User login
Preventing a second bout of acute pancreatitis
ESTES PARK, COLO. – Secondary prevention following a first episode of acute pancreatitis often goes underemphasized.
"If you have somebody who comes in with an MI, TIA, or stroke, you are not going to discharge them from the hospital without further evaluation and a plan for what you’re going to do in the future. Yet I would dare say that many of you have taken care of lots of patients with acute pancreatitis, and you wrote "pancreatitis, did fine," put that on the problem list, but you never addressed that in the future. You need to think about the natural history of acute pancreatitis, which is that 25% of the patients are going to have a recurrence, typically within 12 months," Dr. Peter R. McNally said at a conference on internal medicine sponsored by the University of Colorado.
This high recurrence rate can be reduced by determining the etiology of the pancreatitis and then taking steps to eliminate that trigger.

Either gallstones or consumption of toxic quantities of alcohol underlie 80% of cases of acute pancreatitis. It’s a 50/50 split between the two etiologies. However, alcoholic pancreatitis is five times as common in men as in women, whereas gallstones as a cause of pancreatitis are far more common in women than men. Ultrasound is the best imaging study for finding those stones.
There are twice as many alcoholic men as women in the United States. The reason alcoholic pancreatitis is five times as common in men is that several of the genetic mutations associated with increased risk of chronic pancreatitis are X-linked.
It takes a lot of heavy drinking to trigger pancreatitis, an average of five or more drinks per day for 8-10 years. After a first episode of acute pancreatitis due to alcohol, a patient who becomes completely abstinent has a 14% risk of progressing to chronic pancreatitis, a painful condition caused by irreversible damage to the parenchyma and ducts. If after the first episode of acute pancreatitis the patient continues drinking but cuts back, the risk is 23%. And with no change in alcohol consumption, the risk climbs to 41%.
"These data clearly tell you that, if you don’t send them to inpatient rehabilitation, they will be back. Smoking is an independent and additive factor for relapse. So you really want to stress ‘no alcohol, no tobacco,’ according to Dr. McNally, chief of gastroenterology at Evans Army Hospital in Fort Carson, Colo.
Therapeutic endoscopic cholangiopancreatography is the preferred treatment when gallstones are the cause of acute pancreatitis. That’s fairly straightforward. But pinning down the etiology of the 20% of cases of acute pancreatitis not due to alcohol or gallstones can be challenging. There is a grab bag of potential causes, for which Dr. McNally offered the mnemonic GET SMASH’D. It stands for Gallstones, Ethanol, Trauma, Steroids, Mumps, Autoimmune, Scorpion bites, Hyperlipidemia, and Drugs.
When no other cause for an episode of acute pancreatitis can be identified, it becomes important to perform a medications reconciliation to learn if the patient has been on any of 38 drugs incriminated as probable causes of drug-induced pancreatitis. Many of these agents are widely prescribed, including several statins, tamixofen, trimethoprim/sulfamethoxazole, valproate, and metronidazole.
"If you don’t check their medications against this list, they’re going to be right back in with recurrent pancreatitis," the gastroenterologist advised.
One-quarter to one-third of patients who have had acute pancreatitis will develop exocrine and/or endocrine dysfunction over time.
"If it’s severe pancreatitis, the rate is almost 100%. So you need to look for it. A fecal elastase test 2-3 months after discharge is totally appropriate to see if a patient has fat malabsorption. Check for vitamin D and B12 deficiency as well," Dr. McNally suggested.
Genetic testing is just on the verge of being incorporated into pancreatitis management.
"We’ll be doing genetic tests within the next 5 years on all patients who come in with acute pancreatitis to figure out if they’re in that 10% that will go on to have chronic pancreatitis. And if you have a gene mutation assay that’s positive in a patient with alcoholic pancreatitis, you’ll need to tell them, ‘There’s no way you can drink again,’ " according to Dr. McNally.
He reported having no financial conflicts.
ESTES PARK, COLO. – Secondary prevention following a first episode of acute pancreatitis often goes underemphasized.
"If you have somebody who comes in with an MI, TIA, or stroke, you are not going to discharge them from the hospital without further evaluation and a plan for what you’re going to do in the future. Yet I would dare say that many of you have taken care of lots of patients with acute pancreatitis, and you wrote "pancreatitis, did fine," put that on the problem list, but you never addressed that in the future. You need to think about the natural history of acute pancreatitis, which is that 25% of the patients are going to have a recurrence, typically within 12 months," Dr. Peter R. McNally said at a conference on internal medicine sponsored by the University of Colorado.
This high recurrence rate can be reduced by determining the etiology of the pancreatitis and then taking steps to eliminate that trigger.
Either gallstones or consumption of toxic quantities of alcohol underlie 80% of cases of acute pancreatitis. It’s a 50/50 split between the two etiologies. However, alcoholic pancreatitis is five times as common in men as in women, whereas gallstones as a cause of pancreatitis are far more common in women than men. Ultrasound is the best imaging study for finding those stones.
There are twice as many alcoholic men as women in the United States. The reason alcoholic pancreatitis is five times as common in men is that several of the genetic mutations associated with increased risk of chronic pancreatitis are X-linked.
It takes a lot of heavy drinking to trigger pancreatitis, an average of five or more drinks per day for 8-10 years. After a first episode of acute pancreatitis due to alcohol, a patient who becomes completely abstinent has a 14% risk of progressing to chronic pancreatitis, a painful condition caused by irreversible damage to the parenchyma and ducts. If after the first episode of acute pancreatitis the patient continues drinking but cuts back, the risk is 23%. And with no change in alcohol consumption, the risk climbs to 41%.
"These data clearly tell you that, if you don’t send them to inpatient rehabilitation, they will be back. Smoking is an independent and additive factor for relapse. So you really want to stress ‘no alcohol, no tobacco,’ according to Dr. McNally, chief of gastroenterology at Evans Army Hospital in Fort Carson, Colo.
Therapeutic endoscopic cholangiopancreatography is the preferred treatment when gallstones are the cause of acute pancreatitis. That’s fairly straightforward. But pinning down the etiology of the 20% of cases of acute pancreatitis not due to alcohol or gallstones can be challenging. There is a grab bag of potential causes, for which Dr. McNally offered the mnemonic GET SMASH’D. It stands for Gallstones, Ethanol, Trauma, Steroids, Mumps, Autoimmune, Scorpion bites, Hyperlipidemia, and Drugs.
When no other cause for an episode of acute pancreatitis can be identified, it becomes important to perform a medications reconciliation to learn if the patient has been on any of 38 drugs incriminated as probable causes of drug-induced pancreatitis. Many of these agents are widely prescribed, including several statins, tamixofen, trimethoprim/sulfamethoxazole, valproate, and metronidazole.
"If you don’t check their medications against this list, they’re going to be right back in with recurrent pancreatitis," the gastroenterologist advised.
One-quarter to one-third of patients who have had acute pancreatitis will develop exocrine and/or endocrine dysfunction over time.
"If it’s severe pancreatitis, the rate is almost 100%. So you need to look for it. A fecal elastase test 2-3 months after discharge is totally appropriate to see if a patient has fat malabsorption. Check for vitamin D and B12 deficiency as well," Dr. McNally suggested.
Genetic testing is just on the verge of being incorporated into pancreatitis management.
"We’ll be doing genetic tests within the next 5 years on all patients who come in with acute pancreatitis to figure out if they’re in that 10% that will go on to have chronic pancreatitis. And if you have a gene mutation assay that’s positive in a patient with alcoholic pancreatitis, you’ll need to tell them, ‘There’s no way you can drink again,’ " according to Dr. McNally.
He reported having no financial conflicts.
ESTES PARK, COLO. – Secondary prevention following a first episode of acute pancreatitis often goes underemphasized.
"If you have somebody who comes in with an MI, TIA, or stroke, you are not going to discharge them from the hospital without further evaluation and a plan for what you’re going to do in the future. Yet I would dare say that many of you have taken care of lots of patients with acute pancreatitis, and you wrote "pancreatitis, did fine," put that on the problem list, but you never addressed that in the future. You need to think about the natural history of acute pancreatitis, which is that 25% of the patients are going to have a recurrence, typically within 12 months," Dr. Peter R. McNally said at a conference on internal medicine sponsored by the University of Colorado.
This high recurrence rate can be reduced by determining the etiology of the pancreatitis and then taking steps to eliminate that trigger.
Either gallstones or consumption of toxic quantities of alcohol underlie 80% of cases of acute pancreatitis. It’s a 50/50 split between the two etiologies. However, alcoholic pancreatitis is five times as common in men as in women, whereas gallstones as a cause of pancreatitis are far more common in women than men. Ultrasound is the best imaging study for finding those stones.
There are twice as many alcoholic men as women in the United States. The reason alcoholic pancreatitis is five times as common in men is that several of the genetic mutations associated with increased risk of chronic pancreatitis are X-linked.
It takes a lot of heavy drinking to trigger pancreatitis, an average of five or more drinks per day for 8-10 years. After a first episode of acute pancreatitis due to alcohol, a patient who becomes completely abstinent has a 14% risk of progressing to chronic pancreatitis, a painful condition caused by irreversible damage to the parenchyma and ducts. If after the first episode of acute pancreatitis the patient continues drinking but cuts back, the risk is 23%. And with no change in alcohol consumption, the risk climbs to 41%.
"These data clearly tell you that, if you don’t send them to inpatient rehabilitation, they will be back. Smoking is an independent and additive factor for relapse. So you really want to stress ‘no alcohol, no tobacco,’ according to Dr. McNally, chief of gastroenterology at Evans Army Hospital in Fort Carson, Colo.
Therapeutic endoscopic cholangiopancreatography is the preferred treatment when gallstones are the cause of acute pancreatitis. That’s fairly straightforward. But pinning down the etiology of the 20% of cases of acute pancreatitis not due to alcohol or gallstones can be challenging. There is a grab bag of potential causes, for which Dr. McNally offered the mnemonic GET SMASH’D. It stands for Gallstones, Ethanol, Trauma, Steroids, Mumps, Autoimmune, Scorpion bites, Hyperlipidemia, and Drugs.
When no other cause for an episode of acute pancreatitis can be identified, it becomes important to perform a medications reconciliation to learn if the patient has been on any of 38 drugs incriminated as probable causes of drug-induced pancreatitis. Many of these agents are widely prescribed, including several statins, tamixofen, trimethoprim/sulfamethoxazole, valproate, and metronidazole.
"If you don’t check their medications against this list, they’re going to be right back in with recurrent pancreatitis," the gastroenterologist advised.
One-quarter to one-third of patients who have had acute pancreatitis will develop exocrine and/or endocrine dysfunction over time.
"If it’s severe pancreatitis, the rate is almost 100%. So you need to look for it. A fecal elastase test 2-3 months after discharge is totally appropriate to see if a patient has fat malabsorption. Check for vitamin D and B12 deficiency as well," Dr. McNally suggested.
Genetic testing is just on the verge of being incorporated into pancreatitis management.
"We’ll be doing genetic tests within the next 5 years on all patients who come in with acute pancreatitis to figure out if they’re in that 10% that will go on to have chronic pancreatitis. And if you have a gene mutation assay that’s positive in a patient with alcoholic pancreatitis, you’ll need to tell them, ‘There’s no way you can drink again,’ " according to Dr. McNally.
He reported having no financial conflicts.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Depression, some antidepressants linked to high C. difficile risk
Depression appears to be a novel independent risk factor for Clostridium difficile–associated diarrhea in older adults, according to a large national study.
Moreover, the use of certain antidepressants was associated with an increased risk of hospital-onset C. difficile infection in a separate study simultaneously reported by the same researchers. Although the number of such patients was small, adults on the combination of mirtazapine and trazodone at hospital admission had a whopping 33-fold increased risk of subsequently developing hospital-onset C. difficile infection (CDI), according to Mary A.M. Rogers, Ph.D., and her coinvestigators at the University of Michigan, Ann Arbor (BMC Medicine 2013;11:121).

"While there does appear to be an association between depression and CDI, at this time we cannot completely discern whether it is the pathophysiology of depression itself or the treatment for depression that is the major driver of these findings," Dr. Rogers and her colleagues wrote. "We did not find a class effect for the various antidepressants. Further investigation of the effects of antidepressants on the gut microbiota may be helpful."
One of the two studies was a longitudinal analysis of 16,781 nationally representative older Americans participating in the ongoing National Institute on Aging–sponsored Health and Retirement Study. The rate of subsequent CDI was 282.9 cases/100,000 person-years among study participants with a previous diagnosis of major depressive disorder at any time, compared to 197.1/100,000 person-years in patients without a history of major depression. In a multivariate analysis adjusted for age, sex, race, education, smoking status, body mass index, and comorbid GI or renal disease, the odds of CDI were 36% greater in older subjects with a history of major depressive disorder.
In addition, the risk of CDI was also significantly increased by 54% in subjects who were widowed and by 35% in study participants with a history of any of a broad group of depressive disorders other than major depression. These included diagnoses of brief or prolonged depressive reactions, depressive-type psychosis, bipolar affective disorder with depression, adjustment reaction with anxiety and depression, chronic depressive personality disorder, and depressive disorder not elsewhere classified. Subjects who did not live alone had a 25% lower risk of CDI than those who did.
The mechanism underlying the observed association between depression and CDI in this study is unknown, but a relationship is biologically plausible. It is known that depressed patients have impaired immune responses. In addition, there is evidence that depression and bereavement can alter the gut flora, or microbiome. The brain-gut axis is a hot research area, and the possibility that the relationship is bidirectional has received some research support.
Intrigued by their findings from the longitudinal Health and Retirement Study, Dr. Rogers and her colleagues then conducted a case-control study involving all adults hospitalized during a recent 18-month period in the University of Michigan Health System for any reason other than CDI and who developed diarrhea and other symptoms that prompted stool testing for C. difficile while in-the hospital. A total of 468 patients tested positive and were classified as having hospital-onset CDI, while the remaining 3,579 patients tested negative.
Patients on selected antidepressants at hospital admission had an increased risk of subsequent hospital-onset CDI. The 99 patients on mirtazapine, for example, had an adjusted 2.14-fold increased risk of hospital-onset CDI. And for each dose of mirtazapine they received while in the hospital, their risk increased by 8%. Patients on fluoxetine had nearly a twofold increased risk. So did those on nortriptyline; their risk of hospital-onset CDI climbed by 11% with each dose given. Patients on antidepressant monotherapy with trazodone were not at increased risk.
In a secondary analysis, 17 patients on the combination of trazodone and mirtazapine were at 32.5-fold increased risk.
Other agents in the same antidepressant classes, however, were not associated with hospital-onset CDI.
Interestingly, an identical 57% of patients in the hospital-onset CDI group as well as the C. difficile–negative controls were on a proton pump inhibitor. That observation is noteworthy because it is inconsistent with the Food and Drug Administration’s February 2012 safety warning regarding an association between the use of proton pump inhibitors and CDI in adults.
This project was funded by the National Institute of Allergy and Infectious Diseases. The investigators reported having no conflicts of interest.
Researchers have long been interested in the connection between the brain and the gut. The "gut brain axis" has been studied in a variety of areas, including a recent study that demonstrated ingestion of probiotic-containing yogurt resulted in changes on functional MRIs. Animal studies have demonstrated a relationship between GI flora and anxiety "levels" in mice.

|
| Dr. Michael Pistoria |
This study demonstrates an additional example of what may be a two-way street in the "gut brain axis" - depression as an independent risk factor for Clostridium difficile-associated diarrhea in older patients. Analysis of nearly 17,000 older individuals revealed a 36% increase in C. difficile infection in those individuals with a history of major depressive disorder. Importantly, the risk was not merely increased in those with major depression. Those who were widowed also had increased risk of C. difficile infection (54% increase), as were those with any history of depressive disorders other than major depression (35% increase). Lastly, those who lived with someone had a 25% lower risk of C. difficile infection than did those who lived alone.
Investigators then examined hospitalized patients who developed C. difficile diarrhea during their hospital stay. They found a relationship between specific antidepressants and the development of C. difficile. Patients on mirtazapine, fluoxetine, and nortriptyline all had increased risk of C. difficile. In some instances, this risk increased with each dose of medication given while in the hospital.
This is important news for hospitalists. Many of those for whom we provide care suffer from depressive disorders - either situationally, because of the loss of a spouse, or indicative of underlying major depression. As we work to minimize the risk of C. difficile for our hospitalized patients, this link - and the seeming link between specific medications we use to treat those patients - is important to further investigate and understand as it may drive treatment decisions and precautions.
Dr. Michael Pistoria is chief of hospital medicine at Coordinated Health, Bethlehem, Pa. He is on the advisory board of Hospitalist News.
Researchers have long been interested in the connection between the brain and the gut. The "gut brain axis" has been studied in a variety of areas, including a recent study that demonstrated ingestion of probiotic-containing yogurt resulted in changes on functional MRIs. Animal studies have demonstrated a relationship between GI flora and anxiety "levels" in mice.
|
|
| Dr. Michael Pistoria |
This study demonstrates an additional example of what may be a two-way street in the "gut brain axis" - depression as an independent risk factor for Clostridium difficile-associated diarrhea in older patients. Analysis of nearly 17,000 older individuals revealed a 36% increase in C. difficile infection in those individuals with a history of major depressive disorder. Importantly, the risk was not merely increased in those with major depression. Those who were widowed also had increased risk of C. difficile infection (54% increase), as were those with any history of depressive disorders other than major depression (35% increase). Lastly, those who lived with someone had a 25% lower risk of C. difficile infection than did those who lived alone.
Investigators then examined hospitalized patients who developed C. difficile diarrhea during their hospital stay. They found a relationship between specific antidepressants and the development of C. difficile. Patients on mirtazapine, fluoxetine, and nortriptyline all had increased risk of C. difficile. In some instances, this risk increased with each dose of medication given while in the hospital.
This is important news for hospitalists. Many of those for whom we provide care suffer from depressive disorders - either situationally, because of the loss of a spouse, or indicative of underlying major depression. As we work to minimize the risk of C. difficile for our hospitalized patients, this link - and the seeming link between specific medications we use to treat those patients - is important to further investigate and understand as it may drive treatment decisions and precautions.
