User login
Mitchel is a reporter for MDedge based in the Philadelphia area. He started with the company in 1992, when it was International Medical News Group (IMNG), and has since covered a range of medical specialties. Mitchel trained as a virologist at Roswell Park Memorial Institute in Buffalo, and then worked briefly as a researcher at Boston Children's Hospital before pivoting to journalism as a AAAS Mass Media Fellow in 1980. His first reporting job was with Science Digest magazine, and from the mid-1980s to early-1990s he was a reporter with Medical World News. @mitchelzoler
VIDEO: Decision aids can relay relative risks to lung cancer patients
VIENNA – Many lung cancer patients would like to work with their physicians to reach a shared decision about their care, but often feel inadequately informed to comfortably participate in the decision process.
Patient decision aids offer a way to address this knowledge and participation gap, Laurie E. Gaspar, MD, said in a video interview at the World Conference on Lung Cancer, sponsored by the International Association for the Study of Lung Cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
She and her associates have run an online survey that so far has received responses from 196 lung cancer patients, caregivers of patients, or significant others of patients. One hundred seventeen (60%) said that they faced a difficult management decision, but more than half these patients said they felt they had inadequate information to make their decision. The most popular form of decision making was a shared decision with their physician, favored by 73% of the respondents, but only about half the patients believed they had actually participated in a shared-decision process with their physician, reported Dr. Gaspar, professor of radiation oncology at the University of Colorado in Aurora.
“A majority of the patients felt there was a problem in not having sufficient information, and a majority want to make decisions in a shared way,” she explained.

mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
VIENNA – Many lung cancer patients would like to work with their physicians to reach a shared decision about their care, but often feel inadequately informed to comfortably participate in the decision process.
Patient decision aids offer a way to address this knowledge and participation gap, Laurie E. Gaspar, MD, said in a video interview at the World Conference on Lung Cancer, sponsored by the International Association for the Study of Lung Cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
She and her associates have run an online survey that so far has received responses from 196 lung cancer patients, caregivers of patients, or significant others of patients. One hundred seventeen (60%) said that they faced a difficult management decision, but more than half these patients said they felt they had inadequate information to make their decision. The most popular form of decision making was a shared decision with their physician, favored by 73% of the respondents, but only about half the patients believed they had actually participated in a shared-decision process with their physician, reported Dr. Gaspar, professor of radiation oncology at the University of Colorado in Aurora.
“A majority of the patients felt there was a problem in not having sufficient information, and a majority want to make decisions in a shared way,” she explained.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
VIENNA – Many lung cancer patients would like to work with their physicians to reach a shared decision about their care, but often feel inadequately informed to comfortably participate in the decision process.
Patient decision aids offer a way to address this knowledge and participation gap, Laurie E. Gaspar, MD, said in a video interview at the World Conference on Lung Cancer, sponsored by the International Association for the Study of Lung Cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
She and her associates have run an online survey that so far has received responses from 196 lung cancer patients, caregivers of patients, or significant others of patients. One hundred seventeen (60%) said that they faced a difficult management decision, but more than half these patients said they felt they had inadequate information to make their decision. The most popular form of decision making was a shared decision with their physician, favored by 73% of the respondents, but only about half the patients believed they had actually participated in a shared-decision process with their physician, reported Dr. Gaspar, professor of radiation oncology at the University of Colorado in Aurora.
“A majority of the patients felt there was a problem in not having sufficient information, and a majority want to make decisions in a shared way,” she explained.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
At WCLC 2016
Key clinical point:
Major finding: A shared-decision process received support from 73% of patients, but just half believed they participated in shared decision making.
Data source: Online survey completed by 196 lung cancer patients, caregivers or significant others.
Disclosures: Dr. Gaspar had no disclosures.

U.S. okay looms for third drug-coated PAD balloon
WASHINGTON – Good pivotal-trial performance of a drug-coated balloon for treating superficial femoral and popliteal artery stenoses raised the prospect that it might soon be the third drug-coated balloon on the U.S. market, creating an opportunity for lower prices and competitive improvements for an increasingly used device.
“Having another drug-coated balloon would be useful for several reasons,” commented William A. Gray, MD, during the Transcatheter Cardiovascular Therapeutics annual meeting. The competition should mean lower cost, and accumulating reports on performance might identify a specific drug-coated balloon as most effective. Drug-coated balloons for peripheral artery stenoses “have been introduced over the past 2 years, with a significant increase in use during that time. It’s still not a majority of patients, but it’s increasing,” said Dr. Gray, chief of the division of cardiovascular disease at Main Line Health and president of Main Line Health’s Lankenau Heart Institute in Wynnewood, Pa.

The ILLUMENATE pivotal trial enrolled 300 patients at 43 centers in the United States and Europe. Patients had Rutherford 2, 3 or 4 disease, and averaged about 69 years old. More than 60% had class 3 disease and another 30% had class 2 disease.
The study’s primary safety endpoint was freedom from device- or procedure-related death to 30 days, and freedom from clinically drived target lesion revascularization at 12 months, a 92% rate in the 200 patients who had PTA with the Stellarex drug-coated balloon and 83% in the 100 controls who had PTA with an uncoated balloon. This statistically significant eight percentage point difference met the prespecified criteria for safety superiority.

The two drug-coated balloons already approved for U.S. use are the Lutonix and the IN.PACT Admiral.
“All the drug-coated balloons have worked well. It’s pretty exciting to see them work. It will be interesting to compare them against each other. We need side-by-side comparisons,” commented Craig M. Walker, MD, an interventional cardiologist in Houma, La. and a discussant for Dr. Lyden’s report.
The ILLUMENATE Pivotal trial was funded by Spectranetics, the company that is developing the Stellarex drug-coated balloon. Dr. Lyden has been a consultant to Spectranetics and to Biomet, Endologix, and TVA Medical. He received research support from Spectranetics and several other companies. Dr. Gray has been a consultant to Abbott Vascular, Boston Scientific, Cook, Medtronic, and Shockwave. He has received research support from Gore and Intact Vascular. Dr. Walker has been a consultant to Spectranetics as well as to Abbott Vascular, Bard, Boston Scientific, Cook, Gore, and Medtronic.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
It’s good to have competition among various models of drug-eluting balloons because it will help drive costs down and help drive additional improvements in device design. We win by having a third good drug-coated balloon option available.
Drug-coated balloons are increasingly used in routine U.S. practice. A recent report showed that one of the drug-coated balloons already on the U.S. market outperformed balloon angioplasty out to 3 years of follow-up. Drug-coated balloons hold an advantage over stents by leaving nothing behind. Another attraction of drug-coated balloons is that they can potentially be used as an adjunct to additional interventions for complex lesions, such as atherectomy.

So far, we have not seen a clear winner for safety and efficacy among the two drug-coated balloons already on the U.S. market and this new drug-coated balloon, which may soon be the third option for U.S. practice. But there is no single class effect from these drug-coated balloons; they must be evaluated individually.
D. Christopher Metzger, MD, is an interventional cardiologist and director of cardiac and peripheral vascular catheterization labs at the Wellmont CVA Heart Institute in Kingsport, Tenn. He has been a consultant to and received honoraria from Abbott Vascular, Bard, and Medtronic. He made these comments in an interview.
It’s good to have competition among various models of drug-eluting balloons because it will help drive costs down and help drive additional improvements in device design. We win by having a third good drug-coated balloon option available.
Drug-coated balloons are increasingly used in routine U.S. practice. A recent report showed that one of the drug-coated balloons already on the U.S. market outperformed balloon angioplasty out to 3 years of follow-up. Drug-coated balloons hold an advantage over stents by leaving nothing behind. Another attraction of drug-coated balloons is that they can potentially be used as an adjunct to additional interventions for complex lesions, such as atherectomy.
So far, we have not seen a clear winner for safety and efficacy among the two drug-coated balloons already on the U.S. market and this new drug-coated balloon, which may soon be the third option for U.S. practice. But there is no single class effect from these drug-coated balloons; they must be evaluated individually.
D. Christopher Metzger, MD, is an interventional cardiologist and director of cardiac and peripheral vascular catheterization labs at the Wellmont CVA Heart Institute in Kingsport, Tenn. He has been a consultant to and received honoraria from Abbott Vascular, Bard, and Medtronic. He made these comments in an interview.
It’s good to have competition among various models of drug-eluting balloons because it will help drive costs down and help drive additional improvements in device design. We win by having a third good drug-coated balloon option available.
Drug-coated balloons are increasingly used in routine U.S. practice. A recent report showed that one of the drug-coated balloons already on the U.S. market outperformed balloon angioplasty out to 3 years of follow-up. Drug-coated balloons hold an advantage over stents by leaving nothing behind. Another attraction of drug-coated balloons is that they can potentially be used as an adjunct to additional interventions for complex lesions, such as atherectomy.
So far, we have not seen a clear winner for safety and efficacy among the two drug-coated balloons already on the U.S. market and this new drug-coated balloon, which may soon be the third option for U.S. practice. But there is no single class effect from these drug-coated balloons; they must be evaluated individually.
D. Christopher Metzger, MD, is an interventional cardiologist and director of cardiac and peripheral vascular catheterization labs at the Wellmont CVA Heart Institute in Kingsport, Tenn. He has been a consultant to and received honoraria from Abbott Vascular, Bard, and Medtronic. He made these comments in an interview.
WASHINGTON – Good pivotal-trial performance of a drug-coated balloon for treating superficial femoral and popliteal artery stenoses raised the prospect that it might soon be the third drug-coated balloon on the U.S. market, creating an opportunity for lower prices and competitive improvements for an increasingly used device.
“Having another drug-coated balloon would be useful for several reasons,” commented William A. Gray, MD, during the Transcatheter Cardiovascular Therapeutics annual meeting. The competition should mean lower cost, and accumulating reports on performance might identify a specific drug-coated balloon as most effective. Drug-coated balloons for peripheral artery stenoses “have been introduced over the past 2 years, with a significant increase in use during that time. It’s still not a majority of patients, but it’s increasing,” said Dr. Gray, chief of the division of cardiovascular disease at Main Line Health and president of Main Line Health’s Lankenau Heart Institute in Wynnewood, Pa.
The ILLUMENATE pivotal trial enrolled 300 patients at 43 centers in the United States and Europe. Patients had Rutherford 2, 3 or 4 disease, and averaged about 69 years old. More than 60% had class 3 disease and another 30% had class 2 disease.
The study’s primary safety endpoint was freedom from device- or procedure-related death to 30 days, and freedom from clinically drived target lesion revascularization at 12 months, a 92% rate in the 200 patients who had PTA with the Stellarex drug-coated balloon and 83% in the 100 controls who had PTA with an uncoated balloon. This statistically significant eight percentage point difference met the prespecified criteria for safety superiority.
The two drug-coated balloons already approved for U.S. use are the Lutonix and the IN.PACT Admiral.
“All the drug-coated balloons have worked well. It’s pretty exciting to see them work. It will be interesting to compare them against each other. We need side-by-side comparisons,” commented Craig M. Walker, MD, an interventional cardiologist in Houma, La. and a discussant for Dr. Lyden’s report.
The ILLUMENATE Pivotal trial was funded by Spectranetics, the company that is developing the Stellarex drug-coated balloon. Dr. Lyden has been a consultant to Spectranetics and to Biomet, Endologix, and TVA Medical. He received research support from Spectranetics and several other companies. Dr. Gray has been a consultant to Abbott Vascular, Boston Scientific, Cook, Medtronic, and Shockwave. He has received research support from Gore and Intact Vascular. Dr. Walker has been a consultant to Spectranetics as well as to Abbott Vascular, Bard, Boston Scientific, Cook, Gore, and Medtronic.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
WASHINGTON – Good pivotal-trial performance of a drug-coated balloon for treating superficial femoral and popliteal artery stenoses raised the prospect that it might soon be the third drug-coated balloon on the U.S. market, creating an opportunity for lower prices and competitive improvements for an increasingly used device.
“Having another drug-coated balloon would be useful for several reasons,” commented William A. Gray, MD, during the Transcatheter Cardiovascular Therapeutics annual meeting. The competition should mean lower cost, and accumulating reports on performance might identify a specific drug-coated balloon as most effective. Drug-coated balloons for peripheral artery stenoses “have been introduced over the past 2 years, with a significant increase in use during that time. It’s still not a majority of patients, but it’s increasing,” said Dr. Gray, chief of the division of cardiovascular disease at Main Line Health and president of Main Line Health’s Lankenau Heart Institute in Wynnewood, Pa.
The ILLUMENATE pivotal trial enrolled 300 patients at 43 centers in the United States and Europe. Patients had Rutherford 2, 3 or 4 disease, and averaged about 69 years old. More than 60% had class 3 disease and another 30% had class 2 disease.
The study’s primary safety endpoint was freedom from device- or procedure-related death to 30 days, and freedom from clinically drived target lesion revascularization at 12 months, a 92% rate in the 200 patients who had PTA with the Stellarex drug-coated balloon and 83% in the 100 controls who had PTA with an uncoated balloon. This statistically significant eight percentage point difference met the prespecified criteria for safety superiority.
The two drug-coated balloons already approved for U.S. use are the Lutonix and the IN.PACT Admiral.
“All the drug-coated balloons have worked well. It’s pretty exciting to see them work. It will be interesting to compare them against each other. We need side-by-side comparisons,” commented Craig M. Walker, MD, an interventional cardiologist in Houma, La. and a discussant for Dr. Lyden’s report.
The ILLUMENATE Pivotal trial was funded by Spectranetics, the company that is developing the Stellarex drug-coated balloon. Dr. Lyden has been a consultant to Spectranetics and to Biomet, Endologix, and TVA Medical. He received research support from Spectranetics and several other companies. Dr. Gray has been a consultant to Abbott Vascular, Boston Scientific, Cook, Medtronic, and Shockwave. He has received research support from Gore and Intact Vascular. Dr. Walker has been a consultant to Spectranetics as well as to Abbott Vascular, Bard, Boston Scientific, Cook, Gore, and Medtronic.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
Key clinical point:
Major finding: The primary efficacy endpoint occurred in 76% of patients in the drug-coated balloon arm and 58% of controls.
Data source: The ILLUMENATE pivotal trial, which enrolled 300 patients at 63 U.S. and European centers.
Disclosures: The ILLUMENATE pivotal trial was funded by Spectranetics, the company that is developing the Stellarex drug-coated balloon. Dr. Lyden has been a consultant to Spectranetics and to Biomet, Endologix, and TVA Medical. He received research support from Spectranetics and several other companies. Dr. Gray has been a consultant to Abbott Vascular, Boston Scientific, Cook, Medtronic, and Shockwave. He has received research support from Gore and Intact Vascular. Dr. Walker has been a consultant to Spectranetics as well as to Abbott Vascular, Bard, Boston Scientific, Cook, Gore, and Medtronic.
TAVR valve durability supported in large follow-up
WASHINGTON – First-generation, balloon-expandable transcatheter aortic valves had a less than 1% rate of valve failure in planned echocardiography examinations during follow-up that extended as long as 5 years after valve placement in more than 2,400 patients, a demonstration of durability that experts uniformly called “reassuring.”
This finding from patients who underwent transcatheter aortic valve replacement (TAVR) in the first U.S. pivotal trial for these devices, PARTNER 1 parts A and B, and during the subsequent continued-access program at PARTNER 1 study sites, represents the largest and longest systematic ultrasound follow-up of TAVR patients, Pamela S. Douglas, MD, said at the Transcatheter Cardiovascular Therapeutics annual meeting.

This evaluation of 2,404 TAVR patients in the PARTNER 1 trial examined by echocardiography and encompassing 6,493 patient-years of follow-up is the “largest core-lab based study of transcatheter heart valves to date. These data demonstrate excellent durability of transcatheter heart valves, suggesting that the low 5-year survival observed in this cohort is not related to adverse hemodynamics or transcatheter heart valve deterioration,” said Dr. Douglas, professor of medicine at Duke University, Durham, N.C.
Her findings showed that out of the 2,482 patients treated with TAVR (and including those without echo follow-up) either in the trial or during the continued access program and followed for a median of 2.9 years and an average of 2.6 years, 20 patients (0.8%) required a reintervention. Four of these 20 patients (0.2% of the total cohort) showed a “classic pattern” of aortic valve deterioration marked by an increased valve pressure gradient and a reduced valve area, she reported.
“Reintervention was rare, became less frequent over time, and was usually not due to structural deterioration of the transcatheter heart valve,” she said. But Dr. Douglas also cautioned that among the patients who received the first-generation, balloon expandable Sapien valve in this cohort, just 39% survived to 5 years, and a mere 282 patients (11%) actually underwent echocardiographic examination at 5 years.
“This is one of several steps we need to take to figure out the durability of transcatheter valves,” said Jeffrey J. Popma, MD, professor of medicine and an interventional cardiologist at Beth Israel Deaconess Medical Center, Boston. He noted that data are needed from follow-up periods of 8 or 10 years, but these data will not be available until intermediate- or low-risk patients undergo TAVR in controlled circumstances and have long-term follow-up.

