User login
Expect miracles: New drug for hepatitis C may put treatment in the hands of primary care
ESTES PARK, COLO. – Treatment of hepatitis C infection is likely to shift from gastroenterology and hepatology clinics to primary care physicians’ offices, perhaps as early as next year.
That’s the prediction of Dr. Gregory T. Everson, who cited rapid progress in developing interferon-free treatment regimens as the driving force behind what is anticipated to be a huge change in clinical practice, given that there are an estimated 5 million or more patients with hepatitis C virus (HCV) infection in the United States
Five major pharmaceutical companies are developing oral, interferon-free HCV treatment regimens based upon still-investigational direct-acting antiviral agents (DAAs) that target HCV proteins and their functions. The clinical trials experience to date indicates these DAA-based regimens have substantially higher cure rates, far better tolerability and safety, and a much lower pill burden. Also, they are vastly simpler to administer than are current standard therapies. And all this is being achieved with a 12-week treatment duration instead of the 24 weeks required with standard therapy in 2013, Dr. Everson said at a conference on internal medicine sponsored by the University of Colorado.

"In the past I could say we really had pretty [intolerable] therapy, and it was pretty difficult for patients to take it. Interferon-free therapy is evolving rapidly, and I hope that it will be in primary care physicians’ backyards in the near future. I think this is probably going to be a treatment that you all provide," added Dr. Everson, professor of medicine and director of hepatology at the university.
Indeed, at hepatology clinics around the country, patients with early-stage HCV and their physicians are taking a "wait until next year" attitude toward starting treatment in anticipation that the Food and Drug Administration could approve the first of these new DAAs, sofosbuvir, before the year’s end.
The number of prescriptions for HCV therapy for treatment-naive patients at the University of Colorado clinic has plummeted in 2013 compared with 2012. The only patients starting treatment now are those with advanced HCV liver disease, to halt further disease progression and reduce the risk of developing hepatocellular carcinoma, according to Dr. Everson.
The FDA has granted Gilead Sciences priority review status for sofosbuvir, an oral inhibitor of nucleotide N55b polymerase, with a target decision date in early December. The application for marketing approval is for two indications. One involves sofosbuvir as part of a 12-week, triple-therapy regimen including pegylated interferon and ribavirin in treatment-naive patients with HCV genotypes 1, 4, 5, and 6, based in large part upon the highly favorable results of the phase III NEUTRINO trial (N. Engl. J. Med. 2013;368:1878-87).
The other proposed indication is sofosbuvir in combination with ribavirin as an interferon-free, 12-week regimen in patients with HCV genotypes 2 or 3, based upon the results of the FISSION and POSITRON trials (N. Engl. J. Med. 2013;368:1867-77).
In the NEUTRINO trial, 12 weeks of triple-therapy with sofosbuvir/interferon/ribavirin resulted in a 90% cure rate in patients with HCV genotype 1, which accounts for three-quarters of all HCV infections in the United States. The dropout rate due to side effects was a mere 2%. In contrast, today’s standard therapy, consisting of either of the protease inhibitors telaprevir (Incivek) or boceprevir (Victrelis) combined with pegylated interferon and ribavirin, has a 70%-75% cure rate. And many patients can’t tolerate or are ineligible for interferon.
"When I started treating hepatitis C patients 25 years ago, I was happy because the ALT would normalize in half the patients with genotype 1, but I wasn’t curing anybody. And now triple therapy with sofosbuvir, with a 90% cure rate, could be approved by the end of the year," Dr. Everson marveled.
In the FISSION trial, treatment-naive patients with HCV genotype 2 had a 97% cure rate with 12 weeks of sofosbuvir/ribavirin compared with 78% in those assigned to today’s standard regimen of 24 weeks of pegylated interferon/ribavirin. And sofosbuvir is just one pill per day, coupled with ribavirin at two or three pills twice daily.
In POSITRON, conducted in patients who had relapsed or were nonresponders to the standard 24 weeks of pegylated interferon/ribavirin, 12 weeks of sofosbuvir/ribavirin had an 86% response rate in patients with HCV genotype 2. With an additional 4 weeks of the interferon-free regimen, the cure rate climbed to 94%. Cure rates were lower in genotype 3 patients, but of note, the cure rate in treatment-experienced genotype 3 patients with cirrhosis more than tripled from 19% with 12 weeks of sofosbuvir/ribavirin to 61% with 16 weeks.
Other oral DAAs in the developmental pipeline include simeprevir, daclatasvir, and asunaprevir. The clinical trials experience to date demonstrate that combination therapy with more than one DAA boosts the cure rate even higher than with sofosbuvir/ribavirin. For example, in the phase II, open-label AVIATOR study, 12 weeks of a cocktail comprising three DAAs plus ribavirin brought a 96% cure rate in treatment-naive patients with HCV genotype 1 and a 93% cure rate in those who had previously failed on standard interferon-containing therapy. The AVIATOR cocktail is being formulated as a two-pills-per-day regimen.
Further, Dr. Everson was principal investigator in a Bristol-Myers Squibb–sponsored study of a totally interferon- and ribavirin-free regimen consisting of triple-DAA therapy. Each of the DAAs has a different mechanism of action: Daclatasvir is an inhibitor of the HCV NS5a protein; asunaprevir is an NS3 protease inhibitor; and the agent known for now as BMS-791325 is a nonnucleoside polymerase NS5b inhibitor. The cure rate with 12 weeks of triple-DAA therapy in treatment-naive, noncirrhotic patients with HCV genotype 1 was 94%.
Hepatologists define cure of HCV as an SVR12, or a sustained virologic response featuring no detectable HCV RNA in the blood for 12 weeks after the conclusion of therapy. The likelihood that a patient who achieves an SVR12 will remain HCV free through 10 years is 99%-100% (Gastroenterology 2010;139:1593-1601).
"The future looks pretty good for hepatitis C patients," Dr. Everson observed.
Moreover, curing HCV is going to have major downstream benefits for the health care system, he added. Today, 36% of all patients on the liver transplantation waiting list have HCV; that proportion will drop substantially. There will be fewer cases of hepatocellular carcinoma, B-cell lymphoma, and adult-onset diabetes, a drop in HCV-related autoimmune disorders, and reduced costs of care for patients with chronic HCV.
Dr. Everson reported that he receives research grants from and/or serves as a consultant to or advisory board member for roughly two dozen pharmaceutical companies.
ESTES PARK, COLO. – Treatment of hepatitis C infection is likely to shift from gastroenterology and hepatology clinics to primary care physicians’ offices, perhaps as early as next year.
That’s the prediction of Dr. Gregory T. Everson, who cited rapid progress in developing interferon-free treatment regimens as the driving force behind what is anticipated to be a huge change in clinical practice, given that there are an estimated 5 million or more patients with hepatitis C virus (HCV) infection in the United States
Five major pharmaceutical companies are developing oral, interferon-free HCV treatment regimens based upon still-investigational direct-acting antiviral agents (DAAs) that target HCV proteins and their functions. The clinical trials experience to date indicates these DAA-based regimens have substantially higher cure rates, far better tolerability and safety, and a much lower pill burden. Also, they are vastly simpler to administer than are current standard therapies. And all this is being achieved with a 12-week treatment duration instead of the 24 weeks required with standard therapy in 2013, Dr. Everson said at a conference on internal medicine sponsored by the University of Colorado.
"In the past I could say we really had pretty [intolerable] therapy, and it was pretty difficult for patients to take it. Interferon-free therapy is evolving rapidly, and I hope that it will be in primary care physicians’ backyards in the near future. I think this is probably going to be a treatment that you all provide," added Dr. Everson, professor of medicine and director of hepatology at the university.
Indeed, at hepatology clinics around the country, patients with early-stage HCV and their physicians are taking a "wait until next year" attitude toward starting treatment in anticipation that the Food and Drug Administration could approve the first of these new DAAs, sofosbuvir, before the year’s end.
The number of prescriptions for HCV therapy for treatment-naive patients at the University of Colorado clinic has plummeted in 2013 compared with 2012. The only patients starting treatment now are those with advanced HCV liver disease, to halt further disease progression and reduce the risk of developing hepatocellular carcinoma, according to Dr. Everson.
The FDA has granted Gilead Sciences priority review status for sofosbuvir, an oral inhibitor of nucleotide N55b polymerase, with a target decision date in early December. The application for marketing approval is for two indications. One involves sofosbuvir as part of a 12-week, triple-therapy regimen including pegylated interferon and ribavirin in treatment-naive patients with HCV genotypes 1, 4, 5, and 6, based in large part upon the highly favorable results of the phase III NEUTRINO trial (N. Engl. J. Med. 2013;368:1878-87).
The other proposed indication is sofosbuvir in combination with ribavirin as an interferon-free, 12-week regimen in patients with HCV genotypes 2 or 3, based upon the results of the FISSION and POSITRON trials (N. Engl. J. Med. 2013;368:1867-77).
In the NEUTRINO trial, 12 weeks of triple-therapy with sofosbuvir/interferon/ribavirin resulted in a 90% cure rate in patients with HCV genotype 1, which accounts for three-quarters of all HCV infections in the United States. The dropout rate due to side effects was a mere 2%. In contrast, today’s standard therapy, consisting of either of the protease inhibitors telaprevir (Incivek) or boceprevir (Victrelis) combined with pegylated interferon and ribavirin, has a 70%-75% cure rate. And many patients can’t tolerate or are ineligible for interferon.
"When I started treating hepatitis C patients 25 years ago, I was happy because the ALT would normalize in half the patients with genotype 1, but I wasn’t curing anybody. And now triple therapy with sofosbuvir, with a 90% cure rate, could be approved by the end of the year," Dr. Everson marveled.
In the FISSION trial, treatment-naive patients with HCV genotype 2 had a 97% cure rate with 12 weeks of sofosbuvir/ribavirin compared with 78% in those assigned to today’s standard regimen of 24 weeks of pegylated interferon/ribavirin. And sofosbuvir is just one pill per day, coupled with ribavirin at two or three pills twice daily.
In POSITRON, conducted in patients who had relapsed or were nonresponders to the standard 24 weeks of pegylated interferon/ribavirin, 12 weeks of sofosbuvir/ribavirin had an 86% response rate in patients with HCV genotype 2. With an additional 4 weeks of the interferon-free regimen, the cure rate climbed to 94%. Cure rates were lower in genotype 3 patients, but of note, the cure rate in treatment-experienced genotype 3 patients with cirrhosis more than tripled from 19% with 12 weeks of sofosbuvir/ribavirin to 61% with 16 weeks.
Other oral DAAs in the developmental pipeline include simeprevir, daclatasvir, and asunaprevir. The clinical trials experience to date demonstrate that combination therapy with more than one DAA boosts the cure rate even higher than with sofosbuvir/ribavirin. For example, in the phase II, open-label AVIATOR study, 12 weeks of a cocktail comprising three DAAs plus ribavirin brought a 96% cure rate in treatment-naive patients with HCV genotype 1 and a 93% cure rate in those who had previously failed on standard interferon-containing therapy. The AVIATOR cocktail is being formulated as a two-pills-per-day regimen.
Further, Dr. Everson was principal investigator in a Bristol-Myers Squibb–sponsored study of a totally interferon- and ribavirin-free regimen consisting of triple-DAA therapy. Each of the DAAs has a different mechanism of action: Daclatasvir is an inhibitor of the HCV NS5a protein; asunaprevir is an NS3 protease inhibitor; and the agent known for now as BMS-791325 is a nonnucleoside polymerase NS5b inhibitor. The cure rate with 12 weeks of triple-DAA therapy in treatment-naive, noncirrhotic patients with HCV genotype 1 was 94%.
Hepatologists define cure of HCV as an SVR12, or a sustained virologic response featuring no detectable HCV RNA in the blood for 12 weeks after the conclusion of therapy. The likelihood that a patient who achieves an SVR12 will remain HCV free through 10 years is 99%-100% (Gastroenterology 2010;139:1593-1601).
"The future looks pretty good for hepatitis C patients," Dr. Everson observed.
Moreover, curing HCV is going to have major downstream benefits for the health care system, he added. Today, 36% of all patients on the liver transplantation waiting list have HCV; that proportion will drop substantially. There will be fewer cases of hepatocellular carcinoma, B-cell lymphoma, and adult-onset diabetes, a drop in HCV-related autoimmune disorders, and reduced costs of care for patients with chronic HCV.
Dr. Everson reported that he receives research grants from and/or serves as a consultant to or advisory board member for roughly two dozen pharmaceutical companies.
ESTES PARK, COLO. – Treatment of hepatitis C infection is likely to shift from gastroenterology and hepatology clinics to primary care physicians’ offices, perhaps as early as next year.
That’s the prediction of Dr. Gregory T. Everson, who cited rapid progress in developing interferon-free treatment regimens as the driving force behind what is anticipated to be a huge change in clinical practice, given that there are an estimated 5 million or more patients with hepatitis C virus (HCV) infection in the United States
Five major pharmaceutical companies are developing oral, interferon-free HCV treatment regimens based upon still-investigational direct-acting antiviral agents (DAAs) that target HCV proteins and their functions. The clinical trials experience to date indicates these DAA-based regimens have substantially higher cure rates, far better tolerability and safety, and a much lower pill burden. Also, they are vastly simpler to administer than are current standard therapies. And all this is being achieved with a 12-week treatment duration instead of the 24 weeks required with standard therapy in 2013, Dr. Everson said at a conference on internal medicine sponsored by the University of Colorado.
"In the past I could say we really had pretty [intolerable] therapy, and it was pretty difficult for patients to take it. Interferon-free therapy is evolving rapidly, and I hope that it will be in primary care physicians’ backyards in the near future. I think this is probably going to be a treatment that you all provide," added Dr. Everson, professor of medicine and director of hepatology at the university.
Indeed, at hepatology clinics around the country, patients with early-stage HCV and their physicians are taking a "wait until next year" attitude toward starting treatment in anticipation that the Food and Drug Administration could approve the first of these new DAAs, sofosbuvir, before the year’s end.
The number of prescriptions for HCV therapy for treatment-naive patients at the University of Colorado clinic has plummeted in 2013 compared with 2012. The only patients starting treatment now are those with advanced HCV liver disease, to halt further disease progression and reduce the risk of developing hepatocellular carcinoma, according to Dr. Everson.
The FDA has granted Gilead Sciences priority review status for sofosbuvir, an oral inhibitor of nucleotide N55b polymerase, with a target decision date in early December. The application for marketing approval is for two indications. One involves sofosbuvir as part of a 12-week, triple-therapy regimen including pegylated interferon and ribavirin in treatment-naive patients with HCV genotypes 1, 4, 5, and 6, based in large part upon the highly favorable results of the phase III NEUTRINO trial (N. Engl. J. Med. 2013;368:1878-87).
The other proposed indication is sofosbuvir in combination with ribavirin as an interferon-free, 12-week regimen in patients with HCV genotypes 2 or 3, based upon the results of the FISSION and POSITRON trials (N. Engl. J. Med. 2013;368:1867-77).
In the NEUTRINO trial, 12 weeks of triple-therapy with sofosbuvir/interferon/ribavirin resulted in a 90% cure rate in patients with HCV genotype 1, which accounts for three-quarters of all HCV infections in the United States. The dropout rate due to side effects was a mere 2%. In contrast, today’s standard therapy, consisting of either of the protease inhibitors telaprevir (Incivek) or boceprevir (Victrelis) combined with pegylated interferon and ribavirin, has a 70%-75% cure rate. And many patients can’t tolerate or are ineligible for interferon.