Dr. Michael Pistoria is chief of hospital medicine at Coordinated Health, Bethlehem, Pa. He is on the advisory board of Hospitalist News.
Researchers have long been interested in the connection between the brain and the gut. The "gut brain axis" has been studied in a variety of areas, including a recent study that demonstrated ingestion of probiotic-containing yogurt resulted in changes on functional MRIs. Animal studies have demonstrated a relationship between GI flora and anxiety "levels" in mice.
|
|
| Dr. Michael Pistoria |
This study demonstrates an additional example of what may be a two-way street in the "gut brain axis" - depression as an independent risk factor for Clostridium difficile-associated diarrhea in older patients. Analysis of nearly 17,000 older individuals revealed a 36% increase in C. difficile infection in those individuals with a history of major depressive disorder. Importantly, the risk was not merely increased in those with major depression. Those who were widowed also had increased risk of C. difficile infection (54% increase), as were those with any history of depressive disorders other than major depression (35% increase). Lastly, those who lived with someone had a 25% lower risk of C. difficile infection than did those who lived alone.
Investigators then examined hospitalized patients who developed C. difficile diarrhea during their hospital stay. They found a relationship between specific antidepressants and the development of C. difficile. Patients on mirtazapine, fluoxetine, and nortriptyline all had increased risk of C. difficile. In some instances, this risk increased with each dose of medication given while in the hospital.
This is important news for hospitalists. Many of those for whom we provide care suffer from depressive disorders - either situationally, because of the loss of a spouse, or indicative of underlying major depression. As we work to minimize the risk of C. difficile for our hospitalized patients, this link - and the seeming link between specific medications we use to treat those patients - is important to further investigate and understand as it may drive treatment decisions and precautions.
Dr. Michael Pistoria is chief of hospital medicine at Coordinated Health, Bethlehem, Pa. He is on the advisory board of Hospitalist News.
Depression appears to be a novel independent risk factor for Clostridium difficile–associated diarrhea in older adults, according to a large national study.
Moreover, the use of certain antidepressants was associated with an increased risk of hospital-onset C. difficile infection in a separate study simultaneously reported by the same researchers. Although the number of such patients was small, adults on the combination of mirtazapine and trazodone at hospital admission had a whopping 33-fold increased risk of subsequently developing hospital-onset C. difficile infection (CDI), according to Mary A.M. Rogers, Ph.D., and her coinvestigators at the University of Michigan, Ann Arbor (BMC Medicine 2013;11:121).
"While there does appear to be an association between depression and CDI, at this time we cannot completely discern whether it is the pathophysiology of depression itself or the treatment for depression that is the major driver of these findings," Dr. Rogers and her colleagues wrote. "We did not find a class effect for the various antidepressants. Further investigation of the effects of antidepressants on the gut microbiota may be helpful."
One of the two studies was a longitudinal analysis of 16,781 nationally representative older Americans participating in the ongoing National Institute on Aging–sponsored Health and Retirement Study. The rate of subsequent CDI was 282.9 cases/100,000 person-years among study participants with a previous diagnosis of major depressive disorder at any time, compared to 197.1/100,000 person-years in patients without a history of major depression. In a multivariate analysis adjusted for age, sex, race, education, smoking status, body mass index, and comorbid GI or renal disease, the odds of CDI were 36% greater in older subjects with a history of major depressive disorder.
In addition, the risk of CDI was also significantly increased by 54% in subjects who were widowed and by 35% in study participants with a history of any of a broad group of depressive disorders other than major depression. These included diagnoses of brief or prolonged depressive reactions, depressive-type psychosis, bipolar affective disorder with depression, adjustment reaction with anxiety and depression, chronic depressive personality disorder, and depressive disorder not elsewhere classified. Subjects who did not live alone had a 25% lower risk of CDI than those who did.
The mechanism underlying the observed association between depression and CDI in this study is unknown, but a relationship is biologically plausible. It is known that depressed patients have impaired immune responses. In addition, there is evidence that depression and bereavement can alter the gut flora, or microbiome. The brain-gut axis is a hot research area, and the possibility that the relationship is bidirectional has received some research support.
Intrigued by their findings from the longitudinal Health and Retirement Study, Dr. Rogers and her colleagues then conducted a case-control study involving all adults hospitalized during a recent 18-month period in the University of Michigan Health System for any reason other than CDI and who developed diarrhea and other symptoms that prompted stool testing for C. difficile while in-the hospital. A total of 468 patients tested positive and were classified as having hospital-onset CDI, while the remaining 3,579 patients tested negative.
Patients on selected antidepressants at hospital admission had an increased risk of subsequent hospital-onset CDI. The 99 patients on mirtazapine, for example, had an adjusted 2.14-fold increased risk of hospital-onset CDI. And for each dose of mirtazapine they received while in the hospital, their risk increased by 8%. Patients on fluoxetine had nearly a twofold increased risk. So did those on nortriptyline; their risk of hospital-onset CDI climbed by 11% with each dose given. Patients on antidepressant monotherapy with trazodone were not at increased risk.
In a secondary analysis, 17 patients on the combination of trazodone and mirtazapine were at 32.5-fold increased risk.
Other agents in the same antidepressant classes, however, were not associated with hospital-onset CDI.
Interestingly, an identical 57% of patients in the hospital-onset CDI group as well as the C. difficile–negative controls were on a proton pump inhibitor. That observation is noteworthy because it is inconsistent with the Food and Drug Administration’s February 2012 safety warning regarding an association between the use of proton pump inhibitors and CDI in adults.
This project was funded by the National Institute of Allergy and Infectious Diseases. The investigators reported having no conflicts of interest.
Depression appears to be a novel independent risk factor for Clostridium difficile–associated diarrhea in older adults, according to a large national study.
Moreover, the use of certain antidepressants was associated with an increased risk of hospital-onset C. difficile infection in a separate study simultaneously reported by the same researchers. Although the number of such patients was small, adults on the combination of mirtazapine and trazodone at hospital admission had a whopping 33-fold increased risk of subsequently developing hospital-onset C. difficile infection (CDI), according to Mary A.M. Rogers, Ph.D., and her coinvestigators at the University of Michigan, Ann Arbor (BMC Medicine 2013;11:121).
"While there does appear to be an association between depression and CDI, at this time we cannot completely discern whether it is the pathophysiology of depression itself or the treatment for depression that is the major driver of these findings," Dr. Rogers and her colleagues wrote. "We did not find a class effect for the various antidepressants. Further investigation of the effects of antidepressants on the gut microbiota may be helpful."
One of the two studies was a longitudinal analysis of 16,781 nationally representative older Americans participating in the ongoing National Institute on Aging–sponsored Health and Retirement Study. The rate of subsequent CDI was 282.9 cases/100,000 person-years among study participants with a previous diagnosis of major depressive disorder at any time, compared to 197.1/100,000 person-years in patients without a history of major depression. In a multivariate analysis adjusted for age, sex, race, education, smoking status, body mass index, and comorbid GI or renal disease, the odds of CDI were 36% greater in older subjects with a history of major depressive disorder.
In addition, the risk of CDI was also significantly increased by 54% in subjects who were widowed and by 35% in study participants with a history of any of a broad group of depressive disorders other than major depression. These included diagnoses of brief or prolonged depressive reactions, depressive-type psychosis, bipolar affective disorder with depression, adjustment reaction with anxiety and depression, chronic depressive personality disorder, and depressive disorder not elsewhere classified. Subjects who did not live alone had a 25% lower risk of CDI than those who did.
The mechanism underlying the observed association between depression and CDI in this study is unknown, but a relationship is biologically plausible. It is known that depressed patients have impaired immune responses. In addition, there is evidence that depression and bereavement can alter the gut flora, or microbiome. The brain-gut axis is a hot research area, and the possibility that the relationship is bidirectional has received some research support.
Intrigued by their findings from the longitudinal Health and Retirement Study, Dr. Rogers and her colleagues then conducted a case-control study involving all adults hospitalized during a recent 18-month period in the University of Michigan Health System for any reason other than CDI and who developed diarrhea and other symptoms that prompted stool testing for C. difficile while in-the hospital. A total of 468 patients tested positive and were classified as having hospital-onset CDI, while the remaining 3,579 patients tested negative.
Patients on selected antidepressants at hospital admission had an increased risk of subsequent hospital-onset CDI. The 99 patients on mirtazapine, for example, had an adjusted 2.14-fold increased risk of hospital-onset CDI. And for each dose of mirtazapine they received while in the hospital, their risk increased by 8%. Patients on fluoxetine had nearly a twofold increased risk. So did those on nortriptyline; their risk of hospital-onset CDI climbed by 11% with each dose given. Patients on antidepressant monotherapy with trazodone were not at increased risk.
In a secondary analysis, 17 patients on the combination of trazodone and mirtazapine were at 32.5-fold increased risk.
Other agents in the same antidepressant classes, however, were not associated with hospital-onset CDI.
Interestingly, an identical 57% of patients in the hospital-onset CDI group as well as the C. difficile–negative controls were on a proton pump inhibitor. That observation is noteworthy because it is inconsistent with the Food and Drug Administration’s February 2012 safety warning regarding an association between the use of proton pump inhibitors and CDI in adults.
This project was funded by the National Institute of Allergy and Infectious Diseases. The investigators reported having no conflicts of interest.
FROM BMC MEDICINE
Major finding: Older adults with a history of major depressive disorder were 36% more likely to develop Clostridium difficile–associated diarrhea during longitudinal follow-up than did those without such a history.
Data source: This finding came from analysis of 16,781 older adults participating in the ongoing national Health and Retirement Study.
Disclosures: The Health and Retirement Study is funded by the National Institute on Aging. This analysis was funded by the National Institute of Allergy and Infectious Diseases. The researchers report having no relevant financial conflicts.

Must-knows for quick and simple triage of acute pancreatitis
ESTES PARK, COLO. – With acute pancreatitis now accounting for more than 300,000 hospital admissions per year, it behooves physicians to be adept at early clinical diagnosis and familiar with the newer, user-friendly tools for estimating case severity.
These tasks have been made much easier as a result of the simplified Atlanta consensus diagnostic criteria of 2012 and the development of a couple of quick triage tools – the HAPS and BISAP – which are far better suited for this purpose than the old Ranson criteria and APACHE-II (Acute Physiology and Chronic Health Examination) score, Dr. Peter R. McNally said at a conference on internal medicine sponsored by the University of Colorado.

"Since we solved the riddle of H. pylori and peptic ulcer disease, acute pancreatitis has become the number one GI diagnosis for admission to the hospital," noted Dr. McNally, chief of gastroenterology at Evans Army Hospital in Fort Carson, Colo.
The revised criteria for clinical diagnosis of acute pancreatitis developed by an international panel meeting in Atlanta (Gut 2013;62:102-11) require that two of three criteria be met: typical pain; a serum amylase and/or lipase level at least three times the upper limit of normal; and demonstration of the characteristic findings of acute pancreatitis on imaging, with computed tomography getting the nod as the best imaging modality. However, there are sound reasons for delaying CT imaging until at least the 48-hour mark in most cases. Thus, as a practical matter, early diagnosis requires both typical pain and enzyme elevations.
"The pancreas is located deep in the retroperitoneum. It sits on thoracolumbar vertebrae T12/L1. I want to emphasize that if you have pancreatitis, you have back pain. If you don’t have back pain, just anterior abdominal pain, it’s not pancreatitis," Dr. McNally said.
The classic picture of acute pancreatitis is acute onset of 10/10 pain. When the physician walks into the examination room, the patient is typically in the fetal position in order to relieve the excruciating back pain.
Eighty percent of cases of acute pancreatitis are mild and usually edematous. The other 20% are severe and usually necrotic. Mortality is 3% or less with edematous cases and 15%-25% or more with necrotic pancreatitis.
The HAPS and BISAP scores are enormously helpful in assessing severity early on, unlike the Ranson criteria and APACHE-II score, which are tedious and complicated, and take up to 48 hours to complete, the gastroenterologist observed.
The HAPS (Harmless Acute Pancreatitis Score) can be measured within 30 minutes of hospital admission. There are three criteria for a "harmless" HAPS score: a normal hematocrit, normal serum creatinine, and absence of rebound tenderness. The presence of all three criteria has 96% specificity and 99% positive predictive value for a nonsevere disease course (Pancreatology 2011;11:464-8).
"These are patients you can keep on the general medicine ward or perhaps even on observation status," according to Dr. McNally.
The BISAP (Bedside Index for Severity in Acute Pancreatitis) awards 1 point each for the presence of five possible findings: a urea nitrogen level in excess of 25 mg/dL, indicative of third spacing; impaired mental status defined by a Glasgow Coma Score of even a single point less than the normal 15; age over 60; pleural effusion; and the presence of systemic inflammatory response syndrome, or SIRS.
Sixty percent of patients with acute pancreatitis have SIRS on admission. It resolves within 24 hours in half of cases. Persistent or worsening SIRS is associated with an 11%-25% mortality rate. SIRS is defined by two or more of the following: tachycardia, tachypnea, hypocarbia, fever, and either an elevated or depressed white blood cell count.
A patient with a BISAP score of 1 has less than a 2% risk of mortality. In contrast, a BISAP score of 3 is associated with a 22% mortality rate (Am. J. Gastroenterol. 2009;104:966-71).
"If you’re in Hays, Kan., or Rifle, Colo., and you’re seeing a patient at time zero who already has a BISAP of 3, you probably ought to raise the white flag and ship that patient because you’re going to have a lot of problems otherwise," the gastroenterologist advised.
When the diagnosis of acute pancreatitis is uncertain or the triage tools indicate severe disease, the single best imaging modality for looking at the pancreas is CT using what is known among radiologists as the Balthazar pancreatic protocol. It is utilized to assess pancreatic necrosis, the extent of which predicts mortality. There’s no need for CT in a SIRS-negative patient with mild acute pancreatitis.
A caveat is that CT misses gallstones about 20% of the time because the stones are nonradiolucent – and gallstones are the number one cause of acute pancreatitis in women. The laboratory parameter most predictive of gallstone pancreatitis is an alanine transaminase (ALT) level at least twice the upper limit of normal. Ultrasound is the best imaging method for gallstones and for evaluation of the size of the common bile duct, although it can be difficult to image the pancreas and gallbladder using ultrasound in an obese patient.
As soon as a physician has determined that two of the three Atlanta criteria for acute pancreatitis are present, the crucial next step is to immediately give a 1- to 2-L bolus of intravenous lactated Ringer’s solution, following up at an infusion rate of 250-300 mL/hr. This is the initial intervention in what gastroenterologists have lately begun calling "the golden hours" of management in acute pancreatitis in recognition that taking certain steps in the first 24 hours has a major impact on morbidity and mortality. For example, starting lactated Ringer’s solution in the first hour of acute pancreatitis has been shown to result in an absolute 8.5% reduction in mortality. It is also far more effective than normal saline in preventing or reversing SIRS. The lactated Ringer’s prevents pancreatic enzymes from going hematogenous and causing extrapancreatic tissue breakdown.
In addition to aggressive fluid resuscitation, other elements of "golden hours" management include monitoring of urine output, oxygen, pain control with careful monitoring of oxygen saturation, and monitoring for SIRS. Centers of Excellence where the golden hours approach has been adopted have a 25% reduction in the relative risk of mortality (Gastroenterology 2013;144:1272-81).
In 2013 there is no longer any role for prophylactic antibiotics in patients with acute pancreatitis. Nasogastric decompression, which was once routine, is now done only for symptomatic ileus. Nor is endoscopic cholangiopancreatography appropriate for biliary pancreatitis within the first 24 hours save when ascending cholangitis is present or in the setting of a deteriorating clinical course with worsening liver function tests. Otherwise, the time to perform ERCP, Dr. McNally stressed, is after resolution of acute pancreatitis.
He reported having no financial conflicts.
ESTES PARK, COLO. – With acute pancreatitis now accounting for more than 300,000 hospital admissions per year, it behooves physicians to be adept at early clinical diagnosis and familiar with the newer, user-friendly tools for estimating case severity.
These tasks have been made much easier as a result of the simplified Atlanta consensus diagnostic criteria of 2012 and the development of a couple of quick triage tools – the HAPS and BISAP – which are far better suited for this purpose than the old Ranson criteria and APACHE-II (Acute Physiology and Chronic Health Examination) score, Dr. Peter R. McNally said at a conference on internal medicine sponsored by the University of Colorado.
"Since we solved the riddle of H. pylori and peptic ulcer disease, acute pancreatitis has become the number one GI diagnosis for admission to the hospital," noted Dr. McNally, chief of gastroenterology at Evans Army Hospital in Fort Carson, Colo.
The revised criteria for clinical diagnosis of acute pancreatitis developed by an international panel meeting in Atlanta (Gut 2013;62:102-11) require that two of three criteria be met: typical pain; a serum amylase and/or lipase level at least three times the upper limit of normal; and demonstration of the characteristic findings of acute pancreatitis on imaging, with computed tomography getting the nod as the best imaging modality. However, there are sound reasons for delaying CT imaging until at least the 48-hour mark in most cases. Thus, as a practical matter, early diagnosis requires both typical pain and enzyme elevations.
"The pancreas is located deep in the retroperitoneum. It sits on thoracolumbar vertebrae T12/L1. I want to emphasize that if you have pancreatitis, you have back pain. If you don’t have back pain, just anterior abdominal pain, it’s not pancreatitis," Dr. McNally said.
The classic picture of acute pancreatitis is acute onset of 10/10 pain. When the physician walks into the examination room, the patient is typically in the fetal position in order to relieve the excruciating back pain.
Eighty percent of cases of acute pancreatitis are mild and usually edematous. The other 20% are severe and usually necrotic. Mortality is 3% or less with edematous cases and 15%-25% or more with necrotic pancreatitis.
The HAPS and BISAP scores are enormously helpful in assessing severity early on, unlike the Ranson criteria and APACHE-II score, which are tedious and complicated, and take up to 48 hours to complete, the gastroenterologist observed.
