User login
A Practice Resolution
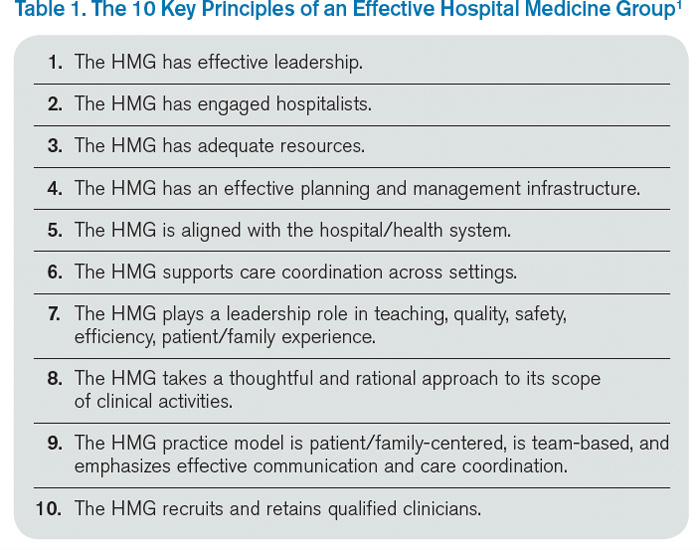
In the heart of the holiday season’s gluttony (and the challenges of staffing the holidays), we need something to get us excited for 2015. Let me suggest that you resolve to use “The Key Principles and Characteristics of an Effective Hospital Medicine Group: An Assessment Guide for Hospitals and Hospitalists” to trim those holiday pounds and make your hospitalist group (HMG) fitter than ever.1
When we published the “Key Principles and Characteristics” in the Journal of Hospital Medicine in February, we intended it to be “aspirational, helping to raise the bar for the specialty of hospital medicine.”1 The author group’s intent was to provide a framework for quality improvement at the HMG level. One can use the 10 principles and 47 characteristics as a basis for self-assessment within the cycle of quality improvement. I will provide an illustration of how a group might utilize the guide to improve its performance using an example and W. Edward Deming’s classic plan-do-study-act (PDSA) cycle.
Principle 6: The HMG supports care coordination across settings.
Characteristic 6.1: The HMG has systems in place to ensure effective and reliable communication with the patient’s primary care provider and/or other providers involved in the patient’s care in the nonacute care setting.
Plan
This phase involves identifying a goal, setting success metrics, and putting a plan into action.
Example: 90% of primary care providers (PCPs) will receive a discharge summary within 24 hours of discharge.
Do
Here the key components of the plan are implemented.
Example: All referring PCPs’ preferred methods of communication and contact information are documented. The HMG has the ability to utilize such communication, e.g. electronic health record (EHR) e-mail or electronic fax. All hospitalists prepare a discharge summary in real time.
Study
In this phase, outcomes are assessed for success and barriers.
Example: Although 97% of discharge summaries are transmitted according to the PCPs’ preferred communication, PCPs state that they received it only 78% of the time.
Act
This is where the lessons learned throughout the process are integrated to adjust the methods, the goal, or the approach in general. Then the entire cycle is repeated.
Example: Even though most PCPs are on the same EHR system as the hospitalists, they don’t check their EHR e-mail (even though during the Plan phase they said they did). Their office staff uses electronic fax, so that will be the method of communication for the PCPs who do not check their EHR e-mail inbox.
In this example, the next time the PDSA cycle is completed, the new approach—using electronic fax for PCPs who don’t check their EHR e-mail while using e-mail for those who check it—will be employed, measured, and further improved in iterative cycles.
Gap Analysis
Another way you can use the “Key Principles and Characteristics” is to do a gap analysis of your HMG. You can assess the current state of your HMG against the “Key Principles and Characteristics,” which can be viewed as an ideal state. The gap between the current and the ideal state can be a roadmap to improvement for your HMG.
For an example of a large HMG’s gap analysis, see “TeamHealth Hospital Medicine Shares Performance Stats” in the August 2014 issue of The Hospitalist.
Strategic Planning
You may be thinking about taking a block of time to devote to your group’s strategic planning. The “Key Principles and Characteristics” is the ideal framework for such planning. You can use the document as a backdrop to your SWOT (strengths, weaknesses, opportunities, and threats) analysis, which forms the basis of your HMG strategic planning activities.
Keep Your Resolution
One of the best ways to maintain your new habit in the New Year is to let others know of your resolution. In the case of your “Key Principles and Characteristics” resolution, announce your plans at the next monthly meeting of your HMG, and find a way to involve other group members in the project. You might assign a single principle or characteristic to each group member, who is tasked with doing a QI project and reporting on the results at a future date. Or, group members can engage in a portion of a gap analysis or SWOT analysis.
No matter how you use the “Key Principles and Characteristics,” I hope they will guide your HMG to a happy, healthy, and effective 2015!

Reference
In the heart of the holiday season’s gluttony (and the challenges of staffing the holidays), we need something to get us excited for 2015. Let me suggest that you resolve to use “The Key Principles and Characteristics of an Effective Hospital Medicine Group: An Assessment Guide for Hospitals and Hospitalists” to trim those holiday pounds and make your hospitalist group (HMG) fitter than ever.1
When we published the “Key Principles and Characteristics” in the Journal of Hospital Medicine in February, we intended it to be “aspirational, helping to raise the bar for the specialty of hospital medicine.”1 The author group’s intent was to provide a framework for quality improvement at the HMG level. One can use the 10 principles and 47 characteristics as a basis for self-assessment within the cycle of quality improvement. I will provide an illustration of how a group might utilize the guide to improve its performance using an example and W. Edward Deming’s classic plan-do-study-act (PDSA) cycle.
Principle 6: The HMG supports care coordination across settings.
Characteristic 6.1: The HMG has systems in place to ensure effective and reliable communication with the patient’s primary care provider and/or other providers involved in the patient’s care in the nonacute care setting.
Plan
This phase involves identifying a goal, setting success metrics, and putting a plan into action.
Example: 90% of primary care providers (PCPs) will receive a discharge summary within 24 hours of discharge.
Do
Here the key components of the plan are implemented.
Example: All referring PCPs’ preferred methods of communication and contact information are documented. The HMG has the ability to utilize such communication, e.g. electronic health record (EHR) e-mail or electronic fax. All hospitalists prepare a discharge summary in real time.
Study
In this phase, outcomes are assessed for success and barriers.
Example: Although 97% of discharge summaries are transmitted according to the PCPs’ preferred communication, PCPs state that they received it only 78% of the time.
Act
This is where the lessons learned throughout the process are integrated to adjust the methods, the goal, or the approach in general. Then the entire cycle is repeated.
Example: Even though most PCPs are on the same EHR system as the hospitalists, they don’t check their EHR e-mail (even though during the Plan phase they said they did). Their office staff uses electronic fax, so that will be the method of communication for the PCPs who do not check their EHR e-mail inbox.
In this example, the next time the PDSA cycle is completed, the new approach—using electronic fax for PCPs who don’t check their EHR e-mail while using e-mail for those who check it—will be employed, measured, and further improved in iterative cycles.
Gap Analysis
Another way you can use the “Key Principles and Characteristics” is to do a gap analysis of your HMG. You can assess the current state of your HMG against the “Key Principles and Characteristics,” which can be viewed as an ideal state. The gap between the current and the ideal state can be a roadmap to improvement for your HMG.
For an example of a large HMG’s gap analysis, see “TeamHealth Hospital Medicine Shares Performance Stats” in the August 2014 issue of The Hospitalist.
Strategic Planning
You may be thinking about taking a block of time to devote to your group’s strategic planning. The “Key Principles and Characteristics” is the ideal framework for such planning. You can use the document as a backdrop to your SWOT (strengths, weaknesses, opportunities, and threats) analysis, which forms the basis of your HMG strategic planning activities.
Keep Your Resolution
One of the best ways to maintain your new habit in the New Year is to let others know of your resolution. In the case of your “Key Principles and Characteristics” resolution, announce your plans at the next monthly meeting of your HMG, and find a way to involve other group members in the project. You might assign a single principle or characteristic to each group member, who is tasked with doing a QI project and reporting on the results at a future date. Or, group members can engage in a portion of a gap analysis or SWOT analysis.
No matter how you use the “Key Principles and Characteristics,” I hope they will guide your HMG to a happy, healthy, and effective 2015!
Reference
In the heart of the holiday season’s gluttony (and the challenges of staffing the holidays), we need something to get us excited for 2015. Let me suggest that you resolve to use “The Key Principles and Characteristics of an Effective Hospital Medicine Group: An Assessment Guide for Hospitals and Hospitalists” to trim those holiday pounds and make your hospitalist group (HMG) fitter than ever.1
When we published the “Key Principles and Characteristics” in the Journal of Hospital Medicine in February, we intended it to be “aspirational, helping to raise the bar for the specialty of hospital medicine.”1 The author group’s intent was to provide a framework for quality improvement at the HMG level. One can use the 10 principles and 47 characteristics as a basis for self-assessment within the cycle of quality improvement. I will provide an illustration of how a group might utilize the guide to improve its performance using an example and W. Edward Deming’s classic plan-do-study-act (PDSA) cycle.
Principle 6: The HMG supports care coordination across settings.
Characteristic 6.1: The HMG has systems in place to ensure effective and reliable communication with the patient’s primary care provider and/or other providers involved in the patient’s care in the nonacute care setting.
Plan
This phase involves identifying a goal, setting success metrics, and putting a plan into action.
Example: 90% of primary care providers (PCPs) will receive a discharge summary within 24 hours of discharge.
Do
Here the key components of the plan are implemented.
Example: All referring PCPs’ preferred methods of communication and contact information are documented. The HMG has the ability to utilize such communication, e.g. electronic health record (EHR) e-mail or electronic fax. All hospitalists prepare a discharge summary in real time.
Study
In this phase, outcomes are assessed for success and barriers.
Example: Although 97% of discharge summaries are transmitted according to the PCPs’ preferred communication, PCPs state that they received it only 78% of the time.
Act
This is where the lessons learned throughout the process are integrated to adjust the methods, the goal, or the approach in general. Then the entire cycle is repeated.
Example: Even though most PCPs are on the same EHR system as the hospitalists, they don’t check their EHR e-mail (even though during the Plan phase they said they did). Their office staff uses electronic fax, so that will be the method of communication for the PCPs who do not check their EHR e-mail inbox.
In this example, the next time the PDSA cycle is completed, the new approach—using electronic fax for PCPs who don’t check their EHR e-mail while using e-mail for those who check it—will be employed, measured, and further improved in iterative cycles.
Gap Analysis
Another way you can use the “Key Principles and Characteristics” is to do a gap analysis of your HMG. You can assess the current state of your HMG against the “Key Principles and Characteristics,” which can be viewed as an ideal state. The gap between the current and the ideal state can be a roadmap to improvement for your HMG.
For an example of a large HMG’s gap analysis, see “TeamHealth Hospital Medicine Shares Performance Stats” in the August 2014 issue of The Hospitalist.
Strategic Planning
You may be thinking about taking a block of time to devote to your group’s strategic planning. The “Key Principles and Characteristics” is the ideal framework for such planning. You can use the document as a backdrop to your SWOT (strengths, weaknesses, opportunities, and threats) analysis, which forms the basis of your HMG strategic planning activities.
Keep Your Resolution
One of the best ways to maintain your new habit in the New Year is to let others know of your resolution. In the case of your “Key Principles and Characteristics” resolution, announce your plans at the next monthly meeting of your HMG, and find a way to involve other group members in the project. You might assign a single principle or characteristic to each group member, who is tasked with doing a QI project and reporting on the results at a future date. Or, group members can engage in a portion of a gap analysis or SWOT analysis.
No matter how you use the “Key Principles and Characteristics,” I hope they will guide your HMG to a happy, healthy, and effective 2015!
Reference
Hospitals' Observation Status Designation May Trigger Malpractice Claims

I’m convinced that observation status is rapidly becoming a meaningful factor in patients’ decision to file a malpractice lawsuit.
First, let me concede that I don’t know of any hard data to support my claim. I even asked the nation’s largest malpractice insurer about this, and they didn’t have any data on it. I think that is because observation status has only become a really big issue in the last couple of years, and since it typically takes several years for a malpractice suit to conclude, it just hasn’t found its way onto their radar yet.
But I’m pretty sure that will change within the next few years.
Implications
As any seasoned practitioner in our field knows, all outpatient and inpatient physician charges for Medicare patients, along with those of other licensed practitioners, are billed through Medicare Part B. After meeting a deductible, patients with traditional fee-for-service Medicare are generally responsible for 20% of all approved Part B charges, with no upper limit. For patients seen by a large number of providers while hospitalized, this 20% can really add up. Some patients have a secondary insurance that pays for this.
Hospital charges for patients on inpatient status are billed through Medicare Part A. Patients have an annual Part A deductible, and only in the case of very long inpatient stays will they have to pay more than that for inpatient care each year.
But hospital charges for patients on observation status are billed through Part B. And because hospital charges add up so quickly, the 20% of this that the patient is responsible for can be a lot of money—thousands of dollars, even for stays of less than 24 hours. Understandably, patients are not at all happy about this.
Let’s say you’re admitted overnight on observation status and your doctor orders your usual Advair inhaler. You use it once. Most hospitals aren’t able to ensure compliance with regulations around dispensing medications for home use like a pharmacy, so they won’t let you take the inhaler home. A few weeks later you’re stunned to learn that the hospital charged $10,000 for all services provided, and you’re responsible for 20% of the allowable amount PLUS the cost of all “self administered” drugs, like inhalers, eye drops, and calcitonin nasal spray. You look over your bill to see that you’re asked to pay $350 for the inhaler you used once and couldn’t even take home with you! Many self-administered medications, including eye drops and calcitonin nasal spray, result in similarly alarming charges to patients.
On top of the unpleasant surprise of a large hospital bill, Medicare won’t pay for skilled nursing facility (SNF) care for patients who are on observation status. That is, observation is not a “qualifying” stay for beneficiaries to access their SNF benefit.
It is easy to see why patients are unhappy about observation status.
The Media Message
News media are making the public aware of the potentially high financial costs they face if placed on observation status. But, too often, they oversimplify the issue, making it seem as though the choice of observation vs. inpatient status is entirely up to the treating doctor.
Saying that this decision is entirely up to the doctor is a lot like saying it is entirely up to you to determine how fast you drive on a freeway. In a sense that is correct, because no one else is in your car to control how fast you go and, in theory, you could choose to go 100 mph or 30 mph. The only problem is that it wouldn’t be long before you’d be in trouble with the law. So you don’t have complete autonomy to choose your speed; you have to comply with the laws. The same is true for doctors choosing observation status. We must comply with regulations in choosing the status or face legal consequences like fines or accusations of fraud.
Most news stories, like this one from NBC news (www.nbcnews.com/video/nightly-news/54511352#54511352) in February, are generally accurate but leave out the important fact that hospitals and doctors have little autonomy to choose the status the patient prefers. Instead, media often simply encourage patients on observation status to argue for a change to inpatient status and “be persistent.” More and more often, patients and families are arguing with the treating doctor; in many cases, that is a hospitalist.
Complaints Surge
At the 2014 SHM annual meeting last spring in Las Vegas, I spoke with many hospitalists who said that, increasingly, they are targets of observation-status complaints. One hospitalist group recently had each doctor list his or her top three frustrations with work; difficult and stressful conversations about observation status topped the list.