"When I started treating hepatitis C patients 25 years ago, I was happy because the ALT would normalize in half the patients with genotype 1, but I wasn’t curing anybody. And now triple therapy with sofosbuvir, with a 90% cure rate, could be approved by the end of the year," Dr. Everson marveled.
In the FISSION trial, treatment-naive patients with HCV genotype 2 had a 97% cure rate with 12 weeks of sofosbuvir/ribavirin compared with 78% in those assigned to today’s standard regimen of 24 weeks of pegylated interferon/ribavirin. And sofosbuvir is just one pill per day, coupled with ribavirin at two or three pills twice daily.
In POSITRON, conducted in patients who had relapsed or were nonresponders to the standard 24 weeks of pegylated interferon/ribavirin, 12 weeks of sofosbuvir/ribavirin had an 86% response rate in patients with HCV genotype 2. With an additional 4 weeks of the interferon-free regimen, the cure rate climbed to 94%. Cure rates were lower in genotype 3 patients, but of note, the cure rate in treatment-experienced genotype 3 patients with cirrhosis more than tripled from 19% with 12 weeks of sofosbuvir/ribavirin to 61% with 16 weeks.
Other oral DAAs in the developmental pipeline include simeprevir, daclatasvir, and asunaprevir. The clinical trials experience to date demonstrate that combination therapy with more than one DAA boosts the cure rate even higher than with sofosbuvir/ribavirin. For example, in the phase II, open-label AVIATOR study, 12 weeks of a cocktail comprising three DAAs plus ribavirin brought a 96% cure rate in treatment-naive patients with HCV genotype 1 and a 93% cure rate in those who had previously failed on standard interferon-containing therapy. The AVIATOR cocktail is being formulated as a two-pills-per-day regimen.
Further, Dr. Everson was principal investigator in a Bristol-Myers Squibb–sponsored study of a totally interferon- and ribavirin-free regimen consisting of triple-DAA therapy. Each of the DAAs has a different mechanism of action: Daclatasvir is an inhibitor of the HCV NS5a protein; asunaprevir is an NS3 protease inhibitor; and the agent known for now as BMS-791325 is a nonnucleoside polymerase NS5b inhibitor. The cure rate with 12 weeks of triple-DAA therapy in treatment-naive, noncirrhotic patients with HCV genotype 1 was 94%.
Hepatologists define cure of HCV as an SVR12, or a sustained virologic response featuring no detectable HCV RNA in the blood for 12 weeks after the conclusion of therapy. The likelihood that a patient who achieves an SVR12 will remain HCV free through 10 years is 99%-100% (Gastroenterology 2010;139:1593-1601).
"The future looks pretty good for hepatitis C patients," Dr. Everson observed.
Moreover, curing HCV is going to have major downstream benefits for the health care system, he added. Today, 36% of all patients on the liver transplantation waiting list have HCV; that proportion will drop substantially. There will be fewer cases of hepatocellular carcinoma, B-cell lymphoma, and adult-onset diabetes, a drop in HCV-related autoimmune disorders, and reduced costs of care for patients with chronic HCV.
Dr. Everson reported that he receives research grants from and/or serves as a consultant to or advisory board member for roughly two dozen pharmaceutical companies.
AT THE ANNUAL INTERNAL MEDICINE PROGRAM

Beware unpasteurized milk and milk products, expert says
VAIL, COLO. – Aged cheese made from unpasteurized milk is not pathogen free and has been responsible for numerous food poisoning outbreaks, Dr. Mary P. Glodé said at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
A common misperception is that the aging or curing process involved in cheese making kills any pathogens present in raw milk. Not so. Last February the Food and Drug Administration and Health Canada jointly published a draft assessment of the risk of listeriosis from soft-ripened cheese. Listeriosis is the third leading cause of death from food poisoning in the United States. The agencies found that the risk of listeriosis was 50-160 times greater per serving if the cheese was made with raw, unpasteurized milk than with pasteurized milk.

The public comment period regarding the draft document has expired, and the FDA is expected to soon announce some sort of action. Possibilities include adopting a European-style approach featuring much closer regulation of animal health and hygiene during the milk collection process so that milk is less contaminated as it comes from the animal, extending the current 60-day aging rule for cheese to 90 days or longer in order to help eliminate pathogens, or banning all cheeses made with raw milk from interstate commerce. The FDA banned interstate commerce of raw milk in 1987, but made an exception for cheese made from raw milk provided it was aged for at least 60 days, noted Dr. Glodé, professor of pediatrics and section head of pediatric infectious diseases at the Children’s Hospital Colorado and the University of Colorado, Denver.
Despite the 26-year-old ban on interstate transport of fluid raw milk, enthusiasts throughout most of the country are still able to obtain it. Raw milk sales are illegal in only a handful of states. Retail sale is legal in 10 states, and on-the-farm sale is legal in another 16. In other states, it’s possible to acquire a share in a raw milk herd or purchase raw milk as "pet food."
A Centers for Disease Control and Prevention analysis concluded that 85% of a series of 239 hospitalizations due to tainted dairy products involved raw milk or cheese made from raw milk. Almost two-thirds of the hospitalized individuals were under age 20.
The CDC estimates that 1.3 million food-borne illnesses due to contaminated dairy products occur annually in the United States, with half involving pathogenic bacteria. Eighty percent of food-borne illness outbreaks involving fluid milk are due to unpasteurized milk, even though less than 1% of milk consumed in the United States is unpasteurized.
Pathogens detected in up to 5%-11% of samples gathered from bulk tank milk used for raw milk cheese production include Escherichia coli 0157, Salmonella, Shigella, Yersinia enterocolitica, Listeria monocytogenes, and Campylobacter jejuni.
Yet raw milk or cheese made from raw milk is by no means always the culprit in food-borne illnesses due to tainted dairy products. For example, a CDC analysis of all reported cases of listeriosis in 2009-2011 implicated cheese in 6 of 12 outbreaks affecting 38 states – but the culprit cheese was made from pasteurized milk in 5 of the 6 outbreaks. Since the cheese was made from pasteurized milk, it is likely that the contamination occurred later, during the cheese-making process. Mexican-style cheeses made from pasteurized milk were implicated in four outbreaks, a chive and white brine cheese made from pasteurized milk was identified as the source in another, and an aged blue cheese made from raw milk was implicated in one multistate outbreak (MMWR 2013;162:448-52).
Raw milk advocates claim the product is more nutritious than pasteurized milk, but this hasn’t held up under scientific scrutiny, Dr. Glodé said.
A more intriguing argument for raw milk, in her view, comes from a single British cross-sectional study, the Study of Asthma and Allergy in Shropshire, which ended up linking consumption of unpasteurized milk to the hygiene hypothesis of atopy.
This was a large-scale study led by investigators at St. George’s University of London. It aimed to determine the explanation for the often-documented observation that farmers’ children have a reduced prevalence of allergic disorders. The investigators queried the parents of nearly 5,000 rural children regarding the kids’ diet, allergic status, and farming exposures, then performed skin prick and blood testing in 879 of the children.
Children who consumed unpasteurized milk, even infrequently, had a 41% reduction in current eczema symptoms as well as a 76% reduction in atopy compared with non–raw milk drinkers. Total IgE levels were 59% lower in the raw milk drinkers, and they also showed greater production of whole blood stimulated interferon-gamma. These benefits were seen regardless of whether the rural raw milk–drinking children were in farming or nonfarming families.
The investigators concluded that unpasteurized milk "might" be a modifiable influence on allergic sensitization in children (J. Allergy Clin. Immunol. 2006;117:1374-81).
"I would say, stay tuned on this. It’s just one study. My main message is that it is very clear that there are serious health dangers associated with consuming nonhuman unpasteurized milk or milk products," Dr. Glodé commented.
She reported having no relevant financial conflicts of interest.
VAIL, COLO. – Aged cheese made from unpasteurized milk is not pathogen free and has been responsible for numerous food poisoning outbreaks, Dr. Mary P. Glodé said at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
A common misperception is that the aging or curing process involved in cheese making kills any pathogens present in raw milk. Not so. Last February the Food and Drug Administration and Health Canada jointly published a draft assessment of the risk of listeriosis from soft-ripened cheese. Listeriosis is the third leading cause of death from food poisoning in the United States. The agencies found that the risk of listeriosis was 50-160 times greater per serving if the cheese was made with raw, unpasteurized milk than with pasteurized milk.
The public comment period regarding the draft document has expired, and the FDA is expected to soon announce some sort of action. Possibilities include adopting a European-style approach featuring much closer regulation of animal health and hygiene during the milk collection process so that milk is less contaminated as it comes from the animal, extending the current 60-day aging rule for cheese to 90 days or longer in order to help eliminate pathogens, or banning all cheeses made with raw milk from interstate commerce. The FDA banned interstate commerce of raw milk in 1987, but made an exception for cheese made from raw milk provided it was aged for at least 60 days, noted Dr. Glodé, professor of pediatrics and section head of pediatric infectious diseases at the Children’s Hospital Colorado and the University of Colorado, Denver.
Despite the 26-year-old ban on interstate transport of fluid raw milk, enthusiasts throughout most of the country are still able to obtain it. Raw milk sales are illegal in only a handful of states. Retail sale is legal in 10 states, and on-the-farm sale is legal in another 16. In other states, it’s possible to acquire a share in a raw milk herd or purchase raw milk as "pet food."
A Centers for Disease Control and Prevention analysis concluded that 85% of a series of 239 hospitalizations due to tainted dairy products involved raw milk or cheese made from raw milk. Almost two-thirds of the hospitalized individuals were under age 20.
The CDC estimates that 1.3 million food-borne illnesses due to contaminated dairy products occur annually in the United States, with half involving pathogenic bacteria. Eighty percent of food-borne illness outbreaks involving fluid milk are due to unpasteurized milk, even though less than 1% of milk consumed in the United States is unpasteurized.
Pathogens detected in up to 5%-11% of samples gathered from bulk tank milk used for raw milk cheese production include Escherichia coli 0157, Salmonella, Shigella, Yersinia enterocolitica, Listeria monocytogenes, and Campylobacter jejuni.
Yet raw milk or cheese made from raw milk is by no means always the culprit in food-borne illnesses due to tainted dairy products. For example, a CDC analysis of all reported cases of listeriosis in 2009-2011 implicated cheese in 6 of 12 outbreaks affecting 38 states – but the culprit cheese was made from pasteurized milk in 5 of the 6 outbreaks. Since the cheese was made from pasteurized milk, it is likely that the contamination occurred later, during the cheese-making process. Mexican-style cheeses made from pasteurized milk were implicated in four outbreaks, a chive and white brine cheese made from pasteurized milk was identified as the source in another, and an aged blue cheese made from raw milk was implicated in one multistate outbreak (MMWR 2013;162:448-52).
Raw milk advocates claim the product is more nutritious than pasteurized milk, but this hasn’t held up under scientific scrutiny, Dr. Glodé said.
A more intriguing argument for raw milk, in her view, comes from a single British cross-sectional study, the Study of Asthma and Allergy in Shropshire, which ended up linking consumption of unpasteurized milk to the hygiene hypothesis of atopy.
This was a large-scale study led by investigators at St. George’s University of London. It aimed to determine the explanation for the often-documented observation that farmers’ children have a reduced prevalence of allergic disorders. The investigators queried the parents of nearly 5,000 rural children regarding the kids’ diet, allergic status, and farming exposures, then performed skin prick and blood testing in 879 of the children.
Children who consumed unpasteurized milk, even infrequently, had a 41% reduction in current eczema symptoms as well as a 76% reduction in atopy compared with non–raw milk drinkers. Total IgE levels were 59% lower in the raw milk drinkers, and they also showed greater production of whole blood stimulated interferon-gamma. These benefits were seen regardless of whether the rural raw milk–drinking children were in farming or nonfarming families.
The investigators concluded that unpasteurized milk "might" be a modifiable influence on allergic sensitization in children (J. Allergy Clin. Immunol. 2006;117:1374-81).
"I would say, stay tuned on this. It’s just one study. My main message is that it is very clear that there are serious health dangers associated with consuming nonhuman unpasteurized milk or milk products," Dr. Glodé commented.
She reported having no relevant financial conflicts of interest.
VAIL, COLO. – Aged cheese made from unpasteurized milk is not pathogen free and has been responsible for numerous food poisoning outbreaks, Dr. Mary P. Glodé said at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
A common misperception is that the aging or curing process involved in cheese making kills any pathogens present in raw milk. Not so. Last February the Food and Drug Administration and Health Canada jointly published a draft assessment of the risk of listeriosis from soft-ripened cheese. Listeriosis is the third leading cause of death from food poisoning in the United States. The agencies found that the risk of listeriosis was 50-160 times greater per serving if the cheese was made with raw, unpasteurized milk than with pasteurized milk.
The public comment period regarding the draft document has expired, and the FDA is expected to soon announce some sort of action. Possibilities include adopting a European-style approach featuring much closer regulation of animal health and hygiene during the milk collection process so that milk is less contaminated as it comes from the animal, extending the current 60-day aging rule for cheese to 90 days or longer in order to help eliminate pathogens, or banning all cheeses made with raw milk from interstate commerce. The FDA banned interstate commerce of raw milk in 1987, but made an exception for cheese made from raw milk provided it was aged for at least 60 days, noted Dr. Glodé, professor of pediatrics and section head of pediatric infectious diseases at the Children’s Hospital Colorado and the University of Colorado, Denver.
Despite the 26-year-old ban on interstate transport of fluid raw milk, enthusiasts throughout most of the country are still able to obtain it. Raw milk sales are illegal in only a handful of states. Retail sale is legal in 10 states, and on-the-farm sale is legal in another 16. In other states, it’s possible to acquire a share in a raw milk herd or purchase raw milk as "pet food."
A Centers for Disease Control and Prevention analysis concluded that 85% of a series of 239 hospitalizations due to tainted dairy products involved raw milk or cheese made from raw milk. Almost two-thirds of the hospitalized individuals were under age 20.
The CDC estimates that 1.3 million food-borne illnesses due to contaminated dairy products occur annually in the United States, with half involving pathogenic bacteria. Eighty percent of food-borne illness outbreaks involving fluid milk are due to unpasteurized milk, even though less than 1% of milk consumed in the United States is unpasteurized.
Pathogens detected in up to 5%-11% of samples gathered from bulk tank milk used for raw milk cheese production include Escherichia coli 0157, Salmonella, Shigella, Yersinia enterocolitica, Listeria monocytogenes, and Campylobacter jejuni.
Yet raw milk or cheese made from raw milk is by no means always the culprit in food-borne illnesses due to tainted dairy products. For example, a CDC analysis of all reported cases of listeriosis in 2009-2011 implicated cheese in 6 of 12 outbreaks affecting 38 states – but the culprit cheese was made from pasteurized milk in 5 of the 6 outbreaks. Since the cheese was made from pasteurized milk, it is likely that the contamination occurred later, during the cheese-making process. Mexican-style cheeses made from pasteurized milk were implicated in four outbreaks, a chive and white brine cheese made from pasteurized milk was identified as the source in another, and an aged blue cheese made from raw milk was implicated in one multistate outbreak (MMWR 2013;162:448-52).
