User login
Cardiovascular complications in pregnancy quickly boost future risk
NEW ORLEANS – Women who experience peripartum cardiomyopathy or any of a variety of hypertensive disorders in pregnancy are at sharply increased risk of acute MI, stroke, or new-onset heart failure beginning within just a few years, Rima Arnaout, MD, reported at the American Heart Association scientific sessions.
“Our study supports the idea that women who have cardiovascular complications in pregnancy really need to be monitored closely for potential primary prevention of cardiovascular events,” said Dr. Arnaout of the University of California, San Francisco.
At a session devoted to “big data” studies in cardiovascular medicine, she presented one of the biggest: a retrospective cohort study of 1.66 million pregnancies during 2005-2009 in California women without any history of congenital or valvular heart disease or prepregnancy cardiovascular events. The California database was created as part of the U.S. Agency for Healthcare Research and Quality’s comprehensive Healthcare Cost and Utilization Project, which included more than 95% of the state’s hospitals. Women who experienced an MI or a stroke, or who were diagnosed with heart failure, during a median of 2.7 years and a maximum of 6 years of follow-up post pregnancy were identified via ICD-9 codes.
There were 111,202 cases of various forms of hypertension in pregnancy, for a 6.9% incidence. Peripartum cardiomyopathy was diagnosed in 562 women, for a rate of 3.5 cases per 10,000 pregnancies.

Indeed, in a multivariate Cox proportional hazards analysis adjusted for numerous potential confounders, peripartum cardiomyopathy was associated with a 16-fold increased risk of acute MI during the relatively short follow-up period, as well as 29-fold increased risks of stroke and heart failure, compared with women with no cardiovascular issues during their pregnancy.
Chronic hypertension, regardless of whether it occurred alone or in combination with preeclampsia or gestational hypertension, was associated with roughly a twofold increased risk of each of the three study outcomes, compared with women who didn’t experience a cardiovascular complication during pregnancy. De novo preeclampsia was also associated with roughly a twofold increased risk of later MI, heart failure, or stroke.
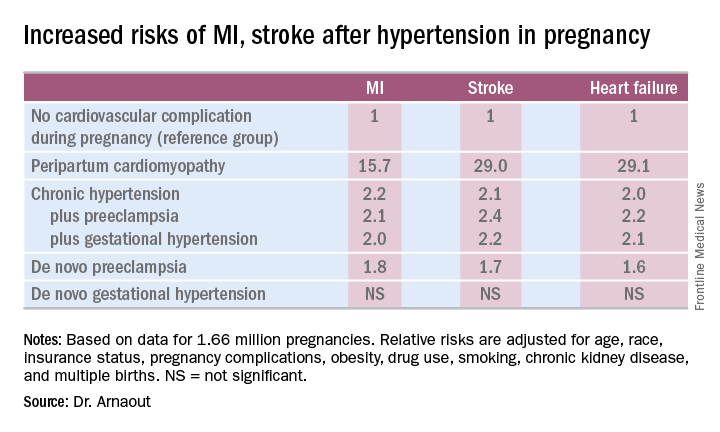
The only form of hypertension in pregnancy that wasn’t associated with a subsequent significantly increased risk of cardiovascular events was de novo gestational hypertension.
Audience member David C. Goff Jr., MD, head of the division of cardiovascular sciences at the National Heart, Lung, and Blood Institute in Bethesda, Md., rose to compliment Dr. Arnaout: “Great work and really important.”
He said that her findings are consistent with the notion that pregnancy constitutes a sort of early-life cardiovascular stress test. He said he wondered, however, just how comfortable Dr. Arnaout is in stating that gestational diabetes isn’t associated with increased subsequent cardiovascular risk, given the relatively short follow-up to date in this population of women who still remain several decades away from the age when cardiovascular event rates really start to climb.
“I completely agree with you,” she replied, noting that other investigators utilizing a different registry have reported an increased longer-term risk for women with gestational diabetes.
Dr. Arnaout said she and her coinvestigators plan to continue to follow the women who experienced peripartum cardiomyopathy or hypertension in pregnancy longer term. They’re also in the process of breaking down the data to look at the risks associated with specific subtypes of MI, stroke, and heart failure.
Dr. Arnaout reported having no financial conflicts regarding her study, which was supported by the American Heart Association and the Sarnoff Cardiovascular Research Foundation.
NEW ORLEANS – Women who experience peripartum cardiomyopathy or any of a variety of hypertensive disorders in pregnancy are at sharply increased risk of acute MI, stroke, or new-onset heart failure beginning within just a few years, Rima Arnaout, MD, reported at the American Heart Association scientific sessions.
“Our study supports the idea that women who have cardiovascular complications in pregnancy really need to be monitored closely for potential primary prevention of cardiovascular events,” said Dr. Arnaout of the University of California, San Francisco.
At a session devoted to “big data” studies in cardiovascular medicine, she presented one of the biggest: a retrospective cohort study of 1.66 million pregnancies during 2005-2009 in California women without any history of congenital or valvular heart disease or prepregnancy cardiovascular events. The California database was created as part of the U.S. Agency for Healthcare Research and Quality’s comprehensive Healthcare Cost and Utilization Project, which included more than 95% of the state’s hospitals. Women who experienced an MI or a stroke, or who were diagnosed with heart failure, during a median of 2.7 years and a maximum of 6 years of follow-up post pregnancy were identified via ICD-9 codes.
There were 111,202 cases of various forms of hypertension in pregnancy, for a 6.9% incidence. Peripartum cardiomyopathy was diagnosed in 562 women, for a rate of 3.5 cases per 10,000 pregnancies.
Indeed, in a multivariate Cox proportional hazards analysis adjusted for numerous potential confounders, peripartum cardiomyopathy was associated with a 16-fold increased risk of acute MI during the relatively short follow-up period, as well as 29-fold increased risks of stroke and heart failure, compared with women with no cardiovascular issues during their pregnancy.
Chronic hypertension, regardless of whether it occurred alone or in combination with preeclampsia or gestational hypertension, was associated with roughly a twofold increased risk of each of the three study outcomes, compared with women who didn’t experience a cardiovascular complication during pregnancy. De novo preeclampsia was also associated with roughly a twofold increased risk of later MI, heart failure, or stroke.
The only form of hypertension in pregnancy that wasn’t associated with a subsequent significantly increased risk of cardiovascular events was de novo gestational hypertension.
Audience member David C. Goff Jr., MD, head of the division of cardiovascular sciences at the National Heart, Lung, and Blood Institute in Bethesda, Md., rose to compliment Dr. Arnaout: “Great work and really important.”
He said that her findings are consistent with the notion that pregnancy constitutes a sort of early-life cardiovascular stress test. He said he wondered, however, just how comfortable Dr. Arnaout is in stating that gestational diabetes isn’t associated with increased subsequent cardiovascular risk, given the relatively short follow-up to date in this population of women who still remain several decades away from the age when cardiovascular event rates really start to climb.
“I completely agree with you,” she replied, noting that other investigators utilizing a different registry have reported an increased longer-term risk for women with gestational diabetes.
Dr. Arnaout said she and her coinvestigators plan to continue to follow the women who experienced peripartum cardiomyopathy or hypertension in pregnancy longer term. They’re also in the process of breaking down the data to look at the risks associated with specific subtypes of MI, stroke, and heart failure.
Dr. Arnaout reported having no financial conflicts regarding her study, which was supported by the American Heart Association and the Sarnoff Cardiovascular Research Foundation.
NEW ORLEANS – Women who experience peripartum cardiomyopathy or any of a variety of hypertensive disorders in pregnancy are at sharply increased risk of acute MI, stroke, or new-onset heart failure beginning within just a few years, Rima Arnaout, MD, reported at the American Heart Association scientific sessions.
“Our study supports the idea that women who have cardiovascular complications in pregnancy really need to be monitored closely for potential primary prevention of cardiovascular events,” said Dr. Arnaout of the University of California, San Francisco.
At a session devoted to “big data” studies in cardiovascular medicine, she presented one of the biggest: a retrospective cohort study of 1.66 million pregnancies during 2005-2009 in California women without any history of congenital or valvular heart disease or prepregnancy cardiovascular events. The California database was created as part of the U.S. Agency for Healthcare Research and Quality’s comprehensive Healthcare Cost and Utilization Project, which included more than 95% of the state’s hospitals. Women who experienced an MI or a stroke, or who were diagnosed with heart failure, during a median of 2.7 years and a maximum of 6 years of follow-up post pregnancy were identified via ICD-9 codes.
There were 111,202 cases of various forms of hypertension in pregnancy, for a 6.9% incidence. Peripartum cardiomyopathy was diagnosed in 562 women, for a rate of 3.5 cases per 10,000 pregnancies.
Indeed, in a multivariate Cox proportional hazards analysis adjusted for numerous potential confounders, peripartum cardiomyopathy was associated with a 16-fold increased risk of acute MI during the relatively short follow-up period, as well as 29-fold increased risks of stroke and heart failure, compared with women with no cardiovascular issues during their pregnancy.
Chronic hypertension, regardless of whether it occurred alone or in combination with preeclampsia or gestational hypertension, was associated with roughly a twofold increased risk of each of the three study outcomes, compared with women who didn’t experience a cardiovascular complication during pregnancy. De novo preeclampsia was also associated with roughly a twofold increased risk of later MI, heart failure, or stroke.
The only form of hypertension in pregnancy that wasn’t associated with a subsequent significantly increased risk of cardiovascular events was de novo gestational hypertension.
Audience member David C. Goff Jr., MD, head of the division of cardiovascular sciences at the National Heart, Lung, and Blood Institute in Bethesda, Md., rose to compliment Dr. Arnaout: “Great work and really important.”
He said that her findings are consistent with the notion that pregnancy constitutes a sort of early-life cardiovascular stress test. He said he wondered, however, just how comfortable Dr. Arnaout is in stating that gestational diabetes isn’t associated with increased subsequent cardiovascular risk, given the relatively short follow-up to date in this population of women who still remain several decades away from the age when cardiovascular event rates really start to climb.
“I completely agree with you,” she replied, noting that other investigators utilizing a different registry have reported an increased longer-term risk for women with gestational diabetes.
Dr. Arnaout said she and her coinvestigators plan to continue to follow the women who experienced peripartum cardiomyopathy or hypertension in pregnancy longer term. They’re also in the process of breaking down the data to look at the risks associated with specific subtypes of MI, stroke, and heart failure.
Dr. Arnaout reported having no financial conflicts regarding her study, which was supported by the American Heart Association and the Sarnoff Cardiovascular Research Foundation.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: California women who developed peripartum cardiomyopathy were at 16- to 29-fold increased risk of experiencing an acute MI, stroke, or heart failure during a median 2.7 years of follow-up.
Data source: A retrospective cohort study of more than 95% of pregnancies in California during 2005-2009.
Disclosures: The presenter reported having no financial conflicts regarding her study, which was supported by the American Heart Association and the Sarnoff Cardiovascular Research Foundation.
Which maternal beta-blockers boost SGA risk?
NEW ORLEANS – The use of labetalol or atenolol in pregnancy is associated with significantly increased risk of having a small-for-gestational-age (SGA) baby; metoprolol and propranolol are not.
And none of these four beta-blockers are associated with increased risk of congenital cardiac anomalies, Angie Ng, MD, reported at the American Heart Association scientific sessions.

Overall, the average birth weight for babies whose mothers were on a beta-blocker was 2,996 g, significantly less than the 3,353 g in 374,391 controls who weren’t exposed to beta-blockers during pregnancy. But beta-blockers are not a monolithic class of drugs; their pharmacokinetics and physical properties differ. And so did their associated incidence of SGA, according to Dr. Ng of Kaiser Permanente Los Angeles.
The rate of SGA below the 10th percentile was 17.6% in the 3,357 women on labetalol during pregnancy and the same in the 638 women on atenolol. In contrast, the SGA rates in women on metoprolol or propranolol – 10.8% and 10.3%, respectively – weren’t significantly different from the 8.7% incidence in controls.
To deal with the possibility of confounding by indication, Dr. Ng and her coinvestigators performed a multivariate analysis adjusted for maternal age, white race, body mass index, gestational age, diabetes, hypertension, arrhythmias, dyslipidemia, and renal insufficiency. The resultant adjusted risk of having an SGA baby was 2.9-fold greater in women on labetalol and 2.4-fold greater in those on atenolol than in controls. Women on the other two beta-blockers faced no increased risk.
The incidence of congenital cardiac anomalies was 5.1% in women exposed to beta-blockers in pregnancy and 1.9% in controls who weren’t. The most commonly diagnosed anomalies – patent ductus arteriosus, atrial septal defect, and ventricular septal defect – were two- to threefold more frequent in the setting of maternal beta-blocker exposure. However, in a multivariate analysis the use of any beta-blocker was no longer associated with significantly elevated risk of congenital cardiac anomalies.
“This suggests that the initial association we see in the unadjusted analysis is likely due to confounders and not due to the beta-blocker exposure,” Dr. Ng said.
Labetalol and atenolol were prescribed during pregnancy most often for hypertension, while metoprolol and propranolol were typically prescribed to control arrhythmias.
Previous reports by other investigators have yielded conflicting results as to whether maternal beta-blocker therapy is associated with increased risk of SGA. A major limitation of those studies was that they examined beta-blockers as a class rather than assessing the impact of specific agents, according to Dr. Ng.
She reported having no financial conflicts of interest regarding her study, which was conducted free of commercial support.
NEW ORLEANS – The use of labetalol or atenolol in pregnancy is associated with significantly increased risk of having a small-for-gestational-age (SGA) baby; metoprolol and propranolol are not.
And none of these four beta-blockers are associated with increased risk of congenital cardiac anomalies, Angie Ng, MD, reported at the American Heart Association scientific sessions.
Overall, the average birth weight for babies whose mothers were on a beta-blocker was 2,996 g, significantly less than the 3,353 g in 374,391 controls who weren’t exposed to beta-blockers during pregnancy. But beta-blockers are not a monolithic class of drugs; their pharmacokinetics and physical properties differ. And so did their associated incidence of SGA, according to Dr. Ng of Kaiser Permanente Los Angeles.
The rate of SGA below the 10th percentile was 17.6% in the 3,357 women on labetalol during pregnancy and the same in the 638 women on atenolol. In contrast, the SGA rates in women on metoprolol or propranolol – 10.8% and 10.3%, respectively – weren’t significantly different from the 8.7% incidence in controls.
To deal with the possibility of confounding by indication, Dr. Ng and her coinvestigators performed a multivariate analysis adjusted for maternal age, white race, body mass index, gestational age, diabetes, hypertension, arrhythmias, dyslipidemia, and renal insufficiency. The resultant adjusted risk of having an SGA baby was 2.9-fold greater in women on labetalol and 2.4-fold greater in those on atenolol than in controls. Women on the other two beta-blockers faced no increased risk.
The incidence of congenital cardiac anomalies was 5.1% in women exposed to beta-blockers in pregnancy and 1.9% in controls who weren’t. The most commonly diagnosed anomalies – patent ductus arteriosus, atrial septal defect, and ventricular septal defect – were two- to threefold more frequent in the setting of maternal beta-blocker exposure. However, in a multivariate analysis the use of any beta-blocker was no longer associated with significantly elevated risk of congenital cardiac anomalies.
“This suggests that the initial association we see in the unadjusted analysis is likely due to confounders and not due to the beta-blocker exposure,” Dr. Ng said.
Labetalol and atenolol were prescribed during pregnancy most often for hypertension, while metoprolol and propranolol were typically prescribed to control arrhythmias.
Previous reports by other investigators have yielded conflicting results as to whether maternal beta-blocker therapy is associated with increased risk of SGA. A major limitation of those studies was that they examined beta-blockers as a class rather than assessing the impact of specific agents, according to Dr. Ng.
She reported having no financial conflicts of interest regarding her study, which was conducted free of commercial support.
NEW ORLEANS – The use of labetalol or atenolol in pregnancy is associated with significantly increased risk of having a small-for-gestational-age (SGA) baby; metoprolol and propranolol are not.
