User login
HPV Vaccination Protects High-risk Girls From Cervical Cancer
Full or partial vaccination with the quadrivalent human papillomavirus vaccine reduced the overall risk of abnormal cervical pathology by 36%, based on data from a retrospective cohort study of just over 4,000 high-risk girls and young adult women.
Early vaccination (ages 11-14 years) was the most protective, with reductions in risk of abnormal cervical pathology of 64% with at least one dose and 73% for three doses (JAMA Pediatr. 2016 March 14. doi: 10.1001/jamapediatrics.2015.3926).

“This study provides crucial information about the HPV vaccine in minority populations and females engaging in high-risk sexual behaviors who arguably were underrepresented in the HPV vaccine clinical trials and postlicensure studies, yet are at increased risk for cervical cancer,” wrote Dr. Annika M. Hofstetter of the University of Washington, Seattle, and her colleagues.
The researchers reviewed data from 4,127 girls and young women aged 11-20 years who were seen at 16 locations in New York City. Most (92%) of the patients were publicly insured, and 58% were Spanish speakers.
Overall, the risk for abnormal cervical pathology was lower in vaccinated vs. unvaccinated individuals, (hazard ratio 0.64) and even lower in those who received all three recommended doses (HR 0.48). Detection rates were 58 per 1,000 person-years in those vaccinated vs. 126 per 1,000 person-years among the unvaccinated.
The next steps for research should include a larger sample and a longer follow-up period after greater uptake of the nonavalent HPV vaccine, the researchers added.
Dr. Hofstetter has received funding for a separate investigator-initiated study from the Pfizer Medical Education Group, and the study was funded in part by a grant from the Merck Investigator-Initiated Studies Program.
Full or partial vaccination with the quadrivalent human papillomavirus vaccine reduced the overall risk of abnormal cervical pathology by 36%, based on data from a retrospective cohort study of just over 4,000 high-risk girls and young adult women.
Early vaccination (ages 11-14 years) was the most protective, with reductions in risk of abnormal cervical pathology of 64% with at least one dose and 73% for three doses (JAMA Pediatr. 2016 March 14. doi: 10.1001/jamapediatrics.2015.3926).
“This study provides crucial information about the HPV vaccine in minority populations and females engaging in high-risk sexual behaviors who arguably were underrepresented in the HPV vaccine clinical trials and postlicensure studies, yet are at increased risk for cervical cancer,” wrote Dr. Annika M. Hofstetter of the University of Washington, Seattle, and her colleagues.
The researchers reviewed data from 4,127 girls and young women aged 11-20 years who were seen at 16 locations in New York City. Most (92%) of the patients were publicly insured, and 58% were Spanish speakers.
Overall, the risk for abnormal cervical pathology was lower in vaccinated vs. unvaccinated individuals, (hazard ratio 0.64) and even lower in those who received all three recommended doses (HR 0.48). Detection rates were 58 per 1,000 person-years in those vaccinated vs. 126 per 1,000 person-years among the unvaccinated.
The next steps for research should include a larger sample and a longer follow-up period after greater uptake of the nonavalent HPV vaccine, the researchers added.
Dr. Hofstetter has received funding for a separate investigator-initiated study from the Pfizer Medical Education Group, and the study was funded in part by a grant from the Merck Investigator-Initiated Studies Program.
Full or partial vaccination with the quadrivalent human papillomavirus vaccine reduced the overall risk of abnormal cervical pathology by 36%, based on data from a retrospective cohort study of just over 4,000 high-risk girls and young adult women.
Early vaccination (ages 11-14 years) was the most protective, with reductions in risk of abnormal cervical pathology of 64% with at least one dose and 73% for three doses (JAMA Pediatr. 2016 March 14. doi: 10.1001/jamapediatrics.2015.3926).
“This study provides crucial information about the HPV vaccine in minority populations and females engaging in high-risk sexual behaviors who arguably were underrepresented in the HPV vaccine clinical trials and postlicensure studies, yet are at increased risk for cervical cancer,” wrote Dr. Annika M. Hofstetter of the University of Washington, Seattle, and her colleagues.
The researchers reviewed data from 4,127 girls and young women aged 11-20 years who were seen at 16 locations in New York City. Most (92%) of the patients were publicly insured, and 58% were Spanish speakers.
Overall, the risk for abnormal cervical pathology was lower in vaccinated vs. unvaccinated individuals, (hazard ratio 0.64) and even lower in those who received all three recommended doses (HR 0.48). Detection rates were 58 per 1,000 person-years in those vaccinated vs. 126 per 1,000 person-years among the unvaccinated.
The next steps for research should include a larger sample and a longer follow-up period after greater uptake of the nonavalent HPV vaccine, the researchers added.
Dr. Hofstetter has received funding for a separate investigator-initiated study from the Pfizer Medical Education Group, and the study was funded in part by a grant from the Merck Investigator-Initiated Studies Program.
FROM JAMA PEDIATRICS

HPV vaccination protects high-risk girls from cervical cancer
Full or partial vaccination with the quadrivalent human papillomavirus vaccine reduced the overall risk of abnormal cervical pathology by 36%, based on data from a retrospective cohort study of just over 4,000 high-risk girls and young adult women.
Early vaccination (ages 11-14 years) was the most protective, with reductions in risk of abnormal cervical pathology of 64% with at least one dose and 73% for three doses (JAMA Pediatr. 2016 March 14. doi: 10.1001/jamapediatrics.2015.3926).

“This study provides crucial information about the HPV vaccine in minority populations and females engaging in high-risk sexual behaviors who arguably were underrepresented in the HPV vaccine clinical trials and postlicensure studies, yet are at increased risk for cervical cancer,” wrote Dr. Annika M. Hofstetter of the University of Washington, Seattle, and her colleagues.
The researchers reviewed data from 4,127 girls and young women aged 11-20 years who were seen at 16 locations in New York City. Most (92%) of the patients were publicly insured, and 58% were Spanish speakers.
Overall, the risk for abnormal cervical pathology was lower in vaccinated vs. unvaccinated individuals, (hazard ratio 0.64) and even lower in those who received all three recommended doses (HR 0.48). Detection rates were 58 per 1,000 person-years in those vaccinated vs. 126 per 1,000 person-years among the unvaccinated.
The next steps for research should include a larger sample and a longer follow-up period after greater uptake of the nonavalent HPV vaccine, the researchers added.
Dr. Hofstetter has received funding for a separate investigator-initiated study from the Pfizer Medical Education Group, and the study was funded in part by a grant from the Merck Investigator-Initiated Studies Program.
Full or partial vaccination with the quadrivalent human papillomavirus vaccine reduced the overall risk of abnormal cervical pathology by 36%, based on data from a retrospective cohort study of just over 4,000 high-risk girls and young adult women.
Early vaccination (ages 11-14 years) was the most protective, with reductions in risk of abnormal cervical pathology of 64% with at least one dose and 73% for three doses (JAMA Pediatr. 2016 March 14. doi: 10.1001/jamapediatrics.2015.3926).
“This study provides crucial information about the HPV vaccine in minority populations and females engaging in high-risk sexual behaviors who arguably were underrepresented in the HPV vaccine clinical trials and postlicensure studies, yet are at increased risk for cervical cancer,” wrote Dr. Annika M. Hofstetter of the University of Washington, Seattle, and her colleagues.
The researchers reviewed data from 4,127 girls and young women aged 11-20 years who were seen at 16 locations in New York City. Most (92%) of the patients were publicly insured, and 58% were Spanish speakers.
Overall, the risk for abnormal cervical pathology was lower in vaccinated vs. unvaccinated individuals, (hazard ratio 0.64) and even lower in those who received all three recommended doses (HR 0.48). Detection rates were 58 per 1,000 person-years in those vaccinated vs. 126 per 1,000 person-years among the unvaccinated.
The next steps for research should include a larger sample and a longer follow-up period after greater uptake of the nonavalent HPV vaccine, the researchers added.
Dr. Hofstetter has received funding for a separate investigator-initiated study from the Pfizer Medical Education Group, and the study was funded in part by a grant from the Merck Investigator-Initiated Studies Program.
Full or partial vaccination with the quadrivalent human papillomavirus vaccine reduced the overall risk of abnormal cervical pathology by 36%, based on data from a retrospective cohort study of just over 4,000 high-risk girls and young adult women.
Early vaccination (ages 11-14 years) was the most protective, with reductions in risk of abnormal cervical pathology of 64% with at least one dose and 73% for three doses (JAMA Pediatr. 2016 March 14. doi: 10.1001/jamapediatrics.2015.3926).
“This study provides crucial information about the HPV vaccine in minority populations and females engaging in high-risk sexual behaviors who arguably were underrepresented in the HPV vaccine clinical trials and postlicensure studies, yet are at increased risk for cervical cancer,” wrote Dr. Annika M. Hofstetter of the University of Washington, Seattle, and her colleagues.