The HAPS (Harmless Acute Pancreatitis Score) can be measured within 30 minutes of hospital admission. There are three criteria for a "harmless" HAPS score: a normal hematocrit, normal serum creatinine, and absence of rebound tenderness. The presence of all three criteria has 96% specificity and 99% positive predictive value for a nonsevere disease course (Pancreatology 2011;11:464-8).
"These are patients you can keep on the general medicine ward or perhaps even on observation status," according to Dr. McNally.
The BISAP (Bedside Index for Severity in Acute Pancreatitis) awards 1 point each for the presence of five possible findings: a urea nitrogen level in excess of 25 mg/dL, indicative of third spacing; impaired mental status defined by a Glasgow Coma Score of even a single point less than the normal 15; age over 60; pleural effusion; and the presence of systemic inflammatory response syndrome, or SIRS.
Sixty percent of patients with acute pancreatitis have SIRS on admission. It resolves within 24 hours in half of cases. Persistent or worsening SIRS is associated with an 11%-25% mortality rate. SIRS is defined by two or more of the following: tachycardia, tachypnea, hypocarbia, fever, and either an elevated or depressed white blood cell count.
A patient with a BISAP score of 1 has less than a 2% risk of mortality. In contrast, a BISAP score of 3 is associated with a 22% mortality rate (Am. J. Gastroenterol. 2009;104:966-71).
"If you’re in Hays, Kan., or Rifle, Colo., and you’re seeing a patient at time zero who already has a BISAP of 3, you probably ought to raise the white flag and ship that patient because you’re going to have a lot of problems otherwise," the gastroenterologist advised.
When the diagnosis of acute pancreatitis is uncertain or the triage tools indicate severe disease, the single best imaging modality for looking at the pancreas is CT using what is known among radiologists as the Balthazar pancreatic protocol. It is utilized to assess pancreatic necrosis, the extent of which predicts mortality. There’s no need for CT in a SIRS-negative patient with mild acute pancreatitis.
A caveat is that CT misses gallstones about 20% of the time because the stones are nonradiolucent – and gallstones are the number one cause of acute pancreatitis in women. The laboratory parameter most predictive of gallstone pancreatitis is an alanine transaminase (ALT) level at least twice the upper limit of normal. Ultrasound is the best imaging method for gallstones and for evaluation of the size of the common bile duct, although it can be difficult to image the pancreas and gallbladder using ultrasound in an obese patient.
As soon as a physician has determined that two of the three Atlanta criteria for acute pancreatitis are present, the crucial next step is to immediately give a 1- to 2-L bolus of intravenous lactated Ringer’s solution, following up at an infusion rate of 250-300 mL/hr. This is the initial intervention in what gastroenterologists have lately begun calling "the golden hours" of management in acute pancreatitis in recognition that taking certain steps in the first 24 hours has a major impact on morbidity and mortality. For example, starting lactated Ringer’s solution in the first hour of acute pancreatitis has been shown to result in an absolute 8.5% reduction in mortality. It is also far more effective than normal saline in preventing or reversing SIRS. The lactated Ringer’s prevents pancreatic enzymes from going hematogenous and causing extrapancreatic tissue breakdown.
In addition to aggressive fluid resuscitation, other elements of "golden hours" management include monitoring of urine output, oxygen, pain control with careful monitoring of oxygen saturation, and monitoring for SIRS. Centers of Excellence where the golden hours approach has been adopted have a 25% reduction in the relative risk of mortality (Gastroenterology 2013;144:1272-81).
In 2013 there is no longer any role for prophylactic antibiotics in patients with acute pancreatitis. Nasogastric decompression, which was once routine, is now done only for symptomatic ileus. Nor is endoscopic cholangiopancreatography appropriate for biliary pancreatitis within the first 24 hours save when ascending cholangitis is present or in the setting of a deteriorating clinical course with worsening liver function tests. Otherwise, the time to perform ERCP, Dr. McNally stressed, is after resolution of acute pancreatitis.
He reported having no financial conflicts.
ESTES PARK, COLO. – With acute pancreatitis now accounting for more than 300,000 hospital admissions per year, it behooves physicians to be adept at early clinical diagnosis and familiar with the newer, user-friendly tools for estimating case severity.
These tasks have been made much easier as a result of the simplified Atlanta consensus diagnostic criteria of 2012 and the development of a couple of quick triage tools – the HAPS and BISAP – which are far better suited for this purpose than the old Ranson criteria and APACHE-II (Acute Physiology and Chronic Health Examination) score, Dr. Peter R. McNally said at a conference on internal medicine sponsored by the University of Colorado.
"Since we solved the riddle of H. pylori and peptic ulcer disease, acute pancreatitis has become the number one GI diagnosis for admission to the hospital," noted Dr. McNally, chief of gastroenterology at Evans Army Hospital in Fort Carson, Colo.
The revised criteria for clinical diagnosis of acute pancreatitis developed by an international panel meeting in Atlanta (Gut 2013;62:102-11) require that two of three criteria be met: typical pain; a serum amylase and/or lipase level at least three times the upper limit of normal; and demonstration of the characteristic findings of acute pancreatitis on imaging, with computed tomography getting the nod as the best imaging modality. However, there are sound reasons for delaying CT imaging until at least the 48-hour mark in most cases. Thus, as a practical matter, early diagnosis requires both typical pain and enzyme elevations.
"The pancreas is located deep in the retroperitoneum. It sits on thoracolumbar vertebrae T12/L1. I want to emphasize that if you have pancreatitis, you have back pain. If you don’t have back pain, just anterior abdominal pain, it’s not pancreatitis," Dr. McNally said.
The classic picture of acute pancreatitis is acute onset of 10/10 pain. When the physician walks into the examination room, the patient is typically in the fetal position in order to relieve the excruciating back pain.
Eighty percent of cases of acute pancreatitis are mild and usually edematous. The other 20% are severe and usually necrotic. Mortality is 3% or less with edematous cases and 15%-25% or more with necrotic pancreatitis.
The HAPS and BISAP scores are enormously helpful in assessing severity early on, unlike the Ranson criteria and APACHE-II score, which are tedious and complicated, and take up to 48 hours to complete, the gastroenterologist observed.
The HAPS (Harmless Acute Pancreatitis Score) can be measured within 30 minutes of hospital admission. There are three criteria for a "harmless" HAPS score: a normal hematocrit, normal serum creatinine, and absence of rebound tenderness. The presence of all three criteria has 96% specificity and 99% positive predictive value for a nonsevere disease course (Pancreatology 2011;11:464-8).
"These are patients you can keep on the general medicine ward or perhaps even on observation status," according to Dr. McNally.
The BISAP (Bedside Index for Severity in Acute Pancreatitis) awards 1 point each for the presence of five possible findings: a urea nitrogen level in excess of 25 mg/dL, indicative of third spacing; impaired mental status defined by a Glasgow Coma Score of even a single point less than the normal 15; age over 60; pleural effusion; and the presence of systemic inflammatory response syndrome, or SIRS.
Sixty percent of patients with acute pancreatitis have SIRS on admission. It resolves within 24 hours in half of cases. Persistent or worsening SIRS is associated with an 11%-25% mortality rate. SIRS is defined by two or more of the following: tachycardia, tachypnea, hypocarbia, fever, and either an elevated or depressed white blood cell count.
A patient with a BISAP score of 1 has less than a 2% risk of mortality. In contrast, a BISAP score of 3 is associated with a 22% mortality rate (Am. J. Gastroenterol. 2009;104:966-71).
"If you’re in Hays, Kan., or Rifle, Colo., and you’re seeing a patient at time zero who already has a BISAP of 3, you probably ought to raise the white flag and ship that patient because you’re going to have a lot of problems otherwise," the gastroenterologist advised.
When the diagnosis of acute pancreatitis is uncertain or the triage tools indicate severe disease, the single best imaging modality for looking at the pancreas is CT using what is known among radiologists as the Balthazar pancreatic protocol. It is utilized to assess pancreatic necrosis, the extent of which predicts mortality. There’s no need for CT in a SIRS-negative patient with mild acute pancreatitis.
A caveat is that CT misses gallstones about 20% of the time because the stones are nonradiolucent – and gallstones are the number one cause of acute pancreatitis in women. The laboratory parameter most predictive of gallstone pancreatitis is an alanine transaminase (ALT) level at least twice the upper limit of normal. Ultrasound is the best imaging method for gallstones and for evaluation of the size of the common bile duct, although it can be difficult to image the pancreas and gallbladder using ultrasound in an obese patient.
As soon as a physician has determined that two of the three Atlanta criteria for acute pancreatitis are present, the crucial next step is to immediately give a 1- to 2-L bolus of intravenous lactated Ringer’s solution, following up at an infusion rate of 250-300 mL/hr. This is the initial intervention in what gastroenterologists have lately begun calling "the golden hours" of management in acute pancreatitis in recognition that taking certain steps in the first 24 hours has a major impact on morbidity and mortality. For example, starting lactated Ringer’s solution in the first hour of acute pancreatitis has been shown to result in an absolute 8.5% reduction in mortality. It is also far more effective than normal saline in preventing or reversing SIRS. The lactated Ringer’s prevents pancreatic enzymes from going hematogenous and causing extrapancreatic tissue breakdown.
In addition to aggressive fluid resuscitation, other elements of "golden hours" management include monitoring of urine output, oxygen, pain control with careful monitoring of oxygen saturation, and monitoring for SIRS. Centers of Excellence where the golden hours approach has been adopted have a 25% reduction in the relative risk of mortality (Gastroenterology 2013;144:1272-81).
In 2013 there is no longer any role for prophylactic antibiotics in patients with acute pancreatitis. Nasogastric decompression, which was once routine, is now done only for symptomatic ileus. Nor is endoscopic cholangiopancreatography appropriate for biliary pancreatitis within the first 24 hours save when ascending cholangitis is present or in the setting of a deteriorating clinical course with worsening liver function tests. Otherwise, the time to perform ERCP, Dr. McNally stressed, is after resolution of acute pancreatitis.
He reported having no financial conflicts.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Five steps to fewer heart failure hospitalizations
ESTES PARK, COLO. – Introducing five evidence-based interventions in patients with heart failure with reduced ejection fraction would dramatically cut admissions for heart failure, according to Dr. JoAnn Lindenfeld, vice president of the Heart Failure Society of America.
Here are the five interventions: recognizing when to switch from furosemide to another oral loop diuretic with far better bioavailability; up-titrating beta-blocker therapy to the maximum recommended dose as quickly as possible; adding a low-dose aldosterone antagonist to the treatment regimen; prescribing digoxin in symptomatic patients with a low ejection fraction; and identifying and treating iron deficiency, Dr. Lindenfeld said at a conference on internal medicine sponsored by the University of Colorado.
• Loop diuretics: Furosemide, everybody’s favorite low-cost loop diuretic, turns out to have an enormously variable oral bioavailability, ranging from 10% to 90% from patient to patient. It also varies substantially from day to day within the same individual. In contrast, torsemide (Demadex) and bumetanide (Bumex) have a consistently high oral bioavailability of roughly 90%. They are useful alternatives in poorly compensated heart failure patients.

"When your patient says they’re not diuresing and you’re pretty sure they’re taking their drugs, or if they’ve had more than one recent admission for heart failure and they’re having trouble with congestion and fluid retention, think about switching to bumetanide or torsemide," said Dr. Lindenfeld, professor of medicine and medical director of the heart transplant program at the university.
"In my own practice, when I have a patient admitted for acute decompensated heart failure with congestion and I don’t find another reversible cause, I will usually switch them," noted Dr. Lindenfeld, who also is codirector of the university’s Center for Women’s Health Research.
In a classic study, 234 patients hospitalized for acute decompensated heart failure were randomized at discharge to torsemide or furosemide in equivalent doses. The torsemide group subsequently had a 52% lower rate of heart failure hospitalization (Am. J. Med. 2001;111:513-21).
Bumetanide is now a pretty inexpensive drug, Dr. Lindenfeld noted. In making the switch, remember that 40 mg of furosemide is equivalent to 1 mg of bumetanide or 20 mg of torsemide.
• Beta-blocker up-titration: Beta-blocker and angiotensin-converting enzyme* (ACE) inhibitor therapy both have a class IA recommendation in heart failure. But what’s the best way to juggle the timing of dual dose increases?
"None of the guidelines says how to manage up-titration, but I strongly believe that once you have somebody on a reasonable dose of an ACE inhibitor – say, 5 mg of lisinopril or the equivalent – then you should go to the beta-blocker and up-titrate it to its maximum," she said. "Then later, come back to the ACE inhibitor and get the patient on the maximum dose of that."
The rationale for this approach is based on a comparison of the outcomes of the landmark beta-blocker trials versus ATLAS, a 3,104-patient trial conducted in the pre-beta-blocker era in which patients were randomized to low-dose lisinopril at 2.5-5 mg/day or high-dose therapy at 32.5-35 mg/day to determine which was better. After 4 years of follow-up, the high-dose group showed a 24% reduction in the risk of heart failure hospitalizations, but no significant advantage in terms of all-cause mortality (Circulation 1999;100:2312-8).
Contrast those results with the outcomes of the major clinical trials for carvedilol, metoprolol, and bisoprolol, each of which featured up-titration to the target dose within 8 weeks whenever possible. All three studies were halted within less than a year because of a roughly 35% reduction in mortality, compared with placebo. And that mortality benefit became apparent at 3 months.
"These are huge reductions in mortality," Dr. Lindenfeld noted. "You don’t want to have a patient come back every 4 weeks to up-titrate their ACE inhibitor for 5 months and miss the opportunity to get the patient on an effective dose of a beta-blocker, when the lifesaving benefit begins so early."
The recommended maximum doses in heart failure patients are carvedilol (Coreg) at 25 mg twice daily, or 50 mg twice daily for patients weighing more than 85 kg; 200 mg/day for extended-release metoprolol (Toprol XL); and 10 mg/day for bisoprolol (Zebeta). The three beta-blockers are similar in their efficacy for treating heart failure, Dr. Lindenfeld said. However, bisoprolol has the fewest pulmonary effects and is thus the best choice in patients with chronic obstructive pulmonary disease (COPD), even though it lacks a specific Food and Drug Administration (FDA)-approved indication for heart failure, she continued.
• Aldosterone antagonists: In terms of mortality benefit, the randomized trial data show that the aldosterone antagonists are nearly as good as beta-blockers. Yet they remain widely underutilized in the United States, according to Dr. Lindenfeld.
Indeed, three major randomized trials showed roughly a 25% reduction in total mortality, compared with placebo, in patients on standard background therapy including a beta-blocker and ACE inhibitor, along with a 20% decrease in risk of sudden cardiac death. The doses used were spironolactone at 12.5-25 mg/day or eplerenone (Inspra) at 25-50 mg/day.
An intriguing retrospective analysis conducted in close to 7,000 patients with heart failure following an acute myocardial infarction concluded that getting the aldosterone antagonist onboard early in that situation is key. Patients who started on the drug less than 7 days post MI had a 29% reduction in total mortality and a 47% decrease in sudden cardiac death, compared with those started on day 7 or later (Eur. J. Heart Fail. 2009;11:1099-1105). That benefit is believed to be the result of early left ventricular remodeling.
A definitive European prospective, randomized trial looking at the impact of starting an aldosterone antagonist within 7 days after acute MI is due to be presented later this year. The inside word is the results are highly favorable, she noted.
Hyperkalemia is a legitimate concern when prescribing an aldosterone antagonist. These agents should be avoided in a patient who has a creatinine level above 2.5 mg/dL or an estimated glomerular filtration rate below 30 mL/min per 1.73 m2, or if other potassium-sparing drugs are onboard. Potassium levels should be checked after the first 3-7 days of therapy, again at 1 month, and then every 3 months, as well as anytime a patient becomes dehydrated.
• Digoxin: In the classic digoxin trial involving close to 7,000 patients, heart failure hospitalization was a prospectively defined endpoint. In patients with a left ventricular ejection fraction of 25%-45%, hospital admission for heart failure was reduced by 26% in patients assigned to digoxin. In those whose ejection fraction was less than 25%, the reduction in hospitalization was 39%.
"So don’t forget that digoxin is still a good drug in patients with low ejection fraction or who have substantial symptoms," Dr. Lindenfeld said. "If we had a drug approved today that didn’t change mortality but reduced hospital admissions by 39%, we’d all be giving it – and we’d be paying a lot for it."
• Role of iron deficiency in heart failure: A new European study is illuminating on this score: Among a cohort of 1,506 patients with chronic heart failure, fully 50% were determined to have iron deficiency, as defined by a ferritin level less than 100 mcg/L, or a ferritin level of 100-299 mcg/L with a transferring saturation lower than 20%. In a multivariate regression analysis, iron deficiency was a strong independent predictor for mortality, associated with a 42% increased risk (Am. Heart J. 2013;165:575-82).
"I think if you restricted the study to hospitalized heart failure patients, the iron deficiency rate would be even higher. It’s just appalling how many people we send home iron deficient without iron replacement therapy," Dr. Lindenfeld asserted.
She noted that in the European FAIR-HF trial involving 459 hospitalized iron-deficient heart failure patients randomized at discharge to intravenous iron corrective and maintenance therapy or to a matching placebo, the iron replacement group demonstrated significant improvement in quality of life and exercise capacity. The benefits were seen regardless of whether a patient’s baseline hemoglobin was high or low.
In addition, the rate of the combined endpoint of first hospitalization for worsening heart failure or death was 7.5% in the iron recipients, compared with 13.9% in placebo-treated controls – a difference that didn’t achieve statistical significance because the study was underpowered to evaluated that endpoint (N. Engl. J. Med. 2009;36:2436-48).
"Iron replacement is a distinct advantage for these patients, so you should be looking for iron deficiency. You probably don’t need to use IV iron, but if your patient is in the hospital anyway, IV iron is pretty benign and will get him iron-repleted almost immediately," Dr. Lindenfeld continued.
Before sending iron-deficient patients home on oral iron, make sure they can absorb it. Many older individuals can’t. Indeed, among patients hospitalized at the University of Colorado heart failure service, only 13% can actually absorb oral iron, she explained.