“Ten-year follow-up data will essentially be impossible” for the high-risk or inoperable patients treated with TAVR in the PARTNER 1 trial, which focused on the sickest patients with aortic stenosis, said Dr. Popma, lead investigator for several studies of TAVR using self-expanding aortic valves and marketed as CoreValve devices.
“We obviously need to follow patients longer. The 5-year results look terrific, and so very reassuring, but we need to keep an eye on this as we move TAVR into less sick and younger patients,” said Dr. Robert O. Bonow, professor of cardiology at Northwestern University, Chicago. “Durability is the remaining frontier in terms of moving TAVR into younger patients,” Dr. Bonow said at the meeting, which was sponsored by the Cardiovascular Research Foundation.

These data continue to show that “transcatheter valves have looked hemodynamically superior to surgically-placed valves with respect to the VARC (Valve Academic Research Consortium)–2 criteria” for prosthetic valve function, Dr. Popma noted. “I think the benefits of surgical valves have been overstated and the benefits of transcatheter valves understated,” he said.
“Surgical valves have not been held to the same [very demanding] standard as transcatheter valves,” Dr. Douglas agreed.
The data Dr. Douglas reported contrast with longer-term follow-up reported in May 2016 for 378 patients who underwent TAVR at either of two pioneering centers in a retrospective review. Those data suggested a valve degeneration rate of about 50% after 8 years, Danny Dvir, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions. Speaking recently in an interview, Dr. Dvir acknowledged some of the challenges in trying to derive valve durability information from a relatively small number of very-high-risk patients who underwent TAVR very early during development of the procedure.
Some TAVR experts have also questioned the criteria that Dr. Dvir used to identify valve structural valve degeneration for this analysis. “The criteria he used were much more stringent that the criteria we have used to assess surgically-placed valves,” said Michael J. Reardon, MD, professor of cardiovascular surgery at Houston Methodist Hospital. “If surgically-placed aortic valves were subjected to the same criteria Dr. Dvir applied then they would perform even worse,” Dr. Reardon said in an interview.
PARTNER 1 was sponsored by Edwards Lifesciences, the company that had marketed the Sapien first-generation, balloon expandable TAVR system. Dr. Douglas has received research support from Edwards. Dr. Bonow had no disclosures. Dr. Popma has been the lead investigator for several studies of a self-expanding TAVR system sponsored by Medtronic, and he has also received research funding from several other companies, has been a consultant to Boston Scientific and Direct Flow, and owns equity in Direct Flow. Dr. Dvir has been a consultant to and received research support from Edwards, Medtronic, and St. Jude. Dr. Reardon has been a consultant to Medtronic.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
The data reported by Dr. Douglas are very important and very reassuring. It isn’t easy to evaluate long-term results in patients who underwent TAVR in the early days because that population of patients was old and at very high risk. Even when patients had successful procedures their longevity wasn’t long. Only about 10% of the starting population of 2,482 patients in Dr. Douglas’ study actually had echocardiography done after 5 years. To assess durability you need longer-term echo follow-up, but it will be very challenging to have enough patients to have statistical power to do that.
I am not nervous about long-term durability of TAVR in octogenarian patients, the most typical age for TAVR patients today and since we began using it. Durability is more of an issue for patients who are 75 or younger, and we will need data from 7- to 10-year follow-up of younger patients to have a reasonable answer. Younger patients who undergo TAVR may face more of a threat from valve deterioration simply because of their longer life expectancy. In addition, with surgical valves we know that younger age is one of the strongest predictors of valve degeneration.

Danny Dvir, MD , is an interventional cardiologist at the University of Washington in Seattle. He has been a consultant to and received research support from Edwards, Medtronic, and St. Jude. He made these comments in an interview.
The data reported by Dr. Douglas are very important and very reassuring. It isn’t easy to evaluate long-term results in patients who underwent TAVR in the early days because that population of patients was old and at very high risk. Even when patients had successful procedures their longevity wasn’t long. Only about 10% of the starting population of 2,482 patients in Dr. Douglas’ study actually had echocardiography done after 5 years. To assess durability you need longer-term echo follow-up, but it will be very challenging to have enough patients to have statistical power to do that.
I am not nervous about long-term durability of TAVR in octogenarian patients, the most typical age for TAVR patients today and since we began using it. Durability is more of an issue for patients who are 75 or younger, and we will need data from 7- to 10-year follow-up of younger patients to have a reasonable answer. Younger patients who undergo TAVR may face more of a threat from valve deterioration simply because of their longer life expectancy. In addition, with surgical valves we know that younger age is one of the strongest predictors of valve degeneration.
Danny Dvir, MD , is an interventional cardiologist at the University of Washington in Seattle. He has been a consultant to and received research support from Edwards, Medtronic, and St. Jude. He made these comments in an interview.
The data reported by Dr. Douglas are very important and very reassuring. It isn’t easy to evaluate long-term results in patients who underwent TAVR in the early days because that population of patients was old and at very high risk. Even when patients had successful procedures their longevity wasn’t long. Only about 10% of the starting population of 2,482 patients in Dr. Douglas’ study actually had echocardiography done after 5 years. To assess durability you need longer-term echo follow-up, but it will be very challenging to have enough patients to have statistical power to do that.
I am not nervous about long-term durability of TAVR in octogenarian patients, the most typical age for TAVR patients today and since we began using it. Durability is more of an issue for patients who are 75 or younger, and we will need data from 7- to 10-year follow-up of younger patients to have a reasonable answer. Younger patients who undergo TAVR may face more of a threat from valve deterioration simply because of their longer life expectancy. In addition, with surgical valves we know that younger age is one of the strongest predictors of valve degeneration.
Danny Dvir, MD , is an interventional cardiologist at the University of Washington in Seattle. He has been a consultant to and received research support from Edwards, Medtronic, and St. Jude. He made these comments in an interview.
WASHINGTON – First-generation, balloon-expandable transcatheter aortic valves had a less than 1% rate of valve failure in planned echocardiography examinations during follow-up that extended as long as 5 years after valve placement in more than 2,400 patients, a demonstration of durability that experts uniformly called “reassuring.”
This finding from patients who underwent transcatheter aortic valve replacement (TAVR) in the first U.S. pivotal trial for these devices, PARTNER 1 parts A and B, and during the subsequent continued-access program at PARTNER 1 study sites, represents the largest and longest systematic ultrasound follow-up of TAVR patients, Pamela S. Douglas, MD, said at the Transcatheter Cardiovascular Therapeutics annual meeting.
This evaluation of 2,404 TAVR patients in the PARTNER 1 trial examined by echocardiography and encompassing 6,493 patient-years of follow-up is the “largest core-lab based study of transcatheter heart valves to date. These data demonstrate excellent durability of transcatheter heart valves, suggesting that the low 5-year survival observed in this cohort is not related to adverse hemodynamics or transcatheter heart valve deterioration,” said Dr. Douglas, professor of medicine at Duke University, Durham, N.C.
Her findings showed that out of the 2,482 patients treated with TAVR (and including those without echo follow-up) either in the trial or during the continued access program and followed for a median of 2.9 years and an average of 2.6 years, 20 patients (0.8%) required a reintervention. Four of these 20 patients (0.2% of the total cohort) showed a “classic pattern” of aortic valve deterioration marked by an increased valve pressure gradient and a reduced valve area, she reported.
“Reintervention was rare, became less frequent over time, and was usually not due to structural deterioration of the transcatheter heart valve,” she said. But Dr. Douglas also cautioned that among the patients who received the first-generation, balloon expandable Sapien valve in this cohort, just 39% survived to 5 years, and a mere 282 patients (11%) actually underwent echocardiographic examination at 5 years.
“This is one of several steps we need to take to figure out the durability of transcatheter valves,” said Jeffrey J. Popma, MD, professor of medicine and an interventional cardiologist at Beth Israel Deaconess Medical Center, Boston. He noted that data are needed from follow-up periods of 8 or 10 years, but these data will not be available until intermediate- or low-risk patients undergo TAVR in controlled circumstances and have long-term follow-up.
“Ten-year follow-up data will essentially be impossible” for the high-risk or inoperable patients treated with TAVR in the PARTNER 1 trial, which focused on the sickest patients with aortic stenosis, said Dr. Popma, lead investigator for several studies of TAVR using self-expanding aortic valves and marketed as CoreValve devices.
“We obviously need to follow patients longer. The 5-year results look terrific, and so very reassuring, but we need to keep an eye on this as we move TAVR into less sick and younger patients,” said Dr. Robert O. Bonow, professor of cardiology at Northwestern University, Chicago. “Durability is the remaining frontier in terms of moving TAVR into younger patients,” Dr. Bonow said at the meeting, which was sponsored by the Cardiovascular Research Foundation.
These data continue to show that “transcatheter valves have looked hemodynamically superior to surgically-placed valves with respect to the VARC (Valve Academic Research Consortium)–2 criteria” for prosthetic valve function, Dr. Popma noted. “I think the benefits of surgical valves have been overstated and the benefits of transcatheter valves understated,” he said.
“Surgical valves have not been held to the same [very demanding] standard as transcatheter valves,” Dr. Douglas agreed.
The data Dr. Douglas reported contrast with longer-term follow-up reported in May 2016 for 378 patients who underwent TAVR at either of two pioneering centers in a retrospective review. Those data suggested a valve degeneration rate of about 50% after 8 years, Danny Dvir, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions. Speaking recently in an interview, Dr. Dvir acknowledged some of the challenges in trying to derive valve durability information from a relatively small number of very-high-risk patients who underwent TAVR very early during development of the procedure.
Some TAVR experts have also questioned the criteria that Dr. Dvir used to identify valve structural valve degeneration for this analysis. “The criteria he used were much more stringent that the criteria we have used to assess surgically-placed valves,” said Michael J. Reardon, MD, professor of cardiovascular surgery at Houston Methodist Hospital. “If surgically-placed aortic valves were subjected to the same criteria Dr. Dvir applied then they would perform even worse,” Dr. Reardon said in an interview.
PARTNER 1 was sponsored by Edwards Lifesciences, the company that had marketed the Sapien first-generation, balloon expandable TAVR system. Dr. Douglas has received research support from Edwards. Dr. Bonow had no disclosures. Dr. Popma has been the lead investigator for several studies of a self-expanding TAVR system sponsored by Medtronic, and he has also received research funding from several other companies, has been a consultant to Boston Scientific and Direct Flow, and owns equity in Direct Flow. Dr. Dvir has been a consultant to and received research support from Edwards, Medtronic, and St. Jude. Dr. Reardon has been a consultant to Medtronic.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
WASHINGTON – First-generation, balloon-expandable transcatheter aortic valves had a less than 1% rate of valve failure in planned echocardiography examinations during follow-up that extended as long as 5 years after valve placement in more than 2,400 patients, a demonstration of durability that experts uniformly called “reassuring.”
This finding from patients who underwent transcatheter aortic valve replacement (TAVR) in the first U.S. pivotal trial for these devices, PARTNER 1 parts A and B, and during the subsequent continued-access program at PARTNER 1 study sites, represents the largest and longest systematic ultrasound follow-up of TAVR patients, Pamela S. Douglas, MD, said at the Transcatheter Cardiovascular Therapeutics annual meeting.
This evaluation of 2,404 TAVR patients in the PARTNER 1 trial examined by echocardiography and encompassing 6,493 patient-years of follow-up is the “largest core-lab based study of transcatheter heart valves to date. These data demonstrate excellent durability of transcatheter heart valves, suggesting that the low 5-year survival observed in this cohort is not related to adverse hemodynamics or transcatheter heart valve deterioration,” said Dr. Douglas, professor of medicine at Duke University, Durham, N.C.
Her findings showed that out of the 2,482 patients treated with TAVR (and including those without echo follow-up) either in the trial or during the continued access program and followed for a median of 2.9 years and an average of 2.6 years, 20 patients (0.8%) required a reintervention. Four of these 20 patients (0.2% of the total cohort) showed a “classic pattern” of aortic valve deterioration marked by an increased valve pressure gradient and a reduced valve area, she reported.
“Reintervention was rare, became less frequent over time, and was usually not due to structural deterioration of the transcatheter heart valve,” she said. But Dr. Douglas also cautioned that among the patients who received the first-generation, balloon expandable Sapien valve in this cohort, just 39% survived to 5 years, and a mere 282 patients (11%) actually underwent echocardiographic examination at 5 years.
“This is one of several steps we need to take to figure out the durability of transcatheter valves,” said Jeffrey J. Popma, MD, professor of medicine and an interventional cardiologist at Beth Israel Deaconess Medical Center, Boston. He noted that data are needed from follow-up periods of 8 or 10 years, but these data will not be available until intermediate- or low-risk patients undergo TAVR in controlled circumstances and have long-term follow-up.
“Ten-year follow-up data will essentially be impossible” for the high-risk or inoperable patients treated with TAVR in the PARTNER 1 trial, which focused on the sickest patients with aortic stenosis, said Dr. Popma, lead investigator for several studies of TAVR using self-expanding aortic valves and marketed as CoreValve devices.
“We obviously need to follow patients longer. The 5-year results look terrific, and so very reassuring, but we need to keep an eye on this as we move TAVR into less sick and younger patients,” said Dr. Robert O. Bonow, professor of cardiology at Northwestern University, Chicago. “Durability is the remaining frontier in terms of moving TAVR into younger patients,” Dr. Bonow said at the meeting, which was sponsored by the Cardiovascular Research Foundation.
These data continue to show that “transcatheter valves have looked hemodynamically superior to surgically-placed valves with respect to the VARC (Valve Academic Research Consortium)–2 criteria” for prosthetic valve function, Dr. Popma noted. “I think the benefits of surgical valves have been overstated and the benefits of transcatheter valves understated,” he said.
“Surgical valves have not been held to the same [very demanding] standard as transcatheter valves,” Dr. Douglas agreed.
The data Dr. Douglas reported contrast with longer-term follow-up reported in May 2016 for 378 patients who underwent TAVR at either of two pioneering centers in a retrospective review. Those data suggested a valve degeneration rate of about 50% after 8 years, Danny Dvir, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions. Speaking recently in an interview, Dr. Dvir acknowledged some of the challenges in trying to derive valve durability information from a relatively small number of very-high-risk patients who underwent TAVR very early during development of the procedure.
Some TAVR experts have also questioned the criteria that Dr. Dvir used to identify valve structural valve degeneration for this analysis. “The criteria he used were much more stringent that the criteria we have used to assess surgically-placed valves,” said Michael J. Reardon, MD, professor of cardiovascular surgery at Houston Methodist Hospital. “If surgically-placed aortic valves were subjected to the same criteria Dr. Dvir applied then they would perform even worse,” Dr. Reardon said in an interview.
PARTNER 1 was sponsored by Edwards Lifesciences, the company that had marketed the Sapien first-generation, balloon expandable TAVR system. Dr. Douglas has received research support from Edwards. Dr. Bonow had no disclosures. Dr. Popma has been the lead investigator for several studies of a self-expanding TAVR system sponsored by Medtronic, and he has also received research funding from several other companies, has been a consultant to Boston Scientific and Direct Flow, and owns equity in Direct Flow. Dr. Dvir has been a consultant to and received research support from Edwards, Medtronic, and St. Jude. Dr. Reardon has been a consultant to Medtronic.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT TCT 2016
Key clinical point:
Major finding: During median follow-up of 2.9 years, 0.2% of patients had valves with classic hemodynamic signs of valve deterioration.
Data source: A total of 2,482 TAVR patients either enrolled in the PARTNER 1 trial or who underwent TAVR during a continued access program.
Disclosures: PARTNER 1 was sponsored by Edwards Lifesciences, the company that had marketed the Sapien first-generation, balloon expandable TAVR system. Dr. Douglas has received research support from Edwards. Dr. Bonow had no disclosures. Dr. Popma has been the lead investigator for several studies of a self-expanding TAVR system sponsored by Medtronic, and he has also received research funding from several other companies, has been a consultant to Boston Scientific and Direct Flow, and owns equity in Direct Flow. Dr. Dvir has been a consultant to and received research support from Edwards, Medtronic, and St. Jude. Dr. Reardon has been a consultant to Medtronic.
New PAD guidelines expected to boost awareness and treatment
NEW ORLEANS – The latest revision of U.S. guidelines for diagnosing and managing lower-extremity peripheral artery disease is seen by several experts as primarily a renewed call to action by American physicians to more diligently identify at-risk people in their practices, diagnose the disease with ankle-brachial index measurement, and appropriately treat patients who have the disease.
The new lower-extremity peripheral artery disease (PAD) guidelines “give us a platform to get something done,” said Heather L. Gornik, MD, vice chair of the guidelines panel and medical director of the noninvasive vascular lab at the Cleveland Clinic. Improved PAD identification and care “starts with the fundamentals of recognizing who is at risk for PAD and then doing some clinical investigation to find it, because it’s there. You just need to ask patients if they have leg symptoms, have them take off their socks and examine their feet,” Dr. Gornik said in an interview following a program devoted to the revised guidelines at the American Heart Association scientific sessions.