The researchers reviewed data from 4,127 girls and young women aged 11-20 years who were seen at 16 locations in New York City. Most (92%) of the patients were publicly insured, and 58% were Spanish speakers.
Overall, the risk for abnormal cervical pathology was lower in vaccinated vs. unvaccinated individuals, (hazard ratio 0.64) and even lower in those who received all three recommended doses (HR 0.48). Detection rates were 58 per 1,000 person-years in those vaccinated vs. 126 per 1,000 person-years among the unvaccinated.
The next steps for research should include a larger sample and a longer follow-up period after greater uptake of the nonavalent HPV vaccine, the researchers added.
Dr. Hofstetter has received funding for a separate investigator-initiated study from the Pfizer Medical Education Group, and the study was funded in part by a grant from the Merck Investigator-Initiated Studies Program.
FROM JAMA PEDIATRICS
Key clinical point: HPV vaccination, even partial vaccination, was protective against cervical cancer in minority girls at increased risk for infection.
Major finding: Abnormal cervical cytology was 36% lower in girls and young women who received any amount of HPV vaccine and 73% lower in those who were fully vaccinated, compared with those who were unvaccinated.
Data source: A retrospective cohort study including data from 4,127 females aged 11-20 years.
Disclosures: Dr. Hofstetter has received funding for a separate investigator-initiated study from the Pfizer Medical Education Group, and the study was funded in part by a grant from the Merck Investigator-Initiated Studies Program.

Study: Two Varicella Vaccination Doses More Effective Than One
Two-dose varicella vaccinations were more effective and resulted in decreased risk of varicella severity and some disease characteristics than did one-dose varicella vaccinations, in a case-control study of children living in two communities in the United States.
Two doses of the vaccine were 93.6% effective against all clinically diagnosed varicella and 97.9% effective against moderate to severe varicella, compared with children receiving no vaccine, among subjects aged 4 years and older. A single dose of the vaccine was 75.6% effective against all clinically diagnosed varicella and 78.1% effective against moderate or severe disease, compared with no vaccine.

Cases of varicella in patients who had two doses of the vaccine were more likely to involve rashes that resolved in less than 1 week (P = .01) and were less likely to involve vesicular rashes (P = .01), among breakthrough cases in patients aged 4 years and older, reported Dana Perella of the Philadelphia Department of Public Health, and her colleagues. They investigated 125 clinically diagnosed cases of varicella and 408 matched controls from May 2009 through June 2011. The study participants, aged 1-18 years, were residents of West Philadelphia and the Antelope Valley are of Northern Los Angeles.
“With superior protection provided by the two-dose varicella vaccination, compared with the one-dose regimen as demonstrated in our study and others, it will be important to expand school immunization requirements to include two-dose varicella vaccination,” the researchers wrote.
Read the study in Pediatrics (doi: 10.1542/peds.2015-2802).
Two-dose varicella vaccinations were more effective and resulted in decreased risk of varicella severity and some disease characteristics than did one-dose varicella vaccinations, in a case-control study of children living in two communities in the United States.
Two doses of the vaccine were 93.6% effective against all clinically diagnosed varicella and 97.9% effective against moderate to severe varicella, compared with children receiving no vaccine, among subjects aged 4 years and older. A single dose of the vaccine was 75.6% effective against all clinically diagnosed varicella and 78.1% effective against moderate or severe disease, compared with no vaccine.
Cases of varicella in patients who had two doses of the vaccine were more likely to involve rashes that resolved in less than 1 week (P = .01) and were less likely to involve vesicular rashes (P = .01), among breakthrough cases in patients aged 4 years and older, reported Dana Perella of the Philadelphia Department of Public Health, and her colleagues. They investigated 125 clinically diagnosed cases of varicella and 408 matched controls from May 2009 through June 2011. The study participants, aged 1-18 years, were residents of West Philadelphia and the Antelope Valley are of Northern Los Angeles.
“With superior protection provided by the two-dose varicella vaccination, compared with the one-dose regimen as demonstrated in our study and others, it will be important to expand school immunization requirements to include two-dose varicella vaccination,” the researchers wrote.
Read the study in Pediatrics (doi: 10.1542/peds.2015-2802).
Two-dose varicella vaccinations were more effective and resulted in decreased risk of varicella severity and some disease characteristics than did one-dose varicella vaccinations, in a case-control study of children living in two communities in the United States.
Two doses of the vaccine were 93.6% effective against all clinically diagnosed varicella and 97.9% effective against moderate to severe varicella, compared with children receiving no vaccine, among subjects aged 4 years and older. A single dose of the vaccine was 75.6% effective against all clinically diagnosed varicella and 78.1% effective against moderate or severe disease, compared with no vaccine.
Cases of varicella in patients who had two doses of the vaccine were more likely to involve rashes that resolved in less than 1 week (P = .01) and were less likely to involve vesicular rashes (P = .01), among breakthrough cases in patients aged 4 years and older, reported Dana Perella of the Philadelphia Department of Public Health, and her colleagues. They investigated 125 clinically diagnosed cases of varicella and 408 matched controls from May 2009 through June 2011. The study participants, aged 1-18 years, were residents of West Philadelphia and the Antelope Valley are of Northern Los Angeles.
“With superior protection provided by the two-dose varicella vaccination, compared with the one-dose regimen as demonstrated in our study and others, it will be important to expand school immunization requirements to include two-dose varicella vaccination,” the researchers wrote.
Read the study in Pediatrics (doi: 10.1542/peds.2015-2802).
FROM PEDIATRICS

Study: Two varicella vaccination doses more effective than one
Two-dose varicella vaccinations were more effective and resulted in decreased risk of varicella severity and some disease characteristics than did one-dose varicella vaccinations, in a case-control study of children living in two communities in the United States.
Two doses of the vaccine were 93.6% effective against all clinically diagnosed varicella and 97.9% effective against moderate to severe varicella, compared with children receiving no vaccine, among subjects aged 4 years and older. A single dose of the vaccine was 75.6% effective against all clinically diagnosed varicella and 78.1% effective against moderate or severe disease, compared with no vaccine.

Cases of varicella in patients who had two doses of the vaccine were more likely to involve rashes that resolved in less than 1 week (P = .01) and were less likely to involve vesicular rashes (P = .01), among breakthrough cases in patients aged 4 years and older, reported Dana Perella of the Philadelphia Department of Public Health, and her colleagues. They investigated 125 clinically diagnosed cases of varicella and 408 matched controls from May 2009 through June 2011. The study participants, aged 1-18 years, were residents of West Philadelphia and the Antelope Valley are of Northern Los Angeles.
“With superior protection provided by the two-dose varicella vaccination, compared with the one-dose regimen as demonstrated in our study and others, it will be important to expand school immunization requirements to include two-dose varicella vaccination,” the researchers wrote.
Read the study in Pediatrics (doi: 10.1542/peds.2015-2802).
Two-dose varicella vaccinations were more effective and resulted in decreased risk of varicella severity and some disease characteristics than did one-dose varicella vaccinations, in a case-control study of children living in two communities in the United States.
Two doses of the vaccine were 93.6% effective against all clinically diagnosed varicella and 97.9% effective against moderate to severe varicella, compared with children receiving no vaccine, among subjects aged 4 years and older. A single dose of the vaccine was 75.6% effective against all clinically diagnosed varicella and 78.1% effective against moderate or severe disease, compared with no vaccine.
Cases of varicella in patients who had two doses of the vaccine were more likely to involve rashes that resolved in less than 1 week (P = .01) and were less likely to involve vesicular rashes (P = .01), among breakthrough cases in patients aged 4 years and older, reported Dana Perella of the Philadelphia Department of Public Health, and her colleagues. They investigated 125 clinically diagnosed cases of varicella and 408 matched controls from May 2009 through June 2011. The study participants, aged 1-18 years, were residents of West Philadelphia and the Antelope Valley are of Northern Los Angeles.
“With superior protection provided by the two-dose varicella vaccination, compared with the one-dose regimen as demonstrated in our study and others, it will be important to expand school immunization requirements to include two-dose varicella vaccination,” the researchers wrote.
Read the study in Pediatrics (doi: 10.1542/peds.2015-2802).
Two-dose varicella vaccinations were more effective and resulted in decreased risk of varicella severity and some disease characteristics than did one-dose varicella vaccinations, in a case-control study of children living in two communities in the United States.
Two doses of the vaccine were 93.6% effective against all clinically diagnosed varicella and 97.9% effective against moderate to severe varicella, compared with children receiving no vaccine, among subjects aged 4 years and older. A single dose of the vaccine was 75.6% effective against all clinically diagnosed varicella and 78.1% effective against moderate or severe disease, compared with no vaccine.
Cases of varicella in patients who had two doses of the vaccine were more likely to involve rashes that resolved in less than 1 week (P = .01) and were less likely to involve vesicular rashes (P = .01), among breakthrough cases in patients aged 4 years and older, reported Dana Perella of the Philadelphia Department of Public Health, and her colleagues. They investigated 125 clinically diagnosed cases of varicella and 408 matched controls from May 2009 through June 2011. The study participants, aged 1-18 years, were residents of West Philadelphia and the Antelope Valley are of Northern Los Angeles.
