User login
Transfusion doesn’t cause NEC, study suggests

Photo by Daniel Gay
Red blood cell (RBC) transfusions do not increase the risk of a serious intestinal disorder in very low-birth-weight (VLBW) infants, according to a study published in JAMA.
Past research has suggested RBC transfusions increase the risk of necrotizing enterocolitis (NEC) among VLBW infants.
But other studies have shown no association between transfusions and NEC or suggested transfusions actually have a protective effect.
So researchers set out to determine whether RBC transfusions or severe anemia were associated with the rate of NEC among VLBW infants. The results suggested a significant association for severe anemia but not RBC transfusion.
To conduct this study, Ravi M. Patel, MD, of the Emory University School of Medicine in Atlanta, Georgia, and his colleagues assessed 598 VLBW infants from 3 neonatal intensive care units in Atlanta.
The team followed the infants for 90 days or until they were discharged from the hospital, transferred to a non-study-affiliated hospital, or died (whichever came first).
Forty-four (7.4%) infants developed NEC, and 32 (5.4%) died (of any cause). Roughly half of the infants (n=319, 53%) received RBC transfusions (n=1430).
The unadjusted cumulative incidence of NEC at week 8 was 9.9% in infants who received transfusions and 4.6% in those who did not.
However, in multivariable analysis, exposure to RBC transfusion in a given week was not significantly related to the rate of NEC. The hazard ratio was 0.44 (P=0.09).
On the other hand, the rate of NEC was significantly higher among infants with severe anemia in a given week than in those without severe anemia. The hazard ratio was 5.99 (P=0.001).
The researchers said these results suggest preventing severe anemia may be more clinically important than minimizing the use of RBC transfusion as a strategy to decrease the risk of NEC in VLBW infants.
However, such a strategy might impact other important neonatal outcomes, so further study is needed. ![]()
Photo by Daniel Gay
Red blood cell (RBC) transfusions do not increase the risk of a serious intestinal disorder in very low-birth-weight (VLBW) infants, according to a study published in JAMA.
Past research has suggested RBC transfusions increase the risk of necrotizing enterocolitis (NEC) among VLBW infants.
But other studies have shown no association between transfusions and NEC or suggested transfusions actually have a protective effect.
So researchers set out to determine whether RBC transfusions or severe anemia were associated with the rate of NEC among VLBW infants. The results suggested a significant association for severe anemia but not RBC transfusion.
To conduct this study, Ravi M. Patel, MD, of the Emory University School of Medicine in Atlanta, Georgia, and his colleagues assessed 598 VLBW infants from 3 neonatal intensive care units in Atlanta.
The team followed the infants for 90 days or until they were discharged from the hospital, transferred to a non-study-affiliated hospital, or died (whichever came first).
Forty-four (7.4%) infants developed NEC, and 32 (5.4%) died (of any cause). Roughly half of the infants (n=319, 53%) received RBC transfusions (n=1430).
The unadjusted cumulative incidence of NEC at week 8 was 9.9% in infants who received transfusions and 4.6% in those who did not.
However, in multivariable analysis, exposure to RBC transfusion in a given week was not significantly related to the rate of NEC. The hazard ratio was 0.44 (P=0.09).
On the other hand, the rate of NEC was significantly higher among infants with severe anemia in a given week than in those without severe anemia. The hazard ratio was 5.99 (P=0.001).
The researchers said these results suggest preventing severe anemia may be more clinically important than minimizing the use of RBC transfusion as a strategy to decrease the risk of NEC in VLBW infants.
However, such a strategy might impact other important neonatal outcomes, so further study is needed. ![]()
Photo by Daniel Gay
Red blood cell (RBC) transfusions do not increase the risk of a serious intestinal disorder in very low-birth-weight (VLBW) infants, according to a study published in JAMA.
Past research has suggested RBC transfusions increase the risk of necrotizing enterocolitis (NEC) among VLBW infants.
But other studies have shown no association between transfusions and NEC or suggested transfusions actually have a protective effect.
So researchers set out to determine whether RBC transfusions or severe anemia were associated with the rate of NEC among VLBW infants. The results suggested a significant association for severe anemia but not RBC transfusion.
To conduct this study, Ravi M. Patel, MD, of the Emory University School of Medicine in Atlanta, Georgia, and his colleagues assessed 598 VLBW infants from 3 neonatal intensive care units in Atlanta.
The team followed the infants for 90 days or until they were discharged from the hospital, transferred to a non-study-affiliated hospital, or died (whichever came first).
Forty-four (7.4%) infants developed NEC, and 32 (5.4%) died (of any cause). Roughly half of the infants (n=319, 53%) received RBC transfusions (n=1430).
The unadjusted cumulative incidence of NEC at week 8 was 9.9% in infants who received transfusions and 4.6% in those who did not.
However, in multivariable analysis, exposure to RBC transfusion in a given week was not significantly related to the rate of NEC. The hazard ratio was 0.44 (P=0.09).
On the other hand, the rate of NEC was significantly higher among infants with severe anemia in a given week than in those without severe anemia. The hazard ratio was 5.99 (P=0.001).
The researchers said these results suggest preventing severe anemia may be more clinically important than minimizing the use of RBC transfusion as a strategy to decrease the risk of NEC in VLBW infants.
However, such a strategy might impact other important neonatal outcomes, so further study is needed. ![]()
High gluten consumption early in life upped risk of celiac disease
Children who were genetically susceptible to celiac disease and consumed high amounts of gluten at 12 months of age were at least twice as likely to develop the autoimmune disorder as genetically predisposed children who consumed less gluten, researchers reported in the March issue of Clinical Gastroenterology and Hepatology.
The association was similar among children who carried any of the major human leukocyte antigen (HLA) risk genotypes for celiac disease, said Dr. Carin Aronsson at Lund University in Sweden and her associates. “Because these HLA risk genotypes are widely distributed in the general population, these findings may have consequence for future infant feeding recommendations,” they said. They recommended repeating the study in other countries to confirm the link.
In order to develop celiac disease, patients must consume gluten and carry at least one of the relevant DR3-DQ2 and DR4-DQ8 HLA risk haplotypes. But because gluten is widely consumed in products containing wheat, rye, and barley, and because about half of whites have at least one of the two haplotypes, gluten intolerance probably depends on other environmental factors, the researchers said. To further study these factors, they compared 3-day food diaries collected at ages 9, 12, 18, and 24 months for 146 children with positive tissue transglutaminase autoantibody (tTGA) assays and biopsy-confirmed celiac disease (cases) and 436 tTGA-negative children (controls). Cases and controls were matched by age, sex, and HLA genotype (Clin Gastroenterol Hepatol. 2015 Oct 7. doi: 10.1016/j.cgh.2015.09.030).
The food diaries revealed higher gluten intake among cases, compared with controls, beginning at the age of 12 months, said the researchers. Notably, cases consumed a median of 4.9 g of gluten a day before tTGA seroconversion, 1 g more than the median amount for controls of the same age (odds ratio, 1.3; 95% confidence interval, 1.1-1.5; P = .0002). Furthermore, significantly more cases than controls consumed the highest tertile of gluten, more than 5 g per day, before seroconversion (OR, 2.7; 95% CI, 1.7-4.1; P less than .0001). These associations were similar among children of all haplotype profiles and trended in the same direction among children with and without first-degree relatives with celiac disease.
Cases and controls resembled each other in terms of breastfeeding duration, age at first introduction to gluten, and total daily caloric intake, the investigators noted. “The prospective design of this birth cohort study enabled us to obtain the diet information before seroconversion of tTGA as a marker of celiac disease,” they said. “This eliminated the risk of reporting biases or a change in feeding habits because of the knowledge of serology results or disease status.” But they did not analyze the number of daily servings of foods that contained gluten. “We cannot exclude the possibility that the number of portions given frequently during the course of the day may have different effects on disease risk,” they said.
The National Institutes of Health, Juvenile Diabetes Research Foundation, and the Centers for Disease Control and Prevention funded the study. The investigators had no disclosures.
Source: American Gastroenterological Association
Long-suffering Swedish children probably have the highest rate of celiac disease in the world. This rate has dramatically increased. Why and why not? Previous studies have shown that it is not breastfeeding. It is not age or timing of introduction of gluten. It is not likely to be infections. This study shows that it is the amount of gluten that drives children with the highest genetic risk for celiac disease to develop the disease early in life. This conversion is preceded by a high intake of gluten. While these results alone should not determine general infant feeding practices, it suggests that if you are a Swedish child who carries these high-risk genes, high quantities of gluten early in life are not for you.
This study also raises the question of the effect high-dose gluten in adults at risk. Previously, studies have shown that the prevalence of celiac disease in adults in Sweden is not much different from the pediatric population. This study needs to be expanded to other Western populations where the rate of celiac disease is not so high. While nutritional engineering on a grand scale should not be undertaken lightly given the possibility of unexpected consequences, it behooves at least the Swedish population to perhaps reexamine their cultural practices of incorporating high gluten-containing cereals early in the lives of children, most especially those at particular risk for celiac disease.
Dr. Joseph A. Murray, AGAF, is professor of medicine, consultant, division of gastroenterology and hepatology, and department of immunology, and director of the Celiac Disease Program at the Mayo Clinic, Rochester, Minn.
Long-suffering Swedish children probably have the highest rate of celiac disease in the world. This rate has dramatically increased. Why and why not? Previous studies have shown that it is not breastfeeding. It is not age or timing of introduction of gluten. It is not likely to be infections. This study shows that it is the amount of gluten that drives children with the highest genetic risk for celiac disease to develop the disease early in life. This conversion is preceded by a high intake of gluten. While these results alone should not determine general infant feeding practices, it suggests that if you are a Swedish child who carries these high-risk genes, high quantities of gluten early in life are not for you.
This study also raises the question of the effect high-dose gluten in adults at risk. Previously, studies have shown that the prevalence of celiac disease in adults in Sweden is not much different from the pediatric population. This study needs to be expanded to other Western populations where the rate of celiac disease is not so high. While nutritional engineering on a grand scale should not be undertaken lightly given the possibility of unexpected consequences, it behooves at least the Swedish population to perhaps reexamine their cultural practices of incorporating high gluten-containing cereals early in the lives of children, most especially those at particular risk for celiac disease.
Dr. Joseph A. Murray, AGAF, is professor of medicine, consultant, division of gastroenterology and hepatology, and department of immunology, and director of the Celiac Disease Program at the Mayo Clinic, Rochester, Minn.
Long-suffering Swedish children probably have the highest rate of celiac disease in the world. This rate has dramatically increased. Why and why not? Previous studies have shown that it is not breastfeeding. It is not age or timing of introduction of gluten. It is not likely to be infections. This study shows that it is the amount of gluten that drives children with the highest genetic risk for celiac disease to develop the disease early in life. This conversion is preceded by a high intake of gluten. While these results alone should not determine general infant feeding practices, it suggests that if you are a Swedish child who carries these high-risk genes, high quantities of gluten early in life are not for you.
This study also raises the question of the effect high-dose gluten in adults at risk. Previously, studies have shown that the prevalence of celiac disease in adults in Sweden is not much different from the pediatric population. This study needs to be expanded to other Western populations where the rate of celiac disease is not so high. While nutritional engineering on a grand scale should not be undertaken lightly given the possibility of unexpected consequences, it behooves at least the Swedish population to perhaps reexamine their cultural practices of incorporating high gluten-containing cereals early in the lives of children, most especially those at particular risk for celiac disease.
Dr. Joseph A. Murray, AGAF, is professor of medicine, consultant, division of gastroenterology and hepatology, and department of immunology, and director of the Celiac Disease Program at the Mayo Clinic, Rochester, Minn.
Children who were genetically susceptible to celiac disease and consumed high amounts of gluten at 12 months of age were at least twice as likely to develop the autoimmune disorder as genetically predisposed children who consumed less gluten, researchers reported in the March issue of Clinical Gastroenterology and Hepatology.
The association was similar among children who carried any of the major human leukocyte antigen (HLA) risk genotypes for celiac disease, said Dr. Carin Aronsson at Lund University in Sweden and her associates. “Because these HLA risk genotypes are widely distributed in the general population, these findings may have consequence for future infant feeding recommendations,” they said. They recommended repeating the study in other countries to confirm the link.
In order to develop celiac disease, patients must consume gluten and carry at least one of the relevant DR3-DQ2 and DR4-DQ8 HLA risk haplotypes. But because gluten is widely consumed in products containing wheat, rye, and barley, and because about half of whites have at least one of the two haplotypes, gluten intolerance probably depends on other environmental factors, the researchers said. To further study these factors, they compared 3-day food diaries collected at ages 9, 12, 18, and 24 months for 146 children with positive tissue transglutaminase autoantibody (tTGA) assays and biopsy-confirmed celiac disease (cases) and 436 tTGA-negative children (controls). Cases and controls were matched by age, sex, and HLA genotype (Clin Gastroenterol Hepatol. 2015 Oct 7. doi: 10.1016/j.cgh.2015.09.030).
The food diaries revealed higher gluten intake among cases, compared with controls, beginning at the age of 12 months, said the researchers. Notably, cases consumed a median of 4.9 g of gluten a day before tTGA seroconversion, 1 g more than the median amount for controls of the same age (odds ratio, 1.3; 95% confidence interval, 1.1-1.5; P = .0002). Furthermore, significantly more cases than controls consumed the highest tertile of gluten, more than 5 g per day, before seroconversion (OR, 2.7; 95% CI, 1.7-4.1; P less than .0001). These associations were similar among children of all haplotype profiles and trended in the same direction among children with and without first-degree relatives with celiac disease.
