Interestingly, the authors showed that this upregulation occurs primarily in cholangiocytes, the cells lining the bile duct. Higher expression of NR0B2 results in reprogramming that alters the metabolic function of these cells and predisposes them to malignancy.
This study, which is the first to look at omics data for PSC, highlights the involvement of genes and pathways that were previously unrecognized in disease pathogenesis. By using data derived from human PSC liver biopsies and animal models of PSC, the authors were able to validate their findings across species, which strengthened their conclusions. This approach also showed that NR0B2 deregulation occurs primarily in cholangiocytes, suggesting that future therapies should be targeted to this cell type. These important findings will improve our understanding of this rare but clinically significant disease.
Kari Nejak-Bowen, PhD, MBA, is associate professor, department of pathology, University of Pittsburgh School of Medicine. She has no relevant conflicts of interest.
Primary sclerosing cholangitis (PSC) is a bile duct disease with few therapeutic options other than liver transplant, and thus its prognosis remains grim. Additionally, the factors that cause the disease are not well understood. Identifying the pathways and genes involved in PSC pathogenesis could help in the development of potential therapeutic targets.
In this report Desterke et al. mined public data sets to identify and define a PSC-specific network. Of the top genes in this list, NR0B2 stood out as a potential player in pathogenesis because of its involvement in regulating bile acid metabolism. The authors showed that upregulation of NR0B2 occurs early in the disease process and in patient tissues is independent of variables such as gender and sex. Interestingly, the authors showed that this upregulation occurs primarily in cholangiocytes, the cells lining the bile duct. Higher expression of NR0B2 results in reprogramming that alters the metabolic function of these cells and predisposes them to malignancy.
This study, which is the first to look at omics data for PSC, highlights the involvement of genes and pathways that were previously unrecognized in disease pathogenesis. By using data derived from human PSC liver biopsies and animal models of PSC, the authors were able to validate their findings across species, which strengthened their conclusions. This approach also showed that NR0B2 deregulation occurs primarily in cholangiocytes, suggesting that future therapies should be targeted to this cell type. These important findings will improve our understanding of this rare but clinically significant disease.
Kari Nejak-Bowen, PhD, MBA, is associate professor, department of pathology, University of Pittsburgh School of Medicine. She has no relevant conflicts of interest.
Primary sclerosing cholangitis (PSC) is a bile duct disease with few therapeutic options other than liver transplant, and thus its prognosis remains grim. Additionally, the factors that cause the disease are not well understood. Identifying the pathways and genes involved in PSC pathogenesis could help in the development of potential therapeutic targets.
In this report Desterke et al. mined public data sets to identify and define a PSC-specific network. Of the top genes in this list, NR0B2 stood out as a potential player in pathogenesis because of its involvement in regulating bile acid metabolism. The authors showed that upregulation of NR0B2 occurs early in the disease process and in patient tissues is independent of variables such as gender and sex. Interestingly, the authors showed that this upregulation occurs primarily in cholangiocytes, the cells lining the bile duct. Higher expression of NR0B2 results in reprogramming that alters the metabolic function of these cells and predisposes them to malignancy.
This study, which is the first to look at omics data for PSC, highlights the involvement of genes and pathways that were previously unrecognized in disease pathogenesis. By using data derived from human PSC liver biopsies and animal models of PSC, the authors were able to validate their findings across species, which strengthened their conclusions. This approach also showed that NR0B2 deregulation occurs primarily in cholangiocytes, suggesting that future therapies should be targeted to this cell type. These important findings will improve our understanding of this rare but clinically significant disease.
Kari Nejak-Bowen, PhD, MBA, is associate professor, department of pathology, University of Pittsburgh School of Medicine. She has no relevant conflicts of interest.
, according to a study published in Gastro Hep Advances.
PSC is very rare, with an incidence of 0-1.3 cases per 100,000 people per year. Because up to 80% of patients with PSC also have inflammatory bowel disease (IBD), a link along the gut-liver axis is suspected. So far, scientists have not understood the causes of PSC, the main complications of which include biliary cirrhosis, bacterial cholangitis, and cholangiocarcinoma.