The new guidelines are “a clarion call to action,” commented Alan T. Hirsch, MD, professor of medicine, epidemiology, and community health and director of the vascular medicine program at the University of Minnesota in Minneapolis. PAD “is the single most morbid and fatal of all cardiovascular diseases, so why in 2016 are we challenged to have every cardiologist trained in basic PAD competency?” asked Dr. Hirsch, who chaired the 2005 guidelines panel.

The AHA wants to “elevate awareness of PAD among the public and health professionals, and we want to better understand how we can be a catalyst for change,” said Terri Wiggins, the organization’s vice president for vascular health programs. AHA publications now stress that clinicians need to have patients “take off their socks and look at the patient’s feet,” she said.
The problem with the way many U.S. physicians handle PAD goes beyond a failure to properly screen and diagnose the disease. Analysis of data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey during 2006-2013 showed that, among an average of 3.9 million patients seen each year with PAD, just 38% received treatment with an antiplatelet drug, 35% received a statin, and among those patients who smoked, 36% received counseling for smoking cessation, Jeffrey S. Berger, MD, reported in a separate talk at the meeting. These rates were roughly constant throughout the 8-year period he examined.

“These data are eye-opening. They highlight a clear opportunity to improve the care of patients with PAD with guideline-directed therapy. PAD is problematic because only 10%-15% of patients have typical symptoms, so many physicians have a false perception that these patients are not at high risk,” Dr. Berger said in an interview. “What the AHA is doing is great” for raising awareness, he added.
The revised 2016 PAD guidelines made several changes, compared with what had been on the books from the 2005 guidelines and 2011 update, including classifying vorapaxar (Zontivity) treatment a class IIb recommendation with “uncertain” incremental benefit when used as an add-on agent on top of standard antiplatelet therapy, endorsement of annual influenza vaccination as something every PAD patient should receive and a class I recommendation, and acknowledgment that selected patients with critical limb ischemia are candidates for an “endovascular first” approach to revascularization,
Perhaps just as important was inclusion for the first time in the new guidelines of three advocacy priorities for initiatives by various professional societies with an interest in PAD: easy availability of ankle-brachial index measurement as the initial test to establish a diagnosis of PAD in patients with physical examination findings suggestive of the disease; access to supervised exercise programs for patients diagnosed with PAD; and incorporation of patient-centered outcomes into the regulatory approval process of new medical therapies and revascularization technologies for treating PAD.
The new guidelines “ form the basis for the AHA establishing a Get With The Guidelines program for PAD so that clinicians can be held accountable for delivering these treatments,” said Naomi M. Hamburg, MD, chief of vascular biology at Boston University and a member of the guidelines panel.

Dr. Gornik has an ownership interest in Summit Doppler Systems and Zin Medical and has received research support from AstraZeneca and Theravasc. Dr. Hamburg has been a consultant to Acceleron and has received research support from Everest Genomics, Hershey’s, Unex, and Welch’s. Dr. Hirsch, Ms. Wiggins, and Dr. Berger had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
NEW ORLEANS – The latest revision of U.S. guidelines for diagnosing and managing lower-extremity peripheral artery disease is seen by several experts as primarily a renewed call to action by American physicians to more diligently identify at-risk people in their practices, diagnose the disease with ankle-brachial index measurement, and appropriately treat patients who have the disease.
The new lower-extremity peripheral artery disease (PAD) guidelines “give us a platform to get something done,” said Heather L. Gornik, MD, vice chair of the guidelines panel and medical director of the noninvasive vascular lab at the Cleveland Clinic. Improved PAD identification and care “starts with the fundamentals of recognizing who is at risk for PAD and then doing some clinical investigation to find it, because it’s there. You just need to ask patients if they have leg symptoms, have them take off their socks and examine their feet,” Dr. Gornik said in an interview following a program devoted to the revised guidelines at the American Heart Association scientific sessions.
The new guidelines are “a clarion call to action,” commented Alan T. Hirsch, MD, professor of medicine, epidemiology, and community health and director of the vascular medicine program at the University of Minnesota in Minneapolis. PAD “is the single most morbid and fatal of all cardiovascular diseases, so why in 2016 are we challenged to have every cardiologist trained in basic PAD competency?” asked Dr. Hirsch, who chaired the 2005 guidelines panel.
The AHA wants to “elevate awareness of PAD among the public and health professionals, and we want to better understand how we can be a catalyst for change,” said Terri Wiggins, the organization’s vice president for vascular health programs. AHA publications now stress that clinicians need to have patients “take off their socks and look at the patient’s feet,” she said.
The problem with the way many U.S. physicians handle PAD goes beyond a failure to properly screen and diagnose the disease. Analysis of data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey during 2006-2013 showed that, among an average of 3.9 million patients seen each year with PAD, just 38% received treatment with an antiplatelet drug, 35% received a statin, and among those patients who smoked, 36% received counseling for smoking cessation, Jeffrey S. Berger, MD, reported in a separate talk at the meeting. These rates were roughly constant throughout the 8-year period he examined.
“These data are eye-opening. They highlight a clear opportunity to improve the care of patients with PAD with guideline-directed therapy. PAD is problematic because only 10%-15% of patients have typical symptoms, so many physicians have a false perception that these patients are not at high risk,” Dr. Berger said in an interview. “What the AHA is doing is great” for raising awareness, he added.
The revised 2016 PAD guidelines made several changes, compared with what had been on the books from the 2005 guidelines and 2011 update, including classifying vorapaxar (Zontivity) treatment a class IIb recommendation with “uncertain” incremental benefit when used as an add-on agent on top of standard antiplatelet therapy, endorsement of annual influenza vaccination as something every PAD patient should receive and a class I recommendation, and acknowledgment that selected patients with critical limb ischemia are candidates for an “endovascular first” approach to revascularization,
Perhaps just as important was inclusion for the first time in the new guidelines of three advocacy priorities for initiatives by various professional societies with an interest in PAD: easy availability of ankle-brachial index measurement as the initial test to establish a diagnosis of PAD in patients with physical examination findings suggestive of the disease; access to supervised exercise programs for patients diagnosed with PAD; and incorporation of patient-centered outcomes into the regulatory approval process of new medical therapies and revascularization technologies for treating PAD.
The new guidelines “ form the basis for the AHA establishing a Get With The Guidelines program for PAD so that clinicians can be held accountable for delivering these treatments,” said Naomi M. Hamburg, MD, chief of vascular biology at Boston University and a member of the guidelines panel.
Dr. Gornik has an ownership interest in Summit Doppler Systems and Zin Medical and has received research support from AstraZeneca and Theravasc. Dr. Hamburg has been a consultant to Acceleron and has received research support from Everest Genomics, Hershey’s, Unex, and Welch’s. Dr. Hirsch, Ms. Wiggins, and Dr. Berger had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
NEW ORLEANS – The latest revision of U.S. guidelines for diagnosing and managing lower-extremity peripheral artery disease is seen by several experts as primarily a renewed call to action by American physicians to more diligently identify at-risk people in their practices, diagnose the disease with ankle-brachial index measurement, and appropriately treat patients who have the disease.
The new lower-extremity peripheral artery disease (PAD) guidelines “give us a platform to get something done,” said Heather L. Gornik, MD, vice chair of the guidelines panel and medical director of the noninvasive vascular lab at the Cleveland Clinic. Improved PAD identification and care “starts with the fundamentals of recognizing who is at risk for PAD and then doing some clinical investigation to find it, because it’s there. You just need to ask patients if they have leg symptoms, have them take off their socks and examine their feet,” Dr. Gornik said in an interview following a program devoted to the revised guidelines at the American Heart Association scientific sessions.
The new guidelines are “a clarion call to action,” commented Alan T. Hirsch, MD, professor of medicine, epidemiology, and community health and director of the vascular medicine program at the University of Minnesota in Minneapolis. PAD “is the single most morbid and fatal of all cardiovascular diseases, so why in 2016 are we challenged to have every cardiologist trained in basic PAD competency?” asked Dr. Hirsch, who chaired the 2005 guidelines panel.
The AHA wants to “elevate awareness of PAD among the public and health professionals, and we want to better understand how we can be a catalyst for change,” said Terri Wiggins, the organization’s vice president for vascular health programs. AHA publications now stress that clinicians need to have patients “take off their socks and look at the patient’s feet,” she said.
The problem with the way many U.S. physicians handle PAD goes beyond a failure to properly screen and diagnose the disease. Analysis of data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey during 2006-2013 showed that, among an average of 3.9 million patients seen each year with PAD, just 38% received treatment with an antiplatelet drug, 35% received a statin, and among those patients who smoked, 36% received counseling for smoking cessation, Jeffrey S. Berger, MD, reported in a separate talk at the meeting. These rates were roughly constant throughout the 8-year period he examined.
“These data are eye-opening. They highlight a clear opportunity to improve the care of patients with PAD with guideline-directed therapy. PAD is problematic because only 10%-15% of patients have typical symptoms, so many physicians have a false perception that these patients are not at high risk,” Dr. Berger said in an interview. “What the AHA is doing is great” for raising awareness, he added.
The revised 2016 PAD guidelines made several changes, compared with what had been on the books from the 2005 guidelines and 2011 update, including classifying vorapaxar (Zontivity) treatment a class IIb recommendation with “uncertain” incremental benefit when used as an add-on agent on top of standard antiplatelet therapy, endorsement of annual influenza vaccination as something every PAD patient should receive and a class I recommendation, and acknowledgment that selected patients with critical limb ischemia are candidates for an “endovascular first” approach to revascularization,
Perhaps just as important was inclusion for the first time in the new guidelines of three advocacy priorities for initiatives by various professional societies with an interest in PAD: easy availability of ankle-brachial index measurement as the initial test to establish a diagnosis of PAD in patients with physical examination findings suggestive of the disease; access to supervised exercise programs for patients diagnosed with PAD; and incorporation of patient-centered outcomes into the regulatory approval process of new medical therapies and revascularization technologies for treating PAD.
The new guidelines “ form the basis for the AHA establishing a Get With The Guidelines program for PAD so that clinicians can be held accountable for delivering these treatments,” said Naomi M. Hamburg, MD, chief of vascular biology at Boston University and a member of the guidelines panel.
Dr. Gornik has an ownership interest in Summit Doppler Systems and Zin Medical and has received research support from AstraZeneca and Theravasc. Dr. Hamburg has been a consultant to Acceleron and has received research support from Everest Genomics, Hershey’s, Unex, and Welch’s. Dr. Hirsch, Ms. Wiggins, and Dr. Berger had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE AHA SCIENTIFIC SESSIONS
VIDEO: HeartMate 3 LVAD solves pump thrombosis
NEW ORLEANS – HeartMate 3, the latest left ventricular assist device in the HeartMate line, appears to have solved the problem of pump thrombosis, a complication that has dogged ventricular pumps since the issue leapt into medical awareness about 3 years ago (New Engl J Med. 2014 Jan 2;370:33-40).
During 6 months of follow-up, none of 152 heart failure patients assigned to receive a HeartMate 3 left ventricular assist device (LVAD) developed suspected or confirmed pump thrombosis, compared with 14 patients (10%) having pump thrombosis out of 138 recipients of the prior-generation HeartMate II LVAD who served as the control group for the study.

“Three years ago, when the issue of pump thrombosis was first revealed, there was a lot of consternation and some drop in LVAD use, especially as destination therapy. We think that seeing no pump thrombosis whatsoever will give people renewed confidence in this technology,” said Dr. Mehra, professor of medicine at Harvard Medical School and medical director of the Heart and Vascular Center of Brigham and Women’s Hospital, both in Boston.
Pump thrombosis has also been a problem for the patients who have received a competitor LVAD, the HeartWare HVAD device (Circulation. 2015 Nov 10;132[suppl 3]:A19675), approved for U.S. use as bridge to transplant. HeartMate II is approved for both bridge to transplant and for destination therapy.
In addition to apparently eliminating pump thrombosis, HeartMate 3’s size and potential implantation approach should make its placement during routine use as quick and minimally invasive as the HeartWare device, features that should further help broader use of HeartMate 3, commented Mark Slaughter, MD, professor and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). But Dr. Slaughter and others were also quick to highlight the shortcomings that remain with both devices that will continue to hamper a broader role for LVAD treatment of patients with advanced heart failure.

