User login
Memory Skills Classes to Address Cognitive Concerns in Older Veterans With a History of Posttraumatic Stress Disorder
The Geriatric Research Education and Clinical Center (GRECC) Memory Disorders Clinic at the VA Puget Sound Health Care System (VAPSHCS) in Seattle, Washington, receives referrals from primary and specialty care. About a decade ago, this clinic began to see an influx of Vietnam-era veterans who presented with a variety of symptoms: not remembering where they were going when driving, forgetting why they went into another room, not remembering what their spouse told them, and feeling “out of it.” These symptoms were not associated with the loss of independence, but they were cause for concern. Family members and care providers typically corroborated the symptom description and perception of decline. Yet during workups, these veterans showed no primary medical causes for cognitive impairments and on neuropsychological evaluation demonstrated essentially normal cognition.
Memory Disorders Clinic staff largely were at a loss to know how to care for these patients. The simple reassurance, “You do not have dementia now,” seemed unsatisfactory given the patients’ ongoing concerns and the established risk factors for neurodegenerative disease.1,2 One theme emerged when talking with these veterans and their families: They all had a diagnosis of or history of treatment for posttraumatic stress disorder (PTSD).
To help these veterans, the VAPSHCS GRECC sought to address their key areas of concern related to memory. With input from veterans and their families, a quality improvement project was developed with the following goals: (1) to educate veterans and their families about PTSD and cognitive changes; (2) to build and field test a psychoeducational class to teach memory skills in this population; and (3) to inform VA staff about PTSD and cognitive change. In this article, the authors focus on how the first 2 goals were addressed and present preliminary results related to quality improvement.
Memory Skills Classes
Several strategies might promote memory skills, including printed materials for self-directed learning, individual sessions, interactive technologies, or groups. Given the patients’ reports about concentration problems, asking them to work through structured materials independently seemed unproductive. Individual clinical evaluations and cognitive interventions likely would not meet the demand or be cost-effective. Groups have long been used to treat PTSD, and Norrie and colleagues reported that at-risk adults benefited from a group psychoeducation program targeting healthy brain aging.3 At the same time, the Memory Disorders Clinic sought to distinguish itself from PTSD groups, because these groups tend to focus on treating active PTSD.
A better fit for this offering was the description of the sessions as classes. Although the focus was on promoting memory skills among those capable of learning them, the authors were mindful that some veterans might truly have prodromal dementia or acute PTSD symptoms that would require clinical management. The classes were not intended to address all these issues, and there was a plan to refer participants either before or during the class if warranted.
There was no formal evaluation of memory prior to starting the class. These classes were not developed as a research intervention and were exempt from institutional review board (IRB) approval requirements, according to prescreening by the VAPSHCS IRB and a memo from the GRECC director.
Core Components of Memory Skills
It may not be evident at first glance that PTSD or a history of PTSD influences memory. The symptom criteria for PTSD (involving reexperiencing, hyperarousal, and avoidance) might be described as “too much remembering” rather than forgetting. Yet problems with attention and concentration often occur in the setting of intrusive memories and alterations in reactivity. Research has found that older adults with PTSD have deficits of memory, especially new learning.
To appreciate these effects, it was important for participants in the memory skills classes to have some understanding of how memory works. The authors developed the Memory Model (Figure) as a visual aid and reference point to discuss the stages of new learning and how different aspects of brain activity are required for new learning and for memory to occur. This straightforward model is based on cognitive science and presented in layman’s terms. An important part of this model is the “filter” stage, which controls the information and stimuli that are available to the brain. Posttraumatic stress disorder involves involuntary emotional responses and efforts to avoid them and selects and colors the information that is processed in some situations (eg, avoidance of situations associated with trauma or dissociation of extreme memories). At other times, such as when a powerful stimulus is presented (eg, a helicopter flying close overhead), the filter may try to block out all inputs in order to preserve safety. The Memory Model also served as a visual aid during class discussions of normal cognitive aging. 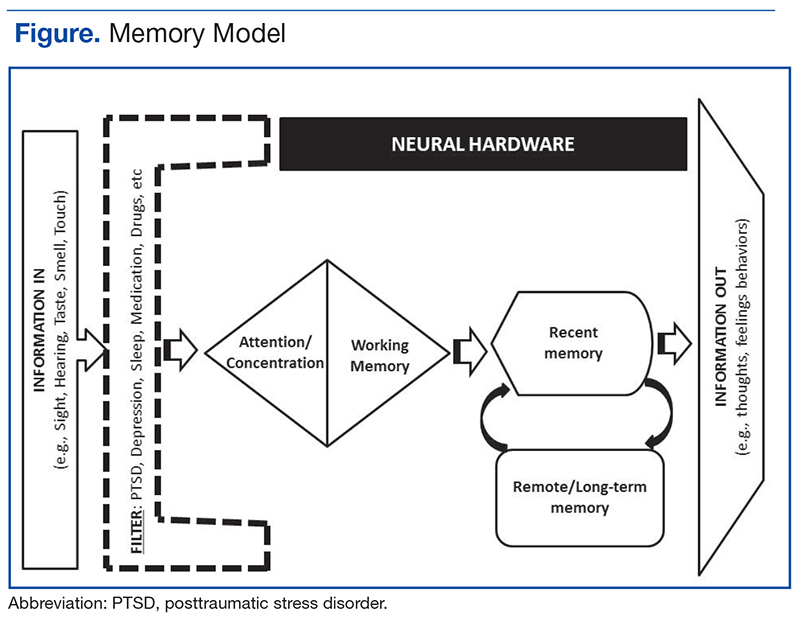
Class sessions incorporated specific, measurable, attainable, realistic, and timely (SMART) goals, regular exercises based on mindfulness-based stress reduction approaches, and principles of behavioral activation.5 The SMART goals structure the sessions and permit customization of learning for participants. Class leaders record a goal for each participant and use these throughout the sessions to build rapport, develop communication, and teach memory skills.
Mindfulness-based stress reduction is an evidence-based treatment used in PTSD.6 It provides a counterpoint to the more didactic memory skills and is a method that even those with objective memory impairments can practice and apply successfully. Being in the current moment and emotional regulation are important skills to teach veterans as they learn to exert 
Organization
Class sessions occurred weekly for 1 hour for a total of 8 sessions. The weekly class topics included introduction to memory; mood disorders, cognition, and cognitive disorders; barriers to effective memory: assessing readiness for change; developing a routine and becoming organized; attention and concentration; memory improvement (strategies internal and external aids); and reassessing goals.
Over the 3 years of classes reported in this article, the class sizes varied from 4 to 12 participants based on veteran interest, retention, and room size. The classes were structured so that important content areas were covered but with enough elasticity so leaders and veterans would develop a rapport and explore in greater depth the topics that resonated most for the attendees. Group participation was strongly encouraged. Veterans were expressly informed that the class was not for treatment of PTSD and that evidence-based therapies were encouraged to address PTSD especially if their symptoms flared up when compared with previous levels. The attendees also understood that they did not receive formal cognitive or memory testing but were encouraged to pursue testing if they showed significant deficits.
Preliminary Findings
From spring 2012 until spring 2015, 69 veterans agreed to participate and attended at least 1 memory skills class. Eighty-seven percent of participants (n = 60) attended 4 or more classes. The mean age (SD) was 67.3 years (4.2). All the participants were men, and the race/ethnic distribution was similar to that of the aging veteran population and very close to racial demographics for Washington state: 80% white, 14% African American, 2% Asian/Pacific Islander, 2% Native American, and 2% unknown.
Attendees were asked, but not required, to complete questionnaires before the classes began and again at completion. These questionnaires included self-assessments of cognitive strategies and compensatory methods used; an assessment of concern regarding cognition, life satisfaction, and community integration; the PTSD CheckList-Civilian Version (PCL-C); and the Geriatric Depression Scale (GDS).7,8 The questionnaire also included open response questions to providefeedback on what attendees liked about the classes and recommendations for improvements. The majority of comments for improvement focused on attendees’ desire for longer sessions and repeat offerings. Five veterans did not complete the full set of questionnaires at the beginning of the classes, and 7 did not complete the questionnaires at completion (the 2 subsets did not perfectly overlap).
At the start of the class, on average, veteran participants were experiencing mild depression and moderate symptoms of PTSD as measured by the GDS (n = 54) and the PCL-C (n = 56), respectively. Preliminary comparisons of ratings pre- and post-classes, using simple paired t tests, indicated a reduction in symptoms of depression on the GDS, improved sense of mastery over their memory symptoms, as well as improved quality of life ratings (all P < .01, no corrections). There was no evidence for a significant reduction in PTSD symptoms or report of elimination of cognitive difficulties. With the small sample and modest effects, the clinical significance of these scores cannot be determined. The authors are planning more detailed analyses on a larger set of participants, including measures of health care utilization before and after the class.
Future Directions
1. Chopra MP, Zhang H, Pless Kaiser A, et al. PTSD is a chronic, fluctuating disorder affecting the mental quality of life in older adults. Am J Geriatr Psychiatry. 2014;22(1):86-97.
2. Donovan NJ, Amariglio RE, Zoller AS, et al. Subjective cognitive concerns and neuropsychiatric predictors of progression to the early clinical stages of Alzheimer disease. Am J Geriatr Psychiatry. 2014;22(12):1642-1651.
3. Norrie LM, Diamond K, Hickie IB, Rogers NL, Fearns S, Naismith SL. Can older “at risk” adults benefit from psychoeducation targeting healthy brain aging? Int Psychogeriatr. 2011;23(3):413-424.
4. Hopko DR, Robertson SMC, Lejuez CW. Behavioral activation for anxiety disorders. Behav Anal Today. 2006;7(2):212-232.
5. Schuitevoerder S, Rosen JW, Twamley EW, et al. A meta-analysis of cognitive functioning in older adults with PTSD. J Anxiety Disord. 2013;27(6):550-558.
6. Polusny MA, Erbes CR, Thuras P, et al. Mindfulness-based stress reduction for posttraumatic stress disorder among veterans: a randomized clinical trial. JAMA. 2015;314(5):456-465.
7. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982-1983;17(1):37-49.
8. Mental Illness Research, Education and Clinical Center. PTSD CheckList-Civilian Version (PCL-C). http://www.mirecc.va.gov/docs/visn6/3_PTSD _CheckList_and_Scoring.pdf Published December 2013. Accessed November 3, 2016.
9. Scott JC, Matt GE, Wrocklage KM, et al. A quantitative meta-analysis of neurocognitive functioning in posttraumatic stress disorder. Psychol Bull. 2015;141(1):105-140.
10. Wrocklage KM, Schweinsburg BC, Krystal JH, et al. Neuropsychological functioning in veterans with posttraumatic stress disorder: associations with performance validity, comorbidities, and functional outcomes. J Int Neuropsychol Soc. 2016;22(4):399-411.
11. Cook JM, O’Donnell C. Assessment and psychological treatment of posttraumatic stress disorder in older adults. J Geriatr Psychiatry Neurol. 2005;18(2):61-71.
12. Mota N, Tsai J, Kirwin PD, et al. Late-life exacerbation of PTSD symptoms in US veterans: results from the National Health and Resilience in Veterans Study. J Clin Psychiatry. 2016;77(3):348-354.
13. Yaffe K, Vittinghoff E, Lindquist K, et al. Posttraumatic stress disorder and risk of dementia among US veterans. Arch Gen Psychiatry. 2010;67(6):608-613.
The Geriatric Research Education and Clinical Center (GRECC) Memory Disorders Clinic at the VA Puget Sound Health Care System (VAPSHCS) in Seattle, Washington, receives referrals from primary and specialty care. About a decade ago, this clinic began to see an influx of Vietnam-era veterans who presented with a variety of symptoms: not remembering where they were going when driving, forgetting why they went into another room, not remembering what their spouse told them, and feeling “out of it.” These symptoms were not associated with the loss of independence, but they were cause for concern. Family members and care providers typically corroborated the symptom description and perception of decline. Yet during workups, these veterans showed no primary medical causes for cognitive impairments and on neuropsychological evaluation demonstrated essentially normal cognition.
Memory Disorders Clinic staff largely were at a loss to know how to care for these patients. The simple reassurance, “You do not have dementia now,” seemed unsatisfactory given the patients’ ongoing concerns and the established risk factors for neurodegenerative disease.1,2 One theme emerged when talking with these veterans and their families: They all had a diagnosis of or history of treatment for posttraumatic stress disorder (PTSD).
To help these veterans, the VAPSHCS GRECC sought to address their key areas of concern related to memory. With input from veterans and their families, a quality improvement project was developed with the following goals: (1) to educate veterans and their families about PTSD and cognitive changes; (2) to build and field test a psychoeducational class to teach memory skills in this population; and (3) to inform VA staff about PTSD and cognitive change. In this article, the authors focus on how the first 2 goals were addressed and present preliminary results related to quality improvement.
Memory Skills Classes
Several strategies might promote memory skills, including printed materials for self-directed learning, individual sessions, interactive technologies, or groups. Given the patients’ reports about concentration problems, asking them to work through structured materials independently seemed unproductive. Individual clinical evaluations and cognitive interventions likely would not meet the demand or be cost-effective. Groups have long been used to treat PTSD, and Norrie and colleagues reported that at-risk adults benefited from a group psychoeducation program targeting healthy brain aging.3 At the same time, the Memory Disorders Clinic sought to distinguish itself from PTSD groups, because these groups tend to focus on treating active PTSD.
A better fit for this offering was the description of the sessions as classes. Although the focus was on promoting memory skills among those capable of learning them, the authors were mindful that some veterans might truly have prodromal dementia or acute PTSD symptoms that would require clinical management. The classes were not intended to address all these issues, and there was a plan to refer participants either before or during the class if warranted.
There was no formal evaluation of memory prior to starting the class. These classes were not developed as a research intervention and were exempt from institutional review board (IRB) approval requirements, according to prescreening by the VAPSHCS IRB and a memo from the GRECC director.
Core Components of Memory Skills
It may not be evident at first glance that PTSD or a history of PTSD influences memory. The symptom criteria for PTSD (involving reexperiencing, hyperarousal, and avoidance) might be described as “too much remembering” rather than forgetting. Yet problems with attention and concentration often occur in the setting of intrusive memories and alterations in reactivity. Research has found that older adults with PTSD have deficits of memory, especially new learning.
To appreciate these effects, it was important for participants in the memory skills classes to have some understanding of how memory works. The authors developed the Memory Model (Figure) as a visual aid and reference point to discuss the stages of new learning and how different aspects of brain activity are required for new learning and for memory to occur. This straightforward model is based on cognitive science and presented in layman’s terms. An important part of this model is the “filter” stage, which controls the information and stimuli that are available to the brain. Posttraumatic stress disorder involves involuntary emotional responses and efforts to avoid them and selects and colors the information that is processed in some situations (eg, avoidance of situations associated with trauma or dissociation of extreme memories). At other times, such as when a powerful stimulus is presented (eg, a helicopter flying close overhead), the filter may try to block out all inputs in order to preserve safety. The Memory Model also served as a visual aid during class discussions of normal cognitive aging.
Class sessions incorporated specific, measurable, attainable, realistic, and timely (SMART) goals, regular exercises based on mindfulness-based stress reduction approaches, and principles of behavioral activation.5 The SMART goals structure the sessions and permit customization of learning for participants. Class leaders record a goal for each participant and use these throughout the sessions to build rapport, develop communication, and teach memory skills.
Mindfulness-based stress reduction is an evidence-based treatment used in PTSD.6 It provides a counterpoint to the more didactic memory skills and is a method that even those with objective memory impairments can practice and apply successfully. Being in the current moment and emotional regulation are important skills to teach veterans as they learn to exert
Organization
Class sessions occurred weekly for 1 hour for a total of 8 sessions. The weekly class topics included introduction to memory; mood disorders, cognition, and cognitive disorders; barriers to effective memory: assessing readiness for change; developing a routine and becoming organized; attention and concentration; memory improvement (strategies internal and external aids); and reassessing goals.
Over the 3 years of classes reported in this article, the class sizes varied from 4 to 12 participants based on veteran interest, retention, and room size. The classes were structured so that important content areas were covered but with enough elasticity so leaders and veterans would develop a rapport and explore in greater depth the topics that resonated most for the attendees. Group participation was strongly encouraged. Veterans were expressly informed that the class was not for treatment of PTSD and that evidence-based therapies were encouraged to address PTSD especially if their symptoms flared up when compared with previous levels. The attendees also understood that they did not receive formal cognitive or memory testing but were encouraged to pursue testing if they showed significant deficits.
Preliminary Findings
From spring 2012 until spring 2015, 69 veterans agreed to participate and attended at least 1 memory skills class. Eighty-seven percent of participants (n = 60) attended 4 or more classes. The mean age (SD) was 67.3 years (4.2). All the participants were men, and the race/ethnic distribution was similar to that of the aging veteran population and very close to racial demographics for Washington state: 80% white, 14% African American, 2% Asian/Pacific Islander, 2% Native American, and 2% unknown.
Attendees were asked, but not required, to complete questionnaires before the classes began and again at completion. These questionnaires included self-assessments of cognitive strategies and compensatory methods used; an assessment of concern regarding cognition, life satisfaction, and community integration; the PTSD CheckList-Civilian Version (PCL-C); and the Geriatric Depression Scale (GDS).7,8 The questionnaire also included open response questions to providefeedback on what attendees liked about the classes and recommendations for improvements. The majority of comments for improvement focused on attendees’ desire for longer sessions and repeat offerings. Five veterans did not complete the full set of questionnaires at the beginning of the classes, and 7 did not complete the questionnaires at completion (the 2 subsets did not perfectly overlap).
At the start of the class, on average, veteran participants were experiencing mild depression and moderate symptoms of PTSD as measured by the GDS (n = 54) and the PCL-C (n = 56), respectively. Preliminary comparisons of ratings pre- and post-classes, using simple paired t tests, indicated a reduction in symptoms of depression on the GDS, improved sense of mastery over their memory symptoms, as well as improved quality of life ratings (all P < .01, no corrections). There was no evidence for a significant reduction in PTSD symptoms or report of elimination of cognitive difficulties. With the small sample and modest effects, the clinical significance of these scores cannot be determined. The authors are planning more detailed analyses on a larger set of participants, including measures of health care utilization before and after the class.
Future Directions
The Geriatric Research Education and Clinical Center (GRECC) Memory Disorders Clinic at the VA Puget Sound Health Care System (VAPSHCS) in Seattle, Washington, receives referrals from primary and specialty care. About a decade ago, this clinic began to see an influx of Vietnam-era veterans who presented with a variety of symptoms: not remembering where they were going when driving, forgetting why they went into another room, not remembering what their spouse told them, and feeling “out of it.” These symptoms were not associated with the loss of independence, but they were cause for concern. Family members and care providers typically corroborated the symptom description and perception of decline. Yet during workups, these veterans showed no primary medical causes for cognitive impairments and on neuropsychological evaluation demonstrated essentially normal cognition.
Memory Disorders Clinic staff largely were at a loss to know how to care for these patients. The simple reassurance, “You do not have dementia now,” seemed unsatisfactory given the patients’ ongoing concerns and the established risk factors for neurodegenerative disease.1,2 One theme emerged when talking with these veterans and their families: They all had a diagnosis of or history of treatment for posttraumatic stress disorder (PTSD).
To help these veterans, the VAPSHCS GRECC sought to address their key areas of concern related to memory. With input from veterans and their families, a quality improvement project was developed with the following goals: (1) to educate veterans and their families about PTSD and cognitive changes; (2) to build and field test a psychoeducational class to teach memory skills in this population; and (3) to inform VA staff about PTSD and cognitive change. In this article, the authors focus on how the first 2 goals were addressed and present preliminary results related to quality improvement.
Memory Skills Classes
Several strategies might promote memory skills, including printed materials for self-directed learning, individual sessions, interactive technologies, or groups. Given the patients’ reports about concentration problems, asking them to work through structured materials independently seemed unproductive. Individual clinical evaluations and cognitive interventions likely would not meet the demand or be cost-effective. Groups have long been used to treat PTSD, and Norrie and colleagues reported that at-risk adults benefited from a group psychoeducation program targeting healthy brain aging.3 At the same time, the Memory Disorders Clinic sought to distinguish itself from PTSD groups, because these groups tend to focus on treating active PTSD.
A better fit for this offering was the description of the sessions as classes. Although the focus was on promoting memory skills among those capable of learning them, the authors were mindful that some veterans might truly have prodromal dementia or acute PTSD symptoms that would require clinical management. The classes were not intended to address all these issues, and there was a plan to refer participants either before or during the class if warranted.
There was no formal evaluation of memory prior to starting the class. These classes were not developed as a research intervention and were exempt from institutional review board (IRB) approval requirements, according to prescreening by the VAPSHCS IRB and a memo from the GRECC director.
Core Components of Memory Skills
It may not be evident at first glance that PTSD or a history of PTSD influences memory. The symptom criteria for PTSD (involving reexperiencing, hyperarousal, and avoidance) might be described as “too much remembering” rather than forgetting. Yet problems with attention and concentration often occur in the setting of intrusive memories and alterations in reactivity. Research has found that older adults with PTSD have deficits of memory, especially new learning.
To appreciate these effects, it was important for participants in the memory skills classes to have some understanding of how memory works. The authors developed the Memory Model (Figure) as a visual aid and reference point to discuss the stages of new learning and how different aspects of brain activity are required for new learning and for memory to occur. This straightforward model is based on cognitive science and presented in layman’s terms. An important part of this model is the “filter” stage, which controls the information and stimuli that are available to the brain. Posttraumatic stress disorder involves involuntary emotional responses and efforts to avoid them and selects and colors the information that is processed in some situations (eg, avoidance of situations associated with trauma or dissociation of extreme memories). At other times, such as when a powerful stimulus is presented (eg, a helicopter flying close overhead), the filter may try to block out all inputs in order to preserve safety. The Memory Model also served as a visual aid during class discussions of normal cognitive aging.
Class sessions incorporated specific, measurable, attainable, realistic, and timely (SMART) goals, regular exercises based on mindfulness-based stress reduction approaches, and principles of behavioral activation.5 The SMART goals structure the sessions and permit customization of learning for participants. Class leaders record a goal for each participant and use these throughout the sessions to build rapport, develop communication, and teach memory skills.
Mindfulness-based stress reduction is an evidence-based treatment used in PTSD.6 It provides a counterpoint to the more didactic memory skills and is a method that even those with objective memory impairments can practice and apply successfully. Being in the current moment and emotional regulation are important skills to teach veterans as they learn to exert
Organization
Class sessions occurred weekly for 1 hour for a total of 8 sessions. The weekly class topics included introduction to memory; mood disorders, cognition, and cognitive disorders; barriers to effective memory: assessing readiness for change; developing a routine and becoming organized; attention and concentration; memory improvement (strategies internal and external aids); and reassessing goals.
Over the 3 years of classes reported in this article, the class sizes varied from 4 to 12 participants based on veteran interest, retention, and room size. The classes were structured so that important content areas were covered but with enough elasticity so leaders and veterans would develop a rapport and explore in greater depth the topics that resonated most for the attendees. Group participation was strongly encouraged. Veterans were expressly informed that the class was not for treatment of PTSD and that evidence-based therapies were encouraged to address PTSD especially if their symptoms flared up when compared with previous levels. The attendees also understood that they did not receive formal cognitive or memory testing but were encouraged to pursue testing if they showed significant deficits.
Preliminary Findings
From spring 2012 until spring 2015, 69 veterans agreed to participate and attended at least 1 memory skills class. Eighty-seven percent of participants (n = 60) attended 4 or more classes. The mean age (SD) was 67.3 years (4.2). All the participants were men, and the race/ethnic distribution was similar to that of the aging veteran population and very close to racial demographics for Washington state: 80% white, 14% African American, 2% Asian/Pacific Islander, 2% Native American, and 2% unknown.
Attendees were asked, but not required, to complete questionnaires before the classes began and again at completion. These questionnaires included self-assessments of cognitive strategies and compensatory methods used; an assessment of concern regarding cognition, life satisfaction, and community integration; the PTSD CheckList-Civilian Version (PCL-C); and the Geriatric Depression Scale (GDS).7,8 The questionnaire also included open response questions to providefeedback on what attendees liked about the classes and recommendations for improvements. The majority of comments for improvement focused on attendees’ desire for longer sessions and repeat offerings. Five veterans did not complete the full set of questionnaires at the beginning of the classes, and 7 did not complete the questionnaires at completion (the 2 subsets did not perfectly overlap).
At the start of the class, on average, veteran participants were experiencing mild depression and moderate symptoms of PTSD as measured by the GDS (n = 54) and the PCL-C (n = 56), respectively. Preliminary comparisons of ratings pre- and post-classes, using simple paired t tests, indicated a reduction in symptoms of depression on the GDS, improved sense of mastery over their memory symptoms, as well as improved quality of life ratings (all P < .01, no corrections). There was no evidence for a significant reduction in PTSD symptoms or report of elimination of cognitive difficulties. With the small sample and modest effects, the clinical significance of these scores cannot be determined. The authors are planning more detailed analyses on a larger set of participants, including measures of health care utilization before and after the class.
Future Directions
1. Chopra MP, Zhang H, Pless Kaiser A, et al. PTSD is a chronic, fluctuating disorder affecting the mental quality of life in older adults. Am J Geriatr Psychiatry. 2014;22(1):86-97.
2. Donovan NJ, Amariglio RE, Zoller AS, et al. Subjective cognitive concerns and neuropsychiatric predictors of progression to the early clinical stages of Alzheimer disease. Am J Geriatr Psychiatry. 2014;22(12):1642-1651.
3. Norrie LM, Diamond K, Hickie IB, Rogers NL, Fearns S, Naismith SL. Can older “at risk” adults benefit from psychoeducation targeting healthy brain aging? Int Psychogeriatr. 2011;23(3):413-424.
4. Hopko DR, Robertson SMC, Lejuez CW. Behavioral activation for anxiety disorders. Behav Anal Today. 2006;7(2):212-232.
5. Schuitevoerder S, Rosen JW, Twamley EW, et al. A meta-analysis of cognitive functioning in older adults with PTSD. J Anxiety Disord. 2013;27(6):550-558.
6. Polusny MA, Erbes CR, Thuras P, et al. Mindfulness-based stress reduction for posttraumatic stress disorder among veterans: a randomized clinical trial. JAMA. 2015;314(5):456-465.
7. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982-1983;17(1):37-49.
8. Mental Illness Research, Education and Clinical Center. PTSD CheckList-Civilian Version (PCL-C). http://www.mirecc.va.gov/docs/visn6/3_PTSD _CheckList_and_Scoring.pdf Published December 2013. Accessed November 3, 2016.
9. Scott JC, Matt GE, Wrocklage KM, et al. A quantitative meta-analysis of neurocognitive functioning in posttraumatic stress disorder. Psychol Bull. 2015;141(1):105-140.
10. Wrocklage KM, Schweinsburg BC, Krystal JH, et al. Neuropsychological functioning in veterans with posttraumatic stress disorder: associations with performance validity, comorbidities, and functional outcomes. J Int Neuropsychol Soc. 2016;22(4):399-411.
11. Cook JM, O’Donnell C. Assessment and psychological treatment of posttraumatic stress disorder in older adults. J Geriatr Psychiatry Neurol. 2005;18(2):61-71.
12. Mota N, Tsai J, Kirwin PD, et al. Late-life exacerbation of PTSD symptoms in US veterans: results from the National Health and Resilience in Veterans Study. J Clin Psychiatry. 2016;77(3):348-354.
13. Yaffe K, Vittinghoff E, Lindquist K, et al. Posttraumatic stress disorder and risk of dementia among US veterans. Arch Gen Psychiatry. 2010;67(6):608-613.
1. Chopra MP, Zhang H, Pless Kaiser A, et al. PTSD is a chronic, fluctuating disorder affecting the mental quality of life in older adults. Am J Geriatr Psychiatry. 2014;22(1):86-97.
2. Donovan NJ, Amariglio RE, Zoller AS, et al. Subjective cognitive concerns and neuropsychiatric predictors of progression to the early clinical stages of Alzheimer disease. Am J Geriatr Psychiatry. 2014;22(12):1642-1651.
3. Norrie LM, Diamond K, Hickie IB, Rogers NL, Fearns S, Naismith SL. Can older “at risk” adults benefit from psychoeducation targeting healthy brain aging? Int Psychogeriatr. 2011;23(3):413-424.
4. Hopko DR, Robertson SMC, Lejuez CW. Behavioral activation for anxiety disorders. Behav Anal Today. 2006;7(2):212-232.
5. Schuitevoerder S, Rosen JW, Twamley EW, et al. A meta-analysis of cognitive functioning in older adults with PTSD. J Anxiety Disord. 2013;27(6):550-558.
6. Polusny MA, Erbes CR, Thuras P, et al. Mindfulness-based stress reduction for posttraumatic stress disorder among veterans: a randomized clinical trial. JAMA. 2015;314(5):456-465.
7. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982-1983;17(1):37-49.
8. Mental Illness Research, Education and Clinical Center. PTSD CheckList-Civilian Version (PCL-C). http://www.mirecc.va.gov/docs/visn6/3_PTSD _CheckList_and_Scoring.pdf Published December 2013. Accessed November 3, 2016.
9. Scott JC, Matt GE, Wrocklage KM, et al. A quantitative meta-analysis of neurocognitive functioning in posttraumatic stress disorder. Psychol Bull. 2015;141(1):105-140.
10. Wrocklage KM, Schweinsburg BC, Krystal JH, et al. Neuropsychological functioning in veterans with posttraumatic stress disorder: associations with performance validity, comorbidities, and functional outcomes. J Int Neuropsychol Soc. 2016;22(4):399-411.
11. Cook JM, O’Donnell C. Assessment and psychological treatment of posttraumatic stress disorder in older adults. J Geriatr Psychiatry Neurol. 2005;18(2):61-71.
12. Mota N, Tsai J, Kirwin PD, et al. Late-life exacerbation of PTSD symptoms in US veterans: results from the National Health and Resilience in Veterans Study. J Clin Psychiatry. 2016;77(3):348-354.
13. Yaffe K, Vittinghoff E, Lindquist K, et al. Posttraumatic stress disorder and risk of dementia among US veterans. Arch Gen Psychiatry. 2010;67(6):608-613.
Ask service members and veterans about sexual health
SILVER SPRING, MD. – Tending to the psychiatric and physical needs of military servicemen, servicewomen, and veterans must include attention to their sexual functioning, according to Col. (Ret.) Elspeth Cameron Ritchie, MD, MPH.
“Think of sexual activity as an activity of daily living,” Dr. Ritchie said at the Trauma Treatment from the Trenches meeting at the Forest Glen Annex in Silver Spring, Md., organized by Sawsan Ghurani, MD, a psychiatrist and Navy captain, and sponsored by the Walter Reed National Military Medical Center in Bethesda, Md.

Despite the deployment of 2.7 million service members over more than 15 years of war in the United States, research on the sexual health of this population has been scant, Dr. Ritchie said. Research has been similarly limited in the civilian population, except for the work that has been done among civilians on the impact of spinal cord injuries on sexual dysfunction, she said (J Spinal Cord Med. 2016 Aug 31:1-12).
Clinicians who work with service members and veterans find that wives complain about the impact of medical interventions on their partners, said Dr. Ritchie, a former Army psychiatry consultant and current chief of Community-Based Outpatient Clinics at the Washington (D.C.) Veterans Affairs Medical Center. “As part of the discussion on sexual health, I remind them that sexual activity is broader than penetration.”
Another issue to be aware of among service members is anger. “Often our patients are angry, and often that anger comes out to us as therapists,” she said. “We need to tell our colleagues about this and get them to expect it.”
Treating post-traumatic stress disorder can be a tricky proposition because of the sexual side effects caused by selective serotonin reuptake inhibitors, Dr. Ritchie said. She prefers bupropion because it is not linked to sexual side effects. Mood stabilizers cause weight gain, as do antipsychotics. Meanwhile, drug holidays lead to problems with adherence, she said. To mitigate side effects, Dr. Ritchie advised “trying one thing at a time and adding trazodone in low doses for sleep.” However, trazodone has been linked to priapism (Gen Hosp Psychiatry. 2015 Jan-Feb;37[1]:40-5), and so must be used with care.
Another treatment for PTSD that is showing promise is stellate ganglion block, which has proven effective for treating hot flashes in postmenopausal women and in addressing estrogen depletion tied to breast cancer treatment in small numbers of patients (Med Hypotheses. 2009 Jun;72[6]:657-61).
“Studies have found a reduction in PTSD symptoms as well as pain,” Dr. Ritchie said. “I’m pushing the VA to do more research in this area.”
In effort to treat sexual dysfunction, Dr. Ritchie said her family practice colleagues prescribe a lot of Viagra and other phosphodiesterase inhibitors. She speculated that flibanserin, a selective agonist for 5-HT1A and an antagonist for 5-HT2A receptors approved in 2015 by the Food and Drug Administration for premenopausal women with hypoactive sexual desire disorder, “will start making its way into the general population,” said Dr. Ritchie, whose comments about using phosphodiesterase inhibitors pertain to VA patients.
Many service members who participated in Operation Iraqi Freedom and Operation Enduring Freedom were aged 18-25 years. Partly because the Department of Defense (DOD) and the VA work with very young families, clinicians are tasked with teaching them about their needs as couples, including the need to discuss intimacy and sexual health. For political reasons, Dr. Ritchie said, in vitro fertilization is not covered by the VA, even though injuries from bomb blasts can make it impossible for couples to conceive naturally.
Toxic and infectious substances faced by troops that are not commonly found in the United States, such as chemicals, pesticides, and motor oils, also need to be acknowledged and addressed by clinicians. “We don’t do a good job about what a veteran thinks about what exposure does to their reproductive systems,” Dr. Ritchie said.
In an interview, Dr. Ghurani said that she came up with the title of the meeting to illustrate the extent to which providers treat PTSD in the military every day. Conference speakers examined the latest treatments on sexual trauma, and the state of the art therapy and research taking place at Walter Reed.
At the meeting, she discussed the distinction between military sexual trauma (MST) and sexual trauma within the civilian population. Research shows that veterans who screen positive for MST “are more likely to have a history of a suicide attempt documented in their VA medical record” (Psychiatry Res. 2016;244:257-65).
A 2008 study found that women are far more likely to screen positive for MST than men. Specifically, the study found that 25% of women and 1.3% of men who are screened for MST within the Veterans Health Administration screen positive (Trauma Violence Abuse. 2008 Oct;9[4]250-69).
Walter Reed’s Interpersonal Recovery Program at the Psychiatry Continuity Service is the only intensive outpatient program within the DOD that provides ongoing treatment for active duty service members with PTSD from a sexual trauma, Dr. Ghurani said.
Earlier during the meeting, Capt. (Ret.) William P. Nash, MD, director of psychological health at the Marine Corps and a 30-year veteran of the Navy, discussed moral injury, and contrasted it with PTSD and other sequelae of psychological trauma. He also described his work on the Moral Injury Events Scale as a tool for recognizing potentially morally injurious events in clinical and research settings.
Dr. Ritchie is the editor of “Intimacy Post-Injury: Combat Trauma and Sexual Health,” (New York: Oxford University Press, 2016). Dr. Ghurani contributed to a chapter in “Intimacy Post Injury,” and Dr. Nash has written extensively about PTSD, particularly among deployed Marines.
SILVER SPRING, MD. – Tending to the psychiatric and physical needs of military servicemen, servicewomen, and veterans must include attention to their sexual functioning, according to Col. (Ret.) Elspeth Cameron Ritchie, MD, MPH.
“Think of sexual activity as an activity of daily living,” Dr. Ritchie said at the Trauma Treatment from the Trenches meeting at the Forest Glen Annex in Silver Spring, Md., organized by Sawsan Ghurani, MD, a psychiatrist and Navy captain, and sponsored by the Walter Reed National Military Medical Center in Bethesda, Md.
Despite the deployment of 2.7 million service members over more than 15 years of war in the United States, research on the sexual health of this population has been scant, Dr. Ritchie said. Research has been similarly limited in the civilian population, except for the work that has been done among civilians on the impact of spinal cord injuries on sexual dysfunction, she said (J Spinal Cord Med. 2016 Aug 31:1-12).
Clinicians who work with service members and veterans find that wives complain about the impact of medical interventions on their partners, said Dr. Ritchie, a former Army psychiatry consultant and current chief of Community-Based Outpatient Clinics at the Washington (D.C.) Veterans Affairs Medical Center. “As part of the discussion on sexual health, I remind them that sexual activity is broader than penetration.”
Another issue to be aware of among service members is anger. “Often our patients are angry, and often that anger comes out to us as therapists,” she said. “We need to tell our colleagues about this and get them to expect it.”
Treating post-traumatic stress disorder can be a tricky proposition because of the sexual side effects caused by selective serotonin reuptake inhibitors, Dr. Ritchie said. She prefers bupropion because it is not linked to sexual side effects. Mood stabilizers cause weight gain, as do antipsychotics. Meanwhile, drug holidays lead to problems with adherence, she said. To mitigate side effects, Dr. Ritchie advised “trying one thing at a time and adding trazodone in low doses for sleep.” However, trazodone has been linked to priapism (Gen Hosp Psychiatry. 2015 Jan-Feb;37[1]:40-5), and so must be used with care.
Another treatment for PTSD that is showing promise is stellate ganglion block, which has proven effective for treating hot flashes in postmenopausal women and in addressing estrogen depletion tied to breast cancer treatment in small numbers of patients (Med Hypotheses. 2009 Jun;72[6]:657-61).
