User login
Secukinumab tames severe scalp psoriasis
VIENNA – Secukinumab proved highly effective specifically for the treatment of moderate to severe scalp psoriasis in a phase IIIb clinical trial, Mark G. Lebwohl, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The scalp is one of the areas most commonly affected by psoriasis, yet few treatment trials have focused on patients with primarily moderate to severe scalp psoriasis. This phase IIIb study was designed to do just that. The 102 participants had psoriasis over a mean of 60% of their scalp for at least 6 months at baseline despite various forms of therapy; 40% had 70% or greater scalp involvement. The study population’s mean baseline Psoriasis Scalp Severity Index score was 34 out of a possible 72, noted Dr. Lebwohl, professor and chairman of the department of dermatology at the Icahn School of Medicine at Mount Sinai, New York.

“The mean involved body surface area was only 11.2%, and the PASI was 8.4. That is below the entry score required for most biologic studies, yet scalp involvement was substantial,” he observed.
Participants in the double-blind trial were randomized to either subcutaneous secukinumab (Cosentyx) at 300 mg on the approved treatment schedule for psoriasis or to placebo, with the primary endpoint being at least a 90% improvement in Psoriasis Area and Severity Index scores (PASI 90 response) at 12 weeks.
“The results were striking. Quite stunning,” Dr. Lebwohl said.
A PASI 90 response was achieved in 53% of secukinumab-treated patients, compared with 2% of controls. Already by week 3 a significant difference was apparent between the two study arms: At that early point, 12% of the secukinumab group, but none of the controls, had a PASI 90 response.
The secondary endpoint was change in the Investigator’s Global Assessment of scalp disease. At baseline, roughly 80% of patients had an IGA of 3 out of a possible 4 and the rest were at 4. At 3 weeks, 26% of the secukinumab group had a score of 0 or 1, signifying a clear or almost clear scalp, compared with 6% of controls. At 12 weeks, 57% of patients on secukinumab had an IGA of 0 or 1, as did 6% of those on placebo.
Side effects of secukinumab in the 12-week study were minimal. There were no serious adverse events. One case of candidiasis occurred in each study arm. Both responded readily to standard therapy.
Secukinumab is a fully human monoclonal antibody that inhibits interleukin-17A. It’s approved for treatment of moderate-to-severe psoriasis, psoriatic arthritis, and ankylosing spondylitis.
This phase IIIb clinical trial was sponsored by Novartis. Dr. Lebwohl reported that his department receives research funding from Novartis and roughly a dozen other pharmaceutical companies.
VIENNA – Secukinumab proved highly effective specifically for the treatment of moderate to severe scalp psoriasis in a phase IIIb clinical trial, Mark G. Lebwohl, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The scalp is one of the areas most commonly affected by psoriasis, yet few treatment trials have focused on patients with primarily moderate to severe scalp psoriasis. This phase IIIb study was designed to do just that. The 102 participants had psoriasis over a mean of 60% of their scalp for at least 6 months at baseline despite various forms of therapy; 40% had 70% or greater scalp involvement. The study population’s mean baseline Psoriasis Scalp Severity Index score was 34 out of a possible 72, noted Dr. Lebwohl, professor and chairman of the department of dermatology at the Icahn School of Medicine at Mount Sinai, New York.
“The mean involved body surface area was only 11.2%, and the PASI was 8.4. That is below the entry score required for most biologic studies, yet scalp involvement was substantial,” he observed.
Participants in the double-blind trial were randomized to either subcutaneous secukinumab (Cosentyx) at 300 mg on the approved treatment schedule for psoriasis or to placebo, with the primary endpoint being at least a 90% improvement in Psoriasis Area and Severity Index scores (PASI 90 response) at 12 weeks.
“The results were striking. Quite stunning,” Dr. Lebwohl said.
A PASI 90 response was achieved in 53% of secukinumab-treated patients, compared with 2% of controls. Already by week 3 a significant difference was apparent between the two study arms: At that early point, 12% of the secukinumab group, but none of the controls, had a PASI 90 response.
The secondary endpoint was change in the Investigator’s Global Assessment of scalp disease. At baseline, roughly 80% of patients had an IGA of 3 out of a possible 4 and the rest were at 4. At 3 weeks, 26% of the secukinumab group had a score of 0 or 1, signifying a clear or almost clear scalp, compared with 6% of controls. At 12 weeks, 57% of patients on secukinumab had an IGA of 0 or 1, as did 6% of those on placebo.
Side effects of secukinumab in the 12-week study were minimal. There were no serious adverse events. One case of candidiasis occurred in each study arm. Both responded readily to standard therapy.
Secukinumab is a fully human monoclonal antibody that inhibits interleukin-17A. It’s approved for treatment of moderate-to-severe psoriasis, psoriatic arthritis, and ankylosing spondylitis.
This phase IIIb clinical trial was sponsored by Novartis. Dr. Lebwohl reported that his department receives research funding from Novartis and roughly a dozen other pharmaceutical companies.
VIENNA – Secukinumab proved highly effective specifically for the treatment of moderate to severe scalp psoriasis in a phase IIIb clinical trial, Mark G. Lebwohl, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The scalp is one of the areas most commonly affected by psoriasis, yet few treatment trials have focused on patients with primarily moderate to severe scalp psoriasis. This phase IIIb study was designed to do just that. The 102 participants had psoriasis over a mean of 60% of their scalp for at least 6 months at baseline despite various forms of therapy; 40% had 70% or greater scalp involvement. The study population’s mean baseline Psoriasis Scalp Severity Index score was 34 out of a possible 72, noted Dr. Lebwohl, professor and chairman of the department of dermatology at the Icahn School of Medicine at Mount Sinai, New York.
“The mean involved body surface area was only 11.2%, and the PASI was 8.4. That is below the entry score required for most biologic studies, yet scalp involvement was substantial,” he observed.
Participants in the double-blind trial were randomized to either subcutaneous secukinumab (Cosentyx) at 300 mg on the approved treatment schedule for psoriasis or to placebo, with the primary endpoint being at least a 90% improvement in Psoriasis Area and Severity Index scores (PASI 90 response) at 12 weeks.
“The results were striking. Quite stunning,” Dr. Lebwohl said.
A PASI 90 response was achieved in 53% of secukinumab-treated patients, compared with 2% of controls. Already by week 3 a significant difference was apparent between the two study arms: At that early point, 12% of the secukinumab group, but none of the controls, had a PASI 90 response.
The secondary endpoint was change in the Investigator’s Global Assessment of scalp disease. At baseline, roughly 80% of patients had an IGA of 3 out of a possible 4 and the rest were at 4. At 3 weeks, 26% of the secukinumab group had a score of 0 or 1, signifying a clear or almost clear scalp, compared with 6% of controls. At 12 weeks, 57% of patients on secukinumab had an IGA of 0 or 1, as did 6% of those on placebo.
Side effects of secukinumab in the 12-week study were minimal. There were no serious adverse events. One case of candidiasis occurred in each study arm. Both responded readily to standard therapy.
Secukinumab is a fully human monoclonal antibody that inhibits interleukin-17A. It’s approved for treatment of moderate-to-severe psoriasis, psoriatic arthritis, and ankylosing spondylitis.
This phase IIIb clinical trial was sponsored by Novartis. Dr. Lebwohl reported that his department receives research funding from Novartis and roughly a dozen other pharmaceutical companies.
AT THE EADV CONGRESS
Key clinical point:
Major finding: 53% of patients with chronic moderate to severe scalp psoriasis experienced at least a 90% improvement after 12 weeks on secukinumab, compared with 2% of controls.
Data source: This prospective, double-blind, phase IIIb clinical trial randomized 102 patients with moderate to severe scalp psoriasis to secukinumab or placebo.
Disclosures: The study was sponsored by Novartis. The presenter reported that his academic department receives research funding from Novartis and roughly a dozen other pharmaceutical companies.
Ixekizumab proves highly effective for palmoplantar, scalp psoriasis
VIENNA – Ixekizumab proved markedly more effective than etanercept for treatment of palmoplantar psoriasis in a head-to-head contest in the landmark phase III UNCOVER-3 trial, Alan Menter, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
Significant improvement in palmoplantar disease was seen as early as week 2 in patients randomized to ixekizumab (Taltz), a humanized monoclonal antibody directed against interleukin-17A. Moreover, the early improvement was maintained out to week 60 with administration of 80 mg of ixekizumab by subcutaneous injection every 4 weeks in the open-label extension phase of UNCOVER-3. This pivotal trial, including 1,346 patients with moderate to severe psoriasis, helped win regulatory approval for ixekizumab for treatment of chronic plaque psoriasis.

The primary results of UNCOVER-3 have been published. At week 60, at least 80% of patients on maintenance therapy with ixekizumab had a PASI 75 response and at least 73% were rated clear or almost clear (N Engl J Med. 2016 Jul 28;375[4]:345-56).
Dr. Menter and Dr. Reich presented new subgroup analyses focused specifically on palmoplantar and scalp psoriasis because these two expressions of the disease are very important in clinical practice, albeit for different reasons.
Scalp psoriasis is extremely common in patients with plaque psoriasis. In fact, nearly 91% of subjects in UNCOVER-3 had scalp involvement.
“That’s a higher percentage than we’re accustomed to seeing in daily practice. It suggests scalp psoriasis may be more common than previously thought in patients with moderate or severe psoriasis,” said Dr. Reich, professor of dermatology at Georg-August-University in Gottingen, Germany, and a partner at the Dermatologikum Hamburg.
At week 60, more than 77% of patients on ixekizumab achieved a Psoriasis Scalp Severity Index 100 response (PSSI 100), meaning they had complete resolution of their scalp psoriasis. More than 80% achieved a PSSI 90 response indicative of complete or near complete resolution of their scalp involvement, the dermatologist reported.

“I often tell my patients that it’s because of palmoplantar psoriasis that I have so many white hairs. It’s certainly a disease that none of us cope with well topically, phototherapy-wise, PUVA-wise, or with systemic therapy. All of the studies done to date with our systemic therapies show significantly lower effect on palmoplantar psoriasis than for psoriasis at other sites. When I did the REVEAL study for Humira [adalimumab], we published a week 16 PASI 75 rate of 71%. When we did the palmoplantar psoriasis cohort, it was less than 40%,” recalled Dr. Menter, who is chair of dermatology at Baylor University Medical Center, Dallas.
“Even though palmoplantar disease affects less than 5% of the body surface area, the quality of life impact for patients with significant palmoplantar pustular or plaque psoriasis is very significant,” Dr. Menter continued. “We’ve worked with our hand surgeons and our foot surgeons to show that the impairment equals that seen in patients with severe rheumatoid arthritis or osteoarthritis of the hands and feet. So it is a huge issue.”
He reported on the 115 UNCOVER-3 participants with palmoplantar involvement. Within 2 weeks after the first 80-mg dose of ixekizumab, recipients had a 60% improvement in their Palmoplantar Psoriasis Area and Severity Index (PPSI) scores.
“It was very dramatic. These are figures that we haven’t seen with methotrexate, with retinoids, or with TNF-alpha blockers,” according to Dr. Menter.
At week 12 in UNCOVER-3, patients randomized to ixekizumab at 80 mg every 2 weeks showed an 85% improvement from baseline in PPSI scores. Those on ixekizumab at 80 mg every 4 weeks had a 78% improvement from baseline, while patients on etanercept at 50 mg twice weekly showed a 52% improvement.
At 60 weeks, PPSI 100 response rates – that is, clear palms and soles – were 60%-70% in the various ixekizumab-treated groups.
“To me, the big issue now is what about palmoplantar pustulosis, a totally different disease, and a disease with equally serious issues for our patients. I’m looking forward to studies in that population. I sincerely hope these new agents such as ixekizumab will have a significant role to play,” he said.
Dr. Menter and Dr. Reich reported receiving research support from and serving as consultants to Eli Lilly, which sponsored the UNCOVER-3 trial and markets ixekizumab, as well as numerous other pharmaceutical companies.
VIENNA – Ixekizumab proved markedly more effective than etanercept for treatment of palmoplantar psoriasis in a head-to-head contest in the landmark phase III UNCOVER-3 trial, Alan Menter, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
Significant improvement in palmoplantar disease was seen as early as week 2 in patients randomized to ixekizumab (Taltz), a humanized monoclonal antibody directed against interleukin-17A. Moreover, the early improvement was maintained out to week 60 with administration of 80 mg of ixekizumab by subcutaneous injection every 4 weeks in the open-label extension phase of UNCOVER-3. This pivotal trial, including 1,346 patients with moderate to severe psoriasis, helped win regulatory approval for ixekizumab for treatment of chronic plaque psoriasis.
The primary results of UNCOVER-3 have been published. At week 60, at least 80% of patients on maintenance therapy with ixekizumab had a PASI 75 response and at least 73% were rated clear or almost clear (N Engl J Med. 2016 Jul 28;375[4]:345-56).
Dr. Menter and Dr. Reich presented new subgroup analyses focused specifically on palmoplantar and scalp psoriasis because these two expressions of the disease are very important in clinical practice, albeit for different reasons.
Scalp psoriasis is extremely common in patients with plaque psoriasis. In fact, nearly 91% of subjects in UNCOVER-3 had scalp involvement.
“That’s a higher percentage than we’re accustomed to seeing in daily practice. It suggests scalp psoriasis may be more common than previously thought in patients with moderate or severe psoriasis,” said Dr. Reich, professor of dermatology at Georg-August-University in Gottingen, Germany, and a partner at the Dermatologikum Hamburg.
At week 60, more than 77% of patients on ixekizumab achieved a Psoriasis Scalp Severity Index 100 response (PSSI 100), meaning they had complete resolution of their scalp psoriasis. More than 80% achieved a PSSI 90 response indicative of complete or near complete resolution of their scalp involvement, the dermatologist reported.
“I often tell my patients that it’s because of palmoplantar psoriasis that I have so many white hairs. It’s certainly a disease that none of us cope with well topically, phototherapy-wise, PUVA-wise, or with systemic therapy. All of the studies done to date with our systemic therapies show significantly lower effect on palmoplantar psoriasis than for psoriasis at other sites. When I did the REVEAL study for Humira [adalimumab], we published a week 16 PASI 75 rate of 71%. When we did the palmoplantar psoriasis cohort, it was less than 40%,” recalled Dr. Menter, who is chair of dermatology at Baylor University Medical Center, Dallas.
“Even though palmoplantar disease affects less than 5% of the body surface area, the quality of life impact for patients with significant palmoplantar pustular or plaque psoriasis is very significant,” Dr. Menter continued. “We’ve worked with our hand surgeons and our foot surgeons to show that the impairment equals that seen in patients with severe rheumatoid arthritis or osteoarthritis of the hands and feet. So it is a huge issue.”
He reported on the 115 UNCOVER-3 participants with palmoplantar involvement. Within 2 weeks after the first 80-mg dose of ixekizumab, recipients had a 60% improvement in their Palmoplantar Psoriasis Area and Severity Index (PPSI) scores.
“It was very dramatic. These are figures that we haven’t seen with methotrexate, with retinoids, or with TNF-alpha blockers,” according to Dr. Menter.
At week 12 in UNCOVER-3, patients randomized to ixekizumab at 80 mg every 2 weeks showed an 85% improvement from baseline in PPSI scores. Those on ixekizumab at 80 mg every 4 weeks had a 78% improvement from baseline, while patients on etanercept at 50 mg twice weekly showed a 52% improvement.
At 60 weeks, PPSI 100 response rates – that is, clear palms and soles – were 60%-70% in the various ixekizumab-treated groups.
“To me, the big issue now is what about palmoplantar pustulosis, a totally different disease, and a disease with equally serious issues for our patients. I’m looking forward to studies in that population. I sincerely hope these new agents such as ixekizumab will have a significant role to play,” he said.
Dr. Menter and Dr. Reich reported receiving research support from and serving as consultants to Eli Lilly, which sponsored the UNCOVER-3 trial and markets ixekizumab, as well as numerous other pharmaceutical companies.
