User login
How To Maximize a Minimal Incision
Mini-incision carotid surgery was first reported (not necessarily performed) by Ascher et al. in 2005. In light of this report and an ever-growing patient demand for minimally invasive procedures, it is surprising that this procedure has not been widely adopted by the vascular surgical community. The reasons for this are probably multifactorial and may include a concern that cranial nerve injuries are more likely to occur as well as an added difficulty in placing a shunt or sewing in a patch. These concerns are mitigated by a thorough knowledge of the usual and variant anatomy of this area and a broad experience in carotid surgery. If performed properly, mini-incision is not synonymous with mini exposure carotid surgery.
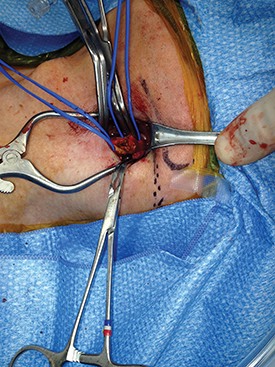
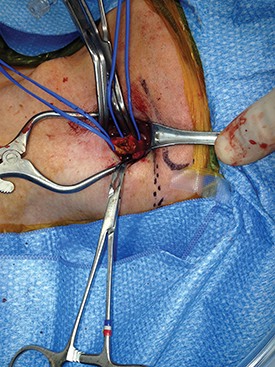
It is important to identify the carotid bifurcation with duplex ultrasound prior to making the skin incision. It is my preference to make a vertical skin incision which extends from approximately 2 cm above to below the carotid bifurcation at a slight outside to inside angle to the anterior border of the sternocleidomastoid muscle (some surgeons prefer a transverse skin incision). The platysma muscle is identified and divided for a short distance between forceps.
The edges of the platysma are grasped with DeBakey forceps while the skin is retracted as far inferiorly as possible.
The platysma is then divided to this point following which this is repeated at the superior aspect of the wound. The extended division of the platysma is what allows for an exposure equal to that of a much larger incision. Now adequate visualization of the common and internal carotid arteries is achieved by use of a small retractor applied alternately to the inferior and superior ends of the wound respectively.
Using this technique, I have easily been able to perform both standard and eversion endarterectomies (as in photo), place a shunt when necessary, and/or sew on a carotid patch.

Once completed the platysma is closed with an absorbable suture and skin is closed with an absorbable monofilament suture.
In my experience, patients have less postoperative pain than those with a larger neck incision. They are also exceptionally pleased with the small, barely visible, neck scar. Finally, I have used the mini-incision for my carotid surgeries for more than 10 years during which time no patient has suffered a permanent cranial nerve injury.
Dr. Dietzek is the chief of the vascular and endovascular surgery section and the Linda and Stephen R. Cohen chair in vascular surgery at Danbury Hospital, Danbury Conn. He is also a clinical associate professor of surgery at the University of Vermont College of Medicine in Burlington.
Editor’s Note: If you would like to submit a similarly useful Tips and Tricks, contact us at vascularspecialist@frontlinemedcom.com.
Mini-incision carotid surgery was first reported (not necessarily performed) by Ascher et al. in 2005. In light of this report and an ever-growing patient demand for minimally invasive procedures, it is surprising that this procedure has not been widely adopted by the vascular surgical community. The reasons for this are probably multifactorial and may include a concern that cranial nerve injuries are more likely to occur as well as an added difficulty in placing a shunt or sewing in a patch. These concerns are mitigated by a thorough knowledge of the usual and variant anatomy of this area and a broad experience in carotid surgery. If performed properly, mini-incision is not synonymous with mini exposure carotid surgery.
It is important to identify the carotid bifurcation with duplex ultrasound prior to making the skin incision. It is my preference to make a vertical skin incision which extends from approximately 2 cm above to below the carotid bifurcation at a slight outside to inside angle to the anterior border of the sternocleidomastoid muscle (some surgeons prefer a transverse skin incision). The platysma muscle is identified and divided for a short distance between forceps.
The edges of the platysma are grasped with DeBakey forceps while the skin is retracted as far inferiorly as possible.
The platysma is then divided to this point following which this is repeated at the superior aspect of the wound. The extended division of the platysma is what allows for an exposure equal to that of a much larger incision. Now adequate visualization of the common and internal carotid arteries is achieved by use of a small retractor applied alternately to the inferior and superior ends of the wound respectively.
Using this technique, I have easily been able to perform both standard and eversion endarterectomies (as in photo), place a shunt when necessary, and/or sew on a carotid patch.
Once completed the platysma is closed with an absorbable suture and skin is closed with an absorbable monofilament suture.
In my experience, patients have less postoperative pain than those with a larger neck incision. They are also exceptionally pleased with the small, barely visible, neck scar. Finally, I have used the mini-incision for my carotid surgeries for more than 10 years during which time no patient has suffered a permanent cranial nerve injury.
Dr. Dietzek is the chief of the vascular and endovascular surgery section and the Linda and Stephen R. Cohen chair in vascular surgery at Danbury Hospital, Danbury Conn. He is also a clinical associate professor of surgery at the University of Vermont College of Medicine in Burlington.
Editor’s Note: If you would like to submit a similarly useful Tips and Tricks, contact us at vascularspecialist@frontlinemedcom.com.
Mini-incision carotid surgery was first reported (not necessarily performed) by Ascher et al. in 2005. In light of this report and an ever-growing patient demand for minimally invasive procedures, it is surprising that this procedure has not been widely adopted by the vascular surgical community. The reasons for this are probably multifactorial and may include a concern that cranial nerve injuries are more likely to occur as well as an added difficulty in placing a shunt or sewing in a patch. These concerns are mitigated by a thorough knowledge of the usual and variant anatomy of this area and a broad experience in carotid surgery. If performed properly, mini-incision is not synonymous with mini exposure carotid surgery.
It is important to identify the carotid bifurcation with duplex ultrasound prior to making the skin incision. It is my preference to make a vertical skin incision which extends from approximately 2 cm above to below the carotid bifurcation at a slight outside to inside angle to the anterior border of the sternocleidomastoid muscle (some surgeons prefer a transverse skin incision). The platysma muscle is identified and divided for a short distance between forceps.
The edges of the platysma are grasped with DeBakey forceps while the skin is retracted as far inferiorly as possible.
The platysma is then divided to this point following which this is repeated at the superior aspect of the wound. The extended division of the platysma is what allows for an exposure equal to that of a much larger incision. Now adequate visualization of the common and internal carotid arteries is achieved by use of a small retractor applied alternately to the inferior and superior ends of the wound respectively.
Using this technique, I have easily been able to perform both standard and eversion endarterectomies (as in photo), place a shunt when necessary, and/or sew on a carotid patch.
Once completed the platysma is closed with an absorbable suture and skin is closed with an absorbable monofilament suture.
In my experience, patients have less postoperative pain than those with a larger neck incision. They are also exceptionally pleased with the small, barely visible, neck scar. Finally, I have used the mini-incision for my carotid surgeries for more than 10 years during which time no patient has suffered a permanent cranial nerve injury.
Dr. Dietzek is the chief of the vascular and endovascular surgery section and the Linda and Stephen R. Cohen chair in vascular surgery at Danbury Hospital, Danbury Conn. He is also a clinical associate professor of surgery at the University of Vermont College of Medicine in Burlington.
Editor’s Note: If you would like to submit a similarly useful Tips and Tricks, contact us at vascularspecialist@frontlinemedcom.com.
Can we believe what we read?
During my mostly enjoyable 14 years as editor of a mainstream surgical publication, one of my less enjoyable but necessary functions was to detect and police author misconduct. Most instances of wrongdoing involved duplicate or redundant publication or the awarding of authorship when it was not deserved. I considered these infractions to be misdemeanors. The more serious sins of plagiarism and fabrication or falsification of data were considerably less common or at least infrequently detected. Based on my experience, one might conclude that most scientific findings are reported accurately and with integrity. In other words, we should be able to believe what we read. Unfortunately this may not be the case.
Compared to prior years, the past decade has seen a 10-fold increase in the number of articles retracted from the scientific literature. Although retractions account for well less than 1% of published articles, it is disturbing that fraudulent research and publishing rather than inadvertent errors underlie up to two-thirds of cases. Of note is that there appears to be a direct correlation between a journal\'s impact factor and the number of articles that are retracted from it. This may be due to a closer scrutiny by the scientific community of what initially were thought to be seminal contributions. Thus the limited number of retracted articles may, and probably does, represent the tip of an iceberg.
Deliberate fraud is an important issue in academic publishing, but an even greater problem is the abundance of poorly designed studies and the misuse of data. A significant fraction of the information available to us for clinical decision-making are underpowered studies with type I or II statistical errors, biased analyses, articles with data that cannot be reproduced by others, inappropriately done meta-analyses based on heterogeneous rather than homogeneous trials, and inaccurate conclusions based on erroneous manipulation of data.
In his analysis of the scientific literature in 2005, John Ioannidis, M.D., Ph.D. (PLoS 2:696-701) postulated that the majority of published articles were inaccurate. Flawed studies were more likely to result when sample sizes were small, the effect between tested variables was small, the number of tested relationships was large (at a P < .05, 5% will be statistically significant by chance), and conflicts of interest were present. Unsound studies were more likely to occur when they took place within popular and highly competitive scientific fields where the timing of publication was of the essence in order to claim primacy.
Compounding this cascade of misleading information is the reluctance of journals to publish negative studies, thereby giving greater weight to positive studies testing the same hypotheses.
These revelations regarding our research enterprise are not widely appreciated. In fact, in surveys of the public who are responsible for funding much of it with their tax dollars, biomedical research occupies an exalted position in comparison to most other endeavors. Why in recent times has it become tainted and what can be done to reverse the present trend? First, and probably most importantly, scientific research has become a highly competitive game. The battle for available research faculty positions in our universities is more intense than ever with room for only one of every six Ph.D. graduates. Once an appointment is attained, promotion and tenure are dependent on obtaining federal funding from an increasingly shrinking pool of money and publishing in high impact journals, many of which have rejection rates in excess of 90%. It is not surprising that minor or even major massaging of data to reach the magic 0.05 P value is probably not uncommon. Surveys of scientists regarding misconduct indicate that up to 20% have either participated in questionable practices themselves or know of colleagues who have.
The onus is not only on the researcher. Journal peer reviewers and editors are exerting much of their effort in looking for the rare seminal paper that would be attractive to their readers. Less attention is paid to the details of scientific rigor. Negative studies and those that are only confirmatory of previously published investigations are generally not given high enough grades to reach the threshold for publication.
Science has and continues to contribute much to the quality of human life. Most research scientists in the academic world operate with integrity and make a sincere effort to uncover truth in their fields. Marginally done and underpowered studies are the culprits leading to misinformation much more often than are issues of scientific honesty.
So what is to be done to right a somewhat listing research enterprise? From the researcher’s perspective, more attention to study design and rigid adherence to it to avoid bias is essential. Pre-study statistical consultation, especially regarding power calculation, is also a key to obtaining reliable results and conclusions. The editorial boards and editors of journals need to be more accepting of negative and confirmatory analyses than they have been in the past. The recent stance of most reputable journals to require registration of all clinical trials and to provide the data from those trials, positive or negative, to one of several web based repositories for review by others is a step in the right direction. It is the responsibility of our academic institutions to detect and police poor research design and implementation in addition to outright academic misconduct and, when necessary, to change the culture within their research establishments. Finally, it behooves us as readers and consumers of new information to realize that science marches forward in only small incremental steps. Important new findings need to be confirmed before they are adopted. The adage of never being the first to accept the new or the last to abandon the old still conveys a great deal of wisdom.
Dr. Rikkers is Editor in Chief of Surgery News.
During my mostly enjoyable 14 years as editor of a mainstream surgical publication, one of my less enjoyable but necessary functions was to detect and police author misconduct. Most instances of wrongdoing involved duplicate or redundant publication or the awarding of authorship when it was not deserved. I considered these infractions to be misdemeanors. The more serious sins of plagiarism and fabrication or falsification of data were considerably less common or at least infrequently detected. Based on my experience, one might conclude that most scientific findings are reported accurately and with integrity. In other words, we should be able to believe what we read. Unfortunately this may not be the case.
Compared to prior years, the past decade has seen a 10-fold increase in the number of articles retracted from the scientific literature. Although retractions account for well less than 1% of published articles, it is disturbing that fraudulent research and publishing rather than inadvertent errors underlie up to two-thirds of cases. Of note is that there appears to be a direct correlation between a journal\'s impact factor and the number of articles that are retracted from it. This may be due to a closer scrutiny by the scientific community of what initially were thought to be seminal contributions. Thus the limited number of retracted articles may, and probably does, represent the tip of an iceberg.
Deliberate fraud is an important issue in academic publishing, but an even greater problem is the abundance of poorly designed studies and the misuse of data. A significant fraction of the information available to us for clinical decision-making are underpowered studies with type I or II statistical errors, biased analyses, articles with data that cannot be reproduced by others, inappropriately done meta-analyses based on heterogeneous rather than homogeneous trials, and inaccurate conclusions based on erroneous manipulation of data.
In his analysis of the scientific literature in 2005, John Ioannidis, M.D., Ph.D. (PLoS 2:696-701) postulated that the majority of published articles were inaccurate. Flawed studies were more likely to result when sample sizes were small, the effect between tested variables was small, the number of tested relationships was large (at a P < .05, 5% will be statistically significant by chance), and conflicts of interest were present. Unsound studies were more likely to occur when they took place within popular and highly competitive scientific fields where the timing of publication was of the essence in order to claim primacy.
Compounding this cascade of misleading information is the reluctance of journals to publish negative studies, thereby giving greater weight to positive studies testing the same hypotheses.
These revelations regarding our research enterprise are not widely appreciated. In fact, in surveys of the public who are responsible for funding much of it with their tax dollars, biomedical research occupies an exalted position in comparison to most other endeavors. Why in recent times has it become tainted and what can be done to reverse the present trend? First, and probably most importantly, scientific research has become a highly competitive game. The battle for available research faculty positions in our universities is more intense than ever with room for only one of every six Ph.D. graduates. Once an appointment is attained, promotion and tenure are dependent on obtaining federal funding from an increasingly shrinking pool of money and publishing in high impact journals, many of which have rejection rates in excess of 90%. It is not surprising that minor or even major massaging of data to reach the magic 0.05 P value is probably not uncommon. Surveys of scientists regarding misconduct indicate that up to 20% have either participated in questionable practices themselves or know of colleagues who have.
The onus is not only on the researcher. Journal peer reviewers and editors are exerting much of their effort in looking for the rare seminal paper that would be attractive to their readers. Less attention is paid to the details of scientific rigor. Negative studies and those that are only confirmatory of previously published investigations are generally not given high enough grades to reach the threshold for publication.
Science has and continues to contribute much to the quality of human life. Most research scientists in the academic world operate with integrity and make a sincere effort to uncover truth in their fields. Marginally done and underpowered studies are the culprits leading to misinformation much more often than are issues of scientific honesty.
So what is to be done to right a somewhat listing research enterprise? From the researcher’s perspective, more attention to study design and rigid adherence to it to avoid bias is essential. Pre-study statistical consultation, especially regarding power calculation, is also a key to obtaining reliable results and conclusions. The editorial boards and editors of journals need to be more accepting of negative and confirmatory analyses than they have been in the past. The recent stance of most reputable journals to require registration of all clinical trials and to provide the data from those trials, positive or negative, to one of several web based repositories for review by others is a step in the right direction. It is the responsibility of our academic institutions to detect and police poor research design and implementation in addition to outright academic misconduct and, when necessary, to change the culture within their research establishments. Finally, it behooves us as readers and consumers of new information to realize that science marches forward in only small incremental steps. Important new findings need to be confirmed before they are adopted. The adage of never being the first to accept the new or the last to abandon the old still conveys a great deal of wisdom.
Dr. Rikkers is Editor in Chief of Surgery News.
During my mostly enjoyable 14 years as editor of a mainstream surgical publication, one of my less enjoyable but necessary functions was to detect and police author misconduct. Most instances of wrongdoing involved duplicate or redundant publication or the awarding of authorship when it was not deserved. I considered these infractions to be misdemeanors. The more serious sins of plagiarism and fabrication or falsification of data were considerably less common or at least infrequently detected. Based on my experience, one might conclude that most scientific findings are reported accurately and with integrity. In other words, we should be able to believe what we read. Unfortunately this may not be the case.
Compared to prior years, the past decade has seen a 10-fold increase in the number of articles retracted from the scientific literature. Although retractions account for well less than 1% of published articles, it is disturbing that fraudulent research and publishing rather than inadvertent errors underlie up to two-thirds of cases. Of note is that there appears to be a direct correlation between a journal\'s impact factor and the number of articles that are retracted from it. This may be due to a closer scrutiny by the scientific community of what initially were thought to be seminal contributions. Thus the limited number of retracted articles may, and probably does, represent the tip of an iceberg.
Deliberate fraud is an important issue in academic publishing, but an even greater problem is the abundance of poorly designed studies and the misuse of data. A significant fraction of the information available to us for clinical decision-making are underpowered studies with type I or II statistical errors, biased analyses, articles with data that cannot be reproduced by others, inappropriately done meta-analyses based on heterogeneous rather than homogeneous trials, and inaccurate conclusions based on erroneous manipulation of data.
In his analysis of the scientific literature in 2005, John Ioannidis, M.D., Ph.D. (PLoS 2:696-701) postulated that the majority of published articles were inaccurate. Flawed studies were more likely to result when sample sizes were small, the effect between tested variables was small, the number of tested relationships was large (at a P < .05, 5% will be statistically significant by chance), and conflicts of interest were present. Unsound studies were more likely to occur when they took place within popular and highly competitive scientific fields where the timing of publication was of the essence in order to claim primacy.
Compounding this cascade of misleading information is the reluctance of journals to publish negative studies, thereby giving greater weight to positive studies testing the same hypotheses.
These revelations regarding our research enterprise are not widely appreciated. In fact, in surveys of the public who are responsible for funding much of it with their tax dollars, biomedical research occupies an exalted position in comparison to most other endeavors. Why in recent times has it become tainted and what can be done to reverse the present trend? First, and probably most importantly, scientific research has become a highly competitive game. The battle for available research faculty positions in our universities is more intense than ever with room for only one of every six Ph.D. graduates. Once an appointment is attained, promotion and tenure are dependent on obtaining federal funding from an increasingly shrinking pool of money and publishing in high impact journals, many of which have rejection rates in excess of 90%. It is not surprising that minor or even major massaging of data to reach the magic 0.05 P value is probably not uncommon. Surveys of scientists regarding misconduct indicate that up to 20% have either participated in questionable practices themselves or know of colleagues who have.
The onus is not only on the researcher. Journal peer reviewers and editors are exerting much of their effort in looking for the rare seminal paper that would be attractive to their readers. Less attention is paid to the details of scientific rigor. Negative studies and those that are only confirmatory of previously published investigations are generally not given high enough grades to reach the threshold for publication.
Science has and continues to contribute much to the quality of human life. Most research scientists in the academic world operate with integrity and make a sincere effort to uncover truth in their fields. Marginally done and underpowered studies are the culprits leading to misinformation much more often than are issues of scientific honesty.
So what is to be done to right a somewhat listing research enterprise? From the researcher’s perspective, more attention to study design and rigid adherence to it to avoid bias is essential. Pre-study statistical consultation, especially regarding power calculation, is also a key to obtaining reliable results and conclusions. The editorial boards and editors of journals need to be more accepting of negative and confirmatory analyses than they have been in the past. The recent stance of most reputable journals to require registration of all clinical trials and to provide the data from those trials, positive or negative, to one of several web based repositories for review by others is a step in the right direction. It is the responsibility of our academic institutions to detect and police poor research design and implementation in addition to outright academic misconduct and, when necessary, to change the culture within their research establishments. Finally, it behooves us as readers and consumers of new information to realize that science marches forward in only small incremental steps. Important new findings need to be confirmed before they are adopted. The adage of never being the first to accept the new or the last to abandon the old still conveys a great deal of wisdom.
Dr. Rikkers is Editor in Chief of Surgery News.

Multi-Site Hospital Medicine Group Leaders Face Similar Challenges

Let’s call them multi-site, hospital medicine group leaders, or just multi-site HMG leaders. Once rare, they’re now becoming common, and among the many people now holding this job are:
- Dr. Doug Apple at Spectrum Health Medical Group in Grand Rapids, Mich;
- Dr. Tierza Stephan at Allina Health in Minneapolis, Minn.;
- Dr. Darren Thomas at St. John Health System in Tulsa, Okla.;
- Dr. Thomas McIlraith at Dignity Health in Sacremento, Calif.; and
- Dr. Rohit Uppal at Ohio Health in Columbus, Ohio.
The career path that led to their current position usually follows a standard pattern. They are a successful leader of a single-site hospitalist program when, through merger or acquisition, their hospital becomes part of a larger system. The executives responsible for this larger system—typically four to eight hospitals—realize that the HMGs serving each hospital in the system vary significantly in their cost, productivity, and performance on things like patient satisfaction and quality metrics. So they tap the leader of the largest (or best performing) HMG in the system to be system-wide hospitalist medical director. They nearly always choose an internal candidate rather than recruiting from outside, which brings some level of cohesion in operations and performance improvement.
Multi-Site Challenges
This is not an easy job. After all, it isn’t easy to serve as lead hospitalist for a single-site group, so it makes sense that the difficulties and challenges only increase when trying to manage groups at different locations.
The new multi-site HMG leader is busy from the first day on the job. The HMG at one site is short on staffing and needs help right away, patient satisfaction scores are poor at the next site, and so on. Although putting out these fires is important, the new leader also needs to think about how to accomplish a broader mission: ensuring greater cohesion across all groups.
I don’t think there is a secret recipe to ensure success in such a job. Prerequisites include the usual leadership skills, such as patience, good listening, and diplomacy (collectively, one’s EQ, or emotional quotient), along with lots of energy and decisive action. But there are a number of practical matters to address that can influence the level of success.
Cohesion vs. Independence
In most situations, a health system will benefit from some common operating principles across all the HMGs who serve its hospitals. For example, it usually makes sense for any portion of compensation tied to performance (e.g., a bonus) to be based on the same performance domains at all sites. For example, if metrics such as the observed-to-expected mortality ratio (O:E ratio) and patient satisfaction are important to the hospital system, then they should probably influence hospitalist compensation at every site. However, it might be reasonable to target a level of performance for any given domain higher at one site than at another.
Among the many things that should be the same across all sites are operational practices: charge capture, coding audits, performance reviews, dashboard elements and format, and credentialing for new hires. Other things, like individual hospitalist productivity, work schedule, and method and amount of compensation, should vary by site because of the unique attributes of the work at each place.
Fixed Locale vs. Rotations
The travel time between hospitals and the value of extensive experience in the details of how each particular hospital operates usually make it most practical for each individual hospitalist to work nearly all of the time at one hospital. But every doctor should be credentialed at every other hospital in the system so that he can cover a staffing shortage elsewhere.
And, hospitalists hired to work primarily at one of the small hospitals would probably benefit from working at the large referral hospital for the first few weeks of employment. This seems like a great way for them to become familiar with the people and operations at the big hospital, especially since they will be transferring patients there periodically.
Governance
Some mix of central control vs. local autonomy in decision making at each site is important for success. There aren’t any clear guidelines here, but providing the local doctors at each location with the ability to make their own decisions on things like work schedule will contribute to their sense of ownership of the practice. That feeling is valuable and supports good performance.
My bias is that each site in a practice could adopt the same “internal governance” guidelines, or rules by which they make decisions when unable to reach consensus (see “Play by the Rules,” December 2007, for sample guidelines.)
There should also be some form of “umbrella” governance structure in which the local site leaders meet regularly with the multi-site HMG leader.
Patient Transfers
One reason hospitals merge into a single system is the hope that they can more effectively meet the needs of all patients in the system’s hospitals. A typical configuration is several small hospitals, along with a single, large, referral center, to which patients are sent if the small hospital can’t meet their needs. The hope is that if all the hospitals are in the same system, the process of transfer can be smoother and more efficient.
A large portion—maybe even the majority—of all transfers in the system will be between a hospitalist at the small hospital and a partner hospitalist at the large hospital. Things will work best when the transferring and receiving hospitalists know something about the strengths and weaknesses of each other’s hospitals. And, you only know one another reasonably well from working together on committees or being on clinical service together at the same hospital, as well as social functions that include hospitalists from all sites.
Therefore, the multi-site HMG leader should think deliberately about how to ensure that the hospitalists interact with one another often, and not just when a transfer needs to take place.
A written agreement outlining the criteria for an appropriate transfer can be helpful. But such agreements cannot address all the situations that will arise, so good relationships between doctors at the different sites are invaluable and worth taking the time to cultivate.
Communication
Like the five people I mentioned above, anyone holding the position of multi-site HMG leader would benefit from talking with others in the same position. I’m working to arrange some forum for such communication, potentially including an in-person meeting at HM14 in Las Vegas in March (www.hospitalmedicine2014.org). If you are a health system-employed, multi-site HMG leader and want to be part of this conversation, I would love to hear from you.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Let’s call them multi-site, hospital medicine group leaders, or just multi-site HMG leaders. Once rare, they’re now becoming common, and among the many people now holding this job are:
- Dr. Doug Apple at Spectrum Health Medical Group in Grand Rapids, Mich;
- Dr. Tierza Stephan at Allina Health in Minneapolis, Minn.;
- Dr. Darren Thomas at St. John Health System in Tulsa, Okla.;
- Dr. Thomas McIlraith at Dignity Health in Sacremento, Calif.; and
- Dr. Rohit Uppal at Ohio Health in Columbus, Ohio.
The career path that led to their current position usually follows a standard pattern. They are a successful leader of a single-site hospitalist program when, through merger or acquisition, their hospital becomes part of a larger system. The executives responsible for this larger system—typically four to eight hospitals—realize that the HMGs serving each hospital in the system vary significantly in their cost, productivity, and performance on things like patient satisfaction and quality metrics. So they tap the leader of the largest (or best performing) HMG in the system to be system-wide hospitalist medical director. They nearly always choose an internal candidate rather than recruiting from outside, which brings some level of cohesion in operations and performance improvement.
Multi-Site Challenges
This is not an easy job. After all, it isn’t easy to serve as lead hospitalist for a single-site group, so it makes sense that the difficulties and challenges only increase when trying to manage groups at different locations.
The new multi-site HMG leader is busy from the first day on the job. The HMG at one site is short on staffing and needs help right away, patient satisfaction scores are poor at the next site, and so on. Although putting out these fires is important, the new leader also needs to think about how to accomplish a broader mission: ensuring greater cohesion across all groups.
I don’t think there is a secret recipe to ensure success in such a job. Prerequisites include the usual leadership skills, such as patience, good listening, and diplomacy (collectively, one’s EQ, or emotional quotient), along with lots of energy and decisive action. But there are a number of practical matters to address that can influence the level of success.
Cohesion vs. Independence
In most situations, a health system will benefit from some common operating principles across all the HMGs who serve its hospitals. For example, it usually makes sense for any portion of compensation tied to performance (e.g., a bonus) to be based on the same performance domains at all sites. For example, if metrics such as the observed-to-expected mortality ratio (O:E ratio) and patient satisfaction are important to the hospital system, then they should probably influence hospitalist compensation at every site. However, it might be reasonable to target a level of performance for any given domain higher at one site than at another.
Among the many things that should be the same across all sites are operational practices: charge capture, coding audits, performance reviews, dashboard elements and format, and credentialing for new hires. Other things, like individual hospitalist productivity, work schedule, and method and amount of compensation, should vary by site because of the unique attributes of the work at each place.
Fixed Locale vs. Rotations
The travel time between hospitals and the value of extensive experience in the details of how each particular hospital operates usually make it most practical for each individual hospitalist to work nearly all of the time at one hospital. But every doctor should be credentialed at every other hospital in the system so that he can cover a staffing shortage elsewhere.
And, hospitalists hired to work primarily at one of the small hospitals would probably benefit from working at the large referral hospital for the first few weeks of employment. This seems like a great way for them to become familiar with the people and operations at the big hospital, especially since they will be transferring patients there periodically.
Governance
Some mix of central control vs. local autonomy in decision making at each site is important for success. There aren’t any clear guidelines here, but providing the local doctors at each location with the ability to make their own decisions on things like work schedule will contribute to their sense of ownership of the practice. That feeling is valuable and supports good performance.
My bias is that each site in a practice could adopt the same “internal governance” guidelines, or rules by which they make decisions when unable to reach consensus (see “Play by the Rules,” December 2007, for sample guidelines.)
There should also be some form of “umbrella” governance structure in which the local site leaders meet regularly with the multi-site HMG leader.
Patient Transfers
One reason hospitals merge into a single system is the hope that they can more effectively meet the needs of all patients in the system’s hospitals. A typical configuration is several small hospitals, along with a single, large, referral center, to which patients are sent if the small hospital can’t meet their needs. The hope is that if all the hospitals are in the same system, the process of transfer can be smoother and more efficient.
A large portion—maybe even the majority—of all transfers in the system will be between a hospitalist at the small hospital and a partner hospitalist at the large hospital. Things will work best when the transferring and receiving hospitalists know something about the strengths and weaknesses of each other’s hospitals. And, you only know one another reasonably well from working together on committees or being on clinical service together at the same hospital, as well as social functions that include hospitalists from all sites.
Therefore, the multi-site HMG leader should think deliberately about how to ensure that the hospitalists interact with one another often, and not just when a transfer needs to take place.
A written agreement outlining the criteria for an appropriate transfer can be helpful. But such agreements cannot address all the situations that will arise, so good relationships between doctors at the different sites are invaluable and worth taking the time to cultivate.
Communication
Like the five people I mentioned above, anyone holding the position of multi-site HMG leader would benefit from talking with others in the same position. I’m working to arrange some forum for such communication, potentially including an in-person meeting at HM14 in Las Vegas in March (www.hospitalmedicine2014.org). If you are a health system-employed, multi-site HMG leader and want to be part of this conversation, I would love to hear from you.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Let’s call them multi-site, hospital medicine group leaders, or just multi-site HMG leaders. Once rare, they’re now becoming common, and among the many people now holding this job are:
- Dr. Doug Apple at Spectrum Health Medical Group in Grand Rapids, Mich;
- Dr. Tierza Stephan at Allina Health in Minneapolis, Minn.;
- Dr. Darren Thomas at St. John Health System in Tulsa, Okla.;
- Dr. Thomas McIlraith at Dignity Health in Sacremento, Calif.; and
- Dr. Rohit Uppal at Ohio Health in Columbus, Ohio.
The career path that led to their current position usually follows a standard pattern. They are a successful leader of a single-site hospitalist program when, through merger or acquisition, their hospital becomes part of a larger system. The executives responsible for this larger system—typically four to eight hospitals—realize that the HMGs serving each hospital in the system vary significantly in their cost, productivity, and performance on things like patient satisfaction and quality metrics. So they tap the leader of the largest (or best performing) HMG in the system to be system-wide hospitalist medical director. They nearly always choose an internal candidate rather than recruiting from outside, which brings some level of cohesion in operations and performance improvement.
Multi-Site Challenges
This is not an easy job. After all, it isn’t easy to serve as lead hospitalist for a single-site group, so it makes sense that the difficulties and challenges only increase when trying to manage groups at different locations.
The new multi-site HMG leader is busy from the first day on the job. The HMG at one site is short on staffing and needs help right away, patient satisfaction scores are poor at the next site, and so on. Although putting out these fires is important, the new leader also needs to think about how to accomplish a broader mission: ensuring greater cohesion across all groups.
I don’t think there is a secret recipe to ensure success in such a job. Prerequisites include the usual leadership skills, such as patience, good listening, and diplomacy (collectively, one’s EQ, or emotional quotient), along with lots of energy and decisive action. But there are a number of practical matters to address that can influence the level of success.
Cohesion vs. Independence
In most situations, a health system will benefit from some common operating principles across all the HMGs who serve its hospitals. For example, it usually makes sense for any portion of compensation tied to performance (e.g., a bonus) to be based on the same performance domains at all sites. For example, if metrics such as the observed-to-expected mortality ratio (O:E ratio) and patient satisfaction are important to the hospital system, then they should probably influence hospitalist compensation at every site. However, it might be reasonable to target a level of performance for any given domain higher at one site than at another.
Among the many things that should be the same across all sites are operational practices: charge capture, coding audits, performance reviews, dashboard elements and format, and credentialing for new hires. Other things, like individual hospitalist productivity, work schedule, and method and amount of compensation, should vary by site because of the unique attributes of the work at each place.
Fixed Locale vs. Rotations
The travel time between hospitals and the value of extensive experience in the details of how each particular hospital operates usually make it most practical for each individual hospitalist to work nearly all of the time at one hospital. But every doctor should be credentialed at every other hospital in the system so that he can cover a staffing shortage elsewhere.
And, hospitalists hired to work primarily at one of the small hospitals would probably benefit from working at the large referral hospital for the first few weeks of employment. This seems like a great way for them to become familiar with the people and operations at the big hospital, especially since they will be transferring patients there periodically.
Governance
Some mix of central control vs. local autonomy in decision making at each site is important for success. There aren’t any clear guidelines here, but providing the local doctors at each location with the ability to make their own decisions on things like work schedule will contribute to their sense of ownership of the practice. That feeling is valuable and supports good performance.
My bias is that each site in a practice could adopt the same “internal governance” guidelines, or rules by which they make decisions when unable to reach consensus (see “Play by the Rules,” December 2007, for sample guidelines.)
There should also be some form of “umbrella” governance structure in which the local site leaders meet regularly with the multi-site HMG leader.
Patient Transfers
One reason hospitals merge into a single system is the hope that they can more effectively meet the needs of all patients in the system’s hospitals. A typical configuration is several small hospitals, along with a single, large, referral center, to which patients are sent if the small hospital can’t meet their needs. The hope is that if all the hospitals are in the same system, the process of transfer can be smoother and more efficient.
A large portion—maybe even the majority—of all transfers in the system will be between a hospitalist at the small hospital and a partner hospitalist at the large hospital. Things will work best when the transferring and receiving hospitalists know something about the strengths and weaknesses of each other’s hospitals. And, you only know one another reasonably well from working together on committees or being on clinical service together at the same hospital, as well as social functions that include hospitalists from all sites.
Therefore, the multi-site HMG leader should think deliberately about how to ensure that the hospitalists interact with one another often, and not just when a transfer needs to take place.
A written agreement outlining the criteria for an appropriate transfer can be helpful. But such agreements cannot address all the situations that will arise, so good relationships between doctors at the different sites are invaluable and worth taking the time to cultivate.
Communication
Like the five people I mentioned above, anyone holding the position of multi-site HMG leader would benefit from talking with others in the same position. I’m working to arrange some forum for such communication, potentially including an in-person meeting at HM14 in Las Vegas in March (www.hospitalmedicine2014.org). If you are a health system-employed, multi-site HMG leader and want to be part of this conversation, I would love to hear from you.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Massachusetts Hospitalists Experiment with Unit-Based Rounding

Today marks the end of the second week of a three-month experiment we are embarking on to improve team-based care. The main elements of our experiment are two early career hospitalists dedicated to a single nursing unit who are present on the unit throughout the day, structured multidisciplinary rounds, pharmacists doing medication histories to help with medical reconciliation, and a veteran hospitalist serving as a coach, broadly overseeing care coordination and throughput on the unit. (I’m going to focus on multidisciplinary care and leave the coaching part for another day.)
Many have written about and many more have tried to establish unit-based hospitalist models, where a hospitalist is assigned to a single nursing unit. These models often incorporate multidisciplinary rounds, where the hospitalist, case management, social services, physical therapy, and perhaps pharmacy meet each day and review each patient’s progress through the hospitalization. The underlying premise for establishing a unit-based model is that all, or nearly all, of the hospitalist’s patients are located on the nursing unit.
It Can’t Be That Hard
Dedicated units and multidisciplinary rounds are designed to achieve better coordination between the hospitalists and the other members of the hospital team. Most healthcare professionals intuitively support this model; however, many hospitalists have concerns.
To provide the best care for their patients while maintaining career satisfaction, these hospitalists may feel the need for flexibility—the ability to be independent and roam unrestricted through the hallways and departments of the hospital. This goal can be at odds with being limited to a single nursing unit.
For these hospitalists to support the unit-based model, there had better be good reasons for doing so.
Measuring the Effects of Teamwork
Jody Hoffer Gittell, PhD, a professor of management at Brandeis University in Waltham, Mass., has studied relational coordination extensively in healthcare and other service industries. Relational coordination can be defined as “coordinating work through relationships of shared goals, shared knowledge and mutual respect, supported by frequent, timely, accurate, problem-solving communication.”1
Dr. Gittell has developed a validated questionnaire to be completed by each member of the healthcare team, quantifying their perspective on these dimensions for others on the team. I think of relational coordination as a rigorous way of quantifying teamwork.
In 2008, Dr. Gittell published an observational study with SHM senior vice president Joe Miller and hospitalist leader Adrienne L. Bennett, MD, PhD, conducted at a suburban Boston hospital.2 The study looked at relational coordination between members of the hospital team under hospitalist care compared to traditional, PCP-based hospital care. They measured relational coordination by asking the attending physician (hospitalist or PCP providing hospital care), medical resident, floor nurse, case manager, social worker, and therapist (occupational, physical, respiratory, speech) to complete questionnaires about the other team members for a cohort of patients.
The study concluded that relational coordination between other members of the team and the physician was significantly higher for patients treated by hospitalists than for patients treated by traditional PCPs. Further, they found that as relational coordination increased, for patients treated either by hospitalists or PCPs, length of stay, cost, and 30-day readmission rates decreased. I will add that the hospitalists were not unit-based in this study, but were assumed to be more available to the care team than traditional PCPs.
Subsequent studies of multidisciplinary rounds on a “hospitalist unit” conducted by Kevin O’Leary, MD, and colleagues at Northwestern University in Chicago have demonstrated a favorable effect on nurses’ ratings of teamwork and collaboration, as well as the rate of adverse events.3,4 The former study did not, however, find decreased costs or length of stay.
Keys to Success
Before our current experiment, I’ve had the privilege to witness, both at my home institution and at a number of outside ones, many permutations of multidisciplinary rounds and unit-based hospitalists. I’ve seen failures, some mixed results, and occasional success stories. In all cases, participants seem to agree that it takes extra effort to execute on this model, especially once the initial enthusiasm wanes. So, for these arrangements to succeed over time, including our current experiment, I see the following four factors as critical:
- Multidisciplinary rounds must be tightly organized, with case manager, nurse, and hospitalist providing input concisely. Average time per patient should not exceed about three minutes. The total time for rounds, no matter how many patients are under discussion, should not exceed one hour.
- Each team member must be prepared to provide critical information for rounds. For example, hospitalists and nurses should have seen/reviewed their patients, case managers should know expected length of stay and key disposition information, and pharmacists should know medical histories and other pertinent information.
- The fundamental concern of multidisciplinary rounds—that someone’s time is being wasted (when not talking about that team member’s patient at that moment)—must be mitigated one way or another. Solutions include rotating nurses or hospitalists in and out of rounds, and allowing hospitalists to enter orders and do other discreet multitasking during rounds. Careful attention to showing up for the rounds on time and on cue is crucial.
- Hospitalist autonomy and need to roam has to be programmed in by allowing them time to get off the unit, see the broader world, and interact with colleagues.
At the conclusion of three months, as a QI project (as opposed to rigorous research), we will measure a number of things, including cost, throughput, patient satisfaction, and team member satisfaction with the model. If you have predictions, please e-mail me. I’ll report our results in a subsequent column.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. E-mail him at wfwhit@comcast.net.
References
- Relational Coordination Research Collaborative. Brandeis University website. Available at: http://rcrc.brandeis.edu/about-rc/What%20is%20Relational%20Coordination.html. Accessed September 23, 2013.
- Gittell JH, Weinberg DB, Bennett AL, Miller JA. Is the doctor in? A relational approach to job design and the coordination of work. Hum Resource Manag J. 2008;47(4):729-755.
- O’Leary KJ, Haviley C, Slade ME, Shah HM, Lee J, Williams MV. Improving teamwork: impact of structured interdisciplinary rounds on a hospitalist unit. J Hosp Med. 2011;6(2):88-93.
- O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684.
Today marks the end of the second week of a three-month experiment we are embarking on to improve team-based care. The main elements of our experiment are two early career hospitalists dedicated to a single nursing unit who are present on the unit throughout the day, structured multidisciplinary rounds, pharmacists doing medication histories to help with medical reconciliation, and a veteran hospitalist serving as a coach, broadly overseeing care coordination and throughput on the unit. (I’m going to focus on multidisciplinary care and leave the coaching part for another day.)
Many have written about and many more have tried to establish unit-based hospitalist models, where a hospitalist is assigned to a single nursing unit. These models often incorporate multidisciplinary rounds, where the hospitalist, case management, social services, physical therapy, and perhaps pharmacy meet each day and review each patient’s progress through the hospitalization. The underlying premise for establishing a unit-based model is that all, or nearly all, of the hospitalist’s patients are located on the nursing unit.
It Can’t Be That Hard
Dedicated units and multidisciplinary rounds are designed to achieve better coordination between the hospitalists and the other members of the hospital team. Most healthcare professionals intuitively support this model; however, many hospitalists have concerns.
To provide the best care for their patients while maintaining career satisfaction, these hospitalists may feel the need for flexibility—the ability to be independent and roam unrestricted through the hallways and departments of the hospital. This goal can be at odds with being limited to a single nursing unit.
For these hospitalists to support the unit-based model, there had better be good reasons for doing so.
Measuring the Effects of Teamwork
Jody Hoffer Gittell, PhD, a professor of management at Brandeis University in Waltham, Mass., has studied relational coordination extensively in healthcare and other service industries. Relational coordination can be defined as “coordinating work through relationships of shared goals, shared knowledge and mutual respect, supported by frequent, timely, accurate, problem-solving communication.”1
Dr. Gittell has developed a validated questionnaire to be completed by each member of the healthcare team, quantifying their perspective on these dimensions for others on the team. I think of relational coordination as a rigorous way of quantifying teamwork.
In 2008, Dr. Gittell published an observational study with SHM senior vice president Joe Miller and hospitalist leader Adrienne L. Bennett, MD, PhD, conducted at a suburban Boston hospital.2 The study looked at relational coordination between members of the hospital team under hospitalist care compared to traditional, PCP-based hospital care. They measured relational coordination by asking the attending physician (hospitalist or PCP providing hospital care), medical resident, floor nurse, case manager, social worker, and therapist (occupational, physical, respiratory, speech) to complete questionnaires about the other team members for a cohort of patients.
The study concluded that relational coordination between other members of the team and the physician was significantly higher for patients treated by hospitalists than for patients treated by traditional PCPs. Further, they found that as relational coordination increased, for patients treated either by hospitalists or PCPs, length of stay, cost, and 30-day readmission rates decreased. I will add that the hospitalists were not unit-based in this study, but were assumed to be more available to the care team than traditional PCPs.
Subsequent studies of multidisciplinary rounds on a “hospitalist unit” conducted by Kevin O’Leary, MD, and colleagues at Northwestern University in Chicago have demonstrated a favorable effect on nurses’ ratings of teamwork and collaboration, as well as the rate of adverse events.3,4 The former study did not, however, find decreased costs or length of stay.
Keys to Success
Before our current experiment, I’ve had the privilege to witness, both at my home institution and at a number of outside ones, many permutations of multidisciplinary rounds and unit-based hospitalists. I’ve seen failures, some mixed results, and occasional success stories. In all cases, participants seem to agree that it takes extra effort to execute on this model, especially once the initial enthusiasm wanes. So, for these arrangements to succeed over time, including our current experiment, I see the following four factors as critical:
- Multidisciplinary rounds must be tightly organized, with case manager, nurse, and hospitalist providing input concisely. Average time per patient should not exceed about three minutes. The total time for rounds, no matter how many patients are under discussion, should not exceed one hour.
- Each team member must be prepared to provide critical information for rounds. For example, hospitalists and nurses should have seen/reviewed their patients, case managers should know expected length of stay and key disposition information, and pharmacists should know medical histories and other pertinent information.
- The fundamental concern of multidisciplinary rounds—that someone’s time is being wasted (when not talking about that team member’s patient at that moment)—must be mitigated one way or another. Solutions include rotating nurses or hospitalists in and out of rounds, and allowing hospitalists to enter orders and do other discreet multitasking during rounds. Careful attention to showing up for the rounds on time and on cue is crucial.
- Hospitalist autonomy and need to roam has to be programmed in by allowing them time to get off the unit, see the broader world, and interact with colleagues.
At the conclusion of three months, as a QI project (as opposed to rigorous research), we will measure a number of things, including cost, throughput, patient satisfaction, and team member satisfaction with the model. If you have predictions, please e-mail me. I’ll report our results in a subsequent column.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. E-mail him at wfwhit@comcast.net.
References
- Relational Coordination Research Collaborative. Brandeis University website. Available at: http://rcrc.brandeis.edu/about-rc/What%20is%20Relational%20Coordination.html. Accessed September 23, 2013.
- Gittell JH, Weinberg DB, Bennett AL, Miller JA. Is the doctor in? A relational approach to job design and the coordination of work. Hum Resource Manag J. 2008;47(4):729-755.
- O’Leary KJ, Haviley C, Slade ME, Shah HM, Lee J, Williams MV. Improving teamwork: impact of structured interdisciplinary rounds on a hospitalist unit. J Hosp Med. 2011;6(2):88-93.
- O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684.
Today marks the end of the second week of a three-month experiment we are embarking on to improve team-based care. The main elements of our experiment are two early career hospitalists dedicated to a single nursing unit who are present on the unit throughout the day, structured multidisciplinary rounds, pharmacists doing medication histories to help with medical reconciliation, and a veteran hospitalist serving as a coach, broadly overseeing care coordination and throughput on the unit. (I’m going to focus on multidisciplinary care and leave the coaching part for another day.)
Many have written about and many more have tried to establish unit-based hospitalist models, where a hospitalist is assigned to a single nursing unit. These models often incorporate multidisciplinary rounds, where the hospitalist, case management, social services, physical therapy, and perhaps pharmacy meet each day and review each patient’s progress through the hospitalization. The underlying premise for establishing a unit-based model is that all, or nearly all, of the hospitalist’s patients are located on the nursing unit.
It Can’t Be That Hard
Dedicated units and multidisciplinary rounds are designed to achieve better coordination between the hospitalists and the other members of the hospital team. Most healthcare professionals intuitively support this model; however, many hospitalists have concerns.
To provide the best care for their patients while maintaining career satisfaction, these hospitalists may feel the need for flexibility—the ability to be independent and roam unrestricted through the hallways and departments of the hospital. This goal can be at odds with being limited to a single nursing unit.
For these hospitalists to support the unit-based model, there had better be good reasons for doing so.
Measuring the Effects of Teamwork
Jody Hoffer Gittell, PhD, a professor of management at Brandeis University in Waltham, Mass., has studied relational coordination extensively in healthcare and other service industries. Relational coordination can be defined as “coordinating work through relationships of shared goals, shared knowledge and mutual respect, supported by frequent, timely, accurate, problem-solving communication.”1
Dr. Gittell has developed a validated questionnaire to be completed by each member of the healthcare team, quantifying their perspective on these dimensions for others on the team. I think of relational coordination as a rigorous way of quantifying teamwork.
In 2008, Dr. Gittell published an observational study with SHM senior vice president Joe Miller and hospitalist leader Adrienne L. Bennett, MD, PhD, conducted at a suburban Boston hospital.2 The study looked at relational coordination between members of the hospital team under hospitalist care compared to traditional, PCP-based hospital care. They measured relational coordination by asking the attending physician (hospitalist or PCP providing hospital care), medical resident, floor nurse, case manager, social worker, and therapist (occupational, physical, respiratory, speech) to complete questionnaires about the other team members for a cohort of patients.
The study concluded that relational coordination between other members of the team and the physician was significantly higher for patients treated by hospitalists than for patients treated by traditional PCPs. Further, they found that as relational coordination increased, for patients treated either by hospitalists or PCPs, length of stay, cost, and 30-day readmission rates decreased. I will add that the hospitalists were not unit-based in this study, but were assumed to be more available to the care team than traditional PCPs.
Subsequent studies of multidisciplinary rounds on a “hospitalist unit” conducted by Kevin O’Leary, MD, and colleagues at Northwestern University in Chicago have demonstrated a favorable effect on nurses’ ratings of teamwork and collaboration, as well as the rate of adverse events.3,4 The former study did not, however, find decreased costs or length of stay.
Keys to Success
Before our current experiment, I’ve had the privilege to witness, both at my home institution and at a number of outside ones, many permutations of multidisciplinary rounds and unit-based hospitalists. I’ve seen failures, some mixed results, and occasional success stories. In all cases, participants seem to agree that it takes extra effort to execute on this model, especially once the initial enthusiasm wanes. So, for these arrangements to succeed over time, including our current experiment, I see the following four factors as critical:
- Multidisciplinary rounds must be tightly organized, with case manager, nurse, and hospitalist providing input concisely. Average time per patient should not exceed about three minutes. The total time for rounds, no matter how many patients are under discussion, should not exceed one hour.
- Each team member must be prepared to provide critical information for rounds. For example, hospitalists and nurses should have seen/reviewed their patients, case managers should know expected length of stay and key disposition information, and pharmacists should know medical histories and other pertinent information.
- The fundamental concern of multidisciplinary rounds—that someone’s time is being wasted (when not talking about that team member’s patient at that moment)—must be mitigated one way or another. Solutions include rotating nurses or hospitalists in and out of rounds, and allowing hospitalists to enter orders and do other discreet multitasking during rounds. Careful attention to showing up for the rounds on time and on cue is crucial.
- Hospitalist autonomy and need to roam has to be programmed in by allowing them time to get off the unit, see the broader world, and interact with colleagues.
At the conclusion of three months, as a QI project (as opposed to rigorous research), we will measure a number of things, including cost, throughput, patient satisfaction, and team member satisfaction with the model. If you have predictions, please e-mail me. I’ll report our results in a subsequent column.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. E-mail him at wfwhit@comcast.net.
References
- Relational Coordination Research Collaborative. Brandeis University website. Available at: http://rcrc.brandeis.edu/about-rc/What%20is%20Relational%20Coordination.html. Accessed September 23, 2013.
- Gittell JH, Weinberg DB, Bennett AL, Miller JA. Is the doctor in? A relational approach to job design and the coordination of work. Hum Resource Manag J. 2008;47(4):729-755.
- O’Leary KJ, Haviley C, Slade ME, Shah HM, Lee J, Williams MV. Improving teamwork: impact of structured interdisciplinary rounds on a hospitalist unit. J Hosp Med. 2011;6(2):88-93.
- O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684.
Global outreach project is not your ordinary mental health clinic
We are in the midst of enormous changes in health care delivery. Implementation of the 2010 Patient Protection and Affordable Care Act will make health care accessible to more people than ever before, and ushers in a cultural shift from a prohibitively expensive interventional health care model to one based on prediction and prevention.
Instead of waiting to get sick and seeking expensive urgent care, we are moving toward identifying vulnerable patient populations early and encouraging them to become active participants in maintaining their health. Whether you like it or not, the Affordable Care Act (or some modification of it) is here to stay, because we simply can’t afford the 20% of our gross domestic product that health care costs us, and it’s not making us any healthier. Psychiatry is not well positioned to respond to this cultural shift, because as a specialty, we are moving in the opposite direction, creating more illnesses and prescribing more drugs. Patients only come to see us now as a last resort because they know we will label them with a disease and prescribe drugs.

Twenty-five percent of all Americans are now diagnosed with a mental illness, and with the recent publication of the DSM-5 and its record-breaking number of mental illnesses, soon 50% of the population might have a diagnosable mental illness. We are perpetuating the myth that if you are feeling anything other than wonderful in every moment, you might be suffering from a mental illness. We are "psychopathologizing" the ordinary ups and downs of the human experience and promoting pills for whatever ails the patient. I believe we would reduce the incidence of mental illness in this country by 90% if we prohibited direct-to-consumer advertising by pharmaceutical companies.
The message to the patient: Are you anxious, shy, sad? Can’t stay focused or can’t stay awake? If so, you could have a disease for which there is a drug (nowadays often more than one). Such messages are good for business, because we’re reimbursed better if we see four patients an hour for 15-minute medication checks than we do for an hour-long psychotherapy session. We are spending less time listening and establishing an intimate rapport, even though this is what most of us like best about what we do and understand as an important aspect of our healing power. Can we do both? Is it possible to make a soulful, human connection in a short time, and could this reduce an epidemic of overprescribing? I believe we can if we expand the ways in which we engage people – and in doing so, move into the new prevention paradigm.
In addition to my degreed credentials, I also am a clown and proudly serve as chief of community mental health at Gesundheit! Institute in Hillsboro, W.Va. The clown/fool/jester/trickster is an archetypal human characteristic that has served the purpose of lightening mood, diffusing anxiety, helping patients look at the familiar from a new perspective. The character can serve as a sacred healer. I clown all over the world with Dr. Patch Adams, perhaps the world’s most recognized humanitarian clown and founder of Gesundheit! Last year, I discussed a 20-minute mental health clinic in which I participated on the streets of Iquitos, Peru.
We did it again this year in Iquitos, and people lined up to see the clown-clinicians; they sat in an open space and talked for 20 minutes to someone they knew was listening to them. Clinicians heard gut-wrenching stories of suffering and challenges, helped people identify their strengths, applauded their resilience, gave advice, and blessed them. Patients felt better, and the clinicians felt better, because it doesn’t take long to make an intimate connection if you are truly present. It is in those moments that we are reminded of our shared humanity and that dreams are possible.
I’m thinking of bringing the Gesundheit! Global Outreach or (GO!) clowns to a mall in America and conducting such mental health clinics. Clowns would play, perform, sit in silence, and talk to anybody who wanted to right out in the open without charge. There would be neither signing of HIPAA compliance forms, nor making diagnoses, nor prescribing drugs. The idea would be to provide clown healers who might inspire people to see their lives from a different perspective.
This would be a community-based, mental health promotion program in which clowns would be supported by local community health agencies; self-help groups of every description (from survivors of violence, burns, and addictions, to parents with attention-deficit/hyperactivity disorder kids who found a way to help them without drugs). There are many untapped resources in communities, and these "clinics" can mobilize them to connect people. By doing this work publicly, we would destigmatize the concept that having ordinary problems of living is the equivalent of being mentally ill, or disabled, and needing only drugs.
You don’t have to be a clown and do this in the street (although you are welcome to join us). Try this approach in your office; use 15-20 minutes to make a heartfelt, therapeutic connection with patients; and remind yourself why you do this work. It will make you feel good and intensify your healing power.
Dr. Hammerschlag is affiliated with the Arizona Health Sciences Center at the University of Arizona, Phoenix, in addition to his role at the Gesundheit! Institute. He also is author of several books on healing, spirituality, and other topics. To get in touch with him, e-mail him at info@healingdoc.com. Those interested in the work of Gesundheit! and clown trips should go to patchadams.org.
<
We are in the midst of enormous changes in health care delivery. Implementation of the 2010 Patient Protection and Affordable Care Act will make health care accessible to more people than ever before, and ushers in a cultural shift from a prohibitively expensive interventional health care model to one based on prediction and prevention.
Instead of waiting to get sick and seeking expensive urgent care, we are moving toward identifying vulnerable patient populations early and encouraging them to become active participants in maintaining their health. Whether you like it or not, the Affordable Care Act (or some modification of it) is here to stay, because we simply can’t afford the 20% of our gross domestic product that health care costs us, and it’s not making us any healthier. Psychiatry is not well positioned to respond to this cultural shift, because as a specialty, we are moving in the opposite direction, creating more illnesses and prescribing more drugs. Patients only come to see us now as a last resort because they know we will label them with a disease and prescribe drugs.
Twenty-five percent of all Americans are now diagnosed with a mental illness, and with the recent publication of the DSM-5 and its record-breaking number of mental illnesses, soon 50% of the population might have a diagnosable mental illness. We are perpetuating the myth that if you are feeling anything other than wonderful in every moment, you might be suffering from a mental illness. We are "psychopathologizing" the ordinary ups and downs of the human experience and promoting pills for whatever ails the patient. I believe we would reduce the incidence of mental illness in this country by 90% if we prohibited direct-to-consumer advertising by pharmaceutical companies.
The message to the patient: Are you anxious, shy, sad? Can’t stay focused or can’t stay awake? If so, you could have a disease for which there is a drug (nowadays often more than one). Such messages are good for business, because we’re reimbursed better if we see four patients an hour for 15-minute medication checks than we do for an hour-long psychotherapy session. We are spending less time listening and establishing an intimate rapport, even though this is what most of us like best about what we do and understand as an important aspect of our healing power. Can we do both? Is it possible to make a soulful, human connection in a short time, and could this reduce an epidemic of overprescribing? I believe we can if we expand the ways in which we engage people – and in doing so, move into the new prevention paradigm.
In addition to my degreed credentials, I also am a clown and proudly serve as chief of community mental health at Gesundheit! Institute in Hillsboro, W.Va. The clown/fool/jester/trickster is an archetypal human characteristic that has served the purpose of lightening mood, diffusing anxiety, helping patients look at the familiar from a new perspective. The character can serve as a sacred healer. I clown all over the world with Dr. Patch Adams, perhaps the world’s most recognized humanitarian clown and founder of Gesundheit! Last year, I discussed a 20-minute mental health clinic in which I participated on the streets of Iquitos, Peru.
We did it again this year in Iquitos, and people lined up to see the clown-clinicians; they sat in an open space and talked for 20 minutes to someone they knew was listening to them. Clinicians heard gut-wrenching stories of suffering and challenges, helped people identify their strengths, applauded their resilience, gave advice, and blessed them. Patients felt better, and the clinicians felt better, because it doesn’t take long to make an intimate connection if you are truly present. It is in those moments that we are reminded of our shared humanity and that dreams are possible.
I’m thinking of bringing the Gesundheit! Global Outreach or (GO!) clowns to a mall in America and conducting such mental health clinics. Clowns would play, perform, sit in silence, and talk to anybody who wanted to right out in the open without charge. There would be neither signing of HIPAA compliance forms, nor making diagnoses, nor prescribing drugs. The idea would be to provide clown healers who might inspire people to see their lives from a different perspective.
This would be a community-based, mental health promotion program in which clowns would be supported by local community health agencies; self-help groups of every description (from survivors of violence, burns, and addictions, to parents with attention-deficit/hyperactivity disorder kids who found a way to help them without drugs). There are many untapped resources in communities, and these "clinics" can mobilize them to connect people. By doing this work publicly, we would destigmatize the concept that having ordinary problems of living is the equivalent of being mentally ill, or disabled, and needing only drugs.
You don’t have to be a clown and do this in the street (although you are welcome to join us). Try this approach in your office; use 15-20 minutes to make a heartfelt, therapeutic connection with patients; and remind yourself why you do this work. It will make you feel good and intensify your healing power.
Dr. Hammerschlag is affiliated with the Arizona Health Sciences Center at the University of Arizona, Phoenix, in addition to his role at the Gesundheit! Institute. He also is author of several books on healing, spirituality, and other topics. To get in touch with him, e-mail him at info@healingdoc.com. Those interested in the work of Gesundheit! and clown trips should go to patchadams.org.
<
We are in the midst of enormous changes in health care delivery. Implementation of the 2010 Patient Protection and Affordable Care Act will make health care accessible to more people than ever before, and ushers in a cultural shift from a prohibitively expensive interventional health care model to one based on prediction and prevention.
Instead of waiting to get sick and seeking expensive urgent care, we are moving toward identifying vulnerable patient populations early and encouraging them to become active participants in maintaining their health. Whether you like it or not, the Affordable Care Act (or some modification of it) is here to stay, because we simply can’t afford the 20% of our gross domestic product that health care costs us, and it’s not making us any healthier. Psychiatry is not well positioned to respond to this cultural shift, because as a specialty, we are moving in the opposite direction, creating more illnesses and prescribing more drugs. Patients only come to see us now as a last resort because they know we will label them with a disease and prescribe drugs.
Twenty-five percent of all Americans are now diagnosed with a mental illness, and with the recent publication of the DSM-5 and its record-breaking number of mental illnesses, soon 50% of the population might have a diagnosable mental illness. We are perpetuating the myth that if you are feeling anything other than wonderful in every moment, you might be suffering from a mental illness. We are "psychopathologizing" the ordinary ups and downs of the human experience and promoting pills for whatever ails the patient. I believe we would reduce the incidence of mental illness in this country by 90% if we prohibited direct-to-consumer advertising by pharmaceutical companies.
The message to the patient: Are you anxious, shy, sad? Can’t stay focused or can’t stay awake? If so, you could have a disease for which there is a drug (nowadays often more than one). Such messages are good for business, because we’re reimbursed better if we see four patients an hour for 15-minute medication checks than we do for an hour-long psychotherapy session. We are spending less time listening and establishing an intimate rapport, even though this is what most of us like best about what we do and understand as an important aspect of our healing power. Can we do both? Is it possible to make a soulful, human connection in a short time, and could this reduce an epidemic of overprescribing? I believe we can if we expand the ways in which we engage people – and in doing so, move into the new prevention paradigm.
In addition to my degreed credentials, I also am a clown and proudly serve as chief of community mental health at Gesundheit! Institute in Hillsboro, W.Va. The clown/fool/jester/trickster is an archetypal human characteristic that has served the purpose of lightening mood, diffusing anxiety, helping patients look at the familiar from a new perspective. The character can serve as a sacred healer. I clown all over the world with Dr. Patch Adams, perhaps the world’s most recognized humanitarian clown and founder of Gesundheit! Last year, I discussed a 20-minute mental health clinic in which I participated on the streets of Iquitos, Peru.
We did it again this year in Iquitos, and people lined up to see the clown-clinicians; they sat in an open space and talked for 20 minutes to someone they knew was listening to them. Clinicians heard gut-wrenching stories of suffering and challenges, helped people identify their strengths, applauded their resilience, gave advice, and blessed them. Patients felt better, and the clinicians felt better, because it doesn’t take long to make an intimate connection if you are truly present. It is in those moments that we are reminded of our shared humanity and that dreams are possible.
I’m thinking of bringing the Gesundheit! Global Outreach or (GO!) clowns to a mall in America and conducting such mental health clinics. Clowns would play, perform, sit in silence, and talk to anybody who wanted to right out in the open without charge. There would be neither signing of HIPAA compliance forms, nor making diagnoses, nor prescribing drugs. The idea would be to provide clown healers who might inspire people to see their lives from a different perspective.
This would be a community-based, mental health promotion program in which clowns would be supported by local community health agencies; self-help groups of every description (from survivors of violence, burns, and addictions, to parents with attention-deficit/hyperactivity disorder kids who found a way to help them without drugs). There are many untapped resources in communities, and these "clinics" can mobilize them to connect people. By doing this work publicly, we would destigmatize the concept that having ordinary problems of living is the equivalent of being mentally ill, or disabled, and needing only drugs.
You don’t have to be a clown and do this in the street (although you are welcome to join us). Try this approach in your office; use 15-20 minutes to make a heartfelt, therapeutic connection with patients; and remind yourself why you do this work. It will make you feel good and intensify your healing power.
Dr. Hammerschlag is affiliated with the Arizona Health Sciences Center at the University of Arizona, Phoenix, in addition to his role at the Gesundheit! Institute. He also is author of several books on healing, spirituality, and other topics. To get in touch with him, e-mail him at info@healingdoc.com. Those interested in the work of Gesundheit! and clown trips should go to patchadams.org.
<

MGMA Surveys Make Hospitalists' Productivity Hard to Assess


The Medical Group Management Association (MGMA) surveys regard both a doctor who works the standard number of annual shifts their practice defines as full time, and a doctor who works many extra shifts, as one full-time equivalent (FTE). This can cause confusion when assessing productivity per FTE (see “SHM and MGMA Survey History,” right).
For example, consider a hospitalist who generated 4,000 wRVUs while working 182 shifts—the standard number of shifts to be full time in that doctor’s practice—during the survey year. In the same practice, another hospitalist worked 39 extra shifts over the same year for a total of 220 shifts, generating 4,860 wRVUs. If the survey contained only these two doctors, it would show them both as full time, with an average productivity per FTE of 4,430 wRVUs. But that would be misleading because 1.0 FTE worth of work as defined by their practice for both doctors would have come to 4,000 wRVUs generated while working 182 shifts.
In prior columns, I’ve highlighted some other numbers in hospitalist productivity and compensation surveys that can lead to confusion. But the MGMA survey methodology, which assigns a particular FTE to a single doctor, may be the most confusing issue, potentially leading to meaningful misunderstandings.
More Details on FTE Definition
MGMA has been conducting physician compensation and productivity surveys across essentially all medical specialties for decades. Competing organizations conduct similar surveys, but most regard the MGMA survey as the most relevant and valuable.
For a long time, MGMA has regarded as “full time” any doctor working 0.75 FTE or greater, using the respondent practice’s definition of an FTE. No single doctor can ever be counted as more than 1.0 FTE, regardless of how much extra the doctor may have worked. Any doctor working 0.35-0.75 FTE is regarded as part time, and those working less than 0.35 FTE are excluded from the survey report. The fact that each practice might have a different definition of what constitutes an FTE is addressed by having a large number of respondents in most medical specialties.
I’m uncertain how MGMA ended up not counting any single doctor as more than 1.0 FTE, even when they work a lot of extra shifts. But my guess is that for the first years, or even decades, that MGMA conducted its survey, few, if any, medical practices even had a strict definition of what constituted 1.0 FTE and simply didn’t keep track of which doctors worked extra shifts or days. So even if MGMA had wanted to know, for example, when a doctor worked extra shifts and should be counted as more than 1.0 FTE, few if any practices even thought about the precise number of shifts or days worked constituting full time versus what was an “extra” shift. So it probably made sense to simply have two categories: full time and part time.
As more practices began assigning FTE with greater precision, like nearly all hospitalist practices do, then using 0.75 FTE to separate full time and part time seemed practical, though imprecise. But keep in mind it also means that all of the doctors who work from 0.75 to 0.99 FTE (that is, something less than 1.0) offset, at least partially, those who work lots of extra shifts (i.e., above 1.0 FTE).
Data Application
My anecdotal experience is that a large portion of hospitalists, probably around half, work more shifts than what their practice regards as full time. I don’t know of any survey database that quantifies this, but my guess is that 25% to 35% of full-time hospitalists work extra shifts at their own practice, and maybe another 15% to 20% moonlight at a different practice. Let’s consider only those in the first category.
Chronic staffing shortages is one of the reasons hospitalists so commonly work extra shifts at their own practice. Extra shifts are sometimes even required by the practice to make up for open positions. And in some places, the hospitalists choose not to fill positions to preserve their ability to continue working more than the number of shifts required to be full time.
It would be great if we had a precise way to adjust the MGMA survey data for hospitalists who work above 1.0 FTE. For example, let’s make three assumptions so that we can then adjust the reported compensation and productivity data to remove the effect of the many doctors working extra shifts, thereby more clearly matching 1.0 FTE. These numbers are my guesses based on lots of anecdotal experience. But they are only guesses. Don’t make too much of them.
Assume 25% of hospitalists nationally work an average of 20% more than the full-time number of shifts for their practice. That is my best guess and intentionally leaves out those who moonlight for a practice other than their own.
Some portion of those working extra shifts (above 1.0 FTE) is offset by survey respondents working between 0.75 and 1.0 FTE, resulting in a wild guess of a net 20% of hospitalists working extra shifts.
Last, let’s assume that their productivity and compensation on extra shifts is identical to their “normal” shifts. This is not true for many practices, but when aggregating the data, it is probably reasonably close.
Using these assumptions (guesses, really), we can decrease both the reported survey mean and median productivity and compensation by about 5% to more accurately reflect results for hospitalists doing only the number of shifts required by the practice to be full time—no extra shifts. I’ll spare you the simple math showing how I arrived at the approximately 5%, but basically it is removing the 20% additional compensation and productivity generated by the net 20% of hospitalists who work extra shifts above 1.0 FTE.
Does It Really Matter?
The whole issue of hospitalists working many extra shifts yet only counting as 1.0 FTE in the MGMA survey might matter a lot for some, and others might see it as useless hand-wringing. As long as a meaningful number of hospitalists work extra shifts, then survey values for productivity and compensation will always be a little higher than the “average” 1.0 FTE hospitalists working no extra shifts. But it may still be well within the range of error of the survey anyway. And the compensation per unit of work (wRVUs or encounters) probably isn’t much affected by this FTE issue.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
The Medical Group Management Association (MGMA) surveys regard both a doctor who works the standard number of annual shifts their practice defines as full time, and a doctor who works many extra shifts, as one full-time equivalent (FTE). This can cause confusion when assessing productivity per FTE (see “SHM and MGMA Survey History,” right).
For example, consider a hospitalist who generated 4,000 wRVUs while working 182 shifts—the standard number of shifts to be full time in that doctor’s practice—during the survey year. In the same practice, another hospitalist worked 39 extra shifts over the same year for a total of 220 shifts, generating 4,860 wRVUs. If the survey contained only these two doctors, it would show them both as full time, with an average productivity per FTE of 4,430 wRVUs. But that would be misleading because 1.0 FTE worth of work as defined by their practice for both doctors would have come to 4,000 wRVUs generated while working 182 shifts.
In prior columns, I’ve highlighted some other numbers in hospitalist productivity and compensation surveys that can lead to confusion. But the MGMA survey methodology, which assigns a particular FTE to a single doctor, may be the most confusing issue, potentially leading to meaningful misunderstandings.
More Details on FTE Definition
MGMA has been conducting physician compensation and productivity surveys across essentially all medical specialties for decades. Competing organizations conduct similar surveys, but most regard the MGMA survey as the most relevant and valuable.
For a long time, MGMA has regarded as “full time” any doctor working 0.75 FTE or greater, using the respondent practice’s definition of an FTE. No single doctor can ever be counted as more than 1.0 FTE, regardless of how much extra the doctor may have worked. Any doctor working 0.35-0.75 FTE is regarded as part time, and those working less than 0.35 FTE are excluded from the survey report. The fact that each practice might have a different definition of what constitutes an FTE is addressed by having a large number of respondents in most medical specialties.
I’m uncertain how MGMA ended up not counting any single doctor as more than 1.0 FTE, even when they work a lot of extra shifts. But my guess is that for the first years, or even decades, that MGMA conducted its survey, few, if any, medical practices even had a strict definition of what constituted 1.0 FTE and simply didn’t keep track of which doctors worked extra shifts or days. So even if MGMA had wanted to know, for example, when a doctor worked extra shifts and should be counted as more than 1.0 FTE, few if any practices even thought about the precise number of shifts or days worked constituting full time versus what was an “extra” shift. So it probably made sense to simply have two categories: full time and part time.
As more practices began assigning FTE with greater precision, like nearly all hospitalist practices do, then using 0.75 FTE to separate full time and part time seemed practical, though imprecise. But keep in mind it also means that all of the doctors who work from 0.75 to 0.99 FTE (that is, something less than 1.0) offset, at least partially, those who work lots of extra shifts (i.e., above 1.0 FTE).
Data Application
My anecdotal experience is that a large portion of hospitalists, probably around half, work more shifts than what their practice regards as full time. I don’t know of any survey database that quantifies this, but my guess is that 25% to 35% of full-time hospitalists work extra shifts at their own practice, and maybe another 15% to 20% moonlight at a different practice. Let’s consider only those in the first category.
Chronic staffing shortages is one of the reasons hospitalists so commonly work extra shifts at their own practice. Extra shifts are sometimes even required by the practice to make up for open positions. And in some places, the hospitalists choose not to fill positions to preserve their ability to continue working more than the number of shifts required to be full time.
It would be great if we had a precise way to adjust the MGMA survey data for hospitalists who work above 1.0 FTE. For example, let’s make three assumptions so that we can then adjust the reported compensation and productivity data to remove the effect of the many doctors working extra shifts, thereby more clearly matching 1.0 FTE. These numbers are my guesses based on lots of anecdotal experience. But they are only guesses. Don’t make too much of them.
Assume 25% of hospitalists nationally work an average of 20% more than the full-time number of shifts for their practice. That is my best guess and intentionally leaves out those who moonlight for a practice other than their own.
Some portion of those working extra shifts (above 1.0 FTE) is offset by survey respondents working between 0.75 and 1.0 FTE, resulting in a wild guess of a net 20% of hospitalists working extra shifts.
Last, let’s assume that their productivity and compensation on extra shifts is identical to their “normal” shifts. This is not true for many practices, but when aggregating the data, it is probably reasonably close.
Using these assumptions (guesses, really), we can decrease both the reported survey mean and median productivity and compensation by about 5% to more accurately reflect results for hospitalists doing only the number of shifts required by the practice to be full time—no extra shifts. I’ll spare you the simple math showing how I arrived at the approximately 5%, but basically it is removing the 20% additional compensation and productivity generated by the net 20% of hospitalists who work extra shifts above 1.0 FTE.
Does It Really Matter?
The whole issue of hospitalists working many extra shifts yet only counting as 1.0 FTE in the MGMA survey might matter a lot for some, and others might see it as useless hand-wringing. As long as a meaningful number of hospitalists work extra shifts, then survey values for productivity and compensation will always be a little higher than the “average” 1.0 FTE hospitalists working no extra shifts. But it may still be well within the range of error of the survey anyway. And the compensation per unit of work (wRVUs or encounters) probably isn’t much affected by this FTE issue.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
The Medical Group Management Association (MGMA) surveys regard both a doctor who works the standard number of annual shifts their practice defines as full time, and a doctor who works many extra shifts, as one full-time equivalent (FTE). This can cause confusion when assessing productivity per FTE (see “SHM and MGMA Survey History,” right).
For example, consider a hospitalist who generated 4,000 wRVUs while working 182 shifts—the standard number of shifts to be full time in that doctor’s practice—during the survey year. In the same practice, another hospitalist worked 39 extra shifts over the same year for a total of 220 shifts, generating 4,860 wRVUs. If the survey contained only these two doctors, it would show them both as full time, with an average productivity per FTE of 4,430 wRVUs. But that would be misleading because 1.0 FTE worth of work as defined by their practice for both doctors would have come to 4,000 wRVUs generated while working 182 shifts.
In prior columns, I’ve highlighted some other numbers in hospitalist productivity and compensation surveys that can lead to confusion. But the MGMA survey methodology, which assigns a particular FTE to a single doctor, may be the most confusing issue, potentially leading to meaningful misunderstandings.
More Details on FTE Definition
MGMA has been conducting physician compensation and productivity surveys across essentially all medical specialties for decades. Competing organizations conduct similar surveys, but most regard the MGMA survey as the most relevant and valuable.
For a long time, MGMA has regarded as “full time” any doctor working 0.75 FTE or greater, using the respondent practice’s definition of an FTE. No single doctor can ever be counted as more than 1.0 FTE, regardless of how much extra the doctor may have worked. Any doctor working 0.35-0.75 FTE is regarded as part time, and those working less than 0.35 FTE are excluded from the survey report. The fact that each practice might have a different definition of what constitutes an FTE is addressed by having a large number of respondents in most medical specialties.
I’m uncertain how MGMA ended up not counting any single doctor as more than 1.0 FTE, even when they work a lot of extra shifts. But my guess is that for the first years, or even decades, that MGMA conducted its survey, few, if any, medical practices even had a strict definition of what constituted 1.0 FTE and simply didn’t keep track of which doctors worked extra shifts or days. So even if MGMA had wanted to know, for example, when a doctor worked extra shifts and should be counted as more than 1.0 FTE, few if any practices even thought about the precise number of shifts or days worked constituting full time versus what was an “extra” shift. So it probably made sense to simply have two categories: full time and part time.
As more practices began assigning FTE with greater precision, like nearly all hospitalist practices do, then using 0.75 FTE to separate full time and part time seemed practical, though imprecise. But keep in mind it also means that all of the doctors who work from 0.75 to 0.99 FTE (that is, something less than 1.0) offset, at least partially, those who work lots of extra shifts (i.e., above 1.0 FTE).
Data Application
My anecdotal experience is that a large portion of hospitalists, probably around half, work more shifts than what their practice regards as full time. I don’t know of any survey database that quantifies this, but my guess is that 25% to 35% of full-time hospitalists work extra shifts at their own practice, and maybe another 15% to 20% moonlight at a different practice. Let’s consider only those in the first category.
Chronic staffing shortages is one of the reasons hospitalists so commonly work extra shifts at their own practice. Extra shifts are sometimes even required by the practice to make up for open positions. And in some places, the hospitalists choose not to fill positions to preserve their ability to continue working more than the number of shifts required to be full time.
It would be great if we had a precise way to adjust the MGMA survey data for hospitalists who work above 1.0 FTE. For example, let’s make three assumptions so that we can then adjust the reported compensation and productivity data to remove the effect of the many doctors working extra shifts, thereby more clearly matching 1.0 FTE. These numbers are my guesses based on lots of anecdotal experience. But they are only guesses. Don’t make too much of them.
Assume 25% of hospitalists nationally work an average of 20% more than the full-time number of shifts for their practice. That is my best guess and intentionally leaves out those who moonlight for a practice other than their own.
Some portion of those working extra shifts (above 1.0 FTE) is offset by survey respondents working between 0.75 and 1.0 FTE, resulting in a wild guess of a net 20% of hospitalists working extra shifts.
Last, let’s assume that their productivity and compensation on extra shifts is identical to their “normal” shifts. This is not true for many practices, but when aggregating the data, it is probably reasonably close.
Using these assumptions (guesses, really), we can decrease both the reported survey mean and median productivity and compensation by about 5% to more accurately reflect results for hospitalists doing only the number of shifts required by the practice to be full time—no extra shifts. I’ll spare you the simple math showing how I arrived at the approximately 5%, but basically it is removing the 20% additional compensation and productivity generated by the net 20% of hospitalists who work extra shifts above 1.0 FTE.
Does It Really Matter?
The whole issue of hospitalists working many extra shifts yet only counting as 1.0 FTE in the MGMA survey might matter a lot for some, and others might see it as useless hand-wringing. As long as a meaningful number of hospitalists work extra shifts, then survey values for productivity and compensation will always be a little higher than the “average” 1.0 FTE hospitalists working no extra shifts. But it may still be well within the range of error of the survey anyway. And the compensation per unit of work (wRVUs or encounters) probably isn’t much affected by this FTE issue.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
New Rules for Value-Based Purchasing, Readmission Penalties, Admissions


The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View from
![]()
Looking for more information to formulate a plan of attack? SHM offers a variety of HVBP resources to orient hospitalists and hospital leaders. The “What Every Hospitalist Should Know About Hospital Value-Based Purchasing” webinar and SHM’s free resource library (www.hospitalmedicine.org/hvbp) offer basic orientation on what to expect on pay-for-performance-related issues. The HVBP resource center also provides multiple case studies from various hospitals across the country, with success stories related to reducing readmissions, increasing evidence-based care focus, and enhancing performance on core measures.
In order to proactively address CMS’ new 30-day readmissions criteria for COPD, SHM’s COPD Resource Center (www.hospitalmedicine.org/copd) provides hospitalists with the most up-to-date guidelines, reviews, and peer-reviewed clinical trials that define evidence-based practice for the care of the COPD patient.
Hospitalists not only are under pressure to help improve hospital-level performance, but also will need to begin reporting physician-level measures. Beginning in 2015, CMS’s Physician Quality Reporting System (PQRS) will apply a penalty to all physicians who do not satisfactorily report data on quality measures for covered professional services.
The time to act is now. Reporting during the 2013 PQRS program year will be used to determine whether a 1.5% penalty applies in 2015. SHM has partnered with CECity to offer discounted access to PQRIwizard, a tool that facilitates PQRS reporting through SHM’s Learning Portal (www.shmlearningportal.org).
October is the beginning of a new year—in this case, fiscal-year 2014 for the Centers for Medicare & Medicaid Services (CMS). It’s a time when the new rules kick in. This month, we’ll look at some highlights, focusing on the new developments affecting your practice. Because you are held accountable for hospital-side performance on programs such as hospital value-based purchasing (HVBP) and the Readmissions Reduction Program, a working knowledge of the 2014 edition of the programs is crucial.
Close the Loop on HVBP
How will your hospital get paid under the 2014 version of HVBP? This past July, your hospital received a report outlining how its Medicare payments will be affected based on your hospital’s performance on process of care (heart failure, pneumonia, myocardial infarction, and surgery), patient experience (HCAHPS), and outcomes (30-day mortality for heart failure, pneumonia, and myocardial infarction).
Here are two hypothetical hospitals and how their performance in the program affects their 2014 payment. As background, in 2014, all hospitals have their base diagnosis related group (DRG) payments reduced by 1.25% for HVBP. They can earn back some, all, or an amount in excess of the 1.25% based on their performance. Payment is based on performance during the April 1 to Dec. 31, 2012, period. Under HVBP, CMS incentive payments occur at the level of individual patients, each of which is assigned a DRG.
Let’s look at two examples:
Hospital 1
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.48%.
- Net change in base DRG payment: +0.23%.
Hospital 2
- Base DRG payment reduction: 1.25% (all hospitals).
- Portion of base DRG earned back based on performance (process/patient experience/outcome metrics): 1.08%.
- Net change in base DRG payment: -0.17%.
Hospital 1 performed relatively well, getting a bump of 0.23% in its base DRG rate. Hospital 2 did not perform so well, so it took a 0.17% hit on its base DRG rate.
In order to determine total dollars made or lost for your hospital, one multiplies the total number of eligible Medicare inpatients for 2014 times the base DRG payment times the percent change in base DRG payment. If Hospital 1 has 10,000 eligible patients in 2014 and a base DRG payment of $5,000, the value is 10,000 x $5,000 x 0.0023 (0.23%) = $115,000 gained. Hospital 2, with the same number of patients and base DRG payment, loses (10,000 x $5,000 x 0.0017 = $85,000).
Readmissions and Penalties
For 2014, CMS is adding 30-day readmissions for COPD to readmissions for heart failure, pneumonia, and myocardial infarction for its penalty program. CMS added COPD because it is the fourth-leading cause of readmissions, according to a recent Medicare Payment Advisory Commission report, and because there is wide variation in the rates (from 18% to 25%) of COPD hospital readmissions.
For 2014, CMS raises the ceiling on readmission penalties to a maximum of 2% of reimbursement for all of a hospital’s Medicare inpatients. (The maximum hit during the first round of readmission penalties, which began in October 2012, was 1%.) More than 2,200 U.S. hospitals will face some financial penalty for excess 30-day readmissions.
Disappointingly, CMS did not add a risk adjustment for socioeconomic status despite being under pressure to do so. There is growing evidence that these factors have a major impact on readmission rates.1,2
New Definition of an Admission
Amidst confusion from many and major blowback from beneficiaries saddled with large out-of-pocket expenses for observation stays and subsequent skilled-nursing-facility stays, CMS is clarifying the definition of an inpatient admission. The agency will define an admission as a hospital stay that spans at least two midnights. If a patient is in the hospital for a shorter period of time, CMS will deem the patient to be on observation status, unless medical record documentation supports a physician’s expectation “that the beneficiary would need care spanning at least two midnights” but unanticipated events led to a shorter stay.
Plan of Attack
For HVBP, make contact with your director of quality to understand your hospital’s performance and payment for 2014. If you have incentive compensation riding on HVBP, make sure you understand how your employer or contracted hospital is calculating the payout (because, for example, the performance period was in 2012!) and that your hospitalist group understands the payout calculation.
For COPD readmissions prevention, ensure patients have a home management plan; appropriate specialist follow-up and that they understand medication use, including inhalers and supplemental oxygen; and that you consider early referral for pulmonary rehabilitation for eligible patients.
For the new definition of inpatient admission, work with your hospital’s physician advisor and case management to ensure your group is getting appropriate guidance on documentation requirements. You are probably being held accountable for your hospital’s total number of observation hours, so remember to track these metrics following implementation of the new rule, as they (hopefully) should decrease. If they do, take some of the credit!
References
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675-681.
- Lindenauer PK, Lagu T, Rothberg MB, et al. Income inequality and 30 day outcomes after acute myocardial infarction, heart failure, and pneumonia: retrospective cohort study. BMJ. 2013;346:f521.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Are Print Publications an Endangered Species?
A paradigm shift in scientific communication occurred in 1450 when Johannes Gutenberg invented the printing press. Before then, dissemination of information depended on the painstaking copying of manuscripts and books by monks in monasteries or the sharing of insights within a limited community by means of letters. A natural spinoff from the ability to mass produce written documents was the invention of the journal, the first one entirely devoted to science being the Philosophical Transactions of the Royal Society of London in 1665. Since then there has been a remarkably steady increase in the number of journals of 3.5% per year that brings us to the 2012 census of approximately 28,100 scholarly, peer-reviewed journals that collectively publish 1.9 million articles a year (The STM Report 2012. The Hague: International Association of Scientific, Technical and Medical Publishers). As a result, the publishing industry has flourished and billions of trees have been sacrificed to the cause of scientific communication.
The first sign of a decline in the paper flood appeared in 1991 when the initial electronic journal was published. The next paradigm shift in communication was about to take place. Now, nearly all of the greater than 28,000 journals have adopted this new technology and are available via the Internet. However, the move away from print publication has been more gradual with many journals still offering print as well as electronic editions.
There have been several reasons, some now outmoded, for preserving the print technology that is now more than half a millennium old. First is the issue of portability. When digital publications could only be read via computer, there was a significant inconvenience factor. But in 2013 there are few surgeons who do not possess one or more of the many portable digital devices that make the surgical literature readily accessible almost anywhere on the planet. Print’s advantage over digital in portability has clearly been negated by these devices. There has been concern in some quarters that without a paper print anchor there is risk that some scientific writings could be lost forever through a major Internet implosion or to a lesser extent from disappearance of a journal’s archives upon cessation of publication or termination of an electronic subscription. Recently developed digital preservation services such as Portico, LOCKSS and CLOCKSS (controlled lots of copies keep stuff safe) have been enlisted by libraries to ensure the safeguarding in perpetuity of the digitally published material they have purchased. These new approaches have proven highly reliable. Finally, advertisers who contribute a significant fraction of the revenue for many journals have been hesitant in some cases to display their wares online rather than in a print format. This appears to be gradually changing.
Despite these barriers, most of them perceived rather than real, there has been an ever-increasing shift from print to digital. Our medical libraries are leading the way. The Ebling Medical Library at the University of Wisconsin is likely typical. Of the 1,200 journals it receives at a cost of $1.2 million, only 37 are in print format. As a result, "the stacks" that represented quiet and comforting study space when we were students are disappearing with considerable savings for these often financially strapped institutions. Access to the majority of these electronic journals is purchased in packages from the major medical publishing houses such as Elsevier, Wolters Kluwer, and Wiley. Two-thirds of Elsevier’s revenue last year was based on digital products ("Global Publishing Leaders 2013: Reed Elsevier Group," Publishers’ Weekly, July 19, 2013. Website accessed 9/13/2013).
At the individual subscription level, a major impetus to keeping print publications afloat is the society owned or sponsored journal. Journals not associated with a society have experienced a marked decline in their print subscriptions over the past decade. As the number of surgeons accessing information from digital mobile devices reaches the tipping point, it is likely that the print edition of many surgical journals, even those affiliated with societies, will eventually disappear.
The logical conclusion from this analysis is that print editions of scientific journals are likely to be either nonexistent or rare within the next decade or two. Digital is less expensive, accessible almost anywhere, and provides increasingly efficient search engines to target one’s reading. Those of you who continue to prefer paper are best advised to purchase a good printer because the printed material you read in the future will likely be produced by you rather than by some distant publishing house.
Dr. Rikkers is Editor in Chief of Surgery News.
A paradigm shift in scientific communication occurred in 1450 when Johannes Gutenberg invented the printing press. Before then, dissemination of information depended on the painstaking copying of manuscripts and books by monks in monasteries or the sharing of insights within a limited community by means of letters. A natural spinoff from the ability to mass produce written documents was the invention of the journal, the first one entirely devoted to science being the Philosophical Transactions of the Royal Society of London in 1665. Since then there has been a remarkably steady increase in the number of journals of 3.5% per year that brings us to the 2012 census of approximately 28,100 scholarly, peer-reviewed journals that collectively publish 1.9 million articles a year (The STM Report 2012. The Hague: International Association of Scientific, Technical and Medical Publishers). As a result, the publishing industry has flourished and billions of trees have been sacrificed to the cause of scientific communication.
The first sign of a decline in the paper flood appeared in 1991 when the initial electronic journal was published. The next paradigm shift in communication was about to take place. Now, nearly all of the greater than 28,000 journals have adopted this new technology and are available via the Internet. However, the move away from print publication has been more gradual with many journals still offering print as well as electronic editions.
There have been several reasons, some now outmoded, for preserving the print technology that is now more than half a millennium old. First is the issue of portability. When digital publications could only be read via computer, there was a significant inconvenience factor. But in 2013 there are few surgeons who do not possess one or more of the many portable digital devices that make the surgical literature readily accessible almost anywhere on the planet. Print’s advantage over digital in portability has clearly been negated by these devices. There has been concern in some quarters that without a paper print anchor there is risk that some scientific writings could be lost forever through a major Internet implosion or to a lesser extent from disappearance of a journal’s archives upon cessation of publication or termination of an electronic subscription. Recently developed digital preservation services such as Portico, LOCKSS and CLOCKSS (controlled lots of copies keep stuff safe) have been enlisted by libraries to ensure the safeguarding in perpetuity of the digitally published material they have purchased. These new approaches have proven highly reliable. Finally, advertisers who contribute a significant fraction of the revenue for many journals have been hesitant in some cases to display their wares online rather than in a print format. This appears to be gradually changing.
Despite these barriers, most of them perceived rather than real, there has been an ever-increasing shift from print to digital. Our medical libraries are leading the way. The Ebling Medical Library at the University of Wisconsin is likely typical. Of the 1,200 journals it receives at a cost of $1.2 million, only 37 are in print format. As a result, "the stacks" that represented quiet and comforting study space when we were students are disappearing with considerable savings for these often financially strapped institutions. Access to the majority of these electronic journals is purchased in packages from the major medical publishing houses such as Elsevier, Wolters Kluwer, and Wiley. Two-thirds of Elsevier’s revenue last year was based on digital products ("Global Publishing Leaders 2013: Reed Elsevier Group," Publishers’ Weekly, July 19, 2013. Website accessed 9/13/2013).
At the individual subscription level, a major impetus to keeping print publications afloat is the society owned or sponsored journal. Journals not associated with a society have experienced a marked decline in their print subscriptions over the past decade. As the number of surgeons accessing information from digital mobile devices reaches the tipping point, it is likely that the print edition of many surgical journals, even those affiliated with societies, will eventually disappear.
The logical conclusion from this analysis is that print editions of scientific journals are likely to be either nonexistent or rare within the next decade or two. Digital is less expensive, accessible almost anywhere, and provides increasingly efficient search engines to target one’s reading. Those of you who continue to prefer paper are best advised to purchase a good printer because the printed material you read in the future will likely be produced by you rather than by some distant publishing house.
Dr. Rikkers is Editor in Chief of Surgery News.
A paradigm shift in scientific communication occurred in 1450 when Johannes Gutenberg invented the printing press. Before then, dissemination of information depended on the painstaking copying of manuscripts and books by monks in monasteries or the sharing of insights within a limited community by means of letters. A natural spinoff from the ability to mass produce written documents was the invention of the journal, the first one entirely devoted to science being the Philosophical Transactions of the Royal Society of London in 1665. Since then there has been a remarkably steady increase in the number of journals of 3.5% per year that brings us to the 2012 census of approximately 28,100 scholarly, peer-reviewed journals that collectively publish 1.9 million articles a year (The STM Report 2012. The Hague: International Association of Scientific, Technical and Medical Publishers). As a result, the publishing industry has flourished and billions of trees have been sacrificed to the cause of scientific communication.
The first sign of a decline in the paper flood appeared in 1991 when the initial electronic journal was published. The next paradigm shift in communication was about to take place. Now, nearly all of the greater than 28,000 journals have adopted this new technology and are available via the Internet. However, the move away from print publication has been more gradual with many journals still offering print as well as electronic editions.
There have been several reasons, some now outmoded, for preserving the print technology that is now more than half a millennium old. First is the issue of portability. When digital publications could only be read via computer, there was a significant inconvenience factor. But in 2013 there are few surgeons who do not possess one or more of the many portable digital devices that make the surgical literature readily accessible almost anywhere on the planet. Print’s advantage over digital in portability has clearly been negated by these devices. There has been concern in some quarters that without a paper print anchor there is risk that some scientific writings could be lost forever through a major Internet implosion or to a lesser extent from disappearance of a journal’s archives upon cessation of publication or termination of an electronic subscription. Recently developed digital preservation services such as Portico, LOCKSS and CLOCKSS (controlled lots of copies keep stuff safe) have been enlisted by libraries to ensure the safeguarding in perpetuity of the digitally published material they have purchased. These new approaches have proven highly reliable. Finally, advertisers who contribute a significant fraction of the revenue for many journals have been hesitant in some cases to display their wares online rather than in a print format. This appears to be gradually changing.
Despite these barriers, most of them perceived rather than real, there has been an ever-increasing shift from print to digital. Our medical libraries are leading the way. The Ebling Medical Library at the University of Wisconsin is likely typical. Of the 1,200 journals it receives at a cost of $1.2 million, only 37 are in print format. As a result, "the stacks" that represented quiet and comforting study space when we were students are disappearing with considerable savings for these often financially strapped institutions. Access to the majority of these electronic journals is purchased in packages from the major medical publishing houses such as Elsevier, Wolters Kluwer, and Wiley. Two-thirds of Elsevier’s revenue last year was based on digital products ("Global Publishing Leaders 2013: Reed Elsevier Group," Publishers’ Weekly, July 19, 2013. Website accessed 9/13/2013).
At the individual subscription level, a major impetus to keeping print publications afloat is the society owned or sponsored journal. Journals not associated with a society have experienced a marked decline in their print subscriptions over the past decade. As the number of surgeons accessing information from digital mobile devices reaches the tipping point, it is likely that the print edition of many surgical journals, even those affiliated with societies, will eventually disappear.
The logical conclusion from this analysis is that print editions of scientific journals are likely to be either nonexistent or rare within the next decade or two. Digital is less expensive, accessible almost anywhere, and provides increasingly efficient search engines to target one’s reading. Those of you who continue to prefer paper are best advised to purchase a good printer because the printed material you read in the future will likely be produced by you rather than by some distant publishing house.
Dr. Rikkers is Editor in Chief of Surgery News.

Ten tips for chronic venous ulcers
The underlying pathophysiology of chronic venous insufficiency is complex and involves many factors. Studies have shown that average venous ulcers may need 6-12 months for complete healing with an anticipated recurrence rate exceeding 2/3 cases in 5 years. These numbers reflect the magnitude of the problem and mandate deploying all efforts to stop progression of the disease. Our group has found the following 10 tips have significantly improved our healing rates.
1. First, rule out any associated arterial, immunologic, endocrine, or other systemic causes for leg/foot ulceration.
2. Be aggressive to stop progression of the disease (fight CEAP 6): any local tenderness at the site of discolored skin at the gaiter area for venous ulcers should initiate a prompt reflux study to evaluate for incompetent perforators.

3. Venous ulcers are associated with an incompetent perforator within 2 cm of the ulcer area.
4. Recurrent venous ulcers at the same location may be associated with venous outflow obstruction, (May-Thurner syndrome is an underestimated pathology) which affects mainly the left leg.
5. When performing iliac vein venograms, make liberal use of intravascular ultrasound.
6. Exudative venous ulcers need multilayer compression dressings and appropriate antibiotics if infection exists.
7. Pentoxifylline (Trental) 800 mg, 3 times daily.
8. Frequent debridement and frequent objective evaluation for ulcer area with each office visit.
9. Bi-layered living cell treatment (Apligraf?) to promote healing.
10. Office/clinic visit every 3 months after complete healing (CEAP 5) and further testing as needed.
Dr. Mousa is an associate professor at the Department of Surgery, West Virginia University, Morgantown.
The underlying pathophysiology of chronic venous insufficiency is complex and involves many factors. Studies have shown that average venous ulcers may need 6-12 months for complete healing with an anticipated recurrence rate exceeding 2/3 cases in 5 years. These numbers reflect the magnitude of the problem and mandate deploying all efforts to stop progression of the disease. Our group has found the following 10 tips have significantly improved our healing rates.
1. First, rule out any associated arterial, immunologic, endocrine, or other systemic causes for leg/foot ulceration.
2. Be aggressive to stop progression of the disease (fight CEAP 6): any local tenderness at the site of discolored skin at the gaiter area for venous ulcers should initiate a prompt reflux study to evaluate for incompetent perforators.
3. Venous ulcers are associated with an incompetent perforator within 2 cm of the ulcer area.
4. Recurrent venous ulcers at the same location may be associated with venous outflow obstruction, (May-Thurner syndrome is an underestimated pathology) which affects mainly the left leg.
5. When performing iliac vein venograms, make liberal use of intravascular ultrasound.
6. Exudative venous ulcers need multilayer compression dressings and appropriate antibiotics if infection exists.
7. Pentoxifylline (Trental) 800 mg, 3 times daily.
8. Frequent debridement and frequent objective evaluation for ulcer area with each office visit.
9. Bi-layered living cell treatment (Apligraf?) to promote healing.
10. Office/clinic visit every 3 months after complete healing (CEAP 5) and further testing as needed.
Dr. Mousa is an associate professor at the Department of Surgery, West Virginia University, Morgantown.
The underlying pathophysiology of chronic venous insufficiency is complex and involves many factors. Studies have shown that average venous ulcers may need 6-12 months for complete healing with an anticipated recurrence rate exceeding 2/3 cases in 5 years. These numbers reflect the magnitude of the problem and mandate deploying all efforts to stop progression of the disease. Our group has found the following 10 tips have significantly improved our healing rates.
1. First, rule out any associated arterial, immunologic, endocrine, or other systemic causes for leg/foot ulceration.
2. Be aggressive to stop progression of the disease (fight CEAP 6): any local tenderness at the site of discolored skin at the gaiter area for venous ulcers should initiate a prompt reflux study to evaluate for incompetent perforators.
3. Venous ulcers are associated with an incompetent perforator within 2 cm of the ulcer area.
4. Recurrent venous ulcers at the same location may be associated with venous outflow obstruction, (May-Thurner syndrome is an underestimated pathology) which affects mainly the left leg.
5. When performing iliac vein venograms, make liberal use of intravascular ultrasound.
6. Exudative venous ulcers need multilayer compression dressings and appropriate antibiotics if infection exists.
7. Pentoxifylline (Trental) 800 mg, 3 times daily.
8. Frequent debridement and frequent objective evaluation for ulcer area with each office visit.
9. Bi-layered living cell treatment (Apligraf?) to promote healing.
10. Office/clinic visit every 3 months after complete healing (CEAP 5) and further testing as needed.
Dr. Mousa is an associate professor at the Department of Surgery, West Virginia University, Morgantown.

Using CBT to decipher dreams
Ms. B is a 23-year-old white, married woman who first sought mental health treatment after experiencing depressive symptoms for 4 weeks following the birth of her first child. She endured guilt, hopelessness, anxiety, ruminative thoughts, and irrational fears of impending doom. Fortunately, her symptoms remitted soon after a trial of low-dose selective serotonin reuptake inhibitors (SSRIs). As the therapeutic relationship grew and Ms. B felt more comfortable with her psychiatrist, she acknowledged that she had endured years of low-grade anxiety and frequently experienced maladaptive thoughts that affected her self-esteem. Ms. B reports that she always had a "fear of failing in life." These beliefs were so entrenched and longstanding that she left college early, married, and started a family. Ms. B feels that her medication "puts her mind more at rest." She has a happier relationship with her husband and feels a greater sense of attachment to her baby. However, Ms. B expresses distress as a result of vivid dreams that began soon after she began treatment with SSRIs.
Ms. B is unable to recall the details of her dreams but is very bothered by them. We provided her with psychoeducation about the relationship between SSRIs and disruptive dreams. We informed her that most dreams that occur shortly before awakening are non-REM dreams, which are typical side effects of SSRIs and differ from REM dreams. She was relieved to learn that her reaction to medication is not unique, just as she was relieved to learn that postpartum depression affects up to 15% of new mothers (MMWR 2008;57:361-6)

We inquired as to whether the dreams are mostly visual or narrative, explaining that non-REM dreams typically tell stories in words rather than images. Non-REM dreams are more like novels than movies or comics. Ms. B maintains that she has little recall of those dreams, apart from the negative emotions that they evoke. She adds that she does not want to begin a "lengthy psychoanalysis" to understand her dreams, since her child care responsibilities leave her with barely enough time for brief 15- to 20-minute psychiatry visits.
We reassured Ms. B that even brief exploration of her dreams might have a therapeutic function. We suggested that she keep an old-fashioned telephone notepad at her bedside, with long, narrow strips that are just wide enough to write a name and number on. The goal is for her to jot down a word or two about her dreams – but nothing more – so that she can fall back asleep quickly. During the day, those few words will likely help jar her memory enough for her to expand upon her recollections. We recommended against her using her smartphone notepad, because the phone’s bright light could make her more alert and obstruct a quick return to sleep.
When Ms. B looked quizzical, we reminded her that this technique of dream note taking is favored by creative people who capture fleeting nighttime images and ideas for projects. Many patients enjoy learning that Romantic Movement poets such as Samuel Coleridge, as well as many Surrealist artists, turned their dreams into art ("Dreams in Myth, Medicine, and Movies," Westport, Conn.: Praeger, 2002).
Ms. B was able to capture the essence or "spirit" of her most disturbing dreams using this technique. She was both proud and embarrassed when she first brought in her notebook – proud, because she completed her assignment but embarrassed because of the dreams’ content. After being reassured that non-REM dreams tend to be bizarre and are not necessarily representative of the dreamer’s personal attitudes, she admitted that she dreamt about child sacrifice. She stressed that she would never harm her child. Nor did she experience similar daytime fantasies. Having observed her interactions with her infant, we were not concerned with an imminent risk of danger to her child. We used this information to normalize Ms. B’s experience while maintaining a nonjudgmental and supportive therapeutic space.
To reassure Ms. B that her unconscious was not the first to coin such unfathomable concepts, we reminded her that the motif of child sacrifice recurs in myth and religion ("The New Golden Bough: A New Abridgement of the Classic Work by Sir James Frazer," New York: Criterion, 1956). For example, Abraham almost sacrificed his son Isaac. The Bible mentions child sacrifice among Near Eastern goddess cults. This made sense to Ms. B, who had studied the Bible in religious school. She also acknowledged that she had wanted to major in anthropology prior to dropping out of college. She linked her ambivalence about bearing a child to her lapsed college studies, correctly perceiving that this conflict predisposed her to postpartum depression.
Had Ms. B expressed interest in exploratory therapy – or if we had doubts about her commitment to her child and ability to be a responsible caretaker – we would have referred her to additional resources. However, we sensed that she could be lost to treatment altogether if we demanded more treatment than she was ready to embrace. We drew inspiration from "High-Yield Cognitive-Behavior Therapy for Brief Sessions" (Arlington, Va.: American Psychiatric Publishing, 2010) and used the limited time available to ask targeted questions. Specifically, how did she react to tragic news about untreated postpartum depression?

We were not surprised to learn of Ms. B’s secret fears that her depression and dreams could progress to the level of Andrea Yates, the Texas woman with untreated psychosis who responded to delusions and hallucinations by murdering her five children in 2001. Again, we reassured Ms. B that many people share such fears, and that was one reason why the Yates case garnered such media attention. We pointed out differences between Ms. Yates’s life and that of Ms. B, stressing that Ms. B’s decision to seek timely treatment (instead of avoiding it), coupled with her husband’s support and the absence of psychosis dramatically distinguished her situation from Ms. Yates’s.
Ms. B accepted this explanation. Her distress subsided, and she gained a greater sense of self-efficacy. She remained in treatment, attending monthly appointments, and expressing joy about her baby. Ms. B revealed to us that she planned to return to college part time when her baby starts preschool.
Dr. Packer is an assistant clinical professor of psychiatry and behavioral sciences at Albert Einstein College of Medicine, New York, and is in private practice. Her most recent book is "Cinemas Sinister Psychiatrists: From Caligari to Hannibal" (Jefferson, N.C.: McFarland, 2012). Dr. Ascher is a postdoctoral fellow in addiction psychiatry at the University of Pennsylvania Perelman School of Medicine, Philadelphia, and a candidate at the New York University postdoctoral program in psychotherapy and psychoanalysis. He is a new Clinical Psychiatry News editorial advisory board member.
Ms. B is a 23-year-old white, married woman who first sought mental health treatment after experiencing depressive symptoms for 4 weeks following the birth of her first child. She endured guilt, hopelessness, anxiety, ruminative thoughts, and irrational fears of impending doom. Fortunately, her symptoms remitted soon after a trial of low-dose selective serotonin reuptake inhibitors (SSRIs). As the therapeutic relationship grew and Ms. B felt more comfortable with her psychiatrist, she acknowledged that she had endured years of low-grade anxiety and frequently experienced maladaptive thoughts that affected her self-esteem. Ms. B reports that she always had a "fear of failing in life." These beliefs were so entrenched and longstanding that she left college early, married, and started a family. Ms. B feels that her medication "puts her mind more at rest." She has a happier relationship with her husband and feels a greater sense of attachment to her baby. However, Ms. B expresses distress as a result of vivid dreams that began soon after she began treatment with SSRIs.
Ms. B is unable to recall the details of her dreams but is very bothered by them. We provided her with psychoeducation about the relationship between SSRIs and disruptive dreams. We informed her that most dreams that occur shortly before awakening are non-REM dreams, which are typical side effects of SSRIs and differ from REM dreams. She was relieved to learn that her reaction to medication is not unique, just as she was relieved to learn that postpartum depression affects up to 15% of new mothers (MMWR 2008;57:361-6)
We inquired as to whether the dreams are mostly visual or narrative, explaining that non-REM dreams typically tell stories in words rather than images. Non-REM dreams are more like novels than movies or comics. Ms. B maintains that she has little recall of those dreams, apart from the negative emotions that they evoke. She adds that she does not want to begin a "lengthy psychoanalysis" to understand her dreams, since her child care responsibilities leave her with barely enough time for brief 15- to 20-minute psychiatry visits.
We reassured Ms. B that even brief exploration of her dreams might have a therapeutic function. We suggested that she keep an old-fashioned telephone notepad at her bedside, with long, narrow strips that are just wide enough to write a name and number on. The goal is for her to jot down a word or two about her dreams – but nothing more – so that she can fall back asleep quickly. During the day, those few words will likely help jar her memory enough for her to expand upon her recollections. We recommended against her using her smartphone notepad, because the phone’s bright light could make her more alert and obstruct a quick return to sleep.
When Ms. B looked quizzical, we reminded her that this technique of dream note taking is favored by creative people who capture fleeting nighttime images and ideas for projects. Many patients enjoy learning that Romantic Movement poets such as Samuel Coleridge, as well as many Surrealist artists, turned their dreams into art ("Dreams in Myth, Medicine, and Movies," Westport, Conn.: Praeger, 2002).
Ms. B was able to capture the essence or "spirit" of her most disturbing dreams using this technique. She was both proud and embarrassed when she first brought in her notebook – proud, because she completed her assignment but embarrassed because of the dreams’ content. After being reassured that non-REM dreams tend to be bizarre and are not necessarily representative of the dreamer’s personal attitudes, she admitted that she dreamt about child sacrifice. She stressed that she would never harm her child. Nor did she experience similar daytime fantasies. Having observed her interactions with her infant, we were not concerned with an imminent risk of danger to her child. We used this information to normalize Ms. B’s experience while maintaining a nonjudgmental and supportive therapeutic space.
To reassure Ms. B that her unconscious was not the first to coin such unfathomable concepts, we reminded her that the motif of child sacrifice recurs in myth and religion ("The New Golden Bough: A New Abridgement of the Classic Work by Sir James Frazer," New York: Criterion, 1956). For example, Abraham almost sacrificed his son Isaac. The Bible mentions child sacrifice among Near Eastern goddess cults. This made sense to Ms. B, who had studied the Bible in religious school. She also acknowledged that she had wanted to major in anthropology prior to dropping out of college. She linked her ambivalence about bearing a child to her lapsed college studies, correctly perceiving that this conflict predisposed her to postpartum depression.
Had Ms. B expressed interest in exploratory therapy – or if we had doubts about her commitment to her child and ability to be a responsible caretaker – we would have referred her to additional resources. However, we sensed that she could be lost to treatment altogether if we demanded more treatment than she was ready to embrace. We drew inspiration from "High-Yield Cognitive-Behavior Therapy for Brief Sessions" (Arlington, Va.: American Psychiatric Publishing, 2010) and used the limited time available to ask targeted questions. Specifically, how did she react to tragic news about untreated postpartum depression?
We were not surprised to learn of Ms. B’s secret fears that her depression and dreams could progress to the level of Andrea Yates, the Texas woman with untreated psychosis who responded to delusions and hallucinations by murdering her five children in 2001. Again, we reassured Ms. B that many people share such fears, and that was one reason why the Yates case garnered such media attention. We pointed out differences between Ms. Yates’s life and that of Ms. B, stressing that Ms. B’s decision to seek timely treatment (instead of avoiding it), coupled with her husband’s support and the absence of psychosis dramatically distinguished her situation from Ms. Yates’s.
Ms. B accepted this explanation. Her distress subsided, and she gained a greater sense of self-efficacy. She remained in treatment, attending monthly appointments, and expressing joy about her baby. Ms. B revealed to us that she planned to return to college part time when her baby starts preschool.
Dr. Packer is an assistant clinical professor of psychiatry and behavioral sciences at Albert Einstein College of Medicine, New York, and is in private practice. Her most recent book is "Cinemas Sinister Psychiatrists: From Caligari to Hannibal" (Jefferson, N.C.: McFarland, 2012). Dr. Ascher is a postdoctoral fellow in addiction psychiatry at the University of Pennsylvania Perelman School of Medicine, Philadelphia, and a candidate at the New York University postdoctoral program in psychotherapy and psychoanalysis. He is a new Clinical Psychiatry News editorial advisory board member.
Ms. B is a 23-year-old white, married woman who first sought mental health treatment after experiencing depressive symptoms for 4 weeks following the birth of her first child. She endured guilt, hopelessness, anxiety, ruminative thoughts, and irrational fears of impending doom. Fortunately, her symptoms remitted soon after a trial of low-dose selective serotonin reuptake inhibitors (SSRIs). As the therapeutic relationship grew and Ms. B felt more comfortable with her psychiatrist, she acknowledged that she had endured years of low-grade anxiety and frequently experienced maladaptive thoughts that affected her self-esteem. Ms. B reports that she always had a "fear of failing in life." These beliefs were so entrenched and longstanding that she left college early, married, and started a family. Ms. B feels that her medication "puts her mind more at rest." She has a happier relationship with her husband and feels a greater sense of attachment to her baby. However, Ms. B expresses distress as a result of vivid dreams that began soon after she began treatment with SSRIs.
Ms. B is unable to recall the details of her dreams but is very bothered by them. We provided her with psychoeducation about the relationship between SSRIs and disruptive dreams. We informed her that most dreams that occur shortly before awakening are non-REM dreams, which are typical side effects of SSRIs and differ from REM dreams. She was relieved to learn that her reaction to medication is not unique, just as she was relieved to learn that postpartum depression affects up to 15% of new mothers (MMWR 2008;57:361-6)
We inquired as to whether the dreams are mostly visual or narrative, explaining that non-REM dreams typically tell stories in words rather than images. Non-REM dreams are more like novels than movies or comics. Ms. B maintains that she has little recall of those dreams, apart from the negative emotions that they evoke. She adds that she does not want to begin a "lengthy psychoanalysis" to understand her dreams, since her child care responsibilities leave her with barely enough time for brief 15- to 20-minute psychiatry visits.
We reassured Ms. B that even brief exploration of her dreams might have a therapeutic function. We suggested that she keep an old-fashioned telephone notepad at her bedside, with long, narrow strips that are just wide enough to write a name and number on. The goal is for her to jot down a word or two about her dreams – but nothing more – so that she can fall back asleep quickly. During the day, those few words will likely help jar her memory enough for her to expand upon her recollections. We recommended against her using her smartphone notepad, because the phone’s bright light could make her more alert and obstruct a quick return to sleep.
When Ms. B looked quizzical, we reminded her that this technique of dream note taking is favored by creative people who capture fleeting nighttime images and ideas for projects. Many patients enjoy learning that Romantic Movement poets such as Samuel Coleridge, as well as many Surrealist artists, turned their dreams into art ("Dreams in Myth, Medicine, and Movies," Westport, Conn.: Praeger, 2002).
Ms. B was able to capture the essence or "spirit" of her most disturbing dreams using this technique. She was both proud and embarrassed when she first brought in her notebook – proud, because she completed her assignment but embarrassed because of the dreams’ content. After being reassured that non-REM dreams tend to be bizarre and are not necessarily representative of the dreamer’s personal attitudes, she admitted that she dreamt about child sacrifice. She stressed that she would never harm her child. Nor did she experience similar daytime fantasies. Having observed her interactions with her infant, we were not concerned with an imminent risk of danger to her child. We used this information to normalize Ms. B’s experience while maintaining a nonjudgmental and supportive therapeutic space.
To reassure Ms. B that her unconscious was not the first to coin such unfathomable concepts, we reminded her that the motif of child sacrifice recurs in myth and religion ("The New Golden Bough: A New Abridgement of the Classic Work by Sir James Frazer," New York: Criterion, 1956). For example, Abraham almost sacrificed his son Isaac. The Bible mentions child sacrifice among Near Eastern goddess cults. This made sense to Ms. B, who had studied the Bible in religious school. She also acknowledged that she had wanted to major in anthropology prior to dropping out of college. She linked her ambivalence about bearing a child to her lapsed college studies, correctly perceiving that this conflict predisposed her to postpartum depression.
Had Ms. B expressed interest in exploratory therapy – or if we had doubts about her commitment to her child and ability to be a responsible caretaker – we would have referred her to additional resources. However, we sensed that she could be lost to treatment altogether if we demanded more treatment than she was ready to embrace. We drew inspiration from "High-Yield Cognitive-Behavior Therapy for Brief Sessions" (Arlington, Va.: American Psychiatric Publishing, 2010) and used the limited time available to ask targeted questions. Specifically, how did she react to tragic news about untreated postpartum depression?
We were not surprised to learn of Ms. B’s secret fears that her depression and dreams could progress to the level of Andrea Yates, the Texas woman with untreated psychosis who responded to delusions and hallucinations by murdering her five children in 2001. Again, we reassured Ms. B that many people share such fears, and that was one reason why the Yates case garnered such media attention. We pointed out differences between Ms. Yates’s life and that of Ms. B, stressing that Ms. B’s decision to seek timely treatment (instead of avoiding it), coupled with her husband’s support and the absence of psychosis dramatically distinguished her situation from Ms. Yates’s.
Ms. B accepted this explanation. Her distress subsided, and she gained a greater sense of self-efficacy. She remained in treatment, attending monthly appointments, and expressing joy about her baby. Ms. B revealed to us that she planned to return to college part time when her baby starts preschool.
Dr. Packer is an assistant clinical professor of psychiatry and behavioral sciences at Albert Einstein College of Medicine, New York, and is in private practice. Her most recent book is "Cinemas Sinister Psychiatrists: From Caligari to Hannibal" (Jefferson, N.C.: McFarland, 2012). Dr. Ascher is a postdoctoral fellow in addiction psychiatry at the University of Pennsylvania Perelman School of Medicine, Philadelphia, and a candidate at the New York University postdoctoral program in psychotherapy and psychoanalysis. He is a new Clinical Psychiatry News editorial advisory board member.
