User login
The power of culture
We psychiatrists should take a biopsychosocial approach to assessing our patients. However, we are enamored with biology and individual psychodynamics. Thus, we often overlook the influence of culture, or the lack thereof, on human behavior.
The assertion of Dr. Douglas K. Novins that using foundational cultural beliefs and practices strengthens interventions with people of color is particularly powerful. Furthermore, Dr. Novins’s findings inform us about the importance of culture in the protective factors and risky behaviors of our patients.

Culture Protects
While doing HIV prevention work in Durban, South Africa, I found it striking that 40% of the black African Zulu people were HIV positive, 6% of the white South Africans were HIV positive, but only 1% of the East Indian South Africans were HIV positive.
As it turns out, the East Indian South African culture (with its intact religious rituals, proscribed clothing customs, age-old mating practices, and so on) protected them. Meanwhile, the black African Zulu culture and its protective cultural influence had been stripped from them, making them vulnerable to activities such as risky sexual behavior, substance abuse, and violence.
In addition, it appears that the white South African culture is eroding, which is resulting in higher levels of HIV-positive individuals.
Culture Destroys
The latest Youth Risk Behavior Surveillance data offer a glimpse into just how paradoxical our world has become. The investigators looked at six categories of health-risk behaviors among young people and young adults.
Among their findings: The prevalence of having carried a weapon in general was higher among white males (27.2%) than among their black counterparts (21%). The prevalence of having carried a weapon onto school property was higher among white males (7.8%) than black males (6.7%). The prevalence of having ever used cocaine was higher among white males (7.6%) than black males (4.2%). Yet, people of color make up a higher proportion of children and young adults who are incarcerated. In fact, in 2010, the imprisonment rate for black non-Hispanic males (3,074/100,000 U.S. black male residents) was almost seven times higher than it was for white non-Hispanic males (459/100,000), according to the U.S. Bureau of Justice Statistics.
Some of these disparities can be deconstructed by looking at housing patterns. Structurally, we understand that most mid- and large-size cities have more absolute numbers of low-income whites than low-income blacks. But few low-income white neighborhoods exist because low-income whites have scattered-site housing, while low-income blacks are concentrated in inner cities. Police have a more difficult time finding and incarcerating illegal drug users when they live in scattered-site housing. Therefore, blacks who use illegal drugs are incarcerated more often than whites who use illegal drugs.
We also must acknowledge that some of these disparities are tied to the human construct of race. Buy-in to this construct explains why law enforcement officers traditionally "hunted" runaway slaves and returned them to their owners. It potentially explains the motivations of former Chicago police officer Jon Burge, who was convicted 2 years ago of lying about the torture of innocent black men in order to get confessions over many decades. Finally, this reality explains the thinking behind this saying in Chicago’s black community: "The police hunt black males!"
International psychiatrist Suman Fernando makes the point in his book "Mental Health, Race and Culture: Third Edition" (New York: Palgrave Macmillan, 2010) that much of Western culture is inherently racist. Derald Wing Sue, Ph.D., the preeminent multicultural scholar, reminds us of "ethnocentric monoculturalism," the notion that the only culture in the Western world that has any value is Western culture, and all other cultural values and practices are "primitive." Dr. Sue points out that ethnocentric monoculturalism and whiteness define a reality that puts those who are white European American males at an advantage (American Psychologist 2004;59:761-9).
In Canada, these destructive, entrenched views led to the removal of children from First Nations communities. This cultural dislocation, in turn, led to the loss of cultural protective factors, which ultimately contributed to the engagement in risky behaviors tied to suicide, intragroup homicide, and substance abuse. As I’ve discussed previously, many of the disruptive behaviors that result in incarceration can be traced back to alcohol consumption (Preventing fetal alcohol syndrome, April 12, 2012). It is well known that this syndrome is a leading cause of speech and language disorders, attention-deficit/hyperactivity disorder, and other developmental/cognitive disorders. These are often responsible for affect dysregulation, which leads to disruptive behaviors – which, in turn, can lead to incarceration.
It is heartening to see research like that produced by Dr. Novins and his colleagues. Their work reaffirms that culture protects. It also is a reminder that psychiatrists need to understand the sociological forces that exacerbate the emotional pain suffered by our patients – particularly those who are marginalized. We must redouble our efforts to incorporate respectful cultural components into our interventions. Doing so will produce better outcomes.
Dr. Bell is president and chief executive officer of Community Mental Health Council Inc. in Chicago. He also serves as director of the Institute for Juvenile Research at the University of Illinois at Chicago, and is director of public health and community psychiatry at the university.
We psychiatrists should take a biopsychosocial approach to assessing our patients. However, we are enamored with biology and individual psychodynamics. Thus, we often overlook the influence of culture, or the lack thereof, on human behavior.
The assertion of Dr. Douglas K. Novins that using foundational cultural beliefs and practices strengthens interventions with people of color is particularly powerful. Furthermore, Dr. Novins’s findings inform us about the importance of culture in the protective factors and risky behaviors of our patients.
Culture Protects
While doing HIV prevention work in Durban, South Africa, I found it striking that 40% of the black African Zulu people were HIV positive, 6% of the white South Africans were HIV positive, but only 1% of the East Indian South Africans were HIV positive.
As it turns out, the East Indian South African culture (with its intact religious rituals, proscribed clothing customs, age-old mating practices, and so on) protected them. Meanwhile, the black African Zulu culture and its protective cultural influence had been stripped from them, making them vulnerable to activities such as risky sexual behavior, substance abuse, and violence.
In addition, it appears that the white South African culture is eroding, which is resulting in higher levels of HIV-positive individuals.
Culture Destroys
The latest Youth Risk Behavior Surveillance data offer a glimpse into just how paradoxical our world has become. The investigators looked at six categories of health-risk behaviors among young people and young adults.
Among their findings: The prevalence of having carried a weapon in general was higher among white males (27.2%) than among their black counterparts (21%). The prevalence of having carried a weapon onto school property was higher among white males (7.8%) than black males (6.7%). The prevalence of having ever used cocaine was higher among white males (7.6%) than black males (4.2%). Yet, people of color make up a higher proportion of children and young adults who are incarcerated. In fact, in 2010, the imprisonment rate for black non-Hispanic males (3,074/100,000 U.S. black male residents) was almost seven times higher than it was for white non-Hispanic males (459/100,000), according to the U.S. Bureau of Justice Statistics.
Some of these disparities can be deconstructed by looking at housing patterns. Structurally, we understand that most mid- and large-size cities have more absolute numbers of low-income whites than low-income blacks. But few low-income white neighborhoods exist because low-income whites have scattered-site housing, while low-income blacks are concentrated in inner cities. Police have a more difficult time finding and incarcerating illegal drug users when they live in scattered-site housing. Therefore, blacks who use illegal drugs are incarcerated more often than whites who use illegal drugs.
We also must acknowledge that some of these disparities are tied to the human construct of race. Buy-in to this construct explains why law enforcement officers traditionally "hunted" runaway slaves and returned them to their owners. It potentially explains the motivations of former Chicago police officer Jon Burge, who was convicted 2 years ago of lying about the torture of innocent black men in order to get confessions over many decades. Finally, this reality explains the thinking behind this saying in Chicago’s black community: "The police hunt black males!"
International psychiatrist Suman Fernando makes the point in his book "Mental Health, Race and Culture: Third Edition" (New York: Palgrave Macmillan, 2010) that much of Western culture is inherently racist. Derald Wing Sue, Ph.D., the preeminent multicultural scholar, reminds us of "ethnocentric monoculturalism," the notion that the only culture in the Western world that has any value is Western culture, and all other cultural values and practices are "primitive." Dr. Sue points out that ethnocentric monoculturalism and whiteness define a reality that puts those who are white European American males at an advantage (American Psychologist 2004;59:761-9).
In Canada, these destructive, entrenched views led to the removal of children from First Nations communities. This cultural dislocation, in turn, led to the loss of cultural protective factors, which ultimately contributed to the engagement in risky behaviors tied to suicide, intragroup homicide, and substance abuse. As I’ve discussed previously, many of the disruptive behaviors that result in incarceration can be traced back to alcohol consumption (Preventing fetal alcohol syndrome, April 12, 2012). It is well known that this syndrome is a leading cause of speech and language disorders, attention-deficit/hyperactivity disorder, and other developmental/cognitive disorders. These are often responsible for affect dysregulation, which leads to disruptive behaviors – which, in turn, can lead to incarceration.
It is heartening to see research like that produced by Dr. Novins and his colleagues. Their work reaffirms that culture protects. It also is a reminder that psychiatrists need to understand the sociological forces that exacerbate the emotional pain suffered by our patients – particularly those who are marginalized. We must redouble our efforts to incorporate respectful cultural components into our interventions. Doing so will produce better outcomes.
Dr. Bell is president and chief executive officer of Community Mental Health Council Inc. in Chicago. He also serves as director of the Institute for Juvenile Research at the University of Illinois at Chicago, and is director of public health and community psychiatry at the university.
We psychiatrists should take a biopsychosocial approach to assessing our patients. However, we are enamored with biology and individual psychodynamics. Thus, we often overlook the influence of culture, or the lack thereof, on human behavior.
The assertion of Dr. Douglas K. Novins that using foundational cultural beliefs and practices strengthens interventions with people of color is particularly powerful. Furthermore, Dr. Novins’s findings inform us about the importance of culture in the protective factors and risky behaviors of our patients.
Culture Protects
While doing HIV prevention work in Durban, South Africa, I found it striking that 40% of the black African Zulu people were HIV positive, 6% of the white South Africans were HIV positive, but only 1% of the East Indian South Africans were HIV positive.
As it turns out, the East Indian South African culture (with its intact religious rituals, proscribed clothing customs, age-old mating practices, and so on) protected them. Meanwhile, the black African Zulu culture and its protective cultural influence had been stripped from them, making them vulnerable to activities such as risky sexual behavior, substance abuse, and violence.
In addition, it appears that the white South African culture is eroding, which is resulting in higher levels of HIV-positive individuals.
Culture Destroys
The latest Youth Risk Behavior Surveillance data offer a glimpse into just how paradoxical our world has become. The investigators looked at six categories of health-risk behaviors among young people and young adults.
Among their findings: The prevalence of having carried a weapon in general was higher among white males (27.2%) than among their black counterparts (21%). The prevalence of having carried a weapon onto school property was higher among white males (7.8%) than black males (6.7%). The prevalence of having ever used cocaine was higher among white males (7.6%) than black males (4.2%). Yet, people of color make up a higher proportion of children and young adults who are incarcerated. In fact, in 2010, the imprisonment rate for black non-Hispanic males (3,074/100,000 U.S. black male residents) was almost seven times higher than it was for white non-Hispanic males (459/100,000), according to the U.S. Bureau of Justice Statistics.
Some of these disparities can be deconstructed by looking at housing patterns. Structurally, we understand that most mid- and large-size cities have more absolute numbers of low-income whites than low-income blacks. But few low-income white neighborhoods exist because low-income whites have scattered-site housing, while low-income blacks are concentrated in inner cities. Police have a more difficult time finding and incarcerating illegal drug users when they live in scattered-site housing. Therefore, blacks who use illegal drugs are incarcerated more often than whites who use illegal drugs.
We also must acknowledge that some of these disparities are tied to the human construct of race. Buy-in to this construct explains why law enforcement officers traditionally "hunted" runaway slaves and returned them to their owners. It potentially explains the motivations of former Chicago police officer Jon Burge, who was convicted 2 years ago of lying about the torture of innocent black men in order to get confessions over many decades. Finally, this reality explains the thinking behind this saying in Chicago’s black community: "The police hunt black males!"
International psychiatrist Suman Fernando makes the point in his book "Mental Health, Race and Culture: Third Edition" (New York: Palgrave Macmillan, 2010) that much of Western culture is inherently racist. Derald Wing Sue, Ph.D., the preeminent multicultural scholar, reminds us of "ethnocentric monoculturalism," the notion that the only culture in the Western world that has any value is Western culture, and all other cultural values and practices are "primitive." Dr. Sue points out that ethnocentric monoculturalism and whiteness define a reality that puts those who are white European American males at an advantage (American Psychologist 2004;59:761-9).
In Canada, these destructive, entrenched views led to the removal of children from First Nations communities. This cultural dislocation, in turn, led to the loss of cultural protective factors, which ultimately contributed to the engagement in risky behaviors tied to suicide, intragroup homicide, and substance abuse. As I’ve discussed previously, many of the disruptive behaviors that result in incarceration can be traced back to alcohol consumption (Preventing fetal alcohol syndrome, April 12, 2012). It is well known that this syndrome is a leading cause of speech and language disorders, attention-deficit/hyperactivity disorder, and other developmental/cognitive disorders. These are often responsible for affect dysregulation, which leads to disruptive behaviors – which, in turn, can lead to incarceration.
It is heartening to see research like that produced by Dr. Novins and his colleagues. Their work reaffirms that culture protects. It also is a reminder that psychiatrists need to understand the sociological forces that exacerbate the emotional pain suffered by our patients – particularly those who are marginalized. We must redouble our efforts to incorporate respectful cultural components into our interventions. Doing so will produce better outcomes.
Dr. Bell is president and chief executive officer of Community Mental Health Council Inc. in Chicago. He also serves as director of the Institute for Juvenile Research at the University of Illinois at Chicago, and is director of public health and community psychiatry at the university.