Raw milk advocates claim the product is more nutritious than pasteurized milk, but this hasn’t held up under scientific scrutiny, Dr. Glodé said.
A more intriguing argument for raw milk, in her view, comes from a single British cross-sectional study, the Study of Asthma and Allergy in Shropshire, which ended up linking consumption of unpasteurized milk to the hygiene hypothesis of atopy.
This was a large-scale study led by investigators at St. George’s University of London. It aimed to determine the explanation for the often-documented observation that farmers’ children have a reduced prevalence of allergic disorders. The investigators queried the parents of nearly 5,000 rural children regarding the kids’ diet, allergic status, and farming exposures, then performed skin prick and blood testing in 879 of the children.
Children who consumed unpasteurized milk, even infrequently, had a 41% reduction in current eczema symptoms as well as a 76% reduction in atopy compared with non–raw milk drinkers. Total IgE levels were 59% lower in the raw milk drinkers, and they also showed greater production of whole blood stimulated interferon-gamma. These benefits were seen regardless of whether the rural raw milk–drinking children were in farming or nonfarming families.
The investigators concluded that unpasteurized milk "might" be a modifiable influence on allergic sensitization in children (J. Allergy Clin. Immunol. 2006;117:1374-81).
"I would say, stay tuned on this. It’s just one study. My main message is that it is very clear that there are serious health dangers associated with consuming nonhuman unpasteurized milk or milk products," Dr. Glodé commented.
She reported having no relevant financial conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL PEDIATRIC INFECTIOUS DISEASES CONFERENCE

Psychiatrists get low marks in assessing adherence
HOLLYWOOD, FLA. – Many American psychiatrists have a bias against long-acting injectable antipsychotic medications, which constitutes a major barrier to broader use of this often advantageous form of therapy, investigators asserted at a meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health.
"There’s a lot of anti-shot sentiment in the U.S., particularly on the part of doctors. They think that the therapeutic alliance will be negatively impacted by talking about an injection. Many of my patients have never been told that there is such a thing as injectable medicines," according to Dawn I. Velligan, Ph.D., professor of psychiatry and director of the division of schizophrenia and related disorders at the University of Texas Health Science Center at San Antonio.
She has participated in studies involving structured observation of psychiatrist-patient encounters that she found revealing – and troubling.

"When doctors do offer a long-acting injectable agent, they’re so uncomfortable about doing it that they stutter and are just clearly uncomfortable. You can see it in linguistic fluency measures. Not only that, but they lead with the modality, rather than the potential benefit. They’ll say, ‘You don’t want a shot, do you?’ Well, of course not. What kind of a question is that? A doctor never starts out by saying, ‘I have these horse pills, and they’re really hard to take.’ They start out by explaining what this medication is going to do for your recovery, and then they mention that they’re horse pills and are hard to swallow," Dr. Velligan said.
Roughly 50% of patients are poorly adherent to oral antipsychotic therapy. Nonadherence results in higher rates of relapse, hospitalization, and disability. When asked, most psychiatrists will say they consider long-acting injectables (LAIs) the way to go when patients are nonadherent. Unfortunately, however, they are not good at all at identifying nonadherent patients.
"They don’t have any idea. I think doctors prescribe antipsychotic medication in an atmosphere of unclear adherence. So what they’re doing is raising the dose and raising the dose. I think they don’t know how much to prescribe," Dr. Velligan declared.
She was on a National Institute of Mental Health–sponsored expert panel that concluded all of the standard methods of assessing adherence are error prone (J. Psychosom. Res. 2010;69:591-9). For example, studies show that patient self-report vastly overestimates adherence and that clinicians are poor at judging the level of adherence. Plasma and urine analysis provide good quality information only about the last 4-5 days, not the past 30-60 days. "Smart" pill containers with electronic monitoring technology don’t work if the patient opens the bottle and forgets to put the top back on. Pill counts work only if the patient remembers to bring in his bottles. And pharmacy records, too, are unreliable in assessing adherence.
"I have people who are 100% adherent, but they haven’t picked up their pills from the pharmacy in 7 months because they had a bunch of pills left over from all the times that they weren’t adherent before," she observed.
An LAI offers numerous potential advantages for the prescriber. For one, it eliminates guesswork about compliance status.
"If patients with a prescription for oral therapy come in and they’re not looking well, you don’t know how much of their medication they’ve been taking. It’s an enormous crap shoot, yet we do it every single day," Dr. Velligan charged.
LAI therapy also alerts the psychiatrist when nonadherence starts, and it’s invaluable in disentangling efficacy from problem adherence.
"If I’m giving you an injection and you’re not doing well and you’ve shown up every time for your shots, this medicine is not working so well. It’s not the right antipsychotic for you," she explained.
Together with Dr. Martha Sajatovic, a psychiatrist at Case Western Reserve University in Cleveland, Dr. Velligan has developed what they call the NOB (individuals Not receiving Optimum Benefit from antipsychotic medication) checklist. It’s intended for implementation by overburdened clinicians in community mental health centers. A "yes" answer to any of the five simple questions (see below) should alert the provider that LAIs might in this case help in clinical decision making and improve patient outcomes.
In a separate presentation, Dr. Steven G. Potkin presented a detailed analysis of 69 recorded psychiatrist-patient community mental health center office visits involving 22 patients being treated with oral antipsychotics and 38 on LAIs. Prescribers spent merely a mean 2% of the visit time discussing adherence with their patients. Moreover, psychiatrists made decisions about antipsychotic treatment without patient or caregiver input in two-thirds of the encounters.
"Collectively, these findings suggest that there is an opportunity for prescribers to increase active patient engagement, address resistance about LAIs, and provide better LAI-relevant information for more individualized options and approaches to treating patients with schizophrenia," concluded Dr. Potkin, professor of psychiatry and director of the brain imaging center at the University of California, Irvine.
Dr. Potkin’s study was funded by Otsuka American Pharmaceutical and H. Lundbeck. He reported receiving research support from roughly 20 pharmaceutical companies. Dr. Velligan reported having no financial conflicts.
The NOB Checklist
The NOB checklist is aimed at helping clinicians working in community health centers to quickly determine whether patients are adherent.
Here is a listing of the five simple questions:
1) Based upon the patient’s report, caregiver report, or your prescribing record, has the patient missed doses such that 30% or more of the medication has been missed?
2) Is the patient currently on more than one antipsychotic (not during a switch)?
3) Has the patient been on more than two antipsychotics in the past 12 months?
4) Has the patient been hospitalized or had a crisis visit in the past 12 months?
5) Is the patient not satisfied with the current level of symptom control?
A "yes" answer to any of these questions warrants offering a long-acting injectable antipsychotic agent to this patient.
Source: Dr. Velligan
HOLLYWOOD, FLA. – Many American psychiatrists have a bias against long-acting injectable antipsychotic medications, which constitutes a major barrier to broader use of this often advantageous form of therapy, investigators asserted at a meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health.
"There’s a lot of anti-shot sentiment in the U.S., particularly on the part of doctors. They think that the therapeutic alliance will be negatively impacted by talking about an injection. Many of my patients have never been told that there is such a thing as injectable medicines," according to Dawn I. Velligan, Ph.D., professor of psychiatry and director of the division of schizophrenia and related disorders at the University of Texas Health Science Center at San Antonio.
She has participated in studies involving structured observation of psychiatrist-patient encounters that she found revealing – and troubling.
"When doctors do offer a long-acting injectable agent, they’re so uncomfortable about doing it that they stutter and are just clearly uncomfortable. You can see it in linguistic fluency measures. Not only that, but they lead with the modality, rather than the potential benefit. They’ll say, ‘You don’t want a shot, do you?’ Well, of course not. What kind of a question is that? A doctor never starts out by saying, ‘I have these horse pills, and they’re really hard to take.’ They start out by explaining what this medication is going to do for your recovery, and then they mention that they’re horse pills and are hard to swallow," Dr. Velligan said.
Roughly 50% of patients are poorly adherent to oral antipsychotic therapy. Nonadherence results in higher rates of relapse, hospitalization, and disability. When asked, most psychiatrists will say they consider long-acting injectables (LAIs) the way to go when patients are nonadherent. Unfortunately, however, they are not good at all at identifying nonadherent patients.
"They don’t have any idea. I think doctors prescribe antipsychotic medication in an atmosphere of unclear adherence. So what they’re doing is raising the dose and raising the dose. I think they don’t know how much to prescribe," Dr. Velligan declared.
She was on a National Institute of Mental Health–sponsored expert panel that concluded all of the standard methods of assessing adherence are error prone (J. Psychosom. Res. 2010;69:591-9). For example, studies show that patient self-report vastly overestimates adherence and that clinicians are poor at judging the level of adherence. Plasma and urine analysis provide good quality information only about the last 4-5 days, not the past 30-60 days. "Smart" pill containers with electronic monitoring technology don’t work if the patient opens the bottle and forgets to put the top back on. Pill counts work only if the patient remembers to bring in his bottles. And pharmacy records, too, are unreliable in assessing adherence.
"I have people who are 100% adherent, but they haven’t picked up their pills from the pharmacy in 7 months because they had a bunch of pills left over from all the times that they weren’t adherent before," she observed.
An LAI offers numerous potential advantages for the prescriber. For one, it eliminates guesswork about compliance status.
"If patients with a prescription for oral therapy come in and they’re not looking well, you don’t know how much of their medication they’ve been taking. It’s an enormous crap shoot, yet we do it every single day," Dr. Velligan charged.
LAI therapy also alerts the psychiatrist when nonadherence starts, and it’s invaluable in disentangling efficacy from problem adherence.
"If I’m giving you an injection and you’re not doing well and you’ve shown up every time for your shots, this medicine is not working so well. It’s not the right antipsychotic for you," she explained.
Together with Dr. Martha Sajatovic, a psychiatrist at Case Western Reserve University in Cleveland, Dr. Velligan has developed what they call the NOB (individuals Not receiving Optimum Benefit from antipsychotic medication) checklist. It’s intended for implementation by overburdened clinicians in community mental health centers. A "yes" answer to any of the five simple questions (see below) should alert the provider that LAIs might in this case help in clinical decision making and improve patient outcomes.
In a separate presentation, Dr. Steven G. Potkin presented a detailed analysis of 69 recorded psychiatrist-patient community mental health center office visits involving 22 patients being treated with oral antipsychotics and 38 on LAIs. Prescribers spent merely a mean 2% of the visit time discussing adherence with their patients. Moreover, psychiatrists made decisions about antipsychotic treatment without patient or caregiver input in two-thirds of the encounters.
"Collectively, these findings suggest that there is an opportunity for prescribers to increase active patient engagement, address resistance about LAIs, and provide better LAI-relevant information for more individualized options and approaches to treating patients with schizophrenia," concluded Dr. Potkin, professor of psychiatry and director of the brain imaging center at the University of California, Irvine.
Dr. Potkin’s study was funded by Otsuka American Pharmaceutical and H. Lundbeck. He reported receiving research support from roughly 20 pharmaceutical companies. Dr. Velligan reported having no financial conflicts.
The NOB Checklist
The NOB checklist is aimed at helping clinicians working in community health centers to quickly determine whether patients are adherent.
Here is a listing of the five simple questions:
1) Based upon the patient’s report, caregiver report, or your prescribing record, has the patient missed doses such that 30% or more of the medication has been missed?
2) Is the patient currently on more than one antipsychotic (not during a switch)?
3) Has the patient been on more than two antipsychotics in the past 12 months?
4) Has the patient been hospitalized or had a crisis visit in the past 12 months?
5) Is the patient not satisfied with the current level of symptom control?
A "yes" answer to any of these questions warrants offering a long-acting injectable antipsychotic agent to this patient.
Source: Dr. Velligan
HOLLYWOOD, FLA. – Many American psychiatrists have a bias against long-acting injectable antipsychotic medications, which constitutes a major barrier to broader use of this often advantageous form of therapy, investigators asserted at a meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health.
"There’s a lot of anti-shot sentiment in the U.S., particularly on the part of doctors. They think that the therapeutic alliance will be negatively impacted by talking about an injection. Many of my patients have never been told that there is such a thing as injectable medicines," according to Dawn I. Velligan, Ph.D., professor of psychiatry and director of the division of schizophrenia and related disorders at the University of Texas Health Science Center at San Antonio.
She has participated in studies involving structured observation of psychiatrist-patient encounters that she found revealing – and troubling.
"When doctors do offer a long-acting injectable agent, they’re so uncomfortable about doing it that they stutter and are just clearly uncomfortable. You can see it in linguistic fluency measures. Not only that, but they lead with the modality, rather than the potential benefit. They’ll say, ‘You don’t want a shot, do you?’ Well, of course not. What kind of a question is that? A doctor never starts out by saying, ‘I have these horse pills, and they’re really hard to take.’ They start out by explaining what this medication is going to do for your recovery, and then they mention that they’re horse pills and are hard to swallow," Dr. Velligan said.
Roughly 50% of patients are poorly adherent to oral antipsychotic therapy. Nonadherence results in higher rates of relapse, hospitalization, and disability. When asked, most psychiatrists will say they consider long-acting injectables (LAIs) the way to go when patients are nonadherent. Unfortunately, however, they are not good at all at identifying nonadherent patients.
"They don’t have any idea. I think doctors prescribe antipsychotic medication in an atmosphere of unclear adherence. So what they’re doing is raising the dose and raising the dose. I think they don’t know how much to prescribe," Dr. Velligan declared.
She was on a National Institute of Mental Health–sponsored expert panel that concluded all of the standard methods of assessing adherence are error prone (J. Psychosom. Res. 2010;69:591-9). For example, studies show that patient self-report vastly overestimates adherence and that clinicians are poor at judging the level of adherence. Plasma and urine analysis provide good quality information only about the last 4-5 days, not the past 30-60 days. "Smart" pill containers with electronic monitoring technology don’t work if the patient opens the bottle and forgets to put the top back on. Pill counts work only if the patient remembers to bring in his bottles. And pharmacy records, too, are unreliable in assessing adherence.
"I have people who are 100% adherent, but they haven’t picked up their pills from the pharmacy in 7 months because they had a bunch of pills left over from all the times that they weren’t adherent before," she observed.
An LAI offers numerous potential advantages for the prescriber. For one, it eliminates guesswork about compliance status.
"If patients with a prescription for oral therapy come in and they’re not looking well, you don’t know how much of their medication they’ve been taking. It’s an enormous crap shoot, yet we do it every single day," Dr. Velligan charged.
LAI therapy also alerts the psychiatrist when nonadherence starts, and it’s invaluable in disentangling efficacy from problem adherence.
"If I’m giving you an injection and you’re not doing well and you’ve shown up every time for your shots, this medicine is not working so well. It’s not the right antipsychotic for you," she explained.
Together with Dr. Martha Sajatovic, a psychiatrist at Case Western Reserve University in Cleveland, Dr. Velligan has developed what they call the NOB (individuals Not receiving Optimum Benefit from antipsychotic medication) checklist. It’s intended for implementation by overburdened clinicians in community mental health centers. A "yes" answer to any of the five simple questions (see below) should alert the provider that LAIs might in this case help in clinical decision making and improve patient outcomes.