VIENNA – Ixekizumab proved markedly more effective than etanercept for treatment of palmoplantar psoriasis in a head-to-head contest in the landmark phase III UNCOVER-3 trial, Alan Menter, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
Significant improvement in palmoplantar disease was seen as early as week 2 in patients randomized to ixekizumab (Taltz), a humanized monoclonal antibody directed against interleukin-17A. Moreover, the early improvement was maintained out to week 60 with administration of 80 mg of ixekizumab by subcutaneous injection every 4 weeks in the open-label extension phase of UNCOVER-3. This pivotal trial, including 1,346 patients with moderate to severe psoriasis, helped win regulatory approval for ixekizumab for treatment of chronic plaque psoriasis.
The primary results of UNCOVER-3 have been published. At week 60, at least 80% of patients on maintenance therapy with ixekizumab had a PASI 75 response and at least 73% were rated clear or almost clear (N Engl J Med. 2016 Jul 28;375[4]:345-56).
Dr. Menter and Dr. Reich presented new subgroup analyses focused specifically on palmoplantar and scalp psoriasis because these two expressions of the disease are very important in clinical practice, albeit for different reasons.
Scalp psoriasis is extremely common in patients with plaque psoriasis. In fact, nearly 91% of subjects in UNCOVER-3 had scalp involvement.
“That’s a higher percentage than we’re accustomed to seeing in daily practice. It suggests scalp psoriasis may be more common than previously thought in patients with moderate or severe psoriasis,” said Dr. Reich, professor of dermatology at Georg-August-University in Gottingen, Germany, and a partner at the Dermatologikum Hamburg.
At week 60, more than 77% of patients on ixekizumab achieved a Psoriasis Scalp Severity Index 100 response (PSSI 100), meaning they had complete resolution of their scalp psoriasis. More than 80% achieved a PSSI 90 response indicative of complete or near complete resolution of their scalp involvement, the dermatologist reported.
“I often tell my patients that it’s because of palmoplantar psoriasis that I have so many white hairs. It’s certainly a disease that none of us cope with well topically, phototherapy-wise, PUVA-wise, or with systemic therapy. All of the studies done to date with our systemic therapies show significantly lower effect on palmoplantar psoriasis than for psoriasis at other sites. When I did the REVEAL study for Humira [adalimumab], we published a week 16 PASI 75 rate of 71%. When we did the palmoplantar psoriasis cohort, it was less than 40%,” recalled Dr. Menter, who is chair of dermatology at Baylor University Medical Center, Dallas.
“Even though palmoplantar disease affects less than 5% of the body surface area, the quality of life impact for patients with significant palmoplantar pustular or plaque psoriasis is very significant,” Dr. Menter continued. “We’ve worked with our hand surgeons and our foot surgeons to show that the impairment equals that seen in patients with severe rheumatoid arthritis or osteoarthritis of the hands and feet. So it is a huge issue.”
He reported on the 115 UNCOVER-3 participants with palmoplantar involvement. Within 2 weeks after the first 80-mg dose of ixekizumab, recipients had a 60% improvement in their Palmoplantar Psoriasis Area and Severity Index (PPSI) scores.
“It was very dramatic. These are figures that we haven’t seen with methotrexate, with retinoids, or with TNF-alpha blockers,” according to Dr. Menter.
At week 12 in UNCOVER-3, patients randomized to ixekizumab at 80 mg every 2 weeks showed an 85% improvement from baseline in PPSI scores. Those on ixekizumab at 80 mg every 4 weeks had a 78% improvement from baseline, while patients on etanercept at 50 mg twice weekly showed a 52% improvement.
At 60 weeks, PPSI 100 response rates – that is, clear palms and soles – were 60%-70% in the various ixekizumab-treated groups.
“To me, the big issue now is what about palmoplantar pustulosis, a totally different disease, and a disease with equally serious issues for our patients. I’m looking forward to studies in that population. I sincerely hope these new agents such as ixekizumab will have a significant role to play,” he said.
Dr. Menter and Dr. Reich reported receiving research support from and serving as consultants to Eli Lilly, which sponsored the UNCOVER-3 trial and markets ixekizumab, as well as numerous other pharmaceutical companies.
EXPERT ANALYSIS FROM THE EADV CONGRESS
Bariatric surgery or total joint replacement: which first?
NEW ORLEANS – Performing bariatric surgery prior to total knee or hip replacement instead of vice versa resulted in significantly shorter orthopedic surgical operating time and length of stay in an observational study, Emanuel E. Nearing II, MD, reported at Obesity Week 2016.
“We propose that strong consideration be given to bariatric surgery as a means of weight loss and BMI [body mass index] reduction in patients with obesity prior to total joint replacement,” he said at the meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.

“A common complaint of patients presenting with obesity is that their osteoarthritis has limited their mobility and that their weight gain is secondary to that reduced mobility. They believe that a new joint will help them regain their mobility and then lose weight. Interestingly, this does not appear to be the case. In fact, the majority of patients in our study actually gained weight following joint replacement. Given that, these patients need to be weight-optimized prior to total joint replacement. Bariatric surgery is a durable way to facilitate this,” he continued.
Dr. Nearing presented a retrospective observational study of 102 patients who underwent either laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy plus a total knee or hip replacement in the Gundersen system. Sixty-six patients had their bariatric surgery first, by a mean of 4.3 years, while the other 36 had arthroplasty a mean of 4.9 years before their bariatric surgery. The two groups were similar in terms of demographics and baseline comorbid conditions.
Patients who had their total joint replacement first had a mean preoperative BMI of 43.7 kg/m2 and a mean pre–bariatric surgery BMI of 46.3 kg/m2. The patients who had bariatric surgery first had a preoperative BMI of 49.6 kg/m2 and a mean pre–orthopedic surgery BMI of 37.6 kgm2. One year after joint replacement surgery, patients who had that operation first had a mean BMI of 43.9 kg/m2, compared with 37.8 kg/m2 for those who waited until after they underwent bariatric surgery.
Mean operative time for total joint replacement when it was the first operation was 113.5 minutes and substantially less at 71 minutes when it was done after bariatric surgery. Mean hospital length of stay for total joint replacement when it followed bariatric surgery was 2.9 days, a full day less than when joint replacement came first.
Rates of complications including skin or soft tissue infection, venous thromboembolism, hematoma, need for transfusion, and periprosthetic infection at 30 and 90 days didn’t differ between the two groups. Neither did the need for late reinterventions.
Dr. Nearing noted that a working group of the American Association of Hip and Knee Surgeons has conducted a review of the orthopedic surgery literature and concluded that all patients with a BMI of 30 kg/m2 or more undergoing total knee or hip arthroplasty are at increased risk for perioperative respiratory complications, thromboembolic events, delayed wound healing, infection, and need for joint revision surgery (J Arthroplasty. 2013 May;28[5]:714-21).
He observed that a retrospective study such as his cannot shed light on the optimal time interval for total joint replacement following bariatric surgery. That key question is being addressed by the ongoing prospective SWIFT (Surgical Weight-Loss to Improve Functional Status Trajectories Following Total Knee Arthroplasty) trial. The study hypothesis is that bariatric surgery prior to the knee replacement surgery will reduce risk and improve long-term outcomes and physical function.
Several audience member commented that, based upon their experience, they would have anticipated that complication rates would have been significantly lower in total joint replacement patients when that operation followed bariatric surgery.
“We were surprised, too,” Dr. Nearing replied. “I think the explanation is that at Gundersen we have three bariatric surgeons and only a handful of orthopedic surgeons, and we use protocols and pathways. We just routinely do our operations the same way each and every time.”
John M. Morton, MD, a former American Society for Metabolic and Bariatric Surgery president, commented that the Gundersen study findings sound a call for more cross-specialty collaboration in steering obese patients with severe knee or hip osteoarthritis to bariatric surgery first in order to maximize the results of the joint replacement surgery.
“I think we’re all seeing weight loss as another form of prehabilitation for other specialties. Our orthopedic colleagues are kind of like us – surgeons – so this seems to be a great place for us to partner with them,” said Dr. Morton, chief of bariatric and minimally invasive surgery at Stanford (Calif.) University.
Dr. Nearing reported having no financial interests relevant to his study.
NEW ORLEANS – Performing bariatric surgery prior to total knee or hip replacement instead of vice versa resulted in significantly shorter orthopedic surgical operating time and length of stay in an observational study, Emanuel E. Nearing II, MD, reported at Obesity Week 2016.
“We propose that strong consideration be given to bariatric surgery as a means of weight loss and BMI [body mass index] reduction in patients with obesity prior to total joint replacement,” he said at the meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
“A common complaint of patients presenting with obesity is that their osteoarthritis has limited their mobility and that their weight gain is secondary to that reduced mobility. They believe that a new joint will help them regain their mobility and then lose weight. Interestingly, this does not appear to be the case. In fact, the majority of patients in our study actually gained weight following joint replacement. Given that, these patients need to be weight-optimized prior to total joint replacement. Bariatric surgery is a durable way to facilitate this,” he continued.
Dr. Nearing presented a retrospective observational study of 102 patients who underwent either laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy plus a total knee or hip replacement in the Gundersen system. Sixty-six patients had their bariatric surgery first, by a mean of 4.3 years, while the other 36 had arthroplasty a mean of 4.9 years before their bariatric surgery. The two groups were similar in terms of demographics and baseline comorbid conditions.
Patients who had their total joint replacement first had a mean preoperative BMI of 43.7 kg/m2 and a mean pre–bariatric surgery BMI of 46.3 kg/m2. The patients who had bariatric surgery first had a preoperative BMI of 49.6 kg/m2 and a mean pre–orthopedic surgery BMI of 37.6 kgm2. One year after joint replacement surgery, patients who had that operation first had a mean BMI of 43.9 kg/m2, compared with 37.8 kg/m2 for those who waited until after they underwent bariatric surgery.
Mean operative time for total joint replacement when it was the first operation was 113.5 minutes and substantially less at 71 minutes when it was done after bariatric surgery. Mean hospital length of stay for total joint replacement when it followed bariatric surgery was 2.9 days, a full day less than when joint replacement came first.
Rates of complications including skin or soft tissue infection, venous thromboembolism, hematoma, need for transfusion, and periprosthetic infection at 30 and 90 days didn’t differ between the two groups. Neither did the need for late reinterventions.
Dr. Nearing noted that a working group of the American Association of Hip and Knee Surgeons has conducted a review of the orthopedic surgery literature and concluded that all patients with a BMI of 30 kg/m2 or more undergoing total knee or hip arthroplasty are at increased risk for perioperative respiratory complications, thromboembolic events, delayed wound healing, infection, and need for joint revision surgery (J Arthroplasty. 2013 May;28[5]:714-21).
He observed that a retrospective study such as his cannot shed light on the optimal time interval for total joint replacement following bariatric surgery. That key question is being addressed by the ongoing prospective SWIFT (Surgical Weight-Loss to Improve Functional Status Trajectories Following Total Knee Arthroplasty) trial. The study hypothesis is that bariatric surgery prior to the knee replacement surgery will reduce risk and improve long-term outcomes and physical function.
Several audience member commented that, based upon their experience, they would have anticipated that complication rates would have been significantly lower in total joint replacement patients when that operation followed bariatric surgery.
“We were surprised, too,” Dr. Nearing replied. “I think the explanation is that at Gundersen we have three bariatric surgeons and only a handful of orthopedic surgeons, and we use protocols and pathways. We just routinely do our operations the same way each and every time.”
John M. Morton, MD, a former American Society for Metabolic and Bariatric Surgery president, commented that the Gundersen study findings sound a call for more cross-specialty collaboration in steering obese patients with severe knee or hip osteoarthritis to bariatric surgery first in order to maximize the results of the joint replacement surgery.
“I think we’re all seeing weight loss as another form of prehabilitation for other specialties. Our orthopedic colleagues are kind of like us – surgeons – so this seems to be a great place for us to partner with them,” said Dr. Morton, chief of bariatric and minimally invasive surgery at Stanford (Calif.) University.
Dr. Nearing reported having no financial interests relevant to his study.
NEW ORLEANS – Performing bariatric surgery prior to total knee or hip replacement instead of vice versa resulted in significantly shorter orthopedic surgical operating time and length of stay in an observational study, Emanuel E. Nearing II, MD, reported at Obesity Week 2016.
“We propose that strong consideration be given to bariatric surgery as a means of weight loss and BMI [body mass index] reduction in patients with obesity prior to total joint replacement,” he said at the meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
“A common complaint of patients presenting with obesity is that their osteoarthritis has limited their mobility and that their weight gain is secondary to that reduced mobility. They believe that a new joint will help them regain their mobility and then lose weight. Interestingly, this does not appear to be the case. In fact, the majority of patients in our study actually gained weight following joint replacement. Given that, these patients need to be weight-optimized prior to total joint replacement. Bariatric surgery is a durable way to facilitate this,” he continued.
Dr. Nearing presented a retrospective observational study of 102 patients who underwent either laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy plus a total knee or hip replacement in the Gundersen system. Sixty-six patients had their bariatric surgery first, by a mean of 4.3 years, while the other 36 had arthroplasty a mean of 4.9 years before their bariatric surgery. The two groups were similar in terms of demographics and baseline comorbid conditions.
Patients who had their total joint replacement first had a mean preoperative BMI of 43.7 kg/m2 and a mean pre–bariatric surgery BMI of 46.3 kg/m2. The patients who had bariatric surgery first had a preoperative BMI of 49.6 kg/m2 and a mean pre–orthopedic surgery BMI of 37.6 kgm2. One year after joint replacement surgery, patients who had that operation first had a mean BMI of 43.9 kg/m2, compared with 37.8 kg/m2 for those who waited until after they underwent bariatric surgery.
Mean operative time for total joint replacement when it was the first operation was 113.5 minutes and substantially less at 71 minutes when it was done after bariatric surgery. Mean hospital length of stay for total joint replacement when it followed bariatric surgery was 2.9 days, a full day less than when joint replacement came first.
Rates of complications including skin or soft tissue infection, venous thromboembolism, hematoma, need for transfusion, and periprosthetic infection at 30 and 90 days didn’t differ between the two groups. Neither did the need for late reinterventions.
Dr. Nearing noted that a working group of the American Association of Hip and Knee Surgeons has conducted a review of the orthopedic surgery literature and concluded that all patients with a BMI of 30 kg/m2 or more undergoing total knee or hip arthroplasty are at increased risk for perioperative respiratory complications, thromboembolic events, delayed wound healing, infection, and need for joint revision surgery (J Arthroplasty. 2013 May;28[5]:714-21).
He observed that a retrospective study such as his cannot shed light on the optimal time interval for total joint replacement following bariatric surgery. That key question is being addressed by the ongoing prospective SWIFT (Surgical Weight-Loss to Improve Functional Status Trajectories Following Total Knee Arthroplasty) trial. The study hypothesis is that bariatric surgery prior to the knee replacement surgery will reduce risk and improve long-term outcomes and physical function.
Several audience member commented that, based upon their experience, they would have anticipated that complication rates would have been significantly lower in total joint replacement patients when that operation followed bariatric surgery.
“We were surprised, too,” Dr. Nearing replied. “I think the explanation is that at Gundersen we have three bariatric surgeons and only a handful of orthopedic surgeons, and we use protocols and pathways. We just routinely do our operations the same way each and every time.”
John M. Morton, MD, a former American Society for Metabolic and Bariatric Surgery president, commented that the Gundersen study findings sound a call for more cross-specialty collaboration in steering obese patients with severe knee or hip osteoarthritis to bariatric surgery first in order to maximize the results of the joint replacement surgery.
“I think we’re all seeing weight loss as another form of prehabilitation for other specialties. Our orthopedic colleagues are kind of like us – surgeons – so this seems to be a great place for us to partner with them,” said Dr. Morton, chief of bariatric and minimally invasive surgery at Stanford (Calif.) University.
Dr. Nearing reported having no financial interests relevant to his study.
AT OBESITY WEEK 2016
Key clinical point:
Major finding: When total joint replacement in obese patients was performed after bariatric surgery, mean hospital length of stay was a full day less than when the orthopedic surgery preceded the bariatric surgery.
Data source: This retrospective observational study included 102 obese patients who underwent bariatric surgery and total knee or hip replacement.