“We thought that if there was less pump thrombosis we’d see less stroke, but that is not what the data suggest. It’s the big puzzle we need to figure out before we see widespread acceptance of this treatment,” Dr. Sweitzer said.
“This will not shift LVAD use substantially,” commented Christopher B. Granger, MD, a professor of medicine and a heart failure specialist at Duke University, Durham, N.C. “Reducing the need for reoperation is good for the field, and is an incremental advance, but it is not transformational,” he said in an interview.
The MOMENTUM 3 (Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy with HeartMate 3) trial randomized 294 patients at 69 U.S. centers. The study’s primary endpoint of 6-month survival free from disabling stroke or reoperation to repair or replace the LVAD occurred in 86% of 152 patients who received a HeartMate 3 and 77% of 142 patients randomized to HeartMate II, a statistical difference that met the prespecified criteria for both noninferiority and superiority. Concurrently with Dr. Mehra’s report at the meeting, a journal article appeared online (New Engl J Med. 2016 Nov 16. doi: 10.1056/NEJMoa1610426). He stated that as far as he understood, St. Jude would submit the 6-month data he reported to the Food and Drug Administration in an application for marketing approval for HeartMate 3.
“I agree that there are still morbid evens [with HeartMate 3] that need to be surmounted, but this is a confidence-building step in the right direction,” Dr. Mehra said.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
By eliminating all episodes of pump thrombosis during 6-month follow-up, the HeartMate 3 appeared to resolve one of the major issues that has stood in the way of patients and physicians feeling comfortable with left ventricular assist devices. The smaller size of the HeartMate 3 pump and its ability to be placed with minimally invasive and fairly rapid surgery is another big advance, putting this device on par with the rival pump, the HeartWare HVAD.
But the performance of the HeartMate 3 left ventricular assist device (LVAD) in MOMENTUM 3 also highlighted the shortcomings that still remain for these devices: the unchanged rates of stroke, gastrointestinal bleeds, and infections with HeartMate 3, compared with HeartMate II in this trial, and similar 6-month survival rates in the two arms of the study.
The HeartMate 3 can be implanted without sternotomy, using an 8 cm incision on the lateral chest wall, resulting in a shorter postoperative stay and fewer perisurgical adverse events. Despite the less invasive surgery and absence of pump thrombosis, some patients and physicians will remain hesitant to use an LVAD unless it is unavoidable because of concern about strokes. Until further design and procedural refinements change the rate of serious strokes and other adverse events, LVADs will not be fully competitive with heart transplantation.
The competition between HeartMate and the HeartWare devices will help drive this field forward, leading to further improvements in outcomes and expanded LVAD use.
Mark Slaughter, MD, is professor of surgery and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). He was an investigator in MOMENTUM 3, he has been a consultant to EvaHeart and Oregon Heart, and he has received research support from Carmat and HeartWare. He made these comments as designated discussant for the report and in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
By eliminating all episodes of pump thrombosis during 6-month follow-up, the HeartMate 3 appeared to resolve one of the major issues that has stood in the way of patients and physicians feeling comfortable with left ventricular assist devices. The smaller size of the HeartMate 3 pump and its ability to be placed with minimally invasive and fairly rapid surgery is another big advance, putting this device on par with the rival pump, the HeartWare HVAD.
But the performance of the HeartMate 3 left ventricular assist device (LVAD) in MOMENTUM 3 also highlighted the shortcomings that still remain for these devices: the unchanged rates of stroke, gastrointestinal bleeds, and infections with HeartMate 3, compared with HeartMate II in this trial, and similar 6-month survival rates in the two arms of the study.
The HeartMate 3 can be implanted without sternotomy, using an 8 cm incision on the lateral chest wall, resulting in a shorter postoperative stay and fewer perisurgical adverse events. Despite the less invasive surgery and absence of pump thrombosis, some patients and physicians will remain hesitant to use an LVAD unless it is unavoidable because of concern about strokes. Until further design and procedural refinements change the rate of serious strokes and other adverse events, LVADs will not be fully competitive with heart transplantation.
The competition between HeartMate and the HeartWare devices will help drive this field forward, leading to further improvements in outcomes and expanded LVAD use.
Mark Slaughter, MD, is professor of surgery and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). He was an investigator in MOMENTUM 3, he has been a consultant to EvaHeart and Oregon Heart, and he has received research support from Carmat and HeartWare. He made these comments as designated discussant for the report and in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
By eliminating all episodes of pump thrombosis during 6-month follow-up, the HeartMate 3 appeared to resolve one of the major issues that has stood in the way of patients and physicians feeling comfortable with left ventricular assist devices. The smaller size of the HeartMate 3 pump and its ability to be placed with minimally invasive and fairly rapid surgery is another big advance, putting this device on par with the rival pump, the HeartWare HVAD.
But the performance of the HeartMate 3 left ventricular assist device (LVAD) in MOMENTUM 3 also highlighted the shortcomings that still remain for these devices: the unchanged rates of stroke, gastrointestinal bleeds, and infections with HeartMate 3, compared with HeartMate II in this trial, and similar 6-month survival rates in the two arms of the study.
The HeartMate 3 can be implanted without sternotomy, using an 8 cm incision on the lateral chest wall, resulting in a shorter postoperative stay and fewer perisurgical adverse events. Despite the less invasive surgery and absence of pump thrombosis, some patients and physicians will remain hesitant to use an LVAD unless it is unavoidable because of concern about strokes. Until further design and procedural refinements change the rate of serious strokes and other adverse events, LVADs will not be fully competitive with heart transplantation.
The competition between HeartMate and the HeartWare devices will help drive this field forward, leading to further improvements in outcomes and expanded LVAD use.
Mark Slaughter, MD, is professor of surgery and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). He was an investigator in MOMENTUM 3, he has been a consultant to EvaHeart and Oregon Heart, and he has received research support from Carmat and HeartWare. He made these comments as designated discussant for the report and in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
NEW ORLEANS – HeartMate 3, the latest left ventricular assist device in the HeartMate line, appears to have solved the problem of pump thrombosis, a complication that has dogged ventricular pumps since the issue leapt into medical awareness about 3 years ago (New Engl J Med. 2014 Jan 2;370:33-40).
During 6 months of follow-up, none of 152 heart failure patients assigned to receive a HeartMate 3 left ventricular assist device (LVAD) developed suspected or confirmed pump thrombosis, compared with 14 patients (10%) having pump thrombosis out of 138 recipients of the prior-generation HeartMate II LVAD who served as the control group for the study.
“Three years ago, when the issue of pump thrombosis was first revealed, there was a lot of consternation and some drop in LVAD use, especially as destination therapy. We think that seeing no pump thrombosis whatsoever will give people renewed confidence in this technology,” said Dr. Mehra, professor of medicine at Harvard Medical School and medical director of the Heart and Vascular Center of Brigham and Women’s Hospital, both in Boston.
Pump thrombosis has also been a problem for the patients who have received a competitor LVAD, the HeartWare HVAD device (Circulation. 2015 Nov 10;132[suppl 3]:A19675), approved for U.S. use as bridge to transplant. HeartMate II is approved for both bridge to transplant and for destination therapy.
In addition to apparently eliminating pump thrombosis, HeartMate 3’s size and potential implantation approach should make its placement during routine use as quick and minimally invasive as the HeartWare device, features that should further help broader use of HeartMate 3, commented Mark Slaughter, MD, professor and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). But Dr. Slaughter and others were also quick to highlight the shortcomings that remain with both devices that will continue to hamper a broader role for LVAD treatment of patients with advanced heart failure.
“We thought that if there was less pump thrombosis we’d see less stroke, but that is not what the data suggest. It’s the big puzzle we need to figure out before we see widespread acceptance of this treatment,” Dr. Sweitzer said.
“This will not shift LVAD use substantially,” commented Christopher B. Granger, MD, a professor of medicine and a heart failure specialist at Duke University, Durham, N.C. “Reducing the need for reoperation is good for the field, and is an incremental advance, but it is not transformational,” he said in an interview.
The MOMENTUM 3 (Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy with HeartMate 3) trial randomized 294 patients at 69 U.S. centers. The study’s primary endpoint of 6-month survival free from disabling stroke or reoperation to repair or replace the LVAD occurred in 86% of 152 patients who received a HeartMate 3 and 77% of 142 patients randomized to HeartMate II, a statistical difference that met the prespecified criteria for both noninferiority and superiority. Concurrently with Dr. Mehra’s report at the meeting, a journal article appeared online (New Engl J Med. 2016 Nov 16. doi: 10.1056/NEJMoa1610426). He stated that as far as he understood, St. Jude would submit the 6-month data he reported to the Food and Drug Administration in an application for marketing approval for HeartMate 3.
“I agree that there are still morbid evens [with HeartMate 3] that need to be surmounted, but this is a confidence-building step in the right direction,” Dr. Mehra said.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
NEW ORLEANS – HeartMate 3, the latest left ventricular assist device in the HeartMate line, appears to have solved the problem of pump thrombosis, a complication that has dogged ventricular pumps since the issue leapt into medical awareness about 3 years ago (New Engl J Med. 2014 Jan 2;370:33-40).
During 6 months of follow-up, none of 152 heart failure patients assigned to receive a HeartMate 3 left ventricular assist device (LVAD) developed suspected or confirmed pump thrombosis, compared with 14 patients (10%) having pump thrombosis out of 138 recipients of the prior-generation HeartMate II LVAD who served as the control group for the study.
“Three years ago, when the issue of pump thrombosis was first revealed, there was a lot of consternation and some drop in LVAD use, especially as destination therapy. We think that seeing no pump thrombosis whatsoever will give people renewed confidence in this technology,” said Dr. Mehra, professor of medicine at Harvard Medical School and medical director of the Heart and Vascular Center of Brigham and Women’s Hospital, both in Boston.
Pump thrombosis has also been a problem for the patients who have received a competitor LVAD, the HeartWare HVAD device (Circulation. 2015 Nov 10;132[suppl 3]:A19675), approved for U.S. use as bridge to transplant. HeartMate II is approved for both bridge to transplant and for destination therapy.
In addition to apparently eliminating pump thrombosis, HeartMate 3’s size and potential implantation approach should make its placement during routine use as quick and minimally invasive as the HeartWare device, features that should further help broader use of HeartMate 3, commented Mark Slaughter, MD, professor and chairman of cardiovascular and thoracic surgery at the University of Louisville (Ky.). But Dr. Slaughter and others were also quick to highlight the shortcomings that remain with both devices that will continue to hamper a broader role for LVAD treatment of patients with advanced heart failure.
“We thought that if there was less pump thrombosis we’d see less stroke, but that is not what the data suggest. It’s the big puzzle we need to figure out before we see widespread acceptance of this treatment,” Dr. Sweitzer said.
“This will not shift LVAD use substantially,” commented Christopher B. Granger, MD, a professor of medicine and a heart failure specialist at Duke University, Durham, N.C. “Reducing the need for reoperation is good for the field, and is an incremental advance, but it is not transformational,” he said in an interview.
The MOMENTUM 3 (Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy with HeartMate 3) trial randomized 294 patients at 69 U.S. centers. The study’s primary endpoint of 6-month survival free from disabling stroke or reoperation to repair or replace the LVAD occurred in 86% of 152 patients who received a HeartMate 3 and 77% of 142 patients randomized to HeartMate II, a statistical difference that met the prespecified criteria for both noninferiority and superiority. Concurrently with Dr. Mehra’s report at the meeting, a journal article appeared online (New Engl J Med. 2016 Nov 16. doi: 10.1056/NEJMoa1610426). He stated that as far as he understood, St. Jude would submit the 6-month data he reported to the Food and Drug Administration in an application for marketing approval for HeartMate 3.
“I agree that there are still morbid evens [with HeartMate 3] that need to be surmounted, but this is a confidence-building step in the right direction,” Dr. Mehra said.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: During 6 months, suspected or confirmed pump thrombosis occurred in no HeartMate 3 patients and in 10% of HeartMate II recipients.
Data source: The MOMENTUM 3 trial, which randomized 294 patients at 69 U.S. centers.
Disclosures: MOMENTUM 3 was sponsored by St. Jude, the company developing the HeartMate 3 LVAD. Dr. Mehra has received travel reimbursements from St. Jude and has been a consultant to Medtronic, Stealth, and Teva. Dr. Sweitzer was an investigator in MOMENTUM 3 and has been a consultant to Acorda and Medtronic and received research support from Bayer, Corvia, and Novartis. Dr. Granger has been a consultant to Boehringer Ingelheim, and received research support from Medtronic and several other drug and device companies. Dr. Slaughter was an investigator in MOMENTUM 3, has been a consultant to EvaHeart and Oregon Heart, and has received research support from Carmat and HeartWare.

VIDEO: Rivaroxaban gives safer protection to atrial fib patients post PCI
NEW ORLEANS – The puzzle of how to safely prevent thrombotic events in patients with atrial fibrillation who receive a coronary stent now has a little more clarity in the era of new oral anticoagulants.
The first randomized trial to compare the safety of a new oral anticoagulant (NOAC, in this case rivaroxaban) against warfarin when paired with one or more antiplatelet drugs showed that the NOAC edged out warfarin for safety by cutting the rate of clinically significant bleeding events while preventing thrombotic events roughly as well as warfarin.

Despite that, the incidence of all major adverse coronary events during the 1-year follow-up was virtually identical in the three groups, ranging from 5.6% to 6.5%, with very low rates of stroke in the three treatment arms, ranging from 1.2%-1.5%, said Dr. Gibson, a professor of medicine at Harvard Medical School and an interventional cardiologist at Beth Israel Deaconess Medical Center, both in Boston.
These results “are a huge step forward and will change practice,” commented Philippe Gabriel Steg, MD, discussant for the report and director of the coronary care unit of Bichat Hospital in Paris. “We’ve gone from having no evidence to having some evidence” for using a NOAC in this setting. “It was a difficult but very important study that truly advances the field.”