A simple way to tell is to draw a serum iron level, give the patient an iron tablet, and check the serum iron level again in 1-3 hours. It should roughly double, Dr. Lindenfeld explained.
Dr. Lindenfeld reported serving as a consultant for Medtronic, St. Jude, and other companies.
*Correction, 8/12/2013: An earlier version of this story misstated the meaning of ACE.
The five-point checklist as noted represents a reliable strategy for ensuring we apply evidence to our clinical practice. I would emphasize the following points:
•Pharmacodynamic issues such bioavailability of loop diuretics are often not well known, and the use of Bumex (bumetanide) can have a meaningful impact on those refractory to furosemide.

|
| Dr. Hiren Shah |
•Up-titration to maximum beta-blockade prior to doing the same with ACE inhibitors is strongly supported by current evidence but not always done in clinical practice.
•Early use of aldosterone antagonists post MI is critical, but in those with chronic HF, it should still be restricted to patients with New York Heart Association (NYHA) class II HF and left ventricular ejection fraction (LVEF) less than or equal to 30% or class III to IV HF and EF less than or equal to 35%.
In addition, aldosterone antagonist therapy should be continued following hospital discharge only in patients who can be carefully monitored for hyperkalemia. Similarly, one should be aware of the occurrence of adverse drug reactions when using digoxin, owing to its narrow therapeutic index requiring serum level monitoring.
•Finally, the most overlooked aspect of HF management on this list is the importance of correcting iron-deficiency anemia, which occurs mainly through chronic renal insufficiency in HF patients.
We also now know that the anemia itself can worsen cardiac function, both because it causes cardiac stress through tachycardia and increased stroke volume, and because it can cause a reduced renal blood flow and fluid retention, adding further stress to the heart. Therefore, it is critical to correct the iron deficiency to break the vicious circle wherein CHF causes anemia, and the anemia causes more CHF, and both damage the kidneys, worsening the anemia and the CHF further.
We should all aim for the preferred strategy of intravenous iron for our hospitalized patients and then convert to oral iron, noting the absorption issues that should be evaluated prior to discharge. Of course, any new iron-deficiency anemia should still be worked up considering other causes such as GI losses.
Dr. Hiren Shah is an assistant professor of medicine in the Feinberg School of Medicine, Northwestern University, Chicago, and a medical director of the Medicine and Cardiac Telemetry Hospitalist Unit at Northwestern Memorial Hospital in Chicago.
The five-point checklist as noted represents a reliable strategy for ensuring we apply evidence to our clinical practice. I would emphasize the following points:
•Pharmacodynamic issues such bioavailability of loop diuretics are often not well known, and the use of Bumex (bumetanide) can have a meaningful impact on those refractory to furosemide.
|
|
| Dr. Hiren Shah |
•Up-titration to maximum beta-blockade prior to doing the same with ACE inhibitors is strongly supported by current evidence but not always done in clinical practice.
•Early use of aldosterone antagonists post MI is critical, but in those with chronic HF, it should still be restricted to patients with New York Heart Association (NYHA) class II HF and left ventricular ejection fraction (LVEF) less than or equal to 30% or class III to IV HF and EF less than or equal to 35%.
In addition, aldosterone antagonist therapy should be continued following hospital discharge only in patients who can be carefully monitored for hyperkalemia. Similarly, one should be aware of the occurrence of adverse drug reactions when using digoxin, owing to its narrow therapeutic index requiring serum level monitoring.
•Finally, the most overlooked aspect of HF management on this list is the importance of correcting iron-deficiency anemia, which occurs mainly through chronic renal insufficiency in HF patients.
We also now know that the anemia itself can worsen cardiac function, both because it causes cardiac stress through tachycardia and increased stroke volume, and because it can cause a reduced renal blood flow and fluid retention, adding further stress to the heart. Therefore, it is critical to correct the iron deficiency to break the vicious circle wherein CHF causes anemia, and the anemia causes more CHF, and both damage the kidneys, worsening the anemia and the CHF further.
We should all aim for the preferred strategy of intravenous iron for our hospitalized patients and then convert to oral iron, noting the absorption issues that should be evaluated prior to discharge. Of course, any new iron-deficiency anemia should still be worked up considering other causes such as GI losses.
Dr. Hiren Shah is an assistant professor of medicine in the Feinberg School of Medicine, Northwestern University, Chicago, and a medical director of the Medicine and Cardiac Telemetry Hospitalist Unit at Northwestern Memorial Hospital in Chicago.
The five-point checklist as noted represents a reliable strategy for ensuring we apply evidence to our clinical practice. I would emphasize the following points:
•Pharmacodynamic issues such bioavailability of loop diuretics are often not well known, and the use of Bumex (bumetanide) can have a meaningful impact on those refractory to furosemide.
|
|
| Dr. Hiren Shah |
•Up-titration to maximum beta-blockade prior to doing the same with ACE inhibitors is strongly supported by current evidence but not always done in clinical practice.
•Early use of aldosterone antagonists post MI is critical, but in those with chronic HF, it should still be restricted to patients with New York Heart Association (NYHA) class II HF and left ventricular ejection fraction (LVEF) less than or equal to 30% or class III to IV HF and EF less than or equal to 35%.
In addition, aldosterone antagonist therapy should be continued following hospital discharge only in patients who can be carefully monitored for hyperkalemia. Similarly, one should be aware of the occurrence of adverse drug reactions when using digoxin, owing to its narrow therapeutic index requiring serum level monitoring.
•Finally, the most overlooked aspect of HF management on this list is the importance of correcting iron-deficiency anemia, which occurs mainly through chronic renal insufficiency in HF patients.
We also now know that the anemia itself can worsen cardiac function, both because it causes cardiac stress through tachycardia and increased stroke volume, and because it can cause a reduced renal blood flow and fluid retention, adding further stress to the heart. Therefore, it is critical to correct the iron deficiency to break the vicious circle wherein CHF causes anemia, and the anemia causes more CHF, and both damage the kidneys, worsening the anemia and the CHF further.
We should all aim for the preferred strategy of intravenous iron for our hospitalized patients and then convert to oral iron, noting the absorption issues that should be evaluated prior to discharge. Of course, any new iron-deficiency anemia should still be worked up considering other causes such as GI losses.
Dr. Hiren Shah is an assistant professor of medicine in the Feinberg School of Medicine, Northwestern University, Chicago, and a medical director of the Medicine and Cardiac Telemetry Hospitalist Unit at Northwestern Memorial Hospital in Chicago.
ESTES PARK, COLO. – Introducing five evidence-based interventions in patients with heart failure with reduced ejection fraction would dramatically cut admissions for heart failure, according to Dr. JoAnn Lindenfeld, vice president of the Heart Failure Society of America.
Here are the five interventions: recognizing when to switch from furosemide to another oral loop diuretic with far better bioavailability; up-titrating beta-blocker therapy to the maximum recommended dose as quickly as possible; adding a low-dose aldosterone antagonist to the treatment regimen; prescribing digoxin in symptomatic patients with a low ejection fraction; and identifying and treating iron deficiency, Dr. Lindenfeld said at a conference on internal medicine sponsored by the University of Colorado.
• Loop diuretics: Furosemide, everybody’s favorite low-cost loop diuretic, turns out to have an enormously variable oral bioavailability, ranging from 10% to 90% from patient to patient. It also varies substantially from day to day within the same individual. In contrast, torsemide (Demadex) and bumetanide (Bumex) have a consistently high oral bioavailability of roughly 90%. They are useful alternatives in poorly compensated heart failure patients.
"When your patient says they’re not diuresing and you’re pretty sure they’re taking their drugs, or if they’ve had more than one recent admission for heart failure and they’re having trouble with congestion and fluid retention, think about switching to bumetanide or torsemide," said Dr. Lindenfeld, professor of medicine and medical director of the heart transplant program at the university.
"In my own practice, when I have a patient admitted for acute decompensated heart failure with congestion and I don’t find another reversible cause, I will usually switch them," noted Dr. Lindenfeld, who also is codirector of the university’s Center for Women’s Health Research.
In a classic study, 234 patients hospitalized for acute decompensated heart failure were randomized at discharge to torsemide or furosemide in equivalent doses. The torsemide group subsequently had a 52% lower rate of heart failure hospitalization (Am. J. Med. 2001;111:513-21).
Bumetanide is now a pretty inexpensive drug, Dr. Lindenfeld noted. In making the switch, remember that 40 mg of furosemide is equivalent to 1 mg of bumetanide or 20 mg of torsemide.
• Beta-blocker up-titration: Beta-blocker and angiotensin-converting enzyme* (ACE) inhibitor therapy both have a class IA recommendation in heart failure. But what’s the best way to juggle the timing of dual dose increases?
"None of the guidelines says how to manage up-titration, but I strongly believe that once you have somebody on a reasonable dose of an ACE inhibitor – say, 5 mg of lisinopril or the equivalent – then you should go to the beta-blocker and up-titrate it to its maximum," she said. "Then later, come back to the ACE inhibitor and get the patient on the maximum dose of that."
The rationale for this approach is based on a comparison of the outcomes of the landmark beta-blocker trials versus ATLAS, a 3,104-patient trial conducted in the pre-beta-blocker era in which patients were randomized to low-dose lisinopril at 2.5-5 mg/day or high-dose therapy at 32.5-35 mg/day to determine which was better. After 4 years of follow-up, the high-dose group showed a 24% reduction in the risk of heart failure hospitalizations, but no significant advantage in terms of all-cause mortality (Circulation 1999;100:2312-8).
Contrast those results with the outcomes of the major clinical trials for carvedilol, metoprolol, and bisoprolol, each of which featured up-titration to the target dose within 8 weeks whenever possible. All three studies were halted within less than a year because of a roughly 35% reduction in mortality, compared with placebo. And that mortality benefit became apparent at 3 months.
"These are huge reductions in mortality," Dr. Lindenfeld noted. "You don’t want to have a patient come back every 4 weeks to up-titrate their ACE inhibitor for 5 months and miss the opportunity to get the patient on an effective dose of a beta-blocker, when the lifesaving benefit begins so early."
The recommended maximum doses in heart failure patients are carvedilol (Coreg) at 25 mg twice daily, or 50 mg twice daily for patients weighing more than 85 kg; 200 mg/day for extended-release metoprolol (Toprol XL); and 10 mg/day for bisoprolol (Zebeta). The three beta-blockers are similar in their efficacy for treating heart failure, Dr. Lindenfeld said. However, bisoprolol has the fewest pulmonary effects and is thus the best choice in patients with chronic obstructive pulmonary disease (COPD), even though it lacks a specific Food and Drug Administration (FDA)-approved indication for heart failure, she continued.
• Aldosterone antagonists: In terms of mortality benefit, the randomized trial data show that the aldosterone antagonists are nearly as good as beta-blockers. Yet they remain widely underutilized in the United States, according to Dr. Lindenfeld.
Indeed, three major randomized trials showed roughly a 25% reduction in total mortality, compared with placebo, in patients on standard background therapy including a beta-blocker and ACE inhibitor, along with a 20% decrease in risk of sudden cardiac death. The doses used were spironolactone at 12.5-25 mg/day or eplerenone (Inspra) at 25-50 mg/day.
An intriguing retrospective analysis conducted in close to 7,000 patients with heart failure following an acute myocardial infarction concluded that getting the aldosterone antagonist onboard early in that situation is key. Patients who started on the drug less than 7 days post MI had a 29% reduction in total mortality and a 47% decrease in sudden cardiac death, compared with those started on day 7 or later (Eur. J. Heart Fail. 2009;11:1099-1105). That benefit is believed to be the result of early left ventricular remodeling.
A definitive European prospective, randomized trial looking at the impact of starting an aldosterone antagonist within 7 days after acute MI is due to be presented later this year. The inside word is the results are highly favorable, she noted.
Hyperkalemia is a legitimate concern when prescribing an aldosterone antagonist. These agents should be avoided in a patient who has a creatinine level above 2.5 mg/dL or an estimated glomerular filtration rate below 30 mL/min per 1.73 m2, or if other potassium-sparing drugs are onboard. Potassium levels should be checked after the first 3-7 days of therapy, again at 1 month, and then every 3 months, as well as anytime a patient becomes dehydrated.
• Digoxin: In the classic digoxin trial involving close to 7,000 patients, heart failure hospitalization was a prospectively defined endpoint. In patients with a left ventricular ejection fraction of 25%-45%, hospital admission for heart failure was reduced by 26% in patients assigned to digoxin. In those whose ejection fraction was less than 25%, the reduction in hospitalization was 39%.
"So don’t forget that digoxin is still a good drug in patients with low ejection fraction or who have substantial symptoms," Dr. Lindenfeld said. "If we had a drug approved today that didn’t change mortality but reduced hospital admissions by 39%, we’d all be giving it – and we’d be paying a lot for it."
• Role of iron deficiency in heart failure: A new European study is illuminating on this score: Among a cohort of 1,506 patients with chronic heart failure, fully 50% were determined to have iron deficiency, as defined by a ferritin level less than 100 mcg/L, or a ferritin level of 100-299 mcg/L with a transferring saturation lower than 20%. In a multivariate regression analysis, iron deficiency was a strong independent predictor for mortality, associated with a 42% increased risk (Am. Heart J. 2013;165:575-82).
"I think if you restricted the study to hospitalized heart failure patients, the iron deficiency rate would be even higher. It’s just appalling how many people we send home iron deficient without iron replacement therapy," Dr. Lindenfeld asserted.
She noted that in the European FAIR-HF trial involving 459 hospitalized iron-deficient heart failure patients randomized at discharge to intravenous iron corrective and maintenance therapy or to a matching placebo, the iron replacement group demonstrated significant improvement in quality of life and exercise capacity. The benefits were seen regardless of whether a patient’s baseline hemoglobin was high or low.
In addition, the rate of the combined endpoint of first hospitalization for worsening heart failure or death was 7.5% in the iron recipients, compared with 13.9% in placebo-treated controls – a difference that didn’t achieve statistical significance because the study was underpowered to evaluated that endpoint (N. Engl. J. Med. 2009;36:2436-48).
"Iron replacement is a distinct advantage for these patients, so you should be looking for iron deficiency. You probably don’t need to use IV iron, but if your patient is in the hospital anyway, IV iron is pretty benign and will get him iron-repleted almost immediately," Dr. Lindenfeld continued.
Before sending iron-deficient patients home on oral iron, make sure they can absorb it. Many older individuals can’t. Indeed, among patients hospitalized at the University of Colorado heart failure service, only 13% can actually absorb oral iron, she explained.
A simple way to tell is to draw a serum iron level, give the patient an iron tablet, and check the serum iron level again in 1-3 hours. It should roughly double, Dr. Lindenfeld explained.
Dr. Lindenfeld reported serving as a consultant for Medtronic, St. Jude, and other companies.
*Correction, 8/12/2013: An earlier version of this story misstated the meaning of ACE.
ESTES PARK, COLO. – Introducing five evidence-based interventions in patients with heart failure with reduced ejection fraction would dramatically cut admissions for heart failure, according to Dr. JoAnn Lindenfeld, vice president of the Heart Failure Society of America.
Here are the five interventions: recognizing when to switch from furosemide to another oral loop diuretic with far better bioavailability; up-titrating beta-blocker therapy to the maximum recommended dose as quickly as possible; adding a low-dose aldosterone antagonist to the treatment regimen; prescribing digoxin in symptomatic patients with a low ejection fraction; and identifying and treating iron deficiency, Dr. Lindenfeld said at a conference on internal medicine sponsored by the University of Colorado.
• Loop diuretics: Furosemide, everybody’s favorite low-cost loop diuretic, turns out to have an enormously variable oral bioavailability, ranging from 10% to 90% from patient to patient. It also varies substantially from day to day within the same individual. In contrast, torsemide (Demadex) and bumetanide (Bumex) have a consistently high oral bioavailability of roughly 90%. They are useful alternatives in poorly compensated heart failure patients.
"When your patient says they’re not diuresing and you’re pretty sure they’re taking their drugs, or if they’ve had more than one recent admission for heart failure and they’re having trouble with congestion and fluid retention, think about switching to bumetanide or torsemide," said Dr. Lindenfeld, professor of medicine and medical director of the heart transplant program at the university.
"In my own practice, when I have a patient admitted for acute decompensated heart failure with congestion and I don’t find another reversible cause, I will usually switch them," noted Dr. Lindenfeld, who also is codirector of the university’s Center for Women’s Health Research.
In a classic study, 234 patients hospitalized for acute decompensated heart failure were randomized at discharge to torsemide or furosemide in equivalent doses. The torsemide group subsequently had a 52% lower rate of heart failure hospitalization (Am. J. Med. 2001;111:513-21).
Bumetanide is now a pretty inexpensive drug, Dr. Lindenfeld noted. In making the switch, remember that 40 mg of furosemide is equivalent to 1 mg of bumetanide or 20 mg of torsemide.
• Beta-blocker up-titration: Beta-blocker and angiotensin-converting enzyme* (ACE) inhibitor therapy both have a class IA recommendation in heart failure. But what’s the best way to juggle the timing of dual dose increases?
"None of the guidelines says how to manage up-titration, but I strongly believe that once you have somebody on a reasonable dose of an ACE inhibitor – say, 5 mg of lisinopril or the equivalent – then you should go to the beta-blocker and up-titrate it to its maximum," she said. "Then later, come back to the ACE inhibitor and get the patient on the maximum dose of that."
The rationale for this approach is based on a comparison of the outcomes of the landmark beta-blocker trials versus ATLAS, a 3,104-patient trial conducted in the pre-beta-blocker era in which patients were randomized to low-dose lisinopril at 2.5-5 mg/day or high-dose therapy at 32.5-35 mg/day to determine which was better. After 4 years of follow-up, the high-dose group showed a 24% reduction in the risk of heart failure hospitalizations, but no significant advantage in terms of all-cause mortality (Circulation 1999;100:2312-8).
Contrast those results with the outcomes of the major clinical trials for carvedilol, metoprolol, and bisoprolol, each of which featured up-titration to the target dose within 8 weeks whenever possible. All three studies were halted within less than a year because of a roughly 35% reduction in mortality, compared with placebo. And that mortality benefit became apparent at 3 months.