Disclosures: The study presenter reported having no financial conflicts of interest.
Ketamine emerging as top treatment for cocaine dependence
VIENNA – The prospect on the horizon of two new effective therapies for chronic cocaine dependence – sustained-release dextroamphetamine and subanesthetic ketamine infusions – was among the top developments of the year in addiction medicine, Wim van den Brink, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
Other highlights on his list included:
• Studies establishing that comorbid attention-deficit/hyperactivity disorder (ADHD) and substance use disorder now can be treated effectively with either extended-release mixed amphetamine salts or high-dose methylphenidate.

• Release of a puzzling array of conflicting studies on the use of high-dose baclofen for treatment of alcohol dependence. It’s tough to reconcile this mishmash of polar opposite results. And that dictates it’s time to declare a moratorium on the use of this therapy in clinical practice, which in many places is now widespread, said Dr. van den Brink, professor of psychiatry and addiction at the University of Amsterdam and director of the Amsterdam Institute for Addiction Research.
“It’s too strange that we have such conflicting evidence out there. Too many people are prescribing crazy-high doses of baclofen with no strong supporting evidence,” Dr. van den Brink said.
Cocaine dependence
Dr. van den Brink was a coinvestigator in a Dutch multicenter randomized, double-blind, placebo-controlled trial of multitreatment-refractory comorbid cocaine dependence in 73 heroin-dependent patients in heroin-assisted treatment. Patients assigned to 60 mg/day of sustained-release dextroamphetamine, in addition to the background methadone and diacetylmorphine all participants were on for their heroin dependence, had significantly fewer days of cocaine use in the 12-week study: a mean of 44.9 days, compared with 60.6 days in placebo-treated controls. Adverse events were transient and well tolerated (Lancet. 2016 May 28;387[10034]:2226-34).
“A lot of medications have been tried for treatment of cocaine dependence, but actually none of them has been shown to be effective with the exception of substitution treatment with stimulants. Ours is one of the most successful trials. These patients were using cocaine an average of 24 days per month along with a lot of other drugs, despite being in heroin treatment for 4 years,” Dr. van den Brink said. “Patients were very willing to take the sustained-release dextroamphetamine. In the last 4 weeks, 84% of them used at least 80% of their medication. And they were blinded to what they were using.
“We saw good effect sizes: 0.6-0.7 for self-report measures and 0.31 for negative urine samples. So this is a very promising approach. But it also means that, like with tobacco dependence or alcohol dependence, we have to start thinking about substitution therapy in stimulant-dependent patients,” he said.
Dr. van den Brink said subanesthetic ketamine as a novel treatment for cocaine dependence is not yet ready for prime time use in clinical practice, because it’s just not practical to bring patients in for a roughly hour-long intravenous infusion on a daily basis, as was done in a highly impressive proof-of-concept study. But new formulations of ketamine are under development that should better lend themselves to use in clinical practice.
In the proof-of-concept study, investigators at the New York State Psychiatric Institute brought into the laboratory cocaine-dependent volunteers not seeking treatment or abstinence and administered 52-minute infusions of ketamine at 0.41 or 71 mg/kg or lorazepam at 2 mg (Biol Psychiatry. 2014 Jul 1;76[1]:40-6). Lorazepam had absolutely no effect on motivation to change, but ketamine was a different story.
“As soon as you give a low dose of ketamine, you see a wonderful effect on motivation to change and on craving ratings in assessments at 24 hours post infusion. This looks like another promising way of treating cocaine dependence,” he said.
Doxazosin for alcoholism
Investigators at the National Institute on Alcohol Abuse and Alcoholism and several U.S. universities hypothesized that the norepinephrine system could be an important treatment target in alcohol dependence. They conducted a double-blind, placebo-controlled randomized trial in which alcohol-dependent patients seeking outpatient treatment were assigned to the alpha1-adrenergic blocker doxazosin (Cardura) titrated to a maximum of 16 mg/day or placebo. They found doxazosin significantly reduced drinks per week and the number of heavy drinking days per week, but only in the subgroup of patients with a strong family history of alcoholism. In patients without such a family history, doxazosin paradoxically increased drinking (Addict Biol. 2016 Jul;21[4]:904-14).
One of the reasons adult ADHD is greatly underrecognized is that it tends to occur in combination with flashier substance use disorders. “Addiction is very comorbid with all kinds of disorders, but especially with externalizing childhood disorders like conduct disorder and ADHD,” Dr. van den Brink said.
It was shown half-a-decade ago that normal doses of methylphenidate have no effect on ADHD symptoms or substance use in comorbid adults. Then Swedish investigators reported that treating criminal offenders with high-dose methylphenidate – roughly three times greater than standard dosing – was effective in reducing both ADHD symptoms and comorbid substance use in criminal offenders. Those findings prompted investigators at the New York State Psychiatric Institute and the University of Minnesota to examine whether prescribing extended-release mixed amphetamine salts in adults with comorbid cocaine use disorder and ADHD would achieve improvement in both conditions. Indeed, it did, Dr. van den Brink said.
One hundred twenty-six affected patients were randomized to 60 or 80 mg/day of extended-release mixed amphetamine salts or placebo for 13 weeks coupled with weekly individual cognitive-behavioral therapy for all in this double-blind, three-arm clinical trial.
“They showed a number-needed-to-treat of about 2.5 in order to achieve a significant reduction in cocaine use and a very nice reduction in ADHD symptoms with a number-needed-to-treat of 3,” Dr. van den Brink said.
The rate of continuous cocaine abstinence in the last 3 weeks of the trial was 30% in the 80-mg group and 17.5% with 60 mg of extended-release mixed amphetamine salts, compared with just 7% with placebo (JAMA Psychiatry. 2015 Jun;72[6]:593-602).
Interpreting baclofen studies
The first high-quality multicenter, randomized, placebo-controlled, double-blind clinical trial, conducted in Germany, showed baclofen (Lioresal) at a mean dose of 180 mg/day was effective in maintaining alcohol abstinence (Eur Neuropsychopharmacol. 2015 Aug;25[8]:1167-77).
“They got wonderful results, with a number-needed-to-treat of 2.3. That is something we’re not used to seeing in the treatment of alcoholism. But there was no dose-response effect, which is a little unusual,” the psychiatrist observed.
Then a multicenter group of Dutch investigators, including Dr. van den Brink, carried out what they believed would be a confirmatory randomized, double-blind, placebo-controlled trial. However, it showed no difference between high- or low-dose baclofen and placebo in time to relapse (Eur Neuropsychopharmacol. 2016 Dec;26[12]:1950-9).
Little further light was shed by the two large French randomized, placebo-controlled clinical trials presented at the 2016 World Congress for Alcohol and Alcoholism in Berlin. One, the BACLOVILLE trial, included 320 patients treated in 60 family practice clinics; it showed strongly positive results for high-dose baclofen. In contrast, the 316-patient ALPADIR study proved negative. These conflicting results were particularly disappointing because France has been at the forefront of using high-dose baclofen to treat alcoholism, Dr. van den Brink said.
“Maybe some 100,000 people have been treated with high-dose baclofen for alcoholism in France,” he said. “What is the conclusion from all these baclofen studies? You can interpret them in many ways. Maybe there are two positive trials and two negative trials, or maybe there are two positive trials and two failed trials. The debate is not closed, even after four randomized trials.”
Dr. van den Brink reported receiving research funding from and/or serving as a consultant to more than half a dozen pharmaceutical companies.
VIENNA – The prospect on the horizon of two new effective therapies for chronic cocaine dependence – sustained-release dextroamphetamine and subanesthetic ketamine infusions – was among the top developments of the year in addiction medicine, Wim van den Brink, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
Other highlights on his list included:
• Studies establishing that comorbid attention-deficit/hyperactivity disorder (ADHD) and substance use disorder now can be treated effectively with either extended-release mixed amphetamine salts or high-dose methylphenidate.
• Release of a puzzling array of conflicting studies on the use of high-dose baclofen for treatment of alcohol dependence. It’s tough to reconcile this mishmash of polar opposite results. And that dictates it’s time to declare a moratorium on the use of this therapy in clinical practice, which in many places is now widespread, said Dr. van den Brink, professor of psychiatry and addiction at the University of Amsterdam and director of the Amsterdam Institute for Addiction Research.
“It’s too strange that we have such conflicting evidence out there. Too many people are prescribing crazy-high doses of baclofen with no strong supporting evidence,” Dr. van den Brink said.
Cocaine dependence
Dr. van den Brink was a coinvestigator in a Dutch multicenter randomized, double-blind, placebo-controlled trial of multitreatment-refractory comorbid cocaine dependence in 73 heroin-dependent patients in heroin-assisted treatment. Patients assigned to 60 mg/day of sustained-release dextroamphetamine, in addition to the background methadone and diacetylmorphine all participants were on for their heroin dependence, had significantly fewer days of cocaine use in the 12-week study: a mean of 44.9 days, compared with 60.6 days in placebo-treated controls. Adverse events were transient and well tolerated (Lancet. 2016 May 28;387[10034]:2226-34).
“A lot of medications have been tried for treatment of cocaine dependence, but actually none of them has been shown to be effective with the exception of substitution treatment with stimulants. Ours is one of the most successful trials. These patients were using cocaine an average of 24 days per month along with a lot of other drugs, despite being in heroin treatment for 4 years,” Dr. van den Brink said. “Patients were very willing to take the sustained-release dextroamphetamine. In the last 4 weeks, 84% of them used at least 80% of their medication. And they were blinded to what they were using.
“We saw good effect sizes: 0.6-0.7 for self-report measures and 0.31 for negative urine samples. So this is a very promising approach. But it also means that, like with tobacco dependence or alcohol dependence, we have to start thinking about substitution therapy in stimulant-dependent patients,” he said.
Dr. van den Brink said subanesthetic ketamine as a novel treatment for cocaine dependence is not yet ready for prime time use in clinical practice, because it’s just not practical to bring patients in for a roughly hour-long intravenous infusion on a daily basis, as was done in a highly impressive proof-of-concept study. But new formulations of ketamine are under development that should better lend themselves to use in clinical practice.
In the proof-of-concept study, investigators at the New York State Psychiatric Institute brought into the laboratory cocaine-dependent volunteers not seeking treatment or abstinence and administered 52-minute infusions of ketamine at 0.41 or 71 mg/kg or lorazepam at 2 mg (Biol Psychiatry. 2014 Jul 1;76[1]:40-6). Lorazepam had absolutely no effect on motivation to change, but ketamine was a different story.
“As soon as you give a low dose of ketamine, you see a wonderful effect on motivation to change and on craving ratings in assessments at 24 hours post infusion. This looks like another promising way of treating cocaine dependence,” he said.
Doxazosin for alcoholism
Investigators at the National Institute on Alcohol Abuse and Alcoholism and several U.S. universities hypothesized that the norepinephrine system could be an important treatment target in alcohol dependence. They conducted a double-blind, placebo-controlled randomized trial in which alcohol-dependent patients seeking outpatient treatment were assigned to the alpha1-adrenergic blocker doxazosin (Cardura) titrated to a maximum of 16 mg/day or placebo. They found doxazosin significantly reduced drinks per week and the number of heavy drinking days per week, but only in the subgroup of patients with a strong family history of alcoholism. In patients without such a family history, doxazosin paradoxically increased drinking (Addict Biol. 2016 Jul;21[4]:904-14).
One of the reasons adult ADHD is greatly underrecognized is that it tends to occur in combination with flashier substance use disorders. “Addiction is very comorbid with all kinds of disorders, but especially with externalizing childhood disorders like conduct disorder and ADHD,” Dr. van den Brink said.
It was shown half-a-decade ago that normal doses of methylphenidate have no effect on ADHD symptoms or substance use in comorbid adults. Then Swedish investigators reported that treating criminal offenders with high-dose methylphenidate – roughly three times greater than standard dosing – was effective in reducing both ADHD symptoms and comorbid substance use in criminal offenders. Those findings prompted investigators at the New York State Psychiatric Institute and the University of Minnesota to examine whether prescribing extended-release mixed amphetamine salts in adults with comorbid cocaine use disorder and ADHD would achieve improvement in both conditions. Indeed, it did, Dr. van den Brink said.
One hundred twenty-six affected patients were randomized to 60 or 80 mg/day of extended-release mixed amphetamine salts or placebo for 13 weeks coupled with weekly individual cognitive-behavioral therapy for all in this double-blind, three-arm clinical trial.
“They showed a number-needed-to-treat of about 2.5 in order to achieve a significant reduction in cocaine use and a very nice reduction in ADHD symptoms with a number-needed-to-treat of 3,” Dr. van den Brink said.
The rate of continuous cocaine abstinence in the last 3 weeks of the trial was 30% in the 80-mg group and 17.5% with 60 mg of extended-release mixed amphetamine salts, compared with just 7% with placebo (JAMA Psychiatry. 2015 Jun;72[6]:593-602).
Interpreting baclofen studies
The first high-quality multicenter, randomized, placebo-controlled, double-blind clinical trial, conducted in Germany, showed baclofen (Lioresal) at a mean dose of 180 mg/day was effective in maintaining alcohol abstinence (Eur Neuropsychopharmacol. 2015 Aug;25[8]:1167-77).
“They got wonderful results, with a number-needed-to-treat of 2.3. That is something we’re not used to seeing in the treatment of alcoholism. But there was no dose-response effect, which is a little unusual,” the psychiatrist observed.
Then a multicenter group of Dutch investigators, including Dr. van den Brink, carried out what they believed would be a confirmatory randomized, double-blind, placebo-controlled trial. However, it showed no difference between high- or low-dose baclofen and placebo in time to relapse (Eur Neuropsychopharmacol. 2016 Dec;26[12]:1950-9).
Little further light was shed by the two large French randomized, placebo-controlled clinical trials presented at the 2016 World Congress for Alcohol and Alcoholism in Berlin. One, the BACLOVILLE trial, included 320 patients treated in 60 family practice clinics; it showed strongly positive results for high-dose baclofen. In contrast, the 316-patient ALPADIR study proved negative. These conflicting results were particularly disappointing because France has been at the forefront of using high-dose baclofen to treat alcoholism, Dr. van den Brink said.
“Maybe some 100,000 people have been treated with high-dose baclofen for alcoholism in France,” he said. “What is the conclusion from all these baclofen studies? You can interpret them in many ways. Maybe there are two positive trials and two negative trials, or maybe there are two positive trials and two failed trials. The debate is not closed, even after four randomized trials.”
Dr. van den Brink reported receiving research funding from and/or serving as a consultant to more than half a dozen pharmaceutical companies.
VIENNA – The prospect on the horizon of two new effective therapies for chronic cocaine dependence – sustained-release dextroamphetamine and subanesthetic ketamine infusions – was among the top developments of the year in addiction medicine, Wim van den Brink, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
Other highlights on his list included:
• Studies establishing that comorbid attention-deficit/hyperactivity disorder (ADHD) and substance use disorder now can be treated effectively with either extended-release mixed amphetamine salts or high-dose methylphenidate.
• Release of a puzzling array of conflicting studies on the use of high-dose baclofen for treatment of alcohol dependence. It’s tough to reconcile this mishmash of polar opposite results. And that dictates it’s time to declare a moratorium on the use of this therapy in clinical practice, which in many places is now widespread, said Dr. van den Brink, professor of psychiatry and addiction at the University of Amsterdam and director of the Amsterdam Institute for Addiction Research.
“It’s too strange that we have such conflicting evidence out there. Too many people are prescribing crazy-high doses of baclofen with no strong supporting evidence,” Dr. van den Brink said.
Cocaine dependence
Dr. van den Brink was a coinvestigator in a Dutch multicenter randomized, double-blind, placebo-controlled trial of multitreatment-refractory comorbid cocaine dependence in 73 heroin-dependent patients in heroin-assisted treatment. Patients assigned to 60 mg/day of sustained-release dextroamphetamine, in addition to the background methadone and diacetylmorphine all participants were on for their heroin dependence, had significantly fewer days of cocaine use in the 12-week study: a mean of 44.9 days, compared with 60.6 days in placebo-treated controls. Adverse events were transient and well tolerated (Lancet. 2016 May 28;387[10034]:2226-34).
“A lot of medications have been tried for treatment of cocaine dependence, but actually none of them has been shown to be effective with the exception of substitution treatment with stimulants. Ours is one of the most successful trials. These patients were using cocaine an average of 24 days per month along with a lot of other drugs, despite being in heroin treatment for 4 years,” Dr. van den Brink said. “Patients were very willing to take the sustained-release dextroamphetamine. In the last 4 weeks, 84% of them used at least 80% of their medication. And they were blinded to what they were using.
“We saw good effect sizes: 0.6-0.7 for self-report measures and 0.31 for negative urine samples. So this is a very promising approach. But it also means that, like with tobacco dependence or alcohol dependence, we have to start thinking about substitution therapy in stimulant-dependent patients,” he said.
Dr. van den Brink said subanesthetic ketamine as a novel treatment for cocaine dependence is not yet ready for prime time use in clinical practice, because it’s just not practical to bring patients in for a roughly hour-long intravenous infusion on a daily basis, as was done in a highly impressive proof-of-concept study. But new formulations of ketamine are under development that should better lend themselves to use in clinical practice.
In the proof-of-concept study, investigators at the New York State Psychiatric Institute brought into the laboratory cocaine-dependent volunteers not seeking treatment or abstinence and administered 52-minute infusions of ketamine at 0.41 or 71 mg/kg or lorazepam at 2 mg (Biol Psychiatry. 2014 Jul 1;76[1]:40-6). Lorazepam had absolutely no effect on motivation to change, but ketamine was a different story.
“As soon as you give a low dose of ketamine, you see a wonderful effect on motivation to change and on craving ratings in assessments at 24 hours post infusion. This looks like another promising way of treating cocaine dependence,” he said.
Doxazosin for alcoholism
Investigators at the National Institute on Alcohol Abuse and Alcoholism and several U.S. universities hypothesized that the norepinephrine system could be an important treatment target in alcohol dependence. They conducted a double-blind, placebo-controlled randomized trial in which alcohol-dependent patients seeking outpatient treatment were assigned to the alpha1-adrenergic blocker doxazosin (Cardura) titrated to a maximum of 16 mg/day or placebo. They found doxazosin significantly reduced drinks per week and the number of heavy drinking days per week, but only in the subgroup of patients with a strong family history of alcoholism. In patients without such a family history, doxazosin paradoxically increased drinking (Addict Biol. 2016 Jul;21[4]:904-14).
One of the reasons adult ADHD is greatly underrecognized is that it tends to occur in combination with flashier substance use disorders. “Addiction is very comorbid with all kinds of disorders, but especially with externalizing childhood disorders like conduct disorder and ADHD,” Dr. van den Brink said.
It was shown half-a-decade ago that normal doses of methylphenidate have no effect on ADHD symptoms or substance use in comorbid adults. Then Swedish investigators reported that treating criminal offenders with high-dose methylphenidate – roughly three times greater than standard dosing – was effective in reducing both ADHD symptoms and comorbid substance use in criminal offenders. Those findings prompted investigators at the New York State Psychiatric Institute and the University of Minnesota to examine whether prescribing extended-release mixed amphetamine salts in adults with comorbid cocaine use disorder and ADHD would achieve improvement in both conditions. Indeed, it did, Dr. van den Brink said.
One hundred twenty-six affected patients were randomized to 60 or 80 mg/day of extended-release mixed amphetamine salts or placebo for 13 weeks coupled with weekly individual cognitive-behavioral therapy for all in this double-blind, three-arm clinical trial.
“They showed a number-needed-to-treat of about 2.5 in order to achieve a significant reduction in cocaine use and a very nice reduction in ADHD symptoms with a number-needed-to-treat of 3,” Dr. van den Brink said.
The rate of continuous cocaine abstinence in the last 3 weeks of the trial was 30% in the 80-mg group and 17.5% with 60 mg of extended-release mixed amphetamine salts, compared with just 7% with placebo (JAMA Psychiatry. 2015 Jun;72[6]:593-602).
Interpreting baclofen studies
The first high-quality multicenter, randomized, placebo-controlled, double-blind clinical trial, conducted in Germany, showed baclofen (Lioresal) at a mean dose of 180 mg/day was effective in maintaining alcohol abstinence (Eur Neuropsychopharmacol. 2015 Aug;25[8]:1167-77).
“They got wonderful results, with a number-needed-to-treat of 2.3. That is something we’re not used to seeing in the treatment of alcoholism. But there was no dose-response effect, which is a little unusual,” the psychiatrist observed.
Then a multicenter group of Dutch investigators, including Dr. van den Brink, carried out what they believed would be a confirmatory randomized, double-blind, placebo-controlled trial. However, it showed no difference between high- or low-dose baclofen and placebo in time to relapse (Eur Neuropsychopharmacol. 2016 Dec;26[12]:1950-9).
Little further light was shed by the two large French randomized, placebo-controlled clinical trials presented at the 2016 World Congress for Alcohol and Alcoholism in Berlin. One, the BACLOVILLE trial, included 320 patients treated in 60 family practice clinics; it showed strongly positive results for high-dose baclofen. In contrast, the 316-patient ALPADIR study proved negative. These conflicting results were particularly disappointing because France has been at the forefront of using high-dose baclofen to treat alcoholism, Dr. van den Brink said.
“Maybe some 100,000 people have been treated with high-dose baclofen for alcoholism in France,” he said. “What is the conclusion from all these baclofen studies? You can interpret them in many ways. Maybe there are two positive trials and two negative trials, or maybe there are two positive trials and two failed trials. The debate is not closed, even after four randomized trials.”
Dr. van den Brink reported receiving research funding from and/or serving as a consultant to more than half a dozen pharmaceutical companies.
EXPERT ANALYSIS FROM THE ECNP CONGRESS

Survey shines new light on weighty comorbidity burden in adult atopic dermatitis
VIENNA – Newly enhanced appreciation of the profound burden of comorbidities associated with adult atopic dermatitis (AD) is provided by the Liberty AD-AWARE study, investigators said at a joint program of the International Eczema Council and the International Psoriasis Council held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
“I think the only reason we thought psoriasis is a systemic disease and atopic dermatitis is not is because people were researching it much more in psoriasis. I think atopic dermatitis will emerge as potentially more systemic than psoriasis, including the comorbidities. It’s just a matter of time before the evidence is put forth for atopic dermatitis,” predicted Emma Guttman-Yassky, MD, PhD, professor and vice chair of the department of dermatology at Mount Sinai School of Medicine in New York.

Dr. Guttman-Yassky noted that 85% of cases of AD begin before 5 years of age. Many cases resolve later in childhood, but for others it becomes a chronic lifelong condition. And while the burden of AD has been well characterized in the pediatric population, that’s not so in affected adults. This was the impetus for the Liberty AD-AWARE (Adults With Atopic Dermatitis Reporting on their Experience) study, an Internet-based cross-sectional survey of more than 1,500 adults with AD receiving their care from dermatologists at eight major U.S. academic medical centers.
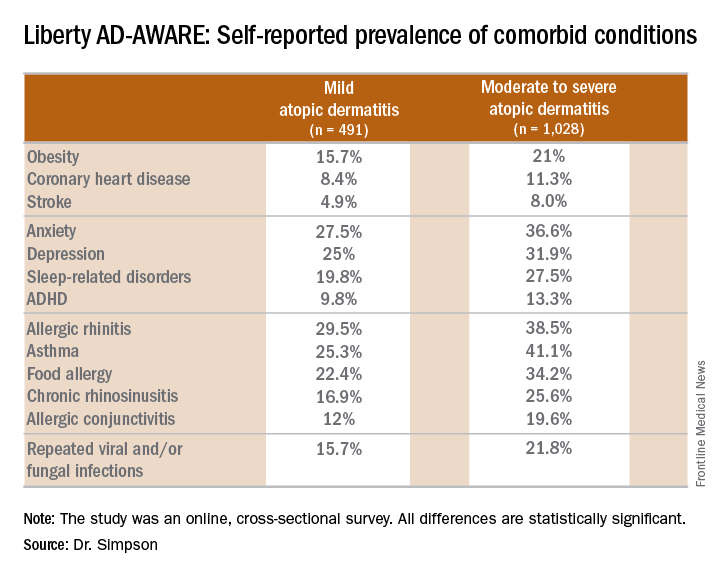
Eric L. Simpson, MD, a coinvestigator with Dr. Guttman-Yassky in Liberty AD-AWARE, observed that the study documented self-reported high rates of a range of psychiatric, cardiovascular, allergic, respiratory, and infectious diseases in participants. And while a cross-sectional study can’t establish causality, it’s important to appreciate that rates of these comorbidities were across the board significantly higher in the 1,028 patients with moderate to severe AD over the prior 12 months than in the 491 classified as having mild AD.
These associations between AD and mental health problems have been confirmed in other studies. For example, a recent analysis of data on more than 354,000 children and nearly 35,000 adults in the United States demonstrated that AD was independently associated with a 14% increased likelihood of attention-deficit/hyperactivity disorder in children and a 61% increased risk in adults. Those risks of ADHD rose far higher in individuals with severe AD and sleep disruption (Br J Dermatol. 2016 Nov;175[5]:920-9).
A number of theories have been put forth to explain these associations, including altered brain development stemming from early exposure to inflammatory cytokines or perhaps shared genetic predisposition, but Dr. Simpson proposed a simpler explanation which carries more optimistic implications.
“I suspect the mental health problems associated with adult atopic dermatitis are probably nonspecific sequelae of any chronic skin disorder involving severe itch and sleep disturbances,” said Dr. Simpson, professor of dermatology at Oregon Health & Science University, Portland.
Moreover, there is good reason to believe that novel therapies targeting inflammation more effectively than what’s been available to date may help improve mental health outcomes, as well as asthma in affected adults with AD, he added. He cited a phase IIb, randomized, double-blind, placebo-controlled study for which he was lead investigator. In this trial, 16 weeks of treatment with dupilumab, a first-in-class investigational blocker of the interleukin-4/interleukin-13 signaling pathway, not only resulted in significant reductions in itch and sleep problems, it also decreased anxiety and depression symptoms and improved multiple validated measures of health-related quality of life (J Am Acad Dermatol. 2016 Sep;75[3]:506-15).
Liberty AD-AWARE provides hints of the profound cumulative negative impact moderate to severe AD can have on a patient’s life course. Among the group with moderate to severe disease, 7.5% said AD had a large negative effect on their pursuit of an education, 10.7% said their disease had influenced their career choice “a lot/very much,” 13.3% were unemployed for reasons other than being retired or a student, and 17.1% reported an annual family income of less than $25,000. All these rates were multifold higher than in patients with mild AD in the study, which didn’t include a non-AD control group.
Dr. Guttman-Yassky observed that 42% of the moderate to severe AD group in Liberty AD-AWARE reported their current treatments were ineffective at controlling their disease, even though study participants were presumably receiving high-quality care at academic medical centers. Twenty-eight percent of patients with inadequately controlled AD had used phototherapy or an immunomodulatory drug within the past 7 days, underscoring the limitations of those forms of therapy in patients with more severe AD as well as the need for new and better treatments.
Dr. Guttman-Yassky has played a key role in the paradigm shift regarding understanding of the pathogenesis of AD as involving not just disordered skin barrier function but also immunologic impairment. She was senior author of a study that showed the nonlesional skin of patients with AD is characterized by high-level expression of inflammatory cytokines, whereas the nonlesional skin of psoriasis patients is not, an observation that serves to highlight the need for proactive treatments for AD (J Allergy Clin Immunol. 2011 Apr;127[4]:954-64.e1-4). Later, she and her coworkers demonstrated that AD is characterized by greater levels of T-cell activation among central and effector CD4+ and CD8+CLA+ and CD8+CLA– memory cell subsets (J Allergy Clin Immunol. 2015 Jul;136[1]:208-11).
More recently, she was also senior author of a landmark study that provides a mechanism to account for the reason AD patients would potentially have more comorbid illnesses than psoriasis patients. The investigators demonstrated that AD is accompanied by systemic expansion of transitional and chronically activated memory B cells, plasmablasts, and IgE-expressing memory B cells in both skin and blood. In other words, AD is characterized by a greater level of systemic immune activation, compared with psoriasis, where activated T cells are largely confined to the skin, and activated central memory B cells don’t figure prominently (J Allergy Clin Immunol. 2016 Jan;137[1]:118-29.e5).
The Liberty AD-AWARE study was sponsored by Sanofi and Regeneron. Dr. Simpson and Dr. Guttman-Yassky reported receiving research grants from and serving as consultants to those and other pharmaceutical companies.
VIENNA – Newly enhanced appreciation of the profound burden of comorbidities associated with adult atopic dermatitis (AD) is provided by the Liberty AD-AWARE study, investigators said at a joint program of the International Eczema Council and the International Psoriasis Council held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
“I think the only reason we thought psoriasis is a systemic disease and atopic dermatitis is not is because people were researching it much more in psoriasis. I think atopic dermatitis will emerge as potentially more systemic than psoriasis, including the comorbidities. It’s just a matter of time before the evidence is put forth for atopic dermatitis,” predicted Emma Guttman-Yassky, MD, PhD, professor and vice chair of the department of dermatology at Mount Sinai School of Medicine in New York.
Dr. Guttman-Yassky noted that 85% of cases of AD begin before 5 years of age. Many cases resolve later in childhood, but for others it becomes a chronic lifelong condition. And while the burden of AD has been well characterized in the pediatric population, that’s not so in affected adults. This was the impetus for the Liberty AD-AWARE (Adults With Atopic Dermatitis Reporting on their Experience) study, an Internet-based cross-sectional survey of more than 1,500 adults with AD receiving their care from dermatologists at eight major U.S. academic medical centers.
Eric L. Simpson, MD, a coinvestigator with Dr. Guttman-Yassky in Liberty AD-AWARE, observed that the study documented self-reported high rates of a range of psychiatric, cardiovascular, allergic, respiratory, and infectious diseases in participants. And while a cross-sectional study can’t establish causality, it’s important to appreciate that rates of these comorbidities were across the board significantly higher in the 1,028 patients with moderate to severe AD over the prior 12 months than in the 491 classified as having mild AD.
These associations between AD and mental health problems have been confirmed in other studies. For example, a recent analysis of data on more than 354,000 children and nearly 35,000 adults in the United States demonstrated that AD was independently associated with a 14% increased likelihood of attention-deficit/hyperactivity disorder in children and a 61% increased risk in adults. Those risks of ADHD rose far higher in individuals with severe AD and sleep disruption (Br J Dermatol. 2016 Nov;175[5]:920-9).
A number of theories have been put forth to explain these associations, including altered brain development stemming from early exposure to inflammatory cytokines or perhaps shared genetic predisposition, but Dr. Simpson proposed a simpler explanation which carries more optimistic implications.
“I suspect the mental health problems associated with adult atopic dermatitis are probably nonspecific sequelae of any chronic skin disorder involving severe itch and sleep disturbances,” said Dr. Simpson, professor of dermatology at Oregon Health & Science University, Portland.
Moreover, there is good reason to believe that novel therapies targeting inflammation more effectively than what’s been available to date may help improve mental health outcomes, as well as asthma in affected adults with AD, he added. He cited a phase IIb, randomized, double-blind, placebo-controlled study for which he was lead investigator. In this trial, 16 weeks of treatment with dupilumab, a first-in-class investigational blocker of the interleukin-4/interleukin-13 signaling pathway, not only resulted in significant reductions in itch and sleep problems, it also decreased anxiety and depression symptoms and improved multiple validated measures of health-related quality of life (J Am Acad Dermatol. 2016 Sep;75[3]:506-15).
Liberty AD-AWARE provides hints of the profound cumulative negative impact moderate to severe AD can have on a patient’s life course. Among the group with moderate to severe disease, 7.5% said AD had a large negative effect on their pursuit of an education, 10.7% said their disease had influenced their career choice “a lot/very much,” 13.3% were unemployed for reasons other than being retired or a student, and 17.1% reported an annual family income of less than $25,000. All these rates were multifold higher than in patients with mild AD in the study, which didn’t include a non-AD control group.
