User login
The Gift That Keeps on Giving
Although unraveling the human genome has been exciting and potentially beneficial, I was a bit dismayed to discover that our genes barely outnumber those of the chimpanzee and, in fact, are only 50% greater in number than those of the fruit fly. If they were able to communicate, even the most discriminating chimpanzee – and especially the humble fruit fly – would likely admit that they are several rungs below us on the animal kingdom ladder. Fortunately, it turns out that this is not the whole story.
The human microbiome project (HMP), close on the heels of the genome undertaking, has found that we have many more genes working for us than those located on the strands of our DNA. The HMP analysis reveals that each of us has more than 100 trillion microorganisms living in the many nooks and crannies of our bodies, with the highest concentration in the gastrointestinal tract. This population of microbes is incredibly diverse, and its exact composition is unique to each of us. Thus, in addition to the individuality granted to us by the genes we receive from our parents, each of us is also a distinctive and rather complex ecosystem.
Not only do these creatures live in and on us peacefully most of the time, they also add to our genetic complement. Whereas our DNA contains only 23,000 genes, these microorganisms in aggregate account for 100 times more genes, several of which transcribe proteins that are essential for our normal daily functioning. For example, they manufacture enzymes that allow digestion of complex carbohydrates that account for more than 10% of our daily calories and that would be indigestible if it were not for the contributions of this microscopic workforce. They also make a variety of vitamins (for example, folic acid, B2, and B12), and they have the capability of gearing production to one’s needs depending on diet and other circumstances. Furthermore, the microbiome likely plays a significant role in the development of our immune system.
When this large population of indigenous bacteria is in appropriate balance, all is well. However, when the equilibrium among species is disrupted by antibiotic therapy or other environmental influences, one or more of a long list of maladies may result. Alterations in the microbiome have been implicated as being a factor in diseases as diverse as colon and pancreatic cancer, diabetes, autism, multiple sclerosis, irritable bowel syndrome, and Clostridium difficile colitis. The latter, usually caused by antibiotic therapy, has even been treated successfully by restoring the microbiome to its normal state by means of a stool transplant from a normal donor. The relationship between the composition of the microbiome and the other disorders is less well understood but is fertile ground for further studies. Such investigations may open doors to future therapies for heretofore untreatable diseases.
Particularly fascinating is the association between the microbiome and the nutritional state. Since microbiomes play an important role in processing what we eat, it makes sense that these microscopic travelers might in part determine our body habitus. Dr. Jeffrey Gordon and his associates at Washington University, St. Louis, have investigated this intriguing prospect (Nature 2006;44:1022-3). They have shown in both animal and human studies that the composition of the microbiome is closely related to the degree of obesity or leanness of the subjects. Of the 100 or so known phyla of bacteria, only two, Bacteroidetes and Firmicutes, account for more than 90% of the microbes in our gastrointestinal tract. Obese mice and humans have a higher ratio of firmicutes to bacteroidetes than do their lean counterparts. Moreover, transplanting the microbiome from obese mice to germ-free animals results in an increase in the body fat of the latter group. Additionally, obese individuals who effectively diet over time increase their intestinal Bacteroidetes-to-Firmicutes ratio.
A common topic of discussion in Surgery News is the worldwide epidemic of obesity and its treatment with a variety of surgical procedures. It is within the realm of possibility that simply altering the microbiome of obese patients might help to resolve this affliction, which impairs the quality of life of so many.
So what is the gift that keeps on giving? It is our microbiome. For more than a century, bacteria have been considered one of the scourges of mankind. It is appropriate as the holiday season approaches that we finally acknowledge the contributions that these usually despised organisms make to our daily welfare. In turn and in the spirit of giving back, we can take some pride in the fact that we provide a warm and hospitable home for these friendly symbionts.
Dr. Rikkers is editor in chief of Surgery News.
Although unraveling the human genome has been exciting and potentially beneficial, I was a bit dismayed to discover that our genes barely outnumber those of the chimpanzee and, in fact, are only 50% greater in number than those of the fruit fly. If they were able to communicate, even the most discriminating chimpanzee – and especially the humble fruit fly – would likely admit that they are several rungs below us on the animal kingdom ladder. Fortunately, it turns out that this is not the whole story.
The human microbiome project (HMP), close on the heels of the genome undertaking, has found that we have many more genes working for us than those located on the strands of our DNA. The HMP analysis reveals that each of us has more than 100 trillion microorganisms living in the many nooks and crannies of our bodies, with the highest concentration in the gastrointestinal tract. This population of microbes is incredibly diverse, and its exact composition is unique to each of us. Thus, in addition to the individuality granted to us by the genes we receive from our parents, each of us is also a distinctive and rather complex ecosystem.
Not only do these creatures live in and on us peacefully most of the time, they also add to our genetic complement. Whereas our DNA contains only 23,000 genes, these microorganisms in aggregate account for 100 times more genes, several of which transcribe proteins that are essential for our normal daily functioning. For example, they manufacture enzymes that allow digestion of complex carbohydrates that account for more than 10% of our daily calories and that would be indigestible if it were not for the contributions of this microscopic workforce. They also make a variety of vitamins (for example, folic acid, B2, and B12), and they have the capability of gearing production to one’s needs depending on diet and other circumstances. Furthermore, the microbiome likely plays a significant role in the development of our immune system.
When this large population of indigenous bacteria is in appropriate balance, all is well. However, when the equilibrium among species is disrupted by antibiotic therapy or other environmental influences, one or more of a long list of maladies may result. Alterations in the microbiome have been implicated as being a factor in diseases as diverse as colon and pancreatic cancer, diabetes, autism, multiple sclerosis, irritable bowel syndrome, and Clostridium difficile colitis. The latter, usually caused by antibiotic therapy, has even been treated successfully by restoring the microbiome to its normal state by means of a stool transplant from a normal donor. The relationship between the composition of the microbiome and the other disorders is less well understood but is fertile ground for further studies. Such investigations may open doors to future therapies for heretofore untreatable diseases.
Particularly fascinating is the association between the microbiome and the nutritional state. Since microbiomes play an important role in processing what we eat, it makes sense that these microscopic travelers might in part determine our body habitus. Dr. Jeffrey Gordon and his associates at Washington University, St. Louis, have investigated this intriguing prospect (Nature 2006;44:1022-3). They have shown in both animal and human studies that the composition of the microbiome is closely related to the degree of obesity or leanness of the subjects. Of the 100 or so known phyla of bacteria, only two, Bacteroidetes and Firmicutes, account for more than 90% of the microbes in our gastrointestinal tract. Obese mice and humans have a higher ratio of firmicutes to bacteroidetes than do their lean counterparts. Moreover, transplanting the microbiome from obese mice to germ-free animals results in an increase in the body fat of the latter group. Additionally, obese individuals who effectively diet over time increase their intestinal Bacteroidetes-to-Firmicutes ratio.
A common topic of discussion in Surgery News is the worldwide epidemic of obesity and its treatment with a variety of surgical procedures. It is within the realm of possibility that simply altering the microbiome of obese patients might help to resolve this affliction, which impairs the quality of life of so many.
So what is the gift that keeps on giving? It is our microbiome. For more than a century, bacteria have been considered one of the scourges of mankind. It is appropriate as the holiday season approaches that we finally acknowledge the contributions that these usually despised organisms make to our daily welfare. In turn and in the spirit of giving back, we can take some pride in the fact that we provide a warm and hospitable home for these friendly symbionts.
Dr. Rikkers is editor in chief of Surgery News.
Although unraveling the human genome has been exciting and potentially beneficial, I was a bit dismayed to discover that our genes barely outnumber those of the chimpanzee and, in fact, are only 50% greater in number than those of the fruit fly. If they were able to communicate, even the most discriminating chimpanzee – and especially the humble fruit fly – would likely admit that they are several rungs below us on the animal kingdom ladder. Fortunately, it turns out that this is not the whole story.
The human microbiome project (HMP), close on the heels of the genome undertaking, has found that we have many more genes working for us than those located on the strands of our DNA. The HMP analysis reveals that each of us has more than 100 trillion microorganisms living in the many nooks and crannies of our bodies, with the highest concentration in the gastrointestinal tract. This population of microbes is incredibly diverse, and its exact composition is unique to each of us. Thus, in addition to the individuality granted to us by the genes we receive from our parents, each of us is also a distinctive and rather complex ecosystem.
Not only do these creatures live in and on us peacefully most of the time, they also add to our genetic complement. Whereas our DNA contains only 23,000 genes, these microorganisms in aggregate account for 100 times more genes, several of which transcribe proteins that are essential for our normal daily functioning. For example, they manufacture enzymes that allow digestion of complex carbohydrates that account for more than 10% of our daily calories and that would be indigestible if it were not for the contributions of this microscopic workforce. They also make a variety of vitamins (for example, folic acid, B2, and B12), and they have the capability of gearing production to one’s needs depending on diet and other circumstances. Furthermore, the microbiome likely plays a significant role in the development of our immune system.
When this large population of indigenous bacteria is in appropriate balance, all is well. However, when the equilibrium among species is disrupted by antibiotic therapy or other environmental influences, one or more of a long list of maladies may result. Alterations in the microbiome have been implicated as being a factor in diseases as diverse as colon and pancreatic cancer, diabetes, autism, multiple sclerosis, irritable bowel syndrome, and Clostridium difficile colitis. The latter, usually caused by antibiotic therapy, has even been treated successfully by restoring the microbiome to its normal state by means of a stool transplant from a normal donor. The relationship between the composition of the microbiome and the other disorders is less well understood but is fertile ground for further studies. Such investigations may open doors to future therapies for heretofore untreatable diseases.
Particularly fascinating is the association between the microbiome and the nutritional state. Since microbiomes play an important role in processing what we eat, it makes sense that these microscopic travelers might in part determine our body habitus. Dr. Jeffrey Gordon and his associates at Washington University, St. Louis, have investigated this intriguing prospect (Nature 2006;44:1022-3). They have shown in both animal and human studies that the composition of the microbiome is closely related to the degree of obesity or leanness of the subjects. Of the 100 or so known phyla of bacteria, only two, Bacteroidetes and Firmicutes, account for more than 90% of the microbes in our gastrointestinal tract. Obese mice and humans have a higher ratio of firmicutes to bacteroidetes than do their lean counterparts. Moreover, transplanting the microbiome from obese mice to germ-free animals results in an increase in the body fat of the latter group. Additionally, obese individuals who effectively diet over time increase their intestinal Bacteroidetes-to-Firmicutes ratio.
A common topic of discussion in Surgery News is the worldwide epidemic of obesity and its treatment with a variety of surgical procedures. It is within the realm of possibility that simply altering the microbiome of obese patients might help to resolve this affliction, which impairs the quality of life of so many.
So what is the gift that keeps on giving? It is our microbiome. For more than a century, bacteria have been considered one of the scourges of mankind. It is appropriate as the holiday season approaches that we finally acknowledge the contributions that these usually despised organisms make to our daily welfare. In turn and in the spirit of giving back, we can take some pride in the fact that we provide a warm and hospitable home for these friendly symbionts.
Dr. Rikkers is editor in chief of Surgery News.

When Terminal Cancer Patients Don't Get the Message
Oh, how disheartening.
I was troubled, but not too surprised, to read recently published conclusions of two large, population-based studies that found many patients with terminal cancer erroneously believe that palliative treatment (chemotherapy or radiation therapy) will likely cure their disease.
What left me truly dismayed was the first study’s powerful association (P = .002) between patients’ inaccurate perceptions of their prognoses and endorsements of their physicians’ communication skills.
That study, published Oct. 25 in the New England Journal of Medicine (2012;367:1616-25), documented beliefs of 1,193 patients who had received palliative chemotherapy for newly diagnosed stage IV lung or colorectal cancer. As oncologists well know, in this context, chemotherapy might extend life a bit (by weeks or perhaps months) and may alleviate pain or other symptoms of the disease. But it is not curative. And that’s the secret that wasn’t conveyed to patients – at least in a way that they could hear or accept.
Fully 81% of patients with metastatic colorectal cancer didn’t get the message. Nearly 70% of patients with metastatic lung cancer didn’t get the message. By disproportionately high percentages, minority patients didn’t get the message.
Most discouragingly, though, was this fact: The higher patients rated the quality of their communication with their physicians, the less likely they were to know the truth.
"This suggests that patients perceive physicians as better communicators when they convey a more optimistic view of chemotherapy," wrote the authors, led by first author Dr. Jane C. Weeks, a medical oncologist at the Dana-Farber Cancer Institute in Boston.
Denial is a familiar companion to anyone who works with patients with cancer, their families, and friends. It was the grief reaction cited first and foremost by Elisabeth Kübler Ross. As noted in an editorial accompanying one New England Journal of Medicine study (N. Engl. J Med. 2012;367:1651-2), "Self-deception [can be] a valuable coping tool."
But, at a certain point for cancer patients, denial has the opposite effect, prolonging exposure to side effects, draining a family’s (and society’s) resources, and wasting precious life moments while someone sits in a chemo chair, hoping for and believing in a cure that will not come.

In their editorial, Dr. Thomas J. Smith and Dr. Dan L. Longo of the Johns Hopkins Sidney Kimmel Cancer Center in Baltimore rightfully pointed out that the study’s design does not allow us to retrospectively tune into those exam rooms to set the record straight. Did the doctors perceived as great communicators simply not state the prognosis? Or did their patients "choose not to believe"?
"These are not trivial issues," they wrote. "Chemotherapy near the end of life is still common, does not improve survival, and is one preventable reason why 25% of all Medicare funds are spent in the last year of life.
"Patients need truthful information in order to make truthful choices."
A second study with strikingly similar results from Dana-Farber Cancer Institute in Boston was presented by radiation oncologist Dr. Aileen B. Chen at a plenary session during the annual meeting of the American Society for Radiation Oncology (ASTRO). In her study, Dr. Chen found that 64% of 384 patients with stage IIIB (wet) or IV lung cancer did not realize that palliative radiation therapy was not likely to cure their disease. In other words, same story, different treatment modality.
Together, these findings raise profoundly serious questions about the role that oncologists play in conveying information that they may not want to share and patients may not seem to want to hear. The implications are vast, both on an individual and societal level.
Dr. Smith and Dr. Longo, fortunately, offered specific guidance in their editorial, based on experience at their institution that has doubled the length of time patients benefit from hospice, kept survival rates steady, and reduced costs.
Here’s their formula for honestly conveying prognostic information, along with use of the "essential" communication skill "ask, tell, ask," that assesses patients’ understanding of a message by asking them to restate it in their own words.
• Clearly state the prognosis at the first visit (and whenever the prognosis changes).
• Assign someone in the office to consistently address advance directives.
• Facilitate a hospice information visit within the first three visits following conveyance of a terminal prognosis.
• Discuss the prognosis and coping ("What is important to you?") at each transition.
"If patients are offered truthful information – repeatedly – on what is going to happen to them. They can choose wisely," concluded the Johns Hopkins physicians. "We have the tools to help patients make these difficult decisions. We just need the gumption and incentives to use them."
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.
Oh, how disheartening.
I was troubled, but not too surprised, to read recently published conclusions of two large, population-based studies that found many patients with terminal cancer erroneously believe that palliative treatment (chemotherapy or radiation therapy) will likely cure their disease.
What left me truly dismayed was the first study’s powerful association (P = .002) between patients’ inaccurate perceptions of their prognoses and endorsements of their physicians’ communication skills.
That study, published Oct. 25 in the New England Journal of Medicine (2012;367:1616-25), documented beliefs of 1,193 patients who had received palliative chemotherapy for newly diagnosed stage IV lung or colorectal cancer. As oncologists well know, in this context, chemotherapy might extend life a bit (by weeks or perhaps months) and may alleviate pain or other symptoms of the disease. But it is not curative. And that’s the secret that wasn’t conveyed to patients – at least in a way that they could hear or accept.
Fully 81% of patients with metastatic colorectal cancer didn’t get the message. Nearly 70% of patients with metastatic lung cancer didn’t get the message. By disproportionately high percentages, minority patients didn’t get the message.
Most discouragingly, though, was this fact: The higher patients rated the quality of their communication with their physicians, the less likely they were to know the truth.
"This suggests that patients perceive physicians as better communicators when they convey a more optimistic view of chemotherapy," wrote the authors, led by first author Dr. Jane C. Weeks, a medical oncologist at the Dana-Farber Cancer Institute in Boston.
Denial is a familiar companion to anyone who works with patients with cancer, their families, and friends. It was the grief reaction cited first and foremost by Elisabeth Kübler Ross. As noted in an editorial accompanying one New England Journal of Medicine study (N. Engl. J Med. 2012;367:1651-2), "Self-deception [can be] a valuable coping tool."
But, at a certain point for cancer patients, denial has the opposite effect, prolonging exposure to side effects, draining a family’s (and society’s) resources, and wasting precious life moments while someone sits in a chemo chair, hoping for and believing in a cure that will not come.
In their editorial, Dr. Thomas J. Smith and Dr. Dan L. Longo of the Johns Hopkins Sidney Kimmel Cancer Center in Baltimore rightfully pointed out that the study’s design does not allow us to retrospectively tune into those exam rooms to set the record straight. Did the doctors perceived as great communicators simply not state the prognosis? Or did their patients "choose not to believe"?
"These are not trivial issues," they wrote. "Chemotherapy near the end of life is still common, does not improve survival, and is one preventable reason why 25% of all Medicare funds are spent in the last year of life.
"Patients need truthful information in order to make truthful choices."
A second study with strikingly similar results from Dana-Farber Cancer Institute in Boston was presented by radiation oncologist Dr. Aileen B. Chen at a plenary session during the annual meeting of the American Society for Radiation Oncology (ASTRO). In her study, Dr. Chen found that 64% of 384 patients with stage IIIB (wet) or IV lung cancer did not realize that palliative radiation therapy was not likely to cure their disease. In other words, same story, different treatment modality.
Together, these findings raise profoundly serious questions about the role that oncologists play in conveying information that they may not want to share and patients may not seem to want to hear. The implications are vast, both on an individual and societal level.
Dr. Smith and Dr. Longo, fortunately, offered specific guidance in their editorial, based on experience at their institution that has doubled the length of time patients benefit from hospice, kept survival rates steady, and reduced costs.
Here’s their formula for honestly conveying prognostic information, along with use of the "essential" communication skill "ask, tell, ask," that assesses patients’ understanding of a message by asking them to restate it in their own words.
• Clearly state the prognosis at the first visit (and whenever the prognosis changes).
• Assign someone in the office to consistently address advance directives.
• Facilitate a hospice information visit within the first three visits following conveyance of a terminal prognosis.
• Discuss the prognosis and coping ("What is important to you?") at each transition.
"If patients are offered truthful information – repeatedly – on what is going to happen to them. They can choose wisely," concluded the Johns Hopkins physicians. "We have the tools to help patients make these difficult decisions. We just need the gumption and incentives to use them."
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.
Oh, how disheartening.
I was troubled, but not too surprised, to read recently published conclusions of two large, population-based studies that found many patients with terminal cancer erroneously believe that palliative treatment (chemotherapy or radiation therapy) will likely cure their disease.
What left me truly dismayed was the first study’s powerful association (P = .002) between patients’ inaccurate perceptions of their prognoses and endorsements of their physicians’ communication skills.
That study, published Oct. 25 in the New England Journal of Medicine (2012;367:1616-25), documented beliefs of 1,193 patients who had received palliative chemotherapy for newly diagnosed stage IV lung or colorectal cancer. As oncologists well know, in this context, chemotherapy might extend life a bit (by weeks or perhaps months) and may alleviate pain or other symptoms of the disease. But it is not curative. And that’s the secret that wasn’t conveyed to patients – at least in a way that they could hear or accept.
Fully 81% of patients with metastatic colorectal cancer didn’t get the message. Nearly 70% of patients with metastatic lung cancer didn’t get the message. By disproportionately high percentages, minority patients didn’t get the message.
Most discouragingly, though, was this fact: The higher patients rated the quality of their communication with their physicians, the less likely they were to know the truth.
"This suggests that patients perceive physicians as better communicators when they convey a more optimistic view of chemotherapy," wrote the authors, led by first author Dr. Jane C. Weeks, a medical oncologist at the Dana-Farber Cancer Institute in Boston.
Denial is a familiar companion to anyone who works with patients with cancer, their families, and friends. It was the grief reaction cited first and foremost by Elisabeth Kübler Ross. As noted in an editorial accompanying one New England Journal of Medicine study (N. Engl. J Med. 2012;367:1651-2), "Self-deception [can be] a valuable coping tool."
But, at a certain point for cancer patients, denial has the opposite effect, prolonging exposure to side effects, draining a family’s (and society’s) resources, and wasting precious life moments while someone sits in a chemo chair, hoping for and believing in a cure that will not come.
In their editorial, Dr. Thomas J. Smith and Dr. Dan L. Longo of the Johns Hopkins Sidney Kimmel Cancer Center in Baltimore rightfully pointed out that the study’s design does not allow us to retrospectively tune into those exam rooms to set the record straight. Did the doctors perceived as great communicators simply not state the prognosis? Or did their patients "choose not to believe"?
"These are not trivial issues," they wrote. "Chemotherapy near the end of life is still common, does not improve survival, and is one preventable reason why 25% of all Medicare funds are spent in the last year of life.
"Patients need truthful information in order to make truthful choices."
A second study with strikingly similar results from Dana-Farber Cancer Institute in Boston was presented by radiation oncologist Dr. Aileen B. Chen at a plenary session during the annual meeting of the American Society for Radiation Oncology (ASTRO). In her study, Dr. Chen found that 64% of 384 patients with stage IIIB (wet) or IV lung cancer did not realize that palliative radiation therapy was not likely to cure their disease. In other words, same story, different treatment modality.
Together, these findings raise profoundly serious questions about the role that oncologists play in conveying information that they may not want to share and patients may not seem to want to hear. The implications are vast, both on an individual and societal level.
Dr. Smith and Dr. Longo, fortunately, offered specific guidance in their editorial, based on experience at their institution that has doubled the length of time patients benefit from hospice, kept survival rates steady, and reduced costs.
Here’s their formula for honestly conveying prognostic information, along with use of the "essential" communication skill "ask, tell, ask," that assesses patients’ understanding of a message by asking them to restate it in their own words.
• Clearly state the prognosis at the first visit (and whenever the prognosis changes).
• Assign someone in the office to consistently address advance directives.
• Facilitate a hospice information visit within the first three visits following conveyance of a terminal prognosis.
• Discuss the prognosis and coping ("What is important to you?") at each transition.
"If patients are offered truthful information – repeatedly – on what is going to happen to them. They can choose wisely," concluded the Johns Hopkins physicians. "We have the tools to help patients make these difficult decisions. We just need the gumption and incentives to use them."
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.

Win Whitcomb: Hospitalists Must Grin and Bear the Hospital-Acquired Conditions Program

The Inpatient Prospective Payment System FY2013 Final Rule charts a different future: By fiscal-year 2015 (October 2014), it will morph into a set of measures that are vetted by the National Quality Forum. Hopefully, this will be an improvement.
In recent years, hospitalists have been deluged with rules about documentation, being asked to use medical vocabulary in ways that were foreign to many of us during our training years. Much of the focus on documentation has been propelled by hospitals’ quest to optimize (“maximize” is a forbidden term) reimbursement, which is purely a function of what is written by “licensed providers” (doctors, physician assistants, and nurse practitioners) in the medical chart.
But another powerful driver of documentation practices of late is the hospital-acquired conditions (HAC) program developed by the Centers for Medicare & Medicaid Services (CMS) and enacted in 2009.
Origins of the HAC List
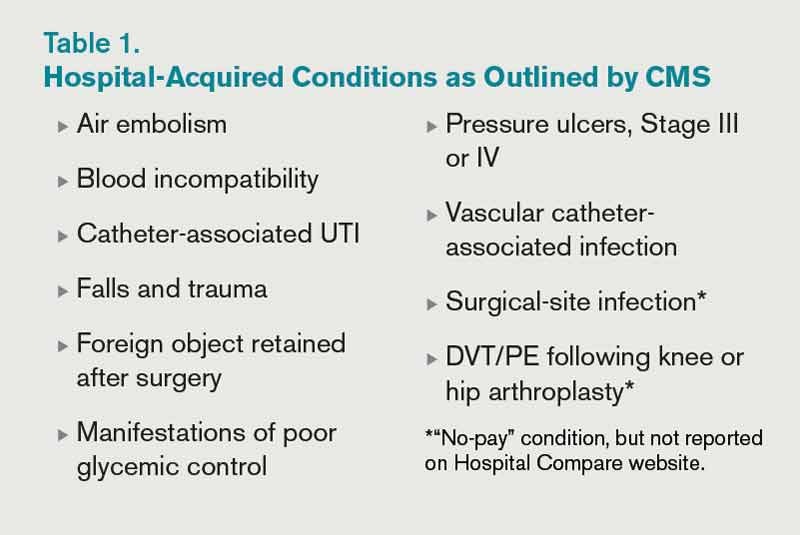
CMS disliked the fact that they were paying for conditions acquired in the hospital that were “reasonably preventable” if evidence-based—or at least “best”—practice was applied. After all, who likes to pay for a punctured gas tank when you brought the minivan in for an oil change? CMS worked with stakeholder groups, including SHM, to create a list of conditions known as hospital-acquired conditions (see Table 1, right).
(As an aside, SHM was supportive of CMS. In fact, we provided direct input into the final rule, recognizing some of the drawbacks of the CMS approach but understanding the larger objective of reengineering a flawed incentive system.)
The idea was that if a hospital submitted a bill to CMS that contained one of these conditions, the hospital would not be paid the amount by which that condition increased total reimbursement for that hospitalization. Note that if you’ve been told your hospital isn’t getting paid at all for patients with one of these conditions, that is not quite correct. Instead, your hospital may not get paid the added amount that is derived from having one of the diagnoses on the list submitted in your hospital’s bill to CMS for a given patient. At the end of the day, this might be a few hundred dollars each time one of these is documented—or $0, if your hospital biller can add another diagnosis in its place to capture the higher payment.
How big a hit to a hospital’s bottom line is this? Meddings and colleagues recently reported that a measly 0.003% of all hospitalizations in Michigan in 2009 saw payments lowered as a result of hospital-acquired catheter-associated UTI, one of the list’s HACs (Ann Int Med. 2012;157:305-312). When all the HACs are added together, one can extrapolate that they haven’t exactly had a big impact on hospital payments.
If the specter of nonpayment for one of these is not enough of a motivator (and it shouldn’t be, given the paltry financial stakes), the rate of HACs are now reported for all hospitals on the Hospital Compare website (www.hospitalcompare.hhs.gov). If a small poke to the pocketbook doesn’t work, maybe public humiliation will.
The Problem with HACs
Although CMS’ intent in creating the HAC program—to eliminate payment for “reasonably preventable” hospital-acquired conditions, thereby improving patient safety—was good, in practice, the program has turned out to be as much about documentation as it is about providing good care. For example, if I forget to write that a Stage III pressure ulcer was present on admission, it gets coded as hospital-acquired and my hospital gets dinged.
It’s important to note that HACs as quality measures were never endorsed by the National Quality Forum (NQF), and without such an endorsement, a quality measure suffers from Rodney Dangerfield syndrome: It don’t get no respect.
Finally, it is disquieting that Meddings et al showed that hospital-acquired catheter-associated UTI rates derived from chart documentation for HACs were but a small fraction of rates determined from rigorous epidemiologic studies, demonstrating that using claims data for determining rates for that specific HAC is flawed. We can only wonder how divergent reported vs. actual rates for the other HACs are.
The Future of the HAC Program
The Affordable Care Act specifies that the lowest-performing quartile of U.S. hospitals for HAC rates will see a 1% Medicare reimbursement reduction beginning in fiscal-year 2015. That’s right: Hospitals facing possible readmissions penalties and losses under value-based purchasing also will face a HAC penalty.
Thankfully, the recently released Inpatient Prospective Payment System FY2013 Final Rule, CMS’ annual update of how hospitals are paid, specifies that the HAC measures are to be removed from public reporting on the Hospital Compare website effective Oct. 1, 2014. They will be replaced by a new set of measures that will (hopefully) be more methodologically sound, because they will require the scrutiny required for endorsement by the NQF. Exactly how these measures will look is not certain, as the rule-making has not yet occurred.
We do know that the three infection measures—catheter-associated UTI, surgical-site infection, and vascular catheter infection—will be generated from clinical data and, therefore, more methodologically sound under the Centers for Disease Control and Prevention’s (CDC) National Healthcare Safety Network. The derivation of the other measures will have to wait until the rule is written next year.
So, until further notice, pay attention to the queries of your hospital’s documentation experts when they approach you about a potential HAC!
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View From
SHM is involved in influencing HAC definitions and the methods in which those definitions are used, in an attempt to “keep it real.” It is important for hospitalists to understand how the HACs can influence care, reimbursement, and their medical center’s strategic priorities. SHM has provided input to CMS, the CDC, and the NQF on the critical role hospitalists have in reducing or preventing HACs. SHM also has played a national role by leading an effort to reduce catheter-associated UTIs through the Partnership for Patients program, a national campaign with a goal of reducing hospital-acquired infections by 40% by the end of 2013.
SHM offers a variety of resources and programs related to reducing HACs, allowing hospitalists to improve patient safety and provide value to their hospital’s leadership. These include:
- Step-by-step implementation guides for reducing hospital-acquired VTE and hyper- and hypoglycemia;
- VTE and glycemic control mentored implementation programs that offer physician experts for tailored coaching on implementing best practices; and
- A fully functioning data repository and reporting engine for glycemic control parameters and hypoglycemia rates and management (eQUIPS).
The Inpatient Prospective Payment System FY2013 Final Rule charts a different future: By fiscal-year 2015 (October 2014), it will morph into a set of measures that are vetted by the National Quality Forum. Hopefully, this will be an improvement.
In recent years, hospitalists have been deluged with rules about documentation, being asked to use medical vocabulary in ways that were foreign to many of us during our training years. Much of the focus on documentation has been propelled by hospitals’ quest to optimize (“maximize” is a forbidden term) reimbursement, which is purely a function of what is written by “licensed providers” (doctors, physician assistants, and nurse practitioners) in the medical chart.
But another powerful driver of documentation practices of late is the hospital-acquired conditions (HAC) program developed by the Centers for Medicare & Medicaid Services (CMS) and enacted in 2009.
Origins of the HAC List
CMS disliked the fact that they were paying for conditions acquired in the hospital that were “reasonably preventable” if evidence-based—or at least “best”—practice was applied. After all, who likes to pay for a punctured gas tank when you brought the minivan in for an oil change? CMS worked with stakeholder groups, including SHM, to create a list of conditions known as hospital-acquired conditions (see Table 1, right).
(As an aside, SHM was supportive of CMS. In fact, we provided direct input into the final rule, recognizing some of the drawbacks of the CMS approach but understanding the larger objective of reengineering a flawed incentive system.)
The idea was that if a hospital submitted a bill to CMS that contained one of these conditions, the hospital would not be paid the amount by which that condition increased total reimbursement for that hospitalization. Note that if you’ve been told your hospital isn’t getting paid at all for patients with one of these conditions, that is not quite correct. Instead, your hospital may not get paid the added amount that is derived from having one of the diagnoses on the list submitted in your hospital’s bill to CMS for a given patient. At the end of the day, this might be a few hundred dollars each time one of these is documented—or $0, if your hospital biller can add another diagnosis in its place to capture the higher payment.
How big a hit to a hospital’s bottom line is this? Meddings and colleagues recently reported that a measly 0.003% of all hospitalizations in Michigan in 2009 saw payments lowered as a result of hospital-acquired catheter-associated UTI, one of the list’s HACs (Ann Int Med. 2012;157:305-312). When all the HACs are added together, one can extrapolate that they haven’t exactly had a big impact on hospital payments.
If the specter of nonpayment for one of these is not enough of a motivator (and it shouldn’t be, given the paltry financial stakes), the rate of HACs are now reported for all hospitals on the Hospital Compare website (www.hospitalcompare.hhs.gov). If a small poke to the pocketbook doesn’t work, maybe public humiliation will.
The Problem with HACs
Although CMS’ intent in creating the HAC program—to eliminate payment for “reasonably preventable” hospital-acquired conditions, thereby improving patient safety—was good, in practice, the program has turned out to be as much about documentation as it is about providing good care. For example, if I forget to write that a Stage III pressure ulcer was present on admission, it gets coded as hospital-acquired and my hospital gets dinged.
It’s important to note that HACs as quality measures were never endorsed by the National Quality Forum (NQF), and without such an endorsement, a quality measure suffers from Rodney Dangerfield syndrome: It don’t get no respect.
Finally, it is disquieting that Meddings et al showed that hospital-acquired catheter-associated UTI rates derived from chart documentation for HACs were but a small fraction of rates determined from rigorous epidemiologic studies, demonstrating that using claims data for determining rates for that specific HAC is flawed. We can only wonder how divergent reported vs. actual rates for the other HACs are.
The Future of the HAC Program
The Affordable Care Act specifies that the lowest-performing quartile of U.S. hospitals for HAC rates will see a 1% Medicare reimbursement reduction beginning in fiscal-year 2015. That’s right: Hospitals facing possible readmissions penalties and losses under value-based purchasing also will face a HAC penalty.
Thankfully, the recently released Inpatient Prospective Payment System FY2013 Final Rule, CMS’ annual update of how hospitals are paid, specifies that the HAC measures are to be removed from public reporting on the Hospital Compare website effective Oct. 1, 2014. They will be replaced by a new set of measures that will (hopefully) be more methodologically sound, because they will require the scrutiny required for endorsement by the NQF. Exactly how these measures will look is not certain, as the rule-making has not yet occurred.
We do know that the three infection measures—catheter-associated UTI, surgical-site infection, and vascular catheter infection—will be generated from clinical data and, therefore, more methodologically sound under the Centers for Disease Control and Prevention’s (CDC) National Healthcare Safety Network. The derivation of the other measures will have to wait until the rule is written next year.
So, until further notice, pay attention to the queries of your hospital’s documentation experts when they approach you about a potential HAC!
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View From
SHM is involved in influencing HAC definitions and the methods in which those definitions are used, in an attempt to “keep it real.” It is important for hospitalists to understand how the HACs can influence care, reimbursement, and their medical center’s strategic priorities. SHM has provided input to CMS, the CDC, and the NQF on the critical role hospitalists have in reducing or preventing HACs. SHM also has played a national role by leading an effort to reduce catheter-associated UTIs through the Partnership for Patients program, a national campaign with a goal of reducing hospital-acquired infections by 40% by the end of 2013.
SHM offers a variety of resources and programs related to reducing HACs, allowing hospitalists to improve patient safety and provide value to their hospital’s leadership. These include:
- Step-by-step implementation guides for reducing hospital-acquired VTE and hyper- and hypoglycemia;
- VTE and glycemic control mentored implementation programs that offer physician experts for tailored coaching on implementing best practices; and
- A fully functioning data repository and reporting engine for glycemic control parameters and hypoglycemia rates and management (eQUIPS).
The Inpatient Prospective Payment System FY2013 Final Rule charts a different future: By fiscal-year 2015 (October 2014), it will morph into a set of measures that are vetted by the National Quality Forum. Hopefully, this will be an improvement.
In recent years, hospitalists have been deluged with rules about documentation, being asked to use medical vocabulary in ways that were foreign to many of us during our training years. Much of the focus on documentation has been propelled by hospitals’ quest to optimize (“maximize” is a forbidden term) reimbursement, which is purely a function of what is written by “licensed providers” (doctors, physician assistants, and nurse practitioners) in the medical chart.
But another powerful driver of documentation practices of late is the hospital-acquired conditions (HAC) program developed by the Centers for Medicare & Medicaid Services (CMS) and enacted in 2009.
Origins of the HAC List
CMS disliked the fact that they were paying for conditions acquired in the hospital that were “reasonably preventable” if evidence-based—or at least “best”—practice was applied. After all, who likes to pay for a punctured gas tank when you brought the minivan in for an oil change? CMS worked with stakeholder groups, including SHM, to create a list of conditions known as hospital-acquired conditions (see Table 1, right).
(As an aside, SHM was supportive of CMS. In fact, we provided direct input into the final rule, recognizing some of the drawbacks of the CMS approach but understanding the larger objective of reengineering a flawed incentive system.)
The idea was that if a hospital submitted a bill to CMS that contained one of these conditions, the hospital would not be paid the amount by which that condition increased total reimbursement for that hospitalization. Note that if you’ve been told your hospital isn’t getting paid at all for patients with one of these conditions, that is not quite correct. Instead, your hospital may not get paid the added amount that is derived from having one of the diagnoses on the list submitted in your hospital’s bill to CMS for a given patient. At the end of the day, this might be a few hundred dollars each time one of these is documented—or $0, if your hospital biller can add another diagnosis in its place to capture the higher payment.
How big a hit to a hospital’s bottom line is this? Meddings and colleagues recently reported that a measly 0.003% of all hospitalizations in Michigan in 2009 saw payments lowered as a result of hospital-acquired catheter-associated UTI, one of the list’s HACs (Ann Int Med. 2012;157:305-312). When all the HACs are added together, one can extrapolate that they haven’t exactly had a big impact on hospital payments.
If the specter of nonpayment for one of these is not enough of a motivator (and it shouldn’t be, given the paltry financial stakes), the rate of HACs are now reported for all hospitals on the Hospital Compare website (www.hospitalcompare.hhs.gov). If a small poke to the pocketbook doesn’t work, maybe public humiliation will.
The Problem with HACs
Although CMS’ intent in creating the HAC program—to eliminate payment for “reasonably preventable” hospital-acquired conditions, thereby improving patient safety—was good, in practice, the program has turned out to be as much about documentation as it is about providing good care. For example, if I forget to write that a Stage III pressure ulcer was present on admission, it gets coded as hospital-acquired and my hospital gets dinged.
It’s important to note that HACs as quality measures were never endorsed by the National Quality Forum (NQF), and without such an endorsement, a quality measure suffers from Rodney Dangerfield syndrome: It don’t get no respect.
Finally, it is disquieting that Meddings et al showed that hospital-acquired catheter-associated UTI rates derived from chart documentation for HACs were but a small fraction of rates determined from rigorous epidemiologic studies, demonstrating that using claims data for determining rates for that specific HAC is flawed. We can only wonder how divergent reported vs. actual rates for the other HACs are.
The Future of the HAC Program
The Affordable Care Act specifies that the lowest-performing quartile of U.S. hospitals for HAC rates will see a 1% Medicare reimbursement reduction beginning in fiscal-year 2015. That’s right: Hospitals facing possible readmissions penalties and losses under value-based purchasing also will face a HAC penalty.
Thankfully, the recently released Inpatient Prospective Payment System FY2013 Final Rule, CMS’ annual update of how hospitals are paid, specifies that the HAC measures are to be removed from public reporting on the Hospital Compare website effective Oct. 1, 2014. They will be replaced by a new set of measures that will (hopefully) be more methodologically sound, because they will require the scrutiny required for endorsement by the NQF. Exactly how these measures will look is not certain, as the rule-making has not yet occurred.
We do know that the three infection measures—catheter-associated UTI, surgical-site infection, and vascular catheter infection—will be generated from clinical data and, therefore, more methodologically sound under the Centers for Disease Control and Prevention’s (CDC) National Healthcare Safety Network. The derivation of the other measures will have to wait until the rule is written next year.
So, until further notice, pay attention to the queries of your hospital’s documentation experts when they approach you about a potential HAC!
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View From
SHM is involved in influencing HAC definitions and the methods in which those definitions are used, in an attempt to “keep it real.” It is important for hospitalists to understand how the HACs can influence care, reimbursement, and their medical center’s strategic priorities. SHM has provided input to CMS, the CDC, and the NQF on the critical role hospitalists have in reducing or preventing HACs. SHM also has played a national role by leading an effort to reduce catheter-associated UTIs through the Partnership for Patients program, a national campaign with a goal of reducing hospital-acquired infections by 40% by the end of 2013.
SHM offers a variety of resources and programs related to reducing HACs, allowing hospitalists to improve patient safety and provide value to their hospital’s leadership. These include:
- Step-by-step implementation guides for reducing hospital-acquired VTE and hyper- and hypoglycemia;
- VTE and glycemic control mentored implementation programs that offer physician experts for tailored coaching on implementing best practices; and
- A fully functioning data repository and reporting engine for glycemic control parameters and hypoglycemia rates and management (eQUIPS).
John Nelson: Learning CPT Coding and Documentation Tricky for Hospitalists

There is a lot to learn when it comes to proper coding and the documentation requirements that go with it. It can even be tricky for a new residency grad to keep the difference in CPT and ICD-9 coding straight, to say nothing of the difference between documentation requirements for physician reimbursement versus hospital reimbursement. This column addresses only physician CPT coding (I’ll save documentation to support hospital billing for another column).
Although I believe that devoting the large number of brain cells required to keep this stuff straight gets in the way of maintaining necessary clinical knowledge, physicians have no real choice but to do it. (One could argue that having a professional coder read charts to determine proper CPT codes relieves a doctor of the burden of documentation and coding headaches. But this is only partially true. The doctor still needs to ensure that the documentation accurately reflects what was done for the coder to be able to select the appropriate codes, so he still needs to know a lot about this topic.)
All providers have a duty to reasonably ensure that submitted claims (bills) are true and accurate. Failing to document and code correctly risks anything from you or your employer having to return money, potentially with a penalty and interest, to being accused of criminal fraud.
Medicare and other payors generally categorize inaccurate claims as follows:
- Erroneous claims include inadvertent mistakes, innocent errors, or even negligence but still require payments associated with the error to be returned.
- Fraudulent claims are ones judged to be intentionally or recklessly false, and are subject to administrative or civil penalties, such as fines.
- Claims associated with criminal intent to defraud are subject to criminal penalties, which could include jail time.
While I haven’t heard of any hospitalists being accused of fraud, I know of several who have undergone audits and been required to return money. Whether your employer would refund the money or you would have to write a personal check to refund the money depends on your employment situation. For example, in most cases, the hospital would be liable to make the repayment for hospitalists it employs. If you’re an independent contractor, there is a good chance you could be stuck making the repayment yourself.
Trend: Increased Use of Higher-Level Codes
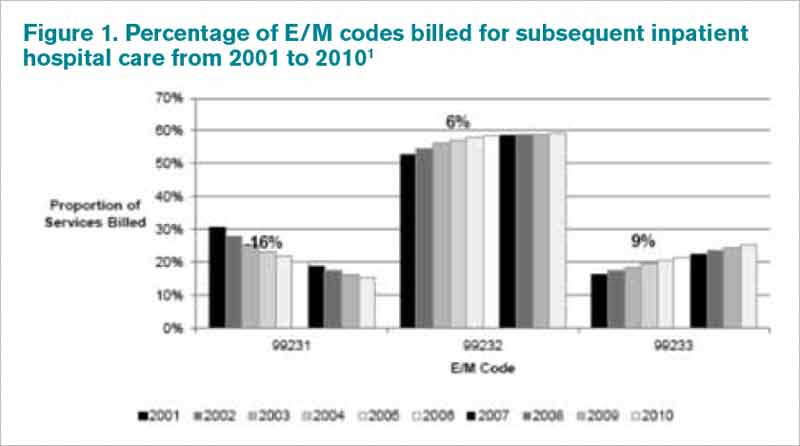
You might have missed it, but there was a recent study of Medicare Part B claims data from 2001 to 2010 showing that “physicians increased their billing of higher-level E/M codes in all types of E/M services.”1 For example, the report showed a steady decrease in use of the 99231 code, the lowest of the three subsequent inpatient hospital care codes, and an increase in the highest level code, 99233 (see Figure 1, below).
I can think of two reasons hospitalists might be increasing the use of higher codes. One, less-sick patients just aren’t seen in the hospital as often as they used to be, so the remaining patients require more intensive services, which could lead to the appropriate use of higher-level codes. Two, doctors have over the past 10 to 15 years invested more energy in learning appropriate documentation and coding, which might have led to correcting historical overuse of lower-level codes.
Did I tell you who conducted the study showing increased use of higher-level codes? It was the federal Office of Inspector General (OIG), which is responsible for preventing and detecting fraud and waste. Although the OIG might agree that the sicker patients and correction of historical undercoding might explain some of the trend, it’s a pretty safe bet they’re also concerned that a significant portion is inappropriate or fraudulent. Some portion of it probably is.
“CMS concurred with [OIG’s] recommendations to (1) continue to educate physicians on proper billing for E/M services and (2) encourage its contractor to review physicians’ billing for E/M services. CMS partially concurred with [OIG’s] third recommendation, to review physicians who bill higher-level E/M codes for appropriate action,” the OIG report noted.1
Plan for Education, Compliance
My sense is that most hospitalists employed by a large entity, such as a hospital or large medical group, have access to a certified coder to perform documentation and coding audits, as well as educational feedback when needed. If your practice doesn’t have access to a certified coder, you should consider photocopying some chart notes (e.g. 10 notes from each of your docs) and send them to an outside coder for an audit. Though they are very valuable, audits usually are not enough to ensure good performance.
In my March 2007 column, I described a reasonably simple chart audit allowing each doctor to compare his or her CPT coding pattern to everyone else in the group. You can compare your own coding to national coding patterns via SHM’s 2012 State of Hospital Medicine Report (www.hospitalmedicine.org/survey) or data from the CMS website, and the Medical Group Management Association (MGMA) will have data in future surveys. Such comparisons might help uncover unusual patterns that are worthy of a closer look.
Other strategies to promote proper documentation and coding include online educational programs, such as:
- SHM’s CODE-H webinars (www.hospitalmedicine.org/codeh), which are available on demand for a fee;
- American Association of Professional Coders Evaluation and Management Online Training (http://www.aapc.com/training/evaluation-management-coding-training.aspx); and
- The American Health Information Management Association’s (AHIMA) Coding Basics Program (www.ahima.org/continuinged/campus/courseinfo/cb.aspx).
If you prefer, an Internet search can turn up in-person courses to learn documentation and coding. Additionally, your in-house or external coding auditors can provide training.
To address tricky issues that come up only occasionally, several in our practice have compiled a “coding manual” by distilling guidance from our certified coders and compliance people on issues as they came up. Some issues would stump all of us, and we’d have to go to the Internet for help. All hospitalists are provided with a copy of the manual during orientation, and an electronic copy is available on the hospital’s Intranet. Topics addressed in the manual include things like how to bill the first inpatient day when a patient has changed from observation status, how to bill initial consult visits for various payors (an issue since Medicare eliminated consult codes a few years ago), how to bill when a patient is seen and discharged from the ED, etc.
Lastly, I suggest someone in your group talk with your hospital’s compliance department about its own coding and billing compliance plan. This could lead to ideas or help develop a compliance plan for your group.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Reference
There is a lot to learn when it comes to proper coding and the documentation requirements that go with it. It can even be tricky for a new residency grad to keep the difference in CPT and ICD-9 coding straight, to say nothing of the difference between documentation requirements for physician reimbursement versus hospital reimbursement. This column addresses only physician CPT coding (I’ll save documentation to support hospital billing for another column).
Although I believe that devoting the large number of brain cells required to keep this stuff straight gets in the way of maintaining necessary clinical knowledge, physicians have no real choice but to do it. (One could argue that having a professional coder read charts to determine proper CPT codes relieves a doctor of the burden of documentation and coding headaches. But this is only partially true. The doctor still needs to ensure that the documentation accurately reflects what was done for the coder to be able to select the appropriate codes, so he still needs to know a lot about this topic.)
All providers have a duty to reasonably ensure that submitted claims (bills) are true and accurate. Failing to document and code correctly risks anything from you or your employer having to return money, potentially with a penalty and interest, to being accused of criminal fraud.
Medicare and other payors generally categorize inaccurate claims as follows:
- Erroneous claims include inadvertent mistakes, innocent errors, or even negligence but still require payments associated with the error to be returned.
- Fraudulent claims are ones judged to be intentionally or recklessly false, and are subject to administrative or civil penalties, such as fines.
- Claims associated with criminal intent to defraud are subject to criminal penalties, which could include jail time.
While I haven’t heard of any hospitalists being accused of fraud, I know of several who have undergone audits and been required to return money. Whether your employer would refund the money or you would have to write a personal check to refund the money depends on your employment situation. For example, in most cases, the hospital would be liable to make the repayment for hospitalists it employs. If you’re an independent contractor, there is a good chance you could be stuck making the repayment yourself.
Trend: Increased Use of Higher-Level Codes
You might have missed it, but there was a recent study of Medicare Part B claims data from 2001 to 2010 showing that “physicians increased their billing of higher-level E/M codes in all types of E/M services.”1 For example, the report showed a steady decrease in use of the 99231 code, the lowest of the three subsequent inpatient hospital care codes, and an increase in the highest level code, 99233 (see Figure 1, below).
I can think of two reasons hospitalists might be increasing the use of higher codes. One, less-sick patients just aren’t seen in the hospital as often as they used to be, so the remaining patients require more intensive services, which could lead to the appropriate use of higher-level codes. Two, doctors have over the past 10 to 15 years invested more energy in learning appropriate documentation and coding, which might have led to correcting historical overuse of lower-level codes.
Did I tell you who conducted the study showing increased use of higher-level codes? It was the federal Office of Inspector General (OIG), which is responsible for preventing and detecting fraud and waste. Although the OIG might agree that the sicker patients and correction of historical undercoding might explain some of the trend, it’s a pretty safe bet they’re also concerned that a significant portion is inappropriate or fraudulent. Some portion of it probably is.
“CMS concurred with [OIG’s] recommendations to (1) continue to educate physicians on proper billing for E/M services and (2) encourage its contractor to review physicians’ billing for E/M services. CMS partially concurred with [OIG’s] third recommendation, to review physicians who bill higher-level E/M codes for appropriate action,” the OIG report noted.1
Plan for Education, Compliance
My sense is that most hospitalists employed by a large entity, such as a hospital or large medical group, have access to a certified coder to perform documentation and coding audits, as well as educational feedback when needed. If your practice doesn’t have access to a certified coder, you should consider photocopying some chart notes (e.g. 10 notes from each of your docs) and send them to an outside coder for an audit. Though they are very valuable, audits usually are not enough to ensure good performance.
In my March 2007 column, I described a reasonably simple chart audit allowing each doctor to compare his or her CPT coding pattern to everyone else in the group. You can compare your own coding to national coding patterns via SHM’s 2012 State of Hospital Medicine Report (www.hospitalmedicine.org/survey) or data from the CMS website, and the Medical Group Management Association (MGMA) will have data in future surveys. Such comparisons might help uncover unusual patterns that are worthy of a closer look.
Other strategies to promote proper documentation and coding include online educational programs, such as:
- SHM’s CODE-H webinars (www.hospitalmedicine.org/codeh), which are available on demand for a fee;
- American Association of Professional Coders Evaluation and Management Online Training (http://www.aapc.com/training/evaluation-management-coding-training.aspx); and
- The American Health Information Management Association’s (AHIMA) Coding Basics Program (www.ahima.org/continuinged/campus/courseinfo/cb.aspx).
If you prefer, an Internet search can turn up in-person courses to learn documentation and coding. Additionally, your in-house or external coding auditors can provide training.
To address tricky issues that come up only occasionally, several in our practice have compiled a “coding manual” by distilling guidance from our certified coders and compliance people on issues as they came up. Some issues would stump all of us, and we’d have to go to the Internet for help. All hospitalists are provided with a copy of the manual during orientation, and an electronic copy is available on the hospital’s Intranet. Topics addressed in the manual include things like how to bill the first inpatient day when a patient has changed from observation status, how to bill initial consult visits for various payors (an issue since Medicare eliminated consult codes a few years ago), how to bill when a patient is seen and discharged from the ED, etc.
Lastly, I suggest someone in your group talk with your hospital’s compliance department about its own coding and billing compliance plan. This could lead to ideas or help develop a compliance plan for your group.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Reference
There is a lot to learn when it comes to proper coding and the documentation requirements that go with it. It can even be tricky for a new residency grad to keep the difference in CPT and ICD-9 coding straight, to say nothing of the difference between documentation requirements for physician reimbursement versus hospital reimbursement. This column addresses only physician CPT coding (I’ll save documentation to support hospital billing for another column).
Although I believe that devoting the large number of brain cells required to keep this stuff straight gets in the way of maintaining necessary clinical knowledge, physicians have no real choice but to do it. (One could argue that having a professional coder read charts to determine proper CPT codes relieves a doctor of the burden of documentation and coding headaches. But this is only partially true. The doctor still needs to ensure that the documentation accurately reflects what was done for the coder to be able to select the appropriate codes, so he still needs to know a lot about this topic.)
All providers have a duty to reasonably ensure that submitted claims (bills) are true and accurate. Failing to document and code correctly risks anything from you or your employer having to return money, potentially with a penalty and interest, to being accused of criminal fraud.
Medicare and other payors generally categorize inaccurate claims as follows:
- Erroneous claims include inadvertent mistakes, innocent errors, or even negligence but still require payments associated with the error to be returned.
- Fraudulent claims are ones judged to be intentionally or recklessly false, and are subject to administrative or civil penalties, such as fines.
- Claims associated with criminal intent to defraud are subject to criminal penalties, which could include jail time.
While I haven’t heard of any hospitalists being accused of fraud, I know of several who have undergone audits and been required to return money. Whether your employer would refund the money or you would have to write a personal check to refund the money depends on your employment situation. For example, in most cases, the hospital would be liable to make the repayment for hospitalists it employs. If you’re an independent contractor, there is a good chance you could be stuck making the repayment yourself.
Trend: Increased Use of Higher-Level Codes
You might have missed it, but there was a recent study of Medicare Part B claims data from 2001 to 2010 showing that “physicians increased their billing of higher-level E/M codes in all types of E/M services.”1 For example, the report showed a steady decrease in use of the 99231 code, the lowest of the three subsequent inpatient hospital care codes, and an increase in the highest level code, 99233 (see Figure 1, below).
I can think of two reasons hospitalists might be increasing the use of higher codes. One, less-sick patients just aren’t seen in the hospital as often as they used to be, so the remaining patients require more intensive services, which could lead to the appropriate use of higher-level codes. Two, doctors have over the past 10 to 15 years invested more energy in learning appropriate documentation and coding, which might have led to correcting historical overuse of lower-level codes.
Did I tell you who conducted the study showing increased use of higher-level codes? It was the federal Office of Inspector General (OIG), which is responsible for preventing and detecting fraud and waste. Although the OIG might agree that the sicker patients and correction of historical undercoding might explain some of the trend, it’s a pretty safe bet they’re also concerned that a significant portion is inappropriate or fraudulent. Some portion of it probably is.
“CMS concurred with [OIG’s] recommendations to (1) continue to educate physicians on proper billing for E/M services and (2) encourage its contractor to review physicians’ billing for E/M services. CMS partially concurred with [OIG’s] third recommendation, to review physicians who bill higher-level E/M codes for appropriate action,” the OIG report noted.1
Plan for Education, Compliance
My sense is that most hospitalists employed by a large entity, such as a hospital or large medical group, have access to a certified coder to perform documentation and coding audits, as well as educational feedback when needed. If your practice doesn’t have access to a certified coder, you should consider photocopying some chart notes (e.g. 10 notes from each of your docs) and send them to an outside coder for an audit. Though they are very valuable, audits usually are not enough to ensure good performance.
In my March 2007 column, I described a reasonably simple chart audit allowing each doctor to compare his or her CPT coding pattern to everyone else in the group. You can compare your own coding to national coding patterns via SHM’s 2012 State of Hospital Medicine Report (www.hospitalmedicine.org/survey) or data from the CMS website, and the Medical Group Management Association (MGMA) will have data in future surveys. Such comparisons might help uncover unusual patterns that are worthy of a closer look.
Other strategies to promote proper documentation and coding include online educational programs, such as:
- SHM’s CODE-H webinars (www.hospitalmedicine.org/codeh), which are available on demand for a fee;
- American Association of Professional Coders Evaluation and Management Online Training (http://www.aapc.com/training/evaluation-management-coding-training.aspx); and
- The American Health Information Management Association’s (AHIMA) Coding Basics Program (www.ahima.org/continuinged/campus/courseinfo/cb.aspx).
If you prefer, an Internet search can turn up in-person courses to learn documentation and coding. Additionally, your in-house or external coding auditors can provide training.
To address tricky issues that come up only occasionally, several in our practice have compiled a “coding manual” by distilling guidance from our certified coders and compliance people on issues as they came up. Some issues would stump all of us, and we’d have to go to the Internet for help. All hospitalists are provided with a copy of the manual during orientation, and an electronic copy is available on the hospital’s Intranet. Topics addressed in the manual include things like how to bill the first inpatient day when a patient has changed from observation status, how to bill initial consult visits for various payors (an issue since Medicare eliminated consult codes a few years ago), how to bill when a patient is seen and discharged from the ED, etc.
Lastly, I suggest someone in your group talk with your hospital’s compliance department about its own coding and billing compliance plan. This could lead to ideas or help develop a compliance plan for your group.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
Reference
John Nelson: Heavy Workloads
Now that HM is moving (or has moved?) from infancy to adolescence or even maturity, you might think that we would have reached some sort of consensus on what a reasonable workload—or patient volume—for a hospitalist is. My sense is that conventional wisdom says a reasonable average daily workload for a daytime rounding/admitting hospitalist is in the range of 12 to 17 billed encounters. And to average this volume, the doctor will have a number of days with more or fewer patients.
After thinking about average workload, the next question is: What is a reasonable upper limit for patient volume on a single day? Here, opinion seems to be a little fuzzier, but I think most would say a hospitalist should be expected to see more than 20 patients in a single day only on rare occasions and on, say, no more than 10 days annually. Keep in mind that a hospitalist who has 22 patients today still has a pretty good chance they will have 20 or more tomorrow, and the day after. High volumes are not a single-day phenomenon, either, because it usually takes a number of days for those patients to reach discharge—and the doctor to realize a decline in workload.
But these numbers are only conventional wisdom. There are little research data to guide our thinking about patient volumes, and thoughtful people sometimes arrive at very different conclusions. As I’ve written in this space previously, I think each individual hospitalist should have significant influence or autonomy to decide the appropriate or optimal patient volume for themselves or their group. This usually requires that doctors are connected to the economic and quality-of-care effects of their patient volume choices, something many hospitalists resist.
Divergence of Opinion
But given lots of autonomy, some hospitalists could make poor choices. I have had the experience of working with hospitalists in three practices around the country who are confident that, at least for themselves, very high patient volumes are safe and reasonable. These high-energy hospitalists see as many as 30 or 40 patients per day, day after day.
At one of these practices, I sat down with the doctors on duty that day at 1 p.m. and talked uninterrupted by pager or patient-care issues for nearly three hours. It was only at the end of the meeting that they explained each of them was seeing around 30 patients that day but had nearly finished rounds before our meeting started. I was stunned. (I probably wouldn’t stop for lunch, to say nothing of a three-hour meeting, to see just 20 patients in a day.)
So I asked just what they saw as an excessive daily patient volume. One of them seemed to deliberate carefully and said, “I probably need help when I have more than 35 patients to see in a day, but I’m OK with anything less than that.”
But the record goes to a really nice, spirited hospitalist who told me that, in addition to his usual workload, he occasionally covered weekends for an internal-medicine group. On a recent weekend, he had 88 patients to see each day, he said. Yes, you read that correctly: 88! (Fortunately, he did see that as a problem and was working to decrease the number.)
Potential Risks
I want to be clear that my own opinion is that the volumes above are unacceptable and dangerous. I think that, in most settings, routinely seeing more than 20 patients in a day probably degrades performance and increases the risk of burnout. While I think most knowledgeable people in our field share this opinion, none of us can point to compelling, generalizable research data to support our opinion.
The way I see it, excessively high workloads risk:
- Adverse patient outcomes due to increased potential for clinical errors and accompanying poor documentation;
- Failure of hospitalists to meet performance and citizenship expectations, such as length of stay (LOS), resource utilization, use of standardized order sets, attention to early discharge times, etc.;
- Lack of any excess capacity to handle transient increases in workload;
- Recruiting and/or retention challenges for hospitalists who might not want to work so hard;
- High risk of hospitalist stress and burnout, which over time could negatively impact a person’s well-being, as well as their attitudes and interactions with other members of the patient care team;
- Overdependence on a few very-hard-working doctors; if one doctor gets sick or has to stop working for a period of time, the hospital must find the equivalent of one-and-a-half doctors to replace him or her; and
- Increased malpractice risk.
Limited Data
There is some research to guide the thinking about workload. I recall one or two abstracts presented at past SHM annual meetings in which doctors in a single practice showed that LOS increased when their patient volume was high. And some sharp hospitalist researchers at Christiana Care Health System in Wilmington, Del., conducted a more robust retrospective cohort study of thousands of non-ICU adult admissions to their 1,100-bed hospital over a three-year period. Their data, which they intend to publish, showed LOS rises as hospitalist workload increases.
Others have assessed the connection between workload and well-being or burnout. Surprisingly, it has been hard to document in the peer-reviewed literature that increasing workloads are associated with increased burnout. Studies of hospitalists published in 2001 and 2011 failed to show a connection between self-reported workload and burnout.1,2 A 2009 systemic review of literature on all physician specialties concluded that “an imbalance between expected and experienced … workload is moderately associated with dissatisfaction, but there is less evidence of a significant association with objective workload.”3 (Emphasis mine.)
Rather than workload, both of the hospitalist studies found that such attributes as organizational solidarity, climate, and fairness; the feeling of being valued by the whole healthcare team; personal time; and compensation were more tightly correlated with whether hospitalists would thrive than workload.
Unfortunately, I’m not aware of any robust studies showing the relationship between hospitalist workload and quality of care (please email me if you know of any). I think the burden of proof is on those who support high workloads to show they don’t adversely affect patient incomes.
If you’d like to discuss workload further, I’ll be moderating a session titled “Who Says 15 is the Right Number?” during HM13, May 17-19, 2013, in Washington, D.C. (www.hospitalmedicine2013.org). I hope to see you there.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
References
2. Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
3. Scheurer D, McKean S, Miller J, Wetterneck T. U.S. physician satisfaction: a systematic review. J Hosp Med. 2009;4(9):560-568.
Now that HM is moving (or has moved?) from infancy to adolescence or even maturity, you might think that we would have reached some sort of consensus on what a reasonable workload—or patient volume—for a hospitalist is. My sense is that conventional wisdom says a reasonable average daily workload for a daytime rounding/admitting hospitalist is in the range of 12 to 17 billed encounters. And to average this volume, the doctor will have a number of days with more or fewer patients.
After thinking about average workload, the next question is: What is a reasonable upper limit for patient volume on a single day? Here, opinion seems to be a little fuzzier, but I think most would say a hospitalist should be expected to see more than 20 patients in a single day only on rare occasions and on, say, no more than 10 days annually. Keep in mind that a hospitalist who has 22 patients today still has a pretty good chance they will have 20 or more tomorrow, and the day after. High volumes are not a single-day phenomenon, either, because it usually takes a number of days for those patients to reach discharge—and the doctor to realize a decline in workload.
But these numbers are only conventional wisdom. There are little research data to guide our thinking about patient volumes, and thoughtful people sometimes arrive at very different conclusions. As I’ve written in this space previously, I think each individual hospitalist should have significant influence or autonomy to decide the appropriate or optimal patient volume for themselves or their group. This usually requires that doctors are connected to the economic and quality-of-care effects of their patient volume choices, something many hospitalists resist.
Divergence of Opinion
But given lots of autonomy, some hospitalists could make poor choices. I have had the experience of working with hospitalists in three practices around the country who are confident that, at least for themselves, very high patient volumes are safe and reasonable. These high-energy hospitalists see as many as 30 or 40 patients per day, day after day.
At one of these practices, I sat down with the doctors on duty that day at 1 p.m. and talked uninterrupted by pager or patient-care issues for nearly three hours. It was only at the end of the meeting that they explained each of them was seeing around 30 patients that day but had nearly finished rounds before our meeting started. I was stunned. (I probably wouldn’t stop for lunch, to say nothing of a three-hour meeting, to see just 20 patients in a day.)
So I asked just what they saw as an excessive daily patient volume. One of them seemed to deliberate carefully and said, “I probably need help when I have more than 35 patients to see in a day, but I’m OK with anything less than that.”
But the record goes to a really nice, spirited hospitalist who told me that, in addition to his usual workload, he occasionally covered weekends for an internal-medicine group. On a recent weekend, he had 88 patients to see each day, he said. Yes, you read that correctly: 88! (Fortunately, he did see that as a problem and was working to decrease the number.)
Potential Risks
I want to be clear that my own opinion is that the volumes above are unacceptable and dangerous. I think that, in most settings, routinely seeing more than 20 patients in a day probably degrades performance and increases the risk of burnout. While I think most knowledgeable people in our field share this opinion, none of us can point to compelling, generalizable research data to support our opinion.
The way I see it, excessively high workloads risk:
- Adverse patient outcomes due to increased potential for clinical errors and accompanying poor documentation;
- Failure of hospitalists to meet performance and citizenship expectations, such as length of stay (LOS), resource utilization, use of standardized order sets, attention to early discharge times, etc.;
- Lack of any excess capacity to handle transient increases in workload;
- Recruiting and/or retention challenges for hospitalists who might not want to work so hard;
- High risk of hospitalist stress and burnout, which over time could negatively impact a person’s well-being, as well as their attitudes and interactions with other members of the patient care team;
- Overdependence on a few very-hard-working doctors; if one doctor gets sick or has to stop working for a period of time, the hospital must find the equivalent of one-and-a-half doctors to replace him or her; and
- Increased malpractice risk.
Limited Data
There is some research to guide the thinking about workload. I recall one or two abstracts presented at past SHM annual meetings in which doctors in a single practice showed that LOS increased when their patient volume was high. And some sharp hospitalist researchers at Christiana Care Health System in Wilmington, Del., conducted a more robust retrospective cohort study of thousands of non-ICU adult admissions to their 1,100-bed hospital over a three-year period. Their data, which they intend to publish, showed LOS rises as hospitalist workload increases.
Others have assessed the connection between workload and well-being or burnout. Surprisingly, it has been hard to document in the peer-reviewed literature that increasing workloads are associated with increased burnout. Studies of hospitalists published in 2001 and 2011 failed to show a connection between self-reported workload and burnout.1,2 A 2009 systemic review of literature on all physician specialties concluded that “an imbalance between expected and experienced … workload is moderately associated with dissatisfaction, but there is less evidence of a significant association with objective workload.”3 (Emphasis mine.)
Rather than workload, both of the hospitalist studies found that such attributes as organizational solidarity, climate, and fairness; the feeling of being valued by the whole healthcare team; personal time; and compensation were more tightly correlated with whether hospitalists would thrive than workload.
Unfortunately, I’m not aware of any robust studies showing the relationship between hospitalist workload and quality of care (please email me if you know of any). I think the burden of proof is on those who support high workloads to show they don’t adversely affect patient incomes.
If you’d like to discuss workload further, I’ll be moderating a session titled “Who Says 15 is the Right Number?” during HM13, May 17-19, 2013, in Washington, D.C. (www.hospitalmedicine2013.org). I hope to see you there.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
References
2. Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
3. Scheurer D, McKean S, Miller J, Wetterneck T. U.S. physician satisfaction: a systematic review. J Hosp Med. 2009;4(9):560-568.
Now that HM is moving (or has moved?) from infancy to adolescence or even maturity, you might think that we would have reached some sort of consensus on what a reasonable workload—or patient volume—for a hospitalist is. My sense is that conventional wisdom says a reasonable average daily workload for a daytime rounding/admitting hospitalist is in the range of 12 to 17 billed encounters. And to average this volume, the doctor will have a number of days with more or fewer patients.
After thinking about average workload, the next question is: What is a reasonable upper limit for patient volume on a single day? Here, opinion seems to be a little fuzzier, but I think most would say a hospitalist should be expected to see more than 20 patients in a single day only on rare occasions and on, say, no more than 10 days annually. Keep in mind that a hospitalist who has 22 patients today still has a pretty good chance they will have 20 or more tomorrow, and the day after. High volumes are not a single-day phenomenon, either, because it usually takes a number of days for those patients to reach discharge—and the doctor to realize a decline in workload.
But these numbers are only conventional wisdom. There are little research data to guide our thinking about patient volumes, and thoughtful people sometimes arrive at very different conclusions. As I’ve written in this space previously, I think each individual hospitalist should have significant influence or autonomy to decide the appropriate or optimal patient volume for themselves or their group. This usually requires that doctors are connected to the economic and quality-of-care effects of their patient volume choices, something many hospitalists resist.
Divergence of Opinion
But given lots of autonomy, some hospitalists could make poor choices. I have had the experience of working with hospitalists in three practices around the country who are confident that, at least for themselves, very high patient volumes are safe and reasonable. These high-energy hospitalists see as many as 30 or 40 patients per day, day after day.
At one of these practices, I sat down with the doctors on duty that day at 1 p.m. and talked uninterrupted by pager or patient-care issues for nearly three hours. It was only at the end of the meeting that they explained each of them was seeing around 30 patients that day but had nearly finished rounds before our meeting started. I was stunned. (I probably wouldn’t stop for lunch, to say nothing of a three-hour meeting, to see just 20 patients in a day.)
So I asked just what they saw as an excessive daily patient volume. One of them seemed to deliberate carefully and said, “I probably need help when I have more than 35 patients to see in a day, but I’m OK with anything less than that.”
But the record goes to a really nice, spirited hospitalist who told me that, in addition to his usual workload, he occasionally covered weekends for an internal-medicine group. On a recent weekend, he had 88 patients to see each day, he said. Yes, you read that correctly: 88! (Fortunately, he did see that as a problem and was working to decrease the number.)
Potential Risks
I want to be clear that my own opinion is that the volumes above are unacceptable and dangerous. I think that, in most settings, routinely seeing more than 20 patients in a day probably degrades performance and increases the risk of burnout. While I think most knowledgeable people in our field share this opinion, none of us can point to compelling, generalizable research data to support our opinion.
The way I see it, excessively high workloads risk:
- Adverse patient outcomes due to increased potential for clinical errors and accompanying poor documentation;
- Failure of hospitalists to meet performance and citizenship expectations, such as length of stay (LOS), resource utilization, use of standardized order sets, attention to early discharge times, etc.;
- Lack of any excess capacity to handle transient increases in workload;
- Recruiting and/or retention challenges for hospitalists who might not want to work so hard;
- High risk of hospitalist stress and burnout, which over time could negatively impact a person’s well-being, as well as their attitudes and interactions with other members of the patient care team;
- Overdependence on a few very-hard-working doctors; if one doctor gets sick or has to stop working for a period of time, the hospital must find the equivalent of one-and-a-half doctors to replace him or her; and
- Increased malpractice risk.
Limited Data
There is some research to guide the thinking about workload. I recall one or two abstracts presented at past SHM annual meetings in which doctors in a single practice showed that LOS increased when their patient volume was high. And some sharp hospitalist researchers at Christiana Care Health System in Wilmington, Del., conducted a more robust retrospective cohort study of thousands of non-ICU adult admissions to their 1,100-bed hospital over a three-year period. Their data, which they intend to publish, showed LOS rises as hospitalist workload increases.
Others have assessed the connection between workload and well-being or burnout. Surprisingly, it has been hard to document in the peer-reviewed literature that increasing workloads are associated with increased burnout. Studies of hospitalists published in 2001 and 2011 failed to show a connection between self-reported workload and burnout.1,2 A 2009 systemic review of literature on all physician specialties concluded that “an imbalance between expected and experienced … workload is moderately associated with dissatisfaction, but there is less evidence of a significant association with objective workload.”3 (Emphasis mine.)
Rather than workload, both of the hospitalist studies found that such attributes as organizational solidarity, climate, and fairness; the feeling of being valued by the whole healthcare team; personal time; and compensation were more tightly correlated with whether hospitalists would thrive than workload.
Unfortunately, I’m not aware of any robust studies showing the relationship between hospitalist workload and quality of care (please email me if you know of any). I think the burden of proof is on those who support high workloads to show they don’t adversely affect patient incomes.
If you’d like to discuss workload further, I’ll be moderating a session titled “Who Says 15 is the Right Number?” during HM13, May 17-19, 2013, in Washington, D.C. (www.hospitalmedicine2013.org). I hope to see you there.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at john.nelson@nelsonflores.com.
References
2. Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
3. Scheurer D, McKean S, Miller J, Wetterneck T. U.S. physician satisfaction: a systematic review. J Hosp Med. 2009;4(9):560-568.
The Value of Listening
It’s becoming the exception for a psychiatrist to spend more than 15 minutes speaking face-to-face with patients. This is the unfortunate concomitant of a medical culture that reimburses us more for 15-minute medication reviews than for talking to patients for an hour.
Yet, we know that connecting with patients at some heartfelt level is critical to doing our work. It is the relationship that inspires their trust and encourages them to dare to imagine that they can create new endings to their old stories. It turns out that listening at that level can actually happen in a short time if you are truly present and paying attention.

I recently participated in a community mental health clinic in the streets of Iquitos, Peru, where I went with Dr. Patch Adams, the world’s most recognized humanitarian clown. One hundred clowns from all over the world participated in a collaborative preventive health project in a desperately impoverished section of town called Belen. They are performers, musicians, artists, teachers, students, entrepreneurs, students, and health workers.
We conducted workshops for children (percussion, dance, acrobatics, puppetry); painted homes and public murals; clowned in hospitals, prisons, and shelters; and supported local health organizations.
For the last 3 years, I’ve worked with Amazon Promise, a nonprofit organization that provides health care to indigenous people in the Amazon. I was the first psychiatrist willing to see patients in an open public space, without privacy or psychiatric drugs. I had a remarkable translator who wove my words into her own meaningful story that touched patients. People waited in line without shame, talking about their problems in full view of their neighbors. We discovered in these sessions that good things can happen – even in 20 minutes.

Among this year’s clown group were 20 clinical health professionals (psychologists, counselors, nurses, doctors, social workers, and body workers). We set up four half-day clinics in the streets of Belen, where we knew people would be gathering. We printed fliers that said health professionals who could offer help would be available for people who were experiencing problems at home (with spouses, children, or parents), couldn’t sleep, or had aches in their body.
Before the first clinic, I met with the clinicians and told them about my experiences over the last several years. In those meetings, the clinicians were in an open setting with no privacy, hearing stories that would make their hearts bleed (abuse, abandonment, sexual trauma), and they would wonder how anything in their training could help them deal with such overwhelming problems. I assured them that, in addition to the symptomatic manifestations of such grinding poverty, they would see a remarkable people with extraordinary resilience.

Perhaps the most significant thing we could do was simply listen to their stories: For many patients, 20 minutes with a compassionate listener was an exceptional event. If, in addition, they could help patients identify some strengths, offer some advice, or inspire hope, that would be an additional dividend.
We had no psychiatric drugs, so at the end of the sessions, we would give them vitamins for themselves and their children. I brought along some necklaces with a small silver medallion of the Virgin of Guadalupe that had been blessed by Huichol and Navajo shamans. I suggested to the clinicians that, if they saw patients who might benefit from having this reminder of their time together, they could share these special amulets with a blessing of their own ... "Whatever your heart prompts you to say at the moment."
We did not dress up in our usual clown regalia – only our clown noses identified us. We set up in a schoolyard, loading dock, and empty rooms. Upon arriving, we passed out the flyers and announced our presence through loudspeakers. Clinicians were paired up and each team huddled in a tight circle with their patient(s) so they could hear above the clamor. Clowns playing with children, veterinarians sterilizing dogs and cats, and laboratory technicians taking blood from kids surrounded the teams – all while the community casually strolled by.

Clinicians saw 200 people over 4 days; they listened to the breadth and depth of the human experience. Twenty minutes is a blink of an eyelash when measured against the length of one’s life, but it’s enough time to feel the pain of another and to reach out to touch them with compassion.
It is those moments, when we are reminded of our shared humanity, that make all suffering bearable. In a short time, in a public place, without privacy, not making diagnoses or prescribing drugs, patients and clinicians connected in a heartfelt way that had a positive impact on both. When we did a post questionnaire, patients said they would come back.
We are psychiatrists. We listen to patients. We reflect and enlighten. And if we really pay attention – even for only 20 minutes – we would be reminded of what we like doing best, and we can magnify our therapeutic efficacy.
Dr. Hammerschlag, a leading proponent of psychoneuroimmunology (mind-body-spirit medicine), is chief of community mental health at the Gesundheit! Institute in Hillsboro, W.Va. He also is affiliated with the Arizona Health Sciences Center at the University of Arizona. In addition, Dr. Hammerschlag is a professional keynote speaker and author of numerous books on healing, spirituality, and other topics. To get in touch with him, e-mail him at info@healingdoc.com.
It’s becoming the exception for a psychiatrist to spend more than 15 minutes speaking face-to-face with patients. This is the unfortunate concomitant of a medical culture that reimburses us more for 15-minute medication reviews than for talking to patients for an hour.
Yet, we know that connecting with patients at some heartfelt level is critical to doing our work. It is the relationship that inspires their trust and encourages them to dare to imagine that they can create new endings to their old stories. It turns out that listening at that level can actually happen in a short time if you are truly present and paying attention.
I recently participated in a community mental health clinic in the streets of Iquitos, Peru, where I went with Dr. Patch Adams, the world’s most recognized humanitarian clown. One hundred clowns from all over the world participated in a collaborative preventive health project in a desperately impoverished section of town called Belen. They are performers, musicians, artists, teachers, students, entrepreneurs, students, and health workers.
We conducted workshops for children (percussion, dance, acrobatics, puppetry); painted homes and public murals; clowned in hospitals, prisons, and shelters; and supported local health organizations.
For the last 3 years, I’ve worked with Amazon Promise, a nonprofit organization that provides health care to indigenous people in the Amazon. I was the first psychiatrist willing to see patients in an open public space, without privacy or psychiatric drugs. I had a remarkable translator who wove my words into her own meaningful story that touched patients. People waited in line without shame, talking about their problems in full view of their neighbors. We discovered in these sessions that good things can happen – even in 20 minutes.
Among this year’s clown group were 20 clinical health professionals (psychologists, counselors, nurses, doctors, social workers, and body workers). We set up four half-day clinics in the streets of Belen, where we knew people would be gathering. We printed fliers that said health professionals who could offer help would be available for people who were experiencing problems at home (with spouses, children, or parents), couldn’t sleep, or had aches in their body.
Before the first clinic, I met with the clinicians and told them about my experiences over the last several years. In those meetings, the clinicians were in an open setting with no privacy, hearing stories that would make their hearts bleed (abuse, abandonment, sexual trauma), and they would wonder how anything in their training could help them deal with such overwhelming problems. I assured them that, in addition to the symptomatic manifestations of such grinding poverty, they would see a remarkable people with extraordinary resilience.
Perhaps the most significant thing we could do was simply listen to their stories: For many patients, 20 minutes with a compassionate listener was an exceptional event. If, in addition, they could help patients identify some strengths, offer some advice, or inspire hope, that would be an additional dividend.
We had no psychiatric drugs, so at the end of the sessions, we would give them vitamins for themselves and their children. I brought along some necklaces with a small silver medallion of the Virgin of Guadalupe that had been blessed by Huichol and Navajo shamans. I suggested to the clinicians that, if they saw patients who might benefit from having this reminder of their time together, they could share these special amulets with a blessing of their own ... "Whatever your heart prompts you to say at the moment."
We did not dress up in our usual clown regalia – only our clown noses identified us. We set up in a schoolyard, loading dock, and empty rooms. Upon arriving, we passed out the flyers and announced our presence through loudspeakers. Clinicians were paired up and each team huddled in a tight circle with their patient(s) so they could hear above the clamor. Clowns playing with children, veterinarians sterilizing dogs and cats, and laboratory technicians taking blood from kids surrounded the teams – all while the community casually strolled by.
Clinicians saw 200 people over 4 days; they listened to the breadth and depth of the human experience. Twenty minutes is a blink of an eyelash when measured against the length of one’s life, but it’s enough time to feel the pain of another and to reach out to touch them with compassion.
It is those moments, when we are reminded of our shared humanity, that make all suffering bearable. In a short time, in a public place, without privacy, not making diagnoses or prescribing drugs, patients and clinicians connected in a heartfelt way that had a positive impact on both. When we did a post questionnaire, patients said they would come back.
We are psychiatrists. We listen to patients. We reflect and enlighten. And if we really pay attention – even for only 20 minutes – we would be reminded of what we like doing best, and we can magnify our therapeutic efficacy.
Dr. Hammerschlag, a leading proponent of psychoneuroimmunology (mind-body-spirit medicine), is chief of community mental health at the Gesundheit! Institute in Hillsboro, W.Va. He also is affiliated with the Arizona Health Sciences Center at the University of Arizona. In addition, Dr. Hammerschlag is a professional keynote speaker and author of numerous books on healing, spirituality, and other topics. To get in touch with him, e-mail him at info@healingdoc.com.
It’s becoming the exception for a psychiatrist to spend more than 15 minutes speaking face-to-face with patients. This is the unfortunate concomitant of a medical culture that reimburses us more for 15-minute medication reviews than for talking to patients for an hour.
Yet, we know that connecting with patients at some heartfelt level is critical to doing our work. It is the relationship that inspires their trust and encourages them to dare to imagine that they can create new endings to their old stories. It turns out that listening at that level can actually happen in a short time if you are truly present and paying attention.
I recently participated in a community mental health clinic in the streets of Iquitos, Peru, where I went with Dr. Patch Adams, the world’s most recognized humanitarian clown. One hundred clowns from all over the world participated in a collaborative preventive health project in a desperately impoverished section of town called Belen. They are performers, musicians, artists, teachers, students, entrepreneurs, students, and health workers.
We conducted workshops for children (percussion, dance, acrobatics, puppetry); painted homes and public murals; clowned in hospitals, prisons, and shelters; and supported local health organizations.
For the last 3 years, I’ve worked with Amazon Promise, a nonprofit organization that provides health care to indigenous people in the Amazon. I was the first psychiatrist willing to see patients in an open public space, without privacy or psychiatric drugs. I had a remarkable translator who wove my words into her own meaningful story that touched patients. People waited in line without shame, talking about their problems in full view of their neighbors. We discovered in these sessions that good things can happen – even in 20 minutes.
Among this year’s clown group were 20 clinical health professionals (psychologists, counselors, nurses, doctors, social workers, and body workers). We set up four half-day clinics in the streets of Belen, where we knew people would be gathering. We printed fliers that said health professionals who could offer help would be available for people who were experiencing problems at home (with spouses, children, or parents), couldn’t sleep, or had aches in their body.
Before the first clinic, I met with the clinicians and told them about my experiences over the last several years. In those meetings, the clinicians were in an open setting with no privacy, hearing stories that would make their hearts bleed (abuse, abandonment, sexual trauma), and they would wonder how anything in their training could help them deal with such overwhelming problems. I assured them that, in addition to the symptomatic manifestations of such grinding poverty, they would see a remarkable people with extraordinary resilience.
Perhaps the most significant thing we could do was simply listen to their stories: For many patients, 20 minutes with a compassionate listener was an exceptional event. If, in addition, they could help patients identify some strengths, offer some advice, or inspire hope, that would be an additional dividend.
We had no psychiatric drugs, so at the end of the sessions, we would give them vitamins for themselves and their children. I brought along some necklaces with a small silver medallion of the Virgin of Guadalupe that had been blessed by Huichol and Navajo shamans. I suggested to the clinicians that, if they saw patients who might benefit from having this reminder of their time together, they could share these special amulets with a blessing of their own ... "Whatever your heart prompts you to say at the moment."
We did not dress up in our usual clown regalia – only our clown noses identified us. We set up in a schoolyard, loading dock, and empty rooms. Upon arriving, we passed out the flyers and announced our presence through loudspeakers. Clinicians were paired up and each team huddled in a tight circle with their patient(s) so they could hear above the clamor. Clowns playing with children, veterinarians sterilizing dogs and cats, and laboratory technicians taking blood from kids surrounded the teams – all while the community casually strolled by.
Clinicians saw 200 people over 4 days; they listened to the breadth and depth of the human experience. Twenty minutes is a blink of an eyelash when measured against the length of one’s life, but it’s enough time to feel the pain of another and to reach out to touch them with compassion.
It is those moments, when we are reminded of our shared humanity, that make all suffering bearable. In a short time, in a public place, without privacy, not making diagnoses or prescribing drugs, patients and clinicians connected in a heartfelt way that had a positive impact on both. When we did a post questionnaire, patients said they would come back.
We are psychiatrists. We listen to patients. We reflect and enlighten. And if we really pay attention – even for only 20 minutes – we would be reminded of what we like doing best, and we can magnify our therapeutic efficacy.
Dr. Hammerschlag, a leading proponent of psychoneuroimmunology (mind-body-spirit medicine), is chief of community mental health at the Gesundheit! Institute in Hillsboro, W.Va. He also is affiliated with the Arizona Health Sciences Center at the University of Arizona. In addition, Dr. Hammerschlag is a professional keynote speaker and author of numerous books on healing, spirituality, and other topics. To get in touch with him, e-mail him at info@healingdoc.com.

Win Whitcomb: Hospital Readmissions Penalties Start Now

The uproar and confusion over readmissions penalties has consumed umpteen hours of senior leaders’ time (especially that of CFOs), not to mention that of front-line nurses, case managers, quality-improvement (QI) coordinators, hospitalists, and others involved in discharge planning and ensuring a safe transition for patients out of the hospital. For many, the math is fuzzy, and for most, the return on investment is even fuzzier. After all, avoided readmissions are lost revenue to those who are running a business known as an acute-care hospital.
Let me start with the conclusion: Eliminating avoidable readmissions is the right thing to do, period. But the financial downside to doing so is probably greater than any upside realized through avoidance of the penalties that began affecting hospital payments on Oct. 1—at least in the fee-for-service world we live in. At some point in the future, when most patients are under a global payment, the math might be clearer, but today, penalties probably won’t offset lost revenue from reduced readmissions added to the cost of paying lots of people to work in meetings (and at the bedside) to devise better care transitions. (Caveat: If your hospital is bursting at the seams with full occupancy, reducing readmissions and replacing them with higher-reimbursing patients, such as those undergoing elective major surgery, likely will be a net financial gain for your hospital.)
Part of the Affordable Care Act (ACA), the Hospital Readmissions Reduction Program (HRRP) will reduce total Medicare DRG reimbursement for hospitals beginning in fiscal-year 2013 based on actual 30-day readmission rates for myocardial infarction (MI), heart failure (HF), and pneumonia that are in excess of risk-adjusted expected rates. The reduction is capped at 1% in 2013, 2% in 2014, and 3% in 2015 and beyond. Hospital readmission rates are based on calculated baseline rates using Medicare data from July 1, 2008, to June 30, 2011.
Cost of a Readmissions-Reduction Program
How much does it cost for a hospital to implement a care-transitions program—such as SHM’s Project BOOST—to reduce readmissions? Last year, I interviewed a dozen hospitals that successfully implemented SHM’s formal mentored implementation program. The result? In the first year of the program, hospitals spent about $170,000 on training and staff time devoted to the project.
Lost Revenue
Let’s look at a sample penalty calculation, then examine a scenario sizing up how revenue is lost when a hospital is successful in reducing readmissions. The ACA defines the payments for excess readmissions as:
The number of patients with the applicable condition (HF, MI, or pneumonia) multiplied by the base DRG payment made for those patients multiplied by the percentage of readmissions beyond the expected.
As an example, let’s take a hospital that treats 500 pneumonia patients (# with the applicable condition), has a base DRG payment for pneumonia of $5,000, and a readmission rate that is 4% higher than expected (in this example, the actual rate is 25% and the expected rate is 24%; 1/25=4%). The penalty is 500 X $5,000 X .04, or $100,000. We’ll assume that the readmission rate for myocardial infarction and heart failure are less than expected, so the total penalty is $100,000.
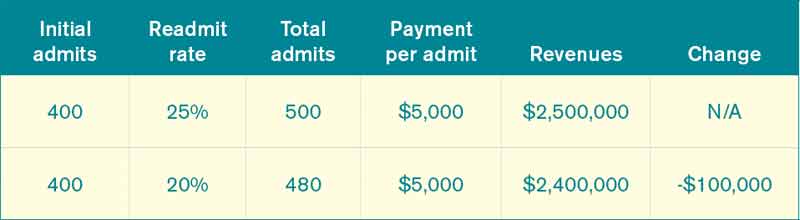
Let’s say the hospital works hard to decrease pneumonia readmissions from 25% to 20% and avoids the penalty. As outlined in Table 1, the hospital will lose $100,000 in revenue (admittedly, reducing readmissions to 20% from 25% represents a big jump, but this is for illustration purposes—we haven’t added in lost revenue from reduced readmissions for other conditions). What’s the final cost of avoiding the $100,000 readmission penalty? Lost revenue of $100,000 plus the cost of implementing the readmission reduction program of $170,000=$270,000.
Why Are We Doing This?
I see the value in care transitions and readmissions-reduction programs, such as Project BOOST, first and foremost as a way to improve patient safety; as such, if implemented effectively, they are likely worth the investment. Second, their value lies in the preparation all hospitals and health systems should be undergoing to remain market-competitive and solvent under global payment systems. Because the penalties in the HRRP might come with lost revenues and the costs of program implementation, be clear about your team’s motivation for reducing readmissions. Your CFO will see to it if I don’t.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View From

SHM is an advocate for the move toward more global payment systems, as well as payment methodologies that reward good outcomes and processes over volume. System improvements require leadership and front-line physicians who are able to implement and evaluate new care-delivery models. SHM offers resources and tools to support the HM community in this era of change through leadership training (www.hospitalmedicine.com/leadership), professional development and mentoring in QI programs (www.hospitalmedicine.org/QI), and other practical tools, such as the value-based purchasing toolkit (www.hospitalmedicine.org/HVBP).
Additionally, the Project BOOST toolkit (www.hospitalmedicine.org/BOOST) includes a return-on-investment calculator to use in your institution’s efforts in reducing readmissions. The calculator is built both for fee-for-service and accountable-care-organization payment models, and it can serve as an adjunct to estimates provided to your hospital of penalties for excess readmissions under HRRP.
The uproar and confusion over readmissions penalties has consumed umpteen hours of senior leaders’ time (especially that of CFOs), not to mention that of front-line nurses, case managers, quality-improvement (QI) coordinators, hospitalists, and others involved in discharge planning and ensuring a safe transition for patients out of the hospital. For many, the math is fuzzy, and for most, the return on investment is even fuzzier. After all, avoided readmissions are lost revenue to those who are running a business known as an acute-care hospital.
Let me start with the conclusion: Eliminating avoidable readmissions is the right thing to do, period. But the financial downside to doing so is probably greater than any upside realized through avoidance of the penalties that began affecting hospital payments on Oct. 1—at least in the fee-for-service world we live in. At some point in the future, when most patients are under a global payment, the math might be clearer, but today, penalties probably won’t offset lost revenue from reduced readmissions added to the cost of paying lots of people to work in meetings (and at the bedside) to devise better care transitions. (Caveat: If your hospital is bursting at the seams with full occupancy, reducing readmissions and replacing them with higher-reimbursing patients, such as those undergoing elective major surgery, likely will be a net financial gain for your hospital.)
Part of the Affordable Care Act (ACA), the Hospital Readmissions Reduction Program (HRRP) will reduce total Medicare DRG reimbursement for hospitals beginning in fiscal-year 2013 based on actual 30-day readmission rates for myocardial infarction (MI), heart failure (HF), and pneumonia that are in excess of risk-adjusted expected rates. The reduction is capped at 1% in 2013, 2% in 2014, and 3% in 2015 and beyond. Hospital readmission rates are based on calculated baseline rates using Medicare data from July 1, 2008, to June 30, 2011.
Cost of a Readmissions-Reduction Program
How much does it cost for a hospital to implement a care-transitions program—such as SHM’s Project BOOST—to reduce readmissions? Last year, I interviewed a dozen hospitals that successfully implemented SHM’s formal mentored implementation program. The result? In the first year of the program, hospitals spent about $170,000 on training and staff time devoted to the project.
Lost Revenue
Let’s look at a sample penalty calculation, then examine a scenario sizing up how revenue is lost when a hospital is successful in reducing readmissions. The ACA defines the payments for excess readmissions as:
The number of patients with the applicable condition (HF, MI, or pneumonia) multiplied by the base DRG payment made for those patients multiplied by the percentage of readmissions beyond the expected.
As an example, let’s take a hospital that treats 500 pneumonia patients (# with the applicable condition), has a base DRG payment for pneumonia of $5,000, and a readmission rate that is 4% higher than expected (in this example, the actual rate is 25% and the expected rate is 24%; 1/25=4%). The penalty is 500 X $5,000 X .04, or $100,000. We’ll assume that the readmission rate for myocardial infarction and heart failure are less than expected, so the total penalty is $100,000.
Let’s say the hospital works hard to decrease pneumonia readmissions from 25% to 20% and avoids the penalty. As outlined in Table 1, the hospital will lose $100,000 in revenue (admittedly, reducing readmissions to 20% from 25% represents a big jump, but this is for illustration purposes—we haven’t added in lost revenue from reduced readmissions for other conditions). What’s the final cost of avoiding the $100,000 readmission penalty? Lost revenue of $100,000 plus the cost of implementing the readmission reduction program of $170,000=$270,000.
Why Are We Doing This?
I see the value in care transitions and readmissions-reduction programs, such as Project BOOST, first and foremost as a way to improve patient safety; as such, if implemented effectively, they are likely worth the investment. Second, their value lies in the preparation all hospitals and health systems should be undergoing to remain market-competitive and solvent under global payment systems. Because the penalties in the HRRP might come with lost revenues and the costs of program implementation, be clear about your team’s motivation for reducing readmissions. Your CFO will see to it if I don’t.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View From
SHM is an advocate for the move toward more global payment systems, as well as payment methodologies that reward good outcomes and processes over volume. System improvements require leadership and front-line physicians who are able to implement and evaluate new care-delivery models. SHM offers resources and tools to support the HM community in this era of change through leadership training (www.hospitalmedicine.com/leadership), professional development and mentoring in QI programs (www.hospitalmedicine.org/QI), and other practical tools, such as the value-based purchasing toolkit (www.hospitalmedicine.org/HVBP).
Additionally, the Project BOOST toolkit (www.hospitalmedicine.org/BOOST) includes a return-on-investment calculator to use in your institution’s efforts in reducing readmissions. The calculator is built both for fee-for-service and accountable-care-organization payment models, and it can serve as an adjunct to estimates provided to your hospital of penalties for excess readmissions under HRRP.
The uproar and confusion over readmissions penalties has consumed umpteen hours of senior leaders’ time (especially that of CFOs), not to mention that of front-line nurses, case managers, quality-improvement (QI) coordinators, hospitalists, and others involved in discharge planning and ensuring a safe transition for patients out of the hospital. For many, the math is fuzzy, and for most, the return on investment is even fuzzier. After all, avoided readmissions are lost revenue to those who are running a business known as an acute-care hospital.
Let me start with the conclusion: Eliminating avoidable readmissions is the right thing to do, period. But the financial downside to doing so is probably greater than any upside realized through avoidance of the penalties that began affecting hospital payments on Oct. 1—at least in the fee-for-service world we live in. At some point in the future, when most patients are under a global payment, the math might be clearer, but today, penalties probably won’t offset lost revenue from reduced readmissions added to the cost of paying lots of people to work in meetings (and at the bedside) to devise better care transitions. (Caveat: If your hospital is bursting at the seams with full occupancy, reducing readmissions and replacing them with higher-reimbursing patients, such as those undergoing elective major surgery, likely will be a net financial gain for your hospital.)
Part of the Affordable Care Act (ACA), the Hospital Readmissions Reduction Program (HRRP) will reduce total Medicare DRG reimbursement for hospitals beginning in fiscal-year 2013 based on actual 30-day readmission rates for myocardial infarction (MI), heart failure (HF), and pneumonia that are in excess of risk-adjusted expected rates. The reduction is capped at 1% in 2013, 2% in 2014, and 3% in 2015 and beyond. Hospital readmission rates are based on calculated baseline rates using Medicare data from July 1, 2008, to June 30, 2011.
Cost of a Readmissions-Reduction Program
How much does it cost for a hospital to implement a care-transitions program—such as SHM’s Project BOOST—to reduce readmissions? Last year, I interviewed a dozen hospitals that successfully implemented SHM’s formal mentored implementation program. The result? In the first year of the program, hospitals spent about $170,000 on training and staff time devoted to the project.
Lost Revenue
Let’s look at a sample penalty calculation, then examine a scenario sizing up how revenue is lost when a hospital is successful in reducing readmissions. The ACA defines the payments for excess readmissions as:
The number of patients with the applicable condition (HF, MI, or pneumonia) multiplied by the base DRG payment made for those patients multiplied by the percentage of readmissions beyond the expected.
As an example, let’s take a hospital that treats 500 pneumonia patients (# with the applicable condition), has a base DRG payment for pneumonia of $5,000, and a readmission rate that is 4% higher than expected (in this example, the actual rate is 25% and the expected rate is 24%; 1/25=4%). The penalty is 500 X $5,000 X .04, or $100,000. We’ll assume that the readmission rate for myocardial infarction and heart failure are less than expected, so the total penalty is $100,000.
Let’s say the hospital works hard to decrease pneumonia readmissions from 25% to 20% and avoids the penalty. As outlined in Table 1, the hospital will lose $100,000 in revenue (admittedly, reducing readmissions to 20% from 25% represents a big jump, but this is for illustration purposes—we haven’t added in lost revenue from reduced readmissions for other conditions). What’s the final cost of avoiding the $100,000 readmission penalty? Lost revenue of $100,000 plus the cost of implementing the readmission reduction program of $170,000=$270,000.
Why Are We Doing This?
I see the value in care transitions and readmissions-reduction programs, such as Project BOOST, first and foremost as a way to improve patient safety; as such, if implemented effectively, they are likely worth the investment. Second, their value lies in the preparation all hospitals and health systems should be undergoing to remain market-competitive and solvent under global payment systems. Because the penalties in the HRRP might come with lost revenues and the costs of program implementation, be clear about your team’s motivation for reducing readmissions. Your CFO will see to it if I don’t.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The View From
SHM is an advocate for the move toward more global payment systems, as well as payment methodologies that reward good outcomes and processes over volume. System improvements require leadership and front-line physicians who are able to implement and evaluate new care-delivery models. SHM offers resources and tools to support the HM community in this era of change through leadership training (www.hospitalmedicine.com/leadership), professional development and mentoring in QI programs (www.hospitalmedicine.org/QI), and other practical tools, such as the value-based purchasing toolkit (www.hospitalmedicine.org/HVBP).
Additionally, the Project BOOST toolkit (www.hospitalmedicine.org/BOOST) includes a return-on-investment calculator to use in your institution’s efforts in reducing readmissions. The calculator is built both for fee-for-service and accountable-care-organization payment models, and it can serve as an adjunct to estimates provided to your hospital of penalties for excess readmissions under HRRP.
Grief -- The Long and the Short of It
The scientific debunking of false beliefs is as relevant today as it was when skeptics took a good look at bloodletting, alchemy, and the balancing of the four humors in the pursuit of good health.
In 1986, after all, Dr. Barry Marshall’s hypothesis that Helicobacter pylori, and not stress, might cause peptic ulcers was deemed "rubbish" – but science prevailed. In 2005, he and his colleague Robin Warren shared the Nobel Prize.
The social sciences, too, depend on science to sort out presumptions from facts.
A prime example was the DARE (Drug Abuse Resistance Education) program widely implemented in schools beginning in the early 1980s. To many, it made sense that police-led drug education and character promotion activities would help vulnerable children "Just Say No" to drugs. But when the program was subjected to well-designed trials, it was determined to be ineffective in preventing drug use and found to have, in some populations, a "boomerang effect" that escalated drug use among children who had participated.
In psychology, as in medicine, the aim is to "do no harm."
That’s why I bring to your attention to a recent article (Curr. Opin. Psychiatry 2012;25:46-51) entitled "Recent trends in the treatment of prolonged grief."
If you think back to a time in your life when you experienced acute grief, you can imagine why it has been assumed that pretty much everyone could benefit from psychotherapy to get them through this profoundly emotional and sometimes physically debilitating experience. Extreme grief can leave people reeling, disoriented, sleepless, and dysregulated. It can make a previously emotionally stable person feel detached and numb or frighteningly out of control.
Now focus your memory on the weeks and months following your acute loss. Chances are that your sleep, appetite, concentration, and mood eventually returned to normal as your exquisitely intense grief reaction subsided into a quieter, more reflective form of longing and sadness.
It turns out, as Dr. Anthony D. Mancini and his associates note in their review, that 50%-60% of people "are resilient and cope remarkably well with loss and would obviously not require professional intervention."
Another 10%-20% come to grips with their grief more slowly, but eventually come to a state of homeostasis on their own timetable.
That leaves a subset of individuals whose symptoms escalate and then persist, perhaps even for years, compromising their function and well-being. People suffering this enduring, complicated grief remain an open and jagged emotional wound. They may become depressed, hopeless, bitter, detached, or wholly focused on their loss.
They need treatment, and benefit from it, just as the small percentage of people who fail to recover after a brush with life-threatening trauma fare better if they receive exposure-based therapy for posttraumatic stress disorder.
Recent meta-analyses of grief therapy for adults conclude that overall effect sizes are vanishingly small to nonexistent when therapy is universally applied.
"By far the most benefit was evidenced in indicated interventions that specifically targeted persons with high levels of distress," the authors wrote. "Curiously, however, even indicated interventions produced effect sizes that were markedly lower than typically found for psychotherapy."
Results were similar in children, although intervening early with grieving children improved efficacy.
So what’s the worst thing that could happen if people not at risk for complicated grief are referred for unnecessary therapy?
Doing harm, of course.
The possibility of introducing iatrogenic pathology is still unresolved, but Dr. Mancini and his associates noted that "grief treatments for unproblematic grief reactions" were included in a review of "potentially harmful" psychological interventions (Perspect. Psychol. Sci. 2007;2:53-70).
Soberingly, there’s a precedent. A specific intervention aimed at preventing PTSD, critical incident stress management, has been shown to interfere with natural recovery.
In a way, it all makes evolutionary sense.
Human life through the ages has been marked by horrific trauma and agonizing sorrow, just as it has been punctuated by moments of ecstatic joy.
Coping well would clearly be a selection-worthy trait in such a context.
The authors recommend that grief therapy be "reserved for children and adults with marked and persistent distress following a loss. The longstanding assumption that grief therapy is appropriate for all grievers is no longer tenable."
When grievers screened for high levels of distress receive exposure-based therapy and the opportunity to cognitively process emotional reactions, there is benefit, several recent studies show. Not surprisingly, antidepressant therapy targeted specifically to grievers suffering symptoms of depression seems to be appropriate as well, since it seems to facilitate participation in recovery.
Specific data are not available to guide in the selection of survivors most at risk for complicated grief, but I think judgment is key.
As a physician, you have seen (and experienced) much grief.
If you detect levels of distress disproportional to the norm, or worry specifically about survivors with pre-existing mental health conditions or a history of many traumas and losses, it would seem reasonable to pay attention and to follow up. Perhaps, like the majority of people coping with loss, they will draw on social supports and inner reserves and heal just fine.
If their distress is extreme and persistent, evidence suggests it would be wise to refer them for psychosocial help in moving on.
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.
The scientific debunking of false beliefs is as relevant today as it was when skeptics took a good look at bloodletting, alchemy, and the balancing of the four humors in the pursuit of good health.
In 1986, after all, Dr. Barry Marshall’s hypothesis that Helicobacter pylori, and not stress, might cause peptic ulcers was deemed "rubbish" – but science prevailed. In 2005, he and his colleague Robin Warren shared the Nobel Prize.
The social sciences, too, depend on science to sort out presumptions from facts.
A prime example was the DARE (Drug Abuse Resistance Education) program widely implemented in schools beginning in the early 1980s. To many, it made sense that police-led drug education and character promotion activities would help vulnerable children "Just Say No" to drugs. But when the program was subjected to well-designed trials, it was determined to be ineffective in preventing drug use and found to have, in some populations, a "boomerang effect" that escalated drug use among children who had participated.
In psychology, as in medicine, the aim is to "do no harm."
That’s why I bring to your attention to a recent article (Curr. Opin. Psychiatry 2012;25:46-51) entitled "Recent trends in the treatment of prolonged grief."
If you think back to a time in your life when you experienced acute grief, you can imagine why it has been assumed that pretty much everyone could benefit from psychotherapy to get them through this profoundly emotional and sometimes physically debilitating experience. Extreme grief can leave people reeling, disoriented, sleepless, and dysregulated. It can make a previously emotionally stable person feel detached and numb or frighteningly out of control.
Now focus your memory on the weeks and months following your acute loss. Chances are that your sleep, appetite, concentration, and mood eventually returned to normal as your exquisitely intense grief reaction subsided into a quieter, more reflective form of longing and sadness.
It turns out, as Dr. Anthony D. Mancini and his associates note in their review, that 50%-60% of people "are resilient and cope remarkably well with loss and would obviously not require professional intervention."
Another 10%-20% come to grips with their grief more slowly, but eventually come to a state of homeostasis on their own timetable.
That leaves a subset of individuals whose symptoms escalate and then persist, perhaps even for years, compromising their function and well-being. People suffering this enduring, complicated grief remain an open and jagged emotional wound. They may become depressed, hopeless, bitter, detached, or wholly focused on their loss.
They need treatment, and benefit from it, just as the small percentage of people who fail to recover after a brush with life-threatening trauma fare better if they receive exposure-based therapy for posttraumatic stress disorder.
Recent meta-analyses of grief therapy for adults conclude that overall effect sizes are vanishingly small to nonexistent when therapy is universally applied.
"By far the most benefit was evidenced in indicated interventions that specifically targeted persons with high levels of distress," the authors wrote. "Curiously, however, even indicated interventions produced effect sizes that were markedly lower than typically found for psychotherapy."
Results were similar in children, although intervening early with grieving children improved efficacy.
So what’s the worst thing that could happen if people not at risk for complicated grief are referred for unnecessary therapy?
Doing harm, of course.
The possibility of introducing iatrogenic pathology is still unresolved, but Dr. Mancini and his associates noted that "grief treatments for unproblematic grief reactions" were included in a review of "potentially harmful" psychological interventions (Perspect. Psychol. Sci. 2007;2:53-70).
Soberingly, there’s a precedent. A specific intervention aimed at preventing PTSD, critical incident stress management, has been shown to interfere with natural recovery.
In a way, it all makes evolutionary sense.
Human life through the ages has been marked by horrific trauma and agonizing sorrow, just as it has been punctuated by moments of ecstatic joy.
Coping well would clearly be a selection-worthy trait in such a context.
The authors recommend that grief therapy be "reserved for children and adults with marked and persistent distress following a loss. The longstanding assumption that grief therapy is appropriate for all grievers is no longer tenable."
When grievers screened for high levels of distress receive exposure-based therapy and the opportunity to cognitively process emotional reactions, there is benefit, several recent studies show. Not surprisingly, antidepressant therapy targeted specifically to grievers suffering symptoms of depression seems to be appropriate as well, since it seems to facilitate participation in recovery.
Specific data are not available to guide in the selection of survivors most at risk for complicated grief, but I think judgment is key.
As a physician, you have seen (and experienced) much grief.
If you detect levels of distress disproportional to the norm, or worry specifically about survivors with pre-existing mental health conditions or a history of many traumas and losses, it would seem reasonable to pay attention and to follow up. Perhaps, like the majority of people coping with loss, they will draw on social supports and inner reserves and heal just fine.
If their distress is extreme and persistent, evidence suggests it would be wise to refer them for psychosocial help in moving on.
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.
The scientific debunking of false beliefs is as relevant today as it was when skeptics took a good look at bloodletting, alchemy, and the balancing of the four humors in the pursuit of good health.
In 1986, after all, Dr. Barry Marshall’s hypothesis that Helicobacter pylori, and not stress, might cause peptic ulcers was deemed "rubbish" – but science prevailed. In 2005, he and his colleague Robin Warren shared the Nobel Prize.
The social sciences, too, depend on science to sort out presumptions from facts.
A prime example was the DARE (Drug Abuse Resistance Education) program widely implemented in schools beginning in the early 1980s. To many, it made sense that police-led drug education and character promotion activities would help vulnerable children "Just Say No" to drugs. But when the program was subjected to well-designed trials, it was determined to be ineffective in preventing drug use and found to have, in some populations, a "boomerang effect" that escalated drug use among children who had participated.
In psychology, as in medicine, the aim is to "do no harm."
That’s why I bring to your attention to a recent article (Curr. Opin. Psychiatry 2012;25:46-51) entitled "Recent trends in the treatment of prolonged grief."
If you think back to a time in your life when you experienced acute grief, you can imagine why it has been assumed that pretty much everyone could benefit from psychotherapy to get them through this profoundly emotional and sometimes physically debilitating experience. Extreme grief can leave people reeling, disoriented, sleepless, and dysregulated. It can make a previously emotionally stable person feel detached and numb or frighteningly out of control.
Now focus your memory on the weeks and months following your acute loss. Chances are that your sleep, appetite, concentration, and mood eventually returned to normal as your exquisitely intense grief reaction subsided into a quieter, more reflective form of longing and sadness.
It turns out, as Dr. Anthony D. Mancini and his associates note in their review, that 50%-60% of people "are resilient and cope remarkably well with loss and would obviously not require professional intervention."
Another 10%-20% come to grips with their grief more slowly, but eventually come to a state of homeostasis on their own timetable.
That leaves a subset of individuals whose symptoms escalate and then persist, perhaps even for years, compromising their function and well-being. People suffering this enduring, complicated grief remain an open and jagged emotional wound. They may become depressed, hopeless, bitter, detached, or wholly focused on their loss.
They need treatment, and benefit from it, just as the small percentage of people who fail to recover after a brush with life-threatening trauma fare better if they receive exposure-based therapy for posttraumatic stress disorder.
Recent meta-analyses of grief therapy for adults conclude that overall effect sizes are vanishingly small to nonexistent when therapy is universally applied.
"By far the most benefit was evidenced in indicated interventions that specifically targeted persons with high levels of distress," the authors wrote. "Curiously, however, even indicated interventions produced effect sizes that were markedly lower than typically found for psychotherapy."
Results were similar in children, although intervening early with grieving children improved efficacy.
So what’s the worst thing that could happen if people not at risk for complicated grief are referred for unnecessary therapy?
Doing harm, of course.
The possibility of introducing iatrogenic pathology is still unresolved, but Dr. Mancini and his associates noted that "grief treatments for unproblematic grief reactions" were included in a review of "potentially harmful" psychological interventions (Perspect. Psychol. Sci. 2007;2:53-70).
Soberingly, there’s a precedent. A specific intervention aimed at preventing PTSD, critical incident stress management, has been shown to interfere with natural recovery.
In a way, it all makes evolutionary sense.
Human life through the ages has been marked by horrific trauma and agonizing sorrow, just as it has been punctuated by moments of ecstatic joy.
Coping well would clearly be a selection-worthy trait in such a context.
The authors recommend that grief therapy be "reserved for children and adults with marked and persistent distress following a loss. The longstanding assumption that grief therapy is appropriate for all grievers is no longer tenable."
When grievers screened for high levels of distress receive exposure-based therapy and the opportunity to cognitively process emotional reactions, there is benefit, several recent studies show. Not surprisingly, antidepressant therapy targeted specifically to grievers suffering symptoms of depression seems to be appropriate as well, since it seems to facilitate participation in recovery.
Specific data are not available to guide in the selection of survivors most at risk for complicated grief, but I think judgment is key.
As a physician, you have seen (and experienced) much grief.
If you detect levels of distress disproportional to the norm, or worry specifically about survivors with pre-existing mental health conditions or a history of many traumas and losses, it would seem reasonable to pay attention and to follow up. Perhaps, like the majority of people coping with loss, they will draw on social supports and inner reserves and heal just fine.
If their distress is extreme and persistent, evidence suggests it would be wise to refer them for psychosocial help in moving on.
Dr. Freed is a psychologist in Santa Barbara, Calif., and a medical journalist.

A Fellowship of Surgeons
My proudest moment as a young surgeon occurred on a clear autumn evening in Atlanta in 1980. On that night I donned the black robe and mortarboard for the last time (finally!) and became a Fellow of the American College of Surgeons. My mentors had emphasized during residency that in order to be recognized as a full-fledged surgeon, attaining fellowship in the College was mandatory. During that era, the honor of becoming a Fellow was sufficient reason to make it a young surgeon’s prime goal.
Over the ensuing 32 years, fellowship in the College has meant much more to me and it has served as a key building block in the foundation of my entire professional career. The annual Clinical Congress, state chapter meetings, and participation in numerous ACS committees have afforded me opportunities to interact and learn from fellow surgeons throughout our country and around the world. Many of these interactions have resulted in lifelong friendships that are renewed at least on an annual basis at the fall Congress and at other ACS events.
Early in my career, I participated in many of the College’s educational offerings. The postgraduate courses and symposia significantly extended and refined what I had learned during residency. In more recent years, under the leadership of Dr. Ajit Sachdeva, the Division of Education has kept pace with the times and now provides Fellows the even greater opportunities to improve and cultivate their skills as well as their knowledge.
Later in my career I was able to participate in the genesis of these educational courses and I have had the privilege of teaching a few – the most memorable being the Surgeons as Leaders course. More than 400 surgeons have participated in this course, which was created to provide them with the skills they need to be more effective leaders in their institutions and in the political arena. Involvement in these ACS educational activities – both as a learner and as a teacher – has been a very satisfying and meaningful aspect of my surgical career.
The ACS mantra of "Inspiring Quality" is so appropriate for this year’s celebration because the College has been in the forefront of promoting quality patient care throughout its 100-year history. Soon after its founding in 1913, the College established the Hospital Standards Committee to develop guidelines for hospitals seeking ACS accreditation. The College was the sole agency for accreditation of hospitals until the 1950s, when the ACS joined with the American Medical Association, American Hospital Association, and American College of Physicians to form the Joint Commission on Accreditation of Hospitals (now The Joint Commission).
The College went on to establish the Committee on Trauma (COT), which set out criteria for accreditation of trauma centers. This program has led to marked improvements in the level of care that trauma patients receive throughout the United States. The COT also established the Advanced Trauma Life Support® (ATLS®) course, which has been presented to thousands of medical professionals throughout the world, saving an untold number of lives.
Most recently, the ACS took responsibility for moving a Veterans Affairs surgical quality improvement program into the private sector. The College’s National Surgical Quality Improvement Program (ACS NSQIP®) is now in place at nearly 500 hospitals of all sizes. It is gaining widespread recognition among health care policy makers as the most effective program for measuring outcomes of care because of its use of risk-adjusted clinical data rather than claims data. Furthermore, evidence is rapidly accumulating that surgical care is significantly improved in those institutions that adopt this program. This initiative is in perfect alignment with the ongoing governmental reforms of the nation’s health care system, and surgeons can proudly claim it as their own.
The government’s involvement in health care started to increase in the 1980s as health care spending started to consume a significant portion of the federal budget. C. Rollins "Rollo" Hanlon, M.D., FACS, recognized the potential effects of government intervention on patient care and established the College’s Washington Office during his term as ACS Director. The capabilities and functions of this office have grown considerably since then under the leadership of subsequent Executive Directors, including Paul Ebert, M.D., FACS, Tom Russell, M.D., FACS, and David B. Hoyt, M.D., FACS. Although progress is not always easily measured in the complex world of political advocacy, surgery’s voice has been heard and has positively influenced national legislation. It is vital that all surgeons, regardless of specialty, support this aspect of the College’s work.
So happy birthday, ACS! I am extremely proud and gratified to have been part of you for nearly a third of your 100-year history. Much has been accomplished, but there is much more to do – especially during the next decade or so as our health care system goes through a major overhaul. Being true to your long-standing principle of promoting patient-centered, quality surgical care, I am certain you will be up to the challenge.
Dr. Layton F. "Bing" Rikkers is Editor in Chief of Surgery News.
My proudest moment as a young surgeon occurred on a clear autumn evening in Atlanta in 1980. On that night I donned the black robe and mortarboard for the last time (finally!) and became a Fellow of the American College of Surgeons. My mentors had emphasized during residency that in order to be recognized as a full-fledged surgeon, attaining fellowship in the College was mandatory. During that era, the honor of becoming a Fellow was sufficient reason to make it a young surgeon’s prime goal.
Over the ensuing 32 years, fellowship in the College has meant much more to me and it has served as a key building block in the foundation of my entire professional career. The annual Clinical Congress, state chapter meetings, and participation in numerous ACS committees have afforded me opportunities to interact and learn from fellow surgeons throughout our country and around the world. Many of these interactions have resulted in lifelong friendships that are renewed at least on an annual basis at the fall Congress and at other ACS events.
Early in my career, I participated in many of the College’s educational offerings. The postgraduate courses and symposia significantly extended and refined what I had learned during residency. In more recent years, under the leadership of Dr. Ajit Sachdeva, the Division of Education has kept pace with the times and now provides Fellows the even greater opportunities to improve and cultivate their skills as well as their knowledge.
Later in my career I was able to participate in the genesis of these educational courses and I have had the privilege of teaching a few – the most memorable being the Surgeons as Leaders course. More than 400 surgeons have participated in this course, which was created to provide them with the skills they need to be more effective leaders in their institutions and in the political arena. Involvement in these ACS educational activities – both as a learner and as a teacher – has been a very satisfying and meaningful aspect of my surgical career.
The ACS mantra of "Inspiring Quality" is so appropriate for this year’s celebration because the College has been in the forefront of promoting quality patient care throughout its 100-year history. Soon after its founding in 1913, the College established the Hospital Standards Committee to develop guidelines for hospitals seeking ACS accreditation. The College was the sole agency for accreditation of hospitals until the 1950s, when the ACS joined with the American Medical Association, American Hospital Association, and American College of Physicians to form the Joint Commission on Accreditation of Hospitals (now The Joint Commission).
The College went on to establish the Committee on Trauma (COT), which set out criteria for accreditation of trauma centers. This program has led to marked improvements in the level of care that trauma patients receive throughout the United States. The COT also established the Advanced Trauma Life Support® (ATLS®) course, which has been presented to thousands of medical professionals throughout the world, saving an untold number of lives.
Most recently, the ACS took responsibility for moving a Veterans Affairs surgical quality improvement program into the private sector. The College’s National Surgical Quality Improvement Program (ACS NSQIP®) is now in place at nearly 500 hospitals of all sizes. It is gaining widespread recognition among health care policy makers as the most effective program for measuring outcomes of care because of its use of risk-adjusted clinical data rather than claims data. Furthermore, evidence is rapidly accumulating that surgical care is significantly improved in those institutions that adopt this program. This initiative is in perfect alignment with the ongoing governmental reforms of the nation’s health care system, and surgeons can proudly claim it as their own.
The government’s involvement in health care started to increase in the 1980s as health care spending started to consume a significant portion of the federal budget. C. Rollins "Rollo" Hanlon, M.D., FACS, recognized the potential effects of government intervention on patient care and established the College’s Washington Office during his term as ACS Director. The capabilities and functions of this office have grown considerably since then under the leadership of subsequent Executive Directors, including Paul Ebert, M.D., FACS, Tom Russell, M.D., FACS, and David B. Hoyt, M.D., FACS. Although progress is not always easily measured in the complex world of political advocacy, surgery’s voice has been heard and has positively influenced national legislation. It is vital that all surgeons, regardless of specialty, support this aspect of the College’s work.
So happy birthday, ACS! I am extremely proud and gratified to have been part of you for nearly a third of your 100-year history. Much has been accomplished, but there is much more to do – especially during the next decade or so as our health care system goes through a major overhaul. Being true to your long-standing principle of promoting patient-centered, quality surgical care, I am certain you will be up to the challenge.
Dr. Layton F. "Bing" Rikkers is Editor in Chief of Surgery News.
My proudest moment as a young surgeon occurred on a clear autumn evening in Atlanta in 1980. On that night I donned the black robe and mortarboard for the last time (finally!) and became a Fellow of the American College of Surgeons. My mentors had emphasized during residency that in order to be recognized as a full-fledged surgeon, attaining fellowship in the College was mandatory. During that era, the honor of becoming a Fellow was sufficient reason to make it a young surgeon’s prime goal.
Over the ensuing 32 years, fellowship in the College has meant much more to me and it has served as a key building block in the foundation of my entire professional career. The annual Clinical Congress, state chapter meetings, and participation in numerous ACS committees have afforded me opportunities to interact and learn from fellow surgeons throughout our country and around the world. Many of these interactions have resulted in lifelong friendships that are renewed at least on an annual basis at the fall Congress and at other ACS events.
Early in my career, I participated in many of the College’s educational offerings. The postgraduate courses and symposia significantly extended and refined what I had learned during residency. In more recent years, under the leadership of Dr. Ajit Sachdeva, the Division of Education has kept pace with the times and now provides Fellows the even greater opportunities to improve and cultivate their skills as well as their knowledge.
Later in my career I was able to participate in the genesis of these educational courses and I have had the privilege of teaching a few – the most memorable being the Surgeons as Leaders course. More than 400 surgeons have participated in this course, which was created to provide them with the skills they need to be more effective leaders in their institutions and in the political arena. Involvement in these ACS educational activities – both as a learner and as a teacher – has been a very satisfying and meaningful aspect of my surgical career.
The ACS mantra of "Inspiring Quality" is so appropriate for this year’s celebration because the College has been in the forefront of promoting quality patient care throughout its 100-year history. Soon after its founding in 1913, the College established the Hospital Standards Committee to develop guidelines for hospitals seeking ACS accreditation. The College was the sole agency for accreditation of hospitals until the 1950s, when the ACS joined with the American Medical Association, American Hospital Association, and American College of Physicians to form the Joint Commission on Accreditation of Hospitals (now The Joint Commission).
The College went on to establish the Committee on Trauma (COT), which set out criteria for accreditation of trauma centers. This program has led to marked improvements in the level of care that trauma patients receive throughout the United States. The COT also established the Advanced Trauma Life Support® (ATLS®) course, which has been presented to thousands of medical professionals throughout the world, saving an untold number of lives.
Most recently, the ACS took responsibility for moving a Veterans Affairs surgical quality improvement program into the private sector. The College’s National Surgical Quality Improvement Program (ACS NSQIP®) is now in place at nearly 500 hospitals of all sizes. It is gaining widespread recognition among health care policy makers as the most effective program for measuring outcomes of care because of its use of risk-adjusted clinical data rather than claims data. Furthermore, evidence is rapidly accumulating that surgical care is significantly improved in those institutions that adopt this program. This initiative is in perfect alignment with the ongoing governmental reforms of the nation’s health care system, and surgeons can proudly claim it as their own.
The government’s involvement in health care started to increase in the 1980s as health care spending started to consume a significant portion of the federal budget. C. Rollins "Rollo" Hanlon, M.D., FACS, recognized the potential effects of government intervention on patient care and established the College’s Washington Office during his term as ACS Director. The capabilities and functions of this office have grown considerably since then under the leadership of subsequent Executive Directors, including Paul Ebert, M.D., FACS, Tom Russell, M.D., FACS, and David B. Hoyt, M.D., FACS. Although progress is not always easily measured in the complex world of political advocacy, surgery’s voice has been heard and has positively influenced national legislation. It is vital that all surgeons, regardless of specialty, support this aspect of the College’s work.
So happy birthday, ACS! I am extremely proud and gratified to have been part of you for nearly a third of your 100-year history. Much has been accomplished, but there is much more to do – especially during the next decade or so as our health care system goes through a major overhaul. Being true to your long-standing principle of promoting patient-centered, quality surgical care, I am certain you will be up to the challenge.
Dr. Layton F. "Bing" Rikkers is Editor in Chief of Surgery News.

Win Whitcomb: Inflexible, Big-Box EHRs Endanger the QI Movement

In “The Lean Startup,” author Eric Ries notes that in its early stages, his gaming company would routinely issue new versions of their software application several times each day. Continuous deployment—the process Ries’ company used—leveraged such Lean principles as reduced batch size and continuous learning based on end-user feedback to achieve rapid improvements in their product.
Ries says companies that learn the quickest about what the customer wants, and can incorporate that information into products more efficiently, stand the greatest chance of succeeding. A software engineer by trade, Ries uses many examples of companies that have succeeded with this approach, none of which are from healthcare.
In stark relief, the chief technology hospitalists interface with daily is the electronic health record (EHR), widely recognized as a system that fails to consider the end-user experience, that is unable to interoperate with other software, and is incapable of using data for quality improvement (QI). The PDSA (“plan, do, study, act”) cycle is the foundation of QI activities and relies on rapidly incorporating observations made by those performing the work to create novel workflows and processes based on learning. EHRs, by digitizing health information, theoretically provide the ideal tool for supporting QI.
The reality is that EHRs have been a colossal disappointment with regard to QI efforts. The space in and around EHR effectively represents “dead zones” for innovation and improvement. Mandl and Kohane note:
EHR companies have followed a business model whereby they control all data, rather than liberating the data for use in innovative applications in clinical care.
Conducting a Google-style search of an EHR database usually requires involvement of a clinician’s information services department and often the specialized knowledge and cooperation of the vendor’s technical teams.
Greg Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Hospital Innovation and Improvement, recently provided testimony to the Office of the National Coordinator for Health Information Technology about the challenges current EHRs present to QI efforts and what features EHRs need to incorporate to better serve the needs of patients and clinicians. Dr. Maynard answered a few questions for The Hospitalist:
Q: What is it about current EHRs that make continuous improvement so difficult?
A: EHRs were built for fiscal and administrative purposes, not for quality improvement and safety. The administrative/fiscal roots of today’s IT systems lead to poor availability of clinical, quality, and safety data. In many medical centers and practices, the great majority of information available is months-old administrative data, which does not lend itself to rapid cycle improvement.
Q: Why is the PDSA cycle endangered in most systems?
A: EHRs often do not facilitate rapid-cycle, PDSA-style improvements on a small pilot scale. Most improvement teams get one shot to get the clinical decision support and data-capture tools correct after months of waiting in queue and development time. Any request for revisions and refinements is treated as a failure of the improvement team, and it is often difficult or impossible to pilot new tools in a limited setting.
Q: What features would you like to see in EHRs that would facilitate QI?
A: We need a user-friendly interface for clinicians and for data analysts/reporters. Other industries have common data formats to allow for sharing of information across disparate systems. We need the same capability for clinical information in healthcare. Also, a change in architecture of EHRs and other health IT tools that allows for not just interoperability but substitutable options is required. In the more “app”-like environment, innovation and flexibility would be the rule. An underlying architecture could have different plug-and-play modules for different functions. Some companies are overcoming the current barriers to provide wonderful, easy-to-generate and useful reports, but most are stymied by proprietary systems.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
In “The Lean Startup,” author Eric Ries notes that in its early stages, his gaming company would routinely issue new versions of their software application several times each day. Continuous deployment—the process Ries’ company used—leveraged such Lean principles as reduced batch size and continuous learning based on end-user feedback to achieve rapid improvements in their product.
Ries says companies that learn the quickest about what the customer wants, and can incorporate that information into products more efficiently, stand the greatest chance of succeeding. A software engineer by trade, Ries uses many examples of companies that have succeeded with this approach, none of which are from healthcare.
In stark relief, the chief technology hospitalists interface with daily is the electronic health record (EHR), widely recognized as a system that fails to consider the end-user experience, that is unable to interoperate with other software, and is incapable of using data for quality improvement (QI). The PDSA (“plan, do, study, act”) cycle is the foundation of QI activities and relies on rapidly incorporating observations made by those performing the work to create novel workflows and processes based on learning. EHRs, by digitizing health information, theoretically provide the ideal tool for supporting QI.
The reality is that EHRs have been a colossal disappointment with regard to QI efforts. The space in and around EHR effectively represents “dead zones” for innovation and improvement. Mandl and Kohane note:
EHR companies have followed a business model whereby they control all data, rather than liberating the data for use in innovative applications in clinical care.
Conducting a Google-style search of an EHR database usually requires involvement of a clinician’s information services department and often the specialized knowledge and cooperation of the vendor’s technical teams.
Greg Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Hospital Innovation and Improvement, recently provided testimony to the Office of the National Coordinator for Health Information Technology about the challenges current EHRs present to QI efforts and what features EHRs need to incorporate to better serve the needs of patients and clinicians. Dr. Maynard answered a few questions for The Hospitalist:
Q: What is it about current EHRs that make continuous improvement so difficult?
A: EHRs were built for fiscal and administrative purposes, not for quality improvement and safety. The administrative/fiscal roots of today’s IT systems lead to poor availability of clinical, quality, and safety data. In many medical centers and practices, the great majority of information available is months-old administrative data, which does not lend itself to rapid cycle improvement.
Q: Why is the PDSA cycle endangered in most systems?
A: EHRs often do not facilitate rapid-cycle, PDSA-style improvements on a small pilot scale. Most improvement teams get one shot to get the clinical decision support and data-capture tools correct after months of waiting in queue and development time. Any request for revisions and refinements is treated as a failure of the improvement team, and it is often difficult or impossible to pilot new tools in a limited setting.
Q: What features would you like to see in EHRs that would facilitate QI?
A: We need a user-friendly interface for clinicians and for data analysts/reporters. Other industries have common data formats to allow for sharing of information across disparate systems. We need the same capability for clinical information in healthcare. Also, a change in architecture of EHRs and other health IT tools that allows for not just interoperability but substitutable options is required. In the more “app”-like environment, innovation and flexibility would be the rule. An underlying architecture could have different plug-and-play modules for different functions. Some companies are overcoming the current barriers to provide wonderful, easy-to-generate and useful reports, but most are stymied by proprietary systems.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
In “The Lean Startup,” author Eric Ries notes that in its early stages, his gaming company would routinely issue new versions of their software application several times each day. Continuous deployment—the process Ries’ company used—leveraged such Lean principles as reduced batch size and continuous learning based on end-user feedback to achieve rapid improvements in their product.
Ries says companies that learn the quickest about what the customer wants, and can incorporate that information into products more efficiently, stand the greatest chance of succeeding. A software engineer by trade, Ries uses many examples of companies that have succeeded with this approach, none of which are from healthcare.
In stark relief, the chief technology hospitalists interface with daily is the electronic health record (EHR), widely recognized as a system that fails to consider the end-user experience, that is unable to interoperate with other software, and is incapable of using data for quality improvement (QI). The PDSA (“plan, do, study, act”) cycle is the foundation of QI activities and relies on rapidly incorporating observations made by those performing the work to create novel workflows and processes based on learning. EHRs, by digitizing health information, theoretically provide the ideal tool for supporting QI.
The reality is that EHRs have been a colossal disappointment with regard to QI efforts. The space in and around EHR effectively represents “dead zones” for innovation and improvement. Mandl and Kohane note:
EHR companies have followed a business model whereby they control all data, rather than liberating the data for use in innovative applications in clinical care.
Conducting a Google-style search of an EHR database usually requires involvement of a clinician’s information services department and often the specialized knowledge and cooperation of the vendor’s technical teams.
Greg Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Hospital Innovation and Improvement, recently provided testimony to the Office of the National Coordinator for Health Information Technology about the challenges current EHRs present to QI efforts and what features EHRs need to incorporate to better serve the needs of patients and clinicians. Dr. Maynard answered a few questions for The Hospitalist:
Q: What is it about current EHRs that make continuous improvement so difficult?
A: EHRs were built for fiscal and administrative purposes, not for quality improvement and safety. The administrative/fiscal roots of today’s IT systems lead to poor availability of clinical, quality, and safety data. In many medical centers and practices, the great majority of information available is months-old administrative data, which does not lend itself to rapid cycle improvement.
Q: Why is the PDSA cycle endangered in most systems?
A: EHRs often do not facilitate rapid-cycle, PDSA-style improvements on a small pilot scale. Most improvement teams get one shot to get the clinical decision support and data-capture tools correct after months of waiting in queue and development time. Any request for revisions and refinements is treated as a failure of the improvement team, and it is often difficult or impossible to pilot new tools in a limited setting.
Q: What features would you like to see in EHRs that would facilitate QI?
A: We need a user-friendly interface for clinicians and for data analysts/reporters. Other industries have common data formats to allow for sharing of information across disparate systems. We need the same capability for clinical information in healthcare. Also, a change in architecture of EHRs and other health IT tools that allows for not just interoperability but substitutable options is required. In the more “app”-like environment, innovation and flexibility would be the rule. An underlying architecture could have different plug-and-play modules for different functions. Some companies are overcoming the current barriers to provide wonderful, easy-to-generate and useful reports, but most are stymied by proprietary systems.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.