Patient anger regarding observation status can turn a satisfied patient into an angry one. We all know that unhappy patients are the ones most likely to pursue malpractice lawsuits. While anger over observation status doesn’t equal medical malpractice, it can change a patient’s opinion of our care, which may in some cases result in a malpractice claim.
Solutions
Medicare is unlikely to do away with observation status, so the best way to prevent complaints is to ensure that all its implications are explained to patients and families, ideally before they’re put into the hospital (e.g., while still in the ED). I think it is best if this message is delivered by someone other than the treating doctor(s): For example, a case manager might handle the discussion. Of course, patients and families are often too overwhelmed in the ED to absorb this information, so the message may need to be repeated later.
Maybe everyone should tell observation patients, “We’re going to observe you” without using any form of the word “admission.” And having these patients stay in distinct observation units probably reduces misunderstandings and complaints compared to the common practice of mixing these patients in “regular” hospital floors housing those on inpatient status.
Unfortunately, I couldn’t find research data to support this idea.
I bet some hospitals have even more elegant and effective ways to reduce misunderstandings and complaints around observation status. I’d love to hear from you if you know of any. E-mail me at john.nelson@nelsonflores.com.

I’m convinced that observation status is rapidly becoming a meaningful factor in patients’ decision to file a malpractice lawsuit.
First, let me concede that I don’t know of any hard data to support my claim. I even asked the nation’s largest malpractice insurer about this, and they didn’t have any data on it. I think that is because observation status has only become a really big issue in the last couple of years, and since it typically takes several years for a malpractice suit to conclude, it just hasn’t found its way onto their radar yet.
But I’m pretty sure that will change within the next few years.
Implications
As any seasoned practitioner in our field knows, all outpatient and inpatient physician charges for Medicare patients, along with those of other licensed practitioners, are billed through Medicare Part B. After meeting a deductible, patients with traditional fee-for-service Medicare are generally responsible for 20% of all approved Part B charges, with no upper limit. For patients seen by a large number of providers while hospitalized, this 20% can really add up. Some patients have a secondary insurance that pays for this.
Hospital charges for patients on inpatient status are billed through Medicare Part A. Patients have an annual Part A deductible, and only in the case of very long inpatient stays will they have to pay more than that for inpatient care each year.
But hospital charges for patients on observation status are billed through Part B. And because hospital charges add up so quickly, the 20% of this that the patient is responsible for can be a lot of money—thousands of dollars, even for stays of less than 24 hours. Understandably, patients are not at all happy about this.
Let’s say you’re admitted overnight on observation status and your doctor orders your usual Advair inhaler. You use it once. Most hospitals aren’t able to ensure compliance with regulations around dispensing medications for home use like a pharmacy, so they won’t let you take the inhaler home. A few weeks later you’re stunned to learn that the hospital charged $10,000 for all services provided, and you’re responsible for 20% of the allowable amount PLUS the cost of all “self administered” drugs, like inhalers, eye drops, and calcitonin nasal spray. You look over your bill to see that you’re asked to pay $350 for the inhaler you used once and couldn’t even take home with you! Many self-administered medications, including eye drops and calcitonin nasal spray, result in similarly alarming charges to patients.
On top of the unpleasant surprise of a large hospital bill, Medicare won’t pay for skilled nursing facility (SNF) care for patients who are on observation status. That is, observation is not a “qualifying” stay for beneficiaries to access their SNF benefit.
It is easy to see why patients are unhappy about observation status.
The Media Message
News media are making the public aware of the potentially high financial costs they face if placed on observation status. But, too often, they oversimplify the issue, making it seem as though the choice of observation vs. inpatient status is entirely up to the treating doctor.
Saying that this decision is entirely up to the doctor is a lot like saying it is entirely up to you to determine how fast you drive on a freeway. In a sense that is correct, because no one else is in your car to control how fast you go and, in theory, you could choose to go 100 mph or 30 mph. The only problem is that it wouldn’t be long before you’d be in trouble with the law. So you don’t have complete autonomy to choose your speed; you have to comply with the laws. The same is true for doctors choosing observation status. We must comply with regulations in choosing the status or face legal consequences like fines or accusations of fraud.
Most news stories, like this one from NBC news (www.nbcnews.com/video/nightly-news/54511352#54511352) in February, are generally accurate but leave out the important fact that hospitals and doctors have little autonomy to choose the status the patient prefers. Instead, media often simply encourage patients on observation status to argue for a change to inpatient status and “be persistent.” More and more often, patients and families are arguing with the treating doctor; in many cases, that is a hospitalist.
Complaints Surge
At the 2014 SHM annual meeting last spring in Las Vegas, I spoke with many hospitalists who said that, increasingly, they are targets of observation-status complaints. One hospitalist group recently had each doctor list his or her top three frustrations with work; difficult and stressful conversations about observation status topped the list.
Patient anger regarding observation status can turn a satisfied patient into an angry one. We all know that unhappy patients are the ones most likely to pursue malpractice lawsuits. While anger over observation status doesn’t equal medical malpractice, it can change a patient’s opinion of our care, which may in some cases result in a malpractice claim.
Solutions
Medicare is unlikely to do away with observation status, so the best way to prevent complaints is to ensure that all its implications are explained to patients and families, ideally before they’re put into the hospital (e.g., while still in the ED). I think it is best if this message is delivered by someone other than the treating doctor(s): For example, a case manager might handle the discussion. Of course, patients and families are often too overwhelmed in the ED to absorb this information, so the message may need to be repeated later.
Maybe everyone should tell observation patients, “We’re going to observe you” without using any form of the word “admission.” And having these patients stay in distinct observation units probably reduces misunderstandings and complaints compared to the common practice of mixing these patients in “regular” hospital floors housing those on inpatient status.
Unfortunately, I couldn’t find research data to support this idea.
I bet some hospitals have even more elegant and effective ways to reduce misunderstandings and complaints around observation status. I’d love to hear from you if you know of any. E-mail me at john.nelson@nelsonflores.com.
I’m convinced that observation status is rapidly becoming a meaningful factor in patients’ decision to file a malpractice lawsuit.
First, let me concede that I don’t know of any hard data to support my claim. I even asked the nation’s largest malpractice insurer about this, and they didn’t have any data on it. I think that is because observation status has only become a really big issue in the last couple of years, and since it typically takes several years for a malpractice suit to conclude, it just hasn’t found its way onto their radar yet.
But I’m pretty sure that will change within the next few years.
Implications
As any seasoned practitioner in our field knows, all outpatient and inpatient physician charges for Medicare patients, along with those of other licensed practitioners, are billed through Medicare Part B. After meeting a deductible, patients with traditional fee-for-service Medicare are generally responsible for 20% of all approved Part B charges, with no upper limit. For patients seen by a large number of providers while hospitalized, this 20% can really add up. Some patients have a secondary insurance that pays for this.
Hospital charges for patients on inpatient status are billed through Medicare Part A. Patients have an annual Part A deductible, and only in the case of very long inpatient stays will they have to pay more than that for inpatient care each year.
But hospital charges for patients on observation status are billed through Part B. And because hospital charges add up so quickly, the 20% of this that the patient is responsible for can be a lot of money—thousands of dollars, even for stays of less than 24 hours. Understandably, patients are not at all happy about this.
Let’s say you’re admitted overnight on observation status and your doctor orders your usual Advair inhaler. You use it once. Most hospitals aren’t able to ensure compliance with regulations around dispensing medications for home use like a pharmacy, so they won’t let you take the inhaler home. A few weeks later you’re stunned to learn that the hospital charged $10,000 for all services provided, and you’re responsible for 20% of the allowable amount PLUS the cost of all “self administered” drugs, like inhalers, eye drops, and calcitonin nasal spray. You look over your bill to see that you’re asked to pay $350 for the inhaler you used once and couldn’t even take home with you! Many self-administered medications, including eye drops and calcitonin nasal spray, result in similarly alarming charges to patients.
On top of the unpleasant surprise of a large hospital bill, Medicare won’t pay for skilled nursing facility (SNF) care for patients who are on observation status. That is, observation is not a “qualifying” stay for beneficiaries to access their SNF benefit.
It is easy to see why patients are unhappy about observation status.
The Media Message
News media are making the public aware of the potentially high financial costs they face if placed on observation status. But, too often, they oversimplify the issue, making it seem as though the choice of observation vs. inpatient status is entirely up to the treating doctor.
Saying that this decision is entirely up to the doctor is a lot like saying it is entirely up to you to determine how fast you drive on a freeway. In a sense that is correct, because no one else is in your car to control how fast you go and, in theory, you could choose to go 100 mph or 30 mph. The only problem is that it wouldn’t be long before you’d be in trouble with the law. So you don’t have complete autonomy to choose your speed; you have to comply with the laws. The same is true for doctors choosing observation status. We must comply with regulations in choosing the status or face legal consequences like fines or accusations of fraud.
Most news stories, like this one from NBC news (www.nbcnews.com/video/nightly-news/54511352#54511352) in February, are generally accurate but leave out the important fact that hospitals and doctors have little autonomy to choose the status the patient prefers. Instead, media often simply encourage patients on observation status to argue for a change to inpatient status and “be persistent.” More and more often, patients and families are arguing with the treating doctor; in many cases, that is a hospitalist.
Complaints Surge
At the 2014 SHM annual meeting last spring in Las Vegas, I spoke with many hospitalists who said that, increasingly, they are targets of observation-status complaints. One hospitalist group recently had each doctor list his or her top three frustrations with work; difficult and stressful conversations about observation status topped the list.
Patient anger regarding observation status can turn a satisfied patient into an angry one. We all know that unhappy patients are the ones most likely to pursue malpractice lawsuits. While anger over observation status doesn’t equal medical malpractice, it can change a patient’s opinion of our care, which may in some cases result in a malpractice claim.
Solutions
Medicare is unlikely to do away with observation status, so the best way to prevent complaints is to ensure that all its implications are explained to patients and families, ideally before they’re put into the hospital (e.g., while still in the ED). I think it is best if this message is delivered by someone other than the treating doctor(s): For example, a case manager might handle the discussion. Of course, patients and families are often too overwhelmed in the ED to absorb this information, so the message may need to be repeated later.
Maybe everyone should tell observation patients, “We’re going to observe you” without using any form of the word “admission.” And having these patients stay in distinct observation units probably reduces misunderstandings and complaints compared to the common practice of mixing these patients in “regular” hospital floors housing those on inpatient status.
Unfortunately, I couldn’t find research data to support this idea.
I bet some hospitals have even more elegant and effective ways to reduce misunderstandings and complaints around observation status. I’d love to hear from you if you know of any. E-mail me at john.nelson@nelsonflores.com.
The Joys of a Life in Surgery
I have been privileged to spend over one half of my 70 years on this planet as a surgeon. Even considering the innumerable highly stressful moments and the occasional failures in patient care that continue to haunt me, I cannot conceive of a more satisfying and enjoyable vocation. It saddens me to know that a significant percentage of those in our profession have not been able to gain a similar level of fulfillment from their lives in surgery as I have.
There is no doubt that a pall of negativity has descended upon the medical profession in recent years. The factors that have caused it are real – declining compensation in face of an increased workload, less autonomy in practice with a steadily increasing number of physicians and surgeons being employees rather than independent practitioners, an oppressive regulatory environment necessitating a seemingly endless amount of paperwork, and finally the uncertainty of what our profession will look like once health care reform settles into its final form.
These issues – along with the always-present stresses that accompany caring for sick patients and the challenge of balancing a too-busy professional life with a meaningful personal existence – have led to a shocking number of our colleagues experiencing the symptoms of burnout; emotional exhaustion, depersonalization, and a sense of low personal accomplishment.
It would be inappropriate for me to in any way minimize the effect that burnout is having on medical professionals. It is now a greater threat to surgeon wellness than any other dynamic, including alcoholism and drug abuse. I will deal with it in some detail in a future editorial. But here I would like to consider some of the unique and positive features that, in my opinion, still make surgery the most noble of professions and a career that we can highly recommend to our children and grandchildren. I sincerely hope that emphasizing the more upbeat and constructive aspects of our profession, most of which are obvious but are unfortunately obscured by the cloud of negativity, will provide at least a small beacon of light for those having difficulty seeing their way forward.
I feel compelled to admit to some important disclaimers. While I do not consider myself a Pollyanna, ever since reading a Dutch study (Giltay et al., Arch. Gen. Psychiatry 2004;61:1126-35) that showed an impressive difference in longevity between optimists and pessimists, I have solidly placed myself in the optimist camp. Additionally, I have spent my entire surgical career within the ivy-covered walls of academe. Finally, I fully realize that what brings joy to one person may not do so to another.
My basic assertion is that, while many aspects of our profession have changed, the basic core – the opportunity to make positive changes in the lives of others – remains solidly intact. As a surgical academician, this was not limited to just patients, but extended to medical students, surgical residents, and surgical faculty. I suspect in the private setting there are also numerous opportunities to mentor young colleagues and lend support to surgeons who are experiencing burnout or other issues that compromise the quality of their lives and their effectiveness as surgeons.
The most satisfying aspect of my practice was the nonmonetary rewards I received from grateful patients. The patient-doctor relationship that surgeons enjoy with their patients is particularly special. We alone among medical professionals have the opportunity to suddenly and dramatically alter the course of patients’ pain, suffering, and prognosis. We alone invade the sacred spaces of their bodies. Although what we do is based on science and anatomy, to many patients, it is almost in the realm of the supernatural. I have always thought that the designing and construction of a complex building is a more challenging feat than removing a diseased gallbladder, but patients don’t see it that way. If we are willing to simply maintain meaningful and kind communication with them, they freely and liberally express their gratitude for even minimal surgical achievements. When a life-threatening situation has been suddenly erased by a surgical operation, many consider it in the domain of the heroic.
Especially amazing to me is the generosity of patients and their families even when complications or death compromise the outcome. Occasionally, gratitude comes in the guise of a gift. The most memorable for me was an envelope labeled “Pennies from Heaven” that contained $2.83 designated for bile duct cancer research given to me by the grandchildren of a woman with that dread disease on whom I had operated. The sum may have been insufficient to have any scientific impact but was more than enough to brighten my day after I observed this lovely woman enduring a long, difficult, and eventually unsuccessful postoperative course (“Pennies from Heaven,” ACS Surgery News, December 2011, p. 18).
Aside from the privilege of caring for patients, the most rewarding element of my professional life has been the opportunity to mentor others. Nearly all of us who have had success in our profession have had one or more valuable mentors. Performing this function for others is not only appropriate, but, in a sense, represents a giving back for what others have done for us. An effective mentor provides a nurturing environment in which the mentee can reach his/her full potential. Whether you are helping a resident or junior associate better adjust to life as a surgeon or find their best career path, assisting them in achieving their goals is nearly as satisfying as successfully seeing a patient through a challenging operation and complicated postoperative course.
As difficult as life in surgery can often be, focusing on the unique positives – the appreciative patient cured of a life-threatening tumor, the skilled and accomplished senior resident who you helped train, the young associate who seeks your wisdom on difficult cases and becomes a better surgeon because of it – rather than the negative background of uncertainty and loss of control may help to confirm that what you are doing is worthwhile and most likely making the world a better place.
Dr. Rikkers is the editor in chief of ACS Surgery News.
I have been privileged to spend over one half of my 70 years on this planet as a surgeon. Even considering the innumerable highly stressful moments and the occasional failures in patient care that continue to haunt me, I cannot conceive of a more satisfying and enjoyable vocation. It saddens me to know that a significant percentage of those in our profession have not been able to gain a similar level of fulfillment from their lives in surgery as I have.
