User login
Narcotic analgesia for breastfeeding women
Editor’s Note: This is the final installment of a six-part series that reviews key concepts and articles that ob.gyns. can use to prepare for the American Board of Obstetrics and Gynecology Maintenance of Certification examination. The series is adapted from Ob/Gyn Board Master (obgynboardmaster.com), an online board review course created by Erudyte. This month’s edition of the Board Corner focuses on narcotic analgesia for breastfeeding women.
The American College of Obstetrics and Gynecologists “Practice Advisories” are released when there is an important clinical issue that needs immediate attention from ob.gyn. clinicians. On April 27, 2017, ACOG joined with the Society for Maternal-Fetal Medicine and the Academy of Breastfeeding Medicine to issue a new practice advisory with recommendations on opiate analgesia in breastfeeding women.1 These Practice Advisories contain material that may be tested on a board exam. We recommend that you read this Practice Advisory and review it carefully.

A. Morphine IV
B. Butorphanol
C. Acetaminophen with codeine
D. Hydromorphone
E. Morphine (given orally)
The correct answer is C.
Acetaminophen with codeine (aka Tylenol #3 or Tylenol #4) is the least appropriate first-choice narcotic in a breastfeeding postpartum patient after Cesarean delivery as it is the only narcotic among the choices that is metabolized by the enzyme CYP2D6. Morphine, butorphanol, and hydromorphone are all metabolized by CYP450. If a narcotic is indicated, it is better to choose one that is not metabolized by CYP2D6 because of potential side effects in both mothers and infants who may be “CYP2D6 ultrametabolizers” or “CYP2D6 poor metabolizers.”
Key points
The key points to remember are:
1. Do not use codeine or tramadol as a first-line narcotic choice in breastfeeding mothers, if possible, because of variable side effects in mothers and infants.
2. The preferred narcotics to use when breastfeeding are butorphanol, morphine, or hydromorphone.

3. If codeine or tramadol is used in breastfeeding women, the clinician should speak with the patient and family about the possible side effects and the recent labeling changes required by the Food and Drug Administration.
Literature summary
In April, the Food and Drug Administration issued a safety alert and said it is requiring labeling changes for prescription medications containing codeine and tramadol. Specifically, the agency warned against use of codeine and tramadol when breastfeeding. This change is the result of the fact that certain people metabolize codeine and tramadol differently. There are some people – considered CYP2D6 “ultrarapid metabolizers” – who can have levels of the drug in their breast milk that can cause excessive sleepiness and depressed breathing in infants. There is one report of an infant death resulting from codeine use. The frequency of these “rapid metabolizers” is about 4%-5% in the United States.
In addition to the effects on breastfed infants, there are effects on the mother as well. This is because 6% of patients in the United States are “poor metabolizers” who have insufficient pain relief, as well as greater side effects.
Hydrocodone and oxycodone are not addressed in the recent labeling changes. However, “ultrarapid metabolizers” do show more pain relief and pupil restriction.
When comparing codeine with nonsteroidal anti-inflammatory medications (NSAIDs) in abdominal surgery, nine randomized trials failed to show that codeine provided superior pain relief.
Hydromorphone, butorphanol, and morphine are not metabolized by CYP2D6 so the problems faced by “ultrarapid metabolizers” or “poor metabolizers” is not an issue.
Ob.gyns. should utilize regional anesthesia, NSAIDs, and acetaminophen (without codeine) to help decrease the risks of anesthesia while still ensuring adequate pain relief. Ob.gyns. should closely monitor their patients on narcotics for any side effects in both mothers and infants, especially central nervous system depression.
Dr. Kairis is an assistant professor in the department of gynecology and obstetrics at Loma Linda (Calif.) University Health and is the director of the Women’s Sexual Medicine Program there. She is on the editorial committee of the Ob/Gyn Board Master. Dr. Siddighi is editor in chief of the Ob/Gyn Board Master and director of female pelvic medicine and reconstructive surgery and director of grand rounds at Loma Linda University Health. Ob.Gyn. News and Ob/Gyn Board Master are owned by the same parent company, Frontline Medical Communications.
Reference
1. Practice Advisory on Codeine and Tramadol for Breastfeeding Women. April 27, 2017. American College of Obstetricians and Gynecologists.
Editor’s Note: This is the final installment of a six-part series that reviews key concepts and articles that ob.gyns. can use to prepare for the American Board of Obstetrics and Gynecology Maintenance of Certification examination. The series is adapted from Ob/Gyn Board Master (obgynboardmaster.com), an online board review course created by Erudyte. This month’s edition of the Board Corner focuses on narcotic analgesia for breastfeeding women.
The American College of Obstetrics and Gynecologists “Practice Advisories” are released when there is an important clinical issue that needs immediate attention from ob.gyn. clinicians. On April 27, 2017, ACOG joined with the Society for Maternal-Fetal Medicine and the Academy of Breastfeeding Medicine to issue a new practice advisory with recommendations on opiate analgesia in breastfeeding women.1 These Practice Advisories contain material that may be tested on a board exam. We recommend that you read this Practice Advisory and review it carefully.
A. Morphine IV
B. Butorphanol
C. Acetaminophen with codeine
D. Hydromorphone
E. Morphine (given orally)
The correct answer is C.
Acetaminophen with codeine (aka Tylenol #3 or Tylenol #4) is the least appropriate first-choice narcotic in a breastfeeding postpartum patient after Cesarean delivery as it is the only narcotic among the choices that is metabolized by the enzyme CYP2D6. Morphine, butorphanol, and hydromorphone are all metabolized by CYP450. If a narcotic is indicated, it is better to choose one that is not metabolized by CYP2D6 because of potential side effects in both mothers and infants who may be “CYP2D6 ultrametabolizers” or “CYP2D6 poor metabolizers.”
Key points
The key points to remember are:
1. Do not use codeine or tramadol as a first-line narcotic choice in breastfeeding mothers, if possible, because of variable side effects in mothers and infants.
2. The preferred narcotics to use when breastfeeding are butorphanol, morphine, or hydromorphone.
3. If codeine or tramadol is used in breastfeeding women, the clinician should speak with the patient and family about the possible side effects and the recent labeling changes required by the Food and Drug Administration.
Literature summary
In April, the Food and Drug Administration issued a safety alert and said it is requiring labeling changes for prescription medications containing codeine and tramadol. Specifically, the agency warned against use of codeine and tramadol when breastfeeding. This change is the result of the fact that certain people metabolize codeine and tramadol differently. There are some people – considered CYP2D6 “ultrarapid metabolizers” – who can have levels of the drug in their breast milk that can cause excessive sleepiness and depressed breathing in infants. There is one report of an infant death resulting from codeine use. The frequency of these “rapid metabolizers” is about 4%-5% in the United States.
In addition to the effects on breastfed infants, there are effects on the mother as well. This is because 6% of patients in the United States are “poor metabolizers” who have insufficient pain relief, as well as greater side effects.
Hydrocodone and oxycodone are not addressed in the recent labeling changes. However, “ultrarapid metabolizers” do show more pain relief and pupil restriction.
When comparing codeine with nonsteroidal anti-inflammatory medications (NSAIDs) in abdominal surgery, nine randomized trials failed to show that codeine provided superior pain relief.
Hydromorphone, butorphanol, and morphine are not metabolized by CYP2D6 so the problems faced by “ultrarapid metabolizers” or “poor metabolizers” is not an issue.
Ob.gyns. should utilize regional anesthesia, NSAIDs, and acetaminophen (without codeine) to help decrease the risks of anesthesia while still ensuring adequate pain relief. Ob.gyns. should closely monitor their patients on narcotics for any side effects in both mothers and infants, especially central nervous system depression.
Dr. Kairis is an assistant professor in the department of gynecology and obstetrics at Loma Linda (Calif.) University Health and is the director of the Women’s Sexual Medicine Program there. She is on the editorial committee of the Ob/Gyn Board Master. Dr. Siddighi is editor in chief of the Ob/Gyn Board Master and director of female pelvic medicine and reconstructive surgery and director of grand rounds at Loma Linda University Health. Ob.Gyn. News and Ob/Gyn Board Master are owned by the same parent company, Frontline Medical Communications.
Reference
1. Practice Advisory on Codeine and Tramadol for Breastfeeding Women. April 27, 2017. American College of Obstetricians and Gynecologists.
Editor’s Note: This is the final installment of a six-part series that reviews key concepts and articles that ob.gyns. can use to prepare for the American Board of Obstetrics and Gynecology Maintenance of Certification examination. The series is adapted from Ob/Gyn Board Master (obgynboardmaster.com), an online board review course created by Erudyte. This month’s edition of the Board Corner focuses on narcotic analgesia for breastfeeding women.
The American College of Obstetrics and Gynecologists “Practice Advisories” are released when there is an important clinical issue that needs immediate attention from ob.gyn. clinicians. On April 27, 2017, ACOG joined with the Society for Maternal-Fetal Medicine and the Academy of Breastfeeding Medicine to issue a new practice advisory with recommendations on opiate analgesia in breastfeeding women.1 These Practice Advisories contain material that may be tested on a board exam. We recommend that you read this Practice Advisory and review it carefully.
A. Morphine IV
B. Butorphanol
C. Acetaminophen with codeine
D. Hydromorphone
E. Morphine (given orally)
The correct answer is C.
Acetaminophen with codeine (aka Tylenol #3 or Tylenol #4) is the least appropriate first-choice narcotic in a breastfeeding postpartum patient after Cesarean delivery as it is the only narcotic among the choices that is metabolized by the enzyme CYP2D6. Morphine, butorphanol, and hydromorphone are all metabolized by CYP450. If a narcotic is indicated, it is better to choose one that is not metabolized by CYP2D6 because of potential side effects in both mothers and infants who may be “CYP2D6 ultrametabolizers” or “CYP2D6 poor metabolizers.”
Key points
The key points to remember are:
1. Do not use codeine or tramadol as a first-line narcotic choice in breastfeeding mothers, if possible, because of variable side effects in mothers and infants.
2. The preferred narcotics to use when breastfeeding are butorphanol, morphine, or hydromorphone.
3. If codeine or tramadol is used in breastfeeding women, the clinician should speak with the patient and family about the possible side effects and the recent labeling changes required by the Food and Drug Administration.
Literature summary
In April, the Food and Drug Administration issued a safety alert and said it is requiring labeling changes for prescription medications containing codeine and tramadol. Specifically, the agency warned against use of codeine and tramadol when breastfeeding. This change is the result of the fact that certain people metabolize codeine and tramadol differently. There are some people – considered CYP2D6 “ultrarapid metabolizers” – who can have levels of the drug in their breast milk that can cause excessive sleepiness and depressed breathing in infants. There is one report of an infant death resulting from codeine use. The frequency of these “rapid metabolizers” is about 4%-5% in the United States.
In addition to the effects on breastfed infants, there are effects on the mother as well. This is because 6% of patients in the United States are “poor metabolizers” who have insufficient pain relief, as well as greater side effects.
Hydrocodone and oxycodone are not addressed in the recent labeling changes. However, “ultrarapid metabolizers” do show more pain relief and pupil restriction.
When comparing codeine with nonsteroidal anti-inflammatory medications (NSAIDs) in abdominal surgery, nine randomized trials failed to show that codeine provided superior pain relief.
Hydromorphone, butorphanol, and morphine are not metabolized by CYP2D6 so the problems faced by “ultrarapid metabolizers” or “poor metabolizers” is not an issue.
Ob.gyns. should utilize regional anesthesia, NSAIDs, and acetaminophen (without codeine) to help decrease the risks of anesthesia while still ensuring adequate pain relief. Ob.gyns. should closely monitor their patients on narcotics for any side effects in both mothers and infants, especially central nervous system depression.
Dr. Kairis is an assistant professor in the department of gynecology and obstetrics at Loma Linda (Calif.) University Health and is the director of the Women’s Sexual Medicine Program there. She is on the editorial committee of the Ob/Gyn Board Master. Dr. Siddighi is editor in chief of the Ob/Gyn Board Master and director of female pelvic medicine and reconstructive surgery and director of grand rounds at Loma Linda University Health. Ob.Gyn. News and Ob/Gyn Board Master are owned by the same parent company, Frontline Medical Communications.
Reference
1. Practice Advisory on Codeine and Tramadol for Breastfeeding Women. April 27, 2017. American College of Obstetricians and Gynecologists.
Endo hubris
I began to write this opinion piece on the red-eye flying back from the outstanding Vascular Annual Meeting, recently held in San Diego. I attended breakfast sessions at 6 a.m., as well as presentations and meetings going on well into the evening. I now have bloodshot eyes, tachycardia, and a heightened perception of things.
It is possible that I am just sleep deprived or maybe it’s a result of inhaling the ubiquitous “medical” marijuana vapors that constantly wafted outside the convention center. Whatever the reason, I have returned in a feverish state of excitement that accompanies a sudden significant insight ... that some of us are under the influence, not of some hallucinogenic, but rather an endovascular- induced euphoria whose spell has made us forget that we are still surgeons.