The trial randomized patients to any of three main treatment regimens: 2.5 mg rivaroxaban b.i.d., 15 mg rivaroxaban once daily, or warfarin taken to maintain an international normalized ratio of 2.0-3.0. During the study, patients in the warfarin arm were in this therapeutic range 65% of the time.
The trial’s design instructed physicians to treat patients who received the lower rivaroxaban dosage to also administer aspirin (75-100 mg daily) plus a thienopyridine of their choice. Patients on the higher rivaroxaban dosage received monotherapy with a thienopyridine of the physician’s choosing, while patients assigned to receive warfarin were also to get aspirin (75-100 mg daily) and a thienopyridine. It turned out that in each of the three treatment arms, 95% of patients received clopidogrel, 4% received ticagrelor (Brilinta), and 1% received prasugrel (Effient).
The trial also left it up to each physician to decide how long each patient should remain on dual antiplatelet therapy. In each of the two treatment arms that used dual therapy, 49% received 12 months of dual treatment, 35% received it for 6 months, and 16% received it for 1 month. Once the period of dual therapy ended, patients continued to receive aspirin (at 75-100 mg/day) for the balance of the 12-month study.
Leaving the choice of thienopyridine and duration of dual therapy up to each physician helped make this a “real world study,” Dr. Gibson said.
The trial was fully powered to prove a difference in safety based on rates of clinically significant bleeding events. The 1-year rates were 17% in patients who received 15 mg of rivaroxaban daily, 18% in those who received 2.5 mg rivaroxaban b.i.d., and 27% in the patients on warfarin: statistically significant differences between the warfarin arm and each of the two rivaroxaban arms. The study was not powered to prove noninferiority of the rivaroxaban regimens for efficacy at preventing stroke or major adverse events (cardiovascular death, MI, or stroke). To do that would require a trial with more than 30,000 patients, Dr. Gibson noted.
Also concurrently with Dr. Gibson’s report, a second article was published online with a post-hoc efficacy analysis that used as an efficacy endpoint the combined 1-year rate of death and all-cause hospitalization for an adverse event (Circulation. 2016 Nov 14. doi: 10.1161/CIRCULATIONAHA.116.025783). In this analysis, each of the two rivaroxaban arms cut the rate of this outcome by about 25% relative to the patients treated with warfarin, statistically significant differences. Both of the rivaroxaban regimens led to significant reductions in hospitalizations both for cardiovascular events and for bleeding events, Dr. Gibson reported.
He speculated that the vast majority of patients in the study wound up receiving clopidogrel because of cost consideration, because many physicians weren’t comfortable pairing a more potent thienopyridine with an anticoagulant, and because clopidogrel remains the most commonly used agent from this class in many parts of the world.
Dr. Gibson suggested that physicians who use these rivaroxaban-based regimens in routine practice tailor their thienopyridine selection and the duration of dual therapy to each patient based on these factors as well as whether the individual patient appears to face a greater danger from bleeding or from an ischemic event. The same approach should also guide choosing between the two rivaroxaban regimens tested. The 2.5-mg b.i.d. dosage used in a triple-therapy strategy that combines it with aspirin and a thienopyridine is better suited to patients at higher risk for ischemic events, while the 15-mg once daily dosage coupled with a thienopyridine but without aspirin is better suited to patients with a high bleeding risk, he said in an interview. Because the 2.5-mg formulation is not currently available for U.S. sales, most American physicians will be limited to only prescribing 15 mg of rivaroxaban daily. And for patients with very poor renal function, with a creatinine clearance rate of less than 15 mL/min, warfarin remains the best option, Dr. Gibson said.
PIONEER AF-PCI was sponsored by Johnson & Johnson (Janssen) and Bayer, the two companies that market rivaroxaban (Xarelto) worldwide. Dr. Gibson has received research support from and has been a consultant to Johnson & Johnson and Bayer and has also received research support and consulted for several other drug companies. Dr. Steg has been a consultant to Bayer and Janssen, and has received research support from or has been a consultant to several other drug companies.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
The results from PIONEER AF-PCI give us important and helpful information now that physicians increasingly prescribe a new oral anticoagulant to treat patients with nonvalvular atrial fibrillation. The trial provides strong evidence that one or two antiplatelet drugs can safely be combined with rivaroxaban when these patients undergo coronary stenting.
Until now, the only data we had on the safety and efficacy of combining an anticoagulant with one or more antiplatelet drugs in these patients involved warfarin-based regimens. Because of this limitation, some clinicians even switched atrial fibrillation patients who were on a new oral anticoagulant to warfarin if they received a coronary stent and therefore needed treatment with antiplatelet drugs.
The study results show that the rivaroxaban-based regimens were safe, even safer than the warfarin-based strategy, and there was no signal of harm in the form on increased strokes or stent thrombosis. Because of the study’s complex design, with many different regimens that included various thienopyridines and various durations of antiplatelet treatment, it is hard to decide from just these results the best approach among all the different combinations tested. But the PIONEER AF-PCI results start to build a data platform for the new oral anticoagulants that clinicians can use to help guide management of these patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Richard C. Becker, MD, is professor of medicine and director of the Heart, Lung and Vascular Institute at the University of Cincinnati. He has received research support from AstraZeneca and Janssen. He made these comments in an interview.
The results from PIONEER AF-PCI give us important and helpful information now that physicians increasingly prescribe a new oral anticoagulant to treat patients with nonvalvular atrial fibrillation. The trial provides strong evidence that one or two antiplatelet drugs can safely be combined with rivaroxaban when these patients undergo coronary stenting.
Until now, the only data we had on the safety and efficacy of combining an anticoagulant with one or more antiplatelet drugs in these patients involved warfarin-based regimens. Because of this limitation, some clinicians even switched atrial fibrillation patients who were on a new oral anticoagulant to warfarin if they received a coronary stent and therefore needed treatment with antiplatelet drugs.
The study results show that the rivaroxaban-based regimens were safe, even safer than the warfarin-based strategy, and there was no signal of harm in the form on increased strokes or stent thrombosis. Because of the study’s complex design, with many different regimens that included various thienopyridines and various durations of antiplatelet treatment, it is hard to decide from just these results the best approach among all the different combinations tested. But the PIONEER AF-PCI results start to build a data platform for the new oral anticoagulants that clinicians can use to help guide management of these patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Richard C. Becker, MD, is professor of medicine and director of the Heart, Lung and Vascular Institute at the University of Cincinnati. He has received research support from AstraZeneca and Janssen. He made these comments in an interview.
The results from PIONEER AF-PCI give us important and helpful information now that physicians increasingly prescribe a new oral anticoagulant to treat patients with nonvalvular atrial fibrillation. The trial provides strong evidence that one or two antiplatelet drugs can safely be combined with rivaroxaban when these patients undergo coronary stenting.
Until now, the only data we had on the safety and efficacy of combining an anticoagulant with one or more antiplatelet drugs in these patients involved warfarin-based regimens. Because of this limitation, some clinicians even switched atrial fibrillation patients who were on a new oral anticoagulant to warfarin if they received a coronary stent and therefore needed treatment with antiplatelet drugs.
The study results show that the rivaroxaban-based regimens were safe, even safer than the warfarin-based strategy, and there was no signal of harm in the form on increased strokes or stent thrombosis. Because of the study’s complex design, with many different regimens that included various thienopyridines and various durations of antiplatelet treatment, it is hard to decide from just these results the best approach among all the different combinations tested. But the PIONEER AF-PCI results start to build a data platform for the new oral anticoagulants that clinicians can use to help guide management of these patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Richard C. Becker, MD, is professor of medicine and director of the Heart, Lung and Vascular Institute at the University of Cincinnati. He has received research support from AstraZeneca and Janssen. He made these comments in an interview.
NEW ORLEANS – The puzzle of how to safely prevent thrombotic events in patients with atrial fibrillation who receive a coronary stent now has a little more clarity in the era of new oral anticoagulants.
The first randomized trial to compare the safety of a new oral anticoagulant (NOAC, in this case rivaroxaban) against warfarin when paired with one or more antiplatelet drugs showed that the NOAC edged out warfarin for safety by cutting the rate of clinically significant bleeding events while preventing thrombotic events roughly as well as warfarin.
Despite that, the incidence of all major adverse coronary events during the 1-year follow-up was virtually identical in the three groups, ranging from 5.6% to 6.5%, with very low rates of stroke in the three treatment arms, ranging from 1.2%-1.5%, said Dr. Gibson, a professor of medicine at Harvard Medical School and an interventional cardiologist at Beth Israel Deaconess Medical Center, both in Boston.
These results “are a huge step forward and will change practice,” commented Philippe Gabriel Steg, MD, discussant for the report and director of the coronary care unit of Bichat Hospital in Paris. “We’ve gone from having no evidence to having some evidence” for using a NOAC in this setting. “It was a difficult but very important study that truly advances the field.”
The trial randomized patients to any of three main treatment regimens: 2.5 mg rivaroxaban b.i.d., 15 mg rivaroxaban once daily, or warfarin taken to maintain an international normalized ratio of 2.0-3.0. During the study, patients in the warfarin arm were in this therapeutic range 65% of the time.
The trial’s design instructed physicians to treat patients who received the lower rivaroxaban dosage to also administer aspirin (75-100 mg daily) plus a thienopyridine of their choice. Patients on the higher rivaroxaban dosage received monotherapy with a thienopyridine of the physician’s choosing, while patients assigned to receive warfarin were also to get aspirin (75-100 mg daily) and a thienopyridine. It turned out that in each of the three treatment arms, 95% of patients received clopidogrel, 4% received ticagrelor (Brilinta), and 1% received prasugrel (Effient).
The trial also left it up to each physician to decide how long each patient should remain on dual antiplatelet therapy. In each of the two treatment arms that used dual therapy, 49% received 12 months of dual treatment, 35% received it for 6 months, and 16% received it for 1 month. Once the period of dual therapy ended, patients continued to receive aspirin (at 75-100 mg/day) for the balance of the 12-month study.
Leaving the choice of thienopyridine and duration of dual therapy up to each physician helped make this a “real world study,” Dr. Gibson said.
The trial was fully powered to prove a difference in safety based on rates of clinically significant bleeding events. The 1-year rates were 17% in patients who received 15 mg of rivaroxaban daily, 18% in those who received 2.5 mg rivaroxaban b.i.d., and 27% in the patients on warfarin: statistically significant differences between the warfarin arm and each of the two rivaroxaban arms. The study was not powered to prove noninferiority of the rivaroxaban regimens for efficacy at preventing stroke or major adverse events (cardiovascular death, MI, or stroke). To do that would require a trial with more than 30,000 patients, Dr. Gibson noted.
Also concurrently with Dr. Gibson’s report, a second article was published online with a post-hoc efficacy analysis that used as an efficacy endpoint the combined 1-year rate of death and all-cause hospitalization for an adverse event (Circulation. 2016 Nov 14. doi: 10.1161/CIRCULATIONAHA.116.025783). In this analysis, each of the two rivaroxaban arms cut the rate of this outcome by about 25% relative to the patients treated with warfarin, statistically significant differences. Both of the rivaroxaban regimens led to significant reductions in hospitalizations both for cardiovascular events and for bleeding events, Dr. Gibson reported.
He speculated that the vast majority of patients in the study wound up receiving clopidogrel because of cost consideration, because many physicians weren’t comfortable pairing a more potent thienopyridine with an anticoagulant, and because clopidogrel remains the most commonly used agent from this class in many parts of the world.
Dr. Gibson suggested that physicians who use these rivaroxaban-based regimens in routine practice tailor their thienopyridine selection and the duration of dual therapy to each patient based on these factors as well as whether the individual patient appears to face a greater danger from bleeding or from an ischemic event. The same approach should also guide choosing between the two rivaroxaban regimens tested. The 2.5-mg b.i.d. dosage used in a triple-therapy strategy that combines it with aspirin and a thienopyridine is better suited to patients at higher risk for ischemic events, while the 15-mg once daily dosage coupled with a thienopyridine but without aspirin is better suited to patients with a high bleeding risk, he said in an interview. Because the 2.5-mg formulation is not currently available for U.S. sales, most American physicians will be limited to only prescribing 15 mg of rivaroxaban daily. And for patients with very poor renal function, with a creatinine clearance rate of less than 15 mL/min, warfarin remains the best option, Dr. Gibson said.
PIONEER AF-PCI was sponsored by Johnson & Johnson (Janssen) and Bayer, the two companies that market rivaroxaban (Xarelto) worldwide. Dr. Gibson has received research support from and has been a consultant to Johnson & Johnson and Bayer and has also received research support and consulted for several other drug companies. Dr. Steg has been a consultant to Bayer and Janssen, and has received research support from or has been a consultant to several other drug companies.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
NEW ORLEANS – The puzzle of how to safely prevent thrombotic events in patients with atrial fibrillation who receive a coronary stent now has a little more clarity in the era of new oral anticoagulants.
The first randomized trial to compare the safety of a new oral anticoagulant (NOAC, in this case rivaroxaban) against warfarin when paired with one or more antiplatelet drugs showed that the NOAC edged out warfarin for safety by cutting the rate of clinically significant bleeding events while preventing thrombotic events roughly as well as warfarin.
Despite that, the incidence of all major adverse coronary events during the 1-year follow-up was virtually identical in the three groups, ranging from 5.6% to 6.5%, with very low rates of stroke in the three treatment arms, ranging from 1.2%-1.5%, said Dr. Gibson, a professor of medicine at Harvard Medical School and an interventional cardiologist at Beth Israel Deaconess Medical Center, both in Boston.
These results “are a huge step forward and will change practice,” commented Philippe Gabriel Steg, MD, discussant for the report and director of the coronary care unit of Bichat Hospital in Paris. “We’ve gone from having no evidence to having some evidence” for using a NOAC in this setting. “It was a difficult but very important study that truly advances the field.”
The trial randomized patients to any of three main treatment regimens: 2.5 mg rivaroxaban b.i.d., 15 mg rivaroxaban once daily, or warfarin taken to maintain an international normalized ratio of 2.0-3.0. During the study, patients in the warfarin arm were in this therapeutic range 65% of the time.
The trial’s design instructed physicians to treat patients who received the lower rivaroxaban dosage to also administer aspirin (75-100 mg daily) plus a thienopyridine of their choice. Patients on the higher rivaroxaban dosage received monotherapy with a thienopyridine of the physician’s choosing, while patients assigned to receive warfarin were also to get aspirin (75-100 mg daily) and a thienopyridine. It turned out that in each of the three treatment arms, 95% of patients received clopidogrel, 4% received ticagrelor (Brilinta), and 1% received prasugrel (Effient).
The trial also left it up to each physician to decide how long each patient should remain on dual antiplatelet therapy. In each of the two treatment arms that used dual therapy, 49% received 12 months of dual treatment, 35% received it for 6 months, and 16% received it for 1 month. Once the period of dual therapy ended, patients continued to receive aspirin (at 75-100 mg/day) for the balance of the 12-month study.
Leaving the choice of thienopyridine and duration of dual therapy up to each physician helped make this a “real world study,” Dr. Gibson said.
The trial was fully powered to prove a difference in safety based on rates of clinically significant bleeding events. The 1-year rates were 17% in patients who received 15 mg of rivaroxaban daily, 18% in those who received 2.5 mg rivaroxaban b.i.d., and 27% in the patients on warfarin: statistically significant differences between the warfarin arm and each of the two rivaroxaban arms. The study was not powered to prove noninferiority of the rivaroxaban regimens for efficacy at preventing stroke or major adverse events (cardiovascular death, MI, or stroke). To do that would require a trial with more than 30,000 patients, Dr. Gibson noted.
Also concurrently with Dr. Gibson’s report, a second article was published online with a post-hoc efficacy analysis that used as an efficacy endpoint the combined 1-year rate of death and all-cause hospitalization for an adverse event (Circulation. 2016 Nov 14. doi: 10.1161/CIRCULATIONAHA.116.025783). In this analysis, each of the two rivaroxaban arms cut the rate of this outcome by about 25% relative to the patients treated with warfarin, statistically significant differences. Both of the rivaroxaban regimens led to significant reductions in hospitalizations both for cardiovascular events and for bleeding events, Dr. Gibson reported.
He speculated that the vast majority of patients in the study wound up receiving clopidogrel because of cost consideration, because many physicians weren’t comfortable pairing a more potent thienopyridine with an anticoagulant, and because clopidogrel remains the most commonly used agent from this class in many parts of the world.
Dr. Gibson suggested that physicians who use these rivaroxaban-based regimens in routine practice tailor their thienopyridine selection and the duration of dual therapy to each patient based on these factors as well as whether the individual patient appears to face a greater danger from bleeding or from an ischemic event. The same approach should also guide choosing between the two rivaroxaban regimens tested. The 2.5-mg b.i.d. dosage used in a triple-therapy strategy that combines it with aspirin and a thienopyridine is better suited to patients at higher risk for ischemic events, while the 15-mg once daily dosage coupled with a thienopyridine but without aspirin is better suited to patients with a high bleeding risk, he said in an interview. Because the 2.5-mg formulation is not currently available for U.S. sales, most American physicians will be limited to only prescribing 15 mg of rivaroxaban daily. And for patients with very poor renal function, with a creatinine clearance rate of less than 15 mL/min, warfarin remains the best option, Dr. Gibson said.
PIONEER AF-PCI was sponsored by Johnson & Johnson (Janssen) and Bayer, the two companies that market rivaroxaban (Xarelto) worldwide. Dr. Gibson has received research support from and has been a consultant to Johnson & Johnson and Bayer and has also received research support and consulted for several other drug companies. Dr. Steg has been a consultant to Bayer and Janssen, and has received research support from or has been a consultant to several other drug companies.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The two tested rivaroxaban regimens cut clinically significant bleeds by about 40%, compared with a warfarin-based regimen.
Data source: PIONEER AF-PCI, an international, multicenter randomized trial with 2,124 patients.
Disclosures: Dr. Gibson has received research support and consulted for Johnson & Johnson (Janssen) and Bayer, the study sponsors that also market rivaroxaban (Xarelto) worldwide, and several other drug companies.
Hypotension ‘dose’ drives mortality in traumatic brain injury
NEW ORLEANS – The severity and duration of hypotension in traumatic brain injury patients during EMS transport to an emergency department has a tight and essentially linear relationship to their mortality rate during subsequent weeks of recovery, according to an analysis of more than 7,500 brain-injured patients.
For each doubling of the combined severity and duration of hypotension during the prehospital period, when systolic blood pressure was less than 90 mm Hg, patient mortality rose by 19%, Daniel W. Spaite, MD, reported at the American Heart Association scientific sessions.
However, the results do not address whether aggressive treatment of hypotension by EMS technicians in a patient with traumatic brain injury (TBI) leads to reduced mortality. That question is being assessed as part of the primary endpoint of the Excellence in Prehospital Injury Care-Traumatic Brain Injury (EPIC-TBI) study, which should have an answer by the end of 2017, said Dr. Spaite, professor of emergency medicine at the University of Arizona in Tuscon.

The innovation introduced by Dr. Spaite and his associates in their analysis of the EPIC-TBI data was to drill down into each patient’s hypotensive event, made possible by the 16,711 patients enrolled in EPIC-TBI.
The calculation they performed was limited to patients with EMS records of at least two blood pressure measurements during prehospital transport. These data allowed them to use both the extent to which systolic blood pressure dropped below 90 mm Hg and the amount of time pressure was below this threshold to better define the total hypotension exposure each patient received.
This meant that a TBI patient with a systolic pressure of 80 mm Hg for 10 minutes had twice the hypotension exposure of both a patient with a pressure of 85 mm Hg for 10 minutes, and a patient with a pressure of 80 mm Hg for 5 minutes.
Their analysis also adjusted the relationship of this total hypotensive dose and subsequent mortality based on several baseline demographic and clinical variables, including age, sex, injury severity, trauma type, and head-region severity score. After adjustment, the researchers found a “strikingly linear relationship” between hypotension dose and mortality, Dr. Spaite said, although a clear dose-response relationship was also evident in the unadjusted data.
EPIC-TBI enrolled TBI patients age 10 years or older during 2007-2014 through participation by dozens of EMS providers throughout Arizona. For the current analysis, the researchers identified 7,521 patients from the total group who had at least two blood pressure measurements taken during their prehospital EMS care and also met other inclusion criteria.
The best way to manage hypotension in TBI patients during the prehospital period remains unclear. Simply raising blood pressure with fluid infusion may not necessarily help, because it could exacerbate a patient’s bleeding, Dr. Spaite noted during an interview.
The primary goal of EPIC-TBI is to assess the impact of the third edition of the traumatic brain injury guidelines released in 2007 by the Brain Trauma Foundation. (The fourth edition of these guidelines came out in August 2016.) The new finding by Dr. Spaite and his associates will allow the full EPIC-TBI analysis to correlate patient outcomes with the impact that acute, prehospital treatment had on the hypotension dose received by each patient, he noted.
“What’s remarkable is that the single, prehospital parameter of hypotension for just a few minutes during transport can have such a strong impact on survival, given all the other factors that can influence outcomes” in TBI patients once they reach a hospital and during the period they remain hospitalized, Dr. Spaite said.
mzoler@frontlinemedcom.com On Twitter @mitchelzoler
NEW ORLEANS – The severity and duration of hypotension in traumatic brain injury patients during EMS transport to an emergency department has a tight and essentially linear relationship to their mortality rate during subsequent weeks of recovery, according to an analysis of more than 7,500 brain-injured patients.
For each doubling of the combined severity and duration of hypotension during the prehospital period, when systolic blood pressure was less than 90 mm Hg, patient mortality rose by 19%, Daniel W. Spaite, MD, reported at the American Heart Association scientific sessions.
However, the results do not address whether aggressive treatment of hypotension by EMS technicians in a patient with traumatic brain injury (TBI) leads to reduced mortality. That question is being assessed as part of the primary endpoint of the Excellence in Prehospital Injury Care-Traumatic Brain Injury (EPIC-TBI) study, which should have an answer by the end of 2017, said Dr. Spaite, professor of emergency medicine at the University of Arizona in Tuscon.
The innovation introduced by Dr. Spaite and his associates in their analysis of the EPIC-TBI data was to drill down into each patient’s hypotensive event, made possible by the 16,711 patients enrolled in EPIC-TBI.
The calculation they performed was limited to patients with EMS records of at least two blood pressure measurements during prehospital transport. These data allowed them to use both the extent to which systolic blood pressure dropped below 90 mm Hg and the amount of time pressure was below this threshold to better define the total hypotension exposure each patient received.
This meant that a TBI patient with a systolic pressure of 80 mm Hg for 10 minutes had twice the hypotension exposure of both a patient with a pressure of 85 mm Hg for 10 minutes, and a patient with a pressure of 80 mm Hg for 5 minutes.
Their analysis also adjusted the relationship of this total hypotensive dose and subsequent mortality based on several baseline demographic and clinical variables, including age, sex, injury severity, trauma type, and head-region severity score. After adjustment, the researchers found a “strikingly linear relationship” between hypotension dose and mortality, Dr. Spaite said, although a clear dose-response relationship was also evident in the unadjusted data.
EPIC-TBI enrolled TBI patients age 10 years or older during 2007-2014 through participation by dozens of EMS providers throughout Arizona. For the current analysis, the researchers identified 7,521 patients from the total group who had at least two blood pressure measurements taken during their prehospital EMS care and also met other inclusion criteria.
The best way to manage hypotension in TBI patients during the prehospital period remains unclear. Simply raising blood pressure with fluid infusion may not necessarily help, because it could exacerbate a patient’s bleeding, Dr. Spaite noted during an interview.
The primary goal of EPIC-TBI is to assess the impact of the third edition of the traumatic brain injury guidelines released in 2007 by the Brain Trauma Foundation. (The fourth edition of these guidelines came out in August 2016.) The new finding by Dr. Spaite and his associates will allow the full EPIC-TBI analysis to correlate patient outcomes with the impact that acute, prehospital treatment had on the hypotension dose received by each patient, he noted.
“What’s remarkable is that the single, prehospital parameter of hypotension for just a few minutes during transport can have such a strong impact on survival, given all the other factors that can influence outcomes” in TBI patients once they reach a hospital and during the period they remain hospitalized, Dr. Spaite said.
mzoler@frontlinemedcom.com On Twitter @mitchelzoler
NEW ORLEANS – The severity and duration of hypotension in traumatic brain injury patients during EMS transport to an emergency department has a tight and essentially linear relationship to their mortality rate during subsequent weeks of recovery, according to an analysis of more than 7,500 brain-injured patients.
For each doubling of the combined severity and duration of hypotension during the prehospital period, when systolic blood pressure was less than 90 mm Hg, patient mortality rose by 19%, Daniel W. Spaite, MD, reported at the American Heart Association scientific sessions.
However, the results do not address whether aggressive treatment of hypotension by EMS technicians in a patient with traumatic brain injury (TBI) leads to reduced mortality. That question is being assessed as part of the primary endpoint of the Excellence in Prehospital Injury Care-Traumatic Brain Injury (EPIC-TBI) study, which should have an answer by the end of 2017, said Dr. Spaite, professor of emergency medicine at the University of Arizona in Tuscon.
The innovation introduced by Dr. Spaite and his associates in their analysis of the EPIC-TBI data was to drill down into each patient’s hypotensive event, made possible by the 16,711 patients enrolled in EPIC-TBI.
The calculation they performed was limited to patients with EMS records of at least two blood pressure measurements during prehospital transport. These data allowed them to use both the extent to which systolic blood pressure dropped below 90 mm Hg and the amount of time pressure was below this threshold to better define the total hypotension exposure each patient received.
This meant that a TBI patient with a systolic pressure of 80 mm Hg for 10 minutes had twice the hypotension exposure of both a patient with a pressure of 85 mm Hg for 10 minutes, and a patient with a pressure of 80 mm Hg for 5 minutes.
Their analysis also adjusted the relationship of this total hypotensive dose and subsequent mortality based on several baseline demographic and clinical variables, including age, sex, injury severity, trauma type, and head-region severity score. After adjustment, the researchers found a “strikingly linear relationship” between hypotension dose and mortality, Dr. Spaite said, although a clear dose-response relationship was also evident in the unadjusted data.
EPIC-TBI enrolled TBI patients age 10 years or older during 2007-2014 through participation by dozens of EMS providers throughout Arizona. For the current analysis, the researchers identified 7,521 patients from the total group who had at least two blood pressure measurements taken during their prehospital EMS care and also met other inclusion criteria.
The best way to manage hypotension in TBI patients during the prehospital period remains unclear. Simply raising blood pressure with fluid infusion may not necessarily help, because it could exacerbate a patient’s bleeding, Dr. Spaite noted during an interview.
The primary goal of EPIC-TBI is to assess the impact of the third edition of the traumatic brain injury guidelines released in 2007 by the Brain Trauma Foundation. (The fourth edition of these guidelines came out in August 2016.) The new finding by Dr. Spaite and his associates will allow the full EPIC-TBI analysis to correlate patient outcomes with the impact that acute, prehospital treatment had on the hypotension dose received by each patient, he noted.
“What’s remarkable is that the single, prehospital parameter of hypotension for just a few minutes during transport can have such a strong impact on survival, given all the other factors that can influence outcomes” in TBI patients once they reach a hospital and during the period they remain hospitalized, Dr. Spaite said.
mzoler@frontlinemedcom.com On Twitter @mitchelzoler
Key clinical point:
Major finding: For each doubling of the dose of prehospital hypotension (a function of severity and duration), mortality rose by 19%.
Data source: EPIC-TBI, a multicenter study with 16,711 patients, including 7,521 who met inclusion criteria for the current analysis.
Disclosures: Dr. Spaite had no disclosures.
Absorb’s problems will revise coronary scaffold standards
One-year outcome results of the first bioresorbable coronary scaffold on the U.S. and world markets, Absorb, failed to show longer-term problems with the device that only became apparent with 3-year follow-up.
The failure of Absorb to show benefits after 3 years in the ABSORB II trial will probably not dampen enthusiasm for the concept of a bioresorbable coronary scaffold (BRS). The idea of treating coronary stenoses with a stent that disappears after a few years once it has done its job is a powerfully attractive idea, and reports from several early-stage clinical tests of new BRSs during TCT 2016 showed that many next-generation versions of these devices are in very active development.