There is no doubt that a pall of negativity has descended upon the medical profession in recent years. The factors that have caused it are real – declining compensation in face of an increased workload, less autonomy in practice with a steadily increasing number of physicians and surgeons being employees rather than independent practitioners, an oppressive regulatory environment necessitating a seemingly endless amount of paperwork, and finally the uncertainty of what our profession will look like once health care reform settles into its final form.
These issues – along with the always-present stresses that accompany caring for sick patients and the challenge of balancing a too-busy professional life with a meaningful personal existence – have led to a shocking number of our colleagues experiencing the symptoms of burnout; emotional exhaustion, depersonalization, and a sense of low personal accomplishment.
It would be inappropriate for me to in any way minimize the effect that burnout is having on medical professionals. It is now a greater threat to surgeon wellness than any other dynamic, including alcoholism and drug abuse. I will deal with it in some detail in a future editorial. But here I would like to consider some of the unique and positive features that, in my opinion, still make surgery the most noble of professions and a career that we can highly recommend to our children and grandchildren. I sincerely hope that emphasizing the more upbeat and constructive aspects of our profession, most of which are obvious but are unfortunately obscured by the cloud of negativity, will provide at least a small beacon of light for those having difficulty seeing their way forward.
I feel compelled to admit to some important disclaimers. While I do not consider myself a Pollyanna, ever since reading a Dutch study (Giltay et al., Arch. Gen. Psychiatry 2004;61:1126-35) that showed an impressive difference in longevity between optimists and pessimists, I have solidly placed myself in the optimist camp. Additionally, I have spent my entire surgical career within the ivy-covered walls of academe. Finally, I fully realize that what brings joy to one person may not do so to another.
My basic assertion is that, while many aspects of our profession have changed, the basic core – the opportunity to make positive changes in the lives of others – remains solidly intact. As a surgical academician, this was not limited to just patients, but extended to medical students, surgical residents, and surgical faculty. I suspect in the private setting there are also numerous opportunities to mentor young colleagues and lend support to surgeons who are experiencing burnout or other issues that compromise the quality of their lives and their effectiveness as surgeons.
The most satisfying aspect of my practice was the nonmonetary rewards I received from grateful patients. The patient-doctor relationship that surgeons enjoy with their patients is particularly special. We alone among medical professionals have the opportunity to suddenly and dramatically alter the course of patients’ pain, suffering, and prognosis. We alone invade the sacred spaces of their bodies. Although what we do is based on science and anatomy, to many patients, it is almost in the realm of the supernatural. I have always thought that the designing and construction of a complex building is a more challenging feat than removing a diseased gallbladder, but patients don’t see it that way. If we are willing to simply maintain meaningful and kind communication with them, they freely and liberally express their gratitude for even minimal surgical achievements. When a life-threatening situation has been suddenly erased by a surgical operation, many consider it in the domain of the heroic.
Especially amazing to me is the generosity of patients and their families even when complications or death compromise the outcome. Occasionally, gratitude comes in the guise of a gift. The most memorable for me was an envelope labeled “Pennies from Heaven” that contained $2.83 designated for bile duct cancer research given to me by the grandchildren of a woman with that dread disease on whom I had operated. The sum may have been insufficient to have any scientific impact but was more than enough to brighten my day after I observed this lovely woman enduring a long, difficult, and eventually unsuccessful postoperative course (“Pennies from Heaven,” ACS Surgery News, December 2011, p. 18).
Aside from the privilege of caring for patients, the most rewarding element of my professional life has been the opportunity to mentor others. Nearly all of us who have had success in our profession have had one or more valuable mentors. Performing this function for others is not only appropriate, but, in a sense, represents a giving back for what others have done for us. An effective mentor provides a nurturing environment in which the mentee can reach his/her full potential. Whether you are helping a resident or junior associate better adjust to life as a surgeon or find their best career path, assisting them in achieving their goals is nearly as satisfying as successfully seeing a patient through a challenging operation and complicated postoperative course.
As difficult as life in surgery can often be, focusing on the unique positives – the appreciative patient cured of a life-threatening tumor, the skilled and accomplished senior resident who you helped train, the young associate who seeks your wisdom on difficult cases and becomes a better surgeon because of it – rather than the negative background of uncertainty and loss of control may help to confirm that what you are doing is worthwhile and most likely making the world a better place.
Dr. Rikkers is the editor in chief of ACS Surgery News.
I have been privileged to spend over one half of my 70 years on this planet as a surgeon. Even considering the innumerable highly stressful moments and the occasional failures in patient care that continue to haunt me, I cannot conceive of a more satisfying and enjoyable vocation. It saddens me to know that a significant percentage of those in our profession have not been able to gain a similar level of fulfillment from their lives in surgery as I have.
There is no doubt that a pall of negativity has descended upon the medical profession in recent years. The factors that have caused it are real – declining compensation in face of an increased workload, less autonomy in practice with a steadily increasing number of physicians and surgeons being employees rather than independent practitioners, an oppressive regulatory environment necessitating a seemingly endless amount of paperwork, and finally the uncertainty of what our profession will look like once health care reform settles into its final form.
These issues – along with the always-present stresses that accompany caring for sick patients and the challenge of balancing a too-busy professional life with a meaningful personal existence – have led to a shocking number of our colleagues experiencing the symptoms of burnout; emotional exhaustion, depersonalization, and a sense of low personal accomplishment.
It would be inappropriate for me to in any way minimize the effect that burnout is having on medical professionals. It is now a greater threat to surgeon wellness than any other dynamic, including alcoholism and drug abuse. I will deal with it in some detail in a future editorial. But here I would like to consider some of the unique and positive features that, in my opinion, still make surgery the most noble of professions and a career that we can highly recommend to our children and grandchildren. I sincerely hope that emphasizing the more upbeat and constructive aspects of our profession, most of which are obvious but are unfortunately obscured by the cloud of negativity, will provide at least a small beacon of light for those having difficulty seeing their way forward.
I feel compelled to admit to some important disclaimers. While I do not consider myself a Pollyanna, ever since reading a Dutch study (Giltay et al., Arch. Gen. Psychiatry 2004;61:1126-35) that showed an impressive difference in longevity between optimists and pessimists, I have solidly placed myself in the optimist camp. Additionally, I have spent my entire surgical career within the ivy-covered walls of academe. Finally, I fully realize that what brings joy to one person may not do so to another.
My basic assertion is that, while many aspects of our profession have changed, the basic core – the opportunity to make positive changes in the lives of others – remains solidly intact. As a surgical academician, this was not limited to just patients, but extended to medical students, surgical residents, and surgical faculty. I suspect in the private setting there are also numerous opportunities to mentor young colleagues and lend support to surgeons who are experiencing burnout or other issues that compromise the quality of their lives and their effectiveness as surgeons.
The most satisfying aspect of my practice was the nonmonetary rewards I received from grateful patients. The patient-doctor relationship that surgeons enjoy with their patients is particularly special. We alone among medical professionals have the opportunity to suddenly and dramatically alter the course of patients’ pain, suffering, and prognosis. We alone invade the sacred spaces of their bodies. Although what we do is based on science and anatomy, to many patients, it is almost in the realm of the supernatural. I have always thought that the designing and construction of a complex building is a more challenging feat than removing a diseased gallbladder, but patients don’t see it that way. If we are willing to simply maintain meaningful and kind communication with them, they freely and liberally express their gratitude for even minimal surgical achievements. When a life-threatening situation has been suddenly erased by a surgical operation, many consider it in the domain of the heroic.
Especially amazing to me is the generosity of patients and their families even when complications or death compromise the outcome. Occasionally, gratitude comes in the guise of a gift. The most memorable for me was an envelope labeled “Pennies from Heaven” that contained $2.83 designated for bile duct cancer research given to me by the grandchildren of a woman with that dread disease on whom I had operated. The sum may have been insufficient to have any scientific impact but was more than enough to brighten my day after I observed this lovely woman enduring a long, difficult, and eventually unsuccessful postoperative course (“Pennies from Heaven,” ACS Surgery News, December 2011, p. 18).
Aside from the privilege of caring for patients, the most rewarding element of my professional life has been the opportunity to mentor others. Nearly all of us who have had success in our profession have had one or more valuable mentors. Performing this function for others is not only appropriate, but, in a sense, represents a giving back for what others have done for us. An effective mentor provides a nurturing environment in which the mentee can reach his/her full potential. Whether you are helping a resident or junior associate better adjust to life as a surgeon or find their best career path, assisting them in achieving their goals is nearly as satisfying as successfully seeing a patient through a challenging operation and complicated postoperative course.
As difficult as life in surgery can often be, focusing on the unique positives – the appreciative patient cured of a life-threatening tumor, the skilled and accomplished senior resident who you helped train, the young associate who seeks your wisdom on difficult cases and becomes a better surgeon because of it – rather than the negative background of uncertainty and loss of control may help to confirm that what you are doing is worthwhile and most likely making the world a better place.
Dr. Rikkers is the editor in chief of ACS Surgery News.

Homecare Will Help You Achieve the Triple Aim

Where there is variation, there is room for improvement. The Institute of Medicine’s report on geographic variation in Medicare spending concluded that the largest contributor to overall spending variation is spending for post-acute care services.1 Furthermore, we know that a significant amount of overall spending is devoted to post-acute care. For example, for patients hospitalized with a flare-up of a chronic condition like COPD or heart failure, Medicare spends nearly as much on post-acute care and readmissions in the first 30 days after discharge as it does on the initial admission.1
What does this mean for hospitalists?
Numerous research articles and quality improvement projects have focused on what makes a good hospital discharge or hand off to the ‘next provider of care’; however, hospitalists are increasingly participating in value-based payment programs like accountable care organizations (ACOs), risk contracts, and bundled payments. This means they must begin to pay attention to the cost side of the value equation (quality divided by cost) as it relates to hospital discharge.
A day of home care represents a more cost-effective alternative than a day of care in a skilled nursing facility (SNF). Hospitalists who can identify those patients who are appropriate to send home with home health services—and who otherwise would have gone to a SNF—will serve the dual goals of improving patient experience and decreasing costs.
Hospitalists will need to develop a decision-making process that determines the appropriate level of care for the patient after discharge. The decision-making process should address questions like:
- What skilled services lead a patient to go to a SNF instead of home with home health?
- Which patients go to a SNF instead of home simply because they don’t have family or a caregiver to help them with activities of daily living?
- Are there services requiring a nurse or a therapist that can’t be delivered in the home?
Hospitalists also will need to develop a more intimate understanding of the following levels of care:
- Skilled nursing includes management of a nursing care plan, assessment of a patient’s changing condition, and services like wound care, infusion therapy, and management of medications, feeding or drainage tubes, and pain.
- Skilled rehabilitation refers to the array of services provided by physical, occupational, speech, and respiratory therapists.
- Custodial care, usually supplied by a home health aid or family member, includes help with activities of daily living (feeding, dressing, bathing, grooming, personal hygiene, and toileting).
It should be noted that most skilled nursing or therapy services can be delivered in the home setting if the patient’s custodial care needs are met—a big ‘if’ in some cases. Some patients go to a SNF because they require three or more skilled nursing or therapy services, and it is therefore impractical for them to go home.
Here are my suggestions to hospitalists seeking to reengineer the discharge process with the goals of “right-sizing” the number of patients who go to SNFs and optimizing the utilization of home healthcare services:
- Become familiar with the range of post-acute care providers and care coordination services in your community.
- Refer any patient who wishes to go home, either directly or after a SNF stay, for a home care evaluation. Home care agencies are experts in determining if and how patients can return home.
- If a need for help with activities of daily living is the major barrier to having a patient discharged to home, create a system in which case management develops a custodial care plan with the patient and caregivers during the inpatient stay. Currently, this step is delayed until well into the SNF stay and may prolong that stay. Such a plan includes a financial analysis, screening for Medicaid eligibility, and evaluating whether a family member can assume some or all of the custodial care needs.
- If a patient is being discharged to a SNF, review the list of needed services leading to the SNF transfer. Ask the case manager if these services can be provided in the home. If not, then why?
- Bed capacity permitting, consider keeping patients who are functionally improving in the hospital an extra day so they can be discharged directly home instead of to a SNF.2
In his seminal work, The Innovator’s Dilemma, Clayton Christensen describes “disruptive innovation” as that which gives rise to products or services that are cheaper, simpler, and more convenient to use. Even though home care has been around for a while, there is a sizeable group of patients, especially in geographic areas of high SNF spending, who might be better served in the home environment. As we create better systems under value-based payment, we should see an increase in the use of home healthcare as a disruptive innovation when applied to appropriate patients transitioning out of the hospital or a SNF.

Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
Where there is variation, there is room for improvement. The Institute of Medicine’s report on geographic variation in Medicare spending concluded that the largest contributor to overall spending variation is spending for post-acute care services.1 Furthermore, we know that a significant amount of overall spending is devoted to post-acute care. For example, for patients hospitalized with a flare-up of a chronic condition like COPD or heart failure, Medicare spends nearly as much on post-acute care and readmissions in the first 30 days after discharge as it does on the initial admission.1
What does this mean for hospitalists?
Numerous research articles and quality improvement projects have focused on what makes a good hospital discharge or hand off to the ‘next provider of care’; however, hospitalists are increasingly participating in value-based payment programs like accountable care organizations (ACOs), risk contracts, and bundled payments. This means they must begin to pay attention to the cost side of the value equation (quality divided by cost) as it relates to hospital discharge.
A day of home care represents a more cost-effective alternative than a day of care in a skilled nursing facility (SNF). Hospitalists who can identify those patients who are appropriate to send home with home health services—and who otherwise would have gone to a SNF—will serve the dual goals of improving patient experience and decreasing costs.
Hospitalists will need to develop a decision-making process that determines the appropriate level of care for the patient after discharge. The decision-making process should address questions like:
- What skilled services lead a patient to go to a SNF instead of home with home health?
- Which patients go to a SNF instead of home simply because they don’t have family or a caregiver to help them with activities of daily living?
- Are there services requiring a nurse or a therapist that can’t be delivered in the home?
Hospitalists also will need to develop a more intimate understanding of the following levels of care:
- Skilled nursing includes management of a nursing care plan, assessment of a patient’s changing condition, and services like wound care, infusion therapy, and management of medications, feeding or drainage tubes, and pain.
- Skilled rehabilitation refers to the array of services provided by physical, occupational, speech, and respiratory therapists.
- Custodial care, usually supplied by a home health aid or family member, includes help with activities of daily living (feeding, dressing, bathing, grooming, personal hygiene, and toileting).
It should be noted that most skilled nursing or therapy services can be delivered in the home setting if the patient’s custodial care needs are met—a big ‘if’ in some cases. Some patients go to a SNF because they require three or more skilled nursing or therapy services, and it is therefore impractical for them to go home.
Here are my suggestions to hospitalists seeking to reengineer the discharge process with the goals of “right-sizing” the number of patients who go to SNFs and optimizing the utilization of home healthcare services:
- Become familiar with the range of post-acute care providers and care coordination services in your community.
- Refer any patient who wishes to go home, either directly or after a SNF stay, for a home care evaluation. Home care agencies are experts in determining if and how patients can return home.
- If a need for help with activities of daily living is the major barrier to having a patient discharged to home, create a system in which case management develops a custodial care plan with the patient and caregivers during the inpatient stay. Currently, this step is delayed until well into the SNF stay and may prolong that stay. Such a plan includes a financial analysis, screening for Medicaid eligibility, and evaluating whether a family member can assume some or all of the custodial care needs.
