User login
Early Mobility Program
“I didn’t get out of bed for 10 days”
—Anonymous patient admitted to a skilled nursing facility post-hospitalization for a COPD exacerbation
Readmission penalties, “Medicare spending per beneficiary” under value-based purchasing, and the move to accountable care are propelling hospitalists to do more to ensure our patients recover well in the least restrictive setting, without returning to the hospital. As we build systems to support patient recovery, we are focused on a medical model, paying attention to managing diseases and reconciling medications. At the same time, there is a growing awareness that functional status and mobility are critical pieces of patient care during and post-hospitalization.
Regardless of principal diagnosis and comorbidities, patients’ functional mobility ultimately determines their trajectory during recovery. To illustrate the importance of functional status and outcomes, one study showed that models predicting readmission based on functional measures outperformed those based on comorbidities.1
The negative effects of hospitalization on patient mobility, and in turn, on recovery, have been recognized for a long time. Immobility is associated with functional decline, which contributes to falls, increased length of stay, delirium, loss of ability to perform activities of daily living, and loss of ambulatory independence. A number of studies have reported successful early mobility programs in critical care and surgical patients.2 Fewer have been reported in general medical patients.3 Taken together, they suggest that a program for mobilizing patients, using a team approach, is an important part of recovery during and after hospitalization.
The purpose of this column is to report the components of one healthcare system’s mobility program for general medical-surgical patients.
Early Mobility: A Case Study
St Luke’s University Health Network (SLUHN) in northeastern Pennsylvania has implemented an early mobility program as part of its broader strategy to reduce readmissions and discharge as many patients home as possible. Although the SLUHN early mobility program depends on nursing, nursing assistants, and the judicious use of therapists, physician leadership during implementation and maintenance of the program has been essential. Moreover, because the program represents a culture shift, especially for nursing, leadership and change management are crucial ingredients for success. Below are the key steps in the SLUHN early mobility program.
Establish baseline functional status. Recording baseline function is an essential first step. For patients admitted through the ED, nurses collect ambulatory status, patient needs for assistance, ambulatory aids/special equipment, and history of falls. They populate an SBAR (situation, background, assessment, recommendation) form with this information and, as part of the handoff, ensure that it is transmitted to the inpatient nurse receiving the patient.
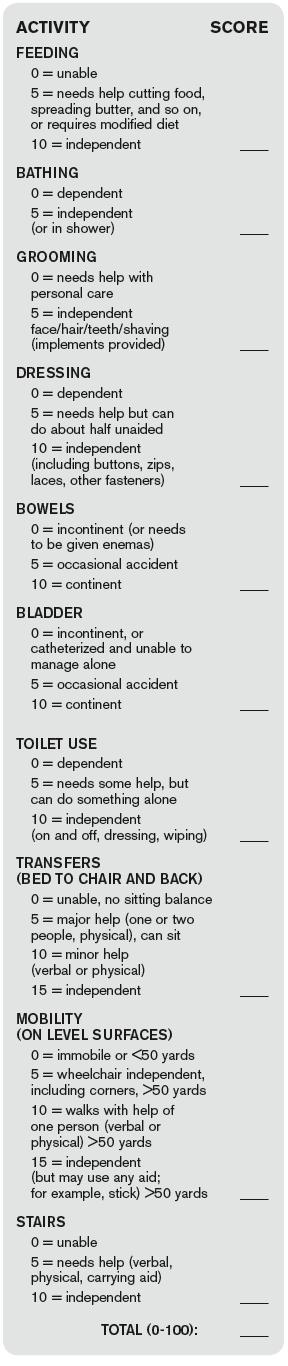
Obtain and document Barthel Index score. SLUHN uses the Barthel Index (see Figure 1) to establish a patient’s degree of independence and need for supervision. The index is scored on a 0-100 scale, with a higher score corresponding to a greater degree of independence. SLUHN created three categories: 0-59, stage 1; 60-84, stage 2; 85-100, stage 3.
Patient mobility plan. Based on the Barthel-derived stage, a patient is assigned a mobility plan.
The role of nursing. The patient’s registered nurse is responsible for implementing the “patient mobility plan.” The nurse initiates an “interdisciplinary plan of care,” in which the mobility stage is written on the SBAR handoff report tool. The report is discussed at change of shift and at multidisciplinary rounds. Nursing also communicates the mobility plan to the nursing assistants and assigns responsibilities for the mobility plan (activities of daily living, out of bed, ambulation, and so on), including verifying documentation of daily activities and assessing the patient’s response to the activity level of the assigned stage.
Further, nursing maintains and revises the mobility status on the SBAR, updates progress toward outcomes on the care plan, consults with the physician and team regarding the discharge plan, and discusses progress with the patient and family.
The role of the nursing/patient care assistant. The nursing assistant is responsible for implementing elements of the plan, such as activities of daily living, getting out of bed, and ambulation, under the guidance of the nurse. The nursing assistant reports patient responses to activity level and reflects mobility goals back to the patient verbally and through white board messaging.
Patient progress in mobility. When a patient sustains progress at one stage for 24 hours, the nurse aims to move the patient to the next stage by reevaluating the Barthel Index and going through the same steps as those followed during the initial scoring. The process moves the patient to higher activity levels, unless there are intervening problems affecting mobility.
In such cases, according to the Barthel Index, the patient may remain at the same—or be moved to a lower—activity level. In practice, patients are assessed each shift, and those with higher function (stage 3) are progressed to unsupervised ambulation.
The role of physical and occupational therapy. Although the role of physical and occupational therapists in the SLUHN mobility program is well codified, it is reserved for patients with complex rehabilitation needs due to the number of patients requiring rehabilitation.
In sum, this patient mobility program–for non-ICU hospitalized patients–relies on:
- Documentation of baseline function;
- Independent scoring using the Barthel Index;
- Creation of clear roles for nursing, nursing assistants, and therapists; and
- Reevaluation of patients at regular intervals based on the Barthel Index, so that they may progress to greater activity levels (or to lower levels in the case of a setback).
A key subsequent step, an evaluation of the program’s performance in terms of readmissions, transfer rates to a skilled nursing facility, and skilled facility length of stay, has shown positive results in all three domains.


References
- Shi SL, Girrard P, Goldstein R, et al. Functional status outperforms comorbidities in predicting acute care readmissions in medically complex patients. J Gen Intern Med. 2015;30(11):1688-1695.
- Dammeyer JA, Baldwin N, Packard D, et al. Mobilizing outcomes: implementation of a nurse-led multidisciplinary mobility program. Crit Care Nurs Q. 2013;36(1):109-119.
- Wood W, Tschannen D, Trotsky A, et al. A mobility program for an inpatient acute care medical unit. Am J Nurs. 2014;114(10):34-40.
- Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65.
“I didn’t get out of bed for 10 days”
—Anonymous patient admitted to a skilled nursing facility post-hospitalization for a COPD exacerbation
Readmission penalties, “Medicare spending per beneficiary” under value-based purchasing, and the move to accountable care are propelling hospitalists to do more to ensure our patients recover well in the least restrictive setting, without returning to the hospital. As we build systems to support patient recovery, we are focused on a medical model, paying attention to managing diseases and reconciling medications. At the same time, there is a growing awareness that functional status and mobility are critical pieces of patient care during and post-hospitalization.
Regardless of principal diagnosis and comorbidities, patients’ functional mobility ultimately determines their trajectory during recovery. To illustrate the importance of functional status and outcomes, one study showed that models predicting readmission based on functional measures outperformed those based on comorbidities.1
The negative effects of hospitalization on patient mobility, and in turn, on recovery, have been recognized for a long time. Immobility is associated with functional decline, which contributes to falls, increased length of stay, delirium, loss of ability to perform activities of daily living, and loss of ambulatory independence. A number of studies have reported successful early mobility programs in critical care and surgical patients.2 Fewer have been reported in general medical patients.3 Taken together, they suggest that a program for mobilizing patients, using a team approach, is an important part of recovery during and after hospitalization.
The purpose of this column is to report the components of one healthcare system’s mobility program for general medical-surgical patients.
Early Mobility: A Case Study
St Luke’s University Health Network (SLUHN) in northeastern Pennsylvania has implemented an early mobility program as part of its broader strategy to reduce readmissions and discharge as many patients home as possible. Although the SLUHN early mobility program depends on nursing, nursing assistants, and the judicious use of therapists, physician leadership during implementation and maintenance of the program has been essential. Moreover, because the program represents a culture shift, especially for nursing, leadership and change management are crucial ingredients for success. Below are the key steps in the SLUHN early mobility program.
Establish baseline functional status. Recording baseline function is an essential first step. For patients admitted through the ED, nurses collect ambulatory status, patient needs for assistance, ambulatory aids/special equipment, and history of falls. They populate an SBAR (situation, background, assessment, recommendation) form with this information and, as part of the handoff, ensure that it is transmitted to the inpatient nurse receiving the patient.
Obtain and document Barthel Index score. SLUHN uses the Barthel Index (see Figure 1) to establish a patient’s degree of independence and need for supervision. The index is scored on a 0-100 scale, with a higher score corresponding to a greater degree of independence. SLUHN created three categories: 0-59, stage 1; 60-84, stage 2; 85-100, stage 3.
Patient mobility plan. Based on the Barthel-derived stage, a patient is assigned a mobility plan.
The role of nursing. The patient’s registered nurse is responsible for implementing the “patient mobility plan.” The nurse initiates an “interdisciplinary plan of care,” in which the mobility stage is written on the SBAR handoff report tool. The report is discussed at change of shift and at multidisciplinary rounds. Nursing also communicates the mobility plan to the nursing assistants and assigns responsibilities for the mobility plan (activities of daily living, out of bed, ambulation, and so on), including verifying documentation of daily activities and assessing the patient’s response to the activity level of the assigned stage.
Further, nursing maintains and revises the mobility status on the SBAR, updates progress toward outcomes on the care plan, consults with the physician and team regarding the discharge plan, and discusses progress with the patient and family.
The role of the nursing/patient care assistant. The nursing assistant is responsible for implementing elements of the plan, such as activities of daily living, getting out of bed, and ambulation, under the guidance of the nurse. The nursing assistant reports patient responses to activity level and reflects mobility goals back to the patient verbally and through white board messaging.
Patient progress in mobility. When a patient sustains progress at one stage for 24 hours, the nurse aims to move the patient to the next stage by reevaluating the Barthel Index and going through the same steps as those followed during the initial scoring. The process moves the patient to higher activity levels, unless there are intervening problems affecting mobility.
In such cases, according to the Barthel Index, the patient may remain at the same—or be moved to a lower—activity level. In practice, patients are assessed each shift, and those with higher function (stage 3) are progressed to unsupervised ambulation.
The role of physical and occupational therapy. Although the role of physical and occupational therapists in the SLUHN mobility program is well codified, it is reserved for patients with complex rehabilitation needs due to the number of patients requiring rehabilitation.
In sum, this patient mobility program–for non-ICU hospitalized patients–relies on:
- Documentation of baseline function;
- Independent scoring using the Barthel Index;
- Creation of clear roles for nursing, nursing assistants, and therapists; and
- Reevaluation of patients at regular intervals based on the Barthel Index, so that they may progress to greater activity levels (or to lower levels in the case of a setback).
A key subsequent step, an evaluation of the program’s performance in terms of readmissions, transfer rates to a skilled nursing facility, and skilled facility length of stay, has shown positive results in all three domains.
References
- Shi SL, Girrard P, Goldstein R, et al. Functional status outperforms comorbidities in predicting acute care readmissions in medically complex patients. J Gen Intern Med. 2015;30(11):1688-1695.
- Dammeyer JA, Baldwin N, Packard D, et al. Mobilizing outcomes: implementation of a nurse-led multidisciplinary mobility program. Crit Care Nurs Q. 2013;36(1):109-119.
- Wood W, Tschannen D, Trotsky A, et al. A mobility program for an inpatient acute care medical unit. Am J Nurs. 2014;114(10):34-40.
- Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65.
“I didn’t get out of bed for 10 days”
—Anonymous patient admitted to a skilled nursing facility post-hospitalization for a COPD exacerbation
Readmission penalties, “Medicare spending per beneficiary” under value-based purchasing, and the move to accountable care are propelling hospitalists to do more to ensure our patients recover well in the least restrictive setting, without returning to the hospital. As we build systems to support patient recovery, we are focused on a medical model, paying attention to managing diseases and reconciling medications. At the same time, there is a growing awareness that functional status and mobility are critical pieces of patient care during and post-hospitalization.
Regardless of principal diagnosis and comorbidities, patients’ functional mobility ultimately determines their trajectory during recovery. To illustrate the importance of functional status and outcomes, one study showed that models predicting readmission based on functional measures outperformed those based on comorbidities.1
The negative effects of hospitalization on patient mobility, and in turn, on recovery, have been recognized for a long time. Immobility is associated with functional decline, which contributes to falls, increased length of stay, delirium, loss of ability to perform activities of daily living, and loss of ambulatory independence. A number of studies have reported successful early mobility programs in critical care and surgical patients.2 Fewer have been reported in general medical patients.3 Taken together, they suggest that a program for mobilizing patients, using a team approach, is an important part of recovery during and after hospitalization.
The purpose of this column is to report the components of one healthcare system’s mobility program for general medical-surgical patients.
Early Mobility: A Case Study
St Luke’s University Health Network (SLUHN) in northeastern Pennsylvania has implemented an early mobility program as part of its broader strategy to reduce readmissions and discharge as many patients home as possible. Although the SLUHN early mobility program depends on nursing, nursing assistants, and the judicious use of therapists, physician leadership during implementation and maintenance of the program has been essential. Moreover, because the program represents a culture shift, especially for nursing, leadership and change management are crucial ingredients for success. Below are the key steps in the SLUHN early mobility program.
Establish baseline functional status. Recording baseline function is an essential first step. For patients admitted through the ED, nurses collect ambulatory status, patient needs for assistance, ambulatory aids/special equipment, and history of falls. They populate an SBAR (situation, background, assessment, recommendation) form with this information and, as part of the handoff, ensure that it is transmitted to the inpatient nurse receiving the patient.
Obtain and document Barthel Index score. SLUHN uses the Barthel Index (see Figure 1) to establish a patient’s degree of independence and need for supervision. The index is scored on a 0-100 scale, with a higher score corresponding to a greater degree of independence. SLUHN created three categories: 0-59, stage 1; 60-84, stage 2; 85-100, stage 3.
Patient mobility plan. Based on the Barthel-derived stage, a patient is assigned a mobility plan.
The role of nursing. The patient’s registered nurse is responsible for implementing the “patient mobility plan.” The nurse initiates an “interdisciplinary plan of care,” in which the mobility stage is written on the SBAR handoff report tool. The report is discussed at change of shift and at multidisciplinary rounds. Nursing also communicates the mobility plan to the nursing assistants and assigns responsibilities for the mobility plan (activities of daily living, out of bed, ambulation, and so on), including verifying documentation of daily activities and assessing the patient’s response to the activity level of the assigned stage.
Further, nursing maintains and revises the mobility status on the SBAR, updates progress toward outcomes on the care plan, consults with the physician and team regarding the discharge plan, and discusses progress with the patient and family.
The role of the nursing/patient care assistant. The nursing assistant is responsible for implementing elements of the plan, such as activities of daily living, getting out of bed, and ambulation, under the guidance of the nurse. The nursing assistant reports patient responses to activity level and reflects mobility goals back to the patient verbally and through white board messaging.
Patient progress in mobility. When a patient sustains progress at one stage for 24 hours, the nurse aims to move the patient to the next stage by reevaluating the Barthel Index and going through the same steps as those followed during the initial scoring. The process moves the patient to higher activity levels, unless there are intervening problems affecting mobility.
In such cases, according to the Barthel Index, the patient may remain at the same—or be moved to a lower—activity level. In practice, patients are assessed each shift, and those with higher function (stage 3) are progressed to unsupervised ambulation.
The role of physical and occupational therapy. Although the role of physical and occupational therapists in the SLUHN mobility program is well codified, it is reserved for patients with complex rehabilitation needs due to the number of patients requiring rehabilitation.
In sum, this patient mobility program–for non-ICU hospitalized patients–relies on:
- Documentation of baseline function;
- Independent scoring using the Barthel Index;
- Creation of clear roles for nursing, nursing assistants, and therapists; and
- Reevaluation of patients at regular intervals based on the Barthel Index, so that they may progress to greater activity levels (or to lower levels in the case of a setback).
A key subsequent step, an evaluation of the program’s performance in terms of readmissions, transfer rates to a skilled nursing facility, and skilled facility length of stay, has shown positive results in all three domains.
References
- Shi SL, Girrard P, Goldstein R, et al. Functional status outperforms comorbidities in predicting acute care readmissions in medically complex patients. J Gen Intern Med. 2015;30(11):1688-1695.
- Dammeyer JA, Baldwin N, Packard D, et al. Mobilizing outcomes: implementation of a nurse-led multidisciplinary mobility program. Crit Care Nurs Q. 2013;36(1):109-119.
- Wood W, Tschannen D, Trotsky A, et al. A mobility program for an inpatient acute care medical unit. Am J Nurs. 2014;114(10):34-40.
- Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65.
Poor Continuity of Patient Care Increases Work for Hospitalist Groups

I think every hospitalist group should diligently try to maximize hospitalist-patient continuity, but many seem to adopt schedules and other operational practices that erode it. Let’s walk through the issue of continuity, starting with some history.
Inpatient Continuity in Old Healthcare System
Proudly carrying a pager nearly the size of a loaf of bread and wearing a white shirt and pants with Converse All Stars, I served as a hospital orderly in the 1970s. This position involved things like getting patients out of bed, placing Foley catheters, performing chest compressions during codes, and transporting the bodies of the deceased to the morgue. I really enjoyed the work, and the experience serves as one of my historical frames of reference for how hospital care has evolved since then.
The way I remember it, nearly everyone at the hospital worked a predictable schedule. RN staffing was the same each day; it didn’t vary based on census. Each full-time RN worked five shifts a week, eight hours each. Most or all would work alternate weekends and would have two compensatory days off during the following work week. This resulted in terrific continuity between nurse and patient, and the long length of stays meant patients and nurses got to know one another really well.
Continuity Takes a Hit
But things have changed. Nurse-patient continuity seems to have declined significantly as a result of two main forces: the hospital’s efforts to reduce staffing costs by varying nurse staffing to match daily patient volume, and nurses’ desire for a wide variety of work schedules. Asking a bedside nurse in today’s hospital whether the patient’s confusion, diarrhea, or appetite is meaningfully different today than yesterday typically yields the same reply. “This is my first day with the patient; I’ll have to look at the chart.”
I couldn’t find many research articles or editorials regarding hospital nurse-patient continuity from one day to the next. But several researchers seem to have begun studying this issue and have recently published a proposed framework for assessing it, and I found one study showing it wasn’t correlated with rates of pressure ulcers.1,2.
My anecdotal experience tells me continuity between the patient and caregivers of all stripes matters a lot. Research will be valuable in helping us to better understand its most significant costs and benefits, but I’m already convinced “Continuity is King” and should be one of the most important factors in the design of work schedules and patient allocation models for nurses and hospitalists alike.
While some might say we should wait for randomized trials of continuity to determine its importance, I’m inclined to see it like the authors of “Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials.” As a ding against those who insist on research data when common sense may be sufficient, they concluded “…that everyone might benefit if the most radical protagonists of evidence-based medicine organised and participated in a double-blind, randomised, placebo-controlled, crossover trial of the parachute.3
Continuity and Hospitalists
On top of what I see as erosion in nurse-patient continuity, the arrival of hospitalists disrupted doctor-patient continuity across the inpatient and outpatient setting. While there was significant concern about this when our field first took off in the 1990s, it seems to be getting a great deal less attention over the last few years. In many hospitalist groups I work with, it is one of the last factors considered when creating a work schedule. Factors that are examined include the following:
- Solely for provider convenience, a group might regularly schedule a provider for only two or three consecutive daytime shifts, or sometimes only single days;
- Groups that use unit-based hospital (a.k.a. “geographic”) staffing might have a patient transfer to a different attending hospitalist solely as a result of moving to a room in a different nursing unit; and
- As part of morning load leveling, some groups reassign existing patients to a new hospitalist.
I think all groups should work hard to avoid doing these things. And while I seem to be a real outlier on this one, I think the benefits of a separate daytime hospitalist admitter shift are not worth the cost of having different doctors always do the admission and first follow-up visit. Most groups should consider moving the admitter into an additional rounder position and allocating daytime admissions across all hospitalists.
One study found that hospitalist discontinuity was not associated with adverse events, and another found it was associated with higher length of stay for selected diagnoses.4,5 But there is too little research to draw hard conclusions. I’m convinced poor continuity increases the possibility of handoff-related errors, likely results in lower patient satisfaction, and increases the overall work of the hospitalist group, because more providers have to take the time to get to know the patient.
Although there will always be some tension between terrific continuity and a sustainable hospitalist lifestyle—a person can work only so many consecutive days before wearing out—every group should thoughtfully consider whether they are doing everything reasonable to maximize continuity. After all, continuity is king.

References
- Stifter J, Yao Y, Lopez KC, Khokhar A, Wilkie DJ, Keenan GM. Proposing a new conceptual model and an exemplar measure using health information technology to examine the impact of relational nurse continuity on hospital-acquired pressure ulcers. ANS Adv Nurs Sci. 2015;38(3):241-251.
- Stifter J, Yao Y, Lodhi MK, et al. Nurse continuity and hospital-acquired pressure ulcers: a comparative analysis using an electronic health record “big data” set. Nurs Res. 2015;64(5):361-371.
- Smith GC, Pell JP. Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. BMJ. 2003;327(7429):1459-1461.
- O’Leary KJ, Turner J, Christensen N, et al. The effect of hospitalist discontinuity on adverse events. J Hosp Med. 2015;10(3):147-151.
- Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-338.
I think every hospitalist group should diligently try to maximize hospitalist-patient continuity, but many seem to adopt schedules and other operational practices that erode it. Let’s walk through the issue of continuity, starting with some history.
Inpatient Continuity in Old Healthcare System
Proudly carrying a pager nearly the size of a loaf of bread and wearing a white shirt and pants with Converse All Stars, I served as a hospital orderly in the 1970s. This position involved things like getting patients out of bed, placing Foley catheters, performing chest compressions during codes, and transporting the bodies of the deceased to the morgue. I really enjoyed the work, and the experience serves as one of my historical frames of reference for how hospital care has evolved since then.
The way I remember it, nearly everyone at the hospital worked a predictable schedule. RN staffing was the same each day; it didn’t vary based on census. Each full-time RN worked five shifts a week, eight hours each. Most or all would work alternate weekends and would have two compensatory days off during the following work week. This resulted in terrific continuity between nurse and patient, and the long length of stays meant patients and nurses got to know one another really well.
Continuity Takes a Hit
But things have changed. Nurse-patient continuity seems to have declined significantly as a result of two main forces: the hospital’s efforts to reduce staffing costs by varying nurse staffing to match daily patient volume, and nurses’ desire for a wide variety of work schedules. Asking a bedside nurse in today’s hospital whether the patient’s confusion, diarrhea, or appetite is meaningfully different today than yesterday typically yields the same reply. “This is my first day with the patient; I’ll have to look at the chart.”
I couldn’t find many research articles or editorials regarding hospital nurse-patient continuity from one day to the next. But several researchers seem to have begun studying this issue and have recently published a proposed framework for assessing it, and I found one study showing it wasn’t correlated with rates of pressure ulcers.1,2.
My anecdotal experience tells me continuity between the patient and caregivers of all stripes matters a lot. Research will be valuable in helping us to better understand its most significant costs and benefits, but I’m already convinced “Continuity is King” and should be one of the most important factors in the design of work schedules and patient allocation models for nurses and hospitalists alike.
While some might say we should wait for randomized trials of continuity to determine its importance, I’m inclined to see it like the authors of “Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials.” As a ding against those who insist on research data when common sense may be sufficient, they concluded “…that everyone might benefit if the most radical protagonists of evidence-based medicine organised and participated in a double-blind, randomised, placebo-controlled, crossover trial of the parachute.3
Continuity and Hospitalists
On top of what I see as erosion in nurse-patient continuity, the arrival of hospitalists disrupted doctor-patient continuity across the inpatient and outpatient setting. While there was significant concern about this when our field first took off in the 1990s, it seems to be getting a great deal less attention over the last few years. In many hospitalist groups I work with, it is one of the last factors considered when creating a work schedule. Factors that are examined include the following:
- Solely for provider convenience, a group might regularly schedule a provider for only two or three consecutive daytime shifts, or sometimes only single days;
- Groups that use unit-based hospital (a.k.a. “geographic”) staffing might have a patient transfer to a different attending hospitalist solely as a result of moving to a room in a different nursing unit; and
- As part of morning load leveling, some groups reassign existing patients to a new hospitalist.
I think all groups should work hard to avoid doing these things. And while I seem to be a real outlier on this one, I think the benefits of a separate daytime hospitalist admitter shift are not worth the cost of having different doctors always do the admission and first follow-up visit. Most groups should consider moving the admitter into an additional rounder position and allocating daytime admissions across all hospitalists.
One study found that hospitalist discontinuity was not associated with adverse events, and another found it was associated with higher length of stay for selected diagnoses.4,5 But there is too little research to draw hard conclusions. I’m convinced poor continuity increases the possibility of handoff-related errors, likely results in lower patient satisfaction, and increases the overall work of the hospitalist group, because more providers have to take the time to get to know the patient.
Although there will always be some tension between terrific continuity and a sustainable hospitalist lifestyle—a person can work only so many consecutive days before wearing out—every group should thoughtfully consider whether they are doing everything reasonable to maximize continuity. After all, continuity is king.
References
- Stifter J, Yao Y, Lopez KC, Khokhar A, Wilkie DJ, Keenan GM. Proposing a new conceptual model and an exemplar measure using health information technology to examine the impact of relational nurse continuity on hospital-acquired pressure ulcers. ANS Adv Nurs Sci. 2015;38(3):241-251.
- Stifter J, Yao Y, Lodhi MK, et al. Nurse continuity and hospital-acquired pressure ulcers: a comparative analysis using an electronic health record “big data” set. Nurs Res. 2015;64(5):361-371.
- Smith GC, Pell JP. Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. BMJ. 2003;327(7429):1459-1461.
- O’Leary KJ, Turner J, Christensen N, et al. The effect of hospitalist discontinuity on adverse events. J Hosp Med. 2015;10(3):147-151.
- Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-338.
I think every hospitalist group should diligently try to maximize hospitalist-patient continuity, but many seem to adopt schedules and other operational practices that erode it. Let’s walk through the issue of continuity, starting with some history.
Inpatient Continuity in Old Healthcare System
Proudly carrying a pager nearly the size of a loaf of bread and wearing a white shirt and pants with Converse All Stars, I served as a hospital orderly in the 1970s. This position involved things like getting patients out of bed, placing Foley catheters, performing chest compressions during codes, and transporting the bodies of the deceased to the morgue. I really enjoyed the work, and the experience serves as one of my historical frames of reference for how hospital care has evolved since then.
The way I remember it, nearly everyone at the hospital worked a predictable schedule. RN staffing was the same each day; it didn’t vary based on census. Each full-time RN worked five shifts a week, eight hours each. Most or all would work alternate weekends and would have two compensatory days off during the following work week. This resulted in terrific continuity between nurse and patient, and the long length of stays meant patients and nurses got to know one another really well.
Continuity Takes a Hit
But things have changed. Nurse-patient continuity seems to have declined significantly as a result of two main forces: the hospital’s efforts to reduce staffing costs by varying nurse staffing to match daily patient volume, and nurses’ desire for a wide variety of work schedules. Asking a bedside nurse in today’s hospital whether the patient’s confusion, diarrhea, or appetite is meaningfully different today than yesterday typically yields the same reply. “This is my first day with the patient; I’ll have to look at the chart.”
I couldn’t find many research articles or editorials regarding hospital nurse-patient continuity from one day to the next. But several researchers seem to have begun studying this issue and have recently published a proposed framework for assessing it, and I found one study showing it wasn’t correlated with rates of pressure ulcers.1,2.
My anecdotal experience tells me continuity between the patient and caregivers of all stripes matters a lot. Research will be valuable in helping us to better understand its most significant costs and benefits, but I’m already convinced “Continuity is King” and should be one of the most important factors in the design of work schedules and patient allocation models for nurses and hospitalists alike.
While some might say we should wait for randomized trials of continuity to determine its importance, I’m inclined to see it like the authors of “Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials.” As a ding against those who insist on research data when common sense may be sufficient, they concluded “…that everyone might benefit if the most radical protagonists of evidence-based medicine organised and participated in a double-blind, randomised, placebo-controlled, crossover trial of the parachute.3
Continuity and Hospitalists
On top of what I see as erosion in nurse-patient continuity, the arrival of hospitalists disrupted doctor-patient continuity across the inpatient and outpatient setting. While there was significant concern about this when our field first took off in the 1990s, it seems to be getting a great deal less attention over the last few years. In many hospitalist groups I work with, it is one of the last factors considered when creating a work schedule. Factors that are examined include the following:
- Solely for provider convenience, a group might regularly schedule a provider for only two or three consecutive daytime shifts, or sometimes only single days;
- Groups that use unit-based hospital (a.k.a. “geographic”) staffing might have a patient transfer to a different attending hospitalist solely as a result of moving to a room in a different nursing unit; and
- As part of morning load leveling, some groups reassign existing patients to a new hospitalist.
I think all groups should work hard to avoid doing these things. And while I seem to be a real outlier on this one, I think the benefits of a separate daytime hospitalist admitter shift are not worth the cost of having different doctors always do the admission and first follow-up visit. Most groups should consider moving the admitter into an additional rounder position and allocating daytime admissions across all hospitalists.
One study found that hospitalist discontinuity was not associated with adverse events, and another found it was associated with higher length of stay for selected diagnoses.4,5 But there is too little research to draw hard conclusions. I’m convinced poor continuity increases the possibility of handoff-related errors, likely results in lower patient satisfaction, and increases the overall work of the hospitalist group, because more providers have to take the time to get to know the patient.
Although there will always be some tension between terrific continuity and a sustainable hospitalist lifestyle—a person can work only so many consecutive days before wearing out—every group should thoughtfully consider whether they are doing everything reasonable to maximize continuity. After all, continuity is king.
References
- Stifter J, Yao Y, Lopez KC, Khokhar A, Wilkie DJ, Keenan GM. Proposing a new conceptual model and an exemplar measure using health information technology to examine the impact of relational nurse continuity on hospital-acquired pressure ulcers. ANS Adv Nurs Sci. 2015;38(3):241-251.
- Stifter J, Yao Y, Lodhi MK, et al. Nurse continuity and hospital-acquired pressure ulcers: a comparative analysis using an electronic health record “big data” set. Nurs Res. 2015;64(5):361-371.
- Smith GC, Pell JP. Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. BMJ. 2003;327(7429):1459-1461.
- O’Leary KJ, Turner J, Christensen N, et al. The effect of hospitalist discontinuity on adverse events. J Hosp Med. 2015;10(3):147-151.
- Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-338.
Eliminations Hospitalist Groups Should Consider

Editor’s note: Second in a continuing series of articles exploring ways hospitalist groups can cut back.
In last month’s column, I made the case that most hospitalist groups should think about doing away with a morning meeting to distribute overnight admissions and changing a daytime admitter shift into another rounder and having all of the day rounders share admissions. Here I’ll describe additional things in place at some hospitalist groups that should probably be eliminated.
Obscuring Attending Hospitalist Name
Some hospitalist groups admit patients to the “blue team” or “gold team” or use a similar system. I encountered one place that had a fuchsia team. Such designations typically take the place of the attending physician’s name and can be convenient when one hospitalist goes off service and is replaced by another; the team name stays the same. Even if the attending hospitalist makes up the entire team (i.e., no residents or students), some groups use the “team” name rather than the attending hospitalist name.
But when the patient’s chart, sign on the door, and other identifying materials all refer only to the team that is caring for the patient, the patients, their families, and most hospital staff don’t have an easy way to identify the responsible physician. Say a worried daughter steps into the hall to ask the nurse, “Which doctor is taking care of my dad?” The nurse might readily see that the blue team is responsible but may not know which hospitalist is working on the blue team today and might have to walk back to the nursing station to look over a sheet of paper (a “decoder ring”) to figure out the hospitalist’s name.
This scenario has all kinds of drawbacks. To the daughter, the name of the doctor in charge is a big deal. It doesn’t inspire confidence if the nurse can’t readily say who that is. And the busy nurse might forget to investigate and provide the name to the daughter in a timely way.
I think groups using a system like this should seriously consider replacing team names with the attending hospitalist name and updating that name in the medical record, whether that is an EHR, a paper chart, or some other form, every time that doctor rotates off service and is replaced by another. Hospital staff, patients, and families should always see the name of the attending physician and not an uninformative color or nondescript team name.
It will require work for someone, the hospitalist in many cases, to go into the EHR and write an order or send a message to ensure that the hospitalist name is kept current every time one doctor replaces another. But it’s worth the effort.
Day Hospitalists Should Round on Patients Admitted after Midnight
Although not exactly common, I’ve come across this scenario often enough that it’s worth mentioning.
Hospitalists, sometimes with a hint of indignity or even chest thumping, have told me they don’t visit or round on patients admitted after midnight by their night doctor. “You can’t bill for a second visit on the same calendar day,” they explain, firmly. “So if I can’t get paid to see the patient, then I won’t.”
This is just crazy.
For one thing, these same doctors are typically employed by the hospital and are being paid to provide whatever care patients need. I think they’ve just latched onto the “can’t bill another visit” as an excuse to get out of some work.
Don’t forget that many of these patients may wait over 30 hours from their admitting visit to the first follow-up visit; this delay is at the beginning of their hospital stay, when they might be most unstable. And it delays initiation of discharge planning and other important steps in patient care.
I don’t see any room for meaningful debate on this. The rounder who picks up a patient admitted the night before should always make a full rounding visit, even if the admission was after midnight.
But if the visit isn’t billable, you are freed from the typical billing-related documentation requirements. No need to document detail in the note that doesn’t meaningfully contribute to the care of the patient. For example, you might omit a chief complaint for this encounter.
Daytime Triage Doctor
Practices larger than about 20 full-time equivalents often have one daytime doctor hold a “triage” or “hot” pager, which others call to make a new referral. This triage doctor will hear about all referrals and keep track of and contact the hospitalist responsible for the next new patient. This can be a very busy job and often comes on top of a full clinical load for that doctor.
As I mentioned in my July 2015 and December 2010 articles, in many or most groups, a clerical person could take over this function, at least during business hours.
Vacation Time
In many or most cases, hospitalists that have specified vacation time are not getting a better deal than those that have no vacation time. What really matters is how many shifts you’re responsible for in a year. For the days you aren’t on shift, in most hospitalist groups it really doesn’t matter whether you label some of them as vacation days or CME days.
I discussed this issue in greater detail in my March 2007 article.
But if you’re in the 30% of hospitalist groups that have a vacation (or PTO) provision currently and it works well, then there certainly isn’t a compelling reason to change or do away with it.
Editor’s note: Second in a continuing series of articles exploring ways hospitalist groups can cut back.
In last month’s column, I made the case that most hospitalist groups should think about doing away with a morning meeting to distribute overnight admissions and changing a daytime admitter shift into another rounder and having all of the day rounders share admissions. Here I’ll describe additional things in place at some hospitalist groups that should probably be eliminated.
Obscuring Attending Hospitalist Name
Some hospitalist groups admit patients to the “blue team” or “gold team” or use a similar system. I encountered one place that had a fuchsia team. Such designations typically take the place of the attending physician’s name and can be convenient when one hospitalist goes off service and is replaced by another; the team name stays the same. Even if the attending hospitalist makes up the entire team (i.e., no residents or students), some groups use the “team” name rather than the attending hospitalist name.
But when the patient’s chart, sign on the door, and other identifying materials all refer only to the team that is caring for the patient, the patients, their families, and most hospital staff don’t have an easy way to identify the responsible physician. Say a worried daughter steps into the hall to ask the nurse, “Which doctor is taking care of my dad?” The nurse might readily see that the blue team is responsible but may not know which hospitalist is working on the blue team today and might have to walk back to the nursing station to look over a sheet of paper (a “decoder ring”) to figure out the hospitalist’s name.
This scenario has all kinds of drawbacks. To the daughter, the name of the doctor in charge is a big deal. It doesn’t inspire confidence if the nurse can’t readily say who that is. And the busy nurse might forget to investigate and provide the name to the daughter in a timely way.
I think groups using a system like this should seriously consider replacing team names with the attending hospitalist name and updating that name in the medical record, whether that is an EHR, a paper chart, or some other form, every time that doctor rotates off service and is replaced by another. Hospital staff, patients, and families should always see the name of the attending physician and not an uninformative color or nondescript team name.
It will require work for someone, the hospitalist in many cases, to go into the EHR and write an order or send a message to ensure that the hospitalist name is kept current every time one doctor replaces another. But it’s worth the effort.
Day Hospitalists Should Round on Patients Admitted after Midnight
Although not exactly common, I’ve come across this scenario often enough that it’s worth mentioning.
Hospitalists, sometimes with a hint of indignity or even chest thumping, have told me they don’t visit or round on patients admitted after midnight by their night doctor. “You can’t bill for a second visit on the same calendar day,” they explain, firmly. “So if I can’t get paid to see the patient, then I won’t.”
This is just crazy.
For one thing, these same doctors are typically employed by the hospital and are being paid to provide whatever care patients need. I think they’ve just latched onto the “can’t bill another visit” as an excuse to get out of some work.
Don’t forget that many of these patients may wait over 30 hours from their admitting visit to the first follow-up visit; this delay is at the beginning of their hospital stay, when they might be most unstable. And it delays initiation of discharge planning and other important steps in patient care.
I don’t see any room for meaningful debate on this. The rounder who picks up a patient admitted the night before should always make a full rounding visit, even if the admission was after midnight.
But if the visit isn’t billable, you are freed from the typical billing-related documentation requirements. No need to document detail in the note that doesn’t meaningfully contribute to the care of the patient. For example, you might omit a chief complaint for this encounter.
Daytime Triage Doctor
Practices larger than about 20 full-time equivalents often have one daytime doctor hold a “triage” or “hot” pager, which others call to make a new referral. This triage doctor will hear about all referrals and keep track of and contact the hospitalist responsible for the next new patient. This can be a very busy job and often comes on top of a full clinical load for that doctor.
As I mentioned in my July 2015 and December 2010 articles, in many or most groups, a clerical person could take over this function, at least during business hours.
Vacation Time
In many or most cases, hospitalists that have specified vacation time are not getting a better deal than those that have no vacation time. What really matters is how many shifts you’re responsible for in a year. For the days you aren’t on shift, in most hospitalist groups it really doesn’t matter whether you label some of them as vacation days or CME days.
I discussed this issue in greater detail in my March 2007 article.
But if you’re in the 30% of hospitalist groups that have a vacation (or PTO) provision currently and it works well, then there certainly isn’t a compelling reason to change or do away with it.
Editor’s note: Second in a continuing series of articles exploring ways hospitalist groups can cut back.
In last month’s column, I made the case that most hospitalist groups should think about doing away with a morning meeting to distribute overnight admissions and changing a daytime admitter shift into another rounder and having all of the day rounders share admissions. Here I’ll describe additional things in place at some hospitalist groups that should probably be eliminated.
Obscuring Attending Hospitalist Name
Some hospitalist groups admit patients to the “blue team” or “gold team” or use a similar system. I encountered one place that had a fuchsia team. Such designations typically take the place of the attending physician’s name and can be convenient when one hospitalist goes off service and is replaced by another; the team name stays the same. Even if the attending hospitalist makes up the entire team (i.e., no residents or students), some groups use the “team” name rather than the attending hospitalist name.
But when the patient’s chart, sign on the door, and other identifying materials all refer only to the team that is caring for the patient, the patients, their families, and most hospital staff don’t have an easy way to identify the responsible physician. Say a worried daughter steps into the hall to ask the nurse, “Which doctor is taking care of my dad?” The nurse might readily see that the blue team is responsible but may not know which hospitalist is working on the blue team today and might have to walk back to the nursing station to look over a sheet of paper (a “decoder ring”) to figure out the hospitalist’s name.
This scenario has all kinds of drawbacks. To the daughter, the name of the doctor in charge is a big deal. It doesn’t inspire confidence if the nurse can’t readily say who that is. And the busy nurse might forget to investigate and provide the name to the daughter in a timely way.
I think groups using a system like this should seriously consider replacing team names with the attending hospitalist name and updating that name in the medical record, whether that is an EHR, a paper chart, or some other form, every time that doctor rotates off service and is replaced by another. Hospital staff, patients, and families should always see the name of the attending physician and not an uninformative color or nondescript team name.
It will require work for someone, the hospitalist in many cases, to go into the EHR and write an order or send a message to ensure that the hospitalist name is kept current every time one doctor replaces another. But it’s worth the effort.
Day Hospitalists Should Round on Patients Admitted after Midnight
Although not exactly common, I’ve come across this scenario often enough that it’s worth mentioning.
Hospitalists, sometimes with a hint of indignity or even chest thumping, have told me they don’t visit or round on patients admitted after midnight by their night doctor. “You can’t bill for a second visit on the same calendar day,” they explain, firmly. “So if I can’t get paid to see the patient, then I won’t.”
This is just crazy.
For one thing, these same doctors are typically employed by the hospital and are being paid to provide whatever care patients need. I think they’ve just latched onto the “can’t bill another visit” as an excuse to get out of some work.
Don’t forget that many of these patients may wait over 30 hours from their admitting visit to the first follow-up visit; this delay is at the beginning of their hospital stay, when they might be most unstable. And it delays initiation of discharge planning and other important steps in patient care.
I don’t see any room for meaningful debate on this. The rounder who picks up a patient admitted the night before should always make a full rounding visit, even if the admission was after midnight.
But if the visit isn’t billable, you are freed from the typical billing-related documentation requirements. No need to document detail in the note that doesn’t meaningfully contribute to the care of the patient. For example, you might omit a chief complaint for this encounter.
Daytime Triage Doctor
Practices larger than about 20 full-time equivalents often have one daytime doctor hold a “triage” or “hot” pager, which others call to make a new referral. This triage doctor will hear about all referrals and keep track of and contact the hospitalist responsible for the next new patient. This can be a very busy job and often comes on top of a full clinical load for that doctor.
As I mentioned in my July 2015 and December 2010 articles, in many or most groups, a clerical person could take over this function, at least during business hours.
Vacation Time
In many or most cases, hospitalists that have specified vacation time are not getting a better deal than those that have no vacation time. What really matters is how many shifts you’re responsible for in a year. For the days you aren’t on shift, in most hospitalist groups it really doesn’t matter whether you label some of them as vacation days or CME days.
I discussed this issue in greater detail in my March 2007 article.
But if you’re in the 30% of hospitalist groups that have a vacation (or PTO) provision currently and it works well, then there certainly isn’t a compelling reason to change or do away with it.
Your College: A Remarkable Organization
Peering out from 28 floors above the busy, early morning streets of downtown Chicago, I was entranced by the view. The rising sun in the east created a shimmering, iridescent play of light on the waters of Lake Michigan that extended as far as the eye could see. The room I was in also commanded my attention. Several rows of desks, each with a computer screen, faced a single elevated line of chairs for the leaders of the deliberations that were about to take place. Above this row on the front wall of this imposing room is emblazoned the seal of our College with its mission statement, “The ACS is dedicated to improving the care of the surgical patient and to safeguarding standards of care in an optimal and ethical practice environment,” to remind those in the room of the ultimate purpose in serving this professional organization. So the Regents room and view appeared to me, a newcomer to these meetings of the leadership of the American College of Surgeons.
I hope I can convince you in the paragraphs that follow that this mission and its execution by Regents, Governors, and Fellows of the ACS, are every bit as noble as the architecture of the room and the view it affords.

