User login
NIAMS Celebrates 25 Years of Advances in Medical Research
BETHESDA, MD. – It’s been 25 years since the establishment of the National Institute of Arthritis and Musculoskeletal and Skin Diseases, and great strides have been made in diagnosis, treatment, and management of numerous conditions, "but you ain’t seen nothing yet," said Dr. Francis Collins, director of the National Institutes of Health.
Opportunities for medical research have never been as great as they are today, said Dr. Collins, who gave the welcome address for NIAMS’ 25th anniversary at the NIH campus in Bethesda, Md.
Although prominent researchers in the field agreed that research has come a long way in the past 25 years, they stressed that there is still a long way to go. Currently, the molecular basis for 4,000 diseases is known, said Dr. Collins. "But we have effective treatment for only 200."
In broad strokes, the day-long event touched upon the past, present, and future of major diseases of bones, joints, muscles, and skin – including muscular dystrophies, osteoporosis, rheumatoid arthritis, and lupus – through panels and discussion involving prominent researchers, physicians, and patient advocates.
"These diseases are chronic, crippling, and common," said Dr. Stephen Katz, director of NIAMS, in his opening address. "They affect every family in the United States."
Among the attendees were many researchers and clinicians who said they felt loyalty and appreciation for receiving funding from NIAMS at some point in their career. For some, the progress in the past 2 decades was quite tangible.
"Public investment in osteoporosis research has really changed how we take care of the patients," said Dr. Sundeep Khosla, president of the American Society for Bone and Mineral Research. Dr. Khosla, professor at the Mayo Medical School, Rochester, Minn., recalled a time more than 2 decades ago when calcium, vitamin D, and estrogen were the only options he could offer to patients with osteoporosis.
A few years later, bisphosphonates became available. Then came anabolic drugs, and now more drugs are in the pipeline. Patient diagnosis also has advanced, he said. Although he agreed that the field still has a long way to go, he was optimistic about more progress. "Who knows what will happen in the next 25 years," he said.
There was talk of individualized therapy, balancing research and treatment, and a closer collaboration among scientists, all in the spirit of bringing better diagnosis and treatment to patients.
"We’re in a different world from when all we had was aspirin," said Dr. Daniel Kastner, a scientific director at the National Human Genome Research Institute. "But what we really want is a cure. And we’re not there yet."
BETHESDA, MD. – It’s been 25 years since the establishment of the National Institute of Arthritis and Musculoskeletal and Skin Diseases, and great strides have been made in diagnosis, treatment, and management of numerous conditions, "but you ain’t seen nothing yet," said Dr. Francis Collins, director of the National Institutes of Health.
Opportunities for medical research have never been as great as they are today, said Dr. Collins, who gave the welcome address for NIAMS’ 25th anniversary at the NIH campus in Bethesda, Md.
Although prominent researchers in the field agreed that research has come a long way in the past 25 years, they stressed that there is still a long way to go. Currently, the molecular basis for 4,000 diseases is known, said Dr. Collins. "But we have effective treatment for only 200."
In broad strokes, the day-long event touched upon the past, present, and future of major diseases of bones, joints, muscles, and skin – including muscular dystrophies, osteoporosis, rheumatoid arthritis, and lupus – through panels and discussion involving prominent researchers, physicians, and patient advocates.
"These diseases are chronic, crippling, and common," said Dr. Stephen Katz, director of NIAMS, in his opening address. "They affect every family in the United States."
Among the attendees were many researchers and clinicians who said they felt loyalty and appreciation for receiving funding from NIAMS at some point in their career. For some, the progress in the past 2 decades was quite tangible.
"Public investment in osteoporosis research has really changed how we take care of the patients," said Dr. Sundeep Khosla, president of the American Society for Bone and Mineral Research. Dr. Khosla, professor at the Mayo Medical School, Rochester, Minn., recalled a time more than 2 decades ago when calcium, vitamin D, and estrogen were the only options he could offer to patients with osteoporosis.
A few years later, bisphosphonates became available. Then came anabolic drugs, and now more drugs are in the pipeline. Patient diagnosis also has advanced, he said. Although he agreed that the field still has a long way to go, he was optimistic about more progress. "Who knows what will happen in the next 25 years," he said.
There was talk of individualized therapy, balancing research and treatment, and a closer collaboration among scientists, all in the spirit of bringing better diagnosis and treatment to patients.
"We’re in a different world from when all we had was aspirin," said Dr. Daniel Kastner, a scientific director at the National Human Genome Research Institute. "But what we really want is a cure. And we’re not there yet."
BETHESDA, MD. – It’s been 25 years since the establishment of the National Institute of Arthritis and Musculoskeletal and Skin Diseases, and great strides have been made in diagnosis, treatment, and management of numerous conditions, "but you ain’t seen nothing yet," said Dr. Francis Collins, director of the National Institutes of Health.
Opportunities for medical research have never been as great as they are today, said Dr. Collins, who gave the welcome address for NIAMS’ 25th anniversary at the NIH campus in Bethesda, Md.
Although prominent researchers in the field agreed that research has come a long way in the past 25 years, they stressed that there is still a long way to go. Currently, the molecular basis for 4,000 diseases is known, said Dr. Collins. "But we have effective treatment for only 200."
In broad strokes, the day-long event touched upon the past, present, and future of major diseases of bones, joints, muscles, and skin – including muscular dystrophies, osteoporosis, rheumatoid arthritis, and lupus – through panels and discussion involving prominent researchers, physicians, and patient advocates.
"These diseases are chronic, crippling, and common," said Dr. Stephen Katz, director of NIAMS, in his opening address. "They affect every family in the United States."
Among the attendees were many researchers and clinicians who said they felt loyalty and appreciation for receiving funding from NIAMS at some point in their career. For some, the progress in the past 2 decades was quite tangible.
"Public investment in osteoporosis research has really changed how we take care of the patients," said Dr. Sundeep Khosla, president of the American Society for Bone and Mineral Research. Dr. Khosla, professor at the Mayo Medical School, Rochester, Minn., recalled a time more than 2 decades ago when calcium, vitamin D, and estrogen were the only options he could offer to patients with osteoporosis.
A few years later, bisphosphonates became available. Then came anabolic drugs, and now more drugs are in the pipeline. Patient diagnosis also has advanced, he said. Although he agreed that the field still has a long way to go, he was optimistic about more progress. "Who knows what will happen in the next 25 years," he said.
There was talk of individualized therapy, balancing research and treatment, and a closer collaboration among scientists, all in the spirit of bringing better diagnosis and treatment to patients.
"We’re in a different world from when all we had was aspirin," said Dr. Daniel Kastner, a scientific director at the National Human Genome Research Institute. "But what we really want is a cure. And we’re not there yet."
FROM A SCIENTIFIC SYMPOSIUM SPONSORED BY NIAMS
Rheumatoid Arthritis Drug Trials Often Lack Comparator Regimens
LONDON – Many recently performed rheumatology drug trials ran into the ethical trap of treating control patients with an ineffective regimen, with the result that some patients experienced ongoing pain and joint dysfunction and continued disease progression.
"I would propose that we change the trial design for the placebo control to use an active comparator against the [investigational] drug," Dr. Aaron Juche said while presenting a poster at the annual European Congress of Rheumatology.

In most cases for current studies testing a new drug aimed at controlling rheumatoid arthritis pain, dysfunction, and progression, "the standard of care would be a tumor necrosis factor [TNF] inhibitor as the active comparator," said Dr. Juche, a rheumatologist at Johanniter Hospital in Treuenbrietzen, Germany. Because TNF inhibitors are so effective, a study that uses this treatment in the comparator arm would likely have to be a noninferiority study and would also probably have to involve a relatively large number of patients, he said in an interview.
Dr. Juche said he first became interested in this issue because he "wondered whether placebo-treated patients [in recent drug trials] were being treated as I would treat a patient in standard practice." The standard approach for drug-trial design in patients with rheumatoid arthritis (RA) in recent years has been to follow a model that’s more than a decade old, dating back to the first studies on TNF inhibitors during the 1990s: "Patients who did not adequately respond to immunosuppressive drugs were randomly assigned to either an experimental condition under which they received the new substance, or to a control condition under which they continued their formerly inefficient treatment and received a placebo."
To more systematically assess the scope of the problem, he and his associate reviewed 17 recent, published clinical trials that drug companies used to document the safety and efficacy of three new drugs, abatacept, golimumab, and tocilizumab, to the European Medicines Agency. Dr. Juche said these studies fairly represented most recently performed drug efficacy trials for patients with RA.
Of the seven studies he reviewed that tested abatacept, none used a control therapy that effectively treated the patients’ disease. In all seven studies, patients remained on treatment with a disease-modifying antirheumatic drug (DMARD) that they had already failed on, most commonly methotrexate. During these studies, "patients experienced a persistent, high disease activity," Dr. Juche reported in his poster.
Among four pivotal studies involving golimumab, one enrolled methotrexate-naive patients and then used methotrexate as the control drug. The other three used control groups that either received placebo and nothing else, or placebo plus methotrexate for enrolled patients who had already failed methotrexate.
A similar pattern existed for the six studies of tocilizumab that Dr. Juche reviewed. One of the six studies used methotrexate as the comparator in a trial that enrolled methotrexate-naive patients. The other five studies used comparator groups on either placebo alone or placebo plus a DMARD to which the patient had already not responded.
Dr. Juche added that he did not believe that rheumatology was a unique medical specialty in having so many of its trials involve ineffective regimens in the control groups, but he did not systematically assess efficacy trials done in other specialties. As a rheumatologist, he focused his attention only on those studies from his specialty.
These designs run counter to the stipulations of the 2008 Declaration of Helsinki of the World Medical Association, Dr. Juche noted. The Declaration said: "The benefits, risks, burdens, and effectiveness of a new intervention must be tested against those of the best current proven intervention, except ... where no current proven intervention exists or where, for compelling and scientifically sound methodological reasons, the use of placebo is necessary to determine the efficacy of an intervention and the patients who receive placebo or no treatment will not be subject to any risk or serious or irreversible harm."
Dr. Juche said that he has received travel expense support from Actelion.
LONDON – Many recently performed rheumatology drug trials ran into the ethical trap of treating control patients with an ineffective regimen, with the result that some patients experienced ongoing pain and joint dysfunction and continued disease progression.
"I would propose that we change the trial design for the placebo control to use an active comparator against the [investigational] drug," Dr. Aaron Juche said while presenting a poster at the annual European Congress of Rheumatology.
In most cases for current studies testing a new drug aimed at controlling rheumatoid arthritis pain, dysfunction, and progression, "the standard of care would be a tumor necrosis factor [TNF] inhibitor as the active comparator," said Dr. Juche, a rheumatologist at Johanniter Hospital in Treuenbrietzen, Germany. Because TNF inhibitors are so effective, a study that uses this treatment in the comparator arm would likely have to be a noninferiority study and would also probably have to involve a relatively large number of patients, he said in an interview.
Dr. Juche said he first became interested in this issue because he "wondered whether placebo-treated patients [in recent drug trials] were being treated as I would treat a patient in standard practice." The standard approach for drug-trial design in patients with rheumatoid arthritis (RA) in recent years has been to follow a model that’s more than a decade old, dating back to the first studies on TNF inhibitors during the 1990s: "Patients who did not adequately respond to immunosuppressive drugs were randomly assigned to either an experimental condition under which they received the new substance, or to a control condition under which they continued their formerly inefficient treatment and received a placebo."
To more systematically assess the scope of the problem, he and his associate reviewed 17 recent, published clinical trials that drug companies used to document the safety and efficacy of three new drugs, abatacept, golimumab, and tocilizumab, to the European Medicines Agency. Dr. Juche said these studies fairly represented most recently performed drug efficacy trials for patients with RA.
Of the seven studies he reviewed that tested abatacept, none used a control therapy that effectively treated the patients’ disease. In all seven studies, patients remained on treatment with a disease-modifying antirheumatic drug (DMARD) that they had already failed on, most commonly methotrexate. During these studies, "patients experienced a persistent, high disease activity," Dr. Juche reported in his poster.
Among four pivotal studies involving golimumab, one enrolled methotrexate-naive patients and then used methotrexate as the control drug. The other three used control groups that either received placebo and nothing else, or placebo plus methotrexate for enrolled patients who had already failed methotrexate.
A similar pattern existed for the six studies of tocilizumab that Dr. Juche reviewed. One of the six studies used methotrexate as the comparator in a trial that enrolled methotrexate-naive patients. The other five studies used comparator groups on either placebo alone or placebo plus a DMARD to which the patient had already not responded.
Dr. Juche added that he did not believe that rheumatology was a unique medical specialty in having so many of its trials involve ineffective regimens in the control groups, but he did not systematically assess efficacy trials done in other specialties. As a rheumatologist, he focused his attention only on those studies from his specialty.
