User login
Evaluation for possible early pregnancy failure
DENVER – There is a slew of ultrasound findings that are equivocal or downright worrisome for the diagnosis of early pregnancy failure, but the list of definitive findings is short – and even those are fraught with controversy, according to Dr. Roxanne Vrees.
"In a highly desired pregnancy, even with ultrasound findings that are perhaps suggestive of early pregnancy failure, I think watchful waiting has a really important role," said Dr. Vrees, an ob.gyn. at Brown University in Providence, R.I.
She is also on the staff at the Women and Infants Hospital in Providence, where she works in a unique women’s emergency department staffed 24/7 exclusively by ob.gyn. attending physicians. Traditional emergency medicine physicians are not in the picture. This busy women’s ED averages nearly 30,000 visits annually, so Dr. Vrees and her colleagues have acquired considerable experience in emergency ob.gyn. However, because the facility is licensed by the state as an ED, by law any patient who comes in must be treated, so medical backup is available around the clock for patients who present with chest pain or otherwise fall outside the generalist ob.gyn.’s scope.

Early pregnancy failure occurs in 15%-20% of clinically recognized pregnancies. The most common symptom is vaginal bleeding, which occurs in one-quarter of all known first-trimester pregnancies, half of which end in pregnancy failure.
Dr. Vrees emphasized that no single aspect of the work-up for early pregnancy failure should drive patient management. That ought to be based upon a combination of the patient’s symptoms, laboratory findings, physical exam, and pelvic ultrasound.
In the setting of worrisome ultrasound findings, the most important step in management is to get a repeat ultrasound under real-time observation. The use of cine loops in order to visualize the entire gestational sac is valuable.
"Most obstetricians underutilize this. You’re unlikely to miss a yolk sac or embryo, and you’re getting a true report of sac diameter, not a random measurement from a snapshot," she explained at the annual meeting of the Society of Ob/Gyn Hospitalists.
Worrisome but nondefinitive findings suggestive of early pregnancy loss include a slow fetal heart rate, an unusual appearance of the uterine lining, and a sac that is small, grossly distorted, enlarged, irregularly contoured, or low in position.
Maternal gestational age is a key consideration in defining a slow fetal heart rate by M-mode ultrasound. At a menstrual age of 6.2 weeks or less, a normal fetal heart rate is 100 bpm or more; less than 90 bpm is considered slow. In contrast, at 6.3-7.0 weeks, normal is defined as 120 bpm or more, and a fetal heart rate of less than 110 bpm is considered slow. When a slow fetal heart rate is detected at 6.0-7.0 weeks, the risk of subsequent first-trimester fetal demise remains elevated at about 25% even if the heart rate is normal at follow-up at 8.0 weeks (Radiology;2005;236:643-6).
The absolute ultrasound criteria for early pregnancy failure used at the Women and Infants Hospital as well as in many other settings are no fetal heart beat in an embryo more than 5 mm in crown-rump length, or menstrual age known to be greater than 6.5 weeks with no heart beat.
However, a group of investigators led by Dr. Yazan Abdallah of Imperial College London has argued that current definitions used to diagnose early pregnancy failure are potentially unsafe and could result in inadvertent termination of wanted pregnancies. Given the inherent inter- and intraobserver variation in ultrasound measurements, they have urged more conservative criteria for the definitive diagnosis of early pregnancy failure: specifically, a crown-rump length cutoff of greater than 7 mm instead of the widely used 5 mm, and a mean gestational sac diameter cutoff of more than 25 mm.
Dr. Abdallah and his coworkers support their argument on the basis of their observational, prospective cross-sectional study involving 1,060 consecutive women diagnosed with intrauterine pregnancy of uncertain viability. This diagnosis was based upon a symptom-generated ultrasound that showed either an empty gestational sac; a gestational sac with a yolk sac but no embryo when the mean gestational sac diameter was either less than 20 mm or less than 30 mm; or an embryo with an absent heart beat and a crown-rump length of either less than 6 mm or less than 8 mm.
The primary endpoint was a viable pregnancy upon routine first-trimester screening ultrasound at 11-14 weeks. At that point, 473 of the women had viable pregnancies and 587 did not.
When neither the yolk sac nor the embryo was visualized on the initial ultrasound, the false-positive rate for diagnosis of early pregnancy failure was 4.4% when a mean gestational sac diameter of 16 mm was used as a cutoff and 0.5% when 20 mm was the cutoff. Only when a cutoff of 21 mm was utilized did the false-positive rate fall to 0.
If a yolk sac was present but an embryo wasn’t, the false-positive rate was 2.6% with a mean gestational sac diameter cutoff of 16 mm and 0.4% with a cutoff of 20 mm. Again, there were no false positives when a cutoff of 21 mm was employed.
When a yolk sac and embryo were visible but a fetal heartbeat was not apparent, the false-positive rate for miscarriage was 8.3% with a crown-rump length cutoff of 5 mm. At a cutoff of 5.3 mm, there were no false-positive results (Ultrasound Obstet. Gynecol. 2011;38:497-502).
When Dr. Vrees asked the audience for a show of hands as to who utilizes a mean gestational sac diameter cutoff of 21 mm to define early pregnancy loss in the absence of both a yolk sac and embryo, only a couple of ob.gyns. responded affirmatively. Some audience members indicated they use a cutoff as low as 16 mm.
"We see great variability at our institution, too, in the definition of early pregnancy failure based upon mean gestational sac diameter," according to Dr. Vrees.
The lack of unanimity on this point, coupled with the remote likelihood of physical harm in waiting 7-10 days to repeat an ultrasound scan, figure prominently in her advocacy of expectant management.
She reported having no relevant financial disclosures.
DENVER – There is a slew of ultrasound findings that are equivocal or downright worrisome for the diagnosis of early pregnancy failure, but the list of definitive findings is short – and even those are fraught with controversy, according to Dr. Roxanne Vrees.
"In a highly desired pregnancy, even with ultrasound findings that are perhaps suggestive of early pregnancy failure, I think watchful waiting has a really important role," said Dr. Vrees, an ob.gyn. at Brown University in Providence, R.I.
She is also on the staff at the Women and Infants Hospital in Providence, where she works in a unique women’s emergency department staffed 24/7 exclusively by ob.gyn. attending physicians. Traditional emergency medicine physicians are not in the picture. This busy women’s ED averages nearly 30,000 visits annually, so Dr. Vrees and her colleagues have acquired considerable experience in emergency ob.gyn. However, because the facility is licensed by the state as an ED, by law any patient who comes in must be treated, so medical backup is available around the clock for patients who present with chest pain or otherwise fall outside the generalist ob.gyn.’s scope.
Early pregnancy failure occurs in 15%-20% of clinically recognized pregnancies. The most common symptom is vaginal bleeding, which occurs in one-quarter of all known first-trimester pregnancies, half of which end in pregnancy failure.
Dr. Vrees emphasized that no single aspect of the work-up for early pregnancy failure should drive patient management. That ought to be based upon a combination of the patient’s symptoms, laboratory findings, physical exam, and pelvic ultrasound.
In the setting of worrisome ultrasound findings, the most important step in management is to get a repeat ultrasound under real-time observation. The use of cine loops in order to visualize the entire gestational sac is valuable.
"Most obstetricians underutilize this. You’re unlikely to miss a yolk sac or embryo, and you’re getting a true report of sac diameter, not a random measurement from a snapshot," she explained at the annual meeting of the Society of Ob/Gyn Hospitalists.
Worrisome but nondefinitive findings suggestive of early pregnancy loss include a slow fetal heart rate, an unusual appearance of the uterine lining, and a sac that is small, grossly distorted, enlarged, irregularly contoured, or low in position.
Maternal gestational age is a key consideration in defining a slow fetal heart rate by M-mode ultrasound. At a menstrual age of 6.2 weeks or less, a normal fetal heart rate is 100 bpm or more; less than 90 bpm is considered slow. In contrast, at 6.3-7.0 weeks, normal is defined as 120 bpm or more, and a fetal heart rate of less than 110 bpm is considered slow. When a slow fetal heart rate is detected at 6.0-7.0 weeks, the risk of subsequent first-trimester fetal demise remains elevated at about 25% even if the heart rate is normal at follow-up at 8.0 weeks (Radiology;2005;236:643-6).
The absolute ultrasound criteria for early pregnancy failure used at the Women and Infants Hospital as well as in many other settings are no fetal heart beat in an embryo more than 5 mm in crown-rump length, or menstrual age known to be greater than 6.5 weeks with no heart beat.
However, a group of investigators led by Dr. Yazan Abdallah of Imperial College London has argued that current definitions used to diagnose early pregnancy failure are potentially unsafe and could result in inadvertent termination of wanted pregnancies. Given the inherent inter- and intraobserver variation in ultrasound measurements, they have urged more conservative criteria for the definitive diagnosis of early pregnancy failure: specifically, a crown-rump length cutoff of greater than 7 mm instead of the widely used 5 mm, and a mean gestational sac diameter cutoff of more than 25 mm.
Dr. Abdallah and his coworkers support their argument on the basis of their observational, prospective cross-sectional study involving 1,060 consecutive women diagnosed with intrauterine pregnancy of uncertain viability. This diagnosis was based upon a symptom-generated ultrasound that showed either an empty gestational sac; a gestational sac with a yolk sac but no embryo when the mean gestational sac diameter was either less than 20 mm or less than 30 mm; or an embryo with an absent heart beat and a crown-rump length of either less than 6 mm or less than 8 mm.
The primary endpoint was a viable pregnancy upon routine first-trimester screening ultrasound at 11-14 weeks. At that point, 473 of the women had viable pregnancies and 587 did not.
When neither the yolk sac nor the embryo was visualized on the initial ultrasound, the false-positive rate for diagnosis of early pregnancy failure was 4.4% when a mean gestational sac diameter of 16 mm was used as a cutoff and 0.5% when 20 mm was the cutoff. Only when a cutoff of 21 mm was utilized did the false-positive rate fall to 0.
If a yolk sac was present but an embryo wasn’t, the false-positive rate was 2.6% with a mean gestational sac diameter cutoff of 16 mm and 0.4% with a cutoff of 20 mm. Again, there were no false positives when a cutoff of 21 mm was employed.
When a yolk sac and embryo were visible but a fetal heartbeat was not apparent, the false-positive rate for miscarriage was 8.3% with a crown-rump length cutoff of 5 mm. At a cutoff of 5.3 mm, there were no false-positive results (Ultrasound Obstet. Gynecol. 2011;38:497-502).
When Dr. Vrees asked the audience for a show of hands as to who utilizes a mean gestational sac diameter cutoff of 21 mm to define early pregnancy loss in the absence of both a yolk sac and embryo, only a couple of ob.gyns. responded affirmatively. Some audience members indicated they use a cutoff as low as 16 mm.
"We see great variability at our institution, too, in the definition of early pregnancy failure based upon mean gestational sac diameter," according to Dr. Vrees.
The lack of unanimity on this point, coupled with the remote likelihood of physical harm in waiting 7-10 days to repeat an ultrasound scan, figure prominently in her advocacy of expectant management.
She reported having no relevant financial disclosures.
DENVER – There is a slew of ultrasound findings that are equivocal or downright worrisome for the diagnosis of early pregnancy failure, but the list of definitive findings is short – and even those are fraught with controversy, according to Dr. Roxanne Vrees.
"In a highly desired pregnancy, even with ultrasound findings that are perhaps suggestive of early pregnancy failure, I think watchful waiting has a really important role," said Dr. Vrees, an ob.gyn. at Brown University in Providence, R.I.
She is also on the staff at the Women and Infants Hospital in Providence, where she works in a unique women’s emergency department staffed 24/7 exclusively by ob.gyn. attending physicians. Traditional emergency medicine physicians are not in the picture. This busy women’s ED averages nearly 30,000 visits annually, so Dr. Vrees and her colleagues have acquired considerable experience in emergency ob.gyn. However, because the facility is licensed by the state as an ED, by law any patient who comes in must be treated, so medical backup is available around the clock for patients who present with chest pain or otherwise fall outside the generalist ob.gyn.’s scope.
Early pregnancy failure occurs in 15%-20% of clinically recognized pregnancies. The most common symptom is vaginal bleeding, which occurs in one-quarter of all known first-trimester pregnancies, half of which end in pregnancy failure.
Dr. Vrees emphasized that no single aspect of the work-up for early pregnancy failure should drive patient management. That ought to be based upon a combination of the patient’s symptoms, laboratory findings, physical exam, and pelvic ultrasound.
In the setting of worrisome ultrasound findings, the most important step in management is to get a repeat ultrasound under real-time observation. The use of cine loops in order to visualize the entire gestational sac is valuable.
"Most obstetricians underutilize this. You’re unlikely to miss a yolk sac or embryo, and you’re getting a true report of sac diameter, not a random measurement from a snapshot," she explained at the annual meeting of the Society of Ob/Gyn Hospitalists.
Worrisome but nondefinitive findings suggestive of early pregnancy loss include a slow fetal heart rate, an unusual appearance of the uterine lining, and a sac that is small, grossly distorted, enlarged, irregularly contoured, or low in position.
Maternal gestational age is a key consideration in defining a slow fetal heart rate by M-mode ultrasound. At a menstrual age of 6.2 weeks or less, a normal fetal heart rate is 100 bpm or more; less than 90 bpm is considered slow. In contrast, at 6.3-7.0 weeks, normal is defined as 120 bpm or more, and a fetal heart rate of less than 110 bpm is considered slow. When a slow fetal heart rate is detected at 6.0-7.0 weeks, the risk of subsequent first-trimester fetal demise remains elevated at about 25% even if the heart rate is normal at follow-up at 8.0 weeks (Radiology;2005;236:643-6).
The absolute ultrasound criteria for early pregnancy failure used at the Women and Infants Hospital as well as in many other settings are no fetal heart beat in an embryo more than 5 mm in crown-rump length, or menstrual age known to be greater than 6.5 weeks with no heart beat.