Cases and controls resembled each other in terms of breastfeeding duration, age at first introduction to gluten, and total daily caloric intake, the investigators noted. “The prospective design of this birth cohort study enabled us to obtain the diet information before seroconversion of tTGA as a marker of celiac disease,” they said. “This eliminated the risk of reporting biases or a change in feeding habits because of the knowledge of serology results or disease status.” But they did not analyze the number of daily servings of foods that contained gluten. “We cannot exclude the possibility that the number of portions given frequently during the course of the day may have different effects on disease risk,” they said.
The National Institutes of Health, Juvenile Diabetes Research Foundation, and the Centers for Disease Control and Prevention funded the study. The investigators had no disclosures.
Source: American Gastroenterological Association
Children who were genetically susceptible to celiac disease and consumed high amounts of gluten at 12 months of age were at least twice as likely to develop the autoimmune disorder as genetically predisposed children who consumed less gluten, researchers reported in the March issue of Clinical Gastroenterology and Hepatology.
The association was similar among children who carried any of the major human leukocyte antigen (HLA) risk genotypes for celiac disease, said Dr. Carin Aronsson at Lund University in Sweden and her associates. “Because these HLA risk genotypes are widely distributed in the general population, these findings may have consequence for future infant feeding recommendations,” they said. They recommended repeating the study in other countries to confirm the link.
In order to develop celiac disease, patients must consume gluten and carry at least one of the relevant DR3-DQ2 and DR4-DQ8 HLA risk haplotypes. But because gluten is widely consumed in products containing wheat, rye, and barley, and because about half of whites have at least one of the two haplotypes, gluten intolerance probably depends on other environmental factors, the researchers said. To further study these factors, they compared 3-day food diaries collected at ages 9, 12, 18, and 24 months for 146 children with positive tissue transglutaminase autoantibody (tTGA) assays and biopsy-confirmed celiac disease (cases) and 436 tTGA-negative children (controls). Cases and controls were matched by age, sex, and HLA genotype (Clin Gastroenterol Hepatol. 2015 Oct 7. doi: 10.1016/j.cgh.2015.09.030).
The food diaries revealed higher gluten intake among cases, compared with controls, beginning at the age of 12 months, said the researchers. Notably, cases consumed a median of 4.9 g of gluten a day before tTGA seroconversion, 1 g more than the median amount for controls of the same age (odds ratio, 1.3; 95% confidence interval, 1.1-1.5; P = .0002). Furthermore, significantly more cases than controls consumed the highest tertile of gluten, more than 5 g per day, before seroconversion (OR, 2.7; 95% CI, 1.7-4.1; P less than .0001). These associations were similar among children of all haplotype profiles and trended in the same direction among children with and without first-degree relatives with celiac disease.
Cases and controls resembled each other in terms of breastfeeding duration, age at first introduction to gluten, and total daily caloric intake, the investigators noted. “The prospective design of this birth cohort study enabled us to obtain the diet information before seroconversion of tTGA as a marker of celiac disease,” they said. “This eliminated the risk of reporting biases or a change in feeding habits because of the knowledge of serology results or disease status.” But they did not analyze the number of daily servings of foods that contained gluten. “We cannot exclude the possibility that the number of portions given frequently during the course of the day may have different effects on disease risk,” they said.
The National Institutes of Health, Juvenile Diabetes Research Foundation, and the Centers for Disease Control and Prevention funded the study. The investigators had no disclosures.
Source: American Gastroenterological Association
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: High levels of gluten consumption in early life significantly increased the risk of celiac disease.
Major finding: The odds of celiac disease were more than twice as high among children who consumed more than 5 g of gluten a day, compared with those who consumed less gluten (OR, 2.65; P less than .0001).
Data source: A 1 to 3 matched nested case-control study of 146 children with biopsy-confirmed celiac disease (cases) and 436 tissue transglutaminase (tTGA)-negative controls.
Disclosures: The National Institutes of Health, Juvenile Diabetes Research Foundation, and the Centers for Disease Control and Prevention funded the study. The investigators had no disclosures.
Sleep problems common among youth with ASD
The majority of children with autism spectrum disorders have sleeping problems and many take medications for sleep, but those taking medications have worse daytime behaviors and poorer quality of life, according to a study published in the February issue of Pediatrics.
“These findings underscore the need for both longitudinal and interventional studies to determine whether improvement of sleep disturbance with medications also improves daytime behaviors and quality of life,” reported Dr. Beth A. Malow of Vanderbilt University in Nashville, and her associates (Pediatrics. 2016;137[S2]:e20152851H).

The researchers analyzed data from parent questionnaires and clinical forms filled out between April 2009 and December 2013 for 1,518 children, aged 4-10 years, in the Autism Speaks Autism Treatment Network Registry. Most of the children were white boys; only 16% were girls and 20% were nonwhite.
Although only 30% of children (P less than .0001) had sleep diagnoses in clinical reports, parents reported that 71% of the children had significant sleep problems, indicated by a score of at least 41 on the Children’s Sleep Habits Questionnaire. The most common sleep diagnosis was sleep disturbance not otherwise specified, followed by inadequate sleep hygiene, behavioral insomnia of childhood, other sleep disorder, and organic insomnia unspecified.
One reason for the discrepancy between diagnoses and parent-reported difficulties, the researchers suggested, was that “sleep concerns may be eclipsed by other needs [of children with ASD], especially in the limited time available at a clinician visit.” At the same time, however, they note that 41 may be too low a scale cutoff for autistic children.
Among those with a sleep diagnosis, 46% were taking any medication for sleep. Just over a third (36%) of those with a sleep diagnosis took melatonin, and 14% took alpha-agonists. Only 2% of those without a sleep diagnosis took alpha-agonists, but 13% took melatonin and 15% took any medication. Other medications children took for sleep included antidepressants, antihistamines, atypical antipsychotics, benzodiazepines, beta-blockers, sedatives, iron supplements, and vitamins/dietary supplements.
The children taking medications for sleep had more insomnia, significantly lower scores for quality of life, and significantly higher scores for irritability and for internalizing and externalizing behaviors.
“It is possible that sleep disturbance itself is driving this relationship,” Dr. Malow and her associates said. “It is also possible that a clinician would be more likely to use a medication for sleep in a child with more difficult daytime behaviors” or that sleep medications influence behaviors and quality of life.
The research was supported by the Autism Speaks Autism Treatment Network, the U.S. Department of Health & Human Services, and the Maternal and Child Health Research Program to the Massachusetts General Hospital. Dr. Malow has received grant funding from Neurim Pharmaceuticals for a study of prolonged release melatonin (Circadin), and Dr. Reynolds has received grant funding from Mead Johnson.
The majority of children with autism spectrum disorders have sleeping problems and many take medications for sleep, but those taking medications have worse daytime behaviors and poorer quality of life, according to a study published in the February issue of Pediatrics.
“These findings underscore the need for both longitudinal and interventional studies to determine whether improvement of sleep disturbance with medications also improves daytime behaviors and quality of life,” reported Dr. Beth A. Malow of Vanderbilt University in Nashville, and her associates (Pediatrics. 2016;137[S2]:e20152851H).
The researchers analyzed data from parent questionnaires and clinical forms filled out between April 2009 and December 2013 for 1,518 children, aged 4-10 years, in the Autism Speaks Autism Treatment Network Registry. Most of the children were white boys; only 16% were girls and 20% were nonwhite.
Although only 30% of children (P less than .0001) had sleep diagnoses in clinical reports, parents reported that 71% of the children had significant sleep problems, indicated by a score of at least 41 on the Children’s Sleep Habits Questionnaire. The most common sleep diagnosis was sleep disturbance not otherwise specified, followed by inadequate sleep hygiene, behavioral insomnia of childhood, other sleep disorder, and organic insomnia unspecified.
One reason for the discrepancy between diagnoses and parent-reported difficulties, the researchers suggested, was that “sleep concerns may be eclipsed by other needs [of children with ASD], especially in the limited time available at a clinician visit.” At the same time, however, they note that 41 may be too low a scale cutoff for autistic children.
Among those with a sleep diagnosis, 46% were taking any medication for sleep. Just over a third (36%) of those with a sleep diagnosis took melatonin, and 14% took alpha-agonists. Only 2% of those without a sleep diagnosis took alpha-agonists, but 13% took melatonin and 15% took any medication. Other medications children took for sleep included antidepressants, antihistamines, atypical antipsychotics, benzodiazepines, beta-blockers, sedatives, iron supplements, and vitamins/dietary supplements.
The children taking medications for sleep had more insomnia, significantly lower scores for quality of life, and significantly higher scores for irritability and for internalizing and externalizing behaviors.
“It is possible that sleep disturbance itself is driving this relationship,” Dr. Malow and her associates said. “It is also possible that a clinician would be more likely to use a medication for sleep in a child with more difficult daytime behaviors” or that sleep medications influence behaviors and quality of life.
The research was supported by the Autism Speaks Autism Treatment Network, the U.S. Department of Health & Human Services, and the Maternal and Child Health Research Program to the Massachusetts General Hospital. Dr. Malow has received grant funding from Neurim Pharmaceuticals for a study of prolonged release melatonin (Circadin), and Dr. Reynolds has received grant funding from Mead Johnson.
The majority of children with autism spectrum disorders have sleeping problems and many take medications for sleep, but those taking medications have worse daytime behaviors and poorer quality of life, according to a study published in the February issue of Pediatrics.
“These findings underscore the need for both longitudinal and interventional studies to determine whether improvement of sleep disturbance with medications also improves daytime behaviors and quality of life,” reported Dr. Beth A. Malow of Vanderbilt University in Nashville, and her associates (Pediatrics. 2016;137[S2]:e20152851H).
The researchers analyzed data from parent questionnaires and clinical forms filled out between April 2009 and December 2013 for 1,518 children, aged 4-10 years, in the Autism Speaks Autism Treatment Network Registry. Most of the children were white boys; only 16% were girls and 20% were nonwhite.
Although only 30% of children (P less than .0001) had sleep diagnoses in clinical reports, parents reported that 71% of the children had significant sleep problems, indicated by a score of at least 41 on the Children’s Sleep Habits Questionnaire. The most common sleep diagnosis was sleep disturbance not otherwise specified, followed by inadequate sleep hygiene, behavioral insomnia of childhood, other sleep disorder, and organic insomnia unspecified.
One reason for the discrepancy between diagnoses and parent-reported difficulties, the researchers suggested, was that “sleep concerns may be eclipsed by other needs [of children with ASD], especially in the limited time available at a clinician visit.” At the same time, however, they note that 41 may be too low a scale cutoff for autistic children.
Among those with a sleep diagnosis, 46% were taking any medication for sleep. Just over a third (36%) of those with a sleep diagnosis took melatonin, and 14% took alpha-agonists. Only 2% of those without a sleep diagnosis took alpha-agonists, but 13% took melatonin and 15% took any medication. Other medications children took for sleep included antidepressants, antihistamines, atypical antipsychotics, benzodiazepines, beta-blockers, sedatives, iron supplements, and vitamins/dietary supplements.
The children taking medications for sleep had more insomnia, significantly lower scores for quality of life, and significantly higher scores for irritability and for internalizing and externalizing behaviors.
“It is possible that sleep disturbance itself is driving this relationship,” Dr. Malow and her associates said. “It is also possible that a clinician would be more likely to use a medication for sleep in a child with more difficult daytime behaviors” or that sleep medications influence behaviors and quality of life.
The research was supported by the Autism Speaks Autism Treatment Network, the U.S. Department of Health & Human Services, and the Maternal and Child Health Research Program to the Massachusetts General Hospital. Dr. Malow has received grant funding from Neurim Pharmaceuticals for a study of prolonged release melatonin (Circadin), and Dr. Reynolds has received grant funding from Mead Johnson.
FROM PEDIATRICS
Key clinical point: Many autistic children have sleeping problems, and many take medications for sleep.
Major finding: 71% of children with autism spectrum disorders have sleeping difficulties, and 30% have a sleep diagnosis, of whom 46% take medications for sleep.
Data source: The findings are based on analysis of questionnaires and clinical reports for 1,518 children, aged 4-10 years, in the Autism Speaks Autism Treatment Network Registry seen between April 2009 and December 2013.
Disclosures: The research was conducted through the Autism Speaks Autism Treatment Network and was supported by the U.S. Department of Health and Human Services, and Massachusetts General Hospital. Dr. Malow has received grant funding from Neurim Pharmaceuticals for a study of prolonged release melatonin (Circadin), and Dr. Reynolds has received grant funding from Mead Johnson.

Children’s cancer survival steadily increasing
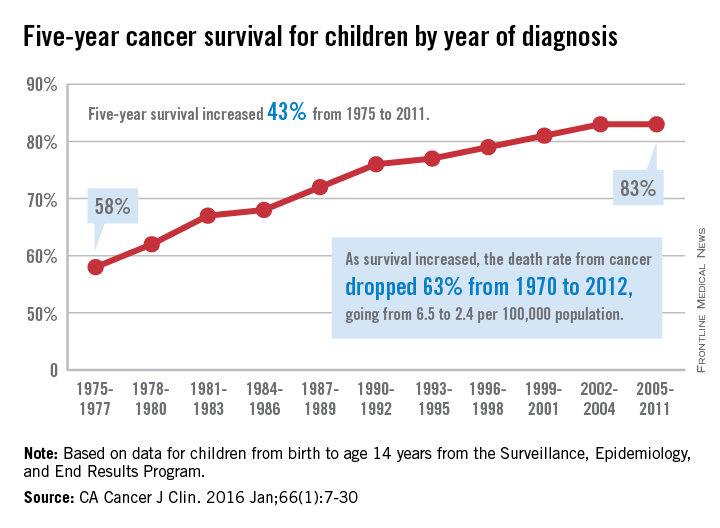
The 5-year cancer survival rate for children younger than 15 years old is up by 43% since 1975, according to investigators from the American Cancer Society.