These designs run counter to the stipulations of the 2008 Declaration of Helsinki of the World Medical Association, Dr. Juche noted. The Declaration said: "The benefits, risks, burdens, and effectiveness of a new intervention must be tested against those of the best current proven intervention, except ... where no current proven intervention exists or where, for compelling and scientifically sound methodological reasons, the use of placebo is necessary to determine the efficacy of an intervention and the patients who receive placebo or no treatment will not be subject to any risk or serious or irreversible harm."
Dr. Juche said that he has received travel expense support from Actelion.
LONDON – Many recently performed rheumatology drug trials ran into the ethical trap of treating control patients with an ineffective regimen, with the result that some patients experienced ongoing pain and joint dysfunction and continued disease progression.
"I would propose that we change the trial design for the placebo control to use an active comparator against the [investigational] drug," Dr. Aaron Juche said while presenting a poster at the annual European Congress of Rheumatology.
In most cases for current studies testing a new drug aimed at controlling rheumatoid arthritis pain, dysfunction, and progression, "the standard of care would be a tumor necrosis factor [TNF] inhibitor as the active comparator," said Dr. Juche, a rheumatologist at Johanniter Hospital in Treuenbrietzen, Germany. Because TNF inhibitors are so effective, a study that uses this treatment in the comparator arm would likely have to be a noninferiority study and would also probably have to involve a relatively large number of patients, he said in an interview.
Dr. Juche said he first became interested in this issue because he "wondered whether placebo-treated patients [in recent drug trials] were being treated as I would treat a patient in standard practice." The standard approach for drug-trial design in patients with rheumatoid arthritis (RA) in recent years has been to follow a model that’s more than a decade old, dating back to the first studies on TNF inhibitors during the 1990s: "Patients who did not adequately respond to immunosuppressive drugs were randomly assigned to either an experimental condition under which they received the new substance, or to a control condition under which they continued their formerly inefficient treatment and received a placebo."
To more systematically assess the scope of the problem, he and his associate reviewed 17 recent, published clinical trials that drug companies used to document the safety and efficacy of three new drugs, abatacept, golimumab, and tocilizumab, to the European Medicines Agency. Dr. Juche said these studies fairly represented most recently performed drug efficacy trials for patients with RA.
Of the seven studies he reviewed that tested abatacept, none used a control therapy that effectively treated the patients’ disease. In all seven studies, patients remained on treatment with a disease-modifying antirheumatic drug (DMARD) that they had already failed on, most commonly methotrexate. During these studies, "patients experienced a persistent, high disease activity," Dr. Juche reported in his poster.
Among four pivotal studies involving golimumab, one enrolled methotrexate-naive patients and then used methotrexate as the control drug. The other three used control groups that either received placebo and nothing else, or placebo plus methotrexate for enrolled patients who had already failed methotrexate.
A similar pattern existed for the six studies of tocilizumab that Dr. Juche reviewed. One of the six studies used methotrexate as the comparator in a trial that enrolled methotrexate-naive patients. The other five studies used comparator groups on either placebo alone or placebo plus a DMARD to which the patient had already not responded.
Dr. Juche added that he did not believe that rheumatology was a unique medical specialty in having so many of its trials involve ineffective regimens in the control groups, but he did not systematically assess efficacy trials done in other specialties. As a rheumatologist, he focused his attention only on those studies from his specialty.
These designs run counter to the stipulations of the 2008 Declaration of Helsinki of the World Medical Association, Dr. Juche noted. The Declaration said: "The benefits, risks, burdens, and effectiveness of a new intervention must be tested against those of the best current proven intervention, except ... where no current proven intervention exists or where, for compelling and scientifically sound methodological reasons, the use of placebo is necessary to determine the efficacy of an intervention and the patients who receive placebo or no treatment will not be subject to any risk or serious or irreversible harm."
Dr. Juche said that he has received travel expense support from Actelion.
FROM THE ANNUAL EUROPEAN CONGRESS OF RHEUMATOLOGY
Major Finding: A review of 17 recent clinical trials for three new rheumatoid arthritis drugs showed that only two of the trials placed patients randomized into the comparator arms on active drug regimens.
Data Source: Review of publicly reported trial data.
Disclosures: Dr. Juche said that he has received travel support from Actelion.
Hereditary Hemochromatosis Linked to Increased Arthropathies and Joint Surgery
LONDON – Patients with hereditary hemochromatosis have a significantly increased prevalence of various arthropathies and an elevated need for joint-replacement surgery, compared with the general population, according to findings from a study of Swedish national registry data.
The analysis also showed that first-degree relatives of people with hereditary hemochromatosis do not have an increased rate of arthropathies or need for joint replacement, even though genetic models predict that a majority of these relatives carry one copy of an autosomal recessive mutation that causes hereditary hemochromatosis.
"This dissociation between the genotype and the phenotype" relative to the risk for arthropathy and need for joint replacement "suggests to me that the gene itself is not involved. It suggests to me that you need more than just the gene" to boost the risk for arthropathy and joint failure, noted Dr. Johan Askling.

Arthropathy is a classic phenotypic feature of patients with hereditary hemochromatosis, a genetic disease in people who carry two mutated copies of the hemochromatosis gene (HFE) associated with iron overload. But the nature of the relationship between the disease and arthropathies remains poorly understood. The new finding that increased arthropathies occur only in homozygous, affected individuals suggests that the risk is linked to iron overload itself, rather than to the causative mutated genes.
Dr. Askling and his associates identified 3,531 patients with a diagnosis of hereditary hemochromatosis from Swedish national records for the period 1999-2006. The investigators also identified another 11,794 first-degree relatives of these patients. They then identified 37,369 people as matched controls for the patients from the general Swedish population and 196,628 people as matched controls for the first-degree relatives.
The researchers then tallied the incidence of consultations or hospitalizations for rheumatoid arthritis, osteoarthritis, and other arthritides in the cases, their first-degree relatives, and the controls during the study period. They calculated a relative risk for these complications in affected people and in their relatives, compared with the controls that adjusted for differences in age, sex, and residence location. The researchers also ran similar analyses for the incidence of various joint-replacement surgeries (see table).
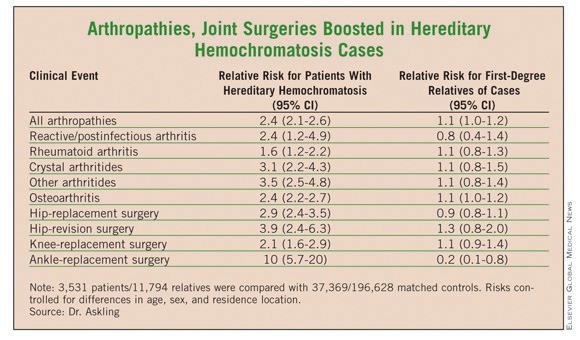
The results showed that the patients with hereditary hemochromatosis had consistent, statistically significant increased rates of arthropathies. For example, for all arthropathies the rate was 2.4-fold higher in the patients than in the controls. But this increased rate did not exist among the first-degree relatives. For all arthropathies, their rate was just 10% higher than among the matched controls, a difference that was not significant, reported Dr. Askling, an epidemiologist at the Karolinska Institute in Stockholm.
A similar pattern existed for joint-replacement surgeries. Hip surgery, for example, was 2.9-fold more frequent among the hereditary hemochromatosis patients than among their matched controls, while among the first-degree relatives the incidence of hip-replacement surgery was 10% less common than among the matched controls, a difference that was not statistically significant.
Dr. Askling said that he had no disclosures.
LONDON – Patients with hereditary hemochromatosis have a significantly increased prevalence of various arthropathies and an elevated need for joint-replacement surgery, compared with the general population, according to findings from a study of Swedish national registry data.
The analysis also showed that first-degree relatives of people with hereditary hemochromatosis do not have an increased rate of arthropathies or need for joint replacement, even though genetic models predict that a majority of these relatives carry one copy of an autosomal recessive mutation that causes hereditary hemochromatosis.
"This dissociation between the genotype and the phenotype" relative to the risk for arthropathy and need for joint replacement "suggests to me that the gene itself is not involved. It suggests to me that you need more than just the gene" to boost the risk for arthropathy and joint failure, noted Dr. Johan Askling.
Arthropathy is a classic phenotypic feature of patients with hereditary hemochromatosis, a genetic disease in people who carry two mutated copies of the hemochromatosis gene (HFE) associated with iron overload. But the nature of the relationship between the disease and arthropathies remains poorly understood. The new finding that increased arthropathies occur only in homozygous, affected individuals suggests that the risk is linked to iron overload itself, rather than to the causative mutated genes.
Dr. Askling and his associates identified 3,531 patients with a diagnosis of hereditary hemochromatosis from Swedish national records for the period 1999-2006. The investigators also identified another 11,794 first-degree relatives of these patients. They then identified 37,369 people as matched controls for the patients from the general Swedish population and 196,628 people as matched controls for the first-degree relatives.
The researchers then tallied the incidence of consultations or hospitalizations for rheumatoid arthritis, osteoarthritis, and other arthritides in the cases, their first-degree relatives, and the controls during the study period. They calculated a relative risk for these complications in affected people and in their relatives, compared with the controls that adjusted for differences in age, sex, and residence location. The researchers also ran similar analyses for the incidence of various joint-replacement surgeries (see table).
The results showed that the patients with hereditary hemochromatosis had consistent, statistically significant increased rates of arthropathies. For example, for all arthropathies the rate was 2.4-fold higher in the patients than in the controls. But this increased rate did not exist among the first-degree relatives. For all arthropathies, their rate was just 10% higher than among the matched controls, a difference that was not significant, reported Dr. Askling, an epidemiologist at the Karolinska Institute in Stockholm.
A similar pattern existed for joint-replacement surgeries. Hip surgery, for example, was 2.9-fold more frequent among the hereditary hemochromatosis patients than among their matched controls, while among the first-degree relatives the incidence of hip-replacement surgery was 10% less common than among the matched controls, a difference that was not statistically significant.
Dr. Askling said that he had no disclosures.
LONDON – Patients with hereditary hemochromatosis have a significantly increased prevalence of various arthropathies and an elevated need for joint-replacement surgery, compared with the general population, according to findings from a study of Swedish national registry data.
The analysis also showed that first-degree relatives of people with hereditary hemochromatosis do not have an increased rate of arthropathies or need for joint replacement, even though genetic models predict that a majority of these relatives carry one copy of an autosomal recessive mutation that causes hereditary hemochromatosis.
"This dissociation between the genotype and the phenotype" relative to the risk for arthropathy and need for joint replacement "suggests to me that the gene itself is not involved. It suggests to me that you need more than just the gene" to boost the risk for arthropathy and joint failure, noted Dr. Johan Askling.
Arthropathy is a classic phenotypic feature of patients with hereditary hemochromatosis, a genetic disease in people who carry two mutated copies of the hemochromatosis gene (HFE) associated with iron overload. But the nature of the relationship between the disease and arthropathies remains poorly understood. The new finding that increased arthropathies occur only in homozygous, affected individuals suggests that the risk is linked to iron overload itself, rather than to the causative mutated genes.
Dr. Askling and his associates identified 3,531 patients with a diagnosis of hereditary hemochromatosis from Swedish national records for the period 1999-2006. The investigators also identified another 11,794 first-degree relatives of these patients. They then identified 37,369 people as matched controls for the patients from the general Swedish population and 196,628 people as matched controls for the first-degree relatives.
The researchers then tallied the incidence of consultations or hospitalizations for rheumatoid arthritis, osteoarthritis, and other arthritides in the cases, their first-degree relatives, and the controls during the study period. They calculated a relative risk for these complications in affected people and in their relatives, compared with the controls that adjusted for differences in age, sex, and residence location. The researchers also ran similar analyses for the incidence of various joint-replacement surgeries (see table).
The results showed that the patients with hereditary hemochromatosis had consistent, statistically significant increased rates of arthropathies. For example, for all arthropathies the rate was 2.4-fold higher in the patients than in the controls. But this increased rate did not exist among the first-degree relatives. For all arthropathies, their rate was just 10% higher than among the matched controls, a difference that was not significant, reported Dr. Askling, an epidemiologist at the Karolinska Institute in Stockholm.
A similar pattern existed for joint-replacement surgeries. Hip surgery, for example, was 2.9-fold more frequent among the hereditary hemochromatosis patients than among their matched controls, while among the first-degree relatives the incidence of hip-replacement surgery was 10% less common than among the matched controls, a difference that was not statistically significant.
Dr. Askling said that he had no disclosures.
FROM THE ANNUAL EUROPEAN CONGRESS OF RHEUMATOLOGY
Major Finding: Patients with hereditary hemochromatosis had a 2.4-fold increased prevalence of arthropathies and a 2.9-fold increased rate of hip surgery, compared with matched controls. In contrast, first-degree relatives of hereditary hemochromatosis patients had no significantly different rates for arthropathy or need for joint-replacement surgery, compared with controls.
Data Source: Case-control study of records from Swedish national registries during 1999-2006, with 3,531 patients diagnosed with hereditary hemochromatosis and 37,369 matched controls, and 11,794 first-degree relatives of the patients and 196,628 matched controls.
Disclosures: Dr. Askling said that he had no disclosures.
RA and SLE Risk Factors Remain for Mothers and Babies
LONDON – Women with both rheumatoid arthritis and systemic lupus erythematosus were more than twice as likely as women without these diseases to have pregnancy-related hypertension, and the risk has not lessened in recent years despite improved treatment, according to 10-years’ worth of admission and discharge data from several Canadian hospitals.
Such women were more likely to undergo a cesarean section, and their newborns were more likely to be born prematurely, be small for gestational age (SGA), and require intensive care, compared with children born to women without RA or SLE.
"We wanted to look at what obstetrical and neonatal outcomes have been like over the past 10 years in both RA and in lupus," study author and rheumatologist Dr. Cheryl Barnabe said in an interview during a poster session at the annual European Congress of Rheumatology.
To do so, Dr. Barnabe and colleagues used an administrative database maintained by the Canadian government to examine the outcomes of 38 women with RA and 95 with SLE who were admitted and discharged from hospitals in Calgary for obstetric reasons. Outcomes were compared with expectant women who did not have either condition, with four times as many controls as cases.
"We found that the RA and lupus patients stayed in hospital longer [after delivery], approximately double the percentage of patients [in both groups] had C-sections done, and there were more postpartum infections in the lupus patients compared to the lupus controls [6.3% vs. 1.3%, P less than .004]," observed Dr. Barnabe, a clinical scholar in the department of medicine at the University of Calgary in Alberta.
Adjusted odds ratios (ORs) for preeclampsia or eclampsia were 2.8 (95% confidence interval 1.0-7.8) for RA and 2.0 (95% CI 1.0-3.7) for SLE.
The mean length of hospital stay was 0.9 days longer for women with RA than for those without (P less than .003) and 1.8 days longer for those with SLE than for those without (P less than .001).
One-third (34.2%) of women with RA and 43.2% of women with SLE underwent cesarean section compared with 21.2% of RA controls and 23.7% of SLE controls. The adjusted ORs for cesarean section in RA and SLE were 2.3 (95% CI 0.9-4.7) and 2.8 (95% CI 1.5-4.0), respectively.
Babies were more frequently premature, with 2.6% vs. 0.7% born between 28 and 34 weeks’ gestation in women with and without RA, and 18.4% vs. 8% born at 34-37 weeks’ gestation. Corresponding values for the children of women with SLE were 8.4% vs. 1.9% at 28-34 weeks and 23.2% vs. 5.1% at 34-37 weeks. Three (3.2%) women with SLE but none without gave birth at less than 28 weeks’ gestation.
The adjusted ORs for premature delivery were 2.7 (95% CI 1.0-7.0) for RA and 6.6 (95% CI 3.5-12.3) for SLE.
Not surprisingly, the need for intensive care was higher among children born to women with RA or SLE than among the babies of women in the control groups. Adjusted ORs for SGA were 3.0 and 2.8 for RA and SLE, respectively.
These findings suggest the need for improved multidisciplinary management of women with arthritic conditions who are pregnant, Dr. Barnabe suggested.
"I think this shows that we can’t just assume that if we treat disease activity well enough we will affect obstetrical outcomes," she said.
"We should liaise with the obstetricians and the maternal-fetal medicine specialists and others to ensure that blood pressures are well controlled during pregnancy and make sure the disease activity is well controlled, and that will hopefully optimize these outcomes," Dr. Barnabe added. "I think a combined clinic is probably the best way to approach this."
Dr. Barnabe disclosed receiving a scholarship from the Arthritis Society, UCB, and the Canadian Rheumatologists Association for her master’s degree. A coauthor has received financial support from Alberta Innovative Health Solutions.
LONDON – Women with both rheumatoid arthritis and systemic lupus erythematosus were more than twice as likely as women without these diseases to have pregnancy-related hypertension, and the risk has not lessened in recent years despite improved treatment, according to 10-years’ worth of admission and discharge data from several Canadian hospitals.
Such women were more likely to undergo a cesarean section, and their newborns were more likely to be born prematurely, be small for gestational age (SGA), and require intensive care, compared with children born to women without RA or SLE.
"We wanted to look at what obstetrical and neonatal outcomes have been like over the past 10 years in both RA and in lupus," study author and rheumatologist Dr. Cheryl Barnabe said in an interview during a poster session at the annual European Congress of Rheumatology.
To do so, Dr. Barnabe and colleagues used an administrative database maintained by the Canadian government to examine the outcomes of 38 women with RA and 95 with SLE who were admitted and discharged from hospitals in Calgary for obstetric reasons. Outcomes were compared with expectant women who did not have either condition, with four times as many controls as cases.
"We found that the RA and lupus patients stayed in hospital longer [after delivery], approximately double the percentage of patients [in both groups] had C-sections done, and there were more postpartum infections in the lupus patients compared to the lupus controls [6.3% vs. 1.3%, P less than .004]," observed Dr. Barnabe, a clinical scholar in the department of medicine at the University of Calgary in Alberta.
Adjusted odds ratios (ORs) for preeclampsia or eclampsia were 2.8 (95% confidence interval 1.0-7.8) for RA and 2.0 (95% CI 1.0-3.7) for SLE.
The mean length of hospital stay was 0.9 days longer for women with RA than for those without (P less than .003) and 1.8 days longer for those with SLE than for those without (P less than .001).
One-third (34.2%) of women with RA and 43.2% of women with SLE underwent cesarean section compared with 21.2% of RA controls and 23.7% of SLE controls. The adjusted ORs for cesarean section in RA and SLE were 2.3 (95% CI 0.9-4.7) and 2.8 (95% CI 1.5-4.0), respectively.
Babies were more frequently premature, with 2.6% vs. 0.7% born between 28 and 34 weeks’ gestation in women with and without RA, and 18.4% vs. 8% born at 34-37 weeks’ gestation. Corresponding values for the children of women with SLE were 8.4% vs. 1.9% at 28-34 weeks and 23.2% vs. 5.1% at 34-37 weeks. Three (3.2%) women with SLE but none without gave birth at less than 28 weeks’ gestation.
The adjusted ORs for premature delivery were 2.7 (95% CI 1.0-7.0) for RA and 6.6 (95% CI 3.5-12.3) for SLE.
Not surprisingly, the need for intensive care was higher among children born to women with RA or SLE than among the babies of women in the control groups. Adjusted ORs for SGA were 3.0 and 2.8 for RA and SLE, respectively.
These findings suggest the need for improved multidisciplinary management of women with arthritic conditions who are pregnant, Dr. Barnabe suggested.
"I think this shows that we can’t just assume that if we treat disease activity well enough we will affect obstetrical outcomes," she said.
"We should liaise with the obstetricians and the maternal-fetal medicine specialists and others to ensure that blood pressures are well controlled during pregnancy and make sure the disease activity is well controlled, and that will hopefully optimize these outcomes," Dr. Barnabe added. "I think a combined clinic is probably the best way to approach this."
Dr. Barnabe disclosed receiving a scholarship from the Arthritis Society, UCB, and the Canadian Rheumatologists Association for her master’s degree. A coauthor has received financial support from Alberta Innovative Health Solutions.
LONDON – Women with both rheumatoid arthritis and systemic lupus erythematosus were more than twice as likely as women without these diseases to have pregnancy-related hypertension, and the risk has not lessened in recent years despite improved treatment, according to 10-years’ worth of admission and discharge data from several Canadian hospitals.
Such women were more likely to undergo a cesarean section, and their newborns were more likely to be born prematurely, be small for gestational age (SGA), and require intensive care, compared with children born to women without RA or SLE.
"We wanted to look at what obstetrical and neonatal outcomes have been like over the past 10 years in both RA and in lupus," study author and rheumatologist Dr. Cheryl Barnabe said in an interview during a poster session at the annual European Congress of Rheumatology.
To do so, Dr. Barnabe and colleagues used an administrative database maintained by the Canadian government to examine the outcomes of 38 women with RA and 95 with SLE who were admitted and discharged from hospitals in Calgary for obstetric reasons. Outcomes were compared with expectant women who did not have either condition, with four times as many controls as cases.
"We found that the RA and lupus patients stayed in hospital longer [after delivery], approximately double the percentage of patients [in both groups] had C-sections done, and there were more postpartum infections in the lupus patients compared to the lupus controls [6.3% vs. 1.3%, P less than .004]," observed Dr. Barnabe, a clinical scholar in the department of medicine at the University of Calgary in Alberta.
Adjusted odds ratios (ORs) for preeclampsia or eclampsia were 2.8 (95% confidence interval 1.0-7.8) for RA and 2.0 (95% CI 1.0-3.7) for SLE.
The mean length of hospital stay was 0.9 days longer for women with RA than for those without (P less than .003) and 1.8 days longer for those with SLE than for those without (P less than .001).
One-third (34.2%) of women with RA and 43.2% of women with SLE underwent cesarean section compared with 21.2% of RA controls and 23.7% of SLE controls. The adjusted ORs for cesarean section in RA and SLE were 2.3 (95% CI 0.9-4.7) and 2.8 (95% CI 1.5-4.0), respectively.
Babies were more frequently premature, with 2.6% vs. 0.7% born between 28 and 34 weeks’ gestation in women with and without RA, and 18.4% vs. 8% born at 34-37 weeks’ gestation. Corresponding values for the children of women with SLE were 8.4% vs. 1.9% at 28-34 weeks and 23.2% vs. 5.1% at 34-37 weeks. Three (3.2%) women with SLE but none without gave birth at less than 28 weeks’ gestation.
The adjusted ORs for premature delivery were 2.7 (95% CI 1.0-7.0) for RA and 6.6 (95% CI 3.5-12.3) for SLE.
Not surprisingly, the need for intensive care was higher among children born to women with RA or SLE than among the babies of women in the control groups. Adjusted ORs for SGA were 3.0 and 2.8 for RA and SLE, respectively.
These findings suggest the need for improved multidisciplinary management of women with arthritic conditions who are pregnant, Dr. Barnabe suggested.
"I think this shows that we can’t just assume that if we treat disease activity well enough we will affect obstetrical outcomes," she said.
"We should liaise with the obstetricians and the maternal-fetal medicine specialists and others to ensure that blood pressures are well controlled during pregnancy and make sure the disease activity is well controlled, and that will hopefully optimize these outcomes," Dr. Barnabe added. "I think a combined clinic is probably the best way to approach this."
Dr. Barnabe disclosed receiving a scholarship from the Arthritis Society, UCB, and the Canadian Rheumatologists Association for her master’s degree. A coauthor has received financial support from Alberta Innovative Health Solutions.
FROM THE ANNUAL EUROPEAN CONGRESS OF RHEUMATOLOGY
Major Finding: Adjusted odds ratios for preeclampsia or eclampsia were 2.8 (95% CI 1.0-7.8) for RA and 2.0 (95% CI 1.0-3.7) for SLE.
Data Source: Inpatient administrative database of obstetric admissions and discharges for 38 women with RA, 95 with SLE, and 525 women with neither condition as controls, between 1998-1999 and 2008-2009.
Disclosures: Dr. Barnabe disclosed receiving a scholarship from the Arthritis Society, UCB, and the Canadian Rheumatologists Association for her master’s degree. A coauthor has received financial support from Alberta Innovative Health Solutions.
GI Perforation Rare in Rheumatoid Arthritis Patients
LONDON – Although a potentially serious complication, perforation of the gastrointestinal tract is rare, judging from the findings of an analysis of more than 140,000 patients with rheumatoid arthritis.
Upper or lower GI tract perforation occurred in 696 (0.5%) of patients, with an overall, unadjusted incidence rate of 1.7 cases per 1,000 person-years, according to a report by Dr. Jeffrey Curtis.
"For [most of] the rheumatoid arthritis patients someone has in their practice, [GI perforation] is going to be very uncommon; I think that should be reassuring," Dr. Curtis said during an interview at the annual European Congress of Rheumatology.
"We also observed that there were cases [of GI perforation] for every biologic group," added Dr. Curtis, a rheumatologist, epidemiologist, and associate professor of medicine at the University of Alabama at Birmingham. This should help dispel any concerns that the adverse event might occur with certain biologic agents used to treat RA, he suggested.
In a retrospective study, Dr. Curtis and his associates analyzed records of 143,433 RA patients from a large U.S.-based administrative claims database for the years 2001-2009. The investigators used a validated algorithm to identify cases of upper and lower GI perforation and to determine predictive factors. The median follow-up was 2.5 years.
Older age was found to be a predictor of GI perforation, with adjusted relative risks of 1.6 and 2.1 for people aged 40-64 years and 65 years, respectively, compared with RA patients younger than 40 years. The mean age of the 142,737 patients who did not have a GI perforation was 57.6 years, and the mean age of the 696 patients who did was 62 years (P less than .01).
Diverticulitis and diverticulosis without diverticulitis were also significantly more common in patients who experienced a GI perforation than in those who did not, although the incidence was still low, with rates of 2.9% vs. 0.3% and 1.4% vs. 0.4%, respectively (both P less than .01). Diverticulitis but not diverticulosis was a significant risk factor for perforation.
The main risk factors among the RA medication groups of most relevance were the use of oral glucocorticosteroids and nonsteroidal anti-inflammatory drugs (NSAIDs), not biologics and not really the disease-modifying antirheumatic drugs (DMARDs), Dr. Curtis said in the interview. Indeed, the incidence of GI perforation was highest in patients who used glucocorticoids in combination with DMARDs other than methotrexate (3.03 per 1,000 patient years).
Steroid monotherapy carried an incidence of 2.86 per 1,000 patient-years. Steroids used in combination with methotrexate and biologics also increased the risk of the GI complications (2.24 and 1.87 per 1,000 patient-years, respectively).
The rates of GI perforations in patients treated with biologics, methotrexate, or other DMARDs without steroids were 1.02, 1.08, and 1.71 per 1,000 patient-years, respectively. NSAID use was associated with an incidence rate of 1.68 per 1,000 patient-years.
"In contrast to about 10 years ago, when there was a lot more GI bleeding with perforation in the upper GI tract, there are population studies now suggesting that we need to be more worried about perforations of the lower GI tract," Dr. Curtis said.
In the study, 80% of the perforations seen were in the lower GI tract, so the use of gastroprotective medications may not be that useful.
"I think that the relative contribution of NSAIDs [to GI perforation] is probably diminished, just because we are seeing more lower now than upper."
Although still important, upper GI bleeding and peptic ulcer disease are perhaps less critical than antecedent diverticulitis and its associated complications.
Minimization of NSAID and steroid use is probably warranted in higher-risk patients, Dr. Curtis advised. "In somebody with a history of diverticulitis, I would be very cautious," he noted.
Dr. Curtis disclosed research and consulting relationships with Abbot, Amgen, BMS, Centocor, CORRONA, Crescendo, Pfizer, Roche, and UCB.
LONDON – Although a potentially serious complication, perforation of the gastrointestinal tract is rare, judging from the findings of an analysis of more than 140,000 patients with rheumatoid arthritis.
Upper or lower GI tract perforation occurred in 696 (0.5%) of patients, with an overall, unadjusted incidence rate of 1.7 cases per 1,000 person-years, according to a report by Dr. Jeffrey Curtis.
"For [most of] the rheumatoid arthritis patients someone has in their practice, [GI perforation] is going to be very uncommon; I think that should be reassuring," Dr. Curtis said during an interview at the annual European Congress of Rheumatology.
"We also observed that there were cases [of GI perforation] for every biologic group," added Dr. Curtis, a rheumatologist, epidemiologist, and associate professor of medicine at the University of Alabama at Birmingham. This should help dispel any concerns that the adverse event might occur with certain biologic agents used to treat RA, he suggested.
In a retrospective study, Dr. Curtis and his associates analyzed records of 143,433 RA patients from a large U.S.-based administrative claims database for the years 2001-2009. The investigators used a validated algorithm to identify cases of upper and lower GI perforation and to determine predictive factors. The median follow-up was 2.5 years.
Older age was found to be a predictor of GI perforation, with adjusted relative risks of 1.6 and 2.1 for people aged 40-64 years and 65 years, respectively, compared with RA patients younger than 40 years. The mean age of the 142,737 patients who did not have a GI perforation was 57.6 years, and the mean age of the 696 patients who did was 62 years (P less than .01).
Diverticulitis and diverticulosis without diverticulitis were also significantly more common in patients who experienced a GI perforation than in those who did not, although the incidence was still low, with rates of 2.9% vs. 0.3% and 1.4% vs. 0.4%, respectively (both P less than .01). Diverticulitis but not diverticulosis was a significant risk factor for perforation.
The main risk factors among the RA medication groups of most relevance were the use of oral glucocorticosteroids and nonsteroidal anti-inflammatory drugs (NSAIDs), not biologics and not really the disease-modifying antirheumatic drugs (DMARDs), Dr. Curtis said in the interview. Indeed, the incidence of GI perforation was highest in patients who used glucocorticoids in combination with DMARDs other than methotrexate (3.03 per 1,000 patient years).
Steroid monotherapy carried an incidence of 2.86 per 1,000 patient-years. Steroids used in combination with methotrexate and biologics also increased the risk of the GI complications (2.24 and 1.87 per 1,000 patient-years, respectively).
The rates of GI perforations in patients treated with biologics, methotrexate, or other DMARDs without steroids were 1.02, 1.08, and 1.71 per 1,000 patient-years, respectively. NSAID use was associated with an incidence rate of 1.68 per 1,000 patient-years.
"In contrast to about 10 years ago, when there was a lot more GI bleeding with perforation in the upper GI tract, there are population studies now suggesting that we need to be more worried about perforations of the lower GI tract," Dr. Curtis said.
In the study, 80% of the perforations seen were in the lower GI tract, so the use of gastroprotective medications may not be that useful.
"I think that the relative contribution of NSAIDs [to GI perforation] is probably diminished, just because we are seeing more lower now than upper."
Although still important, upper GI bleeding and peptic ulcer disease are perhaps less critical than antecedent diverticulitis and its associated complications.
Minimization of NSAID and steroid use is probably warranted in higher-risk patients, Dr. Curtis advised. "In somebody with a history of diverticulitis, I would be very cautious," he noted.
Dr. Curtis disclosed research and consulting relationships with Abbot, Amgen, BMS, Centocor, CORRONA, Crescendo, Pfizer, Roche, and UCB.
LONDON – Although a potentially serious complication, perforation of the gastrointestinal tract is rare, judging from the findings of an analysis of more than 140,000 patients with rheumatoid arthritis.
Upper or lower GI tract perforation occurred in 696 (0.5%) of patients, with an overall, unadjusted incidence rate of 1.7 cases per 1,000 person-years, according to a report by Dr. Jeffrey Curtis.
"For [most of] the rheumatoid arthritis patients someone has in their practice, [GI perforation] is going to be very uncommon; I think that should be reassuring," Dr. Curtis said during an interview at the annual European Congress of Rheumatology.
"We also observed that there were cases [of GI perforation] for every biologic group," added Dr. Curtis, a rheumatologist, epidemiologist, and associate professor of medicine at the University of Alabama at Birmingham. This should help dispel any concerns that the adverse event might occur with certain biologic agents used to treat RA, he suggested.
In a retrospective study, Dr. Curtis and his associates analyzed records of 143,433 RA patients from a large U.S.-based administrative claims database for the years 2001-2009. The investigators used a validated algorithm to identify cases of upper and lower GI perforation and to determine predictive factors. The median follow-up was 2.5 years.
Older age was found to be a predictor of GI perforation, with adjusted relative risks of 1.6 and 2.1 for people aged 40-64 years and 65 years, respectively, compared with RA patients younger than 40 years. The mean age of the 142,737 patients who did not have a GI perforation was 57.6 years, and the mean age of the 696 patients who did was 62 years (P less than .01).
Diverticulitis and diverticulosis without diverticulitis were also significantly more common in patients who experienced a GI perforation than in those who did not, although the incidence was still low, with rates of 2.9% vs. 0.3% and 1.4% vs. 0.4%, respectively (both P less than .01). Diverticulitis but not diverticulosis was a significant risk factor for perforation.
The main risk factors among the RA medication groups of most relevance were the use of oral glucocorticosteroids and nonsteroidal anti-inflammatory drugs (NSAIDs), not biologics and not really the disease-modifying antirheumatic drugs (DMARDs), Dr. Curtis said in the interview. Indeed, the incidence of GI perforation was highest in patients who used glucocorticoids in combination with DMARDs other than methotrexate (3.03 per 1,000 patient years).
Steroid monotherapy carried an incidence of 2.86 per 1,000 patient-years. Steroids used in combination with methotrexate and biologics also increased the risk of the GI complications (2.24 and 1.87 per 1,000 patient-years, respectively).
The rates of GI perforations in patients treated with biologics, methotrexate, or other DMARDs without steroids were 1.02, 1.08, and 1.71 per 1,000 patient-years, respectively. NSAID use was associated with an incidence rate of 1.68 per 1,000 patient-years.
"In contrast to about 10 years ago, when there was a lot more GI bleeding with perforation in the upper GI tract, there are population studies now suggesting that we need to be more worried about perforations of the lower GI tract," Dr. Curtis said.
In the study, 80% of the perforations seen were in the lower GI tract, so the use of gastroprotective medications may not be that useful.
"I think that the relative contribution of NSAIDs [to GI perforation] is probably diminished, just because we are seeing more lower now than upper."
Although still important, upper GI bleeding and peptic ulcer disease are perhaps less critical than antecedent diverticulitis and its associated complications.
Minimization of NSAID and steroid use is probably warranted in higher-risk patients, Dr. Curtis advised. "In somebody with a history of diverticulitis, I would be very cautious," he noted.
Dr. Curtis disclosed research and consulting relationships with Abbot, Amgen, BMS, Centocor, CORRONA, Crescendo, Pfizer, Roche, and UCB.
FROM THE ANNUAL EUROPEAN CONGRESS OF RHEUMATOLOGY
Major Finding: The incidence of GI perforation was highest in patients who used glucocorticoids in combination with DMARDs other than methotrexate (3.03 per 1,000 patient years).
Data Source: Retrospective study of 143,433 patients with rheumatoid arthritis with at least two nondiagnostic claims in a U.S. administrative database filed between 2001 and 2009.
Disclosures: Dr. Curtis disclosed research and consulting relationships with Abbot, Amgen, BMS, Centocor, CORRONA, Crescendo, Pfizer, Roche, and UCB.
Periprosthetic Joint Infections Not Increased by RA Biologics
LONDON – Patients with rheumatoid arthritis who have had total joint replacement are not at greater risk of joint infection if they use biologic agents when compared with conventional disease-modifying drugs.
New data from the German biologics register RABBIT (Rheumatoid Arthritis Observation of Biologic Therapy) show that the overall rate of periprosthetic joint infection is low, at 1%, and remains low regardless of the treatment type.
"A lot of patients with RA have to undergo joint replacement," said Dr. Anja Strangfeld of the German Rheumatism Research Center Berlin, where the biologics register is based.
During an interview, Dr. Strangfeld noted that concern has been voiced about the use of anti-tumor necrosis factor (TNF) agents in patients who need a joint replacement because of the possibility of an increased risk of serious infections.
"It was also thought that in people who already have prostheses, a joint infection will be more likely to occur after starting biologic treatment, especially with anti-TNF agents," Dr. Strangfeld observed.
"The hypothesis was that microorganisms could enter the joint during the surgery [and] form a protective biofilm," but this biofilm might get disrupted when anti-TNF treatment is started, she said. This disruption allows the infective agent to spread and cause infection.
However, of 1,495 total joint replacements in 1,013 patients, very few got infected.
"In our whole register, we only found 15 periprosthetic joint infections, and this means that 1% of the procedures got infected. That’s good news, as it seems that there is not an increased risk for patients," Dr. Strangfeld said.
Until May 2010, 7,536 patients with RA were included in the RABBIT database and were treated with conventional disease-modifying antirheumatic drugs (DMARDs), anti-TNFs, or other biologic agents (tocilizumab, rituximab, abatacept).
Only total replacements of the hip, knee, shoulder, or ankle were included in the analysis, and patients had received joint prostheses both before and after enrollment. The mean exposure to biologic therapy before joint surgery was 2.7 years.
There was no significant difference between the percentage of joints that became infected in patients treated with DMARDs versus those treated with anti-TNF agents (1.5% vs. 1.5%; P = .077)
There was also no significant difference observed among individual anti-TNF drugs, with rates of 1.5%, 1.4%, and 0.9% for adalimumab, etanercept, and infliximab, respectively.
These incidence rates are in line with data from Danish and Finnish arthroplasty registries, in which infection rates of 0.7% and 1.3% have been reported.
In patients treated with tocilizumab, rituximab, or abatacept, no periprosthetic infections occurred, although the number of patient-years of observation were much lower than that for anti-TNFs and DMARDS.
The microorganism responsible for the joint infection was reported in only 10 cases – with Staphylococcus spp. being the most common culprit (6 cases).
When asked whether patients who underwent joint replacement surgery might have to take antibiotic prophylaxis, Dr. Strangfeld noted that this was something that the current analysis could not determine but would be interesting to look at.
These findings suggest that patients who need to have a joint replacement and who are already being treated with a biologic agent should have no great cause to worry about contracting an infection.
"For patients who already have a joint replacement, they also don’t have to worry that much if they start a biologic agent," Dr. Strangfeld said.
RABBIT is supported by a joint, unconditional grant from the following German manufacturers of biologic agents: Abbott, Amgen/Swedish Orphan Biovitrum, Bristol-Myers Squibb, Essex/MSD, Pfizer, Roche, and UCB. Dr. Strangfeld had no personal financial disclosures.
LONDON – Patients with rheumatoid arthritis who have had total joint replacement are not at greater risk of joint infection if they use biologic agents when compared with conventional disease-modifying drugs.
New data from the German biologics register RABBIT (Rheumatoid Arthritis Observation of Biologic Therapy) show that the overall rate of periprosthetic joint infection is low, at 1%, and remains low regardless of the treatment type.
"A lot of patients with RA have to undergo joint replacement," said Dr. Anja Strangfeld of the German Rheumatism Research Center Berlin, where the biologics register is based.
During an interview, Dr. Strangfeld noted that concern has been voiced about the use of anti-tumor necrosis factor (TNF) agents in patients who need a joint replacement because of the possibility of an increased risk of serious infections.
"It was also thought that in people who already have prostheses, a joint infection will be more likely to occur after starting biologic treatment, especially with anti-TNF agents," Dr. Strangfeld observed.
"The hypothesis was that microorganisms could enter the joint during the surgery [and] form a protective biofilm," but this biofilm might get disrupted when anti-TNF treatment is started, she said. This disruption allows the infective agent to spread and cause infection.
However, of 1,495 total joint replacements in 1,013 patients, very few got infected.
"In our whole register, we only found 15 periprosthetic joint infections, and this means that 1% of the procedures got infected. That’s good news, as it seems that there is not an increased risk for patients," Dr. Strangfeld said.
Until May 2010, 7,536 patients with RA were included in the RABBIT database and were treated with conventional disease-modifying antirheumatic drugs (DMARDs), anti-TNFs, or other biologic agents (tocilizumab, rituximab, abatacept).
Only total replacements of the hip, knee, shoulder, or ankle were included in the analysis, and patients had received joint prostheses both before and after enrollment. The mean exposure to biologic therapy before joint surgery was 2.7 years.
There was no significant difference between the percentage of joints that became infected in patients treated with DMARDs versus those treated with anti-TNF agents (1.5% vs. 1.5%; P = .077)
There was also no significant difference observed among individual anti-TNF drugs, with rates of 1.5%, 1.4%, and 0.9% for adalimumab, etanercept, and infliximab, respectively.
These incidence rates are in line with data from Danish and Finnish arthroplasty registries, in which infection rates of 0.7% and 1.3% have been reported.
In patients treated with tocilizumab, rituximab, or abatacept, no periprosthetic infections occurred, although the number of patient-years of observation were much lower than that for anti-TNFs and DMARDS.
The microorganism responsible for the joint infection was reported in only 10 cases – with Staphylococcus spp. being the most common culprit (6 cases).
When asked whether patients who underwent joint replacement surgery might have to take antibiotic prophylaxis, Dr. Strangfeld noted that this was something that the current analysis could not determine but would be interesting to look at.
These findings suggest that patients who need to have a joint replacement and who are already being treated with a biologic agent should have no great cause to worry about contracting an infection.
"For patients who already have a joint replacement, they also don’t have to worry that much if they start a biologic agent," Dr. Strangfeld said.
RABBIT is supported by a joint, unconditional grant from the following German manufacturers of biologic agents: Abbott, Amgen/Swedish Orphan Biovitrum, Bristol-Myers Squibb, Essex/MSD, Pfizer, Roche, and UCB. Dr. Strangfeld had no personal financial disclosures.
LONDON – Patients with rheumatoid arthritis who have had total joint replacement are not at greater risk of joint infection if they use biologic agents when compared with conventional disease-modifying drugs.
New data from the German biologics register RABBIT (Rheumatoid Arthritis Observation of Biologic Therapy) show that the overall rate of periprosthetic joint infection is low, at 1%, and remains low regardless of the treatment type.
"A lot of patients with RA have to undergo joint replacement," said Dr. Anja Strangfeld of the German Rheumatism Research Center Berlin, where the biologics register is based.
During an interview, Dr. Strangfeld noted that concern has been voiced about the use of anti-tumor necrosis factor (TNF) agents in patients who need a joint replacement because of the possibility of an increased risk of serious infections.
"It was also thought that in people who already have prostheses, a joint infection will be more likely to occur after starting biologic treatment, especially with anti-TNF agents," Dr. Strangfeld observed.
"The hypothesis was that microorganisms could enter the joint during the surgery [and] form a protective biofilm," but this biofilm might get disrupted when anti-TNF treatment is started, she said. This disruption allows the infective agent to spread and cause infection.
However, of 1,495 total joint replacements in 1,013 patients, very few got infected.
"In our whole register, we only found 15 periprosthetic joint infections, and this means that 1% of the procedures got infected. That’s good news, as it seems that there is not an increased risk for patients," Dr. Strangfeld said.
Until May 2010, 7,536 patients with RA were included in the RABBIT database and were treated with conventional disease-modifying antirheumatic drugs (DMARDs), anti-TNFs, or other biologic agents (tocilizumab, rituximab, abatacept).
Only total replacements of the hip, knee, shoulder, or ankle were included in the analysis, and patients had received joint prostheses both before and after enrollment. The mean exposure to biologic therapy before joint surgery was 2.7 years.
There was no significant difference between the percentage of joints that became infected in patients treated with DMARDs versus those treated with anti-TNF agents (1.5% vs. 1.5%; P = .077)
There was also no significant difference observed among individual anti-TNF drugs, with rates of 1.5%, 1.4%, and 0.9% for adalimumab, etanercept, and infliximab, respectively.
These incidence rates are in line with data from Danish and Finnish arthroplasty registries, in which infection rates of 0.7% and 1.3% have been reported.
In patients treated with tocilizumab, rituximab, or abatacept, no periprosthetic infections occurred, although the number of patient-years of observation were much lower than that for anti-TNFs and DMARDS.
The microorganism responsible for the joint infection was reported in only 10 cases – with Staphylococcus spp. being the most common culprit (6 cases).
When asked whether patients who underwent joint replacement surgery might have to take antibiotic prophylaxis, Dr. Strangfeld noted that this was something that the current analysis could not determine but would be interesting to look at.
These findings suggest that patients who need to have a joint replacement and who are already being treated with a biologic agent should have no great cause to worry about contracting an infection.
"For patients who already have a joint replacement, they also don’t have to worry that much if they start a biologic agent," Dr. Strangfeld said.
RABBIT is supported by a joint, unconditional grant from the following German manufacturers of biologic agents: Abbott, Amgen/Swedish Orphan Biovitrum, Bristol-Myers Squibb, Essex/MSD, Pfizer, Roche, and UCB. Dr. Strangfeld had no personal financial disclosures.
FROM THE ANNUAL EUROPEAN CONGRESS OF RHEUMATOLOGY
Major Finding: Fifteen joint infections occurred in 1,495 patients, with 1% of conventional DMARD-treated and 1.5% of anti-TNF–treated patients experiencing joint infection (P less than .77).
Data Source: Data analysis of 7,536 RA patients enrolled in the German biologics register RABBIT until May 2010.
Disclosures: RABBIT is supported by a joint, unconditional grant from the following German manufacturers of biologic agents: Abbott, Amgen/Swedish Orphan Biovitrum, Bristol-Myers Squibb, Essex/MSD, Pfizer, Roche, and UCB. Dr. Strangfeld had no personal financial disclosures.
ACPA-Negative RA Incidence Spikes During First Postpartum Year
LONDON – Women who give birth to a child face a twofold increased risk of incident ACPA-negative rheumatoid arthritis, compared with nulliparous women, but they have no increased risk for developing ACPA-positive disease, based on results from a Swedish epidemiologic study
The finding is consistent with a report last year from a Norwegian study that women face about a twofold increased risk for incident rheumatoid arthritis (RA) during the first 2 years after giving birth to a child, compared with their RA risk 2-4 years postpartum (Ann. Rheum. Dis. 2010;69:332-6). The reason why the new analysis, which included more than 1,200 cases and controls, showed a different relationship between partum and the onset of anticitrullinated peptide antibody (ACPA) –positive RH and ACPA-negative RA remains unclear, according to Camilla Bengtsson, Ph.D.
"Why there is only an association with ACPA-negative disease, and which biological mechanisms are involved remains to be elucidated," said Dr. Bengtsson, a researcher at the Karolinska Institute in Stockholm. The way in which this finding might apply to practice also remains unclear, she added.
Dr. Bengtsson’s analysis failed to show an increased incidence of any form of RA in women who were more than a year out from their delivery.
The study used data and blood specimens from Swedish women aged 18-50 years who were enrolled in the Epidemiological Investigation of RA (EIRA) study during 1996-2006. Among the women with incident RA enrolled in EIRA, 547 (95%) agreed to participate and provide blood specimens, and among the control women in the study, 658 (81%) provided blood. The analysis divided the cases and controls into subgroups based on their partum status. The 547 women with new-onset RA included 360 who had given birth and 187 who had not. The parous women included 226 with ACPA-positive RA and 134 with the ACPA-negative form. Among the nulliparous women with RA, 127 had the ACPA-positive form and 60 were ACPA negative.
Among the controls with no RA, 431 had given birth and 227 had never given birth.
The case-control analysis showed that among all women with incident RA, birth status during the year preceding a new RA diagnosis had no statistically significant relationship with RA onset. However, among women who developed ACPA-negative RA, their risk spiked by a statistically significant, 2.4-fold rate during the year following partum, compared with nulliparous women. In contrast, the incidence of ACPA-positive RA showed no significant relationship to partum status during the preceding year.
Further analysis examined the timing between delivery and onset of ACPA-negative RA more closely. Again, the analysis showed that, during the year following giving birth, women faced a statistically significant, 2.4-fold elevated risk for incident ACPA-negative RA, compared with nulliparous women. During the 2-10 years following giving birth, the rate of incident ACPA-negative RA dropped to a 50% higher risk, compared with nulliparous women, but this difference was not considered statistically significant. And women more than 10 years out from their most recent delivery had a risk for incident ACPA-negative RA identical to the nulliparous women, Dr. Bengtsson reported.
Dr. Bengtsson said that she had no disclosures.
LONDON – Women who give birth to a child face a twofold increased risk of incident ACPA-negative rheumatoid arthritis, compared with nulliparous women, but they have no increased risk for developing ACPA-positive disease, based on results from a Swedish epidemiologic study
The finding is consistent with a report last year from a Norwegian study that women face about a twofold increased risk for incident rheumatoid arthritis (RA) during the first 2 years after giving birth to a child, compared with their RA risk 2-4 years postpartum (Ann. Rheum. Dis. 2010;69:332-6). The reason why the new analysis, which included more than 1,200 cases and controls, showed a different relationship between partum and the onset of anticitrullinated peptide antibody (ACPA) –positive RH and ACPA-negative RA remains unclear, according to Camilla Bengtsson, Ph.D.
"Why there is only an association with ACPA-negative disease, and which biological mechanisms are involved remains to be elucidated," said Dr. Bengtsson, a researcher at the Karolinska Institute in Stockholm. The way in which this finding might apply to practice also remains unclear, she added.
Dr. Bengtsson’s analysis failed to show an increased incidence of any form of RA in women who were more than a year out from their delivery.
The study used data and blood specimens from Swedish women aged 18-50 years who were enrolled in the Epidemiological Investigation of RA (EIRA) study during 1996-2006. Among the women with incident RA enrolled in EIRA, 547 (95%) agreed to participate and provide blood specimens, and among the control women in the study, 658 (81%) provided blood. The analysis divided the cases and controls into subgroups based on their partum status. The 547 women with new-onset RA included 360 who had given birth and 187 who had not. The parous women included 226 with ACPA-positive RA and 134 with the ACPA-negative form. Among the nulliparous women with RA, 127 had the ACPA-positive form and 60 were ACPA negative.
Among the controls with no RA, 431 had given birth and 227 had never given birth.
The case-control analysis showed that among all women with incident RA, birth status during the year preceding a new RA diagnosis had no statistically significant relationship with RA onset. However, among women who developed ACPA-negative RA, their risk spiked by a statistically significant, 2.4-fold rate during the year following partum, compared with nulliparous women. In contrast, the incidence of ACPA-positive RA showed no significant relationship to partum status during the preceding year.
Further analysis examined the timing between delivery and onset of ACPA-negative RA more closely. Again, the analysis showed that, during the year following giving birth, women faced a statistically significant, 2.4-fold elevated risk for incident ACPA-negative RA, compared with nulliparous women. During the 2-10 years following giving birth, the rate of incident ACPA-negative RA dropped to a 50% higher risk, compared with nulliparous women, but this difference was not considered statistically significant. And women more than 10 years out from their most recent delivery had a risk for incident ACPA-negative RA identical to the nulliparous women, Dr. Bengtsson reported.
Dr. Bengtsson said that she had no disclosures.
LONDON – Women who give birth to a child face a twofold increased risk of incident ACPA-negative rheumatoid arthritis, compared with nulliparous women, but they have no increased risk for developing ACPA-positive disease, based on results from a Swedish epidemiologic study
The finding is consistent with a report last year from a Norwegian study that women face about a twofold increased risk for incident rheumatoid arthritis (RA) during the first 2 years after giving birth to a child, compared with their RA risk 2-4 years postpartum (Ann. Rheum. Dis. 2010;69:332-6). The reason why the new analysis, which included more than 1,200 cases and controls, showed a different relationship between partum and the onset of anticitrullinated peptide antibody (ACPA) –positive RH and ACPA-negative RA remains unclear, according to Camilla Bengtsson, Ph.D.
"Why there is only an association with ACPA-negative disease, and which biological mechanisms are involved remains to be elucidated," said Dr. Bengtsson, a researcher at the Karolinska Institute in Stockholm. The way in which this finding might apply to practice also remains unclear, she added.
Dr. Bengtsson’s analysis failed to show an increased incidence of any form of RA in women who were more than a year out from their delivery.
The study used data and blood specimens from Swedish women aged 18-50 years who were enrolled in the Epidemiological Investigation of RA (EIRA) study during 1996-2006. Among the women with incident RA enrolled in EIRA, 547 (95%) agreed to participate and provide blood specimens, and among the control women in the study, 658 (81%) provided blood. The analysis divided the cases and controls into subgroups based on their partum status. The 547 women with new-onset RA included 360 who had given birth and 187 who had not. The parous women included 226 with ACPA-positive RA and 134 with the ACPA-negative form. Among the nulliparous women with RA, 127 had the ACPA-positive form and 60 were ACPA negative.
Among the controls with no RA, 431 had given birth and 227 had never given birth.
The case-control analysis showed that among all women with incident RA, birth status during the year preceding a new RA diagnosis had no statistically significant relationship with RA onset. However, among women who developed ACPA-negative RA, their risk spiked by a statistically significant, 2.4-fold rate during the year following partum, compared with nulliparous women. In contrast, the incidence of ACPA-positive RA showed no significant relationship to partum status during the preceding year.
Further analysis examined the timing between delivery and onset of ACPA-negative RA more closely. Again, the analysis showed that, during the year following giving birth, women faced a statistically significant, 2.4-fold elevated risk for incident ACPA-negative RA, compared with nulliparous women. During the 2-10 years following giving birth, the rate of incident ACPA-negative RA dropped to a 50% higher risk, compared with nulliparous women, but this difference was not considered statistically significant. And women more than 10 years out from their most recent delivery had a risk for incident ACPA-negative RA identical to the nulliparous women, Dr. Bengtsson reported.
Dr. Bengtsson said that she had no disclosures.
FROM THE ANNUAL EUROPEAN CONGRESS OF RHEUMATOLOGY
Major Finding: During the year following giving birth, women had a statistically significant, 2.4-fold increased risk of incident ACPA-negative rheumatoid arthritis, compared with nulliparous women.
Data Source: Case-control study of 1,205 Swedish women enrolled in the Epidemiological Investigation of Rheumatoid Arthritis study during 1996-2006.
Disclosures: Dr. Bengtsson said that she had no disclosures.
Opioid Rotation: Convert Tx With Safety-Focused Approach
DESTIN, FLA. – Opioid rotation is a common and potentially beneficial practice for helping to relieve chronic pain in patients who require ongoing opioid therapy, but there are very few data to guide best practice.
The recommended approach, therefore, is one that focuses on safety, according to Dr. Perry Fine. Clinicians should consider opioid rotation when patients on chronic opioid therapy experience intolerable adverse effects, or when benefits are inadequate despite dose increases, according to recently published clinical guidelines (J. Pain 2009;10:113-30).
However, it is important to consider a number of factors before making changes in treatment, including demographic, disease-related, and treatment-related factors, as well as comorbidities, concomitant pharmacotherapy, drug sensitivities, and social situation, said Dr. Fine, professor of anesthesiology at the University of Utah, Salt Lake City.
If a decision is made to convert a patient's treatment, a two-step, safety-focused approach is needed, he said.
Step 1 involves an “automatic safety factor” calculation. That is, the equianalgesic dose of the new opioid should be calculated via an equianalgesic table such as a mu-agonist dose chart, and, with a few exceptions, an automatic dose reduction of 25%–50% should be made, except if the new drug is methadone or transdermal fentanyl.
A 25% reduction for opioids (other than methadone or fentanyl) is adequate in patients with no risk factors and/or if the switch is to a different route of administration of the same drug. A 50% reduction is needed in those receiving a relatively high dose of the current opioid, those who are elderly or frail, and those of Chinese lineage, Dr. Fine said.
If the switch is to methadone, a 75%–90% dose reduction is needed, and if the switch is to transdermal fentanyl, use the reduction that is built into the conversion charts provided in the prescribing information. If an oral transmucosal fentanyl citrate formulation is used, start with the lowest dose, he advised.
The second conversion step involves patient-specific adjustments. The patient should be assessed for pain severity and other medical or psychosocial characteristics, and appropriate additional adjustments should be made to the initial dose of the new opioid.
In patients with specific vulnerabilities such as advanced age, renal insufficiency, or cognitive impairment, consider an additional 10%–30% dose reduction, he said.
Dr. Fine has served as an advisory board member for Ameritox, Covidien, King (now Pfizer), Meda, and Purdue-Pharma. He also is a consultant for Cephalon and Johnson & Johnson.
{kind=link}
Consider opioid rotation when benefits are inadequate despite dose increases.
Source ©Csaba Tóth/iStockphoto.com
Examples of Initial Dose Calculation
▸ To convert controlled-release oxycodone (60 mg oral dose twice daily) to controlled-release morphine:
1. Calculate the total oxycodone 24-hour dose (120 mg).
2. Determine morphine equivalency (20 mg oxycodone = 30 mg morphine).
3. Convert the 24-hour oxycodone dose to the morphine dose (120 mg oxycodone = 180 mg morphine).
4. Reduce the morphine dose by 25% (135 mg morphine).
5. Split the total morphine dose to the twice-daily dose (67.5 mg). Because the controlled-release (extended-release) morphine is not provided in this exact dose, give the closest available dose (60 mg, twice daily).
▸ To convert controlled-release morphine (30 mg oral dose twice daily) to transdermal fentanyl:
1. Calculate the total morphine 24-hour dose (60 mg).
2. Use the prescribing info. to determine the oral equivalent dose of transdermal fentanyl (60 mg oral morphine = 25 mcg/hr fentanyl patch).
3. Prescribe 25 mcg/hr transdermal fentanyl patch to be changed every 3 days. Supply patient with five patches (a 15-day supply); instruct patient on application, and follow up by phone or in office within 2–3 days.
▸ To convert methadone (20 mg oral dose three times daily) to extended-release oxymorphone:
1. Calculate the total methadone 24-hour dose (60 mg daily).
2. Use mu-agonist dose chart to calculate oxymorphone dose equivalency to methadone (5 mg methadone = 10 mg oxymorphone).
3. Convert the 24-hour methadone dose to oxymorphone dose (60 mg methadone = 120 mg oxymorphone).
4. Reduce the dose by 50% and split the 50% total calculated oxymorphone dosage to a twice-daily dose. Prescribe oxymorphone ER (30 mg oral dose every 12 hours).
Source: Dr. Fine
DESTIN, FLA. – Opioid rotation is a common and potentially beneficial practice for helping to relieve chronic pain in patients who require ongoing opioid therapy, but there are very few data to guide best practice.
The recommended approach, therefore, is one that focuses on safety, according to Dr. Perry Fine. Clinicians should consider opioid rotation when patients on chronic opioid therapy experience intolerable adverse effects, or when benefits are inadequate despite dose increases, according to recently published clinical guidelines (J. Pain 2009;10:113-30).
However, it is important to consider a number of factors before making changes in treatment, including demographic, disease-related, and treatment-related factors, as well as comorbidities, concomitant pharmacotherapy, drug sensitivities, and social situation, said Dr. Fine, professor of anesthesiology at the University of Utah, Salt Lake City.
If a decision is made to convert a patient's treatment, a two-step, safety-focused approach is needed, he said.
Step 1 involves an “automatic safety factor” calculation. That is, the equianalgesic dose of the new opioid should be calculated via an equianalgesic table such as a mu-agonist dose chart, and, with a few exceptions, an automatic dose reduction of 25%–50% should be made, except if the new drug is methadone or transdermal fentanyl.
A 25% reduction for opioids (other than methadone or fentanyl) is adequate in patients with no risk factors and/or if the switch is to a different route of administration of the same drug. A 50% reduction is needed in those receiving a relatively high dose of the current opioid, those who are elderly or frail, and those of Chinese lineage, Dr. Fine said.
If the switch is to methadone, a 75%–90% dose reduction is needed, and if the switch is to transdermal fentanyl, use the reduction that is built into the conversion charts provided in the prescribing information. If an oral transmucosal fentanyl citrate formulation is used, start with the lowest dose, he advised.
The second conversion step involves patient-specific adjustments. The patient should be assessed for pain severity and other medical or psychosocial characteristics, and appropriate additional adjustments should be made to the initial dose of the new opioid.
In patients with specific vulnerabilities such as advanced age, renal insufficiency, or cognitive impairment, consider an additional 10%–30% dose reduction, he said.
Dr. Fine has served as an advisory board member for Ameritox, Covidien, King (now Pfizer), Meda, and Purdue-Pharma. He also is a consultant for Cephalon and Johnson & Johnson.
Consider opioid rotation when benefits are inadequate despite dose increases.
Source ©Csaba Tóth/iStockphoto.com
Examples of Initial Dose Calculation
▸ To convert controlled-release oxycodone (60 mg oral dose twice daily) to controlled-release morphine:
1. Calculate the total oxycodone 24-hour dose (120 mg).
2. Determine morphine equivalency (20 mg oxycodone = 30 mg morphine).
3. Convert the 24-hour oxycodone dose to the morphine dose (120 mg oxycodone = 180 mg morphine).
4. Reduce the morphine dose by 25% (135 mg morphine).
5. Split the total morphine dose to the twice-daily dose (67.5 mg). Because the controlled-release (extended-release) morphine is not provided in this exact dose, give the closest available dose (60 mg, twice daily).
▸ To convert controlled-release morphine (30 mg oral dose twice daily) to transdermal fentanyl:
1. Calculate the total morphine 24-hour dose (60 mg).
2. Use the prescribing info. to determine the oral equivalent dose of transdermal fentanyl (60 mg oral morphine = 25 mcg/hr fentanyl patch).
3. Prescribe 25 mcg/hr transdermal fentanyl patch to be changed every 3 days. Supply patient with five patches (a 15-day supply); instruct patient on application, and follow up by phone or in office within 2–3 days.
▸ To convert methadone (20 mg oral dose three times daily) to extended-release oxymorphone:
1. Calculate the total methadone 24-hour dose (60 mg daily).
2. Use mu-agonist dose chart to calculate oxymorphone dose equivalency to methadone (5 mg methadone = 10 mg oxymorphone).
3. Convert the 24-hour methadone dose to oxymorphone dose (60 mg methadone = 120 mg oxymorphone).
4. Reduce the dose by 50% and split the 50% total calculated oxymorphone dosage to a twice-daily dose. Prescribe oxymorphone ER (30 mg oral dose every 12 hours).
Source: Dr. Fine
DESTIN, FLA. – Opioid rotation is a common and potentially beneficial practice for helping to relieve chronic pain in patients who require ongoing opioid therapy, but there are very few data to guide best practice.
The recommended approach, therefore, is one that focuses on safety, according to Dr. Perry Fine. Clinicians should consider opioid rotation when patients on chronic opioid therapy experience intolerable adverse effects, or when benefits are inadequate despite dose increases, according to recently published clinical guidelines (J. Pain 2009;10:113-30).
However, it is important to consider a number of factors before making changes in treatment, including demographic, disease-related, and treatment-related factors, as well as comorbidities, concomitant pharmacotherapy, drug sensitivities, and social situation, said Dr. Fine, professor of anesthesiology at the University of Utah, Salt Lake City.
If a decision is made to convert a patient's treatment, a two-step, safety-focused approach is needed, he said.
Step 1 involves an “automatic safety factor” calculation. That is, the equianalgesic dose of the new opioid should be calculated via an equianalgesic table such as a mu-agonist dose chart, and, with a few exceptions, an automatic dose reduction of 25%–50% should be made, except if the new drug is methadone or transdermal fentanyl.
A 25% reduction for opioids (other than methadone or fentanyl) is adequate in patients with no risk factors and/or if the switch is to a different route of administration of the same drug. A 50% reduction is needed in those receiving a relatively high dose of the current opioid, those who are elderly or frail, and those of Chinese lineage, Dr. Fine said.
If the switch is to methadone, a 75%–90% dose reduction is needed, and if the switch is to transdermal fentanyl, use the reduction that is built into the conversion charts provided in the prescribing information. If an oral transmucosal fentanyl citrate formulation is used, start with the lowest dose, he advised.
The second conversion step involves patient-specific adjustments. The patient should be assessed for pain severity and other medical or psychosocial characteristics, and appropriate additional adjustments should be made to the initial dose of the new opioid.
In patients with specific vulnerabilities such as advanced age, renal insufficiency, or cognitive impairment, consider an additional 10%–30% dose reduction, he said.
Dr. Fine has served as an advisory board member for Ameritox, Covidien, King (now Pfizer), Meda, and Purdue-Pharma. He also is a consultant for Cephalon and Johnson & Johnson.
Consider opioid rotation when benefits are inadequate despite dose increases.
Source ©Csaba Tóth/iStockphoto.com
Examples of Initial Dose Calculation
▸ To convert controlled-release oxycodone (60 mg oral dose twice daily) to controlled-release morphine:
1. Calculate the total oxycodone 24-hour dose (120 mg).
2. Determine morphine equivalency (20 mg oxycodone = 30 mg morphine).
3. Convert the 24-hour oxycodone dose to the morphine dose (120 mg oxycodone = 180 mg morphine).
4. Reduce the morphine dose by 25% (135 mg morphine).
5. Split the total morphine dose to the twice-daily dose (67.5 mg). Because the controlled-release (extended-release) morphine is not provided in this exact dose, give the closest available dose (60 mg, twice daily).
▸ To convert controlled-release morphine (30 mg oral dose twice daily) to transdermal fentanyl:
1. Calculate the total morphine 24-hour dose (60 mg).
2. Use the prescribing info. to determine the oral equivalent dose of transdermal fentanyl (60 mg oral morphine = 25 mcg/hr fentanyl patch).
3. Prescribe 25 mcg/hr transdermal fentanyl patch to be changed every 3 days. Supply patient with five patches (a 15-day supply); instruct patient on application, and follow up by phone or in office within 2–3 days.
▸ To convert methadone (20 mg oral dose three times daily) to extended-release oxymorphone:
1. Calculate the total methadone 24-hour dose (60 mg daily).
2. Use mu-agonist dose chart to calculate oxymorphone dose equivalency to methadone (5 mg methadone = 10 mg oxymorphone).
3. Convert the 24-hour methadone dose to oxymorphone dose (60 mg methadone = 120 mg oxymorphone).
4. Reduce the dose by 50% and split the 50% total calculated oxymorphone dosage to a twice-daily dose. Prescribe oxymorphone ER (30 mg oral dose every 12 hours).
Source: Dr. Fine
RA Drug Trials Often Lack Active Comparator : The proposal is to change the trial design to substitute an active comparator for the placebo.
Major Finding: A review of 17 recent clinical trials for three new rheumatoid arthritis drugs showed that only two of the trials placed patients randomized into the comparator arms on active drug regimens.
Data Source: Review of publicly reported trial data.
Disclosures: Dr. Juche said that he has received travel support from Actelion.
LONDON – Many recently performed rheumatology drug trials have run into the ethical trap of treating control patients with an ineffective regimen, with the result that some patients experienced ongoing pain and joint dysfunction and continued disease progression.
“I would propose that we change the trial design for the placebo control to use an active comparator against the [investigational] drug,” Dr. Aaron Juche said while presenting a poster at the meeting.
For studies testing a new drug aimed at controlling rheumatoid arthritis pain, dysfunction, and progression, “the standard of care would be a tumor necrosis factor [TNF] inhibitor as the active comparator,” said Dr. Juche, a rheumatologist at Johanniter Hospital in Treuenbrietzen, Germany. Because TNF inhibitors are so effective, a study that uses this treatment in the comparator arm would likely have to be a noninferiority study and would also probably have to involve a relatively large number of patients, he said in an interview.
The standard approach for drug-trial design in patients with RA in recent years has been to follow a model that's more than a decade old, dating back to the first studies on TNF inhibitors during the 1990s: “Patients who did not adequately respond to immunosuppressive drugs were randomly assigned to either an experimental condition under which they received the new substance, or to a control condition under which they continued their formerly inefficient treatment and received a placebo.”
To more systematically assess the scope of the problem, he and his associate reviewed 17 recent, published clinical trials that drug companies used to document the safety and efficacy of three new drugs, abatacept, golimumab, and tocilizumab, to the European Medicines Agencies. Dr. Juche said these studies fairly represented most recently performed drug efficacy trials for patients with RA.
Of the seven studies he reviewed that tested abatacept, none used a control therapy that effectively treated the patients' disease. In all seven studies, patients remained on treatment with a disease-modifying antirheumatic drug (DMARD) that they had already failed on, most commonly methotrexate. During these studies, “patients experienced a persistent, high disease activity,” he reported.
Among four pivotal studies involving golimumab, one enrolled methotrexate-naive patients and then used methotrexate as the control drug. The other three used control groups that received placebo and nothing else or placebo plus methotrexate for enrolled patients who had already failed methotrexate.
A similar pattern existed for the six studies of tocilizumab that Dr. Juche reviewed.
One of the six used methotrexate as the comparator in a trial that enrolled methotrexate-naive patients. The other five studies used comparator groups on either placebo alone or placebo plus a DMARD to which the patient had already not responded.
Dr. Juche added that rheumatology is not unique in having so many of its trials involve ineffective regimens in the control groups.
{kind=link}
New drugs should be compared with a TNF inhibitor, suggested Dr. Aaron Juche.
Source Mitchel L. Zoler/Elsevier Global Medical News
Major Finding: A review of 17 recent clinical trials for three new rheumatoid arthritis drugs showed that only two of the trials placed patients randomized into the comparator arms on active drug regimens.
Data Source: Review of publicly reported trial data.
Disclosures: Dr. Juche said that he has received travel support from Actelion.
LONDON – Many recently performed rheumatology drug trials have run into the ethical trap of treating control patients with an ineffective regimen, with the result that some patients experienced ongoing pain and joint dysfunction and continued disease progression.
“I would propose that we change the trial design for the placebo control to use an active comparator against the [investigational] drug,” Dr. Aaron Juche said while presenting a poster at the meeting.
For studies testing a new drug aimed at controlling rheumatoid arthritis pain, dysfunction, and progression, “the standard of care would be a tumor necrosis factor [TNF] inhibitor as the active comparator,” said Dr. Juche, a rheumatologist at Johanniter Hospital in Treuenbrietzen, Germany. Because TNF inhibitors are so effective, a study that uses this treatment in the comparator arm would likely have to be a noninferiority study and would also probably have to involve a relatively large number of patients, he said in an interview.
The standard approach for drug-trial design in patients with RA in recent years has been to follow a model that's more than a decade old, dating back to the first studies on TNF inhibitors during the 1990s: “Patients who did not adequately respond to immunosuppressive drugs were randomly assigned to either an experimental condition under which they received the new substance, or to a control condition under which they continued their formerly inefficient treatment and received a placebo.”
To more systematically assess the scope of the problem, he and his associate reviewed 17 recent, published clinical trials that drug companies used to document the safety and efficacy of three new drugs, abatacept, golimumab, and tocilizumab, to the European Medicines Agencies. Dr. Juche said these studies fairly represented most recently performed drug efficacy trials for patients with RA.
Of the seven studies he reviewed that tested abatacept, none used a control therapy that effectively treated the patients' disease. In all seven studies, patients remained on treatment with a disease-modifying antirheumatic drug (DMARD) that they had already failed on, most commonly methotrexate. During these studies, “patients experienced a persistent, high disease activity,” he reported.
Among four pivotal studies involving golimumab, one enrolled methotrexate-naive patients and then used methotrexate as the control drug. The other three used control groups that received placebo and nothing else or placebo plus methotrexate for enrolled patients who had already failed methotrexate.
A similar pattern existed for the six studies of tocilizumab that Dr. Juche reviewed.
One of the six used methotrexate as the comparator in a trial that enrolled methotrexate-naive patients. The other five studies used comparator groups on either placebo alone or placebo plus a DMARD to which the patient had already not responded.
Dr. Juche added that rheumatology is not unique in having so many of its trials involve ineffective regimens in the control groups.
New drugs should be compared with a TNF inhibitor, suggested Dr. Aaron Juche.
Source Mitchel L. Zoler/Elsevier Global Medical News
Major Finding: A review of 17 recent clinical trials for three new rheumatoid arthritis drugs showed that only two of the trials placed patients randomized into the comparator arms on active drug regimens.
Data Source: Review of publicly reported trial data.
Disclosures: Dr. Juche said that he has received travel support from Actelion.
LONDON – Many recently performed rheumatology drug trials have run into the ethical trap of treating control patients with an ineffective regimen, with the result that some patients experienced ongoing pain and joint dysfunction and continued disease progression.
“I would propose that we change the trial design for the placebo control to use an active comparator against the [investigational] drug,” Dr. Aaron Juche said while presenting a poster at the meeting.
For studies testing a new drug aimed at controlling rheumatoid arthritis pain, dysfunction, and progression, “the standard of care would be a tumor necrosis factor [TNF] inhibitor as the active comparator,” said Dr. Juche, a rheumatologist at Johanniter Hospital in Treuenbrietzen, Germany. Because TNF inhibitors are so effective, a study that uses this treatment in the comparator arm would likely have to be a noninferiority study and would also probably have to involve a relatively large number of patients, he said in an interview.
The standard approach for drug-trial design in patients with RA in recent years has been to follow a model that's more than a decade old, dating back to the first studies on TNF inhibitors during the 1990s: “Patients who did not adequately respond to immunosuppressive drugs were randomly assigned to either an experimental condition under which they received the new substance, or to a control condition under which they continued their formerly inefficient treatment and received a placebo.”
To more systematically assess the scope of the problem, he and his associate reviewed 17 recent, published clinical trials that drug companies used to document the safety and efficacy of three new drugs, abatacept, golimumab, and tocilizumab, to the European Medicines Agencies. Dr. Juche said these studies fairly represented most recently performed drug efficacy trials for patients with RA.
Of the seven studies he reviewed that tested abatacept, none used a control therapy that effectively treated the patients' disease. In all seven studies, patients remained on treatment with a disease-modifying antirheumatic drug (DMARD) that they had already failed on, most commonly methotrexate. During these studies, “patients experienced a persistent, high disease activity,” he reported.
Among four pivotal studies involving golimumab, one enrolled methotrexate-naive patients and then used methotrexate as the control drug. The other three used control groups that received placebo and nothing else or placebo plus methotrexate for enrolled patients who had already failed methotrexate.
A similar pattern existed for the six studies of tocilizumab that Dr. Juche reviewed.
One of the six used methotrexate as the comparator in a trial that enrolled methotrexate-naive patients. The other five studies used comparator groups on either placebo alone or placebo plus a DMARD to which the patient had already not responded.
Dr. Juche added that rheumatology is not unique in having so many of its trials involve ineffective regimens in the control groups.
New drugs should be compared with a TNF inhibitor, suggested Dr. Aaron Juche.
Source Mitchel L. Zoler/Elsevier Global Medical News
Some DMARDs Shown to Lower Diabetes Risk
Major Finding: The hazard ratios for diabetes were 0.62 for patients taking TNF inhibitors and 0.54 for patients taking hydroxychloroquine, compared with patients taking nonbiologic DMARDs to treat their rheumatoid arthritis or psoriasis.
Data Source: A retrospective observational study involving 13,905 adults who had either RA or psoriasis, received a DMARD, and were followed for approximately 6 months for the development of diabetes. Participants were enrolled in one of two health care systems.
Disclosures: This study was supported by Amgen. Dr. Solomon reported ties to Abbott, Amgen, Bristol-Myers Squibb, and Pfizer, and his associates reported ties to numerous industry sources.
Some disease-modifying antirheumatic drugs that are taken for rheumatoid arthritis or psoriasis appear to reduce the rate of incident diabetes.
In a retrospective cohort study of patients who had RA or psoriasis, the use of a tumor necrosis factor (TNF) inhibitor or hydroxychloroquine to treat the systemic inflammatory disorder was associated with a reduced risk of developing diabetes, compared with the use of methotrexate or nonbiologic DMARDs, said Dr. Daniel H. Solomon of the divisions of phamacoepidemiology and rheumatology at Brigham and Women's Hospital, Boston, and his associates.
“Considering these results, in light of prior findings regarding improved insulin and glucose metabolism and reduced diabetes risk with hydroxychloroquine and TNF inhibitors, there is evidence suggesting a possible role for DMARDs and immunosuppression in diabetes prevention,” they noted.
The investigators assessed the relationship between DMARDs and the risk of new-onset diabetes because previous studies have demonstrated that inflammatory conditions such as RA and psoriasis predispose patients to insulin resistance, and that some of these anti-inflammatory medications appear to improve insulin resistance and prevent the onset of diabetes. They analyzed information from the databases of a Canadian health care system and a commercial U.S. health plan to identify 13,905 adults with RA or psoriasis who had filled at least one prescription for a DMARD and could be followed for approximately 6 months.
The DMARDs were divided into four mutually exclusive groups. The four groups were (1) TNF inhibitors such as adalimumab, etanercept, or infliximab; (2) methotrexate; (3) hydroxychloroquine; and (4) other nonbiologic DMARDs such as sulfasalazine, leflunomide, cyclosporine, azathioprine, cyclophosphamide, mycophenolate mofetil, 6-thioguanine, acitretin,
A total of 267 study subjects developed incident diabetes. The incidence was highest among patients who were taking nonbiologic DMARDs.
Patients taking a TNF inhibitor or hydroxychloroquine showed a reduced risk of diabetes, compared with patients taking any other agents.
After accounting for the effects of potentially confounding factors such as patient age, sex, and several clinical variables, investigators found that the hazard ratios for diabetes were 0.62 for TNF inhibitors and 0.54 for hydroxychloroquine, compared with the nonbiologic DMARDs, Dr. Solomon and his colleagues said (JAMA 2011;305:2525-31).
“These findings held up across a variety of sensitivity analyses,” they added.
“Taken in the context of prior research, [our] study supports the potential role for systemic immunosuppression in prevention and control of diabetes.
“If future studies show this convincingly, systemic immunosuppression in such situations would be predicated on a favorable risk-benefit profile.”
For example, the benefit of immunosuppression may outweigh the risk in a patient with a systemic rheumatic disease for which a DMARD is already indicated.
But immunosuppression may not outweigh the risk in a patient who already has diabetes and is prone to infection.
The investigators emphasized that this was an observational epidemiologic study without randomized-treatment assignment, so causation cannot be inferred.
“It is possible that patients receiving a TNF inhibitor or hydroxychloroquine were different from the reference group of other nonbiologic DMARD users in ways that went unmeasured, such as body mass index, exercise participation, family history, or disease severity,” they noted.
They added that the findings warrant confirmation in a randomized, controlled trial to test “the ability of these agents to prevent diabetes among participants with systemic inflammatory disorders.”
View on the News
Confirmation Still Needed
“Prospective trials are needed to confirm [these] observational data and clarify which patients may benefit from these possible pleiotropic effects of specific anti-inflammatories,” said Dr. Tim Bongartz and Dr. Yogish C. Kudva.
If TNF inhibitors or hydroxychloroquine prove to address two complex disease processes at once, “it will be crucial to investigate how much of their potential antidiabetic effects would add to good disease control, the durability of these effects, and the timing of treatment.”
Even if treatment of chronic inflammatory disease can reduce the risk of diabetes, “clinicians still will have to learn how to use specific anti-inflammatory agents to achieve optimal outcomes for both conditions,” they said.
DR. BONGARTZ is in the division of rheumatology and DR. KUDVA is in the division of endocrinology, diabetes, metabolism, and nutrition at the Mayo Clinic in Rochester, Minn. Dr. Bongartz reported ties to Wyeth and Abbott. Dr. Kudva reported no conflicts of interest. These remarks were taken from their editorial accompanying Dr. Solomon's report (JAMA 2011;305:2573-4).
Major Finding: The hazard ratios for diabetes were 0.62 for patients taking TNF inhibitors and 0.54 for patients taking hydroxychloroquine, compared with patients taking nonbiologic DMARDs to treat their rheumatoid arthritis or psoriasis.
Data Source: A retrospective observational study involving 13,905 adults who had either RA or psoriasis, received a DMARD, and were followed for approximately 6 months for the development of diabetes. Participants were enrolled in one of two health care systems.
Disclosures: This study was supported by Amgen. Dr. Solomon reported ties to Abbott, Amgen, Bristol-Myers Squibb, and Pfizer, and his associates reported ties to numerous industry sources.
Some disease-modifying antirheumatic drugs that are taken for rheumatoid arthritis or psoriasis appear to reduce the rate of incident diabetes.
In a retrospective cohort study of patients who had RA or psoriasis, the use of a tumor necrosis factor (TNF) inhibitor or hydroxychloroquine to treat the systemic inflammatory disorder was associated with a reduced risk of developing diabetes, compared with the use of methotrexate or nonbiologic DMARDs, said Dr. Daniel H. Solomon of the divisions of phamacoepidemiology and rheumatology at Brigham and Women's Hospital, Boston, and his associates.
“Considering these results, in light of prior findings regarding improved insulin and glucose metabolism and reduced diabetes risk with hydroxychloroquine and TNF inhibitors, there is evidence suggesting a possible role for DMARDs and immunosuppression in diabetes prevention,” they noted.
The investigators assessed the relationship between DMARDs and the risk of new-onset diabetes because previous studies have demonstrated that inflammatory conditions such as RA and psoriasis predispose patients to insulin resistance, and that some of these anti-inflammatory medications appear to improve insulin resistance and prevent the onset of diabetes. They analyzed information from the databases of a Canadian health care system and a commercial U.S. health plan to identify 13,905 adults with RA or psoriasis who had filled at least one prescription for a DMARD and could be followed for approximately 6 months.
The DMARDs were divided into four mutually exclusive groups. The four groups were (1) TNF inhibitors such as adalimumab, etanercept, or infliximab; (2) methotrexate; (3) hydroxychloroquine; and (4) other nonbiologic DMARDs such as sulfasalazine, leflunomide, cyclosporine, azathioprine, cyclophosphamide, mycophenolate mofetil, 6-thioguanine, acitretin,
A total of 267 study subjects developed incident diabetes. The incidence was highest among patients who were taking nonbiologic DMARDs.
Patients taking a TNF inhibitor or hydroxychloroquine showed a reduced risk of diabetes, compared with patients taking any other agents.
After accounting for the effects of potentially confounding factors such as patient age, sex, and several clinical variables, investigators found that the hazard ratios for diabetes were 0.62 for TNF inhibitors and 0.54 for hydroxychloroquine, compared with the nonbiologic DMARDs, Dr. Solomon and his colleagues said (JAMA 2011;305:2525-31).
“These findings held up across a variety of sensitivity analyses,” they added.
“Taken in the context of prior research, [our] study supports the potential role for systemic immunosuppression in prevention and control of diabetes.
“If future studies show this convincingly, systemic immunosuppression in such situations would be predicated on a favorable risk-benefit profile.”
For example, the benefit of immunosuppression may outweigh the risk in a patient with a systemic rheumatic disease for which a DMARD is already indicated.
But immunosuppression may not outweigh the risk in a patient who already has diabetes and is prone to infection.
The investigators emphasized that this was an observational epidemiologic study without randomized-treatment assignment, so causation cannot be inferred.
“It is possible that patients receiving a TNF inhibitor or hydroxychloroquine were different from the reference group of other nonbiologic DMARD users in ways that went unmeasured, such as body mass index, exercise participation, family history, or disease severity,” they noted.
They added that the findings warrant confirmation in a randomized, controlled trial to test “the ability of these agents to prevent diabetes among participants with systemic inflammatory disorders.”
View on the News
Confirmation Still Needed
“Prospective trials are needed to confirm [these] observational data and clarify which patients may benefit from these possible pleiotropic effects of specific anti-inflammatories,” said Dr. Tim Bongartz and Dr. Yogish C. Kudva.
If TNF inhibitors or hydroxychloroquine prove to address two complex disease processes at once, “it will be crucial to investigate how much of their potential antidiabetic effects would add to good disease control, the durability of these effects, and the timing of treatment.”
Even if treatment of chronic inflammatory disease can reduce the risk of diabetes, “clinicians still will have to learn how to use specific anti-inflammatory agents to achieve optimal outcomes for both conditions,” they said.
DR. BONGARTZ is in the division of rheumatology and DR. KUDVA is in the division of endocrinology, diabetes, metabolism, and nutrition at the Mayo Clinic in Rochester, Minn. Dr. Bongartz reported ties to Wyeth and Abbott. Dr. Kudva reported no conflicts of interest. These remarks were taken from their editorial accompanying Dr. Solomon's report (JAMA 2011;305:2573-4).
Major Finding: The hazard ratios for diabetes were 0.62 for patients taking TNF inhibitors and 0.54 for patients taking hydroxychloroquine, compared with patients taking nonbiologic DMARDs to treat their rheumatoid arthritis or psoriasis.
Data Source: A retrospective observational study involving 13,905 adults who had either RA or psoriasis, received a DMARD, and were followed for approximately 6 months for the development of diabetes. Participants were enrolled in one of two health care systems.
Disclosures: This study was supported by Amgen. Dr. Solomon reported ties to Abbott, Amgen, Bristol-Myers Squibb, and Pfizer, and his associates reported ties to numerous industry sources.
Some disease-modifying antirheumatic drugs that are taken for rheumatoid arthritis or psoriasis appear to reduce the rate of incident diabetes.
In a retrospective cohort study of patients who had RA or psoriasis, the use of a tumor necrosis factor (TNF) inhibitor or hydroxychloroquine to treat the systemic inflammatory disorder was associated with a reduced risk of developing diabetes, compared with the use of methotrexate or nonbiologic DMARDs, said Dr. Daniel H. Solomon of the divisions of phamacoepidemiology and rheumatology at Brigham and Women's Hospital, Boston, and his associates.
“Considering these results, in light of prior findings regarding improved insulin and glucose metabolism and reduced diabetes risk with hydroxychloroquine and TNF inhibitors, there is evidence suggesting a possible role for DMARDs and immunosuppression in diabetes prevention,” they noted.
The investigators assessed the relationship between DMARDs and the risk of new-onset diabetes because previous studies have demonstrated that inflammatory conditions such as RA and psoriasis predispose patients to insulin resistance, and that some of these anti-inflammatory medications appear to improve insulin resistance and prevent the onset of diabetes. They analyzed information from the databases of a Canadian health care system and a commercial U.S. health plan to identify 13,905 adults with RA or psoriasis who had filled at least one prescription for a DMARD and could be followed for approximately 6 months.
The DMARDs were divided into four mutually exclusive groups. The four groups were (1) TNF inhibitors such as adalimumab, etanercept, or infliximab; (2) methotrexate; (3) hydroxychloroquine; and (4) other nonbiologic DMARDs such as sulfasalazine, leflunomide, cyclosporine, azathioprine, cyclophosphamide, mycophenolate mofetil, 6-thioguanine, acitretin,
A total of 267 study subjects developed incident diabetes. The incidence was highest among patients who were taking nonbiologic DMARDs.
Patients taking a TNF inhibitor or hydroxychloroquine showed a reduced risk of diabetes, compared with patients taking any other agents.
After accounting for the effects of potentially confounding factors such as patient age, sex, and several clinical variables, investigators found that the hazard ratios for diabetes were 0.62 for TNF inhibitors and 0.54 for hydroxychloroquine, compared with the nonbiologic DMARDs, Dr. Solomon and his colleagues said (JAMA 2011;305:2525-31).
“These findings held up across a variety of sensitivity analyses,” they added.
“Taken in the context of prior research, [our] study supports the potential role for systemic immunosuppression in prevention and control of diabetes.
“If future studies show this convincingly, systemic immunosuppression in such situations would be predicated on a favorable risk-benefit profile.”
For example, the benefit of immunosuppression may outweigh the risk in a patient with a systemic rheumatic disease for which a DMARD is already indicated.
But immunosuppression may not outweigh the risk in a patient who already has diabetes and is prone to infection.
The investigators emphasized that this was an observational epidemiologic study without randomized-treatment assignment, so causation cannot be inferred.
“It is possible that patients receiving a TNF inhibitor or hydroxychloroquine were different from the reference group of other nonbiologic DMARD users in ways that went unmeasured, such as body mass index, exercise participation, family history, or disease severity,” they noted.
They added that the findings warrant confirmation in a randomized, controlled trial to test “the ability of these agents to prevent diabetes among participants with systemic inflammatory disorders.”
View on the News
Confirmation Still Needed
“Prospective trials are needed to confirm [these] observational data and clarify which patients may benefit from these possible pleiotropic effects of specific anti-inflammatories,” said Dr. Tim Bongartz and Dr. Yogish C. Kudva.
If TNF inhibitors or hydroxychloroquine prove to address two complex disease processes at once, “it will be crucial to investigate how much of their potential antidiabetic effects would add to good disease control, the durability of these effects, and the timing of treatment.”
Even if treatment of chronic inflammatory disease can reduce the risk of diabetes, “clinicians still will have to learn how to use specific anti-inflammatory agents to achieve optimal outcomes for both conditions,” they said.
DR. BONGARTZ is in the division of rheumatology and DR. KUDVA is in the division of endocrinology, diabetes, metabolism, and nutrition at the Mayo Clinic in Rochester, Minn. Dr. Bongartz reported ties to Wyeth and Abbott. Dr. Kudva reported no conflicts of interest. These remarks were taken from their editorial accompanying Dr. Solomon's report (JAMA 2011;305:2573-4).