The exhibition hall had the few customary surgical equipment companies with their surgical loupes, vascular clamps, and needle holders. But it was the expansive displays of every type of endovascular tool, guidewires, catheters, x-ray equipment, endografts, and stents, that attracted the crowds. Not a single vascular ultrasound company showed off their duplex scanners despite the fact that vascular surgeons advanced the use of these instruments and made them as omnipresent as they now are in clinical practice. These companies now find it more profitable to show off their wares at cardiology and radiology meetings.
In the lecture hall, audiences packed in to hear the latest method to treat aortic aneurysms with every variety of endovascular device, but there was not a single presentation on open surgical alternatives. Further, an excellent vascular surgery resident was asked how he would handle a pararenal aneurysm in community practice. He admitted that, unless he could be assisted by an experienced surgeon, he would be uncomfortable performing an open surgical repair. Thus, he would be forced to perform an endovascular treatment even if it would not be the best alternative for the patient. But in the future, will there actually be accomplished surgeons who can assist the newly minted vascular surgeon with open procedures? At a breakfast session dedicated to the aging vascular surgeon, we learned that many will soon be retiring since 46% of the Society are now over the age of 50, and 30% are more than 60 years of age.
Where am I going with this? It is apparent my aphorism that a vascular surgeon can “Operate, Medicate, and Dilate” may no longer hold. Perhaps it should now be “Stent, Ablate, Dilate, and Dilate Again.” Future generations of vascular “surgeons” may be no more than cardiologists who don’t treat the heart, able to perform endovascular revascularizations but unable to perform open operations.
Training paradigms may be affected by middle-aged attending surgeons attempting to prove that they are current by adopting endo-treatments rather than open surgery. Some academic surgeons may see the need to experiment with new endo-techniques to advance their careers. Some may see profit patenting new devices. Some may just be enthralled by what Bruce Brenner refers to as “Endo hubris.” Irrespective, dwindling open procedures will inevitably result in inexperienced open surgeons who will feel comfortable only in an endovascular suite.
Payment inequities that undervalue open procedures and overvalue endovascular ones will promote a preference for endovascular alternatives, many of which are less physically demanding than open surgical procedures and bypasses. Thus, the preference for endovascular procedures will be perpetuated.
Concurrently, our cardiology colleagues will be honing their endovascular skills not only in the coronary arteries but also on the periphery. Soon they will claim superiority. Hospital administrators, already under the spell of Cardiology, will notice the declining profit generated by poorly performed open surgery and resultant prolonged hospitalizations. They will then continue to relegate vascular surgeons to even lesser roles than they now have in so-called Heart and Vascular Centers.
As our open skills deteriorate, patients will be forced to travel to the few centers where some exhausted elderly surgeons will perform the occasional open aortic procedure, distal bypass, or, heaven forbid, some ancient procedure referred to as a carotid endarterectomy.
Of course, some may argue that it is time that endovascular procedures replace “barbaric” or disfiguring open procedures. In fact, this may already be the case for the treatment of thoracic aortic pathology. However, I propose that the time for abandoning surgery has not arrived. There are now sufficient data to show that many endo-procedures are no panacea nor are they without significant limitations. Furthermore, if we abandon open surgery we essentially abandon our raison d’etre. What will then distinguish us from interventional radiologists and cardiologists?
I propose it is time for us to embrace our surgical prowess rather than to treat open procedures like Cinderella’s ugly sisters. I would encourage program directors not to stretch indications for use to justify endovascular treatments but rather adopt standard open procedures. If the volume of indicated open procedures is insufficient, then arrange for the trainee to visit another institution.
We must educate referring physicians and hospital administrators about the benefits of well performed open surgery, and we must make sure that such procedures are, in fact, successfully and expeditiously executed. Non-surgeons also need to be informed about some of the drawbacks of endovascular procedures so that they gain a realistic understanding of the pros and cons.
This does not mean being disparaging, but they should be educated about the occurrence and significance of endoleaks, stent fractures, early recurrence, and other complications. Thus informed, they will better understand the rationale for choosing a vascular surgeon to take care of their patients. They will realize that we remain the only specialists devoted to the understanding and treatment of vascular pathology and consequently able to perform the most appropriate and best treatment for that patient.
I am now fully awake. I am convinced that my evaluation of the events at the meeting were not some sleep-deprived or hallucinogenic aberration. I sincerely believe that it is time for drastic adjustments in our thinking about endovascular and open procedures. If not, vascular surgeons and our specialty may become irrelevant and the repercussions for our survival and that of our patients may be devastating. ■
Russell Samson, MD, a physician in the practice of Sarasota Vascular Specialists, Sarasota, Fl., and a clinical professor of surgery, Florida State University, Tallahassee. He is the medical editor of Vascular Specialist.
I began to write this opinion piece on the red-eye flying back from the outstanding Vascular Annual Meeting, recently held in San Diego. I attended breakfast sessions at 6 a.m., as well as presentations and meetings going on well into the evening. I now have bloodshot eyes, tachycardia, and a heightened perception of things.
It is possible that I am just sleep deprived or maybe it’s a result of inhaling the ubiquitous “medical” marijuana vapors that constantly wafted outside the convention center. Whatever the reason, I have returned in a feverish state of excitement that accompanies a sudden significant insight ... that some of us are under the influence, not of some hallucinogenic, but rather an endovascular- induced euphoria whose spell has made us forget that we are still surgeons.
The exhibition hall had the few customary surgical equipment companies with their surgical loupes, vascular clamps, and needle holders. But it was the expansive displays of every type of endovascular tool, guidewires, catheters, x-ray equipment, endografts, and stents, that attracted the crowds. Not a single vascular ultrasound company showed off their duplex scanners despite the fact that vascular surgeons advanced the use of these instruments and made them as omnipresent as they now are in clinical practice. These companies now find it more profitable to show off their wares at cardiology and radiology meetings.
In the lecture hall, audiences packed in to hear the latest method to treat aortic aneurysms with every variety of endovascular device, but there was not a single presentation on open surgical alternatives. Further, an excellent vascular surgery resident was asked how he would handle a pararenal aneurysm in community practice. He admitted that, unless he could be assisted by an experienced surgeon, he would be uncomfortable performing an open surgical repair. Thus, he would be forced to perform an endovascular treatment even if it would not be the best alternative for the patient. But in the future, will there actually be accomplished surgeons who can assist the newly minted vascular surgeon with open procedures? At a breakfast session dedicated to the aging vascular surgeon, we learned that many will soon be retiring since 46% of the Society are now over the age of 50, and 30% are more than 60 years of age.
Where am I going with this? It is apparent my aphorism that a vascular surgeon can “Operate, Medicate, and Dilate” may no longer hold. Perhaps it should now be “Stent, Ablate, Dilate, and Dilate Again.” Future generations of vascular “surgeons” may be no more than cardiologists who don’t treat the heart, able to perform endovascular revascularizations but unable to perform open operations.
Training paradigms may be affected by middle-aged attending surgeons attempting to prove that they are current by adopting endo-treatments rather than open surgery. Some academic surgeons may see the need to experiment with new endo-techniques to advance their careers. Some may see profit patenting new devices. Some may just be enthralled by what Bruce Brenner refers to as “Endo hubris.” Irrespective, dwindling open procedures will inevitably result in inexperienced open surgeons who will feel comfortable only in an endovascular suite.
Payment inequities that undervalue open procedures and overvalue endovascular ones will promote a preference for endovascular alternatives, many of which are less physically demanding than open surgical procedures and bypasses. Thus, the preference for endovascular procedures will be perpetuated.
Concurrently, our cardiology colleagues will be honing their endovascular skills not only in the coronary arteries but also on the periphery. Soon they will claim superiority. Hospital administrators, already under the spell of Cardiology, will notice the declining profit generated by poorly performed open surgery and resultant prolonged hospitalizations. They will then continue to relegate vascular surgeons to even lesser roles than they now have in so-called Heart and Vascular Centers.
As our open skills deteriorate, patients will be forced to travel to the few centers where some exhausted elderly surgeons will perform the occasional open aortic procedure, distal bypass, or, heaven forbid, some ancient procedure referred to as a carotid endarterectomy.
Of course, some may argue that it is time that endovascular procedures replace “barbaric” or disfiguring open procedures. In fact, this may already be the case for the treatment of thoracic aortic pathology. However, I propose that the time for abandoning surgery has not arrived. There are now sufficient data to show that many endo-procedures are no panacea nor are they without significant limitations. Furthermore, if we abandon open surgery we essentially abandon our raison d’etre. What will then distinguish us from interventional radiologists and cardiologists?
I propose it is time for us to embrace our surgical prowess rather than to treat open procedures like Cinderella’s ugly sisters. I would encourage program directors not to stretch indications for use to justify endovascular treatments but rather adopt standard open procedures. If the volume of indicated open procedures is insufficient, then arrange for the trainee to visit another institution.
We must educate referring physicians and hospital administrators about the benefits of well performed open surgery, and we must make sure that such procedures are, in fact, successfully and expeditiously executed. Non-surgeons also need to be informed about some of the drawbacks of endovascular procedures so that they gain a realistic understanding of the pros and cons.
This does not mean being disparaging, but they should be educated about the occurrence and significance of endoleaks, stent fractures, early recurrence, and other complications. Thus informed, they will better understand the rationale for choosing a vascular surgeon to take care of their patients. They will realize that we remain the only specialists devoted to the understanding and treatment of vascular pathology and consequently able to perform the most appropriate and best treatment for that patient.
I am now fully awake. I am convinced that my evaluation of the events at the meeting were not some sleep-deprived or hallucinogenic aberration. I sincerely believe that it is time for drastic adjustments in our thinking about endovascular and open procedures. If not, vascular surgeons and our specialty may become irrelevant and the repercussions for our survival and that of our patients may be devastating. ■
Russell Samson, MD, a physician in the practice of Sarasota Vascular Specialists, Sarasota, Fl., and a clinical professor of surgery, Florida State University, Tallahassee. He is the medical editor of Vascular Specialist.
I began to write this opinion piece on the red-eye flying back from the outstanding Vascular Annual Meeting, recently held in San Diego. I attended breakfast sessions at 6 a.m., as well as presentations and meetings going on well into the evening. I now have bloodshot eyes, tachycardia, and a heightened perception of things.
It is possible that I am just sleep deprived or maybe it’s a result of inhaling the ubiquitous “medical” marijuana vapors that constantly wafted outside the convention center. Whatever the reason, I have returned in a feverish state of excitement that accompanies a sudden significant insight ... that some of us are under the influence, not of some hallucinogenic, but rather an endovascular- induced euphoria whose spell has made us forget that we are still surgeons.
The exhibition hall had the few customary surgical equipment companies with their surgical loupes, vascular clamps, and needle holders. But it was the expansive displays of every type of endovascular tool, guidewires, catheters, x-ray equipment, endografts, and stents, that attracted the crowds. Not a single vascular ultrasound company showed off their duplex scanners despite the fact that vascular surgeons advanced the use of these instruments and made them as omnipresent as they now are in clinical practice. These companies now find it more profitable to show off their wares at cardiology and radiology meetings.
In the lecture hall, audiences packed in to hear the latest method to treat aortic aneurysms with every variety of endovascular device, but there was not a single presentation on open surgical alternatives. Further, an excellent vascular surgery resident was asked how he would handle a pararenal aneurysm in community practice. He admitted that, unless he could be assisted by an experienced surgeon, he would be uncomfortable performing an open surgical repair. Thus, he would be forced to perform an endovascular treatment even if it would not be the best alternative for the patient. But in the future, will there actually be accomplished surgeons who can assist the newly minted vascular surgeon with open procedures? At a breakfast session dedicated to the aging vascular surgeon, we learned that many will soon be retiring since 46% of the Society are now over the age of 50, and 30% are more than 60 years of age.
Where am I going with this? It is apparent my aphorism that a vascular surgeon can “Operate, Medicate, and Dilate” may no longer hold. Perhaps it should now be “Stent, Ablate, Dilate, and Dilate Again.” Future generations of vascular “surgeons” may be no more than cardiologists who don’t treat the heart, able to perform endovascular revascularizations but unable to perform open operations.
Training paradigms may be affected by middle-aged attending surgeons attempting to prove that they are current by adopting endo-treatments rather than open surgery. Some academic surgeons may see the need to experiment with new endo-techniques to advance their careers. Some may see profit patenting new devices. Some may just be enthralled by what Bruce Brenner refers to as “Endo hubris.” Irrespective, dwindling open procedures will inevitably result in inexperienced open surgeons who will feel comfortable only in an endovascular suite.
Payment inequities that undervalue open procedures and overvalue endovascular ones will promote a preference for endovascular alternatives, many of which are less physically demanding than open surgical procedures and bypasses. Thus, the preference for endovascular procedures will be perpetuated.
Concurrently, our cardiology colleagues will be honing their endovascular skills not only in the coronary arteries but also on the periphery. Soon they will claim superiority. Hospital administrators, already under the spell of Cardiology, will notice the declining profit generated by poorly performed open surgery and resultant prolonged hospitalizations. They will then continue to relegate vascular surgeons to even lesser roles than they now have in so-called Heart and Vascular Centers.
As our open skills deteriorate, patients will be forced to travel to the few centers where some exhausted elderly surgeons will perform the occasional open aortic procedure, distal bypass, or, heaven forbid, some ancient procedure referred to as a carotid endarterectomy.
Of course, some may argue that it is time that endovascular procedures replace “barbaric” or disfiguring open procedures. In fact, this may already be the case for the treatment of thoracic aortic pathology. However, I propose that the time for abandoning surgery has not arrived. There are now sufficient data to show that many endo-procedures are no panacea nor are they without significant limitations. Furthermore, if we abandon open surgery we essentially abandon our raison d’etre. What will then distinguish us from interventional radiologists and cardiologists?
I propose it is time for us to embrace our surgical prowess rather than to treat open procedures like Cinderella’s ugly sisters. I would encourage program directors not to stretch indications for use to justify endovascular treatments but rather adopt standard open procedures. If the volume of indicated open procedures is insufficient, then arrange for the trainee to visit another institution.
We must educate referring physicians and hospital administrators about the benefits of well performed open surgery, and we must make sure that such procedures are, in fact, successfully and expeditiously executed. Non-surgeons also need to be informed about some of the drawbacks of endovascular procedures so that they gain a realistic understanding of the pros and cons.
This does not mean being disparaging, but they should be educated about the occurrence and significance of endoleaks, stent fractures, early recurrence, and other complications. Thus informed, they will better understand the rationale for choosing a vascular surgeon to take care of their patients. They will realize that we remain the only specialists devoted to the understanding and treatment of vascular pathology and consequently able to perform the most appropriate and best treatment for that patient.
I am now fully awake. I am convinced that my evaluation of the events at the meeting were not some sleep-deprived or hallucinogenic aberration. I sincerely believe that it is time for drastic adjustments in our thinking about endovascular and open procedures. If not, vascular surgeons and our specialty may become irrelevant and the repercussions for our survival and that of our patients may be devastating. ■
Russell Samson, MD, a physician in the practice of Sarasota Vascular Specialists, Sarasota, Fl., and a clinical professor of surgery, Florida State University, Tallahassee. He is the medical editor of Vascular Specialist.

Transgender patients face mental health challenges
What I thought would be a typical morning at the major county hospital – if that were ever possible on a psychiatric emergency unit (EU) – quickly turned atypical when I encountered a patient whom I will call Olivia.
Olivia is a 51-year-old male-to-female transgender woman who has not yet undergone gender reassignment surgery. She was brought to the EU by police, after expressing suicidal ideation during a phone call with a tax accountant. This was Olivia’s third visit to the psychiatric emergency unit because of suicide threats within 2 months. Though she was chronically suicidal, her current visit was triggered by a tax audit, which led her to view herself as an unwanted burden on society.

