User login
Dietary Reference Intakes for Vitamin D Caution Against Excess
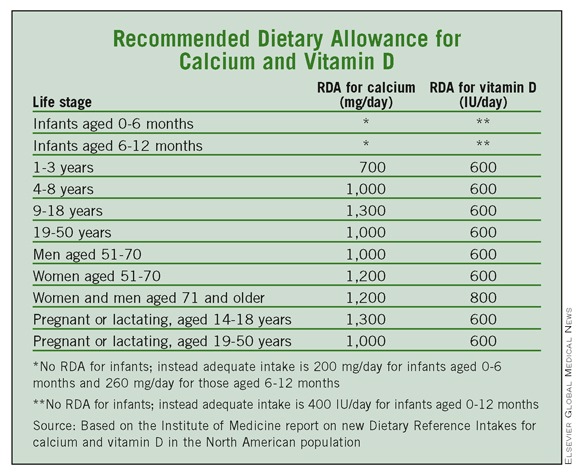
WASHINGTON – Daily doses of 600 international units of vitamin D and between 700 and 1,300 mg of calcium are enough for most children and adults in the United States and Canada, according to a report on new dietary reference intakes issued by the Institute of Medicine.
These new dietary reference intakes for calcium and vitamin D should provide "greater assurance that widespread vitamin D deficiency is not a public health problem," Dr. Steven Clinton, a member of the IOM committee that issued the report. Committee members spoke at a Nov. 30 press briefing.
After reviewing national databases on blood levels from the United States and Canada, the committee determined that most people in both countries are currently meeting their needs for vitamin D. Adequate vitamin D was defined as blood levels of at least 20 ng/mL as measured in the United States (50 nmol/L as measured in Canada).
Dr. Clinton, a medical oncologist at Ohio State University, Columbus, predicted that physicians will become more comfortable using recommended dietary allowances to advise patients about calcium and vitamin D intake and noted that vitamin D screening "probably should not be part of routine medical care."
Previous recommendations for vitamin D and calcium intake were defined in terms of adequate intake, which is not the same as recommended dietary allowance (RDA), noted committee member Patsy Brannon, Ph.D., a professor in the division of nutritional science at Cornell University, Ithaca, N.Y. Although the new values might not look much different, "You can't compare the two sets of numbers," she said. The evidence used to determine the new RDAs for calcium and vitamin D was much more comprehensive, especially data from studies conducted within the past 2 years, she explained.
While calcium and vitamin D are important for health, more is not necessarily better, the reviewers said.
They cautioned against excessive vitamin D supplementation beyond the RDA, but said supplements can be used in combination with diet to meet the RDAs. "The data are not sufficient to conclude that intakes higher than the recommended values would be beneficial," A. Catherine Ross, Ph.D., of Pennsylvania State University, University Park.
To reduce the risk of kidney stones, calcium supplements should be used with caution, Dr. Brannon advised.
The IOM reviewers examined approximately 1,000 published studies and scientific testimonies to determine the levels of calcium and vitamin D needed to maintain health.
Based on their findings, 700 mg/day of calcium is enough for most children aged 1-3 years, and 1,000 mg is appropriate for most children aged 4-8 years. Older children and teens aged 9-18 years need no more than 1,300 mg/day, and most adults aged 19-50 years and men through 71 years need no more than 1,000 mg daily. For women aged 51 years and older and men aged 71 years and older, 1,200 mg of calcium per day is recommended, but more than that is unnecessary, according to the report.
As for vitamin D, the IOM report states that 600 IU/day meets the needs of almost all children and adults aged 1 year through 70 years, including pregnant and lactating women. For men and women aged 71 years and older, the RDA increases to 800 IU/day to accommodate age-related physical and behavioral changes.
The IOM review committee acknowledged the challenges of fitting sun exposure into the equation when estimating dietary reference intake values for vitamin D because of concerns about skin cancer risk. "At this time, the only solution is to proceed on the basis of the assumption of minimal sun exposure and set reference values assuming that all of the vitamin D comes from the diet," the reviewers wrote.
The report lists an upper level for daily vitamin D intake of 1,000 IU for infants up to 6 months of age and 1,500 IU for infants aged 6 months to 12 months. The upper levels for children aged 1-3 years and 4-8 years are 2,500 IU and 3,000 IU, respectively. For all other life stages, the upper level is 4,000 IU.
Upper levels for calcium for adults were based on data related to the formation of kidney stones, and the upper levels for children take adolescent growth spurts into account. The upper level for daily calcium intake for infants aged 0 to 6 months and 6-12 months are 1,000 mg and 1,500 mg, respectively. For children aged 1-8 years and 9-18 years, the upper levels are 2,500 mg and 3,000 mg, respectively, for both boys and girls. Adults aged 19-50 years have an upper level of 2,500 mg that drops to 2,000 mg after age 50 years for both men and women. The upper levels of calcium for pregnant and lactating women aged 14-18 years, 19-30 years, and 31-50 years are 3,000 mg, 2,500 mg, and 2,500 mg, respectively.
"What we have concluded may be surprising to some," Dr. Ross said. "I was surprised to find that vitamin D requirements don't vary much by age."
Dr. Ross noted that the report is not necessarily the last word on the subject, but "we are going to need to do a tremendous amount of research" before drawing any conclusions on additional benefits of vitamin D and calcium.
The study was sponsored by the federal governments of the United States and Canad
WASHINGTON – Daily doses of 600 international units of vitamin D and between 700 and 1,300 mg of calcium are enough for most children and adults in the United States and Canada, according to a report on new dietary reference intakes issued by the Institute of Medicine.
These new dietary reference intakes for calcium and vitamin D should provide "greater assurance that widespread vitamin D deficiency is not a public health problem," Dr. Steven Clinton, a member of the IOM committee that issued the report. Committee members spoke at a Nov. 30 press briefing.
After reviewing national databases on blood levels from the United States and Canada, the committee determined that most people in both countries are currently meeting their needs for vitamin D. Adequate vitamin D was defined as blood levels of at least 20 ng/mL as measured in the United States (50 nmol/L as measured in Canada).
Dr. Clinton, a medical oncologist at Ohio State University, Columbus, predicted that physicians will become more comfortable using recommended dietary allowances to advise patients about calcium and vitamin D intake and noted that vitamin D screening "probably should not be part of routine medical care."
Previous recommendations for vitamin D and calcium intake were defined in terms of adequate intake, which is not the same as recommended dietary allowance (RDA), noted committee member Patsy Brannon, Ph.D., a professor in the division of nutritional science at Cornell University, Ithaca, N.Y. Although the new values might not look much different, "You can't compare the two sets of numbers," she said. The evidence used to determine the new RDAs for calcium and vitamin D was much more comprehensive, especially data from studies conducted within the past 2 years, she explained.
While calcium and vitamin D are important for health, more is not necessarily better, the reviewers said.
They cautioned against excessive vitamin D supplementation beyond the RDA, but said supplements can be used in combination with diet to meet the RDAs. "The data are not sufficient to conclude that intakes higher than the recommended values would be beneficial," A. Catherine Ross, Ph.D., of Pennsylvania State University, University Park.
To reduce the risk of kidney stones, calcium supplements should be used with caution, Dr. Brannon advised.
The IOM reviewers examined approximately 1,000 published studies and scientific testimonies to determine the levels of calcium and vitamin D needed to maintain health.
Based on their findings, 700 mg/day of calcium is enough for most children aged 1-3 years, and 1,000 mg is appropriate for most children aged 4-8 years. Older children and teens aged 9-18 years need no more than 1,300 mg/day, and most adults aged 19-50 years and men through 71 years need no more than 1,000 mg daily. For women aged 51 years and older and men aged 71 years and older, 1,200 mg of calcium per day is recommended, but more than that is unnecessary, according to the report.
As for vitamin D, the IOM report states that 600 IU/day meets the needs of almost all children and adults aged 1 year through 70 years, including pregnant and lactating women. For men and women aged 71 years and older, the RDA increases to 800 IU/day to accommodate age-related physical and behavioral changes.
The IOM review committee acknowledged the challenges of fitting sun exposure into the equation when estimating dietary reference intake values for vitamin D because of concerns about skin cancer risk. "At this time, the only solution is to proceed on the basis of the assumption of minimal sun exposure and set reference values assuming that all of the vitamin D comes from the diet," the reviewers wrote.
The report lists an upper level for daily vitamin D intake of 1,000 IU for infants up to 6 months of age and 1,500 IU for infants aged 6 months to 12 months. The upper levels for children aged 1-3 years and 4-8 years are 2,500 IU and 3,000 IU, respectively. For all other life stages, the upper level is 4,000 IU.
Upper levels for calcium for adults were based on data related to the formation of kidney stones, and the upper levels for children take adolescent growth spurts into account. The upper level for daily calcium intake for infants aged 0 to 6 months and 6-12 months are 1,000 mg and 1,500 mg, respectively. For children aged 1-8 years and 9-18 years, the upper levels are 2,500 mg and 3,000 mg, respectively, for both boys and girls. Adults aged 19-50 years have an upper level of 2,500 mg that drops to 2,000 mg after age 50 years for both men and women. The upper levels of calcium for pregnant and lactating women aged 14-18 years, 19-30 years, and 31-50 years are 3,000 mg, 2,500 mg, and 2,500 mg, respectively.
"What we have concluded may be surprising to some," Dr. Ross said. "I was surprised to find that vitamin D requirements don't vary much by age."
Dr. Ross noted that the report is not necessarily the last word on the subject, but "we are going to need to do a tremendous amount of research" before drawing any conclusions on additional benefits of vitamin D and calcium.
The study was sponsored by the federal governments of the United States and Canad
WASHINGTON – Daily doses of 600 international units of vitamin D and between 700 and 1,300 mg of calcium are enough for most children and adults in the United States and Canada, according to a report on new dietary reference intakes issued by the Institute of Medicine.
These new dietary reference intakes for calcium and vitamin D should provide "greater assurance that widespread vitamin D deficiency is not a public health problem," Dr. Steven Clinton, a member of the IOM committee that issued the report. Committee members spoke at a Nov. 30 press briefing.
After reviewing national databases on blood levels from the United States and Canada, the committee determined that most people in both countries are currently meeting their needs for vitamin D. Adequate vitamin D was defined as blood levels of at least 20 ng/mL as measured in the United States (50 nmol/L as measured in Canada).
Dr. Clinton, a medical oncologist at Ohio State University, Columbus, predicted that physicians will become more comfortable using recommended dietary allowances to advise patients about calcium and vitamin D intake and noted that vitamin D screening "probably should not be part of routine medical care."
Previous recommendations for vitamin D and calcium intake were defined in terms of adequate intake, which is not the same as recommended dietary allowance (RDA), noted committee member Patsy Brannon, Ph.D., a professor in the division of nutritional science at Cornell University, Ithaca, N.Y. Although the new values might not look much different, "You can't compare the two sets of numbers," she said. The evidence used to determine the new RDAs for calcium and vitamin D was much more comprehensive, especially data from studies conducted within the past 2 years, she explained.
While calcium and vitamin D are important for health, more is not necessarily better, the reviewers said.
They cautioned against excessive vitamin D supplementation beyond the RDA, but said supplements can be used in combination with diet to meet the RDAs. "The data are not sufficient to conclude that intakes higher than the recommended values would be beneficial," A. Catherine Ross, Ph.D., of Pennsylvania State University, University Park.
To reduce the risk of kidney stones, calcium supplements should be used with caution, Dr. Brannon advised.
The IOM reviewers examined approximately 1,000 published studies and scientific testimonies to determine the levels of calcium and vitamin D needed to maintain health.
Based on their findings, 700 mg/day of calcium is enough for most children aged 1-3 years, and 1,000 mg is appropriate for most children aged 4-8 years. Older children and teens aged 9-18 years need no more than 1,300 mg/day, and most adults aged 19-50 years and men through 71 years need no more than 1,000 mg daily. For women aged 51 years and older and men aged 71 years and older, 1,200 mg of calcium per day is recommended, but more than that is unnecessary, according to the report.
As for vitamin D, the IOM report states that 600 IU/day meets the needs of almost all children and adults aged 1 year through 70 years, including pregnant and lactating women. For men and women aged 71 years and older, the RDA increases to 800 IU/day to accommodate age-related physical and behavioral changes.
The IOM review committee acknowledged the challenges of fitting sun exposure into the equation when estimating dietary reference intake values for vitamin D because of concerns about skin cancer risk. "At this time, the only solution is to proceed on the basis of the assumption of minimal sun exposure and set reference values assuming that all of the vitamin D comes from the diet," the reviewers wrote.
The report lists an upper level for daily vitamin D intake of 1,000 IU for infants up to 6 months of age and 1,500 IU for infants aged 6 months to 12 months. The upper levels for children aged 1-3 years and 4-8 years are 2,500 IU and 3,000 IU, respectively. For all other life stages, the upper level is 4,000 IU.
Upper levels for calcium for adults were based on data related to the formation of kidney stones, and the upper levels for children take adolescent growth spurts into account. The upper level for daily calcium intake for infants aged 0 to 6 months and 6-12 months are 1,000 mg and 1,500 mg, respectively. For children aged 1-8 years and 9-18 years, the upper levels are 2,500 mg and 3,000 mg, respectively, for both boys and girls. Adults aged 19-50 years have an upper level of 2,500 mg that drops to 2,000 mg after age 50 years for both men and women. The upper levels of calcium for pregnant and lactating women aged 14-18 years, 19-30 years, and 31-50 years are 3,000 mg, 2,500 mg, and 2,500 mg, respectively.
"What we have concluded may be surprising to some," Dr. Ross said. "I was surprised to find that vitamin D requirements don't vary much by age."
Dr. Ross noted that the report is not necessarily the last word on the subject, but "we are going to need to do a tremendous amount of research" before drawing any conclusions on additional benefits of vitamin D and calcium.
The study was sponsored by the federal governments of the United States and Canad
REPORT FROM THE IOM
TNF Inhibitors Protect Against Plaque Buildup in RA Patients
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
TNF Inhibitors Protect Against Plaque Buildup in RA Patients
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
ATLANTA – Patients with rheumatoid arthritis showed significant arterial thickening over a 3-year period, but tumor necrosis factor inhibitor use slowed the progression, based on data from 158 patients. The findings were presented at the annual scientific meeting of the American College of Rheumatology.
"We know that many of our patients with autoimmune disease have higher risk for cardiovascular disease," said Dr. Joan M. Bathon, professor of medicine and director of the Johns Hopkins Arthritis Center at the Johns Hopkins University in Baltimore. But few studies have examined what drives the plaque buildup in these patients.