However, a group of investigators led by Dr. Yazan Abdallah of Imperial College London has argued that current definitions used to diagnose early pregnancy failure are potentially unsafe and could result in inadvertent termination of wanted pregnancies. Given the inherent inter- and intraobserver variation in ultrasound measurements, they have urged more conservative criteria for the definitive diagnosis of early pregnancy failure: specifically, a crown-rump length cutoff of greater than 7 mm instead of the widely used 5 mm, and a mean gestational sac diameter cutoff of more than 25 mm.
Dr. Abdallah and his coworkers support their argument on the basis of their observational, prospective cross-sectional study involving 1,060 consecutive women diagnosed with intrauterine pregnancy of uncertain viability. This diagnosis was based upon a symptom-generated ultrasound that showed either an empty gestational sac; a gestational sac with a yolk sac but no embryo when the mean gestational sac diameter was either less than 20 mm or less than 30 mm; or an embryo with an absent heart beat and a crown-rump length of either less than 6 mm or less than 8 mm.
The primary endpoint was a viable pregnancy upon routine first-trimester screening ultrasound at 11-14 weeks. At that point, 473 of the women had viable pregnancies and 587 did not.
When neither the yolk sac nor the embryo was visualized on the initial ultrasound, the false-positive rate for diagnosis of early pregnancy failure was 4.4% when a mean gestational sac diameter of 16 mm was used as a cutoff and 0.5% when 20 mm was the cutoff. Only when a cutoff of 21 mm was utilized did the false-positive rate fall to 0.
If a yolk sac was present but an embryo wasn’t, the false-positive rate was 2.6% with a mean gestational sac diameter cutoff of 16 mm and 0.4% with a cutoff of 20 mm. Again, there were no false positives when a cutoff of 21 mm was employed.
When a yolk sac and embryo were visible but a fetal heartbeat was not apparent, the false-positive rate for miscarriage was 8.3% with a crown-rump length cutoff of 5 mm. At a cutoff of 5.3 mm, there were no false-positive results (Ultrasound Obstet. Gynecol. 2011;38:497-502).
When Dr. Vrees asked the audience for a show of hands as to who utilizes a mean gestational sac diameter cutoff of 21 mm to define early pregnancy loss in the absence of both a yolk sac and embryo, only a couple of ob.gyns. responded affirmatively. Some audience members indicated they use a cutoff as low as 16 mm.
"We see great variability at our institution, too, in the definition of early pregnancy failure based upon mean gestational sac diameter," according to Dr. Vrees.
The lack of unanimity on this point, coupled with the remote likelihood of physical harm in waiting 7-10 days to repeat an ultrasound scan, figure prominently in her advocacy of expectant management.
She reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM THE SOGH ANNUAL CLINICAL MEETING

REGARDS study suggests optimal elderly SBP of 120-139 mm Hg
AMSTERDAM – The optimal level of systolic blood pressure in all patients above age 55 appears to be 120-139 mm Hg, according to controversial data from a large, observational, U.S. population–based cohort study.
Results from the REGARDS (Reasons for Geographic and Racial Differences in Stroke) study suggest that a systolic blood pressure (SBP) in that range is associated with the lowest rates of cardiovascular events, stroke, and all-cause mortality, even in individuals aged 75 years and up. Since REGARDS is an observational study, this proposed target SBP range should be viewed as a testable hypothesis worthy of confirmation in a large, randomized, antihypertensive treatment study in the elderly, Dr. Maciej Banach said at the annual congress of the European Society of Cardiology (ESC).
REGARDS also turned up evidence supportive of the existence of the long-controversial J-curve, with an increased rate of adverse events noted in subjects with an SBP below 120 mm Hg, added Dr. Banach, professor and head of the department of hypertension at the Medical University of Lodz (Poland).
But discussant Christi Deaton, Ph.D., was quick to slam on the brakes in response to Dr. Banach’s suggestion that 120-139 mm Hg looks like the new optimal in older patients. She noted that the REGARDS proposal is at odds with the latest ESC hypertension guidelines, issued just a couple of months ago.

The evidence-based ESC guidelines (J. Hypertens. 2013;31:1281-357) offer as a class I recommendation an SBP target of 140-150 mm Hg for elderly patients under age 80, with consideration of a target below 140 mm Hg for the subgroup of elderly patients who are fit, noted Dr. Deaton, professor of nursing at the University of Manchester (U.K.), and a member of the ESC Guidelines Committee.
The American College of Cardiology/American Heart Association guidelines, in contrast, recommend a target of less than 140/90 in 65- to 79-year-olds, and an SBP of 140-145 mm Hg, if tolerated, in those aged 80 years and up (Circulation 2011;123:2434-506).

"The hypothesis from this REGARDS analysis is a bold one," she observed. "But we need large, well-designed intervention trials in older patients, particularly in underrepresented groups, before we can set lower blood pressure targets than are currently recommended in our guidelines."
The REGARDS study is a National Institutes of Health–sponsored observational study of 30,329 U.S. subjects aged 45 years or older, with overrepresentation of blacks and residents of the nation’s southeastern "stroke belt." Dr. Banach presented an analysis of 13,948 REGARDS participants aged 55 years or older who were taking antihypertensive medications at baseline. They have thus far been followed for a median of 6 years for all-cause mortality, and slightly less for first occurrence of stroke or coronary heart disease.
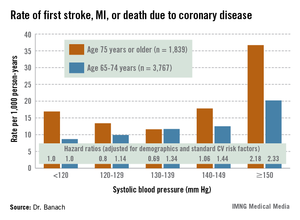
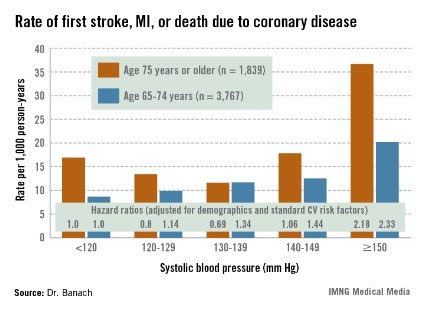
The suggestion of a J-curve was strongest for the composite endpoint of a first stroke, nonfatal myocardial infarction (MI), or death due to coronary heart disease in subjects aged 75 years or older (see graphic). There was no significant relationship between stroke and SBP category for subjects under age 75; however, over age 75, stroke rates were highest in those with an SBP less than 120 or more than 150 mm Hg.
All-cause mortality showed a linear relationship with increasing SBP in subjects aged 55-74 years, but no relationship in those over age 75.
Dr. Deaton applauded the REGARDS investigators for focusing on a high-risk population that’s "certainly underrepresented in our clinical intervention trials," but she cited several major study limitations. One is that only baseline blood pressure measurements were available.
"Importantly," she observed, "we don’t know what happened to blood pressure control during these years of follow-up."
In addition, the incidence rates of stroke, MI, and other major adverse events were relatively low in some subgroups. The planned further follow-up in REGARDS should bring greater clarity, Dr. Deaton added.
Dr. Banach and Dr. Deaton reported having no financial conflicts of interest.
AMSTERDAM – The optimal level of systolic blood pressure in all patients above age 55 appears to be 120-139 mm Hg, according to controversial data from a large, observational, U.S. population–based cohort study.
Results from the REGARDS (Reasons for Geographic and Racial Differences in Stroke) study suggest that a systolic blood pressure (SBP) in that range is associated with the lowest rates of cardiovascular events, stroke, and all-cause mortality, even in individuals aged 75 years and up. Since REGARDS is an observational study, this proposed target SBP range should be viewed as a testable hypothesis worthy of confirmation in a large, randomized, antihypertensive treatment study in the elderly, Dr. Maciej Banach said at the annual congress of the European Society of Cardiology (ESC).
REGARDS also turned up evidence supportive of the existence of the long-controversial J-curve, with an increased rate of adverse events noted in subjects with an SBP below 120 mm Hg, added Dr. Banach, professor and head of the department of hypertension at the Medical University of Lodz (Poland).
But discussant Christi Deaton, Ph.D., was quick to slam on the brakes in response to Dr. Banach’s suggestion that 120-139 mm Hg looks like the new optimal in older patients. She noted that the REGARDS proposal is at odds with the latest ESC hypertension guidelines, issued just a couple of months ago.
The evidence-based ESC guidelines (J. Hypertens. 2013;31:1281-357) offer as a class I recommendation an SBP target of 140-150 mm Hg for elderly patients under age 80, with consideration of a target below 140 mm Hg for the subgroup of elderly patients who are fit, noted Dr. Deaton, professor of nursing at the University of Manchester (U.K.), and a member of the ESC Guidelines Committee.
The American College of Cardiology/American Heart Association guidelines, in contrast, recommend a target of less than 140/90 in 65- to 79-year-olds, and an SBP of 140-145 mm Hg, if tolerated, in those aged 80 years and up (Circulation 2011;123:2434-506).
"The hypothesis from this REGARDS analysis is a bold one," she observed. "But we need large, well-designed intervention trials in older patients, particularly in underrepresented groups, before we can set lower blood pressure targets than are currently recommended in our guidelines."
The REGARDS study is a National Institutes of Health–sponsored observational study of 30,329 U.S. subjects aged 45 years or older, with overrepresentation of blacks and residents of the nation’s southeastern "stroke belt." Dr. Banach presented an analysis of 13,948 REGARDS participants aged 55 years or older who were taking antihypertensive medications at baseline. They have thus far been followed for a median of 6 years for all-cause mortality, and slightly less for first occurrence of stroke or coronary heart disease.
The suggestion of a J-curve was strongest for the composite endpoint of a first stroke, nonfatal myocardial infarction (MI), or death due to coronary heart disease in subjects aged 75 years or older (see graphic). There was no significant relationship between stroke and SBP category for subjects under age 75; however, over age 75, stroke rates were highest in those with an SBP less than 120 or more than 150 mm Hg.
All-cause mortality showed a linear relationship with increasing SBP in subjects aged 55-74 years, but no relationship in those over age 75.
Dr. Deaton applauded the REGARDS investigators for focusing on a high-risk population that’s "certainly underrepresented in our clinical intervention trials," but she cited several major study limitations. One is that only baseline blood pressure measurements were available.
"Importantly," she observed, "we don’t know what happened to blood pressure control during these years of follow-up."
In addition, the incidence rates of stroke, MI, and other major adverse events were relatively low in some subgroups. The planned further follow-up in REGARDS should bring greater clarity, Dr. Deaton added.
Dr. Banach and Dr. Deaton reported having no financial conflicts of interest.
AMSTERDAM – The optimal level of systolic blood pressure in all patients above age 55 appears to be 120-139 mm Hg, according to controversial data from a large, observational, U.S. population–based cohort study.
Results from the REGARDS (Reasons for Geographic and Racial Differences in Stroke) study suggest that a systolic blood pressure (SBP) in that range is associated with the lowest rates of cardiovascular events, stroke, and all-cause mortality, even in individuals aged 75 years and up. Since REGARDS is an observational study, this proposed target SBP range should be viewed as a testable hypothesis worthy of confirmation in a large, randomized, antihypertensive treatment study in the elderly, Dr. Maciej Banach said at the annual congress of the European Society of Cardiology (ESC).
REGARDS also turned up evidence supportive of the existence of the long-controversial J-curve, with an increased rate of adverse events noted in subjects with an SBP below 120 mm Hg, added Dr. Banach, professor and head of the department of hypertension at the Medical University of Lodz (Poland).
But discussant Christi Deaton, Ph.D., was quick to slam on the brakes in response to Dr. Banach’s suggestion that 120-139 mm Hg looks like the new optimal in older patients. She noted that the REGARDS proposal is at odds with the latest ESC hypertension guidelines, issued just a couple of months ago.
The evidence-based ESC guidelines (J. Hypertens. 2013;31:1281-357) offer as a class I recommendation an SBP target of 140-150 mm Hg for elderly patients under age 80, with consideration of a target below 140 mm Hg for the subgroup of elderly patients who are fit, noted Dr. Deaton, professor of nursing at the University of Manchester (U.K.), and a member of the ESC Guidelines Committee.
The American College of Cardiology/American Heart Association guidelines, in contrast, recommend a target of less than 140/90 in 65- to 79-year-olds, and an SBP of 140-145 mm Hg, if tolerated, in those aged 80 years and up (Circulation 2011;123:2434-506).
"The hypothesis from this REGARDS analysis is a bold one," she observed. "But we need large, well-designed intervention trials in older patients, particularly in underrepresented groups, before we can set lower blood pressure targets than are currently recommended in our guidelines."
The REGARDS study is a National Institutes of Health–sponsored observational study of 30,329 U.S. subjects aged 45 years or older, with overrepresentation of blacks and residents of the nation’s southeastern "stroke belt." Dr. Banach presented an analysis of 13,948 REGARDS participants aged 55 years or older who were taking antihypertensive medications at baseline. They have thus far been followed for a median of 6 years for all-cause mortality, and slightly less for first occurrence of stroke or coronary heart disease.
The suggestion of a J-curve was strongest for the composite endpoint of a first stroke, nonfatal myocardial infarction (MI), or death due to coronary heart disease in subjects aged 75 years or older (see graphic). There was no significant relationship between stroke and SBP category for subjects under age 75; however, over age 75, stroke rates were highest in those with an SBP less than 120 or more than 150 mm Hg.
All-cause mortality showed a linear relationship with increasing SBP in subjects aged 55-74 years, but no relationship in those over age 75.
Dr. Deaton applauded the REGARDS investigators for focusing on a high-risk population that’s "certainly underrepresented in our clinical intervention trials," but she cited several major study limitations. One is that only baseline blood pressure measurements were available.
"Importantly," she observed, "we don’t know what happened to blood pressure control during these years of follow-up."
In addition, the incidence rates of stroke, MI, and other major adverse events were relatively low in some subgroups. The planned further follow-up in REGARDS should bring greater clarity, Dr. Deaton added.