And none of these four beta-blockers are associated with increased risk of congenital cardiac anomalies, Angie Ng, MD, reported at the American Heart Association scientific sessions.
Overall, the average birth weight for babies whose mothers were on a beta-blocker was 2,996 g, significantly less than the 3,353 g in 374,391 controls who weren’t exposed to beta-blockers during pregnancy. But beta-blockers are not a monolithic class of drugs; their pharmacokinetics and physical properties differ. And so did their associated incidence of SGA, according to Dr. Ng of Kaiser Permanente Los Angeles.
The rate of SGA below the 10th percentile was 17.6% in the 3,357 women on labetalol during pregnancy and the same in the 638 women on atenolol. In contrast, the SGA rates in women on metoprolol or propranolol – 10.8% and 10.3%, respectively – weren’t significantly different from the 8.7% incidence in controls.
To deal with the possibility of confounding by indication, Dr. Ng and her coinvestigators performed a multivariate analysis adjusted for maternal age, white race, body mass index, gestational age, diabetes, hypertension, arrhythmias, dyslipidemia, and renal insufficiency. The resultant adjusted risk of having an SGA baby was 2.9-fold greater in women on labetalol and 2.4-fold greater in those on atenolol than in controls. Women on the other two beta-blockers faced no increased risk.
The incidence of congenital cardiac anomalies was 5.1% in women exposed to beta-blockers in pregnancy and 1.9% in controls who weren’t. The most commonly diagnosed anomalies – patent ductus arteriosus, atrial septal defect, and ventricular septal defect – were two- to threefold more frequent in the setting of maternal beta-blocker exposure. However, in a multivariate analysis the use of any beta-blocker was no longer associated with significantly elevated risk of congenital cardiac anomalies.
“This suggests that the initial association we see in the unadjusted analysis is likely due to confounders and not due to the beta-blocker exposure,” Dr. Ng said.
Labetalol and atenolol were prescribed during pregnancy most often for hypertension, while metoprolol and propranolol were typically prescribed to control arrhythmias.
Previous reports by other investigators have yielded conflicting results as to whether maternal beta-blocker therapy is associated with increased risk of SGA. A major limitation of those studies was that they examined beta-blockers as a class rather than assessing the impact of specific agents, according to Dr. Ng.
She reported having no financial conflicts of interest regarding her study, which was conducted free of commercial support.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Women on labetalol or atenolol during pregnancy had a 17.6% incidence of small-for-gestational-age babies, a rate more than twice that in women not exposed to a beta-blocker during pregnancy.
Data source: This was a retrospective study of fetal outcomes in nearly 380,000 pregnant women, 4,847 of whom were on beta-blocker therapy during their pregnancy.
Disclosures: The presenter reported having no financial conflicts of interest regarding her study, which was conducted free of commercial support.
Bariatric surgery quality improvement project ‘DROPs’ readmissions
NEW ORLEANS – A significant reduction in 30-day all-cause hospital readmissions after sleeve gastrectomy was accomplished through the first-ever joint national quality improvement collaboration between the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery, John M. Morton, MD, reported at Obesity Week 2016.
The quality improvement program, known as DROP, for Decreasing Readmissions through Opportunities Provided, was developed by the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP). It was put to the test in a year-long study conducted in 128 nationally representative U.S. hospitals. The study involved a comparison of the participating hospitals’ 30-day all-cause readmission rates following bariatric surgery in the year prior to vs. the year after launch of the DROP project.

Overall, the 30-day all-cause readmission rate after primary laparoscopic adjustable gastric banding, laparoscopic sleeve gastrectomy, or laparoscopic Roux-en-Y gastric bypass dropped only modestly, from 4.76% to 4.61%, a relative reduction of 3.2%. But that’s not the whole story. Hidden within that modest overall result were major improvements, Dr. Morton said at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Of particular interest was the finding that the readmission rate following laparoscopic sleeve gastrectomy decreased from 4.02% to 3.54%, a 12% reduction. That’s an important finding, because sleeve gastrectomy is now by far the most frequently performed type of bariatric surgery in the United States. Indeed, it accounted for 54% of the estimated 196,000 bariatric surgery procedures performed in the country in 2015. Roux-en-Y gastric bypass was a distant second at 23%, followed by surgical revisions at 13.6%.
Moreover, the impact of the DROP initiative appeared to accelerate over time. The initiative as tested consisted of a comprehensive bundle of numerous components addressing preoperative, in-hospital, and postoperative care, and it took a while for hospitals to implement. The 30-day readmission rate following laparoscopic sleeve gastrectomy actually increased by 9.2% in the first 3 months following launch of the DROP initiative. But the readmission rate then took a U-turn, declining by 13.2% in the second quarter compared to the year-before rate, by 16.9% in the third quarter, and falling by 27.1% in the final 3 months of the study.
Mean length of stay for patients undergoing laparoscopic sleeve gastrectomy fell significantly, from 1.9 days pre-DROP to 1.79 days. The DROP intervention also achieved a significant decrease in length of stay for laparoscopic adjustable gastric banding, from 0.5 to 0.42 days.
The rate of readmission within 24 hours post discharge in laparoscopic sleeve gastrectomy patients decreased significantly by 19% after introduction of the DROP program. The trend was favorable, albeit not statistically significant, for the other two bariatric procedures studied.
Of note, hospitals in the two quartiles with the lowest preintervention 30-day all-cause readmission rates post bariatric surgery, with rates of 1.34% and 3.15%, respectively, didn’t derive any further reduction by participating in the DROP program. They already were performing many of the elements included in the intervention. But hospitals in the third quartile significantly improved their 30-day readmission rate from 4.84% to 4.13%, and those in the fourth quartile improved from 7.31% preintervention to 4.47% under the DROP program.
The program had no impact on postoperative leak rates or other surgical complications. However, patient satisfaction scores improved after introduction of the DROP intervention.
The preoperative components of the DROP readmission prevention bundle included a standardized 5-minute educational video featuring a surgeon, nutritionist, pharmacist, and psychologist or psychiatrist, with advice on key issues related to the upcoming operation. That’s also when the visits with the surgeon and a nutritionist were to be scheduled for within 30 days post surgery, and when the patient received phone numbers for the clinic and on-call surgeon in case questions arose later.
The in-hospital elements of the DROP intervention included provision of a clinical roadmap to guide patient expectations, as well as a nutritional consultation. The postoperative components included a day-after-discharge phone call from a nurse or physician assistant, a letter sent to the referring physician containing a discharge summary and recommendations, and a system to make sure that the scheduled follow-up appointments with the surgeon and nutritionist actually take place.
Since adherence to the various components of the DROP bundle varied from hospital to hospital, it was possible for Dr. Morton and his coinvestigators to determine which elements made the most difference in improving 30-day readmission rates. They found that the key difference makers were the nurse’s phone call on the day following discharge and the postoperative visits with the surgeon and nutritionist within the first several weeks.
Asked whether the study findings mean that hospitals that already have a 30-day all-cause readmission rate in the lower half of the national average don’t need to adopt the DROP program, Dr. Morton replied: “One size does not fit all. Maybe some centers don’t need to do all this.”
Thirty-day all-cause readmissions were selected for the first quality improvement project by the MBSAQIP in part because the Centers for Medicare & Medicaid Services has identified it as a priority area for surgery in general. Also, Dr. Morton was a coinvestigator in a study that found many readmissions after bariatric surgery are tied to preventable causes, including dietary indiscretions resulting in nausea and vomiting or dehydration, medication side effects, and inappropriate patient expectations (J Gastrointest Surg. 2016 Nov;20[11]:1797-1801).
“I think readmissions are a good outcome to study, because they incorporate many different elements of the patient experience, including patient safety and satisfaction. No surgeon wants to have a patient come back to the ER and be readmitted. And finally, there’s the cost,” Dr. Morton observed.
He noted that members of the MBSAQIP developed the DROP project in a highly efficient and cost-effective manner through a series of webinars and conference calls without the need for face-to-face meetings. The group plans to follow the same approach to its future quality improvement programs.
The DROP study was funded without industry support. Dr. Morton reported serving on advisory boards for Allurion and Novo Nordisk.
NEW ORLEANS – A significant reduction in 30-day all-cause hospital readmissions after sleeve gastrectomy was accomplished through the first-ever joint national quality improvement collaboration between the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery, John M. Morton, MD, reported at Obesity Week 2016.
The quality improvement program, known as DROP, for Decreasing Readmissions through Opportunities Provided, was developed by the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP). It was put to the test in a year-long study conducted in 128 nationally representative U.S. hospitals. The study involved a comparison of the participating hospitals’ 30-day all-cause readmission rates following bariatric surgery in the year prior to vs. the year after launch of the DROP project.
Overall, the 30-day all-cause readmission rate after primary laparoscopic adjustable gastric banding, laparoscopic sleeve gastrectomy, or laparoscopic Roux-en-Y gastric bypass dropped only modestly, from 4.76% to 4.61%, a relative reduction of 3.2%. But that’s not the whole story. Hidden within that modest overall result were major improvements, Dr. Morton said at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Of particular interest was the finding that the readmission rate following laparoscopic sleeve gastrectomy decreased from 4.02% to 3.54%, a 12% reduction. That’s an important finding, because sleeve gastrectomy is now by far the most frequently performed type of bariatric surgery in the United States. Indeed, it accounted for 54% of the estimated 196,000 bariatric surgery procedures performed in the country in 2015. Roux-en-Y gastric bypass was a distant second at 23%, followed by surgical revisions at 13.6%.
Moreover, the impact of the DROP initiative appeared to accelerate over time. The initiative as tested consisted of a comprehensive bundle of numerous components addressing preoperative, in-hospital, and postoperative care, and it took a while for hospitals to implement. The 30-day readmission rate following laparoscopic sleeve gastrectomy actually increased by 9.2% in the first 3 months following launch of the DROP initiative. But the readmission rate then took a U-turn, declining by 13.2% in the second quarter compared to the year-before rate, by 16.9% in the third quarter, and falling by 27.1% in the final 3 months of the study.
Mean length of stay for patients undergoing laparoscopic sleeve gastrectomy fell significantly, from 1.9 days pre-DROP to 1.79 days. The DROP intervention also achieved a significant decrease in length of stay for laparoscopic adjustable gastric banding, from 0.5 to 0.42 days.
The rate of readmission within 24 hours post discharge in laparoscopic sleeve gastrectomy patients decreased significantly by 19% after introduction of the DROP program. The trend was favorable, albeit not statistically significant, for the other two bariatric procedures studied.
Of note, hospitals in the two quartiles with the lowest preintervention 30-day all-cause readmission rates post bariatric surgery, with rates of 1.34% and 3.15%, respectively, didn’t derive any further reduction by participating in the DROP program. They already were performing many of the elements included in the intervention. But hospitals in the third quartile significantly improved their 30-day readmission rate from 4.84% to 4.13%, and those in the fourth quartile improved from 7.31% preintervention to 4.47% under the DROP program.
The program had no impact on postoperative leak rates or other surgical complications. However, patient satisfaction scores improved after introduction of the DROP intervention.
The preoperative components of the DROP readmission prevention bundle included a standardized 5-minute educational video featuring a surgeon, nutritionist, pharmacist, and psychologist or psychiatrist, with advice on key issues related to the upcoming operation. That’s also when the visits with the surgeon and a nutritionist were to be scheduled for within 30 days post surgery, and when the patient received phone numbers for the clinic and on-call surgeon in case questions arose later.
The in-hospital elements of the DROP intervention included provision of a clinical roadmap to guide patient expectations, as well as a nutritional consultation. The postoperative components included a day-after-discharge phone call from a nurse or physician assistant, a letter sent to the referring physician containing a discharge summary and recommendations, and a system to make sure that the scheduled follow-up appointments with the surgeon and nutritionist actually take place.
Since adherence to the various components of the DROP bundle varied from hospital to hospital, it was possible for Dr. Morton and his coinvestigators to determine which elements made the most difference in improving 30-day readmission rates. They found that the key difference makers were the nurse’s phone call on the day following discharge and the postoperative visits with the surgeon and nutritionist within the first several weeks.
Asked whether the study findings mean that hospitals that already have a 30-day all-cause readmission rate in the lower half of the national average don’t need to adopt the DROP program, Dr. Morton replied: “One size does not fit all. Maybe some centers don’t need to do all this.”
Thirty-day all-cause readmissions were selected for the first quality improvement project by the MBSAQIP in part because the Centers for Medicare & Medicaid Services has identified it as a priority area for surgery in general. Also, Dr. Morton was a coinvestigator in a study that found many readmissions after bariatric surgery are tied to preventable causes, including dietary indiscretions resulting in nausea and vomiting or dehydration, medication side effects, and inappropriate patient expectations (J Gastrointest Surg. 2016 Nov;20[11]:1797-1801).
“I think readmissions are a good outcome to study, because they incorporate many different elements of the patient experience, including patient safety and satisfaction. No surgeon wants to have a patient come back to the ER and be readmitted. And finally, there’s the cost,” Dr. Morton observed.
He noted that members of the MBSAQIP developed the DROP project in a highly efficient and cost-effective manner through a series of webinars and conference calls without the need for face-to-face meetings. The group plans to follow the same approach to its future quality improvement programs.
The DROP study was funded without industry support. Dr. Morton reported serving on advisory boards for Allurion and Novo Nordisk.
NEW ORLEANS – A significant reduction in 30-day all-cause hospital readmissions after sleeve gastrectomy was accomplished through the first-ever joint national quality improvement collaboration between the American College of Surgeons and the American Society for Metabolic and Bariatric Surgery, John M. Morton, MD, reported at Obesity Week 2016.
The quality improvement program, known as DROP, for Decreasing Readmissions through Opportunities Provided, was developed by the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP). It was put to the test in a year-long study conducted in 128 nationally representative U.S. hospitals. The study involved a comparison of the participating hospitals’ 30-day all-cause readmission rates following bariatric surgery in the year prior to vs. the year after launch of the DROP project.
Overall, the 30-day all-cause readmission rate after primary laparoscopic adjustable gastric banding, laparoscopic sleeve gastrectomy, or laparoscopic Roux-en-Y gastric bypass dropped only modestly, from 4.76% to 4.61%, a relative reduction of 3.2%. But that’s not the whole story. Hidden within that modest overall result were major improvements, Dr. Morton said at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Of particular interest was the finding that the readmission rate following laparoscopic sleeve gastrectomy decreased from 4.02% to 3.54%, a 12% reduction. That’s an important finding, because sleeve gastrectomy is now by far the most frequently performed type of bariatric surgery in the United States. Indeed, it accounted for 54% of the estimated 196,000 bariatric surgery procedures performed in the country in 2015. Roux-en-Y gastric bypass was a distant second at 23%, followed by surgical revisions at 13.6%.
Moreover, the impact of the DROP initiative appeared to accelerate over time. The initiative as tested consisted of a comprehensive bundle of numerous components addressing preoperative, in-hospital, and postoperative care, and it took a while for hospitals to implement. The 30-day readmission rate following laparoscopic sleeve gastrectomy actually increased by 9.2% in the first 3 months following launch of the DROP initiative. But the readmission rate then took a U-turn, declining by 13.2% in the second quarter compared to the year-before rate, by 16.9% in the third quarter, and falling by 27.1% in the final 3 months of the study.
Mean length of stay for patients undergoing laparoscopic sleeve gastrectomy fell significantly, from 1.9 days pre-DROP to 1.79 days. The DROP intervention also achieved a significant decrease in length of stay for laparoscopic adjustable gastric banding, from 0.5 to 0.42 days.
The rate of readmission within 24 hours post discharge in laparoscopic sleeve gastrectomy patients decreased significantly by 19% after introduction of the DROP program. The trend was favorable, albeit not statistically significant, for the other two bariatric procedures studied.
Of note, hospitals in the two quartiles with the lowest preintervention 30-day all-cause readmission rates post bariatric surgery, with rates of 1.34% and 3.15%, respectively, didn’t derive any further reduction by participating in the DROP program. They already were performing many of the elements included in the intervention. But hospitals in the third quartile significantly improved their 30-day readmission rate from 4.84% to 4.13%, and those in the fourth quartile improved from 7.31% preintervention to 4.47% under the DROP program.