Dr. Guttman-Yassky observed that 42% of the moderate to severe AD group in Liberty AD-AWARE reported their current treatments were ineffective at controlling their disease, even though study participants were presumably receiving high-quality care at academic medical centers. Twenty-eight percent of patients with inadequately controlled AD had used phototherapy or an immunomodulatory drug within the past 7 days, underscoring the limitations of those forms of therapy in patients with more severe AD as well as the need for new and better treatments.
Dr. Guttman-Yassky has played a key role in the paradigm shift regarding understanding of the pathogenesis of AD as involving not just disordered skin barrier function but also immunologic impairment. She was senior author of a study that showed the nonlesional skin of patients with AD is characterized by high-level expression of inflammatory cytokines, whereas the nonlesional skin of psoriasis patients is not, an observation that serves to highlight the need for proactive treatments for AD (J Allergy Clin Immunol. 2011 Apr;127[4]:954-64.e1-4). Later, she and her coworkers demonstrated that AD is characterized by greater levels of T-cell activation among central and effector CD4+ and CD8+CLA+ and CD8+CLA– memory cell subsets (J Allergy Clin Immunol. 2015 Jul;136[1]:208-11).
More recently, she was also senior author of a landmark study that provides a mechanism to account for the reason AD patients would potentially have more comorbid illnesses than psoriasis patients. The investigators demonstrated that AD is accompanied by systemic expansion of transitional and chronically activated memory B cells, plasmablasts, and IgE-expressing memory B cells in both skin and blood. In other words, AD is characterized by a greater level of systemic immune activation, compared with psoriasis, where activated T cells are largely confined to the skin, and activated central memory B cells don’t figure prominently (J Allergy Clin Immunol. 2016 Jan;137[1]:118-29.e5).
The Liberty AD-AWARE study was sponsored by Sanofi and Regeneron. Dr. Simpson and Dr. Guttman-Yassky reported receiving research grants from and serving as consultants to those and other pharmaceutical companies.
VIENNA – Newly enhanced appreciation of the profound burden of comorbidities associated with adult atopic dermatitis (AD) is provided by the Liberty AD-AWARE study, investigators said at a joint program of the International Eczema Council and the International Psoriasis Council held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
“I think the only reason we thought psoriasis is a systemic disease and atopic dermatitis is not is because people were researching it much more in psoriasis. I think atopic dermatitis will emerge as potentially more systemic than psoriasis, including the comorbidities. It’s just a matter of time before the evidence is put forth for atopic dermatitis,” predicted Emma Guttman-Yassky, MD, PhD, professor and vice chair of the department of dermatology at Mount Sinai School of Medicine in New York.
Dr. Guttman-Yassky noted that 85% of cases of AD begin before 5 years of age. Many cases resolve later in childhood, but for others it becomes a chronic lifelong condition. And while the burden of AD has been well characterized in the pediatric population, that’s not so in affected adults. This was the impetus for the Liberty AD-AWARE (Adults With Atopic Dermatitis Reporting on their Experience) study, an Internet-based cross-sectional survey of more than 1,500 adults with AD receiving their care from dermatologists at eight major U.S. academic medical centers.
Eric L. Simpson, MD, a coinvestigator with Dr. Guttman-Yassky in Liberty AD-AWARE, observed that the study documented self-reported high rates of a range of psychiatric, cardiovascular, allergic, respiratory, and infectious diseases in participants. And while a cross-sectional study can’t establish causality, it’s important to appreciate that rates of these comorbidities were across the board significantly higher in the 1,028 patients with moderate to severe AD over the prior 12 months than in the 491 classified as having mild AD.
These associations between AD and mental health problems have been confirmed in other studies. For example, a recent analysis of data on more than 354,000 children and nearly 35,000 adults in the United States demonstrated that AD was independently associated with a 14% increased likelihood of attention-deficit/hyperactivity disorder in children and a 61% increased risk in adults. Those risks of ADHD rose far higher in individuals with severe AD and sleep disruption (Br J Dermatol. 2016 Nov;175[5]:920-9).
A number of theories have been put forth to explain these associations, including altered brain development stemming from early exposure to inflammatory cytokines or perhaps shared genetic predisposition, but Dr. Simpson proposed a simpler explanation which carries more optimistic implications.
“I suspect the mental health problems associated with adult atopic dermatitis are probably nonspecific sequelae of any chronic skin disorder involving severe itch and sleep disturbances,” said Dr. Simpson, professor of dermatology at Oregon Health & Science University, Portland.
Moreover, there is good reason to believe that novel therapies targeting inflammation more effectively than what’s been available to date may help improve mental health outcomes, as well as asthma in affected adults with AD, he added. He cited a phase IIb, randomized, double-blind, placebo-controlled study for which he was lead investigator. In this trial, 16 weeks of treatment with dupilumab, a first-in-class investigational blocker of the interleukin-4/interleukin-13 signaling pathway, not only resulted in significant reductions in itch and sleep problems, it also decreased anxiety and depression symptoms and improved multiple validated measures of health-related quality of life (J Am Acad Dermatol. 2016 Sep;75[3]:506-15).
Liberty AD-AWARE provides hints of the profound cumulative negative impact moderate to severe AD can have on a patient’s life course. Among the group with moderate to severe disease, 7.5% said AD had a large negative effect on their pursuit of an education, 10.7% said their disease had influenced their career choice “a lot/very much,” 13.3% were unemployed for reasons other than being retired or a student, and 17.1% reported an annual family income of less than $25,000. All these rates were multifold higher than in patients with mild AD in the study, which didn’t include a non-AD control group.
Dr. Guttman-Yassky observed that 42% of the moderate to severe AD group in Liberty AD-AWARE reported their current treatments were ineffective at controlling their disease, even though study participants were presumably receiving high-quality care at academic medical centers. Twenty-eight percent of patients with inadequately controlled AD had used phototherapy or an immunomodulatory drug within the past 7 days, underscoring the limitations of those forms of therapy in patients with more severe AD as well as the need for new and better treatments.
Dr. Guttman-Yassky has played a key role in the paradigm shift regarding understanding of the pathogenesis of AD as involving not just disordered skin barrier function but also immunologic impairment. She was senior author of a study that showed the nonlesional skin of patients with AD is characterized by high-level expression of inflammatory cytokines, whereas the nonlesional skin of psoriasis patients is not, an observation that serves to highlight the need for proactive treatments for AD (J Allergy Clin Immunol. 2011 Apr;127[4]:954-64.e1-4). Later, she and her coworkers demonstrated that AD is characterized by greater levels of T-cell activation among central and effector CD4+ and CD8+CLA+ and CD8+CLA– memory cell subsets (J Allergy Clin Immunol. 2015 Jul;136[1]:208-11).
More recently, she was also senior author of a landmark study that provides a mechanism to account for the reason AD patients would potentially have more comorbid illnesses than psoriasis patients. The investigators demonstrated that AD is accompanied by systemic expansion of transitional and chronically activated memory B cells, plasmablasts, and IgE-expressing memory B cells in both skin and blood. In other words, AD is characterized by a greater level of systemic immune activation, compared with psoriasis, where activated T cells are largely confined to the skin, and activated central memory B cells don’t figure prominently (J Allergy Clin Immunol. 2016 Jan;137[1]:118-29.e5).
The Liberty AD-AWARE study was sponsored by Sanofi and Regeneron. Dr. Simpson and Dr. Guttman-Yassky reported receiving research grants from and serving as consultants to those and other pharmaceutical companies.
EXPERT ANALYSIS FROM THE EADV CONGRESS
What referring physicians need to know about bariatric surgery success rates
NEW ORLEANS – About one-third of bariatric surgery patients achieve a body mass index below 30 kg/m2 at 1 year of follow-up, and the strongest predictor of success is having a BMI of 40 kg/m2 or less at the time of surgery, Oliver A. Varban, MD, reported at Obesity Week 2016.
Indeed, patients with a baseline BMI of 40 kg/m2 or less were fully 13.3-fold more likely to have a BMI of less than 30 kg/m2 1 year post surgery in a study of 19,764 patients in the Michigan Bariatric Surgery Collaborative database, according to Dr. Varban, surgical director of the adult bariatric surgery program at the University of Michigan, Ann Arbor.
“In order to optimize outcomes of bariatric surgery, patients should be encouraged to consider it when their BMI is less than 40 kg/m2. And policies that obstruct or delay surgery can actually result in inferior outcomes,” he said at the meeting, which was presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.

“These patients are being referred to us. We don’t seek them out. The biggest impetus for this study was to be able to show referring physicians that outcomes are better when treatment is sought earlier. Every patient who shows up at our clinics with a BMI of 65 must have had a BMI of 35 at some point in time. I think we miss the boat on a lot of those patients,” the surgeon said. “Society at large should recognize that bariatric surgery is the most effective treatment for obesity, but it’s also the most underutilized one.”
The Michigan Bariatric Surgery Collaborative is a unique statewide, payer-funded consortium focused on quality improvement. Dr. Varban presented an analysis of 19,764 patients who underwent a primary bariatric procedure in Michigan during 2006-2015 for whom complete 1-year follow-up data were available. The mean preoperative BMI for the overall group was 48 kg/m2, and the mean postoperative BMI at 1 year was 33 kg/m2.
Thirty-eight percent of patients achieved a BMI below 30 kg/m2 at 1 year; their mean BMI at that time was 26.7 kg/m2. The mean BMI 1 year post surgery in the 62% of patients who didn’t reach the goal was 36.7 kg/m2.
Only 6.2% of patients who didn’t get to a BMI of less than 30 kg/m2 1 year post surgery had a preoperative BMI of 40 kg/m2 or below, whereas 31.7% of patients who achieved the goal did have a baseline BMI of 40 kg/m2 or below.
Among patients with a preoperative BMI of 50-59 kg/m2, only 7.6% reached the target. And among those with a preoperative BMI of 60 kg/m2, only 0.4% had a BMI of less than 30 kg/m2 at 1 year.
“Patients with a BMI of 50 kg/m2 or more should be given realistic expectations about the type of weight loss they’ll have after bariatric surgery,” Dr. Varban said.
Why is a postsurgical BMI below 30 kg/m2 such an important benchmark? Abundant evidence indicates that having a BMI of 30 kg/m2 or higher is associated with a 50%-100% increase in the risk of premature death compared to that of normal-weight individuals. Successful bariatric surgery reduces that risk by 30%-40%.
In the Michigan study, patients who reached the BMI target had a significantly higher rate of resolution of common comorbid conditions associated with morbid obesity, including type 2 diabetes, hypertension, dyslipidemia, and sleep apnea. They also scored higher on a patient satisfaction survey.
The mean percent preoperative weight loss was 2.3% in patients who didn’t achieve the target BMI and similar at 2.5% in those who did. Thus, preoperative weight loss is not a major contributor to postoperative success, Dr. Varban continued.
Failure to reach the postoperative BMI goal was significantly more common among patients who were black or Hispanic, had an annual income below $25,000, or didn’t have private insurance.
Thirty-day perioperative complication rates didn’t differ between patients who attained a BMI below 30 kg/m2 at 1 year and those who did not.
Dr. Varban said it will come to no surprise to bariatric surgeons that the likelihood of attaining the target 1-year BMI varied according to the type of bariatric surgery: Compared to patients who underwent adjustable laparoscopic banding, the success rate was 19-fold higher with Roux-en-Y gastric bypass, 7.2-fold higher with sleeve gastrectomy, and a whopping 72-fold higher in patients who had a duodenal switch procedure.
Neither the mean preoperative nor 1-year postoperative BMI figures changed much over the study period, even though sleeve gastrectomy became much more common after 2010. For example, the mean preoperative BMI was 48.3 kg/m2 in 2006 and 46.9 kg/m2 in 2015, while the mean postoperative BMIs were 32.7 and 32.6 kg/m2, respectively, in those years.
Dr. Varban said that as he ran the numbers, he was surprised to see that the baseline BMI was so high – far higher than he would have guessed. But since then as he has discussed the study findings with referring physicians throughout Michigan, he’s come to understand the explanation: Many of them are content to wait until their morbidly obese patients grow to a BMI above 50 kg/m2 before making the referral because they consider the alternate criterion for bariatric surgery referral – that is, failure to achieve significant weight loss after 1 year of medically supervised attempts – to be too much for them to take on.
Amir A. Ghaferi, MD, a University of Michigan bariatric surgeon and coinvestigator in the study, rose from the audience to urge his colleagues to focus on the health policy implications of the findings.
“Maybe our bariatric surgery criteria aren’t right. We’ve been talking a lot amongst ourselves about pushing the BMI threshold lower and reducing some of the insurance barriers. I think what this study demonstrates from a policy perspective is we need to get these patients sooner, without so many barriers ahead of us and in front of the patients, in order to achieve the best possible outcomes,” Dr. Ghaferi said.
Dr. Varban reported receiving research funding from Blue Cross Blue Shield of Michigan.
NEW ORLEANS – About one-third of bariatric surgery patients achieve a body mass index below 30 kg/m2 at 1 year of follow-up, and the strongest predictor of success is having a BMI of 40 kg/m2 or less at the time of surgery, Oliver A. Varban, MD, reported at Obesity Week 2016.
Indeed, patients with a baseline BMI of 40 kg/m2 or less were fully 13.3-fold more likely to have a BMI of less than 30 kg/m2 1 year post surgery in a study of 19,764 patients in the Michigan Bariatric Surgery Collaborative database, according to Dr. Varban, surgical director of the adult bariatric surgery program at the University of Michigan, Ann Arbor.
“In order to optimize outcomes of bariatric surgery, patients should be encouraged to consider it when their BMI is less than 40 kg/m2. And policies that obstruct or delay surgery can actually result in inferior outcomes,” he said at the meeting, which was presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
“These patients are being referred to us. We don’t seek them out. The biggest impetus for this study was to be able to show referring physicians that outcomes are better when treatment is sought earlier. Every patient who shows up at our clinics with a BMI of 65 must have had a BMI of 35 at some point in time. I think we miss the boat on a lot of those patients,” the surgeon said. “Society at large should recognize that bariatric surgery is the most effective treatment for obesity, but it’s also the most underutilized one.”
The Michigan Bariatric Surgery Collaborative is a unique statewide, payer-funded consortium focused on quality improvement. Dr. Varban presented an analysis of 19,764 patients who underwent a primary bariatric procedure in Michigan during 2006-2015 for whom complete 1-year follow-up data were available. The mean preoperative BMI for the overall group was 48 kg/m2, and the mean postoperative BMI at 1 year was 33 kg/m2.
Thirty-eight percent of patients achieved a BMI below 30 kg/m2 at 1 year; their mean BMI at that time was 26.7 kg/m2. The mean BMI 1 year post surgery in the 62% of patients who didn’t reach the goal was 36.7 kg/m2.
Only 6.2% of patients who didn’t get to a BMI of less than 30 kg/m2 1 year post surgery had a preoperative BMI of 40 kg/m2 or below, whereas 31.7% of patients who achieved the goal did have a baseline BMI of 40 kg/m2 or below.
Among patients with a preoperative BMI of 50-59 kg/m2, only 7.6% reached the target. And among those with a preoperative BMI of 60 kg/m2, only 0.4% had a BMI of less than 30 kg/m2 at 1 year.
“Patients with a BMI of 50 kg/m2 or more should be given realistic expectations about the type of weight loss they’ll have after bariatric surgery,” Dr. Varban said.
Why is a postsurgical BMI below 30 kg/m2 such an important benchmark? Abundant evidence indicates that having a BMI of 30 kg/m2 or higher is associated with a 50%-100% increase in the risk of premature death compared to that of normal-weight individuals. Successful bariatric surgery reduces that risk by 30%-40%.
In the Michigan study, patients who reached the BMI target had a significantly higher rate of resolution of common comorbid conditions associated with morbid obesity, including type 2 diabetes, hypertension, dyslipidemia, and sleep apnea. They also scored higher on a patient satisfaction survey.
The mean percent preoperative weight loss was 2.3% in patients who didn’t achieve the target BMI and similar at 2.5% in those who did. Thus, preoperative weight loss is not a major contributor to postoperative success, Dr. Varban continued.
Failure to reach the postoperative BMI goal was significantly more common among patients who were black or Hispanic, had an annual income below $25,000, or didn’t have private insurance.
Thirty-day perioperative complication rates didn’t differ between patients who attained a BMI below 30 kg/m2 at 1 year and those who did not.
Dr. Varban said it will come to no surprise to bariatric surgeons that the likelihood of attaining the target 1-year BMI varied according to the type of bariatric surgery: Compared to patients who underwent adjustable laparoscopic banding, the success rate was 19-fold higher with Roux-en-Y gastric bypass, 7.2-fold higher with sleeve gastrectomy, and a whopping 72-fold higher in patients who had a duodenal switch procedure.
Neither the mean preoperative nor 1-year postoperative BMI figures changed much over the study period, even though sleeve gastrectomy became much more common after 2010. For example, the mean preoperative BMI was 48.3 kg/m2 in 2006 and 46.9 kg/m2 in 2015, while the mean postoperative BMIs were 32.7 and 32.6 kg/m2, respectively, in those years.
Dr. Varban said that as he ran the numbers, he was surprised to see that the baseline BMI was so high – far higher than he would have guessed. But since then as he has discussed the study findings with referring physicians throughout Michigan, he’s come to understand the explanation: Many of them are content to wait until their morbidly obese patients grow to a BMI above 50 kg/m2 before making the referral because they consider the alternate criterion for bariatric surgery referral – that is, failure to achieve significant weight loss after 1 year of medically supervised attempts – to be too much for them to take on.
Amir A. Ghaferi, MD, a University of Michigan bariatric surgeon and coinvestigator in the study, rose from the audience to urge his colleagues to focus on the health policy implications of the findings.
“Maybe our bariatric surgery criteria aren’t right. We’ve been talking a lot amongst ourselves about pushing the BMI threshold lower and reducing some of the insurance barriers. I think what this study demonstrates from a policy perspective is we need to get these patients sooner, without so many barriers ahead of us and in front of the patients, in order to achieve the best possible outcomes,” Dr. Ghaferi said.
Dr. Varban reported receiving research funding from Blue Cross Blue Shield of Michigan.
NEW ORLEANS – About one-third of bariatric surgery patients achieve a body mass index below 30 kg/m2 at 1 year of follow-up, and the strongest predictor of success is having a BMI of 40 kg/m2 or less at the time of surgery, Oliver A. Varban, MD, reported at Obesity Week 2016.
Indeed, patients with a baseline BMI of 40 kg/m2 or less were fully 13.3-fold more likely to have a BMI of less than 30 kg/m2 1 year post surgery in a study of 19,764 patients in the Michigan Bariatric Surgery Collaborative database, according to Dr. Varban, surgical director of the adult bariatric surgery program at the University of Michigan, Ann Arbor.
“In order to optimize outcomes of bariatric surgery, patients should be encouraged to consider it when their BMI is less than 40 kg/m2. And policies that obstruct or delay surgery can actually result in inferior outcomes,” he said at the meeting, which was presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
“These patients are being referred to us. We don’t seek them out. The biggest impetus for this study was to be able to show referring physicians that outcomes are better when treatment is sought earlier. Every patient who shows up at our clinics with a BMI of 65 must have had a BMI of 35 at some point in time. I think we miss the boat on a lot of those patients,” the surgeon said. “Society at large should recognize that bariatric surgery is the most effective treatment for obesity, but it’s also the most underutilized one.”
The Michigan Bariatric Surgery Collaborative is a unique statewide, payer-funded consortium focused on quality improvement. Dr. Varban presented an analysis of 19,764 patients who underwent a primary bariatric procedure in Michigan during 2006-2015 for whom complete 1-year follow-up data were available. The mean preoperative BMI for the overall group was 48 kg/m2, and the mean postoperative BMI at 1 year was 33 kg/m2.
Thirty-eight percent of patients achieved a BMI below 30 kg/m2 at 1 year; their mean BMI at that time was 26.7 kg/m2. The mean BMI 1 year post surgery in the 62% of patients who didn’t reach the goal was 36.7 kg/m2.
Only 6.2% of patients who didn’t get to a BMI of less than 30 kg/m2 1 year post surgery had a preoperative BMI of 40 kg/m2 or below, whereas 31.7% of patients who achieved the goal did have a baseline BMI of 40 kg/m2 or below.
Among patients with a preoperative BMI of 50-59 kg/m2, only 7.6% reached the target. And among those with a preoperative BMI of 60 kg/m2, only 0.4% had a BMI of less than 30 kg/m2 at 1 year.
“Patients with a BMI of 50 kg/m2 or more should be given realistic expectations about the type of weight loss they’ll have after bariatric surgery,” Dr. Varban said.
Why is a postsurgical BMI below 30 kg/m2 such an important benchmark? Abundant evidence indicates that having a BMI of 30 kg/m2 or higher is associated with a 50%-100% increase in the risk of premature death compared to that of normal-weight individuals. Successful bariatric surgery reduces that risk by 30%-40%.
In the Michigan study, patients who reached the BMI target had a significantly higher rate of resolution of common comorbid conditions associated with morbid obesity, including type 2 diabetes, hypertension, dyslipidemia, and sleep apnea. They also scored higher on a patient satisfaction survey.
The mean percent preoperative weight loss was 2.3% in patients who didn’t achieve the target BMI and similar at 2.5% in those who did. Thus, preoperative weight loss is not a major contributor to postoperative success, Dr. Varban continued.
Failure to reach the postoperative BMI goal was significantly more common among patients who were black or Hispanic, had an annual income below $25,000, or didn’t have private insurance.
Thirty-day perioperative complication rates didn’t differ between patients who attained a BMI below 30 kg/m2 at 1 year and those who did not.
Dr. Varban said it will come to no surprise to bariatric surgeons that the likelihood of attaining the target 1-year BMI varied according to the type of bariatric surgery: Compared to patients who underwent adjustable laparoscopic banding, the success rate was 19-fold higher with Roux-en-Y gastric bypass, 7.2-fold higher with sleeve gastrectomy, and a whopping 72-fold higher in patients who had a duodenal switch procedure.
Neither the mean preoperative nor 1-year postoperative BMI figures changed much over the study period, even though sleeve gastrectomy became much more common after 2010. For example, the mean preoperative BMI was 48.3 kg/m2 in 2006 and 46.9 kg/m2 in 2015, while the mean postoperative BMIs were 32.7 and 32.6 kg/m2, respectively, in those years.
Dr. Varban said that as he ran the numbers, he was surprised to see that the baseline BMI was so high – far higher than he would have guessed. But since then as he has discussed the study findings with referring physicians throughout Michigan, he’s come to understand the explanation: Many of them are content to wait until their morbidly obese patients grow to a BMI above 50 kg/m2 before making the referral because they consider the alternate criterion for bariatric surgery referral – that is, failure to achieve significant weight loss after 1 year of medically supervised attempts – to be too much for them to take on.
Amir A. Ghaferi, MD, a University of Michigan bariatric surgeon and coinvestigator in the study, rose from the audience to urge his colleagues to focus on the health policy implications of the findings.
“Maybe our bariatric surgery criteria aren’t right. We’ve been talking a lot amongst ourselves about pushing the BMI threshold lower and reducing some of the insurance barriers. I think what this study demonstrates from a policy perspective is we need to get these patients sooner, without so many barriers ahead of us and in front of the patients, in order to achieve the best possible outcomes,” Dr. Ghaferi said.
Dr. Varban reported receiving research funding from Blue Cross Blue Shield of Michigan.
OBESITY WEEK 2016
Key clinical point:
Major finding: Patients who underwent bariatric surgery when their BMI was 40 kg/m2 or below were 13.3-fold more likely to have a BMI below 30 kg/m2 1 year later.
Data source: A study of 1-year outcomes in nearly 20,000 patients in the Michigan Bariatric Surgery Collaborative database.
Disclosures: The study presenter reported receiving research funding from Blue Cross Blue Shield of Michigan.
Latest ixekizumab safety data called ‘very reassuring’
VIENNA – Updated longer-term safety data for ixekizumab in patients with moderate to severe plaque psoriasis continue to show no new safety signals, Alexa B. Kimball, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The safety database now includes 4,213 psoriasis patients on ixekizumab (Taltz) for a total of 7,843 patient-years of regular ongoing follow-up in seven different phase I-III clinical trials. And with a large group of patients now having been on the novel humanized monoclonal antibody targeting interleukin-17A for 2 years and smaller numbers out to 5 years, there have been no surprises, according to Dr. Kimball, professor of dermatology at Harvard Medical School, Boston.

The key trends in the safety analysis are that the number of patients with an adverse event resulting in ixekizumab discontinuation is very low, yet adverse event rates are declining over time.
“This is pretty common in clinical trials,” according to the dermatologist. “In those first 12 weeks of a study you are seeing the patients very frequently, asking them very detailed questions, and we often pick up adverse events more frequently as a result. Upper respiratory infections are a good example: In the first month a patient will remember what happened last week. But if you haven’t seen a patient in 3 months they might not remember that 10 weeks ago they had a little cold. That’s why we tend to see URI rates go down over time. Now, if you see adverse events go up over time – especially for things like malignancy – then there is certainly cause for concern that there’s a cumulative problem with toxicity. That is clearly not a problem with this drug.”
Turning to selected adverse events of interest, Dr. Kimball noted that 2.1% of patients have experienced oral candidiasis while on ixekizumab.
“Oral Candida infection is one of the known side effects with this drug. It doesn’t happen very frequently, and to date, the infections have been very manageable, but it is something you want to have in your mind because it does happen,” she noted.
Serious infections have occurred in 105 patients, 2.5% of those on ixekizumab. Major adverse cardiovascular events have occurred in 1.0%, nonmelanoma skin cancers in 0.7%, and other cancers in 1.1%. Of note, only 5 patients (0.1%) have developed Crohn’s disease, 10 have been diagnosed with ulcerative colitis, and there have been no completed suicides.
The safety follow-up is ongoing.
The safety registry is supported by Eli Lilly, which markets ixekizumab. Dr. Kimball reported receiving research funding from and serving as a consultant to Eli Lilly and numerous other pharmaceutical companies.
VIENNA – Updated longer-term safety data for ixekizumab in patients with moderate to severe plaque psoriasis continue to show no new safety signals, Alexa B. Kimball, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The safety database now includes 4,213 psoriasis patients on ixekizumab (Taltz) for a total of 7,843 patient-years of regular ongoing follow-up in seven different phase I-III clinical trials. And with a large group of patients now having been on the novel humanized monoclonal antibody targeting interleukin-17A for 2 years and smaller numbers out to 5 years, there have been no surprises, according to Dr. Kimball, professor of dermatology at Harvard Medical School, Boston.
The key trends in the safety analysis are that the number of patients with an adverse event resulting in ixekizumab discontinuation is very low, yet adverse event rates are declining over time.
“This is pretty common in clinical trials,” according to the dermatologist. “In those first 12 weeks of a study you are seeing the patients very frequently, asking them very detailed questions, and we often pick up adverse events more frequently as a result. Upper respiratory infections are a good example: In the first month a patient will remember what happened last week. But if you haven’t seen a patient in 3 months they might not remember that 10 weeks ago they had a little cold. That’s why we tend to see URI rates go down over time. Now, if you see adverse events go up over time – especially for things like malignancy – then there is certainly cause for concern that there’s a cumulative problem with toxicity. That is clearly not a problem with this drug.”
Turning to selected adverse events of interest, Dr. Kimball noted that 2.1% of patients have experienced oral candidiasis while on ixekizumab.
“Oral Candida infection is one of the known side effects with this drug. It doesn’t happen very frequently, and to date, the infections have been very manageable, but it is something you want to have in your mind because it does happen,” she noted.
Serious infections have occurred in 105 patients, 2.5% of those on ixekizumab. Major adverse cardiovascular events have occurred in 1.0%, nonmelanoma skin cancers in 0.7%, and other cancers in 1.1%. Of note, only 5 patients (0.1%) have developed Crohn’s disease, 10 have been diagnosed with ulcerative colitis, and there have been no completed suicides.
The safety follow-up is ongoing.
The safety registry is supported by Eli Lilly, which markets ixekizumab. Dr. Kimball reported receiving research funding from and serving as a consultant to Eli Lilly and numerous other pharmaceutical companies.
VIENNA – Updated longer-term safety data for ixekizumab in patients with moderate to severe plaque psoriasis continue to show no new safety signals, Alexa B. Kimball, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
The safety database now includes 4,213 psoriasis patients on ixekizumab (Taltz) for a total of 7,843 patient-years of regular ongoing follow-up in seven different phase I-III clinical trials. And with a large group of patients now having been on the novel humanized monoclonal antibody targeting interleukin-17A for 2 years and smaller numbers out to 5 years, there have been no surprises, according to Dr. Kimball, professor of dermatology at Harvard Medical School, Boston.
The key trends in the safety analysis are that the number of patients with an adverse event resulting in ixekizumab discontinuation is very low, yet adverse event rates are declining over time.
“This is pretty common in clinical trials,” according to the dermatologist. “In those first 12 weeks of a study you are seeing the patients very frequently, asking them very detailed questions, and we often pick up adverse events more frequently as a result. Upper respiratory infections are a good example: In the first month a patient will remember what happened last week. But if you haven’t seen a patient in 3 months they might not remember that 10 weeks ago they had a little cold. That’s why we tend to see URI rates go down over time. Now, if you see adverse events go up over time – especially for things like malignancy – then there is certainly cause for concern that there’s a cumulative problem with toxicity. That is clearly not a problem with this drug.”
Turning to selected adverse events of interest, Dr. Kimball noted that 2.1% of patients have experienced oral candidiasis while on ixekizumab.
“Oral Candida infection is one of the known side effects with this drug. It doesn’t happen very frequently, and to date, the infections have been very manageable, but it is something you want to have in your mind because it does happen,” she noted.
Serious infections have occurred in 105 patients, 2.5% of those on ixekizumab. Major adverse cardiovascular events have occurred in 1.0%, nonmelanoma skin cancers in 0.7%, and other cancers in 1.1%. Of note, only 5 patients (0.1%) have developed Crohn’s disease, 10 have been diagnosed with ulcerative colitis, and there have been no completed suicides.
The safety follow-up is ongoing.
The safety registry is supported by Eli Lilly, which markets ixekizumab. Dr. Kimball reported receiving research funding from and serving as a consultant to Eli Lilly and numerous other pharmaceutical companies.
THE EADV CONGRESS
‘Vanishing’ role forecast for whole-brain irradiation for NSCLC metastases
VIENNA – Icotinib proved significantly more effective and less toxic than standard therapy with whole-brain irradiation and chemotherapy in patients with multiple brain metastases from epidermal growth factor receptor (EGFR)–mutated non–small cell lung cancer in the phase III BRAIN trial.
“With favorable objective response and disease control rates, icotinib was superior to whole-brain irradiation with chemotherapy, and therefore icotinib should be used as first-line therapy for advanced EGFR-mutant non–small cell lung cancers with brain metastases,” Yi-long Wu, MD, said in presenting the BRAIN results at the World Congress on Lung Cancer.

Patients with brain metastases are often excluded from participation in clinical trials because their prognosis is so poor. BRAIN is the first phase III trial to report results comparing an EGFR tyrosine kinase inhibitor (TKI) – icotinib – to whole-brain irradiation (WBI) plus chemotherapy, regarded in National Comprehensive Cancer Network guidelines as standard therapy in the setting of brain metastases from NSCLC, noted Dr. Wu of the Guangdong Lung Cancer Institute in Guangzhou, China.
BRAIN was a multicenter Chinese trial in which investigators randomized 158 patients with three or more brain metastases from EGFR-mutated NSCLC to oral icotinib at 125 mg t.i.d. or to WBI with four to six cycles of concurrent or sequential platinum-based chemotherapy.
Icotinib outperformed standard therapy with WBI plus chemotherapy on multiple efficacy endpoints. Median intracranial progression-free survival was 10 months with icotinib, compared with only 4.8 months in patients on WBI with chemotherapy. At 6 months, 72% of patients assigned to icotinib remained free of intracranial disease progression, compared with just 48% of controls on WBI and chemotherapy. Six-month overall PFS, intracranial as well as extracranial, was 6.8 months with icotinib and 3.4 months in the WBI group. The intracranial and overall objective response rates were 67% and 55%, respectively, with icotinib, compared with 41% and 11% with WBI.
In addition, the EGFR TKI had a significantly better safety profile: grade 3 or worse toxicities occurred in just 8% of the icotinib group, compared with 26% of controls on standard therapy, Dr. Wu reported at the meeting sponsored by the International Association for the Study of Lung Cancer.
There was, however, no significant difference between the two study arms in overall survival: 18 months with icotinib, 20.5 months with standard therapy, noted Dr. Wu, who is president of the Chinese Society of Clinical Oncology.
Discussant Jacek Jassem, MD, said “This is potentially, and likely, a practice-changing study.” He added that he’s looking forward to planned future presentation of neurotoxicity and quality of life data from BRAIN. Those important endpoints are also incorporated in the ongoing phase III trials of gefitinib and erlotinib, EGFR TKIs which are far more readily accessible at present to physicians outside the Far East.

“Whole-brain radiotherapy for brain metastases from EGFR-mutated non–small cell lung cancer is a vanishing approach. The remaining role in this setting is as salvage in cases of symptomatic primary or secondary resistance to EGFR TKIs,” said Dr. Jassem, head of the department of oncology and radiotherapy at the Medical University of Gdansk, Poland.
By way of background, he noted that 10%-15% of patients already have brain metastases at the time of diagnosis of NSCLC, and 40% develop them eventually. EGFR-mutated primary tumors are particularly likely to metastasize to the brain.
Remaining questions in the wake of the BRAIN trial include the efficacy of gefitinib and erlotinib versus WBI plus chemotherapy, as well as the broader question of the efficacy of EGFR TKIs in non-Asian patients with brain metastases.
“Most of the studies of EGFR TKIs have been in East Asian populations. These agents are particularly active in East Asians. There’s a question as to whether the BRAIN results can be applied to other populations,” Dr. Jassem said.
The BRAIN study was sponsored by the Guangdong Association of Clinical Trials. Dr. Wu reported serving as a consultant to AstraZeneca, Roche, Eli Lilly, Pfizer, and Sanofi. Dr. Jassem reported having no financial conflicts of interest.
VIENNA – Icotinib proved significantly more effective and less toxic than standard therapy with whole-brain irradiation and chemotherapy in patients with multiple brain metastases from epidermal growth factor receptor (EGFR)–mutated non–small cell lung cancer in the phase III BRAIN trial.
“With favorable objective response and disease control rates, icotinib was superior to whole-brain irradiation with chemotherapy, and therefore icotinib should be used as first-line therapy for advanced EGFR-mutant non–small cell lung cancers with brain metastases,” Yi-long Wu, MD, said in presenting the BRAIN results at the World Congress on Lung Cancer.
Patients with brain metastases are often excluded from participation in clinical trials because their prognosis is so poor. BRAIN is the first phase III trial to report results comparing an EGFR tyrosine kinase inhibitor (TKI) – icotinib – to whole-brain irradiation (WBI) plus chemotherapy, regarded in National Comprehensive Cancer Network guidelines as standard therapy in the setting of brain metastases from NSCLC, noted Dr. Wu of the Guangdong Lung Cancer Institute in Guangzhou, China.
BRAIN was a multicenter Chinese trial in which investigators randomized 158 patients with three or more brain metastases from EGFR-mutated NSCLC to oral icotinib at 125 mg t.i.d. or to WBI with four to six cycles of concurrent or sequential platinum-based chemotherapy.
Icotinib outperformed standard therapy with WBI plus chemotherapy on multiple efficacy endpoints. Median intracranial progression-free survival was 10 months with icotinib, compared with only 4.8 months in patients on WBI with chemotherapy. At 6 months, 72% of patients assigned to icotinib remained free of intracranial disease progression, compared with just 48% of controls on WBI and chemotherapy. Six-month overall PFS, intracranial as well as extracranial, was 6.8 months with icotinib and 3.4 months in the WBI group. The intracranial and overall objective response rates were 67% and 55%, respectively, with icotinib, compared with 41% and 11% with WBI.
In addition, the EGFR TKI had a significantly better safety profile: grade 3 or worse toxicities occurred in just 8% of the icotinib group, compared with 26% of controls on standard therapy, Dr. Wu reported at the meeting sponsored by the International Association for the Study of Lung Cancer.
There was, however, no significant difference between the two study arms in overall survival: 18 months with icotinib, 20.5 months with standard therapy, noted Dr. Wu, who is president of the Chinese Society of Clinical Oncology.
Discussant Jacek Jassem, MD, said “This is potentially, and likely, a practice-changing study.” He added that he’s looking forward to planned future presentation of neurotoxicity and quality of life data from BRAIN. Those important endpoints are also incorporated in the ongoing phase III trials of gefitinib and erlotinib, EGFR TKIs which are far more readily accessible at present to physicians outside the Far East.
“Whole-brain radiotherapy for brain metastases from EGFR-mutated non–small cell lung cancer is a vanishing approach. The remaining role in this setting is as salvage in cases of symptomatic primary or secondary resistance to EGFR TKIs,” said Dr. Jassem, head of the department of oncology and radiotherapy at the Medical University of Gdansk, Poland.
By way of background, he noted that 10%-15% of patients already have brain metastases at the time of diagnosis of NSCLC, and 40% develop them eventually. EGFR-mutated primary tumors are particularly likely to metastasize to the brain.
Remaining questions in the wake of the BRAIN trial include the efficacy of gefitinib and erlotinib versus WBI plus chemotherapy, as well as the broader question of the efficacy of EGFR TKIs in non-Asian patients with brain metastases.
“Most of the studies of EGFR TKIs have been in East Asian populations. These agents are particularly active in East Asians. There’s a question as to whether the BRAIN results can be applied to other populations,” Dr. Jassem said.
The BRAIN study was sponsored by the Guangdong Association of Clinical Trials. Dr. Wu reported serving as a consultant to AstraZeneca, Roche, Eli Lilly, Pfizer, and Sanofi. Dr. Jassem reported having no financial conflicts of interest.
VIENNA – Icotinib proved significantly more effective and less toxic than standard therapy with whole-brain irradiation and chemotherapy in patients with multiple brain metastases from epidermal growth factor receptor (EGFR)–mutated non–small cell lung cancer in the phase III BRAIN trial.
“With favorable objective response and disease control rates, icotinib was superior to whole-brain irradiation with chemotherapy, and therefore icotinib should be used as first-line therapy for advanced EGFR-mutant non–small cell lung cancers with brain metastases,” Yi-long Wu, MD, said in presenting the BRAIN results at the World Congress on Lung Cancer.
Patients with brain metastases are often excluded from participation in clinical trials because their prognosis is so poor. BRAIN is the first phase III trial to report results comparing an EGFR tyrosine kinase inhibitor (TKI) – icotinib – to whole-brain irradiation (WBI) plus chemotherapy, regarded in National Comprehensive Cancer Network guidelines as standard therapy in the setting of brain metastases from NSCLC, noted Dr. Wu of the Guangdong Lung Cancer Institute in Guangzhou, China.
BRAIN was a multicenter Chinese trial in which investigators randomized 158 patients with three or more brain metastases from EGFR-mutated NSCLC to oral icotinib at 125 mg t.i.d. or to WBI with four to six cycles of concurrent or sequential platinum-based chemotherapy.
Icotinib outperformed standard therapy with WBI plus chemotherapy on multiple efficacy endpoints. Median intracranial progression-free survival was 10 months with icotinib, compared with only 4.8 months in patients on WBI with chemotherapy. At 6 months, 72% of patients assigned to icotinib remained free of intracranial disease progression, compared with just 48% of controls on WBI and chemotherapy. Six-month overall PFS, intracranial as well as extracranial, was 6.8 months with icotinib and 3.4 months in the WBI group. The intracranial and overall objective response rates were 67% and 55%, respectively, with icotinib, compared with 41% and 11% with WBI.
In addition, the EGFR TKI had a significantly better safety profile: grade 3 or worse toxicities occurred in just 8% of the icotinib group, compared with 26% of controls on standard therapy, Dr. Wu reported at the meeting sponsored by the International Association for the Study of Lung Cancer.
There was, however, no significant difference between the two study arms in overall survival: 18 months with icotinib, 20.5 months with standard therapy, noted Dr. Wu, who is president of the Chinese Society of Clinical Oncology.
Discussant Jacek Jassem, MD, said “This is potentially, and likely, a practice-changing study.” He added that he’s looking forward to planned future presentation of neurotoxicity and quality of life data from BRAIN. Those important endpoints are also incorporated in the ongoing phase III trials of gefitinib and erlotinib, EGFR TKIs which are far more readily accessible at present to physicians outside the Far East.
“Whole-brain radiotherapy for brain metastases from EGFR-mutated non–small cell lung cancer is a vanishing approach. The remaining role in this setting is as salvage in cases of symptomatic primary or secondary resistance to EGFR TKIs,” said Dr. Jassem, head of the department of oncology and radiotherapy at the Medical University of Gdansk, Poland.
By way of background, he noted that 10%-15% of patients already have brain metastases at the time of diagnosis of NSCLC, and 40% develop them eventually. EGFR-mutated primary tumors are particularly likely to metastasize to the brain.
Remaining questions in the wake of the BRAIN trial include the efficacy of gefitinib and erlotinib versus WBI plus chemotherapy, as well as the broader question of the efficacy of EGFR TKIs in non-Asian patients with brain metastases.
“Most of the studies of EGFR TKIs have been in East Asian populations. These agents are particularly active in East Asians. There’s a question as to whether the BRAIN results can be applied to other populations,” Dr. Jassem said.
The BRAIN study was sponsored by the Guangdong Association of Clinical Trials. Dr. Wu reported serving as a consultant to AstraZeneca, Roche, Eli Lilly, Pfizer, and Sanofi. Dr. Jassem reported having no financial conflicts of interest.
AT WCLC 2016
Key clinical point:
Major finding: Median intracranial progression-free survival in patients with multiple brain metastases from EGFR-mutated NSCLC was 10 months in those randomized to icotinib, compared with 4.8 months with standard-of-care whole-brain irradiation plus chemotherapy.
Data source: This phase III multicenter Chinese trial included 158 patients with multiple brain metastases from EGFR-mutated NSCLC.
Disclosures: The BRAIN study was sponsored by the Guangdong Association of Clinical Trials. The presenter reported serving as a consultant to AstraZeneca, Roche, Eli Lilly, Pfizer, and Sanofi.
Nivolumab plus ipilimumab shines as first-line in advanced NSCLC
VIENNA – The combination of nivolumab and ipilimumab as first-line therapy in patients with advanced non–small cell lung cancer (NSCLC) doubled median progression-free survival time compared with nivolumab monotherapy in updated results from the CheckMate 012 trial, Scott N. Gettinger, MD, reported at the World Congress on Lung Cancer.
This doubling of progression-free survival (PFS) applied to all comers regardless of whether or not their tumor expressed programmed death-ligand 1 (PD-L1). In those patients with any degree of PD-L1 expression – even if just 1% of tumor cells stained positive – combination therapy didn’t just double median PFS, it tripled it, compared with nivolumab alone, added Dr. Gettinger of the Yale Cancer Center in New Haven, Conn.

CheckMate 012 is a phase I study of nivolumab as first-line therapy for advanced NSCLC with numerous treatment arms. Dr. Gettinger presented updated results for 52 patients who received intravenous nivolumab monotherapy at a dose of 3 mg/kg every 2 weeks, 36 patients on nivolumab plus intravenous ipilimumab at 1 mg/kg every 12 weeks, and 39 who received nivolumab plus ipilimumab every 6 weeks. None of the participants had prior chemotherapy for their advanced stage IIIb or IV NSCLC.
Median PFS in the overall study population was 3.6 months with nivolumab monotherapy and 8.0 months with combination therapy. In the roughly 70% of participants who had any degree of tumor PD-L1 expression, median PFS was 3.5 months with monotherapy, compared with 12.7 months in the combined dual therapy arms. And, in the roughly one-quarter of patients whose tumor showed at least 50% PD-L1 expression, median PFS rose to 8.3 months with nivolumab monotherapy and hasn’t yet been reached in patients on combination therapy.
The 1-year overall survival rate in patients on nivolumab monotherapy was 73% in all treated patients, 69% in those with any detectable tumor PD-L1 expression, and 83% in patients with at least 50% PD-L1 expression. In patients on combination therapy, the corresponding figures were higher at 76%, 87%, and 100%.
The clearly enhanced efficacy achieved with the combination of nivolumab plus ipilimumab was accomplished with only a modest increase in toxicity compared with nivolumab alone. At a median follow-up of 22 months in the nivolumab monotherapy group and 16 months for combination therapy, the rate of any treatment-related adverse event leading to study withdrawal was 12% with monotherapy and 18% with combination therapy.
The combination of nivolumab (Opdivo), a PD-L1 immune checkpoint inhibitor, and ipilimumab (Yervoy), a cytotoxic T-lymphocyte–associated protein 4 immune checkpoint inhibitor, is biologically attractive: “The ipilimumab primes the immune system by inducing tumor infiltration of effector T cells while depleting the number of myeloid-derived suppressor cells and suppressive regulatory T cells within the tumor microenvironment,” Dr. Gettinger explained.
Nivolumab is approved for treatment of advanced NSCLC that has progressed despite platinum-based chemotherapy. Of the various toxicities associated with the drug, only dermatologic and GI adverse events occurred more frequently with combination therapy than nivolumab alone.
There were five complete responses in the nivolumab monotherapy group and six with combination therapy. Of note, four of these complete responses occurred in patients without any measurable tumor PD-L1 expression.
Based upon these encouraging results from CheckMate 012, a phase III randomized clinical trial of nivolumab as first-line therapy in patients with advanced NSCLC is underway. In the CheckMate 227 trial, patients with any detectable PD-L1 expression are randomized to nivolumab at 3mg/kg every 2 weeks plus ipilimumab at 1 mg/kg every 6 weeks, nivolumab monotherapy at 240 mg every 2 weeks, or standard platinum-based chemotherapy. Patients with no PD-L1 expression in their tumor are assigned to the nivolumab/ipilimumab combination, or nivolumab at 360 mg every 3 weeks plus chemotherapy, or chemotherapy alone.

“I think we should be cautious despite the excitement about the combination,” argued Dr. Garon, director of thoracic oncology at the University of California, Los Angeles.
He noted that various iterations of the large CheckMate 012 phase I program have been presented repeatedly at major meetings, and the shifting data have raised concerns in his mind about possible patient selection bias stemming from the study design.
“From my perspective, until we see randomized data that can control for these biases, I will remain hopeful but not yet extremely confident that this combination will be the new frontline therapy for metastatic non–small cell lung cancer,” Dr. Garon said.
Dr. Gettinger reported serving as a consultant to Bristol-Myers Squibb, which markets nivolumab.
Dr. Garon reported that his institution receives funding from Bristol-Myers Squibb as well as AstraZeneca, Boehringer Ingelheim, Eli Lilly, Genentech, Mirati, Merck, Pfizer, and Novartis.
VIENNA – The combination of nivolumab and ipilimumab as first-line therapy in patients with advanced non–small cell lung cancer (NSCLC) doubled median progression-free survival time compared with nivolumab monotherapy in updated results from the CheckMate 012 trial, Scott N. Gettinger, MD, reported at the World Congress on Lung Cancer.
This doubling of progression-free survival (PFS) applied to all comers regardless of whether or not their tumor expressed programmed death-ligand 1 (PD-L1). In those patients with any degree of PD-L1 expression – even if just 1% of tumor cells stained positive – combination therapy didn’t just double median PFS, it tripled it, compared with nivolumab alone, added Dr. Gettinger of the Yale Cancer Center in New Haven, Conn.
CheckMate 012 is a phase I study of nivolumab as first-line therapy for advanced NSCLC with numerous treatment arms. Dr. Gettinger presented updated results for 52 patients who received intravenous nivolumab monotherapy at a dose of 3 mg/kg every 2 weeks, 36 patients on nivolumab plus intravenous ipilimumab at 1 mg/kg every 12 weeks, and 39 who received nivolumab plus ipilimumab every 6 weeks. None of the participants had prior chemotherapy for their advanced stage IIIb or IV NSCLC.
Median PFS in the overall study population was 3.6 months with nivolumab monotherapy and 8.0 months with combination therapy. In the roughly 70% of participants who had any degree of tumor PD-L1 expression, median PFS was 3.5 months with monotherapy, compared with 12.7 months in the combined dual therapy arms. And, in the roughly one-quarter of patients whose tumor showed at least 50% PD-L1 expression, median PFS rose to 8.3 months with nivolumab monotherapy and hasn’t yet been reached in patients on combination therapy.
The 1-year overall survival rate in patients on nivolumab monotherapy was 73% in all treated patients, 69% in those with any detectable tumor PD-L1 expression, and 83% in patients with at least 50% PD-L1 expression. In patients on combination therapy, the corresponding figures were higher at 76%, 87%, and 100%.
The clearly enhanced efficacy achieved with the combination of nivolumab plus ipilimumab was accomplished with only a modest increase in toxicity compared with nivolumab alone. At a median follow-up of 22 months in the nivolumab monotherapy group and 16 months for combination therapy, the rate of any treatment-related adverse event leading to study withdrawal was 12% with monotherapy and 18% with combination therapy.
The combination of nivolumab (Opdivo), a PD-L1 immune checkpoint inhibitor, and ipilimumab (Yervoy), a cytotoxic T-lymphocyte–associated protein 4 immune checkpoint inhibitor, is biologically attractive: “The ipilimumab primes the immune system by inducing tumor infiltration of effector T cells while depleting the number of myeloid-derived suppressor cells and suppressive regulatory T cells within the tumor microenvironment,” Dr. Gettinger explained.
Nivolumab is approved for treatment of advanced NSCLC that has progressed despite platinum-based chemotherapy. Of the various toxicities associated with the drug, only dermatologic and GI adverse events occurred more frequently with combination therapy than nivolumab alone.
There were five complete responses in the nivolumab monotherapy group and six with combination therapy. Of note, four of these complete responses occurred in patients without any measurable tumor PD-L1 expression.
Based upon these encouraging results from CheckMate 012, a phase III randomized clinical trial of nivolumab as first-line therapy in patients with advanced NSCLC is underway. In the CheckMate 227 trial, patients with any detectable PD-L1 expression are randomized to nivolumab at 3mg/kg every 2 weeks plus ipilimumab at 1 mg/kg every 6 weeks, nivolumab monotherapy at 240 mg every 2 weeks, or standard platinum-based chemotherapy. Patients with no PD-L1 expression in their tumor are assigned to the nivolumab/ipilimumab combination, or nivolumab at 360 mg every 3 weeks plus chemotherapy, or chemotherapy alone.
“I think we should be cautious despite the excitement about the combination,” argued Dr. Garon, director of thoracic oncology at the University of California, Los Angeles.
He noted that various iterations of the large CheckMate 012 phase I program have been presented repeatedly at major meetings, and the shifting data have raised concerns in his mind about possible patient selection bias stemming from the study design.
“From my perspective, until we see randomized data that can control for these biases, I will remain hopeful but not yet extremely confident that this combination will be the new frontline therapy for metastatic non–small cell lung cancer,” Dr. Garon said.
Dr. Gettinger reported serving as a consultant to Bristol-Myers Squibb, which markets nivolumab.
Dr. Garon reported that his institution receives funding from Bristol-Myers Squibb as well as AstraZeneca, Boehringer Ingelheim, Eli Lilly, Genentech, Mirati, Merck, Pfizer, and Novartis.
VIENNA – The combination of nivolumab and ipilimumab as first-line therapy in patients with advanced non–small cell lung cancer (NSCLC) doubled median progression-free survival time compared with nivolumab monotherapy in updated results from the CheckMate 012 trial, Scott N. Gettinger, MD, reported at the World Congress on Lung Cancer.
This doubling of progression-free survival (PFS) applied to all comers regardless of whether or not their tumor expressed programmed death-ligand 1 (PD-L1). In those patients with any degree of PD-L1 expression – even if just 1% of tumor cells stained positive – combination therapy didn’t just double median PFS, it tripled it, compared with nivolumab alone, added Dr. Gettinger of the Yale Cancer Center in New Haven, Conn.
CheckMate 012 is a phase I study of nivolumab as first-line therapy for advanced NSCLC with numerous treatment arms. Dr. Gettinger presented updated results for 52 patients who received intravenous nivolumab monotherapy at a dose of 3 mg/kg every 2 weeks, 36 patients on nivolumab plus intravenous ipilimumab at 1 mg/kg every 12 weeks, and 39 who received nivolumab plus ipilimumab every 6 weeks. None of the participants had prior chemotherapy for their advanced stage IIIb or IV NSCLC.
Median PFS in the overall study population was 3.6 months with nivolumab monotherapy and 8.0 months with combination therapy. In the roughly 70% of participants who had any degree of tumor PD-L1 expression, median PFS was 3.5 months with monotherapy, compared with 12.7 months in the combined dual therapy arms. And, in the roughly one-quarter of patients whose tumor showed at least 50% PD-L1 expression, median PFS rose to 8.3 months with nivolumab monotherapy and hasn’t yet been reached in patients on combination therapy.
The 1-year overall survival rate in patients on nivolumab monotherapy was 73% in all treated patients, 69% in those with any detectable tumor PD-L1 expression, and 83% in patients with at least 50% PD-L1 expression. In patients on combination therapy, the corresponding figures were higher at 76%, 87%, and 100%.
The clearly enhanced efficacy achieved with the combination of nivolumab plus ipilimumab was accomplished with only a modest increase in toxicity compared with nivolumab alone. At a median follow-up of 22 months in the nivolumab monotherapy group and 16 months for combination therapy, the rate of any treatment-related adverse event leading to study withdrawal was 12% with monotherapy and 18% with combination therapy.
The combination of nivolumab (Opdivo), a PD-L1 immune checkpoint inhibitor, and ipilimumab (Yervoy), a cytotoxic T-lymphocyte–associated protein 4 immune checkpoint inhibitor, is biologically attractive: “The ipilimumab primes the immune system by inducing tumor infiltration of effector T cells while depleting the number of myeloid-derived suppressor cells and suppressive regulatory T cells within the tumor microenvironment,” Dr. Gettinger explained.
Nivolumab is approved for treatment of advanced NSCLC that has progressed despite platinum-based chemotherapy. Of the various toxicities associated with the drug, only dermatologic and GI adverse events occurred more frequently with combination therapy than nivolumab alone.
There were five complete responses in the nivolumab monotherapy group and six with combination therapy. Of note, four of these complete responses occurred in patients without any measurable tumor PD-L1 expression.
Based upon these encouraging results from CheckMate 012, a phase III randomized clinical trial of nivolumab as first-line therapy in patients with advanced NSCLC is underway. In the CheckMate 227 trial, patients with any detectable PD-L1 expression are randomized to nivolumab at 3mg/kg every 2 weeks plus ipilimumab at 1 mg/kg every 6 weeks, nivolumab monotherapy at 240 mg every 2 weeks, or standard platinum-based chemotherapy. Patients with no PD-L1 expression in their tumor are assigned to the nivolumab/ipilimumab combination, or nivolumab at 360 mg every 3 weeks plus chemotherapy, or chemotherapy alone.
“I think we should be cautious despite the excitement about the combination,” argued Dr. Garon, director of thoracic oncology at the University of California, Los Angeles.
He noted that various iterations of the large CheckMate 012 phase I program have been presented repeatedly at major meetings, and the shifting data have raised concerns in his mind about possible patient selection bias stemming from the study design.
“From my perspective, until we see randomized data that can control for these biases, I will remain hopeful but not yet extremely confident that this combination will be the new frontline therapy for metastatic non–small cell lung cancer,” Dr. Garon said.
Dr. Gettinger reported serving as a consultant to Bristol-Myers Squibb, which markets nivolumab.
Dr. Garon reported that his institution receives funding from Bristol-Myers Squibb as well as AstraZeneca, Boehringer Ingelheim, Eli Lilly, Genentech, Mirati, Merck, Pfizer, and Novartis.
AT WCLC 2016
Key clinical point: A combination of two immunotherapy agents with different mechanisms of action produced impressive efficacy and acceptable toxicities as first-line therapy in patients with chemotherapy-naive advanced non–small cell lung cancer.
Major finding: in patients with any detectable tumor PD-L1 expression.
Data source: This analysis from a larger phase I study included 127 patients with no prior chemotherapy for advanced NSCLC.
Disclosures: The study presenter is a consultant to Bristol-Myers Squibb, which sponsored the CheckMate 012 trial.
Observational hospital stays for HF linked to worse outcomes
NEW ORLEANS – The Centers for Medicare & Medicaid Services policy providing financial incentives for hospitals to readmit patients for heart failure for an observational stay rather than as an inpatient is antithetical to the patients’ best interests, according to data presented at the American Heart Association scientific sessions.
“We showed that if you get admitted under observation, the risk of you coming back is much higher than if you’re under an inpatient stay,” said Ahmad Masri, MBBS, of the University of Pittsburgh.

“Since CMS instituted this rule in 2013, there has been a surge in utilization of observational status versus inpatient status,” Dr. Masri noted.
That might make sense if the patients selected for in-hospital observation were less ill at the time than the heart failure patients admitted as inpatients, but that wasn’t the case in his large, retrospective study.
Dr. Masri reported on 21,339 patients with a total of 52,493 admissions for a primary diagnosis of heart failure during 2008-2015 in an 18-hospital health care system. After excluding admissions which involved cardiac surgery or in-hospital mortality, the total was 50,654 admissions.
Of these admissions, 5% were for in-hospital observation; 17% were inpatient admissions with discharge in less than 2 days. The two groups were similar in terms of age, comorbid conditions, and use of guideline-directed medications, although 36% of patients admitted under observation had a left ventricular ejection fraction below 40%, compared with 30% of those with an inpatient admission for less than 2 days.
The majority of patients in both groups were readmitted for heart failure within 1 year; however, the readmission rate was 23% lower in the group with an inpatient stay of less than 2 days, in an analysis adjusted for age, sex, ejection fraction, hypertension, diabetes, pneumonia, chronic obstructive pulmonary disease, liver disease, and renal failure.
Similarly, the group with an inpatient stay of less than 2 days’ duration was 24% less likely to have a cardiac readmission within 1 year than the group admitted for a penalty-free observational stay. The short inpatient stay group’s 1-year all-cause readmission rate was also 24% lower. All of these differences were statistically significant and clinically meaningful.
Yet 1-year all-cause mortality in the two groups was no different.
“This suggests that the difference between these two groups is more of an administrative distinction than a reflection of patient status at time of admission. It looks like it’s just random,” according to Dr. Masri. “There is a real need for a patient-centered, streamlined approach in evaluating and treating patients with heart failure, with a revised treatment-based algorithm and admission rules that guide physicians and shape health care policy.”
He reported having no financial conflicts of interest regarding this study.
NEW ORLEANS – The Centers for Medicare & Medicaid Services policy providing financial incentives for hospitals to readmit patients for heart failure for an observational stay rather than as an inpatient is antithetical to the patients’ best interests, according to data presented at the American Heart Association scientific sessions.
“We showed that if you get admitted under observation, the risk of you coming back is much higher than if you’re under an inpatient stay,” said Ahmad Masri, MBBS, of the University of Pittsburgh.
“Since CMS instituted this rule in 2013, there has been a surge in utilization of observational status versus inpatient status,” Dr. Masri noted.
That might make sense if the patients selected for in-hospital observation were less ill at the time than the heart failure patients admitted as inpatients, but that wasn’t the case in his large, retrospective study.
Dr. Masri reported on 21,339 patients with a total of 52,493 admissions for a primary diagnosis of heart failure during 2008-2015 in an 18-hospital health care system. After excluding admissions which involved cardiac surgery or in-hospital mortality, the total was 50,654 admissions.
Of these admissions, 5% were for in-hospital observation; 17% were inpatient admissions with discharge in less than 2 days. The two groups were similar in terms of age, comorbid conditions, and use of guideline-directed medications, although 36% of patients admitted under observation had a left ventricular ejection fraction below 40%, compared with 30% of those with an inpatient admission for less than 2 days.
The majority of patients in both groups were readmitted for heart failure within 1 year; however, the readmission rate was 23% lower in the group with an inpatient stay of less than 2 days, in an analysis adjusted for age, sex, ejection fraction, hypertension, diabetes, pneumonia, chronic obstructive pulmonary disease, liver disease, and renal failure.
Similarly, the group with an inpatient stay of less than 2 days’ duration was 24% less likely to have a cardiac readmission within 1 year than the group admitted for a penalty-free observational stay. The short inpatient stay group’s 1-year all-cause readmission rate was also 24% lower. All of these differences were statistically significant and clinically meaningful.
Yet 1-year all-cause mortality in the two groups was no different.
“This suggests that the difference between these two groups is more of an administrative distinction than a reflection of patient status at time of admission. It looks like it’s just random,” according to Dr. Masri. “There is a real need for a patient-centered, streamlined approach in evaluating and treating patients with heart failure, with a revised treatment-based algorithm and admission rules that guide physicians and shape health care policy.”
He reported having no financial conflicts of interest regarding this study.
NEW ORLEANS – The Centers for Medicare & Medicaid Services policy providing financial incentives for hospitals to readmit patients for heart failure for an observational stay rather than as an inpatient is antithetical to the patients’ best interests, according to data presented at the American Heart Association scientific sessions.
“We showed that if you get admitted under observation, the risk of you coming back is much higher than if you’re under an inpatient stay,” said Ahmad Masri, MBBS, of the University of Pittsburgh.
“Since CMS instituted this rule in 2013, there has been a surge in utilization of observational status versus inpatient status,” Dr. Masri noted.
That might make sense if the patients selected for in-hospital observation were less ill at the time than the heart failure patients admitted as inpatients, but that wasn’t the case in his large, retrospective study.
Dr. Masri reported on 21,339 patients with a total of 52,493 admissions for a primary diagnosis of heart failure during 2008-2015 in an 18-hospital health care system. After excluding admissions which involved cardiac surgery or in-hospital mortality, the total was 50,654 admissions.
Of these admissions, 5% were for in-hospital observation; 17% were inpatient admissions with discharge in less than 2 days. The two groups were similar in terms of age, comorbid conditions, and use of guideline-directed medications, although 36% of patients admitted under observation had a left ventricular ejection fraction below 40%, compared with 30% of those with an inpatient admission for less than 2 days.
The majority of patients in both groups were readmitted for heart failure within 1 year; however, the readmission rate was 23% lower in the group with an inpatient stay of less than 2 days, in an analysis adjusted for age, sex, ejection fraction, hypertension, diabetes, pneumonia, chronic obstructive pulmonary disease, liver disease, and renal failure.
Similarly, the group with an inpatient stay of less than 2 days’ duration was 24% less likely to have a cardiac readmission within 1 year than the group admitted for a penalty-free observational stay. The short inpatient stay group’s 1-year all-cause readmission rate was also 24% lower. All of these differences were statistically significant and clinically meaningful.
Yet 1-year all-cause mortality in the two groups was no different.
“This suggests that the difference between these two groups is more of an administrative distinction than a reflection of patient status at time of admission. It looks like it’s just random,” according to Dr. Masri. “There is a real need for a patient-centered, streamlined approach in evaluating and treating patients with heart failure, with a revised treatment-based algorithm and admission rules that guide physicians and shape health care policy.”
He reported having no financial conflicts of interest regarding this study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The 1-year rates of readmission for heart failure, cardiac readmission, and all-cause readmission were each 23%-24% lower in heart failure patients admitted for an inpatient stay of less than 2 days’ duration than if they were designated as being admitted under observation.
Data source: A retrospective analysis of more than 50,000 hospital admissions with a primary diagnosis of heart failure in 21,339 patients during 2008-2015.
Disclosures: The presenter reported having no financial conflicts of interest regarding the study.