User login
Continuity of Patient Care: A Value Worth Preserving
Along with many others who are rapidly fading from the American surgical scene, I was born as a baby boomer. Most of us from that generation who embraced surgery as a career held fast to the values of the era. First and foremost among these was a high premium put on hard work, long hours, and an unwavering dedication to our profession and to our patients. We were particularly proud of the continuity of care that we provided to our patients.
During my early years as a surgeon, it was a 24/7 job. Saturday mornings were consumed by Surgery Grand Rounds followed by usually prolonged and detailed patient rounds. Most of us visited our hospitalized patients 7 days a week. When one of my patients developed a complication, I, rather than the surgeon on call, managed it. I missed soccer matches, baseball games, dance recitals, and even some family birthdays because etched into my conscience was the concept that duty to my patients trumped duty to my family. Although there is much to admire in this singular focus on patient care, it took its toll on the other aspects of what should be a more balanced professional life.
Two factors, one of them cultural and the other regulatory, have altered this all-consuming aspect of a surgeon’s life, with implications for the ideal of continuity of care. First was the arrival of freshly minted surgeons from generations X and Y who had a different set of priorities than their predecessors. They insisted on a more even balance between professional and family obligations. In part this resulted from the need for them to be more involved in child rearing since many of their spouses were engaged in time-intensive careers of their own. As they gravitated onto academic surgical faculties and joined private practice groups, they insisted on moving educational programs such as Surgery Grand Rounds to weekdays so they could participate in family activities. They entrusted the care of their patients to their partners, freeing them for entire weekends that could be devoted to family events.
The healthier balance they have brought to a career in surgery is to be admired. Much to the benefit of their senior colleagues, it has become their way of life as well. The trade-off has been some decay of the ideals of patient ownership and continuity of care.
The next and potentially more serious challenge to the cherished concept of continuous care of our patients was the mandate of an 80-hour work week by the Accreditation Council for Graduate Medical Education (ACGME) in 2003. As to its effects on graduate surgical education, I believe the 80-hour work week has been a double-edged sword. On the positive side, at a time when interest in general surgery was waning, institution of duty hours restrictions along with the advent of minimally invasive surgery made our specialty more attractive to medical school graduates, including women, who now constitute 50% of most medical school classes. Another plus was that teaching hospitals were forced to hire physician extenders and other personnel to perform some of the noneducational tasks previously carried out by residents.
On the negative side, since many of the lost hours were in the evenings and weekends, residents’ exposure to urgent and emergency cases was diminished. More significantly, surgery residents began to work in shifts to accommodate increasingly inflexible rules. Ownership of their patients could no longer be held as a high priority in surgical education. Several classes of surgery residents who were educated under these fairly restrictive guidelines have now graduated and have brought a "shift mentality" with them to their positions in private practice groups and on academic faculties.
Since work hour restrictions are highly unlikely to disappear from our training programs and may in fact be applied in the future to all working physicians and surgeons, what can be done to preserve the time-honored value of continuous care of our patients? The answer probably lies in seeking reasonable flexibility within the rules rather than elimination of them. A bright light in this regard is an upcoming randomized controlled trial to assess the feasibility of more flexible work hours rules for general surgery residents. This trial is sponsored by the American Board of Surgery and the American College of Surgeons, and has the support of the ACGME. It will be conducted in hospitals that have instituted the National Surgical Quality Improvement Program (NSQIP) and also sponsor general surgery residencies. Beginning in July 2014, these residencies will be randomized to one of two arms – one using the extensive and rigid present duty hour standards and the second utilizing more flexible standards limited to an 80-hour work week, one night in three on call, and one day in seven free of clinical responsibilities, all averaged over a month. Patient outcomes in each arm will be determined from NSQIP data.
The trial will be conducted over 1 year, with residents’ opinions being surveyed at its midpoint. If patient outcomes are similar in the two arms or superior in the arm with more flexible rules and resident opinion is favorable, this would lend strong support for more flexibility in all general surgery residencies. As of this date, more than 100 general surgery programs have agreed to randomization.
The sponsoring agencies are to be congratulated for designing a trial that for the first time will objectively evaluate just how restrictive work rules need to be. Their efforts may effectively preserve a value that is at the core of our profession – the continuous care of our surgical patients.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.
Along with many others who are rapidly fading from the American surgical scene, I was born as a baby boomer. Most of us from that generation who embraced surgery as a career held fast to the values of the era. First and foremost among these was a high premium put on hard work, long hours, and an unwavering dedication to our profession and to our patients. We were particularly proud of the continuity of care that we provided to our patients.
During my early years as a surgeon, it was a 24/7 job. Saturday mornings were consumed by Surgery Grand Rounds followed by usually prolonged and detailed patient rounds. Most of us visited our hospitalized patients 7 days a week. When one of my patients developed a complication, I, rather than the surgeon on call, managed it. I missed soccer matches, baseball games, dance recitals, and even some family birthdays because etched into my conscience was the concept that duty to my patients trumped duty to my family. Although there is much to admire in this singular focus on patient care, it took its toll on the other aspects of what should be a more balanced professional life.
Two factors, one of them cultural and the other regulatory, have altered this all-consuming aspect of a surgeon’s life, with implications for the ideal of continuity of care. First was the arrival of freshly minted surgeons from generations X and Y who had a different set of priorities than their predecessors. They insisted on a more even balance between professional and family obligations. In part this resulted from the need for them to be more involved in child rearing since many of their spouses were engaged in time-intensive careers of their own. As they gravitated onto academic surgical faculties and joined private practice groups, they insisted on moving educational programs such as Surgery Grand Rounds to weekdays so they could participate in family activities. They entrusted the care of their patients to their partners, freeing them for entire weekends that could be devoted to family events.
The healthier balance they have brought to a career in surgery is to be admired. Much to the benefit of their senior colleagues, it has become their way of life as well. The trade-off has been some decay of the ideals of patient ownership and continuity of care.
The next and potentially more serious challenge to the cherished concept of continuous care of our patients was the mandate of an 80-hour work week by the Accreditation Council for Graduate Medical Education (ACGME) in 2003. As to its effects on graduate surgical education, I believe the 80-hour work week has been a double-edged sword. On the positive side, at a time when interest in general surgery was waning, institution of duty hours restrictions along with the advent of minimally invasive surgery made our specialty more attractive to medical school graduates, including women, who now constitute 50% of most medical school classes. Another plus was that teaching hospitals were forced to hire physician extenders and other personnel to perform some of the noneducational tasks previously carried out by residents.
On the negative side, since many of the lost hours were in the evenings and weekends, residents’ exposure to urgent and emergency cases was diminished. More significantly, surgery residents began to work in shifts to accommodate increasingly inflexible rules. Ownership of their patients could no longer be held as a high priority in surgical education. Several classes of surgery residents who were educated under these fairly restrictive guidelines have now graduated and have brought a "shift mentality" with them to their positions in private practice groups and on academic faculties.
Since work hour restrictions are highly unlikely to disappear from our training programs and may in fact be applied in the future to all working physicians and surgeons, what can be done to preserve the time-honored value of continuous care of our patients? The answer probably lies in seeking reasonable flexibility within the rules rather than elimination of them. A bright light in this regard is an upcoming randomized controlled trial to assess the feasibility of more flexible work hours rules for general surgery residents. This trial is sponsored by the American Board of Surgery and the American College of Surgeons, and has the support of the ACGME. It will be conducted in hospitals that have instituted the National Surgical Quality Improvement Program (NSQIP) and also sponsor general surgery residencies. Beginning in July 2014, these residencies will be randomized to one of two arms – one using the extensive and rigid present duty hour standards and the second utilizing more flexible standards limited to an 80-hour work week, one night in three on call, and one day in seven free of clinical responsibilities, all averaged over a month. Patient outcomes in each arm will be determined from NSQIP data.
The trial will be conducted over 1 year, with residents’ opinions being surveyed at its midpoint. If patient outcomes are similar in the two arms or superior in the arm with more flexible rules and resident opinion is favorable, this would lend strong support for more flexibility in all general surgery residencies. As of this date, more than 100 general surgery programs have agreed to randomization.
The sponsoring agencies are to be congratulated for designing a trial that for the first time will objectively evaluate just how restrictive work rules need to be. Their efforts may effectively preserve a value that is at the core of our profession – the continuous care of our surgical patients.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.
Along with many others who are rapidly fading from the American surgical scene, I was born as a baby boomer. Most of us from that generation who embraced surgery as a career held fast to the values of the era. First and foremost among these was a high premium put on hard work, long hours, and an unwavering dedication to our profession and to our patients. We were particularly proud of the continuity of care that we provided to our patients.
During my early years as a surgeon, it was a 24/7 job. Saturday mornings were consumed by Surgery Grand Rounds followed by usually prolonged and detailed patient rounds. Most of us visited our hospitalized patients 7 days a week. When one of my patients developed a complication, I, rather than the surgeon on call, managed it. I missed soccer matches, baseball games, dance recitals, and even some family birthdays because etched into my conscience was the concept that duty to my patients trumped duty to my family. Although there is much to admire in this singular focus on patient care, it took its toll on the other aspects of what should be a more balanced professional life.
Two factors, one of them cultural and the other regulatory, have altered this all-consuming aspect of a surgeon’s life, with implications for the ideal of continuity of care. First was the arrival of freshly minted surgeons from generations X and Y who had a different set of priorities than their predecessors. They insisted on a more even balance between professional and family obligations. In part this resulted from the need for them to be more involved in child rearing since many of their spouses were engaged in time-intensive careers of their own. As they gravitated onto academic surgical faculties and joined private practice groups, they insisted on moving educational programs such as Surgery Grand Rounds to weekdays so they could participate in family activities. They entrusted the care of their patients to their partners, freeing them for entire weekends that could be devoted to family events.
The healthier balance they have brought to a career in surgery is to be admired. Much to the benefit of their senior colleagues, it has become their way of life as well. The trade-off has been some decay of the ideals of patient ownership and continuity of care.
The next and potentially more serious challenge to the cherished concept of continuous care of our patients was the mandate of an 80-hour work week by the Accreditation Council for Graduate Medical Education (ACGME) in 2003. As to its effects on graduate surgical education, I believe the 80-hour work week has been a double-edged sword. On the positive side, at a time when interest in general surgery was waning, institution of duty hours restrictions along with the advent of minimally invasive surgery made our specialty more attractive to medical school graduates, including women, who now constitute 50% of most medical school classes. Another plus was that teaching hospitals were forced to hire physician extenders and other personnel to perform some of the noneducational tasks previously carried out by residents.
On the negative side, since many of the lost hours were in the evenings and weekends, residents’ exposure to urgent and emergency cases was diminished. More significantly, surgery residents began to work in shifts to accommodate increasingly inflexible rules. Ownership of their patients could no longer be held as a high priority in surgical education. Several classes of surgery residents who were educated under these fairly restrictive guidelines have now graduated and have brought a "shift mentality" with them to their positions in private practice groups and on academic faculties.
Since work hour restrictions are highly unlikely to disappear from our training programs and may in fact be applied in the future to all working physicians and surgeons, what can be done to preserve the time-honored value of continuous care of our patients? The answer probably lies in seeking reasonable flexibility within the rules rather than elimination of them. A bright light in this regard is an upcoming randomized controlled trial to assess the feasibility of more flexible work hours rules for general surgery residents. This trial is sponsored by the American Board of Surgery and the American College of Surgeons, and has the support of the ACGME. It will be conducted in hospitals that have instituted the National Surgical Quality Improvement Program (NSQIP) and also sponsor general surgery residencies. Beginning in July 2014, these residencies will be randomized to one of two arms – one using the extensive and rigid present duty hour standards and the second utilizing more flexible standards limited to an 80-hour work week, one night in three on call, and one day in seven free of clinical responsibilities, all averaged over a month. Patient outcomes in each arm will be determined from NSQIP data.
The trial will be conducted over 1 year, with residents’ opinions being surveyed at its midpoint. If patient outcomes are similar in the two arms or superior in the arm with more flexible rules and resident opinion is favorable, this would lend strong support for more flexibility in all general surgery residencies. As of this date, more than 100 general surgery programs have agreed to randomization.
The sponsoring agencies are to be congratulated for designing a trial that for the first time will objectively evaluate just how restrictive work rules need to be. Their efforts may effectively preserve a value that is at the core of our profession – the continuous care of our surgical patients.
Dr. Rikkers is the Editor in Chief of ACS Surgery News.

Problem Solving In Multi-Site Hospital Medicine Groups


Serving as the lead physician for a hospital medicine group (HMG) makes for challenging work. And the challenges and complexity only increase for anyone who serves as the physician leader for multiple practice sites in the same hospital system. In my November 2013 column on multi-site HMG leaders, I listed a few of the tricky issues they face and will mention a few more here.
Large-Small Friction
Unfortunately, tension between hospitalists at the big hospital and doctors at the small, “feeder” hospitals seems pretty common, and I think it’s due largely to high stress and a wide variation in workload, neither of which are in our direct control. At facilities where there is significant tension, I’m impressed by how vigorously the hospitalists at both the small and large hospitals argue that their own site faces the most stress and challenges. (This is a little like the endless debate about who works harder, those who work with residents and those who don’t.)
The hospitalists at the small site point out that they work with little or no subspecialty help and might even have to take night call from home while working during the day. Those at the big hospital say they are the ones with the very large scope of clinical practice and that, rather than making their life easier, the presence of lots of subspecialists makes for additional work coordinating care and communicating with all parties.
Where it exists, this tension is most evident during a transfer from one of the small hospitals to the large one. After all, one of the reasons to form a system of hospitals is so that nearly all patient needs can be met at one of the facilities in the system. Yet, for many reasons, the hospitalists at the large hospital are—sometimes—not as receptive to transfers as might be ideal. They might be short staffed or facing a high census or an unusually high number of admissions from their own ED. Or, perhaps, they’re concerned that the subspecialty services for which the patient is being transferred (e.g. to be scoped by a GI doctor) won’t be as helpful or prompt as needed. Or maybe they’ve felt “burned” by their colleagues at the small hospital for past transfers that didn’t seem necessary.
The result can be that the doctors at the smaller hospital complain that the “mother ship” hospitalists often are unfriendly and unreceptive to transfer requests. Although there may not be a definitive “cure” for this issue, there are several ways to help address the problem.
- In my last column, I mentioned the value of one or more in-person meetings between those who tend to be on the sending and receiving end of transfers, to establish some criteria regarding transfers that are appropriate and review the process of requesting a transfer and making the associated arrangements. In most cases there will be value in the parties meeting routinely—perhaps two to four times annually—to review how the system is working and address any difficulties.
- Periodic social meetings among the hospitalists at each site will help to form relationships that can make it less likely that any conversation about transfers will go in an unhelpful direction. Things can be very different when the people on each end of the phone call know each other personally.
- Record the phone calls between those seeking and accepting/declining each transfer. Scott Rissmiller, MD, the lead hospitalist for the 17 practice sites in Carolinas Healthcare, has said that having underperforming doctors listen to recordings of their phone calls about transfers has, in most cases he’s been involved with, proven to be a very effective way to encourage improvement.
Shared Staffing
The small hospitals in many systems sometimes struggle to find a way to provide economical night coverage. Hospitals below a certain size find it very difficult to justify a separate, in-house night provider. Some hospital systems have had success sharing night staffing, with the large hospital’s night hospitalist, nurse practitioner, or physician assistant providing telephone coverage for “cross cover” issues that arise after hours.
For example, when a nurse at the small hospital needs to contact a night hospitalist, staff will page the provider at the big hospital, and, in many cases, the issue can be managed effectively by phone. This works best when both hospitals are on the same electronic medical record, so that the responding provider can look through the record as needed.
The hospitalist at the small hospital typically stays on back-up call and is contacted if bedside attention is required.
Or, if the large and small hospitals are a short drive apart, the night hospitalist at the large facility might make the short drive to the small hospital when needed. In the case of emergencies (i.e., a code blue), the in-house night ED physician is relied on as the first responder.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Serving as the lead physician for a hospital medicine group (HMG) makes for challenging work. And the challenges and complexity only increase for anyone who serves as the physician leader for multiple practice sites in the same hospital system. In my November 2013 column on multi-site HMG leaders, I listed a few of the tricky issues they face and will mention a few more here.
Large-Small Friction
Unfortunately, tension between hospitalists at the big hospital and doctors at the small, “feeder” hospitals seems pretty common, and I think it’s due largely to high stress and a wide variation in workload, neither of which are in our direct control. At facilities where there is significant tension, I’m impressed by how vigorously the hospitalists at both the small and large hospitals argue that their own site faces the most stress and challenges. (This is a little like the endless debate about who works harder, those who work with residents and those who don’t.)
The hospitalists at the small site point out that they work with little or no subspecialty help and might even have to take night call from home while working during the day. Those at the big hospital say they are the ones with the very large scope of clinical practice and that, rather than making their life easier, the presence of lots of subspecialists makes for additional work coordinating care and communicating with all parties.
Where it exists, this tension is most evident during a transfer from one of the small hospitals to the large one. After all, one of the reasons to form a system of hospitals is so that nearly all patient needs can be met at one of the facilities in the system. Yet, for many reasons, the hospitalists at the large hospital are—sometimes—not as receptive to transfers as might be ideal. They might be short staffed or facing a high census or an unusually high number of admissions from their own ED. Or, perhaps, they’re concerned that the subspecialty services for which the patient is being transferred (e.g. to be scoped by a GI doctor) won’t be as helpful or prompt as needed. Or maybe they’ve felt “burned” by their colleagues at the small hospital for past transfers that didn’t seem necessary.
The result can be that the doctors at the smaller hospital complain that the “mother ship” hospitalists often are unfriendly and unreceptive to transfer requests. Although there may not be a definitive “cure” for this issue, there are several ways to help address the problem.
- In my last column, I mentioned the value of one or more in-person meetings between those who tend to be on the sending and receiving end of transfers, to establish some criteria regarding transfers that are appropriate and review the process of requesting a transfer and making the associated arrangements. In most cases there will be value in the parties meeting routinely—perhaps two to four times annually—to review how the system is working and address any difficulties.
- Periodic social meetings among the hospitalists at each site will help to form relationships that can make it less likely that any conversation about transfers will go in an unhelpful direction. Things can be very different when the people on each end of the phone call know each other personally.
- Record the phone calls between those seeking and accepting/declining each transfer. Scott Rissmiller, MD, the lead hospitalist for the 17 practice sites in Carolinas Healthcare, has said that having underperforming doctors listen to recordings of their phone calls about transfers has, in most cases he’s been involved with, proven to be a very effective way to encourage improvement.
Shared Staffing
The small hospitals in many systems sometimes struggle to find a way to provide economical night coverage. Hospitals below a certain size find it very difficult to justify a separate, in-house night provider. Some hospital systems have had success sharing night staffing, with the large hospital’s night hospitalist, nurse practitioner, or physician assistant providing telephone coverage for “cross cover” issues that arise after hours.
For example, when a nurse at the small hospital needs to contact a night hospitalist, staff will page the provider at the big hospital, and, in many cases, the issue can be managed effectively by phone. This works best when both hospitals are on the same electronic medical record, so that the responding provider can look through the record as needed.
The hospitalist at the small hospital typically stays on back-up call and is contacted if bedside attention is required.
Or, if the large and small hospitals are a short drive apart, the night hospitalist at the large facility might make the short drive to the small hospital when needed. In the case of emergencies (i.e., a code blue), the in-house night ED physician is relied on as the first responder.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Serving as the lead physician for a hospital medicine group (HMG) makes for challenging work. And the challenges and complexity only increase for anyone who serves as the physician leader for multiple practice sites in the same hospital system. In my November 2013 column on multi-site HMG leaders, I listed a few of the tricky issues they face and will mention a few more here.
Large-Small Friction
Unfortunately, tension between hospitalists at the big hospital and doctors at the small, “feeder” hospitals seems pretty common, and I think it’s due largely to high stress and a wide variation in workload, neither of which are in our direct control. At facilities where there is significant tension, I’m impressed by how vigorously the hospitalists at both the small and large hospitals argue that their own site faces the most stress and challenges. (This is a little like the endless debate about who works harder, those who work with residents and those who don’t.)
The hospitalists at the small site point out that they work with little or no subspecialty help and might even have to take night call from home while working during the day. Those at the big hospital say they are the ones with the very large scope of clinical practice and that, rather than making their life easier, the presence of lots of subspecialists makes for additional work coordinating care and communicating with all parties.
Where it exists, this tension is most evident during a transfer from one of the small hospitals to the large one. After all, one of the reasons to form a system of hospitals is so that nearly all patient needs can be met at one of the facilities in the system. Yet, for many reasons, the hospitalists at the large hospital are—sometimes—not as receptive to transfers as might be ideal. They might be short staffed or facing a high census or an unusually high number of admissions from their own ED. Or, perhaps, they’re concerned that the subspecialty services for which the patient is being transferred (e.g. to be scoped by a GI doctor) won’t be as helpful or prompt as needed. Or maybe they’ve felt “burned” by their colleagues at the small hospital for past transfers that didn’t seem necessary.
The result can be that the doctors at the smaller hospital complain that the “mother ship” hospitalists often are unfriendly and unreceptive to transfer requests. Although there may not be a definitive “cure” for this issue, there are several ways to help address the problem.
- In my last column, I mentioned the value of one or more in-person meetings between those who tend to be on the sending and receiving end of transfers, to establish some criteria regarding transfers that are appropriate and review the process of requesting a transfer and making the associated arrangements. In most cases there will be value in the parties meeting routinely—perhaps two to four times annually—to review how the system is working and address any difficulties.
- Periodic social meetings among the hospitalists at each site will help to form relationships that can make it less likely that any conversation about transfers will go in an unhelpful direction. Things can be very different when the people on each end of the phone call know each other personally.
- Record the phone calls between those seeking and accepting/declining each transfer. Scott Rissmiller, MD, the lead hospitalist for the 17 practice sites in Carolinas Healthcare, has said that having underperforming doctors listen to recordings of their phone calls about transfers has, in most cases he’s been involved with, proven to be a very effective way to encourage improvement.
Shared Staffing
The small hospitals in many systems sometimes struggle to find a way to provide economical night coverage. Hospitals below a certain size find it very difficult to justify a separate, in-house night provider. Some hospital systems have had success sharing night staffing, with the large hospital’s night hospitalist, nurse practitioner, or physician assistant providing telephone coverage for “cross cover” issues that arise after hours.
For example, when a nurse at the small hospital needs to contact a night hospitalist, staff will page the provider at the big hospital, and, in many cases, the issue can be managed effectively by phone. This works best when both hospitals are on the same electronic medical record, so that the responding provider can look through the record as needed.
The hospitalist at the small hospital typically stays on back-up call and is contacted if bedside attention is required.
Or, if the large and small hospitals are a short drive apart, the night hospitalist at the large facility might make the short drive to the small hospital when needed. In the case of emergencies (i.e., a code blue), the in-house night ED physician is relied on as the first responder.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Beware Mid-Career
Middle age is typically a difficult passage for many professionals. It is a developmental phase involving the mourning of lost opportunities and the acceptance of one’s limits. One also reflects on his or her identity, takes note of regrets, and reevaluates how one will apportion time in the future.—Glen Gabbard, MD1

Hospital medicine is a relatively young specialty, but we are growing up, with many hospitalists now firmly in the middle phase of their careers. In 1999, 15% of our peers had been hospitalists for more than five years; by 2010, that number had grown to 50%.2 As the ranks of hospitalists grow older, we are faced with questions reflecting a life station marked by a little more wisdom, a few more gray hairs, and an occasional reflection on the legacy we will leave.
Drybye and colleagues recently released further analysis on a survey that had been previously reported, shedding new light on mid-career physician satisfaction and burnout and revealing important implications for hospital medicine.3 The study looked at responses to the Maslach Burnout Inventory for physicians from a range of specialties who had been in practice 10 years or less (early career), 11 to 20 years (mid-career), and 21 years or more (late career).
The study demonstrated that while early and late career have their challenges, middle career is a particularly difficult time for physicians. Mid-career physicians had the lowest satisfaction with their specialty choice and their work-life balance and the highest rates of emotional exhaustion and burnout. Strikingly, mid-career physicians were more than twice as likely as those in early and late career to plan to leave the practice of medicine for reasons other than retirement in the next 24 months.
What does this mean for hospital medicine? Because the survey findings are drawn from multiple specialties, we must use caution in extrapolating the results to hospitalists; however, if hospitalists are leaving the specialty mid-career, a more pressing problem may exist for hospital medicine than for other specialties. Why? First, the specialty has grown so rapidly over the last 15 years that it has been difficult to generate a sufficient supply of physicians to meet the demand. If a large number of mid-career hospitalists leave the specialty, our field may be stuck in a state of “arrested development” without the sufficient presence of mature clinicians. Second, effective hospitalists possess “system” skills that are learned on the job, so seasoned hospitalists often play an integrative and problem-solving role within the hospital. Third, there could be a downward spiral of career satisfaction in the specialty if onlookers like trainees and stakeholders in the healthcare ecosystem see hospitalists as dissatisfied and disengaged. Will the promise of hospital medicine be fulfilled?
In an accompanying editorial, Spinelli suggests three principles for physician well-being, which hospitalist programs would do well to consider:4
- Elevate well-being metrics to the same level of importance as financial, quality, and patient satisfaction metrics. (Place such metrics on the organizational dashboard.)
- Design system and care processes that include intentional plans for physician and staff wellness. (Redesign of care models and workflows should consider physician and staff wellness.)
- Adopt a robust set of self-care strategies for those experiencing burnout.
SHM’s Role
SHM has taken up the issue of hospitalist career satisfaction on a number of occasions over the years, initially engendered by field observations of the stressful nature of hospitalist work and a 2001 study reporting that 25% of hospitalists were “at risk” of burnout and 13% were “burned out.”5 Subsequently, SHM released a white paper with a number of specific recommendations organized around a career satisfaction framework consisting of autonomy, reward/recognition, occupational solidarity, and connection with one’s professional and broader community.6
Recently, the SHM Practice Management Committee has once again taken up the issue of “physician engagement.” Over the next few months, the committee plans to:
- Create a repository of related resources on the SHM website, including physician engagement profiles for some hospitalist practices;
- Initiate a dialogue on the topic of physician engagement on HMX (connect.hospitalmedicine.org), SHM’s social networking platform; and
- Publish a “public domain” survey questionnaire that hospitalist practices can use. This is a crucial matter that remains a central concern for our specialty and for the safety and well-being of our patients.
Conclusion
The Institute for Healthcare Improvement advanced the idea of the Triple Aim (better care, better health, lower costs) several years ago as a guiding principle in the transformation of healthcare. More recently, a growing number of voices suggest that physician satisfaction is a crucial foundation of the Triple Aim.4 I submit that for hospitalists to fulfill their potential as healthcare change agents, we will need to build a professional experience that enables them to traverse mid-career challenges and make it to the professional finish line as engaged and well-adjusted members of the healthcare community.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
- Gabbard GO. Medicine and its discontents. Mayo Clin Proc. 2013;88(12):1347-1349.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: Toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
- Drybye LN, Varkey P, Boone SL, Satele DV, Sloan JA, Shanafelt TD. Physician satisfaction and burnout at different career stages. Mayo Clin Proc. 2013;88(12):1358-1367.
- Spinelli WM. The phantom limb of the triple aim. Mayo Clin Proc. 2013;88(12):1356-1357.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Society of Hospital Medicine. A challenge for a new specialty: a white paper on hospitalist career satisfaction. Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Publications/WhitePapers/White_Papers.htm. Accessed January 4, 2014.
Middle age is typically a difficult passage for many professionals. It is a developmental phase involving the mourning of lost opportunities and the acceptance of one’s limits. One also reflects on his or her identity, takes note of regrets, and reevaluates how one will apportion time in the future.—Glen Gabbard, MD1
Hospital medicine is a relatively young specialty, but we are growing up, with many hospitalists now firmly in the middle phase of their careers. In 1999, 15% of our peers had been hospitalists for more than five years; by 2010, that number had grown to 50%.2 As the ranks of hospitalists grow older, we are faced with questions reflecting a life station marked by a little more wisdom, a few more gray hairs, and an occasional reflection on the legacy we will leave.
Drybye and colleagues recently released further analysis on a survey that had been previously reported, shedding new light on mid-career physician satisfaction and burnout and revealing important implications for hospital medicine.3 The study looked at responses to the Maslach Burnout Inventory for physicians from a range of specialties who had been in practice 10 years or less (early career), 11 to 20 years (mid-career), and 21 years or more (late career).
The study demonstrated that while early and late career have their challenges, middle career is a particularly difficult time for physicians. Mid-career physicians had the lowest satisfaction with their specialty choice and their work-life balance and the highest rates of emotional exhaustion and burnout. Strikingly, mid-career physicians were more than twice as likely as those in early and late career to plan to leave the practice of medicine for reasons other than retirement in the next 24 months.
What does this mean for hospital medicine? Because the survey findings are drawn from multiple specialties, we must use caution in extrapolating the results to hospitalists; however, if hospitalists are leaving the specialty mid-career, a more pressing problem may exist for hospital medicine than for other specialties. Why? First, the specialty has grown so rapidly over the last 15 years that it has been difficult to generate a sufficient supply of physicians to meet the demand. If a large number of mid-career hospitalists leave the specialty, our field may be stuck in a state of “arrested development” without the sufficient presence of mature clinicians. Second, effective hospitalists possess “system” skills that are learned on the job, so seasoned hospitalists often play an integrative and problem-solving role within the hospital. Third, there could be a downward spiral of career satisfaction in the specialty if onlookers like trainees and stakeholders in the healthcare ecosystem see hospitalists as dissatisfied and disengaged. Will the promise of hospital medicine be fulfilled?
In an accompanying editorial, Spinelli suggests three principles for physician well-being, which hospitalist programs would do well to consider:4
- Elevate well-being metrics to the same level of importance as financial, quality, and patient satisfaction metrics. (Place such metrics on the organizational dashboard.)
- Design system and care processes that include intentional plans for physician and staff wellness. (Redesign of care models and workflows should consider physician and staff wellness.)
- Adopt a robust set of self-care strategies for those experiencing burnout.
SHM’s Role
SHM has taken up the issue of hospitalist career satisfaction on a number of occasions over the years, initially engendered by field observations of the stressful nature of hospitalist work and a 2001 study reporting that 25% of hospitalists were “at risk” of burnout and 13% were “burned out.”5 Subsequently, SHM released a white paper with a number of specific recommendations organized around a career satisfaction framework consisting of autonomy, reward/recognition, occupational solidarity, and connection with one’s professional and broader community.6
Recently, the SHM Practice Management Committee has once again taken up the issue of “physician engagement.” Over the next few months, the committee plans to:
- Create a repository of related resources on the SHM website, including physician engagement profiles for some hospitalist practices;
- Initiate a dialogue on the topic of physician engagement on HMX (connect.hospitalmedicine.org), SHM’s social networking platform; and
- Publish a “public domain” survey questionnaire that hospitalist practices can use. This is a crucial matter that remains a central concern for our specialty and for the safety and well-being of our patients.
Conclusion
The Institute for Healthcare Improvement advanced the idea of the Triple Aim (better care, better health, lower costs) several years ago as a guiding principle in the transformation of healthcare. More recently, a growing number of voices suggest that physician satisfaction is a crucial foundation of the Triple Aim.4 I submit that for hospitalists to fulfill their potential as healthcare change agents, we will need to build a professional experience that enables them to traverse mid-career challenges and make it to the professional finish line as engaged and well-adjusted members of the healthcare community.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
- Gabbard GO. Medicine and its discontents. Mayo Clin Proc. 2013;88(12):1347-1349.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: Toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
- Drybye LN, Varkey P, Boone SL, Satele DV, Sloan JA, Shanafelt TD. Physician satisfaction and burnout at different career stages. Mayo Clin Proc. 2013;88(12):1358-1367.
- Spinelli WM. The phantom limb of the triple aim. Mayo Clin Proc. 2013;88(12):1356-1357.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Society of Hospital Medicine. A challenge for a new specialty: a white paper on hospitalist career satisfaction. Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Publications/WhitePapers/White_Papers.htm. Accessed January 4, 2014.
Middle age is typically a difficult passage for many professionals. It is a developmental phase involving the mourning of lost opportunities and the acceptance of one’s limits. One also reflects on his or her identity, takes note of regrets, and reevaluates how one will apportion time in the future.—Glen Gabbard, MD1
Hospital medicine is a relatively young specialty, but we are growing up, with many hospitalists now firmly in the middle phase of their careers. In 1999, 15% of our peers had been hospitalists for more than five years; by 2010, that number had grown to 50%.2 As the ranks of hospitalists grow older, we are faced with questions reflecting a life station marked by a little more wisdom, a few more gray hairs, and an occasional reflection on the legacy we will leave.
Drybye and colleagues recently released further analysis on a survey that had been previously reported, shedding new light on mid-career physician satisfaction and burnout and revealing important implications for hospital medicine.3 The study looked at responses to the Maslach Burnout Inventory for physicians from a range of specialties who had been in practice 10 years or less (early career), 11 to 20 years (mid-career), and 21 years or more (late career).
The study demonstrated that while early and late career have their challenges, middle career is a particularly difficult time for physicians. Mid-career physicians had the lowest satisfaction with their specialty choice and their work-life balance and the highest rates of emotional exhaustion and burnout. Strikingly, mid-career physicians were more than twice as likely as those in early and late career to plan to leave the practice of medicine for reasons other than retirement in the next 24 months.
What does this mean for hospital medicine? Because the survey findings are drawn from multiple specialties, we must use caution in extrapolating the results to hospitalists; however, if hospitalists are leaving the specialty mid-career, a more pressing problem may exist for hospital medicine than for other specialties. Why? First, the specialty has grown so rapidly over the last 15 years that it has been difficult to generate a sufficient supply of physicians to meet the demand. If a large number of mid-career hospitalists leave the specialty, our field may be stuck in a state of “arrested development” without the sufficient presence of mature clinicians. Second, effective hospitalists possess “system” skills that are learned on the job, so seasoned hospitalists often play an integrative and problem-solving role within the hospital. Third, there could be a downward spiral of career satisfaction in the specialty if onlookers like trainees and stakeholders in the healthcare ecosystem see hospitalists as dissatisfied and disengaged. Will the promise of hospital medicine be fulfilled?
In an accompanying editorial, Spinelli suggests three principles for physician well-being, which hospitalist programs would do well to consider:4
- Elevate well-being metrics to the same level of importance as financial, quality, and patient satisfaction metrics. (Place such metrics on the organizational dashboard.)
- Design system and care processes that include intentional plans for physician and staff wellness. (Redesign of care models and workflows should consider physician and staff wellness.)
- Adopt a robust set of self-care strategies for those experiencing burnout.
SHM’s Role
SHM has taken up the issue of hospitalist career satisfaction on a number of occasions over the years, initially engendered by field observations of the stressful nature of hospitalist work and a 2001 study reporting that 25% of hospitalists were “at risk” of burnout and 13% were “burned out.”5 Subsequently, SHM released a white paper with a number of specific recommendations organized around a career satisfaction framework consisting of autonomy, reward/recognition, occupational solidarity, and connection with one’s professional and broader community.6
Recently, the SHM Practice Management Committee has once again taken up the issue of “physician engagement.” Over the next few months, the committee plans to:
- Create a repository of related resources on the SHM website, including physician engagement profiles for some hospitalist practices;
- Initiate a dialogue on the topic of physician engagement on HMX (connect.hospitalmedicine.org), SHM’s social networking platform; and
- Publish a “public domain” survey questionnaire that hospitalist practices can use. This is a crucial matter that remains a central concern for our specialty and for the safety and well-being of our patients.
Conclusion
The Institute for Healthcare Improvement advanced the idea of the Triple Aim (better care, better health, lower costs) several years ago as a guiding principle in the transformation of healthcare. More recently, a growing number of voices suggest that physician satisfaction is a crucial foundation of the Triple Aim.4 I submit that for hospitalists to fulfill their potential as healthcare change agents, we will need to build a professional experience that enables them to traverse mid-career challenges and make it to the professional finish line as engaged and well-adjusted members of the healthcare community.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
- Gabbard GO. Medicine and its discontents. Mayo Clin Proc. 2013;88(12):1347-1349.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: Toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
- Drybye LN, Varkey P, Boone SL, Satele DV, Sloan JA, Shanafelt TD. Physician satisfaction and burnout at different career stages. Mayo Clin Proc. 2013;88(12):1358-1367.
- Spinelli WM. The phantom limb of the triple aim. Mayo Clin Proc. 2013;88(12):1356-1357.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Society of Hospital Medicine. A challenge for a new specialty: a white paper on hospitalist career satisfaction. Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Publications/WhitePapers/White_Papers.htm. Accessed January 4, 2014.
Percutaneous closure
Editor’s Note: I urge readers unfamiliar with the Perclose Proglide® device to pay special attention to the instructions for use and to follow them carefully. The device is relatively simple to use but it is a complex piece of equipment and so it is also easy to misuse it with dire consequences. I suggest that one at least read the section on "Troubleshooting," since preventing some of these problems can be lifesaving.
The key to successful percutaneous closure is selecting the appropriate site of entry into the common femoral artery (CFA). Using ultrasound (in transverse and longitudinal planes) and fluoroscopy, I gain access at a noncalcified spot 1 cm above the bifurcation of the CFA (Fig. 1). This is immediately confirmed with an oblique angiogram while pulling the 5F sheath to the ipsilateral side (Fig. 2). This small last maneuver allows me to see exactly where the puncture was and confirms that I will be able to use a closure device.

If using a sheath larger than 12F, I would dilate the track and cut any skin bridges within the puncture site using 11 blade. Doing this maneuver at the end of the procedure could result in inadvertently cutting the sutures. The Proglide device is then inserted and the sutures deployed as per the instructions for use.
At the end of the case, the sheath is pulled over a nonstiff wire while pulling on the nonrail (blue end) wire in a coaxial fashion. I can’t stress enough the need to be calm and not to pull too hard on the suture. This can result in the suture breaking or being pulled out of the artery. The knot pusher is then used on each suture sequentially. At this point, I tug on the wire to make sure it is "snug" within the arteriotomy. This signifies adequate closure but I also check briefly to ensure that there is no significant bleeding. Then I can go ahead and remove the wire and slide the knot pusher again.
The final step is to advance the knot pusher over the two sutures and cut the suture just under the skin. There is no need to slide the knot pusher all the way down to cut the suture as this may inadvertently cut the knot. Steristrips and Band-Aid are applied and I reverse the heparin after confirming the status of distal pulses
Dr. Mussa is an assistant professor of surgery at New York University School of Medicine and Langone Medical Center.
Editor’s Note: I urge readers unfamiliar with the Perclose Proglide® device to pay special attention to the instructions for use and to follow them carefully. The device is relatively simple to use but it is a complex piece of equipment and so it is also easy to misuse it with dire consequences. I suggest that one at least read the section on "Troubleshooting," since preventing some of these problems can be lifesaving.
The key to successful percutaneous closure is selecting the appropriate site of entry into the common femoral artery (CFA). Using ultrasound (in transverse and longitudinal planes) and fluoroscopy, I gain access at a noncalcified spot 1 cm above the bifurcation of the CFA (Fig. 1). This is immediately confirmed with an oblique angiogram while pulling the 5F sheath to the ipsilateral side (Fig. 2). This small last maneuver allows me to see exactly where the puncture was and confirms that I will be able to use a closure device.
If using a sheath larger than 12F, I would dilate the track and cut any skin bridges within the puncture site using 11 blade. Doing this maneuver at the end of the procedure could result in inadvertently cutting the sutures. The Proglide device is then inserted and the sutures deployed as per the instructions for use.
At the end of the case, the sheath is pulled over a nonstiff wire while pulling on the nonrail (blue end) wire in a coaxial fashion. I can’t stress enough the need to be calm and not to pull too hard on the suture. This can result in the suture breaking or being pulled out of the artery. The knot pusher is then used on each suture sequentially. At this point, I tug on the wire to make sure it is "snug" within the arteriotomy. This signifies adequate closure but I also check briefly to ensure that there is no significant bleeding. Then I can go ahead and remove the wire and slide the knot pusher again.
The final step is to advance the knot pusher over the two sutures and cut the suture just under the skin. There is no need to slide the knot pusher all the way down to cut the suture as this may inadvertently cut the knot. Steristrips and Band-Aid are applied and I reverse the heparin after confirming the status of distal pulses
Dr. Mussa is an assistant professor of surgery at New York University School of Medicine and Langone Medical Center.
Editor’s Note: I urge readers unfamiliar with the Perclose Proglide® device to pay special attention to the instructions for use and to follow them carefully. The device is relatively simple to use but it is a complex piece of equipment and so it is also easy to misuse it with dire consequences. I suggest that one at least read the section on "Troubleshooting," since preventing some of these problems can be lifesaving.
The key to successful percutaneous closure is selecting the appropriate site of entry into the common femoral artery (CFA). Using ultrasound (in transverse and longitudinal planes) and fluoroscopy, I gain access at a noncalcified spot 1 cm above the bifurcation of the CFA (Fig. 1). This is immediately confirmed with an oblique angiogram while pulling the 5F sheath to the ipsilateral side (Fig. 2). This small last maneuver allows me to see exactly where the puncture was and confirms that I will be able to use a closure device.
If using a sheath larger than 12F, I would dilate the track and cut any skin bridges within the puncture site using 11 blade. Doing this maneuver at the end of the procedure could result in inadvertently cutting the sutures. The Proglide device is then inserted and the sutures deployed as per the instructions for use.
At the end of the case, the sheath is pulled over a nonstiff wire while pulling on the nonrail (blue end) wire in a coaxial fashion. I can’t stress enough the need to be calm and not to pull too hard on the suture. This can result in the suture breaking or being pulled out of the artery. The knot pusher is then used on each suture sequentially. At this point, I tug on the wire to make sure it is "snug" within the arteriotomy. This signifies adequate closure but I also check briefly to ensure that there is no significant bleeding. Then I can go ahead and remove the wire and slide the knot pusher again.
The final step is to advance the knot pusher over the two sutures and cut the suture just under the skin. There is no need to slide the knot pusher all the way down to cut the suture as this may inadvertently cut the knot. Steristrips and Band-Aid are applied and I reverse the heparin after confirming the status of distal pulses
Dr. Mussa is an assistant professor of surgery at New York University School of Medicine and Langone Medical Center.
Smoking cessation and psychiatry
Proving that cigarette smoking leads to negative health consequences has taken many years. It was President John F. Kennedy who in 1962 created a blue ribbon panel to study the effects of smoking and lung cancer, as well as other cancers and cardiovascular disease. Starting with the seminal 1964 report, numerous surgeons general have made strong cases for these links. The downward trend of cigarette smoking among physicians suggests that we have heeded these warnings.
In the late 1940s, 60% of physicians smoked cigarettes. By the time the surgeon general issued the 1964 report on the health benefits of smoking cessation, 30% of physicians smoked. The prevalence of smoking among physicians continued to decline in the 1960s. In the early 1980s, surveys showed that 5%-10% of physicians smoked cigarettes. By 2006-2007, the prevalence of physicians who smoked cigarettes had declined to 2% (Nicotine Tob. Res. 2010;12:1167-71).

Smoking never appealed to me, and I never started. However, early in my career, I grew concerned about smoking as a public health issue. When I told my father, an eye surgeon (who also did not smoke), that I wanted to pursue psychiatry, he encouraged me to learn an aspect of the specialty that few others knew and to develop that area as a subspecialty. That proved to be great advice. After all, I was underwhelmed by the absolute unsubstantiated dogma that dominated traditional talk therapies in psychiatric training at the time.
Soon after my residency, I started learning about hypnosis, behavior modification, and the emerging discipline of cognitive-behavioral therapy. I spent several years learning and working with the late Dr. Herbert Spiegel, a superb psychiatrist and nationally known expert in hypnosis. Dr. Spiegel and his son, Dr. David Spiegel, wrote the classic book Trance and Treatment: Clinical Uses of Hypnosis, 2nd edition (Washington: American Psychiatric Association, 2003). From there, I started a short-term psychotherapy program in the mid-1970s at NYU Langone Medical Center/Bellevue – first using hypnosis in the treatment of smoking cessation. I continue to use this strategy today.
Although I have modified my approach to smoking cessation from the original Spiegel technique, after almost 4 decades of using hypnosis for smoking cessation, I still find the Hypnotic Induction Profile (HIP), as developed by the Spiegels, to be the easiest way to measure hypnotizability. This technique involves teaching the patient self-hypnosis within a 5- to 10-minute period after taking his health and smoking history.
Besides aiming to help motivated people stop the life-threatening and addictive smoking habit, the use of hypnosis in treating smoking cessation empowers the patient to take control of the addiction and habituation that smoking creates. Instructing the individual in what can be a lifelong process in the use of hypnosis regularly on his own reinforces the original treatment program and makes this approach successful. This is comparable to following a diet-exercise plan.
Another great advantage of using medical hypnosis for smoking cessation is that doing so eliminates the use of powerful medications, including patches, and even needles (as in acupuncture). Such medications have potential side effects.
During the first 10 years of my smoking cessation work, follow-up phone calls were used to determine success. My team and I discovered a success rate of about 30% with responders over a 6-month period.
Today, we understand that smoking affects almost every organ system and is the No. 1 cause of preventable disease and death worldwide.
In the current political environment – in which the emphasis on austerity is leading to enormous cutbacks in health care funding and restrictions by insurers at all levels of care – it would seem that recognizing cigarette smoking as the leading preventable cause of death and disease would be addressed and controlled in a logical way. In fact, if a food or beverage had a fraction of the toxins found in cigarettes, they would be taken off the market. This is how we handle medications that show the slightest bit of danger. Why the double standard for cigarettes?
In addition, electronic cigarettes, or e-cigarettes, are rising in popularity. These products deliver nicotine with secondhand vapor, and the science hasn’t been done on the implications of long-term use. I, for one, would not want to be in a car, restaurant, or movie theater having to inhale microscopic particles of vapor.
Another issue that we must consider is the prevalence of smoking among people with mental illness. A recent report showed that the nationwide decline in cigarette smoking has not extended to our patients (JAMA 2014 [doi:10.1001/jama.2013.284985]). The investigators noted in that study that the smoking rate fell among adults without mental illness from 19.2% in 2004 to 16.5% in 2011. But among adults with mental illness, the rate barely fell, from 25.3% to 24.9%.
Looking back, I am pleased to have started my career focusing on the behavior modification aspect of smoking cessation. I continue to believe that mastering smoking cessation techniques gives us as psychiatrists a way to affect public health in a positive way.
Dr. London is a psychiatrist affiliated with the New York University Langone Medical Center. He said he has no conflicts of interest to disclose.
Proving that cigarette smoking leads to negative health consequences has taken many years. It was President John F. Kennedy who in 1962 created a blue ribbon panel to study the effects of smoking and lung cancer, as well as other cancers and cardiovascular disease. Starting with the seminal 1964 report, numerous surgeons general have made strong cases for these links. The downward trend of cigarette smoking among physicians suggests that we have heeded these warnings.
In the late 1940s, 60% of physicians smoked cigarettes. By the time the surgeon general issued the 1964 report on the health benefits of smoking cessation, 30% of physicians smoked. The prevalence of smoking among physicians continued to decline in the 1960s. In the early 1980s, surveys showed that 5%-10% of physicians smoked cigarettes. By 2006-2007, the prevalence of physicians who smoked cigarettes had declined to 2% (Nicotine Tob. Res. 2010;12:1167-71).
Smoking never appealed to me, and I never started. However, early in my career, I grew concerned about smoking as a public health issue. When I told my father, an eye surgeon (who also did not smoke), that I wanted to pursue psychiatry, he encouraged me to learn an aspect of the specialty that few others knew and to develop that area as a subspecialty. That proved to be great advice. After all, I was underwhelmed by the absolute unsubstantiated dogma that dominated traditional talk therapies in psychiatric training at the time.
Soon after my residency, I started learning about hypnosis, behavior modification, and the emerging discipline of cognitive-behavioral therapy. I spent several years learning and working with the late Dr. Herbert Spiegel, a superb psychiatrist and nationally known expert in hypnosis. Dr. Spiegel and his son, Dr. David Spiegel, wrote the classic book Trance and Treatment: Clinical Uses of Hypnosis, 2nd edition (Washington: American Psychiatric Association, 2003). From there, I started a short-term psychotherapy program in the mid-1970s at NYU Langone Medical Center/Bellevue – first using hypnosis in the treatment of smoking cessation. I continue to use this strategy today.
Although I have modified my approach to smoking cessation from the original Spiegel technique, after almost 4 decades of using hypnosis for smoking cessation, I still find the Hypnotic Induction Profile (HIP), as developed by the Spiegels, to be the easiest way to measure hypnotizability. This technique involves teaching the patient self-hypnosis within a 5- to 10-minute period after taking his health and smoking history.
Besides aiming to help motivated people stop the life-threatening and addictive smoking habit, the use of hypnosis in treating smoking cessation empowers the patient to take control of the addiction and habituation that smoking creates. Instructing the individual in what can be a lifelong process in the use of hypnosis regularly on his own reinforces the original treatment program and makes this approach successful. This is comparable to following a diet-exercise plan.
Another great advantage of using medical hypnosis for smoking cessation is that doing so eliminates the use of powerful medications, including patches, and even needles (as in acupuncture). Such medications have potential side effects.
During the first 10 years of my smoking cessation work, follow-up phone calls were used to determine success. My team and I discovered a success rate of about 30% with responders over a 6-month period.
Today, we understand that smoking affects almost every organ system and is the No. 1 cause of preventable disease and death worldwide.
In the current political environment – in which the emphasis on austerity is leading to enormous cutbacks in health care funding and restrictions by insurers at all levels of care – it would seem that recognizing cigarette smoking as the leading preventable cause of death and disease would be addressed and controlled in a logical way. In fact, if a food or beverage had a fraction of the toxins found in cigarettes, they would be taken off the market. This is how we handle medications that show the slightest bit of danger. Why the double standard for cigarettes?
In addition, electronic cigarettes, or e-cigarettes, are rising in popularity. These products deliver nicotine with secondhand vapor, and the science hasn’t been done on the implications of long-term use. I, for one, would not want to be in a car, restaurant, or movie theater having to inhale microscopic particles of vapor.
Another issue that we must consider is the prevalence of smoking among people with mental illness. A recent report showed that the nationwide decline in cigarette smoking has not extended to our patients (JAMA 2014 [doi:10.1001/jama.2013.284985]). The investigators noted in that study that the smoking rate fell among adults without mental illness from 19.2% in 2004 to 16.5% in 2011. But among adults with mental illness, the rate barely fell, from 25.3% to 24.9%.
Looking back, I am pleased to have started my career focusing on the behavior modification aspect of smoking cessation. I continue to believe that mastering smoking cessation techniques gives us as psychiatrists a way to affect public health in a positive way.
Dr. London is a psychiatrist affiliated with the New York University Langone Medical Center. He said he has no conflicts of interest to disclose.
Proving that cigarette smoking leads to negative health consequences has taken many years. It was President John F. Kennedy who in 1962 created a blue ribbon panel to study the effects of smoking and lung cancer, as well as other cancers and cardiovascular disease. Starting with the seminal 1964 report, numerous surgeons general have made strong cases for these links. The downward trend of cigarette smoking among physicians suggests that we have heeded these warnings.
In the late 1940s, 60% of physicians smoked cigarettes. By the time the surgeon general issued the 1964 report on the health benefits of smoking cessation, 30% of physicians smoked. The prevalence of smoking among physicians continued to decline in the 1960s. In the early 1980s, surveys showed that 5%-10% of physicians smoked cigarettes. By 2006-2007, the prevalence of physicians who smoked cigarettes had declined to 2% (Nicotine Tob. Res. 2010;12:1167-71).
Smoking never appealed to me, and I never started. However, early in my career, I grew concerned about smoking as a public health issue. When I told my father, an eye surgeon (who also did not smoke), that I wanted to pursue psychiatry, he encouraged me to learn an aspect of the specialty that few others knew and to develop that area as a subspecialty. That proved to be great advice. After all, I was underwhelmed by the absolute unsubstantiated dogma that dominated traditional talk therapies in psychiatric training at the time.
Soon after my residency, I started learning about hypnosis, behavior modification, and the emerging discipline of cognitive-behavioral therapy. I spent several years learning and working with the late Dr. Herbert Spiegel, a superb psychiatrist and nationally known expert in hypnosis. Dr. Spiegel and his son, Dr. David Spiegel, wrote the classic book Trance and Treatment: Clinical Uses of Hypnosis, 2nd edition (Washington: American Psychiatric Association, 2003). From there, I started a short-term psychotherapy program in the mid-1970s at NYU Langone Medical Center/Bellevue – first using hypnosis in the treatment of smoking cessation. I continue to use this strategy today.
Although I have modified my approach to smoking cessation from the original Spiegel technique, after almost 4 decades of using hypnosis for smoking cessation, I still find the Hypnotic Induction Profile (HIP), as developed by the Spiegels, to be the easiest way to measure hypnotizability. This technique involves teaching the patient self-hypnosis within a 5- to 10-minute period after taking his health and smoking history.
Besides aiming to help motivated people stop the life-threatening and addictive smoking habit, the use of hypnosis in treating smoking cessation empowers the patient to take control of the addiction and habituation that smoking creates. Instructing the individual in what can be a lifelong process in the use of hypnosis regularly on his own reinforces the original treatment program and makes this approach successful. This is comparable to following a diet-exercise plan.
Another great advantage of using medical hypnosis for smoking cessation is that doing so eliminates the use of powerful medications, including patches, and even needles (as in acupuncture). Such medications have potential side effects.
During the first 10 years of my smoking cessation work, follow-up phone calls were used to determine success. My team and I discovered a success rate of about 30% with responders over a 6-month period.
Today, we understand that smoking affects almost every organ system and is the No. 1 cause of preventable disease and death worldwide.
In the current political environment – in which the emphasis on austerity is leading to enormous cutbacks in health care funding and restrictions by insurers at all levels of care – it would seem that recognizing cigarette smoking as the leading preventable cause of death and disease would be addressed and controlled in a logical way. In fact, if a food or beverage had a fraction of the toxins found in cigarettes, they would be taken off the market. This is how we handle medications that show the slightest bit of danger. Why the double standard for cigarettes?
In addition, electronic cigarettes, or e-cigarettes, are rising in popularity. These products deliver nicotine with secondhand vapor, and the science hasn’t been done on the implications of long-term use. I, for one, would not want to be in a car, restaurant, or movie theater having to inhale microscopic particles of vapor.
Another issue that we must consider is the prevalence of smoking among people with mental illness. A recent report showed that the nationwide decline in cigarette smoking has not extended to our patients (JAMA 2014 [doi:10.1001/jama.2013.284985]). The investigators noted in that study that the smoking rate fell among adults without mental illness from 19.2% in 2004 to 16.5% in 2011. But among adults with mental illness, the rate barely fell, from 25.3% to 24.9%.
Looking back, I am pleased to have started my career focusing on the behavior modification aspect of smoking cessation. I continue to believe that mastering smoking cessation techniques gives us as psychiatrists a way to affect public health in a positive way.
Dr. London is a psychiatrist affiliated with the New York University Langone Medical Center. He said he has no conflicts of interest to disclose.

Treatment courts for veterans deserve our support
Over the last 5 years, Veterans Treatment Courts have been established across the country to address the unique challenges posed by our nation’s veterans who suffer from addiction, psychiatric illness, and/or co-occurring disorders, and who also run afoul of the law.
One study of almost 250,000 veterans who had returned from Iraq and Afghanistan and were under Veterans Affairs care found that 35% of them had received mental health diagnoses, including adjustment disorder, depression, and substance use disorders. The most prevalent mental health diagnosis was posttraumatic stress disorder (J. Gen. Intern. Med. 2010;25:18-24).
Meanwhile, a Bureau of Justice Statistics Special Report found that 9.3% of people incarcerated in jails are veterans and the majority of those serving time were for nonviolent crimes. More than 29% of the violent offenses among offenders who were in military correctional facilities came under the categories of rape and "other sexual assault." The report estimates that at least 90,000 of the 9 million inmates annually released from U.S. jails are veterans and that 82% are eligible for VA services.
Reintegrating into civilian life can be profoundly challenging for veterans, particularly when they also suffer from psychiatric illness, substance use disorders, and/or traumatic brain injury. Veterans often return to a life lacking in adequate support, which may result in unemployment, limited social connectedness, and housing problems. The physical and emotional scars that many veterans acquire during active duty also can be the catalyst for progressive mental health decline. Returning service members are at increased risk of engaging in unsafe risk-taking behaviors, such as reckless driving and heavy drinking (Drug Court Rev. 2011;3:171-208). Furthermore, many veterans live in rural areas with limited access to mental health care. To make matters worse, there continues to be a stigma among veterans that is associated with mental health treatment. Veterans Treatment Courts (VTCs) help to divert veteran defendants into community-based treatments where they are offered access to a comprehensive package of medical and mental health resources through the VA, as well as peer support services.
VTCs grew out of the drug court movement. The first VTC was formed in Buffalo, N.Y., in 2008 by Judge Robert Russell, who grew frustrated with the number of nonviolent veteran offenders forced to enter the criminal justice system after being arrested for crimes related to substance and mental health problems. Opponents of VTCs argue that all citizens, regardless of veteran status, should be afforded equal protection under the law and treated the same. However, while there have been no elegant outcome studies done thus far, state reports indicate that VTCs save taxpayers money and contribute to lower rates of recidivism.
Because of the many complexities of treating veterans, clinicians should embrace a culture of recovery. In particular, contingency management and the use of positive-reinforcement systems should be a standard and central practice in all treatment settings. Servicemen and -women have experienced trauma in order to protect our freedoms and ensure our safety, and it is our collective job to support a compassionate system that makes every effort to help our veterans avoid incarceration, which can be a retraumatizing experience. Many patients who are eligible for VA services are not connected to those services and clinicians should make appropriate referrals if necessary.
Dr. Ascher is a postdoctoral fellow at the Philadelphia VA Medical Center and clinical instructor in psychiatry at the University of Pennsylvania, Philadelphia.
Over the last 5 years, Veterans Treatment Courts have been established across the country to address the unique challenges posed by our nation’s veterans who suffer from addiction, psychiatric illness, and/or co-occurring disorders, and who also run afoul of the law.
One study of almost 250,000 veterans who had returned from Iraq and Afghanistan and were under Veterans Affairs care found that 35% of them had received mental health diagnoses, including adjustment disorder, depression, and substance use disorders. The most prevalent mental health diagnosis was posttraumatic stress disorder (J. Gen. Intern. Med. 2010;25:18-24).
Meanwhile, a Bureau of Justice Statistics Special Report found that 9.3% of people incarcerated in jails are veterans and the majority of those serving time were for nonviolent crimes. More than 29% of the violent offenses among offenders who were in military correctional facilities came under the categories of rape and "other sexual assault." The report estimates that at least 90,000 of the 9 million inmates annually released from U.S. jails are veterans and that 82% are eligible for VA services.
Reintegrating into civilian life can be profoundly challenging for veterans, particularly when they also suffer from psychiatric illness, substance use disorders, and/or traumatic brain injury. Veterans often return to a life lacking in adequate support, which may result in unemployment, limited social connectedness, and housing problems. The physical and emotional scars that many veterans acquire during active duty also can be the catalyst for progressive mental health decline. Returning service members are at increased risk of engaging in unsafe risk-taking behaviors, such as reckless driving and heavy drinking (Drug Court Rev. 2011;3:171-208). Furthermore, many veterans live in rural areas with limited access to mental health care. To make matters worse, there continues to be a stigma among veterans that is associated with mental health treatment. Veterans Treatment Courts (VTCs) help to divert veteran defendants into community-based treatments where they are offered access to a comprehensive package of medical and mental health resources through the VA, as well as peer support services.
VTCs grew out of the drug court movement. The first VTC was formed in Buffalo, N.Y., in 2008 by Judge Robert Russell, who grew frustrated with the number of nonviolent veteran offenders forced to enter the criminal justice system after being arrested for crimes related to substance and mental health problems. Opponents of VTCs argue that all citizens, regardless of veteran status, should be afforded equal protection under the law and treated the same. However, while there have been no elegant outcome studies done thus far, state reports indicate that VTCs save taxpayers money and contribute to lower rates of recidivism.
Because of the many complexities of treating veterans, clinicians should embrace a culture of recovery. In particular, contingency management and the use of positive-reinforcement systems should be a standard and central practice in all treatment settings. Servicemen and -women have experienced trauma in order to protect our freedoms and ensure our safety, and it is our collective job to support a compassionate system that makes every effort to help our veterans avoid incarceration, which can be a retraumatizing experience. Many patients who are eligible for VA services are not connected to those services and clinicians should make appropriate referrals if necessary.
Dr. Ascher is a postdoctoral fellow at the Philadelphia VA Medical Center and clinical instructor in psychiatry at the University of Pennsylvania, Philadelphia.
Over the last 5 years, Veterans Treatment Courts have been established across the country to address the unique challenges posed by our nation’s veterans who suffer from addiction, psychiatric illness, and/or co-occurring disorders, and who also run afoul of the law.
One study of almost 250,000 veterans who had returned from Iraq and Afghanistan and were under Veterans Affairs care found that 35% of them had received mental health diagnoses, including adjustment disorder, depression, and substance use disorders. The most prevalent mental health diagnosis was posttraumatic stress disorder (J. Gen. Intern. Med. 2010;25:18-24).
Meanwhile, a Bureau of Justice Statistics Special Report found that 9.3% of people incarcerated in jails are veterans and the majority of those serving time were for nonviolent crimes. More than 29% of the violent offenses among offenders who were in military correctional facilities came under the categories of rape and "other sexual assault." The report estimates that at least 90,000 of the 9 million inmates annually released from U.S. jails are veterans and that 82% are eligible for VA services.
Reintegrating into civilian life can be profoundly challenging for veterans, particularly when they also suffer from psychiatric illness, substance use disorders, and/or traumatic brain injury. Veterans often return to a life lacking in adequate support, which may result in unemployment, limited social connectedness, and housing problems. The physical and emotional scars that many veterans acquire during active duty also can be the catalyst for progressive mental health decline. Returning service members are at increased risk of engaging in unsafe risk-taking behaviors, such as reckless driving and heavy drinking (Drug Court Rev. 2011;3:171-208). Furthermore, many veterans live in rural areas with limited access to mental health care. To make matters worse, there continues to be a stigma among veterans that is associated with mental health treatment. Veterans Treatment Courts (VTCs) help to divert veteran defendants into community-based treatments where they are offered access to a comprehensive package of medical and mental health resources through the VA, as well as peer support services.
VTCs grew out of the drug court movement. The first VTC was formed in Buffalo, N.Y., in 2008 by Judge Robert Russell, who grew frustrated with the number of nonviolent veteran offenders forced to enter the criminal justice system after being arrested for crimes related to substance and mental health problems. Opponents of VTCs argue that all citizens, regardless of veteran status, should be afforded equal protection under the law and treated the same. However, while there have been no elegant outcome studies done thus far, state reports indicate that VTCs save taxpayers money and contribute to lower rates of recidivism.
Because of the many complexities of treating veterans, clinicians should embrace a culture of recovery. In particular, contingency management and the use of positive-reinforcement systems should be a standard and central practice in all treatment settings. Servicemen and -women have experienced trauma in order to protect our freedoms and ensure our safety, and it is our collective job to support a compassionate system that makes every effort to help our veterans avoid incarceration, which can be a retraumatizing experience. Many patients who are eligible for VA services are not connected to those services and clinicians should make appropriate referrals if necessary.
Dr. Ascher is a postdoctoral fellow at the Philadelphia VA Medical Center and clinical instructor in psychiatry at the University of Pennsylvania, Philadelphia.

Electronic Health Records Can Complicate Who Does What in a Hospital


The accumulated wisdom, research data, and opinions regarding the use of electronic health records (EHRs) are vast. A quick Internet search turns up many informative articles on their positive and negative effects. But I haven’t found many that explicitly review the unanticipated effects EHRs have on who does what in the hospital.
For example, when reports such as admission and discharge notes are done via recorded dictation and transcription, the author would typically dictate where copies of the report should be sent (“copy to Dr. Matheny”) and rely on others to ensure it reached its intended destination. In many hospitals, such reports are now typed directly into the EHR, often using speech recognition software, and it is up to the author to click several buttons to ensure that it is routed to the intended recipients. So now a clerical function, sending reports, is handled by providers. This can be a good thing—reduced clerical staffing costs, faster transmission of reports—but often means that there is no documentation within the report itself of whom it was sent to (i.e., no list of “cc’s”). It also means that when the recipient isn’t easy to find, the report author is likely to give up, and the report may never be sent.
Any hospitalist using an EHR could easily list dozens of similar unanticipated effects, both good and bad. The magnitude and risk of these are difficult to quantify.
Altered Referral Patterns, Division of Labor
A hospitalist-specific side effect of EHR adoption is that they tend to cause many other doctors to resist serving as attending physician, instead asking hospitalists to replace them in that role. Even without EHRs, shifting attending responsibility to hospitalists has been a trend at nearly every hospital for years, but it can be accelerated dramatically at the time of a “go live.” So, in addition to the stress of adapting to the new EHR, hospitalists typically face higher than usual patient volumes resulting from increased referrals from other doctors.
If you’re a hospitalist facing an upcoming “go live,” it would be worth talking to other doctors in multiple specialties regarding your capacity to handle additional work. Keep in mind the possibility of higher than typical winter 2014 patient volumes that could result from patients who are newly insured through health exchanges.
Many factors, in addition to EHRs, are moving physicians away from a willingness to serve as attending, including the complexity of managing inpatient vs. observation status, keeping up with ever-changing documentation, pay-for-performance initiatives, the stress of ED call, and so on. As I’ve written before (see my January 2011 column, “Health IT Hurdles,”), I think effective management of hospital systems is becoming as complicated as safely piloting a jumbo jet. It will be increasingly difficult for doctors in any specialty to stay proficient at “piloting” a hospital unless they do it all or most of the time. And, staying proficient at multiple hospitals simultaneously may not be feasible at some point. We’ll see.
When Do Things Get Done?
A friend of mine, Dr. John Maa, is a general surgeon who was instrumental in establishing one of the first general surgery hospitalist practices. He tells a very personal and tragic story of his mother’s death, which, he has come to believe, might have been made more likely because of the unintended effect of an EHR.
She was a healthy 69-year-old who developed new onset atrial fibrillation and went to “one of the most highly regarded academic medical centers on the West Coast,” albeit not a facility where John was practicing. She was admitted with orders for anticoagulation but spent her first night on a stretcher in the ED because no inpatient bed was available. She went to a hospital room the next day, but her late arrival there delayed the planned transesophageal echo and cardioversion by another day.
Tragically, before the cardioversion could be done, she had a very large embolic stroke that led to brain herniation. A short time later, John and his father made the wrenching decision to discontinue mechanical ventilation. She died 112 hours after walking into the hospital.
What John later learned is that the admission orders written while she was in the ED were put into “sign and hold” status in the hospital’s EHR. Her caregivers had not anticipated a significant delay in moving her to an inpatient bed, and for the 18 or so hours she spent boarding in the ED, her admission orders were not acted on, and anticoagulation was delayed many hours. She might have had the same outcome even if anticoagulation had been started promptly, but it would have been much less likely.
John believes that the “sign and hold” status of the admission orders was a major contributor to the treatment delay. It increased the risk that the ED caregivers never acted on those orders, and may not have even seen them, since the EHR essentially holds them for presentation to the receiving inpatient unit.
John only recognized this vulnerability three years after his mother’s passing, when he underwent the physician training for the same EHR system. The course teachers agreed that this problem could arise if a patient was boarded in the ED for a prolonged period but felt that the responsibility rested with hospital administrators to minimize overcrowding in the ED. John also raised the issue with hospital leadership, who shared his concern but believed that a software remedy should be the solution. Ultimately, the answer may come from medical hospitalists, who recognize that every day and night, patients across America are at risk for a repeat of the incident John’s family suffered nearly five years ago.
In a very well written and moving essay, John describes his mother’s care.1 Though he doesn’t specifically mention the likely contribution of the “sign and hold” orders, it is one more example of EHR-related confusion that can arise around who does what and when they should do it. Clearly, the same sort of confusion exists in a non-EHR hospital, but it is the EHR-related change in the previous way of doing things that likely increases risk.
It can be very difficult—even impossible—to see all of these issues in advance. Even when acknowledged, the challenges can be difficult to address. But the first step is to recognize a problem, or potential problem, and think carefully about how it should be addressed.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Reference
The accumulated wisdom, research data, and opinions regarding the use of electronic health records (EHRs) are vast. A quick Internet search turns up many informative articles on their positive and negative effects. But I haven’t found many that explicitly review the unanticipated effects EHRs have on who does what in the hospital.
For example, when reports such as admission and discharge notes are done via recorded dictation and transcription, the author would typically dictate where copies of the report should be sent (“copy to Dr. Matheny”) and rely on others to ensure it reached its intended destination. In many hospitals, such reports are now typed directly into the EHR, often using speech recognition software, and it is up to the author to click several buttons to ensure that it is routed to the intended recipients. So now a clerical function, sending reports, is handled by providers. This can be a good thing—reduced clerical staffing costs, faster transmission of reports—but often means that there is no documentation within the report itself of whom it was sent to (i.e., no list of “cc’s”). It also means that when the recipient isn’t easy to find, the report author is likely to give up, and the report may never be sent.
Any hospitalist using an EHR could easily list dozens of similar unanticipated effects, both good and bad. The magnitude and risk of these are difficult to quantify.
Altered Referral Patterns, Division of Labor
A hospitalist-specific side effect of EHR adoption is that they tend to cause many other doctors to resist serving as attending physician, instead asking hospitalists to replace them in that role. Even without EHRs, shifting attending responsibility to hospitalists has been a trend at nearly every hospital for years, but it can be accelerated dramatically at the time of a “go live.” So, in addition to the stress of adapting to the new EHR, hospitalists typically face higher than usual patient volumes resulting from increased referrals from other doctors.
If you’re a hospitalist facing an upcoming “go live,” it would be worth talking to other doctors in multiple specialties regarding your capacity to handle additional work. Keep in mind the possibility of higher than typical winter 2014 patient volumes that could result from patients who are newly insured through health exchanges.
Many factors, in addition to EHRs, are moving physicians away from a willingness to serve as attending, including the complexity of managing inpatient vs. observation status, keeping up with ever-changing documentation, pay-for-performance initiatives, the stress of ED call, and so on. As I’ve written before (see my January 2011 column, “Health IT Hurdles,”), I think effective management of hospital systems is becoming as complicated as safely piloting a jumbo jet. It will be increasingly difficult for doctors in any specialty to stay proficient at “piloting” a hospital unless they do it all or most of the time. And, staying proficient at multiple hospitals simultaneously may not be feasible at some point. We’ll see.
When Do Things Get Done?
A friend of mine, Dr. John Maa, is a general surgeon who was instrumental in establishing one of the first general surgery hospitalist practices. He tells a very personal and tragic story of his mother’s death, which, he has come to believe, might have been made more likely because of the unintended effect of an EHR.
She was a healthy 69-year-old who developed new onset atrial fibrillation and went to “one of the most highly regarded academic medical centers on the West Coast,” albeit not a facility where John was practicing. She was admitted with orders for anticoagulation but spent her first night on a stretcher in the ED because no inpatient bed was available. She went to a hospital room the next day, but her late arrival there delayed the planned transesophageal echo and cardioversion by another day.
Tragically, before the cardioversion could be done, she had a very large embolic stroke that led to brain herniation. A short time later, John and his father made the wrenching decision to discontinue mechanical ventilation. She died 112 hours after walking into the hospital.
What John later learned is that the admission orders written while she was in the ED were put into “sign and hold” status in the hospital’s EHR. Her caregivers had not anticipated a significant delay in moving her to an inpatient bed, and for the 18 or so hours she spent boarding in the ED, her admission orders were not acted on, and anticoagulation was delayed many hours. She might have had the same outcome even if anticoagulation had been started promptly, but it would have been much less likely.
John believes that the “sign and hold” status of the admission orders was a major contributor to the treatment delay. It increased the risk that the ED caregivers never acted on those orders, and may not have even seen them, since the EHR essentially holds them for presentation to the receiving inpatient unit.
John only recognized this vulnerability three years after his mother’s passing, when he underwent the physician training for the same EHR system. The course teachers agreed that this problem could arise if a patient was boarded in the ED for a prolonged period but felt that the responsibility rested with hospital administrators to minimize overcrowding in the ED. John also raised the issue with hospital leadership, who shared his concern but believed that a software remedy should be the solution. Ultimately, the answer may come from medical hospitalists, who recognize that every day and night, patients across America are at risk for a repeat of the incident John’s family suffered nearly five years ago.
In a very well written and moving essay, John describes his mother’s care.1 Though he doesn’t specifically mention the likely contribution of the “sign and hold” orders, it is one more example of EHR-related confusion that can arise around who does what and when they should do it. Clearly, the same sort of confusion exists in a non-EHR hospital, but it is the EHR-related change in the previous way of doing things that likely increases risk.
It can be very difficult—even impossible—to see all of these issues in advance. Even when acknowledged, the challenges can be difficult to address. But the first step is to recognize a problem, or potential problem, and think carefully about how it should be addressed.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Reference
The accumulated wisdom, research data, and opinions regarding the use of electronic health records (EHRs) are vast. A quick Internet search turns up many informative articles on their positive and negative effects. But I haven’t found many that explicitly review the unanticipated effects EHRs have on who does what in the hospital.
For example, when reports such as admission and discharge notes are done via recorded dictation and transcription, the author would typically dictate where copies of the report should be sent (“copy to Dr. Matheny”) and rely on others to ensure it reached its intended destination. In many hospitals, such reports are now typed directly into the EHR, often using speech recognition software, and it is up to the author to click several buttons to ensure that it is routed to the intended recipients. So now a clerical function, sending reports, is handled by providers. This can be a good thing—reduced clerical staffing costs, faster transmission of reports—but often means that there is no documentation within the report itself of whom it was sent to (i.e., no list of “cc’s”). It also means that when the recipient isn’t easy to find, the report author is likely to give up, and the report may never be sent.
Any hospitalist using an EHR could easily list dozens of similar unanticipated effects, both good and bad. The magnitude and risk of these are difficult to quantify.
Altered Referral Patterns, Division of Labor
A hospitalist-specific side effect of EHR adoption is that they tend to cause many other doctors to resist serving as attending physician, instead asking hospitalists to replace them in that role. Even without EHRs, shifting attending responsibility to hospitalists has been a trend at nearly every hospital for years, but it can be accelerated dramatically at the time of a “go live.” So, in addition to the stress of adapting to the new EHR, hospitalists typically face higher than usual patient volumes resulting from increased referrals from other doctors.
If you’re a hospitalist facing an upcoming “go live,” it would be worth talking to other doctors in multiple specialties regarding your capacity to handle additional work. Keep in mind the possibility of higher than typical winter 2014 patient volumes that could result from patients who are newly insured through health exchanges.
Many factors, in addition to EHRs, are moving physicians away from a willingness to serve as attending, including the complexity of managing inpatient vs. observation status, keeping up with ever-changing documentation, pay-for-performance initiatives, the stress of ED call, and so on. As I’ve written before (see my January 2011 column, “Health IT Hurdles,”), I think effective management of hospital systems is becoming as complicated as safely piloting a jumbo jet. It will be increasingly difficult for doctors in any specialty to stay proficient at “piloting” a hospital unless they do it all or most of the time. And, staying proficient at multiple hospitals simultaneously may not be feasible at some point. We’ll see.
When Do Things Get Done?
A friend of mine, Dr. John Maa, is a general surgeon who was instrumental in establishing one of the first general surgery hospitalist practices. He tells a very personal and tragic story of his mother’s death, which, he has come to believe, might have been made more likely because of the unintended effect of an EHR.
She was a healthy 69-year-old who developed new onset atrial fibrillation and went to “one of the most highly regarded academic medical centers on the West Coast,” albeit not a facility where John was practicing. She was admitted with orders for anticoagulation but spent her first night on a stretcher in the ED because no inpatient bed was available. She went to a hospital room the next day, but her late arrival there delayed the planned transesophageal echo and cardioversion by another day.
Tragically, before the cardioversion could be done, she had a very large embolic stroke that led to brain herniation. A short time later, John and his father made the wrenching decision to discontinue mechanical ventilation. She died 112 hours after walking into the hospital.
What John later learned is that the admission orders written while she was in the ED were put into “sign and hold” status in the hospital’s EHR. Her caregivers had not anticipated a significant delay in moving her to an inpatient bed, and for the 18 or so hours she spent boarding in the ED, her admission orders were not acted on, and anticoagulation was delayed many hours. She might have had the same outcome even if anticoagulation had been started promptly, but it would have been much less likely.
John believes that the “sign and hold” status of the admission orders was a major contributor to the treatment delay. It increased the risk that the ED caregivers never acted on those orders, and may not have even seen them, since the EHR essentially holds them for presentation to the receiving inpatient unit.
John only recognized this vulnerability three years after his mother’s passing, when he underwent the physician training for the same EHR system. The course teachers agreed that this problem could arise if a patient was boarded in the ED for a prolonged period but felt that the responsibility rested with hospital administrators to minimize overcrowding in the ED. John also raised the issue with hospital leadership, who shared his concern but believed that a software remedy should be the solution. Ultimately, the answer may come from medical hospitalists, who recognize that every day and night, patients across America are at risk for a repeat of the incident John’s family suffered nearly five years ago.
In a very well written and moving essay, John describes his mother’s care.1 Though he doesn’t specifically mention the likely contribution of the “sign and hold” orders, it is one more example of EHR-related confusion that can arise around who does what and when they should do it. Clearly, the same sort of confusion exists in a non-EHR hospital, but it is the EHR-related change in the previous way of doing things that likely increases risk.
It can be very difficult—even impossible—to see all of these issues in advance. Even when acknowledged, the challenges can be difficult to address. But the first step is to recognize a problem, or potential problem, and think carefully about how it should be addressed.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Reference
Performance Evaluation Program for Individual Physicians Directional at Best


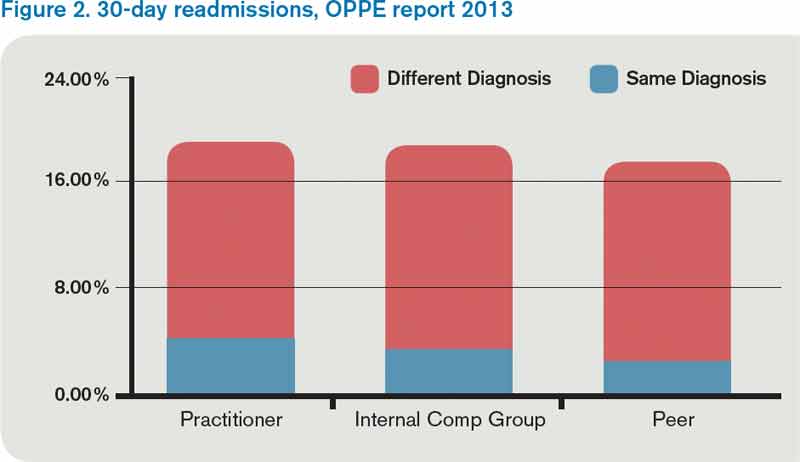
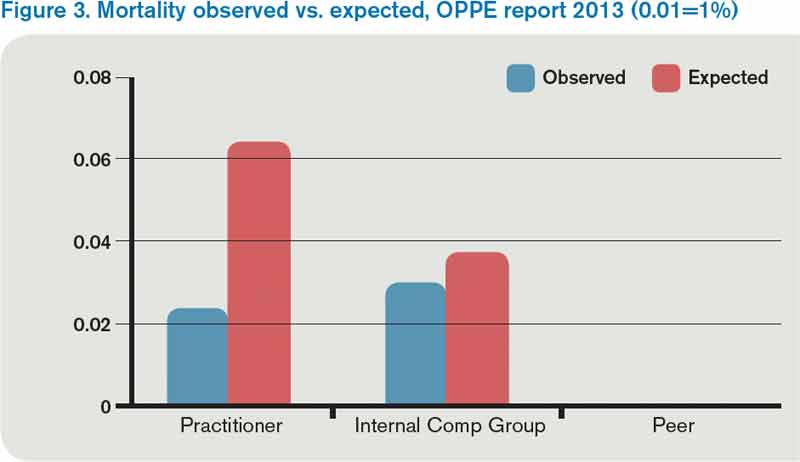
What makes a great doctor? Heck if I know. Maybe it’s like pornography. A great physician, well, “You know one when you see one.” That approach worked from the time of Hippocrates until the recent past, when the Centers for Medicare & Medicaid Services (CMS), the Joint Commission, and others embarked on programs to measure and report physician quality. Of course, bodies like the American Board of Internal Medicine have been certifying physicians for a long time.
Ongoing Professional Practice Evaluation (OPPE) is one such measurement program, now over four years old, with standards put forth by the Joint Commission in an effort to monitor individual physician—and non-physician provider—performance across a number of domains. The program requires accredited hospitals to monitor and report performance to the physician/provider at least every 11 months, and to use such information in the credentialing process.
This year, I received two OPPE reports, causing me to reflect on how helpful these reports are in judging and improving the quality of my practice. Before I discuss some of the “grades” I received, let me start with my conclusion: Physician quality measurement is in its infancy, and the measures are at best “directional” for most physicians, including hospitalists. Some measurement is better than none at all, however, and selected measures, such as surgical site infection and other measures of harm, may be grounds for closer monitoring, or even corrective action, of a physician’s practice. Unfortunately, my stance that OPPE quality measures are “directional” might not help a physician whose privileges are on the line.
Attribution
For hospitalists, the first concern in measuring and reporting quality is, “How can I attribute quality to an individual hospitalist, when several different hospitalists see the patient?” My perspective is that unless a quality measure can be attributed to an individual hospitalist (e.g. discharge medication reconciliation), it should be attributed at the group level.
However, the OPPE program is specifically intended to address the individual physician/provider for purposes of credentialing, and group attribution is a non-starter. In my performance examples below, I believe that attributing outcomes like mortality, readmissions, or resource utilization to individual hospitalists does not make sense—and is probably unfair.
Resource Utilization
The report lists my performance (Practitioner) compared to an Internal Comparison Group for a specified time period (see Figure 1). The comparison group is described as “practitioners in your specialty...from within your health system.” My data were generated based on only 45 cases (I see patients only part time), while the comparison group was based on 4,530 cases. What I take home from this is that, for cost/resource, I look favorable in “supplies” and “pharmacy”; for most of the others, I’m expensive in comparison.
Will this change my practice? Maybe I will think twice about incurring laboratory or pharmacy costs, but I can’t say I am going to fundamentally rethink how or what I order. And I take all these data with a grain of salt, because I share responsibility for patients with several other hospitalists.
Readmissions
My 30-day readmissions performance (see Figure 2) is weak compared to the Internal Comp Group, which I defined above, and the Peer group, which in my report is defined as derived from practitioners at facilities with 501 beds or more (my facility has 700-plus beds). I accept the “directional” nature of the data, meaning that it provides a general idea but not a precise measurement, and vow to reflect on the processes underlying my approach to hospital discharge (teach back, medication reconciliation, PCP communication, and so on).
Mortality
For this category (see Figure 3), I’m looking better. The blue bar is “observed,” while the red bar is “expected.” Although my patients are sicker (higher “expected” mortality), my “observed” mortality is lower than the comparison group. I’m not sure why my observed mortality is lower, but I’m convinced that part of the reason for a higher expected mortality is that my documentation is better than the comparison group.
Will OPPE Change My Practice?
There are other data in my report, including process (core) measures, length of stay, hospital-acquired conditions, and patient flow measures. The OPPE report is but one of a growing number of physician report cards: The Massachusetts Board of Medicine, Physician Compare (CMS), and Health Grades are just a few of the organizations that have public websites reporting my performance. Perhaps at this stage, the primary impact of these reports is through the oft-invoked “Hawthorne Effect,” where subjects modify behavior simply because they are being observed, as opposed to any particular piece of feedback.
My sense is that hospitalists are particularly open to the type of feedback offered in OPPE and similar reports, as long as the data are credible, even if reflecting group level performance. The 2012 SHM State of Hospital Medicine survey shows that the percent of hospitalist compensation based on performance (other than production/billings) increased to 7% from 4% in 2011. It seems that performance measurement with consequences, be it for credentialing or compensation, is here to stay.
Dr. Whitcombis Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
What makes a great doctor? Heck if I know. Maybe it’s like pornography. A great physician, well, “You know one when you see one.” That approach worked from the time of Hippocrates until the recent past, when the Centers for Medicare & Medicaid Services (CMS), the Joint Commission, and others embarked on programs to measure and report physician quality. Of course, bodies like the American Board of Internal Medicine have been certifying physicians for a long time.
Ongoing Professional Practice Evaluation (OPPE) is one such measurement program, now over four years old, with standards put forth by the Joint Commission in an effort to monitor individual physician—and non-physician provider—performance across a number of domains. The program requires accredited hospitals to monitor and report performance to the physician/provider at least every 11 months, and to use such information in the credentialing process.
This year, I received two OPPE reports, causing me to reflect on how helpful these reports are in judging and improving the quality of my practice. Before I discuss some of the “grades” I received, let me start with my conclusion: Physician quality measurement is in its infancy, and the measures are at best “directional” for most physicians, including hospitalists. Some measurement is better than none at all, however, and selected measures, such as surgical site infection and other measures of harm, may be grounds for closer monitoring, or even corrective action, of a physician’s practice. Unfortunately, my stance that OPPE quality measures are “directional” might not help a physician whose privileges are on the line.
Attribution
For hospitalists, the first concern in measuring and reporting quality is, “How can I attribute quality to an individual hospitalist, when several different hospitalists see the patient?” My perspective is that unless a quality measure can be attributed to an individual hospitalist (e.g. discharge medication reconciliation), it should be attributed at the group level.
However, the OPPE program is specifically intended to address the individual physician/provider for purposes of credentialing, and group attribution is a non-starter. In my performance examples below, I believe that attributing outcomes like mortality, readmissions, or resource utilization to individual hospitalists does not make sense—and is probably unfair.
Resource Utilization
The report lists my performance (Practitioner) compared to an Internal Comparison Group for a specified time period (see Figure 1). The comparison group is described as “practitioners in your specialty...from within your health system.” My data were generated based on only 45 cases (I see patients only part time), while the comparison group was based on 4,530 cases. What I take home from this is that, for cost/resource, I look favorable in “supplies” and “pharmacy”; for most of the others, I’m expensive in comparison.
Will this change my practice? Maybe I will think twice about incurring laboratory or pharmacy costs, but I can’t say I am going to fundamentally rethink how or what I order. And I take all these data with a grain of salt, because I share responsibility for patients with several other hospitalists.
Readmissions
My 30-day readmissions performance (see Figure 2) is weak compared to the Internal Comp Group, which I defined above, and the Peer group, which in my report is defined as derived from practitioners at facilities with 501 beds or more (my facility has 700-plus beds). I accept the “directional” nature of the data, meaning that it provides a general idea but not a precise measurement, and vow to reflect on the processes underlying my approach to hospital discharge (teach back, medication reconciliation, PCP communication, and so on).
Mortality
For this category (see Figure 3), I’m looking better. The blue bar is “observed,” while the red bar is “expected.” Although my patients are sicker (higher “expected” mortality), my “observed” mortality is lower than the comparison group. I’m not sure why my observed mortality is lower, but I’m convinced that part of the reason for a higher expected mortality is that my documentation is better than the comparison group.
Will OPPE Change My Practice?
There are other data in my report, including process (core) measures, length of stay, hospital-acquired conditions, and patient flow measures. The OPPE report is but one of a growing number of physician report cards: The Massachusetts Board of Medicine, Physician Compare (CMS), and Health Grades are just a few of the organizations that have public websites reporting my performance. Perhaps at this stage, the primary impact of these reports is through the oft-invoked “Hawthorne Effect,” where subjects modify behavior simply because they are being observed, as opposed to any particular piece of feedback.
My sense is that hospitalists are particularly open to the type of feedback offered in OPPE and similar reports, as long as the data are credible, even if reflecting group level performance. The 2012 SHM State of Hospital Medicine survey shows that the percent of hospitalist compensation based on performance (other than production/billings) increased to 7% from 4% in 2011. It seems that performance measurement with consequences, be it for credentialing or compensation, is here to stay.
Dr. Whitcombis Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
What makes a great doctor? Heck if I know. Maybe it’s like pornography. A great physician, well, “You know one when you see one.” That approach worked from the time of Hippocrates until the recent past, when the Centers for Medicare & Medicaid Services (CMS), the Joint Commission, and others embarked on programs to measure and report physician quality. Of course, bodies like the American Board of Internal Medicine have been certifying physicians for a long time.
Ongoing Professional Practice Evaluation (OPPE) is one such measurement program, now over four years old, with standards put forth by the Joint Commission in an effort to monitor individual physician—and non-physician provider—performance across a number of domains. The program requires accredited hospitals to monitor and report performance to the physician/provider at least every 11 months, and to use such information in the credentialing process.
This year, I received two OPPE reports, causing me to reflect on how helpful these reports are in judging and improving the quality of my practice. Before I discuss some of the “grades” I received, let me start with my conclusion: Physician quality measurement is in its infancy, and the measures are at best “directional” for most physicians, including hospitalists. Some measurement is better than none at all, however, and selected measures, such as surgical site infection and other measures of harm, may be grounds for closer monitoring, or even corrective action, of a physician’s practice. Unfortunately, my stance that OPPE quality measures are “directional” might not help a physician whose privileges are on the line.
Attribution
For hospitalists, the first concern in measuring and reporting quality is, “How can I attribute quality to an individual hospitalist, when several different hospitalists see the patient?” My perspective is that unless a quality measure can be attributed to an individual hospitalist (e.g. discharge medication reconciliation), it should be attributed at the group level.
However, the OPPE program is specifically intended to address the individual physician/provider for purposes of credentialing, and group attribution is a non-starter. In my performance examples below, I believe that attributing outcomes like mortality, readmissions, or resource utilization to individual hospitalists does not make sense—and is probably unfair.
Resource Utilization
The report lists my performance (Practitioner) compared to an Internal Comparison Group for a specified time period (see Figure 1). The comparison group is described as “practitioners in your specialty...from within your health system.” My data were generated based on only 45 cases (I see patients only part time), while the comparison group was based on 4,530 cases. What I take home from this is that, for cost/resource, I look favorable in “supplies” and “pharmacy”; for most of the others, I’m expensive in comparison.
Will this change my practice? Maybe I will think twice about incurring laboratory or pharmacy costs, but I can’t say I am going to fundamentally rethink how or what I order. And I take all these data with a grain of salt, because I share responsibility for patients with several other hospitalists.
Readmissions
My 30-day readmissions performance (see Figure 2) is weak compared to the Internal Comp Group, which I defined above, and the Peer group, which in my report is defined as derived from practitioners at facilities with 501 beds or more (my facility has 700-plus beds). I accept the “directional” nature of the data, meaning that it provides a general idea but not a precise measurement, and vow to reflect on the processes underlying my approach to hospital discharge (teach back, medication reconciliation, PCP communication, and so on).
Mortality
For this category (see Figure 3), I’m looking better. The blue bar is “observed,” while the red bar is “expected.” Although my patients are sicker (higher “expected” mortality), my “observed” mortality is lower than the comparison group. I’m not sure why my observed mortality is lower, but I’m convinced that part of the reason for a higher expected mortality is that my documentation is better than the comparison group.
Will OPPE Change My Practice?
There are other data in my report, including process (core) measures, length of stay, hospital-acquired conditions, and patient flow measures. The OPPE report is but one of a growing number of physician report cards: The Massachusetts Board of Medicine, Physician Compare (CMS), and Health Grades are just a few of the organizations that have public websites reporting my performance. Perhaps at this stage, the primary impact of these reports is through the oft-invoked “Hawthorne Effect,” where subjects modify behavior simply because they are being observed, as opposed to any particular piece of feedback.
My sense is that hospitalists are particularly open to the type of feedback offered in OPPE and similar reports, as long as the data are credible, even if reflecting group level performance. The 2012 SHM State of Hospital Medicine survey shows that the percent of hospitalist compensation based on performance (other than production/billings) increased to 7% from 4% in 2011. It seems that performance measurement with consequences, be it for credentialing or compensation, is here to stay.
Dr. Whitcombis Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Get Ready for Transition to ICD-10 Medical Coding

By now, I’m sure you’re knowledgeable about things like healthcare exchanges and other parts of the Accountable Care Act, the increasing number of metrics within hospital value-based purchasing, the physician value-based payment modifier, the physician quality reporting system (PQRS), how to use your hospital’s new EHR efficiently, the new “two-midnight rule” to determine inpatient vs. observation status, and so on.
You’re to be commended if you’re staying on top of all these things and have effective plans in place to ensure good performance on each. And if you haven’t already, you should add at least one more important issue to this list—the transition to ICD-10 coding on Oct. 1, 2014.
An Overview
ICD stands for International Classification of Diseases, and the U.S. has been using the 9th revision (ICD-9) since 1978. ICD-9 is now significantly out of step with current medical knowledge and has run out of codes in some disease sections (“chapters”). This might mean, for example, that new codes for heart diseases would be assigned to the chapter for eye disease, because the former is full.
ICD-10 provides a way to fix these problems and, through more specific coding of diseases, should be able to yield more useful “big data” to measure things like safety and efficacy of care and more accurately identify diagnosis trends and epidemics. And, in theory, it could reduce the number of rejected billing claims, though I’m waiting to see if that happens. I worry that even after fixing all the initial bugs related to the ICD-10 transition, we will see more claim rejections than we experience today.
ICD codes can be thought of as diagnosis codes. CPT codes (Current Procedural Terminology) are an entirely separate set of codes that we use to report the work we do for the purposes of billing. We need to be familiar with both, but it is the ICD codes that are changing.
ICD-10 Basics and Trivia
The World Health Organization issued the ICD-10 in 1994, and it is already in use in many countries. Like some other countries, the U.S. made modifications to the WHO’s original code set, so we refer to ICD-10-CM (Clinical Modification), which contains diagnosis codes. The National Center for Health Statistics, a department of the CDC, is responsible for these modifications.
The WHO version of ICD-10 doesn’t have any procedure codes, so CMS developed ICD-10-PCS (Procedure Coding System) to report procedures, such as surgeries, done in U.S. hospitals. Most hospitalists won’t use these procedure codes often.
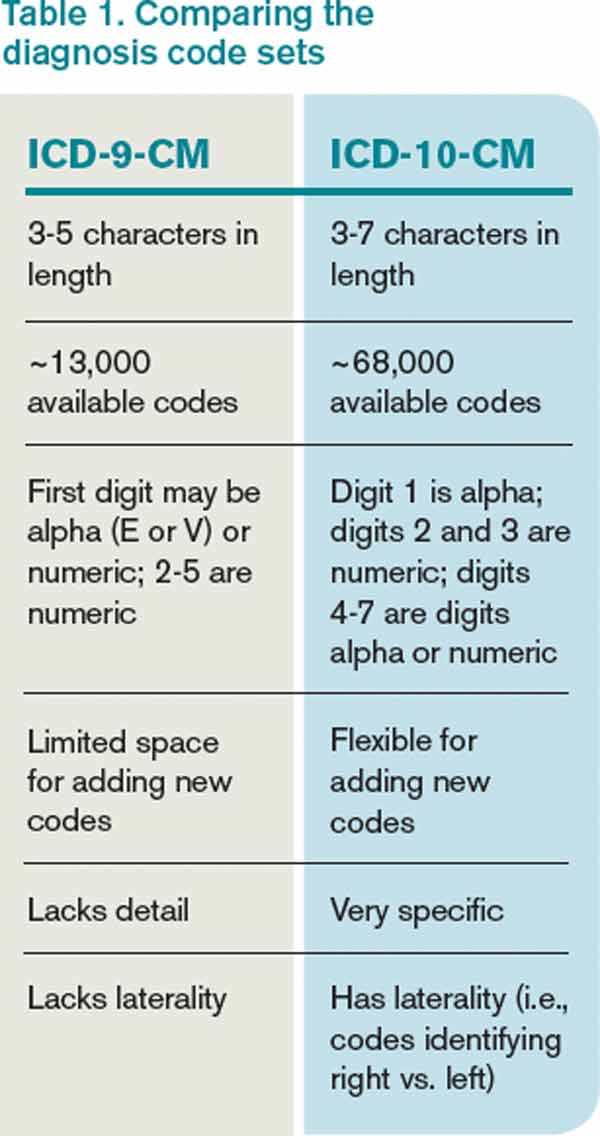
Table 1 (left) compares ICD-10-CM to ICD-9-CM. Most of the additional codes in the new version simply add information regarding whether the diagnosis is on the left or right of the body, acute or chronic, or an initial or subsequent visit for the condition. But the standard structure for each code had to be modified significantly to capture this additional information. Some highlights of the seven-character code structure are:
- Characters 1–3: category; first digit always a letter, second digit always a number, all other digits can be either; not case sensitive;
- Characters 4–6: etiology, anatomic site, severity, or other clinical detail; for example, 1=right, 2=left, 3-bilateral, and 0 or 9=unspecified; and
- Character 7: extension (i.e., A=initial encounter, D=subsequent encounter, S=sequelae).
- A placeholder “x” is used as needed to fill in empty characters to ensure that the seventh character stays in the seventh position. For example, T79.1xxA equates to “fat embolism, initial encounter.” (Note that the “dummy” characters could create problems for some IT systems.)
An example of more information contained in additional characters:
- S52=fracture of forearm.
- S52.5=fracture of lower end of radius.
- S52.52=torus fracture of lower end of radius.
- S52.521=torus fracture of lower end of right radius.
- S52.521A=torus fracture of lower end of right radius, initial encounter for closed fracture.
Compared to its predecessor, ICD-10 expands use of combination codes. These are single codes that can be used to classify either two diagnoses, a diagnosis with an associated secondary process, or a diagnosis with an associated complication. For example, rather than reporting acute cor pulmonale and septic pulmonary embolism separately, ICD-10 allows use of the code I26.01: septic pulmonary embolism with acute cor pulmonale.
Resources
In addition to resources on the SHM website, both the American Medical Association (www.ama-assn.org, search “ICD-10”) and the Centers for Medicare and Medicaid Services (www.cms.gov/icd10) have very informative microsites offering detailed ICD-10 information. Much of the information in this column, including the examples above, comes from those sites.
What to Expect
Your hospital and your employer are probably already working in earnest to prepare for the change. In some cases, hospitalists are actively involved in these preparations, but in most cases they will simply wait for an organization to notify them that they should begin training to understand the new coding system. Experts say that most physicians will need two to four hours of training on ICD-10, but because we use a universe of diagnosis codes that is much larger than many specialties, I wonder if hospitalists may need additional training.
Like nearly all the programs I listed at the beginning, the transition to ICD-10 has me concerned. Managing it poorly could mean significant loss in hospital and physician professional fee revenue, as well as lots of tedious and time-consuming work. So, doing it right is important. But, it is also important to do well on all the programs I listed at the beginning of this column, and many others, and there is a limit to just how much we can do effectively as individuals.
Collectively, these programs risk taking too much time and too many brain cells away from keeping up with clinical medicine. So, I wonder if, for many of us, ICD-10 will serve as a tipping point that results in physicians hiring professional coders to choose our diagnosis codes and CPT codes rather than doing it ourselves.
As with EHRs, ICD-10 is said to have many benefits. But the introduction of EHRs in many hospitals had the unintended effect of significantly reducing the number of doctors who were willing to serve as admitting and attending physicians; instead, many chose to refer to hospitalists. In a similar way, ICD-10 might lead many organizations to relieve physicians of the responsibility of looking up and entering codes for each patient, leaving them with more time and energy to be clinicians. We’ll have to wait and see.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
By now, I’m sure you’re knowledgeable about things like healthcare exchanges and other parts of the Accountable Care Act, the increasing number of metrics within hospital value-based purchasing, the physician value-based payment modifier, the physician quality reporting system (PQRS), how to use your hospital’s new EHR efficiently, the new “two-midnight rule” to determine inpatient vs. observation status, and so on.
You’re to be commended if you’re staying on top of all these things and have effective plans in place to ensure good performance on each. And if you haven’t already, you should add at least one more important issue to this list—the transition to ICD-10 coding on Oct. 1, 2014.
An Overview
ICD stands for International Classification of Diseases, and the U.S. has been using the 9th revision (ICD-9) since 1978. ICD-9 is now significantly out of step with current medical knowledge and has run out of codes in some disease sections (“chapters”). This might mean, for example, that new codes for heart diseases would be assigned to the chapter for eye disease, because the former is full.
ICD-10 provides a way to fix these problems and, through more specific coding of diseases, should be able to yield more useful “big data” to measure things like safety and efficacy of care and more accurately identify diagnosis trends and epidemics. And, in theory, it could reduce the number of rejected billing claims, though I’m waiting to see if that happens. I worry that even after fixing all the initial bugs related to the ICD-10 transition, we will see more claim rejections than we experience today.
ICD codes can be thought of as diagnosis codes. CPT codes (Current Procedural Terminology) are an entirely separate set of codes that we use to report the work we do for the purposes of billing. We need to be familiar with both, but it is the ICD codes that are changing.
ICD-10 Basics and Trivia
The World Health Organization issued the ICD-10 in 1994, and it is already in use in many countries. Like some other countries, the U.S. made modifications to the WHO’s original code set, so we refer to ICD-10-CM (Clinical Modification), which contains diagnosis codes. The National Center for Health Statistics, a department of the CDC, is responsible for these modifications.
The WHO version of ICD-10 doesn’t have any procedure codes, so CMS developed ICD-10-PCS (Procedure Coding System) to report procedures, such as surgeries, done in U.S. hospitals. Most hospitalists won’t use these procedure codes often.
Table 1 (left) compares ICD-10-CM to ICD-9-CM. Most of the additional codes in the new version simply add information regarding whether the diagnosis is on the left or right of the body, acute or chronic, or an initial or subsequent visit for the condition. But the standard structure for each code had to be modified significantly to capture this additional information. Some highlights of the seven-character code structure are:
- Characters 1–3: category; first digit always a letter, second digit always a number, all other digits can be either; not case sensitive;
- Characters 4–6: etiology, anatomic site, severity, or other clinical detail; for example, 1=right, 2=left, 3-bilateral, and 0 or 9=unspecified; and
- Character 7: extension (i.e., A=initial encounter, D=subsequent encounter, S=sequelae).
- A placeholder “x” is used as needed to fill in empty characters to ensure that the seventh character stays in the seventh position. For example, T79.1xxA equates to “fat embolism, initial encounter.” (Note that the “dummy” characters could create problems for some IT systems.)
An example of more information contained in additional characters:
- S52=fracture of forearm.
- S52.5=fracture of lower end of radius.
- S52.52=torus fracture of lower end of radius.
- S52.521=torus fracture of lower end of right radius.
- S52.521A=torus fracture of lower end of right radius, initial encounter for closed fracture.
Compared to its predecessor, ICD-10 expands use of combination codes. These are single codes that can be used to classify either two diagnoses, a diagnosis with an associated secondary process, or a diagnosis with an associated complication. For example, rather than reporting acute cor pulmonale and septic pulmonary embolism separately, ICD-10 allows use of the code I26.01: septic pulmonary embolism with acute cor pulmonale.
Resources
In addition to resources on the SHM website, both the American Medical Association (www.ama-assn.org, search “ICD-10”) and the Centers for Medicare and Medicaid Services (www.cms.gov/icd10) have very informative microsites offering detailed ICD-10 information. Much of the information in this column, including the examples above, comes from those sites.
What to Expect
Your hospital and your employer are probably already working in earnest to prepare for the change. In some cases, hospitalists are actively involved in these preparations, but in most cases they will simply wait for an organization to notify them that they should begin training to understand the new coding system. Experts say that most physicians will need two to four hours of training on ICD-10, but because we use a universe of diagnosis codes that is much larger than many specialties, I wonder if hospitalists may need additional training.
Like nearly all the programs I listed at the beginning, the transition to ICD-10 has me concerned. Managing it poorly could mean significant loss in hospital and physician professional fee revenue, as well as lots of tedious and time-consuming work. So, doing it right is important. But, it is also important to do well on all the programs I listed at the beginning of this column, and many others, and there is a limit to just how much we can do effectively as individuals.
Collectively, these programs risk taking too much time and too many brain cells away from keeping up with clinical medicine. So, I wonder if, for many of us, ICD-10 will serve as a tipping point that results in physicians hiring professional coders to choose our diagnosis codes and CPT codes rather than doing it ourselves.
As with EHRs, ICD-10 is said to have many benefits. But the introduction of EHRs in many hospitals had the unintended effect of significantly reducing the number of doctors who were willing to serve as admitting and attending physicians; instead, many chose to refer to hospitalists. In a similar way, ICD-10 might lead many organizations to relieve physicians of the responsibility of looking up and entering codes for each patient, leaving them with more time and energy to be clinicians. We’ll have to wait and see.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
By now, I’m sure you’re knowledgeable about things like healthcare exchanges and other parts of the Accountable Care Act, the increasing number of metrics within hospital value-based purchasing, the physician value-based payment modifier, the physician quality reporting system (PQRS), how to use your hospital’s new EHR efficiently, the new “two-midnight rule” to determine inpatient vs. observation status, and so on.
You’re to be commended if you’re staying on top of all these things and have effective plans in place to ensure good performance on each. And if you haven’t already, you should add at least one more important issue to this list—the transition to ICD-10 coding on Oct. 1, 2014.
An Overview
ICD stands for International Classification of Diseases, and the U.S. has been using the 9th revision (ICD-9) since 1978. ICD-9 is now significantly out of step with current medical knowledge and has run out of codes in some disease sections (“chapters”). This might mean, for example, that new codes for heart diseases would be assigned to the chapter for eye disease, because the former is full.
ICD-10 provides a way to fix these problems and, through more specific coding of diseases, should be able to yield more useful “big data” to measure things like safety and efficacy of care and more accurately identify diagnosis trends and epidemics. And, in theory, it could reduce the number of rejected billing claims, though I’m waiting to see if that happens. I worry that even after fixing all the initial bugs related to the ICD-10 transition, we will see more claim rejections than we experience today.
ICD codes can be thought of as diagnosis codes. CPT codes (Current Procedural Terminology) are an entirely separate set of codes that we use to report the work we do for the purposes of billing. We need to be familiar with both, but it is the ICD codes that are changing.
ICD-10 Basics and Trivia
The World Health Organization issued the ICD-10 in 1994, and it is already in use in many countries. Like some other countries, the U.S. made modifications to the WHO’s original code set, so we refer to ICD-10-CM (Clinical Modification), which contains diagnosis codes. The National Center for Health Statistics, a department of the CDC, is responsible for these modifications.
The WHO version of ICD-10 doesn’t have any procedure codes, so CMS developed ICD-10-PCS (Procedure Coding System) to report procedures, such as surgeries, done in U.S. hospitals. Most hospitalists won’t use these procedure codes often.
Table 1 (left) compares ICD-10-CM to ICD-9-CM. Most of the additional codes in the new version simply add information regarding whether the diagnosis is on the left or right of the body, acute or chronic, or an initial or subsequent visit for the condition. But the standard structure for each code had to be modified significantly to capture this additional information. Some highlights of the seven-character code structure are:
- Characters 1–3: category; first digit always a letter, second digit always a number, all other digits can be either; not case sensitive;
- Characters 4–6: etiology, anatomic site, severity, or other clinical detail; for example, 1=right, 2=left, 3-bilateral, and 0 or 9=unspecified; and
- Character 7: extension (i.e., A=initial encounter, D=subsequent encounter, S=sequelae).
- A placeholder “x” is used as needed to fill in empty characters to ensure that the seventh character stays in the seventh position. For example, T79.1xxA equates to “fat embolism, initial encounter.” (Note that the “dummy” characters could create problems for some IT systems.)
An example of more information contained in additional characters:
- S52=fracture of forearm.
- S52.5=fracture of lower end of radius.
- S52.52=torus fracture of lower end of radius.
- S52.521=torus fracture of lower end of right radius.
- S52.521A=torus fracture of lower end of right radius, initial encounter for closed fracture.
Compared to its predecessor, ICD-10 expands use of combination codes. These are single codes that can be used to classify either two diagnoses, a diagnosis with an associated secondary process, or a diagnosis with an associated complication. For example, rather than reporting acute cor pulmonale and septic pulmonary embolism separately, ICD-10 allows use of the code I26.01: septic pulmonary embolism with acute cor pulmonale.
Resources
In addition to resources on the SHM website, both the American Medical Association (www.ama-assn.org, search “ICD-10”) and the Centers for Medicare and Medicaid Services (www.cms.gov/icd10) have very informative microsites offering detailed ICD-10 information. Much of the information in this column, including the examples above, comes from those sites.
What to Expect
Your hospital and your employer are probably already working in earnest to prepare for the change. In some cases, hospitalists are actively involved in these preparations, but in most cases they will simply wait for an organization to notify them that they should begin training to understand the new coding system. Experts say that most physicians will need two to four hours of training on ICD-10, but because we use a universe of diagnosis codes that is much larger than many specialties, I wonder if hospitalists may need additional training.
Like nearly all the programs I listed at the beginning, the transition to ICD-10 has me concerned. Managing it poorly could mean significant loss in hospital and physician professional fee revenue, as well as lots of tedious and time-consuming work. So, doing it right is important. But, it is also important to do well on all the programs I listed at the beginning of this column, and many others, and there is a limit to just how much we can do effectively as individuals.
Collectively, these programs risk taking too much time and too many brain cells away from keeping up with clinical medicine. So, I wonder if, for many of us, ICD-10 will serve as a tipping point that results in physicians hiring professional coders to choose our diagnosis codes and CPT codes rather than doing it ourselves.
As with EHRs, ICD-10 is said to have many benefits. But the introduction of EHRs in many hospitals had the unintended effect of significantly reducing the number of doctors who were willing to serve as admitting and attending physicians; instead, many chose to refer to hospitalists. In a similar way, ICD-10 might lead many organizations to relieve physicians of the responsibility of looking up and entering codes for each patient, leaving them with more time and energy to be clinicians. We’ll have to wait and see.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Workflow Interruptions Threaten Patient Safety, Hospitalists' Job Satisfaction


When I visit hospitalist programs, one of the things I am most interested in learning about is the degree to which the hospitalists enjoy their work and why. On a recent visit, in my usual meeting with the hospitalist group, we talked a lot about what it is like to be a hospitalist. When I asked them what the greatest threat to their job satisfaction was, there was a chorus of consistency in their answers: interruptions. The hospitalists were deeply frustrated by minute-to-minute intrusions into their workflow. The emergency department, nurses, pharmacy, the admitting department, the lab, radiology—you name it, everyone wants a piece of them.
Constant interruptions are a career satisfaction issue for hospitalists. But for patients, the interruptions represent a safety and quality of care issue. Why?
The Myth of Multi-tasking
Some of us take pride in our ability to multi-task. Others freely admit they aren’t very good at it. In any case, we know through cognitive psychology that the brain cannot multi-task, at least in the realm of conscious work. (The brain, of course, carries out basic, life-sustaining functions while we are doing other work cognitively.) The brain is actually a “sequential processor,” and multi-tasking actually is “task-switching.” Those of us who “multi-task” well are able to switch tasks easily and effectively.
But, task switching comes at a cost. When we switch tasks, we are prone to errors in the performance of those tasks. Two psychologists, Rogers and Monsell, demonstrated this in a study that looked at error rates when subjects performed tasks involving numerical or letter manipulations.1 The tasks involved classifying either the digit member of a pair of characters as even/odd or the letter member as consonant/vowel. When subjects performed the tasks while switching among multiple tasks, the error rate was fourfold the rate with no task switching (see Figure 1).1 These findings have been replicated since the original study. Further, there is now well-developed literature devoted to interruptions and patient safety.
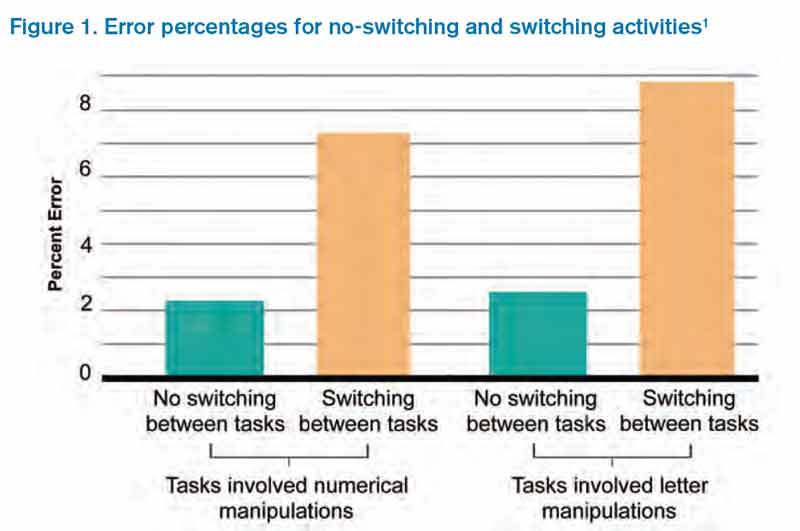
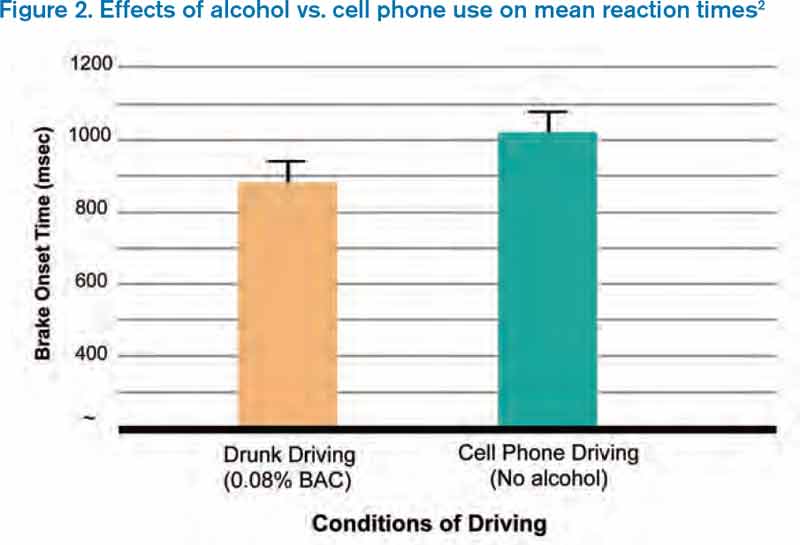
It Takes Time
We also know that switching between tasks takes time. Why? Because changing one’s attention from one subject to another involves neurologic processes that are not instantaneous. In a simulated driving study comparing mean reaction times between intoxicated subjects (blood alcohol 0.08%) and those talking on a cell phone, Strayer and Drews found the mean time to brake onset was significantly slower in the cell phone group than in the drunk driving group, presumably because cell phone users had to switch tasks.2
How Can We Tame Interruptions?
I submit that we need to be realistic about our ability to control the number of interruptions hospitalists experience in a given workday. One approach is to identify “high stakes moments” that are protected from excessive interruptions. Taking an example from aviation, airplane takeoffs and landings are “no interruption” zones, meaning that no needless talking or tasking is allowed in the cockpit during these tasks. Potential “no interruption” zones in hospital medicine might include times when hospitalists are developing an assessment and plan, engaged in complex decision-making, or performing medication reconciliation.
But is it realistic to think that we can cordon off hospitalists during these tasks?
Another approach is to establish practices that may decrease interruptions. Interruptions likely are reduced by:
- Having unit-based hospitalist staffing;
- Holding multidisciplinary rounds;
- Training nurses to batch pages;
- Conducting structured evening and night rounds on all nursing units for non-urgent matters; and
- Developing paging “levels” so that a receiving physician knows if a call back is needed and, if so, if it is urgent or not.
In talking to hospitalists who cite interruptions as job dissatisfiers, it occurs to me that anything that erodes career engagement also threatens patient safety. If we could figure out how to control interruptions, we would kill two birds with one stone.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
When I visit hospitalist programs, one of the things I am most interested in learning about is the degree to which the hospitalists enjoy their work and why. On a recent visit, in my usual meeting with the hospitalist group, we talked a lot about what it is like to be a hospitalist. When I asked them what the greatest threat to their job satisfaction was, there was a chorus of consistency in their answers: interruptions. The hospitalists were deeply frustrated by minute-to-minute intrusions into their workflow. The emergency department, nurses, pharmacy, the admitting department, the lab, radiology—you name it, everyone wants a piece of them.
Constant interruptions are a career satisfaction issue for hospitalists. But for patients, the interruptions represent a safety and quality of care issue. Why?
The Myth of Multi-tasking
Some of us take pride in our ability to multi-task. Others freely admit they aren’t very good at it. In any case, we know through cognitive psychology that the brain cannot multi-task, at least in the realm of conscious work. (The brain, of course, carries out basic, life-sustaining functions while we are doing other work cognitively.) The brain is actually a “sequential processor,” and multi-tasking actually is “task-switching.” Those of us who “multi-task” well are able to switch tasks easily and effectively.
But, task switching comes at a cost. When we switch tasks, we are prone to errors in the performance of those tasks. Two psychologists, Rogers and Monsell, demonstrated this in a study that looked at error rates when subjects performed tasks involving numerical or letter manipulations.1 The tasks involved classifying either the digit member of a pair of characters as even/odd or the letter member as consonant/vowel. When subjects performed the tasks while switching among multiple tasks, the error rate was fourfold the rate with no task switching (see Figure 1).1 These findings have been replicated since the original study. Further, there is now well-developed literature devoted to interruptions and patient safety.
It Takes Time
We also know that switching between tasks takes time. Why? Because changing one’s attention from one subject to another involves neurologic processes that are not instantaneous. In a simulated driving study comparing mean reaction times between intoxicated subjects (blood alcohol 0.08%) and those talking on a cell phone, Strayer and Drews found the mean time to brake onset was significantly slower in the cell phone group than in the drunk driving group, presumably because cell phone users had to switch tasks.2
How Can We Tame Interruptions?
I submit that we need to be realistic about our ability to control the number of interruptions hospitalists experience in a given workday. One approach is to identify “high stakes moments” that are protected from excessive interruptions. Taking an example from aviation, airplane takeoffs and landings are “no interruption” zones, meaning that no needless talking or tasking is allowed in the cockpit during these tasks. Potential “no interruption” zones in hospital medicine might include times when hospitalists are developing an assessment and plan, engaged in complex decision-making, or performing medication reconciliation.
But is it realistic to think that we can cordon off hospitalists during these tasks?
Another approach is to establish practices that may decrease interruptions. Interruptions likely are reduced by:
- Having unit-based hospitalist staffing;
- Holding multidisciplinary rounds;
- Training nurses to batch pages;
- Conducting structured evening and night rounds on all nursing units for non-urgent matters; and
- Developing paging “levels” so that a receiving physician knows if a call back is needed and, if so, if it is urgent or not.
In talking to hospitalists who cite interruptions as job dissatisfiers, it occurs to me that anything that erodes career engagement also threatens patient safety. If we could figure out how to control interruptions, we would kill two birds with one stone.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
References
When I visit hospitalist programs, one of the things I am most interested in learning about is the degree to which the hospitalists enjoy their work and why. On a recent visit, in my usual meeting with the hospitalist group, we talked a lot about what it is like to be a hospitalist. When I asked them what the greatest threat to their job satisfaction was, there was a chorus of consistency in their answers: interruptions. The hospitalists were deeply frustrated by minute-to-minute intrusions into their workflow. The emergency department, nurses, pharmacy, the admitting department, the lab, radiology—you name it, everyone wants a piece of them.
Constant interruptions are a career satisfaction issue for hospitalists. But for patients, the interruptions represent a safety and quality of care issue. Why?
The Myth of Multi-tasking
Some of us take pride in our ability to multi-task. Others freely admit they aren’t very good at it. In any case, we know through cognitive psychology that the brain cannot multi-task, at least in the realm of conscious work. (The brain, of course, carries out basic, life-sustaining functions while we are doing other work cognitively.) The brain is actually a “sequential processor,” and multi-tasking actually is “task-switching.” Those of us who “multi-task” well are able to switch tasks easily and effectively.
But, task switching comes at a cost. When we switch tasks, we are prone to errors in the performance of those tasks. Two psychologists, Rogers and Monsell, demonstrated this in a study that looked at error rates when subjects performed tasks involving numerical or letter manipulations.1 The tasks involved classifying either the digit member of a pair of characters as even/odd or the letter member as consonant/vowel. When subjects performed the tasks while switching among multiple tasks, the error rate was fourfold the rate with no task switching (see Figure 1).1 These findings have been replicated since the original study. Further, there is now well-developed literature devoted to interruptions and patient safety.
It Takes Time
We also know that switching between tasks takes time. Why? Because changing one’s attention from one subject to another involves neurologic processes that are not instantaneous. In a simulated driving study comparing mean reaction times between intoxicated subjects (blood alcohol 0.08%) and those talking on a cell phone, Strayer and Drews found the mean time to brake onset was significantly slower in the cell phone group than in the drunk driving group, presumably because cell phone users had to switch tasks.2
How Can We Tame Interruptions?
I submit that we need to be realistic about our ability to control the number of interruptions hospitalists experience in a given workday. One approach is to identify “high stakes moments” that are protected from excessive interruptions. Taking an example from aviation, airplane takeoffs and landings are “no interruption” zones, meaning that no needless talking or tasking is allowed in the cockpit during these tasks. Potential “no interruption” zones in hospital medicine might include times when hospitalists are developing an assessment and plan, engaged in complex decision-making, or performing medication reconciliation.
But is it realistic to think that we can cordon off hospitalists during these tasks?
Another approach is to establish practices that may decrease interruptions. Interruptions likely are reduced by:
- Having unit-based hospitalist staffing;
- Holding multidisciplinary rounds;
- Training nurses to batch pages;
- Conducting structured evening and night rounds on all nursing units for non-urgent matters; and
- Developing paging “levels” so that a receiving physician knows if a call back is needed and, if so, if it is urgent or not.
In talking to hospitalists who cite interruptions as job dissatisfiers, it occurs to me that anything that erodes career engagement also threatens patient safety. If we could figure out how to control interruptions, we would kill two birds with one stone.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.