I have been a Fellow of the American College of Surgeons since 1980. My membership in this extraordinary association has provided me many benefits and numerous opportunities. In the early years, I significantly expanded the knowledge base I had gained in residency by attending every fall Clinical Congress and consuming as many educational offerings as time would permit during this nearly week-long learning marathon. After a few years, I was granted the privilege of being on the instructor end of several of these educational exchanges. At that time in my career, it appeared to me that the ACS’s main and almost sole purpose was to provide continuing education for surgeons who attended the annual Clinical Congress. I have subsequently found that it is so much more.
In 2005, I was invited to represent one of my specialist surgical societies as a Governor. During my 6-year term, I came to realize that the key purpose of the Board of Governors (BOG) is to provide an effective communication conduit between the Fellows and the sole policy-making body of the ACS, the Board of Regents (BOR). In recent years, most of the Regents have attended the annual BOG meeting in order to facilitate this interaction.
In 2012, I was elected First Vice-President of the ACS. Now as an officer of the College, I was invited for 2 years to attend all BOR meetings and to be in the mainstream of all communications relating to strategy and policy. These opportunities provided me with an intimate, inside look at how this large organization of nearly 80,000 members functions to serve the entire surgical profession including each of its many specialties. What I learned about the internal workings of the leadership and those who dedicate their time to this work has reinforced my own commitment to the ACS. It is a remarkable organization.
This brings us back to the well-designed and impressive Regents’ room high above Chicago. The hum of numerous disjointed conversations ceased as the Chair of the ACS Board of Regents called the June 2012 meeting to order. My attention is now focused on the proceedings rather than on the beauty of Lake Michigan below. Although every surgical specialty is represented among the 22 Regents, all discussion was invariably directed toward the betterment of the surgical profession as a whole rather than about any specific specialty’s interests.
The Regents are dedicated servants of the ACS. In addition to three one-and-a-half day meetings annually, each of which requires hours of reading in preparation, most of the Regents serve on at least two committees of the Board. Regents are nominated by Fellows, advisory councils, and committees, and are elected by the much larger BOG which represents every state and Canadian province, several countries, and many surgery specialist societies. In addition to assuring that all surgical specialties are represented, bylaws of the ACS state that the President of the ACS and two Canadian Fellows must be among the BOR membership. Based on my 2-year experience, the BOG has exhibited considerable wisdom in their choice of Regents.
The officers of the ACS (President-Elect, First and Second Vice-Presidents and Vice-Presidents-Elect, Secretary, Treasurer), and the officers of the BOG (Chair, Vice-Chair, and Secretary/Treasurer) attend all BOR meetings and serve in an advisory capacity. Also in attendance and providing essential input are executive members of the ACS staff and, representing the younger ACS membership, the chairs of the Resident Associates Society (RAS) and the Young Fellows Association (YAF). Although only Regents can vote and are therefore responsible for establishing ACS policy, I discovered they welcome participation from all in attendance. I always felt that my contributions and those of other non-voting attendees were thoughtfully and carefully considered.
Much of the preparatory work for BOR meetings is done in the committees that meet just prior to the full Board meeting. I had the pleasure of being on the Honors Committee that selects Honorary Fellows of the ACS from regions throughout the world and selects Fellows for special awards such as the Distinguished Service Award, and on the Members Services Liaison Committee that concentrates on expanding ACS membership and on more fully informing the Fellows of BOR activities. Among several other important committees are the Central Judiciary Committee that is responsible for disciplining Fellows who breach the ethical standards of our College and the Finance Committee that assures responsible fiscal stewardship of the ACS. Deliberations of all of the committees are brought before the full Board for final approval
Although the BOR has been the policy-making body since the founding of the ACS 102 years ago, the structure of our society has evolved considerably, especially during the past 2 decades. The ACS is organized around five major Divisions: Advocacy and Health Policy, Education, Integrated Communications, Member Services, and Research and Optimal Patient Care. The Directors of these Divisions report on a regular basis to the BOR to keep the Regents’ knowledge up-to-date and to assist them in determining the strategic direction of the ACS. Much of the discussion, modifications, and innovations center around these Divisions, also represented as pillars in the recent BOG re-organization. I trust you are aware of the many achievements that have resulted: NSQIP, legislative elimination of the flawed Sustainable Growth Rate (SGR) formula, reorganization of the Clinical Congress, and a re-emphasis on global surgery and the Operation Giving Back Program to name but a few.
Finally, a key role of the BOR is to select the Executive Director of the ACS who manages the day-to-day operations of the College with the Board’s strategic guidance. The ACS has been blessed with a number of excellent Directors, none more visionary and competent than the present Director, David Hoyt, MD, FACS, who is 1 year into his second 5-year term.
I hope that this discussion provides you with a better understanding of the role and functioning of the BOR and the College of which you are a member. The grandeur of the BOR room appropriately parallels the excellence of what takes place within it.
Take time to visit the next time you are in Chicago. I am certain the ACS staff would be pleased and proud to meet you, show you around, and have you experience what I have tried to describe in this brief discourse.
Dr. Rikkers is Editor in Chief of ACS Surgery News.
Peering out from 28 floors above the busy, early morning streets of downtown Chicago, I was entranced by the view. The rising sun in the east created a shimmering, iridescent play of light on the waters of Lake Michigan that extended as far as the eye could see. The room I was in also commanded my attention. Several rows of desks, each with a computer screen, faced a single elevated line of chairs for the leaders of the deliberations that were about to take place. Above this row on the front wall of this imposing room is emblazoned the seal of our College with its mission statement, “The ACS is dedicated to improving the care of the surgical patient and to safeguarding standards of care in an optimal and ethical practice environment,” to remind those in the room of the ultimate purpose in serving this professional organization. So the Regents room and view appeared to me, a newcomer to these meetings of the leadership of the American College of Surgeons.
I hope I can convince you in the paragraphs that follow that this mission and its execution by Regents, Governors, and Fellows of the ACS, are every bit as noble as the architecture of the room and the view it affords.
I have been a Fellow of the American College of Surgeons since 1980. My membership in this extraordinary association has provided me many benefits and numerous opportunities. In the early years, I significantly expanded the knowledge base I had gained in residency by attending every fall Clinical Congress and consuming as many educational offerings as time would permit during this nearly week-long learning marathon. After a few years, I was granted the privilege of being on the instructor end of several of these educational exchanges. At that time in my career, it appeared to me that the ACS’s main and almost sole purpose was to provide continuing education for surgeons who attended the annual Clinical Congress. I have subsequently found that it is so much more.
In 2005, I was invited to represent one of my specialist surgical societies as a Governor. During my 6-year term, I came to realize that the key purpose of the Board of Governors (BOG) is to provide an effective communication conduit between the Fellows and the sole policy-making body of the ACS, the Board of Regents (BOR). In recent years, most of the Regents have attended the annual BOG meeting in order to facilitate this interaction.
In 2012, I was elected First Vice-President of the ACS. Now as an officer of the College, I was invited for 2 years to attend all BOR meetings and to be in the mainstream of all communications relating to strategy and policy. These opportunities provided me with an intimate, inside look at how this large organization of nearly 80,000 members functions to serve the entire surgical profession including each of its many specialties. What I learned about the internal workings of the leadership and those who dedicate their time to this work has reinforced my own commitment to the ACS. It is a remarkable organization.
This brings us back to the well-designed and impressive Regents’ room high above Chicago. The hum of numerous disjointed conversations ceased as the Chair of the ACS Board of Regents called the June 2012 meeting to order. My attention is now focused on the proceedings rather than on the beauty of Lake Michigan below. Although every surgical specialty is represented among the 22 Regents, all discussion was invariably directed toward the betterment of the surgical profession as a whole rather than about any specific specialty’s interests.
The Regents are dedicated servants of the ACS. In addition to three one-and-a-half day meetings annually, each of which requires hours of reading in preparation, most of the Regents serve on at least two committees of the Board. Regents are nominated by Fellows, advisory councils, and committees, and are elected by the much larger BOG which represents every state and Canadian province, several countries, and many surgery specialist societies. In addition to assuring that all surgical specialties are represented, bylaws of the ACS state that the President of the ACS and two Canadian Fellows must be among the BOR membership. Based on my 2-year experience, the BOG has exhibited considerable wisdom in their choice of Regents.
The officers of the ACS (President-Elect, First and Second Vice-Presidents and Vice-Presidents-Elect, Secretary, Treasurer), and the officers of the BOG (Chair, Vice-Chair, and Secretary/Treasurer) attend all BOR meetings and serve in an advisory capacity. Also in attendance and providing essential input are executive members of the ACS staff and, representing the younger ACS membership, the chairs of the Resident Associates Society (RAS) and the Young Fellows Association (YAF). Although only Regents can vote and are therefore responsible for establishing ACS policy, I discovered they welcome participation from all in attendance. I always felt that my contributions and those of other non-voting attendees were thoughtfully and carefully considered.
Much of the preparatory work for BOR meetings is done in the committees that meet just prior to the full Board meeting. I had the pleasure of being on the Honors Committee that selects Honorary Fellows of the ACS from regions throughout the world and selects Fellows for special awards such as the Distinguished Service Award, and on the Members Services Liaison Committee that concentrates on expanding ACS membership and on more fully informing the Fellows of BOR activities. Among several other important committees are the Central Judiciary Committee that is responsible for disciplining Fellows who breach the ethical standards of our College and the Finance Committee that assures responsible fiscal stewardship of the ACS. Deliberations of all of the committees are brought before the full Board for final approval
Although the BOR has been the policy-making body since the founding of the ACS 102 years ago, the structure of our society has evolved considerably, especially during the past 2 decades. The ACS is organized around five major Divisions: Advocacy and Health Policy, Education, Integrated Communications, Member Services, and Research and Optimal Patient Care. The Directors of these Divisions report on a regular basis to the BOR to keep the Regents’ knowledge up-to-date and to assist them in determining the strategic direction of the ACS. Much of the discussion, modifications, and innovations center around these Divisions, also represented as pillars in the recent BOG re-organization. I trust you are aware of the many achievements that have resulted: NSQIP, legislative elimination of the flawed Sustainable Growth Rate (SGR) formula, reorganization of the Clinical Congress, and a re-emphasis on global surgery and the Operation Giving Back Program to name but a few.
Finally, a key role of the BOR is to select the Executive Director of the ACS who manages the day-to-day operations of the College with the Board’s strategic guidance. The ACS has been blessed with a number of excellent Directors, none more visionary and competent than the present Director, David Hoyt, MD, FACS, who is 1 year into his second 5-year term.
I hope that this discussion provides you with a better understanding of the role and functioning of the BOR and the College of which you are a member. The grandeur of the BOR room appropriately parallels the excellence of what takes place within it.
Take time to visit the next time you are in Chicago. I am certain the ACS staff would be pleased and proud to meet you, show you around, and have you experience what I have tried to describe in this brief discourse.
Dr. Rikkers is Editor in Chief of ACS Surgery News.
Peering out from 28 floors above the busy, early morning streets of downtown Chicago, I was entranced by the view. The rising sun in the east created a shimmering, iridescent play of light on the waters of Lake Michigan that extended as far as the eye could see. The room I was in also commanded my attention. Several rows of desks, each with a computer screen, faced a single elevated line of chairs for the leaders of the deliberations that were about to take place. Above this row on the front wall of this imposing room is emblazoned the seal of our College with its mission statement, “The ACS is dedicated to improving the care of the surgical patient and to safeguarding standards of care in an optimal and ethical practice environment,” to remind those in the room of the ultimate purpose in serving this professional organization. So the Regents room and view appeared to me, a newcomer to these meetings of the leadership of the American College of Surgeons.
I hope I can convince you in the paragraphs that follow that this mission and its execution by Regents, Governors, and Fellows of the ACS, are every bit as noble as the architecture of the room and the view it affords.
I have been a Fellow of the American College of Surgeons since 1980. My membership in this extraordinary association has provided me many benefits and numerous opportunities. In the early years, I significantly expanded the knowledge base I had gained in residency by attending every fall Clinical Congress and consuming as many educational offerings as time would permit during this nearly week-long learning marathon. After a few years, I was granted the privilege of being on the instructor end of several of these educational exchanges. At that time in my career, it appeared to me that the ACS’s main and almost sole purpose was to provide continuing education for surgeons who attended the annual Clinical Congress. I have subsequently found that it is so much more.
In 2005, I was invited to represent one of my specialist surgical societies as a Governor. During my 6-year term, I came to realize that the key purpose of the Board of Governors (BOG) is to provide an effective communication conduit between the Fellows and the sole policy-making body of the ACS, the Board of Regents (BOR). In recent years, most of the Regents have attended the annual BOG meeting in order to facilitate this interaction.
In 2012, I was elected First Vice-President of the ACS. Now as an officer of the College, I was invited for 2 years to attend all BOR meetings and to be in the mainstream of all communications relating to strategy and policy. These opportunities provided me with an intimate, inside look at how this large organization of nearly 80,000 members functions to serve the entire surgical profession including each of its many specialties. What I learned about the internal workings of the leadership and those who dedicate their time to this work has reinforced my own commitment to the ACS. It is a remarkable organization.
This brings us back to the well-designed and impressive Regents’ room high above Chicago. The hum of numerous disjointed conversations ceased as the Chair of the ACS Board of Regents called the June 2012 meeting to order. My attention is now focused on the proceedings rather than on the beauty of Lake Michigan below. Although every surgical specialty is represented among the 22 Regents, all discussion was invariably directed toward the betterment of the surgical profession as a whole rather than about any specific specialty’s interests.
The Regents are dedicated servants of the ACS. In addition to three one-and-a-half day meetings annually, each of which requires hours of reading in preparation, most of the Regents serve on at least two committees of the Board. Regents are nominated by Fellows, advisory councils, and committees, and are elected by the much larger BOG which represents every state and Canadian province, several countries, and many surgery specialist societies. In addition to assuring that all surgical specialties are represented, bylaws of the ACS state that the President of the ACS and two Canadian Fellows must be among the BOR membership. Based on my 2-year experience, the BOG has exhibited considerable wisdom in their choice of Regents.
The officers of the ACS (President-Elect, First and Second Vice-Presidents and Vice-Presidents-Elect, Secretary, Treasurer), and the officers of the BOG (Chair, Vice-Chair, and Secretary/Treasurer) attend all BOR meetings and serve in an advisory capacity. Also in attendance and providing essential input are executive members of the ACS staff and, representing the younger ACS membership, the chairs of the Resident Associates Society (RAS) and the Young Fellows Association (YAF). Although only Regents can vote and are therefore responsible for establishing ACS policy, I discovered they welcome participation from all in attendance. I always felt that my contributions and those of other non-voting attendees were thoughtfully and carefully considered.
Much of the preparatory work for BOR meetings is done in the committees that meet just prior to the full Board meeting. I had the pleasure of being on the Honors Committee that selects Honorary Fellows of the ACS from regions throughout the world and selects Fellows for special awards such as the Distinguished Service Award, and on the Members Services Liaison Committee that concentrates on expanding ACS membership and on more fully informing the Fellows of BOR activities. Among several other important committees are the Central Judiciary Committee that is responsible for disciplining Fellows who breach the ethical standards of our College and the Finance Committee that assures responsible fiscal stewardship of the ACS. Deliberations of all of the committees are brought before the full Board for final approval
Although the BOR has been the policy-making body since the founding of the ACS 102 years ago, the structure of our society has evolved considerably, especially during the past 2 decades. The ACS is organized around five major Divisions: Advocacy and Health Policy, Education, Integrated Communications, Member Services, and Research and Optimal Patient Care. The Directors of these Divisions report on a regular basis to the BOR to keep the Regents’ knowledge up-to-date and to assist them in determining the strategic direction of the ACS. Much of the discussion, modifications, and innovations center around these Divisions, also represented as pillars in the recent BOG re-organization. I trust you are aware of the many achievements that have resulted: NSQIP, legislative elimination of the flawed Sustainable Growth Rate (SGR) formula, reorganization of the Clinical Congress, and a re-emphasis on global surgery and the Operation Giving Back Program to name but a few.
Finally, a key role of the BOR is to select the Executive Director of the ACS who manages the day-to-day operations of the College with the Board’s strategic guidance. The ACS has been blessed with a number of excellent Directors, none more visionary and competent than the present Director, David Hoyt, MD, FACS, who is 1 year into his second 5-year term.
I hope that this discussion provides you with a better understanding of the role and functioning of the BOR and the College of which you are a member. The grandeur of the BOR room appropriately parallels the excellence of what takes place within it.
Take time to visit the next time you are in Chicago. I am certain the ACS staff would be pleased and proud to meet you, show you around, and have you experience what I have tried to describe in this brief discourse.
Dr. Rikkers is Editor in Chief of ACS Surgery News.

