User login
New IPF guidelines limit treatment choices
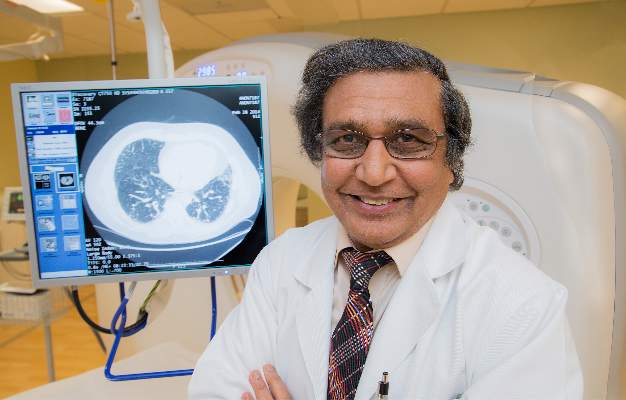
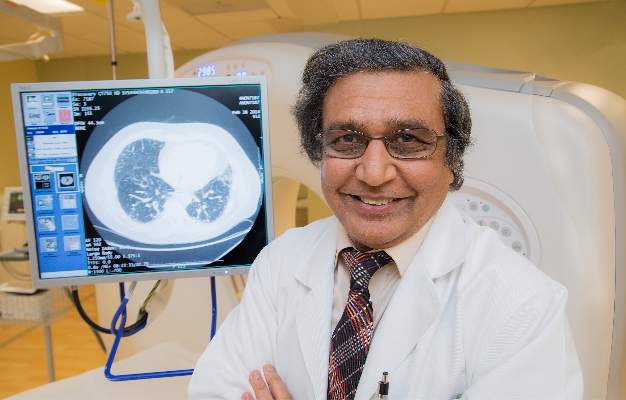
Idiopathic pulmonary fibrosis patients and physicians have two new medication choices but fewer options among established treatments, according to updated clinical practice guidelines published by an international working group. The update of the 2011 guidelines was released by the American Thoracic Society in conjunction with the European Respiratory Society, the Japanese Respiratory Society, and the Latin American Thoracic Association.
The tyrosine kinase inhibitor nintedanib (Ofev) received a conditional recommendation for use in idiopathic pulmonary fibrosis (IPF), a progressive, restrictive lung disorder characterized by increasing fibrosis and findings of usual interstitial pneumonia on CT scan. Pirfenidone (Esbriet), an orally administered pleiotropic antifibrotic medication, also received a conditional positive recommendation in the guidelines (Am J Respir Crit Care Med. 2015;192[2]:e3-19), which were formulated by a panel led by first author Dr. Ganesh Raghu of the University of Washington, Seattle.
Antacid therapy to reduce the potentially harmful effects of microaspiration of acidic stomach contents from gastroesophageal reflux received a conditional positive recommendation. Abnormal gastroesophageal reflux occurs in up to 90% of IPF patients, according to Dr. Raghu and his coauthors.
No other treatments show efficacy when rigorously examined, Dr. Raghu said. “We haven’t shown that any treatment regimen affects how patients feel or function. We haven’t improved survivability or quality of life.”
Dr. Raghu and the guideline coauthors issued a strong recommendation against use of prednisone, azathioprine, and N-acetylcysteine as triple therapy, noting “a clear negative effect…for multiple patient–important outcomes” in a trial that was stopped early for harm. In discussion, they recommended revisiting the diagnosis in instances where IPF patients seem to be receiving benefit from triple therapy.
The use of N-acetylcysteine as monotherapy for IPF showed no improvement in mortality, lung function studies, or quality of life in three studies, although two studies showed improvement on the 6-minute walk test. Dr. Raghu and his coauthors thus issued a conditional recommendation against using N-acetylcysteine as monotherapy.
The 2015 clinical practice guidelines also strengthened the recommendation against using warfarin for anticoagulation to treat IPF; Warfarin had received a conditional recommendation against treatment in the previous guidelines released in 2011. Although studies provide “biological plausibility for a mechanistic link between thrombosis and lung fibrosis,” Dr. Raghu and his coauthors noted increased mortality and no improvement in lung function in some studies comparing warfarin with placebo as an IPF treatment. However, warfarin should still be used as clinically indicated in patients with other indications for its use as an anticoagulant.
Endothelin receptors (ERs) can promote epithelial to mesenchymal transition via cytokine mediators, a process associated with organ fibrosis. Thus, ER antagonists have been studied to treat IPF. Ambrisentan (Letairis) is a selective ER type-A antagonist that, in a single, randomized, controlled trial, was associated with worsening respiratory function and increased mortality. The guidelines thus strongly recommend against the use of ambrisentan for IPF.
The dual-acting ER antagonists bosentan (Tracleer) and macitentan (Opsumit) target both ER-A and ER-B sites and were examined together in the guidelines. Dr. Raghu and his coauthors pooled results of three studies examining one or the other of the two dual-acting ER antagonists, finding no overall effect on mortality but a small improvement in the composite outcome of death or disease; they issued a conditional recommendation against using either bosentan or macitentan. For the subset of IPF patients with pulmonary hypertension (PH), “[t]he committee felt that patients with PH secondary to IPF might benefit … however, the evidence did not allow a specific subgroup recommendation.”
Sildenafil (Revatio) is a phosphodiesterase-5 inhibitor that has been used in patients with PH and right ventricular dysfunction; however, in the limited data available for its use in patients with IPF, no benefit on mortality, dyspnea, or IPF exacerbations was seen. There was a slight benefit on quality of life, but Dr. Raghu and his fellow committee members gave sildenafil a qualified negative recommendation. No specific subgroup recommendations were made for patients with PH and/or right ventricular dysfunction.
Finally, Dr. Raghu and his coauthors did not make a recommendation regarding single, compared with bilateral, lung transplantation for individuals with moderate or severe IPF. “The shortage of organs is a universal problem, and the decision to give bilateral lung transplantation to a single patient rather than give single-lung transplantation to two patients, including the effect on health inequity, must be considered,” they said, calling for randomized, controlled trials to address the question.
“Evidence surrounding the clinical management of IPF is rapidly evolving,” Dr. Raghu and his coauthors said; accordingly, they envision the guideline as a “ ‘living document,’ allowing new evidence to be incorporated as available.”
The authors of the guidelines followed a strict protocol to recuse themselves from deliberation or voting when conflicts existed. Dr. Raghu said, “The non-IPF experts were able to make unbiased recommendations.”
A patient with IPF, William Cunningham, was also a fully involved panel member, bringing his perspective into the guideline formation process. “Mr. Cunningham was incredible and he was a gentleman and a scholar. When he spoke, everyone just listened, and his input was always well thought out. He really was instrumental in the guideline-development process.” Mr. Cunningham died from his disease shortly after the committee’s work was completed. The full list of conflicts of interest and a detailed protocol description may be found in the full text of the guidelines.
On Twitter @karioakes
The new IPF guidelines set a critical framework for the path forward. The international task force that formulated the 2015 update of the clinical practice guidelines for IPF have done tremendous work, moving much further toward answering the kinds of questions that the research and clinical community will not be able to address unless they work together. These guidelines are a critical appraisal of where we are and of the need to push forward.

|
Dr. Gregory P. Cosgrove |
As we push as fast as we can toward more and better treatments, we should be aware that care of IPF patients should be multifaceted, and not just pharmacologic. In order to address the suffering associated with this disease, we need to use all available modalities: supplemental oxygen; physical therapy; and psychological support. We can help patients in so many different ways; lung fibrosis is a heterogeneous disease, and by focusing on how individual patients are affected, we can help meet their needs. The fund of available knowledge has been addressed in an evidence-based fashion. Unfortunately, this is the state of affairs; however, now we can begin to answer the questions that need to be answered.
Dr. Gregory P. Cosgrove is the chief medical officer of the Pulmonary Fibrosis Foundation and holds the endowed chair of interstitial lung disease at National Jewish Health in Denver. His comments are summarized from an interview.
The new IPF guidelines set a critical framework for the path forward. The international task force that formulated the 2015 update of the clinical practice guidelines for IPF have done tremendous work, moving much further toward answering the kinds of questions that the research and clinical community will not be able to address unless they work together. These guidelines are a critical appraisal of where we are and of the need to push forward.
|
|
Dr. Gregory P. Cosgrove |
As we push as fast as we can toward more and better treatments, we should be aware that care of IPF patients should be multifaceted, and not just pharmacologic. In order to address the suffering associated with this disease, we need to use all available modalities: supplemental oxygen; physical therapy; and psychological support. We can help patients in so many different ways; lung fibrosis is a heterogeneous disease, and by focusing on how individual patients are affected, we can help meet their needs. The fund of available knowledge has been addressed in an evidence-based fashion. Unfortunately, this is the state of affairs; however, now we can begin to answer the questions that need to be answered.
Dr. Gregory P. Cosgrove is the chief medical officer of the Pulmonary Fibrosis Foundation and holds the endowed chair of interstitial lung disease at National Jewish Health in Denver. His comments are summarized from an interview.
The new IPF guidelines set a critical framework for the path forward. The international task force that formulated the 2015 update of the clinical practice guidelines for IPF have done tremendous work, moving much further toward answering the kinds of questions that the research and clinical community will not be able to address unless they work together. These guidelines are a critical appraisal of where we are and of the need to push forward.
|
|
Dr. Gregory P. Cosgrove |
As we push as fast as we can toward more and better treatments, we should be aware that care of IPF patients should be multifaceted, and not just pharmacologic. In order to address the suffering associated with this disease, we need to use all available modalities: supplemental oxygen; physical therapy; and psychological support. We can help patients in so many different ways; lung fibrosis is a heterogeneous disease, and by focusing on how individual patients are affected, we can help meet their needs. The fund of available knowledge has been addressed in an evidence-based fashion. Unfortunately, this is the state of affairs; however, now we can begin to answer the questions that need to be answered.
Dr. Gregory P. Cosgrove is the chief medical officer of the Pulmonary Fibrosis Foundation and holds the endowed chair of interstitial lung disease at National Jewish Health in Denver. His comments are summarized from an interview.
Idiopathic pulmonary fibrosis patients and physicians have two new medication choices but fewer options among established treatments, according to updated clinical practice guidelines published by an international working group. The update of the 2011 guidelines was released by the American Thoracic Society in conjunction with the European Respiratory Society, the Japanese Respiratory Society, and the Latin American Thoracic Association.
The tyrosine kinase inhibitor nintedanib (Ofev) received a conditional recommendation for use in idiopathic pulmonary fibrosis (IPF), a progressive, restrictive lung disorder characterized by increasing fibrosis and findings of usual interstitial pneumonia on CT scan. Pirfenidone (Esbriet), an orally administered pleiotropic antifibrotic medication, also received a conditional positive recommendation in the guidelines (Am J Respir Crit Care Med. 2015;192[2]:e3-19), which were formulated by a panel led by first author Dr. Ganesh Raghu of the University of Washington, Seattle.
Antacid therapy to reduce the potentially harmful effects of microaspiration of acidic stomach contents from gastroesophageal reflux received a conditional positive recommendation. Abnormal gastroesophageal reflux occurs in up to 90% of IPF patients, according to Dr. Raghu and his coauthors.
No other treatments show efficacy when rigorously examined, Dr. Raghu said. “We haven’t shown that any treatment regimen affects how patients feel or function. We haven’t improved survivability or quality of life.”
Dr. Raghu and the guideline coauthors issued a strong recommendation against use of prednisone, azathioprine, and N-acetylcysteine as triple therapy, noting “a clear negative effect…for multiple patient–important outcomes” in a trial that was stopped early for harm. In discussion, they recommended revisiting the diagnosis in instances where IPF patients seem to be receiving benefit from triple therapy.
The use of N-acetylcysteine as monotherapy for IPF showed no improvement in mortality, lung function studies, or quality of life in three studies, although two studies showed improvement on the 6-minute walk test. Dr. Raghu and his coauthors thus issued a conditional recommendation against using N-acetylcysteine as monotherapy.
The 2015 clinical practice guidelines also strengthened the recommendation against using warfarin for anticoagulation to treat IPF; Warfarin had received a conditional recommendation against treatment in the previous guidelines released in 2011. Although studies provide “biological plausibility for a mechanistic link between thrombosis and lung fibrosis,” Dr. Raghu and his coauthors noted increased mortality and no improvement in lung function in some studies comparing warfarin with placebo as an IPF treatment. However, warfarin should still be used as clinically indicated in patients with other indications for its use as an anticoagulant.
Endothelin receptors (ERs) can promote epithelial to mesenchymal transition via cytokine mediators, a process associated with organ fibrosis. Thus, ER antagonists have been studied to treat IPF. Ambrisentan (Letairis) is a selective ER type-A antagonist that, in a single, randomized, controlled trial, was associated with worsening respiratory function and increased mortality. The guidelines thus strongly recommend against the use of ambrisentan for IPF.
The dual-acting ER antagonists bosentan (Tracleer) and macitentan (Opsumit) target both ER-A and ER-B sites and were examined together in the guidelines. Dr. Raghu and his coauthors pooled results of three studies examining one or the other of the two dual-acting ER antagonists, finding no overall effect on mortality but a small improvement in the composite outcome of death or disease; they issued a conditional recommendation against using either bosentan or macitentan. For the subset of IPF patients with pulmonary hypertension (PH), “[t]he committee felt that patients with PH secondary to IPF might benefit … however, the evidence did not allow a specific subgroup recommendation.”
Sildenafil (Revatio) is a phosphodiesterase-5 inhibitor that has been used in patients with PH and right ventricular dysfunction; however, in the limited data available for its use in patients with IPF, no benefit on mortality, dyspnea, or IPF exacerbations was seen. There was a slight benefit on quality of life, but Dr. Raghu and his fellow committee members gave sildenafil a qualified negative recommendation. No specific subgroup recommendations were made for patients with PH and/or right ventricular dysfunction.
Finally, Dr. Raghu and his coauthors did not make a recommendation regarding single, compared with bilateral, lung transplantation for individuals with moderate or severe IPF. “The shortage of organs is a universal problem, and the decision to give bilateral lung transplantation to a single patient rather than give single-lung transplantation to two patients, including the effect on health inequity, must be considered,” they said, calling for randomized, controlled trials to address the question.
“Evidence surrounding the clinical management of IPF is rapidly evolving,” Dr. Raghu and his coauthors said; accordingly, they envision the guideline as a “ ‘living document,’ allowing new evidence to be incorporated as available.”
The authors of the guidelines followed a strict protocol to recuse themselves from deliberation or voting when conflicts existed. Dr. Raghu said, “The non-IPF experts were able to make unbiased recommendations.”
A patient with IPF, William Cunningham, was also a fully involved panel member, bringing his perspective into the guideline formation process. “Mr. Cunningham was incredible and he was a gentleman and a scholar. When he spoke, everyone just listened, and his input was always well thought out. He really was instrumental in the guideline-development process.” Mr. Cunningham died from his disease shortly after the committee’s work was completed. The full list of conflicts of interest and a detailed protocol description may be found in the full text of the guidelines.
On Twitter @karioakes
Idiopathic pulmonary fibrosis patients and physicians have two new medication choices but fewer options among established treatments, according to updated clinical practice guidelines published by an international working group. The update of the 2011 guidelines was released by the American Thoracic Society in conjunction with the European Respiratory Society, the Japanese Respiratory Society, and the Latin American Thoracic Association.
The tyrosine kinase inhibitor nintedanib (Ofev) received a conditional recommendation for use in idiopathic pulmonary fibrosis (IPF), a progressive, restrictive lung disorder characterized by increasing fibrosis and findings of usual interstitial pneumonia on CT scan. Pirfenidone (Esbriet), an orally administered pleiotropic antifibrotic medication, also received a conditional positive recommendation in the guidelines (Am J Respir Crit Care Med. 2015;192[2]:e3-19), which were formulated by a panel led by first author Dr. Ganesh Raghu of the University of Washington, Seattle.
Antacid therapy to reduce the potentially harmful effects of microaspiration of acidic stomach contents from gastroesophageal reflux received a conditional positive recommendation. Abnormal gastroesophageal reflux occurs in up to 90% of IPF patients, according to Dr. Raghu and his coauthors.
No other treatments show efficacy when rigorously examined, Dr. Raghu said. “We haven’t shown that any treatment regimen affects how patients feel or function. We haven’t improved survivability or quality of life.”
Dr. Raghu and the guideline coauthors issued a strong recommendation against use of prednisone, azathioprine, and N-acetylcysteine as triple therapy, noting “a clear negative effect…for multiple patient–important outcomes” in a trial that was stopped early for harm. In discussion, they recommended revisiting the diagnosis in instances where IPF patients seem to be receiving benefit from triple therapy.
The use of N-acetylcysteine as monotherapy for IPF showed no improvement in mortality, lung function studies, or quality of life in three studies, although two studies showed improvement on the 6-minute walk test. Dr. Raghu and his coauthors thus issued a conditional recommendation against using N-acetylcysteine as monotherapy.
The 2015 clinical practice guidelines also strengthened the recommendation against using warfarin for anticoagulation to treat IPF; Warfarin had received a conditional recommendation against treatment in the previous guidelines released in 2011. Although studies provide “biological plausibility for a mechanistic link between thrombosis and lung fibrosis,” Dr. Raghu and his coauthors noted increased mortality and no improvement in lung function in some studies comparing warfarin with placebo as an IPF treatment. However, warfarin should still be used as clinically indicated in patients with other indications for its use as an anticoagulant.
Endothelin receptors (ERs) can promote epithelial to mesenchymal transition via cytokine mediators, a process associated with organ fibrosis. Thus, ER antagonists have been studied to treat IPF. Ambrisentan (Letairis) is a selective ER type-A antagonist that, in a single, randomized, controlled trial, was associated with worsening respiratory function and increased mortality. The guidelines thus strongly recommend against the use of ambrisentan for IPF.
The dual-acting ER antagonists bosentan (Tracleer) and macitentan (Opsumit) target both ER-A and ER-B sites and were examined together in the guidelines. Dr. Raghu and his coauthors pooled results of three studies examining one or the other of the two dual-acting ER antagonists, finding no overall effect on mortality but a small improvement in the composite outcome of death or disease; they issued a conditional recommendation against using either bosentan or macitentan. For the subset of IPF patients with pulmonary hypertension (PH), “[t]he committee felt that patients with PH secondary to IPF might benefit … however, the evidence did not allow a specific subgroup recommendation.”
Sildenafil (Revatio) is a phosphodiesterase-5 inhibitor that has been used in patients with PH and right ventricular dysfunction; however, in the limited data available for its use in patients with IPF, no benefit on mortality, dyspnea, or IPF exacerbations was seen. There was a slight benefit on quality of life, but Dr. Raghu and his fellow committee members gave sildenafil a qualified negative recommendation. No specific subgroup recommendations were made for patients with PH and/or right ventricular dysfunction.
Finally, Dr. Raghu and his coauthors did not make a recommendation regarding single, compared with bilateral, lung transplantation for individuals with moderate or severe IPF. “The shortage of organs is a universal problem, and the decision to give bilateral lung transplantation to a single patient rather than give single-lung transplantation to two patients, including the effect on health inequity, must be considered,” they said, calling for randomized, controlled trials to address the question.
“Evidence surrounding the clinical management of IPF is rapidly evolving,” Dr. Raghu and his coauthors said; accordingly, they envision the guideline as a “ ‘living document,’ allowing new evidence to be incorporated as available.”
The authors of the guidelines followed a strict protocol to recuse themselves from deliberation or voting when conflicts existed. Dr. Raghu said, “The non-IPF experts were able to make unbiased recommendations.”
A patient with IPF, William Cunningham, was also a fully involved panel member, bringing his perspective into the guideline formation process. “Mr. Cunningham was incredible and he was a gentleman and a scholar. When he spoke, everyone just listened, and his input was always well thought out. He really was instrumental in the guideline-development process.” Mr. Cunningham died from his disease shortly after the committee’s work was completed. The full list of conflicts of interest and a detailed protocol description may be found in the full text of the guidelines.
On Twitter @karioakes
FROM THE AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Time a significant factor in assessing RA patients’ symptoms
Reliability of patient-reported outcomes for pain, fatigue, and other disease activity measurements in rheumatoid arthritis patients decreased as time intervals between assessments increased, according to research published in Rheumatology.
It is unclear to what degree variability between the measurements is explainable by within-patient variability and measurement error, reported Dr. Paul Studenic of the Medical University of Vienna (Austria) and his associates.

They assessed 40 rheumatoid arthritis patients and gathered self-assessed pain, fatigue, and patient global assessment (PGA) scores three times per day for 2 months. Twenty patients recorded their assessments over the phone, and 20 kept a diary. PGA was assessed on a 100-mm visual analog scale (VAS), using no disease activity and highly active disease as anchors. The investigators calculated intraclass correlation coefficients (ICCs) and the smallest detectable differences (SDDs) for 1-, 7-, 14- and 28-day testing intervals.
Overall, the SDD and ICC were 25 mm and 0.67 for pain, 25 mm and 0.71 for PGA, and 30 mm and 0.66 for fatigue, respectively. SDD was higher with longer time periods between assessments, ranging from 19 mm (1-day intervals) to 30 mm (28-day intervals) for pain, 19-33 mm for PGA, and 26-34 mm for fatigue. Meanwhile, ICC was smaller with longer intervals, and ranged between the 1- and the 28-day interval from 0.80 to 0.50 for pain, 0.83 to 0.57 for PGA, and 0.76 to 0.58 for fatigue. In general, higher reliability according to ICC coincided with smaller SDD. The researchers noted that pain scores had a significant effect on the patient’s estimation of disease activity.
“The results of this study suggest that, in stable RA patients, a 25-mm change on the VAS for pain or PGA and a 30-mm change for fatigue may identify true change; however, this is clearly dependent on (and can be refined based on) the starting measurement level. It is also apparent that in patients who are assessed less frequently, the evaluation of measurement differences as indicating changes is more difficult,” the investigators concluded.
Read the full article here.
Reliability of patient-reported outcomes for pain, fatigue, and other disease activity measurements in rheumatoid arthritis patients decreased as time intervals between assessments increased, according to research published in Rheumatology.
It is unclear to what degree variability between the measurements is explainable by within-patient variability and measurement error, reported Dr. Paul Studenic of the Medical University of Vienna (Austria) and his associates.
They assessed 40 rheumatoid arthritis patients and gathered self-assessed pain, fatigue, and patient global assessment (PGA) scores three times per day for 2 months. Twenty patients recorded their assessments over the phone, and 20 kept a diary. PGA was assessed on a 100-mm visual analog scale (VAS), using no disease activity and highly active disease as anchors. The investigators calculated intraclass correlation coefficients (ICCs) and the smallest detectable differences (SDDs) for 1-, 7-, 14- and 28-day testing intervals.
Overall, the SDD and ICC were 25 mm and 0.67 for pain, 25 mm and 0.71 for PGA, and 30 mm and 0.66 for fatigue, respectively. SDD was higher with longer time periods between assessments, ranging from 19 mm (1-day intervals) to 30 mm (28-day intervals) for pain, 19-33 mm for PGA, and 26-34 mm for fatigue. Meanwhile, ICC was smaller with longer intervals, and ranged between the 1- and the 28-day interval from 0.80 to 0.50 for pain, 0.83 to 0.57 for PGA, and 0.76 to 0.58 for fatigue. In general, higher reliability according to ICC coincided with smaller SDD. The researchers noted that pain scores had a significant effect on the patient’s estimation of disease activity.
“The results of this study suggest that, in stable RA patients, a 25-mm change on the VAS for pain or PGA and a 30-mm change for fatigue may identify true change; however, this is clearly dependent on (and can be refined based on) the starting measurement level. It is also apparent that in patients who are assessed less frequently, the evaluation of measurement differences as indicating changes is more difficult,” the investigators concluded.
Read the full article here.
Reliability of patient-reported outcomes for pain, fatigue, and other disease activity measurements in rheumatoid arthritis patients decreased as time intervals between assessments increased, according to research published in Rheumatology.
It is unclear to what degree variability between the measurements is explainable by within-patient variability and measurement error, reported Dr. Paul Studenic of the Medical University of Vienna (Austria) and his associates.
They assessed 40 rheumatoid arthritis patients and gathered self-assessed pain, fatigue, and patient global assessment (PGA) scores three times per day for 2 months. Twenty patients recorded their assessments over the phone, and 20 kept a diary. PGA was assessed on a 100-mm visual analog scale (VAS), using no disease activity and highly active disease as anchors. The investigators calculated intraclass correlation coefficients (ICCs) and the smallest detectable differences (SDDs) for 1-, 7-, 14- and 28-day testing intervals.
Overall, the SDD and ICC were 25 mm and 0.67 for pain, 25 mm and 0.71 for PGA, and 30 mm and 0.66 for fatigue, respectively. SDD was higher with longer time periods between assessments, ranging from 19 mm (1-day intervals) to 30 mm (28-day intervals) for pain, 19-33 mm for PGA, and 26-34 mm for fatigue. Meanwhile, ICC was smaller with longer intervals, and ranged between the 1- and the 28-day interval from 0.80 to 0.50 for pain, 0.83 to 0.57 for PGA, and 0.76 to 0.58 for fatigue. In general, higher reliability according to ICC coincided with smaller SDD. The researchers noted that pain scores had a significant effect on the patient’s estimation of disease activity.
“The results of this study suggest that, in stable RA patients, a 25-mm change on the VAS for pain or PGA and a 30-mm change for fatigue may identify true change; however, this is clearly dependent on (and can be refined based on) the starting measurement level. It is also apparent that in patients who are assessed less frequently, the evaluation of measurement differences as indicating changes is more difficult,” the investigators concluded.
Read the full article here.

Tofacitinib proves effective in RA when biologics don’t work
The oral Janus kinase inhibitor tofacitinib was effective at treating rheumatoid arthritis in patients who had never before taken or had an inadequate response to biological disease-modifying antirheumatic drugs, according to a combined analysis of results from four phase II and five phase III trials conducted by Dr. Christina Charles-Schoeman and her associates.
Each of the two main study groups, consisting of 2,812 patients naive to biological disease-modifying antirheumatic drugs (bDMARDs) and 705 bDMARD patients with an inadequate response (IR), was further split into three subgroups: a placebo group, a group receiving 5 mg tofacitinib twice daily, and a group receiving 10 mg tofacitinib twice daily. All subgroups receiving medication had a significantly improved clinical response over the placebo group, although tofacitinib had greater efficacy in the bDMARD-naive group.
The rate of adverse events was similar in all groups receiving tofacitinib, though the numerical amount of both adverse events and clinical responses was somewhat higher in the 10-mg twice-daily group. In addition, a subpopulation of patients who also were receiving glucocorticoids tended to have more serious adverse events and discontinuations as a result of serious infections and herpes zoster.
Although bDMARD-IR patients did not respond as well to tofacitinib, “bDMARD-IR patients had longer disease duration and slightly greater disease activity at baseline compared with bDMARD-naive patients, which could have influenced these results,” the investigators noted.
Find the full study in Annals of the Rheumatic Diseases (doi: 10.1136/annrheumdis-2014-207178).
The oral Janus kinase inhibitor tofacitinib was effective at treating rheumatoid arthritis in patients who had never before taken or had an inadequate response to biological disease-modifying antirheumatic drugs, according to a combined analysis of results from four phase II and five phase III trials conducted by Dr. Christina Charles-Schoeman and her associates.
Each of the two main study groups, consisting of 2,812 patients naive to biological disease-modifying antirheumatic drugs (bDMARDs) and 705 bDMARD patients with an inadequate response (IR), was further split into three subgroups: a placebo group, a group receiving 5 mg tofacitinib twice daily, and a group receiving 10 mg tofacitinib twice daily. All subgroups receiving medication had a significantly improved clinical response over the placebo group, although tofacitinib had greater efficacy in the bDMARD-naive group.
The rate of adverse events was similar in all groups receiving tofacitinib, though the numerical amount of both adverse events and clinical responses was somewhat higher in the 10-mg twice-daily group. In addition, a subpopulation of patients who also were receiving glucocorticoids tended to have more serious adverse events and discontinuations as a result of serious infections and herpes zoster.
Although bDMARD-IR patients did not respond as well to tofacitinib, “bDMARD-IR patients had longer disease duration and slightly greater disease activity at baseline compared with bDMARD-naive patients, which could have influenced these results,” the investigators noted.
Find the full study in Annals of the Rheumatic Diseases (doi: 10.1136/annrheumdis-2014-207178).
The oral Janus kinase inhibitor tofacitinib was effective at treating rheumatoid arthritis in patients who had never before taken or had an inadequate response to biological disease-modifying antirheumatic drugs, according to a combined analysis of results from four phase II and five phase III trials conducted by Dr. Christina Charles-Schoeman and her associates.
Each of the two main study groups, consisting of 2,812 patients naive to biological disease-modifying antirheumatic drugs (bDMARDs) and 705 bDMARD patients with an inadequate response (IR), was further split into three subgroups: a placebo group, a group receiving 5 mg tofacitinib twice daily, and a group receiving 10 mg tofacitinib twice daily. All subgroups receiving medication had a significantly improved clinical response over the placebo group, although tofacitinib had greater efficacy in the bDMARD-naive group.
The rate of adverse events was similar in all groups receiving tofacitinib, though the numerical amount of both adverse events and clinical responses was somewhat higher in the 10-mg twice-daily group. In addition, a subpopulation of patients who also were receiving glucocorticoids tended to have more serious adverse events and discontinuations as a result of serious infections and herpes zoster.
Although bDMARD-IR patients did not respond as well to tofacitinib, “bDMARD-IR patients had longer disease duration and slightly greater disease activity at baseline compared with bDMARD-naive patients, which could have influenced these results,” the investigators noted.
Find the full study in Annals of the Rheumatic Diseases (doi: 10.1136/annrheumdis-2014-207178).
Long-term RA remission can restore physical function
Long-term remission of rheumatoid arthritis for 24 weeks allowed 58%-73% of patients to regain full physical function, depending on which disease activity index is used, researchers reported online in Arthritis Research & Therapy.
“Physical function continues to improve over time when remission is maintained,” wrote Dr. Helga Radner and her associates at the Medical University of Vienna. Patients with DAS28 (Disease Activity Score using 28-joint counts including C-reactive protein) remission of at least 24 weeks improved by an average of 0.08 on the Health Assessment Questionnaire (HAQ), while those with sustained SDAI (Simplified Disease Activity Index) remissions improved by an average of 0.04, the investigators said.

The changes might seem small, but reflected the “very good” functional status of rheumatoid arthritis (RA) patients who achieve long-term remission, they noted, adding that, “on the group level in this population, the relative further improvement was between a quarter and a third of the initial HAQ assessment.”
Remission is a common treatment goal in RA, but maintaining it is the best way to slow or stop further joint damage. To better understand physical function within the context of sustained remission, the investigators analyzed HAQ disability index functional scores for 4,364 patients with active baseline disease who participated in the ASPIRE, ATTRACT, PREMIER, DE019, ERA, TEMPO, and leflunomide trials (Arthritis Res Ther. 2015;17:203).
In all, 14% of patients remained in DAS28 remission (scoring 2.6 or less) for at least 24 consecutive weeks and 5.8% achieved sustained SDAI remission (3.3 or less), Dr. Radner and her associates reported. Lower baseline disease activity, rheumatoid factor levels, and disease duration all predicted sustained remission (P less than .05 for all associations).
Full physical function, defined as a score of zero on the HAQ, occurred in 58% of patients in DAS28 remission for 24 weeks and in 73% of patients in SDAI remission for 24 weeks. Among patients in sustained DAS28 remission, women were significantly more likely than men to regain full physical function (hazard ratio, 1.41; 95% confidence interval, 1.13-1.76), as were patients with early (less than 2 years), compared with longer-term, disease (HR, 1.29; 95% CI, 1.01-1.65). Seropositivity and treatment regimen did not significantly affect the chances of regaining full function.
The researchers may not have captured some disease fluctuations because of the study design, they said. They also did not account for factors such as psychological status and comorbidities, which can affect physical disability.
The Medical University of Vienna funded the study. The investigators declared no competing interests.
Long-term remission of rheumatoid arthritis for 24 weeks allowed 58%-73% of patients to regain full physical function, depending on which disease activity index is used, researchers reported online in Arthritis Research & Therapy.
“Physical function continues to improve over time when remission is maintained,” wrote Dr. Helga Radner and her associates at the Medical University of Vienna. Patients with DAS28 (Disease Activity Score using 28-joint counts including C-reactive protein) remission of at least 24 weeks improved by an average of 0.08 on the Health Assessment Questionnaire (HAQ), while those with sustained SDAI (Simplified Disease Activity Index) remissions improved by an average of 0.04, the investigators said.
The changes might seem small, but reflected the “very good” functional status of rheumatoid arthritis (RA) patients who achieve long-term remission, they noted, adding that, “on the group level in this population, the relative further improvement was between a quarter and a third of the initial HAQ assessment.”
Remission is a common treatment goal in RA, but maintaining it is the best way to slow or stop further joint damage. To better understand physical function within the context of sustained remission, the investigators analyzed HAQ disability index functional scores for 4,364 patients with active baseline disease who participated in the ASPIRE, ATTRACT, PREMIER, DE019, ERA, TEMPO, and leflunomide trials (Arthritis Res Ther. 2015;17:203).
In all, 14% of patients remained in DAS28 remission (scoring 2.6 or less) for at least 24 consecutive weeks and 5.8% achieved sustained SDAI remission (3.3 or less), Dr. Radner and her associates reported. Lower baseline disease activity, rheumatoid factor levels, and disease duration all predicted sustained remission (P less than .05 for all associations).
Full physical function, defined as a score of zero on the HAQ, occurred in 58% of patients in DAS28 remission for 24 weeks and in 73% of patients in SDAI remission for 24 weeks. Among patients in sustained DAS28 remission, women were significantly more likely than men to regain full physical function (hazard ratio, 1.41; 95% confidence interval, 1.13-1.76), as were patients with early (less than 2 years), compared with longer-term, disease (HR, 1.29; 95% CI, 1.01-1.65). Seropositivity and treatment regimen did not significantly affect the chances of regaining full function.
The researchers may not have captured some disease fluctuations because of the study design, they said. They also did not account for factors such as psychological status and comorbidities, which can affect physical disability.
The Medical University of Vienna funded the study. The investigators declared no competing interests.
Long-term remission of rheumatoid arthritis for 24 weeks allowed 58%-73% of patients to regain full physical function, depending on which disease activity index is used, researchers reported online in Arthritis Research & Therapy.
“Physical function continues to improve over time when remission is maintained,” wrote Dr. Helga Radner and her associates at the Medical University of Vienna. Patients with DAS28 (Disease Activity Score using 28-joint counts including C-reactive protein) remission of at least 24 weeks improved by an average of 0.08 on the Health Assessment Questionnaire (HAQ), while those with sustained SDAI (Simplified Disease Activity Index) remissions improved by an average of 0.04, the investigators said.
The changes might seem small, but reflected the “very good” functional status of rheumatoid arthritis (RA) patients who achieve long-term remission, they noted, adding that, “on the group level in this population, the relative further improvement was between a quarter and a third of the initial HAQ assessment.”
Remission is a common treatment goal in RA, but maintaining it is the best way to slow or stop further joint damage. To better understand physical function within the context of sustained remission, the investigators analyzed HAQ disability index functional scores for 4,364 patients with active baseline disease who participated in the ASPIRE, ATTRACT, PREMIER, DE019, ERA, TEMPO, and leflunomide trials (Arthritis Res Ther. 2015;17:203).
In all, 14% of patients remained in DAS28 remission (scoring 2.6 or less) for at least 24 consecutive weeks and 5.8% achieved sustained SDAI remission (3.3 or less), Dr. Radner and her associates reported. Lower baseline disease activity, rheumatoid factor levels, and disease duration all predicted sustained remission (P less than .05 for all associations).
Full physical function, defined as a score of zero on the HAQ, occurred in 58% of patients in DAS28 remission for 24 weeks and in 73% of patients in SDAI remission for 24 weeks. Among patients in sustained DAS28 remission, women were significantly more likely than men to regain full physical function (hazard ratio, 1.41; 95% confidence interval, 1.13-1.76), as were patients with early (less than 2 years), compared with longer-term, disease (HR, 1.29; 95% CI, 1.01-1.65). Seropositivity and treatment regimen did not significantly affect the chances of regaining full function.
The researchers may not have captured some disease fluctuations because of the study design, they said. They also did not account for factors such as psychological status and comorbidities, which can affect physical disability.
The Medical University of Vienna funded the study. The investigators declared no competing interests.
FROM ARTHRITIS RESEARCH & THERAPY
Key clinical point: Patients with rheumatoid arthritis can regain full physical functioning after achieving sustained clinical remission.
Major finding: Full physical function, defined as a score of zero on the HAQ, occurred in 58% of patients in DAS28 remission for 24 weeks and in 73% of patients in SDAI remission for 24 weeks.
Data source: Combined analysis of data for 4,364 patients from the ASPIRE, ATTRACT, PREMIER, DE019, ERA, TEMPO, and leflunomide trials.
Disclosures: The Medical University of Vienna funded the study. The investigators declared no competing interests.

OCs may ease inflammatory arthritis severity
Oral contraceptive use may improve symptoms of inflammatory arthritis in women, according to a cohort study conducted in Germany between 2010 and 2013.
The researchers analyzed reports on 273 18- to 60-year-old women who had arthritis for fewer than 6 months, from both a rheumatologist and the patients. The rheumatologist followed patients for 24 months, conducting standardized assessments at 0, 3, 6, 12, 18, and 24 months. Patients reported outcomes at 0, 6, 12, and 24 months.

Of the patients studied, 50 (18%) had never used OCs, 170 (62%) had used OCs in the past, and 53 (19%) used OCs at the time of the study.
Inflammatory arthritis patients who were taking OCs at the time of the study or had previously taken OCs reported better outcomes within the first 2 years of disease, compared with patients who had never used OCs.
After adjustment for age, education, and body mass index, current or previous OC use was associated with better scores on the patient-reported Rheumatoid Arthritis Impact of Disease Score (RAID), Profile of Mood and Discomfort (PROFAD), Rheumatoid Arthritis Disease Activity Index (RADAI), and Hannover Functional Assessment (FFbH) at 12 months (P less than .05). In addition, over 2 years, average RAID scores were significantly better in women who had used or were using OCs (P less than .001).
Although better disease activity scores “seemed to be associated with the use of OCs, the parameters of active inflammation were not,” noted Dr. Katinka Albrecht of German Rheumatism Research Centre, Berlin, and her colleagues.
“The positive effects of past or current OC use on patient-reported outcomes within the first 2 years after the onset of inflammatory arthritis may be explained by long-lasting programming of [central nervous system] function,” but further research is needed to confirm this,” the researchers concluded.
The study was sponsored by a grant from Pfizer. The authors declared no conflicts of interest. Read the full study in Arthritis Care & Research (doi: 10.1002/acr.22667).
Oral contraceptive use may improve symptoms of inflammatory arthritis in women, according to a cohort study conducted in Germany between 2010 and 2013.
The researchers analyzed reports on 273 18- to 60-year-old women who had arthritis for fewer than 6 months, from both a rheumatologist and the patients. The rheumatologist followed patients for 24 months, conducting standardized assessments at 0, 3, 6, 12, 18, and 24 months. Patients reported outcomes at 0, 6, 12, and 24 months.
Of the patients studied, 50 (18%) had never used OCs, 170 (62%) had used OCs in the past, and 53 (19%) used OCs at the time of the study.
Inflammatory arthritis patients who were taking OCs at the time of the study or had previously taken OCs reported better outcomes within the first 2 years of disease, compared with patients who had never used OCs.
After adjustment for age, education, and body mass index, current or previous OC use was associated with better scores on the patient-reported Rheumatoid Arthritis Impact of Disease Score (RAID), Profile of Mood and Discomfort (PROFAD), Rheumatoid Arthritis Disease Activity Index (RADAI), and Hannover Functional Assessment (FFbH) at 12 months (P less than .05). In addition, over 2 years, average RAID scores were significantly better in women who had used or were using OCs (P less than .001).
Although better disease activity scores “seemed to be associated with the use of OCs, the parameters of active inflammation were not,” noted Dr. Katinka Albrecht of German Rheumatism Research Centre, Berlin, and her colleagues.
“The positive effects of past or current OC use on patient-reported outcomes within the first 2 years after the onset of inflammatory arthritis may be explained by long-lasting programming of [central nervous system] function,” but further research is needed to confirm this,” the researchers concluded.
The study was sponsored by a grant from Pfizer. The authors declared no conflicts of interest. Read the full study in Arthritis Care & Research (doi: 10.1002/acr.22667).
Oral contraceptive use may improve symptoms of inflammatory arthritis in women, according to a cohort study conducted in Germany between 2010 and 2013.
The researchers analyzed reports on 273 18- to 60-year-old women who had arthritis for fewer than 6 months, from both a rheumatologist and the patients. The rheumatologist followed patients for 24 months, conducting standardized assessments at 0, 3, 6, 12, 18, and 24 months. Patients reported outcomes at 0, 6, 12, and 24 months.
Of the patients studied, 50 (18%) had never used OCs, 170 (62%) had used OCs in the past, and 53 (19%) used OCs at the time of the study.
Inflammatory arthritis patients who were taking OCs at the time of the study or had previously taken OCs reported better outcomes within the first 2 years of disease, compared with patients who had never used OCs.
After adjustment for age, education, and body mass index, current or previous OC use was associated with better scores on the patient-reported Rheumatoid Arthritis Impact of Disease Score (RAID), Profile of Mood and Discomfort (PROFAD), Rheumatoid Arthritis Disease Activity Index (RADAI), and Hannover Functional Assessment (FFbH) at 12 months (P less than .05). In addition, over 2 years, average RAID scores were significantly better in women who had used or were using OCs (P less than .001).
Although better disease activity scores “seemed to be associated with the use of OCs, the parameters of active inflammation were not,” noted Dr. Katinka Albrecht of German Rheumatism Research Centre, Berlin, and her colleagues.
“The positive effects of past or current OC use on patient-reported outcomes within the first 2 years after the onset of inflammatory arthritis may be explained by long-lasting programming of [central nervous system] function,” but further research is needed to confirm this,” the researchers concluded.
The study was sponsored by a grant from Pfizer. The authors declared no conflicts of interest. Read the full study in Arthritis Care & Research (doi: 10.1002/acr.22667).
FROM ARTHRITIS CARE & RESEARCH
Predictors identified for progression of moderate RA on methotrexate
Patients with moderately active rheumatoid arthritis who were positive for rheumatoid factor and had baseline C-reactive protein levels above 40 mg/L had about a 60% chance of progressing on methotrexate monotherapy, investigators reported in RMD Open.
Elevated C-reactive protein (CRP) levels are known to predict radiographic progression in active rheumatoid arthritis (RA), but this study is the first to extend the finding to moderately active disease, said Dr. Bruno Fautrel of Pierre and Marie Curie University, Paris, and his associates. Understanding baseline predictors of radiographic progression could help clinicians to decide which patients need early, aggressive treatment and who can be spared intensive therapies, the researchers added.

“Studies investigating the risk of disease progression in patients with established and stable moderate disease activity are very limited,” they noted. “While it is established that moderate disease activity is not an adequate target for patients with RA, in real life, those with moderate RA represent a substantial proportion of patients in clinical practice.”
The study was a subgroup analysis of 96 patients with moderate RA from the methotrexate arm of the multicenter, phase III, randomized, double-blind, TEMPO (Trial of Etanercept and Methotrexate with Radiographic Patient Outcomes) trial. Patients had sustained moderate RA, defined as mean disease activity score in 28 joints ranging from 3.2 to 5.1 during the last 6 months of the first year. The researchers scored radiographs of hands, wrists, and feet based on the modified Total Sharp Score (mTSS) method, and defined radiographic progression as an increase from baseline mTSS of at least 3.0 after at least 2 years of methotrexate treatment. Patients averaged 55 years of age, and 84% were women, the investigators said (RMD Open 2015;1:e000018 doi: 10.1136/rmdopen-2014-000018).
Overall, about 26% of patients had signs of significant radiographic progression after 2 years of methotrexate treatment, and 34% had significantly progressed after 3 years, the researchers reported. Stratifying patients by baseline rheumatoid factor (RF) and CRP levels showed that those who were RF-positive at baseline with CRP levels above 40 mg/L were significantly more likely to progress at year 2 (51%; 95% confidence interval, 32%-69%) and year 3 (61%; 95% CI, 42%-78%) than were other patients, they said. In fact, only 33% of patients who were RF-positive and had baseline CRP levels below 10 mg/L had significantly progressed at year 3, as had only 10% of patients who were RF-negative and had baseline CRP levels below 10 mg/L. The median change in mTSS at year 3 was 3.6 for the highest-risk group, compared with zero for the lowest-risk group. Baseline erosion scores did not predict radiographic progression, probably because TEMPO patients had erosive disease at baseline, the researchers said.
The study was a post hoc analysis with a small sample size, and the mean methotrexate dose at baseline was only 7.5 mg/week, although the weekly dose rose to an average of 15 mg by week 24 of the study. Future studies should examine progression on etanercept monotherapy and on methotrexate-etanercept dual therapy, the investigators said.
Pfizer supported the research. Dr. Fautrel reported financial relationships with Pfizer, AbbVie, Bristol-Myers Squibb, Merck Sharp & Dohme, Roche, Sobi, and UCB. All three coauthors reported current or former employment with Pfizer.
Patients with moderately active rheumatoid arthritis who were positive for rheumatoid factor and had baseline C-reactive protein levels above 40 mg/L had about a 60% chance of progressing on methotrexate monotherapy, investigators reported in RMD Open.
Elevated C-reactive protein (CRP) levels are known to predict radiographic progression in active rheumatoid arthritis (RA), but this study is the first to extend the finding to moderately active disease, said Dr. Bruno Fautrel of Pierre and Marie Curie University, Paris, and his associates. Understanding baseline predictors of radiographic progression could help clinicians to decide which patients need early, aggressive treatment and who can be spared intensive therapies, the researchers added.
“Studies investigating the risk of disease progression in patients with established and stable moderate disease activity are very limited,” they noted. “While it is established that moderate disease activity is not an adequate target for patients with RA, in real life, those with moderate RA represent a substantial proportion of patients in clinical practice.”
The study was a subgroup analysis of 96 patients with moderate RA from the methotrexate arm of the multicenter, phase III, randomized, double-blind, TEMPO (Trial of Etanercept and Methotrexate with Radiographic Patient Outcomes) trial. Patients had sustained moderate RA, defined as mean disease activity score in 28 joints ranging from 3.2 to 5.1 during the last 6 months of the first year. The researchers scored radiographs of hands, wrists, and feet based on the modified Total Sharp Score (mTSS) method, and defined radiographic progression as an increase from baseline mTSS of at least 3.0 after at least 2 years of methotrexate treatment. Patients averaged 55 years of age, and 84% were women, the investigators said (RMD Open 2015;1:e000018 doi: 10.1136/rmdopen-2014-000018).
Overall, about 26% of patients had signs of significant radiographic progression after 2 years of methotrexate treatment, and 34% had significantly progressed after 3 years, the researchers reported. Stratifying patients by baseline rheumatoid factor (RF) and CRP levels showed that those who were RF-positive at baseline with CRP levels above 40 mg/L were significantly more likely to progress at year 2 (51%; 95% confidence interval, 32%-69%) and year 3 (61%; 95% CI, 42%-78%) than were other patients, they said. In fact, only 33% of patients who were RF-positive and had baseline CRP levels below 10 mg/L had significantly progressed at year 3, as had only 10% of patients who were RF-negative and had baseline CRP levels below 10 mg/L. The median change in mTSS at year 3 was 3.6 for the highest-risk group, compared with zero for the lowest-risk group. Baseline erosion scores did not predict radiographic progression, probably because TEMPO patients had erosive disease at baseline, the researchers said.
The study was a post hoc analysis with a small sample size, and the mean methotrexate dose at baseline was only 7.5 mg/week, although the weekly dose rose to an average of 15 mg by week 24 of the study. Future studies should examine progression on etanercept monotherapy and on methotrexate-etanercept dual therapy, the investigators said.
Pfizer supported the research. Dr. Fautrel reported financial relationships with Pfizer, AbbVie, Bristol-Myers Squibb, Merck Sharp & Dohme, Roche, Sobi, and UCB. All three coauthors reported current or former employment with Pfizer.
Patients with moderately active rheumatoid arthritis who were positive for rheumatoid factor and had baseline C-reactive protein levels above 40 mg/L had about a 60% chance of progressing on methotrexate monotherapy, investigators reported in RMD Open.
Elevated C-reactive protein (CRP) levels are known to predict radiographic progression in active rheumatoid arthritis (RA), but this study is the first to extend the finding to moderately active disease, said Dr. Bruno Fautrel of Pierre and Marie Curie University, Paris, and his associates. Understanding baseline predictors of radiographic progression could help clinicians to decide which patients need early, aggressive treatment and who can be spared intensive therapies, the researchers added.
“Studies investigating the risk of disease progression in patients with established and stable moderate disease activity are very limited,” they noted. “While it is established that moderate disease activity is not an adequate target for patients with RA, in real life, those with moderate RA represent a substantial proportion of patients in clinical practice.”
The study was a subgroup analysis of 96 patients with moderate RA from the methotrexate arm of the multicenter, phase III, randomized, double-blind, TEMPO (Trial of Etanercept and Methotrexate with Radiographic Patient Outcomes) trial. Patients had sustained moderate RA, defined as mean disease activity score in 28 joints ranging from 3.2 to 5.1 during the last 6 months of the first year. The researchers scored radiographs of hands, wrists, and feet based on the modified Total Sharp Score (mTSS) method, and defined radiographic progression as an increase from baseline mTSS of at least 3.0 after at least 2 years of methotrexate treatment. Patients averaged 55 years of age, and 84% were women, the investigators said (RMD Open 2015;1:e000018 doi: 10.1136/rmdopen-2014-000018).
Overall, about 26% of patients had signs of significant radiographic progression after 2 years of methotrexate treatment, and 34% had significantly progressed after 3 years, the researchers reported. Stratifying patients by baseline rheumatoid factor (RF) and CRP levels showed that those who were RF-positive at baseline with CRP levels above 40 mg/L were significantly more likely to progress at year 2 (51%; 95% confidence interval, 32%-69%) and year 3 (61%; 95% CI, 42%-78%) than were other patients, they said. In fact, only 33% of patients who were RF-positive and had baseline CRP levels below 10 mg/L had significantly progressed at year 3, as had only 10% of patients who were RF-negative and had baseline CRP levels below 10 mg/L. The median change in mTSS at year 3 was 3.6 for the highest-risk group, compared with zero for the lowest-risk group. Baseline erosion scores did not predict radiographic progression, probably because TEMPO patients had erosive disease at baseline, the researchers said.
The study was a post hoc analysis with a small sample size, and the mean methotrexate dose at baseline was only 7.5 mg/week, although the weekly dose rose to an average of 15 mg by week 24 of the study. Future studies should examine progression on etanercept monotherapy and on methotrexate-etanercept dual therapy, the investigators said.
Pfizer supported the research. Dr. Fautrel reported financial relationships with Pfizer, AbbVie, Bristol-Myers Squibb, Merck Sharp & Dohme, Roche, Sobi, and UCB. All three coauthors reported current or former employment with Pfizer.
FROM RMD OPEN
Key clinical point:Elevated C-reactive protein and rheumatoid factor levels predicted radiographic progression of moderate rheumatoid arthritis despite methotrexate treatment.
Major finding: RF positivity and baseline CRP levels above 40 mg/L predicted significant radiographic progression after 2 and 3 years (P less than .05 for all associations).
Data source: Subgroup analysis of 96 patients from the methotrexate arm of the multicenter, double-blind, randomized, 3-year TEMPO study.
Disclosures: Pfizer supported the research. Dr. Fautrel reported financial relationships with Pfizer, AbbVie, Bristol-Myers Squibb, Merck Sharp & Dohme, Roche, Sobi, and UCB. All three coauthors reported current or former employment with Pfizer.

Yet another insurer demand: patient care notifications
Some insurance companies recently started sending notifications about patient care. For example, one recently sent my boss a letter about one of his patients with rheumatoid arthritis, asking why the patient is not on a disease modifier. There is an invitation to explain why by ticking any one of several boxes. Is the patient perhaps not compliant? Did the patient discontinue the medication against the doctor’s advice? Has the patient passed away? Does the patient not have rheumatoid arthritis?
Oh, to be a fly on the wall when the insurance company decided that they would start doing this! This must impose a financial burden on the insurer, one that I cannot imagine they take on out of sheer altruism. What is the end game? What do they do with this information? Will they hold this information against the patient somehow, raise their premium in the next enrollment period? Or hold it against the physician, perhaps ding their reimbursement or use the information to include or exclude physicians from their panels?
When I decided to come to the United States, one of the biggest draws was the availability of health insurance. Most of my medical school education came from American textbooks, after all, so I thought it would be fabulous to be able to practice medicine the way it should be practiced because insurance will pay for it. (I know I sound like your elderly aunt that likes to repeat herself, but if you have not read any of my columns before, I come from the Philippines where health care is mostly paid for out of pocket, so how we treated patients was severely limited by how much the patient could afford.) I was wrong. I had no idea that part of my job description would include having to ask a corporate entity’s permission to administer treatments.
My boss replied to the letter. He said: “Patient is on dialysis and cannot be on methotrexate. He was prescribed a biologic, but your insurance does not cover its cost sufficiently to make it affordable. We had obtained the biologic through foundation support, but they ran out of money. So when you send out a letter like this blaming either the patient or MD for a compliance issue, I urge you to do some soul-searching.”
Dr. Chan practices rheumatology in Pawtucket, R.I.
Some insurance companies recently started sending notifications about patient care. For example, one recently sent my boss a letter about one of his patients with rheumatoid arthritis, asking why the patient is not on a disease modifier. There is an invitation to explain why by ticking any one of several boxes. Is the patient perhaps not compliant? Did the patient discontinue the medication against the doctor’s advice? Has the patient passed away? Does the patient not have rheumatoid arthritis?
Oh, to be a fly on the wall when the insurance company decided that they would start doing this! This must impose a financial burden on the insurer, one that I cannot imagine they take on out of sheer altruism. What is the end game? What do they do with this information? Will they hold this information against the patient somehow, raise their premium in the next enrollment period? Or hold it against the physician, perhaps ding their reimbursement or use the information to include or exclude physicians from their panels?
When I decided to come to the United States, one of the biggest draws was the availability of health insurance. Most of my medical school education came from American textbooks, after all, so I thought it would be fabulous to be able to practice medicine the way it should be practiced because insurance will pay for it. (I know I sound like your elderly aunt that likes to repeat herself, but if you have not read any of my columns before, I come from the Philippines where health care is mostly paid for out of pocket, so how we treated patients was severely limited by how much the patient could afford.) I was wrong. I had no idea that part of my job description would include having to ask a corporate entity’s permission to administer treatments.
My boss replied to the letter. He said: “Patient is on dialysis and cannot be on methotrexate. He was prescribed a biologic, but your insurance does not cover its cost sufficiently to make it affordable. We had obtained the biologic through foundation support, but they ran out of money. So when you send out a letter like this blaming either the patient or MD for a compliance issue, I urge you to do some soul-searching.”
Dr. Chan practices rheumatology in Pawtucket, R.I.
Some insurance companies recently started sending notifications about patient care. For example, one recently sent my boss a letter about one of his patients with rheumatoid arthritis, asking why the patient is not on a disease modifier. There is an invitation to explain why by ticking any one of several boxes. Is the patient perhaps not compliant? Did the patient discontinue the medication against the doctor’s advice? Has the patient passed away? Does the patient not have rheumatoid arthritis?
Oh, to be a fly on the wall when the insurance company decided that they would start doing this! This must impose a financial burden on the insurer, one that I cannot imagine they take on out of sheer altruism. What is the end game? What do they do with this information? Will they hold this information against the patient somehow, raise their premium in the next enrollment period? Or hold it against the physician, perhaps ding their reimbursement or use the information to include or exclude physicians from their panels?
When I decided to come to the United States, one of the biggest draws was the availability of health insurance. Most of my medical school education came from American textbooks, after all, so I thought it would be fabulous to be able to practice medicine the way it should be practiced because insurance will pay for it. (I know I sound like your elderly aunt that likes to repeat herself, but if you have not read any of my columns before, I come from the Philippines where health care is mostly paid for out of pocket, so how we treated patients was severely limited by how much the patient could afford.) I was wrong. I had no idea that part of my job description would include having to ask a corporate entity’s permission to administer treatments.
My boss replied to the letter. He said: “Patient is on dialysis and cannot be on methotrexate. He was prescribed a biologic, but your insurance does not cover its cost sufficiently to make it affordable. We had obtained the biologic through foundation support, but they ran out of money. So when you send out a letter like this blaming either the patient or MD for a compliance issue, I urge you to do some soul-searching.”
Dr. Chan practices rheumatology in Pawtucket, R.I.

Study links statin use to lower mortality in RA patients
Among adults with rheumatoid arthritis, starting a statin prescription led to a 21% drop in risk of dying from any cause, compared with not using statins, according to a study published online Aug. 5 in Annals of the Rheumatic Diseases.
The size of the protective effect resembled results from trials of patients without RA and somewhat exceeded those from population-level analyses of statins as preventive therapy, reported Dr. Sara Schoenfeld of Harvard Medical School, Boston.
“Although the differences were small, this finding may not be surprising, as patients with RA are at a higher risk for cardiovascular disease than the general population, and might benefit from the dual anti-inflammatory and lipid-lowering effects of statins in a way that the general population might not,” wrote Dr. Schoenfeld and her colleagues.

Few studies have examined statin use in patients with RA, and a recent randomized trial, TRACE-RA (Ann Rheum Dis. 2015;74:688), was halted early because of a low event rate, the investigators noted.
To further explore the issue, they compared matched cohorts of RA patients who were at least 20 years old, were listed in a general practice medical records database from the United Kingdom, had used at least one disease-modifying antirheumatic drug between 2000 and 2012, and had either started statins or not during the year they were added to the study.
The investigators excluded current or former statin users to help prevent selection bias, and they excluded patients with missing data on relevant risk factors, such as body mass index or smoking status (Ann Rheum Dis. 2015 Aug. 5 doi: 10.1136/annrheumdis-2015-207714).
Over a median of 4.5 years of follow-up, 432 of 2,943 patients with RA who started statins died, for an incidence rate of 32.6 deaths per 1,000 person-years, which was substantially less than the rate of 40.6 per 1,000 person-years among those who did not use statins, the investigators reported. Thus, starting statins was linked to a 21% lower likelihood of all-cause mortality (hazard ratio, 0.79; 95% confidence interval, 0.68 to 0.91), they said. The hazard ratio was similar when they defined RA based on diagnostic code only, without requiring use of DMARDs for the case definition (HR, 0.81; 95% CI, 0.74 to 0.90).
“Our findings expand previous evidence for the beneficial effects of statins in RA, which have been indirectly drawn from studies evaluating intermediate markers of cardiovascular disease and premature mortality in RA, antirheumatic and lipid findings from studies evaluating RA disease outcomes, and studies evaluating statin effects in other patient populations, such as the JUPITER trial,” the researchers said.
The comparison groups were well balanced in terms of baseline demographic traits, comorbidities, total cholesterol levels, and use of cardiovascular medications, nonsteroidal anti-inflammatory drugs, glucocorticoids, and biological agents, but the medical records database usually lacked information on cause of death, the researchers noted. “We hypothesize that the lower mortality rate associated with statin use stems from the reduction of cardiovascular-specific mortality in patients with RA, and this speculation calls for future studies that examine cause-specific mortality outcomes,” they concluded.
The National Institutes of Health partly funded the work. The investigators declared having no competing interests.
Among adults with rheumatoid arthritis, starting a statin prescription led to a 21% drop in risk of dying from any cause, compared with not using statins, according to a study published online Aug. 5 in Annals of the Rheumatic Diseases.
The size of the protective effect resembled results from trials of patients without RA and somewhat exceeded those from population-level analyses of statins as preventive therapy, reported Dr. Sara Schoenfeld of Harvard Medical School, Boston.
“Although the differences were small, this finding may not be surprising, as patients with RA are at a higher risk for cardiovascular disease than the general population, and might benefit from the dual anti-inflammatory and lipid-lowering effects of statins in a way that the general population might not,” wrote Dr. Schoenfeld and her colleagues.
Few studies have examined statin use in patients with RA, and a recent randomized trial, TRACE-RA (Ann Rheum Dis. 2015;74:688), was halted early because of a low event rate, the investigators noted.
To further explore the issue, they compared matched cohorts of RA patients who were at least 20 years old, were listed in a general practice medical records database from the United Kingdom, had used at least one disease-modifying antirheumatic drug between 2000 and 2012, and had either started statins or not during the year they were added to the study.
The investigators excluded current or former statin users to help prevent selection bias, and they excluded patients with missing data on relevant risk factors, such as body mass index or smoking status (Ann Rheum Dis. 2015 Aug. 5 doi: 10.1136/annrheumdis-2015-207714).
Over a median of 4.5 years of follow-up, 432 of 2,943 patients with RA who started statins died, for an incidence rate of 32.6 deaths per 1,000 person-years, which was substantially less than the rate of 40.6 per 1,000 person-years among those who did not use statins, the investigators reported. Thus, starting statins was linked to a 21% lower likelihood of all-cause mortality (hazard ratio, 0.79; 95% confidence interval, 0.68 to 0.91), they said. The hazard ratio was similar when they defined RA based on diagnostic code only, without requiring use of DMARDs for the case definition (HR, 0.81; 95% CI, 0.74 to 0.90).
“Our findings expand previous evidence for the beneficial effects of statins in RA, which have been indirectly drawn from studies evaluating intermediate markers of cardiovascular disease and premature mortality in RA, antirheumatic and lipid findings from studies evaluating RA disease outcomes, and studies evaluating statin effects in other patient populations, such as the JUPITER trial,” the researchers said.
The comparison groups were well balanced in terms of baseline demographic traits, comorbidities, total cholesterol levels, and use of cardiovascular medications, nonsteroidal anti-inflammatory drugs, glucocorticoids, and biological agents, but the medical records database usually lacked information on cause of death, the researchers noted. “We hypothesize that the lower mortality rate associated with statin use stems from the reduction of cardiovascular-specific mortality in patients with RA, and this speculation calls for future studies that examine cause-specific mortality outcomes,” they concluded.
The National Institutes of Health partly funded the work. The investigators declared having no competing interests.
Among adults with rheumatoid arthritis, starting a statin prescription led to a 21% drop in risk of dying from any cause, compared with not using statins, according to a study published online Aug. 5 in Annals of the Rheumatic Diseases.
The size of the protective effect resembled results from trials of patients without RA and somewhat exceeded those from population-level analyses of statins as preventive therapy, reported Dr. Sara Schoenfeld of Harvard Medical School, Boston.
“Although the differences were small, this finding may not be surprising, as patients with RA are at a higher risk for cardiovascular disease than the general population, and might benefit from the dual anti-inflammatory and lipid-lowering effects of statins in a way that the general population might not,” wrote Dr. Schoenfeld and her colleagues.
Few studies have examined statin use in patients with RA, and a recent randomized trial, TRACE-RA (Ann Rheum Dis. 2015;74:688), was halted early because of a low event rate, the investigators noted.
To further explore the issue, they compared matched cohorts of RA patients who were at least 20 years old, were listed in a general practice medical records database from the United Kingdom, had used at least one disease-modifying antirheumatic drug between 2000 and 2012, and had either started statins or not during the year they were added to the study.
The investigators excluded current or former statin users to help prevent selection bias, and they excluded patients with missing data on relevant risk factors, such as body mass index or smoking status (Ann Rheum Dis. 2015 Aug. 5 doi: 10.1136/annrheumdis-2015-207714).
Over a median of 4.5 years of follow-up, 432 of 2,943 patients with RA who started statins died, for an incidence rate of 32.6 deaths per 1,000 person-years, which was substantially less than the rate of 40.6 per 1,000 person-years among those who did not use statins, the investigators reported. Thus, starting statins was linked to a 21% lower likelihood of all-cause mortality (hazard ratio, 0.79; 95% confidence interval, 0.68 to 0.91), they said. The hazard ratio was similar when they defined RA based on diagnostic code only, without requiring use of DMARDs for the case definition (HR, 0.81; 95% CI, 0.74 to 0.90).
“Our findings expand previous evidence for the beneficial effects of statins in RA, which have been indirectly drawn from studies evaluating intermediate markers of cardiovascular disease and premature mortality in RA, antirheumatic and lipid findings from studies evaluating RA disease outcomes, and studies evaluating statin effects in other patient populations, such as the JUPITER trial,” the researchers said.
The comparison groups were well balanced in terms of baseline demographic traits, comorbidities, total cholesterol levels, and use of cardiovascular medications, nonsteroidal anti-inflammatory drugs, glucocorticoids, and biological agents, but the medical records database usually lacked information on cause of death, the researchers noted. “We hypothesize that the lower mortality rate associated with statin use stems from the reduction of cardiovascular-specific mortality in patients with RA, and this speculation calls for future studies that examine cause-specific mortality outcomes,” they concluded.
The National Institutes of Health partly funded the work. The investigators declared having no competing interests.
FROM ANNALS OF THE RHEUMATIC DISEASES
Key clinical point:Starting statins might substantially decrease mortality among adults with rheumatoid arthritis.
Major finding: Patients who started statins had a subsequent 21% lower risk of all-cause mortality than did those who did not.
Data source: Matched cohort study of 5,886 patients with rheumatoid arthritis who at baseline had never used statins.
Disclosures: The National Institutes of Health partly funded the work. The investigators declared no competing interests.

Recommended RA targets tied to better health outcomes
Patients with rheumatoid arthritis who achieved recommended targets on measures of disease activity functioned better, had better quality of life, and used fewer health care resources, compared with patients with low disease activity levels, according to researchers.
Relevant targets included scoring 3.3 or less on the Simplified Disease Activity Index (SDAI), 2.8 or less on the Clinical Disease Activity Index (CDAI), and less than 2.6 on the Disease Activity Score in 28 joints using C-reactive protein (DAS28-CRP), said Dr. Evo Alemao of Bristol-Myers Squibb, Princeton, N.J., and associates. If patient-clinician teams cannot meet these targets, they should aim for low levels of disease activity because higher levels were associated with even worse physical functioning and health-related quality of life, they said.

Clinical studies have increasingly focused on target measures of RA activity, but their short durations and highly adherent, severely affected patient populations have limited generalizability, the investigators noted. To bridge the gap, they analyzed outcomes data from the observational, longitudinal, prospective Brigham and Women’s Hospital Rheumatoid Arthritis Sequential Study, which has followed almost 1,300 RA patients seen at a single hospital center for up to 5 years.
The average age of the patients was 56 years. They had experienced RA symptoms for a median of 15 years (Arthritis Care Res. (Hoboken) 2015 Aug 3 doi: 10.1002/acr.22678). In the controlled analysis, patients who met recommended SDAI and CDAI targets functioned better physically than did those with low disease activity (average improvement on the Modified Health Activity Questionnaire, .047 and .073, respectively; P values, .01 and .0003), the researchers reported. The DAS28-CRP target did not show that effect, but all three targets were linked to better EQ-5D scores compared with low, moderate, or high disease activity (range of improvement, .022 to .096; P less than .003).
Furthermore, patients who met recommended targets were 36%-45% less likely to be hospitalized (P less than .05) and 23%-45% less likely to report using durable medical equipment (P less than .01) than were patients with residual disease activity, the researchers said.
Future work should look at relationships between target measures and pain, fatigue, and Total Sharp Score outcomes, and also should analyze cost data, the investigators said.
Bristol-Myers Squibb funded the study and write-up, and Crescendo Bioscience and UCB funded the BRASS Registry. Dr. Alemao reported being employed by BMS. Four coauthors reported financial ties with BMS, Amgen, AbbVie, Genentech, Crescendo Bioscience, Medimmune, and UCB. The rest reported having no conflicts of interest.
Patients with rheumatoid arthritis who achieved recommended targets on measures of disease activity functioned better, had better quality of life, and used fewer health care resources, compared with patients with low disease activity levels, according to researchers.
Relevant targets included scoring 3.3 or less on the Simplified Disease Activity Index (SDAI), 2.8 or less on the Clinical Disease Activity Index (CDAI), and less than 2.6 on the Disease Activity Score in 28 joints using C-reactive protein (DAS28-CRP), said Dr. Evo Alemao of Bristol-Myers Squibb, Princeton, N.J., and associates. If patient-clinician teams cannot meet these targets, they should aim for low levels of disease activity because higher levels were associated with even worse physical functioning and health-related quality of life, they said.
Clinical studies have increasingly focused on target measures of RA activity, but their short durations and highly adherent, severely affected patient populations have limited generalizability, the investigators noted. To bridge the gap, they analyzed outcomes data from the observational, longitudinal, prospective Brigham and Women’s Hospital Rheumatoid Arthritis Sequential Study, which has followed almost 1,300 RA patients seen at a single hospital center for up to 5 years.
The average age of the patients was 56 years. They had experienced RA symptoms for a median of 15 years (Arthritis Care Res. (Hoboken) 2015 Aug 3 doi: 10.1002/acr.22678). In the controlled analysis, patients who met recommended SDAI and CDAI targets functioned better physically than did those with low disease activity (average improvement on the Modified Health Activity Questionnaire, .047 and .073, respectively; P values, .01 and .0003), the researchers reported. The DAS28-CRP target did not show that effect, but all three targets were linked to better EQ-5D scores compared with low, moderate, or high disease activity (range of improvement, .022 to .096; P less than .003).
Furthermore, patients who met recommended targets were 36%-45% less likely to be hospitalized (P less than .05) and 23%-45% less likely to report using durable medical equipment (P less than .01) than were patients with residual disease activity, the researchers said.
Future work should look at relationships between target measures and pain, fatigue, and Total Sharp Score outcomes, and also should analyze cost data, the investigators said.
Bristol-Myers Squibb funded the study and write-up, and Crescendo Bioscience and UCB funded the BRASS Registry. Dr. Alemao reported being employed by BMS. Four coauthors reported financial ties with BMS, Amgen, AbbVie, Genentech, Crescendo Bioscience, Medimmune, and UCB. The rest reported having no conflicts of interest.
Patients with rheumatoid arthritis who achieved recommended targets on measures of disease activity functioned better, had better quality of life, and used fewer health care resources, compared with patients with low disease activity levels, according to researchers.
Relevant targets included scoring 3.3 or less on the Simplified Disease Activity Index (SDAI), 2.8 or less on the Clinical Disease Activity Index (CDAI), and less than 2.6 on the Disease Activity Score in 28 joints using C-reactive protein (DAS28-CRP), said Dr. Evo Alemao of Bristol-Myers Squibb, Princeton, N.J., and associates. If patient-clinician teams cannot meet these targets, they should aim for low levels of disease activity because higher levels were associated with even worse physical functioning and health-related quality of life, they said.
Clinical studies have increasingly focused on target measures of RA activity, but their short durations and highly adherent, severely affected patient populations have limited generalizability, the investigators noted. To bridge the gap, they analyzed outcomes data from the observational, longitudinal, prospective Brigham and Women’s Hospital Rheumatoid Arthritis Sequential Study, which has followed almost 1,300 RA patients seen at a single hospital center for up to 5 years.
The average age of the patients was 56 years. They had experienced RA symptoms for a median of 15 years (Arthritis Care Res. (Hoboken) 2015 Aug 3 doi: 10.1002/acr.22678). In the controlled analysis, patients who met recommended SDAI and CDAI targets functioned better physically than did those with low disease activity (average improvement on the Modified Health Activity Questionnaire, .047 and .073, respectively; P values, .01 and .0003), the researchers reported. The DAS28-CRP target did not show that effect, but all three targets were linked to better EQ-5D scores compared with low, moderate, or high disease activity (range of improvement, .022 to .096; P less than .003).
Furthermore, patients who met recommended targets were 36%-45% less likely to be hospitalized (P less than .05) and 23%-45% less likely to report using durable medical equipment (P less than .01) than were patients with residual disease activity, the researchers said.
Future work should look at relationships between target measures and pain, fatigue, and Total Sharp Score outcomes, and also should analyze cost data, the investigators said.
Bristol-Myers Squibb funded the study and write-up, and Crescendo Bioscience and UCB funded the BRASS Registry. Dr. Alemao reported being employed by BMS. Four coauthors reported financial ties with BMS, Amgen, AbbVie, Genentech, Crescendo Bioscience, Medimmune, and UCB. The rest reported having no conflicts of interest.
FROM ARTHRITIS CARE & RESEARCH
Key clinical point: Patients with rheumatoid arthritis who achieved recommended disease activity targets had significantly better physical functioning, health-related quality of life, and use of health care resources than did those with low disease activity.
Major finding: Modified Health Activity Questionnaire scores were significantly better for patients who scored 3.3 or less on the Simplified Disease Activity Index and 2.8 or less on the Clinical Disease Activity Index (P values, .01 and .0003), compared with patients with low disease activity.
Data source: Analysis of outcomes for 1,297 patients from the prospective, observational, longitudinal Brigham and Women’s Hospital Rheumatoid Arthritis Sequential Study.
Disclosures: Bristol-Myers Squibb funded the study and write-up, and Crescendo Bioscience and UCB funded the BRASS Registry. Dr. Alemao reported being employed by BMS. Four coauthors reported financial ties with BMS, Amgen, AbbVie, Genentech, Crescendo Bioscience, Medimmune, and UCB. The rest reported having no conflicts of interest.

Pain, quality of life measures improve more in OA than RA after knee arthroplasty
Total knee arthroplasty provides osteoarthritis patients with greater improvement in pain and health-related quality of life than it does for rheumatoid arthritis patients, possibly relating to the lower pain and younger age of RA patients at the time of surgery, according to a study based on patients’ responses to semiannual questionnaires.
The study included 834 patients diagnosed with RA and 315 patients diagnosed with osteoarthritis (OA), who had a primary total knee arthroplasty (TKA) between Jan. 1, 1999, and June 30, 2012. The patients were probed on their demographic characteristics, disease duration, mental health, functional status, health-related quality of life (HRQoL), pain, and usage of pain medication. All study participants participated in at least three consecutive sampling intervals: a 6-month preoperative period, a 6-month immediate postoperative period, and a subsequent 6-month “recovery” period. Of the patients who underwent a TKA, 144 (11%) did not complete all three sampling intervals.

At baseline, compared with OA patients, RA patients had significantly less severe scores for measures of pain, lesser usage of pain medications, and significantly more severe scores for measures of disease activity.
After recovering from a TKA, the RA and OA patients improved in almost all outcome measures of pain, function, and HRQoL. The surgery had a larger beneficial effect in OA patients than in RA patients for all measures of pain and HRQoL indices, except for the RA disease activity index (RADAI)/total joint count. In contrast to the OA patients, RA patients showed greater improvements in joint involvement.
For both groups, all outcome measures of pain and function worsened a year before TKA and improved immediately after the surgery; however, the improvement leveled off in the 6-12 months after the procedure.
“After adjusting for preoperative variables, post TKA, a diagnosis of RA (vs. OA) (P = .03), income (P < .01), and anxiety (P = .03) were most useful in predicting the reduction in [visual analog scale] pain scores,” noted Dr. Anand Dusad of the Veterans Affairs Nebraska–Western Iowa Health Care System, Omaha, and his colleagues.
“In summary, using a large cohort of arthritis patients, we have shown that TKA is performed in patients with severe disease and leads to marked improvements in pain function and HRQoL,” according to the researchers.
Read the full study published online July 20 in Arthritis & Rheumatology (doi:10.1002/art.39221).
Total knee arthroplasty provides osteoarthritis patients with greater improvement in pain and health-related quality of life than it does for rheumatoid arthritis patients, possibly relating to the lower pain and younger age of RA patients at the time of surgery, according to a study based on patients’ responses to semiannual questionnaires.
The study included 834 patients diagnosed with RA and 315 patients diagnosed with osteoarthritis (OA), who had a primary total knee arthroplasty (TKA) between Jan. 1, 1999, and June 30, 2012. The patients were probed on their demographic characteristics, disease duration, mental health, functional status, health-related quality of life (HRQoL), pain, and usage of pain medication. All study participants participated in at least three consecutive sampling intervals: a 6-month preoperative period, a 6-month immediate postoperative period, and a subsequent 6-month “recovery” period. Of the patients who underwent a TKA, 144 (11%) did not complete all three sampling intervals.
At baseline, compared with OA patients, RA patients had significantly less severe scores for measures of pain, lesser usage of pain medications, and significantly more severe scores for measures of disease activity.
After recovering from a TKA, the RA and OA patients improved in almost all outcome measures of pain, function, and HRQoL. The surgery had a larger beneficial effect in OA patients than in RA patients for all measures of pain and HRQoL indices, except for the RA disease activity index (RADAI)/total joint count. In contrast to the OA patients, RA patients showed greater improvements in joint involvement.
For both groups, all outcome measures of pain and function worsened a year before TKA and improved immediately after the surgery; however, the improvement leveled off in the 6-12 months after the procedure.
“After adjusting for preoperative variables, post TKA, a diagnosis of RA (vs. OA) (P = .03), income (P < .01), and anxiety (P = .03) were most useful in predicting the reduction in [visual analog scale] pain scores,” noted Dr. Anand Dusad of the Veterans Affairs Nebraska–Western Iowa Health Care System, Omaha, and his colleagues.
“In summary, using a large cohort of arthritis patients, we have shown that TKA is performed in patients with severe disease and leads to marked improvements in pain function and HRQoL,” according to the researchers.
Read the full study published online July 20 in Arthritis & Rheumatology (doi:10.1002/art.39221).
Total knee arthroplasty provides osteoarthritis patients with greater improvement in pain and health-related quality of life than it does for rheumatoid arthritis patients, possibly relating to the lower pain and younger age of RA patients at the time of surgery, according to a study based on patients’ responses to semiannual questionnaires.
The study included 834 patients diagnosed with RA and 315 patients diagnosed with osteoarthritis (OA), who had a primary total knee arthroplasty (TKA) between Jan. 1, 1999, and June 30, 2012. The patients were probed on their demographic characteristics, disease duration, mental health, functional status, health-related quality of life (HRQoL), pain, and usage of pain medication. All study participants participated in at least three consecutive sampling intervals: a 6-month preoperative period, a 6-month immediate postoperative period, and a subsequent 6-month “recovery” period. Of the patients who underwent a TKA, 144 (11%) did not complete all three sampling intervals.
At baseline, compared with OA patients, RA patients had significantly less severe scores for measures of pain, lesser usage of pain medications, and significantly more severe scores for measures of disease activity.
After recovering from a TKA, the RA and OA patients improved in almost all outcome measures of pain, function, and HRQoL. The surgery had a larger beneficial effect in OA patients than in RA patients for all measures of pain and HRQoL indices, except for the RA disease activity index (RADAI)/total joint count. In contrast to the OA patients, RA patients showed greater improvements in joint involvement.
For both groups, all outcome measures of pain and function worsened a year before TKA and improved immediately after the surgery; however, the improvement leveled off in the 6-12 months after the procedure.
“After adjusting for preoperative variables, post TKA, a diagnosis of RA (vs. OA) (P = .03), income (P < .01), and anxiety (P = .03) were most useful in predicting the reduction in [visual analog scale] pain scores,” noted Dr. Anand Dusad of the Veterans Affairs Nebraska–Western Iowa Health Care System, Omaha, and his colleagues.
“In summary, using a large cohort of arthritis patients, we have shown that TKA is performed in patients with severe disease and leads to marked improvements in pain function and HRQoL,” according to the researchers.
Read the full study published online July 20 in Arthritis & Rheumatology (doi:10.1002/art.39221).
FROM ARTHRITIS & RHEUMATOLOGY