The surprising ABSORB II results showed more than just a failure of the Absorb BRS to produce 3 years after placement the improved coronary artery vasomotion and reduced late lumen loss that were the two primary efficacy endpoints of the trial.
The results also showed troubling signs of harm from the BRS, including significantly worse late lumen loss, compared with a contemporary drug-eluting metallic stent. In addition, there was a shocking 1%/year rate of late stent thrombosis during both the second and third years following Absorb placement in coronary arteries, the period when the Absorb BRS was in the process of disappearing, and which did not occur in the study’s control patients who received a conventional, metallic drug-eluting stent.
Patrick W. Serruys, MD, lead investigator of ABSORB II, attributed these adverse outcomes to the “highly thrombogenic” proteoglycan material that formed as the Absorb BRS resorbed, and a “structural discontinuity” of the BRS as it resorbed in some patients, resulting in parts of the scaffold remnant sticking out from the coronary artery wall toward the center of the vessel.
These late flaws in the bioresorption process will now need closer scrutiny during future studies of next-generation BRSs, and will surely mean longer follow-up of pivotal trials and a shift from the 1-year follow-up data used by the Food and Drug Administration when it approved the Absorb BRS last July.
“The challenge for the field [of BRS development] is the late results, as we saw in ABSORB II,” commented David J. Cohen, MD, an interventional cardiologist at Saint Luke’s Health System in Kansas City, Mo. The ABSORB II results “will lead to reexamination of the trial design and endpoints for the next generation of BRSs,” Dr. Cohen predicted at the meeting, sponsored by the Cardiovascular Research Foundation.

“It’s not clear that BRS reduces the duration for DAPT,” Dr. Cohen noted, at least for the Absorb device, which is not full resorbed until it’s been in patients for about 3 years.
A striking property of the next-generation BRSs reported at the meeting was their use of thinner struts and faster resorption times. “These iterations hold immense promise for improving late outcomes,” commented Dean J. Kereiakes, MD, an interventional cardiologist at the Christ Hospital in Cincinnati who helped lead the large U.S. clinical trial of the Absorb BRS, ABSORB III.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
One-year outcome results of the first bioresorbable coronary scaffold on the U.S. and world markets, Absorb, failed to show longer-term problems with the device that only became apparent with 3-year follow-up.
The failure of Absorb to show benefits after 3 years in the ABSORB II trial will probably not dampen enthusiasm for the concept of a bioresorbable coronary scaffold (BRS). The idea of treating coronary stenoses with a stent that disappears after a few years once it has done its job is a powerfully attractive idea, and reports from several early-stage clinical tests of new BRSs during TCT 2016 showed that many next-generation versions of these devices are in very active development.
The surprising ABSORB II results showed more than just a failure of the Absorb BRS to produce 3 years after placement the improved coronary artery vasomotion and reduced late lumen loss that were the two primary efficacy endpoints of the trial.
The results also showed troubling signs of harm from the BRS, including significantly worse late lumen loss, compared with a contemporary drug-eluting metallic stent. In addition, there was a shocking 1%/year rate of late stent thrombosis during both the second and third years following Absorb placement in coronary arteries, the period when the Absorb BRS was in the process of disappearing, and which did not occur in the study’s control patients who received a conventional, metallic drug-eluting stent.
Patrick W. Serruys, MD, lead investigator of ABSORB II, attributed these adverse outcomes to the “highly thrombogenic” proteoglycan material that formed as the Absorb BRS resorbed, and a “structural discontinuity” of the BRS as it resorbed in some patients, resulting in parts of the scaffold remnant sticking out from the coronary artery wall toward the center of the vessel.
These late flaws in the bioresorption process will now need closer scrutiny during future studies of next-generation BRSs, and will surely mean longer follow-up of pivotal trials and a shift from the 1-year follow-up data used by the Food and Drug Administration when it approved the Absorb BRS last July.
“The challenge for the field [of BRS development] is the late results, as we saw in ABSORB II,” commented David J. Cohen, MD, an interventional cardiologist at Saint Luke’s Health System in Kansas City, Mo. The ABSORB II results “will lead to reexamination of the trial design and endpoints for the next generation of BRSs,” Dr. Cohen predicted at the meeting, sponsored by the Cardiovascular Research Foundation.
“It’s not clear that BRS reduces the duration for DAPT,” Dr. Cohen noted, at least for the Absorb device, which is not full resorbed until it’s been in patients for about 3 years.
A striking property of the next-generation BRSs reported at the meeting was their use of thinner struts and faster resorption times. “These iterations hold immense promise for improving late outcomes,” commented Dean J. Kereiakes, MD, an interventional cardiologist at the Christ Hospital in Cincinnati who helped lead the large U.S. clinical trial of the Absorb BRS, ABSORB III.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
One-year outcome results of the first bioresorbable coronary scaffold on the U.S. and world markets, Absorb, failed to show longer-term problems with the device that only became apparent with 3-year follow-up.
The failure of Absorb to show benefits after 3 years in the ABSORB II trial will probably not dampen enthusiasm for the concept of a bioresorbable coronary scaffold (BRS). The idea of treating coronary stenoses with a stent that disappears after a few years once it has done its job is a powerfully attractive idea, and reports from several early-stage clinical tests of new BRSs during TCT 2016 showed that many next-generation versions of these devices are in very active development.
The surprising ABSORB II results showed more than just a failure of the Absorb BRS to produce 3 years after placement the improved coronary artery vasomotion and reduced late lumen loss that were the two primary efficacy endpoints of the trial.
The results also showed troubling signs of harm from the BRS, including significantly worse late lumen loss, compared with a contemporary drug-eluting metallic stent. In addition, there was a shocking 1%/year rate of late stent thrombosis during both the second and third years following Absorb placement in coronary arteries, the period when the Absorb BRS was in the process of disappearing, and which did not occur in the study’s control patients who received a conventional, metallic drug-eluting stent.
Patrick W. Serruys, MD, lead investigator of ABSORB II, attributed these adverse outcomes to the “highly thrombogenic” proteoglycan material that formed as the Absorb BRS resorbed, and a “structural discontinuity” of the BRS as it resorbed in some patients, resulting in parts of the scaffold remnant sticking out from the coronary artery wall toward the center of the vessel.
These late flaws in the bioresorption process will now need closer scrutiny during future studies of next-generation BRSs, and will surely mean longer follow-up of pivotal trials and a shift from the 1-year follow-up data used by the Food and Drug Administration when it approved the Absorb BRS last July.
“The challenge for the field [of BRS development] is the late results, as we saw in ABSORB II,” commented David J. Cohen, MD, an interventional cardiologist at Saint Luke’s Health System in Kansas City, Mo. The ABSORB II results “will lead to reexamination of the trial design and endpoints for the next generation of BRSs,” Dr. Cohen predicted at the meeting, sponsored by the Cardiovascular Research Foundation.
“It’s not clear that BRS reduces the duration for DAPT,” Dr. Cohen noted, at least for the Absorb device, which is not full resorbed until it’s been in patients for about 3 years.
A striking property of the next-generation BRSs reported at the meeting was their use of thinner struts and faster resorption times. “These iterations hold immense promise for improving late outcomes,” commented Dean J. Kereiakes, MD, an interventional cardiologist at the Christ Hospital in Cincinnati who helped lead the large U.S. clinical trial of the Absorb BRS, ABSORB III.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
VIDEO: PCI outcomes lag in women, minorities
WASHINGTON – The relatively low number of women and minority-group patients enrolled into cardiovascular disease clinical trials may skew the results, based on a comparison of outcomes following coronary stenting in an analysis of more than 4,000 patients.
During 12 months following coronary-disease treatment with percutaneous coronary intervention (PCI), women of diverse racial and ethnic backgrounds had a statistically significant 60% relative increase in death and myocardial infarctions, compared with white men, after adjustment for known baseline variables, Wayne B. Batchelor, MD, reported at the Transcatheter Cardiovascular Therapeutics annual meeting.
Minority patients, a mix of women and men, had a 90% relative rise in death and MIs, and a 60% higher rate of MIs after adjustment, both statistically significant differences.
Dr. Batchelor and his associates have not yet analyzed what factors are behind these worse outcomes in women and minority patients. But he suspects social and economic factors may provide at least some explanation, including income, education, language fluency, exercise habits, and access to health care.
“I think the trends we saw are real; the question is what accounts for the differences,” said Dr. Batchelor, an interventional cardiologist in Tallahassee, Fla. Regardless of the causes, he believes that the outcome differences have important immediate messages.
“We need to ensure better representation of women and minorities in clinical trials,” he said in an interview. “We don’t collect enough data from women and minorities. Historically, they have been underrepresented in trials.”
Another lesson is the importance of putting women and minority patients with cardiovascular disease on guideline-directed treatment, including dual antiplatelet therapy, lipid-lowering drugs, and antihypertensive drugs. The results show potential opportunity to further improve outcomes in women and minority patients, Dr. Batchelor said at the meeting, sponsored by the Cardiovascular Research Foundation.
The PLATINUM Diversity trial enrolled 1,501 women and men from minority groups with coronary disease who required PCI at one of 52 U.S. sites. For his analysis, Dr. Batchelor combined the 12-month outcomes of these patients with 12-month data from 2,687 unselected patients enrolled in the PROMUS Element Plus post-marketing approval study, a group of mostly white men.
The PLATINUM Diversity trial was sponsored by Boston Scientific. Dr. Batchelor has received research support from and has been a speaker for and consultant to Boston Scientific. He also has been a speaker for and consultant to Abbott Vascular and Medtronic.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com On Twitter @mitchelzoler
WASHINGTON – The relatively low number of women and minority-group patients enrolled into cardiovascular disease clinical trials may skew the results, based on a comparison of outcomes following coronary stenting in an analysis of more than 4,000 patients.
During 12 months following coronary-disease treatment with percutaneous coronary intervention (PCI), women of diverse racial and ethnic backgrounds had a statistically significant 60% relative increase in death and myocardial infarctions, compared with white men, after adjustment for known baseline variables, Wayne B. Batchelor, MD, reported at the Transcatheter Cardiovascular Therapeutics annual meeting.
Minority patients, a mix of women and men, had a 90% relative rise in death and MIs, and a 60% higher rate of MIs after adjustment, both statistically significant differences.
Dr. Batchelor and his associates have not yet analyzed what factors are behind these worse outcomes in women and minority patients. But he suspects social and economic factors may provide at least some explanation, including income, education, language fluency, exercise habits, and access to health care.
“I think the trends we saw are real; the question is what accounts for the differences,” said Dr. Batchelor, an interventional cardiologist in Tallahassee, Fla. Regardless of the causes, he believes that the outcome differences have important immediate messages.
“We need to ensure better representation of women and minorities in clinical trials,” he said in an interview. “We don’t collect enough data from women and minorities. Historically, they have been underrepresented in trials.”
Another lesson is the importance of putting women and minority patients with cardiovascular disease on guideline-directed treatment, including dual antiplatelet therapy, lipid-lowering drugs, and antihypertensive drugs. The results show potential opportunity to further improve outcomes in women and minority patients, Dr. Batchelor said at the meeting, sponsored by the Cardiovascular Research Foundation.
The PLATINUM Diversity trial enrolled 1,501 women and men from minority groups with coronary disease who required PCI at one of 52 U.S. sites. For his analysis, Dr. Batchelor combined the 12-month outcomes of these patients with 12-month data from 2,687 unselected patients enrolled in the PROMUS Element Plus post-marketing approval study, a group of mostly white men.
The PLATINUM Diversity trial was sponsored by Boston Scientific. Dr. Batchelor has received research support from and has been a speaker for and consultant to Boston Scientific. He also has been a speaker for and consultant to Abbott Vascular and Medtronic.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com On Twitter @mitchelzoler
WASHINGTON – The relatively low number of women and minority-group patients enrolled into cardiovascular disease clinical trials may skew the results, based on a comparison of outcomes following coronary stenting in an analysis of more than 4,000 patients.
During 12 months following coronary-disease treatment with percutaneous coronary intervention (PCI), women of diverse racial and ethnic backgrounds had a statistically significant 60% relative increase in death and myocardial infarctions, compared with white men, after adjustment for known baseline variables, Wayne B. Batchelor, MD, reported at the Transcatheter Cardiovascular Therapeutics annual meeting.
Minority patients, a mix of women and men, had a 90% relative rise in death and MIs, and a 60% higher rate of MIs after adjustment, both statistically significant differences.
Dr. Batchelor and his associates have not yet analyzed what factors are behind these worse outcomes in women and minority patients. But he suspects social and economic factors may provide at least some explanation, including income, education, language fluency, exercise habits, and access to health care.
“I think the trends we saw are real; the question is what accounts for the differences,” said Dr. Batchelor, an interventional cardiologist in Tallahassee, Fla. Regardless of the causes, he believes that the outcome differences have important immediate messages.
“We need to ensure better representation of women and minorities in clinical trials,” he said in an interview. “We don’t collect enough data from women and minorities. Historically, they have been underrepresented in trials.”
Another lesson is the importance of putting women and minority patients with cardiovascular disease on guideline-directed treatment, including dual antiplatelet therapy, lipid-lowering drugs, and antihypertensive drugs. The results show potential opportunity to further improve outcomes in women and minority patients, Dr. Batchelor said at the meeting, sponsored by the Cardiovascular Research Foundation.
The PLATINUM Diversity trial enrolled 1,501 women and men from minority groups with coronary disease who required PCI at one of 52 U.S. sites. For his analysis, Dr. Batchelor combined the 12-month outcomes of these patients with 12-month data from 2,687 unselected patients enrolled in the PROMUS Element Plus post-marketing approval study, a group of mostly white men.
The PLATINUM Diversity trial was sponsored by Boston Scientific. Dr. Batchelor has received research support from and has been a speaker for and consultant to Boston Scientific. He also has been a speaker for and consultant to Abbott Vascular and Medtronic.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com On Twitter @mitchelzoler
Key clinical point:
Major finding: One year after percutaneous coronary intervention, death or myocardial infarction was 60% higher in women and 90% higher in minorities, compared with white men.
Data source: PLATINUM Diversity, a multicenter, single-arm study with 1,501 patients, and the PROMUS Element Plus U.S. postmarketing approval study with 2,683 patients.
Disclosures: The PLATINUM Diversity trial was sponsored by Boston Scientific. Dr. Batchelor has received research support from and has been a speaker for and consultant to Boston Scientific. He also has been a speaker for and consultant to Abbott Vascular and Medtronic.
Diabetes drugs with cardiovascular benefits broaden cardiology’s turf
The dramatic reduction in cardiovascular death and heart failure hospitalization seen during treatment with empagliflozin (Jardiance) in the EMPA-REG OUTCOME (Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients) trial, for example, has prompted some cardiologists in the year since the first EMPA-REG report to become active prescribers of the drug to their patients who have type 2 diabetes and cardiovascular disease. The same evidence has driven other cardiologists who may not feel fully comfortable prescribing an antidiabetic drug on their own to enter into active partnerships with endocrinologists to work as a team to put diabetes patients with cardiovascular disease on empagliflozin.