“Studies have found a reduction in PTSD symptoms as well as pain,” Dr. Ritchie said. “I’m pushing the VA to do more research in this area.”
In effort to treat sexual dysfunction, Dr. Ritchie said her family practice colleagues prescribe a lot of Viagra and other phosphodiesterase inhibitors. She speculated that flibanserin, a selective agonist for 5-HT1A and an antagonist for 5-HT2A receptors approved in 2015 by the Food and Drug Administration for premenopausal women with hypoactive sexual desire disorder, “will start making its way into the general population,” said Dr. Ritchie, whose comments about using phosphodiesterase inhibitors pertain to VA patients.
Many service members who participated in Operation Iraqi Freedom and Operation Enduring Freedom were aged 18-25 years. Partly because the Department of Defense (DOD) and the VA work with very young families, clinicians are tasked with teaching them about their needs as couples, including the need to discuss intimacy and sexual health. For political reasons, Dr. Ritchie said, in vitro fertilization is not covered by the VA, even though injuries from bomb blasts can make it impossible for couples to conceive naturally.
Toxic and infectious substances faced by troops that are not commonly found in the United States, such as chemicals, pesticides, and motor oils, also need to be acknowledged and addressed by clinicians. “We don’t do a good job about what a veteran thinks about what exposure does to their reproductive systems,” Dr. Ritchie said.
In an interview, Dr. Ghurani said that she came up with the title of the meeting to illustrate the extent to which providers treat PTSD in the military every day. Conference speakers examined the latest treatments on sexual trauma, and the state of the art therapy and research taking place at Walter Reed.
At the meeting, she discussed the distinction between military sexual trauma (MST) and sexual trauma within the civilian population. Research shows that veterans who screen positive for MST “are more likely to have a history of a suicide attempt documented in their VA medical record” (Psychiatry Res. 2016;244:257-65).
A 2008 study found that women are far more likely to screen positive for MST than men. Specifically, the study found that 25% of women and 1.3% of men who are screened for MST within the Veterans Health Administration screen positive (Trauma Violence Abuse. 2008 Oct;9[4]250-69).
Walter Reed’s Interpersonal Recovery Program at the Psychiatry Continuity Service is the only intensive outpatient program within the DOD that provides ongoing treatment for active duty service members with PTSD from a sexual trauma, Dr. Ghurani said.
Earlier during the meeting, Capt. (Ret.) William P. Nash, MD, director of psychological health at the Marine Corps and a 30-year veteran of the Navy, discussed moral injury, and contrasted it with PTSD and other sequelae of psychological trauma. He also described his work on the Moral Injury Events Scale as a tool for recognizing potentially morally injurious events in clinical and research settings.
Dr. Ritchie is the editor of “Intimacy Post-Injury: Combat Trauma and Sexual Health,” (New York: Oxford University Press, 2016). Dr. Ghurani contributed to a chapter in “Intimacy Post Injury,” and Dr. Nash has written extensively about PTSD, particularly among deployed Marines.
SILVER SPRING, MD. – Tending to the psychiatric and physical needs of military servicemen, servicewomen, and veterans must include attention to their sexual functioning, according to Col. (Ret.) Elspeth Cameron Ritchie, MD, MPH.
“Think of sexual activity as an activity of daily living,” Dr. Ritchie said at the Trauma Treatment from the Trenches meeting at the Forest Glen Annex in Silver Spring, Md., organized by Sawsan Ghurani, MD, a psychiatrist and Navy captain, and sponsored by the Walter Reed National Military Medical Center in Bethesda, Md.
Despite the deployment of 2.7 million service members over more than 15 years of war in the United States, research on the sexual health of this population has been scant, Dr. Ritchie said. Research has been similarly limited in the civilian population, except for the work that has been done among civilians on the impact of spinal cord injuries on sexual dysfunction, she said (J Spinal Cord Med. 2016 Aug 31:1-12).
Clinicians who work with service members and veterans find that wives complain about the impact of medical interventions on their partners, said Dr. Ritchie, a former Army psychiatry consultant and current chief of Community-Based Outpatient Clinics at the Washington (D.C.) Veterans Affairs Medical Center. “As part of the discussion on sexual health, I remind them that sexual activity is broader than penetration.”
Another issue to be aware of among service members is anger. “Often our patients are angry, and often that anger comes out to us as therapists,” she said. “We need to tell our colleagues about this and get them to expect it.”
Treating post-traumatic stress disorder can be a tricky proposition because of the sexual side effects caused by selective serotonin reuptake inhibitors, Dr. Ritchie said. She prefers bupropion because it is not linked to sexual side effects. Mood stabilizers cause weight gain, as do antipsychotics. Meanwhile, drug holidays lead to problems with adherence, she said. To mitigate side effects, Dr. Ritchie advised “trying one thing at a time and adding trazodone in low doses for sleep.” However, trazodone has been linked to priapism (Gen Hosp Psychiatry. 2015 Jan-Feb;37[1]:40-5), and so must be used with care.
Another treatment for PTSD that is showing promise is stellate ganglion block, which has proven effective for treating hot flashes in postmenopausal women and in addressing estrogen depletion tied to breast cancer treatment in small numbers of patients (Med Hypotheses. 2009 Jun;72[6]:657-61).
“Studies have found a reduction in PTSD symptoms as well as pain,” Dr. Ritchie said. “I’m pushing the VA to do more research in this area.”
In effort to treat sexual dysfunction, Dr. Ritchie said her family practice colleagues prescribe a lot of Viagra and other phosphodiesterase inhibitors. She speculated that flibanserin, a selective agonist for 5-HT1A and an antagonist for 5-HT2A receptors approved in 2015 by the Food and Drug Administration for premenopausal women with hypoactive sexual desire disorder, “will start making its way into the general population,” said Dr. Ritchie, whose comments about using phosphodiesterase inhibitors pertain to VA patients.
Many service members who participated in Operation Iraqi Freedom and Operation Enduring Freedom were aged 18-25 years. Partly because the Department of Defense (DOD) and the VA work with very young families, clinicians are tasked with teaching them about their needs as couples, including the need to discuss intimacy and sexual health. For political reasons, Dr. Ritchie said, in vitro fertilization is not covered by the VA, even though injuries from bomb blasts can make it impossible for couples to conceive naturally.
Toxic and infectious substances faced by troops that are not commonly found in the United States, such as chemicals, pesticides, and motor oils, also need to be acknowledged and addressed by clinicians. “We don’t do a good job about what a veteran thinks about what exposure does to their reproductive systems,” Dr. Ritchie said.
In an interview, Dr. Ghurani said that she came up with the title of the meeting to illustrate the extent to which providers treat PTSD in the military every day. Conference speakers examined the latest treatments on sexual trauma, and the state of the art therapy and research taking place at Walter Reed.
At the meeting, she discussed the distinction between military sexual trauma (MST) and sexual trauma within the civilian population. Research shows that veterans who screen positive for MST “are more likely to have a history of a suicide attempt documented in their VA medical record” (Psychiatry Res. 2016;244:257-65).
A 2008 study found that women are far more likely to screen positive for MST than men. Specifically, the study found that 25% of women and 1.3% of men who are screened for MST within the Veterans Health Administration screen positive (Trauma Violence Abuse. 2008 Oct;9[4]250-69).
Walter Reed’s Interpersonal Recovery Program at the Psychiatry Continuity Service is the only intensive outpatient program within the DOD that provides ongoing treatment for active duty service members with PTSD from a sexual trauma, Dr. Ghurani said.
Earlier during the meeting, Capt. (Ret.) William P. Nash, MD, director of psychological health at the Marine Corps and a 30-year veteran of the Navy, discussed moral injury, and contrasted it with PTSD and other sequelae of psychological trauma. He also described his work on the Moral Injury Events Scale as a tool for recognizing potentially morally injurious events in clinical and research settings.
Dr. Ritchie is the editor of “Intimacy Post-Injury: Combat Trauma and Sexual Health,” (New York: Oxford University Press, 2016). Dr. Ghurani contributed to a chapter in “Intimacy Post Injury,” and Dr. Nash has written extensively about PTSD, particularly among deployed Marines.
FROM TRAUMA TREATMENT FROM THE TRENCHES
Posttraumatic Stress Disorder, Depression, and Other Comorbidities: Clinical and Systems Approaches to Diagnostic Uncertainties
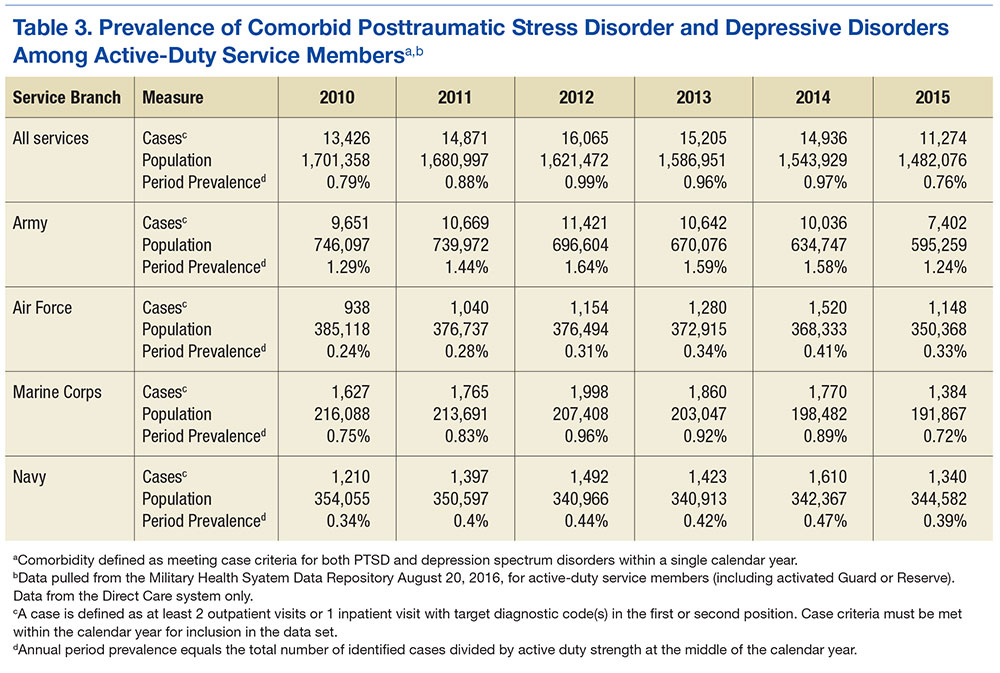
Over the past decade, nationwide attention has focused on mental health conditions associated with military service. Recent legal mandates have led to changes in the DoD, VA, and HHS health systems aimed at increasing access to care, decreasing barriers to care, and expanding research on mental health conditions commonly seen in service members and veterans. On August 31, 2012, President Barack Obama signed the Improving Access to Mental Health Services for Veterans, Service Members, and Military Families executive order, establishing an interagency task force from the VA, DoD, and HHS.1 The task force was charged with addressing quality of care and provider training in the management of commonly comorbid conditions, including (among other conditions) posttraumatic stress disorder (PTSD) and depression.
Depression and PTSD present major health burdens in both military and veteran cohorts. Overlap in clinical presentation and significant rates of comorbidity complicate effective management of these conditions. This article offers a brief review of the diagnostic and epidemiologic complexities associated with PTSD and depression, a summary of research relevant to these issues, and a description of recent system-level developments within the Military Health System (MHS) designed to improve care through better approaches in identification, management, and research of these conditions.
Diagnostic Uncertainty
Both PTSD and major depressive disorder (MDD) have been recognized as mental health disorders since the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM) discarded its previous etiologically based approach to diagnostic classification in 1980 in favor of a system in which diagnosis is based on observable symptoms.2,3 With the release of DSM-5 in 2013, the diagnostic criteria for PTSD underwent a substantial transformation.4 Previously, PTSD was described as an anxiety disorder, and some of its manifestations overlapped descriptively (and in many cases, etiologically) with anxiety and depressive illnesses.5
Clinicians also often described shorter-lived, developmental, formes fruste, or otherwise subsyndromal manifestations of trauma associated with PTSD. In DSM-5, PTSD was removed from the anxiety disorders section and placed in a new category of disorders labeled Trauma and Stressor-Related Disorders. This new category also included reactive attachment disorder (in children), acute stress disorder, adjustment disorders, and unspecified or other trauma and stressor-related disorders. Other major changes to the PTSD diagnostic criteria included modification to the DSM-IV-TR (text revision) trauma definition (making the construct more specific), removal of the requirement for explicit subjective emotional reaction to a traumatic event, and greater emphasis on negative cognitions and mood. Debate surrounds the updated symptom criteria with critics questioning whether there is any improvement in the clinical utility of the diagnosis, especially in light of the substantial policy and practice implications the change engenders.6
Recently, Hoge and colleagues examined the psychometric implications of the diagnostic changes (between DSM-IV-TR and DSM-5) in the PTSD definition.6 The authors found that although the 2 definitions showed nearly identical association with other psychiatric disorders (including depression) and functional impairment, 30% of soldiers who met DSM-IV-TR criteria for PTSD failed to meet criteria in DSM-5, and another 20% met only DSM-5 criteria. Recognizing discordance in PTSD and associated diagnoses, the U.S. Army Medical Command mandated that its clinicians familiarize themselves with the controversies surrounding the discordant diagnoses and coding of subthreshold PTSD.7
Adding to the problem of diagnostic uncertainty, the clinical presentation of MDD includes significant overlap with that of PTSD. Specifically, symptoms of guilt, diminished interests, problems with concentration, and sleep disturbances are descriptive of both disorders. Furthermore, the criteria set for several subthreshold forms of MDD evidence considerable overlap with PTSD symptoms. For example, diagnostic criteria for disruptive mood dysregulation disorder include behavioral outbursts and irritability, and diagnostic criteria for dysthymia include sleep disturbances and concentration problems.
Adjustment disorders are categorized as trauma and stressor-related disorders in DSM-5 and hold many emotional and behavioral symptoms in common with PTSD. The “acute” and “chronic” adjustment disorder specifiers contribute to problems in diagnostic certainty for PTSD. In general, issues pertaining to diagnostic uncertainty and overlap likely reflect the limits of using a diagnostic classification system that relies exclusively on observational and subjective reports of psychological symptoms.8,9
In a treatment environment where a veteran or active-duty patient has presented for care, in the face of these shared symptom sets, clinicians frequently offer initial diagnoses. These diagnoses are often based on perceived etiologic factors derived from patients’ descriptions of stressors encountered during military service. This tendency likely contributes to considerable inconsistencies and potential inaccuracies in diagnoses, and much of the variance can be attributed to the clinicians’ degree of familiarity with military exposures, perceptions of what constitutes trauma, and outside pressure to assign or avoid specific diagnoses.
Importantly, the phenomenologic differences between PTSD and depressive disorders increase the likelihood of poorly aligned and inconsistent treatment plans, and this lack of clarity may, in turn, compromise effective patient care. To address some of these diagnostic challenges, the VA and DoD incorporate military culture training into clinicians’ curriculum to increase provider familiarity with the common stressors and challenges of military life, mandate the use of validated measures to support diagnostic decision making, and regularly review policies that influence diagnostic practices.
Epidemiology
The prevalence rates for PTSD are increasing in the military, possibly stemming from the demands on service members engaged in years’ long wars. Despite the increased attention on this phenomenon, research has demonstrated that the majority of service members who deploy do not develop PTSD or significant trauma-related functional impairment.10 Furthermore, many cases of PTSD diagnosed in the MHS stem from traumatic experiences other than combat exposure, including childhood abuse and neglect, sexual and other assaults, accidents and health care exposures, domestic abuse, and bullying. Depression arguably has received less attention despite comparable prevalence rates in military populations, high co-occurrence of PTSD and depression, and depression being associated with a greater odds ratio for mortality that includes death by suicide in military service members.11
Estimates of the prevalence of PTSD from the U.S. Army suggest that it exists in 3% to 6% of military members who have not deployed and in 6% to 25% of service members with combat deployment histories. The frequency and intensity of combat are strong predictors of risk.7 A recent epidemiologic study using inpatient and outpatient encounter records showed that the prevalence of PTSD in the active military component was 2.0% in the middle of calendar year (CY) 2010; a two-thirds increase from 1.2% in CY 2007.12 The incidence of PTSD 
Epidemiologic studies and prevalence/incidence rates derived from administrative data rely on strict case definitions. Consequently, such administrative investigations include data only from service members 
PTSD and Depression Treatment
Despite the high rates of PTSD and MDD comorbidity, few treatments have been developed for and tested on an exclusively comorbid sample of patients.13 However, psychopharmacologic agents targeting depression have been applied to the treatment of PTSD, and PTSD psychotherapy trials typically include depression response as a secondary outcome. The generalizability of findings to a truly comorbid population may be limited based on study sampling frames and the unique characteristics of patients with comorbid PTSD and depression.14-16 Several psychopharmacologic treatments for depression have been evaluated as frontline treatments for PTSD. The 3 pharmacologic treatments that demonstrate efficacy in treating PTSD include fluoxetine, paroxetine, and venlafaxine.17
Although these pharmacologic agents represent good candidate treatments for comorbid patients, the effect size of pharmacologic treatments are generally smaller than those of psychotherapeutic treatments for PTSD.17,18 This observation, however, is based on indirect comparisons, and a recent systematic review concluded that the evidence was insufficient to determine the comparative effectiveness between psychotherapy and pharmacotherapy for PTSD.19 Evidence indicates that trauma-focused cognitive behavioral therapies consistently demonstrate efficacy and effectiveness in treating PTSD.19,20 These treatments also have been shown to significantly reduce depressive symptoms among PTSD samples.21
Based on strong bodies of evidence, these pharmacologic and psychological treatments have received the highest level of recommendation in the VA and DoD.22,23 Accordingly, both agencies have invested considerable resources in large-scale efforts to improve patient access to these particular treatments. Despite these impressive implementation efforts, however, the limitations of relying exclusively on these treatments as frontline approaches within large health care systems have become evident.24-26
Penetration of Therapies
Penetration of these evidence-based treatments (EBTs) within the DoD and VHA remains limited. For instance, one study showed that VA clinicians in mental health specialty care clinics may provide only about 4 hours of EBT per week.27
Other reports suggest that only about 60% of treatment-seeking patients in PTSD clinics receive any type of evidence-based therapy and that within-session care quality is questionable based on a systematic review of chart notes.28,29 Attrition in trauma-focused therapy is a recognized limitation, with 1 out of 3 treatment-seeking patients not completing a full dose of evidence-based treatment.30-33 Large-scale analyses of VHA and DoD utilization data suggest that the majority of PTSD patients do not receive a sufficient number of sessions to be characterized as an adequate dose of EBT, with a majority of dropouts occur- ring after just a few sessions.34-37
Hoge and colleagues found that < 50% of soldiers meeting criteria for PTSD received any mental health care within the prior 6 months with one-quarter of those patients dropping out of care prematurely.38 Among a large cohort of soldiers engaged in care for the treatment of PTSD, only about 40% received a number of EBT treatment sessions that could qualify as an adequate dose.38 Thus, although major advancements in the development and implementation of effective treatments for PTSD and depression have occurred, the penetration of these treatments is limited, and the majority of patients in need of treatment potentially receive inadequate care.39
System level approaches that integrate behavioral health services into the primary care system have been proposed to address these care gaps for service members and veterans.40-42 Fundamentally, system-level approaches seek to improve the reach and effectiveness of care through large-scale screening efforts, a greater emphasis on the quality of patient care, and enhanced care continuity across episodes of treatment.
Primary Care
With the primary care setting considered the de facto mental health system, integrated approaches enhance the reach of care by incorporating uniform mental health screening and referral for patients coming through primary care. Specific evidence-based treatments can be integrated into this approach within a stepped-care framework that aims to match patients strategically to the right type of care and leverage specialty care resources as needed. Integrated care approaches for the treatment of PTSD and depression have been developed and evaluated inside and outside of the MHS. Findings indicate that integrated treatment approaches can improve care access, care continuity, patient satisfaction, quality of care,and in several trials, PTSD and depression outcomes.43-47
Recently, an integrated care approach targeting U.S. Army soldiers who screened positive for PTSD or depression in primary care was evaluated in a multisite effectiveness trial.48 Patients randomized to the treatment approach experienced significant improvements in both PTSD and depression symptoms relative to patients in usual care.43 In addition, patients treated in this care model received significantly more mental health services; the patterns of care indicated that patients with comorbid PTSD and depression were more likely to be triaged to specialty care, whereas patients with a single diagnosis were more likely to be managed in primary care.49 This trial suggests that integrated care models feasibly can be implemented in the U.S. Army care system, yielding increased uptake of mental health care, more efficiently matched care based on patient comorbidities, and improved PTSD and depression outcomes.
Treatment Research
The MHS supports a large portfolio of research in PTSD and depression through DoD/VA research consortia (eg, the Congressionally Directed Medical Research Program, the Consortium to Alleviate PTSD, the Injury and Traumatic Stress Clinical Consortium). The U.S. Army Medical Research and Materiel Command (USAMRMC) executes and manages the portfolio of research, relying on a joint program committee of DoD and non-DoD experts to make funding recommendations based on identified research priorities, policy guidance, and knowledge translation needs.
Health systems research on PTSD and MDD in federal health care settings is expanding. For example, the RAND Corporation recently evaluated a candidate set of quality measures for PTSD and MDD, using an operational definition of an episode of care.37 This work is intended to inform efforts to measure and improve the quality of care for PTSD and depression across the enterprise.
The DoD Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury is simultaneously completing an inferential assessment of adjunctive mental health care services, many focused on PTSD and depression, throughout the health care enterprise. Along with the substantial resources devoted to research on PTSD and depression, the MHS is implementing strategies to improve the system of care for service members with mental health conditions.
Army Care System Innovations
The U.S. Army is engaged in a variety of strategies to improve the identification of patients with mental health conditions, increase access to mental health services, and enhance the quality of care that soldiers receive for PTSD and depression. To improve the coordination of mental health care, the U.S. Army Medical Command implemented a wide-scale innovative transformation of its mental health care system through the establishment of the Behavioral Health Service Line program management office.
This move eliminated separate departments of psychiatry, psychology, and social work in favor of integrated behavioral health departments that are now responsible for all mental health care delivered to soldiers, including inpatient, outpatient, partial hospitalization, residential, embedded care in garrison, and primary care settings. This transformation ensured coordination of care for soldiers, eliminating potential miscommunication with patients, commands, and other clinicians while clearly defining performance indicators in process (eg, productivity, scheduling, access to care, and patient satisfaction) and outcome measures.49 In conjunction with the development of its service line, the U.S. Army created a Behavioral Health Data Portal (BHDP), an electronic and standardized means to assess clinical outcomes for common conditions.
To promote higher quality mental health care, the Office of the Surgeon General of the U.S. Army provided direct guidance on the treatment of PTSD and depression. U.S. Army policy mandates that providers treating mental health conditions adhere to the VA/DoD clinical practice guidelines (CPGs) and that soldiers with PTSD and depression be offered treatments with the highest level of scientific support and that outcome measures be routinely administered. In line with the CPGs, U.S. Army policy also recommends the use of both integrated and embedded mental health care approaches to address PTSD, depression, and other common physical and psychological health conditions.
To reduce stigma and improve mental health care access, the U.S. Army began implementing integrated care approaches in 2007 with its Re-Engineering Systems of Primary Care Treatment in the Military (RESPECT-Mil) program, an evidence-based collaborative care model.51-55 This approach included structured screening and diagnostic procedures, predictable follow-up schedules for patients, and the coordination of the divisions of responsibility among and between primary care providers, paraprofessionals, and behavioral health care providers. From 2007 to 2013, this collaborative care model was rolled out across 96 clinics worldwide and provided PTSD and depression screening to more than 1 million encounters per year.52,53
More recently, the U.S. Army led DoD in integrating behavioral health personnel in patient centered medical homes (PCMH) in compliance with DoD Instruction 6490.15.56 This hybrid integrated care model combines collaborative care elements developed in the RESPECT-Mil program with elements of the U.S. Air Force Behavioral Health Optimization project colocating behavioral health providers in primary care settings to provide brief consultative services.
MHS Care Enhancements
Many of the innovations deployed throughout the U.S. Army system of behavioral health care have driven changes across the MHS as a whole. The DoD and the VA have made substantive systemwide policy and practice changes to improve care for beneficiaries with PTSD, depression, and comorbid PTSD and depression. In particular, significant implementation efforts have addressed population screening strategies, outcome monitoring to support measurement-based care, increased access to effective care, and revision of the disability evaluation system.
To improve the identification and referral of soldiers with deployment-related mental health concerns, the DoD implemented a comprehensive program that screens service members prior to deployment, immediately on redeployment, and then again 6 months after returning from deployment. Additionally, annual primary care- based screening requirements have been instituted as part of the DoD PCMH initiative. Both deployment-related and primary care-based screenings include an instrumentation to detect symptoms of PTSD and depression and extend the reach of mental health screening to the entire MHS population.
Building on the success of BHDP, former Assistant Secretary of Defense for Health Affairs Jonathan Woodson mandated BHDP use across the MHS for all patients in DoD behavioral health clinics and the use of outcome measures for the treatment of PTSD, anxiety, depression, and alcohol use disorders.57 A DoD-wide requirement to use the PTSD checklist and patient health questionnaire to monitor PTSD and depression symptoms at mental health intakes and regularly at follow-up visits is being implemented. The Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury, through its Practice-Based Implementation Network (underwritten by a Joint Incentive Fund managed between DoD and VA), has worked across the MHS and the VA to facilitate the implementation, uptake, and adoption of this initiative.
The DoD established the Center for Deployment Psychology (CDP) in 2006 to promote clinician training in EBTs with the aim of increasing service members’ access to effective psychological treatments. Since its inception, the CDP has provided EBT training to more than 40,000 behavioral health providers. Although the impact of these and other efforts on improving the quality of care that patients receive is unknown, a recent study documented widespread self-reported usage of EBT components in U.S. Army clinics and that providers formally trained in EBTs were more likely to deliver EBTs.58
Finally, systemwide changes to the VA Schedule of Ratings for Disability (VASRD) and integration of DoD and VA disability evaluation systems have led to shifts in diagnosis toward PTSD that usually merit a minimum 50% disability rating. Mandates in law require military clinicians to evaluate patients who have deployed for PTSD and TBI prior to taking any actions associated with administrative separation. The practice of attributing PTSD symptoms to character pathology or personality disorders, even when these symptoms did not clearly manifest or worsen with military service, has likely been eliminated from practice in military and veteran populations.
Robust policy changes to limit personality disorder discharges started in fiscal year 2007, when there were 4,127 personality disorder separations across DoD. This number was reduced to 300 within 5 years. Policy changes regarding separation not only seem to have affected discharges, but also may have shaped diagnostic practice. The incidence rate of personality disorder diagnoses declined from 513 per 100,000 person-years in 2007 to 284 per 100,000 person-years by 2011.59 The VASRD recognizes chronic adjustment disorder as a disability, and the National Defense Authorization Act of 2008 mandated that DoD follow disability guidelines promulgated by VA.
As stated in the memorandum Clinical Policy Guidance for Assessment and Treatment of Post-Traumatic Stress Disorders (August 24, 2012), DoD recognizes chronic adjustment disorder as an unfitting condition that merits referral to its disability evaluation system.60 Acute adjustment disorders may still lead to administrative separations, as many service members manifest emotional symptoms stemming from the failure to adjust to the routine vicissitudes of military life. Finally, many court jurisdictions, including veteran’s courts, military courts, and commanders empowered to adjudicate nonjudicial infractions under the Uniform Code of Military Justice, have recognized PTSD as grounds for the mitigation of penalties associated with a wide array of criminal and administrative infractions.
Conclusion
In response to the increased mental health burden following a decade of war and the associated pressures stemming from federal mandates, the MHS has invested unprecedented resources into improving care for military service members. The U.S. Army has played a prominent role in this endeavor by investing in clinical research efforts to accelerate discovery on the causes and cures for these conditions, enacting policies that mandate best practices, and implementing evidence-based care approaches across the system of care. Despite this progress, however, understanding and effectively treating the most prevalent mental health conditions remain a challenge across the DoD and VHA health care systems. Many service members and veterans still do not receive timely, high-quality care for PTSD, depression, and other common comorbidities associated with military experience, and controversies in diagnostic clarification abound.
In short, great strides have been made, yet there is still a large distance to go. The vision of an effective, efficient, comprehensive care system for mental health conditions will continue to be pursued and achieved through collaborations across key agencies and the scientific community, implementation of health system approaches that support population care, and the sustained efforts of dedicated clinicians, staff, and clinic leaders who deliver the care to our service members and veterans.
1. The White House, Office of the Press Secretary. Executive Order 13625: Improving Access to Mental Health Services for Veterans, Service Members, and Military Families. https://www.whitehouse.gov/the-press-office/2012/08/31/executive-order-improving-access-mental-health-services-veterans-service. Published August 31, 2012. Accessed September 20, 2016.
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. Arlington, VA: American Psychiatric Association Press; 1980.
3. Mayes R, Horwitz AV. DSM-III and the revolution in the classification of mental illness. J Hist Behav Sci. 2005;41(3):249-267.
4. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association Press; 2013.
5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed., text rev. Arlington, VA: American Psychiatric Association Press; 2000.
6. Hoge CW, Riviere LA, Wilk JE, Herrell RK, Weathers FW. The prevalence of post-traumatic stress disorder (PTSD) in US combat soldiers: a head-to-head comparison of DSM-5 versus DSM-IV-TR symptom criteria with the PTSD checklist. Lancet Psychiatry. 2014;1(4):269-277.
7. OTSG-MEDCOM. Policy Memo 14-094: Policy Guidance on the Assessment and Treatment of Posttraumatic Stress Disorder (PTSD). Published December 18, 2014.
8. Insel T, Cuthbert B, Garvey M, et al. Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry, 2010;167(7):748-751.
9. National Institute of Mental Health. NIMH strategic plan for research. http://www.nimh.nih.gov/about/strategic-planning-reports/index.shtml. Revised 2015. Accessed September 20, 2016.
10. Colston M, Hocter W. Forensic aspects of posttraumatic stress disorder. In: Ritchie EC, ed. Forensic and Ethical Issues in Military Behavioral Health. Washington, DC: U.S. Department of the Army; 2015:97-110.
11. Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury. National Center for Telehealth and Technology. Department of Defense suicide event report: calendar year 2013 annual report. http://t2health.dcoe.mil/programs/dodser. Published January 13, 2015. Accessed September 20, 2016.
12. Otto JL, O’Donnell FL, Ford SA, Ritschard HV. Selected mental health disorders among active component members, US Armed Forces, 2007-2010. MSMR. 2010;17(11):2-5.
13. Gutner CA, Galovski T, Bovin MJ, Schnurr PP. Emergence of transdiagnostic treatments for PTSD and posttraumatic distress. Curr Psychiatry Rep. 2016;18(10):95-101.
14. Campbell DG, Felker BL, Liu CF, et al. Prevalence of depression-PTSD comorbidity: implications for clinical practice guidelines and primary care-based interventions. J Gen Intern Med. 2007;22(6):711-718.
15. Chan D, Cheadle AD, Reiber G, Unützer J, Chaney EF. Health care utilization and its costs for depressed veterans with and without comorbid PTSD symptoms. Psychiatr Serv. 2009;60(12):1612-1617.
16. Maguen S, Cohen B, Cohen G, Madden E, Bertenthal D, Seal K. Gender differences in health service utilization among Iraq and Afghanistan veterans with posttraumatic stress disorder. J Womens Health (Larchmt). 2012;21(6):666-673.
17. Hoskins M, Pearce J, Bethell A, et al. Pharmacotherapy for post-traumatic stress disorder: systematic review and meta-analysis. Br J Psychiatry. 2015;206(2):93-100.
18. Puetz TW, Youngstedt SD, Herring MP. Effects of pharmacotherapy on combat-related PTSD, anxiety, and depression: a systematic review and meta-regression analysis. PLoS One. 2015;10(5):e0126529.
19. Jonas DE, Cusack K, Forneris CA, et al. Psychological and pharmacological treatments for adults with posttraumatic stress disorder (PTSD). Comparative effectiveness review no. 92. https://effectivehealthcare.ahrq.gov/ehc/products/347/1435/PTSD-adult-treatment-report-130403.pdf. Published April 3, 2013. Accessed September 20, 2016.
20. Haagen JFG, Smid GE, Knipscheer JW, Kleber RJ. The efficacy of recommended treatments for veterans with PTSD: a metaregression analysis. Clin Psychol Rev. 2015;40:184-194.
21. Tran K, Moulton K, Santesso N, Rabb D. Cognitive processing therapy for post-traumatic stress disorder: a systematic review and meta-analysis. https://www.cadth.ca/cognitive-processing-therapy-post-traumatic-stress-disorder-systematic-review-and-meta-analysis. Published August 11, 2015. Accessed September 20, 2016.
22. VA/DoD Management of Post-Traumatic Stress Working Group. VA/DoD Clinical Practice Guideline for Management of Post-Traumatic Stress. Version 2. http://www.healthquality.va.gov/guidelines/MH/ptsd/. Published October, 2010. Accessed September 20, 2016.
23. VA/DoD Management of Major Depressive Disorder Working Group. VA/DoD Clinical Practice Guideline for the Management of Major Depressive Disorder. Version 3. http://www.healthquality.va.gov/guidelines/mh/mdd/index.asp. Published April 2016. Accessed September 20, 2016.
24. Zatzick DF, Galea S. An epidemiologic approach to the development of early trauma focused intervention. J Trauma Stress. 2007;20(4):401-412.
25. Zatzick DF, Koepsell T, Rivara FP. Using target population specification, effect size, and reach to estimate and compare the population impact of two PTSD preventive interventions. Psychiatry. 2009;72(4):346-359.
26. Glasgow RE, Nelson CC, Strycker LA, King DK. Using RE-AIM metrics to evaluate diabetes self-management support interventions. Am J Prev Med. 2006;30(1):67-73.
27. Finley EP, Garcia HA, Ketchum NS, et al. Utilization of evidence-based psychotherapies in Veterans Affairs posttraumatic stress disorder outpatient clinics. Psychol Serv. 2015;12(1):73-82.
28. Mott JM, Mondragon S, Hundt NE, Beason-Smith M, Grady RH, Teng EJ. Characteristics of U.S. veterans who begin and complete prolonged exposure and cognitive processing therapy for PTSD. J Trauma Stress. 2014;27(3):265-273.
29. Shiner B, D’Avolio LW, Nguyen TM, et al. Measuring use of evidence based psychotherapy for PTSD. Adm Policy Ment Health. 2013;40(4):311-318.
30. Schnurr PP, Friedman MJ, Engel CC, et al. Cognitive behavioral therapy for posttraumatic stress disorder in women: a randomized controlled trial. JAMA. 2007;297(8):820-830.
31. Tuerk PW, Yoder M, Grubaugh A, Myrick H, Hamner M, Acierno R. Prolonged exposure therapy for combat-related posttraumatic stress disorder: an examination of treatment effectiveness for veterans of the wars in Afghanistan and Iraq. J Anxiety Disord. 2011;25(3):397-403.
32. Chard KM, Schumm JA, Owens GP, Cottingham SM. A comparison of OEF and OIF veterans and Vietnam veterans receiving cognitive processing therapy. J Trauma Stress. 2010;23(1):25-32.
33. Monson CM, Schnurr PP, Resick PA, Friedman MJ, Young-Xu Y, Stevens SP. Cognitive processing therapy for veterans with military-related posttraumatic stress disorder. J Consult Clin Psychol. 2006;74(5):898-907.
34. Mott JM, Hundt NE, Sansgiry S, Mignogna J, Cully JA. Changes in psychotherapy utilization among veterans with depression, anxiety, and PTSD. Psychiatr Serv. 2014;65(1):106-112.
35. Seal KH, Maguen S, Cohen B, et al. VA mental health services utilization in Iraq and Afghanistan veterans in the first year of receiving new mental health diagnoses. J Trauma Stress. 2010;23(1):5-16.
36. Russell M, Silver SM. Training needs for the treatment of combat-related posttraumatic stress disorder: a survey of Department of Defense clinicians. Traumatology. 2007;13(3):4-10.
37. Schell TL, Marshall GN. Survey of individuals previously deployed for OEF/OIF. In: Tanielian T, Jaycox LH, eds. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND Corporation; 2008:87-118.
38. Hoge CW, Grossman SH, Auchterlonie JL, Riviere LA, Milliken CS, >Wilk JE. PTSD treatment for soldiers after combat deployment: low utilization of mental health care and reasons for dropout. Psychiatr Serv. 2014;65(8):997-1004.
39. Committee on the Assessment of Ongoing Efforts in the Treatment of Posttraumatic Stress Disorder, Board on the Health of Select Populations, Institute of Medicine. Treatment for Posttraumatic Stress Disorder in Military and Veteran Populations: Final Assessment. Washington, DC: National Academies Press; 2014.
40. Schnurr PP. Extending collaborative care for posttraumatic mental health. JAMA Intern Med. 2016;176(7):956-957.
41. Hoge CW. Interventions for war-related posttraumatic stress disorder: meeting veterans where they are. JAMA. 2011;306(5):549-551.
42. Engel CC. Improving primary care for military personnel and veterans with posttraumatic stress disorder: the road ahead. Gen Hosp Psychiatry. 2005;27(3):158-160.
43. Engel CC, Jaycox LH, Freed MC, et al. Centrally assisted collaborative telecare management for posttraumatic stress disorder and depression in military primary care: a randomized controlled trial. JAMA Intern Med. 2016;176(7):948-956.
44. Fortney JC, Pyne JM, Kimbrell TA, et al. Telemedicine-based collaborative care for posttraumatic stress disorder: a randomized clinical trial. JAMA Psychiatry. 2015;72(1):58-67.
45. Schnurr PP, Friedman MJ, Oxman TE, et al. RESPECT-PTSD: re-engineering systems for the primary care treatment of PTSD, a randomized controlled trial. J Gen Intern Med. 2013;28(1):32-40.
46. Zatzick D, Roy-Byrne P, Russo J, et al. A randomized effectiveness trial of stepped collaborative care for acutely injured trauma survivors. Arch Gen Psychiatry. 2004;61(5):498-506.
47. Zatzick D, O’Connor SS, Russo J, et al. Technology-enhanced stepped collaborative care targeting posttraumatic stress disorder and comorbidity after injury: a randomized controlled trial. J Trauma Stress. 2015;28(5):391-400.
48. Engel CC, Bray RM, Jaycox LH, et al. Implementing collaborative primary care for depression and posttraumatic stress disorder: design and sample for a randomized trial in the U.S. Military Health System. Contemp Clin Trials. 2014;39(2):310-319.
49. Belsher BE, Jaycox LH, Freed MC, et al. Mental health utilization patterns during a stepped, collaborative care effectiveness trial for PTSD and depression in the military health system. Med Care. 2016;54(7):706-713.
50. Hepner KA, Roth CP, Farris C, et al. Measuring the Quality of Care for Psychological Health Conditions in the Military Health System: Candidate Quality Measures for Posttraumatic Stress Disorder and Major Depressive Disorder. Santa Monica, CA: RAND Corporation; 2015.
51. Engel C, Oxman T, Yamamoto C, et al. RESPECT-Mil: feasibility of a systems-level collaborative care approach to depression and post-traumatic stress disorder in military primary care. Mil Med. 2008;173(10):935-940.
52. Belsher BE, Curry J, McCutchan P, et al. Implementation of a collaborative care initiative for PTSD and depression in the Army primary care system. Soc Work Ment Health. 2014;12(5-6):500-522.
53. Wong EC, Jaycox LH, Ayer L, et al. Evaluating the Implementation of the Re-Engineering Systems of Primary Care Treatment in the Military (RESPECT-Mil). Santa Monica, CA: RAND Corporation; 2015.
54. Archer J, Bower P, Gilbody S, et al. Collaborative care for depression and anxiety problems. Cochrane Database Syst Rev. 2012;10:CD006525.
55. Woltmann E, Grogan-Kaylor A, Perron B, Georges H, Kilbourne AM, Bauer MS. Comparative effectiveness of collaborative chronic care models for mental health conditions across primary, specialty, and behavioral health care settings: systematic review and meta-analysis. Am J Psychiatry. 2012;169(8):790-804.
56. Wright JL. DoD Directive 6490.15. www.dtic.mil/whs/directives/corres/pdf/649015p.pdf.Revised November 20, 2014. Accessed October 3, 2016. 57. Woodson J. Military treatment facility mental health clinical outcomes guidance. http://dcoe.mil/Libraries/Documents/MentalHealthClinicalOutcomesGuidance_Woodson.pdf. Published September 9, 2013. Accessed October 4, 2016.
58. Wilk JE, West JC, Duffy FF, Herrell RK, Rae DS, Hoge CW. Use of evidence-based treatment for posttraumatic stress disorder in Army behavioral healthcare. Psychiatry. 2013;76(4):336-348.
59. Stockton PN, Olsen ET, Hayford S, et al. Security from within: independent review of the Washington Navy Yard shooting. http://archive.defense.gov/pubs/Independent-Review-of-the-WNY-Shooting-14-Nov-2013.pdf. Published November, 2013. Accessed September 20, 2016.
60. Woodson J. ASD(HA) Memorandum: Clinical Policy Guidance for Assessment and Treatment of Posttraumatic Stress Disorder. August 24, 2012.
Over the past decade, nationwide attention has focused on mental health conditions associated with military service. Recent legal mandates have led to changes in the DoD, VA, and HHS health systems aimed at increasing access to care, decreasing barriers to care, and expanding research on mental health conditions commonly seen in service members and veterans. On August 31, 2012, President Barack Obama signed the Improving Access to Mental Health Services for Veterans, Service Members, and Military Families executive order, establishing an interagency task force from the VA, DoD, and HHS.1 The task force was charged with addressing quality of care and provider training in the management of commonly comorbid conditions, including (among other conditions) posttraumatic stress disorder (PTSD) and depression.
Depression and PTSD present major health burdens in both military and veteran cohorts. Overlap in clinical presentation and significant rates of comorbidity complicate effective management of these conditions. This article offers a brief review of the diagnostic and epidemiologic complexities associated with PTSD and depression, a summary of research relevant to these issues, and a description of recent system-level developments within the Military Health System (MHS) designed to improve care through better approaches in identification, management, and research of these conditions.
Diagnostic Uncertainty
Both PTSD and major depressive disorder (MDD) have been recognized as mental health disorders since the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM) discarded its previous etiologically based approach to diagnostic classification in 1980 in favor of a system in which diagnosis is based on observable symptoms.2,3 With the release of DSM-5 in 2013, the diagnostic criteria for PTSD underwent a substantial transformation.4 Previously, PTSD was described as an anxiety disorder, and some of its manifestations overlapped descriptively (and in many cases, etiologically) with anxiety and depressive illnesses.5
Clinicians also often described shorter-lived, developmental, formes fruste, or otherwise subsyndromal manifestations of trauma associated with PTSD. In DSM-5, PTSD was removed from the anxiety disorders section and placed in a new category of disorders labeled Trauma and Stressor-Related Disorders. This new category also included reactive attachment disorder (in children), acute stress disorder, adjustment disorders, and unspecified or other trauma and stressor-related disorders. Other major changes to the PTSD diagnostic criteria included modification to the DSM-IV-TR (text revision) trauma definition (making the construct more specific), removal of the requirement for explicit subjective emotional reaction to a traumatic event, and greater emphasis on negative cognitions and mood. Debate surrounds the updated symptom criteria with critics questioning whether there is any improvement in the clinical utility of the diagnosis, especially in light of the substantial policy and practice implications the change engenders.6
Recently, Hoge and colleagues examined the psychometric implications of the diagnostic changes (between DSM-IV-TR and DSM-5) in the PTSD definition.6 The authors found that although the 2 definitions showed nearly identical association with other psychiatric disorders (including depression) and functional impairment, 30% of soldiers who met DSM-IV-TR criteria for PTSD failed to meet criteria in DSM-5, and another 20% met only DSM-5 criteria. Recognizing discordance in PTSD and associated diagnoses, the U.S. Army Medical Command mandated that its clinicians familiarize themselves with the controversies surrounding the discordant diagnoses and coding of subthreshold PTSD.7
Adding to the problem of diagnostic uncertainty, the clinical presentation of MDD includes significant overlap with that of PTSD. Specifically, symptoms of guilt, diminished interests, problems with concentration, and sleep disturbances are descriptive of both disorders. Furthermore, the criteria set for several subthreshold forms of MDD evidence considerable overlap with PTSD symptoms. For example, diagnostic criteria for disruptive mood dysregulation disorder include behavioral outbursts and irritability, and diagnostic criteria for dysthymia include sleep disturbances and concentration problems.
Adjustment disorders are categorized as trauma and stressor-related disorders in DSM-5 and hold many emotional and behavioral symptoms in common with PTSD. The “acute” and “chronic” adjustment disorder specifiers contribute to problems in diagnostic certainty for PTSD. In general, issues pertaining to diagnostic uncertainty and overlap likely reflect the limits of using a diagnostic classification system that relies exclusively on observational and subjective reports of psychological symptoms.8,9
In a treatment environment where a veteran or active-duty patient has presented for care, in the face of these shared symptom sets, clinicians frequently offer initial diagnoses. These diagnoses are often based on perceived etiologic factors derived from patients’ descriptions of stressors encountered during military service. This tendency likely contributes to considerable inconsistencies and potential inaccuracies in diagnoses, and much of the variance can be attributed to the clinicians’ degree of familiarity with military exposures, perceptions of what constitutes trauma, and outside pressure to assign or avoid specific diagnoses.
Importantly, the phenomenologic differences between PTSD and depressive disorders increase the likelihood of poorly aligned and inconsistent treatment plans, and this lack of clarity may, in turn, compromise effective patient care. To address some of these diagnostic challenges, the VA and DoD incorporate military culture training into clinicians’ curriculum to increase provider familiarity with the common stressors and challenges of military life, mandate the use of validated measures to support diagnostic decision making, and regularly review policies that influence diagnostic practices.
Epidemiology
The prevalence rates for PTSD are increasing in the military, possibly stemming from the demands on service members engaged in years’ long wars. Despite the increased attention on this phenomenon, research has demonstrated that the majority of service members who deploy do not develop PTSD or significant trauma-related functional impairment.10 Furthermore, many cases of PTSD diagnosed in the MHS stem from traumatic experiences other than combat exposure, including childhood abuse and neglect, sexual and other assaults, accidents and health care exposures, domestic abuse, and bullying. Depression arguably has received less attention despite comparable prevalence rates in military populations, high co-occurrence of PTSD and depression, and depression being associated with a greater odds ratio for mortality that includes death by suicide in military service members.11
Estimates of the prevalence of PTSD from the U.S. Army suggest that it exists in 3% to 6% of military members who have not deployed and in 6% to 25% of service members with combat deployment histories. The frequency and intensity of combat are strong predictors of risk.7 A recent epidemiologic study using inpatient and outpatient encounter records showed that the prevalence of PTSD in the active military component was 2.0% in the middle of calendar year (CY) 2010; a two-thirds increase from 1.2% in CY 2007.12 The incidence of PTSD
Epidemiologic studies and prevalence/incidence rates derived from administrative data rely on strict case definitions. Consequently, such administrative investigations include data only from service members
PTSD and Depression Treatment
Despite the high rates of PTSD and MDD comorbidity, few treatments have been developed for and tested on an exclusively comorbid sample of patients.13 However, psychopharmacologic agents targeting depression have been applied to the treatment of PTSD, and PTSD psychotherapy trials typically include depression response as a secondary outcome. The generalizability of findings to a truly comorbid population may be limited based on study sampling frames and the unique characteristics of patients with comorbid PTSD and depression.14-16 Several psychopharmacologic treatments for depression have been evaluated as frontline treatments for PTSD. The 3 pharmacologic treatments that demonstrate efficacy in treating PTSD include fluoxetine, paroxetine, and venlafaxine.17
Although these pharmacologic agents represent good candidate treatments for comorbid patients, the effect size of pharmacologic treatments are generally smaller than those of psychotherapeutic treatments for PTSD.17,18 This observation, however, is based on indirect comparisons, and a recent systematic review concluded that the evidence was insufficient to determine the comparative effectiveness between psychotherapy and pharmacotherapy for PTSD.19 Evidence indicates that trauma-focused cognitive behavioral therapies consistently demonstrate efficacy and effectiveness in treating PTSD.19,20 These treatments also have been shown to significantly reduce depressive symptoms among PTSD samples.21
Based on strong bodies of evidence, these pharmacologic and psychological treatments have received the highest level of recommendation in the VA and DoD.22,23 Accordingly, both agencies have invested considerable resources in large-scale efforts to improve patient access to these particular treatments. Despite these impressive implementation efforts, however, the limitations of relying exclusively on these treatments as frontline approaches within large health care systems have become evident.24-26
Penetration of Therapies
Penetration of these evidence-based treatments (EBTs) within the DoD and VHA remains limited. For instance, one study showed that VA clinicians in mental health specialty care clinics may provide only about 4 hours of EBT per week.27
Other reports suggest that only about 60% of treatment-seeking patients in PTSD clinics receive any type of evidence-based therapy and that within-session care quality is questionable based on a systematic review of chart notes.28,29 Attrition in trauma-focused therapy is a recognized limitation, with 1 out of 3 treatment-seeking patients not completing a full dose of evidence-based treatment.30-33 Large-scale analyses of VHA and DoD utilization data suggest that the majority of PTSD patients do not receive a sufficient number of sessions to be characterized as an adequate dose of EBT, with a majority of dropouts occur- ring after just a few sessions.34-37
Hoge and colleagues found that < 50% of soldiers meeting criteria for PTSD received any mental health care within the prior 6 months with one-quarter of those patients dropping out of care prematurely.38 Among a large cohort of soldiers engaged in care for the treatment of PTSD, only about 40% received a number of EBT treatment sessions that could qualify as an adequate dose.38 Thus, although major advancements in the development and implementation of effective treatments for PTSD and depression have occurred, the penetration of these treatments is limited, and the majority of patients in need of treatment potentially receive inadequate care.39
System level approaches that integrate behavioral health services into the primary care system have been proposed to address these care gaps for service members and veterans.40-42 Fundamentally, system-level approaches seek to improve the reach and effectiveness of care through large-scale screening efforts, a greater emphasis on the quality of patient care, and enhanced care continuity across episodes of treatment.
Primary Care
With the primary care setting considered the de facto mental health system, integrated approaches enhance the reach of care by incorporating uniform mental health screening and referral for patients coming through primary care. Specific evidence-based treatments can be integrated into this approach within a stepped-care framework that aims to match patients strategically to the right type of care and leverage specialty care resources as needed. Integrated care approaches for the treatment of PTSD and depression have been developed and evaluated inside and outside of the MHS. Findings indicate that integrated treatment approaches can improve care access, care continuity, patient satisfaction, quality of care,and in several trials, PTSD and depression outcomes.43-47
Recently, an integrated care approach targeting U.S. Army soldiers who screened positive for PTSD or depression in primary care was evaluated in a multisite effectiveness trial.48 Patients randomized to the treatment approach experienced significant improvements in both PTSD and depression symptoms relative to patients in usual care.43 In addition, patients treated in this care model received significantly more mental health services; the patterns of care indicated that patients with comorbid PTSD and depression were more likely to be triaged to specialty care, whereas patients with a single diagnosis were more likely to be managed in primary care.49 This trial suggests that integrated care models feasibly can be implemented in the U.S. Army care system, yielding increased uptake of mental health care, more efficiently matched care based on patient comorbidities, and improved PTSD and depression outcomes.
Treatment Research
The MHS supports a large portfolio of research in PTSD and depression through DoD/VA research consortia (eg, the Congressionally Directed Medical Research Program, the Consortium to Alleviate PTSD, the Injury and Traumatic Stress Clinical Consortium). The U.S. Army Medical Research and Materiel Command (USAMRMC) executes and manages the portfolio of research, relying on a joint program committee of DoD and non-DoD experts to make funding recommendations based on identified research priorities, policy guidance, and knowledge translation needs.
Health systems research on PTSD and MDD in federal health care settings is expanding. For example, the RAND Corporation recently evaluated a candidate set of quality measures for PTSD and MDD, using an operational definition of an episode of care.37 This work is intended to inform efforts to measure and improve the quality of care for PTSD and depression across the enterprise.
The DoD Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury is simultaneously completing an inferential assessment of adjunctive mental health care services, many focused on PTSD and depression, throughout the health care enterprise. Along with the substantial resources devoted to research on PTSD and depression, the MHS is implementing strategies to improve the system of care for service members with mental health conditions.
Army Care System Innovations
The U.S. Army is engaged in a variety of strategies to improve the identification of patients with mental health conditions, increase access to mental health services, and enhance the quality of care that soldiers receive for PTSD and depression. To improve the coordination of mental health care, the U.S. Army Medical Command implemented a wide-scale innovative transformation of its mental health care system through the establishment of the Behavioral Health Service Line program management office.
This move eliminated separate departments of psychiatry, psychology, and social work in favor of integrated behavioral health departments that are now responsible for all mental health care delivered to soldiers, including inpatient, outpatient, partial hospitalization, residential, embedded care in garrison, and primary care settings. This transformation ensured coordination of care for soldiers, eliminating potential miscommunication with patients, commands, and other clinicians while clearly defining performance indicators in process (eg, productivity, scheduling, access to care, and patient satisfaction) and outcome measures.49 In conjunction with the development of its service line, the U.S. Army created a Behavioral Health Data Portal (BHDP), an electronic and standardized means to assess clinical outcomes for common conditions.
To promote higher quality mental health care, the Office of the Surgeon General of the U.S. Army provided direct guidance on the treatment of PTSD and depression. U.S. Army policy mandates that providers treating mental health conditions adhere to the VA/DoD clinical practice guidelines (CPGs) and that soldiers with PTSD and depression be offered treatments with the highest level of scientific support and that outcome measures be routinely administered. In line with the CPGs, U.S. Army policy also recommends the use of both integrated and embedded mental health care approaches to address PTSD, depression, and other common physical and psychological health conditions.
To reduce stigma and improve mental health care access, the U.S. Army began implementing integrated care approaches in 2007 with its Re-Engineering Systems of Primary Care Treatment in the Military (RESPECT-Mil) program, an evidence-based collaborative care model.51-55 This approach included structured screening and diagnostic procedures, predictable follow-up schedules for patients, and the coordination of the divisions of responsibility among and between primary care providers, paraprofessionals, and behavioral health care providers. From 2007 to 2013, this collaborative care model was rolled out across 96 clinics worldwide and provided PTSD and depression screening to more than 1 million encounters per year.52,53
More recently, the U.S. Army led DoD in integrating behavioral health personnel in patient centered medical homes (PCMH) in compliance with DoD Instruction 6490.15.56 This hybrid integrated care model combines collaborative care elements developed in the RESPECT-Mil program with elements of the U.S. Air Force Behavioral Health Optimization project colocating behavioral health providers in primary care settings to provide brief consultative services.
MHS Care Enhancements
Many of the innovations deployed throughout the U.S. Army system of behavioral health care have driven changes across the MHS as a whole. The DoD and the VA have made substantive systemwide policy and practice changes to improve care for beneficiaries with PTSD, depression, and comorbid PTSD and depression. In particular, significant implementation efforts have addressed population screening strategies, outcome monitoring to support measurement-based care, increased access to effective care, and revision of the disability evaluation system.
To improve the identification and referral of soldiers with deployment-related mental health concerns, the DoD implemented a comprehensive program that screens service members prior to deployment, immediately on redeployment, and then again 6 months after returning from deployment. Additionally, annual primary care- based screening requirements have been instituted as part of the DoD PCMH initiative. Both deployment-related and primary care-based screenings include an instrumentation to detect symptoms of PTSD and depression and extend the reach of mental health screening to the entire MHS population.
Building on the success of BHDP, former Assistant Secretary of Defense for Health Affairs Jonathan Woodson mandated BHDP use across the MHS for all patients in DoD behavioral health clinics and the use of outcome measures for the treatment of PTSD, anxiety, depression, and alcohol use disorders.57 A DoD-wide requirement to use the PTSD checklist and patient health questionnaire to monitor PTSD and depression symptoms at mental health intakes and regularly at follow-up visits is being implemented. The Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury, through its Practice-Based Implementation Network (underwritten by a Joint Incentive Fund managed between DoD and VA), has worked across the MHS and the VA to facilitate the implementation, uptake, and adoption of this initiative.
The DoD established the Center for Deployment Psychology (CDP) in 2006 to promote clinician training in EBTs with the aim of increasing service members’ access to effective psychological treatments. Since its inception, the CDP has provided EBT training to more than 40,000 behavioral health providers. Although the impact of these and other efforts on improving the quality of care that patients receive is unknown, a recent study documented widespread self-reported usage of EBT components in U.S. Army clinics and that providers formally trained in EBTs were more likely to deliver EBTs.58
Finally, systemwide changes to the VA Schedule of Ratings for Disability (VASRD) and integration of DoD and VA disability evaluation systems have led to shifts in diagnosis toward PTSD that usually merit a minimum 50% disability rating. Mandates in law require military clinicians to evaluate patients who have deployed for PTSD and TBI prior to taking any actions associated with administrative separation. The practice of attributing PTSD symptoms to character pathology or personality disorders, even when these symptoms did not clearly manifest or worsen with military service, has likely been eliminated from practice in military and veteran populations.
Robust policy changes to limit personality disorder discharges started in fiscal year 2007, when there were 4,127 personality disorder separations across DoD. This number was reduced to 300 within 5 years. Policy changes regarding separation not only seem to have affected discharges, but also may have shaped diagnostic practice. The incidence rate of personality disorder diagnoses declined from 513 per 100,000 person-years in 2007 to 284 per 100,000 person-years by 2011.59 The VASRD recognizes chronic adjustment disorder as a disability, and the National Defense Authorization Act of 2008 mandated that DoD follow disability guidelines promulgated by VA.
As stated in the memorandum Clinical Policy Guidance for Assessment and Treatment of Post-Traumatic Stress Disorders (August 24, 2012), DoD recognizes chronic adjustment disorder as an unfitting condition that merits referral to its disability evaluation system.60 Acute adjustment disorders may still lead to administrative separations, as many service members manifest emotional symptoms stemming from the failure to adjust to the routine vicissitudes of military life. Finally, many court jurisdictions, including veteran’s courts, military courts, and commanders empowered to adjudicate nonjudicial infractions under the Uniform Code of Military Justice, have recognized PTSD as grounds for the mitigation of penalties associated with a wide array of criminal and administrative infractions.
Conclusion
In response to the increased mental health burden following a decade of war and the associated pressures stemming from federal mandates, the MHS has invested unprecedented resources into improving care for military service members. The U.S. Army has played a prominent role in this endeavor by investing in clinical research efforts to accelerate discovery on the causes and cures for these conditions, enacting policies that mandate best practices, and implementing evidence-based care approaches across the system of care. Despite this progress, however, understanding and effectively treating the most prevalent mental health conditions remain a challenge across the DoD and VHA health care systems. Many service members and veterans still do not receive timely, high-quality care for PTSD, depression, and other common comorbidities associated with military experience, and controversies in diagnostic clarification abound.
In short, great strides have been made, yet there is still a large distance to go. The vision of an effective, efficient, comprehensive care system for mental health conditions will continue to be pursued and achieved through collaborations across key agencies and the scientific community, implementation of health system approaches that support population care, and the sustained efforts of dedicated clinicians, staff, and clinic leaders who deliver the care to our service members and veterans.
Over the past decade, nationwide attention has focused on mental health conditions associated with military service. Recent legal mandates have led to changes in the DoD, VA, and HHS health systems aimed at increasing access to care, decreasing barriers to care, and expanding research on mental health conditions commonly seen in service members and veterans. On August 31, 2012, President Barack Obama signed the Improving Access to Mental Health Services for Veterans, Service Members, and Military Families executive order, establishing an interagency task force from the VA, DoD, and HHS.1 The task force was charged with addressing quality of care and provider training in the management of commonly comorbid conditions, including (among other conditions) posttraumatic stress disorder (PTSD) and depression.
Depression and PTSD present major health burdens in both military and veteran cohorts. Overlap in clinical presentation and significant rates of comorbidity complicate effective management of these conditions. This article offers a brief review of the diagnostic and epidemiologic complexities associated with PTSD and depression, a summary of research relevant to these issues, and a description of recent system-level developments within the Military Health System (MHS) designed to improve care through better approaches in identification, management, and research of these conditions.
Diagnostic Uncertainty
Both PTSD and major depressive disorder (MDD) have been recognized as mental health disorders since the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM) discarded its previous etiologically based approach to diagnostic classification in 1980 in favor of a system in which diagnosis is based on observable symptoms.2,3 With the release of DSM-5 in 2013, the diagnostic criteria for PTSD underwent a substantial transformation.4 Previously, PTSD was described as an anxiety disorder, and some of its manifestations overlapped descriptively (and in many cases, etiologically) with anxiety and depressive illnesses.5
Clinicians also often described shorter-lived, developmental, formes fruste, or otherwise subsyndromal manifestations of trauma associated with PTSD. In DSM-5, PTSD was removed from the anxiety disorders section and placed in a new category of disorders labeled Trauma and Stressor-Related Disorders. This new category also included reactive attachment disorder (in children), acute stress disorder, adjustment disorders, and unspecified or other trauma and stressor-related disorders. Other major changes to the PTSD diagnostic criteria included modification to the DSM-IV-TR (text revision) trauma definition (making the construct more specific), removal of the requirement for explicit subjective emotional reaction to a traumatic event, and greater emphasis on negative cognitions and mood. Debate surrounds the updated symptom criteria with critics questioning whether there is any improvement in the clinical utility of the diagnosis, especially in light of the substantial policy and practice implications the change engenders.6
Recently, Hoge and colleagues examined the psychometric implications of the diagnostic changes (between DSM-IV-TR and DSM-5) in the PTSD definition.6 The authors found that although the 2 definitions showed nearly identical association with other psychiatric disorders (including depression) and functional impairment, 30% of soldiers who met DSM-IV-TR criteria for PTSD failed to meet criteria in DSM-5, and another 20% met only DSM-5 criteria. Recognizing discordance in PTSD and associated diagnoses, the U.S. Army Medical Command mandated that its clinicians familiarize themselves with the controversies surrounding the discordant diagnoses and coding of subthreshold PTSD.7
Adding to the problem of diagnostic uncertainty, the clinical presentation of MDD includes significant overlap with that of PTSD. Specifically, symptoms of guilt, diminished interests, problems with concentration, and sleep disturbances are descriptive of both disorders. Furthermore, the criteria set for several subthreshold forms of MDD evidence considerable overlap with PTSD symptoms. For example, diagnostic criteria for disruptive mood dysregulation disorder include behavioral outbursts and irritability, and diagnostic criteria for dysthymia include sleep disturbances and concentration problems.
Adjustment disorders are categorized as trauma and stressor-related disorders in DSM-5 and hold many emotional and behavioral symptoms in common with PTSD. The “acute” and “chronic” adjustment disorder specifiers contribute to problems in diagnostic certainty for PTSD. In general, issues pertaining to diagnostic uncertainty and overlap likely reflect the limits of using a diagnostic classification system that relies exclusively on observational and subjective reports of psychological symptoms.8,9
In a treatment environment where a veteran or active-duty patient has presented for care, in the face of these shared symptom sets, clinicians frequently offer initial diagnoses. These diagnoses are often based on perceived etiologic factors derived from patients’ descriptions of stressors encountered during military service. This tendency likely contributes to considerable inconsistencies and potential inaccuracies in diagnoses, and much of the variance can be attributed to the clinicians’ degree of familiarity with military exposures, perceptions of what constitutes trauma, and outside pressure to assign or avoid specific diagnoses.
Importantly, the phenomenologic differences between PTSD and depressive disorders increase the likelihood of poorly aligned and inconsistent treatment plans, and this lack of clarity may, in turn, compromise effective patient care. To address some of these diagnostic challenges, the VA and DoD incorporate military culture training into clinicians’ curriculum to increase provider familiarity with the common stressors and challenges of military life, mandate the use of validated measures to support diagnostic decision making, and regularly review policies that influence diagnostic practices.
Epidemiology
The prevalence rates for PTSD are increasing in the military, possibly stemming from the demands on service members engaged in years’ long wars. Despite the increased attention on this phenomenon, research has demonstrated that the majority of service members who deploy do not develop PTSD or significant trauma-related functional impairment.10 Furthermore, many cases of PTSD diagnosed in the MHS stem from traumatic experiences other than combat exposure, including childhood abuse and neglect, sexual and other assaults, accidents and health care exposures, domestic abuse, and bullying. Depression arguably has received less attention despite comparable prevalence rates in military populations, high co-occurrence of PTSD and depression, and depression being associated with a greater odds ratio for mortality that includes death by suicide in military service members.11
Estimates of the prevalence of PTSD from the U.S. Army suggest that it exists in 3% to 6% of military members who have not deployed and in 6% to 25% of service members with combat deployment histories. The frequency and intensity of combat are strong predictors of risk.7 A recent epidemiologic study using inpatient and outpatient encounter records showed that the prevalence of PTSD in the active military component was 2.0% in the middle of calendar year (CY) 2010; a two-thirds increase from 1.2% in CY 2007.12 The incidence of PTSD
Epidemiologic studies and prevalence/incidence rates derived from administrative data rely on strict case definitions. Consequently, such administrative investigations include data only from service members
PTSD and Depression Treatment
Despite the high rates of PTSD and MDD comorbidity, few treatments have been developed for and tested on an exclusively comorbid sample of patients.13 However, psychopharmacologic agents targeting depression have been applied to the treatment of PTSD, and PTSD psychotherapy trials typically include depression response as a secondary outcome. The generalizability of findings to a truly comorbid population may be limited based on study sampling frames and the unique characteristics of patients with comorbid PTSD and depression.14-16 Several psychopharmacologic treatments for depression have been evaluated as frontline treatments for PTSD. The 3 pharmacologic treatments that demonstrate efficacy in treating PTSD include fluoxetine, paroxetine, and venlafaxine.17
Although these pharmacologic agents represent good candidate treatments for comorbid patients, the effect size of pharmacologic treatments are generally smaller than those of psychotherapeutic treatments for PTSD.17,18 This observation, however, is based on indirect comparisons, and a recent systematic review concluded that the evidence was insufficient to determine the comparative effectiveness between psychotherapy and pharmacotherapy for PTSD.19 Evidence indicates that trauma-focused cognitive behavioral therapies consistently demonstrate efficacy and effectiveness in treating PTSD.19,20 These treatments also have been shown to significantly reduce depressive symptoms among PTSD samples.21
Based on strong bodies of evidence, these pharmacologic and psychological treatments have received the highest level of recommendation in the VA and DoD.22,23 Accordingly, both agencies have invested considerable resources in large-scale efforts to improve patient access to these particular treatments. Despite these impressive implementation efforts, however, the limitations of relying exclusively on these treatments as frontline approaches within large health care systems have become evident.24-26
Penetration of Therapies
Penetration of these evidence-based treatments (EBTs) within the DoD and VHA remains limited. For instance, one study showed that VA clinicians in mental health specialty care clinics may provide only about 4 hours of EBT per week.27
Other reports suggest that only about 60% of treatment-seeking patients in PTSD clinics receive any type of evidence-based therapy and that within-session care quality is questionable based on a systematic review of chart notes.28,29 Attrition in trauma-focused therapy is a recognized limitation, with 1 out of 3 treatment-seeking patients not completing a full dose of evidence-based treatment.30-33 Large-scale analyses of VHA and DoD utilization data suggest that the majority of PTSD patients do not receive a sufficient number of sessions to be characterized as an adequate dose of EBT, with a majority of dropouts occur- ring after just a few sessions.34-37
Hoge and colleagues found that < 50% of soldiers meeting criteria for PTSD received any mental health care within the prior 6 months with one-quarter of those patients dropping out of care prematurely.38 Among a large cohort of soldiers engaged in care for the treatment of PTSD, only about 40% received a number of EBT treatment sessions that could qualify as an adequate dose.38 Thus, although major advancements in the development and implementation of effective treatments for PTSD and depression have occurred, the penetration of these treatments is limited, and the majority of patients in need of treatment potentially receive inadequate care.39
System level approaches that integrate behavioral health services into the primary care system have been proposed to address these care gaps for service members and veterans.40-42 Fundamentally, system-level approaches seek to improve the reach and effectiveness of care through large-scale screening efforts, a greater emphasis on the quality of patient care, and enhanced care continuity across episodes of treatment.
Primary Care
With the primary care setting considered the de facto mental health system, integrated approaches enhance the reach of care by incorporating uniform mental health screening and referral for patients coming through primary care. Specific evidence-based treatments can be integrated into this approach within a stepped-care framework that aims to match patients strategically to the right type of care and leverage specialty care resources as needed. Integrated care approaches for the treatment of PTSD and depression have been developed and evaluated inside and outside of the MHS. Findings indicate that integrated treatment approaches can improve care access, care continuity, patient satisfaction, quality of care,and in several trials, PTSD and depression outcomes.43-47
Recently, an integrated care approach targeting U.S. Army soldiers who screened positive for PTSD or depression in primary care was evaluated in a multisite effectiveness trial.48 Patients randomized to the treatment approach experienced significant improvements in both PTSD and depression symptoms relative to patients in usual care.43 In addition, patients treated in this care model received significantly more mental health services; the patterns of care indicated that patients with comorbid PTSD and depression were more likely to be triaged to specialty care, whereas patients with a single diagnosis were more likely to be managed in primary care.49 This trial suggests that integrated care models feasibly can be implemented in the U.S. Army care system, yielding increased uptake of mental health care, more efficiently matched care based on patient comorbidities, and improved PTSD and depression outcomes.
Treatment Research
The MHS supports a large portfolio of research in PTSD and depression through DoD/VA research consortia (eg, the Congressionally Directed Medical Research Program, the Consortium to Alleviate PTSD, the Injury and Traumatic Stress Clinical Consortium). The U.S. Army Medical Research and Materiel Command (USAMRMC) executes and manages the portfolio of research, relying on a joint program committee of DoD and non-DoD experts to make funding recommendations based on identified research priorities, policy guidance, and knowledge translation needs.
Health systems research on PTSD and MDD in federal health care settings is expanding. For example, the RAND Corporation recently evaluated a candidate set of quality measures for PTSD and MDD, using an operational definition of an episode of care.37 This work is intended to inform efforts to measure and improve the quality of care for PTSD and depression across the enterprise.
The DoD Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury is simultaneously completing an inferential assessment of adjunctive mental health care services, many focused on PTSD and depression, throughout the health care enterprise. Along with the substantial resources devoted to research on PTSD and depression, the MHS is implementing strategies to improve the system of care for service members with mental health conditions.
Army Care System Innovations
The U.S. Army is engaged in a variety of strategies to improve the identification of patients with mental health conditions, increase access to mental health services, and enhance the quality of care that soldiers receive for PTSD and depression. To improve the coordination of mental health care, the U.S. Army Medical Command implemented a wide-scale innovative transformation of its mental health care system through the establishment of the Behavioral Health Service Line program management office.
This move eliminated separate departments of psychiatry, psychology, and social work in favor of integrated behavioral health departments that are now responsible for all mental health care delivered to soldiers, including inpatient, outpatient, partial hospitalization, residential, embedded care in garrison, and primary care settings. This transformation ensured coordination of care for soldiers, eliminating potential miscommunication with patients, commands, and other clinicians while clearly defining performance indicators in process (eg, productivity, scheduling, access to care, and patient satisfaction) and outcome measures.49 In conjunction with the development of its service line, the U.S. Army created a Behavioral Health Data Portal (BHDP), an electronic and standardized means to assess clinical outcomes for common conditions.
To promote higher quality mental health care, the Office of the Surgeon General of the U.S. Army provided direct guidance on the treatment of PTSD and depression. U.S. Army policy mandates that providers treating mental health conditions adhere to the VA/DoD clinical practice guidelines (CPGs) and that soldiers with PTSD and depression be offered treatments with the highest level of scientific support and that outcome measures be routinely administered. In line with the CPGs, U.S. Army policy also recommends the use of both integrated and embedded mental health care approaches to address PTSD, depression, and other common physical and psychological health conditions.
To reduce stigma and improve mental health care access, the U.S. Army began implementing integrated care approaches in 2007 with its Re-Engineering Systems of Primary Care Treatment in the Military (RESPECT-Mil) program, an evidence-based collaborative care model.51-55 This approach included structured screening and diagnostic procedures, predictable follow-up schedules for patients, and the coordination of the divisions of responsibility among and between primary care providers, paraprofessionals, and behavioral health care providers. From 2007 to 2013, this collaborative care model was rolled out across 96 clinics worldwide and provided PTSD and depression screening to more than 1 million encounters per year.52,53
More recently, the U.S. Army led DoD in integrating behavioral health personnel in patient centered medical homes (PCMH) in compliance with DoD Instruction 6490.15.56 This hybrid integrated care model combines collaborative care elements developed in the RESPECT-Mil program with elements of the U.S. Air Force Behavioral Health Optimization project colocating behavioral health providers in primary care settings to provide brief consultative services.
MHS Care Enhancements
Many of the innovations deployed throughout the U.S. Army system of behavioral health care have driven changes across the MHS as a whole. The DoD and the VA have made substantive systemwide policy and practice changes to improve care for beneficiaries with PTSD, depression, and comorbid PTSD and depression. In particular, significant implementation efforts have addressed population screening strategies, outcome monitoring to support measurement-based care, increased access to effective care, and revision of the disability evaluation system.
To improve the identification and referral of soldiers with deployment-related mental health concerns, the DoD implemented a comprehensive program that screens service members prior to deployment, immediately on redeployment, and then again 6 months after returning from deployment. Additionally, annual primary care- based screening requirements have been instituted as part of the DoD PCMH initiative. Both deployment-related and primary care-based screenings include an instrumentation to detect symptoms of PTSD and depression and extend the reach of mental health screening to the entire MHS population.
Building on the success of BHDP, former Assistant Secretary of Defense for Health Affairs Jonathan Woodson mandated BHDP use across the MHS for all patients in DoD behavioral health clinics and the use of outcome measures for the treatment of PTSD, anxiety, depression, and alcohol use disorders.57 A DoD-wide requirement to use the PTSD checklist and patient health questionnaire to monitor PTSD and depression symptoms at mental health intakes and regularly at follow-up visits is being implemented. The Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury, through its Practice-Based Implementation Network (underwritten by a Joint Incentive Fund managed between DoD and VA), has worked across the MHS and the VA to facilitate the implementation, uptake, and adoption of this initiative.
The DoD established the Center for Deployment Psychology (CDP) in 2006 to promote clinician training in EBTs with the aim of increasing service members’ access to effective psychological treatments. Since its inception, the CDP has provided EBT training to more than 40,000 behavioral health providers. Although the impact of these and other efforts on improving the quality of care that patients receive is unknown, a recent study documented widespread self-reported usage of EBT components in U.S. Army clinics and that providers formally trained in EBTs were more likely to deliver EBTs.58
Finally, systemwide changes to the VA Schedule of Ratings for Disability (VASRD) and integration of DoD and VA disability evaluation systems have led to shifts in diagnosis toward PTSD that usually merit a minimum 50% disability rating. Mandates in law require military clinicians to evaluate patients who have deployed for PTSD and TBI prior to taking any actions associated with administrative separation. The practice of attributing PTSD symptoms to character pathology or personality disorders, even when these symptoms did not clearly manifest or worsen with military service, has likely been eliminated from practice in military and veteran populations.
Robust policy changes to limit personality disorder discharges started in fiscal year 2007, when there were 4,127 personality disorder separations across DoD. This number was reduced to 300 within 5 years. Policy changes regarding separation not only seem to have affected discharges, but also may have shaped diagnostic practice. The incidence rate of personality disorder diagnoses declined from 513 per 100,000 person-years in 2007 to 284 per 100,000 person-years by 2011.59 The VASRD recognizes chronic adjustment disorder as a disability, and the National Defense Authorization Act of 2008 mandated that DoD follow disability guidelines promulgated by VA.
As stated in the memorandum Clinical Policy Guidance for Assessment and Treatment of Post-Traumatic Stress Disorders (August 24, 2012), DoD recognizes chronic adjustment disorder as an unfitting condition that merits referral to its disability evaluation system.60 Acute adjustment disorders may still lead to administrative separations, as many service members manifest emotional symptoms stemming from the failure to adjust to the routine vicissitudes of military life. Finally, many court jurisdictions, including veteran’s courts, military courts, and commanders empowered to adjudicate nonjudicial infractions under the Uniform Code of Military Justice, have recognized PTSD as grounds for the mitigation of penalties associated with a wide array of criminal and administrative infractions.
Conclusion
In response to the increased mental health burden following a decade of war and the associated pressures stemming from federal mandates, the MHS has invested unprecedented resources into improving care for military service members. The U.S. Army has played a prominent role in this endeavor by investing in clinical research efforts to accelerate discovery on the causes and cures for these conditions, enacting policies that mandate best practices, and implementing evidence-based care approaches across the system of care. Despite this progress, however, understanding and effectively treating the most prevalent mental health conditions remain a challenge across the DoD and VHA health care systems. Many service members and veterans still do not receive timely, high-quality care for PTSD, depression, and other common comorbidities associated with military experience, and controversies in diagnostic clarification abound.
In short, great strides have been made, yet there is still a large distance to go. The vision of an effective, efficient, comprehensive care system for mental health conditions will continue to be pursued and achieved through collaborations across key agencies and the scientific community, implementation of health system approaches that support population care, and the sustained efforts of dedicated clinicians, staff, and clinic leaders who deliver the care to our service members and veterans.
1. The White House, Office of the Press Secretary. Executive Order 13625: Improving Access to Mental Health Services for Veterans, Service Members, and Military Families. https://www.whitehouse.gov/the-press-office/2012/08/31/executive-order-improving-access-mental-health-services-veterans-service. Published August 31, 2012. Accessed September 20, 2016.
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. Arlington, VA: American Psychiatric Association Press; 1980.
3. Mayes R, Horwitz AV. DSM-III and the revolution in the classification of mental illness. J Hist Behav Sci. 2005;41(3):249-267.
4. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association Press; 2013.
5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed., text rev. Arlington, VA: American Psychiatric Association Press; 2000.
6. Hoge CW, Riviere LA, Wilk JE, Herrell RK, Weathers FW. The prevalence of post-traumatic stress disorder (PTSD) in US combat soldiers: a head-to-head comparison of DSM-5 versus DSM-IV-TR symptom criteria with the PTSD checklist. Lancet Psychiatry. 2014;1(4):269-277.
7. OTSG-MEDCOM. Policy Memo 14-094: Policy Guidance on the Assessment and Treatment of Posttraumatic Stress Disorder (PTSD). Published December 18, 2014.
8. Insel T, Cuthbert B, Garvey M, et al. Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry, 2010;167(7):748-751.
9. National Institute of Mental Health. NIMH strategic plan for research. http://www.nimh.nih.gov/about/strategic-planning-reports/index.shtml. Revised 2015. Accessed September 20, 2016.
10. Colston M, Hocter W. Forensic aspects of posttraumatic stress disorder. In: Ritchie EC, ed. Forensic and Ethical Issues in Military Behavioral Health. Washington, DC: U.S. Department of the Army; 2015:97-110.
11. Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury. National Center for Telehealth and Technology. Department of Defense suicide event report: calendar year 2013 annual report. http://t2health.dcoe.mil/programs/dodser. Published January 13, 2015. Accessed September 20, 2016.
12. Otto JL, O’Donnell FL, Ford SA, Ritschard HV. Selected mental health disorders among active component members, US Armed Forces, 2007-2010. MSMR. 2010;17(11):2-5.
13. Gutner CA, Galovski T, Bovin MJ, Schnurr PP. Emergence of transdiagnostic treatments for PTSD and posttraumatic distress. Curr Psychiatry Rep. 2016;18(10):95-101.
14. Campbell DG, Felker BL, Liu CF, et al. Prevalence of depression-PTSD comorbidity: implications for clinical practice guidelines and primary care-based interventions. J Gen Intern Med. 2007;22(6):711-718.
15. Chan D, Cheadle AD, Reiber G, Unützer J, Chaney EF. Health care utilization and its costs for depressed veterans with and without comorbid PTSD symptoms. Psychiatr Serv. 2009;60(12):1612-1617.
16. Maguen S, Cohen B, Cohen G, Madden E, Bertenthal D, Seal K. Gender differences in health service utilization among Iraq and Afghanistan veterans with posttraumatic stress disorder. J Womens Health (Larchmt). 2012;21(6):666-673.
17. Hoskins M, Pearce J, Bethell A, et al. Pharmacotherapy for post-traumatic stress disorder: systematic review and meta-analysis. Br J Psychiatry. 2015;206(2):93-100.
18. Puetz TW, Youngstedt SD, Herring MP. Effects of pharmacotherapy on combat-related PTSD, anxiety, and depression: a systematic review and meta-regression analysis. PLoS One. 2015;10(5):e0126529.
19. Jonas DE, Cusack K, Forneris CA, et al. Psychological and pharmacological treatments for adults with posttraumatic stress disorder (PTSD). Comparative effectiveness review no. 92. https://effectivehealthcare.ahrq.gov/ehc/products/347/1435/PTSD-adult-treatment-report-130403.pdf. Published April 3, 2013. Accessed September 20, 2016.
20. Haagen JFG, Smid GE, Knipscheer JW, Kleber RJ. The efficacy of recommended treatments for veterans with PTSD: a metaregression analysis. Clin Psychol Rev. 2015;40:184-194.
21. Tran K, Moulton K, Santesso N, Rabb D. Cognitive processing therapy for post-traumatic stress disorder: a systematic review and meta-analysis. https://www.cadth.ca/cognitive-processing-therapy-post-traumatic-stress-disorder-systematic-review-and-meta-analysis. Published August 11, 2015. Accessed September 20, 2016.
22. VA/DoD Management of Post-Traumatic Stress Working Group. VA/DoD Clinical Practice Guideline for Management of Post-Traumatic Stress. Version 2. http://www.healthquality.va.gov/guidelines/MH/ptsd/. Published October, 2010. Accessed September 20, 2016.
23. VA/DoD Management of Major Depressive Disorder Working Group. VA/DoD Clinical Practice Guideline for the Management of Major Depressive Disorder. Version 3. http://www.healthquality.va.gov/guidelines/mh/mdd/index.asp. Published April 2016. Accessed September 20, 2016.
24. Zatzick DF, Galea S. An epidemiologic approach to the development of early trauma focused intervention. J Trauma Stress. 2007;20(4):401-412.
25. Zatzick DF, Koepsell T, Rivara FP. Using target population specification, effect size, and reach to estimate and compare the population impact of two PTSD preventive interventions. Psychiatry. 2009;72(4):346-359.
26. Glasgow RE, Nelson CC, Strycker LA, King DK. Using RE-AIM metrics to evaluate diabetes self-management support interventions. Am J Prev Med. 2006;30(1):67-73.
27. Finley EP, Garcia HA, Ketchum NS, et al. Utilization of evidence-based psychotherapies in Veterans Affairs posttraumatic stress disorder outpatient clinics. Psychol Serv. 2015;12(1):73-82.
28. Mott JM, Mondragon S, Hundt NE, Beason-Smith M, Grady RH, Teng EJ. Characteristics of U.S. veterans who begin and complete prolonged exposure and cognitive processing therapy for PTSD. J Trauma Stress. 2014;27(3):265-273.
29. Shiner B, D’Avolio LW, Nguyen TM, et al. Measuring use of evidence based psychotherapy for PTSD. Adm Policy Ment Health. 2013;40(4):311-318.
30. Schnurr PP, Friedman MJ, Engel CC, et al. Cognitive behavioral therapy for posttraumatic stress disorder in women: a randomized controlled trial. JAMA. 2007;297(8):820-830.
31. Tuerk PW, Yoder M, Grubaugh A, Myrick H, Hamner M, Acierno R. Prolonged exposure therapy for combat-related posttraumatic stress disorder: an examination of treatment effectiveness for veterans of the wars in Afghanistan and Iraq. J Anxiety Disord. 2011;25(3):397-403.
32. Chard KM, Schumm JA, Owens GP, Cottingham SM. A comparison of OEF and OIF veterans and Vietnam veterans receiving cognitive processing therapy. J Trauma Stress. 2010;23(1):25-32.
33. Monson CM, Schnurr PP, Resick PA, Friedman MJ, Young-Xu Y, Stevens SP. Cognitive processing therapy for veterans with military-related posttraumatic stress disorder. J Consult Clin Psychol. 2006;74(5):898-907.
34. Mott JM, Hundt NE, Sansgiry S, Mignogna J, Cully JA. Changes in psychotherapy utilization among veterans with depression, anxiety, and PTSD. Psychiatr Serv. 2014;65(1):106-112.
35. Seal KH, Maguen S, Cohen B, et al. VA mental health services utilization in Iraq and Afghanistan veterans in the first year of receiving new mental health diagnoses. J Trauma Stress. 2010;23(1):5-16.
36. Russell M, Silver SM. Training needs for the treatment of combat-related posttraumatic stress disorder: a survey of Department of Defense clinicians. Traumatology. 2007;13(3):4-10.
37. Schell TL, Marshall GN. Survey of individuals previously deployed for OEF/OIF. In: Tanielian T, Jaycox LH, eds. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND Corporation; 2008:87-118.
38. Hoge CW, Grossman SH, Auchterlonie JL, Riviere LA, Milliken CS, >Wilk JE. PTSD treatment for soldiers after combat deployment: low utilization of mental health care and reasons for dropout. Psychiatr Serv. 2014;65(8):997-1004.
39. Committee on the Assessment of Ongoing Efforts in the Treatment of Posttraumatic Stress Disorder, Board on the Health of Select Populations, Institute of Medicine. Treatment for Posttraumatic Stress Disorder in Military and Veteran Populations: Final Assessment. Washington, DC: National Academies Press; 2014.
40. Schnurr PP. Extending collaborative care for posttraumatic mental health. JAMA Intern Med. 2016;176(7):956-957.
41. Hoge CW. Interventions for war-related posttraumatic stress disorder: meeting veterans where they are. JAMA. 2011;306(5):549-551.
42. Engel CC. Improving primary care for military personnel and veterans with posttraumatic stress disorder: the road ahead. Gen Hosp Psychiatry. 2005;27(3):158-160.
43. Engel CC, Jaycox LH, Freed MC, et al. Centrally assisted collaborative telecare management for posttraumatic stress disorder and depression in military primary care: a randomized controlled trial. JAMA Intern Med. 2016;176(7):948-956.
44. Fortney JC, Pyne JM, Kimbrell TA, et al. Telemedicine-based collaborative care for posttraumatic stress disorder: a randomized clinical trial. JAMA Psychiatry. 2015;72(1):58-67.
45. Schnurr PP, Friedman MJ, Oxman TE, et al. RESPECT-PTSD: re-engineering systems for the primary care treatment of PTSD, a randomized controlled trial. J Gen Intern Med. 2013;28(1):32-40.
46. Zatzick D, Roy-Byrne P, Russo J, et al. A randomized effectiveness trial of stepped collaborative care for acutely injured trauma survivors. Arch Gen Psychiatry. 2004;61(5):498-506.
47. Zatzick D, O’Connor SS, Russo J, et al. Technology-enhanced stepped collaborative care targeting posttraumatic stress disorder and comorbidity after injury: a randomized controlled trial. J Trauma Stress. 2015;28(5):391-400.
48. Engel CC, Bray RM, Jaycox LH, et al. Implementing collaborative primary care for depression and posttraumatic stress disorder: design and sample for a randomized trial in the U.S. Military Health System. Contemp Clin Trials. 2014;39(2):310-319.
49. Belsher BE, Jaycox LH, Freed MC, et al. Mental health utilization patterns during a stepped, collaborative care effectiveness trial for PTSD and depression in the military health system. Med Care. 2016;54(7):706-713.
50. Hepner KA, Roth CP, Farris C, et al. Measuring the Quality of Care for Psychological Health Conditions in the Military Health System: Candidate Quality Measures for Posttraumatic Stress Disorder and Major Depressive Disorder. Santa Monica, CA: RAND Corporation; 2015.
51. Engel C, Oxman T, Yamamoto C, et al. RESPECT-Mil: feasibility of a systems-level collaborative care approach to depression and post-traumatic stress disorder in military primary care. Mil Med. 2008;173(10):935-940.
52. Belsher BE, Curry J, McCutchan P, et al. Implementation of a collaborative care initiative for PTSD and depression in the Army primary care system. Soc Work Ment Health. 2014;12(5-6):500-522.
53. Wong EC, Jaycox LH, Ayer L, et al. Evaluating the Implementation of the Re-Engineering Systems of Primary Care Treatment in the Military (RESPECT-Mil). Santa Monica, CA: RAND Corporation; 2015.
54. Archer J, Bower P, Gilbody S, et al. Collaborative care for depression and anxiety problems. Cochrane Database Syst Rev. 2012;10:CD006525.
55. Woltmann E, Grogan-Kaylor A, Perron B, Georges H, Kilbourne AM, Bauer MS. Comparative effectiveness of collaborative chronic care models for mental health conditions across primary, specialty, and behavioral health care settings: systematic review and meta-analysis. Am J Psychiatry. 2012;169(8):790-804.
56. Wright JL. DoD Directive 6490.15. www.dtic.mil/whs/directives/corres/pdf/649015p.pdf.Revised November 20, 2014. Accessed October 3, 2016. 57. Woodson J. Military treatment facility mental health clinical outcomes guidance. http://dcoe.mil/Libraries/Documents/MentalHealthClinicalOutcomesGuidance_Woodson.pdf. Published September 9, 2013. Accessed October 4, 2016.
58. Wilk JE, West JC, Duffy FF, Herrell RK, Rae DS, Hoge CW. Use of evidence-based treatment for posttraumatic stress disorder in Army behavioral healthcare. Psychiatry. 2013;76(4):336-348.
59. Stockton PN, Olsen ET, Hayford S, et al. Security from within: independent review of the Washington Navy Yard shooting. http://archive.defense.gov/pubs/Independent-Review-of-the-WNY-Shooting-14-Nov-2013.pdf. Published November, 2013. Accessed September 20, 2016.
60. Woodson J. ASD(HA) Memorandum: Clinical Policy Guidance for Assessment and Treatment of Posttraumatic Stress Disorder. August 24, 2012.
1. The White House, Office of the Press Secretary. Executive Order 13625: Improving Access to Mental Health Services for Veterans, Service Members, and Military Families. https://www.whitehouse.gov/the-press-office/2012/08/31/executive-order-improving-access-mental-health-services-veterans-service. Published August 31, 2012. Accessed September 20, 2016.
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. Arlington, VA: American Psychiatric Association Press; 1980.
3. Mayes R, Horwitz AV. DSM-III and the revolution in the classification of mental illness. J Hist Behav Sci. 2005;41(3):249-267.
4. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association Press; 2013.
5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed., text rev. Arlington, VA: American Psychiatric Association Press; 2000.
6. Hoge CW, Riviere LA, Wilk JE, Herrell RK, Weathers FW. The prevalence of post-traumatic stress disorder (PTSD) in US combat soldiers: a head-to-head comparison of DSM-5 versus DSM-IV-TR symptom criteria with the PTSD checklist. Lancet Psychiatry. 2014;1(4):269-277.
7. OTSG-MEDCOM. Policy Memo 14-094: Policy Guidance on the Assessment and Treatment of Posttraumatic Stress Disorder (PTSD). Published December 18, 2014.
8. Insel T, Cuthbert B, Garvey M, et al. Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry, 2010;167(7):748-751.
9. National Institute of Mental Health. NIMH strategic plan for research. http://www.nimh.nih.gov/about/strategic-planning-reports/index.shtml. Revised 2015. Accessed September 20, 2016.
10. Colston M, Hocter W. Forensic aspects of posttraumatic stress disorder. In: Ritchie EC, ed. Forensic and Ethical Issues in Military Behavioral Health. Washington, DC: U.S. Department of the Army; 2015:97-110.
11. Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury. National Center for Telehealth and Technology. Department of Defense suicide event report: calendar year 2013 annual report. http://t2health.dcoe.mil/programs/dodser. Published January 13, 2015. Accessed September 20, 2016.
12. Otto JL, O’Donnell FL, Ford SA, Ritschard HV. Selected mental health disorders among active component members, US Armed Forces, 2007-2010. MSMR. 2010;17(11):2-5.
13. Gutner CA, Galovski T, Bovin MJ, Schnurr PP. Emergence of transdiagnostic treatments for PTSD and posttraumatic distress. Curr Psychiatry Rep. 2016;18(10):95-101.
14. Campbell DG, Felker BL, Liu CF, et al. Prevalence of depression-PTSD comorbidity: implications for clinical practice guidelines and primary care-based interventions. J Gen Intern Med. 2007;22(6):711-718.
15. Chan D, Cheadle AD, Reiber G, Unützer J, Chaney EF. Health care utilization and its costs for depressed veterans with and without comorbid PTSD symptoms. Psychiatr Serv. 2009;60(12):1612-1617.
16. Maguen S, Cohen B, Cohen G, Madden E, Bertenthal D, Seal K. Gender differences in health service utilization among Iraq and Afghanistan veterans with posttraumatic stress disorder. J Womens Health (Larchmt). 2012;21(6):666-673.
17. Hoskins M, Pearce J, Bethell A, et al. Pharmacotherapy for post-traumatic stress disorder: systematic review and meta-analysis. Br J Psychiatry. 2015;206(2):93-100.
18. Puetz TW, Youngstedt SD, Herring MP. Effects of pharmacotherapy on combat-related PTSD, anxiety, and depression: a systematic review and meta-regression analysis. PLoS One. 2015;10(5):e0126529.
19. Jonas DE, Cusack K, Forneris CA, et al. Psychological and pharmacological treatments for adults with posttraumatic stress disorder (PTSD). Comparative effectiveness review no. 92. https://effectivehealthcare.ahrq.gov/ehc/products/347/1435/PTSD-adult-treatment-report-130403.pdf. Published April 3, 2013. Accessed September 20, 2016.
20. Haagen JFG, Smid GE, Knipscheer JW, Kleber RJ. The efficacy of recommended treatments for veterans with PTSD: a metaregression analysis. Clin Psychol Rev. 2015;40:184-194.
21. Tran K, Moulton K, Santesso N, Rabb D. Cognitive processing therapy for post-traumatic stress disorder: a systematic review and meta-analysis. https://www.cadth.ca/cognitive-processing-therapy-post-traumatic-stress-disorder-systematic-review-and-meta-analysis. Published August 11, 2015. Accessed September 20, 2016.
22. VA/DoD Management of Post-Traumatic Stress Working Group. VA/DoD Clinical Practice Guideline for Management of Post-Traumatic Stress. Version 2. http://www.healthquality.va.gov/guidelines/MH/ptsd/. Published October, 2010. Accessed September 20, 2016.
23. VA/DoD Management of Major Depressive Disorder Working Group. VA/DoD Clinical Practice Guideline for the Management of Major Depressive Disorder. Version 3. http://www.healthquality.va.gov/guidelines/mh/mdd/index.asp. Published April 2016. Accessed September 20, 2016.
24. Zatzick DF, Galea S. An epidemiologic approach to the development of early trauma focused intervention. J Trauma Stress. 2007;20(4):401-412.
25. Zatzick DF, Koepsell T, Rivara FP. Using target population specification, effect size, and reach to estimate and compare the population impact of two PTSD preventive interventions. Psychiatry. 2009;72(4):346-359.
26. Glasgow RE, Nelson CC, Strycker LA, King DK. Using RE-AIM metrics to evaluate diabetes self-management support interventions. Am J Prev Med. 2006;30(1):67-73.
27. Finley EP, Garcia HA, Ketchum NS, et al. Utilization of evidence-based psychotherapies in Veterans Affairs posttraumatic stress disorder outpatient clinics. Psychol Serv. 2015;12(1):73-82.
28. Mott JM, Mondragon S, Hundt NE, Beason-Smith M, Grady RH, Teng EJ. Characteristics of U.S. veterans who begin and complete prolonged exposure and cognitive processing therapy for PTSD. J Trauma Stress. 2014;27(3):265-273.
29. Shiner B, D’Avolio LW, Nguyen TM, et al. Measuring use of evidence based psychotherapy for PTSD. Adm Policy Ment Health. 2013;40(4):311-318.
30. Schnurr PP, Friedman MJ, Engel CC, et al. Cognitive behavioral therapy for posttraumatic stress disorder in women: a randomized controlled trial. JAMA. 2007;297(8):820-830.
31. Tuerk PW, Yoder M, Grubaugh A, Myrick H, Hamner M, Acierno R. Prolonged exposure therapy for combat-related posttraumatic stress disorder: an examination of treatment effectiveness for veterans of the wars in Afghanistan and Iraq. J Anxiety Disord. 2011;25(3):397-403.
32. Chard KM, Schumm JA, Owens GP, Cottingham SM. A comparison of OEF and OIF veterans and Vietnam veterans receiving cognitive processing therapy. J Trauma Stress. 2010;23(1):25-32.
33. Monson CM, Schnurr PP, Resick PA, Friedman MJ, Young-Xu Y, Stevens SP. Cognitive processing therapy for veterans with military-related posttraumatic stress disorder. J Consult Clin Psychol. 2006;74(5):898-907.
34. Mott JM, Hundt NE, Sansgiry S, Mignogna J, Cully JA. Changes in psychotherapy utilization among veterans with depression, anxiety, and PTSD. Psychiatr Serv. 2014;65(1):106-112.
35. Seal KH, Maguen S, Cohen B, et al. VA mental health services utilization in Iraq and Afghanistan veterans in the first year of receiving new mental health diagnoses. J Trauma Stress. 2010;23(1):5-16.
36. Russell M, Silver SM. Training needs for the treatment of combat-related posttraumatic stress disorder: a survey of Department of Defense clinicians. Traumatology. 2007;13(3):4-10.
37. Schell TL, Marshall GN. Survey of individuals previously deployed for OEF/OIF. In: Tanielian T, Jaycox LH, eds. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND Corporation; 2008:87-118.
38. Hoge CW, Grossman SH, Auchterlonie JL, Riviere LA, Milliken CS, >Wilk JE. PTSD treatment for soldiers after combat deployment: low utilization of mental health care and reasons for dropout. Psychiatr Serv. 2014;65(8):997-1004.
39. Committee on the Assessment of Ongoing Efforts in the Treatment of Posttraumatic Stress Disorder, Board on the Health of Select Populations, Institute of Medicine. Treatment for Posttraumatic Stress Disorder in Military and Veteran Populations: Final Assessment. Washington, DC: National Academies Press; 2014.
40. Schnurr PP. Extending collaborative care for posttraumatic mental health. JAMA Intern Med. 2016;176(7):956-957.
41. Hoge CW. Interventions for war-related posttraumatic stress disorder: meeting veterans where they are. JAMA. 2011;306(5):549-551.
42. Engel CC. Improving primary care for military personnel and veterans with posttraumatic stress disorder: the road ahead. Gen Hosp Psychiatry. 2005;27(3):158-160.
43. Engel CC, Jaycox LH, Freed MC, et al. Centrally assisted collaborative telecare management for posttraumatic stress disorder and depression in military primary care: a randomized controlled trial. JAMA Intern Med. 2016;176(7):948-956.
44. Fortney JC, Pyne JM, Kimbrell TA, et al. Telemedicine-based collaborative care for posttraumatic stress disorder: a randomized clinical trial. JAMA Psychiatry. 2015;72(1):58-67.
45. Schnurr PP, Friedman MJ, Oxman TE, et al. RESPECT-PTSD: re-engineering systems for the primary care treatment of PTSD, a randomized controlled trial. J Gen Intern Med. 2013;28(1):32-40.
46. Zatzick D, Roy-Byrne P, Russo J, et al. A randomized effectiveness trial of stepped collaborative care for acutely injured trauma survivors. Arch Gen Psychiatry. 2004;61(5):498-506.
47. Zatzick D, O’Connor SS, Russo J, et al. Technology-enhanced stepped collaborative care targeting posttraumatic stress disorder and comorbidity after injury: a randomized controlled trial. J Trauma Stress. 2015;28(5):391-400.
48. Engel CC, Bray RM, Jaycox LH, et al. Implementing collaborative primary care for depression and posttraumatic stress disorder: design and sample for a randomized trial in the U.S. Military Health System. Contemp Clin Trials. 2014;39(2):310-319.
49. Belsher BE, Jaycox LH, Freed MC, et al. Mental health utilization patterns during a stepped, collaborative care effectiveness trial for PTSD and depression in the military health system. Med Care. 2016;54(7):706-713.
50. Hepner KA, Roth CP, Farris C, et al. Measuring the Quality of Care for Psychological Health Conditions in the Military Health System: Candidate Quality Measures for Posttraumatic Stress Disorder and Major Depressive Disorder. Santa Monica, CA: RAND Corporation; 2015.
51. Engel C, Oxman T, Yamamoto C, et al. RESPECT-Mil: feasibility of a systems-level collaborative care approach to depression and post-traumatic stress disorder in military primary care. Mil Med. 2008;173(10):935-940.
52. Belsher BE, Curry J, McCutchan P, et al. Implementation of a collaborative care initiative for PTSD and depression in the Army primary care system. Soc Work Ment Health. 2014;12(5-6):500-522.
53. Wong EC, Jaycox LH, Ayer L, et al. Evaluating the Implementation of the Re-Engineering Systems of Primary Care Treatment in the Military (RESPECT-Mil). Santa Monica, CA: RAND Corporation; 2015.
54. Archer J, Bower P, Gilbody S, et al. Collaborative care for depression and anxiety problems. Cochrane Database Syst Rev. 2012;10:CD006525.
55. Woltmann E, Grogan-Kaylor A, Perron B, Georges H, Kilbourne AM, Bauer MS. Comparative effectiveness of collaborative chronic care models for mental health conditions across primary, specialty, and behavioral health care settings: systematic review and meta-analysis. Am J Psychiatry. 2012;169(8):790-804.
56. Wright JL. DoD Directive 6490.15. www.dtic.mil/whs/directives/corres/pdf/649015p.pdf.Revised November 20, 2014. Accessed October 3, 2016. 57. Woodson J. Military treatment facility mental health clinical outcomes guidance. http://dcoe.mil/Libraries/Documents/MentalHealthClinicalOutcomesGuidance_Woodson.pdf. Published September 9, 2013. Accessed October 4, 2016.
58. Wilk JE, West JC, Duffy FF, Herrell RK, Rae DS, Hoge CW. Use of evidence-based treatment for posttraumatic stress disorder in Army behavioral healthcare. Psychiatry. 2013;76(4):336-348.
59. Stockton PN, Olsen ET, Hayford S, et al. Security from within: independent review of the Washington Navy Yard shooting. http://archive.defense.gov/pubs/Independent-Review-of-the-WNY-Shooting-14-Nov-2013.pdf. Published November, 2013. Accessed September 20, 2016.
60. Woodson J. ASD(HA) Memorandum: Clinical Policy Guidance for Assessment and Treatment of Posttraumatic Stress Disorder. August 24, 2012.
Preventive Treatment for Posttraumatic Stress Disorder
Identifying people who might be at risk for posttraumatic stress disorder (PTSD) before the trauma—and teaching them preventive coping skills—could reduce or prevent long-term effects, according to University of Oxford in Oxford, United Kingdom, and King’s College London, United Kingdom, researchers.
They assessed 453 newly recruited paramedics every 4 months for 2 years. Of those, 386 paramedics participated in follow-up interviews.
Related: Let’s Dance: A Holistic Approach to Treating Veterans With Posttraumatic Stress Disorder
Over the 2 years, 32 participants (8.3%) had an episode of PTSD, and 41 participants had (10.6%) an episode of major depression (MD). Most of the episodes were moderate and short lived. In most cases, the participant had recovered by the next 4-month assessment. However, at 2 years, those who had experienced episodes of PTSD or MD during the follow-up period reported more days off work, poorer sleep, poorer quality of life, and greater burn out as well as weight gain (mean gain, 6.9 kg) for those with P
Ten participants who developed PTSD received treatment during follow-up, as did 12 participants who developed MD. Five of 9 participants who had recurrent P
Related: Telehealth for Native Americans With PTSD
The researchers tested a number of possible pretrauma predictors of PTSD and MD. They correlated several: cognitive style (eg, suppression, rumination, intentional numbing), coping style (eg, avoidant styles, such as wishful thinking), and psychological traits (eg, neuroticism). However, they found rumination about memories of stressful events uniquely predicted an episode of PTSD. Perceived resilience uniquely predicted an episode of MD.
Interestingly, about 42% of the study participants had a psychiatric history before training—more than the general population. That might be a factor that draws them to emergency work, the researchers suggest.
Some predictors, such as psychiatric history, are fixed, the researchers note. But others, such as cognitive styles, can be modified or taught. Studies have shown that rumination can be redirected through training in concrete thinking, for instance, and psychoeducation and cognitive behavioral techniques (eg, modifying interpretations of stressful events) have been used to strengthen resilience. The predictors they identified in their study could serve as targets, the researchers suggest, for modifying future resilience programs.
Source:
Wild J, Smith KV, Thompson E, Béar F, Lommen MJ, Ehlers A. Psychol Med. 2016;46(12):2571-2582. doi: 10.1017/S0033291716000532.
Identifying people who might be at risk for posttraumatic stress disorder (PTSD) before the trauma—and teaching them preventive coping skills—could reduce or prevent long-term effects, according to University of Oxford in Oxford, United Kingdom, and King’s College London, United Kingdom, researchers.
They assessed 453 newly recruited paramedics every 4 months for 2 years. Of those, 386 paramedics participated in follow-up interviews.
Related: Let’s Dance: A Holistic Approach to Treating Veterans With Posttraumatic Stress Disorder
Over the 2 years, 32 participants (8.3%) had an episode of PTSD, and 41 participants had (10.6%) an episode of major depression (MD). Most of the episodes were moderate and short lived. In most cases, the participant had recovered by the next 4-month assessment. However, at 2 years, those who had experienced episodes of PTSD or MD during the follow-up period reported more days off work, poorer sleep, poorer quality of life, and greater burn out as well as weight gain (mean gain, 6.9 kg) for those with P
Ten participants who developed PTSD received treatment during follow-up, as did 12 participants who developed MD. Five of 9 participants who had recurrent P
Related: Telehealth for Native Americans With PTSD
The researchers tested a number of possible pretrauma predictors of PTSD and MD. They correlated several: cognitive style (eg, suppression, rumination, intentional numbing), coping style (eg, avoidant styles, such as wishful thinking), and psychological traits (eg, neuroticism). However, they found rumination about memories of stressful events uniquely predicted an episode of PTSD. Perceived resilience uniquely predicted an episode of MD.
Interestingly, about 42% of the study participants had a psychiatric history before training—more than the general population. That might be a factor that draws them to emergency work, the researchers suggest.
Some predictors, such as psychiatric history, are fixed, the researchers note. But others, such as cognitive styles, can be modified or taught. Studies have shown that rumination can be redirected through training in concrete thinking, for instance, and psychoeducation and cognitive behavioral techniques (eg, modifying interpretations of stressful events) have been used to strengthen resilience. The predictors they identified in their study could serve as targets, the researchers suggest, for modifying future resilience programs.
Source:
Wild J, Smith KV, Thompson E, Béar F, Lommen MJ, Ehlers A. Psychol Med. 2016;46(12):2571-2582. doi: 10.1017/S0033291716000532.
Identifying people who might be at risk for posttraumatic stress disorder (PTSD) before the trauma—and teaching them preventive coping skills—could reduce or prevent long-term effects, according to University of Oxford in Oxford, United Kingdom, and King’s College London, United Kingdom, researchers.
They assessed 453 newly recruited paramedics every 4 months for 2 years. Of those, 386 paramedics participated in follow-up interviews.
Related: Let’s Dance: A Holistic Approach to Treating Veterans With Posttraumatic Stress Disorder
Over the 2 years, 32 participants (8.3%) had an episode of PTSD, and 41 participants had (10.6%) an episode of major depression (MD). Most of the episodes were moderate and short lived. In most cases, the participant had recovered by the next 4-month assessment. However, at 2 years, those who had experienced episodes of PTSD or MD during the follow-up period reported more days off work, poorer sleep, poorer quality of life, and greater burn out as well as weight gain (mean gain, 6.9 kg) for those with P
Ten participants who developed PTSD received treatment during follow-up, as did 12 participants who developed MD. Five of 9 participants who had recurrent P
Related: Telehealth for Native Americans With PTSD
The researchers tested a number of possible pretrauma predictors of PTSD and MD. They correlated several: cognitive style (eg, suppression, rumination, intentional numbing), coping style (eg, avoidant styles, such as wishful thinking), and psychological traits (eg, neuroticism). However, they found rumination about memories of stressful events uniquely predicted an episode of PTSD. Perceived resilience uniquely predicted an episode of MD.
Interestingly, about 42% of the study participants had a psychiatric history before training—more than the general population. That might be a factor that draws them to emergency work, the researchers suggest.
Some predictors, such as psychiatric history, are fixed, the researchers note. But others, such as cognitive styles, can be modified or taught. Studies have shown that rumination can be redirected through training in concrete thinking, for instance, and psychoeducation and cognitive behavioral techniques (eg, modifying interpretations of stressful events) have been used to strengthen resilience. The predictors they identified in their study could serve as targets, the researchers suggest, for modifying future resilience programs.
Source:
Wild J, Smith KV, Thompson E, Béar F, Lommen MJ, Ehlers A. Psychol Med. 2016;46(12):2571-2582. doi: 10.1017/S0033291716000532.
Brief screen helps identify patients with PTSD, depression
WAIKOLOA, HAWAII – A new nine-item tool known as the Injured Trauma Survivor Screen demonstrated strong sensitivity and specificity for predicting posttraumatic stress disorder and depression in trauma patients.
At the annual meeting of the American Association for the Surgery of Trauma, Terri deRoon-Cassini, PhD, said that the rates of PTSD among trauma patients range from 10% to 42%, depending on the type of injury sustained. “There is significant life impairment, including an increased risk for suicide and an increased risk for morbidity and mortality,” said Dr. deRoon-Cassini, a clinical psychologist and associate professor with the division of trauma and critical care at the Medical College of Wisconsin, Milwaukee.
The ACS Committee on Trauma currently recommends PTSD screening by trauma centers, including the 20-item PTSD Checklist and the nine-item PHD-9 for depression. However, these symptom-based screens were not validated in hospitalized trauma patients. “This becomes important, because according to the symptom trajectory of PTSD after trauma, about 22% of people experience chronic disease and about 16%-18% of people who have symptoms at baseline do not translate to symptoms by 6 months, so screening with a symptom-based measure isn’t always the best route,” she said.

In an effort to create a brief screening tool to identify those at risk for PTSD and depression following traumatic injury, Dr. deRoon-Cassini and her associates scoured existing medical literature on the topic to review risk factors and created an item pool of questions based on those risk factors. They came up with 47 items and statistically “funneled out the items to create the most parsimonious model predicting who goes on to develop PTSD and depression separately,” she explained. They then created the Injured Trauma Survivor Screen (ITSS), a nine-item list of yes/no questions that takes about 5 minutes to administer: five items for PTSD and five items for depression, with one item that overlaps. The five ITSS PTSD questions are:
• Did you think you were going to die? (risk factor being perceived life threat; odds ratio 6.32).
• Do you think this was done to you intentionally? (risk factor being intentionality; OR, 4.24).
• Have you felt more restless, tense, or jumpy than usual? (risk factor being assessment of arousal; OR, 5.31).
• Have you found yourself unable to stop worrying? (risk factor being worry/rumination; OR, 4.49).
• Do you find yourself thinking that the world is unsafe and that people are not to be trusted? (risk factor being negative alterations in cognition; OR, 5.52).
The five ITSS depression questions are:
• Have you ever taken medication for, or been given a mental health diagnosis? (risk factor being preexisting psychopathology; OR, 10.58).
• Has there ever been a time in your life you have been bothered by feeling down or hopeless or lost all interest in things you usually enjoyed for more than 2 weeks? (risk factor being premorbid depression; OR, 3.78).
• Did you think you were going to die? (risk factor being perceived life threat; OR, 9.69).
• Have you felt emotionally detached from your loved ones? (risk factor being negative alteration in mood; OR, 8.03).
• Do you find yourself crying and are unsure why? (risk factor being mood/depression; OR, 9.18).
The researchers administered the survey to 139 patients at two trauma centers. More than half (69%) were male, 48% were white, 40% were African American, and the remainder were from other ethnic backgrounds. The three most common mechanisms of injury were motor vehicle crashes (29%), motorcycle/all-terrain vehicle crashes (19%), and falls (13%). Dr. deRoon-Cassini reported that administration of the ITSS within 4 days of injury demonstrated a 75% sensitivity for identifying the risk for PTSD and depression, a 94% specificity for PTSD, and a 96% specificity for depression, with a cutoff score of 2 out of 5 for both subscales based on a receiver operating characteristic (ROC) curve analysis.
One month following administration of the ITSS, 20% of patients were diagnosed with depression and 29% were diagnosed with PTSD. Of those diagnosed with PTSD, 55% met criteria for concomitant depression “so we are seeing a high comorbidity between PTSD and depression, which is consistent with the medical literature,” she said.
“The ITSS represents a brief way that we can screen for PTSD and depression within a trauma system,” Dr. deRoon-Cassini said. “At our institution, social workers administer the tool. They have a flow sheet in our EMR system where they enter the responses. If someone screens positive, a best practice recommendation is put into the patient’s chart, which gets funneled to a trauma psychology consult. On the treatment side we try to intervene by triaging the severity of the current distress the person is experiencing, past comorbidities, and past trauma histories. From there we decide whether to do a brief intervention or more intensive evidence-based interventions for PTSD or depression together or separately.”
The study was funded by a grant from the Medical College of Wisconsin. Coauthors included Joshua Hunt, PhD, of the Medical College of Wisconsin, Milwaukee; Ann Marie Warren, PhD, of Baylor Medical Center, Dallas; and Karen Brasel, MD, FACS, of Oregon Health & Science University, Portland. Dr. deRoon-Cassini reported having no financial disclosures.
WAIKOLOA, HAWAII – A new nine-item tool known as the Injured Trauma Survivor Screen demonstrated strong sensitivity and specificity for predicting posttraumatic stress disorder and depression in trauma patients.
At the annual meeting of the American Association for the Surgery of Trauma, Terri deRoon-Cassini, PhD, said that the rates of PTSD among trauma patients range from 10% to 42%, depending on the type of injury sustained. “There is significant life impairment, including an increased risk for suicide and an increased risk for morbidity and mortality,” said Dr. deRoon-Cassini, a clinical psychologist and associate professor with the division of trauma and critical care at the Medical College of Wisconsin, Milwaukee.
The ACS Committee on Trauma currently recommends PTSD screening by trauma centers, including the 20-item PTSD Checklist and the nine-item PHD-9 for depression. However, these symptom-based screens were not validated in hospitalized trauma patients. “This becomes important, because according to the symptom trajectory of PTSD after trauma, about 22% of people experience chronic disease and about 16%-18% of people who have symptoms at baseline do not translate to symptoms by 6 months, so screening with a symptom-based measure isn’t always the best route,” she said.
In an effort to create a brief screening tool to identify those at risk for PTSD and depression following traumatic injury, Dr. deRoon-Cassini and her associates scoured existing medical literature on the topic to review risk factors and created an item pool of questions based on those risk factors. They came up with 47 items and statistically “funneled out the items to create the most parsimonious model predicting who goes on to develop PTSD and depression separately,” she explained. They then created the Injured Trauma Survivor Screen (ITSS), a nine-item list of yes/no questions that takes about 5 minutes to administer: five items for PTSD and five items for depression, with one item that overlaps. The five ITSS PTSD questions are:
• Did you think you were going to die? (risk factor being perceived life threat; odds ratio 6.32).
• Do you think this was done to you intentionally? (risk factor being intentionality; OR, 4.24).
• Have you felt more restless, tense, or jumpy than usual? (risk factor being assessment of arousal; OR, 5.31).
• Have you found yourself unable to stop worrying? (risk factor being worry/rumination; OR, 4.49).
• Do you find yourself thinking that the world is unsafe and that people are not to be trusted? (risk factor being negative alterations in cognition; OR, 5.52).
The five ITSS depression questions are:
• Have you ever taken medication for, or been given a mental health diagnosis? (risk factor being preexisting psychopathology; OR, 10.58).
• Has there ever been a time in your life you have been bothered by feeling down or hopeless or lost all interest in things you usually enjoyed for more than 2 weeks? (risk factor being premorbid depression; OR, 3.78).
• Did you think you were going to die? (risk factor being perceived life threat; OR, 9.69).
• Have you felt emotionally detached from your loved ones? (risk factor being negative alteration in mood; OR, 8.03).
• Do you find yourself crying and are unsure why? (risk factor being mood/depression; OR, 9.18).
The researchers administered the survey to 139 patients at two trauma centers. More than half (69%) were male, 48% were white, 40% were African American, and the remainder were from other ethnic backgrounds. The three most common mechanisms of injury were motor vehicle crashes (29%), motorcycle/all-terrain vehicle crashes (19%), and falls (13%). Dr. deRoon-Cassini reported that administration of the ITSS within 4 days of injury demonstrated a 75% sensitivity for identifying the risk for PTSD and depression, a 94% specificity for PTSD, and a 96% specificity for depression, with a cutoff score of 2 out of 5 for both subscales based on a receiver operating characteristic (ROC) curve analysis.
One month following administration of the ITSS, 20% of patients were diagnosed with depression and 29% were diagnosed with PTSD. Of those diagnosed with PTSD, 55% met criteria for concomitant depression “so we are seeing a high comorbidity between PTSD and depression, which is consistent with the medical literature,” she said.
“The ITSS represents a brief way that we can screen for PTSD and depression within a trauma system,” Dr. deRoon-Cassini said. “At our institution, social workers administer the tool. They have a flow sheet in our EMR system where they enter the responses. If someone screens positive, a best practice recommendation is put into the patient’s chart, which gets funneled to a trauma psychology consult. On the treatment side we try to intervene by triaging the severity of the current distress the person is experiencing, past comorbidities, and past trauma histories. From there we decide whether to do a brief intervention or more intensive evidence-based interventions for PTSD or depression together or separately.”
The study was funded by a grant from the Medical College of Wisconsin. Coauthors included Joshua Hunt, PhD, of the Medical College of Wisconsin, Milwaukee; Ann Marie Warren, PhD, of Baylor Medical Center, Dallas; and Karen Brasel, MD, FACS, of Oregon Health & Science University, Portland. Dr. deRoon-Cassini reported having no financial disclosures.
WAIKOLOA, HAWAII – A new nine-item tool known as the Injured Trauma Survivor Screen demonstrated strong sensitivity and specificity for predicting posttraumatic stress disorder and depression in trauma patients.
At the annual meeting of the American Association for the Surgery of Trauma, Terri deRoon-Cassini, PhD, said that the rates of PTSD among trauma patients range from 10% to 42%, depending on the type of injury sustained. “There is significant life impairment, including an increased risk for suicide and an increased risk for morbidity and mortality,” said Dr. deRoon-Cassini, a clinical psychologist and associate professor with the division of trauma and critical care at the Medical College of Wisconsin, Milwaukee.
The ACS Committee on Trauma currently recommends PTSD screening by trauma centers, including the 20-item PTSD Checklist and the nine-item PHD-9 for depression. However, these symptom-based screens were not validated in hospitalized trauma patients. “This becomes important, because according to the symptom trajectory of PTSD after trauma, about 22% of people experience chronic disease and about 16%-18% of people who have symptoms at baseline do not translate to symptoms by 6 months, so screening with a symptom-based measure isn’t always the best route,” she said.
In an effort to create a brief screening tool to identify those at risk for PTSD and depression following traumatic injury, Dr. deRoon-Cassini and her associates scoured existing medical literature on the topic to review risk factors and created an item pool of questions based on those risk factors. They came up with 47 items and statistically “funneled out the items to create the most parsimonious model predicting who goes on to develop PTSD and depression separately,” she explained. They then created the Injured Trauma Survivor Screen (ITSS), a nine-item list of yes/no questions that takes about 5 minutes to administer: five items for PTSD and five items for depression, with one item that overlaps. The five ITSS PTSD questions are:
• Did you think you were going to die? (risk factor being perceived life threat; odds ratio 6.32).
• Do you think this was done to you intentionally? (risk factor being intentionality; OR, 4.24).
• Have you felt more restless, tense, or jumpy than usual? (risk factor being assessment of arousal; OR, 5.31).
• Have you found yourself unable to stop worrying? (risk factor being worry/rumination; OR, 4.49).
• Do you find yourself thinking that the world is unsafe and that people are not to be trusted? (risk factor being negative alterations in cognition; OR, 5.52).
The five ITSS depression questions are:
• Have you ever taken medication for, or been given a mental health diagnosis? (risk factor being preexisting psychopathology; OR, 10.58).
• Has there ever been a time in your life you have been bothered by feeling down or hopeless or lost all interest in things you usually enjoyed for more than 2 weeks? (risk factor being premorbid depression; OR, 3.78).
• Did you think you were going to die? (risk factor being perceived life threat; OR, 9.69).
• Have you felt emotionally detached from your loved ones? (risk factor being negative alteration in mood; OR, 8.03).
• Do you find yourself crying and are unsure why? (risk factor being mood/depression; OR, 9.18).
The researchers administered the survey to 139 patients at two trauma centers. More than half (69%) were male, 48% were white, 40% were African American, and the remainder were from other ethnic backgrounds. The three most common mechanisms of injury were motor vehicle crashes (29%), motorcycle/all-terrain vehicle crashes (19%), and falls (13%). Dr. deRoon-Cassini reported that administration of the ITSS within 4 days of injury demonstrated a 75% sensitivity for identifying the risk for PTSD and depression, a 94% specificity for PTSD, and a 96% specificity for depression, with a cutoff score of 2 out of 5 for both subscales based on a receiver operating characteristic (ROC) curve analysis.
One month following administration of the ITSS, 20% of patients were diagnosed with depression and 29% were diagnosed with PTSD. Of those diagnosed with PTSD, 55% met criteria for concomitant depression “so we are seeing a high comorbidity between PTSD and depression, which is consistent with the medical literature,” she said.
“The ITSS represents a brief way that we can screen for PTSD and depression within a trauma system,” Dr. deRoon-Cassini said. “At our institution, social workers administer the tool. They have a flow sheet in our EMR system where they enter the responses. If someone screens positive, a best practice recommendation is put into the patient’s chart, which gets funneled to a trauma psychology consult. On the treatment side we try to intervene by triaging the severity of the current distress the person is experiencing, past comorbidities, and past trauma histories. From there we decide whether to do a brief intervention or more intensive evidence-based interventions for PTSD or depression together or separately.”
The study was funded by a grant from the Medical College of Wisconsin. Coauthors included Joshua Hunt, PhD, of the Medical College of Wisconsin, Milwaukee; Ann Marie Warren, PhD, of Baylor Medical Center, Dallas; and Karen Brasel, MD, FACS, of Oregon Health & Science University, Portland. Dr. deRoon-Cassini reported having no financial disclosures.
Key clinical point:
Major finding: Administration of the Injured Trauma Survivor Screen (ITSS) within 4 days of injury demonstrated a 75% sensitivity for identifying the risk for PTSD and depression, a 94% specificity for PTSD, and a 96% specificity for depression.
Data source: An analysis of 139 patients from two trauma centers who completed the ITSS.
Disclosures: The study was funded by a grant from the Medical College of Wisconsin. Dr. deRoon-Cassini reported having no financial disclosures.
Ostracism is a growing concern as mechanism of poor health outcomes in military
WASHINGTON – The role of ostracism in overall poor health outcomes in service personnel is a growing concern, according to a panel of military experts.
“Think about the primary mechanism of suicide in kids who are bullied: It’s ostracism,” Kate McGraw, PhD, said in an interview at the American Psychiatric Association’s Institute on Psychiatric Services. Dr. McGraw is the interim director of the Deployment Health Clinical Center, a Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury.

Although the literature is scant at this point because the effects of being left out are “common sense,” said Dr. McGraw, “we need to take it seriously.”
While ostracism as a clinical term doesn’t actually exist and direct data on its impact are not numerous, its inherent psychological risks include suicide, depression, and trauma, according to another of the panelists, Jacqueline Garrick, acting director of the Defense Suicide Prevention Office in the Department of Defense.
Dr. McGraw defined ostracism as group behavior “designed to isolate or deprive another individual of being part of that group.”
Women in the military are particularly at risk for ostracism simply because they tend to be outnumbered by their male counterparts in a combat unit, according to Dr. McGraw. This, combined with a wariness of women after sexual assault awareness education, can exacerbate the segregation.

Add to the mix the separation from the male group that female biology can sometimes cause, whether due to menstrual cycles or toilet needs, Ms. Garrick said. This can widen the gap.
Additionally, service personnel – men or women – who report sexual assault are at risk of being isolated or can suffer retaliation, despite there being antiharassment and antibullying policies in place.
In the interview, Dr. McGraw said she recommends assessing the level of social support a serviceman or servicewoman has by asking directly: “How included do you feel in your group?” She also suggested looking for evidence of ostracism such as the patient endorsing a sense that they do not belong, or being friendless.
If a clinician suspects that a person who says “I am stressed” actually means, “My feelings are hurt,” Dr. McGraw suggested going deeper: Seek clues as to whether the person is experiencing ostracism either covertly, such as being bullied in private, or overtly such as not being given information that ends up making the person appear foolish or unprepared for a task.
“Ask some very pointed questions, such as ‘Are people behaving toward you in a certain way?’ and ‘Do you feel targeted?’ ”
The challenge, she said, is to maintain what is known as “military bearing” – essentially, cultivated stoicism, while also admitting that one’s functionality is suffering because of having been isolated. A dialogue between patient and clinician about being ostracized can lead to helping the person develop strategies for coping with its effects, such as making the commanding officer aware of what is happening.
“Most military personnel are not going to say their feelings are hurt, but they can address the behavior,” Dr. McGraw said.
Although Dr. McGraw admitted when asked that reporting the behavior to a superior could result in further ostracism, she said she has faith in the power of leadership to evoke cultural change. “In a military environment, if the leaders are aware of what is happening, and they take steps to mitigate or eliminate it as a unit, then they can create a healthier environment in the unit, improving morale and esprit de corps.”
None of the presenters had any relevant financial disclosures and said their presentations represented their own opinions, not those of the U.S. Armed Forces.
WASHINGTON – The role of ostracism in overall poor health outcomes in service personnel is a growing concern, according to a panel of military experts.
“Think about the primary mechanism of suicide in kids who are bullied: It’s ostracism,” Kate McGraw, PhD, said in an interview at the American Psychiatric Association’s Institute on Psychiatric Services. Dr. McGraw is the interim director of the Deployment Health Clinical Center, a Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury.
Although the literature is scant at this point because the effects of being left out are “common sense,” said Dr. McGraw, “we need to take it seriously.”
While ostracism as a clinical term doesn’t actually exist and direct data on its impact are not numerous, its inherent psychological risks include suicide, depression, and trauma, according to another of the panelists, Jacqueline Garrick, acting director of the Defense Suicide Prevention Office in the Department of Defense.
Dr. McGraw defined ostracism as group behavior “designed to isolate or deprive another individual of being part of that group.”
Women in the military are particularly at risk for ostracism simply because they tend to be outnumbered by their male counterparts in a combat unit, according to Dr. McGraw. This, combined with a wariness of women after sexual assault awareness education, can exacerbate the segregation.
Add to the mix the separation from the male group that female biology can sometimes cause, whether due to menstrual cycles or toilet needs, Ms. Garrick said. This can widen the gap.
Additionally, service personnel – men or women – who report sexual assault are at risk of being isolated or can suffer retaliation, despite there being antiharassment and antibullying policies in place.
In the interview, Dr. McGraw said she recommends assessing the level of social support a serviceman or servicewoman has by asking directly: “How included do you feel in your group?” She also suggested looking for evidence of ostracism such as the patient endorsing a sense that they do not belong, or being friendless.
If a clinician suspects that a person who says “I am stressed” actually means, “My feelings are hurt,” Dr. McGraw suggested going deeper: Seek clues as to whether the person is experiencing ostracism either covertly, such as being bullied in private, or overtly such as not being given information that ends up making the person appear foolish or unprepared for a task.
“Ask some very pointed questions, such as ‘Are people behaving toward you in a certain way?’ and ‘Do you feel targeted?’ ”
The challenge, she said, is to maintain what is known as “military bearing” – essentially, cultivated stoicism, while also admitting that one’s functionality is suffering because of having been isolated. A dialogue between patient and clinician about being ostracized can lead to helping the person develop strategies for coping with its effects, such as making the commanding officer aware of what is happening.
“Most military personnel are not going to say their feelings are hurt, but they can address the behavior,” Dr. McGraw said.
Although Dr. McGraw admitted when asked that reporting the behavior to a superior could result in further ostracism, she said she has faith in the power of leadership to evoke cultural change. “In a military environment, if the leaders are aware of what is happening, and they take steps to mitigate or eliminate it as a unit, then they can create a healthier environment in the unit, improving morale and esprit de corps.”
None of the presenters had any relevant financial disclosures and said their presentations represented their own opinions, not those of the U.S. Armed Forces.
WASHINGTON – The role of ostracism in overall poor health outcomes in service personnel is a growing concern, according to a panel of military experts.
“Think about the primary mechanism of suicide in kids who are bullied: It’s ostracism,” Kate McGraw, PhD, said in an interview at the American Psychiatric Association’s Institute on Psychiatric Services. Dr. McGraw is the interim director of the Deployment Health Clinical Center, a Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury.
Although the literature is scant at this point because the effects of being left out are “common sense,” said Dr. McGraw, “we need to take it seriously.”
While ostracism as a clinical term doesn’t actually exist and direct data on its impact are not numerous, its inherent psychological risks include suicide, depression, and trauma, according to another of the panelists, Jacqueline Garrick, acting director of the Defense Suicide Prevention Office in the Department of Defense.
Dr. McGraw defined ostracism as group behavior “designed to isolate or deprive another individual of being part of that group.”
Women in the military are particularly at risk for ostracism simply because they tend to be outnumbered by their male counterparts in a combat unit, according to Dr. McGraw. This, combined with a wariness of women after sexual assault awareness education, can exacerbate the segregation.
Add to the mix the separation from the male group that female biology can sometimes cause, whether due to menstrual cycles or toilet needs, Ms. Garrick said. This can widen the gap.
Additionally, service personnel – men or women – who report sexual assault are at risk of being isolated or can suffer retaliation, despite there being antiharassment and antibullying policies in place.
In the interview, Dr. McGraw said she recommends assessing the level of social support a serviceman or servicewoman has by asking directly: “How included do you feel in your group?” She also suggested looking for evidence of ostracism such as the patient endorsing a sense that they do not belong, or being friendless.
If a clinician suspects that a person who says “I am stressed” actually means, “My feelings are hurt,” Dr. McGraw suggested going deeper: Seek clues as to whether the person is experiencing ostracism either covertly, such as being bullied in private, or overtly such as not being given information that ends up making the person appear foolish or unprepared for a task.
“Ask some very pointed questions, such as ‘Are people behaving toward you in a certain way?’ and ‘Do you feel targeted?’ ”
The challenge, she said, is to maintain what is known as “military bearing” – essentially, cultivated stoicism, while also admitting that one’s functionality is suffering because of having been isolated. A dialogue between patient and clinician about being ostracized can lead to helping the person develop strategies for coping with its effects, such as making the commanding officer aware of what is happening.
“Most military personnel are not going to say their feelings are hurt, but they can address the behavior,” Dr. McGraw said.
Although Dr. McGraw admitted when asked that reporting the behavior to a superior could result in further ostracism, she said she has faith in the power of leadership to evoke cultural change. “In a military environment, if the leaders are aware of what is happening, and they take steps to mitigate or eliminate it as a unit, then they can create a healthier environment in the unit, improving morale and esprit de corps.”
None of the presenters had any relevant financial disclosures and said their presentations represented their own opinions, not those of the U.S. Armed Forces.
EXPERT ANALYSIS FROM THE INSTITUTE ON PSYCHIATRIC SERVICES
Sublingual cyclobenzaprine may be effective, safe for military-related PTSD
SCOTTSDALE, ARIZ. – A sublingual formulation of cyclobenzaprine taken at bedtime was significantly better than placebo at reducing symptoms of military-related posttraumatic stress disorder, and study participants taking cyclobenzaprine also reported better sleep, a study showed.
After 12 weeks of nightly use at bedtime, 5.6 mg of sublingual cyclobenzaprine (CBP) resulted in a significant reduction on the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5), compared with placebo. Under several different analytic and data imputation methods, CAPS-5 values improved by 20.2 to 22.6 points from baseline for the 5.6-mg group, compared with reductions of 17.4 to 20.6 for the placebo group (P value range, 0.038-0.016). Improvement in the CAPS-5 was the study’s primary efficacy outcome measure.
Patients also saw significantly improved global symptoms, as assessed by the Clinician Global Impression – Improvement scale (CGI-I; 63.3% responders cyclobenzaprine versus 44.6% placebo, P = 0.041).
Significant reductions in hyperarousal (P less than 0.05) and exaggerated startle (P =0.015) symptoms also were seen in the 5.6-mg cyclobenzaprine group, and those participants also had significantly less symptom-related disruption in work/school, and in social/leisure activities, as measured by those domains on the Sheehan Disability Scale (for both, P less than 0.050).
Gregory M. Sullivan, MD, chief medical officer of Tonix Pharmaceuticals, presented these findings from AtEase, a randomized, placebo-controlled, double-blind study of sublingual cyclobenzaprine for military PTSD, at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Drug Clinical Evaluation Unit meeting.
The phase II safety, efficacy, and dose-ranging study of 245 patients (231 in the modified intent-to-treat population, and 237 in the safety population) also compared 2.8- and 5.6-mg sublingual doses. At the end of the 12-week study period, those on the lower dose did not experience significantly improved sleep or PTSD symptoms.
The AtEase participants were current or former servicemembers with PTSD. Ninety-three percent of the patients were male and had been deployed an average of 2.3 times. The index trauma occurred a mean of 7 years ago. Demographic distribution was representative of the U.S. military, according to Dr. Sullivan. The mean CAPS-5 and Montgomery-Åsberg Depression Rating Scale (MADRS) scores were similar across treatment arms. The mean CAPS-5 score for participants in the study was 39.5 representing “severe” PTSD. “These people are quite ill,” said Seth Lederman, MD, Tonix CEO, in an interview.
Oral symptoms were the most frequent side effects reported in the safety analysis. Of those taking the 2.8-mg cyclobenzaprine dose, 38.7% (36/93) experienced oral hypoesthesia, as did 36% (18/50) of the 5.6-mg dosing group. This compared with 2.1% (2/94) of the placebo group. Somnolence was noted by 11.8% (11/93) of the lower dose group, by 16% (8/50) of the higher dose group, and by 6.4% (6/94) of the placebo group. No participants discontinued the study because of adverse events.
Military traumatic brain injury may be different from most civilian TBI, said Dr. Lederman, because of both the intensity and duration of the events that precipitated the condition. Most military-related trauma stems from combat, and most patients with military-related trauma are men; in the civilian population, PTSD patients are predominantly women. “Especially in today’s military, servicemembers are deploying multiple times,” he noted. “Everyone has their breaking point.”
Effective medical treatments for military PTSD are lacking, said Dr. Sullivan. One multicenter trial found that sertraline not effective for PTSD in military veterans (J Clin Psychiatry. 2007 May;68[5]:711-20), and selective serotonin reuptake inhibitors are associated with sexual dysfunction and insomnia for some patients.
Cyclobenzaprine is thought to interact with several receptors thought to be important for sleep, including 5-HT2A, alpha-1 adrenergic, and H1 histamine receptors.
Problems with sleep for individuals with PTSD may include nightmares, as well as sleep disturbances associated with the hyperarousal that characterizes the disorder. Sleep disruption may contribute to “attenuated extinction consolidation, or a delay in the processing of emotionally charged memories,” Dr. Sullivan said. Sleep disturbances in those with PTSD also are associated with depression, substance use disorders, and suicidal behavior.
“Processing memories is an essential part of learning and extinction,” Dr. Lederman said. “We saw startle improve” in the clinical trial of sublingual cyclobenzaprine, an indication of diminished hyperarousal, he said.
The sublingual formulation, said Dr. Lederman, avoids first-pass metabolism of cyclobenzaprine, which converts large amounts of the dose to norcyclobenzaprine. This metabolite has a much longer half-life than cyclobenzaprine and is responsible, in large part, for the persistent grogginess many patients report when taking the oral formulation of the medication. Previous work showed that the exposure ratio for cyclobenzaprine/norcyclobenzaprine for oral immediate-release cyclobenzaprine was 1.2, compared with 1.9 for sublingual cyclobenzaprine
“With the sublingual formulation, we hope to achieve a true ‘on-off’ effect, really helping sleep quality and improving sleep architecture,” Dr. Lederman said.
“Early effects on sleep and hyperarousal are consistent with the mechanistic hypothesis that TNX-102 SL’s primary actions on sleep architecture and autonomic balance underlie the observed PTSD treatment effect,” wrote Dr. Sullivan. The later reduction in exaggerated startle is consistent with the memory consolidation hypothesis, he said.
Sublingual cyclobenzaprine also is being trialed for fibromyalgia, another condition where significant sleep disruption can be a prominent symptom. Next steps for military PTSD include a larger clinical trial that plans to enroll 450 patients, said Dr. Lederman.
Dr. Lederman and Dr. Sullivan are both employed by Tonix Pharmaceuticals, which was the sponsor of the AtEase study.
On Twitter @karioakes
SCOTTSDALE, ARIZ. – A sublingual formulation of cyclobenzaprine taken at bedtime was significantly better than placebo at reducing symptoms of military-related posttraumatic stress disorder, and study participants taking cyclobenzaprine also reported better sleep, a study showed.
After 12 weeks of nightly use at bedtime, 5.6 mg of sublingual cyclobenzaprine (CBP) resulted in a significant reduction on the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5), compared with placebo. Under several different analytic and data imputation methods, CAPS-5 values improved by 20.2 to 22.6 points from baseline for the 5.6-mg group, compared with reductions of 17.4 to 20.6 for the placebo group (P value range, 0.038-0.016). Improvement in the CAPS-5 was the study’s primary efficacy outcome measure.
Patients also saw significantly improved global symptoms, as assessed by the Clinician Global Impression – Improvement scale (CGI-I; 63.3% responders cyclobenzaprine versus 44.6% placebo, P = 0.041).
Significant reductions in hyperarousal (P less than 0.05) and exaggerated startle (P =0.015) symptoms also were seen in the 5.6-mg cyclobenzaprine group, and those participants also had significantly less symptom-related disruption in work/school, and in social/leisure activities, as measured by those domains on the Sheehan Disability Scale (for both, P less than 0.050).
Gregory M. Sullivan, MD, chief medical officer of Tonix Pharmaceuticals, presented these findings from AtEase, a randomized, placebo-controlled, double-blind study of sublingual cyclobenzaprine for military PTSD, at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Drug Clinical Evaluation Unit meeting.
The phase II safety, efficacy, and dose-ranging study of 245 patients (231 in the modified intent-to-treat population, and 237 in the safety population) also compared 2.8- and 5.6-mg sublingual doses. At the end of the 12-week study period, those on the lower dose did not experience significantly improved sleep or PTSD symptoms.
The AtEase participants were current or former servicemembers with PTSD. Ninety-three percent of the patients were male and had been deployed an average of 2.3 times. The index trauma occurred a mean of 7 years ago. Demographic distribution was representative of the U.S. military, according to Dr. Sullivan. The mean CAPS-5 and Montgomery-Åsberg Depression Rating Scale (MADRS) scores were similar across treatment arms. The mean CAPS-5 score for participants in the study was 39.5 representing “severe” PTSD. “These people are quite ill,” said Seth Lederman, MD, Tonix CEO, in an interview.
Oral symptoms were the most frequent side effects reported in the safety analysis. Of those taking the 2.8-mg cyclobenzaprine dose, 38.7% (36/93) experienced oral hypoesthesia, as did 36% (18/50) of the 5.6-mg dosing group. This compared with 2.1% (2/94) of the placebo group. Somnolence was noted by 11.8% (11/93) of the lower dose group, by 16% (8/50) of the higher dose group, and by 6.4% (6/94) of the placebo group. No participants discontinued the study because of adverse events.
Military traumatic brain injury may be different from most civilian TBI, said Dr. Lederman, because of both the intensity and duration of the events that precipitated the condition. Most military-related trauma stems from combat, and most patients with military-related trauma are men; in the civilian population, PTSD patients are predominantly women. “Especially in today’s military, servicemembers are deploying multiple times,” he noted. “Everyone has their breaking point.”
Effective medical treatments for military PTSD are lacking, said Dr. Sullivan. One multicenter trial found that sertraline not effective for PTSD in military veterans (J Clin Psychiatry. 2007 May;68[5]:711-20), and selective serotonin reuptake inhibitors are associated with sexual dysfunction and insomnia for some patients.
Cyclobenzaprine is thought to interact with several receptors thought to be important for sleep, including 5-HT2A, alpha-1 adrenergic, and H1 histamine receptors.
Problems with sleep for individuals with PTSD may include nightmares, as well as sleep disturbances associated with the hyperarousal that characterizes the disorder. Sleep disruption may contribute to “attenuated extinction consolidation, or a delay in the processing of emotionally charged memories,” Dr. Sullivan said. Sleep disturbances in those with PTSD also are associated with depression, substance use disorders, and suicidal behavior.
“Processing memories is an essential part of learning and extinction,” Dr. Lederman said. “We saw startle improve” in the clinical trial of sublingual cyclobenzaprine, an indication of diminished hyperarousal, he said.
The sublingual formulation, said Dr. Lederman, avoids first-pass metabolism of cyclobenzaprine, which converts large amounts of the dose to norcyclobenzaprine. This metabolite has a much longer half-life than cyclobenzaprine and is responsible, in large part, for the persistent grogginess many patients report when taking the oral formulation of the medication. Previous work showed that the exposure ratio for cyclobenzaprine/norcyclobenzaprine for oral immediate-release cyclobenzaprine was 1.2, compared with 1.9 for sublingual cyclobenzaprine
“With the sublingual formulation, we hope to achieve a true ‘on-off’ effect, really helping sleep quality and improving sleep architecture,” Dr. Lederman said.
“Early effects on sleep and hyperarousal are consistent with the mechanistic hypothesis that TNX-102 SL’s primary actions on sleep architecture and autonomic balance underlie the observed PTSD treatment effect,” wrote Dr. Sullivan. The later reduction in exaggerated startle is consistent with the memory consolidation hypothesis, he said.
Sublingual cyclobenzaprine also is being trialed for fibromyalgia, another condition where significant sleep disruption can be a prominent symptom. Next steps for military PTSD include a larger clinical trial that plans to enroll 450 patients, said Dr. Lederman.
Dr. Lederman and Dr. Sullivan are both employed by Tonix Pharmaceuticals, which was the sponsor of the AtEase study.
On Twitter @karioakes
SCOTTSDALE, ARIZ. – A sublingual formulation of cyclobenzaprine taken at bedtime was significantly better than placebo at reducing symptoms of military-related posttraumatic stress disorder, and study participants taking cyclobenzaprine also reported better sleep, a study showed.
After 12 weeks of nightly use at bedtime, 5.6 mg of sublingual cyclobenzaprine (CBP) resulted in a significant reduction on the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5), compared with placebo. Under several different analytic and data imputation methods, CAPS-5 values improved by 20.2 to 22.6 points from baseline for the 5.6-mg group, compared with reductions of 17.4 to 20.6 for the placebo group (P value range, 0.038-0.016). Improvement in the CAPS-5 was the study’s primary efficacy outcome measure.
Patients also saw significantly improved global symptoms, as assessed by the Clinician Global Impression – Improvement scale (CGI-I; 63.3% responders cyclobenzaprine versus 44.6% placebo, P = 0.041).
Significant reductions in hyperarousal (P less than 0.05) and exaggerated startle (P =0.015) symptoms also were seen in the 5.6-mg cyclobenzaprine group, and those participants also had significantly less symptom-related disruption in work/school, and in social/leisure activities, as measured by those domains on the Sheehan Disability Scale (for both, P less than 0.050).
Gregory M. Sullivan, MD, chief medical officer of Tonix Pharmaceuticals, presented these findings from AtEase, a randomized, placebo-controlled, double-blind study of sublingual cyclobenzaprine for military PTSD, at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Drug Clinical Evaluation Unit meeting.
The phase II safety, efficacy, and dose-ranging study of 245 patients (231 in the modified intent-to-treat population, and 237 in the safety population) also compared 2.8- and 5.6-mg sublingual doses. At the end of the 12-week study period, those on the lower dose did not experience significantly improved sleep or PTSD symptoms.
The AtEase participants were current or former servicemembers with PTSD. Ninety-three percent of the patients were male and had been deployed an average of 2.3 times. The index trauma occurred a mean of 7 years ago. Demographic distribution was representative of the U.S. military, according to Dr. Sullivan. The mean CAPS-5 and Montgomery-Åsberg Depression Rating Scale (MADRS) scores were similar across treatment arms. The mean CAPS-5 score for participants in the study was 39.5 representing “severe” PTSD. “These people are quite ill,” said Seth Lederman, MD, Tonix CEO, in an interview.
Oral symptoms were the most frequent side effects reported in the safety analysis. Of those taking the 2.8-mg cyclobenzaprine dose, 38.7% (36/93) experienced oral hypoesthesia, as did 36% (18/50) of the 5.6-mg dosing group. This compared with 2.1% (2/94) of the placebo group. Somnolence was noted by 11.8% (11/93) of the lower dose group, by 16% (8/50) of the higher dose group, and by 6.4% (6/94) of the placebo group. No participants discontinued the study because of adverse events.
Military traumatic brain injury may be different from most civilian TBI, said Dr. Lederman, because of both the intensity and duration of the events that precipitated the condition. Most military-related trauma stems from combat, and most patients with military-related trauma are men; in the civilian population, PTSD patients are predominantly women. “Especially in today’s military, servicemembers are deploying multiple times,” he noted. “Everyone has their breaking point.”
Effective medical treatments for military PTSD are lacking, said Dr. Sullivan. One multicenter trial found that sertraline not effective for PTSD in military veterans (J Clin Psychiatry. 2007 May;68[5]:711-20), and selective serotonin reuptake inhibitors are associated with sexual dysfunction and insomnia for some patients.
Cyclobenzaprine is thought to interact with several receptors thought to be important for sleep, including 5-HT2A, alpha-1 adrenergic, and H1 histamine receptors.
Problems with sleep for individuals with PTSD may include nightmares, as well as sleep disturbances associated with the hyperarousal that characterizes the disorder. Sleep disruption may contribute to “attenuated extinction consolidation, or a delay in the processing of emotionally charged memories,” Dr. Sullivan said. Sleep disturbances in those with PTSD also are associated with depression, substance use disorders, and suicidal behavior.
“Processing memories is an essential part of learning and extinction,” Dr. Lederman said. “We saw startle improve” in the clinical trial of sublingual cyclobenzaprine, an indication of diminished hyperarousal, he said.
The sublingual formulation, said Dr. Lederman, avoids first-pass metabolism of cyclobenzaprine, which converts large amounts of the dose to norcyclobenzaprine. This metabolite has a much longer half-life than cyclobenzaprine and is responsible, in large part, for the persistent grogginess many patients report when taking the oral formulation of the medication. Previous work showed that the exposure ratio for cyclobenzaprine/norcyclobenzaprine for oral immediate-release cyclobenzaprine was 1.2, compared with 1.9 for sublingual cyclobenzaprine
“With the sublingual formulation, we hope to achieve a true ‘on-off’ effect, really helping sleep quality and improving sleep architecture,” Dr. Lederman said.
“Early effects on sleep and hyperarousal are consistent with the mechanistic hypothesis that TNX-102 SL’s primary actions on sleep architecture and autonomic balance underlie the observed PTSD treatment effect,” wrote Dr. Sullivan. The later reduction in exaggerated startle is consistent with the memory consolidation hypothesis, he said.
Sublingual cyclobenzaprine also is being trialed for fibromyalgia, another condition where significant sleep disruption can be a prominent symptom. Next steps for military PTSD include a larger clinical trial that plans to enroll 450 patients, said Dr. Lederman.
Dr. Lederman and Dr. Sullivan are both employed by Tonix Pharmaceuticals, which was the sponsor of the AtEase study.
On Twitter @karioakes
AT THE ASCP ANNUAL MEETING
Key clinical point: Sublingual cyclobenzaprine improved sleep and reduced hyperarousal symptoms in military-related PTSD.
Major finding: Global symptom improvement was seen in 63.3% of those taking 5.6 mg sublingual cyclobenzaprine compared with 44.6% of those taking placebo (P=0.041).
Data source: Randomized double-blind placebo-controlled trial of 245 patients with military-related PTSD, comparing two doses of nightly sublingual cyclobenzaprine to placebo.
Disclosures: The study was funded by Tonix Pharmaceuticals, which employs Dr. Sullivan and Dr. Lederman.
PTSD, eating disorders tied to suppressing negative emotions
A pathway from posttraumatic stress disorder to eating disorders might be through the maladaptive coping mechanism of expressive suppression, a study of 860 older veterans shows.
“Expressive suppression reflects attempts to reduce outward expression of emotion and may be adaptive in the short term; however, this strategy becomes less effective over the long term,” wrote Karen S. Mitchell, PhD, and Erika J. Wolf, PhD., both of the National Center for PTSD, VA Boston Healthcare System. “This finding aligns with previous ... work suggesting that in some individuals, [eating disorder] symptoms may be used to cope with negative affect.”
“We weren’t surprised by the findings,” Dr. Mitchell said in an interview. “They were consistent with our hypothesis that for some people, disordered eating may be used to cope with PTSD symptoms.”
She said the clinical implications of the study are direct. “It is important to assess eating habits and other potentially harmful coping strategies among patients with trauma histories and PTSD. On the other hand, it would be helpful to assess trauma histories in patients with eating disorders to determine if trauma reminders or other PTSD symptoms serve as a maintaining factor for the eating disorder.”
Dr. Mitchell and Dr. Wolf randomly selected 1,126 veterans who had reported trauma exposure in the GfK Knowledge Networks study (Depress Anxiety. 2013 May;30[5]:432-4), which looked at psychological resilience in a sample of U.S. veterans aged 60 and older. The veterans in the randomly selected group were asked to participate in a survey about PTSD, dissociation, and disordered eating, and 860 responded, 787 of whom were men (Psychiatry Res. 2016;243:23-9).
The participants’ age range was 22-96 years; mean age was 63. Most were white (85%) and married (77%), and had attended some college (87%).
Participants were asked to complete several surveys, including the Eating Disorder Diagnostic Scale (EDDS), the Yale Food Addiction Scale, the Emotion Regulation Questionnaire, and the National Stressful Events Survey (NSES).
The investigators said the sudden, unexpected death of a loved one (17.5%), and the aftermath of combat (13.6%) were cited as the worst traumatic experiences most cited by the participants. They also cited the violent death of a loved one (7.3%), the witnessing of dead bodies or body parts (6.3%), and physical or sexual assault (5.5%) as traumatic experiences.
Meanwhile, 23 participants (18 men [2.8%] and 5 women [9.1%]) met the criteria for bulimia nervosa; 20 met the criteria for binge eating disorder (16 men [2.5%] and 4 women [7.3%]); and 16 people (12 men [1.9%] and 4 women [7.3%]) met the proposed criteria for food addiction, reported Dr. Mitchell and Dr. Wolf, who also both are affiliated with the department of psychiatry at Boston University.
After analyzing the data, the researchers found that “the indirect path from PTSD to expressive suppression to [eating disorder] symptoms was significant in the full sample (P = .002; 95% confidence interval, 0.069-0.314) and in the male subsample (P = .029; 95% CI, 0.014-0.255).”
The researchers cited several limitations. For example, the participants’ diagnoses were not confirmed by interviews. In addition, “the validity of DSM-5 diagnoses using the EDDS and NSES has not yet been established,” they wrote.
Nevertheless, Dr. Mitchell and Dr. Wolf wrote, their findings highlight the importance of looking at eating disorders and food addiction in populations that traditionally have been underserved.
The study was funded by National Institutes of Health grant and an award from the Department of Veterans Affairs.
A pathway from posttraumatic stress disorder to eating disorders might be through the maladaptive coping mechanism of expressive suppression, a study of 860 older veterans shows.
“Expressive suppression reflects attempts to reduce outward expression of emotion and may be adaptive in the short term; however, this strategy becomes less effective over the long term,” wrote Karen S. Mitchell, PhD, and Erika J. Wolf, PhD., both of the National Center for PTSD, VA Boston Healthcare System. “This finding aligns with previous ... work suggesting that in some individuals, [eating disorder] symptoms may be used to cope with negative affect.”
“We weren’t surprised by the findings,” Dr. Mitchell said in an interview. “They were consistent with our hypothesis that for some people, disordered eating may be used to cope with PTSD symptoms.”
She said the clinical implications of the study are direct. “It is important to assess eating habits and other potentially harmful coping strategies among patients with trauma histories and PTSD. On the other hand, it would be helpful to assess trauma histories in patients with eating disorders to determine if trauma reminders or other PTSD symptoms serve as a maintaining factor for the eating disorder.”
Dr. Mitchell and Dr. Wolf randomly selected 1,126 veterans who had reported trauma exposure in the GfK Knowledge Networks study (Depress Anxiety. 2013 May;30[5]:432-4), which looked at psychological resilience in a sample of U.S. veterans aged 60 and older. The veterans in the randomly selected group were asked to participate in a survey about PTSD, dissociation, and disordered eating, and 860 responded, 787 of whom were men (Psychiatry Res. 2016;243:23-9).
The participants’ age range was 22-96 years; mean age was 63. Most were white (85%) and married (77%), and had attended some college (87%).
Participants were asked to complete several surveys, including the Eating Disorder Diagnostic Scale (EDDS), the Yale Food Addiction Scale, the Emotion Regulation Questionnaire, and the National Stressful Events Survey (NSES).
The investigators said the sudden, unexpected death of a loved one (17.5%), and the aftermath of combat (13.6%) were cited as the worst traumatic experiences most cited by the participants. They also cited the violent death of a loved one (7.3%), the witnessing of dead bodies or body parts (6.3%), and physical or sexual assault (5.5%) as traumatic experiences.
Meanwhile, 23 participants (18 men [2.8%] and 5 women [9.1%]) met the criteria for bulimia nervosa; 20 met the criteria for binge eating disorder (16 men [2.5%] and 4 women [7.3%]); and 16 people (12 men [1.9%] and 4 women [7.3%]) met the proposed criteria for food addiction, reported Dr. Mitchell and Dr. Wolf, who also both are affiliated with the department of psychiatry at Boston University.
After analyzing the data, the researchers found that “the indirect path from PTSD to expressive suppression to [eating disorder] symptoms was significant in the full sample (P = .002; 95% confidence interval, 0.069-0.314) and in the male subsample (P = .029; 95% CI, 0.014-0.255).”
The researchers cited several limitations. For example, the participants’ diagnoses were not confirmed by interviews. In addition, “the validity of DSM-5 diagnoses using the EDDS and NSES has not yet been established,” they wrote.
Nevertheless, Dr. Mitchell and Dr. Wolf wrote, their findings highlight the importance of looking at eating disorders and food addiction in populations that traditionally have been underserved.
The study was funded by National Institutes of Health grant and an award from the Department of Veterans Affairs.
A pathway from posttraumatic stress disorder to eating disorders might be through the maladaptive coping mechanism of expressive suppression, a study of 860 older veterans shows.
“Expressive suppression reflects attempts to reduce outward expression of emotion and may be adaptive in the short term; however, this strategy becomes less effective over the long term,” wrote Karen S. Mitchell, PhD, and Erika J. Wolf, PhD., both of the National Center for PTSD, VA Boston Healthcare System. “This finding aligns with previous ... work suggesting that in some individuals, [eating disorder] symptoms may be used to cope with negative affect.”
“We weren’t surprised by the findings,” Dr. Mitchell said in an interview. “They were consistent with our hypothesis that for some people, disordered eating may be used to cope with PTSD symptoms.”
She said the clinical implications of the study are direct. “It is important to assess eating habits and other potentially harmful coping strategies among patients with trauma histories and PTSD. On the other hand, it would be helpful to assess trauma histories in patients with eating disorders to determine if trauma reminders or other PTSD symptoms serve as a maintaining factor for the eating disorder.”
Dr. Mitchell and Dr. Wolf randomly selected 1,126 veterans who had reported trauma exposure in the GfK Knowledge Networks study (Depress Anxiety. 2013 May;30[5]:432-4), which looked at psychological resilience in a sample of U.S. veterans aged 60 and older. The veterans in the randomly selected group were asked to participate in a survey about PTSD, dissociation, and disordered eating, and 860 responded, 787 of whom were men (Psychiatry Res. 2016;243:23-9).
The participants’ age range was 22-96 years; mean age was 63. Most were white (85%) and married (77%), and had attended some college (87%).
Participants were asked to complete several surveys, including the Eating Disorder Diagnostic Scale (EDDS), the Yale Food Addiction Scale, the Emotion Regulation Questionnaire, and the National Stressful Events Survey (NSES).
The investigators said the sudden, unexpected death of a loved one (17.5%), and the aftermath of combat (13.6%) were cited as the worst traumatic experiences most cited by the participants. They also cited the violent death of a loved one (7.3%), the witnessing of dead bodies or body parts (6.3%), and physical or sexual assault (5.5%) as traumatic experiences.
Meanwhile, 23 participants (18 men [2.8%] and 5 women [9.1%]) met the criteria for bulimia nervosa; 20 met the criteria for binge eating disorder (16 men [2.5%] and 4 women [7.3%]); and 16 people (12 men [1.9%] and 4 women [7.3%]) met the proposed criteria for food addiction, reported Dr. Mitchell and Dr. Wolf, who also both are affiliated with the department of psychiatry at Boston University.
After analyzing the data, the researchers found that “the indirect path from PTSD to expressive suppression to [eating disorder] symptoms was significant in the full sample (P = .002; 95% confidence interval, 0.069-0.314) and in the male subsample (P = .029; 95% CI, 0.014-0.255).”
The researchers cited several limitations. For example, the participants’ diagnoses were not confirmed by interviews. In addition, “the validity of DSM-5 diagnoses using the EDDS and NSES has not yet been established,” they wrote.
Nevertheless, Dr. Mitchell and Dr. Wolf wrote, their findings highlight the importance of looking at eating disorders and food addiction in populations that traditionally have been underserved.
The study was funded by National Institutes of Health grant and an award from the Department of Veterans Affairs.
FROM PSYCHIATRY RESEARCH
Key clinical point: Older veterans with posttraumatic stress disorder might cope with their trauma symptoms by suppressing their emotions, and developing eating disorders and food addictions.
Major finding: The indirect path from PTSD to expressive suppression to [eating disorder] symptoms was significant in the full sample (P = .002; 95% confidence interval, 0.069-0.314) and in the male subsample” (P = .029; 95% CI, 0.014-0.255).
Data source: A subset of 1,126 veterans who had been selected to participate in the GfK Knowledge Networks study, which examined psychological resilience among U.S. veterans aged 60 and older.
Disclosures: The study was funded by a National Institutes of Health grant and an award from the Department of Veterans Affairs.
Let’s Dance: A Holistic Approach to Treating Veterans With Posttraumatic Stress Disorder
Dance holds value as a cathartic, therapeutic act.1 Dance and movement therapies may help reduce symptoms of several medical conditions and aid overall motor functioning. Studies have shown that they have been used to improve gait and balance in patients with Parkinson disease.2,3
Many theorists believe in the psychological healing power of dance/movement therapies, and researchers have begun to examine the ability of these therapies to enhance well-being and quality of life. Their findings suggest that dance fosters a sense of well-being, community, mastery, and joy.3-8 Bräuninger found that a 10-week dance/movement intervention reduced stress and improved social relations, general life satisfaction, and physical and psychological health.9 Other research has shown that subjective well-being is maintained through dance in elderly adults.10,11
Dance/movement also has been found helpful in reducing symptoms associated with several psychiatric conditions. Kline and colleagues reported that movement therapy reduced anxiety in populations with severe mental illness.12 Koch and colleagues found larger reductions on depression measures and higher vitality ratings in a dance intervention group compared with music-only and exercise groups.13 An approach integrating yoga and dance/movement was found to improve stress-management skills in people affected by several mental illnesses.14
Compared with the amount of data demonstrating that dance and movement are helpful treatment modalities for psychiatric conditions, there is relatively little empirical evidence that dance or movement is effective in treating posttraumatic stress disorder (PTSD). This is particularly surprising given the somatic or bodily nature of PTSD. Traumatic events trigger significant bodily reactions—flight, fight, or freeze reactions—and PTSD involves reexperiencing bodily sensations, such as hypervigilance, agitation, and elevated arousal.15 Although dance/movement has consistently been used to treat PTSD, the evidence for its effectiveness comes mainly from case studies.16 Further empirical studies are needed to determine whether dance/movement therapies are effective in treating PTSD.
Recently, as part of the VHA patient-centered, innovative care initiative, efforts have been made to augment treating disease with improving wellness and health. For example, the VA Greater Los Angeles Healthcare System (VAGLAHS) has supported Dance for Veterans (DFV), a dance/movement program that uses movement, creativity, relaxation, and social cohesion to treat veterans with serious mental illnesses. In a recent VAGLAHS study of the effect of DFV on patients with chronic schizophrenia, bipolar disorder, major depression, PTSD, and other serious mental illnesses, Wilbur and colleagues found a 25% decrease in stress, self-rated at the beginning and end of each class; in addition, veterans indicated they received long-term benefits from taking the class.17
This pilot study investigated the effectiveness of DFV as an adjunctive treatment for PTSD. The goal of the study was to assess whether the dance class helped reduce stress symptoms in veterans diagnosed with PTSD. As rates of PTSD are much higher in veterans than in the general population, the VA has taken particular interest in the diagnosis and has prioritized treatment of this disorder.18

Toward that end, the VA began a wide-scale national dissemination of 2 empirically validated PTSD-specific treatments: prolonged exposure therapy and cognitive processing therapy. These evidence-based therapies produce clinically significant reductions in PTSD symptoms among veterans.19,20 Nevertheless, concern exists about the dropout rates and tolerability of these manualized trauma-focused treatments.19,21 Patient-centered, integrative treatments are considered less demanding and more enjoyable, but there is little evidence of their effectiveness in PTSD treatment. The VA Los Angeles Ambulatory Care Center (LAACC) had been using DFV as an adjunct treatment for veterans diagnosed with PTSD. This pilot study examined whether participating in the program reduced veterans’ stress levels.
Methods
Development of DFV was a collaborative effort of members of the department of psychiatry at VAGLAHS, dancers in the community, and graduate students in the department of World Arts and Cultures/Dance at the University of California, Los Angeles (UCLA). The first class, in January 2011, was offered to patients in the Psychosocial Rehabilitation and Recovery Program at the West Los Angeles campus of VAGLAHS. The program quickly spread to LAACC, the Sepulveda Ambulatory Care Center, the East Los Angeles Clinic, and other VAGLAHS campuses.
The goals of DFV were to introduce techniques for stress management, enhance participants’ commitment to self-worth, increase participants’ faith in their physical capabilities, encourage focus and self-discipline, build confidence, have participants discover the value of learning new skills, challenge participants to use a variety of learning styles (eg, kinesthetic, aural, musical, visual), create opportunities for active watching and listening, decrease feelings of isolation, improve group (social) and personal awareness, cultivate expressive and emotional range, develop group trust, and improve large and small muscle coordination.22
Class Format
The DFV classes were standardized, and each week followed a consistent structure. Dance for Veterans is a 1-hour class that begins with a greeting and an expression of gratitude as represented by movements developed by individual class members. After listening to an introduction, the seated participants perform yogalike stretches that promote relaxation and improve flexibility. The stretches are followed by rhythm games. Participants repeat and change rhythms to the sounds of upbeat songs, thereby enhancing their observation and listening skills, creativity, and sense of mastery. Then, in Brain Dance, the middle part of the class, memory and coordination are challenged as participants learn a 7-part movement progression.23 Last is a group creative exploration call-and-response activity, usually a game in which the group coordinates participants’ names with their specific individual movements. Each participant says his or her name and creates an individual movement to represent himself or herself; the group then echoes that participant’s name and movement. This activity fosters group cohesion and creativity while improving attention, memory, and a sense of self-worth.
Instructor Training
The 12-week course of DFV classes was led by Dr. Steinberg-Oren and Dr. Krasnova as part of the LAACC general mental health program. The instructors received intensive training in DFV implementation from Sarah Wilbur, a doctoral student in the UCLA department of World Arts and Cultures/Dance and one of the founders of DFV. Training involved written materials and a half-day retreat. Ms. Wilbur modeled the class for 8 weeks. Then she observed the teachers and provided corrective feedback for another 4 weeks. After the 12-week training period, Ms. Wilbur attended class periodically to monitor how closely the instructors were following the prescribed class format and to provide helpful suggestions and new exercises.
Participants
Veterans receiving outpatient psychiatric care for PTSD at LAACC were recruited for the DFV class. They had undergone a thorough psychiatric interview and been found to meet the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM) criteria for PTSD. All underwent physical screening by a primary care provider to rule out preexisting medical conditions that would contraindicate taking the class. Participation was voluntary. Data analysis was approved by the institutional review board of VAGLAHCS.
Data Collection
Sixty-one veterans entered the class on a rolling basis from August 2012 to November 2014. At the participants first class, they completed a demographic questionnaire. For each of the first 12 sessions attended, they were asked to complete the State-Trait Anxiety Inventory (STAI) form Y before and immediately after class.24 The STAI is a self-report questionnaire that measures short-term state anxiety and long-term trait anxiety as characterized by tension, apprehension, nervousness, and worry. It lists the same 20 items twice, first for state anxiety and then for trait anxiety. This valid and reliable measure of generalized anxiety, which has been used in hundreds of research studies, has test–retest intervals ranging from 1 hour to more than 3 months.24,25 Veterans in the study were also asked to provide qualitative feedback on any mood or sense-of-self changes experienced from the time they entered class to once it was completed.
For data analysis, a final sample of 20 veterans was selected. These veterans had completed at least 12 preclass and postclass STAI ratings within the 4-month period. The other 41 veterans in the study were not included in the data analysis because of inconsistent attendance, tardiness, or leaving class without completing a questionnaire. Further, because a large amount of STAI trait data was missing, only state items were analyzed. The data of the veterans who completed their ratings were double-entered to minimize recording errors.
Of the 20 completers (all men), 7 (35%) were African American, 7 (35%) were Hispanic, 5 (25%) were white, and 1 (5%) declined to report race. Completers’ ages ranged from the 40s to the late 70s; 40% (the largest grouping) were between ages 60 and 69 years. Noncompleters’ demographic data were comparable. Of the 41 noncompleters, 14 (34%) were African American, 15 (37%) were Hispanic, 8 (19%) were white, and 4 (10%) were Asian or Pacific Islander. Noncompleters’ ages also ranged from the 40s to the late 70s, with the largest grouping (58%) between ages 60 and 69 years. Thus, the authors did not find any significant differences between completers and noncompleters.
Results
A mixed-effects linear model was used to assess whether participation length (in weeks), testing time (preclass vs postclass), or the interaction of these two variables were significant predictors of state anxiety as measured by STAI. This model included a random intercept by participant to account for differences in baseline stress levels. Analyses revealed a significant main effect of testing time on STAI state scores, t(458) = 7.48, P < .0001, such that class participation appeared to be associated with a mean decrease of 11 points on the state scale (Figure). However, participation length was not a significant predictor of STAI state scores, t(458) = 1.20, P = .233, and there was no interaction effect, t(458) = –0.57, P = .567.
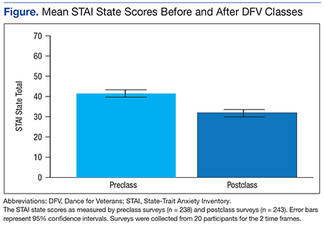
Qualitative Results
Study participants unanimously reported improvements in outlook, well-being, mood, sense of well-being, and interpersonal relationships as a result of taking the DFV class. The most commonly reported preclass–postclass change was an increased sense of camaraderie and belonging. Many participants also expressed reductions in anger and isolation as well as an increase in self/other acceptance. Participants’ comments about the DFV class included, “It makes me forget about everything, and I enjoy myself.” “It relaxes me, makes me smile.” “I’ve made new friends.” “When I came here and tried this group, I felt very nervous. But I came over and over. I am so much more at ease.” “I come to class upset, and I leave with a smile on my face.” “I enjoy the camaraderie. I feel I am part of something.” “The class is helping me by body movement: moving my arms and legs—my attitude just changes.” “It’s a lot of fun!”
Discussion
This hypothesis-generating study examined whether an adjunctive, holistic intervention (dance class) could reduce stress in veterans with PTSD. Results showed significant reductions in state stress levels after DFV class participation. The finding of a significant effect of short-term reduction in state stress levels corroborates the findings from Wilbur and colleagues but with use of a comprehensive, reliable, well-validated measure of stress.17,24,25 This study’s qualitative results are also consistent with the prior qualitative data suggesting improvements in social connection and sense of well-being.
Some experts believe that PTSD-associated symptoms are fairly intractable and that trauma-focused treatments are required to reduce symptoms and promote a sense of well-being. This study did not show sustained reductions in stress levels across class sessions. Nevertheless, the significant state stress reductions that occurred after class suggest that this dance/movement intervention is a helpful adjunctive treatment for enhancing well-being, at least temporarily, in veterans with PTSD. The findings also suggest that veterans can benefit from a single session and need not attend class regularly to see results. Thus, DFV shows promise even on a drop-in basis. Overall, the results of this study provide further impetus to develop and provide more holistic, arts-based programs for veterans diagnosed with PTSD.
Study Limitations
At the beginning of this study, the authors did not expect strong participation of male veterans in a dance class. Surprisingly, 61 veterans enrolled over a period of 2 years 3 months. Nevertheless, the research sample was small, as empirical difficulties were encountered secondary to veterans’ inconsistent attendance and failure to complete ratings in a consistent and timely manner. Therefore, the sample may not have been representative. Research is needed to validate and expand the findings of this study.
Another methodologic concern was lack of a control group. Future studies might use a no-intervention control group and/or comparison groups, including support, meditation, and trauma-focused groups. In addition, veterans were not blinded to the intervention, and the STAI is a self-report survey with face-valid items. Thus, participants may have tried to please the instructors, bringing into question how much social desirability may have accounted for the reductions in stress levels.
The authors also did not examine confounding variables with regard to additional mental health treatments. It would have been helpful to address whether stress reductions were larger for veterans who were also receiving psychiatric medications and/or participating in other mental health groups or individual psychotherapies. The effect of comorbid diagnoses on the reduction in state stress levels also was not examined. Last, the authors did not investigate actual PTSD symptoms (eg, flashbacks, nightmares, hypervigilance, and avoidance). Further studies are needed to measure reductions on the PTSD Checklist for DSM 5 or on other empirical measures of PTSD as a consequence of this class in order to examine its effectiveness in reducing PTSD symptoms.
Qualitative responses from the veterans suggested that DFV promoted quality-of-life and well-being improvements. It would be helpful to assess this quantitatively through control or comparison group studies using measurements that minimize face validity. To understand the mechanism by which this class is effective, research also needs to examine what class-related factors are most effective in promoting positive change. The qualitative data provide glimpses into these factors, but empirical investigation could provide substantive proof of what specific factors are therapeutic.
Conclusion
The VHA has introduced several integrative adjunctive PTSD treatments, including dance, tai chi, mindfulness meditation, breathing/stretching/relaxation, yoga, healing touch, and others with the goal of maximizing veterans’ physical and psychological wellness. Although it seems unlikely that integrative once-a-week treatments lead to sustained reductions in PTSD and other serious psychiatric conditions, it is possible that participating in DFV classes more regularly, as part of adjunctive treatment, could promote a sustained sense of well-being, self-compassion, self-confidence, and sense of belonging. The question still remains whether such programs are effective in promoting well-being. The present study was not conclusive enough to substantiate that claim, but it represents a small step (a dance step) in the right direction, toward a holistic, creative, and well-rounded approach to the treatment of PTSD in veterans.
Acknowledgments
The authors thank the many people involved in Dance for Veterans. Robert Rubin, MD, had the creative foresight to assemble the program; Donna Ames, MD, invited her coauthors to undergo training and provided them with research support; Sarah Wilbur, PhD, (program in Culture and Performance, Department of World Arts and Cultures/Dance, University of California, Los Angeles) developed the class and handbook as well as showed the authors how to run it; Sandra Robertson, RN, MSN, PH-CNS, (principal investigator, Integrative Health and Healing Project, VA T21 Center of Innovation Grant for Patient-Centered Care) provided the funding and initiative to develop and implement the class; and (Christine Suarez Suarez Dance Theatre, Santa Monica, California) developed the class and the handbook and trained instructors.
The authors also thank all the VAGLAHS veterans and staff for their help with the class—especially Andrea Serafin, LCSW; Rosie Dominguez, LCSW; Retha de Johnette, LCSW; and Donna Ames, MD, all part of the Psychosocial Rehabilitation and Recovery Programs; Dana Melching, LCSW, Mental Health Intensive Case Management; and Vanessa Baumann, PhD (Vet Center).
1. Levy FJ. Dance/Movement Therapy: A Healing Art. Reston, VA: American Alliance for Health, Physical Education, Recreation, and Dance; 1992.
2. Marigold DS, Misiaszek JE. Whole-body responses: neural control and implications for rehabilitation and fall prevention. Neuroscientist. 2009;15(1):36-46.
3. Hackney ME, Kantorovich S, Levin R, Earhart GM. Effects of tango on functional mobility in Parkinson's disease: a preliminary study. J Neurol Phys Ther. 2007;31(4):173-179.
4. Ravelin T, Kylmä J, Korhonen T. Dance in mental health nursing: a hybrid concept analysis. Issues Ment Health Nurs. 2006;27(3):307-317.
5. Hackney ME, Earhart GM. Effects of dance on gait and balance in Parkinson's disease: a comparison of partnered and nonpartnered dance movement. Neurorehabil Neural Repair. 2010;24(4):384-392.
6. Heiberger L, Maurer C, Amtage F, et al. Impact of a weekly dance class on the functional mobility and on the quality of life of individuals with Parkinson's disease. Front Aging Neurosci. 2011;3:14.
7. Houston S, McGill A. A mixed-methods study into ballet for people living with Parkinson's. Arts Health. 2013;5(2):103-119.
8. Westheimer O. Why dance for Parkinson's disease. Top Geriatr Rehabil. 2008;24(2):127-140.
9. Bräuninger I. Dance movement therapy group intervention in stress treatment: a randomized controlled trial (RCT). Arts Psychother. 2012;39(5):443-450.
10. Kattenstroth, JC, Kalisch T, Holt S, Tegenthoff M, Dinse HR. Six months of dance intervention enhances postural, sensorimotor, and cognitive performance in elderly without affecting cardio-respiratory functions. Front Aging Neurosci. 2013;5:5.
11. Kattenstroth J-C, Kolankowska I, Kalisch T, Dinse HR. Superior sensory, motor, and cognitive performance in elderly individuals with multi-year dancing activities. Front Aging Neurosci. 2010;2:31.
12. Kline F, Burgoyne RW, Staples F, Moredock P, Snyder V, Ioerger M. A report on the use of movement therapy for chronic, severely disabled outpatients. Arts Psychother. 1977;4(4-5):181-183.
13. Koch SC, Morlinghaus K, Fuchs T. The joy dance: specific effects of a single dance intervention on psychiatric patients with depression. Arts Psychother. 2007;34(4):340-349.
14. Barton EJ. Movement and mindfulness: a formative evaluation of a dance/movement and yoga therapy program with participants experiencing severe mental illness. Am J Dance Ther. 2011;33(2):157-181.
15. van der Kolk BA, McFarlane AC, Weisaeth L, eds. Traumatic Stress: The Effects of Overwhelming Experience on Mind, Body, and Society. New York, NY: Guilford Press; 1996.
16. Foa EB, Keane TM, Friedman MJ, Cohen JA, eds. Effective Treatments for PTSD: Practice Guidelines From the International Society for Traumatic Stress Studies. 2nd ed. New York, NY: Guilford Press; 2009.
17. Wilbur S, Meyer HB, Baker MR, et al. Dance for Veterans: a complementary health program for veterans with serious mental illness. Arts Health. 2015;7(2):96-108.
18. Gradus JL. Epidemiology of PTSD. U.S. Department of Veterans Affairs, PTSD: National Center for PTSD website. http://www.ptsd.va.gov/professional/PTSD-overview/epidemiological-facts-ptsd.asp. Published January 30, 2014. Accessed August 20, 2015.
19. Eftekhari A, Ruzek JI, Crowley JJ, Rosen CS, Greenbaum MA, Karlin BE. Effectiveness of national implementation of prolonged exposure therapy in Veterans Affairs care. JAMA Psychiatry. 2013;70(9):949-955.
20. Monson CM, Schnurr PP, Resick PA, Friedman MJ, Young-Xu Y, Stevens SP. Cognitive processing therapy for veterans with military-related posttraumatic stress disorder. J Consult Clin Psychol. 2006;74(5):898-907.
21. Schottenbauer MA, Glass CR, Arnkoff DB, Tendick V, Gray SH. Nonresponse and dropout rates in outcome studies on PTSD: review and methodological considerations. Psychiatry. 2008;71(2):134-168.
22. Suarez CA, Wilbur S, Smiarowski K, Rubin RT, Ames D. Dance for Veterans: Music, Movement & Rhythm Manual for Instruction. 2nd ed. Publisher unknown; 2014.
23. Gilbert AG, Gilbert BA, Rossano A. Brain-Compatible Dance Education. Reston, VA: National Dance Association; 2006.
24. Spielberger C. Manual for the State-Trait Anxiety Inventory. Rev ed. Palo Alto, CA: Consulting Psychologists Press; 1983.
25. Julian LJ. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res. 2011;63(suppl 11):S467-S472.
Dance holds value as a cathartic, therapeutic act.1 Dance and movement therapies may help reduce symptoms of several medical conditions and aid overall motor functioning. Studies have shown that they have been used to improve gait and balance in patients with Parkinson disease.2,3
Many theorists believe in the psychological healing power of dance/movement therapies, and researchers have begun to examine the ability of these therapies to enhance well-being and quality of life. Their findings suggest that dance fosters a sense of well-being, community, mastery, and joy.3-8 Bräuninger found that a 10-week dance/movement intervention reduced stress and improved social relations, general life satisfaction, and physical and psychological health.9 Other research has shown that subjective well-being is maintained through dance in elderly adults.10,11
Dance/movement also has been found helpful in reducing symptoms associated with several psychiatric conditions. Kline and colleagues reported that movement therapy reduced anxiety in populations with severe mental illness.12 Koch and colleagues found larger reductions on depression measures and higher vitality ratings in a dance intervention group compared with music-only and exercise groups.13 An approach integrating yoga and dance/movement was found to improve stress-management skills in people affected by several mental illnesses.14
Compared with the amount of data demonstrating that dance and movement are helpful treatment modalities for psychiatric conditions, there is relatively little empirical evidence that dance or movement is effective in treating posttraumatic stress disorder (PTSD). This is particularly surprising given the somatic or bodily nature of PTSD. Traumatic events trigger significant bodily reactions—flight, fight, or freeze reactions—and PTSD involves reexperiencing bodily sensations, such as hypervigilance, agitation, and elevated arousal.15 Although dance/movement has consistently been used to treat PTSD, the evidence for its effectiveness comes mainly from case studies.16 Further empirical studies are needed to determine whether dance/movement therapies are effective in treating PTSD.
Recently, as part of the VHA patient-centered, innovative care initiative, efforts have been made to augment treating disease with improving wellness and health. For example, the VA Greater Los Angeles Healthcare System (VAGLAHS) has supported Dance for Veterans (DFV), a dance/movement program that uses movement, creativity, relaxation, and social cohesion to treat veterans with serious mental illnesses. In a recent VAGLAHS study of the effect of DFV on patients with chronic schizophrenia, bipolar disorder, major depression, PTSD, and other serious mental illnesses, Wilbur and colleagues found a 25% decrease in stress, self-rated at the beginning and end of each class; in addition, veterans indicated they received long-term benefits from taking the class.17
This pilot study investigated the effectiveness of DFV as an adjunctive treatment for PTSD. The goal of the study was to assess whether the dance class helped reduce stress symptoms in veterans diagnosed with PTSD. As rates of PTSD are much higher in veterans than in the general population, the VA has taken particular interest in the diagnosis and has prioritized treatment of this disorder.18
Toward that end, the VA began a wide-scale national dissemination of 2 empirically validated PTSD-specific treatments: prolonged exposure therapy and cognitive processing therapy. These evidence-based therapies produce clinically significant reductions in PTSD symptoms among veterans.19,20 Nevertheless, concern exists about the dropout rates and tolerability of these manualized trauma-focused treatments.19,21 Patient-centered, integrative treatments are considered less demanding and more enjoyable, but there is little evidence of their effectiveness in PTSD treatment. The VA Los Angeles Ambulatory Care Center (LAACC) had been using DFV as an adjunct treatment for veterans diagnosed with PTSD. This pilot study examined whether participating in the program reduced veterans’ stress levels.
Methods
Development of DFV was a collaborative effort of members of the department of psychiatry at VAGLAHS, dancers in the community, and graduate students in the department of World Arts and Cultures/Dance at the University of California, Los Angeles (UCLA). The first class, in January 2011, was offered to patients in the Psychosocial Rehabilitation and Recovery Program at the West Los Angeles campus of VAGLAHS. The program quickly spread to LAACC, the Sepulveda Ambulatory Care Center, the East Los Angeles Clinic, and other VAGLAHS campuses.
The goals of DFV were to introduce techniques for stress management, enhance participants’ commitment to self-worth, increase participants’ faith in their physical capabilities, encourage focus and self-discipline, build confidence, have participants discover the value of learning new skills, challenge participants to use a variety of learning styles (eg, kinesthetic, aural, musical, visual), create opportunities for active watching and listening, decrease feelings of isolation, improve group (social) and personal awareness, cultivate expressive and emotional range, develop group trust, and improve large and small muscle coordination.22
Class Format
The DFV classes were standardized, and each week followed a consistent structure. Dance for Veterans is a 1-hour class that begins with a greeting and an expression of gratitude as represented by movements developed by individual class members. After listening to an introduction, the seated participants perform yogalike stretches that promote relaxation and improve flexibility. The stretches are followed by rhythm games. Participants repeat and change rhythms to the sounds of upbeat songs, thereby enhancing their observation and listening skills, creativity, and sense of mastery. Then, in Brain Dance, the middle part of the class, memory and coordination are challenged as participants learn a 7-part movement progression.23 Last is a group creative exploration call-and-response activity, usually a game in which the group coordinates participants’ names with their specific individual movements. Each participant says his or her name and creates an individual movement to represent himself or herself; the group then echoes that participant’s name and movement. This activity fosters group cohesion and creativity while improving attention, memory, and a sense of self-worth.
Instructor Training
The 12-week course of DFV classes was led by Dr. Steinberg-Oren and Dr. Krasnova as part of the LAACC general mental health program. The instructors received intensive training in DFV implementation from Sarah Wilbur, a doctoral student in the UCLA department of World Arts and Cultures/Dance and one of the founders of DFV. Training involved written materials and a half-day retreat. Ms. Wilbur modeled the class for 8 weeks. Then she observed the teachers and provided corrective feedback for another 4 weeks. After the 12-week training period, Ms. Wilbur attended class periodically to monitor how closely the instructors were following the prescribed class format and to provide helpful suggestions and new exercises.
Participants
Veterans receiving outpatient psychiatric care for PTSD at LAACC were recruited for the DFV class. They had undergone a thorough psychiatric interview and been found to meet the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM) criteria for PTSD. All underwent physical screening by a primary care provider to rule out preexisting medical conditions that would contraindicate taking the class. Participation was voluntary. Data analysis was approved by the institutional review board of VAGLAHCS.
Data Collection
Sixty-one veterans entered the class on a rolling basis from August 2012 to November 2014. At the participants first class, they completed a demographic questionnaire. For each of the first 12 sessions attended, they were asked to complete the State-Trait Anxiety Inventory (STAI) form Y before and immediately after class.24 The STAI is a self-report questionnaire that measures short-term state anxiety and long-term trait anxiety as characterized by tension, apprehension, nervousness, and worry. It lists the same 20 items twice, first for state anxiety and then for trait anxiety. This valid and reliable measure of generalized anxiety, which has been used in hundreds of research studies, has test–retest intervals ranging from 1 hour to more than 3 months.24,25 Veterans in the study were also asked to provide qualitative feedback on any mood or sense-of-self changes experienced from the time they entered class to once it was completed.
For data analysis, a final sample of 20 veterans was selected. These veterans had completed at least 12 preclass and postclass STAI ratings within the 4-month period. The other 41 veterans in the study were not included in the data analysis because of inconsistent attendance, tardiness, or leaving class without completing a questionnaire. Further, because a large amount of STAI trait data was missing, only state items were analyzed. The data of the veterans who completed their ratings were double-entered to minimize recording errors.
Of the 20 completers (all men), 7 (35%) were African American, 7 (35%) were Hispanic, 5 (25%) were white, and 1 (5%) declined to report race. Completers’ ages ranged from the 40s to the late 70s; 40% (the largest grouping) were between ages 60 and 69 years. Noncompleters’ demographic data were comparable. Of the 41 noncompleters, 14 (34%) were African American, 15 (37%) were Hispanic, 8 (19%) were white, and 4 (10%) were Asian or Pacific Islander. Noncompleters’ ages also ranged from the 40s to the late 70s, with the largest grouping (58%) between ages 60 and 69 years. Thus, the authors did not find any significant differences between completers and noncompleters.
Results
A mixed-effects linear model was used to assess whether participation length (in weeks), testing time (preclass vs postclass), or the interaction of these two variables were significant predictors of state anxiety as measured by STAI. This model included a random intercept by participant to account for differences in baseline stress levels. Analyses revealed a significant main effect of testing time on STAI state scores, t(458) = 7.48, P < .0001, such that class participation appeared to be associated with a mean decrease of 11 points on the state scale (Figure). However, participation length was not a significant predictor of STAI state scores, t(458) = 1.20, P = .233, and there was no interaction effect, t(458) = –0.57, P = .567.
Qualitative Results
Study participants unanimously reported improvements in outlook, well-being, mood, sense of well-being, and interpersonal relationships as a result of taking the DFV class. The most commonly reported preclass–postclass change was an increased sense of camaraderie and belonging. Many participants also expressed reductions in anger and isolation as well as an increase in self/other acceptance. Participants’ comments about the DFV class included, “It makes me forget about everything, and I enjoy myself.” “It relaxes me, makes me smile.” “I’ve made new friends.” “When I came here and tried this group, I felt very nervous. But I came over and over. I am so much more at ease.” “I come to class upset, and I leave with a smile on my face.” “I enjoy the camaraderie. I feel I am part of something.” “The class is helping me by body movement: moving my arms and legs—my attitude just changes.” “It’s a lot of fun!”
Discussion
This hypothesis-generating study examined whether an adjunctive, holistic intervention (dance class) could reduce stress in veterans with PTSD. Results showed significant reductions in state stress levels after DFV class participation. The finding of a significant effect of short-term reduction in state stress levels corroborates the findings from Wilbur and colleagues but with use of a comprehensive, reliable, well-validated measure of stress.17,24,25 This study’s qualitative results are also consistent with the prior qualitative data suggesting improvements in social connection and sense of well-being.
Some experts believe that PTSD-associated symptoms are fairly intractable and that trauma-focused treatments are required to reduce symptoms and promote a sense of well-being. This study did not show sustained reductions in stress levels across class sessions. Nevertheless, the significant state stress reductions that occurred after class suggest that this dance/movement intervention is a helpful adjunctive treatment for enhancing well-being, at least temporarily, in veterans with PTSD. The findings also suggest that veterans can benefit from a single session and need not attend class regularly to see results. Thus, DFV shows promise even on a drop-in basis. Overall, the results of this study provide further impetus to develop and provide more holistic, arts-based programs for veterans diagnosed with PTSD.
Study Limitations
At the beginning of this study, the authors did not expect strong participation of male veterans in a dance class. Surprisingly, 61 veterans enrolled over a period of 2 years 3 months. Nevertheless, the research sample was small, as empirical difficulties were encountered secondary to veterans’ inconsistent attendance and failure to complete ratings in a consistent and timely manner. Therefore, the sample may not have been representative. Research is needed to validate and expand the findings of this study.
Another methodologic concern was lack of a control group. Future studies might use a no-intervention control group and/or comparison groups, including support, meditation, and trauma-focused groups. In addition, veterans were not blinded to the intervention, and the STAI is a self-report survey with face-valid items. Thus, participants may have tried to please the instructors, bringing into question how much social desirability may have accounted for the reductions in stress levels.
The authors also did not examine confounding variables with regard to additional mental health treatments. It would have been helpful to address whether stress reductions were larger for veterans who were also receiving psychiatric medications and/or participating in other mental health groups or individual psychotherapies. The effect of comorbid diagnoses on the reduction in state stress levels also was not examined. Last, the authors did not investigate actual PTSD symptoms (eg, flashbacks, nightmares, hypervigilance, and avoidance). Further studies are needed to measure reductions on the PTSD Checklist for DSM 5 or on other empirical measures of PTSD as a consequence of this class in order to examine its effectiveness in reducing PTSD symptoms.
Qualitative responses from the veterans suggested that DFV promoted quality-of-life and well-being improvements. It would be helpful to assess this quantitatively through control or comparison group studies using measurements that minimize face validity. To understand the mechanism by which this class is effective, research also needs to examine what class-related factors are most effective in promoting positive change. The qualitative data provide glimpses into these factors, but empirical investigation could provide substantive proof of what specific factors are therapeutic.
Conclusion
The VHA has introduced several integrative adjunctive PTSD treatments, including dance, tai chi, mindfulness meditation, breathing/stretching/relaxation, yoga, healing touch, and others with the goal of maximizing veterans’ physical and psychological wellness. Although it seems unlikely that integrative once-a-week treatments lead to sustained reductions in PTSD and other serious psychiatric conditions, it is possible that participating in DFV classes more regularly, as part of adjunctive treatment, could promote a sustained sense of well-being, self-compassion, self-confidence, and sense of belonging. The question still remains whether such programs are effective in promoting well-being. The present study was not conclusive enough to substantiate that claim, but it represents a small step (a dance step) in the right direction, toward a holistic, creative, and well-rounded approach to the treatment of PTSD in veterans.
Acknowledgments
The authors thank the many people involved in Dance for Veterans. Robert Rubin, MD, had the creative foresight to assemble the program; Donna Ames, MD, invited her coauthors to undergo training and provided them with research support; Sarah Wilbur, PhD, (program in Culture and Performance, Department of World Arts and Cultures/Dance, University of California, Los Angeles) developed the class and handbook as well as showed the authors how to run it; Sandra Robertson, RN, MSN, PH-CNS, (principal investigator, Integrative Health and Healing Project, VA T21 Center of Innovation Grant for Patient-Centered Care) provided the funding and initiative to develop and implement the class; and (Christine Suarez Suarez Dance Theatre, Santa Monica, California) developed the class and the handbook and trained instructors.
The authors also thank all the VAGLAHS veterans and staff for their help with the class—especially Andrea Serafin, LCSW; Rosie Dominguez, LCSW; Retha de Johnette, LCSW; and Donna Ames, MD, all part of the Psychosocial Rehabilitation and Recovery Programs; Dana Melching, LCSW, Mental Health Intensive Case Management; and Vanessa Baumann, PhD (Vet Center).
Dance holds value as a cathartic, therapeutic act.1 Dance and movement therapies may help reduce symptoms of several medical conditions and aid overall motor functioning. Studies have shown that they have been used to improve gait and balance in patients with Parkinson disease.2,3
Many theorists believe in the psychological healing power of dance/movement therapies, and researchers have begun to examine the ability of these therapies to enhance well-being and quality of life. Their findings suggest that dance fosters a sense of well-being, community, mastery, and joy.3-8 Bräuninger found that a 10-week dance/movement intervention reduced stress and improved social relations, general life satisfaction, and physical and psychological health.9 Other research has shown that subjective well-being is maintained through dance in elderly adults.10,11
Dance/movement also has been found helpful in reducing symptoms associated with several psychiatric conditions. Kline and colleagues reported that movement therapy reduced anxiety in populations with severe mental illness.12 Koch and colleagues found larger reductions on depression measures and higher vitality ratings in a dance intervention group compared with music-only and exercise groups.13 An approach integrating yoga and dance/movement was found to improve stress-management skills in people affected by several mental illnesses.14
Compared with the amount of data demonstrating that dance and movement are helpful treatment modalities for psychiatric conditions, there is relatively little empirical evidence that dance or movement is effective in treating posttraumatic stress disorder (PTSD). This is particularly surprising given the somatic or bodily nature of PTSD. Traumatic events trigger significant bodily reactions—flight, fight, or freeze reactions—and PTSD involves reexperiencing bodily sensations, such as hypervigilance, agitation, and elevated arousal.15 Although dance/movement has consistently been used to treat PTSD, the evidence for its effectiveness comes mainly from case studies.16 Further empirical studies are needed to determine whether dance/movement therapies are effective in treating PTSD.
Recently, as part of the VHA patient-centered, innovative care initiative, efforts have been made to augment treating disease with improving wellness and health. For example, the VA Greater Los Angeles Healthcare System (VAGLAHS) has supported Dance for Veterans (DFV), a dance/movement program that uses movement, creativity, relaxation, and social cohesion to treat veterans with serious mental illnesses. In a recent VAGLAHS study of the effect of DFV on patients with chronic schizophrenia, bipolar disorder, major depression, PTSD, and other serious mental illnesses, Wilbur and colleagues found a 25% decrease in stress, self-rated at the beginning and end of each class; in addition, veterans indicated they received long-term benefits from taking the class.17
This pilot study investigated the effectiveness of DFV as an adjunctive treatment for PTSD. The goal of the study was to assess whether the dance class helped reduce stress symptoms in veterans diagnosed with PTSD. As rates of PTSD are much higher in veterans than in the general population, the VA has taken particular interest in the diagnosis and has prioritized treatment of this disorder.18
Toward that end, the VA began a wide-scale national dissemination of 2 empirically validated PTSD-specific treatments: prolonged exposure therapy and cognitive processing therapy. These evidence-based therapies produce clinically significant reductions in PTSD symptoms among veterans.19,20 Nevertheless, concern exists about the dropout rates and tolerability of these manualized trauma-focused treatments.19,21 Patient-centered, integrative treatments are considered less demanding and more enjoyable, but there is little evidence of their effectiveness in PTSD treatment. The VA Los Angeles Ambulatory Care Center (LAACC) had been using DFV as an adjunct treatment for veterans diagnosed with PTSD. This pilot study examined whether participating in the program reduced veterans’ stress levels.
Methods
Development of DFV was a collaborative effort of members of the department of psychiatry at VAGLAHS, dancers in the community, and graduate students in the department of World Arts and Cultures/Dance at the University of California, Los Angeles (UCLA). The first class, in January 2011, was offered to patients in the Psychosocial Rehabilitation and Recovery Program at the West Los Angeles campus of VAGLAHS. The program quickly spread to LAACC, the Sepulveda Ambulatory Care Center, the East Los Angeles Clinic, and other VAGLAHS campuses.
The goals of DFV were to introduce techniques for stress management, enhance participants’ commitment to self-worth, increase participants’ faith in their physical capabilities, encourage focus and self-discipline, build confidence, have participants discover the value of learning new skills, challenge participants to use a variety of learning styles (eg, kinesthetic, aural, musical, visual), create opportunities for active watching and listening, decrease feelings of isolation, improve group (social) and personal awareness, cultivate expressive and emotional range, develop group trust, and improve large and small muscle coordination.22
Class Format
The DFV classes were standardized, and each week followed a consistent structure. Dance for Veterans is a 1-hour class that begins with a greeting and an expression of gratitude as represented by movements developed by individual class members. After listening to an introduction, the seated participants perform yogalike stretches that promote relaxation and improve flexibility. The stretches are followed by rhythm games. Participants repeat and change rhythms to the sounds of upbeat songs, thereby enhancing their observation and listening skills, creativity, and sense of mastery. Then, in Brain Dance, the middle part of the class, memory and coordination are challenged as participants learn a 7-part movement progression.23 Last is a group creative exploration call-and-response activity, usually a game in which the group coordinates participants’ names with their specific individual movements. Each participant says his or her name and creates an individual movement to represent himself or herself; the group then echoes that participant’s name and movement. This activity fosters group cohesion and creativity while improving attention, memory, and a sense of self-worth.
Instructor Training
The 12-week course of DFV classes was led by Dr. Steinberg-Oren and Dr. Krasnova as part of the LAACC general mental health program. The instructors received intensive training in DFV implementation from Sarah Wilbur, a doctoral student in the UCLA department of World Arts and Cultures/Dance and one of the founders of DFV. Training involved written materials and a half-day retreat. Ms. Wilbur modeled the class for 8 weeks. Then she observed the teachers and provided corrective feedback for another 4 weeks. After the 12-week training period, Ms. Wilbur attended class periodically to monitor how closely the instructors were following the prescribed class format and to provide helpful suggestions and new exercises.
Participants
Veterans receiving outpatient psychiatric care for PTSD at LAACC were recruited for the DFV class. They had undergone a thorough psychiatric interview and been found to meet the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM) criteria for PTSD. All underwent physical screening by a primary care provider to rule out preexisting medical conditions that would contraindicate taking the class. Participation was voluntary. Data analysis was approved by the institutional review board of VAGLAHCS.
Data Collection
Sixty-one veterans entered the class on a rolling basis from August 2012 to November 2014. At the participants first class, they completed a demographic questionnaire. For each of the first 12 sessions attended, they were asked to complete the State-Trait Anxiety Inventory (STAI) form Y before and immediately after class.24 The STAI is a self-report questionnaire that measures short-term state anxiety and long-term trait anxiety as characterized by tension, apprehension, nervousness, and worry. It lists the same 20 items twice, first for state anxiety and then for trait anxiety. This valid and reliable measure of generalized anxiety, which has been used in hundreds of research studies, has test–retest intervals ranging from 1 hour to more than 3 months.24,25 Veterans in the study were also asked to provide qualitative feedback on any mood or sense-of-self changes experienced from the time they entered class to once it was completed.
For data analysis, a final sample of 20 veterans was selected. These veterans had completed at least 12 preclass and postclass STAI ratings within the 4-month period. The other 41 veterans in the study were not included in the data analysis because of inconsistent attendance, tardiness, or leaving class without completing a questionnaire. Further, because a large amount of STAI trait data was missing, only state items were analyzed. The data of the veterans who completed their ratings were double-entered to minimize recording errors.
Of the 20 completers (all men), 7 (35%) were African American, 7 (35%) were Hispanic, 5 (25%) were white, and 1 (5%) declined to report race. Completers’ ages ranged from the 40s to the late 70s; 40% (the largest grouping) were between ages 60 and 69 years. Noncompleters’ demographic data were comparable. Of the 41 noncompleters, 14 (34%) were African American, 15 (37%) were Hispanic, 8 (19%) were white, and 4 (10%) were Asian or Pacific Islander. Noncompleters’ ages also ranged from the 40s to the late 70s, with the largest grouping (58%) between ages 60 and 69 years. Thus, the authors did not find any significant differences between completers and noncompleters.
Results
A mixed-effects linear model was used to assess whether participation length (in weeks), testing time (preclass vs postclass), or the interaction of these two variables were significant predictors of state anxiety as measured by STAI. This model included a random intercept by participant to account for differences in baseline stress levels. Analyses revealed a significant main effect of testing time on STAI state scores, t(458) = 7.48, P < .0001, such that class participation appeared to be associated with a mean decrease of 11 points on the state scale (Figure). However, participation length was not a significant predictor of STAI state scores, t(458) = 1.20, P = .233, and there was no interaction effect, t(458) = –0.57, P = .567.
Qualitative Results
Study participants unanimously reported improvements in outlook, well-being, mood, sense of well-being, and interpersonal relationships as a result of taking the DFV class. The most commonly reported preclass–postclass change was an increased sense of camaraderie and belonging. Many participants also expressed reductions in anger and isolation as well as an increase in self/other acceptance. Participants’ comments about the DFV class included, “It makes me forget about everything, and I enjoy myself.” “It relaxes me, makes me smile.” “I’ve made new friends.” “When I came here and tried this group, I felt very nervous. But I came over and over. I am so much more at ease.” “I come to class upset, and I leave with a smile on my face.” “I enjoy the camaraderie. I feel I am part of something.” “The class is helping me by body movement: moving my arms and legs—my attitude just changes.” “It’s a lot of fun!”
Discussion
This hypothesis-generating study examined whether an adjunctive, holistic intervention (dance class) could reduce stress in veterans with PTSD. Results showed significant reductions in state stress levels after DFV class participation. The finding of a significant effect of short-term reduction in state stress levels corroborates the findings from Wilbur and colleagues but with use of a comprehensive, reliable, well-validated measure of stress.17,24,25 This study’s qualitative results are also consistent with the prior qualitative data suggesting improvements in social connection and sense of well-being.
Some experts believe that PTSD-associated symptoms are fairly intractable and that trauma-focused treatments are required to reduce symptoms and promote a sense of well-being. This study did not show sustained reductions in stress levels across class sessions. Nevertheless, the significant state stress reductions that occurred after class suggest that this dance/movement intervention is a helpful adjunctive treatment for enhancing well-being, at least temporarily, in veterans with PTSD. The findings also suggest that veterans can benefit from a single session and need not attend class regularly to see results. Thus, DFV shows promise even on a drop-in basis. Overall, the results of this study provide further impetus to develop and provide more holistic, arts-based programs for veterans diagnosed with PTSD.
Study Limitations
At the beginning of this study, the authors did not expect strong participation of male veterans in a dance class. Surprisingly, 61 veterans enrolled over a period of 2 years 3 months. Nevertheless, the research sample was small, as empirical difficulties were encountered secondary to veterans’ inconsistent attendance and failure to complete ratings in a consistent and timely manner. Therefore, the sample may not have been representative. Research is needed to validate and expand the findings of this study.
Another methodologic concern was lack of a control group. Future studies might use a no-intervention control group and/or comparison groups, including support, meditation, and trauma-focused groups. In addition, veterans were not blinded to the intervention, and the STAI is a self-report survey with face-valid items. Thus, participants may have tried to please the instructors, bringing into question how much social desirability may have accounted for the reductions in stress levels.
The authors also did not examine confounding variables with regard to additional mental health treatments. It would have been helpful to address whether stress reductions were larger for veterans who were also receiving psychiatric medications and/or participating in other mental health groups or individual psychotherapies. The effect of comorbid diagnoses on the reduction in state stress levels also was not examined. Last, the authors did not investigate actual PTSD symptoms (eg, flashbacks, nightmares, hypervigilance, and avoidance). Further studies are needed to measure reductions on the PTSD Checklist for DSM 5 or on other empirical measures of PTSD as a consequence of this class in order to examine its effectiveness in reducing PTSD symptoms.
Qualitative responses from the veterans suggested that DFV promoted quality-of-life and well-being improvements. It would be helpful to assess this quantitatively through control or comparison group studies using measurements that minimize face validity. To understand the mechanism by which this class is effective, research also needs to examine what class-related factors are most effective in promoting positive change. The qualitative data provide glimpses into these factors, but empirical investigation could provide substantive proof of what specific factors are therapeutic.
Conclusion
The VHA has introduced several integrative adjunctive PTSD treatments, including dance, tai chi, mindfulness meditation, breathing/stretching/relaxation, yoga, healing touch, and others with the goal of maximizing veterans’ physical and psychological wellness. Although it seems unlikely that integrative once-a-week treatments lead to sustained reductions in PTSD and other serious psychiatric conditions, it is possible that participating in DFV classes more regularly, as part of adjunctive treatment, could promote a sustained sense of well-being, self-compassion, self-confidence, and sense of belonging. The question still remains whether such programs are effective in promoting well-being. The present study was not conclusive enough to substantiate that claim, but it represents a small step (a dance step) in the right direction, toward a holistic, creative, and well-rounded approach to the treatment of PTSD in veterans.
Acknowledgments
The authors thank the many people involved in Dance for Veterans. Robert Rubin, MD, had the creative foresight to assemble the program; Donna Ames, MD, invited her coauthors to undergo training and provided them with research support; Sarah Wilbur, PhD, (program in Culture and Performance, Department of World Arts and Cultures/Dance, University of California, Los Angeles) developed the class and handbook as well as showed the authors how to run it; Sandra Robertson, RN, MSN, PH-CNS, (principal investigator, Integrative Health and Healing Project, VA T21 Center of Innovation Grant for Patient-Centered Care) provided the funding and initiative to develop and implement the class; and (Christine Suarez Suarez Dance Theatre, Santa Monica, California) developed the class and the handbook and trained instructors.
The authors also thank all the VAGLAHS veterans and staff for their help with the class—especially Andrea Serafin, LCSW; Rosie Dominguez, LCSW; Retha de Johnette, LCSW; and Donna Ames, MD, all part of the Psychosocial Rehabilitation and Recovery Programs; Dana Melching, LCSW, Mental Health Intensive Case Management; and Vanessa Baumann, PhD (Vet Center).
1. Levy FJ. Dance/Movement Therapy: A Healing Art. Reston, VA: American Alliance for Health, Physical Education, Recreation, and Dance; 1992.
2. Marigold DS, Misiaszek JE. Whole-body responses: neural control and implications for rehabilitation and fall prevention. Neuroscientist. 2009;15(1):36-46.
3. Hackney ME, Kantorovich S, Levin R, Earhart GM. Effects of tango on functional mobility in Parkinson's disease: a preliminary study. J Neurol Phys Ther. 2007;31(4):173-179.
4. Ravelin T, Kylmä J, Korhonen T. Dance in mental health nursing: a hybrid concept analysis. Issues Ment Health Nurs. 2006;27(3):307-317.
5. Hackney ME, Earhart GM. Effects of dance on gait and balance in Parkinson's disease: a comparison of partnered and nonpartnered dance movement. Neurorehabil Neural Repair. 2010;24(4):384-392.
6. Heiberger L, Maurer C, Amtage F, et al. Impact of a weekly dance class on the functional mobility and on the quality of life of individuals with Parkinson's disease. Front Aging Neurosci. 2011;3:14.
7. Houston S, McGill A. A mixed-methods study into ballet for people living with Parkinson's. Arts Health. 2013;5(2):103-119.
8. Westheimer O. Why dance for Parkinson's disease. Top Geriatr Rehabil. 2008;24(2):127-140.
9. Bräuninger I. Dance movement therapy group intervention in stress treatment: a randomized controlled trial (RCT). Arts Psychother. 2012;39(5):443-450.
10. Kattenstroth, JC, Kalisch T, Holt S, Tegenthoff M, Dinse HR. Six months of dance intervention enhances postural, sensorimotor, and cognitive performance in elderly without affecting cardio-respiratory functions. Front Aging Neurosci. 2013;5:5.
11. Kattenstroth J-C, Kolankowska I, Kalisch T, Dinse HR. Superior sensory, motor, and cognitive performance in elderly individuals with multi-year dancing activities. Front Aging Neurosci. 2010;2:31.
12. Kline F, Burgoyne RW, Staples F, Moredock P, Snyder V, Ioerger M. A report on the use of movement therapy for chronic, severely disabled outpatients. Arts Psychother. 1977;4(4-5):181-183.
13. Koch SC, Morlinghaus K, Fuchs T. The joy dance: specific effects of a single dance intervention on psychiatric patients with depression. Arts Psychother. 2007;34(4):340-349.
14. Barton EJ. Movement and mindfulness: a formative evaluation of a dance/movement and yoga therapy program with participants experiencing severe mental illness. Am J Dance Ther. 2011;33(2):157-181.
15. van der Kolk BA, McFarlane AC, Weisaeth L, eds. Traumatic Stress: The Effects of Overwhelming Experience on Mind, Body, and Society. New York, NY: Guilford Press; 1996.
16. Foa EB, Keane TM, Friedman MJ, Cohen JA, eds. Effective Treatments for PTSD: Practice Guidelines From the International Society for Traumatic Stress Studies. 2nd ed. New York, NY: Guilford Press; 2009.
17. Wilbur S, Meyer HB, Baker MR, et al. Dance for Veterans: a complementary health program for veterans with serious mental illness. Arts Health. 2015;7(2):96-108.
18. Gradus JL. Epidemiology of PTSD. U.S. Department of Veterans Affairs, PTSD: National Center for PTSD website. http://www.ptsd.va.gov/professional/PTSD-overview/epidemiological-facts-ptsd.asp. Published January 30, 2014. Accessed August 20, 2015.
19. Eftekhari A, Ruzek JI, Crowley JJ, Rosen CS, Greenbaum MA, Karlin BE. Effectiveness of national implementation of prolonged exposure therapy in Veterans Affairs care. JAMA Psychiatry. 2013;70(9):949-955.
20. Monson CM, Schnurr PP, Resick PA, Friedman MJ, Young-Xu Y, Stevens SP. Cognitive processing therapy for veterans with military-related posttraumatic stress disorder. J Consult Clin Psychol. 2006;74(5):898-907.
21. Schottenbauer MA, Glass CR, Arnkoff DB, Tendick V, Gray SH. Nonresponse and dropout rates in outcome studies on PTSD: review and methodological considerations. Psychiatry. 2008;71(2):134-168.
22. Suarez CA, Wilbur S, Smiarowski K, Rubin RT, Ames D. Dance for Veterans: Music, Movement & Rhythm Manual for Instruction. 2nd ed. Publisher unknown; 2014.
23. Gilbert AG, Gilbert BA, Rossano A. Brain-Compatible Dance Education. Reston, VA: National Dance Association; 2006.
24. Spielberger C. Manual for the State-Trait Anxiety Inventory. Rev ed. Palo Alto, CA: Consulting Psychologists Press; 1983.
25. Julian LJ. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res. 2011;63(suppl 11):S467-S472.
1. Levy FJ. Dance/Movement Therapy: A Healing Art. Reston, VA: American Alliance for Health, Physical Education, Recreation, and Dance; 1992.
2. Marigold DS, Misiaszek JE. Whole-body responses: neural control and implications for rehabilitation and fall prevention. Neuroscientist. 2009;15(1):36-46.
3. Hackney ME, Kantorovich S, Levin R, Earhart GM. Effects of tango on functional mobility in Parkinson's disease: a preliminary study. J Neurol Phys Ther. 2007;31(4):173-179.
4. Ravelin T, Kylmä J, Korhonen T. Dance in mental health nursing: a hybrid concept analysis. Issues Ment Health Nurs. 2006;27(3):307-317.
5. Hackney ME, Earhart GM. Effects of dance on gait and balance in Parkinson's disease: a comparison of partnered and nonpartnered dance movement. Neurorehabil Neural Repair. 2010;24(4):384-392.
6. Heiberger L, Maurer C, Amtage F, et al. Impact of a weekly dance class on the functional mobility and on the quality of life of individuals with Parkinson's disease. Front Aging Neurosci. 2011;3:14.
7. Houston S, McGill A. A mixed-methods study into ballet for people living with Parkinson's. Arts Health. 2013;5(2):103-119.
8. Westheimer O. Why dance for Parkinson's disease. Top Geriatr Rehabil. 2008;24(2):127-140.
9. Bräuninger I. Dance movement therapy group intervention in stress treatment: a randomized controlled trial (RCT). Arts Psychother. 2012;39(5):443-450.
10. Kattenstroth, JC, Kalisch T, Holt S, Tegenthoff M, Dinse HR. Six months of dance intervention enhances postural, sensorimotor, and cognitive performance in elderly without affecting cardio-respiratory functions. Front Aging Neurosci. 2013;5:5.
11. Kattenstroth J-C, Kolankowska I, Kalisch T, Dinse HR. Superior sensory, motor, and cognitive performance in elderly individuals with multi-year dancing activities. Front Aging Neurosci. 2010;2:31.
12. Kline F, Burgoyne RW, Staples F, Moredock P, Snyder V, Ioerger M. A report on the use of movement therapy for chronic, severely disabled outpatients. Arts Psychother. 1977;4(4-5):181-183.
13. Koch SC, Morlinghaus K, Fuchs T. The joy dance: specific effects of a single dance intervention on psychiatric patients with depression. Arts Psychother. 2007;34(4):340-349.
14. Barton EJ. Movement and mindfulness: a formative evaluation of a dance/movement and yoga therapy program with participants experiencing severe mental illness. Am J Dance Ther. 2011;33(2):157-181.
15. van der Kolk BA, McFarlane AC, Weisaeth L, eds. Traumatic Stress: The Effects of Overwhelming Experience on Mind, Body, and Society. New York, NY: Guilford Press; 1996.
16. Foa EB, Keane TM, Friedman MJ, Cohen JA, eds. Effective Treatments for PTSD: Practice Guidelines From the International Society for Traumatic Stress Studies. 2nd ed. New York, NY: Guilford Press; 2009.
17. Wilbur S, Meyer HB, Baker MR, et al. Dance for Veterans: a complementary health program for veterans with serious mental illness. Arts Health. 2015;7(2):96-108.
18. Gradus JL. Epidemiology of PTSD. U.S. Department of Veterans Affairs, PTSD: National Center for PTSD website. http://www.ptsd.va.gov/professional/PTSD-overview/epidemiological-facts-ptsd.asp. Published January 30, 2014. Accessed August 20, 2015.
19. Eftekhari A, Ruzek JI, Crowley JJ, Rosen CS, Greenbaum MA, Karlin BE. Effectiveness of national implementation of prolonged exposure therapy in Veterans Affairs care. JAMA Psychiatry. 2013;70(9):949-955.
20. Monson CM, Schnurr PP, Resick PA, Friedman MJ, Young-Xu Y, Stevens SP. Cognitive processing therapy for veterans with military-related posttraumatic stress disorder. J Consult Clin Psychol. 2006;74(5):898-907.
21. Schottenbauer MA, Glass CR, Arnkoff DB, Tendick V, Gray SH. Nonresponse and dropout rates in outcome studies on PTSD: review and methodological considerations. Psychiatry. 2008;71(2):134-168.
22. Suarez CA, Wilbur S, Smiarowski K, Rubin RT, Ames D. Dance for Veterans: Music, Movement & Rhythm Manual for Instruction. 2nd ed. Publisher unknown; 2014.
23. Gilbert AG, Gilbert BA, Rossano A. Brain-Compatible Dance Education. Reston, VA: National Dance Association; 2006.
24. Spielberger C. Manual for the State-Trait Anxiety Inventory. Rev ed. Palo Alto, CA: Consulting Psychologists Press; 1983.
25. Julian LJ. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res. 2011;63(suppl 11):S467-S472.
Academic Reasonable Accommodations for Post-9/11 Veterans With Psychiatric Diagnoses, Part 2
Among the ever increasing number of post-9/11 veterans pursuing higher education are many who carry psychological injuries, which include depression, anxiety, and posttraumatic stress disorder (PTSD). The effects of these mental health issues can create acquired learning disabilities involving impairments in memory, attention, concentration, and abstract thinking.1-4 Such learning disabilities can prevent a soldier from successfully transitioning to student-veteran.
Academic reasonable accommodations for veterans with psychiatric diagnoses can strategically enhance student-veteran role integration. Similar to reasonable accommodations for physical diagnoses, academic accommodations for psychiatric conditions enhance qualifying student-veterans’ abilities to successfully pursue higher education by enabling them to compensate for deficits in memory, recall, concentration, and abstract thinking. Such assistance for veterans with disabilities has been advocated in order to promote academic progression and student empowerment.5,6 Although academic accommodations enable veterans to compensate for learning disabilities, such interventions are not routinely requested for a variety of reasons. There are several key factors influencing veterans’ decisions to request such accommodations.
To promote a healthy transition to the student-veteran role, health care providers (HCPs) should initiate conversations about potential acquired learning disabilities with post-9/11 veterans with psychiatric diagnoses who are or will become students. Unfortunately, the medical literature includes little information on this topic or on how to have these conversations. To date, there is no suggested theoretical framework for guiding such discussions.
As a foundation for such discussion, Part 1 of this article explained the implications of psychiatric diagnoses and other common factors that can significantly impede adult learning among post-9/11 veterans who are separated from service.7 Part 1 also addressed the fundamentals of academic reasonable accommodations, which are outlined in Table 1.
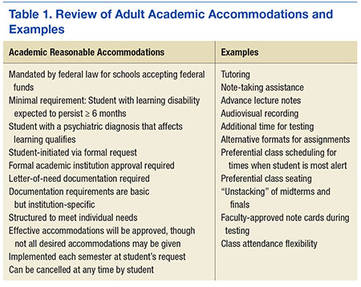
Through use of a theoretical model, part 2 of this study defines key factors influencing post-9/11 veterans’ decision to request academic reasonable accommodations for psychiatric diagnoses. It also provides practical advice for facilitating clinical conversations at each stage of the model to promote the acceptance of academic reasonable accommodations among eligible post-9/11 veterans.
Health Belief Model
The health belief model (HBM) can be adopted to understand the steps of veterans’ decision-making processes involving reasonable accommodations. The model outlines determinants of human behavior that influence the potential health care decision to deliberately mitigate harm from a perceived health threat.8,9 The 6 primary components are perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy.8,9 The HBM previously has been applied to a diverse range of health behaviors involving prevention, medical regimen adherence, and utilization of health care services.10 Its application to learning impairment and academic reasonable accommodations is outlined in Table 2.
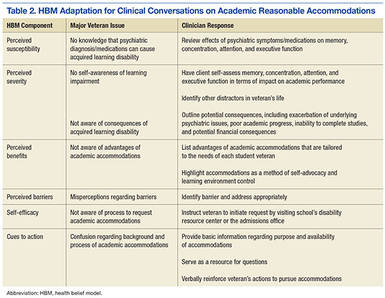
When the HBM framework is applied to academic accommodations, the perceived health threat is acquired learning disability. The desired health care decision is the act of requesting academic reasonable accommodations. The targeted population at risk is the post-9/11 veteran cohort with symptomatic psychiatric diagnoses who are enrolled in, or who are considering, postsecondary education.
The initial perceived susceptibility step determines the degree to which these veterans judge themselves as being at risk for learning impairment because of psychiatric diagnoses. During this step, it is imperative that HCPs educate veterans on how mental health conditions can alter adult learning styles. Clinicians should describe the negative effects of psychiatric symptoms on memory, concentration, focus, attention, and abstract thinking. Insight is developed in this step as veterans recognize that their academic endeavors potentially could be affected by underlying mental health symptoms.
Perceived Severity
Recognition of the perceived severity of impaired learning is the next step in HBM. Veterans will need to self-evaluate their actual or potential academic performance based on their current state of memory, concentration, focus, and attention. Although many veterans might determine that the impact is transient or minimal, a significant number of veterans will observe that their learning abilities are greatly affected. If veterans identify with loss of those skills since the onset of serious mental health issues, there should be further discussion regarding the existence of academic accommodations that address any learning impairment expected to last longer than 6 months.
As discussed in part 1, mental health diagnoses involving mood, though possessing individually distinct diagnostic criteria, create potentially similar global learning impairments in terms of decreased memory, poor concentration, and slowed executive functioning.1-4 Insight into the impact of any acquired learning disability from these mental health conditions and/or associated pharmacologic treatment can be encouraged if the clinician and client jointly review the client’s self-described premorbid learning style and compare it with the client’s current functioning in day-to-day activities requiring memory, concentration, and decision making. A clinician can use a gentle emphasis on the incongruities between premorbid learning ability and present-day impairments as a springboard for discussion about ways to compensate for learning impairments.
Additional insight can be elicited by providing practical examples of how other factors can accentuate the learning difficulties caused by serious or persistent psychiatric symptoms. By discussing these issues, clinicians can provide veterans with a more realistic understanding of potential obstacles in the postsecondary setting and the need for a strategic plan to address such challenges. For example, if a veteran takes prescription medications to manage underlying psychiatric conditions, a discussion regarding pertinent pharmacologic adverse effects (AEs) can highlight how academic performance might be affected. As outlined in part 1, fatigue, drowsiness, restlessness, mental grogginess, and insomnia are just a few medication AEs that may impair academic performance by negatively affecting memory, concentration, and executive functioning.
There are multiple circumstances that can increase the degree to which psychiatric symptoms impede recall, memory, insight, judgment, concentration, attention, organization, and abstract thinking. Impaired memory, poor concentration, irritability, and decreased attention can occur in the normal postmilitary transition period or as residual effects from mild-to-moderate traumatic brain injury. Multiple role responsibilities, such as being a spouse and parent, also can present significant mental distractions from academic endeavors. A physical impairment, such as tinnitus, hearing loss, or chronic pain, can impede classroom participation.
At this juncture, HCPs also should identify the academic consequences of impaired learning. Knowing these consequences will help veterans decide whether a course of action is needed to compensate for any learning disability that may be present. Inability to finish timed tests, difficulty taking notes, and inefficient studying are some of the more serious potential sequelae. Feared long-term consequences include a lack of progress through the required course load and, ultimately, failing courses.
A basic explanation of the potential financial effects of poor academic achievement provides another practical method for clinicians to outline negative consequences of an acquired learning disability. The student’s sole income for basic necessities is often the post-9/11 GI Bill, which pays for up to 36 months of education benefits and includes a living allowance and book stipend.
Unfortunately, given their financial dependence on the GI Bill, many veterans who withdraw from classes due to academic difficulties face economic uncertainty. If their withdrawal is not approved by the GI Bill program, these veterans must pay back all the money granted during the semester. Veterans who remain in school despite receiving failing marks cannot recover money spent on failed courses. This potentially results in veterans exceeding their entire GI Bill allotment before completing course requirements for their desired certificate or degree. Many veterans logically conclude that the potential financial devastation is a sufficiently severe consequence of impaired learning ability, and those who believe they have significantly impaired learning ability may become more motivated to reduce any risk of academic failure by pursuing academic accommodations.
In tandem with reviewing the potential severity of the problem, clinicians always should emphasize the availability of academic accommodations to circumvent the negative consequences of an acquired learning disability. Veterans who experience academic difficulties but are unaware of academic interventions may decide to forgo postsecondary education. By understanding basic details about accommodations, veterans can make the informed decision to pursue these interventions as part of a plan for academic success.
Perceived Benefits
Although identifying perceived susceptibility and perceived severity are necessary for veterans to consider academic reasonable accommodation use, eligible veterans still may not understand how these accommodations can apply to their situation. In the next step of HBM, veterans must view formal academic accommodations as a desirable solution to mitigate the effects of impaired learning ability. Veterans must appreciate the perceived benefits of such requests before they elect to pursue them.
At this point, HCPs should provide examples of academic accommodations to illustrate the simplicity and ease of such interventions. Tutoring, note-taking assistance, and providing additional time for testing are examples of a few types of accommodations featuring advantages that should be readily apparent to veterans returning to school. These measures not only lessen the likelihood of struggling academically, but also afford an opportunity to excel. By painting accommodations as a powerful method of self-advocacy, HCPs can inform veterans that accommodations enable a measure of control within the academic setting and assist with planning.
Perceived Barriers
Although identifying perceived benefits may be persuasive, discerning perceived barriers is an important HBM step that influences whether veterans will seek academic accommodations. Fortunately, many of the common barriers to accommodation requests are simply misconceptions that clinicians can address easily. For example, some veterans misconstrue reasonable accommodations as giving them an unfair advantage, which they find offensive to their personal integrity and pride. Clinicians should point out to these veterans that accommodations address deficits in learning abilities and merely level the academic playing field so the student-veteran is on par with those students without such impairments. The core work needed to pass the class remains unchanged by such accommodations.
Often a barrier is erected when veterans subscribe to the traditional military definition of disability, which is equated with having overwhelming physical injuries or paralyzing psychological states. These veterans are reluctant to request any formal accommodations, because they do not see themselves as having a disability under this restrictive definition. For these veterans, HCPs need to explain that the broad federal definition of disability does not imply veterans must be disabled in any other aspect of his or her life except for learning.
Some veterans do not want to draw attention to themselves either as a veteran or as a student with learning difficulties.11,12 Aware of civilian stereotyping of veterans, they prefer to remain anonymous. In this instance, clinicians should emphasize that psychiatric diagnoses are confidential and that only the reasonable accommodations are shared with the professor—not the underlying medical problem. The clinician also should emphasize that the accommodations are open to all eligible adult students, not just student-veterans. Therefore, use of such accommodations is not a disclosure of veteran status.
In conjunction with addressing client fears about stereotyping of both veterans and students with learning disabilities, HCPs should be mindful that mental health stigma is a significant barrier to seeking mental health services among military personnel, post-9/11 veterans, and college students.13,14 Therefore, clinicians should emphasize that academic accommodations for psychiatric diagnoses are not self-disclosing of psychiatric concerns and are usually the same accommodations used to address learning disabilities caused by other factors.
Veterans may believe that documentation obtained in support of reasonable accommodations is too intimidating or too personal to reveal. Not realizing that federal law prevents institutions from requesting in-depth documentation, veterans mistakenly believe that they must provide all medical documents in order to qualify for academic accommodations. To assuage these fears, clinicians should inform veterans that schools generally require only a documentation letter from a qualified provider and usually do not require other medical records.
To further alleviate veteran fears and promote a measure of client control, providers may find it beneficial to review the proposed medical documentation letter with the veteran and have the veteran approve the content. Figures 1 and 2 illustrate a basic medical documentation letter with optional institution-specific criteria. To ensure compliance with any applicable federal privacy regulations or local facility policy, clinicians should obtain an information release form from the veteran. The medical documentation letter can then be released to the veteran for hand delivery to the academic institution.
Veterans might be concerned about the potential lack of confidentiality regarding the diagnosis contributing to their learning disability. They also may worry that accommodations will prevent them from entering the field of their choice when they graduate, especially for law enforcement careers. These veterans can be reassured by informing them that use of academic accommodations is completely confidential during their school years and will not appear on their school graduation records. Recommending that veterans confirm the established confidentiality process with their schools may help allay fears about inadvertent release of private information by the institution.
Self-Efficacy and Cues to Action
Even after perceived benefits and barriers are identified, veterans still may not act unless they believe that they can intervene appropriately to address the problem. The HBM refers to this step as self-efficacy. Student-veterans must feel empowered to effectively make reasonable accommodation requests and negotiate any potential setbacks to the implementation of those accommodations. Health care providers should inform veterans about the availability of a disability resource center or other counseling service at each school that can help the student-veteran through the process of accommodation approval. Ideally, student-veterans also should receive guidance on how to approach professors regarding both the request for and the implementation of the approved reasonable accommodations.15 Counselors at the institution should offer this guidance and help veterans select the appropriate accommodations.
In the HBM, cues to action occur at every step. These cues consist of the influential factors promoting the desired behavior. Providing answers to common veteran questions about academic accommodations is one cue to action. Another is providing a written step-by-step guide explaining academic accommodations to veterans. (The author has created a veteran-centric guide to academic accommodations. The guide, which explains basic concepts and addresses common barriers to requesting such accommodations, is available upon request from Katherine.Mitchell1@va.gov).
At all times, positive feedback from clinicians is important in motivating veterans to complete the entire process. Discussion may be stalled at any point if veterans overestimate current academic abilities or underestimate their level of impaired learning ability. Motivational interviewing techniques may help resolve this impasse. However, even if eligible veterans are not interested in pursuing academic accommodations, HCPs should leave the option open for consideration. Although interventions are most beneficial when instituted early in the student’s coursework, veterans can formally request academic accommodations at any stage of their academic career.
Conclusion
Formal academic accommodations are viable tools for cultivating academic success among student-veterans with significant psychiatric conditions. The adoption of such interventions requires understanding post-9/11 veterans’ motivation and concerns about formal academic accommodation requests. Application of the HBM can guide clinicians in their discussions with post-9/11 veterans. By understanding the veterans’ perspectives on the subject, HCPs can directly address the factors influencing the decision to seek academic accommodations.
Ensuring successful transition to the student-veteran role is of prime importance for veterans who bear emotional scars from military service. To this author’s knowledge, no structured educational programs currently exist that inform either post-9/11 veterans or their HCPs about pertinent aspects of academic accommodations for student-veterans with symptomatic psychiatric diagnoses that impede learning. Future endeavors need to include development of programs to inform veterans and providers about this important topic. Such programs should not only promote the dissemination of general information, but also explore specific ways to tailor accommodations to the cognitive needs of each veteran.
1. Burriss L, Ayers E, Ginsberg J, Powell DA. Learning and memory impairment in PTSD: relationship to depression. Depress Anxiety. 2008;25(2):149-157.
2. Sweeney JA, Kmiec JA, Kupfer DJ. Neuropsychologic impairments in bipolar and unipolar mood disorders on the CANTAB neurocognitive battery. Biol Psychiatry. 2000;48(7):674-684.
3. Chamberlain SR, Sahakian BJ. The neuropsychology of mood disorders. Curr Psychiatry Rep. 2006;8(6):458-463.
4. Jaeger J, Berns S, Uzelac S, Davis-Conway S. Neurocognitive deficits and disability in major depressive disorder. Psychiatry Res. 2006;145(1):39-48.
5. Branker C. Deserving design: the new generation of student veterans. J Postsecond Educ Disabil. 2009;22(1):59-66.
6. Burnett SE, Segoria J. Collaboration for military transition students from combat to college: it takes a community. J Postsecond Educ and Disabil. 2009;22(1):53-58.
7. Mitchell K. Understanding academic reasonable accommodations for post-9/11 veterans with psychiatric diagnoses—part 1, the foundation. Fed Pract. 2016;33(4):33-39.
8. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health Educ Q. 1988;15(2):175-183.
9. Glanz K, Rimer BK. Theory at a Glance: A Guide for Health Promotion Practice. 2nd ed. Bethesda, MD: U.S. Deptartment of Health and Human Services, National Institutes of Health, National Cancer Institute; 2005.
10. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. 1984;11(1):1-47.
11. Salzer MS, Wick LC, Rogers JA. Familiarity with and use of accommodations and supports among postsecondary students with mental illnesses. Psychiatr Serv. 2008;59(4):370-375.
12. Shackelford AL. Documenting the needs of student veterans with disabilities: intersection roadblocks, solutions, and legal realities. J Postsecond Educ Disabil. 2009;22(1):36-42.
13. Eisenberg D, Downs MF, Golberstein E, Zivin K. Stigma and help seeking for mental health among college students. Med Care Res Rev. 2009;66(5):522-541.
14. Vogt D. Mental health related beliefs as a barrier to service use for military personnel and veterans: a review. Psychiatr Serv. 2011;62(2):135-142.
15. Palmer C, Roessler RT. Requesting classroom accommodations: self-advocacy and conflict resolution training for college students with disabilities. J Rehabil. 2000;66(3):38-43.
Among the ever increasing number of post-9/11 veterans pursuing higher education are many who carry psychological injuries, which include depression, anxiety, and posttraumatic stress disorder (PTSD). The effects of these mental health issues can create acquired learning disabilities involving impairments in memory, attention, concentration, and abstract thinking.1-4 Such learning disabilities can prevent a soldier from successfully transitioning to student-veteran.
Academic reasonable accommodations for veterans with psychiatric diagnoses can strategically enhance student-veteran role integration. Similar to reasonable accommodations for physical diagnoses, academic accommodations for psychiatric conditions enhance qualifying student-veterans’ abilities to successfully pursue higher education by enabling them to compensate for deficits in memory, recall, concentration, and abstract thinking. Such assistance for veterans with disabilities has been advocated in order to promote academic progression and student empowerment.5,6 Although academic accommodations enable veterans to compensate for learning disabilities, such interventions are not routinely requested for a variety of reasons. There are several key factors influencing veterans’ decisions to request such accommodations.
To promote a healthy transition to the student-veteran role, health care providers (HCPs) should initiate conversations about potential acquired learning disabilities with post-9/11 veterans with psychiatric diagnoses who are or will become students. Unfortunately, the medical literature includes little information on this topic or on how to have these conversations. To date, there is no suggested theoretical framework for guiding such discussions.
As a foundation for such discussion, Part 1 of this article explained the implications of psychiatric diagnoses and other common factors that can significantly impede adult learning among post-9/11 veterans who are separated from service.7 Part 1 also addressed the fundamentals of academic reasonable accommodations, which are outlined in Table 1.
Through use of a theoretical model, part 2 of this study defines key factors influencing post-9/11 veterans’ decision to request academic reasonable accommodations for psychiatric diagnoses. It also provides practical advice for facilitating clinical conversations at each stage of the model to promote the acceptance of academic reasonable accommodations among eligible post-9/11 veterans.
Health Belief Model
The health belief model (HBM) can be adopted to understand the steps of veterans’ decision-making processes involving reasonable accommodations. The model outlines determinants of human behavior that influence the potential health care decision to deliberately mitigate harm from a perceived health threat.8,9 The 6 primary components are perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy.8,9 The HBM previously has been applied to a diverse range of health behaviors involving prevention, medical regimen adherence, and utilization of health care services.10 Its application to learning impairment and academic reasonable accommodations is outlined in Table 2.
When the HBM framework is applied to academic accommodations, the perceived health threat is acquired learning disability. The desired health care decision is the act of requesting academic reasonable accommodations. The targeted population at risk is the post-9/11 veteran cohort with symptomatic psychiatric diagnoses who are enrolled in, or who are considering, postsecondary education.
The initial perceived susceptibility step determines the degree to which these veterans judge themselves as being at risk for learning impairment because of psychiatric diagnoses. During this step, it is imperative that HCPs educate veterans on how mental health conditions can alter adult learning styles. Clinicians should describe the negative effects of psychiatric symptoms on memory, concentration, focus, attention, and abstract thinking. Insight is developed in this step as veterans recognize that their academic endeavors potentially could be affected by underlying mental health symptoms.
Perceived Severity
Recognition of the perceived severity of impaired learning is the next step in HBM. Veterans will need to self-evaluate their actual or potential academic performance based on their current state of memory, concentration, focus, and attention. Although many veterans might determine that the impact is transient or minimal, a significant number of veterans will observe that their learning abilities are greatly affected. If veterans identify with loss of those skills since the onset of serious mental health issues, there should be further discussion regarding the existence of academic accommodations that address any learning impairment expected to last longer than 6 months.
As discussed in part 1, mental health diagnoses involving mood, though possessing individually distinct diagnostic criteria, create potentially similar global learning impairments in terms of decreased memory, poor concentration, and slowed executive functioning.1-4 Insight into the impact of any acquired learning disability from these mental health conditions and/or associated pharmacologic treatment can be encouraged if the clinician and client jointly review the client’s self-described premorbid learning style and compare it with the client’s current functioning in day-to-day activities requiring memory, concentration, and decision making. A clinician can use a gentle emphasis on the incongruities between premorbid learning ability and present-day impairments as a springboard for discussion about ways to compensate for learning impairments.
Additional insight can be elicited by providing practical examples of how other factors can accentuate the learning difficulties caused by serious or persistent psychiatric symptoms. By discussing these issues, clinicians can provide veterans with a more realistic understanding of potential obstacles in the postsecondary setting and the need for a strategic plan to address such challenges. For example, if a veteran takes prescription medications to manage underlying psychiatric conditions, a discussion regarding pertinent pharmacologic adverse effects (AEs) can highlight how academic performance might be affected. As outlined in part 1, fatigue, drowsiness, restlessness, mental grogginess, and insomnia are just a few medication AEs that may impair academic performance by negatively affecting memory, concentration, and executive functioning.
There are multiple circumstances that can increase the degree to which psychiatric symptoms impede recall, memory, insight, judgment, concentration, attention, organization, and abstract thinking. Impaired memory, poor concentration, irritability, and decreased attention can occur in the normal postmilitary transition period or as residual effects from mild-to-moderate traumatic brain injury. Multiple role responsibilities, such as being a spouse and parent, also can present significant mental distractions from academic endeavors. A physical impairment, such as tinnitus, hearing loss, or chronic pain, can impede classroom participation.
At this juncture, HCPs also should identify the academic consequences of impaired learning. Knowing these consequences will help veterans decide whether a course of action is needed to compensate for any learning disability that may be present. Inability to finish timed tests, difficulty taking notes, and inefficient studying are some of the more serious potential sequelae. Feared long-term consequences include a lack of progress through the required course load and, ultimately, failing courses.
A basic explanation of the potential financial effects of poor academic achievement provides another practical method for clinicians to outline negative consequences of an acquired learning disability. The student’s sole income for basic necessities is often the post-9/11 GI Bill, which pays for up to 36 months of education benefits and includes a living allowance and book stipend.
Unfortunately, given their financial dependence on the GI Bill, many veterans who withdraw from classes due to academic difficulties face economic uncertainty. If their withdrawal is not approved by the GI Bill program, these veterans must pay back all the money granted during the semester. Veterans who remain in school despite receiving failing marks cannot recover money spent on failed courses. This potentially results in veterans exceeding their entire GI Bill allotment before completing course requirements for their desired certificate or degree. Many veterans logically conclude that the potential financial devastation is a sufficiently severe consequence of impaired learning ability, and those who believe they have significantly impaired learning ability may become more motivated to reduce any risk of academic failure by pursuing academic accommodations.
In tandem with reviewing the potential severity of the problem, clinicians always should emphasize the availability of academic accommodations to circumvent the negative consequences of an acquired learning disability. Veterans who experience academic difficulties but are unaware of academic interventions may decide to forgo postsecondary education. By understanding basic details about accommodations, veterans can make the informed decision to pursue these interventions as part of a plan for academic success.
Perceived Benefits
Although identifying perceived susceptibility and perceived severity are necessary for veterans to consider academic reasonable accommodation use, eligible veterans still may not understand how these accommodations can apply to their situation. In the next step of HBM, veterans must view formal academic accommodations as a desirable solution to mitigate the effects of impaired learning ability. Veterans must appreciate the perceived benefits of such requests before they elect to pursue them.
At this point, HCPs should provide examples of academic accommodations to illustrate the simplicity and ease of such interventions. Tutoring, note-taking assistance, and providing additional time for testing are examples of a few types of accommodations featuring advantages that should be readily apparent to veterans returning to school. These measures not only lessen the likelihood of struggling academically, but also afford an opportunity to excel. By painting accommodations as a powerful method of self-advocacy, HCPs can inform veterans that accommodations enable a measure of control within the academic setting and assist with planning.
Perceived Barriers
Although identifying perceived benefits may be persuasive, discerning perceived barriers is an important HBM step that influences whether veterans will seek academic accommodations. Fortunately, many of the common barriers to accommodation requests are simply misconceptions that clinicians can address easily. For example, some veterans misconstrue reasonable accommodations as giving them an unfair advantage, which they find offensive to their personal integrity and pride. Clinicians should point out to these veterans that accommodations address deficits in learning abilities and merely level the academic playing field so the student-veteran is on par with those students without such impairments. The core work needed to pass the class remains unchanged by such accommodations.
Often a barrier is erected when veterans subscribe to the traditional military definition of disability, which is equated with having overwhelming physical injuries or paralyzing psychological states. These veterans are reluctant to request any formal accommodations, because they do not see themselves as having a disability under this restrictive definition. For these veterans, HCPs need to explain that the broad federal definition of disability does not imply veterans must be disabled in any other aspect of his or her life except for learning.
Some veterans do not want to draw attention to themselves either as a veteran or as a student with learning difficulties.11,12 Aware of civilian stereotyping of veterans, they prefer to remain anonymous. In this instance, clinicians should emphasize that psychiatric diagnoses are confidential and that only the reasonable accommodations are shared with the professor—not the underlying medical problem. The clinician also should emphasize that the accommodations are open to all eligible adult students, not just student-veterans. Therefore, use of such accommodations is not a disclosure of veteran status.
In conjunction with addressing client fears about stereotyping of both veterans and students with learning disabilities, HCPs should be mindful that mental health stigma is a significant barrier to seeking mental health services among military personnel, post-9/11 veterans, and college students.13,14 Therefore, clinicians should emphasize that academic accommodations for psychiatric diagnoses are not self-disclosing of psychiatric concerns and are usually the same accommodations used to address learning disabilities caused by other factors.
Veterans may believe that documentation obtained in support of reasonable accommodations is too intimidating or too personal to reveal. Not realizing that federal law prevents institutions from requesting in-depth documentation, veterans mistakenly believe that they must provide all medical documents in order to qualify for academic accommodations. To assuage these fears, clinicians should inform veterans that schools generally require only a documentation letter from a qualified provider and usually do not require other medical records.
To further alleviate veteran fears and promote a measure of client control, providers may find it beneficial to review the proposed medical documentation letter with the veteran and have the veteran approve the content. Figures 1 and 2 illustrate a basic medical documentation letter with optional institution-specific criteria. To ensure compliance with any applicable federal privacy regulations or local facility policy, clinicians should obtain an information release form from the veteran. The medical documentation letter can then be released to the veteran for hand delivery to the academic institution.
Veterans might be concerned about the potential lack of confidentiality regarding the diagnosis contributing to their learning disability. They also may worry that accommodations will prevent them from entering the field of their choice when they graduate, especially for law enforcement careers. These veterans can be reassured by informing them that use of academic accommodations is completely confidential during their school years and will not appear on their school graduation records. Recommending that veterans confirm the established confidentiality process with their schools may help allay fears about inadvertent release of private information by the institution.
Self-Efficacy and Cues to Action
Even after perceived benefits and barriers are identified, veterans still may not act unless they believe that they can intervene appropriately to address the problem. The HBM refers to this step as self-efficacy. Student-veterans must feel empowered to effectively make reasonable accommodation requests and negotiate any potential setbacks to the implementation of those accommodations. Health care providers should inform veterans about the availability of a disability resource center or other counseling service at each school that can help the student-veteran through the process of accommodation approval. Ideally, student-veterans also should receive guidance on how to approach professors regarding both the request for and the implementation of the approved reasonable accommodations.15 Counselors at the institution should offer this guidance and help veterans select the appropriate accommodations.
In the HBM, cues to action occur at every step. These cues consist of the influential factors promoting the desired behavior. Providing answers to common veteran questions about academic accommodations is one cue to action. Another is providing a written step-by-step guide explaining academic accommodations to veterans. (The author has created a veteran-centric guide to academic accommodations. The guide, which explains basic concepts and addresses common barriers to requesting such accommodations, is available upon request from Katherine.Mitchell1@va.gov).
At all times, positive feedback from clinicians is important in motivating veterans to complete the entire process. Discussion may be stalled at any point if veterans overestimate current academic abilities or underestimate their level of impaired learning ability. Motivational interviewing techniques may help resolve this impasse. However, even if eligible veterans are not interested in pursuing academic accommodations, HCPs should leave the option open for consideration. Although interventions are most beneficial when instituted early in the student’s coursework, veterans can formally request academic accommodations at any stage of their academic career.
Conclusion
Formal academic accommodations are viable tools for cultivating academic success among student-veterans with significant psychiatric conditions. The adoption of such interventions requires understanding post-9/11 veterans’ motivation and concerns about formal academic accommodation requests. Application of the HBM can guide clinicians in their discussions with post-9/11 veterans. By understanding the veterans’ perspectives on the subject, HCPs can directly address the factors influencing the decision to seek academic accommodations.
Ensuring successful transition to the student-veteran role is of prime importance for veterans who bear emotional scars from military service. To this author’s knowledge, no structured educational programs currently exist that inform either post-9/11 veterans or their HCPs about pertinent aspects of academic accommodations for student-veterans with symptomatic psychiatric diagnoses that impede learning. Future endeavors need to include development of programs to inform veterans and providers about this important topic. Such programs should not only promote the dissemination of general information, but also explore specific ways to tailor accommodations to the cognitive needs of each veteran.
Among the ever increasing number of post-9/11 veterans pursuing higher education are many who carry psychological injuries, which include depression, anxiety, and posttraumatic stress disorder (PTSD). The effects of these mental health issues can create acquired learning disabilities involving impairments in memory, attention, concentration, and abstract thinking.1-4 Such learning disabilities can prevent a soldier from successfully transitioning to student-veteran.
Academic reasonable accommodations for veterans with psychiatric diagnoses can strategically enhance student-veteran role integration. Similar to reasonable accommodations for physical diagnoses, academic accommodations for psychiatric conditions enhance qualifying student-veterans’ abilities to successfully pursue higher education by enabling them to compensate for deficits in memory, recall, concentration, and abstract thinking. Such assistance for veterans with disabilities has been advocated in order to promote academic progression and student empowerment.5,6 Although academic accommodations enable veterans to compensate for learning disabilities, such interventions are not routinely requested for a variety of reasons. There are several key factors influencing veterans’ decisions to request such accommodations.
To promote a healthy transition to the student-veteran role, health care providers (HCPs) should initiate conversations about potential acquired learning disabilities with post-9/11 veterans with psychiatric diagnoses who are or will become students. Unfortunately, the medical literature includes little information on this topic or on how to have these conversations. To date, there is no suggested theoretical framework for guiding such discussions.
As a foundation for such discussion, Part 1 of this article explained the implications of psychiatric diagnoses and other common factors that can significantly impede adult learning among post-9/11 veterans who are separated from service.7 Part 1 also addressed the fundamentals of academic reasonable accommodations, which are outlined in Table 1.
Through use of a theoretical model, part 2 of this study defines key factors influencing post-9/11 veterans’ decision to request academic reasonable accommodations for psychiatric diagnoses. It also provides practical advice for facilitating clinical conversations at each stage of the model to promote the acceptance of academic reasonable accommodations among eligible post-9/11 veterans.
Health Belief Model
The health belief model (HBM) can be adopted to understand the steps of veterans’ decision-making processes involving reasonable accommodations. The model outlines determinants of human behavior that influence the potential health care decision to deliberately mitigate harm from a perceived health threat.8,9 The 6 primary components are perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy.8,9 The HBM previously has been applied to a diverse range of health behaviors involving prevention, medical regimen adherence, and utilization of health care services.10 Its application to learning impairment and academic reasonable accommodations is outlined in Table 2.
When the HBM framework is applied to academic accommodations, the perceived health threat is acquired learning disability. The desired health care decision is the act of requesting academic reasonable accommodations. The targeted population at risk is the post-9/11 veteran cohort with symptomatic psychiatric diagnoses who are enrolled in, or who are considering, postsecondary education.
The initial perceived susceptibility step determines the degree to which these veterans judge themselves as being at risk for learning impairment because of psychiatric diagnoses. During this step, it is imperative that HCPs educate veterans on how mental health conditions can alter adult learning styles. Clinicians should describe the negative effects of psychiatric symptoms on memory, concentration, focus, attention, and abstract thinking. Insight is developed in this step as veterans recognize that their academic endeavors potentially could be affected by underlying mental health symptoms.
Perceived Severity
Recognition of the perceived severity of impaired learning is the next step in HBM. Veterans will need to self-evaluate their actual or potential academic performance based on their current state of memory, concentration, focus, and attention. Although many veterans might determine that the impact is transient or minimal, a significant number of veterans will observe that their learning abilities are greatly affected. If veterans identify with loss of those skills since the onset of serious mental health issues, there should be further discussion regarding the existence of academic accommodations that address any learning impairment expected to last longer than 6 months.
As discussed in part 1, mental health diagnoses involving mood, though possessing individually distinct diagnostic criteria, create potentially similar global learning impairments in terms of decreased memory, poor concentration, and slowed executive functioning.1-4 Insight into the impact of any acquired learning disability from these mental health conditions and/or associated pharmacologic treatment can be encouraged if the clinician and client jointly review the client’s self-described premorbid learning style and compare it with the client’s current functioning in day-to-day activities requiring memory, concentration, and decision making. A clinician can use a gentle emphasis on the incongruities between premorbid learning ability and present-day impairments as a springboard for discussion about ways to compensate for learning impairments.
Additional insight can be elicited by providing practical examples of how other factors can accentuate the learning difficulties caused by serious or persistent psychiatric symptoms. By discussing these issues, clinicians can provide veterans with a more realistic understanding of potential obstacles in the postsecondary setting and the need for a strategic plan to address such challenges. For example, if a veteran takes prescription medications to manage underlying psychiatric conditions, a discussion regarding pertinent pharmacologic adverse effects (AEs) can highlight how academic performance might be affected. As outlined in part 1, fatigue, drowsiness, restlessness, mental grogginess, and insomnia are just a few medication AEs that may impair academic performance by negatively affecting memory, concentration, and executive functioning.
There are multiple circumstances that can increase the degree to which psychiatric symptoms impede recall, memory, insight, judgment, concentration, attention, organization, and abstract thinking. Impaired memory, poor concentration, irritability, and decreased attention can occur in the normal postmilitary transition period or as residual effects from mild-to-moderate traumatic brain injury. Multiple role responsibilities, such as being a spouse and parent, also can present significant mental distractions from academic endeavors. A physical impairment, such as tinnitus, hearing loss, or chronic pain, can impede classroom participation.
At this juncture, HCPs also should identify the academic consequences of impaired learning. Knowing these consequences will help veterans decide whether a course of action is needed to compensate for any learning disability that may be present. Inability to finish timed tests, difficulty taking notes, and inefficient studying are some of the more serious potential sequelae. Feared long-term consequences include a lack of progress through the required course load and, ultimately, failing courses.
A basic explanation of the potential financial effects of poor academic achievement provides another practical method for clinicians to outline negative consequences of an acquired learning disability. The student’s sole income for basic necessities is often the post-9/11 GI Bill, which pays for up to 36 months of education benefits and includes a living allowance and book stipend.
Unfortunately, given their financial dependence on the GI Bill, many veterans who withdraw from classes due to academic difficulties face economic uncertainty. If their withdrawal is not approved by the GI Bill program, these veterans must pay back all the money granted during the semester. Veterans who remain in school despite receiving failing marks cannot recover money spent on failed courses. This potentially results in veterans exceeding their entire GI Bill allotment before completing course requirements for their desired certificate or degree. Many veterans logically conclude that the potential financial devastation is a sufficiently severe consequence of impaired learning ability, and those who believe they have significantly impaired learning ability may become more motivated to reduce any risk of academic failure by pursuing academic accommodations.
In tandem with reviewing the potential severity of the problem, clinicians always should emphasize the availability of academic accommodations to circumvent the negative consequences of an acquired learning disability. Veterans who experience academic difficulties but are unaware of academic interventions may decide to forgo postsecondary education. By understanding basic details about accommodations, veterans can make the informed decision to pursue these interventions as part of a plan for academic success.
Perceived Benefits
Although identifying perceived susceptibility and perceived severity are necessary for veterans to consider academic reasonable accommodation use, eligible veterans still may not understand how these accommodations can apply to their situation. In the next step of HBM, veterans must view formal academic accommodations as a desirable solution to mitigate the effects of impaired learning ability. Veterans must appreciate the perceived benefits of such requests before they elect to pursue them.
At this point, HCPs should provide examples of academic accommodations to illustrate the simplicity and ease of such interventions. Tutoring, note-taking assistance, and providing additional time for testing are examples of a few types of accommodations featuring advantages that should be readily apparent to veterans returning to school. These measures not only lessen the likelihood of struggling academically, but also afford an opportunity to excel. By painting accommodations as a powerful method of self-advocacy, HCPs can inform veterans that accommodations enable a measure of control within the academic setting and assist with planning.
Perceived Barriers
Although identifying perceived benefits may be persuasive, discerning perceived barriers is an important HBM step that influences whether veterans will seek academic accommodations. Fortunately, many of the common barriers to accommodation requests are simply misconceptions that clinicians can address easily. For example, some veterans misconstrue reasonable accommodations as giving them an unfair advantage, which they find offensive to their personal integrity and pride. Clinicians should point out to these veterans that accommodations address deficits in learning abilities and merely level the academic playing field so the student-veteran is on par with those students without such impairments. The core work needed to pass the class remains unchanged by such accommodations.
Often a barrier is erected when veterans subscribe to the traditional military definition of disability, which is equated with having overwhelming physical injuries or paralyzing psychological states. These veterans are reluctant to request any formal accommodations, because they do not see themselves as having a disability under this restrictive definition. For these veterans, HCPs need to explain that the broad federal definition of disability does not imply veterans must be disabled in any other aspect of his or her life except for learning.
Some veterans do not want to draw attention to themselves either as a veteran or as a student with learning difficulties.11,12 Aware of civilian stereotyping of veterans, they prefer to remain anonymous. In this instance, clinicians should emphasize that psychiatric diagnoses are confidential and that only the reasonable accommodations are shared with the professor—not the underlying medical problem. The clinician also should emphasize that the accommodations are open to all eligible adult students, not just student-veterans. Therefore, use of such accommodations is not a disclosure of veteran status.
In conjunction with addressing client fears about stereotyping of both veterans and students with learning disabilities, HCPs should be mindful that mental health stigma is a significant barrier to seeking mental health services among military personnel, post-9/11 veterans, and college students.13,14 Therefore, clinicians should emphasize that academic accommodations for psychiatric diagnoses are not self-disclosing of psychiatric concerns and are usually the same accommodations used to address learning disabilities caused by other factors.
Veterans may believe that documentation obtained in support of reasonable accommodations is too intimidating or too personal to reveal. Not realizing that federal law prevents institutions from requesting in-depth documentation, veterans mistakenly believe that they must provide all medical documents in order to qualify for academic accommodations. To assuage these fears, clinicians should inform veterans that schools generally require only a documentation letter from a qualified provider and usually do not require other medical records.
To further alleviate veteran fears and promote a measure of client control, providers may find it beneficial to review the proposed medical documentation letter with the veteran and have the veteran approve the content. Figures 1 and 2 illustrate a basic medical documentation letter with optional institution-specific criteria. To ensure compliance with any applicable federal privacy regulations or local facility policy, clinicians should obtain an information release form from the veteran. The medical documentation letter can then be released to the veteran for hand delivery to the academic institution.
Veterans might be concerned about the potential lack of confidentiality regarding the diagnosis contributing to their learning disability. They also may worry that accommodations will prevent them from entering the field of their choice when they graduate, especially for law enforcement careers. These veterans can be reassured by informing them that use of academic accommodations is completely confidential during their school years and will not appear on their school graduation records. Recommending that veterans confirm the established confidentiality process with their schools may help allay fears about inadvertent release of private information by the institution.
Self-Efficacy and Cues to Action
Even after perceived benefits and barriers are identified, veterans still may not act unless they believe that they can intervene appropriately to address the problem. The HBM refers to this step as self-efficacy. Student-veterans must feel empowered to effectively make reasonable accommodation requests and negotiate any potential setbacks to the implementation of those accommodations. Health care providers should inform veterans about the availability of a disability resource center or other counseling service at each school that can help the student-veteran through the process of accommodation approval. Ideally, student-veterans also should receive guidance on how to approach professors regarding both the request for and the implementation of the approved reasonable accommodations.15 Counselors at the institution should offer this guidance and help veterans select the appropriate accommodations.
In the HBM, cues to action occur at every step. These cues consist of the influential factors promoting the desired behavior. Providing answers to common veteran questions about academic accommodations is one cue to action. Another is providing a written step-by-step guide explaining academic accommodations to veterans. (The author has created a veteran-centric guide to academic accommodations. The guide, which explains basic concepts and addresses common barriers to requesting such accommodations, is available upon request from Katherine.Mitchell1@va.gov).
At all times, positive feedback from clinicians is important in motivating veterans to complete the entire process. Discussion may be stalled at any point if veterans overestimate current academic abilities or underestimate their level of impaired learning ability. Motivational interviewing techniques may help resolve this impasse. However, even if eligible veterans are not interested in pursuing academic accommodations, HCPs should leave the option open for consideration. Although interventions are most beneficial when instituted early in the student’s coursework, veterans can formally request academic accommodations at any stage of their academic career.
Conclusion
Formal academic accommodations are viable tools for cultivating academic success among student-veterans with significant psychiatric conditions. The adoption of such interventions requires understanding post-9/11 veterans’ motivation and concerns about formal academic accommodation requests. Application of the HBM can guide clinicians in their discussions with post-9/11 veterans. By understanding the veterans’ perspectives on the subject, HCPs can directly address the factors influencing the decision to seek academic accommodations.
Ensuring successful transition to the student-veteran role is of prime importance for veterans who bear emotional scars from military service. To this author’s knowledge, no structured educational programs currently exist that inform either post-9/11 veterans or their HCPs about pertinent aspects of academic accommodations for student-veterans with symptomatic psychiatric diagnoses that impede learning. Future endeavors need to include development of programs to inform veterans and providers about this important topic. Such programs should not only promote the dissemination of general information, but also explore specific ways to tailor accommodations to the cognitive needs of each veteran.
1. Burriss L, Ayers E, Ginsberg J, Powell DA. Learning and memory impairment in PTSD: relationship to depression. Depress Anxiety. 2008;25(2):149-157.
2. Sweeney JA, Kmiec JA, Kupfer DJ. Neuropsychologic impairments in bipolar and unipolar mood disorders on the CANTAB neurocognitive battery. Biol Psychiatry. 2000;48(7):674-684.
3. Chamberlain SR, Sahakian BJ. The neuropsychology of mood disorders. Curr Psychiatry Rep. 2006;8(6):458-463.
4. Jaeger J, Berns S, Uzelac S, Davis-Conway S. Neurocognitive deficits and disability in major depressive disorder. Psychiatry Res. 2006;145(1):39-48.
5. Branker C. Deserving design: the new generation of student veterans. J Postsecond Educ Disabil. 2009;22(1):59-66.
6. Burnett SE, Segoria J. Collaboration for military transition students from combat to college: it takes a community. J Postsecond Educ and Disabil. 2009;22(1):53-58.
7. Mitchell K. Understanding academic reasonable accommodations for post-9/11 veterans with psychiatric diagnoses—part 1, the foundation. Fed Pract. 2016;33(4):33-39.
8. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health Educ Q. 1988;15(2):175-183.
9. Glanz K, Rimer BK. Theory at a Glance: A Guide for Health Promotion Practice. 2nd ed. Bethesda, MD: U.S. Deptartment of Health and Human Services, National Institutes of Health, National Cancer Institute; 2005.
10. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. 1984;11(1):1-47.
11. Salzer MS, Wick LC, Rogers JA. Familiarity with and use of accommodations and supports among postsecondary students with mental illnesses. Psychiatr Serv. 2008;59(4):370-375.
12. Shackelford AL. Documenting the needs of student veterans with disabilities: intersection roadblocks, solutions, and legal realities. J Postsecond Educ Disabil. 2009;22(1):36-42.
13. Eisenberg D, Downs MF, Golberstein E, Zivin K. Stigma and help seeking for mental health among college students. Med Care Res Rev. 2009;66(5):522-541.
14. Vogt D. Mental health related beliefs as a barrier to service use for military personnel and veterans: a review. Psychiatr Serv. 2011;62(2):135-142.
15. Palmer C, Roessler RT. Requesting classroom accommodations: self-advocacy and conflict resolution training for college students with disabilities. J Rehabil. 2000;66(3):38-43.
1. Burriss L, Ayers E, Ginsberg J, Powell DA. Learning and memory impairment in PTSD: relationship to depression. Depress Anxiety. 2008;25(2):149-157.
2. Sweeney JA, Kmiec JA, Kupfer DJ. Neuropsychologic impairments in bipolar and unipolar mood disorders on the CANTAB neurocognitive battery. Biol Psychiatry. 2000;48(7):674-684.
3. Chamberlain SR, Sahakian BJ. The neuropsychology of mood disorders. Curr Psychiatry Rep. 2006;8(6):458-463.
4. Jaeger J, Berns S, Uzelac S, Davis-Conway S. Neurocognitive deficits and disability in major depressive disorder. Psychiatry Res. 2006;145(1):39-48.
5. Branker C. Deserving design: the new generation of student veterans. J Postsecond Educ Disabil. 2009;22(1):59-66.
6. Burnett SE, Segoria J. Collaboration for military transition students from combat to college: it takes a community. J Postsecond Educ and Disabil. 2009;22(1):53-58.
7. Mitchell K. Understanding academic reasonable accommodations for post-9/11 veterans with psychiatric diagnoses—part 1, the foundation. Fed Pract. 2016;33(4):33-39.
8. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health Educ Q. 1988;15(2):175-183.
9. Glanz K, Rimer BK. Theory at a Glance: A Guide for Health Promotion Practice. 2nd ed. Bethesda, MD: U.S. Deptartment of Health and Human Services, National Institutes of Health, National Cancer Institute; 2005.
10. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. 1984;11(1):1-47.
11. Salzer MS, Wick LC, Rogers JA. Familiarity with and use of accommodations and supports among postsecondary students with mental illnesses. Psychiatr Serv. 2008;59(4):370-375.
12. Shackelford AL. Documenting the needs of student veterans with disabilities: intersection roadblocks, solutions, and legal realities. J Postsecond Educ Disabil. 2009;22(1):36-42.
13. Eisenberg D, Downs MF, Golberstein E, Zivin K. Stigma and help seeking for mental health among college students. Med Care Res Rev. 2009;66(5):522-541.
14. Vogt D. Mental health related beliefs as a barrier to service use for military personnel and veterans: a review. Psychiatr Serv. 2011;62(2):135-142.
15. Palmer C, Roessler RT. Requesting classroom accommodations: self-advocacy and conflict resolution training for college students with disabilities. J Rehabil. 2000;66(3):38-43.