In a separate presentation, Dr. Steven G. Potkin presented a detailed analysis of 69 recorded psychiatrist-patient community mental health center office visits involving 22 patients being treated with oral antipsychotics and 38 on LAIs. Prescribers spent merely a mean 2% of the visit time discussing adherence with their patients. Moreover, psychiatrists made decisions about antipsychotic treatment without patient or caregiver input in two-thirds of the encounters.
"Collectively, these findings suggest that there is an opportunity for prescribers to increase active patient engagement, address resistance about LAIs, and provide better LAI-relevant information for more individualized options and approaches to treating patients with schizophrenia," concluded Dr. Potkin, professor of psychiatry and director of the brain imaging center at the University of California, Irvine.
Dr. Potkin’s study was funded by Otsuka American Pharmaceutical and H. Lundbeck. He reported receiving research support from roughly 20 pharmaceutical companies. Dr. Velligan reported having no financial conflicts.
The NOB Checklist
The NOB checklist is aimed at helping clinicians working in community health centers to quickly determine whether patients are adherent.
Here is a listing of the five simple questions:
1) Based upon the patient’s report, caregiver report, or your prescribing record, has the patient missed doses such that 30% or more of the medication has been missed?
2) Is the patient currently on more than one antipsychotic (not during a switch)?
3) Has the patient been on more than two antipsychotics in the past 12 months?
4) Has the patient been hospitalized or had a crisis visit in the past 12 months?
5) Is the patient not satisfied with the current level of symptom control?
A "yes" answer to any of these questions warrants offering a long-acting injectable antipsychotic agent to this patient.
Source: Dr. Velligan
EXPERT ANALYSIS FROM THE NCDEU MEETING

Adult ADHD: Nonpharmacologic interventions are useful adjuncts
ESTES PARK, COLO. – Hands down, the most effective treatment for adult attention-deficit/hyperactivity disorder is psychostimulants.
The nonstimulant medications are a second-line alternative with less robust benefits, but they come in quite handy in selected situations, Dr. Robert D. Davies noted at a conference on internal medicine sponsored by the University of Colorado.
Also, a wealth of nonpharmacologic treatments are available. These include mindfulness exercises, cognitive behavioral therapy, life coaching, psychoeducational self-help audio books, and support groups.
"They’re great adjunct treatments, but in and of themselves not great solo treatments," according to Dr. Davies. "There’s an analogy to having poor near vision, so you never learned to read, and then suddenly you get glasses. That’s kind of like getting on medications: You still wouldn’t know how to read, but now you could learn how. So trying the nonpharmacologic interventions will be pretty frustrating for somebody who wants to avoid medications. You can try using those tools to help them with organization and those sorts of things, but it’s usually a huge struggle. Instead, put them on meds, teach them some of those things, and then see if off meds they can maintain those gains," advised Dr. Davies, a psychiatrist at the university.

A tip on self-help books geared to adults with attention-deficit/hyperactivity disorder (ADHD): "If you have a patient who’s never been able to get through a book in their life, don’t recommend a book that’s going to help them. ADHD folks do better with books on tape." Among the many on the market, Dr. Davies mentioned "Driven to Distraction" by Dr. Edward M. Hallowell and Dr. John J. Ratey as particularly good.
The psychostimulants fall into two categories: methylphenidate formulations and dextroamphetamine formulations. They’re equally effective, with the caveat that 20% of the population doesn’t respond to the methylphenidate drugs; however, they do respond to the dextroamphetamines. It’s a class effect, so when a patient isn’t doing well on a methylphenidate, don’t bother switching to a different methylphenidate drug; move on to a dextroamphetamine formulation.
Only four stimulants are approved by the Food and Drug Administration for adults: Adderal XR (dextroamphetamine/amphetamine), with a 9-hour duration of action and 15- to 30-mg dosage range; Focalin XR (dexmethylphenidate), with an 8- to 12-hour duration of action and dosage range of 20-40 mg; Vyvanse (lisdexamfetamine dimesylate), with a duration of 12 hours and dosing at 30-70 mg; and Concerta (methylphenidate extended-release), with a 12-hour duration of action and dosage range of 18-54 mg.
A history of drug abuse is a consideration in choosing a pharmacologic agent, but it isn’t necessarily a deal breaker in prescribing a stimulant. Some individuals with ADHD used stimulants or cocaine illicitly while students as a form of self-medication to enhance academic performance; they may be reasonable candidates for Concerta or Vyvanse, which have extremely low abuse potential. On the other hand, Dr. Davies recommended against prescribing stimulants for adult ADHD patients with a history of opiate or methamphetamine abuse.
Other situations where stimulant medications are best avoided include patients with medical conditions including heart disease, hypertension, and seizure disorders.
Only one nonstimulant medication is approved in adults: Strattera (atomoxetine). The reduction in ADHD symptoms is roughly 30% less than with stimulants. However, it is a once-daily drug, which is an advantage.
"When I’m treating anxiety or ADHD, especially in adults, a longer-acting drug is better. I always try to get patients away from that on-off phenomenon. That’s a feeling they don’t like," the psychiatrist continued.
Adults with ADHD may need pharmacologic assistance not only during a lengthy workday, but in the evening as well.
Nonstimulants that are sometimes used off-label in adults include Wellbutrin (bupropion), which is approved for children with ADHD. It is about half as effective as a stimulant medication. Effexor (venlafaxine) and Provigil (modafanil) are other nonstimulants used off-label; neither has been well studied in adult ADHD, according to Dr. Davies.
Adults with ADHD don’t develop tolerance to stimulant medications, unlike amphetamine abusers. Asked if there is an upper age limit for the use of psychostimulants in treating ADHD, the psychiatrist replied no.
"My oldest patient is 75 and I’ve been treating him for the last 15 years," he added.
Dr. Davies reported having no financial conflicts.
ESTES PARK, COLO. – Hands down, the most effective treatment for adult attention-deficit/hyperactivity disorder is psychostimulants.
The nonstimulant medications are a second-line alternative with less robust benefits, but they come in quite handy in selected situations, Dr. Robert D. Davies noted at a conference on internal medicine sponsored by the University of Colorado.
Also, a wealth of nonpharmacologic treatments are available. These include mindfulness exercises, cognitive behavioral therapy, life coaching, psychoeducational self-help audio books, and support groups.
"They’re great adjunct treatments, but in and of themselves not great solo treatments," according to Dr. Davies. "There’s an analogy to having poor near vision, so you never learned to read, and then suddenly you get glasses. That’s kind of like getting on medications: You still wouldn’t know how to read, but now you could learn how. So trying the nonpharmacologic interventions will be pretty frustrating for somebody who wants to avoid medications. You can try using those tools to help them with organization and those sorts of things, but it’s usually a huge struggle. Instead, put them on meds, teach them some of those things, and then see if off meds they can maintain those gains," advised Dr. Davies, a psychiatrist at the university.
A tip on self-help books geared to adults with attention-deficit/hyperactivity disorder (ADHD): "If you have a patient who’s never been able to get through a book in their life, don’t recommend a book that’s going to help them. ADHD folks do better with books on tape." Among the many on the market, Dr. Davies mentioned "Driven to Distraction" by Dr. Edward M. Hallowell and Dr. John J. Ratey as particularly good.
The psychostimulants fall into two categories: methylphenidate formulations and dextroamphetamine formulations. They’re equally effective, with the caveat that 20% of the population doesn’t respond to the methylphenidate drugs; however, they do respond to the dextroamphetamines. It’s a class effect, so when a patient isn’t doing well on a methylphenidate, don’t bother switching to a different methylphenidate drug; move on to a dextroamphetamine formulation.
Only four stimulants are approved by the Food and Drug Administration for adults: Adderal XR (dextroamphetamine/amphetamine), with a 9-hour duration of action and 15- to 30-mg dosage range; Focalin XR (dexmethylphenidate), with an 8- to 12-hour duration of action and dosage range of 20-40 mg; Vyvanse (lisdexamfetamine dimesylate), with a duration of 12 hours and dosing at 30-70 mg; and Concerta (methylphenidate extended-release), with a 12-hour duration of action and dosage range of 18-54 mg.
A history of drug abuse is a consideration in choosing a pharmacologic agent, but it isn’t necessarily a deal breaker in prescribing a stimulant. Some individuals with ADHD used stimulants or cocaine illicitly while students as a form of self-medication to enhance academic performance; they may be reasonable candidates for Concerta or Vyvanse, which have extremely low abuse potential. On the other hand, Dr. Davies recommended against prescribing stimulants for adult ADHD patients with a history of opiate or methamphetamine abuse.
Other situations where stimulant medications are best avoided include patients with medical conditions including heart disease, hypertension, and seizure disorders.
Only one nonstimulant medication is approved in adults: Strattera (atomoxetine). The reduction in ADHD symptoms is roughly 30% less than with stimulants. However, it is a once-daily drug, which is an advantage.
"When I’m treating anxiety or ADHD, especially in adults, a longer-acting drug is better. I always try to get patients away from that on-off phenomenon. That’s a feeling they don’t like," the psychiatrist continued.
Adults with ADHD may need pharmacologic assistance not only during a lengthy workday, but in the evening as well.
Nonstimulants that are sometimes used off-label in adults include Wellbutrin (bupropion), which is approved for children with ADHD. It is about half as effective as a stimulant medication. Effexor (venlafaxine) and Provigil (modafanil) are other nonstimulants used off-label; neither has been well studied in adult ADHD, according to Dr. Davies.
Adults with ADHD don’t develop tolerance to stimulant medications, unlike amphetamine abusers. Asked if there is an upper age limit for the use of psychostimulants in treating ADHD, the psychiatrist replied no.
"My oldest patient is 75 and I’ve been treating him for the last 15 years," he added.
Dr. Davies reported having no financial conflicts.
ESTES PARK, COLO. – Hands down, the most effective treatment for adult attention-deficit/hyperactivity disorder is psychostimulants.
The nonstimulant medications are a second-line alternative with less robust benefits, but they come in quite handy in selected situations, Dr. Robert D. Davies noted at a conference on internal medicine sponsored by the University of Colorado.
Also, a wealth of nonpharmacologic treatments are available. These include mindfulness exercises, cognitive behavioral therapy, life coaching, psychoeducational self-help audio books, and support groups.
"They’re great adjunct treatments, but in and of themselves not great solo treatments," according to Dr. Davies. "There’s an analogy to having poor near vision, so you never learned to read, and then suddenly you get glasses. That’s kind of like getting on medications: You still wouldn’t know how to read, but now you could learn how. So trying the nonpharmacologic interventions will be pretty frustrating for somebody who wants to avoid medications. You can try using those tools to help them with organization and those sorts of things, but it’s usually a huge struggle. Instead, put them on meds, teach them some of those things, and then see if off meds they can maintain those gains," advised Dr. Davies, a psychiatrist at the university.
A tip on self-help books geared to adults with attention-deficit/hyperactivity disorder (ADHD): "If you have a patient who’s never been able to get through a book in their life, don’t recommend a book that’s going to help them. ADHD folks do better with books on tape." Among the many on the market, Dr. Davies mentioned "Driven to Distraction" by Dr. Edward M. Hallowell and Dr. John J. Ratey as particularly good.
The psychostimulants fall into two categories: methylphenidate formulations and dextroamphetamine formulations. They’re equally effective, with the caveat that 20% of the population doesn’t respond to the methylphenidate drugs; however, they do respond to the dextroamphetamines. It’s a class effect, so when a patient isn’t doing well on a methylphenidate, don’t bother switching to a different methylphenidate drug; move on to a dextroamphetamine formulation.
Only four stimulants are approved by the Food and Drug Administration for adults: Adderal XR (dextroamphetamine/amphetamine), with a 9-hour duration of action and 15- to 30-mg dosage range; Focalin XR (dexmethylphenidate), with an 8- to 12-hour duration of action and dosage range of 20-40 mg; Vyvanse (lisdexamfetamine dimesylate), with a duration of 12 hours and dosing at 30-70 mg; and Concerta (methylphenidate extended-release), with a 12-hour duration of action and dosage range of 18-54 mg.
A history of drug abuse is a consideration in choosing a pharmacologic agent, but it isn’t necessarily a deal breaker in prescribing a stimulant. Some individuals with ADHD used stimulants or cocaine illicitly while students as a form of self-medication to enhance academic performance; they may be reasonable candidates for Concerta or Vyvanse, which have extremely low abuse potential. On the other hand, Dr. Davies recommended against prescribing stimulants for adult ADHD patients with a history of opiate or methamphetamine abuse.
Other situations where stimulant medications are best avoided include patients with medical conditions including heart disease, hypertension, and seizure disorders.
Only one nonstimulant medication is approved in adults: Strattera (atomoxetine). The reduction in ADHD symptoms is roughly 30% less than with stimulants. However, it is a once-daily drug, which is an advantage.
"When I’m treating anxiety or ADHD, especially in adults, a longer-acting drug is better. I always try to get patients away from that on-off phenomenon. That’s a feeling they don’t like," the psychiatrist continued.
Adults with ADHD may need pharmacologic assistance not only during a lengthy workday, but in the evening as well.
Nonstimulants that are sometimes used off-label in adults include Wellbutrin (bupropion), which is approved for children with ADHD. It is about half as effective as a stimulant medication. Effexor (venlafaxine) and Provigil (modafanil) are other nonstimulants used off-label; neither has been well studied in adult ADHD, according to Dr. Davies.
Adults with ADHD don’t develop tolerance to stimulant medications, unlike amphetamine abusers. Asked if there is an upper age limit for the use of psychostimulants in treating ADHD, the psychiatrist replied no.
"My oldest patient is 75 and I’ve been treating him for the last 15 years," he added.
Dr. Davies reported having no financial conflicts.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Trochanteric bursitis: Easily misdiagnosed, readily treatable
ESTES PARK, COLO. – Trochanteric bursitis is an often overlooked cause of hip pain that’s sometimes so severe it can mimic a septic hip.
This overuse syndrome, common among weekend warriors, is also often mistaken for lumbar radiculopathy. The distinction is this: The pseudoradiculopathy of trochanteric bursitis doesn’t extend below the knee, while lumbar radiculopathy with sciatica typically goes past the knee laterally and runs down the leg, often as far as the foot, Dr. Robert W. Janson said at a conference on internal medicine sponsored by the University of Colorado.
Patients with trochanteric bursitis report pain over the trochanteric area and lateral thigh. This lateral hip pain is accentuated by walking, climbing stairs, or sitting in a deep chair. Patients report discomfort sleeping on the affected side. The range of motion in the hip joint is normal, but there is local point tenderness over the greater tuberosity that is exacerbated with external rotation of the hip and hip abduction against resistance.
"It just takes a second. Feel the greater tuberosity. You push in there, and they respond with the positive chandelier sign," the rheumatologist said, using a term for a pain response so sudden and electrifying that the patient figuratively rises up off the examination table and grabs for the ceiling lights.
The etiology of trochanteric bursitis is often a gait abnormality from a leg-length discrepancy. A difference of 2 cm or more is deemed clinically significant. The two static anatomic landmarks used in measuring leg-length discrepancy are the anterior superior iliac spine located right under the belt line and the medial malleolus.
"We’re concerned if the difference between the two legs is more than 2 cm. We typically work with a podiatrist to give the patient an insert or shoe lift. Remember, if you have a 2-cm leg-length discrepancy, you don’t replace all 2 cm. The podiatrist will start at one-eighth or one-quarter of an inch and work up as tolerated," according to Dr. Janson, chief of the rheumatology section at the Denver Veterans Affairs Medical Center.
Other common causes of trochanteric bursitis include osteoarthritis of the hip or lumbosacral spine, scoliosis, or a pathologically tight tensor fascia latae caused by running. This common running overuse injury entails tightness of the iliotibial band, with resultant inflammation of the bursa from repeated snapping of the shortened band over the greater tuberosity.
Treatment, beyond correction of any biomechanical causes, involves the usual general measures employed in overuse injuries: rest, with possible partial weight bearing; ice; full-anti-inflammatory-dose NSAIDs for at least several weeks; and physical therapy directed at stretching the gluteus medius and a possibly tight iliotibial band.
A local injection of 10-20 mg of long-acting methylprednisolone mixed with a few milliliters of lidocaine will bring much-appreciated symptomatic relief.
"The greater tuberosity is about the size of a silver dollar. When you inject the bursa, mark the greater tuberosity and go straight down the center as the patient lies laterally. A few seconds spent palpating that area and outlining the greater tuberosity can really be beneficial for your steroid injection," Dr. Janson commented.
Use a long needle, and bear in mind a time-honored rheumatologic pearl: "All injections in rheumatology should flow easily. If you find you’re against resistance, you’re in the wrong place," according to Dr. Janson.
He reported having no financial conflicts.
ESTES PARK, COLO. – Trochanteric bursitis is an often overlooked cause of hip pain that’s sometimes so severe it can mimic a septic hip.
This overuse syndrome, common among weekend warriors, is also often mistaken for lumbar radiculopathy. The distinction is this: The pseudoradiculopathy of trochanteric bursitis doesn’t extend below the knee, while lumbar radiculopathy with sciatica typically goes past the knee laterally and runs down the leg, often as far as the foot, Dr. Robert W. Janson said at a conference on internal medicine sponsored by the University of Colorado.
Patients with trochanteric bursitis report pain over the trochanteric area and lateral thigh. This lateral hip pain is accentuated by walking, climbing stairs, or sitting in a deep chair. Patients report discomfort sleeping on the affected side. The range of motion in the hip joint is normal, but there is local point tenderness over the greater tuberosity that is exacerbated with external rotation of the hip and hip abduction against resistance.
"It just takes a second. Feel the greater tuberosity. You push in there, and they respond with the positive chandelier sign," the rheumatologist said, using a term for a pain response so sudden and electrifying that the patient figuratively rises up off the examination table and grabs for the ceiling lights.
The etiology of trochanteric bursitis is often a gait abnormality from a leg-length discrepancy. A difference of 2 cm or more is deemed clinically significant. The two static anatomic landmarks used in measuring leg-length discrepancy are the anterior superior iliac spine located right under the belt line and the medial malleolus.
"We’re concerned if the difference between the two legs is more than 2 cm. We typically work with a podiatrist to give the patient an insert or shoe lift. Remember, if you have a 2-cm leg-length discrepancy, you don’t replace all 2 cm. The podiatrist will start at one-eighth or one-quarter of an inch and work up as tolerated," according to Dr. Janson, chief of the rheumatology section at the Denver Veterans Affairs Medical Center.
Other common causes of trochanteric bursitis include osteoarthritis of the hip or lumbosacral spine, scoliosis, or a pathologically tight tensor fascia latae caused by running. This common running overuse injury entails tightness of the iliotibial band, with resultant inflammation of the bursa from repeated snapping of the shortened band over the greater tuberosity.
Treatment, beyond correction of any biomechanical causes, involves the usual general measures employed in overuse injuries: rest, with possible partial weight bearing; ice; full-anti-inflammatory-dose NSAIDs for at least several weeks; and physical therapy directed at stretching the gluteus medius and a possibly tight iliotibial band.
A local injection of 10-20 mg of long-acting methylprednisolone mixed with a few milliliters of lidocaine will bring much-appreciated symptomatic relief.
"The greater tuberosity is about the size of a silver dollar. When you inject the bursa, mark the greater tuberosity and go straight down the center as the patient lies laterally. A few seconds spent palpating that area and outlining the greater tuberosity can really be beneficial for your steroid injection," Dr. Janson commented.
Use a long needle, and bear in mind a time-honored rheumatologic pearl: "All injections in rheumatology should flow easily. If you find you’re against resistance, you’re in the wrong place," according to Dr. Janson.
He reported having no financial conflicts.
ESTES PARK, COLO. – Trochanteric bursitis is an often overlooked cause of hip pain that’s sometimes so severe it can mimic a septic hip.
This overuse syndrome, common among weekend warriors, is also often mistaken for lumbar radiculopathy. The distinction is this: The pseudoradiculopathy of trochanteric bursitis doesn’t extend below the knee, while lumbar radiculopathy with sciatica typically goes past the knee laterally and runs down the leg, often as far as the foot, Dr. Robert W. Janson said at a conference on internal medicine sponsored by the University of Colorado.
Patients with trochanteric bursitis report pain over the trochanteric area and lateral thigh. This lateral hip pain is accentuated by walking, climbing stairs, or sitting in a deep chair. Patients report discomfort sleeping on the affected side. The range of motion in the hip joint is normal, but there is local point tenderness over the greater tuberosity that is exacerbated with external rotation of the hip and hip abduction against resistance.
"It just takes a second. Feel the greater tuberosity. You push in there, and they respond with the positive chandelier sign," the rheumatologist said, using a term for a pain response so sudden and electrifying that the patient figuratively rises up off the examination table and grabs for the ceiling lights.
The etiology of trochanteric bursitis is often a gait abnormality from a leg-length discrepancy. A difference of 2 cm or more is deemed clinically significant. The two static anatomic landmarks used in measuring leg-length discrepancy are the anterior superior iliac spine located right under the belt line and the medial malleolus.
"We’re concerned if the difference between the two legs is more than 2 cm. We typically work with a podiatrist to give the patient an insert or shoe lift. Remember, if you have a 2-cm leg-length discrepancy, you don’t replace all 2 cm. The podiatrist will start at one-eighth or one-quarter of an inch and work up as tolerated," according to Dr. Janson, chief of the rheumatology section at the Denver Veterans Affairs Medical Center.
Other common causes of trochanteric bursitis include osteoarthritis of the hip or lumbosacral spine, scoliosis, or a pathologically tight tensor fascia latae caused by running. This common running overuse injury entails tightness of the iliotibial band, with resultant inflammation of the bursa from repeated snapping of the shortened band over the greater tuberosity.
Treatment, beyond correction of any biomechanical causes, involves the usual general measures employed in overuse injuries: rest, with possible partial weight bearing; ice; full-anti-inflammatory-dose NSAIDs for at least several weeks; and physical therapy directed at stretching the gluteus medius and a possibly tight iliotibial band.
A local injection of 10-20 mg of long-acting methylprednisolone mixed with a few milliliters of lidocaine will bring much-appreciated symptomatic relief.
"The greater tuberosity is about the size of a silver dollar. When you inject the bursa, mark the greater tuberosity and go straight down the center as the patient lies laterally. A few seconds spent palpating that area and outlining the greater tuberosity can really be beneficial for your steroid injection," Dr. Janson commented.
Use a long needle, and bear in mind a time-honored rheumatologic pearl: "All injections in rheumatology should flow easily. If you find you’re against resistance, you’re in the wrong place," according to Dr. Janson.
He reported having no financial conflicts.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Trochanteric bursitis: Easily misdiagnosed, readily treatable
ESTES PARK, COLO. – Trochanteric bursitis is an often overlooked cause of hip pain that’s sometimes so severe it can mimic a septic hip.
This overuse syndrome, common among weekend warriors, is also often mistaken for lumbar radiculopathy. The distinction is this: The pseudoradiculopathy of trochanteric bursitis doesn’t extend below the knee, while lumbar radiculopathy with sciatica typically goes past the knee laterally and runs down the leg, often as far as the foot, Dr. Robert W. Janson said at a conference on internal medicine sponsored by the University of Colorado.
Patients with trochanteric bursitis report pain over the trochanteric area and lateral thigh. This lateral hip pain is accentuated by walking, climbing stairs, or sitting in a deep chair. Patients report discomfort sleeping on the affected side. The range of motion in the hip joint is normal, but there is local point tenderness over the greater tuberosity that is exacerbated with external rotation of the hip and hip abduction against resistance.

"It just takes a second. Feel the greater tuberosity. You push in there, and they respond with the positive chandelier sign," the rheumatologist said, using a term for a pain response so sudden and electrifying that the patient figuratively rises up off the examination table and grabs for the ceiling lights.
The etiology of trochanteric bursitis is often a gait abnormality from a leg-length discrepancy. A difference of 2 cm or more is deemed clinically significant. The two static anatomic landmarks used in measuring leg-length discrepancy are the anterior superior iliac spine located right under the belt line and the medial malleolus.
"We’re concerned if the difference between the two legs is more than 2 cm. We typically work with a podiatrist to give the patient an insert or shoe lift. Remember, if you have a 2-cm leg-length discrepancy, you don’t replace all 2 cm. The podiatrist will start at one-eighth or one-quarter of an inch and work up as tolerated," according to Dr. Janson, chief of the rheumatology section at the Denver Veterans Affairs Medical Center.
Other common causes of trochanteric bursitis include osteoarthritis of the hip or lumbosacral spine, scoliosis, or a pathologically tight tensor fascia latae caused by running. This common running overuse injury entails tightness of the iliotibial band, with resultant inflammation of the bursa from repeated snapping of the shortened band over the greater tuberosity.
Treatment, beyond correction of any biomechanical causes, involves the usual general measures employed in overuse injuries: rest, with possible partial weight bearing; ice; full-anti-inflammatory-dose NSAIDs for at least several weeks; and physical therapy directed at stretching the gluteus medius and a possibly tight iliotibial band.
A local injection of 10-20 mg of long-acting methylprednisolone mixed with a few milliliters of lidocaine will bring much-appreciated symptomatic relief.
"The greater tuberosity is about the size of a silver dollar. When you inject the bursa, mark the greater tuberosity and go straight down the center as the patient lies laterally. A few seconds spent palpating that area and outlining the greater tuberosity can really be beneficial for your steroid injection," Dr. Janson commented.
Use a long needle, and bear in mind a time-honored rheumatologic pearl: "All injections in rheumatology should flow easily. If you find you’re against resistance, you’re in the wrong place," according to Dr. Janson.
He reported having no financial conflicts.
ESTES PARK, COLO. – Trochanteric bursitis is an often overlooked cause of hip pain that’s sometimes so severe it can mimic a septic hip.
This overuse syndrome, common among weekend warriors, is also often mistaken for lumbar radiculopathy. The distinction is this: The pseudoradiculopathy of trochanteric bursitis doesn’t extend below the knee, while lumbar radiculopathy with sciatica typically goes past the knee laterally and runs down the leg, often as far as the foot, Dr. Robert W. Janson said at a conference on internal medicine sponsored by the University of Colorado.
Patients with trochanteric bursitis report pain over the trochanteric area and lateral thigh. This lateral hip pain is accentuated by walking, climbing stairs, or sitting in a deep chair. Patients report discomfort sleeping on the affected side. The range of motion in the hip joint is normal, but there is local point tenderness over the greater tuberosity that is exacerbated with external rotation of the hip and hip abduction against resistance.
"It just takes a second. Feel the greater tuberosity. You push in there, and they respond with the positive chandelier sign," the rheumatologist said, using a term for a pain response so sudden and electrifying that the patient figuratively rises up off the examination table and grabs for the ceiling lights.
The etiology of trochanteric bursitis is often a gait abnormality from a leg-length discrepancy. A difference of 2 cm or more is deemed clinically significant. The two static anatomic landmarks used in measuring leg-length discrepancy are the anterior superior iliac spine located right under the belt line and the medial malleolus.
"We’re concerned if the difference between the two legs is more than 2 cm. We typically work with a podiatrist to give the patient an insert or shoe lift. Remember, if you have a 2-cm leg-length discrepancy, you don’t replace all 2 cm. The podiatrist will start at one-eighth or one-quarter of an inch and work up as tolerated," according to Dr. Janson, chief of the rheumatology section at the Denver Veterans Affairs Medical Center.
Other common causes of trochanteric bursitis include osteoarthritis of the hip or lumbosacral spine, scoliosis, or a pathologically tight tensor fascia latae caused by running. This common running overuse injury entails tightness of the iliotibial band, with resultant inflammation of the bursa from repeated snapping of the shortened band over the greater tuberosity.
Treatment, beyond correction of any biomechanical causes, involves the usual general measures employed in overuse injuries: rest, with possible partial weight bearing; ice; full-anti-inflammatory-dose NSAIDs for at least several weeks; and physical therapy directed at stretching the gluteus medius and a possibly tight iliotibial band.
A local injection of 10-20 mg of long-acting methylprednisolone mixed with a few milliliters of lidocaine will bring much-appreciated symptomatic relief.
"The greater tuberosity is about the size of a silver dollar. When you inject the bursa, mark the greater tuberosity and go straight down the center as the patient lies laterally. A few seconds spent palpating that area and outlining the greater tuberosity can really be beneficial for your steroid injection," Dr. Janson commented.
Use a long needle, and bear in mind a time-honored rheumatologic pearl: "All injections in rheumatology should flow easily. If you find you’re against resistance, you’re in the wrong place," according to Dr. Janson.
He reported having no financial conflicts.
ESTES PARK, COLO. – Trochanteric bursitis is an often overlooked cause of hip pain that’s sometimes so severe it can mimic a septic hip.
This overuse syndrome, common among weekend warriors, is also often mistaken for lumbar radiculopathy. The distinction is this: The pseudoradiculopathy of trochanteric bursitis doesn’t extend below the knee, while lumbar radiculopathy with sciatica typically goes past the knee laterally and runs down the leg, often as far as the foot, Dr. Robert W. Janson said at a conference on internal medicine sponsored by the University of Colorado.
Patients with trochanteric bursitis report pain over the trochanteric area and lateral thigh. This lateral hip pain is accentuated by walking, climbing stairs, or sitting in a deep chair. Patients report discomfort sleeping on the affected side. The range of motion in the hip joint is normal, but there is local point tenderness over the greater tuberosity that is exacerbated with external rotation of the hip and hip abduction against resistance.
"It just takes a second. Feel the greater tuberosity. You push in there, and they respond with the positive chandelier sign," the rheumatologist said, using a term for a pain response so sudden and electrifying that the patient figuratively rises up off the examination table and grabs for the ceiling lights.
The etiology of trochanteric bursitis is often a gait abnormality from a leg-length discrepancy. A difference of 2 cm or more is deemed clinically significant. The two static anatomic landmarks used in measuring leg-length discrepancy are the anterior superior iliac spine located right under the belt line and the medial malleolus.
"We’re concerned if the difference between the two legs is more than 2 cm. We typically work with a podiatrist to give the patient an insert or shoe lift. Remember, if you have a 2-cm leg-length discrepancy, you don’t replace all 2 cm. The podiatrist will start at one-eighth or one-quarter of an inch and work up as tolerated," according to Dr. Janson, chief of the rheumatology section at the Denver Veterans Affairs Medical Center.