No treatment is currently available for PSC, but the findings of this genomics study suggest several targets that may be worth pursuing, particularly the gene NR0B2.
“The therapeutic targeting of NR0B2 may potentiate that of FXR [farnesoid X receptor] and enable action on early events of the disease and prevent its progression,” wrote Christophe Desterke, PhD, of the Paul-Brousse Hospital, the French National Institute of Health and Medical Research, and the University of Paris-Saclay in Villejuif, France, and his associates.
The researchers used an algorithmic tool to mine the MEDLINE/PubMed/NCBI database using the three key symptoms of PSC – biliary fibrosis, biliary inflammation, and biliary stasis – as their keywords. This approach allowed them to discover the genes and potential pathways related to PSC in published research text or in clinical, animal, and cellular models.
The researchers initially found 525 genes linked to PSC and then compared them to RNA data from liver biopsies taken from patients with liver disease from various causes. This process led to a ranking of the 10 best markers of PSC, based on the data-mining method and the genes’ association with one or more of the three PSC symptoms.
At the top of the list is NR1H4, also called FXR, which ranks most highly with biliary fibrosis and biliary stasis. NR1H4 is already a clear target for cholestatic and fatty liver diseases, the authors noted. The other genes, in descending order of relevance, are: ABCB4, ABCB11, TGFB1, IFNL3, PNPLA3, IL6, TLR4, GPBAR1, and IL17A. In addition, complications of PSC were significantly associated with upregulation of TNFRS12A, SOX9, ANXA2, MMP7, and LCN2.
Separately, investigation of the 525 initially identified genes in mouse models of PSC revealed that NR0B2 is also a key player in the pathogenesis of PSC.
"NR0B2 was upregulated in PSC livers independent of gender, age, and body mass index,” the authors reported. “Importantly, it was not dependent on the severity of PSC in the prognostic cohort, suggesting that this may be an early event during the disease.”
The researchers also found a possible pathway explaining the autoimmunity of PSC – the involvement of CD274, also known as the PDL1 immune checkpoint. The authors noted that the PDL1 inhibitor pembrolizumab has previously been reported as a cause of sclerosing cholangitis.
Further, the researchers discovered overexpression of FOXP3 in the livers of patients with PSC. Because FOXP3 determines what T-cell subtypes look like, the finding suggests that an “imbalance between Foxp3þ regulatory T cells and Th17 cells may be involved in IBD and PSC,” they wrote.
Also of note was the overexpression of SOX9 in the livers of patients with PSC whose profiles suggested the worst clinical prognoses.
Finally, the researchers identified three genes as potentially involved in development of cholangiocarcinoma: GSTA3, ID2 (which is overexpressed in biliary tract cancer), and especially TMEM45A, a protein in cells’ Golgi apparatus that is already known to be involved in the development of several other cancers.
The research was funded by the French National Institute of Health and Medical Research. The authors reported no conflicts of interest.
, according to a study published in Gastro Hep Advances.
PSC is very rare, with an incidence of 0-1.3 cases per 100,000 people per year. Because up to 80% of patients with PSC also have inflammatory bowel disease (IBD), a link along the gut-liver axis is suspected. So far, scientists have not understood the causes of PSC, the main complications of which include biliary cirrhosis, bacterial cholangitis, and cholangiocarcinoma.
No treatment is currently available for PSC, but the findings of this genomics study suggest several targets that may be worth pursuing, particularly the gene NR0B2.
“The therapeutic targeting of NR0B2 may potentiate that of FXR [farnesoid X receptor] and enable action on early events of the disease and prevent its progression,” wrote Christophe Desterke, PhD, of the Paul-Brousse Hospital, the French National Institute of Health and Medical Research, and the University of Paris-Saclay in Villejuif, France, and his associates.
The researchers used an algorithmic tool to mine the MEDLINE/PubMed/NCBI database using the three key symptoms of PSC – biliary fibrosis, biliary inflammation, and biliary stasis – as their keywords. This approach allowed them to discover the genes and potential pathways related to PSC in published research text or in clinical, animal, and cellular models.
The researchers initially found 525 genes linked to PSC and then compared them to RNA data from liver biopsies taken from patients with liver disease from various causes. This process led to a ranking of the 10 best markers of PSC, based on the data-mining method and the genes’ association with one or more of the three PSC symptoms.
At the top of the list is NR1H4, also called FXR, which ranks most highly with biliary fibrosis and biliary stasis. NR1H4 is already a clear target for cholestatic and fatty liver diseases, the authors noted. The other genes, in descending order of relevance, are: ABCB4, ABCB11, TGFB1, IFNL3, PNPLA3, IL6, TLR4, GPBAR1, and IL17A. In addition, complications of PSC were significantly associated with upregulation of TNFRS12A, SOX9, ANXA2, MMP7, and LCN2.
Separately, investigation of the 525 initially identified genes in mouse models of PSC revealed that NR0B2 is also a key player in the pathogenesis of PSC.
"NR0B2 was upregulated in PSC livers independent of gender, age, and body mass index,” the authors reported. “Importantly, it was not dependent on the severity of PSC in the prognostic cohort, suggesting that this may be an early event during the disease.”
The researchers also found a possible pathway explaining the autoimmunity of PSC – the involvement of CD274, also known as the PDL1 immune checkpoint. The authors noted that the PDL1 inhibitor pembrolizumab has previously been reported as a cause of sclerosing cholangitis.
Further, the researchers discovered overexpression of FOXP3 in the livers of patients with PSC. Because FOXP3 determines what T-cell subtypes look like, the finding suggests that an “imbalance between Foxp3þ regulatory T cells and Th17 cells may be involved in IBD and PSC,” they wrote.
Also of note was the overexpression of SOX9 in the livers of patients with PSC whose profiles suggested the worst clinical prognoses.
Finally, the researchers identified three genes as potentially involved in development of cholangiocarcinoma: GSTA3, ID2 (which is overexpressed in biliary tract cancer), and especially TMEM45A, a protein in cells’ Golgi apparatus that is already known to be involved in the development of several other cancers.
The research was funded by the French National Institute of Health and Medical Research. The authors reported no conflicts of interest.
FROM GASTRO HEP ADVANCES
Scar overgrowth

Dermatopathology was consistent with a diagnosis of cutaneous myxoma (CM). There are very few dermoscopic descriptions of CM in the literature, so diagnostic features are not established. However, the absence of more diagnostic features of basal cell carcinoma or squamous cell carcinoma (SCC) increases the likelihood of a rare diagnosis, such as CM.
CMs are rare benign neoplasms that manifest most commonly in young adults as small (< 1 cm) flesh-colored to blue papules on the head, neck, and trunk. The size of this particular CM was an outlier. CMs may be associated with Carney Complex (CNC), a rare inherited syndrome that has been linked to multiple endocrine neoplasias—namely, pituitary adenomas, testicular Sertoli cell tumors, thyroid tumors, and cardiac atrial myxomas.1 Additionally, in CNC, lentigines and multiple blue nevi develop on the skin and mucosal surfaces.
The differential diagnosis for a large, pink to flesh-colored nodule of this size includes benign histiocytoma, SCC, CM, and dermatofibrosarcoma protuberans. Benign histiocytomas and SCCs are much more common than CM. Clinical features only hint at the correct diagnosis, which must be made histologically.
Patients with CMs benefit from ongoing dermatology surveillance to monitor for the development of atypical nevi or new CMs. In this case, a wide excision with generous margins was planned with plastic surgery. (CMs have been reported to recur after surgery, which is why wide margins are essential.)
