User login
Does caffeine intake during pregnancy affect birth weight?
No. Reducing caffeinated coffee consumption by 180 mg of caffeine (the equivalent of 2 cups) per day after 16 weeks’ gestation doesn’t affect birth weight. Consuming more than 300 mg of caffeine per day is associated with a clinically trivial, and statistically insignificant (less than 1 ounce), reduction in birth weight, compared with consuming no caffeine (strength of recommendation: B, randomized controlled trial [RCT] and large prospective cohort study).
EVIDENCE SUMMARY
A Cochrane systematic review of the effects of caffeine on pregnancy identified 2 studies, only one of which addressed the question of maternal caffeine intake and infant birth weight.1 The double-blind RCT evaluating caffeine intake during pregnancy found no significant differences in birth weight or length of gestation between women who drank regular coffee and women who drank decaffeinated coffee.2
At 16 weeks’ gestation, investigators randomized 1207 pregnant women who reported daily intake of at least 3 cups of regular coffee to drink unlabeled instant coffee (which was either regular or decaffeinated) for the rest of their pregnancy. The women were allowed to request as much of their assigned instant coffee as they wanted.
Subjects were recruited from among all women with uncomplicated, singleton pregnancies who were expected to deliver at a Danish university hospital during the study period. Investigators interviewed the women at 20, 25, and 34 weeks to determine coffee consumption (including both coffee provided by the investigators and other coffee), consumption of other caffeinated beverages, and smoking status.
The difference in caffeine intake between the groups didn’t correspond to significant differences in birth weight (16 g lighter with caffeinated coffee; 95% confidence interval [CI], −40 g to 73 g; P=.48) or birth length (0.03 cm longer with caffeinated coffee; 95% CI, −0.29 to 0.22) among infants born to the 1150 women who completed the study.
Limitations of the study include randomizing women after 16 weeks’ gestation and the observation that many women correctly guessed which type of coffee they received (35% of women drinking caffeinated coffee and 49% of women drinking decaf).
A caffeine effect, but with study limitations
The Cochrane systematic review (described above) and a meta-analysis of 9 prospective cohort studies with a total of 90,000 patients that evaluated maternal caffeine intake found that it was associated with increased low birth weight, intrauterine growth restriction (IUGR), or small for gestational age (SGA) infants.3
Researchers assessed caffeine consumption from coffee or other sources either by questionnaire (5 studies) or interview (4 studies) at various times during pregnancy, mostly in the first or second trimester, and assigned subjects to 4 intake categories: none, low (50-149 mg/d), moderate (150-349 mg/d), and high (>350 mg/d).
Compared with no caffeine, all levels of caffeine intake were associated with increased rates of low birth weight, IUGR, or SGA (low intake: relative risk [RR]=1.13; 95% CI, 1.06-1.21; moderate intake: RR=1.38; 95% CI, 1.18-1.62; high intake: RR=1.60; 95% CI, 1.24-2.08).
A major limitation of the meta-analysis was that 8 of the included studies were identified by the reviewers as having quality problems. The reviewers also identified additional cohort studies, not included in the meta-analysis, which failed to show any association between caffeine intake and poor pregnancy outcomes.
Results of best-quality study prove clinically trivial
The best-quality prospective cohort study in the review described above was also the largest, comprising two-thirds of the total patients. It found a statistically significant, but clinically trivial, association between caffeine intake and birth weight.4
Investigators from Norway’s Institute of Public Health mailed surveys to 106,707 pregnant Norwegian women and recruited 59,123 with uncomplicated singleton pregnancies. The survey assessed diet and lifestyle at several stages of pregnancy and correlated caffeine intake with birth weight, gestational length, and SGA deliveries. Investigators calculated caffeine intake from coffee and other dietary sources (tea and chocolate).
Higher caffeine intake was associated with a small reduction in birth weight (8 g/100 mg/d of additional caffeine intake; 95% CI, −10 to −6 g/100 mg/d). Higher intake was also associated with increasing likelihood of SGA birth, a finding of borderline significance (odds ratio [OR]=1.18; 95% CI, 1.00-1.38, comparing intake <50 mg/d with 51-200 mg/d; OR=1.62; 95% CI, 1.26-2.29, comparing <50 mg/d with 201-300 mg/d; and OR=1.62; 95% CI, 1.15-2.29, comparing <50 mg/d with >300 mg/d).
1. Jahanfar S, Jaafar SH. Effects of restricted caffeine intake by mother on fetal, neonatal and pregnancy outcome. Cochrane Database Syst Rev. 2013;(2):CD006965.
2. Bech BH, Obel C, Henriksen TB, et al. Effect of reducing caffeine intake on birth weight and length of gestation: randomised controlled trial. BMJ. 2007;334:409.
3. Chen LW, Wu Y, Neelakantan N, et al. Maternal caffeine intake during pregnancy is associated with risk of low birth weight: a systematic review and dose-response meta-analysis. BMC Medicine. 2014;12:174-176.
4. Sengpiel V, Elind E, Bacelis J, et al. Maternal caffeine intake during pregnancy is associated with birth weight but not with gestational length: results form a large prospective observational cohort trial. BMC Medicine. 2013;11:42.
No. Reducing caffeinated coffee consumption by 180 mg of caffeine (the equivalent of 2 cups) per day after 16 weeks’ gestation doesn’t affect birth weight. Consuming more than 300 mg of caffeine per day is associated with a clinically trivial, and statistically insignificant (less than 1 ounce), reduction in birth weight, compared with consuming no caffeine (strength of recommendation: B, randomized controlled trial [RCT] and large prospective cohort study).
EVIDENCE SUMMARY
A Cochrane systematic review of the effects of caffeine on pregnancy identified 2 studies, only one of which addressed the question of maternal caffeine intake and infant birth weight.1 The double-blind RCT evaluating caffeine intake during pregnancy found no significant differences in birth weight or length of gestation between women who drank regular coffee and women who drank decaffeinated coffee.2
At 16 weeks’ gestation, investigators randomized 1207 pregnant women who reported daily intake of at least 3 cups of regular coffee to drink unlabeled instant coffee (which was either regular or decaffeinated) for the rest of their pregnancy. The women were allowed to request as much of their assigned instant coffee as they wanted.
Subjects were recruited from among all women with uncomplicated, singleton pregnancies who were expected to deliver at a Danish university hospital during the study period. Investigators interviewed the women at 20, 25, and 34 weeks to determine coffee consumption (including both coffee provided by the investigators and other coffee), consumption of other caffeinated beverages, and smoking status.
The difference in caffeine intake between the groups didn’t correspond to significant differences in birth weight (16 g lighter with caffeinated coffee; 95% confidence interval [CI], −40 g to 73 g; P=.48) or birth length (0.03 cm longer with caffeinated coffee; 95% CI, −0.29 to 0.22) among infants born to the 1150 women who completed the study.
Limitations of the study include randomizing women after 16 weeks’ gestation and the observation that many women correctly guessed which type of coffee they received (35% of women drinking caffeinated coffee and 49% of women drinking decaf).
A caffeine effect, but with study limitations
The Cochrane systematic review (described above) and a meta-analysis of 9 prospective cohort studies with a total of 90,000 patients that evaluated maternal caffeine intake found that it was associated with increased low birth weight, intrauterine growth restriction (IUGR), or small for gestational age (SGA) infants.3
Researchers assessed caffeine consumption from coffee or other sources either by questionnaire (5 studies) or interview (4 studies) at various times during pregnancy, mostly in the first or second trimester, and assigned subjects to 4 intake categories: none, low (50-149 mg/d), moderate (150-349 mg/d), and high (>350 mg/d).
Compared with no caffeine, all levels of caffeine intake were associated with increased rates of low birth weight, IUGR, or SGA (low intake: relative risk [RR]=1.13; 95% CI, 1.06-1.21; moderate intake: RR=1.38; 95% CI, 1.18-1.62; high intake: RR=1.60; 95% CI, 1.24-2.08).
A major limitation of the meta-analysis was that 8 of the included studies were identified by the reviewers as having quality problems. The reviewers also identified additional cohort studies, not included in the meta-analysis, which failed to show any association between caffeine intake and poor pregnancy outcomes.
Results of best-quality study prove clinically trivial
The best-quality prospective cohort study in the review described above was also the largest, comprising two-thirds of the total patients. It found a statistically significant, but clinically trivial, association between caffeine intake and birth weight.4
Investigators from Norway’s Institute of Public Health mailed surveys to 106,707 pregnant Norwegian women and recruited 59,123 with uncomplicated singleton pregnancies. The survey assessed diet and lifestyle at several stages of pregnancy and correlated caffeine intake with birth weight, gestational length, and SGA deliveries. Investigators calculated caffeine intake from coffee and other dietary sources (tea and chocolate).
Higher caffeine intake was associated with a small reduction in birth weight (8 g/100 mg/d of additional caffeine intake; 95% CI, −10 to −6 g/100 mg/d). Higher intake was also associated with increasing likelihood of SGA birth, a finding of borderline significance (odds ratio [OR]=1.18; 95% CI, 1.00-1.38, comparing intake <50 mg/d with 51-200 mg/d; OR=1.62; 95% CI, 1.26-2.29, comparing <50 mg/d with 201-300 mg/d; and OR=1.62; 95% CI, 1.15-2.29, comparing <50 mg/d with >300 mg/d).
No. Reducing caffeinated coffee consumption by 180 mg of caffeine (the equivalent of 2 cups) per day after 16 weeks’ gestation doesn’t affect birth weight. Consuming more than 300 mg of caffeine per day is associated with a clinically trivial, and statistically insignificant (less than 1 ounce), reduction in birth weight, compared with consuming no caffeine (strength of recommendation: B, randomized controlled trial [RCT] and large prospective cohort study).
EVIDENCE SUMMARY
A Cochrane systematic review of the effects of caffeine on pregnancy identified 2 studies, only one of which addressed the question of maternal caffeine intake and infant birth weight.1 The double-blind RCT evaluating caffeine intake during pregnancy found no significant differences in birth weight or length of gestation between women who drank regular coffee and women who drank decaffeinated coffee.2
At 16 weeks’ gestation, investigators randomized 1207 pregnant women who reported daily intake of at least 3 cups of regular coffee to drink unlabeled instant coffee (which was either regular or decaffeinated) for the rest of their pregnancy. The women were allowed to request as much of their assigned instant coffee as they wanted.
Subjects were recruited from among all women with uncomplicated, singleton pregnancies who were expected to deliver at a Danish university hospital during the study period. Investigators interviewed the women at 20, 25, and 34 weeks to determine coffee consumption (including both coffee provided by the investigators and other coffee), consumption of other caffeinated beverages, and smoking status.
The difference in caffeine intake between the groups didn’t correspond to significant differences in birth weight (16 g lighter with caffeinated coffee; 95% confidence interval [CI], −40 g to 73 g; P=.48) or birth length (0.03 cm longer with caffeinated coffee; 95% CI, −0.29 to 0.22) among infants born to the 1150 women who completed the study.
Limitations of the study include randomizing women after 16 weeks’ gestation and the observation that many women correctly guessed which type of coffee they received (35% of women drinking caffeinated coffee and 49% of women drinking decaf).
A caffeine effect, but with study limitations
The Cochrane systematic review (described above) and a meta-analysis of 9 prospective cohort studies with a total of 90,000 patients that evaluated maternal caffeine intake found that it was associated with increased low birth weight, intrauterine growth restriction (IUGR), or small for gestational age (SGA) infants.3
Researchers assessed caffeine consumption from coffee or other sources either by questionnaire (5 studies) or interview (4 studies) at various times during pregnancy, mostly in the first or second trimester, and assigned subjects to 4 intake categories: none, low (50-149 mg/d), moderate (150-349 mg/d), and high (>350 mg/d).
Compared with no caffeine, all levels of caffeine intake were associated with increased rates of low birth weight, IUGR, or SGA (low intake: relative risk [RR]=1.13; 95% CI, 1.06-1.21; moderate intake: RR=1.38; 95% CI, 1.18-1.62; high intake: RR=1.60; 95% CI, 1.24-2.08).
A major limitation of the meta-analysis was that 8 of the included studies were identified by the reviewers as having quality problems. The reviewers also identified additional cohort studies, not included in the meta-analysis, which failed to show any association between caffeine intake and poor pregnancy outcomes.
Results of best-quality study prove clinically trivial
The best-quality prospective cohort study in the review described above was also the largest, comprising two-thirds of the total patients. It found a statistically significant, but clinically trivial, association between caffeine intake and birth weight.4
Investigators from Norway’s Institute of Public Health mailed surveys to 106,707 pregnant Norwegian women and recruited 59,123 with uncomplicated singleton pregnancies. The survey assessed diet and lifestyle at several stages of pregnancy and correlated caffeine intake with birth weight, gestational length, and SGA deliveries. Investigators calculated caffeine intake from coffee and other dietary sources (tea and chocolate).
Higher caffeine intake was associated with a small reduction in birth weight (8 g/100 mg/d of additional caffeine intake; 95% CI, −10 to −6 g/100 mg/d). Higher intake was also associated with increasing likelihood of SGA birth, a finding of borderline significance (odds ratio [OR]=1.18; 95% CI, 1.00-1.38, comparing intake <50 mg/d with 51-200 mg/d; OR=1.62; 95% CI, 1.26-2.29, comparing <50 mg/d with 201-300 mg/d; and OR=1.62; 95% CI, 1.15-2.29, comparing <50 mg/d with >300 mg/d).
1. Jahanfar S, Jaafar SH. Effects of restricted caffeine intake by mother on fetal, neonatal and pregnancy outcome. Cochrane Database Syst Rev. 2013;(2):CD006965.
2. Bech BH, Obel C, Henriksen TB, et al. Effect of reducing caffeine intake on birth weight and length of gestation: randomised controlled trial. BMJ. 2007;334:409.
3. Chen LW, Wu Y, Neelakantan N, et al. Maternal caffeine intake during pregnancy is associated with risk of low birth weight: a systematic review and dose-response meta-analysis. BMC Medicine. 2014;12:174-176.
4. Sengpiel V, Elind E, Bacelis J, et al. Maternal caffeine intake during pregnancy is associated with birth weight but not with gestational length: results form a large prospective observational cohort trial. BMC Medicine. 2013;11:42.
1. Jahanfar S, Jaafar SH. Effects of restricted caffeine intake by mother on fetal, neonatal and pregnancy outcome. Cochrane Database Syst Rev. 2013;(2):CD006965.
2. Bech BH, Obel C, Henriksen TB, et al. Effect of reducing caffeine intake on birth weight and length of gestation: randomised controlled trial. BMJ. 2007;334:409.
3. Chen LW, Wu Y, Neelakantan N, et al. Maternal caffeine intake during pregnancy is associated with risk of low birth weight: a systematic review and dose-response meta-analysis. BMC Medicine. 2014;12:174-176.
4. Sengpiel V, Elind E, Bacelis J, et al. Maternal caffeine intake during pregnancy is associated with birth weight but not with gestational length: results form a large prospective observational cohort trial. BMC Medicine. 2013;11:42.
Evidence-based answers from the Family Physicians Inquiries Network

Portal inflammation in pediatric NAFLD linked to fibrosis
Portal inflammation in children with nonalcoholic fatty liver disease is associated with more than a threefold greater risk of more advanced fibrosis, according to a paper published in Hepatology.
A cross-sectional study in 430 children with nonalcoholic fatty liver disease – 12% with type 1 disease, 22% with type 2, and 66% with an overlap of both – found that the presence of portal inflammation was associated with a significant independent association with stage 2-4 fibrosis (odds ratio, 3.70; 95% confidence interval, 1.40-5.21; P = .003), after adjustment for age and sex.

Stage 2-4 fibrosis was associated with a greater incidence of steatosis (OR, 1.81; P less than .0001), lobular inflammation (OR, 1.40; P less than .0001) and a twofold greater incidence of ballooning (P less than .0001).
While children with type 2 or overlap nonalcoholic fatty liver disease typically had lower alanine aminotransferase, aspartate aminotransferase, and bilirubin scores than those with type 1, they had a higher adjusted body mass index and waist circumference, lower HDL cholesterol and higher triglycerides (Hepatology. March 2016;63:745-53).
“Our data highlight that patients with type 2 and overlap NAFLD, in particular portal inflammation and high BMI or waist circumference, may be at increased risk of hepatic or metabolic complications,” wrote Dr. Jake P. Mann from the University of Cambridge, England, and his coauthors, suggesting that an elevated waist circumference could serve as a noninvasive indicator of risk of portal inflammation and fibrosis.
No conflicts of interest were declared.
Portal inflammation in children with nonalcoholic fatty liver disease is associated with more than a threefold greater risk of more advanced fibrosis, according to a paper published in Hepatology.
A cross-sectional study in 430 children with nonalcoholic fatty liver disease – 12% with type 1 disease, 22% with type 2, and 66% with an overlap of both – found that the presence of portal inflammation was associated with a significant independent association with stage 2-4 fibrosis (odds ratio, 3.70; 95% confidence interval, 1.40-5.21; P = .003), after adjustment for age and sex.
Stage 2-4 fibrosis was associated with a greater incidence of steatosis (OR, 1.81; P less than .0001), lobular inflammation (OR, 1.40; P less than .0001) and a twofold greater incidence of ballooning (P less than .0001).
While children with type 2 or overlap nonalcoholic fatty liver disease typically had lower alanine aminotransferase, aspartate aminotransferase, and bilirubin scores than those with type 1, they had a higher adjusted body mass index and waist circumference, lower HDL cholesterol and higher triglycerides (Hepatology. March 2016;63:745-53).
“Our data highlight that patients with type 2 and overlap NAFLD, in particular portal inflammation and high BMI or waist circumference, may be at increased risk of hepatic or metabolic complications,” wrote Dr. Jake P. Mann from the University of Cambridge, England, and his coauthors, suggesting that an elevated waist circumference could serve as a noninvasive indicator of risk of portal inflammation and fibrosis.
No conflicts of interest were declared.
Portal inflammation in children with nonalcoholic fatty liver disease is associated with more than a threefold greater risk of more advanced fibrosis, according to a paper published in Hepatology.
A cross-sectional study in 430 children with nonalcoholic fatty liver disease – 12% with type 1 disease, 22% with type 2, and 66% with an overlap of both – found that the presence of portal inflammation was associated with a significant independent association with stage 2-4 fibrosis (odds ratio, 3.70; 95% confidence interval, 1.40-5.21; P = .003), after adjustment for age and sex.
Stage 2-4 fibrosis was associated with a greater incidence of steatosis (OR, 1.81; P less than .0001), lobular inflammation (OR, 1.40; P less than .0001) and a twofold greater incidence of ballooning (P less than .0001).
While children with type 2 or overlap nonalcoholic fatty liver disease typically had lower alanine aminotransferase, aspartate aminotransferase, and bilirubin scores than those with type 1, they had a higher adjusted body mass index and waist circumference, lower HDL cholesterol and higher triglycerides (Hepatology. March 2016;63:745-53).
“Our data highlight that patients with type 2 and overlap NAFLD, in particular portal inflammation and high BMI or waist circumference, may be at increased risk of hepatic or metabolic complications,” wrote Dr. Jake P. Mann from the University of Cambridge, England, and his coauthors, suggesting that an elevated waist circumference could serve as a noninvasive indicator of risk of portal inflammation and fibrosis.
No conflicts of interest were declared.
FROM HEPATOLOGY
Key clinical point: Portal inflammation in children with nonalcoholic fatty liver disease is associated with more advanced fibrosis and a worse metabolic phenotype.
Major finding: Portal inflammation in children with NAFLD is associated with a more than threefold greater risk of more advanced fibrosis.
Data source: A cross-sectional study in 430 children with NAFLD.
Disclosures: No conflicts of interest were declared.

More teens complete HPV vaccine series when parents choose reminder methods
Asking parents how they want to be reminded of the need for their child’s second dose of the human papillomavirus (HPV) vaccine appears to increase the likelihood of their child completing the three-dose series, a recent study found.
“For the promise of the HPV vaccine to be realized, rates of vaccine initiation and series completion must be markedly increased,” wrote Dr. Allison Kempe of the University of Colorado, Aurora, and her associates. “Results of this study demonstrate that preference-based recall could have a major impact on increasing HPV series completion rates and in increasing the timeliness of full vaccination” (Pediatrics. 2016 Feb 26. doi: 10.1542/peds.2015-2857). “The intervention was most effective for younger adolescents, and reminding the adolescent, in addition to the parent, did not increase effectiveness.”

The researchers randomly assigned three pediatric practices from Kaiser Permanente Colorado to offer usual care and four practices to the intervention, during January to June 2013. They limited the practices to those with a similar proportion of African American and Hispanic patients, a similar number of patients aged 11-17 years, and a similar proportion of Medicaid-covered patients. At the start of the study, the intervention sites had an 18% rate for the first dose of the HPV vaccine and a 6% series completion rate, compared with 20% and 7%, respectively, at the control sites.
When parents brought their children in for the first dose of the HPV vaccine, staff at the intervention practices asked the parents if they wanted to receive a reminder about the next dose. If they did, they chose whether they wanted a text message, an email, or an automated phone message (they could choose up to two) and whether they wanted their child contacted as well. Parents of 43% of the 867 eligible adolescents participated.
The researchers compared HPV vaccines series completion rates between those 374 adolescents and the 555 eligible adolescents at the control practices. At the intervention practices, 83% of the teens received the second dose, and 63% completed the vaccine series. At the control practice, 71% of the teens received the second dose, and 38% completed the series – similar to the 33% completion rate of unenrolled teens at the intervention practices. Overall, 46% of all the teens – enrolled and unenrolled – at the intervention practices completed the series, compared with 38% at the control practices – for an adjusted risk ratio of 1.22 (P less than .01)
The most popular recall method was text messaging alone, requested by 39% of parents and particularly preferred by parents of Hispanic adolescents. Both text and email were requested by 19% of parents, while 18% of parents requested email only, 9% requested text and phone, and 9% requested phone only. Only 6% requested phone and email, yet this was the only recall method associated with higher series completion rates that significantly differed from the other methods. Nearly one in five parents (19%) requested the practice to remind their child too, but these reminders had no apparent impact on completion rates.
“Whether this method [of preference-based recall] could also increase initiation of the series also should be examined, as barriers to initiation and to completion have been shown to differ,” the authors wrote.
The Centers for Disease Control and Prevention funded the study. The authors reported no disclosures.
Asking parents how they want to be reminded of the need for their child’s second dose of the human papillomavirus (HPV) vaccine appears to increase the likelihood of their child completing the three-dose series, a recent study found.
“For the promise of the HPV vaccine to be realized, rates of vaccine initiation and series completion must be markedly increased,” wrote Dr. Allison Kempe of the University of Colorado, Aurora, and her associates. “Results of this study demonstrate that preference-based recall could have a major impact on increasing HPV series completion rates and in increasing the timeliness of full vaccination” (Pediatrics. 2016 Feb 26. doi: 10.1542/peds.2015-2857). “The intervention was most effective for younger adolescents, and reminding the adolescent, in addition to the parent, did not increase effectiveness.”
The researchers randomly assigned three pediatric practices from Kaiser Permanente Colorado to offer usual care and four practices to the intervention, during January to June 2013. They limited the practices to those with a similar proportion of African American and Hispanic patients, a similar number of patients aged 11-17 years, and a similar proportion of Medicaid-covered patients. At the start of the study, the intervention sites had an 18% rate for the first dose of the HPV vaccine and a 6% series completion rate, compared with 20% and 7%, respectively, at the control sites.
When parents brought their children in for the first dose of the HPV vaccine, staff at the intervention practices asked the parents if they wanted to receive a reminder about the next dose. If they did, they chose whether they wanted a text message, an email, or an automated phone message (they could choose up to two) and whether they wanted their child contacted as well. Parents of 43% of the 867 eligible adolescents participated.
The researchers compared HPV vaccines series completion rates between those 374 adolescents and the 555 eligible adolescents at the control practices. At the intervention practices, 83% of the teens received the second dose, and 63% completed the vaccine series. At the control practice, 71% of the teens received the second dose, and 38% completed the series – similar to the 33% completion rate of unenrolled teens at the intervention practices. Overall, 46% of all the teens – enrolled and unenrolled – at the intervention practices completed the series, compared with 38% at the control practices – for an adjusted risk ratio of 1.22 (P less than .01)
The most popular recall method was text messaging alone, requested by 39% of parents and particularly preferred by parents of Hispanic adolescents. Both text and email were requested by 19% of parents, while 18% of parents requested email only, 9% requested text and phone, and 9% requested phone only. Only 6% requested phone and email, yet this was the only recall method associated with higher series completion rates that significantly differed from the other methods. Nearly one in five parents (19%) requested the practice to remind their child too, but these reminders had no apparent impact on completion rates.
“Whether this method [of preference-based recall] could also increase initiation of the series also should be examined, as barriers to initiation and to completion have been shown to differ,” the authors wrote.
The Centers for Disease Control and Prevention funded the study. The authors reported no disclosures.
Asking parents how they want to be reminded of the need for their child’s second dose of the human papillomavirus (HPV) vaccine appears to increase the likelihood of their child completing the three-dose series, a recent study found.
“For the promise of the HPV vaccine to be realized, rates of vaccine initiation and series completion must be markedly increased,” wrote Dr. Allison Kempe of the University of Colorado, Aurora, and her associates. “Results of this study demonstrate that preference-based recall could have a major impact on increasing HPV series completion rates and in increasing the timeliness of full vaccination” (Pediatrics. 2016 Feb 26. doi: 10.1542/peds.2015-2857). “The intervention was most effective for younger adolescents, and reminding the adolescent, in addition to the parent, did not increase effectiveness.”
The researchers randomly assigned three pediatric practices from Kaiser Permanente Colorado to offer usual care and four practices to the intervention, during January to June 2013. They limited the practices to those with a similar proportion of African American and Hispanic patients, a similar number of patients aged 11-17 years, and a similar proportion of Medicaid-covered patients. At the start of the study, the intervention sites had an 18% rate for the first dose of the HPV vaccine and a 6% series completion rate, compared with 20% and 7%, respectively, at the control sites.
When parents brought their children in for the first dose of the HPV vaccine, staff at the intervention practices asked the parents if they wanted to receive a reminder about the next dose. If they did, they chose whether they wanted a text message, an email, or an automated phone message (they could choose up to two) and whether they wanted their child contacted as well. Parents of 43% of the 867 eligible adolescents participated.
The researchers compared HPV vaccines series completion rates between those 374 adolescents and the 555 eligible adolescents at the control practices. At the intervention practices, 83% of the teens received the second dose, and 63% completed the vaccine series. At the control practice, 71% of the teens received the second dose, and 38% completed the series – similar to the 33% completion rate of unenrolled teens at the intervention practices. Overall, 46% of all the teens – enrolled and unenrolled – at the intervention practices completed the series, compared with 38% at the control practices – for an adjusted risk ratio of 1.22 (P less than .01)
The most popular recall method was text messaging alone, requested by 39% of parents and particularly preferred by parents of Hispanic adolescents. Both text and email were requested by 19% of parents, while 18% of parents requested email only, 9% requested text and phone, and 9% requested phone only. Only 6% requested phone and email, yet this was the only recall method associated with higher series completion rates that significantly differed from the other methods. Nearly one in five parents (19%) requested the practice to remind their child too, but these reminders had no apparent impact on completion rates.
“Whether this method [of preference-based recall] could also increase initiation of the series also should be examined, as barriers to initiation and to completion have been shown to differ,” the authors wrote.
The Centers for Disease Control and Prevention funded the study. The authors reported no disclosures.
FROM PEDIATRICS
Key clinical point: Preference-based reminders increased HPV vaccine series completion rates.
Major finding: 46% of adolescents at intervention practices completed the series, compared with 38% at practices providing usual care.
Data source: The findings are based on a cluster randomized trial of seven pediatric practices in the Kaiser Permanent Colorado system involving 1,422 patients aged 11-17 years.
Disclosures: The Centers for Disease Control and Prevention funded the study. The authors reported no disclosures.

Efavirenz linked with higher bone mass in children with HIV
BOSTON – Switching HIV-infected South African children from ritonavir-boosted lopinavir (LPV/r) to efavirenz (EFV)-based antiretroviral therapy improved bone mineral content in the children, compared with remaining on LPV/r, according to a study presented at the Conference on Retroviruses and Opportunistic Infections.
HIV infection affects bone accrual but there are limited data on how to optimize antiretrovirals to improve bone outcomes in HIV-infected children, said Dr. Stephen Arpadi, professor of pediatrics at Columbia University (N.Y.) Medical Center, and lead author of the study. To determine whether a preemptive switch from LPV/r to EFV antiretroviral therapy might be associated with beneficial outcomes in terms of children’s bone development, his team reviewed the results of a randomized clinical trial of HIV-infected children undertaken in Johannesburg, South Africa.

Two hundred twenty HIV-infected children aged 5-10 years (mean 6.4 years) were enrolled 1-4 years (mean 2.1 years) after randomization in the trial, while 180 similarly-aged HIV-uninfected children were recruited at the same site in Johannesburg for comparison. Among HIV-infected children, 110 were on EFV and 110 LPV/r at the time of assessment. All children also were on two nucleoside reverse transcriptase inhibitors, including 3TC (lamivudine) and ABC (abacavir), AZT, or d4T (stavudine). None were on TDF (tenofovir).
The investigators – part of the CHANGES Bone Study Team – assessed the children’s bone mineral content (BMC), fat mass, and lean body mass of the whole body by Dual-energy X-ray absorptiometry. Sex-specific BMC-for-height Z-scores for the infected children were generated using the BMC-for-height distribution of the uninfected controls. The children with HIV currently receiving EFV were compared with those on LPV/r.
Dr. Arpadi told CROI attendees that the BMC Z score was –0.49 in the EFV group and –1.07 in the LPV/r group, and that this association remained significant (P less than .001) and of a similar magnitude (Z-score difference, 0.58) after adjustment for age, fat mass, lean mass, vigorous physical activity, dietary vitamin D and calcium, CD4, and viral load. Sex-stratified analysis showed similar size effects in both boys and girls.
Higher fat and lean body mass also were independently associated with better bone mass outcomes in the children, Dr. Arpadi affirmed. “The use of bone friendly drugs may be beneficial for bone health in children with HIV,” he concluded.
The study was supported by the National Institutes of Health. Dr. Arpadi reported no conflicts of interest.
On Twitter @richpizzi
BOSTON – Switching HIV-infected South African children from ritonavir-boosted lopinavir (LPV/r) to efavirenz (EFV)-based antiretroviral therapy improved bone mineral content in the children, compared with remaining on LPV/r, according to a study presented at the Conference on Retroviruses and Opportunistic Infections.
HIV infection affects bone accrual but there are limited data on how to optimize antiretrovirals to improve bone outcomes in HIV-infected children, said Dr. Stephen Arpadi, professor of pediatrics at Columbia University (N.Y.) Medical Center, and lead author of the study. To determine whether a preemptive switch from LPV/r to EFV antiretroviral therapy might be associated with beneficial outcomes in terms of children’s bone development, his team reviewed the results of a randomized clinical trial of HIV-infected children undertaken in Johannesburg, South Africa.
Two hundred twenty HIV-infected children aged 5-10 years (mean 6.4 years) were enrolled 1-4 years (mean 2.1 years) after randomization in the trial, while 180 similarly-aged HIV-uninfected children were recruited at the same site in Johannesburg for comparison. Among HIV-infected children, 110 were on EFV and 110 LPV/r at the time of assessment. All children also were on two nucleoside reverse transcriptase inhibitors, including 3TC (lamivudine) and ABC (abacavir), AZT, or d4T (stavudine). None were on TDF (tenofovir).
The investigators – part of the CHANGES Bone Study Team – assessed the children’s bone mineral content (BMC), fat mass, and lean body mass of the whole body by Dual-energy X-ray absorptiometry. Sex-specific BMC-for-height Z-scores for the infected children were generated using the BMC-for-height distribution of the uninfected controls. The children with HIV currently receiving EFV were compared with those on LPV/r.
Dr. Arpadi told CROI attendees that the BMC Z score was –0.49 in the EFV group and –1.07 in the LPV/r group, and that this association remained significant (P less than .001) and of a similar magnitude (Z-score difference, 0.58) after adjustment for age, fat mass, lean mass, vigorous physical activity, dietary vitamin D and calcium, CD4, and viral load. Sex-stratified analysis showed similar size effects in both boys and girls.
Higher fat and lean body mass also were independently associated with better bone mass outcomes in the children, Dr. Arpadi affirmed. “The use of bone friendly drugs may be beneficial for bone health in children with HIV,” he concluded.
The study was supported by the National Institutes of Health. Dr. Arpadi reported no conflicts of interest.
On Twitter @richpizzi
BOSTON – Switching HIV-infected South African children from ritonavir-boosted lopinavir (LPV/r) to efavirenz (EFV)-based antiretroviral therapy improved bone mineral content in the children, compared with remaining on LPV/r, according to a study presented at the Conference on Retroviruses and Opportunistic Infections.
HIV infection affects bone accrual but there are limited data on how to optimize antiretrovirals to improve bone outcomes in HIV-infected children, said Dr. Stephen Arpadi, professor of pediatrics at Columbia University (N.Y.) Medical Center, and lead author of the study. To determine whether a preemptive switch from LPV/r to EFV antiretroviral therapy might be associated with beneficial outcomes in terms of children’s bone development, his team reviewed the results of a randomized clinical trial of HIV-infected children undertaken in Johannesburg, South Africa.
Two hundred twenty HIV-infected children aged 5-10 years (mean 6.4 years) were enrolled 1-4 years (mean 2.1 years) after randomization in the trial, while 180 similarly-aged HIV-uninfected children were recruited at the same site in Johannesburg for comparison. Among HIV-infected children, 110 were on EFV and 110 LPV/r at the time of assessment. All children also were on two nucleoside reverse transcriptase inhibitors, including 3TC (lamivudine) and ABC (abacavir), AZT, or d4T (stavudine). None were on TDF (tenofovir).
The investigators – part of the CHANGES Bone Study Team – assessed the children’s bone mineral content (BMC), fat mass, and lean body mass of the whole body by Dual-energy X-ray absorptiometry. Sex-specific BMC-for-height Z-scores for the infected children were generated using the BMC-for-height distribution of the uninfected controls. The children with HIV currently receiving EFV were compared with those on LPV/r.
Dr. Arpadi told CROI attendees that the BMC Z score was –0.49 in the EFV group and –1.07 in the LPV/r group, and that this association remained significant (P less than .001) and of a similar magnitude (Z-score difference, 0.58) after adjustment for age, fat mass, lean mass, vigorous physical activity, dietary vitamin D and calcium, CD4, and viral load. Sex-stratified analysis showed similar size effects in both boys and girls.
Higher fat and lean body mass also were independently associated with better bone mass outcomes in the children, Dr. Arpadi affirmed. “The use of bone friendly drugs may be beneficial for bone health in children with HIV,” he concluded.
The study was supported by the National Institutes of Health. Dr. Arpadi reported no conflicts of interest.
On Twitter @richpizzi
AT CROI 2016
Key clinical point: Switching HIV-infected children from ritonavir-boosted lopinavir to efavirenz-based antiretroviral therapy may increase bone mass.
Major finding: The Bone Mineral Content Z score was –0.49 in the EFV group and –1.07 in the LPV/r group, and the association remained significant (P less than .001) and of a similar magnitude (Z-score difference, 0.58) after adjustment for age, fat mass, lean mass, vigorous physical activity, dietary vitamin D and calcium, CD4, and viral load.
Data source: A randomized clinical trial of 220 HIV-infected children aged 5-10 years (mean 6.4 years) enrolled 1-4 years (mean 2.1 years) after randomization in the trial, and 180 similarly-aged HIV-uninfected children at the same site for comparison. Among HIV-infected children, 110 were on EFV and 110 LPV/r at the time of assessment.
Disclosures: The study was supported by the National Institutes of Health. Dr. Arpadi reported no conflicts of interest.

Donor human milk availability to VLBW infants associated with decreased NEC
For very low birth weight infants, the availability of donor human milk to newborns was associated with a decreased incidence of necrotizing enterocolitis and an increased rate of breastfeeding at discharge from a neonatal intensive care unit.

The researchers based their findings on data obtained from the California Perinatal Quality Care Collaborative, which gathers information on the care of greater than 90% of California’s neonatal intensive care unit (NICU) admissions of very low birth weight (VLBW) infants (defined as weighing less than or equal to 1.5 kg at birth), and the Mother’s Milk Bank of San Jose, a human milk bank serving 94 hospitals across several states, including California. All of the data was collected between 2007 and 2013 in over 42,000 VLBW babies. Babies were classified as breastfeeding at discharge, if they were feeding with human milk or human milk with fortifier or formula, but not if they were only feeding with formula.
Agata Kantorowska, a medical student at the University of Rochester (N.Y.) School of Medicine and Dentistry, and her colleagues noted that they did not know if donor human milk (DHM) was used primarily as a back-up feeding if mother’s milk was unavailable, in another way, or in conjunction with human milk-derived fortifiers; the proportion of VLBW infants within each NICU that received DHM; or the length of time that an individual received DHM.
Among the 22 hospitals studied that went from not having DHM available to making it available, on average, the rate of breastfeeding at discharge increased by 10% after DHM became available (P less than .0001). Among these same hospitals, the mean change in necrotizing enterocolitis (NEC) prevalence, following the introduction of DHM, was a 2.6% decrease (P = .0006). Before DHM became available in the 22 hospitals, 52.8% of VLBW infants were breastfeeding at discharge, compared with 61.7% after DHM became available. The rate of NEC was 6.6% among VLBW infants prior to DHM having becoming available at a hospital, versus 4.3% following the introduction of DHM to a hospital.
Following risk adjustment, not having DHM available in a hospital was a negative predictor for breastfeeding at discharge (odds ratio, 0.70) and a positive predictor of NEC (odds ratio, 1.15).
Ms. Kantorowska and her associates said while they found “a significant association between a hospital’s DHM status and increased breastfeeding and decreased NEC rates among VLBW infants,” factors other than the availability of DHM contributed to changes in breastfeeding and NEC rates that occurred. They also noted that they saw an increased rate of breastfeeding and a similar decreasing rate of NEC in hospitals that did not transition to using DHM.
“Societal attitudes toward breastfeeding are likely influencing mothers’ attempts to provide breast milk to their VLBW infants. ... The NICU battle against NEC is ongoing, and other advances in care that occurred from 2007 to 2013 could be contributing to the observed decrease in NEC rate in hospitals that acquired DHM,” the researchers said.
Read the full study in Pediatrics (doi: 10.1542/peds.2015-3123).
For very low birth weight infants, the availability of donor human milk to newborns was associated with a decreased incidence of necrotizing enterocolitis and an increased rate of breastfeeding at discharge from a neonatal intensive care unit.
The researchers based their findings on data obtained from the California Perinatal Quality Care Collaborative, which gathers information on the care of greater than 90% of California’s neonatal intensive care unit (NICU) admissions of very low birth weight (VLBW) infants (defined as weighing less than or equal to 1.5 kg at birth), and the Mother’s Milk Bank of San Jose, a human milk bank serving 94 hospitals across several states, including California. All of the data was collected between 2007 and 2013 in over 42,000 VLBW babies. Babies were classified as breastfeeding at discharge, if they were feeding with human milk or human milk with fortifier or formula, but not if they were only feeding with formula.
Agata Kantorowska, a medical student at the University of Rochester (N.Y.) School of Medicine and Dentistry, and her colleagues noted that they did not know if donor human milk (DHM) was used primarily as a back-up feeding if mother’s milk was unavailable, in another way, or in conjunction with human milk-derived fortifiers; the proportion of VLBW infants within each NICU that received DHM; or the length of time that an individual received DHM.
Among the 22 hospitals studied that went from not having DHM available to making it available, on average, the rate of breastfeeding at discharge increased by 10% after DHM became available (P less than .0001). Among these same hospitals, the mean change in necrotizing enterocolitis (NEC) prevalence, following the introduction of DHM, was a 2.6% decrease (P = .0006). Before DHM became available in the 22 hospitals, 52.8% of VLBW infants were breastfeeding at discharge, compared with 61.7% after DHM became available. The rate of NEC was 6.6% among VLBW infants prior to DHM having becoming available at a hospital, versus 4.3% following the introduction of DHM to a hospital.
Following risk adjustment, not having DHM available in a hospital was a negative predictor for breastfeeding at discharge (odds ratio, 0.70) and a positive predictor of NEC (odds ratio, 1.15).
Ms. Kantorowska and her associates said while they found “a significant association between a hospital’s DHM status and increased breastfeeding and decreased NEC rates among VLBW infants,” factors other than the availability of DHM contributed to changes in breastfeeding and NEC rates that occurred. They also noted that they saw an increased rate of breastfeeding and a similar decreasing rate of NEC in hospitals that did not transition to using DHM.
“Societal attitudes toward breastfeeding are likely influencing mothers’ attempts to provide breast milk to their VLBW infants. ... The NICU battle against NEC is ongoing, and other advances in care that occurred from 2007 to 2013 could be contributing to the observed decrease in NEC rate in hospitals that acquired DHM,” the researchers said.
Read the full study in Pediatrics (doi: 10.1542/peds.2015-3123).
For very low birth weight infants, the availability of donor human milk to newborns was associated with a decreased incidence of necrotizing enterocolitis and an increased rate of breastfeeding at discharge from a neonatal intensive care unit.
The researchers based their findings on data obtained from the California Perinatal Quality Care Collaborative, which gathers information on the care of greater than 90% of California’s neonatal intensive care unit (NICU) admissions of very low birth weight (VLBW) infants (defined as weighing less than or equal to 1.5 kg at birth), and the Mother’s Milk Bank of San Jose, a human milk bank serving 94 hospitals across several states, including California. All of the data was collected between 2007 and 2013 in over 42,000 VLBW babies. Babies were classified as breastfeeding at discharge, if they were feeding with human milk or human milk with fortifier or formula, but not if they were only feeding with formula.
Agata Kantorowska, a medical student at the University of Rochester (N.Y.) School of Medicine and Dentistry, and her colleagues noted that they did not know if donor human milk (DHM) was used primarily as a back-up feeding if mother’s milk was unavailable, in another way, or in conjunction with human milk-derived fortifiers; the proportion of VLBW infants within each NICU that received DHM; or the length of time that an individual received DHM.
Among the 22 hospitals studied that went from not having DHM available to making it available, on average, the rate of breastfeeding at discharge increased by 10% after DHM became available (P less than .0001). Among these same hospitals, the mean change in necrotizing enterocolitis (NEC) prevalence, following the introduction of DHM, was a 2.6% decrease (P = .0006). Before DHM became available in the 22 hospitals, 52.8% of VLBW infants were breastfeeding at discharge, compared with 61.7% after DHM became available. The rate of NEC was 6.6% among VLBW infants prior to DHM having becoming available at a hospital, versus 4.3% following the introduction of DHM to a hospital.
Following risk adjustment, not having DHM available in a hospital was a negative predictor for breastfeeding at discharge (odds ratio, 0.70) and a positive predictor of NEC (odds ratio, 1.15).
Ms. Kantorowska and her associates said while they found “a significant association between a hospital’s DHM status and increased breastfeeding and decreased NEC rates among VLBW infants,” factors other than the availability of DHM contributed to changes in breastfeeding and NEC rates that occurred. They also noted that they saw an increased rate of breastfeeding and a similar decreasing rate of NEC in hospitals that did not transition to using DHM.
“Societal attitudes toward breastfeeding are likely influencing mothers’ attempts to provide breast milk to their VLBW infants. ... The NICU battle against NEC is ongoing, and other advances in care that occurred from 2007 to 2013 could be contributing to the observed decrease in NEC rate in hospitals that acquired DHM,” the researchers said.
Read the full study in Pediatrics (doi: 10.1542/peds.2015-3123).
FROM PEDIATRICS

Data on two-dose 9-valent HPV vaccinations encouraging, but more needed
Studies of two-dose and three-dose 9-valent human papillomavirus (HPV) vaccines in youth aged 9-14 years and in those up to age 26 found the vaccines to be “generally well tolerated in all vaccination groups,” according to a report at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
There were no vaccine-related severe adverse events, deaths, or discontinuations due to an adverse event.
The key points for ACIP to consider were the time interval between the first and second vaccine doses, the duration of protection provided by a two-dose regimen, and that it is imperative for patients to complete the entire series of vaccinations. A longer-term follow-up is planned, explained Dr. Alain Luxembourg, who spoke about the studies on behalf of Merck. “9-valent [vaccine] has now been licensed in more than 30 countries, [and] the ACIP recommended gardasil-9 for vaccination in 2015, so we continue to look at further developments in terms of licensure and recommendations,” he said.
The first of two 9vHPV two-dose studies was an open-label trial that examined five cohorts of 300 children; cohorts 1-3 and 5 were of children ages 9-14 years, and cohort 4 – the control – was of children and adults aged 16-26 years. All individuals in cohorts 1, 4, and 5 were female, all children in cohort 2 were male, and cohort 3 comprised males and females.
Children in cohorts 1 and 2 were put on dosing regimens lasting either 0 or 6 months. Children in cohort 3 were placed in regimens lasting either 0 or 12 months, while those in cohorts 4 and 5 were in regimens of either 0, 2, or 6 months. Vaccine administration was done over two or three visits, within a 4-week window of month 6 and month 12; those who were on a 2-month regimen were vaccinated within 3 weeks of reaching 2 months. In addition, one dose of 9vHPV was administered at 36 months to “assess immune memory.”
The second study was a 37-month trial that examined noninferiority of measured geometric mean titer (GMT) concentrations – the metric used for both studies to determine HPV concentration – at 1 month after last dose in both girls and boys who were on a two-dose regimen, and compared them with young women who received a three-dose regimen.
The results indicated that noninferior HPV concentrations at 1 month after administration of the final dose in both girls and boys “supports extending efficacy findings in women who received three doses to girls and boys who received two doses.” Furthermore, lower measure GMTs were found in girls who received only two doses versus three, although Dr. Luxembourg said the clinical significance of this finding is as yet unknown.
Dr. Luxembourg is an employee of Merck.
Studies of two-dose and three-dose 9-valent human papillomavirus (HPV) vaccines in youth aged 9-14 years and in those up to age 26 found the vaccines to be “generally well tolerated in all vaccination groups,” according to a report at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
There were no vaccine-related severe adverse events, deaths, or discontinuations due to an adverse event.
The key points for ACIP to consider were the time interval between the first and second vaccine doses, the duration of protection provided by a two-dose regimen, and that it is imperative for patients to complete the entire series of vaccinations. A longer-term follow-up is planned, explained Dr. Alain Luxembourg, who spoke about the studies on behalf of Merck. “9-valent [vaccine] has now been licensed in more than 30 countries, [and] the ACIP recommended gardasil-9 for vaccination in 2015, so we continue to look at further developments in terms of licensure and recommendations,” he said.
The first of two 9vHPV two-dose studies was an open-label trial that examined five cohorts of 300 children; cohorts 1-3 and 5 were of children ages 9-14 years, and cohort 4 – the control – was of children and adults aged 16-26 years. All individuals in cohorts 1, 4, and 5 were female, all children in cohort 2 were male, and cohort 3 comprised males and females.
Children in cohorts 1 and 2 were put on dosing regimens lasting either 0 or 6 months. Children in cohort 3 were placed in regimens lasting either 0 or 12 months, while those in cohorts 4 and 5 were in regimens of either 0, 2, or 6 months. Vaccine administration was done over two or three visits, within a 4-week window of month 6 and month 12; those who were on a 2-month regimen were vaccinated within 3 weeks of reaching 2 months. In addition, one dose of 9vHPV was administered at 36 months to “assess immune memory.”
The second study was a 37-month trial that examined noninferiority of measured geometric mean titer (GMT) concentrations – the metric used for both studies to determine HPV concentration – at 1 month after last dose in both girls and boys who were on a two-dose regimen, and compared them with young women who received a three-dose regimen.
The results indicated that noninferior HPV concentrations at 1 month after administration of the final dose in both girls and boys “supports extending efficacy findings in women who received three doses to girls and boys who received two doses.” Furthermore, lower measure GMTs were found in girls who received only two doses versus three, although Dr. Luxembourg said the clinical significance of this finding is as yet unknown.
Dr. Luxembourg is an employee of Merck.
Studies of two-dose and three-dose 9-valent human papillomavirus (HPV) vaccines in youth aged 9-14 years and in those up to age 26 found the vaccines to be “generally well tolerated in all vaccination groups,” according to a report at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
There were no vaccine-related severe adverse events, deaths, or discontinuations due to an adverse event.
The key points for ACIP to consider were the time interval between the first and second vaccine doses, the duration of protection provided by a two-dose regimen, and that it is imperative for patients to complete the entire series of vaccinations. A longer-term follow-up is planned, explained Dr. Alain Luxembourg, who spoke about the studies on behalf of Merck. “9-valent [vaccine] has now been licensed in more than 30 countries, [and] the ACIP recommended gardasil-9 for vaccination in 2015, so we continue to look at further developments in terms of licensure and recommendations,” he said.
The first of two 9vHPV two-dose studies was an open-label trial that examined five cohorts of 300 children; cohorts 1-3 and 5 were of children ages 9-14 years, and cohort 4 – the control – was of children and adults aged 16-26 years. All individuals in cohorts 1, 4, and 5 were female, all children in cohort 2 were male, and cohort 3 comprised males and females.
Children in cohorts 1 and 2 were put on dosing regimens lasting either 0 or 6 months. Children in cohort 3 were placed in regimens lasting either 0 or 12 months, while those in cohorts 4 and 5 were in regimens of either 0, 2, or 6 months. Vaccine administration was done over two or three visits, within a 4-week window of month 6 and month 12; those who were on a 2-month regimen were vaccinated within 3 weeks of reaching 2 months. In addition, one dose of 9vHPV was administered at 36 months to “assess immune memory.”
The second study was a 37-month trial that examined noninferiority of measured geometric mean titer (GMT) concentrations – the metric used for both studies to determine HPV concentration – at 1 month after last dose in both girls and boys who were on a two-dose regimen, and compared them with young women who received a three-dose regimen.
The results indicated that noninferior HPV concentrations at 1 month after administration of the final dose in both girls and boys “supports extending efficacy findings in women who received three doses to girls and boys who received two doses.” Furthermore, lower measure GMTs were found in girls who received only two doses versus three, although Dr. Luxembourg said the clinical significance of this finding is as yet unknown.
Dr. Luxembourg is an employee of Merck.
FROM AN ACIP MEETING
Poverty tied to early relapse in kids with ALL

Photo by Logan Tuttle
A new study suggests children with acute lymphoblastic leukemia (ALL) are more likely to suffer early relapse if they live in high-poverty areas.
All of the children studied received the same treatment, and the rates of relapse were similar regardless of poverty level.
But early relapse was more common among children from poorer areas. These children also had a lower rate of 5-year overall survival, but the difference was not significant.
Kira Bona, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts, and her colleagues reported these results in Pediatric Blood & Cancer.
The team examined outcomes for 575 children, ages 1 to 18, with newly diagnosed ALL who were treated on Dana-Farber Cancer Institute ALL Consortium Protocols at 7 major academic medical centers in the US between 2000 and 2010.
Using US Census Bureau criteria, the investigators defined high-poverty areas as zip codes where 20% or more of residents have incomes below the federal poverty level. For a family of 4, this translates to an annual income of $24,250 or less.
Dr Bona and her colleagues found the overall rates of relapse were similar between children from low-poverty areas and those from high-poverty areas.
However, the timing of relapse differed significantly. Ninety-two percent of children from high-poverty areas who relapsed suffered early relapse (less than 36 months after first achieving complete remission), while 48% of the other children who relapsed did so early (P=0.008).
The 5-year overall survival was 85% for children from high-poverty areas and 92% for children from low-poverty areas. This difference is statistically significant when considered on its own (P=0.02) but not when the analysis is adjusted for other factors (P=0.07).
Still, the investigators said this suggests a possible disparity in survival.
“These children are getting the same best possible care at well-resourced institutions from highly trained clinicians, and we’re still seeing disparities,” Dr Bona said. “In trying to improve cure rates, we, as a field, have focused almost exclusively on biology. If we want to move forward, we also have to look at social determinants.”
Next steps
Dr Bona and her colleagues are undertaking further research designed to delve deeper into the relationship between socioeconomic status and outcomes and to allow for the development of poverty-targeted interventions.
As part of a prospective trial for children with ALL, the researchers will investigate associations between disease outcomes and the socioeconomic status of patients’ families, using a targetable measure of socioeconomic status called material hardship (food, housing, and/or energy insecurity).
The researchers will also investigate possible mechanisms underlying the relationship between socioeconomic status and early relapse, including adherence to oral chemotherapy and delays or dose reductions in chemotherapy due to a child’s underlying health.
In another study, investigators will conduct in-depth interviews with patients’ families, probing their knowledge and experience to pinpoint factors that might explain the disparity in outcomes and identify factors that can be targeted with interventions.
“Doing these next 2 studies is incredibly important,” Dr Bona said. “This study told us that simply providing the current best treatment regimen is not good enough if our goal is to cure every child with cancer.”
“At the same time that we develop new drugs and new treatment protocols, we need to address social determinants of health. Findings from these next studies will help us develop specific interventions to address disparities in outcomes. That’s an amazing opportunity.” ![]()
Photo by Logan Tuttle
A new study suggests children with acute lymphoblastic leukemia (ALL) are more likely to suffer early relapse if they live in high-poverty areas.
All of the children studied received the same treatment, and the rates of relapse were similar regardless of poverty level.
But early relapse was more common among children from poorer areas. These children also had a lower rate of 5-year overall survival, but the difference was not significant.
Kira Bona, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts, and her colleagues reported these results in Pediatric Blood & Cancer.
The team examined outcomes for 575 children, ages 1 to 18, with newly diagnosed ALL who were treated on Dana-Farber Cancer Institute ALL Consortium Protocols at 7 major academic medical centers in the US between 2000 and 2010.
Using US Census Bureau criteria, the investigators defined high-poverty areas as zip codes where 20% or more of residents have incomes below the federal poverty level. For a family of 4, this translates to an annual income of $24,250 or less.
Dr Bona and her colleagues found the overall rates of relapse were similar between children from low-poverty areas and those from high-poverty areas.
However, the timing of relapse differed significantly. Ninety-two percent of children from high-poverty areas who relapsed suffered early relapse (less than 36 months after first achieving complete remission), while 48% of the other children who relapsed did so early (P=0.008).
The 5-year overall survival was 85% for children from high-poverty areas and 92% for children from low-poverty areas. This difference is statistically significant when considered on its own (P=0.02) but not when the analysis is adjusted for other factors (P=0.07).
Still, the investigators said this suggests a possible disparity in survival.
“These children are getting the same best possible care at well-resourced institutions from highly trained clinicians, and we’re still seeing disparities,” Dr Bona said. “In trying to improve cure rates, we, as a field, have focused almost exclusively on biology. If we want to move forward, we also have to look at social determinants.”
Next steps
Dr Bona and her colleagues are undertaking further research designed to delve deeper into the relationship between socioeconomic status and outcomes and to allow for the development of poverty-targeted interventions.
As part of a prospective trial for children with ALL, the researchers will investigate associations between disease outcomes and the socioeconomic status of patients’ families, using a targetable measure of socioeconomic status called material hardship (food, housing, and/or energy insecurity).
The researchers will also investigate possible mechanisms underlying the relationship between socioeconomic status and early relapse, including adherence to oral chemotherapy and delays or dose reductions in chemotherapy due to a child’s underlying health.
In another study, investigators will conduct in-depth interviews with patients’ families, probing their knowledge and experience to pinpoint factors that might explain the disparity in outcomes and identify factors that can be targeted with interventions.
“Doing these next 2 studies is incredibly important,” Dr Bona said. “This study told us that simply providing the current best treatment regimen is not good enough if our goal is to cure every child with cancer.”
“At the same time that we develop new drugs and new treatment protocols, we need to address social determinants of health. Findings from these next studies will help us develop specific interventions to address disparities in outcomes. That’s an amazing opportunity.” ![]()
Photo by Logan Tuttle
A new study suggests children with acute lymphoblastic leukemia (ALL) are more likely to suffer early relapse if they live in high-poverty areas.
All of the children studied received the same treatment, and the rates of relapse were similar regardless of poverty level.
But early relapse was more common among children from poorer areas. These children also had a lower rate of 5-year overall survival, but the difference was not significant.
Kira Bona, MD, of Dana-Farber Cancer Institute in Boston, Massachusetts, and her colleagues reported these results in Pediatric Blood & Cancer.
The team examined outcomes for 575 children, ages 1 to 18, with newly diagnosed ALL who were treated on Dana-Farber Cancer Institute ALL Consortium Protocols at 7 major academic medical centers in the US between 2000 and 2010.
Using US Census Bureau criteria, the investigators defined high-poverty areas as zip codes where 20% or more of residents have incomes below the federal poverty level. For a family of 4, this translates to an annual income of $24,250 or less.
Dr Bona and her colleagues found the overall rates of relapse were similar between children from low-poverty areas and those from high-poverty areas.
However, the timing of relapse differed significantly. Ninety-two percent of children from high-poverty areas who relapsed suffered early relapse (less than 36 months after first achieving complete remission), while 48% of the other children who relapsed did so early (P=0.008).
The 5-year overall survival was 85% for children from high-poverty areas and 92% for children from low-poverty areas. This difference is statistically significant when considered on its own (P=0.02) but not when the analysis is adjusted for other factors (P=0.07).
Still, the investigators said this suggests a possible disparity in survival.
“These children are getting the same best possible care at well-resourced institutions from highly trained clinicians, and we’re still seeing disparities,” Dr Bona said. “In trying to improve cure rates, we, as a field, have focused almost exclusively on biology. If we want to move forward, we also have to look at social determinants.”
Next steps
Dr Bona and her colleagues are undertaking further research designed to delve deeper into the relationship between socioeconomic status and outcomes and to allow for the development of poverty-targeted interventions.
As part of a prospective trial for children with ALL, the researchers will investigate associations between disease outcomes and the socioeconomic status of patients’ families, using a targetable measure of socioeconomic status called material hardship (food, housing, and/or energy insecurity).
The researchers will also investigate possible mechanisms underlying the relationship between socioeconomic status and early relapse, including adherence to oral chemotherapy and delays or dose reductions in chemotherapy due to a child’s underlying health.
In another study, investigators will conduct in-depth interviews with patients’ families, probing their knowledge and experience to pinpoint factors that might explain the disparity in outcomes and identify factors that can be targeted with interventions.
“Doing these next 2 studies is incredibly important,” Dr Bona said. “This study told us that simply providing the current best treatment regimen is not good enough if our goal is to cure every child with cancer.”
“At the same time that we develop new drugs and new treatment protocols, we need to address social determinants of health. Findings from these next studies will help us develop specific interventions to address disparities in outcomes. That’s an amazing opportunity.” ![]()
#payattention
Social media consumes the attention of the majority of teens. It is a place to express yourself, flirt, intimidate, and keep them up to date with the latest happenings in the social circles. But, teens are using social media for much more.

Instagram, a social media site comprising photographs followed by comments, is one of the most common sites used by teens. They post everything from the meal they are eating to the new love in their life and everything in between.
A hashtag is a type of label or metadata tag used on social networks and microblogging services, which makes it easier for users to find messages with a specific theme or content. Users create hashtags by placing the hash character # (the number sign) in front of a word or unspaced phrase, either in the main text of a message or at the end. Searching for that hashtag will then present each message that has been tagged with it.1 Although teens seem to prefer simple phrases, these hashtags are used to link users to what many refer to as “Secret Society.”
For example, if a teen girl was “cutting” or interested in connecting with other teens that cut, putting #cat would link her to several social communities with the related topic. Similarly, #selfharm was the initial term used to connect to this secret society. When that was shut down by the social media site, it resurfaced as #selfharmmm2.
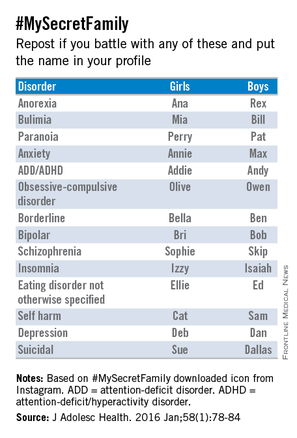
#MySecretFamily is a very popular hashtag that connects teens struggling with a variety of mental illnesses. Teens are instructed to put various names in their profile to identify which mental illness they are battling. For example, depression would be identified as “DEB” for a girl and “DAN” for a boy. The chart below lists various disorders.2
Nonsuicidal self-injury (NSSI) or deliberate destruction of one’s body in the absence of suicidal intent3 is most common in the middle school ages, and exposure to peer NSSI may increase the risk of engaging these behaviors.2,4 Although distinct from suicidal behaviors, there is a comorbidity between them. The normalization of these behaviors through social media and acceptance into the this “Secret Society” can only augment the risk of NSSI.
Parents not only need to be educated about the importance of monitoring their children’s social media but also about what to look for that may be a sign that something more serious is going on with them.
Although we hear so much of the negative impact of social media, it also can be a tool for early intervention.
References
1. Oxford English Dictionary, definition of “hashtag.”
2. J Adolesc Health. 2016 Jan;58(1):78-84.
4. Dev Psychol. 2006 May;42(3):407-17.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
Social media consumes the attention of the majority of teens. It is a place to express yourself, flirt, intimidate, and keep them up to date with the latest happenings in the social circles. But, teens are using social media for much more.
Instagram, a social media site comprising photographs followed by comments, is one of the most common sites used by teens. They post everything from the meal they are eating to the new love in their life and everything in between.
A hashtag is a type of label or metadata tag used on social networks and microblogging services, which makes it easier for users to find messages with a specific theme or content. Users create hashtags by placing the hash character # (the number sign) in front of a word or unspaced phrase, either in the main text of a message or at the end. Searching for that hashtag will then present each message that has been tagged with it.1 Although teens seem to prefer simple phrases, these hashtags are used to link users to what many refer to as “Secret Society.”
For example, if a teen girl was “cutting” or interested in connecting with other teens that cut, putting #cat would link her to several social communities with the related topic. Similarly, #selfharm was the initial term used to connect to this secret society. When that was shut down by the social media site, it resurfaced as #selfharmmm2.
#MySecretFamily is a very popular hashtag that connects teens struggling with a variety of mental illnesses. Teens are instructed to put various names in their profile to identify which mental illness they are battling. For example, depression would be identified as “DEB” for a girl and “DAN” for a boy. The chart below lists various disorders.2
Nonsuicidal self-injury (NSSI) or deliberate destruction of one’s body in the absence of suicidal intent3 is most common in the middle school ages, and exposure to peer NSSI may increase the risk of engaging these behaviors.2,4 Although distinct from suicidal behaviors, there is a comorbidity between them. The normalization of these behaviors through social media and acceptance into the this “Secret Society” can only augment the risk of NSSI.
Parents not only need to be educated about the importance of monitoring their children’s social media but also about what to look for that may be a sign that something more serious is going on with them.
Although we hear so much of the negative impact of social media, it also can be a tool for early intervention.
References
1. Oxford English Dictionary, definition of “hashtag.”
2. J Adolesc Health. 2016 Jan;58(1):78-84.
4. Dev Psychol. 2006 May;42(3):407-17.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
Social media consumes the attention of the majority of teens. It is a place to express yourself, flirt, intimidate, and keep them up to date with the latest happenings in the social circles. But, teens are using social media for much more.
Instagram, a social media site comprising photographs followed by comments, is one of the most common sites used by teens. They post everything from the meal they are eating to the new love in their life and everything in between.
A hashtag is a type of label or metadata tag used on social networks and microblogging services, which makes it easier for users to find messages with a specific theme or content. Users create hashtags by placing the hash character # (the number sign) in front of a word or unspaced phrase, either in the main text of a message or at the end. Searching for that hashtag will then present each message that has been tagged with it.1 Although teens seem to prefer simple phrases, these hashtags are used to link users to what many refer to as “Secret Society.”
For example, if a teen girl was “cutting” or interested in connecting with other teens that cut, putting #cat would link her to several social communities with the related topic. Similarly, #selfharm was the initial term used to connect to this secret society. When that was shut down by the social media site, it resurfaced as #selfharmmm2.
#MySecretFamily is a very popular hashtag that connects teens struggling with a variety of mental illnesses. Teens are instructed to put various names in their profile to identify which mental illness they are battling. For example, depression would be identified as “DEB” for a girl and “DAN” for a boy. The chart below lists various disorders.2
Nonsuicidal self-injury (NSSI) or deliberate destruction of one’s body in the absence of suicidal intent3 is most common in the middle school ages, and exposure to peer NSSI may increase the risk of engaging these behaviors.2,4 Although distinct from suicidal behaviors, there is a comorbidity between them. The normalization of these behaviors through social media and acceptance into the this “Secret Society” can only augment the risk of NSSI.
Parents not only need to be educated about the importance of monitoring their children’s social media but also about what to look for that may be a sign that something more serious is going on with them.
Although we hear so much of the negative impact of social media, it also can be a tool for early intervention.
References
1. Oxford English Dictionary, definition of “hashtag.”
2. J Adolesc Health. 2016 Jan;58(1):78-84.
4. Dev Psychol. 2006 May;42(3):407-17.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.

MRI assessment of pulmonary vein stenosis predicts outcomes
A retrospective analysis of children who underwent pulmonary vein stenosis repair with preoperative computed tomography and magnetic resonance imaging from 1990 to 2012 showed that smaller upstream or downstream total cross-sectional area indexed (TCSAi) for body surface area led to poorer survival.
The study of 31 patients at a single institution also indicated that early survival seemed especially poor for patients with a greater number of stenotic veins and upstream pulmonary vein (PV) involvement. The study was published in the March issue of the Journal of Thoracic and Cardiovascular Surgery.
Dr. Mauro Lo Rito and his colleagues at The Hospital for Sick Children, Toronto, retrospectively assessed the 31 patients out of 145 who underwent surgical repair who had had preoperative CT and MRI imaging. Complete sutureless repair was done in 18 (58%), single-side sutureless repair in 12 (39%), and pericardial patch reconstruction in 1 (3%). The mean follow-up was 4.3 years; the median patient age at time of operation was 226 days. Stenosis was bilateral in 45% of patients and unilateral in 55 (J Thorac Cardiovasc Surg. 2016;151:657-66).
In-hospital mortality was 9.7%, with an overall survival of 75%, 69%, and 64% at 1, 3, and 5 years, respectively. Univariate analysis showed that a younger age at operation, lower body surface area, smaller upstream TCSAi, and greater number of PV with stenosis/occlusion were associated with an increased risk of death.
Multivariate analysis showed that smaller upstream TCSAi for body surface area (P = .030) and greater number of stenotic PVs (P = .007) were associated with poor early (less than 1 year) survival. There was a nonsignificant tendency for smaller downstream TCSAi to be associated with poor late survival (greater than 1 year). None of the different PV morphologies were found to influence survival, according to Dr. Lo Rito and his colleagues.
Among the 28 hospital survivors, restenosis occurred in 10 patients, 7 of whom did not undergo further surgery (3 of these were alive at last follow-up and 4 died secondary to disease progression). Of the 3 patients who underwent subsequent intervention, 2 were alive at last follow-up.
“Risk stratification for patients with PV stenosis is currently challenging because of the variability in the anatomic configuration and the unknown relationship between these anatomic variants and survival. Our study demonstrates that by using cross-sectional areas, pulmonary vein cross-sectional area indexed to body surface area (PVCSAi) and TCSAi and tabulating the number of stenotic PVs, we can identify high-risk subsets of patients with high predicted mortality.” Dr. Lo Rito and his colleagues stated.
“The upstream total cross-sectional area and the number of stenotic PVs influence early survival and can be used to guide counseling. Smaller downstream cross-sectional area influences late survival, and those patients should be monitored with close follow-up. This methodology could aid in risk stratification for future clinical trials of pharmacologic agents designed to target upstream pulmonary vasculopathy,” the investigators concluded.
The authors reported that they had no conflicts of interest.
A webcast of the original presentation of these results at the 95th American Association for Thoracic Surgery Annual Meeting is available online (http://webcast.aats.org/2015/Video/Tuesday/04-28-15_6A_1615_Lo_Rito.mp4).
“The Toronto group has contributed significantly to our knowledge and management of pulmonary vein stenosis during the past decade. This article by Dr. Lo Rito and coworkers continues that contribution by reinforcing the values of MRI in imaging PVs before intervention and providing a valuable “hint” that preoperative PV size measurements are related to outcome,” Dr. William M. DeCampli wrote in his invited commentary (J Thorac Cardiovasc Surg. 2016;1510:667-8).
“The task of definitively demonstrating this relationship is daunting for any single institution, however, because 1) PVS is relatively rare, 2) MRI and computed tomography are relatively recently used diagnostic modalities, and 3) MRI is not easily used in an important subset of the cohort, small infants.” This limited the study to a small number of covariates,” noted Dr. DeCampli, and prevented the researchers from taking into account a myriad of additional covariates commonly associated with survival in complex congenital heart disease.

|
Dr. William M. DeCampli |
Such covariates included in a sufficiently large model could significantly alter the observed odds ratios otherwise calculated for the included variables in this study, he added, citing a study of PVS by Boston Children’s Hospital (J Thorac Cardiovasc Surg. 2015;150:911-7), which found a different set of covariates associated with death; in that case, age younger than 6 months at operation, weight less than 3 kg at operation, and lesser preoperative right ventricular systolic pressure.
“The challenges in studying PVS encountered by these two high-volume, research-oriented programs leads us to suggest that PVS should be studied in a different way. Perhaps it is time to consider a multi-institutional, mixed or inception cohort registry for PVS. The spring 2015 Society of Thoracic Surgeons Congenital Heart Database report lists 506 cases of PVS repair as the primary procedure between January 2011 and December 2014. If a study were to enroll just one-third of these subjects it would accrue more than 40 subjects per year. Five years hence with an anticipated 50-80 events (deaths), it would be possible to carry out more robust risk-hazard analyses,” Dr. DeCampli suggested.
Dr. DeCampli is a congenital heart surgeon at the department of clinical sciences, University of Central Florida, and the Heart Center at Arnold Palmer Hospital for Children, both in Orlando. He reported having no conflicts.
“The Toronto group has contributed significantly to our knowledge and management of pulmonary vein stenosis during the past decade. This article by Dr. Lo Rito and coworkers continues that contribution by reinforcing the values of MRI in imaging PVs before intervention and providing a valuable “hint” that preoperative PV size measurements are related to outcome,” Dr. William M. DeCampli wrote in his invited commentary (J Thorac Cardiovasc Surg. 2016;1510:667-8).
“The task of definitively demonstrating this relationship is daunting for any single institution, however, because 1) PVS is relatively rare, 2) MRI and computed tomography are relatively recently used diagnostic modalities, and 3) MRI is not easily used in an important subset of the cohort, small infants.” This limited the study to a small number of covariates,” noted Dr. DeCampli, and prevented the researchers from taking into account a myriad of additional covariates commonly associated with survival in complex congenital heart disease.
|
|
Dr. William M. DeCampli |
Such covariates included in a sufficiently large model could significantly alter the observed odds ratios otherwise calculated for the included variables in this study, he added, citing a study of PVS by Boston Children’s Hospital (J Thorac Cardiovasc Surg. 2015;150:911-7), which found a different set of covariates associated with death; in that case, age younger than 6 months at operation, weight less than 3 kg at operation, and lesser preoperative right ventricular systolic pressure.
“The challenges in studying PVS encountered by these two high-volume, research-oriented programs leads us to suggest that PVS should be studied in a different way. Perhaps it is time to consider a multi-institutional, mixed or inception cohort registry for PVS. The spring 2015 Society of Thoracic Surgeons Congenital Heart Database report lists 506 cases of PVS repair as the primary procedure between January 2011 and December 2014. If a study were to enroll just one-third of these subjects it would accrue more than 40 subjects per year. Five years hence with an anticipated 50-80 events (deaths), it would be possible to carry out more robust risk-hazard analyses,” Dr. DeCampli suggested.
Dr. DeCampli is a congenital heart surgeon at the department of clinical sciences, University of Central Florida, and the Heart Center at Arnold Palmer Hospital for Children, both in Orlando. He reported having no conflicts.
“The Toronto group has contributed significantly to our knowledge and management of pulmonary vein stenosis during the past decade. This article by Dr. Lo Rito and coworkers continues that contribution by reinforcing the values of MRI in imaging PVs before intervention and providing a valuable “hint” that preoperative PV size measurements are related to outcome,” Dr. William M. DeCampli wrote in his invited commentary (J Thorac Cardiovasc Surg. 2016;1510:667-8).
“The task of definitively demonstrating this relationship is daunting for any single institution, however, because 1) PVS is relatively rare, 2) MRI and computed tomography are relatively recently used diagnostic modalities, and 3) MRI is not easily used in an important subset of the cohort, small infants.” This limited the study to a small number of covariates,” noted Dr. DeCampli, and prevented the researchers from taking into account a myriad of additional covariates commonly associated with survival in complex congenital heart disease.
|
|
Dr. William M. DeCampli |
Such covariates included in a sufficiently large model could significantly alter the observed odds ratios otherwise calculated for the included variables in this study, he added, citing a study of PVS by Boston Children’s Hospital (J Thorac Cardiovasc Surg. 2015;150:911-7), which found a different set of covariates associated with death; in that case, age younger than 6 months at operation, weight less than 3 kg at operation, and lesser preoperative right ventricular systolic pressure.
“The challenges in studying PVS encountered by these two high-volume, research-oriented programs leads us to suggest that PVS should be studied in a different way. Perhaps it is time to consider a multi-institutional, mixed or inception cohort registry for PVS. The spring 2015 Society of Thoracic Surgeons Congenital Heart Database report lists 506 cases of PVS repair as the primary procedure between January 2011 and December 2014. If a study were to enroll just one-third of these subjects it would accrue more than 40 subjects per year. Five years hence with an anticipated 50-80 events (deaths), it would be possible to carry out more robust risk-hazard analyses,” Dr. DeCampli suggested.
Dr. DeCampli is a congenital heart surgeon at the department of clinical sciences, University of Central Florida, and the Heart Center at Arnold Palmer Hospital for Children, both in Orlando. He reported having no conflicts.
A retrospective analysis of children who underwent pulmonary vein stenosis repair with preoperative computed tomography and magnetic resonance imaging from 1990 to 2012 showed that smaller upstream or downstream total cross-sectional area indexed (TCSAi) for body surface area led to poorer survival.
The study of 31 patients at a single institution also indicated that early survival seemed especially poor for patients with a greater number of stenotic veins and upstream pulmonary vein (PV) involvement. The study was published in the March issue of the Journal of Thoracic and Cardiovascular Surgery.
Dr. Mauro Lo Rito and his colleagues at The Hospital for Sick Children, Toronto, retrospectively assessed the 31 patients out of 145 who underwent surgical repair who had had preoperative CT and MRI imaging. Complete sutureless repair was done in 18 (58%), single-side sutureless repair in 12 (39%), and pericardial patch reconstruction in 1 (3%). The mean follow-up was 4.3 years; the median patient age at time of operation was 226 days. Stenosis was bilateral in 45% of patients and unilateral in 55 (J Thorac Cardiovasc Surg. 2016;151:657-66).
In-hospital mortality was 9.7%, with an overall survival of 75%, 69%, and 64% at 1, 3, and 5 years, respectively. Univariate analysis showed that a younger age at operation, lower body surface area, smaller upstream TCSAi, and greater number of PV with stenosis/occlusion were associated with an increased risk of death.
Multivariate analysis showed that smaller upstream TCSAi for body surface area (P = .030) and greater number of stenotic PVs (P = .007) were associated with poor early (less than 1 year) survival. There was a nonsignificant tendency for smaller downstream TCSAi to be associated with poor late survival (greater than 1 year). None of the different PV morphologies were found to influence survival, according to Dr. Lo Rito and his colleagues.
Among the 28 hospital survivors, restenosis occurred in 10 patients, 7 of whom did not undergo further surgery (3 of these were alive at last follow-up and 4 died secondary to disease progression). Of the 3 patients who underwent subsequent intervention, 2 were alive at last follow-up.
“Risk stratification for patients with PV stenosis is currently challenging because of the variability in the anatomic configuration and the unknown relationship between these anatomic variants and survival. Our study demonstrates that by using cross-sectional areas, pulmonary vein cross-sectional area indexed to body surface area (PVCSAi) and TCSAi and tabulating the number of stenotic PVs, we can identify high-risk subsets of patients with high predicted mortality.” Dr. Lo Rito and his colleagues stated.
“The upstream total cross-sectional area and the number of stenotic PVs influence early survival and can be used to guide counseling. Smaller downstream cross-sectional area influences late survival, and those patients should be monitored with close follow-up. This methodology could aid in risk stratification for future clinical trials of pharmacologic agents designed to target upstream pulmonary vasculopathy,” the investigators concluded.
The authors reported that they had no conflicts of interest.
A webcast of the original presentation of these results at the 95th American Association for Thoracic Surgery Annual Meeting is available online (http://webcast.aats.org/2015/Video/Tuesday/04-28-15_6A_1615_Lo_Rito.mp4).
A retrospective analysis of children who underwent pulmonary vein stenosis repair with preoperative computed tomography and magnetic resonance imaging from 1990 to 2012 showed that smaller upstream or downstream total cross-sectional area indexed (TCSAi) for body surface area led to poorer survival.
The study of 31 patients at a single institution also indicated that early survival seemed especially poor for patients with a greater number of stenotic veins and upstream pulmonary vein (PV) involvement. The study was published in the March issue of the Journal of Thoracic and Cardiovascular Surgery.
Dr. Mauro Lo Rito and his colleagues at The Hospital for Sick Children, Toronto, retrospectively assessed the 31 patients out of 145 who underwent surgical repair who had had preoperative CT and MRI imaging. Complete sutureless repair was done in 18 (58%), single-side sutureless repair in 12 (39%), and pericardial patch reconstruction in 1 (3%). The mean follow-up was 4.3 years; the median patient age at time of operation was 226 days. Stenosis was bilateral in 45% of patients and unilateral in 55 (J Thorac Cardiovasc Surg. 2016;151:657-66).
In-hospital mortality was 9.7%, with an overall survival of 75%, 69%, and 64% at 1, 3, and 5 years, respectively. Univariate analysis showed that a younger age at operation, lower body surface area, smaller upstream TCSAi, and greater number of PV with stenosis/occlusion were associated with an increased risk of death.
Multivariate analysis showed that smaller upstream TCSAi for body surface area (P = .030) and greater number of stenotic PVs (P = .007) were associated with poor early (less than 1 year) survival. There was a nonsignificant tendency for smaller downstream TCSAi to be associated with poor late survival (greater than 1 year). None of the different PV morphologies were found to influence survival, according to Dr. Lo Rito and his colleagues.
Among the 28 hospital survivors, restenosis occurred in 10 patients, 7 of whom did not undergo further surgery (3 of these were alive at last follow-up and 4 died secondary to disease progression). Of the 3 patients who underwent subsequent intervention, 2 were alive at last follow-up.
“Risk stratification for patients with PV stenosis is currently challenging because of the variability in the anatomic configuration and the unknown relationship between these anatomic variants and survival. Our study demonstrates that by using cross-sectional areas, pulmonary vein cross-sectional area indexed to body surface area (PVCSAi) and TCSAi and tabulating the number of stenotic PVs, we can identify high-risk subsets of patients with high predicted mortality.” Dr. Lo Rito and his colleagues stated.
“The upstream total cross-sectional area and the number of stenotic PVs influence early survival and can be used to guide counseling. Smaller downstream cross-sectional area influences late survival, and those patients should be monitored with close follow-up. This methodology could aid in risk stratification for future clinical trials of pharmacologic agents designed to target upstream pulmonary vasculopathy,” the investigators concluded.
The authors reported that they had no conflicts of interest.
A webcast of the original presentation of these results at the 95th American Association for Thoracic Surgery Annual Meeting is available online (http://webcast.aats.org/2015/Video/Tuesday/04-28-15_6A_1615_Lo_Rito.mp4).
FROM JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Survival after pulmonary vein stenosis repair was adversely affected by smaller upstream cross-sectional area indexed to body surface area.
Major finding: Smaller upstream total cross-sectional area indexed for body surface area (P = .30) and greater number of stenotic pulmonary veins (P = .007) were associated with increased early risk of death.
Data source: Researchers reviewed the outcomes of 31/145 patients who underwent surgical repair of pulmonary stenosis who had preoperative computed tomography and magnetic resonance imaging between 1990 and 2012.
Disclosures: The authors reported that they had no conflicts of interest.

Watch for failure to thrive in children with eosinophilic esophagitis
Be on the lookout for failure to thrive among pediatric patients with eosinophilic esophagitis, according to a letter to the editor of Annals of Allergy, Asthma & Immunology by Dr. Brenda Paquet of Sainte-Justine University Hospital Center in Montreal, and her colleagues.
These investigators reviewed charts for all children referred to their allergy clinic with a diagnosis of eosinophilic esophagitis (EoE) from 2004 to 2012. In addition to a standard clinical evaluation, patients had undergone a series of food and respiratory skin prick tests and food patch testing. Dr. Paquet and her associates also reviewed anthropometric measurements for the children and applied failure to thrive (FTT) criteria to all growth parameters available from birth.
Of 62 patients referred to the clinic, 15 (24%) met at least one of the six criteria for FTT, and more than half (n = 8) met at least two criteria. The most frequent FTT criterion met was a weight deceleration crossing two major percentile lines.
FTT should be assessed through different growth characteristics, such as weight, length, growth velocity, and body mass index, Dr Paquet and her associates wrote. “Because no single clinical feature can accurately predict it, it is important to maintain a high level of suspicion for FTT in children with a confirmed or suspected diagnosis of EoE, and inversely, EoE should be included in the differential diagnosis of FTT.” Although FTT usually resolves, it can persist in some children despite medical treatment, “highlighting the need for research and new therapies.”
Read the article in Annals of Allergy, Asthma & Immunology (2016 Jan. doi: 10.1016/j.anai.2015.09.015).
Be on the lookout for failure to thrive among pediatric patients with eosinophilic esophagitis, according to a letter to the editor of Annals of Allergy, Asthma & Immunology by Dr. Brenda Paquet of Sainte-Justine University Hospital Center in Montreal, and her colleagues.
These investigators reviewed charts for all children referred to their allergy clinic with a diagnosis of eosinophilic esophagitis (EoE) from 2004 to 2012. In addition to a standard clinical evaluation, patients had undergone a series of food and respiratory skin prick tests and food patch testing. Dr. Paquet and her associates also reviewed anthropometric measurements for the children and applied failure to thrive (FTT) criteria to all growth parameters available from birth.
Of 62 patients referred to the clinic, 15 (24%) met at least one of the six criteria for FTT, and more than half (n = 8) met at least two criteria. The most frequent FTT criterion met was a weight deceleration crossing two major percentile lines.
FTT should be assessed through different growth characteristics, such as weight, length, growth velocity, and body mass index, Dr Paquet and her associates wrote. “Because no single clinical feature can accurately predict it, it is important to maintain a high level of suspicion for FTT in children with a confirmed or suspected diagnosis of EoE, and inversely, EoE should be included in the differential diagnosis of FTT.” Although FTT usually resolves, it can persist in some children despite medical treatment, “highlighting the need for research and new therapies.”
Read the article in Annals of Allergy, Asthma & Immunology (2016 Jan. doi: 10.1016/j.anai.2015.09.015).
Be on the lookout for failure to thrive among pediatric patients with eosinophilic esophagitis, according to a letter to the editor of Annals of Allergy, Asthma & Immunology by Dr. Brenda Paquet of Sainte-Justine University Hospital Center in Montreal, and her colleagues.
These investigators reviewed charts for all children referred to their allergy clinic with a diagnosis of eosinophilic esophagitis (EoE) from 2004 to 2012. In addition to a standard clinical evaluation, patients had undergone a series of food and respiratory skin prick tests and food patch testing. Dr. Paquet and her associates also reviewed anthropometric measurements for the children and applied failure to thrive (FTT) criteria to all growth parameters available from birth.
Of 62 patients referred to the clinic, 15 (24%) met at least one of the six criteria for FTT, and more than half (n = 8) met at least two criteria. The most frequent FTT criterion met was a weight deceleration crossing two major percentile lines.
FTT should be assessed through different growth characteristics, such as weight, length, growth velocity, and body mass index, Dr Paquet and her associates wrote. “Because no single clinical feature can accurately predict it, it is important to maintain a high level of suspicion for FTT in children with a confirmed or suspected diagnosis of EoE, and inversely, EoE should be included in the differential diagnosis of FTT.” Although FTT usually resolves, it can persist in some children despite medical treatment, “highlighting the need for research and new therapies.”
Read the article in Annals of Allergy, Asthma & Immunology (2016 Jan. doi: 10.1016/j.anai.2015.09.015).
FROM ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY