User login
Rapid-Response Teams Help Hospitalists Manage Non-Medical Distress
A team that could respond quickly to social and behavioral concerns—and not medical issues per se—would have tremendous benefits for patients and caregivers.
I think there has been a steady increase, over the last 20 years or so, in the number of very unhappy, angry, or misbehaving patients (e.g. abusive/threatening to staff). In some cases, the hospital and caregivers have failed the patient. In other cases, their frustration arises out of things outside the hospital’s direct control, such as Medicare observation status, or perhaps the patient or family is just unreasonable or suffering from a psychiatric or substance abuse disorder.
I’m not talking about the common occurrence of a disappointed patient or family who might calmly complain about something. Instead, I want to focus on those patients who, whether we perceive them as justifiably unhappy or not, are so angry that they become very time consuming and distressing to deal with. Maybe they shout about how their lawyer will be suing us and the newspaper will be writing a story about how awful we are. Or they shout and throw things, and staff become afraid of them.
In my May 2013 column, I discussed care plans for patients like this who are admitted frequently, but such plans are not sufficient in every case.
A Haphazard Approach
Most hospitals have an informal process of dealing with these patients; it starts with the bedside nurse and/or doctor trying to apologize or make adjustments to satisfy and calm the patient. If that fails, then perhaps the manager of the nursing unit gets involved. Others may be recruited, such as someone from the hospital’s risk management or “patient advocate” departments and hospital executives such as the CNO, CMO, or CEO. Sometimes several of these people may meet as a group in an effort to come up with a plan to address the situation. But, most institutions do not have a clear and consistent approach to this important work, so the hospital personnel involved end up “reinventing the wheel” each time.
The growing awareness that hospital personnel don’t seem to have a robust and confident approach to addressing this type of situation can increase a patient’s distress, and it may embolden some to become even more demanding or threatening.
And all of this takes a significant toll on bedside caregivers, who often spend so much time dealing with the angry patient that they have less time to devote to other patients, who are in turn at least a little more likely to become unhappy or suffer as a result of a distressed and busy caregiver.
A Consistent Approach: RRT for Non-Medical Distress
I think the potential benefit for patients and caregivers is significant enough that hospitals should develop a standardized approach to managing such patients, and rapid response teams (RRTs) could serve as a model. To be clear, I’m not advocating that RRTs add management of very angry or distressed patients to their current role. Let’s call it an “RRT for non-medical distress.” And, while I think it is a worthwhile idea, and I am in the early steps of trying to develop it at “my” hospital, I’m not aware of any such team in place anywhere now.
To make it practical, I think this team should be available only during weekday business hours and would comprise something like six to 10 people with clinical backgrounds who do mostly administrative work. For example, the team members could include two nursing unit directors, a risk manager, a patient advocate (or patient satisfaction “czar”), a psychiatrist, the hospitalist medical director, the chief medical officer, and a few other individuals selected for their communication skills.
One of the team members would be on call for a day or week at a time and would carry the team’s pager during business hours. Any hospital caregiver could send a page requesting the team’s assistance, and the on-call team member would respond immediately by phone or, if possible, in person. After the on-call team member’s initial assessment, the whole team would meet later the same day or early the next day. On most days, a few members of the team would be off and unable to attend the meeting. So, if the team has eight members, each meeting of the team might average about five participants.
Non-Medical Distress RRT Processes
When meeting to establish a plan for addressing an extraordinarily distressed patient/family, the team should follow a standardized written approach. A designated person should lead the conversation—perhaps the on-call team member who responded first—and another should take notes. Using a form developed for this purpose, the note-taker would capture a standardized data set that is likely to be useful in determining a course of action, as well as valuable in helping the team fine-tune its approach by reviewing trends in aggregate data. The form might include things like patient demographics; the patient’s complaints and demands; potential complicating patient issues such as substance abuse, psychoactive drugs, or psychiatric history; location in the hospital; and names of bedside caregivers. Every effort should be made to keep the meetings efficient and as brief as practical—typically 30-60 minutes.
I’m convinced that when deciding how to respond to the situation, the team should try to limit itself to choosing one or more of eight to 10 standard interventions, rather than aiming for an entirely customized response in every case. Among the standardized interventions:
- Service recovery tools, such as a handwritten apology letter;
- A meeting between the patient/family and the hospital CEO or CMO;
- Security guard(s) at the door, on “high alert” to help if called; or
- A behavioral contract specifying the expectations for both patient and hospital staff behavior.
You might think of additional “tools” this team could have in their standardized response set.
Why limit the team as much as possible to a small set of standardized interventions? Developing customized responses in each situation is time consuming and, arguably, has a higher risk of failure, since it will be difficult to ensure that all staff caring for the patient can understand and execute them effectively. And the small set of interventions will make it easier to track their effectiveness over multiple patients so that the whole process can be improved over time.
Set a High Bar
The team should not be activated for every unhappy or difficult patient; that would be overkill and would result in many activations requiring dedicated staff with no other duties to serve on the team each day. Instead, I think the team should be activated only for the most difficult and distressing cases, at least for the first few years. In a 300-bed hospital, this would be approximately one to 1.5 activations per week.
Bedside caregivers would likely feel some reassurance knowing that they can reliably get help managing the most difficult patients, and, if the plan is executed well, these patients may get care that is safer for both themselves and staff. Who knows, medical outcomes might be improved for these patients also.

A team that could respond quickly to social and behavioral concerns—and not medical issues per se—would have tremendous benefits for patients and caregivers.
I think there has been a steady increase, over the last 20 years or so, in the number of very unhappy, angry, or misbehaving patients (e.g. abusive/threatening to staff). In some cases, the hospital and caregivers have failed the patient. In other cases, their frustration arises out of things outside the hospital’s direct control, such as Medicare observation status, or perhaps the patient or family is just unreasonable or suffering from a psychiatric or substance abuse disorder.
I’m not talking about the common occurrence of a disappointed patient or family who might calmly complain about something. Instead, I want to focus on those patients who, whether we perceive them as justifiably unhappy or not, are so angry that they become very time consuming and distressing to deal with. Maybe they shout about how their lawyer will be suing us and the newspaper will be writing a story about how awful we are. Or they shout and throw things, and staff become afraid of them.
In my May 2013 column, I discussed care plans for patients like this who are admitted frequently, but such plans are not sufficient in every case.
A Haphazard Approach
Most hospitals have an informal process of dealing with these patients; it starts with the bedside nurse and/or doctor trying to apologize or make adjustments to satisfy and calm the patient. If that fails, then perhaps the manager of the nursing unit gets involved. Others may be recruited, such as someone from the hospital’s risk management or “patient advocate” departments and hospital executives such as the CNO, CMO, or CEO. Sometimes several of these people may meet as a group in an effort to come up with a plan to address the situation. But, most institutions do not have a clear and consistent approach to this important work, so the hospital personnel involved end up “reinventing the wheel” each time.
The growing awareness that hospital personnel don’t seem to have a robust and confident approach to addressing this type of situation can increase a patient’s distress, and it may embolden some to become even more demanding or threatening.
And all of this takes a significant toll on bedside caregivers, who often spend so much time dealing with the angry patient that they have less time to devote to other patients, who are in turn at least a little more likely to become unhappy or suffer as a result of a distressed and busy caregiver.
A Consistent Approach: RRT for Non-Medical Distress
I think the potential benefit for patients and caregivers is significant enough that hospitals should develop a standardized approach to managing such patients, and rapid response teams (RRTs) could serve as a model. To be clear, I’m not advocating that RRTs add management of very angry or distressed patients to their current role. Let’s call it an “RRT for non-medical distress.” And, while I think it is a worthwhile idea, and I am in the early steps of trying to develop it at “my” hospital, I’m not aware of any such team in place anywhere now.
To make it practical, I think this team should be available only during weekday business hours and would comprise something like six to 10 people with clinical backgrounds who do mostly administrative work. For example, the team members could include two nursing unit directors, a risk manager, a patient advocate (or patient satisfaction “czar”), a psychiatrist, the hospitalist medical director, the chief medical officer, and a few other individuals selected for their communication skills.
One of the team members would be on call for a day or week at a time and would carry the team’s pager during business hours. Any hospital caregiver could send a page requesting the team’s assistance, and the on-call team member would respond immediately by phone or, if possible, in person. After the on-call team member’s initial assessment, the whole team would meet later the same day or early the next day. On most days, a few members of the team would be off and unable to attend the meeting. So, if the team has eight members, each meeting of the team might average about five participants.
Non-Medical Distress RRT Processes
When meeting to establish a plan for addressing an extraordinarily distressed patient/family, the team should follow a standardized written approach. A designated person should lead the conversation—perhaps the on-call team member who responded first—and another should take notes. Using a form developed for this purpose, the note-taker would capture a standardized data set that is likely to be useful in determining a course of action, as well as valuable in helping the team fine-tune its approach by reviewing trends in aggregate data. The form might include things like patient demographics; the patient’s complaints and demands; potential complicating patient issues such as substance abuse, psychoactive drugs, or psychiatric history; location in the hospital; and names of bedside caregivers. Every effort should be made to keep the meetings efficient and as brief as practical—typically 30-60 minutes.
I’m convinced that when deciding how to respond to the situation, the team should try to limit itself to choosing one or more of eight to 10 standard interventions, rather than aiming for an entirely customized response in every case. Among the standardized interventions:
- Service recovery tools, such as a handwritten apology letter;
- A meeting between the patient/family and the hospital CEO or CMO;
- Security guard(s) at the door, on “high alert” to help if called; or
- A behavioral contract specifying the expectations for both patient and hospital staff behavior.
You might think of additional “tools” this team could have in their standardized response set.
Why limit the team as much as possible to a small set of standardized interventions? Developing customized responses in each situation is time consuming and, arguably, has a higher risk of failure, since it will be difficult to ensure that all staff caring for the patient can understand and execute them effectively. And the small set of interventions will make it easier to track their effectiveness over multiple patients so that the whole process can be improved over time.
Set a High Bar
The team should not be activated for every unhappy or difficult patient; that would be overkill and would result in many activations requiring dedicated staff with no other duties to serve on the team each day. Instead, I think the team should be activated only for the most difficult and distressing cases, at least for the first few years. In a 300-bed hospital, this would be approximately one to 1.5 activations per week.
Bedside caregivers would likely feel some reassurance knowing that they can reliably get help managing the most difficult patients, and, if the plan is executed well, these patients may get care that is safer for both themselves and staff. Who knows, medical outcomes might be improved for these patients also.
A team that could respond quickly to social and behavioral concerns—and not medical issues per se—would have tremendous benefits for patients and caregivers.
I think there has been a steady increase, over the last 20 years or so, in the number of very unhappy, angry, or misbehaving patients (e.g. abusive/threatening to staff). In some cases, the hospital and caregivers have failed the patient. In other cases, their frustration arises out of things outside the hospital’s direct control, such as Medicare observation status, or perhaps the patient or family is just unreasonable or suffering from a psychiatric or substance abuse disorder.
I’m not talking about the common occurrence of a disappointed patient or family who might calmly complain about something. Instead, I want to focus on those patients who, whether we perceive them as justifiably unhappy or not, are so angry that they become very time consuming and distressing to deal with. Maybe they shout about how their lawyer will be suing us and the newspaper will be writing a story about how awful we are. Or they shout and throw things, and staff become afraid of them.
In my May 2013 column, I discussed care plans for patients like this who are admitted frequently, but such plans are not sufficient in every case.
A Haphazard Approach
Most hospitals have an informal process of dealing with these patients; it starts with the bedside nurse and/or doctor trying to apologize or make adjustments to satisfy and calm the patient. If that fails, then perhaps the manager of the nursing unit gets involved. Others may be recruited, such as someone from the hospital’s risk management or “patient advocate” departments and hospital executives such as the CNO, CMO, or CEO. Sometimes several of these people may meet as a group in an effort to come up with a plan to address the situation. But, most institutions do not have a clear and consistent approach to this important work, so the hospital personnel involved end up “reinventing the wheel” each time.
The growing awareness that hospital personnel don’t seem to have a robust and confident approach to addressing this type of situation can increase a patient’s distress, and it may embolden some to become even more demanding or threatening.
And all of this takes a significant toll on bedside caregivers, who often spend so much time dealing with the angry patient that they have less time to devote to other patients, who are in turn at least a little more likely to become unhappy or suffer as a result of a distressed and busy caregiver.
A Consistent Approach: RRT for Non-Medical Distress
I think the potential benefit for patients and caregivers is significant enough that hospitals should develop a standardized approach to managing such patients, and rapid response teams (RRTs) could serve as a model. To be clear, I’m not advocating that RRTs add management of very angry or distressed patients to their current role. Let’s call it an “RRT for non-medical distress.” And, while I think it is a worthwhile idea, and I am in the early steps of trying to develop it at “my” hospital, I’m not aware of any such team in place anywhere now.
To make it practical, I think this team should be available only during weekday business hours and would comprise something like six to 10 people with clinical backgrounds who do mostly administrative work. For example, the team members could include two nursing unit directors, a risk manager, a patient advocate (or patient satisfaction “czar”), a psychiatrist, the hospitalist medical director, the chief medical officer, and a few other individuals selected for their communication skills.
One of the team members would be on call for a day or week at a time and would carry the team’s pager during business hours. Any hospital caregiver could send a page requesting the team’s assistance, and the on-call team member would respond immediately by phone or, if possible, in person. After the on-call team member’s initial assessment, the whole team would meet later the same day or early the next day. On most days, a few members of the team would be off and unable to attend the meeting. So, if the team has eight members, each meeting of the team might average about five participants.
Non-Medical Distress RRT Processes
When meeting to establish a plan for addressing an extraordinarily distressed patient/family, the team should follow a standardized written approach. A designated person should lead the conversation—perhaps the on-call team member who responded first—and another should take notes. Using a form developed for this purpose, the note-taker would capture a standardized data set that is likely to be useful in determining a course of action, as well as valuable in helping the team fine-tune its approach by reviewing trends in aggregate data. The form might include things like patient demographics; the patient’s complaints and demands; potential complicating patient issues such as substance abuse, psychoactive drugs, or psychiatric history; location in the hospital; and names of bedside caregivers. Every effort should be made to keep the meetings efficient and as brief as practical—typically 30-60 minutes.
I’m convinced that when deciding how to respond to the situation, the team should try to limit itself to choosing one or more of eight to 10 standard interventions, rather than aiming for an entirely customized response in every case. Among the standardized interventions:
- Service recovery tools, such as a handwritten apology letter;
- A meeting between the patient/family and the hospital CEO or CMO;
- Security guard(s) at the door, on “high alert” to help if called; or
- A behavioral contract specifying the expectations for both patient and hospital staff behavior.
You might think of additional “tools” this team could have in their standardized response set.
Why limit the team as much as possible to a small set of standardized interventions? Developing customized responses in each situation is time consuming and, arguably, has a higher risk of failure, since it will be difficult to ensure that all staff caring for the patient can understand and execute them effectively. And the small set of interventions will make it easier to track their effectiveness over multiple patients so that the whole process can be improved over time.
Set a High Bar
The team should not be activated for every unhappy or difficult patient; that would be overkill and would result in many activations requiring dedicated staff with no other duties to serve on the team each day. Instead, I think the team should be activated only for the most difficult and distressing cases, at least for the first few years. In a 300-bed hospital, this would be approximately one to 1.5 activations per week.
Bedside caregivers would likely feel some reassurance knowing that they can reliably get help managing the most difficult patients, and, if the plan is executed well, these patients may get care that is safer for both themselves and staff. Who knows, medical outcomes might be improved for these patients also.
Trading in work-life balance for a well-balanced life
My residency supervisor candidly asked me today – Isn’t stressing out about writing an article on work-life balance kind of missing the point? Well, yeah, that’s why she’s my supervisor. This brings me to one of the lesser advertised tips to avoiding burnout, which is: Get yourself a great mensch. But I’m getting ahead of myself here. The plan was to have 10 perfectly delineated rules, because if it worked for Letterman and Moses, it should work for residency. More to come on that.

Another part of the plan was to have this article finished by last weekend, but long call was Saturday. This was followed by long call recovery consisting of sleeping in so late my dad texted and left a voicemail asking, what happened? I haven’t heard from you all weekend. Then there was the obligatory run on the treadmill so the gooey cinnamon rolls the nurses baked and generously invited me to on Thursday would not stick around long enough for my husband to wonder if this was the beginning of me letting myself go. Isn’t that a lovely phrase?
Monday was Monday. How does anyone get anything done on Mondays? I had a new team, two new patients to learn and discharge. Plus, it was the first day that cracked 50 degrees in 5 months. I had to meet up with a friend, grab some coffee, and gossip walk around the lake. This was before we found out another friend was being slammed with consults in the emergency room. So there I was right back at the hospital Monday night with a cream cheese cherry pastry to cheer up my compatriot in the struggle.
This brings me to Tuesday. I had planned to be at the editing stage of this article on Tuesday. But didactics ran long due to everyone being so engaged in our formulations lecture, I didn’t have a shot at looking at this thing until lunchtime. Lunchtime came, and as I opened Microsoft Word among my dollar turkey sandwich and mini Purell bottles stationed around me like glorious little sergeants, I heard the gingerly utterings of a medical student: Um, if you have a moment, could you tell me the difference between the side-effect profile of first-generation and second-generation antipsychotics?
An hour later, I was informed that an admit was on the way and was traveling from out of state, set to arrive a half-hour before shift’s end. Did I mention he arrived with two family members in tow who wanted to talk about how things went wrong starting 20 years ago? Then there was the patient to see who I knew would pout if I didn’t spend at least a half-hour checking in. You know, the one the nurses always try to save me from even though I secretly never wanted to be saved.
I finally drove home 2 hours later than anticipated with a smile on my face. I should repeat that, WITH A SMILE ON MY FACE. I felt good because I’d done good. After all, there’s even a little sunlight left. When I walk in the front door, I kiss my husband and then immediately delve into a new story from the day. We laugh. We warm up leftovers, sit on the couch with our bare feet on the table, and catch an hour of American Idol (talent never gets old). Then it’s time to meet this maker.
The strange thing is, the person who began this column with all of her well-intentioned plans feels very different from the person who has made it to the deadline. There is a whole life lived in between. All of the readings I had done, notations I had made, seem kind of beside the point. I could pepper you with statistics and evidence-based outcomes warning of divorce, substance abuse, physician suicide, patient errors, and the like, which are all very real outcomes of poorly balanced lives. But I think we know all of that. It’s the in between space, the living part where so many of us lose our way. So instead of referenced journals, I offer you my journey. Because I can truly say that for the last 3 months of the most difficult year of residency, I have been happy. May this piece be also with you.
Dr. Schmidt, a second-year psychiatry resident at the Mayo Clinic in Rochester, Minn., is interested in psychodynamic therapy and in pursuing a fellowship in addictions. After obtaining a bachelor of arts at the University of California, Berkeley, she earned a master of arts degree in philosophy and humanities at the University of Chicago. She attended medical school at the University of Illinois College of Medicine at Peoria.
My residency supervisor candidly asked me today – Isn’t stressing out about writing an article on work-life balance kind of missing the point? Well, yeah, that’s why she’s my supervisor. This brings me to one of the lesser advertised tips to avoiding burnout, which is: Get yourself a great mensch. But I’m getting ahead of myself here. The plan was to have 10 perfectly delineated rules, because if it worked for Letterman and Moses, it should work for residency. More to come on that.
Another part of the plan was to have this article finished by last weekend, but long call was Saturday. This was followed by long call recovery consisting of sleeping in so late my dad texted and left a voicemail asking, what happened? I haven’t heard from you all weekend. Then there was the obligatory run on the treadmill so the gooey cinnamon rolls the nurses baked and generously invited me to on Thursday would not stick around long enough for my husband to wonder if this was the beginning of me letting myself go. Isn’t that a lovely phrase?
Monday was Monday. How does anyone get anything done on Mondays? I had a new team, two new patients to learn and discharge. Plus, it was the first day that cracked 50 degrees in 5 months. I had to meet up with a friend, grab some coffee, and gossip walk around the lake. This was before we found out another friend was being slammed with consults in the emergency room. So there I was right back at the hospital Monday night with a cream cheese cherry pastry to cheer up my compatriot in the struggle.
This brings me to Tuesday. I had planned to be at the editing stage of this article on Tuesday. But didactics ran long due to everyone being so engaged in our formulations lecture, I didn’t have a shot at looking at this thing until lunchtime. Lunchtime came, and as I opened Microsoft Word among my dollar turkey sandwich and mini Purell bottles stationed around me like glorious little sergeants, I heard the gingerly utterings of a medical student: Um, if you have a moment, could you tell me the difference between the side-effect profile of first-generation and second-generation antipsychotics?
An hour later, I was informed that an admit was on the way and was traveling from out of state, set to arrive a half-hour before shift’s end. Did I mention he arrived with two family members in tow who wanted to talk about how things went wrong starting 20 years ago? Then there was the patient to see who I knew would pout if I didn’t spend at least a half-hour checking in. You know, the one the nurses always try to save me from even though I secretly never wanted to be saved.
I finally drove home 2 hours later than anticipated with a smile on my face. I should repeat that, WITH A SMILE ON MY FACE. I felt good because I’d done good. After all, there’s even a little sunlight left. When I walk in the front door, I kiss my husband and then immediately delve into a new story from the day. We laugh. We warm up leftovers, sit on the couch with our bare feet on the table, and catch an hour of American Idol (talent never gets old). Then it’s time to meet this maker.
The strange thing is, the person who began this column with all of her well-intentioned plans feels very different from the person who has made it to the deadline. There is a whole life lived in between. All of the readings I had done, notations I had made, seem kind of beside the point. I could pepper you with statistics and evidence-based outcomes warning of divorce, substance abuse, physician suicide, patient errors, and the like, which are all very real outcomes of poorly balanced lives. But I think we know all of that. It’s the in between space, the living part where so many of us lose our way. So instead of referenced journals, I offer you my journey. Because I can truly say that for the last 3 months of the most difficult year of residency, I have been happy. May this piece be also with you.
Dr. Schmidt, a second-year psychiatry resident at the Mayo Clinic in Rochester, Minn., is interested in psychodynamic therapy and in pursuing a fellowship in addictions. After obtaining a bachelor of arts at the University of California, Berkeley, she earned a master of arts degree in philosophy and humanities at the University of Chicago. She attended medical school at the University of Illinois College of Medicine at Peoria.
My residency supervisor candidly asked me today – Isn’t stressing out about writing an article on work-life balance kind of missing the point? Well, yeah, that’s why she’s my supervisor. This brings me to one of the lesser advertised tips to avoiding burnout, which is: Get yourself a great mensch. But I’m getting ahead of myself here. The plan was to have 10 perfectly delineated rules, because if it worked for Letterman and Moses, it should work for residency. More to come on that.
Another part of the plan was to have this article finished by last weekend, but long call was Saturday. This was followed by long call recovery consisting of sleeping in so late my dad texted and left a voicemail asking, what happened? I haven’t heard from you all weekend. Then there was the obligatory run on the treadmill so the gooey cinnamon rolls the nurses baked and generously invited me to on Thursday would not stick around long enough for my husband to wonder if this was the beginning of me letting myself go. Isn’t that a lovely phrase?
Monday was Monday. How does anyone get anything done on Mondays? I had a new team, two new patients to learn and discharge. Plus, it was the first day that cracked 50 degrees in 5 months. I had to meet up with a friend, grab some coffee, and gossip walk around the lake. This was before we found out another friend was being slammed with consults in the emergency room. So there I was right back at the hospital Monday night with a cream cheese cherry pastry to cheer up my compatriot in the struggle.
This brings me to Tuesday. I had planned to be at the editing stage of this article on Tuesday. But didactics ran long due to everyone being so engaged in our formulations lecture, I didn’t have a shot at looking at this thing until lunchtime. Lunchtime came, and as I opened Microsoft Word among my dollar turkey sandwich and mini Purell bottles stationed around me like glorious little sergeants, I heard the gingerly utterings of a medical student: Um, if you have a moment, could you tell me the difference between the side-effect profile of first-generation and second-generation antipsychotics?
An hour later, I was informed that an admit was on the way and was traveling from out of state, set to arrive a half-hour before shift’s end. Did I mention he arrived with two family members in tow who wanted to talk about how things went wrong starting 20 years ago? Then there was the patient to see who I knew would pout if I didn’t spend at least a half-hour checking in. You know, the one the nurses always try to save me from even though I secretly never wanted to be saved.
I finally drove home 2 hours later than anticipated with a smile on my face. I should repeat that, WITH A SMILE ON MY FACE. I felt good because I’d done good. After all, there’s even a little sunlight left. When I walk in the front door, I kiss my husband and then immediately delve into a new story from the day. We laugh. We warm up leftovers, sit on the couch with our bare feet on the table, and catch an hour of American Idol (talent never gets old). Then it’s time to meet this maker.
The strange thing is, the person who began this column with all of her well-intentioned plans feels very different from the person who has made it to the deadline. There is a whole life lived in between. All of the readings I had done, notations I had made, seem kind of beside the point. I could pepper you with statistics and evidence-based outcomes warning of divorce, substance abuse, physician suicide, patient errors, and the like, which are all very real outcomes of poorly balanced lives. But I think we know all of that. It’s the in between space, the living part where so many of us lose our way. So instead of referenced journals, I offer you my journey. Because I can truly say that for the last 3 months of the most difficult year of residency, I have been happy. May this piece be also with you.
Dr. Schmidt, a second-year psychiatry resident at the Mayo Clinic in Rochester, Minn., is interested in psychodynamic therapy and in pursuing a fellowship in addictions. After obtaining a bachelor of arts at the University of California, Berkeley, she earned a master of arts degree in philosophy and humanities at the University of Chicago. She attended medical school at the University of Illinois College of Medicine at Peoria.

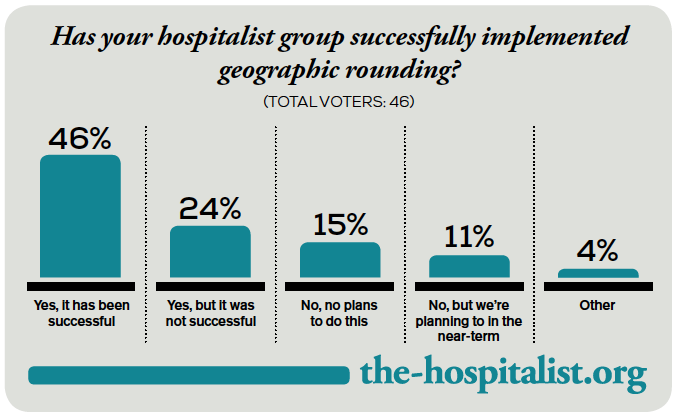
Geographic Rounding of Hospital Nurses Challenges Unit-Based Theory
Nurses, of course, have always been assigned by unit—that is, geographically. So it should come as no surprise that searching “unit-based” at the-hospitalist.org returns many articles about assigning hospitalists geographically, but not nurses, partly because few would consider it a new idea. But this article is about a new wrinkle in assigning nurses.
Although there likely are a number of hospitals doing something similar, I’ll describe a place I was lucky enough to see up close.
Bassett Medical Center
On a cold day last December, I was part of a team that spent a few days in Cooperstown, N.Y. This is a place that is so pretty that I didn’t immediately recognize we had arrived at the Bassett Medical Center Campus, since the entrance we used looked more like a library topped by a pretty cupola and warmly decorated for the holidays. We met so many nice people, including Kai Mebust, MD, FHM, who I’m convinced works full-time for the local Chamber of Commerce and tourism industry. If he doesn’t, then they should put him on their payroll.
Not long after our arrival, Dr. Mebust led us outside in the winter air without our coats to see the very beautiful view from the patio adjacent to the hospital cafeteria. And before we left for home he climbed in our car to direct us on a tour of the town. I’m sold. What a beautiful place. So much more than the Baseball Hall of Fame for which Cooperstown is known.
When not promoting his town’s tourism or enthusiastically describing his eighth-grade son playing with the Preservation Hall Jazz Band in New Orleans, he seems to find time to serve as the chief of this academic hospital’s hospital medicine practice. He was the principal engineer of the geographic assignment of nurses and describes it with an enthusiasm that matches his service as tour guide.
Geographic Care: Single RN Caring for Five Adjacent Patients
The idea is simple and best described using an illustration. A single nurse cares for five patients in adjacent rooms referred to as a “pod.” A second nurse is responsible for the next pod of five consecutive patients, and a single hospitalist cares for all 10 in both pods. There are currently four pods on a single floor of 36 beds; however, they hope to expand this system to most of the medical-surgical beds in the hospital.
The nurses eligible to care for patients in these pods are all trained to be able to provide “step down” level of care, meaning patients don’t need to transfer to a different location for more frequent monitoring and such therapies as vasopressors, mask ventilation, and the like.
Each hospitalist caring for two pods of 10 adjacent patients will typically have additional patients in other locations. This is the hospital’s way of finding the sweet spot between the competing interests of “load leveling” patient volume across hospitalists and rigidly assigning each doctor to a single location, though if they succeed in expanding the model through most of the hospital, the hospitalists will likely need to figure out how to assign themselves more rigidly to three or four pods.
Additional Components
Each morning, the hospitalist meets with the two pod nurses. They briefly discuss overnight events and plans for the day.
Much later in the morning, they also conduct daily multidisciplinary rounds involving nurse, case manager, pharmacist, dietician, social worker, respiratory therapist, and hospitalist. These follow a standard format, which is posted on the wall, and are done in a workroom that allows most participants to be in front of a computer, so they can enter notes and orders into the electronic health record (EHR) as they discuss patients.
What Is the Big Deal Here?
A lot of smart people have developed and written about systems that assign hospitalists geographically, but in most cases this has not been accompanied by adjustments in the way nurses are assigned. On nursing units at most hospitals, this means that even if a hospitalist has all of her patients on the same floor, she is still interacting with five to seven nurses caring for her patients. That usually means the hospitalist and nurse have less awareness of each other’s thinking and doing than if the ratio is reduced to no more than three or four nurses for a single hospitalist.
Dr. Mebust provided a document enumerating the goals for the program:
- Improve communication;
- Reduce patient bed moves;
- Improve patient and staff satisfaction; and
- Provide more efficient care as measured in time-of-discharge, decreased physician time-per-patient, and possibly length of stay.
Because of a number of problems teasing out the effects of this program and its limited duration to this point, Dr. Mebust and staff can’t provide robust statistics to document success in these goals. But anecdotal information is very encouraging, and clearly the nurses love it.
A major barrier to assigning nurses based rigidly on patients in adjacent rooms is the inability to ensure that each nurse has a workload of roughly equivalent complexity, but they’ve found this is a much less significant problem than feared. The nurse I spoke with said any risk of ending up with unusually complex and time-consuming patients is essentially offset by the efficiency gained by having the same attending hospitalist for all of her patients.
In fact, the nurses love it so much that they much prefer being assigned to a pod rather than a traditional assortment of patients with different attending physicians, even if the latter offers a chance to address uneven acuity.
The Big Picture
I’ve often wished that I could incorporate into hospitalist work some of the efficient ways a doctor and nurse can work together seeing scheduled patients in an outpatient setting. Surely assigning hospitalists geographically does this to some degree and has a number of advantages that others have written about. But it comes at the cost of difficult tradeoffs for hospitalists, and I know of many groups that have abandoned it after concluding that the challenges of the system exceeded its benefits.
But when it is coupled with assigning nurses geographically, I think the benefits are even greater, not only for the hospitalists, but also for patients, nurses, and other hospital staff.
Next time you’re in Cooperstown, be sure you don’t just visit the Baseball Hall of Fame. Look up Dr. Mebust, Komron Ostovar, MD, and their colleagues at Bassett Medical Center. I betcha you’ll be persuaded to see the value of their geographic model.
And maybe you’ll even fall so far under the spell of how they all talk about where they work and live that you’ll be ready to move there and join them.
Nurses, of course, have always been assigned by unit—that is, geographically. So it should come as no surprise that searching “unit-based” at the-hospitalist.org returns many articles about assigning hospitalists geographically, but not nurses, partly because few would consider it a new idea. But this article is about a new wrinkle in assigning nurses.
Although there likely are a number of hospitals doing something similar, I’ll describe a place I was lucky enough to see up close.
Bassett Medical Center
On a cold day last December, I was part of a team that spent a few days in Cooperstown, N.Y. This is a place that is so pretty that I didn’t immediately recognize we had arrived at the Bassett Medical Center Campus, since the entrance we used looked more like a library topped by a pretty cupola and warmly decorated for the holidays. We met so many nice people, including Kai Mebust, MD, FHM, who I’m convinced works full-time for the local Chamber of Commerce and tourism industry. If he doesn’t, then they should put him on their payroll.
Not long after our arrival, Dr. Mebust led us outside in the winter air without our coats to see the very beautiful view from the patio adjacent to the hospital cafeteria. And before we left for home he climbed in our car to direct us on a tour of the town. I’m sold. What a beautiful place. So much more than the Baseball Hall of Fame for which Cooperstown is known.
When not promoting his town’s tourism or enthusiastically describing his eighth-grade son playing with the Preservation Hall Jazz Band in New Orleans, he seems to find time to serve as the chief of this academic hospital’s hospital medicine practice. He was the principal engineer of the geographic assignment of nurses and describes it with an enthusiasm that matches his service as tour guide.
Geographic Care: Single RN Caring for Five Adjacent Patients
The idea is simple and best described using an illustration. A single nurse cares for five patients in adjacent rooms referred to as a “pod.” A second nurse is responsible for the next pod of five consecutive patients, and a single hospitalist cares for all 10 in both pods. There are currently four pods on a single floor of 36 beds; however, they hope to expand this system to most of the medical-surgical beds in the hospital.
The nurses eligible to care for patients in these pods are all trained to be able to provide “step down” level of care, meaning patients don’t need to transfer to a different location for more frequent monitoring and such therapies as vasopressors, mask ventilation, and the like.
Each hospitalist caring for two pods of 10 adjacent patients will typically have additional patients in other locations. This is the hospital’s way of finding the sweet spot between the competing interests of “load leveling” patient volume across hospitalists and rigidly assigning each doctor to a single location, though if they succeed in expanding the model through most of the hospital, the hospitalists will likely need to figure out how to assign themselves more rigidly to three or four pods.
Additional Components
Each morning, the hospitalist meets with the two pod nurses. They briefly discuss overnight events and plans for the day.
Much later in the morning, they also conduct daily multidisciplinary rounds involving nurse, case manager, pharmacist, dietician, social worker, respiratory therapist, and hospitalist. These follow a standard format, which is posted on the wall, and are done in a workroom that allows most participants to be in front of a computer, so they can enter notes and orders into the electronic health record (EHR) as they discuss patients.
What Is the Big Deal Here?
A lot of smart people have developed and written about systems that assign hospitalists geographically, but in most cases this has not been accompanied by adjustments in the way nurses are assigned. On nursing units at most hospitals, this means that even if a hospitalist has all of her patients on the same floor, she is still interacting with five to seven nurses caring for her patients. That usually means the hospitalist and nurse have less awareness of each other’s thinking and doing than if the ratio is reduced to no more than three or four nurses for a single hospitalist.
Dr. Mebust provided a document enumerating the goals for the program:
- Improve communication;
- Reduce patient bed moves;
- Improve patient and staff satisfaction; and
- Provide more efficient care as measured in time-of-discharge, decreased physician time-per-patient, and possibly length of stay.
Because of a number of problems teasing out the effects of this program and its limited duration to this point, Dr. Mebust and staff can’t provide robust statistics to document success in these goals. But anecdotal information is very encouraging, and clearly the nurses love it.
A major barrier to assigning nurses based rigidly on patients in adjacent rooms is the inability to ensure that each nurse has a workload of roughly equivalent complexity, but they’ve found this is a much less significant problem than feared. The nurse I spoke with said any risk of ending up with unusually complex and time-consuming patients is essentially offset by the efficiency gained by having the same attending hospitalist for all of her patients.
In fact, the nurses love it so much that they much prefer being assigned to a pod rather than a traditional assortment of patients with different attending physicians, even if the latter offers a chance to address uneven acuity.
The Big Picture
I’ve often wished that I could incorporate into hospitalist work some of the efficient ways a doctor and nurse can work together seeing scheduled patients in an outpatient setting. Surely assigning hospitalists geographically does this to some degree and has a number of advantages that others have written about. But it comes at the cost of difficult tradeoffs for hospitalists, and I know of many groups that have abandoned it after concluding that the challenges of the system exceeded its benefits.
But when it is coupled with assigning nurses geographically, I think the benefits are even greater, not only for the hospitalists, but also for patients, nurses, and other hospital staff.
Next time you’re in Cooperstown, be sure you don’t just visit the Baseball Hall of Fame. Look up Dr. Mebust, Komron Ostovar, MD, and their colleagues at Bassett Medical Center. I betcha you’ll be persuaded to see the value of their geographic model.
And maybe you’ll even fall so far under the spell of how they all talk about where they work and live that you’ll be ready to move there and join them.
Nurses, of course, have always been assigned by unit—that is, geographically. So it should come as no surprise that searching “unit-based” at the-hospitalist.org returns many articles about assigning hospitalists geographically, but not nurses, partly because few would consider it a new idea. But this article is about a new wrinkle in assigning nurses.
Although there likely are a number of hospitals doing something similar, I’ll describe a place I was lucky enough to see up close.
Bassett Medical Center
On a cold day last December, I was part of a team that spent a few days in Cooperstown, N.Y. This is a place that is so pretty that I didn’t immediately recognize we had arrived at the Bassett Medical Center Campus, since the entrance we used looked more like a library topped by a pretty cupola and warmly decorated for the holidays. We met so many nice people, including Kai Mebust, MD, FHM, who I’m convinced works full-time for the local Chamber of Commerce and tourism industry. If he doesn’t, then they should put him on their payroll.
Not long after our arrival, Dr. Mebust led us outside in the winter air without our coats to see the very beautiful view from the patio adjacent to the hospital cafeteria. And before we left for home he climbed in our car to direct us on a tour of the town. I’m sold. What a beautiful place. So much more than the Baseball Hall of Fame for which Cooperstown is known.
When not promoting his town’s tourism or enthusiastically describing his eighth-grade son playing with the Preservation Hall Jazz Band in New Orleans, he seems to find time to serve as the chief of this academic hospital’s hospital medicine practice. He was the principal engineer of the geographic assignment of nurses and describes it with an enthusiasm that matches his service as tour guide.
Geographic Care: Single RN Caring for Five Adjacent Patients
The idea is simple and best described using an illustration. A single nurse cares for five patients in adjacent rooms referred to as a “pod.” A second nurse is responsible for the next pod of five consecutive patients, and a single hospitalist cares for all 10 in both pods. There are currently four pods on a single floor of 36 beds; however, they hope to expand this system to most of the medical-surgical beds in the hospital.
The nurses eligible to care for patients in these pods are all trained to be able to provide “step down” level of care, meaning patients don’t need to transfer to a different location for more frequent monitoring and such therapies as vasopressors, mask ventilation, and the like.
Each hospitalist caring for two pods of 10 adjacent patients will typically have additional patients in other locations. This is the hospital’s way of finding the sweet spot between the competing interests of “load leveling” patient volume across hospitalists and rigidly assigning each doctor to a single location, though if they succeed in expanding the model through most of the hospital, the hospitalists will likely need to figure out how to assign themselves more rigidly to three or four pods.
Additional Components
Each morning, the hospitalist meets with the two pod nurses. They briefly discuss overnight events and plans for the day.
Much later in the morning, they also conduct daily multidisciplinary rounds involving nurse, case manager, pharmacist, dietician, social worker, respiratory therapist, and hospitalist. These follow a standard format, which is posted on the wall, and are done in a workroom that allows most participants to be in front of a computer, so they can enter notes and orders into the electronic health record (EHR) as they discuss patients.
What Is the Big Deal Here?
A lot of smart people have developed and written about systems that assign hospitalists geographically, but in most cases this has not been accompanied by adjustments in the way nurses are assigned. On nursing units at most hospitals, this means that even if a hospitalist has all of her patients on the same floor, she is still interacting with five to seven nurses caring for her patients. That usually means the hospitalist and nurse have less awareness of each other’s thinking and doing than if the ratio is reduced to no more than three or four nurses for a single hospitalist.
Dr. Mebust provided a document enumerating the goals for the program:
- Improve communication;
- Reduce patient bed moves;
- Improve patient and staff satisfaction; and
- Provide more efficient care as measured in time-of-discharge, decreased physician time-per-patient, and possibly length of stay.
Because of a number of problems teasing out the effects of this program and its limited duration to this point, Dr. Mebust and staff can’t provide robust statistics to document success in these goals. But anecdotal information is very encouraging, and clearly the nurses love it.
A major barrier to assigning nurses based rigidly on patients in adjacent rooms is the inability to ensure that each nurse has a workload of roughly equivalent complexity, but they’ve found this is a much less significant problem than feared. The nurse I spoke with said any risk of ending up with unusually complex and time-consuming patients is essentially offset by the efficiency gained by having the same attending hospitalist for all of her patients.
In fact, the nurses love it so much that they much prefer being assigned to a pod rather than a traditional assortment of patients with different attending physicians, even if the latter offers a chance to address uneven acuity.
The Big Picture
I’ve often wished that I could incorporate into hospitalist work some of the efficient ways a doctor and nurse can work together seeing scheduled patients in an outpatient setting. Surely assigning hospitalists geographically does this to some degree and has a number of advantages that others have written about. But it comes at the cost of difficult tradeoffs for hospitalists, and I know of many groups that have abandoned it after concluding that the challenges of the system exceeded its benefits.
But when it is coupled with assigning nurses geographically, I think the benefits are even greater, not only for the hospitalists, but also for patients, nurses, and other hospital staff.
Next time you’re in Cooperstown, be sure you don’t just visit the Baseball Hall of Fame. Look up Dr. Mebust, Komron Ostovar, MD, and their colleagues at Bassett Medical Center. I betcha you’ll be persuaded to see the value of their geographic model.
And maybe you’ll even fall so far under the spell of how they all talk about where they work and live that you’ll be ready to move there and join them.
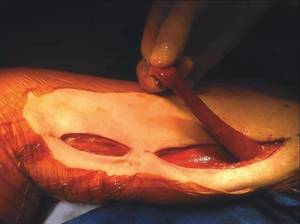
Using the gracilis muscle flap
Muscle flaps have come to play an invaluable role in the management of complex groin wounds (Figure 1). We have found that the gracilis muscle offers significant advantages over other local muscle flaps. In comparison to the segmental blood supply of the sartorius muscle which can be disrupted during mobilization, the gracilis muscle has a single vascular pedicle that arises reliably from the medial femoral circumflex vessels. Unlike the sartorius muscle which may be damaged by the infectious/inflammatory process in the groin, the gracilis muscle is remote from the groin wound itself. In addition, the procedure is relatively simple and can be completed in less than thirty minutes.

The procedure is performed with the patient in the supine position with the knee slightly flexed. The gracilis muscle can be palpated along the medial aspect of the thigh and the longitudinal incision is placed directly over the muscle . After the deep fascia is divided, the muscle can be easily freed from surrounding attachments (Figure 2). We completely mobilize the distal two-thirds of the muscle and divide it at the musculotendinous insertion on the femur. We do not mobilize the proximal one-third of the muscle to avoid injury to the vascular pedicle). The muscle is retroflexed into the groin wound using a ringed-forceps. The muscle provides excellent coverage of the femoral triangle. A vacuum dressing may be applied without concern for injury to the femoral vessels.
We used the gracilis flap to treat complex groin wounds in 68 limbs in 64 patients at the University of Arkansas for Medical Sciences, Little Rock. Complete healing was achieved in 91%. In six patients (9%), recurrent or persistent infection led to bleeding that required surgical management. Limb salvage was achieved in 86%.
The presence of autogenous vascular reconstruction was associated with a reduced risk of persistent/recurrent infection in comparison to synthetic grafts (2.3% vs 23.8%, P = .006). Age greater than 75 years was associated with worse outcomes overall. Wound problems (infection, hematoma, seroma) at the harvest site were rare.
We prefer the gracilis flap to the sartorius or other groin muscle flaps in the management of complex groin wounds. The procedure is simple enough for a vascular surgeon, the muscle is reliable in location and blood supply, and the results are satisfactory given the complexity of the problem.
Dr. Eidt is at Greenville Health System, University of South Carolina School of Medicine Greenville, and Dr. Ali is at University of Arkansas for Medical Sciences, Little Rock.
Muscle flaps have come to play an invaluable role in the management of complex groin wounds (Figure 1). We have found that the gracilis muscle offers significant advantages over other local muscle flaps. In comparison to the segmental blood supply of the sartorius muscle which can be disrupted during mobilization, the gracilis muscle has a single vascular pedicle that arises reliably from the medial femoral circumflex vessels. Unlike the sartorius muscle which may be damaged by the infectious/inflammatory process in the groin, the gracilis muscle is remote from the groin wound itself. In addition, the procedure is relatively simple and can be completed in less than thirty minutes.
The procedure is performed with the patient in the supine position with the knee slightly flexed. The gracilis muscle can be palpated along the medial aspect of the thigh and the longitudinal incision is placed directly over the muscle . After the deep fascia is divided, the muscle can be easily freed from surrounding attachments (Figure 2). We completely mobilize the distal two-thirds of the muscle and divide it at the musculotendinous insertion on the femur. We do not mobilize the proximal one-third of the muscle to avoid injury to the vascular pedicle). The muscle is retroflexed into the groin wound using a ringed-forceps. The muscle provides excellent coverage of the femoral triangle. A vacuum dressing may be applied without concern for injury to the femoral vessels.
We used the gracilis flap to treat complex groin wounds in 68 limbs in 64 patients at the University of Arkansas for Medical Sciences, Little Rock. Complete healing was achieved in 91%. In six patients (9%), recurrent or persistent infection led to bleeding that required surgical management. Limb salvage was achieved in 86%.
The presence of autogenous vascular reconstruction was associated with a reduced risk of persistent/recurrent infection in comparison to synthetic grafts (2.3% vs 23.8%, P = .006). Age greater than 75 years was associated with worse outcomes overall. Wound problems (infection, hematoma, seroma) at the harvest site were rare.
We prefer the gracilis flap to the sartorius or other groin muscle flaps in the management of complex groin wounds. The procedure is simple enough for a vascular surgeon, the muscle is reliable in location and blood supply, and the results are satisfactory given the complexity of the problem.
Dr. Eidt is at Greenville Health System, University of South Carolina School of Medicine Greenville, and Dr. Ali is at University of Arkansas for Medical Sciences, Little Rock.
Muscle flaps have come to play an invaluable role in the management of complex groin wounds (Figure 1). We have found that the gracilis muscle offers significant advantages over other local muscle flaps. In comparison to the segmental blood supply of the sartorius muscle which can be disrupted during mobilization, the gracilis muscle has a single vascular pedicle that arises reliably from the medial femoral circumflex vessels. Unlike the sartorius muscle which may be damaged by the infectious/inflammatory process in the groin, the gracilis muscle is remote from the groin wound itself. In addition, the procedure is relatively simple and can be completed in less than thirty minutes.
The procedure is performed with the patient in the supine position with the knee slightly flexed. The gracilis muscle can be palpated along the medial aspect of the thigh and the longitudinal incision is placed directly over the muscle . After the deep fascia is divided, the muscle can be easily freed from surrounding attachments (Figure 2). We completely mobilize the distal two-thirds of the muscle and divide it at the musculotendinous insertion on the femur. We do not mobilize the proximal one-third of the muscle to avoid injury to the vascular pedicle). The muscle is retroflexed into the groin wound using a ringed-forceps. The muscle provides excellent coverage of the femoral triangle. A vacuum dressing may be applied without concern for injury to the femoral vessels.
We used the gracilis flap to treat complex groin wounds in 68 limbs in 64 patients at the University of Arkansas for Medical Sciences, Little Rock. Complete healing was achieved in 91%. In six patients (9%), recurrent or persistent infection led to bleeding that required surgical management. Limb salvage was achieved in 86%.
The presence of autogenous vascular reconstruction was associated with a reduced risk of persistent/recurrent infection in comparison to synthetic grafts (2.3% vs 23.8%, P = .006). Age greater than 75 years was associated with worse outcomes overall. Wound problems (infection, hematoma, seroma) at the harvest site were rare.
We prefer the gracilis flap to the sartorius or other groin muscle flaps in the management of complex groin wounds. The procedure is simple enough for a vascular surgeon, the muscle is reliable in location and blood supply, and the results are satisfactory given the complexity of the problem.
Dr. Eidt is at Greenville Health System, University of South Carolina School of Medicine Greenville, and Dr. Ali is at University of Arkansas for Medical Sciences, Little Rock.
Shyness vs. social anxiety
Many advocating for more attention to psychosocial issues by primary care pediatricians focus on serious conditions and the value of early recognition. For example, early recognition of autism spectrum disorder could lead to earlier intensive treatment that might impact the long-term course. Early diagnosis and appropriate treatment of attention-deficit/hyperactivity disorder very likely will lessen symptoms and also maintain self-esteem under the withering ordeal – often punctuated by teacher comments – of trying to pay attention hour after hour in school
Are there seemingly less serious conditions very likely worthy of early diagnosis, even those on the edge of normal developmental hurdles? One of the essential tasks of childhood is mastering the anxiety that emerges as children face the new challenges of each developmental stage, so parents, teachers, and clinicians are (or need to be) used to bearing anxiety in the children with whom they work. Intense shyness and anxiety around separation from parents are routine and healthy in infants and toddlers from 6-18 months. Anxiety in new social situations, such as the first day of preschool, is the rule, not the exception. School-age children commonly experience a surge of anxiety around performance and independence, as they are managing and mastering new skills in these domains every day. This anxiety can cause distress, but it should get better every time a child faces it, as they become better at managing the situation. When a child has an anxious temperament, poor coping skills, or parents who struggle to manage their own anxiety, children may have a harder time mastering new, anxiety-provoking challenges across settings. But, with time, and even just one adult who patiently models good coping, they will face and manage challenges. Social anxiety disorder is present when specific social or performance situations provoke the same intense anxiety and avoidance over and over, and for more than 6 months.
Most infants and young children who are more timid and fearful seem to grow into a normal range of social behavior, although few become extroverts. Some of these shy children are cautious in new situations for a period of time measured in minutes, but once the situations are familiar, these children are indistinguishable from their peers. However, some of these temperamentally timid children emerge consistently more anxious with greater likelihood to have phobias and to have social anxiety that can seriously impact long term happiness, achievement, and increase risk taking behaviors. A pediatrician should watch and note the emerging pattern of a timid toddler to see if the shyness eases or impacts social functioning; by bending the course of social interactions, social anxiety disorder critically affects developing social skills, self-regulation, affect tolerance, emerging identity, and confidence. Recognition and effective treatment of social anxiety will keep a child on the optimal developmental trajectory.
Anxiety disorders are the most common psychiatric illnesses in the United States, and social anxiety disorder (previously labeled as social phobia) is the third most common psychiatric disorder in U.S. adults (after depression and alcohol dependence). Most persistent anxiety disorders begin in childhood, and social anxiety is no exception. The mean age of onset for social anxiety is 13 years old, and it rarely begins after the age of 25, with an annual prevalence around 7% in childhood and adolescence (Psychiatr. Clin. North Am. 2009;32;483-524).The DSM-5 criteria for social anxiety disorder include, “a marked and persistent fear of one or more social or performance situations in which the person is exposed to unfamiliar people or to possible scrutiny by others,” and exposure to those situations provokes intense anxiety, which in children can be marked by severe or prolonged crying, freezing, tantrums, shrinking from social situations, refusing to speak, or clinging to parents. In adolescents, it may trigger panic attacks. The avoidance and distress interfere with the child’s function in school, social activities, or relationships, and must have lasted for at least 6 months. To ensure that there is not another problem of social relatedness, the child should have shown some capacity to have normal peer relationships.
Will social anxiety disorder be vividly apparent to teachers, parents, and clinicians? No. The feeling of anxiety is an internal experience, not easily observed, and anxious children and teens are rarely eager or comfortable communicators about their own anxiety. Indeed, in a 2007 survey of patients in treatment for anxiety, 36% of people with social anxiety disorder reported experiencing symptoms for 10 or more years before seeking help. It’s true that the distress children experience when feeling intensely anxious will probably be observable, but all of those behaviors (clinging, crying, tantrums) are common and normal expressions of distress in childhood. Even in adolescence, while having a panic attack may prompt the teenager to seek care, she may not connect it with the anxiety she was feeling about being called on in class or talking to peers, especially if that is an anxiety she has experienced for a long time as a daily part of her lives and routines.
Social anxiety disorder is treatable. The first-line treatment in mild to moderate cases, particularly with younger children, is cognitive-behavioral therapy. This is a practical variant of psychotherapy in which children develop and practice skills at recognizing and labeling their own feelings of anxiety, identifying the situations that trigger them, and practicing relaxation strategies that help them to face and manage the anxiety-provoking situations rather than avoiding them.
When symptoms or the degree of impairment are more severe, medications can become an important part of treatment. SSRIs are the first-line medications used to treat social anxiety disorder, and the effective doses are often higher than effective antidepressant doses, although we often titrate toward those doses more slowly with anxious patients to avoid side effects that might increase or exacerbate their anxiety.
Even with effective medication treatment, though, psychotherapy will be an essential part of treatment. These young patients need to build the essential skills of anxiety management, although it is in the nature of anxiety that such patients often wish to dissolve their anxiety by simply using a pill.
Anxiety disorders are typically chronic and will persist without effective treatment. Failure to recognize and treat social anxiety disorder can distort or even derail healthy development and may result in major psychiatric complications. As a pediatrician, you are trying to stop or modify a chain of potential events. Imagine a socially anxious young woman who enters puberty in high school. Will she withdraw from social activities? Will she avoid new opportunities or interests? Will alcohol become a necessary social lubricant? Will she be at increased risk for sexual assault at a party or poor grades in school? Will social anxiety affect her choice of college, fearful of leaving home? The incidence of secondary depression and substance abuse disorders is substantially higher in adolescents with untreated anxiety disorders. Although a depressed, alcohol-dependent teenager is more likely to be recognized as needing treatment, once they have developed those complications, effective treatment of the underlying anxiety will be much more complicated and slow to treat. Prevention starting before puberty is a much more desirable approach.
Pediatricians truly do have the opportunity to improve outcomes for these patients, by learning to recognize this sometimes-invisible disorder. Children suffering from anxiety disorders are more likely to identify a physical concern than a psychological one. (They have a lot of headaches and tummy aches!) When you are seeing a “shy” school-age child who has persistent crying spells around attending school on test days or before each sporting event despite loving practice, it is useful to gather more history. Is there a family history of anxiety or depression? What are the circumstances of their crying jags or persistent tantrums? Ask teenagers about episodes of shortness of breath, tachycardia, dizziness or sweating that leave them feeling like they are going to die (panic attacks). See if they can rank their anxiety on a scale from 1-10, and find out of there are consistent situations where their anxiety seems disproportionate. Children or teens may recognize that their anxiety is not merited, or they may not. If their parent also suffers from anxiety, they are less likely to recognize that this intense, persistent “shyness” in their child represents a treatable symptom. When you simply have a high index of suspicion, it is worth a referral to a mental health expert to evaluate their anxiety.
Reassuring parents and children that this is a common, treatable problem in childhood will go a long way to diminishing the secrecy and shame that can accompany paralyzing anxiety, and help your patients toward a track that optimizes their psychosocial development.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston.
Many advocating for more attention to psychosocial issues by primary care pediatricians focus on serious conditions and the value of early recognition. For example, early recognition of autism spectrum disorder could lead to earlier intensive treatment that might impact the long-term course. Early diagnosis and appropriate treatment of attention-deficit/hyperactivity disorder very likely will lessen symptoms and also maintain self-esteem under the withering ordeal – often punctuated by teacher comments – of trying to pay attention hour after hour in school
Are there seemingly less serious conditions very likely worthy of early diagnosis, even those on the edge of normal developmental hurdles? One of the essential tasks of childhood is mastering the anxiety that emerges as children face the new challenges of each developmental stage, so parents, teachers, and clinicians are (or need to be) used to bearing anxiety in the children with whom they work. Intense shyness and anxiety around separation from parents are routine and healthy in infants and toddlers from 6-18 months. Anxiety in new social situations, such as the first day of preschool, is the rule, not the exception. School-age children commonly experience a surge of anxiety around performance and independence, as they are managing and mastering new skills in these domains every day. This anxiety can cause distress, but it should get better every time a child faces it, as they become better at managing the situation. When a child has an anxious temperament, poor coping skills, or parents who struggle to manage their own anxiety, children may have a harder time mastering new, anxiety-provoking challenges across settings. But, with time, and even just one adult who patiently models good coping, they will face and manage challenges. Social anxiety disorder is present when specific social or performance situations provoke the same intense anxiety and avoidance over and over, and for more than 6 months.
Most infants and young children who are more timid and fearful seem to grow into a normal range of social behavior, although few become extroverts. Some of these shy children are cautious in new situations for a period of time measured in minutes, but once the situations are familiar, these children are indistinguishable from their peers. However, some of these temperamentally timid children emerge consistently more anxious with greater likelihood to have phobias and to have social anxiety that can seriously impact long term happiness, achievement, and increase risk taking behaviors. A pediatrician should watch and note the emerging pattern of a timid toddler to see if the shyness eases or impacts social functioning; by bending the course of social interactions, social anxiety disorder critically affects developing social skills, self-regulation, affect tolerance, emerging identity, and confidence. Recognition and effective treatment of social anxiety will keep a child on the optimal developmental trajectory.
Anxiety disorders are the most common psychiatric illnesses in the United States, and social anxiety disorder (previously labeled as social phobia) is the third most common psychiatric disorder in U.S. adults (after depression and alcohol dependence). Most persistent anxiety disorders begin in childhood, and social anxiety is no exception. The mean age of onset for social anxiety is 13 years old, and it rarely begins after the age of 25, with an annual prevalence around 7% in childhood and adolescence (Psychiatr. Clin. North Am. 2009;32;483-524).The DSM-5 criteria for social anxiety disorder include, “a marked and persistent fear of one or more social or performance situations in which the person is exposed to unfamiliar people or to possible scrutiny by others,” and exposure to those situations provokes intense anxiety, which in children can be marked by severe or prolonged crying, freezing, tantrums, shrinking from social situations, refusing to speak, or clinging to parents. In adolescents, it may trigger panic attacks. The avoidance and distress interfere with the child’s function in school, social activities, or relationships, and must have lasted for at least 6 months. To ensure that there is not another problem of social relatedness, the child should have shown some capacity to have normal peer relationships.
Will social anxiety disorder be vividly apparent to teachers, parents, and clinicians? No. The feeling of anxiety is an internal experience, not easily observed, and anxious children and teens are rarely eager or comfortable communicators about their own anxiety. Indeed, in a 2007 survey of patients in treatment for anxiety, 36% of people with social anxiety disorder reported experiencing symptoms for 10 or more years before seeking help. It’s true that the distress children experience when feeling intensely anxious will probably be observable, but all of those behaviors (clinging, crying, tantrums) are common and normal expressions of distress in childhood. Even in adolescence, while having a panic attack may prompt the teenager to seek care, she may not connect it with the anxiety she was feeling about being called on in class or talking to peers, especially if that is an anxiety she has experienced for a long time as a daily part of her lives and routines.
Social anxiety disorder is treatable. The first-line treatment in mild to moderate cases, particularly with younger children, is cognitive-behavioral therapy. This is a practical variant of psychotherapy in which children develop and practice skills at recognizing and labeling their own feelings of anxiety, identifying the situations that trigger them, and practicing relaxation strategies that help them to face and manage the anxiety-provoking situations rather than avoiding them.
When symptoms or the degree of impairment are more severe, medications can become an important part of treatment. SSRIs are the first-line medications used to treat social anxiety disorder, and the effective doses are often higher than effective antidepressant doses, although we often titrate toward those doses more slowly with anxious patients to avoid side effects that might increase or exacerbate their anxiety.
Even with effective medication treatment, though, psychotherapy will be an essential part of treatment. These young patients need to build the essential skills of anxiety management, although it is in the nature of anxiety that such patients often wish to dissolve their anxiety by simply using a pill.
Anxiety disorders are typically chronic and will persist without effective treatment. Failure to recognize and treat social anxiety disorder can distort or even derail healthy development and may result in major psychiatric complications. As a pediatrician, you are trying to stop or modify a chain of potential events. Imagine a socially anxious young woman who enters puberty in high school. Will she withdraw from social activities? Will she avoid new opportunities or interests? Will alcohol become a necessary social lubricant? Will she be at increased risk for sexual assault at a party or poor grades in school? Will social anxiety affect her choice of college, fearful of leaving home? The incidence of secondary depression and substance abuse disorders is substantially higher in adolescents with untreated anxiety disorders. Although a depressed, alcohol-dependent teenager is more likely to be recognized as needing treatment, once they have developed those complications, effective treatment of the underlying anxiety will be much more complicated and slow to treat. Prevention starting before puberty is a much more desirable approach.
Pediatricians truly do have the opportunity to improve outcomes for these patients, by learning to recognize this sometimes-invisible disorder. Children suffering from anxiety disorders are more likely to identify a physical concern than a psychological one. (They have a lot of headaches and tummy aches!) When you are seeing a “shy” school-age child who has persistent crying spells around attending school on test days or before each sporting event despite loving practice, it is useful to gather more history. Is there a family history of anxiety or depression? What are the circumstances of their crying jags or persistent tantrums? Ask teenagers about episodes of shortness of breath, tachycardia, dizziness or sweating that leave them feeling like they are going to die (panic attacks). See if they can rank their anxiety on a scale from 1-10, and find out of there are consistent situations where their anxiety seems disproportionate. Children or teens may recognize that their anxiety is not merited, or they may not. If their parent also suffers from anxiety, they are less likely to recognize that this intense, persistent “shyness” in their child represents a treatable symptom. When you simply have a high index of suspicion, it is worth a referral to a mental health expert to evaluate their anxiety.
Reassuring parents and children that this is a common, treatable problem in childhood will go a long way to diminishing the secrecy and shame that can accompany paralyzing anxiety, and help your patients toward a track that optimizes their psychosocial development.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston.
Many advocating for more attention to psychosocial issues by primary care pediatricians focus on serious conditions and the value of early recognition. For example, early recognition of autism spectrum disorder could lead to earlier intensive treatment that might impact the long-term course. Early diagnosis and appropriate treatment of attention-deficit/hyperactivity disorder very likely will lessen symptoms and also maintain self-esteem under the withering ordeal – often punctuated by teacher comments – of trying to pay attention hour after hour in school
Are there seemingly less serious conditions very likely worthy of early diagnosis, even those on the edge of normal developmental hurdles? One of the essential tasks of childhood is mastering the anxiety that emerges as children face the new challenges of each developmental stage, so parents, teachers, and clinicians are (or need to be) used to bearing anxiety in the children with whom they work. Intense shyness and anxiety around separation from parents are routine and healthy in infants and toddlers from 6-18 months. Anxiety in new social situations, such as the first day of preschool, is the rule, not the exception. School-age children commonly experience a surge of anxiety around performance and independence, as they are managing and mastering new skills in these domains every day. This anxiety can cause distress, but it should get better every time a child faces it, as they become better at managing the situation. When a child has an anxious temperament, poor coping skills, or parents who struggle to manage their own anxiety, children may have a harder time mastering new, anxiety-provoking challenges across settings. But, with time, and even just one adult who patiently models good coping, they will face and manage challenges. Social anxiety disorder is present when specific social or performance situations provoke the same intense anxiety and avoidance over and over, and for more than 6 months.
Most infants and young children who are more timid and fearful seem to grow into a normal range of social behavior, although few become extroverts. Some of these shy children are cautious in new situations for a period of time measured in minutes, but once the situations are familiar, these children are indistinguishable from their peers. However, some of these temperamentally timid children emerge consistently more anxious with greater likelihood to have phobias and to have social anxiety that can seriously impact long term happiness, achievement, and increase risk taking behaviors. A pediatrician should watch and note the emerging pattern of a timid toddler to see if the shyness eases or impacts social functioning; by bending the course of social interactions, social anxiety disorder critically affects developing social skills, self-regulation, affect tolerance, emerging identity, and confidence. Recognition and effective treatment of social anxiety will keep a child on the optimal developmental trajectory.
Anxiety disorders are the most common psychiatric illnesses in the United States, and social anxiety disorder (previously labeled as social phobia) is the third most common psychiatric disorder in U.S. adults (after depression and alcohol dependence). Most persistent anxiety disorders begin in childhood, and social anxiety is no exception. The mean age of onset for social anxiety is 13 years old, and it rarely begins after the age of 25, with an annual prevalence around 7% in childhood and adolescence (Psychiatr. Clin. North Am. 2009;32;483-524).The DSM-5 criteria for social anxiety disorder include, “a marked and persistent fear of one or more social or performance situations in which the person is exposed to unfamiliar people or to possible scrutiny by others,” and exposure to those situations provokes intense anxiety, which in children can be marked by severe or prolonged crying, freezing, tantrums, shrinking from social situations, refusing to speak, or clinging to parents. In adolescents, it may trigger panic attacks. The avoidance and distress interfere with the child’s function in school, social activities, or relationships, and must have lasted for at least 6 months. To ensure that there is not another problem of social relatedness, the child should have shown some capacity to have normal peer relationships.
Will social anxiety disorder be vividly apparent to teachers, parents, and clinicians? No. The feeling of anxiety is an internal experience, not easily observed, and anxious children and teens are rarely eager or comfortable communicators about their own anxiety. Indeed, in a 2007 survey of patients in treatment for anxiety, 36% of people with social anxiety disorder reported experiencing symptoms for 10 or more years before seeking help. It’s true that the distress children experience when feeling intensely anxious will probably be observable, but all of those behaviors (clinging, crying, tantrums) are common and normal expressions of distress in childhood. Even in adolescence, while having a panic attack may prompt the teenager to seek care, she may not connect it with the anxiety she was feeling about being called on in class or talking to peers, especially if that is an anxiety she has experienced for a long time as a daily part of her lives and routines.
Social anxiety disorder is treatable. The first-line treatment in mild to moderate cases, particularly with younger children, is cognitive-behavioral therapy. This is a practical variant of psychotherapy in which children develop and practice skills at recognizing and labeling their own feelings of anxiety, identifying the situations that trigger them, and practicing relaxation strategies that help them to face and manage the anxiety-provoking situations rather than avoiding them.
When symptoms or the degree of impairment are more severe, medications can become an important part of treatment. SSRIs are the first-line medications used to treat social anxiety disorder, and the effective doses are often higher than effective antidepressant doses, although we often titrate toward those doses more slowly with anxious patients to avoid side effects that might increase or exacerbate their anxiety.
Even with effective medication treatment, though, psychotherapy will be an essential part of treatment. These young patients need to build the essential skills of anxiety management, although it is in the nature of anxiety that such patients often wish to dissolve their anxiety by simply using a pill.
Anxiety disorders are typically chronic and will persist without effective treatment. Failure to recognize and treat social anxiety disorder can distort or even derail healthy development and may result in major psychiatric complications. As a pediatrician, you are trying to stop or modify a chain of potential events. Imagine a socially anxious young woman who enters puberty in high school. Will she withdraw from social activities? Will she avoid new opportunities or interests? Will alcohol become a necessary social lubricant? Will she be at increased risk for sexual assault at a party or poor grades in school? Will social anxiety affect her choice of college, fearful of leaving home? The incidence of secondary depression and substance abuse disorders is substantially higher in adolescents with untreated anxiety disorders. Although a depressed, alcohol-dependent teenager is more likely to be recognized as needing treatment, once they have developed those complications, effective treatment of the underlying anxiety will be much more complicated and slow to treat. Prevention starting before puberty is a much more desirable approach.
Pediatricians truly do have the opportunity to improve outcomes for these patients, by learning to recognize this sometimes-invisible disorder. Children suffering from anxiety disorders are more likely to identify a physical concern than a psychological one. (They have a lot of headaches and tummy aches!) When you are seeing a “shy” school-age child who has persistent crying spells around attending school on test days or before each sporting event despite loving practice, it is useful to gather more history. Is there a family history of anxiety or depression? What are the circumstances of their crying jags or persistent tantrums? Ask teenagers about episodes of shortness of breath, tachycardia, dizziness or sweating that leave them feeling like they are going to die (panic attacks). See if they can rank their anxiety on a scale from 1-10, and find out of there are consistent situations where their anxiety seems disproportionate. Children or teens may recognize that their anxiety is not merited, or they may not. If their parent also suffers from anxiety, they are less likely to recognize that this intense, persistent “shyness” in their child represents a treatable symptom. When you simply have a high index of suspicion, it is worth a referral to a mental health expert to evaluate their anxiety.
Reassuring parents and children that this is a common, treatable problem in childhood will go a long way to diminishing the secrecy and shame that can accompany paralyzing anxiety, and help your patients toward a track that optimizes their psychosocial development.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston.

Reducing radiation exposure
SCOTTSDALE, Ariz.– “It’s surprising to me today, when I go proctor or watch a case, how people don’t understand the impact of radiation,” Dr. Mark A. Farber, professor of surgery and radiology at the University of North Carolina, Chapel Hill, said at the Southern Association for Vascular Surgery annual meeting. “Many times, I see people’s hands underneath the machine and on the fluoroscopy image.”
This flouting of the so-called ALARA (as low as reasonably achievable) principle happens in part because the number of complex procedures performed by vascular surgeons is increasing, despite what presenter Dr. Melissa Kirkwood, a vascular surgeon at the University of Texas Southwestern Medical Center, Dallas, told the audience is a lack of training in radiation dose terminology and basic safety principles. Yet, practicing excellent radiation safety protocols is “paramount” according to Dr. Farber who, along with Dr. Kirkwood, shared insights on how to minimize dose to both patients and vascular specialists, whether it be from primary, leakage, or scatter radiation.

Table up, detector down
Minimizing the air gap by as little as 100 mm – from 700 mm to 600 mm, for example – can reduce the dose of radiation from 17%-29%, whereas a 10-cm increase in the air gap can result in as much as a 20%-38% increase in the radiation skin dose. This is essentially the application of the inverse square law, according to Dr. Kirkwood.
Dr. Farber said that some of the newer, more advanced machines have sensors that automatically detect where the collector should be in relation to the patient, but if your machine doesn’t have these “bells and whistles … remember that the skin dose decreases as the air gap decreases.”

Another advantage to using new imaging systems, according to Dr. Farber, is that they allow the use of pulsed fluoroscopy for as few as 2 or 3 pulses/sec. The selected pulse rate determines the number of fluoroscopic image frames that are generated by the machine per second. This is significant when the dose savings are essential and when performing simpler procedures, he said. “If you go from 7.5 frames down to 3 frames/sec, you can decrease the exposure for both you and your patient.”
Use between 15 and 30 pulses/sec for critical procedures where precision is crucial, but reducing the rate to 7.5 pulses/sec may result in as much as 70% less of a skin dose.
Add radiation barriers
Don’t assume that the lead shielding is doing the job. “It’s important that you keep up on this and have it tested regularly,” said Dr. Farber, who recently discovered his thyroid shield was cracked and needed to be replaced. Also, consider the lead shielding of your staff, which, even if it is not used as frequently as the physician’s, can suffer from improper handling. “They fold it or crinkle it up and drop it on the floor. This can lead to problems,” he said. And be sure to remember leaded glasses, lead drapes for the sides of the table, and leaded ceiling-mounted or standing shields.
For extra protection, Dr. Farber recommended the use of disposable protective drapes with cut-outs that allow access to the patient while helping to reduce the amount of scatter radiation exposure to the operator’s limbs. At a tally of anywhere from 1 to 10 mGy/hour, scatter radiation emanating from the patient is a particular risk to the operator’s legs from the knees down, said Dr. Kirkwood, “depending on how tall you are.”
Using the disposable drapes also can result in a 12-fold decrease in the amount of scatter on the eyes, a 25-fold decrease in thyroid exposure to scatter, and a 29-fold decrease in the hands being exposed. “They can be cumbersome at times, I admit,” Dr. Farber said. “But there is no substitute for using protective drapes.”
Leaded aprons also help cut radiation transmission rates, even if they are not foolproof. Wearing two-piece leaded apron systems can help cut down the body strain from the weight of the aprons; however, Dr. Farber said that, at his institution, they use a suspended body shield system operated by a boom so there is no physical stress on the clinician. Because the weightless system also provides additional protection for the specialist’s head and limbs, Dr. Farber said that the hefty price tag is justified. “The way I sold it to the hospital was I told them I could stop doing procedures, or they could get me one of these systems so I could do more procedures,” he said, adding he is having a weightless system installed on each side of the table. “They’ll get their money’s worth by the fact that you’re not over your exposure limit.”
And finally, don’t forget to protect the anesthesiologist! A standing shield that gives broad coverage area should suffice, Dr. Farber said.
Alter the intensifier position
Altering the angle can help ensure that one area of the patient’s body isn’t being overexposed to radiation. Since previously irradiated skin reacts abnormally when re-exposed to radiation because the regeneration and repair of the dermis can take up to several weeks after the initial insult, the timing of the intervals between exposures is critical, said Dr. Kirkwood, adding that the Joint Commission recommended that all doses of fluoroscopically guided interventions performed within the past 6-12 months should be considered when assessing potential skin injury risk.
Use collimation
Making it tighter, for example, can help improve image quality and reduce the radiation dose to both the patient and the operator, as can varying the acquisition rates.
Exit the room during DSA
During digital subtraction angiography, Dr. Farber said to “get away from the table if you can! It’s a huge dose you don’t need to be exposed to if you don’t need to be right next to the machine.” Dr. Kirkwood agreed: “Angiography is 10-100 times more dose than fluoroscopy.”
Reduce magnification
Using a larger monitor allows the operator to see more detail without increasing the magnification, which also increases the dose in the amount of the diameter over the diameter squared. “By not magnifying up [from a field of view of 14 to 28], you will save yourself a factor of at least 4,” Dr. Farber said. “And the actual dose may be even less.”
Optimize imaging
Today’s advanced imaging systems make it easy to produce many high-quality images – CT scans and ultrasounds – that allow a more comprehensive picture. Having various image sources on screen at once is “practice changing” because it can help clinicians see more possibilities for “how to do the case,” said Dr. Farber. “I’ve never heard anyone say, ’Well, I wish I didn’t have that extra imaging next to me.’ ”
Save images
But once you get it, don’t forget to keep it. “Many times you do an acquisition, you move the machine, and you realize you forget to save the image and now you’ve got to go back and do it all over again,” Dr. Farber lamented. But by once again making technology your friend, with functions that allow auto-return to previous positions, among other auto-commands, you can save the needed information and reduce any unnecessary dose exposure for both yourself and the patient, he said.
Protect your eyes
Cataracts are still all too common in the field, according to Dr. Farber. “It’s important that you have side shields on your glasses to cut down on the amount of radiation that comes in and around the glasses.” Eschew glasses that don’t overtly hug your face.
Geometric differences
Don’t forget that, if you’re standing on the side of the imaging source, the scattering effect will be greater than if you’re on the side of the image receptor. Once again, an understanding of the inverse square law can be protective, according to Dr. Kirkwood: “As x-rays exit the source, there is an exponential decrease in the number of x-rays per unit area as the distance from the source increases.”
“It’s simple stuff,” concluded Dr. Farber. “If you get in the habit of doing these things you will cut down your radiation exposure.”
Neither Dr. Farber nor Dr. Kirkwood had any relevant disclosures.
wmcknight@frontlinemedcom.com On Twitter @whitneymcknight
SCOTTSDALE, Ariz.– “It’s surprising to me today, when I go proctor or watch a case, how people don’t understand the impact of radiation,” Dr. Mark A. Farber, professor of surgery and radiology at the University of North Carolina, Chapel Hill, said at the Southern Association for Vascular Surgery annual meeting. “Many times, I see people’s hands underneath the machine and on the fluoroscopy image.”
This flouting of the so-called ALARA (as low as reasonably achievable) principle happens in part because the number of complex procedures performed by vascular surgeons is increasing, despite what presenter Dr. Melissa Kirkwood, a vascular surgeon at the University of Texas Southwestern Medical Center, Dallas, told the audience is a lack of training in radiation dose terminology and basic safety principles. Yet, practicing excellent radiation safety protocols is “paramount” according to Dr. Farber who, along with Dr. Kirkwood, shared insights on how to minimize dose to both patients and vascular specialists, whether it be from primary, leakage, or scatter radiation.
Table up, detector down
Minimizing the air gap by as little as 100 mm – from 700 mm to 600 mm, for example – can reduce the dose of radiation from 17%-29%, whereas a 10-cm increase in the air gap can result in as much as a 20%-38% increase in the radiation skin dose. This is essentially the application of the inverse square law, according to Dr. Kirkwood.
Dr. Farber said that some of the newer, more advanced machines have sensors that automatically detect where the collector should be in relation to the patient, but if your machine doesn’t have these “bells and whistles … remember that the skin dose decreases as the air gap decreases.”
Another advantage to using new imaging systems, according to Dr. Farber, is that they allow the use of pulsed fluoroscopy for as few as 2 or 3 pulses/sec. The selected pulse rate determines the number of fluoroscopic image frames that are generated by the machine per second. This is significant when the dose savings are essential and when performing simpler procedures, he said. “If you go from 7.5 frames down to 3 frames/sec, you can decrease the exposure for both you and your patient.”
Use between 15 and 30 pulses/sec for critical procedures where precision is crucial, but reducing the rate to 7.5 pulses/sec may result in as much as 70% less of a skin dose.
Add radiation barriers
Don’t assume that the lead shielding is doing the job. “It’s important that you keep up on this and have it tested regularly,” said Dr. Farber, who recently discovered his thyroid shield was cracked and needed to be replaced. Also, consider the lead shielding of your staff, which, even if it is not used as frequently as the physician’s, can suffer from improper handling. “They fold it or crinkle it up and drop it on the floor. This can lead to problems,” he said. And be sure to remember leaded glasses, lead drapes for the sides of the table, and leaded ceiling-mounted or standing shields.
For extra protection, Dr. Farber recommended the use of disposable protective drapes with cut-outs that allow access to the patient while helping to reduce the amount of scatter radiation exposure to the operator’s limbs. At a tally of anywhere from 1 to 10 mGy/hour, scatter radiation emanating from the patient is a particular risk to the operator’s legs from the knees down, said Dr. Kirkwood, “depending on how tall you are.”
Using the disposable drapes also can result in a 12-fold decrease in the amount of scatter on the eyes, a 25-fold decrease in thyroid exposure to scatter, and a 29-fold decrease in the hands being exposed. “They can be cumbersome at times, I admit,” Dr. Farber said. “But there is no substitute for using protective drapes.”
Leaded aprons also help cut radiation transmission rates, even if they are not foolproof. Wearing two-piece leaded apron systems can help cut down the body strain from the weight of the aprons; however, Dr. Farber said that, at his institution, they use a suspended body shield system operated by a boom so there is no physical stress on the clinician. Because the weightless system also provides additional protection for the specialist’s head and limbs, Dr. Farber said that the hefty price tag is justified. “The way I sold it to the hospital was I told them I could stop doing procedures, or they could get me one of these systems so I could do more procedures,” he said, adding he is having a weightless system installed on each side of the table. “They’ll get their money’s worth by the fact that you’re not over your exposure limit.”
And finally, don’t forget to protect the anesthesiologist! A standing shield that gives broad coverage area should suffice, Dr. Farber said.
Alter the intensifier position
Altering the angle can help ensure that one area of the patient’s body isn’t being overexposed to radiation. Since previously irradiated skin reacts abnormally when re-exposed to radiation because the regeneration and repair of the dermis can take up to several weeks after the initial insult, the timing of the intervals between exposures is critical, said Dr. Kirkwood, adding that the Joint Commission recommended that all doses of fluoroscopically guided interventions performed within the past 6-12 months should be considered when assessing potential skin injury risk.
Use collimation
Making it tighter, for example, can help improve image quality and reduce the radiation dose to both the patient and the operator, as can varying the acquisition rates.
Exit the room during DSA
During digital subtraction angiography, Dr. Farber said to “get away from the table if you can! It’s a huge dose you don’t need to be exposed to if you don’t need to be right next to the machine.” Dr. Kirkwood agreed: “Angiography is 10-100 times more dose than fluoroscopy.”
Reduce magnification
Using a larger monitor allows the operator to see more detail without increasing the magnification, which also increases the dose in the amount of the diameter over the diameter squared. “By not magnifying up [from a field of view of 14 to 28], you will save yourself a factor of at least 4,” Dr. Farber said. “And the actual dose may be even less.”
Optimize imaging
Today’s advanced imaging systems make it easy to produce many high-quality images – CT scans and ultrasounds – that allow a more comprehensive picture. Having various image sources on screen at once is “practice changing” because it can help clinicians see more possibilities for “how to do the case,” said Dr. Farber. “I’ve never heard anyone say, ’Well, I wish I didn’t have that extra imaging next to me.’ ”
Save images
But once you get it, don’t forget to keep it. “Many times you do an acquisition, you move the machine, and you realize you forget to save the image and now you’ve got to go back and do it all over again,” Dr. Farber lamented. But by once again making technology your friend, with functions that allow auto-return to previous positions, among other auto-commands, you can save the needed information and reduce any unnecessary dose exposure for both yourself and the patient, he said.
Protect your eyes
Cataracts are still all too common in the field, according to Dr. Farber. “It’s important that you have side shields on your glasses to cut down on the amount of radiation that comes in and around the glasses.” Eschew glasses that don’t overtly hug your face.
Geometric differences
Don’t forget that, if you’re standing on the side of the imaging source, the scattering effect will be greater than if you’re on the side of the image receptor. Once again, an understanding of the inverse square law can be protective, according to Dr. Kirkwood: “As x-rays exit the source, there is an exponential decrease in the number of x-rays per unit area as the distance from the source increases.”
“It’s simple stuff,” concluded Dr. Farber. “If you get in the habit of doing these things you will cut down your radiation exposure.”
Neither Dr. Farber nor Dr. Kirkwood had any relevant disclosures.
wmcknight@frontlinemedcom.com On Twitter @whitneymcknight
SCOTTSDALE, Ariz.– “It’s surprising to me today, when I go proctor or watch a case, how people don’t understand the impact of radiation,” Dr. Mark A. Farber, professor of surgery and radiology at the University of North Carolina, Chapel Hill, said at the Southern Association for Vascular Surgery annual meeting. “Many times, I see people’s hands underneath the machine and on the fluoroscopy image.”
This flouting of the so-called ALARA (as low as reasonably achievable) principle happens in part because the number of complex procedures performed by vascular surgeons is increasing, despite what presenter Dr. Melissa Kirkwood, a vascular surgeon at the University of Texas Southwestern Medical Center, Dallas, told the audience is a lack of training in radiation dose terminology and basic safety principles. Yet, practicing excellent radiation safety protocols is “paramount” according to Dr. Farber who, along with Dr. Kirkwood, shared insights on how to minimize dose to both patients and vascular specialists, whether it be from primary, leakage, or scatter radiation.
Table up, detector down
Minimizing the air gap by as little as 100 mm – from 700 mm to 600 mm, for example – can reduce the dose of radiation from 17%-29%, whereas a 10-cm increase in the air gap can result in as much as a 20%-38% increase in the radiation skin dose. This is essentially the application of the inverse square law, according to Dr. Kirkwood.
Dr. Farber said that some of the newer, more advanced machines have sensors that automatically detect where the collector should be in relation to the patient, but if your machine doesn’t have these “bells and whistles … remember that the skin dose decreases as the air gap decreases.”
Another advantage to using new imaging systems, according to Dr. Farber, is that they allow the use of pulsed fluoroscopy for as few as 2 or 3 pulses/sec. The selected pulse rate determines the number of fluoroscopic image frames that are generated by the machine per second. This is significant when the dose savings are essential and when performing simpler procedures, he said. “If you go from 7.5 frames down to 3 frames/sec, you can decrease the exposure for both you and your patient.”
Use between 15 and 30 pulses/sec for critical procedures where precision is crucial, but reducing the rate to 7.5 pulses/sec may result in as much as 70% less of a skin dose.
Add radiation barriers
Don’t assume that the lead shielding is doing the job. “It’s important that you keep up on this and have it tested regularly,” said Dr. Farber, who recently discovered his thyroid shield was cracked and needed to be replaced. Also, consider the lead shielding of your staff, which, even if it is not used as frequently as the physician’s, can suffer from improper handling. “They fold it or crinkle it up and drop it on the floor. This can lead to problems,” he said. And be sure to remember leaded glasses, lead drapes for the sides of the table, and leaded ceiling-mounted or standing shields.
For extra protection, Dr. Farber recommended the use of disposable protective drapes with cut-outs that allow access to the patient while helping to reduce the amount of scatter radiation exposure to the operator’s limbs. At a tally of anywhere from 1 to 10 mGy/hour, scatter radiation emanating from the patient is a particular risk to the operator’s legs from the knees down, said Dr. Kirkwood, “depending on how tall you are.”
Using the disposable drapes also can result in a 12-fold decrease in the amount of scatter on the eyes, a 25-fold decrease in thyroid exposure to scatter, and a 29-fold decrease in the hands being exposed. “They can be cumbersome at times, I admit,” Dr. Farber said. “But there is no substitute for using protective drapes.”
Leaded aprons also help cut radiation transmission rates, even if they are not foolproof. Wearing two-piece leaded apron systems can help cut down the body strain from the weight of the aprons; however, Dr. Farber said that, at his institution, they use a suspended body shield system operated by a boom so there is no physical stress on the clinician. Because the weightless system also provides additional protection for the specialist’s head and limbs, Dr. Farber said that the hefty price tag is justified. “The way I sold it to the hospital was I told them I could stop doing procedures, or they could get me one of these systems so I could do more procedures,” he said, adding he is having a weightless system installed on each side of the table. “They’ll get their money’s worth by the fact that you’re not over your exposure limit.”
And finally, don’t forget to protect the anesthesiologist! A standing shield that gives broad coverage area should suffice, Dr. Farber said.
Alter the intensifier position
Altering the angle can help ensure that one area of the patient’s body isn’t being overexposed to radiation. Since previously irradiated skin reacts abnormally when re-exposed to radiation because the regeneration and repair of the dermis can take up to several weeks after the initial insult, the timing of the intervals between exposures is critical, said Dr. Kirkwood, adding that the Joint Commission recommended that all doses of fluoroscopically guided interventions performed within the past 6-12 months should be considered when assessing potential skin injury risk.
Use collimation
Making it tighter, for example, can help improve image quality and reduce the radiation dose to both the patient and the operator, as can varying the acquisition rates.
Exit the room during DSA
During digital subtraction angiography, Dr. Farber said to “get away from the table if you can! It’s a huge dose you don’t need to be exposed to if you don’t need to be right next to the machine.” Dr. Kirkwood agreed: “Angiography is 10-100 times more dose than fluoroscopy.”
Reduce magnification
Using a larger monitor allows the operator to see more detail without increasing the magnification, which also increases the dose in the amount of the diameter over the diameter squared. “By not magnifying up [from a field of view of 14 to 28], you will save yourself a factor of at least 4,” Dr. Farber said. “And the actual dose may be even less.”
Optimize imaging
Today’s advanced imaging systems make it easy to produce many high-quality images – CT scans and ultrasounds – that allow a more comprehensive picture. Having various image sources on screen at once is “practice changing” because it can help clinicians see more possibilities for “how to do the case,” said Dr. Farber. “I’ve never heard anyone say, ’Well, I wish I didn’t have that extra imaging next to me.’ ”
Save images
But once you get it, don’t forget to keep it. “Many times you do an acquisition, you move the machine, and you realize you forget to save the image and now you’ve got to go back and do it all over again,” Dr. Farber lamented. But by once again making technology your friend, with functions that allow auto-return to previous positions, among other auto-commands, you can save the needed information and reduce any unnecessary dose exposure for both yourself and the patient, he said.
Protect your eyes
Cataracts are still all too common in the field, according to Dr. Farber. “It’s important that you have side shields on your glasses to cut down on the amount of radiation that comes in and around the glasses.” Eschew glasses that don’t overtly hug your face.
Geometric differences
Don’t forget that, if you’re standing on the side of the imaging source, the scattering effect will be greater than if you’re on the side of the image receptor. Once again, an understanding of the inverse square law can be protective, according to Dr. Kirkwood: “As x-rays exit the source, there is an exponential decrease in the number of x-rays per unit area as the distance from the source increases.”
“It’s simple stuff,” concluded Dr. Farber. “If you get in the habit of doing these things you will cut down your radiation exposure.”
Neither Dr. Farber nor Dr. Kirkwood had any relevant disclosures.
wmcknight@frontlinemedcom.com On Twitter @whitneymcknight

Much Ado about Hospital Quality
I have reported previously on major incentive programs under Medicare and the Affordable Care Act that affect hospitals and, by extension, their affiliated hospitalists. I’d like to provide you with an update on these programs. The bad news is that hospitals have more revenue than ever that is at risk based on performance. The good news is that such risk, and its mitigation, centers on performance measures in the sweet spot of hospitalists and the teams they work with to improve patient care.

Hospital-Acquired Conditions
On Dec. 17, 2014, the Centers for Medicare and Medicaid Services (CMS) announced that 724 U.S. hospitals—the lowest quartile—will have 1% of their reimbursement docked effective Oct. 1, 2014, as part of the Hospital-Acquired Condition Reduction Program (HACRP). The HACRP is divided into the following domains:
- 35%, Agency for Healthcare Research and Quality Patient Safety Indicators (PSI-90). This is a composite of eight claims-based harm measures.
- 65%, CDC National Health Safety Network measures. These are clinically derived metrics, currently central line-associated blood stream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI).
The HACRP program, which debuted in October 2014, will continue at least through 2020. The 65% weight domain will change in FY16 with the addition of surgical site infections (colon, hysterectomy) and in FY17 with the addition of MRSA and Clostridium difficile infections.
The full list of U.S. hospitals and their performance in the HACRP and the Hospital Value-Based Purchasing (VBP) program is available at www.modernhealthcare.com/article/20141108/INFO/141109959.
Just two weeks prior to the CMS announcement, AHRQ announced some major accomplishments in efforts to address patient safety at U.S. hospitals. The agency reported that the number of hospital-acquired conditions in the Partnership for Patients (PfP) program in the U.S. declined 9% over a one-year period (2012 to 2013) and 17% over a three-year period (2010 to 2013). Hospital-acquired conditions are defined somewhat differently in the PfP than in the HACRP, with PfP targeting certain hospital-acquired infections, pressure ulcers, falls, and adverse drug effects.
The report noted that reductions in adverse drug events and pressure ulcers were the largest contributors to a reported 50,000 fewer in-hospital deaths over the 2010-2013 period.
Hospital Value-Based Purchasing
The Hospital VBP program continues to evolve. See Table 1 for a breakdown of the program for the next two years.
Unlike the HACRP and the Hospital Readmissions Reduction Program, which are pure penalty programs, VBP has hospitals at risk for 1.5% (for 2015) of Medicare payments, but they may earn back some, all, or an amount in excess of the 1.5% based on performance. For the years noted above, the VBP program metrics are as follows:
- Clinical Process: selected heart failure (HF), pneumonia (PN), myocardial infarction (MI), and surgical care measures.
- Patient Experience: a subset of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey questions.
- Outcomes: HF, PN, MI, 30-day mortality, CLABSI, and PSI-90.
- Efficiency: Medicare spending per beneficiary (spending from three days prior to an inpatient hospital admission through 30 days after discharge)
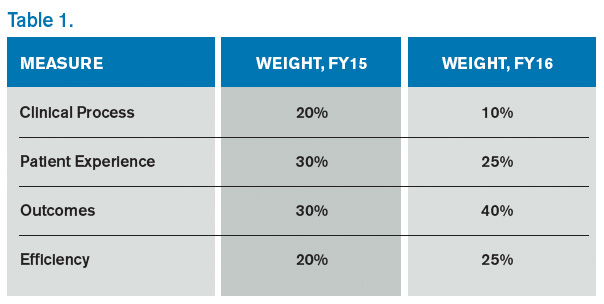
Readmission Penalties
CMS announced that in the latest round of the Hospital Readmissions Reduction Program, 2,610 hospitals were penalized in total, while 39 hospitals will receive the largest penalty allowed. For FY15, the program added chronic obstructive pulmonary disease and hip and knee arthroplasty to HF, PN, and MI as the conditions counting toward excess readmissions.
For FY15, the number of hospitals penalized and the amount of the penalty are expected to increase. In addition, 1% of hospitals are anticipated to receive the maximum penalty, while 77% are expected to have some penalty, and 22% will likely have no penalty. The maximum penalty has topped out at 3% of Medicare inpatient payments.
HCAHPS Star Ratings
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures. The initial ratings will be based on discharges during the period ranging from July 2013 through June 2014.
What’s a Hospitalist to Do?
The latest version of CMS incentive programs should serve to reinforce your hospital medicine group’s strategy to be agents of collaboration and change. Link up with your quality department to align priorities, and make sure you have hospitalist representatives on key patient safety, patient experience, and quality improvement committees.
Because dollars are at stake for your hospital, have a clear understanding of the value your hospitalist group brings to the table, so you can secure the appropriate financial support for the time and work expended on these initiatives.
And don’t forget to keep the patient at the center of your efforts.

I have reported previously on major incentive programs under Medicare and the Affordable Care Act that affect hospitals and, by extension, their affiliated hospitalists. I’d like to provide you with an update on these programs. The bad news is that hospitals have more revenue than ever that is at risk based on performance. The good news is that such risk, and its mitigation, centers on performance measures in the sweet spot of hospitalists and the teams they work with to improve patient care.
Hospital-Acquired Conditions
On Dec. 17, 2014, the Centers for Medicare and Medicaid Services (CMS) announced that 724 U.S. hospitals—the lowest quartile—will have 1% of their reimbursement docked effective Oct. 1, 2014, as part of the Hospital-Acquired Condition Reduction Program (HACRP). The HACRP is divided into the following domains:
- 35%, Agency for Healthcare Research and Quality Patient Safety Indicators (PSI-90). This is a composite of eight claims-based harm measures.
- 65%, CDC National Health Safety Network measures. These are clinically derived metrics, currently central line-associated blood stream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI).
The HACRP program, which debuted in October 2014, will continue at least through 2020. The 65% weight domain will change in FY16 with the addition of surgical site infections (colon, hysterectomy) and in FY17 with the addition of MRSA and Clostridium difficile infections.
The full list of U.S. hospitals and their performance in the HACRP and the Hospital Value-Based Purchasing (VBP) program is available at www.modernhealthcare.com/article/20141108/INFO/141109959.
Just two weeks prior to the CMS announcement, AHRQ announced some major accomplishments in efforts to address patient safety at U.S. hospitals. The agency reported that the number of hospital-acquired conditions in the Partnership for Patients (PfP) program in the U.S. declined 9% over a one-year period (2012 to 2013) and 17% over a three-year period (2010 to 2013). Hospital-acquired conditions are defined somewhat differently in the PfP than in the HACRP, with PfP targeting certain hospital-acquired infections, pressure ulcers, falls, and adverse drug effects.
The report noted that reductions in adverse drug events and pressure ulcers were the largest contributors to a reported 50,000 fewer in-hospital deaths over the 2010-2013 period.
Hospital Value-Based Purchasing
The Hospital VBP program continues to evolve. See Table 1 for a breakdown of the program for the next two years.
Unlike the HACRP and the Hospital Readmissions Reduction Program, which are pure penalty programs, VBP has hospitals at risk for 1.5% (for 2015) of Medicare payments, but they may earn back some, all, or an amount in excess of the 1.5% based on performance. For the years noted above, the VBP program metrics are as follows:
- Clinical Process: selected heart failure (HF), pneumonia (PN), myocardial infarction (MI), and surgical care measures.
- Patient Experience: a subset of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey questions.
- Outcomes: HF, PN, MI, 30-day mortality, CLABSI, and PSI-90.
- Efficiency: Medicare spending per beneficiary (spending from three days prior to an inpatient hospital admission through 30 days after discharge)
Readmission Penalties
CMS announced that in the latest round of the Hospital Readmissions Reduction Program, 2,610 hospitals were penalized in total, while 39 hospitals will receive the largest penalty allowed. For FY15, the program added chronic obstructive pulmonary disease and hip and knee arthroplasty to HF, PN, and MI as the conditions counting toward excess readmissions.
For FY15, the number of hospitals penalized and the amount of the penalty are expected to increase. In addition, 1% of hospitals are anticipated to receive the maximum penalty, while 77% are expected to have some penalty, and 22% will likely have no penalty. The maximum penalty has topped out at 3% of Medicare inpatient payments.
HCAHPS Star Ratings
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures. The initial ratings will be based on discharges during the period ranging from July 2013 through June 2014.
What’s a Hospitalist to Do?
The latest version of CMS incentive programs should serve to reinforce your hospital medicine group’s strategy to be agents of collaboration and change. Link up with your quality department to align priorities, and make sure you have hospitalist representatives on key patient safety, patient experience, and quality improvement committees.
Because dollars are at stake for your hospital, have a clear understanding of the value your hospitalist group brings to the table, so you can secure the appropriate financial support for the time and work expended on these initiatives.
And don’t forget to keep the patient at the center of your efforts.
I have reported previously on major incentive programs under Medicare and the Affordable Care Act that affect hospitals and, by extension, their affiliated hospitalists. I’d like to provide you with an update on these programs. The bad news is that hospitals have more revenue than ever that is at risk based on performance. The good news is that such risk, and its mitigation, centers on performance measures in the sweet spot of hospitalists and the teams they work with to improve patient care.
Hospital-Acquired Conditions
On Dec. 17, 2014, the Centers for Medicare and Medicaid Services (CMS) announced that 724 U.S. hospitals—the lowest quartile—will have 1% of their reimbursement docked effective Oct. 1, 2014, as part of the Hospital-Acquired Condition Reduction Program (HACRP). The HACRP is divided into the following domains:
- 35%, Agency for Healthcare Research and Quality Patient Safety Indicators (PSI-90). This is a composite of eight claims-based harm measures.
- 65%, CDC National Health Safety Network measures. These are clinically derived metrics, currently central line-associated blood stream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI).
The HACRP program, which debuted in October 2014, will continue at least through 2020. The 65% weight domain will change in FY16 with the addition of surgical site infections (colon, hysterectomy) and in FY17 with the addition of MRSA and Clostridium difficile infections.
The full list of U.S. hospitals and their performance in the HACRP and the Hospital Value-Based Purchasing (VBP) program is available at www.modernhealthcare.com/article/20141108/INFO/141109959.
Just two weeks prior to the CMS announcement, AHRQ announced some major accomplishments in efforts to address patient safety at U.S. hospitals. The agency reported that the number of hospital-acquired conditions in the Partnership for Patients (PfP) program in the U.S. declined 9% over a one-year period (2012 to 2013) and 17% over a three-year period (2010 to 2013). Hospital-acquired conditions are defined somewhat differently in the PfP than in the HACRP, with PfP targeting certain hospital-acquired infections, pressure ulcers, falls, and adverse drug effects.
The report noted that reductions in adverse drug events and pressure ulcers were the largest contributors to a reported 50,000 fewer in-hospital deaths over the 2010-2013 period.
Hospital Value-Based Purchasing
The Hospital VBP program continues to evolve. See Table 1 for a breakdown of the program for the next two years.
Unlike the HACRP and the Hospital Readmissions Reduction Program, which are pure penalty programs, VBP has hospitals at risk for 1.5% (for 2015) of Medicare payments, but they may earn back some, all, or an amount in excess of the 1.5% based on performance. For the years noted above, the VBP program metrics are as follows:
- Clinical Process: selected heart failure (HF), pneumonia (PN), myocardial infarction (MI), and surgical care measures.
- Patient Experience: a subset of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey questions.
- Outcomes: HF, PN, MI, 30-day mortality, CLABSI, and PSI-90.
- Efficiency: Medicare spending per beneficiary (spending from three days prior to an inpatient hospital admission through 30 days after discharge)
Readmission Penalties
CMS announced that in the latest round of the Hospital Readmissions Reduction Program, 2,610 hospitals were penalized in total, while 39 hospitals will receive the largest penalty allowed. For FY15, the program added chronic obstructive pulmonary disease and hip and knee arthroplasty to HF, PN, and MI as the conditions counting toward excess readmissions.
For FY15, the number of hospitals penalized and the amount of the penalty are expected to increase. In addition, 1% of hospitals are anticipated to receive the maximum penalty, while 77% are expected to have some penalty, and 22% will likely have no penalty. The maximum penalty has topped out at 3% of Medicare inpatient payments.
HCAHPS Star Ratings
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures. The initial ratings will be based on discharges during the period ranging from July 2013 through June 2014.
What’s a Hospitalist to Do?
The latest version of CMS incentive programs should serve to reinforce your hospital medicine group’s strategy to be agents of collaboration and change. Link up with your quality department to align priorities, and make sure you have hospitalist representatives on key patient safety, patient experience, and quality improvement committees.
Because dollars are at stake for your hospital, have a clear understanding of the value your hospitalist group brings to the table, so you can secure the appropriate financial support for the time and work expended on these initiatives.
And don’t forget to keep the patient at the center of your efforts.
How to Use Hospitalist Productivity, Compensation Survey Data
The 2014 State of Hospital Medicine report (SOHM), published by SHM in the fall of even years, is unquestionably the most robust and informative data available to understand the hospitalist workforce marketplace. And if you are the person who returned a completed survey for your practice, you get a free copy of the report mailed to you.
Keep in mind that the Medical Group Management Association (MGMA) surveys and reports data on hospitalist productivity and compensation every year. And the data acquired by MGMA in even years is simply folded into the SOHM, along with a ton of additional information added by a separate SHM survey, including things like the amount of financial support provided to hospitalist groups by hospitals (now up to a median of $156, 063 per full-time equivalent, or FTE).
I’ve written previously about some of the ways that the data reported in both of these surveys can be tricky to interpret (September 2013 and October 2013), and in this column I’ll go a little deeper into how to use the data reported on number of shifts worked and productivity.
A Common Question
Assume that, to address a staffing shortage or simply as a way to boost their income, some of the doctors in your group are willing to work more shifts than required for full-time status. And, in your group, some portion of a doctor’s compensation is a function of their individual work relevant value unit (wRVU) productivity—for example, a bonus for wRVUs above a certain threshold. You want to know whether the wRVU productivity generated by a doctor on their extra shifts should factor into compensation the same way it does for “regular” shifts.
You might turn to the MGMA and SOHM surveys to see how other groups handle this issue. But here is where it gets tricky.
First, you need to realize that the MGMA surveys, and similar ones from the American Medical Group Association and others, report wRVUs and compensation per physician, not per FTE. So wRVUs generated by these doctors on extra shifts are included, and you can’t tell from the aggregate data what portion of wRVUs came from regular shifts and what portion came from extra shifts.
And it is critical to keep in mind that any doctor who works at least 0.8 FTE as defined by that particular practice is reported as full time. Those working 79% or less of full time are counted by MGMA as part time.
To summarize: The MGMA and similar surveys don’t provide data on wRVU productivity per FTE, even though in most cases that is how everyone describes the data. Instead, the surveys provide data per individual doctor, many of whom work more or less than 1.0 FTE. So, despite the fact that most people, including me, tend to quote data from the surveys as though it is per FTE, as in “The 2014 MGMA data shows median hospitalist compensation is $253,977 per FTE,” we should say “per doctor” instead.
Theoretically, doctors working slightly less than 1.0 FTE should offset the doctors working slightly more than 1.0 FTE. But, while I think that’s a reasonable assumption for most specialties, such a significant portion of hospitalist groups have had chronic staffing shortages that a lot of hospitalists across the country are working extra shifts, probably more than are working between 0.8 and 1.0 FTE. So the hospitalist survey wRVU data is probably at least a little higher than it would be if it were reported per FTE.
Unfortunately, there is no way to confirm my suspicion, because MGMA doesn’t allow any individual doctor to be reported as more than 1.0 FTE, even if he works far more shifts than the number that defines full time for that practice. In other words, extra shifts just aren’t accounted for in the MGMA survey.
Implications of Individual vs. FTE
For most purposes, it probably doesn’t make any difference if you are erroneously thinking about the compensation and productivity survey numbers on a per FTE basis. But, for some purposes, and for those who work significantly more shifts than most hospitalists, it can start to matter.
Now back to the original question. You’re thinking about whether wRVUs generated by the doctors in your group on extra shifts should count toward the wRVU bonus just like those generated on regular shifts. You’d like to handle this the same way as other groups, but, unfortunately, survey data just isn’t helpful here. You’ll have to decide this for yourself.
I think some, but probably not all, extra shift productivity should count toward your wRVU bonus. You might, for example, say that productivity for somewhere between three or five extra shifts per quarter—that’s totally arbitrary, and of course this would be a negotiation between you and hospital leadership—should count toward the productivity target, and the rest wouldn’t, or that those extra shifts above an agreed-upon number would result in an increase in the wRVU target. The biggest problem with this is that it would be a nightmare to administer—essentially impossible for many practices. But you could accomplish the same thing by including the first few shifts per quarter in the “base” FTE calculation and then, after that, adjusting each person’s FTE value up as they work more shifts.
One more thing about productivity targets…
It’s also important to remember that productivity targets make the most sense at the group—not the individual—level. The MGMA data includes hospitalists who work night shifts (including nocturnists) and doctors who work low-production shifts (i.e., pager or ED triage shifts), as well as daytime rounding doctors. So, if you have a doctor who only works days, you would expect him to generate wRVUs in excess of the global target of wRVUs per FTE to make up for the low-productivity shifts that other doctors have to work.
For example, your practice might decide the group as a whole is expected to generate the MGMA yearly median 4,298 wRVUs per doctor, multiplied by the number of FTEs in the group. But the nocturnists would be expected to generate fewer, while those who work most or all of their shifts in a daytime rounder would be expected to generate more. So the threshold to begin paying the wRVU bonus for daytime rounding doctors might be adjusted up to something like 4,500 wRVUs.
The above example is just as an illustration, of course, and there are all kinds of reasons it might be more appropriate to choose different thresholds for your practice. But it’s a good place to start the thinking.

The 2014 State of Hospital Medicine report (SOHM), published by SHM in the fall of even years, is unquestionably the most robust and informative data available to understand the hospitalist workforce marketplace. And if you are the person who returned a completed survey for your practice, you get a free copy of the report mailed to you.
Keep in mind that the Medical Group Management Association (MGMA) surveys and reports data on hospitalist productivity and compensation every year. And the data acquired by MGMA in even years is simply folded into the SOHM, along with a ton of additional information added by a separate SHM survey, including things like the amount of financial support provided to hospitalist groups by hospitals (now up to a median of $156, 063 per full-time equivalent, or FTE).
I’ve written previously about some of the ways that the data reported in both of these surveys can be tricky to interpret (September 2013 and October 2013), and in this column I’ll go a little deeper into how to use the data reported on number of shifts worked and productivity.
A Common Question
Assume that, to address a staffing shortage or simply as a way to boost their income, some of the doctors in your group are willing to work more shifts than required for full-time status. And, in your group, some portion of a doctor’s compensation is a function of their individual work relevant value unit (wRVU) productivity—for example, a bonus for wRVUs above a certain threshold. You want to know whether the wRVU productivity generated by a doctor on their extra shifts should factor into compensation the same way it does for “regular” shifts.
You might turn to the MGMA and SOHM surveys to see how other groups handle this issue. But here is where it gets tricky.
First, you need to realize that the MGMA surveys, and similar ones from the American Medical Group Association and others, report wRVUs and compensation per physician, not per FTE. So wRVUs generated by these doctors on extra shifts are included, and you can’t tell from the aggregate data what portion of wRVUs came from regular shifts and what portion came from extra shifts.
And it is critical to keep in mind that any doctor who works at least 0.8 FTE as defined by that particular practice is reported as full time. Those working 79% or less of full time are counted by MGMA as part time.
To summarize: The MGMA and similar surveys don’t provide data on wRVU productivity per FTE, even though in most cases that is how everyone describes the data. Instead, the surveys provide data per individual doctor, many of whom work more or less than 1.0 FTE. So, despite the fact that most people, including me, tend to quote data from the surveys as though it is per FTE, as in “The 2014 MGMA data shows median hospitalist compensation is $253,977 per FTE,” we should say “per doctor” instead.
Theoretically, doctors working slightly less than 1.0 FTE should offset the doctors working slightly more than 1.0 FTE. But, while I think that’s a reasonable assumption for most specialties, such a significant portion of hospitalist groups have had chronic staffing shortages that a lot of hospitalists across the country are working extra shifts, probably more than are working between 0.8 and 1.0 FTE. So the hospitalist survey wRVU data is probably at least a little higher than it would be if it were reported per FTE.
Unfortunately, there is no way to confirm my suspicion, because MGMA doesn’t allow any individual doctor to be reported as more than 1.0 FTE, even if he works far more shifts than the number that defines full time for that practice. In other words, extra shifts just aren’t accounted for in the MGMA survey.
Implications of Individual vs. FTE
For most purposes, it probably doesn’t make any difference if you are erroneously thinking about the compensation and productivity survey numbers on a per FTE basis. But, for some purposes, and for those who work significantly more shifts than most hospitalists, it can start to matter.
Now back to the original question. You’re thinking about whether wRVUs generated by the doctors in your group on extra shifts should count toward the wRVU bonus just like those generated on regular shifts. You’d like to handle this the same way as other groups, but, unfortunately, survey data just isn’t helpful here. You’ll have to decide this for yourself.
I think some, but probably not all, extra shift productivity should count toward your wRVU bonus. You might, for example, say that productivity for somewhere between three or five extra shifts per quarter—that’s totally arbitrary, and of course this would be a negotiation between you and hospital leadership—should count toward the productivity target, and the rest wouldn’t, or that those extra shifts above an agreed-upon number would result in an increase in the wRVU target. The biggest problem with this is that it would be a nightmare to administer—essentially impossible for many practices. But you could accomplish the same thing by including the first few shifts per quarter in the “base” FTE calculation and then, after that, adjusting each person’s FTE value up as they work more shifts.
One more thing about productivity targets…
It’s also important to remember that productivity targets make the most sense at the group—not the individual—level. The MGMA data includes hospitalists who work night shifts (including nocturnists) and doctors who work low-production shifts (i.e., pager or ED triage shifts), as well as daytime rounding doctors. So, if you have a doctor who only works days, you would expect him to generate wRVUs in excess of the global target of wRVUs per FTE to make up for the low-productivity shifts that other doctors have to work.
For example, your practice might decide the group as a whole is expected to generate the MGMA yearly median 4,298 wRVUs per doctor, multiplied by the number of FTEs in the group. But the nocturnists would be expected to generate fewer, while those who work most or all of their shifts in a daytime rounder would be expected to generate more. So the threshold to begin paying the wRVU bonus for daytime rounding doctors might be adjusted up to something like 4,500 wRVUs.
The above example is just as an illustration, of course, and there are all kinds of reasons it might be more appropriate to choose different thresholds for your practice. But it’s a good place to start the thinking.
The 2014 State of Hospital Medicine report (SOHM), published by SHM in the fall of even years, is unquestionably the most robust and informative data available to understand the hospitalist workforce marketplace. And if you are the person who returned a completed survey for your practice, you get a free copy of the report mailed to you.
Keep in mind that the Medical Group Management Association (MGMA) surveys and reports data on hospitalist productivity and compensation every year. And the data acquired by MGMA in even years is simply folded into the SOHM, along with a ton of additional information added by a separate SHM survey, including things like the amount of financial support provided to hospitalist groups by hospitals (now up to a median of $156, 063 per full-time equivalent, or FTE).
I’ve written previously about some of the ways that the data reported in both of these surveys can be tricky to interpret (September 2013 and October 2013), and in this column I’ll go a little deeper into how to use the data reported on number of shifts worked and productivity.
A Common Question
Assume that, to address a staffing shortage or simply as a way to boost their income, some of the doctors in your group are willing to work more shifts than required for full-time status. And, in your group, some portion of a doctor’s compensation is a function of their individual work relevant value unit (wRVU) productivity—for example, a bonus for wRVUs above a certain threshold. You want to know whether the wRVU productivity generated by a doctor on their extra shifts should factor into compensation the same way it does for “regular” shifts.
You might turn to the MGMA and SOHM surveys to see how other groups handle this issue. But here is where it gets tricky.
First, you need to realize that the MGMA surveys, and similar ones from the American Medical Group Association and others, report wRVUs and compensation per physician, not per FTE. So wRVUs generated by these doctors on extra shifts are included, and you can’t tell from the aggregate data what portion of wRVUs came from regular shifts and what portion came from extra shifts.
And it is critical to keep in mind that any doctor who works at least 0.8 FTE as defined by that particular practice is reported as full time. Those working 79% or less of full time are counted by MGMA as part time.
To summarize: The MGMA and similar surveys don’t provide data on wRVU productivity per FTE, even though in most cases that is how everyone describes the data. Instead, the surveys provide data per individual doctor, many of whom work more or less than 1.0 FTE. So, despite the fact that most people, including me, tend to quote data from the surveys as though it is per FTE, as in “The 2014 MGMA data shows median hospitalist compensation is $253,977 per FTE,” we should say “per doctor” instead.
Theoretically, doctors working slightly less than 1.0 FTE should offset the doctors working slightly more than 1.0 FTE. But, while I think that’s a reasonable assumption for most specialties, such a significant portion of hospitalist groups have had chronic staffing shortages that a lot of hospitalists across the country are working extra shifts, probably more than are working between 0.8 and 1.0 FTE. So the hospitalist survey wRVU data is probably at least a little higher than it would be if it were reported per FTE.
Unfortunately, there is no way to confirm my suspicion, because MGMA doesn’t allow any individual doctor to be reported as more than 1.0 FTE, even if he works far more shifts than the number that defines full time for that practice. In other words, extra shifts just aren’t accounted for in the MGMA survey.
Implications of Individual vs. FTE
For most purposes, it probably doesn’t make any difference if you are erroneously thinking about the compensation and productivity survey numbers on a per FTE basis. But, for some purposes, and for those who work significantly more shifts than most hospitalists, it can start to matter.
Now back to the original question. You’re thinking about whether wRVUs generated by the doctors in your group on extra shifts should count toward the wRVU bonus just like those generated on regular shifts. You’d like to handle this the same way as other groups, but, unfortunately, survey data just isn’t helpful here. You’ll have to decide this for yourself.
I think some, but probably not all, extra shift productivity should count toward your wRVU bonus. You might, for example, say that productivity for somewhere between three or five extra shifts per quarter—that’s totally arbitrary, and of course this would be a negotiation between you and hospital leadership—should count toward the productivity target, and the rest wouldn’t, or that those extra shifts above an agreed-upon number would result in an increase in the wRVU target. The biggest problem with this is that it would be a nightmare to administer—essentially impossible for many practices. But you could accomplish the same thing by including the first few shifts per quarter in the “base” FTE calculation and then, after that, adjusting each person’s FTE value up as they work more shifts.
One more thing about productivity targets…
It’s also important to remember that productivity targets make the most sense at the group—not the individual—level. The MGMA data includes hospitalists who work night shifts (including nocturnists) and doctors who work low-production shifts (i.e., pager or ED triage shifts), as well as daytime rounding doctors. So, if you have a doctor who only works days, you would expect him to generate wRVUs in excess of the global target of wRVUs per FTE to make up for the low-productivity shifts that other doctors have to work.
For example, your practice might decide the group as a whole is expected to generate the MGMA yearly median 4,298 wRVUs per doctor, multiplied by the number of FTEs in the group. But the nocturnists would be expected to generate fewer, while those who work most or all of their shifts in a daytime rounder would be expected to generate more. So the threshold to begin paying the wRVU bonus for daytime rounding doctors might be adjusted up to something like 4,500 wRVUs.
The above example is just as an illustration, of course, and there are all kinds of reasons it might be more appropriate to choose different thresholds for your practice. But it’s a good place to start the thinking.
Curbside Consult: A new column for Clinical Psychiatry News
We are pleased to introduce Curbside Consult with the Group for the Advancement of Psychiatry's (GAP) Family and Cultural committees. The column is inspired by the DSM-5's emphasis on developing a cultural formulation of patients' illnesses and addressing family dynamics and resilience in promoting care that fosters prevention and recovery.
What is GAP?
GAP was formed in 1946 under the leadership of Dr. William Menninger by a group of young psychiatrists who had served in World War II. They returned to the United States to find an inadequate system of civilian care. They were eager to professionalize the field and collaboratively develop new and creative thinking. They developed an organization that met as a whole twice a year, organized into committees of particular interest to the members and crucial to the needs of psychiatric care. The committees wrote monographs that formed a crucial role in the development of modern psychiatric thought.
Mission of GAP
- Bring together top psychiatrists of all disciplines
- Offer an objective, critical perspective on current issues facing psychiatry
- Develop smart analysis and recommendations
- Shape psychiatric thinking, clinical practice, and mental health programs
- Advocate for necessary changes in the psychiatric field
- Inspire the next generation of leading psychiatric thinkers
The Family and Cultural Psychiatry committees want to focus psychiatrists on the resilience inherent in the families and cultures of our patients in order to promote psychiatric care that focuses on prevention and recovery.

The Family and Cultural Psychiatry committees see every patient as connected to family members and belonging to a network of cultures that might include their national origin, race/ethnicity, religion/spirituality, language, occupation, age, sexual orientation and gender identity, or any other element of the person's background and collective life.
Over time, these family and cultural influences have shaped all aspects of the person’s response to adversity, experience of illness, and expectations of help seeking, even among patients who are currently living alone or do not recognize their background as explicitly cultural. This influence is highly individual; each person has his/her own combination of family and cultural experiences. How does the psychiatrist access this experience and use it to help develop resilience in our patients? How do we encourage them to use strengths/support from their family and culture, and to identify narratives that are helpful?
We see this column as one way to help answer these questions. We will bring to bear both family and cultural perspectives on the care of patients in everyday clinical practice through our comments on case vignettes sent in by readers. It can be challenging to integrate an understanding of family and culture into each patient encounter.

Our committees will work together to develop a coherent response that integrates both family and cultural perspectives and can be applied in real-world patient situations by clinicians who might not have access to specialized consultation. We aim to contribute to the growing awareness in our field of the cultural complexity of our patients, as developed and transmitted in the nexus of their families, which requires from us as clinicians a more inclusive and holistic approach to care.
This column helps to meet the goals of accreditation bodies such as The Joint Commission and the Accreditation Council for Graduate Medical Education (ACGME) for cultural and linguistic competence and patient- and family-centered care. Understanding how to think about, assess, and engage in treatment with the diversity of our patients’ cultural and family backgrounds constitutes important educational topics for all psychiatric trainees. In conjunction with formal didactics, these cases can be used as a focus for discussion in psychiatric residency training programs, ACGME Clinical Learning Environment Review (CLER), health care quality improvement activities, and faculty development programs.

Practicing clinicians also will find the DSM-5 Outline for Cultural Formulation and Cultural Formulation Interview to be a helpful clinical tool for eliciting and organizing cultural information, and in differential diagnosis and treatment planning.
The following is a list of the guiding principles we will use for assessment:
1. Heterogeneity and diversity exists within all families, cultures, and societies.
2. Avoid stereotyping, essentializing, and overgeneralizing.
3. Individualize and tailor diagnostic assessment, treatment, and care.
4. Address any language access barriers through the use of qualified medical interpreters and appropriately translated educational and informational materials.
5. Employ plain language in communicating with patients with limited health and mental health literacy.
6. Recognize the impact on both the patient and the clinician of our families of origin.
7. Engage in reflective, mindful practice and attend to cultural countertransference to provide insight into one’s own values, beliefs, and behaviors.
8. Cultivate cultural humility – the realization that our understanding of the other person’s background is always limited and incomplete.
9. Every encounter is a cross-cultural one.
10. Developing cultural competence is a lifelong journey and not a final destination.
Guidelines for Case Submission

We are requesting that you submit cases to cpnews@frontlinemedcom.com in which your understanding and treatment are affected by challenging cultural and family issues. We will then write back with our best answers about how one might proceed in such a case. Your case and our response will be published in Clinical Psychiatry News. Please limit your case description to 250 words and please include the following details:
1. Patient’s presenting problem or reason for the visit.
2. Patient’s age and gender.
3. Indicators of the patient’s identity – self-identified race/ethnicity, culture, religion/spirituality, socioeconomic status, education, among other variables.
4. Patient’s living situation, family composition, and genogram information (if available).
5. Patient’s geographic location (rural, suburban, urban) and occupation.
6. Patient’s and family’s degree of participation in their identified culture.
7. Questions of the individual submitting the case, including concerns about the role of the family and culture in the case, diagnosis, and treatment planning.
8. Please follow local ethical requirements, disguise the case to protect confidentiality and attend to HIPAA requirements, so that patients or family members reading the article would not recognize themselves.
Additional information might be requested, and editing of the case, questions, and commentary might be needed prior to final publication.
Please note that the opinions expressed in the case commentaries should not be seen as formal medical consultations and do not represent the opinions of GAP, CPN, or the institutions where the authors are employed or with which they are affiliated.
Contributors:
Michael S. Ascher, M.D. – University of Pennsylvania, Perelman School of Medicine
Alison M. Heru, M.D. – University of Colorado at Denver, Aurora
Roberto Lewis-Fernández, M.D. – Columbia University and New York State Psychiatric Institute
Robert C. Like, M.D., M.S. – Rutgers University, Robert Wood Johnson Medical School
Resources:
DSM-5 – Outline for Cultural Formulation and Cultural Formulation Interview: http://www.psychiatry.org/practice/dsm/dsm5/online-assessment-measures#Cultural
Clinical Manual of Couples and Family Therapy, Washington: American Psychiatric Publishing Inc., 2009.
Thinking Through Cultures: Expeditions in Cultural Psychology. Cambridge, Mass.: Harvard University Press, 1991.
Clinical Manual of Cultural Psychiatry, 2nd Edition, Washington: American Psychiatric Publishing Inc., 2015.
We are pleased to introduce Curbside Consult with the Group for the Advancement of Psychiatry's (GAP) Family and Cultural committees. The column is inspired by the DSM-5's emphasis on developing a cultural formulation of patients' illnesses and addressing family dynamics and resilience in promoting care that fosters prevention and recovery.
What is GAP?
GAP was formed in 1946 under the leadership of Dr. William Menninger by a group of young psychiatrists who had served in World War II. They returned to the United States to find an inadequate system of civilian care. They were eager to professionalize the field and collaboratively develop new and creative thinking. They developed an organization that met as a whole twice a year, organized into committees of particular interest to the members and crucial to the needs of psychiatric care. The committees wrote monographs that formed a crucial role in the development of modern psychiatric thought.
Mission of GAP
- Bring together top psychiatrists of all disciplines
- Offer an objective, critical perspective on current issues facing psychiatry
- Develop smart analysis and recommendations
- Shape psychiatric thinking, clinical practice, and mental health programs
- Advocate for necessary changes in the psychiatric field
- Inspire the next generation of leading psychiatric thinkers
The Family and Cultural Psychiatry committees want to focus psychiatrists on the resilience inherent in the families and cultures of our patients in order to promote psychiatric care that focuses on prevention and recovery.
The Family and Cultural Psychiatry committees see every patient as connected to family members and belonging to a network of cultures that might include their national origin, race/ethnicity, religion/spirituality, language, occupation, age, sexual orientation and gender identity, or any other element of the person's background and collective life.
Over time, these family and cultural influences have shaped all aspects of the person’s response to adversity, experience of illness, and expectations of help seeking, even among patients who are currently living alone or do not recognize their background as explicitly cultural. This influence is highly individual; each person has his/her own combination of family and cultural experiences. How does the psychiatrist access this experience and use it to help develop resilience in our patients? How do we encourage them to use strengths/support from their family and culture, and to identify narratives that are helpful?
We see this column as one way to help answer these questions. We will bring to bear both family and cultural perspectives on the care of patients in everyday clinical practice through our comments on case vignettes sent in by readers. It can be challenging to integrate an understanding of family and culture into each patient encounter.
Our committees will work together to develop a coherent response that integrates both family and cultural perspectives and can be applied in real-world patient situations by clinicians who might not have access to specialized consultation. We aim to contribute to the growing awareness in our field of the cultural complexity of our patients, as developed and transmitted in the nexus of their families, which requires from us as clinicians a more inclusive and holistic approach to care.
This column helps to meet the goals of accreditation bodies such as The Joint Commission and the Accreditation Council for Graduate Medical Education (ACGME) for cultural and linguistic competence and patient- and family-centered care. Understanding how to think about, assess, and engage in treatment with the diversity of our patients’ cultural and family backgrounds constitutes important educational topics for all psychiatric trainees. In conjunction with formal didactics, these cases can be used as a focus for discussion in psychiatric residency training programs, ACGME Clinical Learning Environment Review (CLER), health care quality improvement activities, and faculty development programs.
Practicing clinicians also will find the DSM-5 Outline for Cultural Formulation and Cultural Formulation Interview to be a helpful clinical tool for eliciting and organizing cultural information, and in differential diagnosis and treatment planning.
The following is a list of the guiding principles we will use for assessment:
1. Heterogeneity and diversity exists within all families, cultures, and societies.
2. Avoid stereotyping, essentializing, and overgeneralizing.
3. Individualize and tailor diagnostic assessment, treatment, and care.
4. Address any language access barriers through the use of qualified medical interpreters and appropriately translated educational and informational materials.
5. Employ plain language in communicating with patients with limited health and mental health literacy.
6. Recognize the impact on both the patient and the clinician of our families of origin.
7. Engage in reflective, mindful practice and attend to cultural countertransference to provide insight into one’s own values, beliefs, and behaviors.
8. Cultivate cultural humility – the realization that our understanding of the other person’s background is always limited and incomplete.
9. Every encounter is a cross-cultural one.
10. Developing cultural competence is a lifelong journey and not a final destination.
Guidelines for Case Submission
We are requesting that you submit cases to cpnews@frontlinemedcom.com in which your understanding and treatment are affected by challenging cultural and family issues. We will then write back with our best answers about how one might proceed in such a case. Your case and our response will be published in Clinical Psychiatry News. Please limit your case description to 250 words and please include the following details:
1. Patient’s presenting problem or reason for the visit.
2. Patient’s age and gender.
3. Indicators of the patient’s identity – self-identified race/ethnicity, culture, religion/spirituality, socioeconomic status, education, among other variables.
4. Patient’s living situation, family composition, and genogram information (if available).
5. Patient’s geographic location (rural, suburban, urban) and occupation.
6. Patient’s and family’s degree of participation in their identified culture.
7. Questions of the individual submitting the case, including concerns about the role of the family and culture in the case, diagnosis, and treatment planning.
8. Please follow local ethical requirements, disguise the case to protect confidentiality and attend to HIPAA requirements, so that patients or family members reading the article would not recognize themselves.
Additional information might be requested, and editing of the case, questions, and commentary might be needed prior to final publication.
Please note that the opinions expressed in the case commentaries should not be seen as formal medical consultations and do not represent the opinions of GAP, CPN, or the institutions where the authors are employed or with which they are affiliated.
Contributors:
Michael S. Ascher, M.D. – University of Pennsylvania, Perelman School of Medicine
Alison M. Heru, M.D. – University of Colorado at Denver, Aurora
Roberto Lewis-Fernández, M.D. – Columbia University and New York State Psychiatric Institute
Robert C. Like, M.D., M.S. – Rutgers University, Robert Wood Johnson Medical School
Resources:
DSM-5 – Outline for Cultural Formulation and Cultural Formulation Interview: http://www.psychiatry.org/practice/dsm/dsm5/online-assessment-measures#Cultural
Clinical Manual of Couples and Family Therapy, Washington: American Psychiatric Publishing Inc., 2009.
Thinking Through Cultures: Expeditions in Cultural Psychology. Cambridge, Mass.: Harvard University Press, 1991.
Clinical Manual of Cultural Psychiatry, 2nd Edition, Washington: American Psychiatric Publishing Inc., 2015.
We are pleased to introduce Curbside Consult with the Group for the Advancement of Psychiatry's (GAP) Family and Cultural committees. The column is inspired by the DSM-5's emphasis on developing a cultural formulation of patients' illnesses and addressing family dynamics and resilience in promoting care that fosters prevention and recovery.
What is GAP?
GAP was formed in 1946 under the leadership of Dr. William Menninger by a group of young psychiatrists who had served in World War II. They returned to the United States to find an inadequate system of civilian care. They were eager to professionalize the field and collaboratively develop new and creative thinking. They developed an organization that met as a whole twice a year, organized into committees of particular interest to the members and crucial to the needs of psychiatric care. The committees wrote monographs that formed a crucial role in the development of modern psychiatric thought.
Mission of GAP
- Bring together top psychiatrists of all disciplines
- Offer an objective, critical perspective on current issues facing psychiatry
- Develop smart analysis and recommendations
- Shape psychiatric thinking, clinical practice, and mental health programs
- Advocate for necessary changes in the psychiatric field
- Inspire the next generation of leading psychiatric thinkers
The Family and Cultural Psychiatry committees want to focus psychiatrists on the resilience inherent in the families and cultures of our patients in order to promote psychiatric care that focuses on prevention and recovery.
The Family and Cultural Psychiatry committees see every patient as connected to family members and belonging to a network of cultures that might include their national origin, race/ethnicity, religion/spirituality, language, occupation, age, sexual orientation and gender identity, or any other element of the person's background and collective life.
Over time, these family and cultural influences have shaped all aspects of the person’s response to adversity, experience of illness, and expectations of help seeking, even among patients who are currently living alone or do not recognize their background as explicitly cultural. This influence is highly individual; each person has his/her own combination of family and cultural experiences. How does the psychiatrist access this experience and use it to help develop resilience in our patients? How do we encourage them to use strengths/support from their family and culture, and to identify narratives that are helpful?
We see this column as one way to help answer these questions. We will bring to bear both family and cultural perspectives on the care of patients in everyday clinical practice through our comments on case vignettes sent in by readers. It can be challenging to integrate an understanding of family and culture into each patient encounter.
Our committees will work together to develop a coherent response that integrates both family and cultural perspectives and can be applied in real-world patient situations by clinicians who might not have access to specialized consultation. We aim to contribute to the growing awareness in our field of the cultural complexity of our patients, as developed and transmitted in the nexus of their families, which requires from us as clinicians a more inclusive and holistic approach to care.
This column helps to meet the goals of accreditation bodies such as The Joint Commission and the Accreditation Council for Graduate Medical Education (ACGME) for cultural and linguistic competence and patient- and family-centered care. Understanding how to think about, assess, and engage in treatment with the diversity of our patients’ cultural and family backgrounds constitutes important educational topics for all psychiatric trainees. In conjunction with formal didactics, these cases can be used as a focus for discussion in psychiatric residency training programs, ACGME Clinical Learning Environment Review (CLER), health care quality improvement activities, and faculty development programs.
Practicing clinicians also will find the DSM-5 Outline for Cultural Formulation and Cultural Formulation Interview to be a helpful clinical tool for eliciting and organizing cultural information, and in differential diagnosis and treatment planning.
The following is a list of the guiding principles we will use for assessment:
1. Heterogeneity and diversity exists within all families, cultures, and societies.
2. Avoid stereotyping, essentializing, and overgeneralizing.
3. Individualize and tailor diagnostic assessment, treatment, and care.
4. Address any language access barriers through the use of qualified medical interpreters and appropriately translated educational and informational materials.
5. Employ plain language in communicating with patients with limited health and mental health literacy.
6. Recognize the impact on both the patient and the clinician of our families of origin.
7. Engage in reflective, mindful practice and attend to cultural countertransference to provide insight into one’s own values, beliefs, and behaviors.
8. Cultivate cultural humility – the realization that our understanding of the other person’s background is always limited and incomplete.
9. Every encounter is a cross-cultural one.
10. Developing cultural competence is a lifelong journey and not a final destination.
Guidelines for Case Submission
We are requesting that you submit cases to cpnews@frontlinemedcom.com in which your understanding and treatment are affected by challenging cultural and family issues. We will then write back with our best answers about how one might proceed in such a case. Your case and our response will be published in Clinical Psychiatry News. Please limit your case description to 250 words and please include the following details:
1. Patient’s presenting problem or reason for the visit.
2. Patient’s age and gender.
3. Indicators of the patient’s identity – self-identified race/ethnicity, culture, religion/spirituality, socioeconomic status, education, among other variables.
4. Patient’s living situation, family composition, and genogram information (if available).
5. Patient’s geographic location (rural, suburban, urban) and occupation.
6. Patient’s and family’s degree of participation in their identified culture.
7. Questions of the individual submitting the case, including concerns about the role of the family and culture in the case, diagnosis, and treatment planning.
8. Please follow local ethical requirements, disguise the case to protect confidentiality and attend to HIPAA requirements, so that patients or family members reading the article would not recognize themselves.
Additional information might be requested, and editing of the case, questions, and commentary might be needed prior to final publication.
Please note that the opinions expressed in the case commentaries should not be seen as formal medical consultations and do not represent the opinions of GAP, CPN, or the institutions where the authors are employed or with which they are affiliated.
Contributors:
Michael S. Ascher, M.D. – University of Pennsylvania, Perelman School of Medicine
Alison M. Heru, M.D. – University of Colorado at Denver, Aurora
Roberto Lewis-Fernández, M.D. – Columbia University and New York State Psychiatric Institute
Robert C. Like, M.D., M.S. – Rutgers University, Robert Wood Johnson Medical School
Resources:
DSM-5 – Outline for Cultural Formulation and Cultural Formulation Interview: http://www.psychiatry.org/practice/dsm/dsm5/online-assessment-measures#Cultural
Clinical Manual of Couples and Family Therapy, Washington: American Psychiatric Publishing Inc., 2009.
Thinking Through Cultures: Expeditions in Cultural Psychology. Cambridge, Mass.: Harvard University Press, 1991.
Clinical Manual of Cultural Psychiatry, 2nd Edition, Washington: American Psychiatric Publishing Inc., 2015.

Human experimentation: The good, the bad, and the ugly
Ever since the earliest medical practitioners treated the first patients, a tension has existed between potentially beneficial innovation and unintentional harm. For many centuries doctors relied on their own experience or intuition to determine what was best for those whom they treated. It was not until the 17th century that Francis Bacon introduced the scientific method that consisted of systematic observation and testing of hypotheses. In the case of clinical science, this provided an objective means of determining which treatments would be in the best interest of patients. Since then, society has greatly benefited from remarkable medical advancements based on what is essentially human experimentation, much of it noble, but unfortunately some episodes quite tragic, misguided, and even demonic.
The most notorious human research abuses were those perpetrated by the Nazi regime during the Holocaust. There were only 200 survivors from the 1,500 sets of twins forced to participate in Josef Mengele’s infamous twin experiments at the Auschwitz concentration camp. Many of these investigations were genetic experiments intended to prove the superiority of the Aryan race. Little useful scientific information was gained from these inhumane and evil studies.
However, totalitarianism is not a prerequisite for mistreatment of human subjects. The American research community has its own checkered past. Possibly the most well-known abuse is the Tuskegee syphilis experiments that were conducted between 1932 and 1972 by the U.S. Public Health Service. Four hundred impoverished African American males infected with syphilis, who were not fully informed about their disease, were closely followed in order to record the natural history of this deadly and debilitating illness. These patients were not treated with penicillin although the drug became available in 1947. As a result, over one-third of the subjects died of their disease, many of their wives contracted syphilis, and numerous children were unnecessarily born with congenital syphilis.
On the other end of the ethical scale are a number of noble researchers scattered throughout history who insisted on experimenting on themselves before submitting others to their treatments or procedures. A prime example is a courageous and creative German surgical intern, Werner Forssmann, who paved the path to heart surgery through self-experimentation. Even into the 20th century, it was taboo for a physician to touch the living heart. Thus, much of its physiology and pathophysiology remained shrouded in mystery. In 1929, Dr. Forssmann did a cut-down on his antecubital vein, inserted a ureteral catheter into the right side of his heart, and then descended a flight of stairs to confirm its position by x-ray. Later experiments, also performed on him, resulted in the first cardiac angiograms. Although heavily criticized by his superiors and the German medical establishment, Dr. Forssmann, an obscure urologist and general surgeon at the time, was eventually rewarded by sharing the Nobel Prize in 1956.
From the very beginning of surgery as a clinical science, surgeons have sat on the precipice of beneficial innovation versus unintentional harm to their patients. Because of the very nature of what they do, it has not usually been possible for them to self-experiment before testing their ideas on others. Every operation ever devised, occasionally with, but often without, animal experimentation, has had its initial human guinea pigs. In fact, surgeons have generally been given freer rein to try new and untested procedures or to modify older accepted ones. They have had greater license than have their counterparts who innovate with drugs and medical devices and are thus more tightly regulated by agencies such as the Food and Drug Administration.
In the best of circumstances, surgical patients are fully informed as to the potential consequences of a novel operation, both good and bad, and the results are carefully recorded to determine the benefit/harm ratio of the procedure. Ideally, though it is often not possible, the new approach is compared to a proven alternative therapy in a carefully designed trial. Unfortunately, such careful analysis has not always been done.
A glaring example of surgical human experimentation gone wrong is the frontal lobotomy story. In the early part of the 20th century, mental institutions in this country and throughout the world were filled with desperate patients for whom there were few therapeutic alternatives available. Many of these patients were incapable of giving meaningful informed consent. In 1935, frontal lobotomy was introduced by Antonio Moniz, a Portuguese neurologist, who later shared in a highly controversial Nobel Prize for his discovery. In 1946, an American neuropsychiatrist, Walter Freeman, modified the procedure so it could be done by psychiatrists with an ice pick–like instrument via a transorbital approach. A neurosurgeon performing a craniotomy, general anesthesia, and an operating room were no longer necessary, resulting in the rapid proliferation of this simpler operation despite its increasingly well-known and devastating side effects of loss of personality, decreased cognition, and even death. Only after more than 40,000 procedures were done in the United States did mounting criticism eventually lead to a ban on most lobotomies..
On the more noble side of surgical innovation, if Dr. Thomas Starzl and Dr. C. Walton Lillehei had not persisted despite failure after failure and death after death, liver transplantation and cardiac surgery would not have evolved to the lifesaving therapies they are today. These surgical pioneers and many others like them, who have persisted in the face of failure to develop new and useful approaches to surgical disease, can hardly be condemned for their human experiments that were disasters in the short term but enduring medical advancements in the long-term. Their initial patients were courageous, desperate, and hopefully well informed.
What separates these successful forerunners from those who promoted the lobotomy debacle? One factor may be history itself. Passed by Congress in response to the atrocities that had occurred earlier in the century, the National Research Act of 1974 mandated Institutional Review Boards (IRBs) in institutions conducting human research. Although the initial attempts at operating on the heart and transplanting the liver predated IRBs, much of the development of these specialties as we know them today took place under the watchful eye of these committees.
Whereas Freeman’s modifications made lobotomy a procedure that could be performed by almost anyone, cardiac surgery and liver transplantation required resources that could be provided only by major academic institutions.
While lobotomy almost became a traveling sideshow with poor documentation of results, the earliest attempts at heart surgery and liver transplantation were carefully recorded in the surgical literature for the entire academic community to analyze and ponder.
We owe much to those surgeons who persisted against great odds to develop our craft and to those patients with the courage to be a part of the great enterprise of surgical innovation. Without their daring, perseverance, and creativity, surgery would not have evolved to the diverse and noble specialty it is today. It is now incumbent upon us to make certain that future surgical innovation transpires only under an umbrella of safe, well-informed, and satisfactorily documented and controlled human experimentation.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.
Ever since the earliest medical practitioners treated the first patients, a tension has existed between potentially beneficial innovation and unintentional harm. For many centuries doctors relied on their own experience or intuition to determine what was best for those whom they treated. It was not until the 17th century that Francis Bacon introduced the scientific method that consisted of systematic observation and testing of hypotheses. In the case of clinical science, this provided an objective means of determining which treatments would be in the best interest of patients. Since then, society has greatly benefited from remarkable medical advancements based on what is essentially human experimentation, much of it noble, but unfortunately some episodes quite tragic, misguided, and even demonic.
The most notorious human research abuses were those perpetrated by the Nazi regime during the Holocaust. There were only 200 survivors from the 1,500 sets of twins forced to participate in Josef Mengele’s infamous twin experiments at the Auschwitz concentration camp. Many of these investigations were genetic experiments intended to prove the superiority of the Aryan race. Little useful scientific information was gained from these inhumane and evil studies.
However, totalitarianism is not a prerequisite for mistreatment of human subjects. The American research community has its own checkered past. Possibly the most well-known abuse is the Tuskegee syphilis experiments that were conducted between 1932 and 1972 by the U.S. Public Health Service. Four hundred impoverished African American males infected with syphilis, who were not fully informed about their disease, were closely followed in order to record the natural history of this deadly and debilitating illness. These patients were not treated with penicillin although the drug became available in 1947. As a result, over one-third of the subjects died of their disease, many of their wives contracted syphilis, and numerous children were unnecessarily born with congenital syphilis.
On the other end of the ethical scale are a number of noble researchers scattered throughout history who insisted on experimenting on themselves before submitting others to their treatments or procedures. A prime example is a courageous and creative German surgical intern, Werner Forssmann, who paved the path to heart surgery through self-experimentation. Even into the 20th century, it was taboo for a physician to touch the living heart. Thus, much of its physiology and pathophysiology remained shrouded in mystery. In 1929, Dr. Forssmann did a cut-down on his antecubital vein, inserted a ureteral catheter into the right side of his heart, and then descended a flight of stairs to confirm its position by x-ray. Later experiments, also performed on him, resulted in the first cardiac angiograms. Although heavily criticized by his superiors and the German medical establishment, Dr. Forssmann, an obscure urologist and general surgeon at the time, was eventually rewarded by sharing the Nobel Prize in 1956.
From the very beginning of surgery as a clinical science, surgeons have sat on the precipice of beneficial innovation versus unintentional harm to their patients. Because of the very nature of what they do, it has not usually been possible for them to self-experiment before testing their ideas on others. Every operation ever devised, occasionally with, but often without, animal experimentation, has had its initial human guinea pigs. In fact, surgeons have generally been given freer rein to try new and untested procedures or to modify older accepted ones. They have had greater license than have their counterparts who innovate with drugs and medical devices and are thus more tightly regulated by agencies such as the Food and Drug Administration.
In the best of circumstances, surgical patients are fully informed as to the potential consequences of a novel operation, both good and bad, and the results are carefully recorded to determine the benefit/harm ratio of the procedure. Ideally, though it is often not possible, the new approach is compared to a proven alternative therapy in a carefully designed trial. Unfortunately, such careful analysis has not always been done.
A glaring example of surgical human experimentation gone wrong is the frontal lobotomy story. In the early part of the 20th century, mental institutions in this country and throughout the world were filled with desperate patients for whom there were few therapeutic alternatives available. Many of these patients were incapable of giving meaningful informed consent. In 1935, frontal lobotomy was introduced by Antonio Moniz, a Portuguese neurologist, who later shared in a highly controversial Nobel Prize for his discovery. In 1946, an American neuropsychiatrist, Walter Freeman, modified the procedure so it could be done by psychiatrists with an ice pick–like instrument via a transorbital approach. A neurosurgeon performing a craniotomy, general anesthesia, and an operating room were no longer necessary, resulting in the rapid proliferation of this simpler operation despite its increasingly well-known and devastating side effects of loss of personality, decreased cognition, and even death. Only after more than 40,000 procedures were done in the United States did mounting criticism eventually lead to a ban on most lobotomies..
On the more noble side of surgical innovation, if Dr. Thomas Starzl and Dr. C. Walton Lillehei had not persisted despite failure after failure and death after death, liver transplantation and cardiac surgery would not have evolved to the lifesaving therapies they are today. These surgical pioneers and many others like them, who have persisted in the face of failure to develop new and useful approaches to surgical disease, can hardly be condemned for their human experiments that were disasters in the short term but enduring medical advancements in the long-term. Their initial patients were courageous, desperate, and hopefully well informed.
What separates these successful forerunners from those who promoted the lobotomy debacle? One factor may be history itself. Passed by Congress in response to the atrocities that had occurred earlier in the century, the National Research Act of 1974 mandated Institutional Review Boards (IRBs) in institutions conducting human research. Although the initial attempts at operating on the heart and transplanting the liver predated IRBs, much of the development of these specialties as we know them today took place under the watchful eye of these committees.
Whereas Freeman’s modifications made lobotomy a procedure that could be performed by almost anyone, cardiac surgery and liver transplantation required resources that could be provided only by major academic institutions.
While lobotomy almost became a traveling sideshow with poor documentation of results, the earliest attempts at heart surgery and liver transplantation were carefully recorded in the surgical literature for the entire academic community to analyze and ponder.
We owe much to those surgeons who persisted against great odds to develop our craft and to those patients with the courage to be a part of the great enterprise of surgical innovation. Without their daring, perseverance, and creativity, surgery would not have evolved to the diverse and noble specialty it is today. It is now incumbent upon us to make certain that future surgical innovation transpires only under an umbrella of safe, well-informed, and satisfactorily documented and controlled human experimentation.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.
Ever since the earliest medical practitioners treated the first patients, a tension has existed between potentially beneficial innovation and unintentional harm. For many centuries doctors relied on their own experience or intuition to determine what was best for those whom they treated. It was not until the 17th century that Francis Bacon introduced the scientific method that consisted of systematic observation and testing of hypotheses. In the case of clinical science, this provided an objective means of determining which treatments would be in the best interest of patients. Since then, society has greatly benefited from remarkable medical advancements based on what is essentially human experimentation, much of it noble, but unfortunately some episodes quite tragic, misguided, and even demonic.
The most notorious human research abuses were those perpetrated by the Nazi regime during the Holocaust. There were only 200 survivors from the 1,500 sets of twins forced to participate in Josef Mengele’s infamous twin experiments at the Auschwitz concentration camp. Many of these investigations were genetic experiments intended to prove the superiority of the Aryan race. Little useful scientific information was gained from these inhumane and evil studies.
However, totalitarianism is not a prerequisite for mistreatment of human subjects. The American research community has its own checkered past. Possibly the most well-known abuse is the Tuskegee syphilis experiments that were conducted between 1932 and 1972 by the U.S. Public Health Service. Four hundred impoverished African American males infected with syphilis, who were not fully informed about their disease, were closely followed in order to record the natural history of this deadly and debilitating illness. These patients were not treated with penicillin although the drug became available in 1947. As a result, over one-third of the subjects died of their disease, many of their wives contracted syphilis, and numerous children were unnecessarily born with congenital syphilis.
On the other end of the ethical scale are a number of noble researchers scattered throughout history who insisted on experimenting on themselves before submitting others to their treatments or procedures. A prime example is a courageous and creative German surgical intern, Werner Forssmann, who paved the path to heart surgery through self-experimentation. Even into the 20th century, it was taboo for a physician to touch the living heart. Thus, much of its physiology and pathophysiology remained shrouded in mystery. In 1929, Dr. Forssmann did a cut-down on his antecubital vein, inserted a ureteral catheter into the right side of his heart, and then descended a flight of stairs to confirm its position by x-ray. Later experiments, also performed on him, resulted in the first cardiac angiograms. Although heavily criticized by his superiors and the German medical establishment, Dr. Forssmann, an obscure urologist and general surgeon at the time, was eventually rewarded by sharing the Nobel Prize in 1956.
From the very beginning of surgery as a clinical science, surgeons have sat on the precipice of beneficial innovation versus unintentional harm to their patients. Because of the very nature of what they do, it has not usually been possible for them to self-experiment before testing their ideas on others. Every operation ever devised, occasionally with, but often without, animal experimentation, has had its initial human guinea pigs. In fact, surgeons have generally been given freer rein to try new and untested procedures or to modify older accepted ones. They have had greater license than have their counterparts who innovate with drugs and medical devices and are thus more tightly regulated by agencies such as the Food and Drug Administration.
In the best of circumstances, surgical patients are fully informed as to the potential consequences of a novel operation, both good and bad, and the results are carefully recorded to determine the benefit/harm ratio of the procedure. Ideally, though it is often not possible, the new approach is compared to a proven alternative therapy in a carefully designed trial. Unfortunately, such careful analysis has not always been done.
A glaring example of surgical human experimentation gone wrong is the frontal lobotomy story. In the early part of the 20th century, mental institutions in this country and throughout the world were filled with desperate patients for whom there were few therapeutic alternatives available. Many of these patients were incapable of giving meaningful informed consent. In 1935, frontal lobotomy was introduced by Antonio Moniz, a Portuguese neurologist, who later shared in a highly controversial Nobel Prize for his discovery. In 1946, an American neuropsychiatrist, Walter Freeman, modified the procedure so it could be done by psychiatrists with an ice pick–like instrument via a transorbital approach. A neurosurgeon performing a craniotomy, general anesthesia, and an operating room were no longer necessary, resulting in the rapid proliferation of this simpler operation despite its increasingly well-known and devastating side effects of loss of personality, decreased cognition, and even death. Only after more than 40,000 procedures were done in the United States did mounting criticism eventually lead to a ban on most lobotomies..
On the more noble side of surgical innovation, if Dr. Thomas Starzl and Dr. C. Walton Lillehei had not persisted despite failure after failure and death after death, liver transplantation and cardiac surgery would not have evolved to the lifesaving therapies they are today. These surgical pioneers and many others like them, who have persisted in the face of failure to develop new and useful approaches to surgical disease, can hardly be condemned for their human experiments that were disasters in the short term but enduring medical advancements in the long-term. Their initial patients were courageous, desperate, and hopefully well informed.
What separates these successful forerunners from those who promoted the lobotomy debacle? One factor may be history itself. Passed by Congress in response to the atrocities that had occurred earlier in the century, the National Research Act of 1974 mandated Institutional Review Boards (IRBs) in institutions conducting human research. Although the initial attempts at operating on the heart and transplanting the liver predated IRBs, much of the development of these specialties as we know them today took place under the watchful eye of these committees.
Whereas Freeman’s modifications made lobotomy a procedure that could be performed by almost anyone, cardiac surgery and liver transplantation required resources that could be provided only by major academic institutions.
While lobotomy almost became a traveling sideshow with poor documentation of results, the earliest attempts at heart surgery and liver transplantation were carefully recorded in the surgical literature for the entire academic community to analyze and ponder.
We owe much to those surgeons who persisted against great odds to develop our craft and to those patients with the courage to be a part of the great enterprise of surgical innovation. Without their daring, perseverance, and creativity, surgery would not have evolved to the diverse and noble specialty it is today. It is now incumbent upon us to make certain that future surgical innovation transpires only under an umbrella of safe, well-informed, and satisfactorily documented and controlled human experimentation.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.