Other common causes of trochanteric bursitis include osteoarthritis of the hip or lumbosacral spine, scoliosis, or a pathologically tight tensor fascia latae caused by running. This common running overuse injury entails tightness of the iliotibial band, with resultant inflammation of the bursa from repeated snapping of the shortened band over the greater tuberosity.
Treatment, beyond correction of any biomechanical causes, involves the usual general measures employed in overuse injuries: rest, with possible partial weight bearing; ice; full-anti-inflammatory-dose NSAIDs for at least several weeks; and physical therapy directed at stretching the gluteus medius and a possibly tight iliotibial band.
A local injection of 10-20 mg of long-acting methylprednisolone mixed with a few milliliters of lidocaine will bring much-appreciated symptomatic relief.
"The greater tuberosity is about the size of a silver dollar. When you inject the bursa, mark the greater tuberosity and go straight down the center as the patient lies laterally. A few seconds spent palpating that area and outlining the greater tuberosity can really be beneficial for your steroid injection," Dr. Janson commented.
Use a long needle, and bear in mind a time-honored rheumatologic pearl: "All injections in rheumatology should flow easily. If you find you’re against resistance, you’re in the wrong place," according to Dr. Janson.
He reported having no financial conflicts.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Adult ADHD: Making the diagnosis
ESTES PARK, COLO. – Adult attention-deficit/hyperactivity disorder is a common and treatable psychiatric condition the diagnosis of which is made more challenging because the disorder looks different than the classic picture in children.
Trying to apply the Diagnostic and Statistical Manual of Mental Disorders diagnostic criteria for attention-deficit/hyperactivity disorder (ADHD) to adults is problematic. The DSM-IV symptoms focus mainly on childhood activities, particularly school and play. Plus, hyperactivity – the most recognizable symptom of ADHD in childhood – tends to diminish with age, becoming a more subjective experience of internal restlessness, Dr. Robert D. Davies explained at a conference on internal medicine sponsored by the University of Colorado.
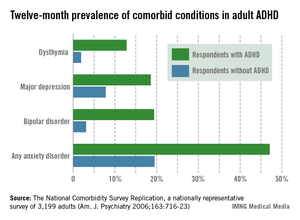
Yet ADHD by definition always first develops in childhood, even if an affected adult hasn’t previously been diagnosed and doesn’t recall the early impairment.
"Very often patients first present in adulthood because things have changed in their life, but if you go back and look carefully, it has been there since childhood. If you have a patient who comes in saying, ‘In the last few years all of a sudden I can’t concentrate, I can’t focus, I’m not doing well at work’ and there’s never been any hint of that before, I don’t know what it is, but it’s not ADHD," declared Dr. Davies, a psychiatrist at the university.
The adult presentation of ADHD is more subtle than in children. It includes disorganization and poor time-management skills; impulsivity with poor self-control often demonstrated via rude comments and frequent interruption of others; emotional difficulties rooted in low self-esteem and poor affect regulation; and difficulty in concentrating and completing even simple tasks.

"Adults with ADHD make great salespeople. They can really close the sale. But I’ve had so many salespeople I’ve treated who are failing at work because they never get the paperwork in and actually file the order. They don’t follow up on those things, but they’re great at the beginning," he observed.
The hyperactivity component can look much like mania: thrill seeking, racing thoughts, excessive talking, and difficulty in falling asleep.
All these adult ADHD symptoms add up to increased risks of divorce, difficulties at work, substance abuse, incarceration, a poor driving history – "lots of fender benders," according to Dr. Davies – and high rates of comorbid depression and anxiety that have been well documented in a landmark national study sponsored by the National Institute of Mental Health. The study, the National Comorbidity Survey Replication, placed the prevalence of adult ADHD among the general population at 4.4% (see accompanying graphic).
Substance abuse, hearing loss, and hyperthyroidism need to be ruled out before arriving at the diagnosis of adult ADHD. More challenging is to sort out adult ADHD from several commonly comorbid psychiatric conditions, most notably bipolar disorder, generalized anxiety disorder, and personality disorder.
The patient’s sleep pattern can provide useful information in this regard. Adult ADHD is characterized by a phase shift: The internal hyperactivity leads to difficulty in falling asleep until quite late, with subsequent trouble in waking up in the morning. In contrast, the manic phase of bipolar disorder is marked by a decreased sleep requirement. Patients with generalized anxiety disorder, unlike those with bipolar mania, really need their sleep, but their difficulty in falling asleep stems from worries about what might happen in the future. Individuals with adult ADHD typically can’t sleep because they’re ruminating about mistakes they’ve made.
"They’re worried about things that are real: what they forgot to do, who they’ve offended. In contrast, anytime you’re talking to a patient and they’re saying a lot of ‘what ifs,’ that’s a clue that the problem is generalized anxiety disorder," he explained.
While ADHD is a lifelong condition that begins in childhood, bipolar disorder is episodic and starts in the late teen years or later.
As for the differential between adult ADHD and borderline personality disorder, patients with ADHD typically have a sense of self as being harmed by their own failures and shortcomings coupled with the negative way others perceive them. In contrast, individuals with personality disorders often don’t have any real sense of self. The chaotic life that figures so prominently in the personal histories of many patients with adult ADHD dates back to childhood and results from their impulsivity and inattention, whereas the chaotic life of the patient with borderline personality disorder often starts in adolescence and is the result of their poor interpersonal relationships and rigid thinking.
Lots of adults are coming to the offices of primary care physicians and psychiatrists seeking help for what they believe is ADHD, brandishing their scores on self-report screening scales they find in popular magazines. Dr. Davies advises not attaching much weight to the self-report scales.
"I don’t use them routinely," he said. "If you think about the symptoms of ADHD, especially the ones that come out of magazines that they’re going to bring in to you, almost everybody at some point is going to fill these criteria. You want to ask people about those big, core ADHD symptoms: Are they really causing problems in your life?"
Dr. Davies acknowledged that adult ADHD is a disorder surrounded by considerable professional skepticism, even though the prevalence, serious consequences, and treatment responsiveness of adult ADHD are now well established.
"It’s a very controversial area outside of psychiatry but also inside psychiatry," according to Dr. Davies. "A psychiatric colleague of mine had diagnosed an adult patient with ADHD and then wanted to refer him to me. I asked why. He said, ‘Because I don’t believe in it.’"
Dr. Davies reported having no financial conflicts.
ESTES PARK, COLO. – Adult attention-deficit/hyperactivity disorder is a common and treatable psychiatric condition the diagnosis of which is made more challenging because the disorder looks different than the classic picture in children.
Trying to apply the Diagnostic and Statistical Manual of Mental Disorders diagnostic criteria for attention-deficit/hyperactivity disorder (ADHD) to adults is problematic. The DSM-IV symptoms focus mainly on childhood activities, particularly school and play. Plus, hyperactivity – the most recognizable symptom of ADHD in childhood – tends to diminish with age, becoming a more subjective experience of internal restlessness, Dr. Robert D. Davies explained at a conference on internal medicine sponsored by the University of Colorado.
Yet ADHD by definition always first develops in childhood, even if an affected adult hasn’t previously been diagnosed and doesn’t recall the early impairment.
"Very often patients first present in adulthood because things have changed in their life, but if you go back and look carefully, it has been there since childhood. If you have a patient who comes in saying, ‘In the last few years all of a sudden I can’t concentrate, I can’t focus, I’m not doing well at work’ and there’s never been any hint of that before, I don’t know what it is, but it’s not ADHD," declared Dr. Davies, a psychiatrist at the university.
The adult presentation of ADHD is more subtle than in children. It includes disorganization and poor time-management skills; impulsivity with poor self-control often demonstrated via rude comments and frequent interruption of others; emotional difficulties rooted in low self-esteem and poor affect regulation; and difficulty in concentrating and completing even simple tasks.
"Adults with ADHD make great salespeople. They can really close the sale. But I’ve had so many salespeople I’ve treated who are failing at work because they never get the paperwork in and actually file the order. They don’t follow up on those things, but they’re great at the beginning," he observed.
The hyperactivity component can look much like mania: thrill seeking, racing thoughts, excessive talking, and difficulty in falling asleep.
All these adult ADHD symptoms add up to increased risks of divorce, difficulties at work, substance abuse, incarceration, a poor driving history – "lots of fender benders," according to Dr. Davies – and high rates of comorbid depression and anxiety that have been well documented in a landmark national study sponsored by the National Institute of Mental Health. The study, the National Comorbidity Survey Replication, placed the prevalence of adult ADHD among the general population at 4.4% (see accompanying graphic).
Substance abuse, hearing loss, and hyperthyroidism need to be ruled out before arriving at the diagnosis of adult ADHD. More challenging is to sort out adult ADHD from several commonly comorbid psychiatric conditions, most notably bipolar disorder, generalized anxiety disorder, and personality disorder.
The patient’s sleep pattern can provide useful information in this regard. Adult ADHD is characterized by a phase shift: The internal hyperactivity leads to difficulty in falling asleep until quite late, with subsequent trouble in waking up in the morning. In contrast, the manic phase of bipolar disorder is marked by a decreased sleep requirement. Patients with generalized anxiety disorder, unlike those with bipolar mania, really need their sleep, but their difficulty in falling asleep stems from worries about what might happen in the future. Individuals with adult ADHD typically can’t sleep because they’re ruminating about mistakes they’ve made.
"They’re worried about things that are real: what they forgot to do, who they’ve offended. In contrast, anytime you’re talking to a patient and they’re saying a lot of ‘what ifs,’ that’s a clue that the problem is generalized anxiety disorder," he explained.
While ADHD is a lifelong condition that begins in childhood, bipolar disorder is episodic and starts in the late teen years or later.
As for the differential between adult ADHD and borderline personality disorder, patients with ADHD typically have a sense of self as being harmed by their own failures and shortcomings coupled with the negative way others perceive them. In contrast, individuals with personality disorders often don’t have any real sense of self. The chaotic life that figures so prominently in the personal histories of many patients with adult ADHD dates back to childhood and results from their impulsivity and inattention, whereas the chaotic life of the patient with borderline personality disorder often starts in adolescence and is the result of their poor interpersonal relationships and rigid thinking.
Lots of adults are coming to the offices of primary care physicians and psychiatrists seeking help for what they believe is ADHD, brandishing their scores on self-report screening scales they find in popular magazines. Dr. Davies advises not attaching much weight to the self-report scales.
"I don’t use them routinely," he said. "If you think about the symptoms of ADHD, especially the ones that come out of magazines that they’re going to bring in to you, almost everybody at some point is going to fill these criteria. You want to ask people about those big, core ADHD symptoms: Are they really causing problems in your life?"
Dr. Davies acknowledged that adult ADHD is a disorder surrounded by considerable professional skepticism, even though the prevalence, serious consequences, and treatment responsiveness of adult ADHD are now well established.
"It’s a very controversial area outside of psychiatry but also inside psychiatry," according to Dr. Davies. "A psychiatric colleague of mine had diagnosed an adult patient with ADHD and then wanted to refer him to me. I asked why. He said, ‘Because I don’t believe in it.’"
Dr. Davies reported having no financial conflicts.
ESTES PARK, COLO. – Adult attention-deficit/hyperactivity disorder is a common and treatable psychiatric condition the diagnosis of which is made more challenging because the disorder looks different than the classic picture in children.
Trying to apply the Diagnostic and Statistical Manual of Mental Disorders diagnostic criteria for attention-deficit/hyperactivity disorder (ADHD) to adults is problematic. The DSM-IV symptoms focus mainly on childhood activities, particularly school and play. Plus, hyperactivity – the most recognizable symptom of ADHD in childhood – tends to diminish with age, becoming a more subjective experience of internal restlessness, Dr. Robert D. Davies explained at a conference on internal medicine sponsored by the University of Colorado.
Yet ADHD by definition always first develops in childhood, even if an affected adult hasn’t previously been diagnosed and doesn’t recall the early impairment.
"Very often patients first present in adulthood because things have changed in their life, but if you go back and look carefully, it has been there since childhood. If you have a patient who comes in saying, ‘In the last few years all of a sudden I can’t concentrate, I can’t focus, I’m not doing well at work’ and there’s never been any hint of that before, I don’t know what it is, but it’s not ADHD," declared Dr. Davies, a psychiatrist at the university.
The adult presentation of ADHD is more subtle than in children. It includes disorganization and poor time-management skills; impulsivity with poor self-control often demonstrated via rude comments and frequent interruption of others; emotional difficulties rooted in low self-esteem and poor affect regulation; and difficulty in concentrating and completing even simple tasks.
"Adults with ADHD make great salespeople. They can really close the sale. But I’ve had so many salespeople I’ve treated who are failing at work because they never get the paperwork in and actually file the order. They don’t follow up on those things, but they’re great at the beginning," he observed.
The hyperactivity component can look much like mania: thrill seeking, racing thoughts, excessive talking, and difficulty in falling asleep.
All these adult ADHD symptoms add up to increased risks of divorce, difficulties at work, substance abuse, incarceration, a poor driving history – "lots of fender benders," according to Dr. Davies – and high rates of comorbid depression and anxiety that have been well documented in a landmark national study sponsored by the National Institute of Mental Health. The study, the National Comorbidity Survey Replication, placed the prevalence of adult ADHD among the general population at 4.4% (see accompanying graphic).
Substance abuse, hearing loss, and hyperthyroidism need to be ruled out before arriving at the diagnosis of adult ADHD. More challenging is to sort out adult ADHD from several commonly comorbid psychiatric conditions, most notably bipolar disorder, generalized anxiety disorder, and personality disorder.
The patient’s sleep pattern can provide useful information in this regard. Adult ADHD is characterized by a phase shift: The internal hyperactivity leads to difficulty in falling asleep until quite late, with subsequent trouble in waking up in the morning. In contrast, the manic phase of bipolar disorder is marked by a decreased sleep requirement. Patients with generalized anxiety disorder, unlike those with bipolar mania, really need their sleep, but their difficulty in falling asleep stems from worries about what might happen in the future. Individuals with adult ADHD typically can’t sleep because they’re ruminating about mistakes they’ve made.
"They’re worried about things that are real: what they forgot to do, who they’ve offended. In contrast, anytime you’re talking to a patient and they’re saying a lot of ‘what ifs,’ that’s a clue that the problem is generalized anxiety disorder," he explained.
While ADHD is a lifelong condition that begins in childhood, bipolar disorder is episodic and starts in the late teen years or later.
As for the differential between adult ADHD and borderline personality disorder, patients with ADHD typically have a sense of self as being harmed by their own failures and shortcomings coupled with the negative way others perceive them. In contrast, individuals with personality disorders often don’t have any real sense of self. The chaotic life that figures so prominently in the personal histories of many patients with adult ADHD dates back to childhood and results from their impulsivity and inattention, whereas the chaotic life of the patient with borderline personality disorder often starts in adolescence and is the result of their poor interpersonal relationships and rigid thinking.
Lots of adults are coming to the offices of primary care physicians and psychiatrists seeking help for what they believe is ADHD, brandishing their scores on self-report screening scales they find in popular magazines. Dr. Davies advises not attaching much weight to the self-report scales.
"I don’t use them routinely," he said. "If you think about the symptoms of ADHD, especially the ones that come out of magazines that they’re going to bring in to you, almost everybody at some point is going to fill these criteria. You want to ask people about those big, core ADHD symptoms: Are they really causing problems in your life?"