Know Thyself
"Thank you all for agreeing to what I think is an excellent plan." Thus concluded the meeting led by one of the division heads in our department of surgery. The key agenda item was developing consensus on a highly controversial academic incentive plan that would transfer revenue from the busy clinicians who produced it to the faculty who were more engaged in the academic and educational missions of the division.
Several faculty members later related to me that the division head had dominated the conversation, belittled suggestions from his younger and less powerful colleagues, and "convinced" them to accept his plan with minimal alterations. They were irritated and frustrated. The division head reported to me that the meeting had gone extremely well and that he was able to gain consensus on a controversial and difficult issue. He was very pleased with himself.
I think we have all experienced this scenario – a person who is highly competent and possibly even pleasant in a social setting enters a meeting and, within minutes, irritates and comes into conflict with nearly everyone present, but sadly does not realize he has done so. What is lacking here?
The ancient Greeks called it "nothi auton" or "know thyself," and the modern parlance for it is self-awareness: the essential core of emotional intelligence and one of the most valuable attributes you can possess as a human being. In essence, it represents opening a door to your mind and discovering your own reality.
If self-awareness is so valuable, what exactly is it, why do you need it, and how do you get it if you don’t have it? Self-awareness consists of a number of components. First, it is an objective recognition of your strengths and weaknesses, values and beliefs, motives, and emotions. It also consists of an ability to continuously compare your current behavior to your core values and objectively assess whether that behavior reflects those values. Self-awareness also helps you to understand other people and how they perceive you. It helps you to recognize when you are stressed, and is a prerequisite for effective communication and interpersonal relations.
Why do you need self-awareness? Having self-awareness is required for you to be able to accept who you really are, to change those aspects of your personality that need to change, and to build on your strengths and clearly define your weaknesses. It is an important ingredient for effectively communicating with the world around you. In fact, it is difficult to imagine a happy human existence without a reasonable dose of this essential elixir.
Also, knowing oneself is the component of emotional intelligence that effective leaders possess in abundance. When I have encountered a failure of leadership in my surgical world, 90% of the time it has been due to a relative lack of self-awareness. (By the way, the division head described at the beginning of this editorial is now working elsewhere and the incentive plan for which he thought he had gained consensus is on the trash heap of unrealized objectives.)
How do you get self-awareness? In my experience, it is extremely difficult to instill self-awareness in people who are starting on empty. For individuals in leadership positions, the complete lack of this attribute may be a fatal flaw. For most of us, it is a natural part of maturation and can be improved by spending time in self-reflection, a practice few surgeons utilize because of their busy lives. Self-reflection should include spending quiet time, asking yourself difficult questions, and giving honest answers. Did I live to my core values during the meeting I just led? What could I have done better to lower the temperature in the room and avoid the conflicts that ensued? This requires commitment and courage. Also helpful is to have a sounding board of friends, colleagues, and/or mentors who are willing to critique you and provide honest feedback regarding your conduct during meetings, in the operating room, and even when having informal conversations.
So if you haven’t had the opportunity or acquired the tools to introduce yourself to yourself, it is never too late. It is not an easy process, but I believe you will be pleased with the result – a happier and more productive life.
Dr. Rikkers is Editor in Chief of Surgery News.
"Thank you all for agreeing to what I think is an excellent plan." Thus concluded the meeting led by one of the division heads in our department of surgery. The key agenda item was developing consensus on a highly controversial academic incentive plan that would transfer revenue from the busy clinicians who produced it to the faculty who were more engaged in the academic and educational missions of the division.
Several faculty members later related to me that the division head had dominated the conversation, belittled suggestions from his younger and less powerful colleagues, and "convinced" them to accept his plan with minimal alterations. They were irritated and frustrated. The division head reported to me that the meeting had gone extremely well and that he was able to gain consensus on a controversial and difficult issue. He was very pleased with himself.
I think we have all experienced this scenario – a person who is highly competent and possibly even pleasant in a social setting enters a meeting and, within minutes, irritates and comes into conflict with nearly everyone present, but sadly does not realize he has done so. What is lacking here?
The ancient Greeks called it "nothi auton" or "know thyself," and the modern parlance for it is self-awareness: the essential core of emotional intelligence and one of the most valuable attributes you can possess as a human being. In essence, it represents opening a door to your mind and discovering your own reality.
If self-awareness is so valuable, what exactly is it, why do you need it, and how do you get it if you don’t have it? Self-awareness consists of a number of components. First, it is an objective recognition of your strengths and weaknesses, values and beliefs, motives, and emotions. It also consists of an ability to continuously compare your current behavior to your core values and objectively assess whether that behavior reflects those values. Self-awareness also helps you to understand other people and how they perceive you. It helps you to recognize when you are stressed, and is a prerequisite for effective communication and interpersonal relations.
Why do you need self-awareness? Having self-awareness is required for you to be able to accept who you really are, to change those aspects of your personality that need to change, and to build on your strengths and clearly define your weaknesses. It is an important ingredient for effectively communicating with the world around you. In fact, it is difficult to imagine a happy human existence without a reasonable dose of this essential elixir.
Also, knowing oneself is the component of emotional intelligence that effective leaders possess in abundance. When I have encountered a failure of leadership in my surgical world, 90% of the time it has been due to a relative lack of self-awareness. (By the way, the division head described at the beginning of this editorial is now working elsewhere and the incentive plan for which he thought he had gained consensus is on the trash heap of unrealized objectives.)
How do you get self-awareness? In my experience, it is extremely difficult to instill self-awareness in people who are starting on empty. For individuals in leadership positions, the complete lack of this attribute may be a fatal flaw. For most of us, it is a natural part of maturation and can be improved by spending time in self-reflection, a practice few surgeons utilize because of their busy lives. Self-reflection should include spending quiet time, asking yourself difficult questions, and giving honest answers. Did I live to my core values during the meeting I just led? What could I have done better to lower the temperature in the room and avoid the conflicts that ensued? This requires commitment and courage. Also helpful is to have a sounding board of friends, colleagues, and/or mentors who are willing to critique you and provide honest feedback regarding your conduct during meetings, in the operating room, and even when having informal conversations.
So if you haven’t had the opportunity or acquired the tools to introduce yourself to yourself, it is never too late. It is not an easy process, but I believe you will be pleased with the result – a happier and more productive life.
Dr. Rikkers is Editor in Chief of Surgery News.
"Thank you all for agreeing to what I think is an excellent plan." Thus concluded the meeting led by one of the division heads in our department of surgery. The key agenda item was developing consensus on a highly controversial academic incentive plan that would transfer revenue from the busy clinicians who produced it to the faculty who were more engaged in the academic and educational missions of the division.
Several faculty members later related to me that the division head had dominated the conversation, belittled suggestions from his younger and less powerful colleagues, and "convinced" them to accept his plan with minimal alterations. They were irritated and frustrated. The division head reported to me that the meeting had gone extremely well and that he was able to gain consensus on a controversial and difficult issue. He was very pleased with himself.
I think we have all experienced this scenario – a person who is highly competent and possibly even pleasant in a social setting enters a meeting and, within minutes, irritates and comes into conflict with nearly everyone present, but sadly does not realize he has done so. What is lacking here?
The ancient Greeks called it "nothi auton" or "know thyself," and the modern parlance for it is self-awareness: the essential core of emotional intelligence and one of the most valuable attributes you can possess as a human being. In essence, it represents opening a door to your mind and discovering your own reality.
If self-awareness is so valuable, what exactly is it, why do you need it, and how do you get it if you don’t have it? Self-awareness consists of a number of components. First, it is an objective recognition of your strengths and weaknesses, values and beliefs, motives, and emotions. It also consists of an ability to continuously compare your current behavior to your core values and objectively assess whether that behavior reflects those values. Self-awareness also helps you to understand other people and how they perceive you. It helps you to recognize when you are stressed, and is a prerequisite for effective communication and interpersonal relations.
Why do you need self-awareness? Having self-awareness is required for you to be able to accept who you really are, to change those aspects of your personality that need to change, and to build on your strengths and clearly define your weaknesses. It is an important ingredient for effectively communicating with the world around you. In fact, it is difficult to imagine a happy human existence without a reasonable dose of this essential elixir.
Also, knowing oneself is the component of emotional intelligence that effective leaders possess in abundance. When I have encountered a failure of leadership in my surgical world, 90% of the time it has been due to a relative lack of self-awareness. (By the way, the division head described at the beginning of this editorial is now working elsewhere and the incentive plan for which he thought he had gained consensus is on the trash heap of unrealized objectives.)
How do you get self-awareness? In my experience, it is extremely difficult to instill self-awareness in people who are starting on empty. For individuals in leadership positions, the complete lack of this attribute may be a fatal flaw. For most of us, it is a natural part of maturation and can be improved by spending time in self-reflection, a practice few surgeons utilize because of their busy lives. Self-reflection should include spending quiet time, asking yourself difficult questions, and giving honest answers. Did I live to my core values during the meeting I just led? What could I have done better to lower the temperature in the room and avoid the conflicts that ensued? This requires commitment and courage. Also helpful is to have a sounding board of friends, colleagues, and/or mentors who are willing to critique you and provide honest feedback regarding your conduct during meetings, in the operating room, and even when having informal conversations.
So if you haven’t had the opportunity or acquired the tools to introduce yourself to yourself, it is never too late. It is not an easy process, but I believe you will be pleased with the result – a happier and more productive life.
Dr. Rikkers is Editor in Chief of Surgery News.

Win Whitcomb: Hospitalists Central to Helping Hospitals Meet Performance Goals, Avoid Financial Penalities


After a long wait, the time where quality really matters to the finance department has arrived. Why? Because now a lot of money is on the line based on hospitals’ ability to demonstrate performance on quality, patient safety, and patient satisfaction measures. And there is no physician group more central to the hospital’s performance on these measures than hospitalists.
To make this point, I will discuss the financial implications of three programs that are part of the Affordable Care Act: hospital value-based purchasing (HVBP), readmission penalties, and hospital-acquired conditions (HACs). Although many have found fault with these programs, especially the ones that only penalize hospitals (HACs and readmissions*), the dollars at risk can represent a new business case for hospitalist programs. High-performing hospitalist programs can positively impact their institution’s income statement.
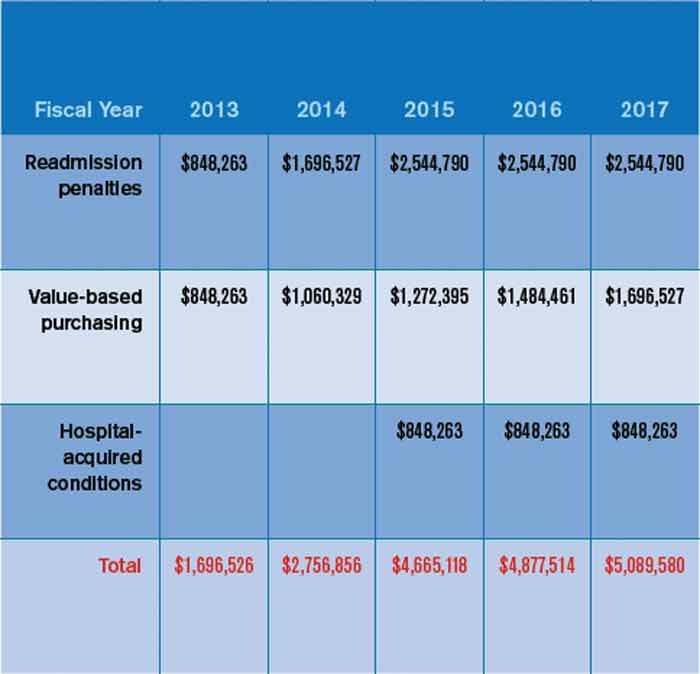
In October 2012, readmissions penalties and VBP payments/penalties went into effect. In October 2014, a 1% penalty for groups in the worst-performing quartile in the HACs will be in force. Taken together, as Table 1 demonstrates, the total payments at risk will grow such that by fiscal-year 2017, 6% of a hospital’s inpatient payments from Medicare will be at risk. To put this in perspective, Table 2 models the dollars at risk for each of the five years beginning in 2013 for the three programs in a hypothetical, 327-bed hospital. While the risk in 2013 is a modest $1.7 million, by 2017, this hospital has more than $5 million at risk.
So where should hospitalists be focusing their efforts with these three programs and the monies that accompany them? First, for those designing incentive compensation for hospitalists, the incentives should address the applicable elements of these programs. Second, the components of VBP will evolve. For example, 2013 VPB payments are based on 70% process measures (a subset of the core measure set for heart failure, myocardial infarction, pneumonia, and surgery) and 30% patient satisfaction measures. In 2015, VBP will add such outcomes measures as central-line-associated bloodstream infections, catheter UTIs, mortality rates, and the new efficiency measure, Medicare spending per beneficiary. Third, readmissions penalties, while encompassing heart failure, myocardial infarction, and pneumonia for fiscal-year 2013 payments, will expand in fiscal-year 2015 to include chronic obstructive pulmonary disease, coronary artery bypass grafting, percutaneous coronary intervention, and other vascular conditions.
While all this can be hard to keep track of, not to mention address in the course of daily patient care, I suggest hospitalists set the following priorities to enable high performance for their hospitals under these programs:
- Catheter UTIs. Work with nursing, the ED, and other areas to ensure that catheters are indicated, insertion is sterile, there is a mechanism for their prompt removal, specimens are collected and handled appropriately, and that “present on admission” is documented if appropriate.
- Central-line-associated bloodstream infections. Ensure your hospital has the systems in place to support the central-line insertion bundle, and that the bundle elements are followed and documented.
- Readmissions. Focus on heart failure, pneumonia, myocardial infarction, and COPD; work with nursing and case management to identify those at high risk for readmission; perform targeted interventions based on that risk (e.g. palliative care or clinical pharmacy consultation); prioritize medication reconciliation; provide timely communication of discharge summary to the next provider of care; and contact the patient soon after discharge to ensure they are following their plan of care.
- Patient satisfaction. Have a system for high performance on the questions comprising the “doctor communication” domain. These are “How often did doctors treat you with courtesy and respect/listen carefully to you/explain things in a way you could understand?”
Medicare’s Message
Clearly, the financial impacts of hospital quality, satisfaction, and safety are growing, conveying the message from the Centers for Medicare & Medicaid Services (CMS) that quality matters, making a business case for quality. Our focus as leaders in hospital systems improvement will only sharpen as we see hospital payments increasingly affected as a direct consequence of our efforts. If that doesn’t get the attention of the finance department, what will?
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
After a long wait, the time where quality really matters to the finance department has arrived. Why? Because now a lot of money is on the line based on hospitals’ ability to demonstrate performance on quality, patient safety, and patient satisfaction measures. And there is no physician group more central to the hospital’s performance on these measures than hospitalists.
To make this point, I will discuss the financial implications of three programs that are part of the Affordable Care Act: hospital value-based purchasing (HVBP), readmission penalties, and hospital-acquired conditions (HACs). Although many have found fault with these programs, especially the ones that only penalize hospitals (HACs and readmissions*), the dollars at risk can represent a new business case for hospitalist programs. High-performing hospitalist programs can positively impact their institution’s income statement.
In October 2012, readmissions penalties and VBP payments/penalties went into effect. In October 2014, a 1% penalty for groups in the worst-performing quartile in the HACs will be in force. Taken together, as Table 1 demonstrates, the total payments at risk will grow such that by fiscal-year 2017, 6% of a hospital’s inpatient payments from Medicare will be at risk. To put this in perspective, Table 2 models the dollars at risk for each of the five years beginning in 2013 for the three programs in a hypothetical, 327-bed hospital. While the risk in 2013 is a modest $1.7 million, by 2017, this hospital has more than $5 million at risk.
So where should hospitalists be focusing their efforts with these three programs and the monies that accompany them? First, for those designing incentive compensation for hospitalists, the incentives should address the applicable elements of these programs. Second, the components of VBP will evolve. For example, 2013 VPB payments are based on 70% process measures (a subset of the core measure set for heart failure, myocardial infarction, pneumonia, and surgery) and 30% patient satisfaction measures. In 2015, VBP will add such outcomes measures as central-line-associated bloodstream infections, catheter UTIs, mortality rates, and the new efficiency measure, Medicare spending per beneficiary. Third, readmissions penalties, while encompassing heart failure, myocardial infarction, and pneumonia for fiscal-year 2013 payments, will expand in fiscal-year 2015 to include chronic obstructive pulmonary disease, coronary artery bypass grafting, percutaneous coronary intervention, and other vascular conditions.
While all this can be hard to keep track of, not to mention address in the course of daily patient care, I suggest hospitalists set the following priorities to enable high performance for their hospitals under these programs:
- Catheter UTIs. Work with nursing, the ED, and other areas to ensure that catheters are indicated, insertion is sterile, there is a mechanism for their prompt removal, specimens are collected and handled appropriately, and that “present on admission” is documented if appropriate.
- Central-line-associated bloodstream infections. Ensure your hospital has the systems in place to support the central-line insertion bundle, and that the bundle elements are followed and documented.
- Readmissions. Focus on heart failure, pneumonia, myocardial infarction, and COPD; work with nursing and case management to identify those at high risk for readmission; perform targeted interventions based on that risk (e.g. palliative care or clinical pharmacy consultation); prioritize medication reconciliation; provide timely communication of discharge summary to the next provider of care; and contact the patient soon after discharge to ensure they are following their plan of care.
- Patient satisfaction. Have a system for high performance on the questions comprising the “doctor communication” domain. These are “How often did doctors treat you with courtesy and respect/listen carefully to you/explain things in a way you could understand?”
Medicare’s Message
Clearly, the financial impacts of hospital quality, satisfaction, and safety are growing, conveying the message from the Centers for Medicare & Medicaid Services (CMS) that quality matters, making a business case for quality. Our focus as leaders in hospital systems improvement will only sharpen as we see hospital payments increasingly affected as a direct consequence of our efforts. If that doesn’t get the attention of the finance department, what will?
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
After a long wait, the time where quality really matters to the finance department has arrived. Why? Because now a lot of money is on the line based on hospitals’ ability to demonstrate performance on quality, patient safety, and patient satisfaction measures. And there is no physician group more central to the hospital’s performance on these measures than hospitalists.
To make this point, I will discuss the financial implications of three programs that are part of the Affordable Care Act: hospital value-based purchasing (HVBP), readmission penalties, and hospital-acquired conditions (HACs). Although many have found fault with these programs, especially the ones that only penalize hospitals (HACs and readmissions*), the dollars at risk can represent a new business case for hospitalist programs. High-performing hospitalist programs can positively impact their institution’s income statement.
In October 2012, readmissions penalties and VBP payments/penalties went into effect. In October 2014, a 1% penalty for groups in the worst-performing quartile in the HACs will be in force. Taken together, as Table 1 demonstrates, the total payments at risk will grow such that by fiscal-year 2017, 6% of a hospital’s inpatient payments from Medicare will be at risk. To put this in perspective, Table 2 models the dollars at risk for each of the five years beginning in 2013 for the three programs in a hypothetical, 327-bed hospital. While the risk in 2013 is a modest $1.7 million, by 2017, this hospital has more than $5 million at risk.
So where should hospitalists be focusing their efforts with these three programs and the monies that accompany them? First, for those designing incentive compensation for hospitalists, the incentives should address the applicable elements of these programs. Second, the components of VBP will evolve. For example, 2013 VPB payments are based on 70% process measures (a subset of the core measure set for heart failure, myocardial infarction, pneumonia, and surgery) and 30% patient satisfaction measures. In 2015, VBP will add such outcomes measures as central-line-associated bloodstream infections, catheter UTIs, mortality rates, and the new efficiency measure, Medicare spending per beneficiary. Third, readmissions penalties, while encompassing heart failure, myocardial infarction, and pneumonia for fiscal-year 2013 payments, will expand in fiscal-year 2015 to include chronic obstructive pulmonary disease, coronary artery bypass grafting, percutaneous coronary intervention, and other vascular conditions.
While all this can be hard to keep track of, not to mention address in the course of daily patient care, I suggest hospitalists set the following priorities to enable high performance for their hospitals under these programs:
- Catheter UTIs. Work with nursing, the ED, and other areas to ensure that catheters are indicated, insertion is sterile, there is a mechanism for their prompt removal, specimens are collected and handled appropriately, and that “present on admission” is documented if appropriate.
- Central-line-associated bloodstream infections. Ensure your hospital has the systems in place to support the central-line insertion bundle, and that the bundle elements are followed and documented.
- Readmissions. Focus on heart failure, pneumonia, myocardial infarction, and COPD; work with nursing and case management to identify those at high risk for readmission; perform targeted interventions based on that risk (e.g. palliative care or clinical pharmacy consultation); prioritize medication reconciliation; provide timely communication of discharge summary to the next provider of care; and contact the patient soon after discharge to ensure they are following their plan of care.
- Patient satisfaction. Have a system for high performance on the questions comprising the “doctor communication” domain. These are “How often did doctors treat you with courtesy and respect/listen carefully to you/explain things in a way you could understand?”
Medicare’s Message
Clearly, the financial impacts of hospital quality, satisfaction, and safety are growing, conveying the message from the Centers for Medicare & Medicaid Services (CMS) that quality matters, making a business case for quality. Our focus as leaders in hospital systems improvement will only sharpen as we see hospital payments increasingly affected as a direct consequence of our efforts. If that doesn’t get the attention of the finance department, what will?
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
John Nelson, MD: A New Hospitalist