Dr. Banach and Dr. Deaton reported having no financial conflicts of interest.
AT THE ESC CONGRESS 2013
Major finding: The adjusted risk of a first stroke, MI, or cardiovascular death in individuals aged 75 years or older on antihypertensive therapy was 20% lower in those with a systolic blood pressure of 120-129 mm Hg than in those with an SBP less than 120, and 31% lower in those with an SBP of 130-139 mm Hg. In contrast, the risk was 2.2-fold greater in those with an SBP of 150 mm Hg or more than in subjects with an SBP below 120 mm Hg.
Data source: This was a secondary analysis involving nearly 14,000 participants in the prospective observational REGARDS study, all at least 55 years old and on antihypertensive medication at baseline.
Disclosures: Dr. Banach and Dr. Deaton reported having no financial conflicts of interest.
Implementing hospital laborist program cut cesarean rates
DENVER – The newly published first data showing improved clinical outcomes after adoption of a full-time hospital laborist program was roundly celebrated at the annual meeting of the Society of Ob/Gyn Hospitalists.
Dr. Thomas J. Garite presented highlights of this freshly published retrospective observational study (Am. J. Obstet. Gynecol. 2013;209:251.e1-6) conducted at a large-delivery-volume tertiary hospital in Las Vegas. Dr. Garite and his coinvestigators, led by Dr. Brian K. Iriye, compared hospital-wide cesarean delivery rates for 6,206 nulliparous, term, singleton live births during 2006-2011.

This was a period of change in how labor and delivery was organized at the hospital. During the first 16 months of the study period, the traditional private-practice model of patient care was in place, with ob.gyns. on call and no laborists in the house. This was followed by a 14-month interlude in which local private-practice ob.gyns. got together and made sure that a community physician was continuously in-hospital to provide laborist coverage.
"I call that the doc-in-a-box model," said Dr. Garite, professor emeritus and former chair of obstetrics and gynecology at the University of California, Irvine.
Finally came a 24-month period with full-time laborists – that is, ob.gyns. without a private practice – providing in-hospital coverage 24/7.
In a multivariate logistic regression analysis adjusted for potential confounders, the hospital’s cesarean section rate was roughly 25% lower after implementation of the full-time laborist program than in either of the other two periods.
"I haven’t seen other studies to date that demonstrate these kinds of outcome advantages for this kind of practice. I think we’re going to see a lot more. But until we do, a lot of people who don’t like change are going to be saying, ‘Wait, where’s the proof?’ Well, this is the beginning of the proof of something I believe in strongly," declared Dr. Garite, who is also editor-in-chief of the American Journal of Obstetrics and Gynecology and chief clinical officer at PeriGen, a provider of fetal surveillance systems.
Society of Ob/Gyn Hospitalists (SOGH) board member Dr. Jennifer Tessmer-Tuck hailed the new study as "the best and almost the only" clinical outcome data to date showing the advantages of the ob.gyn. hospitalist model of care. And it was a long time coming, she noted: a full 10½ years since Dr. Louis Weinstein of the Medical College of Ohio, Toledo, heralded the birth of a radically different form of ob.gyn. practice in his seminal essay "The laborist: A new focus of practice for the obstetrician" (Am. J. Obstet. Gynecol. 2003;188:310-2).
"We have a lot to do. SOGH would really like to have more of a research platform and be able to put ourselves out there. There’s really a gap in care, and we’re hoping to jump in and fill it," said Dr. Tessmer-Tuck, director of North Memorial Medical Center Laborist Associates in Robbinsdale, Minn.
But while the SOGH leadership is eager to see the field assume a bigger research presence, it’s a challenge. Most society members, when they talk about why they became hospitalists, say they had burned out in traditional private practice, with its demanding on-call schedule. They sought well-defined hours, perhaps more family time. Given those priorities, taking on a research project can sound daunting, even though the fruits of such a project might enhance the standing of the young subspecialty.
Dr. Garite reported that the cesarean section rate at the tertiary center was 33.2% during the 24 months when full-time laborists were on hand, compared with 39.2% under the traditional private practice model with no laborists, and 38.7% with laborist coverage by community staff. In a multivariate logistic regression analysis adjusted for maternal age, physician age, race, gestational age, induction of labor, birth weight, and maternal weight, the hospital’s cesarean section rate after the introduction of full-time laborists was 27% lower than in the earlier period of no laborists and 23% less than with community laborist care.
There were no differences between the three groups in rates of low Apgar scores, metabolic acidosis, or any other parameters of adverse neonatal or maternal outcome.
During the study years of 2006-2011, cesarean section rates at the other hospitals in the city were either stable or rising.
Asked why hospital-wide cesarean section rates dropped significantly once full-time obstetric hospitalists were in place, Dr. Garite replied, "It’s not, for example, the patient with abruption who comes in the door; she’s going to get a cesarean section whether a hospitalist is there or some other doctor is covering. Instead, it’s the patient who has what I call ‘failure to wait,’ a.k.a. failure to progress, or the 4 o’clock induction that hasn’t made any progress ... There are lots of examples of why cesarean section rates change with a hospitalist in place, especially if you look at the correlation between cesarean sections and time of day."
Dr. Tessmer-Tuck said she found the Las Vegas study highly relevant because lots of hospitals throughout the country are now going through a similar transition from traditional on-call practice to around-the-clock coverage provided by rotating private practice community laborists, while pondering a possible move to full-time laborists.

"This is where many of our hospitals are at: They’re in the middle phase, with private-practice docs being paid to stay in-house 24 hours in case there’s an emergency," according to Dr. Tessmer-Tuck.
She said she found particularly impressive the investigators’ calculation that a full-time laborist resulted in an average of one fewer cesarean section every 2 days in a population of primiparous, term, singleton patients, with a resultant estimated savings in patient care costs of $2,823-$3,305 per day. Because a laborist might be paid $2,500 per 24-hour shift, the reduced cesarean section rate alone covers the laborist’s salary. Those are the sort of numbers hospital administrators find persuasive.
"This is a message you guys should take home with you when you go back to your own program," she said.
While the Las Vegas study provides the first evidence to be published in a major peer-reviewed journal demonstrating superior clinical outcomes with the full-time laborist model, Dr. Tessmer-Tuck noted that in addition there are several published studies suggesting that hospitals experience fewer adverse events and markedly lower payouts for bad outcomes after they implement multipronged, comprehensive obstetric patient safety programs that include bringing a laborist on board.
"Liability has become a huge issue for us. Many hospitals implement hospitalist programs mainly in order to reduce liability," according to Dr. Tessmer-Tuck.
She cited a study by ob.gyns. at New York Presbyterian/Weill Cornell Medical Center in which they analyzed the impact of a comprehensive patient safety program initiated in stages beginning in 2003. The interventions included mandatory labor and delivery team training aimed at enhancing physician/nurse communication, development of standardized management protocols, training in fetal heart rate monitoring interpretation, creation of a patient safety nurse position, and, in 2006, introduction of a laborist.
It’s not possible to parse out just how much of the improvement in response to the multipronged safety program was the result of adopting the laborist model, Dr. Tessmer-Tuck said, but she noted the average yearly compensation payments for patient claims or lawsuits were $27.6 million during 2003-2006, plummeting to $2.5 million per year in 2007-2009, after the laborist was in place. Moreover, sentinel adverse events such as maternal death or severe neurodevelopmental impairment in a child decreased from five in the year 2000 to none in 2008 and 2009 (Am. J. Obstet. Gynecol. 2011;204:97-105).
Ob.gyns. at Yale–New Haven (Conn.) Hospital introduced a similar comprehensive patient safety program, also including implementation of a 24-hour obstetrics hospitalist, during 2004-2006. During 3 years of prospective follow-up involving nearly 14,000 deliveries, they documented a significant linear decline in obstetric adverse outcomes (Am. J. Obstet. Gynecol. 2009;200:492e1-8). They also administered a validated workplace safety attitude questionnaire four times during 2004-2009 and documented marked improvement over time in favorable scores in the domains of job satisfaction, teamwork, and safety culture (Am J. Obstet. Gynecol. 2011;204:216.e1-6).
Dr. Garite and Dr. Tessmer-Tuck reported having no germane financial relationships.
DENVER – The newly published first data showing improved clinical outcomes after adoption of a full-time hospital laborist program was roundly celebrated at the annual meeting of the Society of Ob/Gyn Hospitalists.
Dr. Thomas J. Garite presented highlights of this freshly published retrospective observational study (Am. J. Obstet. Gynecol. 2013;209:251.e1-6) conducted at a large-delivery-volume tertiary hospital in Las Vegas. Dr. Garite and his coinvestigators, led by Dr. Brian K. Iriye, compared hospital-wide cesarean delivery rates for 6,206 nulliparous, term, singleton live births during 2006-2011.
This was a period of change in how labor and delivery was organized at the hospital. During the first 16 months of the study period, the traditional private-practice model of patient care was in place, with ob.gyns. on call and no laborists in the house. This was followed by a 14-month interlude in which local private-practice ob.gyns. got together and made sure that a community physician was continuously in-hospital to provide laborist coverage.
"I call that the doc-in-a-box model," said Dr. Garite, professor emeritus and former chair of obstetrics and gynecology at the University of California, Irvine.
Finally came a 24-month period with full-time laborists – that is, ob.gyns. without a private practice – providing in-hospital coverage 24/7.
In a multivariate logistic regression analysis adjusted for potential confounders, the hospital’s cesarean section rate was roughly 25% lower after implementation of the full-time laborist program than in either of the other two periods.
"I haven’t seen other studies to date that demonstrate these kinds of outcome advantages for this kind of practice. I think we’re going to see a lot more. But until we do, a lot of people who don’t like change are going to be saying, ‘Wait, where’s the proof?’ Well, this is the beginning of the proof of something I believe in strongly," declared Dr. Garite, who is also editor-in-chief of the American Journal of Obstetrics and Gynecology and chief clinical officer at PeriGen, a provider of fetal surveillance systems.
Society of Ob/Gyn Hospitalists (SOGH) board member Dr. Jennifer Tessmer-Tuck hailed the new study as "the best and almost the only" clinical outcome data to date showing the advantages of the ob.gyn. hospitalist model of care. And it was a long time coming, she noted: a full 10½ years since Dr. Louis Weinstein of the Medical College of Ohio, Toledo, heralded the birth of a radically different form of ob.gyn. practice in his seminal essay "The laborist: A new focus of practice for the obstetrician" (Am. J. Obstet. Gynecol. 2003;188:310-2).
"We have a lot to do. SOGH would really like to have more of a research platform and be able to put ourselves out there. There’s really a gap in care, and we’re hoping to jump in and fill it," said Dr. Tessmer-Tuck, director of North Memorial Medical Center Laborist Associates in Robbinsdale, Minn.
But while the SOGH leadership is eager to see the field assume a bigger research presence, it’s a challenge. Most society members, when they talk about why they became hospitalists, say they had burned out in traditional private practice, with its demanding on-call schedule. They sought well-defined hours, perhaps more family time. Given those priorities, taking on a research project can sound daunting, even though the fruits of such a project might enhance the standing of the young subspecialty.
Dr. Garite reported that the cesarean section rate at the tertiary center was 33.2% during the 24 months when full-time laborists were on hand, compared with 39.2% under the traditional private practice model with no laborists, and 38.7% with laborist coverage by community staff. In a multivariate logistic regression analysis adjusted for maternal age, physician age, race, gestational age, induction of labor, birth weight, and maternal weight, the hospital’s cesarean section rate after the introduction of full-time laborists was 27% lower than in the earlier period of no laborists and 23% less than with community laborist care.
There were no differences between the three groups in rates of low Apgar scores, metabolic acidosis, or any other parameters of adverse neonatal or maternal outcome.
During the study years of 2006-2011, cesarean section rates at the other hospitals in the city were either stable or rising.
Asked why hospital-wide cesarean section rates dropped significantly once full-time obstetric hospitalists were in place, Dr. Garite replied, "It’s not, for example, the patient with abruption who comes in the door; she’s going to get a cesarean section whether a hospitalist is there or some other doctor is covering. Instead, it’s the patient who has what I call ‘failure to wait,’ a.k.a. failure to progress, or the 4 o’clock induction that hasn’t made any progress ... There are lots of examples of why cesarean section rates change with a hospitalist in place, especially if you look at the correlation between cesarean sections and time of day."
Dr. Tessmer-Tuck said she found the Las Vegas study highly relevant because lots of hospitals throughout the country are now going through a similar transition from traditional on-call practice to around-the-clock coverage provided by rotating private practice community laborists, while pondering a possible move to full-time laborists.
"This is where many of our hospitals are at: They’re in the middle phase, with private-practice docs being paid to stay in-house 24 hours in case there’s an emergency," according to Dr. Tessmer-Tuck.
She said she found particularly impressive the investigators’ calculation that a full-time laborist resulted in an average of one fewer cesarean section every 2 days in a population of primiparous, term, singleton patients, with a resultant estimated savings in patient care costs of $2,823-$3,305 per day. Because a laborist might be paid $2,500 per 24-hour shift, the reduced cesarean section rate alone covers the laborist’s salary. Those are the sort of numbers hospital administrators find persuasive.
"This is a message you guys should take home with you when you go back to your own program," she said.
While the Las Vegas study provides the first evidence to be published in a major peer-reviewed journal demonstrating superior clinical outcomes with the full-time laborist model, Dr. Tessmer-Tuck noted that in addition there are several published studies suggesting that hospitals experience fewer adverse events and markedly lower payouts for bad outcomes after they implement multipronged, comprehensive obstetric patient safety programs that include bringing a laborist on board.
"Liability has become a huge issue for us. Many hospitals implement hospitalist programs mainly in order to reduce liability," according to Dr. Tessmer-Tuck.
She cited a study by ob.gyns. at New York Presbyterian/Weill Cornell Medical Center in which they analyzed the impact of a comprehensive patient safety program initiated in stages beginning in 2003. The interventions included mandatory labor and delivery team training aimed at enhancing physician/nurse communication, development of standardized management protocols, training in fetal heart rate monitoring interpretation, creation of a patient safety nurse position, and, in 2006, introduction of a laborist.
It’s not possible to parse out just how much of the improvement in response to the multipronged safety program was the result of adopting the laborist model, Dr. Tessmer-Tuck said, but she noted the average yearly compensation payments for patient claims or lawsuits were $27.6 million during 2003-2006, plummeting to $2.5 million per year in 2007-2009, after the laborist was in place. Moreover, sentinel adverse events such as maternal death or severe neurodevelopmental impairment in a child decreased from five in the year 2000 to none in 2008 and 2009 (Am. J. Obstet. Gynecol. 2011;204:97-105).
Ob.gyns. at Yale–New Haven (Conn.) Hospital introduced a similar comprehensive patient safety program, also including implementation of a 24-hour obstetrics hospitalist, during 2004-2006. During 3 years of prospective follow-up involving nearly 14,000 deliveries, they documented a significant linear decline in obstetric adverse outcomes (Am. J. Obstet. Gynecol. 2009;200:492e1-8). They also administered a validated workplace safety attitude questionnaire four times during 2004-2009 and documented marked improvement over time in favorable scores in the domains of job satisfaction, teamwork, and safety culture (Am J. Obstet. Gynecol. 2011;204:216.e1-6).
Dr. Garite and Dr. Tessmer-Tuck reported having no germane financial relationships.
DENVER – The newly published first data showing improved clinical outcomes after adoption of a full-time hospital laborist program was roundly celebrated at the annual meeting of the Society of Ob/Gyn Hospitalists.
Dr. Thomas J. Garite presented highlights of this freshly published retrospective observational study (Am. J. Obstet. Gynecol. 2013;209:251.e1-6) conducted at a large-delivery-volume tertiary hospital in Las Vegas. Dr. Garite and his coinvestigators, led by Dr. Brian K. Iriye, compared hospital-wide cesarean delivery rates for 6,206 nulliparous, term, singleton live births during 2006-2011.
This was a period of change in how labor and delivery was organized at the hospital. During the first 16 months of the study period, the traditional private-practice model of patient care was in place, with ob.gyns. on call and no laborists in the house. This was followed by a 14-month interlude in which local private-practice ob.gyns. got together and made sure that a community physician was continuously in-hospital to provide laborist coverage.
"I call that the doc-in-a-box model," said Dr. Garite, professor emeritus and former chair of obstetrics and gynecology at the University of California, Irvine.
Finally came a 24-month period with full-time laborists – that is, ob.gyns. without a private practice – providing in-hospital coverage 24/7.
In a multivariate logistic regression analysis adjusted for potential confounders, the hospital’s cesarean section rate was roughly 25% lower after implementation of the full-time laborist program than in either of the other two periods.
"I haven’t seen other studies to date that demonstrate these kinds of outcome advantages for this kind of practice. I think we’re going to see a lot more. But until we do, a lot of people who don’t like change are going to be saying, ‘Wait, where’s the proof?’ Well, this is the beginning of the proof of something I believe in strongly," declared Dr. Garite, who is also editor-in-chief of the American Journal of Obstetrics and Gynecology and chief clinical officer at PeriGen, a provider of fetal surveillance systems.
Society of Ob/Gyn Hospitalists (SOGH) board member Dr. Jennifer Tessmer-Tuck hailed the new study as "the best and almost the only" clinical outcome data to date showing the advantages of the ob.gyn. hospitalist model of care. And it was a long time coming, she noted: a full 10½ years since Dr. Louis Weinstein of the Medical College of Ohio, Toledo, heralded the birth of a radically different form of ob.gyn. practice in his seminal essay "The laborist: A new focus of practice for the obstetrician" (Am. J. Obstet. Gynecol. 2003;188:310-2).
"We have a lot to do. SOGH would really like to have more of a research platform and be able to put ourselves out there. There’s really a gap in care, and we’re hoping to jump in and fill it," said Dr. Tessmer-Tuck, director of North Memorial Medical Center Laborist Associates in Robbinsdale, Minn.
But while the SOGH leadership is eager to see the field assume a bigger research presence, it’s a challenge. Most society members, when they talk about why they became hospitalists, say they had burned out in traditional private practice, with its demanding on-call schedule. They sought well-defined hours, perhaps more family time. Given those priorities, taking on a research project can sound daunting, even though the fruits of such a project might enhance the standing of the young subspecialty.
Dr. Garite reported that the cesarean section rate at the tertiary center was 33.2% during the 24 months when full-time laborists were on hand, compared with 39.2% under the traditional private practice model with no laborists, and 38.7% with laborist coverage by community staff. In a multivariate logistic regression analysis adjusted for maternal age, physician age, race, gestational age, induction of labor, birth weight, and maternal weight, the hospital’s cesarean section rate after the introduction of full-time laborists was 27% lower than in the earlier period of no laborists and 23% less than with community laborist care.
There were no differences between the three groups in rates of low Apgar scores, metabolic acidosis, or any other parameters of adverse neonatal or maternal outcome.
During the study years of 2006-2011, cesarean section rates at the other hospitals in the city were either stable or rising.
Asked why hospital-wide cesarean section rates dropped significantly once full-time obstetric hospitalists were in place, Dr. Garite replied, "It’s not, for example, the patient with abruption who comes in the door; she’s going to get a cesarean section whether a hospitalist is there or some other doctor is covering. Instead, it’s the patient who has what I call ‘failure to wait,’ a.k.a. failure to progress, or the 4 o’clock induction that hasn’t made any progress ... There are lots of examples of why cesarean section rates change with a hospitalist in place, especially if you look at the correlation between cesarean sections and time of day."
Dr. Tessmer-Tuck said she found the Las Vegas study highly relevant because lots of hospitals throughout the country are now going through a similar transition from traditional on-call practice to around-the-clock coverage provided by rotating private practice community laborists, while pondering a possible move to full-time laborists.
"This is where many of our hospitals are at: They’re in the middle phase, with private-practice docs being paid to stay in-house 24 hours in case there’s an emergency," according to Dr. Tessmer-Tuck.
She said she found particularly impressive the investigators’ calculation that a full-time laborist resulted in an average of one fewer cesarean section every 2 days in a population of primiparous, term, singleton patients, with a resultant estimated savings in patient care costs of $2,823-$3,305 per day. Because a laborist might be paid $2,500 per 24-hour shift, the reduced cesarean section rate alone covers the laborist’s salary. Those are the sort of numbers hospital administrators find persuasive.
"This is a message you guys should take home with you when you go back to your own program," she said.
While the Las Vegas study provides the first evidence to be published in a major peer-reviewed journal demonstrating superior clinical outcomes with the full-time laborist model, Dr. Tessmer-Tuck noted that in addition there are several published studies suggesting that hospitals experience fewer adverse events and markedly lower payouts for bad outcomes after they implement multipronged, comprehensive obstetric patient safety programs that include bringing a laborist on board.
"Liability has become a huge issue for us. Many hospitals implement hospitalist programs mainly in order to reduce liability," according to Dr. Tessmer-Tuck.
She cited a study by ob.gyns. at New York Presbyterian/Weill Cornell Medical Center in which they analyzed the impact of a comprehensive patient safety program initiated in stages beginning in 2003. The interventions included mandatory labor and delivery team training aimed at enhancing physician/nurse communication, development of standardized management protocols, training in fetal heart rate monitoring interpretation, creation of a patient safety nurse position, and, in 2006, introduction of a laborist.
It’s not possible to parse out just how much of the improvement in response to the multipronged safety program was the result of adopting the laborist model, Dr. Tessmer-Tuck said, but she noted the average yearly compensation payments for patient claims or lawsuits were $27.6 million during 2003-2006, plummeting to $2.5 million per year in 2007-2009, after the laborist was in place. Moreover, sentinel adverse events such as maternal death or severe neurodevelopmental impairment in a child decreased from five in the year 2000 to none in 2008 and 2009 (Am. J. Obstet. Gynecol. 2011;204:97-105).
Ob.gyns. at Yale–New Haven (Conn.) Hospital introduced a similar comprehensive patient safety program, also including implementation of a 24-hour obstetrics hospitalist, during 2004-2006. During 3 years of prospective follow-up involving nearly 14,000 deliveries, they documented a significant linear decline in obstetric adverse outcomes (Am. J. Obstet. Gynecol. 2009;200:492e1-8). They also administered a validated workplace safety attitude questionnaire four times during 2004-2009 and documented marked improvement over time in favorable scores in the domains of job satisfaction, teamwork, and safety culture (Am J. Obstet. Gynecol. 2011;204:216.e1-6).
Dr. Garite and Dr. Tessmer-Tuck reported having no germane financial relationships.
AT THE SOGH ANNUAL CLINICAL MEETING

HDL hypothesis takes yet another hit
AMSTERDAM – A novel oral drug that raises HDL cholesterol levels by upregulating hepatic synthesis of apolipoprotein A1 failed to significantly reduce coronary atheroma volume in a large phase II study.
The lack of efficacy for the drug known as RVX-208 in the ASSURE trial (ApoA1 Synthesis Stimulation and Intravascular Ultrasound for Coronary Atheroma Regression Evaluation) was "disappointing and surprising, given promising earlier findings," Dr. Stephen J. Nicholls observed in presenting the trial results at the annual congress of the European Society of Cardiology.
The study involved 323 patients with symptomatic coronary artery disease and low HDL cholesterol who were randomized 3:1 to 26 weeks of RVX-208 at 100 mg twice daily or placebo. All subjects were on atorvastatin or rosuvastatin. The RVX-208 group experienced a mean 10.9% increase in HDL over baseline, a 12.8% rise in ApoA-1, and a 16% drop in LDL. But these beneficial lipid changes weren’t significantly different than in the placebo group, which showed a 7.7% increase in HDL, a 10.6% bump in ApoA-1, and a 17.6% fall in LDL.

The primary study endpoint was change from baseline in atheroma volume. The median drop was 40% in the RVX-208 group and not statistically different from the 30% decrease in placebo-treated controls. Nor was there a significant difference between the two study arms in reduction in atheroma volume within the most-diseased 10-mm coronary segment, reported Dr. Nicholls, professor of medicine at the University of Adelaide and deputy director of the South Australian Health and Medical Research Institute.
Moreover, RVX-208 was associated with liver enzyme elevations in the great majority of treated patients, exceeding three times the upper limit of normal in 7.1% of them.
"This drug had been developed with the thought that it would be a potent oral compound from the perspective of an HDL therapeutic and would be comparable to the HDL infusional approaches that were previously seen to regress plaque. That’s clearly not the case. We saw no biochemical or plaque improvement whatsoever above and beyond the placebo group. So RVX-208 does not appear to be a potent approach to HDL therapeutics," Dr. Nicholls concluded.
Nonetheless, he expressed some regret that the trial hadn’t been designed to be lengthier. It’s possible that with another 6 months or more of treatment the trends favoring the investigational agent might have achieved statistical significance.
Asked if the negative result in ASSURE, coming on top of a steady flow of consistently negative clinical trials for niacin, torcetrapib, and other HDL-raising agents, means that the HDL-raising hypothesis of cardiovascular prevention is dead, Dr. Deepak L. Bhatt replied, "I think that’s a good question. The hypothesis has always been a good one, but I believe that in patients who are statin treated, no one has really shown an incremental benefit of HDL-raising. Of course, there are older data in patients not on statins to show that drugs like niacin are useful, but these drugs also have an effect on other lipid parameters, like LDL.
"It does appear that low HDL is a risk marker. But it may not be a modifiable risk factor. I think for the time being, the HDL hypothesis remains a hypothesis with a lot of holes in it. Moving forward, we’ll probably have more to gain by reducing LDL incrementally beyond the levels obtained with statins than with solely trying to raise HDL, unless those HDL-raising compounds we study in the future also have LDL-reduction or other properties," added Dr. Bhatt, professor of medicine at Harvard Medical School, Boston, and chief of cardiology at Veterans Affairs Boston Healthcare System.
Dr. Nicholls conceded that "this continues to be a field with a lot of uncertainty." But he asserted "there continues to be immense interest in the development of therapies targeting HDL."
Noting that, in ASSURE, RVX-208 wasn’t significantly better at raising HDL than was state-of-the-art background medical therapy including statins in the placebo arm, he said, "I think we haven’t really tested the HDL hypothesis yet." Advancing an investigational agent to phase III testing with clinical outcomes will require that the drug first demonstrate atheroma regression in a solid phase II study, he added.
The ASSURE trial was sponsored by Resverlogix. Dr. Nicholls has received research support from, and serves as a consultant to, Resverlogix and more than half a dozen other pharmaceutical companies.
AMSTERDAM – A novel oral drug that raises HDL cholesterol levels by upregulating hepatic synthesis of apolipoprotein A1 failed to significantly reduce coronary atheroma volume in a large phase II study.
The lack of efficacy for the drug known as RVX-208 in the ASSURE trial (ApoA1 Synthesis Stimulation and Intravascular Ultrasound for Coronary Atheroma Regression Evaluation) was "disappointing and surprising, given promising earlier findings," Dr. Stephen J. Nicholls observed in presenting the trial results at the annual congress of the European Society of Cardiology.
The study involved 323 patients with symptomatic coronary artery disease and low HDL cholesterol who were randomized 3:1 to 26 weeks of RVX-208 at 100 mg twice daily or placebo. All subjects were on atorvastatin or rosuvastatin. The RVX-208 group experienced a mean 10.9% increase in HDL over baseline, a 12.8% rise in ApoA-1, and a 16% drop in LDL. But these beneficial lipid changes weren’t significantly different than in the placebo group, which showed a 7.7% increase in HDL, a 10.6% bump in ApoA-1, and a 17.6% fall in LDL.
The primary study endpoint was change from baseline in atheroma volume. The median drop was 40% in the RVX-208 group and not statistically different from the 30% decrease in placebo-treated controls. Nor was there a significant difference between the two study arms in reduction in atheroma volume within the most-diseased 10-mm coronary segment, reported Dr. Nicholls, professor of medicine at the University of Adelaide and deputy director of the South Australian Health and Medical Research Institute.
Moreover, RVX-208 was associated with liver enzyme elevations in the great majority of treated patients, exceeding three times the upper limit of normal in 7.1% of them.
"This drug had been developed with the thought that it would be a potent oral compound from the perspective of an HDL therapeutic and would be comparable to the HDL infusional approaches that were previously seen to regress plaque. That’s clearly not the case. We saw no biochemical or plaque improvement whatsoever above and beyond the placebo group. So RVX-208 does not appear to be a potent approach to HDL therapeutics," Dr. Nicholls concluded.
Nonetheless, he expressed some regret that the trial hadn’t been designed to be lengthier. It’s possible that with another 6 months or more of treatment the trends favoring the investigational agent might have achieved statistical significance.
Asked if the negative result in ASSURE, coming on top of a steady flow of consistently negative clinical trials for niacin, torcetrapib, and other HDL-raising agents, means that the HDL-raising hypothesis of cardiovascular prevention is dead, Dr. Deepak L. Bhatt replied, "I think that’s a good question. The hypothesis has always been a good one, but I believe that in patients who are statin treated, no one has really shown an incremental benefit of HDL-raising. Of course, there are older data in patients not on statins to show that drugs like niacin are useful, but these drugs also have an effect on other lipid parameters, like LDL.
"It does appear that low HDL is a risk marker. But it may not be a modifiable risk factor. I think for the time being, the HDL hypothesis remains a hypothesis with a lot of holes in it. Moving forward, we’ll probably have more to gain by reducing LDL incrementally beyond the levels obtained with statins than with solely trying to raise HDL, unless those HDL-raising compounds we study in the future also have LDL-reduction or other properties," added Dr. Bhatt, professor of medicine at Harvard Medical School, Boston, and chief of cardiology at Veterans Affairs Boston Healthcare System.
Dr. Nicholls conceded that "this continues to be a field with a lot of uncertainty." But he asserted "there continues to be immense interest in the development of therapies targeting HDL."
Noting that, in ASSURE, RVX-208 wasn’t significantly better at raising HDL than was state-of-the-art background medical therapy including statins in the placebo arm, he said, "I think we haven’t really tested the HDL hypothesis yet." Advancing an investigational agent to phase III testing with clinical outcomes will require that the drug first demonstrate atheroma regression in a solid phase II study, he added.
The ASSURE trial was sponsored by Resverlogix. Dr. Nicholls has received research support from, and serves as a consultant to, Resverlogix and more than half a dozen other pharmaceutical companies.
AMSTERDAM – A novel oral drug that raises HDL cholesterol levels by upregulating hepatic synthesis of apolipoprotein A1 failed to significantly reduce coronary atheroma volume in a large phase II study.
The lack of efficacy for the drug known as RVX-208 in the ASSURE trial (ApoA1 Synthesis Stimulation and Intravascular Ultrasound for Coronary Atheroma Regression Evaluation) was "disappointing and surprising, given promising earlier findings," Dr. Stephen J. Nicholls observed in presenting the trial results at the annual congress of the European Society of Cardiology.
The study involved 323 patients with symptomatic coronary artery disease and low HDL cholesterol who were randomized 3:1 to 26 weeks of RVX-208 at 100 mg twice daily or placebo. All subjects were on atorvastatin or rosuvastatin. The RVX-208 group experienced a mean 10.9% increase in HDL over baseline, a 12.8% rise in ApoA-1, and a 16% drop in LDL. But these beneficial lipid changes weren’t significantly different than in the placebo group, which showed a 7.7% increase in HDL, a 10.6% bump in ApoA-1, and a 17.6% fall in LDL.
The primary study endpoint was change from baseline in atheroma volume. The median drop was 40% in the RVX-208 group and not statistically different from the 30% decrease in placebo-treated controls. Nor was there a significant difference between the two study arms in reduction in atheroma volume within the most-diseased 10-mm coronary segment, reported Dr. Nicholls, professor of medicine at the University of Adelaide and deputy director of the South Australian Health and Medical Research Institute.
Moreover, RVX-208 was associated with liver enzyme elevations in the great majority of treated patients, exceeding three times the upper limit of normal in 7.1% of them.
"This drug had been developed with the thought that it would be a potent oral compound from the perspective of an HDL therapeutic and would be comparable to the HDL infusional approaches that were previously seen to regress plaque. That’s clearly not the case. We saw no biochemical or plaque improvement whatsoever above and beyond the placebo group. So RVX-208 does not appear to be a potent approach to HDL therapeutics," Dr. Nicholls concluded.
Nonetheless, he expressed some regret that the trial hadn’t been designed to be lengthier. It’s possible that with another 6 months or more of treatment the trends favoring the investigational agent might have achieved statistical significance.
Asked if the negative result in ASSURE, coming on top of a steady flow of consistently negative clinical trials for niacin, torcetrapib, and other HDL-raising agents, means that the HDL-raising hypothesis of cardiovascular prevention is dead, Dr. Deepak L. Bhatt replied, "I think that’s a good question. The hypothesis has always been a good one, but I believe that in patients who are statin treated, no one has really shown an incremental benefit of HDL-raising. Of course, there are older data in patients not on statins to show that drugs like niacin are useful, but these drugs also have an effect on other lipid parameters, like LDL.
"It does appear that low HDL is a risk marker. But it may not be a modifiable risk factor. I think for the time being, the HDL hypothesis remains a hypothesis with a lot of holes in it. Moving forward, we’ll probably have more to gain by reducing LDL incrementally beyond the levels obtained with statins than with solely trying to raise HDL, unless those HDL-raising compounds we study in the future also have LDL-reduction or other properties," added Dr. Bhatt, professor of medicine at Harvard Medical School, Boston, and chief of cardiology at Veterans Affairs Boston Healthcare System.
Dr. Nicholls conceded that "this continues to be a field with a lot of uncertainty." But he asserted "there continues to be immense interest in the development of therapies targeting HDL."
Noting that, in ASSURE, RVX-208 wasn’t significantly better at raising HDL than was state-of-the-art background medical therapy including statins in the placebo arm, he said, "I think we haven’t really tested the HDL hypothesis yet." Advancing an investigational agent to phase III testing with clinical outcomes will require that the drug first demonstrate atheroma regression in a solid phase II study, he added.
The ASSURE trial was sponsored by Resverlogix. Dr. Nicholls has received research support from, and serves as a consultant to, Resverlogix and more than half a dozen other pharmaceutical companies.
AT THE ESC CONGRESS 2013
Major finding: The investigational oral HDL-raising agent RVX-208 reduced percent atheroma volume as measured by IVUS by 40% from baseline, a nonsignificant difference from the 30% reduction in placebo patients.
Data source: ASSURE, a 26-week, randomized, placebo-controlled study in which 323 patients with symptomatic coronary artery disease were randomized 3:1 to RVX-208 or placebo.
Disclosures: The study was sponsored by Resverlogix. The presenter has received research funding from, and is a paid consultant to, the company.

Losartan shown effective in Marfan syndrome
AMSTERDAM – Daily losartan significantly slowed the aortic root dilatation rate in adults with Marfan syndrome in a 3-year randomized clinical trial.
"I think we can be positive about this treatment. We can now recommend losartan in clinical practice," Dr. Maarten Groenink said at the annual congress of the European Society of Cardiology.
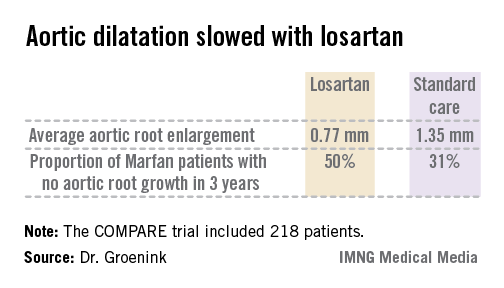
The COMPARE (Cozaar in Marfan Patients Reduces Aortic Enlargement) trial included 218 patients at all four university Marfan centers in the Netherlands. Patients were randomized to oral losartan at a target dose of 100 mg/day or no losartan in addition to standard-of-care treatment with beta-blockers. Roughly half of the patients in the losartan group were unable to tolerate the full dose of losartan in addition to a beta-blocker; those patients were maintained on losartan at 50 mg/day. Aortic root diameter was measured by MRI at enrollment and after 3 years of prospective follow-up. The aortic dilatation rate was significantly lower in the losartan group than in controls both in the patients with a native root and in those who had undergone aortic root replacement surgery, reported Dr. Groenink, a cardiologist at the Academic Medical Center, Amsterdam.

There were no aortic dissections in the losartan group and two in the control arm. Elective aortic replacement surgery was performed in a similar number of patients in both groups.
Blood pressure was lower in the losartan group, yet blood pressure didn’t correlate with the aortic dilatation rate. Dr. Groenink speculated that losartan’s chief mechanism of benefit in Marfan syndrome is its ability to curb overexpression of transforming growth factor-beta, which weakens the structure of the media layer of the aortic wall.
Dr. Groenink said it’s unknown whether losartan’s benefits are specific to that drug or are a class effect obtainable with other angiotensin II receptor antagonists, though he suspects it’s a class effect.
Ongoing clinical trials are evaluating losartan in children and adolescents with Marfan syndrome, he said, adding that there is a solid rationale for beginning treatment as early in life as possible.
"I believe the adverse effects on the aortic wall in Marfan syndrome are caused by the fibrillin defect but also by wear and tear due to cyclic stress by the beating heart. So you can hypothesize that the earlier you start treatment, the better the results," he explained.
Marfan syndrome is a genetic connective tissue disorder affecting multiple organ systems. The prognosis is mainly determined by the aortic complications, including dilatation, aneurysm formation, and possible acute dissection. Affected individuals tend to be tall, long-limbed, and have distinctively long, thin fingers. The prevalence of Marfan syndrome has been estimated at 1 in 5,000, but Dr. Groenink suspects the syndrome may actually be more common than that.
Simultaneous with Dr. Groenink’s presentation at the ESC, the COMPARE results were published online (Eur. Heart J. 2013 [doi:10.1093/eurheartj/eht334]).
The COMPARE trial was funded by the Dutch Heart Association. Dr. Groenink reported having no relevant financial interests.
*CORRECTION 11/14/13: The first version of this story had Dr. Groenink's name misspelled.

|
Bruce Jancin/IMNG Medical Media
|
COMPARE is a very important study whose results are going to mean a paradigm shift for the management of Marfan syndrome.
It is intriguing to consider that the benefits of losartan might possibly also extend to patients with thoracic aortic disease in general, a worthy topic for future investigation.
Dr. John Gordon Harold is with Cedars-Sinai Heart Institute, Los Angeles, and president of the American College of Cardiology. He had no relevant financial disclosures.
|
|
Bruce Jancin/IMNG Medical Media
|
COMPARE is a very important study whose results are going to mean a paradigm shift for the management of Marfan syndrome.
It is intriguing to consider that the benefits of losartan might possibly also extend to patients with thoracic aortic disease in general, a worthy topic for future investigation.
Dr. John Gordon Harold is with Cedars-Sinai Heart Institute, Los Angeles, and president of the American College of Cardiology. He had no relevant financial disclosures.
|
|
Bruce Jancin/IMNG Medical Media
|
COMPARE is a very important study whose results are going to mean a paradigm shift for the management of Marfan syndrome.
It is intriguing to consider that the benefits of losartan might possibly also extend to patients with thoracic aortic disease in general, a worthy topic for future investigation.
Dr. John Gordon Harold is with Cedars-Sinai Heart Institute, Los Angeles, and president of the American College of Cardiology. He had no relevant financial disclosures.
AMSTERDAM – Daily losartan significantly slowed the aortic root dilatation rate in adults with Marfan syndrome in a 3-year randomized clinical trial.
"I think we can be positive about this treatment. We can now recommend losartan in clinical practice," Dr. Maarten Groenink said at the annual congress of the European Society of Cardiology.
The COMPARE (Cozaar in Marfan Patients Reduces Aortic Enlargement) trial included 218 patients at all four university Marfan centers in the Netherlands. Patients were randomized to oral losartan at a target dose of 100 mg/day or no losartan in addition to standard-of-care treatment with beta-blockers. Roughly half of the patients in the losartan group were unable to tolerate the full dose of losartan in addition to a beta-blocker; those patients were maintained on losartan at 50 mg/day. Aortic root diameter was measured by MRI at enrollment and after 3 years of prospective follow-up. The aortic dilatation rate was significantly lower in the losartan group than in controls both in the patients with a native root and in those who had undergone aortic root replacement surgery, reported Dr. Groenink, a cardiologist at the Academic Medical Center, Amsterdam.
There were no aortic dissections in the losartan group and two in the control arm. Elective aortic replacement surgery was performed in a similar number of patients in both groups.
Blood pressure was lower in the losartan group, yet blood pressure didn’t correlate with the aortic dilatation rate. Dr. Groenink speculated that losartan’s chief mechanism of benefit in Marfan syndrome is its ability to curb overexpression of transforming growth factor-beta, which weakens the structure of the media layer of the aortic wall.
Dr. Groenink said it’s unknown whether losartan’s benefits are specific to that drug or are a class effect obtainable with other angiotensin II receptor antagonists, though he suspects it’s a class effect.
Ongoing clinical trials are evaluating losartan in children and adolescents with Marfan syndrome, he said, adding that there is a solid rationale for beginning treatment as early in life as possible.
"I believe the adverse effects on the aortic wall in Marfan syndrome are caused by the fibrillin defect but also by wear and tear due to cyclic stress by the beating heart. So you can hypothesize that the earlier you start treatment, the better the results," he explained.
Marfan syndrome is a genetic connective tissue disorder affecting multiple organ systems. The prognosis is mainly determined by the aortic complications, including dilatation, aneurysm formation, and possible acute dissection. Affected individuals tend to be tall, long-limbed, and have distinctively long, thin fingers. The prevalence of Marfan syndrome has been estimated at 1 in 5,000, but Dr. Groenink suspects the syndrome may actually be more common than that.
Simultaneous with Dr. Groenink’s presentation at the ESC, the COMPARE results were published online (Eur. Heart J. 2013 [doi:10.1093/eurheartj/eht334]).
The COMPARE trial was funded by the Dutch Heart Association. Dr. Groenink reported having no relevant financial interests.
*CORRECTION 11/14/13: The first version of this story had Dr. Groenink's name misspelled.
AMSTERDAM – Daily losartan significantly slowed the aortic root dilatation rate in adults with Marfan syndrome in a 3-year randomized clinical trial.
"I think we can be positive about this treatment. We can now recommend losartan in clinical practice," Dr. Maarten Groenink said at the annual congress of the European Society of Cardiology.
The COMPARE (Cozaar in Marfan Patients Reduces Aortic Enlargement) trial included 218 patients at all four university Marfan centers in the Netherlands. Patients were randomized to oral losartan at a target dose of 100 mg/day or no losartan in addition to standard-of-care treatment with beta-blockers. Roughly half of the patients in the losartan group were unable to tolerate the full dose of losartan in addition to a beta-blocker; those patients were maintained on losartan at 50 mg/day. Aortic root diameter was measured by MRI at enrollment and after 3 years of prospective follow-up. The aortic dilatation rate was significantly lower in the losartan group than in controls both in the patients with a native root and in those who had undergone aortic root replacement surgery, reported Dr. Groenink, a cardiologist at the Academic Medical Center, Amsterdam.
There were no aortic dissections in the losartan group and two in the control arm. Elective aortic replacement surgery was performed in a similar number of patients in both groups.
Blood pressure was lower in the losartan group, yet blood pressure didn’t correlate with the aortic dilatation rate. Dr. Groenink speculated that losartan’s chief mechanism of benefit in Marfan syndrome is its ability to curb overexpression of transforming growth factor-beta, which weakens the structure of the media layer of the aortic wall.
Dr. Groenink said it’s unknown whether losartan’s benefits are specific to that drug or are a class effect obtainable with other angiotensin II receptor antagonists, though he suspects it’s a class effect.
Ongoing clinical trials are evaluating losartan in children and adolescents with Marfan syndrome, he said, adding that there is a solid rationale for beginning treatment as early in life as possible.
"I believe the adverse effects on the aortic wall in Marfan syndrome are caused by the fibrillin defect but also by wear and tear due to cyclic stress by the beating heart. So you can hypothesize that the earlier you start treatment, the better the results," he explained.
Marfan syndrome is a genetic connective tissue disorder affecting multiple organ systems. The prognosis is mainly determined by the aortic complications, including dilatation, aneurysm formation, and possible acute dissection. Affected individuals tend to be tall, long-limbed, and have distinctively long, thin fingers. The prevalence of Marfan syndrome has been estimated at 1 in 5,000, but Dr. Groenink suspects the syndrome may actually be more common than that.
Simultaneous with Dr. Groenink’s presentation at the ESC, the COMPARE results were published online (Eur. Heart J. 2013 [doi:10.1093/eurheartj/eht334]).
The COMPARE trial was funded by the Dutch Heart Association. Dr. Groenink reported having no relevant financial interests.
*CORRECTION 11/14/13: The first version of this story had Dr. Groenink's name misspelled.
AT THE ESC CONGRESS 2013
Major finding: The rate of aortic root enlargement during 3 years of prospective follow-up was 0.77 mm in losartan-treated patients with Marfan syndrome, significantly less than the 1.35 mm in patients on standard-of-care treatment with no losartan.
Data source: The COMPARE trial was a randomized, prospective, open-label multicenter study in which 218 patients with Marfan syndrome were randomized to losartan at a target dose of 100 mg or to no losartan and followed for 3 years with the aortic root dilatation rate as measured by MRI the primary endpoint.
Disclosures: The COMPARE trial was supported by the Dutch Heart Association. Dr. Groenink reported having no financial conflicts.
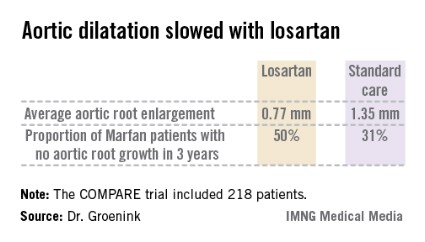
CLARIFY'ed: Angina's impact on outcomes in stable CAD
AMSTERDAM – Sixty percent of all myocardial infarctions and cardiovascular deaths in a large population of stable outpatients with coronary artery disease occurred in patients with neither anginal symptoms in daily life nor evidence of silent myocardial ischemia.
"This emphasizes the need to enforce secondary prevention measures, even in stable asymptomatic patients, Dr. Phillipe G. Steg observed at the annual congress of the European Society of Cardiology.
The risk of these adverse events was significantly greater in patients with stable coronary artery disease (CAD) who had angina than in those with neither angina nor silent myocardial ischemia, and higher still in those with both angina and silent ischemia. But in patients with silent ischemia and no angina, the risk of adverse clinical outcomes wasn’t significantly different than in patients with neither angina nor ischemia, added Dr. Steg, professor of cardiology at the University of Paris.
He presented an analysis from the CLARIFY registry, a prospective registry including 32,396 patients with stable CAD enrolled during 2009-2010 in 45 countries and followed up for 2 years. Participants had to have a baseline history of MI, chest pain with evidence of myocardial ischemia, evidence of CAD on coronary angiography, or prior PCI or CABG surgery.
For this analysis, Dr. Steg focused on the 20,402 CLARIFY participants who underwent noninvasive testing for myocardial ischemia within 1 year prior to enrollment and didn’t undergo revascularization as a result of the findings. These patients fell into four categories: 65% had neither angina nor myocardial ischemia at baseline, 9% had angina without ischemia, 15% had ischemia and no angina, and 11% had both angina and ischemia.
The absolute risk of the primary composite endpoint – cardiovascular death or nonfatal MI – was just under 4% in 2 years of follow-up in the patients with both angina and ischemia.
"I think that low rate corresponds to the modern environment of a well-treated patient population. Even though this was a global registry, patients were remarkably well treated, with a high rate of use of antiplatelet agents, lipid-lowering therapies, ACE inhibitors, and beta-blockers. I think it’s striking that two-thirds of the population had neither angina nor ischemia," he added.
In a multivariate analysis adjusted for demographics, smoking status, dyslipidemia, and diabetes, patients with angina but not silent ischemia had a statistically significant 46% greater risk of cardiovascular death or nonfatal MI than did those with neither angina nor ischemia. Patients with both angina and ischemia had a 76% greater risk than did the comparison group.
For the secondary composite endpoint consisting of cardiovascular death, MI, stroke, or revascularization, the angina-only group was at 38% increased risk and the angina-plus-ischemia group had a 58% greater risk than did patients with neither angina nor ischemia.
Importantly, major bleeding was not linked to the presence of ischemia, angina, or both.
The CLARIFY registry was supported by Servier. Dr. Steg has received research funding from and served as a consultant to the company. He has also consulted for a dozen other pharmaceutical or medical device companies.
AMSTERDAM – Sixty percent of all myocardial infarctions and cardiovascular deaths in a large population of stable outpatients with coronary artery disease occurred in patients with neither anginal symptoms in daily life nor evidence of silent myocardial ischemia.
"This emphasizes the need to enforce secondary prevention measures, even in stable asymptomatic patients, Dr. Phillipe G. Steg observed at the annual congress of the European Society of Cardiology.
The risk of these adverse events was significantly greater in patients with stable coronary artery disease (CAD) who had angina than in those with neither angina nor silent myocardial ischemia, and higher still in those with both angina and silent ischemia. But in patients with silent ischemia and no angina, the risk of adverse clinical outcomes wasn’t significantly different than in patients with neither angina nor ischemia, added Dr. Steg, professor of cardiology at the University of Paris.
He presented an analysis from the CLARIFY registry, a prospective registry including 32,396 patients with stable CAD enrolled during 2009-2010 in 45 countries and followed up for 2 years. Participants had to have a baseline history of MI, chest pain with evidence of myocardial ischemia, evidence of CAD on coronary angiography, or prior PCI or CABG surgery.
For this analysis, Dr. Steg focused on the 20,402 CLARIFY participants who underwent noninvasive testing for myocardial ischemia within 1 year prior to enrollment and didn’t undergo revascularization as a result of the findings. These patients fell into four categories: 65% had neither angina nor myocardial ischemia at baseline, 9% had angina without ischemia, 15% had ischemia and no angina, and 11% had both angina and ischemia.
The absolute risk of the primary composite endpoint – cardiovascular death or nonfatal MI – was just under 4% in 2 years of follow-up in the patients with both angina and ischemia.
"I think that low rate corresponds to the modern environment of a well-treated patient population. Even though this was a global registry, patients were remarkably well treated, with a high rate of use of antiplatelet agents, lipid-lowering therapies, ACE inhibitors, and beta-blockers. I think it’s striking that two-thirds of the population had neither angina nor ischemia," he added.
In a multivariate analysis adjusted for demographics, smoking status, dyslipidemia, and diabetes, patients with angina but not silent ischemia had a statistically significant 46% greater risk of cardiovascular death or nonfatal MI than did those with neither angina nor ischemia. Patients with both angina and ischemia had a 76% greater risk than did the comparison group.
For the secondary composite endpoint consisting of cardiovascular death, MI, stroke, or revascularization, the angina-only group was at 38% increased risk and the angina-plus-ischemia group had a 58% greater risk than did patients with neither angina nor ischemia.
Importantly, major bleeding was not linked to the presence of ischemia, angina, or both.
The CLARIFY registry was supported by Servier. Dr. Steg has received research funding from and served as a consultant to the company. He has also consulted for a dozen other pharmaceutical or medical device companies.
AMSTERDAM – Sixty percent of all myocardial infarctions and cardiovascular deaths in a large population of stable outpatients with coronary artery disease occurred in patients with neither anginal symptoms in daily life nor evidence of silent myocardial ischemia.
"This emphasizes the need to enforce secondary prevention measures, even in stable asymptomatic patients, Dr. Phillipe G. Steg observed at the annual congress of the European Society of Cardiology.
The risk of these adverse events was significantly greater in patients with stable coronary artery disease (CAD) who had angina than in those with neither angina nor silent myocardial ischemia, and higher still in those with both angina and silent ischemia. But in patients with silent ischemia and no angina, the risk of adverse clinical outcomes wasn’t significantly different than in patients with neither angina nor ischemia, added Dr. Steg, professor of cardiology at the University of Paris.
He presented an analysis from the CLARIFY registry, a prospective registry including 32,396 patients with stable CAD enrolled during 2009-2010 in 45 countries and followed up for 2 years. Participants had to have a baseline history of MI, chest pain with evidence of myocardial ischemia, evidence of CAD on coronary angiography, or prior PCI or CABG surgery.
For this analysis, Dr. Steg focused on the 20,402 CLARIFY participants who underwent noninvasive testing for myocardial ischemia within 1 year prior to enrollment and didn’t undergo revascularization as a result of the findings. These patients fell into four categories: 65% had neither angina nor myocardial ischemia at baseline, 9% had angina without ischemia, 15% had ischemia and no angina, and 11% had both angina and ischemia.
The absolute risk of the primary composite endpoint – cardiovascular death or nonfatal MI – was just under 4% in 2 years of follow-up in the patients with both angina and ischemia.
"I think that low rate corresponds to the modern environment of a well-treated patient population. Even though this was a global registry, patients were remarkably well treated, with a high rate of use of antiplatelet agents, lipid-lowering therapies, ACE inhibitors, and beta-blockers. I think it’s striking that two-thirds of the population had neither angina nor ischemia," he added.
In a multivariate analysis adjusted for demographics, smoking status, dyslipidemia, and diabetes, patients with angina but not silent ischemia had a statistically significant 46% greater risk of cardiovascular death or nonfatal MI than did those with neither angina nor ischemia. Patients with both angina and ischemia had a 76% greater risk than did the comparison group.
For the secondary composite endpoint consisting of cardiovascular death, MI, stroke, or revascularization, the angina-only group was at 38% increased risk and the angina-plus-ischemia group had a 58% greater risk than did patients with neither angina nor ischemia.
Importantly, major bleeding was not linked to the presence of ischemia, angina, or both.
The CLARIFY registry was supported by Servier. Dr. Steg has received research funding from and served as a consultant to the company. He has also consulted for a dozen other pharmaceutical or medical device companies.
AT THE ESC CONGRESS 2013
Major finding: Patients with stable coronary artery disease who had angina in their daily life but not silent ischemia had a 46% greater 2-year risk of cardiovascular death or nonfatal MI than did those with neither angina nor ischemia. Those with both angina and ischemia were at 76% increased risk of the composite endpoint.
Data source: This was a prospective registry with 2-year follow-up of more than 32,000 patients with stable coronary artery disease in 45 countries.
Disclosures: The CLARIFY registry was supported by Servier. The presenter is a consultant to the company.
Just over a third of hypertensive kidney patients are at target BP
AMSTERDAM – Eighty percent of Americans with chronic kidney disease have comorbid hypertension, which is controlled in only 36% of cases, according to a large national study.
This is an area of significant unmet medical need in spite of the wide availability of antihypertensive medications, Panagiotis Mavros, Ph.D., said at the annual congress of the European Society of Cardiology.
He presented a cross-sectional study involving 159,306 American adults with stage 1-4 chronic kidney disease (CKD) identified in the GE Centricity electronic medical record database. Fifty-seven percent were in stage 3 and 29% were in stage 2 CKD.
Roughly 43% of this very large group of CKD patients carried the diagnosis of diabetes mellitus. Eighty percent of the CKD population had hypertension, including 10% of the overall study population with previously undiagnosed hypertension. Among the CKD patients with hypertension, 15% were not being treated for it, said Dr. Mavros of Merck in Whitehouse Station, N.J.
Blood pressure was controlled to the target of less than 130/80 mm Hg in 36% of patients with diagnosed hypertension.
Seventy-three percent of treated hypertensive patients with CKD were on combination therapy, typically with three different classes of antihypertensive drugs. Patients on more than three different classes of antihypertensive medications tended to have more advanced CKD. However, the proportion of treated patients with good blood pressure control did not differ according to CKD stage.
This cross-sectional study was funded by Merck. Dr. Mavros is a full-time company employee.
AMSTERDAM – Eighty percent of Americans with chronic kidney disease have comorbid hypertension, which is controlled in only 36% of cases, according to a large national study.
This is an area of significant unmet medical need in spite of the wide availability of antihypertensive medications, Panagiotis Mavros, Ph.D., said at the annual congress of the European Society of Cardiology.
He presented a cross-sectional study involving 159,306 American adults with stage 1-4 chronic kidney disease (CKD) identified in the GE Centricity electronic medical record database. Fifty-seven percent were in stage 3 and 29% were in stage 2 CKD.
Roughly 43% of this very large group of CKD patients carried the diagnosis of diabetes mellitus. Eighty percent of the CKD population had hypertension, including 10% of the overall study population with previously undiagnosed hypertension. Among the CKD patients with hypertension, 15% were not being treated for it, said Dr. Mavros of Merck in Whitehouse Station, N.J.
Blood pressure was controlled to the target of less than 130/80 mm Hg in 36% of patients with diagnosed hypertension.
Seventy-three percent of treated hypertensive patients with CKD were on combination therapy, typically with three different classes of antihypertensive drugs. Patients on more than three different classes of antihypertensive medications tended to have more advanced CKD. However, the proportion of treated patients with good blood pressure control did not differ according to CKD stage.
This cross-sectional study was funded by Merck. Dr. Mavros is a full-time company employee.
AMSTERDAM – Eighty percent of Americans with chronic kidney disease have comorbid hypertension, which is controlled in only 36% of cases, according to a large national study.
This is an area of significant unmet medical need in spite of the wide availability of antihypertensive medications, Panagiotis Mavros, Ph.D., said at the annual congress of the European Society of Cardiology.
He presented a cross-sectional study involving 159,306 American adults with stage 1-4 chronic kidney disease (CKD) identified in the GE Centricity electronic medical record database. Fifty-seven percent were in stage 3 and 29% were in stage 2 CKD.
Roughly 43% of this very large group of CKD patients carried the diagnosis of diabetes mellitus. Eighty percent of the CKD population had hypertension, including 10% of the overall study population with previously undiagnosed hypertension. Among the CKD patients with hypertension, 15% were not being treated for it, said Dr. Mavros of Merck in Whitehouse Station, N.J.
Blood pressure was controlled to the target of less than 130/80 mm Hg in 36% of patients with diagnosed hypertension.
Seventy-three percent of treated hypertensive patients with CKD were on combination therapy, typically with three different classes of antihypertensive drugs. Patients on more than three different classes of antihypertensive medications tended to have more advanced CKD. However, the proportion of treated patients with good blood pressure control did not differ according to CKD stage.
This cross-sectional study was funded by Merck. Dr. Mavros is a full-time company employee.
AT THE ESC CONGRESS 2013
Just over a third of hypertensive kidney patients are at target BP
AMSTERDAM – Eighty percent of Americans with chronic kidney disease have comorbid hypertension, which is controlled in only 36% of cases, according to a large national study.
This is an area of significant unmet medical need in spite of the wide availability of antihypertensive medications, Panagiotis Mavros, Ph.D., said at the annual congress of the European Society of Cardiology.
He presented a cross-sectional study involving 159,306 American adults with stage 1-4 chronic kidney disease (CKD) identified in the GE Centricity electronic medical record database. Fifty-seven percent were in stage 3 and 29% were in stage 2 CKD.
Roughly 43% of this very large group of CKD patients carried the diagnosis of diabetes mellitus. Eighty percent of the CKD population had hypertension, including 10% of the overall study population with previously undiagnosed hypertension. Among the CKD patients with hypertension, 15% were not being treated for it, said Dr. Mavros of Merck in Whitehouse Station, N.J.
Blood pressure was controlled to the target of less than 130/80 mm Hg in 36% of patients with diagnosed hypertension.
Seventy-three percent of treated hypertensive patients with CKD were on combination therapy, typically with three different classes of antihypertensive drugs. Patients on more than three different classes of antihypertensive medications tended to have more advanced CKD. However, the proportion of treated patients with good blood pressure control did not differ according to CKD stage.
This cross-sectional study was funded by Merck. Dr. Mavros is a full-time company employee.
AMSTERDAM – Eighty percent of Americans with chronic kidney disease have comorbid hypertension, which is controlled in only 36% of cases, according to a large national study.
This is an area of significant unmet medical need in spite of the wide availability of antihypertensive medications, Panagiotis Mavros, Ph.D., said at the annual congress of the European Society of Cardiology.
He presented a cross-sectional study involving 159,306 American adults with stage 1-4 chronic kidney disease (CKD) identified in the GE Centricity electronic medical record database. Fifty-seven percent were in stage 3 and 29% were in stage 2 CKD.
Roughly 43% of this very large group of CKD patients carried the diagnosis of diabetes mellitus. Eighty percent of the CKD population had hypertension, including 10% of the overall study population with previously undiagnosed hypertension. Among the CKD patients with hypertension, 15% were not being treated for it, said Dr. Mavros of Merck in Whitehouse Station, N.J.
Blood pressure was controlled to the target of less than 130/80 mm Hg in 36% of patients with diagnosed hypertension.
Seventy-three percent of treated hypertensive patients with CKD were on combination therapy, typically with three different classes of antihypertensive drugs. Patients on more than three different classes of antihypertensive medications tended to have more advanced CKD. However, the proportion of treated patients with good blood pressure control did not differ according to CKD stage.
This cross-sectional study was funded by Merck. Dr. Mavros is a full-time company employee.
AMSTERDAM – Eighty percent of Americans with chronic kidney disease have comorbid hypertension, which is controlled in only 36% of cases, according to a large national study.
This is an area of significant unmet medical need in spite of the wide availability of antihypertensive medications, Panagiotis Mavros, Ph.D., said at the annual congress of the European Society of Cardiology.
He presented a cross-sectional study involving 159,306 American adults with stage 1-4 chronic kidney disease (CKD) identified in the GE Centricity electronic medical record database. Fifty-seven percent were in stage 3 and 29% were in stage 2 CKD.
Roughly 43% of this very large group of CKD patients carried the diagnosis of diabetes mellitus. Eighty percent of the CKD population had hypertension, including 10% of the overall study population with previously undiagnosed hypertension. Among the CKD patients with hypertension, 15% were not being treated for it, said Dr. Mavros of Merck in Whitehouse Station, N.J.
Blood pressure was controlled to the target of less than 130/80 mm Hg in 36% of patients with diagnosed hypertension.
Seventy-three percent of treated hypertensive patients with CKD were on combination therapy, typically with three different classes of antihypertensive drugs. Patients on more than three different classes of antihypertensive medications tended to have more advanced CKD. However, the proportion of treated patients with good blood pressure control did not differ according to CKD stage.
This cross-sectional study was funded by Merck. Dr. Mavros is a full-time company employee.
AT THE ESC CONGRESS 2013
Major finding: Of a large group of patients with chronic kidney disease and comorbid hypertension, 36% were at the blood pressure goal of less than 130/80 mm Hg.
Data source: A cross-sectional study involving more than 159,000 U.S. adults with stage 1-4 chronic kidney disease, 80% of whom had comorbid hypertension.
Disclosures: The study was funded by Merck. The presenter is a full-time employee of the pharmaceutical company.
CHA2DS2-VASc score performs best in assessing atrial fibrillation stroke risk
AMSTERDAM – Use of the CHA2DS2-VASc score markedly improves classification of atrial fibrillation patients who are truly at low risk of stroke, compared with the commonly used CHADS2 score, a German national study found.
"We do not feel that a CHADS2 risk score of 0 or 1 is suitable to identify low-risk patients. The CHA2DS2-VASc score provides a more refined risk stratification in low-risk patients. In the real life, prospective German AFNET [German Competence Network on Atrial Fibrillation] registry, a CHA2DS2-VASc score of 0 identifies a subgroup of patients with very low stroke risk unlikely to benefit from oral anticoagulation therapy," Dr. Michael Näbauer said at the annual congress of the European Society of Cardiology.
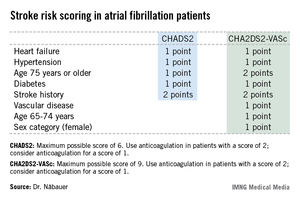
Among 795 patients in the AFNET registry who had a CHA2DS2-VASc score of 0, only 8 correctly categorized patients had a nonprocedurally related stroke, transient ischemic attack (TIA), or thromboembolism during 5 years of prospective follow-up, reported Dr. Näbauer, head of the echocardiographic unit at Ludwig Maximilians University Hospital, Munich.
A transcontinental split exists at present regarding the best clinical decision tool for assessing stroke risk in patients with atrial fibrillation (AF), and thus identifying those in whom oral anticoagulation is or is not warranted. Current American guidelines recommend using the CHADS2 score, while more recent ESC guidelines released last year advocate superseding CHADS2 with the newer CHA2DS2-VASc scoring system (Eur. Heart J. 2012;33:2719-47).

Dr. Näbauer’s report from the German AFNET registry highlighted the advantages of using CHA2DS2-VASc. Among 8,847 patients with nonvalvular AF participating in the registry run by physicians having a special interest in atrial fibrillation, 16.2% were assigned a CHADS2 score of 0 and 31.5% had a score of 1, meaning their stroke risk going forward was too low to justify the routine use of prophylactic oral anticoagulation therapy, with its attendant bleeding risk.
Here’s the deal killer for the CHADS2 scoring system, he said: Of the 403 stroke, TIA, and thromboembolic events that occurred in the nearly 9,000 AF patients during 5 years of prospective follow-up, 36% occurred in patients with a CHADS2 score of 0 or 1.
"This finding suggests that CHADS2 classes 0 and 1 contain subgroups of patients with significant stroke risk that may be identified by refined stroke risk classification," the cardiologist noted.
Application of the CHA2DS2-VASc score to the AFNET population resulted in reclassification of 126 of the 145 CHADS2 class 0 or 1 patients who had a stroke, TIA, or thromboembolism to a higher-risk CHA2DS2-VASc category where oral anticoagulation is appropriate.
Of the 45 stroke events that occurred among 1,430 patients who were CHADS2 class 0, 12 events occurred in patients who were CHA2DS2-VASc class 2 and 14 in CHA2DS2-VASc class 1 – groups in which oral anticoagulation is recommended.
Moreover, 4 of the 19 stroke events occurring in the 795 patients who were CHA2DS2-VASc class 0 happened in association with AF ablation or cardioversion procedures, when oral anticoagulation is temporarily discontinued. Another seven stroke events occurred in patients whose true CHA2DS2-VASc score had increased from 0 during follow-up, mainly because of advancing age. So ultimately only 8 of 795 patients correctly classified as CHA2DS2-VASc 0 had a stroke event unrelated to a cardiac procedure during 5 years of follow-up.

Session cochair Dr. Robert Hatala said that the AFNET experience highlights an important clinical lesson: Stroke risk in AF patients is not static. It changes over time, and periodic reassessment is essential.
"All of the risk scores are imperfect. It’s really very important to relook at your patients and not give them a fixed stamp forever. The risk scores change over time as patients get older, perhaps receive a diagnosis of hypertension, or develop congestive heart failure, maybe with preserved systolic function. So restratify," urged Dr. Hatala, head of cardiology and director of the arrhythmia and pacing center at Slovak Medical University, Bratislava, Slovakia.
Dr. Näbauer and Dr. Hatala reported having no relevant financial conflicts.
AMSTERDAM – Use of the CHA2DS2-VASc score markedly improves classification of atrial fibrillation patients who are truly at low risk of stroke, compared with the commonly used CHADS2 score, a German national study found.
"We do not feel that a CHADS2 risk score of 0 or 1 is suitable to identify low-risk patients. The CHA2DS2-VASc score provides a more refined risk stratification in low-risk patients. In the real life, prospective German AFNET [German Competence Network on Atrial Fibrillation] registry, a CHA2DS2-VASc score of 0 identifies a subgroup of patients with very low stroke risk unlikely to benefit from oral anticoagulation therapy," Dr. Michael Näbauer said at the annual congress of the European Society of Cardiology.
Among 795 patients in the AFNET registry who had a CHA2DS2-VASc score of 0, only 8 correctly categorized patients had a nonprocedurally related stroke, transient ischemic attack (TIA), or thromboembolism during 5 years of prospective follow-up, reported Dr. Näbauer, head of the echocardiographic unit at Ludwig Maximilians University Hospital, Munich.
A transcontinental split exists at present regarding the best clinical decision tool for assessing stroke risk in patients with atrial fibrillation (AF), and thus identifying those in whom oral anticoagulation is or is not warranted. Current American guidelines recommend using the CHADS2 score, while more recent ESC guidelines released last year advocate superseding CHADS2 with the newer CHA2DS2-VASc scoring system (Eur. Heart J. 2012;33:2719-47).
Dr. Näbauer’s report from the German AFNET registry highlighted the advantages of using CHA2DS2-VASc. Among 8,847 patients with nonvalvular AF participating in the registry run by physicians having a special interest in atrial fibrillation, 16.2% were assigned a CHADS2 score of 0 and 31.5% had a score of 1, meaning their stroke risk going forward was too low to justify the routine use of prophylactic oral anticoagulation therapy, with its attendant bleeding risk.
Here’s the deal killer for the CHADS2 scoring system, he said: Of the 403 stroke, TIA, and thromboembolic events that occurred in the nearly 9,000 AF patients during 5 years of prospective follow-up, 36% occurred in patients with a CHADS2 score of 0 or 1.
"This finding suggests that CHADS2 classes 0 and 1 contain subgroups of patients with significant stroke risk that may be identified by refined stroke risk classification," the cardiologist noted.
Application of the CHA2DS2-VASc score to the AFNET population resulted in reclassification of 126 of the 145 CHADS2 class 0 or 1 patients who had a stroke, TIA, or thromboembolism to a higher-risk CHA2DS2-VASc category where oral anticoagulation is appropriate.
Of the 45 stroke events that occurred among 1,430 patients who were CHADS2 class 0, 12 events occurred in patients who were CHA2DS2-VASc class 2 and 14 in CHA2DS2-VASc class 1 – groups in which oral anticoagulation is recommended.
Moreover, 4 of the 19 stroke events occurring in the 795 patients who were CHA2DS2-VASc class 0 happened in association with AF ablation or cardioversion procedures, when oral anticoagulation is temporarily discontinued. Another seven stroke events occurred in patients whose true CHA2DS2-VASc score had increased from 0 during follow-up, mainly because of advancing age. So ultimately only 8 of 795 patients correctly classified as CHA2DS2-VASc 0 had a stroke event unrelated to a cardiac procedure during 5 years of follow-up.
Session cochair Dr. Robert Hatala said that the AFNET experience highlights an important clinical lesson: Stroke risk in AF patients is not static. It changes over time, and periodic reassessment is essential.
"All of the risk scores are imperfect. It’s really very important to relook at your patients and not give them a fixed stamp forever. The risk scores change over time as patients get older, perhaps receive a diagnosis of hypertension, or develop congestive heart failure, maybe with preserved systolic function. So restratify," urged Dr. Hatala, head of cardiology and director of the arrhythmia and pacing center at Slovak Medical University, Bratislava, Slovakia.
Dr. Näbauer and Dr. Hatala reported having no relevant financial conflicts.
AMSTERDAM – Use of the CHA2DS2-VASc score markedly improves classification of atrial fibrillation patients who are truly at low risk of stroke, compared with the commonly used CHADS2 score, a German national study found.
"We do not feel that a CHADS2 risk score of 0 or 1 is suitable to identify low-risk patients. The CHA2DS2-VASc score provides a more refined risk stratification in low-risk patients. In the real life, prospective German AFNET [German Competence Network on Atrial Fibrillation] registry, a CHA2DS2-VASc score of 0 identifies a subgroup of patients with very low stroke risk unlikely to benefit from oral anticoagulation therapy," Dr. Michael Näbauer said at the annual congress of the European Society of Cardiology.
Among 795 patients in the AFNET registry who had a CHA2DS2-VASc score of 0, only 8 correctly categorized patients had a nonprocedurally related stroke, transient ischemic attack (TIA), or thromboembolism during 5 years of prospective follow-up, reported Dr. Näbauer, head of the echocardiographic unit at Ludwig Maximilians University Hospital, Munich.
A transcontinental split exists at present regarding the best clinical decision tool for assessing stroke risk in patients with atrial fibrillation (AF), and thus identifying those in whom oral anticoagulation is or is not warranted. Current American guidelines recommend using the CHADS2 score, while more recent ESC guidelines released last year advocate superseding CHADS2 with the newer CHA2DS2-VASc scoring system (Eur. Heart J. 2012;33:2719-47).
Dr. Näbauer’s report from the German AFNET registry highlighted the advantages of using CHA2DS2-VASc. Among 8,847 patients with nonvalvular AF participating in the registry run by physicians having a special interest in atrial fibrillation, 16.2% were assigned a CHADS2 score of 0 and 31.5% had a score of 1, meaning their stroke risk going forward was too low to justify the routine use of prophylactic oral anticoagulation therapy, with its attendant bleeding risk.
Here’s the deal killer for the CHADS2 scoring system, he said: Of the 403 stroke, TIA, and thromboembolic events that occurred in the nearly 9,000 AF patients during 5 years of prospective follow-up, 36% occurred in patients with a CHADS2 score of 0 or 1.
"This finding suggests that CHADS2 classes 0 and 1 contain subgroups of patients with significant stroke risk that may be identified by refined stroke risk classification," the cardiologist noted.
Application of the CHA2DS2-VASc score to the AFNET population resulted in reclassification of 126 of the 145 CHADS2 class 0 or 1 patients who had a stroke, TIA, or thromboembolism to a higher-risk CHA2DS2-VASc category where oral anticoagulation is appropriate.
Of the 45 stroke events that occurred among 1,430 patients who were CHADS2 class 0, 12 events occurred in patients who were CHA2DS2-VASc class 2 and 14 in CHA2DS2-VASc class 1 – groups in which oral anticoagulation is recommended.
Moreover, 4 of the 19 stroke events occurring in the 795 patients who were CHA2DS2-VASc class 0 happened in association with AF ablation or cardioversion procedures, when oral anticoagulation is temporarily discontinued. Another seven stroke events occurred in patients whose true CHA2DS2-VASc score had increased from 0 during follow-up, mainly because of advancing age. So ultimately only 8 of 795 patients correctly classified as CHA2DS2-VASc 0 had a stroke event unrelated to a cardiac procedure during 5 years of follow-up.
Session cochair Dr. Robert Hatala said that the AFNET experience highlights an important clinical lesson: Stroke risk in AF patients is not static. It changes over time, and periodic reassessment is essential.
"All of the risk scores are imperfect. It’s really very important to relook at your patients and not give them a fixed stamp forever. The risk scores change over time as patients get older, perhaps receive a diagnosis of hypertension, or develop congestive heart failure, maybe with preserved systolic function. So restratify," urged Dr. Hatala, head of cardiology and director of the arrhythmia and pacing center at Slovak Medical University, Bratislava, Slovakia.
Dr. Näbauer and Dr. Hatala reported having no relevant financial conflicts.
AT THE ESC CONGRESS 2013
Major finding: During 5 years of prospective follow-up of patients with nonvalvular atrial fibrillation, 145 patients who had a stroke, transient ischemic attack, or thromboembolism also had a CHADS2 score indicating a low risk for stroke, compared with only 19 who had one of those events and were classified as low risk by the CHA2DS2-VASc stroke risk scoring system.
Data source: The German AFNET registry, a real-world, prospective national registry including 8,847 patients with nonvalvular atrial fibrillation.
Disclosures: The AFNET registry is publically funded by the German Federal Ministry for Education and Research. Dr. Näbauer and Dr. Hatala reported having no relevant financial conflicts.
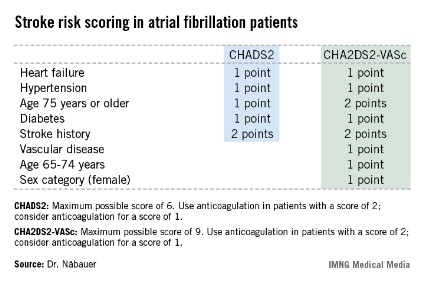
Diabetic Patients' Stroke Risk Post MI has Plummeted
AMSTERDAM – The risk of ischemic stroke following an acute myocardial infarction in diabetes patients dropped markedly during a recent 10-year period, according to a nationwide Swedish study.
Indeed, the reduction in ischemic stroke risk during the first year after an MI was significantly larger in diabetic than in nondiabetic patients over the course of a decade, Stina Jakobsson said at the annual congress of the European Society of Cardiology.
"We believe that the larger risk reduction seen in the diabetic patients may indicate that they have gained more from the increased use of evidence-based secondary preventive treatment," added Ms. Jakobsson, a medical student at Umea (Sweden) University.
She presented an analysis of all 173,233 patients discharged from Swedish coronary care units after an acute MI during 1998-2008. A total of 19% of them had a previous diagnosis of diabetes.
Among diabetes patients with an MI in 1998-2000, ischemic stroke occurred in 7.1% within 1 year after their coronary event. However, the 1-year ischemic stroke rate in such patients whose MI occurred in 2007-2008 dropped to 4.7%. This was a much more impressive improvement than occurred in the same time span among nondiabetic patients, where the ischemic stroke rate during the first year after an acute MI was 4.2% in 1998-2000, nudging downward to 3.7% in 2007-2008.
Ms. Jakobsson stressed that there is definitely room for improvement in the use of reperfusion therapy and secondary preventive medications among diabetes patients with an MI. Although the use of these key interventions increased over time in both diabetic and nondiabetic MI patients, rates still remained lower in the diabetic group in the most recent study years.
The 4.7% 1-year incidence of ischemic stroke among Swedish diabetes patients with an acute MI in 2007-2008 was significantly greater than the 3.7% rate among nondiabetic patients. Moreover, even among patients on optimized secondary prevention therapies, the ischemic stroke rate was higher in the diabetic group. That’s not surprising because they more often had a history of prior cardiovascular disease at the time of their acute MI.
"They were sicker to start with," Ms. Jakobsson observed.
The most powerful predictors of increased risk of ischemic stroke post MI included older age, atrial fibrillation, an ST-elevation MI, and prior ischemic stroke.
This study was supported by Swedish governmental research funds. Ms. Jakobsson reported having no financial conflicts of interest.
AMSTERDAM – The risk of ischemic stroke following an acute myocardial infarction in diabetes patients dropped markedly during a recent 10-year period, according to a nationwide Swedish study.
Indeed, the reduction in ischemic stroke risk during the first year after an MI was significantly larger in diabetic than in nondiabetic patients over the course of a decade, Stina Jakobsson said at the annual congress of the European Society of Cardiology.
"We believe that the larger risk reduction seen in the diabetic patients may indicate that they have gained more from the increased use of evidence-based secondary preventive treatment," added Ms. Jakobsson, a medical student at Umea (Sweden) University.
She presented an analysis of all 173,233 patients discharged from Swedish coronary care units after an acute MI during 1998-2008. A total of 19% of them had a previous diagnosis of diabetes.
Among diabetes patients with an MI in 1998-2000, ischemic stroke occurred in 7.1% within 1 year after their coronary event. However, the 1-year ischemic stroke rate in such patients whose MI occurred in 2007-2008 dropped to 4.7%. This was a much more impressive improvement than occurred in the same time span among nondiabetic patients, where the ischemic stroke rate during the first year after an acute MI was 4.2% in 1998-2000, nudging downward to 3.7% in 2007-2008.
Ms. Jakobsson stressed that there is definitely room for improvement in the use of reperfusion therapy and secondary preventive medications among diabetes patients with an MI. Although the use of these key interventions increased over time in both diabetic and nondiabetic MI patients, rates still remained lower in the diabetic group in the most recent study years.
The 4.7% 1-year incidence of ischemic stroke among Swedish diabetes patients with an acute MI in 2007-2008 was significantly greater than the 3.7% rate among nondiabetic patients. Moreover, even among patients on optimized secondary prevention therapies, the ischemic stroke rate was higher in the diabetic group. That’s not surprising because they more often had a history of prior cardiovascular disease at the time of their acute MI.
"They were sicker to start with," Ms. Jakobsson observed.
The most powerful predictors of increased risk of ischemic stroke post MI included older age, atrial fibrillation, an ST-elevation MI, and prior ischemic stroke.
This study was supported by Swedish governmental research funds. Ms. Jakobsson reported having no financial conflicts of interest.
AMSTERDAM – The risk of ischemic stroke following an acute myocardial infarction in diabetes patients dropped markedly during a recent 10-year period, according to a nationwide Swedish study.
Indeed, the reduction in ischemic stroke risk during the first year after an MI was significantly larger in diabetic than in nondiabetic patients over the course of a decade, Stina Jakobsson said at the annual congress of the European Society of Cardiology.
"We believe that the larger risk reduction seen in the diabetic patients may indicate that they have gained more from the increased use of evidence-based secondary preventive treatment," added Ms. Jakobsson, a medical student at Umea (Sweden) University.
She presented an analysis of all 173,233 patients discharged from Swedish coronary care units after an acute MI during 1998-2008. A total of 19% of them had a previous diagnosis of diabetes.
Among diabetes patients with an MI in 1998-2000, ischemic stroke occurred in 7.1% within 1 year after their coronary event. However, the 1-year ischemic stroke rate in such patients whose MI occurred in 2007-2008 dropped to 4.7%. This was a much more impressive improvement than occurred in the same time span among nondiabetic patients, where the ischemic stroke rate during the first year after an acute MI was 4.2% in 1998-2000, nudging downward to 3.7% in 2007-2008.
Ms. Jakobsson stressed that there is definitely room for improvement in the use of reperfusion therapy and secondary preventive medications among diabetes patients with an MI. Although the use of these key interventions increased over time in both diabetic and nondiabetic MI patients, rates still remained lower in the diabetic group in the most recent study years.
The 4.7% 1-year incidence of ischemic stroke among Swedish diabetes patients with an acute MI in 2007-2008 was significantly greater than the 3.7% rate among nondiabetic patients. Moreover, even among patients on optimized secondary prevention therapies, the ischemic stroke rate was higher in the diabetic group. That’s not surprising because they more often had a history of prior cardiovascular disease at the time of their acute MI.
"They were sicker to start with," Ms. Jakobsson observed.
The most powerful predictors of increased risk of ischemic stroke post MI included older age, atrial fibrillation, an ST-elevation MI, and prior ischemic stroke.
This study was supported by Swedish governmental research funds. Ms. Jakobsson reported having no financial conflicts of interest.
AT THE ESC CONGRESS 2013