The program had no impact on postoperative leak rates or other surgical complications. However, patient satisfaction scores improved after introduction of the DROP intervention.
The preoperative components of the DROP readmission prevention bundle included a standardized 5-minute educational video featuring a surgeon, nutritionist, pharmacist, and psychologist or psychiatrist, with advice on key issues related to the upcoming operation. That’s also when the visits with the surgeon and a nutritionist were to be scheduled for within 30 days post surgery, and when the patient received phone numbers for the clinic and on-call surgeon in case questions arose later.
The in-hospital elements of the DROP intervention included provision of a clinical roadmap to guide patient expectations, as well as a nutritional consultation. The postoperative components included a day-after-discharge phone call from a nurse or physician assistant, a letter sent to the referring physician containing a discharge summary and recommendations, and a system to make sure that the scheduled follow-up appointments with the surgeon and nutritionist actually take place.
Since adherence to the various components of the DROP bundle varied from hospital to hospital, it was possible for Dr. Morton and his coinvestigators to determine which elements made the most difference in improving 30-day readmission rates. They found that the key difference makers were the nurse’s phone call on the day following discharge and the postoperative visits with the surgeon and nutritionist within the first several weeks.
Asked whether the study findings mean that hospitals that already have a 30-day all-cause readmission rate in the lower half of the national average don’t need to adopt the DROP program, Dr. Morton replied: “One size does not fit all. Maybe some centers don’t need to do all this.”
Thirty-day all-cause readmissions were selected for the first quality improvement project by the MBSAQIP in part because the Centers for Medicare & Medicaid Services has identified it as a priority area for surgery in general. Also, Dr. Morton was a coinvestigator in a study that found many readmissions after bariatric surgery are tied to preventable causes, including dietary indiscretions resulting in nausea and vomiting or dehydration, medication side effects, and inappropriate patient expectations (J Gastrointest Surg. 2016 Nov;20[11]:1797-1801).
“I think readmissions are a good outcome to study, because they incorporate many different elements of the patient experience, including patient safety and satisfaction. No surgeon wants to have a patient come back to the ER and be readmitted. And finally, there’s the cost,” Dr. Morton observed.
He noted that members of the MBSAQIP developed the DROP project in a highly efficient and cost-effective manner through a series of webinars and conference calls without the need for face-to-face meetings. The group plans to follow the same approach to its future quality improvement programs.
The DROP study was funded without industry support. Dr. Morton reported serving on advisory boards for Allurion and Novo Nordisk.
Key clinical point:
Major finding: In a large national study, the 30-day all-cause readmission rate after laparoscopic sleeve gastrectomy improved by 12% in the year after introduction of a quality improvement program targeting that outcome.
Data source: The DROP study involved a comparison of 30-day all-cause readmission rates after bariatric surgery at 128 nationally representative hospitals during the year prior to vs. the year following launch of a comprehensive package of quality improvement steps.
Disclosures: The DROP study received no industry funding. Dr. Morton reported serving on advisory boards for Allurion and Novo Nordisk.
Malpractice issues tied to bariatric surgery explored
NEW ORLEANS – The first-ever analysis of medical malpractice closed claims involving bariatric surgeons spotlights key opportunities for improvement for the surgical specialty, Eric J. DeMaria, MD, declared at Obesity Week 2016.
Four of the nation’s largest medical malpractice insurance companies agreed to allow members of an American Society for Metabolic and Bariatric Surgery task force to make site visits to their corporate offices, where the surgeons sat in closed rooms to read and take notes on a total of 175 cases closed during 2010-2015. Those case notes were later shared with the full task force, which sifted through the details in order to identify common causal themes and opportunities for improvement, explained Dr. DeMaria, a bariatric surgeon in Suffolk, Va.

Among the key findings:
• The defense prevailed in 63% of cases. The mean expense for defending a lawsuit was $91,836.
• In the 37% of cases involving monetary awards, the mean figure was $293,500, ranging from $20,000 to $8 million.
• Mortality was involved in 35% of cases. Other notable complications resulting in lawsuits included leak in 18% of cases, bowel obstruction in 10%, bleeding in 5.3%, retained foreign body in 5.3%, and vascular injury from access in 4.4%.
• Preoperative issues such as informed consent and disclosure of information were rare.
• The defendant surgeon was a foreign medical graduate in 27.5% of cases, board certified in 75.9%, and only 43% of the hospitals where the surgery took place were accredited. All those figures are at odds with national norms.
• The panel determined that the cause of the complication was provider-related in 50% of cases, system-related in 29%, and intrinsic to the patient’s disease in 21%.
• In the panel’s view, the complication was preventable by the surgeon in nearly 60% of cases and not preventable by the surgeon in 20%, with the remainder of cases deemed impossible to judge.
• Better preoperative care would have prevented the complication in 20% of cases, in the panel’s view. Better postoperative care would have prevented the complication in 45%.
• Just over 5% of the malpractice claims involved nonstandard malabsorptive operations. “Some of them I’d never heard of before,” according to Dr. DeMaria.
• Care was deemed by the panel to be appropriate in roughly 21% of the malpractice cases and grossly negligent or incompetent in 8%. Twenty-three percent of lawsuits involved preventable error of such magnitude that significant coaching and instruction would be required in order to prevent a recurrence.
Dr. DeMaria observed that this analysis of closed claims suggests that in order to reduce future malpractice claims against bariatric surgeons, it makes sense to focus on a few key areas of practice where most of the serious problems occur.
“We found the same themes repeated over and over; for example, delays in diagnosis and treatment of leaks,” he said.
A substantial number of the lawsuits could have been prevented through the use of preinsufflation and optical trocars, or access away from the midline, he added.
But the number one theme to emerge from the lawsuit analysis was poor communication with the health care team and/or family. The experts on the task force considered the communication performance to be appropriate in only 20% of cases.
“I would emphasize the strong contribution of communication issues, and the strong contribution of coverage and handoff issues,” Dr. DeMaria said. “One example of an intervention that might be introduced would be to standardize the language used in the operating room just before you start to staple the stomach, very similar to what airplane pilots do in their communication. We saw cases over and over again where the anesthesia person was asked to take out the [nasogastric] tube didn’t realize that meant the esophageal stethoscope, too.
“We need to do a better job of not just making sure a coverage person has been identified, but actually communicating with that person and doing a standardized handoff procedure,” Dr. DeMaria continued. “Management of postoperative phone calls is another important area: Who answers the phone? What are they supposed to do with that information? How do you get patients to appropriate care?”
Discussant Ramsey M. Dallal, MD, congratulated Dr. DeMaria and his fellow ASMBS task force members on “the massive amount of work” entailed in this project. And he urged his colleagues to take to heart the lessons learned.
“People hear the word ‘malpractice’ and they get fearful. They think of lawyers and of being attacked. The reality is this is not a malpractice study; this is a patient safety study. A study like this is an excellent way to improve patient safety. The problem with registry data is we don’t get the details – and it’s the case details that point out problems and potential solutions,” said Dr. Dallal, director of bariatrics and vice chair of the department of surgery at the Einstein Healthcare Network in the Philadelphia area.
The closed claims analysis was conducted free of commercial support. Dr. DeMaria reported serving as a consultant to Covidien and Ethicon.
NEW ORLEANS – The first-ever analysis of medical malpractice closed claims involving bariatric surgeons spotlights key opportunities for improvement for the surgical specialty, Eric J. DeMaria, MD, declared at Obesity Week 2016.
Four of the nation’s largest medical malpractice insurance companies agreed to allow members of an American Society for Metabolic and Bariatric Surgery task force to make site visits to their corporate offices, where the surgeons sat in closed rooms to read and take notes on a total of 175 cases closed during 2010-2015. Those case notes were later shared with the full task force, which sifted through the details in order to identify common causal themes and opportunities for improvement, explained Dr. DeMaria, a bariatric surgeon in Suffolk, Va.
Among the key findings:
• The defense prevailed in 63% of cases. The mean expense for defending a lawsuit was $91,836.
• In the 37% of cases involving monetary awards, the mean figure was $293,500, ranging from $20,000 to $8 million.
• Mortality was involved in 35% of cases. Other notable complications resulting in lawsuits included leak in 18% of cases, bowel obstruction in 10%, bleeding in 5.3%, retained foreign body in 5.3%, and vascular injury from access in 4.4%.
• Preoperative issues such as informed consent and disclosure of information were rare.
• The defendant surgeon was a foreign medical graduate in 27.5% of cases, board certified in 75.9%, and only 43% of the hospitals where the surgery took place were accredited. All those figures are at odds with national norms.
• The panel determined that the cause of the complication was provider-related in 50% of cases, system-related in 29%, and intrinsic to the patient’s disease in 21%.
• In the panel’s view, the complication was preventable by the surgeon in nearly 60% of cases and not preventable by the surgeon in 20%, with the remainder of cases deemed impossible to judge.
• Better preoperative care would have prevented the complication in 20% of cases, in the panel’s view. Better postoperative care would have prevented the complication in 45%.
• Just over 5% of the malpractice claims involved nonstandard malabsorptive operations. “Some of them I’d never heard of before,” according to Dr. DeMaria.
• Care was deemed by the panel to be appropriate in roughly 21% of the malpractice cases and grossly negligent or incompetent in 8%. Twenty-three percent of lawsuits involved preventable error of such magnitude that significant coaching and instruction would be required in order to prevent a recurrence.
Dr. DeMaria observed that this analysis of closed claims suggests that in order to reduce future malpractice claims against bariatric surgeons, it makes sense to focus on a few key areas of practice where most of the serious problems occur.
“We found the same themes repeated over and over; for example, delays in diagnosis and treatment of leaks,” he said.
A substantial number of the lawsuits could have been prevented through the use of preinsufflation and optical trocars, or access away from the midline, he added.
But the number one theme to emerge from the lawsuit analysis was poor communication with the health care team and/or family. The experts on the task force considered the communication performance to be appropriate in only 20% of cases.
“I would emphasize the strong contribution of communication issues, and the strong contribution of coverage and handoff issues,” Dr. DeMaria said. “One example of an intervention that might be introduced would be to standardize the language used in the operating room just before you start to staple the stomach, very similar to what airplane pilots do in their communication. We saw cases over and over again where the anesthesia person was asked to take out the [nasogastric] tube didn’t realize that meant the esophageal stethoscope, too.
“We need to do a better job of not just making sure a coverage person has been identified, but actually communicating with that person and doing a standardized handoff procedure,” Dr. DeMaria continued. “Management of postoperative phone calls is another important area: Who answers the phone? What are they supposed to do with that information? How do you get patients to appropriate care?”
Discussant Ramsey M. Dallal, MD, congratulated Dr. DeMaria and his fellow ASMBS task force members on “the massive amount of work” entailed in this project. And he urged his colleagues to take to heart the lessons learned.
“People hear the word ‘malpractice’ and they get fearful. They think of lawyers and of being attacked. The reality is this is not a malpractice study; this is a patient safety study. A study like this is an excellent way to improve patient safety. The problem with registry data is we don’t get the details – and it’s the case details that point out problems and potential solutions,” said Dr. Dallal, director of bariatrics and vice chair of the department of surgery at the Einstein Healthcare Network in the Philadelphia area.
The closed claims analysis was conducted free of commercial support. Dr. DeMaria reported serving as a consultant to Covidien and Ethicon.
NEW ORLEANS – The first-ever analysis of medical malpractice closed claims involving bariatric surgeons spotlights key opportunities for improvement for the surgical specialty, Eric J. DeMaria, MD, declared at Obesity Week 2016.
Four of the nation’s largest medical malpractice insurance companies agreed to allow members of an American Society for Metabolic and Bariatric Surgery task force to make site visits to their corporate offices, where the surgeons sat in closed rooms to read and take notes on a total of 175 cases closed during 2010-2015. Those case notes were later shared with the full task force, which sifted through the details in order to identify common causal themes and opportunities for improvement, explained Dr. DeMaria, a bariatric surgeon in Suffolk, Va.
Among the key findings:
• The defense prevailed in 63% of cases. The mean expense for defending a lawsuit was $91,836.
• In the 37% of cases involving monetary awards, the mean figure was $293,500, ranging from $20,000 to $8 million.
• Mortality was involved in 35% of cases. Other notable complications resulting in lawsuits included leak in 18% of cases, bowel obstruction in 10%, bleeding in 5.3%, retained foreign body in 5.3%, and vascular injury from access in 4.4%.
• Preoperative issues such as informed consent and disclosure of information were rare.
• The defendant surgeon was a foreign medical graduate in 27.5% of cases, board certified in 75.9%, and only 43% of the hospitals where the surgery took place were accredited. All those figures are at odds with national norms.
• The panel determined that the cause of the complication was provider-related in 50% of cases, system-related in 29%, and intrinsic to the patient’s disease in 21%.
• In the panel’s view, the complication was preventable by the surgeon in nearly 60% of cases and not preventable by the surgeon in 20%, with the remainder of cases deemed impossible to judge.
• Better preoperative care would have prevented the complication in 20% of cases, in the panel’s view. Better postoperative care would have prevented the complication in 45%.
• Just over 5% of the malpractice claims involved nonstandard malabsorptive operations. “Some of them I’d never heard of before,” according to Dr. DeMaria.
• Care was deemed by the panel to be appropriate in roughly 21% of the malpractice cases and grossly negligent or incompetent in 8%. Twenty-three percent of lawsuits involved preventable error of such magnitude that significant coaching and instruction would be required in order to prevent a recurrence.
Dr. DeMaria observed that this analysis of closed claims suggests that in order to reduce future malpractice claims against bariatric surgeons, it makes sense to focus on a few key areas of practice where most of the serious problems occur.
“We found the same themes repeated over and over; for example, delays in diagnosis and treatment of leaks,” he said.
A substantial number of the lawsuits could have been prevented through the use of preinsufflation and optical trocars, or access away from the midline, he added.
But the number one theme to emerge from the lawsuit analysis was poor communication with the health care team and/or family. The experts on the task force considered the communication performance to be appropriate in only 20% of cases.
“I would emphasize the strong contribution of communication issues, and the strong contribution of coverage and handoff issues,” Dr. DeMaria said. “One example of an intervention that might be introduced would be to standardize the language used in the operating room just before you start to staple the stomach, very similar to what airplane pilots do in their communication. We saw cases over and over again where the anesthesia person was asked to take out the [nasogastric] tube didn’t realize that meant the esophageal stethoscope, too.
“We need to do a better job of not just making sure a coverage person has been identified, but actually communicating with that person and doing a standardized handoff procedure,” Dr. DeMaria continued. “Management of postoperative phone calls is another important area: Who answers the phone? What are they supposed to do with that information? How do you get patients to appropriate care?”
Discussant Ramsey M. Dallal, MD, congratulated Dr. DeMaria and his fellow ASMBS task force members on “the massive amount of work” entailed in this project. And he urged his colleagues to take to heart the lessons learned.
“People hear the word ‘malpractice’ and they get fearful. They think of lawyers and of being attacked. The reality is this is not a malpractice study; this is a patient safety study. A study like this is an excellent way to improve patient safety. The problem with registry data is we don’t get the details – and it’s the case details that point out problems and potential solutions,” said Dr. Dallal, director of bariatrics and vice chair of the department of surgery at the Einstein Healthcare Network in the Philadelphia area.
The closed claims analysis was conducted free of commercial support. Dr. DeMaria reported serving as a consultant to Covidien and Ethicon.
Key clinical point:
Major finding: Communication with the health care team and the patient’s family was deemed appropriate in only 20% of a large series of medical malpractice lawsuits filed against bariatric surgeons.
Data source: This analysis of malpractice insurers’ files on 175 closed malpractice claims against bariatric surgeons was conducted by an American Society for Metabolic and Bariatric Surgery task force.
Disclosures: The study was conducted free of industry support.
Insurance-mandated diet pre–bariatric surgery deemed harmful
NEW ORLEANS – The widespread health insurance industry practice of requiring obese patients to spend months on a physician-supervised strict weight-loss diet prior to approving coverage of bariatric surgery accomplishes nothing constructive, Charles J. Keith Jr., MD, reported at Obesity Week 2016.