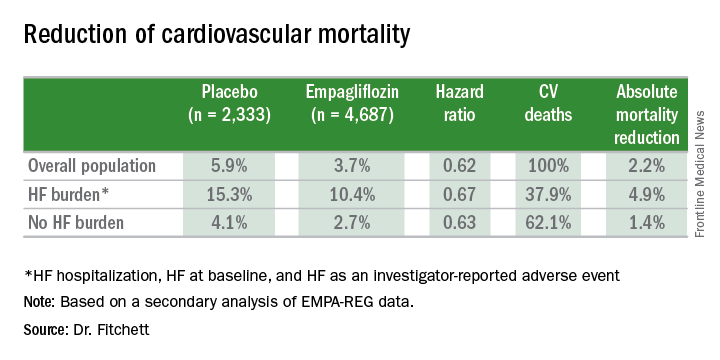
In Dr. Fitchett’s practice, “if a patient with type 2 diabetes has an endocrinologist, then I will send a letter to that physician saying I think the patient should be on one of these drugs,” empagliflozin or liraglutide, he said. “If the patient is being treated by a primary care physician, then I will prescribe empagliflozin myself because most primary care physicians are not willing to prescribe it. I think more and more cardiologists are doing this. The great thing about empagliflozin and liraglutide is that they do not cause hypoglycemia and the adverse effect profiles are relatively good. As long as drug cost is not an issue, then as cardiologists we need to adjust glycemia control with cardiovascular benefit as we did years ago with statin treatment,” explained Dr. Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a senior collaborator and coauthor on the EMPA-REG study.
When results from the 4S [Scandinavian Simvastatin Survival Study] came out in 1994, proving that long-term statin treatment was both safe and increased survival in patients with coronary heart disease, “cardiologists took over lipid management from endocrinologists,” he recalled. “We now have a safe and simple treatment for glucose lowering that also cuts cardiovascular disease events, so cardiologists have to also be involved, at least to some extent. Their degree of involvement depends on their practice and who provides a patient’s primary diabetes care,” he said.
Cardiologists vary on empagliflozin
Other cardiologists are mixed in their take on personally prescribing antidiabetic drugs to high-risk patients with type 2 diabetes. Greg C. Fonarow, MD, has also aggressively taken to empagliflozin over the past year, especially for his patients with heart failure or at high risk for developing heart failure. The EMPA-REG results showed that empagliflozin’s potent impact on reducing cardiovascular death in patients linked closely with a reduction in heart failure hospitalizations. In his recent experience, endocrinologists as well as other physicians who care for patients with type 2 diabetes “are often reluctant to make any changes [in a patient’s hypoglycemic regimen], and in general they have not gravitated toward the treatments that have been shown to improve cardiovascular outcomes and instead focus solely on a patient’s hemoglobin A1c,” Dr. Fonarow said in an interview at the recent annual meeting of the Heart Failure Society of America.

He said he prescribes empagliflozin to patients with type 2 diabetes if they are hospitalized for heart failure or as outpatients, and he targets it to patients diagnosed with heart failure – including heart failure with preserved ejection fraction – as well as to patients with other forms of cardiovascular disease, closely following the EMPA-REG enrollment criteria. It’s too early in the experience with empagliflozin to use it preferentially in diabetes patients without cardiovascular disease or patients who in any other way fall outside the enrollment criteria for EMPA-REG, he said.
“I am happy to consult with their endocrinologist, or I tell patients to discuss this treatment with their endocrinologist. If the endocrinologist prescribes empagliflozin, great; if not, I feel an obligation to provide the best care I can to my patients. This is not a hard medication to use. The safety profile is good. Treatment with empagliflozin obviously has renal-function considerations, but that’s true for many drugs. The biggest challenge is what is covered by the patient’s insurance. We often need preauthorization.
“So far I have seen excellent responses in patients for both metabolic control and clinical responses in patients with heart failure. Their symptoms seem to improve,” said Dr. Fonarow, professor of medicine and co-chief of cardiology at the University of Southern California , Los Angeles.
While Dr. Fonarow cautioned that he also would not start empagliflozin in a patient with a HbA1c below 7%, he would seriously consider swapping out a patient’s drug for empagliflozin if it were a sulfonylurea or a dipeptidyl peptidase-4 inhibitor. He stopped short of suggesting a substitution of empagliflozin for metformin. In Dr. Fonarow’s opinion, the evidence for empagliflozin is also “more robust” than it has been for liraglutide or semaglutide. With what’s now known about the clinical impact of these drugs, he foresees a time when a combination between a SGLT-2 inhibitor, with its effect on heart failure, and a GLP-1 analogue, with its effect on atherosclerotic disease, may seem an ideal initial drug pairing for patients with type 2 diabetes and significant cardiovascular disease risk, with metformin relegated to a second-line role.
Other cardiologists endorsed a more collaborative approach to prescribing empagliflozin and liraglutide.

Another team-approach advocate is Robert O. Bonow, MD, cardiologist and professor of medicine at Northwestern University in Chicago. “Cardiologists are comfortable prescribing metformin and telling patients about lifestyle, but when it comes to newer antidiabetic drugs, that’s a new field, and a team approach may be best,” he said in an interview. “If possible, a cardiologist should have a friendly partnership with a diabetologist or endocrinologist who is expert in treating diabetes.” Many cardiologists now work in and for hospitals, and easy access to an endocrinologist is probably available, he noted.

But new analyses of the EMPA-REG data reported by Dr. Fitchett at the ESC congress showed that empagliflozin treatment exerted a similar benefit of reduced cardiovascular death regardless of whether patients had prevalent heart failure at entry into the study, incident heart failure during follow-up, or no heart failure of any sort.
Impact of heart failure in EMPA-REG
Roughly 10% of the 7,020 patients enrolled in EMPA-REG had heart failure at the time they entered the trial. During a median follow-up of just over 3 years, the incidence of new-onset heart failure – tallied as either a new heart failure hospitalization or a clinical episode deemed to be heart failure by an investigator – occurred in 4.6% of patients on empagliflozin and in 6.5% of patients in the placebo arm, a 1.9-percentage-point difference and a 30% relative risk reduction linked with empagliflozin use, Dr. Fitchett reported.
The main EMPA-REG outcome was a composite of cardiovascular death, nonfatal MI, and nonfatal stroke. This positive outcome in favor of empagliflozin treatment was primarily driven by a difference in the rate of cardiovascular death. In the new analysis, the relative reduction in cardiovascular deaths with empagliflozin compared with placebo was 29% among patients with prevalent heart failure at baseline, 35% among those who had an incident heart failure hospitalization during follow-up, 27% among patients with an incident heart failure episode diagnosed by an investigator during follow-up, 33% among the combined group of trial patients with any form of heart failure at trial entry or during the trial (those with prevalent heart failure at baseline plus those with an incident event), and 37% among the large number of patients in the trial who remained free from any indication of heart failure during follow-up.
In short, treatment with empagliflozin “reduced cardiovascular mortality by the same relative amount” regardless of whether patients did or did not have heart failure during the trial,” Dr. Fitchett concluded.
Additional secondary analyses from EMPA-REG reported at the ESC congress in August also documented that the benefit from empagliflozin treatment was roughly the same regardless of the age of patients enrolled in the trial and regardless of patients’ blood level of LDL cholesterol at entry into the study. These findings provide “confidence in the consistency of the effect” by empagliflozin, Dr. Fitchett said.
The endocrinologists’ view

“Most cardiologists are not thoroughly familiar with the full palette of medications for hyperglycemia. Selection of medication should not be made solely on the basis of results from a cardiovascular outcomes trial,” said Helena W. Rodbard, MD, a clinical endocrinologist in Rockville, Md.

“The EMPA-REG OUTCOMES and LEADER results are very exciting and encouraging. When all other factors are equal, the cardiovascular results could sway the decision about which medication to use. But an endocrinologist is in the best position to balance the many factors when choosing combination therapy and to set a target level for HbA1c, fasting blood glucose, and postprandial glucose, and to adjust therapy to minimize the risk of hypoglycemia,” Dr. Rodbard said in an interview.

He called empagliflozin a drug with “interesting promise,” especially for patients with incipient heart failure. The extra cardiovascular benefit from the GLP-1 analogues is “less settled,” although the liraglutide and semaglutide trial results are important and mean these drugs need more consideration and study. The EMPA-REG results were more clearly positive, he said.