- If a patient is being discharged to a SNF, review the list of needed services leading to the SNF transfer. Ask the case manager if these services can be provided in the home. If not, then why?
- Bed capacity permitting, consider keeping patients who are functionally improving in the hospital an extra day so they can be discharged directly home instead of to a SNF.2
In his seminal work, The Innovator’s Dilemma, Clayton Christensen describes “disruptive innovation” as that which gives rise to products or services that are cheaper, simpler, and more convenient to use. Even though home care has been around for a while, there is a sizeable group of patients, especially in geographic areas of high SNF spending, who might be better served in the home environment. As we create better systems under value-based payment, we should see an increase in the use of home healthcare as a disruptive innovation when applied to appropriate patients transitioning out of the hospital or a SNF.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
Where there is variation, there is room for improvement. The Institute of Medicine’s report on geographic variation in Medicare spending concluded that the largest contributor to overall spending variation is spending for post-acute care services.1 Furthermore, we know that a significant amount of overall spending is devoted to post-acute care. For example, for patients hospitalized with a flare-up of a chronic condition like COPD or heart failure, Medicare spends nearly as much on post-acute care and readmissions in the first 30 days after discharge as it does on the initial admission.1
What does this mean for hospitalists?
Numerous research articles and quality improvement projects have focused on what makes a good hospital discharge or hand off to the ‘next provider of care’; however, hospitalists are increasingly participating in value-based payment programs like accountable care organizations (ACOs), risk contracts, and bundled payments. This means they must begin to pay attention to the cost side of the value equation (quality divided by cost) as it relates to hospital discharge.
A day of home care represents a more cost-effective alternative than a day of care in a skilled nursing facility (SNF). Hospitalists who can identify those patients who are appropriate to send home with home health services—and who otherwise would have gone to a SNF—will serve the dual goals of improving patient experience and decreasing costs.
Hospitalists will need to develop a decision-making process that determines the appropriate level of care for the patient after discharge. The decision-making process should address questions like:
- What skilled services lead a patient to go to a SNF instead of home with home health?
- Which patients go to a SNF instead of home simply because they don’t have family or a caregiver to help them with activities of daily living?
- Are there services requiring a nurse or a therapist that can’t be delivered in the home?
Hospitalists also will need to develop a more intimate understanding of the following levels of care:
- Skilled nursing includes management of a nursing care plan, assessment of a patient’s changing condition, and services like wound care, infusion therapy, and management of medications, feeding or drainage tubes, and pain.
- Skilled rehabilitation refers to the array of services provided by physical, occupational, speech, and respiratory therapists.
- Custodial care, usually supplied by a home health aid or family member, includes help with activities of daily living (feeding, dressing, bathing, grooming, personal hygiene, and toileting).
It should be noted that most skilled nursing or therapy services can be delivered in the home setting if the patient’s custodial care needs are met—a big ‘if’ in some cases. Some patients go to a SNF because they require three or more skilled nursing or therapy services, and it is therefore impractical for them to go home.
Here are my suggestions to hospitalists seeking to reengineer the discharge process with the goals of “right-sizing” the number of patients who go to SNFs and optimizing the utilization of home healthcare services:
- Become familiar with the range of post-acute care providers and care coordination services in your community.
- Refer any patient who wishes to go home, either directly or after a SNF stay, for a home care evaluation. Home care agencies are experts in determining if and how patients can return home.
- If a need for help with activities of daily living is the major barrier to having a patient discharged to home, create a system in which case management develops a custodial care plan with the patient and caregivers during the inpatient stay. Currently, this step is delayed until well into the SNF stay and may prolong that stay. Such a plan includes a financial analysis, screening for Medicaid eligibility, and evaluating whether a family member can assume some or all of the custodial care needs.
- If a patient is being discharged to a SNF, review the list of needed services leading to the SNF transfer. Ask the case manager if these services can be provided in the home. If not, then why?
- Bed capacity permitting, consider keeping patients who are functionally improving in the hospital an extra day so they can be discharged directly home instead of to a SNF.2
In his seminal work, The Innovator’s Dilemma, Clayton Christensen describes “disruptive innovation” as that which gives rise to products or services that are cheaper, simpler, and more convenient to use. Even though home care has been around for a while, there is a sizeable group of patients, especially in geographic areas of high SNF spending, who might be better served in the home environment. As we create better systems under value-based payment, we should see an increase in the use of home healthcare as a disruptive innovation when applied to appropriate patients transitioning out of the hospital or a SNF.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
Put Key Principles, Characteristics of Effective Hospital Medicine Groups to Work


I hope you’re already familiar with “The Key Principles and Characteristics of an Effective Hospital Medicine Group: An Assessment Guide for Hospitals and Hospitalists” [www.hospitalmedicine.org/keychar] and have spent at least a few minutes reviewing the list of 10 “principles” and 47 “characteristics” thought to be associated with effective hospital medicine groups (HMGs). (Full disclosure: I was one of the authors of the article published in February 2014 in the Journal of Hospital Medicine.) Most of us are very busy, so the temptation might be high to set the article aside and risk forgetting it. But I hope many in our field, both clinicians and administrators, will look at it more carefully. There are a number of ways you could use the guide to stimulate thinking or change in your practice.
Grading Our Specialty
I just returned from a meeting of about 10 hospitalist leaders from different organizations around the country. Attendees represented the diversity of our field, including hospital-employed HMGs, large hospitalist management companies, and academic programs. We spent a portion of the meeting discussing what grade we as a group would give the whole specialty of hospital medicine on each of the 10 “principles.” Essentially, we generated a report card for the U.S. hospitalist movement.
This wasn’t a rigorous scientific exercise; instead, it was a robust and thought-provoking discussion around what grade to assign. Opinions regarding the appropriate grade varied significantly, but a common theme was that our specialty really “owns” the importance of pursuing many or most of the principles listed in the article and is devoting time and resources to them even if many individual HMGs might have a long way to go to perform optimally.
For example, meeting attendees thought our field has for a long time worked diligently to “support care coordination across the care continuum” (Principle 6). No one thought that all HMGs do this optimally, but the consensus was that most HMGs have invested effort to do it well. And most were concerned that many HMGs still lack “adequate resources” (Principle 3) and sufficiently “engaged hospitalists” (Principle 2)—and that the former contributes to the latter.
The opinion of the hospitalist leaders who happened to attend the meeting where this conversation took place doesn’t represent the final word on how our specialty is performing, but I think all involved found value in having the conversation, hearing different perspectives about what we’re doing well and where we should focus energy and resources to improve.
Grading Your HM Group
You might want to do something similar within your own group, but make it more relevant by grading how your own practice performs on each of the 10 principles. You could do this on your own just to stimulate your thinking, or you could have each member of your HMG generate a report card of your group’s performance—then discuss where there is agreement or disagreement within the group.
You could structure this sort of individual or group assessment simply as an exercise to generate ideas and conversation about the practice, or your group could take a more formal approach and use it as part of a planning process to determine future practice management-related goals. I know of some groups that scheduled strategic planning meetings specifically to discuss which of the elements to make a priority.
Discussion Document for Leadership
In addition to using the article to generate conversation among hospitalists within your group, it can be a really valuable tool in guiding conversations with hospital leaders and the entity that employs the hospitalists. For example, you could use the article to generate or update the job description of the lead hospitalist or practice manager. Or during annual budgeting for the hospitalist practice, the guide could be used as a checklist to think about whether there are important areas that would benefit from more resources.
Of course, there is a risk that hospital leaders or those who employ the hospitalists could use the article primarily to criticize a hospitalist group and its leader for not already having excellent performance on every one of the principles and characteristics listed. That would be pretty unfortunate; there probably isn’t a single group that performs well on every domain, and the real value of the article is to “be aspirational, helping to raise the bar” for each HMG and our specialty as a whole.
And, as discussed in the article, an HMG doesn’t need to be a stellar performer on all 47 characteristics to be effective. Some of the characteristics listed in the article may not apply to all groups, so all involved in the management of any individual HMG should think about whether to set some aside when assessing their own group.
Where to Go from Here
The article is based on expert opinion, with the help of many more people than those listed as author, and I’m hopeful it will stimulate researchers to study some of these principles and characteristics. For many reasons, we will probably never have robust data, but I’d be happy for whatever we can get.
There is a pretty good chance that the evolution in the work we do and the nature of the hospital setting mean that the principles and characteristics may need to be revised periodically. I would love to know how they might be different in 10 or 20 years.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
I hope you’re already familiar with “The Key Principles and Characteristics of an Effective Hospital Medicine Group: An Assessment Guide for Hospitals and Hospitalists” [www.hospitalmedicine.org/keychar] and have spent at least a few minutes reviewing the list of 10 “principles” and 47 “characteristics” thought to be associated with effective hospital medicine groups (HMGs). (Full disclosure: I was one of the authors of the article published in February 2014 in the Journal of Hospital Medicine.) Most of us are very busy, so the temptation might be high to set the article aside and risk forgetting it. But I hope many in our field, both clinicians and administrators, will look at it more carefully. There are a number of ways you could use the guide to stimulate thinking or change in your practice.
Grading Our Specialty
I just returned from a meeting of about 10 hospitalist leaders from different organizations around the country. Attendees represented the diversity of our field, including hospital-employed HMGs, large hospitalist management companies, and academic programs. We spent a portion of the meeting discussing what grade we as a group would give the whole specialty of hospital medicine on each of the 10 “principles.” Essentially, we generated a report card for the U.S. hospitalist movement.
This wasn’t a rigorous scientific exercise; instead, it was a robust and thought-provoking discussion around what grade to assign. Opinions regarding the appropriate grade varied significantly, but a common theme was that our specialty really “owns” the importance of pursuing many or most of the principles listed in the article and is devoting time and resources to them even if many individual HMGs might have a long way to go to perform optimally.
For example, meeting attendees thought our field has for a long time worked diligently to “support care coordination across the care continuum” (Principle 6). No one thought that all HMGs do this optimally, but the consensus was that most HMGs have invested effort to do it well. And most were concerned that many HMGs still lack “adequate resources” (Principle 3) and sufficiently “engaged hospitalists” (Principle 2)—and that the former contributes to the latter.
The opinion of the hospitalist leaders who happened to attend the meeting where this conversation took place doesn’t represent the final word on how our specialty is performing, but I think all involved found value in having the conversation, hearing different perspectives about what we’re doing well and where we should focus energy and resources to improve.
Grading Your HM Group
You might want to do something similar within your own group, but make it more relevant by grading how your own practice performs on each of the 10 principles. You could do this on your own just to stimulate your thinking, or you could have each member of your HMG generate a report card of your group’s performance—then discuss where there is agreement or disagreement within the group.
You could structure this sort of individual or group assessment simply as an exercise to generate ideas and conversation about the practice, or your group could take a more formal approach and use it as part of a planning process to determine future practice management-related goals. I know of some groups that scheduled strategic planning meetings specifically to discuss which of the elements to make a priority.
Discussion Document for Leadership
In addition to using the article to generate conversation among hospitalists within your group, it can be a really valuable tool in guiding conversations with hospital leaders and the entity that employs the hospitalists. For example, you could use the article to generate or update the job description of the lead hospitalist or practice manager. Or during annual budgeting for the hospitalist practice, the guide could be used as a checklist to think about whether there are important areas that would benefit from more resources.
Of course, there is a risk that hospital leaders or those who employ the hospitalists could use the article primarily to criticize a hospitalist group and its leader for not already having excellent performance on every one of the principles and characteristics listed. That would be pretty unfortunate; there probably isn’t a single group that performs well on every domain, and the real value of the article is to “be aspirational, helping to raise the bar” for each HMG and our specialty as a whole.
And, as discussed in the article, an HMG doesn’t need to be a stellar performer on all 47 characteristics to be effective. Some of the characteristics listed in the article may not apply to all groups, so all involved in the management of any individual HMG should think about whether to set some aside when assessing their own group.
Where to Go from Here
The article is based on expert opinion, with the help of many more people than those listed as author, and I’m hopeful it will stimulate researchers to study some of these principles and characteristics. For many reasons, we will probably never have robust data, but I’d be happy for whatever we can get.
There is a pretty good chance that the evolution in the work we do and the nature of the hospital setting mean that the principles and characteristics may need to be revised periodically. I would love to know how they might be different in 10 or 20 years.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
I hope you’re already familiar with “The Key Principles and Characteristics of an Effective Hospital Medicine Group: An Assessment Guide for Hospitals and Hospitalists” [www.hospitalmedicine.org/keychar] and have spent at least a few minutes reviewing the list of 10 “principles” and 47 “characteristics” thought to be associated with effective hospital medicine groups (HMGs). (Full disclosure: I was one of the authors of the article published in February 2014 in the Journal of Hospital Medicine.) Most of us are very busy, so the temptation might be high to set the article aside and risk forgetting it. But I hope many in our field, both clinicians and administrators, will look at it more carefully. There are a number of ways you could use the guide to stimulate thinking or change in your practice.
Grading Our Specialty
I just returned from a meeting of about 10 hospitalist leaders from different organizations around the country. Attendees represented the diversity of our field, including hospital-employed HMGs, large hospitalist management companies, and academic programs. We spent a portion of the meeting discussing what grade we as a group would give the whole specialty of hospital medicine on each of the 10 “principles.” Essentially, we generated a report card for the U.S. hospitalist movement.
This wasn’t a rigorous scientific exercise; instead, it was a robust and thought-provoking discussion around what grade to assign. Opinions regarding the appropriate grade varied significantly, but a common theme was that our specialty really “owns” the importance of pursuing many or most of the principles listed in the article and is devoting time and resources to them even if many individual HMGs might have a long way to go to perform optimally.
For example, meeting attendees thought our field has for a long time worked diligently to “support care coordination across the care continuum” (Principle 6). No one thought that all HMGs do this optimally, but the consensus was that most HMGs have invested effort to do it well. And most were concerned that many HMGs still lack “adequate resources” (Principle 3) and sufficiently “engaged hospitalists” (Principle 2)—and that the former contributes to the latter.
The opinion of the hospitalist leaders who happened to attend the meeting where this conversation took place doesn’t represent the final word on how our specialty is performing, but I think all involved found value in having the conversation, hearing different perspectives about what we’re doing well and where we should focus energy and resources to improve.
Grading Your HM Group
You might want to do something similar within your own group, but make it more relevant by grading how your own practice performs on each of the 10 principles. You could do this on your own just to stimulate your thinking, or you could have each member of your HMG generate a report card of your group’s performance—then discuss where there is agreement or disagreement within the group.
You could structure this sort of individual or group assessment simply as an exercise to generate ideas and conversation about the practice, or your group could take a more formal approach and use it as part of a planning process to determine future practice management-related goals. I know of some groups that scheduled strategic planning meetings specifically to discuss which of the elements to make a priority.
Discussion Document for Leadership
In addition to using the article to generate conversation among hospitalists within your group, it can be a really valuable tool in guiding conversations with hospital leaders and the entity that employs the hospitalists. For example, you could use the article to generate or update the job description of the lead hospitalist or practice manager. Or during annual budgeting for the hospitalist practice, the guide could be used as a checklist to think about whether there are important areas that would benefit from more resources.
Of course, there is a risk that hospital leaders or those who employ the hospitalists could use the article primarily to criticize a hospitalist group and its leader for not already having excellent performance on every one of the principles and characteristics listed. That would be pretty unfortunate; there probably isn’t a single group that performs well on every domain, and the real value of the article is to “be aspirational, helping to raise the bar” for each HMG and our specialty as a whole.
And, as discussed in the article, an HMG doesn’t need to be a stellar performer on all 47 characteristics to be effective. Some of the characteristics listed in the article may not apply to all groups, so all involved in the management of any individual HMG should think about whether to set some aside when assessing their own group.
Where to Go from Here
The article is based on expert opinion, with the help of many more people than those listed as author, and I’m hopeful it will stimulate researchers to study some of these principles and characteristics. For many reasons, we will probably never have robust data, but I’d be happy for whatever we can get.
There is a pretty good chance that the evolution in the work we do and the nature of the hospital setting mean that the principles and characteristics may need to be revised periodically. I would love to know how they might be different in 10 or 20 years.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Many eyes are better
Peer review is the filter that determines what is published in the scientific literature and what is not allowed to see the light of day. It has been considered "the gatekeeper of science." In modern times, peer review has consisted of a journal editor sending a submitted article to a limited number of experts in the field who then judge its worth for publication. Many specialists see reviewing manuscripts as a service to their profession, put considerable effort into their analysis, and provide extensive comments on revisions needed to strengthen papers.
However, the value of this venerable process as it is presently constituted has been questioned by numerous critics. Because manuscripts are reviewed by a limited number of often rival scientists in a highly specialized field, the practice is prone to bias. Innovation may be stifled when reviewers reject outlier concepts that may be correct but that do not fit into the mainstream of thought. Critiques are often superficial as they are performed by otherwise busy individuals who receive no compensation for their efforts. Finally, journal editors are given undue power in the process. Not only do they make the final decision to publish or reject a manuscript, they are also responsible for selecting reviewers and are then free to ignore or accept their recommendations.
These criticisms of this time-honored system have led to a strong impetus for change. Coincident with the motivation for modifying this essential component of the publication process have been technological advancements that are facilitating new approaches. The Internet has provided a mechanism for making peer review a more open, inclusive process with any member of the scientific community who so desires having the opportunity to contribute to the evaluation of published work. A recent incident highlights how uninvited, but valuable, input from the wider scientific community can rapidly and effectively improve the accuracy of the literature.
On July 2, 2014, National Public Radio’s Morning Edition broadcast "Easy method for making stem cells was too good to be true" and a New York Times headline proclaimed "Stem cell research papers are retracted." In January 2014, Haruko Obokata of the RIKEN Centre for Developmental Biology in Japan published an innovative and considerably simpler method of producing stem cells than extracting them from embryos or making them from skin cells in a complicated and prolonged process (Nature 2014;505: 641-7). At the time of publication, the work was viewed by many to be potentially Nobel Prize-worthy research—that is, until the stem cell research community chimed in with its extensive and detailed post-publication peer review.
A number of research groups questioned Obokata’s conclusions. Some even attempted to replicate the experiments, but with no success. Soon the critics’ findings and opinions appeared on a variety of websites and blogs, including the Nature website. The RIKEN Centre took notice and appointed a committee to investigate the research. The committee found that Obokata had manipulated her data on at least two occasions and concluded that she had participated in research misconduct. Pressure mounted, which led to the recent voluntary retraction of the article by its authors.
This case represents an extreme outcome resulting from a failure of pre-publication vetting followed by a successful post-hoc peer review. But it demonstrates how the emerging and more comprehensive means of evaluating published research is rapidly working its way into the fabric of how science and the reporting of it operate. It would be ideal if this extensive vetting of potentially important research could be done prior to rather than after its release to the general public. Physics academicians have accomplished this by posting their research papers as pre-prints on-line for their colleagues to evaluate. Only after a successful conclusion of this process is a work deemed acceptable for entry into the physics literature. Submission of biomedical research to a similar process has a significant downside in that new, possibly harmful therapies, not yet peer-reviewed, could be adopted by practitioners and/or patients before their time. However, some modification of it will likely evolve and lead to a more accurate assessment of submitted work than the present process allows.
How publications are valued is also being modified thanks to the omnibus means of rapid communication allowed by an ever-expanding Internet. Bibliometrics, most notably the number of times an article is subsequently cited in print, has been the mainstay in determining the value of individual articles. The journal impact factor, which has historically been the main measure of a journal\'s standing compared to that of others in its field, is derived from the aggregate of citations for all articles over a period of time. With the advent of the Internet, a new set of alternative metrics (altmetrics) is now contributing to the evaluation of published work. While print citations take years to accumulate, article downloads, mentions on Facebook, number of tweets on Twitter, and numerous other altmetrics have the considerable advantage of immediacy and can be logged by any reader, not only those authors who decide to subsequently cite certain publications. Although these new metrics are unlikely to replace traditional citations in assigning value to individual articles, along with them, they will be helpful in determining what must be read to maintain currency in one’s specialty.
So, readers of the surgical literature feel your newly found power and exert it. You along with your colleagues around the globe can, and in fact have an obligation to, play a role in determining what is worth reading from an ever-expanding volume of new information. Many eyes will almost certainly be better than relying solely on the opinions of a chosen few.
Dr. Rikkers is Editor in Chief of ACS Surgery News.
Peer review is the filter that determines what is published in the scientific literature and what is not allowed to see the light of day. It has been considered "the gatekeeper of science." In modern times, peer review has consisted of a journal editor sending a submitted article to a limited number of experts in the field who then judge its worth for publication. Many specialists see reviewing manuscripts as a service to their profession, put considerable effort into their analysis, and provide extensive comments on revisions needed to strengthen papers.
However, the value of this venerable process as it is presently constituted has been questioned by numerous critics. Because manuscripts are reviewed by a limited number of often rival scientists in a highly specialized field, the practice is prone to bias. Innovation may be stifled when reviewers reject outlier concepts that may be correct but that do not fit into the mainstream of thought. Critiques are often superficial as they are performed by otherwise busy individuals who receive no compensation for their efforts. Finally, journal editors are given undue power in the process. Not only do they make the final decision to publish or reject a manuscript, they are also responsible for selecting reviewers and are then free to ignore or accept their recommendations.
These criticisms of this time-honored system have led to a strong impetus for change. Coincident with the motivation for modifying this essential component of the publication process have been technological advancements that are facilitating new approaches. The Internet has provided a mechanism for making peer review a more open, inclusive process with any member of the scientific community who so desires having the opportunity to contribute to the evaluation of published work. A recent incident highlights how uninvited, but valuable, input from the wider scientific community can rapidly and effectively improve the accuracy of the literature.
On July 2, 2014, National Public Radio’s Morning Edition broadcast "Easy method for making stem cells was too good to be true" and a New York Times headline proclaimed "Stem cell research papers are retracted." In January 2014, Haruko Obokata of the RIKEN Centre for Developmental Biology in Japan published an innovative and considerably simpler method of producing stem cells than extracting them from embryos or making them from skin cells in a complicated and prolonged process (Nature 2014;505: 641-7). At the time of publication, the work was viewed by many to be potentially Nobel Prize-worthy research—that is, until the stem cell research community chimed in with its extensive and detailed post-publication peer review.
A number of research groups questioned Obokata’s conclusions. Some even attempted to replicate the experiments, but with no success. Soon the critics’ findings and opinions appeared on a variety of websites and blogs, including the Nature website. The RIKEN Centre took notice and appointed a committee to investigate the research. The committee found that Obokata had manipulated her data on at least two occasions and concluded that she had participated in research misconduct. Pressure mounted, which led to the recent voluntary retraction of the article by its authors.
This case represents an extreme outcome resulting from a failure of pre-publication vetting followed by a successful post-hoc peer review. But it demonstrates how the emerging and more comprehensive means of evaluating published research is rapidly working its way into the fabric of how science and the reporting of it operate. It would be ideal if this extensive vetting of potentially important research could be done prior to rather than after its release to the general public. Physics academicians have accomplished this by posting their research papers as pre-prints on-line for their colleagues to evaluate. Only after a successful conclusion of this process is a work deemed acceptable for entry into the physics literature. Submission of biomedical research to a similar process has a significant downside in that new, possibly harmful therapies, not yet peer-reviewed, could be adopted by practitioners and/or patients before their time. However, some modification of it will likely evolve and lead to a more accurate assessment of submitted work than the present process allows.
How publications are valued is also being modified thanks to the omnibus means of rapid communication allowed by an ever-expanding Internet. Bibliometrics, most notably the number of times an article is subsequently cited in print, has been the mainstay in determining the value of individual articles. The journal impact factor, which has historically been the main measure of a journal\'s standing compared to that of others in its field, is derived from the aggregate of citations for all articles over a period of time. With the advent of the Internet, a new set of alternative metrics (altmetrics) is now contributing to the evaluation of published work. While print citations take years to accumulate, article downloads, mentions on Facebook, number of tweets on Twitter, and numerous other altmetrics have the considerable advantage of immediacy and can be logged by any reader, not only those authors who decide to subsequently cite certain publications. Although these new metrics are unlikely to replace traditional citations in assigning value to individual articles, along with them, they will be helpful in determining what must be read to maintain currency in one’s specialty.
So, readers of the surgical literature feel your newly found power and exert it. You along with your colleagues around the globe can, and in fact have an obligation to, play a role in determining what is worth reading from an ever-expanding volume of new information. Many eyes will almost certainly be better than relying solely on the opinions of a chosen few.
Dr. Rikkers is Editor in Chief of ACS Surgery News.
Peer review is the filter that determines what is published in the scientific literature and what is not allowed to see the light of day. It has been considered "the gatekeeper of science." In modern times, peer review has consisted of a journal editor sending a submitted article to a limited number of experts in the field who then judge its worth for publication. Many specialists see reviewing manuscripts as a service to their profession, put considerable effort into their analysis, and provide extensive comments on revisions needed to strengthen papers.
However, the value of this venerable process as it is presently constituted has been questioned by numerous critics. Because manuscripts are reviewed by a limited number of often rival scientists in a highly specialized field, the practice is prone to bias. Innovation may be stifled when reviewers reject outlier concepts that may be correct but that do not fit into the mainstream of thought. Critiques are often superficial as they are performed by otherwise busy individuals who receive no compensation for their efforts. Finally, journal editors are given undue power in the process. Not only do they make the final decision to publish or reject a manuscript, they are also responsible for selecting reviewers and are then free to ignore or accept their recommendations.
These criticisms of this time-honored system have led to a strong impetus for change. Coincident with the motivation for modifying this essential component of the publication process have been technological advancements that are facilitating new approaches. The Internet has provided a mechanism for making peer review a more open, inclusive process with any member of the scientific community who so desires having the opportunity to contribute to the evaluation of published work. A recent incident highlights how uninvited, but valuable, input from the wider scientific community can rapidly and effectively improve the accuracy of the literature.
On July 2, 2014, National Public Radio’s Morning Edition broadcast "Easy method for making stem cells was too good to be true" and a New York Times headline proclaimed "Stem cell research papers are retracted." In January 2014, Haruko Obokata of the RIKEN Centre for Developmental Biology in Japan published an innovative and considerably simpler method of producing stem cells than extracting them from embryos or making them from skin cells in a complicated and prolonged process (Nature 2014;505: 641-7). At the time of publication, the work was viewed by many to be potentially Nobel Prize-worthy research—that is, until the stem cell research community chimed in with its extensive and detailed post-publication peer review.
A number of research groups questioned Obokata’s conclusions. Some even attempted to replicate the experiments, but with no success. Soon the critics’ findings and opinions appeared on a variety of websites and blogs, including the Nature website. The RIKEN Centre took notice and appointed a committee to investigate the research. The committee found that Obokata had manipulated her data on at least two occasions and concluded that she had participated in research misconduct. Pressure mounted, which led to the recent voluntary retraction of the article by its authors.
This case represents an extreme outcome resulting from a failure of pre-publication vetting followed by a successful post-hoc peer review. But it demonstrates how the emerging and more comprehensive means of evaluating published research is rapidly working its way into the fabric of how science and the reporting of it operate. It would be ideal if this extensive vetting of potentially important research could be done prior to rather than after its release to the general public. Physics academicians have accomplished this by posting their research papers as pre-prints on-line for their colleagues to evaluate. Only after a successful conclusion of this process is a work deemed acceptable for entry into the physics literature. Submission of biomedical research to a similar process has a significant downside in that new, possibly harmful therapies, not yet peer-reviewed, could be adopted by practitioners and/or patients before their time. However, some modification of it will likely evolve and lead to a more accurate assessment of submitted work than the present process allows.
How publications are valued is also being modified thanks to the omnibus means of rapid communication allowed by an ever-expanding Internet. Bibliometrics, most notably the number of times an article is subsequently cited in print, has been the mainstay in determining the value of individual articles. The journal impact factor, which has historically been the main measure of a journal\'s standing compared to that of others in its field, is derived from the aggregate of citations for all articles over a period of time. With the advent of the Internet, a new set of alternative metrics (altmetrics) is now contributing to the evaluation of published work. While print citations take years to accumulate, article downloads, mentions on Facebook, number of tweets on Twitter, and numerous other altmetrics have the considerable advantage of immediacy and can be logged by any reader, not only those authors who decide to subsequently cite certain publications. Although these new metrics are unlikely to replace traditional citations in assigning value to individual articles, along with them, they will be helpful in determining what must be read to maintain currency in one’s specialty.
So, readers of the surgical literature feel your newly found power and exert it. You along with your colleagues around the globe can, and in fact have an obligation to, play a role in determining what is worth reading from an ever-expanding volume of new information. Many eyes will almost certainly be better than relying solely on the opinions of a chosen few.
Dr. Rikkers is Editor in Chief of ACS Surgery News.

Proper Inpatient Documentation, Coding Essential to Avoid a Medicare Audit

Several years ago we sent a CPT coding auditor 15 chart notes generated by each doctor in our group. Among each doctors’ 15 notes were at least one or two billed as initial hospital care, follow up, discharge, critical care, and so on. This coding expert returned a report showing that, out of all the notes reviewed, a significant portion were not billed at the correct level. Most of the incorrectly billed notes were judged to reflect “up-coding,” and a few were seen as “down-coded.”
This was distressing and hard to believe.
So I took the same set of notes and paid a second coding expert for an independent review. She didn’t know about the first audit but returned a report that showed a nearly identical portion of incorrectly coded notes.
Two independent audits showing nearly the same portion of notes coded incorrectly was alarming. But it was difficult for my partners and me to address, because the auditors didn’t agree on the correct code for many of the notes. In some cases, both flagged a note as incorrectly coded but didn’t agree on the correct code. For a number of the notes, one auditor said the visit was “up-coded,” while the other said it was “down-coded.” There was so little agreement between the two of them that we had a hard time coming up with any firm conclusions about what we should do to improve our performance.
If experts who think about coding all the time can’t agree on the right code for a given note, how can hospitalists be expected to code nearly all of our visits accurately?
RAC: Recovery Audit Contractor
Despite what I believe is poor inter-rater reliability among coding auditors, we need to work diligently to comply with coding guidelines. A 2003 Federal law mandated a program of Recovery Audit Contractors, or RAC for short, to find cases of “up-coding” or other overbilling and require the provider to repay any resulting loss.
A number of companies are in the business of conducting RAC audits (one of them, CGI, is the Canadian company blamed for the failed “Obamacare” exchange websites), and there is a reasonable chance one of these companies has reviewed some of your charges—or those of your hospitalist colleagues.
The RAC auditors review information about your charges, and if they determine that you up-coded or overbilled, they send a “demand letter” summarizing their findings, along with the amount of money they have determined you should pay back. (Theoretically, they could notify you of “under-coding,” so that you can be paid more for past work, but I haven’t yet come across an example of that.)
It is common to appeal the RAC findings, but that can be a long process, and many organizations decide to pay back all the money requested by the RAC as quickly as possible to avoid paying interest on a delayed payment if the appeal is unsuccessful. In the case of a successful appeal, the money previously refunded by the doctor would be returned.
Page 338 of the CMS Fiscal Year 2015 “Justification of Estimates for Appropriations Committees” says that “…about 50 percent of the estimated 43,000 appeals [of adverse RAC audit findings] were fully or partially overturned…” This could mean the RACs are a sort of loose cannon, accusing many providers of overbilling while knowing that some won’t bother to appeal because they don’t understand the process or because the dollar amount involved for a single provider is too small to justify the time and expense of conducting the appeal. In this way, a RAC audit is like the $15 rebate on the last electronic gadget you bought. The seller knows that many people, including me, will fail to do the work required to claim the rebate.
Accuracy Strategies
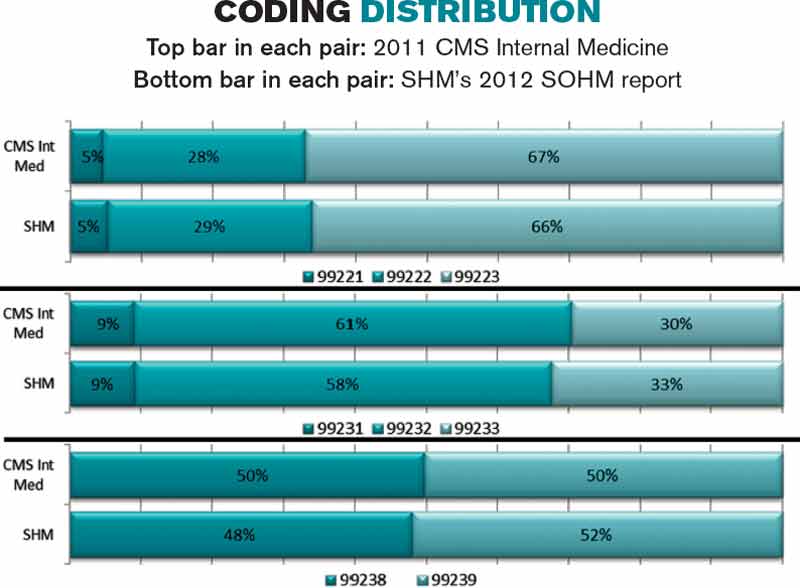
There are a number of ways to help your group ensure appropriate CPT coding and reduce the chance a RAC will ask for money back.
Education. There are many ways to help providers in your practice understand the elements of documentation and coding. Periodic training classes (e.g. during orientation and annually thereafter) are useful but may not be enough. For me, this is a little like learning a foreign language by going to a couple of classes. Instead, I think “immersion training” is more effective. That might mean a doctor spends a few minutes with a certified coder on most working days for a few weeks. For example, they could meet for 15 minutes near lunchtime and review how the doctor plans to bill visits made that morning. Lastly, consider targeted education for each doctor, based on any problems found in an audit of his/her coding.
Review coding patterns. As I wrote in my August 2007 column, there is value in ensuring that each doctor in the group can see how her coding pattern differs from the group as a whole or any individual in the group. That is, what portion of follow-up visits was billed at the lowest, middle, and highest levels? What about admissions, discharges, and so on? I provided a sample report in that same column.
It also is worth taking the time to compare each doctor’s coding pattern to both the CMS Internal Medicine data and SHM’s State of Hospital Medicine report. The accompanying figure shows the most current data sets available.
Keep in mind that the goal is not to simply ensure that your coding pattern matches these external data sets; knowing where yours differs from these sets can suggest where you might want to investigate further or seek additional education.
Coding audits. Having a certified coder audit your performance at least annually is a good idea. It can help uncover areas in which you’d benefit from further review and training, and if, heaven forbid, questions are ever raised about whether you’re intentionally up-coding (fraud), showing that you’re audited regularly could help demonstrate your efforts to code correctly. In the latter case, it is probably more valuable if the audit is done independently of your employer.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Several years ago we sent a CPT coding auditor 15 chart notes generated by each doctor in our group. Among each doctors’ 15 notes were at least one or two billed as initial hospital care, follow up, discharge, critical care, and so on. This coding expert returned a report showing that, out of all the notes reviewed, a significant portion were not billed at the correct level. Most of the incorrectly billed notes were judged to reflect “up-coding,” and a few were seen as “down-coded.”
This was distressing and hard to believe.
So I took the same set of notes and paid a second coding expert for an independent review. She didn’t know about the first audit but returned a report that showed a nearly identical portion of incorrectly coded notes.
Two independent audits showing nearly the same portion of notes coded incorrectly was alarming. But it was difficult for my partners and me to address, because the auditors didn’t agree on the correct code for many of the notes. In some cases, both flagged a note as incorrectly coded but didn’t agree on the correct code. For a number of the notes, one auditor said the visit was “up-coded,” while the other said it was “down-coded.” There was so little agreement between the two of them that we had a hard time coming up with any firm conclusions about what we should do to improve our performance.
If experts who think about coding all the time can’t agree on the right code for a given note, how can hospitalists be expected to code nearly all of our visits accurately?
RAC: Recovery Audit Contractor
Despite what I believe is poor inter-rater reliability among coding auditors, we need to work diligently to comply with coding guidelines. A 2003 Federal law mandated a program of Recovery Audit Contractors, or RAC for short, to find cases of “up-coding” or other overbilling and require the provider to repay any resulting loss.
A number of companies are in the business of conducting RAC audits (one of them, CGI, is the Canadian company blamed for the failed “Obamacare” exchange websites), and there is a reasonable chance one of these companies has reviewed some of your charges—or those of your hospitalist colleagues.
The RAC auditors review information about your charges, and if they determine that you up-coded or overbilled, they send a “demand letter” summarizing their findings, along with the amount of money they have determined you should pay back. (Theoretically, they could notify you of “under-coding,” so that you can be paid more for past work, but I haven’t yet come across an example of that.)
It is common to appeal the RAC findings, but that can be a long process, and many organizations decide to pay back all the money requested by the RAC as quickly as possible to avoid paying interest on a delayed payment if the appeal is unsuccessful. In the case of a successful appeal, the money previously refunded by the doctor would be returned.
Page 338 of the CMS Fiscal Year 2015 “Justification of Estimates for Appropriations Committees” says that “…about 50 percent of the estimated 43,000 appeals [of adverse RAC audit findings] were fully or partially overturned…” This could mean the RACs are a sort of loose cannon, accusing many providers of overbilling while knowing that some won’t bother to appeal because they don’t understand the process or because the dollar amount involved for a single provider is too small to justify the time and expense of conducting the appeal. In this way, a RAC audit is like the $15 rebate on the last electronic gadget you bought. The seller knows that many people, including me, will fail to do the work required to claim the rebate.
Accuracy Strategies
There are a number of ways to help your group ensure appropriate CPT coding and reduce the chance a RAC will ask for money back.
Education. There are many ways to help providers in your practice understand the elements of documentation and coding. Periodic training classes (e.g. during orientation and annually thereafter) are useful but may not be enough. For me, this is a little like learning a foreign language by going to a couple of classes. Instead, I think “immersion training” is more effective. That might mean a doctor spends a few minutes with a certified coder on most working days for a few weeks. For example, they could meet for 15 minutes near lunchtime and review how the doctor plans to bill visits made that morning. Lastly, consider targeted education for each doctor, based on any problems found in an audit of his/her coding.
Review coding patterns. As I wrote in my August 2007 column, there is value in ensuring that each doctor in the group can see how her coding pattern differs from the group as a whole or any individual in the group. That is, what portion of follow-up visits was billed at the lowest, middle, and highest levels? What about admissions, discharges, and so on? I provided a sample report in that same column.
It also is worth taking the time to compare each doctor’s coding pattern to both the CMS Internal Medicine data and SHM’s State of Hospital Medicine report. The accompanying figure shows the most current data sets available.
Keep in mind that the goal is not to simply ensure that your coding pattern matches these external data sets; knowing where yours differs from these sets can suggest where you might want to investigate further or seek additional education.
Coding audits. Having a certified coder audit your performance at least annually is a good idea. It can help uncover areas in which you’d benefit from further review and training, and if, heaven forbid, questions are ever raised about whether you’re intentionally up-coding (fraud), showing that you’re audited regularly could help demonstrate your efforts to code correctly. In the latter case, it is probably more valuable if the audit is done independently of your employer.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Several years ago we sent a CPT coding auditor 15 chart notes generated by each doctor in our group. Among each doctors’ 15 notes were at least one or two billed as initial hospital care, follow up, discharge, critical care, and so on. This coding expert returned a report showing that, out of all the notes reviewed, a significant portion were not billed at the correct level. Most of the incorrectly billed notes were judged to reflect “up-coding,” and a few were seen as “down-coded.”
This was distressing and hard to believe.
So I took the same set of notes and paid a second coding expert for an independent review. She didn’t know about the first audit but returned a report that showed a nearly identical portion of incorrectly coded notes.
Two independent audits showing nearly the same portion of notes coded incorrectly was alarming. But it was difficult for my partners and me to address, because the auditors didn’t agree on the correct code for many of the notes. In some cases, both flagged a note as incorrectly coded but didn’t agree on the correct code. For a number of the notes, one auditor said the visit was “up-coded,” while the other said it was “down-coded.” There was so little agreement between the two of them that we had a hard time coming up with any firm conclusions about what we should do to improve our performance.
If experts who think about coding all the time can’t agree on the right code for a given note, how can hospitalists be expected to code nearly all of our visits accurately?
RAC: Recovery Audit Contractor
Despite what I believe is poor inter-rater reliability among coding auditors, we need to work diligently to comply with coding guidelines. A 2003 Federal law mandated a program of Recovery Audit Contractors, or RAC for short, to find cases of “up-coding” or other overbilling and require the provider to repay any resulting loss.
A number of companies are in the business of conducting RAC audits (one of them, CGI, is the Canadian company blamed for the failed “Obamacare” exchange websites), and there is a reasonable chance one of these companies has reviewed some of your charges—or those of your hospitalist colleagues.
The RAC auditors review information about your charges, and if they determine that you up-coded or overbilled, they send a “demand letter” summarizing their findings, along with the amount of money they have determined you should pay back. (Theoretically, they could notify you of “under-coding,” so that you can be paid more for past work, but I haven’t yet come across an example of that.)
It is common to appeal the RAC findings, but that can be a long process, and many organizations decide to pay back all the money requested by the RAC as quickly as possible to avoid paying interest on a delayed payment if the appeal is unsuccessful. In the case of a successful appeal, the money previously refunded by the doctor would be returned.
Page 338 of the CMS Fiscal Year 2015 “Justification of Estimates for Appropriations Committees” says that “…about 50 percent of the estimated 43,000 appeals [of adverse RAC audit findings] were fully or partially overturned…” This could mean the RACs are a sort of loose cannon, accusing many providers of overbilling while knowing that some won’t bother to appeal because they don’t understand the process or because the dollar amount involved for a single provider is too small to justify the time and expense of conducting the appeal. In this way, a RAC audit is like the $15 rebate on the last electronic gadget you bought. The seller knows that many people, including me, will fail to do the work required to claim the rebate.
Accuracy Strategies
There are a number of ways to help your group ensure appropriate CPT coding and reduce the chance a RAC will ask for money back.
Education. There are many ways to help providers in your practice understand the elements of documentation and coding. Periodic training classes (e.g. during orientation and annually thereafter) are useful but may not be enough. For me, this is a little like learning a foreign language by going to a couple of classes. Instead, I think “immersion training” is more effective. That might mean a doctor spends a few minutes with a certified coder on most working days for a few weeks. For example, they could meet for 15 minutes near lunchtime and review how the doctor plans to bill visits made that morning. Lastly, consider targeted education for each doctor, based on any problems found in an audit of his/her coding.
Review coding patterns. As I wrote in my August 2007 column, there is value in ensuring that each doctor in the group can see how her coding pattern differs from the group as a whole or any individual in the group. That is, what portion of follow-up visits was billed at the lowest, middle, and highest levels? What about admissions, discharges, and so on? I provided a sample report in that same column.
It also is worth taking the time to compare each doctor’s coding pattern to both the CMS Internal Medicine data and SHM’s State of Hospital Medicine report. The accompanying figure shows the most current data sets available.
Keep in mind that the goal is not to simply ensure that your coding pattern matches these external data sets; knowing where yours differs from these sets can suggest where you might want to investigate further or seek additional education.
Coding audits. Having a certified coder audit your performance at least annually is a good idea. It can help uncover areas in which you’d benefit from further review and training, and if, heaven forbid, questions are ever raised about whether you’re intentionally up-coding (fraud), showing that you’re audited regularly could help demonstrate your efforts to code correctly. In the latter case, it is probably more valuable if the audit is done independently of your employer.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Doing it right
“It is concluded that nasogastric suction should not be used routinely following abdominal surgery." This is the concluding statement from a paper presented at the Pacific Coast Surgical Association and published in the American Journal of Surgery more than 50 years ago (Am. J. Surg 1957;94:257-61).
Since then innumerable randomized controlled trials and meta-analyses have confirmed that nasogastric tubes inserted prophylactically after abdominal surgery, even when gastrointestinal anastomoses have been constructed, are unnecessary. So how did this incontrovertible evidence impact my practice and that of most of my surgical colleagues? Not at all, at least not for many years. We continued our routine of torturing postoperative patients with nasogastric tubes because it had been drummed into us during residency and because we were uncomfortable not doing so. But why did we persist after convincing evidence to the contrary emerged?
Unfortunately it is not uncommon that even when good evidence exists, we fail to incorporate it into decision-making. The comfort we enjoy with our standard way of doing things is often preferred to the discomfort – cognitive dissonance – we experience when confronted with mounting empirical evidence that challenges our beliefs. All too often, the cognitive dissonance is reduced by holding on to those notions with which we are most comfortable and ignoring or rejecting new information no matter how valid.
What is the harm? In the case of prophylactic nasogastric tubes, considerable discomfort has unnecessarily complicated the postoperative courses of millions of patients. Many trials have shown that aspiration and pneumonia, the adverse events for which the tubes were placed to prevent, occurred more frequently in patients with than those without nasogastric tubes.
Prophylactic gastric decompression is but one of many practices that have been continued long after their efficacy was disproven. How many radical mastectomies were performed after modified radical mastectomy, and then later partial mastectomy with radiation were shown with irrefutable data to provide equal survival with less disfigurement and fewer complications such as arm lymphedema? For many years after the indications for tonsillectomy were narrowed, this procedure continued to be more commonly done than was appropriate based on the evidence available.
Some hold on to their cherished habits more persistently and longer than others. In order to maintain consonance and avoid the stress of dissonance, I have known surgeons who have retained nearly all of the practices they learned from their mentors during residency long past their utility. Such individuals may insist that they alone prep their patients and that long outmoded suture and instruments be maintained on the operating room supply list. When new, and often proven to be superior, instruments, sutures, and pathways of care for their patients are introduced in their institutions, they find it difficult or even impossible to change.
In an era when the few controlled trials and meta-analyses available were buried within a surgical literature that was difficult to access and the term evidence-based surgery was not yet a part of our lexicon, such a rigid posture was often tolerated. I would hope that in most institutions and departments of surgery this is no longer the case. We live in a time when the imperatives of renewal and reevaluation of our practices are increasing. Therefore, reviewing new evidence, even that which goes against our established notions, and incorporating new proven methods, are essential to maintaining the highest standard of patient care.
Although many gray areas remain and there is often more than one best way to manage a surgical patient, our treatments should be based on the best evidence available rather than on what we learned 5, 10, or even 30 years ago. Fortunately, such evidence is now readily accessible. A notable example is “Evidence-based decisions in surgery,” surgical practice guidelines recently introduced by the American College of Surgeons (ACS) under the guidance of Dr. Lewis Flint.
“Evidence-based decisions in surgery” presently consists of 15 modules of the most common diseases and conditions encountered by general surgeons. These modules can be easily accessed by ACS Fellows on any mobile device at the point-of-care (http://ebds.facs.org). Surgical recommendations along with the strength of evidence (weak, moderate, or strong) for each are presented in an easy-to-interpret format. The modules have been developed by American College of Surgeons staff and been peer-reviewed by the Best Practices Workgroup of the College’s Board of Governors and by representatives of the Advisory Council for General Surgery. A consensus of the reviewers was used to determine the content of each module. It is emphasized that the purpose of these modules is to guide rather than dictate decision-making.
In addition to the strength of evidence for each recommendation, a clinical decision algorithm for a typical patient, suggested talking points for patient education, and key references on which the recommendations are based are also provided. Although clinical practice guidelines have been developed by a number of specialty surgical societies, I have found none that are as easy to digest and use in a busy clinical practice as “Evidence-based decisions in surgery.
So we no longer have an excuse to hold on to our cherished and venerable practices that are outmoded and possibly not in the best interest of our patients. The information needed to do it right is virtually one click of a mouse away. Try applying “Evidence-based decisions in surgery” in your practice. I am convinced you will find them valuable as you make decisions for the most appropriate care of your patients.
Dr. Rikkers is Editor in Chief of ACS Surgery News
“It is concluded that nasogastric suction should not be used routinely following abdominal surgery." This is the concluding statement from a paper presented at the Pacific Coast Surgical Association and published in the American Journal of Surgery more than 50 years ago (Am. J. Surg 1957;94:257-61).
Since then innumerable randomized controlled trials and meta-analyses have confirmed that nasogastric tubes inserted prophylactically after abdominal surgery, even when gastrointestinal anastomoses have been constructed, are unnecessary. So how did this incontrovertible evidence impact my practice and that of most of my surgical colleagues? Not at all, at least not for many years. We continued our routine of torturing postoperative patients with nasogastric tubes because it had been drummed into us during residency and because we were uncomfortable not doing so. But why did we persist after convincing evidence to the contrary emerged?
Unfortunately it is not uncommon that even when good evidence exists, we fail to incorporate it into decision-making. The comfort we enjoy with our standard way of doing things is often preferred to the discomfort – cognitive dissonance – we experience when confronted with mounting empirical evidence that challenges our beliefs. All too often, the cognitive dissonance is reduced by holding on to those notions with which we are most comfortable and ignoring or rejecting new information no matter how valid.
What is the harm? In the case of prophylactic nasogastric tubes, considerable discomfort has unnecessarily complicated the postoperative courses of millions of patients. Many trials have shown that aspiration and pneumonia, the adverse events for which the tubes were placed to prevent, occurred more frequently in patients with than those without nasogastric tubes.
Prophylactic gastric decompression is but one of many practices that have been continued long after their efficacy was disproven. How many radical mastectomies were performed after modified radical mastectomy, and then later partial mastectomy with radiation were shown with irrefutable data to provide equal survival with less disfigurement and fewer complications such as arm lymphedema? For many years after the indications for tonsillectomy were narrowed, this procedure continued to be more commonly done than was appropriate based on the evidence available.
Some hold on to their cherished habits more persistently and longer than others. In order to maintain consonance and avoid the stress of dissonance, I have known surgeons who have retained nearly all of the practices they learned from their mentors during residency long past their utility. Such individuals may insist that they alone prep their patients and that long outmoded suture and instruments be maintained on the operating room supply list. When new, and often proven to be superior, instruments, sutures, and pathways of care for their patients are introduced in their institutions, they find it difficult or even impossible to change.
In an era when the few controlled trials and meta-analyses available were buried within a surgical literature that was difficult to access and the term evidence-based surgery was not yet a part of our lexicon, such a rigid posture was often tolerated. I would hope that in most institutions and departments of surgery this is no longer the case. We live in a time when the imperatives of renewal and reevaluation of our practices are increasing. Therefore, reviewing new evidence, even that which goes against our established notions, and incorporating new proven methods, are essential to maintaining the highest standard of patient care.
Although many gray areas remain and there is often more than one best way to manage a surgical patient, our treatments should be based on the best evidence available rather than on what we learned 5, 10, or even 30 years ago. Fortunately, such evidence is now readily accessible. A notable example is “Evidence-based decisions in surgery,” surgical practice guidelines recently introduced by the American College of Surgeons (ACS) under the guidance of Dr. Lewis Flint.
“Evidence-based decisions in surgery” presently consists of 15 modules of the most common diseases and conditions encountered by general surgeons. These modules can be easily accessed by ACS Fellows on any mobile device at the point-of-care (http://ebds.facs.org). Surgical recommendations along with the strength of evidence (weak, moderate, or strong) for each are presented in an easy-to-interpret format. The modules have been developed by American College of Surgeons staff and been peer-reviewed by the Best Practices Workgroup of the College’s Board of Governors and by representatives of the Advisory Council for General Surgery. A consensus of the reviewers was used to determine the content of each module. It is emphasized that the purpose of these modules is to guide rather than dictate decision-making.
In addition to the strength of evidence for each recommendation, a clinical decision algorithm for a typical patient, suggested talking points for patient education, and key references on which the recommendations are based are also provided. Although clinical practice guidelines have been developed by a number of specialty surgical societies, I have found none that are as easy to digest and use in a busy clinical practice as “Evidence-based decisions in surgery.
So we no longer have an excuse to hold on to our cherished and venerable practices that are outmoded and possibly not in the best interest of our patients. The information needed to do it right is virtually one click of a mouse away. Try applying “Evidence-based decisions in surgery” in your practice. I am convinced you will find them valuable as you make decisions for the most appropriate care of your patients.
Dr. Rikkers is Editor in Chief of ACS Surgery News
“It is concluded that nasogastric suction should not be used routinely following abdominal surgery." This is the concluding statement from a paper presented at the Pacific Coast Surgical Association and published in the American Journal of Surgery more than 50 years ago (Am. J. Surg 1957;94:257-61).
Since then innumerable randomized controlled trials and meta-analyses have confirmed that nasogastric tubes inserted prophylactically after abdominal surgery, even when gastrointestinal anastomoses have been constructed, are unnecessary. So how did this incontrovertible evidence impact my practice and that of most of my surgical colleagues? Not at all, at least not for many years. We continued our routine of torturing postoperative patients with nasogastric tubes because it had been drummed into us during residency and because we were uncomfortable not doing so. But why did we persist after convincing evidence to the contrary emerged?
Unfortunately it is not uncommon that even when good evidence exists, we fail to incorporate it into decision-making. The comfort we enjoy with our standard way of doing things is often preferred to the discomfort – cognitive dissonance – we experience when confronted with mounting empirical evidence that challenges our beliefs. All too often, the cognitive dissonance is reduced by holding on to those notions with which we are most comfortable and ignoring or rejecting new information no matter how valid.
What is the harm? In the case of prophylactic nasogastric tubes, considerable discomfort has unnecessarily complicated the postoperative courses of millions of patients. Many trials have shown that aspiration and pneumonia, the adverse events for which the tubes were placed to prevent, occurred more frequently in patients with than those without nasogastric tubes.
Prophylactic gastric decompression is but one of many practices that have been continued long after their efficacy was disproven. How many radical mastectomies were performed after modified radical mastectomy, and then later partial mastectomy with radiation were shown with irrefutable data to provide equal survival with less disfigurement and fewer complications such as arm lymphedema? For many years after the indications for tonsillectomy were narrowed, this procedure continued to be more commonly done than was appropriate based on the evidence available.
Some hold on to their cherished habits more persistently and longer than others. In order to maintain consonance and avoid the stress of dissonance, I have known surgeons who have retained nearly all of the practices they learned from their mentors during residency long past their utility. Such individuals may insist that they alone prep their patients and that long outmoded suture and instruments be maintained on the operating room supply list. When new, and often proven to be superior, instruments, sutures, and pathways of care for their patients are introduced in their institutions, they find it difficult or even impossible to change.
In an era when the few controlled trials and meta-analyses available were buried within a surgical literature that was difficult to access and the term evidence-based surgery was not yet a part of our lexicon, such a rigid posture was often tolerated. I would hope that in most institutions and departments of surgery this is no longer the case. We live in a time when the imperatives of renewal and reevaluation of our practices are increasing. Therefore, reviewing new evidence, even that which goes against our established notions, and incorporating new proven methods, are essential to maintaining the highest standard of patient care.
Although many gray areas remain and there is often more than one best way to manage a surgical patient, our treatments should be based on the best evidence available rather than on what we learned 5, 10, or even 30 years ago. Fortunately, such evidence is now readily accessible. A notable example is “Evidence-based decisions in surgery,” surgical practice guidelines recently introduced by the American College of Surgeons (ACS) under the guidance of Dr. Lewis Flint.
“Evidence-based decisions in surgery” presently consists of 15 modules of the most common diseases and conditions encountered by general surgeons. These modules can be easily accessed by ACS Fellows on any mobile device at the point-of-care (http://ebds.facs.org). Surgical recommendations along with the strength of evidence (weak, moderate, or strong) for each are presented in an easy-to-interpret format. The modules have been developed by American College of Surgeons staff and been peer-reviewed by the Best Practices Workgroup of the College’s Board of Governors and by representatives of the Advisory Council for General Surgery. A consensus of the reviewers was used to determine the content of each module. It is emphasized that the purpose of these modules is to guide rather than dictate decision-making.
In addition to the strength of evidence for each recommendation, a clinical decision algorithm for a typical patient, suggested talking points for patient education, and key references on which the recommendations are based are also provided. Although clinical practice guidelines have been developed by a number of specialty surgical societies, I have found none that are as easy to digest and use in a busy clinical practice as “Evidence-based decisions in surgery.
So we no longer have an excuse to hold on to our cherished and venerable practices that are outmoded and possibly not in the best interest of our patients. The information needed to do it right is virtually one click of a mouse away. Try applying “Evidence-based decisions in surgery” in your practice. I am convinced you will find them valuable as you make decisions for the most appropriate care of your patients.
Dr. Rikkers is Editor in Chief of ACS Surgery News

'Walk out the snot'
Balloon embolectomy revolutionized the treatment of acute thromboembolism involving peripheral arteries. However, an often overlooked method that actually may be more beneficial is to "walk out the snot."
This may sound somewhat disgusting but as can be seen from the accompanying photograph, the surgeon can often retrieve the entire clot from the main artery including extensions into collateral vessels.
In this picture of a patient undergoing femoral embolectomy with this technique, we retrieved a cast of the entire superficial femoral artery as well as the peroneal and posterior tibial arteries and two major collaterals.
The technique is simple. With proximal control of the inflow artery, the visible clot is gently pulled out of the arteriotomy in a slow but deliberate fashion, hand over hand. Often back bleeding will aid in pushing the specimen out of the arteriotomy. The maneuver is very similar to what children do when they feel the need to empty their nostrils! (No adult would do that – would they?)
Retrieval of a specimen like the one in the photo will usually reassure the surgeon that there will not be more thrombus left behind.
The technique also prevents possible arterial injury from a balloon catheter. For both reasons a postcompletion arteriogram may sometimes be avoided.
Dr. Showalter is clinical assistant professor of surgery at Florida State University Medical School and attending vascular surgeon, Sarasota Vascular Specialists.
Dr. Samson is clinical professor of surgery at Florida State University Medical School, attending vascular surgeon, Sarasota Vascular Specialists, and the medical editor of Vascular Specialist.
Balloon embolectomy revolutionized the treatment of acute thromboembolism involving peripheral arteries. However, an often overlooked method that actually may be more beneficial is to "walk out the snot."
This may sound somewhat disgusting but as can be seen from the accompanying photograph, the surgeon can often retrieve the entire clot from the main artery including extensions into collateral vessels.
In this picture of a patient undergoing femoral embolectomy with this technique, we retrieved a cast of the entire superficial femoral artery as well as the peroneal and posterior tibial arteries and two major collaterals.
The technique is simple. With proximal control of the inflow artery, the visible clot is gently pulled out of the arteriotomy in a slow but deliberate fashion, hand over hand. Often back bleeding will aid in pushing the specimen out of the arteriotomy. The maneuver is very similar to what children do when they feel the need to empty their nostrils! (No adult would do that – would they?)
Retrieval of a specimen like the one in the photo will usually reassure the surgeon that there will not be more thrombus left behind.
The technique also prevents possible arterial injury from a balloon catheter. For both reasons a postcompletion arteriogram may sometimes be avoided.
Dr. Showalter is clinical assistant professor of surgery at Florida State University Medical School and attending vascular surgeon, Sarasota Vascular Specialists.
Dr. Samson is clinical professor of surgery at Florida State University Medical School, attending vascular surgeon, Sarasota Vascular Specialists, and the medical editor of Vascular Specialist.
Balloon embolectomy revolutionized the treatment of acute thromboembolism involving peripheral arteries. However, an often overlooked method that actually may be more beneficial is to "walk out the snot."
This may sound somewhat disgusting but as can be seen from the accompanying photograph, the surgeon can often retrieve the entire clot from the main artery including extensions into collateral vessels.
In this picture of a patient undergoing femoral embolectomy with this technique, we retrieved a cast of the entire superficial femoral artery as well as the peroneal and posterior tibial arteries and two major collaterals.
The technique is simple. With proximal control of the inflow artery, the visible clot is gently pulled out of the arteriotomy in a slow but deliberate fashion, hand over hand. Often back bleeding will aid in pushing the specimen out of the arteriotomy. The maneuver is very similar to what children do when they feel the need to empty their nostrils! (No adult would do that – would they?)
Retrieval of a specimen like the one in the photo will usually reassure the surgeon that there will not be more thrombus left behind.
The technique also prevents possible arterial injury from a balloon catheter. For both reasons a postcompletion arteriogram may sometimes be avoided.
Dr. Showalter is clinical assistant professor of surgery at Florida State University Medical School and attending vascular surgeon, Sarasota Vascular Specialists.
Dr. Samson is clinical professor of surgery at Florida State University Medical School, attending vascular surgeon, Sarasota Vascular Specialists, and the medical editor of Vascular Specialist.
Nurturing values: An inevitable part of parenting
If you ask the parents in your practice what their most important task is with their children, they will probably say something about keeping their child safe and developing their child’s character. They might speak about wanting to raise children who are ready to live independently, happily, and successfully. Beyond independence, they may also observe that they want to raise children of good character, with a deeply held value system that reflects their own core principles. The details of such a value system will vary from family to family, but often will include descriptive ideals such as being ethical, empathic, courageous, generous, ambitious, responsible, and having integrity. Because the everyday tasks of life with children can be so demanding, this larger task often does not get much direct attention from physicians and may not even be explicitly discussed between parents. A few questions from their physician can be profoundly helpful to parents as they reflect on practical strategies to cultivate the qualities of character that will prepare their children to live independent, happy, purposeful, and meaningful adult lives.
