User login
APA-IPS: Disaster psychiatry – Nepal, Ebola, and beyond
NEW YORK – After the earthquake in Nepal earlier this year, Disaster Psychiatry Outreach sent in volunteers who found preexisting issues that made their mental health response challenging at best, Dr. Ram Suresh Mahato reported at the American Psychiatric Association’s Institute on Psychiatric Services.
Nepal was recovering from armed conflict that lasted from 1996 to 2006 and resulted in what some have called a “postconflict identity crisis” (Int J Educ Dev. 2014;34:42-50). The caste system in the country was abolished in 1963, but social inequality continued to persist. In addition, more than 60 languages are spoken in Nepal, and at least 25% of the population lives below the poverty line, said Dr. Mahato, a Disaster Psychiatry Outreach (DPO) volunteer who was part of the needs-assessment team dispatched to the country in May.

Other complicating factors included high rates of domestic violence. Nepali women are at greater risk of depression, anxiety, and posttraumatic stress than are males (Lancet. 2008 May;371[9625]:1664) and (J Affect Disord. 2007 Sep;102[1-3]:219-25), and a culture of silence prevails, Dr. Mahato said. The literature describes informal social networks in Nepal in which community members share their distress and symptoms, “as well as traditional (shamanistic) healing practices for those suffering mental health complaints in relation to political violence” (Soc Sci Med. 2010 Jan;70[1]:35-44).
Dr. Mahato spoke at a workshop, sponsored by DPO, aimed at urging psychiatrists to be prepared in providing mental health services to disaster survivors across the globe and here at home. “The room was full last year,” said Dr. Sander Koyfman, DPO’s president, referring to the intense interest in Ebola at the height of the outbreak in 2014. “This year, it’s more of a challenge, as interest wanes from disaster to disaster,” but their organization would like to “sustain the desire in mental health providers and disaster responders to learn how to help most effectively,” Dr. Koyfman said in an interview.
The presentation focused on the mental health aspects of the Ebola response and the more recent DPO work following the earthquake in Nepal that killed 10,000 people. In a striking similarity, about 10,900 people died in the wake of the Ebola epidemic in West Africa and its rolling impact across many regions. (In May, the World Health Organization declared Liberia free of Ebola but said on Oct. 14 that a preliminary study published in the New England Journal of Medicine shows that the virus can persist in the semen of some survivors for at least 9 months.)
Vulnerable suffer most
Over the last 10 years, more than 1.4 million people have been injured and about 23 million have been left homeless across the globe because of man-made and natural disasters, according to a 2015 United Nations report. “Overall, more than 1.5 billion people have been affected by disasters in various ways, with women, children, and people in vulnerable situations disproportionately affected,” the report says.
DPO, a New York–based nonprofit, launched in 1998, has sent volunteers to an average of one disaster per year, said Dr. Koyfman, also medical director for EmblemHealth Insurance, New York.
“We at DPO learn to caution folks and say, ‘Look, it’s important and it’s critical to do everything you can, but do appreciate one thing: The key is what happens 3 to 6 months from today,’ ” he said. “The mental health component will happen then. This is very different from a typical disaster mentality.”
Before the earthquake in Nepal, manpower and resources were limited: The country has about 80 psychiatrists, or about 1 for every million people, said Dr. Mahato, chief psychiatry resident, PGY-4, at Mount Sinai/Elmhurst Hospital Center, New York. After the earthquake and more than 300 aftershocks, about 2.8 million people were in need of humanitarian assistance. The DPO team partnered with the Psychiatrists’ Association of Nepal by visiting affected districts and participating in health camps. “The challenges we saw involved developing communication and training materials in a culturally appropriate framework,” Dr. Mahato said.
Portable intervention used
One intervention used by DPO teams in Nepal was Psychological First Aid (PFA), Dr. Javier Garcia said.
PFA has grown in popularity and acceptance, especially when it became increasingly clear after the attacks of Sept. 11, 2001, that psychological debriefing was not as universally useful or safe modality as it was once thought to be, said Dr. Garcia of Richmond University Medical Center, New York.
In contrast, PFA is an intervention based on principles of resilience that focuses on safety, calming, connectedness, self-community, efficacy, and hope. “PFA assumes that people can have maladaptive reactions,” Dr. Garcia said. “ But is designed to reduce the initial distress and foster short- and long-term adaptive functioning.” He said all first responders, including fire, police and crisis response teams, health care professionals, and paraprofessionals can be trained to use PFA. In fact, another model of PFA was created for school staff in the 1990s in response to school shootings.
The first goal after a disaster is to ensure physical safety. After that, teams try to protect those traumatized from additional trauma. Emotionally overwhelmed and disoriented survivors must be stabilized, and medications generally are not recommended during this part of the process. Medications might be helpful in cases involving addiction or sleep, but such cases are exceptions, Dr. Garcia said. In general, the same strict clinical criteria for use of psychiatric medications are applicable in postdisaster environments and are specific to the episode and the individual. PFA attempts to be culturally informed and delivered in a flexible manner, Dr. Garcia said. “It’s evidence informed but not evidence based. So, we need more research.”
PFA, along with effective risk communications, frequently are the mainstay of an effective mental health response. Where PFA informs the “what” of the mental health conversation, risk communications, as Dr. Grant H. Brenner pointed out at the meeting, is the key “how” of getting the right message out the right way. Dr. Brenner, DPO board member, is a faculty member of Mount Sinai Hospital, director of the William Alanson White Institute Trauma Service, and an editor of Creating Spiritual and Psychological Resilience: Integrating Care in Disaster Relief Work (New York: Routledge, 2009).
After the Ebola work on the ground, volunteers often found complicated terrain in the United States. As the example of the single New York City Ebola patient showed, medical and psychological preparedness and the ability of the authorities to effectively communicate safety information to the public were tested. DPO worked with a nonprofit group called More Than Me to offer mental health support services to returning volunteers and to the few people who were under quarantine orders in New York.
Each disaster is different, but a few common themes are apparent. “There’s huge value in presence and human touch,” Dr. Koyfman said.
DPO offers training sessions for new volunteers. Psychiatrists interested in volunteering can send a message to info@disasterpsych.org or call 646-867-3514. For more on risk communication, check out the information on emergency preparedness and response provided by the Centers for Disease Control and Prevention. Other useful resources are the American Psychiatric Association’s Committee on Psychiatric Dimensions of Disaster and Resiliency in the Face of Disaster and Terrorism: 10 Things to Do to Survive (Personhood Press, 2005).
ghenderson@frontlinemedcom.com
On Twitter @ginalhenderson
NEW YORK – After the earthquake in Nepal earlier this year, Disaster Psychiatry Outreach sent in volunteers who found preexisting issues that made their mental health response challenging at best, Dr. Ram Suresh Mahato reported at the American Psychiatric Association’s Institute on Psychiatric Services.
Nepal was recovering from armed conflict that lasted from 1996 to 2006 and resulted in what some have called a “postconflict identity crisis” (Int J Educ Dev. 2014;34:42-50). The caste system in the country was abolished in 1963, but social inequality continued to persist. In addition, more than 60 languages are spoken in Nepal, and at least 25% of the population lives below the poverty line, said Dr. Mahato, a Disaster Psychiatry Outreach (DPO) volunteer who was part of the needs-assessment team dispatched to the country in May.
Other complicating factors included high rates of domestic violence. Nepali women are at greater risk of depression, anxiety, and posttraumatic stress than are males (Lancet. 2008 May;371[9625]:1664) and (J Affect Disord. 2007 Sep;102[1-3]:219-25), and a culture of silence prevails, Dr. Mahato said. The literature describes informal social networks in Nepal in which community members share their distress and symptoms, “as well as traditional (shamanistic) healing practices for those suffering mental health complaints in relation to political violence” (Soc Sci Med. 2010 Jan;70[1]:35-44).
Dr. Mahato spoke at a workshop, sponsored by DPO, aimed at urging psychiatrists to be prepared in providing mental health services to disaster survivors across the globe and here at home. “The room was full last year,” said Dr. Sander Koyfman, DPO’s president, referring to the intense interest in Ebola at the height of the outbreak in 2014. “This year, it’s more of a challenge, as interest wanes from disaster to disaster,” but their organization would like to “sustain the desire in mental health providers and disaster responders to learn how to help most effectively,” Dr. Koyfman said in an interview.
The presentation focused on the mental health aspects of the Ebola response and the more recent DPO work following the earthquake in Nepal that killed 10,000 people. In a striking similarity, about 10,900 people died in the wake of the Ebola epidemic in West Africa and its rolling impact across many regions. (In May, the World Health Organization declared Liberia free of Ebola but said on Oct. 14 that a preliminary study published in the New England Journal of Medicine shows that the virus can persist in the semen of some survivors for at least 9 months.)
Vulnerable suffer most
Over the last 10 years, more than 1.4 million people have been injured and about 23 million have been left homeless across the globe because of man-made and natural disasters, according to a 2015 United Nations report. “Overall, more than 1.5 billion people have been affected by disasters in various ways, with women, children, and people in vulnerable situations disproportionately affected,” the report says.
DPO, a New York–based nonprofit, launched in 1998, has sent volunteers to an average of one disaster per year, said Dr. Koyfman, also medical director for EmblemHealth Insurance, New York.
“We at DPO learn to caution folks and say, ‘Look, it’s important and it’s critical to do everything you can, but do appreciate one thing: The key is what happens 3 to 6 months from today,’ ” he said. “The mental health component will happen then. This is very different from a typical disaster mentality.”
Before the earthquake in Nepal, manpower and resources were limited: The country has about 80 psychiatrists, or about 1 for every million people, said Dr. Mahato, chief psychiatry resident, PGY-4, at Mount Sinai/Elmhurst Hospital Center, New York. After the earthquake and more than 300 aftershocks, about 2.8 million people were in need of humanitarian assistance. The DPO team partnered with the Psychiatrists’ Association of Nepal by visiting affected districts and participating in health camps. “The challenges we saw involved developing communication and training materials in a culturally appropriate framework,” Dr. Mahato said.
Portable intervention used
One intervention used by DPO teams in Nepal was Psychological First Aid (PFA), Dr. Javier Garcia said.
PFA has grown in popularity and acceptance, especially when it became increasingly clear after the attacks of Sept. 11, 2001, that psychological debriefing was not as universally useful or safe modality as it was once thought to be, said Dr. Garcia of Richmond University Medical Center, New York.
In contrast, PFA is an intervention based on principles of resilience that focuses on safety, calming, connectedness, self-community, efficacy, and hope. “PFA assumes that people can have maladaptive reactions,” Dr. Garcia said. “ But is designed to reduce the initial distress and foster short- and long-term adaptive functioning.” He said all first responders, including fire, police and crisis response teams, health care professionals, and paraprofessionals can be trained to use PFA. In fact, another model of PFA was created for school staff in the 1990s in response to school shootings.
The first goal after a disaster is to ensure physical safety. After that, teams try to protect those traumatized from additional trauma. Emotionally overwhelmed and disoriented survivors must be stabilized, and medications generally are not recommended during this part of the process. Medications might be helpful in cases involving addiction or sleep, but such cases are exceptions, Dr. Garcia said. In general, the same strict clinical criteria for use of psychiatric medications are applicable in postdisaster environments and are specific to the episode and the individual. PFA attempts to be culturally informed and delivered in a flexible manner, Dr. Garcia said. “It’s evidence informed but not evidence based. So, we need more research.”
PFA, along with effective risk communications, frequently are the mainstay of an effective mental health response. Where PFA informs the “what” of the mental health conversation, risk communications, as Dr. Grant H. Brenner pointed out at the meeting, is the key “how” of getting the right message out the right way. Dr. Brenner, DPO board member, is a faculty member of Mount Sinai Hospital, director of the William Alanson White Institute Trauma Service, and an editor of Creating Spiritual and Psychological Resilience: Integrating Care in Disaster Relief Work (New York: Routledge, 2009).
After the Ebola work on the ground, volunteers often found complicated terrain in the United States. As the example of the single New York City Ebola patient showed, medical and psychological preparedness and the ability of the authorities to effectively communicate safety information to the public were tested. DPO worked with a nonprofit group called More Than Me to offer mental health support services to returning volunteers and to the few people who were under quarantine orders in New York.
Each disaster is different, but a few common themes are apparent. “There’s huge value in presence and human touch,” Dr. Koyfman said.
DPO offers training sessions for new volunteers. Psychiatrists interested in volunteering can send a message to info@disasterpsych.org or call 646-867-3514. For more on risk communication, check out the information on emergency preparedness and response provided by the Centers for Disease Control and Prevention. Other useful resources are the American Psychiatric Association’s Committee on Psychiatric Dimensions of Disaster and Resiliency in the Face of Disaster and Terrorism: 10 Things to Do to Survive (Personhood Press, 2005).
ghenderson@frontlinemedcom.com
On Twitter @ginalhenderson
NEW YORK – After the earthquake in Nepal earlier this year, Disaster Psychiatry Outreach sent in volunteers who found preexisting issues that made their mental health response challenging at best, Dr. Ram Suresh Mahato reported at the American Psychiatric Association’s Institute on Psychiatric Services.
Nepal was recovering from armed conflict that lasted from 1996 to 2006 and resulted in what some have called a “postconflict identity crisis” (Int J Educ Dev. 2014;34:42-50). The caste system in the country was abolished in 1963, but social inequality continued to persist. In addition, more than 60 languages are spoken in Nepal, and at least 25% of the population lives below the poverty line, said Dr. Mahato, a Disaster Psychiatry Outreach (DPO) volunteer who was part of the needs-assessment team dispatched to the country in May.
Other complicating factors included high rates of domestic violence. Nepali women are at greater risk of depression, anxiety, and posttraumatic stress than are males (Lancet. 2008 May;371[9625]:1664) and (J Affect Disord. 2007 Sep;102[1-3]:219-25), and a culture of silence prevails, Dr. Mahato said. The literature describes informal social networks in Nepal in which community members share their distress and symptoms, “as well as traditional (shamanistic) healing practices for those suffering mental health complaints in relation to political violence” (Soc Sci Med. 2010 Jan;70[1]:35-44).
Dr. Mahato spoke at a workshop, sponsored by DPO, aimed at urging psychiatrists to be prepared in providing mental health services to disaster survivors across the globe and here at home. “The room was full last year,” said Dr. Sander Koyfman, DPO’s president, referring to the intense interest in Ebola at the height of the outbreak in 2014. “This year, it’s more of a challenge, as interest wanes from disaster to disaster,” but their organization would like to “sustain the desire in mental health providers and disaster responders to learn how to help most effectively,” Dr. Koyfman said in an interview.
The presentation focused on the mental health aspects of the Ebola response and the more recent DPO work following the earthquake in Nepal that killed 10,000 people. In a striking similarity, about 10,900 people died in the wake of the Ebola epidemic in West Africa and its rolling impact across many regions. (In May, the World Health Organization declared Liberia free of Ebola but said on Oct. 14 that a preliminary study published in the New England Journal of Medicine shows that the virus can persist in the semen of some survivors for at least 9 months.)
Vulnerable suffer most
Over the last 10 years, more than 1.4 million people have been injured and about 23 million have been left homeless across the globe because of man-made and natural disasters, according to a 2015 United Nations report. “Overall, more than 1.5 billion people have been affected by disasters in various ways, with women, children, and people in vulnerable situations disproportionately affected,” the report says.
DPO, a New York–based nonprofit, launched in 1998, has sent volunteers to an average of one disaster per year, said Dr. Koyfman, also medical director for EmblemHealth Insurance, New York.
“We at DPO learn to caution folks and say, ‘Look, it’s important and it’s critical to do everything you can, but do appreciate one thing: The key is what happens 3 to 6 months from today,’ ” he said. “The mental health component will happen then. This is very different from a typical disaster mentality.”
Before the earthquake in Nepal, manpower and resources were limited: The country has about 80 psychiatrists, or about 1 for every million people, said Dr. Mahato, chief psychiatry resident, PGY-4, at Mount Sinai/Elmhurst Hospital Center, New York. After the earthquake and more than 300 aftershocks, about 2.8 million people were in need of humanitarian assistance. The DPO team partnered with the Psychiatrists’ Association of Nepal by visiting affected districts and participating in health camps. “The challenges we saw involved developing communication and training materials in a culturally appropriate framework,” Dr. Mahato said.
Portable intervention used
One intervention used by DPO teams in Nepal was Psychological First Aid (PFA), Dr. Javier Garcia said.
PFA has grown in popularity and acceptance, especially when it became increasingly clear after the attacks of Sept. 11, 2001, that psychological debriefing was not as universally useful or safe modality as it was once thought to be, said Dr. Garcia of Richmond University Medical Center, New York.
In contrast, PFA is an intervention based on principles of resilience that focuses on safety, calming, connectedness, self-community, efficacy, and hope. “PFA assumes that people can have maladaptive reactions,” Dr. Garcia said. “ But is designed to reduce the initial distress and foster short- and long-term adaptive functioning.” He said all first responders, including fire, police and crisis response teams, health care professionals, and paraprofessionals can be trained to use PFA. In fact, another model of PFA was created for school staff in the 1990s in response to school shootings.
The first goal after a disaster is to ensure physical safety. After that, teams try to protect those traumatized from additional trauma. Emotionally overwhelmed and disoriented survivors must be stabilized, and medications generally are not recommended during this part of the process. Medications might be helpful in cases involving addiction or sleep, but such cases are exceptions, Dr. Garcia said. In general, the same strict clinical criteria for use of psychiatric medications are applicable in postdisaster environments and are specific to the episode and the individual. PFA attempts to be culturally informed and delivered in a flexible manner, Dr. Garcia said. “It’s evidence informed but not evidence based. So, we need more research.”
PFA, along with effective risk communications, frequently are the mainstay of an effective mental health response. Where PFA informs the “what” of the mental health conversation, risk communications, as Dr. Grant H. Brenner pointed out at the meeting, is the key “how” of getting the right message out the right way. Dr. Brenner, DPO board member, is a faculty member of Mount Sinai Hospital, director of the William Alanson White Institute Trauma Service, and an editor of Creating Spiritual and Psychological Resilience: Integrating Care in Disaster Relief Work (New York: Routledge, 2009).
After the Ebola work on the ground, volunteers often found complicated terrain in the United States. As the example of the single New York City Ebola patient showed, medical and psychological preparedness and the ability of the authorities to effectively communicate safety information to the public were tested. DPO worked with a nonprofit group called More Than Me to offer mental health support services to returning volunteers and to the few people who were under quarantine orders in New York.
Each disaster is different, but a few common themes are apparent. “There’s huge value in presence and human touch,” Dr. Koyfman said.
DPO offers training sessions for new volunteers. Psychiatrists interested in volunteering can send a message to info@disasterpsych.org or call 646-867-3514. For more on risk communication, check out the information on emergency preparedness and response provided by the Centers for Disease Control and Prevention. Other useful resources are the American Psychiatric Association’s Committee on Psychiatric Dimensions of Disaster and Resiliency in the Face of Disaster and Terrorism: 10 Things to Do to Survive (Personhood Press, 2005).
ghenderson@frontlinemedcom.com
On Twitter @ginalhenderson
EXPERT ANALYSIS AT THE INSTITUTE ON PSYCHIATRIC SERVICES

Yoga-Based Classes for Veterans With Severe Mental Illness: Development, Dissemination, and Assessment
There is growing interest in developing a holistic and integrative approach for the treatment of severe mental illnesses (SMI), such as schizophrenia, major depression, posttraumatic stress disorder (PTSD), and anxiety disorders. Western medicine has traditionally focused on the direct treatment of symptoms and separated the management of physical and mental health, but increasing attention is being given to complementary and alternative medicine (CAM) for patients with SMI.
Recognizing the connectedness of the mind and body, these complementary or alternative approaches incorporate nontraditional therapeutic techniques with mainstream treatment methods, including psychopharmacology and psychotherapy.1 Patients with SMI may particularly benefit from a mind-body therapeutic approach, because they often experience psychological symptoms such as stress, anxiety, depression and psychosis, as well as a preponderance of medical comorbidities, including obesity, diabetes mellitus, and cardiovascular disease, some of which are compounded by adverse effects (AEs) of essential pharmacologic treatments.2-4 Mind-body interventions might also be particularly advantageous for veterans, who often experience a range of interconnected physical and psychological difficulties due to trauma exposure and challenges transitioning from military to civilian life.5
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
In 2002, the White House Commission on Complementary and Alternative Medicine Policy issued a report supporting CAM research and integration into existing medical systems.6 The DoD later established Total Force Fitness, a holistic health care program for active-duty military personnel.7 The VA has also incorporated mind-body and holistic strategies into veteran care.8 One such mind-body intervention, yoga, is becoming increasingly popular within the health care field.
Recent research has documented the effectiveness of yoga, underscoring its utility as a mind-body therapeutic approach. Yoga is associated with improvement in balance and flexibility,9 fatigue,10 blood pressure,11 sleep,12 strength,13 and pain14 in both healthy individuals and patients with medical and psychiatric disorders.15 The literature also illustrates that yoga has led to significant improvements in stress and psychiatric symptoms in individuals with PTSD, schizophrenia, depression, and anxiety.16-22 A previous meta-analysis conducted by the authors, which considered studies of the effectiveness of yoga as an adjunctive treatment for patients with mental illness, found that 212 studies with null results would need to be located and incorporated to negate the positive effects of yoga found in the literature.17
Because yoga emphasizes the practice of mindfulness and timing movement with breath awareness, it is a calming practice that may decrease stress and relieve psychiatric symptoms not treated through psychopharmacology and psychotherapy.17,21 Recent research has postulated that the physiological mechanisms by which this occurs may include (a) reduction in sympathetic and increase in parasympathetic activity23,24; (b) increases in heart-rate variability and respiratory sinus arrhythmia, low levels of which are associated with anxiety, panic disorder, and depression23,24; (c) increases in melatonin and serotonin 25-27; and (d) decrease in cortisol.28,29
Related: Enhancing Patient Satisfaction Through the Use of Complementary Therapies
As yoga may calm the autonomic nervous system and reduce stress, it may benefit patients with SMI, whose symptoms are often aggravated by stress.30 In addition, veterans experience both acute stressors and high levels of chronic stress.5 Therefore, because they experience mind-body comorbid illnesses as well as high levels of stress, the authors believe that veterans with SMI could benefit greatly from a tailored yoga-based program as part of a holistic approach that includes necessary medication and evidence-based therapies.
In order to evaluate the effects of a yoga program on veterans receiving mental health treatment across the VA Greater Los Angeles Healthcare System (VAGLAHS), the authors developed a set of yoga-based wellness classes called Breathing, Stretching, Relaxation (BSR) classes. This article describes the process of developing these classes and outlines the procedures and results of a study to assess their effects.
BSR Classes
The development of BSR classes took place at the West Los Angeles VA Medical Center (WLAVAMC), within the Psychosocial Rehabilitation and Recovery Center (PRRC) program. The PRRC is a psychoeducational program that focuses on the biological, psychological, social, and spiritual aspects of life in order to help veterans with SMI rehabilitate and reintegrate into the community. The program allows veterans to create their own recovery curriculum by selecting from diverse classes led by program staff members, including physicians, psychologists, nurses, social workers, nutritionists, and recreational therapists.
Development of BSR Protocols
The primary goal of this project was to develop a yoga-based program tailored to the specific needs of veterans with SMI. To the authors’ knowledge, BSR is the first yoga-based program customized for SMI. The BSR classes were developed within interdisciplinary focus groups that included professional yoga teachers, the director of the PRRC, psychiatrists, psychologists, nurses, occupational therapists, and physical therapists. Drawing on their experience with SMI and yoga, members of the focus groups identified 3 aspects of yoga that would be most beneficial to veterans with SMI, and the program was designed to optimize these effects. Because SMI can both create and be exacerbated by stress, BSR classes were designed to reduce stress and provide veterans with the tools to monitor and manage their stress.
Breathing and meditative techniques were adapted from yoga in order to facilitate stress reduction. In addition, aerobic elements of yoga have the potential to help veterans manage their incidence of medical diseases, such as cardiovascular disease, obesity, and diabetes. Patients with SMI are at a greater risk for developing these diseases, so classes were designed to incorporate physical stretching elements to promote overall health.4,31-33 Finally BSR was designed to improve veteran self- efficacy and self-esteem, and to place veterans at the center of their care by equipping them with skills to practice BSR independently.
Related: Mindfulness to Reduce Stress
The focus groups also identified the logistic requirements when implementing a yoga-based program for veterans with SMI, including (a) obtaining participant or conservator consent; (b) obtaining medical clearance from care providers, given the high prevalence of medical comorbidities; (c) removing the traditional yoga terms, taking a secular approach, and naming the class “Breathing, Stretching, Relaxation” without directly referencing yoga; (d) asking veterans’ permission before incorporating physical contact into demonstrations, because veterans with SMI, especially those with PTSD, might be uncomfortable with touching from instructors; (e) creating protocols of varying duration and intensity so that BSR was approachable for veterans with diverse levels of physical ability; and (f) ensuring that a clinician who regularly works with SMI patients be present to supervise classes for the safety of patients and instructors.
Yoga instructors and clinicians collaborated to create adaptable 30- and 50-minute protocols that reflected best practices for an SMI population. The 30-minute seated BSR class protocol is included in eAppendix A. Once protocols were finalized, a Train the Trainer program was established to facilitate dissemination of BSR to clinicians working with veterans with SMI throughout the VAGLAHS.
Interested clinicians were given protocols and trained to lead BSR classes on their own. Subsequently, clinician-led BSR classes of various lengths (depending on clinician preference and program scheduling) were established at PRRCs and other mental health programs, such as Mental Health Recovery and Intensive Treatment and Dual Diagnosis Treatment Program, throughout the VAGLAHS. These programs were selected, because they are centered on recovery and improvements in symptoms of SMI. The adoption of a Train the Trainer model, through which VA clinicians were trained by professional yoga instructors, allowed for seamless integration of BSR into VA usual care for veterans with SMI.
Assessment of Classes
The authors conducted a study to assess the quality and effectiveness of BSR classes. This survey research was approved by the VAGLAHS institutional review board for human subjects. The authors hypothesized that there would be significant improvements in veterans’ stress, pain, well-being, and perception of the benefits of BSR over 8 weeks of participation in classes. Also hypothesized was that there would be greater benefits in veterans who participated in longer classes and who attended classes more frequently.
Methods
A total of 120 veterans completed surveys after participating in clinician- and yoga instructor-led BSR classes at the 3 sites within the VAGLAHS: WLAVAMC, Los Angeles Ambulatory Care Center (LAACC), and Sepulveda Ambulatory Care Center (SACC). At the WLAVAMC, surveys were collected at 10-, 30-, 60-, and 90-minute classes. At LAACC, surveys were collected at 30- and 60-minute classes. At SACC, surveys were collected at 20- and 45-minute classes. A researcher noted the duration of the class and was available to assist with comprehension. Veterans completed identical surveys after classes at a designated week 0 (baseline), week 4, and week 8. Of the 120 patients with an initial survey, 82 completed at least 1 follow-up survey and 49 completed both follow-up surveys.
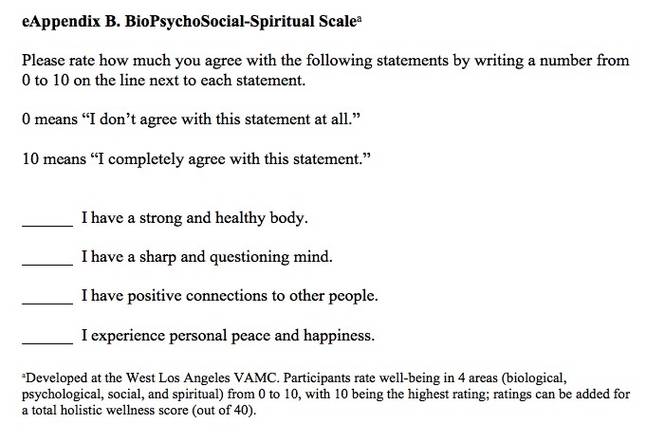
Survey packets included (a) demographic questions, including age, gender, and ethnicity; (b) class participation questions, including frequency of class attendance, patients’ favorite aspect of class, and dura tion of class attendance (in months of prior participation); (c) a pain rating from 0 (no pain) to 10 (the worst pain imaginable); (d) the BioPsychoSocial-Spiritual (BPSS) Scale (eAppendix B), developed at the WLAVAMC, which provides wellness scores from 0 (low) to 10 (high) in 4 areas as well as a holistic wellness score from 0 (low) to 40 (high); (e) the Perceived Stress Scale (PSS), developed by Cohen and colleagues, which generates a stress score for the past month from 0 (low) to 40 (high)34; and (f) the Perceived Benefits of Yoga Questionnaire (PBYQ) (eAppendix C), which rates participants’ opinions about the benefits of yoga from 12 (low) to 60 (high) and is based on the Perceived Benefits of Dance Questionnaire.35
Statistical Analysis
Pearson’s r correlation coefficients were calculated between PBYQ scores and quantitative survey items at each time point (weeks 0, 4, and 8). Linear mixed-effects models were used to test for effects of multiple predictor variables on individual outcomes. Each model had a random intercept by participant, and regressors included main effects for the following: survey week (0, 4, or 8), class duration (in minutes), age, sex, ethnicity, frequency of attendance (in days per week), and duration of attendance (in months). For all statistical analyses, a 2-tailed significance criterion of α = .05 was used.
Results
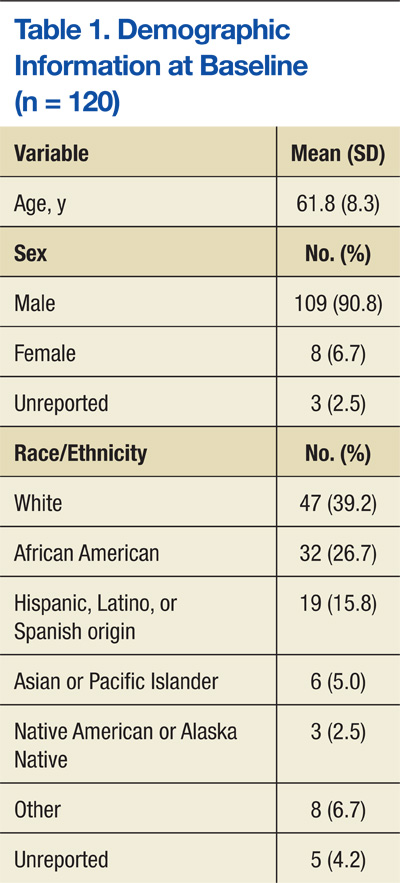
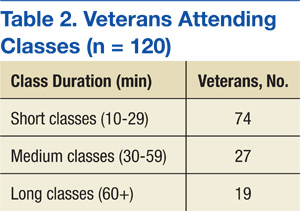
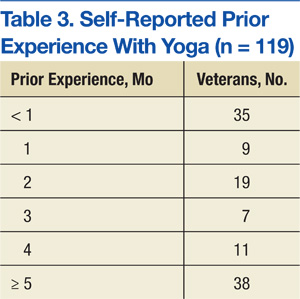
Veterans who completed surveys were predominantly male (90.8%) and averaged 61.4 years of age. Table 1 shows demographic information. Table 2 displays the number of participants who were involved in short (< 30 min), medium (30-59 min), and long (> 60 min) classes. Veteran participants also had a wide range of prior BSR experience (Table 3).
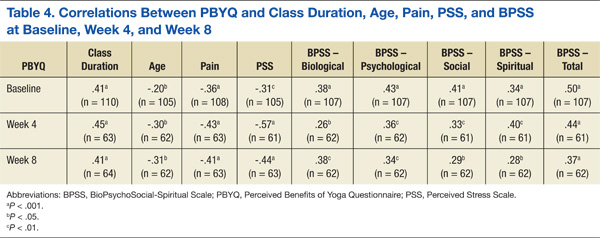
At all time points, PBYQ scores were significantly positively correlated with class duration and biological, psychological, social, spiritual, and total well-being as measured by the BPSS. The PBYQ scores at all time points were also significantly negatively correlated with age, pain ratings, and PSS scores. Table 4 includes specific Pearson’s r values.
Survey week was not significantly associated with any individual outcome measures. There were no significant regressors for total PSS score or total BPSS score within the linear models. However, participants’ PBYQ scores were significantly associated with age (t(98) = -2.13, P = .036), frequency of attendance (t(103) = 2.10, P = .038), and class duration (t(98) = 4.35, P < .001). Additionally, class duration was significantly associated with pain (t(98) = -3.01, P = .003), with longer duration associated with less pain. Ethnicity was also associated with pain, with African American veterans reporting less pain than did white (t(98) = -2.41, P = .017) and Hispanic (t(98) = -2.31, P = .023) veterans. Because ethnicity was significantly associated with class duration (F(5,339) = 3.81, P = .002), the authors used an analysis of covariance to test for a mediating effect of ethnicity on the relationship between class duration and pain. Although there was a partial mediation (F(5,203) = 2.57, P = .028), the main effect of class duration remained significant.
Discussion and Limitations
The goals of this project were to develop a yoga-based program tailored for veterans with SMI and assess the program in a sample of veterans with SMI on subjective reports of stress, pain, well-being, and benefits of yoga. The authors hypothesized that significant improvements in these measures in veterans with SMI would be observed over 8 weeks of participation in BSR classes and that there would be greater benefits in veterans who participated in longer classes and who attended classes more frequently.
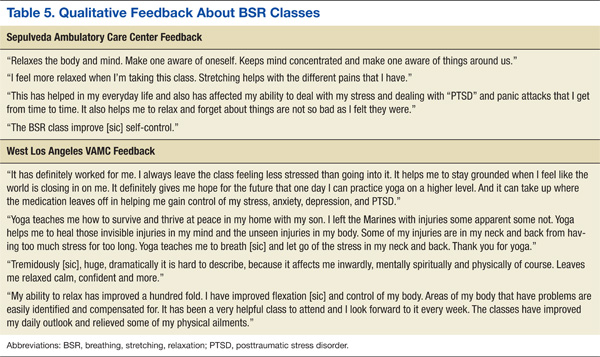
The authors succeeded in developing an adaptable yoga-based wellness program for veterans with SMI that can be both practiced in structured classes and incorporated into veterans’ everyday routines. The BSR classes were well tolerated by veterans with SMI, caused no discernible AEs, and are readily available for dissemination across other mental health programs. Veterans described integrating the tools they learned within BSR classes into their daily lives, helping them to manage pain; feel more flexible; reduce stress, anxiety, depression, and PTSD symptoms; and increase relaxation and feelings of self-control and confidence. Table 5 shows qualitative feedback collected from veterans. In addition, the Train the Trainer model optimized clinical applicability and flexibility, demonstrating that clinicians can seamlessly integrate BSR classes into a health care plan for veterans with SMI.
In assessing quantitative measures of stress, pain, well-being, and perceived benefits of a yoga-based program, veterans who reported BSR classes as beneficial experienced lower levels of pain and stress and higher levels of biological, psychological, social, spiritual, and overall well-being. Those veterans who perceived BSR as more beneficial tended to be younger and attend longer classes with greater frequency. Veterans who attended longer classes also reported experiencing less pain. This may be because the more rigorous stretching and posing involved in longer BSR classes made them more effective at reducing pain; however, it is also possible that veterans who were experiencing more pain avoided these longer classes due to their rigor and length.
Results suggest that longer classes attended with greater regularity may be more beneficial to veterans than short and infrequent classes, particularly in regards to their pain. Despite the relationships between class and outcome variables, the authors did not find significant improvements in measures of wellness, pain, stress, or perceived benefits of BSR over time, as was hypothesized. This may be because the data collection for this study began after classes had been established for some time. In fact, only 35 of 120 veterans included in this study reported having < 1 month of BSR experience at week 0, suggesting that results collected from week 0 did not represent a true baseline measurement. Although no relationship was found between prior duration of attendance and any outcome measures, the fact that most veterans in the sample had attended classes for several months prior to completing surveys may have biased the results by favoring the responses of veterans who were more invested in the classes. Improvements may have been better captured in a BSR-naïve sample.
The finding that the PBYQ score was significantly correlated with all other outcome measures (pain, BPSS score, and PSS score) raises some questions about the ways in which these classes were beneficial to veterans. It may be that veterans who experienced more positive outcomes from classes saw BSR as more beneficial, but it is also possible that veterans who entered classes with greater expectations experienced better outcomes due to a placebo effect—that is, outcomes may have been influenced more by the expectation than by the content of the classes. In the case of well-being (BPSS scores) and stress (PSS score), this could explain why these outcomes were significantly correlated with perceived benefits of BSR but were not significantly related to any class-related variables such as duration and frequency of attendance. Pain ratings, however, were related to class variables and perceived benefits of BSR.
In a post hoc analysis, the main effect of the PBYQ score as a regressor was added to the linear model for pain, resulting in the PBYQ score having a significant main effect (t(100) = -2.98, P = .004). The main effect of class duration remained significant (t(97) = -1.99, P = .050) but was less substantial when the PBYQ score was added, suggesting some correlation between class duration and pain, independent of BSR’s perceived benefits. Future research should consider the possible mediating effect of perceptions of the effectiveness of a yoga-based program a priori or control for placebo effects in order to address the degree to which outcomes are influenced by participant expectations.
This study had a few other notable limitations. Because it was an observational study administered within a clinical mental health program, a control group was not included. Measurement began after BSR classes were established, so veterans had varying levels of prior experience. Specific SMI and medical diagnosis information was not collected from individual veterans. Data were collected from classes of varying length and intensity. The BSR classes often took place within larger programs at the VA, which offered comprehensive care, so some effects of the BSR classes might have been confounded with concurrent evidenced-based treatments or other holistic care programs. Due to these limitations, particularly the absence of a control group, the relationships between BSR participation and health outcomes cannot be assumed to be causal, because a multitude of other variables, such as patient contact and expectancy effects, may have influenced outcomes.
Future Directions
Future research should aim to utilize a control group and collect data from classes of the same intensity and length to better examine whether BSR can be causally linked with improvements in measures of stress, pain, and well-being and to attempt to control for expectancy and contact effects. In addition, future research should aim to recruit a BSR-naïve sample to account for prior experience. Future studies should also aim to parse out whether BSR is differentially effective for each SMI or medical diagnosis, whether there is a relationship between class time and outcomes (as these results suggest that longer class times might be more beneficial for pain), and whether any pain-management benefits from BSR influence other measures of functionality and well-being. Finally, future research can further divide BSR into its active components, such as meditative breathing and aerobic stretching, in order to examine which aspect leads to the greatest effect on each measure; the current results imply that the more rigorous components of BSR classes have the greatest effects on pain.
Conclusion
A yoga-based class affects the mind and body, making it particularly useful for veterans with SMI who experience a range of physical and psychological symptoms and comorbidities.4 Other studies have demonstrated that when practiced alone, yoga leads to improvements in both physical and psychological symptoms.15,17 Looking forward, yoga-based classes may be implemented as part of a larger biopsychosocial-spiritual care plan that is being embraced both within and outside of the VA.7,8,36,37 This integrative health care model suggests that psychosocial and CAM modalities are additive and should be practiced concurrently.37
Although little research has assessed the effects of comprehensive psychosocial and CAM treatment programs, initial research indicates that these programs are associated with reductions in symptoms of medical and mental illness.37-40 Participants in BSR classes may derive further benefits if classes are incorporated into a larger holistic health care plan that includes both traditional psychiatric treatment modalities and CAM therapies that integrate biopsychosocial-spiritual components.
Acknowledgements
The authors would like to thank Nancy Mohler, Anne Platt, and Matthew Crowder, all professional yoga instructors, for their integral role in developing classes, providing classes to veterans, and assisting VA staff with training. The authors also acknowledge Rosie Dominguez, LCSW, for expertly leading BSR classes at LAACC. The authors also thank Irina Arnold, MS, MD, and Vanessa Streiff, MA, for their vital assistance with data collection at SACC.
Funding for the development of BSR protocols, quality improvement research, and expenses associated with classes was provided by the Disabled American Veterans Charitable Service Trust. Support for dissemination of classes to multiple VA programs was provided by a grant from the VA Center of Innovation for Patient Centered Care, headed by Sandra Robertson, RN, MSN, PH-CNS.
The authors are very grateful to the veterans and staff of the Mental Health Intensive Case Management, Psychosocial Rehabilitation and Recovery Centers, Mental Health Clinics, and Domiciliary throughout Greater Los Angeles for their support of the BSR classes.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.


1. National Center for Complementary and Integrative Health. Complementary, alternative, or integrative health: what's in a name? U.S. Department of Health and Human Services, National Institutes of Health Website. http://nccam.nih.gov/health/whatiscam. Updated March 2015. Accessed August 27, 2015.
2. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):617-627.
3. Fleischhacker WW, Cetkovich-Bakmas M, De Hert M, et al. Comorbid somatic illnesses in patients with severe mental disorders: clinical, policy, and research challenges. J Clin Psychiatry. 2008;69(4):514-519.
4. Wirshing DA, Boyd JA, Meng LR, Ballon JS, Marder SR, Wirshing WC. The effects of novel antipsychotics on glucose and lipid levels. J Clin Psychiatry. 2002;63(10):856-865.
5. Tanielian T, Jaycox LH, eds. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND Corporation; 2008.
6. White House Commission on Complementary and Alternative Medicine Policy. Final Report. Washington, DC: White House Commission on Complementary and Alternative Medicine Policy; 2002.
7. Land BC. Current Department of Defense guidance for total force fitness. Mil Med. 2010;175(suppl 8):3-5.
8. U.S. Department of Veterans Affairs, Veterans Health Administration. Pain Management. VHA Directive 2009-053. Washington, DC: U.S. Department of Veterans Affairs, Veterans Health Administration; 2009.
9. Oken BS, Zajdel D, Kishiyama S, et al. Randomized, controlled, six-month trial of yoga in healthy seniors: effects on cognition and quality of life. Altern Ther Health Med. 2006;12(1):40-47.
10. Bower JE, Garet D, Sternlieb B, et al. Yoga for persistent fatigue in breast cancer survivors: a randomized controlled trial. Cancer. 2012;118(15):3766-3775.
11. Cade WT, Reeds DN, Mondy KE, et al. Yoga lifestyle intervention reduces blood pressure in HIV-infected adults with cardiovascular disease risk factors. HIV Med. 2010;11(6):379-388.
12. Innes KE, Selfe TK. The effects of a gentle yoga program on sleep, mood, and blood pressure in older women with restless leg syndrome (RLS): a preliminary randomized controlled trial. Evid Based Complement Alternat Med. 2012;2012:294058.
13. Van Puymbroeck M, Payne LL, Hsieh PC. A phase I feasibility study of yoga on the physical health and coping of informal caregivers. Evid Based Complement Alternat Med. 2007;4(4):519-529.
14. Rani K, Tiwari SC, Singh U, Agrawal GG, Srivastava N. Six-month trial of Yoga Nidra in menstrual disorder patients: effects on somatoform symptoms. Ind Psychiatry J. 2011;20(2):97-102.
15. Ross A, Thomas S. The health benefits of yoga and exercise: a review of comparison studies. J Altern Complement Med. 2010;16(1):3-12.
16. Banerjee B, Vadiraj HS, Ram A, et al. Effects of an integrated yoga program in modulating psychological stress and radiation-induced genotoxic stress in breast cancer patients undergoing radiotherapy. Integr Cancer Ther. 2007;6(3):242-250.
17. Cabral P, Meyer HB, Ames D. Effectiveness of yoga therapy as a complementary treatment for major psychiatric disorders: a meta-analysis. Prim Care Companion CNS Disord. 2011;13(4):doi:10.4088/PCC.10r01068.
18. Katzman MA, Vermani M, Gerbarg PL, et al. A multicomponent yoga-based, breath intervention program as an adjunctive treatment in patients suffering from generalized anxiety disorder with or without comorbidities. Int J Yoga. 2012;5(1):57-65.
19. Köhn M, Persson Lundholm U, Bryngelsson IL, Anderzén-Carlsson A, Westerdahl E. Medical yoga for patients with stress-related symptoms and diagnoses in primary health care: a randomized controlled trial. Evid Based Complement Alternat Med. 2013;2013:215348.
20. Krishnamurthy MN, Telles S. Assessing depression following two ancient Indian interventions: effects of yoga and ayurveda on older adults in a residential home. J Gerontol Nurs. 2007;33(2):17-23.
21. Meyer HB, Katsman A, Sones AC, Auerbach DE, Ames D, Rubin RT. Yoga as an ancillary treatment for neurological and psychiatric disorders: a review. J Neuropsychiatry Clin Neurosci. 2012;24(2):152-164.
22. Visceglia E, Lewis S. Yoga therapy as an adjunctive treatment for schizophrenia: a randomized, controlled pilot study. J Altern Complement Med. 2011;17(7):601-607.
23. Brown RP, Gerbarg PL. Sudarshan Kriya yogic breathing in the treatment of stress, anxiety, and depression, part I-neurophysiologic model. J Altern Complement Med. 2005;11(1):189-201.
24. Brown RP, Gerbarg PL. Yoga breathing, meditation, and longevity. Ann N Y Acad Sci. 2009;1172:54-62.
25. Harinath K, Malhotra AS, Pal K, et al. Effects of hatha yoga and Omkar meditation on cardiorespiratory performance, psychologic profile, and melatonin secretion. J Altern Complement Med. 2004;10(2):261-268.
26. Tooley GA, Armstrong SM, Norman TR, Sali A. Acute increases in night-time plasma melatonin levels following a period of meditation. Biol Psychol. 2000;53(1):69-78.
27. Walton KG, Pugh ND, Gelderloos P, Macrae P. Stress reduction and preventing hypertension: preliminary support of a psychoneuroendocrine mechanism. J Altern Complement Med. 1995;1(3):263-283.
28. Banasik J, Williams H, Haberman M, Blank SE, Bendel R. Effect of Iyengar yoga practice on fatigue and diurnal salivary cortisol concentration in breast cancer survivors. J Am Acad Nurse Pract. 2011;23(3):135-142.
29. Vadiraja HS, Raghavendra RM, Nagarathna R, et al. Effects of a yoga program on cortisol rhythm and mood states in early breast cancer patients undergoing adjuvant radiotherapy: a randomized controlled trial. Integr Cancer Ther. 2009;8(1):37-46.
30. Esch T, Stefano GB, Fricchione GL, Benson H. The role of stress in neurodegenerative diseases and mental disorders. Neuro Endocrinol Lett. 2002;23(3):199-208.
31. Lingjaerde O, Ahlfors UG, Bech P, Dencker SJ, Elgen K. The UKU side effect rating scale. A new comprehensive rating scale for psychotropic drugs and a cross-sectional study of side effects in neuroleptic-treated patients. Acta Psychiatr Scand Suppl. 1987;334:1-100.
32. Schwartz TL, Nihalani N, Jindal S, Virk S, Jones N. Psychiatric medication-induced obesity: a review. Obes Rev. 2004;5(2):115-121.
33. Wirshing DA, Spellberg BJ, Erhart SM, Marder SR, Wirshing WC. Novel antipsychotics and new onset diabetes. Biol Psychiatry. 1998;44(8):778-783.
34. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385-396.
35. Quiroga Murcia C, Kreutz G, Clift S, Bongard S. Shall we dance? An exploration of the perceived benefits of dancing on well-being. Arts Health. 2010;2(2):149-163.
36. The Duke Center for Integrative Medicine; Liebowitz R, Smith L. The Duke Encyclopedia of New Medicine: Conventional and Alternative Medicine for All Ages. London, UK: Rodale Books International; 2006.
37. Walsh R. Lifestyle and mental health. Am Psychol. 2011;66(7):579-592.
38. Frattaroli J, Weidner G, Dnistrian AM, et al. Clinical events in prostate cancer lifestyle trial: results from two years of follow-up. Urology. 2008;72(6):1319-1323.
39. Khaw KT, Wareham N, Bingham S, Welch A, Luben R, Day N. Combined impact of health behaviours and mortality in men and women: the EPIC-Norfolk prospective population study. PLoS Med. 2008;5(1):e12.
40. Sidhu KS, Vandana P, Balon R. Exercise prescription: a practical, effective therapy for depression. Curr Psychiatr. 2009;8(6):38-51.
There is growing interest in developing a holistic and integrative approach for the treatment of severe mental illnesses (SMI), such as schizophrenia, major depression, posttraumatic stress disorder (PTSD), and anxiety disorders. Western medicine has traditionally focused on the direct treatment of symptoms and separated the management of physical and mental health, but increasing attention is being given to complementary and alternative medicine (CAM) for patients with SMI.
Recognizing the connectedness of the mind and body, these complementary or alternative approaches incorporate nontraditional therapeutic techniques with mainstream treatment methods, including psychopharmacology and psychotherapy.1 Patients with SMI may particularly benefit from a mind-body therapeutic approach, because they often experience psychological symptoms such as stress, anxiety, depression and psychosis, as well as a preponderance of medical comorbidities, including obesity, diabetes mellitus, and cardiovascular disease, some of which are compounded by adverse effects (AEs) of essential pharmacologic treatments.2-4 Mind-body interventions might also be particularly advantageous for veterans, who often experience a range of interconnected physical and psychological difficulties due to trauma exposure and challenges transitioning from military to civilian life.5
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
In 2002, the White House Commission on Complementary and Alternative Medicine Policy issued a report supporting CAM research and integration into existing medical systems.6 The DoD later established Total Force Fitness, a holistic health care program for active-duty military personnel.7 The VA has also incorporated mind-body and holistic strategies into veteran care.8 One such mind-body intervention, yoga, is becoming increasingly popular within the health care field.
Recent research has documented the effectiveness of yoga, underscoring its utility as a mind-body therapeutic approach. Yoga is associated with improvement in balance and flexibility,9 fatigue,10 blood pressure,11 sleep,12 strength,13 and pain14 in both healthy individuals and patients with medical and psychiatric disorders.15 The literature also illustrates that yoga has led to significant improvements in stress and psychiatric symptoms in individuals with PTSD, schizophrenia, depression, and anxiety.16-22 A previous meta-analysis conducted by the authors, which considered studies of the effectiveness of yoga as an adjunctive treatment for patients with mental illness, found that 212 studies with null results would need to be located and incorporated to negate the positive effects of yoga found in the literature.17
Because yoga emphasizes the practice of mindfulness and timing movement with breath awareness, it is a calming practice that may decrease stress and relieve psychiatric symptoms not treated through psychopharmacology and psychotherapy.17,21 Recent research has postulated that the physiological mechanisms by which this occurs may include (a) reduction in sympathetic and increase in parasympathetic activity23,24; (b) increases in heart-rate variability and respiratory sinus arrhythmia, low levels of which are associated with anxiety, panic disorder, and depression23,24; (c) increases in melatonin and serotonin 25-27; and (d) decrease in cortisol.28,29
Related: Enhancing Patient Satisfaction Through the Use of Complementary Therapies
As yoga may calm the autonomic nervous system and reduce stress, it may benefit patients with SMI, whose symptoms are often aggravated by stress.30 In addition, veterans experience both acute stressors and high levels of chronic stress.5 Therefore, because they experience mind-body comorbid illnesses as well as high levels of stress, the authors believe that veterans with SMI could benefit greatly from a tailored yoga-based program as part of a holistic approach that includes necessary medication and evidence-based therapies.
In order to evaluate the effects of a yoga program on veterans receiving mental health treatment across the VA Greater Los Angeles Healthcare System (VAGLAHS), the authors developed a set of yoga-based wellness classes called Breathing, Stretching, Relaxation (BSR) classes. This article describes the process of developing these classes and outlines the procedures and results of a study to assess their effects.
BSR Classes
The development of BSR classes took place at the West Los Angeles VA Medical Center (WLAVAMC), within the Psychosocial Rehabilitation and Recovery Center (PRRC) program. The PRRC is a psychoeducational program that focuses on the biological, psychological, social, and spiritual aspects of life in order to help veterans with SMI rehabilitate and reintegrate into the community. The program allows veterans to create their own recovery curriculum by selecting from diverse classes led by program staff members, including physicians, psychologists, nurses, social workers, nutritionists, and recreational therapists.
Development of BSR Protocols
The primary goal of this project was to develop a yoga-based program tailored to the specific needs of veterans with SMI. To the authors’ knowledge, BSR is the first yoga-based program customized for SMI. The BSR classes were developed within interdisciplinary focus groups that included professional yoga teachers, the director of the PRRC, psychiatrists, psychologists, nurses, occupational therapists, and physical therapists. Drawing on their experience with SMI and yoga, members of the focus groups identified 3 aspects of yoga that would be most beneficial to veterans with SMI, and the program was designed to optimize these effects. Because SMI can both create and be exacerbated by stress, BSR classes were designed to reduce stress and provide veterans with the tools to monitor and manage their stress.
Breathing and meditative techniques were adapted from yoga in order to facilitate stress reduction. In addition, aerobic elements of yoga have the potential to help veterans manage their incidence of medical diseases, such as cardiovascular disease, obesity, and diabetes. Patients with SMI are at a greater risk for developing these diseases, so classes were designed to incorporate physical stretching elements to promote overall health.4,31-33 Finally BSR was designed to improve veteran self- efficacy and self-esteem, and to place veterans at the center of their care by equipping them with skills to practice BSR independently.
Related: Mindfulness to Reduce Stress
The focus groups also identified the logistic requirements when implementing a yoga-based program for veterans with SMI, including (a) obtaining participant or conservator consent; (b) obtaining medical clearance from care providers, given the high prevalence of medical comorbidities; (c) removing the traditional yoga terms, taking a secular approach, and naming the class “Breathing, Stretching, Relaxation” without directly referencing yoga; (d) asking veterans’ permission before incorporating physical contact into demonstrations, because veterans with SMI, especially those with PTSD, might be uncomfortable with touching from instructors; (e) creating protocols of varying duration and intensity so that BSR was approachable for veterans with diverse levels of physical ability; and (f) ensuring that a clinician who regularly works with SMI patients be present to supervise classes for the safety of patients and instructors.
Yoga instructors and clinicians collaborated to create adaptable 30- and 50-minute protocols that reflected best practices for an SMI population. The 30-minute seated BSR class protocol is included in eAppendix A. Once protocols were finalized, a Train the Trainer program was established to facilitate dissemination of BSR to clinicians working with veterans with SMI throughout the VAGLAHS.
Interested clinicians were given protocols and trained to lead BSR classes on their own. Subsequently, clinician-led BSR classes of various lengths (depending on clinician preference and program scheduling) were established at PRRCs and other mental health programs, such as Mental Health Recovery and Intensive Treatment and Dual Diagnosis Treatment Program, throughout the VAGLAHS. These programs were selected, because they are centered on recovery and improvements in symptoms of SMI. The adoption of a Train the Trainer model, through which VA clinicians were trained by professional yoga instructors, allowed for seamless integration of BSR into VA usual care for veterans with SMI.
Assessment of Classes
The authors conducted a study to assess the quality and effectiveness of BSR classes. This survey research was approved by the VAGLAHS institutional review board for human subjects. The authors hypothesized that there would be significant improvements in veterans’ stress, pain, well-being, and perception of the benefits of BSR over 8 weeks of participation in classes. Also hypothesized was that there would be greater benefits in veterans who participated in longer classes and who attended classes more frequently.
Methods
A total of 120 veterans completed surveys after participating in clinician- and yoga instructor-led BSR classes at the 3 sites within the VAGLAHS: WLAVAMC, Los Angeles Ambulatory Care Center (LAACC), and Sepulveda Ambulatory Care Center (SACC). At the WLAVAMC, surveys were collected at 10-, 30-, 60-, and 90-minute classes. At LAACC, surveys were collected at 30- and 60-minute classes. At SACC, surveys were collected at 20- and 45-minute classes. A researcher noted the duration of the class and was available to assist with comprehension. Veterans completed identical surveys after classes at a designated week 0 (baseline), week 4, and week 8. Of the 120 patients with an initial survey, 82 completed at least 1 follow-up survey and 49 completed both follow-up surveys.
Survey packets included (a) demographic questions, including age, gender, and ethnicity; (b) class participation questions, including frequency of class attendance, patients’ favorite aspect of class, and dura tion of class attendance (in months of prior participation); (c) a pain rating from 0 (no pain) to 10 (the worst pain imaginable); (d) the BioPsychoSocial-Spiritual (BPSS) Scale (eAppendix B), developed at the WLAVAMC, which provides wellness scores from 0 (low) to 10 (high) in 4 areas as well as a holistic wellness score from 0 (low) to 40 (high); (e) the Perceived Stress Scale (PSS), developed by Cohen and colleagues, which generates a stress score for the past month from 0 (low) to 40 (high)34; and (f) the Perceived Benefits of Yoga Questionnaire (PBYQ) (eAppendix C), which rates participants’ opinions about the benefits of yoga from 12 (low) to 60 (high) and is based on the Perceived Benefits of Dance Questionnaire.35
Statistical Analysis
Pearson’s r correlation coefficients were calculated between PBYQ scores and quantitative survey items at each time point (weeks 0, 4, and 8). Linear mixed-effects models were used to test for effects of multiple predictor variables on individual outcomes. Each model had a random intercept by participant, and regressors included main effects for the following: survey week (0, 4, or 8), class duration (in minutes), age, sex, ethnicity, frequency of attendance (in days per week), and duration of attendance (in months). For all statistical analyses, a 2-tailed significance criterion of α = .05 was used.
Results
Veterans who completed surveys were predominantly male (90.8%) and averaged 61.4 years of age. Table 1 shows demographic information. Table 2 displays the number of participants who were involved in short (< 30 min), medium (30-59 min), and long (> 60 min) classes. Veteran participants also had a wide range of prior BSR experience (Table 3).
At all time points, PBYQ scores were significantly positively correlated with class duration and biological, psychological, social, spiritual, and total well-being as measured by the BPSS. The PBYQ scores at all time points were also significantly negatively correlated with age, pain ratings, and PSS scores. Table 4 includes specific Pearson’s r values.
Survey week was not significantly associated with any individual outcome measures. There were no significant regressors for total PSS score or total BPSS score within the linear models. However, participants’ PBYQ scores were significantly associated with age (t(98) = -2.13, P = .036), frequency of attendance (t(103) = 2.10, P = .038), and class duration (t(98) = 4.35, P < .001). Additionally, class duration was significantly associated with pain (t(98) = -3.01, P = .003), with longer duration associated with less pain. Ethnicity was also associated with pain, with African American veterans reporting less pain than did white (t(98) = -2.41, P = .017) and Hispanic (t(98) = -2.31, P = .023) veterans. Because ethnicity was significantly associated with class duration (F(5,339) = 3.81, P = .002), the authors used an analysis of covariance to test for a mediating effect of ethnicity on the relationship between class duration and pain. Although there was a partial mediation (F(5,203) = 2.57, P = .028), the main effect of class duration remained significant.
Discussion and Limitations
The goals of this project were to develop a yoga-based program tailored for veterans with SMI and assess the program in a sample of veterans with SMI on subjective reports of stress, pain, well-being, and benefits of yoga. The authors hypothesized that significant improvements in these measures in veterans with SMI would be observed over 8 weeks of participation in BSR classes and that there would be greater benefits in veterans who participated in longer classes and who attended classes more frequently.
The authors succeeded in developing an adaptable yoga-based wellness program for veterans with SMI that can be both practiced in structured classes and incorporated into veterans’ everyday routines. The BSR classes were well tolerated by veterans with SMI, caused no discernible AEs, and are readily available for dissemination across other mental health programs. Veterans described integrating the tools they learned within BSR classes into their daily lives, helping them to manage pain; feel more flexible; reduce stress, anxiety, depression, and PTSD symptoms; and increase relaxation and feelings of self-control and confidence. Table 5 shows qualitative feedback collected from veterans. In addition, the Train the Trainer model optimized clinical applicability and flexibility, demonstrating that clinicians can seamlessly integrate BSR classes into a health care plan for veterans with SMI.
In assessing quantitative measures of stress, pain, well-being, and perceived benefits of a yoga-based program, veterans who reported BSR classes as beneficial experienced lower levels of pain and stress and higher levels of biological, psychological, social, spiritual, and overall well-being. Those veterans who perceived BSR as more beneficial tended to be younger and attend longer classes with greater frequency. Veterans who attended longer classes also reported experiencing less pain. This may be because the more rigorous stretching and posing involved in longer BSR classes made them more effective at reducing pain; however, it is also possible that veterans who were experiencing more pain avoided these longer classes due to their rigor and length.
Results suggest that longer classes attended with greater regularity may be more beneficial to veterans than short and infrequent classes, particularly in regards to their pain. Despite the relationships between class and outcome variables, the authors did not find significant improvements in measures of wellness, pain, stress, or perceived benefits of BSR over time, as was hypothesized. This may be because the data collection for this study began after classes had been established for some time. In fact, only 35 of 120 veterans included in this study reported having < 1 month of BSR experience at week 0, suggesting that results collected from week 0 did not represent a true baseline measurement. Although no relationship was found between prior duration of attendance and any outcome measures, the fact that most veterans in the sample had attended classes for several months prior to completing surveys may have biased the results by favoring the responses of veterans who were more invested in the classes. Improvements may have been better captured in a BSR-naïve sample.
The finding that the PBYQ score was significantly correlated with all other outcome measures (pain, BPSS score, and PSS score) raises some questions about the ways in which these classes were beneficial to veterans. It may be that veterans who experienced more positive outcomes from classes saw BSR as more beneficial, but it is also possible that veterans who entered classes with greater expectations experienced better outcomes due to a placebo effect—that is, outcomes may have been influenced more by the expectation than by the content of the classes. In the case of well-being (BPSS scores) and stress (PSS score), this could explain why these outcomes were significantly correlated with perceived benefits of BSR but were not significantly related to any class-related variables such as duration and frequency of attendance. Pain ratings, however, were related to class variables and perceived benefits of BSR.
In a post hoc analysis, the main effect of the PBYQ score as a regressor was added to the linear model for pain, resulting in the PBYQ score having a significant main effect (t(100) = -2.98, P = .004). The main effect of class duration remained significant (t(97) = -1.99, P = .050) but was less substantial when the PBYQ score was added, suggesting some correlation between class duration and pain, independent of BSR’s perceived benefits. Future research should consider the possible mediating effect of perceptions of the effectiveness of a yoga-based program a priori or control for placebo effects in order to address the degree to which outcomes are influenced by participant expectations.
This study had a few other notable limitations. Because it was an observational study administered within a clinical mental health program, a control group was not included. Measurement began after BSR classes were established, so veterans had varying levels of prior experience. Specific SMI and medical diagnosis information was not collected from individual veterans. Data were collected from classes of varying length and intensity. The BSR classes often took place within larger programs at the VA, which offered comprehensive care, so some effects of the BSR classes might have been confounded with concurrent evidenced-based treatments or other holistic care programs. Due to these limitations, particularly the absence of a control group, the relationships between BSR participation and health outcomes cannot be assumed to be causal, because a multitude of other variables, such as patient contact and expectancy effects, may have influenced outcomes.
Future Directions
Future research should aim to utilize a control group and collect data from classes of the same intensity and length to better examine whether BSR can be causally linked with improvements in measures of stress, pain, and well-being and to attempt to control for expectancy and contact effects. In addition, future research should aim to recruit a BSR-naïve sample to account for prior experience. Future studies should also aim to parse out whether BSR is differentially effective for each SMI or medical diagnosis, whether there is a relationship between class time and outcomes (as these results suggest that longer class times might be more beneficial for pain), and whether any pain-management benefits from BSR influence other measures of functionality and well-being. Finally, future research can further divide BSR into its active components, such as meditative breathing and aerobic stretching, in order to examine which aspect leads to the greatest effect on each measure; the current results imply that the more rigorous components of BSR classes have the greatest effects on pain.
Conclusion
A yoga-based class affects the mind and body, making it particularly useful for veterans with SMI who experience a range of physical and psychological symptoms and comorbidities.4 Other studies have demonstrated that when practiced alone, yoga leads to improvements in both physical and psychological symptoms.15,17 Looking forward, yoga-based classes may be implemented as part of a larger biopsychosocial-spiritual care plan that is being embraced both within and outside of the VA.7,8,36,37 This integrative health care model suggests that psychosocial and CAM modalities are additive and should be practiced concurrently.37
Although little research has assessed the effects of comprehensive psychosocial and CAM treatment programs, initial research indicates that these programs are associated with reductions in symptoms of medical and mental illness.37-40 Participants in BSR classes may derive further benefits if classes are incorporated into a larger holistic health care plan that includes both traditional psychiatric treatment modalities and CAM therapies that integrate biopsychosocial-spiritual components.
Acknowledgements
The authors would like to thank Nancy Mohler, Anne Platt, and Matthew Crowder, all professional yoga instructors, for their integral role in developing classes, providing classes to veterans, and assisting VA staff with training. The authors also acknowledge Rosie Dominguez, LCSW, for expertly leading BSR classes at LAACC. The authors also thank Irina Arnold, MS, MD, and Vanessa Streiff, MA, for their vital assistance with data collection at SACC.
Funding for the development of BSR protocols, quality improvement research, and expenses associated with classes was provided by the Disabled American Veterans Charitable Service Trust. Support for dissemination of classes to multiple VA programs was provided by a grant from the VA Center of Innovation for Patient Centered Care, headed by Sandra Robertson, RN, MSN, PH-CNS.
The authors are very grateful to the veterans and staff of the Mental Health Intensive Case Management, Psychosocial Rehabilitation and Recovery Centers, Mental Health Clinics, and Domiciliary throughout Greater Los Angeles for their support of the BSR classes.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
There is growing interest in developing a holistic and integrative approach for the treatment of severe mental illnesses (SMI), such as schizophrenia, major depression, posttraumatic stress disorder (PTSD), and anxiety disorders. Western medicine has traditionally focused on the direct treatment of symptoms and separated the management of physical and mental health, but increasing attention is being given to complementary and alternative medicine (CAM) for patients with SMI.
Recognizing the connectedness of the mind and body, these complementary or alternative approaches incorporate nontraditional therapeutic techniques with mainstream treatment methods, including psychopharmacology and psychotherapy.1 Patients with SMI may particularly benefit from a mind-body therapeutic approach, because they often experience psychological symptoms such as stress, anxiety, depression and psychosis, as well as a preponderance of medical comorbidities, including obesity, diabetes mellitus, and cardiovascular disease, some of which are compounded by adverse effects (AEs) of essential pharmacologic treatments.2-4 Mind-body interventions might also be particularly advantageous for veterans, who often experience a range of interconnected physical and psychological difficulties due to trauma exposure and challenges transitioning from military to civilian life.5
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
In 2002, the White House Commission on Complementary and Alternative Medicine Policy issued a report supporting CAM research and integration into existing medical systems.6 The DoD later established Total Force Fitness, a holistic health care program for active-duty military personnel.7 The VA has also incorporated mind-body and holistic strategies into veteran care.8 One such mind-body intervention, yoga, is becoming increasingly popular within the health care field.
Recent research has documented the effectiveness of yoga, underscoring its utility as a mind-body therapeutic approach. Yoga is associated with improvement in balance and flexibility,9 fatigue,10 blood pressure,11 sleep,12 strength,13 and pain14 in both healthy individuals and patients with medical and psychiatric disorders.15 The literature also illustrates that yoga has led to significant improvements in stress and psychiatric symptoms in individuals with PTSD, schizophrenia, depression, and anxiety.16-22 A previous meta-analysis conducted by the authors, which considered studies of the effectiveness of yoga as an adjunctive treatment for patients with mental illness, found that 212 studies with null results would need to be located and incorporated to negate the positive effects of yoga found in the literature.17
Because yoga emphasizes the practice of mindfulness and timing movement with breath awareness, it is a calming practice that may decrease stress and relieve psychiatric symptoms not treated through psychopharmacology and psychotherapy.17,21 Recent research has postulated that the physiological mechanisms by which this occurs may include (a) reduction in sympathetic and increase in parasympathetic activity23,24; (b) increases in heart-rate variability and respiratory sinus arrhythmia, low levels of which are associated with anxiety, panic disorder, and depression23,24; (c) increases in melatonin and serotonin 25-27; and (d) decrease in cortisol.28,29
Related: Enhancing Patient Satisfaction Through the Use of Complementary Therapies
As yoga may calm the autonomic nervous system and reduce stress, it may benefit patients with SMI, whose symptoms are often aggravated by stress.30 In addition, veterans experience both acute stressors and high levels of chronic stress.5 Therefore, because they experience mind-body comorbid illnesses as well as high levels of stress, the authors believe that veterans with SMI could benefit greatly from a tailored yoga-based program as part of a holistic approach that includes necessary medication and evidence-based therapies.
In order to evaluate the effects of a yoga program on veterans receiving mental health treatment across the VA Greater Los Angeles Healthcare System (VAGLAHS), the authors developed a set of yoga-based wellness classes called Breathing, Stretching, Relaxation (BSR) classes. This article describes the process of developing these classes and outlines the procedures and results of a study to assess their effects.
BSR Classes
The development of BSR classes took place at the West Los Angeles VA Medical Center (WLAVAMC), within the Psychosocial Rehabilitation and Recovery Center (PRRC) program. The PRRC is a psychoeducational program that focuses on the biological, psychological, social, and spiritual aspects of life in order to help veterans with SMI rehabilitate and reintegrate into the community. The program allows veterans to create their own recovery curriculum by selecting from diverse classes led by program staff members, including physicians, psychologists, nurses, social workers, nutritionists, and recreational therapists.
Development of BSR Protocols
The primary goal of this project was to develop a yoga-based program tailored to the specific needs of veterans with SMI. To the authors’ knowledge, BSR is the first yoga-based program customized for SMI. The BSR classes were developed within interdisciplinary focus groups that included professional yoga teachers, the director of the PRRC, psychiatrists, psychologists, nurses, occupational therapists, and physical therapists. Drawing on their experience with SMI and yoga, members of the focus groups identified 3 aspects of yoga that would be most beneficial to veterans with SMI, and the program was designed to optimize these effects. Because SMI can both create and be exacerbated by stress, BSR classes were designed to reduce stress and provide veterans with the tools to monitor and manage their stress.
Breathing and meditative techniques were adapted from yoga in order to facilitate stress reduction. In addition, aerobic elements of yoga have the potential to help veterans manage their incidence of medical diseases, such as cardiovascular disease, obesity, and diabetes. Patients with SMI are at a greater risk for developing these diseases, so classes were designed to incorporate physical stretching elements to promote overall health.4,31-33 Finally BSR was designed to improve veteran self- efficacy and self-esteem, and to place veterans at the center of their care by equipping them with skills to practice BSR independently.
Related: Mindfulness to Reduce Stress
The focus groups also identified the logistic requirements when implementing a yoga-based program for veterans with SMI, including (a) obtaining participant or conservator consent; (b) obtaining medical clearance from care providers, given the high prevalence of medical comorbidities; (c) removing the traditional yoga terms, taking a secular approach, and naming the class “Breathing, Stretching, Relaxation” without directly referencing yoga; (d) asking veterans’ permission before incorporating physical contact into demonstrations, because veterans with SMI, especially those with PTSD, might be uncomfortable with touching from instructors; (e) creating protocols of varying duration and intensity so that BSR was approachable for veterans with diverse levels of physical ability; and (f) ensuring that a clinician who regularly works with SMI patients be present to supervise classes for the safety of patients and instructors.
Yoga instructors and clinicians collaborated to create adaptable 30- and 50-minute protocols that reflected best practices for an SMI population. The 30-minute seated BSR class protocol is included in eAppendix A. Once protocols were finalized, a Train the Trainer program was established to facilitate dissemination of BSR to clinicians working with veterans with SMI throughout the VAGLAHS.
Interested clinicians were given protocols and trained to lead BSR classes on their own. Subsequently, clinician-led BSR classes of various lengths (depending on clinician preference and program scheduling) were established at PRRCs and other mental health programs, such as Mental Health Recovery and Intensive Treatment and Dual Diagnosis Treatment Program, throughout the VAGLAHS. These programs were selected, because they are centered on recovery and improvements in symptoms of SMI. The adoption of a Train the Trainer model, through which VA clinicians were trained by professional yoga instructors, allowed for seamless integration of BSR into VA usual care for veterans with SMI.
Assessment of Classes
The authors conducted a study to assess the quality and effectiveness of BSR classes. This survey research was approved by the VAGLAHS institutional review board for human subjects. The authors hypothesized that there would be significant improvements in veterans’ stress, pain, well-being, and perception of the benefits of BSR over 8 weeks of participation in classes. Also hypothesized was that there would be greater benefits in veterans who participated in longer classes and who attended classes more frequently.
Methods
A total of 120 veterans completed surveys after participating in clinician- and yoga instructor-led BSR classes at the 3 sites within the VAGLAHS: WLAVAMC, Los Angeles Ambulatory Care Center (LAACC), and Sepulveda Ambulatory Care Center (SACC). At the WLAVAMC, surveys were collected at 10-, 30-, 60-, and 90-minute classes. At LAACC, surveys were collected at 30- and 60-minute classes. At SACC, surveys were collected at 20- and 45-minute classes. A researcher noted the duration of the class and was available to assist with comprehension. Veterans completed identical surveys after classes at a designated week 0 (baseline), week 4, and week 8. Of the 120 patients with an initial survey, 82 completed at least 1 follow-up survey and 49 completed both follow-up surveys.
Survey packets included (a) demographic questions, including age, gender, and ethnicity; (b) class participation questions, including frequency of class attendance, patients’ favorite aspect of class, and dura tion of class attendance (in months of prior participation); (c) a pain rating from 0 (no pain) to 10 (the worst pain imaginable); (d) the BioPsychoSocial-Spiritual (BPSS) Scale (eAppendix B), developed at the WLAVAMC, which provides wellness scores from 0 (low) to 10 (high) in 4 areas as well as a holistic wellness score from 0 (low) to 40 (high); (e) the Perceived Stress Scale (PSS), developed by Cohen and colleagues, which generates a stress score for the past month from 0 (low) to 40 (high)34; and (f) the Perceived Benefits of Yoga Questionnaire (PBYQ) (eAppendix C), which rates participants’ opinions about the benefits of yoga from 12 (low) to 60 (high) and is based on the Perceived Benefits of Dance Questionnaire.35
Statistical Analysis
Pearson’s r correlation coefficients were calculated between PBYQ scores and quantitative survey items at each time point (weeks 0, 4, and 8). Linear mixed-effects models were used to test for effects of multiple predictor variables on individual outcomes. Each model had a random intercept by participant, and regressors included main effects for the following: survey week (0, 4, or 8), class duration (in minutes), age, sex, ethnicity, frequency of attendance (in days per week), and duration of attendance (in months). For all statistical analyses, a 2-tailed significance criterion of α = .05 was used.
Results
Veterans who completed surveys were predominantly male (90.8%) and averaged 61.4 years of age. Table 1 shows demographic information. Table 2 displays the number of participants who were involved in short (< 30 min), medium (30-59 min), and long (> 60 min) classes. Veteran participants also had a wide range of prior BSR experience (Table 3).
At all time points, PBYQ scores were significantly positively correlated with class duration and biological, psychological, social, spiritual, and total well-being as measured by the BPSS. The PBYQ scores at all time points were also significantly negatively correlated with age, pain ratings, and PSS scores. Table 4 includes specific Pearson’s r values.
Survey week was not significantly associated with any individual outcome measures. There were no significant regressors for total PSS score or total BPSS score within the linear models. However, participants’ PBYQ scores were significantly associated with age (t(98) = -2.13, P = .036), frequency of attendance (t(103) = 2.10, P = .038), and class duration (t(98) = 4.35, P < .001). Additionally, class duration was significantly associated with pain (t(98) = -3.01, P = .003), with longer duration associated with less pain. Ethnicity was also associated with pain, with African American veterans reporting less pain than did white (t(98) = -2.41, P = .017) and Hispanic (t(98) = -2.31, P = .023) veterans. Because ethnicity was significantly associated with class duration (F(5,339) = 3.81, P = .002), the authors used an analysis of covariance to test for a mediating effect of ethnicity on the relationship between class duration and pain. Although there was a partial mediation (F(5,203) = 2.57, P = .028), the main effect of class duration remained significant.
Discussion and Limitations
The goals of this project were to develop a yoga-based program tailored for veterans with SMI and assess the program in a sample of veterans with SMI on subjective reports of stress, pain, well-being, and benefits of yoga. The authors hypothesized that significant improvements in these measures in veterans with SMI would be observed over 8 weeks of participation in BSR classes and that there would be greater benefits in veterans who participated in longer classes and who attended classes more frequently.
The authors succeeded in developing an adaptable yoga-based wellness program for veterans with SMI that can be both practiced in structured classes and incorporated into veterans’ everyday routines. The BSR classes were well tolerated by veterans with SMI, caused no discernible AEs, and are readily available for dissemination across other mental health programs. Veterans described integrating the tools they learned within BSR classes into their daily lives, helping them to manage pain; feel more flexible; reduce stress, anxiety, depression, and PTSD symptoms; and increase relaxation and feelings of self-control and confidence. Table 5 shows qualitative feedback collected from veterans. In addition, the Train the Trainer model optimized clinical applicability and flexibility, demonstrating that clinicians can seamlessly integrate BSR classes into a health care plan for veterans with SMI.
In assessing quantitative measures of stress, pain, well-being, and perceived benefits of a yoga-based program, veterans who reported BSR classes as beneficial experienced lower levels of pain and stress and higher levels of biological, psychological, social, spiritual, and overall well-being. Those veterans who perceived BSR as more beneficial tended to be younger and attend longer classes with greater frequency. Veterans who attended longer classes also reported experiencing less pain. This may be because the more rigorous stretching and posing involved in longer BSR classes made them more effective at reducing pain; however, it is also possible that veterans who were experiencing more pain avoided these longer classes due to their rigor and length.
Results suggest that longer classes attended with greater regularity may be more beneficial to veterans than short and infrequent classes, particularly in regards to their pain. Despite the relationships between class and outcome variables, the authors did not find significant improvements in measures of wellness, pain, stress, or perceived benefits of BSR over time, as was hypothesized. This may be because the data collection for this study began after classes had been established for some time. In fact, only 35 of 120 veterans included in this study reported having < 1 month of BSR experience at week 0, suggesting that results collected from week 0 did not represent a true baseline measurement. Although no relationship was found between prior duration of attendance and any outcome measures, the fact that most veterans in the sample had attended classes for several months prior to completing surveys may have biased the results by favoring the responses of veterans who were more invested in the classes. Improvements may have been better captured in a BSR-naïve sample.
The finding that the PBYQ score was significantly correlated with all other outcome measures (pain, BPSS score, and PSS score) raises some questions about the ways in which these classes were beneficial to veterans. It may be that veterans who experienced more positive outcomes from classes saw BSR as more beneficial, but it is also possible that veterans who entered classes with greater expectations experienced better outcomes due to a placebo effect—that is, outcomes may have been influenced more by the expectation than by the content of the classes. In the case of well-being (BPSS scores) and stress (PSS score), this could explain why these outcomes were significantly correlated with perceived benefits of BSR but were not significantly related to any class-related variables such as duration and frequency of attendance. Pain ratings, however, were related to class variables and perceived benefits of BSR.
In a post hoc analysis, the main effect of the PBYQ score as a regressor was added to the linear model for pain, resulting in the PBYQ score having a significant main effect (t(100) = -2.98, P = .004). The main effect of class duration remained significant (t(97) = -1.99, P = .050) but was less substantial when the PBYQ score was added, suggesting some correlation between class duration and pain, independent of BSR’s perceived benefits. Future research should consider the possible mediating effect of perceptions of the effectiveness of a yoga-based program a priori or control for placebo effects in order to address the degree to which outcomes are influenced by participant expectations.
This study had a few other notable limitations. Because it was an observational study administered within a clinical mental health program, a control group was not included. Measurement began after BSR classes were established, so veterans had varying levels of prior experience. Specific SMI and medical diagnosis information was not collected from individual veterans. Data were collected from classes of varying length and intensity. The BSR classes often took place within larger programs at the VA, which offered comprehensive care, so some effects of the BSR classes might have been confounded with concurrent evidenced-based treatments or other holistic care programs. Due to these limitations, particularly the absence of a control group, the relationships between BSR participation and health outcomes cannot be assumed to be causal, because a multitude of other variables, such as patient contact and expectancy effects, may have influenced outcomes.
Future Directions
Future research should aim to utilize a control group and collect data from classes of the same intensity and length to better examine whether BSR can be causally linked with improvements in measures of stress, pain, and well-being and to attempt to control for expectancy and contact effects. In addition, future research should aim to recruit a BSR-naïve sample to account for prior experience. Future studies should also aim to parse out whether BSR is differentially effective for each SMI or medical diagnosis, whether there is a relationship between class time and outcomes (as these results suggest that longer class times might be more beneficial for pain), and whether any pain-management benefits from BSR influence other measures of functionality and well-being. Finally, future research can further divide BSR into its active components, such as meditative breathing and aerobic stretching, in order to examine which aspect leads to the greatest effect on each measure; the current results imply that the more rigorous components of BSR classes have the greatest effects on pain.
Conclusion
A yoga-based class affects the mind and body, making it particularly useful for veterans with SMI who experience a range of physical and psychological symptoms and comorbidities.4 Other studies have demonstrated that when practiced alone, yoga leads to improvements in both physical and psychological symptoms.15,17 Looking forward, yoga-based classes may be implemented as part of a larger biopsychosocial-spiritual care plan that is being embraced both within and outside of the VA.7,8,36,37 This integrative health care model suggests that psychosocial and CAM modalities are additive and should be practiced concurrently.37
Although little research has assessed the effects of comprehensive psychosocial and CAM treatment programs, initial research indicates that these programs are associated with reductions in symptoms of medical and mental illness.37-40 Participants in BSR classes may derive further benefits if classes are incorporated into a larger holistic health care plan that includes both traditional psychiatric treatment modalities and CAM therapies that integrate biopsychosocial-spiritual components.
Acknowledgements
The authors would like to thank Nancy Mohler, Anne Platt, and Matthew Crowder, all professional yoga instructors, for their integral role in developing classes, providing classes to veterans, and assisting VA staff with training. The authors also acknowledge Rosie Dominguez, LCSW, for expertly leading BSR classes at LAACC. The authors also thank Irina Arnold, MS, MD, and Vanessa Streiff, MA, for their vital assistance with data collection at SACC.
Funding for the development of BSR protocols, quality improvement research, and expenses associated with classes was provided by the Disabled American Veterans Charitable Service Trust. Support for dissemination of classes to multiple VA programs was provided by a grant from the VA Center of Innovation for Patient Centered Care, headed by Sandra Robertson, RN, MSN, PH-CNS.
The authors are very grateful to the veterans and staff of the Mental Health Intensive Case Management, Psychosocial Rehabilitation and Recovery Centers, Mental Health Clinics, and Domiciliary throughout Greater Los Angeles for their support of the BSR classes.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. National Center for Complementary and Integrative Health. Complementary, alternative, or integrative health: what's in a name? U.S. Department of Health and Human Services, National Institutes of Health Website. http://nccam.nih.gov/health/whatiscam. Updated March 2015. Accessed August 27, 2015.
2. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):617-627.
3. Fleischhacker WW, Cetkovich-Bakmas M, De Hert M, et al. Comorbid somatic illnesses in patients with severe mental disorders: clinical, policy, and research challenges. J Clin Psychiatry. 2008;69(4):514-519.
4. Wirshing DA, Boyd JA, Meng LR, Ballon JS, Marder SR, Wirshing WC. The effects of novel antipsychotics on glucose and lipid levels. J Clin Psychiatry. 2002;63(10):856-865.
5. Tanielian T, Jaycox LH, eds. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND Corporation; 2008.
6. White House Commission on Complementary and Alternative Medicine Policy. Final Report. Washington, DC: White House Commission on Complementary and Alternative Medicine Policy; 2002.
7. Land BC. Current Department of Defense guidance for total force fitness. Mil Med. 2010;175(suppl 8):3-5.
8. U.S. Department of Veterans Affairs, Veterans Health Administration. Pain Management. VHA Directive 2009-053. Washington, DC: U.S. Department of Veterans Affairs, Veterans Health Administration; 2009.
9. Oken BS, Zajdel D, Kishiyama S, et al. Randomized, controlled, six-month trial of yoga in healthy seniors: effects on cognition and quality of life. Altern Ther Health Med. 2006;12(1):40-47.
10. Bower JE, Garet D, Sternlieb B, et al. Yoga for persistent fatigue in breast cancer survivors: a randomized controlled trial. Cancer. 2012;118(15):3766-3775.
11. Cade WT, Reeds DN, Mondy KE, et al. Yoga lifestyle intervention reduces blood pressure in HIV-infected adults with cardiovascular disease risk factors. HIV Med. 2010;11(6):379-388.
12. Innes KE, Selfe TK. The effects of a gentle yoga program on sleep, mood, and blood pressure in older women with restless leg syndrome (RLS): a preliminary randomized controlled trial. Evid Based Complement Alternat Med. 2012;2012:294058.
13. Van Puymbroeck M, Payne LL, Hsieh PC. A phase I feasibility study of yoga on the physical health and coping of informal caregivers. Evid Based Complement Alternat Med. 2007;4(4):519-529.
14. Rani K, Tiwari SC, Singh U, Agrawal GG, Srivastava N. Six-month trial of Yoga Nidra in menstrual disorder patients: effects on somatoform symptoms. Ind Psychiatry J. 2011;20(2):97-102.
15. Ross A, Thomas S. The health benefits of yoga and exercise: a review of comparison studies. J Altern Complement Med. 2010;16(1):3-12.
16. Banerjee B, Vadiraj HS, Ram A, et al. Effects of an integrated yoga program in modulating psychological stress and radiation-induced genotoxic stress in breast cancer patients undergoing radiotherapy. Integr Cancer Ther. 2007;6(3):242-250.
17. Cabral P, Meyer HB, Ames D. Effectiveness of yoga therapy as a complementary treatment for major psychiatric disorders: a meta-analysis. Prim Care Companion CNS Disord. 2011;13(4):doi:10.4088/PCC.10r01068.
18. Katzman MA, Vermani M, Gerbarg PL, et al. A multicomponent yoga-based, breath intervention program as an adjunctive treatment in patients suffering from generalized anxiety disorder with or without comorbidities. Int J Yoga. 2012;5(1):57-65.
19. Köhn M, Persson Lundholm U, Bryngelsson IL, Anderzén-Carlsson A, Westerdahl E. Medical yoga for patients with stress-related symptoms and diagnoses in primary health care: a randomized controlled trial. Evid Based Complement Alternat Med. 2013;2013:215348.
20. Krishnamurthy MN, Telles S. Assessing depression following two ancient Indian interventions: effects of yoga and ayurveda on older adults in a residential home. J Gerontol Nurs. 2007;33(2):17-23.
21. Meyer HB, Katsman A, Sones AC, Auerbach DE, Ames D, Rubin RT. Yoga as an ancillary treatment for neurological and psychiatric disorders: a review. J Neuropsychiatry Clin Neurosci. 2012;24(2):152-164.
22. Visceglia E, Lewis S. Yoga therapy as an adjunctive treatment for schizophrenia: a randomized, controlled pilot study. J Altern Complement Med. 2011;17(7):601-607.
23. Brown RP, Gerbarg PL. Sudarshan Kriya yogic breathing in the treatment of stress, anxiety, and depression, part I-neurophysiologic model. J Altern Complement Med. 2005;11(1):189-201.
24. Brown RP, Gerbarg PL. Yoga breathing, meditation, and longevity. Ann N Y Acad Sci. 2009;1172:54-62.
25. Harinath K, Malhotra AS, Pal K, et al. Effects of hatha yoga and Omkar meditation on cardiorespiratory performance, psychologic profile, and melatonin secretion. J Altern Complement Med. 2004;10(2):261-268.
26. Tooley GA, Armstrong SM, Norman TR, Sali A. Acute increases in night-time plasma melatonin levels following a period of meditation. Biol Psychol. 2000;53(1):69-78.
27. Walton KG, Pugh ND, Gelderloos P, Macrae P. Stress reduction and preventing hypertension: preliminary support of a psychoneuroendocrine mechanism. J Altern Complement Med. 1995;1(3):263-283.
28. Banasik J, Williams H, Haberman M, Blank SE, Bendel R. Effect of Iyengar yoga practice on fatigue and diurnal salivary cortisol concentration in breast cancer survivors. J Am Acad Nurse Pract. 2011;23(3):135-142.
29. Vadiraja HS, Raghavendra RM, Nagarathna R, et al. Effects of a yoga program on cortisol rhythm and mood states in early breast cancer patients undergoing adjuvant radiotherapy: a randomized controlled trial. Integr Cancer Ther. 2009;8(1):37-46.
30. Esch T, Stefano GB, Fricchione GL, Benson H. The role of stress in neurodegenerative diseases and mental disorders. Neuro Endocrinol Lett. 2002;23(3):199-208.
31. Lingjaerde O, Ahlfors UG, Bech P, Dencker SJ, Elgen K. The UKU side effect rating scale. A new comprehensive rating scale for psychotropic drugs and a cross-sectional study of side effects in neuroleptic-treated patients. Acta Psychiatr Scand Suppl. 1987;334:1-100.
32. Schwartz TL, Nihalani N, Jindal S, Virk S, Jones N. Psychiatric medication-induced obesity: a review. Obes Rev. 2004;5(2):115-121.
33. Wirshing DA, Spellberg BJ, Erhart SM, Marder SR, Wirshing WC. Novel antipsychotics and new onset diabetes. Biol Psychiatry. 1998;44(8):778-783.
34. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385-396.
35. Quiroga Murcia C, Kreutz G, Clift S, Bongard S. Shall we dance? An exploration of the perceived benefits of dancing on well-being. Arts Health. 2010;2(2):149-163.
36. The Duke Center for Integrative Medicine; Liebowitz R, Smith L. The Duke Encyclopedia of New Medicine: Conventional and Alternative Medicine for All Ages. London, UK: Rodale Books International; 2006.
37. Walsh R. Lifestyle and mental health. Am Psychol. 2011;66(7):579-592.
38. Frattaroli J, Weidner G, Dnistrian AM, et al. Clinical events in prostate cancer lifestyle trial: results from two years of follow-up. Urology. 2008;72(6):1319-1323.
39. Khaw KT, Wareham N, Bingham S, Welch A, Luben R, Day N. Combined impact of health behaviours and mortality in men and women: the EPIC-Norfolk prospective population study. PLoS Med. 2008;5(1):e12.
40. Sidhu KS, Vandana P, Balon R. Exercise prescription: a practical, effective therapy for depression. Curr Psychiatr. 2009;8(6):38-51.
1. National Center for Complementary and Integrative Health. Complementary, alternative, or integrative health: what's in a name? U.S. Department of Health and Human Services, National Institutes of Health Website. http://nccam.nih.gov/health/whatiscam. Updated March 2015. Accessed August 27, 2015.
2. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):617-627.
3. Fleischhacker WW, Cetkovich-Bakmas M, De Hert M, et al. Comorbid somatic illnesses in patients with severe mental disorders: clinical, policy, and research challenges. J Clin Psychiatry. 2008;69(4):514-519.
4. Wirshing DA, Boyd JA, Meng LR, Ballon JS, Marder SR, Wirshing WC. The effects of novel antipsychotics on glucose and lipid levels. J Clin Psychiatry. 2002;63(10):856-865.
5. Tanielian T, Jaycox LH, eds. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND Corporation; 2008.
6. White House Commission on Complementary and Alternative Medicine Policy. Final Report. Washington, DC: White House Commission on Complementary and Alternative Medicine Policy; 2002.
7. Land BC. Current Department of Defense guidance for total force fitness. Mil Med. 2010;175(suppl 8):3-5.
8. U.S. Department of Veterans Affairs, Veterans Health Administration. Pain Management. VHA Directive 2009-053. Washington, DC: U.S. Department of Veterans Affairs, Veterans Health Administration; 2009.
9. Oken BS, Zajdel D, Kishiyama S, et al. Randomized, controlled, six-month trial of yoga in healthy seniors: effects on cognition and quality of life. Altern Ther Health Med. 2006;12(1):40-47.
10. Bower JE, Garet D, Sternlieb B, et al. Yoga for persistent fatigue in breast cancer survivors: a randomized controlled trial. Cancer. 2012;118(15):3766-3775.
11. Cade WT, Reeds DN, Mondy KE, et al. Yoga lifestyle intervention reduces blood pressure in HIV-infected adults with cardiovascular disease risk factors. HIV Med. 2010;11(6):379-388.
12. Innes KE, Selfe TK. The effects of a gentle yoga program on sleep, mood, and blood pressure in older women with restless leg syndrome (RLS): a preliminary randomized controlled trial. Evid Based Complement Alternat Med. 2012;2012:294058.
13. Van Puymbroeck M, Payne LL, Hsieh PC. A phase I feasibility study of yoga on the physical health and coping of informal caregivers. Evid Based Complement Alternat Med. 2007;4(4):519-529.
14. Rani K, Tiwari SC, Singh U, Agrawal GG, Srivastava N. Six-month trial of Yoga Nidra in menstrual disorder patients: effects on somatoform symptoms. Ind Psychiatry J. 2011;20(2):97-102.
15. Ross A, Thomas S. The health benefits of yoga and exercise: a review of comparison studies. J Altern Complement Med. 2010;16(1):3-12.
16. Banerjee B, Vadiraj HS, Ram A, et al. Effects of an integrated yoga program in modulating psychological stress and radiation-induced genotoxic stress in breast cancer patients undergoing radiotherapy. Integr Cancer Ther. 2007;6(3):242-250.
17. Cabral P, Meyer HB, Ames D. Effectiveness of yoga therapy as a complementary treatment for major psychiatric disorders: a meta-analysis. Prim Care Companion CNS Disord. 2011;13(4):doi:10.4088/PCC.10r01068.
18. Katzman MA, Vermani M, Gerbarg PL, et al. A multicomponent yoga-based, breath intervention program as an adjunctive treatment in patients suffering from generalized anxiety disorder with or without comorbidities. Int J Yoga. 2012;5(1):57-65.
19. Köhn M, Persson Lundholm U, Bryngelsson IL, Anderzén-Carlsson A, Westerdahl E. Medical yoga for patients with stress-related symptoms and diagnoses in primary health care: a randomized controlled trial. Evid Based Complement Alternat Med. 2013;2013:215348.
20. Krishnamurthy MN, Telles S. Assessing depression following two ancient Indian interventions: effects of yoga and ayurveda on older adults in a residential home. J Gerontol Nurs. 2007;33(2):17-23.
21. Meyer HB, Katsman A, Sones AC, Auerbach DE, Ames D, Rubin RT. Yoga as an ancillary treatment for neurological and psychiatric disorders: a review. J Neuropsychiatry Clin Neurosci. 2012;24(2):152-164.
22. Visceglia E, Lewis S. Yoga therapy as an adjunctive treatment for schizophrenia: a randomized, controlled pilot study. J Altern Complement Med. 2011;17(7):601-607.
23. Brown RP, Gerbarg PL. Sudarshan Kriya yogic breathing in the treatment of stress, anxiety, and depression, part I-neurophysiologic model. J Altern Complement Med. 2005;11(1):189-201.
24. Brown RP, Gerbarg PL. Yoga breathing, meditation, and longevity. Ann N Y Acad Sci. 2009;1172:54-62.
25. Harinath K, Malhotra AS, Pal K, et al. Effects of hatha yoga and Omkar meditation on cardiorespiratory performance, psychologic profile, and melatonin secretion. J Altern Complement Med. 2004;10(2):261-268.
26. Tooley GA, Armstrong SM, Norman TR, Sali A. Acute increases in night-time plasma melatonin levels following a period of meditation. Biol Psychol. 2000;53(1):69-78.
27. Walton KG, Pugh ND, Gelderloos P, Macrae P. Stress reduction and preventing hypertension: preliminary support of a psychoneuroendocrine mechanism. J Altern Complement Med. 1995;1(3):263-283.
28. Banasik J, Williams H, Haberman M, Blank SE, Bendel R. Effect of Iyengar yoga practice on fatigue and diurnal salivary cortisol concentration in breast cancer survivors. J Am Acad Nurse Pract. 2011;23(3):135-142.
29. Vadiraja HS, Raghavendra RM, Nagarathna R, et al. Effects of a yoga program on cortisol rhythm and mood states in early breast cancer patients undergoing adjuvant radiotherapy: a randomized controlled trial. Integr Cancer Ther. 2009;8(1):37-46.
30. Esch T, Stefano GB, Fricchione GL, Benson H. The role of stress in neurodegenerative diseases and mental disorders. Neuro Endocrinol Lett. 2002;23(3):199-208.
31. Lingjaerde O, Ahlfors UG, Bech P, Dencker SJ, Elgen K. The UKU side effect rating scale. A new comprehensive rating scale for psychotropic drugs and a cross-sectional study of side effects in neuroleptic-treated patients. Acta Psychiatr Scand Suppl. 1987;334:1-100.
32. Schwartz TL, Nihalani N, Jindal S, Virk S, Jones N. Psychiatric medication-induced obesity: a review. Obes Rev. 2004;5(2):115-121.
33. Wirshing DA, Spellberg BJ, Erhart SM, Marder SR, Wirshing WC. Novel antipsychotics and new onset diabetes. Biol Psychiatry. 1998;44(8):778-783.
34. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385-396.
35. Quiroga Murcia C, Kreutz G, Clift S, Bongard S. Shall we dance? An exploration of the perceived benefits of dancing on well-being. Arts Health. 2010;2(2):149-163.
36. The Duke Center for Integrative Medicine; Liebowitz R, Smith L. The Duke Encyclopedia of New Medicine: Conventional and Alternative Medicine for All Ages. London, UK: Rodale Books International; 2006.
37. Walsh R. Lifestyle and mental health. Am Psychol. 2011;66(7):579-592.
38. Frattaroli J, Weidner G, Dnistrian AM, et al. Clinical events in prostate cancer lifestyle trial: results from two years of follow-up. Urology. 2008;72(6):1319-1323.
39. Khaw KT, Wareham N, Bingham S, Welch A, Luben R, Day N. Combined impact of health behaviours and mortality in men and women: the EPIC-Norfolk prospective population study. PLoS Med. 2008;5(1):e12.
40. Sidhu KS, Vandana P, Balon R. Exercise prescription: a practical, effective therapy for depression. Curr Psychiatr. 2009;8(6):38-51.
Caring for refugees requires flexibility, cultural humility
When the recent photo of a drowned Syrian toddler woke up the world to the Syrian refugee crisis more viscerally than ever before, multiple nations announced plans to take in more refugees. According to the U.S. State Department, approximately 10,000 Syrian refugees are already in processing, eventually headed to cities that may include Atlanta, San Diego, Houston, Dallas, Chicago, Boston, Boise, Nashville, Tucson, Buffalo, and Erie.
To pediatricians, that boy on the beach represents a child who might have ended up in their practice with diverse, complex needs greatly exceeding the typical needs of a U.S. child coming in for a well-child visit.

“Families are coming from a country that has been ravaged by civil war for over 4 years,” Dr. Susan S. Reines, a pediatrician with the Southeast Kaiser Permanente Medical Group and lead pediatrician for the Refugee Pediatric Clinic at DeKalb County Board of Health in Decatur, Georgia, said in an interview. “Cities have been destroyed, and millions have been forced to leave their homes and are displaced either within Syria or in neighboring countries.”
About a third of the more than 58,000 refugees admitted to the United States in 2012 were under 18 years old. Although the majority that year hailed from Bhutan, Burma, and Iraq, an increasing number of children have been coming from war-torn Syria since June 2014. The proposed ceiling for all refugees in the United States 2015 fiscal year is 70,000, a “significant number” of whom will be children with their families, according to a State Department spokesperson.
These children come with “unique medical, developmental and psychosocial needs,” noted Dr. Thomas J. Seery and fellow authors of “Caring for Refugee Children,” a Pediatrics in Review article recommended by Dr. Reines for pediatricians who may be caring for refugee children.
“The health care infrastructure of Syria is broken and many hospitals have closed, medications are difficult to obtain, and numerous doctors have fled the violence,” Dr. Reines said. She compared the anticipated health care problems of these children with those seen among Iraqi refugee children:
• Undernutrition and micronutrient deficiencies.
• Infectious diseases such as vaccine-preventable diseases like measles, but also typhoid, tuberculosis, and parasitic infections.
• Dental disease.
• Surgically amenable congenital anomalies such as congenital heart disease, myelomeningocele, and others that have not been repaired.
• Neurologic problems, such as cerebral palsy, intellectual disability, and autism.
• Hearing loss.
• Posttraumatic stress disorder (PTSD),depression, and anxiety.
• Trauma such as gunshot wounds, shrapnel injuries, and genital trauma secondary to sexual violence.
• Sequelae from illnesses that previously were easily treated, such as hearing loss and ear complications from otitis media, and rheumatic fever from inadequately treated strep throat.
• Underimmunization.
Various resources listed below, including Dr. Seery’s paper, can help guide providers in assessing and meeting these needs, and navigating paperwork and the U.S. refugee system. These resources also can help practitioners address the mental health concerns these patients and their families may face.
Mental health needs
Even children in the best physical shape will have experienced significant upheaval that could lead to depression, anxiety, and PTSD – conditions more common among refugee children than in the general population, research has shown.
“Mental health conditions will be especially present in these children uprooted from their homes and families, and exposed to the violence of war,” Dr. Francis E. Rushton Jr. of the department of pediatrics at the University of South Carolina, Columbia, and a member of the American Academy of Pediatrics Committee on Community Health Services, said in an interview. Of the four major areas of health care need he described for these children, two relate to mental health: toxic mental stress and fractured families and the lack of nurture.
One challenge pediatricians face, however, is recognizing these conditions despite cultural differences that could obscure them.
“It is not uncommon for teens and adults to deny symptoms of depression, stress, and anxiety in early encounters,” Dr. Reines said. “Many cultures stigmatize psychiatric or mental health problems, and refugees may be reluctant to admit they are having difficulties.”
One way around this obstacle is to ask patients and their parents about sleep, energy level, appetite, weight changes, and thoughts of harming one’s self, she said. Mental stress also manifests as somatic symptoms, such as headaches, stomach aches, and back pain, particularly in teens.
“Infants and toddlers are generally most adaptable as long as parents are coping well, and can provide a buffer for stress with a safe and nurturing environment,” Dr. Reines said. Children of parents with depression or PTSD, or who have lost a parent, may feel abandoned and experience depression or developmental delays.
Although school-age children may have nightmares, show anxiety, and cling to their parents, they usually transition well to their new homes. Adolescents face the biggest difficulties, especially if they have lost a parent, must care for their siblings, or have experienced sexual trauma. “They may have more vivid memories of disturbing events and a greater understanding of what their family has endured,” Dr. Reines said. Further, language and educational deficits can lead to alienation and embarrassment, yet families may rebuff behavioral health referrals.
“In these cases, it’s best to keep communication open, encourage dialogue with family, and try to find an activity or sport the refugee can participate in to improve self-esteem,” Dr. Reines said.
Avoiding cultural confusion
While cultural challenges are obvious – language barriers may necessitate translators or bicultural caseworkers – others may be more subtle. Developmental screening questions that rely on blocks, certain pictures, or other culturally specific bases, for example, may not adequately capture a child’s development.
Dr. Reines stresses a strategy for managing cultural differences that is recommended in Dr. Seery’s article: striving for cultural humility rather than cultural competence.
“It is impossible for U.S. physicians who have never practiced outside of our culture and are not bicultural or bilingual to become truly culturally competent in health care delivery for so many refugee populations,” Dr. Reines said. Instead then, cultural humility emphasizes showing respect, interest, and a willingness to learn from patients, she explained.
Cultural humility is a “lifelong process” that also demands flexibility and “allows the practitioner to release the false sense of security associated with stereotyping,” Dr. Seery and his colleagues wrote.
At the same time, pediatricians are guarding against inadvertent stereotyping; however, they can be aware of some cultural generalities that may apply to their Syrian refugee patients.
“Arab communities stress the importance of family rather than the individual and are often more modest than Westerners,” Dr. Rushton said. Further, “Arab families frequently experience discrimination on the basis of their religion in the United States, and pediatricians should be aware of ongoing traumatization even after arrival in America,” he said.
Teens may become embarrassed with discussions about sex or alcohol because few teens from the Middle East drink or become sexually active before marriage, Dr. Reines added. She noted that a Muslim male may not shake hands with females outside his family – a practice providers should respect – and that important religious holidays such as Ramadan may influence a family’s compliance with a treatment plan.
Perhaps the most important commonality, however, is one universal to most refugee families, regardless of their home country.
“The vast majority of families that we meet show incredible courage and resilience, and caring for their children is their highest priority,” Dr. Reines said. “We can learn a great deal from these families, and caring for their children is a tremendously rewarding experience.”
Other cultural resources:
Bridging Refugee Youth and Children’s Services
“The Middle of Everywhere: Helping Refugees Enter the American Community,” by Mary Pipher (Orlando: Mariner Books, 2003)
“Immigrant Medicine,” a textbook by Patricia Walker, M.D., and Elizabeth Barnett, M.D. (New York, N.Y.: Elsevier, 2007)
“Opening cultural doors: Providing culturally sensitive healthcare to Arab American and American Muslim patients” (Am J Obstet Gynecol. 2005 Oct;193]:1307-11).
When the recent photo of a drowned Syrian toddler woke up the world to the Syrian refugee crisis more viscerally than ever before, multiple nations announced plans to take in more refugees. According to the U.S. State Department, approximately 10,000 Syrian refugees are already in processing, eventually headed to cities that may include Atlanta, San Diego, Houston, Dallas, Chicago, Boston, Boise, Nashville, Tucson, Buffalo, and Erie.
To pediatricians, that boy on the beach represents a child who might have ended up in their practice with diverse, complex needs greatly exceeding the typical needs of a U.S. child coming in for a well-child visit.
“Families are coming from a country that has been ravaged by civil war for over 4 years,” Dr. Susan S. Reines, a pediatrician with the Southeast Kaiser Permanente Medical Group and lead pediatrician for the Refugee Pediatric Clinic at DeKalb County Board of Health in Decatur, Georgia, said in an interview. “Cities have been destroyed, and millions have been forced to leave their homes and are displaced either within Syria or in neighboring countries.”
About a third of the more than 58,000 refugees admitted to the United States in 2012 were under 18 years old. Although the majority that year hailed from Bhutan, Burma, and Iraq, an increasing number of children have been coming from war-torn Syria since June 2014. The proposed ceiling for all refugees in the United States 2015 fiscal year is 70,000, a “significant number” of whom will be children with their families, according to a State Department spokesperson.
These children come with “unique medical, developmental and psychosocial needs,” noted Dr. Thomas J. Seery and fellow authors of “Caring for Refugee Children,” a Pediatrics in Review article recommended by Dr. Reines for pediatricians who may be caring for refugee children.
“The health care infrastructure of Syria is broken and many hospitals have closed, medications are difficult to obtain, and numerous doctors have fled the violence,” Dr. Reines said. She compared the anticipated health care problems of these children with those seen among Iraqi refugee children:
• Undernutrition and micronutrient deficiencies.
• Infectious diseases such as vaccine-preventable diseases like measles, but also typhoid, tuberculosis, and parasitic infections.
• Dental disease.
• Surgically amenable congenital anomalies such as congenital heart disease, myelomeningocele, and others that have not been repaired.
• Neurologic problems, such as cerebral palsy, intellectual disability, and autism.
• Hearing loss.
• Posttraumatic stress disorder (PTSD),depression, and anxiety.
• Trauma such as gunshot wounds, shrapnel injuries, and genital trauma secondary to sexual violence.
• Sequelae from illnesses that previously were easily treated, such as hearing loss and ear complications from otitis media, and rheumatic fever from inadequately treated strep throat.
• Underimmunization.
Various resources listed below, including Dr. Seery’s paper, can help guide providers in assessing and meeting these needs, and navigating paperwork and the U.S. refugee system. These resources also can help practitioners address the mental health concerns these patients and their families may face.
Mental health needs
Even children in the best physical shape will have experienced significant upheaval that could lead to depression, anxiety, and PTSD – conditions more common among refugee children than in the general population, research has shown.
“Mental health conditions will be especially present in these children uprooted from their homes and families, and exposed to the violence of war,” Dr. Francis E. Rushton Jr. of the department of pediatrics at the University of South Carolina, Columbia, and a member of the American Academy of Pediatrics Committee on Community Health Services, said in an interview. Of the four major areas of health care need he described for these children, two relate to mental health: toxic mental stress and fractured families and the lack of nurture.
One challenge pediatricians face, however, is recognizing these conditions despite cultural differences that could obscure them.
“It is not uncommon for teens and adults to deny symptoms of depression, stress, and anxiety in early encounters,” Dr. Reines said. “Many cultures stigmatize psychiatric or mental health problems, and refugees may be reluctant to admit they are having difficulties.”
One way around this obstacle is to ask patients and their parents about sleep, energy level, appetite, weight changes, and thoughts of harming one’s self, she said. Mental stress also manifests as somatic symptoms, such as headaches, stomach aches, and back pain, particularly in teens.
“Infants and toddlers are generally most adaptable as long as parents are coping well, and can provide a buffer for stress with a safe and nurturing environment,” Dr. Reines said. Children of parents with depression or PTSD, or who have lost a parent, may feel abandoned and experience depression or developmental delays.
Although school-age children may have nightmares, show anxiety, and cling to their parents, they usually transition well to their new homes. Adolescents face the biggest difficulties, especially if they have lost a parent, must care for their siblings, or have experienced sexual trauma. “They may have more vivid memories of disturbing events and a greater understanding of what their family has endured,” Dr. Reines said. Further, language and educational deficits can lead to alienation and embarrassment, yet families may rebuff behavioral health referrals.
“In these cases, it’s best to keep communication open, encourage dialogue with family, and try to find an activity or sport the refugee can participate in to improve self-esteem,” Dr. Reines said.
Avoiding cultural confusion
While cultural challenges are obvious – language barriers may necessitate translators or bicultural caseworkers – others may be more subtle. Developmental screening questions that rely on blocks, certain pictures, or other culturally specific bases, for example, may not adequately capture a child’s development.
Dr. Reines stresses a strategy for managing cultural differences that is recommended in Dr. Seery’s article: striving for cultural humility rather than cultural competence.
“It is impossible for U.S. physicians who have never practiced outside of our culture and are not bicultural or bilingual to become truly culturally competent in health care delivery for so many refugee populations,” Dr. Reines said. Instead then, cultural humility emphasizes showing respect, interest, and a willingness to learn from patients, she explained.
Cultural humility is a “lifelong process” that also demands flexibility and “allows the practitioner to release the false sense of security associated with stereotyping,” Dr. Seery and his colleagues wrote.
At the same time, pediatricians are guarding against inadvertent stereotyping; however, they can be aware of some cultural generalities that may apply to their Syrian refugee patients.
“Arab communities stress the importance of family rather than the individual and are often more modest than Westerners,” Dr. Rushton said. Further, “Arab families frequently experience discrimination on the basis of their religion in the United States, and pediatricians should be aware of ongoing traumatization even after arrival in America,” he said.
Teens may become embarrassed with discussions about sex or alcohol because few teens from the Middle East drink or become sexually active before marriage, Dr. Reines added. She noted that a Muslim male may not shake hands with females outside his family – a practice providers should respect – and that important religious holidays such as Ramadan may influence a family’s compliance with a treatment plan.
Perhaps the most important commonality, however, is one universal to most refugee families, regardless of their home country.
“The vast majority of families that we meet show incredible courage and resilience, and caring for their children is their highest priority,” Dr. Reines said. “We can learn a great deal from these families, and caring for their children is a tremendously rewarding experience.”
Other cultural resources:
Bridging Refugee Youth and Children’s Services
“The Middle of Everywhere: Helping Refugees Enter the American Community,” by Mary Pipher (Orlando: Mariner Books, 2003)
“Immigrant Medicine,” a textbook by Patricia Walker, M.D., and Elizabeth Barnett, M.D. (New York, N.Y.: Elsevier, 2007)
“Opening cultural doors: Providing culturally sensitive healthcare to Arab American and American Muslim patients” (Am J Obstet Gynecol. 2005 Oct;193]:1307-11).
When the recent photo of a drowned Syrian toddler woke up the world to the Syrian refugee crisis more viscerally than ever before, multiple nations announced plans to take in more refugees. According to the U.S. State Department, approximately 10,000 Syrian refugees are already in processing, eventually headed to cities that may include Atlanta, San Diego, Houston, Dallas, Chicago, Boston, Boise, Nashville, Tucson, Buffalo, and Erie.
To pediatricians, that boy on the beach represents a child who might have ended up in their practice with diverse, complex needs greatly exceeding the typical needs of a U.S. child coming in for a well-child visit.
“Families are coming from a country that has been ravaged by civil war for over 4 years,” Dr. Susan S. Reines, a pediatrician with the Southeast Kaiser Permanente Medical Group and lead pediatrician for the Refugee Pediatric Clinic at DeKalb County Board of Health in Decatur, Georgia, said in an interview. “Cities have been destroyed, and millions have been forced to leave their homes and are displaced either within Syria or in neighboring countries.”
About a third of the more than 58,000 refugees admitted to the United States in 2012 were under 18 years old. Although the majority that year hailed from Bhutan, Burma, and Iraq, an increasing number of children have been coming from war-torn Syria since June 2014. The proposed ceiling for all refugees in the United States 2015 fiscal year is 70,000, a “significant number” of whom will be children with their families, according to a State Department spokesperson.
These children come with “unique medical, developmental and psychosocial needs,” noted Dr. Thomas J. Seery and fellow authors of “Caring for Refugee Children,” a Pediatrics in Review article recommended by Dr. Reines for pediatricians who may be caring for refugee children.
“The health care infrastructure of Syria is broken and many hospitals have closed, medications are difficult to obtain, and numerous doctors have fled the violence,” Dr. Reines said. She compared the anticipated health care problems of these children with those seen among Iraqi refugee children:
• Undernutrition and micronutrient deficiencies.
• Infectious diseases such as vaccine-preventable diseases like measles, but also typhoid, tuberculosis, and parasitic infections.
• Dental disease.
• Surgically amenable congenital anomalies such as congenital heart disease, myelomeningocele, and others that have not been repaired.
• Neurologic problems, such as cerebral palsy, intellectual disability, and autism.
• Hearing loss.
• Posttraumatic stress disorder (PTSD),depression, and anxiety.
• Trauma such as gunshot wounds, shrapnel injuries, and genital trauma secondary to sexual violence.
• Sequelae from illnesses that previously were easily treated, such as hearing loss and ear complications from otitis media, and rheumatic fever from inadequately treated strep throat.
• Underimmunization.
Various resources listed below, including Dr. Seery’s paper, can help guide providers in assessing and meeting these needs, and navigating paperwork and the U.S. refugee system. These resources also can help practitioners address the mental health concerns these patients and their families may face.
Mental health needs
Even children in the best physical shape will have experienced significant upheaval that could lead to depression, anxiety, and PTSD – conditions more common among refugee children than in the general population, research has shown.
“Mental health conditions will be especially present in these children uprooted from their homes and families, and exposed to the violence of war,” Dr. Francis E. Rushton Jr. of the department of pediatrics at the University of South Carolina, Columbia, and a member of the American Academy of Pediatrics Committee on Community Health Services, said in an interview. Of the four major areas of health care need he described for these children, two relate to mental health: toxic mental stress and fractured families and the lack of nurture.
One challenge pediatricians face, however, is recognizing these conditions despite cultural differences that could obscure them.
“It is not uncommon for teens and adults to deny symptoms of depression, stress, and anxiety in early encounters,” Dr. Reines said. “Many cultures stigmatize psychiatric or mental health problems, and refugees may be reluctant to admit they are having difficulties.”
One way around this obstacle is to ask patients and their parents about sleep, energy level, appetite, weight changes, and thoughts of harming one’s self, she said. Mental stress also manifests as somatic symptoms, such as headaches, stomach aches, and back pain, particularly in teens.
“Infants and toddlers are generally most adaptable as long as parents are coping well, and can provide a buffer for stress with a safe and nurturing environment,” Dr. Reines said. Children of parents with depression or PTSD, or who have lost a parent, may feel abandoned and experience depression or developmental delays.
Although school-age children may have nightmares, show anxiety, and cling to their parents, they usually transition well to their new homes. Adolescents face the biggest difficulties, especially if they have lost a parent, must care for their siblings, or have experienced sexual trauma. “They may have more vivid memories of disturbing events and a greater understanding of what their family has endured,” Dr. Reines said. Further, language and educational deficits can lead to alienation and embarrassment, yet families may rebuff behavioral health referrals.
“In these cases, it’s best to keep communication open, encourage dialogue with family, and try to find an activity or sport the refugee can participate in to improve self-esteem,” Dr. Reines said.
Avoiding cultural confusion
While cultural challenges are obvious – language barriers may necessitate translators or bicultural caseworkers – others may be more subtle. Developmental screening questions that rely on blocks, certain pictures, or other culturally specific bases, for example, may not adequately capture a child’s development.
Dr. Reines stresses a strategy for managing cultural differences that is recommended in Dr. Seery’s article: striving for cultural humility rather than cultural competence.
“It is impossible for U.S. physicians who have never practiced outside of our culture and are not bicultural or bilingual to become truly culturally competent in health care delivery for so many refugee populations,” Dr. Reines said. Instead then, cultural humility emphasizes showing respect, interest, and a willingness to learn from patients, she explained.
Cultural humility is a “lifelong process” that also demands flexibility and “allows the practitioner to release the false sense of security associated with stereotyping,” Dr. Seery and his colleagues wrote.
At the same time, pediatricians are guarding against inadvertent stereotyping; however, they can be aware of some cultural generalities that may apply to their Syrian refugee patients.
“Arab communities stress the importance of family rather than the individual and are often more modest than Westerners,” Dr. Rushton said. Further, “Arab families frequently experience discrimination on the basis of their religion in the United States, and pediatricians should be aware of ongoing traumatization even after arrival in America,” he said.
Teens may become embarrassed with discussions about sex or alcohol because few teens from the Middle East drink or become sexually active before marriage, Dr. Reines added. She noted that a Muslim male may not shake hands with females outside his family – a practice providers should respect – and that important religious holidays such as Ramadan may influence a family’s compliance with a treatment plan.
Perhaps the most important commonality, however, is one universal to most refugee families, regardless of their home country.
“The vast majority of families that we meet show incredible courage and resilience, and caring for their children is their highest priority,” Dr. Reines said. “We can learn a great deal from these families, and caring for their children is a tremendously rewarding experience.”
Other cultural resources:
Bridging Refugee Youth and Children’s Services
“The Middle of Everywhere: Helping Refugees Enter the American Community,” by Mary Pipher (Orlando: Mariner Books, 2003)
“Immigrant Medicine,” a textbook by Patricia Walker, M.D., and Elizabeth Barnett, M.D. (New York, N.Y.: Elsevier, 2007)
“Opening cultural doors: Providing culturally sensitive healthcare to Arab American and American Muslim patients” (Am J Obstet Gynecol. 2005 Oct;193]:1307-11).

Female Service Members in the Long War
September 11, 2001, is a day burned into the consciousness of all Americans old enough to remember that day. For members of the U.S. military, it was also the beginning of more than 14 years of war, variously called the war on terror, Operation Enduring Freedom (Afghanistan), Operation Iraqi Freedom (Iraq), Operation New Dawn (Iraq) and the Long War. The Long War encapsulates the repeated deployments into combat zones in Afghanistan and Iraq, as well as the Horn of Africa and to humanitarian assistance operations.
For women, 9/11 also ushered in a steadily increasing role in the U.S. military. No longer mainly nurses, as in the Vietnam War, or primarily in support roles, as in the Gulf War, female service members have been in the thick of the conflicts in Iraq and Afghanistan.
Only recently have women officially been allowed into the Military Occupational Specialty (MOS) of combat occupations. Combat occupations are typically the “warfighters”; however, it is now widely accepted that women have been in combat since long before 9/11. For example, the deployment to Somalia in 1993 started as a humanitarian assistance operation and was later turned into a combat mission. More recently, in the Long War, numerous roles open to women, such as military police and truckers, have been frequently involved in firefights.
New Research
Research and data about women in the military have had a relapsing course. After the first Gulf War, there were a number of articles focusing on the health issues of women deployed there. The main reasons for redeployment to the U.S. were abnormal pap smears gathered before deployment and positive pregnancy screens. In the late 1990s, there was a considerable amount of research, mainly covered under the loose rubric of the Defense Women’s Health Research Project.1
In 2002, I organized a symposium at the Women in Military Service Memorial, which focused on the prevention of urinary tract infections in the field, unintended pregnancy while deployed, and stress fractures. Partly because of the repeal of the combat exclusion rule and partly because the Long War seems to be winding down, recently there have been a number of activities and publications about women in combat. With COL Anne L. Naclerio, MD, MPH, I recently coedited Women at War, a collection of 19 articles that bring together much of the available information and experience on women service members’ health and mental health.2 We hope that it will further spur interest and research on the topic.
The lack of data on female service members is in contrast to the extensive scientific literature on male service members. The Walter Reed Army Institute of Research and the Mental Health Advisory teams both have focused on combat troops, which have been primarily male. The Millennium Study includes women, but its results are just beginning to emerge. The VA has data on female veterans, but only a small number of female veterans go to the VA, and VA studies on women have focused primarily on military sexual assault. Although this area is very important, there are many other issues that female service members deal with, including reproductive and genitourinary concerns.
The Women at War volume begins to address this problem. Chapters examine data on deployment-related issues, posttraumatic stress disorder (PTSD) in female service members, and intimate partner violence. Due to a lack of quantitative data, other chapters summarize either civilian data or data on male service members, then move to extrapolate for service women. A few chapters are more anecdotal, describing the experience of being a female sailor on a ship or a mother on deployment.
Reproduction and Gynecology
Much of the current discussion about women in the military focuses on physical strength. Can she carry a 60-round rucksack? Can she load artillery rounds? In contrast, issues about reproduction and gynecology are understudied in the recent literature on female service members.
Urinary tract infections (UTIs) are a major issue for women in the field. Much of the concerns that female service members have are about bathrooms. Is the latrine—maybe used by many other service members—clean enough to sit on? Women often restrict fluids to avoid going to the filthy or nonexistent bathrooms and thus get UTIs or become dehydrated. Managing menses in austere conditions is another dilemma. Can I change my tampon while driving on the roads in Iraq? Should I be on oral contraception while deployed to regulate menses?
Although sexual assault has received considerable attention, consensual sex has received much less. A taboo area seems to be the sexual desires of women who deploy. But young women—and most women who deploy are young—do have sexual desires, perhaps heightened by the daily exposure to death and close bonding in the combat zone. The literature is totally devoid on this topic. If contraception is scarce, pregnancies happen. In the worst cases, this results in ectopic pregnancies, resulting in life-threatening emergencies and expensive medical evacuations. In the best cases, unexpected pregnancy results in an evacuation from the war zone. There is no systematic data on availability of birth control.
Motherhood is also a major issue for female service members who are normally in their prime reproductive years. Concerns about pregnancy, being a mother, and breast-feeding are central, and being a mother and/or wife deploying not only leads to all types of emotional issues, but also personal growth.
Sexual Assault and Mental Health Disorders
Military sexual assault is a highly publicized area that is covered widely in both the scientific literature and the media. The number of cases reported has been rising, but this may be partially due to better reporting. In the military, as in the civilian world, this is not a simple issue, and many sexual activities are partially consensual, partially coercive. Sexual assault can lead to a myriad of mental health issues, including guilt, depression, PTSD, and substance abuse. In many cases, it can also lead to an exit from military service for both parties.
Posttraumatic stress disorder is a common consequence of combat. It has been studied widely in military men after Vietnam and during the Long War. It has also been widely studied in civilian women, especially after sexual assault. Far less is known about combat-related PTSD in military women; however, the available statistics show that military women have rates of combat-related PTSD at about the same rate as men. What we do not know is whether their PTSD symptoms are similar or different. Depression, suicide, and traumatic brain injury are also common sequelae that are covered in Women at War. Substance abuse and homelessness are likewise critically important areas but areas that need more research.
Conclusions
Medical and academic volumes rely on scientific evidence, which should lead to evidence-based practice. From that standpoint, Women at War has been a challenging one to put together, chiefly because there has been so little recent comprehensive data on the psychological and physical health of female service members. Nonetheless, this volume seeks to gather the data that are available, add anecdotal but universal information, translate it into actionable information for clinicians, and make recommendations for future research. Important take-home messages for the clinician include asking their patient about their overall military service, their experiences in the theater of war, and the positive and negative effects of that service.
Female service members are a vital part of the nation’s military and have been heavily deployed beside their male counterparts since the Persian Gulf War in 1990. The tragedy of 9/11 dramatically increased the operational tempo for all the troops.
It is hoped that this volume will stimulate more understanding of the experiences of female service members, women at war, in order to have the experience be a better one. Throughout this volume is implicit and/or explicit commentary on the lack of research data on gender issues in the military. Clearly, more targeted understanding is needed.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs.
1. Friedl KE. Biomedical research on health and performance of military women: accomplishments of the Defense Women’s Health Research Program (DWHRP). J Womens Health (Larchmt). 2005;14(9):764-802.
2. Ritchie EC, Naclerio AL, eds. Women at War. New York, NY: Oxford University Press; 2015.
September 11, 2001, is a day burned into the consciousness of all Americans old enough to remember that day. For members of the U.S. military, it was also the beginning of more than 14 years of war, variously called the war on terror, Operation Enduring Freedom (Afghanistan), Operation Iraqi Freedom (Iraq), Operation New Dawn (Iraq) and the Long War. The Long War encapsulates the repeated deployments into combat zones in Afghanistan and Iraq, as well as the Horn of Africa and to humanitarian assistance operations.
For women, 9/11 also ushered in a steadily increasing role in the U.S. military. No longer mainly nurses, as in the Vietnam War, or primarily in support roles, as in the Gulf War, female service members have been in the thick of the conflicts in Iraq and Afghanistan.
Only recently have women officially been allowed into the Military Occupational Specialty (MOS) of combat occupations. Combat occupations are typically the “warfighters”; however, it is now widely accepted that women have been in combat since long before 9/11. For example, the deployment to Somalia in 1993 started as a humanitarian assistance operation and was later turned into a combat mission. More recently, in the Long War, numerous roles open to women, such as military police and truckers, have been frequently involved in firefights.
New Research
Research and data about women in the military have had a relapsing course. After the first Gulf War, there were a number of articles focusing on the health issues of women deployed there. The main reasons for redeployment to the U.S. were abnormal pap smears gathered before deployment and positive pregnancy screens. In the late 1990s, there was a considerable amount of research, mainly covered under the loose rubric of the Defense Women’s Health Research Project.1
In 2002, I organized a symposium at the Women in Military Service Memorial, which focused on the prevention of urinary tract infections in the field, unintended pregnancy while deployed, and stress fractures. Partly because of the repeal of the combat exclusion rule and partly because the Long War seems to be winding down, recently there have been a number of activities and publications about women in combat. With COL Anne L. Naclerio, MD, MPH, I recently coedited Women at War, a collection of 19 articles that bring together much of the available information and experience on women service members’ health and mental health.2 We hope that it will further spur interest and research on the topic.
The lack of data on female service members is in contrast to the extensive scientific literature on male service members. The Walter Reed Army Institute of Research and the Mental Health Advisory teams both have focused on combat troops, which have been primarily male. The Millennium Study includes women, but its results are just beginning to emerge. The VA has data on female veterans, but only a small number of female veterans go to the VA, and VA studies on women have focused primarily on military sexual assault. Although this area is very important, there are many other issues that female service members deal with, including reproductive and genitourinary concerns.
The Women at War volume begins to address this problem. Chapters examine data on deployment-related issues, posttraumatic stress disorder (PTSD) in female service members, and intimate partner violence. Due to a lack of quantitative data, other chapters summarize either civilian data or data on male service members, then move to extrapolate for service women. A few chapters are more anecdotal, describing the experience of being a female sailor on a ship or a mother on deployment.
Reproduction and Gynecology
Much of the current discussion about women in the military focuses on physical strength. Can she carry a 60-round rucksack? Can she load artillery rounds? In contrast, issues about reproduction and gynecology are understudied in the recent literature on female service members.
Urinary tract infections (UTIs) are a major issue for women in the field. Much of the concerns that female service members have are about bathrooms. Is the latrine—maybe used by many other service members—clean enough to sit on? Women often restrict fluids to avoid going to the filthy or nonexistent bathrooms and thus get UTIs or become dehydrated. Managing menses in austere conditions is another dilemma. Can I change my tampon while driving on the roads in Iraq? Should I be on oral contraception while deployed to regulate menses?
Although sexual assault has received considerable attention, consensual sex has received much less. A taboo area seems to be the sexual desires of women who deploy. But young women—and most women who deploy are young—do have sexual desires, perhaps heightened by the daily exposure to death and close bonding in the combat zone. The literature is totally devoid on this topic. If contraception is scarce, pregnancies happen. In the worst cases, this results in ectopic pregnancies, resulting in life-threatening emergencies and expensive medical evacuations. In the best cases, unexpected pregnancy results in an evacuation from the war zone. There is no systematic data on availability of birth control.
Motherhood is also a major issue for female service members who are normally in their prime reproductive years. Concerns about pregnancy, being a mother, and breast-feeding are central, and being a mother and/or wife deploying not only leads to all types of emotional issues, but also personal growth.
Sexual Assault and Mental Health Disorders
Military sexual assault is a highly publicized area that is covered widely in both the scientific literature and the media. The number of cases reported has been rising, but this may be partially due to better reporting. In the military, as in the civilian world, this is not a simple issue, and many sexual activities are partially consensual, partially coercive. Sexual assault can lead to a myriad of mental health issues, including guilt, depression, PTSD, and substance abuse. In many cases, it can also lead to an exit from military service for both parties.
Posttraumatic stress disorder is a common consequence of combat. It has been studied widely in military men after Vietnam and during the Long War. It has also been widely studied in civilian women, especially after sexual assault. Far less is known about combat-related PTSD in military women; however, the available statistics show that military women have rates of combat-related PTSD at about the same rate as men. What we do not know is whether their PTSD symptoms are similar or different. Depression, suicide, and traumatic brain injury are also common sequelae that are covered in Women at War. Substance abuse and homelessness are likewise critically important areas but areas that need more research.
Conclusions
Medical and academic volumes rely on scientific evidence, which should lead to evidence-based practice. From that standpoint, Women at War has been a challenging one to put together, chiefly because there has been so little recent comprehensive data on the psychological and physical health of female service members. Nonetheless, this volume seeks to gather the data that are available, add anecdotal but universal information, translate it into actionable information for clinicians, and make recommendations for future research. Important take-home messages for the clinician include asking their patient about their overall military service, their experiences in the theater of war, and the positive and negative effects of that service.
Female service members are a vital part of the nation’s military and have been heavily deployed beside their male counterparts since the Persian Gulf War in 1990. The tragedy of 9/11 dramatically increased the operational tempo for all the troops.
It is hoped that this volume will stimulate more understanding of the experiences of female service members, women at war, in order to have the experience be a better one. Throughout this volume is implicit and/or explicit commentary on the lack of research data on gender issues in the military. Clearly, more targeted understanding is needed.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs.
September 11, 2001, is a day burned into the consciousness of all Americans old enough to remember that day. For members of the U.S. military, it was also the beginning of more than 14 years of war, variously called the war on terror, Operation Enduring Freedom (Afghanistan), Operation Iraqi Freedom (Iraq), Operation New Dawn (Iraq) and the Long War. The Long War encapsulates the repeated deployments into combat zones in Afghanistan and Iraq, as well as the Horn of Africa and to humanitarian assistance operations.
For women, 9/11 also ushered in a steadily increasing role in the U.S. military. No longer mainly nurses, as in the Vietnam War, or primarily in support roles, as in the Gulf War, female service members have been in the thick of the conflicts in Iraq and Afghanistan.
Only recently have women officially been allowed into the Military Occupational Specialty (MOS) of combat occupations. Combat occupations are typically the “warfighters”; however, it is now widely accepted that women have been in combat since long before 9/11. For example, the deployment to Somalia in 1993 started as a humanitarian assistance operation and was later turned into a combat mission. More recently, in the Long War, numerous roles open to women, such as military police and truckers, have been frequently involved in firefights.
New Research
Research and data about women in the military have had a relapsing course. After the first Gulf War, there were a number of articles focusing on the health issues of women deployed there. The main reasons for redeployment to the U.S. were abnormal pap smears gathered before deployment and positive pregnancy screens. In the late 1990s, there was a considerable amount of research, mainly covered under the loose rubric of the Defense Women’s Health Research Project.1
In 2002, I organized a symposium at the Women in Military Service Memorial, which focused on the prevention of urinary tract infections in the field, unintended pregnancy while deployed, and stress fractures. Partly because of the repeal of the combat exclusion rule and partly because the Long War seems to be winding down, recently there have been a number of activities and publications about women in combat. With COL Anne L. Naclerio, MD, MPH, I recently coedited Women at War, a collection of 19 articles that bring together much of the available information and experience on women service members’ health and mental health.2 We hope that it will further spur interest and research on the topic.
The lack of data on female service members is in contrast to the extensive scientific literature on male service members. The Walter Reed Army Institute of Research and the Mental Health Advisory teams both have focused on combat troops, which have been primarily male. The Millennium Study includes women, but its results are just beginning to emerge. The VA has data on female veterans, but only a small number of female veterans go to the VA, and VA studies on women have focused primarily on military sexual assault. Although this area is very important, there are many other issues that female service members deal with, including reproductive and genitourinary concerns.
The Women at War volume begins to address this problem. Chapters examine data on deployment-related issues, posttraumatic stress disorder (PTSD) in female service members, and intimate partner violence. Due to a lack of quantitative data, other chapters summarize either civilian data or data on male service members, then move to extrapolate for service women. A few chapters are more anecdotal, describing the experience of being a female sailor on a ship or a mother on deployment.
Reproduction and Gynecology
Much of the current discussion about women in the military focuses on physical strength. Can she carry a 60-round rucksack? Can she load artillery rounds? In contrast, issues about reproduction and gynecology are understudied in the recent literature on female service members.
Urinary tract infections (UTIs) are a major issue for women in the field. Much of the concerns that female service members have are about bathrooms. Is the latrine—maybe used by many other service members—clean enough to sit on? Women often restrict fluids to avoid going to the filthy or nonexistent bathrooms and thus get UTIs or become dehydrated. Managing menses in austere conditions is another dilemma. Can I change my tampon while driving on the roads in Iraq? Should I be on oral contraception while deployed to regulate menses?
Although sexual assault has received considerable attention, consensual sex has received much less. A taboo area seems to be the sexual desires of women who deploy. But young women—and most women who deploy are young—do have sexual desires, perhaps heightened by the daily exposure to death and close bonding in the combat zone. The literature is totally devoid on this topic. If contraception is scarce, pregnancies happen. In the worst cases, this results in ectopic pregnancies, resulting in life-threatening emergencies and expensive medical evacuations. In the best cases, unexpected pregnancy results in an evacuation from the war zone. There is no systematic data on availability of birth control.
Motherhood is also a major issue for female service members who are normally in their prime reproductive years. Concerns about pregnancy, being a mother, and breast-feeding are central, and being a mother and/or wife deploying not only leads to all types of emotional issues, but also personal growth.
Sexual Assault and Mental Health Disorders
Military sexual assault is a highly publicized area that is covered widely in both the scientific literature and the media. The number of cases reported has been rising, but this may be partially due to better reporting. In the military, as in the civilian world, this is not a simple issue, and many sexual activities are partially consensual, partially coercive. Sexual assault can lead to a myriad of mental health issues, including guilt, depression, PTSD, and substance abuse. In many cases, it can also lead to an exit from military service for both parties.
Posttraumatic stress disorder is a common consequence of combat. It has been studied widely in military men after Vietnam and during the Long War. It has also been widely studied in civilian women, especially after sexual assault. Far less is known about combat-related PTSD in military women; however, the available statistics show that military women have rates of combat-related PTSD at about the same rate as men. What we do not know is whether their PTSD symptoms are similar or different. Depression, suicide, and traumatic brain injury are also common sequelae that are covered in Women at War. Substance abuse and homelessness are likewise critically important areas but areas that need more research.
Conclusions
Medical and academic volumes rely on scientific evidence, which should lead to evidence-based practice. From that standpoint, Women at War has been a challenging one to put together, chiefly because there has been so little recent comprehensive data on the psychological and physical health of female service members. Nonetheless, this volume seeks to gather the data that are available, add anecdotal but universal information, translate it into actionable information for clinicians, and make recommendations for future research. Important take-home messages for the clinician include asking their patient about their overall military service, their experiences in the theater of war, and the positive and negative effects of that service.
Female service members are a vital part of the nation’s military and have been heavily deployed beside their male counterparts since the Persian Gulf War in 1990. The tragedy of 9/11 dramatically increased the operational tempo for all the troops.
It is hoped that this volume will stimulate more understanding of the experiences of female service members, women at war, in order to have the experience be a better one. Throughout this volume is implicit and/or explicit commentary on the lack of research data on gender issues in the military. Clearly, more targeted understanding is needed.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs.
1. Friedl KE. Biomedical research on health and performance of military women: accomplishments of the Defense Women’s Health Research Program (DWHRP). J Womens Health (Larchmt). 2005;14(9):764-802.
2. Ritchie EC, Naclerio AL, eds. Women at War. New York, NY: Oxford University Press; 2015.
1. Friedl KE. Biomedical research on health and performance of military women: accomplishments of the Defense Women’s Health Research Program (DWHRP). J Womens Health (Larchmt). 2005;14(9):764-802.
2. Ritchie EC, Naclerio AL, eds. Women at War. New York, NY: Oxford University Press; 2015.

Communication key to helping kids after disasters
Posttraumatic stress disorder can be hard to spot in kids after natural or manmade disasters.
They may not understand that intrusive thoughts, panic attacks, and other symptoms are problems that can be addressed, and are unlikely to mention them.
As a result, parents, teachers, and others often underestimate children’s distress levels and overestimate their resilience. One way around the problem is to ask children how they’re doing, and probe for signs of trouble. It helps to let them know that PTSD and adjustment problems are normal after a frightening event, and to teach them how to anticipate and cope with PTSD triggers.
That’s just a small fraction of the useful advice in new guidance from the American Academy of Pediatrics on the psychosocial support of children and families after disasters, published online Sept. 14 (Pediatrics. 2015 Sept. 14. doi:10.1542/peds.2015-2861).
“Children are particularly vulnerable to the effects of disasters and other traumatic events because of a lack of experience, skills, and resources to be able to independently meet their developmental, socioemotional, mental, and behavioral health needs,” said the authors, led by Dr. David Schonfeld of St. Christopher’s Hospital for Children, and Thomas Demaria, Ph.D., of Long Island (N.Y.) University.
Mental health triage should come right after medical stabilization. Dissociative symptoms; extreme confusion or inability to concentrate or make even simple decisions; intense fear, anxiety, panic, helplessness, or horror; depression at the time of the event; uncontrollable and intense grief; suicidal ideation; and marked somatization are among the warning signs that kids are in trouble.
Psychiatric medications to blunt such reactions are usually the wrong call. “Children need to develop an understanding of the event and learn to express and cope with their reactions.” If medication does seem necessary, its best to let an expert in childhood trauma make the decision, the authors said.
Dismissing children’s concerns is a mistake. “In reality, if children feel worried, then they are worried. Telling them that they should not be worried is usually ineffective.” It’s also a mistake to avoid talking about grief for fear of making it worse. Children’s “distress is caused by the reaction to the death itself, rather than any question or invitation to talk. Talking may provide some relief if not coerced. Avoiding discussion is rarely helpful and often isolates children at a time when they are most in need of support and assistance,” they said.
Simple, basic facts about the event – as long as they’re not graphic or overwhelming – will help children make sense of what they’ve been through, and reassurance that things will eventually be okay can be healing. Kids also have to know that the situation isn’t their fault, and how to cope with it.
Parents can share how they’re upset about losing their home, for instance, but then discuss how talking to another trusted adult, getting exercise, meditating, and helping others makes them feel better. Pediatricians can boost spirits by saying something like “the tornado created a big mess, but we are pulling together as a community” or “living in a shelter with all the other children in the neighborhood must have been a real adventure,” the authors said.
Having children contribute to food drives or draw hopeful pictures for victims in the hospital can help them regain a sense of control and usefulness. Resuming their routines as soon as possible will also help bring back a sense of normalcy.
Bereavement counseling is in order when children are struggling with the loss of a loved one, and cognitive behavioral therapy for kids with PTSD.
Posttraumatic stress disorder can be hard to spot in kids after natural or manmade disasters.
They may not understand that intrusive thoughts, panic attacks, and other symptoms are problems that can be addressed, and are unlikely to mention them.
As a result, parents, teachers, and others often underestimate children’s distress levels and overestimate their resilience. One way around the problem is to ask children how they’re doing, and probe for signs of trouble. It helps to let them know that PTSD and adjustment problems are normal after a frightening event, and to teach them how to anticipate and cope with PTSD triggers.
That’s just a small fraction of the useful advice in new guidance from the American Academy of Pediatrics on the psychosocial support of children and families after disasters, published online Sept. 14 (Pediatrics. 2015 Sept. 14. doi:10.1542/peds.2015-2861).
“Children are particularly vulnerable to the effects of disasters and other traumatic events because of a lack of experience, skills, and resources to be able to independently meet their developmental, socioemotional, mental, and behavioral health needs,” said the authors, led by Dr. David Schonfeld of St. Christopher’s Hospital for Children, and Thomas Demaria, Ph.D., of Long Island (N.Y.) University.
Mental health triage should come right after medical stabilization. Dissociative symptoms; extreme confusion or inability to concentrate or make even simple decisions; intense fear, anxiety, panic, helplessness, or horror; depression at the time of the event; uncontrollable and intense grief; suicidal ideation; and marked somatization are among the warning signs that kids are in trouble.
Psychiatric medications to blunt such reactions are usually the wrong call. “Children need to develop an understanding of the event and learn to express and cope with their reactions.” If medication does seem necessary, its best to let an expert in childhood trauma make the decision, the authors said.
Dismissing children’s concerns is a mistake. “In reality, if children feel worried, then they are worried. Telling them that they should not be worried is usually ineffective.” It’s also a mistake to avoid talking about grief for fear of making it worse. Children’s “distress is caused by the reaction to the death itself, rather than any question or invitation to talk. Talking may provide some relief if not coerced. Avoiding discussion is rarely helpful and often isolates children at a time when they are most in need of support and assistance,” they said.
Simple, basic facts about the event – as long as they’re not graphic or overwhelming – will help children make sense of what they’ve been through, and reassurance that things will eventually be okay can be healing. Kids also have to know that the situation isn’t their fault, and how to cope with it.
Parents can share how they’re upset about losing their home, for instance, but then discuss how talking to another trusted adult, getting exercise, meditating, and helping others makes them feel better. Pediatricians can boost spirits by saying something like “the tornado created a big mess, but we are pulling together as a community” or “living in a shelter with all the other children in the neighborhood must have been a real adventure,” the authors said.
Having children contribute to food drives or draw hopeful pictures for victims in the hospital can help them regain a sense of control and usefulness. Resuming their routines as soon as possible will also help bring back a sense of normalcy.
Bereavement counseling is in order when children are struggling with the loss of a loved one, and cognitive behavioral therapy for kids with PTSD.
Posttraumatic stress disorder can be hard to spot in kids after natural or manmade disasters.
They may not understand that intrusive thoughts, panic attacks, and other symptoms are problems that can be addressed, and are unlikely to mention them.
As a result, parents, teachers, and others often underestimate children’s distress levels and overestimate their resilience. One way around the problem is to ask children how they’re doing, and probe for signs of trouble. It helps to let them know that PTSD and adjustment problems are normal after a frightening event, and to teach them how to anticipate and cope with PTSD triggers.
That’s just a small fraction of the useful advice in new guidance from the American Academy of Pediatrics on the psychosocial support of children and families after disasters, published online Sept. 14 (Pediatrics. 2015 Sept. 14. doi:10.1542/peds.2015-2861).
“Children are particularly vulnerable to the effects of disasters and other traumatic events because of a lack of experience, skills, and resources to be able to independently meet their developmental, socioemotional, mental, and behavioral health needs,” said the authors, led by Dr. David Schonfeld of St. Christopher’s Hospital for Children, and Thomas Demaria, Ph.D., of Long Island (N.Y.) University.
Mental health triage should come right after medical stabilization. Dissociative symptoms; extreme confusion or inability to concentrate or make even simple decisions; intense fear, anxiety, panic, helplessness, or horror; depression at the time of the event; uncontrollable and intense grief; suicidal ideation; and marked somatization are among the warning signs that kids are in trouble.
Psychiatric medications to blunt such reactions are usually the wrong call. “Children need to develop an understanding of the event and learn to express and cope with their reactions.” If medication does seem necessary, its best to let an expert in childhood trauma make the decision, the authors said.
Dismissing children’s concerns is a mistake. “In reality, if children feel worried, then they are worried. Telling them that they should not be worried is usually ineffective.” It’s also a mistake to avoid talking about grief for fear of making it worse. Children’s “distress is caused by the reaction to the death itself, rather than any question or invitation to talk. Talking may provide some relief if not coerced. Avoiding discussion is rarely helpful and often isolates children at a time when they are most in need of support and assistance,” they said.
Simple, basic facts about the event – as long as they’re not graphic or overwhelming – will help children make sense of what they’ve been through, and reassurance that things will eventually be okay can be healing. Kids also have to know that the situation isn’t their fault, and how to cope with it.
Parents can share how they’re upset about losing their home, for instance, but then discuss how talking to another trusted adult, getting exercise, meditating, and helping others makes them feel better. Pediatricians can boost spirits by saying something like “the tornado created a big mess, but we are pulling together as a community” or “living in a shelter with all the other children in the neighborhood must have been a real adventure,” the authors said.
Having children contribute to food drives or draw hopeful pictures for victims in the hospital can help them regain a sense of control and usefulness. Resuming their routines as soon as possible will also help bring back a sense of normalcy.
Bereavement counseling is in order when children are struggling with the loss of a loved one, and cognitive behavioral therapy for kids with PTSD.
FROM PEDIATRICS
Banking on Vets for Better PTSD Research
Veterans can now help advance PTSD research by enrolling in a “brain bank.” A consortium led by the VA National Center for Posttraumatic Stress Disorder has launched the first brain tissue repository to support research into causes, progression, and treatment of PTSD.
Related: PTSD Campaign: Caring and Sharing
The Leahy-Friedman National PTSD Brain Bank is the fruit of 12 years of labor by Senator Patrick Leahy (D-VT) and Dr. Matthew Friedman, senior advisor to the VA PTSD Center and its former executive director. Dr. Friedman is directing the consortium, which will have sites across the U.S.
Brain bank researchers will follow the health of enrolled participants during their lifetime; participants will donate brain and body tissue after death. Any veteran with PTSD living in the U.S. is eligible to enroll—as are veterans without PTSD, who are needed for purposes of comparison.
Related: Evidence-Based Psychotherapy Telemental Health Center and Regional Pilot
Participation involves filling out surveys by telephone, mail, or a secure Internet website. Surveys ask about exposure to chemicals at home, work, or during military service. Participants are also asked about mental health and given brief tests of memory and concentration. Information collected is labeled with a code that does not identify the veteran directly; all information is kept confidential. The veteran has the right to withdraw at any time, even after signing consent forms. VA benefits and VA health care will not be influenced in any way by agreeing or refusing to participate. Next of kin can give consent immediately following a veteran’s death.
Related: Attention-Deficit/Hyperactivity Disorder in a VA Polytrauma Clinic
The data will expand knowledge about a significant health concern for veterans: In 2013, 533,720 veterans with a primary or secondary diagnosis of PTSD were treated at VAMCs and clinics. “Although we have learned a great deal about abnormalities in brain structure and function from brain imaging research, there is no substitute for looking at the neurons themselves,” said Dr. Friedman. “Understanding the cellular and circuit contributions to abnormal brain activity in PTSD is critical in the search for potential biomarkers of susceptibility, illness, and treatment response and for developing new treatments targeting the conditions at the cellular level.”
Veterans interested in learning more about the brain bank and enrollment can call (800) 762-6609 or visit www.research.va.gov/programs/tissue_banking/PTSD/default.cfm.
Veterans can now help advance PTSD research by enrolling in a “brain bank.” A consortium led by the VA National Center for Posttraumatic Stress Disorder has launched the first brain tissue repository to support research into causes, progression, and treatment of PTSD.
Related: PTSD Campaign: Caring and Sharing
The Leahy-Friedman National PTSD Brain Bank is the fruit of 12 years of labor by Senator Patrick Leahy (D-VT) and Dr. Matthew Friedman, senior advisor to the VA PTSD Center and its former executive director. Dr. Friedman is directing the consortium, which will have sites across the U.S.
Brain bank researchers will follow the health of enrolled participants during their lifetime; participants will donate brain and body tissue after death. Any veteran with PTSD living in the U.S. is eligible to enroll—as are veterans without PTSD, who are needed for purposes of comparison.
Related: Evidence-Based Psychotherapy Telemental Health Center and Regional Pilot
Participation involves filling out surveys by telephone, mail, or a secure Internet website. Surveys ask about exposure to chemicals at home, work, or during military service. Participants are also asked about mental health and given brief tests of memory and concentration. Information collected is labeled with a code that does not identify the veteran directly; all information is kept confidential. The veteran has the right to withdraw at any time, even after signing consent forms. VA benefits and VA health care will not be influenced in any way by agreeing or refusing to participate. Next of kin can give consent immediately following a veteran’s death.
Related: Attention-Deficit/Hyperactivity Disorder in a VA Polytrauma Clinic
The data will expand knowledge about a significant health concern for veterans: In 2013, 533,720 veterans with a primary or secondary diagnosis of PTSD were treated at VAMCs and clinics. “Although we have learned a great deal about abnormalities in brain structure and function from brain imaging research, there is no substitute for looking at the neurons themselves,” said Dr. Friedman. “Understanding the cellular and circuit contributions to abnormal brain activity in PTSD is critical in the search for potential biomarkers of susceptibility, illness, and treatment response and for developing new treatments targeting the conditions at the cellular level.”
Veterans interested in learning more about the brain bank and enrollment can call (800) 762-6609 or visit www.research.va.gov/programs/tissue_banking/PTSD/default.cfm.
Veterans can now help advance PTSD research by enrolling in a “brain bank.” A consortium led by the VA National Center for Posttraumatic Stress Disorder has launched the first brain tissue repository to support research into causes, progression, and treatment of PTSD.
Related: PTSD Campaign: Caring and Sharing
The Leahy-Friedman National PTSD Brain Bank is the fruit of 12 years of labor by Senator Patrick Leahy (D-VT) and Dr. Matthew Friedman, senior advisor to the VA PTSD Center and its former executive director. Dr. Friedman is directing the consortium, which will have sites across the U.S.
Brain bank researchers will follow the health of enrolled participants during their lifetime; participants will donate brain and body tissue after death. Any veteran with PTSD living in the U.S. is eligible to enroll—as are veterans without PTSD, who are needed for purposes of comparison.
Related: Evidence-Based Psychotherapy Telemental Health Center and Regional Pilot
Participation involves filling out surveys by telephone, mail, or a secure Internet website. Surveys ask about exposure to chemicals at home, work, or during military service. Participants are also asked about mental health and given brief tests of memory and concentration. Information collected is labeled with a code that does not identify the veteran directly; all information is kept confidential. The veteran has the right to withdraw at any time, even after signing consent forms. VA benefits and VA health care will not be influenced in any way by agreeing or refusing to participate. Next of kin can give consent immediately following a veteran’s death.
Related: Attention-Deficit/Hyperactivity Disorder in a VA Polytrauma Clinic
The data will expand knowledge about a significant health concern for veterans: In 2013, 533,720 veterans with a primary or secondary diagnosis of PTSD were treated at VAMCs and clinics. “Although we have learned a great deal about abnormalities in brain structure and function from brain imaging research, there is no substitute for looking at the neurons themselves,” said Dr. Friedman. “Understanding the cellular and circuit contributions to abnormal brain activity in PTSD is critical in the search for potential biomarkers of susceptibility, illness, and treatment response and for developing new treatments targeting the conditions at the cellular level.”
Veterans interested in learning more about the brain bank and enrollment can call (800) 762-6609 or visit www.research.va.gov/programs/tissue_banking/PTSD/default.cfm.
VA Hospital Deficiencies Contributed to Marine’s Death
On August 30, 2014, a 35-year-old marine died during inpatient treatment for mental health at the Tomah VAMC in Wisconsin. A year later, the VA Office of Inspector General (OIG) Office of Healthcare Inspections determined a number of deficiencies in hospital operations as a result of the investigation of this patient’s death.
Among these deficiencies were a lack of documenting patient consent for treatment and insufficient response to the patient’s cardiopulmonary emergency.
“We are deeply saddened by the tragic, avoidable death of this veteran and are committed to learning from this event and making improvements in the care we provide to our veterans,” the Tomah VAMC said in a statement.
Related: Negligence Settlement Reached After Army Hospital Death
Neither of the 2 psychiatrists treating the patient, Jason Simcakoski, obtained informed consent, verbal or written, for the buprenorphine/naloxone, according to both the patient’s electronic health record and the treating psychiatrists’ accounts. The prescription was administered to the patient with an off-label indication beginning the day prior to his death.
In addition, when the patient was found unresponsive in his room, “unit staff did not immediately assess the patient and determine the need for cardiopulmonary resuscitation,” nor did they use the in-room emergency call system or determine cardiac activity with the automatic external defibrillator, as noted in the OIG report.
Mr. Simcakoski served with the U.S. Marine Corp from 1998 until his honorable discharge in 2002. Mr. Simcakoski established VA medical care in 2003, according to the OIG report. Two years later, he sought help for his addiction to oxycodone, a medication he said he obtained from a friend; no VA provider ever prescribed Mr. Simcakoski oxycodone or other Schedule II opioid analgesic. The patient was treated for addiction at a non-VA clinic through 2007 and again in 2010.
Related: VISN 22 Evidence-Based Psychotherapy Telemental Health Center and Regional Pilot
The patient’s psychiatric diagnoses included posttraumatic stress disorder, bipolar I disorder, generalized anxiety disorder, attention deficit/hyperactivity disorder, panic disorder, opioid dependence, and alcohol and benzodiazepine abuse.
As a result of OIG recommendations, one of the psychiatrists involved in this case was terminated and the second awaits administrative proceedings. Under the direction of the Tomah VAMC acting chief of staff, all appropriate providers will be required to take relevant VHA training on informed consent, and all patients currently on buprenorphine will be reviewed to ensure consent has been obtained, both of which have an October 2015 target date of completion.
“I feel some comfort knowing they have admitted they failed Jason,” Heather Fluty Simcakoski, the victim’s widow, told Gannett Wisconsin Media. “It doesn't bring him back, but I know it's a step closer to getting justice for him.”
On August 30, 2014, a 35-year-old marine died during inpatient treatment for mental health at the Tomah VAMC in Wisconsin. A year later, the VA Office of Inspector General (OIG) Office of Healthcare Inspections determined a number of deficiencies in hospital operations as a result of the investigation of this patient’s death.
Among these deficiencies were a lack of documenting patient consent for treatment and insufficient response to the patient’s cardiopulmonary emergency.
“We are deeply saddened by the tragic, avoidable death of this veteran and are committed to learning from this event and making improvements in the care we provide to our veterans,” the Tomah VAMC said in a statement.
Related: Negligence Settlement Reached After Army Hospital Death
Neither of the 2 psychiatrists treating the patient, Jason Simcakoski, obtained informed consent, verbal or written, for the buprenorphine/naloxone, according to both the patient’s electronic health record and the treating psychiatrists’ accounts. The prescription was administered to the patient with an off-label indication beginning the day prior to his death.
In addition, when the patient was found unresponsive in his room, “unit staff did not immediately assess the patient and determine the need for cardiopulmonary resuscitation,” nor did they use the in-room emergency call system or determine cardiac activity with the automatic external defibrillator, as noted in the OIG report.
Mr. Simcakoski served with the U.S. Marine Corp from 1998 until his honorable discharge in 2002. Mr. Simcakoski established VA medical care in 2003, according to the OIG report. Two years later, he sought help for his addiction to oxycodone, a medication he said he obtained from a friend; no VA provider ever prescribed Mr. Simcakoski oxycodone or other Schedule II opioid analgesic. The patient was treated for addiction at a non-VA clinic through 2007 and again in 2010.
Related: VISN 22 Evidence-Based Psychotherapy Telemental Health Center and Regional Pilot
The patient’s psychiatric diagnoses included posttraumatic stress disorder, bipolar I disorder, generalized anxiety disorder, attention deficit/hyperactivity disorder, panic disorder, opioid dependence, and alcohol and benzodiazepine abuse.
As a result of OIG recommendations, one of the psychiatrists involved in this case was terminated and the second awaits administrative proceedings. Under the direction of the Tomah VAMC acting chief of staff, all appropriate providers will be required to take relevant VHA training on informed consent, and all patients currently on buprenorphine will be reviewed to ensure consent has been obtained, both of which have an October 2015 target date of completion.
“I feel some comfort knowing they have admitted they failed Jason,” Heather Fluty Simcakoski, the victim’s widow, told Gannett Wisconsin Media. “It doesn't bring him back, but I know it's a step closer to getting justice for him.”
On August 30, 2014, a 35-year-old marine died during inpatient treatment for mental health at the Tomah VAMC in Wisconsin. A year later, the VA Office of Inspector General (OIG) Office of Healthcare Inspections determined a number of deficiencies in hospital operations as a result of the investigation of this patient’s death.
Among these deficiencies were a lack of documenting patient consent for treatment and insufficient response to the patient’s cardiopulmonary emergency.
“We are deeply saddened by the tragic, avoidable death of this veteran and are committed to learning from this event and making improvements in the care we provide to our veterans,” the Tomah VAMC said in a statement.
Related: Negligence Settlement Reached After Army Hospital Death
Neither of the 2 psychiatrists treating the patient, Jason Simcakoski, obtained informed consent, verbal or written, for the buprenorphine/naloxone, according to both the patient’s electronic health record and the treating psychiatrists’ accounts. The prescription was administered to the patient with an off-label indication beginning the day prior to his death.
In addition, when the patient was found unresponsive in his room, “unit staff did not immediately assess the patient and determine the need for cardiopulmonary resuscitation,” nor did they use the in-room emergency call system or determine cardiac activity with the automatic external defibrillator, as noted in the OIG report.
Mr. Simcakoski served with the U.S. Marine Corp from 1998 until his honorable discharge in 2002. Mr. Simcakoski established VA medical care in 2003, according to the OIG report. Two years later, he sought help for his addiction to oxycodone, a medication he said he obtained from a friend; no VA provider ever prescribed Mr. Simcakoski oxycodone or other Schedule II opioid analgesic. The patient was treated for addiction at a non-VA clinic through 2007 and again in 2010.
Related: VISN 22 Evidence-Based Psychotherapy Telemental Health Center and Regional Pilot
The patient’s psychiatric diagnoses included posttraumatic stress disorder, bipolar I disorder, generalized anxiety disorder, attention deficit/hyperactivity disorder, panic disorder, opioid dependence, and alcohol and benzodiazepine abuse.
As a result of OIG recommendations, one of the psychiatrists involved in this case was terminated and the second awaits administrative proceedings. Under the direction of the Tomah VAMC acting chief of staff, all appropriate providers will be required to take relevant VHA training on informed consent, and all patients currently on buprenorphine will be reviewed to ensure consent has been obtained, both of which have an October 2015 target date of completion.
“I feel some comfort knowing they have admitted they failed Jason,” Heather Fluty Simcakoski, the victim’s widow, told Gannett Wisconsin Media. “It doesn't bring him back, but I know it's a step closer to getting justice for him.”

VIDEO: Three veterans describe impact of mindfulness therapy
Mindfulness-based stress reduction therapy teaches patients to be in the present moment in nonjudgmental, accepting ways. Researchers at the Minneapolis Veterans Affairs Medical Center decided to compare a mindfulness intervention with present-centered group therapy of 116 veterans with post-traumatic stress disorder.
Those in the mindfulness group had eight weekly 2.5-hour sessions and one day-long retreat. Veterans in the present-centered group attended nine weekly 1.5-hour group sessions focusing on current problems. The results found that the veterans who used the mindfulness techniques experienced a greater decrease in the severity of their PTSD symptoms than did those in the other group.
In this video, Melissa A. Polusny, Ph.D., and Dr. Kelvin O. Lim, both of the medical center, talk with three veterans with PTSD about how mindfulness changed their quality of life and helped them find peace of mind.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Mindfulness-based stress reduction therapy teaches patients to be in the present moment in nonjudgmental, accepting ways. Researchers at the Minneapolis Veterans Affairs Medical Center decided to compare a mindfulness intervention with present-centered group therapy of 116 veterans with post-traumatic stress disorder.
Those in the mindfulness group had eight weekly 2.5-hour sessions and one day-long retreat. Veterans in the present-centered group attended nine weekly 1.5-hour group sessions focusing on current problems. The results found that the veterans who used the mindfulness techniques experienced a greater decrease in the severity of their PTSD symptoms than did those in the other group.
In this video, Melissa A. Polusny, Ph.D., and Dr. Kelvin O. Lim, both of the medical center, talk with three veterans with PTSD about how mindfulness changed their quality of life and helped them find peace of mind.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Mindfulness-based stress reduction therapy teaches patients to be in the present moment in nonjudgmental, accepting ways. Researchers at the Minneapolis Veterans Affairs Medical Center decided to compare a mindfulness intervention with present-centered group therapy of 116 veterans with post-traumatic stress disorder.
Those in the mindfulness group had eight weekly 2.5-hour sessions and one day-long retreat. Veterans in the present-centered group attended nine weekly 1.5-hour group sessions focusing on current problems. The results found that the veterans who used the mindfulness techniques experienced a greater decrease in the severity of their PTSD symptoms than did those in the other group.
In this video, Melissa A. Polusny, Ph.D., and Dr. Kelvin O. Lim, both of the medical center, talk with three veterans with PTSD about how mindfulness changed their quality of life and helped them find peace of mind.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Stopping intergenerational cycles of trauma
Understanding the root of stress and trauma experienced by patients as individuals is a key charge of psychiatry. But patients also can experience psychological distress because of the traumatic experiences of previous generations. The mental health community must be prepared to treat patients who fall into the latter category.
My colleagues and I recently analyzed representative samples of First Nations adults and youth living on a reserve in Canada. We found that the number of previous generations in which families were forced to attend Indian residential schools was cumulatively linked with higher levels of psychological distress and suicidal ideation among those who did not attend themselves (Transcultural Psychiatry. 2014, 51:320-338).
The forced removal of Indigenous children from their homes for the purposes of assimilation occurred over generations in many countries around the world. In Canada, these government-mandated church-run residential schools ran from the mid-1800s until 1996, and resulted in generations of indigenous children being exposed to chronic neglect, abuse, trauma, racism, and cultural shaming (“Honouring the Truth: Reconciling for the Future,” Truth and Reconciliation Commission of Canada, 2015).

Some of our more recent analyses revealed that having a family history of residential school attendance has been linked to a greater likelihood of early-onset mental health symptoms, which in turn, has been tied to an increased risk of suicidality and other unique outcomes that have implications for treatment and prevention. Furthermore, other negative outcomes experienced by indigenous peoples, such as low family income and limited educational opportunities, also appear to be involved in the intergenerational transmission of residential school trauma.
Against this backdrop in Canada, we have a prevailing sense of blaming the victim that is counterproductive to healing. According to a 2014 report by the Royal Canadian Mounted Police (RCMP), 1,017 indigenous women and girls were murdered between 1980 and 2012 across Canada. About one-third of the women died as a result of physical beating, and more than 90% of the victims had a “previous relationship” with the person who killed them, according to the RCMP report. Yet, despite evidence to the contrary, the prime minister of Canada shared his view last year that those staggering numbers should be viewed as a criminal issue and not a “sociological phenomenon” (CBC News, Aug. 21, 2014).
Members of other groups whose previous generations also were exposed indirectly to unspeakable trauma include Americans of African descent, Native Americans, and adult offspring of Holocaust survivors. Rachel Yehuda, Ph.D., has studied the latter group extensively.
In one study, Dr. Yehuda and her associates found significantly reduced cortisol excretion in Holocaust offspring, compared with controls (Psychoneuroendocrinology. 2014 Oct;48:1-10). In another study of the adult offspring of Holocaust survivors, Dr. Yehuda, professor of psychiatry at the Icahn School of Medicine at Mount Sinai in New York, found that “offspring with paternal [posttraumatic stress disorder] showed higher GR-1F promoter methylation, whereas offspring with both maternal and paternal PTSD showed lower methylation.” Furthermore, lower methylation was tied to greater suppression of cortisol (Am J Psychiatry. 2014 Aug;171(8)872-880).
An appreciation for the power of epigenetics, or “soul wounds,” can help us stop blaming indigenous and other traumatized populations, and start tending to their mental health needs. Furthermore, getting individuals to understand these concepts can be yet another step on the path toward healing.
A study of 19 staff members and clients in a Native American healing lodge who began a discourse on the legacy of historical trauma found that counselors understood that their clients carried pain “leading to adult dysfunction, including substance abuse” (J Consult Clin Psychol. 2009 Aug;77(4):751-762). Second, the counselors believed that the pain needed to be confessed. Third, the counselors thought that expressing the pain would help the clients become more introspective. Finally, the process included reclaiming “indigenous heritage, identity, and spirituality that program staff thought would neutralize the pathogenic effects of colonization.”
We do not know the extent to which epigenetics are involved in specific diseases. Epigenetic mechanisms have not yet been tested as pathways involved in the intergenerational transmission of trauma in indigenous peoples. But Dr. Yehuda’s work with the children of Holocaust survivors shows that these mechanisms do indeed exist.
In light of what we do understand and the DSM-5’s emphasis on cultural competency, mental health professionals have a role to play in reversing the negative intergenerational cycles experienced by people across the globe. Only when we start paying attention to the plight of indigenous peoples across the globe will true healing begin.
Dr. Bombay is assistant professor of psychiatry at Dalhousie University, Halifax, N.S.
Understanding the root of stress and trauma experienced by patients as individuals is a key charge of psychiatry. But patients also can experience psychological distress because of the traumatic experiences of previous generations. The mental health community must be prepared to treat patients who fall into the latter category.
My colleagues and I recently analyzed representative samples of First Nations adults and youth living on a reserve in Canada. We found that the number of previous generations in which families were forced to attend Indian residential schools was cumulatively linked with higher levels of psychological distress and suicidal ideation among those who did not attend themselves (Transcultural Psychiatry. 2014, 51:320-338).
The forced removal of Indigenous children from their homes for the purposes of assimilation occurred over generations in many countries around the world. In Canada, these government-mandated church-run residential schools ran from the mid-1800s until 1996, and resulted in generations of indigenous children being exposed to chronic neglect, abuse, trauma, racism, and cultural shaming (“Honouring the Truth: Reconciling for the Future,” Truth and Reconciliation Commission of Canada, 2015).
Some of our more recent analyses revealed that having a family history of residential school attendance has been linked to a greater likelihood of early-onset mental health symptoms, which in turn, has been tied to an increased risk of suicidality and other unique outcomes that have implications for treatment and prevention. Furthermore, other negative outcomes experienced by indigenous peoples, such as low family income and limited educational opportunities, also appear to be involved in the intergenerational transmission of residential school trauma.
Against this backdrop in Canada, we have a prevailing sense of blaming the victim that is counterproductive to healing. According to a 2014 report by the Royal Canadian Mounted Police (RCMP), 1,017 indigenous women and girls were murdered between 1980 and 2012 across Canada. About one-third of the women died as a result of physical beating, and more than 90% of the victims had a “previous relationship” with the person who killed them, according to the RCMP report. Yet, despite evidence to the contrary, the prime minister of Canada shared his view last year that those staggering numbers should be viewed as a criminal issue and not a “sociological phenomenon” (CBC News, Aug. 21, 2014).
Members of other groups whose previous generations also were exposed indirectly to unspeakable trauma include Americans of African descent, Native Americans, and adult offspring of Holocaust survivors. Rachel Yehuda, Ph.D., has studied the latter group extensively.
In one study, Dr. Yehuda and her associates found significantly reduced cortisol excretion in Holocaust offspring, compared with controls (Psychoneuroendocrinology. 2014 Oct;48:1-10). In another study of the adult offspring of Holocaust survivors, Dr. Yehuda, professor of psychiatry at the Icahn School of Medicine at Mount Sinai in New York, found that “offspring with paternal [posttraumatic stress disorder] showed higher GR-1F promoter methylation, whereas offspring with both maternal and paternal PTSD showed lower methylation.” Furthermore, lower methylation was tied to greater suppression of cortisol (Am J Psychiatry. 2014 Aug;171(8)872-880).
An appreciation for the power of epigenetics, or “soul wounds,” can help us stop blaming indigenous and other traumatized populations, and start tending to their mental health needs. Furthermore, getting individuals to understand these concepts can be yet another step on the path toward healing.
A study of 19 staff members and clients in a Native American healing lodge who began a discourse on the legacy of historical trauma found that counselors understood that their clients carried pain “leading to adult dysfunction, including substance abuse” (J Consult Clin Psychol. 2009 Aug;77(4):751-762). Second, the counselors believed that the pain needed to be confessed. Third, the counselors thought that expressing the pain would help the clients become more introspective. Finally, the process included reclaiming “indigenous heritage, identity, and spirituality that program staff thought would neutralize the pathogenic effects of colonization.”
We do not know the extent to which epigenetics are involved in specific diseases. Epigenetic mechanisms have not yet been tested as pathways involved in the intergenerational transmission of trauma in indigenous peoples. But Dr. Yehuda’s work with the children of Holocaust survivors shows that these mechanisms do indeed exist.
In light of what we do understand and the DSM-5’s emphasis on cultural competency, mental health professionals have a role to play in reversing the negative intergenerational cycles experienced by people across the globe. Only when we start paying attention to the plight of indigenous peoples across the globe will true healing begin.
Dr. Bombay is assistant professor of psychiatry at Dalhousie University, Halifax, N.S.
Understanding the root of stress and trauma experienced by patients as individuals is a key charge of psychiatry. But patients also can experience psychological distress because of the traumatic experiences of previous generations. The mental health community must be prepared to treat patients who fall into the latter category.
My colleagues and I recently analyzed representative samples of First Nations adults and youth living on a reserve in Canada. We found that the number of previous generations in which families were forced to attend Indian residential schools was cumulatively linked with higher levels of psychological distress and suicidal ideation among those who did not attend themselves (Transcultural Psychiatry. 2014, 51:320-338).
The forced removal of Indigenous children from their homes for the purposes of assimilation occurred over generations in many countries around the world. In Canada, these government-mandated church-run residential schools ran from the mid-1800s until 1996, and resulted in generations of indigenous children being exposed to chronic neglect, abuse, trauma, racism, and cultural shaming (“Honouring the Truth: Reconciling for the Future,” Truth and Reconciliation Commission of Canada, 2015).
Some of our more recent analyses revealed that having a family history of residential school attendance has been linked to a greater likelihood of early-onset mental health symptoms, which in turn, has been tied to an increased risk of suicidality and other unique outcomes that have implications for treatment and prevention. Furthermore, other negative outcomes experienced by indigenous peoples, such as low family income and limited educational opportunities, also appear to be involved in the intergenerational transmission of residential school trauma.
Against this backdrop in Canada, we have a prevailing sense of blaming the victim that is counterproductive to healing. According to a 2014 report by the Royal Canadian Mounted Police (RCMP), 1,017 indigenous women and girls were murdered between 1980 and 2012 across Canada. About one-third of the women died as a result of physical beating, and more than 90% of the victims had a “previous relationship” with the person who killed them, according to the RCMP report. Yet, despite evidence to the contrary, the prime minister of Canada shared his view last year that those staggering numbers should be viewed as a criminal issue and not a “sociological phenomenon” (CBC News, Aug. 21, 2014).
Members of other groups whose previous generations also were exposed indirectly to unspeakable trauma include Americans of African descent, Native Americans, and adult offspring of Holocaust survivors. Rachel Yehuda, Ph.D., has studied the latter group extensively.
In one study, Dr. Yehuda and her associates found significantly reduced cortisol excretion in Holocaust offspring, compared with controls (Psychoneuroendocrinology. 2014 Oct;48:1-10). In another study of the adult offspring of Holocaust survivors, Dr. Yehuda, professor of psychiatry at the Icahn School of Medicine at Mount Sinai in New York, found that “offspring with paternal [posttraumatic stress disorder] showed higher GR-1F promoter methylation, whereas offspring with both maternal and paternal PTSD showed lower methylation.” Furthermore, lower methylation was tied to greater suppression of cortisol (Am J Psychiatry. 2014 Aug;171(8)872-880).
An appreciation for the power of epigenetics, or “soul wounds,” can help us stop blaming indigenous and other traumatized populations, and start tending to their mental health needs. Furthermore, getting individuals to understand these concepts can be yet another step on the path toward healing.
A study of 19 staff members and clients in a Native American healing lodge who began a discourse on the legacy of historical trauma found that counselors understood that their clients carried pain “leading to adult dysfunction, including substance abuse” (J Consult Clin Psychol. 2009 Aug;77(4):751-762). Second, the counselors believed that the pain needed to be confessed. Third, the counselors thought that expressing the pain would help the clients become more introspective. Finally, the process included reclaiming “indigenous heritage, identity, and spirituality that program staff thought would neutralize the pathogenic effects of colonization.”
We do not know the extent to which epigenetics are involved in specific diseases. Epigenetic mechanisms have not yet been tested as pathways involved in the intergenerational transmission of trauma in indigenous peoples. But Dr. Yehuda’s work with the children of Holocaust survivors shows that these mechanisms do indeed exist.
In light of what we do understand and the DSM-5’s emphasis on cultural competency, mental health professionals have a role to play in reversing the negative intergenerational cycles experienced by people across the globe. Only when we start paying attention to the plight of indigenous peoples across the globe will true healing begin.
Dr. Bombay is assistant professor of psychiatry at Dalhousie University, Halifax, N.S.

PTSD Campaign: Caring and Sharing
“Learn, connect, and share”—that’s the theme of this year’s VA PTSD awareness campaign. The campaign is focused on online materials about how posttraumatic stress disorder (PTSD) treatment can help and encourages the general public to reach out to someone and share the information. The VA National Center for PTSD website (http://www.ptsd.va.gov/about/PTSD-awareness) offers a number of resources to help with that mission:
- PTSD Coach Online and the PTSD Coach mobile app, providing strategies to manage symptoms
- AboutFace, a video gallery of veterans talking about how treatment can turn lives around
- Whiteboards, short animated videos to learn about PTSD and effective treatments
Providers will also find continuing education and CME opportunities, such as PTSD 101 courses and the PTSD Monthly Update, offering the latest information about PTSD and trauma.
“Learn, connect, and share”—that’s the theme of this year’s VA PTSD awareness campaign. The campaign is focused on online materials about how posttraumatic stress disorder (PTSD) treatment can help and encourages the general public to reach out to someone and share the information. The VA National Center for PTSD website (http://www.ptsd.va.gov/about/PTSD-awareness) offers a number of resources to help with that mission:
- PTSD Coach Online and the PTSD Coach mobile app, providing strategies to manage symptoms
- AboutFace, a video gallery of veterans talking about how treatment can turn lives around
- Whiteboards, short animated videos to learn about PTSD and effective treatments
Providers will also find continuing education and CME opportunities, such as PTSD 101 courses and the PTSD Monthly Update, offering the latest information about PTSD and trauma.
“Learn, connect, and share”—that’s the theme of this year’s VA PTSD awareness campaign. The campaign is focused on online materials about how posttraumatic stress disorder (PTSD) treatment can help and encourages the general public to reach out to someone and share the information. The VA National Center for PTSD website (http://www.ptsd.va.gov/about/PTSD-awareness) offers a number of resources to help with that mission:
- PTSD Coach Online and the PTSD Coach mobile app, providing strategies to manage symptoms
- AboutFace, a video gallery of veterans talking about how treatment can turn lives around
- Whiteboards, short animated videos to learn about PTSD and effective treatments
Providers will also find continuing education and CME opportunities, such as PTSD 101 courses and the PTSD Monthly Update, offering the latest information about PTSD and trauma.