The 5-year survival rate for all cancers showed a statistically significant rise from 58% in 1975 to 83% in 2011, said Rebecca L. Siegel and her associates at the ACS (CA Cancer J Clin. 2016 Jan;66[1]:7-30).
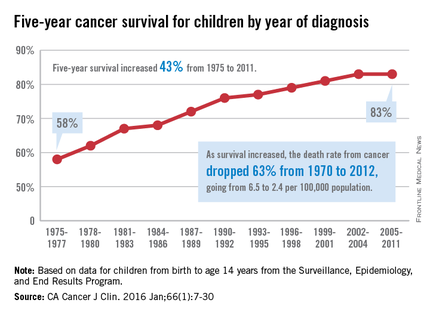
“The substantial progress for all of the major childhood cancers reflects both improvements in treatment and high levels of participation in clinical trials,” they wrote.
Survival for cancers of the brain and nervous system – now the leading cause of cancer death for those younger than 20 years old – increased from 57% in 1975 to 74% in 2011. The next-most-common cause of cancer death in children and adolescents is leukemia, and 5-year survival for acute myeloid leukemia went from 19% in 1975 to 67% in 2011, while 5-year survival for acute lymphocytic leukemia rose from 57% to 91% over that time period, the investigators reported.
The authors reported no conflicts of interest.
The 5-year cancer survival rate for children younger than 15 years old is up by 43% since 1975, according to investigators from the American Cancer Society.
The 5-year survival rate for all cancers showed a statistically significant rise from 58% in 1975 to 83% in 2011, said Rebecca L. Siegel and her associates at the ACS (CA Cancer J Clin. 2016 Jan;66[1]:7-30).
“The substantial progress for all of the major childhood cancers reflects both improvements in treatment and high levels of participation in clinical trials,” they wrote.
Survival for cancers of the brain and nervous system – now the leading cause of cancer death for those younger than 20 years old – increased from 57% in 1975 to 74% in 2011. The next-most-common cause of cancer death in children and adolescents is leukemia, and 5-year survival for acute myeloid leukemia went from 19% in 1975 to 67% in 2011, while 5-year survival for acute lymphocytic leukemia rose from 57% to 91% over that time period, the investigators reported.
The authors reported no conflicts of interest.
The 5-year cancer survival rate for children younger than 15 years old is up by 43% since 1975, according to investigators from the American Cancer Society.
The 5-year survival rate for all cancers showed a statistically significant rise from 58% in 1975 to 83% in 2011, said Rebecca L. Siegel and her associates at the ACS (CA Cancer J Clin. 2016 Jan;66[1]:7-30).
“The substantial progress for all of the major childhood cancers reflects both improvements in treatment and high levels of participation in clinical trials,” they wrote.
Survival for cancers of the brain and nervous system – now the leading cause of cancer death for those younger than 20 years old – increased from 57% in 1975 to 74% in 2011. The next-most-common cause of cancer death in children and adolescents is leukemia, and 5-year survival for acute myeloid leukemia went from 19% in 1975 to 67% in 2011, while 5-year survival for acute lymphocytic leukemia rose from 57% to 91% over that time period, the investigators reported.
The authors reported no conflicts of interest.
FROM CA: A CANCER JOURNAL FOR CLINICIANS
Bedside asthma medication delivery tied to lower ED readmissions
A bedside medication delivery service increased the percentage of asthma patients discharged with medications in hand from 0% to 75%, which helped prevent emergency department readmissions within the next month, according to an exploratory, retrospective analysis.
“To our knowledge this report is the first to detail specific strategies to reliably discharge patients with meds in hand,” said Dr. Jonathan Hatoun of Boston University Medical Center and his associates. “Although this study was not designed to detect adherence, families may feel more comfortable administering medications after receiving teaching from and having questions answered by their inpatient nurse, using the same medications and equipment they will use at home.”
Before the intervention, the hospital previously had routinely discharged asthma patients without medications in hand, and in 2011, a survey showed that 37% never filled their prescriptions. Concerned that patients were “unnecessarily suffering,” Dr. Hatoun and his associates assembled a multidisciplinary team that worked for 2 years to improve this outcome measure. They initially asked residents to write prescriptions at least a day before discharge, but they were concerned that treatment plans could change. Next, they asked families to pick up medications at the hospital pharmacy, but parents were reluctant to leave their sick child’s bedside. Therefore, the researchers designed an in-room service in which pharmacists delivered the medications to the child’s room when a parent was present (Pediatrics 2016 Feb 24. doi: 10.1542/peds.2015-0461). “Copayments were collected in the room, either in cash or with a mobile credit payment system purchased by the pharmacy,” the researchers explained. “Unlike traditional pharmacy pickup, the delivery service allows the patient, parent, nurse, and pharmacist to be together in the patient’s hospital room for teaching with the actual medications available for demonstration.”
The delivery service not only met the project goal to increase the “meds in hand” rate from 0% to 75%, but an analysis of patients with complete insurance claims showed that patients discharged with medications in hand were significantly less likely to return to the emergency department within 30 days of discharge, for any reason, compared with patients who received usual care (odds ratio, 0.22; 95% confidence interval, 0.05-0.99).
“Although more evidence on the impact of being discharged in possession of discharge medications is needed, a service that provides admitted patients with their outpatient medications before they leave the hospital has many potential benefits,” the investigators noted. “Additional areas of exploration could include how the Meds-in-Hand service affects the patient experience, hospital finances, and clinical outcomes for other medical conditions.”
The authors had no external funding sources or disclosures.
A bedside medication delivery service increased the percentage of asthma patients discharged with medications in hand from 0% to 75%, which helped prevent emergency department readmissions within the next month, according to an exploratory, retrospective analysis.
“To our knowledge this report is the first to detail specific strategies to reliably discharge patients with meds in hand,” said Dr. Jonathan Hatoun of Boston University Medical Center and his associates. “Although this study was not designed to detect adherence, families may feel more comfortable administering medications after receiving teaching from and having questions answered by their inpatient nurse, using the same medications and equipment they will use at home.”
Before the intervention, the hospital previously had routinely discharged asthma patients without medications in hand, and in 2011, a survey showed that 37% never filled their prescriptions. Concerned that patients were “unnecessarily suffering,” Dr. Hatoun and his associates assembled a multidisciplinary team that worked for 2 years to improve this outcome measure. They initially asked residents to write prescriptions at least a day before discharge, but they were concerned that treatment plans could change. Next, they asked families to pick up medications at the hospital pharmacy, but parents were reluctant to leave their sick child’s bedside. Therefore, the researchers designed an in-room service in which pharmacists delivered the medications to the child’s room when a parent was present (Pediatrics 2016 Feb 24. doi: 10.1542/peds.2015-0461). “Copayments were collected in the room, either in cash or with a mobile credit payment system purchased by the pharmacy,” the researchers explained. “Unlike traditional pharmacy pickup, the delivery service allows the patient, parent, nurse, and pharmacist to be together in the patient’s hospital room for teaching with the actual medications available for demonstration.”
The delivery service not only met the project goal to increase the “meds in hand” rate from 0% to 75%, but an analysis of patients with complete insurance claims showed that patients discharged with medications in hand were significantly less likely to return to the emergency department within 30 days of discharge, for any reason, compared with patients who received usual care (odds ratio, 0.22; 95% confidence interval, 0.05-0.99).
“Although more evidence on the impact of being discharged in possession of discharge medications is needed, a service that provides admitted patients with their outpatient medications before they leave the hospital has many potential benefits,” the investigators noted. “Additional areas of exploration could include how the Meds-in-Hand service affects the patient experience, hospital finances, and clinical outcomes for other medical conditions.”
The authors had no external funding sources or disclosures.
A bedside medication delivery service increased the percentage of asthma patients discharged with medications in hand from 0% to 75%, which helped prevent emergency department readmissions within the next month, according to an exploratory, retrospective analysis.
“To our knowledge this report is the first to detail specific strategies to reliably discharge patients with meds in hand,” said Dr. Jonathan Hatoun of Boston University Medical Center and his associates. “Although this study was not designed to detect adherence, families may feel more comfortable administering medications after receiving teaching from and having questions answered by their inpatient nurse, using the same medications and equipment they will use at home.”
Before the intervention, the hospital previously had routinely discharged asthma patients without medications in hand, and in 2011, a survey showed that 37% never filled their prescriptions. Concerned that patients were “unnecessarily suffering,” Dr. Hatoun and his associates assembled a multidisciplinary team that worked for 2 years to improve this outcome measure. They initially asked residents to write prescriptions at least a day before discharge, but they were concerned that treatment plans could change. Next, they asked families to pick up medications at the hospital pharmacy, but parents were reluctant to leave their sick child’s bedside. Therefore, the researchers designed an in-room service in which pharmacists delivered the medications to the child’s room when a parent was present (Pediatrics 2016 Feb 24. doi: 10.1542/peds.2015-0461). “Copayments were collected in the room, either in cash or with a mobile credit payment system purchased by the pharmacy,” the researchers explained. “Unlike traditional pharmacy pickup, the delivery service allows the patient, parent, nurse, and pharmacist to be together in the patient’s hospital room for teaching with the actual medications available for demonstration.”
The delivery service not only met the project goal to increase the “meds in hand” rate from 0% to 75%, but an analysis of patients with complete insurance claims showed that patients discharged with medications in hand were significantly less likely to return to the emergency department within 30 days of discharge, for any reason, compared with patients who received usual care (odds ratio, 0.22; 95% confidence interval, 0.05-0.99).
“Although more evidence on the impact of being discharged in possession of discharge medications is needed, a service that provides admitted patients with their outpatient medications before they leave the hospital has many potential benefits,” the investigators noted. “Additional areas of exploration could include how the Meds-in-Hand service affects the patient experience, hospital finances, and clinical outcomes for other medical conditions.”
The authors had no external funding sources or disclosures.
FROM PEDIATRICS
Key clinical point: A bedside medication delivery service ensured that most children hospitalized with asthma left with medications in hand, helping prevent 30-day readmissions.
Major finding: The rate of discharge with medications in hand rose from 0% to 75%. Discharge with medications in hand was associated with significantly decreased odds of 30-day all-cause emergency department readmission, compared with usual care (odds ratio, 0.22; 95% confidence interval, 0.05-0.99).
Data source: A single-center exploratory retrospective study.
Disclosures: The researchers had no external funding sources and no disclosures.
Keep cancer prominent in differential diagnoses of pediatric rheumatic complaints
MAUI, HAWAII – The first thing nonpediatric rheumatologists need to understand about a child who presents with rheumatic complaints is the importance of ruling out malignancy, Dr. Anne M. Stevens stressed at the 2016 Rheumatology Winter Clinical Symposium.
“This is something I think we in pediatric rheumatology worry about a lot more than adult rheumatologists: malignancy and how to distinguish it from rheumatic diseases,” said Dr. Stevens, a pediatric rheumatologist at Seattle Children’s Hospital and the University of Washington.

And with there being only about 250 pediatric rheumatologists in the entire United States, and a handful of states having none at all, it’s important that physicians in other specialties be familiar with key differences between pediatric and adult rheumatic diseases, she added.
A diverse group of malignancies in children and teens can present with swollen joints or other rheumatic features. One of the biggest red flags suggestive of an underlying malignancy is disproportionate pain, especially nonarticular bone pain or tenderness or back pain as a major presenting feature.
The source of this bone or back pain may be a reactive arthritis in response to local bony changes caused by an osteosarcoma or neuroblastoma, or malignant effusions as a result of leukemia or lymphoma, Dr. Stevens explained.
Other atypical features that get her thinking about the possibility of underlying malignancy rather than juvenile idiopathic arthritis include weight loss, night sweats, fatigue, fever, and night pain. Overall, young patients with an undetected cancer just seem sicker than those with rheumatic disease, she continued.
In a classic retrospective study of 29 children and teens who initially presented to pediatric rheumatologists at the University of British Columbia and were ultimately found to have malignancy, the most common provisional rheumatologic diagnosis was juvenile rheumatoid arthritis in 12 of the 29. Five patients were thought by referring physicians to have a connective tissue disease, and three each were believed to have discitis or spondyloarthropathy. Other provisional diagnoses included systemic lupus erythematosus in two patients; Kawasaki disease in two; and Lyme disease, mixed connective tissue disease, and dermatomyositis in one each.
The final diagnoses included leukemia in 13 patients, neuroblastoma in 6, lymphoma in 3, Ewing sarcoma in 3, and single cases of ependymoma, thalamic glioma, epithelioma, and sarcoma (J Pediatr. 1999 Jan;134[1]:53-7).
Working backwards, the investigators developed a set of clinical clues helpful in detecting malignancy. Nonarticular bone pain was a prominent presenting complaint in 20 of the 29, bone tenderness in 8, and back pain in 9.