Additionally, 2 factors prompted an echocardiogram: the association between CMs and possible cardiac tumors and the patient’s need to undergo future orthopedic surgery under general anesthesia. No cardiac tumors were visible on echocardiogram. Thyroid imaging and genetic evaluation were planned but not completed.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
1. Zou Y, Billings SD. Myxoid cutaneous tumors: a review. J Cutan Pathol. 2016;43:903-18. doi: 10.1111/cup.12749.
Dermatopathology was consistent with a diagnosis of cutaneous myxoma (CM). There are very few dermoscopic descriptions of CM in the literature, so diagnostic features are not established. However, the absence of more diagnostic features of basal cell carcinoma or squamous cell carcinoma (SCC) increases the likelihood of a rare diagnosis, such as CM.
CMs are rare benign neoplasms that manifest most commonly in young adults as small (< 1 cm) flesh-colored to blue papules on the head, neck, and trunk. The size of this particular CM was an outlier. CMs may be associated with Carney Complex (CNC), a rare inherited syndrome that has been linked to multiple endocrine neoplasias—namely, pituitary adenomas, testicular Sertoli cell tumors, thyroid tumors, and cardiac atrial myxomas.1 Additionally, in CNC, lentigines and multiple blue nevi develop on the skin and mucosal surfaces.
The differential diagnosis for a large, pink to flesh-colored nodule of this size includes benign histiocytoma, SCC, CM, and dermatofibrosarcoma protuberans. Benign histiocytomas and SCCs are much more common than CM. Clinical features only hint at the correct diagnosis, which must be made histologically.
Patients with CMs benefit from ongoing dermatology surveillance to monitor for the development of atypical nevi or new CMs. In this case, a wide excision with generous margins was planned with plastic surgery. (CMs have been reported to recur after surgery, which is why wide margins are essential.)
Additionally, 2 factors prompted an echocardiogram: the association between CMs and possible cardiac tumors and the patient’s need to undergo future orthopedic surgery under general anesthesia. No cardiac tumors were visible on echocardiogram. Thyroid imaging and genetic evaluation were planned but not completed.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
Dermatopathology was consistent with a diagnosis of cutaneous myxoma (CM). There are very few dermoscopic descriptions of CM in the literature, so diagnostic features are not established. However, the absence of more diagnostic features of basal cell carcinoma or squamous cell carcinoma (SCC) increases the likelihood of a rare diagnosis, such as CM.
CMs are rare benign neoplasms that manifest most commonly in young adults as small (< 1 cm) flesh-colored to blue papules on the head, neck, and trunk. The size of this particular CM was an outlier. CMs may be associated with Carney Complex (CNC), a rare inherited syndrome that has been linked to multiple endocrine neoplasias—namely, pituitary adenomas, testicular Sertoli cell tumors, thyroid tumors, and cardiac atrial myxomas.1 Additionally, in CNC, lentigines and multiple blue nevi develop on the skin and mucosal surfaces.
The differential diagnosis for a large, pink to flesh-colored nodule of this size includes benign histiocytoma, SCC, CM, and dermatofibrosarcoma protuberans. Benign histiocytomas and SCCs are much more common than CM. Clinical features only hint at the correct diagnosis, which must be made histologically.
Patients with CMs benefit from ongoing dermatology surveillance to monitor for the development of atypical nevi or new CMs. In this case, a wide excision with generous margins was planned with plastic surgery. (CMs have been reported to recur after surgery, which is why wide margins are essential.)
Additionally, 2 factors prompted an echocardiogram: the association between CMs and possible cardiac tumors and the patient’s need to undergo future orthopedic surgery under general anesthesia. No cardiac tumors were visible on echocardiogram. Thyroid imaging and genetic evaluation were planned but not completed.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
1. Zou Y, Billings SD. Myxoid cutaneous tumors: a review. J Cutan Pathol. 2016;43:903-18. doi: 10.1111/cup.12749.
1. Zou Y, Billings SD. Myxoid cutaneous tumors: a review. J Cutan Pathol. 2016;43:903-18. doi: 10.1111/cup.12749.