“We found that insurance-mandated preoperative diets were associated with a significant delay in treatment, no improvement in postoperative complication rates, and also no improvement in weight loss outcomes. If anything, after adjusting for potential confounding variables, the outcomes were inferior to the group that wasn’t required to diet,” said Dr. Keith of the University of Alabama at Birmingham.

Dr. Keith presented a retrospective review from the prospectively collected Alabama University bariatric surgery database, which included all 284 patients who underwent laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy during 2009-2013. A total of 79% of the patients had private health insurance that required their participation in a preoperative physician-guided diet program, typically for 6 months. The other 21% did not have a mandatory preoperative diet requirement; the great majority of this group were covered under Medicare, which doesn’t require a diet program before bariatric surgery. The two groups weren’t significantly different in initial or immediately preoperative weight or body mass index, obesity-related comorbid conditions, type of bariatric surgery, or socioeconomic status.
The mean time from initial clinic visit to bariatric surgery was significantly shorter in the group with no mandated preoperative diet, at 154 vs. 218 days. In a multivariate analysis adjusted for age, sex, race, operation type, and comorbidities, the no-mandatory-diet group had a significantly greater reduction in BMI 6 months post surgery: a mean loss of 12.2 kg/m2, compared with 10.9 kg/m2 in the group required to participate in a preoperative diet. The difference was even greater at 2 years follow-up: a mean decrease of 14.9 kg/m2 in the no-diet group, vs. 10.7 kg/m2 in the mandatory diet group. The no-diet group experienced a mean 33% weight loss at 2 years, significantly better than the 25% weight loss in the mandatory diet group, Dr. Keith reported at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Audience discussion showed that the insurance-mandated preoperative diet requirement is a hot button issue in the bariatric surgical community.
“I think these insurance programs are specifically designed to delay care,” one surgeon asserted.
Another bariatric surgeon commented that while Dr. Keith’s study will be helpful in advocating for removal of the mandatory preoperative diet requirement, what’s really needed are studies that demonstrate just how often this requirement results in drop out from bariatric programs by patients who’ve grown discouraged by yet-another unsuccessful attempt at nonsurgical weight loss.
Dr. Keith reported having no financial conflicts of interest regarding his study.
NEW ORLEANS – The widespread health insurance industry practice of requiring obese patients to spend months on a physician-supervised strict weight-loss diet prior to approving coverage of bariatric surgery accomplishes nothing constructive, Charles J. Keith Jr., MD, reported at Obesity Week 2016.
“We found that insurance-mandated preoperative diets were associated with a significant delay in treatment, no improvement in postoperative complication rates, and also no improvement in weight loss outcomes. If anything, after adjusting for potential confounding variables, the outcomes were inferior to the group that wasn’t required to diet,” said Dr. Keith of the University of Alabama at Birmingham.
Dr. Keith presented a retrospective review from the prospectively collected Alabama University bariatric surgery database, which included all 284 patients who underwent laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy during 2009-2013. A total of 79% of the patients had private health insurance that required their participation in a preoperative physician-guided diet program, typically for 6 months. The other 21% did not have a mandatory preoperative diet requirement; the great majority of this group were covered under Medicare, which doesn’t require a diet program before bariatric surgery. The two groups weren’t significantly different in initial or immediately preoperative weight or body mass index, obesity-related comorbid conditions, type of bariatric surgery, or socioeconomic status.
The mean time from initial clinic visit to bariatric surgery was significantly shorter in the group with no mandated preoperative diet, at 154 vs. 218 days. In a multivariate analysis adjusted for age, sex, race, operation type, and comorbidities, the no-mandatory-diet group had a significantly greater reduction in BMI 6 months post surgery: a mean loss of 12.2 kg/m2, compared with 10.9 kg/m2 in the group required to participate in a preoperative diet. The difference was even greater at 2 years follow-up: a mean decrease of 14.9 kg/m2 in the no-diet group, vs. 10.7 kg/m2 in the mandatory diet group. The no-diet group experienced a mean 33% weight loss at 2 years, significantly better than the 25% weight loss in the mandatory diet group, Dr. Keith reported at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Audience discussion showed that the insurance-mandated preoperative diet requirement is a hot button issue in the bariatric surgical community.
“I think these insurance programs are specifically designed to delay care,” one surgeon asserted.
Another bariatric surgeon commented that while Dr. Keith’s study will be helpful in advocating for removal of the mandatory preoperative diet requirement, what’s really needed are studies that demonstrate just how often this requirement results in drop out from bariatric programs by patients who’ve grown discouraged by yet-another unsuccessful attempt at nonsurgical weight loss.
Dr. Keith reported having no financial conflicts of interest regarding his study.
NEW ORLEANS – The widespread health insurance industry practice of requiring obese patients to spend months on a physician-supervised strict weight-loss diet prior to approving coverage of bariatric surgery accomplishes nothing constructive, Charles J. Keith Jr., MD, reported at Obesity Week 2016.
“We found that insurance-mandated preoperative diets were associated with a significant delay in treatment, no improvement in postoperative complication rates, and also no improvement in weight loss outcomes. If anything, after adjusting for potential confounding variables, the outcomes were inferior to the group that wasn’t required to diet,” said Dr. Keith of the University of Alabama at Birmingham.
Dr. Keith presented a retrospective review from the prospectively collected Alabama University bariatric surgery database, which included all 284 patients who underwent laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy during 2009-2013. A total of 79% of the patients had private health insurance that required their participation in a preoperative physician-guided diet program, typically for 6 months. The other 21% did not have a mandatory preoperative diet requirement; the great majority of this group were covered under Medicare, which doesn’t require a diet program before bariatric surgery. The two groups weren’t significantly different in initial or immediately preoperative weight or body mass index, obesity-related comorbid conditions, type of bariatric surgery, or socioeconomic status.
The mean time from initial clinic visit to bariatric surgery was significantly shorter in the group with no mandated preoperative diet, at 154 vs. 218 days. In a multivariate analysis adjusted for age, sex, race, operation type, and comorbidities, the no-mandatory-diet group had a significantly greater reduction in BMI 6 months post surgery: a mean loss of 12.2 kg/m2, compared with 10.9 kg/m2 in the group required to participate in a preoperative diet. The difference was even greater at 2 years follow-up: a mean decrease of 14.9 kg/m2 in the no-diet group, vs. 10.7 kg/m2 in the mandatory diet group. The no-diet group experienced a mean 33% weight loss at 2 years, significantly better than the 25% weight loss in the mandatory diet group, Dr. Keith reported at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Audience discussion showed that the insurance-mandated preoperative diet requirement is a hot button issue in the bariatric surgical community.
“I think these insurance programs are specifically designed to delay care,” one surgeon asserted.
Another bariatric surgeon commented that while Dr. Keith’s study will be helpful in advocating for removal of the mandatory preoperative diet requirement, what’s really needed are studies that demonstrate just how often this requirement results in drop out from bariatric programs by patients who’ve grown discouraged by yet-another unsuccessful attempt at nonsurgical weight loss.
Dr. Keith reported having no financial conflicts of interest regarding his study.
Key clinical point:
Major finding: At follow-up 2 years after bariatric surgery, patients who were required by their insurance company to participate in a physician-supervised preoperative diet program had an adjusted mean 25% weight loss, a significantly worse outcome than the mean 33% weight loss among patients with no such requirement.
Data source: This was a retrospective analysis of 284 patients in a prospectively collected university bariatric surgery database.
Disclosures: The study presenter reported having no relevant financial interests.
MDMA – the love drug – makes a therapeutic comeback
VIENNA – What a difference a decade can make in the world of psychiatry.
Take, for example, the case of 3,4-methylenedioxymethamphetamine, better known as MDMA or, when used recreationally, as ecstasy, the love drug.
“Ten years ago at pretty much every scientific meeting where MDMA was being discussed, people were looking to find problems with it. People were dredging around trying to vilify this drug, because there was a hope that it might cause brain damage, which would justify having made its use illicit. Ten years later, we’ve changed direction completely, from fear and hating MDMA to loving it. Now we’re talking about the possibility that MDMA might actually heal the brain, and restoring MDMA to the therapeutic armamentarium,” David Nutt, MD, observed at the annual congress of the European College of Neuropsychopharmacology.
Indeed, the drug’s potential as an adjunct to psychotherapy in patients with posttraumatic stress disorder was the topic of a packed-to-the-gills session in the largest hall at the ECNP Congress, where Dr. Nutt highlighted recent insights into the psychopharmacology of MDMA and other speakers described evidence of the drug’s salutary effects on autobiographical memory and social cognition.
“The biggest problem with MDMA is its name,” quipped Dr. Nutt, professor of neuropsychopharmacology at Imperial College London.
“It used to be called ‘empathy,’ but when it started being used recreationally at raves and in the clubs, the dealers decided to change its name to ‘ecstasy.’ And that created havoc, because there’s nothing that aged editors of newspapers hate more than young people having ecstasy. They hated the term, and so the drug had to go,” according to the psychiatrist.
MDMA’s comeback as a potentially valuable medication in psychiatry can be traced to the first report of the drug’s impressive success when used as an adjunct to psychotherapy in a randomized, placebo-controlled pilot study. Michael C. Mithoefer, MD, a psychiatrist in private practice in South Carolina, and his coinvestigators stunned the psychiatric world by reporting that 10 of 12 patients with chronic PTSD refractory to both medications and psychotherapy showed significant clinical improvement in response to just two sessions of MDMA-assisted psychotherapy supplementing a more conventional course of psychotherapy (J Psychopharmacology. 2011 Apr;25[4]:439-52).
Moreover, the benefits proved durable: In a subsequent paper, the investigators reported the clinical benefit of this two-dose treatment program persisted at a mean 3.8 years of follow-up and no safety concerns had been seen (J Psychopharmacol. 2013 Jan;27[1]:28-39).
This study, which eventually drew the attention of military veterans’ groups with political clout, proved hugely influential, especially since PTSD is so common and often is highly treatment resistant.
“We’re now living in a very strange world where trauma has in some ways become the No. 1 problem facing many societies,” Dr. Nutt observed.
He predicted that with the Food and Drug Administration’s recent approval of clinical trials of MDMA in patients with PTSD, the drug will be licensed for that indication “within the next couple years.”
How MDMA works
The pharmacology of MDMA is complex, he continued. The drug is chiefly a serotonin-releasing agent and 5HT reuptake blocker, but it also acts as an agonist on alpha-adrenergic receptors, has muscarinic and histamine-blocking effects, and promotes release of oxytocin.
Animal studies have demonstrated that MDMA facilitates extinction of fear memories through a mechanism involving changes in levels of brain-derived neurotrophic factor. Experience in humans has shown that the drug has diverse pro-social effects: It is activating, enhances mood, promotes more flexible thinking, boosts tactile experiences, and increases empathy, which in turn aids patients in bonding with their therapists.
Dr. Nutt and his coinvestigators performed the first whole-brain study of the effects of MDMA using functional MRI. This double-blind, placebo-controlled, crossover study in healthy volunteers used measurements obtained through arterial spin labeling and analysis of blood oxygen level–dependent resting state functional connectivity. The investigators documented that the marked increase in positive mood and decreased magnitude of negative personal memories produced by MDMA was accompanied by profound reduction of cerebral blood flow in the right amygdala and hippocampus. Cerebral blood flow also was reduced in the right medial temporal lobe, thalamus, and inferior visual cortex. MDMA also resulted in decreased amygdala-cortical connectivity (Biol Psychiatry. 2015 Oct 15;78[8]:554-62; Int J Neuropsychopharmacol. 2014 Apr;17[4]:527-40).
The changes in those particular brain systems are consistent with and most likely underlie the drug’s therapeutic effects, he said. Taken together, they could serve to assist a patient in re-engaging with traumatic memories with less interference from emotional centers, thereby helping to gain executive control of the memory of the trauma.
H. Valerie Curran, PhD, a coinvestigator in the brain imaging study, cautioned the rapt audience that while there are abundant favorable anecdotal reports from psychotherapists going back as far as the 1970s, the actual evidence base for MDMA as a therapeutic adjunct to psychotherapy for PTSD is still pretty thin. She noted that in their groundbreaking study, Dr. Mithoefer and his colleagues used an unconventional form of psychotherapy modeled on the LSD therapy developed by Stanislav Grof, MD, PhD. The two MDMA-assisted sessions were each 8 hours long and included shamanistic techniques and specialized breathing to promote diminished oxygen to the brain. Also, the patient sat on a futon listening to music with a male therapist on one side and a female therapist on the other. As a clinical psychologist herself, she assured the audience that this is not standard practice in her field.
Only one other randomized, double-blind, placebo-controlled study of MDMA-assisted psychotherapy has been published to date (J Psychopharmacol. 2013 Jan;27[1]:40-52). With just 12 participants, it was too small to be conclusive. So there is a definite need for additional controlled studies on the interaction between MDMA and evidence-based forms of psychotherapy. Fortunately, additional clinical trials are ongoing, noted Dr. Curran, professor of psychopharmacology at University College London.
She presented highlights of a study she and her coinvestigators carried out to determine how MDMA affects the encoding and recall of emotional autobiographical memories, since the core of most psychotherapy for PTSD entails controlled revisiting of traumatic memories. The nonblinded study included a group of recreational MDMA users who – on two separate occasions, one under the influence of street-quality MDMA of uncertain dose and purity, the other on placebo – were tasked with responding to self-threatening scenarios, exposure to compassionate imagery, and a large series of positive and negative adjectives addressed at themselves or another person (J Psychopharmacol. 2015 Sep;29[9]:961-70).
The investigators found that MDMA enhanced the emotional intensity, vividness, and positivity of the subjects’ best autobiographical memories while modestly reducing the negativity of their worst memories. Structured ratings of compassion markedly increased while on MDMA. Overall, the drug’s effects were similar to those obtained through rigorous cognitive training methods developed in venerable Eastern contemplative practices in pursuit of a compassionate mindset, according to Dr. Curran.
The study results suggest a mechanism by which MDMA might enhance psychotherapy not only by improving the therapeutic alliance but also by reducing self-referential emotional processing without diminishing declarative memory, she added.
Findings of Swiss studies
Matthias E. Liechti, MD, head of the psychopharmacology research unit at the University of Basel, explained that at present Switzerland is the only country in the world where it’s legal to prescribe MDMA. Ditto LSD. Psychiatrists can do so on a case-by-case basis outside of a clinical trial setting in patients with treatment-resistant PTSD or anxiety disorders.
Dr. Liechti and his coinvestigators are interested in examining how MDMA affects social cognition as assessed by outcome measures, including a structured face emotion recognition test, the multifaceted empathy test, and a sexual arousal task.

In a series of studies in which they exposed subjects to MDMA, alcohol, methamphetamine, or LSD, they have established that both MDMA and LSD produce empathogenic effects that are possibly serotonin mediated. On a visual analog scale, subjects on those drugs gave high marks for feeling happy, open, trusting, and extroverted, and having a sense of well-being. MDMA impaired recognition of fearful, angry, and sad faces.
In contrast, methamphetamine, a pure stimulant that activates the norepinephrine/dopamine system, produced no empathogenic effects, but it enhanced recognition of sad or fearful faces. Alcohol slightly increased self-ratings for trust, happiness, and openness.
Methamphetamine increased ratings of sexual arousal in response to explicit sexual stimuli, while MDMA had no effect on sexual arousal.
MDMA and LSD increased oxytocin, prolactin, and cortisol levels consistent with their serotonergic effects. Methylphenidate did not, Dr. Liechti said.
A neuroscientist in the audience raised a possible safety concern regarding MDMA: If the drug has an agonist effect on serotonin receptors, couldn’t it have cardiac side effects similar to those of fenfluramine, a drug now banned because it stimulated the abundant 5HT-2b receptors present in the heart, resulting in increased risk of pulmonary hypertension and other adverse cardiovascular effects?
Dr. Nutt replied that there are multitudes of serotonin receptor subtypes, and it’s not yet known whether MDMA acts upon the 5HT-2b receptor. In any case, it shouldn’t be an issue for the drug’s medicinal use.