"These are huge reductions in mortality," Dr. Lindenfeld noted. "You don’t want to have a patient come back every 4 weeks to up-titrate their ACE inhibitor for 5 months and miss the opportunity to get the patient on an effective dose of a beta-blocker, when the lifesaving benefit begins so early."
The recommended maximum doses in heart failure patients are carvedilol (Coreg) at 25 mg twice daily, or 50 mg twice daily for patients weighing more than 85 kg; 200 mg/day for extended-release metoprolol (Toprol XL); and 10 mg/day for bisoprolol (Zebeta). The three beta-blockers are similar in their efficacy for treating heart failure, Dr. Lindenfeld said. However, bisoprolol has the fewest pulmonary effects and is thus the best choice in patients with chronic obstructive pulmonary disease (COPD), even though it lacks a specific Food and Drug Administration (FDA)-approved indication for heart failure, she continued.
• Aldosterone antagonists: In terms of mortality benefit, the randomized trial data show that the aldosterone antagonists are nearly as good as beta-blockers. Yet they remain widely underutilized in the United States, according to Dr. Lindenfeld.
Indeed, three major randomized trials showed roughly a 25% reduction in total mortality, compared with placebo, in patients on standard background therapy including a beta-blocker and ACE inhibitor, along with a 20% decrease in risk of sudden cardiac death. The doses used were spironolactone at 12.5-25 mg/day or eplerenone (Inspra) at 25-50 mg/day.
An intriguing retrospective analysis conducted in close to 7,000 patients with heart failure following an acute myocardial infarction concluded that getting the aldosterone antagonist onboard early in that situation is key. Patients who started on the drug less than 7 days post MI had a 29% reduction in total mortality and a 47% decrease in sudden cardiac death, compared with those started on day 7 or later (Eur. J. Heart Fail. 2009;11:1099-1105). That benefit is believed to be the result of early left ventricular remodeling.
A definitive European prospective, randomized trial looking at the impact of starting an aldosterone antagonist within 7 days after acute MI is due to be presented later this year. The inside word is the results are highly favorable, she noted.
Hyperkalemia is a legitimate concern when prescribing an aldosterone antagonist. These agents should be avoided in a patient who has a creatinine level above 2.5 mg/dL or an estimated glomerular filtration rate below 30 mL/min per 1.73 m2, or if other potassium-sparing drugs are onboard. Potassium levels should be checked after the first 3-7 days of therapy, again at 1 month, and then every 3 months, as well as anytime a patient becomes dehydrated.
• Digoxin: In the classic digoxin trial involving close to 7,000 patients, heart failure hospitalization was a prospectively defined endpoint. In patients with a left ventricular ejection fraction of 25%-45%, hospital admission for heart failure was reduced by 26% in patients assigned to digoxin. In those whose ejection fraction was less than 25%, the reduction in hospitalization was 39%.
"So don’t forget that digoxin is still a good drug in patients with low ejection fraction or who have substantial symptoms," Dr. Lindenfeld said. "If we had a drug approved today that didn’t change mortality but reduced hospital admissions by 39%, we’d all be giving it – and we’d be paying a lot for it."
• Role of iron deficiency in heart failure: A new European study is illuminating on this score: Among a cohort of 1,506 patients with chronic heart failure, fully 50% were determined to have iron deficiency, as defined by a ferritin level less than 100 mcg/L, or a ferritin level of 100-299 mcg/L with a transferring saturation lower than 20%. In a multivariate regression analysis, iron deficiency was a strong independent predictor for mortality, associated with a 42% increased risk (Am. Heart J. 2013;165:575-82).
"I think if you restricted the study to hospitalized heart failure patients, the iron deficiency rate would be even higher. It’s just appalling how many people we send home iron deficient without iron replacement therapy," Dr. Lindenfeld asserted.
She noted that in the European FAIR-HF trial involving 459 hospitalized iron-deficient heart failure patients randomized at discharge to intravenous iron corrective and maintenance therapy or to a matching placebo, the iron replacement group demonstrated significant improvement in quality of life and exercise capacity. The benefits were seen regardless of whether a patient’s baseline hemoglobin was high or low.
In addition, the rate of the combined endpoint of first hospitalization for worsening heart failure or death was 7.5% in the iron recipients, compared with 13.9% in placebo-treated controls – a difference that didn’t achieve statistical significance because the study was underpowered to evaluated that endpoint (N. Engl. J. Med. 2009;36:2436-48).
"Iron replacement is a distinct advantage for these patients, so you should be looking for iron deficiency. You probably don’t need to use IV iron, but if your patient is in the hospital anyway, IV iron is pretty benign and will get him iron-repleted almost immediately," Dr. Lindenfeld continued.
Before sending iron-deficient patients home on oral iron, make sure they can absorb it. Many older individuals can’t. Indeed, among patients hospitalized at the University of Colorado heart failure service, only 13% can actually absorb oral iron, she explained.
A simple way to tell is to draw a serum iron level, give the patient an iron tablet, and check the serum iron level again in 1-3 hours. It should roughly double, Dr. Lindenfeld explained.
Dr. Lindenfeld reported serving as a consultant for Medtronic, St. Jude, and other companies.
*Correction, 8/12/2013: An earlier version of this story misstated the meaning of ACE.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Prevention: Probiotics cut C. difficile risk
VAIL, COLO. – The strategy of a short course of probiotics prescribed to prevent development of Clostridium difficile–associated diarrhea in patients on antibiotic therapy for any of myriad indications is attracting serious attention in both pediatrics and adult medicine.
Interest in this low-cost and demonstrably low-risk preventive strategy has been driven by a recent favorable meta-analysis by the Cochrane Collaboration.
The Cochrane analysis included all 23 randomized controlled trials of probiotics for the prevention of C. difficile–associated diarrhea in adults or children taking antibiotics. The trials, three of which were conducted in children, included 4,213 subjects, none of whom were immunocompromised, severely ill, or had an underlying gastrointestinal disorder.
The incidence of C. difficile–associated diarrhea was 2.0% in patients randomized to probiotics, compared with 5.5% in controls, for a highly significant 64% reduction in risk. Moreover, the risk of adverse GI events such as abdominal cramping, nausea, fever, taste disturbance, or flatulence was reduced by 20% in the probiotics group (Cochrane Database Syst. Rev. 2013 May 31 [doi: 10.1002/14651858.CD006095.pub3]).
The benefit of prophylactic probiotics was similar in magnitude in children and adults.
"Moderate-quality evidence suggests that probiotics are both safe and effective for preventing C. difficile–associated diarrhea when used along with antibiotics in patients who are not immunocompromised or severely debilitated," the Cochrane investigators concluded.
Neither the current American College of Gastroenterology practice guidelines on C. difficile–associated diarrhea (Am. J. Gastroenterol. 2013;108:478-98) nor the Infectious Diseases Society of America guidelines (Infect. Control Hosp. Epidemiol. 2010;31:431-55) recommend using prophylactic probiotics. However, both guidelines were published before the Cochrane meta-analysis was released, Dr. Samuel R. Dominguez pointed out at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
"Interestingly, a larger effect size was seen in studies of probiotics that contained multiple species compared to a single species, although the data set wasn’t large enough for investigators to be able to look at different specific formulations," added Dr. Dominguez, a pediatric infectious diseases specialist at the University of Colorado, Denver.
He noted that the incidence, severity, and mortality of C. difficile infections have increased dramatically since 2000. Even in children, a population traditionally considered at low risk, a recent population-based study conducted in Olmsted County, Minn., by investigators at the Mayo Clinic concluded that the age- and gender-adjusted incidence of C. difficile infection jumped nearly 13-fold from 1991 to 2009, when it reached 32.6 per 100,000 persons. Three-quarters of the 92 cases were community acquired. Prior studies of C. difficile disease in children may have underestimated the incidence because they were largely based on hospital-acquired cases (Clin. Infect. Dis. 2013;56:1401-6).
Another recent study highlights the serious nature of C. difficile in children, Dr. Dominguez continued. This retrospective cohort study conducted at 41 children’s hospitals included 4,474 patients hospitalized with C. difficile infection and 8,821 matched controls. The in-hospital mortality rate was 1.43% in children with C. difficile infection, compared with 0.66% in controls. In the subgroup of children with hospital-onset C. difficile infection, the mortality risk was an adjusted 6.7-fold higher than in matched controls.
Patients with community-onset C. difficile infection had a mean hospital length of stay that was 5.6 days longer and total hospital costs that were $18,900 greater than those of controls. In patients with hospital-onset C. difficile infection, the differences were even more dramatic: a mean 21.6-day longer length of stay than for controls, and a $93,600 greater hospital cost (Clin. Infect. Dis. 2013;57:1-8).
Dr. Dominguez said that although there is no set policy at Children’s Hospital, his own practice is to recommend probiotics to healthy children who are going to be taking antibiotics.
At a separate conference devoted to adult medicine, Dr. Mel L. Anderson cited both the Cochrane Collaboration meta-analysis and a separate one led by investigators at Toronto’s Hospital for Sick Children that concluded probiotics reduced the incidence of C. difficile–associated diarrhea by 66% (Ann. Intern. Med. 2012;157:878-88).
"If you look at these randomized controlled trials, I think the evidence is fairly convincing. And it’s not an expensive treatment. We use a lot of it in our inpatient service to reduce the risk of antibiotic-associated diarrhea, and C. difficile in particular," said Dr. Anderson, chief of the hospital medicine section at the Denver VA Medical Center.
Prophylactic probiotics are not for the surgical patient who is merely getting a dose or two of perioperative antibiotic coverage. But the preventive therapy is worth at least considering in pretty much everybody else getting a prescription for antibiotics. The randomized trials included in the two meta-analyses basically included patients receiving 3 days or more of antibiotics. Classes of antibiotics identified in previous work as posing an increased risk of C. difficile–associated diarrhea included the beta-lactams, cephalosporins, fluoroquinolones, and clindamycin – "pretty much everything you prescribe" – Dr. Anderson observed in Estes Park, Colo., at a conference on internal medicine sponsored by the University of Colorado.
"I have to say, if someone comes in with uncomplicated community-acquired pneumonia, I oftentimes don’t prescribe prophylactic probiotics unless they’ve had C. difficile–associated diarrhea before or they’re very fragile. But if something is even a little bit wrong with you, bad diarrheal illness can be the straw that breaks the camel’s back. And I strongly think about prophylactic probiotics in folks on long-term antibiotics, like for a diabetic foot ulcer," he noted.
Dr. Anderson said his typical prescription is for two Lactobacillus acidophilus capsules twice daily.
"The randomized studies done to date don’t let us know the optimal mix of critters or how much is enough," according to the hospitalist.
While preventive probiotic therapy is low cost, Dr. Dominguez noted that a more high-tech therapy for secondary prevention of C. difficile infection is in the developmental pipeline.
A pair of neutralizing, fully human monoclonal antibodies against C. difficile toxins A and B administered together in a single infusion in a randomized, double-blind, placebo-controlled, phase II clinical trial in patients with C. difficile–associated diarrhea didn’t have any effect on duration of hospitalization for that episode. However, it did result in a highly significant 72% reduction in recurrence, according to investigators at Medarex in Princeton, N.J., and the University of Massachusetts, Boston (N. Engl. J. Med. 2010;362:197-205).
"This may be a useful tool in the future for preventing recurrences," Dr. Dominguez commented.
Dr. Dominguez and Dr. Anderson reported having no financial conflicts of interest.
VAIL, COLO. – The strategy of a short course of probiotics prescribed to prevent development of Clostridium difficile–associated diarrhea in patients on antibiotic therapy for any of myriad indications is attracting serious attention in both pediatrics and adult medicine.
Interest in this low-cost and demonstrably low-risk preventive strategy has been driven by a recent favorable meta-analysis by the Cochrane Collaboration.
The Cochrane analysis included all 23 randomized controlled trials of probiotics for the prevention of C. difficile–associated diarrhea in adults or children taking antibiotics. The trials, three of which were conducted in children, included 4,213 subjects, none of whom were immunocompromised, severely ill, or had an underlying gastrointestinal disorder.
The incidence of C. difficile–associated diarrhea was 2.0% in patients randomized to probiotics, compared with 5.5% in controls, for a highly significant 64% reduction in risk. Moreover, the risk of adverse GI events such as abdominal cramping, nausea, fever, taste disturbance, or flatulence was reduced by 20% in the probiotics group (Cochrane Database Syst. Rev. 2013 May 31 [doi: 10.1002/14651858.CD006095.pub3]).
The benefit of prophylactic probiotics was similar in magnitude in children and adults.
"Moderate-quality evidence suggests that probiotics are both safe and effective for preventing C. difficile–associated diarrhea when used along with antibiotics in patients who are not immunocompromised or severely debilitated," the Cochrane investigators concluded.
Neither the current American College of Gastroenterology practice guidelines on C. difficile–associated diarrhea (Am. J. Gastroenterol. 2013;108:478-98) nor the Infectious Diseases Society of America guidelines (Infect. Control Hosp. Epidemiol. 2010;31:431-55) recommend using prophylactic probiotics. However, both guidelines were published before the Cochrane meta-analysis was released, Dr. Samuel R. Dominguez pointed out at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
"Interestingly, a larger effect size was seen in studies of probiotics that contained multiple species compared to a single species, although the data set wasn’t large enough for investigators to be able to look at different specific formulations," added Dr. Dominguez, a pediatric infectious diseases specialist at the University of Colorado, Denver.
He noted that the incidence, severity, and mortality of C. difficile infections have increased dramatically since 2000. Even in children, a population traditionally considered at low risk, a recent population-based study conducted in Olmsted County, Minn., by investigators at the Mayo Clinic concluded that the age- and gender-adjusted incidence of C. difficile infection jumped nearly 13-fold from 1991 to 2009, when it reached 32.6 per 100,000 persons. Three-quarters of the 92 cases were community acquired. Prior studies of C. difficile disease in children may have underestimated the incidence because they were largely based on hospital-acquired cases (Clin. Infect. Dis. 2013;56:1401-6).
Another recent study highlights the serious nature of C. difficile in children, Dr. Dominguez continued. This retrospective cohort study conducted at 41 children’s hospitals included 4,474 patients hospitalized with C. difficile infection and 8,821 matched controls. The in-hospital mortality rate was 1.43% in children with C. difficile infection, compared with 0.66% in controls. In the subgroup of children with hospital-onset C. difficile infection, the mortality risk was an adjusted 6.7-fold higher than in matched controls.
Patients with community-onset C. difficile infection had a mean hospital length of stay that was 5.6 days longer and total hospital costs that were $18,900 greater than those of controls. In patients with hospital-onset C. difficile infection, the differences were even more dramatic: a mean 21.6-day longer length of stay than for controls, and a $93,600 greater hospital cost (Clin. Infect. Dis. 2013;57:1-8).
Dr. Dominguez said that although there is no set policy at Children’s Hospital, his own practice is to recommend probiotics to healthy children who are going to be taking antibiotics.
At a separate conference devoted to adult medicine, Dr. Mel L. Anderson cited both the Cochrane Collaboration meta-analysis and a separate one led by investigators at Toronto’s Hospital for Sick Children that concluded probiotics reduced the incidence of C. difficile–associated diarrhea by 66% (Ann. Intern. Med. 2012;157:878-88).
"If you look at these randomized controlled trials, I think the evidence is fairly convincing. And it’s not an expensive treatment. We use a lot of it in our inpatient service to reduce the risk of antibiotic-associated diarrhea, and C. difficile in particular," said Dr. Anderson, chief of the hospital medicine section at the Denver VA Medical Center.
Prophylactic probiotics are not for the surgical patient who is merely getting a dose or two of perioperative antibiotic coverage. But the preventive therapy is worth at least considering in pretty much everybody else getting a prescription for antibiotics. The randomized trials included in the two meta-analyses basically included patients receiving 3 days or more of antibiotics. Classes of antibiotics identified in previous work as posing an increased risk of C. difficile–associated diarrhea included the beta-lactams, cephalosporins, fluoroquinolones, and clindamycin – "pretty much everything you prescribe" – Dr. Anderson observed in Estes Park, Colo., at a conference on internal medicine sponsored by the University of Colorado.
"I have to say, if someone comes in with uncomplicated community-acquired pneumonia, I oftentimes don’t prescribe prophylactic probiotics unless they’ve had C. difficile–associated diarrhea before or they’re very fragile. But if something is even a little bit wrong with you, bad diarrheal illness can be the straw that breaks the camel’s back. And I strongly think about prophylactic probiotics in folks on long-term antibiotics, like for a diabetic foot ulcer," he noted.
Dr. Anderson said his typical prescription is for two Lactobacillus acidophilus capsules twice daily.
"The randomized studies done to date don’t let us know the optimal mix of critters or how much is enough," according to the hospitalist.
While preventive probiotic therapy is low cost, Dr. Dominguez noted that a more high-tech therapy for secondary prevention of C. difficile infection is in the developmental pipeline.
A pair of neutralizing, fully human monoclonal antibodies against C. difficile toxins A and B administered together in a single infusion in a randomized, double-blind, placebo-controlled, phase II clinical trial in patients with C. difficile–associated diarrhea didn’t have any effect on duration of hospitalization for that episode. However, it did result in a highly significant 72% reduction in recurrence, according to investigators at Medarex in Princeton, N.J., and the University of Massachusetts, Boston (N. Engl. J. Med. 2010;362:197-205).
"This may be a useful tool in the future for preventing recurrences," Dr. Dominguez commented.
Dr. Dominguez and Dr. Anderson reported having no financial conflicts of interest.
VAIL, COLO. – The strategy of a short course of probiotics prescribed to prevent development of Clostridium difficile–associated diarrhea in patients on antibiotic therapy for any of myriad indications is attracting serious attention in both pediatrics and adult medicine.
Interest in this low-cost and demonstrably low-risk preventive strategy has been driven by a recent favorable meta-analysis by the Cochrane Collaboration.
The Cochrane analysis included all 23 randomized controlled trials of probiotics for the prevention of C. difficile–associated diarrhea in adults or children taking antibiotics. The trials, three of which were conducted in children, included 4,213 subjects, none of whom were immunocompromised, severely ill, or had an underlying gastrointestinal disorder.
The incidence of C. difficile–associated diarrhea was 2.0% in patients randomized to probiotics, compared with 5.5% in controls, for a highly significant 64% reduction in risk. Moreover, the risk of adverse GI events such as abdominal cramping, nausea, fever, taste disturbance, or flatulence was reduced by 20% in the probiotics group (Cochrane Database Syst. Rev. 2013 May 31 [doi: 10.1002/14651858.CD006095.pub3]).
The benefit of prophylactic probiotics was similar in magnitude in children and adults.
"Moderate-quality evidence suggests that probiotics are both safe and effective for preventing C. difficile–associated diarrhea when used along with antibiotics in patients who are not immunocompromised or severely debilitated," the Cochrane investigators concluded.
Neither the current American College of Gastroenterology practice guidelines on C. difficile–associated diarrhea (Am. J. Gastroenterol. 2013;108:478-98) nor the Infectious Diseases Society of America guidelines (Infect. Control Hosp. Epidemiol. 2010;31:431-55) recommend using prophylactic probiotics. However, both guidelines were published before the Cochrane meta-analysis was released, Dr. Samuel R. Dominguez pointed out at a conference on pediatric infectious diseases sponsored by the Children’s Hospital Colorado.
"Interestingly, a larger effect size was seen in studies of probiotics that contained multiple species compared to a single species, although the data set wasn’t large enough for investigators to be able to look at different specific formulations," added Dr. Dominguez, a pediatric infectious diseases specialist at the University of Colorado, Denver.
He noted that the incidence, severity, and mortality of C. difficile infections have increased dramatically since 2000. Even in children, a population traditionally considered at low risk, a recent population-based study conducted in Olmsted County, Minn., by investigators at the Mayo Clinic concluded that the age- and gender-adjusted incidence of C. difficile infection jumped nearly 13-fold from 1991 to 2009, when it reached 32.6 per 100,000 persons. Three-quarters of the 92 cases were community acquired. Prior studies of C. difficile disease in children may have underestimated the incidence because they were largely based on hospital-acquired cases (Clin. Infect. Dis. 2013;56:1401-6).
Another recent study highlights the serious nature of C. difficile in children, Dr. Dominguez continued. This retrospective cohort study conducted at 41 children’s hospitals included 4,474 patients hospitalized with C. difficile infection and 8,821 matched controls. The in-hospital mortality rate was 1.43% in children with C. difficile infection, compared with 0.66% in controls. In the subgroup of children with hospital-onset C. difficile infection, the mortality risk was an adjusted 6.7-fold higher than in matched controls.
Patients with community-onset C. difficile infection had a mean hospital length of stay that was 5.6 days longer and total hospital costs that were $18,900 greater than those of controls. In patients with hospital-onset C. difficile infection, the differences were even more dramatic: a mean 21.6-day longer length of stay than for controls, and a $93,600 greater hospital cost (Clin. Infect. Dis. 2013;57:1-8).
Dr. Dominguez said that although there is no set policy at Children’s Hospital, his own practice is to recommend probiotics to healthy children who are going to be taking antibiotics.
At a separate conference devoted to adult medicine, Dr. Mel L. Anderson cited both the Cochrane Collaboration meta-analysis and a separate one led by investigators at Toronto’s Hospital for Sick Children that concluded probiotics reduced the incidence of C. difficile–associated diarrhea by 66% (Ann. Intern. Med. 2012;157:878-88).
"If you look at these randomized controlled trials, I think the evidence is fairly convincing. And it’s not an expensive treatment. We use a lot of it in our inpatient service to reduce the risk of antibiotic-associated diarrhea, and C. difficile in particular," said Dr. Anderson, chief of the hospital medicine section at the Denver VA Medical Center.
Prophylactic probiotics are not for the surgical patient who is merely getting a dose or two of perioperative antibiotic coverage. But the preventive therapy is worth at least considering in pretty much everybody else getting a prescription for antibiotics. The randomized trials included in the two meta-analyses basically included patients receiving 3 days or more of antibiotics. Classes of antibiotics identified in previous work as posing an increased risk of C. difficile–associated diarrhea included the beta-lactams, cephalosporins, fluoroquinolones, and clindamycin – "pretty much everything you prescribe" – Dr. Anderson observed in Estes Park, Colo., at a conference on internal medicine sponsored by the University of Colorado.
"I have to say, if someone comes in with uncomplicated community-acquired pneumonia, I oftentimes don’t prescribe prophylactic probiotics unless they’ve had C. difficile–associated diarrhea before or they’re very fragile. But if something is even a little bit wrong with you, bad diarrheal illness can be the straw that breaks the camel’s back. And I strongly think about prophylactic probiotics in folks on long-term antibiotics, like for a diabetic foot ulcer," he noted.
Dr. Anderson said his typical prescription is for two Lactobacillus acidophilus capsules twice daily.
"The randomized studies done to date don’t let us know the optimal mix of critters or how much is enough," according to the hospitalist.
While preventive probiotic therapy is low cost, Dr. Dominguez noted that a more high-tech therapy for secondary prevention of C. difficile infection is in the developmental pipeline.
A pair of neutralizing, fully human monoclonal antibodies against C. difficile toxins A and B administered together in a single infusion in a randomized, double-blind, placebo-controlled, phase II clinical trial in patients with C. difficile–associated diarrhea didn’t have any effect on duration of hospitalization for that episode. However, it did result in a highly significant 72% reduction in recurrence, according to investigators at Medarex in Princeton, N.J., and the University of Massachusetts, Boston (N. Engl. J. Med. 2010;362:197-205).
"This may be a useful tool in the future for preventing recurrences," Dr. Dominguez commented.
Dr. Dominguez and Dr. Anderson reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL PEDIATRIC INFECTIOUS DISEASES CONFERENCE
Novel intervention improves outcomes in homeless schizophrenia patients
HOLLYWOOD, FLA. – A manualized psychosocial intervention known as customized adherence enhancement coupled with long-acting injectable antipsychotic medication produced marked improvement in adherence to concomitant oral medication as well as in psychiatric symptoms and functional status in urban homeless people with schizophrenia in a small prospective observational study.
Moreover, the intervention also achieved an impressive improvement in a domain not often considered in psychiatric studies, but one of great practical value to patients and their families: housing conditions, Dr. Martha Sajatovic said at a meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health
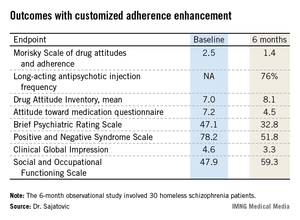
The mean time spent in suboptimal housing – living outdoors or in jail – changed from 56% during the 6 months prior to study enrollment to 41% in the first 3 months of the intervention and a mere 14% in the second 3 months of the study, reported Dr. Sajatovic, professor of psychiatry and neurology at Case Western Reserve University, Cleveland.
"What I think is most interesting about our study are the housing data. Our intervention did not include anything about housing – no housing placement or outreach or anything like that. People used whatever was available in the community. And Cleveland has the dubious distinction of being one of the poorest cities in America, so we have services, but not a lot of them," she noted.
Customized adherence enhancement (CAE) is a needs-based, flexibly dosed psychosocial intervention originally developed by Dr. Sajatovic and her colleagues to improve medication adherence in individuals with bipolar disorder receiving antipsychotic therapy. Following a 6-month study demonstrating its benefits in this population (Bipolar Disord. 2012;14:291-300), the investigators adapted the manualized CAE program for application in a particularly challenging patient population: homeless people with schizophrenia/schizoaffective disorder and poor adherence to their prescribed oral antipsychotic medication.

This 6-month, observational, uncontrolled study involved 30 homeless schizophrenic patients. The CAE consisted of once-monthly brief interventions matched to core adherence vulnerabilities identified at baseline. The CAE entailed psychoeducation, modified motivational enhancement therapy, and coaching on communication with providers and medication routines.
At the time of the monthly CAE session, patients also received a dose of long-acting injectable antipsychotic medication. Because the study was funded by a small nonprofit charitable organization, investigators employed the least expensive long-acting antipsychotic available: intramuscular haloperidol decanoate. This resulted in a high rate of side effects, most prominently restlessness because of akathisia in 40% of subjects, dry mouth in 33%, and muscle twitching in 33%. The mean monthly dose at 24 weeks was 68 mg, with a range of 50-100 mg.
The study population was typical of homeless individuals with major mental illness. Their mean age was 42 years, roughly half were women, 97% had a history of substance abuse, 97% had a history of incarceration, most subjects had not finished high school, and 70% were single or never married.
All patients remained on oral medication in addition to their new long-acting injectable antipsychotic regimen. Adherence to oral medication improved dramatically during the 6-month intervention: At baseline, patients had missed 46% of their oral medication during the past month, compared with just 10% at week 25. Adherence to long-acting injectable therapy was good: 76% at 6 months.
Twenty of 30 patients completed the 6-month study. Of the 10 nonfinishers, 3 were incarcerated, 2 relocated elsewhere, 1 discontinued because of drug-induced akathisia, and 4 were lost to follow-up.
Participants showed significant improvement in numerous measures of adherence behavior, treatment attitudes, psychiatric symptoms, and functioning (see chart).
For Dr. Sajatovic, the take-home message from this study was clear: "I would say that when we think about adherence, we can talk about relapse, but it’s very hard to have relapse as an outcome measure in these kinds of patients. They start out in relapse. So we should also consider those outcome components that patients and families really value, like functioning and housing."
Discussant Dr. Stephen R. Marder concurred: "Adherence is not necessarily the goal; it’s the path to better outcomes. And looking at things that are distal to relapse and symptoms – things like housing – shows an advantage. We need to tell patients that preventing relapse is just one of the reasons to be adherent. Long-term outcomes, whether it’s housing, work, school, or independent living, seem to be better for people who are adherent to medication. With adherence, rehabilitation can start.
"Without adherence, it’s really impossible to do," commented Dr. Marder, professor of psychiatry and behavioral sciences and director of the section on psychosis at the University of California, Los Angeles, Neuropsychiatric Institute.
He serves as a consultant to or recipient of research funding from roughly a dozen pharmaceutical companies. Dr. Sajatovic reported having no conflicts of interest.
HOLLYWOOD, FLA. – A manualized psychosocial intervention known as customized adherence enhancement coupled with long-acting injectable antipsychotic medication produced marked improvement in adherence to concomitant oral medication as well as in psychiatric symptoms and functional status in urban homeless people with schizophrenia in a small prospective observational study.
Moreover, the intervention also achieved an impressive improvement in a domain not often considered in psychiatric studies, but one of great practical value to patients and their families: housing conditions, Dr. Martha Sajatovic said at a meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health
The mean time spent in suboptimal housing – living outdoors or in jail – changed from 56% during the 6 months prior to study enrollment to 41% in the first 3 months of the intervention and a mere 14% in the second 3 months of the study, reported Dr. Sajatovic, professor of psychiatry and neurology at Case Western Reserve University, Cleveland.
"What I think is most interesting about our study are the housing data. Our intervention did not include anything about housing – no housing placement or outreach or anything like that. People used whatever was available in the community. And Cleveland has the dubious distinction of being one of the poorest cities in America, so we have services, but not a lot of them," she noted.
Customized adherence enhancement (CAE) is a needs-based, flexibly dosed psychosocial intervention originally developed by Dr. Sajatovic and her colleagues to improve medication adherence in individuals with bipolar disorder receiving antipsychotic therapy. Following a 6-month study demonstrating its benefits in this population (Bipolar Disord. 2012;14:291-300), the investigators adapted the manualized CAE program for application in a particularly challenging patient population: homeless people with schizophrenia/schizoaffective disorder and poor adherence to their prescribed oral antipsychotic medication.
This 6-month, observational, uncontrolled study involved 30 homeless schizophrenic patients. The CAE consisted of once-monthly brief interventions matched to core adherence vulnerabilities identified at baseline. The CAE entailed psychoeducation, modified motivational enhancement therapy, and coaching on communication with providers and medication routines.
At the time of the monthly CAE session, patients also received a dose of long-acting injectable antipsychotic medication. Because the study was funded by a small nonprofit charitable organization, investigators employed the least expensive long-acting antipsychotic available: intramuscular haloperidol decanoate. This resulted in a high rate of side effects, most prominently restlessness because of akathisia in 40% of subjects, dry mouth in 33%, and muscle twitching in 33%. The mean monthly dose at 24 weeks was 68 mg, with a range of 50-100 mg.
The study population was typical of homeless individuals with major mental illness. Their mean age was 42 years, roughly half were women, 97% had a history of substance abuse, 97% had a history of incarceration, most subjects had not finished high school, and 70% were single or never married.
All patients remained on oral medication in addition to their new long-acting injectable antipsychotic regimen. Adherence to oral medication improved dramatically during the 6-month intervention: At baseline, patients had missed 46% of their oral medication during the past month, compared with just 10% at week 25. Adherence to long-acting injectable therapy was good: 76% at 6 months.
Twenty of 30 patients completed the 6-month study. Of the 10 nonfinishers, 3 were incarcerated, 2 relocated elsewhere, 1 discontinued because of drug-induced akathisia, and 4 were lost to follow-up.
Participants showed significant improvement in numerous measures of adherence behavior, treatment attitudes, psychiatric symptoms, and functioning (see chart).
For Dr. Sajatovic, the take-home message from this study was clear: "I would say that when we think about adherence, we can talk about relapse, but it’s very hard to have relapse as an outcome measure in these kinds of patients. They start out in relapse. So we should also consider those outcome components that patients and families really value, like functioning and housing."
Discussant Dr. Stephen R. Marder concurred: "Adherence is not necessarily the goal; it’s the path to better outcomes. And looking at things that are distal to relapse and symptoms – things like housing – shows an advantage. We need to tell patients that preventing relapse is just one of the reasons to be adherent. Long-term outcomes, whether it’s housing, work, school, or independent living, seem to be better for people who are adherent to medication. With adherence, rehabilitation can start.
"Without adherence, it’s really impossible to do," commented Dr. Marder, professor of psychiatry and behavioral sciences and director of the section on psychosis at the University of California, Los Angeles, Neuropsychiatric Institute.
He serves as a consultant to or recipient of research funding from roughly a dozen pharmaceutical companies. Dr. Sajatovic reported having no conflicts of interest.
HOLLYWOOD, FLA. – A manualized psychosocial intervention known as customized adherence enhancement coupled with long-acting injectable antipsychotic medication produced marked improvement in adherence to concomitant oral medication as well as in psychiatric symptoms and functional status in urban homeless people with schizophrenia in a small prospective observational study.
Moreover, the intervention also achieved an impressive improvement in a domain not often considered in psychiatric studies, but one of great practical value to patients and their families: housing conditions, Dr. Martha Sajatovic said at a meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health
The mean time spent in suboptimal housing – living outdoors or in jail – changed from 56% during the 6 months prior to study enrollment to 41% in the first 3 months of the intervention and a mere 14% in the second 3 months of the study, reported Dr. Sajatovic, professor of psychiatry and neurology at Case Western Reserve University, Cleveland.
"What I think is most interesting about our study are the housing data. Our intervention did not include anything about housing – no housing placement or outreach or anything like that. People used whatever was available in the community. And Cleveland has the dubious distinction of being one of the poorest cities in America, so we have services, but not a lot of them," she noted.
Customized adherence enhancement (CAE) is a needs-based, flexibly dosed psychosocial intervention originally developed by Dr. Sajatovic and her colleagues to improve medication adherence in individuals with bipolar disorder receiving antipsychotic therapy. Following a 6-month study demonstrating its benefits in this population (Bipolar Disord. 2012;14:291-300), the investigators adapted the manualized CAE program for application in a particularly challenging patient population: homeless people with schizophrenia/schizoaffective disorder and poor adherence to their prescribed oral antipsychotic medication.
This 6-month, observational, uncontrolled study involved 30 homeless schizophrenic patients. The CAE consisted of once-monthly brief interventions matched to core adherence vulnerabilities identified at baseline. The CAE entailed psychoeducation, modified motivational enhancement therapy, and coaching on communication with providers and medication routines.
At the time of the monthly CAE session, patients also received a dose of long-acting injectable antipsychotic medication. Because the study was funded by a small nonprofit charitable organization, investigators employed the least expensive long-acting antipsychotic available: intramuscular haloperidol decanoate. This resulted in a high rate of side effects, most prominently restlessness because of akathisia in 40% of subjects, dry mouth in 33%, and muscle twitching in 33%. The mean monthly dose at 24 weeks was 68 mg, with a range of 50-100 mg.
The study population was typical of homeless individuals with major mental illness. Their mean age was 42 years, roughly half were women, 97% had a history of substance abuse, 97% had a history of incarceration, most subjects had not finished high school, and 70% were single or never married.
All patients remained on oral medication in addition to their new long-acting injectable antipsychotic regimen. Adherence to oral medication improved dramatically during the 6-month intervention: At baseline, patients had missed 46% of their oral medication during the past month, compared with just 10% at week 25. Adherence to long-acting injectable therapy was good: 76% at 6 months.
Twenty of 30 patients completed the 6-month study. Of the 10 nonfinishers, 3 were incarcerated, 2 relocated elsewhere, 1 discontinued because of drug-induced akathisia, and 4 were lost to follow-up.
Participants showed significant improvement in numerous measures of adherence behavior, treatment attitudes, psychiatric symptoms, and functioning (see chart).
For Dr. Sajatovic, the take-home message from this study was clear: "I would say that when we think about adherence, we can talk about relapse, but it’s very hard to have relapse as an outcome measure in these kinds of patients. They start out in relapse. So we should also consider those outcome components that patients and families really value, like functioning and housing."
Discussant Dr. Stephen R. Marder concurred: "Adherence is not necessarily the goal; it’s the path to better outcomes. And looking at things that are distal to relapse and symptoms – things like housing – shows an advantage. We need to tell patients that preventing relapse is just one of the reasons to be adherent. Long-term outcomes, whether it’s housing, work, school, or independent living, seem to be better for people who are adherent to medication. With adherence, rehabilitation can start.
"Without adherence, it’s really impossible to do," commented Dr. Marder, professor of psychiatry and behavioral sciences and director of the section on psychosis at the University of California, Los Angeles, Neuropsychiatric Institute.
He serves as a consultant to or recipient of research funding from roughly a dozen pharmaceutical companies. Dr. Sajatovic reported having no conflicts of interest.
AT THE NCDEU MEETING
Major finding: Homeless patients with schizophrenia missed 46% of their oral medication in the month prior to a customized psychosocial intervention. After the intervention, the percentage of missed medication dropped sharply to just 10% in the final month of a 6-month study.
Data source: This was a 6-month, prospective, uncontrolled study involving 30 homeless individuals with schizophrenia or schizoaffective disorder.
Disclosures: The study was supported by a grant from the Reuter Foundation. The presenter reported having no financial conflicts.
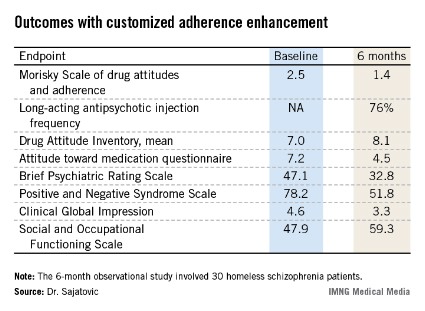
Recognizing and treating inflammatory subtype of osteoarthritis
ESTES PARK, COLO. – Thinking outside the evidence-based guidelines is the only way to manage erosive, inflammatory osteoarthritis of the hand, which is an aggressive subtype of primary osteoarthritis frequently misdiagnosed as rheumatoid arthritis or psoriatic arthritis.
This inflammatory destructive joint disease accounts for 5%-10% of all cases of primary OA. The inflammation waxes and wanes over the course of years, resulting in knobbly, painful, inflamed knuckles and finger deformities of the distal and proximal interphalangeal joints.
This form of OA most often affects white women in their 40s and 50s. A strong genetic component is involved: Two-thirds of patients with the erosive, inflammatory subtype of OA have a positive family history, Dr. Sterling West noted at a conference on internal medicine sponsored by the University of Colorado.
Misdiagnosis as rheumatoid arthritis or psoriatic arthritis can be avoided by bearing in mind that despite its aggressive nature, inflammatory OA is still a form of OA. As such, the serology is normal: There is no elevation in erythrocyte sedimentation rate (ESR) or C-reactive protein, and antinuclear antibody and rheumatoid factor testing will be negative. Unlike in rheumatoid arthritis or secondary OA due to hemochromatosis, calcium pyrophosphate disease, or trauma, there is no metacarpophalangeal joint or wrist involvement, stressed Dr. West, professor of medicine and fellowship program director at the university.
X-rays are extremely useful in making the diagnosis. A hallmark of the erosive, inflammatory subtype of OA is the gull-wing sign, a distinctive pattern of central subchondral erosions of the interphalangeal joints evocative of a seagull’s wing.
Unfortunately, OA therapy "really hasn’t changed in 100 years," according to Dr. West. But the aggressive inflammatory nature of the erosive subtype often necessitates moving beyond evidence-based, guideline-recommended treatment.
While acetaminophen at up to 4 g/day is guideline-endorsed as first-line treatment for OA because it can safely achieve up to about a 30% reduction in pain, it doesn’t work as monotherapy in the erosive, inflammatory subtype. It’s best paired with other evidence-based therapies: topical 1% diclofenac gel at 2-4 g four times daily and/or an oral nonsteroidal anti-inflammatory drug (NSAID).
"Salsalate is something that tends to get shunted off to the side. It’s certainly not our strongest NSAID, but it is one of our safest ones," the rheumatologist said.
Celecoxib (Celebrex) and other prescription NSAIDs are more potent but pose safety concerns in patients with cardiovascular disease or renal impairment. Under those circumstances, Dr. West tends not to use them, opting instead for tramadol (Ultram) or duloxetine (Cymbalta). There is good evidence for their efficacy in OA, where their pain-modulating effect is achieved via serotonin/norepinephrine reuptake inhibition.
"They’re expensive. Insurance companies often will not pay for them. Keep in mind that venlafaxine (Effexor) is another [serotonin/norepinephrine reuptake inhibitor]. And while it’s not approved for use in osteoarthritis, it certainly is less expensive and works very similarly to duloxetine and tramadol," according to Dr. West.
His go-to, non–evidence-based therapies for erosive, inflammatory OA include isotoner gloves at night. "The warmth and compression help with morning stiffness," Dr. West explained.
He also recommends application of heated paraffin wax in the morning for the same reason.
Hydroxychloroquine (Plaquenil) often effectively addresses the inflammatory component of the erosive subtype of OA. And intra-articular corticosteroid injections are "a very important treatment" that’s safe so long as a joint isn’t injected more than three or four times per year, the rheumatologist continued.
Case reports describe treatment success with anakinra (Kineret) and adalimumab (Humira). "This is a very expensive way to go. We don’t use that," he said.
Dr. West reported having no conflicts of interest.
ESTES PARK, COLO. – Thinking outside the evidence-based guidelines is the only way to manage erosive, inflammatory osteoarthritis of the hand, which is an aggressive subtype of primary osteoarthritis frequently misdiagnosed as rheumatoid arthritis or psoriatic arthritis.
This inflammatory destructive joint disease accounts for 5%-10% of all cases of primary OA. The inflammation waxes and wanes over the course of years, resulting in knobbly, painful, inflamed knuckles and finger deformities of the distal and proximal interphalangeal joints.
This form of OA most often affects white women in their 40s and 50s. A strong genetic component is involved: Two-thirds of patients with the erosive, inflammatory subtype of OA have a positive family history, Dr. Sterling West noted at a conference on internal medicine sponsored by the University of Colorado.
Misdiagnosis as rheumatoid arthritis or psoriatic arthritis can be avoided by bearing in mind that despite its aggressive nature, inflammatory OA is still a form of OA. As such, the serology is normal: There is no elevation in erythrocyte sedimentation rate (ESR) or C-reactive protein, and antinuclear antibody and rheumatoid factor testing will be negative. Unlike in rheumatoid arthritis or secondary OA due to hemochromatosis, calcium pyrophosphate disease, or trauma, there is no metacarpophalangeal joint or wrist involvement, stressed Dr. West, professor of medicine and fellowship program director at the university.
X-rays are extremely useful in making the diagnosis. A hallmark of the erosive, inflammatory subtype of OA is the gull-wing sign, a distinctive pattern of central subchondral erosions of the interphalangeal joints evocative of a seagull’s wing.
Unfortunately, OA therapy "really hasn’t changed in 100 years," according to Dr. West. But the aggressive inflammatory nature of the erosive subtype often necessitates moving beyond evidence-based, guideline-recommended treatment.
While acetaminophen at up to 4 g/day is guideline-endorsed as first-line treatment for OA because it can safely achieve up to about a 30% reduction in pain, it doesn’t work as monotherapy in the erosive, inflammatory subtype. It’s best paired with other evidence-based therapies: topical 1% diclofenac gel at 2-4 g four times daily and/or an oral nonsteroidal anti-inflammatory drug (NSAID).
"Salsalate is something that tends to get shunted off to the side. It’s certainly not our strongest NSAID, but it is one of our safest ones," the rheumatologist said.
Celecoxib (Celebrex) and other prescription NSAIDs are more potent but pose safety concerns in patients with cardiovascular disease or renal impairment. Under those circumstances, Dr. West tends not to use them, opting instead for tramadol (Ultram) or duloxetine (Cymbalta). There is good evidence for their efficacy in OA, where their pain-modulating effect is achieved via serotonin/norepinephrine reuptake inhibition.
"They’re expensive. Insurance companies often will not pay for them. Keep in mind that venlafaxine (Effexor) is another [serotonin/norepinephrine reuptake inhibitor]. And while it’s not approved for use in osteoarthritis, it certainly is less expensive and works very similarly to duloxetine and tramadol," according to Dr. West.
His go-to, non–evidence-based therapies for erosive, inflammatory OA include isotoner gloves at night. "The warmth and compression help with morning stiffness," Dr. West explained.
He also recommends application of heated paraffin wax in the morning for the same reason.
Hydroxychloroquine (Plaquenil) often effectively addresses the inflammatory component of the erosive subtype of OA. And intra-articular corticosteroid injections are "a very important treatment" that’s safe so long as a joint isn’t injected more than three or four times per year, the rheumatologist continued.
Case reports describe treatment success with anakinra (Kineret) and adalimumab (Humira). "This is a very expensive way to go. We don’t use that," he said.
Dr. West reported having no conflicts of interest.
ESTES PARK, COLO. – Thinking outside the evidence-based guidelines is the only way to manage erosive, inflammatory osteoarthritis of the hand, which is an aggressive subtype of primary osteoarthritis frequently misdiagnosed as rheumatoid arthritis or psoriatic arthritis.
This inflammatory destructive joint disease accounts for 5%-10% of all cases of primary OA. The inflammation waxes and wanes over the course of years, resulting in knobbly, painful, inflamed knuckles and finger deformities of the distal and proximal interphalangeal joints.
This form of OA most often affects white women in their 40s and 50s. A strong genetic component is involved: Two-thirds of patients with the erosive, inflammatory subtype of OA have a positive family history, Dr. Sterling West noted at a conference on internal medicine sponsored by the University of Colorado.
Misdiagnosis as rheumatoid arthritis or psoriatic arthritis can be avoided by bearing in mind that despite its aggressive nature, inflammatory OA is still a form of OA. As such, the serology is normal: There is no elevation in erythrocyte sedimentation rate (ESR) or C-reactive protein, and antinuclear antibody and rheumatoid factor testing will be negative. Unlike in rheumatoid arthritis or secondary OA due to hemochromatosis, calcium pyrophosphate disease, or trauma, there is no metacarpophalangeal joint or wrist involvement, stressed Dr. West, professor of medicine and fellowship program director at the university.
X-rays are extremely useful in making the diagnosis. A hallmark of the erosive, inflammatory subtype of OA is the gull-wing sign, a distinctive pattern of central subchondral erosions of the interphalangeal joints evocative of a seagull’s wing.
Unfortunately, OA therapy "really hasn’t changed in 100 years," according to Dr. West. But the aggressive inflammatory nature of the erosive subtype often necessitates moving beyond evidence-based, guideline-recommended treatment.
While acetaminophen at up to 4 g/day is guideline-endorsed as first-line treatment for OA because it can safely achieve up to about a 30% reduction in pain, it doesn’t work as monotherapy in the erosive, inflammatory subtype. It’s best paired with other evidence-based therapies: topical 1% diclofenac gel at 2-4 g four times daily and/or an oral nonsteroidal anti-inflammatory drug (NSAID).
"Salsalate is something that tends to get shunted off to the side. It’s certainly not our strongest NSAID, but it is one of our safest ones," the rheumatologist said.
Celecoxib (Celebrex) and other prescription NSAIDs are more potent but pose safety concerns in patients with cardiovascular disease or renal impairment. Under those circumstances, Dr. West tends not to use them, opting instead for tramadol (Ultram) or duloxetine (Cymbalta). There is good evidence for their efficacy in OA, where their pain-modulating effect is achieved via serotonin/norepinephrine reuptake inhibition.
"They’re expensive. Insurance companies often will not pay for them. Keep in mind that venlafaxine (Effexor) is another [serotonin/norepinephrine reuptake inhibitor]. And while it’s not approved for use in osteoarthritis, it certainly is less expensive and works very similarly to duloxetine and tramadol," according to Dr. West.
His go-to, non–evidence-based therapies for erosive, inflammatory OA include isotoner gloves at night. "The warmth and compression help with morning stiffness," Dr. West explained.
He also recommends application of heated paraffin wax in the morning for the same reason.
Hydroxychloroquine (Plaquenil) often effectively addresses the inflammatory component of the erosive subtype of OA. And intra-articular corticosteroid injections are "a very important treatment" that’s safe so long as a joint isn’t injected more than three or four times per year, the rheumatologist continued.
Case reports describe treatment success with anakinra (Kineret) and adalimumab (Humira). "This is a very expensive way to go. We don’t use that," he said.
Dr. West reported having no conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM
Recognizing and treating inflammatory subtype of osteoarthritis
ESTES PARK, COLO. – Thinking outside the evidence-based guidelines is the only way to manage erosive, inflammatory osteoarthritis of the hand, which is an aggressive subtype of primary osteoarthritis frequently misdiagnosed as rheumatoid arthritis or psoriatic arthritis.
This inflammatory destructive joint disease accounts for 5%-10% of all cases of primary OA. The inflammation waxes and wanes over the course of years, resulting in knobbly, painful, inflamed knuckles and finger deformities of the distal and proximal interphalangeal joints.

This form of OA most often affects white women in their 40s and 50s. A strong genetic component is involved: Two-thirds of patients with the erosive, inflammatory subtype of OA have a positive family history, Dr. Sterling West noted at a conference on internal medicine sponsored by the University of Colorado.
Misdiagnosis as rheumatoid arthritis or psoriatic arthritis can be avoided by bearing in mind that despite its aggressive nature, inflammatory OA is still a form of OA. As such, the serology is normal: There is no elevation in erythrocyte sedimentation rate (ESR) or C-reactive protein, and antinuclear antibody and rheumatoid factor testing will be negative. Unlike in rheumatoid arthritis or secondary OA due to hemochromatosis, calcium pyrophosphate disease, or trauma, there is no metacarpophalangeal joint or wrist involvement, stressed Dr. West, professor of medicine and fellowship program director at the university.
X-rays are extremely useful in making the diagnosis. A hallmark of the erosive, inflammatory subtype of OA is the gull-wing sign, a distinctive pattern of central subchondral erosions of the interphalangeal joints evocative of a seagull’s wing.
Unfortunately, OA therapy "really hasn’t changed in 100 years," according to Dr. West. But the aggressive inflammatory nature of the erosive subtype often necessitates moving beyond evidence-based, guideline-recommended treatment.
While acetaminophen at up to 4 g/day is guideline-endorsed as first-line treatment for OA because it can safely achieve up to about a 30% reduction in pain, it doesn’t work as monotherapy in the erosive, inflammatory subtype. It’s best paired with other evidence-based therapies: topical 1% diclofenac gel at 2-4 g four times daily and/or an oral nonsteroidal anti-inflammatory drug (NSAID).
"Salsalate is something that tends to get shunted off to the side. It’s certainly not our strongest NSAID, but it is one of our safest ones," the rheumatologist said.
Celecoxib (Celebrex) and other prescription NSAIDs are more potent but pose safety concerns in patients with cardiovascular disease or renal impairment. Under those circumstances, Dr. West tends not to use them, opting instead for tramadol (Ultram) or duloxetine (Cymbalta). There is good evidence for their efficacy in OA, where their pain-modulating effect is achieved via serotonin/norepinephrine reuptake inhibition.
"They’re expensive. Insurance companies often will not pay for them. Keep in mind that venlafaxine (Effexor) is another [serotonin/norepinephrine reuptake inhibitor]. And while it’s not approved for use in osteoarthritis, it certainly is less expensive and works very similarly to duloxetine and tramadol," according to Dr. West.
His go-to, non–evidence-based therapies for erosive, inflammatory OA include isotoner gloves at night. "The warmth and compression help with morning stiffness," Dr. West explained.
He also recommends application of heated paraffin wax in the morning for the same reason.
Hydroxychloroquine (Plaquenil) often effectively addresses the inflammatory component of the erosive subtype of OA. And intra-articular corticosteroid injections are "a very important treatment" that’s safe so long as a joint isn’t injected more than three or four times per year, the rheumatologist continued.
Case reports describe treatment success with anakinra (Kineret) and adalimumab (Humira). "This is a very expensive way to go. We don’t use that," he said.
Dr. West reported having no conflicts of interest.
ESTES PARK, COLO. – Thinking outside the evidence-based guidelines is the only way to manage erosive, inflammatory osteoarthritis of the hand, which is an aggressive subtype of primary osteoarthritis frequently misdiagnosed as rheumatoid arthritis or psoriatic arthritis.
This inflammatory destructive joint disease accounts for 5%-10% of all cases of primary OA. The inflammation waxes and wanes over the course of years, resulting in knobbly, painful, inflamed knuckles and finger deformities of the distal and proximal interphalangeal joints.
This form of OA most often affects white women in their 40s and 50s. A strong genetic component is involved: Two-thirds of patients with the erosive, inflammatory subtype of OA have a positive family history, Dr. Sterling West noted at a conference on internal medicine sponsored by the University of Colorado.
Misdiagnosis as rheumatoid arthritis or psoriatic arthritis can be avoided by bearing in mind that despite its aggressive nature, inflammatory OA is still a form of OA. As such, the serology is normal: There is no elevation in erythrocyte sedimentation rate (ESR) or C-reactive protein, and antinuclear antibody and rheumatoid factor testing will be negative. Unlike in rheumatoid arthritis or secondary OA due to hemochromatosis, calcium pyrophosphate disease, or trauma, there is no metacarpophalangeal joint or wrist involvement, stressed Dr. West, professor of medicine and fellowship program director at the university.
X-rays are extremely useful in making the diagnosis. A hallmark of the erosive, inflammatory subtype of OA is the gull-wing sign, a distinctive pattern of central subchondral erosions of the interphalangeal joints evocative of a seagull’s wing.
Unfortunately, OA therapy "really hasn’t changed in 100 years," according to Dr. West. But the aggressive inflammatory nature of the erosive subtype often necessitates moving beyond evidence-based, guideline-recommended treatment.
While acetaminophen at up to 4 g/day is guideline-endorsed as first-line treatment for OA because it can safely achieve up to about a 30% reduction in pain, it doesn’t work as monotherapy in the erosive, inflammatory subtype. It’s best paired with other evidence-based therapies: topical 1% diclofenac gel at 2-4 g four times daily and/or an oral nonsteroidal anti-inflammatory drug (NSAID).
"Salsalate is something that tends to get shunted off to the side. It’s certainly not our strongest NSAID, but it is one of our safest ones," the rheumatologist said.