One way to get a sense of how parents are preparing their children for independence is to ask how they are they teaching their children about the value of money. Do they give their children a predictable allowance? Is it contingent on chores or responsibilities? Do their children have a bank account or a piggy bank? Do they spend time talking with their children about how they manage their money or plan for large purchases? Money is often a charged subject for families. Asking about it explicitly can help support open, thoughtful communication within the family. Parents will be very interested to learn that such discussions and efforts can powerfully support the development of independence, self-confidence, patience, good judgment, and responsibility in their children. You might inform parents that they can consider their child’s natural temperament when having these discussions. An anxious child, who may be prone to worries about poverty and perfection, might benefit from hearing that money is something that everyone needs to learn how to manage, and it is a tool that can make life easier, but it is not a measure of a person’s worth. On the other hand, a very easygoing child may benefit from having an allowance that is contingent on chores or an adolescent could be urged to get a job rather than depend on allowance. This is how they will learn the real value of work and will cultivate discipline, planning, and the meaningful confidence that they know how to work hard. Whether a family is struggling or can afford more than they choose to spend, the values inherent in financial decisions will be very meaningful for the preadolescent or teenager.
While all parents would likely agree that they hope to raise children who are disciplined, responsible, and independent, the other values that they hope their children appreciate and integrate will cover a wider territory. If you understand what the parents in your practice consider to be their most important values, it also will enhance your understanding of that family’s priorities and how they will manage challenges. You might ask them, "What three values, such as caring about others, honesty, or bravery, would you most like to cultivate in your children?" For those parents that have not actively reflected on their values and behavior or where there are differences between parents concerning values, this may be the start of an important conversation at home.
With ethical qualities that are interpersonal, such as empathy or generosity, there is a growing body of evidence in the psychological literature that suggests that children are much more likely to emulate their parents’ behavior than to follow their suggestions. In a classic experiment published in 1975, the psychologist J. Philippe Rushton observed how school-age children’s generous behaviors correspond with the generous (or selfish) behaviors or suggestions of parents and teachers. Rushton found that there was a very robust relationship between what the adults did and what the children did, one that could powerfully counteract what the adults said (when they disagreed). It seems actions truly do speak louder than words.
Clearly, parents should actively pay attention to how they are living their values, demonstrating them to their children in choices they make, both large and small. Then they can consider what experiences might encourage these values for their children. If they value empathy, what sorts of experiences will give their children the chance to experience and develop empathy for others? They might think about school-based activities or hobbies that can foster empathy. Is there an activity dedicated to helping children in need or to partnering with children with physical disabilities? Perhaps there is a group of children that work toward a chosen public service. If there is not such a group at their children’s school, they should consider starting one. By living these values, by doing it in a way that teaches these values to other children, and by being involved in their children’s school experience, parents can very powerfully nourish the development of these values and behaviors in their children.
Parents also might keep these important values in mind as they are helping their older children choose extracurricular activities or apply for summer jobs. While their children are considering what is most interesting to them, what will "look good" on a college application, or how to make the most money, parents might keep in mind how important values, such as empathy, generosity, bravery, discipline, or patience might be nurtured by the various experiences. Ultimately, these will be their teenager’s choices to make, but parents can still have a powerful influence by showing an interest and highlighting the importance of principles beyond dollars or college ambitions.
Emphasizing the potency of modeling treasured values does not mean that parents shouldn’t also talk about these values and even mixed feelings as they approach difficult, value-laden decisions in their own lives. What matters is how such values are discussed. Praise is powerful, and it appears that when parents praise a child’s character, it is even more powerful than when they praise a behavior. This is especially true for younger children (6- to 12-year-olds), when children lightly try on many different behaviors but are considering the kinds of people they wish to be. Likewise, when children fail to live up to their parents’ values, it is effective for parents to share their disappointment, but they should take care not to shame their children, which leave children feeling discouraged and powerless to change.
Beyond praise and reproach, when parents talk openly and with curiosity about these complex, nuanced topics, and genuinely listen to their children’s questions, thoughts, and opinions about them, they are communicating that their child’s thinking, feelings, and character are valued. Parents should look for opportunities to discuss values one step removed from their children. They could discuss characters’ choices in a movie or book, issues faced by their or their children’s friends, challenges managed by a celebrated athlete or celebrity or even events in a reality television show they have watched together. With these conversations, they are helping their children nurture their own ideas about values and demonstrating genuine confidence that their children can develop their own opinions about such complex matters. They also contribute to a climate in which their children appreciate that values should be carefully considered and may evolve over time. These conversations will be most helpful as their teenagers become more autonomous and face choices on their own in late high school, college, and young adulthood. They will build a strong foundation on which their children will gradually construct their own considered, individual value system, one they can reflect upon and modify over their lifetime.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at pdnews@frontlinemedcom.com.
If you ask the parents in your practice what their most important task is with their children, they will probably say something about keeping their child safe and developing their child’s character. They might speak about wanting to raise children who are ready to live independently, happily, and successfully. Beyond independence, they may also observe that they want to raise children of good character, with a deeply held value system that reflects their own core principles. The details of such a value system will vary from family to family, but often will include descriptive ideals such as being ethical, empathic, courageous, generous, ambitious, responsible, and having integrity. Because the everyday tasks of life with children can be so demanding, this larger task often does not get much direct attention from physicians and may not even be explicitly discussed between parents. A few questions from their physician can be profoundly helpful to parents as they reflect on practical strategies to cultivate the qualities of character that will prepare their children to live independent, happy, purposeful, and meaningful adult lives.
One way to get a sense of how parents are preparing their children for independence is to ask how they are they teaching their children about the value of money. Do they give their children a predictable allowance? Is it contingent on chores or responsibilities? Do their children have a bank account or a piggy bank? Do they spend time talking with their children about how they manage their money or plan for large purchases? Money is often a charged subject for families. Asking about it explicitly can help support open, thoughtful communication within the family. Parents will be very interested to learn that such discussions and efforts can powerfully support the development of independence, self-confidence, patience, good judgment, and responsibility in their children. You might inform parents that they can consider their child’s natural temperament when having these discussions. An anxious child, who may be prone to worries about poverty and perfection, might benefit from hearing that money is something that everyone needs to learn how to manage, and it is a tool that can make life easier, but it is not a measure of a person’s worth. On the other hand, a very easygoing child may benefit from having an allowance that is contingent on chores or an adolescent could be urged to get a job rather than depend on allowance. This is how they will learn the real value of work and will cultivate discipline, planning, and the meaningful confidence that they know how to work hard. Whether a family is struggling or can afford more than they choose to spend, the values inherent in financial decisions will be very meaningful for the preadolescent or teenager.
While all parents would likely agree that they hope to raise children who are disciplined, responsible, and independent, the other values that they hope their children appreciate and integrate will cover a wider territory. If you understand what the parents in your practice consider to be their most important values, it also will enhance your understanding of that family’s priorities and how they will manage challenges. You might ask them, "What three values, such as caring about others, honesty, or bravery, would you most like to cultivate in your children?" For those parents that have not actively reflected on their values and behavior or where there are differences between parents concerning values, this may be the start of an important conversation at home.
With ethical qualities that are interpersonal, such as empathy or generosity, there is a growing body of evidence in the psychological literature that suggests that children are much more likely to emulate their parents’ behavior than to follow their suggestions. In a classic experiment published in 1975, the psychologist J. Philippe Rushton observed how school-age children’s generous behaviors correspond with the generous (or selfish) behaviors or suggestions of parents and teachers. Rushton found that there was a very robust relationship between what the adults did and what the children did, one that could powerfully counteract what the adults said (when they disagreed). It seems actions truly do speak louder than words.
Clearly, parents should actively pay attention to how they are living their values, demonstrating them to their children in choices they make, both large and small. Then they can consider what experiences might encourage these values for their children. If they value empathy, what sorts of experiences will give their children the chance to experience and develop empathy for others? They might think about school-based activities or hobbies that can foster empathy. Is there an activity dedicated to helping children in need or to partnering with children with physical disabilities? Perhaps there is a group of children that work toward a chosen public service. If there is not such a group at their children’s school, they should consider starting one. By living these values, by doing it in a way that teaches these values to other children, and by being involved in their children’s school experience, parents can very powerfully nourish the development of these values and behaviors in their children.
Parents also might keep these important values in mind as they are helping their older children choose extracurricular activities or apply for summer jobs. While their children are considering what is most interesting to them, what will "look good" on a college application, or how to make the most money, parents might keep in mind how important values, such as empathy, generosity, bravery, discipline, or patience might be nurtured by the various experiences. Ultimately, these will be their teenager’s choices to make, but parents can still have a powerful influence by showing an interest and highlighting the importance of principles beyond dollars or college ambitions.
Emphasizing the potency of modeling treasured values does not mean that parents shouldn’t also talk about these values and even mixed feelings as they approach difficult, value-laden decisions in their own lives. What matters is how such values are discussed. Praise is powerful, and it appears that when parents praise a child’s character, it is even more powerful than when they praise a behavior. This is especially true for younger children (6- to 12-year-olds), when children lightly try on many different behaviors but are considering the kinds of people they wish to be. Likewise, when children fail to live up to their parents’ values, it is effective for parents to share their disappointment, but they should take care not to shame their children, which leave children feeling discouraged and powerless to change.
Beyond praise and reproach, when parents talk openly and with curiosity about these complex, nuanced topics, and genuinely listen to their children’s questions, thoughts, and opinions about them, they are communicating that their child’s thinking, feelings, and character are valued. Parents should look for opportunities to discuss values one step removed from their children. They could discuss characters’ choices in a movie or book, issues faced by their or their children’s friends, challenges managed by a celebrated athlete or celebrity or even events in a reality television show they have watched together. With these conversations, they are helping their children nurture their own ideas about values and demonstrating genuine confidence that their children can develop their own opinions about such complex matters. They also contribute to a climate in which their children appreciate that values should be carefully considered and may evolve over time. These conversations will be most helpful as their teenagers become more autonomous and face choices on their own in late high school, college, and young adulthood. They will build a strong foundation on which their children will gradually construct their own considered, individual value system, one they can reflect upon and modify over their lifetime.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at pdnews@frontlinemedcom.com.
If you ask the parents in your practice what their most important task is with their children, they will probably say something about keeping their child safe and developing their child’s character. They might speak about wanting to raise children who are ready to live independently, happily, and successfully. Beyond independence, they may also observe that they want to raise children of good character, with a deeply held value system that reflects their own core principles. The details of such a value system will vary from family to family, but often will include descriptive ideals such as being ethical, empathic, courageous, generous, ambitious, responsible, and having integrity. Because the everyday tasks of life with children can be so demanding, this larger task often does not get much direct attention from physicians and may not even be explicitly discussed between parents. A few questions from their physician can be profoundly helpful to parents as they reflect on practical strategies to cultivate the qualities of character that will prepare their children to live independent, happy, purposeful, and meaningful adult lives.
One way to get a sense of how parents are preparing their children for independence is to ask how they are they teaching their children about the value of money. Do they give their children a predictable allowance? Is it contingent on chores or responsibilities? Do their children have a bank account or a piggy bank? Do they spend time talking with their children about how they manage their money or plan for large purchases? Money is often a charged subject for families. Asking about it explicitly can help support open, thoughtful communication within the family. Parents will be very interested to learn that such discussions and efforts can powerfully support the development of independence, self-confidence, patience, good judgment, and responsibility in their children. You might inform parents that they can consider their child’s natural temperament when having these discussions. An anxious child, who may be prone to worries about poverty and perfection, might benefit from hearing that money is something that everyone needs to learn how to manage, and it is a tool that can make life easier, but it is not a measure of a person’s worth. On the other hand, a very easygoing child may benefit from having an allowance that is contingent on chores or an adolescent could be urged to get a job rather than depend on allowance. This is how they will learn the real value of work and will cultivate discipline, planning, and the meaningful confidence that they know how to work hard. Whether a family is struggling or can afford more than they choose to spend, the values inherent in financial decisions will be very meaningful for the preadolescent or teenager.
While all parents would likely agree that they hope to raise children who are disciplined, responsible, and independent, the other values that they hope their children appreciate and integrate will cover a wider territory. If you understand what the parents in your practice consider to be their most important values, it also will enhance your understanding of that family’s priorities and how they will manage challenges. You might ask them, "What three values, such as caring about others, honesty, or bravery, would you most like to cultivate in your children?" For those parents that have not actively reflected on their values and behavior or where there are differences between parents concerning values, this may be the start of an important conversation at home.
With ethical qualities that are interpersonal, such as empathy or generosity, there is a growing body of evidence in the psychological literature that suggests that children are much more likely to emulate their parents’ behavior than to follow their suggestions. In a classic experiment published in 1975, the psychologist J. Philippe Rushton observed how school-age children’s generous behaviors correspond with the generous (or selfish) behaviors or suggestions of parents and teachers. Rushton found that there was a very robust relationship between what the adults did and what the children did, one that could powerfully counteract what the adults said (when they disagreed). It seems actions truly do speak louder than words.
Clearly, parents should actively pay attention to how they are living their values, demonstrating them to their children in choices they make, both large and small. Then they can consider what experiences might encourage these values for their children. If they value empathy, what sorts of experiences will give their children the chance to experience and develop empathy for others? They might think about school-based activities or hobbies that can foster empathy. Is there an activity dedicated to helping children in need or to partnering with children with physical disabilities? Perhaps there is a group of children that work toward a chosen public service. If there is not such a group at their children’s school, they should consider starting one. By living these values, by doing it in a way that teaches these values to other children, and by being involved in their children’s school experience, parents can very powerfully nourish the development of these values and behaviors in their children.
Parents also might keep these important values in mind as they are helping their older children choose extracurricular activities or apply for summer jobs. While their children are considering what is most interesting to them, what will "look good" on a college application, or how to make the most money, parents might keep in mind how important values, such as empathy, generosity, bravery, discipline, or patience might be nurtured by the various experiences. Ultimately, these will be their teenager’s choices to make, but parents can still have a powerful influence by showing an interest and highlighting the importance of principles beyond dollars or college ambitions.
Emphasizing the potency of modeling treasured values does not mean that parents shouldn’t also talk about these values and even mixed feelings as they approach difficult, value-laden decisions in their own lives. What matters is how such values are discussed. Praise is powerful, and it appears that when parents praise a child’s character, it is even more powerful than when they praise a behavior. This is especially true for younger children (6- to 12-year-olds), when children lightly try on many different behaviors but are considering the kinds of people they wish to be. Likewise, when children fail to live up to their parents’ values, it is effective for parents to share their disappointment, but they should take care not to shame their children, which leave children feeling discouraged and powerless to change.
Beyond praise and reproach, when parents talk openly and with curiosity about these complex, nuanced topics, and genuinely listen to their children’s questions, thoughts, and opinions about them, they are communicating that their child’s thinking, feelings, and character are valued. Parents should look for opportunities to discuss values one step removed from their children. They could discuss characters’ choices in a movie or book, issues faced by their or their children’s friends, challenges managed by a celebrated athlete or celebrity or even events in a reality television show they have watched together. With these conversations, they are helping their children nurture their own ideas about values and demonstrating genuine confidence that their children can develop their own opinions about such complex matters. They also contribute to a climate in which their children appreciate that values should be carefully considered and may evolve over time. These conversations will be most helpful as their teenagers become more autonomous and face choices on their own in late high school, college, and young adulthood. They will build a strong foundation on which their children will gradually construct their own considered, individual value system, one they can reflect upon and modify over their lifetime.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor of psychiatry and of pediatrics at Harvard Medical School, Boston. E-mail them at pdnews@frontlinemedcom.com.