Dr. Bathon and her colleagues examined a subgroup of patients enrolled in a larger study of cardiovascular disease and RA. They used ultrasound to measure the thickness of the walls of the common carotid artery (CCA) and internal carotid artery (ICA) and compared data on each patient at two visits approximately 3 years apart. The average age of the patients was 60 years, 36% were male, and the average duration of RA at baseline was 8.5 years.
Thickening of the CCA occurred in 82% of the patients over 3 years, with a median yearly increase of 16 mcm. Thickening of the ICA occurred in 70% of the patients, with median yearly increase of 25 mcm.
However, patients who used a tumor necrosis factor inhibitor (TNFi) agents at baseline had a 37% lower rate of CCA thickening compared to those who did not use a TNFi agent (14 mcm/year vs. 22 mcm/year), after controlling for demographic variables, cardiovascular risk factors, and baseline arterial thickening.
"We found that progression in the common carotid was much more pronounced in patients with early disease than in later disease," said Dr. Bathon. "There seems to be a particular risk when the disease first starts."
Thickening of the ICA was independently associated with prednisone use, but progression was significantly lower in patients who were taking statins at baseline, Dr. Bathon said.
A total of 68 patients showed at least some plaque development, and 14% of patients developed new plaque during the study period. Patients who developed plaque over time had higher average swollen joint counts and higher average C-reactive protein levels than those who did not show atherosclerosis progression, Dr. Bathon noted.
"The data need to be confirmed in other studies," Dr. Bathon said, "but they suggest that prednisone promotes atherosclerosis in RA, even in the tiny doses that we use." But the findings also support the protective value of statins and TNFi agents against atherosclerosis in RA patients, she said.
The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF RHEUMATOLOGY
Major Finding: Limiting inflammation with TNFi agents reduced the progression of carotid artery atherosclerosis by 37% in rheumatoid arthritis patients.
Data Source: A prospective study of 158 adults with rheumatoid arthritis
Disclosures: The study was supported in part by the American College of Rheumatology Research and Education Foundation. Dr. Bathon said she had no financial conflicts to disclose.
Foot Deformities Are Highly Heritable
ATLANTA – Got bunions? Thank your parents. Bunions were inherited in 89% of adults younger than 60 years, according to genetic data from more than 2,000 adults that were presented at the annual scientific meeting of the American College of Rheumatology.
Bunions and other foot disorders can limit mobility and exacerbate other musculoskeletal weaknesses, but interventions are available, and they are most effective if foot deformities are identified early, said Marian Hannan, D.Sc., of Harvard Medical School, Boston.
Foot disorders occur in 20%-60% of adults, and researchers have long suspected genetic involvement, but this study is the first to examine specific associations between genes and foot deformities, Dr. Hannan said.
Dr. Hannan and her colleagues reviewed data from 959 men and 1,220 women in the Framingham Foot Study of 2002-2005. A trained examiner evaluated the study participants for any of 20 different foot disorders. In this study, Dr. Hannan reported data about the most common and least common of the disorders: hallux valgus (bunions) and pes cavus (high arches).
Overall, 675 individuals (31%) had bunions and 154 (7%) had high arches. A bunion was defined as a big toe angled at least 15 degrees toward the first metatarsal. High arches were identified by calculating weight-bearing arch width.
The researchers used statistical genetics software to determine the heritability of the two conditions. Across all ages, 39% of women and 38% of men inherited their bunions, and 68% of women and 20% of men inherited their high arches. Among individuals younger than 60 years, 99% of women and 63% of men inherited their high arches. The heritability estimates were statistically significant for both conditions.
The average age of the study participants was 66 years, and 57% were women.
"Known interventions can slow the progression of disease" for patients with foot problems, Dr. Hannan emphasized. "We are continuing with research within the Framingham Foot Study to look at the other 18 foot conditions," she added. "We are also looking at specific genetic analyses to see what specific gene might be behind what is going on."
Dr. Hannan had no financial conflicts to disclose.
ATLANTA – Got bunions? Thank your parents. Bunions were inherited in 89% of adults younger than 60 years, according to genetic data from more than 2,000 adults that were presented at the annual scientific meeting of the American College of Rheumatology.
Bunions and other foot disorders can limit mobility and exacerbate other musculoskeletal weaknesses, but interventions are available, and they are most effective if foot deformities are identified early, said Marian Hannan, D.Sc., of Harvard Medical School, Boston.
Foot disorders occur in 20%-60% of adults, and researchers have long suspected genetic involvement, but this study is the first to examine specific associations between genes and foot deformities, Dr. Hannan said.
Dr. Hannan and her colleagues reviewed data from 959 men and 1,220 women in the Framingham Foot Study of 2002-2005. A trained examiner evaluated the study participants for any of 20 different foot disorders. In this study, Dr. Hannan reported data about the most common and least common of the disorders: hallux valgus (bunions) and pes cavus (high arches).
Overall, 675 individuals (31%) had bunions and 154 (7%) had high arches. A bunion was defined as a big toe angled at least 15 degrees toward the first metatarsal. High arches were identified by calculating weight-bearing arch width.
The researchers used statistical genetics software to determine the heritability of the two conditions. Across all ages, 39% of women and 38% of men inherited their bunions, and 68% of women and 20% of men inherited their high arches. Among individuals younger than 60 years, 99% of women and 63% of men inherited their high arches. The heritability estimates were statistically significant for both conditions.
The average age of the study participants was 66 years, and 57% were women.
"Known interventions can slow the progression of disease" for patients with foot problems, Dr. Hannan emphasized. "We are continuing with research within the Framingham Foot Study to look at the other 18 foot conditions," she added. "We are also looking at specific genetic analyses to see what specific gene might be behind what is going on."
Dr. Hannan had no financial conflicts to disclose.
ATLANTA – Got bunions? Thank your parents. Bunions were inherited in 89% of adults younger than 60 years, according to genetic data from more than 2,000 adults that were presented at the annual scientific meeting of the American College of Rheumatology.
Bunions and other foot disorders can limit mobility and exacerbate other musculoskeletal weaknesses, but interventions are available, and they are most effective if foot deformities are identified early, said Marian Hannan, D.Sc., of Harvard Medical School, Boston.
Foot disorders occur in 20%-60% of adults, and researchers have long suspected genetic involvement, but this study is the first to examine specific associations between genes and foot deformities, Dr. Hannan said.
Dr. Hannan and her colleagues reviewed data from 959 men and 1,220 women in the Framingham Foot Study of 2002-2005. A trained examiner evaluated the study participants for any of 20 different foot disorders. In this study, Dr. Hannan reported data about the most common and least common of the disorders: hallux valgus (bunions) and pes cavus (high arches).
Overall, 675 individuals (31%) had bunions and 154 (7%) had high arches. A bunion was defined as a big toe angled at least 15 degrees toward the first metatarsal. High arches were identified by calculating weight-bearing arch width.
The researchers used statistical genetics software to determine the heritability of the two conditions. Across all ages, 39% of women and 38% of men inherited their bunions, and 68% of women and 20% of men inherited their high arches. Among individuals younger than 60 years, 99% of women and 63% of men inherited their high arches. The heritability estimates were statistically significant for both conditions.
The average age of the study participants was 66 years, and 57% were women.
"Known interventions can slow the progression of disease" for patients with foot problems, Dr. Hannan emphasized. "We are continuing with research within the Framingham Foot Study to look at the other 18 foot conditions," she added. "We are also looking at specific genetic analyses to see what specific gene might be behind what is going on."
Dr. Hannan had no financial conflicts to disclose.
Major Finding: Of adults younger than age 60 years who have bunions, 89% inherited the condition.
Data Source: A genetic analysis and foot examination of 2,179 adults.
Disclosures: Dr. Hannan had no financial conflicts to disclose.
FDA Committee Considers Gardasil for Anal Cancer Prevention
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
FROM A MEETING OF THE FOOD AND DRUG ADMINISTRATION’S VACCINE AND RELATED BIOLOGICAL PRODUCTS ADVISORY COMMITTEE
FDA Committee Considers Gardasil for Anal Cancer Prevention
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
SILVER SPRING, Md. – The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
FROM A MEETING OF THE FOOD AND DRUG ADMINISTRATION’S VACCINE AND RELATED BIOLOGICAL PRODUCTS ADVISORY COMMITTEE
FDA Committee Considers Gardasil for Anal Cancer Prevention
SILVER SPRING, Md. - The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
Body text goes here
Doctor’s Bio
Body text goes here
Doctor’s Bio
Body text goes here
Doctor’s Bio
SILVER SPRING, Md. - The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
SILVER SPRING, Md. - The human papillomavirus vaccine Gardasil moved closer to an indication for anal cancer prevention after a meeting of the Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Nov. 17.
The vaccine, manufactured by Merck & Co. Inc., is approved for the prevention of cervical, vulvar, and vaginal cancers and precancerous lesions in females aged 9-26 years, and for the prevention of genital warts in males and females aged 9-26 years. The company is seeking an indication for the prevention of anal cancer in males and females aged 9-26 years.
Previous studies have shown that anal cancer and cervical cancer are biologically similar, and both are associated with HPV infections, Dr. Joel Palefsky, professor of medicine at the University of California, San Francisco, said at the meeting.
The primary data supporting an anal cancer indication for Gardasil came from a randomized, controlled trial of 602 men who have sex with men (MSM), who were part of the larger study that led to the indication for preventing genital warts in boys and men. The participants received three doses of vaccine or a placebo.
The vaccine showed 78% effectiveness, compared with placebo in preventing anal intraepithelial neoplasms related to human papillomavirus types 6, 11, 16, and 18. These lesions are considered precursors to anal cancer, Dr. Palefsky said.
Although MSM are at increased risk for HPV-associated anal cancer, they are not the only population at risk. Data from the National Cancer Institute presented at the meeting showed that anal cancer incidence in the United States is increasing by a rate of approximately 2% per year, and that approximately 60% of cases and deaths occur in women.
A majority of the committee members expressed opinions in favor of the indication, but no formal vote was taken. The FDA will consider the committee’s recommendations. If the indication is approved before the February 2011 meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, the ACIP might revisit its previous recommendation against routine HPV vaccination for boys and men for genital wart prevention. ACIP has given a permissive recommendation for HPV vaccination for boys and men aged 9-26 years at the discretion of the physician.
Dr. Palefsky has served as a consultant and clinical investigator for Merck & Co. Inc.
FROM A MEETING OF THE FOOD AND DRUG ADMINISTRATION’S VACCINE AND RELATED BIOLOGICAL PRODUCTS ADVISORY COMMITTEE
One-Third of Medicare Patients With Cancer Die in Hospitals
Approximately 29% of Medicare patients with cancer died in a hospital, and hospice care was inconsistent among medical centers in the United States, according to a report published Nov. 16 by the Dartmouth Institute for Health Policy & Clinical Practice.
The rate of hospital deaths varied widely by region, ranging from 47% in Manhattan (New York City) to 7% in Mason City, Iowa.
"The bottom line is that the care patients receive has less to do with what they want and more to do with the hospital they seek care from," Dr. David Goodman of Dartmouth University, Hanover, N.H., said in a press briefing. "We as physicians often make assumptions about what patients and families want for their lives. What patients really want is for a physician to be honest with them and to share the full range of options with them."
The report, "Quality of End-of-Life Cancer Care for Medicare Beneficiaries: Regional and Hospital-Specific Analyses," is the first to focus on cancer care at the end of life for the Medicare population in particular. The report was produced by the Dartmouth Atlas Project, which has been documenting the use of medical resources in the United States for more than 2 decades.
Researchers reviewed data from 235,821 Medicare patients (aged 65 years and older) with metastatic or aggressive cancer who died in 2003-2007. They identified regional trends as well as information about specific academic medical centers.
Nationwide, approximately 61% of cancer patients were hospitalized at least once during their last month of life. Hospital admissions varied from approximately 70% of cancer patients in Detroit to 46% of cancer patients in San Angelo, Tex.
The researchers identified the highest rates of hospitalization during the last month of life (more than 75%) among cancer patients at two hospitals in Detroit: St. John Hospital and Medical Center and Sinai-Grace Hospital. The lowest rate of hospitalization during the last month of life was 45% of cancer patients at the University of Washington Medical Center in Seattle.
Chemotherapy was part of care during the last 2 weeks of life in approximately 6% of patients nationwide, but the rate exceeded 10% in eight areas, including Olympia, Wash. (12%), and San Antonio (11%).
The researchers also found that fewer than 50% of cancer patients with a poor prognosis received hospice care, and some centers provided hospice care only in the last few days of life.
The degree of variation in the findings is too great to be explained by racial or ethnic preferences for aggressive end-of-life care, and adjustment for socioeconomic status does not change the results, said Dr. Goodman said.
But the data show that investment in beds, ICU facilities, and palliative care services is quite different from one health care system to another, he said.
The report highlights the need for doctors and health systems "to take a look at themselves and examine where they need to make their investments," said Dr. Goodman, who added that clinicians "need to look at ourselves in terms of how we communicate with patients" about cancer care options.
In a commentary accompanying the report, Dr. Joan Teno of Brown University in Providence, R.I., emphasized the need for health care providers to educate patients about their prognoses and to provide hospice options.
"If opportunities to improve are identified, hospitals should work with the local hospice or existing palliative care consult service, and/or start a palliative care consult service," to ensure that the institution is delivering high-quality care, Dr. Teno wrote.
Conversations about end-of-life care need to be started early in the course of treatment, Dr. Goodman said. "Our preferences can certainly change, but opening up the conversation early allows the conversation to evolve over time. The tragedy is when those conversations start near the end."
In a statement, Dr. George W. Sledge Jr., president of the American Society of Clinical Oncology said, "While saving lives is the oncologist’s goal, helping individuals live their final days in comfort and dignity is one of the most valuable and important responsibilities of our profession.
"Options to enhance a patient’s quality of life should be discussed throughout the course of their treatment. It is critical that we increase medical training in end-of-life patient communication and planning, and that Medicare and other insurers cover the costs of these essential conversations," Dr. Sledge noted.
The study was supported in part by the Robert Wood Johnson Foundation.
Approximately 29% of Medicare patients with cancer died in a hospital, and hospice care was inconsistent among medical centers in the United States, according to a report published Nov. 16 by the Dartmouth Institute for Health Policy & Clinical Practice.
The rate of hospital deaths varied widely by region, ranging from 47% in Manhattan (New York City) to 7% in Mason City, Iowa.
"The bottom line is that the care patients receive has less to do with what they want and more to do with the hospital they seek care from," Dr. David Goodman of Dartmouth University, Hanover, N.H., said in a press briefing. "We as physicians often make assumptions about what patients and families want for their lives. What patients really want is for a physician to be honest with them and to share the full range of options with them."
The report, "Quality of End-of-Life Cancer Care for Medicare Beneficiaries: Regional and Hospital-Specific Analyses," is the first to focus on cancer care at the end of life for the Medicare population in particular. The report was produced by the Dartmouth Atlas Project, which has been documenting the use of medical resources in the United States for more than 2 decades.
Researchers reviewed data from 235,821 Medicare patients (aged 65 years and older) with metastatic or aggressive cancer who died in 2003-2007. They identified regional trends as well as information about specific academic medical centers.
Nationwide, approximately 61% of cancer patients were hospitalized at least once during their last month of life. Hospital admissions varied from approximately 70% of cancer patients in Detroit to 46% of cancer patients in San Angelo, Tex.
The researchers identified the highest rates of hospitalization during the last month of life (more than 75%) among cancer patients at two hospitals in Detroit: St. John Hospital and Medical Center and Sinai-Grace Hospital. The lowest rate of hospitalization during the last month of life was 45% of cancer patients at the University of Washington Medical Center in Seattle.
Chemotherapy was part of care during the last 2 weeks of life in approximately 6% of patients nationwide, but the rate exceeded 10% in eight areas, including Olympia, Wash. (12%), and San Antonio (11%).
The researchers also found that fewer than 50% of cancer patients with a poor prognosis received hospice care, and some centers provided hospice care only in the last few days of life.
The degree of variation in the findings is too great to be explained by racial or ethnic preferences for aggressive end-of-life care, and adjustment for socioeconomic status does not change the results, said Dr. Goodman said.
But the data show that investment in beds, ICU facilities, and palliative care services is quite different from one health care system to another, he said.
The report highlights the need for doctors and health systems "to take a look at themselves and examine where they need to make their investments," said Dr. Goodman, who added that clinicians "need to look at ourselves in terms of how we communicate with patients" about cancer care options.
In a commentary accompanying the report, Dr. Joan Teno of Brown University in Providence, R.I., emphasized the need for health care providers to educate patients about their prognoses and to provide hospice options.
"If opportunities to improve are identified, hospitals should work with the local hospice or existing palliative care consult service, and/or start a palliative care consult service," to ensure that the institution is delivering high-quality care, Dr. Teno wrote.
Conversations about end-of-life care need to be started early in the course of treatment, Dr. Goodman said. "Our preferences can certainly change, but opening up the conversation early allows the conversation to evolve over time. The tragedy is when those conversations start near the end."
In a statement, Dr. George W. Sledge Jr., president of the American Society of Clinical Oncology said, "While saving lives is the oncologist’s goal, helping individuals live their final days in comfort and dignity is one of the most valuable and important responsibilities of our profession.
"Options to enhance a patient’s quality of life should be discussed throughout the course of their treatment. It is critical that we increase medical training in end-of-life patient communication and planning, and that Medicare and other insurers cover the costs of these essential conversations," Dr. Sledge noted.
The study was supported in part by the Robert Wood Johnson Foundation.
Approximately 29% of Medicare patients with cancer died in a hospital, and hospice care was inconsistent among medical centers in the United States, according to a report published Nov. 16 by the Dartmouth Institute for Health Policy & Clinical Practice.
The rate of hospital deaths varied widely by region, ranging from 47% in Manhattan (New York City) to 7% in Mason City, Iowa.
"The bottom line is that the care patients receive has less to do with what they want and more to do with the hospital they seek care from," Dr. David Goodman of Dartmouth University, Hanover, N.H., said in a press briefing. "We as physicians often make assumptions about what patients and families want for their lives. What patients really want is for a physician to be honest with them and to share the full range of options with them."
The report, "Quality of End-of-Life Cancer Care for Medicare Beneficiaries: Regional and Hospital-Specific Analyses," is the first to focus on cancer care at the end of life for the Medicare population in particular. The report was produced by the Dartmouth Atlas Project, which has been documenting the use of medical resources in the United States for more than 2 decades.
Researchers reviewed data from 235,821 Medicare patients (aged 65 years and older) with metastatic or aggressive cancer who died in 2003-2007. They identified regional trends as well as information about specific academic medical centers.
Nationwide, approximately 61% of cancer patients were hospitalized at least once during their last month of life. Hospital admissions varied from approximately 70% of cancer patients in Detroit to 46% of cancer patients in San Angelo, Tex.
The researchers identified the highest rates of hospitalization during the last month of life (more than 75%) among cancer patients at two hospitals in Detroit: St. John Hospital and Medical Center and Sinai-Grace Hospital. The lowest rate of hospitalization during the last month of life was 45% of cancer patients at the University of Washington Medical Center in Seattle.
Chemotherapy was part of care during the last 2 weeks of life in approximately 6% of patients nationwide, but the rate exceeded 10% in eight areas, including Olympia, Wash. (12%), and San Antonio (11%).
The researchers also found that fewer than 50% of cancer patients with a poor prognosis received hospice care, and some centers provided hospice care only in the last few days of life.
The degree of variation in the findings is too great to be explained by racial or ethnic preferences for aggressive end-of-life care, and adjustment for socioeconomic status does not change the results, said Dr. Goodman said.
But the data show that investment in beds, ICU facilities, and palliative care services is quite different from one health care system to another, he said.
The report highlights the need for doctors and health systems "to take a look at themselves and examine where they need to make their investments," said Dr. Goodman, who added that clinicians "need to look at ourselves in terms of how we communicate with patients" about cancer care options.
In a commentary accompanying the report, Dr. Joan Teno of Brown University in Providence, R.I., emphasized the need for health care providers to educate patients about their prognoses and to provide hospice options.
"If opportunities to improve are identified, hospitals should work with the local hospice or existing palliative care consult service, and/or start a palliative care consult service," to ensure that the institution is delivering high-quality care, Dr. Teno wrote.
Conversations about end-of-life care need to be started early in the course of treatment, Dr. Goodman said. "Our preferences can certainly change, but opening up the conversation early allows the conversation to evolve over time. The tragedy is when those conversations start near the end."
In a statement, Dr. George W. Sledge Jr., president of the American Society of Clinical Oncology said, "While saving lives is the oncologist’s goal, helping individuals live their final days in comfort and dignity is one of the most valuable and important responsibilities of our profession.
"Options to enhance a patient’s quality of life should be discussed throughout the course of their treatment. It is critical that we increase medical training in end-of-life patient communication and planning, and that Medicare and other insurers cover the costs of these essential conversations," Dr. Sledge noted.
The study was supported in part by the Robert Wood Johnson Foundation.
One-Third of Medicare Patients With Cancer Die in Hospitals
Approximately 29% of Medicare patients with cancer died in a hospital, and hospice care was inconsistent among medical centers in the United States, according to a report published Nov. 16 by the Dartmouth Institute for Health Policy & Clinical Practice.
The rate of hospital deaths varied widely by region, ranging from 47% in Manhattan (New York City) to 7% in Mason City, Iowa.
"The bottom line is that the care patients receive has less to do with what they want and more to do with the hospital they seek care from," Dr. David Goodman of Dartmouth University, Hanover, N.H., said in a press briefing. "We as physicians often make assumptions about what patients and families want for their lives. What patients really want is for a physician to be honest with them and to share the full range of options with them."
The report, "Quality of End-of-Life Cancer Care for Medicare Beneficiaries: Regional and Hospital-Specific Analyses," is the first to focus on cancer care at the end of life for the Medicare population in particular. The report was produced by the Dartmouth Atlas Project, which has been documenting the use of medical resources in the United States for more than 2 decades.
Researchers reviewed data from 235,821 Medicare patients (aged 65 years and older) with metastatic or aggressive cancer who died in 2003-2007. They identified regional trends as well as information about specific academic medical centers.
Nationwide, approximately 61% of cancer patients were hospitalized at least once during their last month of life. Hospital admissions varied from approximately 70% of cancer patients in Detroit to 46% of cancer patients in San Angelo, Tex.
The researchers identified the highest rates of hospitalization during the last month of life (more than 75%) among cancer patients at two hospitals in Detroit: St. John Hospital and Medical Center and Sinai-Grace Hospital. The lowest rate of hospitalization during the last month of life was 45% of cancer patients at the University of Washington Medical Center in Seattle.
Chemotherapy was part of care during the last 2 weeks of life in approximately 6% of patients nationwide, but the rate exceeded 10% in eight areas, including Olympia, Wash. (12%), and San Antonio (11%).
The researchers also found that fewer than 50% of cancer patients with a poor prognosis received hospice care, and some centers provided hospice care only in the last few days of life.
The degree of variation in the findings is too great to be explained by racial or ethnic preferences for aggressive end-of-life care, and adjustment for socioeconomic status does not change the results, said Dr. Goodman said.
But the data show that investment in beds, ICU facilities, and palliative care services is quite different from one health care system to another, he said.
The report highlights the need for doctors and health systems "to take a look at themselves and examine where they need to make their investments," said Dr. Goodman, who added that clinicians "need to look at ourselves in terms of how we communicate with patients" about cancer care options.
In a commentary accompanying the report, Dr. Joan Teno of Brown University in Providence, R.I., emphasized the need for health care providers to educate patients about their prognoses and to provide hospice options.
"If opportunities to improve are identified, hospitals should work with the local hospice or existing palliative care consult service, and/or start a palliative care consult service," to ensure that the institution is delivering high-quality care, Dr. Teno wrote.
Conversations about end-of-life care need to be started early in the course of treatment, Dr. Goodman said. "Our preferences can certainly change, but opening up the conversation early allows the conversation to evolve over time. The tragedy is when those conversations start near the end."
In a statement, Dr. George W. Sledge Jr., president of the American Society of Clinical Oncology said, "While saving lives is the oncologist’s goal, helping individuals live their final days in comfort and dignity is one of the most valuable and important responsibilities of our profession.
"Options to enhance a patient’s quality of life should be discussed throughout the course of their treatment. It is critical that we increase medical training in end-of-life patient communication and planning, and that Medicare and other insurers cover the costs of these essential conversations," Dr. Sledge noted.
The study was supported in part by the Robert Wood Johnson Foundation.
Approximately 29% of Medicare patients with cancer died in a hospital, and hospice care was inconsistent among medical centers in the United States, according to a report published Nov. 16 by the Dartmouth Institute for Health Policy & Clinical Practice.
The rate of hospital deaths varied widely by region, ranging from 47% in Manhattan (New York City) to 7% in Mason City, Iowa.
"The bottom line is that the care patients receive has less to do with what they want and more to do with the hospital they seek care from," Dr. David Goodman of Dartmouth University, Hanover, N.H., said in a press briefing. "We as physicians often make assumptions about what patients and families want for their lives. What patients really want is for a physician to be honest with them and to share the full range of options with them."
The report, "Quality of End-of-Life Cancer Care for Medicare Beneficiaries: Regional and Hospital-Specific Analyses," is the first to focus on cancer care at the end of life for the Medicare population in particular. The report was produced by the Dartmouth Atlas Project, which has been documenting the use of medical resources in the United States for more than 2 decades.
Researchers reviewed data from 235,821 Medicare patients (aged 65 years and older) with metastatic or aggressive cancer who died in 2003-2007. They identified regional trends as well as information about specific academic medical centers.
Nationwide, approximately 61% of cancer patients were hospitalized at least once during their last month of life. Hospital admissions varied from approximately 70% of cancer patients in Detroit to 46% of cancer patients in San Angelo, Tex.
The researchers identified the highest rates of hospitalization during the last month of life (more than 75%) among cancer patients at two hospitals in Detroit: St. John Hospital and Medical Center and Sinai-Grace Hospital. The lowest rate of hospitalization during the last month of life was 45% of cancer patients at the University of Washington Medical Center in Seattle.
Chemotherapy was part of care during the last 2 weeks of life in approximately 6% of patients nationwide, but the rate exceeded 10% in eight areas, including Olympia, Wash. (12%), and San Antonio (11%).
The researchers also found that fewer than 50% of cancer patients with a poor prognosis received hospice care, and some centers provided hospice care only in the last few days of life.
The degree of variation in the findings is too great to be explained by racial or ethnic preferences for aggressive end-of-life care, and adjustment for socioeconomic status does not change the results, said Dr. Goodman said.
But the data show that investment in beds, ICU facilities, and palliative care services is quite different from one health care system to another, he said.
The report highlights the need for doctors and health systems "to take a look at themselves and examine where they need to make their investments," said Dr. Goodman, who added that clinicians "need to look at ourselves in terms of how we communicate with patients" about cancer care options.
In a commentary accompanying the report, Dr. Joan Teno of Brown University in Providence, R.I., emphasized the need for health care providers to educate patients about their prognoses and to provide hospice options.
"If opportunities to improve are identified, hospitals should work with the local hospice or existing palliative care consult service, and/or start a palliative care consult service," to ensure that the institution is delivering high-quality care, Dr. Teno wrote.
Conversations about end-of-life care need to be started early in the course of treatment, Dr. Goodman said. "Our preferences can certainly change, but opening up the conversation early allows the conversation to evolve over time. The tragedy is when those conversations start near the end."
In a statement, Dr. George W. Sledge Jr., president of the American Society of Clinical Oncology said, "While saving lives is the oncologist’s goal, helping individuals live their final days in comfort and dignity is one of the most valuable and important responsibilities of our profession.
"Options to enhance a patient’s quality of life should be discussed throughout the course of their treatment. It is critical that we increase medical training in end-of-life patient communication and planning, and that Medicare and other insurers cover the costs of these essential conversations," Dr. Sledge noted.
The study was supported in part by the Robert Wood Johnson Foundation.
Approximately 29% of Medicare patients with cancer died in a hospital, and hospice care was inconsistent among medical centers in the United States, according to a report published Nov. 16 by the Dartmouth Institute for Health Policy & Clinical Practice.
The rate of hospital deaths varied widely by region, ranging from 47% in Manhattan (New York City) to 7% in Mason City, Iowa.
"The bottom line is that the care patients receive has less to do with what they want and more to do with the hospital they seek care from," Dr. David Goodman of Dartmouth University, Hanover, N.H., said in a press briefing. "We as physicians often make assumptions about what patients and families want for their lives. What patients really want is for a physician to be honest with them and to share the full range of options with them."
The report, "Quality of End-of-Life Cancer Care for Medicare Beneficiaries: Regional and Hospital-Specific Analyses," is the first to focus on cancer care at the end of life for the Medicare population in particular. The report was produced by the Dartmouth Atlas Project, which has been documenting the use of medical resources in the United States for more than 2 decades.
Researchers reviewed data from 235,821 Medicare patients (aged 65 years and older) with metastatic or aggressive cancer who died in 2003-2007. They identified regional trends as well as information about specific academic medical centers.
Nationwide, approximately 61% of cancer patients were hospitalized at least once during their last month of life. Hospital admissions varied from approximately 70% of cancer patients in Detroit to 46% of cancer patients in San Angelo, Tex.
The researchers identified the highest rates of hospitalization during the last month of life (more than 75%) among cancer patients at two hospitals in Detroit: St. John Hospital and Medical Center and Sinai-Grace Hospital. The lowest rate of hospitalization during the last month of life was 45% of cancer patients at the University of Washington Medical Center in Seattle.
Chemotherapy was part of care during the last 2 weeks of life in approximately 6% of patients nationwide, but the rate exceeded 10% in eight areas, including Olympia, Wash. (12%), and San Antonio (11%).
The researchers also found that fewer than 50% of cancer patients with a poor prognosis received hospice care, and some centers provided hospice care only in the last few days of life.
The degree of variation in the findings is too great to be explained by racial or ethnic preferences for aggressive end-of-life care, and adjustment for socioeconomic status does not change the results, said Dr. Goodman said.
But the data show that investment in beds, ICU facilities, and palliative care services is quite different from one health care system to another, he said.
The report highlights the need for doctors and health systems "to take a look at themselves and examine where they need to make their investments," said Dr. Goodman, who added that clinicians "need to look at ourselves in terms of how we communicate with patients" about cancer care options.
In a commentary accompanying the report, Dr. Joan Teno of Brown University in Providence, R.I., emphasized the need for health care providers to educate patients about their prognoses and to provide hospice options.
"If opportunities to improve are identified, hospitals should work with the local hospice or existing palliative care consult service, and/or start a palliative care consult service," to ensure that the institution is delivering high-quality care, Dr. Teno wrote.
Conversations about end-of-life care need to be started early in the course of treatment, Dr. Goodman said. "Our preferences can certainly change, but opening up the conversation early allows the conversation to evolve over time. The tragedy is when those conversations start near the end."
In a statement, Dr. George W. Sledge Jr., president of the American Society of Clinical Oncology said, "While saving lives is the oncologist’s goal, helping individuals live their final days in comfort and dignity is one of the most valuable and important responsibilities of our profession.
"Options to enhance a patient’s quality of life should be discussed throughout the course of their treatment. It is critical that we increase medical training in end-of-life patient communication and planning, and that Medicare and other insurers cover the costs of these essential conversations," Dr. Sledge noted.
The study was supported in part by the Robert Wood Johnson Foundation.
Major Finding: For patients with aggressive or metastatic cancer, hospital admission in the last month varied from about 70% of those in the Detroit area to 46% of those in San Angelo, Tex.
Data Source: Medicare data sets including the Medicare Denominator file, the 20% Carrier file, the MedPAR file, the Outpatient file, and the Hospital file.
Disclosures: Supported in part by the Robert Wood Johnson Foundation.
Program Improves Medical Training in Uganda
After receiving medical training at the University of Wisconsin, Madison, and the University of Pennsylvania, Philadelphia, Dr. Asghar Rastegar returned to his native Iran, taught medical school, and collaborated with several American institutions, including Yale University in New Haven, Conn. During that time, he says that he developed a sense of what strategies are the most effective at improving physician training.
Since his return to the United States 25 years ago, Dr. Rastegar, who is currently professor of medicine in nephrology and director of global health in the department of medicine at Yale, has devoted himself to improving medical training globally.
In 1995, he and his colleagues developed a collaborative program with Kazan (Russian Federation) State Medical University, aimed at boosting that institution's capacity to train their own physicians. Fifteen years later, Dr. Rastegar and his colleagues are still working with the Russian medical school to help them define their needs and improve medical training.
In an interview, Dr. Rastegar discussed a similar program in Uganda.
How did you get started with the physician-training program in Uganda?
After the success of the collaborative model in Russia, Dr. Majid Sadigh, also of the department of medicine at Yale and a close colleague who had worked extensively on this model, became interested in creating a similar program in Africa.
For decades, Yale's department of internal medicine has sent residents to work overseas for 4- to 6-week periods at as many as 16 different sites.
Four years ago, the International Health Program in the department of medicine, which has been funded by Johnson & Johnson as well as our own institution, decided to develop more in-depth collaborative programs with five sites. We applied the Russian model to Makerere University in Kampala, Uganda, with a capacity-building focus. As in Russia, the plan was to help enhance physician training with the goal of improving patient care. Makerere is one of the oldest medical schools in Africa, and probably the best known medical school outside of South Africa.
Mulago Hospital, which is affiliated with Makerere, is the main referral hospital for patients from all parts of Uganda. It has about 2,000 beds, and it handles up to 5,000 patients. It is a very underresourced hospital, and unfortunately about half the patients have HIV disease. Our goal has been to train their physicians so they can train their own specialists and subspecialists within 10 years.
What are the main elements of the physician-training program at Makerere?
Under Dr. Sadigh's leadership, we have an exchange program with Makerere that involves students and faculty. At any one time, we have two to four faculty members from Makerere who spend anywhere from 4 to 12 months at Yale. These faculty members come to receive specialized training in areas such as cardiology, kidney disease, and emergency medicine.
In addition, faculty from Yale and from other medical schools go to Makerere; we have medical residents there at all times, funded through the Yale/Stanford Johnson & Johnson Global Health Scholars Program. The idea is to help the Makerere faculty define what they need, and then find the resources to respond to that need.
What are the challenges of developing a training program in another country?
The key is to find the right partner and develop a relationship based on mutual respect. We didn't go to Mulago to do research; we went to improve patient care through education. There are other medical schools from the United States and Europe doing work with Makerere, but we were surprised that very few had become directly involved in providing the hands-on training to improve patient care. Research is critical to improving patient care, but often the fruit of such discoveries is not translated to improvement in patient care locally.
The people we have worked with at Makerere are as committed and intelligent as anyone I have worked with anywhere in the world. They know what to do to improve care, but they don't have the capacity to train specialists, so they are missing individuals with badly needed knowledge and skills in specific areas. That's the part we are playing.
How can other physicians in the United States get involved to volunteer on a short-term basis?
They can get involved through the Yale/Stanford Johnson & Johnson Global Health Scholars Program, which we at Yale codirect with Dr. Michele Barry, professor and senior associate dean for Global Health at Stanford (Calif.) University. The program is funded by Johnson & Johnson, and it selects residents and career physicians through a competitive application process. The funded scholars receive a travel award on completion of their 6-week assignments. More information is available on our Web site (http://medicine.yale.edu/intmed/globalhealthscholars
{kind=link}
Ugandan students and faculty visit Yale University as part of the exchange program.
Source Courtesy Dr. Asghar Rastegar
After receiving medical training at the University of Wisconsin, Madison, and the University of Pennsylvania, Philadelphia, Dr. Asghar Rastegar returned to his native Iran, taught medical school, and collaborated with several American institutions, including Yale University in New Haven, Conn. During that time, he says that he developed a sense of what strategies are the most effective at improving physician training.
Since his return to the United States 25 years ago, Dr. Rastegar, who is currently professor of medicine in nephrology and director of global health in the department of medicine at Yale, has devoted himself to improving medical training globally.
In 1995, he and his colleagues developed a collaborative program with Kazan (Russian Federation) State Medical University, aimed at boosting that institution's capacity to train their own physicians. Fifteen years later, Dr. Rastegar and his colleagues are still working with the Russian medical school to help them define their needs and improve medical training.
In an interview, Dr. Rastegar discussed a similar program in Uganda.
How did you get started with the physician-training program in Uganda?
After the success of the collaborative model in Russia, Dr. Majid Sadigh, also of the department of medicine at Yale and a close colleague who had worked extensively on this model, became interested in creating a similar program in Africa.
For decades, Yale's department of internal medicine has sent residents to work overseas for 4- to 6-week periods at as many as 16 different sites.
Four years ago, the International Health Program in the department of medicine, which has been funded by Johnson & Johnson as well as our own institution, decided to develop more in-depth collaborative programs with five sites. We applied the Russian model to Makerere University in Kampala, Uganda, with a capacity-building focus. As in Russia, the plan was to help enhance physician training with the goal of improving patient care. Makerere is one of the oldest medical schools in Africa, and probably the best known medical school outside of South Africa.
Mulago Hospital, which is affiliated with Makerere, is the main referral hospital for patients from all parts of Uganda. It has about 2,000 beds, and it handles up to 5,000 patients. It is a very underresourced hospital, and unfortunately about half the patients have HIV disease. Our goal has been to train their physicians so they can train their own specialists and subspecialists within 10 years.
What are the main elements of the physician-training program at Makerere?
Under Dr. Sadigh's leadership, we have an exchange program with Makerere that involves students and faculty. At any one time, we have two to four faculty members from Makerere who spend anywhere from 4 to 12 months at Yale. These faculty members come to receive specialized training in areas such as cardiology, kidney disease, and emergency medicine.
In addition, faculty from Yale and from other medical schools go to Makerere; we have medical residents there at all times, funded through the Yale/Stanford Johnson & Johnson Global Health Scholars Program. The idea is to help the Makerere faculty define what they need, and then find the resources to respond to that need.
What are the challenges of developing a training program in another country?
The key is to find the right partner and develop a relationship based on mutual respect. We didn't go to Mulago to do research; we went to improve patient care through education. There are other medical schools from the United States and Europe doing work with Makerere, but we were surprised that very few had become directly involved in providing the hands-on training to improve patient care. Research is critical to improving patient care, but often the fruit of such discoveries is not translated to improvement in patient care locally.
The people we have worked with at Makerere are as committed and intelligent as anyone I have worked with anywhere in the world. They know what to do to improve care, but they don't have the capacity to train specialists, so they are missing individuals with badly needed knowledge and skills in specific areas. That's the part we are playing.
How can other physicians in the United States get involved to volunteer on a short-term basis?
They can get involved through the Yale/Stanford Johnson & Johnson Global Health Scholars Program, which we at Yale codirect with Dr. Michele Barry, professor and senior associate dean for Global Health at Stanford (Calif.) University. The program is funded by Johnson & Johnson, and it selects residents and career physicians through a competitive application process. The funded scholars receive a travel award on completion of their 6-week assignments. More information is available on our Web site (http://medicine.yale.edu/intmed/globalhealthscholars
Ugandan students and faculty visit Yale University as part of the exchange program.
Source Courtesy Dr. Asghar Rastegar
After receiving medical training at the University of Wisconsin, Madison, and the University of Pennsylvania, Philadelphia, Dr. Asghar Rastegar returned to his native Iran, taught medical school, and collaborated with several American institutions, including Yale University in New Haven, Conn. During that time, he says that he developed a sense of what strategies are the most effective at improving physician training.
Since his return to the United States 25 years ago, Dr. Rastegar, who is currently professor of medicine in nephrology and director of global health in the department of medicine at Yale, has devoted himself to improving medical training globally.
In 1995, he and his colleagues developed a collaborative program with Kazan (Russian Federation) State Medical University, aimed at boosting that institution's capacity to train their own physicians. Fifteen years later, Dr. Rastegar and his colleagues are still working with the Russian medical school to help them define their needs and improve medical training.
In an interview, Dr. Rastegar discussed a similar program in Uganda.
How did you get started with the physician-training program in Uganda?
After the success of the collaborative model in Russia, Dr. Majid Sadigh, also of the department of medicine at Yale and a close colleague who had worked extensively on this model, became interested in creating a similar program in Africa.
For decades, Yale's department of internal medicine has sent residents to work overseas for 4- to 6-week periods at as many as 16 different sites.
Four years ago, the International Health Program in the department of medicine, which has been funded by Johnson & Johnson as well as our own institution, decided to develop more in-depth collaborative programs with five sites. We applied the Russian model to Makerere University in Kampala, Uganda, with a capacity-building focus. As in Russia, the plan was to help enhance physician training with the goal of improving patient care. Makerere is one of the oldest medical schools in Africa, and probably the best known medical school outside of South Africa.
Mulago Hospital, which is affiliated with Makerere, is the main referral hospital for patients from all parts of Uganda. It has about 2,000 beds, and it handles up to 5,000 patients. It is a very underresourced hospital, and unfortunately about half the patients have HIV disease. Our goal has been to train their physicians so they can train their own specialists and subspecialists within 10 years.
What are the main elements of the physician-training program at Makerere?
Under Dr. Sadigh's leadership, we have an exchange program with Makerere that involves students and faculty. At any one time, we have two to four faculty members from Makerere who spend anywhere from 4 to 12 months at Yale. These faculty members come to receive specialized training in areas such as cardiology, kidney disease, and emergency medicine.
In addition, faculty from Yale and from other medical schools go to Makerere; we have medical residents there at all times, funded through the Yale/Stanford Johnson & Johnson Global Health Scholars Program. The idea is to help the Makerere faculty define what they need, and then find the resources to respond to that need.
What are the challenges of developing a training program in another country?
The key is to find the right partner and develop a relationship based on mutual respect. We didn't go to Mulago to do research; we went to improve patient care through education. There are other medical schools from the United States and Europe doing work with Makerere, but we were surprised that very few had become directly involved in providing the hands-on training to improve patient care. Research is critical to improving patient care, but often the fruit of such discoveries is not translated to improvement in patient care locally.
The people we have worked with at Makerere are as committed and intelligent as anyone I have worked with anywhere in the world. They know what to do to improve care, but they don't have the capacity to train specialists, so they are missing individuals with badly needed knowledge and skills in specific areas. That's the part we are playing.
How can other physicians in the United States get involved to volunteer on a short-term basis?
They can get involved through the Yale/Stanford Johnson & Johnson Global Health Scholars Program, which we at Yale codirect with Dr. Michele Barry, professor and senior associate dean for Global Health at Stanford (Calif.) University. The program is funded by Johnson & Johnson, and it selects residents and career physicians through a competitive application process. The funded scholars receive a travel award on completion of their 6-week assignments. More information is available on our Web site (http://medicine.yale.edu/intmed/globalhealthscholars
Ugandan students and faculty visit Yale University as part of the exchange program.
Source Courtesy Dr. Asghar Rastegar