“Metformin is still the initial drug” for most patients with type 2 diabetes, echoed Dr. Levy. Drugs like empagliflozin and liraglutide are usually used in combination with metformin.
“Like many endocrinologists, I have for some time used the oral SGLT-2 inhibitors and GLP-1 analogues in combination with metformin. It made sense before the recent cardiovascular data appeared, and it makes even more sense now,” said Dr. Jellinger, professor of clinical medicine and an endocrinologist at the University of Miami.
“Endocrinologists and diabetologists are aware that cardiologists have been taking a larger role in the care of patients with diabetes,” noted Dr. Rodbard. “I favor cardiologists and endocrinologists working in concert to improve the care of patients with diabetes.”
“Over the next few years, we will need to decide whether to treat patients with type 2 diabetes with an agent with proven benefits,” said Dr. Fitchett. “Until the results from EMPA-REG and the LEADER trial came out, there was no specific glucose-lowering agent that also reduced cardiovascular events. Some cardiologists might ask when they should get involved in managing patients with type 2 diabetes. What I would do for patients with a history of cardiovascular disease who develop new type 2 diabetes is start empagliflozin as their first drug,” Dr. Fitchett said, though he admitted that no evidence yet exists to back that approach.
The EMPA-REG trial was sponsored by Boehringer Ingelheim and by Eli Lilly, the companies that market empagliflozin. The LEADER trial was sponsored in part by Novo Nordisk, the company that markets liraglutide. Dr. Fitchett and Dr. Mentz were both researchers for EMPA-REG. Dr. Fitchett has been a consultant to AstraZeneca, Merck, and Amgen. Dr. Mentz has been an adviser to Boehringer Ingelheim. Dr. Fonarow has been an adviser to Amgen, Janssen, Novartis, and ZS Pharma. Dr. Bozkurt had no disclosures. Dr. Bonow has been a consultant to Gilead. Dr. Jellinger has been a speaker on behalf of Boehringer-Ingelheim, Novo Nordisk, Merck, and Janssen. Dr. Rodbard has been a consultant to or speaker for several drug companies including Boehringer-Ingelheim, Eli Lilly, and Novo Nordisk. Dr. Levy has been a speaker on behalf of Boehringer-Ingelheim, Eli Lilly, Novo Nordisk, and AstraZeneca. Dr. Hellman had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
The dramatic reduction in cardiovascular death and heart failure hospitalization seen during treatment with empagliflozin (Jardiance) in the EMPA-REG OUTCOME (Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients) trial, for example, has prompted some cardiologists in the year since the first EMPA-REG report to become active prescribers of the drug to their patients who have type 2 diabetes and cardiovascular disease. The same evidence has driven other cardiologists who may not feel fully comfortable prescribing an antidiabetic drug on their own to enter into active partnerships with endocrinologists to work as a team to put diabetes patients with cardiovascular disease on empagliflozin.
In Dr. Fitchett’s practice, “if a patient with type 2 diabetes has an endocrinologist, then I will send a letter to that physician saying I think the patient should be on one of these drugs,” empagliflozin or liraglutide, he said. “If the patient is being treated by a primary care physician, then I will prescribe empagliflozin myself because most primary care physicians are not willing to prescribe it. I think more and more cardiologists are doing this. The great thing about empagliflozin and liraglutide is that they do not cause hypoglycemia and the adverse effect profiles are relatively good. As long as drug cost is not an issue, then as cardiologists we need to adjust glycemia control with cardiovascular benefit as we did years ago with statin treatment,” explained Dr. Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a senior collaborator and coauthor on the EMPA-REG study.
When results from the 4S [Scandinavian Simvastatin Survival Study] came out in 1994, proving that long-term statin treatment was both safe and increased survival in patients with coronary heart disease, “cardiologists took over lipid management from endocrinologists,” he recalled. “We now have a safe and simple treatment for glucose lowering that also cuts cardiovascular disease events, so cardiologists have to also be involved, at least to some extent. Their degree of involvement depends on their practice and who provides a patient’s primary diabetes care,” he said.
Cardiologists vary on empagliflozin
Other cardiologists are mixed in their take on personally prescribing antidiabetic drugs to high-risk patients with type 2 diabetes. Greg C. Fonarow, MD, has also aggressively taken to empagliflozin over the past year, especially for his patients with heart failure or at high risk for developing heart failure. The EMPA-REG results showed that empagliflozin’s potent impact on reducing cardiovascular death in patients linked closely with a reduction in heart failure hospitalizations. In his recent experience, endocrinologists as well as other physicians who care for patients with type 2 diabetes “are often reluctant to make any changes [in a patient’s hypoglycemic regimen], and in general they have not gravitated toward the treatments that have been shown to improve cardiovascular outcomes and instead focus solely on a patient’s hemoglobin A1c,” Dr. Fonarow said in an interview at the recent annual meeting of the Heart Failure Society of America.
He said he prescribes empagliflozin to patients with type 2 diabetes if they are hospitalized for heart failure or as outpatients, and he targets it to patients diagnosed with heart failure – including heart failure with preserved ejection fraction – as well as to patients with other forms of cardiovascular disease, closely following the EMPA-REG enrollment criteria. It’s too early in the experience with empagliflozin to use it preferentially in diabetes patients without cardiovascular disease or patients who in any other way fall outside the enrollment criteria for EMPA-REG, he said.
“I am happy to consult with their endocrinologist, or I tell patients to discuss this treatment with their endocrinologist. If the endocrinologist prescribes empagliflozin, great; if not, I feel an obligation to provide the best care I can to my patients. This is not a hard medication to use. The safety profile is good. Treatment with empagliflozin obviously has renal-function considerations, but that’s true for many drugs. The biggest challenge is what is covered by the patient’s insurance. We often need preauthorization.
“So far I have seen excellent responses in patients for both metabolic control and clinical responses in patients with heart failure. Their symptoms seem to improve,” said Dr. Fonarow, professor of medicine and co-chief of cardiology at the University of Southern California , Los Angeles.
While Dr. Fonarow cautioned that he also would not start empagliflozin in a patient with a HbA1c below 7%, he would seriously consider swapping out a patient’s drug for empagliflozin if it were a sulfonylurea or a dipeptidyl peptidase-4 inhibitor. He stopped short of suggesting a substitution of empagliflozin for metformin. In Dr. Fonarow’s opinion, the evidence for empagliflozin is also “more robust” than it has been for liraglutide or semaglutide. With what’s now known about the clinical impact of these drugs, he foresees a time when a combination between a SGLT-2 inhibitor, with its effect on heart failure, and a GLP-1 analogue, with its effect on atherosclerotic disease, may seem an ideal initial drug pairing for patients with type 2 diabetes and significant cardiovascular disease risk, with metformin relegated to a second-line role.
Other cardiologists endorsed a more collaborative approach to prescribing empagliflozin and liraglutide.
Another team-approach advocate is Robert O. Bonow, MD, cardiologist and professor of medicine at Northwestern University in Chicago. “Cardiologists are comfortable prescribing metformin and telling patients about lifestyle, but when it comes to newer antidiabetic drugs, that’s a new field, and a team approach may be best,” he said in an interview. “If possible, a cardiologist should have a friendly partnership with a diabetologist or endocrinologist who is expert in treating diabetes.” Many cardiologists now work in and for hospitals, and easy access to an endocrinologist is probably available, he noted.
But new analyses of the EMPA-REG data reported by Dr. Fitchett at the ESC congress showed that empagliflozin treatment exerted a similar benefit of reduced cardiovascular death regardless of whether patients had prevalent heart failure at entry into the study, incident heart failure during follow-up, or no heart failure of any sort.
Impact of heart failure in EMPA-REG
Roughly 10% of the 7,020 patients enrolled in EMPA-REG had heart failure at the time they entered the trial. During a median follow-up of just over 3 years, the incidence of new-onset heart failure – tallied as either a new heart failure hospitalization or a clinical episode deemed to be heart failure by an investigator – occurred in 4.6% of patients on empagliflozin and in 6.5% of patients in the placebo arm, a 1.9-percentage-point difference and a 30% relative risk reduction linked with empagliflozin use, Dr. Fitchett reported.
The main EMPA-REG outcome was a composite of cardiovascular death, nonfatal MI, and nonfatal stroke. This positive outcome in favor of empagliflozin treatment was primarily driven by a difference in the rate of cardiovascular death. In the new analysis, the relative reduction in cardiovascular deaths with empagliflozin compared with placebo was 29% among patients with prevalent heart failure at baseline, 35% among those who had an incident heart failure hospitalization during follow-up, 27% among patients with an incident heart failure episode diagnosed by an investigator during follow-up, 33% among the combined group of trial patients with any form of heart failure at trial entry or during the trial (those with prevalent heart failure at baseline plus those with an incident event), and 37% among the large number of patients in the trial who remained free from any indication of heart failure during follow-up.
In short, treatment with empagliflozin “reduced cardiovascular mortality by the same relative amount” regardless of whether patients did or did not have heart failure during the trial,” Dr. Fitchett concluded.
Additional secondary analyses from EMPA-REG reported at the ESC congress in August also documented that the benefit from empagliflozin treatment was roughly the same regardless of the age of patients enrolled in the trial and regardless of patients’ blood level of LDL cholesterol at entry into the study. These findings provide “confidence in the consistency of the effect” by empagliflozin, Dr. Fitchett said.
The endocrinologists’ view
“Most cardiologists are not thoroughly familiar with the full palette of medications for hyperglycemia. Selection of medication should not be made solely on the basis of results from a cardiovascular outcomes trial,” said Helena W. Rodbard, MD, a clinical endocrinologist in Rockville, Md.
“The EMPA-REG OUTCOMES and LEADER results are very exciting and encouraging. When all other factors are equal, the cardiovascular results could sway the decision about which medication to use. But an endocrinologist is in the best position to balance the many factors when choosing combination therapy and to set a target level for HbA1c, fasting blood glucose, and postprandial glucose, and to adjust therapy to minimize the risk of hypoglycemia,” Dr. Rodbard said in an interview.
He called empagliflozin a drug with “interesting promise,” especially for patients with incipient heart failure. The extra cardiovascular benefit from the GLP-1 analogues is “less settled,” although the liraglutide and semaglutide trial results are important and mean these drugs need more consideration and study. The EMPA-REG results were more clearly positive, he said.
“Metformin is still the initial drug” for most patients with type 2 diabetes, echoed Dr. Levy. Drugs like empagliflozin and liraglutide are usually used in combination with metformin.
“Like many endocrinologists, I have for some time used the oral SGLT-2 inhibitors and GLP-1 analogues in combination with metformin. It made sense before the recent cardiovascular data appeared, and it makes even more sense now,” said Dr. Jellinger, professor of clinical medicine and an endocrinologist at the University of Miami.
“Endocrinologists and diabetologists are aware that cardiologists have been taking a larger role in the care of patients with diabetes,” noted Dr. Rodbard. “I favor cardiologists and endocrinologists working in concert to improve the care of patients with diabetes.”
“Over the next few years, we will need to decide whether to treat patients with type 2 diabetes with an agent with proven benefits,” said Dr. Fitchett. “Until the results from EMPA-REG and the LEADER trial came out, there was no specific glucose-lowering agent that also reduced cardiovascular events. Some cardiologists might ask when they should get involved in managing patients with type 2 diabetes. What I would do for patients with a history of cardiovascular disease who develop new type 2 diabetes is start empagliflozin as their first drug,” Dr. Fitchett said, though he admitted that no evidence yet exists to back that approach.
The EMPA-REG trial was sponsored by Boehringer Ingelheim and by Eli Lilly, the companies that market empagliflozin. The LEADER trial was sponsored in part by Novo Nordisk, the company that markets liraglutide. Dr. Fitchett and Dr. Mentz were both researchers for EMPA-REG. Dr. Fitchett has been a consultant to AstraZeneca, Merck, and Amgen. Dr. Mentz has been an adviser to Boehringer Ingelheim. Dr. Fonarow has been an adviser to Amgen, Janssen, Novartis, and ZS Pharma. Dr. Bozkurt had no disclosures. Dr. Bonow has been a consultant to Gilead. Dr. Jellinger has been a speaker on behalf of Boehringer-Ingelheim, Novo Nordisk, Merck, and Janssen. Dr. Rodbard has been a consultant to or speaker for several drug companies including Boehringer-Ingelheim, Eli Lilly, and Novo Nordisk. Dr. Levy has been a speaker on behalf of Boehringer-Ingelheim, Eli Lilly, Novo Nordisk, and AstraZeneca. Dr. Hellman had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
The dramatic reduction in cardiovascular death and heart failure hospitalization seen during treatment with empagliflozin (Jardiance) in the EMPA-REG OUTCOME (Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients) trial, for example, has prompted some cardiologists in the year since the first EMPA-REG report to become active prescribers of the drug to their patients who have type 2 diabetes and cardiovascular disease. The same evidence has driven other cardiologists who may not feel fully comfortable prescribing an antidiabetic drug on their own to enter into active partnerships with endocrinologists to work as a team to put diabetes patients with cardiovascular disease on empagliflozin.
In Dr. Fitchett’s practice, “if a patient with type 2 diabetes has an endocrinologist, then I will send a letter to that physician saying I think the patient should be on one of these drugs,” empagliflozin or liraglutide, he said. “If the patient is being treated by a primary care physician, then I will prescribe empagliflozin myself because most primary care physicians are not willing to prescribe it. I think more and more cardiologists are doing this. The great thing about empagliflozin and liraglutide is that they do not cause hypoglycemia and the adverse effect profiles are relatively good. As long as drug cost is not an issue, then as cardiologists we need to adjust glycemia control with cardiovascular benefit as we did years ago with statin treatment,” explained Dr. Fitchett, a cardiologist at St. Michael’s Hospital in Toronto and a senior collaborator and coauthor on the EMPA-REG study.
When results from the 4S [Scandinavian Simvastatin Survival Study] came out in 1994, proving that long-term statin treatment was both safe and increased survival in patients with coronary heart disease, “cardiologists took over lipid management from endocrinologists,” he recalled. “We now have a safe and simple treatment for glucose lowering that also cuts cardiovascular disease events, so cardiologists have to also be involved, at least to some extent. Their degree of involvement depends on their practice and who provides a patient’s primary diabetes care,” he said.
Cardiologists vary on empagliflozin
Other cardiologists are mixed in their take on personally prescribing antidiabetic drugs to high-risk patients with type 2 diabetes. Greg C. Fonarow, MD, has also aggressively taken to empagliflozin over the past year, especially for his patients with heart failure or at high risk for developing heart failure. The EMPA-REG results showed that empagliflozin’s potent impact on reducing cardiovascular death in patients linked closely with a reduction in heart failure hospitalizations. In his recent experience, endocrinologists as well as other physicians who care for patients with type 2 diabetes “are often reluctant to make any changes [in a patient’s hypoglycemic regimen], and in general they have not gravitated toward the treatments that have been shown to improve cardiovascular outcomes and instead focus solely on a patient’s hemoglobin A1c,” Dr. Fonarow said in an interview at the recent annual meeting of the Heart Failure Society of America.
He said he prescribes empagliflozin to patients with type 2 diabetes if they are hospitalized for heart failure or as outpatients, and he targets it to patients diagnosed with heart failure – including heart failure with preserved ejection fraction – as well as to patients with other forms of cardiovascular disease, closely following the EMPA-REG enrollment criteria. It’s too early in the experience with empagliflozin to use it preferentially in diabetes patients without cardiovascular disease or patients who in any other way fall outside the enrollment criteria for EMPA-REG, he said.
“I am happy to consult with their endocrinologist, or I tell patients to discuss this treatment with their endocrinologist. If the endocrinologist prescribes empagliflozin, great; if not, I feel an obligation to provide the best care I can to my patients. This is not a hard medication to use. The safety profile is good. Treatment with empagliflozin obviously has renal-function considerations, but that’s true for many drugs. The biggest challenge is what is covered by the patient’s insurance. We often need preauthorization.
“So far I have seen excellent responses in patients for both metabolic control and clinical responses in patients with heart failure. Their symptoms seem to improve,” said Dr. Fonarow, professor of medicine and co-chief of cardiology at the University of Southern California , Los Angeles.
While Dr. Fonarow cautioned that he also would not start empagliflozin in a patient with a HbA1c below 7%, he would seriously consider swapping out a patient’s drug for empagliflozin if it were a sulfonylurea or a dipeptidyl peptidase-4 inhibitor. He stopped short of suggesting a substitution of empagliflozin for metformin. In Dr. Fonarow’s opinion, the evidence for empagliflozin is also “more robust” than it has been for liraglutide or semaglutide. With what’s now known about the clinical impact of these drugs, he foresees a time when a combination between a SGLT-2 inhibitor, with its effect on heart failure, and a GLP-1 analogue, with its effect on atherosclerotic disease, may seem an ideal initial drug pairing for patients with type 2 diabetes and significant cardiovascular disease risk, with metformin relegated to a second-line role.
Other cardiologists endorsed a more collaborative approach to prescribing empagliflozin and liraglutide.
Another team-approach advocate is Robert O. Bonow, MD, cardiologist and professor of medicine at Northwestern University in Chicago. “Cardiologists are comfortable prescribing metformin and telling patients about lifestyle, but when it comes to newer antidiabetic drugs, that’s a new field, and a team approach may be best,” he said in an interview. “If possible, a cardiologist should have a friendly partnership with a diabetologist or endocrinologist who is expert in treating diabetes.” Many cardiologists now work in and for hospitals, and easy access to an endocrinologist is probably available, he noted.
But new analyses of the EMPA-REG data reported by Dr. Fitchett at the ESC congress showed that empagliflozin treatment exerted a similar benefit of reduced cardiovascular death regardless of whether patients had prevalent heart failure at entry into the study, incident heart failure during follow-up, or no heart failure of any sort.
Impact of heart failure in EMPA-REG
Roughly 10% of the 7,020 patients enrolled in EMPA-REG had heart failure at the time they entered the trial. During a median follow-up of just over 3 years, the incidence of new-onset heart failure – tallied as either a new heart failure hospitalization or a clinical episode deemed to be heart failure by an investigator – occurred in 4.6% of patients on empagliflozin and in 6.5% of patients in the placebo arm, a 1.9-percentage-point difference and a 30% relative risk reduction linked with empagliflozin use, Dr. Fitchett reported.
The main EMPA-REG outcome was a composite of cardiovascular death, nonfatal MI, and nonfatal stroke. This positive outcome in favor of empagliflozin treatment was primarily driven by a difference in the rate of cardiovascular death. In the new analysis, the relative reduction in cardiovascular deaths with empagliflozin compared with placebo was 29% among patients with prevalent heart failure at baseline, 35% among those who had an incident heart failure hospitalization during follow-up, 27% among patients with an incident heart failure episode diagnosed by an investigator during follow-up, 33% among the combined group of trial patients with any form of heart failure at trial entry or during the trial (those with prevalent heart failure at baseline plus those with an incident event), and 37% among the large number of patients in the trial who remained free from any indication of heart failure during follow-up.
In short, treatment with empagliflozin “reduced cardiovascular mortality by the same relative amount” regardless of whether patients did or did not have heart failure during the trial,” Dr. Fitchett concluded.
Additional secondary analyses from EMPA-REG reported at the ESC congress in August also documented that the benefit from empagliflozin treatment was roughly the same regardless of the age of patients enrolled in the trial and regardless of patients’ blood level of LDL cholesterol at entry into the study. These findings provide “confidence in the consistency of the effect” by empagliflozin, Dr. Fitchett said.
The endocrinologists’ view
“Most cardiologists are not thoroughly familiar with the full palette of medications for hyperglycemia. Selection of medication should not be made solely on the basis of results from a cardiovascular outcomes trial,” said Helena W. Rodbard, MD, a clinical endocrinologist in Rockville, Md.
“The EMPA-REG OUTCOMES and LEADER results are very exciting and encouraging. When all other factors are equal, the cardiovascular results could sway the decision about which medication to use. But an endocrinologist is in the best position to balance the many factors when choosing combination therapy and to set a target level for HbA1c, fasting blood glucose, and postprandial glucose, and to adjust therapy to minimize the risk of hypoglycemia,” Dr. Rodbard said in an interview.
He called empagliflozin a drug with “interesting promise,” especially for patients with incipient heart failure. The extra cardiovascular benefit from the GLP-1 analogues is “less settled,” although the liraglutide and semaglutide trial results are important and mean these drugs need more consideration and study. The EMPA-REG results were more clearly positive, he said.
“Metformin is still the initial drug” for most patients with type 2 diabetes, echoed Dr. Levy. Drugs like empagliflozin and liraglutide are usually used in combination with metformin.
“Like many endocrinologists, I have for some time used the oral SGLT-2 inhibitors and GLP-1 analogues in combination with metformin. It made sense before the recent cardiovascular data appeared, and it makes even more sense now,” said Dr. Jellinger, professor of clinical medicine and an endocrinologist at the University of Miami.
“Endocrinologists and diabetologists are aware that cardiologists have been taking a larger role in the care of patients with diabetes,” noted Dr. Rodbard. “I favor cardiologists and endocrinologists working in concert to improve the care of patients with diabetes.”
“Over the next few years, we will need to decide whether to treat patients with type 2 diabetes with an agent with proven benefits,” said Dr. Fitchett. “Until the results from EMPA-REG and the LEADER trial came out, there was no specific glucose-lowering agent that also reduced cardiovascular events. Some cardiologists might ask when they should get involved in managing patients with type 2 diabetes. What I would do for patients with a history of cardiovascular disease who develop new type 2 diabetes is start empagliflozin as their first drug,” Dr. Fitchett said, though he admitted that no evidence yet exists to back that approach.
The EMPA-REG trial was sponsored by Boehringer Ingelheim and by Eli Lilly, the companies that market empagliflozin. The LEADER trial was sponsored in part by Novo Nordisk, the company that markets liraglutide. Dr. Fitchett and Dr. Mentz were both researchers for EMPA-REG. Dr. Fitchett has been a consultant to AstraZeneca, Merck, and Amgen. Dr. Mentz has been an adviser to Boehringer Ingelheim. Dr. Fonarow has been an adviser to Amgen, Janssen, Novartis, and ZS Pharma. Dr. Bozkurt had no disclosures. Dr. Bonow has been a consultant to Gilead. Dr. Jellinger has been a speaker on behalf of Boehringer-Ingelheim, Novo Nordisk, Merck, and Janssen. Dr. Rodbard has been a consultant to or speaker for several drug companies including Boehringer-Ingelheim, Eli Lilly, and Novo Nordisk. Dr. Levy has been a speaker on behalf of Boehringer-Ingelheim, Eli Lilly, Novo Nordisk, and AstraZeneca. Dr. Hellman had no disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler