User login
MGMA Physician Compensation Survey Raises Questions About Performance Pay

Sorting out whether a hospitalist’s bonus and other compensation elements are in line with survey data often leads to confusion. The 2013 MGMA Physician Compensation and Production Survey report, based on 2012 data, shows median compensation of $240,352 for internal-medicine hospitalists (I’ll round it to $240,000 for the rest of this piece). So is your compensation in line with survey medians if your base pay is $230,000 and you have a performance bonus of up to $20,000?
The problem is that you can’t know in advance how much of the $20,000 performance bonus you will earn. And isn’t a bonus supposed to be on top of typical compensation? To be in line with the survey, shouldn’t your base pay equal the $240,000 median, with any available bonus dollars on top of that? (Base pay means all forms of compensation other than a performance bonus; it could be productivity-based compensation, pay connected to numbers of shifts or hours worked, or a fixed annual salary, etc.)
The short answer is no, and to demonstrate why, I’ll first review some facts about the survey itself, then apply that knowledge to the hospitalist marketplace.
I want to emphasize that in this article, I’m not taking a position on the right amount of workload, compensation, or bonus for any hospitalist practice. And I’m using survey medians just to simplify the discussion, not because they’re optimal for any particular practice.
Survey Data
The most important thing to know about the survey data is that the $240,000 figure takes into account all forms of pay, including extra shift pay and any bonuses that might have been paid to each provider in the data set. Such benefits as health insurance and retirement-plan contribution are not included in this figure.
There are several ways a hospitalist might have earned compensation that matches the survey median. He or she might have a fixed annual salary equal to the median with no bonus available or had a meaningful bonus (e.g. $10,000 to $20,000) available and failed to earn any of it. Or the base might have come to $230,000, and he or she earned half of the available $20,000 performance bonus. Many other permutations of bonus and other salary elements could occur to arrive at the same $240,000 figure.
The important thing to remember is that whatever bonus dollars were paid, they are included in the salary figure from the survey—not added on top of that figure. So if all bonus dollars earned were subtracted from the survey, the total “nonbonus” compensation would be lower than $240,000.
How much lower?
Typical Hospitalist Bonus Amounts
The MGMA survey doesn’t report the portion of compensation tied to a bonus, but SHM’s does. SHM’s 2012 State of Hospital Medicine Report, based on 2011 data (www.hospitalmedicine.org/survey), is based on the most recent data available, and it showed (on page 60) that an average of 7% of pay was tied to performance for nonacademic hospitalist groups serving adults only. This included any payments for good individual or group performance on quality, efficiency, service, satisfaction, and/or other nonproduction measures. In conversation, this often is referred to as a “bonus” rather than “performance compensation.”
One way to estimate the nonbonus compensation would be to reduce the total pay by 7%, which comes to $223,200. Keep in mind that there are all kinds of mathematical and methodological problems in manipulating the reported survey numbers from two separate surveys to derive additional benchmarks. But this seems like a reasonable guess.
An increasing portion of hospitalist groups have some pay tied to performance, and the portion of total pay tied to performance seems to be going up at least a little. It was 5% of pay in 2010 and 4% in 2011, compared with 7% in the 2012 survey.
Keep in mind two things. First, this 7% reflects the performance or bonus dollars actually paid out, not the total amount available. In other words, even if the median total bonus dollars available were 20% of compensation, hospitalists earned less than that. Some hospitalists earned all dollars available, and some earned only a portion of what was available. And second, some hospitalists fail to earn any bonus or don’t have one available at all. So the survey would show for them zero compensation tied to bonus.
Making Sense of the Numbers
If you follow the reasoning above, then you probably agree that if your goal is to match mean compensation from the MGMA survey (I’m not suggesting that is the best goal, merely using it for simplicity), then you would set nonbonus compensation 7% below median—as long as you’re likely to get the same portion of a bonus as the median practice.
In some practices, performance thresholds are set at a level that is very easy to achieve, meaning the hospitalists are almost guaranteed to get all of the bonus compensation available. To be consistent with survey medians, it would be appropriate for them to set nonbonus compensation by subtracting all bonus dollars from the survey median. For example, if a $20,000 bonus is available and all of it is likely to be earned by the hospitalists, then total nonbonus compensation would be $220,000.
However, what if the bonus requires significant improvements in performance by the doctors (which seems most appropriate to me; why have a bonus otherwise?) and it is likely they will earn only 25% of all bonus dollars available? If the total available bonus is $20,000, then something like 25%, or $5,000, should be subtracted from the median to yield a total nonbonus compensation of $235,000.
Simple Thinking
I think it makes most sense to set total nonbonus compensation below the targeted total compensation. Failure to achieve any performance thresholds means no bonus and compensation will be below target that year. Meeting some thresholds (some improvement in performance) should result in matching the target compensation, and truly terrific performance that meets or exceeds all thresholds should result in the doctor being paid above the target.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Sorting out whether a hospitalist’s bonus and other compensation elements are in line with survey data often leads to confusion. The 2013 MGMA Physician Compensation and Production Survey report, based on 2012 data, shows median compensation of $240,352 for internal-medicine hospitalists (I’ll round it to $240,000 for the rest of this piece). So is your compensation in line with survey medians if your base pay is $230,000 and you have a performance bonus of up to $20,000?
The problem is that you can’t know in advance how much of the $20,000 performance bonus you will earn. And isn’t a bonus supposed to be on top of typical compensation? To be in line with the survey, shouldn’t your base pay equal the $240,000 median, with any available bonus dollars on top of that? (Base pay means all forms of compensation other than a performance bonus; it could be productivity-based compensation, pay connected to numbers of shifts or hours worked, or a fixed annual salary, etc.)
The short answer is no, and to demonstrate why, I’ll first review some facts about the survey itself, then apply that knowledge to the hospitalist marketplace.
I want to emphasize that in this article, I’m not taking a position on the right amount of workload, compensation, or bonus for any hospitalist practice. And I’m using survey medians just to simplify the discussion, not because they’re optimal for any particular practice.
Survey Data
The most important thing to know about the survey data is that the $240,000 figure takes into account all forms of pay, including extra shift pay and any bonuses that might have been paid to each provider in the data set. Such benefits as health insurance and retirement-plan contribution are not included in this figure.
There are several ways a hospitalist might have earned compensation that matches the survey median. He or she might have a fixed annual salary equal to the median with no bonus available or had a meaningful bonus (e.g. $10,000 to $20,000) available and failed to earn any of it. Or the base might have come to $230,000, and he or she earned half of the available $20,000 performance bonus. Many other permutations of bonus and other salary elements could occur to arrive at the same $240,000 figure.
The important thing to remember is that whatever bonus dollars were paid, they are included in the salary figure from the survey—not added on top of that figure. So if all bonus dollars earned were subtracted from the survey, the total “nonbonus” compensation would be lower than $240,000.
How much lower?
Typical Hospitalist Bonus Amounts
The MGMA survey doesn’t report the portion of compensation tied to a bonus, but SHM’s does. SHM’s 2012 State of Hospital Medicine Report, based on 2011 data (www.hospitalmedicine.org/survey), is based on the most recent data available, and it showed (on page 60) that an average of 7% of pay was tied to performance for nonacademic hospitalist groups serving adults only. This included any payments for good individual or group performance on quality, efficiency, service, satisfaction, and/or other nonproduction measures. In conversation, this often is referred to as a “bonus” rather than “performance compensation.”
One way to estimate the nonbonus compensation would be to reduce the total pay by 7%, which comes to $223,200. Keep in mind that there are all kinds of mathematical and methodological problems in manipulating the reported survey numbers from two separate surveys to derive additional benchmarks. But this seems like a reasonable guess.
An increasing portion of hospitalist groups have some pay tied to performance, and the portion of total pay tied to performance seems to be going up at least a little. It was 5% of pay in 2010 and 4% in 2011, compared with 7% in the 2012 survey.
Keep in mind two things. First, this 7% reflects the performance or bonus dollars actually paid out, not the total amount available. In other words, even if the median total bonus dollars available were 20% of compensation, hospitalists earned less than that. Some hospitalists earned all dollars available, and some earned only a portion of what was available. And second, some hospitalists fail to earn any bonus or don’t have one available at all. So the survey would show for them zero compensation tied to bonus.
Making Sense of the Numbers
If you follow the reasoning above, then you probably agree that if your goal is to match mean compensation from the MGMA survey (I’m not suggesting that is the best goal, merely using it for simplicity), then you would set nonbonus compensation 7% below median—as long as you’re likely to get the same portion of a bonus as the median practice.
In some practices, performance thresholds are set at a level that is very easy to achieve, meaning the hospitalists are almost guaranteed to get all of the bonus compensation available. To be consistent with survey medians, it would be appropriate for them to set nonbonus compensation by subtracting all bonus dollars from the survey median. For example, if a $20,000 bonus is available and all of it is likely to be earned by the hospitalists, then total nonbonus compensation would be $220,000.
However, what if the bonus requires significant improvements in performance by the doctors (which seems most appropriate to me; why have a bonus otherwise?) and it is likely they will earn only 25% of all bonus dollars available? If the total available bonus is $20,000, then something like 25%, or $5,000, should be subtracted from the median to yield a total nonbonus compensation of $235,000.
Simple Thinking
I think it makes most sense to set total nonbonus compensation below the targeted total compensation. Failure to achieve any performance thresholds means no bonus and compensation will be below target that year. Meeting some thresholds (some improvement in performance) should result in matching the target compensation, and truly terrific performance that meets or exceeds all thresholds should result in the doctor being paid above the target.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Sorting out whether a hospitalist’s bonus and other compensation elements are in line with survey data often leads to confusion. The 2013 MGMA Physician Compensation and Production Survey report, based on 2012 data, shows median compensation of $240,352 for internal-medicine hospitalists (I’ll round it to $240,000 for the rest of this piece). So is your compensation in line with survey medians if your base pay is $230,000 and you have a performance bonus of up to $20,000?
The problem is that you can’t know in advance how much of the $20,000 performance bonus you will earn. And isn’t a bonus supposed to be on top of typical compensation? To be in line with the survey, shouldn’t your base pay equal the $240,000 median, with any available bonus dollars on top of that? (Base pay means all forms of compensation other than a performance bonus; it could be productivity-based compensation, pay connected to numbers of shifts or hours worked, or a fixed annual salary, etc.)
The short answer is no, and to demonstrate why, I’ll first review some facts about the survey itself, then apply that knowledge to the hospitalist marketplace.
I want to emphasize that in this article, I’m not taking a position on the right amount of workload, compensation, or bonus for any hospitalist practice. And I’m using survey medians just to simplify the discussion, not because they’re optimal for any particular practice.
Survey Data
The most important thing to know about the survey data is that the $240,000 figure takes into account all forms of pay, including extra shift pay and any bonuses that might have been paid to each provider in the data set. Such benefits as health insurance and retirement-plan contribution are not included in this figure.
There are several ways a hospitalist might have earned compensation that matches the survey median. He or she might have a fixed annual salary equal to the median with no bonus available or had a meaningful bonus (e.g. $10,000 to $20,000) available and failed to earn any of it. Or the base might have come to $230,000, and he or she earned half of the available $20,000 performance bonus. Many other permutations of bonus and other salary elements could occur to arrive at the same $240,000 figure.
The important thing to remember is that whatever bonus dollars were paid, they are included in the salary figure from the survey—not added on top of that figure. So if all bonus dollars earned were subtracted from the survey, the total “nonbonus” compensation would be lower than $240,000.
How much lower?
Typical Hospitalist Bonus Amounts
The MGMA survey doesn’t report the portion of compensation tied to a bonus, but SHM’s does. SHM’s 2012 State of Hospital Medicine Report, based on 2011 data (www.hospitalmedicine.org/survey), is based on the most recent data available, and it showed (on page 60) that an average of 7% of pay was tied to performance for nonacademic hospitalist groups serving adults only. This included any payments for good individual or group performance on quality, efficiency, service, satisfaction, and/or other nonproduction measures. In conversation, this often is referred to as a “bonus” rather than “performance compensation.”
One way to estimate the nonbonus compensation would be to reduce the total pay by 7%, which comes to $223,200. Keep in mind that there are all kinds of mathematical and methodological problems in manipulating the reported survey numbers from two separate surveys to derive additional benchmarks. But this seems like a reasonable guess.
An increasing portion of hospitalist groups have some pay tied to performance, and the portion of total pay tied to performance seems to be going up at least a little. It was 5% of pay in 2010 and 4% in 2011, compared with 7% in the 2012 survey.
Keep in mind two things. First, this 7% reflects the performance or bonus dollars actually paid out, not the total amount available. In other words, even if the median total bonus dollars available were 20% of compensation, hospitalists earned less than that. Some hospitalists earned all dollars available, and some earned only a portion of what was available. And second, some hospitalists fail to earn any bonus or don’t have one available at all. So the survey would show for them zero compensation tied to bonus.
Making Sense of the Numbers
If you follow the reasoning above, then you probably agree that if your goal is to match mean compensation from the MGMA survey (I’m not suggesting that is the best goal, merely using it for simplicity), then you would set nonbonus compensation 7% below median—as long as you’re likely to get the same portion of a bonus as the median practice.
In some practices, performance thresholds are set at a level that is very easy to achieve, meaning the hospitalists are almost guaranteed to get all of the bonus compensation available. To be consistent with survey medians, it would be appropriate for them to set nonbonus compensation by subtracting all bonus dollars from the survey median. For example, if a $20,000 bonus is available and all of it is likely to be earned by the hospitalists, then total nonbonus compensation would be $220,000.
However, what if the bonus requires significant improvements in performance by the doctors (which seems most appropriate to me; why have a bonus otherwise?) and it is likely they will earn only 25% of all bonus dollars available? If the total available bonus is $20,000, then something like 25%, or $5,000, should be subtracted from the median to yield a total nonbonus compensation of $235,000.
Simple Thinking
I think it makes most sense to set total nonbonus compensation below the targeted total compensation. Failure to achieve any performance thresholds means no bonus and compensation will be below target that year. Meeting some thresholds (some improvement in performance) should result in matching the target compensation, and truly terrific performance that meets or exceeds all thresholds should result in the doctor being paid above the target.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Patient Satisfaction Surveys Not Accurate Measure of Hospitalists’ Performance

Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
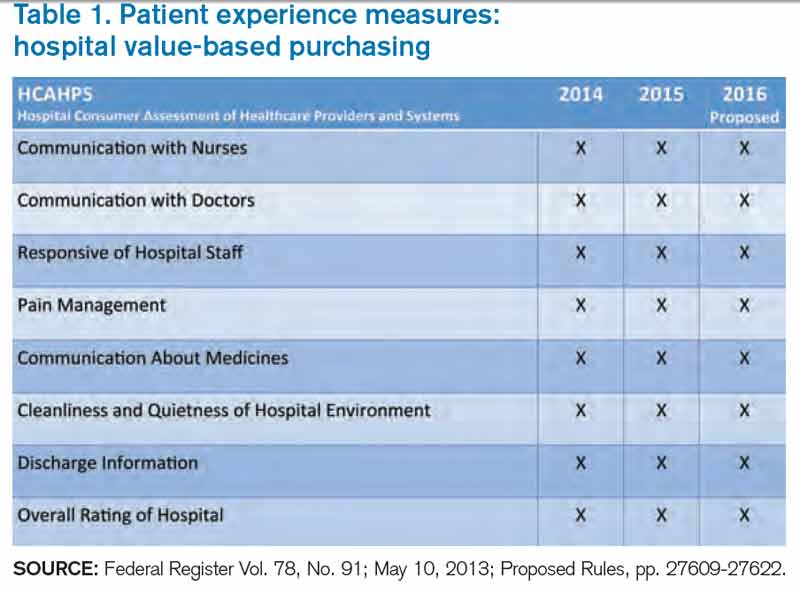
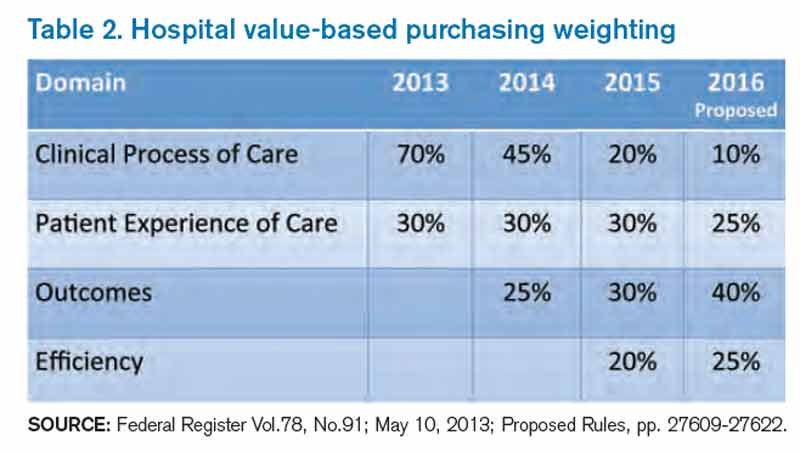
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Silencing science
Ever since the "age of enlightenment" dawned in the 17th century and emphasized an objective view of the natural world by means of the scientific method, free societies everywhere have prided themselves on making research findings from their laboratories readily available to all through the scientific literature. Such openness has had an incalculable beneficial effect on the advancement of science in all of its domains. Discoveries in one study often form the basis for novel lines of investigation by other research groups. The widespread accessibility to new findings has played a key role in the explosion of scientific knowledge that has occurred during the past three centuries.
Because of this cherished legacy of open access to new information, the scientific world was taken aback by the National Science Advisory Board for Biosecurity (NSABB) recommendation in late 2011 that manuscripts from two virology research groups – one at my home base, the University of Wisconsin-Madison, and the other at Rotterdam’s Erasmus Medical Centre – be revised prior to publication (Kawaoka Y: Flu transmission work is urgent. Nature 2012;482:155). The Board requested that the methodological details regarding the transmission of H5N1 virus in mammals be deleted from the manuscripts. The NSABB’s contention was that if such information became available to malefactors, it had the potential to be used for harmful rather than beneficial purposes.
Because of the lethality of the H5N1 virus in humans, these studies and future investigations engendered by them are of central importance. One only needs to recount the devastating effects of the "Spanish flu" that claimed up to 100 million lives early in the 20th century. Of the 570 known cases of H5N1 flu in humans, 60% have been fatal. All of these illnesses resulted from bird to human transmission. The key question the contentious investigations were attempting to answer is whether transmission of the virus is possible between mammals. The ferret that is evidently much like Homo sapiens when it comes to flu transmission was the experimental animal used.
The NSABB’s recommendation was highly controversial among scientists. Some supported a ban on such research until global guidelines could be developed for high-risk virus studies, while others contended that the benefits of making the detailed research findings widely available far outweighed the risks. They believed that even temporary suspension of research would delay the important scientific groundwork needed to be completed for H5N1 flu pandemic preparedness. The two involved scientists agreed to a voluntary ban on further investigations until guidelines were developed by the World Health Organization. These were published in 2012, and work on this key problem was resumed in laboratories able to meet the appropriate biosafety and biosecurity standards. Fortunately neither an increased number of cases nor an H5N1 flu pandemic developed in the interim.
The obvious ethical question underlying this imposed research moratorium is when, if ever, should free societies condone suppression of science? In the physical sciences that more frequently deal with matters of national security, such as weapons development, the boundaries of when to and when not to control research findings are much clearer. In contrast, when to impose limitations in the medical sciences is considerably murkier. In the example cited above, the NSABB felt compelled to act for two reasons. First, they wanted assurance that laboratories conducting this high-risk viral research met established biosafety and biosecurity standards. Few would question the appropriateness of such action. Second, they wished to prevent publication and thereby wide accessibility of newly acquired scientific information to avoid the remote possibility that it might be used for other than noble purposes. This consideration represents a much slipperier slope. In view of the virulence of the virus being tested, there is no doubt that H5N1 transmission studies are high risk. On the other hand, to withhold important, recently acquired information about this potentially deadly agent may impede research by other virologists who could contribute to eventual eradication of the threat, e.g., by development of an effective vaccine.
While the conundrum presented here has little to do with surgical science per se, it should make all of us in the greater scientific community ponder whether, when, and by whom limitations on communication of important research discoveries should be enforced. Offhand I cannot provide a scenario of a similar situation occurring within the surgical realm. However, seminal advancements in our craft have often depended on innovations in fields far removed from surgery. Only through the collective efforts of basic scientists and clinicians at the bedside and in the operating room can we unravel those secrets of nature so necessary to provide optimal care to our patients. How and when these discoveries are made available for the greater good does command our careful and thoughtful consideration.
Dr. Rikkers is Editor in Chief of Surgery News.
Ever since the "age of enlightenment" dawned in the 17th century and emphasized an objective view of the natural world by means of the scientific method, free societies everywhere have prided themselves on making research findings from their laboratories readily available to all through the scientific literature. Such openness has had an incalculable beneficial effect on the advancement of science in all of its domains. Discoveries in one study often form the basis for novel lines of investigation by other research groups. The widespread accessibility to new findings has played a key role in the explosion of scientific knowledge that has occurred during the past three centuries.
Because of this cherished legacy of open access to new information, the scientific world was taken aback by the National Science Advisory Board for Biosecurity (NSABB) recommendation in late 2011 that manuscripts from two virology research groups – one at my home base, the University of Wisconsin-Madison, and the other at Rotterdam’s Erasmus Medical Centre – be revised prior to publication (Kawaoka Y: Flu transmission work is urgent. Nature 2012;482:155). The Board requested that the methodological details regarding the transmission of H5N1 virus in mammals be deleted from the manuscripts. The NSABB’s contention was that if such information became available to malefactors, it had the potential to be used for harmful rather than beneficial purposes.
Because of the lethality of the H5N1 virus in humans, these studies and future investigations engendered by them are of central importance. One only needs to recount the devastating effects of the "Spanish flu" that claimed up to 100 million lives early in the 20th century. Of the 570 known cases of H5N1 flu in humans, 60% have been fatal. All of these illnesses resulted from bird to human transmission. The key question the contentious investigations were attempting to answer is whether transmission of the virus is possible between mammals. The ferret that is evidently much like Homo sapiens when it comes to flu transmission was the experimental animal used.
The NSABB’s recommendation was highly controversial among scientists. Some supported a ban on such research until global guidelines could be developed for high-risk virus studies, while others contended that the benefits of making the detailed research findings widely available far outweighed the risks. They believed that even temporary suspension of research would delay the important scientific groundwork needed to be completed for H5N1 flu pandemic preparedness. The two involved scientists agreed to a voluntary ban on further investigations until guidelines were developed by the World Health Organization. These were published in 2012, and work on this key problem was resumed in laboratories able to meet the appropriate biosafety and biosecurity standards. Fortunately neither an increased number of cases nor an H5N1 flu pandemic developed in the interim.
The obvious ethical question underlying this imposed research moratorium is when, if ever, should free societies condone suppression of science? In the physical sciences that more frequently deal with matters of national security, such as weapons development, the boundaries of when to and when not to control research findings are much clearer. In contrast, when to impose limitations in the medical sciences is considerably murkier. In the example cited above, the NSABB felt compelled to act for two reasons. First, they wanted assurance that laboratories conducting this high-risk viral research met established biosafety and biosecurity standards. Few would question the appropriateness of such action. Second, they wished to prevent publication and thereby wide accessibility of newly acquired scientific information to avoid the remote possibility that it might be used for other than noble purposes. This consideration represents a much slipperier slope. In view of the virulence of the virus being tested, there is no doubt that H5N1 transmission studies are high risk. On the other hand, to withhold important, recently acquired information about this potentially deadly agent may impede research by other virologists who could contribute to eventual eradication of the threat, e.g., by development of an effective vaccine.
While the conundrum presented here has little to do with surgical science per se, it should make all of us in the greater scientific community ponder whether, when, and by whom limitations on communication of important research discoveries should be enforced. Offhand I cannot provide a scenario of a similar situation occurring within the surgical realm. However, seminal advancements in our craft have often depended on innovations in fields far removed from surgery. Only through the collective efforts of basic scientists and clinicians at the bedside and in the operating room can we unravel those secrets of nature so necessary to provide optimal care to our patients. How and when these discoveries are made available for the greater good does command our careful and thoughtful consideration.
Dr. Rikkers is Editor in Chief of Surgery News.
Ever since the "age of enlightenment" dawned in the 17th century and emphasized an objective view of the natural world by means of the scientific method, free societies everywhere have prided themselves on making research findings from their laboratories readily available to all through the scientific literature. Such openness has had an incalculable beneficial effect on the advancement of science in all of its domains. Discoveries in one study often form the basis for novel lines of investigation by other research groups. The widespread accessibility to new findings has played a key role in the explosion of scientific knowledge that has occurred during the past three centuries.
Because of this cherished legacy of open access to new information, the scientific world was taken aback by the National Science Advisory Board for Biosecurity (NSABB) recommendation in late 2011 that manuscripts from two virology research groups – one at my home base, the University of Wisconsin-Madison, and the other at Rotterdam’s Erasmus Medical Centre – be revised prior to publication (Kawaoka Y: Flu transmission work is urgent. Nature 2012;482:155). The Board requested that the methodological details regarding the transmission of H5N1 virus in mammals be deleted from the manuscripts. The NSABB’s contention was that if such information became available to malefactors, it had the potential to be used for harmful rather than beneficial purposes.
Because of the lethality of the H5N1 virus in humans, these studies and future investigations engendered by them are of central importance. One only needs to recount the devastating effects of the "Spanish flu" that claimed up to 100 million lives early in the 20th century. Of the 570 known cases of H5N1 flu in humans, 60% have been fatal. All of these illnesses resulted from bird to human transmission. The key question the contentious investigations were attempting to answer is whether transmission of the virus is possible between mammals. The ferret that is evidently much like Homo sapiens when it comes to flu transmission was the experimental animal used.
The NSABB’s recommendation was highly controversial among scientists. Some supported a ban on such research until global guidelines could be developed for high-risk virus studies, while others contended that the benefits of making the detailed research findings widely available far outweighed the risks. They believed that even temporary suspension of research would delay the important scientific groundwork needed to be completed for H5N1 flu pandemic preparedness. The two involved scientists agreed to a voluntary ban on further investigations until guidelines were developed by the World Health Organization. These were published in 2012, and work on this key problem was resumed in laboratories able to meet the appropriate biosafety and biosecurity standards. Fortunately neither an increased number of cases nor an H5N1 flu pandemic developed in the interim.
The obvious ethical question underlying this imposed research moratorium is when, if ever, should free societies condone suppression of science? In the physical sciences that more frequently deal with matters of national security, such as weapons development, the boundaries of when to and when not to control research findings are much clearer. In contrast, when to impose limitations in the medical sciences is considerably murkier. In the example cited above, the NSABB felt compelled to act for two reasons. First, they wanted assurance that laboratories conducting this high-risk viral research met established biosafety and biosecurity standards. Few would question the appropriateness of such action. Second, they wished to prevent publication and thereby wide accessibility of newly acquired scientific information to avoid the remote possibility that it might be used for other than noble purposes. This consideration represents a much slipperier slope. In view of the virulence of the virus being tested, there is no doubt that H5N1 transmission studies are high risk. On the other hand, to withhold important, recently acquired information about this potentially deadly agent may impede research by other virologists who could contribute to eventual eradication of the threat, e.g., by development of an effective vaccine.
While the conundrum presented here has little to do with surgical science per se, it should make all of us in the greater scientific community ponder whether, when, and by whom limitations on communication of important research discoveries should be enforced. Offhand I cannot provide a scenario of a similar situation occurring within the surgical realm. However, seminal advancements in our craft have often depended on innovations in fields far removed from surgery. Only through the collective efforts of basic scientists and clinicians at the bedside and in the operating room can we unravel those secrets of nature so necessary to provide optimal care to our patients. How and when these discoveries are made available for the greater good does command our careful and thoughtful consideration.
Dr. Rikkers is Editor in Chief of Surgery News.

Bundled-Payment Program Basics

With general agreement that health-care costs in the U.S. are unsustainable, the Centers for Medicare & Medicaid Services (CMS), through the Center for Medicare and Medicaid Innovation (CMMI), and the private sector are embarking on new approaches to cost containment. On the one hand, we have value-based purchasing (VBP), which rests on the existing fee-for-service system and aims for incremental change. On the other hand, we have accountable-care organizations (ACOs), which provide a global payment for a population of patients, and bundled-payment programs, which provide a single payment for an episode of care. These reimbursement models represent a fundamental change in how we pay for health care.
On a broad scale, ACOs may be further along in development than bundled-payment programs, even though pockets of bundling prototypes have existed for years. Examples include the Prometheus payment system, Geisinger’s ProvenCare, and CMS’ Acute Care Episode demonstration project, which bundled Part A (hospital) and Part B (doctors, others) payments for cardiac and orthopedic surgery procedures. Over the past two years, we have seen a dramatic uptick in bundling activity, including programs in a number of states (including Arkansas, California, and Massachusetts). Here at Baystate Health in Massachusetts, we kicked off a total-hip-replacement bundle with our subsidiary health plan in January 2011.

Perhaps most notably, bundled payments are part of the Affordable Care Act. The Bundled Payments for Care Improvement initiative, launched earlier this year by CMMI, is enrolling traditional Medicare patients in bundled-payment programs across the country at more than 400 health systems.
How Bundled Payments Work
Bundled-payment programs provide a single payment to hospitals, doctors, post-acute providers, and other providers (for home care, lab, medical equipment, etc.) for a defined episode of care. Most bundles encompass at least an acute hospital episode and physician payments for the episode; many include some period after hospitalization, covering rehabilitation at a facility or at home and doctors’ visits during recovery. Bundling goes beyond Medicare’s diagnosis-related group (DRG) payments, which reimburse hospitals for all elements of an inpatient hospital stay for a given diagnosis but do not include services performed by nonhospital providers.
How do the finances work in a bundled-payment program? A single price for an episode of care is determined based on historical performance, factoring in all the services one wishes to include in a bundle (e.g. hospital, doctor visits in hospital, home physical therapy, follow-up doctor visits, follow up X-ray and labs for a defined time period). If the hospital, doctors, and others in the bundle generate new efficiencies in care (e.g. due to better care coordination, less wasteful test ordering, or lower implant/device costs), the savings are then distributed to these providers. What if spending exceeds the predetermined price? In some instances, the health plan bears the financial risk; in other instances, the hospital, physicians, and other bundle providers must pay back the shortfall. Important to note is that all sharing of savings is contingent on attainment of or improvement in demonstrated quality-of-care measures relevant to the bundle. In the future, bundling will evolve from shared savings to a single prospective payment for a care episode.
For now, most bundles encompass surgical procedures, although CMMI is working with health systems on several medical bundles, including acute MI, COPD, and stroke. All of these bundles are initiated by an acute hospitalization. Other types of bundles exist, such as with chronic conditions or with post-acute care only. In Massachusetts, a pediatric asthma bundle is being implemented through Medicaid, covering that population for a year or longer. The aim is to redirect dollars that normally would pay for ED visits and inpatient care to pay for interventions that promote better control of the disease and prevent acute flare-ups that lead to hospital visits.
How Hospitalists Fit In
To date, there has been little discussion of how physicians other than the surgeons doing the procedure (most bundles are for surgeries) fit into the clinical or financial model underpinning the program. However, with most patients in surgical or medical bundles being discharged to home, we now recognize that primary-care physicians (PCPs) will be essential to the success of a bundle.
Similarly, with medically complex patients enrolling in surgical bundles, hospitalists will be essential to the pre- and perioperative care of these patients. Also, transitioning bundle patients to home or to a rehabilitation will benefit from the involvement of a hospitalist.
What You Can Do Today
Although this might seem abstract for hospitalists practicing in the here and now, there are compelling opportunities for hospitalists who get involved in bundled-payment programs. Here’s what I suggest:
Find out if your hospital or post-acute facility is participating in bundling by looking at a map of CMMI bundle programs here: http://innovation.cms.gov/initiatives/bundled-payments;
- Get a seat at the table working on the bundle; and
- Negotiate a portion of the bundle’s shared savings on the basis of 1) increased efficiency and quality resulting from hospitalist involvement and 2) hospitalist direct oversight of bundled patients in post-acute facilities (if you choose).
Post-acute care may be new for your hospitalist program. Bundling programs are an important new business case for hospitalists in this setting.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
With general agreement that health-care costs in the U.S. are unsustainable, the Centers for Medicare & Medicaid Services (CMS), through the Center for Medicare and Medicaid Innovation (CMMI), and the private sector are embarking on new approaches to cost containment. On the one hand, we have value-based purchasing (VBP), which rests on the existing fee-for-service system and aims for incremental change. On the other hand, we have accountable-care organizations (ACOs), which provide a global payment for a population of patients, and bundled-payment programs, which provide a single payment for an episode of care. These reimbursement models represent a fundamental change in how we pay for health care.
On a broad scale, ACOs may be further along in development than bundled-payment programs, even though pockets of bundling prototypes have existed for years. Examples include the Prometheus payment system, Geisinger’s ProvenCare, and CMS’ Acute Care Episode demonstration project, which bundled Part A (hospital) and Part B (doctors, others) payments for cardiac and orthopedic surgery procedures. Over the past two years, we have seen a dramatic uptick in bundling activity, including programs in a number of states (including Arkansas, California, and Massachusetts). Here at Baystate Health in Massachusetts, we kicked off a total-hip-replacement bundle with our subsidiary health plan in January 2011.
Perhaps most notably, bundled payments are part of the Affordable Care Act. The Bundled Payments for Care Improvement initiative, launched earlier this year by CMMI, is enrolling traditional Medicare patients in bundled-payment programs across the country at more than 400 health systems.
How Bundled Payments Work
Bundled-payment programs provide a single payment to hospitals, doctors, post-acute providers, and other providers (for home care, lab, medical equipment, etc.) for a defined episode of care. Most bundles encompass at least an acute hospital episode and physician payments for the episode; many include some period after hospitalization, covering rehabilitation at a facility or at home and doctors’ visits during recovery. Bundling goes beyond Medicare’s diagnosis-related group (DRG) payments, which reimburse hospitals for all elements of an inpatient hospital stay for a given diagnosis but do not include services performed by nonhospital providers.
How do the finances work in a bundled-payment program? A single price for an episode of care is determined based on historical performance, factoring in all the services one wishes to include in a bundle (e.g. hospital, doctor visits in hospital, home physical therapy, follow-up doctor visits, follow up X-ray and labs for a defined time period). If the hospital, doctors, and others in the bundle generate new efficiencies in care (e.g. due to better care coordination, less wasteful test ordering, or lower implant/device costs), the savings are then distributed to these providers. What if spending exceeds the predetermined price? In some instances, the health plan bears the financial risk; in other instances, the hospital, physicians, and other bundle providers must pay back the shortfall. Important to note is that all sharing of savings is contingent on attainment of or improvement in demonstrated quality-of-care measures relevant to the bundle. In the future, bundling will evolve from shared savings to a single prospective payment for a care episode.
For now, most bundles encompass surgical procedures, although CMMI is working with health systems on several medical bundles, including acute MI, COPD, and stroke. All of these bundles are initiated by an acute hospitalization. Other types of bundles exist, such as with chronic conditions or with post-acute care only. In Massachusetts, a pediatric asthma bundle is being implemented through Medicaid, covering that population for a year or longer. The aim is to redirect dollars that normally would pay for ED visits and inpatient care to pay for interventions that promote better control of the disease and prevent acute flare-ups that lead to hospital visits.
How Hospitalists Fit In
To date, there has been little discussion of how physicians other than the surgeons doing the procedure (most bundles are for surgeries) fit into the clinical or financial model underpinning the program. However, with most patients in surgical or medical bundles being discharged to home, we now recognize that primary-care physicians (PCPs) will be essential to the success of a bundle.
Similarly, with medically complex patients enrolling in surgical bundles, hospitalists will be essential to the pre- and perioperative care of these patients. Also, transitioning bundle patients to home or to a rehabilitation will benefit from the involvement of a hospitalist.
What You Can Do Today
Although this might seem abstract for hospitalists practicing in the here and now, there are compelling opportunities for hospitalists who get involved in bundled-payment programs. Here’s what I suggest:
Find out if your hospital or post-acute facility is participating in bundling by looking at a map of CMMI bundle programs here: http://innovation.cms.gov/initiatives/bundled-payments;
- Get a seat at the table working on the bundle; and
- Negotiate a portion of the bundle’s shared savings on the basis of 1) increased efficiency and quality resulting from hospitalist involvement and 2) hospitalist direct oversight of bundled patients in post-acute facilities (if you choose).
Post-acute care may be new for your hospitalist program. Bundling programs are an important new business case for hospitalists in this setting.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
With general agreement that health-care costs in the U.S. are unsustainable, the Centers for Medicare & Medicaid Services (CMS), through the Center for Medicare and Medicaid Innovation (CMMI), and the private sector are embarking on new approaches to cost containment. On the one hand, we have value-based purchasing (VBP), which rests on the existing fee-for-service system and aims for incremental change. On the other hand, we have accountable-care organizations (ACOs), which provide a global payment for a population of patients, and bundled-payment programs, which provide a single payment for an episode of care. These reimbursement models represent a fundamental change in how we pay for health care.
On a broad scale, ACOs may be further along in development than bundled-payment programs, even though pockets of bundling prototypes have existed for years. Examples include the Prometheus payment system, Geisinger’s ProvenCare, and CMS’ Acute Care Episode demonstration project, which bundled Part A (hospital) and Part B (doctors, others) payments for cardiac and orthopedic surgery procedures. Over the past two years, we have seen a dramatic uptick in bundling activity, including programs in a number of states (including Arkansas, California, and Massachusetts). Here at Baystate Health in Massachusetts, we kicked off a total-hip-replacement bundle with our subsidiary health plan in January 2011.
Perhaps most notably, bundled payments are part of the Affordable Care Act. The Bundled Payments for Care Improvement initiative, launched earlier this year by CMMI, is enrolling traditional Medicare patients in bundled-payment programs across the country at more than 400 health systems.
How Bundled Payments Work
Bundled-payment programs provide a single payment to hospitals, doctors, post-acute providers, and other providers (for home care, lab, medical equipment, etc.) for a defined episode of care. Most bundles encompass at least an acute hospital episode and physician payments for the episode; many include some period after hospitalization, covering rehabilitation at a facility or at home and doctors’ visits during recovery. Bundling goes beyond Medicare’s diagnosis-related group (DRG) payments, which reimburse hospitals for all elements of an inpatient hospital stay for a given diagnosis but do not include services performed by nonhospital providers.
How do the finances work in a bundled-payment program? A single price for an episode of care is determined based on historical performance, factoring in all the services one wishes to include in a bundle (e.g. hospital, doctor visits in hospital, home physical therapy, follow-up doctor visits, follow up X-ray and labs for a defined time period). If the hospital, doctors, and others in the bundle generate new efficiencies in care (e.g. due to better care coordination, less wasteful test ordering, or lower implant/device costs), the savings are then distributed to these providers. What if spending exceeds the predetermined price? In some instances, the health plan bears the financial risk; in other instances, the hospital, physicians, and other bundle providers must pay back the shortfall. Important to note is that all sharing of savings is contingent on attainment of or improvement in demonstrated quality-of-care measures relevant to the bundle. In the future, bundling will evolve from shared savings to a single prospective payment for a care episode.
For now, most bundles encompass surgical procedures, although CMMI is working with health systems on several medical bundles, including acute MI, COPD, and stroke. All of these bundles are initiated by an acute hospitalization. Other types of bundles exist, such as with chronic conditions or with post-acute care only. In Massachusetts, a pediatric asthma bundle is being implemented through Medicaid, covering that population for a year or longer. The aim is to redirect dollars that normally would pay for ED visits and inpatient care to pay for interventions that promote better control of the disease and prevent acute flare-ups that lead to hospital visits.
How Hospitalists Fit In
To date, there has been little discussion of how physicians other than the surgeons doing the procedure (most bundles are for surgeries) fit into the clinical or financial model underpinning the program. However, with most patients in surgical or medical bundles being discharged to home, we now recognize that primary-care physicians (PCPs) will be essential to the success of a bundle.
Similarly, with medically complex patients enrolling in surgical bundles, hospitalists will be essential to the pre- and perioperative care of these patients. Also, transitioning bundle patients to home or to a rehabilitation will benefit from the involvement of a hospitalist.
What You Can Do Today
Although this might seem abstract for hospitalists practicing in the here and now, there are compelling opportunities for hospitalists who get involved in bundled-payment programs. Here’s what I suggest:
Find out if your hospital or post-acute facility is participating in bundling by looking at a map of CMMI bundle programs here: http://innovation.cms.gov/initiatives/bundled-payments;
- Get a seat at the table working on the bundle; and
- Negotiate a portion of the bundle’s shared savings on the basis of 1) increased efficiency and quality resulting from hospitalist involvement and 2) hospitalist direct oversight of bundled patients in post-acute facilities (if you choose).
Post-acute care may be new for your hospitalist program. Bundling programs are an important new business case for hospitalists in this setting.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Why Hospitalists Should Provide Patients with Discharge Summaries

I continue to believe that hospitalists should routinely provide patients a copy of their discharge summary. I made the case for this in a 2006 column (“Keeping Patients in the Loop,” October 2006, p. 74), but I don’t see the idea catching on. I bet this simple act would have all kinds of benefits, including at least modest reductions in overall health-care expenditures and readmissions.
The whole dynamic of this issue seems to be changing as a result of “patient portals” allowing direct access to review test results and, in some cases, physician documentation. Typically, these are integrated with or at least connected to an electronic health record (EHR) and allow a patient, and those provided access (e.g. the password) by the patient, to review records. My own PCP provides access to a portal that I’ve found very useful, but I think, like most others, it doesn’t provide access to physician notes.
So there still is a case to be made for hospitalists (and all specialties) to provide copies of the discharge summary directly to patients and perhaps other forms of documentation as well.
Timeliness
I think all discharge summaries should be completed before the patient leaves the hospital and amended as needed to capture any last-minute changes and details. The act of generating the summary often leads the discharging doctor to notice, and have a chance to address, important details that may have dropped off the daily problem list. Things like the need to recheck a lab test to ensure normalization prior to discharge, or make arrangements for outpatient colonoscopy to pursue the heme-positive stool found on admission, have sometimes slipped off the radar during the hospital stay and can be caught when preparing discharge summary.
Preparing a discharge summary the night before anticipated discharge can have many advantages, including improving early discharge times the next morning. And it means the doctor can prepare the summary late in the day after routine rounding is finished and interruptions are less likely. Although I think quality of care is enhanced by generating the summary the night before (and amending it as needed), I worked with a hospital that was cited by the Centers for Medicare & Medicaid Services (CMS) for doing this and was told they can’t be done prior to the calendar day of discharge.
Creation of the discharge summary isn’t the only relevant step. It should be transcribed on a stat basis (e.g. within two to four hours) and pushed to the PCP and other treating physicians. It isn’t enough that the document is available to the PCP via an EHR; these doctors need some sort of notice, such as an email.
To take advantage of the new “transitional-care management” codes (99495 and 99496), PCPs must make telephone contact with patients within two days of discharge and must have a face-to-face visit within one or two weeks of discharge (depending on whether the patient is high- or moderate-risk). Making the summary available to the PCP quickly can be crucial in ensuring these phone calls and visits are meaningful. (For an excellent review of the TCM codes, see Dr. Lauren Doctoroff’s article “New Codes Bridge Hospitals’ Post-Discharge Billing Gap” in the February 2013 issue of The Hospitalist.)
So I think both patients and other treating physicians should get the discharge summary on the day of discharge or no more than a day or two after. I bet this improves quality of care and readmissions, but one study found no association, and another found a trend toward reduced readmissions that did not reach statistical significance.1,2
Content
Just what information should go in a discharge summary? There are lots of opinions here, but it is worth starting with the components required by The Joint Commission. (You were aware of these, right?) The commission requires:
- Reason for hospitalization;
- Significant findings;
- Procedures and treatment provided;
- Patient’s discharge condition;
- Patient and family instructions; and
- Attending physician’s signature
To this list, I would add enumeration of tests pending at discharge.
The May/June 2005 issue of The Hospitalist has a terrific article by three thoughtful hospitalists titled “Advancing Toward the Ideal Hospital Discharge for the Elderly Patient.” It summarizes a 2005 workshop at the SHM annual meeting that produced a checklist of elements to consider including in every summary.
Brevity is a worthwhile goal but not at the expense of conveying the thought processes behind decisions. Things like how a decision was made to pursue watchful waiting versus aggressive workup now should be spelled out. Was it simply patient preference? It is common to start a trial of a medical therapy during a hospital stay, and it should be made clear that its effect should be assessed and a deliberate decision regarding continuing or stopping the therapy will be needed after discharge.
Lots of things need context and explanation for subsequent caregivers.
Format
The hospital in which I practice recently switched to a new EHR, and our hospitalist group has talked some about all of us using the same basic template for our notes. This should be valuable to all other caregivers who read a reasonable number of our notes and might improve our communication with one another around handoffs, etc. Although we haven’t reached a final decision about this, I’m an advocate for a shared template rather than each doctor using his or her own. This would be a worthwhile thing for all groups to consider.

Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
References
I continue to believe that hospitalists should routinely provide patients a copy of their discharge summary. I made the case for this in a 2006 column (“Keeping Patients in the Loop,” October 2006, p. 74), but I don’t see the idea catching on. I bet this simple act would have all kinds of benefits, including at least modest reductions in overall health-care expenditures and readmissions.
The whole dynamic of this issue seems to be changing as a result of “patient portals” allowing direct access to review test results and, in some cases, physician documentation. Typically, these are integrated with or at least connected to an electronic health record (EHR) and allow a patient, and those provided access (e.g. the password) by the patient, to review records. My own PCP provides access to a portal that I’ve found very useful, but I think, like most others, it doesn’t provide access to physician notes.
So there still is a case to be made for hospitalists (and all specialties) to provide copies of the discharge summary directly to patients and perhaps other forms of documentation as well.
Timeliness
I think all discharge summaries should be completed before the patient leaves the hospital and amended as needed to capture any last-minute changes and details. The act of generating the summary often leads the discharging doctor to notice, and have a chance to address, important details that may have dropped off the daily problem list. Things like the need to recheck a lab test to ensure normalization prior to discharge, or make arrangements for outpatient colonoscopy to pursue the heme-positive stool found on admission, have sometimes slipped off the radar during the hospital stay and can be caught when preparing discharge summary.
Preparing a discharge summary the night before anticipated discharge can have many advantages, including improving early discharge times the next morning. And it means the doctor can prepare the summary late in the day after routine rounding is finished and interruptions are less likely. Although I think quality of care is enhanced by generating the summary the night before (and amending it as needed), I worked with a hospital that was cited by the Centers for Medicare & Medicaid Services (CMS) for doing this and was told they can’t be done prior to the calendar day of discharge.
Creation of the discharge summary isn’t the only relevant step. It should be transcribed on a stat basis (e.g. within two to four hours) and pushed to the PCP and other treating physicians. It isn’t enough that the document is available to the PCP via an EHR; these doctors need some sort of notice, such as an email.
To take advantage of the new “transitional-care management” codes (99495 and 99496), PCPs must make telephone contact with patients within two days of discharge and must have a face-to-face visit within one or two weeks of discharge (depending on whether the patient is high- or moderate-risk). Making the summary available to the PCP quickly can be crucial in ensuring these phone calls and visits are meaningful. (For an excellent review of the TCM codes, see Dr. Lauren Doctoroff’s article “New Codes Bridge Hospitals’ Post-Discharge Billing Gap” in the February 2013 issue of The Hospitalist.)
So I think both patients and other treating physicians should get the discharge summary on the day of discharge or no more than a day or two after. I bet this improves quality of care and readmissions, but one study found no association, and another found a trend toward reduced readmissions that did not reach statistical significance.1,2
Content
Just what information should go in a discharge summary? There are lots of opinions here, but it is worth starting with the components required by The Joint Commission. (You were aware of these, right?) The commission requires:
- Reason for hospitalization;
- Significant findings;
- Procedures and treatment provided;
- Patient’s discharge condition;
- Patient and family instructions; and
- Attending physician’s signature
To this list, I would add enumeration of tests pending at discharge.
The May/June 2005 issue of The Hospitalist has a terrific article by three thoughtful hospitalists titled “Advancing Toward the Ideal Hospital Discharge for the Elderly Patient.” It summarizes a 2005 workshop at the SHM annual meeting that produced a checklist of elements to consider including in every summary.
Brevity is a worthwhile goal but not at the expense of conveying the thought processes behind decisions. Things like how a decision was made to pursue watchful waiting versus aggressive workup now should be spelled out. Was it simply patient preference? It is common to start a trial of a medical therapy during a hospital stay, and it should be made clear that its effect should be assessed and a deliberate decision regarding continuing or stopping the therapy will be needed after discharge.
Lots of things need context and explanation for subsequent caregivers.
Format
The hospital in which I practice recently switched to a new EHR, and our hospitalist group has talked some about all of us using the same basic template for our notes. This should be valuable to all other caregivers who read a reasonable number of our notes and might improve our communication with one another around handoffs, etc. Although we haven’t reached a final decision about this, I’m an advocate for a shared template rather than each doctor using his or her own. This would be a worthwhile thing for all groups to consider.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
References
I continue to believe that hospitalists should routinely provide patients a copy of their discharge summary. I made the case for this in a 2006 column (“Keeping Patients in the Loop,” October 2006, p. 74), but I don’t see the idea catching on. I bet this simple act would have all kinds of benefits, including at least modest reductions in overall health-care expenditures and readmissions.
The whole dynamic of this issue seems to be changing as a result of “patient portals” allowing direct access to review test results and, in some cases, physician documentation. Typically, these are integrated with or at least connected to an electronic health record (EHR) and allow a patient, and those provided access (e.g. the password) by the patient, to review records. My own PCP provides access to a portal that I’ve found very useful, but I think, like most others, it doesn’t provide access to physician notes.
So there still is a case to be made for hospitalists (and all specialties) to provide copies of the discharge summary directly to patients and perhaps other forms of documentation as well.
Timeliness
I think all discharge summaries should be completed before the patient leaves the hospital and amended as needed to capture any last-minute changes and details. The act of generating the summary often leads the discharging doctor to notice, and have a chance to address, important details that may have dropped off the daily problem list. Things like the need to recheck a lab test to ensure normalization prior to discharge, or make arrangements for outpatient colonoscopy to pursue the heme-positive stool found on admission, have sometimes slipped off the radar during the hospital stay and can be caught when preparing discharge summary.
Preparing a discharge summary the night before anticipated discharge can have many advantages, including improving early discharge times the next morning. And it means the doctor can prepare the summary late in the day after routine rounding is finished and interruptions are less likely. Although I think quality of care is enhanced by generating the summary the night before (and amending it as needed), I worked with a hospital that was cited by the Centers for Medicare & Medicaid Services (CMS) for doing this and was told they can’t be done prior to the calendar day of discharge.
Creation of the discharge summary isn’t the only relevant step. It should be transcribed on a stat basis (e.g. within two to four hours) and pushed to the PCP and other treating physicians. It isn’t enough that the document is available to the PCP via an EHR; these doctors need some sort of notice, such as an email.
To take advantage of the new “transitional-care management” codes (99495 and 99496), PCPs must make telephone contact with patients within two days of discharge and must have a face-to-face visit within one or two weeks of discharge (depending on whether the patient is high- or moderate-risk). Making the summary available to the PCP quickly can be crucial in ensuring these phone calls and visits are meaningful. (For an excellent review of the TCM codes, see Dr. Lauren Doctoroff’s article “New Codes Bridge Hospitals’ Post-Discharge Billing Gap” in the February 2013 issue of The Hospitalist.)
So I think both patients and other treating physicians should get the discharge summary on the day of discharge or no more than a day or two after. I bet this improves quality of care and readmissions, but one study found no association, and another found a trend toward reduced readmissions that did not reach statistical significance.1,2
Content
Just what information should go in a discharge summary? There are lots of opinions here, but it is worth starting with the components required by The Joint Commission. (You were aware of these, right?) The commission requires:
- Reason for hospitalization;
- Significant findings;
- Procedures and treatment provided;
- Patient’s discharge condition;
- Patient and family instructions; and
- Attending physician’s signature
To this list, I would add enumeration of tests pending at discharge.
The May/June 2005 issue of The Hospitalist has a terrific article by three thoughtful hospitalists titled “Advancing Toward the Ideal Hospital Discharge for the Elderly Patient.” It summarizes a 2005 workshop at the SHM annual meeting that produced a checklist of elements to consider including in every summary.
Brevity is a worthwhile goal but not at the expense of conveying the thought processes behind decisions. Things like how a decision was made to pursue watchful waiting versus aggressive workup now should be spelled out. Was it simply patient preference? It is common to start a trial of a medical therapy during a hospital stay, and it should be made clear that its effect should be assessed and a deliberate decision regarding continuing or stopping the therapy will be needed after discharge.
Lots of things need context and explanation for subsequent caregivers.
Format
The hospital in which I practice recently switched to a new EHR, and our hospitalist group has talked some about all of us using the same basic template for our notes. This should be valuable to all other caregivers who read a reasonable number of our notes and might improve our communication with one another around handoffs, etc. Although we haven’t reached a final decision about this, I’m an advocate for a shared template rather than each doctor using his or her own. This would be a worthwhile thing for all groups to consider.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
References
CBT underused, undervalued
Recently, I conducted a rather unscientific survey. I asked a few psychotherapists how they would treat a patient with whom I had worked successfully in the past.
The patient is a 39-year-old single woman who is a successful attorney. Despite her career success, the patient’s personal and social life had been replete with conflicts, especially surrounding her relationships with men. In our work together, these issues resolved when I used a cognitive-behavioral approach with her. But just as we were wrapping things up, an unexpected issue surfaced.

She told me that at age 20, she had studied abroad for a year in Europe with her closest female friend. It seems that my patient’s friend was successfully married and the mother of four children – all under age 10. She also was an attorney but was now working part time. And now, years later, the patient reported despair and unhappiness about "not seeing her anymore."
My survey began by asking numerous therapists what their approach would be to this woman’s dilemma. All of them knew about cognitive-behavioral therapy (CBT), reported using it, and endorsed using the technique to help this patient. However, the more we talked, it became clear that they were discussing traditional psychodynamic psychotherapy rather than the type of therapy started by Albert Ellis, Ph.D., in the 1950s as rational emotive behavior therapy, and later refined and codified as CBT by Dr. Aaron T. Beck in the 1960s and 1970s. In other words, my colleagues were not viewing this patient’s fears, distress, and even anger about losing her longtime friend in "here and now" terms.
They told me that they would ask questions like "How does that make you feel?" and "What memories came to mind?" as well as the usual series of exploratory, open-ended questions and interpretations. "You need to discuss this with her and ‘get it out there,’ " one of the therapists suggested. Wrong.
Admittedly, my patient’s past was marked by perceived abandonment, including a parental divorce; the loss of an older sister; and the constant switching of schools, because her mother moved several times. I agree that a psychodynamic style in this particular case might indeed have gotten to the root of the problem – at some point. But this approach is different from CBT, which circumscribes the problem, challenges faulty beliefs, and develops avenues for change in a reasonably short period of time.
I was able to make quick progress with this patient by asking her a simple question: "When did you last see your friend?" The answer, not surprising for "all or nothing" responders, was that she had seen her the previous week – but only for a quick 45-minute lunch. And the week before that, the two had met up at the local gym and taken a class together, but "we didn’t talk much," my patient observed. My response to the patient was that she did indeed see and spend time with her friend, but not as much as she had when the friend was single and childless. Isn’t this the case? I asked. "Yes, yes that’s the case, I do see her, but, but, but ..."
As the patient and I proceeded through the thinking therapy of CBT, she was able to recognize that she did see her friend but not as much. It became easier for the patient to understand that her friend’s life had changed dramatically and that her availability was limited because her friend’s family and work responsibilities kept her busy. The patient also began to realize that her own availability also had become more limited since she was 20.
The process of working with this patient using CBT involved more than one question and answer. The approach starts out as homing in on the "all or nothing" negative-type generalized thinking, and is clearly aimed at resolving the patient’s distortions, and focusing on developing a new perspective and new way of thinking about this particular issue. Changing the thought process in this particular context is aimed at getting the patient to extrapolate to better processing in other contexts.
In addition, it is important to note that a psychodynamic approach can be incorporated into CBT as a teaching model. In this case, I found that bringing into the picture past events that had influenced the patient’s current distorted thinking helped the patient get a more honest picture of this long friendship. Her newfound perspective on that relationship spilled over into other aspects of my patient’s life in a positive way.
CBT is not only helpful for patients dealing with anxiety, depression, or lifetime personality styles and behaviors that cause them some form of distress in everyday living. A study soon to be published in the Journal of Behavior Therapy and Experimental Psychiatry suggests that CBT also might prove beneficial for negative symptoms in outpatients with disorders on the schizophrenia spectrum.
After 20 sessions of CBT over a 6-month period, the investigators found that patients reported a decrease in the number of dysfunctional beliefs about their own "cognitive abilities, performance, emotional experience, and social exclusion" (J. Behav. Ther. Exp. Psychiatry 2013;44:300-6). This was a small study (n = 21), and as the investigators noted, randomized controlled trials are needed. Still, this study is a reminder that focusing on problem resolution in a few highly focused sessions also can help patients with serious mental illness.
Those findings notwithstanding, CBT is certainly no panacea for numerous psychotic disorders. But in light of its superb track record of resolving many emotional problems, I believe that it should be used more as a mainstay of treatment and that anyone coming out of a mental health training program – whether psychiatrists, psychologists, mental health social workers, or psychiatric nurse practitioners – should be just as adept at using CBT as they are in using psychodynamic psychotherapy or medication management.
Dr. London is a psychiatrist affiliated with the New York University Langone Medical Center. He has no conflicts of interest to disclose.
Recently, I conducted a rather unscientific survey. I asked a few psychotherapists how they would treat a patient with whom I had worked successfully in the past.
The patient is a 39-year-old single woman who is a successful attorney. Despite her career success, the patient’s personal and social life had been replete with conflicts, especially surrounding her relationships with men. In our work together, these issues resolved when I used a cognitive-behavioral approach with her. But just as we were wrapping things up, an unexpected issue surfaced.
She told me that at age 20, she had studied abroad for a year in Europe with her closest female friend. It seems that my patient’s friend was successfully married and the mother of four children – all under age 10. She also was an attorney but was now working part time. And now, years later, the patient reported despair and unhappiness about "not seeing her anymore."
My survey began by asking numerous therapists what their approach would be to this woman’s dilemma. All of them knew about cognitive-behavioral therapy (CBT), reported using it, and endorsed using the technique to help this patient. However, the more we talked, it became clear that they were discussing traditional psychodynamic psychotherapy rather than the type of therapy started by Albert Ellis, Ph.D., in the 1950s as rational emotive behavior therapy, and later refined and codified as CBT by Dr. Aaron T. Beck in the 1960s and 1970s. In other words, my colleagues were not viewing this patient’s fears, distress, and even anger about losing her longtime friend in "here and now" terms.
They told me that they would ask questions like "How does that make you feel?" and "What memories came to mind?" as well as the usual series of exploratory, open-ended questions and interpretations. "You need to discuss this with her and ‘get it out there,’ " one of the therapists suggested. Wrong.
Admittedly, my patient’s past was marked by perceived abandonment, including a parental divorce; the loss of an older sister; and the constant switching of schools, because her mother moved several times. I agree that a psychodynamic style in this particular case might indeed have gotten to the root of the problem – at some point. But this approach is different from CBT, which circumscribes the problem, challenges faulty beliefs, and develops avenues for change in a reasonably short period of time.
I was able to make quick progress with this patient by asking her a simple question: "When did you last see your friend?" The answer, not surprising for "all or nothing" responders, was that she had seen her the previous week – but only for a quick 45-minute lunch. And the week before that, the two had met up at the local gym and taken a class together, but "we didn’t talk much," my patient observed. My response to the patient was that she did indeed see and spend time with her friend, but not as much as she had when the friend was single and childless. Isn’t this the case? I asked. "Yes, yes that’s the case, I do see her, but, but, but ..."
As the patient and I proceeded through the thinking therapy of CBT, she was able to recognize that she did see her friend but not as much. It became easier for the patient to understand that her friend’s life had changed dramatically and that her availability was limited because her friend’s family and work responsibilities kept her busy. The patient also began to realize that her own availability also had become more limited since she was 20.
The process of working with this patient using CBT involved more than one question and answer. The approach starts out as homing in on the "all or nothing" negative-type generalized thinking, and is clearly aimed at resolving the patient’s distortions, and focusing on developing a new perspective and new way of thinking about this particular issue. Changing the thought process in this particular context is aimed at getting the patient to extrapolate to better processing in other contexts.
In addition, it is important to note that a psychodynamic approach can be incorporated into CBT as a teaching model. In this case, I found that bringing into the picture past events that had influenced the patient’s current distorted thinking helped the patient get a more honest picture of this long friendship. Her newfound perspective on that relationship spilled over into other aspects of my patient’s life in a positive way.
CBT is not only helpful for patients dealing with anxiety, depression, or lifetime personality styles and behaviors that cause them some form of distress in everyday living. A study soon to be published in the Journal of Behavior Therapy and Experimental Psychiatry suggests that CBT also might prove beneficial for negative symptoms in outpatients with disorders on the schizophrenia spectrum.
After 20 sessions of CBT over a 6-month period, the investigators found that patients reported a decrease in the number of dysfunctional beliefs about their own "cognitive abilities, performance, emotional experience, and social exclusion" (J. Behav. Ther. Exp. Psychiatry 2013;44:300-6). This was a small study (n = 21), and as the investigators noted, randomized controlled trials are needed. Still, this study is a reminder that focusing on problem resolution in a few highly focused sessions also can help patients with serious mental illness.
Those findings notwithstanding, CBT is certainly no panacea for numerous psychotic disorders. But in light of its superb track record of resolving many emotional problems, I believe that it should be used more as a mainstay of treatment and that anyone coming out of a mental health training program – whether psychiatrists, psychologists, mental health social workers, or psychiatric nurse practitioners – should be just as adept at using CBT as they are in using psychodynamic psychotherapy or medication management.
Dr. London is a psychiatrist affiliated with the New York University Langone Medical Center. He has no conflicts of interest to disclose.
Recently, I conducted a rather unscientific survey. I asked a few psychotherapists how they would treat a patient with whom I had worked successfully in the past.
The patient is a 39-year-old single woman who is a successful attorney. Despite her career success, the patient’s personal and social life had been replete with conflicts, especially surrounding her relationships with men. In our work together, these issues resolved when I used a cognitive-behavioral approach with her. But just as we were wrapping things up, an unexpected issue surfaced.
She told me that at age 20, she had studied abroad for a year in Europe with her closest female friend. It seems that my patient’s friend was successfully married and the mother of four children – all under age 10. She also was an attorney but was now working part time. And now, years later, the patient reported despair and unhappiness about "not seeing her anymore."
My survey began by asking numerous therapists what their approach would be to this woman’s dilemma. All of them knew about cognitive-behavioral therapy (CBT), reported using it, and endorsed using the technique to help this patient. However, the more we talked, it became clear that they were discussing traditional psychodynamic psychotherapy rather than the type of therapy started by Albert Ellis, Ph.D., in the 1950s as rational emotive behavior therapy, and later refined and codified as CBT by Dr. Aaron T. Beck in the 1960s and 1970s. In other words, my colleagues were not viewing this patient’s fears, distress, and even anger about losing her longtime friend in "here and now" terms.
They told me that they would ask questions like "How does that make you feel?" and "What memories came to mind?" as well as the usual series of exploratory, open-ended questions and interpretations. "You need to discuss this with her and ‘get it out there,’ " one of the therapists suggested. Wrong.
Admittedly, my patient’s past was marked by perceived abandonment, including a parental divorce; the loss of an older sister; and the constant switching of schools, because her mother moved several times. I agree that a psychodynamic style in this particular case might indeed have gotten to the root of the problem – at some point. But this approach is different from CBT, which circumscribes the problem, challenges faulty beliefs, and develops avenues for change in a reasonably short period of time.
I was able to make quick progress with this patient by asking her a simple question: "When did you last see your friend?" The answer, not surprising for "all or nothing" responders, was that she had seen her the previous week – but only for a quick 45-minute lunch. And the week before that, the two had met up at the local gym and taken a class together, but "we didn’t talk much," my patient observed. My response to the patient was that she did indeed see and spend time with her friend, but not as much as she had when the friend was single and childless. Isn’t this the case? I asked. "Yes, yes that’s the case, I do see her, but, but, but ..."
As the patient and I proceeded through the thinking therapy of CBT, she was able to recognize that she did see her friend but not as much. It became easier for the patient to understand that her friend’s life had changed dramatically and that her availability was limited because her friend’s family and work responsibilities kept her busy. The patient also began to realize that her own availability also had become more limited since she was 20.
The process of working with this patient using CBT involved more than one question and answer. The approach starts out as homing in on the "all or nothing" negative-type generalized thinking, and is clearly aimed at resolving the patient’s distortions, and focusing on developing a new perspective and new way of thinking about this particular issue. Changing the thought process in this particular context is aimed at getting the patient to extrapolate to better processing in other contexts.
In addition, it is important to note that a psychodynamic approach can be incorporated into CBT as a teaching model. In this case, I found that bringing into the picture past events that had influenced the patient’s current distorted thinking helped the patient get a more honest picture of this long friendship. Her newfound perspective on that relationship spilled over into other aspects of my patient’s life in a positive way.
CBT is not only helpful for patients dealing with anxiety, depression, or lifetime personality styles and behaviors that cause them some form of distress in everyday living. A study soon to be published in the Journal of Behavior Therapy and Experimental Psychiatry suggests that CBT also might prove beneficial for negative symptoms in outpatients with disorders on the schizophrenia spectrum.
After 20 sessions of CBT over a 6-month period, the investigators found that patients reported a decrease in the number of dysfunctional beliefs about their own "cognitive abilities, performance, emotional experience, and social exclusion" (J. Behav. Ther. Exp. Psychiatry 2013;44:300-6). This was a small study (n = 21), and as the investigators noted, randomized controlled trials are needed. Still, this study is a reminder that focusing on problem resolution in a few highly focused sessions also can help patients with serious mental illness.
Those findings notwithstanding, CBT is certainly no panacea for numerous psychotic disorders. But in light of its superb track record of resolving many emotional problems, I believe that it should be used more as a mainstay of treatment and that anyone coming out of a mental health training program – whether psychiatrists, psychologists, mental health social workers, or psychiatric nurse practitioners – should be just as adept at using CBT as they are in using psychodynamic psychotherapy or medication management.
Dr. London is a psychiatrist affiliated with the New York University Langone Medical Center. He has no conflicts of interest to disclose.

Stopping the ooze
Many of us will do anything or use any product available to stop oozing from suture needle holes. After all, waiting for bleeding to stop is usually not something most vascular surgeons enjoy. Most hemostatic agents are quite expensive and some don’t work very well at all.

Our group has found a cheap alternative that is freely available in every OR and, although not perfect, works well enough in most cases – the standard ultrasonic transmission Doppler gel that you use to listen to arteries in the operative field. We usually have these available in sterile packets (Fig. 1). We cut off one end and squeeze the contents as a large glob onto the patch or anastomosis (Fig. 2). Presumably the weight of the material is enough to stop the needle-hole bleeds.
Active bleeding will usually only occur between stitches and is evidence that another stitch would be prudent. Since the gel is clear, any bleeding is easily seen. We routinely also use protamine reversal for our carotid artery endarterectomies and bypasses and so we leave the jelly on until all the protamine has been given. By that time, the bleeding has almost always stopped.

The jelly can be sucked away (it makes a great sounding noise in the suction!) or just diluted out with saline. I do note on the package insert that Doppler gel is not for internal use, and it is not FDA approved for this indication, but I believe we all use it anyway?
Dr. Samson is a clinical associate professor of surgery (vascular), Florida State University Medical School and a member of Sarasota Vascular Specialists, Sarasota, Fl., and the Medical Editor of Vascular Specialist.
[Editor’s Note: Please submit your own helpful tips and tricks for inclusion in this column to vascularspecialist@frontlinemedcom.com.]
Many of us will do anything or use any product available to stop oozing from suture needle holes. After all, waiting for bleeding to stop is usually not something most vascular surgeons enjoy. Most hemostatic agents are quite expensive and some don’t work very well at all.
Our group has found a cheap alternative that is freely available in every OR and, although not perfect, works well enough in most cases – the standard ultrasonic transmission Doppler gel that you use to listen to arteries in the operative field. We usually have these available in sterile packets (Fig. 1). We cut off one end and squeeze the contents as a large glob onto the patch or anastomosis (Fig. 2). Presumably the weight of the material is enough to stop the needle-hole bleeds.
Active bleeding will usually only occur between stitches and is evidence that another stitch would be prudent. Since the gel is clear, any bleeding is easily seen. We routinely also use protamine reversal for our carotid artery endarterectomies and bypasses and so we leave the jelly on until all the protamine has been given. By that time, the bleeding has almost always stopped.
The jelly can be sucked away (it makes a great sounding noise in the suction!) or just diluted out with saline. I do note on the package insert that Doppler gel is not for internal use, and it is not FDA approved for this indication, but I believe we all use it anyway?
Dr. Samson is a clinical associate professor of surgery (vascular), Florida State University Medical School and a member of Sarasota Vascular Specialists, Sarasota, Fl., and the Medical Editor of Vascular Specialist.
[Editor’s Note: Please submit your own helpful tips and tricks for inclusion in this column to vascularspecialist@frontlinemedcom.com.]
Many of us will do anything or use any product available to stop oozing from suture needle holes. After all, waiting for bleeding to stop is usually not something most vascular surgeons enjoy. Most hemostatic agents are quite expensive and some don’t work very well at all.
Our group has found a cheap alternative that is freely available in every OR and, although not perfect, works well enough in most cases – the standard ultrasonic transmission Doppler gel that you use to listen to arteries in the operative field. We usually have these available in sterile packets (Fig. 1). We cut off one end and squeeze the contents as a large glob onto the patch or anastomosis (Fig. 2). Presumably the weight of the material is enough to stop the needle-hole bleeds.
Active bleeding will usually only occur between stitches and is evidence that another stitch would be prudent. Since the gel is clear, any bleeding is easily seen. We routinely also use protamine reversal for our carotid artery endarterectomies and bypasses and so we leave the jelly on until all the protamine has been given. By that time, the bleeding has almost always stopped.
The jelly can be sucked away (it makes a great sounding noise in the suction!) or just diluted out with saline. I do note on the package insert that Doppler gel is not for internal use, and it is not FDA approved for this indication, but I believe we all use it anyway?
Dr. Samson is a clinical associate professor of surgery (vascular), Florida State University Medical School and a member of Sarasota Vascular Specialists, Sarasota, Fl., and the Medical Editor of Vascular Specialist.
[Editor’s Note: Please submit your own helpful tips and tricks for inclusion in this column to vascularspecialist@frontlinemedcom.com.]
Commemorating Round-the-Clock Hospital Medicine Programs


The steam engine. The telephone. Television. ATMs. The Internet. Smartphones. The 24/7 hospitalist program.
Perhaps the single most important innovation along the road to where we are now in HM has been the development of the hospital-sponsored, 24/7, on-site hospitalist program. And the father of this invention may be the most significant figure in HM you’ve never heard of: John Holbrook, MD, FACEP. An emergency-medicine physician since the mid-1970s, Dr. Holbrook did something in July 1993 that was considered off the wall, yet proved to be revolutionary: From nothing, he launched a 24/7 hospitalist program staffed with board-eligible and board-certified internists at Mercy Hospital in Springfield, Mass. The inpatient physicians (this was before the word “hospitalist” came to be) were employed by a subsidiary of the hospital and worked in place of community primary-care physicians (PCPs), taking care of hospitalized patients who did not have a PCP, or whose PCP chose not to come to the hospital.
Of great significance, from the beginning, and perhaps by unintentional design, these physicians were agents of change and improvement for the hospital itself.
To be sure, in places like Southern California, 24/7, on-site hospitalist programs were in place in the late 1980s. Some claim those programs may have been the birthplace of the hospitalist model. However, such programs came to be in order to help medical groups manage full capitated risk delegated to them from HMOs on a population of patients, and were not supported by the hospital, per se. This is distinct from hospitalist programs—such as Mercy’s—sponsored by hospitals (whether employed or contracted) in predominantly fee-for-service markets, which then comprised the lion’s share of the U.S. market.
I had the extraordinary good fortune to happen along in July 1994, get hired by Dr. Holbrook, and soon after begin serving as medical director for the Mercy program, which I would do for the next decade. To this day, Dr. Holbrook is a mentor and trusted advisor to me. I caught up with him in recognition of the 20th anniversary of the Mercy Inpatient Medicine Service.

Question: What gave you the idea to launch what was, at the time, considered such an unconventional program?
Answer: Before the specialty of emergency medicine, a patient’s private physician would be called in most cases when a patient present in the ED: 25 or 50 doctors might be called over 24 hours, each to see one patient each. The inefficiency and disruption caused by this system was a natural and logical stimulus to develop the specialty of emergency medicine. I saw hospitalist medicine as an exact analogy.
Q: What were you observing in the healthcare environment that drove you to create the Mercy Inpatient Medicine Service?
A: Working for many years in the emergency department of a community hospital without a house staff, the ED docs would admit a patient at night or on the weekend and the attending physician would often plan to see the patient “in the morning.” When the patient would decompensate in the middle of the night, the ED doc would get a call to run to the floor to “Band-Aid” the situation.
Q: How did you convince the board of trustees to fund it?
A: The reasons were primarily economic. No. 1, the hospital was losing market share because local physicians would prefer to admit to the teaching hospital [a nearby competitor], where they were not required to come in during the middle of the night. No. 2, the cost of a hospitalization managed by a hospitalist was less expensive than either a hospital stay managed by house staff or managed over the telephone by a private attending at home.
Q: What was the most difficult operational challenge for the program?
A: Effective and timely communication with the community physicians was the most difficult operational challenge. Access to outpatient medical treatment immediately prior to a hospitalization and timely communication to the community physician were both challenges that we never adequately solved in the early days. I understand that these issues can still be problematic.
Q: How was it received by patients?
A: Overall, patients were very happy with the system. In the old system, with a typical four-physician practice, a patient had only a 1 in 4 chance of being admitted by the doctor who was familiar with the case. The fact that the hospitalist was available in the hospital made the improvement in quality apparent to most patients.
Q: How did you get the medical staff to buy into the program?
A: I personally visited every private physician who participated. Physicians were given the option of not participating, or of part-time participation—for example, on weekends or holidays only. The word spread. Physicians came up to me and told me that the program enabled them to continue practicing for another five years. Physicians’ spouses thanked me.
Q: Are you surprised HM as a field has grown so quickly?
A: I am not really that surprised. It is a better way to organize health care. I am surprised that it did not occur sooner. We talked about instituting this system for 10 years before 1993.
Q: What big challenges remain for hospital medicine? What are some solutions?
A: I believe that the biggest global challenge for hospital medicine remains communication with community-based providers, both before the hospitalization as well as during hospitalization and immediately after discharge. In the era of the EMR, the Internet, and the iPhone and Android, this should be easier. HIPAA has not helped.
The other growing challenge will become apparent as hospitalists age in the profession: Disruption of the diurnal sleep cycle becomes increasingly problematic for many physicians after the age of 50 and can easily lead to burnout. The early hospitalists were all in their 30s. The attractive lifestyle choice for the 30-year-old can lead to burnout for the 55-year-old. The emergency-medicine literature has noted a similar problem of shift work/sleep fragmentation.
Final Thoughts
I believe Dr. Holbrook’s assessments on the future of our specialty are on target. As HM continues to mature, we need to continue to focus on how we communicate with providers outside the four walls of the hospital and how to address barriers to making HM a sustainable career.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
(Editor's note: Updated July 12, 2013.)
The steam engine. The telephone. Television. ATMs. The Internet. Smartphones. The 24/7 hospitalist program.
Perhaps the single most important innovation along the road to where we are now in HM has been the development of the hospital-sponsored, 24/7, on-site hospitalist program. And the father of this invention may be the most significant figure in HM you’ve never heard of: John Holbrook, MD, FACEP. An emergency-medicine physician since the mid-1970s, Dr. Holbrook did something in July 1993 that was considered off the wall, yet proved to be revolutionary: From nothing, he launched a 24/7 hospitalist program staffed with board-eligible and board-certified internists at Mercy Hospital in Springfield, Mass. The inpatient physicians (this was before the word “hospitalist” came to be) were employed by a subsidiary of the hospital and worked in place of community primary-care physicians (PCPs), taking care of hospitalized patients who did not have a PCP, or whose PCP chose not to come to the hospital.
Of great significance, from the beginning, and perhaps by unintentional design, these physicians were agents of change and improvement for the hospital itself.
To be sure, in places like Southern California, 24/7, on-site hospitalist programs were in place in the late 1980s. Some claim those programs may have been the birthplace of the hospitalist model. However, such programs came to be in order to help medical groups manage full capitated risk delegated to them from HMOs on a population of patients, and were not supported by the hospital, per se. This is distinct from hospitalist programs—such as Mercy’s—sponsored by hospitals (whether employed or contracted) in predominantly fee-for-service markets, which then comprised the lion’s share of the U.S. market.
I had the extraordinary good fortune to happen along in July 1994, get hired by Dr. Holbrook, and soon after begin serving as medical director for the Mercy program, which I would do for the next decade. To this day, Dr. Holbrook is a mentor and trusted advisor to me. I caught up with him in recognition of the 20th anniversary of the Mercy Inpatient Medicine Service.
Question: What gave you the idea to launch what was, at the time, considered such an unconventional program?
Answer: Before the specialty of emergency medicine, a patient’s private physician would be called in most cases when a patient present in the ED: 25 or 50 doctors might be called over 24 hours, each to see one patient each. The inefficiency and disruption caused by this system was a natural and logical stimulus to develop the specialty of emergency medicine. I saw hospitalist medicine as an exact analogy.
Q: What were you observing in the healthcare environment that drove you to create the Mercy Inpatient Medicine Service?
A: Working for many years in the emergency department of a community hospital without a house staff, the ED docs would admit a patient at night or on the weekend and the attending physician would often plan to see the patient “in the morning.” When the patient would decompensate in the middle of the night, the ED doc would get a call to run to the floor to “Band-Aid” the situation.
Q: How did you convince the board of trustees to fund it?
A: The reasons were primarily economic. No. 1, the hospital was losing market share because local physicians would prefer to admit to the teaching hospital [a nearby competitor], where they were not required to come in during the middle of the night. No. 2, the cost of a hospitalization managed by a hospitalist was less expensive than either a hospital stay managed by house staff or managed over the telephone by a private attending at home.
Q: What was the most difficult operational challenge for the program?
A: Effective and timely communication with the community physicians was the most difficult operational challenge. Access to outpatient medical treatment immediately prior to a hospitalization and timely communication to the community physician were both challenges that we never adequately solved in the early days. I understand that these issues can still be problematic.
Q: How was it received by patients?
A: Overall, patients were very happy with the system. In the old system, with a typical four-physician practice, a patient had only a 1 in 4 chance of being admitted by the doctor who was familiar with the case. The fact that the hospitalist was available in the hospital made the improvement in quality apparent to most patients.
Q: How did you get the medical staff to buy into the program?
A: I personally visited every private physician who participated. Physicians were given the option of not participating, or of part-time participation—for example, on weekends or holidays only. The word spread. Physicians came up to me and told me that the program enabled them to continue practicing for another five years. Physicians’ spouses thanked me.
Q: Are you surprised HM as a field has grown so quickly?
A: I am not really that surprised. It is a better way to organize health care. I am surprised that it did not occur sooner. We talked about instituting this system for 10 years before 1993.
Q: What big challenges remain for hospital medicine? What are some solutions?
A: I believe that the biggest global challenge for hospital medicine remains communication with community-based providers, both before the hospitalization as well as during hospitalization and immediately after discharge. In the era of the EMR, the Internet, and the iPhone and Android, this should be easier. HIPAA has not helped.
The other growing challenge will become apparent as hospitalists age in the profession: Disruption of the diurnal sleep cycle becomes increasingly problematic for many physicians after the age of 50 and can easily lead to burnout. The early hospitalists were all in their 30s. The attractive lifestyle choice for the 30-year-old can lead to burnout for the 55-year-old. The emergency-medicine literature has noted a similar problem of shift work/sleep fragmentation.
Final Thoughts
I believe Dr. Holbrook’s assessments on the future of our specialty are on target. As HM continues to mature, we need to continue to focus on how we communicate with providers outside the four walls of the hospital and how to address barriers to making HM a sustainable career.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
(Editor's note: Updated July 12, 2013.)
The steam engine. The telephone. Television. ATMs. The Internet. Smartphones. The 24/7 hospitalist program.
Perhaps the single most important innovation along the road to where we are now in HM has been the development of the hospital-sponsored, 24/7, on-site hospitalist program. And the father of this invention may be the most significant figure in HM you’ve never heard of: John Holbrook, MD, FACEP. An emergency-medicine physician since the mid-1970s, Dr. Holbrook did something in July 1993 that was considered off the wall, yet proved to be revolutionary: From nothing, he launched a 24/7 hospitalist program staffed with board-eligible and board-certified internists at Mercy Hospital in Springfield, Mass. The inpatient physicians (this was before the word “hospitalist” came to be) were employed by a subsidiary of the hospital and worked in place of community primary-care physicians (PCPs), taking care of hospitalized patients who did not have a PCP, or whose PCP chose not to come to the hospital.
Of great significance, from the beginning, and perhaps by unintentional design, these physicians were agents of change and improvement for the hospital itself.
To be sure, in places like Southern California, 24/7, on-site hospitalist programs were in place in the late 1980s. Some claim those programs may have been the birthplace of the hospitalist model. However, such programs came to be in order to help medical groups manage full capitated risk delegated to them from HMOs on a population of patients, and were not supported by the hospital, per se. This is distinct from hospitalist programs—such as Mercy’s—sponsored by hospitals (whether employed or contracted) in predominantly fee-for-service markets, which then comprised the lion’s share of the U.S. market.
I had the extraordinary good fortune to happen along in July 1994, get hired by Dr. Holbrook, and soon after begin serving as medical director for the Mercy program, which I would do for the next decade. To this day, Dr. Holbrook is a mentor and trusted advisor to me. I caught up with him in recognition of the 20th anniversary of the Mercy Inpatient Medicine Service.
Question: What gave you the idea to launch what was, at the time, considered such an unconventional program?
Answer: Before the specialty of emergency medicine, a patient’s private physician would be called in most cases when a patient present in the ED: 25 or 50 doctors might be called over 24 hours, each to see one patient each. The inefficiency and disruption caused by this system was a natural and logical stimulus to develop the specialty of emergency medicine. I saw hospitalist medicine as an exact analogy.
Q: What were you observing in the healthcare environment that drove you to create the Mercy Inpatient Medicine Service?
A: Working for many years in the emergency department of a community hospital without a house staff, the ED docs would admit a patient at night or on the weekend and the attending physician would often plan to see the patient “in the morning.” When the patient would decompensate in the middle of the night, the ED doc would get a call to run to the floor to “Band-Aid” the situation.
Q: How did you convince the board of trustees to fund it?
A: The reasons were primarily economic. No. 1, the hospital was losing market share because local physicians would prefer to admit to the teaching hospital [a nearby competitor], where they were not required to come in during the middle of the night. No. 2, the cost of a hospitalization managed by a hospitalist was less expensive than either a hospital stay managed by house staff or managed over the telephone by a private attending at home.
Q: What was the most difficult operational challenge for the program?
A: Effective and timely communication with the community physicians was the most difficult operational challenge. Access to outpatient medical treatment immediately prior to a hospitalization and timely communication to the community physician were both challenges that we never adequately solved in the early days. I understand that these issues can still be problematic.
Q: How was it received by patients?
A: Overall, patients were very happy with the system. In the old system, with a typical four-physician practice, a patient had only a 1 in 4 chance of being admitted by the doctor who was familiar with the case. The fact that the hospitalist was available in the hospital made the improvement in quality apparent to most patients.
Q: How did you get the medical staff to buy into the program?
A: I personally visited every private physician who participated. Physicians were given the option of not participating, or of part-time participation—for example, on weekends or holidays only. The word spread. Physicians came up to me and told me that the program enabled them to continue practicing for another five years. Physicians’ spouses thanked me.
Q: Are you surprised HM as a field has grown so quickly?
A: I am not really that surprised. It is a better way to organize health care. I am surprised that it did not occur sooner. We talked about instituting this system for 10 years before 1993.
Q: What big challenges remain for hospital medicine? What are some solutions?
A: I believe that the biggest global challenge for hospital medicine remains communication with community-based providers, both before the hospitalization as well as during hospitalization and immediately after discharge. In the era of the EMR, the Internet, and the iPhone and Android, this should be easier. HIPAA has not helped.
The other growing challenge will become apparent as hospitalists age in the profession: Disruption of the diurnal sleep cycle becomes increasingly problematic for many physicians after the age of 50 and can easily lead to burnout. The early hospitalists were all in their 30s. The attractive lifestyle choice for the 30-year-old can lead to burnout for the 55-year-old. The emergency-medicine literature has noted a similar problem of shift work/sleep fragmentation.
Final Thoughts
I believe Dr. Holbrook’s assessments on the future of our specialty are on target. As HM continues to mature, we need to continue to focus on how we communicate with providers outside the four walls of the hospital and how to address barriers to making HM a sustainable career.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
(Editor's note: Updated July 12, 2013.)
Steps Hospitalists Should Take to Reduce Turnaround Time of Death Certificates

Funeral-home representatives sometimes make multiple trips to a hospital or doctor’s office to get a death certificate signed, often waiting in the lobby for hours. I first realized this in the 1980s when starting post-residency practice as a hospitalist. I began asking these guys (they are nearly always men, in my experience) how much time they typically invest getting each certificate signed. They told of walking halfway across a golf course to catch the doctor on the 13th hole or making the 90-minute drive (each way) to a doctor’s office, sometimes finding the doctor had just left, only to repeat the process several times before getting the signature.
When the Clinton administration made electronic signatures via the Internet valid, I thought about starting a business charging funeral homes something like $200 for getting the doctor to sign it electronically within 48 hours. I would use about half of the $200 to provide an incentive for the doctor to sign quickly (sign within 48 hours, and you’ll get a $100 gift card!), then use the rest to fund the company. Since funeral homes probably spend much more than $200 per certificate paying their staff to drive around getting signatures on paper, I thought they would jump at this idea.
I never pursued it, but that doesn’t stop me from loudly proclaiming to friends and family that it was a “can’t-miss” blockbuster Internet business idea. Of course, I never tested that theory, but it makes for fun chest-thumping at parties.
A number of states, including Florida, Texas, and others, now have in place online completion of death certificates. Indiana has required use of its online death certificate since 2011; there is no option to use paper. I suspect nearly every state will do the same before long. But that alone won’t ensure timely completion. Doctors and others who complete the certificates need to ensure they respond quickly, something they often fail to do.
It Really Matters
Lack of a death certificate can hold up burial or cremation, and things like life-insurance payouts and estate settlement are delayed. For a grieving family, these things only add to their pain.
I’m aware of a tragic case from a few years ago in which a certificate was passed around to a number of doctors, each of whom thought with some justification that someone else should sign it. It sat in two different mailboxes for many days while the intended recipients were vacationing. All of this delayed the burial, and the poor family had to send updates to loved ones saying, “We don’t know when Dad’s funeral will be.” About three weeks later, the certificate was completed and the funeral held. What a terribly sad story!
Some states have laws governing how quickly certificates must be signed. A thought-provoking 2004 Medical Staff Update from Stanford University says that California requires a signature within 15 hours of death, though I wonder how often this is enforced.
Improving Turnaround Time
There are several things hospitalists could consider to improve timely completion of death certificates:
- Ensure doctors liberally complete them for one another. Don’t let one doctor’s absence delay, even for a day, getting it completed and signed. This means the “covering” doctor has access to the discharge (death) summary in the medical record.
- When several doctors in different specialties are caring for a patient at the time of death, nearly any of them could reasonably sign the certificate. It might be appropriate to adopt a policy that whichever doctor (e.g. hospitalist, intensivist, or oncologist) who had contact with the patient and is presented with the certificate should go ahead and sign it rather than passing it along to one of the other specialties, regardless of which served as attending.
- Consider creating a central access point at your hospital for receipt of death certificates. Ideally, a funeral-home representative can deliver it to one person at the hospital who will do the leg work of getting a doctor to sign it quickly. Delays are likely if the funeral-home representative has to “shop it around” to different departments and physician offices. A hospital staffer should be able to navigate this quickly.
- Pressure EMR vendors to include some sort of death-certificate functionality in the future. I don’t know if some have it already, but it seems like it shouldn’t be too difficult for an EMR to spit out a prefilled certificate in much the same way e-prescribing works. It could even be delivered electronically to the funeral home.
- For hospitalists with 24-hour, on-site presence, it could be reasonable to have an on-duty hospitalist complete the certificate at the time of death rather than waiting for the funeral home to initiate the process. This was standard when I was a resident, and it may be a practical approach in many settings.
- Consider copying one hospital I worked with previously: They created a hospitalist salary bonus for timely completion. I assure you this policy was very effective.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Funeral-home representatives sometimes make multiple trips to a hospital or doctor’s office to get a death certificate signed, often waiting in the lobby for hours. I first realized this in the 1980s when starting post-residency practice as a hospitalist. I began asking these guys (they are nearly always men, in my experience) how much time they typically invest getting each certificate signed. They told of walking halfway across a golf course to catch the doctor on the 13th hole or making the 90-minute drive (each way) to a doctor’s office, sometimes finding the doctor had just left, only to repeat the process several times before getting the signature.
When the Clinton administration made electronic signatures via the Internet valid, I thought about starting a business charging funeral homes something like $200 for getting the doctor to sign it electronically within 48 hours. I would use about half of the $200 to provide an incentive for the doctor to sign quickly (sign within 48 hours, and you’ll get a $100 gift card!), then use the rest to fund the company. Since funeral homes probably spend much more than $200 per certificate paying their staff to drive around getting signatures on paper, I thought they would jump at this idea.
I never pursued it, but that doesn’t stop me from loudly proclaiming to friends and family that it was a “can’t-miss” blockbuster Internet business idea. Of course, I never tested that theory, but it makes for fun chest-thumping at parties.
A number of states, including Florida, Texas, and others, now have in place online completion of death certificates. Indiana has required use of its online death certificate since 2011; there is no option to use paper. I suspect nearly every state will do the same before long. But that alone won’t ensure timely completion. Doctors and others who complete the certificates need to ensure they respond quickly, something they often fail to do.
It Really Matters
Lack of a death certificate can hold up burial or cremation, and things like life-insurance payouts and estate settlement are delayed. For a grieving family, these things only add to their pain.
I’m aware of a tragic case from a few years ago in which a certificate was passed around to a number of doctors, each of whom thought with some justification that someone else should sign it. It sat in two different mailboxes for many days while the intended recipients were vacationing. All of this delayed the burial, and the poor family had to send updates to loved ones saying, “We don’t know when Dad’s funeral will be.” About three weeks later, the certificate was completed and the funeral held. What a terribly sad story!
Some states have laws governing how quickly certificates must be signed. A thought-provoking 2004 Medical Staff Update from Stanford University says that California requires a signature within 15 hours of death, though I wonder how often this is enforced.
Improving Turnaround Time
There are several things hospitalists could consider to improve timely completion of death certificates:
- Ensure doctors liberally complete them for one another. Don’t let one doctor’s absence delay, even for a day, getting it completed and signed. This means the “covering” doctor has access to the discharge (death) summary in the medical record.
- When several doctors in different specialties are caring for a patient at the time of death, nearly any of them could reasonably sign the certificate. It might be appropriate to adopt a policy that whichever doctor (e.g. hospitalist, intensivist, or oncologist) who had contact with the patient and is presented with the certificate should go ahead and sign it rather than passing it along to one of the other specialties, regardless of which served as attending.
- Consider creating a central access point at your hospital for receipt of death certificates. Ideally, a funeral-home representative can deliver it to one person at the hospital who will do the leg work of getting a doctor to sign it quickly. Delays are likely if the funeral-home representative has to “shop it around” to different departments and physician offices. A hospital staffer should be able to navigate this quickly.
- Pressure EMR vendors to include some sort of death-certificate functionality in the future. I don’t know if some have it already, but it seems like it shouldn’t be too difficult for an EMR to spit out a prefilled certificate in much the same way e-prescribing works. It could even be delivered electronically to the funeral home.
- For hospitalists with 24-hour, on-site presence, it could be reasonable to have an on-duty hospitalist complete the certificate at the time of death rather than waiting for the funeral home to initiate the process. This was standard when I was a resident, and it may be a practical approach in many settings.
- Consider copying one hospital I worked with previously: They created a hospitalist salary bonus for timely completion. I assure you this policy was very effective.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Funeral-home representatives sometimes make multiple trips to a hospital or doctor’s office to get a death certificate signed, often waiting in the lobby for hours. I first realized this in the 1980s when starting post-residency practice as a hospitalist. I began asking these guys (they are nearly always men, in my experience) how much time they typically invest getting each certificate signed. They told of walking halfway across a golf course to catch the doctor on the 13th hole or making the 90-minute drive (each way) to a doctor’s office, sometimes finding the doctor had just left, only to repeat the process several times before getting the signature.
When the Clinton administration made electronic signatures via the Internet valid, I thought about starting a business charging funeral homes something like $200 for getting the doctor to sign it electronically within 48 hours. I would use about half of the $200 to provide an incentive for the doctor to sign quickly (sign within 48 hours, and you’ll get a $100 gift card!), then use the rest to fund the company. Since funeral homes probably spend much more than $200 per certificate paying their staff to drive around getting signatures on paper, I thought they would jump at this idea.
I never pursued it, but that doesn’t stop me from loudly proclaiming to friends and family that it was a “can’t-miss” blockbuster Internet business idea. Of course, I never tested that theory, but it makes for fun chest-thumping at parties.
A number of states, including Florida, Texas, and others, now have in place online completion of death certificates. Indiana has required use of its online death certificate since 2011; there is no option to use paper. I suspect nearly every state will do the same before long. But that alone won’t ensure timely completion. Doctors and others who complete the certificates need to ensure they respond quickly, something they often fail to do.
It Really Matters
Lack of a death certificate can hold up burial or cremation, and things like life-insurance payouts and estate settlement are delayed. For a grieving family, these things only add to their pain.
I’m aware of a tragic case from a few years ago in which a certificate was passed around to a number of doctors, each of whom thought with some justification that someone else should sign it. It sat in two different mailboxes for many days while the intended recipients were vacationing. All of this delayed the burial, and the poor family had to send updates to loved ones saying, “We don’t know when Dad’s funeral will be.” About three weeks later, the certificate was completed and the funeral held. What a terribly sad story!
Some states have laws governing how quickly certificates must be signed. A thought-provoking 2004 Medical Staff Update from Stanford University says that California requires a signature within 15 hours of death, though I wonder how often this is enforced.
Improving Turnaround Time
There are several things hospitalists could consider to improve timely completion of death certificates:
- Ensure doctors liberally complete them for one another. Don’t let one doctor’s absence delay, even for a day, getting it completed and signed. This means the “covering” doctor has access to the discharge (death) summary in the medical record.
- When several doctors in different specialties are caring for a patient at the time of death, nearly any of them could reasonably sign the certificate. It might be appropriate to adopt a policy that whichever doctor (e.g. hospitalist, intensivist, or oncologist) who had contact with the patient and is presented with the certificate should go ahead and sign it rather than passing it along to one of the other specialties, regardless of which served as attending.
- Consider creating a central access point at your hospital for receipt of death certificates. Ideally, a funeral-home representative can deliver it to one person at the hospital who will do the leg work of getting a doctor to sign it quickly. Delays are likely if the funeral-home representative has to “shop it around” to different departments and physician offices. A hospital staffer should be able to navigate this quickly.
- Pressure EMR vendors to include some sort of death-certificate functionality in the future. I don’t know if some have it already, but it seems like it shouldn’t be too difficult for an EMR to spit out a prefilled certificate in much the same way e-prescribing works. It could even be delivered electronically to the funeral home.
- For hospitalists with 24-hour, on-site presence, it could be reasonable to have an on-duty hospitalist complete the certificate at the time of death rather than waiting for the funeral home to initiate the process. This was standard when I was a resident, and it may be a practical approach in many settings.
- Consider copying one hospital I worked with previously: They created a hospitalist salary bonus for timely completion. I assure you this policy was very effective.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Effective Clinical Documentation Can Influence Medicare Reimbursement

Back in the 1980s, I would go by medical records every day or two and find, on the front of the charts of my recently discharged patients, a form listing the diagnoses the hospital was billing to Medicare. Before the hospital could submit a patient’s bill, the attending physician was required to review the form and, by signing it, indicate agreement.
The requirement for this signature by the physician went away a long time ago and in my memory is one of the very few examples of reducing a doctor’s paperwork.
For my first few months in practice, I regularly would seek out the people who completed the form and explain they had misunderstood the patient’s clinical situation. “The main issue was a urinary tract infection,” I would say, “but you listed diabetes as the principal diagnosis.”
I don’t ever remember them changing anything based on my feedback. Instead, they explained to me that, for billing purposes, it was legitimate to list diabetes as the principal diagnosis because it had the additional benefit of resulting in a higher payment to the hospital than having “urinary tract infection” listed first.
Such was my introduction to the world of documentation and coding for hospital billing purposes and how it can sometimes differ significantly from the way a doctor sees the clinical picture. Things have evolved a lot since then, but the way doctors document medical conditions still has a huge influence on hospital reimbursement.
Hospital CDI Programs
About 80% of hospitals have formal clinical documentation improvement (CDI) programs to help ensure all clinical conditions are captured and described in the medical record in ways that are valuable for billing and other recordkeeping purposes. These programs might lead to you receive queries about your documentation. For example, you might be asked to clarify whether your patient’s pneumonia might be on the basis of aspiration.
Within SHM’s Code-H program, Dr. Richard Pinson, a former ED physician who now works with Houston-based HCQ Consulting, has a good presentation explaining these documentation issues. In it, he makes the point that, in addition to influencing how hospitals are paid, the way various conditions are documented also influences quality ratings.
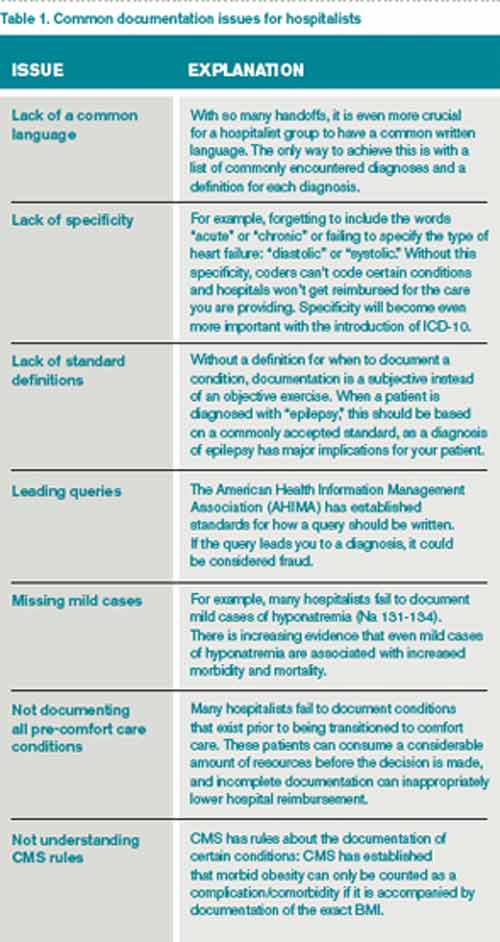
Novel Approach
The most common approach to engaging hospitalists in CDI initiatives is to have them attend a presentation on the topic, then put in place documentation specialists who generate queries asking the doctor to clarify diagnoses when it might influence payment, severity of illness determination, etc. Dr. Kenji Asakura, a Seattle hospitalist, and Erik Ordal, MBA, have a company called ClinIntell that analyzes each hospitalist (or other specialty) group’s historical patient mix and trains them on the documentation issues that they see most often. The idea of this focused approach is to make “documentation queries” unnecessary, or at least much less necessary. The benefits of this approach are many, including reducing or eliminating the risk of “leading queries”—that is, queries that seem to encourage the doctor to document a diagnosis because it is an advantage to the hospital rather than a well-considered medical opinion. Leading queries can be regarded as fraudulent and can get a lot of people in trouble.
I asked Kenji and Erik if they could provide me with a list of common documentation issues that most hospitalists need to know more about. Table 1 is what they came up with. I hope it helps you and your practice.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at john.nelson@nelsonflores.com.
Back in the 1980s, I would go by medical records every day or two and find, on the front of the charts of my recently discharged patients, a form listing the diagnoses the hospital was billing to Medicare. Before the hospital could submit a patient’s bill, the attending physician was required to review the form and, by signing it, indicate agreement.
The requirement for this signature by the physician went away a long time ago and in my memory is one of the very few examples of reducing a doctor’s paperwork.
For my first few months in practice, I regularly would seek out the people who completed the form and explain they had misunderstood the patient’s clinical situation. “The main issue was a urinary tract infection,” I would say, “but you listed diabetes as the principal diagnosis.”
I don’t ever remember them changing anything based on my feedback. Instead, they explained to me that, for billing purposes, it was legitimate to list diabetes as the principal diagnosis because it had the additional benefit of resulting in a higher payment to the hospital than having “urinary tract infection” listed first.
Such was my introduction to the world of documentation and coding for hospital billing purposes and how it can sometimes differ significantly from the way a doctor sees the clinical picture. Things have evolved a lot since then, but the way doctors document medical conditions still has a huge influence on hospital reimbursement.
Hospital CDI Programs
About 80% of hospitals have formal clinical documentation improvement (CDI) programs to help ensure all clinical conditions are captured and described in the medical record in ways that are valuable for billing and other recordkeeping purposes. These programs might lead to you receive queries about your documentation. For example, you might be asked to clarify whether your patient’s pneumonia might be on the basis of aspiration.
Within SHM’s Code-H program, Dr. Richard Pinson, a former ED physician who now works with Houston-based HCQ Consulting, has a good presentation explaining these documentation issues. In it, he makes the point that, in addition to influencing how hospitals are paid, the way various conditions are documented also influences quality ratings.
Novel Approach
The most common approach to engaging hospitalists in CDI initiatives is to have them attend a presentation on the topic, then put in place documentation specialists who generate queries asking the doctor to clarify diagnoses when it might influence payment, severity of illness determination, etc. Dr. Kenji Asakura, a Seattle hospitalist, and Erik Ordal, MBA, have a company called ClinIntell that analyzes each hospitalist (or other specialty) group’s historical patient mix and trains them on the documentation issues that they see most often. The idea of this focused approach is to make “documentation queries” unnecessary, or at least much less necessary. The benefits of this approach are many, including reducing or eliminating the risk of “leading queries”—that is, queries that seem to encourage the doctor to document a diagnosis because it is an advantage to the hospital rather than a well-considered medical opinion. Leading queries can be regarded as fraudulent and can get a lot of people in trouble.
I asked Kenji and Erik if they could provide me with a list of common documentation issues that most hospitalists need to know more about. Table 1 is what they came up with. I hope it helps you and your practice.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at john.nelson@nelsonflores.com.
Back in the 1980s, I would go by medical records every day or two and find, on the front of the charts of my recently discharged patients, a form listing the diagnoses the hospital was billing to Medicare. Before the hospital could submit a patient’s bill, the attending physician was required to review the form and, by signing it, indicate agreement.
The requirement for this signature by the physician went away a long time ago and in my memory is one of the very few examples of reducing a doctor’s paperwork.
For my first few months in practice, I regularly would seek out the people who completed the form and explain they had misunderstood the patient’s clinical situation. “The main issue was a urinary tract infection,” I would say, “but you listed diabetes as the principal diagnosis.”
I don’t ever remember them changing anything based on my feedback. Instead, they explained to me that, for billing purposes, it was legitimate to list diabetes as the principal diagnosis because it had the additional benefit of resulting in a higher payment to the hospital than having “urinary tract infection” listed first.
Such was my introduction to the world of documentation and coding for hospital billing purposes and how it can sometimes differ significantly from the way a doctor sees the clinical picture. Things have evolved a lot since then, but the way doctors document medical conditions still has a huge influence on hospital reimbursement.
Hospital CDI Programs
About 80% of hospitals have formal clinical documentation improvement (CDI) programs to help ensure all clinical conditions are captured and described in the medical record in ways that are valuable for billing and other recordkeeping purposes. These programs might lead to you receive queries about your documentation. For example, you might be asked to clarify whether your patient’s pneumonia might be on the basis of aspiration.
Within SHM’s Code-H program, Dr. Richard Pinson, a former ED physician who now works with Houston-based HCQ Consulting, has a good presentation explaining these documentation issues. In it, he makes the point that, in addition to influencing how hospitals are paid, the way various conditions are documented also influences quality ratings.
Novel Approach
The most common approach to engaging hospitalists in CDI initiatives is to have them attend a presentation on the topic, then put in place documentation specialists who generate queries asking the doctor to clarify diagnoses when it might influence payment, severity of illness determination, etc. Dr. Kenji Asakura, a Seattle hospitalist, and Erik Ordal, MBA, have a company called ClinIntell that analyzes each hospitalist (or other specialty) group’s historical patient mix and trains them on the documentation issues that they see most often. The idea of this focused approach is to make “documentation queries” unnecessary, or at least much less necessary. The benefits of this approach are many, including reducing or eliminating the risk of “leading queries”—that is, queries that seem to encourage the doctor to document a diagnosis because it is an advantage to the hospital rather than a well-considered medical opinion. Leading queries can be regarded as fraudulent and can get a lot of people in trouble.
I asked Kenji and Erik if they could provide me with a list of common documentation issues that most hospitalists need to know more about. Table 1 is what they came up with. I hope it helps you and your practice.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at john.nelson@nelsonflores.com.