As a male-to-female transgender woman, Olivia faced discrimination in various aspects of her life. Despite her professional competence as an accountant, she was unable to find an employer accepting of her transgender status. Her efforts to align her legal identity with her experienced gender by legally changing her name were met by a web of bureaucratic complications. In the face of numerous challenges, Olivia had minimal social support to rely on during her gender-affirming transition. In short, nothing – not work, family, or finances – was simple for Olivia.
Olivia’s case is not atypical. My purpose in describing Olivia’s circumstances is to highlight the issues faced by many transgender men and women in every aspect of their day-to-day lives. To protect her identity, I have been careful to change several specifics related to her case.
Historical perspective
Societal views of transgendered people vary. On one end of the spectrum is acceptance; in the middle is perhaps tolerance or mild discomfort at perceived abnormality; and at the other extreme are virulent hatred, discrimination, and invalidation of these individuals’ gender-affirming efforts.
Awareness of these hostile attitudes creates a vicious cycle of marginalization and mental illness among many transgender individuals.
Controversies surrounding sexual minorities are rooted in societal perceptions of gender delineations, and prevailing societal norms surrounding ethical and moral conduct. Most societies have a narrow perspective on gender, and seek to maintain a strict delineation of male and female identities, which contributes to the rejection of those with gender identity issues.1,2 This often results in the invalidation of or active opposition to transgender individuals’ transition efforts. The reasons behind the rejection of transgender men and women are multifactorial, and can include a lack of awareness, homophobia, religious dogma, social stigmatization, and perceived non-employability – all often stemming largely from the lack of awareness that sexual identity and orientation are not a choice, but rather are predetermined by biological mechanisms. The intensifying familial, societal, political, and financial pressures all contribute to increased mental health issues, including increased incidence of suicide among sexual minorities.
Globally, sexual minorities continue to be subjected to gross human rights violations. Against the backdrop of prevalent social discrimination, transgender people experience a roughly threefold increase in the risk of developing anxiety disorders, which impair self-esteem and interpersonal functioning.3 The lifetime risk of attempted suicide is four times higher among transgender men, and two times higher among transgender women, than it is among cisgender men and women, respectively. Institutional discrimination in the public and private sectors results from laws and policies that impose inequities, or fail to protect sexual minorities. Examples are current policies denying medical coverage for sex reassignment surgery, denying health care by a provider because of transgender identity and numerous obstacles to obtain health insurance coverage.4
Impact of low acceptance
Recall Olivia’s need to delay the vocal cord surgery that arguably would have had a positive impact on her self-esteem. The transgender population faces increased health risks and barriers to appropriate mental health evaluation and inclusive care, particularly individuals with low acceptance from family, friends, and partners.5
A century ago, changing one’s gender was considered both highly disreputable and an impossible feat.6 Today, sex reassignment is the focus of political debate, with activists seeking equal rights for transgender individuals, despite the high rate of mental disorders in the community. While there is some positive public perception of transgender people, most still hold religious or moral objections to sex reassignment. Olivia’s family, for example, is typical in their rejection of her gender-affirming efforts. One example of this rejection is forbidding her to wear women’s clothing, stating that it makes them feel ashamed and subjects them to social ridicule.
As a result, Olivia lacks the social support that could work to remedy, to some extent, her suicidal ideation. Efforts to alleviate financial burdens that result from workplace discrimination, impediments to the pursuit of health, security, and happiness and the bureaucratic hurdles to gender affirmation are needed.7,8 According to research by Kristen Clements-Nolle, PhD, MPH, and her associates, suicidality may be largely a reaction to the absence of legally secure equal rights for transgender men and women.9 In Olivia’s case, financial struggles with her mortgage, medical expenses for her autistic son, and anxiety about potentially losing the disability benefits on which she depends have added to her insecurity.
Financial insecurity resulting from her unemployment likely has exacerbated her feelings of inadequacy and depression. For example, because of her lack of financial resources, she had to delay the vocal cord surgery she desired. What would her prognosis be if her legal rights, including employment protection, were firmly in place? Likewise, the demands of parenting an autistic son posed another significant stressor that likely contributes to reciprocal stress for the child, resulting in the worsening of his autism symptoms.
In summary, transgender individuals face bias and discrimination in response to their gender-affirming efforts, which creates a vicious cycle of mental illness, suicidality, and societal marginalization. Addressing these endemic issues requires a multifaceted approach. Preventive strategies, including identification of mental health issues, and integration of mental health service with primary health care, are needed. Case registration, as a research measure to help understand the prevalence and severity of suicide among the LGBT population, would be beneficial.
Monitoring and follow-up of identified cases for supportive care (for example, gatekeeper training similar to the World Health Organization’s Suicide Prevention Initiative) also are needed to identify protective factors, in order to foster resilience in LGBT individuals facing negative reactions to disclosure of their sexual minority status. Legislation aimed at better facilitating a seamless integration of transgender men and women into mainstream society also is necessary. Supportive measures, particularly social supports promoting better mental health in trans individuals, could help reduce suicide rates. Finally, governmental initiatives to protect the human and constitutional rights of transgender people are key to minimizing the incidence of mental health issues and suicides among this vulnerable sexual minority group.
The path to addressing the issues faced by transgender individuals begins with education, which then leads to understanding. From understanding comes acceptance. Acceptance leads to equality – social, legal, and thereby, economic. Ensuring acceptance of all sexes as equal could mitigate the marginalization – in all its forms – experienced by gender-affirming individuals, with the end result being less mental illness and reduced rates of suicidality in this vulnerable population.7
Dr. Ahmed is a second-year resident in the department of psychiatry at the Nassau University Medical Center, East Meadow, New York. His interests include public social psychiatry, health care policy, health disparities, mental health stigma, and addiction psychiatry. Dr. Ahmed is a member of the American Psychiatric Association, the American Society of Clinical Psychopharmacology, and the American Association for Social Psychiatry.
References
1. LGBT Health. 2014 Jun;1(2):98-106.
2. Signs: Journal of Women in Culture and Society. 2006;32(1):83-111.
3. Int J Transgenderism. 2016:18(1):16-26.
4. Am J Public Health. 2014 Mar;104(3):e31-8.
5. Int J Transgenderism. 2017;18(1):104-18.
6. “Suicide attempts among transgender and gender non-conforming adults,” American Foundation for Suicide Prevention, 2014.
7. “Injustice at every turn: A report of the national transgender discrimination survey,” National Center for Transgender Equality, 2011.
8. J Gay Lesbian Soc Serv. 2014;26(2):186-206.
9. J Homosex. 2006;51(3):53-69.
What I thought would be a typical morning at the major county hospital – if that were ever possible on a psychiatric emergency unit (EU) – quickly turned atypical when I encountered a patient whom I will call Olivia.
Olivia is a 51-year-old male-to-female transgender woman who has not yet undergone gender reassignment surgery. She was brought to the EU by police, after expressing suicidal ideation during a phone call with a tax accountant. This was Olivia’s third visit to the psychiatric emergency unit because of suicide threats within 2 months. Though she was chronically suicidal, her current visit was triggered by a tax audit, which led her to view herself as an unwanted burden on society.
As a male-to-female transgender woman, Olivia faced discrimination in various aspects of her life. Despite her professional competence as an accountant, she was unable to find an employer accepting of her transgender status. Her efforts to align her legal identity with her experienced gender by legally changing her name were met by a web of bureaucratic complications. In the face of numerous challenges, Olivia had minimal social support to rely on during her gender-affirming transition. In short, nothing – not work, family, or finances – was simple for Olivia.
Olivia’s case is not atypical. My purpose in describing Olivia’s circumstances is to highlight the issues faced by many transgender men and women in every aspect of their day-to-day lives. To protect her identity, I have been careful to change several specifics related to her case.
Historical perspective
Societal views of transgendered people vary. On one end of the spectrum is acceptance; in the middle is perhaps tolerance or mild discomfort at perceived abnormality; and at the other extreme are virulent hatred, discrimination, and invalidation of these individuals’ gender-affirming efforts.
Awareness of these hostile attitudes creates a vicious cycle of marginalization and mental illness among many transgender individuals.
Controversies surrounding sexual minorities are rooted in societal perceptions of gender delineations, and prevailing societal norms surrounding ethical and moral conduct. Most societies have a narrow perspective on gender, and seek to maintain a strict delineation of male and female identities, which contributes to the rejection of those with gender identity issues.1,2 This often results in the invalidation of or active opposition to transgender individuals’ transition efforts. The reasons behind the rejection of transgender men and women are multifactorial, and can include a lack of awareness, homophobia, religious dogma, social stigmatization, and perceived non-employability – all often stemming largely from the lack of awareness that sexual identity and orientation are not a choice, but rather are predetermined by biological mechanisms. The intensifying familial, societal, political, and financial pressures all contribute to increased mental health issues, including increased incidence of suicide among sexual minorities.
Globally, sexual minorities continue to be subjected to gross human rights violations. Against the backdrop of prevalent social discrimination, transgender people experience a roughly threefold increase in the risk of developing anxiety disorders, which impair self-esteem and interpersonal functioning.3 The lifetime risk of attempted suicide is four times higher among transgender men, and two times higher among transgender women, than it is among cisgender men and women, respectively. Institutional discrimination in the public and private sectors results from laws and policies that impose inequities, or fail to protect sexual minorities. Examples are current policies denying medical coverage for sex reassignment surgery, denying health care by a provider because of transgender identity and numerous obstacles to obtain health insurance coverage.4
Impact of low acceptance
Recall Olivia’s need to delay the vocal cord surgery that arguably would have had a positive impact on her self-esteem. The transgender population faces increased health risks and barriers to appropriate mental health evaluation and inclusive care, particularly individuals with low acceptance from family, friends, and partners.5
A century ago, changing one’s gender was considered both highly disreputable and an impossible feat.6 Today, sex reassignment is the focus of political debate, with activists seeking equal rights for transgender individuals, despite the high rate of mental disorders in the community. While there is some positive public perception of transgender people, most still hold religious or moral objections to sex reassignment. Olivia’s family, for example, is typical in their rejection of her gender-affirming efforts. One example of this rejection is forbidding her to wear women’s clothing, stating that it makes them feel ashamed and subjects them to social ridicule.
As a result, Olivia lacks the social support that could work to remedy, to some extent, her suicidal ideation. Efforts to alleviate financial burdens that result from workplace discrimination, impediments to the pursuit of health, security, and happiness and the bureaucratic hurdles to gender affirmation are needed.7,8 According to research by Kristen Clements-Nolle, PhD, MPH, and her associates, suicidality may be largely a reaction to the absence of legally secure equal rights for transgender men and women.9 In Olivia’s case, financial struggles with her mortgage, medical expenses for her autistic son, and anxiety about potentially losing the disability benefits on which she depends have added to her insecurity.
Financial insecurity resulting from her unemployment likely has exacerbated her feelings of inadequacy and depression. For example, because of her lack of financial resources, she had to delay the vocal cord surgery she desired. What would her prognosis be if her legal rights, including employment protection, were firmly in place? Likewise, the demands of parenting an autistic son posed another significant stressor that likely contributes to reciprocal stress for the child, resulting in the worsening of his autism symptoms.
In summary, transgender individuals face bias and discrimination in response to their gender-affirming efforts, which creates a vicious cycle of mental illness, suicidality, and societal marginalization. Addressing these endemic issues requires a multifaceted approach. Preventive strategies, including identification of mental health issues, and integration of mental health service with primary health care, are needed. Case registration, as a research measure to help understand the prevalence and severity of suicide among the LGBT population, would be beneficial.
Monitoring and follow-up of identified cases for supportive care (for example, gatekeeper training similar to the World Health Organization’s Suicide Prevention Initiative) also are needed to identify protective factors, in order to foster resilience in LGBT individuals facing negative reactions to disclosure of their sexual minority status. Legislation aimed at better facilitating a seamless integration of transgender men and women into mainstream society also is necessary. Supportive measures, particularly social supports promoting better mental health in trans individuals, could help reduce suicide rates. Finally, governmental initiatives to protect the human and constitutional rights of transgender people are key to minimizing the incidence of mental health issues and suicides among this vulnerable sexual minority group.
The path to addressing the issues faced by transgender individuals begins with education, which then leads to understanding. From understanding comes acceptance. Acceptance leads to equality – social, legal, and thereby, economic. Ensuring acceptance of all sexes as equal could mitigate the marginalization – in all its forms – experienced by gender-affirming individuals, with the end result being less mental illness and reduced rates of suicidality in this vulnerable population.7
Dr. Ahmed is a second-year resident in the department of psychiatry at the Nassau University Medical Center, East Meadow, New York. His interests include public social psychiatry, health care policy, health disparities, mental health stigma, and addiction psychiatry. Dr. Ahmed is a member of the American Psychiatric Association, the American Society of Clinical Psychopharmacology, and the American Association for Social Psychiatry.
References
1. LGBT Health. 2014 Jun;1(2):98-106.
2. Signs: Journal of Women in Culture and Society. 2006;32(1):83-111.
3. Int J Transgenderism. 2016:18(1):16-26.
4. Am J Public Health. 2014 Mar;104(3):e31-8.
5. Int J Transgenderism. 2017;18(1):104-18.
6. “Suicide attempts among transgender and gender non-conforming adults,” American Foundation for Suicide Prevention, 2014.
7. “Injustice at every turn: A report of the national transgender discrimination survey,” National Center for Transgender Equality, 2011.
8. J Gay Lesbian Soc Serv. 2014;26(2):186-206.
9. J Homosex. 2006;51(3):53-69.
What I thought would be a typical morning at the major county hospital – if that were ever possible on a psychiatric emergency unit (EU) – quickly turned atypical when I encountered a patient whom I will call Olivia.
Olivia is a 51-year-old male-to-female transgender woman who has not yet undergone gender reassignment surgery. She was brought to the EU by police, after expressing suicidal ideation during a phone call with a tax accountant. This was Olivia’s third visit to the psychiatric emergency unit because of suicide threats within 2 months. Though she was chronically suicidal, her current visit was triggered by a tax audit, which led her to view herself as an unwanted burden on society.
As a male-to-female transgender woman, Olivia faced discrimination in various aspects of her life. Despite her professional competence as an accountant, she was unable to find an employer accepting of her transgender status. Her efforts to align her legal identity with her experienced gender by legally changing her name were met by a web of bureaucratic complications. In the face of numerous challenges, Olivia had minimal social support to rely on during her gender-affirming transition. In short, nothing – not work, family, or finances – was simple for Olivia.
Olivia’s case is not atypical. My purpose in describing Olivia’s circumstances is to highlight the issues faced by many transgender men and women in every aspect of their day-to-day lives. To protect her identity, I have been careful to change several specifics related to her case.
Historical perspective
Societal views of transgendered people vary. On one end of the spectrum is acceptance; in the middle is perhaps tolerance or mild discomfort at perceived abnormality; and at the other extreme are virulent hatred, discrimination, and invalidation of these individuals’ gender-affirming efforts.
Awareness of these hostile attitudes creates a vicious cycle of marginalization and mental illness among many transgender individuals.
Controversies surrounding sexual minorities are rooted in societal perceptions of gender delineations, and prevailing societal norms surrounding ethical and moral conduct. Most societies have a narrow perspective on gender, and seek to maintain a strict delineation of male and female identities, which contributes to the rejection of those with gender identity issues.1,2 This often results in the invalidation of or active opposition to transgender individuals’ transition efforts. The reasons behind the rejection of transgender men and women are multifactorial, and can include a lack of awareness, homophobia, religious dogma, social stigmatization, and perceived non-employability – all often stemming largely from the lack of awareness that sexual identity and orientation are not a choice, but rather are predetermined by biological mechanisms. The intensifying familial, societal, political, and financial pressures all contribute to increased mental health issues, including increased incidence of suicide among sexual minorities.
Globally, sexual minorities continue to be subjected to gross human rights violations. Against the backdrop of prevalent social discrimination, transgender people experience a roughly threefold increase in the risk of developing anxiety disorders, which impair self-esteem and interpersonal functioning.3 The lifetime risk of attempted suicide is four times higher among transgender men, and two times higher among transgender women, than it is among cisgender men and women, respectively. Institutional discrimination in the public and private sectors results from laws and policies that impose inequities, or fail to protect sexual minorities. Examples are current policies denying medical coverage for sex reassignment surgery, denying health care by a provider because of transgender identity and numerous obstacles to obtain health insurance coverage.4
Impact of low acceptance
Recall Olivia’s need to delay the vocal cord surgery that arguably would have had a positive impact on her self-esteem. The transgender population faces increased health risks and barriers to appropriate mental health evaluation and inclusive care, particularly individuals with low acceptance from family, friends, and partners.5
A century ago, changing one’s gender was considered both highly disreputable and an impossible feat.6 Today, sex reassignment is the focus of political debate, with activists seeking equal rights for transgender individuals, despite the high rate of mental disorders in the community. While there is some positive public perception of transgender people, most still hold religious or moral objections to sex reassignment. Olivia’s family, for example, is typical in their rejection of her gender-affirming efforts. One example of this rejection is forbidding her to wear women’s clothing, stating that it makes them feel ashamed and subjects them to social ridicule.
As a result, Olivia lacks the social support that could work to remedy, to some extent, her suicidal ideation. Efforts to alleviate financial burdens that result from workplace discrimination, impediments to the pursuit of health, security, and happiness and the bureaucratic hurdles to gender affirmation are needed.7,8 According to research by Kristen Clements-Nolle, PhD, MPH, and her associates, suicidality may be largely a reaction to the absence of legally secure equal rights for transgender men and women.9 In Olivia’s case, financial struggles with her mortgage, medical expenses for her autistic son, and anxiety about potentially losing the disability benefits on which she depends have added to her insecurity.
Financial insecurity resulting from her unemployment likely has exacerbated her feelings of inadequacy and depression. For example, because of her lack of financial resources, she had to delay the vocal cord surgery she desired. What would her prognosis be if her legal rights, including employment protection, were firmly in place? Likewise, the demands of parenting an autistic son posed another significant stressor that likely contributes to reciprocal stress for the child, resulting in the worsening of his autism symptoms.
In summary, transgender individuals face bias and discrimination in response to their gender-affirming efforts, which creates a vicious cycle of mental illness, suicidality, and societal marginalization. Addressing these endemic issues requires a multifaceted approach. Preventive strategies, including identification of mental health issues, and integration of mental health service with primary health care, are needed. Case registration, as a research measure to help understand the prevalence and severity of suicide among the LGBT population, would be beneficial.
Monitoring and follow-up of identified cases for supportive care (for example, gatekeeper training similar to the World Health Organization’s Suicide Prevention Initiative) also are needed to identify protective factors, in order to foster resilience in LGBT individuals facing negative reactions to disclosure of their sexual minority status. Legislation aimed at better facilitating a seamless integration of transgender men and women into mainstream society also is necessary. Supportive measures, particularly social supports promoting better mental health in trans individuals, could help reduce suicide rates. Finally, governmental initiatives to protect the human and constitutional rights of transgender people are key to minimizing the incidence of mental health issues and suicides among this vulnerable sexual minority group.
The path to addressing the issues faced by transgender individuals begins with education, which then leads to understanding. From understanding comes acceptance. Acceptance leads to equality – social, legal, and thereby, economic. Ensuring acceptance of all sexes as equal could mitigate the marginalization – in all its forms – experienced by gender-affirming individuals, with the end result being less mental illness and reduced rates of suicidality in this vulnerable population.7
Dr. Ahmed is a second-year resident in the department of psychiatry at the Nassau University Medical Center, East Meadow, New York. His interests include public social psychiatry, health care policy, health disparities, mental health stigma, and addiction psychiatry. Dr. Ahmed is a member of the American Psychiatric Association, the American Society of Clinical Psychopharmacology, and the American Association for Social Psychiatry.
References
1. LGBT Health. 2014 Jun;1(2):98-106.
2. Signs: Journal of Women in Culture and Society. 2006;32(1):83-111.
3. Int J Transgenderism. 2016:18(1):16-26.
4. Am J Public Health. 2014 Mar;104(3):e31-8.
5. Int J Transgenderism. 2017;18(1):104-18.
6. “Suicide attempts among transgender and gender non-conforming adults,” American Foundation for Suicide Prevention, 2014.
7. “Injustice at every turn: A report of the national transgender discrimination survey,” National Center for Transgender Equality, 2011.
8. J Gay Lesbian Soc Serv. 2014;26(2):186-206.
9. J Homosex. 2006;51(3):53-69.
The latest news on pediatric migraine
Migraine is the most common disabling neurologic disease, with an estimated 1 billion sufferers worldwide.1 In children aged 5-15 years, migraine prevalence is 10%, and these children miss more school than their peers.2,3 Research specific to the child and adolescent migraine population is imperative, as the findings in adult studies do not always correlate or translate to pediatrics. The American Headache Society (AHS) held its 59th annual scientific meeting in Boston in June 2017, a meeting designed to showcase the latest advances in the field of headache medicine. Several interesting pediatric headache studies were presented.

Pediatric patient, parent goals and preferences for preventive treatment
There is a general consensus among headache specialists that migraine preventive treatment should be instituted when a migraineur has at least four headache days per month. Clinically, and in most research trials, migraine preventive treatment is considered effective when a 50% reduction in headache days or the headache frequency is reduced to no more than four headache days per month.

Perhaps not surprisingly, patients and families expect treatment to result in very few headaches with minimal side effects. It is helpful to understand patient and family treatment goals as clinicians so we can to better provide realistic expectations of care, improve treatment adherence, and reduce patient/parent frustration.
Premonitory symptoms
Migraine is disabling not simply because of the headache but because of the range of symptoms that occur around the headache. Migraine may involve four phases: premonitory, aura, headache, and postdrome. The premonitory phase involves symptoms that may occur hours to days prior to the headache. Functional imaging studies reveal hypothalamic activation during this phase.4 In a large retrospective study, premonitory symptoms occurred in approximately three-quarters of pediatric and adult migraineurs.5 In a prior pediatric chart review, the most common premonitory symptoms in order of decreasing frequency were fatigue, mood change, neck stiffness, and yawning.6

Understanding and identifying premonitory signs is important for better understanding the pathophysiology of migraine and to help our patients recognize when a migraine may be coming.
Mapping pain in pediatric migraine
Diagnosis of migraine is based on the International Classification of Headache Disorders 3rd edition beta (ICHD-3b). For adults with migraine, part of the diagnostic criteria requires at least two of a number of features: unilateral location, pulsating quality, moderate or severe pain intensity, or aggravation by or avoidance of routine physical activity. The comments section of the ICHD-3b mentions that, in children under 18 years, the pain may be bilateral.
This study sought to characterize the location and quality of headache pain in the pediatric and young adult population. Sixty migraineurs were enrolled and divided into three age groups: children (7-11 years), adolescents (12-18), and young adults (19-26). The patients were guided to use a diagram to draw pain location and quality. The pain was bilateral for the majority of patients in all age groups. Of the young adult group, 85% had bilateral headache. This is of interest, as adults with migraine are conventionally thought to have unilateral headache. The main descriptors among all three groups were throbbing, pounding, and pressing. In children, tightening was more common than throbbing.
When diagnosing migraine, it is helpful to take these differences into consideration. Overall, this study provides a better understanding of the quality and location of migraine in the pediatric and young adult population.
Efficacy of zolmitriptan nasal spray in adolescents
Zolmitriptan nasal spray (NS) was approved by the Food and Drug Administration in 2015 for acute migraine treatment in adolescents ages 12-17 years. This was the first triptan NS approved for use in pediatric migraine. The NS route benefits migraineurs who need a rapidly absorbed triptan or those who do not tolerate oral triptans because of significant nausea or emesis with their migraine. The efficacy of zolmitriptan NS in adolescents was established in a multicenter, double-blind, randomized placebo controlled study with 798 participants.7 The primary endpoint of pain freedom at 2 hours after treatment for the 5-mg dose was superior to placebo, 30% vs. 17%, respectively (P less than .001; odds ratio, 2.18; 95% confidence interval, 1.40, 3.39). Patients with migraine going from moderate or severe to mild or no headache at 2 hours post treatment were 51% vs. 39%, respectively (P = .010).
The follow-up study presented at AHS was a subgroup analysis of the above data in younger (12-14 years) and older (15-17 years) adolescents. The primary efficacy endpoint of being pain free at 2 hours post treatment was similarly better for zolmitriptan 5 mg, compared with placebo, in both the younger and older adolescent migraineurs.
This study reinforces that zolmitriptan 5-mg NS is an effective abortive migraine treatment in adolescents and is generally well tolerated.
New migraine treatments
Although not pediatric studies, several presentations addressed exciting new preventive treatments that target one of the main neuropeptides implicated in migraine pathophysiology, calcitonin gene related peptide. Four drug companies have completed phase II and phase III adult trials in which they have developed humanized monoclonal antibodies that bind to CGRP or its receptor. These medications have shown great promise and appear to be very well tolerated. These are the first medications developed specifically for migraine prevention, as opposed to current medications which we borrow from other fields of medicine. It is anticipated they will be available for use in adult migraineurs later this year.
Dr. Qubty is a pediatric headache specialist and an assistant professor of neurology at the University of California, San Francisco, and he is a member of the American Headache Society. He said he had no relevant financial disclosures.
*Correction, 8/10/2017: An earlier version of this article misstated the percentage of pediatric migraine patients who had premonitory signs, and how common premonitory signs were among episodic migraineurs with and without aura.
References
1. Lancet. 2016 Oct 8;388(10053):1545-1602.
2. Dev Med Child Neurol. 2010 Dec;52(12):1088-97.
3. Neurology. 2012 Oct 30;79(18):1881-8.
4. Brain. 2014 Jan;137(Pt 1):232-41.
5. Cephalalgia 2016;36:951-959.
6. J Headache Pain. 2016 Dec;17(1):94.
7. Headache. 2016 Jul;56(7):1107-19.
Migraine is the most common disabling neurologic disease, with an estimated 1 billion sufferers worldwide.1 In children aged 5-15 years, migraine prevalence is 10%, and these children miss more school than their peers.2,3 Research specific to the child and adolescent migraine population is imperative, as the findings in adult studies do not always correlate or translate to pediatrics. The American Headache Society (AHS) held its 59th annual scientific meeting in Boston in June 2017, a meeting designed to showcase the latest advances in the field of headache medicine. Several interesting pediatric headache studies were presented.
Pediatric patient, parent goals and preferences for preventive treatment
There is a general consensus among headache specialists that migraine preventive treatment should be instituted when a migraineur has at least four headache days per month. Clinically, and in most research trials, migraine preventive treatment is considered effective when a 50% reduction in headache days or the headache frequency is reduced to no more than four headache days per month.
Perhaps not surprisingly, patients and families expect treatment to result in very few headaches with minimal side effects. It is helpful to understand patient and family treatment goals as clinicians so we can to better provide realistic expectations of care, improve treatment adherence, and reduce patient/parent frustration.
Premonitory symptoms
Migraine is disabling not simply because of the headache but because of the range of symptoms that occur around the headache. Migraine may involve four phases: premonitory, aura, headache, and postdrome. The premonitory phase involves symptoms that may occur hours to days prior to the headache. Functional imaging studies reveal hypothalamic activation during this phase.4 In a large retrospective study, premonitory symptoms occurred in approximately three-quarters of pediatric and adult migraineurs.5 In a prior pediatric chart review, the most common premonitory symptoms in order of decreasing frequency were fatigue, mood change, neck stiffness, and yawning.6
Understanding and identifying premonitory signs is important for better understanding the pathophysiology of migraine and to help our patients recognize when a migraine may be coming.
Mapping pain in pediatric migraine
Diagnosis of migraine is based on the International Classification of Headache Disorders 3rd edition beta (ICHD-3b). For adults with migraine, part of the diagnostic criteria requires at least two of a number of features: unilateral location, pulsating quality, moderate or severe pain intensity, or aggravation by or avoidance of routine physical activity. The comments section of the ICHD-3b mentions that, in children under 18 years, the pain may be bilateral.
This study sought to characterize the location and quality of headache pain in the pediatric and young adult population. Sixty migraineurs were enrolled and divided into three age groups: children (7-11 years), adolescents (12-18), and young adults (19-26). The patients were guided to use a diagram to draw pain location and quality. The pain was bilateral for the majority of patients in all age groups. Of the young adult group, 85% had bilateral headache. This is of interest, as adults with migraine are conventionally thought to have unilateral headache. The main descriptors among all three groups were throbbing, pounding, and pressing. In children, tightening was more common than throbbing.
When diagnosing migraine, it is helpful to take these differences into consideration. Overall, this study provides a better understanding of the quality and location of migraine in the pediatric and young adult population.
Efficacy of zolmitriptan nasal spray in adolescents
Zolmitriptan nasal spray (NS) was approved by the Food and Drug Administration in 2015 for acute migraine treatment in adolescents ages 12-17 years. This was the first triptan NS approved for use in pediatric migraine. The NS route benefits migraineurs who need a rapidly absorbed triptan or those who do not tolerate oral triptans because of significant nausea or emesis with their migraine. The efficacy of zolmitriptan NS in adolescents was established in a multicenter, double-blind, randomized placebo controlled study with 798 participants.7 The primary endpoint of pain freedom at 2 hours after treatment for the 5-mg dose was superior to placebo, 30% vs. 17%, respectively (P less than .001; odds ratio, 2.18; 95% confidence interval, 1.40, 3.39). Patients with migraine going from moderate or severe to mild or no headache at 2 hours post treatment were 51% vs. 39%, respectively (P = .010).
The follow-up study presented at AHS was a subgroup analysis of the above data in younger (12-14 years) and older (15-17 years) adolescents. The primary efficacy endpoint of being pain free at 2 hours post treatment was similarly better for zolmitriptan 5 mg, compared with placebo, in both the younger and older adolescent migraineurs.
This study reinforces that zolmitriptan 5-mg NS is an effective abortive migraine treatment in adolescents and is generally well tolerated.
New migraine treatments
Although not pediatric studies, several presentations addressed exciting new preventive treatments that target one of the main neuropeptides implicated in migraine pathophysiology, calcitonin gene related peptide. Four drug companies have completed phase II and phase III adult trials in which they have developed humanized monoclonal antibodies that bind to CGRP or its receptor. These medications have shown great promise and appear to be very well tolerated. These are the first medications developed specifically for migraine prevention, as opposed to current medications which we borrow from other fields of medicine. It is anticipated they will be available for use in adult migraineurs later this year.
Dr. Qubty is a pediatric headache specialist and an assistant professor of neurology at the University of California, San Francisco, and he is a member of the American Headache Society. He said he had no relevant financial disclosures.
*Correction, 8/10/2017: An earlier version of this article misstated the percentage of pediatric migraine patients who had premonitory signs, and how common premonitory signs were among episodic migraineurs with and without aura.
References
1. Lancet. 2016 Oct 8;388(10053):1545-1602.
2. Dev Med Child Neurol. 2010 Dec;52(12):1088-97.
3. Neurology. 2012 Oct 30;79(18):1881-8.
4. Brain. 2014 Jan;137(Pt 1):232-41.
5. Cephalalgia 2016;36:951-959.
6. J Headache Pain. 2016 Dec;17(1):94.
7. Headache. 2016 Jul;56(7):1107-19.
Migraine is the most common disabling neurologic disease, with an estimated 1 billion sufferers worldwide.1 In children aged 5-15 years, migraine prevalence is 10%, and these children miss more school than their peers.2,3 Research specific to the child and adolescent migraine population is imperative, as the findings in adult studies do not always correlate or translate to pediatrics. The American Headache Society (AHS) held its 59th annual scientific meeting in Boston in June 2017, a meeting designed to showcase the latest advances in the field of headache medicine. Several interesting pediatric headache studies were presented.
Pediatric patient, parent goals and preferences for preventive treatment
There is a general consensus among headache specialists that migraine preventive treatment should be instituted when a migraineur has at least four headache days per month. Clinically, and in most research trials, migraine preventive treatment is considered effective when a 50% reduction in headache days or the headache frequency is reduced to no more than four headache days per month.
Perhaps not surprisingly, patients and families expect treatment to result in very few headaches with minimal side effects. It is helpful to understand patient and family treatment goals as clinicians so we can to better provide realistic expectations of care, improve treatment adherence, and reduce patient/parent frustration.
Premonitory symptoms
Migraine is disabling not simply because of the headache but because of the range of symptoms that occur around the headache. Migraine may involve four phases: premonitory, aura, headache, and postdrome. The premonitory phase involves symptoms that may occur hours to days prior to the headache. Functional imaging studies reveal hypothalamic activation during this phase.4 In a large retrospective study, premonitory symptoms occurred in approximately three-quarters of pediatric and adult migraineurs.5 In a prior pediatric chart review, the most common premonitory symptoms in order of decreasing frequency were fatigue, mood change, neck stiffness, and yawning.6
Understanding and identifying premonitory signs is important for better understanding the pathophysiology of migraine and to help our patients recognize when a migraine may be coming.
Mapping pain in pediatric migraine
Diagnosis of migraine is based on the International Classification of Headache Disorders 3rd edition beta (ICHD-3b). For adults with migraine, part of the diagnostic criteria requires at least two of a number of features: unilateral location, pulsating quality, moderate or severe pain intensity, or aggravation by or avoidance of routine physical activity. The comments section of the ICHD-3b mentions that, in children under 18 years, the pain may be bilateral.
This study sought to characterize the location and quality of headache pain in the pediatric and young adult population. Sixty migraineurs were enrolled and divided into three age groups: children (7-11 years), adolescents (12-18), and young adults (19-26). The patients were guided to use a diagram to draw pain location and quality. The pain was bilateral for the majority of patients in all age groups. Of the young adult group, 85% had bilateral headache. This is of interest, as adults with migraine are conventionally thought to have unilateral headache. The main descriptors among all three groups were throbbing, pounding, and pressing. In children, tightening was more common than throbbing.
When diagnosing migraine, it is helpful to take these differences into consideration. Overall, this study provides a better understanding of the quality and location of migraine in the pediatric and young adult population.
Efficacy of zolmitriptan nasal spray in adolescents
Zolmitriptan nasal spray (NS) was approved by the Food and Drug Administration in 2015 for acute migraine treatment in adolescents ages 12-17 years. This was the first triptan NS approved for use in pediatric migraine. The NS route benefits migraineurs who need a rapidly absorbed triptan or those who do not tolerate oral triptans because of significant nausea or emesis with their migraine. The efficacy of zolmitriptan NS in adolescents was established in a multicenter, double-blind, randomized placebo controlled study with 798 participants.7 The primary endpoint of pain freedom at 2 hours after treatment for the 5-mg dose was superior to placebo, 30% vs. 17%, respectively (P less than .001; odds ratio, 2.18; 95% confidence interval, 1.40, 3.39). Patients with migraine going from moderate or severe to mild or no headache at 2 hours post treatment were 51% vs. 39%, respectively (P = .010).
The follow-up study presented at AHS was a subgroup analysis of the above data in younger (12-14 years) and older (15-17 years) adolescents. The primary efficacy endpoint of being pain free at 2 hours post treatment was similarly better for zolmitriptan 5 mg, compared with placebo, in both the younger and older adolescent migraineurs.
This study reinforces that zolmitriptan 5-mg NS is an effective abortive migraine treatment in adolescents and is generally well tolerated.
New migraine treatments
Although not pediatric studies, several presentations addressed exciting new preventive treatments that target one of the main neuropeptides implicated in migraine pathophysiology, calcitonin gene related peptide. Four drug companies have completed phase II and phase III adult trials in which they have developed humanized monoclonal antibodies that bind to CGRP or its receptor. These medications have shown great promise and appear to be very well tolerated. These are the first medications developed specifically for migraine prevention, as opposed to current medications which we borrow from other fields of medicine. It is anticipated they will be available for use in adult migraineurs later this year.
Dr. Qubty is a pediatric headache specialist and an assistant professor of neurology at the University of California, San Francisco, and he is a member of the American Headache Society. He said he had no relevant financial disclosures.
*Correction, 8/10/2017: An earlier version of this article misstated the percentage of pediatric migraine patients who had premonitory signs, and how common premonitory signs were among episodic migraineurs with and without aura.
References
1. Lancet. 2016 Oct 8;388(10053):1545-1602.
2. Dev Med Child Neurol. 2010 Dec;52(12):1088-97.
3. Neurology. 2012 Oct 30;79(18):1881-8.
4. Brain. 2014 Jan;137(Pt 1):232-41.
5. Cephalalgia 2016;36:951-959.
6. J Headache Pain. 2016 Dec;17(1):94.
7. Headache. 2016 Jul;56(7):1107-19.
Keep a symptom diary!
A friend sent me an article from the New Yorker called “The Algorithm Will See You Now,” in which Siddhartha Mukherjee, MD, author of the magisterial “The Emperor of All Maladies,” ponders the effect artificial intelligence may have on medicine. One possible outcome may be that computers replace radiologists and dermatologists. (They already beat top humans at Jeopardy, chess, and Go, so why not lick Homo sapiens at pattern recognition?)
No worries for me. When Watson takes over, I will be off somewhere playing shuffleboard.

“It’s a particularly bad case. But, the question is why it appeared now, and why it’s getting worse.” She asked the patient about new hair products or family stress. The man said he’d just lost his job.
“Keep a diary,” she advised. “We can determine if there’s a link.”
Thus was my pedagogic legacy shattered in an instant. I’ve spent decades advising students not to tell patients they have a bad case of anything and never to ask them to keep diaries. Then, a foremost medical writer in a leading cultural journal endorses the reverse of both lessons. What was I thinking all these years?
I counseled students not to call any case “bad” because I saw how patients took it personally if I told them that. No matter how mild their diagnosis – rosacea and seborrhea, maladies less emperors than footmen– patients who heard theirs called “bad” looked sad, even insulted. Sad and insulted patients may give up and don’t follow treatment advice. (With such a bad case, why bother?) I didn’t urge patients to think that way. I just couldn’t ignore that they did. By contrast, assuring people that their case “wasn’t bad at all!” made them light up like Halloween pumpkins.
As for diaries, I’ve filed a few that patients handed me over the years. I showed these detailed chronicles to students to illustrate the lengths to which people will go to explain the unexplainable, like the ups and downs of idiopathic urticaria, eczema, and so forth:
- Thursday, August 6th, had sushi at a restaurant with friends.
- Sunday, September 3rd, watched science-fiction movie, unable to sleep that night.
- Monday, October 2nd, discarded fourth new detergent.
And so on.
In the meantime, several times each working day patients would troop in with randomly reoccurring conditions, atopic dermatitis above all, prompting dialogues like these:
“This is crazy! I never had anything like this before!”
“Well, actually, Ms. Jones, I treated you for the same thing in 2006.”
*********************
“This is bizarre! I never had this, and no one in my family ever did either.”
“I see. Well, here’s a prescription.”
“Come to think of it, my Mom had sensitive skin, and I get these dry patches on my arms and legs every winter.”
********************
“I’ve changed my soap three times and thrown out my makeup four times, and the rash keeps coming back. What should I do?”
“Stop throwing out your soap and makeup?”
And so on and on.
Sometimes, of course, semi-plausible causes seem to surface, such as stress. The question is, How useful is it to point this out? Consider the New Yorker case. Once the doctor “determined there is a link,” how might the conversation go?
“We have found the trigger, Mr. Smith. It’s stress.”
“Great! What should I do?”
“Don’t get laid off.”
No doctor (I hope) would ever say that, but patients present reports like the following all the time:
“As a kid, I was allergic to milk, but I’m not anymore.” (No, he wasn’t – he had infantile eczema that got blamed on milk.)
“Penicillin gave me hives.” (But, the hives lasted 6 weeks after the penicillin was stopped, which showed that the hives were idiopathic.)
“I’m very sensitive. I can’t use any moisturizer, any makeup, or all pills.” (People generate long litanies of sensitivities, piling one spurious correlation on another.)
Who benefits from “determining the link” when there isn’t any? Not the patients I’ve been seeing for forty years. Your patients? Maybe detergent manufacturers?
As to my errant pedagogy, with any luck, my students don’t remember a word I told them, a safe assumption for any teacher.
Either that or they don’t read the New Yorker.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@frontlinemedcom.com.
A friend sent me an article from the New Yorker called “The Algorithm Will See You Now,” in which Siddhartha Mukherjee, MD, author of the magisterial “The Emperor of All Maladies,” ponders the effect artificial intelligence may have on medicine. One possible outcome may be that computers replace radiologists and dermatologists. (They already beat top humans at Jeopardy, chess, and Go, so why not lick Homo sapiens at pattern recognition?)
No worries for me. When Watson takes over, I will be off somewhere playing shuffleboard.
“It’s a particularly bad case. But, the question is why it appeared now, and why it’s getting worse.” She asked the patient about new hair products or family stress. The man said he’d just lost his job.
“Keep a diary,” she advised. “We can determine if there’s a link.”
Thus was my pedagogic legacy shattered in an instant. I’ve spent decades advising students not to tell patients they have a bad case of anything and never to ask them to keep diaries. Then, a foremost medical writer in a leading cultural journal endorses the reverse of both lessons. What was I thinking all these years?
I counseled students not to call any case “bad” because I saw how patients took it personally if I told them that. No matter how mild their diagnosis – rosacea and seborrhea, maladies less emperors than footmen– patients who heard theirs called “bad” looked sad, even insulted. Sad and insulted patients may give up and don’t follow treatment advice. (With such a bad case, why bother?) I didn’t urge patients to think that way. I just couldn’t ignore that they did. By contrast, assuring people that their case “wasn’t bad at all!” made them light up like Halloween pumpkins.
As for diaries, I’ve filed a few that patients handed me over the years. I showed these detailed chronicles to students to illustrate the lengths to which people will go to explain the unexplainable, like the ups and downs of idiopathic urticaria, eczema, and so forth:
- Thursday, August 6th, had sushi at a restaurant with friends.
- Sunday, September 3rd, watched science-fiction movie, unable to sleep that night.
- Monday, October 2nd, discarded fourth new detergent.
And so on.
In the meantime, several times each working day patients would troop in with randomly reoccurring conditions, atopic dermatitis above all, prompting dialogues like these:
“This is crazy! I never had anything like this before!”
“Well, actually, Ms. Jones, I treated you for the same thing in 2006.”
*********************
“This is bizarre! I never had this, and no one in my family ever did either.”
“I see. Well, here’s a prescription.”
“Come to think of it, my Mom had sensitive skin, and I get these dry patches on my arms and legs every winter.”
********************
“I’ve changed my soap three times and thrown out my makeup four times, and the rash keeps coming back. What should I do?”
“Stop throwing out your soap and makeup?”
And so on and on.
Sometimes, of course, semi-plausible causes seem to surface, such as stress. The question is, How useful is it to point this out? Consider the New Yorker case. Once the doctor “determined there is a link,” how might the conversation go?
“We have found the trigger, Mr. Smith. It’s stress.”
“Great! What should I do?”
“Don’t get laid off.”
No doctor (I hope) would ever say that, but patients present reports like the following all the time:
“As a kid, I was allergic to milk, but I’m not anymore.” (No, he wasn’t – he had infantile eczema that got blamed on milk.)
“Penicillin gave me hives.” (But, the hives lasted 6 weeks after the penicillin was stopped, which showed that the hives were idiopathic.)
“I’m very sensitive. I can’t use any moisturizer, any makeup, or all pills.” (People generate long litanies of sensitivities, piling one spurious correlation on another.)
Who benefits from “determining the link” when there isn’t any? Not the patients I’ve been seeing for forty years. Your patients? Maybe detergent manufacturers?
As to my errant pedagogy, with any luck, my students don’t remember a word I told them, a safe assumption for any teacher.
Either that or they don’t read the New Yorker.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@frontlinemedcom.com.
A friend sent me an article from the New Yorker called “The Algorithm Will See You Now,” in which Siddhartha Mukherjee, MD, author of the magisterial “The Emperor of All Maladies,” ponders the effect artificial intelligence may have on medicine. One possible outcome may be that computers replace radiologists and dermatologists. (They already beat top humans at Jeopardy, chess, and Go, so why not lick Homo sapiens at pattern recognition?)
No worries for me. When Watson takes over, I will be off somewhere playing shuffleboard.
“It’s a particularly bad case. But, the question is why it appeared now, and why it’s getting worse.” She asked the patient about new hair products or family stress. The man said he’d just lost his job.
“Keep a diary,” she advised. “We can determine if there’s a link.”
Thus was my pedagogic legacy shattered in an instant. I’ve spent decades advising students not to tell patients they have a bad case of anything and never to ask them to keep diaries. Then, a foremost medical writer in a leading cultural journal endorses the reverse of both lessons. What was I thinking all these years?
I counseled students not to call any case “bad” because I saw how patients took it personally if I told them that. No matter how mild their diagnosis – rosacea and seborrhea, maladies less emperors than footmen– patients who heard theirs called “bad” looked sad, even insulted. Sad and insulted patients may give up and don’t follow treatment advice. (With such a bad case, why bother?) I didn’t urge patients to think that way. I just couldn’t ignore that they did. By contrast, assuring people that their case “wasn’t bad at all!” made them light up like Halloween pumpkins.
As for diaries, I’ve filed a few that patients handed me over the years. I showed these detailed chronicles to students to illustrate the lengths to which people will go to explain the unexplainable, like the ups and downs of idiopathic urticaria, eczema, and so forth:
- Thursday, August 6th, had sushi at a restaurant with friends.
- Sunday, September 3rd, watched science-fiction movie, unable to sleep that night.
- Monday, October 2nd, discarded fourth new detergent.
And so on.
In the meantime, several times each working day patients would troop in with randomly reoccurring conditions, atopic dermatitis above all, prompting dialogues like these:
“This is crazy! I never had anything like this before!”
“Well, actually, Ms. Jones, I treated you for the same thing in 2006.”
*********************
“This is bizarre! I never had this, and no one in my family ever did either.”
“I see. Well, here’s a prescription.”
“Come to think of it, my Mom had sensitive skin, and I get these dry patches on my arms and legs every winter.”
********************
“I’ve changed my soap three times and thrown out my makeup four times, and the rash keeps coming back. What should I do?”
“Stop throwing out your soap and makeup?”
And so on and on.
Sometimes, of course, semi-plausible causes seem to surface, such as stress. The question is, How useful is it to point this out? Consider the New Yorker case. Once the doctor “determined there is a link,” how might the conversation go?
“We have found the trigger, Mr. Smith. It’s stress.”
“Great! What should I do?”
“Don’t get laid off.”
No doctor (I hope) would ever say that, but patients present reports like the following all the time:
“As a kid, I was allergic to milk, but I’m not anymore.” (No, he wasn’t – he had infantile eczema that got blamed on milk.)
“Penicillin gave me hives.” (But, the hives lasted 6 weeks after the penicillin was stopped, which showed that the hives were idiopathic.)
“I’m very sensitive. I can’t use any moisturizer, any makeup, or all pills.” (People generate long litanies of sensitivities, piling one spurious correlation on another.)
Who benefits from “determining the link” when there isn’t any? Not the patients I’ve been seeing for forty years. Your patients? Maybe detergent manufacturers?
As to my errant pedagogy, with any luck, my students don’t remember a word I told them, a safe assumption for any teacher.
Either that or they don’t read the New Yorker.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@frontlinemedcom.com.
Digital cohorts within the social mediome to circumvent conventional research challenges?
We are becoming comfortable with the concept of a sharing economy, where resources are shared among many individuals using online forums. Whether activities involve sharing rides (Uber, Lyft, and others), accommodations (Airbnb), or information (social media), underlying attributes include reduced transactional costs, enhanced information transparency, dynamic feedback, and socialization of opportunity. As health care systems realize that they are changing from direct-to-business to a direct-to-customer model, their ability to connect directly with individuals will become a foundational strategy.
This month’s column introduces us to social media as a research tool. Information derived from social media sites can be harvested for critical clinical information (the Centers for Disease and Control and Prevention tracks the spread of influenza using social media analytic tools), research data (patient preferences), and as a recruitment method for clinical studies. Kulanthaivel and colleagues have described their experiences and literature review to help us imagine new ways to collect data at markedly reduced transaction costs (compared to a formal clinical trial). While there are many cautions about the use of social media in your practice or research, we are only beginning to understand its potential.
John I. Allen, MD, MBA, AGAF
Editor in Chief
Medical knowledge, culminating from the collection and translation of patient data, is the primary objective of the clinical research paradigm. The successful conduct of this traditional model has become even more challenging with expansion of costs and a dwindling research infrastructure. Beyond systemic issues, conventional research methods are burdened further by minimal patient engagement, inadequate staffing, and geographic limitations to recruitment. Clinical research also has failed to keep pace with patient demands, and the limited scope of well-funded, disease-specific investigations have left many patients feeling disenfranchised. Social media venues may represent a viable option to surpass these current and evolving barriers when used as an adjunctive approach to traditional clinical investigation.

Advantages and pitfalls in social media research
SM is a new frontier containing a wide spectrum of clinical and qualitative data from connected users (patients). Collection and examination of either individuals’ or groups’ SM information use can provide insight into qualitative life experiences, just as analysis of biologic samples can enable dissection of genetic disease underpinnings. This mediome is analogous to the human genome, both in content and utility.1 Analyzing data streams from SM for interpersonal interactions, message content, and even frequency can provide digital investigators with volumes of information that otherwise would remain unattainable.

Several limitations and potential risks of SM for medical research should be addressed, including the possible compromise of privacy and confidentiality, the use and dissemination of medical advice and information, potential demographic biases, and a required trust of the investigator by patients. Many of these challenges can be similar to traditional methods, however, as in the conventional model, careful management can drastically reduce unwanted study issues.
The risk of Health Insurance Portability and Accountability Act violations must be considered seriously in the context of patient–researcher interactions on SM. Because of the relatively public nature of these venues, patient confidentiality may be at risk if patients choose to divulge personal medical information. However, if proper protective measures are taken to ensure that the venue is secure (e.g., a private or closed group on Facebook or a by-invitation-only online Internet forum), and the researcher vets all patients who request entrance into the group, this risk may be minimized. Moreover, to further reduce any legal liability, the researcher should not provide any medical advice to patients who participate in a SM study. The drive to provide medical direction in study patients with clinical need may be strong because collaborative relationships between investigator and patients are likely to form. Furthermore, digital access to investigators on SM commonly becomes easy for patients. Safe approaches to communication could include redirecting patients to consult with their own doctor for advice, unbiased dissemination of disease-specific educational materials, or depiction of only institutional review board–approved study materials.7,8

The perception that only younger populations use SM may appear to be a significant limitation for its implementation in clinical research. However, this limitation is rapidly becoming less significant because recent studies have shown that the use of SM has become increasingly common among older adults. As of 2014, more than half of the US adult population used Facebook, including 73% and 63% of Internet-using adults ages 30–49 and 50–64 years, respectively.10 SM may not be suitable for all diseases, however, there is likely significant demographic overlap for many disease populations.
Finally, it is imperative for researchers to gain the trust of patients on SM to effectively use these venues for research purposes. Because patient–researcher interaction does not occur face-to-face on these platforms, gaining the trust of patients may be more difficult than it would be in a clinical setting. Thus, patient–patient and patient–researcher communications within SM platforms must be cultivated carefully to instill participant confidence in the research being performed on their behalf. One of the authors (C.L.) has established an SM educational model for this exchange.4 Specifically, he provides patients with a distillation of current field research by posting updates in a research-specific Facebook group and on Twitter. This model not only empowers patients with disease education, it also solidifies the importance of patient investment in disease-specific research. Furthermore, invested patients bring ideas to research, take a more educated and proactive role in their care team, and, ultimately, return to seek more study involvement.

Social media in rare disease research
Rare diseases (conditions with a prevalence of less than 200,000 patients in North America), in particular, are prime for high-yield results and community impact using novel SM approaches. This is the result of established digital support groups, publications with historically low study numbers, and few focused investigators. Several studies of rare diseases have shown considerable advantages of using SM as a study tool. For instance, an existing neuroendocrine cervical cancer Facebook support group recently was used to recruit a geographically widespread cohort of patients with this rare cancer. Through an online survey posted in the Facebook group, patients were able to provide specific information on their treatment, disease, and symptom history, current disease status, and quality of life, including various psychological factors. Without the use of SM, collecting this information would have been virtually impossible because the patients were treated at 51 cancer centers across the country.14
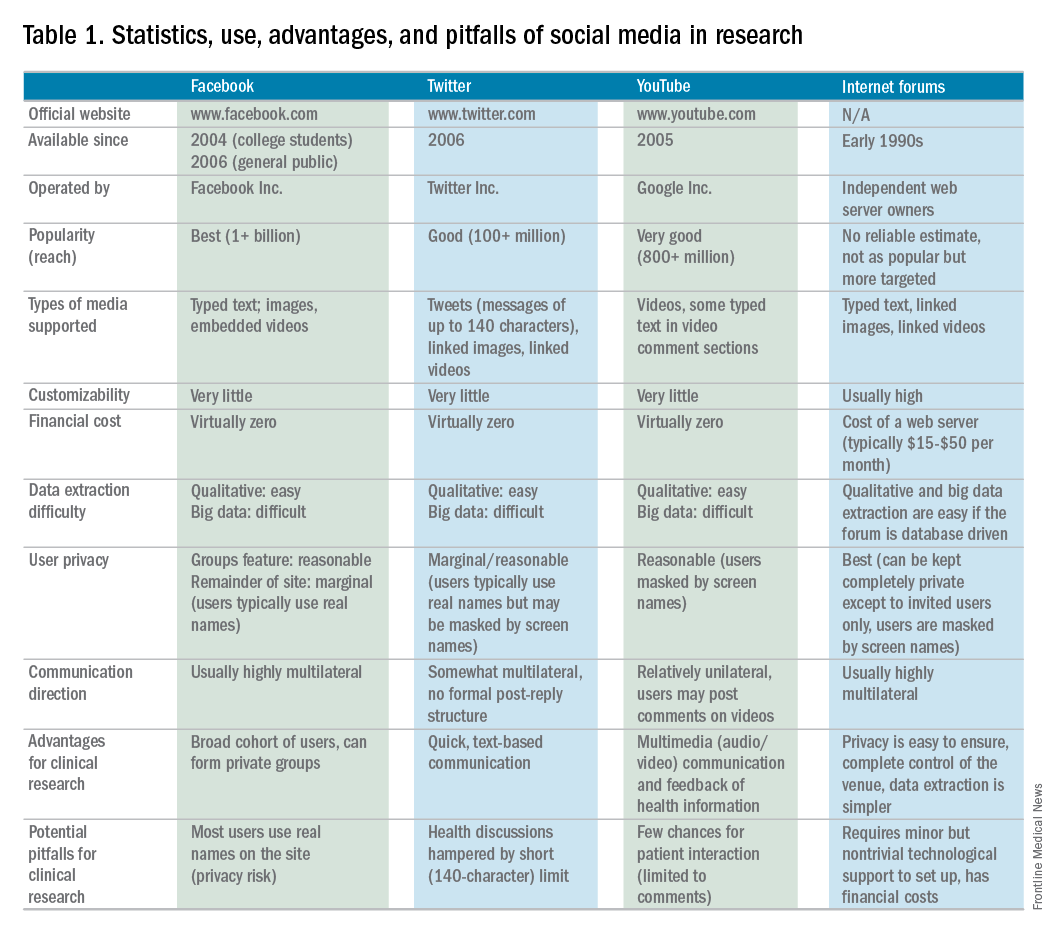
Currently, the use of SM in hepatology research, focused specifically on autoimmune hepatitis (AIH), is under exploration at Indiana University. AIH is a rare autoimmune liver disease that results in immune-mediated destruction of liver cells, possibly resulting in fibrosis, cirrhosis, or liver failure if treatment is unsuccessful. One of the authors (C.L.) used both Facebook and Twitter to construct a large study group of individuals affected with AIH called the Autoimmune Hepatitis Research Network (AHRN; 1,500 members) during the past 2 years.4 Interested individuals have joined this research group after searching for AIH online support groups or reading shared AHRN posts on other media platforms. Between April 2015 and April 2016, there were posts by more than 750 unique active members (more than 50% of the group contributes to discussions), most of whom appear to be either caregivers of AIH patients or AIH patients themselves.
Preliminary informational analysis on this group has shown that C.L. and study collaborators have been able to uncover rich clinical and nonclinical information that otherwise would remain unknown. This research was performed by semi-automated download of the Facebook group’s content and subsequent semantic analysis. Qualitative analysis also was performed by direct reading of patient narratives. Collected clinical information has included histories of medication side effects, familial autoimmune diseases, and comorbid conditions. The most common factors that patients were unlikely to discuss with a provider (e.g., financial issues, employment, personal relationships, use of supplements, and alcohol use) frequently were discussed in the AHRN group, allowing a more transparent view of the complete disease experience.
Beyond research conducted in the current paradigm, the AHRN has provided a rich community construct in which patients offer each other social support. The patient impression of AHRN on Facebook has been overwhelmingly positive, and patients often wonder why such a model has not been used with other diseases. The close digital interaction the author (C.L.) has had with numerous patients and families has promoted other benefits of this methodology: more than 40 new AIH patients from outside Indiana have traveled to Indiana University for medical consultation despite no advertisement.
Conclusions
SM has the potential to transform health care research as a supplement to traditional research methods. Compared with a conventional research model, this methodology has proven to be cost and time effective, wide reaching, and similarly capable of data collection. Use of SM in research has tremendous potential to direct patient-centered research because invested patient collaborators can take an active role in their own disease and may hone investigatory focus on stakeholder priorities. Limitations to this method are known, however; if implemented cautiously, these can be mitigated. Investment in and application of the social mediome by investigators and patients has the potential to support and transform research that otherwise would be impossible.
Acknowledgments
The authors wish to extend their gratitude to the members of the Autoimmune Hepatitis Research Network for their continued proactivity and engagement in autoimmune hepatitis research. Furthermore, the authors are grateful to Dr. Naga Chalasani for his continued mentorship and extensive contributions to the development of social media approaches in clinical investigation.
References
1. Asch, D.A., Rader, D.J., Merchant, R.M. Mining the social mediome. Trends Mol Med. 2015;21:528-9.
2. Brotherton, C.S., Martin, C.A., Long, M.D. et al. Avoidance of fiber is associated with greater risk of Crohn’s disease flare in a 6-month period. Clin Gastroenterol Hepatol. 2016;14:1130-6.
3. Fenner, Y., Garland, S.M., Moore, E.E., et al. Web-based recruiting for health research using a social networking site: an exploratory study. J Med Internet Res. 2012;14:e20.
4. Lammert, C., Comerford, M., Love, J., et al. Investigation gone viral: application of the social mediasphere in research. Gastroenterology. 2015;149:839-43.
5. Wicks, P., Massagli, M., Frost, J., et al. Sharing health data for better outcomes on PatientsLikeMe. J Med Internet Res. 2010;12:e19.
6. Admon, L., Haefner, J.K., Kolenic, G.E., et al. Recruiting pregnant patients for survey research: a head to head comparison of social media-based versus clinic-based approaches. J Med Internet Res. 2016;18:e326.
7. Farnan, J.M., Sulmasy, L.S., Chaudhry, H. Online medical professionalism. Ann Intern Med. 2013;159:158-9.
8. Massachusetts Medical Society: Social Media Guidelines for Physicians. Available from: http://www.massmed.org/Physicians/Legal-and-Regulatory/Social-Media-Guidelines-for-Physicians/#. Accessed: January 3, 2017.
9. Pirraglia, P.A. Kravitz, R.L. Social media: new opportunities, new ethical concerns. J Gen Intern Med. 2013;28:165-6.
10. Duggan, M., Ellison, N.B., Lampe, C. et al. Demographics of key social networking platforms. (Available from:) (Accessed: January 4, 2017) Pew Res Cent Internet Sci Tech. 2015; http://www.pewinternet.org/2015/01/09/demographics-of-key-social-networking-platforms-2
11. Kang, X., Zhao, L., Leung, F., et al. Delivery of Instructions via mobile social media app increases quality of bowel preparation. Clin Gastroenterol Hepatol. 2016;14:429-35.
12. Bajaj, J.S., Heuman, D.M., Sterling, R.K., et al. Validation of EncephalApp, Smartphone-based Stroop test, for the diagnosis of covert hepatic encephalopathy. Clin Gastroenterol Hepatol. 2015;13:1828-35.
13. Riaz, M.S. Atreja, A. Personalized technologies in chronic gastrointestinal disorders: self-monitoring and remote sensor technologies. Clin Gastroenterol Hepatol. 2016;14:1697-705.
14. Zaid, T., Burzawa, J., Basen-Engquist, K., et al. Use of social media to conduct a cross-sectional epidemiologic and quality of life survey of patients with neuroendocrine carcinoma of the cervix: a feasibility study. Gynecol Oncol. 2014;132:149-53.
15. Schumacher, K.R., Stringer, K.A., Donohue, J.E., et al. Social media methods for studying rare diseases. Pediatrics. 2014;133:e1345–53.
Dr. Kulanthaivel and Dr. Jones are in the school of informatics and computing, Purdue University, Indiana University, Indianapolis; Dr. Fogel and Dr. Lammert are in the department of digestive and liver diseases, Indiana University School of Medicine, Indianapolis. This study was supported by KL2TR001106 and UL1TR001108 from the National Institutes of Health, and the Clinical and Translational Sciences Award from the National Center for Advancing Translational Sciences (C.L.). The authors disclose no conflicts.
We are becoming comfortable with the concept of a sharing economy, where resources are shared among many individuals using online forums. Whether activities involve sharing rides (Uber, Lyft, and others), accommodations (Airbnb), or information (social media), underlying attributes include reduced transactional costs, enhanced information transparency, dynamic feedback, and socialization of opportunity. As health care systems realize that they are changing from direct-to-business to a direct-to-customer model, their ability to connect directly with individuals will become a foundational strategy.
This month’s column introduces us to social media as a research tool. Information derived from social media sites can be harvested for critical clinical information (the Centers for Disease and Control and Prevention tracks the spread of influenza using social media analytic tools), research data (patient preferences), and as a recruitment method for clinical studies. Kulanthaivel and colleagues have described their experiences and literature review to help us imagine new ways to collect data at markedly reduced transaction costs (compared to a formal clinical trial). While there are many cautions about the use of social media in your practice or research, we are only beginning to understand its potential.
John I. Allen, MD, MBA, AGAF
Editor in Chief
Medical knowledge, culminating from the collection and translation of patient data, is the primary objective of the clinical research paradigm. The successful conduct of this traditional model has become even more challenging with expansion of costs and a dwindling research infrastructure. Beyond systemic issues, conventional research methods are burdened further by minimal patient engagement, inadequate staffing, and geographic limitations to recruitment. Clinical research also has failed to keep pace with patient demands, and the limited scope of well-funded, disease-specific investigations have left many patients feeling disenfranchised. Social media venues may represent a viable option to surpass these current and evolving barriers when used as an adjunctive approach to traditional clinical investigation.
Advantages and pitfalls in social media research
SM is a new frontier containing a wide spectrum of clinical and qualitative data from connected users (patients). Collection and examination of either individuals’ or groups’ SM information use can provide insight into qualitative life experiences, just as analysis of biologic samples can enable dissection of genetic disease underpinnings. This mediome is analogous to the human genome, both in content and utility.1 Analyzing data streams from SM for interpersonal interactions, message content, and even frequency can provide digital investigators with volumes of information that otherwise would remain unattainable.
Several limitations and potential risks of SM for medical research should be addressed, including the possible compromise of privacy and confidentiality, the use and dissemination of medical advice and information, potential demographic biases, and a required trust of the investigator by patients. Many of these challenges can be similar to traditional methods, however, as in the conventional model, careful management can drastically reduce unwanted study issues.
The risk of Health Insurance Portability and Accountability Act violations must be considered seriously in the context of patient–researcher interactions on SM. Because of the relatively public nature of these venues, patient confidentiality may be at risk if patients choose to divulge personal medical information. However, if proper protective measures are taken to ensure that the venue is secure (e.g., a private or closed group on Facebook or a by-invitation-only online Internet forum), and the researcher vets all patients who request entrance into the group, this risk may be minimized. Moreover, to further reduce any legal liability, the researcher should not provide any medical advice to patients who participate in a SM study. The drive to provide medical direction in study patients with clinical need may be strong because collaborative relationships between investigator and patients are likely to form. Furthermore, digital access to investigators on SM commonly becomes easy for patients. Safe approaches to communication could include redirecting patients to consult with their own doctor for advice, unbiased dissemination of disease-specific educational materials, or depiction of only institutional review board–approved study materials.7,8
The perception that only younger populations use SM may appear to be a significant limitation for its implementation in clinical research. However, this limitation is rapidly becoming less significant because recent studies have shown that the use of SM has become increasingly common among older adults. As of 2014, more than half of the US adult population used Facebook, including 73% and 63% of Internet-using adults ages 30–49 and 50–64 years, respectively.10 SM may not be suitable for all diseases, however, there is likely significant demographic overlap for many disease populations.
Finally, it is imperative for researchers to gain the trust of patients on SM to effectively use these venues for research purposes. Because patient–researcher interaction does not occur face-to-face on these platforms, gaining the trust of patients may be more difficult than it would be in a clinical setting. Thus, patient–patient and patient–researcher communications within SM platforms must be cultivated carefully to instill participant confidence in the research being performed on their behalf. One of the authors (C.L.) has established an SM educational model for this exchange.4 Specifically, he provides patients with a distillation of current field research by posting updates in a research-specific Facebook group and on Twitter. This model not only empowers patients with disease education, it also solidifies the importance of patient investment in disease-specific research. Furthermore, invested patients bring ideas to research, take a more educated and proactive role in their care team, and, ultimately, return to seek more study involvement.
Social media in rare disease research
Rare diseases (conditions with a prevalence of less than 200,000 patients in North America), in particular, are prime for high-yield results and community impact using novel SM approaches. This is the result of established digital support groups, publications with historically low study numbers, and few focused investigators. Several studies of rare diseases have shown considerable advantages of using SM as a study tool. For instance, an existing neuroendocrine cervical cancer Facebook support group recently was used to recruit a geographically widespread cohort of patients with this rare cancer. Through an online survey posted in the Facebook group, patients were able to provide specific information on their treatment, disease, and symptom history, current disease status, and quality of life, including various psychological factors. Without the use of SM, collecting this information would have been virtually impossible because the patients were treated at 51 cancer centers across the country.14
Currently, the use of SM in hepatology research, focused specifically on autoimmune hepatitis (AIH), is under exploration at Indiana University. AIH is a rare autoimmune liver disease that results in immune-mediated destruction of liver cells, possibly resulting in fibrosis, cirrhosis, or liver failure if treatment is unsuccessful. One of the authors (C.L.) used both Facebook and Twitter to construct a large study group of individuals affected with AIH called the Autoimmune Hepatitis Research Network (AHRN; 1,500 members) during the past 2 years.4 Interested individuals have joined this research group after searching for AIH online support groups or reading shared AHRN posts on other media platforms. Between April 2015 and April 2016, there were posts by more than 750 unique active members (more than 50% of the group contributes to discussions), most of whom appear to be either caregivers of AIH patients or AIH patients themselves.
Preliminary informational analysis on this group has shown that C.L. and study collaborators have been able to uncover rich clinical and nonclinical information that otherwise would remain unknown. This research was performed by semi-automated download of the Facebook group’s content and subsequent semantic analysis. Qualitative analysis also was performed by direct reading of patient narratives. Collected clinical information has included histories of medication side effects, familial autoimmune diseases, and comorbid conditions. The most common factors that patients were unlikely to discuss with a provider (e.g., financial issues, employment, personal relationships, use of supplements, and alcohol use) frequently were discussed in the AHRN group, allowing a more transparent view of the complete disease experience.
Beyond research conducted in the current paradigm, the AHRN has provided a rich community construct in which patients offer each other social support. The patient impression of AHRN on Facebook has been overwhelmingly positive, and patients often wonder why such a model has not been used with other diseases. The close digital interaction the author (C.L.) has had with numerous patients and families has promoted other benefits of this methodology: more than 40 new AIH patients from outside Indiana have traveled to Indiana University for medical consultation despite no advertisement.
Conclusions
SM has the potential to transform health care research as a supplement to traditional research methods. Compared with a conventional research model, this methodology has proven to be cost and time effective, wide reaching, and similarly capable of data collection. Use of SM in research has tremendous potential to direct patient-centered research because invested patient collaborators can take an active role in their own disease and may hone investigatory focus on stakeholder priorities. Limitations to this method are known, however; if implemented cautiously, these can be mitigated. Investment in and application of the social mediome by investigators and patients has the potential to support and transform research that otherwise would be impossible.
Acknowledgments
The authors wish to extend their gratitude to the members of the Autoimmune Hepatitis Research Network for their continued proactivity and engagement in autoimmune hepatitis research. Furthermore, the authors are grateful to Dr. Naga Chalasani for his continued mentorship and extensive contributions to the development of social media approaches in clinical investigation.
References
1. Asch, D.A., Rader, D.J., Merchant, R.M. Mining the social mediome. Trends Mol Med. 2015;21:528-9.
2. Brotherton, C.S., Martin, C.A., Long, M.D. et al. Avoidance of fiber is associated with greater risk of Crohn’s disease flare in a 6-month period. Clin Gastroenterol Hepatol. 2016;14:1130-6.
3. Fenner, Y., Garland, S.M., Moore, E.E., et al. Web-based recruiting for health research using a social networking site: an exploratory study. J Med Internet Res. 2012;14:e20.
4. Lammert, C., Comerford, M., Love, J., et al. Investigation gone viral: application of the social mediasphere in research. Gastroenterology. 2015;149:839-43.
5. Wicks, P., Massagli, M., Frost, J., et al. Sharing health data for better outcomes on PatientsLikeMe. J Med Internet Res. 2010;12:e19.
6. Admon, L., Haefner, J.K., Kolenic, G.E., et al. Recruiting pregnant patients for survey research: a head to head comparison of social media-based versus clinic-based approaches. J Med Internet Res. 2016;18:e326.
7. Farnan, J.M., Sulmasy, L.S., Chaudhry, H. Online medical professionalism. Ann Intern Med. 2013;159:158-9.
8. Massachusetts Medical Society: Social Media Guidelines for Physicians. Available from: http://www.massmed.org/Physicians/Legal-and-Regulatory/Social-Media-Guidelines-for-Physicians/#. Accessed: January 3, 2017.
9. Pirraglia, P.A. Kravitz, R.L. Social media: new opportunities, new ethical concerns. J Gen Intern Med. 2013;28:165-6.
10. Duggan, M., Ellison, N.B., Lampe, C. et al. Demographics of key social networking platforms. (Available from:) (Accessed: January 4, 2017) Pew Res Cent Internet Sci Tech. 2015; http://www.pewinternet.org/2015/01/09/demographics-of-key-social-networking-platforms-2
11. Kang, X., Zhao, L., Leung, F., et al. Delivery of Instructions via mobile social media app increases quality of bowel preparation. Clin Gastroenterol Hepatol. 2016;14:429-35.
12. Bajaj, J.S., Heuman, D.M., Sterling, R.K., et al. Validation of EncephalApp, Smartphone-based Stroop test, for the diagnosis of covert hepatic encephalopathy. Clin Gastroenterol Hepatol. 2015;13:1828-35.
13. Riaz, M.S. Atreja, A. Personalized technologies in chronic gastrointestinal disorders: self-monitoring and remote sensor technologies. Clin Gastroenterol Hepatol. 2016;14:1697-705.
14. Zaid, T., Burzawa, J., Basen-Engquist, K., et al. Use of social media to conduct a cross-sectional epidemiologic and quality of life survey of patients with neuroendocrine carcinoma of the cervix: a feasibility study. Gynecol Oncol. 2014;132:149-53.
15. Schumacher, K.R., Stringer, K.A., Donohue, J.E., et al. Social media methods for studying rare diseases. Pediatrics. 2014;133:e1345–53.
Dr. Kulanthaivel and Dr. Jones are in the school of informatics and computing, Purdue University, Indiana University, Indianapolis; Dr. Fogel and Dr. Lammert are in the department of digestive and liver diseases, Indiana University School of Medicine, Indianapolis. This study was supported by KL2TR001106 and UL1TR001108 from the National Institutes of Health, and the Clinical and Translational Sciences Award from the National Center for Advancing Translational Sciences (C.L.). The authors disclose no conflicts.
We are becoming comfortable with the concept of a sharing economy, where resources are shared among many individuals using online forums. Whether activities involve sharing rides (Uber, Lyft, and others), accommodations (Airbnb), or information (social media), underlying attributes include reduced transactional costs, enhanced information transparency, dynamic feedback, and socialization of opportunity. As health care systems realize that they are changing from direct-to-business to a direct-to-customer model, their ability to connect directly with individuals will become a foundational strategy.
This month’s column introduces us to social media as a research tool. Information derived from social media sites can be harvested for critical clinical information (the Centers for Disease and Control and Prevention tracks the spread of influenza using social media analytic tools), research data (patient preferences), and as a recruitment method for clinical studies. Kulanthaivel and colleagues have described their experiences and literature review to help us imagine new ways to collect data at markedly reduced transaction costs (compared to a formal clinical trial). While there are many cautions about the use of social media in your practice or research, we are only beginning to understand its potential.
John I. Allen, MD, MBA, AGAF
Editor in Chief
Medical knowledge, culminating from the collection and translation of patient data, is the primary objective of the clinical research paradigm. The successful conduct of this traditional model has become even more challenging with expansion of costs and a dwindling research infrastructure. Beyond systemic issues, conventional research methods are burdened further by minimal patient engagement, inadequate staffing, and geographic limitations to recruitment. Clinical research also has failed to keep pace with patient demands, and the limited scope of well-funded, disease-specific investigations have left many patients feeling disenfranchised. Social media venues may represent a viable option to surpass these current and evolving barriers when used as an adjunctive approach to traditional clinical investigation.
Advantages and pitfalls in social media research
SM is a new frontier containing a wide spectrum of clinical and qualitative data from connected users (patients). Collection and examination of either individuals’ or groups’ SM information use can provide insight into qualitative life experiences, just as analysis of biologic samples can enable dissection of genetic disease underpinnings. This mediome is analogous to the human genome, both in content and utility.1 Analyzing data streams from SM for interpersonal interactions, message content, and even frequency can provide digital investigators with volumes of information that otherwise would remain unattainable.
Several limitations and potential risks of SM for medical research should be addressed, including the possible compromise of privacy and confidentiality, the use and dissemination of medical advice and information, potential demographic biases, and a required trust of the investigator by patients. Many of these challenges can be similar to traditional methods, however, as in the conventional model, careful management can drastically reduce unwanted study issues.
The risk of Health Insurance Portability and Accountability Act violations must be considered seriously in the context of patient–researcher interactions on SM. Because of the relatively public nature of these venues, patient confidentiality may be at risk if patients choose to divulge personal medical information. However, if proper protective measures are taken to ensure that the venue is secure (e.g., a private or closed group on Facebook or a by-invitation-only online Internet forum), and the researcher vets all patients who request entrance into the group, this risk may be minimized. Moreover, to further reduce any legal liability, the researcher should not provide any medical advice to patients who participate in a SM study. The drive to provide medical direction in study patients with clinical need may be strong because collaborative relationships between investigator and patients are likely to form. Furthermore, digital access to investigators on SM commonly becomes easy for patients. Safe approaches to communication could include redirecting patients to consult with their own doctor for advice, unbiased dissemination of disease-specific educational materials, or depiction of only institutional review board–approved study materials.7,8
The perception that only younger populations use SM may appear to be a significant limitation for its implementation in clinical research. However, this limitation is rapidly becoming less significant because recent studies have shown that the use of SM has become increasingly common among older adults. As of 2014, more than half of the US adult population used Facebook, including 73% and 63% of Internet-using adults ages 30–49 and 50–64 years, respectively.10 SM may not be suitable for all diseases, however, there is likely significant demographic overlap for many disease populations.
Finally, it is imperative for researchers to gain the trust of patients on SM to effectively use these venues for research purposes. Because patient–researcher interaction does not occur face-to-face on these platforms, gaining the trust of patients may be more difficult than it would be in a clinical setting. Thus, patient–patient and patient–researcher communications within SM platforms must be cultivated carefully to instill participant confidence in the research being performed on their behalf. One of the authors (C.L.) has established an SM educational model for this exchange.4 Specifically, he provides patients with a distillation of current field research by posting updates in a research-specific Facebook group and on Twitter. This model not only empowers patients with disease education, it also solidifies the importance of patient investment in disease-specific research. Furthermore, invested patients bring ideas to research, take a more educated and proactive role in their care team, and, ultimately, return to seek more study involvement.
Social media in rare disease research
Rare diseases (conditions with a prevalence of less than 200,000 patients in North America), in particular, are prime for high-yield results and community impact using novel SM approaches. This is the result of established digital support groups, publications with historically low study numbers, and few focused investigators. Several studies of rare diseases have shown considerable advantages of using SM as a study tool. For instance, an existing neuroendocrine cervical cancer Facebook support group recently was used to recruit a geographically widespread cohort of patients with this rare cancer. Through an online survey posted in the Facebook group, patients were able to provide specific information on their treatment, disease, and symptom history, current disease status, and quality of life, including various psychological factors. Without the use of SM, collecting this information would have been virtually impossible because the patients were treated at 51 cancer centers across the country.14
Currently, the use of SM in hepatology research, focused specifically on autoimmune hepatitis (AIH), is under exploration at Indiana University. AIH is a rare autoimmune liver disease that results in immune-mediated destruction of liver cells, possibly resulting in fibrosis, cirrhosis, or liver failure if treatment is unsuccessful. One of the authors (C.L.) used both Facebook and Twitter to construct a large study group of individuals affected with AIH called the Autoimmune Hepatitis Research Network (AHRN; 1,500 members) during the past 2 years.4 Interested individuals have joined this research group after searching for AIH online support groups or reading shared AHRN posts on other media platforms. Between April 2015 and April 2016, there were posts by more than 750 unique active members (more than 50% of the group contributes to discussions), most of whom appear to be either caregivers of AIH patients or AIH patients themselves.
Preliminary informational analysis on this group has shown that C.L. and study collaborators have been able to uncover rich clinical and nonclinical information that otherwise would remain unknown. This research was performed by semi-automated download of the Facebook group’s content and subsequent semantic analysis. Qualitative analysis also was performed by direct reading of patient narratives. Collected clinical information has included histories of medication side effects, familial autoimmune diseases, and comorbid conditions. The most common factors that patients were unlikely to discuss with a provider (e.g., financial issues, employment, personal relationships, use of supplements, and alcohol use) frequently were discussed in the AHRN group, allowing a more transparent view of the complete disease experience.
Beyond research conducted in the current paradigm, the AHRN has provided a rich community construct in which patients offer each other social support. The patient impression of AHRN on Facebook has been overwhelmingly positive, and patients often wonder why such a model has not been used with other diseases. The close digital interaction the author (C.L.) has had with numerous patients and families has promoted other benefits of this methodology: more than 40 new AIH patients from outside Indiana have traveled to Indiana University for medical consultation despite no advertisement.
Conclusions
SM has the potential to transform health care research as a supplement to traditional research methods. Compared with a conventional research model, this methodology has proven to be cost and time effective, wide reaching, and similarly capable of data collection. Use of SM in research has tremendous potential to direct patient-centered research because invested patient collaborators can take an active role in their own disease and may hone investigatory focus on stakeholder priorities. Limitations to this method are known, however; if implemented cautiously, these can be mitigated. Investment in and application of the social mediome by investigators and patients has the potential to support and transform research that otherwise would be impossible.
Acknowledgments
The authors wish to extend their gratitude to the members of the Autoimmune Hepatitis Research Network for their continued proactivity and engagement in autoimmune hepatitis research. Furthermore, the authors are grateful to Dr. Naga Chalasani for his continued mentorship and extensive contributions to the development of social media approaches in clinical investigation.
References
1. Asch, D.A., Rader, D.J., Merchant, R.M. Mining the social mediome. Trends Mol Med. 2015;21:528-9.
2. Brotherton, C.S., Martin, C.A., Long, M.D. et al. Avoidance of fiber is associated with greater risk of Crohn’s disease flare in a 6-month period. Clin Gastroenterol Hepatol. 2016;14:1130-6.
3. Fenner, Y., Garland, S.M., Moore, E.E., et al. Web-based recruiting for health research using a social networking site: an exploratory study. J Med Internet Res. 2012;14:e20.
4. Lammert, C., Comerford, M., Love, J., et al. Investigation gone viral: application of the social mediasphere in research. Gastroenterology. 2015;149:839-43.
5. Wicks, P., Massagli, M., Frost, J., et al. Sharing health data for better outcomes on PatientsLikeMe. J Med Internet Res. 2010;12:e19.
6. Admon, L., Haefner, J.K., Kolenic, G.E., et al. Recruiting pregnant patients for survey research: a head to head comparison of social media-based versus clinic-based approaches. J Med Internet Res. 2016;18:e326.
7. Farnan, J.M., Sulmasy, L.S., Chaudhry, H. Online medical professionalism. Ann Intern Med. 2013;159:158-9.
8. Massachusetts Medical Society: Social Media Guidelines for Physicians. Available from: http://www.massmed.org/Physicians/Legal-and-Regulatory/Social-Media-Guidelines-for-Physicians/#. Accessed: January 3, 2017.
9. Pirraglia, P.A. Kravitz, R.L. Social media: new opportunities, new ethical concerns. J Gen Intern Med. 2013;28:165-6.
10. Duggan, M., Ellison, N.B., Lampe, C. et al. Demographics of key social networking platforms. (Available from:) (Accessed: January 4, 2017) Pew Res Cent Internet Sci Tech. 2015; http://www.pewinternet.org/2015/01/09/demographics-of-key-social-networking-platforms-2
11. Kang, X., Zhao, L., Leung, F., et al. Delivery of Instructions via mobile social media app increases quality of bowel preparation. Clin Gastroenterol Hepatol. 2016;14:429-35.
12. Bajaj, J.S., Heuman, D.M., Sterling, R.K., et al. Validation of EncephalApp, Smartphone-based Stroop test, for the diagnosis of covert hepatic encephalopathy. Clin Gastroenterol Hepatol. 2015;13:1828-35.
13. Riaz, M.S. Atreja, A. Personalized technologies in chronic gastrointestinal disorders: self-monitoring and remote sensor technologies. Clin Gastroenterol Hepatol. 2016;14:1697-705.
14. Zaid, T., Burzawa, J., Basen-Engquist, K., et al. Use of social media to conduct a cross-sectional epidemiologic and quality of life survey of patients with neuroendocrine carcinoma of the cervix: a feasibility study. Gynecol Oncol. 2014;132:149-53.
15. Schumacher, K.R., Stringer, K.A., Donohue, J.E., et al. Social media methods for studying rare diseases. Pediatrics. 2014;133:e1345–53.
Dr. Kulanthaivel and Dr. Jones are in the school of informatics and computing, Purdue University, Indiana University, Indianapolis; Dr. Fogel and Dr. Lammert are in the department of digestive and liver diseases, Indiana University School of Medicine, Indianapolis. This study was supported by KL2TR001106 and UL1TR001108 from the National Institutes of Health, and the Clinical and Translational Sciences Award from the National Center for Advancing Translational Sciences (C.L.). The authors disclose no conflicts.
Points/Counterpoint: Should surgeons operate on functional tricuspid regurgitation?
Yes, functional TR is worth repairing (David H. Adams, MD)
Functional tricuspid regurgitation is a common finding in patients undergoing degenerative mitral valve repair. Severe tricuspid regurgitation is unusual, and clearly there is little debate on the merits of concomitant tricuspid repair for these patients. Moderate tricuspid regurgitation is identified preoperatively in around 15% of patients undergoing degenerative mitral repair (J Thorac Cardiovasc Surg. 2011;142:608-13), and concomitant tricuspid repair in these patients is certainly supported by both the American and European guidelines (J Am Coll Cardiol. 2017. doi: 10.1016/j.jacc.2017.03.011; Eur Heart J. 2012;33:2451-96).
What experience and evidence has led us to a more aggressive approach? One of the most important influences on our early adoption of tricuspid repair at the time of mitral surgery was linked to observations that tricuspid regurgitation (TR) sometimes progressed after isolated mitral valve repair (MVR), with some patients developing moderate or worse insufficiency. Certainly, the impact of significant tricuspid regurgitation on the quality and length of patients’ lives and the challenges of reoperation for isolated tricuspid regurgitation are well known to all surgeons.

Consequently, the importance of treating significant annular dilatation, even without significant tricuspid regurgitation, is supported by the guidelines. Our own experience with an aggressive approach to functional tricuspid regurgitation (FTR) at the time of mitral surgery put an exclamation point on this (J Am Coll Cardiol. 2015;65:1931-8). We found that concomitant tricuspid repair in patients who were worse off before surgery with more TR and higher rates of atrial fibrillation and right-sided dysfunction, actually did better during 5 years of follow-up than the isolated mitral repair patients who started with completely normal tricuspid valve anatomy and ventricular function.
Benign neglect is always an option (J Thorac Cardiovasc Surg. 2017;154:125-6), but we agree with Roberto Dion, MD – despite our friends’ opinions in Toronto and Rochester – we would much prefer to have minimal TR and a normal sized tricuspid valve after MVR. Ask yourself: would you rather have no TR and a normal sized tricuspid valve after you undergo a mitral operation, or a very dilated annulus and perhaps moderate FTR? I am pretty sure I know the answer, but if you are not sure, read our paper.
Dr. Adams is cardiac surgeon-in-chief, Mount Sinai Health System, and Marie-Josée and Henry R. Kravis Professor and Chairman, department of cardiovascular surgery, Icahn School of Medicine at Mount Sinai and The Mount Sinai Hospital, and president-elect of the American Association for Thoracic Surgery. He disclosed he is the national co-principal investigator for the Medtronic NeoChord trial, and receives royalties from Medtronic and Edwards Lifesciences. The Icahn School of Medicine at Mount Sinai receives royalty payments from Edwards Lifesciences and Medtronic for intellectual property related to Dr. Adams’ involvement in the development of 2 mitral valve repair rings and 1 tricuspid valve repair ring.
No, a patient with FTR does not necessarily need repair (Tirone David, MD)
In our clinic, a patient who undergoes MVR and has FTR generally goes home without an annuloplasty. We now have 12 years or more of follow-up in these patients, and they do not develop TR if their MVR is competent. We have reported that preoperative TR in patients who had MVR is associated with mitral valve disease and often improves after the operation (J Thorac Cardiovasc Surg. 2017;154:110-22). New postoperative TR is uncommon.
Ninety percent of my mitral valve repair patients today have no symptoms. Of those patients, a small proportion have moderate TR.

Dr. David is a professor of surgery at Toronto General Hospital. He reported no financial relationships.
Yes, but repair of FTR requires caution (Gilles Dreyfus, MD)
The controversy surrounding the legitimacy of concomitant tricuspid annuloplasty for functional TR during MVR begs for a clinical trial, but before we can conduct a clinical trial, we must define the primary and secondary endpoints. We’ve seen recent prospective, randomized trials that have reported faulty conclusions because the primary endpoints were wrong.
We need a strong debate to agree on those endpoints. Mortality as an endpoint will probably take a very long time to arrive at.
We’re mixing up many different factors. We’re mixing up TR grading, and we know that grading is unreliable. We have all seen patients with full-fledged TR, and after we put them on Lasix (furosemide, Sanofi), 3 days later they have mild TR. So the same patient with no treatment becomes let’s say a “Dreyfus indication,” and then suddenly in 3 days the patient doesn’t need surgery. At any further stage of his life this patient can experience severe TR again; tricuspid annuloplasty will prevent that from happening.

Moderate TR according to the common definition does not exist. If you look at the reports in echocardiography and if you ask any cardiologist, everything between no TR and severe TR is considered moderate. We have proposed a new staging system for evaluating FTR that uses three factors: TR severity; annular dilatation; and extent of tethering, or mode of leaflet coaptation (J Am Coll Cardiol. 2015;65:2331-6).
Dr. Dreyfus is director of the medical and surgical team at the Cardiothoracic Centre of Monaco in Monte Carlo and professor of cardiothoracic surgery at Paris V University and the Imperial College of London. He disclosed receiving speaker fees from Edwards Lifesciences, LivaNova, and Medtronic.
No, few FTR patients at risk after MVR (Hartzell Schaff, MD)
Echocardiography can provide a great deal of information about when concomitant repair for TR is indicated during MVR. We’ve found that if the patient has no right-sided signs, has normal right atrial pressure, and has mild or mild/moderate TR at the time of repair to the journey mitral valve, the chance of him returning for a tricuspid valve procedure is near zero.
A few patients do return after MVR. They develop atrial fibrillation and may need a pacemaker, but we see very few patients return for tricuspid surgery.

It’s fair to say we cannot demonstrate any benefit of correcting functional mitral regurgitation. Why would we think there’s a benefit of correcting FTR? We can say we’re going to look at grade of TR down the road, or we could look at some other endpoint, but think about it this way: If we cannot prove that correcting functional mitral regurgitation is helpful, why is correcting FTR going to help?
Dr. Schaff is a cardiothoracic surgeon at Mayo Clinic Foundation, Rochester, Minn. He reported no financial relationships.
Yes, functional TR is worth repairing (David H. Adams, MD)
Functional tricuspid regurgitation is a common finding in patients undergoing degenerative mitral valve repair. Severe tricuspid regurgitation is unusual, and clearly there is little debate on the merits of concomitant tricuspid repair for these patients. Moderate tricuspid regurgitation is identified preoperatively in around 15% of patients undergoing degenerative mitral repair (J Thorac Cardiovasc Surg. 2011;142:608-13), and concomitant tricuspid repair in these patients is certainly supported by both the American and European guidelines (J Am Coll Cardiol. 2017. doi: 10.1016/j.jacc.2017.03.011; Eur Heart J. 2012;33:2451-96).
What experience and evidence has led us to a more aggressive approach? One of the most important influences on our early adoption of tricuspid repair at the time of mitral surgery was linked to observations that tricuspid regurgitation (TR) sometimes progressed after isolated mitral valve repair (MVR), with some patients developing moderate or worse insufficiency. Certainly, the impact of significant tricuspid regurgitation on the quality and length of patients’ lives and the challenges of reoperation for isolated tricuspid regurgitation are well known to all surgeons.
Consequently, the importance of treating significant annular dilatation, even without significant tricuspid regurgitation, is supported by the guidelines. Our own experience with an aggressive approach to functional tricuspid regurgitation (FTR) at the time of mitral surgery put an exclamation point on this (J Am Coll Cardiol. 2015;65:1931-8). We found that concomitant tricuspid repair in patients who were worse off before surgery with more TR and higher rates of atrial fibrillation and right-sided dysfunction, actually did better during 5 years of follow-up than the isolated mitral repair patients who started with completely normal tricuspid valve anatomy and ventricular function.
Benign neglect is always an option (J Thorac Cardiovasc Surg. 2017;154:125-6), but we agree with Roberto Dion, MD – despite our friends’ opinions in Toronto and Rochester – we would much prefer to have minimal TR and a normal sized tricuspid valve after MVR. Ask yourself: would you rather have no TR and a normal sized tricuspid valve after you undergo a mitral operation, or a very dilated annulus and perhaps moderate FTR? I am pretty sure I know the answer, but if you are not sure, read our paper.
Dr. Adams is cardiac surgeon-in-chief, Mount Sinai Health System, and Marie-Josée and Henry R. Kravis Professor and Chairman, department of cardiovascular surgery, Icahn School of Medicine at Mount Sinai and The Mount Sinai Hospital, and president-elect of the American Association for Thoracic Surgery. He disclosed he is the national co-principal investigator for the Medtronic NeoChord trial, and receives royalties from Medtronic and Edwards Lifesciences. The Icahn School of Medicine at Mount Sinai receives royalty payments from Edwards Lifesciences and Medtronic for intellectual property related to Dr. Adams’ involvement in the development of 2 mitral valve repair rings and 1 tricuspid valve repair ring.
No, a patient with FTR does not necessarily need repair (Tirone David, MD)
In our clinic, a patient who undergoes MVR and has FTR generally goes home without an annuloplasty. We now have 12 years or more of follow-up in these patients, and they do not develop TR if their MVR is competent. We have reported that preoperative TR in patients who had MVR is associated with mitral valve disease and often improves after the operation (J Thorac Cardiovasc Surg. 2017;154:110-22). New postoperative TR is uncommon.
Ninety percent of my mitral valve repair patients today have no symptoms. Of those patients, a small proportion have moderate TR.
Dr. David is a professor of surgery at Toronto General Hospital. He reported no financial relationships.
Yes, but repair of FTR requires caution (Gilles Dreyfus, MD)
The controversy surrounding the legitimacy of concomitant tricuspid annuloplasty for functional TR during MVR begs for a clinical trial, but before we can conduct a clinical trial, we must define the primary and secondary endpoints. We’ve seen recent prospective, randomized trials that have reported faulty conclusions because the primary endpoints were wrong.
We need a strong debate to agree on those endpoints. Mortality as an endpoint will probably take a very long time to arrive at.
We’re mixing up many different factors. We’re mixing up TR grading, and we know that grading is unreliable. We have all seen patients with full-fledged TR, and after we put them on Lasix (furosemide, Sanofi), 3 days later they have mild TR. So the same patient with no treatment becomes let’s say a “Dreyfus indication,” and then suddenly in 3 days the patient doesn’t need surgery. At any further stage of his life this patient can experience severe TR again; tricuspid annuloplasty will prevent that from happening.
Moderate TR according to the common definition does not exist. If you look at the reports in echocardiography and if you ask any cardiologist, everything between no TR and severe TR is considered moderate. We have proposed a new staging system for evaluating FTR that uses three factors: TR severity; annular dilatation; and extent of tethering, or mode of leaflet coaptation (J Am Coll Cardiol. 2015;65:2331-6).
Dr. Dreyfus is director of the medical and surgical team at the Cardiothoracic Centre of Monaco in Monte Carlo and professor of cardiothoracic surgery at Paris V University and the Imperial College of London. He disclosed receiving speaker fees from Edwards Lifesciences, LivaNova, and Medtronic.
No, few FTR patients at risk after MVR (Hartzell Schaff, MD)
Echocardiography can provide a great deal of information about when concomitant repair for TR is indicated during MVR. We’ve found that if the patient has no right-sided signs, has normal right atrial pressure, and has mild or mild/moderate TR at the time of repair to the journey mitral valve, the chance of him returning for a tricuspid valve procedure is near zero.
A few patients do return after MVR. They develop atrial fibrillation and may need a pacemaker, but we see very few patients return for tricuspid surgery.
It’s fair to say we cannot demonstrate any benefit of correcting functional mitral regurgitation. Why would we think there’s a benefit of correcting FTR? We can say we’re going to look at grade of TR down the road, or we could look at some other endpoint, but think about it this way: If we cannot prove that correcting functional mitral regurgitation is helpful, why is correcting FTR going to help?
Dr. Schaff is a cardiothoracic surgeon at Mayo Clinic Foundation, Rochester, Minn. He reported no financial relationships.
Yes, functional TR is worth repairing (David H. Adams, MD)
Functional tricuspid regurgitation is a common finding in patients undergoing degenerative mitral valve repair. Severe tricuspid regurgitation is unusual, and clearly there is little debate on the merits of concomitant tricuspid repair for these patients. Moderate tricuspid regurgitation is identified preoperatively in around 15% of patients undergoing degenerative mitral repair (J Thorac Cardiovasc Surg. 2011;142:608-13), and concomitant tricuspid repair in these patients is certainly supported by both the American and European guidelines (J Am Coll Cardiol. 2017. doi: 10.1016/j.jacc.2017.03.011; Eur Heart J. 2012;33:2451-96).
What experience and evidence has led us to a more aggressive approach? One of the most important influences on our early adoption of tricuspid repair at the time of mitral surgery was linked to observations that tricuspid regurgitation (TR) sometimes progressed after isolated mitral valve repair (MVR), with some patients developing moderate or worse insufficiency. Certainly, the impact of significant tricuspid regurgitation on the quality and length of patients’ lives and the challenges of reoperation for isolated tricuspid regurgitation are well known to all surgeons.
Consequently, the importance of treating significant annular dilatation, even without significant tricuspid regurgitation, is supported by the guidelines. Our own experience with an aggressive approach to functional tricuspid regurgitation (FTR) at the time of mitral surgery put an exclamation point on this (J Am Coll Cardiol. 2015;65:1931-8). We found that concomitant tricuspid repair in patients who were worse off before surgery with more TR and higher rates of atrial fibrillation and right-sided dysfunction, actually did better during 5 years of follow-up than the isolated mitral repair patients who started with completely normal tricuspid valve anatomy and ventricular function.
Benign neglect is always an option (J Thorac Cardiovasc Surg. 2017;154:125-6), but we agree with Roberto Dion, MD – despite our friends’ opinions in Toronto and Rochester – we would much prefer to have minimal TR and a normal sized tricuspid valve after MVR. Ask yourself: would you rather have no TR and a normal sized tricuspid valve after you undergo a mitral operation, or a very dilated annulus and perhaps moderate FTR? I am pretty sure I know the answer, but if you are not sure, read our paper.
Dr. Adams is cardiac surgeon-in-chief, Mount Sinai Health System, and Marie-Josée and Henry R. Kravis Professor and Chairman, department of cardiovascular surgery, Icahn School of Medicine at Mount Sinai and The Mount Sinai Hospital, and president-elect of the American Association for Thoracic Surgery. He disclosed he is the national co-principal investigator for the Medtronic NeoChord trial, and receives royalties from Medtronic and Edwards Lifesciences. The Icahn School of Medicine at Mount Sinai receives royalty payments from Edwards Lifesciences and Medtronic for intellectual property related to Dr. Adams’ involvement in the development of 2 mitral valve repair rings and 1 tricuspid valve repair ring.
No, a patient with FTR does not necessarily need repair (Tirone David, MD)
In our clinic, a patient who undergoes MVR and has FTR generally goes home without an annuloplasty. We now have 12 years or more of follow-up in these patients, and they do not develop TR if their MVR is competent. We have reported that preoperative TR in patients who had MVR is associated with mitral valve disease and often improves after the operation (J Thorac Cardiovasc Surg. 2017;154:110-22). New postoperative TR is uncommon.
Ninety percent of my mitral valve repair patients today have no symptoms. Of those patients, a small proportion have moderate TR.
Dr. David is a professor of surgery at Toronto General Hospital. He reported no financial relationships.
Yes, but repair of FTR requires caution (Gilles Dreyfus, MD)
The controversy surrounding the legitimacy of concomitant tricuspid annuloplasty for functional TR during MVR begs for a clinical trial, but before we can conduct a clinical trial, we must define the primary and secondary endpoints. We’ve seen recent prospective, randomized trials that have reported faulty conclusions because the primary endpoints were wrong.
We need a strong debate to agree on those endpoints. Mortality as an endpoint will probably take a very long time to arrive at.
We’re mixing up many different factors. We’re mixing up TR grading, and we know that grading is unreliable. We have all seen patients with full-fledged TR, and after we put them on Lasix (furosemide, Sanofi), 3 days later they have mild TR. So the same patient with no treatment becomes let’s say a “Dreyfus indication,” and then suddenly in 3 days the patient doesn’t need surgery. At any further stage of his life this patient can experience severe TR again; tricuspid annuloplasty will prevent that from happening.
Moderate TR according to the common definition does not exist. If you look at the reports in echocardiography and if you ask any cardiologist, everything between no TR and severe TR is considered moderate. We have proposed a new staging system for evaluating FTR that uses three factors: TR severity; annular dilatation; and extent of tethering, or mode of leaflet coaptation (J Am Coll Cardiol. 2015;65:2331-6).
Dr. Dreyfus is director of the medical and surgical team at the Cardiothoracic Centre of Monaco in Monte Carlo and professor of cardiothoracic surgery at Paris V University and the Imperial College of London. He disclosed receiving speaker fees from Edwards Lifesciences, LivaNova, and Medtronic.
No, few FTR patients at risk after MVR (Hartzell Schaff, MD)
Echocardiography can provide a great deal of information about when concomitant repair for TR is indicated during MVR. We’ve found that if the patient has no right-sided signs, has normal right atrial pressure, and has mild or mild/moderate TR at the time of repair to the journey mitral valve, the chance of him returning for a tricuspid valve procedure is near zero.
A few patients do return after MVR. They develop atrial fibrillation and may need a pacemaker, but we see very few patients return for tricuspid surgery.
It’s fair to say we cannot demonstrate any benefit of correcting functional mitral regurgitation. Why would we think there’s a benefit of correcting FTR? We can say we’re going to look at grade of TR down the road, or we could look at some other endpoint, but think about it this way: If we cannot prove that correcting functional mitral regurgitation is helpful, why is correcting FTR going to help?
Dr. Schaff is a cardiothoracic surgeon at Mayo Clinic Foundation, Rochester, Minn. He reported no financial relationships.
AT THE AATS MITRAL CONCLAVE 2017
Sneak Peek: Journal of Hospital Medicine – July 2017
BACKGROUND: Medicare patients account for approximately 50% of hospital days. Hospitalization in older adults often results in poor outcomes.
OBJECTIVE: To test the feasibility and impact of using Assessing Care of Vulnerable Elders (ACOVE) quality indicators (QIs) as a therapeutic intervention to improve care of hospitalized older adults.
SETTING: Large tertiary hospital in the greater New York Metropolitan area.
PATIENTS: Hospitalized patients, 75 and over, admitted to medical units.
INTERVENTION: A checklist, comprised of four ACOVE QIs, administered during daily interdisciplinary rounds: venous thrombosis prophylaxis (VTE) (QI 1), indwelling bladder catheters (QI 2), mobilization (QI 3), and delirium evaluation (QI 4).
MEASUREMENTS: Variables were extracted from electronic medical records with QI compliance as the primary outcome, and length of stay (LOS), discharge disposition, and readmissions as secondary outcomes. Generalized linear mixed models for binary clustered data were used to estimate compliance rates for each group (intervention group or control group) in the postintervention period, along with their corresponding 95% confidence intervals.
RESULTS: Of the 2,396 patients, 530 were on an intervention unit. In those patients not already compliant with VTE, the compliance rate was 57% in intervention vs. 39% in control (P less than .0056). For indwelling catheters, mobilization, and delirium evaluation, overall compliance was significantly higher in the intervention group 72.2% vs. 54.4% (P = .1061), 62.9% vs. 48.2% (P less than .0001), and 27.9% vs. 21.7% (P = .0027), respectively.
CONCLUSIONS: The study demonstrates the feasibility and effectiveness of integrating ACOVE QIs to improve the quality of care in hospitalized older adults.
Also in JHM
Use of simulation to assess incoming interns’ recognition of opportunities to choose wisely
AUTHORS: Kathleen M. Wiest, Jeanne M. Farnan, MD, MHPE, Ellen Byrne, Lukas Matern, Melissa Cappaert, MA, Kristen Hirsch, Vineet M. Arora, MD, MAPP
Clinician attitudes regarding ICD deactivation in DNR/DNI patients
AUTHORS: Andrew J. Bradley, MD, Adam D. Marks, MD, MPH
Using standardized patients to assess hospitalist communication skills
AUTHORS: Dennis T. Chang, MD, Micah Mann, MD, Terry Sommer, BFA, Robert Fallar, PhD, Alan Weinberg, MS, Erica Friedman, MD
Techniques and behaviors associated with exemplary inpatient general medicine teaching: An exploratory qualitative study
AUTHORS: Nathan Houchens, MD, Molly Harrod, PhD, Stephanie Moody, PhD, Karen E. Fowler, MPH, Sanjay Saint, MD, MPH
A simple algorithm for predicting bacteremia using food consumption and shaking chills: A prospective observational study
AUTHORS: Takayuki Komatsu, MD, PhD, Erika Takahashi, MD, Kentaro Mishima, MD, Takeo Toyoda, MD, Fumihiro Saitoh, MD, Akari Yasuda, RN, Joe Matsuoka, PhD, Manabu Sugita, MD, PhD, Joel Branch, MD, Makoto Aoki, MD, Lawrence M. Tierney Jr., MD, Kenji Inoue, MD, PhD
For more articles and subscription information, visit www.journalofhospitalmedicine.com.
BACKGROUND: Medicare patients account for approximately 50% of hospital days. Hospitalization in older adults often results in poor outcomes.
OBJECTIVE: To test the feasibility and impact of using Assessing Care of Vulnerable Elders (ACOVE) quality indicators (QIs) as a therapeutic intervention to improve care of hospitalized older adults.
SETTING: Large tertiary hospital in the greater New York Metropolitan area.
PATIENTS: Hospitalized patients, 75 and over, admitted to medical units.
INTERVENTION: A checklist, comprised of four ACOVE QIs, administered during daily interdisciplinary rounds: venous thrombosis prophylaxis (VTE) (QI 1), indwelling bladder catheters (QI 2), mobilization (QI 3), and delirium evaluation (QI 4).
MEASUREMENTS: Variables were extracted from electronic medical records with QI compliance as the primary outcome, and length of stay (LOS), discharge disposition, and readmissions as secondary outcomes. Generalized linear mixed models for binary clustered data were used to estimate compliance rates for each group (intervention group or control group) in the postintervention period, along with their corresponding 95% confidence intervals.
RESULTS: Of the 2,396 patients, 530 were on an intervention unit. In those patients not already compliant with VTE, the compliance rate was 57% in intervention vs. 39% in control (P less than .0056). For indwelling catheters, mobilization, and delirium evaluation, overall compliance was significantly higher in the intervention group 72.2% vs. 54.4% (P = .1061), 62.9% vs. 48.2% (P less than .0001), and 27.9% vs. 21.7% (P = .0027), respectively.
CONCLUSIONS: The study demonstrates the feasibility and effectiveness of integrating ACOVE QIs to improve the quality of care in hospitalized older adults.
Also in JHM
Use of simulation to assess incoming interns’ recognition of opportunities to choose wisely
AUTHORS: Kathleen M. Wiest, Jeanne M. Farnan, MD, MHPE, Ellen Byrne, Lukas Matern, Melissa Cappaert, MA, Kristen Hirsch, Vineet M. Arora, MD, MAPP
Clinician attitudes regarding ICD deactivation in DNR/DNI patients
AUTHORS: Andrew J. Bradley, MD, Adam D. Marks, MD, MPH
Using standardized patients to assess hospitalist communication skills
AUTHORS: Dennis T. Chang, MD, Micah Mann, MD, Terry Sommer, BFA, Robert Fallar, PhD, Alan Weinberg, MS, Erica Friedman, MD
Techniques and behaviors associated with exemplary inpatient general medicine teaching: An exploratory qualitative study
AUTHORS: Nathan Houchens, MD, Molly Harrod, PhD, Stephanie Moody, PhD, Karen E. Fowler, MPH, Sanjay Saint, MD, MPH
A simple algorithm for predicting bacteremia using food consumption and shaking chills: A prospective observational study
AUTHORS: Takayuki Komatsu, MD, PhD, Erika Takahashi, MD, Kentaro Mishima, MD, Takeo Toyoda, MD, Fumihiro Saitoh, MD, Akari Yasuda, RN, Joe Matsuoka, PhD, Manabu Sugita, MD, PhD, Joel Branch, MD, Makoto Aoki, MD, Lawrence M. Tierney Jr., MD, Kenji Inoue, MD, PhD
For more articles and subscription information, visit www.journalofhospitalmedicine.com.
BACKGROUND: Medicare patients account for approximately 50% of hospital days. Hospitalization in older adults often results in poor outcomes.
OBJECTIVE: To test the feasibility and impact of using Assessing Care of Vulnerable Elders (ACOVE) quality indicators (QIs) as a therapeutic intervention to improve care of hospitalized older adults.
SETTING: Large tertiary hospital in the greater New York Metropolitan area.
PATIENTS: Hospitalized patients, 75 and over, admitted to medical units.
INTERVENTION: A checklist, comprised of four ACOVE QIs, administered during daily interdisciplinary rounds: venous thrombosis prophylaxis (VTE) (QI 1), indwelling bladder catheters (QI 2), mobilization (QI 3), and delirium evaluation (QI 4).
MEASUREMENTS: Variables were extracted from electronic medical records with QI compliance as the primary outcome, and length of stay (LOS), discharge disposition, and readmissions as secondary outcomes. Generalized linear mixed models for binary clustered data were used to estimate compliance rates for each group (intervention group or control group) in the postintervention period, along with their corresponding 95% confidence intervals.
RESULTS: Of the 2,396 patients, 530 were on an intervention unit. In those patients not already compliant with VTE, the compliance rate was 57% in intervention vs. 39% in control (P less than .0056). For indwelling catheters, mobilization, and delirium evaluation, overall compliance was significantly higher in the intervention group 72.2% vs. 54.4% (P = .1061), 62.9% vs. 48.2% (P less than .0001), and 27.9% vs. 21.7% (P = .0027), respectively.
CONCLUSIONS: The study demonstrates the feasibility and effectiveness of integrating ACOVE QIs to improve the quality of care in hospitalized older adults.
Also in JHM
Use of simulation to assess incoming interns’ recognition of opportunities to choose wisely
AUTHORS: Kathleen M. Wiest, Jeanne M. Farnan, MD, MHPE, Ellen Byrne, Lukas Matern, Melissa Cappaert, MA, Kristen Hirsch, Vineet M. Arora, MD, MAPP
Clinician attitudes regarding ICD deactivation in DNR/DNI patients
AUTHORS: Andrew J. Bradley, MD, Adam D. Marks, MD, MPH
Using standardized patients to assess hospitalist communication skills
AUTHORS: Dennis T. Chang, MD, Micah Mann, MD, Terry Sommer, BFA, Robert Fallar, PhD, Alan Weinberg, MS, Erica Friedman, MD
Techniques and behaviors associated with exemplary inpatient general medicine teaching: An exploratory qualitative study
AUTHORS: Nathan Houchens, MD, Molly Harrod, PhD, Stephanie Moody, PhD, Karen E. Fowler, MPH, Sanjay Saint, MD, MPH
A simple algorithm for predicting bacteremia using food consumption and shaking chills: A prospective observational study
AUTHORS: Takayuki Komatsu, MD, PhD, Erika Takahashi, MD, Kentaro Mishima, MD, Takeo Toyoda, MD, Fumihiro Saitoh, MD, Akari Yasuda, RN, Joe Matsuoka, PhD, Manabu Sugita, MD, PhD, Joel Branch, MD, Makoto Aoki, MD, Lawrence M. Tierney Jr., MD, Kenji Inoue, MD, PhD
For more articles and subscription information, visit www.journalofhospitalmedicine.com.
The hype behind facial oils
The therapeutic benefits of plant oils have been documented for hundreds of years. The properties of medicinal and aromatic plants have been explored for their essential oils. Essential oils are synthesized and used in a multibillion dollar global market for their curative properties, which include antimicrobial, antioxidant, anti-inflammatory, chemoprotective, antiproliferative, antiatherogenic, and antidiabetic properties. More than 80% of the global population depends on traditional plant-based medicine for treating health problems. There are currently over 3,000 known essential oils, among which 300 are commercially available for food, pharmaceutical, cosmetic, sanitary, and perfume industries. The extraction of these oils and their use in cosmeceuticals has increased in the last decade, as minor ingredients in creams and skin cleansing preparations.
However, these oils are now being marketed for direct application on the skin. What’s the hype about facial oils and why are there hundreds currently on the market?

Choosing the right oil, however, is not easy. Most consumers shy away from pure oils because they fear breakouts or increased “oiliness” of their skin. Understanding the properties of the oils can help determine which oils will benefit specific skin types. Argan oil and sunflower oil, for example, are rich in essential fatty acids and vitamin E, which hydrate the skin and have antiaging properties. Tea tree oil has antibacterial and anti-inflammatory qualities which are great for acne-prone skin. Oils such as these are particularly effective if acne medications are used. Acne medications can strip the natural barrier of the skin and without proper hydration excess sebum is produced and can cause clogging of pores.

Essential oils have antiaging properties as well. A study of sixty postmenopausal women who received oral or topical argan oil had significantly improved elasticity of the skin after 60 days, compared with the consumption of olive oil, which produced no improvement of skin elasticity. Sunflower oil has been used in skin preparations for its rich antioxidant properties, which decrease free radical damage from UV radiation.
The use of oils is multidimensional. Oils are highly effective for removing makeup and are the best source for cleansing of dry, dehydrated, or sensitive skin. Similarly, oils applied to the hair can help restore the natural oils of the hair, which are often stripped from overwashing and from chemical hair treatments. Facial oils also help improve skin hydration and restore the natural barrier of the skin. In addition, facial oils can be used in place of moisturizers or under a moisturizer to help prevent transepidermal water loss in dehydrated or atopic skin.
But these oils have a downside. Fragrant plant-based oils can cause skin irritation, photosensitivity, and potentially, allergic reactions. Consumers with plant-based allergies or sensitive skin should therefore steer clear of fragrant oils and test every oil on their inner forearm prior to applying them on the face.
I am a believer in these products. Oils have come a long way in cosmetic products and their manufacturing process has been improved over the last decade, making them easy to use, noncomedogenic, and nongreasy. They are an essential part of skin care for anyone with inflamed, dry, or irritated skin. More cosmetically elegant than their predecessors, when used correctly, oils are among the best products in the cosmeceutical market today.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
References
J Pharm Pharmacol. 2010 Dec;62(12):1669-75.
Inflamm Allergy Drug Targets. 2014;13(3):168-76.
Issue Biol. Sci. Pharm. Res. 2(1):001-007.
Evid Based Complement Alternat Med. 2017;2017:4517971.
Clin Interv Aging. 2015; 10: 339-49.
Evid Based Complement Alternat Med. 2013;2013:827248.
Dermatoendocrinol. 2012 Jul 1;4(3):298-307.
http://www.circulating-oils-library.com/en/start.
The therapeutic benefits of plant oils have been documented for hundreds of years. The properties of medicinal and aromatic plants have been explored for their essential oils. Essential oils are synthesized and used in a multibillion dollar global market for their curative properties, which include antimicrobial, antioxidant, anti-inflammatory, chemoprotective, antiproliferative, antiatherogenic, and antidiabetic properties. More than 80% of the global population depends on traditional plant-based medicine for treating health problems. There are currently over 3,000 known essential oils, among which 300 are commercially available for food, pharmaceutical, cosmetic, sanitary, and perfume industries. The extraction of these oils and their use in cosmeceuticals has increased in the last decade, as minor ingredients in creams and skin cleansing preparations.
However, these oils are now being marketed for direct application on the skin. What’s the hype about facial oils and why are there hundreds currently on the market?
Choosing the right oil, however, is not easy. Most consumers shy away from pure oils because they fear breakouts or increased “oiliness” of their skin. Understanding the properties of the oils can help determine which oils will benefit specific skin types. Argan oil and sunflower oil, for example, are rich in essential fatty acids and vitamin E, which hydrate the skin and have antiaging properties. Tea tree oil has antibacterial and anti-inflammatory qualities which are great for acne-prone skin. Oils such as these are particularly effective if acne medications are used. Acne medications can strip the natural barrier of the skin and without proper hydration excess sebum is produced and can cause clogging of pores.
Essential oils have antiaging properties as well. A study of sixty postmenopausal women who received oral or topical argan oil had significantly improved elasticity of the skin after 60 days, compared with the consumption of olive oil, which produced no improvement of skin elasticity. Sunflower oil has been used in skin preparations for its rich antioxidant properties, which decrease free radical damage from UV radiation.
The use of oils is multidimensional. Oils are highly effective for removing makeup and are the best source for cleansing of dry, dehydrated, or sensitive skin. Similarly, oils applied to the hair can help restore the natural oils of the hair, which are often stripped from overwashing and from chemical hair treatments. Facial oils also help improve skin hydration and restore the natural barrier of the skin. In addition, facial oils can be used in place of moisturizers or under a moisturizer to help prevent transepidermal water loss in dehydrated or atopic skin.
But these oils have a downside. Fragrant plant-based oils can cause skin irritation, photosensitivity, and potentially, allergic reactions. Consumers with plant-based allergies or sensitive skin should therefore steer clear of fragrant oils and test every oil on their inner forearm prior to applying them on the face.
I am a believer in these products. Oils have come a long way in cosmetic products and their manufacturing process has been improved over the last decade, making them easy to use, noncomedogenic, and nongreasy. They are an essential part of skin care for anyone with inflamed, dry, or irritated skin. More cosmetically elegant than their predecessors, when used correctly, oils are among the best products in the cosmeceutical market today.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
References
J Pharm Pharmacol. 2010 Dec;62(12):1669-75.
Inflamm Allergy Drug Targets. 2014;13(3):168-76.
Issue Biol. Sci. Pharm. Res. 2(1):001-007.
Evid Based Complement Alternat Med. 2017;2017:4517971.
Clin Interv Aging. 2015; 10: 339-49.
Evid Based Complement Alternat Med. 2013;2013:827248.
Dermatoendocrinol. 2012 Jul 1;4(3):298-307.
http://www.circulating-oils-library.com/en/start.
The therapeutic benefits of plant oils have been documented for hundreds of years. The properties of medicinal and aromatic plants have been explored for their essential oils. Essential oils are synthesized and used in a multibillion dollar global market for their curative properties, which include antimicrobial, antioxidant, anti-inflammatory, chemoprotective, antiproliferative, antiatherogenic, and antidiabetic properties. More than 80% of the global population depends on traditional plant-based medicine for treating health problems. There are currently over 3,000 known essential oils, among which 300 are commercially available for food, pharmaceutical, cosmetic, sanitary, and perfume industries. The extraction of these oils and their use in cosmeceuticals has increased in the last decade, as minor ingredients in creams and skin cleansing preparations.
However, these oils are now being marketed for direct application on the skin. What’s the hype about facial oils and why are there hundreds currently on the market?
Choosing the right oil, however, is not easy. Most consumers shy away from pure oils because they fear breakouts or increased “oiliness” of their skin. Understanding the properties of the oils can help determine which oils will benefit specific skin types. Argan oil and sunflower oil, for example, are rich in essential fatty acids and vitamin E, which hydrate the skin and have antiaging properties. Tea tree oil has antibacterial and anti-inflammatory qualities which are great for acne-prone skin. Oils such as these are particularly effective if acne medications are used. Acne medications can strip the natural barrier of the skin and without proper hydration excess sebum is produced and can cause clogging of pores.
Essential oils have antiaging properties as well. A study of sixty postmenopausal women who received oral or topical argan oil had significantly improved elasticity of the skin after 60 days, compared with the consumption of olive oil, which produced no improvement of skin elasticity. Sunflower oil has been used in skin preparations for its rich antioxidant properties, which decrease free radical damage from UV radiation.
The use of oils is multidimensional. Oils are highly effective for removing makeup and are the best source for cleansing of dry, dehydrated, or sensitive skin. Similarly, oils applied to the hair can help restore the natural oils of the hair, which are often stripped from overwashing and from chemical hair treatments. Facial oils also help improve skin hydration and restore the natural barrier of the skin. In addition, facial oils can be used in place of moisturizers or under a moisturizer to help prevent transepidermal water loss in dehydrated or atopic skin.
But these oils have a downside. Fragrant plant-based oils can cause skin irritation, photosensitivity, and potentially, allergic reactions. Consumers with plant-based allergies or sensitive skin should therefore steer clear of fragrant oils and test every oil on their inner forearm prior to applying them on the face.
I am a believer in these products. Oils have come a long way in cosmetic products and their manufacturing process has been improved over the last decade, making them easy to use, noncomedogenic, and nongreasy. They are an essential part of skin care for anyone with inflamed, dry, or irritated skin. More cosmetically elegant than their predecessors, when used correctly, oils are among the best products in the cosmeceutical market today.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
References
J Pharm Pharmacol. 2010 Dec;62(12):1669-75.
Inflamm Allergy Drug Targets. 2014;13(3):168-76.
Issue Biol. Sci. Pharm. Res. 2(1):001-007.
Evid Based Complement Alternat Med. 2017;2017:4517971.
Clin Interv Aging. 2015; 10: 339-49.
Evid Based Complement Alternat Med. 2013;2013:827248.
Dermatoendocrinol. 2012 Jul 1;4(3):298-307.
http://www.circulating-oils-library.com/en/start.
How patients want their biopsy results
I had just done an ED&C, scraping the friable tumor gently from her tissue paper–thin skin. “Yes,” I replied more loudly than our close proximity would warrant. “This is probably another basal cell carcinoma. When I get the pathology back, I’ll call you.” As my medical assistant was putting on the Band-Aid, my patient exclaimed, “Oh, no! “Don’t call me! Just send me an email, honey.”
At the time of the biopsy, she was 84 years old. My 84-year-old patient just chastised me for not using her preferred method of communication. She didn’t want a follow-up visit or a phone call. She wanted an email.

A certain trend is that patients want speed and convenience. Patients, like all humans, hate to wait. They hate to wait for an appointment. They hate to wait in waiting rooms. They hate to wait for answers. They also hate phone tag and long lines at the TSA (the latter will not be covered in this column).
For most of my biopsy results, I send a secure message – essentially an email – to my patients. I do this for benign results, as well as for treated cancerous growths. For serious diagnoses such as melanoma, I call them and sometimes arrange for a follow-up appointment.
Securely emailing results saves my patients, and me, bags of time. In fact, I not only send them the diagnosis, I include the pathology report. This might seem risky: What will patients make of “atypical melanocytic hyperplasia” or “cannot rule out invasive carcinoma” in their result? I can tell you, not much. After thousands of such emails, I’ve learned that follow-up replies are rare. And I cannot recall any follow-up question that was unhelpful. I’ve even had one correct our report (“Doc, it was on the left arm, not the right”) and at least one that led to a great discussion of different treatments based on my patient’s research.
If nothing else, I hope sending path reports directly to patients will eradicate the unhelpful past medical history of “skin cancer of unknown type or stage.” One biopsy result at a time, thousands of results later, each of my patients has his or her own copy to print and share with their next dermatologist, who might just be you.
“Yes, ma’am, I’ll email the result as soon as it’s back,” I replied, trying to save face. “Great!” she said, showing me her new iPhone, which was one generation advanced from my own. “I’ll get it right here!”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com.
I had just done an ED&C, scraping the friable tumor gently from her tissue paper–thin skin. “Yes,” I replied more loudly than our close proximity would warrant. “This is probably another basal cell carcinoma. When I get the pathology back, I’ll call you.” As my medical assistant was putting on the Band-Aid, my patient exclaimed, “Oh, no! “Don’t call me! Just send me an email, honey.”
At the time of the biopsy, she was 84 years old. My 84-year-old patient just chastised me for not using her preferred method of communication. She didn’t want a follow-up visit or a phone call. She wanted an email.
A certain trend is that patients want speed and convenience. Patients, like all humans, hate to wait. They hate to wait for an appointment. They hate to wait in waiting rooms. They hate to wait for answers. They also hate phone tag and long lines at the TSA (the latter will not be covered in this column).
For most of my biopsy results, I send a secure message – essentially an email – to my patients. I do this for benign results, as well as for treated cancerous growths. For serious diagnoses such as melanoma, I call them and sometimes arrange for a follow-up appointment.
Securely emailing results saves my patients, and me, bags of time. In fact, I not only send them the diagnosis, I include the pathology report. This might seem risky: What will patients make of “atypical melanocytic hyperplasia” or “cannot rule out invasive carcinoma” in their result? I can tell you, not much. After thousands of such emails, I’ve learned that follow-up replies are rare. And I cannot recall any follow-up question that was unhelpful. I’ve even had one correct our report (“Doc, it was on the left arm, not the right”) and at least one that led to a great discussion of different treatments based on my patient’s research.
If nothing else, I hope sending path reports directly to patients will eradicate the unhelpful past medical history of “skin cancer of unknown type or stage.” One biopsy result at a time, thousands of results later, each of my patients has his or her own copy to print and share with their next dermatologist, who might just be you.
“Yes, ma’am, I’ll email the result as soon as it’s back,” I replied, trying to save face. “Great!” she said, showing me her new iPhone, which was one generation advanced from my own. “I’ll get it right here!”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com.
I had just done an ED&C, scraping the friable tumor gently from her tissue paper–thin skin. “Yes,” I replied more loudly than our close proximity would warrant. “This is probably another basal cell carcinoma. When I get the pathology back, I’ll call you.” As my medical assistant was putting on the Band-Aid, my patient exclaimed, “Oh, no! “Don’t call me! Just send me an email, honey.”
At the time of the biopsy, she was 84 years old. My 84-year-old patient just chastised me for not using her preferred method of communication. She didn’t want a follow-up visit or a phone call. She wanted an email.
A certain trend is that patients want speed and convenience. Patients, like all humans, hate to wait. They hate to wait for an appointment. They hate to wait in waiting rooms. They hate to wait for answers. They also hate phone tag and long lines at the TSA (the latter will not be covered in this column).
For most of my biopsy results, I send a secure message – essentially an email – to my patients. I do this for benign results, as well as for treated cancerous growths. For serious diagnoses such as melanoma, I call them and sometimes arrange for a follow-up appointment.
Securely emailing results saves my patients, and me, bags of time. In fact, I not only send them the diagnosis, I include the pathology report. This might seem risky: What will patients make of “atypical melanocytic hyperplasia” or “cannot rule out invasive carcinoma” in their result? I can tell you, not much. After thousands of such emails, I’ve learned that follow-up replies are rare. And I cannot recall any follow-up question that was unhelpful. I’ve even had one correct our report (“Doc, it was on the left arm, not the right”) and at least one that led to a great discussion of different treatments based on my patient’s research.
If nothing else, I hope sending path reports directly to patients will eradicate the unhelpful past medical history of “skin cancer of unknown type or stage.” One biopsy result at a time, thousands of results later, each of my patients has his or her own copy to print and share with their next dermatologist, who might just be you.
“Yes, ma’am, I’ll email the result as soon as it’s back,” I replied, trying to save face. “Great!” she said, showing me her new iPhone, which was one generation advanced from my own. “I’ll get it right here!”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com.