Celecoxib (Celebrex) and other prescription NSAIDs are more potent but pose safety concerns in patients with cardiovascular disease or renal impairment. Under those circumstances, Dr. West tends not to use them, opting instead for tramadol (Ultram) or duloxetine (Cymbalta). There is good evidence for their efficacy in OA, where their pain-modulating effect is achieved via serotonin/norepinephrine reuptake inhibition.
"They’re expensive. Insurance companies often will not pay for them. Keep in mind that venlafaxine (Effexor) is another [serotonin/norepinephrine reuptake inhibitor]. And while it’s not approved for use in osteoarthritis, it certainly is less expensive and works very similarly to duloxetine and tramadol," according to Dr. West.
His go-to, non–evidence-based therapies for erosive, inflammatory OA include isotoner gloves at night. "The warmth and compression help with morning stiffness," Dr. West explained.
He also recommends application of heated paraffin wax in the morning for the same reason.
Hydroxychloroquine (Plaquenil) often effectively addresses the inflammatory component of the erosive subtype of OA. And intra-articular corticosteroid injections are "a very important treatment" that’s safe so long as a joint isn’t injected more than three or four times per year, the rheumatologist continued.
Case reports describe treatment success with anakinra (Kineret) and adalimumab (Humira). "This is a very expensive way to go. We don’t use that," he said.
Dr. West reported having no conflicts of interest.
ESTES PARK, COLO. – Thinking outside the evidence-based guidelines is the only way to manage erosive, inflammatory osteoarthritis of the hand, which is an aggressive subtype of primary osteoarthritis frequently misdiagnosed as rheumatoid arthritis or psoriatic arthritis.
This inflammatory destructive joint disease accounts for 5%-10% of all cases of primary OA. The inflammation waxes and wanes over the course of years, resulting in knobbly, painful, inflamed knuckles and finger deformities of the distal and proximal interphalangeal joints.
This form of OA most often affects white women in their 40s and 50s. A strong genetic component is involved: Two-thirds of patients with the erosive, inflammatory subtype of OA have a positive family history, Dr. Sterling West noted at a conference on internal medicine sponsored by the University of Colorado.
Misdiagnosis as rheumatoid arthritis or psoriatic arthritis can be avoided by bearing in mind that despite its aggressive nature, inflammatory OA is still a form of OA. As such, the serology is normal: There is no elevation in erythrocyte sedimentation rate (ESR) or C-reactive protein, and antinuclear antibody and rheumatoid factor testing will be negative. Unlike in rheumatoid arthritis or secondary OA due to hemochromatosis, calcium pyrophosphate disease, or trauma, there is no metacarpophalangeal joint or wrist involvement, stressed Dr. West, professor of medicine and fellowship program director at the university.
X-rays are extremely useful in making the diagnosis. A hallmark of the erosive, inflammatory subtype of OA is the gull-wing sign, a distinctive pattern of central subchondral erosions of the interphalangeal joints evocative of a seagull’s wing.
Unfortunately, OA therapy "really hasn’t changed in 100 years," according to Dr. West. But the aggressive inflammatory nature of the erosive subtype often necessitates moving beyond evidence-based, guideline-recommended treatment.
While acetaminophen at up to 4 g/day is guideline-endorsed as first-line treatment for OA because it can safely achieve up to about a 30% reduction in pain, it doesn’t work as monotherapy in the erosive, inflammatory subtype. It’s best paired with other evidence-based therapies: topical 1% diclofenac gel at 2-4 g four times daily and/or an oral nonsteroidal anti-inflammatory drug (NSAID).
"Salsalate is something that tends to get shunted off to the side. It’s certainly not our strongest NSAID, but it is one of our safest ones," the rheumatologist said.
Celecoxib (Celebrex) and other prescription NSAIDs are more potent but pose safety concerns in patients with cardiovascular disease or renal impairment. Under those circumstances, Dr. West tends not to use them, opting instead for tramadol (Ultram) or duloxetine (Cymbalta). There is good evidence for their efficacy in OA, where their pain-modulating effect is achieved via serotonin/norepinephrine reuptake inhibition.
"They’re expensive. Insurance companies often will not pay for them. Keep in mind that venlafaxine (Effexor) is another [serotonin/norepinephrine reuptake inhibitor]. And while it’s not approved for use in osteoarthritis, it certainly is less expensive and works very similarly to duloxetine and tramadol," according to Dr. West.
His go-to, non–evidence-based therapies for erosive, inflammatory OA include isotoner gloves at night. "The warmth and compression help with morning stiffness," Dr. West explained.
He also recommends application of heated paraffin wax in the morning for the same reason.
Hydroxychloroquine (Plaquenil) often effectively addresses the inflammatory component of the erosive subtype of OA. And intra-articular corticosteroid injections are "a very important treatment" that’s safe so long as a joint isn’t injected more than three or four times per year, the rheumatologist continued.
Case reports describe treatment success with anakinra (Kineret) and adalimumab (Humira). "This is a very expensive way to go. We don’t use that," he said.
Dr. West reported having no conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Smokin': Report finds marijuana has negligible effects on lungs
LOS ANGELES – The pulmonary consequences of regularly smoking marijuana are far less than for tobacco, according a review of the published evidence conducted by Dr. Donald P. Tashkin, emeritus professor of medicine and medical director of the pulmonary function laboratory at the University of California, Los Angeles.
Habitual use of marijuana alone doesn’t appear to lead to significant abnormalities in lung function, nor does it increase the risks of COPD or either lung or upper airway cancer. It is associated with an increase in symptoms of chronic bronchitis; however the symptoms go away upon discontinuation of use, according to Dr. Tashkin (Ann. Am. Thorac. Soc. 2013;10:239-47).

"The accumulated weight of evidence implies far lower risks for pulmonary complications of even regular heavy use of marijuana, compared with the grave pulmonary consequences of tobacco," he concluded.
In an accompanying editorial, Dr. Mark A. Ware called Dr. Tashkin’s article "the most comprehensive and authoritative review of the subject ever published."
Dr. Tashkin’s conclusion that smoking marijuana is not a major risk factor for airway cancer or COPD "will affect the way health professionals interact with patients, parents with teenagers, and policy makers with their constituents," predicted Dr. Ware, a family physician and anesthesiologist who is director of clinical research at the Alan Edwards Pain Management Unit at McGill University in Montreal.
Dr. Tashkin reported having no conflicts of interest. Dr. Ware has received lecture fees from the Canadian Consortium for the Investigation of the Cannabinoids and a research grant and honoraria from Valeant for conducting a randomized trial of nabilone in fibromyalgia patients.
LOS ANGELES – The pulmonary consequences of regularly smoking marijuana are far less than for tobacco, according a review of the published evidence conducted by Dr. Donald P. Tashkin, emeritus professor of medicine and medical director of the pulmonary function laboratory at the University of California, Los Angeles.
Habitual use of marijuana alone doesn’t appear to lead to significant abnormalities in lung function, nor does it increase the risks of COPD or either lung or upper airway cancer. It is associated with an increase in symptoms of chronic bronchitis; however the symptoms go away upon discontinuation of use, according to Dr. Tashkin (Ann. Am. Thorac. Soc. 2013;10:239-47).
"The accumulated weight of evidence implies far lower risks for pulmonary complications of even regular heavy use of marijuana, compared with the grave pulmonary consequences of tobacco," he concluded.
In an accompanying editorial, Dr. Mark A. Ware called Dr. Tashkin’s article "the most comprehensive and authoritative review of the subject ever published."
Dr. Tashkin’s conclusion that smoking marijuana is not a major risk factor for airway cancer or COPD "will affect the way health professionals interact with patients, parents with teenagers, and policy makers with their constituents," predicted Dr. Ware, a family physician and anesthesiologist who is director of clinical research at the Alan Edwards Pain Management Unit at McGill University in Montreal.
Dr. Tashkin reported having no conflicts of interest. Dr. Ware has received lecture fees from the Canadian Consortium for the Investigation of the Cannabinoids and a research grant and honoraria from Valeant for conducting a randomized trial of nabilone in fibromyalgia patients.
LOS ANGELES – The pulmonary consequences of regularly smoking marijuana are far less than for tobacco, according a review of the published evidence conducted by Dr. Donald P. Tashkin, emeritus professor of medicine and medical director of the pulmonary function laboratory at the University of California, Los Angeles.
Habitual use of marijuana alone doesn’t appear to lead to significant abnormalities in lung function, nor does it increase the risks of COPD or either lung or upper airway cancer. It is associated with an increase in symptoms of chronic bronchitis; however the symptoms go away upon discontinuation of use, according to Dr. Tashkin (Ann. Am. Thorac. Soc. 2013;10:239-47).
"The accumulated weight of evidence implies far lower risks for pulmonary complications of even regular heavy use of marijuana, compared with the grave pulmonary consequences of tobacco," he concluded.
In an accompanying editorial, Dr. Mark A. Ware called Dr. Tashkin’s article "the most comprehensive and authoritative review of the subject ever published."
Dr. Tashkin’s conclusion that smoking marijuana is not a major risk factor for airway cancer or COPD "will affect the way health professionals interact with patients, parents with teenagers, and policy makers with their constituents," predicted Dr. Ware, a family physician and anesthesiologist who is director of clinical research at the Alan Edwards Pain Management Unit at McGill University in Montreal.
Dr. Tashkin reported having no conflicts of interest. Dr. Ware has received lecture fees from the Canadian Consortium for the Investigation of the Cannabinoids and a research grant and honoraria from Valeant for conducting a randomized trial of nabilone in fibromyalgia patients.
Levomilnacipran SR for major depression also improves attention deficits
HOLLYWOOD, FLA. – Levomilnacipran SR resulted in significant improvement in cognitive measures of attention and information processing in a phase 3 trial conducted in patients with major depressive disorder; the drug was approved July 25 by the Food and Drug Administration under the trade name Fetzima.*
Attention deficits are commonplace in patients with major depressive disorder (MDD). In the phase 3 study, improvement in MDD in levomilnacipran SR–treated patients was accompanied by gains in measures of attention. A question that will need to be addressed in future studies is whether the observed improvement in attention deficits results from a direct drug effect upon brain structures controlling attention or is a secondary by-product of reduced depressive symptoms, Keith A. Wesnes, Ph.D., noted at a meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health.

Levomilnacipran SR is a selective serotonin and norepinephrine reuptake inhibitor. Its norepinephrine reuptake potency is twice as great as its serotonin reuptake potency. In addition, levomilnacipran SR is greater than 10-fold more selective for norepinephrine reuptake inhibition than either duloxetine or venlafaxine.
The 8-week, double-blind, phase 3 clinical trial included 429 patients with MDD who were randomized to once-daily levomilnacipran SR at 40-120 mg or placebo. This was a severely depressed population as reflected in their mean baseline Montgomery-Åsberg Depression Rating Scale (MADRS) score of 35, said Dr. Wesnes, professor of psychology at Northumbria University in Newcastle, England, and an employee of Bracket, a pharmaceutical industry consulting firm.
A MADRS total score reduction of at least 50% was achieved in 42% of the levomilnacipran SR group compared with 29% of controls. These MADRS responders on levomilnacipran SR also displayed significant improvement from baseline in several measures of attention. In contrast, placebo-treated controls and MADRS nonresponders on levomilnacipran SR did not.
During the course of the 8-week study, cognitive assessments carried out using the Cognitive Drug Research System for Attention demonstrated that MADRS responders on levomilnacipran SR had significant improvement over time on computerized tasks measuring power of attention, continuity of attention, reaction time variability, and digit vigilance task accuracy.
For example, levomilnacipran SR–treated MADRS responders improved their digit vigilance task accuracy by 3.1-U over baseline, while levomilnacipran SR–treated MADRS nonresponders had a 0.8-U decrease in performance, placebo-treated MADRS nonresponders averaged a 1.8-U decrease, and placebo-treated MADRS responders had a 1.5-U decline.
Arguing in favor of the possibility that the antidepressant medication improves attention deficits in MDD through direct action upon brain structures controlling attention is the observation that baseline measures of cognition correlated poorly with baseline MADRS depression symptoms or with changes in depressive symptoms during treatment, according to Dr. Wesnes.
He is an employee of Bracket, which was funded by Forest Laboratories and Pierre Fabre to conduct this analysis.
*This story was updated 7/29/2013.
HOLLYWOOD, FLA. – Levomilnacipran SR resulted in significant improvement in cognitive measures of attention and information processing in a phase 3 trial conducted in patients with major depressive disorder; the drug was approved July 25 by the Food and Drug Administration under the trade name Fetzima.*
Attention deficits are commonplace in patients with major depressive disorder (MDD). In the phase 3 study, improvement in MDD in levomilnacipran SR–treated patients was accompanied by gains in measures of attention. A question that will need to be addressed in future studies is whether the observed improvement in attention deficits results from a direct drug effect upon brain structures controlling attention or is a secondary by-product of reduced depressive symptoms, Keith A. Wesnes, Ph.D., noted at a meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health.
Levomilnacipran SR is a selective serotonin and norepinephrine reuptake inhibitor. Its norepinephrine reuptake potency is twice as great as its serotonin reuptake potency. In addition, levomilnacipran SR is greater than 10-fold more selective for norepinephrine reuptake inhibition than either duloxetine or venlafaxine.
The 8-week, double-blind, phase 3 clinical trial included 429 patients with MDD who were randomized to once-daily levomilnacipran SR at 40-120 mg or placebo. This was a severely depressed population as reflected in their mean baseline Montgomery-Åsberg Depression Rating Scale (MADRS) score of 35, said Dr. Wesnes, professor of psychology at Northumbria University in Newcastle, England, and an employee of Bracket, a pharmaceutical industry consulting firm.
A MADRS total score reduction of at least 50% was achieved in 42% of the levomilnacipran SR group compared with 29% of controls. These MADRS responders on levomilnacipran SR also displayed significant improvement from baseline in several measures of attention. In contrast, placebo-treated controls and MADRS nonresponders on levomilnacipran SR did not.
During the course of the 8-week study, cognitive assessments carried out using the Cognitive Drug Research System for Attention demonstrated that MADRS responders on levomilnacipran SR had significant improvement over time on computerized tasks measuring power of attention, continuity of attention, reaction time variability, and digit vigilance task accuracy.
For example, levomilnacipran SR–treated MADRS responders improved their digit vigilance task accuracy by 3.1-U over baseline, while levomilnacipran SR–treated MADRS nonresponders had a 0.8-U decrease in performance, placebo-treated MADRS nonresponders averaged a 1.8-U decrease, and placebo-treated MADRS responders had a 1.5-U decline.
Arguing in favor of the possibility that the antidepressant medication improves attention deficits in MDD through direct action upon brain structures controlling attention is the observation that baseline measures of cognition correlated poorly with baseline MADRS depression symptoms or with changes in depressive symptoms during treatment, according to Dr. Wesnes.
He is an employee of Bracket, which was funded by Forest Laboratories and Pierre Fabre to conduct this analysis.
*This story was updated 7/29/2013.
HOLLYWOOD, FLA. – Levomilnacipran SR resulted in significant improvement in cognitive measures of attention and information processing in a phase 3 trial conducted in patients with major depressive disorder; the drug was approved July 25 by the Food and Drug Administration under the trade name Fetzima.*
Attention deficits are commonplace in patients with major depressive disorder (MDD). In the phase 3 study, improvement in MDD in levomilnacipran SR–treated patients was accompanied by gains in measures of attention. A question that will need to be addressed in future studies is whether the observed improvement in attention deficits results from a direct drug effect upon brain structures controlling attention or is a secondary by-product of reduced depressive symptoms, Keith A. Wesnes, Ph.D., noted at a meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health.
Levomilnacipran SR is a selective serotonin and norepinephrine reuptake inhibitor. Its norepinephrine reuptake potency is twice as great as its serotonin reuptake potency. In addition, levomilnacipran SR is greater than 10-fold more selective for norepinephrine reuptake inhibition than either duloxetine or venlafaxine.
The 8-week, double-blind, phase 3 clinical trial included 429 patients with MDD who were randomized to once-daily levomilnacipran SR at 40-120 mg or placebo. This was a severely depressed population as reflected in their mean baseline Montgomery-Åsberg Depression Rating Scale (MADRS) score of 35, said Dr. Wesnes, professor of psychology at Northumbria University in Newcastle, England, and an employee of Bracket, a pharmaceutical industry consulting firm.
A MADRS total score reduction of at least 50% was achieved in 42% of the levomilnacipran SR group compared with 29% of controls. These MADRS responders on levomilnacipran SR also displayed significant improvement from baseline in several measures of attention. In contrast, placebo-treated controls and MADRS nonresponders on levomilnacipran SR did not.
During the course of the 8-week study, cognitive assessments carried out using the Cognitive Drug Research System for Attention demonstrated that MADRS responders on levomilnacipran SR had significant improvement over time on computerized tasks measuring power of attention, continuity of attention, reaction time variability, and digit vigilance task accuracy.
For example, levomilnacipran SR–treated MADRS responders improved their digit vigilance task accuracy by 3.1-U over baseline, while levomilnacipran SR–treated MADRS nonresponders had a 0.8-U decrease in performance, placebo-treated MADRS nonresponders averaged a 1.8-U decrease, and placebo-treated MADRS responders had a 1.5-U decline.
Arguing in favor of the possibility that the antidepressant medication improves attention deficits in MDD through direct action upon brain structures controlling attention is the observation that baseline measures of cognition correlated poorly with baseline MADRS depression symptoms or with changes in depressive symptoms during treatment, according to Dr. Wesnes.
He is an employee of Bracket, which was funded by Forest Laboratories and Pierre Fabre to conduct this analysis.
*This story was updated 7/29/2013.
AT THE NCDEU MEETING
Major finding: Patients with severe major depressive disorder who had a significant clinical response to the investigational antidepressant levomilnacipran SR also showed significant improvement in baseline attention deficits.
Data source: An 8-week, double-blind, phase 3 clinical trial involving 429 patients with major depressive disorder who were randomized to once-daily levomilnacipran SR or placebo.
Disclosures: Dr. Wesnes is an employee of Bracket, which was funded by Forest Laboratories and Pierre Fabre to conduct this analysis.