“Bone tenderness is not seen in juvenile idiopathic arthritis at all, and children under about age 10 just don’t get low back pain. That really alerts us to malignancy concern,” Dr. Stevens said.
Night sweats were present in four patients, severe constitutional symptoms in nine.
Two patients had true juvenile idiopathic arthritis, so that finding doesn’t rule out malignancy.
Surprisingly, the CBC was normal in three-quarters of patients. Antinuclear antibody testing is not helpful, as it can be strongly positive in the setting of pediatric malignancy, but lactate dehydrogenase and uric acid tests are important in making the differential diagnosis.
If there are any surprising findings raising concerns about possible malignancy, a bone marrow biopsy is essential.
“We have a lot of fights with our hematologists when we’re trying to get a bone marrow biopsy and they say, ‘No, the CBC is normal so you don’t need a bone marrow biopsy.’ But you have to get that bone marrow biopsy. A strategy that works is for us to say, ‘Could you please include a note in the chart that it’s okay for us to give steroids because you’re sure it’s not a lymphoma?’ Then we usually get it scheduled for the next day,” Dr. Stevens said.
She reported having no relevant financial disclosures.
MAUI, HAWAII – The first thing nonpediatric rheumatologists need to understand about a child who presents with rheumatic complaints is the importance of ruling out malignancy, Dr. Anne M. Stevens stressed at the 2016 Rheumatology Winter Clinical Symposium.
“This is something I think we in pediatric rheumatology worry about a lot more than adult rheumatologists: malignancy and how to distinguish it from rheumatic diseases,” said Dr. Stevens, a pediatric rheumatologist at Seattle Children’s Hospital and the University of Washington.
And with there being only about 250 pediatric rheumatologists in the entire United States, and a handful of states having none at all, it’s important that physicians in other specialties be familiar with key differences between pediatric and adult rheumatic diseases, she added.
A diverse group of malignancies in children and teens can present with swollen joints or other rheumatic features. One of the biggest red flags suggestive of an underlying malignancy is disproportionate pain, especially nonarticular bone pain or tenderness or back pain as a major presenting feature.
The source of this bone or back pain may be a reactive arthritis in response to local bony changes caused by an osteosarcoma or neuroblastoma, or malignant effusions as a result of leukemia or lymphoma, Dr. Stevens explained.
Other atypical features that get her thinking about the possibility of underlying malignancy rather than juvenile idiopathic arthritis include weight loss, night sweats, fatigue, fever, and night pain. Overall, young patients with an undetected cancer just seem sicker than those with rheumatic disease, she continued.
In a classic retrospective study of 29 children and teens who initially presented to pediatric rheumatologists at the University of British Columbia and were ultimately found to have malignancy, the most common provisional rheumatologic diagnosis was juvenile rheumatoid arthritis in 12 of the 29. Five patients were thought by referring physicians to have a connective tissue disease, and three each were believed to have discitis or spondyloarthropathy. Other provisional diagnoses included systemic lupus erythematosus in two patients; Kawasaki disease in two; and Lyme disease, mixed connective tissue disease, and dermatomyositis in one each.
The final diagnoses included leukemia in 13 patients, neuroblastoma in 6, lymphoma in 3, Ewing sarcoma in 3, and single cases of ependymoma, thalamic glioma, epithelioma, and sarcoma (J Pediatr. 1999 Jan;134[1]:53-7).
Working backwards, the investigators developed a set of clinical clues helpful in detecting malignancy. Nonarticular bone pain was a prominent presenting complaint in 20 of the 29, bone tenderness in 8, and back pain in 9.
“Bone tenderness is not seen in juvenile idiopathic arthritis at all, and children under about age 10 just don’t get low back pain. That really alerts us to malignancy concern,” Dr. Stevens said.
Night sweats were present in four patients, severe constitutional symptoms in nine.
Two patients had true juvenile idiopathic arthritis, so that finding doesn’t rule out malignancy.
Surprisingly, the CBC was normal in three-quarters of patients. Antinuclear antibody testing is not helpful, as it can be strongly positive in the setting of pediatric malignancy, but lactate dehydrogenase and uric acid tests are important in making the differential diagnosis.
If there are any surprising findings raising concerns about possible malignancy, a bone marrow biopsy is essential.
“We have a lot of fights with our hematologists when we’re trying to get a bone marrow biopsy and they say, ‘No, the CBC is normal so you don’t need a bone marrow biopsy.’ But you have to get that bone marrow biopsy. A strategy that works is for us to say, ‘Could you please include a note in the chart that it’s okay for us to give steroids because you’re sure it’s not a lymphoma?’ Then we usually get it scheduled for the next day,” Dr. Stevens said.
She reported having no relevant financial disclosures.
MAUI, HAWAII – The first thing nonpediatric rheumatologists need to understand about a child who presents with rheumatic complaints is the importance of ruling out malignancy, Dr. Anne M. Stevens stressed at the 2016 Rheumatology Winter Clinical Symposium.
“This is something I think we in pediatric rheumatology worry about a lot more than adult rheumatologists: malignancy and how to distinguish it from rheumatic diseases,” said Dr. Stevens, a pediatric rheumatologist at Seattle Children’s Hospital and the University of Washington.
And with there being only about 250 pediatric rheumatologists in the entire United States, and a handful of states having none at all, it’s important that physicians in other specialties be familiar with key differences between pediatric and adult rheumatic diseases, she added.
A diverse group of malignancies in children and teens can present with swollen joints or other rheumatic features. One of the biggest red flags suggestive of an underlying malignancy is disproportionate pain, especially nonarticular bone pain or tenderness or back pain as a major presenting feature.
The source of this bone or back pain may be a reactive arthritis in response to local bony changes caused by an osteosarcoma or neuroblastoma, or malignant effusions as a result of leukemia or lymphoma, Dr. Stevens explained.
Other atypical features that get her thinking about the possibility of underlying malignancy rather than juvenile idiopathic arthritis include weight loss, night sweats, fatigue, fever, and night pain. Overall, young patients with an undetected cancer just seem sicker than those with rheumatic disease, she continued.
In a classic retrospective study of 29 children and teens who initially presented to pediatric rheumatologists at the University of British Columbia and were ultimately found to have malignancy, the most common provisional rheumatologic diagnosis was juvenile rheumatoid arthritis in 12 of the 29. Five patients were thought by referring physicians to have a connective tissue disease, and three each were believed to have discitis or spondyloarthropathy. Other provisional diagnoses included systemic lupus erythematosus in two patients; Kawasaki disease in two; and Lyme disease, mixed connective tissue disease, and dermatomyositis in one each.
The final diagnoses included leukemia in 13 patients, neuroblastoma in 6, lymphoma in 3, Ewing sarcoma in 3, and single cases of ependymoma, thalamic glioma, epithelioma, and sarcoma (J Pediatr. 1999 Jan;134[1]:53-7).
Working backwards, the investigators developed a set of clinical clues helpful in detecting malignancy. Nonarticular bone pain was a prominent presenting complaint in 20 of the 29, bone tenderness in 8, and back pain in 9.
“Bone tenderness is not seen in juvenile idiopathic arthritis at all, and children under about age 10 just don’t get low back pain. That really alerts us to malignancy concern,” Dr. Stevens said.
Night sweats were present in four patients, severe constitutional symptoms in nine.
Two patients had true juvenile idiopathic arthritis, so that finding doesn’t rule out malignancy.
Surprisingly, the CBC was normal in three-quarters of patients. Antinuclear antibody testing is not helpful, as it can be strongly positive in the setting of pediatric malignancy, but lactate dehydrogenase and uric acid tests are important in making the differential diagnosis.
If there are any surprising findings raising concerns about possible malignancy, a bone marrow biopsy is essential.
“We have a lot of fights with our hematologists when we’re trying to get a bone marrow biopsy and they say, ‘No, the CBC is normal so you don’t need a bone marrow biopsy.’ But you have to get that bone marrow biopsy. A strategy that works is for us to say, ‘Could you please include a note in the chart that it’s okay for us to give steroids because you’re sure it’s not a lymphoma?’ Then we usually get it scheduled for the next day,” Dr. Stevens said.
She reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM RWCS 2016

Resilience
It has been clear for a long time that a child who grows up in an environment dominated by adversity is more likely to enter adulthood scarred psychologically, and as a result is less likely to succeed. This well-described association has in the last few years become a hot button topic. A 2012 American Academy of Pediatrics policy statement alerted pediatricians to their potential role in identifying and managing what is now referred to as “toxic stress” (“Early Childhood Adversity, Toxic Stress, and the Role of the Pediatrician: Translating Developmental Science Into Lifelong Health”).
Although a childhood in which challenges outnumber advantages is often followed by an adult life characterized by failure and dysfunction, there are a few individuals who not only survive a disadvantaged childhood unscathed but somehow manage to thrive in its wake. For example, Joe Rantz, the central figure in Daniel James Brown’s nonfiction best seller “The Boys in the Boat” (New York: Viking Press, 2013) was abandoned several times by his family but emerged to power the University of Washington crew team to victory in the 1936 Olympics. Intrigued by these outliers, a developmental psychologist and clinician from the University of Minnesota named Norman Garmezy began looking for features that may have allowed these exceptional people to succeed and even excel despite incredibly difficult circumstances (“How People Learn to Become Resilient,” Maria Konnikova, The New Yorker, Feb. 11, 2016). His search for the characteristics that might have protected these individuals as children from the acute and chronic environmental threats of their disadvantaged childhoods has spawned a breed of developmental psychologists who devote their research to a quality now referred to as “resilience.”
In 1989, Emmy E. Werner, Ph.D., published a study of 698 children on the island of Kauai in Hawaii and identified several elements that might predict resilience (“Children of the Garden Island,” Sci Am. 1989;260[4]:106-11). Not surprisingly, one factor was the good luck of having formed a strong bond with a supportive person such as a caregiver or mentor. However, Dr. Werner also discovered that resilient individuals possessed a set of psychological characteristics that included a positive social orientation prompting them to “meet the world on their own terms.” They were likely to be autonomous and independent and had the attitude that “they, and not their circumstances, affected their achievements.”
These findings lead to the obvious question of whether those attributes that can protect against adversity can be taught. George Bonanno, a clinical psychologist at Columbia University’s Teachers College, found that an individual’s perception of the situation is the key element in resilience. In the New Yorker article on resilience, he was quoted in an interview as saying, “Events are not traumatic until we experience them as traumatic.” In his studies he has found that individuals can be taught how to reframe an event in positive terms that was initially perceived as negative. Unfortunately, the reverse can occur, and as Dr. Bonanno also said in the interview, “We can create or exaggerate stressors very easily in our own minds.” Every event is potentially traumatic if we perceive it that way.
Could it be that in some situations our behavior as adults, parents, and professionals creates an environment that transforms an event into one that is more easily perceived by a child as traumatizing? While it is important to be on the lookout for children who have been emotionally traumatized by an unfortunate event such as a school shooting, we must be careful to keep our responses measured and positive. Children should be reminded that it is they who control their own behavior and achievements, not the circumstances in which they find themselves.
Parents should be reminded that hovering and overinvolvement in their children’s lives is preventing the development of independence and a sense of autonomy, two important characteristics of resilience. The trend in education that emphasizes group solutions may be helping some children learn to cooperate with others and function as a team. But, we must also remember to offer each individual child abundant opportunities to learn so that he or she can also rely on himself or herself to solve problems.
Few of us will ever have the capacity for resiliency demonstrated by Louis Zamperini in the nonfiction best seller Unbroken, but we can and should be doing a better job helping children learn that even in the most adverse conditions, they have some control – if not over the circumstance, then at least over their perception of it.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
It has been clear for a long time that a child who grows up in an environment dominated by adversity is more likely to enter adulthood scarred psychologically, and as a result is less likely to succeed. This well-described association has in the last few years become a hot button topic. A 2012 American Academy of Pediatrics policy statement alerted pediatricians to their potential role in identifying and managing what is now referred to as “toxic stress” (“Early Childhood Adversity, Toxic Stress, and the Role of the Pediatrician: Translating Developmental Science Into Lifelong Health”).
Although a childhood in which challenges outnumber advantages is often followed by an adult life characterized by failure and dysfunction, there are a few individuals who not only survive a disadvantaged childhood unscathed but somehow manage to thrive in its wake. For example, Joe Rantz, the central figure in Daniel James Brown’s nonfiction best seller “The Boys in the Boat” (New York: Viking Press, 2013) was abandoned several times by his family but emerged to power the University of Washington crew team to victory in the 1936 Olympics. Intrigued by these outliers, a developmental psychologist and clinician from the University of Minnesota named Norman Garmezy began looking for features that may have allowed these exceptional people to succeed and even excel despite incredibly difficult circumstances (“How People Learn to Become Resilient,” Maria Konnikova, The New Yorker, Feb. 11, 2016). His search for the characteristics that might have protected these individuals as children from the acute and chronic environmental threats of their disadvantaged childhoods has spawned a breed of developmental psychologists who devote their research to a quality now referred to as “resilience.”
In 1989, Emmy E. Werner, Ph.D., published a study of 698 children on the island of Kauai in Hawaii and identified several elements that might predict resilience (“Children of the Garden Island,” Sci Am. 1989;260[4]:106-11). Not surprisingly, one factor was the good luck of having formed a strong bond with a supportive person such as a caregiver or mentor. However, Dr. Werner also discovered that resilient individuals possessed a set of psychological characteristics that included a positive social orientation prompting them to “meet the world on their own terms.” They were likely to be autonomous and independent and had the attitude that “they, and not their circumstances, affected their achievements.”
These findings lead to the obvious question of whether those attributes that can protect against adversity can be taught. George Bonanno, a clinical psychologist at Columbia University’s Teachers College, found that an individual’s perception of the situation is the key element in resilience. In the New Yorker article on resilience, he was quoted in an interview as saying, “Events are not traumatic until we experience them as traumatic.” In his studies he has found that individuals can be taught how to reframe an event in positive terms that was initially perceived as negative. Unfortunately, the reverse can occur, and as Dr. Bonanno also said in the interview, “We can create or exaggerate stressors very easily in our own minds.” Every event is potentially traumatic if we perceive it that way.
Could it be that in some situations our behavior as adults, parents, and professionals creates an environment that transforms an event into one that is more easily perceived by a child as traumatizing? While it is important to be on the lookout for children who have been emotionally traumatized by an unfortunate event such as a school shooting, we must be careful to keep our responses measured and positive. Children should be reminded that it is they who control their own behavior and achievements, not the circumstances in which they find themselves.
Parents should be reminded that hovering and overinvolvement in their children’s lives is preventing the development of independence and a sense of autonomy, two important characteristics of resilience. The trend in education that emphasizes group solutions may be helping some children learn to cooperate with others and function as a team. But, we must also remember to offer each individual child abundant opportunities to learn so that he or she can also rely on himself or herself to solve problems.
Few of us will ever have the capacity for resiliency demonstrated by Louis Zamperini in the nonfiction best seller Unbroken, but we can and should be doing a better job helping children learn that even in the most adverse conditions, they have some control – if not over the circumstance, then at least over their perception of it.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
It has been clear for a long time that a child who grows up in an environment dominated by adversity is more likely to enter adulthood scarred psychologically, and as a result is less likely to succeed. This well-described association has in the last few years become a hot button topic. A 2012 American Academy of Pediatrics policy statement alerted pediatricians to their potential role in identifying and managing what is now referred to as “toxic stress” (“Early Childhood Adversity, Toxic Stress, and the Role of the Pediatrician: Translating Developmental Science Into Lifelong Health”).
Although a childhood in which challenges outnumber advantages is often followed by an adult life characterized by failure and dysfunction, there are a few individuals who not only survive a disadvantaged childhood unscathed but somehow manage to thrive in its wake. For example, Joe Rantz, the central figure in Daniel James Brown’s nonfiction best seller “The Boys in the Boat” (New York: Viking Press, 2013) was abandoned several times by his family but emerged to power the University of Washington crew team to victory in the 1936 Olympics. Intrigued by these outliers, a developmental psychologist and clinician from the University of Minnesota named Norman Garmezy began looking for features that may have allowed these exceptional people to succeed and even excel despite incredibly difficult circumstances (“How People Learn to Become Resilient,” Maria Konnikova, The New Yorker, Feb. 11, 2016). His search for the characteristics that might have protected these individuals as children from the acute and chronic environmental threats of their disadvantaged childhoods has spawned a breed of developmental psychologists who devote their research to a quality now referred to as “resilience.”
In 1989, Emmy E. Werner, Ph.D., published a study of 698 children on the island of Kauai in Hawaii and identified several elements that might predict resilience (“Children of the Garden Island,” Sci Am. 1989;260[4]:106-11). Not surprisingly, one factor was the good luck of having formed a strong bond with a supportive person such as a caregiver or mentor. However, Dr. Werner also discovered that resilient individuals possessed a set of psychological characteristics that included a positive social orientation prompting them to “meet the world on their own terms.” They were likely to be autonomous and independent and had the attitude that “they, and not their circumstances, affected their achievements.”
These findings lead to the obvious question of whether those attributes that can protect against adversity can be taught. George Bonanno, a clinical psychologist at Columbia University’s Teachers College, found that an individual’s perception of the situation is the key element in resilience. In the New Yorker article on resilience, he was quoted in an interview as saying, “Events are not traumatic until we experience them as traumatic.” In his studies he has found that individuals can be taught how to reframe an event in positive terms that was initially perceived as negative. Unfortunately, the reverse can occur, and as Dr. Bonanno also said in the interview, “We can create or exaggerate stressors very easily in our own minds.” Every event is potentially traumatic if we perceive it that way.
Could it be that in some situations our behavior as adults, parents, and professionals creates an environment that transforms an event into one that is more easily perceived by a child as traumatizing? While it is important to be on the lookout for children who have been emotionally traumatized by an unfortunate event such as a school shooting, we must be careful to keep our responses measured and positive. Children should be reminded that it is they who control their own behavior and achievements, not the circumstances in which they find themselves.
Parents should be reminded that hovering and overinvolvement in their children’s lives is preventing the development of independence and a sense of autonomy, two important characteristics of resilience. The trend in education that emphasizes group solutions may be helping some children learn to cooperate with others and function as a team. But, we must also remember to offer each individual child abundant opportunities to learn so that he or she can also rely on himself or herself to solve problems.
Few of us will ever have the capacity for resiliency demonstrated by Louis Zamperini in the nonfiction best seller Unbroken, but we can and should be doing a better job helping children learn that even in the most adverse conditions, they have some control – if not over the circumstance, then at least over their perception of it.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”

The Challenges of Type 1 Diabetes: A Case-based Review
IN THIS ARTICLE
- Progress and treatment timeline with long- and rapid-acting insulin
- Progress and treatment timeline with continuous subcutaneous insulin infusion
- American Diabetes Association criteria for diagnosis of diabetes
- Blood glucose and A1C goals for type 1 diabetes by age-group
A 5-year-old Caucasian girl presents to the primary care practitioner’s office with chief complaints of polydipsia, polyuria with nocturia, polyphagia, and weight loss over the past three weeks. Her medical history includes a four-year history of keratosis pilaris (KP). The child experienced a KP flare-up two weeks ago; application of triamcinolone acetonide cream yielded no improvement. She also has xerosis, which is treated daily with OTC moisturizing lotion. She was born vaginally and breast-fed and is up to date on her immunizations. There is no family history of diabetes or autoimmune diseases.
Physical examination reveals a weight of 54 lb (95th percentile); height, 47 in (97th percentile); and BMI, 17.2. Vital signs include a blood pressure of 105/55 mm Hg; pulse, 85 beats/min and regular; temperature, 98.2°F; and respiratory rate, 22 breaths/min. KP is noted on the patient’s eyebrows, bilateral upper arms, and bilateral cheeks; the affected skin is erythemic and rough to the touch. Her physical examination findings are otherwise unremarkable.
The child’s urine is tested in the office for glucose and ketones, with results of 4+ glucose and 3+ ketones. These results and the child’s history prompt her admission to the pediatric ICU at a nearby hospital for further treatment with a diagnosis of new-onset type 1 diabetes (T1D) and diabetic ketoacidosis (DKA).
The diagnosis is confirmed at the hospital with laboratory results that include venous glucose, 418 mg/dL (normal range, 70 to 100 mg/dL) and A1C, 10.5% (range, 4.0% to 5.6%). Venous blood gas results include pH, 7.278 (7.32 to 7.42); PCO2, 29.6 mm Hg (39 to 54 mm Hg); HCO3, 13.8 mEq/L (19 to 25 mEq/L); base excess, –12 mmol/L (–4 to +2 mmol/L); beta hydroxybutyrate, 6.0 mmol/L (0.4 to 0.5 mmol/L); insulin antibody, 0.9 U/mL (< 0.4 U/mL); glutamic acid decarboxylase, 166 U/mL (< 0.5 U/mL); and venous lactate, 1.79 mmol/L (0.69 to 2.75 mmol/L).
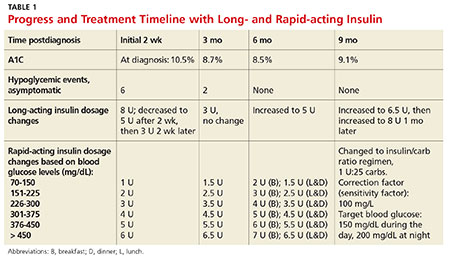
The child is treated initially with an IV insulin infusion for 24 hours, then transitioned to subcutaneous insulin therapy once the DKA resolves and glucose levels are within normal limits. The child remains hospitalized for four days. Discharge medications include insulin glargine, 8 U/d, and insulin lispro before each meal, at bedtime, and at 0200 hours, with dosing based on sliding scales. Dietary orders include 45 to 60 g carbohydrates per meal, along with two snacks of 15 g carbohydrates.
The child is instructed to exercise at least 30 min/d (unless hypoglycemic events occur more than once per week or ketones are found in the blood or urine), drink plenty of water, and avoid concentrated sweets. Education is provided via the Diabetes Educator; the family takes home the beginner T1D booklet and is instructed to log the child’s blood glucose levels and return with this information in two weeks.
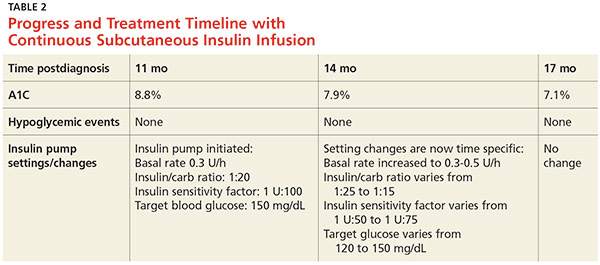
In the first three months, the patient experiences eight asymptomatic hypoglycemic events; for the next seven months, after dosing changes, she remains hyperglycemic most of the time (see Table 1). Insulin doses are adjusted, ranging from weekly to every three months, but glycemic goals are not achieved with the subcutaneous insulin injections. Use of continuous subcutaneous insulin infusion, the “insulin pump,” is then considered. Ten months postdiagnosis, the child begins a five-day-long saline (placebo) pump trial to determine whether the pump is appropriate for her and her lifestyle. After the trial, the decision is made to move forward with the insulin pump, initiated 11 months postdiagnosis.
The practitioner remains in frequent communication with the child’s mother in an effort to maintain glycemic control. After three months on the insulin pump, the child’s A1C is reduced to 7.9%, which is within the target range for her age-group (see Table 2). The child is now maintaining glycemic goals with the use of the insulin pump and close monitoring by the practitioner.
Continue for the discussion >>
DISCUSSION
According to the Juvenile Diabetes Research Foundation, as many as 1.25 million Americans are currently living with T1D; from 2001 to 2009, the prevalence of T1D in people younger than 20 increased by 23%.1 The overall prevalence of diabetes (both types 1 and 2) is predicted to be one in every three people by 2050 if current trends continue.2 According to the American Diabetes Association (ADA), 18,436 US youths are diagnosed with T1D every year, and T1D accounts for about 5% of diabetes cases in the US population.2
Diagnosis
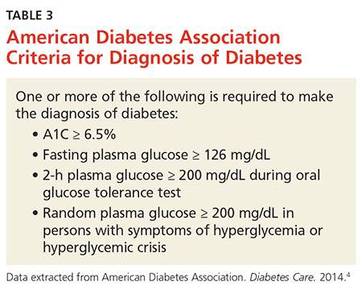
Diabetes is diagnosed based on blood test results that fall within the parameters set by the ADA diagnostic criteria (see Table 3).3 In addition to diagnostic testing for diabetes recommended by the ADA guidelines, blood tests are ordered for autoantibodies that are associated with T1D, to distinguish between type 1 and type 2 diabetes. (T1D results from cellular-mediated autoimmune destruction of the insulin-producing beta cells in the pancreas.4) Upon initial diagnosis, about 85% to 90% of T1D patients have one or more autoantibodies present in blood work, such as autoantibodies to islet cells or to insulin, glutamic acid decarboxylase (GAD65), or tyrosine phosphatases IA-2 and IA-2B.4
In this case study, the child had an elevated GAD65 value and a positive screening for an insulin autoantibody, which explained the destruction of her beta cells. The patient also had KP and xerosis, which are clinical manifestations commonly seen in T1D. In one study of children with T1D, 22% had xerosis, compared with 3% of healthy, age-matched controls, and KP was also significantly more common in T1D patients than in controls (12% vs 1.5%).5
The presence of ketones in the case patient’s urine also suggests T1D, rather than type 2.4 The differential diagnosis for T1D includes type 2 diabetes mellitus, monogenic diabetes mellitus (formerly known as maturity-onset diabetes of the young), secondary hyperglycemia, and other endocrine disorders.6
Acute complications associated with T1D include hypoglycemia, hyperglycemia, and DKA. Long-term complications may include diabetic retinopathy, cataracts, gastroparesis, hypertension, renal failure, coronary artery disease, peripheral vascular disease, diabetic neuropathy, and increased risk for infection.7 These complications can likely be prevented by good glycemic control, proper diet, exercise, and avoidance of nicotine.7
Unfortunately, T1D cannot currently be prevented, although research studies are under way. TrialNet is currently conducting a “Pathway to Prevention” trial; the researchers are testing ways to delay and prevent T1D, as well as slow its progression after diagnosis.8 Potential participants (family members of a T1D patient) are screened for T1D autoantibodies. If test results are positive, these participants are included in the prevention pathway study.
Continue for management >>
Management
Most cases of T1D are diagnosed in patients younger than 18.9 Management of the child with T1D involves many challenges. The patient will experience an initial honeymoon period, that is, a brief remission during which the pancreas begins to secrete some insulin again and exogenous insulin demands are lower. However, this period is temporary, lasting only a few weeks, months, or years. Once pancreatic insulin secretion stops (as a result of complete beta-cell destruction), the exogenous insulin demands increase. In the case study, the child’s insulin demands were initially low, and she experienced hypoglycemia. Once she transitioned out of the honeymoon period, however, her blood glucose levels rose because her pancreas was producing little to no insulin.
As the patient ages, physical growth and hormone changes also alter the demand for insulin. A key factor to keep in mind is lifestyle changes: The child may need age-appropriate supervision and adjustments in exercise, diet, and diabetes education regimens when school routines and self-care capacities change. The child with T1D can only be educated as far as his or her cognitive ability will allow, but autonomy should increase with age.
Helping the patient reach glycemic goals requires special consideration, based on the child’s age. Whereas the target A1C for an adult with diabetes is below 7%, that for a young child is either < 7.5% or < 8.5%, depending on age (see Table 4).9 According to Danne et al, approximately 60% of children younger than 6 years have an imperfect awareness of hypoglycemia. 10 Because the risk for a hypoglycemic event is increased in this age-group, their target A1C is higher.10
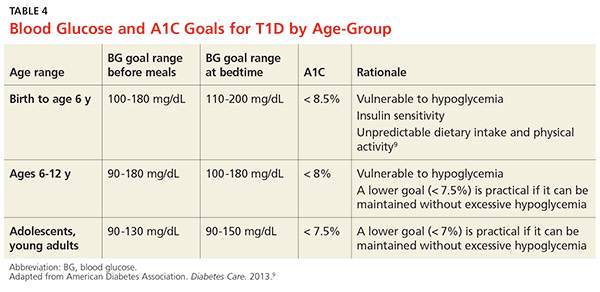
This is also an important age for brain development: The metabolism of glucose in the brain of a young child occurs at double the rate of that in an adult brain.11 Between ages 1 and 6 years, the brain increases in size dramatically, reaching 90% of its adult volume by age 6.11 In retrospective studies reviewed by Arbelaez et al,data show that frequent, severe hypoglycemic and hyperglycemic events are associated with poor cognitive function, particularly memory and attention.11 Due to the timing of brain development and the risk for glycemic extremes in young children, practitioners are advised to follow the ADA recommendations shown in Table 4.9
Continue for the conclusion >>
CONCLUSION
T1D is the most common chronic, serious, potentially life-threatening disease among children and adolescents. This lifelong illness is challenging to control, especially when managing the honeymoon period and addressing the increasing insulin demands in a growing child. Once a diagnosis is confirmed, the challenges persist, as each patient needs an individualized treatment regimen with ongoing adjustments. Knowledge of the ADA guidelines for age-appropriate A1C goals is essential for the practitioner who manages a growing child with T1D in order to achieve glycemic control while avoiding hypoglycemia. Preventing hypoglycemia is of the utmost importance, especially in a child too young to recognize symptoms.
Considering all the changes that a child with T1D is likely to experience, it is also important to remember that the foremost goal is for this child to live a healthy life. Thus, practitioners must educate both patients and parents regarding the complications that can arise with poor glycemic control and encourage adherence to the insulin therapy.
T1D requires vigilant monitoring and ongoing adjusted insulin therapy. Understanding age-appropriate treatment and maintaining good communications with patients and their parents are key to successful management of this disease.
REFERENCES
1. Juvenile Diabetes Research Foundation. Type 1 diabetes facts (2014). http://jdrf.org/about-jdrf/fact-sheets/type-1-diabetes-facts/. Accessed February 8, 2016.
2. American Diabetes Association. Fast facts: data and statistics about diabetes (2015). http://professional2.diabetes.org/admin/UserFiles/0%20-%20Sean/Documents/Fast_Facts_12-2015a.pdf. Accessed February 8, 2016.
3. American Diabetes Association. Executive summary: standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S5-S13.
4. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(1):81-90.
5. Pavlovic MD, Milenkovic T, Dinic M, et al. The prevalence of cutaneous manifestations in young patients with type 1 diabetes. Diabetes Care. 2007;30(8):1964-1967.
6. Khardori R. Type 1 diabetes mellitus differential diagnosis (updated 2015). http://emedicine.medscape.com/article/117739-differential. Accessed February 8, 2016.
7. Lamb WH. Pediatric type 1 diabetes mellitus (updated 2015). http://emedicine.medscape.com/article/919999-overview. Accessed February 8, 2016.
8. Type 1 Diabetes TrialNet. TrialNet Pathway to Prevention (2014). www.pathway2prevention.org/study/. Accessed February 8, 2016.
9. American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care. 2013;36(suppl 1):S11-S66. VIII. Diabetes care in specific populations. http://care.diabetesjournals.org/content/36/Supplement_1/S11.full#sec-128. Accessed February 8, 2016.
10. Danne T, Philotheou A, Goldman D, et al. A randomized trial comparing the rate of hypoglycemia—assessed using continuous glucose monitoring—in 125 preschool children with type 1 diabetes treated with insulin glargine or NPH insulin (the PRESCHOOL study). Pediatr Diabetes. 2013;14(8):593-601.
11. Arbelaez AM, Semenkovich K, Hershey T. Glycemic extremes in youth with T1DM: the structural and functional integrity of the developing brain. Pediatr Diabetes. 2013;14(8):541-553.
IN THIS ARTICLE
- Progress and treatment timeline with long- and rapid-acting insulin
- Progress and treatment timeline with continuous subcutaneous insulin infusion
- American Diabetes Association criteria for diagnosis of diabetes
- Blood glucose and A1C goals for type 1 diabetes by age-group
A 5-year-old Caucasian girl presents to the primary care practitioner’s office with chief complaints of polydipsia, polyuria with nocturia, polyphagia, and weight loss over the past three weeks. Her medical history includes a four-year history of keratosis pilaris (KP). The child experienced a KP flare-up two weeks ago; application of triamcinolone acetonide cream yielded no improvement. She also has xerosis, which is treated daily with OTC moisturizing lotion. She was born vaginally and breast-fed and is up to date on her immunizations. There is no family history of diabetes or autoimmune diseases.
Physical examination reveals a weight of 54 lb (95th percentile); height, 47 in (97th percentile); and BMI, 17.2. Vital signs include a blood pressure of 105/55 mm Hg; pulse, 85 beats/min and regular; temperature, 98.2°F; and respiratory rate, 22 breaths/min. KP is noted on the patient’s eyebrows, bilateral upper arms, and bilateral cheeks; the affected skin is erythemic and rough to the touch. Her physical examination findings are otherwise unremarkable.
The child’s urine is tested in the office for glucose and ketones, with results of 4+ glucose and 3+ ketones. These results and the child’s history prompt her admission to the pediatric ICU at a nearby hospital for further treatment with a diagnosis of new-onset type 1 diabetes (T1D) and diabetic ketoacidosis (DKA).
The diagnosis is confirmed at the hospital with laboratory results that include venous glucose, 418 mg/dL (normal range, 70 to 100 mg/dL) and A1C, 10.5% (range, 4.0% to 5.6%). Venous blood gas results include pH, 7.278 (7.32 to 7.42); PCO2, 29.6 mm Hg (39 to 54 mm Hg); HCO3, 13.8 mEq/L (19 to 25 mEq/L); base excess, –12 mmol/L (–4 to +2 mmol/L); beta hydroxybutyrate, 6.0 mmol/L (0.4 to 0.5 mmol/L); insulin antibody, 0.9 U/mL (< 0.4 U/mL); glutamic acid decarboxylase, 166 U/mL (< 0.5 U/mL); and venous lactate, 1.79 mmol/L (0.69 to 2.75 mmol/L).
The child is treated initially with an IV insulin infusion for 24 hours, then transitioned to subcutaneous insulin therapy once the DKA resolves and glucose levels are within normal limits. The child remains hospitalized for four days. Discharge medications include insulin glargine, 8 U/d, and insulin lispro before each meal, at bedtime, and at 0200 hours, with dosing based on sliding scales. Dietary orders include 45 to 60 g carbohydrates per meal, along with two snacks of 15 g carbohydrates.
The child is instructed to exercise at least 30 min/d (unless hypoglycemic events occur more than once per week or ketones are found in the blood or urine), drink plenty of water, and avoid concentrated sweets. Education is provided via the Diabetes Educator; the family takes home the beginner T1D booklet and is instructed to log the child’s blood glucose levels and return with this information in two weeks.
In the first three months, the patient experiences eight asymptomatic hypoglycemic events; for the next seven months, after dosing changes, she remains hyperglycemic most of the time (see Table 1). Insulin doses are adjusted, ranging from weekly to every three months, but glycemic goals are not achieved with the subcutaneous insulin injections. Use of continuous subcutaneous insulin infusion, the “insulin pump,” is then considered. Ten months postdiagnosis, the child begins a five-day-long saline (placebo) pump trial to determine whether the pump is appropriate for her and her lifestyle. After the trial, the decision is made to move forward with the insulin pump, initiated 11 months postdiagnosis.
The practitioner remains in frequent communication with the child’s mother in an effort to maintain glycemic control. After three months on the insulin pump, the child’s A1C is reduced to 7.9%, which is within the target range for her age-group (see Table 2). The child is now maintaining glycemic goals with the use of the insulin pump and close monitoring by the practitioner.
Continue for the discussion >>
DISCUSSION
According to the Juvenile Diabetes Research Foundation, as many as 1.25 million Americans are currently living with T1D; from 2001 to 2009, the prevalence of T1D in people younger than 20 increased by 23%.1 The overall prevalence of diabetes (both types 1 and 2) is predicted to be one in every three people by 2050 if current trends continue.2 According to the American Diabetes Association (ADA), 18,436 US youths are diagnosed with T1D every year, and T1D accounts for about 5% of diabetes cases in the US population.2
Diagnosis
Diabetes is diagnosed based on blood test results that fall within the parameters set by the ADA diagnostic criteria (see Table 3).3 In addition to diagnostic testing for diabetes recommended by the ADA guidelines, blood tests are ordered for autoantibodies that are associated with T1D, to distinguish between type 1 and type 2 diabetes. (T1D results from cellular-mediated autoimmune destruction of the insulin-producing beta cells in the pancreas.4) Upon initial diagnosis, about 85% to 90% of T1D patients have one or more autoantibodies present in blood work, such as autoantibodies to islet cells or to insulin, glutamic acid decarboxylase (GAD65), or tyrosine phosphatases IA-2 and IA-2B.4
In this case study, the child had an elevated GAD65 value and a positive screening for an insulin autoantibody, which explained the destruction of her beta cells. The patient also had KP and xerosis, which are clinical manifestations commonly seen in T1D. In one study of children with T1D, 22% had xerosis, compared with 3% of healthy, age-matched controls, and KP was also significantly more common in T1D patients than in controls (12% vs 1.5%).5
The presence of ketones in the case patient’s urine also suggests T1D, rather than type 2.4 The differential diagnosis for T1D includes type 2 diabetes mellitus, monogenic diabetes mellitus (formerly known as maturity-onset diabetes of the young), secondary hyperglycemia, and other endocrine disorders.6
Acute complications associated with T1D include hypoglycemia, hyperglycemia, and DKA. Long-term complications may include diabetic retinopathy, cataracts, gastroparesis, hypertension, renal failure, coronary artery disease, peripheral vascular disease, diabetic neuropathy, and increased risk for infection.7 These complications can likely be prevented by good glycemic control, proper diet, exercise, and avoidance of nicotine.7
Unfortunately, T1D cannot currently be prevented, although research studies are under way. TrialNet is currently conducting a “Pathway to Prevention” trial; the researchers are testing ways to delay and prevent T1D, as well as slow its progression after diagnosis.8 Potential participants (family members of a T1D patient) are screened for T1D autoantibodies. If test results are positive, these participants are included in the prevention pathway study.
Continue for management >>
Management
Most cases of T1D are diagnosed in patients younger than 18.9 Management of the child with T1D involves many challenges. The patient will experience an initial honeymoon period, that is, a brief remission during which the pancreas begins to secrete some insulin again and exogenous insulin demands are lower. However, this period is temporary, lasting only a few weeks, months, or years. Once pancreatic insulin secretion stops (as a result of complete beta-cell destruction), the exogenous insulin demands increase. In the case study, the child’s insulin demands were initially low, and she experienced hypoglycemia. Once she transitioned out of the honeymoon period, however, her blood glucose levels rose because her pancreas was producing little to no insulin.
As the patient ages, physical growth and hormone changes also alter the demand for insulin. A key factor to keep in mind is lifestyle changes: The child may need age-appropriate supervision and adjustments in exercise, diet, and diabetes education regimens when school routines and self-care capacities change. The child with T1D can only be educated as far as his or her cognitive ability will allow, but autonomy should increase with age.
Helping the patient reach glycemic goals requires special consideration, based on the child’s age. Whereas the target A1C for an adult with diabetes is below 7%, that for a young child is either < 7.5% or < 8.5%, depending on age (see Table 4).9 According to Danne et al, approximately 60% of children younger than 6 years have an imperfect awareness of hypoglycemia. 10 Because the risk for a hypoglycemic event is increased in this age-group, their target A1C is higher.10
This is also an important age for brain development: The metabolism of glucose in the brain of a young child occurs at double the rate of that in an adult brain.11 Between ages 1 and 6 years, the brain increases in size dramatically, reaching 90% of its adult volume by age 6.11 In retrospective studies reviewed by Arbelaez et al,data show that frequent, severe hypoglycemic and hyperglycemic events are associated with poor cognitive function, particularly memory and attention.11 Due to the timing of brain development and the risk for glycemic extremes in young children, practitioners are advised to follow the ADA recommendations shown in Table 4.9
Continue for the conclusion >>
CONCLUSION
T1D is the most common chronic, serious, potentially life-threatening disease among children and adolescents. This lifelong illness is challenging to control, especially when managing the honeymoon period and addressing the increasing insulin demands in a growing child. Once a diagnosis is confirmed, the challenges persist, as each patient needs an individualized treatment regimen with ongoing adjustments. Knowledge of the ADA guidelines for age-appropriate A1C goals is essential for the practitioner who manages a growing child with T1D in order to achieve glycemic control while avoiding hypoglycemia. Preventing hypoglycemia is of the utmost importance, especially in a child too young to recognize symptoms.
Considering all the changes that a child with T1D is likely to experience, it is also important to remember that the foremost goal is for this child to live a healthy life. Thus, practitioners must educate both patients and parents regarding the complications that can arise with poor glycemic control and encourage adherence to the insulin therapy.
T1D requires vigilant monitoring and ongoing adjusted insulin therapy. Understanding age-appropriate treatment and maintaining good communications with patients and their parents are key to successful management of this disease.
REFERENCES
1. Juvenile Diabetes Research Foundation. Type 1 diabetes facts (2014). http://jdrf.org/about-jdrf/fact-sheets/type-1-diabetes-facts/. Accessed February 8, 2016.
2. American Diabetes Association. Fast facts: data and statistics about diabetes (2015). http://professional2.diabetes.org/admin/UserFiles/0%20-%20Sean/Documents/Fast_Facts_12-2015a.pdf. Accessed February 8, 2016.
3. American Diabetes Association. Executive summary: standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S5-S13.
4. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(1):81-90.
5. Pavlovic MD, Milenkovic T, Dinic M, et al. The prevalence of cutaneous manifestations in young patients with type 1 diabetes. Diabetes Care. 2007;30(8):1964-1967.
6. Khardori R. Type 1 diabetes mellitus differential diagnosis (updated 2015). http://emedicine.medscape.com/article/117739-differential. Accessed February 8, 2016.
7. Lamb WH. Pediatric type 1 diabetes mellitus (updated 2015). http://emedicine.medscape.com/article/919999-overview. Accessed February 8, 2016.
8. Type 1 Diabetes TrialNet. TrialNet Pathway to Prevention (2014). www.pathway2prevention.org/study/. Accessed February 8, 2016.
9. American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care. 2013;36(suppl 1):S11-S66. VIII. Diabetes care in specific populations. http://care.diabetesjournals.org/content/36/Supplement_1/S11.full#sec-128. Accessed February 8, 2016.
10. Danne T, Philotheou A, Goldman D, et al. A randomized trial comparing the rate of hypoglycemia—assessed using continuous glucose monitoring—in 125 preschool children with type 1 diabetes treated with insulin glargine or NPH insulin (the PRESCHOOL study). Pediatr Diabetes. 2013;14(8):593-601.
11. Arbelaez AM, Semenkovich K, Hershey T. Glycemic extremes in youth with T1DM: the structural and functional integrity of the developing brain. Pediatr Diabetes. 2013;14(8):541-553.
IN THIS ARTICLE
- Progress and treatment timeline with long- and rapid-acting insulin
- Progress and treatment timeline with continuous subcutaneous insulin infusion
- American Diabetes Association criteria for diagnosis of diabetes
- Blood glucose and A1C goals for type 1 diabetes by age-group
A 5-year-old Caucasian girl presents to the primary care practitioner’s office with chief complaints of polydipsia, polyuria with nocturia, polyphagia, and weight loss over the past three weeks. Her medical history includes a four-year history of keratosis pilaris (KP). The child experienced a KP flare-up two weeks ago; application of triamcinolone acetonide cream yielded no improvement. She also has xerosis, which is treated daily with OTC moisturizing lotion. She was born vaginally and breast-fed and is up to date on her immunizations. There is no family history of diabetes or autoimmune diseases.
Physical examination reveals a weight of 54 lb (95th percentile); height, 47 in (97th percentile); and BMI, 17.2. Vital signs include a blood pressure of 105/55 mm Hg; pulse, 85 beats/min and regular; temperature, 98.2°F; and respiratory rate, 22 breaths/min. KP is noted on the patient’s eyebrows, bilateral upper arms, and bilateral cheeks; the affected skin is erythemic and rough to the touch. Her physical examination findings are otherwise unremarkable.
The child’s urine is tested in the office for glucose and ketones, with results of 4+ glucose and 3+ ketones. These results and the child’s history prompt her admission to the pediatric ICU at a nearby hospital for further treatment with a diagnosis of new-onset type 1 diabetes (T1D) and diabetic ketoacidosis (DKA).
The diagnosis is confirmed at the hospital with laboratory results that include venous glucose, 418 mg/dL (normal range, 70 to 100 mg/dL) and A1C, 10.5% (range, 4.0% to 5.6%). Venous blood gas results include pH, 7.278 (7.32 to 7.42); PCO2, 29.6 mm Hg (39 to 54 mm Hg); HCO3, 13.8 mEq/L (19 to 25 mEq/L); base excess, –12 mmol/L (–4 to +2 mmol/L); beta hydroxybutyrate, 6.0 mmol/L (0.4 to 0.5 mmol/L); insulin antibody, 0.9 U/mL (< 0.4 U/mL); glutamic acid decarboxylase, 166 U/mL (< 0.5 U/mL); and venous lactate, 1.79 mmol/L (0.69 to 2.75 mmol/L).
The child is treated initially with an IV insulin infusion for 24 hours, then transitioned to subcutaneous insulin therapy once the DKA resolves and glucose levels are within normal limits. The child remains hospitalized for four days. Discharge medications include insulin glargine, 8 U/d, and insulin lispro before each meal, at bedtime, and at 0200 hours, with dosing based on sliding scales. Dietary orders include 45 to 60 g carbohydrates per meal, along with two snacks of 15 g carbohydrates.
The child is instructed to exercise at least 30 min/d (unless hypoglycemic events occur more than once per week or ketones are found in the blood or urine), drink plenty of water, and avoid concentrated sweets. Education is provided via the Diabetes Educator; the family takes home the beginner T1D booklet and is instructed to log the child’s blood glucose levels and return with this information in two weeks.
In the first three months, the patient experiences eight asymptomatic hypoglycemic events; for the next seven months, after dosing changes, she remains hyperglycemic most of the time (see Table 1). Insulin doses are adjusted, ranging from weekly to every three months, but glycemic goals are not achieved with the subcutaneous insulin injections. Use of continuous subcutaneous insulin infusion, the “insulin pump,” is then considered. Ten months postdiagnosis, the child begins a five-day-long saline (placebo) pump trial to determine whether the pump is appropriate for her and her lifestyle. After the trial, the decision is made to move forward with the insulin pump, initiated 11 months postdiagnosis.
The practitioner remains in frequent communication with the child’s mother in an effort to maintain glycemic control. After three months on the insulin pump, the child’s A1C is reduced to 7.9%, which is within the target range for her age-group (see Table 2). The child is now maintaining glycemic goals with the use of the insulin pump and close monitoring by the practitioner.
Continue for the discussion >>
DISCUSSION
According to the Juvenile Diabetes Research Foundation, as many as 1.25 million Americans are currently living with T1D; from 2001 to 2009, the prevalence of T1D in people younger than 20 increased by 23%.1 The overall prevalence of diabetes (both types 1 and 2) is predicted to be one in every three people by 2050 if current trends continue.2 According to the American Diabetes Association (ADA), 18,436 US youths are diagnosed with T1D every year, and T1D accounts for about 5% of diabetes cases in the US population.2
Diagnosis
Diabetes is diagnosed based on blood test results that fall within the parameters set by the ADA diagnostic criteria (see Table 3).3 In addition to diagnostic testing for diabetes recommended by the ADA guidelines, blood tests are ordered for autoantibodies that are associated with T1D, to distinguish between type 1 and type 2 diabetes. (T1D results from cellular-mediated autoimmune destruction of the insulin-producing beta cells in the pancreas.4) Upon initial diagnosis, about 85% to 90% of T1D patients have one or more autoantibodies present in blood work, such as autoantibodies to islet cells or to insulin, glutamic acid decarboxylase (GAD65), or tyrosine phosphatases IA-2 and IA-2B.4
In this case study, the child had an elevated GAD65 value and a positive screening for an insulin autoantibody, which explained the destruction of her beta cells. The patient also had KP and xerosis, which are clinical manifestations commonly seen in T1D. In one study of children with T1D, 22% had xerosis, compared with 3% of healthy, age-matched controls, and KP was also significantly more common in T1D patients than in controls (12% vs 1.5%).5
The presence of ketones in the case patient’s urine also suggests T1D, rather than type 2.4 The differential diagnosis for T1D includes type 2 diabetes mellitus, monogenic diabetes mellitus (formerly known as maturity-onset diabetes of the young), secondary hyperglycemia, and other endocrine disorders.6
Acute complications associated with T1D include hypoglycemia, hyperglycemia, and DKA. Long-term complications may include diabetic retinopathy, cataracts, gastroparesis, hypertension, renal failure, coronary artery disease, peripheral vascular disease, diabetic neuropathy, and increased risk for infection.7 These complications can likely be prevented by good glycemic control, proper diet, exercise, and avoidance of nicotine.7
Unfortunately, T1D cannot currently be prevented, although research studies are under way. TrialNet is currently conducting a “Pathway to Prevention” trial; the researchers are testing ways to delay and prevent T1D, as well as slow its progression after diagnosis.8 Potential participants (family members of a T1D patient) are screened for T1D autoantibodies. If test results are positive, these participants are included in the prevention pathway study.
Continue for management >>
Management
Most cases of T1D are diagnosed in patients younger than 18.9 Management of the child with T1D involves many challenges. The patient will experience an initial honeymoon period, that is, a brief remission during which the pancreas begins to secrete some insulin again and exogenous insulin demands are lower. However, this period is temporary, lasting only a few weeks, months, or years. Once pancreatic insulin secretion stops (as a result of complete beta-cell destruction), the exogenous insulin demands increase. In the case study, the child’s insulin demands were initially low, and she experienced hypoglycemia. Once she transitioned out of the honeymoon period, however, her blood glucose levels rose because her pancreas was producing little to no insulin.
As the patient ages, physical growth and hormone changes also alter the demand for insulin. A key factor to keep in mind is lifestyle changes: The child may need age-appropriate supervision and adjustments in exercise, diet, and diabetes education regimens when school routines and self-care capacities change. The child with T1D can only be educated as far as his or her cognitive ability will allow, but autonomy should increase with age.
Helping the patient reach glycemic goals requires special consideration, based on the child’s age. Whereas the target A1C for an adult with diabetes is below 7%, that for a young child is either < 7.5% or < 8.5%, depending on age (see Table 4).9 According to Danne et al, approximately 60% of children younger than 6 years have an imperfect awareness of hypoglycemia. 10 Because the risk for a hypoglycemic event is increased in this age-group, their target A1C is higher.10
This is also an important age for brain development: The metabolism of glucose in the brain of a young child occurs at double the rate of that in an adult brain.11 Between ages 1 and 6 years, the brain increases in size dramatically, reaching 90% of its adult volume by age 6.11 In retrospective studies reviewed by Arbelaez et al,data show that frequent, severe hypoglycemic and hyperglycemic events are associated with poor cognitive function, particularly memory and attention.11 Due to the timing of brain development and the risk for glycemic extremes in young children, practitioners are advised to follow the ADA recommendations shown in Table 4.9
Continue for the conclusion >>
CONCLUSION
T1D is the most common chronic, serious, potentially life-threatening disease among children and adolescents. This lifelong illness is challenging to control, especially when managing the honeymoon period and addressing the increasing insulin demands in a growing child. Once a diagnosis is confirmed, the challenges persist, as each patient needs an individualized treatment regimen with ongoing adjustments. Knowledge of the ADA guidelines for age-appropriate A1C goals is essential for the practitioner who manages a growing child with T1D in order to achieve glycemic control while avoiding hypoglycemia. Preventing hypoglycemia is of the utmost importance, especially in a child too young to recognize symptoms.
Considering all the changes that a child with T1D is likely to experience, it is also important to remember that the foremost goal is for this child to live a healthy life. Thus, practitioners must educate both patients and parents regarding the complications that can arise with poor glycemic control and encourage adherence to the insulin therapy.
T1D requires vigilant monitoring and ongoing adjusted insulin therapy. Understanding age-appropriate treatment and maintaining good communications with patients and their parents are key to successful management of this disease.
REFERENCES
1. Juvenile Diabetes Research Foundation. Type 1 diabetes facts (2014). http://jdrf.org/about-jdrf/fact-sheets/type-1-diabetes-facts/. Accessed February 8, 2016.
2. American Diabetes Association. Fast facts: data and statistics about diabetes (2015). http://professional2.diabetes.org/admin/UserFiles/0%20-%20Sean/Documents/Fast_Facts_12-2015a.pdf. Accessed February 8, 2016.
3. American Diabetes Association. Executive summary: standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S5-S13.
4. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(1):81-90.
5. Pavlovic MD, Milenkovic T, Dinic M, et al. The prevalence of cutaneous manifestations in young patients with type 1 diabetes. Diabetes Care. 2007;30(8):1964-1967.
6. Khardori R. Type 1 diabetes mellitus differential diagnosis (updated 2015). http://emedicine.medscape.com/article/117739-differential. Accessed February 8, 2016.
7. Lamb WH. Pediatric type 1 diabetes mellitus (updated 2015). http://emedicine.medscape.com/article/919999-overview. Accessed February 8, 2016.
8. Type 1 Diabetes TrialNet. TrialNet Pathway to Prevention (2014). www.pathway2prevention.org/study/. Accessed February 8, 2016.
9. American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care. 2013;36(suppl 1):S11-S66. VIII. Diabetes care in specific populations. http://care.diabetesjournals.org/content/36/Supplement_1/S11.full#sec-128. Accessed February 8, 2016.
10. Danne T, Philotheou A, Goldman D, et al. A randomized trial comparing the rate of hypoglycemia—assessed using continuous glucose monitoring—in 125 preschool children with type 1 diabetes treated with insulin glargine or NPH insulin (the PRESCHOOL study). Pediatr Diabetes. 2013;14(8):593-601.
11. Arbelaez AM, Semenkovich K, Hershey T. Glycemic extremes in youth with T1DM: the structural and functional integrity of the developing brain. Pediatr Diabetes. 2013;14(8):541-553.
The hunger game
How do you feel about hunger? Do you trust in its power? Having written one book on picky eating based solely on my mother’s wisdom, supplemented with a scanty amount of Internet-based research, I have spent and continue to spend a good bit of time thinking about hunger.
I have concluded that it is a very powerful force and that when a child gets hungry enough, he will eat, even foods that he has previously rejected. It is that assumption that is at the core of my advice to parents of picky eaters. I suspect that many of you share that same philosophy and recommend a strategy that is heavy on patience. Of course the problem lies in getting parents to adopt that attitude and accept the fact that if they just present a healthy diet and step back, hunger will eventually win, and the child will eat.

However, the devil is in the details. Have the parents set rules that will prevent the child from overdrinking? Have they really stopped talking about what the child, and everyone else in the family, is or isn’t eating? Are the parents setting good examples with their own eating habits and comments about food?
Because 99% of my patient population have been healthy, I have always felt comfortable relying on the power of hunger to win the battle over picky eating. If properly managed, none of my patients was going to die or suffer permanent consequences from picky eating. However, I have always wondered whether hunger could be leveraged to safely manage selective eating in children with serious health problems. I have a suspicion that it would succeed, but luckily I have never been presented with a case to test my hunch.
I recently read a very personal account written by the mother of a child with severe congenital cardiac disease that supports my gut feeling that when carefully monitored, starvation can be an effective strategy in managing selective eating (“When Your Baby Won’t Eat,” by Virginia Sole-Smith, The New York Times Magazine, Feb. 4, 2016). Three surgeries in the first few months of life necessitated that the child be fed by gavage. Attempts at breastfeeding failed, as it often does in situations like this. Struggles with gavage tube placement at home became such an emotionally traumatic ordeal that eventually a gastrostomy tube was placed when the child was 6 months old.
The family was led to believe that an important window in the child’s oral development had closed as a result of interventions necessitated by the child’s cardiac malformations. Although she was neurologically and physically capable of eating, getting her to do so was going to require long-term behavior modification, and there was no guarantee that this approach would completely undo what bad luck and prior management strategies had created. She might never relate to food as a normal child does.
After several attempts at behavior management using one-to-one reinforcement, this mother began to do some research. She discovered that of the nearly 30 feeding programs in children’s hospitals and private clinics, almost all use variations of a similar behavior modification strategy that had not worked for her daughter. As she observed: “This behavioral model presumes that children who don’t eat need external motivation.”
Eventually, the family found help in one of the few feeding programs in the United States that has adopted a dramatically different “child-centered” approach in which “therapists believe that all children have some internal motivation to eat, as well as an innate ability to effectively self-regulate their intake.” The solution to this child’s problem didn’t occur overnight. It began by exposing the child to a variety of foods in situations free of attempts to get her to eat – no coercion or rewards, regardless of how subtle they might have seemed. Once the child was experimenting with food, her tube feedings were gradually decreased in volume and caloric content. And, voila! Hunger won and the child began meeting her total nutritional needs by eating, in some cases with gusto.
Of course I was easy to convince because the results confirmed my hunch. But, do you believe that hunger can and should be used as the centerpiece in the management of selective eating, even in cases well beyond the parameters of garden variety picky eating? Are you willing to play the hunger game along with me?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
How do you feel about hunger? Do you trust in its power? Having written one book on picky eating based solely on my mother’s wisdom, supplemented with a scanty amount of Internet-based research, I have spent and continue to spend a good bit of time thinking about hunger.
I have concluded that it is a very powerful force and that when a child gets hungry enough, he will eat, even foods that he has previously rejected. It is that assumption that is at the core of my advice to parents of picky eaters. I suspect that many of you share that same philosophy and recommend a strategy that is heavy on patience. Of course the problem lies in getting parents to adopt that attitude and accept the fact that if they just present a healthy diet and step back, hunger will eventually win, and the child will eat.
However, the devil is in the details. Have the parents set rules that will prevent the child from overdrinking? Have they really stopped talking about what the child, and everyone else in the family, is or isn’t eating? Are the parents setting good examples with their own eating habits and comments about food?
Because 99% of my patient population have been healthy, I have always felt comfortable relying on the power of hunger to win the battle over picky eating. If properly managed, none of my patients was going to die or suffer permanent consequences from picky eating. However, I have always wondered whether hunger could be leveraged to safely manage selective eating in children with serious health problems. I have a suspicion that it would succeed, but luckily I have never been presented with a case to test my hunch.
I recently read a very personal account written by the mother of a child with severe congenital cardiac disease that supports my gut feeling that when carefully monitored, starvation can be an effective strategy in managing selective eating (“When Your Baby Won’t Eat,” by Virginia Sole-Smith, The New York Times Magazine, Feb. 4, 2016). Three surgeries in the first few months of life necessitated that the child be fed by gavage. Attempts at breastfeeding failed, as it often does in situations like this. Struggles with gavage tube placement at home became such an emotionally traumatic ordeal that eventually a gastrostomy tube was placed when the child was 6 months old.
The family was led to believe that an important window in the child’s oral development had closed as a result of interventions necessitated by the child’s cardiac malformations. Although she was neurologically and physically capable of eating, getting her to do so was going to require long-term behavior modification, and there was no guarantee that this approach would completely undo what bad luck and prior management strategies had created. She might never relate to food as a normal child does.
After several attempts at behavior management using one-to-one reinforcement, this mother began to do some research. She discovered that of the nearly 30 feeding programs in children’s hospitals and private clinics, almost all use variations of a similar behavior modification strategy that had not worked for her daughter. As she observed: “This behavioral model presumes that children who don’t eat need external motivation.”
Eventually, the family found help in one of the few feeding programs in the United States that has adopted a dramatically different “child-centered” approach in which “therapists believe that all children have some internal motivation to eat, as well as an innate ability to effectively self-regulate their intake.” The solution to this child’s problem didn’t occur overnight. It began by exposing the child to a variety of foods in situations free of attempts to get her to eat – no coercion or rewards, regardless of how subtle they might have seemed. Once the child was experimenting with food, her tube feedings were gradually decreased in volume and caloric content. And, voila! Hunger won and the child began meeting her total nutritional needs by eating, in some cases with gusto.
Of course I was easy to convince because the results confirmed my hunch. But, do you believe that hunger can and should be used as the centerpiece in the management of selective eating, even in cases well beyond the parameters of garden variety picky eating? Are you willing to play the hunger game along with me?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
How do you feel about hunger? Do you trust in its power? Having written one book on picky eating based solely on my mother’s wisdom, supplemented with a scanty amount of Internet-based research, I have spent and continue to spend a good bit of time thinking about hunger.
I have concluded that it is a very powerful force and that when a child gets hungry enough, he will eat, even foods that he has previously rejected. It is that assumption that is at the core of my advice to parents of picky eaters. I suspect that many of you share that same philosophy and recommend a strategy that is heavy on patience. Of course the problem lies in getting parents to adopt that attitude and accept the fact that if they just present a healthy diet and step back, hunger will eventually win, and the child will eat.
However, the devil is in the details. Have the parents set rules that will prevent the child from overdrinking? Have they really stopped talking about what the child, and everyone else in the family, is or isn’t eating? Are the parents setting good examples with their own eating habits and comments about food?
Because 99% of my patient population have been healthy, I have always felt comfortable relying on the power of hunger to win the battle over picky eating. If properly managed, none of my patients was going to die or suffer permanent consequences from picky eating. However, I have always wondered whether hunger could be leveraged to safely manage selective eating in children with serious health problems. I have a suspicion that it would succeed, but luckily I have never been presented with a case to test my hunch.
I recently read a very personal account written by the mother of a child with severe congenital cardiac disease that supports my gut feeling that when carefully monitored, starvation can be an effective strategy in managing selective eating (“When Your Baby Won’t Eat,” by Virginia Sole-Smith, The New York Times Magazine, Feb. 4, 2016). Three surgeries in the first few months of life necessitated that the child be fed by gavage. Attempts at breastfeeding failed, as it often does in situations like this. Struggles with gavage tube placement at home became such an emotionally traumatic ordeal that eventually a gastrostomy tube was placed when the child was 6 months old.
The family was led to believe that an important window in the child’s oral development had closed as a result of interventions necessitated by the child’s cardiac malformations. Although she was neurologically and physically capable of eating, getting her to do so was going to require long-term behavior modification, and there was no guarantee that this approach would completely undo what bad luck and prior management strategies had created. She might never relate to food as a normal child does.
After several attempts at behavior management using one-to-one reinforcement, this mother began to do some research. She discovered that of the nearly 30 feeding programs in children’s hospitals and private clinics, almost all use variations of a similar behavior modification strategy that had not worked for her daughter. As she observed: “This behavioral model presumes that children who don’t eat need external motivation.”
Eventually, the family found help in one of the few feeding programs in the United States that has adopted a dramatically different “child-centered” approach in which “therapists believe that all children have some internal motivation to eat, as well as an innate ability to effectively self-regulate their intake.” The solution to this child’s problem didn’t occur overnight. It began by exposing the child to a variety of foods in situations free of attempts to get her to eat – no coercion or rewards, regardless of how subtle they might have seemed. Once the child was experimenting with food, her tube feedings were gradually decreased in volume and caloric content. And, voila! Hunger won and the child began meeting her total nutritional needs by eating, in some cases with gusto.
Of course I was easy to convince because the results confirmed my hunch. But, do you believe that hunger can and should be used as the centerpiece in the management of selective eating, even in cases well beyond the parameters of garden variety picky eating? Are you willing to play the hunger game along with me?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”

Asthma hospitalizations linked to prevalence of common cold in children
Daily viral prevalence was the greatest predictor of asthma hospitalizations in children, according to Rosalind M. Eggo and her associates.
Asthma hospitalizations in children occurred most frequently during the school year, and dropped off dramatically when school was out. Increases were not driven by triggers within the school environment, but by increased transmission and prevalence of viruses such as the common cold, the researchers noted. Common cold transmission rates were 45% lower during school holidays and breaks, and asthma hospitalizations decreased accordingly.
In adults, asthma hospitalizations were greatest during the winter and were most influenced by influenza prevalence. Low temperatures were an important risk factor for both groups; however, ozone and particulate matter were not.
“In general, future risk assessments and interventions for asthma, particularly in children, should explicitly consider both the school calendar and the seasonal dynamic of infectious triggers, either through spatiotemporal modeling or when possible, viral surveillance data,” the investigators concluded.
Find the study in PNAS (doi: 10.1073/pnas.1518677113).
Daily viral prevalence was the greatest predictor of asthma hospitalizations in children, according to Rosalind M. Eggo and her associates.
Asthma hospitalizations in children occurred most frequently during the school year, and dropped off dramatically when school was out. Increases were not driven by triggers within the school environment, but by increased transmission and prevalence of viruses such as the common cold, the researchers noted. Common cold transmission rates were 45% lower during school holidays and breaks, and asthma hospitalizations decreased accordingly.
In adults, asthma hospitalizations were greatest during the winter and were most influenced by influenza prevalence. Low temperatures were an important risk factor for both groups; however, ozone and particulate matter were not.
“In general, future risk assessments and interventions for asthma, particularly in children, should explicitly consider both the school calendar and the seasonal dynamic of infectious triggers, either through spatiotemporal modeling or when possible, viral surveillance data,” the investigators concluded.
Find the study in PNAS (doi: 10.1073/pnas.1518677113).
Daily viral prevalence was the greatest predictor of asthma hospitalizations in children, according to Rosalind M. Eggo and her associates.
Asthma hospitalizations in children occurred most frequently during the school year, and dropped off dramatically when school was out. Increases were not driven by triggers within the school environment, but by increased transmission and prevalence of viruses such as the common cold, the researchers noted. Common cold transmission rates were 45% lower during school holidays and breaks, and asthma hospitalizations decreased accordingly.
In adults, asthma hospitalizations were greatest during the winter and were most influenced by influenza prevalence. Low temperatures were an important risk factor for both groups; however, ozone and particulate matter were not.
“In general, future risk assessments and interventions for asthma, particularly in children, should explicitly consider both the school calendar and the seasonal dynamic of infectious triggers, either through spatiotemporal modeling or when possible, viral surveillance data,” the investigators concluded.
Find the study in PNAS (doi: 10.1073/pnas.1518677113).
FROM PNAS