Empathy, Patients, and Caregivers
Empathy—the feeling that you understand and share another person’s experiences and emotions: the ability to share someone else’s feelings.
—Merriam-Webster
By the time I became a third-year medical resident, I had mastered the repertoire of “don’t tread on me” behaviors that seemed essential to survive as a senior level trainee. I emulated my supervisors, mostly residents, as they advocated for themselves in the face of an onslaught of demand from other departments and from patients. I remember one occasion when, in front of my intern, I firmly “told off” a patient who was obviously poor and possibly homeless and who I thought was faking pain in order to get admitted to the hospital and receive analgesics. I was pleased with myself when I informed the ED staff that I would not accept the patient onto the medical service.
In retrospect, I wonder how and why I had become a “tough guy”? What had happened to my desire to “be there” for patients in their hour of need? Had I lost my aspiration to care for others, fueled by role models like my father, an internist and pillar in the community?
Does Empathy Decrease over Time?
A number of studies support my personal observation that physician empathy decreases during the training years and later persists at lower levels.1
Yet, perhaps ironically, increased empathy is associated with fewer medical errors, increased patient satisfaction, fewer malpractice claims, and improved clinical outcomes.1
Can We Increase Empathy?
In a 2012 study, Helen Reiss and colleagues randomized residents from several specialties into two groups, one receiving standard post-graduate education and a second whose education included three 60-minute empathy training modules. The empathy training consisted of the following elements:
- Neurobiology of empathy;
- Approaches to increase awareness of the physiology of emotions during patient encounters;
- Skills involved in interpreting the meaning of facial expressions; and
- Breathing exercises and mindfulness practices to enhance empathic responses to patients.
Using a validated instrument to measure empathy as rated by patients, the study reported increased empathy scores for the residents who participated in the empathy training program. An important skill the residents learned in the training was the ability to read/decode the facial expressions of patients and use that information to alter their behavior, thereby increasing patient-reported empathy.1
The authors point to the need for more studies to learn if, and to what extent, empathy training can improve performance in key areas like patient outcomes, malpractice claims, physician well-being, and patient satisfaction. Furthermore, they concluded that “long-lasting improvements in empathic clinical care cannot be sustained without organizational changes at all levels of healthcare. Such cultural changes require a commitment from clinical and administrative leaders to place empathic care at the forefront of institutional missions.”
Committing to Enhancing Physician Empathy
The Cleveland Clinic has addressed empathy as an important element of its institutional mission. Consider the following initiatives and interventions:
- The health system’s CEO publicly prioritizes empathy as a path to better patient experience and caregiver well-being.
- There is a chief experience officer position.
- All employees receive specialized H.E.A.R.T. (Hear, Empathize, Apologize, Respond, Thank) training; embedded approaches and practices support ongoing prioritization of empathy.
- All employees are trained to see themselves as caregivers.
- Physicians and trainees receive training in communication with patients.
- The health system holds an annual national summit on empathy and patient experience.
If you haven’t seen the Cleveland Clinic video that has gone viral, Google “Empathy: The Human Connection to Patient Care.” The video takes advantage of a universal human trait: When we truly know what another person is experiencing and feeling, we can experience and feel the same thing.
Can Hospitalists Retain an Empathic Approach over the Long Term?
I believe hospitalists can retain or regain the empathy that led to our choice of medicine as a career. To do this, we should consider a few critical practices, some of which occur at work and some at home. These include the following strategies:
- Find ways to be fully present in your human encounters with patients and co-workers. This includes minimizing interruptions whenever possible, sitting with people, making eye contact, and putting your phone away.
- Reward yourself for hard work. Make rewards, which needn’t always be expensive, a regular part of your life.
- Take measures to avoid overwork. Know when to say “no” to added responsibilities. Find time to add a wellness practice to your life, such as exercise, art, literature, spending time with your spouse/children, or community service.
- Express the gratitude you are feeling to those you work and live with.
Resources for Empathy Training
Empathetics.com offers CME and nursing continuing education credits for training in “how to detect and manage the emotional states of patients and how to respond with empathy and compassion, even in difficult interactions.”
PaulEkman.com has a series of training modules geared to detecting the “unspoken feelings” of others by recognizing the meaning of facial expressions.
Reference
- Reiss H, Kelley JM, Bailey RW, Dunn EJ, Phillips M. Empathy training for resident physicians: a randomized controlled trial of a neuroscience-informed curriculum. J Gen Intern Med. 2012;27(10):1280-1286.
Empathy—the feeling that you understand and share another person’s experiences and emotions: the ability to share someone else’s feelings.
—Merriam-Webster
By the time I became a third-year medical resident, I had mastered the repertoire of “don’t tread on me” behaviors that seemed essential to survive as a senior level trainee. I emulated my supervisors, mostly residents, as they advocated for themselves in the face of an onslaught of demand from other departments and from patients. I remember one occasion when, in front of my intern, I firmly “told off” a patient who was obviously poor and possibly homeless and who I thought was faking pain in order to get admitted to the hospital and receive analgesics. I was pleased with myself when I informed the ED staff that I would not accept the patient onto the medical service.
In retrospect, I wonder how and why I had become a “tough guy”? What had happened to my desire to “be there” for patients in their hour of need? Had I lost my aspiration to care for others, fueled by role models like my father, an internist and pillar in the community?
Does Empathy Decrease over Time?
A number of studies support my personal observation that physician empathy decreases during the training years and later persists at lower levels.1
Yet, perhaps ironically, increased empathy is associated with fewer medical errors, increased patient satisfaction, fewer malpractice claims, and improved clinical outcomes.1
Can We Increase Empathy?
In a 2012 study, Helen Reiss and colleagues randomized residents from several specialties into two groups, one receiving standard post-graduate education and a second whose education included three 60-minute empathy training modules. The empathy training consisted of the following elements:
- Neurobiology of empathy;
- Approaches to increase awareness of the physiology of emotions during patient encounters;
- Skills involved in interpreting the meaning of facial expressions; and
- Breathing exercises and mindfulness practices to enhance empathic responses to patients.
Using a validated instrument to measure empathy as rated by patients, the study reported increased empathy scores for the residents who participated in the empathy training program. An important skill the residents learned in the training was the ability to read/decode the facial expressions of patients and use that information to alter their behavior, thereby increasing patient-reported empathy.1
The authors point to the need for more studies to learn if, and to what extent, empathy training can improve performance in key areas like patient outcomes, malpractice claims, physician well-being, and patient satisfaction. Furthermore, they concluded that “long-lasting improvements in empathic clinical care cannot be sustained without organizational changes at all levels of healthcare. Such cultural changes require a commitment from clinical and administrative leaders to place empathic care at the forefront of institutional missions.”
Committing to Enhancing Physician Empathy
The Cleveland Clinic has addressed empathy as an important element of its institutional mission. Consider the following initiatives and interventions:
- The health system’s CEO publicly prioritizes empathy as a path to better patient experience and caregiver well-being.
- There is a chief experience officer position.
- All employees receive specialized H.E.A.R.T. (Hear, Empathize, Apologize, Respond, Thank) training; embedded approaches and practices support ongoing prioritization of empathy.
- All employees are trained to see themselves as caregivers.
- Physicians and trainees receive training in communication with patients.
- The health system holds an annual national summit on empathy and patient experience.
If you haven’t seen the Cleveland Clinic video that has gone viral, Google “Empathy: The Human Connection to Patient Care.” The video takes advantage of a universal human trait: When we truly know what another person is experiencing and feeling, we can experience and feel the same thing.
Can Hospitalists Retain an Empathic Approach over the Long Term?
I believe hospitalists can retain or regain the empathy that led to our choice of medicine as a career. To do this, we should consider a few critical practices, some of which occur at work and some at home. These include the following strategies:
- Find ways to be fully present in your human encounters with patients and co-workers. This includes minimizing interruptions whenever possible, sitting with people, making eye contact, and putting your phone away.
- Reward yourself for hard work. Make rewards, which needn’t always be expensive, a regular part of your life.
- Take measures to avoid overwork. Know when to say “no” to added responsibilities. Find time to add a wellness practice to your life, such as exercise, art, literature, spending time with your spouse/children, or community service.
- Express the gratitude you are feeling to those you work and live with.
Resources for Empathy Training
Empathetics.com offers CME and nursing continuing education credits for training in “how to detect and manage the emotional states of patients and how to respond with empathy and compassion, even in difficult interactions.”
PaulEkman.com has a series of training modules geared to detecting the “unspoken feelings” of others by recognizing the meaning of facial expressions.
Reference
- Reiss H, Kelley JM, Bailey RW, Dunn EJ, Phillips M. Empathy training for resident physicians: a randomized controlled trial of a neuroscience-informed curriculum. J Gen Intern Med. 2012;27(10):1280-1286.
Empathy—the feeling that you understand and share another person’s experiences and emotions: the ability to share someone else’s feelings.
—Merriam-Webster
By the time I became a third-year medical resident, I had mastered the repertoire of “don’t tread on me” behaviors that seemed essential to survive as a senior level trainee. I emulated my supervisors, mostly residents, as they advocated for themselves in the face of an onslaught of demand from other departments and from patients. I remember one occasion when, in front of my intern, I firmly “told off” a patient who was obviously poor and possibly homeless and who I thought was faking pain in order to get admitted to the hospital and receive analgesics. I was pleased with myself when I informed the ED staff that I would not accept the patient onto the medical service.
In retrospect, I wonder how and why I had become a “tough guy”? What had happened to my desire to “be there” for patients in their hour of need? Had I lost my aspiration to care for others, fueled by role models like my father, an internist and pillar in the community?
Does Empathy Decrease over Time?
A number of studies support my personal observation that physician empathy decreases during the training years and later persists at lower levels.1
Yet, perhaps ironically, increased empathy is associated with fewer medical errors, increased patient satisfaction, fewer malpractice claims, and improved clinical outcomes.1
Can We Increase Empathy?
In a 2012 study, Helen Reiss and colleagues randomized residents from several specialties into two groups, one receiving standard post-graduate education and a second whose education included three 60-minute empathy training modules. The empathy training consisted of the following elements:
- Neurobiology of empathy;
- Approaches to increase awareness of the physiology of emotions during patient encounters;
- Skills involved in interpreting the meaning of facial expressions; and
- Breathing exercises and mindfulness practices to enhance empathic responses to patients.
Using a validated instrument to measure empathy as rated by patients, the study reported increased empathy scores for the residents who participated in the empathy training program. An important skill the residents learned in the training was the ability to read/decode the facial expressions of patients and use that information to alter their behavior, thereby increasing patient-reported empathy.1
The authors point to the need for more studies to learn if, and to what extent, empathy training can improve performance in key areas like patient outcomes, malpractice claims, physician well-being, and patient satisfaction. Furthermore, they concluded that “long-lasting improvements in empathic clinical care cannot be sustained without organizational changes at all levels of healthcare. Such cultural changes require a commitment from clinical and administrative leaders to place empathic care at the forefront of institutional missions.”
Committing to Enhancing Physician Empathy
The Cleveland Clinic has addressed empathy as an important element of its institutional mission. Consider the following initiatives and interventions:
- The health system’s CEO publicly prioritizes empathy as a path to better patient experience and caregiver well-being.
- There is a chief experience officer position.
- All employees receive specialized H.E.A.R.T. (Hear, Empathize, Apologize, Respond, Thank) training; embedded approaches and practices support ongoing prioritization of empathy.
- All employees are trained to see themselves as caregivers.
- Physicians and trainees receive training in communication with patients.
- The health system holds an annual national summit on empathy and patient experience.
If you haven’t seen the Cleveland Clinic video that has gone viral, Google “Empathy: The Human Connection to Patient Care.” The video takes advantage of a universal human trait: When we truly know what another person is experiencing and feeling, we can experience and feel the same thing.
Can Hospitalists Retain an Empathic Approach over the Long Term?
I believe hospitalists can retain or regain the empathy that led to our choice of medicine as a career. To do this, we should consider a few critical practices, some of which occur at work and some at home. These include the following strategies:
- Find ways to be fully present in your human encounters with patients and co-workers. This includes minimizing interruptions whenever possible, sitting with people, making eye contact, and putting your phone away.
- Reward yourself for hard work. Make rewards, which needn’t always be expensive, a regular part of your life.
- Take measures to avoid overwork. Know when to say “no” to added responsibilities. Find time to add a wellness practice to your life, such as exercise, art, literature, spending time with your spouse/children, or community service.
- Express the gratitude you are feeling to those you work and live with.
Resources for Empathy Training
Empathetics.com offers CME and nursing continuing education credits for training in “how to detect and manage the emotional states of patients and how to respond with empathy and compassion, even in difficult interactions.”
PaulEkman.com has a series of training modules geared to detecting the “unspoken feelings” of others by recognizing the meaning of facial expressions.
Reference
- Reiss H, Kelley JM, Bailey RW, Dunn EJ, Phillips M. Empathy training for resident physicians: a randomized controlled trial of a neuroscience-informed curriculum. J Gen Intern Med. 2012;27(10):1280-1286.
Hospital Groups Might Do Better Without Daytime Admission Shifts, Morning Meetings
You shouldn’t maintain things that do not deliver the value you anticipated when you first put them in place. For example, I thought Netflix streaming would be terrific, but I have used it so infrequently that it probably costs me $50 per movie or show watched. I should probably dump it.
Your hospitalist group might have some operational practices that are not as valuable as they seem and could be replaced with something better. For many groups, this might include doing away with a separate daytime admitter shift and a morning meeting to distribute the overnight admissions.
Daytime Admission Shift
My experience is that hospitalist groups with more than about five daytime doctors almost always have a day-shift person dedicated to seeing new admissions. In most cases, this procedure is implemented with the idea of reducing the stress of other day-shift doctors, who don’t have to interrupt rounds to admit a new patient. Some see a dedicated admitter as a tool to improve ED throughput, because this doctor isn’t tied up with rounds and can immediately start seeing a new admission.
I think an admitter shift does deliver both of these benefits, but its costs make it suboptimal in most settings. For example, a single admitter will impede ED throughput any time more than one new admission is waiting to be seen, and for most groups that will be much of the day. In fact, improved ED throughput is best achieved by having many hospitalists available for admissions, not just a single admitter. (There are many other factors influencing ED throughput, such as whether ED doctors simply send patients to their “floor” bed prior to being seen by a hospitalist. But for this article, I’m just considering the influence of a dedicated admitter.)
I think “silo-ing” work into different roles, such as separating rounding and admitting, makes it more difficult to ensure that each is always working productively. There are likely to be times when the admitter has little or nothing to do, even though the rounders are very busy. Or perhaps the rounders aren’t very busy, but the admitter has just been asked to admit four ED patients at the same time.
While protecting rounders from the stress of admissions is valuable, it comes at the cost of a net increase in hospitalist work, because a new doctor must get to know the patient on the day following admission. And this admitter-to-rounder handoff serves as another opportunity for errors—and probably lowers patient satisfaction.
I think most groups should consider moving the admitter shift into an additional rounder position, dividing admissions across all of the doctors working during the daytime. For example, a group that has six rounders and a separate admitter would change to seven rounders, each available to admit every seventh daytime admission. Each would bear the meaningful stress of having rounds interrupted to admit a new patient, but accepting every seventh daytime admission shouldn’t be too difficult on most days.
Don’t forget that eliminating the admitter means that the list of new patients you take on each morning will be shorter. Mornings may be a little less stressful.
A.M. Distribution
The daytime doctors at many hospitalist groups meet each morning to discuss how the new admissions from the prior night (or even the last 24 hours) will be distributed. Or perhaps one person, sometimes a nurse or clerical staff, arrives very early each day to do this.
Although it might take some careful planning, I think most groups that use this sort of morning distribution should abandon it for a better system. Consider a group in which all six daytime doctors spend an average of 20 minutes distributing patients each morning. Twenty minutes (0.33 hours) times six doctors times 365 days comes to 730 hours annually.
Assuming these doctors are compensated at typical rates, the practice is spending more than $100,000 annually just so the doctors can distribute patients each morning. On top of this, nurses and others at the hospital are usually delayed in learning which daytime hospitalist is caring for each patient. These costs seem unreasonably high.
An alternative is to develop a system by which any admitter, such as a night doctor, who will not be providing subsequent care to a patient can identify by name the doctor who will be providing that care. During the admission encounter, the admitter can tell patient/family, “Dr. Boswell will be taking over your care starting tomorrow. He’s a great guy and has been named one of Portland’s best doctors.” This seems so much better than saying, “One of my partners will be taking over tomorrow. I don’t know which of my partners it will be, but they’re all good doctors.” And Dr. Boswell’s name can be entered into the attending physician field of the EHR so that all hospital staff will know without delay.
MedAptus has recently launched software they call “Assign” that may be able to replace the morning meeting and automate assigning new admissions to each hospitalist. I haven’t seen it in operation, so I can’t speak for its effectiveness, but it might be worthwhile for some groups.
Practical Considerations
The changes I’ve described above might not be optimal for every group, and they may take meaningful work to implement. But I don’t think the difficulty of these things is the biggest barrier. The biggest barrier is probably just inertia in most cases, the same reason I’m still a Netflix streaming subscriber even though I almost never watch it. I did, however, really enjoy the Nexflix original series Lilyhammer.
You shouldn’t maintain things that do not deliver the value you anticipated when you first put them in place. For example, I thought Netflix streaming would be terrific, but I have used it so infrequently that it probably costs me $50 per movie or show watched. I should probably dump it.
Your hospitalist group might have some operational practices that are not as valuable as they seem and could be replaced with something better. For many groups, this might include doing away with a separate daytime admitter shift and a morning meeting to distribute the overnight admissions.
Daytime Admission Shift
My experience is that hospitalist groups with more than about five daytime doctors almost always have a day-shift person dedicated to seeing new admissions. In most cases, this procedure is implemented with the idea of reducing the stress of other day-shift doctors, who don’t have to interrupt rounds to admit a new patient. Some see a dedicated admitter as a tool to improve ED throughput, because this doctor isn’t tied up with rounds and can immediately start seeing a new admission.
I think an admitter shift does deliver both of these benefits, but its costs make it suboptimal in most settings. For example, a single admitter will impede ED throughput any time more than one new admission is waiting to be seen, and for most groups that will be much of the day. In fact, improved ED throughput is best achieved by having many hospitalists available for admissions, not just a single admitter. (There are many other factors influencing ED throughput, such as whether ED doctors simply send patients to their “floor” bed prior to being seen by a hospitalist. But for this article, I’m just considering the influence of a dedicated admitter.)
I think “silo-ing” work into different roles, such as separating rounding and admitting, makes it more difficult to ensure that each is always working productively. There are likely to be times when the admitter has little or nothing to do, even though the rounders are very busy. Or perhaps the rounders aren’t very busy, but the admitter has just been asked to admit four ED patients at the same time.
While protecting rounders from the stress of admissions is valuable, it comes at the cost of a net increase in hospitalist work, because a new doctor must get to know the patient on the day following admission. And this admitter-to-rounder handoff serves as another opportunity for errors—and probably lowers patient satisfaction.
I think most groups should consider moving the admitter shift into an additional rounder position, dividing admissions across all of the doctors working during the daytime. For example, a group that has six rounders and a separate admitter would change to seven rounders, each available to admit every seventh daytime admission. Each would bear the meaningful stress of having rounds interrupted to admit a new patient, but accepting every seventh daytime admission shouldn’t be too difficult on most days.
Don’t forget that eliminating the admitter means that the list of new patients you take on each morning will be shorter. Mornings may be a little less stressful.
A.M. Distribution
The daytime doctors at many hospitalist groups meet each morning to discuss how the new admissions from the prior night (or even the last 24 hours) will be distributed. Or perhaps one person, sometimes a nurse or clerical staff, arrives very early each day to do this.
Although it might take some careful planning, I think most groups that use this sort of morning distribution should abandon it for a better system. Consider a group in which all six daytime doctors spend an average of 20 minutes distributing patients each morning. Twenty minutes (0.33 hours) times six doctors times 365 days comes to 730 hours annually.
Assuming these doctors are compensated at typical rates, the practice is spending more than $100,000 annually just so the doctors can distribute patients each morning. On top of this, nurses and others at the hospital are usually delayed in learning which daytime hospitalist is caring for each patient. These costs seem unreasonably high.
An alternative is to develop a system by which any admitter, such as a night doctor, who will not be providing subsequent care to a patient can identify by name the doctor who will be providing that care. During the admission encounter, the admitter can tell patient/family, “Dr. Boswell will be taking over your care starting tomorrow. He’s a great guy and has been named one of Portland’s best doctors.” This seems so much better than saying, “One of my partners will be taking over tomorrow. I don’t know which of my partners it will be, but they’re all good doctors.” And Dr. Boswell’s name can be entered into the attending physician field of the EHR so that all hospital staff will know without delay.
MedAptus has recently launched software they call “Assign” that may be able to replace the morning meeting and automate assigning new admissions to each hospitalist. I haven’t seen it in operation, so I can’t speak for its effectiveness, but it might be worthwhile for some groups.
Practical Considerations
The changes I’ve described above might not be optimal for every group, and they may take meaningful work to implement. But I don’t think the difficulty of these things is the biggest barrier. The biggest barrier is probably just inertia in most cases, the same reason I’m still a Netflix streaming subscriber even though I almost never watch it. I did, however, really enjoy the Nexflix original series Lilyhammer.
You shouldn’t maintain things that do not deliver the value you anticipated when you first put them in place. For example, I thought Netflix streaming would be terrific, but I have used it so infrequently that it probably costs me $50 per movie or show watched. I should probably dump it.
Your hospitalist group might have some operational practices that are not as valuable as they seem and could be replaced with something better. For many groups, this might include doing away with a separate daytime admitter shift and a morning meeting to distribute the overnight admissions.
Daytime Admission Shift
My experience is that hospitalist groups with more than about five daytime doctors almost always have a day-shift person dedicated to seeing new admissions. In most cases, this procedure is implemented with the idea of reducing the stress of other day-shift doctors, who don’t have to interrupt rounds to admit a new patient. Some see a dedicated admitter as a tool to improve ED throughput, because this doctor isn’t tied up with rounds and can immediately start seeing a new admission.
I think an admitter shift does deliver both of these benefits, but its costs make it suboptimal in most settings. For example, a single admitter will impede ED throughput any time more than one new admission is waiting to be seen, and for most groups that will be much of the day. In fact, improved ED throughput is best achieved by having many hospitalists available for admissions, not just a single admitter. (There are many other factors influencing ED throughput, such as whether ED doctors simply send patients to their “floor” bed prior to being seen by a hospitalist. But for this article, I’m just considering the influence of a dedicated admitter.)
I think “silo-ing” work into different roles, such as separating rounding and admitting, makes it more difficult to ensure that each is always working productively. There are likely to be times when the admitter has little or nothing to do, even though the rounders are very busy. Or perhaps the rounders aren’t very busy, but the admitter has just been asked to admit four ED patients at the same time.
While protecting rounders from the stress of admissions is valuable, it comes at the cost of a net increase in hospitalist work, because a new doctor must get to know the patient on the day following admission. And this admitter-to-rounder handoff serves as another opportunity for errors—and probably lowers patient satisfaction.
I think most groups should consider moving the admitter shift into an additional rounder position, dividing admissions across all of the doctors working during the daytime. For example, a group that has six rounders and a separate admitter would change to seven rounders, each available to admit every seventh daytime admission. Each would bear the meaningful stress of having rounds interrupted to admit a new patient, but accepting every seventh daytime admission shouldn’t be too difficult on most days.
Don’t forget that eliminating the admitter means that the list of new patients you take on each morning will be shorter. Mornings may be a little less stressful.
A.M. Distribution
The daytime doctors at many hospitalist groups meet each morning to discuss how the new admissions from the prior night (or even the last 24 hours) will be distributed. Or perhaps one person, sometimes a nurse or clerical staff, arrives very early each day to do this.
Although it might take some careful planning, I think most groups that use this sort of morning distribution should abandon it for a better system. Consider a group in which all six daytime doctors spend an average of 20 minutes distributing patients each morning. Twenty minutes (0.33 hours) times six doctors times 365 days comes to 730 hours annually.
Assuming these doctors are compensated at typical rates, the practice is spending more than $100,000 annually just so the doctors can distribute patients each morning. On top of this, nurses and others at the hospital are usually delayed in learning which daytime hospitalist is caring for each patient. These costs seem unreasonably high.
An alternative is to develop a system by which any admitter, such as a night doctor, who will not be providing subsequent care to a patient can identify by name the doctor who will be providing that care. During the admission encounter, the admitter can tell patient/family, “Dr. Boswell will be taking over your care starting tomorrow. He’s a great guy and has been named one of Portland’s best doctors.” This seems so much better than saying, “One of my partners will be taking over tomorrow. I don’t know which of my partners it will be, but they’re all good doctors.” And Dr. Boswell’s name can be entered into the attending physician field of the EHR so that all hospital staff will know without delay.
MedAptus has recently launched software they call “Assign” that may be able to replace the morning meeting and automate assigning new admissions to each hospitalist. I haven’t seen it in operation, so I can’t speak for its effectiveness, but it might be worthwhile for some groups.
Practical Considerations
The changes I’ve described above might not be optimal for every group, and they may take meaningful work to implement. But I don’t think the difficulty of these things is the biggest barrier. The biggest barrier is probably just inertia in most cases, the same reason I’m still a Netflix streaming subscriber even though I almost never watch it. I did, however, really enjoy the Nexflix original series Lilyhammer.
Why Hospitalist Morale is Declining and Ways to Improve It

Using quotes to ensure that the results were only those that include the two words adjacent to one another, rather than separated, I entered the following phrases into my Google search engine:
- “hospitalist burnout” = 1,580 results
- “hospitalist morale” = 208 results
- “hospitalist well-being” = 0 results
I think the number of results suggests the level of interest in each topic and, if that is the case, clearly thinking about how hospitalists are doing in their careers is more commonly done through the paradigm of burnout than the other two terms. (Of course, there may be other terms that I didn’t consider.) In fact, there have been a handful of published studies of hospitalist burnout and job satisfaction.1,2
Those studies generally have shown both reasonably high levels of job satisfaction and troubling levels of burnout.
But I’ve been thinking about hospitalist morale for a while. I think morale is reasonably distinct from both burnout and job satisfaction.
Causes of a National Decline in Hospitalist Morale
I think hospitalist morale has declined some over the past two or three years across the country. This observation is meaningful because it comes from my experience working with a lot of hospitalist groups coast to coast. But I’m the first to admit it is just anecdotal and is subject to my own biases.
I can think of several things contributing to a decline in morale.
EHR adoption. Near the top of the list is the adoption of EHRs in many hospitals, which typically leads doctors in other specialties to seek hospitalist assistance with EHR-related tasks (e.g. medicine reconciliation and order writing) even in cases where there is little or no clinical reason for hospitalist involvement. Lots of hospitalists complain about this. To be clear, in many hospitals the hospitalists are reasonably content with using the EHR, but they experience ongoing frustration and low morale resulting from nonclinical work other doctors pressure them to take over.
Observation status. Many hospitals began classifying a larger portion of patients as observation status over the last few years; at the same time, patients and families have become more aware of how much of a disadvantage this is. In many cases, it is the hospitalist who takes the brunt of patient and family frustration. This can get awfully stressful and frustrating, and I think it is a contributor to allegations of malpractice.
Budgetary stress. Ever since SHM began collecting survey data in the late 1990s, the financial support hospitals have been providing to hospitalists has increased dramatically. The most recent State of Hospital Medicine report, published in 2104, showed median support provided by hospitals of $156,063 per FTE hospitalist, per year. Some hospitals have begun to resist providing more support, and this translates into stress and lower morale for hospitalists. This is far from a universal issue, but it does lead to lower morale for hospitalists who face it.
Many other factors may be contributing to a national decline in morale, but I think these are some of the most important.
What Can Be Done?
Some hospitalist groups have great morale now and don’t need to do much of anything right now, but some groups should think about a deliberate strategy to improve it.
Sadly, there isn’t a prescription that is sure to work. But there are some things you can try.
Self-care. The field of palliative care has thought a lot about caring for caregivers, and hospitalist groups might want to adopt some of their practices. Search the Internet on “self-care” + “palliative care,” and you’ll find a lot of interesting things. The group I’m part of launched a deliberate program of professionally led and facilitated hospitalist self-care, with high hopes that included mindful meditation, among other things. As soon as we had designed our program, the Mayo Clinic published their favorable experience with a program that was very similar to what we had planned, and I thought we would see similar benefits.3
But, while all who attended the sessions thought they were valuable, attendance was so poor that we ended up cancelling the program. The hospitalists were interested in attending but were either on service and busy seeing patients, or were off and didn’t want to drive in to work solely for the purpose of reducing work stress.
I’m convinced a self-care program is valuable but very tricky to schedule effectively. Maybe others have come up with effective ways of overcoming this problem.
Social connections. Some hospitalist groups seem to have little social and personal connection to other physicians and hospital leaders. I think this results in lower hospitalist morale and tends to be self-reinforcing. If you’re in such a group, you and your hospitalist colleagues should deliberately seek better relationships with other doctors and hospital administrative leaders. Ensure that you visit with others at lunch, talk with them at committee meetings, ask about their vacation and personal activities, and pursue activities with them outside of work.
When these sorts of social connections are strong, work is far more satisfying and you’re much more likely to be treated as a peer by other doctors. I think this is really important and shouldn’t be overlooked if your group is suffering from low morale.
Adaptive work. Lastly, you might want to approach changes to your work and morale as “adaptive work,” rather than “technical work.” Space doesn’t permit a description of these, but it is worth reading about how they differ. Many groups will find value in reframing their approach to aspects of work they don’t like as adaptive work.
References
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- West CP, Dyrbye LN, Rabatin JT, et al. Intervention to promote physician well-being, job satisfaction, and professionalism: a randomized clinical trial. JAMA Intern Med. 2014;174(4):527-533.
Using quotes to ensure that the results were only those that include the two words adjacent to one another, rather than separated, I entered the following phrases into my Google search engine:
- “hospitalist burnout” = 1,580 results
- “hospitalist morale” = 208 results
- “hospitalist well-being” = 0 results
I think the number of results suggests the level of interest in each topic and, if that is the case, clearly thinking about how hospitalists are doing in their careers is more commonly done through the paradigm of burnout than the other two terms. (Of course, there may be other terms that I didn’t consider.) In fact, there have been a handful of published studies of hospitalist burnout and job satisfaction.1,2
Those studies generally have shown both reasonably high levels of job satisfaction and troubling levels of burnout.
But I’ve been thinking about hospitalist morale for a while. I think morale is reasonably distinct from both burnout and job satisfaction.
Causes of a National Decline in Hospitalist Morale
I think hospitalist morale has declined some over the past two or three years across the country. This observation is meaningful because it comes from my experience working with a lot of hospitalist groups coast to coast. But I’m the first to admit it is just anecdotal and is subject to my own biases.
I can think of several things contributing to a decline in morale.
EHR adoption. Near the top of the list is the adoption of EHRs in many hospitals, which typically leads doctors in other specialties to seek hospitalist assistance with EHR-related tasks (e.g. medicine reconciliation and order writing) even in cases where there is little or no clinical reason for hospitalist involvement. Lots of hospitalists complain about this. To be clear, in many hospitals the hospitalists are reasonably content with using the EHR, but they experience ongoing frustration and low morale resulting from nonclinical work other doctors pressure them to take over.
Observation status. Many hospitals began classifying a larger portion of patients as observation status over the last few years; at the same time, patients and families have become more aware of how much of a disadvantage this is. In many cases, it is the hospitalist who takes the brunt of patient and family frustration. This can get awfully stressful and frustrating, and I think it is a contributor to allegations of malpractice.
Budgetary stress. Ever since SHM began collecting survey data in the late 1990s, the financial support hospitals have been providing to hospitalists has increased dramatically. The most recent State of Hospital Medicine report, published in 2104, showed median support provided by hospitals of $156,063 per FTE hospitalist, per year. Some hospitals have begun to resist providing more support, and this translates into stress and lower morale for hospitalists. This is far from a universal issue, but it does lead to lower morale for hospitalists who face it.
Many other factors may be contributing to a national decline in morale, but I think these are some of the most important.
What Can Be Done?
Some hospitalist groups have great morale now and don’t need to do much of anything right now, but some groups should think about a deliberate strategy to improve it.
Sadly, there isn’t a prescription that is sure to work. But there are some things you can try.
Self-care. The field of palliative care has thought a lot about caring for caregivers, and hospitalist groups might want to adopt some of their practices. Search the Internet on “self-care” + “palliative care,” and you’ll find a lot of interesting things. The group I’m part of launched a deliberate program of professionally led and facilitated hospitalist self-care, with high hopes that included mindful meditation, among other things. As soon as we had designed our program, the Mayo Clinic published their favorable experience with a program that was very similar to what we had planned, and I thought we would see similar benefits.3
But, while all who attended the sessions thought they were valuable, attendance was so poor that we ended up cancelling the program. The hospitalists were interested in attending but were either on service and busy seeing patients, or were off and didn’t want to drive in to work solely for the purpose of reducing work stress.
I’m convinced a self-care program is valuable but very tricky to schedule effectively. Maybe others have come up with effective ways of overcoming this problem.
Social connections. Some hospitalist groups seem to have little social and personal connection to other physicians and hospital leaders. I think this results in lower hospitalist morale and tends to be self-reinforcing. If you’re in such a group, you and your hospitalist colleagues should deliberately seek better relationships with other doctors and hospital administrative leaders. Ensure that you visit with others at lunch, talk with them at committee meetings, ask about their vacation and personal activities, and pursue activities with them outside of work.
When these sorts of social connections are strong, work is far more satisfying and you’re much more likely to be treated as a peer by other doctors. I think this is really important and shouldn’t be overlooked if your group is suffering from low morale.
Adaptive work. Lastly, you might want to approach changes to your work and morale as “adaptive work,” rather than “technical work.” Space doesn’t permit a description of these, but it is worth reading about how they differ. Many groups will find value in reframing their approach to aspects of work they don’t like as adaptive work.
References
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- West CP, Dyrbye LN, Rabatin JT, et al. Intervention to promote physician well-being, job satisfaction, and professionalism: a randomized clinical trial. JAMA Intern Med. 2014;174(4):527-533.
Using quotes to ensure that the results were only those that include the two words adjacent to one another, rather than separated, I entered the following phrases into my Google search engine:
- “hospitalist burnout” = 1,580 results
- “hospitalist morale” = 208 results
- “hospitalist well-being” = 0 results
I think the number of results suggests the level of interest in each topic and, if that is the case, clearly thinking about how hospitalists are doing in their careers is more commonly done through the paradigm of burnout than the other two terms. (Of course, there may be other terms that I didn’t consider.) In fact, there have been a handful of published studies of hospitalist burnout and job satisfaction.1,2
Those studies generally have shown both reasonably high levels of job satisfaction and troubling levels of burnout.
But I’ve been thinking about hospitalist morale for a while. I think morale is reasonably distinct from both burnout and job satisfaction.
Causes of a National Decline in Hospitalist Morale
I think hospitalist morale has declined some over the past two or three years across the country. This observation is meaningful because it comes from my experience working with a lot of hospitalist groups coast to coast. But I’m the first to admit it is just anecdotal and is subject to my own biases.
I can think of several things contributing to a decline in morale.
EHR adoption. Near the top of the list is the adoption of EHRs in many hospitals, which typically leads doctors in other specialties to seek hospitalist assistance with EHR-related tasks (e.g. medicine reconciliation and order writing) even in cases where there is little or no clinical reason for hospitalist involvement. Lots of hospitalists complain about this. To be clear, in many hospitals the hospitalists are reasonably content with using the EHR, but they experience ongoing frustration and low morale resulting from nonclinical work other doctors pressure them to take over.
Observation status. Many hospitals began classifying a larger portion of patients as observation status over the last few years; at the same time, patients and families have become more aware of how much of a disadvantage this is. In many cases, it is the hospitalist who takes the brunt of patient and family frustration. This can get awfully stressful and frustrating, and I think it is a contributor to allegations of malpractice.
Budgetary stress. Ever since SHM began collecting survey data in the late 1990s, the financial support hospitals have been providing to hospitalists has increased dramatically. The most recent State of Hospital Medicine report, published in 2104, showed median support provided by hospitals of $156,063 per FTE hospitalist, per year. Some hospitals have begun to resist providing more support, and this translates into stress and lower morale for hospitalists. This is far from a universal issue, but it does lead to lower morale for hospitalists who face it.
Many other factors may be contributing to a national decline in morale, but I think these are some of the most important.
What Can Be Done?
Some hospitalist groups have great morale now and don’t need to do much of anything right now, but some groups should think about a deliberate strategy to improve it.
Sadly, there isn’t a prescription that is sure to work. But there are some things you can try.
Self-care. The field of palliative care has thought a lot about caring for caregivers, and hospitalist groups might want to adopt some of their practices. Search the Internet on “self-care” + “palliative care,” and you’ll find a lot of interesting things. The group I’m part of launched a deliberate program of professionally led and facilitated hospitalist self-care, with high hopes that included mindful meditation, among other things. As soon as we had designed our program, the Mayo Clinic published their favorable experience with a program that was very similar to what we had planned, and I thought we would see similar benefits.3
But, while all who attended the sessions thought they were valuable, attendance was so poor that we ended up cancelling the program. The hospitalists were interested in attending but were either on service and busy seeing patients, or were off and didn’t want to drive in to work solely for the purpose of reducing work stress.
I’m convinced a self-care program is valuable but very tricky to schedule effectively. Maybe others have come up with effective ways of overcoming this problem.
Social connections. Some hospitalist groups seem to have little social and personal connection to other physicians and hospital leaders. I think this results in lower hospitalist morale and tends to be self-reinforcing. If you’re in such a group, you and your hospitalist colleagues should deliberately seek better relationships with other doctors and hospital administrative leaders. Ensure that you visit with others at lunch, talk with them at committee meetings, ask about their vacation and personal activities, and pursue activities with them outside of work.
When these sorts of social connections are strong, work is far more satisfying and you’re much more likely to be treated as a peer by other doctors. I think this is really important and shouldn’t be overlooked if your group is suffering from low morale.
Adaptive work. Lastly, you might want to approach changes to your work and morale as “adaptive work,” rather than “technical work.” Space doesn’t permit a description of these, but it is worth reading about how they differ. Many groups will find value in reframing their approach to aspects of work they don’t like as adaptive work.
References
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- West CP, Dyrbye LN, Rabatin JT, et al. Intervention to promote physician well-being, job satisfaction, and professionalism: a randomized clinical trial. JAMA Intern Med. 2014;174(4):527-533.
Using a retrojugular approach to the carotid
Carotid endarterectomy is one of the most common operations for vascular surgeons. The standard approach, anteriorly, requires division of the facial vein, frequently additional small tributaries, and sacrifice of the ansa cervicalis.
The facial vein is not infrequently the cause of bleeding on patients returned to the OR who truly have surgical bleeding. The vagus nerve is not well visualized during the standard approach, unless maneuvers are taken to specifically identify it. Although this approach gives good access to the common carotid artery, and to the external carotid, it requires additional maneuvers in order to gain access to the distal internal carotid artery (ICA), which is located more posterolaterally.

This frequently requires ligation of the vascular bundle around the hypoglossal nerve, which can lead to bleeding if not properly addressed. Visualization of the distal ICA is not ideal with this approach.
An alternative: The retrojugular approach
The surgery is performed with the patient prepped in the same fashion as for standard CEA. Skin incision and initial dissection is identical for standard CEA approach, and is made along the sternocleidomastoid, with division of the platysma.
Dissection is carried out just along the border of the SCM until the carotid sheath is encountered. At this point, the dissection differs. Dissection is continued along the lateral border of the internal jugular vein, which is gently dissected from the surrounding tissue.
There are rarely branches along the lateral or posterior border that require ligation. This area is sharply dissected due to the proximity of nervous structures. The vagus nerve is easily visualized utilizing this approach, and left lateral to the carotid artery. Once a sufficient length of jugular has been mobilized, a blunt whietlander is placed, retracting the vein medially. The Carotid artery is then easily visualized, with a long segment of the ICA easily visible.
The hypoglossal nerve and facial vein are not visualized. The ansa cervicalis is not divided. Standard mobilization of the CCA, ICA, and ECA is then performed. With this approach, the ICA is anterior.
Visualization of the ECA is slightly more limited with this approach, but the proximal ECA and superior thyroidal arteries are easily identified and looped. CEA, either with eversion or standard longitudinal incision, is completed in standard fashion. After completion of the CEA, and confirmation of adequate hemostasis, the IJ is simply allowed to return to its normal position. The wound is then closed in standard fashion.
This approach permits significant exposure to a markedly longer segment of the ICA, without division of additional vascular branches, nor mobilization of nerves. There is slightly less visibility of the ECA, but more than adequate for the necessary vascular control. The approach also has less risk of postoperative bleed, and has been reported to be slightly faster than the anterior approach.
Dr. Harris is division chief, Vascular Surgery, at the State University of New York at Buffalo, and an associate medical editor of Vascular Specialist.
Carotid endarterectomy is one of the most common operations for vascular surgeons. The standard approach, anteriorly, requires division of the facial vein, frequently additional small tributaries, and sacrifice of the ansa cervicalis.
The facial vein is not infrequently the cause of bleeding on patients returned to the OR who truly have surgical bleeding. The vagus nerve is not well visualized during the standard approach, unless maneuvers are taken to specifically identify it. Although this approach gives good access to the common carotid artery, and to the external carotid, it requires additional maneuvers in order to gain access to the distal internal carotid artery (ICA), which is located more posterolaterally.
This frequently requires ligation of the vascular bundle around the hypoglossal nerve, which can lead to bleeding if not properly addressed. Visualization of the distal ICA is not ideal with this approach.
An alternative: The retrojugular approach
The surgery is performed with the patient prepped in the same fashion as for standard CEA. Skin incision and initial dissection is identical for standard CEA approach, and is made along the sternocleidomastoid, with division of the platysma.
Dissection is carried out just along the border of the SCM until the carotid sheath is encountered. At this point, the dissection differs. Dissection is continued along the lateral border of the internal jugular vein, which is gently dissected from the surrounding tissue.
There are rarely branches along the lateral or posterior border that require ligation. This area is sharply dissected due to the proximity of nervous structures. The vagus nerve is easily visualized utilizing this approach, and left lateral to the carotid artery. Once a sufficient length of jugular has been mobilized, a blunt whietlander is placed, retracting the vein medially. The Carotid artery is then easily visualized, with a long segment of the ICA easily visible.
The hypoglossal nerve and facial vein are not visualized. The ansa cervicalis is not divided. Standard mobilization of the CCA, ICA, and ECA is then performed. With this approach, the ICA is anterior.
Visualization of the ECA is slightly more limited with this approach, but the proximal ECA and superior thyroidal arteries are easily identified and looped. CEA, either with eversion or standard longitudinal incision, is completed in standard fashion. After completion of the CEA, and confirmation of adequate hemostasis, the IJ is simply allowed to return to its normal position. The wound is then closed in standard fashion.
This approach permits significant exposure to a markedly longer segment of the ICA, without division of additional vascular branches, nor mobilization of nerves. There is slightly less visibility of the ECA, but more than adequate for the necessary vascular control. The approach also has less risk of postoperative bleed, and has been reported to be slightly faster than the anterior approach.
Dr. Harris is division chief, Vascular Surgery, at the State University of New York at Buffalo, and an associate medical editor of Vascular Specialist.
Carotid endarterectomy is one of the most common operations for vascular surgeons. The standard approach, anteriorly, requires division of the facial vein, frequently additional small tributaries, and sacrifice of the ansa cervicalis.
The facial vein is not infrequently the cause of bleeding on patients returned to the OR who truly have surgical bleeding. The vagus nerve is not well visualized during the standard approach, unless maneuvers are taken to specifically identify it. Although this approach gives good access to the common carotid artery, and to the external carotid, it requires additional maneuvers in order to gain access to the distal internal carotid artery (ICA), which is located more posterolaterally.
This frequently requires ligation of the vascular bundle around the hypoglossal nerve, which can lead to bleeding if not properly addressed. Visualization of the distal ICA is not ideal with this approach.
An alternative: The retrojugular approach
The surgery is performed with the patient prepped in the same fashion as for standard CEA. Skin incision and initial dissection is identical for standard CEA approach, and is made along the sternocleidomastoid, with division of the platysma.
Dissection is carried out just along the border of the SCM until the carotid sheath is encountered. At this point, the dissection differs. Dissection is continued along the lateral border of the internal jugular vein, which is gently dissected from the surrounding tissue.
There are rarely branches along the lateral or posterior border that require ligation. This area is sharply dissected due to the proximity of nervous structures. The vagus nerve is easily visualized utilizing this approach, and left lateral to the carotid artery. Once a sufficient length of jugular has been mobilized, a blunt whietlander is placed, retracting the vein medially. The Carotid artery is then easily visualized, with a long segment of the ICA easily visible.
The hypoglossal nerve and facial vein are not visualized. The ansa cervicalis is not divided. Standard mobilization of the CCA, ICA, and ECA is then performed. With this approach, the ICA is anterior.
Visualization of the ECA is slightly more limited with this approach, but the proximal ECA and superior thyroidal arteries are easily identified and looped. CEA, either with eversion or standard longitudinal incision, is completed in standard fashion. After completion of the CEA, and confirmation of adequate hemostasis, the IJ is simply allowed to return to its normal position. The wound is then closed in standard fashion.
This approach permits significant exposure to a markedly longer segment of the ICA, without division of additional vascular branches, nor mobilization of nerves. There is slightly less visibility of the ECA, but more than adequate for the necessary vascular control. The approach also has less risk of postoperative bleed, and has been reported to be slightly faster than the anterior approach.
Dr. Harris is division chief, Vascular Surgery, at the State University of New York at Buffalo, and an associate medical editor of Vascular Specialist.

Grandparents and the new baby
A couple having a baby brings together two family traditions that themselves blended the previous generations’ experiences and perspectives. Each of the new parents has been raised by two parents with their own histories, values, successes, and crises all available and potentially playing a part in the new baby’s future. A baby’s arrival can call forth memories of past successes, failures, hopes, and dreams – some fulfilled and some not.
As the pediatrician, you serve as an authority and a resource for the new parents. You will hear questions that have roots that may go back one, two, or more generations. Some may involve discipline, approaches to food, religious issues, or more subtle concerns relating to control and autonomy. And you may find that they will bring you the challenge of managing the beliefs, values, and expectations of the new grandparents. You may even find these new grandparents in your office! You have a unique opportunity to help new parents set a course with their own parents or in-laws that can promote family cohesion and honor family traditions or values, while empowering parents to trust themselves and truly be in charge of raising their own children.

Imagine this scenario: A young couple has just had their first baby, a son. The paternal grandfather, who played soccer in high school and college, presents his first grandchild with his own college soccer ball, proclaiming with great emotion that soccer will certainly be a part of his grandson’s future.
While this simple act may seem touching, it might also be perceived by the new parents as intrusive or controlling. How does the new father (who was maybe more bookish than athletic) feel the burden of this expectation? Perhaps the mother may wish her son to be more of a scholar than an athlete, or may want no expectation set, but may feel uncomfortable speaking honestly with her father-in-law. And this scenario is just about the gift of a soccer ball!
Grandparents (like parents) come with expectations, with beliefs about what practices worked and what failed over a wide range of areas from child rearing to managing finances to career to marriage. The arrival of a new grandchild will likely prompt them to share these beliefs, and do so in the way they usually communicate with their own children, be it blunt, emotional, indirect, or mute. These views might be forcefully presented, if a grandparent feels guilty or unfulfilled because a meaningful hope for their own child did not materialize: The new grandchild is their “last chance.” While their love and interest, their experience and wisdom can be invaluable, they might also arouse insecurity in a new parent or be disruptive. If they share opinions in a way that is stressful, devaluing, or confusing for new parents, that can translate into anxious, uncertain interactions with their new baby or a climate at home that is full of conflict instead of calm.
Parents are already blending their two styles and values, challenging enough before also trying to blend the elements of four grandparents.
The first weeks after the arrival of the new baby is a crucial time in the baby’s development, as well as in the development of the new parents, as all are rapidly acquiring new skills, adjusting to a new schedule, and learning how to understand and respond to each other. During these hard early days, grandparents often will be present, staying in the home or nearby to offer support to their children. Very commonly, they will share their opinions about such basics as nutrition and sleep. These are areas that are fundamentally important for a baby’s healthy development, but can be mysterious and challenging for new parents. They may seek out guidance from friends, books, websites, and pediatricians, as well as the new grandparents.
While their accumulated wisdom may be as helpful as their helping with laundry or meal preparation (think, “sleep when the baby sleeps”), it also might not. Perhaps the opinions are misguided (think, “sleeping on the tummy was always fine in my day”). And grandparents who are inadvertently undermining (“I don’t understand the difficulty, nursing was so easy for me”), or highly anxious might add to the new parents’ stress and uncertainty rather than alleviate it.
Grandparents also may come with strong cultural beliefs about child rearing. In families that are only one or two generations removed from immigration to this country, there may be powerfully held ideas about newborns, ones that might be inextricably linked for the grandparents with their drive to preserve their own cultural background. These may include ideas about when a child can eat solid food or what he or she should start eating. They may include beliefs that a child should never be put down or should be left to cry for long periods, lest they be “spoiled.” They might include ideas about when a baby can swim or how best to bathe them, what sorts of toys are appropriate or when their hair can be cut. While many of these beliefs have cultural value and no medical implications (like the timing of the first haircut), some may fly in the face of current scientific evidence (such as eating solids before they are able). And even when they are “safe,” new parents may experience these beliefs as fraught directives: ones that they may not believe in, but which will make them guilty of some cultural betrayal if they do not follow them.
Along a similar vein, grandparents may enter the home of their new grandchild with passionately held religious beliefs. While few of these may have direct medical implications for the new baby (such as circumcision), they can still have profound implications for life in the family’s home. When parents and grandparents all share the same religious beliefs, there is less possibility of conflict. But when new parents come from different religious traditions or no longer share their parents’ faith, there is high potential for emotionally charged differences. And if the new parents have not anticipated these conversations (say, whether or not to circumcise a baby boy when one parent is Jewish and the other is Protestant), trying to sort out these matters while also learning to change diapers or nurse a colicky baby can make a challenging situation into an overwhelming one.
Lastly, about 1% of all households have same-sex partners or marriages and about one in four are raising children. While same-sex parenthood has rapidly gained cultural acceptance over the past decade, it is possible that some grandparents will not have fully accepted the reality of their own child’s sexual orientation and committed relationship. If the parents speak to you about such a fraught situation, listen supportively. When it sounds like there is ambivalence in the grandparents, the new parents can try to nurture the love that is there and be patient when their own parents still struggle. They should nurture the connections with those in their families that offer unconditional support and who can model love and acceptance for the new grandparents. In situations in which there is deeper alienation and little or no contact, offer that they might want to find a way to share photos and stories through one who remains close to their parents and periodically offer opportunities to rebuild relationships. A new grandchild can be a loving moment to take a fresh look at unresolved anger and loss, and as clinicians we have seen families resolve differences as they look to a new baby’s future.
Pediatricians are in a unique position of both neutrality and authority with their new patient’s parents and grandparents. When parents come to a newborn check or well-baby check, it can be invaluable to determine “who else is helping you?” After finding out about nursing or feeding the baby and about sleep, inquire about where they are getting any guidance or support. Friends or siblings with children? Books or websites? Grandparents? What has been helpful and what has not? When you hear about grandparents and see an eye-roll or hear a deep sigh, be curious about what has been helpful and what has been challenging. It is vitally helpful to first-time parents to be validated in their feeling that their own parents are a valuable resource, but not without their challenges.
While it may be important to offer a “medical” opinion about certain matters (back-sleeping, cosleeping, and introducing solids, for example), on most matters, the pediatrician’s role will be to help parents set a framework that will help them to cultivate what is precious and helpful from grandparents while minimizing conflict or unnecessary stress. For new parents, this may be as simple as reminding them that while this is an vital time for the baby’s development, it is also a big transition for them into parenthood and a significant transition for their parents or in-laws into grandparenthood. Help the new parents to understand that there is sometimes no one “right” way to handle certain decisions or challenges, and they will have to try a variety of strategies before finding the one that fits them as parents to this particular child. Remind them that parenting is a learning curve and it is common to feel stressed in new territory with high stakes. But they will find the right rhythm with being attuned to their new baby and eventually managing routines and limits. They are allowed to embrace the support that they find helpful and limit that which they experience as deeply undermining, dismissive, or judgmental.
When you notice that parents sound very angry at or alienated from grandparents, particularly when it is causing some marital conflict, it can be powerful for you to suggest that they should sort out their wishes and beliefs as parents first and then find a clear and loving way to communicate these to the grandparents. Remind them that they are becoming the experts on their children and that they will best be able to set appropriate routines and expectations. But remind them also that grandparents are potentially a treasure to their grandchildren, beyond the help with laundry and meal preparation at the very start of a child’s life.
There can never be enough loving, interested adults in a child’s orbit or a big enough cheering section. And grandparents can be uniquely passionate, patient, curious, and supportive to their growing grandchildren. They bring perspective on a family’s history, wonderful as a growing child builds a story about who they are and where they come from. And their interest and love will help a growing child build a sense of what characteristics make them a treasure to others. Few people can do this as well as grandparents, and letting them begin this involvement at the start of their grandchild’s life only supports this role.
While the arrival of a new baby will be a joyful event for a family, it will also be emotionally complex. Providing your patient’s parents with support and even some language that may help them cultivate the grandparents’ interest and love, while building healthy boundaries around their own parenting, may help set the stage for the healthiest development of your very young patient.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at pdnews@frontlinemedcom.com.
A couple having a baby brings together two family traditions that themselves blended the previous generations’ experiences and perspectives. Each of the new parents has been raised by two parents with their own histories, values, successes, and crises all available and potentially playing a part in the new baby’s future. A baby’s arrival can call forth memories of past successes, failures, hopes, and dreams – some fulfilled and some not.
As the pediatrician, you serve as an authority and a resource for the new parents. You will hear questions that have roots that may go back one, two, or more generations. Some may involve discipline, approaches to food, religious issues, or more subtle concerns relating to control and autonomy. And you may find that they will bring you the challenge of managing the beliefs, values, and expectations of the new grandparents. You may even find these new grandparents in your office! You have a unique opportunity to help new parents set a course with their own parents or in-laws that can promote family cohesion and honor family traditions or values, while empowering parents to trust themselves and truly be in charge of raising their own children.
Imagine this scenario: A young couple has just had their first baby, a son. The paternal grandfather, who played soccer in high school and college, presents his first grandchild with his own college soccer ball, proclaiming with great emotion that soccer will certainly be a part of his grandson’s future.
While this simple act may seem touching, it might also be perceived by the new parents as intrusive or controlling. How does the new father (who was maybe more bookish than athletic) feel the burden of this expectation? Perhaps the mother may wish her son to be more of a scholar than an athlete, or may want no expectation set, but may feel uncomfortable speaking honestly with her father-in-law. And this scenario is just about the gift of a soccer ball!
Grandparents (like parents) come with expectations, with beliefs about what practices worked and what failed over a wide range of areas from child rearing to managing finances to career to marriage. The arrival of a new grandchild will likely prompt them to share these beliefs, and do so in the way they usually communicate with their own children, be it blunt, emotional, indirect, or mute. These views might be forcefully presented, if a grandparent feels guilty or unfulfilled because a meaningful hope for their own child did not materialize: The new grandchild is their “last chance.” While their love and interest, their experience and wisdom can be invaluable, they might also arouse insecurity in a new parent or be disruptive. If they share opinions in a way that is stressful, devaluing, or confusing for new parents, that can translate into anxious, uncertain interactions with their new baby or a climate at home that is full of conflict instead of calm.
Parents are already blending their two styles and values, challenging enough before also trying to blend the elements of four grandparents.
The first weeks after the arrival of the new baby is a crucial time in the baby’s development, as well as in the development of the new parents, as all are rapidly acquiring new skills, adjusting to a new schedule, and learning how to understand and respond to each other. During these hard early days, grandparents often will be present, staying in the home or nearby to offer support to their children. Very commonly, they will share their opinions about such basics as nutrition and sleep. These are areas that are fundamentally important for a baby’s healthy development, but can be mysterious and challenging for new parents. They may seek out guidance from friends, books, websites, and pediatricians, as well as the new grandparents.
While their accumulated wisdom may be as helpful as their helping with laundry or meal preparation (think, “sleep when the baby sleeps”), it also might not. Perhaps the opinions are misguided (think, “sleeping on the tummy was always fine in my day”). And grandparents who are inadvertently undermining (“I don’t understand the difficulty, nursing was so easy for me”), or highly anxious might add to the new parents’ stress and uncertainty rather than alleviate it.
Grandparents also may come with strong cultural beliefs about child rearing. In families that are only one or two generations removed from immigration to this country, there may be powerfully held ideas about newborns, ones that might be inextricably linked for the grandparents with their drive to preserve their own cultural background. These may include ideas about when a child can eat solid food or what he or she should start eating. They may include beliefs that a child should never be put down or should be left to cry for long periods, lest they be “spoiled.” They might include ideas about when a baby can swim or how best to bathe them, what sorts of toys are appropriate or when their hair can be cut. While many of these beliefs have cultural value and no medical implications (like the timing of the first haircut), some may fly in the face of current scientific evidence (such as eating solids before they are able). And even when they are “safe,” new parents may experience these beliefs as fraught directives: ones that they may not believe in, but which will make them guilty of some cultural betrayal if they do not follow them.
Along a similar vein, grandparents may enter the home of their new grandchild with passionately held religious beliefs. While few of these may have direct medical implications for the new baby (such as circumcision), they can still have profound implications for life in the family’s home. When parents and grandparents all share the same religious beliefs, there is less possibility of conflict. But when new parents come from different religious traditions or no longer share their parents’ faith, there is high potential for emotionally charged differences. And if the new parents have not anticipated these conversations (say, whether or not to circumcise a baby boy when one parent is Jewish and the other is Protestant), trying to sort out these matters while also learning to change diapers or nurse a colicky baby can make a challenging situation into an overwhelming one.
Lastly, about 1% of all households have same-sex partners or marriages and about one in four are raising children. While same-sex parenthood has rapidly gained cultural acceptance over the past decade, it is possible that some grandparents will not have fully accepted the reality of their own child’s sexual orientation and committed relationship. If the parents speak to you about such a fraught situation, listen supportively. When it sounds like there is ambivalence in the grandparents, the new parents can try to nurture the love that is there and be patient when their own parents still struggle. They should nurture the connections with those in their families that offer unconditional support and who can model love and acceptance for the new grandparents. In situations in which there is deeper alienation and little or no contact, offer that they might want to find a way to share photos and stories through one who remains close to their parents and periodically offer opportunities to rebuild relationships. A new grandchild can be a loving moment to take a fresh look at unresolved anger and loss, and as clinicians we have seen families resolve differences as they look to a new baby’s future.
Pediatricians are in a unique position of both neutrality and authority with their new patient’s parents and grandparents. When parents come to a newborn check or well-baby check, it can be invaluable to determine “who else is helping you?” After finding out about nursing or feeding the baby and about sleep, inquire about where they are getting any guidance or support. Friends or siblings with children? Books or websites? Grandparents? What has been helpful and what has not? When you hear about grandparents and see an eye-roll or hear a deep sigh, be curious about what has been helpful and what has been challenging. It is vitally helpful to first-time parents to be validated in their feeling that their own parents are a valuable resource, but not without their challenges.
While it may be important to offer a “medical” opinion about certain matters (back-sleeping, cosleeping, and introducing solids, for example), on most matters, the pediatrician’s role will be to help parents set a framework that will help them to cultivate what is precious and helpful from grandparents while minimizing conflict or unnecessary stress. For new parents, this may be as simple as reminding them that while this is an vital time for the baby’s development, it is also a big transition for them into parenthood and a significant transition for their parents or in-laws into grandparenthood. Help the new parents to understand that there is sometimes no one “right” way to handle certain decisions or challenges, and they will have to try a variety of strategies before finding the one that fits them as parents to this particular child. Remind them that parenting is a learning curve and it is common to feel stressed in new territory with high stakes. But they will find the right rhythm with being attuned to their new baby and eventually managing routines and limits. They are allowed to embrace the support that they find helpful and limit that which they experience as deeply undermining, dismissive, or judgmental.
When you notice that parents sound very angry at or alienated from grandparents, particularly when it is causing some marital conflict, it can be powerful for you to suggest that they should sort out their wishes and beliefs as parents first and then find a clear and loving way to communicate these to the grandparents. Remind them that they are becoming the experts on their children and that they will best be able to set appropriate routines and expectations. But remind them also that grandparents are potentially a treasure to their grandchildren, beyond the help with laundry and meal preparation at the very start of a child’s life.
There can never be enough loving, interested adults in a child’s orbit or a big enough cheering section. And grandparents can be uniquely passionate, patient, curious, and supportive to their growing grandchildren. They bring perspective on a family’s history, wonderful as a growing child builds a story about who they are and where they come from. And their interest and love will help a growing child build a sense of what characteristics make them a treasure to others. Few people can do this as well as grandparents, and letting them begin this involvement at the start of their grandchild’s life only supports this role.
While the arrival of a new baby will be a joyful event for a family, it will also be emotionally complex. Providing your patient’s parents with support and even some language that may help them cultivate the grandparents’ interest and love, while building healthy boundaries around their own parenting, may help set the stage for the healthiest development of your very young patient.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at pdnews@frontlinemedcom.com.
A couple having a baby brings together two family traditions that themselves blended the previous generations’ experiences and perspectives. Each of the new parents has been raised by two parents with their own histories, values, successes, and crises all available and potentially playing a part in the new baby’s future. A baby’s arrival can call forth memories of past successes, failures, hopes, and dreams – some fulfilled and some not.
As the pediatrician, you serve as an authority and a resource for the new parents. You will hear questions that have roots that may go back one, two, or more generations. Some may involve discipline, approaches to food, religious issues, or more subtle concerns relating to control and autonomy. And you may find that they will bring you the challenge of managing the beliefs, values, and expectations of the new grandparents. You may even find these new grandparents in your office! You have a unique opportunity to help new parents set a course with their own parents or in-laws that can promote family cohesion and honor family traditions or values, while empowering parents to trust themselves and truly be in charge of raising their own children.
Imagine this scenario: A young couple has just had their first baby, a son. The paternal grandfather, who played soccer in high school and college, presents his first grandchild with his own college soccer ball, proclaiming with great emotion that soccer will certainly be a part of his grandson’s future.
While this simple act may seem touching, it might also be perceived by the new parents as intrusive or controlling. How does the new father (who was maybe more bookish than athletic) feel the burden of this expectation? Perhaps the mother may wish her son to be more of a scholar than an athlete, or may want no expectation set, but may feel uncomfortable speaking honestly with her father-in-law. And this scenario is just about the gift of a soccer ball!
Grandparents (like parents) come with expectations, with beliefs about what practices worked and what failed over a wide range of areas from child rearing to managing finances to career to marriage. The arrival of a new grandchild will likely prompt them to share these beliefs, and do so in the way they usually communicate with their own children, be it blunt, emotional, indirect, or mute. These views might be forcefully presented, if a grandparent feels guilty or unfulfilled because a meaningful hope for their own child did not materialize: The new grandchild is their “last chance.” While their love and interest, their experience and wisdom can be invaluable, they might also arouse insecurity in a new parent or be disruptive. If they share opinions in a way that is stressful, devaluing, or confusing for new parents, that can translate into anxious, uncertain interactions with their new baby or a climate at home that is full of conflict instead of calm.
Parents are already blending their two styles and values, challenging enough before also trying to blend the elements of four grandparents.
The first weeks after the arrival of the new baby is a crucial time in the baby’s development, as well as in the development of the new parents, as all are rapidly acquiring new skills, adjusting to a new schedule, and learning how to understand and respond to each other. During these hard early days, grandparents often will be present, staying in the home or nearby to offer support to their children. Very commonly, they will share their opinions about such basics as nutrition and sleep. These are areas that are fundamentally important for a baby’s healthy development, but can be mysterious and challenging for new parents. They may seek out guidance from friends, books, websites, and pediatricians, as well as the new grandparents.
While their accumulated wisdom may be as helpful as their helping with laundry or meal preparation (think, “sleep when the baby sleeps”), it also might not. Perhaps the opinions are misguided (think, “sleeping on the tummy was always fine in my day”). And grandparents who are inadvertently undermining (“I don’t understand the difficulty, nursing was so easy for me”), or highly anxious might add to the new parents’ stress and uncertainty rather than alleviate it.
Grandparents also may come with strong cultural beliefs about child rearing. In families that are only one or two generations removed from immigration to this country, there may be powerfully held ideas about newborns, ones that might be inextricably linked for the grandparents with their drive to preserve their own cultural background. These may include ideas about when a child can eat solid food or what he or she should start eating. They may include beliefs that a child should never be put down or should be left to cry for long periods, lest they be “spoiled.” They might include ideas about when a baby can swim or how best to bathe them, what sorts of toys are appropriate or when their hair can be cut. While many of these beliefs have cultural value and no medical implications (like the timing of the first haircut), some may fly in the face of current scientific evidence (such as eating solids before they are able). And even when they are “safe,” new parents may experience these beliefs as fraught directives: ones that they may not believe in, but which will make them guilty of some cultural betrayal if they do not follow them.
Along a similar vein, grandparents may enter the home of their new grandchild with passionately held religious beliefs. While few of these may have direct medical implications for the new baby (such as circumcision), they can still have profound implications for life in the family’s home. When parents and grandparents all share the same religious beliefs, there is less possibility of conflict. But when new parents come from different religious traditions or no longer share their parents’ faith, there is high potential for emotionally charged differences. And if the new parents have not anticipated these conversations (say, whether or not to circumcise a baby boy when one parent is Jewish and the other is Protestant), trying to sort out these matters while also learning to change diapers or nurse a colicky baby can make a challenging situation into an overwhelming one.
Lastly, about 1% of all households have same-sex partners or marriages and about one in four are raising children. While same-sex parenthood has rapidly gained cultural acceptance over the past decade, it is possible that some grandparents will not have fully accepted the reality of their own child’s sexual orientation and committed relationship. If the parents speak to you about such a fraught situation, listen supportively. When it sounds like there is ambivalence in the grandparents, the new parents can try to nurture the love that is there and be patient when their own parents still struggle. They should nurture the connections with those in their families that offer unconditional support and who can model love and acceptance for the new grandparents. In situations in which there is deeper alienation and little or no contact, offer that they might want to find a way to share photos and stories through one who remains close to their parents and periodically offer opportunities to rebuild relationships. A new grandchild can be a loving moment to take a fresh look at unresolved anger and loss, and as clinicians we have seen families resolve differences as they look to a new baby’s future.
Pediatricians are in a unique position of both neutrality and authority with their new patient’s parents and grandparents. When parents come to a newborn check or well-baby check, it can be invaluable to determine “who else is helping you?” After finding out about nursing or feeding the baby and about sleep, inquire about where they are getting any guidance or support. Friends or siblings with children? Books or websites? Grandparents? What has been helpful and what has not? When you hear about grandparents and see an eye-roll or hear a deep sigh, be curious about what has been helpful and what has been challenging. It is vitally helpful to first-time parents to be validated in their feeling that their own parents are a valuable resource, but not without their challenges.
While it may be important to offer a “medical” opinion about certain matters (back-sleeping, cosleeping, and introducing solids, for example), on most matters, the pediatrician’s role will be to help parents set a framework that will help them to cultivate what is precious and helpful from grandparents while minimizing conflict or unnecessary stress. For new parents, this may be as simple as reminding them that while this is an vital time for the baby’s development, it is also a big transition for them into parenthood and a significant transition for their parents or in-laws into grandparenthood. Help the new parents to understand that there is sometimes no one “right” way to handle certain decisions or challenges, and they will have to try a variety of strategies before finding the one that fits them as parents to this particular child. Remind them that parenting is a learning curve and it is common to feel stressed in new territory with high stakes. But they will find the right rhythm with being attuned to their new baby and eventually managing routines and limits. They are allowed to embrace the support that they find helpful and limit that which they experience as deeply undermining, dismissive, or judgmental.
When you notice that parents sound very angry at or alienated from grandparents, particularly when it is causing some marital conflict, it can be powerful for you to suggest that they should sort out their wishes and beliefs as parents first and then find a clear and loving way to communicate these to the grandparents. Remind them that they are becoming the experts on their children and that they will best be able to set appropriate routines and expectations. But remind them also that grandparents are potentially a treasure to their grandchildren, beyond the help with laundry and meal preparation at the very start of a child’s life.
There can never be enough loving, interested adults in a child’s orbit or a big enough cheering section. And grandparents can be uniquely passionate, patient, curious, and supportive to their growing grandchildren. They bring perspective on a family’s history, wonderful as a growing child builds a story about who they are and where they come from. And their interest and love will help a growing child build a sense of what characteristics make them a treasure to others. Few people can do this as well as grandparents, and letting them begin this involvement at the start of their grandchild’s life only supports this role.
While the arrival of a new baby will be a joyful event for a family, it will also be emotionally complex. Providing your patient’s parents with support and even some language that may help them cultivate the grandparents’ interest and love, while building healthy boundaries around their own parenting, may help set the stage for the healthiest development of your very young patient.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at pdnews@frontlinemedcom.com.

Postpartum psychosis and ill-advised discharge
Muslim Bangladeshi female presents
The patient is a 31-year-old married Muslim Bangladeshi female homemaker admitted to an inpatient unit in a private hospital in a large urban area in the northeastern United States because of postpartum psychosis. She recently had immigrated to the United States and spoke no English. She lived with her husband, his parents, and his siblings in a city neighborhood predominantly comprised of South Asian immigrants. Her sole source of financial support was her husband, who worked as a cab driver. Both patient and her husband were uninsured. They identified strongly with their religion and culture of origin.
Key questions
Communication was a challenge and was accomplished using an interpreter, who was not always available. The patient did not seem to respond to treatment, and there was a question about the possibility that she was “cheeking” her medications. Her husband requested her discharge against medical advice, despite her still showing signs of psychosis. He appeared ambivalent about outpatient follow-up.
What is the duty of care in this situation, given the complexities inherent in a cross-cultural situation, the presence of communication barriers, the question of patient and infant safety, the husband’s role (given the understanding that his actions were probably culturally sanctioned and consistent with his role), issues regarding financing their current and follow-up care, and their ambivalence toward follow-up care?
Family perspective
Working with a qualified medical interpreter is imperative, and hospitals and health care providers who accept federal funds are obliged to provide language assistance services under Title VI of the Civil Rights Act of 1964.
First, it is important to accurately assess the woman’s psychosis, including risk of self-harm, risk of harming the infant or others, and capacity to care adequately and safely for the infant.
Second, the team should assess the patient’s and husband’s beliefs about the illness, hospitalization, and treatment. For some Muslim patients, the daily practice of Islam may necessitate the separation of sexes, meaning that female nurses and physicians might be optimal. Accessing professional spiritual or pastoral care in meeting the patient’s and family’s religious needs should be considered. Additional cultural practices that might help increase the acceptability of inpatient psychiatric care for the family include practices regarding diet, dress, hygiene, and prayer. The husband also might want to stay and sleep in the patient’s room during her hospitalization.

It also might be challenging for some North American therapists to understand and focus on the entire family as a functioning unit, rather than seeing the issues as only between husband and wife. Learning about how “normal family functioning” is defined, especially in terms of roles, hierarchy, and intimacy, is critical to supporting this mother and baby. Cultivating “cultural humility” in working with patients and families from diverse backgrounds is extremely important.
During the hospitalization as the patient improves, a plan for care needs to be developed with the patient and her family. This plan should include adequate support of the mother and her baby. The husband should bring his parents and siblings to an initial meeting early during the hospitalization, being mindful of addressing any HIPAA-related issues. This will allow for a uniform understanding of the patient’s illness and treatment. At this meeting, all family members should express their concerns, worries, beliefs, and perceived barriers to optimal care. If the family members feel listened to, they are more likely to feel understood and adhere to recommendations.

At the initial meeting and subsequent ones, the following questions might be helpful to ask to gather information in negotiating a mutually acceptable treatment plan:
1. What is the family’s understanding of her illness? What do they think may have caused it? How do they understand postpartum psychosis? Do they think there is a role for medication? Are any other alternative healing modalities being considered or used?
2. Who is caring for the baby now? Is the baby healthy? Does the family understand how the mother’s illness affects the baby? Can the family provide adequate care for the baby?
3. How are decisions made in the family? Are there any other issues in the family, such as ill health in a parent?
4. Was this an arranged marriage? How long have they known the patient? Do they care for her? What is the family’s attitude toward her?
5. Besides the mother-in-law, are there other adult females (for example, her husband’s sisters and his brothers’ wives) living in the household? How old is the mother-in-law? Who runs the household? Who does all the work? If possible, it will be important to interview anyone else in the household. How long have the couple and the family been in the United States? Did they all come at the same time?
6. Does the family have a supportive community? What are their beliefs about mental illness? Whom do they trust in their community? A religious leader? A local doctor? Who treats the women in the community?
7. If there is time, other issues can be explored. For example, what were the circumstances of their immigration? What has the transition from Bangladesh to life in the United States been like for the family?
8. Who will care for her at home? Who will ensure she takes her medications? Who will take her to follow-up visits?
There are many unknowns in this case that require further exploration. Time taken to arrange for a medically qualified interpreter and an extended family meeting will help the physician and psychiatric team understand the current situation and set up an appropriate plan of care.
Cultural perspective
The case material raises many questions. In the first place, there is no need to assume that the husband was behaving in a “culturally sanctioned and consistent way.” In a large population like that of Bangladeshi Muslims, significant heterogeneity exists, and there are more ways than one to respond. Although access to care is increasing for some population segments, Bangladesh still has limited mental health services and resources.

What were the reasons for the patient to be admitted to a psychiatric unit? How many days after the delivery? Were there any hostile actions or reactions to the baby? What is the patient’s pregnancy history? What meaning was ascribed to the symptoms and behavior that the patient manifested prior to hospitalization? Was this the first episode of psychiatric illness for the patient? Has she shown any dangerous behaviors before?
The reason why the husband is taking the wife home against medical advice is unclear. What reason did the husband give for this decision? Could stigma toward mental illness or hospitalization play a role? Was an interpreter used to help understand his reasoning? Was the husband dissatisfied about something? This is important, because it is likely that the husband brought the wife for hospitalization in the first place. Were the inpatient physician and nurses male or female, and could gender-related issues have been a barrier to accepting care? Might there have been a Muslim chaplain in the hospital or in the community or someone else who could have served as a cultural broker earlier in the hospitalization to have prevented this impasse?

The Cultural Formulation Interview (CFI) in the DSM-5 and the CFI-Informant Version for family members provide a framework to explore these questions and the questions recommended in the Family Perspective throughout the course of treatment.
Additional relevant questions include the following: What are cultural norms for their expectations for support of a new mother during the postpartum period? What are the norms for who, besides the mother, provides infant care? Are normative postpartum practices possible, or have they been disrupted in the hospital setting and/or in their home? If the mother and baby are both on the unit, is the request motivated by a desire to bring the baby home? If the baby is not on the unit, is this driving the family’s concern?
How isolated will the woman feel when she is home with the baby and her husband is out working as a taxi driver? Are there community-based organizations that the clinicians could collaborate with to provide resources and support for this woman (for example, women’s groups, immigrant groups, religious groups)? This would require learning more about what appeals to her, which groups she might identify with, and what is available in her neighborhood/community that aligns with what appeals to her.
It also would be important to determine if the patient was having any side effects from her psychotropic medications. Many South Asians have a low tolerance for side effects. Did the patient or family have any religious or cultural concerns about how the medications were manufactured or their composition (for example, worries about alcohol content)? Could any of these factors be related to the patient’s possible “cheeking” of her medications?

The major ethical/legal question to address is the patient’s attitude toward and relationship with the baby, and whether she was and is currently a danger to herself or others. Was the baby with the patient in the hospital? Did she feed the baby? What were the signs of psychosis that the patient exhibited, and what were the bases of her diagnosis? Was there an opportunity to discuss these issues with the husband? If so, what was his response?
Unless the patient is found to be dangerous to herself or others, including the baby, there is no option but to discharge. If a Bengali-speaking psychiatrist/therapist could be located within a reasonable driving distance, every effort should be made to connect the two. Husband and wife certainly should be instructed at the first sign of trouble to seek medical/psychiatric assistance, with or without insurance. Is there a possibility of home visits with an interpreter given the potential risks of patient and infant safety? Close follow-up and coordination of care with the patient’s and baby’s primary care physician is needed. Seeking support from the patient’s religious community also is worth considering.
Contributors
Alison M. Heru, M.D. – University of Colorado Denver, Aurora
Ellen Berman, M.D. – University of Pennsylvania, Philadelphia
Annelle B. Primm, M.D., M.P.H. – Johns Hopkins University, Baltimore (adjunct faculty)
Anne E. Becker, M.D., Ph.D. – Harvard Medical School, Boston
Robert C. Like, M.D., M.S. – Rutgers University, Robert Wood Johnson Medical School, New Brunswick
Resources
Farooq S., Fear C. Working Through Interpreters. (Adv Psychiatr Treat. 2003 Mar;9[2]:104-9. doi: 10.1192/apt.01.12 http://apt.rcpsych.org/content/9/2/104.full.)
Chandra P.S. Postpartum Psychiatric Care in India: The need for Integration and Innovation. (World Psychiatry. 2004;3[2]:99-100.)
Ahmad F., Shik A., Vanza R., Cheung A.M., George U, Stewart D.E. Voices of South Asian Women: Immigration and Mental Health. (Women Health 2004; 40[4]:113-130.)
Mantle F. Developing a Culture-Specific Tool to Assess Postnatal Depression in the Indian Community. (Br J Community Nurs. 2003;8[4]:176-180.)
To read about the goals of Curbside Consult, the guiding principles for assessment, and the guidelines for case submission, see “Considering patients’ family, culture,” Clinical Psychiatry News, January 2015, p. 12. The contributors have revised selected patient details to shield the identities of the patients/cases and to comply with HIPAA requirements. This column is meant to be educational and does not constitute medical advice. The opinions expressed are those of the contributors and do not represent those of the organizations they are employed by or affiliated with or the Group for the Advancement of Psychiatry (GAP).
This column is in memory of Dr. Prakash N. Desai, who contributed to this piece before his death earlier this year.
Muslim Bangladeshi female presents
The patient is a 31-year-old married Muslim Bangladeshi female homemaker admitted to an inpatient unit in a private hospital in a large urban area in the northeastern United States because of postpartum psychosis. She recently had immigrated to the United States and spoke no English. She lived with her husband, his parents, and his siblings in a city neighborhood predominantly comprised of South Asian immigrants. Her sole source of financial support was her husband, who worked as a cab driver. Both patient and her husband were uninsured. They identified strongly with their religion and culture of origin.
Key questions
Communication was a challenge and was accomplished using an interpreter, who was not always available. The patient did not seem to respond to treatment, and there was a question about the possibility that she was “cheeking” her medications. Her husband requested her discharge against medical advice, despite her still showing signs of psychosis. He appeared ambivalent about outpatient follow-up.
What is the duty of care in this situation, given the complexities inherent in a cross-cultural situation, the presence of communication barriers, the question of patient and infant safety, the husband’s role (given the understanding that his actions were probably culturally sanctioned and consistent with his role), issues regarding financing their current and follow-up care, and their ambivalence toward follow-up care?
Family perspective
Working with a qualified medical interpreter is imperative, and hospitals and health care providers who accept federal funds are obliged to provide language assistance services under Title VI of the Civil Rights Act of 1964.
First, it is important to accurately assess the woman’s psychosis, including risk of self-harm, risk of harming the infant or others, and capacity to care adequately and safely for the infant.
Second, the team should assess the patient’s and husband’s beliefs about the illness, hospitalization, and treatment. For some Muslim patients, the daily practice of Islam may necessitate the separation of sexes, meaning that female nurses and physicians might be optimal. Accessing professional spiritual or pastoral care in meeting the patient’s and family’s religious needs should be considered. Additional cultural practices that might help increase the acceptability of inpatient psychiatric care for the family include practices regarding diet, dress, hygiene, and prayer. The husband also might want to stay and sleep in the patient’s room during her hospitalization.
It also might be challenging for some North American therapists to understand and focus on the entire family as a functioning unit, rather than seeing the issues as only between husband and wife. Learning about how “normal family functioning” is defined, especially in terms of roles, hierarchy, and intimacy, is critical to supporting this mother and baby. Cultivating “cultural humility” in working with patients and families from diverse backgrounds is extremely important.
During the hospitalization as the patient improves, a plan for care needs to be developed with the patient and her family. This plan should include adequate support of the mother and her baby. The husband should bring his parents and siblings to an initial meeting early during the hospitalization, being mindful of addressing any HIPAA-related issues. This will allow for a uniform understanding of the patient’s illness and treatment. At this meeting, all family members should express their concerns, worries, beliefs, and perceived barriers to optimal care. If the family members feel listened to, they are more likely to feel understood and adhere to recommendations.
At the initial meeting and subsequent ones, the following questions might be helpful to ask to gather information in negotiating a mutually acceptable treatment plan:
1. What is the family’s understanding of her illness? What do they think may have caused it? How do they understand postpartum psychosis? Do they think there is a role for medication? Are any other alternative healing modalities being considered or used?
2. Who is caring for the baby now? Is the baby healthy? Does the family understand how the mother’s illness affects the baby? Can the family provide adequate care for the baby?
3. How are decisions made in the family? Are there any other issues in the family, such as ill health in a parent?
4. Was this an arranged marriage? How long have they known the patient? Do they care for her? What is the family’s attitude toward her?
5. Besides the mother-in-law, are there other adult females (for example, her husband’s sisters and his brothers’ wives) living in the household? How old is the mother-in-law? Who runs the household? Who does all the work? If possible, it will be important to interview anyone else in the household. How long have the couple and the family been in the United States? Did they all come at the same time?
6. Does the family have a supportive community? What are their beliefs about mental illness? Whom do they trust in their community? A religious leader? A local doctor? Who treats the women in the community?
7. If there is time, other issues can be explored. For example, what were the circumstances of their immigration? What has the transition from Bangladesh to life in the United States been like for the family?
8. Who will care for her at home? Who will ensure she takes her medications? Who will take her to follow-up visits?
There are many unknowns in this case that require further exploration. Time taken to arrange for a medically qualified interpreter and an extended family meeting will help the physician and psychiatric team understand the current situation and set up an appropriate plan of care.
Cultural perspective
The case material raises many questions. In the first place, there is no need to assume that the husband was behaving in a “culturally sanctioned and consistent way.” In a large population like that of Bangladeshi Muslims, significant heterogeneity exists, and there are more ways than one to respond. Although access to care is increasing for some population segments, Bangladesh still has limited mental health services and resources.
What were the reasons for the patient to be admitted to a psychiatric unit? How many days after the delivery? Were there any hostile actions or reactions to the baby? What is the patient’s pregnancy history? What meaning was ascribed to the symptoms and behavior that the patient manifested prior to hospitalization? Was this the first episode of psychiatric illness for the patient? Has she shown any dangerous behaviors before?
The reason why the husband is taking the wife home against medical advice is unclear. What reason did the husband give for this decision? Could stigma toward mental illness or hospitalization play a role? Was an interpreter used to help understand his reasoning? Was the husband dissatisfied about something? This is important, because it is likely that the husband brought the wife for hospitalization in the first place. Were the inpatient physician and nurses male or female, and could gender-related issues have been a barrier to accepting care? Might there have been a Muslim chaplain in the hospital or in the community or someone else who could have served as a cultural broker earlier in the hospitalization to have prevented this impasse?
The Cultural Formulation Interview (CFI) in the DSM-5 and the CFI-Informant Version for family members provide a framework to explore these questions and the questions recommended in the Family Perspective throughout the course of treatment.
Additional relevant questions include the following: What are cultural norms for their expectations for support of a new mother during the postpartum period? What are the norms for who, besides the mother, provides infant care? Are normative postpartum practices possible, or have they been disrupted in the hospital setting and/or in their home? If the mother and baby are both on the unit, is the request motivated by a desire to bring the baby home? If the baby is not on the unit, is this driving the family’s concern?
How isolated will the woman feel when she is home with the baby and her husband is out working as a taxi driver? Are there community-based organizations that the clinicians could collaborate with to provide resources and support for this woman (for example, women’s groups, immigrant groups, religious groups)? This would require learning more about what appeals to her, which groups she might identify with, and what is available in her neighborhood/community that aligns with what appeals to her.
It also would be important to determine if the patient was having any side effects from her psychotropic medications. Many South Asians have a low tolerance for side effects. Did the patient or family have any religious or cultural concerns about how the medications were manufactured or their composition (for example, worries about alcohol content)? Could any of these factors be related to the patient’s possible “cheeking” of her medications?
The major ethical/legal question to address is the patient’s attitude toward and relationship with the baby, and whether she was and is currently a danger to herself or others. Was the baby with the patient in the hospital? Did she feed the baby? What were the signs of psychosis that the patient exhibited, and what were the bases of her diagnosis? Was there an opportunity to discuss these issues with the husband? If so, what was his response?
Unless the patient is found to be dangerous to herself or others, including the baby, there is no option but to discharge. If a Bengali-speaking psychiatrist/therapist could be located within a reasonable driving distance, every effort should be made to connect the two. Husband and wife certainly should be instructed at the first sign of trouble to seek medical/psychiatric assistance, with or without insurance. Is there a possibility of home visits with an interpreter given the potential risks of patient and infant safety? Close follow-up and coordination of care with the patient’s and baby’s primary care physician is needed. Seeking support from the patient’s religious community also is worth considering.
Contributors
Alison M. Heru, M.D. – University of Colorado Denver, Aurora
Ellen Berman, M.D. – University of Pennsylvania, Philadelphia
Annelle B. Primm, M.D., M.P.H. – Johns Hopkins University, Baltimore (adjunct faculty)
Anne E. Becker, M.D., Ph.D. – Harvard Medical School, Boston
Robert C. Like, M.D., M.S. – Rutgers University, Robert Wood Johnson Medical School, New Brunswick
Resources
Farooq S., Fear C. Working Through Interpreters. (Adv Psychiatr Treat. 2003 Mar;9[2]:104-9. doi: 10.1192/apt.01.12 http://apt.rcpsych.org/content/9/2/104.full.)
Chandra P.S. Postpartum Psychiatric Care in India: The need for Integration and Innovation. (World Psychiatry. 2004;3[2]:99-100.)
Ahmad F., Shik A., Vanza R., Cheung A.M., George U, Stewart D.E. Voices of South Asian Women: Immigration and Mental Health. (Women Health 2004; 40[4]:113-130.)
Mantle F. Developing a Culture-Specific Tool to Assess Postnatal Depression in the Indian Community. (Br J Community Nurs. 2003;8[4]:176-180.)
To read about the goals of Curbside Consult, the guiding principles for assessment, and the guidelines for case submission, see “Considering patients’ family, culture,” Clinical Psychiatry News, January 2015, p. 12. The contributors have revised selected patient details to shield the identities of the patients/cases and to comply with HIPAA requirements. This column is meant to be educational and does not constitute medical advice. The opinions expressed are those of the contributors and do not represent those of the organizations they are employed by or affiliated with or the Group for the Advancement of Psychiatry (GAP).
This column is in memory of Dr. Prakash N. Desai, who contributed to this piece before his death earlier this year.
Muslim Bangladeshi female presents
The patient is a 31-year-old married Muslim Bangladeshi female homemaker admitted to an inpatient unit in a private hospital in a large urban area in the northeastern United States because of postpartum psychosis. She recently had immigrated to the United States and spoke no English. She lived with her husband, his parents, and his siblings in a city neighborhood predominantly comprised of South Asian immigrants. Her sole source of financial support was her husband, who worked as a cab driver. Both patient and her husband were uninsured. They identified strongly with their religion and culture of origin.
Key questions
Communication was a challenge and was accomplished using an interpreter, who was not always available. The patient did not seem to respond to treatment, and there was a question about the possibility that she was “cheeking” her medications. Her husband requested her discharge against medical advice, despite her still showing signs of psychosis. He appeared ambivalent about outpatient follow-up.
What is the duty of care in this situation, given the complexities inherent in a cross-cultural situation, the presence of communication barriers, the question of patient and infant safety, the husband’s role (given the understanding that his actions were probably culturally sanctioned and consistent with his role), issues regarding financing their current and follow-up care, and their ambivalence toward follow-up care?
Family perspective
Working with a qualified medical interpreter is imperative, and hospitals and health care providers who accept federal funds are obliged to provide language assistance services under Title VI of the Civil Rights Act of 1964.
First, it is important to accurately assess the woman’s psychosis, including risk of self-harm, risk of harming the infant or others, and capacity to care adequately and safely for the infant.
Second, the team should assess the patient’s and husband’s beliefs about the illness, hospitalization, and treatment. For some Muslim patients, the daily practice of Islam may necessitate the separation of sexes, meaning that female nurses and physicians might be optimal. Accessing professional spiritual or pastoral care in meeting the patient’s and family’s religious needs should be considered. Additional cultural practices that might help increase the acceptability of inpatient psychiatric care for the family include practices regarding diet, dress, hygiene, and prayer. The husband also might want to stay and sleep in the patient’s room during her hospitalization.
It also might be challenging for some North American therapists to understand and focus on the entire family as a functioning unit, rather than seeing the issues as only between husband and wife. Learning about how “normal family functioning” is defined, especially in terms of roles, hierarchy, and intimacy, is critical to supporting this mother and baby. Cultivating “cultural humility” in working with patients and families from diverse backgrounds is extremely important.
During the hospitalization as the patient improves, a plan for care needs to be developed with the patient and her family. This plan should include adequate support of the mother and her baby. The husband should bring his parents and siblings to an initial meeting early during the hospitalization, being mindful of addressing any HIPAA-related issues. This will allow for a uniform understanding of the patient’s illness and treatment. At this meeting, all family members should express their concerns, worries, beliefs, and perceived barriers to optimal care. If the family members feel listened to, they are more likely to feel understood and adhere to recommendations.
At the initial meeting and subsequent ones, the following questions might be helpful to ask to gather information in negotiating a mutually acceptable treatment plan:
1. What is the family’s understanding of her illness? What do they think may have caused it? How do they understand postpartum psychosis? Do they think there is a role for medication? Are any other alternative healing modalities being considered or used?
2. Who is caring for the baby now? Is the baby healthy? Does the family understand how the mother’s illness affects the baby? Can the family provide adequate care for the baby?
3. How are decisions made in the family? Are there any other issues in the family, such as ill health in a parent?
4. Was this an arranged marriage? How long have they known the patient? Do they care for her? What is the family’s attitude toward her?
5. Besides the mother-in-law, are there other adult females (for example, her husband’s sisters and his brothers’ wives) living in the household? How old is the mother-in-law? Who runs the household? Who does all the work? If possible, it will be important to interview anyone else in the household. How long have the couple and the family been in the United States? Did they all come at the same time?
6. Does the family have a supportive community? What are their beliefs about mental illness? Whom do they trust in their community? A religious leader? A local doctor? Who treats the women in the community?
7. If there is time, other issues can be explored. For example, what were the circumstances of their immigration? What has the transition from Bangladesh to life in the United States been like for the family?
8. Who will care for her at home? Who will ensure she takes her medications? Who will take her to follow-up visits?
There are many unknowns in this case that require further exploration. Time taken to arrange for a medically qualified interpreter and an extended family meeting will help the physician and psychiatric team understand the current situation and set up an appropriate plan of care.
Cultural perspective
The case material raises many questions. In the first place, there is no need to assume that the husband was behaving in a “culturally sanctioned and consistent way.” In a large population like that of Bangladeshi Muslims, significant heterogeneity exists, and there are more ways than one to respond. Although access to care is increasing for some population segments, Bangladesh still has limited mental health services and resources.
What were the reasons for the patient to be admitted to a psychiatric unit? How many days after the delivery? Were there any hostile actions or reactions to the baby? What is the patient’s pregnancy history? What meaning was ascribed to the symptoms and behavior that the patient manifested prior to hospitalization? Was this the first episode of psychiatric illness for the patient? Has she shown any dangerous behaviors before?
The reason why the husband is taking the wife home against medical advice is unclear. What reason did the husband give for this decision? Could stigma toward mental illness or hospitalization play a role? Was an interpreter used to help understand his reasoning? Was the husband dissatisfied about something? This is important, because it is likely that the husband brought the wife for hospitalization in the first place. Were the inpatient physician and nurses male or female, and could gender-related issues have been a barrier to accepting care? Might there have been a Muslim chaplain in the hospital or in the community or someone else who could have served as a cultural broker earlier in the hospitalization to have prevented this impasse?
The Cultural Formulation Interview (CFI) in the DSM-5 and the CFI-Informant Version for family members provide a framework to explore these questions and the questions recommended in the Family Perspective throughout the course of treatment.
Additional relevant questions include the following: What are cultural norms for their expectations for support of a new mother during the postpartum period? What are the norms for who, besides the mother, provides infant care? Are normative postpartum practices possible, or have they been disrupted in the hospital setting and/or in their home? If the mother and baby are both on the unit, is the request motivated by a desire to bring the baby home? If the baby is not on the unit, is this driving the family’s concern?
How isolated will the woman feel when she is home with the baby and her husband is out working as a taxi driver? Are there community-based organizations that the clinicians could collaborate with to provide resources and support for this woman (for example, women’s groups, immigrant groups, religious groups)? This would require learning more about what appeals to her, which groups she might identify with, and what is available in her neighborhood/community that aligns with what appeals to her.
It also would be important to determine if the patient was having any side effects from her psychotropic medications. Many South Asians have a low tolerance for side effects. Did the patient or family have any religious or cultural concerns about how the medications were manufactured or their composition (for example, worries about alcohol content)? Could any of these factors be related to the patient’s possible “cheeking” of her medications?
The major ethical/legal question to address is the patient’s attitude toward and relationship with the baby, and whether she was and is currently a danger to herself or others. Was the baby with the patient in the hospital? Did she feed the baby? What were the signs of psychosis that the patient exhibited, and what were the bases of her diagnosis? Was there an opportunity to discuss these issues with the husband? If so, what was his response?
Unless the patient is found to be dangerous to herself or others, including the baby, there is no option but to discharge. If a Bengali-speaking psychiatrist/therapist could be located within a reasonable driving distance, every effort should be made to connect the two. Husband and wife certainly should be instructed at the first sign of trouble to seek medical/psychiatric assistance, with or without insurance. Is there a possibility of home visits with an interpreter given the potential risks of patient and infant safety? Close follow-up and coordination of care with the patient’s and baby’s primary care physician is needed. Seeking support from the patient’s religious community also is worth considering.
Contributors
Alison M. Heru, M.D. – University of Colorado Denver, Aurora
Ellen Berman, M.D. – University of Pennsylvania, Philadelphia
Annelle B. Primm, M.D., M.P.H. – Johns Hopkins University, Baltimore (adjunct faculty)
Anne E. Becker, M.D., Ph.D. – Harvard Medical School, Boston
Robert C. Like, M.D., M.S. – Rutgers University, Robert Wood Johnson Medical School, New Brunswick
Resources
Farooq S., Fear C. Working Through Interpreters. (Adv Psychiatr Treat. 2003 Mar;9[2]:104-9. doi: 10.1192/apt.01.12 http://apt.rcpsych.org/content/9/2/104.full.)
Chandra P.S. Postpartum Psychiatric Care in India: The need for Integration and Innovation. (World Psychiatry. 2004;3[2]:99-100.)
Ahmad F., Shik A., Vanza R., Cheung A.M., George U, Stewart D.E. Voices of South Asian Women: Immigration and Mental Health. (Women Health 2004; 40[4]:113-130.)
Mantle F. Developing a Culture-Specific Tool to Assess Postnatal Depression in the Indian Community. (Br J Community Nurs. 2003;8[4]:176-180.)
To read about the goals of Curbside Consult, the guiding principles for assessment, and the guidelines for case submission, see “Considering patients’ family, culture,” Clinical Psychiatry News, January 2015, p. 12. The contributors have revised selected patient details to shield the identities of the patients/cases and to comply with HIPAA requirements. This column is meant to be educational and does not constitute medical advice. The opinions expressed are those of the contributors and do not represent those of the organizations they are employed by or affiliated with or the Group for the Advancement of Psychiatry (GAP).
This column is in memory of Dr. Prakash N. Desai, who contributed to this piece before his death earlier this year.