Dr. Davies acknowledged that adult ADHD is a disorder surrounded by considerable professional skepticism, even though the prevalence, serious consequences, and treatment responsiveness of adult ADHD are now well established.
"It’s a very controversial area outside of psychiatry but also inside psychiatry," according to Dr. Davies. "A psychiatric colleague of mine had diagnosed an adult patient with ADHD and then wanted to refer him to me. I asked why. He said, ‘Because I don’t believe in it.’"
Dr. Davies reported having no financial conflicts.
AT THE ANNUAL INTERNAL MEDICINE PROGRAM
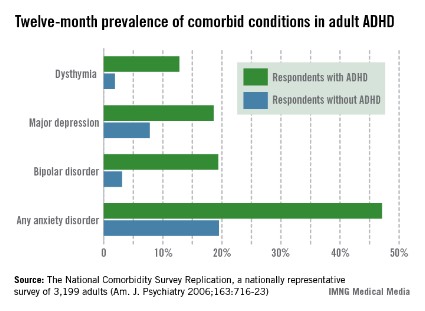
Think ‘ceftaroline’ in suspected drug-resistant CAP
ESTES PARK, COLO. – For primary care physicians, ceftaroline is hands-down the most exciting and important of the four systemic antibacterial agents to reach the U.S. market since the great 7-year drought in approvals ended in 2008, an infectious disease expert observed.
Ceftaroline (Teflaro) is a novel cephalosporin with unique binding to penicillin-binding proteins, including the altered versions that confer resistance in methicillin-resistant Staphylococcus aureus and penicillin- and cephalosporin-resistant Streptococcus pneumoniae. Thus, ceftaroline is a potent and effective drug in the increasingly common situation of beta-lactam-resistant community-acquired pneumonia (CAP) or complicated skin and soft tissue infections, noted Dr. Mary T. Bessesen, chief of the infectious diseases section at Denver V.A. Medical Center.

In the pivotal FOCUS 1 and FOCUS 2 trials conducted in patients with CAP not due to MRSA, ceftaroline proved noninferior overall to ceftriaxone (Rocephin). Of note, in the 14% of FOCUS participants with CAP due to S. aureus, ceftaroline proved to be significantly more effective than ceftriaxone. Importantly, the same was true among the one-third of FOCUS participants in whom S. pneumoniae was isolated (Clin. Infect. Dis. 2010;51:1395-405).
"I think if you’re going to impact mortality in CAP, pneumococcus has to be the primary target. Ceftaroline is a good alternative when penicillin-resistant S. pneumoniae is suspected or proven," Dr. Bessesen said at a conference on internal medicine sponsored by the University of Colorado.
Other common pathogens in CAP that are sensitive to ceftaroline are Hemophilus influenza and Moraxella catarrhalis. The Gram-negative pathogens E. coli, Klebsiella pneumoniae, and Enterobacter cloacae are also ceftaroline sensitive, with activity similar to ceftriaxone and ceftazidime (Fortaz).
Not only is MRSA sensitive to ceftaroline, so are methicillin-sensitive S. aureus, vancomycin-intermediate S. aureus, vancomycin-resistant S. aureus, linezolid (Zyvox)-resistant S. aureus, and daptomycin (Cubicin)-nonsusceptible S. aureus.
Ceftaroline does not cover the atypical pneumonia pathogens Mycoplasma pneumoniae, Chlamydia pneumoniae, and Legionella pneumoniae, nor does it cover Pseudomonas aeruginosa or extended-spectrum beta-lactamase-producing Enterobacteriaceae, stressed Dr. Bessesen.
The current CAP guidelines don’t include recommendations for ceftaroline, because the drug received Food and Drug Administration approval for treatment of CAP and complicated skin and soft tissue infections after the guidelines were issued.
Clinical trials investigating ceftaroline in CAP caused by MRSA would be welcome, Dr. Bessesen noted, because the current CAP guidelines don’t include any recommendations for CAP pneumonia.
"It really leaves us wondering in high-risk cases what’s best to do," she said. "There’s been some controversy about vancomycin versus linezolid when you suspect MRSA pneumonia. Ceftaroline would be a nice way to get around all of that."
Ceftaroline is administered intravenously twice daily, with dose adjustment for renal function. The drug’s pharmacokinetics are favorable for intramuscular injection, but there are limited clinical data for this route, and it is not FDA approved.
Ceftaroline costs about $84 per day, or four times more than ceftriaxone, Dr. Bessesen said. As a result, formulary committees are reluctant to put ceftaroline on the list.
That makes Dr. Bessesen see red.
"I’ve never been on a drug company speakers bureau. I’ve never had any research money from drug companies. I speak only as someone who’s interested in us being able to continue to treat bacterial infections when I say we’ve got to change our attitude. We have to be willing to pay something for these antibiotics," she asserted.
The antibiotic development pipeline has failed as pharmaceutical companies have abandoned the field, Dr. Bessesen continued. There are three reasons for this. One is that all the easy drugs have already been discovered. Another is that the FDA regulatory approval system for antibacterial agents is seriously outdated; the European Medicines Agency is much more forward thinking in this area and would be a useful model for FDA modernization, she noted.
But the biggest reason for the broken pipeline is that antibiotics are not a good financial investment for pharmaceutical companies. "It’s much more profitable for them to develop a drug like lovastatin that you’re going to take every day for the rest of your life than to develop an antibiotic you’re going to prescribe for a week or two. And society expects antibiotics to be cheap," Dr. Bessesen observed.
Contrast the roughly $1,600 cost of 4 weeks of ceftriaxone for S. viridans endocarditis – a serious infection – with the $54,000 price tag for 1 year of trastuzumab for breast cancer or $240,000 for a course of induction therapy with ipilimumab for melanoma, Dr. Bessesen noted.
"I’m not saying drugs should cost that much. I’m simply pointing out how society looks differently at these," she said.
With regard to the other three systemic antibiotics approved by the FDA in the 5 years since the 7-year drought ended, bedaquiline (Sirturo) is the most important globally, because it is indicated for multidrug-resistant tuberculosis. However, few U.S. physicians will have occasion to prescribe it.
Fidaxomicin (Dificid) is an effective drug for Clostridium difficile diarrhea; it’s eight times more potent than vancomycin against C. difficile, has minimal systemic absorption, and offers the major advantage of producing little negative impact on favorable gut flora. Telavancin (Vibativ) is a once-daily agent for hospital-acquired and ventilator-associated bacterial pneumonia.
Dr. Bessesen reported having no conflicts of interest.
ESTES PARK, COLO. – For primary care physicians, ceftaroline is hands-down the most exciting and important of the four systemic antibacterial agents to reach the U.S. market since the great 7-year drought in approvals ended in 2008, an infectious disease expert observed.
Ceftaroline (Teflaro) is a novel cephalosporin with unique binding to penicillin-binding proteins, including the altered versions that confer resistance in methicillin-resistant Staphylococcus aureus and penicillin- and cephalosporin-resistant Streptococcus pneumoniae. Thus, ceftaroline is a potent and effective drug in the increasingly common situation of beta-lactam-resistant community-acquired pneumonia (CAP) or complicated skin and soft tissue infections, noted Dr. Mary T. Bessesen, chief of the infectious diseases section at Denver V.A. Medical Center.
In the pivotal FOCUS 1 and FOCUS 2 trials conducted in patients with CAP not due to MRSA, ceftaroline proved noninferior overall to ceftriaxone (Rocephin). Of note, in the 14% of FOCUS participants with CAP due to S. aureus, ceftaroline proved to be significantly more effective than ceftriaxone. Importantly, the same was true among the one-third of FOCUS participants in whom S. pneumoniae was isolated (Clin. Infect. Dis. 2010;51:1395-405).
"I think if you’re going to impact mortality in CAP, pneumococcus has to be the primary target. Ceftaroline is a good alternative when penicillin-resistant S. pneumoniae is suspected or proven," Dr. Bessesen said at a conference on internal medicine sponsored by the University of Colorado.
Other common pathogens in CAP that are sensitive to ceftaroline are Hemophilus influenza and Moraxella catarrhalis. The Gram-negative pathogens E. coli, Klebsiella pneumoniae, and Enterobacter cloacae are also ceftaroline sensitive, with activity similar to ceftriaxone and ceftazidime (Fortaz).
Not only is MRSA sensitive to ceftaroline, so are methicillin-sensitive S. aureus, vancomycin-intermediate S. aureus, vancomycin-resistant S. aureus, linezolid (Zyvox)-resistant S. aureus, and daptomycin (Cubicin)-nonsusceptible S. aureus.
Ceftaroline does not cover the atypical pneumonia pathogens Mycoplasma pneumoniae, Chlamydia pneumoniae, and Legionella pneumoniae, nor does it cover Pseudomonas aeruginosa or extended-spectrum beta-lactamase-producing Enterobacteriaceae, stressed Dr. Bessesen.
The current CAP guidelines don’t include recommendations for ceftaroline, because the drug received Food and Drug Administration approval for treatment of CAP and complicated skin and soft tissue infections after the guidelines were issued.
Clinical trials investigating ceftaroline in CAP caused by MRSA would be welcome, Dr. Bessesen noted, because the current CAP guidelines don’t include any recommendations for CAP pneumonia.
"It really leaves us wondering in high-risk cases what’s best to do," she said. "There’s been some controversy about vancomycin versus linezolid when you suspect MRSA pneumonia. Ceftaroline would be a nice way to get around all of that."
Ceftaroline is administered intravenously twice daily, with dose adjustment for renal function. The drug’s pharmacokinetics are favorable for intramuscular injection, but there are limited clinical data for this route, and it is not FDA approved.
Ceftaroline costs about $84 per day, or four times more than ceftriaxone, Dr. Bessesen said. As a result, formulary committees are reluctant to put ceftaroline on the list.
That makes Dr. Bessesen see red.
"I’ve never been on a drug company speakers bureau. I’ve never had any research money from drug companies. I speak only as someone who’s interested in us being able to continue to treat bacterial infections when I say we’ve got to change our attitude. We have to be willing to pay something for these antibiotics," she asserted.
The antibiotic development pipeline has failed as pharmaceutical companies have abandoned the field, Dr. Bessesen continued. There are three reasons for this. One is that all the easy drugs have already been discovered. Another is that the FDA regulatory approval system for antibacterial agents is seriously outdated; the European Medicines Agency is much more forward thinking in this area and would be a useful model for FDA modernization, she noted.
But the biggest reason for the broken pipeline is that antibiotics are not a good financial investment for pharmaceutical companies. "It’s much more profitable for them to develop a drug like lovastatin that you’re going to take every day for the rest of your life than to develop an antibiotic you’re going to prescribe for a week or two. And society expects antibiotics to be cheap," Dr. Bessesen observed.
Contrast the roughly $1,600 cost of 4 weeks of ceftriaxone for S. viridans endocarditis – a serious infection – with the $54,000 price tag for 1 year of trastuzumab for breast cancer or $240,000 for a course of induction therapy with ipilimumab for melanoma, Dr. Bessesen noted.
"I’m not saying drugs should cost that much. I’m simply pointing out how society looks differently at these," she said.
With regard to the other three systemic antibiotics approved by the FDA in the 5 years since the 7-year drought ended, bedaquiline (Sirturo) is the most important globally, because it is indicated for multidrug-resistant tuberculosis. However, few U.S. physicians will have occasion to prescribe it.
Fidaxomicin (Dificid) is an effective drug for Clostridium difficile diarrhea; it’s eight times more potent than vancomycin against C. difficile, has minimal systemic absorption, and offers the major advantage of producing little negative impact on favorable gut flora. Telavancin (Vibativ) is a once-daily agent for hospital-acquired and ventilator-associated bacterial pneumonia.
Dr. Bessesen reported having no conflicts of interest.
ESTES PARK, COLO. – For primary care physicians, ceftaroline is hands-down the most exciting and important of the four systemic antibacterial agents to reach the U.S. market since the great 7-year drought in approvals ended in 2008, an infectious disease expert observed.
Ceftaroline (Teflaro) is a novel cephalosporin with unique binding to penicillin-binding proteins, including the altered versions that confer resistance in methicillin-resistant Staphylococcus aureus and penicillin- and cephalosporin-resistant Streptococcus pneumoniae. Thus, ceftaroline is a potent and effective drug in the increasingly common situation of beta-lactam-resistant community-acquired pneumonia (CAP) or complicated skin and soft tissue infections, noted Dr. Mary T. Bessesen, chief of the infectious diseases section at Denver V.A. Medical Center.
In the pivotal FOCUS 1 and FOCUS 2 trials conducted in patients with CAP not due to MRSA, ceftaroline proved noninferior overall to ceftriaxone (Rocephin). Of note, in the 14% of FOCUS participants with CAP due to S. aureus, ceftaroline proved to be significantly more effective than ceftriaxone. Importantly, the same was true among the one-third of FOCUS participants in whom S. pneumoniae was isolated (Clin. Infect. Dis. 2010;51:1395-405).
"I think if you’re going to impact mortality in CAP, pneumococcus has to be the primary target. Ceftaroline is a good alternative when penicillin-resistant S. pneumoniae is suspected or proven," Dr. Bessesen said at a conference on internal medicine sponsored by the University of Colorado.
Other common pathogens in CAP that are sensitive to ceftaroline are Hemophilus influenza and Moraxella catarrhalis. The Gram-negative pathogens E. coli, Klebsiella pneumoniae, and Enterobacter cloacae are also ceftaroline sensitive, with activity similar to ceftriaxone and ceftazidime (Fortaz).
Not only is MRSA sensitive to ceftaroline, so are methicillin-sensitive S. aureus, vancomycin-intermediate S. aureus, vancomycin-resistant S. aureus, linezolid (Zyvox)-resistant S. aureus, and daptomycin (Cubicin)-nonsusceptible S. aureus.
Ceftaroline does not cover the atypical pneumonia pathogens Mycoplasma pneumoniae, Chlamydia pneumoniae, and Legionella pneumoniae, nor does it cover Pseudomonas aeruginosa or extended-spectrum beta-lactamase-producing Enterobacteriaceae, stressed Dr. Bessesen.
The current CAP guidelines don’t include recommendations for ceftaroline, because the drug received Food and Drug Administration approval for treatment of CAP and complicated skin and soft tissue infections after the guidelines were issued.
Clinical trials investigating ceftaroline in CAP caused by MRSA would be welcome, Dr. Bessesen noted, because the current CAP guidelines don’t include any recommendations for CAP pneumonia.
"It really leaves us wondering in high-risk cases what’s best to do," she said. "There’s been some controversy about vancomycin versus linezolid when you suspect MRSA pneumonia. Ceftaroline would be a nice way to get around all of that."
Ceftaroline is administered intravenously twice daily, with dose adjustment for renal function. The drug’s pharmacokinetics are favorable for intramuscular injection, but there are limited clinical data for this route, and it is not FDA approved.
Ceftaroline costs about $84 per day, or four times more than ceftriaxone, Dr. Bessesen said. As a result, formulary committees are reluctant to put ceftaroline on the list.
That makes Dr. Bessesen see red.
"I’ve never been on a drug company speakers bureau. I’ve never had any research money from drug companies. I speak only as someone who’s interested in us being able to continue to treat bacterial infections when I say we’ve got to change our attitude. We have to be willing to pay something for these antibiotics," she asserted.
The antibiotic development pipeline has failed as pharmaceutical companies have abandoned the field, Dr. Bessesen continued. There are three reasons for this. One is that all the easy drugs have already been discovered. Another is that the FDA regulatory approval system for antibacterial agents is seriously outdated; the European Medicines Agency is much more forward thinking in this area and would be a useful model for FDA modernization, she noted.
But the biggest reason for the broken pipeline is that antibiotics are not a good financial investment for pharmaceutical companies. "It’s much more profitable for them to develop a drug like lovastatin that you’re going to take every day for the rest of your life than to develop an antibiotic you’re going to prescribe for a week or two. And society expects antibiotics to be cheap," Dr. Bessesen observed.
Contrast the roughly $1,600 cost of 4 weeks of ceftriaxone for S. viridans endocarditis – a serious infection – with the $54,000 price tag for 1 year of trastuzumab for breast cancer or $240,000 for a course of induction therapy with ipilimumab for melanoma, Dr. Bessesen noted.
"I’m not saying drugs should cost that much. I’m simply pointing out how society looks differently at these," she said.
With regard to the other three systemic antibiotics approved by the FDA in the 5 years since the 7-year drought ended, bedaquiline (Sirturo) is the most important globally, because it is indicated for multidrug-resistant tuberculosis. However, few U.S. physicians will have occasion to prescribe it.
Fidaxomicin (Dificid) is an effective drug for Clostridium difficile diarrhea; it’s eight times more potent than vancomycin against C. difficile, has minimal systemic absorption, and offers the major advantage of producing little negative impact on favorable gut flora. Telavancin (Vibativ) is a once-daily agent for hospital-acquired and ventilator-associated bacterial pneumonia.
Dr. Bessesen reported having no conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Itching on opiates is not allergic
ESTES PARK, COLO. – Patients who report itching like crazy while on opiates or in response to radiocontrast media are appropriately managed by their primary care physician without referral to an allergist, Dr. Mark A. Ebadi stressed at a conference on internal medicine sponsored by the University of Colorado.
That’s because these are not true IgE-mediated allergic reactions. No one is allergic to opiates or radiocontrast media. These agents are direct mast cell histamine-releasing agents. Hence, there is no role for allergy testing and desensitization therapy. The right treatment is vastly less expensive and laborious than that, explained Dr. Ebadi of the Colorado Allergy and Asthma Center, Denver.
Between 20%-25% of patients experience intense itching when they take opiates. Sometimes they are told they should undergo desensitization therapy before having a planned surgical procedure.

"I see patients like this every week," the allergist said.
The solution is simple: Have the patient start taking high-dose fexofenadine the day before surgery and continue on the antihistamine until a couple of days after stopping the opiate medication.
"I’ve never had a patient call me back and say it didn’t work. So don’t send your patients who itch on opiates to the allergist. I never even skin test these patients for opiates; a skin test will always be positive, since opiates are direct mast cell histamine releasers," he said.
His preferred histamine-1/histamine-2 blocker is fexofenadine because it doesn’t cross the blood-brain barrier at all. He tells patients to get generic fexofenadine because it is far less expensive than brand-name Allegra.
"You can get 365 pills for $14 at Costco!" he said.
His recommended dosing is 180 mg t.i.d.
Many patients who have had the frightening experience of erupting in intense flushing, itching, and hives when undergoing medical imaging with radiocontrast media have been told that they’re allergic to iodine and must never again receive radiocontrast material or eat shellfish.
That’s just plain wrong, according to Dr. Ebadi. This is not an IgE-mediated reaction, and the shellfish prohibition is simply a medical myth with no basis in fact, he continued.
Once again, the best management option is well within the purview of nonallergists: Prep the patient with diphenhydramine and oral prednisone before the next infusion of radiocontrast media. The dosing schedule is 50 mg of diphenhydramine and 20 mg of prednisone taken 12 hours, 7 hours, and 1 hour prior to the scheduled infusion.
"No allergy consult is warranted, but I would recommend that all future imaging studies with radiocontrast media in these patients be done in the hospital with the ER doc alerted just in case, instead of in an outpatient imaging center. These anaphylactoid reactions can be severe. I have had a few patients that, even with the prep, got kind of sick," said Dr. Ebadi.
He reported having no financial conflicts.
ESTES PARK, COLO. – Patients who report itching like crazy while on opiates or in response to radiocontrast media are appropriately managed by their primary care physician without referral to an allergist, Dr. Mark A. Ebadi stressed at a conference on internal medicine sponsored by the University of Colorado.
That’s because these are not true IgE-mediated allergic reactions. No one is allergic to opiates or radiocontrast media. These agents are direct mast cell histamine-releasing agents. Hence, there is no role for allergy testing and desensitization therapy. The right treatment is vastly less expensive and laborious than that, explained Dr. Ebadi of the Colorado Allergy and Asthma Center, Denver.
Between 20%-25% of patients experience intense itching when they take opiates. Sometimes they are told they should undergo desensitization therapy before having a planned surgical procedure.
"I see patients like this every week," the allergist said.
The solution is simple: Have the patient start taking high-dose fexofenadine the day before surgery and continue on the antihistamine until a couple of days after stopping the opiate medication.
"I’ve never had a patient call me back and say it didn’t work. So don’t send your patients who itch on opiates to the allergist. I never even skin test these patients for opiates; a skin test will always be positive, since opiates are direct mast cell histamine releasers," he said.
His preferred histamine-1/histamine-2 blocker is fexofenadine because it doesn’t cross the blood-brain barrier at all. He tells patients to get generic fexofenadine because it is far less expensive than brand-name Allegra.
"You can get 365 pills for $14 at Costco!" he said.
His recommended dosing is 180 mg t.i.d.
Many patients who have had the frightening experience of erupting in intense flushing, itching, and hives when undergoing medical imaging with radiocontrast media have been told that they’re allergic to iodine and must never again receive radiocontrast material or eat shellfish.
That’s just plain wrong, according to Dr. Ebadi. This is not an IgE-mediated reaction, and the shellfish prohibition is simply a medical myth with no basis in fact, he continued.
Once again, the best management option is well within the purview of nonallergists: Prep the patient with diphenhydramine and oral prednisone before the next infusion of radiocontrast media. The dosing schedule is 50 mg of diphenhydramine and 20 mg of prednisone taken 12 hours, 7 hours, and 1 hour prior to the scheduled infusion.
"No allergy consult is warranted, but I would recommend that all future imaging studies with radiocontrast media in these patients be done in the hospital with the ER doc alerted just in case, instead of in an outpatient imaging center. These anaphylactoid reactions can be severe. I have had a few patients that, even with the prep, got kind of sick," said Dr. Ebadi.
He reported having no financial conflicts.
ESTES PARK, COLO. – Patients who report itching like crazy while on opiates or in response to radiocontrast media are appropriately managed by their primary care physician without referral to an allergist, Dr. Mark A. Ebadi stressed at a conference on internal medicine sponsored by the University of Colorado.
That’s because these are not true IgE-mediated allergic reactions. No one is allergic to opiates or radiocontrast media. These agents are direct mast cell histamine-releasing agents. Hence, there is no role for allergy testing and desensitization therapy. The right treatment is vastly less expensive and laborious than that, explained Dr. Ebadi of the Colorado Allergy and Asthma Center, Denver.
Between 20%-25% of patients experience intense itching when they take opiates. Sometimes they are told they should undergo desensitization therapy before having a planned surgical procedure.
"I see patients like this every week," the allergist said.
The solution is simple: Have the patient start taking high-dose fexofenadine the day before surgery and continue on the antihistamine until a couple of days after stopping the opiate medication.
"I’ve never had a patient call me back and say it didn’t work. So don’t send your patients who itch on opiates to the allergist. I never even skin test these patients for opiates; a skin test will always be positive, since opiates are direct mast cell histamine releasers," he said.
His preferred histamine-1/histamine-2 blocker is fexofenadine because it doesn’t cross the blood-brain barrier at all. He tells patients to get generic fexofenadine because it is far less expensive than brand-name Allegra.
"You can get 365 pills for $14 at Costco!" he said.
His recommended dosing is 180 mg t.i.d.
Many patients who have had the frightening experience of erupting in intense flushing, itching, and hives when undergoing medical imaging with radiocontrast media have been told that they’re allergic to iodine and must never again receive radiocontrast material or eat shellfish.
That’s just plain wrong, according to Dr. Ebadi. This is not an IgE-mediated reaction, and the shellfish prohibition is simply a medical myth with no basis in fact, he continued.
Once again, the best management option is well within the purview of nonallergists: Prep the patient with diphenhydramine and oral prednisone before the next infusion of radiocontrast media. The dosing schedule is 50 mg of diphenhydramine and 20 mg of prednisone taken 12 hours, 7 hours, and 1 hour prior to the scheduled infusion.
"No allergy consult is warranted, but I would recommend that all future imaging studies with radiocontrast media in these patients be done in the hospital with the ER doc alerted just in case, instead of in an outpatient imaging center. These anaphylactoid reactions can be severe. I have had a few patients that, even with the prep, got kind of sick," said Dr. Ebadi.
He reported having no financial conflicts.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM
Stinging insect reactions: Who needs referral?
ESTES PARK, COLO. – Recognizing which patients with even a breathtakingly dramatic reaction to a hymenoptera sting can be appropriately managed by their primary care physician and which ones need referral to an allergy specialist is the key to avoiding a potential lawsuit that’s essentially indefensible.
A patient needs referral for allergy testing and desensitization therapy only if the swelling or hives occurred in a discontinuous pattern from the site of the sting or if there was anaphylaxis. Otherwise the patient is best managed in his or her medical home by a primary care physician using reassurance, a short course of oral prednisone and, if infection is present, a beta-lactam antibiotic, Dr. Mark A. Ebadi said at a conference on internal medicine sponsored by the University of Colorado.

"I see a patient with an incredibly swollen hand, neck, or leg due to a hymenoptera sting every day during the summer. I tell patients that if you’re stung on the hand, even if it swells all the way up your arm and into your neck, that’s still a local reaction. That does not portend an anaphylactic reaction the next time you get stung. You’re supposed to react to a hymenoptera sting, it’s not a big deal," explained Dr. Ebadi of the Colorado Allergy and Asthma Center, Denver.
On the other hand, a patient who got stung on the foot and minutes later experienced facial swelling in a discontinuous pattern, perhaps accompanied by widespread hives and difficulty breathing, has had a systemic reaction with production of IgE in response to hymenoptera of some kind.
"The standard of care in internal medicine for hymenoptera anaphylaxis is referral to a specialist for testing and allergen desensitization. You don’t have a leg to stand on if you just give the patient an epi pen and tell them to keep it with them at all times, and then they get stung when they forgot to carry it and they get laryngeal angioedema, airway compromise, and die. I see cases like that probably twice a year when attorneys consult with me. I’ll review the chart and tell the attorney, ‘You should probably settle,’ " the allergist continued.
For the results of RAST (radioallergosorbent) testing to be meaningful, the testing should be delayed until 1 month after the sting. It’s an excellent idea to give the patient an epi pen and instructions to carry it at all times while waiting for the specialist appointment, he added.
Dr. Ebadi reported having no financial conflicts of interest.
ESTES PARK, COLO. – Recognizing which patients with even a breathtakingly dramatic reaction to a hymenoptera sting can be appropriately managed by their primary care physician and which ones need referral to an allergy specialist is the key to avoiding a potential lawsuit that’s essentially indefensible.
A patient needs referral for allergy testing and desensitization therapy only if the swelling or hives occurred in a discontinuous pattern from the site of the sting or if there was anaphylaxis. Otherwise the patient is best managed in his or her medical home by a primary care physician using reassurance, a short course of oral prednisone and, if infection is present, a beta-lactam antibiotic, Dr. Mark A. Ebadi said at a conference on internal medicine sponsored by the University of Colorado.
"I see a patient with an incredibly swollen hand, neck, or leg due to a hymenoptera sting every day during the summer. I tell patients that if you’re stung on the hand, even if it swells all the way up your arm and into your neck, that’s still a local reaction. That does not portend an anaphylactic reaction the next time you get stung. You’re supposed to react to a hymenoptera sting, it’s not a big deal," explained Dr. Ebadi of the Colorado Allergy and Asthma Center, Denver.
On the other hand, a patient who got stung on the foot and minutes later experienced facial swelling in a discontinuous pattern, perhaps accompanied by widespread hives and difficulty breathing, has had a systemic reaction with production of IgE in response to hymenoptera of some kind.
"The standard of care in internal medicine for hymenoptera anaphylaxis is referral to a specialist for testing and allergen desensitization. You don’t have a leg to stand on if you just give the patient an epi pen and tell them to keep it with them at all times, and then they get stung when they forgot to carry it and they get laryngeal angioedema, airway compromise, and die. I see cases like that probably twice a year when attorneys consult with me. I’ll review the chart and tell the attorney, ‘You should probably settle,’ " the allergist continued.
For the results of RAST (radioallergosorbent) testing to be meaningful, the testing should be delayed until 1 month after the sting. It’s an excellent idea to give the patient an epi pen and instructions to carry it at all times while waiting for the specialist appointment, he added.
Dr. Ebadi reported having no financial conflicts of interest.
ESTES PARK, COLO. – Recognizing which patients with even a breathtakingly dramatic reaction to a hymenoptera sting can be appropriately managed by their primary care physician and which ones need referral to an allergy specialist is the key to avoiding a potential lawsuit that’s essentially indefensible.
A patient needs referral for allergy testing and desensitization therapy only if the swelling or hives occurred in a discontinuous pattern from the site of the sting or if there was anaphylaxis. Otherwise the patient is best managed in his or her medical home by a primary care physician using reassurance, a short course of oral prednisone and, if infection is present, a beta-lactam antibiotic, Dr. Mark A. Ebadi said at a conference on internal medicine sponsored by the University of Colorado.
"I see a patient with an incredibly swollen hand, neck, or leg due to a hymenoptera sting every day during the summer. I tell patients that if you’re stung on the hand, even if it swells all the way up your arm and into your neck, that’s still a local reaction. That does not portend an anaphylactic reaction the next time you get stung. You’re supposed to react to a hymenoptera sting, it’s not a big deal," explained Dr. Ebadi of the Colorado Allergy and Asthma Center, Denver.
On the other hand, a patient who got stung on the foot and minutes later experienced facial swelling in a discontinuous pattern, perhaps accompanied by widespread hives and difficulty breathing, has had a systemic reaction with production of IgE in response to hymenoptera of some kind.
"The standard of care in internal medicine for hymenoptera anaphylaxis is referral to a specialist for testing and allergen desensitization. You don’t have a leg to stand on if you just give the patient an epi pen and tell them to keep it with them at all times, and then they get stung when they forgot to carry it and they get laryngeal angioedema, airway compromise, and die. I see cases like that probably twice a year when attorneys consult with me. I’ll review the chart and tell the attorney, ‘You should probably settle,’ " the allergist continued.
For the results of RAST (radioallergosorbent) testing to be meaningful, the testing should be delayed until 1 month after the sting. It’s an excellent idea to give the patient an epi pen and instructions to carry it at all times while waiting for the specialist appointment, he added.
Dr. Ebadi reported having no financial conflicts of interest.
EXPERYT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM
