User login
The Three-Year Plan
Although 2019 may seem like a long way away, it isn’t too soon to start thinking about and preparing for the Merit-based Incentive Payment System (MIPS) or its (seemingly preferable) alternative, participation in an alternative payment model (APM) such as an ACO, a medical home, or a bundled payment program.
In April, Congress permanently repealed Medicare’s sustainable growth rate (SGR) formula for controlling physician payment. In yet another sign that we are in the midst of the biggest healthcare transformation in a generation, the 18-year-old SGR formula will be replaced by a far-reaching package of payment reforms. Here we will focus on the MIPS and its alternative, an APM, which involves assuming risk for financial loss or gain and measuring and reporting on quality.
The MIPS replaces three existing quality measurement programs that, to greater and lesser degrees, physicians have struggled with:
- Physician Quality Reporting System (PQRS);
- Value-based payment modifier; and
- Meaningful use of electronic health records.
MIPS will not totally eliminate these programs but will instead incorporate yet-to-be-defined elements of them and, presumably, though it is yet unclear, add new elements. For 2015-2018, the current payment system will remain intact. For 2019, physicians will have a choice. Either they must participate in MIPS, which will likely be complex and involve some administrative burden, or derive at least 25% of their practice revenue from an APM.
For those participating in MIPS, physician payment rates will be subject to an up or down adjustment based on performance in four categories: quality, meaningful use of EHRs, resource use, and clinical practice improvement.
There is an opportunity to avoid MIPS altogether, however. One of the most notable elements of the SGR fix is its push for physicians to participate in APMs such as ACOs, medical homes, bundled payment arrangements, and other payment models now being evaluated by the CMS Innovation Center. Physicians who gain a substantial portion—this means 25% in 2019 and 2020, and likely more thereafter—of their revenue through APMs like these will have the dual benefit of being exempt from MIPS participation and receiving a 5% annual bonus through 2024. After that, physicians in APMs will receive annual fee increases of 0.75%, while all other physicians will receive only a 0.25% increase.1
Strategic Thinking for Hospitalists: Enter an APM
If you’re asking yourself where you want your hospitalist practice to be in three years, I would suggest the answer is “in an alternative payment model of one kind or another.”
If you are an employed practice, strategic planning will involve assessing the APMs your hospital or health system is participating in and planning how your hospitalist practice can become a formal member of the arrangement.
If you are a freestanding practice, you should become a student of the APM policy coming from the CMS Innovation Center, and determine the best “insertion point” for your practice, such that you gain at least a quarter of your revenue through an APM within three years.

Reference
- Steinbrook R. The repeal of Medicare’s sustainable growth rate for physician payment. JAMA. 2015;313(20):2025-2026.
Obituary
Remembering Frank Michota, 1967-2015

Frank founded the “Update in Hospital Medicine” series at SHM annual meetings and in the Annals of Internal Medicine. He was a prolific speaker, writer, and teacher. More than that, Frank was an original kind of persona, one who collaborated often and led frequently, but rarely followed. Yet he had the humility to engage and contribute whenever he was asked.
I had the good fortune of working with him on a number of speaking and writing projects in the early days. I recall his charisma, irreverence, and larger-than-life presence whenever he addressed an audience.
Frank’s signature is etched forever on hospital medicine; our patients and hospitalists everywhere are the lucky beneficiaries of his work.
Although 2019 may seem like a long way away, it isn’t too soon to start thinking about and preparing for the Merit-based Incentive Payment System (MIPS) or its (seemingly preferable) alternative, participation in an alternative payment model (APM) such as an ACO, a medical home, or a bundled payment program.
In April, Congress permanently repealed Medicare’s sustainable growth rate (SGR) formula for controlling physician payment. In yet another sign that we are in the midst of the biggest healthcare transformation in a generation, the 18-year-old SGR formula will be replaced by a far-reaching package of payment reforms. Here we will focus on the MIPS and its alternative, an APM, which involves assuming risk for financial loss or gain and measuring and reporting on quality.
The MIPS replaces three existing quality measurement programs that, to greater and lesser degrees, physicians have struggled with:
- Physician Quality Reporting System (PQRS);
- Value-based payment modifier; and
- Meaningful use of electronic health records.
MIPS will not totally eliminate these programs but will instead incorporate yet-to-be-defined elements of them and, presumably, though it is yet unclear, add new elements. For 2015-2018, the current payment system will remain intact. For 2019, physicians will have a choice. Either they must participate in MIPS, which will likely be complex and involve some administrative burden, or derive at least 25% of their practice revenue from an APM.
For those participating in MIPS, physician payment rates will be subject to an up or down adjustment based on performance in four categories: quality, meaningful use of EHRs, resource use, and clinical practice improvement.
There is an opportunity to avoid MIPS altogether, however. One of the most notable elements of the SGR fix is its push for physicians to participate in APMs such as ACOs, medical homes, bundled payment arrangements, and other payment models now being evaluated by the CMS Innovation Center. Physicians who gain a substantial portion—this means 25% in 2019 and 2020, and likely more thereafter—of their revenue through APMs like these will have the dual benefit of being exempt from MIPS participation and receiving a 5% annual bonus through 2024. After that, physicians in APMs will receive annual fee increases of 0.75%, while all other physicians will receive only a 0.25% increase.1
Strategic Thinking for Hospitalists: Enter an APM
If you’re asking yourself where you want your hospitalist practice to be in three years, I would suggest the answer is “in an alternative payment model of one kind or another.”
If you are an employed practice, strategic planning will involve assessing the APMs your hospital or health system is participating in and planning how your hospitalist practice can become a formal member of the arrangement.
If you are a freestanding practice, you should become a student of the APM policy coming from the CMS Innovation Center, and determine the best “insertion point” for your practice, such that you gain at least a quarter of your revenue through an APM within three years.
Reference
- Steinbrook R. The repeal of Medicare’s sustainable growth rate for physician payment. JAMA. 2015;313(20):2025-2026.
Obituary
Remembering Frank Michota, 1967-2015
Frank founded the “Update in Hospital Medicine” series at SHM annual meetings and in the Annals of Internal Medicine. He was a prolific speaker, writer, and teacher. More than that, Frank was an original kind of persona, one who collaborated often and led frequently, but rarely followed. Yet he had the humility to engage and contribute whenever he was asked.
I had the good fortune of working with him on a number of speaking and writing projects in the early days. I recall his charisma, irreverence, and larger-than-life presence whenever he addressed an audience.
Frank’s signature is etched forever on hospital medicine; our patients and hospitalists everywhere are the lucky beneficiaries of his work.
Although 2019 may seem like a long way away, it isn’t too soon to start thinking about and preparing for the Merit-based Incentive Payment System (MIPS) or its (seemingly preferable) alternative, participation in an alternative payment model (APM) such as an ACO, a medical home, or a bundled payment program.
In April, Congress permanently repealed Medicare’s sustainable growth rate (SGR) formula for controlling physician payment. In yet another sign that we are in the midst of the biggest healthcare transformation in a generation, the 18-year-old SGR formula will be replaced by a far-reaching package of payment reforms. Here we will focus on the MIPS and its alternative, an APM, which involves assuming risk for financial loss or gain and measuring and reporting on quality.
The MIPS replaces three existing quality measurement programs that, to greater and lesser degrees, physicians have struggled with:
- Physician Quality Reporting System (PQRS);
- Value-based payment modifier; and
- Meaningful use of electronic health records.
MIPS will not totally eliminate these programs but will instead incorporate yet-to-be-defined elements of them and, presumably, though it is yet unclear, add new elements. For 2015-2018, the current payment system will remain intact. For 2019, physicians will have a choice. Either they must participate in MIPS, which will likely be complex and involve some administrative burden, or derive at least 25% of their practice revenue from an APM.
For those participating in MIPS, physician payment rates will be subject to an up or down adjustment based on performance in four categories: quality, meaningful use of EHRs, resource use, and clinical practice improvement.
There is an opportunity to avoid MIPS altogether, however. One of the most notable elements of the SGR fix is its push for physicians to participate in APMs such as ACOs, medical homes, bundled payment arrangements, and other payment models now being evaluated by the CMS Innovation Center. Physicians who gain a substantial portion—this means 25% in 2019 and 2020, and likely more thereafter—of their revenue through APMs like these will have the dual benefit of being exempt from MIPS participation and receiving a 5% annual bonus through 2024. After that, physicians in APMs will receive annual fee increases of 0.75%, while all other physicians will receive only a 0.25% increase.1
Strategic Thinking for Hospitalists: Enter an APM
If you’re asking yourself where you want your hospitalist practice to be in three years, I would suggest the answer is “in an alternative payment model of one kind or another.”
If you are an employed practice, strategic planning will involve assessing the APMs your hospital or health system is participating in and planning how your hospitalist practice can become a formal member of the arrangement.
If you are a freestanding practice, you should become a student of the APM policy coming from the CMS Innovation Center, and determine the best “insertion point” for your practice, such that you gain at least a quarter of your revenue through an APM within three years.
Reference
- Steinbrook R. The repeal of Medicare’s sustainable growth rate for physician payment. JAMA. 2015;313(20):2025-2026.
Obituary
Remembering Frank Michota, 1967-2015
Frank founded the “Update in Hospital Medicine” series at SHM annual meetings and in the Annals of Internal Medicine. He was a prolific speaker, writer, and teacher. More than that, Frank was an original kind of persona, one who collaborated often and led frequently, but rarely followed. Yet he had the humility to engage and contribute whenever he was asked.
I had the good fortune of working with him on a number of speaking and writing projects in the early days. I recall his charisma, irreverence, and larger-than-life presence whenever he addressed an audience.
Frank’s signature is etched forever on hospital medicine; our patients and hospitalists everywhere are the lucky beneficiaries of his work.
Tips for Hospitalists on Spending More of Their Time at the Top of Their License

Hospitalists spend too little time working at the top of their license. Put differently, I think a hospitalist often spends only about 1.5 to two hours in a 10- or 12-hour workday making use of the knowledge base and skills developed in training. (I wrote about this and referenced some hospitalist time-motion studies in my December 2010 column.)
The remaining hours are typically spent in activities such as figuring out which surgeon is on call and tracking her down, managing patient lists, filling out paper or electronic forms, explaining observation status to patients, and so on.
When I first became a hospitalist in the 1980s, there was already a lot of talk about the paperwork burden faced by doctors across all specialties. I recall the gnashing of teeth that ensued—lots of articles and seminars, and it seems to me even a few legislative proposals, focused on the topic. It appears that nearly every recruitment ad at the time mentioned something like “Let us take care of running the business, so you can focus solely on patient care.” Clearly, doctors were seeking relief from the burden of nonclinical work even back then.
I can’t recall reading or hearing anyone talk about the “paperwork” burden of physician practice in the past few years. This isn’t because things have gotten better; in fact, I think the burden of “non-doctoring activities” has steadily increased. We hear less about the problem of excessive paperwork simply because, more recently, it has been framed differently—it is now typically referred to as the problem of too little time spent practicing at the top of license.
Search the Internet for “top of license” and a number of interesting things turn up. Most are healthcare related—maybe other professions don’t use the term—and there are just as many links referring to nurses as physicians. Much is written about the need for primary care physicians to spend more time working at the top of their license, but I couldn’t find anything addressing this issue specifically for hospitalists.
What Can Be Done?
Moving your work as a hospitalist more to the top of your license isn’t a simple thing, and our whole field will need to work on this over time. The most effective interventions will vary some from place to place, but here are some ideas that may be relevant for many hospitalist groups.
Medication reconciliation. I fully support the idea of careful medication reconciliation, but, given that such a large portion of hospitalist patients are on so many medications, this is a time-consuming task. And, in many or most hospitals, the task suffers from diffusion of responsibility; for example, the ED nurse makes only a half-hearted attempt to get an accurate list, and the hospitalist believes that whatever the ED nurse entered into the record regarding patient medications is probably the best obtainable list.
A pharmacy technician stationed in the ED and charged with recording the best obtainable list of medicines on patient arrival can address both of these problems (for more information, the American Society of Health-System Pharmacists offers webinars and other resources on this topic). This would include calling family members, pharmacies, and physician offices for clarification in some cases. Hospitalists working in such an environment nearly always say it is extremely valuable in reducing inaccuracies in the pre-hospital medication list, as well as saving hospitalists time when they are admitting patients.
Unfortunately, hospitals may resist adding pharmacy technicians because of the expense or, in some cases, because of concerns that such work may exceed the legal scope of work for technicians.
Post-hospital appointments. I think arranging post-hospital appointments should be no more difficult for the hospitalist than ordering a complete blood count (CBC). It shouldn’t matter whether I want the patient to follow up with the PCP he has been seeing for years, or see a neurologist or diabetes educator as a new patient consult. Any treating doctor in the hospital should be able to arrange such post-hospital visits with just a click or two in the EHR, or a stroke of the pen. And the patient should leave the hospital with a written date and time of the appointment that has been made for them.
Few hospitals can reliably provide this, however, so, all too often, hospitalists spend their time calling clerical staff at outpatient clinics to arrange appointments, writing them down, and delivering them to patients. This is far from what anyone would consider top of license work. (I wrote a little more about this in last month’s column.)
Medicare benefits specialist. Many hospitalists end up spending significant time explaining to patients and families the reason a patient is on observation status and trying to defuse the resulting frustration and anger. As I stated in my November 2014 column, I think observation status is so frustrating to patients that it is often the root cause of complaints about care and, potentially, the source of malpractice suits.
Physicians have an unavoidable role in determining observation versus inpatient status, but I think hospitals should work hard to ensure that someone other than the doctor is available to explain to patients and families the reason for observation status, along with its implications, and to provide sympathy for their frustrations. This allows the doctor to stay focused on clinical care.
Limit reliance on a “triage hospitalist.” Hospitalist groups larger than about 20 providers often have one provider devoted through much of a daytime shift to triaging and assigning new referrals across all providers working that day. For larger practices, this triage work may consume all of the provider’s shift, so that person has no time left for clinical care. It is hard for me to see this as top of license work that only a physician or advanced practice clinician can do. In my December 2010 column, I provided some potential alternatives to dedicating a physician or other provider to a triage role.
Your list of important changes that are needed to move hospitalists toward more time spent working at the top of their license will likely differ a lot from the issues above. But every group could benefit from deliberately thinking about what would be most valuable for them and trying to make that a reality.

Hospitalists spend too little time working at the top of their license. Put differently, I think a hospitalist often spends only about 1.5 to two hours in a 10- or 12-hour workday making use of the knowledge base and skills developed in training. (I wrote about this and referenced some hospitalist time-motion studies in my December 2010 column.)
The remaining hours are typically spent in activities such as figuring out which surgeon is on call and tracking her down, managing patient lists, filling out paper or electronic forms, explaining observation status to patients, and so on.
When I first became a hospitalist in the 1980s, there was already a lot of talk about the paperwork burden faced by doctors across all specialties. I recall the gnashing of teeth that ensued—lots of articles and seminars, and it seems to me even a few legislative proposals, focused on the topic. It appears that nearly every recruitment ad at the time mentioned something like “Let us take care of running the business, so you can focus solely on patient care.” Clearly, doctors were seeking relief from the burden of nonclinical work even back then.
I can’t recall reading or hearing anyone talk about the “paperwork” burden of physician practice in the past few years. This isn’t because things have gotten better; in fact, I think the burden of “non-doctoring activities” has steadily increased. We hear less about the problem of excessive paperwork simply because, more recently, it has been framed differently—it is now typically referred to as the problem of too little time spent practicing at the top of license.
Search the Internet for “top of license” and a number of interesting things turn up. Most are healthcare related—maybe other professions don’t use the term—and there are just as many links referring to nurses as physicians. Much is written about the need for primary care physicians to spend more time working at the top of their license, but I couldn’t find anything addressing this issue specifically for hospitalists.
What Can Be Done?
Moving your work as a hospitalist more to the top of your license isn’t a simple thing, and our whole field will need to work on this over time. The most effective interventions will vary some from place to place, but here are some ideas that may be relevant for many hospitalist groups.
Medication reconciliation. I fully support the idea of careful medication reconciliation, but, given that such a large portion of hospitalist patients are on so many medications, this is a time-consuming task. And, in many or most hospitals, the task suffers from diffusion of responsibility; for example, the ED nurse makes only a half-hearted attempt to get an accurate list, and the hospitalist believes that whatever the ED nurse entered into the record regarding patient medications is probably the best obtainable list.
A pharmacy technician stationed in the ED and charged with recording the best obtainable list of medicines on patient arrival can address both of these problems (for more information, the American Society of Health-System Pharmacists offers webinars and other resources on this topic). This would include calling family members, pharmacies, and physician offices for clarification in some cases. Hospitalists working in such an environment nearly always say it is extremely valuable in reducing inaccuracies in the pre-hospital medication list, as well as saving hospitalists time when they are admitting patients.
Unfortunately, hospitals may resist adding pharmacy technicians because of the expense or, in some cases, because of concerns that such work may exceed the legal scope of work for technicians.
Post-hospital appointments. I think arranging post-hospital appointments should be no more difficult for the hospitalist than ordering a complete blood count (CBC). It shouldn’t matter whether I want the patient to follow up with the PCP he has been seeing for years, or see a neurologist or diabetes educator as a new patient consult. Any treating doctor in the hospital should be able to arrange such post-hospital visits with just a click or two in the EHR, or a stroke of the pen. And the patient should leave the hospital with a written date and time of the appointment that has been made for them.
Few hospitals can reliably provide this, however, so, all too often, hospitalists spend their time calling clerical staff at outpatient clinics to arrange appointments, writing them down, and delivering them to patients. This is far from what anyone would consider top of license work. (I wrote a little more about this in last month’s column.)
Medicare benefits specialist. Many hospitalists end up spending significant time explaining to patients and families the reason a patient is on observation status and trying to defuse the resulting frustration and anger. As I stated in my November 2014 column, I think observation status is so frustrating to patients that it is often the root cause of complaints about care and, potentially, the source of malpractice suits.
Physicians have an unavoidable role in determining observation versus inpatient status, but I think hospitals should work hard to ensure that someone other than the doctor is available to explain to patients and families the reason for observation status, along with its implications, and to provide sympathy for their frustrations. This allows the doctor to stay focused on clinical care.
Limit reliance on a “triage hospitalist.” Hospitalist groups larger than about 20 providers often have one provider devoted through much of a daytime shift to triaging and assigning new referrals across all providers working that day. For larger practices, this triage work may consume all of the provider’s shift, so that person has no time left for clinical care. It is hard for me to see this as top of license work that only a physician or advanced practice clinician can do. In my December 2010 column, I provided some potential alternatives to dedicating a physician or other provider to a triage role.
Your list of important changes that are needed to move hospitalists toward more time spent working at the top of their license will likely differ a lot from the issues above. But every group could benefit from deliberately thinking about what would be most valuable for them and trying to make that a reality.
Hospitalists spend too little time working at the top of their license. Put differently, I think a hospitalist often spends only about 1.5 to two hours in a 10- or 12-hour workday making use of the knowledge base and skills developed in training. (I wrote about this and referenced some hospitalist time-motion studies in my December 2010 column.)
The remaining hours are typically spent in activities such as figuring out which surgeon is on call and tracking her down, managing patient lists, filling out paper or electronic forms, explaining observation status to patients, and so on.
When I first became a hospitalist in the 1980s, there was already a lot of talk about the paperwork burden faced by doctors across all specialties. I recall the gnashing of teeth that ensued—lots of articles and seminars, and it seems to me even a few legislative proposals, focused on the topic. It appears that nearly every recruitment ad at the time mentioned something like “Let us take care of running the business, so you can focus solely on patient care.” Clearly, doctors were seeking relief from the burden of nonclinical work even back then.
I can’t recall reading or hearing anyone talk about the “paperwork” burden of physician practice in the past few years. This isn’t because things have gotten better; in fact, I think the burden of “non-doctoring activities” has steadily increased. We hear less about the problem of excessive paperwork simply because, more recently, it has been framed differently—it is now typically referred to as the problem of too little time spent practicing at the top of license.
Search the Internet for “top of license” and a number of interesting things turn up. Most are healthcare related—maybe other professions don’t use the term—and there are just as many links referring to nurses as physicians. Much is written about the need for primary care physicians to spend more time working at the top of their license, but I couldn’t find anything addressing this issue specifically for hospitalists.
What Can Be Done?
Moving your work as a hospitalist more to the top of your license isn’t a simple thing, and our whole field will need to work on this over time. The most effective interventions will vary some from place to place, but here are some ideas that may be relevant for many hospitalist groups.
Medication reconciliation. I fully support the idea of careful medication reconciliation, but, given that such a large portion of hospitalist patients are on so many medications, this is a time-consuming task. And, in many or most hospitals, the task suffers from diffusion of responsibility; for example, the ED nurse makes only a half-hearted attempt to get an accurate list, and the hospitalist believes that whatever the ED nurse entered into the record regarding patient medications is probably the best obtainable list.
A pharmacy technician stationed in the ED and charged with recording the best obtainable list of medicines on patient arrival can address both of these problems (for more information, the American Society of Health-System Pharmacists offers webinars and other resources on this topic). This would include calling family members, pharmacies, and physician offices for clarification in some cases. Hospitalists working in such an environment nearly always say it is extremely valuable in reducing inaccuracies in the pre-hospital medication list, as well as saving hospitalists time when they are admitting patients.
Unfortunately, hospitals may resist adding pharmacy technicians because of the expense or, in some cases, because of concerns that such work may exceed the legal scope of work for technicians.
Post-hospital appointments. I think arranging post-hospital appointments should be no more difficult for the hospitalist than ordering a complete blood count (CBC). It shouldn’t matter whether I want the patient to follow up with the PCP he has been seeing for years, or see a neurologist or diabetes educator as a new patient consult. Any treating doctor in the hospital should be able to arrange such post-hospital visits with just a click or two in the EHR, or a stroke of the pen. And the patient should leave the hospital with a written date and time of the appointment that has been made for them.
Few hospitals can reliably provide this, however, so, all too often, hospitalists spend their time calling clerical staff at outpatient clinics to arrange appointments, writing them down, and delivering them to patients. This is far from what anyone would consider top of license work. (I wrote a little more about this in last month’s column.)
Medicare benefits specialist. Many hospitalists end up spending significant time explaining to patients and families the reason a patient is on observation status and trying to defuse the resulting frustration and anger. As I stated in my November 2014 column, I think observation status is so frustrating to patients that it is often the root cause of complaints about care and, potentially, the source of malpractice suits.
Physicians have an unavoidable role in determining observation versus inpatient status, but I think hospitals should work hard to ensure that someone other than the doctor is available to explain to patients and families the reason for observation status, along with its implications, and to provide sympathy for their frustrations. This allows the doctor to stay focused on clinical care.
Limit reliance on a “triage hospitalist.” Hospitalist groups larger than about 20 providers often have one provider devoted through much of a daytime shift to triaging and assigning new referrals across all providers working that day. For larger practices, this triage work may consume all of the provider’s shift, so that person has no time left for clinical care. It is hard for me to see this as top of license work that only a physician or advanced practice clinician can do. In my December 2010 column, I provided some potential alternatives to dedicating a physician or other provider to a triage role.
Your list of important changes that are needed to move hospitalists toward more time spent working at the top of their license will likely differ a lot from the issues above. But every group could benefit from deliberately thinking about what would be most valuable for them and trying to make that a reality.
Hospital Medicine's Old Practices Become New Again
The musty collections of National Geographic magazines once found in so many basements are largely gone. Replacing them are dusty sets of the Advisory Board binders and booklets found in hospital administration offices around the country. I think the same principle drives the impulse to collect both publications—the idea that they contain worthwhile information that one day will be reviewed. But I think it’s more likely they will be ignored until it is time to move and someone has to decide what to do with the painfully heavy pile of paper.
Lots of old and largely forgotten things are making a comeback in healthcare. I suppose this is always happening, but I sense we’re now experiencing more of this than usual. It’s a renaissance of sorts.
I first heard about fecal transplant for Clostridium difficile infection (instilling a “better” microbiome in the hope of realizing many benefits) about six or eight years ago. Although I was sure this was a new idea, my retired internist father told me this had been around when he was in training. Wikipedia says that four Colorado surgeons published a paper about it in 1958 and that the Chinese were doing this 1,600 years ago.
PCPs Visit Hospitalized Patients
Writing in the NEJM earlier this year, Goroll and Hunt proposed that primary care physicians visit their hospitalized patients in the role of consultant while the hospitalist remains attending. As they note, this idea surfaced as soon as the hospitalist model began taking hold. Back then, we usually referred to it as a “social visit” by the PCP. Anecdotal experience from my work with hundreds of hospitalist groups tells me that such visits have all but disappeared. But nearly every such PCP visit on a patient I’ve cared for has seemed worthwhile; in many cases, these hospital calls simply reassure a nervous patient or family member, and occasionally they ensure that the PCP and I arrive at a more effective plan of care than we might otherwise.
Perhaps new forms of healthcare reimbursement, accountable care, and population health may make “continuity visits” economically viable for PCPs. Wouldn’t it be interesting if PCP visits to hospitalized patients and hospitalist visits to outpatients, such as those occurring in a pre-op clinic or a skilled nursing facility, become commonplace? The trick in all of this will be to ensure the right amount of overlap, or shared visits, between PCP and hospitalist without expensive duplication of effort or errors stemming from too many cooks in the kitchen.
Post-Hospital Follow-Up Schedules
When I began practicing as a hospitalist in the 1980s, doctors routinely wrote orders similar to this one: “Have patient follow up with Dr. Smith (PCP or specialist) in 1-2 weeks.” The unit secretary or other hospital clerical staff would contact the physician’s office to schedule the appointment, and the patient would leave the hospital with a written reminder in hand. My sense is that nearly all hospitals had been doing this for decades; somehow this practice has nearly disappeared over the last 10-20 years, however, and I sometimes hear this old practice discussed as a new idea.
I think making sure the patient has a follow-up appointment in hand when leaving the hospital is likely good for clinical outcomes, readmissions, and patient satisfaction. In my view, it is hardly worth lots of research to prove the benefit of what should be a relatively low-cost intervention. Why not just have providers write orders detailing follow-up with a specific doctor or clinic and a timeframe, and have unit secretaries communicate with outpatient clinics to schedule the appointments and ensure that the details are provided to the patient, maybe via an EHR-generated after visit summary? Seems pretty easy, right?
Turns out it isn’t easy at all for most hospitals. Lots of energetic hospitalists have taken on a project like this, only to run into so many brick walls. One hospitalist told me recently that the unit secretary’s labor union at her hospital refused to allow it. So some hospitals have turned to a single person, or a small group of people, who make appointments for all hospital patients. Some hospitalist groups have one of their own staff make appointments for hospitalist patients. This relieves the unit secretaries of the task but requires additional funding for the salaries of these people.
Maybe, at some time not so far off, EHRs will be so user-friendly and patients/families so accustomed to using them that it will be common for patients/families to arrange the appointments on their own. It could even be a required step—a hard stop—in the discharge process.
Whatever emerges as the most common method of making these appointments, I think it is safe to say this old practice will become “new” and common within the next few years.
Multidisciplinary Rounds
While working as an orderly in the 1970s, I would often visit with the nurses in their break room. When a doctor arrived to make rounds on the floor, the RN would jump up, stub out her cigarette, and round with the doctor. I sometimes tagged along as an observer. The nurse let the doctor know just how the patient had been doing and provided test results and any other relevant information the doctor might need. The doctor would provide orders, and sometimes the nurse wrote them into the chart (think of today’s medical scribes). Although their interaction was much less collaborative than is typical today, they did ask lots of questions of one another to clarify ambiguities.
I think these 1970s caregivers were doing effective multidisciplinary rounds. But by the late 1980s or so, as both doctor and nurse became busier, they stopped rounding together.
I smile when I hear descriptions of this “new” idea of doctor and nurse (and often other caregivers) rounding together. Today’s hospital culture is less hierarchical than the 1970s, though some would say it still has a ways to go, so teamwork and multidisciplinary rounds may yield more benefit than decades ago. But the idea of rounding together certainly isn’t new.
As we try to figure out the best way to thrive in a rapidly changing healthcare environment, we may find value in returning to the old ways of doing some things.

The musty collections of National Geographic magazines once found in so many basements are largely gone. Replacing them are dusty sets of the Advisory Board binders and booklets found in hospital administration offices around the country. I think the same principle drives the impulse to collect both publications—the idea that they contain worthwhile information that one day will be reviewed. But I think it’s more likely they will be ignored until it is time to move and someone has to decide what to do with the painfully heavy pile of paper.
Lots of old and largely forgotten things are making a comeback in healthcare. I suppose this is always happening, but I sense we’re now experiencing more of this than usual. It’s a renaissance of sorts.
I first heard about fecal transplant for Clostridium difficile infection (instilling a “better” microbiome in the hope of realizing many benefits) about six or eight years ago. Although I was sure this was a new idea, my retired internist father told me this had been around when he was in training. Wikipedia says that four Colorado surgeons published a paper about it in 1958 and that the Chinese were doing this 1,600 years ago.
PCPs Visit Hospitalized Patients
Writing in the NEJM earlier this year, Goroll and Hunt proposed that primary care physicians visit their hospitalized patients in the role of consultant while the hospitalist remains attending. As they note, this idea surfaced as soon as the hospitalist model began taking hold. Back then, we usually referred to it as a “social visit” by the PCP. Anecdotal experience from my work with hundreds of hospitalist groups tells me that such visits have all but disappeared. But nearly every such PCP visit on a patient I’ve cared for has seemed worthwhile; in many cases, these hospital calls simply reassure a nervous patient or family member, and occasionally they ensure that the PCP and I arrive at a more effective plan of care than we might otherwise.
Perhaps new forms of healthcare reimbursement, accountable care, and population health may make “continuity visits” economically viable for PCPs. Wouldn’t it be interesting if PCP visits to hospitalized patients and hospitalist visits to outpatients, such as those occurring in a pre-op clinic or a skilled nursing facility, become commonplace? The trick in all of this will be to ensure the right amount of overlap, or shared visits, between PCP and hospitalist without expensive duplication of effort or errors stemming from too many cooks in the kitchen.
Post-Hospital Follow-Up Schedules
When I began practicing as a hospitalist in the 1980s, doctors routinely wrote orders similar to this one: “Have patient follow up with Dr. Smith (PCP or specialist) in 1-2 weeks.” The unit secretary or other hospital clerical staff would contact the physician’s office to schedule the appointment, and the patient would leave the hospital with a written reminder in hand. My sense is that nearly all hospitals had been doing this for decades; somehow this practice has nearly disappeared over the last 10-20 years, however, and I sometimes hear this old practice discussed as a new idea.
I think making sure the patient has a follow-up appointment in hand when leaving the hospital is likely good for clinical outcomes, readmissions, and patient satisfaction. In my view, it is hardly worth lots of research to prove the benefit of what should be a relatively low-cost intervention. Why not just have providers write orders detailing follow-up with a specific doctor or clinic and a timeframe, and have unit secretaries communicate with outpatient clinics to schedule the appointments and ensure that the details are provided to the patient, maybe via an EHR-generated after visit summary? Seems pretty easy, right?
Turns out it isn’t easy at all for most hospitals. Lots of energetic hospitalists have taken on a project like this, only to run into so many brick walls. One hospitalist told me recently that the unit secretary’s labor union at her hospital refused to allow it. So some hospitals have turned to a single person, or a small group of people, who make appointments for all hospital patients. Some hospitalist groups have one of their own staff make appointments for hospitalist patients. This relieves the unit secretaries of the task but requires additional funding for the salaries of these people.
Maybe, at some time not so far off, EHRs will be so user-friendly and patients/families so accustomed to using them that it will be common for patients/families to arrange the appointments on their own. It could even be a required step—a hard stop—in the discharge process.
Whatever emerges as the most common method of making these appointments, I think it is safe to say this old practice will become “new” and common within the next few years.
Multidisciplinary Rounds
While working as an orderly in the 1970s, I would often visit with the nurses in their break room. When a doctor arrived to make rounds on the floor, the RN would jump up, stub out her cigarette, and round with the doctor. I sometimes tagged along as an observer. The nurse let the doctor know just how the patient had been doing and provided test results and any other relevant information the doctor might need. The doctor would provide orders, and sometimes the nurse wrote them into the chart (think of today’s medical scribes). Although their interaction was much less collaborative than is typical today, they did ask lots of questions of one another to clarify ambiguities.
I think these 1970s caregivers were doing effective multidisciplinary rounds. But by the late 1980s or so, as both doctor and nurse became busier, they stopped rounding together.
I smile when I hear descriptions of this “new” idea of doctor and nurse (and often other caregivers) rounding together. Today’s hospital culture is less hierarchical than the 1970s, though some would say it still has a ways to go, so teamwork and multidisciplinary rounds may yield more benefit than decades ago. But the idea of rounding together certainly isn’t new.
As we try to figure out the best way to thrive in a rapidly changing healthcare environment, we may find value in returning to the old ways of doing some things.
The musty collections of National Geographic magazines once found in so many basements are largely gone. Replacing them are dusty sets of the Advisory Board binders and booklets found in hospital administration offices around the country. I think the same principle drives the impulse to collect both publications—the idea that they contain worthwhile information that one day will be reviewed. But I think it’s more likely they will be ignored until it is time to move and someone has to decide what to do with the painfully heavy pile of paper.
Lots of old and largely forgotten things are making a comeback in healthcare. I suppose this is always happening, but I sense we’re now experiencing more of this than usual. It’s a renaissance of sorts.
I first heard about fecal transplant for Clostridium difficile infection (instilling a “better” microbiome in the hope of realizing many benefits) about six or eight years ago. Although I was sure this was a new idea, my retired internist father told me this had been around when he was in training. Wikipedia says that four Colorado surgeons published a paper about it in 1958 and that the Chinese were doing this 1,600 years ago.
PCPs Visit Hospitalized Patients
Writing in the NEJM earlier this year, Goroll and Hunt proposed that primary care physicians visit their hospitalized patients in the role of consultant while the hospitalist remains attending. As they note, this idea surfaced as soon as the hospitalist model began taking hold. Back then, we usually referred to it as a “social visit” by the PCP. Anecdotal experience from my work with hundreds of hospitalist groups tells me that such visits have all but disappeared. But nearly every such PCP visit on a patient I’ve cared for has seemed worthwhile; in many cases, these hospital calls simply reassure a nervous patient or family member, and occasionally they ensure that the PCP and I arrive at a more effective plan of care than we might otherwise.
Perhaps new forms of healthcare reimbursement, accountable care, and population health may make “continuity visits” economically viable for PCPs. Wouldn’t it be interesting if PCP visits to hospitalized patients and hospitalist visits to outpatients, such as those occurring in a pre-op clinic or a skilled nursing facility, become commonplace? The trick in all of this will be to ensure the right amount of overlap, or shared visits, between PCP and hospitalist without expensive duplication of effort or errors stemming from too many cooks in the kitchen.
Post-Hospital Follow-Up Schedules
When I began practicing as a hospitalist in the 1980s, doctors routinely wrote orders similar to this one: “Have patient follow up with Dr. Smith (PCP or specialist) in 1-2 weeks.” The unit secretary or other hospital clerical staff would contact the physician’s office to schedule the appointment, and the patient would leave the hospital with a written reminder in hand. My sense is that nearly all hospitals had been doing this for decades; somehow this practice has nearly disappeared over the last 10-20 years, however, and I sometimes hear this old practice discussed as a new idea.
I think making sure the patient has a follow-up appointment in hand when leaving the hospital is likely good for clinical outcomes, readmissions, and patient satisfaction. In my view, it is hardly worth lots of research to prove the benefit of what should be a relatively low-cost intervention. Why not just have providers write orders detailing follow-up with a specific doctor or clinic and a timeframe, and have unit secretaries communicate with outpatient clinics to schedule the appointments and ensure that the details are provided to the patient, maybe via an EHR-generated after visit summary? Seems pretty easy, right?
Turns out it isn’t easy at all for most hospitals. Lots of energetic hospitalists have taken on a project like this, only to run into so many brick walls. One hospitalist told me recently that the unit secretary’s labor union at her hospital refused to allow it. So some hospitals have turned to a single person, or a small group of people, who make appointments for all hospital patients. Some hospitalist groups have one of their own staff make appointments for hospitalist patients. This relieves the unit secretaries of the task but requires additional funding for the salaries of these people.
Maybe, at some time not so far off, EHRs will be so user-friendly and patients/families so accustomed to using them that it will be common for patients/families to arrange the appointments on their own. It could even be a required step—a hard stop—in the discharge process.
Whatever emerges as the most common method of making these appointments, I think it is safe to say this old practice will become “new” and common within the next few years.
Multidisciplinary Rounds
While working as an orderly in the 1970s, I would often visit with the nurses in their break room. When a doctor arrived to make rounds on the floor, the RN would jump up, stub out her cigarette, and round with the doctor. I sometimes tagged along as an observer. The nurse let the doctor know just how the patient had been doing and provided test results and any other relevant information the doctor might need. The doctor would provide orders, and sometimes the nurse wrote them into the chart (think of today’s medical scribes). Although their interaction was much less collaborative than is typical today, they did ask lots of questions of one another to clarify ambiguities.
I think these 1970s caregivers were doing effective multidisciplinary rounds. But by the late 1980s or so, as both doctor and nurse became busier, they stopped rounding together.
I smile when I hear descriptions of this “new” idea of doctor and nurse (and often other caregivers) rounding together. Today’s hospital culture is less hierarchical than the 1970s, though some would say it still has a ways to go, so teamwork and multidisciplinary rounds may yield more benefit than decades ago. But the idea of rounding together certainly isn’t new.
As we try to figure out the best way to thrive in a rapidly changing healthcare environment, we may find value in returning to the old ways of doing some things.
Bundled Payment and Hospital Medicine, Pt. 2
Editor’s note: Second in a two-part series examining bundled payments and hospital medicine. In full disclosure, Dr. Whitcomb works for a company that is an Awardee Convener in the CMS Bundled Payments for Care Improvement (BPCI) Initiative.
In part one of this series, we discussed the basics of the BPCI program. Now we will delve into specific roles and opportunities for hospitalists in bundled payment programs in general, and the BPCI program in particular.
The bundled payment model can be hard to explain. One example that might make it clearer is that of LASIK vision correction surgery, where a single bundled payment covers the fees of the ophthalmologist, the operating facility, and any other services (like optometry) and medications (like eye drops). Another example is the diagnosis-related group (DRG) payment for hospital care, in which all facility costs are bundled together into a single payment.
A simplistic way to differentiate bundled payment from accountable care organization (ACOs) is that the former is typically initiated by an acute medical or surgical event and concludes after a recovery period—often 30, 60, or 90 days. Conversely, the latter generally covers the care of individuals within a population over time, often focusing on the management of chronic conditions.
The Opportunity
Two major opportunities for hospitalists to improve value (quality/cost) present themselves through the BPCI initiative. One is in post-acute facility utilization, and the other is in reducing readmissions. Figure 1 shows that for 30-day episodes starting with a hospitalization for five common conditions, payments for post-acute care are surprisingly close in amount to those for the preceding hospitalization.1
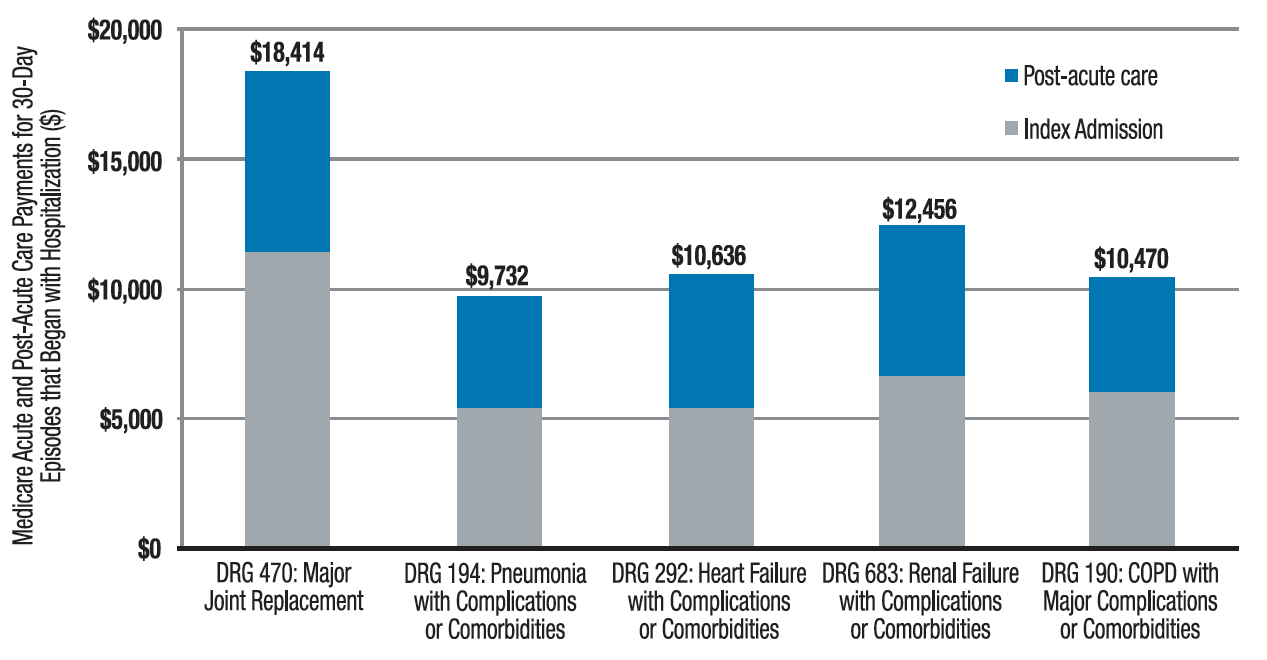
Much of the cost of post-acute care comes from skilled nursing facilities (SNFs) and, to a lesser degree, inpatient rehabilitation facilities. A broad range of research studies has demonstrated that inpatient care managed by hospitalists—compared with the traditional model—is associated with a decrease in inpatient costs; however, recent research indicates that the hospital cost savings generated by hospitalists are offset by more spending in the 30 days post discharge, specifically on more SNF care and increased readmissions.2 As another indicator that post-acute care needs a closer look, a 2013 Institute of Medicine report concluded that spending on post-acute care was responsible for the majority of Medicare’s overall regional variation in spending.1,3
Of course, success in a bundled payment model will also be derived from reducing costs in the hospital setting, such as those stemming from unnecessary or duplicative testing and imaging, injudicious use of consultants, and practices identified in programs such as Choosing Wisely.
How Your Practice Can Drive Bundled Payment Success
The aforementioned observations point to the need to improve the value of post-acute care by optimizing post-acute spending—driven mostly by SNF costs—and minimizing avoidable readmissions. I offer the following inpatient interventions to achieve these goals:
- Speak with patients early and often regarding expectations for recovery post discharge. When possible, set a goal of home discharge with the needed support.
- Write orders for early ambulation. Develop an early ambulation program with nursing and physical therapy.
- Address goals of care during the patient/family meeting. For appropriate patients with life-limiting illness, involve the palliative care service or equivalent and discuss the role of future aggressive interventions, including hospitalization, so that the course set is consistent with the patients’ goals and wishes.
- Lead the in-hospital team, instead of defaulting to others, like case management, in making an informed decision about ideal post-discharge location by factoring in caregiver availability, independence, and SNF needs. Marshal resources to enable a home recovery (i.e., home health evaluation), whether or not there is an intervening SNF stay. If patients go to a SNF, set expectations for length of stay in the facility.
- Adhere to best practices for care transitions, such as those in Project BOOST, including thorough medication reconciliation.
Beyond the Four Walls
As you aim for a high-value (high quality and affordable) discharge, your hospital medicine practice may consider new approaches to filling longstanding gaps in post-acute care. Forward-looking hospitalist groups have implemented the following approaches:
- Establish a post-discharge clinic where patients are seen after discharge, in the interim before they have an opportunity for primary care follow-up;
- Send teams to work in SNFs;
- Call patients after discharge to ensure they are following their plan of care;
- Leverage newer current procedural terminology (CPT) codes, like the Transitional Care Management or Chronic Care Management codes, to support your transitional care services;
- Provide home visits for high-risk patients; and
- Access waivers for G-codes for home visits and/or telemedicine outside of rural areas. These waivers exist under the BPCI initiative.
Shift from ‘Traditional’ Hospitalist to ‘Value’ Hospitalist
If some of the changes in practice needed to succeed in a bundled payment world seem daunting to you, it may be helpful to realize that with the challenge comes an opportunity. This opportunity for hospitalists parallels that of the early days of the specialty, when reducing length of stay created substantial support from hospital leaders and was a factor leading to the rapid growth in the number of hospitalists. In January, the U.S. Secretary of Health and Human Services set a goal to tie 50% of Medicare payments to ‘alternative payment models’ like bundled payments by 2018. In April, as part of the sustainable growth rate fix, Medicare announced it would create substantial new bonuses for physicians who have at least 25% of their revenue in such models.1
As healthcare policy aligns behind ‘alternative payment models,’ bundled payment programs are likely to be a potent driver of an evolving hospitalist specialty. Next-generation hospitalists will be asked to take a leadership role in addressing ‘value’ with responsibility for improving care coordination and affordability over an episode of illness.
Now may be the time to take to heart the words of computer scientist Alan Kay: “The best way to predict the future is to invent it.”

References
- Mechanic R. Post-acute care–the next frontier for controlling Medicare spending. N Engl J Med. 2014;370(8):692-694.
- Kuo YF, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3):152-159.
- Newhouse JP, Garber AM. Geographic variation in Medicare services. N Engl J Med. 2013;368(16):1465-1468.
Editor’s note: Second in a two-part series examining bundled payments and hospital medicine. In full disclosure, Dr. Whitcomb works for a company that is an Awardee Convener in the CMS Bundled Payments for Care Improvement (BPCI) Initiative.
In part one of this series, we discussed the basics of the BPCI program. Now we will delve into specific roles and opportunities for hospitalists in bundled payment programs in general, and the BPCI program in particular.
The bundled payment model can be hard to explain. One example that might make it clearer is that of LASIK vision correction surgery, where a single bundled payment covers the fees of the ophthalmologist, the operating facility, and any other services (like optometry) and medications (like eye drops). Another example is the diagnosis-related group (DRG) payment for hospital care, in which all facility costs are bundled together into a single payment.
A simplistic way to differentiate bundled payment from accountable care organization (ACOs) is that the former is typically initiated by an acute medical or surgical event and concludes after a recovery period—often 30, 60, or 90 days. Conversely, the latter generally covers the care of individuals within a population over time, often focusing on the management of chronic conditions.
The Opportunity
Two major opportunities for hospitalists to improve value (quality/cost) present themselves through the BPCI initiative. One is in post-acute facility utilization, and the other is in reducing readmissions. Figure 1 shows that for 30-day episodes starting with a hospitalization for five common conditions, payments for post-acute care are surprisingly close in amount to those for the preceding hospitalization.1
Much of the cost of post-acute care comes from skilled nursing facilities (SNFs) and, to a lesser degree, inpatient rehabilitation facilities. A broad range of research studies has demonstrated that inpatient care managed by hospitalists—compared with the traditional model—is associated with a decrease in inpatient costs; however, recent research indicates that the hospital cost savings generated by hospitalists are offset by more spending in the 30 days post discharge, specifically on more SNF care and increased readmissions.2 As another indicator that post-acute care needs a closer look, a 2013 Institute of Medicine report concluded that spending on post-acute care was responsible for the majority of Medicare’s overall regional variation in spending.1,3
Of course, success in a bundled payment model will also be derived from reducing costs in the hospital setting, such as those stemming from unnecessary or duplicative testing and imaging, injudicious use of consultants, and practices identified in programs such as Choosing Wisely.
How Your Practice Can Drive Bundled Payment Success
The aforementioned observations point to the need to improve the value of post-acute care by optimizing post-acute spending—driven mostly by SNF costs—and minimizing avoidable readmissions. I offer the following inpatient interventions to achieve these goals:
- Speak with patients early and often regarding expectations for recovery post discharge. When possible, set a goal of home discharge with the needed support.
- Write orders for early ambulation. Develop an early ambulation program with nursing and physical therapy.
- Address goals of care during the patient/family meeting. For appropriate patients with life-limiting illness, involve the palliative care service or equivalent and discuss the role of future aggressive interventions, including hospitalization, so that the course set is consistent with the patients’ goals and wishes.
- Lead the in-hospital team, instead of defaulting to others, like case management, in making an informed decision about ideal post-discharge location by factoring in caregiver availability, independence, and SNF needs. Marshal resources to enable a home recovery (i.e., home health evaluation), whether or not there is an intervening SNF stay. If patients go to a SNF, set expectations for length of stay in the facility.
- Adhere to best practices for care transitions, such as those in Project BOOST, including thorough medication reconciliation.
Beyond the Four Walls
As you aim for a high-value (high quality and affordable) discharge, your hospital medicine practice may consider new approaches to filling longstanding gaps in post-acute care. Forward-looking hospitalist groups have implemented the following approaches:
- Establish a post-discharge clinic where patients are seen after discharge, in the interim before they have an opportunity for primary care follow-up;
- Send teams to work in SNFs;
- Call patients after discharge to ensure they are following their plan of care;
- Leverage newer current procedural terminology (CPT) codes, like the Transitional Care Management or Chronic Care Management codes, to support your transitional care services;
- Provide home visits for high-risk patients; and
- Access waivers for G-codes for home visits and/or telemedicine outside of rural areas. These waivers exist under the BPCI initiative.
Shift from ‘Traditional’ Hospitalist to ‘Value’ Hospitalist
If some of the changes in practice needed to succeed in a bundled payment world seem daunting to you, it may be helpful to realize that with the challenge comes an opportunity. This opportunity for hospitalists parallels that of the early days of the specialty, when reducing length of stay created substantial support from hospital leaders and was a factor leading to the rapid growth in the number of hospitalists. In January, the U.S. Secretary of Health and Human Services set a goal to tie 50% of Medicare payments to ‘alternative payment models’ like bundled payments by 2018. In April, as part of the sustainable growth rate fix, Medicare announced it would create substantial new bonuses for physicians who have at least 25% of their revenue in such models.1
As healthcare policy aligns behind ‘alternative payment models,’ bundled payment programs are likely to be a potent driver of an evolving hospitalist specialty. Next-generation hospitalists will be asked to take a leadership role in addressing ‘value’ with responsibility for improving care coordination and affordability over an episode of illness.
Now may be the time to take to heart the words of computer scientist Alan Kay: “The best way to predict the future is to invent it.”
References
- Mechanic R. Post-acute care–the next frontier for controlling Medicare spending. N Engl J Med. 2014;370(8):692-694.
- Kuo YF, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3):152-159.
- Newhouse JP, Garber AM. Geographic variation in Medicare services. N Engl J Med. 2013;368(16):1465-1468.
Editor’s note: Second in a two-part series examining bundled payments and hospital medicine. In full disclosure, Dr. Whitcomb works for a company that is an Awardee Convener in the CMS Bundled Payments for Care Improvement (BPCI) Initiative.
In part one of this series, we discussed the basics of the BPCI program. Now we will delve into specific roles and opportunities for hospitalists in bundled payment programs in general, and the BPCI program in particular.
The bundled payment model can be hard to explain. One example that might make it clearer is that of LASIK vision correction surgery, where a single bundled payment covers the fees of the ophthalmologist, the operating facility, and any other services (like optometry) and medications (like eye drops). Another example is the diagnosis-related group (DRG) payment for hospital care, in which all facility costs are bundled together into a single payment.
A simplistic way to differentiate bundled payment from accountable care organization (ACOs) is that the former is typically initiated by an acute medical or surgical event and concludes after a recovery period—often 30, 60, or 90 days. Conversely, the latter generally covers the care of individuals within a population over time, often focusing on the management of chronic conditions.
The Opportunity
Two major opportunities for hospitalists to improve value (quality/cost) present themselves through the BPCI initiative. One is in post-acute facility utilization, and the other is in reducing readmissions. Figure 1 shows that for 30-day episodes starting with a hospitalization for five common conditions, payments for post-acute care are surprisingly close in amount to those for the preceding hospitalization.1
Much of the cost of post-acute care comes from skilled nursing facilities (SNFs) and, to a lesser degree, inpatient rehabilitation facilities. A broad range of research studies has demonstrated that inpatient care managed by hospitalists—compared with the traditional model—is associated with a decrease in inpatient costs; however, recent research indicates that the hospital cost savings generated by hospitalists are offset by more spending in the 30 days post discharge, specifically on more SNF care and increased readmissions.2 As another indicator that post-acute care needs a closer look, a 2013 Institute of Medicine report concluded that spending on post-acute care was responsible for the majority of Medicare’s overall regional variation in spending.1,3
Of course, success in a bundled payment model will also be derived from reducing costs in the hospital setting, such as those stemming from unnecessary or duplicative testing and imaging, injudicious use of consultants, and practices identified in programs such as Choosing Wisely.
How Your Practice Can Drive Bundled Payment Success
The aforementioned observations point to the need to improve the value of post-acute care by optimizing post-acute spending—driven mostly by SNF costs—and minimizing avoidable readmissions. I offer the following inpatient interventions to achieve these goals:
- Speak with patients early and often regarding expectations for recovery post discharge. When possible, set a goal of home discharge with the needed support.
- Write orders for early ambulation. Develop an early ambulation program with nursing and physical therapy.
- Address goals of care during the patient/family meeting. For appropriate patients with life-limiting illness, involve the palliative care service or equivalent and discuss the role of future aggressive interventions, including hospitalization, so that the course set is consistent with the patients’ goals and wishes.
- Lead the in-hospital team, instead of defaulting to others, like case management, in making an informed decision about ideal post-discharge location by factoring in caregiver availability, independence, and SNF needs. Marshal resources to enable a home recovery (i.e., home health evaluation), whether or not there is an intervening SNF stay. If patients go to a SNF, set expectations for length of stay in the facility.
- Adhere to best practices for care transitions, such as those in Project BOOST, including thorough medication reconciliation.
Beyond the Four Walls
As you aim for a high-value (high quality and affordable) discharge, your hospital medicine practice may consider new approaches to filling longstanding gaps in post-acute care. Forward-looking hospitalist groups have implemented the following approaches:
- Establish a post-discharge clinic where patients are seen after discharge, in the interim before they have an opportunity for primary care follow-up;
- Send teams to work in SNFs;
- Call patients after discharge to ensure they are following their plan of care;
- Leverage newer current procedural terminology (CPT) codes, like the Transitional Care Management or Chronic Care Management codes, to support your transitional care services;
- Provide home visits for high-risk patients; and
- Access waivers for G-codes for home visits and/or telemedicine outside of rural areas. These waivers exist under the BPCI initiative.
Shift from ‘Traditional’ Hospitalist to ‘Value’ Hospitalist
If some of the changes in practice needed to succeed in a bundled payment world seem daunting to you, it may be helpful to realize that with the challenge comes an opportunity. This opportunity for hospitalists parallels that of the early days of the specialty, when reducing length of stay created substantial support from hospital leaders and was a factor leading to the rapid growth in the number of hospitalists. In January, the U.S. Secretary of Health and Human Services set a goal to tie 50% of Medicare payments to ‘alternative payment models’ like bundled payments by 2018. In April, as part of the sustainable growth rate fix, Medicare announced it would create substantial new bonuses for physicians who have at least 25% of their revenue in such models.1
As healthcare policy aligns behind ‘alternative payment models,’ bundled payment programs are likely to be a potent driver of an evolving hospitalist specialty. Next-generation hospitalists will be asked to take a leadership role in addressing ‘value’ with responsibility for improving care coordination and affordability over an episode of illness.
Now may be the time to take to heart the words of computer scientist Alan Kay: “The best way to predict the future is to invent it.”
References
- Mechanic R. Post-acute care–the next frontier for controlling Medicare spending. N Engl J Med. 2014;370(8):692-694.
- Kuo YF, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3):152-159.
- Newhouse JP, Garber AM. Geographic variation in Medicare services. N Engl J Med. 2013;368(16):1465-1468.
Standard Text Messaging for Smartphones Not HIPAA Compliant

Doctors were the first to begin using pagers and, along with drug dealers, appear to be the last to give them up. But we really need to get rid of them.
Sadly, for the foreseeable future, we will need a pager replacement, but, in the longer term, I’m hopeful that we can:
- Reduce the frequency of electronic interruptions—all forms of interruptions—and the adverse effects that reliably accompany them, and
- Ensure that each interruption has value—that is, reduce or eliminate the many low value and non-urgent messages we all get (e.g. the ones informing you of a lab result you’ve already seen).
Death to the Pager
I can’t imagine anyone who will be more pleased than I will if pagers go the way of now rare hospital-wide PA announcements. Some hospitals have eliminated these announcements entirely, and even critical messages like “code blue” announcements are sent directly to each responder via a pager or other personal device.
Around the time the first iPhone was born, hospital signs banning cell phones began coming down. It seems the fear that they would disrupt hospital electronics, such as telemetry and other monitoring devices, has proven largely unfounded (though, along with things like computer keyboards and stethoscopes, pagers and cell phones can serve as dangerous repositories of bacteria).
Now nearly everyone, from staff to patients, keeps a cell phone with them while in the hospital. I think that is the most important step toward getting rid of pagers. Many doctors already are using the standard text messaging apps that come with the phone to communicate with one another efficiently.
“Regular” Texting Won’t Cut It
Unfortunately, the standard text messaging that comes with every smartphone is not HIPAA compliant. Though I certainly don’t know how anyone would do it, it is apparently too easy for another person to intercept the message. So, if you’re texting information related to your clinical work, you need to make sure it doesn’t include anything that could be considered protected health information. It isn’t enough just to leave the patient’s name off the message. If you’re in the habit of regularly texting doctors, nurses, and other healthcare personnel about patient care, you are at high risk of violating HIPAA, even if you try hard to avoid it.
Another big drawback is that there isn’t a good way to turn off work-related texting when you’re off duty, while leaving your texting app open for communication with your friends and family. Hospital staff will sometimes fail to check whether you’re on duty before texting, and that will lead to your personal time being interrupted by work reminders.
I think these shortcomings mean that none of us should rely on the standard text messaging apps that come with our phones.
But in order for a different app or service to be of any value, we will need to ensure that most providers associated with our hospital are on the same messaging system. That is a tall order, but fortunately there are a lot of companies trying to produce an attractive product that makes it as easy as possible to attract a critical mass of users at your institution.
HIPAA-Compliant Texting Vendors
Many healthcare tech companies provide secure messaging, usually at no additional cost, as an add-on to their main products, such as charge capture software (e.g. IngeniousMed), or physician social networking (e.g. Doximity). Something like 30 companies now offer a dedicated HIPAA-compliant texting option, including IM Your Doc, Voalte, Telmediq, PerfectServe, Vocera, and TigerText. There are so many that it is awfully tough to understand all of their strengths and shortcomings in detail, but I’m having fun trying to do just that. And I anticipate there will be significant consolidation in vendors within the next two to three years.
The dedicated HIPAA-compliant texting services range in price from free for basic features to a monthly fee per user that varies depending on the features you choose to enable. Some offer integration with the hospital’s EHR, which can let a message sender who only knows the patient’s name to see which doctor, nurse, or other caregiver is currently responsible for the patient. Some offer integration with a call schedule and answering service, or even replace an answering service.
No pager replacement will be viable if there are sites in the hospital or elsewhere where it is out of contact; a solution that works on both cellular networks and Wi-Fi is essential. Some vendors offer the ability for messages not delivered to or acknowledged by the recipient to escalate to other forms of delivery after a specified period of time.
I would love to see a feature that I don’t think any vendor offers yet. It would be great if all messages the sender hasn’t marked “stat” or “urgent” first went to a queue in the EHR rather than immediately interrupting the recipient. That way a doctor or other caregiver could see messages while already working in the EHR, rather than glancing at each new message as it arrives, something that all too often needlessly interrupts another important task such as talking with a patient.
And, since most work in EHRs is done in front of a larger device with a full keyboard, it would be easier to type a quick reply message than it would be to rely on a smartphone keyboard for return messaging. Protocols could be established such that messages waiting in the EHR without a reply or dismissal after a specified time would then be sent to the recipient’s personal device.
A Texting Ecosystem
In nearly every case, the hospital will select the text messaging vendor, though hospitalists and nurses, who will typically be among the highest-volume users, should participate in the decision. But the real value of the system hinges on ensuring its wide adoption by most, or nearly all, hospital caregivers and affiliated ambulatory providers.
I would enjoy hearing from those who are already using a HIPAA-secure texting and pager replacement service now, as well as those still researching their options. This has the potential to meaningfully change the way hospitalists and others do their work.
Doctors were the first to begin using pagers and, along with drug dealers, appear to be the last to give them up. But we really need to get rid of them.
Sadly, for the foreseeable future, we will need a pager replacement, but, in the longer term, I’m hopeful that we can:
- Reduce the frequency of electronic interruptions—all forms of interruptions—and the adverse effects that reliably accompany them, and
- Ensure that each interruption has value—that is, reduce or eliminate the many low value and non-urgent messages we all get (e.g. the ones informing you of a lab result you’ve already seen).
Death to the Pager
I can’t imagine anyone who will be more pleased than I will if pagers go the way of now rare hospital-wide PA announcements. Some hospitals have eliminated these announcements entirely, and even critical messages like “code blue” announcements are sent directly to each responder via a pager or other personal device.
Around the time the first iPhone was born, hospital signs banning cell phones began coming down. It seems the fear that they would disrupt hospital electronics, such as telemetry and other monitoring devices, has proven largely unfounded (though, along with things like computer keyboards and stethoscopes, pagers and cell phones can serve as dangerous repositories of bacteria).
Now nearly everyone, from staff to patients, keeps a cell phone with them while in the hospital. I think that is the most important step toward getting rid of pagers. Many doctors already are using the standard text messaging apps that come with the phone to communicate with one another efficiently.
“Regular” Texting Won’t Cut It
Unfortunately, the standard text messaging that comes with every smartphone is not HIPAA compliant. Though I certainly don’t know how anyone would do it, it is apparently too easy for another person to intercept the message. So, if you’re texting information related to your clinical work, you need to make sure it doesn’t include anything that could be considered protected health information. It isn’t enough just to leave the patient’s name off the message. If you’re in the habit of regularly texting doctors, nurses, and other healthcare personnel about patient care, you are at high risk of violating HIPAA, even if you try hard to avoid it.
Another big drawback is that there isn’t a good way to turn off work-related texting when you’re off duty, while leaving your texting app open for communication with your friends and family. Hospital staff will sometimes fail to check whether you’re on duty before texting, and that will lead to your personal time being interrupted by work reminders.
I think these shortcomings mean that none of us should rely on the standard text messaging apps that come with our phones.
But in order for a different app or service to be of any value, we will need to ensure that most providers associated with our hospital are on the same messaging system. That is a tall order, but fortunately there are a lot of companies trying to produce an attractive product that makes it as easy as possible to attract a critical mass of users at your institution.
HIPAA-Compliant Texting Vendors
Many healthcare tech companies provide secure messaging, usually at no additional cost, as an add-on to their main products, such as charge capture software (e.g. IngeniousMed), or physician social networking (e.g. Doximity). Something like 30 companies now offer a dedicated HIPAA-compliant texting option, including IM Your Doc, Voalte, Telmediq, PerfectServe, Vocera, and TigerText. There are so many that it is awfully tough to understand all of their strengths and shortcomings in detail, but I’m having fun trying to do just that. And I anticipate there will be significant consolidation in vendors within the next two to three years.
The dedicated HIPAA-compliant texting services range in price from free for basic features to a monthly fee per user that varies depending on the features you choose to enable. Some offer integration with the hospital’s EHR, which can let a message sender who only knows the patient’s name to see which doctor, nurse, or other caregiver is currently responsible for the patient. Some offer integration with a call schedule and answering service, or even replace an answering service.
No pager replacement will be viable if there are sites in the hospital or elsewhere where it is out of contact; a solution that works on both cellular networks and Wi-Fi is essential. Some vendors offer the ability for messages not delivered to or acknowledged by the recipient to escalate to other forms of delivery after a specified period of time.
I would love to see a feature that I don’t think any vendor offers yet. It would be great if all messages the sender hasn’t marked “stat” or “urgent” first went to a queue in the EHR rather than immediately interrupting the recipient. That way a doctor or other caregiver could see messages while already working in the EHR, rather than glancing at each new message as it arrives, something that all too often needlessly interrupts another important task such as talking with a patient.
And, since most work in EHRs is done in front of a larger device with a full keyboard, it would be easier to type a quick reply message than it would be to rely on a smartphone keyboard for return messaging. Protocols could be established such that messages waiting in the EHR without a reply or dismissal after a specified time would then be sent to the recipient’s personal device.
A Texting Ecosystem
In nearly every case, the hospital will select the text messaging vendor, though hospitalists and nurses, who will typically be among the highest-volume users, should participate in the decision. But the real value of the system hinges on ensuring its wide adoption by most, or nearly all, hospital caregivers and affiliated ambulatory providers.
I would enjoy hearing from those who are already using a HIPAA-secure texting and pager replacement service now, as well as those still researching their options. This has the potential to meaningfully change the way hospitalists and others do their work.
Doctors were the first to begin using pagers and, along with drug dealers, appear to be the last to give them up. But we really need to get rid of them.
Sadly, for the foreseeable future, we will need a pager replacement, but, in the longer term, I’m hopeful that we can:
- Reduce the frequency of electronic interruptions—all forms of interruptions—and the adverse effects that reliably accompany them, and
- Ensure that each interruption has value—that is, reduce or eliminate the many low value and non-urgent messages we all get (e.g. the ones informing you of a lab result you’ve already seen).
Death to the Pager
I can’t imagine anyone who will be more pleased than I will if pagers go the way of now rare hospital-wide PA announcements. Some hospitals have eliminated these announcements entirely, and even critical messages like “code blue” announcements are sent directly to each responder via a pager or other personal device.
Around the time the first iPhone was born, hospital signs banning cell phones began coming down. It seems the fear that they would disrupt hospital electronics, such as telemetry and other monitoring devices, has proven largely unfounded (though, along with things like computer keyboards and stethoscopes, pagers and cell phones can serve as dangerous repositories of bacteria).
Now nearly everyone, from staff to patients, keeps a cell phone with them while in the hospital. I think that is the most important step toward getting rid of pagers. Many doctors already are using the standard text messaging apps that come with the phone to communicate with one another efficiently.
“Regular” Texting Won’t Cut It
Unfortunately, the standard text messaging that comes with every smartphone is not HIPAA compliant. Though I certainly don’t know how anyone would do it, it is apparently too easy for another person to intercept the message. So, if you’re texting information related to your clinical work, you need to make sure it doesn’t include anything that could be considered protected health information. It isn’t enough just to leave the patient’s name off the message. If you’re in the habit of regularly texting doctors, nurses, and other healthcare personnel about patient care, you are at high risk of violating HIPAA, even if you try hard to avoid it.
Another big drawback is that there isn’t a good way to turn off work-related texting when you’re off duty, while leaving your texting app open for communication with your friends and family. Hospital staff will sometimes fail to check whether you’re on duty before texting, and that will lead to your personal time being interrupted by work reminders.
I think these shortcomings mean that none of us should rely on the standard text messaging apps that come with our phones.
But in order for a different app or service to be of any value, we will need to ensure that most providers associated with our hospital are on the same messaging system. That is a tall order, but fortunately there are a lot of companies trying to produce an attractive product that makes it as easy as possible to attract a critical mass of users at your institution.
HIPAA-Compliant Texting Vendors
Many healthcare tech companies provide secure messaging, usually at no additional cost, as an add-on to their main products, such as charge capture software (e.g. IngeniousMed), or physician social networking (e.g. Doximity). Something like 30 companies now offer a dedicated HIPAA-compliant texting option, including IM Your Doc, Voalte, Telmediq, PerfectServe, Vocera, and TigerText. There are so many that it is awfully tough to understand all of their strengths and shortcomings in detail, but I’m having fun trying to do just that. And I anticipate there will be significant consolidation in vendors within the next two to three years.
The dedicated HIPAA-compliant texting services range in price from free for basic features to a monthly fee per user that varies depending on the features you choose to enable. Some offer integration with the hospital’s EHR, which can let a message sender who only knows the patient’s name to see which doctor, nurse, or other caregiver is currently responsible for the patient. Some offer integration with a call schedule and answering service, or even replace an answering service.
No pager replacement will be viable if there are sites in the hospital or elsewhere where it is out of contact; a solution that works on both cellular networks and Wi-Fi is essential. Some vendors offer the ability for messages not delivered to or acknowledged by the recipient to escalate to other forms of delivery after a specified period of time.
I would love to see a feature that I don’t think any vendor offers yet. It would be great if all messages the sender hasn’t marked “stat” or “urgent” first went to a queue in the EHR rather than immediately interrupting the recipient. That way a doctor or other caregiver could see messages while already working in the EHR, rather than glancing at each new message as it arrives, something that all too often needlessly interrupts another important task such as talking with a patient.
And, since most work in EHRs is done in front of a larger device with a full keyboard, it would be easier to type a quick reply message than it would be to rely on a smartphone keyboard for return messaging. Protocols could be established such that messages waiting in the EHR without a reply or dismissal after a specified time would then be sent to the recipient’s personal device.
A Texting Ecosystem
In nearly every case, the hospital will select the text messaging vendor, though hospitalists and nurses, who will typically be among the highest-volume users, should participate in the decision. But the real value of the system hinges on ensuring its wide adoption by most, or nearly all, hospital caregivers and affiliated ambulatory providers.
I would enjoy hearing from those who are already using a HIPAA-secure texting and pager replacement service now, as well as those still researching their options. This has the potential to meaningfully change the way hospitalists and others do their work.
Tips for assessing, managing temper tantrums
Concerns about tantrums come up a lot in pediatric care. We all know about telling parents to ignore tantrums in toddlers and not to give in. But what about when this advice does not work?
I like to think of tantrums as emotions that go beyond the child’s control. This reframing helps families consider that not all tantrums are an attempt by the child to manipulate them. That is an important first step in avoiding a solely punitive response and instead encouraging parents to look for the source of the imbalance.
Temper tantrums are most common when a child is making developmental spurts in abilities or thinking that are typically unevenly matched with self-control. There is a lot of unevenness in children’s ability to do, say, or tolerate feelings between the early tantrums of the 9-month-old until the greater coping of the 6-year-old. For example, 87% of 18- to 24-month-olds have tantrums just as they acquire autonomy and some language, yet can’t really speak their feelings, while 91% of 30- to 36-month-olds have tantrums because they can imagine big things, but are only capable of or allowed small ones. Even at 42-48 months, more than half have tantrums, which often are associated with the stress and fatigue from dropping their nap.
Life is frustrating for kids. Young children want to try to use their new skills such as climbing, opening things, or scribbling, but parents – at first delighted – suddenly want them to stop! At first, every new word is celebrated, but then toddler talk gets routine, and toddlers may be ignored or even shushed. When the child has a strong desire, the words may not be there, or emotions may make it hard to talk at all, leading to frustration.
With the development of a sense of self, the song is “I want,” “mine,” and “no!” Sharing is not in the child’s repertoire until age 3 years or older. Temperamentally more intense children give up less easily or are not readily distracted.
The threshold for frustration depends on the child’s overall state. Is the child hungry? Tired? Stressed? In pain? Here is where the differential diagnosis of excessive tantrums needs to also include pain from a medical condition such as celiac disease, arthritis, migraine, or sickle cell disease. Children under age 7 years commonly have a low tolerance for sensations as simple as loud noises and elastic waistbands, but those with sensory integration disorder are at the extreme in what sounds, feelings, or motions they cannot bear at any age and may need specific intervention by occupational or physical therapists. Mental health conditions such as attention-deficit/hyperactivity disorder, depression, anxiety, and bipolar disorder also predispose to irritable responses to even normal stresses, often in combination with lagging skills and poor sleep. Consider these when tantrums are extreme.

An age period of tantrums may be expected and accepted by parents, thus the name “terrible twos,” but if tantrums persist, they can wear out even a patient parent. Signs that a child’s tantrums are beyond the usual range include a frequency of more than once a day, a duration of more than the typical 5 minutes, or persistence after age 6 years. When you are asked if a child’s tantrums are “normal,” these are useful parameters. It also helps to explain to parents the natural course of anger arousal that starts with a trigger, peaks within 3 minutes, then subsides rapidly (usually a total of 90 seconds), and although starting with anger, ends up with sadness. Asking parents to collect this information helps them avoid interfering with or reinforcing tantrums.
Understanding the child’s temperament and needs, and avoiding triggers, can prevent many tantrums. What was she doing just before the tantrum started? What were the triggers such as fatigue, hunger, inability to express herself, or a buildup of jealousy from repeated sibling intrusions? Are there skill deficits setting him off, especially fine motor or language delays? Management then needs to focus on avoiding these triggers, if possible, and diagnosing and treating developmental delays.
Next, parents can try to distract by jollying, making a joke, or singing. These are useful moments of modeling. Some parents are worried that distracting the child with something more fun to do will interfere with his learning to cope. If distraction works, they should use it!
Often nothing works, and the child has to explode and recover on her own. Talking, cajoling, or scolding during the fit is useless – like trying to squash dynamite after the flame has hit the powder.
While standing by silently ignoring tantrums is usually the fastest way to reduce them, some children calm down faster if held. This does not reinforce the fits as long as the child’s demand is not fulfilled. Instead, it lends adult “ego support” to reassure the child that all is well and life goes on. Children quickly go from angry to sad; older children are even embarrassed by their loss of control. Comfort is appropriate and kind, as long as at least one parent can do this authentically.
Point out that frustrations in small doses are crucial for learning frustration tolerance. Parents who overprotect their child from any little stress to avoid fits is doing him a disservice. Instead, attention, praise, or marks for little bits of self-control effort or for “using your words” builds self-control over time. Times of transitions such as coming for dinner or going to brush teeth are often times of tantrums; these deserve a 2-minute warning and praise or marks for success in “moving on.”(Stopping electronics without a fit is another . Hint: If the child has a fit, he gets no electronics the next day.)
Adult management may be reinforcing tantrums. When parents give the child what she was screaming for, or remove a demand – such as to take a bath – that had sparked a fit, they can count on having an even worse reaction the next time.
I coach parents to think together about the six main things that set off their child’s tantrums and decide in advance on which ones they will hold their ground. Then, when the child just begins to beg for that snack, the parent should decide instantly if this is a “yes” or a “no” (aiming for more yeses). Parental “giving in” before a tantrum starts models positive flexibility for the child and avoids reinforcement. When an event on the “no” list comes up, both parents are then better able to have an unequivocal response and then walk away.
“But when should we teach him a lesson?” parents often ask. If parents interpret a tantrum as manipulative, a moral failing, or an evil tendency, they tend to react with anger and even loss of control themselves. Be alert for risks of excessive punishment in these cases. Not only is their response a poor model and scary for the child, it can even become an exciting, reinforcing display. If parents are depressed or tend to ignore the child as a norm, it may be worth it to the child to throw a fit to bring them to life. You can emphasize that positive attention to good behavior and silent ignoring of fits is more effective and avoids these side effects.
Parents may experience tantrums as a battle of wills that they are not willing to lose, imagining a future rebellious teen. They need education on the normal imbalances of childhood and on both prevention and intervention strategies. What they can lose in the present is their child’s confidence in adult kindness, the opportunity to model flexibility and self-control, and a relationship with their child that conveys acceptance.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical Communications.
Concerns about tantrums come up a lot in pediatric care. We all know about telling parents to ignore tantrums in toddlers and not to give in. But what about when this advice does not work?
I like to think of tantrums as emotions that go beyond the child’s control. This reframing helps families consider that not all tantrums are an attempt by the child to manipulate them. That is an important first step in avoiding a solely punitive response and instead encouraging parents to look for the source of the imbalance.
Temper tantrums are most common when a child is making developmental spurts in abilities or thinking that are typically unevenly matched with self-control. There is a lot of unevenness in children’s ability to do, say, or tolerate feelings between the early tantrums of the 9-month-old until the greater coping of the 6-year-old. For example, 87% of 18- to 24-month-olds have tantrums just as they acquire autonomy and some language, yet can’t really speak their feelings, while 91% of 30- to 36-month-olds have tantrums because they can imagine big things, but are only capable of or allowed small ones. Even at 42-48 months, more than half have tantrums, which often are associated with the stress and fatigue from dropping their nap.
Life is frustrating for kids. Young children want to try to use their new skills such as climbing, opening things, or scribbling, but parents – at first delighted – suddenly want them to stop! At first, every new word is celebrated, but then toddler talk gets routine, and toddlers may be ignored or even shushed. When the child has a strong desire, the words may not be there, or emotions may make it hard to talk at all, leading to frustration.
With the development of a sense of self, the song is “I want,” “mine,” and “no!” Sharing is not in the child’s repertoire until age 3 years or older. Temperamentally more intense children give up less easily or are not readily distracted.
The threshold for frustration depends on the child’s overall state. Is the child hungry? Tired? Stressed? In pain? Here is where the differential diagnosis of excessive tantrums needs to also include pain from a medical condition such as celiac disease, arthritis, migraine, or sickle cell disease. Children under age 7 years commonly have a low tolerance for sensations as simple as loud noises and elastic waistbands, but those with sensory integration disorder are at the extreme in what sounds, feelings, or motions they cannot bear at any age and may need specific intervention by occupational or physical therapists. Mental health conditions such as attention-deficit/hyperactivity disorder, depression, anxiety, and bipolar disorder also predispose to irritable responses to even normal stresses, often in combination with lagging skills and poor sleep. Consider these when tantrums are extreme.
An age period of tantrums may be expected and accepted by parents, thus the name “terrible twos,” but if tantrums persist, they can wear out even a patient parent. Signs that a child’s tantrums are beyond the usual range include a frequency of more than once a day, a duration of more than the typical 5 minutes, or persistence after age 6 years. When you are asked if a child’s tantrums are “normal,” these are useful parameters. It also helps to explain to parents the natural course of anger arousal that starts with a trigger, peaks within 3 minutes, then subsides rapidly (usually a total of 90 seconds), and although starting with anger, ends up with sadness. Asking parents to collect this information helps them avoid interfering with or reinforcing tantrums.
Understanding the child’s temperament and needs, and avoiding triggers, can prevent many tantrums. What was she doing just before the tantrum started? What were the triggers such as fatigue, hunger, inability to express herself, or a buildup of jealousy from repeated sibling intrusions? Are there skill deficits setting him off, especially fine motor or language delays? Management then needs to focus on avoiding these triggers, if possible, and diagnosing and treating developmental delays.
Next, parents can try to distract by jollying, making a joke, or singing. These are useful moments of modeling. Some parents are worried that distracting the child with something more fun to do will interfere with his learning to cope. If distraction works, they should use it!
Often nothing works, and the child has to explode and recover on her own. Talking, cajoling, or scolding during the fit is useless – like trying to squash dynamite after the flame has hit the powder.
While standing by silently ignoring tantrums is usually the fastest way to reduce them, some children calm down faster if held. This does not reinforce the fits as long as the child’s demand is not fulfilled. Instead, it lends adult “ego support” to reassure the child that all is well and life goes on. Children quickly go from angry to sad; older children are even embarrassed by their loss of control. Comfort is appropriate and kind, as long as at least one parent can do this authentically.
Point out that frustrations in small doses are crucial for learning frustration tolerance. Parents who overprotect their child from any little stress to avoid fits is doing him a disservice. Instead, attention, praise, or marks for little bits of self-control effort or for “using your words” builds self-control over time. Times of transitions such as coming for dinner or going to brush teeth are often times of tantrums; these deserve a 2-minute warning and praise or marks for success in “moving on.”(Stopping electronics without a fit is another . Hint: If the child has a fit, he gets no electronics the next day.)
Adult management may be reinforcing tantrums. When parents give the child what she was screaming for, or remove a demand – such as to take a bath – that had sparked a fit, they can count on having an even worse reaction the next time.
I coach parents to think together about the six main things that set off their child’s tantrums and decide in advance on which ones they will hold their ground. Then, when the child just begins to beg for that snack, the parent should decide instantly if this is a “yes” or a “no” (aiming for more yeses). Parental “giving in” before a tantrum starts models positive flexibility for the child and avoids reinforcement. When an event on the “no” list comes up, both parents are then better able to have an unequivocal response and then walk away.
“But when should we teach him a lesson?” parents often ask. If parents interpret a tantrum as manipulative, a moral failing, or an evil tendency, they tend to react with anger and even loss of control themselves. Be alert for risks of excessive punishment in these cases. Not only is their response a poor model and scary for the child, it can even become an exciting, reinforcing display. If parents are depressed or tend to ignore the child as a norm, it may be worth it to the child to throw a fit to bring them to life. You can emphasize that positive attention to good behavior and silent ignoring of fits is more effective and avoids these side effects.
Parents may experience tantrums as a battle of wills that they are not willing to lose, imagining a future rebellious teen. They need education on the normal imbalances of childhood and on both prevention and intervention strategies. What they can lose in the present is their child’s confidence in adult kindness, the opportunity to model flexibility and self-control, and a relationship with their child that conveys acceptance.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical Communications.
Concerns about tantrums come up a lot in pediatric care. We all know about telling parents to ignore tantrums in toddlers and not to give in. But what about when this advice does not work?
I like to think of tantrums as emotions that go beyond the child’s control. This reframing helps families consider that not all tantrums are an attempt by the child to manipulate them. That is an important first step in avoiding a solely punitive response and instead encouraging parents to look for the source of the imbalance.
Temper tantrums are most common when a child is making developmental spurts in abilities or thinking that are typically unevenly matched with self-control. There is a lot of unevenness in children’s ability to do, say, or tolerate feelings between the early tantrums of the 9-month-old until the greater coping of the 6-year-old. For example, 87% of 18- to 24-month-olds have tantrums just as they acquire autonomy and some language, yet can’t really speak their feelings, while 91% of 30- to 36-month-olds have tantrums because they can imagine big things, but are only capable of or allowed small ones. Even at 42-48 months, more than half have tantrums, which often are associated with the stress and fatigue from dropping their nap.
Life is frustrating for kids. Young children want to try to use their new skills such as climbing, opening things, or scribbling, but parents – at first delighted – suddenly want them to stop! At first, every new word is celebrated, but then toddler talk gets routine, and toddlers may be ignored or even shushed. When the child has a strong desire, the words may not be there, or emotions may make it hard to talk at all, leading to frustration.
With the development of a sense of self, the song is “I want,” “mine,” and “no!” Sharing is not in the child’s repertoire until age 3 years or older. Temperamentally more intense children give up less easily or are not readily distracted.
The threshold for frustration depends on the child’s overall state. Is the child hungry? Tired? Stressed? In pain? Here is where the differential diagnosis of excessive tantrums needs to also include pain from a medical condition such as celiac disease, arthritis, migraine, or sickle cell disease. Children under age 7 years commonly have a low tolerance for sensations as simple as loud noises and elastic waistbands, but those with sensory integration disorder are at the extreme in what sounds, feelings, or motions they cannot bear at any age and may need specific intervention by occupational or physical therapists. Mental health conditions such as attention-deficit/hyperactivity disorder, depression, anxiety, and bipolar disorder also predispose to irritable responses to even normal stresses, often in combination with lagging skills and poor sleep. Consider these when tantrums are extreme.
An age period of tantrums may be expected and accepted by parents, thus the name “terrible twos,” but if tantrums persist, they can wear out even a patient parent. Signs that a child’s tantrums are beyond the usual range include a frequency of more than once a day, a duration of more than the typical 5 minutes, or persistence after age 6 years. When you are asked if a child’s tantrums are “normal,” these are useful parameters. It also helps to explain to parents the natural course of anger arousal that starts with a trigger, peaks within 3 minutes, then subsides rapidly (usually a total of 90 seconds), and although starting with anger, ends up with sadness. Asking parents to collect this information helps them avoid interfering with or reinforcing tantrums.
Understanding the child’s temperament and needs, and avoiding triggers, can prevent many tantrums. What was she doing just before the tantrum started? What were the triggers such as fatigue, hunger, inability to express herself, or a buildup of jealousy from repeated sibling intrusions? Are there skill deficits setting him off, especially fine motor or language delays? Management then needs to focus on avoiding these triggers, if possible, and diagnosing and treating developmental delays.
Next, parents can try to distract by jollying, making a joke, or singing. These are useful moments of modeling. Some parents are worried that distracting the child with something more fun to do will interfere with his learning to cope. If distraction works, they should use it!
Often nothing works, and the child has to explode and recover on her own. Talking, cajoling, or scolding during the fit is useless – like trying to squash dynamite after the flame has hit the powder.
While standing by silently ignoring tantrums is usually the fastest way to reduce them, some children calm down faster if held. This does not reinforce the fits as long as the child’s demand is not fulfilled. Instead, it lends adult “ego support” to reassure the child that all is well and life goes on. Children quickly go from angry to sad; older children are even embarrassed by their loss of control. Comfort is appropriate and kind, as long as at least one parent can do this authentically.
Point out that frustrations in small doses are crucial for learning frustration tolerance. Parents who overprotect their child from any little stress to avoid fits is doing him a disservice. Instead, attention, praise, or marks for little bits of self-control effort or for “using your words” builds self-control over time. Times of transitions such as coming for dinner or going to brush teeth are often times of tantrums; these deserve a 2-minute warning and praise or marks for success in “moving on.”(Stopping electronics without a fit is another . Hint: If the child has a fit, he gets no electronics the next day.)
Adult management may be reinforcing tantrums. When parents give the child what she was screaming for, or remove a demand – such as to take a bath – that had sparked a fit, they can count on having an even worse reaction the next time.
I coach parents to think together about the six main things that set off their child’s tantrums and decide in advance on which ones they will hold their ground. Then, when the child just begins to beg for that snack, the parent should decide instantly if this is a “yes” or a “no” (aiming for more yeses). Parental “giving in” before a tantrum starts models positive flexibility for the child and avoids reinforcement. When an event on the “no” list comes up, both parents are then better able to have an unequivocal response and then walk away.
“But when should we teach him a lesson?” parents often ask. If parents interpret a tantrum as manipulative, a moral failing, or an evil tendency, they tend to react with anger and even loss of control themselves. Be alert for risks of excessive punishment in these cases. Not only is their response a poor model and scary for the child, it can even become an exciting, reinforcing display. If parents are depressed or tend to ignore the child as a norm, it may be worth it to the child to throw a fit to bring them to life. You can emphasize that positive attention to good behavior and silent ignoring of fits is more effective and avoids these side effects.
Parents may experience tantrums as a battle of wills that they are not willing to lose, imagining a future rebellious teen. They need education on the normal imbalances of childhood and on both prevention and intervention strategies. What they can lose in the present is their child’s confidence in adult kindness, the opportunity to model flexibility and self-control, and a relationship with their child that conveys acceptance.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical Communications.
Do unto others...
In his most recent bestseller, Being Mortal, Dr. Atul Gawande has again raised social awareness of the inadequacies of our health care system in assisting patients with end-of-life decisions and care. In his treatise, he laments his own lack of training in medical school and residency regarding what he has emphasized should be a key component of any physician’s education.
To some degree, there has been a greater emphasis on palliative care training in our medical schools since Dr. Gawande graduated two decades or so ago. The subject of physician-patient communication, including those difficult discussions that should occur near the end of life, is now incorporated into most medical school curricula. Additionally, palliative care has become a respected and growing subspecialty within both medicine and surgery.* Despite these improvements, still far too many patients die while receiving futile end-of-life care in our nation’s intensive care units and hospital wards rather than in the comfort of their homes surrounded by loved ones. Although referrals have increased, too few patients are afforded the opportunity to utilize hospice care and, those that do, are often referred too late in the course of their terminal disease to obtain full benefit
Why are we not doing better? Two likely contributors include a physician mindset that only cure is success and death represents failure, and unrealistic expectations of patients as to what modern medicine can accomplish. A more fixable and probably more important factor is the failure of doctors to effectively communicate during these highly stressful circumstances. As emphasized by Gawande and from my own experience, the key to negotiating a sensible path in hopeless, end-of-life situations is frequent, reasonable, and realistic consultation with our patients.
Not only are the conversations usually difficult and demanding, but the choices of whether to pursue treatment or remove life-sustaining efforts are frequently not well-defined. While these challenging clinical scenarios are often painted as black and white in the lay press, any physician or surgeon who has cared for such patients realizes that there is a delicate and precarious balance between providing hope, administering appropriate aggressive treatment, and ensuring patient comfort. In a well-intentioned attempt to leave some remnant of hope, we physicians too frequently paint an unrealistic picture for our patients.
Advance patient directives have been promoted as one means for patients to avoid futile, uncomfortable, and unnecessary care during the last stage of their lives. Though I by no means wish to discourage these often useful legal documents, they should not be entered into naively. For example, aggressive life-sustaining care for a patient with extensive metastatic lung cancer is likely inappropriate. On the other hand, short-term ventilator assistance for an elderly unconscious person recovering from an automobile accident may result in many additional years of enjoyable and productive life. Patients need to understand that all grave clinical situations are not equal and that their advance directives should be flexible enough to cover a variety of circumstances.
It has been well established that most patients and families have selective hearing and understanding. Even when the details of a major operation with a greater likelihood of a negative rather than a positive outcome are carefully and clearly presented using lay language, the potential positive outcomes frequently push the more probable adverse consequences into hidden recesses of the brain. In my experience, the more desperate the situation, the more often it is that the possibility of an unsuccessful outcome will be masked or denied by patients or their family members. Even though in my practice I carefully explained the high probability of eventual recurrence when operating on patients with pancreatic cancer, many of them were surprised and some were even quite indignant when this disappointing consequence developed. In my opinion, the most effective means to avoid such misunderstandings is to always have the patient and/or family relate their comprehension of the just-completed conversation. It is then essential to re-emphasize the important details that they suppressed and pushed to the background from your initial explanation.
In these challenging end-of-life moments, what advice should we offer? One question that should almost never be asked of the patient or his/her representative is: “Would you like everything possible done?” Especially for a family member who may take on considerable guilt by answering in the negative, the response will nearly always be “yes” no matter how unlikely a successful outcome. Rather, I believe that recommending only reasonable options, including and possibly emphasizing the choice of comfort therapy alone despite the certainty of death, is our obligation. We should be cognizant of the fact that the decision made by the patient is often highly dependent on how the alternatives are presented by his/her doctor. After clearly presenting the therapeutic options and their likely consequences, it may be helpful to relate what you would do yourself for a loved one in the same circumstances.
As in many other aspects of our lives, a useful guidepost in these situations is the Golden Rule: “Do unto others as you would have done unto yourself.” Interestingly, most probably based on our intimate exposure to numerous unnecessarily complicated and uncomfortable deaths, there is evidence that we physicians choose to die differently than our patients. In a recent essay, Dr. Ken Murray presented data from the John Hopkins Precursors Study that suggested doctors are less likely than their patients to submit themselves to futile end-of-life care. (Murray K: Doctors really do die differently. Zocalopublicsquare.org; accessed March 29, 2015). The proof he presents is from a survey of graduates of Johns Hopkins School of Medicine between 1948 and 1964. It revealed that 65% of them had written their own advance directives in comparison to 20% for the public at large. In addition, only 10% of the graduates would opt for cardiopulmonary resuscitation if they were comatose, compared with 75% of the general population.
I suspect that most surgeons, desiring a dignified death for themselves, are not surprised by these statistics. Therefore, we owe it to our patients to be as compassionate and thoughtful in managing the last stage of their lives as we have traditionally been trained to do in earlier phases when cure was a realistic expectation.
Dr. Rikkers is Editor in Chief of ACS Surgery News.
*Recognizing the importance of end-of-life issues in a surgeon’s education, in 2012 ACS Surgery News initiated a series of articles on various aspects of palliative care.
In his most recent bestseller, Being Mortal, Dr. Atul Gawande has again raised social awareness of the inadequacies of our health care system in assisting patients with end-of-life decisions and care. In his treatise, he laments his own lack of training in medical school and residency regarding what he has emphasized should be a key component of any physician’s education.
To some degree, there has been a greater emphasis on palliative care training in our medical schools since Dr. Gawande graduated two decades or so ago. The subject of physician-patient communication, including those difficult discussions that should occur near the end of life, is now incorporated into most medical school curricula. Additionally, palliative care has become a respected and growing subspecialty within both medicine and surgery.* Despite these improvements, still far too many patients die while receiving futile end-of-life care in our nation’s intensive care units and hospital wards rather than in the comfort of their homes surrounded by loved ones. Although referrals have increased, too few patients are afforded the opportunity to utilize hospice care and, those that do, are often referred too late in the course of their terminal disease to obtain full benefit
Why are we not doing better? Two likely contributors include a physician mindset that only cure is success and death represents failure, and unrealistic expectations of patients as to what modern medicine can accomplish. A more fixable and probably more important factor is the failure of doctors to effectively communicate during these highly stressful circumstances. As emphasized by Gawande and from my own experience, the key to negotiating a sensible path in hopeless, end-of-life situations is frequent, reasonable, and realistic consultation with our patients.
Not only are the conversations usually difficult and demanding, but the choices of whether to pursue treatment or remove life-sustaining efforts are frequently not well-defined. While these challenging clinical scenarios are often painted as black and white in the lay press, any physician or surgeon who has cared for such patients realizes that there is a delicate and precarious balance between providing hope, administering appropriate aggressive treatment, and ensuring patient comfort. In a well-intentioned attempt to leave some remnant of hope, we physicians too frequently paint an unrealistic picture for our patients.
Advance patient directives have been promoted as one means for patients to avoid futile, uncomfortable, and unnecessary care during the last stage of their lives. Though I by no means wish to discourage these often useful legal documents, they should not be entered into naively. For example, aggressive life-sustaining care for a patient with extensive metastatic lung cancer is likely inappropriate. On the other hand, short-term ventilator assistance for an elderly unconscious person recovering from an automobile accident may result in many additional years of enjoyable and productive life. Patients need to understand that all grave clinical situations are not equal and that their advance directives should be flexible enough to cover a variety of circumstances.
It has been well established that most patients and families have selective hearing and understanding. Even when the details of a major operation with a greater likelihood of a negative rather than a positive outcome are carefully and clearly presented using lay language, the potential positive outcomes frequently push the more probable adverse consequences into hidden recesses of the brain. In my experience, the more desperate the situation, the more often it is that the possibility of an unsuccessful outcome will be masked or denied by patients or their family members. Even though in my practice I carefully explained the high probability of eventual recurrence when operating on patients with pancreatic cancer, many of them were surprised and some were even quite indignant when this disappointing consequence developed. In my opinion, the most effective means to avoid such misunderstandings is to always have the patient and/or family relate their comprehension of the just-completed conversation. It is then essential to re-emphasize the important details that they suppressed and pushed to the background from your initial explanation.
In these challenging end-of-life moments, what advice should we offer? One question that should almost never be asked of the patient or his/her representative is: “Would you like everything possible done?” Especially for a family member who may take on considerable guilt by answering in the negative, the response will nearly always be “yes” no matter how unlikely a successful outcome. Rather, I believe that recommending only reasonable options, including and possibly emphasizing the choice of comfort therapy alone despite the certainty of death, is our obligation. We should be cognizant of the fact that the decision made by the patient is often highly dependent on how the alternatives are presented by his/her doctor. After clearly presenting the therapeutic options and their likely consequences, it may be helpful to relate what you would do yourself for a loved one in the same circumstances.
As in many other aspects of our lives, a useful guidepost in these situations is the Golden Rule: “Do unto others as you would have done unto yourself.” Interestingly, most probably based on our intimate exposure to numerous unnecessarily complicated and uncomfortable deaths, there is evidence that we physicians choose to die differently than our patients. In a recent essay, Dr. Ken Murray presented data from the John Hopkins Precursors Study that suggested doctors are less likely than their patients to submit themselves to futile end-of-life care. (Murray K: Doctors really do die differently. Zocalopublicsquare.org; accessed March 29, 2015). The proof he presents is from a survey of graduates of Johns Hopkins School of Medicine between 1948 and 1964. It revealed that 65% of them had written their own advance directives in comparison to 20% for the public at large. In addition, only 10% of the graduates would opt for cardiopulmonary resuscitation if they were comatose, compared with 75% of the general population.
I suspect that most surgeons, desiring a dignified death for themselves, are not surprised by these statistics. Therefore, we owe it to our patients to be as compassionate and thoughtful in managing the last stage of their lives as we have traditionally been trained to do in earlier phases when cure was a realistic expectation.
Dr. Rikkers is Editor in Chief of ACS Surgery News.
*Recognizing the importance of end-of-life issues in a surgeon’s education, in 2012 ACS Surgery News initiated a series of articles on various aspects of palliative care.
In his most recent bestseller, Being Mortal, Dr. Atul Gawande has again raised social awareness of the inadequacies of our health care system in assisting patients with end-of-life decisions and care. In his treatise, he laments his own lack of training in medical school and residency regarding what he has emphasized should be a key component of any physician’s education.
To some degree, there has been a greater emphasis on palliative care training in our medical schools since Dr. Gawande graduated two decades or so ago. The subject of physician-patient communication, including those difficult discussions that should occur near the end of life, is now incorporated into most medical school curricula. Additionally, palliative care has become a respected and growing subspecialty within both medicine and surgery.* Despite these improvements, still far too many patients die while receiving futile end-of-life care in our nation’s intensive care units and hospital wards rather than in the comfort of their homes surrounded by loved ones. Although referrals have increased, too few patients are afforded the opportunity to utilize hospice care and, those that do, are often referred too late in the course of their terminal disease to obtain full benefit
Why are we not doing better? Two likely contributors include a physician mindset that only cure is success and death represents failure, and unrealistic expectations of patients as to what modern medicine can accomplish. A more fixable and probably more important factor is the failure of doctors to effectively communicate during these highly stressful circumstances. As emphasized by Gawande and from my own experience, the key to negotiating a sensible path in hopeless, end-of-life situations is frequent, reasonable, and realistic consultation with our patients.
Not only are the conversations usually difficult and demanding, but the choices of whether to pursue treatment or remove life-sustaining efforts are frequently not well-defined. While these challenging clinical scenarios are often painted as black and white in the lay press, any physician or surgeon who has cared for such patients realizes that there is a delicate and precarious balance between providing hope, administering appropriate aggressive treatment, and ensuring patient comfort. In a well-intentioned attempt to leave some remnant of hope, we physicians too frequently paint an unrealistic picture for our patients.
Advance patient directives have been promoted as one means for patients to avoid futile, uncomfortable, and unnecessary care during the last stage of their lives. Though I by no means wish to discourage these often useful legal documents, they should not be entered into naively. For example, aggressive life-sustaining care for a patient with extensive metastatic lung cancer is likely inappropriate. On the other hand, short-term ventilator assistance for an elderly unconscious person recovering from an automobile accident may result in many additional years of enjoyable and productive life. Patients need to understand that all grave clinical situations are not equal and that their advance directives should be flexible enough to cover a variety of circumstances.
It has been well established that most patients and families have selective hearing and understanding. Even when the details of a major operation with a greater likelihood of a negative rather than a positive outcome are carefully and clearly presented using lay language, the potential positive outcomes frequently push the more probable adverse consequences into hidden recesses of the brain. In my experience, the more desperate the situation, the more often it is that the possibility of an unsuccessful outcome will be masked or denied by patients or their family members. Even though in my practice I carefully explained the high probability of eventual recurrence when operating on patients with pancreatic cancer, many of them were surprised and some were even quite indignant when this disappointing consequence developed. In my opinion, the most effective means to avoid such misunderstandings is to always have the patient and/or family relate their comprehension of the just-completed conversation. It is then essential to re-emphasize the important details that they suppressed and pushed to the background from your initial explanation.
In these challenging end-of-life moments, what advice should we offer? One question that should almost never be asked of the patient or his/her representative is: “Would you like everything possible done?” Especially for a family member who may take on considerable guilt by answering in the negative, the response will nearly always be “yes” no matter how unlikely a successful outcome. Rather, I believe that recommending only reasonable options, including and possibly emphasizing the choice of comfort therapy alone despite the certainty of death, is our obligation. We should be cognizant of the fact that the decision made by the patient is often highly dependent on how the alternatives are presented by his/her doctor. After clearly presenting the therapeutic options and their likely consequences, it may be helpful to relate what you would do yourself for a loved one in the same circumstances.
As in many other aspects of our lives, a useful guidepost in these situations is the Golden Rule: “Do unto others as you would have done unto yourself.” Interestingly, most probably based on our intimate exposure to numerous unnecessarily complicated and uncomfortable deaths, there is evidence that we physicians choose to die differently than our patients. In a recent essay, Dr. Ken Murray presented data from the John Hopkins Precursors Study that suggested doctors are less likely than their patients to submit themselves to futile end-of-life care. (Murray K: Doctors really do die differently. Zocalopublicsquare.org; accessed March 29, 2015). The proof he presents is from a survey of graduates of Johns Hopkins School of Medicine between 1948 and 1964. It revealed that 65% of them had written their own advance directives in comparison to 20% for the public at large. In addition, only 10% of the graduates would opt for cardiopulmonary resuscitation if they were comatose, compared with 75% of the general population.
I suspect that most surgeons, desiring a dignified death for themselves, are not surprised by these statistics. Therefore, we owe it to our patients to be as compassionate and thoughtful in managing the last stage of their lives as we have traditionally been trained to do in earlier phases when cure was a realistic expectation.
Dr. Rikkers is Editor in Chief of ACS Surgery News.
*Recognizing the importance of end-of-life issues in a surgeon’s education, in 2012 ACS Surgery News initiated a series of articles on various aspects of palliative care.
Good medical care for psychiatric patients is imperative
The first year of residency came faster than I had expected and concluded just as quickly. At times, it felt like medical school, with different rotations, adjusting to newly formed teams, dealing with the pressures of getting the right diagnosis and treatment, managing the unrelenting speed of rounds, and trying to make a difference for the better. I must be honest – there were times when I was counting down the days for the rotation to end so that I could begin focusing and working directly in the mental health field.
Now, in my second year, the pace has improved, and the rotations resemble the work and patient population that I chose during the match process. Nonetheless, I am thankful for the time spent and the knowledge gained during my intern year, because it is only now that I understand the true value of my first-year experiences and the need to continue getting a well-rounded medical education for the benefit of my patients.
During my second year of residency, I have come across multiple instances of health disparities for people with mental illness. While working in several inpatient units, I have witnessed delayed time of visit from medical/surgical or ob.gyn. consults, shorter evaluation times from visiting consulting personnel, and postponed follow-up appointments for general medical conditions. I remember one occasion when a patient with urinary incontinence waited 3 days until internal medicine completed its consult. These experiences remind me of the conversations I had in medical school. Some of my colleagues would say, “Psychiatric patients are difficult.” Others were honest in admitting that they were scared to even enter a psychiatric inpatient unit.
Medical comorbidities common
During one 24-hour shift, I was paged to the inpatient unit. A new admission from that afternoon was complaining of “toe pain.”
The patient had been admitted for suicidal ideation and alcohol withdrawal. He reported tripping over a concrete step 2 weeks prior to admission. Under examination, he had an open laceration with purulent, foul-smelling discharge, erythema, and edema around the wound. The patient had signs of cellulitis, had a possible fracture of the phalanx, and was at risk for osteomyelitis.
He had been medically cleared at another facility prior to his admission, where he also had complained of toe pain. At that time, however, he was told, “You are not here for that,” and the extremity was not examined during the medical clearance. I ordered a referral, imaging was completed, and antibiotic treatment was started for his infection. Unfortunately, this is not an incidental or isolated case; situations similar to this one have become more frequent than we would like for those with mental illness.
Often, psychiatric patients are overlooked and undertreated. We frequently are the only physicians who evaluate the patient and help improve their quality of life. After reviewing the literature, I found countless studies concluding that patients who have a psychiatric diagnosis often have increased medical comorbidity and even increased mortality. A review and meta-analysis published earlier this year suggested that “people with mental disorders often do not receive preventive services, such as immunizations, cancer screenings, and tobacco counseling, and often receive a lower quality of care for medical conditions” (JAMA Psychiatry 2015;72:334-41). The researchers also found that “mortality was significantly higher among people with mental disorders than among the comparison population.”
Focusing on mind, body
I knew I wanted to be a psychiatrist since my early years in training. Initially, I was drawn toward psychology, in which I completed a bachelor’s degree, but my world turned around after a conversation with the father of a high school classmate. He told me: “I commend you on your decision to want to help people; however, I would like to give you food for thought. If your goal is to be of service to your patients and provide care, it would be to their benefit to address not only the mind but also the body” (which, coincidentally, is the theme of this year’s American Psychiatric Association meeting in Toronto.)
At that time, I was weighing becoming a clinician versus a physician; after all, both have instrumental roles in treatment. Yet, those words resonate now in my life for a new reason, namely, that my duty as an advocate for mental health is not only to treat psychiatric disorders but also to work toward treating general medical conditions.
I have been fortunate to cross paths with mentors who helped strengthen my commitment to well-rounded care and a multidisciplinary approach for the mentally ill. I am thankful to have worked with Dr. Jill Williams, who stressed the need to treat tobacco dependence, and Dr. Anthony Tobia, who emphasized the need to rule out substance- and medication-induced disorders prior to treatment. I have had the pleasure of working with many other attending psychiatrists who not only focused on psychiatric symptoms and diagnosis but stressed the need to address the medical care of our patients.
If I can understand my patients by learning about human behavior, conditioning, defense mechanisms, and interpersonal relationships and also focus on pathophysiology, comorbid conditions, differential diagnosis, and exacerbating medical conditions, I will be able to give them the best medical care possible.
Dr. Poulsen, a second-year psychiatry resident at the Robert Wood Johnson Medical School, Piscataway, N.J., is interested in cultural psychiatry and advocacy, and in pursuing a fellowship in child and adolescent psychiatry. After obtaining a bachelor of science degree at the University of Florida, Gainesville, he earned a medical degree at the University of Puerto Rico. He is currently serving in multiple leadership positions, including vice president of the New Jersey Psychiatric Association (NJPA) Residents Chapter and NJPA chapter advocacy coordinator. In addition, he has been selected as resident-fellow representative of the APA’s Area 3.
The first year of residency came faster than I had expected and concluded just as quickly. At times, it felt like medical school, with different rotations, adjusting to newly formed teams, dealing with the pressures of getting the right diagnosis and treatment, managing the unrelenting speed of rounds, and trying to make a difference for the better. I must be honest – there were times when I was counting down the days for the rotation to end so that I could begin focusing and working directly in the mental health field.
Now, in my second year, the pace has improved, and the rotations resemble the work and patient population that I chose during the match process. Nonetheless, I am thankful for the time spent and the knowledge gained during my intern year, because it is only now that I understand the true value of my first-year experiences and the need to continue getting a well-rounded medical education for the benefit of my patients.
During my second year of residency, I have come across multiple instances of health disparities for people with mental illness. While working in several inpatient units, I have witnessed delayed time of visit from medical/surgical or ob.gyn. consults, shorter evaluation times from visiting consulting personnel, and postponed follow-up appointments for general medical conditions. I remember one occasion when a patient with urinary incontinence waited 3 days until internal medicine completed its consult. These experiences remind me of the conversations I had in medical school. Some of my colleagues would say, “Psychiatric patients are difficult.” Others were honest in admitting that they were scared to even enter a psychiatric inpatient unit.
Medical comorbidities common
During one 24-hour shift, I was paged to the inpatient unit. A new admission from that afternoon was complaining of “toe pain.”
The patient had been admitted for suicidal ideation and alcohol withdrawal. He reported tripping over a concrete step 2 weeks prior to admission. Under examination, he had an open laceration with purulent, foul-smelling discharge, erythema, and edema around the wound. The patient had signs of cellulitis, had a possible fracture of the phalanx, and was at risk for osteomyelitis.
He had been medically cleared at another facility prior to his admission, where he also had complained of toe pain. At that time, however, he was told, “You are not here for that,” and the extremity was not examined during the medical clearance. I ordered a referral, imaging was completed, and antibiotic treatment was started for his infection. Unfortunately, this is not an incidental or isolated case; situations similar to this one have become more frequent than we would like for those with mental illness.
Often, psychiatric patients are overlooked and undertreated. We frequently are the only physicians who evaluate the patient and help improve their quality of life. After reviewing the literature, I found countless studies concluding that patients who have a psychiatric diagnosis often have increased medical comorbidity and even increased mortality. A review and meta-analysis published earlier this year suggested that “people with mental disorders often do not receive preventive services, such as immunizations, cancer screenings, and tobacco counseling, and often receive a lower quality of care for medical conditions” (JAMA Psychiatry 2015;72:334-41). The researchers also found that “mortality was significantly higher among people with mental disorders than among the comparison population.”
Focusing on mind, body
I knew I wanted to be a psychiatrist since my early years in training. Initially, I was drawn toward psychology, in which I completed a bachelor’s degree, but my world turned around after a conversation with the father of a high school classmate. He told me: “I commend you on your decision to want to help people; however, I would like to give you food for thought. If your goal is to be of service to your patients and provide care, it would be to their benefit to address not only the mind but also the body” (which, coincidentally, is the theme of this year’s American Psychiatric Association meeting in Toronto.)
At that time, I was weighing becoming a clinician versus a physician; after all, both have instrumental roles in treatment. Yet, those words resonate now in my life for a new reason, namely, that my duty as an advocate for mental health is not only to treat psychiatric disorders but also to work toward treating general medical conditions.
I have been fortunate to cross paths with mentors who helped strengthen my commitment to well-rounded care and a multidisciplinary approach for the mentally ill. I am thankful to have worked with Dr. Jill Williams, who stressed the need to treat tobacco dependence, and Dr. Anthony Tobia, who emphasized the need to rule out substance- and medication-induced disorders prior to treatment. I have had the pleasure of working with many other attending psychiatrists who not only focused on psychiatric symptoms and diagnosis but stressed the need to address the medical care of our patients.
If I can understand my patients by learning about human behavior, conditioning, defense mechanisms, and interpersonal relationships and also focus on pathophysiology, comorbid conditions, differential diagnosis, and exacerbating medical conditions, I will be able to give them the best medical care possible.
Dr. Poulsen, a second-year psychiatry resident at the Robert Wood Johnson Medical School, Piscataway, N.J., is interested in cultural psychiatry and advocacy, and in pursuing a fellowship in child and adolescent psychiatry. After obtaining a bachelor of science degree at the University of Florida, Gainesville, he earned a medical degree at the University of Puerto Rico. He is currently serving in multiple leadership positions, including vice president of the New Jersey Psychiatric Association (NJPA) Residents Chapter and NJPA chapter advocacy coordinator. In addition, he has been selected as resident-fellow representative of the APA’s Area 3.
The first year of residency came faster than I had expected and concluded just as quickly. At times, it felt like medical school, with different rotations, adjusting to newly formed teams, dealing with the pressures of getting the right diagnosis and treatment, managing the unrelenting speed of rounds, and trying to make a difference for the better. I must be honest – there were times when I was counting down the days for the rotation to end so that I could begin focusing and working directly in the mental health field.
Now, in my second year, the pace has improved, and the rotations resemble the work and patient population that I chose during the match process. Nonetheless, I am thankful for the time spent and the knowledge gained during my intern year, because it is only now that I understand the true value of my first-year experiences and the need to continue getting a well-rounded medical education for the benefit of my patients.
During my second year of residency, I have come across multiple instances of health disparities for people with mental illness. While working in several inpatient units, I have witnessed delayed time of visit from medical/surgical or ob.gyn. consults, shorter evaluation times from visiting consulting personnel, and postponed follow-up appointments for general medical conditions. I remember one occasion when a patient with urinary incontinence waited 3 days until internal medicine completed its consult. These experiences remind me of the conversations I had in medical school. Some of my colleagues would say, “Psychiatric patients are difficult.” Others were honest in admitting that they were scared to even enter a psychiatric inpatient unit.
Medical comorbidities common
During one 24-hour shift, I was paged to the inpatient unit. A new admission from that afternoon was complaining of “toe pain.”
The patient had been admitted for suicidal ideation and alcohol withdrawal. He reported tripping over a concrete step 2 weeks prior to admission. Under examination, he had an open laceration with purulent, foul-smelling discharge, erythema, and edema around the wound. The patient had signs of cellulitis, had a possible fracture of the phalanx, and was at risk for osteomyelitis.
He had been medically cleared at another facility prior to his admission, where he also had complained of toe pain. At that time, however, he was told, “You are not here for that,” and the extremity was not examined during the medical clearance. I ordered a referral, imaging was completed, and antibiotic treatment was started for his infection. Unfortunately, this is not an incidental or isolated case; situations similar to this one have become more frequent than we would like for those with mental illness.
Often, psychiatric patients are overlooked and undertreated. We frequently are the only physicians who evaluate the patient and help improve their quality of life. After reviewing the literature, I found countless studies concluding that patients who have a psychiatric diagnosis often have increased medical comorbidity and even increased mortality. A review and meta-analysis published earlier this year suggested that “people with mental disorders often do not receive preventive services, such as immunizations, cancer screenings, and tobacco counseling, and often receive a lower quality of care for medical conditions” (JAMA Psychiatry 2015;72:334-41). The researchers also found that “mortality was significantly higher among people with mental disorders than among the comparison population.”
Focusing on mind, body
I knew I wanted to be a psychiatrist since my early years in training. Initially, I was drawn toward psychology, in which I completed a bachelor’s degree, but my world turned around after a conversation with the father of a high school classmate. He told me: “I commend you on your decision to want to help people; however, I would like to give you food for thought. If your goal is to be of service to your patients and provide care, it would be to their benefit to address not only the mind but also the body” (which, coincidentally, is the theme of this year’s American Psychiatric Association meeting in Toronto.)
At that time, I was weighing becoming a clinician versus a physician; after all, both have instrumental roles in treatment. Yet, those words resonate now in my life for a new reason, namely, that my duty as an advocate for mental health is not only to treat psychiatric disorders but also to work toward treating general medical conditions.
I have been fortunate to cross paths with mentors who helped strengthen my commitment to well-rounded care and a multidisciplinary approach for the mentally ill. I am thankful to have worked with Dr. Jill Williams, who stressed the need to treat tobacco dependence, and Dr. Anthony Tobia, who emphasized the need to rule out substance- and medication-induced disorders prior to treatment. I have had the pleasure of working with many other attending psychiatrists who not only focused on psychiatric symptoms and diagnosis but stressed the need to address the medical care of our patients.
If I can understand my patients by learning about human behavior, conditioning, defense mechanisms, and interpersonal relationships and also focus on pathophysiology, comorbid conditions, differential diagnosis, and exacerbating medical conditions, I will be able to give them the best medical care possible.
Dr. Poulsen, a second-year psychiatry resident at the Robert Wood Johnson Medical School, Piscataway, N.J., is interested in cultural psychiatry and advocacy, and in pursuing a fellowship in child and adolescent psychiatry. After obtaining a bachelor of science degree at the University of Florida, Gainesville, he earned a medical degree at the University of Puerto Rico. He is currently serving in multiple leadership positions, including vice president of the New Jersey Psychiatric Association (NJPA) Residents Chapter and NJPA chapter advocacy coordinator. In addition, he has been selected as resident-fellow representative of the APA’s Area 3.

Treating a Japanese patient with family pressures
Editors’ Note: This is the first installment of Curbside Consult, written by two Group for the Advancement of Psychiatry (GAP) committees – the Committee on Family Psychiatry and the Committee on Cultural Psychiatry.
Come back home
The patient is an unmarried Japanese man in his early 40s who presents with symptoms of social phobia. He was born and raised in Japan, and migrated to the United States to pursue a PhD. In Japan, he enjoyed middle-class status, but after immigrating to the United States, he has faced many financial difficulties. His language barriers have made him uncomfortable in front of his colleagues and supervisors and he has not been able to do well in his PhD program, ultimately leading to his expulsion. He does not want to go back to Japan, thinking he will not have a “good life” there. He believes that there is no respect for a person’s individuality in Japan. He is currently living in an urban location of New Jersey and works odd jobs. He states that his family does not understand his feelings about not returning to Japan, and instead they want him to support them. He has engaged in supportive psychotherapy and cognitive-behavioral therapy in the outpatient clinic along with psychopharmacological treatment.
Key questions
1. How is Japanese culture different from U.S. culture in terms of respecting a person’s individuality?
2. The expectations of the patient’s family are considered excessive by the patient. What is the role of Japanese culture in this situation?
3. In moving forward with treatment planning, what aspects of the patient’s culture should the clinician keep in mind?
Family perspective
This middle-aged Japanese man has had a challenging time since coming to the United States to study. He lives here alone. He has failed to achieve his goal of earning a PhD. He has had financial difficulties because of his job challenges. He has had the courage to seek mental health treatment, although the goals of his treatment are unclear. He is in contact with his family in Japan, who has asked that he come home, presumably to support his somewhat older parents. It is unclear who constitutes his “family.”

From a family perspective, it seems that the family/parents in Japan are expecting that family obligation will draw the man home while the patient is defying that expectation by seeking and building individuality in the United States. A family-oriented therapist would consider the patient’s relationship with his family and help him consider how to make his decision on where to live. The therapist also would support the patient in maintaining a connection with his family. The therapist would help the patient avoid both passively capitulating to his family and defiantly cutting off from them. This would entail discussing the role of family in the United States and Japan. It would be important to empower the patient to explore his reasons for wanting to stay in the United States, what he means by “a good life,” and what he senses as his obligation to his family.
The history of this man’s life in Japan, including recollections of his childhood and an understanding of the job history of other members of his family, will help the therapist understand this man and his experience of his family. The telling of the family narrative, from his perspective, may help the patient understand his wishes and his fears. Exploring his relationships with his mother and his father will help the therapist and the patient understand some of the problems he has had in the United States.
Given his current life circumstances, work, and social stresses, lack of social support, and problems functioning, he also should be clinically assessed for depression and any other significant mental health problems. Additional questions to explore include: Does he define himself as a “failure,” and what would it be like going back to Japan? Are there concerns about “losing face”? If his parents want him to support them, do they know about his financial situation? Would he be able to get a job in Japan, or would he end up living with his parents? Are their requests that he “come home” based on their need for support, or are they afraid that he really needs their help given his difficulties establishing a life here? As the patient explores these issues in more detail, he can begin the process of resolving his future.
Cultural psychiatry perspective
This case raises important cultural questions, which deserve further exploration in psychotherapy. Alternate approaches to evaluating culture in clinical settings have moved away from conceptualizing “U.S.” or “Japanese” cultures monolithically to understand how cultural dynamics matter to the individual.

Notably, clarifying what the patient means by the “individuality” that is “not respected in Japan” would be essential, as well as what he perceives as “excessive” in his family’s demands. Alan Roland, Ph.D., in his book “In Search of Self in India and Japan: Toward a Cross-Cultural Psychology” describes marked differences between traditional Japanese and U.S. expectations of family obligation and relationship: “dependence and interdependence with close emotional connectedness versus independence and autonomy; receptivity and deference to superiors in hierarchical relationships versus self-assertion and self-promotion in egalitarian-contractual relationships; communication on multiple levels and by innuendo versus verbal articulateness and forthrightness; maintaining and enhancing esteem at all costs versus forthright criticism and expressing the truth of the matter” (pp. 292-3).
Of course, these are intentionally polarized descriptions; yet many Japanese in the United States find themselves negotiating contrasting expectations about what it means to be a person in a family and a society, some finding value in at least parts of each tradition, some holding on to traditional Japanese values, and some adopting values related to the new environment.

A key question in this case is what made the situation so difficult for this patient. Going forward, the clinician will want to characterize the biopsychosocial etiologies of his symptoms. Are the social phobia symptoms related to premorbid developmental issues hindering communication, planning, and sociability? Were they exacerbated by language difficulties and the acculturation challenges of finding himself in a new country and institution with potentially different expectations of fulfillment and success?
One wonders how he was accepted into this PhD program and why his performance led to expulsion so quickly. Are there additional symptoms and impairments beyond the breakdown in communication? For example, are there depressive symptoms? Does he have other somatic symptomatology as part of his idiom of distress that may be magnifying his impairment? Were academic supports in place that could have prevented his expulsion? Does he have other social supports and relationships? Is he struggling with intense isolation and, potentially, individuation issues triggered by his new setting?
The DSM-5 Cultural Formulation Interview (CFI), a standardized method for conducting a cultural assessment in mental health care, could help the clinician elicit the patient’s understandings of the problem, its causes and contextual stressors and supports, cultural identity, the cultural features of the relationship between the patient and the clinician, and options for self-coping and clinical care. This exploration of the patient’s lifeworld may clarify how to intervene. Selected supplementary modules to the CFI also may also be useful to ‘amplify’ the core CFI and to further explore the patient’s perception of the family’s role in his illness, including the Social Network Module and the Psychosocial Stressors Module.
Contributors
John Sargent, M.D. – Tufts University School of Medicine
Ellen Berman, M.D. – University of Pennsylvania, Perelman School of Medicine
Roberto Lewis-Fernández, M.D. – Columbia University and New York State Psychiatric Institute
Robert C. Like, M.D., M.S. – Rutgers University, Robert Wood Johnson Medical School
Resources
Lewis-Fernández R., Aggarwal N.K., Baarnhielm, S., et al. Culture and Psychiatric Evaluation: Operationalizing Cultural Formulation for DSM-5 (Psychiatry 2014;77:130-54).
Roland A. In Search of Self in India and Japan: Toward a Cross-Cultural Psychology (Princeton,
N.J.: Princeton University Press, 1988).
Shibusawa T. Japanese Families, in Ethnicity and Family Therapy, 3rd edition. Edited by McGoldrick M., Giordano J., and Garcia-Preto. (New York: Guilford Press, 2005, pp. 339-48).
Tseng W.S., Chang S.C., Nishizono M., eds. Asian Culture and Psychotherapy: Implications for East and West (Honolulu: University of Hawai’i Press).
To read about the goals of Curbside Consult, the guiding principles for assessment, and the guidelines for case submission, see “Considering patients’ family, culture,” Clinical Psychiatry News, January 2015, p. 12. To contribute a case, send it to cpnews@frontlinemedcom.com. The contributors have revised selected patient details to shield the identities of the patients/cases and to comply with HIPAA requirements. This column is meant to be educational and does not constitute medical advice. The opinions expressed are those of the contributors and do not represent those of the organizations they employed by or affiliated with or the Group for the Advancement of Psychiatry (GAP).
Editors’ Note: This is the first installment of Curbside Consult, written by two Group for the Advancement of Psychiatry (GAP) committees – the Committee on Family Psychiatry and the Committee on Cultural Psychiatry.
Come back home
The patient is an unmarried Japanese man in his early 40s who presents with symptoms of social phobia. He was born and raised in Japan, and migrated to the United States to pursue a PhD. In Japan, he enjoyed middle-class status, but after immigrating to the United States, he has faced many financial difficulties. His language barriers have made him uncomfortable in front of his colleagues and supervisors and he has not been able to do well in his PhD program, ultimately leading to his expulsion. He does not want to go back to Japan, thinking he will not have a “good life” there. He believes that there is no respect for a person’s individuality in Japan. He is currently living in an urban location of New Jersey and works odd jobs. He states that his family does not understand his feelings about not returning to Japan, and instead they want him to support them. He has engaged in supportive psychotherapy and cognitive-behavioral therapy in the outpatient clinic along with psychopharmacological treatment.
Key questions
1. How is Japanese culture different from U.S. culture in terms of respecting a person’s individuality?
2. The expectations of the patient’s family are considered excessive by the patient. What is the role of Japanese culture in this situation?
3. In moving forward with treatment planning, what aspects of the patient’s culture should the clinician keep in mind?
Family perspective
This middle-aged Japanese man has had a challenging time since coming to the United States to study. He lives here alone. He has failed to achieve his goal of earning a PhD. He has had financial difficulties because of his job challenges. He has had the courage to seek mental health treatment, although the goals of his treatment are unclear. He is in contact with his family in Japan, who has asked that he come home, presumably to support his somewhat older parents. It is unclear who constitutes his “family.”
From a family perspective, it seems that the family/parents in Japan are expecting that family obligation will draw the man home while the patient is defying that expectation by seeking and building individuality in the United States. A family-oriented therapist would consider the patient’s relationship with his family and help him consider how to make his decision on where to live. The therapist also would support the patient in maintaining a connection with his family. The therapist would help the patient avoid both passively capitulating to his family and defiantly cutting off from them. This would entail discussing the role of family in the United States and Japan. It would be important to empower the patient to explore his reasons for wanting to stay in the United States, what he means by “a good life,” and what he senses as his obligation to his family.
The history of this man’s life in Japan, including recollections of his childhood and an understanding of the job history of other members of his family, will help the therapist understand this man and his experience of his family. The telling of the family narrative, from his perspective, may help the patient understand his wishes and his fears. Exploring his relationships with his mother and his father will help the therapist and the patient understand some of the problems he has had in the United States.
Given his current life circumstances, work, and social stresses, lack of social support, and problems functioning, he also should be clinically assessed for depression and any other significant mental health problems. Additional questions to explore include: Does he define himself as a “failure,” and what would it be like going back to Japan? Are there concerns about “losing face”? If his parents want him to support them, do they know about his financial situation? Would he be able to get a job in Japan, or would he end up living with his parents? Are their requests that he “come home” based on their need for support, or are they afraid that he really needs their help given his difficulties establishing a life here? As the patient explores these issues in more detail, he can begin the process of resolving his future.
Cultural psychiatry perspective
This case raises important cultural questions, which deserve further exploration in psychotherapy. Alternate approaches to evaluating culture in clinical settings have moved away from conceptualizing “U.S.” or “Japanese” cultures monolithically to understand how cultural dynamics matter to the individual.
Notably, clarifying what the patient means by the “individuality” that is “not respected in Japan” would be essential, as well as what he perceives as “excessive” in his family’s demands. Alan Roland, Ph.D., in his book “In Search of Self in India and Japan: Toward a Cross-Cultural Psychology” describes marked differences between traditional Japanese and U.S. expectations of family obligation and relationship: “dependence and interdependence with close emotional connectedness versus independence and autonomy; receptivity and deference to superiors in hierarchical relationships versus self-assertion and self-promotion in egalitarian-contractual relationships; communication on multiple levels and by innuendo versus verbal articulateness and forthrightness; maintaining and enhancing esteem at all costs versus forthright criticism and expressing the truth of the matter” (pp. 292-3).
Of course, these are intentionally polarized descriptions; yet many Japanese in the United States find themselves negotiating contrasting expectations about what it means to be a person in a family and a society, some finding value in at least parts of each tradition, some holding on to traditional Japanese values, and some adopting values related to the new environment.
A key question in this case is what made the situation so difficult for this patient. Going forward, the clinician will want to characterize the biopsychosocial etiologies of his symptoms. Are the social phobia symptoms related to premorbid developmental issues hindering communication, planning, and sociability? Were they exacerbated by language difficulties and the acculturation challenges of finding himself in a new country and institution with potentially different expectations of fulfillment and success?
One wonders how he was accepted into this PhD program and why his performance led to expulsion so quickly. Are there additional symptoms and impairments beyond the breakdown in communication? For example, are there depressive symptoms? Does he have other somatic symptomatology as part of his idiom of distress that may be magnifying his impairment? Were academic supports in place that could have prevented his expulsion? Does he have other social supports and relationships? Is he struggling with intense isolation and, potentially, individuation issues triggered by his new setting?
The DSM-5 Cultural Formulation Interview (CFI), a standardized method for conducting a cultural assessment in mental health care, could help the clinician elicit the patient’s understandings of the problem, its causes and contextual stressors and supports, cultural identity, the cultural features of the relationship between the patient and the clinician, and options for self-coping and clinical care. This exploration of the patient’s lifeworld may clarify how to intervene. Selected supplementary modules to the CFI also may also be useful to ‘amplify’ the core CFI and to further explore the patient’s perception of the family’s role in his illness, including the Social Network Module and the Psychosocial Stressors Module.
Contributors
John Sargent, M.D. – Tufts University School of Medicine
Ellen Berman, M.D. – University of Pennsylvania, Perelman School of Medicine
Roberto Lewis-Fernández, M.D. – Columbia University and New York State Psychiatric Institute
Robert C. Like, M.D., M.S. – Rutgers University, Robert Wood Johnson Medical School
Resources
Lewis-Fernández R., Aggarwal N.K., Baarnhielm, S., et al. Culture and Psychiatric Evaluation: Operationalizing Cultural Formulation for DSM-5 (Psychiatry 2014;77:130-54).
Roland A. In Search of Self in India and Japan: Toward a Cross-Cultural Psychology (Princeton,
N.J.: Princeton University Press, 1988).
Shibusawa T. Japanese Families, in Ethnicity and Family Therapy, 3rd edition. Edited by McGoldrick M., Giordano J., and Garcia-Preto. (New York: Guilford Press, 2005, pp. 339-48).
Tseng W.S., Chang S.C., Nishizono M., eds. Asian Culture and Psychotherapy: Implications for East and West (Honolulu: University of Hawai’i Press).
To read about the goals of Curbside Consult, the guiding principles for assessment, and the guidelines for case submission, see “Considering patients’ family, culture,” Clinical Psychiatry News, January 2015, p. 12. To contribute a case, send it to cpnews@frontlinemedcom.com. The contributors have revised selected patient details to shield the identities of the patients/cases and to comply with HIPAA requirements. This column is meant to be educational and does not constitute medical advice. The opinions expressed are those of the contributors and do not represent those of the organizations they employed by or affiliated with or the Group for the Advancement of Psychiatry (GAP).
Editors’ Note: This is the first installment of Curbside Consult, written by two Group for the Advancement of Psychiatry (GAP) committees – the Committee on Family Psychiatry and the Committee on Cultural Psychiatry.
Come back home
The patient is an unmarried Japanese man in his early 40s who presents with symptoms of social phobia. He was born and raised in Japan, and migrated to the United States to pursue a PhD. In Japan, he enjoyed middle-class status, but after immigrating to the United States, he has faced many financial difficulties. His language barriers have made him uncomfortable in front of his colleagues and supervisors and he has not been able to do well in his PhD program, ultimately leading to his expulsion. He does not want to go back to Japan, thinking he will not have a “good life” there. He believes that there is no respect for a person’s individuality in Japan. He is currently living in an urban location of New Jersey and works odd jobs. He states that his family does not understand his feelings about not returning to Japan, and instead they want him to support them. He has engaged in supportive psychotherapy and cognitive-behavioral therapy in the outpatient clinic along with psychopharmacological treatment.
Key questions
1. How is Japanese culture different from U.S. culture in terms of respecting a person’s individuality?
2. The expectations of the patient’s family are considered excessive by the patient. What is the role of Japanese culture in this situation?
3. In moving forward with treatment planning, what aspects of the patient’s culture should the clinician keep in mind?
Family perspective
This middle-aged Japanese man has had a challenging time since coming to the United States to study. He lives here alone. He has failed to achieve his goal of earning a PhD. He has had financial difficulties because of his job challenges. He has had the courage to seek mental health treatment, although the goals of his treatment are unclear. He is in contact with his family in Japan, who has asked that he come home, presumably to support his somewhat older parents. It is unclear who constitutes his “family.”
From a family perspective, it seems that the family/parents in Japan are expecting that family obligation will draw the man home while the patient is defying that expectation by seeking and building individuality in the United States. A family-oriented therapist would consider the patient’s relationship with his family and help him consider how to make his decision on where to live. The therapist also would support the patient in maintaining a connection with his family. The therapist would help the patient avoid both passively capitulating to his family and defiantly cutting off from them. This would entail discussing the role of family in the United States and Japan. It would be important to empower the patient to explore his reasons for wanting to stay in the United States, what he means by “a good life,” and what he senses as his obligation to his family.
The history of this man’s life in Japan, including recollections of his childhood and an understanding of the job history of other members of his family, will help the therapist understand this man and his experience of his family. The telling of the family narrative, from his perspective, may help the patient understand his wishes and his fears. Exploring his relationships with his mother and his father will help the therapist and the patient understand some of the problems he has had in the United States.
Given his current life circumstances, work, and social stresses, lack of social support, and problems functioning, he also should be clinically assessed for depression and any other significant mental health problems. Additional questions to explore include: Does he define himself as a “failure,” and what would it be like going back to Japan? Are there concerns about “losing face”? If his parents want him to support them, do they know about his financial situation? Would he be able to get a job in Japan, or would he end up living with his parents? Are their requests that he “come home” based on their need for support, or are they afraid that he really needs their help given his difficulties establishing a life here? As the patient explores these issues in more detail, he can begin the process of resolving his future.
Cultural psychiatry perspective
This case raises important cultural questions, which deserve further exploration in psychotherapy. Alternate approaches to evaluating culture in clinical settings have moved away from conceptualizing “U.S.” or “Japanese” cultures monolithically to understand how cultural dynamics matter to the individual.
Notably, clarifying what the patient means by the “individuality” that is “not respected in Japan” would be essential, as well as what he perceives as “excessive” in his family’s demands. Alan Roland, Ph.D., in his book “In Search of Self in India and Japan: Toward a Cross-Cultural Psychology” describes marked differences between traditional Japanese and U.S. expectations of family obligation and relationship: “dependence and interdependence with close emotional connectedness versus independence and autonomy; receptivity and deference to superiors in hierarchical relationships versus self-assertion and self-promotion in egalitarian-contractual relationships; communication on multiple levels and by innuendo versus verbal articulateness and forthrightness; maintaining and enhancing esteem at all costs versus forthright criticism and expressing the truth of the matter” (pp. 292-3).
Of course, these are intentionally polarized descriptions; yet many Japanese in the United States find themselves negotiating contrasting expectations about what it means to be a person in a family and a society, some finding value in at least parts of each tradition, some holding on to traditional Japanese values, and some adopting values related to the new environment.
A key question in this case is what made the situation so difficult for this patient. Going forward, the clinician will want to characterize the biopsychosocial etiologies of his symptoms. Are the social phobia symptoms related to premorbid developmental issues hindering communication, planning, and sociability? Were they exacerbated by language difficulties and the acculturation challenges of finding himself in a new country and institution with potentially different expectations of fulfillment and success?
One wonders how he was accepted into this PhD program and why his performance led to expulsion so quickly. Are there additional symptoms and impairments beyond the breakdown in communication? For example, are there depressive symptoms? Does he have other somatic symptomatology as part of his idiom of distress that may be magnifying his impairment? Were academic supports in place that could have prevented his expulsion? Does he have other social supports and relationships? Is he struggling with intense isolation and, potentially, individuation issues triggered by his new setting?
The DSM-5 Cultural Formulation Interview (CFI), a standardized method for conducting a cultural assessment in mental health care, could help the clinician elicit the patient’s understandings of the problem, its causes and contextual stressors and supports, cultural identity, the cultural features of the relationship between the patient and the clinician, and options for self-coping and clinical care. This exploration of the patient’s lifeworld may clarify how to intervene. Selected supplementary modules to the CFI also may also be useful to ‘amplify’ the core CFI and to further explore the patient’s perception of the family’s role in his illness, including the Social Network Module and the Psychosocial Stressors Module.
Contributors
John Sargent, M.D. – Tufts University School of Medicine
Ellen Berman, M.D. – University of Pennsylvania, Perelman School of Medicine
Roberto Lewis-Fernández, M.D. – Columbia University and New York State Psychiatric Institute
Robert C. Like, M.D., M.S. – Rutgers University, Robert Wood Johnson Medical School
Resources
Lewis-Fernández R., Aggarwal N.K., Baarnhielm, S., et al. Culture and Psychiatric Evaluation: Operationalizing Cultural Formulation for DSM-5 (Psychiatry 2014;77:130-54).
Roland A. In Search of Self in India and Japan: Toward a Cross-Cultural Psychology (Princeton,
N.J.: Princeton University Press, 1988).
Shibusawa T. Japanese Families, in Ethnicity and Family Therapy, 3rd edition. Edited by McGoldrick M., Giordano J., and Garcia-Preto. (New York: Guilford Press, 2005, pp. 339-48).
Tseng W.S., Chang S.C., Nishizono M., eds. Asian Culture and Psychotherapy: Implications for East and West (Honolulu: University of Hawai’i Press).
To read about the goals of Curbside Consult, the guiding principles for assessment, and the guidelines for case submission, see “Considering patients’ family, culture,” Clinical Psychiatry News, January 2015, p. 12. To contribute a case, send it to cpnews@frontlinemedcom.com. The contributors have revised selected patient details to shield the identities of the patients/cases and to comply with HIPAA requirements. This column is meant to be educational and does not constitute medical advice. The opinions expressed are those of the contributors and do not represent those of the organizations they employed by or affiliated with or the Group for the Advancement of Psychiatry (GAP).

The Biggest Thing in Hospital Medicine Since Patient Safety?
Editor’s note: First of a two-part series examining bundled payments and hospital medicine. Additionally, Dr. Whitcomb works for a company that is an Awardee Convener in the CMS Bundled Payments for Care Improvement (BPCI) Initiative.
The Centers for Medicare and Medicaid Services’ (CMS) bundled payment initiative was announced in August 2011 and has been “live” since October 2013, when a handful of healthcare systems launched bundled payment programs. In 2014, the CMS initiative grew substantially as a result of large-scale interest on the part of hospitals, physician groups, skilled nursing facilities (SNFs), and others in testing the model, which can be described as a single payment for an episode of care.
The BPCI initiative will be a large-scale program by July 1; it starts with an April 1 cohort launch and will result in the program’s presence in all 50 states, with hundreds of physician practices and hospitals participating. The 2015 cohort will involve a large number of hospitalist practices, participating as “episode initiators” that bear clinical and economic responsibility for the bundle, or as “gainsharers” who are eligible to receive incentive payments if they can reduce costs while maintaining measurable quality for an episode of care.
How Does Bundled Payment Work?
The BPCI initiative is a large-scale, three- to five-year demonstration to test bundled payment in patients with fee-for-service Medicare. The most common model, referred to as Model 2, involves an inpatient hospitalization for one of 48 defined episodes, which include both medical and surgical conditions, followed by a recovery period lasting 30, 60, or 90 days.
Each hospital or physician practice that is considering entering the BPCI program receives prices for all 48 episodes based on a 2009-2012 historical average of Medicare part A and B claims associated with that hospital or physician group. After analyzing those prices, the hospital or physician practice may elect to choose the bundles that have a good chance of being successful—where actual spending comes in under the historical target price—based on care improvement expectations in their local system. In Model 2, CMS takes 2% off the target price for 90-day episodes and 3% off the target price for 30- and 60-day episodes, making it all the more important to choose bundles that demonstrate a high likelihood of success.
The revenue cycle for hospitals and physicians in the program does not change. They submit claims for their services and receive reimbursement as they always have; however, after the end of each quarter, when the majority of part A and B claims have been processed, a “look back” at actual spending for all participating episodes is reconciled against the baseline price derived from 2009-2012. If there is a net savings compared to the baseline, monies can be distributed to the participating providers—the hospital or physician practice—and those providers may further share some of the savings with other physicians/providers who have signed a gainsharing contract.
Hospitalists and BPCI
Hospitalist practices participate in the CMS program either as episode initiators or gainsharers. As episode initiators, they “own” the bundle, which means they bear economic risk for the program. In this capacity, overall savings will mean the hospitalist practice has a new revenue stream, which could be substantial; however, the practice is also responsible for any losses.
Other hospitalist practices have become gainsharers in the program, which means they have signed an agreement enabling them to receive payments in addition to professional fee revenues for activities that reduce costs while maintaining or improving quality. Such activities are referred to as “care redesign” in the program. Gainsharers do not bear financial risk.
Where Will Savings Come From?
Perhaps ironically for hospitalists, the main source of savings in the BPCI program comes from post-acute care and readmissions. For example, for common conditions like heart failure, COPD, and pneumonia, Medicare spends almost as much on post-acute care and readmissions in the first 30 days after discharge as it does on the index hospitalization.1 As a result, the BPCI program adds further emphasis on preventing readmissions when added to existing pressures, and there is a new premium placed on “right-sizing” the usage of SNF and other post-acute facilities, such as inpatient rehabilitation and long-term acute care hospitals. For hospitalists, this means that new rigor is needed to connect to the post-acute setting, such as determining why a patient is being discharged to a skilled facility.
Another savings pool, called “internal cost savings,” is available to reward decreasing inpatient utilization from, for example, testing, imaging, and implantable devices.
Conclusion
Bundled payment might be the biggest thing to come along for hospitalists since the patient safety movement launched some 16 years ago. Why? Although accountable care organizations have largely focused on ambulatory practice, bundled payment has a major focus on hospital care and on the post-acute care decisions that are made during the hospitalization. If bundled payment proves to be an effective way to pay for—and organize—care, hospitalists will play a central role in the success of this innovation.
In part two of this series, I will explore specific roles hospitalists play in successful bundled payment programs.
Reference
Editor’s note: First of a two-part series examining bundled payments and hospital medicine. Additionally, Dr. Whitcomb works for a company that is an Awardee Convener in the CMS Bundled Payments for Care Improvement (BPCI) Initiative.
The Centers for Medicare and Medicaid Services’ (CMS) bundled payment initiative was announced in August 2011 and has been “live” since October 2013, when a handful of healthcare systems launched bundled payment programs. In 2014, the CMS initiative grew substantially as a result of large-scale interest on the part of hospitals, physician groups, skilled nursing facilities (SNFs), and others in testing the model, which can be described as a single payment for an episode of care.
The BPCI initiative will be a large-scale program by July 1; it starts with an April 1 cohort launch and will result in the program’s presence in all 50 states, with hundreds of physician practices and hospitals participating. The 2015 cohort will involve a large number of hospitalist practices, participating as “episode initiators” that bear clinical and economic responsibility for the bundle, or as “gainsharers” who are eligible to receive incentive payments if they can reduce costs while maintaining measurable quality for an episode of care.
How Does Bundled Payment Work?
The BPCI initiative is a large-scale, three- to five-year demonstration to test bundled payment in patients with fee-for-service Medicare. The most common model, referred to as Model 2, involves an inpatient hospitalization for one of 48 defined episodes, which include both medical and surgical conditions, followed by a recovery period lasting 30, 60, or 90 days.
Each hospital or physician practice that is considering entering the BPCI program receives prices for all 48 episodes based on a 2009-2012 historical average of Medicare part A and B claims associated with that hospital or physician group. After analyzing those prices, the hospital or physician practice may elect to choose the bundles that have a good chance of being successful—where actual spending comes in under the historical target price—based on care improvement expectations in their local system. In Model 2, CMS takes 2% off the target price for 90-day episodes and 3% off the target price for 30- and 60-day episodes, making it all the more important to choose bundles that demonstrate a high likelihood of success.
The revenue cycle for hospitals and physicians in the program does not change. They submit claims for their services and receive reimbursement as they always have; however, after the end of each quarter, when the majority of part A and B claims have been processed, a “look back” at actual spending for all participating episodes is reconciled against the baseline price derived from 2009-2012. If there is a net savings compared to the baseline, monies can be distributed to the participating providers—the hospital or physician practice—and those providers may further share some of the savings with other physicians/providers who have signed a gainsharing contract.
Hospitalists and BPCI
Hospitalist practices participate in the CMS program either as episode initiators or gainsharers. As episode initiators, they “own” the bundle, which means they bear economic risk for the program. In this capacity, overall savings will mean the hospitalist practice has a new revenue stream, which could be substantial; however, the practice is also responsible for any losses.
Other hospitalist practices have become gainsharers in the program, which means they have signed an agreement enabling them to receive payments in addition to professional fee revenues for activities that reduce costs while maintaining or improving quality. Such activities are referred to as “care redesign” in the program. Gainsharers do not bear financial risk.
Where Will Savings Come From?
Perhaps ironically for hospitalists, the main source of savings in the BPCI program comes from post-acute care and readmissions. For example, for common conditions like heart failure, COPD, and pneumonia, Medicare spends almost as much on post-acute care and readmissions in the first 30 days after discharge as it does on the index hospitalization.1 As a result, the BPCI program adds further emphasis on preventing readmissions when added to existing pressures, and there is a new premium placed on “right-sizing” the usage of SNF and other post-acute facilities, such as inpatient rehabilitation and long-term acute care hospitals. For hospitalists, this means that new rigor is needed to connect to the post-acute setting, such as determining why a patient is being discharged to a skilled facility.
Another savings pool, called “internal cost savings,” is available to reward decreasing inpatient utilization from, for example, testing, imaging, and implantable devices.
Conclusion
Bundled payment might be the biggest thing to come along for hospitalists since the patient safety movement launched some 16 years ago. Why? Although accountable care organizations have largely focused on ambulatory practice, bundled payment has a major focus on hospital care and on the post-acute care decisions that are made during the hospitalization. If bundled payment proves to be an effective way to pay for—and organize—care, hospitalists will play a central role in the success of this innovation.
In part two of this series, I will explore specific roles hospitalists play in successful bundled payment programs.
Reference
Editor’s note: First of a two-part series examining bundled payments and hospital medicine. Additionally, Dr. Whitcomb works for a company that is an Awardee Convener in the CMS Bundled Payments for Care Improvement (BPCI) Initiative.
The Centers for Medicare and Medicaid Services’ (CMS) bundled payment initiative was announced in August 2011 and has been “live” since October 2013, when a handful of healthcare systems launched bundled payment programs. In 2014, the CMS initiative grew substantially as a result of large-scale interest on the part of hospitals, physician groups, skilled nursing facilities (SNFs), and others in testing the model, which can be described as a single payment for an episode of care.
The BPCI initiative will be a large-scale program by July 1; it starts with an April 1 cohort launch and will result in the program’s presence in all 50 states, with hundreds of physician practices and hospitals participating. The 2015 cohort will involve a large number of hospitalist practices, participating as “episode initiators” that bear clinical and economic responsibility for the bundle, or as “gainsharers” who are eligible to receive incentive payments if they can reduce costs while maintaining measurable quality for an episode of care.
How Does Bundled Payment Work?
The BPCI initiative is a large-scale, three- to five-year demonstration to test bundled payment in patients with fee-for-service Medicare. The most common model, referred to as Model 2, involves an inpatient hospitalization for one of 48 defined episodes, which include both medical and surgical conditions, followed by a recovery period lasting 30, 60, or 90 days.
Each hospital or physician practice that is considering entering the BPCI program receives prices for all 48 episodes based on a 2009-2012 historical average of Medicare part A and B claims associated with that hospital or physician group. After analyzing those prices, the hospital or physician practice may elect to choose the bundles that have a good chance of being successful—where actual spending comes in under the historical target price—based on care improvement expectations in their local system. In Model 2, CMS takes 2% off the target price for 90-day episodes and 3% off the target price for 30- and 60-day episodes, making it all the more important to choose bundles that demonstrate a high likelihood of success.
The revenue cycle for hospitals and physicians in the program does not change. They submit claims for their services and receive reimbursement as they always have; however, after the end of each quarter, when the majority of part A and B claims have been processed, a “look back” at actual spending for all participating episodes is reconciled against the baseline price derived from 2009-2012. If there is a net savings compared to the baseline, monies can be distributed to the participating providers—the hospital or physician practice—and those providers may further share some of the savings with other physicians/providers who have signed a gainsharing contract.
Hospitalists and BPCI
Hospitalist practices participate in the CMS program either as episode initiators or gainsharers. As episode initiators, they “own” the bundle, which means they bear economic risk for the program. In this capacity, overall savings will mean the hospitalist practice has a new revenue stream, which could be substantial; however, the practice is also responsible for any losses.
Other hospitalist practices have become gainsharers in the program, which means they have signed an agreement enabling them to receive payments in addition to professional fee revenues for activities that reduce costs while maintaining or improving quality. Such activities are referred to as “care redesign” in the program. Gainsharers do not bear financial risk.
Where Will Savings Come From?
Perhaps ironically for hospitalists, the main source of savings in the BPCI program comes from post-acute care and readmissions. For example, for common conditions like heart failure, COPD, and pneumonia, Medicare spends almost as much on post-acute care and readmissions in the first 30 days after discharge as it does on the index hospitalization.1 As a result, the BPCI program adds further emphasis on preventing readmissions when added to existing pressures, and there is a new premium placed on “right-sizing” the usage of SNF and other post-acute facilities, such as inpatient rehabilitation and long-term acute care hospitals. For hospitalists, this means that new rigor is needed to connect to the post-acute setting, such as determining why a patient is being discharged to a skilled facility.
Another savings pool, called “internal cost savings,” is available to reward decreasing inpatient utilization from, for example, testing, imaging, and implantable devices.
Conclusion
Bundled payment might be the biggest thing to come along for hospitalists since the patient safety movement launched some 16 years ago. Why? Although accountable care organizations have largely focused on ambulatory practice, bundled payment has a major focus on hospital care and on the post-acute care decisions that are made during the hospitalization. If bundled payment proves to be an effective way to pay for—and organize—care, hospitalists will play a central role in the success of this innovation.
In part two of this series, I will explore specific roles hospitalists play in successful bundled payment programs.