User login
Save Your Tickets
To me the most daunting of speaking assignments is the after-dinner presentation. By the time the speech begins, the audience has been well fed, and many have emptied their wine glasses and refilled them several times. Bedtime is approaching, and the often somnolent listeners are nowhere near the peak of their powers of comprehension.
I have heard many such presentations, usually at surgical meetings and several from notable, even famous, personalities who had considerable wisdom to convey. Unfortunately, although I do remember the names of many of the speakers, their messages, if they were captured by the memory circuits of my brain, have since escaped me. There is one notable exception: a talk entitled "Tickets" given by Dr. Jerry Shuck, who was then professor and chairman of surgery at Case Western Reserve University. The occasion was the annual dinner of Surgical Biology Club III that is held during the American College of Surgeons fall Congress. This meeting occurred in the mid-1980s soon after I had assumed a major administrative responsibility as chair of a department of surgery. At the time I was the definition of a young, unseasoned, and inexperienced leader. The wisdom so unexpectedly imparted that evening goes to the core of exemplary leadership and has served me well over many years. In fact, I consider the message I received so important that it became a central tenet of a publication I wrote on surgical leadership several years later (Rikkers LF: Surgical leadership: lessons learned. Surgery 2004;140:717-24).
Virtually all surgeons are expected to be leaders. This responsibility may be limited to leading their operating room team or as extensive as guiding a large multidisciplinary health care team or a major academic department of surgery. Unfortunately leadership skills are not a component of the curriculum of most surgical residencies. Many surgeons have leadership responsibilities suddenly thrust upon them, and they are often ill-prepared. Courses in leadership offered nationally are usually expensive both in the cost of participating as well as time away from work. An exception is the ACS’s Surgeons As Leaders course that is conducted over a 3-day span. Thus, whenever a pearl regarding this challenging responsibility that we all face unexpectedly appears, it is essential to tuck it away into the recesses of one’s brain so that it can be quickly mobilized when needed. That evening at the Surgical Biology Club III dinner so many years ago was one such opportunity for me.
Shuck’s thesis was that a leader is presented with a gift of tickets when taking on a new position. In a sense, the tickets represent the goodwill freely given from the institution and the unit led at the beginning of one’s term. This is often defined as the "honeymoon period." Subsequent success or failure of the leader is greatly dependent on how these tickets are spent. Unfortunately, there are hard and fast rules of this ticket game that must be adhered to. Most importantly, once tickets are spent, they cannot be replenished. Second, one is never told exactly how many tickets he or she has been given. The bottom line is that one must be extremely careful in how the tickets are used. In other words, throughout the course of one’s leadership, issues and battles that require expenditure of tickets must be carefully chosen. Ticket spendthrifts tend to squander their tickets on relatively insignificant concerns early in their tenure with none left when a truly game-changing matter arises. A key concept that must be understood early on by inexperienced leaders is that most apparent crises are not crises at all. The tincture of time resolves or modulates most of them. Careful study followed by benign neglect is a wise course in many cases. Immediate and decisive action not preceded by detailed analysis, although occasionally merited, usually results in an unwise and unnecessary disbursement of tickets. The supposed crisis of today is often forgotten by tomorrow, even by those who were embroiled in it.
Another important notion for the unseasoned leader to grasp is the fact that we live in a gray world and that black or white issues are quite uncommon. The art of compromise, so poorly understood by our present national leaders, can be a crucial ticket saver. Rapid, definitive, and possibly risky decision-making is warranted only when one’s most cherished values are threatened. However, such instances should be infrequently encountered even during a long career in leadership. One absolute in ticket spending is to never waste tickets on those things that cannot be changed. The Alcoholics Anonymous serenity prayer provides sage advice for successful leadership: "God, grant me the serenity to accept the things I cannot change, the courage to change the things I can, and wisdom to know the difference."
In my personal leadership odyssey as a department chair that spanned 24 years, I confronted only two controversies that merited expenditure of my valuable tickets. When it was all over, no one could tell me how many I had left, but I am happy to pass the residual on to my successor. He may need them in the increasingly complex world in which surgeons live.
So the next time you purposely or inadvertently happen upon an after-dinner presentation, refuse that second glass of wine and tune your antenna into whatever rare bit of wisdom might be forthcoming. Although I can promise nothing, you just might gain an insight that will serve you well the rest of your life.
To me the most daunting of speaking assignments is the after-dinner presentation. By the time the speech begins, the audience has been well fed, and many have emptied their wine glasses and refilled them several times. Bedtime is approaching, and the often somnolent listeners are nowhere near the peak of their powers of comprehension.
I have heard many such presentations, usually at surgical meetings and several from notable, even famous, personalities who had considerable wisdom to convey. Unfortunately, although I do remember the names of many of the speakers, their messages, if they were captured by the memory circuits of my brain, have since escaped me. There is one notable exception: a talk entitled "Tickets" given by Dr. Jerry Shuck, who was then professor and chairman of surgery at Case Western Reserve University. The occasion was the annual dinner of Surgical Biology Club III that is held during the American College of Surgeons fall Congress. This meeting occurred in the mid-1980s soon after I had assumed a major administrative responsibility as chair of a department of surgery. At the time I was the definition of a young, unseasoned, and inexperienced leader. The wisdom so unexpectedly imparted that evening goes to the core of exemplary leadership and has served me well over many years. In fact, I consider the message I received so important that it became a central tenet of a publication I wrote on surgical leadership several years later (Rikkers LF: Surgical leadership: lessons learned. Surgery 2004;140:717-24).
Virtually all surgeons are expected to be leaders. This responsibility may be limited to leading their operating room team or as extensive as guiding a large multidisciplinary health care team or a major academic department of surgery. Unfortunately leadership skills are not a component of the curriculum of most surgical residencies. Many surgeons have leadership responsibilities suddenly thrust upon them, and they are often ill-prepared. Courses in leadership offered nationally are usually expensive both in the cost of participating as well as time away from work. An exception is the ACS’s Surgeons As Leaders course that is conducted over a 3-day span. Thus, whenever a pearl regarding this challenging responsibility that we all face unexpectedly appears, it is essential to tuck it away into the recesses of one’s brain so that it can be quickly mobilized when needed. That evening at the Surgical Biology Club III dinner so many years ago was one such opportunity for me.
Shuck’s thesis was that a leader is presented with a gift of tickets when taking on a new position. In a sense, the tickets represent the goodwill freely given from the institution and the unit led at the beginning of one’s term. This is often defined as the "honeymoon period." Subsequent success or failure of the leader is greatly dependent on how these tickets are spent. Unfortunately, there are hard and fast rules of this ticket game that must be adhered to. Most importantly, once tickets are spent, they cannot be replenished. Second, one is never told exactly how many tickets he or she has been given. The bottom line is that one must be extremely careful in how the tickets are used. In other words, throughout the course of one’s leadership, issues and battles that require expenditure of tickets must be carefully chosen. Ticket spendthrifts tend to squander their tickets on relatively insignificant concerns early in their tenure with none left when a truly game-changing matter arises. A key concept that must be understood early on by inexperienced leaders is that most apparent crises are not crises at all. The tincture of time resolves or modulates most of them. Careful study followed by benign neglect is a wise course in many cases. Immediate and decisive action not preceded by detailed analysis, although occasionally merited, usually results in an unwise and unnecessary disbursement of tickets. The supposed crisis of today is often forgotten by tomorrow, even by those who were embroiled in it.
Another important notion for the unseasoned leader to grasp is the fact that we live in a gray world and that black or white issues are quite uncommon. The art of compromise, so poorly understood by our present national leaders, can be a crucial ticket saver. Rapid, definitive, and possibly risky decision-making is warranted only when one’s most cherished values are threatened. However, such instances should be infrequently encountered even during a long career in leadership. One absolute in ticket spending is to never waste tickets on those things that cannot be changed. The Alcoholics Anonymous serenity prayer provides sage advice for successful leadership: "God, grant me the serenity to accept the things I cannot change, the courage to change the things I can, and wisdom to know the difference."
In my personal leadership odyssey as a department chair that spanned 24 years, I confronted only two controversies that merited expenditure of my valuable tickets. When it was all over, no one could tell me how many I had left, but I am happy to pass the residual on to my successor. He may need them in the increasingly complex world in which surgeons live.
So the next time you purposely or inadvertently happen upon an after-dinner presentation, refuse that second glass of wine and tune your antenna into whatever rare bit of wisdom might be forthcoming. Although I can promise nothing, you just might gain an insight that will serve you well the rest of your life.
To me the most daunting of speaking assignments is the after-dinner presentation. By the time the speech begins, the audience has been well fed, and many have emptied their wine glasses and refilled them several times. Bedtime is approaching, and the often somnolent listeners are nowhere near the peak of their powers of comprehension.
I have heard many such presentations, usually at surgical meetings and several from notable, even famous, personalities who had considerable wisdom to convey. Unfortunately, although I do remember the names of many of the speakers, their messages, if they were captured by the memory circuits of my brain, have since escaped me. There is one notable exception: a talk entitled "Tickets" given by Dr. Jerry Shuck, who was then professor and chairman of surgery at Case Western Reserve University. The occasion was the annual dinner of Surgical Biology Club III that is held during the American College of Surgeons fall Congress. This meeting occurred in the mid-1980s soon after I had assumed a major administrative responsibility as chair of a department of surgery. At the time I was the definition of a young, unseasoned, and inexperienced leader. The wisdom so unexpectedly imparted that evening goes to the core of exemplary leadership and has served me well over many years. In fact, I consider the message I received so important that it became a central tenet of a publication I wrote on surgical leadership several years later (Rikkers LF: Surgical leadership: lessons learned. Surgery 2004;140:717-24).
Virtually all surgeons are expected to be leaders. This responsibility may be limited to leading their operating room team or as extensive as guiding a large multidisciplinary health care team or a major academic department of surgery. Unfortunately leadership skills are not a component of the curriculum of most surgical residencies. Many surgeons have leadership responsibilities suddenly thrust upon them, and they are often ill-prepared. Courses in leadership offered nationally are usually expensive both in the cost of participating as well as time away from work. An exception is the ACS’s Surgeons As Leaders course that is conducted over a 3-day span. Thus, whenever a pearl regarding this challenging responsibility that we all face unexpectedly appears, it is essential to tuck it away into the recesses of one’s brain so that it can be quickly mobilized when needed. That evening at the Surgical Biology Club III dinner so many years ago was one such opportunity for me.
Shuck’s thesis was that a leader is presented with a gift of tickets when taking on a new position. In a sense, the tickets represent the goodwill freely given from the institution and the unit led at the beginning of one’s term. This is often defined as the "honeymoon period." Subsequent success or failure of the leader is greatly dependent on how these tickets are spent. Unfortunately, there are hard and fast rules of this ticket game that must be adhered to. Most importantly, once tickets are spent, they cannot be replenished. Second, one is never told exactly how many tickets he or she has been given. The bottom line is that one must be extremely careful in how the tickets are used. In other words, throughout the course of one’s leadership, issues and battles that require expenditure of tickets must be carefully chosen. Ticket spendthrifts tend to squander their tickets on relatively insignificant concerns early in their tenure with none left when a truly game-changing matter arises. A key concept that must be understood early on by inexperienced leaders is that most apparent crises are not crises at all. The tincture of time resolves or modulates most of them. Careful study followed by benign neglect is a wise course in many cases. Immediate and decisive action not preceded by detailed analysis, although occasionally merited, usually results in an unwise and unnecessary disbursement of tickets. The supposed crisis of today is often forgotten by tomorrow, even by those who were embroiled in it.
Another important notion for the unseasoned leader to grasp is the fact that we live in a gray world and that black or white issues are quite uncommon. The art of compromise, so poorly understood by our present national leaders, can be a crucial ticket saver. Rapid, definitive, and possibly risky decision-making is warranted only when one’s most cherished values are threatened. However, such instances should be infrequently encountered even during a long career in leadership. One absolute in ticket spending is to never waste tickets on those things that cannot be changed. The Alcoholics Anonymous serenity prayer provides sage advice for successful leadership: "God, grant me the serenity to accept the things I cannot change, the courage to change the things I can, and wisdom to know the difference."
In my personal leadership odyssey as a department chair that spanned 24 years, I confronted only two controversies that merited expenditure of my valuable tickets. When it was all over, no one could tell me how many I had left, but I am happy to pass the residual on to my successor. He may need them in the increasingly complex world in which surgeons live.
So the next time you purposely or inadvertently happen upon an after-dinner presentation, refuse that second glass of wine and tune your antenna into whatever rare bit of wisdom might be forthcoming. Although I can promise nothing, you just might gain an insight that will serve you well the rest of your life.

Coordinated Approach May Help in Caring for Hospitals’ Neediest Patients

To my way of thinking, a person’s diagnosis or pathophysiology is not as strong a predictor of needing inpatient hospital care as it might have been 10 or 20 years ago. Rather than the clinical diagnosis (e.g. pneumonia), it seems to me that frailty or social complexity often are the principal determinants of which patients are admitted to a hospital for medical conditions.
Some of these patients are admitted frequently but appear to realize little or no benefit from hospitalization. These patients typically have little or no social support, and they often have either significant mental health disorders or substance abuse, or both. Much has been written about these patients, and I recommend an article by Dr. Atul Gawande in the Jan. 24, 2011, issue of The New Yorker titled “The Hot Spotters: Can We Lower Medical Costs by Giving the Neediest Patients Better Care?”
The Agency for Healthcare Research and Quality’s “Statistical Brief 354” on how health-care expenditures are allocated across the population reported that 1% of the population accounted for more than 22% of health-care spending in 2008. One in 5 of those were in that category again in 2009. Some of these patients would benefit from care plans.
The Role of Care Plans
It seems that there may be few effective inpatient interventions that will benefit these patients. After all, they have chronic issues that require ongoing relationships with outpatient providers, something that many of these patients lack. But for some (most?) of these patients, it seems clear that frequent hospitalizations don’t help and sometimes just perpetuate or worsen the patient’s dependence on the hospital at a high financial cost to society—and significant frustration and burnout on the part of hospital caregivers, including hospitalists.
For most hospitals, this problem is significant enough to require some sort of coordinated approach to the care of the dozens of types of patients in this category. Implementing whatever plan of care seems appropriate to the caregivers during each admission is frustrating, ensures lots of variation in care, and makes it easier for manipulative patients to abuse the hospital resources and personnel.