Ben was just accepted to med school!!! Hopefully, more acceptances will be forthcoming. We are very proud of Ben for all his hard work. Another doctor in the family.
I was delighted to find the above message from an old friend in my inbox. It got me thinking: Will Ben become a hospitalist? Will he join his dad’s hospitalist group? Will his dad encourage him to pursue a hospitalist career or something else?
Early Hospitalist Practice
The author of that email was Ben’s dad, Chuck Wilson. Chuck is the reason I’m a hospitalist. He was a year ahead of me in residency, and while still a resident, he somehow connected with a really busy family physician in town who was looking for someone to manage his hospital patients. Not one to be bound by convention, Chuck agreed to what was at the time a nearly unheard-of arrangement. He finished residency, joined the staff of the community hospital across town from our residency, and began caring for the family physician’s hospital patients. Within days, he was fielding calls from other doctors asking him to do the same for them. Within weeks of arriving, he had begun accepting essentially all unassigned medical admissions from the ED. This was in the 1980s; Chuck was among the nation’s first real hospitalists.
I don’t think Chuck spent any time worrying about how his practice was so different from the traditional internists and family physicians in the community. He was confident he was providing a valuable service to his patients and the medical community. The rapid growth in his patient census was an indicator he was on to something, and soon he and I began talking. He was looking for a partner.
In November of my third year of residency, I decided I would put off my endocrinology fellowship for a year or two and join Chuck in his new practice. From our conversations, I anticipated that I would care for exactly the kinds of patients that filled nearly all of my time as a resident. I wouldn’t need to learn the new skills in ambulatory medicine, and wouldn’t need to make the long-term commitment expected to join a traditional primary-care practice. And I would earn a competitive compensation and have a flexible lifestyle. I soon realized that hospitalist practice provided me with all of these advantages, so more than two decades later, I still haven’t gotten around to completing the application for an endocrine fellowship.
A Loose Arrangement
For the first few years, Chuck and I didn’t bother to have any sort of legal agreement with each other. We shook hands and agreed to a “reap what you till” form of compensation, which meant we didn’t have to work exactly the same amount, and never had disagreements about how practice revenue was divided between us.
Because of Chuck’s influence, we had miniscule overhead expenses, most likely less than 10% of revenue. We each bought our own malpractice insurance, paid our biller a percent of collections, and rented a pager. That was about it for overhead.
We had no rigid scheduling algorithm, the only requirement being that at least one of us needed to be working every day. Both of us worked most weekdays, but we took time off whenever it suited us. Our scheduling meetings were usually held when we bumped into one another while rounding and went something like this:
“You OK if I take five days off starting tomorrow?”
“Sure. That’s fine.”
Meeting adjourned.
For years, we had no official name for our practice. This became a bigger issue when our group had grown to four doctors, so we defaulted to referring to the group by the first letter of the last name of each doctor, in order of tenure: The WNKL Group. A more formal name was to follow a few years later when the group was even larger, but I’ve taken delight in hearing that WNKL has persisted in some places and documents around the hospital years later, even though N, K, and L left the group long ago.
In the first few years, we never thought about developing clinical protocols or measuring our efficiency or clinical effectiveness. Chuck was confident that compared to the traditional primary-care model, we were providing higher-quality care at a lower cost. But I wasn’t so sure. After a few years, we began seeing hospital data showing that our cost per case tended to be lower, and what little data we could get regarding our quality of care suggested that it was about the same, and in some cases might be better.
A principal reason the practice has survived more than 25 years is that other than a small “tax” during their first 18 months (mainly to cover the cost of recruiting them), new doctors were regarded as equals in the business. Chuck and subsequent doctors never tried to gain an advantage over newer doctors by trying to claim a greater share of the practice’s revenue or decision-making authority.
Chuck is still in the same group he founded. In 2000, I was lured away by the chance to start a new group and live in a place that both my wife and I love. He and I have enjoyed watching our field grow up, and we take satisfaction in our roles in its evolution.
Lessons Learned
The hospitalist model of practice didn’t have a single inventor or place of origin, and anyone involved in starting a practice in the 1980s or before should be proud to have invented their practice when no blueprint existed. Creative thinking and openness to a new way of doing things were critical in developing the first hospitalist practices. They also are useful traits in trying to improve modern hospitalist practices or other segments of our healthcare system.
Like many new developments in medicine, the economic effects of our practice—lower hospital cost per case—became apparent, especially to Chuck, before data regarding quality surfaced. I wish we had gotten more serious early on about capturing whatever quality data might have been available—clearly less than what is available today—and those in new healthcare endeavors today should try to measure quality at the outset. Unlike the 1980s, the current marketplace will help ensure that happens.
Coda
There is one other really cool thing about Chuck’s email at the beginning of this column: those three exclamation points! Chuck is typically laconic and understated, and not given to such displays of emotion, but there are few things that generate more enthusiasm than a parent sharing news of a child’s success.
So, Ben, as you start med school next year, I wish you the best. You can be sure I’ll be asking for updates about your progress. The most important thing is that you find a life and career that engages you to do good work for others and provides satisfaction. And whatever you choose to do after med school, I know you’ll continue to make your parents proud.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Ben was just accepted to med school!!! Hopefully, more acceptances will be forthcoming. We are very proud of Ben for all his hard work. Another doctor in the family.
I was delighted to find the above message from an old friend in my inbox. It got me thinking: Will Ben become a hospitalist? Will he join his dad’s hospitalist group? Will his dad encourage him to pursue a hospitalist career or something else?
Early Hospitalist Practice
The author of that email was Ben’s dad, Chuck Wilson. Chuck is the reason I’m a hospitalist. He was a year ahead of me in residency, and while still a resident, he somehow connected with a really busy family physician in town who was looking for someone to manage his hospital patients. Not one to be bound by convention, Chuck agreed to what was at the time a nearly unheard-of arrangement. He finished residency, joined the staff of the community hospital across town from our residency, and began caring for the family physician’s hospital patients. Within days, he was fielding calls from other doctors asking him to do the same for them. Within weeks of arriving, he had begun accepting essentially all unassigned medical admissions from the ED. This was in the 1980s; Chuck was among the nation’s first real hospitalists.
I don’t think Chuck spent any time worrying about how his practice was so different from the traditional internists and family physicians in the community. He was confident he was providing a valuable service to his patients and the medical community. The rapid growth in his patient census was an indicator he was on to something, and soon he and I began talking. He was looking for a partner.
In November of my third year of residency, I decided I would put off my endocrinology fellowship for a year or two and join Chuck in his new practice. From our conversations, I anticipated that I would care for exactly the kinds of patients that filled nearly all of my time as a resident. I wouldn’t need to learn the new skills in ambulatory medicine, and wouldn’t need to make the long-term commitment expected to join a traditional primary-care practice. And I would earn a competitive compensation and have a flexible lifestyle. I soon realized that hospitalist practice provided me with all of these advantages, so more than two decades later, I still haven’t gotten around to completing the application for an endocrine fellowship.
A Loose Arrangement
For the first few years, Chuck and I didn’t bother to have any sort of legal agreement with each other. We shook hands and agreed to a “reap what you till” form of compensation, which meant we didn’t have to work exactly the same amount, and never had disagreements about how practice revenue was divided between us.
Because of Chuck’s influence, we had miniscule overhead expenses, most likely less than 10% of revenue. We each bought our own malpractice insurance, paid our biller a percent of collections, and rented a pager. That was about it for overhead.
We had no rigid scheduling algorithm, the only requirement being that at least one of us needed to be working every day. Both of us worked most weekdays, but we took time off whenever it suited us. Our scheduling meetings were usually held when we bumped into one another while rounding and went something like this:
“You OK if I take five days off starting tomorrow?”
“Sure. That’s fine.”
Meeting adjourned.
For years, we had no official name for our practice. This became a bigger issue when our group had grown to four doctors, so we defaulted to referring to the group by the first letter of the last name of each doctor, in order of tenure: The WNKL Group. A more formal name was to follow a few years later when the group was even larger, but I’ve taken delight in hearing that WNKL has persisted in some places and documents around the hospital years later, even though N, K, and L left the group long ago.
In the first few years, we never thought about developing clinical protocols or measuring our efficiency or clinical effectiveness. Chuck was confident that compared to the traditional primary-care model, we were providing higher-quality care at a lower cost. But I wasn’t so sure. After a few years, we began seeing hospital data showing that our cost per case tended to be lower, and what little data we could get regarding our quality of care suggested that it was about the same, and in some cases might be better.
A principal reason the practice has survived more than 25 years is that other than a small “tax” during their first 18 months (mainly to cover the cost of recruiting them), new doctors were regarded as equals in the business. Chuck and subsequent doctors never tried to gain an advantage over newer doctors by trying to claim a greater share of the practice’s revenue or decision-making authority.
Chuck is still in the same group he founded. In 2000, I was lured away by the chance to start a new group and live in a place that both my wife and I love. He and I have enjoyed watching our field grow up, and we take satisfaction in our roles in its evolution.
Lessons Learned
The hospitalist model of practice didn’t have a single inventor or place of origin, and anyone involved in starting a practice in the 1980s or before should be proud to have invented their practice when no blueprint existed. Creative thinking and openness to a new way of doing things were critical in developing the first hospitalist practices. They also are useful traits in trying to improve modern hospitalist practices or other segments of our healthcare system.
Like many new developments in medicine, the economic effects of our practice—lower hospital cost per case—became apparent, especially to Chuck, before data regarding quality surfaced. I wish we had gotten more serious early on about capturing whatever quality data might have been available—clearly less than what is available today—and those in new healthcare endeavors today should try to measure quality at the outset. Unlike the 1980s, the current marketplace will help ensure that happens.
Coda
There is one other really cool thing about Chuck’s email at the beginning of this column: those three exclamation points! Chuck is typically laconic and understated, and not given to such displays of emotion, but there are few things that generate more enthusiasm than a parent sharing news of a child’s success.
So, Ben, as you start med school next year, I wish you the best. You can be sure I’ll be asking for updates about your progress. The most important thing is that you find a life and career that engages you to do good work for others and provides satisfaction. And whatever you choose to do after med school, I know you’ll continue to make your parents proud.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Ben was just accepted to med school!!! Hopefully, more acceptances will be forthcoming. We are very proud of Ben for all his hard work. Another doctor in the family.
I was delighted to find the above message from an old friend in my inbox. It got me thinking: Will Ben become a hospitalist? Will he join his dad’s hospitalist group? Will his dad encourage him to pursue a hospitalist career or something else?
Early Hospitalist Practice
The author of that email was Ben’s dad, Chuck Wilson. Chuck is the reason I’m a hospitalist. He was a year ahead of me in residency, and while still a resident, he somehow connected with a really busy family physician in town who was looking for someone to manage his hospital patients. Not one to be bound by convention, Chuck agreed to what was at the time a nearly unheard-of arrangement. He finished residency, joined the staff of the community hospital across town from our residency, and began caring for the family physician’s hospital patients. Within days, he was fielding calls from other doctors asking him to do the same for them. Within weeks of arriving, he had begun accepting essentially all unassigned medical admissions from the ED. This was in the 1980s; Chuck was among the nation’s first real hospitalists.
I don’t think Chuck spent any time worrying about how his practice was so different from the traditional internists and family physicians in the community. He was confident he was providing a valuable service to his patients and the medical community. The rapid growth in his patient census was an indicator he was on to something, and soon he and I began talking. He was looking for a partner.
In November of my third year of residency, I decided I would put off my endocrinology fellowship for a year or two and join Chuck in his new practice. From our conversations, I anticipated that I would care for exactly the kinds of patients that filled nearly all of my time as a resident. I wouldn’t need to learn the new skills in ambulatory medicine, and wouldn’t need to make the long-term commitment expected to join a traditional primary-care practice. And I would earn a competitive compensation and have a flexible lifestyle. I soon realized that hospitalist practice provided me with all of these advantages, so more than two decades later, I still haven’t gotten around to completing the application for an endocrine fellowship.
A Loose Arrangement
For the first few years, Chuck and I didn’t bother to have any sort of legal agreement with each other. We shook hands and agreed to a “reap what you till” form of compensation, which meant we didn’t have to work exactly the same amount, and never had disagreements about how practice revenue was divided between us.
Because of Chuck’s influence, we had miniscule overhead expenses, most likely less than 10% of revenue. We each bought our own malpractice insurance, paid our biller a percent of collections, and rented a pager. That was about it for overhead.
We had no rigid scheduling algorithm, the only requirement being that at least one of us needed to be working every day. Both of us worked most weekdays, but we took time off whenever it suited us. Our scheduling meetings were usually held when we bumped into one another while rounding and went something like this:
“You OK if I take five days off starting tomorrow?”
“Sure. That’s fine.”
Meeting adjourned.
For years, we had no official name for our practice. This became a bigger issue when our group had grown to four doctors, so we defaulted to referring to the group by the first letter of the last name of each doctor, in order of tenure: The WNKL Group. A more formal name was to follow a few years later when the group was even larger, but I’ve taken delight in hearing that WNKL has persisted in some places and documents around the hospital years later, even though N, K, and L left the group long ago.
In the first few years, we never thought about developing clinical protocols or measuring our efficiency or clinical effectiveness. Chuck was confident that compared to the traditional primary-care model, we were providing higher-quality care at a lower cost. But I wasn’t so sure. After a few years, we began seeing hospital data showing that our cost per case tended to be lower, and what little data we could get regarding our quality of care suggested that it was about the same, and in some cases might be better.
A principal reason the practice has survived more than 25 years is that other than a small “tax” during their first 18 months (mainly to cover the cost of recruiting them), new doctors were regarded as equals in the business. Chuck and subsequent doctors never tried to gain an advantage over newer doctors by trying to claim a greater share of the practice’s revenue or decision-making authority.
Chuck is still in the same group he founded. In 2000, I was lured away by the chance to start a new group and live in a place that both my wife and I love. He and I have enjoyed watching our field grow up, and we take satisfaction in our roles in its evolution.
Lessons Learned
The hospitalist model of practice didn’t have a single inventor or place of origin, and anyone involved in starting a practice in the 1980s or before should be proud to have invented their practice when no blueprint existed. Creative thinking and openness to a new way of doing things were critical in developing the first hospitalist practices. They also are useful traits in trying to improve modern hospitalist practices or other segments of our healthcare system.
Like many new developments in medicine, the economic effects of our practice—lower hospital cost per case—became apparent, especially to Chuck, before data regarding quality surfaced. I wish we had gotten more serious early on about capturing whatever quality data might have been available—clearly less than what is available today—and those in new healthcare endeavors today should try to measure quality at the outset. Unlike the 1980s, the current marketplace will help ensure that happens.
Coda
There is one other really cool thing about Chuck’s email at the beginning of this column: those three exclamation points! Chuck is typically laconic and understated, and not given to such displays of emotion, but there are few things that generate more enthusiasm than a parent sharing news of a child’s success.
So, Ben, as you start med school next year, I wish you the best. You can be sure I’ll be asking for updates about your progress. The most important thing is that you find a life and career that engages you to do good work for others and provides satisfaction. And whatever you choose to do after med school, I know you’ll continue to make your parents proud.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Poverty's Effect on Mental Health
The greatest of evils and the worst of crimes is poverty.
– George Bernard Shaw, 1856-1950
"I don’t care" was the response from Gerardo when I asked, "Of the people you know, is there anyone who loves you?"
Gerardo was a 17-year-old high school senior who had grown up in poverty. He was planning to attend Stony Brook University on scholarship. Gerardo had been referred for psychiatric evaluation because he slapped his mother, slammed a refrigerator door against her back, and cursed at her.

He was eager to leave his family, including his Ecuadorian mother, who sold burritos from a street stand; his 19-year-old sister, Lola, who lived primarily with her 21-year-old boyfriend; and his 9-year-old half-sister, the daughter of the man who beat him repeatedly.
His biological father, an alcoholic and drug addict, had left when he was 3; his stepfather, Manuel, subsequently became violent toward him, and his mother at times held him down during beatings.
After Manuel left the home, his mother took another man into the house. Fred, a cook in a Chinese restaurant, helped with rent and kept to his room.
Gerardo blamed his mother. "She was never around" and was out selling food. His mother overlooked Manuel’s molestation of Gerardo’s older sister Lola and enabled her son’s abuse. Why?
It was only when Lola took an overdose that New York City’s Administration for Children’s Services learned of the distressed family and intervened.
Gerardo talked about his commitment to school as an entrée into a good position. Still, he was cynical. In a provocative manner, he called school, "boring." He added, "The other option is to find a minimum wage job." With anger, he said, "I am preparing to live in corporate America." His disdain encompassed personal, academic, and family areas.
Is the diagnosis of Gerardo depression or a nascent personality disorder? Does he have posttraumatic stress disorder? One thing was clear: Gerardo, an intelligent adolescent, was emerging from childhood scarred by his experience.
The Toll of Poverty
Poverty is common in the United States. Peter Edelman in his book "So Rich, So Poor: Why It’s So Hard to End Poverty in America" (New York: The New Press, 2012) details that 46 million Americans live in poverty, defined as earning no more than $23,050 yearly for a family of four. Food stamps and housing assistance programs are helpful, but with cutbacks in welfare, there are 6 million people living solely on food stamps.
Edelman, a professor at Georgetown University Law Center, Washington, says that good-paying jobs have gone overseas; the number of single-parent households is on the rise; and the wealthiest have created disadvantages for the poor, resulting in economic crises such as the housing bubble. At present, children rather than the elderly are more likely in poverty. More than 40% of families headed by single mothers are poor.
We view poverty as an economic dilemma, but its psychological consequences are profound. Do poor people develop mental illness or does mental illness cause a slide into poverty? Much controversy exists on this question, but both probably are true. Poverty has far-reaching consequences and creates vulnerabilities. It negatively affects mental health.
Many of the social ills associated with poverty confound with mental illness. Poverty is depressing.
A 63-year-old Hispanic patient described her struggle. Glenda suffers from rheumatoid arthritis, depression, diabetes, and osteoporosis. From supplemental security income, she receives $716 a month. She receives food stamps amounting to $200 monthly. Were it not for her daughter, a school crossing guard, sharing the apartment, Glenda could not afford the rent of $604 a month. "Even clothes, buying a pair of jeans for $35, would stop me from getting things for the house," she said. "I’m angry; it gets me irritated. I like to listen to music, go to concerts, Central Park, but I have no financial means."
She planned to go to a local food pantry in Long Island City because grocery prices are rising.
According to Susan Grange, a social worker and assistant director at a family services agency in Queens: "Poverty leads to depression and hopelessness – no expectations in clients. They are burnt out before they can grow up. Most don’t make it through high school."
The inner-city youth she sees abuse drugs and become sexually active by age 12 or 13 years. If the children succeed, it is because "someone is there emotionally for them." Some recognize the importance of school; others have the financial resources to get mental health assistance.
Apathy among the young is significant as illustrated by Gerardo’s outlook. Domestic violence and sexual abuse wreak havoc in these families.
Education for All
Many focus on formal education of youth as a means of curbing poverty, but the picture is complex. Chaotic family life erodes early brain development.
Neurobiologists find that stress and trauma impinge on development of executive function and impulse control. With these deficits, children fail at school, and a cycle of failure ensues. Evidence suggests that the poorest children do worse as students.
Journalist Paul Tough, the author of "How Children Succeed: Grit, Curiosity, and the Hidden Power of Character" (New York: Houghton Mifflin Harcourt, 2012), studied poor families in Chicago and the ways in which children grow up in poverty.
He emphasizes that youngsters in stressful homes are not able to develop normally. Character traits such as perseverance, grit, self-discipline, and the ability to conquer adversity are survival skills. They get fostered in mentoring programs geared for inner-city youth.
There already are isolated community-based projects such as the Harlem Children’s Zone, which have raised awareness of education’s value and the need for family involvement. Unfortunately, funding for such projects remains scarce.
Young people such as Gerardo are channeling their grit – despite cynicism – into an education. Others in similar circumstances commit crimes and cause us to wonder whether they lack humanity. They live on "the edge of the law, the edge of the economy, the edge of family structure and communities," according to then Sen. Barack Obama in his speech at Hampton University in 2007. Depression, posttraumatic stress disorder, and character disorders abound in this population.
Remedies Through Education
Education is cited as the first step in curbing poverty. Learning leads to awareness and the acquisition of marketable skills. But education is a family matter. It should extend to the parents of children at risk. Adults need to know that their children require peace and safety to get homework done and to thrive. Working, devoted parents are role models. The way in which parents eat determines what children consume.
I see in my practice parents whose misconceptions prevent their children from benefiting from learning opportunities. Tutoring is available in public schools but overwhelm parents who say their child’s teacher never advised it. The same reasoning applies to summer school and sponsored summer camps such as the Fresh Air Fund. Sometimes parents fear after-school activities or church groups because they hear of incidents of child abuse on the news. Instead, children languish in front of a TV or play video games; they fall behind academically after inactive summers.
Parent education can make the adults advocates. It should be broadly available in schools and social service agencies. If adults become knowledgeable and improve their judgment, the needs of youngsters will be met.
This is where we psychiatrists have a role. As mental health professionals, we can help parents change their behaviors. We also can work with young people such as Gerardo so that they are able to come to terms with their circumstances and go on to lead prosperous and fulfilling lives. Education and mental health services can help patients overcome poverty.
Dr. Cohen is in private practice in New York. She consults at New York Presbyterian Hospital-Cornell and at the Hospital for Special Surgery.
The greatest of evils and the worst of crimes is poverty.
– George Bernard Shaw, 1856-1950
"I don’t care" was the response from Gerardo when I asked, "Of the people you know, is there anyone who loves you?"
Gerardo was a 17-year-old high school senior who had grown up in poverty. He was planning to attend Stony Brook University on scholarship. Gerardo had been referred for psychiatric evaluation because he slapped his mother, slammed a refrigerator door against her back, and cursed at her.
He was eager to leave his family, including his Ecuadorian mother, who sold burritos from a street stand; his 19-year-old sister, Lola, who lived primarily with her 21-year-old boyfriend; and his 9-year-old half-sister, the daughter of the man who beat him repeatedly.
His biological father, an alcoholic and drug addict, had left when he was 3; his stepfather, Manuel, subsequently became violent toward him, and his mother at times held him down during beatings.
After Manuel left the home, his mother took another man into the house. Fred, a cook in a Chinese restaurant, helped with rent and kept to his room.
Gerardo blamed his mother. "She was never around" and was out selling food. His mother overlooked Manuel’s molestation of Gerardo’s older sister Lola and enabled her son’s abuse. Why?
It was only when Lola took an overdose that New York City’s Administration for Children’s Services learned of the distressed family and intervened.
Gerardo talked about his commitment to school as an entrée into a good position. Still, he was cynical. In a provocative manner, he called school, "boring." He added, "The other option is to find a minimum wage job." With anger, he said, "I am preparing to live in corporate America." His disdain encompassed personal, academic, and family areas.
Is the diagnosis of Gerardo depression or a nascent personality disorder? Does he have posttraumatic stress disorder? One thing was clear: Gerardo, an intelligent adolescent, was emerging from childhood scarred by his experience.
The Toll of Poverty
Poverty is common in the United States. Peter Edelman in his book "So Rich, So Poor: Why It’s So Hard to End Poverty in America" (New York: The New Press, 2012) details that 46 million Americans live in poverty, defined as earning no more than $23,050 yearly for a family of four. Food stamps and housing assistance programs are helpful, but with cutbacks in welfare, there are 6 million people living solely on food stamps.
Edelman, a professor at Georgetown University Law Center, Washington, says that good-paying jobs have gone overseas; the number of single-parent households is on the rise; and the wealthiest have created disadvantages for the poor, resulting in economic crises such as the housing bubble. At present, children rather than the elderly are more likely in poverty. More than 40% of families headed by single mothers are poor.
We view poverty as an economic dilemma, but its psychological consequences are profound. Do poor people develop mental illness or does mental illness cause a slide into poverty? Much controversy exists on this question, but both probably are true. Poverty has far-reaching consequences and creates vulnerabilities. It negatively affects mental health.
Many of the social ills associated with poverty confound with mental illness. Poverty is depressing.
A 63-year-old Hispanic patient described her struggle. Glenda suffers from rheumatoid arthritis, depression, diabetes, and osteoporosis. From supplemental security income, she receives $716 a month. She receives food stamps amounting to $200 monthly. Were it not for her daughter, a school crossing guard, sharing the apartment, Glenda could not afford the rent of $604 a month. "Even clothes, buying a pair of jeans for $35, would stop me from getting things for the house," she said. "I’m angry; it gets me irritated. I like to listen to music, go to concerts, Central Park, but I have no financial means."
She planned to go to a local food pantry in Long Island City because grocery prices are rising.
According to Susan Grange, a social worker and assistant director at a family services agency in Queens: "Poverty leads to depression and hopelessness – no expectations in clients. They are burnt out before they can grow up. Most don’t make it through high school."
The inner-city youth she sees abuse drugs and become sexually active by age 12 or 13 years. If the children succeed, it is because "someone is there emotionally for them." Some recognize the importance of school; others have the financial resources to get mental health assistance.
Apathy among the young is significant as illustrated by Gerardo’s outlook. Domestic violence and sexual abuse wreak havoc in these families.
Education for All
Many focus on formal education of youth as a means of curbing poverty, but the picture is complex. Chaotic family life erodes early brain development.
Neurobiologists find that stress and trauma impinge on development of executive function and impulse control. With these deficits, children fail at school, and a cycle of failure ensues. Evidence suggests that the poorest children do worse as students.
Journalist Paul Tough, the author of "How Children Succeed: Grit, Curiosity, and the Hidden Power of Character" (New York: Houghton Mifflin Harcourt, 2012), studied poor families in Chicago and the ways in which children grow up in poverty.
He emphasizes that youngsters in stressful homes are not able to develop normally. Character traits such as perseverance, grit, self-discipline, and the ability to conquer adversity are survival skills. They get fostered in mentoring programs geared for inner-city youth.
There already are isolated community-based projects such as the Harlem Children’s Zone, which have raised awareness of education’s value and the need for family involvement. Unfortunately, funding for such projects remains scarce.
Young people such as Gerardo are channeling their grit – despite cynicism – into an education. Others in similar circumstances commit crimes and cause us to wonder whether they lack humanity. They live on "the edge of the law, the edge of the economy, the edge of family structure and communities," according to then Sen. Barack Obama in his speech at Hampton University in 2007. Depression, posttraumatic stress disorder, and character disorders abound in this population.
Remedies Through Education
Education is cited as the first step in curbing poverty. Learning leads to awareness and the acquisition of marketable skills. But education is a family matter. It should extend to the parents of children at risk. Adults need to know that their children require peace and safety to get homework done and to thrive. Working, devoted parents are role models. The way in which parents eat determines what children consume.
I see in my practice parents whose misconceptions prevent their children from benefiting from learning opportunities. Tutoring is available in public schools but overwhelm parents who say their child’s teacher never advised it. The same reasoning applies to summer school and sponsored summer camps such as the Fresh Air Fund. Sometimes parents fear after-school activities or church groups because they hear of incidents of child abuse on the news. Instead, children languish in front of a TV or play video games; they fall behind academically after inactive summers.
Parent education can make the adults advocates. It should be broadly available in schools and social service agencies. If adults become knowledgeable and improve their judgment, the needs of youngsters will be met.
This is where we psychiatrists have a role. As mental health professionals, we can help parents change their behaviors. We also can work with young people such as Gerardo so that they are able to come to terms with their circumstances and go on to lead prosperous and fulfilling lives. Education and mental health services can help patients overcome poverty.
Dr. Cohen is in private practice in New York. She consults at New York Presbyterian Hospital-Cornell and at the Hospital for Special Surgery.
The greatest of evils and the worst of crimes is poverty.
– George Bernard Shaw, 1856-1950
"I don’t care" was the response from Gerardo when I asked, "Of the people you know, is there anyone who loves you?"
Gerardo was a 17-year-old high school senior who had grown up in poverty. He was planning to attend Stony Brook University on scholarship. Gerardo had been referred for psychiatric evaluation because he slapped his mother, slammed a refrigerator door against her back, and cursed at her.
He was eager to leave his family, including his Ecuadorian mother, who sold burritos from a street stand; his 19-year-old sister, Lola, who lived primarily with her 21-year-old boyfriend; and his 9-year-old half-sister, the daughter of the man who beat him repeatedly.
His biological father, an alcoholic and drug addict, had left when he was 3; his stepfather, Manuel, subsequently became violent toward him, and his mother at times held him down during beatings.
After Manuel left the home, his mother took another man into the house. Fred, a cook in a Chinese restaurant, helped with rent and kept to his room.
Gerardo blamed his mother. "She was never around" and was out selling food. His mother overlooked Manuel’s molestation of Gerardo’s older sister Lola and enabled her son’s abuse. Why?
It was only when Lola took an overdose that New York City’s Administration for Children’s Services learned of the distressed family and intervened.
Gerardo talked about his commitment to school as an entrée into a good position. Still, he was cynical. In a provocative manner, he called school, "boring." He added, "The other option is to find a minimum wage job." With anger, he said, "I am preparing to live in corporate America." His disdain encompassed personal, academic, and family areas.
Is the diagnosis of Gerardo depression or a nascent personality disorder? Does he have posttraumatic stress disorder? One thing was clear: Gerardo, an intelligent adolescent, was emerging from childhood scarred by his experience.
The Toll of Poverty
Poverty is common in the United States. Peter Edelman in his book "So Rich, So Poor: Why It’s So Hard to End Poverty in America" (New York: The New Press, 2012) details that 46 million Americans live in poverty, defined as earning no more than $23,050 yearly for a family of four. Food stamps and housing assistance programs are helpful, but with cutbacks in welfare, there are 6 million people living solely on food stamps.
Edelman, a professor at Georgetown University Law Center, Washington, says that good-paying jobs have gone overseas; the number of single-parent households is on the rise; and the wealthiest have created disadvantages for the poor, resulting in economic crises such as the housing bubble. At present, children rather than the elderly are more likely in poverty. More than 40% of families headed by single mothers are poor.
We view poverty as an economic dilemma, but its psychological consequences are profound. Do poor people develop mental illness or does mental illness cause a slide into poverty? Much controversy exists on this question, but both probably are true. Poverty has far-reaching consequences and creates vulnerabilities. It negatively affects mental health.
Many of the social ills associated with poverty confound with mental illness. Poverty is depressing.
A 63-year-old Hispanic patient described her struggle. Glenda suffers from rheumatoid arthritis, depression, diabetes, and osteoporosis. From supplemental security income, she receives $716 a month. She receives food stamps amounting to $200 monthly. Were it not for her daughter, a school crossing guard, sharing the apartment, Glenda could not afford the rent of $604 a month. "Even clothes, buying a pair of jeans for $35, would stop me from getting things for the house," she said. "I’m angry; it gets me irritated. I like to listen to music, go to concerts, Central Park, but I have no financial means."
She planned to go to a local food pantry in Long Island City because grocery prices are rising.
According to Susan Grange, a social worker and assistant director at a family services agency in Queens: "Poverty leads to depression and hopelessness – no expectations in clients. They are burnt out before they can grow up. Most don’t make it through high school."
The inner-city youth she sees abuse drugs and become sexually active by age 12 or 13 years. If the children succeed, it is because "someone is there emotionally for them." Some recognize the importance of school; others have the financial resources to get mental health assistance.
Apathy among the young is significant as illustrated by Gerardo’s outlook. Domestic violence and sexual abuse wreak havoc in these families.
Education for All
Many focus on formal education of youth as a means of curbing poverty, but the picture is complex. Chaotic family life erodes early brain development.
Neurobiologists find that stress and trauma impinge on development of executive function and impulse control. With these deficits, children fail at school, and a cycle of failure ensues. Evidence suggests that the poorest children do worse as students.
Journalist Paul Tough, the author of "How Children Succeed: Grit, Curiosity, and the Hidden Power of Character" (New York: Houghton Mifflin Harcourt, 2012), studied poor families in Chicago and the ways in which children grow up in poverty.
He emphasizes that youngsters in stressful homes are not able to develop normally. Character traits such as perseverance, grit, self-discipline, and the ability to conquer adversity are survival skills. They get fostered in mentoring programs geared for inner-city youth.
There already are isolated community-based projects such as the Harlem Children’s Zone, which have raised awareness of education’s value and the need for family involvement. Unfortunately, funding for such projects remains scarce.
Young people such as Gerardo are channeling their grit – despite cynicism – into an education. Others in similar circumstances commit crimes and cause us to wonder whether they lack humanity. They live on "the edge of the law, the edge of the economy, the edge of family structure and communities," according to then Sen. Barack Obama in his speech at Hampton University in 2007. Depression, posttraumatic stress disorder, and character disorders abound in this population.
Remedies Through Education
Education is cited as the first step in curbing poverty. Learning leads to awareness and the acquisition of marketable skills. But education is a family matter. It should extend to the parents of children at risk. Adults need to know that their children require peace and safety to get homework done and to thrive. Working, devoted parents are role models. The way in which parents eat determines what children consume.
I see in my practice parents whose misconceptions prevent their children from benefiting from learning opportunities. Tutoring is available in public schools but overwhelm parents who say their child’s teacher never advised it. The same reasoning applies to summer school and sponsored summer camps such as the Fresh Air Fund. Sometimes parents fear after-school activities or church groups because they hear of incidents of child abuse on the news. Instead, children languish in front of a TV or play video games; they fall behind academically after inactive summers.
Parent education can make the adults advocates. It should be broadly available in schools and social service agencies. If adults become knowledgeable and improve their judgment, the needs of youngsters will be met.
This is where we psychiatrists have a role. As mental health professionals, we can help parents change their behaviors. We also can work with young people such as Gerardo so that they are able to come to terms with their circumstances and go on to lead prosperous and fulfilling lives. Education and mental health services can help patients overcome poverty.
Dr. Cohen is in private practice in New York. She consults at New York Presbyterian Hospital-Cornell and at the Hospital for Special Surgery.

Preventing suicide preceded by mass murder
As the country struggles to process the horrific massacre in Newtown, Conn., those of us who treat patients with mental illness must keep several facts in mind.
We know that 20,000 out of 100,000 people in the United States have a mental illness and that much of this is depression. In addition, an estimated 1 million adults in the United States reported making a suicide attempt in the past year.
Finally, it turns out that overall, for the last 30 years, the suicide rates run around 11/100,000 people across all age ranges and 20/100,000 for young adults. This makes suicide the third-leading cause of death among young people. Yet, suicide is actually a rare event. Furthermore, the likelihood of a person committing a single homicide before committing suicide is even rarer.

As an expert in violence prevention who has been investigating these phenomena for 45 years, I view such incidents as "suicides preceded by mass murder" (mass murder defined as three or more people being killed). The problem is there is no solid evidence for this theory. Also, these kinds of suicides are even rarer and even more difficult to study with the goal of preventing these tragedies.
Of course, if people get their understanding about public health and the frequency of certain events from the media, they believe such events are not rare, but rather are quite common. These difficulties make it tricky for public psychiatrists to inform public policy and public opinion to do things that prevent these horrible events from occurring and repeating.
When an individual commits suicide and the media give that suicide a great deal of coverage, shortly afterward, there are what are called "copycat" or "contagion" suicides – this was David Phillips’s seminal work back in the 1970s. The proof is so strong that the American Foundation for Suicide Prevention, the American Association of Suicidology, and the Annenberg Public Policy Center have provided "Reporting on Suicide: Recommendations for the Media." These guidelines suggest that the media not give a great deal of attention to the phenomenon of suicide, and it begins with the assertion that "Suicide contagion is real."
Those of us who work with these patients know that when the media provide details about these suicides, they provide depressed, hurt individuals who express their pain through anger and violence with a blueprint for what to do with their suicidal ideation. We know that a huge dynamic in the thinking of suicidal people is often: "I’ll fix you; I’ll kill myself." Unfortunately, some people take this a step further and think: "I’ll show you; not only will I kill myself, but I will kill a bunch of other people first." Fortunately, as I said earlier, this is an extremely rare event – despite the perception perpetuated by the mainstream media that this is common.
In light of these facts, I have several recommendations:
• First, I realize that the media cannot ignore these horrific events, but it could report on them differently to minimize what I suspect is contagion.
• Second, we can increase the protective factors that generally prevent more suicides from occurring.
Here are four steps we can take to stop these events:
1. We can increase the social fabric surrounding mentally ill people, which entails not being afraid of them and not stigmatizing them.
2. We can ensure that all youth are strongly connected to people so they will be able to feel good about their relationships and about themselves. Such support systems help ease some of the pain caused by depression.
3. We can teach all of our children social and emotional skills such as "affect regulation" so that "hurt people will not hurt people."
4. We can monitor our young adults (that is, anyone under 26), because research shows that brain development is a gradual process. The limbic system (the flight, fight, or freeze system of the brain) is the first to develop. The frontal lobes, where thinking, judgment, and wisdom occur, are not fully developed until age 26 – in other words, young adults tend to be all gasoline and no brakes or steering wheel. Thus, it is up to families, schools, friends, and neighbors to supply the brakes and steering wheels for young adults in a loving manner – not a punitive one – so they are influenced by formal and informal social controls that prevent risky behaviors.
• Lastly, the 2012 National Strategy for Suicide Prevention: Goals and Objectives for Action, if followed, could prevent "suicides preceded by mass murder."
Dr. Bell is professor of public health and director of the Institute for Juvenile Research in the department of psychiatry at the University of Illinois at Chicago. He has written extensively on the issue of suicide and homicide, and was appointed to serve on the Institute of Medicine’s Board of Neuroscience and Behavioral Health study on pathophysiology and prevention of adolescent and adult suicide in 2000 that produced the seminal IOM report "Reducing Suicide" in 2002. Dr. Bell also worked with former U.S. Surgeon General David Satcher on "Youth Violence: A Report of the Surgeon General" in 2001.
As the country struggles to process the horrific massacre in Newtown, Conn., those of us who treat patients with mental illness must keep several facts in mind.
We know that 20,000 out of 100,000 people in the United States have a mental illness and that much of this is depression. In addition, an estimated 1 million adults in the United States reported making a suicide attempt in the past year.
Finally, it turns out that overall, for the last 30 years, the suicide rates run around 11/100,000 people across all age ranges and 20/100,000 for young adults. This makes suicide the third-leading cause of death among young people. Yet, suicide is actually a rare event. Furthermore, the likelihood of a person committing a single homicide before committing suicide is even rarer.
As an expert in violence prevention who has been investigating these phenomena for 45 years, I view such incidents as "suicides preceded by mass murder" (mass murder defined as three or more people being killed). The problem is there is no solid evidence for this theory. Also, these kinds of suicides are even rarer and even more difficult to study with the goal of preventing these tragedies.
Of course, if people get their understanding about public health and the frequency of certain events from the media, they believe such events are not rare, but rather are quite common. These difficulties make it tricky for public psychiatrists to inform public policy and public opinion to do things that prevent these horrible events from occurring and repeating.
When an individual commits suicide and the media give that suicide a great deal of coverage, shortly afterward, there are what are called "copycat" or "contagion" suicides – this was David Phillips’s seminal work back in the 1970s. The proof is so strong that the American Foundation for Suicide Prevention, the American Association of Suicidology, and the Annenberg Public Policy Center have provided "Reporting on Suicide: Recommendations for the Media." These guidelines suggest that the media not give a great deal of attention to the phenomenon of suicide, and it begins with the assertion that "Suicide contagion is real."
Those of us who work with these patients know that when the media provide details about these suicides, they provide depressed, hurt individuals who express their pain through anger and violence with a blueprint for what to do with their suicidal ideation. We know that a huge dynamic in the thinking of suicidal people is often: "I’ll fix you; I’ll kill myself." Unfortunately, some people take this a step further and think: "I’ll show you; not only will I kill myself, but I will kill a bunch of other people first." Fortunately, as I said earlier, this is an extremely rare event – despite the perception perpetuated by the mainstream media that this is common.
In light of these facts, I have several recommendations:
• First, I realize that the media cannot ignore these horrific events, but it could report on them differently to minimize what I suspect is contagion.
• Second, we can increase the protective factors that generally prevent more suicides from occurring.
Here are four steps we can take to stop these events:
1. We can increase the social fabric surrounding mentally ill people, which entails not being afraid of them and not stigmatizing them.
2. We can ensure that all youth are strongly connected to people so they will be able to feel good about their relationships and about themselves. Such support systems help ease some of the pain caused by depression.
3. We can teach all of our children social and emotional skills such as "affect regulation" so that "hurt people will not hurt people."
4. We can monitor our young adults (that is, anyone under 26), because research shows that brain development is a gradual process. The limbic system (the flight, fight, or freeze system of the brain) is the first to develop. The frontal lobes, where thinking, judgment, and wisdom occur, are not fully developed until age 26 – in other words, young adults tend to be all gasoline and no brakes or steering wheel. Thus, it is up to families, schools, friends, and neighbors to supply the brakes and steering wheels for young adults in a loving manner – not a punitive one – so they are influenced by formal and informal social controls that prevent risky behaviors.
• Lastly, the 2012 National Strategy for Suicide Prevention: Goals and Objectives for Action, if followed, could prevent "suicides preceded by mass murder."
Dr. Bell is professor of public health and director of the Institute for Juvenile Research in the department of psychiatry at the University of Illinois at Chicago. He has written extensively on the issue of suicide and homicide, and was appointed to serve on the Institute of Medicine’s Board of Neuroscience and Behavioral Health study on pathophysiology and prevention of adolescent and adult suicide in 2000 that produced the seminal IOM report "Reducing Suicide" in 2002. Dr. Bell also worked with former U.S. Surgeon General David Satcher on "Youth Violence: A Report of the Surgeon General" in 2001.
As the country struggles to process the horrific massacre in Newtown, Conn., those of us who treat patients with mental illness must keep several facts in mind.
We know that 20,000 out of 100,000 people in the United States have a mental illness and that much of this is depression. In addition, an estimated 1 million adults in the United States reported making a suicide attempt in the past year.
Finally, it turns out that overall, for the last 30 years, the suicide rates run around 11/100,000 people across all age ranges and 20/100,000 for young adults. This makes suicide the third-leading cause of death among young people. Yet, suicide is actually a rare event. Furthermore, the likelihood of a person committing a single homicide before committing suicide is even rarer.
As an expert in violence prevention who has been investigating these phenomena for 45 years, I view such incidents as "suicides preceded by mass murder" (mass murder defined as three or more people being killed). The problem is there is no solid evidence for this theory. Also, these kinds of suicides are even rarer and even more difficult to study with the goal of preventing these tragedies.
Of course, if people get their understanding about public health and the frequency of certain events from the media, they believe such events are not rare, but rather are quite common. These difficulties make it tricky for public psychiatrists to inform public policy and public opinion to do things that prevent these horrible events from occurring and repeating.
When an individual commits suicide and the media give that suicide a great deal of coverage, shortly afterward, there are what are called "copycat" or "contagion" suicides – this was David Phillips’s seminal work back in the 1970s. The proof is so strong that the American Foundation for Suicide Prevention, the American Association of Suicidology, and the Annenberg Public Policy Center have provided "Reporting on Suicide: Recommendations for the Media." These guidelines suggest that the media not give a great deal of attention to the phenomenon of suicide, and it begins with the assertion that "Suicide contagion is real."
Those of us who work with these patients know that when the media provide details about these suicides, they provide depressed, hurt individuals who express their pain through anger and violence with a blueprint for what to do with their suicidal ideation. We know that a huge dynamic in the thinking of suicidal people is often: "I’ll fix you; I’ll kill myself." Unfortunately, some people take this a step further and think: "I’ll show you; not only will I kill myself, but I will kill a bunch of other people first." Fortunately, as I said earlier, this is an extremely rare event – despite the perception perpetuated by the mainstream media that this is common.
In light of these facts, I have several recommendations:
• First, I realize that the media cannot ignore these horrific events, but it could report on them differently to minimize what I suspect is contagion.
• Second, we can increase the protective factors that generally prevent more suicides from occurring.
Here are four steps we can take to stop these events:
1. We can increase the social fabric surrounding mentally ill people, which entails not being afraid of them and not stigmatizing them.
2. We can ensure that all youth are strongly connected to people so they will be able to feel good about their relationships and about themselves. Such support systems help ease some of the pain caused by depression.
3. We can teach all of our children social and emotional skills such as "affect regulation" so that "hurt people will not hurt people."
4. We can monitor our young adults (that is, anyone under 26), because research shows that brain development is a gradual process. The limbic system (the flight, fight, or freeze system of the brain) is the first to develop. The frontal lobes, where thinking, judgment, and wisdom occur, are not fully developed until age 26 – in other words, young adults tend to be all gasoline and no brakes or steering wheel. Thus, it is up to families, schools, friends, and neighbors to supply the brakes and steering wheels for young adults in a loving manner – not a punitive one – so they are influenced by formal and informal social controls that prevent risky behaviors.
• Lastly, the 2012 National Strategy for Suicide Prevention: Goals and Objectives for Action, if followed, could prevent "suicides preceded by mass murder."
Dr. Bell is professor of public health and director of the Institute for Juvenile Research in the department of psychiatry at the University of Illinois at Chicago. He has written extensively on the issue of suicide and homicide, and was appointed to serve on the Institute of Medicine’s Board of Neuroscience and Behavioral Health study on pathophysiology and prevention of adolescent and adult suicide in 2000 that produced the seminal IOM report "Reducing Suicide" in 2002. Dr. Bell also worked with former U.S. Surgeon General David Satcher on "Youth Violence: A Report of the Surgeon General" in 2001.

Prevention Continues to Gain Traction in Psychiatry
As a prevention-focused, public health psychiatrist, I am committed to proactively addressing the needs of patients with mental health problems. In light of this commitment, I want to bring to your attention several recent advances in prevention in psychiatry.
When Dr. David Satcher served as the 16th surgeon general, during his 2000 Conference on Children’s Mental Health, he suggested three areas of focus for mental health professionals that would lead to improving the public’s health: protective services, special education, and juvenile justice. Taking his advice, many of us have been working in these areas and gaining some ground.

Child Protective Services
More than a decade ago, some disturbing trends became apparent in downstate Illinois in McLean County. Although the statewide average of removing children from their families was 4/1,000, child protective services in that county were removing 40/1,000 children from their families.
The director of the Department of Children and Family Services (DCFS) learned about this problem and sent Community Mental Health Council (CMHC), and Urban Services, downstate to fix this problem. CMHC is a mental health center that uses evidence-based practices to serve its community in Chicago, and Urban Services is a social service agency that seeks to support communities by improving their social cohesion and control. By using a seven-field principle model that strengthened families, we were able to reduce the number of children being removed dropped from 24.1/1,000 down to 11.1/1,000.
Furthermore, follow-up studies indicated children and families in the intervention were far less likely to have subsequent hotline calls, compared with those not in the intervention. Thanks to the leadership of several subsequent DCFS directors, slowly but surely, Illinois began to infuse intact family services into their agency.
The result was Illinois was able to reduce the number of children being removed from their homes from 4/1,000 down to 1.8/1,000. Fortunately, for the nation, President Barack Obama appointed Bryan Samuels, a former DCFS directors who infused a prevention into Illinois DCFS, as the commissioner of the Administration of Children, Youth, and Families, and he is on a mission to spread what he started in Illinois to the entire nation.
Youth in Special Education
Earlier this year, I realized that fetal alcohol syndrome (FAS) was a serious contributor to the four major and common problems children have (speech and language disorders, attention-deficit/hyperactivity disorder, specific learning disorders, and mild mental retardation).
It is interesting to me how focused psychiatry is on neuropsychiatry and brain imaging, but as far as I know, there is no objective test available to diagnose FAS other than the characteristic facies with which a child with serious FAS is born but gradually outgrows, making it difficult to diagnose an adolescent or adult.
Someone once suggested that if I suspected any of the four major and common problems of children, I ask to see a baby picture to see whether I can recognize the characteristic facies of FAS. While I am more a fan of clinical medicine/psychiatry than I am of laboratory medicine/psychiatry, I wonder why our neuropsychiatric researchers have not tackled this common problem.
Regardless, the problem of FAS does seem to be on federal radar as a potentially major prevention initiative, and the Substance Abuse and Mental Health Administration is certainly aware of the problem as the agency cites fetal alcohol spectrum disorders as more common than autism. Fortunately, some states are ahead of the curve (for example, Alaska and Washington states), and there is a National Organization on Fetal Alcohol Syndrome (NOFAS). Hopefully, the observations about the huge impact that FAS makes on special education will pan out, and we will see some prevention traction in the area of special education – as we did with cretinism and phenylketonuria.
Youth in Juvenile Justice
For me, providing treatment to young people who have wound up in the juvenile justice system has been the toughest challenge, because the psychiatrist’s ability to influence such systems is minimal. However, a recent National Academy of Sciences (NAS) report – "Reforming Juvenile Justice: A Developmental Approach" – has just been released, and, if this report gains footing in the United States, we will all be much better off.
As director of the Institute for Juvenile Research (IJR) – where child psychiatry started – I am familiar with the development of the first juvenile court in the United States. It was shortly thereafter that the same group of women (led by Nobel Prize–winning social workers Jane Addams and Julia Lathrop) who developed that special court began IJR to study delinquency. It turns out more than 100 years later, we are rediscovering their wisdom as the new NAS report illustrates.
So, prevention is alive and well in psychiatry. The construct of prevention in psychiatry has even made its way beyond the specialty. Take, for example, the Wikipedia entry on mental disorders – which has a subsection on prevention.
Dr. Bell is president and chief executive officer of Community Mental Health Council Inc. in Chicago. In addition to serving as director of the Institute for Juvenile Research at the University of Illinois at Chicago, he is director of public and community psychiatry at the university.
As a prevention-focused, public health psychiatrist, I am committed to proactively addressing the needs of patients with mental health problems. In light of this commitment, I want to bring to your attention several recent advances in prevention in psychiatry.
When Dr. David Satcher served as the 16th surgeon general, during his 2000 Conference on Children’s Mental Health, he suggested three areas of focus for mental health professionals that would lead to improving the public’s health: protective services, special education, and juvenile justice. Taking his advice, many of us have been working in these areas and gaining some ground.
Child Protective Services
More than a decade ago, some disturbing trends became apparent in downstate Illinois in McLean County. Although the statewide average of removing children from their families was 4/1,000, child protective services in that county were removing 40/1,000 children from their families.
The director of the Department of Children and Family Services (DCFS) learned about this problem and sent Community Mental Health Council (CMHC), and Urban Services, downstate to fix this problem. CMHC is a mental health center that uses evidence-based practices to serve its community in Chicago, and Urban Services is a social service agency that seeks to support communities by improving their social cohesion and control. By using a seven-field principle model that strengthened families, we were able to reduce the number of children being removed dropped from 24.1/1,000 down to 11.1/1,000.
Furthermore, follow-up studies indicated children and families in the intervention were far less likely to have subsequent hotline calls, compared with those not in the intervention. Thanks to the leadership of several subsequent DCFS directors, slowly but surely, Illinois began to infuse intact family services into their agency.
The result was Illinois was able to reduce the number of children being removed from their homes from 4/1,000 down to 1.8/1,000. Fortunately, for the nation, President Barack Obama appointed Bryan Samuels, a former DCFS directors who infused a prevention into Illinois DCFS, as the commissioner of the Administration of Children, Youth, and Families, and he is on a mission to spread what he started in Illinois to the entire nation.
Youth in Special Education
Earlier this year, I realized that fetal alcohol syndrome (FAS) was a serious contributor to the four major and common problems children have (speech and language disorders, attention-deficit/hyperactivity disorder, specific learning disorders, and mild mental retardation).
It is interesting to me how focused psychiatry is on neuropsychiatry and brain imaging, but as far as I know, there is no objective test available to diagnose FAS other than the characteristic facies with which a child with serious FAS is born but gradually outgrows, making it difficult to diagnose an adolescent or adult.
Someone once suggested that if I suspected any of the four major and common problems of children, I ask to see a baby picture to see whether I can recognize the characteristic facies of FAS. While I am more a fan of clinical medicine/psychiatry than I am of laboratory medicine/psychiatry, I wonder why our neuropsychiatric researchers have not tackled this common problem.
Regardless, the problem of FAS does seem to be on federal radar as a potentially major prevention initiative, and the Substance Abuse and Mental Health Administration is certainly aware of the problem as the agency cites fetal alcohol spectrum disorders as more common than autism. Fortunately, some states are ahead of the curve (for example, Alaska and Washington states), and there is a National Organization on Fetal Alcohol Syndrome (NOFAS). Hopefully, the observations about the huge impact that FAS makes on special education will pan out, and we will see some prevention traction in the area of special education – as we did with cretinism and phenylketonuria.
Youth in Juvenile Justice
For me, providing treatment to young people who have wound up in the juvenile justice system has been the toughest challenge, because the psychiatrist’s ability to influence such systems is minimal. However, a recent National Academy of Sciences (NAS) report – "Reforming Juvenile Justice: A Developmental Approach" – has just been released, and, if this report gains footing in the United States, we will all be much better off.
As director of the Institute for Juvenile Research (IJR) – where child psychiatry started – I am familiar with the development of the first juvenile court in the United States. It was shortly thereafter that the same group of women (led by Nobel Prize–winning social workers Jane Addams and Julia Lathrop) who developed that special court began IJR to study delinquency. It turns out more than 100 years later, we are rediscovering their wisdom as the new NAS report illustrates.
So, prevention is alive and well in psychiatry. The construct of prevention in psychiatry has even made its way beyond the specialty. Take, for example, the Wikipedia entry on mental disorders – which has a subsection on prevention.
Dr. Bell is president and chief executive officer of Community Mental Health Council Inc. in Chicago. In addition to serving as director of the Institute for Juvenile Research at the University of Illinois at Chicago, he is director of public and community psychiatry at the university.
As a prevention-focused, public health psychiatrist, I am committed to proactively addressing the needs of patients with mental health problems. In light of this commitment, I want to bring to your attention several recent advances in prevention in psychiatry.
When Dr. David Satcher served as the 16th surgeon general, during his 2000 Conference on Children’s Mental Health, he suggested three areas of focus for mental health professionals that would lead to improving the public’s health: protective services, special education, and juvenile justice. Taking his advice, many of us have been working in these areas and gaining some ground.
Child Protective Services
More than a decade ago, some disturbing trends became apparent in downstate Illinois in McLean County. Although the statewide average of removing children from their families was 4/1,000, child protective services in that county were removing 40/1,000 children from their families.
The director of the Department of Children and Family Services (DCFS) learned about this problem and sent Community Mental Health Council (CMHC), and Urban Services, downstate to fix this problem. CMHC is a mental health center that uses evidence-based practices to serve its community in Chicago, and Urban Services is a social service agency that seeks to support communities by improving their social cohesion and control. By using a seven-field principle model that strengthened families, we were able to reduce the number of children being removed dropped from 24.1/1,000 down to 11.1/1,000.
Furthermore, follow-up studies indicated children and families in the intervention were far less likely to have subsequent hotline calls, compared with those not in the intervention. Thanks to the leadership of several subsequent DCFS directors, slowly but surely, Illinois began to infuse intact family services into their agency.
The result was Illinois was able to reduce the number of children being removed from their homes from 4/1,000 down to 1.8/1,000. Fortunately, for the nation, President Barack Obama appointed Bryan Samuels, a former DCFS directors who infused a prevention into Illinois DCFS, as the commissioner of the Administration of Children, Youth, and Families, and he is on a mission to spread what he started in Illinois to the entire nation.
Youth in Special Education
Earlier this year, I realized that fetal alcohol syndrome (FAS) was a serious contributor to the four major and common problems children have (speech and language disorders, attention-deficit/hyperactivity disorder, specific learning disorders, and mild mental retardation).
It is interesting to me how focused psychiatry is on neuropsychiatry and brain imaging, but as far as I know, there is no objective test available to diagnose FAS other than the characteristic facies with which a child with serious FAS is born but gradually outgrows, making it difficult to diagnose an adolescent or adult.
Someone once suggested that if I suspected any of the four major and common problems of children, I ask to see a baby picture to see whether I can recognize the characteristic facies of FAS. While I am more a fan of clinical medicine/psychiatry than I am of laboratory medicine/psychiatry, I wonder why our neuropsychiatric researchers have not tackled this common problem.
Regardless, the problem of FAS does seem to be on federal radar as a potentially major prevention initiative, and the Substance Abuse and Mental Health Administration is certainly aware of the problem as the agency cites fetal alcohol spectrum disorders as more common than autism. Fortunately, some states are ahead of the curve (for example, Alaska and Washington states), and there is a National Organization on Fetal Alcohol Syndrome (NOFAS). Hopefully, the observations about the huge impact that FAS makes on special education will pan out, and we will see some prevention traction in the area of special education – as we did with cretinism and phenylketonuria.
Youth in Juvenile Justice
For me, providing treatment to young people who have wound up in the juvenile justice system has been the toughest challenge, because the psychiatrist’s ability to influence such systems is minimal. However, a recent National Academy of Sciences (NAS) report – "Reforming Juvenile Justice: A Developmental Approach" – has just been released, and, if this report gains footing in the United States, we will all be much better off.
As director of the Institute for Juvenile Research (IJR) – where child psychiatry started – I am familiar with the development of the first juvenile court in the United States. It was shortly thereafter that the same group of women (led by Nobel Prize–winning social workers Jane Addams and Julia Lathrop) who developed that special court began IJR to study delinquency. It turns out more than 100 years later, we are rediscovering their wisdom as the new NAS report illustrates.
So, prevention is alive and well in psychiatry. The construct of prevention in psychiatry has even made its way beyond the specialty. Take, for example, the Wikipedia entry on mental disorders – which has a subsection on prevention.
Dr. Bell is president and chief executive officer of Community Mental Health Council Inc. in Chicago. In addition to serving as director of the Institute for Juvenile Research at the University of Illinois at Chicago, he is director of public and community psychiatry at the university.

Win Whitcomb: Introducing Neuroquality and Neurosafety

The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
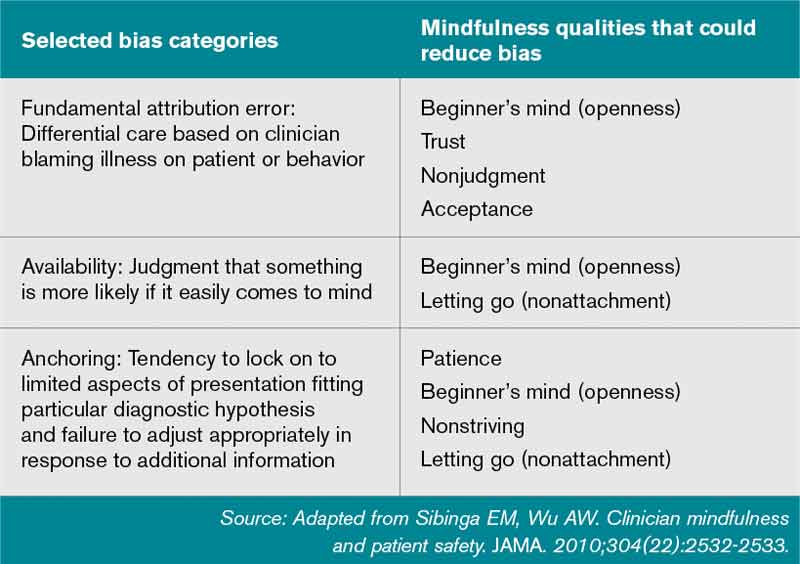
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
John Nelson: Peformance Key to Federal Value-Based Payment Modifier Plan

For years, your hospital was paid additional money by Medicare to report its performance on such things as core measures. Medicare then shared that information with the public via www.hospitalcompare.hhs.gov. Even if the hospital never gave Pneumovax when indicated, it was paid more simply for reporting that fact. (Fortunately, there were lots of reasons hospitals wanted to perform well.)
The days of hospitals being paid more simply for reporting ended a long time ago. Now performance, e.g., how often Pneumovax was given when indicated, influences payment. That is, things have transitioned from pay-for-reporting to a pay-for-performance program called hospital value-based purchasing (VBP).
I hope that at least one member of your hospitalist group is keeping up with hospital VBP. It got a lot of attention in the fall because it was the first time Medicare Part A payments to hospitals were adjusted based on performance on some core measures and patient satisfaction domains, as well as readmission rates for congestive heart failure (CHF), acute myocardial infarction (AMI), and pneumonia patients. The dollars at stake and performance metrics change will change every year, so plan to pay attention to hospital VBP on an ongoing basis.
Physicians’ Turn
Medicare payment to physicians is evolving along the same trajectory as hospitals. For several years, doctors have had the option to voluntarily participate in the Physician Quality Reporting System (PQRS). As long as a doctor reported quality performance on a sufficient portion of certain patient types, Medicare would provide a “bonus” at the end of the year. From 2012 through 2014, the “bonus” is 0.5% of that doctor’s total allowable Medicare charges. For example, if that doctor generated $150,000 of Medicare allowable charges over the calendar year, the additional payment for successful reporting PQRS would be $750 (0.5% of $150,000).
Although $750 is only a tiny fraction of collections, the right charge-capture system can make it pretty easy to achieve. And an extra payment of $750 sure is better than the 1.5% penalty for not participating; that program starts in 2015 and increases to a 2% penalty in 2016. If you are still not participating successfully in PQRS in 2015, the reimbursement for that $150,000 in charges will be reduced by $2,250 (1.5% of $150,000). So I strongly recommend that you begin reporting in 2013 so that you have time to work out the kinks well ahead of 2015. Don’t delay, but don’t panic, either, because you can still succeed in 2013 even if you don’t start capturing or reporting PQRS data until late winter or early spring.
At some point in the next year or so, data from as early as January 2013 for doctors reporting through PQRS will be made public on the Centers for Medicare & Medicaid’s (CMS) physician compare website: www.medicare.gov/find-a-doctor/provider-search.aspx. For example, should you choose to report the portion of stroke patients for whom you prescribed DVT prophylaxis, the public will be able to see your data.
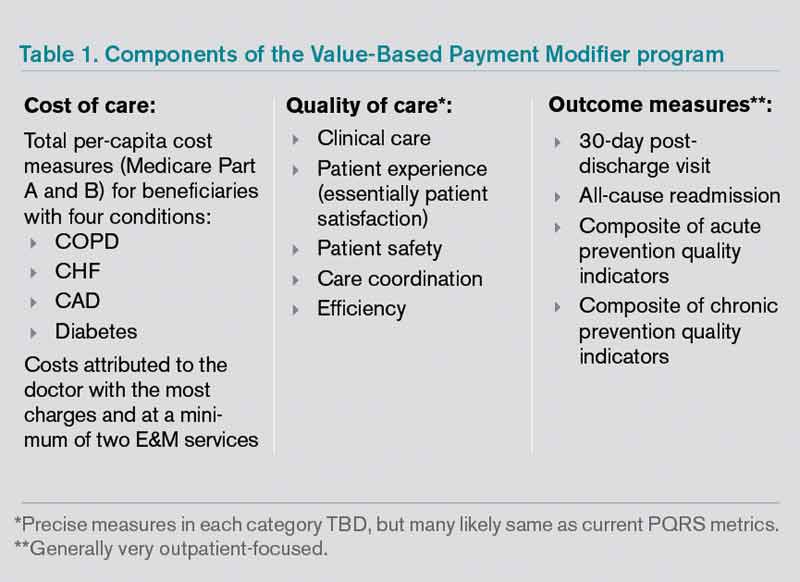
The Next Wave of Physician Pay for Performance
As the name implies, PQRS is a program based on reporting. Now CMS is adding the Value-Based Payment Modifier (VBPM) program, in which performance determines payments (see Table 1). It incorporates quality measures from PQRS, but is for now a separate program. It is very similar in name and structure to the hospital VBP program mentioned above, but incorporates cost of care data as well as quality performance. So it is really about value and not just quality performance (hence the name).
For providers in groups of more than 100 that bill under the same tax ID number (they don’t have to be in the same specialty), VBPM will first influence Part B Medicare reimbursement for physician services in 2015. It will expand to include all providers in 2017.
But don’t think you have until 2015 or 2017 to learn about all of this. There is a two-year lag, so payments in 2015 are based on performance in 2013 and 2017 payments presumably will be based on 2015 performance. In the fall of 2013, CMS plans to provide group-level (not individual) performance reports to all doctors in groups of 100 or more under the same tax ID number. These performance reports are known as quality resource use reports (QRURs). QRURs were trialed on physicians in a few states who received reports in 2012 based on 2011 performance, but in 2013, reports based on 2012 performance will be distributed to all doctors who practice in groups of 100 or more.
The calculation to determine whether a doctor is due additional payment for good performance (more accurately, good value) is awfully complicated. But providers have a choice to make. They can choose to:
- Not report data and accept a 1% penalty (likely to increase in successive years and in addition to the penalty for not reporting PQRS data, for a total penalty of 2.5%);
- Report data but not compete for financial upside or downside; or
- Compete for additional payments (amount to be determined) and risk a penalty of 0.5% or 1% for poor performance.
Look for more details about the VBPM program in future columns and other articles in The Hospitalist. There are a number of good online resources, including a CMS presentation titled “CMS Proposals for the Physician Value-Based Payment Modifier under the Medicare Physician Fee Schedule.” Type “Value-Based Payment Modifier” and “CMS” into any search engine to locate the video.
Parting Recommendations
Just about every hospitalist group should:
- Designate someone in your group to keep up with evolving pay-for-performance programs. It doesn’t have to be an MD, but you do need someone local that can guide your group through it. Consider becoming the most expert physician at your hospital on this topic.
- Start reporting through PQRS in 2013 if you haven’t already.
- Support SHM’s efforts to provide feedback to CMS to ensure that the metrics are meaningful for the type of care we provide.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Author’s note: For helping to explain all this pay-for-performance stuff, I once again owe thanks to Dr. Pat Torcson, a hospitalist in Covington, La., and member of SHM’s Public Policy Committee. He does an amazing job of keeping up with the evolving pay-for-performance programs, advocating on behalf of hospitalists and the patients we serve, and graciously answers my tedious questions with thoughtful and informative replies. He is a really pleasant guy and a terrific asset to SHM and hospital medicine.
For years, your hospital was paid additional money by Medicare to report its performance on such things as core measures. Medicare then shared that information with the public via www.hospitalcompare.hhs.gov. Even if the hospital never gave Pneumovax when indicated, it was paid more simply for reporting that fact. (Fortunately, there were lots of reasons hospitals wanted to perform well.)
The days of hospitals being paid more simply for reporting ended a long time ago. Now performance, e.g., how often Pneumovax was given when indicated, influences payment. That is, things have transitioned from pay-for-reporting to a pay-for-performance program called hospital value-based purchasing (VBP).
I hope that at least one member of your hospitalist group is keeping up with hospital VBP. It got a lot of attention in the fall because it was the first time Medicare Part A payments to hospitals were adjusted based on performance on some core measures and patient satisfaction domains, as well as readmission rates for congestive heart failure (CHF), acute myocardial infarction (AMI), and pneumonia patients. The dollars at stake and performance metrics change will change every year, so plan to pay attention to hospital VBP on an ongoing basis.
Physicians’ Turn
Medicare payment to physicians is evolving along the same trajectory as hospitals. For several years, doctors have had the option to voluntarily participate in the Physician Quality Reporting System (PQRS). As long as a doctor reported quality performance on a sufficient portion of certain patient types, Medicare would provide a “bonus” at the end of the year. From 2012 through 2014, the “bonus” is 0.5% of that doctor’s total allowable Medicare charges. For example, if that doctor generated $150,000 of Medicare allowable charges over the calendar year, the additional payment for successful reporting PQRS would be $750 (0.5% of $150,000).
Although $750 is only a tiny fraction of collections, the right charge-capture system can make it pretty easy to achieve. And an extra payment of $750 sure is better than the 1.5% penalty for not participating; that program starts in 2015 and increases to a 2% penalty in 2016. If you are still not participating successfully in PQRS in 2015, the reimbursement for that $150,000 in charges will be reduced by $2,250 (1.5% of $150,000). So I strongly recommend that you begin reporting in 2013 so that you have time to work out the kinks well ahead of 2015. Don’t delay, but don’t panic, either, because you can still succeed in 2013 even if you don’t start capturing or reporting PQRS data until late winter or early spring.
At some point in the next year or so, data from as early as January 2013 for doctors reporting through PQRS will be made public on the Centers for Medicare & Medicaid’s (CMS) physician compare website: www.medicare.gov/find-a-doctor/provider-search.aspx. For example, should you choose to report the portion of stroke patients for whom you prescribed DVT prophylaxis, the public will be able to see your data.
The Next Wave of Physician Pay for Performance
As the name implies, PQRS is a program based on reporting. Now CMS is adding the Value-Based Payment Modifier (VBPM) program, in which performance determines payments (see Table 1). It incorporates quality measures from PQRS, but is for now a separate program. It is very similar in name and structure to the hospital VBP program mentioned above, but incorporates cost of care data as well as quality performance. So it is really about value and not just quality performance (hence the name).
For providers in groups of more than 100 that bill under the same tax ID number (they don’t have to be in the same specialty), VBPM will first influence Part B Medicare reimbursement for physician services in 2015. It will expand to include all providers in 2017.
But don’t think you have until 2015 or 2017 to learn about all of this. There is a two-year lag, so payments in 2015 are based on performance in 2013 and 2017 payments presumably will be based on 2015 performance. In the fall of 2013, CMS plans to provide group-level (not individual) performance reports to all doctors in groups of 100 or more under the same tax ID number. These performance reports are known as quality resource use reports (QRURs). QRURs were trialed on physicians in a few states who received reports in 2012 based on 2011 performance, but in 2013, reports based on 2012 performance will be distributed to all doctors who practice in groups of 100 or more.
The calculation to determine whether a doctor is due additional payment for good performance (more accurately, good value) is awfully complicated. But providers have a choice to make. They can choose to:
- Not report data and accept a 1% penalty (likely to increase in successive years and in addition to the penalty for not reporting PQRS data, for a total penalty of 2.5%);
- Report data but not compete for financial upside or downside; or
- Compete for additional payments (amount to be determined) and risk a penalty of 0.5% or 1% for poor performance.
Look for more details about the VBPM program in future columns and other articles in The Hospitalist. There are a number of good online resources, including a CMS presentation titled “CMS Proposals for the Physician Value-Based Payment Modifier under the Medicare Physician Fee Schedule.” Type “Value-Based Payment Modifier” and “CMS” into any search engine to locate the video.
Parting Recommendations
Just about every hospitalist group should:
- Designate someone in your group to keep up with evolving pay-for-performance programs. It doesn’t have to be an MD, but you do need someone local that can guide your group through it. Consider becoming the most expert physician at your hospital on this topic.
- Start reporting through PQRS in 2013 if you haven’t already.
- Support SHM’s efforts to provide feedback to CMS to ensure that the metrics are meaningful for the type of care we provide.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Author’s note: For helping to explain all this pay-for-performance stuff, I once again owe thanks to Dr. Pat Torcson, a hospitalist in Covington, La., and member of SHM’s Public Policy Committee. He does an amazing job of keeping up with the evolving pay-for-performance programs, advocating on behalf of hospitalists and the patients we serve, and graciously answers my tedious questions with thoughtful and informative replies. He is a really pleasant guy and a terrific asset to SHM and hospital medicine.
For years, your hospital was paid additional money by Medicare to report its performance on such things as core measures. Medicare then shared that information with the public via www.hospitalcompare.hhs.gov. Even if the hospital never gave Pneumovax when indicated, it was paid more simply for reporting that fact. (Fortunately, there were lots of reasons hospitals wanted to perform well.)
The days of hospitals being paid more simply for reporting ended a long time ago. Now performance, e.g., how often Pneumovax was given when indicated, influences payment. That is, things have transitioned from pay-for-reporting to a pay-for-performance program called hospital value-based purchasing (VBP).
I hope that at least one member of your hospitalist group is keeping up with hospital VBP. It got a lot of attention in the fall because it was the first time Medicare Part A payments to hospitals were adjusted based on performance on some core measures and patient satisfaction domains, as well as readmission rates for congestive heart failure (CHF), acute myocardial infarction (AMI), and pneumonia patients. The dollars at stake and performance metrics change will change every year, so plan to pay attention to hospital VBP on an ongoing basis.
Physicians’ Turn
Medicare payment to physicians is evolving along the same trajectory as hospitals. For several years, doctors have had the option to voluntarily participate in the Physician Quality Reporting System (PQRS). As long as a doctor reported quality performance on a sufficient portion of certain patient types, Medicare would provide a “bonus” at the end of the year. From 2012 through 2014, the “bonus” is 0.5% of that doctor’s total allowable Medicare charges. For example, if that doctor generated $150,000 of Medicare allowable charges over the calendar year, the additional payment for successful reporting PQRS would be $750 (0.5% of $150,000).
Although $750 is only a tiny fraction of collections, the right charge-capture system can make it pretty easy to achieve. And an extra payment of $750 sure is better than the 1.5% penalty for not participating; that program starts in 2015 and increases to a 2% penalty in 2016. If you are still not participating successfully in PQRS in 2015, the reimbursement for that $150,000 in charges will be reduced by $2,250 (1.5% of $150,000). So I strongly recommend that you begin reporting in 2013 so that you have time to work out the kinks well ahead of 2015. Don’t delay, but don’t panic, either, because you can still succeed in 2013 even if you don’t start capturing or reporting PQRS data until late winter or early spring.
At some point in the next year or so, data from as early as January 2013 for doctors reporting through PQRS will be made public on the Centers for Medicare & Medicaid’s (CMS) physician compare website: www.medicare.gov/find-a-doctor/provider-search.aspx. For example, should you choose to report the portion of stroke patients for whom you prescribed DVT prophylaxis, the public will be able to see your data.
The Next Wave of Physician Pay for Performance
As the name implies, PQRS is a program based on reporting. Now CMS is adding the Value-Based Payment Modifier (VBPM) program, in which performance determines payments (see Table 1). It incorporates quality measures from PQRS, but is for now a separate program. It is very similar in name and structure to the hospital VBP program mentioned above, but incorporates cost of care data as well as quality performance. So it is really about value and not just quality performance (hence the name).
For providers in groups of more than 100 that bill under the same tax ID number (they don’t have to be in the same specialty), VBPM will first influence Part B Medicare reimbursement for physician services in 2015. It will expand to include all providers in 2017.
But don’t think you have until 2015 or 2017 to learn about all of this. There is a two-year lag, so payments in 2015 are based on performance in 2013 and 2017 payments presumably will be based on 2015 performance. In the fall of 2013, CMS plans to provide group-level (not individual) performance reports to all doctors in groups of 100 or more under the same tax ID number. These performance reports are known as quality resource use reports (QRURs). QRURs were trialed on physicians in a few states who received reports in 2012 based on 2011 performance, but in 2013, reports based on 2012 performance will be distributed to all doctors who practice in groups of 100 or more.
The calculation to determine whether a doctor is due additional payment for good performance (more accurately, good value) is awfully complicated. But providers have a choice to make. They can choose to:
- Not report data and accept a 1% penalty (likely to increase in successive years and in addition to the penalty for not reporting PQRS data, for a total penalty of 2.5%);
- Report data but not compete for financial upside or downside; or
- Compete for additional payments (amount to be determined) and risk a penalty of 0.5% or 1% for poor performance.
Look for more details about the VBPM program in future columns and other articles in The Hospitalist. There are a number of good online resources, including a CMS presentation titled “CMS Proposals for the Physician Value-Based Payment Modifier under the Medicare Physician Fee Schedule.” Type “Value-Based Payment Modifier” and “CMS” into any search engine to locate the video.
Parting Recommendations
Just about every hospitalist group should:
- Designate someone in your group to keep up with evolving pay-for-performance programs. It doesn’t have to be an MD, but you do need someone local that can guide your group through it. Consider becoming the most expert physician at your hospital on this topic.
- Start reporting through PQRS in 2013 if you haven’t already.
- Support SHM’s efforts to provide feedback to CMS to ensure that the metrics are meaningful for the type of care we provide.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Author’s note: For helping to explain all this pay-for-performance stuff, I once again owe thanks to Dr. Pat Torcson, a hospitalist in Covington, La., and member of SHM’s Public Policy Committee. He does an amazing job of keeping up with the evolving pay-for-performance programs, advocating on behalf of hospitalists and the patients we serve, and graciously answers my tedious questions with thoughtful and informative replies. He is a really pleasant guy and a terrific asset to SHM and hospital medicine.
Hurricane Sandy and PTSD
As Hurricane Sandy was predicted to hit the New York/New Jersey area, I was able to make what I believed were more than adequate preparations. I needed to stock up on food, especially the nonperishable foods and water; make sure that I had flashlights and enough batteries; keep a battery radio around; and have a bag of essentials packed – in addition to a place to retreat to if my safety was at stake.
Indeed, I prepared. This was not going to be a hurricane Andrew or Katrina for me. I would weather it with ease as I’ve done in the past. Secure in my New York City apartment, opposite the NYU Langone Medical Center, where I trained and remain on the faculty, I was secure and offered comfort to many of my neighbors as their worries increased with the impending storm.

I watched and listened to New York City’s mayor, and the New York and New Jersey governors with their warnings and advice on storm preparations and realized I was in good shape. At around 8:30 Monday evening, the night the storm hit, my apartment lights dimmed for a brief moment. Soon after, I noticed a medical center housing complex nearby go dark. Following that, momentarily, the lights dimmed on the NYU Langone Medical and subsequently went out. I waited for the medical center’s generators to kick in as I watched from my window. It never happened.
At 8:50 p.m., my electricity went out. "Worry not," I said to myself. This is New York City, and all the power lines are underground, and there’s a deli or bodega on every corner.
I was comfortable in my darkened apartment when a friend and neighbor explained that when the lights went out, the water stopped – as the basement pumps could not work without electricity. This bothered me a bit, but I realized the power would be on soon. This was New York City.
As the hours passed, I checked the food and water, which remained cold in my refrigerator. I tuned onto an all-talk news station on my battery-operated radio, even though finding the station with one hand and the other hand holding a flashlight proved frustrating. Little did I know how my frustration would grow.
As the evening moved into night, it was reported on the news that the power from ConEdison electric station at the 14th Street was flooded, had an explosion, and that all power was out across Manhattan from 39th Street to the bottom of our crowded island. This affected a large residential and commercial part of the city.

There were no traffic lights; no food stores were open; gasoline stations were not able to pump and, in the building where I live, total darkness surrounded us, as hall and stair well emergency lighting is good for only 2 hours. Adding to this, sirens began to sound around the streets below, and ambulances were lining up in front of the NYU Langone Medical Center. As I watched, my heart sank. The hospital was being evacuated by hospital staff and EMS workers with the help of fire fighters and police officers. At the height of the storm, with the elevators not running, hundreds of patients were being carried down stairways, placed in ambulances, and sent to other hospitals.
This was the legendary NYU Medical Center where I had trained, treated patients, and supervised residents. It is where my sons were born. My father, an eye surgeon died there and recently, my four grandchildren were born there. In addition, this is an institution at which I have lifelong friendships and professional relationships. As I witnessed this evacuation, I began to feel a great loss. During that night, I slept very little and found myself watching from my window as the evacuation continued well into the next day.
On that next day, a sense of frustration and some despair began with electricity still off, no computer, the food in the refrigerator warming, the cell phone and iPad discharged, and the bathroom facilities not working because of a lack of water. This was starting to affect my emotions.
I still had a landline, and both my sons – one of whom had full power – had opened up their homes to me. But I just knew that things would get back to normal soon. This was New York City.
By Wednesday, the best information was it would be days before power would be back on. With no cell phone, computer, iPad, water, food, or electricity, I gave up and asked one of my sons to pick me up and take me to his home. During my multiple story descent in the dark, with a flashlight and a suitcase, I nearly fell – and luckily avoided a major injury.
At my son’s home, the ominous aspects of this storm became painfully clear from the TV reports: I could see people’s despair in light of destroyed homes and businesses. Some people were injured and other dying. I was lucky. Still, I felt a sense of helplessness and alienation from the two previous days and nights. Now after watching the despair that people were experiencing on TV, I felt a sense of despair as well knowing that my professional and personal routines would be changing for days and weeks to come.
I was far from having posttraumatic stress disorder or a PTSD experience, but I began to think of the PTSD patients I’ve treated using nonmedicinal approaches and the psychological toll that Sandy was bound to have on my community. Certainly Sandy, not unlike Katrina, the earthquake in Haiti, and the BP oil spill – to name a few disasters, both natural and manmade – inevitably led to numerous PTSD cases.
My concern, as always, is who will treat these PTSD patients with the most appropriate treatments, such as cognitive-behavioral therapy [CBT], behavior modification [BM], or hypnosis coupled with behavior modification and guided imagery. With so few clinicians using or knowing these techniques, it concerns me that those suffering will be treated with a variety of psychotropics, which only rarely have been successful as studies have shown.
In light of the increasing number of manmade and natural disasters as well as the many other factors that lead to PTSD, such as war experience, incarceration, torture, abuse, and near-death experiences plus the subclinical/subthreshold variations of PTSD that I’ve written about, we need to establish treatment guidelines that work best and are used first once and for all.
Mental health professionals, whether psychiatrists, psychologists, social workers, or psychiatric nurse practitioners, should be expert in the CBT, BM, and hypnotic/guided imagery techniques that have the best outcomes.
Dr. London is a psychiatrist with the New York University Langone Medical Center. He has no conflicts of interest to disclose.
As Hurricane Sandy was predicted to hit the New York/New Jersey area, I was able to make what I believed were more than adequate preparations. I needed to stock up on food, especially the nonperishable foods and water; make sure that I had flashlights and enough batteries; keep a battery radio around; and have a bag of essentials packed – in addition to a place to retreat to if my safety was at stake.
Indeed, I prepared. This was not going to be a hurricane Andrew or Katrina for me. I would weather it with ease as I’ve done in the past. Secure in my New York City apartment, opposite the NYU Langone Medical Center, where I trained and remain on the faculty, I was secure and offered comfort to many of my neighbors as their worries increased with the impending storm.
I watched and listened to New York City’s mayor, and the New York and New Jersey governors with their warnings and advice on storm preparations and realized I was in good shape. At around 8:30 Monday evening, the night the storm hit, my apartment lights dimmed for a brief moment. Soon after, I noticed a medical center housing complex nearby go dark. Following that, momentarily, the lights dimmed on the NYU Langone Medical and subsequently went out. I waited for the medical center’s generators to kick in as I watched from my window. It never happened.
At 8:50 p.m., my electricity went out. "Worry not," I said to myself. This is New York City, and all the power lines are underground, and there’s a deli or bodega on every corner.
I was comfortable in my darkened apartment when a friend and neighbor explained that when the lights went out, the water stopped – as the basement pumps could not work without electricity. This bothered me a bit, but I realized the power would be on soon. This was New York City.
As the hours passed, I checked the food and water, which remained cold in my refrigerator. I tuned onto an all-talk news station on my battery-operated radio, even though finding the station with one hand and the other hand holding a flashlight proved frustrating. Little did I know how my frustration would grow.
As the evening moved into night, it was reported on the news that the power from ConEdison electric station at the 14th Street was flooded, had an explosion, and that all power was out across Manhattan from 39th Street to the bottom of our crowded island. This affected a large residential and commercial part of the city.
There were no traffic lights; no food stores were open; gasoline stations were not able to pump and, in the building where I live, total darkness surrounded us, as hall and stair well emergency lighting is good for only 2 hours. Adding to this, sirens began to sound around the streets below, and ambulances were lining up in front of the NYU Langone Medical Center. As I watched, my heart sank. The hospital was being evacuated by hospital staff and EMS workers with the help of fire fighters and police officers. At the height of the storm, with the elevators not running, hundreds of patients were being carried down stairways, placed in ambulances, and sent to other hospitals.
This was the legendary NYU Medical Center where I had trained, treated patients, and supervised residents. It is where my sons were born. My father, an eye surgeon died there and recently, my four grandchildren were born there. In addition, this is an institution at which I have lifelong friendships and professional relationships. As I witnessed this evacuation, I began to feel a great loss. During that night, I slept very little and found myself watching from my window as the evacuation continued well into the next day.
On that next day, a sense of frustration and some despair began with electricity still off, no computer, the food in the refrigerator warming, the cell phone and iPad discharged, and the bathroom facilities not working because of a lack of water. This was starting to affect my emotions.
I still had a landline, and both my sons – one of whom had full power – had opened up their homes to me. But I just knew that things would get back to normal soon. This was New York City.
By Wednesday, the best information was it would be days before power would be back on. With no cell phone, computer, iPad, water, food, or electricity, I gave up and asked one of my sons to pick me up and take me to his home. During my multiple story descent in the dark, with a flashlight and a suitcase, I nearly fell – and luckily avoided a major injury.
At my son’s home, the ominous aspects of this storm became painfully clear from the TV reports: I could see people’s despair in light of destroyed homes and businesses. Some people were injured and other dying. I was lucky. Still, I felt a sense of helplessness and alienation from the two previous days and nights. Now after watching the despair that people were experiencing on TV, I felt a sense of despair as well knowing that my professional and personal routines would be changing for days and weeks to come.
I was far from having posttraumatic stress disorder or a PTSD experience, but I began to think of the PTSD patients I’ve treated using nonmedicinal approaches and the psychological toll that Sandy was bound to have on my community. Certainly Sandy, not unlike Katrina, the earthquake in Haiti, and the BP oil spill – to name a few disasters, both natural and manmade – inevitably led to numerous PTSD cases.
My concern, as always, is who will treat these PTSD patients with the most appropriate treatments, such as cognitive-behavioral therapy [CBT], behavior modification [BM], or hypnosis coupled with behavior modification and guided imagery. With so few clinicians using or knowing these techniques, it concerns me that those suffering will be treated with a variety of psychotropics, which only rarely have been successful as studies have shown.
In light of the increasing number of manmade and natural disasters as well as the many other factors that lead to PTSD, such as war experience, incarceration, torture, abuse, and near-death experiences plus the subclinical/subthreshold variations of PTSD that I’ve written about, we need to establish treatment guidelines that work best and are used first once and for all.
Mental health professionals, whether psychiatrists, psychologists, social workers, or psychiatric nurse practitioners, should be expert in the CBT, BM, and hypnotic/guided imagery techniques that have the best outcomes.
Dr. London is a psychiatrist with the New York University Langone Medical Center. He has no conflicts of interest to disclose.
As Hurricane Sandy was predicted to hit the New York/New Jersey area, I was able to make what I believed were more than adequate preparations. I needed to stock up on food, especially the nonperishable foods and water; make sure that I had flashlights and enough batteries; keep a battery radio around; and have a bag of essentials packed – in addition to a place to retreat to if my safety was at stake.
Indeed, I prepared. This was not going to be a hurricane Andrew or Katrina for me. I would weather it with ease as I’ve done in the past. Secure in my New York City apartment, opposite the NYU Langone Medical Center, where I trained and remain on the faculty, I was secure and offered comfort to many of my neighbors as their worries increased with the impending storm.
I watched and listened to New York City’s mayor, and the New York and New Jersey governors with their warnings and advice on storm preparations and realized I was in good shape. At around 8:30 Monday evening, the night the storm hit, my apartment lights dimmed for a brief moment. Soon after, I noticed a medical center housing complex nearby go dark. Following that, momentarily, the lights dimmed on the NYU Langone Medical and subsequently went out. I waited for the medical center’s generators to kick in as I watched from my window. It never happened.
At 8:50 p.m., my electricity went out. "Worry not," I said to myself. This is New York City, and all the power lines are underground, and there’s a deli or bodega on every corner.
I was comfortable in my darkened apartment when a friend and neighbor explained that when the lights went out, the water stopped – as the basement pumps could not work without electricity. This bothered me a bit, but I realized the power would be on soon. This was New York City.
As the hours passed, I checked the food and water, which remained cold in my refrigerator. I tuned onto an all-talk news station on my battery-operated radio, even though finding the station with one hand and the other hand holding a flashlight proved frustrating. Little did I know how my frustration would grow.
As the evening moved into night, it was reported on the news that the power from ConEdison electric station at the 14th Street was flooded, had an explosion, and that all power was out across Manhattan from 39th Street to the bottom of our crowded island. This affected a large residential and commercial part of the city.
There were no traffic lights; no food stores were open; gasoline stations were not able to pump and, in the building where I live, total darkness surrounded us, as hall and stair well emergency lighting is good for only 2 hours. Adding to this, sirens began to sound around the streets below, and ambulances were lining up in front of the NYU Langone Medical Center. As I watched, my heart sank. The hospital was being evacuated by hospital staff and EMS workers with the help of fire fighters and police officers. At the height of the storm, with the elevators not running, hundreds of patients were being carried down stairways, placed in ambulances, and sent to other hospitals.
This was the legendary NYU Medical Center where I had trained, treated patients, and supervised residents. It is where my sons were born. My father, an eye surgeon died there and recently, my four grandchildren were born there. In addition, this is an institution at which I have lifelong friendships and professional relationships. As I witnessed this evacuation, I began to feel a great loss. During that night, I slept very little and found myself watching from my window as the evacuation continued well into the next day.
On that next day, a sense of frustration and some despair began with electricity still off, no computer, the food in the refrigerator warming, the cell phone and iPad discharged, and the bathroom facilities not working because of a lack of water. This was starting to affect my emotions.
I still had a landline, and both my sons – one of whom had full power – had opened up their homes to me. But I just knew that things would get back to normal soon. This was New York City.
By Wednesday, the best information was it would be days before power would be back on. With no cell phone, computer, iPad, water, food, or electricity, I gave up and asked one of my sons to pick me up and take me to his home. During my multiple story descent in the dark, with a flashlight and a suitcase, I nearly fell – and luckily avoided a major injury.
At my son’s home, the ominous aspects of this storm became painfully clear from the TV reports: I could see people’s despair in light of destroyed homes and businesses. Some people were injured and other dying. I was lucky. Still, I felt a sense of helplessness and alienation from the two previous days and nights. Now after watching the despair that people were experiencing on TV, I felt a sense of despair as well knowing that my professional and personal routines would be changing for days and weeks to come.
I was far from having posttraumatic stress disorder or a PTSD experience, but I began to think of the PTSD patients I’ve treated using nonmedicinal approaches and the psychological toll that Sandy was bound to have on my community. Certainly Sandy, not unlike Katrina, the earthquake in Haiti, and the BP oil spill – to name a few disasters, both natural and manmade – inevitably led to numerous PTSD cases.
My concern, as always, is who will treat these PTSD patients with the most appropriate treatments, such as cognitive-behavioral therapy [CBT], behavior modification [BM], or hypnosis coupled with behavior modification and guided imagery. With so few clinicians using or knowing these techniques, it concerns me that those suffering will be treated with a variety of psychotropics, which only rarely have been successful as studies have shown.
In light of the increasing number of manmade and natural disasters as well as the many other factors that lead to PTSD, such as war experience, incarceration, torture, abuse, and near-death experiences plus the subclinical/subthreshold variations of PTSD that I’ve written about, we need to establish treatment guidelines that work best and are used first once and for all.
Mental health professionals, whether psychiatrists, psychologists, social workers, or psychiatric nurse practitioners, should be expert in the CBT, BM, and hypnotic/guided imagery techniques that have the best outcomes.
Dr. London is a psychiatrist with the New York University Langone Medical Center. He has no conflicts of interest to disclose.