“Luckily, the effects of MDMA wear off quickly, and when it’s used with psychotherapy we may be giving only one or two doses in a lifetime, so it shouldn’t be a concern,” he said.
Dr. Nutt reported that the functional MRI brain imaging study was funded by a British television station and a private foundation.
“The reason for that is we’ve found it impossible to get any money from any traditional government funders to study drugs like MDMA unless you write grants to show they’re harmful,” he asserted.
Dr. Curran reported having no financial conflicts of interest regarding her studies. Dr. Liechti’s work is supported by the Swiss National Science Foundation.
VIENNA – What a difference a decade can make in the world of psychiatry.
Take, for example, the case of 3,4-methylenedioxymethamphetamine, better known as MDMA or, when used recreationally, as ecstasy, the love drug.
“Ten years ago at pretty much every scientific meeting where MDMA was being discussed, people were looking to find problems with it. People were dredging around trying to vilify this drug, because there was a hope that it might cause brain damage, which would justify having made its use illicit. Ten years later, we’ve changed direction completely, from fear and hating MDMA to loving it. Now we’re talking about the possibility that MDMA might actually heal the brain, and restoring MDMA to the therapeutic armamentarium,” David Nutt, MD, observed at the annual congress of the European College of Neuropsychopharmacology.
Indeed, the drug’s potential as an adjunct to psychotherapy in patients with posttraumatic stress disorder was the topic of a packed-to-the-gills session in the largest hall at the ECNP Congress, where Dr. Nutt highlighted recent insights into the psychopharmacology of MDMA and other speakers described evidence of the drug’s salutary effects on autobiographical memory and social cognition.
“The biggest problem with MDMA is its name,” quipped Dr. Nutt, professor of neuropsychopharmacology at Imperial College London.
“It used to be called ‘empathy,’ but when it started being used recreationally at raves and in the clubs, the dealers decided to change its name to ‘ecstasy.’ And that created havoc, because there’s nothing that aged editors of newspapers hate more than young people having ecstasy. They hated the term, and so the drug had to go,” according to the psychiatrist.
MDMA’s comeback as a potentially valuable medication in psychiatry can be traced to the first report of the drug’s impressive success when used as an adjunct to psychotherapy in a randomized, placebo-controlled pilot study. Michael C. Mithoefer, MD, a psychiatrist in private practice in South Carolina, and his coinvestigators stunned the psychiatric world by reporting that 10 of 12 patients with chronic PTSD refractory to both medications and psychotherapy showed significant clinical improvement in response to just two sessions of MDMA-assisted psychotherapy supplementing a more conventional course of psychotherapy (J Psychopharmacology. 2011 Apr;25[4]:439-52).
Moreover, the benefits proved durable: In a subsequent paper, the investigators reported the clinical benefit of this two-dose treatment program persisted at a mean 3.8 years of follow-up and no safety concerns had been seen (J Psychopharmacol. 2013 Jan;27[1]:28-39).
This study, which eventually drew the attention of military veterans’ groups with political clout, proved hugely influential, especially since PTSD is so common and often is highly treatment resistant.
“We’re now living in a very strange world where trauma has in some ways become the No. 1 problem facing many societies,” Dr. Nutt observed.
He predicted that with the Food and Drug Administration’s recent approval of clinical trials of MDMA in patients with PTSD, the drug will be licensed for that indication “within the next couple years.”
How MDMA works
The pharmacology of MDMA is complex, he continued. The drug is chiefly a serotonin-releasing agent and 5HT reuptake blocker, but it also acts as an agonist on alpha-adrenergic receptors, has muscarinic and histamine-blocking effects, and promotes release of oxytocin.
Animal studies have demonstrated that MDMA facilitates extinction of fear memories through a mechanism involving changes in levels of brain-derived neurotrophic factor. Experience in humans has shown that the drug has diverse pro-social effects: It is activating, enhances mood, promotes more flexible thinking, boosts tactile experiences, and increases empathy, which in turn aids patients in bonding with their therapists.
Dr. Nutt and his coinvestigators performed the first whole-brain study of the effects of MDMA using functional MRI. This double-blind, placebo-controlled, crossover study in healthy volunteers used measurements obtained through arterial spin labeling and analysis of blood oxygen level–dependent resting state functional connectivity. The investigators documented that the marked increase in positive mood and decreased magnitude of negative personal memories produced by MDMA was accompanied by profound reduction of cerebral blood flow in the right amygdala and hippocampus. Cerebral blood flow also was reduced in the right medial temporal lobe, thalamus, and inferior visual cortex. MDMA also resulted in decreased amygdala-cortical connectivity (Biol Psychiatry. 2015 Oct 15;78[8]:554-62; Int J Neuropsychopharmacol. 2014 Apr;17[4]:527-40).
The changes in those particular brain systems are consistent with and most likely underlie the drug’s therapeutic effects, he said. Taken together, they could serve to assist a patient in re-engaging with traumatic memories with less interference from emotional centers, thereby helping to gain executive control of the memory of the trauma.
H. Valerie Curran, PhD, a coinvestigator in the brain imaging study, cautioned the rapt audience that while there are abundant favorable anecdotal reports from psychotherapists going back as far as the 1970s, the actual evidence base for MDMA as a therapeutic adjunct to psychotherapy for PTSD is still pretty thin. She noted that in their groundbreaking study, Dr. Mithoefer and his colleagues used an unconventional form of psychotherapy modeled on the LSD therapy developed by Stanislav Grof, MD, PhD. The two MDMA-assisted sessions were each 8 hours long and included shamanistic techniques and specialized breathing to promote diminished oxygen to the brain. Also, the patient sat on a futon listening to music with a male therapist on one side and a female therapist on the other. As a clinical psychologist herself, she assured the audience that this is not standard practice in her field.
Only one other randomized, double-blind, placebo-controlled study of MDMA-assisted psychotherapy has been published to date (J Psychopharmacol. 2013 Jan;27[1]:40-52). With just 12 participants, it was too small to be conclusive. So there is a definite need for additional controlled studies on the interaction between MDMA and evidence-based forms of psychotherapy. Fortunately, additional clinical trials are ongoing, noted Dr. Curran, professor of psychopharmacology at University College London.
She presented highlights of a study she and her coinvestigators carried out to determine how MDMA affects the encoding and recall of emotional autobiographical memories, since the core of most psychotherapy for PTSD entails controlled revisiting of traumatic memories. The nonblinded study included a group of recreational MDMA users who – on two separate occasions, one under the influence of street-quality MDMA of uncertain dose and purity, the other on placebo – were tasked with responding to self-threatening scenarios, exposure to compassionate imagery, and a large series of positive and negative adjectives addressed at themselves or another person (J Psychopharmacol. 2015 Sep;29[9]:961-70).
The investigators found that MDMA enhanced the emotional intensity, vividness, and positivity of the subjects’ best autobiographical memories while modestly reducing the negativity of their worst memories. Structured ratings of compassion markedly increased while on MDMA. Overall, the drug’s effects were similar to those obtained through rigorous cognitive training methods developed in venerable Eastern contemplative practices in pursuit of a compassionate mindset, according to Dr. Curran.
The study results suggest a mechanism by which MDMA might enhance psychotherapy not only by improving the therapeutic alliance but also by reducing self-referential emotional processing without diminishing declarative memory, she added.
Findings of Swiss studies
Matthias E. Liechti, MD, head of the psychopharmacology research unit at the University of Basel, explained that at present Switzerland is the only country in the world where it’s legal to prescribe MDMA. Ditto LSD. Psychiatrists can do so on a case-by-case basis outside of a clinical trial setting in patients with treatment-resistant PTSD or anxiety disorders.
Dr. Liechti and his coinvestigators are interested in examining how MDMA affects social cognition as assessed by outcome measures, including a structured face emotion recognition test, the multifaceted empathy test, and a sexual arousal task.
In a series of studies in which they exposed subjects to MDMA, alcohol, methamphetamine, or LSD, they have established that both MDMA and LSD produce empathogenic effects that are possibly serotonin mediated. On a visual analog scale, subjects on those drugs gave high marks for feeling happy, open, trusting, and extroverted, and having a sense of well-being. MDMA impaired recognition of fearful, angry, and sad faces.
In contrast, methamphetamine, a pure stimulant that activates the norepinephrine/dopamine system, produced no empathogenic effects, but it enhanced recognition of sad or fearful faces. Alcohol slightly increased self-ratings for trust, happiness, and openness.
Methamphetamine increased ratings of sexual arousal in response to explicit sexual stimuli, while MDMA had no effect on sexual arousal.
MDMA and LSD increased oxytocin, prolactin, and cortisol levels consistent with their serotonergic effects. Methylphenidate did not, Dr. Liechti said.
A neuroscientist in the audience raised a possible safety concern regarding MDMA: If the drug has an agonist effect on serotonin receptors, couldn’t it have cardiac side effects similar to those of fenfluramine, a drug now banned because it stimulated the abundant 5HT-2b receptors present in the heart, resulting in increased risk of pulmonary hypertension and other adverse cardiovascular effects?
Dr. Nutt replied that there are multitudes of serotonin receptor subtypes, and it’s not yet known whether MDMA acts upon the 5HT-2b receptor. In any case, it shouldn’t be an issue for the drug’s medicinal use.
“Luckily, the effects of MDMA wear off quickly, and when it’s used with psychotherapy we may be giving only one or two doses in a lifetime, so it shouldn’t be a concern,” he said.
Dr. Nutt reported that the functional MRI brain imaging study was funded by a British television station and a private foundation.
“The reason for that is we’ve found it impossible to get any money from any traditional government funders to study drugs like MDMA unless you write grants to show they’re harmful,” he asserted.
Dr. Curran reported having no financial conflicts of interest regarding her studies. Dr. Liechti’s work is supported by the Swiss National Science Foundation.
VIENNA – What a difference a decade can make in the world of psychiatry.
Take, for example, the case of 3,4-methylenedioxymethamphetamine, better known as MDMA or, when used recreationally, as ecstasy, the love drug.
“Ten years ago at pretty much every scientific meeting where MDMA was being discussed, people were looking to find problems with it. People were dredging around trying to vilify this drug, because there was a hope that it might cause brain damage, which would justify having made its use illicit. Ten years later, we’ve changed direction completely, from fear and hating MDMA to loving it. Now we’re talking about the possibility that MDMA might actually heal the brain, and restoring MDMA to the therapeutic armamentarium,” David Nutt, MD, observed at the annual congress of the European College of Neuropsychopharmacology.
Indeed, the drug’s potential as an adjunct to psychotherapy in patients with posttraumatic stress disorder was the topic of a packed-to-the-gills session in the largest hall at the ECNP Congress, where Dr. Nutt highlighted recent insights into the psychopharmacology of MDMA and other speakers described evidence of the drug’s salutary effects on autobiographical memory and social cognition.
“The biggest problem with MDMA is its name,” quipped Dr. Nutt, professor of neuropsychopharmacology at Imperial College London.
“It used to be called ‘empathy,’ but when it started being used recreationally at raves and in the clubs, the dealers decided to change its name to ‘ecstasy.’ And that created havoc, because there’s nothing that aged editors of newspapers hate more than young people having ecstasy. They hated the term, and so the drug had to go,” according to the psychiatrist.
MDMA’s comeback as a potentially valuable medication in psychiatry can be traced to the first report of the drug’s impressive success when used as an adjunct to psychotherapy in a randomized, placebo-controlled pilot study. Michael C. Mithoefer, MD, a psychiatrist in private practice in South Carolina, and his coinvestigators stunned the psychiatric world by reporting that 10 of 12 patients with chronic PTSD refractory to both medications and psychotherapy showed significant clinical improvement in response to just two sessions of MDMA-assisted psychotherapy supplementing a more conventional course of psychotherapy (J Psychopharmacology. 2011 Apr;25[4]:439-52).
Moreover, the benefits proved durable: In a subsequent paper, the investigators reported the clinical benefit of this two-dose treatment program persisted at a mean 3.8 years of follow-up and no safety concerns had been seen (J Psychopharmacol. 2013 Jan;27[1]:28-39).
This study, which eventually drew the attention of military veterans’ groups with political clout, proved hugely influential, especially since PTSD is so common and often is highly treatment resistant.
“We’re now living in a very strange world where trauma has in some ways become the No. 1 problem facing many societies,” Dr. Nutt observed.
He predicted that with the Food and Drug Administration’s recent approval of clinical trials of MDMA in patients with PTSD, the drug will be licensed for that indication “within the next couple years.”
How MDMA works
The pharmacology of MDMA is complex, he continued. The drug is chiefly a serotonin-releasing agent and 5HT reuptake blocker, but it also acts as an agonist on alpha-adrenergic receptors, has muscarinic and histamine-blocking effects, and promotes release of oxytocin.
Animal studies have demonstrated that MDMA facilitates extinction of fear memories through a mechanism involving changes in levels of brain-derived neurotrophic factor. Experience in humans has shown that the drug has diverse pro-social effects: It is activating, enhances mood, promotes more flexible thinking, boosts tactile experiences, and increases empathy, which in turn aids patients in bonding with their therapists.
Dr. Nutt and his coinvestigators performed the first whole-brain study of the effects of MDMA using functional MRI. This double-blind, placebo-controlled, crossover study in healthy volunteers used measurements obtained through arterial spin labeling and analysis of blood oxygen level–dependent resting state functional connectivity. The investigators documented that the marked increase in positive mood and decreased magnitude of negative personal memories produced by MDMA was accompanied by profound reduction of cerebral blood flow in the right amygdala and hippocampus. Cerebral blood flow also was reduced in the right medial temporal lobe, thalamus, and inferior visual cortex. MDMA also resulted in decreased amygdala-cortical connectivity (Biol Psychiatry. 2015 Oct 15;78[8]:554-62; Int J Neuropsychopharmacol. 2014 Apr;17[4]:527-40).
The changes in those particular brain systems are consistent with and most likely underlie the drug’s therapeutic effects, he said. Taken together, they could serve to assist a patient in re-engaging with traumatic memories with less interference from emotional centers, thereby helping to gain executive control of the memory of the trauma.
H. Valerie Curran, PhD, a coinvestigator in the brain imaging study, cautioned the rapt audience that while there are abundant favorable anecdotal reports from psychotherapists going back as far as the 1970s, the actual evidence base for MDMA as a therapeutic adjunct to psychotherapy for PTSD is still pretty thin. She noted that in their groundbreaking study, Dr. Mithoefer and his colleagues used an unconventional form of psychotherapy modeled on the LSD therapy developed by Stanislav Grof, MD, PhD. The two MDMA-assisted sessions were each 8 hours long and included shamanistic techniques and specialized breathing to promote diminished oxygen to the brain. Also, the patient sat on a futon listening to music with a male therapist on one side and a female therapist on the other. As a clinical psychologist herself, she assured the audience that this is not standard practice in her field.
Only one other randomized, double-blind, placebo-controlled study of MDMA-assisted psychotherapy has been published to date (J Psychopharmacol. 2013 Jan;27[1]:40-52). With just 12 participants, it was too small to be conclusive. So there is a definite need for additional controlled studies on the interaction between MDMA and evidence-based forms of psychotherapy. Fortunately, additional clinical trials are ongoing, noted Dr. Curran, professor of psychopharmacology at University College London.
She presented highlights of a study she and her coinvestigators carried out to determine how MDMA affects the encoding and recall of emotional autobiographical memories, since the core of most psychotherapy for PTSD entails controlled revisiting of traumatic memories. The nonblinded study included a group of recreational MDMA users who – on two separate occasions, one under the influence of street-quality MDMA of uncertain dose and purity, the other on placebo – were tasked with responding to self-threatening scenarios, exposure to compassionate imagery, and a large series of positive and negative adjectives addressed at themselves or another person (J Psychopharmacol. 2015 Sep;29[9]:961-70).
The investigators found that MDMA enhanced the emotional intensity, vividness, and positivity of the subjects’ best autobiographical memories while modestly reducing the negativity of their worst memories. Structured ratings of compassion markedly increased while on MDMA. Overall, the drug’s effects were similar to those obtained through rigorous cognitive training methods developed in venerable Eastern contemplative practices in pursuit of a compassionate mindset, according to Dr. Curran.
The study results suggest a mechanism by which MDMA might enhance psychotherapy not only by improving the therapeutic alliance but also by reducing self-referential emotional processing without diminishing declarative memory, she added.
Findings of Swiss studies
Matthias E. Liechti, MD, head of the psychopharmacology research unit at the University of Basel, explained that at present Switzerland is the only country in the world where it’s legal to prescribe MDMA. Ditto LSD. Psychiatrists can do so on a case-by-case basis outside of a clinical trial setting in patients with treatment-resistant PTSD or anxiety disorders.
Dr. Liechti and his coinvestigators are interested in examining how MDMA affects social cognition as assessed by outcome measures, including a structured face emotion recognition test, the multifaceted empathy test, and a sexual arousal task.
In a series of studies in which they exposed subjects to MDMA, alcohol, methamphetamine, or LSD, they have established that both MDMA and LSD produce empathogenic effects that are possibly serotonin mediated. On a visual analog scale, subjects on those drugs gave high marks for feeling happy, open, trusting, and extroverted, and having a sense of well-being. MDMA impaired recognition of fearful, angry, and sad faces.
In contrast, methamphetamine, a pure stimulant that activates the norepinephrine/dopamine system, produced no empathogenic effects, but it enhanced recognition of sad or fearful faces. Alcohol slightly increased self-ratings for trust, happiness, and openness.
Methamphetamine increased ratings of sexual arousal in response to explicit sexual stimuli, while MDMA had no effect on sexual arousal.
MDMA and LSD increased oxytocin, prolactin, and cortisol levels consistent with their serotonergic effects. Methylphenidate did not, Dr. Liechti said.
A neuroscientist in the audience raised a possible safety concern regarding MDMA: If the drug has an agonist effect on serotonin receptors, couldn’t it have cardiac side effects similar to those of fenfluramine, a drug now banned because it stimulated the abundant 5HT-2b receptors present in the heart, resulting in increased risk of pulmonary hypertension and other adverse cardiovascular effects?
Dr. Nutt replied that there are multitudes of serotonin receptor subtypes, and it’s not yet known whether MDMA acts upon the 5HT-2b receptor. In any case, it shouldn’t be an issue for the drug’s medicinal use.
“Luckily, the effects of MDMA wear off quickly, and when it’s used with psychotherapy we may be giving only one or two doses in a lifetime, so it shouldn’t be a concern,” he said.
Dr. Nutt reported that the functional MRI brain imaging study was funded by a British television station and a private foundation.
“The reason for that is we’ve found it impossible to get any money from any traditional government funders to study drugs like MDMA unless you write grants to show they’re harmful,” he asserted.
Dr. Curran reported having no financial conflicts of interest regarding her studies. Dr. Liechti’s work is supported by the Swiss National Science Foundation.
What’s next for deep brain stimulation in OCD?
VIENNA – Even though deep brain stimulation has been used to treat obsessive-compulsive disorder in fewer than 300 patients worldwide, the therapy has had a huge impact on understanding of the disorder, Damiaan Denys, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
Indeed, the efficacy of deep brain stimulation (DBS) in the most severe, treatment-refractory cases of OCD casts doubt upon the fundamental construct clinicians have relied upon for decades to comprehend OCD: Namely, that affected patients first experience obsessions, which induce anxiety, which then stimulates compulsions, and engaging in those compulsions brings relief and reward, and then the whole cycle starts over again.

That construct may not actually be true.
“Deep brain stimulation will force us to rethink OCD,” predicted Dr. Denys, professor and head of psychiatry at the University of Amsterdam.
What does DBS change, and is there a temporal order? It varies, the psychiatrist said.
“In some patients, anxiety is the first thing that changes. In others, it starts with obsessions. Compulsions do decrease, but it’s difficult. It takes some time, and often we need supplemental cognitive-behavioral therapy (CBT). What changes, mainly, in my experience, is not symptoms, but something outside of OCD: namely, mood. Deep brain stimulation has a huge impact on mood. That’s an interesting finding, because it suggests the possibility that you can change a psychiatric disorder by changing symptoms that are thought of as being outside the disorder,” Dr. Denys observed.
“Another interesting thing is that deep brain stimulation changes things that are not even within psychiatry. When we ask our patients what has been the most profound impact deep brain stimulation has had on their lives, all of them say, ‘It increases my self-confidence.’ And that’s not something that is included in our scales. We assess patients using the HAM-D [Hamilton Rating Scale for Depression] and Y-BOCS [Yale-Brown Obsessive Compulsive Scale] and other measures, but there are still some very important aspects we are not taking into account and that have a profound effect on symptoms. In this case, using deep brain stimulation, we improve self-confidence and thereby change a whole chain of symptoms,” he continued.
Among the 60 highly refractory OCD patients treated by DBS by Dr. Denys and his colleagues at the Amsterdam center over the past 15 years, 15% were cured as a result.
“I purposely use the word ‘cured,’ because they don’t have obsessive-compulsive symptoms, anymore, which is, of course, extraordinary,” Dr. Denys noted.
An additional 35% of patients had a good response, defined as 60%-80% improvement on the Y-BOCS. Ten percent of patients were partial responders, with a 20%-40% improvement on the Y-BOCS. And 15% were nonresponders.
Closed-loop system coming
DBS entails implantation of electrodes deep within the brain to interrupt dysfunctional brain signals in local areas and across neural networks. This dysfunctional brain activity is expressed as symptoms. To date, DBS has been used in what’s called an open-loop system: Patients report the symptoms they’re experiencing and the clinician then adjusts the electrode settings in order to quell those symptoms. This approach is about to change. The technology has improved vastly since the early days, when the electrodes had four contact points. Now they have 64 contact points, and are capable of sending and receiving electrical signals.
“The next step in deep brain stimulation will be a closed-loop system. We will remove the clinician and the patient, and attempt to use a device capable of recording what happens in the brain and then changing electrical activity in response to the recordings. Our purpose will be to block these brain signals in advance of obsessions and compulsions so patients don’t have these symptoms. It’s technically possible. It has been done in Parkinson’s, and I think it’s the next step in psychiatry,” Dr. Denys said.
Indeed, he and his coinvestigators are planning formal studies of closed-loop DBS. For him, the prospect raises three key questions: What are the neural correlates of OCD symptoms? What about the ethics of implanting a device in the brain which by itself results in different life experiences? And will closed-loop DBS have superior efficacy, compared with open-loop DBS?
“How is the mind rooted in the brain, and how is the brain expressed in the mind? It’s the most fascinating question; it’s why we all love psychiatry, and up until now, there are no answers,” he observed.
Significant progress already has been made on the neural correlates question. Dr. Denys and his colleagues have found that when OCD patients with deep brain electrodes engage in cleaning compulsions, their local field potentials in the striatal area show peaks of roughly 9 Hz in the alpha range and in the beta/low gamma range. These patterns may represent compulsive behavior and likely could be useful in steering a closed-loop system. Also, the Dutch investigators have found that 3- to 8-Hz theta oscillations in local field potentials in the striatal area may represent a neural signature for anxiety and/or obsessions.
Using a closed-loop system, he continued, investigators plan to test two quite different hypotheses about the fundamental nature of OCD. One is that obsessions, anxiety, compulsions, and relief are each separately related to different brain areas. The other hypothesis is that one central brain stimulus drives the chain of symptoms that characterize OCD, and that by identifying and blocking that primary signal, the whole pathologic process can be stopped.
Current status of procedure
While Dr. Denys focused on the near future of DBS for OCD, another speaker at the session, Sina Kohl, PhD, addressed DBS for OCD as it exists today, particularly the who, how, and where.
The “who” is the relatively rare patient with truly refractory OCD after multiple drug trials of agents in different antidepressant classes, one of which should be clomipramine, as well as a failed course of CBT provided by an expert in CBT for OCD, of which there are relatively few. In a study led by investigators at Brown University, Providence, R.I., only 2 of 325 patients with OCD were deemed truly refractory (J Neuropsychiatry Clin Neurosci. 2014 Winter;26[1]:81-6). That sounds about right, according to Dr. Kohl, a psychologist at the University of Cologne, in Germany.

The “how” is to deliver DBS in conjunction with CBT. Response rates are higher at centers where that practice is routine, she added.
The “where” is an unsettled question. In Dr. Kohl’s meta-analysis of 25 published DBS studies, electrode placement in four different DBS target structures produced similar results: the nucleus accumbens, the anterior limb of the internal capsule, the ventral striatum, and the subthalamic nucleus. Stimulation of the inferior thalamic peduncle appeared to achieve better results, but this is a sketchy conclusion based upon two studies totaling just six patients (BMC Psychiatry. 2014 Aug 2;14:214. doi: 10.1186/s12888-014-0214-y).
Recently, Belgian investigators have reported particularly promising results – the best so far – for DBS targeting the bed nucleus of the stria terminalis (Mol Psychiatry. 2016 Sep;21[9]:1272-80).
Bilateral DBS appears to be more effective than unilateral.
Dr. Kohl and her colleagues in Cologne recently completed a study of DBS in 20 patients. She noted that it took 5 years to collect these 20 patients, underscoring the high bar that’s appropriate for resort to DBS, even though the therapy is approved for OCD by both the Food and Drug Administration and European regulatory authorities. Forty percent of the patients were DBS responders, with a mean 30% improvement in Y-BOCS scores. That’s a lower responder rate than in Dr. Denys’s and some other series, which Dr. Kohl attributed to the fact that in Germany, postimplantation CBT is not yet routine.
Asked about DBS side effects, the speakers agreed that they’re transient and fall off after initial stimulation parameters are changed.
“The most consistent and impressive side effect is that initially after surgical implantation of the electrodes and stimulation of the nucleus accumbens, patients experience 3 or 4 days of hypomania, which then disappears,” Dr. Denys said. “It causes a kind of imprinting, because even a decade later, patients ask us, ‘Could you bring back that really nice feeling?’ It’s 3 days of love, peace, and hypomania. It’s a side effect, but people like it.”
Dr. Denys and Dr. Kohl reported no financial conflicts of interest regarding their presentations.
VIENNA – Even though deep brain stimulation has been used to treat obsessive-compulsive disorder in fewer than 300 patients worldwide, the therapy has had a huge impact on understanding of the disorder, Damiaan Denys, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
Indeed, the efficacy of deep brain stimulation (DBS) in the most severe, treatment-refractory cases of OCD casts doubt upon the fundamental construct clinicians have relied upon for decades to comprehend OCD: Namely, that affected patients first experience obsessions, which induce anxiety, which then stimulates compulsions, and engaging in those compulsions brings relief and reward, and then the whole cycle starts over again.
That construct may not actually be true.
“Deep brain stimulation will force us to rethink OCD,” predicted Dr. Denys, professor and head of psychiatry at the University of Amsterdam.
What does DBS change, and is there a temporal order? It varies, the psychiatrist said.
“In some patients, anxiety is the first thing that changes. In others, it starts with obsessions. Compulsions do decrease, but it’s difficult. It takes some time, and often we need supplemental cognitive-behavioral therapy (CBT). What changes, mainly, in my experience, is not symptoms, but something outside of OCD: namely, mood. Deep brain stimulation has a huge impact on mood. That’s an interesting finding, because it suggests the possibility that you can change a psychiatric disorder by changing symptoms that are thought of as being outside the disorder,” Dr. Denys observed.
“Another interesting thing is that deep brain stimulation changes things that are not even within psychiatry. When we ask our patients what has been the most profound impact deep brain stimulation has had on their lives, all of them say, ‘It increases my self-confidence.’ And that’s not something that is included in our scales. We assess patients using the HAM-D [Hamilton Rating Scale for Depression] and Y-BOCS [Yale-Brown Obsessive Compulsive Scale] and other measures, but there are still some very important aspects we are not taking into account and that have a profound effect on symptoms. In this case, using deep brain stimulation, we improve self-confidence and thereby change a whole chain of symptoms,” he continued.
Among the 60 highly refractory OCD patients treated by DBS by Dr. Denys and his colleagues at the Amsterdam center over the past 15 years, 15% were cured as a result.
“I purposely use the word ‘cured,’ because they don’t have obsessive-compulsive symptoms, anymore, which is, of course, extraordinary,” Dr. Denys noted.
An additional 35% of patients had a good response, defined as 60%-80% improvement on the Y-BOCS. Ten percent of patients were partial responders, with a 20%-40% improvement on the Y-BOCS. And 15% were nonresponders.
Closed-loop system coming
DBS entails implantation of electrodes deep within the brain to interrupt dysfunctional brain signals in local areas and across neural networks. This dysfunctional brain activity is expressed as symptoms. To date, DBS has been used in what’s called an open-loop system: Patients report the symptoms they’re experiencing and the clinician then adjusts the electrode settings in order to quell those symptoms. This approach is about to change. The technology has improved vastly since the early days, when the electrodes had four contact points. Now they have 64 contact points, and are capable of sending and receiving electrical signals.
“The next step in deep brain stimulation will be a closed-loop system. We will remove the clinician and the patient, and attempt to use a device capable of recording what happens in the brain and then changing electrical activity in response to the recordings. Our purpose will be to block these brain signals in advance of obsessions and compulsions so patients don’t have these symptoms. It’s technically possible. It has been done in Parkinson’s, and I think it’s the next step in psychiatry,” Dr. Denys said.
Indeed, he and his coinvestigators are planning formal studies of closed-loop DBS. For him, the prospect raises three key questions: What are the neural correlates of OCD symptoms? What about the ethics of implanting a device in the brain which by itself results in different life experiences? And will closed-loop DBS have superior efficacy, compared with open-loop DBS?
“How is the mind rooted in the brain, and how is the brain expressed in the mind? It’s the most fascinating question; it’s why we all love psychiatry, and up until now, there are no answers,” he observed.
Significant progress already has been made on the neural correlates question. Dr. Denys and his colleagues have found that when OCD patients with deep brain electrodes engage in cleaning compulsions, their local field potentials in the striatal area show peaks of roughly 9 Hz in the alpha range and in the beta/low gamma range. These patterns may represent compulsive behavior and likely could be useful in steering a closed-loop system. Also, the Dutch investigators have found that 3- to 8-Hz theta oscillations in local field potentials in the striatal area may represent a neural signature for anxiety and/or obsessions.
Using a closed-loop system, he continued, investigators plan to test two quite different hypotheses about the fundamental nature of OCD. One is that obsessions, anxiety, compulsions, and relief are each separately related to different brain areas. The other hypothesis is that one central brain stimulus drives the chain of symptoms that characterize OCD, and that by identifying and blocking that primary signal, the whole pathologic process can be stopped.
Current status of procedure
While Dr. Denys focused on the near future of DBS for OCD, another speaker at the session, Sina Kohl, PhD, addressed DBS for OCD as it exists today, particularly the who, how, and where.
The “who” is the relatively rare patient with truly refractory OCD after multiple drug trials of agents in different antidepressant classes, one of which should be clomipramine, as well as a failed course of CBT provided by an expert in CBT for OCD, of which there are relatively few. In a study led by investigators at Brown University, Providence, R.I., only 2 of 325 patients with OCD were deemed truly refractory (J Neuropsychiatry Clin Neurosci. 2014 Winter;26[1]:81-6). That sounds about right, according to Dr. Kohl, a psychologist at the University of Cologne, in Germany.
The “how” is to deliver DBS in conjunction with CBT. Response rates are higher at centers where that practice is routine, she added.
The “where” is an unsettled question. In Dr. Kohl’s meta-analysis of 25 published DBS studies, electrode placement in four different DBS target structures produced similar results: the nucleus accumbens, the anterior limb of the internal capsule, the ventral striatum, and the subthalamic nucleus. Stimulation of the inferior thalamic peduncle appeared to achieve better results, but this is a sketchy conclusion based upon two studies totaling just six patients (BMC Psychiatry. 2014 Aug 2;14:214. doi: 10.1186/s12888-014-0214-y).
Recently, Belgian investigators have reported particularly promising results – the best so far – for DBS targeting the bed nucleus of the stria terminalis (Mol Psychiatry. 2016 Sep;21[9]:1272-80).
Bilateral DBS appears to be more effective than unilateral.
Dr. Kohl and her colleagues in Cologne recently completed a study of DBS in 20 patients. She noted that it took 5 years to collect these 20 patients, underscoring the high bar that’s appropriate for resort to DBS, even though the therapy is approved for OCD by both the Food and Drug Administration and European regulatory authorities. Forty percent of the patients were DBS responders, with a mean 30% improvement in Y-BOCS scores. That’s a lower responder rate than in Dr. Denys’s and some other series, which Dr. Kohl attributed to the fact that in Germany, postimplantation CBT is not yet routine.
Asked about DBS side effects, the speakers agreed that they’re transient and fall off after initial stimulation parameters are changed.
“The most consistent and impressive side effect is that initially after surgical implantation of the electrodes and stimulation of the nucleus accumbens, patients experience 3 or 4 days of hypomania, which then disappears,” Dr. Denys said. “It causes a kind of imprinting, because even a decade later, patients ask us, ‘Could you bring back that really nice feeling?’ It’s 3 days of love, peace, and hypomania. It’s a side effect, but people like it.”
Dr. Denys and Dr. Kohl reported no financial conflicts of interest regarding their presentations.
VIENNA – Even though deep brain stimulation has been used to treat obsessive-compulsive disorder in fewer than 300 patients worldwide, the therapy has had a huge impact on understanding of the disorder, Damiaan Denys, MD, PhD, said at the annual congress of the European College of Neuropsychopharmacology.
Indeed, the efficacy of deep brain stimulation (DBS) in the most severe, treatment-refractory cases of OCD casts doubt upon the fundamental construct clinicians have relied upon for decades to comprehend OCD: Namely, that affected patients first experience obsessions, which induce anxiety, which then stimulates compulsions, and engaging in those compulsions brings relief and reward, and then the whole cycle starts over again.
That construct may not actually be true.
“Deep brain stimulation will force us to rethink OCD,” predicted Dr. Denys, professor and head of psychiatry at the University of Amsterdam.
What does DBS change, and is there a temporal order? It varies, the psychiatrist said.
“In some patients, anxiety is the first thing that changes. In others, it starts with obsessions. Compulsions do decrease, but it’s difficult. It takes some time, and often we need supplemental cognitive-behavioral therapy (CBT). What changes, mainly, in my experience, is not symptoms, but something outside of OCD: namely, mood. Deep brain stimulation has a huge impact on mood. That’s an interesting finding, because it suggests the possibility that you can change a psychiatric disorder by changing symptoms that are thought of as being outside the disorder,” Dr. Denys observed.
“Another interesting thing is that deep brain stimulation changes things that are not even within psychiatry. When we ask our patients what has been the most profound impact deep brain stimulation has had on their lives, all of them say, ‘It increases my self-confidence.’ And that’s not something that is included in our scales. We assess patients using the HAM-D [Hamilton Rating Scale for Depression] and Y-BOCS [Yale-Brown Obsessive Compulsive Scale] and other measures, but there are still some very important aspects we are not taking into account and that have a profound effect on symptoms. In this case, using deep brain stimulation, we improve self-confidence and thereby change a whole chain of symptoms,” he continued.
Among the 60 highly refractory OCD patients treated by DBS by Dr. Denys and his colleagues at the Amsterdam center over the past 15 years, 15% were cured as a result.
“I purposely use the word ‘cured,’ because they don’t have obsessive-compulsive symptoms, anymore, which is, of course, extraordinary,” Dr. Denys noted.
An additional 35% of patients had a good response, defined as 60%-80% improvement on the Y-BOCS. Ten percent of patients were partial responders, with a 20%-40% improvement on the Y-BOCS. And 15% were nonresponders.
Closed-loop system coming
DBS entails implantation of electrodes deep within the brain to interrupt dysfunctional brain signals in local areas and across neural networks. This dysfunctional brain activity is expressed as symptoms. To date, DBS has been used in what’s called an open-loop system: Patients report the symptoms they’re experiencing and the clinician then adjusts the electrode settings in order to quell those symptoms. This approach is about to change. The technology has improved vastly since the early days, when the electrodes had four contact points. Now they have 64 contact points, and are capable of sending and receiving electrical signals.
“The next step in deep brain stimulation will be a closed-loop system. We will remove the clinician and the patient, and attempt to use a device capable of recording what happens in the brain and then changing electrical activity in response to the recordings. Our purpose will be to block these brain signals in advance of obsessions and compulsions so patients don’t have these symptoms. It’s technically possible. It has been done in Parkinson’s, and I think it’s the next step in psychiatry,” Dr. Denys said.
Indeed, he and his coinvestigators are planning formal studies of closed-loop DBS. For him, the prospect raises three key questions: What are the neural correlates of OCD symptoms? What about the ethics of implanting a device in the brain which by itself results in different life experiences? And will closed-loop DBS have superior efficacy, compared with open-loop DBS?
“How is the mind rooted in the brain, and how is the brain expressed in the mind? It’s the most fascinating question; it’s why we all love psychiatry, and up until now, there are no answers,” he observed.
Significant progress already has been made on the neural correlates question. Dr. Denys and his colleagues have found that when OCD patients with deep brain electrodes engage in cleaning compulsions, their local field potentials in the striatal area show peaks of roughly 9 Hz in the alpha range and in the beta/low gamma range. These patterns may represent compulsive behavior and likely could be useful in steering a closed-loop system. Also, the Dutch investigators have found that 3- to 8-Hz theta oscillations in local field potentials in the striatal area may represent a neural signature for anxiety and/or obsessions.
Using a closed-loop system, he continued, investigators plan to test two quite different hypotheses about the fundamental nature of OCD. One is that obsessions, anxiety, compulsions, and relief are each separately related to different brain areas. The other hypothesis is that one central brain stimulus drives the chain of symptoms that characterize OCD, and that by identifying and blocking that primary signal, the whole pathologic process can be stopped.
Current status of procedure
While Dr. Denys focused on the near future of DBS for OCD, another speaker at the session, Sina Kohl, PhD, addressed DBS for OCD as it exists today, particularly the who, how, and where.
The “who” is the relatively rare patient with truly refractory OCD after multiple drug trials of agents in different antidepressant classes, one of which should be clomipramine, as well as a failed course of CBT provided by an expert in CBT for OCD, of which there are relatively few. In a study led by investigators at Brown University, Providence, R.I., only 2 of 325 patients with OCD were deemed truly refractory (J Neuropsychiatry Clin Neurosci. 2014 Winter;26[1]:81-6). That sounds about right, according to Dr. Kohl, a psychologist at the University of Cologne, in Germany.
The “how” is to deliver DBS in conjunction with CBT. Response rates are higher at centers where that practice is routine, she added.
The “where” is an unsettled question. In Dr. Kohl’s meta-analysis of 25 published DBS studies, electrode placement in four different DBS target structures produced similar results: the nucleus accumbens, the anterior limb of the internal capsule, the ventral striatum, and the subthalamic nucleus. Stimulation of the inferior thalamic peduncle appeared to achieve better results, but this is a sketchy conclusion based upon two studies totaling just six patients (BMC Psychiatry. 2014 Aug 2;14:214. doi: 10.1186/s12888-014-0214-y).
Recently, Belgian investigators have reported particularly promising results – the best so far – for DBS targeting the bed nucleus of the stria terminalis (Mol Psychiatry. 2016 Sep;21[9]:1272-80).
Bilateral DBS appears to be more effective than unilateral.
Dr. Kohl and her colleagues in Cologne recently completed a study of DBS in 20 patients. She noted that it took 5 years to collect these 20 patients, underscoring the high bar that’s appropriate for resort to DBS, even though the therapy is approved for OCD by both the Food and Drug Administration and European regulatory authorities. Forty percent of the patients were DBS responders, with a mean 30% improvement in Y-BOCS scores. That’s a lower responder rate than in Dr. Denys’s and some other series, which Dr. Kohl attributed to the fact that in Germany, postimplantation CBT is not yet routine.
Asked about DBS side effects, the speakers agreed that they’re transient and fall off after initial stimulation parameters are changed.
“The most consistent and impressive side effect is that initially after surgical implantation of the electrodes and stimulation of the nucleus accumbens, patients experience 3 or 4 days of hypomania, which then disappears,” Dr. Denys said. “It causes a kind of imprinting, because even a decade later, patients ask us, ‘Could you bring back that really nice feeling?’ It’s 3 days of love, peace, and hypomania. It’s a side effect, but people like it.”
Dr. Denys and Dr. Kohl reported no financial conflicts of interest regarding their presentations.
Prepregnancy overweight boosts risk of depressive symptoms in pregnancy
NEW ORLEANS – Prepregnancy overweight and obesity are associated with increased incidence and severity of depressive symptoms during pregnancy, independent of preeclampsia and other hypertensive pregnancy disorders or gestational diabetes, Satu Kumpulainen reported at Obesity Week 2016.
The implications of this novel finding are clear: “Prepregnancy interventions targeting overweight and obesity and mental health will not only benefit the pregnant mother’s health but will also provide optimal odds for healthy development of the fetus as well,” said Ms. Kumpulainen, a doctoral student at the University of Helsinki Institute of Behavioral Sciences.
It’s well established that prepregnancy obesity is a risk factor for gestational diabetes, preeclampsia, and depression during pregnancy. This study was carried out to learn if a high prepregnancy BMI boosts the risk of prenatal depression independent of the cardiometabolic complications of pregnancy, Ms. Kumpulainen explained at the meeting, which was presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
This proved to be the case in the Finnish women, 67.3% of whom were normal weight before pregnancy; 19.1% were overweight and 13.6% obese. Gestational diabetes occurred in 10.6% of the PREDO participants, and hypertension-spectrum disorders of pregnancy occurred in 8.2%.
The women who were obese or overweight prepregnancy reported higher rates of clinically meaningful depressive symptoms throughout pregnancy, compared with women who were normal weight. Using a CES-D score of 16 or more to define clinically significant depressive symptoms, such symptoms were reported as early as gestational week 12 and on multiple occasions thereafter by 19.9% of the women who were normal weight before pregnancy, 23.3% of those who were overweight, and 27.4% of those who were obese. The differences were statistically significant.
The risk of clinically significant depressive symptoms during pregnancy was no higher in prepregnancy normal-weight women who developed gestational diabetes or preeclampsia than in those who did not, Ms. Kumpulainen reported.
“Our findings suggest that cardiometabolic pregnancy disorders per se don’t trigger higher levels of depressive symptoms, but women with prepregnancy overweight and obesity feel more depressed right from the beginning of pregnancy,” Ms. Kumpulainen said.
She reported having no financial conflicts of interest related to the study, which was supported by Finnish scientific research grants.
NEW ORLEANS – Prepregnancy overweight and obesity are associated with increased incidence and severity of depressive symptoms during pregnancy, independent of preeclampsia and other hypertensive pregnancy disorders or gestational diabetes, Satu Kumpulainen reported at Obesity Week 2016.
The implications of this novel finding are clear: “Prepregnancy interventions targeting overweight and obesity and mental health will not only benefit the pregnant mother’s health but will also provide optimal odds for healthy development of the fetus as well,” said Ms. Kumpulainen, a doctoral student at the University of Helsinki Institute of Behavioral Sciences.
It’s well established that prepregnancy obesity is a risk factor for gestational diabetes, preeclampsia, and depression during pregnancy. This study was carried out to learn if a high prepregnancy BMI boosts the risk of prenatal depression independent of the cardiometabolic complications of pregnancy, Ms. Kumpulainen explained at the meeting, which was presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
This proved to be the case in the Finnish women, 67.3% of whom were normal weight before pregnancy; 19.1% were overweight and 13.6% obese. Gestational diabetes occurred in 10.6% of the PREDO participants, and hypertension-spectrum disorders of pregnancy occurred in 8.2%.
The women who were obese or overweight prepregnancy reported higher rates of clinically meaningful depressive symptoms throughout pregnancy, compared with women who were normal weight. Using a CES-D score of 16 or more to define clinically significant depressive symptoms, such symptoms were reported as early as gestational week 12 and on multiple occasions thereafter by 19.9% of the women who were normal weight before pregnancy, 23.3% of those who were overweight, and 27.4% of those who were obese. The differences were statistically significant.
The risk of clinically significant depressive symptoms during pregnancy was no higher in prepregnancy normal-weight women who developed gestational diabetes or preeclampsia than in those who did not, Ms. Kumpulainen reported.
“Our findings suggest that cardiometabolic pregnancy disorders per se don’t trigger higher levels of depressive symptoms, but women with prepregnancy overweight and obesity feel more depressed right from the beginning of pregnancy,” Ms. Kumpulainen said.
She reported having no financial conflicts of interest related to the study, which was supported by Finnish scientific research grants.
NEW ORLEANS – Prepregnancy overweight and obesity are associated with increased incidence and severity of depressive symptoms during pregnancy, independent of preeclampsia and other hypertensive pregnancy disorders or gestational diabetes, Satu Kumpulainen reported at Obesity Week 2016.
The implications of this novel finding are clear: “Prepregnancy interventions targeting overweight and obesity and mental health will not only benefit the pregnant mother’s health but will also provide optimal odds for healthy development of the fetus as well,” said Ms. Kumpulainen, a doctoral student at the University of Helsinki Institute of Behavioral Sciences.
It’s well established that prepregnancy obesity is a risk factor for gestational diabetes, preeclampsia, and depression during pregnancy. This study was carried out to learn if a high prepregnancy BMI boosts the risk of prenatal depression independent of the cardiometabolic complications of pregnancy, Ms. Kumpulainen explained at the meeting, which was presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
This proved to be the case in the Finnish women, 67.3% of whom were normal weight before pregnancy; 19.1% were overweight and 13.6% obese. Gestational diabetes occurred in 10.6% of the PREDO participants, and hypertension-spectrum disorders of pregnancy occurred in 8.2%.
The women who were obese or overweight prepregnancy reported higher rates of clinically meaningful depressive symptoms throughout pregnancy, compared with women who were normal weight. Using a CES-D score of 16 or more to define clinically significant depressive symptoms, such symptoms were reported as early as gestational week 12 and on multiple occasions thereafter by 19.9% of the women who were normal weight before pregnancy, 23.3% of those who were overweight, and 27.4% of those who were obese. The differences were statistically significant.
The risk of clinically significant depressive symptoms during pregnancy was no higher in prepregnancy normal-weight women who developed gestational diabetes or preeclampsia than in those who did not, Ms. Kumpulainen reported.
“Our findings suggest that cardiometabolic pregnancy disorders per se don’t trigger higher levels of depressive symptoms, but women with prepregnancy overweight and obesity feel more depressed right from the beginning of pregnancy,” Ms. Kumpulainen said.
She reported having no financial conflicts of interest related to the study, which was supported by Finnish scientific research grants.
AT OBESITY WEEK 2016
Key clinical point:
Major finding: Women who were obese prior to pregnancy were over 50% more likely to experience clinically significant depressive symptoms throughout pregnancy, compared with women who were normal weight before pregnancy, independent of whether the women developed gestational diabetes or preeclampsia.
Data source: This was a secondary analysis from a prospective study of more than 3,000 pregnant Finnish women.
Disclosures: The study was supported by Finnish scientific research grants. The presenter reported having no financial conflicts of interest related to the study.
Unless it is diagnosed, obesity won’t be treated
NEW ORLEANS – Obesity has been formally diagnosed in less than half of patients with a body-mass index of 30 kg/m2 or higher in the Cleveland Clinic’s large multispecialty database, and Bartolome Burguera, MD, believes it’s the same story elsewhere.
“I think pretty much all over the country obesity is really not well diagnosed,” Dr. Burguera, director of obesity programs at the Cleveland Clinic, said at Obesity Week 2016.
And that which hasn’t been diagnosed doesn’t get treated.

The diagnosis rate went up with higher BMIs; still, of the 25,137 patients with obesity class 3 as defined by a BMI of 40 kg/m2 or higher, only 75% had a formal diagnosis of obesity in their record, the endocrinologist said at the meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
“For many years, physicians thought that obesity is not a disease. And even though it was considered a disease by some, they didn’t feel they had the tools, the knowledge, the support, the medications, or the time to take care of obesity, especially when they thought of it as a self-inflicted disease,” Dr. Burguera explained in an interview. He believes physician attitudes are slowly changing.
“In our clinic we’ve taken measures to change attitudes, for sure. Now, when we look in the electronic health record we get an automatic alert if the patient has a BMI of 30 or more,” he said.
“I think, in general, many more people now think of obesity as a disease. But it’s a chronic disease and you have to have chronic therapy. We have to make sure we make the diagnosis, and once you make the diagnosis you have to discuss treatment with the patient. If you don’t feel comfortable for whatever reason, I think you have to refer the patient to a colleague to take care of the obesity. Because when you take care of the obesity all the comorbidities get better: the diabetes, the blood pressure, the cholesterol. Obesity is the primary problem in so many other comorbidities. We have put little effort to this point in taking care of the obesity. We’ve put more effort into treating the diabetes and the other comorbidities,” Dr. Burguera said.

The Medicare obesity benefit provides reimbursement in primary care settings for intensive behavioral therapy with face-to-face counseling and motivational interviewing. The billing code is G0447. Coverage is provided for 22 visits over the course of a year, each lasting 15 minutes.
Dr. Batsis presented highlights of his published serial cross-sectional analysis of fee-for-service Medicare claims data for 2012 and 2013. Among Medicare beneficiaries eligible for the obesity benefit because they had a BMI of 30 kg/m2 or above, only 0.35% used the benefit in 2012. There was a tiny uptick to 0.6% in 2013, but even in the tiny fraction of eligible patients who availed themselves of the benefit, the average number of behavioral therapy sessions was just 2.1 visits out of the 22 for which physician reimbursement is available (Obesity. 2016 Sep;24[9]:1983-8).
“Let’s hope the 2014 data look a little better,” commented Dr. Batsis of the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H.
There was marked regional variation in utilization of the Medicare obesity benefit across the U.S. in 2013. Rates were highest in Colorado – the state with the lowest obesity rate in the country – as well as Nebraska, Wisconsin, Vermont, and New Hampshire. Rates were lowest across the Southwest.
Dr. Burguera’s study was funded by Novo Nordisk. Dr. Batsis reported having no financial conflicts of interest.
NEW ORLEANS – Obesity has been formally diagnosed in less than half of patients with a body-mass index of 30 kg/m2 or higher in the Cleveland Clinic’s large multispecialty database, and Bartolome Burguera, MD, believes it’s the same story elsewhere.
“I think pretty much all over the country obesity is really not well diagnosed,” Dr. Burguera, director of obesity programs at the Cleveland Clinic, said at Obesity Week 2016.
And that which hasn’t been diagnosed doesn’t get treated.
The diagnosis rate went up with higher BMIs; still, of the 25,137 patients with obesity class 3 as defined by a BMI of 40 kg/m2 or higher, only 75% had a formal diagnosis of obesity in their record, the endocrinologist said at the meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
“For many years, physicians thought that obesity is not a disease. And even though it was considered a disease by some, they didn’t feel they had the tools, the knowledge, the support, the medications, or the time to take care of obesity, especially when they thought of it as a self-inflicted disease,” Dr. Burguera explained in an interview. He believes physician attitudes are slowly changing.
“In our clinic we’ve taken measures to change attitudes, for sure. Now, when we look in the electronic health record we get an automatic alert if the patient has a BMI of 30 or more,” he said.
“I think, in general, many more people now think of obesity as a disease. But it’s a chronic disease and you have to have chronic therapy. We have to make sure we make the diagnosis, and once you make the diagnosis you have to discuss treatment with the patient. If you don’t feel comfortable for whatever reason, I think you have to refer the patient to a colleague to take care of the obesity. Because when you take care of the obesity all the comorbidities get better: the diabetes, the blood pressure, the cholesterol. Obesity is the primary problem in so many other comorbidities. We have put little effort to this point in taking care of the obesity. We’ve put more effort into treating the diabetes and the other comorbidities,” Dr. Burguera said.
The Medicare obesity benefit provides reimbursement in primary care settings for intensive behavioral therapy with face-to-face counseling and motivational interviewing. The billing code is G0447. Coverage is provided for 22 visits over the course of a year, each lasting 15 minutes.
Dr. Batsis presented highlights of his published serial cross-sectional analysis of fee-for-service Medicare claims data for 2012 and 2013. Among Medicare beneficiaries eligible for the obesity benefit because they had a BMI of 30 kg/m2 or above, only 0.35% used the benefit in 2012. There was a tiny uptick to 0.6% in 2013, but even in the tiny fraction of eligible patients who availed themselves of the benefit, the average number of behavioral therapy sessions was just 2.1 visits out of the 22 for which physician reimbursement is available (Obesity. 2016 Sep;24[9]:1983-8).
“Let’s hope the 2014 data look a little better,” commented Dr. Batsis of the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H.
There was marked regional variation in utilization of the Medicare obesity benefit across the U.S. in 2013. Rates were highest in Colorado – the state with the lowest obesity rate in the country – as well as Nebraska, Wisconsin, Vermont, and New Hampshire. Rates were lowest across the Southwest.
Dr. Burguera’s study was funded by Novo Nordisk. Dr. Batsis reported having no financial conflicts of interest.
NEW ORLEANS – Obesity has been formally diagnosed in less than half of patients with a body-mass index of 30 kg/m2 or higher in the Cleveland Clinic’s large multispecialty database, and Bartolome Burguera, MD, believes it’s the same story elsewhere.
“I think pretty much all over the country obesity is really not well diagnosed,” Dr. Burguera, director of obesity programs at the Cleveland Clinic, said at Obesity Week 2016.
And that which hasn’t been diagnosed doesn’t get treated.
The diagnosis rate went up with higher BMIs; still, of the 25,137 patients with obesity class 3 as defined by a BMI of 40 kg/m2 or higher, only 75% had a formal diagnosis of obesity in their record, the endocrinologist said at the meeting presented by the Obesity Society and the American Society for Metabolic and Bariatric Surgery.
“For many years, physicians thought that obesity is not a disease. And even though it was considered a disease by some, they didn’t feel they had the tools, the knowledge, the support, the medications, or the time to take care of obesity, especially when they thought of it as a self-inflicted disease,” Dr. Burguera explained in an interview. He believes physician attitudes are slowly changing.
“In our clinic we’ve taken measures to change attitudes, for sure. Now, when we look in the electronic health record we get an automatic alert if the patient has a BMI of 30 or more,” he said.
“I think, in general, many more people now think of obesity as a disease. But it’s a chronic disease and you have to have chronic therapy. We have to make sure we make the diagnosis, and once you make the diagnosis you have to discuss treatment with the patient. If you don’t feel comfortable for whatever reason, I think you have to refer the patient to a colleague to take care of the obesity. Because when you take care of the obesity all the comorbidities get better: the diabetes, the blood pressure, the cholesterol. Obesity is the primary problem in so many other comorbidities. We have put little effort to this point in taking care of the obesity. We’ve put more effort into treating the diabetes and the other comorbidities,” Dr. Burguera said.
The Medicare obesity benefit provides reimbursement in primary care settings for intensive behavioral therapy with face-to-face counseling and motivational interviewing. The billing code is G0447. Coverage is provided for 22 visits over the course of a year, each lasting 15 minutes.
Dr. Batsis presented highlights of his published serial cross-sectional analysis of fee-for-service Medicare claims data for 2012 and 2013. Among Medicare beneficiaries eligible for the obesity benefit because they had a BMI of 30 kg/m2 or above, only 0.35% used the benefit in 2012. There was a tiny uptick to 0.6% in 2013, but even in the tiny fraction of eligible patients who availed themselves of the benefit, the average number of behavioral therapy sessions was just 2.1 visits out of the 22 for which physician reimbursement is available (Obesity. 2016 Sep;24[9]:1983-8).
“Let’s hope the 2014 data look a little better,” commented Dr. Batsis of the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H.
There was marked regional variation in utilization of the Medicare obesity benefit across the U.S. in 2013. Rates were highest in Colorado – the state with the lowest obesity rate in the country – as well as Nebraska, Wisconsin, Vermont, and New Hampshire. Rates were lowest across the Southwest.
Dr. Burguera’s study was funded by Novo Nordisk. Dr. Batsis reported having no financial conflicts of interest.
AT OBESITY WEEK 2016
Key clinical point:
Major finding: Only 48% of a large group of patients with a BMI of 30 kg/m2 or higher had a formal diagnosis of obesity in their medical record.
Data source: This was a cross-sectional study of the electronic health records of nearly 325,000 active patients in the Cleveland Clinic database, 41.5% of whom had a BMI of 30 kg/m2 or higher.
Disclosures: The study was funded by Novo Nordisk.
Initial suboptimal responders to secukinumab usually bloom later
VIENNA – When the occasional patient on secukinumab for moderate to severe psoriasis fails to achieve a PASI 75 response initially, don’t despair: Continuing treatment with the biologic usually gets them over that bar, Christopher E. Griffiths, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
A new secondary pooled analysis of four phase III, 52-week, pivotal clinical trials of secukinumab (Cosentyx) indicates that more than three-quarters of initial suboptimal responders will go on to achieve a PASI 75 response. Moreover, more than one-third will have a PASI 90 response by week 16, which is sustained through week 52. And almost one in five slow responders will have a PASI 100 response – clear skin – at week 52, according to Dr. Griffiths, professor of dermatology at the University of Manchester, England.

He presented a secondary analysis of four phase III studies: ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis), FEATURE (First Study of Secukinumab in Pre-filled Syringes in Subjects With Chronic Plaque-type Psoriasis: Response at 12 Weeks), FIXTURE (Full Year Investigative Examination of Secukinumab vs. Etanercept Using Two Dosing Regimens to Determine Efficacy in Psoriasis), and JUNCTURE (Judging the Efficacy of Secukinumab in Patients With Psoriasis Using AutoiNjector: a Clinical Trial Evaluating Treatment Results). The analysis was conducted to provide additional perspective on the product labeling statement that treatment discontinuation should be considered in patients who haven’t responded to secukinumab by week 16.
The four studies featured a total of 2,405 patients with moderate to severe psoriasis on secukinumab at the approved dosing schedule.
The key findings: At week 12 – the primary endpoint in the four trials – only 5.2% of patients on secukinumab had not achieved a PASI 75 response. Yet just 4 weeks later, at week 16, 56% of this group had managed to get there. Seventy-seven percent of early non- or partial responders achieved a PASI 75 response at some point during weeks 13-52, and 55% had a PASI 75 response at 52 weeks.
Thirty-five percent of early poor responders achieved PASI 90 at 16 weeks and 37% at 52 weeks. Twelve percent of patients who didn’t get to PASI 75 at 12 weeks had a PASI 100 response by 16 weeks, and nearly 18% did by week 52.
This analysis was supported by secukinumab manufacturer Novartis. Dr. Griffiths reported receiving research funds from and serving as a consultant to Novartis and numerous other pharmaceutical companies.
VIENNA – When the occasional patient on secukinumab for moderate to severe psoriasis fails to achieve a PASI 75 response initially, don’t despair: Continuing treatment with the biologic usually gets them over that bar, Christopher E. Griffiths, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
A new secondary pooled analysis of four phase III, 52-week, pivotal clinical trials of secukinumab (Cosentyx) indicates that more than three-quarters of initial suboptimal responders will go on to achieve a PASI 75 response. Moreover, more than one-third will have a PASI 90 response by week 16, which is sustained through week 52. And almost one in five slow responders will have a PASI 100 response – clear skin – at week 52, according to Dr. Griffiths, professor of dermatology at the University of Manchester, England.
He presented a secondary analysis of four phase III studies: ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis), FEATURE (First Study of Secukinumab in Pre-filled Syringes in Subjects With Chronic Plaque-type Psoriasis: Response at 12 Weeks), FIXTURE (Full Year Investigative Examination of Secukinumab vs. Etanercept Using Two Dosing Regimens to Determine Efficacy in Psoriasis), and JUNCTURE (Judging the Efficacy of Secukinumab in Patients With Psoriasis Using AutoiNjector: a Clinical Trial Evaluating Treatment Results). The analysis was conducted to provide additional perspective on the product labeling statement that treatment discontinuation should be considered in patients who haven’t responded to secukinumab by week 16.
The four studies featured a total of 2,405 patients with moderate to severe psoriasis on secukinumab at the approved dosing schedule.
The key findings: At week 12 – the primary endpoint in the four trials – only 5.2% of patients on secukinumab had not achieved a PASI 75 response. Yet just 4 weeks later, at week 16, 56% of this group had managed to get there. Seventy-seven percent of early non- or partial responders achieved a PASI 75 response at some point during weeks 13-52, and 55% had a PASI 75 response at 52 weeks.
Thirty-five percent of early poor responders achieved PASI 90 at 16 weeks and 37% at 52 weeks. Twelve percent of patients who didn’t get to PASI 75 at 12 weeks had a PASI 100 response by 16 weeks, and nearly 18% did by week 52.
This analysis was supported by secukinumab manufacturer Novartis. Dr. Griffiths reported receiving research funds from and serving as a consultant to Novartis and numerous other pharmaceutical companies.
VIENNA – When the occasional patient on secukinumab for moderate to severe psoriasis fails to achieve a PASI 75 response initially, don’t despair: Continuing treatment with the biologic usually gets them over that bar, Christopher E. Griffiths, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
A new secondary pooled analysis of four phase III, 52-week, pivotal clinical trials of secukinumab (Cosentyx) indicates that more than three-quarters of initial suboptimal responders will go on to achieve a PASI 75 response. Moreover, more than one-third will have a PASI 90 response by week 16, which is sustained through week 52. And almost one in five slow responders will have a PASI 100 response – clear skin – at week 52, according to Dr. Griffiths, professor of dermatology at the University of Manchester, England.
He presented a secondary analysis of four phase III studies: ERASURE (Efficacy of Response and Safety of Two Fixed Secukinumab Regimens in Psoriasis), FEATURE (First Study of Secukinumab in Pre-filled Syringes in Subjects With Chronic Plaque-type Psoriasis: Response at 12 Weeks), FIXTURE (Full Year Investigative Examination of Secukinumab vs. Etanercept Using Two Dosing Regimens to Determine Efficacy in Psoriasis), and JUNCTURE (Judging the Efficacy of Secukinumab in Patients With Psoriasis Using AutoiNjector: a Clinical Trial Evaluating Treatment Results). The analysis was conducted to provide additional perspective on the product labeling statement that treatment discontinuation should be considered in patients who haven’t responded to secukinumab by week 16.
The four studies featured a total of 2,405 patients with moderate to severe psoriasis on secukinumab at the approved dosing schedule.
The key findings: At week 12 – the primary endpoint in the four trials – only 5.2% of patients on secukinumab had not achieved a PASI 75 response. Yet just 4 weeks later, at week 16, 56% of this group had managed to get there. Seventy-seven percent of early non- or partial responders achieved a PASI 75 response at some point during weeks 13-52, and 55% had a PASI 75 response at 52 weeks.
Thirty-five percent of early poor responders achieved PASI 90 at 16 weeks and 37% at 52 weeks. Twelve percent of patients who didn’t get to PASI 75 at 12 weeks had a PASI 100 response by 16 weeks, and nearly 18% did by week 52.
This analysis was supported by secukinumab manufacturer Novartis. Dr. Griffiths reported receiving research funds from and serving as a consultant to Novartis and numerous other pharmaceutical companies.
AT THE EADV CONGRESS
Key clinical point:
Major finding: Most psoriasis patients who don’t achieve a PASI 75 response by week 12 on secukinumab will do so by week 16 and will maintain that response through week 52.
Data source: A pooled secondary analysis of PASI response rates in four phase III randomized clinical trials of secukinumab featuring 2,405 patients with moderate to severe psoriasis who were on the biologic for 52 weeks, including the 119 who did not achieve a PASI 75 response by week 12.
Disclosures: This analysis of four phase III clinical trials was sponsored by Novartis, as were the trials. The presenter reported receiving research funding from and serving as a consultant to Novartis and other pharmaceutical companies.