A better approach is to follow the same plan of care from one hospital visit to the next. You already knew that. But developing a care plan to follow during each ED visit and admission is time-consuming and often fraught with uncertainty about where boundaries should be set. So if you’re like me, you might just try to guide the patient to discharge this time and hope that whoever sees the patient on the next admission will take the initiative to develop the care plan. The result is that few such plans are developed.
Your Hospital Needs a Care Plan
Relying on individual doctors or nurses to take the initiative to develop care plans will almost always mean few plans are developed, they will vary in their effectiveness, and other providers may not be aware a plan exists. This was the case at the hospital where I practice until I heard Dr. Rick Hilger, MD, SFHM, a hospitalist at Regions Hospital in Minneapolis, present on this topic at HM12 in San Diego.
Dr. Hilger led a multidisciplinary team to develop care plans (they call them “restriction care plans”) and found that they dramatically reduced the rate of hospital admissions and ED visits for these patients. Hearing about this experience served as a kick in the pants for me, so I did much the same thing at “my” hospital. We have now developed plans for more than 20 patients and found that they visit our ED and are admitted less often. And, anecdotally at least, hospitalists and other hospital staff find that the care plans reduce, at least a little, the stress of caring for these patients.
Unanswered Questions
Although it seems clear that care plans reduce visits to the hospital that develops them, I suspect that some of these patients aren’t consuming any fewer health-care resources. They may just seek care from a different hospital.
My home state of Washington is working to develop individual patient care plans available to all hospitals in the state. A system called the Emergency Department Information Exchange (EDIE) has been adopted by nearly all the hospitals in the state. It allows them to share information on ED visits and such things as care plans with one another. For example, through EDIE, each hospital could see the opiate dosing schedule and admission criteria agreed to by patient and primary-care physician.
So it seems that care plans and the technology to share them can make it more difficult for patients to harm themselves by visiting many hospitals to get excessive opiate prescriptions, for example. This should benefit the patient and lower ED and hospital expenditures for these patients. But we don’t know what portion of costs simply is shifted to other settings, so there is no easy way to know the net effect on health-care costs.
An important unanswered question is whether these care plans improve patient well-being. It seems clear they do in some cases, but it is hard to know whether some patients may be worse off because of the plan.
Conclusion
I think nearly every hospital would benefit from a care plan committee composed of at least one hospitalist, ED physician, a nursing representative, and potentially other disciplines (see “Care Plan Attributes,” above). Our committee includes our inpatient psychiatrist, a really valuable contributor.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
To my way of thinking, a person’s diagnosis or pathophysiology is not as strong a predictor of needing inpatient hospital care as it might have been 10 or 20 years ago. Rather than the clinical diagnosis (e.g. pneumonia), it seems to me that frailty or social complexity often are the principal determinants of which patients are admitted to a hospital for medical conditions.
Some of these patients are admitted frequently but appear to realize little or no benefit from hospitalization. These patients typically have little or no social support, and they often have either significant mental health disorders or substance abuse, or both. Much has been written about these patients, and I recommend an article by Dr. Atul Gawande in the Jan. 24, 2011, issue of The New Yorker titled “The Hot Spotters: Can We Lower Medical Costs by Giving the Neediest Patients Better Care?”
The Agency for Healthcare Research and Quality’s “Statistical Brief 354” on how health-care expenditures are allocated across the population reported that 1% of the population accounted for more than 22% of health-care spending in 2008. One in 5 of those were in that category again in 2009. Some of these patients would benefit from care plans.
The Role of Care Plans
It seems that there may be few effective inpatient interventions that will benefit these patients. After all, they have chronic issues that require ongoing relationships with outpatient providers, something that many of these patients lack. But for some (most?) of these patients, it seems clear that frequent hospitalizations don’t help and sometimes just perpetuate or worsen the patient’s dependence on the hospital at a high financial cost to society—and significant frustration and burnout on the part of hospital caregivers, including hospitalists.
For most hospitals, this problem is significant enough to require some sort of coordinated approach to the care of the dozens of types of patients in this category. Implementing whatever plan of care seems appropriate to the caregivers during each admission is frustrating, ensures lots of variation in care, and makes it easier for manipulative patients to abuse the hospital resources and personnel.
A better approach is to follow the same plan of care from one hospital visit to the next. You already knew that. But developing a care plan to follow during each ED visit and admission is time-consuming and often fraught with uncertainty about where boundaries should be set. So if you’re like me, you might just try to guide the patient to discharge this time and hope that whoever sees the patient on the next admission will take the initiative to develop the care plan. The result is that few such plans are developed.
Your Hospital Needs a Care Plan
Relying on individual doctors or nurses to take the initiative to develop care plans will almost always mean few plans are developed, they will vary in their effectiveness, and other providers may not be aware a plan exists. This was the case at the hospital where I practice until I heard Dr. Rick Hilger, MD, SFHM, a hospitalist at Regions Hospital in Minneapolis, present on this topic at HM12 in San Diego.
Dr. Hilger led a multidisciplinary team to develop care plans (they call them “restriction care plans”) and found that they dramatically reduced the rate of hospital admissions and ED visits for these patients. Hearing about this experience served as a kick in the pants for me, so I did much the same thing at “my” hospital. We have now developed plans for more than 20 patients and found that they visit our ED and are admitted less often. And, anecdotally at least, hospitalists and other hospital staff find that the care plans reduce, at least a little, the stress of caring for these patients.
Unanswered Questions
Although it seems clear that care plans reduce visits to the hospital that develops them, I suspect that some of these patients aren’t consuming any fewer health-care resources. They may just seek care from a different hospital.
My home state of Washington is working to develop individual patient care plans available to all hospitals in the state. A system called the Emergency Department Information Exchange (EDIE) has been adopted by nearly all the hospitals in the state. It allows them to share information on ED visits and such things as care plans with one another. For example, through EDIE, each hospital could see the opiate dosing schedule and admission criteria agreed to by patient and primary-care physician.
So it seems that care plans and the technology to share them can make it more difficult for patients to harm themselves by visiting many hospitals to get excessive opiate prescriptions, for example. This should benefit the patient and lower ED and hospital expenditures for these patients. But we don’t know what portion of costs simply is shifted to other settings, so there is no easy way to know the net effect on health-care costs.
An important unanswered question is whether these care plans improve patient well-being. It seems clear they do in some cases, but it is hard to know whether some patients may be worse off because of the plan.
Conclusion
I think nearly every hospital would benefit from a care plan committee composed of at least one hospitalist, ED physician, a nursing representative, and potentially other disciplines (see “Care Plan Attributes,” above). Our committee includes our inpatient psychiatrist, a really valuable contributor.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
To my way of thinking, a person’s diagnosis or pathophysiology is not as strong a predictor of needing inpatient hospital care as it might have been 10 or 20 years ago. Rather than the clinical diagnosis (e.g. pneumonia), it seems to me that frailty or social complexity often are the principal determinants of which patients are admitted to a hospital for medical conditions.
Some of these patients are admitted frequently but appear to realize little or no benefit from hospitalization. These patients typically have little or no social support, and they often have either significant mental health disorders or substance abuse, or both. Much has been written about these patients, and I recommend an article by Dr. Atul Gawande in the Jan. 24, 2011, issue of The New Yorker titled “The Hot Spotters: Can We Lower Medical Costs by Giving the Neediest Patients Better Care?”
The Agency for Healthcare Research and Quality’s “Statistical Brief 354” on how health-care expenditures are allocated across the population reported that 1% of the population accounted for more than 22% of health-care spending in 2008. One in 5 of those were in that category again in 2009. Some of these patients would benefit from care plans.
The Role of Care Plans
It seems that there may be few effective inpatient interventions that will benefit these patients. After all, they have chronic issues that require ongoing relationships with outpatient providers, something that many of these patients lack. But for some (most?) of these patients, it seems clear that frequent hospitalizations don’t help and sometimes just perpetuate or worsen the patient’s dependence on the hospital at a high financial cost to society—and significant frustration and burnout on the part of hospital caregivers, including hospitalists.
For most hospitals, this problem is significant enough to require some sort of coordinated approach to the care of the dozens of types of patients in this category. Implementing whatever plan of care seems appropriate to the caregivers during each admission is frustrating, ensures lots of variation in care, and makes it easier for manipulative patients to abuse the hospital resources and personnel.
A better approach is to follow the same plan of care from one hospital visit to the next. You already knew that. But developing a care plan to follow during each ED visit and admission is time-consuming and often fraught with uncertainty about where boundaries should be set. So if you’re like me, you might just try to guide the patient to discharge this time and hope that whoever sees the patient on the next admission will take the initiative to develop the care plan. The result is that few such plans are developed.
Your Hospital Needs a Care Plan
Relying on individual doctors or nurses to take the initiative to develop care plans will almost always mean few plans are developed, they will vary in their effectiveness, and other providers may not be aware a plan exists. This was the case at the hospital where I practice until I heard Dr. Rick Hilger, MD, SFHM, a hospitalist at Regions Hospital in Minneapolis, present on this topic at HM12 in San Diego.
Dr. Hilger led a multidisciplinary team to develop care plans (they call them “restriction care plans”) and found that they dramatically reduced the rate of hospital admissions and ED visits for these patients. Hearing about this experience served as a kick in the pants for me, so I did much the same thing at “my” hospital. We have now developed plans for more than 20 patients and found that they visit our ED and are admitted less often. And, anecdotally at least, hospitalists and other hospital staff find that the care plans reduce, at least a little, the stress of caring for these patients.
Unanswered Questions
Although it seems clear that care plans reduce visits to the hospital that develops them, I suspect that some of these patients aren’t consuming any fewer health-care resources. They may just seek care from a different hospital.
My home state of Washington is working to develop individual patient care plans available to all hospitals in the state. A system called the Emergency Department Information Exchange (EDIE) has been adopted by nearly all the hospitals in the state. It allows them to share information on ED visits and such things as care plans with one another. For example, through EDIE, each hospital could see the opiate dosing schedule and admission criteria agreed to by patient and primary-care physician.
So it seems that care plans and the technology to share them can make it more difficult for patients to harm themselves by visiting many hospitals to get excessive opiate prescriptions, for example. This should benefit the patient and lower ED and hospital expenditures for these patients. But we don’t know what portion of costs simply is shifted to other settings, so there is no easy way to know the net effect on health-care costs.
An important unanswered question is whether these care plans improve patient well-being. It seems clear they do in some cases, but it is hard to know whether some patients may be worse off because of the plan.
Conclusion
I think nearly every hospital would benefit from a care plan committee composed of at least one hospitalist, ED physician, a nursing representative, and potentially other disciplines (see “Care Plan Attributes,” above). Our committee includes our inpatient psychiatrist, a really valuable contributor.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Communication Key to Peaceful Coexistence for Competing Hospital Medicine Groups

Experienced hospitalists and medical directors agree that the key to multiple hospitalist groups coexisting effectively under one roof—whether directly competing or not—is good communication. Effective communication can take time to build.
“Start by working together on something—anything, [such as] a hospital committee of some sort where there’s not likely to be much tension,” says hospitalist pioneer and practice consultant John Nelson, MD, MHM.
Dr. Nelson practices at Overlake Hospital in Bellevue, Wash., which has a hospitalist group employed by the hospital and another employed by Group Health Cooperative, a nonprofit health system in Washington state. It is important to put some trust in the trust bank, he says, “and that’s hard if you have no social connections at all. At my hospital, we enjoy each other’s company, we visit each other at lunch, and we even tried to have a journal club.” The two hospitalist groups work together on developing care protocols. Dr. Nelson says it also makes sense for the groups’ leaders to sit down together on a regular basis and have a venue for discussing important issues and solving problems that may arise.
Other suggestions for hospitalist groups working together under one roof include:
- Clearly define each group’s territory. The groups’ representatives can go out and try to persuade health plans or physician groups to shift their hospitalist allegiances, but there should be no “trolling” or “poaching” of patients going on inside the hospital’s walls. That will only confuse patients and disrupt the hospital’s larger service goals.
- Inform the ED and other key staff of your schedules. It’s important that everyone know exactly who is supposed to get which patients, and how these referrals get made. But recognize that mistakes happen and, hopefully, these will even out between the groups over time.
- Transparency, honesty, and even-handed treatment of all hospitalists can prevent resentment. Clearly defined guidelines and expectations are helpful. If the policy spells out transfers for an incorrectly referred patient, both sides should be accessible and cooperative with that process.
- Identify areas of common interest and agree to work together on these areas (i.e. competition-free zones). It might be possible, for example, for competing groups to take each others’ after-hours call on a rotating basis, with a firm commitment not to steal patients along the way.
- Spell out responsibilities in a way that everyone can agree is fair, such as alternating referrals or taking call on alternating days. For example, if subsidies are paid to more than one hospitalist group, is this done equitably, such as based on the number of hospitalist FTEs or shifts?
- Restrictive covenants and contractual noncompete clauses could become an issue in areas where multiple groups practice. Rather than using overly broad, blanket language, it could be clarified that such pacts apply only to the hospital where the physician currently works, and within a reasonable time frame. But everyone involved should be aware of what these covenants contain and, if they appear unreasonable, don’t sign them.
—Larry Beresford
Experienced hospitalists and medical directors agree that the key to multiple hospitalist groups coexisting effectively under one roof—whether directly competing or not—is good communication. Effective communication can take time to build.
“Start by working together on something—anything, [such as] a hospital committee of some sort where there’s not likely to be much tension,” says hospitalist pioneer and practice consultant John Nelson, MD, MHM.
Dr. Nelson practices at Overlake Hospital in Bellevue, Wash., which has a hospitalist group employed by the hospital and another employed by Group Health Cooperative, a nonprofit health system in Washington state. It is important to put some trust in the trust bank, he says, “and that’s hard if you have no social connections at all. At my hospital, we enjoy each other’s company, we visit each other at lunch, and we even tried to have a journal club.” The two hospitalist groups work together on developing care protocols. Dr. Nelson says it also makes sense for the groups’ leaders to sit down together on a regular basis and have a venue for discussing important issues and solving problems that may arise.
Other suggestions for hospitalist groups working together under one roof include:
- Clearly define each group’s territory. The groups’ representatives can go out and try to persuade health plans or physician groups to shift their hospitalist allegiances, but there should be no “trolling” or “poaching” of patients going on inside the hospital’s walls. That will only confuse patients and disrupt the hospital’s larger service goals.
- Inform the ED and other key staff of your schedules. It’s important that everyone know exactly who is supposed to get which patients, and how these referrals get made. But recognize that mistakes happen and, hopefully, these will even out between the groups over time.
- Transparency, honesty, and even-handed treatment of all hospitalists can prevent resentment. Clearly defined guidelines and expectations are helpful. If the policy spells out transfers for an incorrectly referred patient, both sides should be accessible and cooperative with that process.
- Identify areas of common interest and agree to work together on these areas (i.e. competition-free zones). It might be possible, for example, for competing groups to take each others’ after-hours call on a rotating basis, with a firm commitment not to steal patients along the way.
- Spell out responsibilities in a way that everyone can agree is fair, such as alternating referrals or taking call on alternating days. For example, if subsidies are paid to more than one hospitalist group, is this done equitably, such as based on the number of hospitalist FTEs or shifts?
- Restrictive covenants and contractual noncompete clauses could become an issue in areas where multiple groups practice. Rather than using overly broad, blanket language, it could be clarified that such pacts apply only to the hospital where the physician currently works, and within a reasonable time frame. But everyone involved should be aware of what these covenants contain and, if they appear unreasonable, don’t sign them.
—Larry Beresford
Experienced hospitalists and medical directors agree that the key to multiple hospitalist groups coexisting effectively under one roof—whether directly competing or not—is good communication. Effective communication can take time to build.
“Start by working together on something—anything, [such as] a hospital committee of some sort where there’s not likely to be much tension,” says hospitalist pioneer and practice consultant John Nelson, MD, MHM.
Dr. Nelson practices at Overlake Hospital in Bellevue, Wash., which has a hospitalist group employed by the hospital and another employed by Group Health Cooperative, a nonprofit health system in Washington state. It is important to put some trust in the trust bank, he says, “and that’s hard if you have no social connections at all. At my hospital, we enjoy each other’s company, we visit each other at lunch, and we even tried to have a journal club.” The two hospitalist groups work together on developing care protocols. Dr. Nelson says it also makes sense for the groups’ leaders to sit down together on a regular basis and have a venue for discussing important issues and solving problems that may arise.
Other suggestions for hospitalist groups working together under one roof include:
- Clearly define each group’s territory. The groups’ representatives can go out and try to persuade health plans or physician groups to shift their hospitalist allegiances, but there should be no “trolling” or “poaching” of patients going on inside the hospital’s walls. That will only confuse patients and disrupt the hospital’s larger service goals.
- Inform the ED and other key staff of your schedules. It’s important that everyone know exactly who is supposed to get which patients, and how these referrals get made. But recognize that mistakes happen and, hopefully, these will even out between the groups over time.
- Transparency, honesty, and even-handed treatment of all hospitalists can prevent resentment. Clearly defined guidelines and expectations are helpful. If the policy spells out transfers for an incorrectly referred patient, both sides should be accessible and cooperative with that process.
- Identify areas of common interest and agree to work together on these areas (i.e. competition-free zones). It might be possible, for example, for competing groups to take each others’ after-hours call on a rotating basis, with a firm commitment not to steal patients along the way.
- Spell out responsibilities in a way that everyone can agree is fair, such as alternating referrals or taking call on alternating days. For example, if subsidies are paid to more than one hospitalist group, is this done equitably, such as based on the number of hospitalist FTEs or shifts?
- Restrictive covenants and contractual noncompete clauses could become an issue in areas where multiple groups practice. Rather than using overly broad, blanket language, it could be clarified that such pacts apply only to the hospital where the physician currently works, and within a reasonable time frame. But everyone involved should be aware of what these covenants contain and, if they appear unreasonable, don’t sign them.
—Larry Beresford
What's for dessert?
Hemingway once remarked: “Retirement is the ugliest word in the language.” Since most surgeons as well as many others would agree with his assessment, I believe it is time to retire the word retirement and look to another, more positive means of depicting the twilight years of our lives. Shakespeare, writing several centuries before Hemingway, considered the world a stage on which the days of our existence are played out.
<[stk 3]>My rather simplistic view of the surgeon’s life is that of a three-act play or a three-course meal. Act I, the appetizer, represents a surgeon’s approximately 33 years of education and may be, at least in the early years, in part directed by his parents. Act II, the main course and also 33 years give or take a few, is our vocational phase during which we deliver surgical care to our patients. Act III, the dessert, and for symmetry’s sake, can also approach 33 years, is what we formerly called retirement. With appropriate planning and foresight, each of these acts can be and should be gratifying and fulfilling. <[etk]>
<[stk 3]>For most of us a great deal of thought and meticulous planning are responsible for whatever success and satisfaction we have gained from Acts I and II. Unfortunately, such is not the case for Act III, that can be suddenly thrust upon us because of illness or disability. The pundits recommend careful preparation for Act III but their counsel is usually limited to financial considerations. This is an important aspect of Act III, but we all know that a secure economic future does not guarantee happiness or fulfillment. <[etk]>
So what can one do during Act II to make it more likely that the years of Act III are filled with contentment and purpose rather than frustration and regret? Realizing that no formula for Act III fits all, some recommendations and observations may be helpful. Most economic considerations for Act III are obvious and well documented. In nearly all situations, it is wise to never live to or beyond one’s income, to maximize retirement contributions, and to allow carefully chosen professionals rather than ourselves to manage our finances. If too much is consumed during the main course, little will be left for dessert.
A<[stk 3]>ll surgeons have spent much of their lives in service to others, and it is important for most of us that this continue after laying aside our scalpels. For some, this need is met by medical missionary work here or abroad or by service in one or more volunteer organizations. Funding a family foundation during the higher income years of Act II permits you to be a substantial player in philanthropy throughout the years of Act III. If this is done fairly early, even rather modest contributions will grow to an impressive sum by the time Act III arrives, permitting you to make a significant difference in a worthy agency or institution or in the lives of people in need.<[etk]>
<[stk -3]>Life as a surgeon can be all-consuming. An essential activity during Act II is to develop interests, even passions, outside of surgery. It is tempting to put this off until one has more leisure time, but this can be a fatal mistake. Suddenly or even gradually confronting Act III with no appealing substitutes for the many hours spent in the clinic and operating room can lead to an unfulfilling existence. Ideally one or more of these interests should be initiated during Act II, but if that is not possible because of time restrictions, ideas should be carefully recorded as they come to mind so they are not forgotten when the time for action arrives. Preferably some of these should be relevant to the significant other in your life to solidify a relationship that may have suffered from years of separation caused by a demanding work schedule. <[etk]>
<[stk -3]>The most difficult aspect of the transition to Act III can be the loss of identity as a surgeon. Nurturing new interests and passions provides the opportunity to reinvent yourself in a new and exciting way that may be just as satisfying as your former professional life. <[etk]>
Most would agree that nothing in life is more important than relationships. Those with friends and especially family can be stressed and even frayed during the rigorous years of training and work as a surgeon. These must be repaired before or during Act III.
One of the joys that can occupy these later years is the luxury of meaningful time spent with your mate, adult children, grandchildren, and friends. If romance with that important person in your life has waned during the harried years of surgery, Act III is the time to reinvigorate it and bring it to a new and refreshing pinnacle.
<[stk 3]>Finally, a key consideration is timing. When is it time to end your life as a surgeon? Should it be done abruptly or gradually? Gradually is often a challenge as many partnerships are not prone to include a part-time surgeon who does not participate in the call schedule. Again, no size fits all, but it is far preferable to quit when one is near the peak of his/her skills than when associates notice decline that may or may not be verbalized. <[etk]>
<[stk 3]>Rather than emphasizing the ending, in my opinion it is advantageous, even essential, to highlight a new beginning – one in which the skills and talents gained during a life in surgery can be redirected toward novel pursuits and opportunities to help society in new and exciting ways. To get there requires careful planning. As we all know, dessert can be delicious and enjoyable, but it all depends on what w<[ker -3]>e order. <[etk]>
Dr. Rikkers is Editor in Chief of Surgery News.
Hemingway once remarked: “Retirement is the ugliest word in the language.” Since most surgeons as well as many others would agree with his assessment, I believe it is time to retire the word retirement and look to another, more positive means of depicting the twilight years of our lives. Shakespeare, writing several centuries before Hemingway, considered the world a stage on which the days of our existence are played out.
<[stk 3]>My rather simplistic view of the surgeon’s life is that of a three-act play or a three-course meal. Act I, the appetizer, represents a surgeon’s approximately 33 years of education and may be, at least in the early years, in part directed by his parents. Act II, the main course and also 33 years give or take a few, is our vocational phase during which we deliver surgical care to our patients. Act III, the dessert, and for symmetry’s sake, can also approach 33 years, is what we formerly called retirement. With appropriate planning and foresight, each of these acts can be and should be gratifying and fulfilling. <[etk]>
<[stk 3]>For most of us a great deal of thought and meticulous planning are responsible for whatever success and satisfaction we have gained from Acts I and II. Unfortunately, such is not the case for Act III, that can be suddenly thrust upon us because of illness or disability. The pundits recommend careful preparation for Act III but their counsel is usually limited to financial considerations. This is an important aspect of Act III, but we all know that a secure economic future does not guarantee happiness or fulfillment. <[etk]>
So what can one do during Act II to make it more likely that the years of Act III are filled with contentment and purpose rather than frustration and regret? Realizing that no formula for Act III fits all, some recommendations and observations may be helpful. Most economic considerations for Act III are obvious and well documented. In nearly all situations, it is wise to never live to or beyond one’s income, to maximize retirement contributions, and to allow carefully chosen professionals rather than ourselves to manage our finances. If too much is consumed during the main course, little will be left for dessert.
A<[stk 3]>ll surgeons have spent much of their lives in service to others, and it is important for most of us that this continue after laying aside our scalpels. For some, this need is met by medical missionary work here or abroad or by service in one or more volunteer organizations. Funding a family foundation during the higher income years of Act II permits you to be a substantial player in philanthropy throughout the years of Act III. If this is done fairly early, even rather modest contributions will grow to an impressive sum by the time Act III arrives, permitting you to make a significant difference in a worthy agency or institution or in the lives of people in need.<[etk]>
<[stk -3]>Life as a surgeon can be all-consuming. An essential activity during Act II is to develop interests, even passions, outside of surgery. It is tempting to put this off until one has more leisure time, but this can be a fatal mistake. Suddenly or even gradually confronting Act III with no appealing substitutes for the many hours spent in the clinic and operating room can lead to an unfulfilling existence. Ideally one or more of these interests should be initiated during Act II, but if that is not possible because of time restrictions, ideas should be carefully recorded as they come to mind so they are not forgotten when the time for action arrives. Preferably some of these should be relevant to the significant other in your life to solidify a relationship that may have suffered from years of separation caused by a demanding work schedule. <[etk]>
<[stk -3]>The most difficult aspect of the transition to Act III can be the loss of identity as a surgeon. Nurturing new interests and passions provides the opportunity to reinvent yourself in a new and exciting way that may be just as satisfying as your former professional life. <[etk]>
Most would agree that nothing in life is more important than relationships. Those with friends and especially family can be stressed and even frayed during the rigorous years of training and work as a surgeon. These must be repaired before or during Act III.
One of the joys that can occupy these later years is the luxury of meaningful time spent with your mate, adult children, grandchildren, and friends. If romance with that important person in your life has waned during the harried years of surgery, Act III is the time to reinvigorate it and bring it to a new and refreshing pinnacle.
<[stk 3]>Finally, a key consideration is timing. When is it time to end your life as a surgeon? Should it be done abruptly or gradually? Gradually is often a challenge as many partnerships are not prone to include a part-time surgeon who does not participate in the call schedule. Again, no size fits all, but it is far preferable to quit when one is near the peak of his/her skills than when associates notice decline that may or may not be verbalized. <[etk]>
<[stk 3]>Rather than emphasizing the ending, in my opinion it is advantageous, even essential, to highlight a new beginning – one in which the skills and talents gained during a life in surgery can be redirected toward novel pursuits and opportunities to help society in new and exciting ways. To get there requires careful planning. As we all know, dessert can be delicious and enjoyable, but it all depends on what w<[ker -3]>e order. <[etk]>
Dr. Rikkers is Editor in Chief of Surgery News.
Hemingway once remarked: “Retirement is the ugliest word in the language.” Since most surgeons as well as many others would agree with his assessment, I believe it is time to retire the word retirement and look to another, more positive means of depicting the twilight years of our lives. Shakespeare, writing several centuries before Hemingway, considered the world a stage on which the days of our existence are played out.
<[stk 3]>My rather simplistic view of the surgeon’s life is that of a three-act play or a three-course meal. Act I, the appetizer, represents a surgeon’s approximately 33 years of education and may be, at least in the early years, in part directed by his parents. Act II, the main course and also 33 years give or take a few, is our vocational phase during which we deliver surgical care to our patients. Act III, the dessert, and for symmetry’s sake, can also approach 33 years, is what we formerly called retirement. With appropriate planning and foresight, each of these acts can be and should be gratifying and fulfilling. <[etk]>
<[stk 3]>For most of us a great deal of thought and meticulous planning are responsible for whatever success and satisfaction we have gained from Acts I and II. Unfortunately, such is not the case for Act III, that can be suddenly thrust upon us because of illness or disability. The pundits recommend careful preparation for Act III but their counsel is usually limited to financial considerations. This is an important aspect of Act III, but we all know that a secure economic future does not guarantee happiness or fulfillment. <[etk]>
So what can one do during Act II to make it more likely that the years of Act III are filled with contentment and purpose rather than frustration and regret? Realizing that no formula for Act III fits all, some recommendations and observations may be helpful. Most economic considerations for Act III are obvious and well documented. In nearly all situations, it is wise to never live to or beyond one’s income, to maximize retirement contributions, and to allow carefully chosen professionals rather than ourselves to manage our finances. If too much is consumed during the main course, little will be left for dessert.
A<[stk 3]>ll surgeons have spent much of their lives in service to others, and it is important for most of us that this continue after laying aside our scalpels. For some, this need is met by medical missionary work here or abroad or by service in one or more volunteer organizations. Funding a family foundation during the higher income years of Act II permits you to be a substantial player in philanthropy throughout the years of Act III. If this is done fairly early, even rather modest contributions will grow to an impressive sum by the time Act III arrives, permitting you to make a significant difference in a worthy agency or institution or in the lives of people in need.<[etk]>
<[stk -3]>Life as a surgeon can be all-consuming. An essential activity during Act II is to develop interests, even passions, outside of surgery. It is tempting to put this off until one has more leisure time, but this can be a fatal mistake. Suddenly or even gradually confronting Act III with no appealing substitutes for the many hours spent in the clinic and operating room can lead to an unfulfilling existence. Ideally one or more of these interests should be initiated during Act II, but if that is not possible because of time restrictions, ideas should be carefully recorded as they come to mind so they are not forgotten when the time for action arrives. Preferably some of these should be relevant to the significant other in your life to solidify a relationship that may have suffered from years of separation caused by a demanding work schedule. <[etk]>
<[stk -3]>The most difficult aspect of the transition to Act III can be the loss of identity as a surgeon. Nurturing new interests and passions provides the opportunity to reinvent yourself in a new and exciting way that may be just as satisfying as your former professional life. <[etk]>
Most would agree that nothing in life is more important than relationships. Those with friends and especially family can be stressed and even frayed during the rigorous years of training and work as a surgeon. These must be repaired before or during Act III.
One of the joys that can occupy these later years is the luxury of meaningful time spent with your mate, adult children, grandchildren, and friends. If romance with that important person in your life has waned during the harried years of surgery, Act III is the time to reinvigorate it and bring it to a new and refreshing pinnacle.
<[stk 3]>Finally, a key consideration is timing. When is it time to end your life as a surgeon? Should it be done abruptly or gradually? Gradually is often a challenge as many partnerships are not prone to include a part-time surgeon who does not participate in the call schedule. Again, no size fits all, but it is far preferable to quit when one is near the peak of his/her skills than when associates notice decline that may or may not be verbalized. <[etk]>
<[stk 3]>Rather than emphasizing the ending, in my opinion it is advantageous, even essential, to highlight a new beginning – one in which the skills and talents gained during a life in surgery can be redirected toward novel pursuits and opportunities to help society in new and exciting ways. To get there requires careful planning. As we all know, dessert can be delicious and enjoyable, but it all depends on what w<[ker -3]>e order. <[etk]>
Dr. Rikkers is Editor in Chief of Surgery News.

Win Whitcomb: Front-Line Hospitalists Fight Against Health Care-Associated Infections (HAIs)

2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
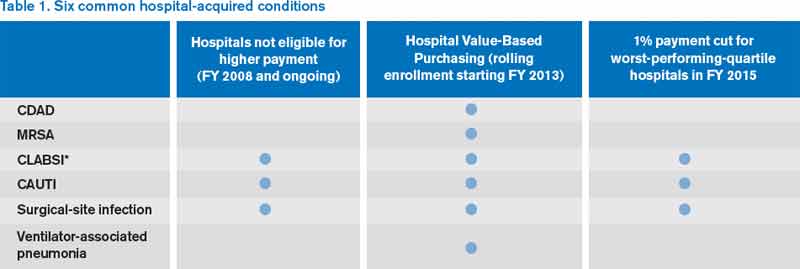
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
2013 marks a turning point in the way hospitals are held accountable for the prevention of healthcare-associated infections (HAIs). It has been known for some time that HAIs are a serious cause of morbidity, with 1 in 20 hospital patients in the U.S. acquiring one. That represents 1.7 million Americans and accounts for about 100,000 lives lost each year. On a personal note, my father died of an HAI after surgery in 2000.
Now, with the Affordable Care Act coming into full swing, hospitals must get serious about preventing HAIs. This presents a major opportunity for hospitalists. There are three ways that hospitals will be affected:
- Since 2008, hospitals have not been reimbursed at a higher rate for vascular catheter-associated infections, catheter-associated urinary tract infections (UTIs), or surgical-site infections when acquired in the hospital.
- Over the next few years, Medicare’s Hospital Value-Based Purchasing (HVBP) program will begin to pay hospitals more or less, depending on how they perform, on six HAIs.
- Beginning in October 2014, in a roll-up measure for hospital-acquired conditions (which include infections), the worst-performing quartile of U.S. hospitals will be penalized 1% of their Medicare inpatient payments (see Table 1, below).
There are six HAIs that will be increasingly tied to hospital reimbursement. Each can be partially or completely prevented based on sets of practices, or care bundles, that require teamwork both in the planning stages and at the bedside. And, of course, the single most important way to reduce the spread of HAIs is to clean your hands before and after each patient encounter.
Clostridium-Difficile-Associated Disease (CDAD)
It is likely that your hospital has some type of CDAD prevention program. Here are a few things to keep in mind for CDAD prevention:
- Avoid alcohol-based hand rubs, because they do not kill C. diff spores. Vigorous hand washing with soap and water is the best approach.
- Use clindamycin, fluoroquinolones, and third-generation cephalosporins judiciously, as their restriction has been associated with reduced rates of CDAD.
- Place patients with suspected or proven C. diff infection on contact precautions, including gloves and gowns.
Methicillin-Resistant Staphylococcus Aureus (MRSA)
This includes hospital-acquired MRSA bacteremia. This topic will be discussed in future columns. Approaches to prevention include hand hygiene, cohorting patients, effective environmental cleaning, and antibiotic stewardship.
Central-Line-Associated Bloodstream Infection (CLABSI)
Adherence to the central-line insertion bundle has been conclusively shown to prevent CLABSI. It will become a process measure for HVBP in the near future. Prevention measures include hand hygiene, maximal barrier precautions during insertion, skin antisepsis with chlorhexidine, avoidance of the femoral vein, and daily assessment for readiness to discontinue the central line (which should involve every hospitalist).
Catheter-Associated Urinary Tract Infection (CAUTI)
CAUTI has been mentioned frequently in this column, and for good reason: It is the most common HAI. Although the evidence supporting practices that prevent CAUTI is not as strong as for CLABSI, every institution should have a bundle of practices embedded in nurses’ and doctors’ workflow to prevent CAUTI (see “Quality Meets Finance,” January 2013, p. 31).
Surgical-Site Infection (SSI)
For the most part, SSI can be left to the surgeons and other operating room professionals. However, with increasing involvement of hospitalists in surgical cases, we must have an understanding of how SSIs are prevented. The World Health Organization surgical checklist (www.who.int/patientsafety/safesurgery) is a great starting point for any organization.
Ventilator-Associated Pneumonia (VAP)
For hospitalists who provide critical care, adherence to a VAP prevention bundle includes:
- Elevation of the head of the bed;
- Daily “sedation vacation” and readiness to extubate;
- Oral care with chlorhexidine; and
- Peptic ulcer disease and venous thromboembolism prophylaxis.
In 2009, the U.S. Department of Health and Human Services (HHS) launched an action plan to prevent HAIs. As part of this effort, the Agency for Health Research and Quality (AHRQ) created a comprehensive unit-based safety program (CUSP) aimed at preventing CLABSI and CAUTI. The effort also focuses on safety culture and teamwork. For those interested in participating, visit www.onthecuspstophai.org.
Another way to get involved is to work Partnership for Patients, a public-private partnership led by HHS (http://partnershipforpatients.cms.gov), if a team at your hospital is participating. The Partnership for Patients seeks to reduce harm, including HAIs, by 40% by the end of 2013 compared with a 2010 baseline.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View from The Center
As many of you know, SHM recently submitted five recommendations to the American Board of Internal Medicine Foundation’s Choosing Wisely campaign. This campaign encourages physicians and patients to have crucial conversations about appropriate utilization of tests and treatments. Seventeen specialty societies released lists in the second phase of the campaign. Many of the lists, including SHM’s, include recommendations that can help reduce hospital-acquired infections.
For example, one of SHM’s recommendations suggests not placing, or leaving in place, urinary catheters for any reason other than those indicated by the guidelines (e.g. bladder outlet obstruction, acute urinary retention, patient requires prolonged immobilization, to improve comfort for end of life, selected perioperative conditions). As Dr. Whitcomb indicates above, CAUTIs are low-hanging fruit when it comes to improving this condition—the guidelines are clear-cut, and relatively simple protocols can be put into place to prevent CAUTI.
Among the American Academy of Family Physicians and other society recommendations is avoidance of routine prescriptions of antibiotics for acute sinusitis or upper respiratory infections. Good antimicrobial stewardship policies are another approach to reduce or eliminate harmful antibiotic-resistant infections.
SHM will be offering multiple opportunities in the coming months to support your institution in Choosing Wisely. A daylong pre-course and two breakout sessions will be offered at HM13 (www.hospitalmedicine2013.org) addressing how you can implement the various recommendations. Additionally, publications are in the works describing the evidence base for SHM’s “avoid lists.” For resources, more information about SHM’s recommendations, and the latest Choosing Wisely developments, visit www.hospitalmedicine.org/choosingwisely.
John Nelson: Excessive Workload a Concern for Many Hospitalists

“Forty percent of physicians reported that their typical inpatient census exceeded safe levels at least monthly.”1
This quote is taken from an article by Henry Michtalik and colleagues that appeared at the end of January this year in JAMA Internal Medicine. In 2010 the authors conducted an on-line survey asking hospitalists their perceptions of their workload. Respondents indicated that with concerning frequency a high workload prevented them from adequately discussing with patients treatment options or answering questions, delay admitting or discharging patients until the next day or shift, or in some other way risk patient safety or the overall quality of their work.
This alarming finding matches my anecdotal experience working with many different hospitalist groups around the country. I think few hospitalists were surprised by the survey’s findings. Excess hospitalist workloads are indeed a problem in some settings, and those who bear them are typically not shy about speaking out.
The demand for hospitalists has exceeded the supply of doctors available to do the work throughout the history of the field. Under the weight of stunningly rapid growth in referral volume, from about 1995 to 2002, it was reasonably common for the original doctors in a hospitalist practice to become overwhelmed and leave for other work after a year or two, sometimes resulting in the collapse of the practice. Most practices are no longer in such a rapid-growth phase, but for many of them, staffing has not yet caught up with workload. The result can be chronic excess work, and even if daily patient volume is not seen as being unsafe, the number of days or shifts worked might be excessive and lead to fatigue and poor performance.
Other Workload Data
The respondents to the Michtalik survey reported that regardless of any assistance, “they could safely see 15 patients per shift, if their effort was 100% clinical.” What we don’t know is how long their shifts were, whether they included things like ICU coverage, and how many shifts they work consecutively or in a year.
SHM’s 2012 State of Hospital Medicine report, which is based on 2011 data, provides additional context. It shows that hospitalists serving adult patients report a median 2,092 billed encounters annually (mean 2,245, standard deviation 1,161). They spread this work over a median 185 shifts (“work periods”) annually (mean 192). While there are lots of methodological problems in manipulating those numbers further, 2,092 encounters divided by 185 shifts yields 11.3 encounters per shift. These numbers exclude academicians who typically spend significant time in activities other than direct patient care, and I’m intentionally ignoring such issues as the night-shift doctor, who typically has low productivity, bringing down the average per full-time doctor in a practice.
The numbers from both surveys are sort of fuzzy because they aren’t audited or verified, but the 2012 State of Hospital Medicine data suggest that typical workloads aren’t too high in most practices, yet 40% of respondents in the Michtalik survey said they were high enough—unreasonably high—to risk quality and safety at least once a month.
One way to reconcile these findings is to take into account the standard deviation in daily volume in a single practice of about 30% to 40% on above or below the mean. If a hospitalist averages 14 encounters each day shift, then he should expect that the daily number might vary between about eight and 20. The Michtalik survey responses were likely reflecting the shifts on the high end.
Perspective
I wonder what a survey of physician workload opinions in other specialties would show, or what a survey of workers across all segments of the U.S. workforce in and out of healthcare would show. Of course, many or most jobs outside of healthcare don’t risk another’s health or well-being as significantly as ours do, but it would still be instructive to know how people in general think about the work they do.
I suspect a significant number of people across many different jobs feel like too much work is expected of them, and they can point to the ways their performance suffers as a result. It is difficult to know what portion of those who report too much work is just complaining versus a thoughtful self-reflection of the determinants of their performance. Lots of hospitalists do face worrisome high workloads, but some would probably still complain even with a much lower workload.
What Can Be Done?
For those practices facing remarkably high patient volumes, the solution is to make sure you’re recruiting additional doctors, and/or NPs/PAs, as fast as you can. But a portion of these practices must first convince their employers that more staff is needed. Some practices face a real uphill battle in getting the required additional funding, and the place to start is with a careful analysis of your current workload—based on hard numbers from your practice, not just anecdotes and estimates.
Don’t forget that some hospitalists put themselves in the position of having to manage high daily patient volumes by choosing a schedule of relatively few worked days annually. For example, a group working a seven-on/seven-off schedule that also has 14 shifts of time off means that each doctor will work only 168.5 shifts annually. Compressing a year’s worth of work into only 168 shifts means that each shift will be busy, and many will involve patient volumes that exceed what is seen as safe.
It could make more sense to titrate that same work volume over more annual shifts so that the average shift is less busy. I would love to see the Michtalik data segregated by those who work many shifts annually versus those who work few shifts. It is possible that those working more shifts have reported excessive workloads less often.
SHM has a role in influencing hospitalist workloads and promotes dissemination of data and opinions about it. At HM13 next month in Washington, D.C., I am leading a session titled “Hospitalist Workload: Is 15 the Right Number?” Although it won’t provide the “right” workload for all hospitalists, it will offer worthwhile data and food for thought.
It is much more difficult to do studies of how workload influences performance than something like effects of sleep deprivation on performance, so we may never get clear answers. You could take some consolation in the fact that successive surveys have shown little change or even modest decreases in annual patient encounters. But then again, maybe that hasn’t helped with excess work since providing hospital care gets harder and more complex every year.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at john.nelson@nelsonflores.com.
Reference
“Forty percent of physicians reported that their typical inpatient census exceeded safe levels at least monthly.”1
This quote is taken from an article by Henry Michtalik and colleagues that appeared at the end of January this year in JAMA Internal Medicine. In 2010 the authors conducted an on-line survey asking hospitalists their perceptions of their workload. Respondents indicated that with concerning frequency a high workload prevented them from adequately discussing with patients treatment options or answering questions, delay admitting or discharging patients until the next day or shift, or in some other way risk patient safety or the overall quality of their work.
This alarming finding matches my anecdotal experience working with many different hospitalist groups around the country. I think few hospitalists were surprised by the survey’s findings. Excess hospitalist workloads are indeed a problem in some settings, and those who bear them are typically not shy about speaking out.
The demand for hospitalists has exceeded the supply of doctors available to do the work throughout the history of the field. Under the weight of stunningly rapid growth in referral volume, from about 1995 to 2002, it was reasonably common for the original doctors in a hospitalist practice to become overwhelmed and leave for other work after a year or two, sometimes resulting in the collapse of the practice. Most practices are no longer in such a rapid-growth phase, but for many of them, staffing has not yet caught up with workload. The result can be chronic excess work, and even if daily patient volume is not seen as being unsafe, the number of days or shifts worked might be excessive and lead to fatigue and poor performance.
Other Workload Data
The respondents to the Michtalik survey reported that regardless of any assistance, “they could safely see 15 patients per shift, if their effort was 100% clinical.” What we don’t know is how long their shifts were, whether they included things like ICU coverage, and how many shifts they work consecutively or in a year.
SHM’s 2012 State of Hospital Medicine report, which is based on 2011 data, provides additional context. It shows that hospitalists serving adult patients report a median 2,092 billed encounters annually (mean 2,245, standard deviation 1,161). They spread this work over a median 185 shifts (“work periods”) annually (mean 192). While there are lots of methodological problems in manipulating those numbers further, 2,092 encounters divided by 185 shifts yields 11.3 encounters per shift. These numbers exclude academicians who typically spend significant time in activities other than direct patient care, and I’m intentionally ignoring such issues as the night-shift doctor, who typically has low productivity, bringing down the average per full-time doctor in a practice.
The numbers from both surveys are sort of fuzzy because they aren’t audited or verified, but the 2012 State of Hospital Medicine data suggest that typical workloads aren’t too high in most practices, yet 40% of respondents in the Michtalik survey said they were high enough—unreasonably high—to risk quality and safety at least once a month.
One way to reconcile these findings is to take into account the standard deviation in daily volume in a single practice of about 30% to 40% on above or below the mean. If a hospitalist averages 14 encounters each day shift, then he should expect that the daily number might vary between about eight and 20. The Michtalik survey responses were likely reflecting the shifts on the high end.
Perspective
I wonder what a survey of physician workload opinions in other specialties would show, or what a survey of workers across all segments of the U.S. workforce in and out of healthcare would show. Of course, many or most jobs outside of healthcare don’t risk another’s health or well-being as significantly as ours do, but it would still be instructive to know how people in general think about the work they do.
I suspect a significant number of people across many different jobs feel like too much work is expected of them, and they can point to the ways their performance suffers as a result. It is difficult to know what portion of those who report too much work is just complaining versus a thoughtful self-reflection of the determinants of their performance. Lots of hospitalists do face worrisome high workloads, but some would probably still complain even with a much lower workload.
What Can Be Done?
For those practices facing remarkably high patient volumes, the solution is to make sure you’re recruiting additional doctors, and/or NPs/PAs, as fast as you can. But a portion of these practices must first convince their employers that more staff is needed. Some practices face a real uphill battle in getting the required additional funding, and the place to start is with a careful analysis of your current workload—based on hard numbers from your practice, not just anecdotes and estimates.
Don’t forget that some hospitalists put themselves in the position of having to manage high daily patient volumes by choosing a schedule of relatively few worked days annually. For example, a group working a seven-on/seven-off schedule that also has 14 shifts of time off means that each doctor will work only 168.5 shifts annually. Compressing a year’s worth of work into only 168 shifts means that each shift will be busy, and many will involve patient volumes that exceed what is seen as safe.
It could make more sense to titrate that same work volume over more annual shifts so that the average shift is less busy. I would love to see the Michtalik data segregated by those who work many shifts annually versus those who work few shifts. It is possible that those working more shifts have reported excessive workloads less often.
SHM has a role in influencing hospitalist workloads and promotes dissemination of data and opinions about it. At HM13 next month in Washington, D.C., I am leading a session titled “Hospitalist Workload: Is 15 the Right Number?” Although it won’t provide the “right” workload for all hospitalists, it will offer worthwhile data and food for thought.
It is much more difficult to do studies of how workload influences performance than something like effects of sleep deprivation on performance, so we may never get clear answers. You could take some consolation in the fact that successive surveys have shown little change or even modest decreases in annual patient encounters. But then again, maybe that hasn’t helped with excess work since providing hospital care gets harder and more complex every year.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at john.nelson@nelsonflores.com.
Reference
“Forty percent of physicians reported that their typical inpatient census exceeded safe levels at least monthly.”1
This quote is taken from an article by Henry Michtalik and colleagues that appeared at the end of January this year in JAMA Internal Medicine. In 2010 the authors conducted an on-line survey asking hospitalists their perceptions of their workload. Respondents indicated that with concerning frequency a high workload prevented them from adequately discussing with patients treatment options or answering questions, delay admitting or discharging patients until the next day or shift, or in some other way risk patient safety or the overall quality of their work.
This alarming finding matches my anecdotal experience working with many different hospitalist groups around the country. I think few hospitalists were surprised by the survey’s findings. Excess hospitalist workloads are indeed a problem in some settings, and those who bear them are typically not shy about speaking out.
The demand for hospitalists has exceeded the supply of doctors available to do the work throughout the history of the field. Under the weight of stunningly rapid growth in referral volume, from about 1995 to 2002, it was reasonably common for the original doctors in a hospitalist practice to become overwhelmed and leave for other work after a year or two, sometimes resulting in the collapse of the practice. Most practices are no longer in such a rapid-growth phase, but for many of them, staffing has not yet caught up with workload. The result can be chronic excess work, and even if daily patient volume is not seen as being unsafe, the number of days or shifts worked might be excessive and lead to fatigue and poor performance.
Other Workload Data
The respondents to the Michtalik survey reported that regardless of any assistance, “they could safely see 15 patients per shift, if their effort was 100% clinical.” What we don’t know is how long their shifts were, whether they included things like ICU coverage, and how many shifts they work consecutively or in a year.
SHM’s 2012 State of Hospital Medicine report, which is based on 2011 data, provides additional context. It shows that hospitalists serving adult patients report a median 2,092 billed encounters annually (mean 2,245, standard deviation 1,161). They spread this work over a median 185 shifts (“work periods”) annually (mean 192). While there are lots of methodological problems in manipulating those numbers further, 2,092 encounters divided by 185 shifts yields 11.3 encounters per shift. These numbers exclude academicians who typically spend significant time in activities other than direct patient care, and I’m intentionally ignoring such issues as the night-shift doctor, who typically has low productivity, bringing down the average per full-time doctor in a practice.
The numbers from both surveys are sort of fuzzy because they aren’t audited or verified, but the 2012 State of Hospital Medicine data suggest that typical workloads aren’t too high in most practices, yet 40% of respondents in the Michtalik survey said they were high enough—unreasonably high—to risk quality and safety at least once a month.
One way to reconcile these findings is to take into account the standard deviation in daily volume in a single practice of about 30% to 40% on above or below the mean. If a hospitalist averages 14 encounters each day shift, then he should expect that the daily number might vary between about eight and 20. The Michtalik survey responses were likely reflecting the shifts on the high end.
Perspective
I wonder what a survey of physician workload opinions in other specialties would show, or what a survey of workers across all segments of the U.S. workforce in and out of healthcare would show. Of course, many or most jobs outside of healthcare don’t risk another’s health or well-being as significantly as ours do, but it would still be instructive to know how people in general think about the work they do.
I suspect a significant number of people across many different jobs feel like too much work is expected of them, and they can point to the ways their performance suffers as a result. It is difficult to know what portion of those who report too much work is just complaining versus a thoughtful self-reflection of the determinants of their performance. Lots of hospitalists do face worrisome high workloads, but some would probably still complain even with a much lower workload.
What Can Be Done?
For those practices facing remarkably high patient volumes, the solution is to make sure you’re recruiting additional doctors, and/or NPs/PAs, as fast as you can. But a portion of these practices must first convince their employers that more staff is needed. Some practices face a real uphill battle in getting the required additional funding, and the place to start is with a careful analysis of your current workload—based on hard numbers from your practice, not just anecdotes and estimates.
Don’t forget that some hospitalists put themselves in the position of having to manage high daily patient volumes by choosing a schedule of relatively few worked days annually. For example, a group working a seven-on/seven-off schedule that also has 14 shifts of time off means that each doctor will work only 168.5 shifts annually. Compressing a year’s worth of work into only 168 shifts means that each shift will be busy, and many will involve patient volumes that exceed what is seen as safe.
It could make more sense to titrate that same work volume over more annual shifts so that the average shift is less busy. I would love to see the Michtalik data segregated by those who work many shifts annually versus those who work few shifts. It is possible that those working more shifts have reported excessive workloads less often.
SHM has a role in influencing hospitalist workloads and promotes dissemination of data and opinions about it. At HM13 next month in Washington, D.C., I am leading a session titled “Hospitalist Workload: Is 15 the Right Number?” Although it won’t provide the “right” workload for all hospitalists, it will offer worthwhile data and food for thought.
It is much more difficult to do studies of how workload influences performance than something like effects of sleep deprivation on performance, so we may never get clear answers. You could take some consolation in the fact that successive surveys have shown little change or even modest decreases in annual patient encounters. But then again, maybe that hasn’t helped with excess work since providing hospital care gets harder and more complex every year.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM's "Best Practices in Managing a Hospital Medicine Program" course. Write to him at john.nelson@nelsonflores.com.
Reference
Win Whitcomb: Hospital Value-Based Purchasing Program Adds Measure in Efficiency Domain

HVBP’s First Efficiency Measure
Move over, cost, LOS—make room for ‘Medicare spending per beneficiary’
The unwritten rule in hospitalist circles is that lower cost and length of stay (LOS) mean higher efficiency, with hospitalists (me included) often pointing to one or both of these as a yardstick of performance in the efficiency domain. But if we lower hospital length of stay and costs while shifting costs to post-hospital care, have we solved anything?
This very question was raised by Kuo and Goodwin’s observational study that revealed that decreased hospital costs and LOS were offset by higher utilization and costs after discharge under hospitalist care.1
Efficiency As a Domain of Quality
Using the Institute of Medicine’s (IOM) six domains of quality as a framework (see Table 1, right), the Centers for Medicare & Medicaid Services’ (CMS) Hospital Value-Based Purchasing (HVBP) program seeks to encourage enhanced quality in all of the IOM domains. For HVBP 2015, we see the addition of the first measure in the domain of efficiency.
You may be saying to yourself, “It’s only 2013. Why should I worry about HVBP 2015?” Here’s why: The measurement periods for HVBP 2015 are May to December 2011 (baseline) and May to December 2013 (performance). Hospitals can succeed under HVBP if they demonstrate improvement from baseline or attainment, which indicates maintenance of a high level of performance despite no substantial improvement from baseline. Medicare spending per beneficiary (MSPB) will make up 20% of the 2015 HVBP incentive pool for hospitals.
Medicare Spending Per Beneficiary Instead of Costs or LOS
Why did CMS choose to use MSPB as a measure and not simply hospital costs or length of stay? Measuring efficiency of hospital care has proven to be a sticky wicket. If one simply measures and rewards decreased hospital costs and/or length of stay (which you might legitimately argue is exactly what the current DRG system does by paying a case rate to the hospital), one runs the risk of shifting costs to settings beyond the four walls of the hospital, or even fueling higher rates of hospital readmissions. Also, physician costs and other costs (therapy, home care) are not accounted for; they are accounted for under MSPB (described below). Finally, hospital costs and LOS vary substantially across regions and by severity of illness of the patients being analyzed. This makes it difficult to compare, for example, LOS in California versus Massachusetts.
The MSPB is designed to be a comprehensive and equitable metric:
- It seeks to eliminate cost-shifting among settings by widening the time period from three days prior to 30 days post-inpatient-care episode;
- It looks at the full cost of care by including expenses from both Medicare Part A (hospital) and Part B (doctors, PT, OT, home health, others);
- It incorporates risk adjustment by taking into account differences in patient health status; and
- It seeks to level the playing field by using a price standardization methodology that factors in geographic payment differences in wages, practice costs, and payments for indirect medical education and disproportionate share hospitals (those that treat large numbers of the indigent population).
Driving High Performance in Medicare Spending Per Beneficiary
Hospitalists straddle the Part A and Part B elements of Medicare; they have one foot in the hospital and one foot in the physician practice world. They should be able to improve their hospitals’ performance under the MSPB yardstick. Since the performance measurement period starts in May, now is the time to sharpen your focus on MSPB.
Here are the top priorities for MSPB that I recommend for hospitalists:
Reduction of marginally beneficial resource utilization. This is a process of analyzing resource (e.g. pharmacy, radiology, laboratory, blood products) utilization for the purpose of minimizing costly practices that do not benefit the patient. This is an essential practice of a high-functioning hospitalist program. Through its participation in the Choosing Wisely campaign (see “Stop! Think Twice Before You Order,” p. 46), SHM has helped hospitalists have conversations about these practices with patients.
Hospital throughput. Work on “front end” throughput with the ED by having a process in place to quickly evaluate and facilitate potential admissions. Work with case management to assure timely (and early in the day) discharges.
Safe-discharge processes. We reviewed key elements of a safe discharge last month and provided a link to SHM’s Project BOOST (www.hospitalmedicine.org/boost). From the MSPB perspective: A safe discharge minimizes exorbitant spending after discharge.
Documentation integrity. Because MSPB is risk-adjusted, the more the record reflects patient severity of illness, the better your hospital will perform, all else being equal. Work collaboratively with your documentation integrity professionals!
Much of the success of the HM specialty has been built on the tenet that the hospitalist model delivers efficient inpatient care. In the coming years, the specialty’s contribution will increasingly be gauged by the MSPB measure.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
HVBP’s First Efficiency Measure
Move over, cost, LOS—make room for ‘Medicare spending per beneficiary’
The unwritten rule in hospitalist circles is that lower cost and length of stay (LOS) mean higher efficiency, with hospitalists (me included) often pointing to one or both of these as a yardstick of performance in the efficiency domain. But if we lower hospital length of stay and costs while shifting costs to post-hospital care, have we solved anything?
This very question was raised by Kuo and Goodwin’s observational study that revealed that decreased hospital costs and LOS were offset by higher utilization and costs after discharge under hospitalist care.1
Efficiency As a Domain of Quality
Using the Institute of Medicine’s (IOM) six domains of quality as a framework (see Table 1, right), the Centers for Medicare & Medicaid Services’ (CMS) Hospital Value-Based Purchasing (HVBP) program seeks to encourage enhanced quality in all of the IOM domains. For HVBP 2015, we see the addition of the first measure in the domain of efficiency.
You may be saying to yourself, “It’s only 2013. Why should I worry about HVBP 2015?” Here’s why: The measurement periods for HVBP 2015 are May to December 2011 (baseline) and May to December 2013 (performance). Hospitals can succeed under HVBP if they demonstrate improvement from baseline or attainment, which indicates maintenance of a high level of performance despite no substantial improvement from baseline. Medicare spending per beneficiary (MSPB) will make up 20% of the 2015 HVBP incentive pool for hospitals.
Medicare Spending Per Beneficiary Instead of Costs or LOS
Why did CMS choose to use MSPB as a measure and not simply hospital costs or length of stay? Measuring efficiency of hospital care has proven to be a sticky wicket. If one simply measures and rewards decreased hospital costs and/or length of stay (which you might legitimately argue is exactly what the current DRG system does by paying a case rate to the hospital), one runs the risk of shifting costs to settings beyond the four walls of the hospital, or even fueling higher rates of hospital readmissions. Also, physician costs and other costs (therapy, home care) are not accounted for; they are accounted for under MSPB (described below). Finally, hospital costs and LOS vary substantially across regions and by severity of illness of the patients being analyzed. This makes it difficult to compare, for example, LOS in California versus Massachusetts.
The MSPB is designed to be a comprehensive and equitable metric:
- It seeks to eliminate cost-shifting among settings by widening the time period from three days prior to 30 days post-inpatient-care episode;
- It looks at the full cost of care by including expenses from both Medicare Part A (hospital) and Part B (doctors, PT, OT, home health, others);
- It incorporates risk adjustment by taking into account differences in patient health status; and
- It seeks to level the playing field by using a price standardization methodology that factors in geographic payment differences in wages, practice costs, and payments for indirect medical education and disproportionate share hospitals (those that treat large numbers of the indigent population).
Driving High Performance in Medicare Spending Per Beneficiary
Hospitalists straddle the Part A and Part B elements of Medicare; they have one foot in the hospital and one foot in the physician practice world. They should be able to improve their hospitals’ performance under the MSPB yardstick. Since the performance measurement period starts in May, now is the time to sharpen your focus on MSPB.
Here are the top priorities for MSPB that I recommend for hospitalists:
Reduction of marginally beneficial resource utilization. This is a process of analyzing resource (e.g. pharmacy, radiology, laboratory, blood products) utilization for the purpose of minimizing costly practices that do not benefit the patient. This is an essential practice of a high-functioning hospitalist program. Through its participation in the Choosing Wisely campaign (see “Stop! Think Twice Before You Order,” p. 46), SHM has helped hospitalists have conversations about these practices with patients.
Hospital throughput. Work on “front end” throughput with the ED by having a process in place to quickly evaluate and facilitate potential admissions. Work with case management to assure timely (and early in the day) discharges.
Safe-discharge processes. We reviewed key elements of a safe discharge last month and provided a link to SHM’s Project BOOST (www.hospitalmedicine.org/boost). From the MSPB perspective: A safe discharge minimizes exorbitant spending after discharge.
Documentation integrity. Because MSPB is risk-adjusted, the more the record reflects patient severity of illness, the better your hospital will perform, all else being equal. Work collaboratively with your documentation integrity professionals!
Much of the success of the HM specialty has been built on the tenet that the hospitalist model delivers efficient inpatient care. In the coming years, the specialty’s contribution will increasingly be gauged by the MSPB measure.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
HVBP’s First Efficiency Measure
Move over, cost, LOS—make room for ‘Medicare spending per beneficiary’
The unwritten rule in hospitalist circles is that lower cost and length of stay (LOS) mean higher efficiency, with hospitalists (me included) often pointing to one or both of these as a yardstick of performance in the efficiency domain. But if we lower hospital length of stay and costs while shifting costs to post-hospital care, have we solved anything?
This very question was raised by Kuo and Goodwin’s observational study that revealed that decreased hospital costs and LOS were offset by higher utilization and costs after discharge under hospitalist care.1
Efficiency As a Domain of Quality
Using the Institute of Medicine’s (IOM) six domains of quality as a framework (see Table 1, right), the Centers for Medicare & Medicaid Services’ (CMS) Hospital Value-Based Purchasing (HVBP) program seeks to encourage enhanced quality in all of the IOM domains. For HVBP 2015, we see the addition of the first measure in the domain of efficiency.
You may be saying to yourself, “It’s only 2013. Why should I worry about HVBP 2015?” Here’s why: The measurement periods for HVBP 2015 are May to December 2011 (baseline) and May to December 2013 (performance). Hospitals can succeed under HVBP if they demonstrate improvement from baseline or attainment, which indicates maintenance of a high level of performance despite no substantial improvement from baseline. Medicare spending per beneficiary (MSPB) will make up 20% of the 2015 HVBP incentive pool for hospitals.
Medicare Spending Per Beneficiary Instead of Costs or LOS
Why did CMS choose to use MSPB as a measure and not simply hospital costs or length of stay? Measuring efficiency of hospital care has proven to be a sticky wicket. If one simply measures and rewards decreased hospital costs and/or length of stay (which you might legitimately argue is exactly what the current DRG system does by paying a case rate to the hospital), one runs the risk of shifting costs to settings beyond the four walls of the hospital, or even fueling higher rates of hospital readmissions. Also, physician costs and other costs (therapy, home care) are not accounted for; they are accounted for under MSPB (described below). Finally, hospital costs and LOS vary substantially across regions and by severity of illness of the patients being analyzed. This makes it difficult to compare, for example, LOS in California versus Massachusetts.
The MSPB is designed to be a comprehensive and equitable metric:
- It seeks to eliminate cost-shifting among settings by widening the time period from three days prior to 30 days post-inpatient-care episode;
- It looks at the full cost of care by including expenses from both Medicare Part A (hospital) and Part B (doctors, PT, OT, home health, others);
- It incorporates risk adjustment by taking into account differences in patient health status; and
- It seeks to level the playing field by using a price standardization methodology that factors in geographic payment differences in wages, practice costs, and payments for indirect medical education and disproportionate share hospitals (those that treat large numbers of the indigent population).
Driving High Performance in Medicare Spending Per Beneficiary
Hospitalists straddle the Part A and Part B elements of Medicare; they have one foot in the hospital and one foot in the physician practice world. They should be able to improve their hospitals’ performance under the MSPB yardstick. Since the performance measurement period starts in May, now is the time to sharpen your focus on MSPB.
Here are the top priorities for MSPB that I recommend for hospitalists:
Reduction of marginally beneficial resource utilization. This is a process of analyzing resource (e.g. pharmacy, radiology, laboratory, blood products) utilization for the purpose of minimizing costly practices that do not benefit the patient. This is an essential practice of a high-functioning hospitalist program. Through its participation in the Choosing Wisely campaign (see “Stop! Think Twice Before You Order,” p. 46), SHM has helped hospitalists have conversations about these practices with patients.
Hospital throughput. Work on “front end” throughput with the ED by having a process in place to quickly evaluate and facilitate potential admissions. Work with case management to assure timely (and early in the day) discharges.
Safe-discharge processes. We reviewed key elements of a safe discharge last month and provided a link to SHM’s Project BOOST (www.hospitalmedicine.org/boost). From the MSPB perspective: A safe discharge minimizes exorbitant spending after discharge.
Documentation integrity. Because MSPB is risk-adjusted, the more the record reflects patient severity of illness, the better your hospital will perform, all else being equal. Work collaboratively with your documentation integrity professionals!
Much of the success of the HM specialty has been built on the tenet that the hospitalist model delivers efficient inpatient care. In the coming years, the specialty’s contribution will increasingly be gauged by the MSPB measure.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Benefits of oxytocin for kids with autism remain unclear
If you are a child psychiatrist and haven’t heard of oxytocin for autism, you will.
Parents might soon ask you to put their autistic child on it, if they haven’t done so already, according to Lawrence Scahill, Ph.D.
"There’s a huge amount of interest in oxytocin. If you haven’t heard about this from your families, you will, believe me. It’s a hot topic," said Dr. Scahill, a pediatrics professor at Emory University and the Marcus Autism Center, both in Atlanta.
But "I’m not sure if [the interest] is warranted. There’s much, much more [that needs to be] learned about oxytocin," he said at the American Academy of Child and Adolescent Psychiatry’s Psychopharmacology Update Institute in Washington.
Some parents are getting the peptide hormone from compounding pharmacies and giving perhaps 18-24 IU intranasally to their autistic children daily in the hopes that it will help. But there’s just not enough data to know whether those children will benefit, or even whether oxytocin is safe to give to kids with autism.
Oxytocin plays an important role in child birth and lactation. Most agree it also has a role in emotion regulation and social interaction; the fact that plasma levels are low in autism has led "some to wonder if" supplements will help. "Ten minutes after a [24 IU] intranasal injection, plasma levels double" in autistic people. "They don’t normalize, but they double; the amount that gets through the blood-brain barrier is completely unclear at the moment," Dr. Scahill said (Proc. Natl. Acad. Sci. USA 2010;107:4389-94).
There’s also been "no great" human studies so far on benefit. In most, investigators gave single doses to healthy adults "and then did laboratory measurements of social interaction" with computer or gambling games. "That’s the state of the art," Dr. Scahill said.
Oxytocin seemed to increase trust in some of those studies. In another, a one-time dose of 18-24 IU appeared to slightly boost the ability of autistic boys to identify emotions from eye expressions, but it wasn’t "a very big effect," about a 5% increase in the number of correct answers, he said (Biol. Psychiatry 2010;67:692-4).
At this point, "we know next to nothing" about daily dosing, what parents are most likely to request. "If a parent said to me ‘I want my child on oxytocin,’ I would say we don’t know anything about how to dose it," and "as far as I know, it’s not been given to children younger than 12 in published studies. We don’t know anything about [using it in] young children," Dr. Scahill said.
Upcoming trials of oxytocin for autism should provide answers. Among them is a 5-year, multimillion dollar, National Institutes of Health–funded study that will test daily nasal dosing in 300 autistic children aged 3-17 years old.
In the meantime, Dr. Scahill reminded his audience that "in the 1990s, secretin was going to be the cure for autism" until a series of placebo-controlled studies showed no benefit. "Now it looks like oxytocin is the new cure. Is it really? I don’t know," he said.
For more information, he referred his audience to a recent investigation in the magazine Science (2013;339:267-9).
Dr. Scahill is a consultant for Biomarin and Roche. He also receives research funding form Pfizer, Roche, and Shire Pharmaceuticals.
BY M. ALEXANDER OTTO

If you are a child psychiatrist and haven’t heard of oxytocin for autism, you will.
Parents might soon ask you to put their autistic child on it, if they haven’t done so already, according to Lawrence Scahill, Ph.D.
"There’s a huge amount of interest in oxytocin. If you haven’t heard about this from your families, you will, believe me. It’s a hot topic," said Dr. Scahill, a pediatrics professor at Emory University and the Marcus Autism Center, both in Atlanta.
But "I’m not sure if [the interest] is warranted. There’s much, much more [that needs to be] learned about oxytocin," he said at the American Academy of Child and Adolescent Psychiatry’s Psychopharmacology Update Institute in Washington.
Some parents are getting the peptide hormone from compounding pharmacies and giving perhaps 18-24 IU intranasally to their autistic children daily in the hopes that it will help. But there’s just not enough data to know whether those children will benefit, or even whether oxytocin is safe to give to kids with autism.
Oxytocin plays an important role in child birth and lactation. Most agree it also has a role in emotion regulation and social interaction; the fact that plasma levels are low in autism has led "some to wonder if" supplements will help. "Ten minutes after a [24 IU] intranasal injection, plasma levels double" in autistic people. "They don’t normalize, but they double; the amount that gets through the blood-brain barrier is completely unclear at the moment," Dr. Scahill said (Proc. Natl. Acad. Sci. USA 2010;107:4389-94).
There’s also been "no great" human studies so far on benefit. In most, investigators gave single doses to healthy adults "and then did laboratory measurements of social interaction" with computer or gambling games. "That’s the state of the art," Dr. Scahill said.
Oxytocin seemed to increase trust in some of those studies. In another, a one-time dose of 18-24 IU appeared to slightly boost the ability of autistic boys to identify emotions from eye expressions, but it wasn’t "a very big effect," about a 5% increase in the number of correct answers, he said (Biol. Psychiatry 2010;67:692-4).
At this point, "we know next to nothing" about daily dosing, what parents are most likely to request. "If a parent said to me ‘I want my child on oxytocin,’ I would say we don’t know anything about how to dose it," and "as far as I know, it’s not been given to children younger than 12 in published studies. We don’t know anything about [using it in] young children," Dr. Scahill said.
Upcoming trials of oxytocin for autism should provide answers. Among them is a 5-year, multimillion dollar, National Institutes of Health–funded study that will test daily nasal dosing in 300 autistic children aged 3-17 years old.
In the meantime, Dr. Scahill reminded his audience that "in the 1990s, secretin was going to be the cure for autism" until a series of placebo-controlled studies showed no benefit. "Now it looks like oxytocin is the new cure. Is it really? I don’t know," he said.
For more information, he referred his audience to a recent investigation in the magazine Science (2013;339:267-9).
Dr. Scahill is a consultant for Biomarin and Roche. He also receives research funding form Pfizer, Roche, and Shire Pharmaceuticals.
BY M. ALEXANDER OTTO
If you are a child psychiatrist and haven’t heard of oxytocin for autism, you will.
Parents might soon ask you to put their autistic child on it, if they haven’t done so already, according to Lawrence Scahill, Ph.D.
"There’s a huge amount of interest in oxytocin. If you haven’t heard about this from your families, you will, believe me. It’s a hot topic," said Dr. Scahill, a pediatrics professor at Emory University and the Marcus Autism Center, both in Atlanta.
But "I’m not sure if [the interest] is warranted. There’s much, much more [that needs to be] learned about oxytocin," he said at the American Academy of Child and Adolescent Psychiatry’s Psychopharmacology Update Institute in Washington.
Some parents are getting the peptide hormone from compounding pharmacies and giving perhaps 18-24 IU intranasally to their autistic children daily in the hopes that it will help. But there’s just not enough data to know whether those children will benefit, or even whether oxytocin is safe to give to kids with autism.
Oxytocin plays an important role in child birth and lactation. Most agree it also has a role in emotion regulation and social interaction; the fact that plasma levels are low in autism has led "some to wonder if" supplements will help. "Ten minutes after a [24 IU] intranasal injection, plasma levels double" in autistic people. "They don’t normalize, but they double; the amount that gets through the blood-brain barrier is completely unclear at the moment," Dr. Scahill said (Proc. Natl. Acad. Sci. USA 2010;107:4389-94).
There’s also been "no great" human studies so far on benefit. In most, investigators gave single doses to healthy adults "and then did laboratory measurements of social interaction" with computer or gambling games. "That’s the state of the art," Dr. Scahill said.
Oxytocin seemed to increase trust in some of those studies. In another, a one-time dose of 18-24 IU appeared to slightly boost the ability of autistic boys to identify emotions from eye expressions, but it wasn’t "a very big effect," about a 5% increase in the number of correct answers, he said (Biol. Psychiatry 2010;67:692-4).
At this point, "we know next to nothing" about daily dosing, what parents are most likely to request. "If a parent said to me ‘I want my child on oxytocin,’ I would say we don’t know anything about how to dose it," and "as far as I know, it’s not been given to children younger than 12 in published studies. We don’t know anything about [using it in] young children," Dr. Scahill said.
Upcoming trials of oxytocin for autism should provide answers. Among them is a 5-year, multimillion dollar, National Institutes of Health–funded study that will test daily nasal dosing in 300 autistic children aged 3-17 years old.
In the meantime, Dr. Scahill reminded his audience that "in the 1990s, secretin was going to be the cure for autism" until a series of placebo-controlled studies showed no benefit. "Now it looks like oxytocin is the new cure. Is it really? I don’t know," he said.
For more information, he referred his audience to a recent investigation in the magazine Science (2013;339:267-9).
Dr. Scahill is a consultant for Biomarin and Roche. He also receives research funding form Pfizer, Roche, and Shire Pharmaceuticals.
BY M. ALEXANDER OTTO

John Nelson: Why Spinal Epidural Abcess Poses A Particular Liability Risk for Hospitalists

Delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA): that will be the case over which you are sued.
Over the last 15 years, I’ve served as an expert witness for six or seven malpractice cases. Most were related to spinal cord injuries, and in all but one of those, the etiology was epidural abscess. I’ve been asked to review about 40 or 50 additional cases, and while I’ve turned them down (I just don’t have time to do reviews), I nearly always ask about the clinical picture in every case. A significant number have been SEA-related. This experience has convinced me that SEA poses a particular liability risk for hospitalists.
Of course, it is patients who bear the real risk and unfortunate consequences of SEA. Being a defendant physician in a lawsuit is stressful, but it’s nothing compared to the distress of permanent loss of neurologic function. To prevent permanent sequelae, we need to maintain a very high index of suspicion to try to make a prompt diagnosis, and ensure immediate intervention once the diagnosis is made.
Data from Malpractice Insurers
I had the pleasure of getting to know a number of leaders at The Doctor’s Company, a large malpractice insurer that provides malpractice policies for all specialties, including a lot of hospitalists. From 2007 to 2011, they closed 28 SEA-related claims, for which they spent an average of $212,000 defending each one. Eleven of the 28 resulted in indemnity payments averaging $754,000 each (median was $455,000). These dollar amounts are roughly double what might be seen for all other claims and reflect only the payments made on behalf of the company’s insured doctors. The total award to each patient was likely much higher, because in most cases, several defendants (other doctors and a hospital) probably paid money to the patient.
The Physician Insurers Association of America (PIAA) “is the insurance industry trade association representing domestic and international medical professional liability insurance companies.” Their member malpractice insurance companies have the opportunity to report claims data that PIAA aggregates and makes available. Data from 2002 to 2011 showed 312 closed claims related to any diagnosis (not just SEA) for hospitalists, with an average indemnity payment of $272,553 (the highest hospitalist-related payment was $1.4 million). The most common allegations related to paid claims were 1) “errors in diagnosis,” 2) “failure/delay in referral or consultation,” and 3) “failure to supervise/monitor case.” Although only three of the 312 claims were related to “diseases of the spinal cord,” that was exceeded in frequency only by “diabetes.”
I think these numbers from the malpractice insurance industry support my concern that SEA is a high-risk area, but it doesn’t really support my anecdotal experience that SEA is clearly hospitalists’ highest-risk area. Maybe SEA is only one of several high-risk areas. Nevertheless, I’m going to stick to my sensationalist guns to get your attention.
Why Is Epidural Abscess a High Risk?
There likely are several reasons SEA is a treacherous liability problem. It can lead to devastating permanent disabling neurologic deficits in people who were previously healthy, and if the medical care was substandard, then significant financial compensation seems appropriate.
Delays in diagnosis of SEA are common. It can be a very sneaky illness that in the early stages is very easy to confuse with less-serious causes of back pain or fever. Even though I think about this particular diagnosis all the time, just last year I had a patient who reported an increase in his usual back pain. I felt reassured that he had no neurologic deficit or fever, and took the time to explain why there was no reason to repeat the spine MRI that had been done about two weeks prior to admission. But he was insistent that he have another MRI, and after a day or two I finally agreed to order it, assuring him it would not explain the cause of his pain. But it did. He had a significant SEA and went to emergency surgery. I was stunned, and profoundly relieved that he had no neurologic sequelae.
One of the remarkable things I’ve seen in the cases I’ve reviewed is that even when there is clear cause for concern, there is too often no action taken. In a number of cases, the nurses’ note indicates increasing back pain, loss of ability to stand, urinary retention, and other alarming signs. Yet the doctors either never learn of these issues, or they choose to attribute them to other causes.
Even when the diagnosis of SEA is clearly established, it is all too common for doctors caring for the patient not to act on this information. In several cases I reviewed, a radiologist had documented reporting the diagnosis to the hospitalist (and in one case the neurosurgeon as well), yet nothing was done for 12 hours or more. It is hard to imagine that establishing this diagnosis doesn’t reliably lead to an emergent response, but it doesn’t. (In some cases, nonsurgical management may be an option, but in these malpractices cases, there was just a failure to act on the diagnosis with any sort of plan.)
Practice Management Perspective
I usually discuss hospitalist practice operations in this space—things like work schedules and compensation. But attending to risk management is one component of effective practice operations, so I thought I’d raise the topic here. Obviously, there is a lot more to hospitalist risk management than one diagnosis, but a column on the whole universe of risk management would probably serve no purpose other than as a sleep aid. I hope that by focusing solely on SEA, there is some chance that you’ll remember it, and you’ll make sure that you disprove my first two sentences.
Lowering your risk of a malpractice lawsuit is valuable and worth spending time on. But far more important is that by keeping the diagnosis in mind, and ensuring that you act emergently when there is cause for concern, you might save someone from the devastating consequences of this disease.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA): that will be the case over which you are sued.
Over the last 15 years, I’ve served as an expert witness for six or seven malpractice cases. Most were related to spinal cord injuries, and in all but one of those, the etiology was epidural abscess. I’ve been asked to review about 40 or 50 additional cases, and while I’ve turned them down (I just don’t have time to do reviews), I nearly always ask about the clinical picture in every case. A significant number have been SEA-related. This experience has convinced me that SEA poses a particular liability risk for hospitalists.
Of course, it is patients who bear the real risk and unfortunate consequences of SEA. Being a defendant physician in a lawsuit is stressful, but it’s nothing compared to the distress of permanent loss of neurologic function. To prevent permanent sequelae, we need to maintain a very high index of suspicion to try to make a prompt diagnosis, and ensure immediate intervention once the diagnosis is made.
Data from Malpractice Insurers
I had the pleasure of getting to know a number of leaders at The Doctor’s Company, a large malpractice insurer that provides malpractice policies for all specialties, including a lot of hospitalists. From 2007 to 2011, they closed 28 SEA-related claims, for which they spent an average of $212,000 defending each one. Eleven of the 28 resulted in indemnity payments averaging $754,000 each (median was $455,000). These dollar amounts are roughly double what might be seen for all other claims and reflect only the payments made on behalf of the company’s insured doctors. The total award to each patient was likely much higher, because in most cases, several defendants (other doctors and a hospital) probably paid money to the patient.
The Physician Insurers Association of America (PIAA) “is the insurance industry trade association representing domestic and international medical professional liability insurance companies.” Their member malpractice insurance companies have the opportunity to report claims data that PIAA aggregates and makes available. Data from 2002 to 2011 showed 312 closed claims related to any diagnosis (not just SEA) for hospitalists, with an average indemnity payment of $272,553 (the highest hospitalist-related payment was $1.4 million). The most common allegations related to paid claims were 1) “errors in diagnosis,” 2) “failure/delay in referral or consultation,” and 3) “failure to supervise/monitor case.” Although only three of the 312 claims were related to “diseases of the spinal cord,” that was exceeded in frequency only by “diabetes.”
I think these numbers from the malpractice insurance industry support my concern that SEA is a high-risk area, but it doesn’t really support my anecdotal experience that SEA is clearly hospitalists’ highest-risk area. Maybe SEA is only one of several high-risk areas. Nevertheless, I’m going to stick to my sensationalist guns to get your attention.
Why Is Epidural Abscess a High Risk?
There likely are several reasons SEA is a treacherous liability problem. It can lead to devastating permanent disabling neurologic deficits in people who were previously healthy, and if the medical care was substandard, then significant financial compensation seems appropriate.
Delays in diagnosis of SEA are common. It can be a very sneaky illness that in the early stages is very easy to confuse with less-serious causes of back pain or fever. Even though I think about this particular diagnosis all the time, just last year I had a patient who reported an increase in his usual back pain. I felt reassured that he had no neurologic deficit or fever, and took the time to explain why there was no reason to repeat the spine MRI that had been done about two weeks prior to admission. But he was insistent that he have another MRI, and after a day or two I finally agreed to order it, assuring him it would not explain the cause of his pain. But it did. He had a significant SEA and went to emergency surgery. I was stunned, and profoundly relieved that he had no neurologic sequelae.
One of the remarkable things I’ve seen in the cases I’ve reviewed is that even when there is clear cause for concern, there is too often no action taken. In a number of cases, the nurses’ note indicates increasing back pain, loss of ability to stand, urinary retention, and other alarming signs. Yet the doctors either never learn of these issues, or they choose to attribute them to other causes.
Even when the diagnosis of SEA is clearly established, it is all too common for doctors caring for the patient not to act on this information. In several cases I reviewed, a radiologist had documented reporting the diagnosis to the hospitalist (and in one case the neurosurgeon as well), yet nothing was done for 12 hours or more. It is hard to imagine that establishing this diagnosis doesn’t reliably lead to an emergent response, but it doesn’t. (In some cases, nonsurgical management may be an option, but in these malpractices cases, there was just a failure to act on the diagnosis with any sort of plan.)
Practice Management Perspective
I usually discuss hospitalist practice operations in this space—things like work schedules and compensation. But attending to risk management is one component of effective practice operations, so I thought I’d raise the topic here. Obviously, there is a lot more to hospitalist risk management than one diagnosis, but a column on the whole universe of risk management would probably serve no purpose other than as a sleep aid. I hope that by focusing solely on SEA, there is some chance that you’ll remember it, and you’ll make sure that you disprove my first two sentences.
Lowering your risk of a malpractice lawsuit is valuable and worth spending time on. But far more important is that by keeping the diagnosis in mind, and ensuring that you act emergently when there is cause for concern, you might save someone from the devastating consequences of this disease.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA): that will be the case over which you are sued.
Over the last 15 years, I’ve served as an expert witness for six or seven malpractice cases. Most were related to spinal cord injuries, and in all but one of those, the etiology was epidural abscess. I’ve been asked to review about 40 or 50 additional cases, and while I’ve turned them down (I just don’t have time to do reviews), I nearly always ask about the clinical picture in every case. A significant number have been SEA-related. This experience has convinced me that SEA poses a particular liability risk for hospitalists.
Of course, it is patients who bear the real risk and unfortunate consequences of SEA. Being a defendant physician in a lawsuit is stressful, but it’s nothing compared to the distress of permanent loss of neurologic function. To prevent permanent sequelae, we need to maintain a very high index of suspicion to try to make a prompt diagnosis, and ensure immediate intervention once the diagnosis is made.
Data from Malpractice Insurers
I had the pleasure of getting to know a number of leaders at The Doctor’s Company, a large malpractice insurer that provides malpractice policies for all specialties, including a lot of hospitalists. From 2007 to 2011, they closed 28 SEA-related claims, for which they spent an average of $212,000 defending each one. Eleven of the 28 resulted in indemnity payments averaging $754,000 each (median was $455,000). These dollar amounts are roughly double what might be seen for all other claims and reflect only the payments made on behalf of the company’s insured doctors. The total award to each patient was likely much higher, because in most cases, several defendants (other doctors and a hospital) probably paid money to the patient.
The Physician Insurers Association of America (PIAA) “is the insurance industry trade association representing domestic and international medical professional liability insurance companies.” Their member malpractice insurance companies have the opportunity to report claims data that PIAA aggregates and makes available. Data from 2002 to 2011 showed 312 closed claims related to any diagnosis (not just SEA) for hospitalists, with an average indemnity payment of $272,553 (the highest hospitalist-related payment was $1.4 million). The most common allegations related to paid claims were 1) “errors in diagnosis,” 2) “failure/delay in referral or consultation,” and 3) “failure to supervise/monitor case.” Although only three of the 312 claims were related to “diseases of the spinal cord,” that was exceeded in frequency only by “diabetes.”
I think these numbers from the malpractice insurance industry support my concern that SEA is a high-risk area, but it doesn’t really support my anecdotal experience that SEA is clearly hospitalists’ highest-risk area. Maybe SEA is only one of several high-risk areas. Nevertheless, I’m going to stick to my sensationalist guns to get your attention.
Why Is Epidural Abscess a High Risk?
There likely are several reasons SEA is a treacherous liability problem. It can lead to devastating permanent disabling neurologic deficits in people who were previously healthy, and if the medical care was substandard, then significant financial compensation seems appropriate.
Delays in diagnosis of SEA are common. It can be a very sneaky illness that in the early stages is very easy to confuse with less-serious causes of back pain or fever. Even though I think about this particular diagnosis all the time, just last year I had a patient who reported an increase in his usual back pain. I felt reassured that he had no neurologic deficit or fever, and took the time to explain why there was no reason to repeat the spine MRI that had been done about two weeks prior to admission. But he was insistent that he have another MRI, and after a day or two I finally agreed to order it, assuring him it would not explain the cause of his pain. But it did. He had a significant SEA and went to emergency surgery. I was stunned, and profoundly relieved that he had no neurologic sequelae.
One of the remarkable things I’ve seen in the cases I’ve reviewed is that even when there is clear cause for concern, there is too often no action taken. In a number of cases, the nurses’ note indicates increasing back pain, loss of ability to stand, urinary retention, and other alarming signs. Yet the doctors either never learn of these issues, or they choose to attribute them to other causes.
Even when the diagnosis of SEA is clearly established, it is all too common for doctors caring for the patient not to act on this information. In several cases I reviewed, a radiologist had documented reporting the diagnosis to the hospitalist (and in one case the neurosurgeon as well), yet nothing was done for 12 hours or more. It is hard to imagine that establishing this diagnosis doesn’t reliably lead to an emergent response, but it doesn’t. (In some cases, nonsurgical management may be an option, but in these malpractices cases, there was just a failure to act on the diagnosis with any sort of plan.)
Practice Management Perspective
I usually discuss hospitalist practice operations in this space—things like work schedules and compensation. But attending to risk management is one component of effective practice operations, so I thought I’d raise the topic here. Obviously, there is a lot more to hospitalist risk management than one diagnosis, but a column on the whole universe of risk management would probably serve no purpose other than as a sleep aid. I hope that by focusing solely on SEA, there is some chance that you’ll remember it, and you’ll make sure that you disprove my first two sentences.
Lowering your risk of a malpractice lawsuit is valuable and worth spending time on. But far more important is that by keeping the diagnosis in mind, and ensuring that you act emergently when there is cause for concern, you might save someone from the devastating consequences of this disease.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Win Whitcomb: Mortality Rates Become a Measuring Stick for Hospital Performance

—Blue Oyster Cult
The designers of the hospital value-based purchasing (HVBP) program sought to include outcomes measures in 2014, and when they did, mortality was their choice. Specifically, HVBP for fiscal-year 2014 (starting October 2013) will include 30-day mortality rates for myocardial infarction, heart failure, and pneumonia. The weighting for the mortality domain will be 25% (see Table 1).
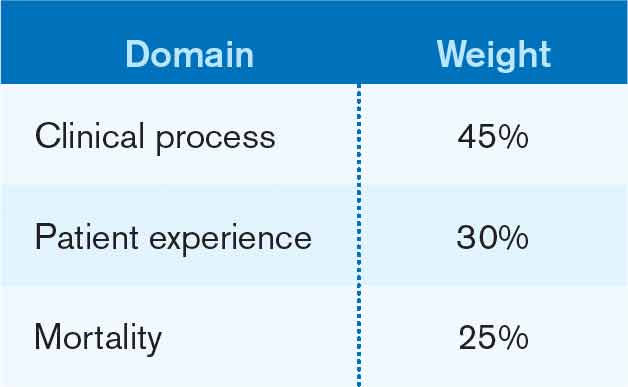
To review the requirements for the HVBP program in FY2014: All hospitals will have 1.25% of their Medicare inpatient payments withheld. They can earn back none, some, all, or an amount in excess of the 1.25%, depending on performance in the performance domains. To put it in perspective, 1.25% of Medicare inpatient payments for a 320-bed hospital are about $1 million. Such a hospital will have about $250,000 at risk in the mortality domain in FY2014.
Given the role hospitalists play in quality and safety initiatives, and the importance of medical record documentation in defining the risk of mortality and severity of illness, we can be crucial players in how our hospitals perform with regard to mortality.
Focus Areas for Mortality Reduction
Although many hospitalists might think that reducing mortality is like “boiling the ocean,” there are some areas where we can clearly focus our attention. There are four priority areas we should target in the coming years (also see Figure 1):
Reduce harm. This may take the form of reducing hospital-acquired infections, such as catheter-related UTIs, Clostridium difficile, and central-line-associated bloodstream infections, or reducing hospital-acquired VTE, falls, and delirium. Many hospital-acquired conditions have a collection, or bundle, of preventive practices. Hospitalists can work both in an institutional leadership capacity and in the course of daily clinical practice to implement bundles and best practices to reduce patient harm.
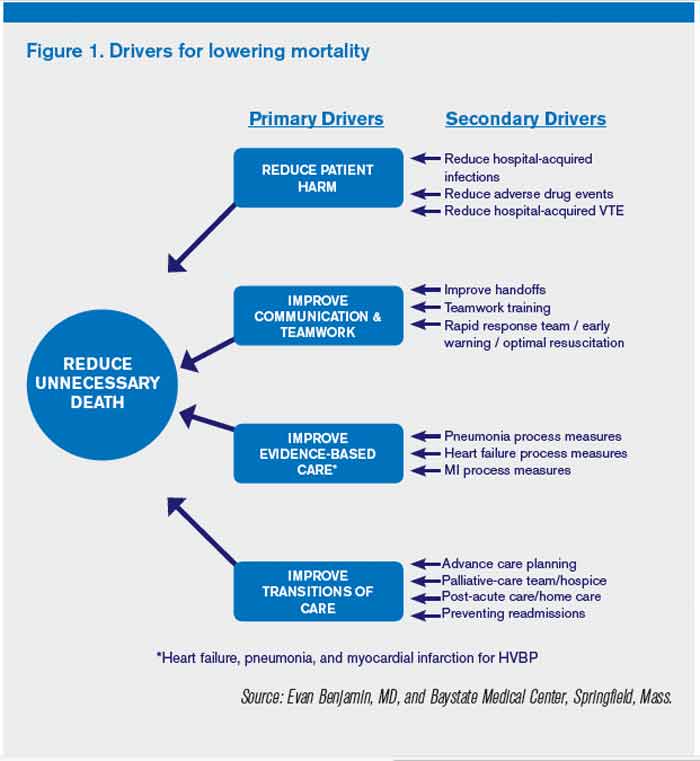
Improve teamwork. With hospitalists, “you started to have teams caring for inpatients in a coordinated way. So I regard this as [hospitalists] coming into their own, their vision of the future starting to really take hold,” said Brent James, coauthor of the recent Institute of Medicine report “Best Care at Lower Cost: The Path to Continuously Learning Health Care in America.” Partly, we’ve accomplished this through simply “showing up” and partly we’ve done it through becoming students of the art and science of teamwork. An example of teamwork training, developed by the Defense Department and the Agency for Healthcare Quality and Research (AHRQ), is TeamSTEPPS, which offers a systematic approach to cooperation, coordination, and communication among team members. Optimal patient resuscitation, in-hospital handoffs, rapid-response teams, and early-warning systems are essential pieces of teamwork that may reduce mortality.
Improve evidence-based care. This domain covers process measures aimed at optimizing care, including reducing mortality. For HVBP in particular, myocardial infarction, heart failure, and pneumonia are the focus.
Improve transitions of care. Best practices for care transitions and reducing readmissions, including advance-care planning, involvement of palliative care and hospice, and coordination with post-acute care, can be a key part of reducing 30-day mortality.
Documentation Integrity
Accurately capturing a patient’s condition in the medical record is crucial to assigning severity of illness and risk of mortality. Because mortality rates are severity-adjusted, accurate documentation is another important dimension to potentially improving a hospital’s performance with regard to the mortality domain. This is one more reason to work closely with your hospital’s documentation specialists.
Don’t Be Afraid...
Proponents of mortality as a quality measure point to it as the ultimate reflection of the care provided. While moving the needle might seem like a task too big to undertake, a disciplined approach to the elements of the driver diagram combined with a robust documentation program can provide your institution with a tangible focus on this definitive measure.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
—Blue Oyster Cult
The designers of the hospital value-based purchasing (HVBP) program sought to include outcomes measures in 2014, and when they did, mortality was their choice. Specifically, HVBP for fiscal-year 2014 (starting October 2013) will include 30-day mortality rates for myocardial infarction, heart failure, and pneumonia. The weighting for the mortality domain will be 25% (see Table 1).
To review the requirements for the HVBP program in FY2014: All hospitals will have 1.25% of their Medicare inpatient payments withheld. They can earn back none, some, all, or an amount in excess of the 1.25%, depending on performance in the performance domains. To put it in perspective, 1.25% of Medicare inpatient payments for a 320-bed hospital are about $1 million. Such a hospital will have about $250,000 at risk in the mortality domain in FY2014.
Given the role hospitalists play in quality and safety initiatives, and the importance of medical record documentation in defining the risk of mortality and severity of illness, we can be crucial players in how our hospitals perform with regard to mortality.
Focus Areas for Mortality Reduction
Although many hospitalists might think that reducing mortality is like “boiling the ocean,” there are some areas where we can clearly focus our attention. There are four priority areas we should target in the coming years (also see Figure 1):
Reduce harm. This may take the form of reducing hospital-acquired infections, such as catheter-related UTIs, Clostridium difficile, and central-line-associated bloodstream infections, or reducing hospital-acquired VTE, falls, and delirium. Many hospital-acquired conditions have a collection, or bundle, of preventive practices. Hospitalists can work both in an institutional leadership capacity and in the course of daily clinical practice to implement bundles and best practices to reduce patient harm.
Improve teamwork. With hospitalists, “you started to have teams caring for inpatients in a coordinated way. So I regard this as [hospitalists] coming into their own, their vision of the future starting to really take hold,” said Brent James, coauthor of the recent Institute of Medicine report “Best Care at Lower Cost: The Path to Continuously Learning Health Care in America.” Partly, we’ve accomplished this through simply “showing up” and partly we’ve done it through becoming students of the art and science of teamwork. An example of teamwork training, developed by the Defense Department and the Agency for Healthcare Quality and Research (AHRQ), is TeamSTEPPS, which offers a systematic approach to cooperation, coordination, and communication among team members. Optimal patient resuscitation, in-hospital handoffs, rapid-response teams, and early-warning systems are essential pieces of teamwork that may reduce mortality.
Improve evidence-based care. This domain covers process measures aimed at optimizing care, including reducing mortality. For HVBP in particular, myocardial infarction, heart failure, and pneumonia are the focus.
Improve transitions of care. Best practices for care transitions and reducing readmissions, including advance-care planning, involvement of palliative care and hospice, and coordination with post-acute care, can be a key part of reducing 30-day mortality.
Documentation Integrity
Accurately capturing a patient’s condition in the medical record is crucial to assigning severity of illness and risk of mortality. Because mortality rates are severity-adjusted, accurate documentation is another important dimension to potentially improving a hospital’s performance with regard to the mortality domain. This is one more reason to work closely with your hospital’s documentation specialists.
Don’t Be Afraid...
Proponents of mortality as a quality measure point to it as the ultimate reflection of the care provided. While moving the needle might seem like a task too big to undertake, a disciplined approach to the elements of the driver diagram combined with a robust documentation program can provide your institution with a tangible focus on this definitive measure.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
—Blue Oyster Cult
The designers of the hospital value-based purchasing (HVBP) program sought to include outcomes measures in 2014, and when they did, mortality was their choice. Specifically, HVBP for fiscal-year 2014 (starting October 2013) will include 30-day mortality rates for myocardial infarction, heart failure, and pneumonia. The weighting for the mortality domain will be 25% (see Table 1).
To review the requirements for the HVBP program in FY2014: All hospitals will have 1.25% of their Medicare inpatient payments withheld. They can earn back none, some, all, or an amount in excess of the 1.25%, depending on performance in the performance domains. To put it in perspective, 1.25% of Medicare inpatient payments for a 320-bed hospital are about $1 million. Such a hospital will have about $250,000 at risk in the mortality domain in FY2014.
Given the role hospitalists play in quality and safety initiatives, and the importance of medical record documentation in defining the risk of mortality and severity of illness, we can be crucial players in how our hospitals perform with regard to mortality.
Focus Areas for Mortality Reduction
Although many hospitalists might think that reducing mortality is like “boiling the ocean,” there are some areas where we can clearly focus our attention. There are four priority areas we should target in the coming years (also see Figure 1):
Reduce harm. This may take the form of reducing hospital-acquired infections, such as catheter-related UTIs, Clostridium difficile, and central-line-associated bloodstream infections, or reducing hospital-acquired VTE, falls, and delirium. Many hospital-acquired conditions have a collection, or bundle, of preventive practices. Hospitalists can work both in an institutional leadership capacity and in the course of daily clinical practice to implement bundles and best practices to reduce patient harm.
Improve teamwork. With hospitalists, “you started to have teams caring for inpatients in a coordinated way. So I regard this as [hospitalists] coming into their own, their vision of the future starting to really take hold,” said Brent James, coauthor of the recent Institute of Medicine report “Best Care at Lower Cost: The Path to Continuously Learning Health Care in America.” Partly, we’ve accomplished this through simply “showing up” and partly we’ve done it through becoming students of the art and science of teamwork. An example of teamwork training, developed by the Defense Department and the Agency for Healthcare Quality and Research (AHRQ), is TeamSTEPPS, which offers a systematic approach to cooperation, coordination, and communication among team members. Optimal patient resuscitation, in-hospital handoffs, rapid-response teams, and early-warning systems are essential pieces of teamwork that may reduce mortality.
Improve evidence-based care. This domain covers process measures aimed at optimizing care, including reducing mortality. For HVBP in particular, myocardial infarction, heart failure, and pneumonia are the focus.
Improve transitions of care. Best practices for care transitions and reducing readmissions, including advance-care planning, involvement of palliative care and hospice, and coordination with post-acute care, can be a key part of reducing 30-day mortality.
Documentation Integrity
Accurately capturing a patient’s condition in the medical record is crucial to assigning severity of illness and risk of mortality. Because mortality rates are severity-adjusted, accurate documentation is another important dimension to potentially improving a hospital’s performance with regard to the mortality domain. This is one more reason to work closely with your hospital’s documentation specialists.
Don’t Be Afraid...
Proponents of mortality as a quality measure point to it as the ultimate reflection of the care provided. While moving the needle might seem like a task too big to undertake, a disciplined approach to the elements of the driver diagram combined with a robust documentation program can provide your institution with a tangible focus on this definitive measure.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.