“With superior protection provided by the two-dose varicella vaccination, compared with the one-dose regimen as demonstrated in our study and others, it will be important to expand school immunization requirements to include two-dose varicella vaccination,” the researchers wrote.
Read the study in Pediatrics (doi: 10.1542/peds.2015-2802).
FROM PEDIATRICS

As varicella recedes, zoster rises: The question is ‘why?’
WASHINGTON – As the number of children vaccinated against varicella has risen, the number of chicken pox cases has proportionally declined.
No news there.
But, as the number of kids getting chickenpox gets smaller, the number of adults getting shingles is growing – and no one really knows why, Dr. Vikash Oza said at the annual meeting of the American Academy of Dermatology.
“Varicella vaccination has had a dramatic impact on the incidence of chickenpox,” said Dr. Oza, a pediatric dermatologist at New York University Langone Medical Center. “In fact, as a resident I saw not one case of chickenpox. That’s pretty astounding considering how common it used to be.”
Introduced in 1995, the vaccine now covers about 90% of children in this country – an achievement almost exactly mirrored by the decrease in disease incidence. In fact, according to a 2013 study, the bang for the vaccine buck may be even bigger, achieving 98% decreases in two regions examined (Pediatrics. 2013 Nov;132[5]:e1134-40).
That study also found that vaccinated children who did get chickenpox had much milder infections that resolved more quickly.

Again, that’s good news, but not particularly surprising, said Dr. Oza. The more intriguing change is the steady increase in herpes zoster among older adults occurring in tandem with the decreased incidence of chickenpox. Cases were up a total of 39% from 1992 to 2010 among adults 65 and older, according to the Centers for Disease Control and Prevention (Ann Intern Med. 2013;159[11]:739-45).
“This thing that’s happening in adults is quite interesting,” Dr. Oza said. “Although zoster in children is uncommon, we do know that children are much less likely to develop it if they’ve been vaccinated against varicella. What we don’t really know is what this means for adults. One of the effects of the vaccine, of course, is less circulating varicella zoster virus in our communities. It’s possible that a benefit of having some circulating VZV gives adults an immune boost that keeps zoster in check, and without that, developing shingles is more likely.”
Several recent studies have documented the association. A 2005 study found that during 1998-2003, the incidence of chickenpox in Massachusetts went down by 79%, while the incidence of shingles increased by 90% (BMC Public Health 2005;5:68. doi: 10.1186/1471-2458-5-68). But a shifting age-related immune response is only one possible explanation, the authors wrote. “There are several possible explanations, which may be operating in combination. Other possible explanations include increases in the proportion of people with immunosuppressive conditions and therapies, in the duration of those conditions and treatments, and/or in the prevalence of other triggering factors.”
The shifting incidences of chickenpox and shingles, however, were predicted years before they occurred. A mathematical model from 1992 predicted a long-term elevation of up to 20% in the shingles rate, relative to pre-vaccination incidence (Epidemiol Infect. 1992 Jun;108[3]:513–28). A 2001 paper predicted that shingles would increase for 30-50 years after mass varicella vaccination, rising to a maximum of about 50% above pre-vaccination rates, before falling below baseline levels (Epidemiol Infect. 2001 Oct;127[2]:305–14).
The CDC refutes any causative link between varicella vaccinations and shingles. “This proposed explanation seems unlikely based on two CDC studies which found that shingles rates started increasing before chickenpox vaccine was introduced in the United States, and after the routine chickenpox vaccination program started,” the agency’s surveillance pagenotes. “Other countries without routine chickenpox vaccination programs, have observed similar increases in shingles rates.”
Regardless of the “why” behind the association, Dr. Oza expects it to level out as vaccinated children come of shingles age. “As the Millenials take over, with their heightened immunity to varicella virus, we will eventually get to the point where zoster has less of an impact on clinical practice and the healthcare industry.”
He had no financial disclosures.
On Twitter @Alz_Gal
WASHINGTON – As the number of children vaccinated against varicella has risen, the number of chicken pox cases has proportionally declined.
No news there.
But, as the number of kids getting chickenpox gets smaller, the number of adults getting shingles is growing – and no one really knows why, Dr. Vikash Oza said at the annual meeting of the American Academy of Dermatology.
“Varicella vaccination has had a dramatic impact on the incidence of chickenpox,” said Dr. Oza, a pediatric dermatologist at New York University Langone Medical Center. “In fact, as a resident I saw not one case of chickenpox. That’s pretty astounding considering how common it used to be.”
Introduced in 1995, the vaccine now covers about 90% of children in this country – an achievement almost exactly mirrored by the decrease in disease incidence. In fact, according to a 2013 study, the bang for the vaccine buck may be even bigger, achieving 98% decreases in two regions examined (Pediatrics. 2013 Nov;132[5]:e1134-40).
That study also found that vaccinated children who did get chickenpox had much milder infections that resolved more quickly.
Again, that’s good news, but not particularly surprising, said Dr. Oza. The more intriguing change is the steady increase in herpes zoster among older adults occurring in tandem with the decreased incidence of chickenpox. Cases were up a total of 39% from 1992 to 2010 among adults 65 and older, according to the Centers for Disease Control and Prevention (Ann Intern Med. 2013;159[11]:739-45).
“This thing that’s happening in adults is quite interesting,” Dr. Oza said. “Although zoster in children is uncommon, we do know that children are much less likely to develop it if they’ve been vaccinated against varicella. What we don’t really know is what this means for adults. One of the effects of the vaccine, of course, is less circulating varicella zoster virus in our communities. It’s possible that a benefit of having some circulating VZV gives adults an immune boost that keeps zoster in check, and without that, developing shingles is more likely.”
Several recent studies have documented the association. A 2005 study found that during 1998-2003, the incidence of chickenpox in Massachusetts went down by 79%, while the incidence of shingles increased by 90% (BMC Public Health 2005;5:68. doi: 10.1186/1471-2458-5-68). But a shifting age-related immune response is only one possible explanation, the authors wrote. “There are several possible explanations, which may be operating in combination. Other possible explanations include increases in the proportion of people with immunosuppressive conditions and therapies, in the duration of those conditions and treatments, and/or in the prevalence of other triggering factors.”
The shifting incidences of chickenpox and shingles, however, were predicted years before they occurred. A mathematical model from 1992 predicted a long-term elevation of up to 20% in the shingles rate, relative to pre-vaccination incidence (Epidemiol Infect. 1992 Jun;108[3]:513–28). A 2001 paper predicted that shingles would increase for 30-50 years after mass varicella vaccination, rising to a maximum of about 50% above pre-vaccination rates, before falling below baseline levels (Epidemiol Infect. 2001 Oct;127[2]:305–14).
The CDC refutes any causative link between varicella vaccinations and shingles. “This proposed explanation seems unlikely based on two CDC studies which found that shingles rates started increasing before chickenpox vaccine was introduced in the United States, and after the routine chickenpox vaccination program started,” the agency’s surveillance pagenotes. “Other countries without routine chickenpox vaccination programs, have observed similar increases in shingles rates.”
Regardless of the “why” behind the association, Dr. Oza expects it to level out as vaccinated children come of shingles age. “As the Millenials take over, with their heightened immunity to varicella virus, we will eventually get to the point where zoster has less of an impact on clinical practice and the healthcare industry.”
He had no financial disclosures.
On Twitter @Alz_Gal
WASHINGTON – As the number of children vaccinated against varicella has risen, the number of chicken pox cases has proportionally declined.
No news there.
But, as the number of kids getting chickenpox gets smaller, the number of adults getting shingles is growing – and no one really knows why, Dr. Vikash Oza said at the annual meeting of the American Academy of Dermatology.
“Varicella vaccination has had a dramatic impact on the incidence of chickenpox,” said Dr. Oza, a pediatric dermatologist at New York University Langone Medical Center. “In fact, as a resident I saw not one case of chickenpox. That’s pretty astounding considering how common it used to be.”
Introduced in 1995, the vaccine now covers about 90% of children in this country – an achievement almost exactly mirrored by the decrease in disease incidence. In fact, according to a 2013 study, the bang for the vaccine buck may be even bigger, achieving 98% decreases in two regions examined (Pediatrics. 2013 Nov;132[5]:e1134-40).
That study also found that vaccinated children who did get chickenpox had much milder infections that resolved more quickly.
Again, that’s good news, but not particularly surprising, said Dr. Oza. The more intriguing change is the steady increase in herpes zoster among older adults occurring in tandem with the decreased incidence of chickenpox. Cases were up a total of 39% from 1992 to 2010 among adults 65 and older, according to the Centers for Disease Control and Prevention (Ann Intern Med. 2013;159[11]:739-45).
“This thing that’s happening in adults is quite interesting,” Dr. Oza said. “Although zoster in children is uncommon, we do know that children are much less likely to develop it if they’ve been vaccinated against varicella. What we don’t really know is what this means for adults. One of the effects of the vaccine, of course, is less circulating varicella zoster virus in our communities. It’s possible that a benefit of having some circulating VZV gives adults an immune boost that keeps zoster in check, and without that, developing shingles is more likely.”
Several recent studies have documented the association. A 2005 study found that during 1998-2003, the incidence of chickenpox in Massachusetts went down by 79%, while the incidence of shingles increased by 90% (BMC Public Health 2005;5:68. doi: 10.1186/1471-2458-5-68). But a shifting age-related immune response is only one possible explanation, the authors wrote. “There are several possible explanations, which may be operating in combination. Other possible explanations include increases in the proportion of people with immunosuppressive conditions and therapies, in the duration of those conditions and treatments, and/or in the prevalence of other triggering factors.”
The shifting incidences of chickenpox and shingles, however, were predicted years before they occurred. A mathematical model from 1992 predicted a long-term elevation of up to 20% in the shingles rate, relative to pre-vaccination incidence (Epidemiol Infect. 1992 Jun;108[3]:513–28). A 2001 paper predicted that shingles would increase for 30-50 years after mass varicella vaccination, rising to a maximum of about 50% above pre-vaccination rates, before falling below baseline levels (Epidemiol Infect. 2001 Oct;127[2]:305–14).
The CDC refutes any causative link between varicella vaccinations and shingles. “This proposed explanation seems unlikely based on two CDC studies which found that shingles rates started increasing before chickenpox vaccine was introduced in the United States, and after the routine chickenpox vaccination program started,” the agency’s surveillance pagenotes. “Other countries without routine chickenpox vaccination programs, have observed similar increases in shingles rates.”
Regardless of the “why” behind the association, Dr. Oza expects it to level out as vaccinated children come of shingles age. “As the Millenials take over, with their heightened immunity to varicella virus, we will eventually get to the point where zoster has less of an impact on clinical practice and the healthcare industry.”
He had no financial disclosures.
On Twitter @Alz_Gal
EXPERT ANALYSIS FROM AAD 2016

14-Year-Old Boy With Mild Antecedent Neck Pain in Setting of Acute Trauma: A Rare Case of Benign Fibrous Histiocytoma of the Spine
Benign fibrous histiocytoma (BFH) is a rare, well-recognized, primary skeletal tumor accounting for approximately 1% of all benign bone tumors. Spinal involvement is exceedingly rare with only 11 cases reported in the literature.1,2 We present a case of BFH located in the cervical spine of a pediatric patient that was successfully treated with curretage through an anterior surgical approach, along with a review of the literature and appropriate management concerning BFH of the spine.
Case Report
A 14-year-old boy was tackled while playing football and noticed immediate neck pain and subjective paresthesia in the upper extremities. Examination revealed a nontender spine (cervical, thoracic, lumbar) and normal strength and range of motion in all extremities. Sensation was diffusely intact, long tract signs were absent, and gait was normal. On questioning, the patient endorsed mild antecedent neck pain but denied prior history of any trauma. Neck pain did not radiate and was slightly worsened by activity but was mostly intermittent and random. As the neck pain was very mild and was not interfering with daily activities, the patient had not sought care before presenting to the emergency department. He had no pertinent past medical or surgical history.
The patient presented with a computed tomography (CT) scan of his head and cervical spine and a magnetic resonance imaging (MRI) scan of the cervical spine. A magnetic resonance angiography (MRA) scan of the neck was ordered after his arrival.
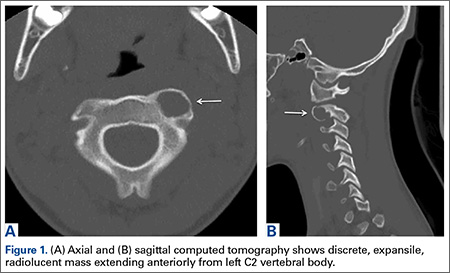
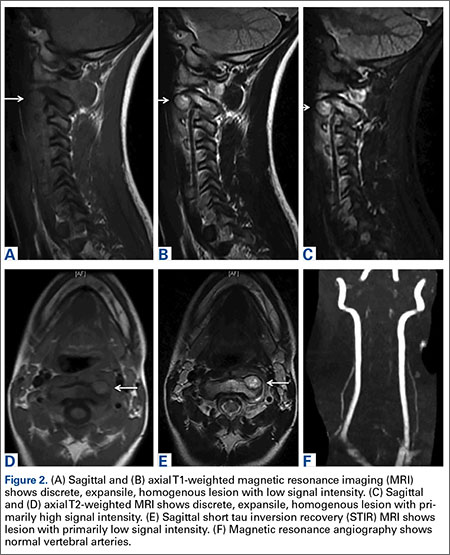
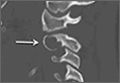
Axial and sagittal CT (Figures 1A, 1B) showed a 1×1.2-cm discrete, expansile, lytic, radiolucent mass extending anterior from the left C2 vertebral body. The mass appeared to abut the left vertebral artery foramen. The cortical bone surrounding the lesion was thin but uniform. Sagittal and axial T1-weighted MRI (Figures 2A, 2B) showed the discrete, expansile, homogenous lesion with the same intensity as normal bone marrow. Sagittal and axial T2-weighted MRI (Figures 2C, 2D) showed a discrete, expansile, homogenous lesion with primarily high signal intensity. Sagittal short tau inversion recovery (STIR) MRI (Figure 2E) again showed the lesion with primarily low intensity. Given the close proximity of the lesion to the vertebral foramen, MRA was ordered; it showed the lesion was not interfering with the vertebral artery (Figure 2F).
The tumor’s location, in the left anterior aspect of the C2 vertebral body, was not conducive to percutaneous biopsy for establishing tissue diagnosis, so the decision was made to surgically excise the lesion. A left-sided anterior incision was made 2 fingerbreadths inferior to the jaw line in a neck crease. A head and neck surgeon assisted with dissection. Dissection was carried down through the skin, subcutaneous tissue, and platysma on to the anterior part of the spine medial to the carotid sheath. Superior thyroid nerve and vessels and superior laryngeal nerve were identified and preserved. Fluoroscopy confirmed correct location at C2. The tumor was easily visualized, and the outer shell broke easily with palpation. Gentle curettage was necessary when removing the tumor off the vertebral artery. A portion of the specimen was sent during surgery for frozen section, which showed infrequent mitotic figures and no other findings concerning for malignancy. No instability was created after curettage and excision of the tumor, so no grafting or instrumentation was necessary.
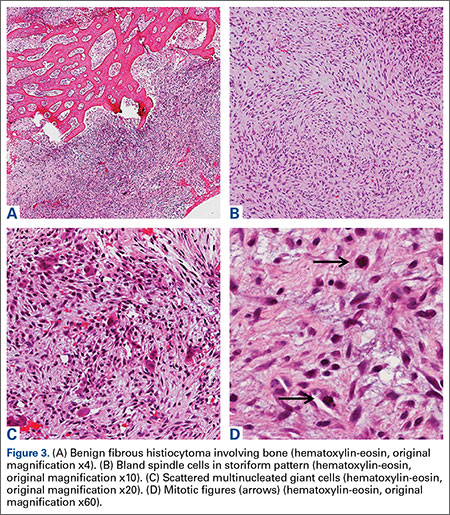
Grossly, the tumor was pale tan and firm. Histologic examination with hematoxylin-eosin staining revealed a bland spindle-cell neoplasm that focally involved bone. A storiform pattern was present. The cells had scant cytoplasm and oval to elongate nuclei with tapered ends. Significant nuclear pleomorphism was not seen. The stroma was loose, with focal myxoid change. Benign multinucleated giant cells were present. Mitotic activity was infrequent (Figures 3A–3D). Two attending pathologists reviewed the case material and the frozen and formalin-fixed specimens independently and concurred with the diagnosis of BFH. In addition, the case was reviewed at the surgical pathology consensus conference; the reviewers agreed on BFH, and additional studies were deemed unnecessary.
Given the patient’s complete clinical picture, the differential diagnosis included nonossifying fibroma (NOF), eosinophilic granuloma (EG), BFH, fibrous dysplasia, giant cell tumor (GCT), aneurysmal bone cyst (ABC), and osteoblastoma (OB).
Discussion
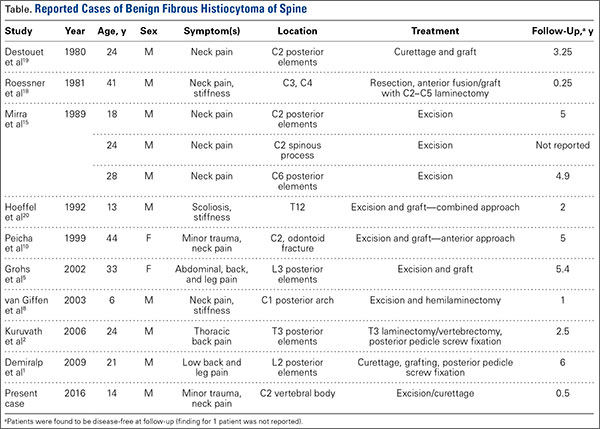
BFH is an extremely rare bone lesion, accounting for only 1% of all surgically managed bone tumors; not counting the present case, only 11 spine cases have been reported in the literature.1,2 BFH of the spine traditionally causes nonspecific, poorly localized pain. The Table lists the reported cases of spinal BFH and their presenting symptoms, location, and treatment. BFH usually occurs in young adults, but the age range is 5 to 75 years.2-4 Mean age of the 12 patients with spinal BFH in the literature (including ours) is 25 years.1 In addition, spinal BFH appears to have no predilection for sex.
Skeletal BFH presents as a discrete, well-defined, osteolytic lesion with sharp borders and potentially a sclerotic rim.4-6 Cortical expansion and even cortical disruption with invasion into adjacent tissue have occurred in flat bones.7 Histologically, BFHs contain spindle cells, multinucleated giant cells, and foam cells in storiform pattern.6
BFH shares many of its radiologic and histologic characteristics and clinical symptoms with other benign bone lesions (the tumors listed above). Therefore, accurate diagnosis of BFH requires appropriate correlation of clinical, radiographic, and histologic data.2,3,8 Below is a comparison of BFH with related bone lesions.
Spinal BFH causes a nonspecific, poorly localized pain similar to that of EG, ABC, GCT, and OB.3,9 NOF and fibrous dysplasia generally do not cause pain, unless these lesions are discovered secondary to a pathologic fracture.8,10,11 Our patient had minor antecedent neck pain, which was brought to light by his football accident. ABC and OB are more locally aggressive than BFH and can cause neurologic symptoms by mass effect and spinal cord or nerve root compression.1,8 In this case and in the 6 other cases of BFH of the cervical spine, there were no neurologic changes.4,10
Of the tumors mentioned, NOF and EG almost always occur in children. However, NOF usually occurs in the metaphyseal region of long bones, and EG is usually accompanied by systemic symptoms, such as lymphadenopathy, hepatomegaly, and increased inflammatory markers.1,8 Fibrous dysplasia usually presents in childhood but does not become symptomatic until adulthood. GCTs and OB predominantly occur in adulthood.12,13 Our patient’s age and lack of other systemic symptoms supported the diagnosis of BFH.
Appearance on MRI is reported less with BFH than with other tumors, but heterogenous signal intensity similar to that of skeletal muscle on T1-weighted images and high signal intensity on T2-weighted images is typically reported.8,14 NOF and fibrous dysplasia do not disrupt the bony cortex unless a pathologic fracture has occurred.4 GCTs are more aggressive lytic lesions with more aggressive radiologic features. GCTs generally cause cortical expansion/attenuation, and lack a sclerotic rim. GCTs also have a heterogenous appearance on MRI and give a low to intermediate signal on both T1- and T2-weighted images.12,15 The appearance of EG is similar to that of BFH as an osteolytic lesion with a sclerotic rim, though EGs typically break through the cortex and acquire a “punched-out” look.1,8 ABC typically is described as an expansile osteolytic lesion with a “soap-bubble” appearance on radiographs; periosteal elevation and cortical attenuation can also be visualized. MRI shows the typical multilobular appearance of the lesion with fluid levels.13
OB appears as a radiolucent lesion, with or without calcifications, surrounded by a thin margin of reactive bone.14,16 A distinguishing characteristic of OB was thought to be intense radioisotope uptake on bone scintigraphy, but recently a bony BFH demonstrated intense uptake.17 OBs typically demonstrate nonspecific MRI results similar to those of BFH: low to intermediate signal on T1-weighted images and intermediate to high signal on T2-weighted images.13 In our patient’s case, the radiographic appearance and lack of specific radiographic findings consistent with the other tumors supported the diagnosis of BFH.
Histologically, BFHs contain spindle cells, multinucleated giant cells, and foam cells in a storiform pattern6 which was demonstrated in our patient’s case. In addition, significant nuclear pleomorphism, mitotic activity, and necrosis were absent—a difference between BFH and malignant fibrous histiocytoma.4,15 The microscopic characteristics of BFH readily differentiate it from OB, ABC, EG, and GCT, but not from NOF on microscopic appearance alone. Clinical and radiographic findings must be consistent, as mentioned.7,18
Complete surgical excision is the reported treatment for BFH. Prognosis after resection or curettage is usually good, and recurrences have been rare.1,2 Depending on the intraspinous location of BFH, stabilization after resection or curettage may be necessary to prevent residual instability. Three of the 11 reported cases of spinal BFH required stabilization by anterior fusion or posterior pedicle screw fixation after resection.1,2 The other 8 cases underwent excision alone or excision and grafting. All 11 patients were disease-free at a mean follow-up of 3.5 years.1 In nonspinal BFH, however, both local recurrence and lung metastasis have been reported.2,5,9,19 Clarke and colleagues9 reported local recurrences in 3 of 8 cases. These recurrences involved BFH in long bones of the leg, which had been treated with curettage and grafting. There has been no reliable report of a malignant change in BFH.2,9 The only case of lung metastasis, reported by Unni and Dahlin6 in their study of 10 cases, occurred 2 years after local recurrence in the distal femur.Our patient was doing well at most recent follow-up, 6 months after surgery. He had no pain and had returned to normal activities. Although there are no reported cases of spinal BFH recurrence, we will follow this patient with imaging on an annual basis. His case is of particular interest to orthopedic surgeons because they encounter benign bone lesions every day, and many of these lesions are in difficult anatomical locations. Knowing the characteristics, differential diagnoses, and appropriate diagnostic workups for benign bone lesions is important for optimal and timely patient care.
1. Demiralp B, Kose O, Oguz E, Sanal T, Ozcan A, Sehirlioglu A. Benign fibrous histiocytoma of the lumbar vertebrae. Skeletal Radiol. 2009;38(2):187-191.
2. Kuruvath S, O’Donovan DG, Aspoas AR, David KM. Benign fibrous histiocytoma of the thoracic spine: case report and review of the literature. J Neurosurg Spine. 2006;4(3):260-264.
3. Ceroni D, Dayer R, De Coulon G, Kaelin A. Benign fibrous histiocytoma of bone in a paediatric population: a report of 6 cases. Musculoskelet Surg. 2011;95(2):107-114.
4. Dorfman HD, Czerniak B. Bone Tumors. St. Louis, MO: Mosby; 1998.
5. Grohs JG, Nicolakis M, Kainberger F, Lang S, Kotz R. Benign fibrous histiocytoma of bone: a report of ten cases and review of literature. Wien Klin Wochenschr. 2002;114(1-2):56-63.
6. Unni KK, Dahlin DC. Dahlin’s Bone Tumors. 5th ed. Philadelphia, PA: Lippincott-Raven; 1996.
7. Balasubramanian C, Rajaraman G, Singh CS, Baliga DK. Benign fibrous histiocytoma of the sacrum—diagnostic difficulties facing this rare bone tumor. Pediatr Neurosurg. 2005;41(5):253-257.
8. van Giffen NH, van Rhijn LW, van Ooij A, et al. Benign fibrous histiocytoma of the posterior arch of C1 in a 6-year old boy: a case report. Spine. 2003;28(18):E359-E363.
9. Clarke BE, Xipell JM, Thomas DP. Benign fibrous histiocytoma of bone. Am J Surg Pathol. 1985;9(11):806-815.
10. Peicha G, Siebert FJ, Bratschitsch G, Fankhauser F, Grechenig W. Pathologic odontoid fracture and benign fibrous histiocytoma of bone. Eur Spine J. 1999;8(2):161-163.
11. Unni KK, Inwards CY, Bridge JA, Kindblom LG, Wold LE. Tumors of the Bones and Joints (AFIP Atlas of Tumor Pathology Series IV). Annapolis Junction, MD: American Registry of Pathology Press; 2005.
12. Dee R. Principles of Orthopaedic Practice. 2nd ed. New York, NY: McGraw-Hill; 1997.
13. Murphey M, Andrews C, Flemming D, Temple HT, Smith WS, Smirniotopoulos JG. Primary tumors of the spine: radiologic–pathologic correlation. Radiographics. 1996;16(5):1131-1158.
14. Hamada T, Ito H, Araki Y, Fujii K, Inoue M, Ishida O. Benign fibrous histiocytoma of the femur: review of three cases. Skeletal Radiol. 1996;25(1):25-29.
15. Mirra JM, Picci P, Gold RH. Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Vol 1. Philadelphia, PA: Lea & Febiger; 1989.
16. Theodorou DJ, Theodorou SJ, Sartoris DJ. An imaging overview of primary tumors of the spine: part 1. Benign tumors. Clin Imaging. 2008;32(3):196-203.
17. Li X, Meng Z, Li D, Tan J, Song X. Benign fibrous histiocytoma of a rib. Clin Nucl Med. 2014;39(9): 837-841.
18. Roessner A, Immenkamp M, Weidner A, Hobik HP, Grundmann E. Benign fibrous histiocytoma of bone. Light- and electron-microscopic observations. J Cancer Res Clin Oncol. 1981;101(2):191-202.
19. Destouet JM, Kyriakos M, Gilula LA. Fibrous histiocytoma (fibroxanthoma) of a cervical vertebra. A report with a review of the literature. Skeletal Radiol. 1980;5(4):241-246.
20. Hoeffel JC, Bomand-Ferrand F, Tachet F, Lascombes P, Czorny A, Bernard C. So-called benign fibrous histiocytoma: report of a case. J Pediatr Surg. 1992;27(5):672-674.
Benign fibrous histiocytoma (BFH) is a rare, well-recognized, primary skeletal tumor accounting for approximately 1% of all benign bone tumors. Spinal involvement is exceedingly rare with only 11 cases reported in the literature.1,2 We present a case of BFH located in the cervical spine of a pediatric patient that was successfully treated with curretage through an anterior surgical approach, along with a review of the literature and appropriate management concerning BFH of the spine.
Case Report
A 14-year-old boy was tackled while playing football and noticed immediate neck pain and subjective paresthesia in the upper extremities. Examination revealed a nontender spine (cervical, thoracic, lumbar) and normal strength and range of motion in all extremities. Sensation was diffusely intact, long tract signs were absent, and gait was normal. On questioning, the patient endorsed mild antecedent neck pain but denied prior history of any trauma. Neck pain did not radiate and was slightly worsened by activity but was mostly intermittent and random. As the neck pain was very mild and was not interfering with daily activities, the patient had not sought care before presenting to the emergency department. He had no pertinent past medical or surgical history.
The patient presented with a computed tomography (CT) scan of his head and cervical spine and a magnetic resonance imaging (MRI) scan of the cervical spine. A magnetic resonance angiography (MRA) scan of the neck was ordered after his arrival.
Axial and sagittal CT (Figures 1A, 1B) showed a 1×1.2-cm discrete, expansile, lytic, radiolucent mass extending anterior from the left C2 vertebral body. The mass appeared to abut the left vertebral artery foramen. The cortical bone surrounding the lesion was thin but uniform. Sagittal and axial T1-weighted MRI (Figures 2A, 2B) showed the discrete, expansile, homogenous lesion with the same intensity as normal bone marrow. Sagittal and axial T2-weighted MRI (Figures 2C, 2D) showed a discrete, expansile, homogenous lesion with primarily high signal intensity. Sagittal short tau inversion recovery (STIR) MRI (Figure 2E) again showed the lesion with primarily low intensity. Given the close proximity of the lesion to the vertebral foramen, MRA was ordered; it showed the lesion was not interfering with the vertebral artery (Figure 2F).
The tumor’s location, in the left anterior aspect of the C2 vertebral body, was not conducive to percutaneous biopsy for establishing tissue diagnosis, so the decision was made to surgically excise the lesion. A left-sided anterior incision was made 2 fingerbreadths inferior to the jaw line in a neck crease. A head and neck surgeon assisted with dissection. Dissection was carried down through the skin, subcutaneous tissue, and platysma on to the anterior part of the spine medial to the carotid sheath. Superior thyroid nerve and vessels and superior laryngeal nerve were identified and preserved. Fluoroscopy confirmed correct location at C2. The tumor was easily visualized, and the outer shell broke easily with palpation. Gentle curettage was necessary when removing the tumor off the vertebral artery. A portion of the specimen was sent during surgery for frozen section, which showed infrequent mitotic figures and no other findings concerning for malignancy. No instability was created after curettage and excision of the tumor, so no grafting or instrumentation was necessary.
Grossly, the tumor was pale tan and firm. Histologic examination with hematoxylin-eosin staining revealed a bland spindle-cell neoplasm that focally involved bone. A storiform pattern was present. The cells had scant cytoplasm and oval to elongate nuclei with tapered ends. Significant nuclear pleomorphism was not seen. The stroma was loose, with focal myxoid change. Benign multinucleated giant cells were present. Mitotic activity was infrequent (Figures 3A–3D). Two attending pathologists reviewed the case material and the frozen and formalin-fixed specimens independently and concurred with the diagnosis of BFH. In addition, the case was reviewed at the surgical pathology consensus conference; the reviewers agreed on BFH, and additional studies were deemed unnecessary.
Given the patient’s complete clinical picture, the differential diagnosis included nonossifying fibroma (NOF), eosinophilic granuloma (EG), BFH, fibrous dysplasia, giant cell tumor (GCT), aneurysmal bone cyst (ABC), and osteoblastoma (OB).
Discussion
BFH is an extremely rare bone lesion, accounting for only 1% of all surgically managed bone tumors; not counting the present case, only 11 spine cases have been reported in the literature.1,2 BFH of the spine traditionally causes nonspecific, poorly localized pain. The Table lists the reported cases of spinal BFH and their presenting symptoms, location, and treatment. BFH usually occurs in young adults, but the age range is 5 to 75 years.2-4 Mean age of the 12 patients with spinal BFH in the literature (including ours) is 25 years.1 In addition, spinal BFH appears to have no predilection for sex.
Skeletal BFH presents as a discrete, well-defined, osteolytic lesion with sharp borders and potentially a sclerotic rim.4-6 Cortical expansion and even cortical disruption with invasion into adjacent tissue have occurred in flat bones.7 Histologically, BFHs contain spindle cells, multinucleated giant cells, and foam cells in storiform pattern.6
BFH shares many of its radiologic and histologic characteristics and clinical symptoms with other benign bone lesions (the tumors listed above). Therefore, accurate diagnosis of BFH requires appropriate correlation of clinical, radiographic, and histologic data.2,3,8 Below is a comparison of BFH with related bone lesions.
Spinal BFH causes a nonspecific, poorly localized pain similar to that of EG, ABC, GCT, and OB.3,9 NOF and fibrous dysplasia generally do not cause pain, unless these lesions are discovered secondary to a pathologic fracture.8,10,11 Our patient had minor antecedent neck pain, which was brought to light by his football accident. ABC and OB are more locally aggressive than BFH and can cause neurologic symptoms by mass effect and spinal cord or nerve root compression.1,8 In this case and in the 6 other cases of BFH of the cervical spine, there were no neurologic changes.4,10
Of the tumors mentioned, NOF and EG almost always occur in children. However, NOF usually occurs in the metaphyseal region of long bones, and EG is usually accompanied by systemic symptoms, such as lymphadenopathy, hepatomegaly, and increased inflammatory markers.1,8 Fibrous dysplasia usually presents in childhood but does not become symptomatic until adulthood. GCTs and OB predominantly occur in adulthood.12,13 Our patient’s age and lack of other systemic symptoms supported the diagnosis of BFH.
Appearance on MRI is reported less with BFH than with other tumors, but heterogenous signal intensity similar to that of skeletal muscle on T1-weighted images and high signal intensity on T2-weighted images is typically reported.8,14 NOF and fibrous dysplasia do not disrupt the bony cortex unless a pathologic fracture has occurred.4 GCTs are more aggressive lytic lesions with more aggressive radiologic features. GCTs generally cause cortical expansion/attenuation, and lack a sclerotic rim. GCTs also have a heterogenous appearance on MRI and give a low to intermediate signal on both T1- and T2-weighted images.12,15 The appearance of EG is similar to that of BFH as an osteolytic lesion with a sclerotic rim, though EGs typically break through the cortex and acquire a “punched-out” look.1,8 ABC typically is described as an expansile osteolytic lesion with a “soap-bubble” appearance on radiographs; periosteal elevation and cortical attenuation can also be visualized. MRI shows the typical multilobular appearance of the lesion with fluid levels.13
OB appears as a radiolucent lesion, with or without calcifications, surrounded by a thin margin of reactive bone.14,16 A distinguishing characteristic of OB was thought to be intense radioisotope uptake on bone scintigraphy, but recently a bony BFH demonstrated intense uptake.17 OBs typically demonstrate nonspecific MRI results similar to those of BFH: low to intermediate signal on T1-weighted images and intermediate to high signal on T2-weighted images.13 In our patient’s case, the radiographic appearance and lack of specific radiographic findings consistent with the other tumors supported the diagnosis of BFH.
Histologically, BFHs contain spindle cells, multinucleated giant cells, and foam cells in a storiform pattern6 which was demonstrated in our patient’s case. In addition, significant nuclear pleomorphism, mitotic activity, and necrosis were absent—a difference between BFH and malignant fibrous histiocytoma.4,15 The microscopic characteristics of BFH readily differentiate it from OB, ABC, EG, and GCT, but not from NOF on microscopic appearance alone. Clinical and radiographic findings must be consistent, as mentioned.7,18
Complete surgical excision is the reported treatment for BFH. Prognosis after resection or curettage is usually good, and recurrences have been rare.1,2 Depending on the intraspinous location of BFH, stabilization after resection or curettage may be necessary to prevent residual instability. Three of the 11 reported cases of spinal BFH required stabilization by anterior fusion or posterior pedicle screw fixation after resection.1,2 The other 8 cases underwent excision alone or excision and grafting. All 11 patients were disease-free at a mean follow-up of 3.5 years.1 In nonspinal BFH, however, both local recurrence and lung metastasis have been reported.2,5,9,19 Clarke and colleagues9 reported local recurrences in 3 of 8 cases. These recurrences involved BFH in long bones of the leg, which had been treated with curettage and grafting. There has been no reliable report of a malignant change in BFH.2,9 The only case of lung metastasis, reported by Unni and Dahlin6 in their study of 10 cases, occurred 2 years after local recurrence in the distal femur.Our patient was doing well at most recent follow-up, 6 months after surgery. He had no pain and had returned to normal activities. Although there are no reported cases of spinal BFH recurrence, we will follow this patient with imaging on an annual basis. His case is of particular interest to orthopedic surgeons because they encounter benign bone lesions every day, and many of these lesions are in difficult anatomical locations. Knowing the characteristics, differential diagnoses, and appropriate diagnostic workups for benign bone lesions is important for optimal and timely patient care.
Benign fibrous histiocytoma (BFH) is a rare, well-recognized, primary skeletal tumor accounting for approximately 1% of all benign bone tumors. Spinal involvement is exceedingly rare with only 11 cases reported in the literature.1,2 We present a case of BFH located in the cervical spine of a pediatric patient that was successfully treated with curretage through an anterior surgical approach, along with a review of the literature and appropriate management concerning BFH of the spine.
Case Report
A 14-year-old boy was tackled while playing football and noticed immediate neck pain and subjective paresthesia in the upper extremities. Examination revealed a nontender spine (cervical, thoracic, lumbar) and normal strength and range of motion in all extremities. Sensation was diffusely intact, long tract signs were absent, and gait was normal. On questioning, the patient endorsed mild antecedent neck pain but denied prior history of any trauma. Neck pain did not radiate and was slightly worsened by activity but was mostly intermittent and random. As the neck pain was very mild and was not interfering with daily activities, the patient had not sought care before presenting to the emergency department. He had no pertinent past medical or surgical history.
The patient presented with a computed tomography (CT) scan of his head and cervical spine and a magnetic resonance imaging (MRI) scan of the cervical spine. A magnetic resonance angiography (MRA) scan of the neck was ordered after his arrival.
Axial and sagittal CT (Figures 1A, 1B) showed a 1×1.2-cm discrete, expansile, lytic, radiolucent mass extending anterior from the left C2 vertebral body. The mass appeared to abut the left vertebral artery foramen. The cortical bone surrounding the lesion was thin but uniform. Sagittal and axial T1-weighted MRI (Figures 2A, 2B) showed the discrete, expansile, homogenous lesion with the same intensity as normal bone marrow. Sagittal and axial T2-weighted MRI (Figures 2C, 2D) showed a discrete, expansile, homogenous lesion with primarily high signal intensity. Sagittal short tau inversion recovery (STIR) MRI (Figure 2E) again showed the lesion with primarily low intensity. Given the close proximity of the lesion to the vertebral foramen, MRA was ordered; it showed the lesion was not interfering with the vertebral artery (Figure 2F).
The tumor’s location, in the left anterior aspect of the C2 vertebral body, was not conducive to percutaneous biopsy for establishing tissue diagnosis, so the decision was made to surgically excise the lesion. A left-sided anterior incision was made 2 fingerbreadths inferior to the jaw line in a neck crease. A head and neck surgeon assisted with dissection. Dissection was carried down through the skin, subcutaneous tissue, and platysma on to the anterior part of the spine medial to the carotid sheath. Superior thyroid nerve and vessels and superior laryngeal nerve were identified and preserved. Fluoroscopy confirmed correct location at C2. The tumor was easily visualized, and the outer shell broke easily with palpation. Gentle curettage was necessary when removing the tumor off the vertebral artery. A portion of the specimen was sent during surgery for frozen section, which showed infrequent mitotic figures and no other findings concerning for malignancy. No instability was created after curettage and excision of the tumor, so no grafting or instrumentation was necessary.
Grossly, the tumor was pale tan and firm. Histologic examination with hematoxylin-eosin staining revealed a bland spindle-cell neoplasm that focally involved bone. A storiform pattern was present. The cells had scant cytoplasm and oval to elongate nuclei with tapered ends. Significant nuclear pleomorphism was not seen. The stroma was loose, with focal myxoid change. Benign multinucleated giant cells were present. Mitotic activity was infrequent (Figures 3A–3D). Two attending pathologists reviewed the case material and the frozen and formalin-fixed specimens independently and concurred with the diagnosis of BFH. In addition, the case was reviewed at the surgical pathology consensus conference; the reviewers agreed on BFH, and additional studies were deemed unnecessary.
Given the patient’s complete clinical picture, the differential diagnosis included nonossifying fibroma (NOF), eosinophilic granuloma (EG), BFH, fibrous dysplasia, giant cell tumor (GCT), aneurysmal bone cyst (ABC), and osteoblastoma (OB).
Discussion
BFH is an extremely rare bone lesion, accounting for only 1% of all surgically managed bone tumors; not counting the present case, only 11 spine cases have been reported in the literature.1,2 BFH of the spine traditionally causes nonspecific, poorly localized pain. The Table lists the reported cases of spinal BFH and their presenting symptoms, location, and treatment. BFH usually occurs in young adults, but the age range is 5 to 75 years.2-4 Mean age of the 12 patients with spinal BFH in the literature (including ours) is 25 years.1 In addition, spinal BFH appears to have no predilection for sex.
Skeletal BFH presents as a discrete, well-defined, osteolytic lesion with sharp borders and potentially a sclerotic rim.4-6 Cortical expansion and even cortical disruption with invasion into adjacent tissue have occurred in flat bones.7 Histologically, BFHs contain spindle cells, multinucleated giant cells, and foam cells in storiform pattern.6
BFH shares many of its radiologic and histologic characteristics and clinical symptoms with other benign bone lesions (the tumors listed above). Therefore, accurate diagnosis of BFH requires appropriate correlation of clinical, radiographic, and histologic data.2,3,8 Below is a comparison of BFH with related bone lesions.
Spinal BFH causes a nonspecific, poorly localized pain similar to that of EG, ABC, GCT, and OB.3,9 NOF and fibrous dysplasia generally do not cause pain, unless these lesions are discovered secondary to a pathologic fracture.8,10,11 Our patient had minor antecedent neck pain, which was brought to light by his football accident. ABC and OB are more locally aggressive than BFH and can cause neurologic symptoms by mass effect and spinal cord or nerve root compression.1,8 In this case and in the 6 other cases of BFH of the cervical spine, there were no neurologic changes.4,10
Of the tumors mentioned, NOF and EG almost always occur in children. However, NOF usually occurs in the metaphyseal region of long bones, and EG is usually accompanied by systemic symptoms, such as lymphadenopathy, hepatomegaly, and increased inflammatory markers.1,8 Fibrous dysplasia usually presents in childhood but does not become symptomatic until adulthood. GCTs and OB predominantly occur in adulthood.12,13 Our patient’s age and lack of other systemic symptoms supported the diagnosis of BFH.
Appearance on MRI is reported less with BFH than with other tumors, but heterogenous signal intensity similar to that of skeletal muscle on T1-weighted images and high signal intensity on T2-weighted images is typically reported.8,14 NOF and fibrous dysplasia do not disrupt the bony cortex unless a pathologic fracture has occurred.4 GCTs are more aggressive lytic lesions with more aggressive radiologic features. GCTs generally cause cortical expansion/attenuation, and lack a sclerotic rim. GCTs also have a heterogenous appearance on MRI and give a low to intermediate signal on both T1- and T2-weighted images.12,15 The appearance of EG is similar to that of BFH as an osteolytic lesion with a sclerotic rim, though EGs typically break through the cortex and acquire a “punched-out” look.1,8 ABC typically is described as an expansile osteolytic lesion with a “soap-bubble” appearance on radiographs; periosteal elevation and cortical attenuation can also be visualized. MRI shows the typical multilobular appearance of the lesion with fluid levels.13
OB appears as a radiolucent lesion, with or without calcifications, surrounded by a thin margin of reactive bone.14,16 A distinguishing characteristic of OB was thought to be intense radioisotope uptake on bone scintigraphy, but recently a bony BFH demonstrated intense uptake.17 OBs typically demonstrate nonspecific MRI results similar to those of BFH: low to intermediate signal on T1-weighted images and intermediate to high signal on T2-weighted images.13 In our patient’s case, the radiographic appearance and lack of specific radiographic findings consistent with the other tumors supported the diagnosis of BFH.
Histologically, BFHs contain spindle cells, multinucleated giant cells, and foam cells in a storiform pattern6 which was demonstrated in our patient’s case. In addition, significant nuclear pleomorphism, mitotic activity, and necrosis were absent—a difference between BFH and malignant fibrous histiocytoma.4,15 The microscopic characteristics of BFH readily differentiate it from OB, ABC, EG, and GCT, but not from NOF on microscopic appearance alone. Clinical and radiographic findings must be consistent, as mentioned.7,18
Complete surgical excision is the reported treatment for BFH. Prognosis after resection or curettage is usually good, and recurrences have been rare.1,2 Depending on the intraspinous location of BFH, stabilization after resection or curettage may be necessary to prevent residual instability. Three of the 11 reported cases of spinal BFH required stabilization by anterior fusion or posterior pedicle screw fixation after resection.1,2 The other 8 cases underwent excision alone or excision and grafting. All 11 patients were disease-free at a mean follow-up of 3.5 years.1 In nonspinal BFH, however, both local recurrence and lung metastasis have been reported.2,5,9,19 Clarke and colleagues9 reported local recurrences in 3 of 8 cases. These recurrences involved BFH in long bones of the leg, which had been treated with curettage and grafting. There has been no reliable report of a malignant change in BFH.2,9 The only case of lung metastasis, reported by Unni and Dahlin6 in their study of 10 cases, occurred 2 years after local recurrence in the distal femur.Our patient was doing well at most recent follow-up, 6 months after surgery. He had no pain and had returned to normal activities. Although there are no reported cases of spinal BFH recurrence, we will follow this patient with imaging on an annual basis. His case is of particular interest to orthopedic surgeons because they encounter benign bone lesions every day, and many of these lesions are in difficult anatomical locations. Knowing the characteristics, differential diagnoses, and appropriate diagnostic workups for benign bone lesions is important for optimal and timely patient care.
1. Demiralp B, Kose O, Oguz E, Sanal T, Ozcan A, Sehirlioglu A. Benign fibrous histiocytoma of the lumbar vertebrae. Skeletal Radiol. 2009;38(2):187-191.
2. Kuruvath S, O’Donovan DG, Aspoas AR, David KM. Benign fibrous histiocytoma of the thoracic spine: case report and review of the literature. J Neurosurg Spine. 2006;4(3):260-264.
3. Ceroni D, Dayer R, De Coulon G, Kaelin A. Benign fibrous histiocytoma of bone in a paediatric population: a report of 6 cases. Musculoskelet Surg. 2011;95(2):107-114.
4. Dorfman HD, Czerniak B. Bone Tumors. St. Louis, MO: Mosby; 1998.
5. Grohs JG, Nicolakis M, Kainberger F, Lang S, Kotz R. Benign fibrous histiocytoma of bone: a report of ten cases and review of literature. Wien Klin Wochenschr. 2002;114(1-2):56-63.
6. Unni KK, Dahlin DC. Dahlin’s Bone Tumors. 5th ed. Philadelphia, PA: Lippincott-Raven; 1996.
7. Balasubramanian C, Rajaraman G, Singh CS, Baliga DK. Benign fibrous histiocytoma of the sacrum—diagnostic difficulties facing this rare bone tumor. Pediatr Neurosurg. 2005;41(5):253-257.
8. van Giffen NH, van Rhijn LW, van Ooij A, et al. Benign fibrous histiocytoma of the posterior arch of C1 in a 6-year old boy: a case report. Spine. 2003;28(18):E359-E363.
9. Clarke BE, Xipell JM, Thomas DP. Benign fibrous histiocytoma of bone. Am J Surg Pathol. 1985;9(11):806-815.
10. Peicha G, Siebert FJ, Bratschitsch G, Fankhauser F, Grechenig W. Pathologic odontoid fracture and benign fibrous histiocytoma of bone. Eur Spine J. 1999;8(2):161-163.
11. Unni KK, Inwards CY, Bridge JA, Kindblom LG, Wold LE. Tumors of the Bones and Joints (AFIP Atlas of Tumor Pathology Series IV). Annapolis Junction, MD: American Registry of Pathology Press; 2005.
12. Dee R. Principles of Orthopaedic Practice. 2nd ed. New York, NY: McGraw-Hill; 1997.
13. Murphey M, Andrews C, Flemming D, Temple HT, Smith WS, Smirniotopoulos JG. Primary tumors of the spine: radiologic–pathologic correlation. Radiographics. 1996;16(5):1131-1158.
14. Hamada T, Ito H, Araki Y, Fujii K, Inoue M, Ishida O. Benign fibrous histiocytoma of the femur: review of three cases. Skeletal Radiol. 1996;25(1):25-29.
15. Mirra JM, Picci P, Gold RH. Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Vol 1. Philadelphia, PA: Lea & Febiger; 1989.
16. Theodorou DJ, Theodorou SJ, Sartoris DJ. An imaging overview of primary tumors of the spine: part 1. Benign tumors. Clin Imaging. 2008;32(3):196-203.
17. Li X, Meng Z, Li D, Tan J, Song X. Benign fibrous histiocytoma of a rib. Clin Nucl Med. 2014;39(9): 837-841.
18. Roessner A, Immenkamp M, Weidner A, Hobik HP, Grundmann E. Benign fibrous histiocytoma of bone. Light- and electron-microscopic observations. J Cancer Res Clin Oncol. 1981;101(2):191-202.
19. Destouet JM, Kyriakos M, Gilula LA. Fibrous histiocytoma (fibroxanthoma) of a cervical vertebra. A report with a review of the literature. Skeletal Radiol. 1980;5(4):241-246.
20. Hoeffel JC, Bomand-Ferrand F, Tachet F, Lascombes P, Czorny A, Bernard C. So-called benign fibrous histiocytoma: report of a case. J Pediatr Surg. 1992;27(5):672-674.
1. Demiralp B, Kose O, Oguz E, Sanal T, Ozcan A, Sehirlioglu A. Benign fibrous histiocytoma of the lumbar vertebrae. Skeletal Radiol. 2009;38(2):187-191.
2. Kuruvath S, O’Donovan DG, Aspoas AR, David KM. Benign fibrous histiocytoma of the thoracic spine: case report and review of the literature. J Neurosurg Spine. 2006;4(3):260-264.
3. Ceroni D, Dayer R, De Coulon G, Kaelin A. Benign fibrous histiocytoma of bone in a paediatric population: a report of 6 cases. Musculoskelet Surg. 2011;95(2):107-114.
4. Dorfman HD, Czerniak B. Bone Tumors. St. Louis, MO: Mosby; 1998.
5. Grohs JG, Nicolakis M, Kainberger F, Lang S, Kotz R. Benign fibrous histiocytoma of bone: a report of ten cases and review of literature. Wien Klin Wochenschr. 2002;114(1-2):56-63.
6. Unni KK, Dahlin DC. Dahlin’s Bone Tumors. 5th ed. Philadelphia, PA: Lippincott-Raven; 1996.
7. Balasubramanian C, Rajaraman G, Singh CS, Baliga DK. Benign fibrous histiocytoma of the sacrum—diagnostic difficulties facing this rare bone tumor. Pediatr Neurosurg. 2005;41(5):253-257.
8. van Giffen NH, van Rhijn LW, van Ooij A, et al. Benign fibrous histiocytoma of the posterior arch of C1 in a 6-year old boy: a case report. Spine. 2003;28(18):E359-E363.
9. Clarke BE, Xipell JM, Thomas DP. Benign fibrous histiocytoma of bone. Am J Surg Pathol. 1985;9(11):806-815.
10. Peicha G, Siebert FJ, Bratschitsch G, Fankhauser F, Grechenig W. Pathologic odontoid fracture and benign fibrous histiocytoma of bone. Eur Spine J. 1999;8(2):161-163.
11. Unni KK, Inwards CY, Bridge JA, Kindblom LG, Wold LE. Tumors of the Bones and Joints (AFIP Atlas of Tumor Pathology Series IV). Annapolis Junction, MD: American Registry of Pathology Press; 2005.
12. Dee R. Principles of Orthopaedic Practice. 2nd ed. New York, NY: McGraw-Hill; 1997.
13. Murphey M, Andrews C, Flemming D, Temple HT, Smith WS, Smirniotopoulos JG. Primary tumors of the spine: radiologic–pathologic correlation. Radiographics. 1996;16(5):1131-1158.
14. Hamada T, Ito H, Araki Y, Fujii K, Inoue M, Ishida O. Benign fibrous histiocytoma of the femur: review of three cases. Skeletal Radiol. 1996;25(1):25-29.
15. Mirra JM, Picci P, Gold RH. Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Vol 1. Philadelphia, PA: Lea & Febiger; 1989.
16. Theodorou DJ, Theodorou SJ, Sartoris DJ. An imaging overview of primary tumors of the spine: part 1. Benign tumors. Clin Imaging. 2008;32(3):196-203.
17. Li X, Meng Z, Li D, Tan J, Song X. Benign fibrous histiocytoma of a rib. Clin Nucl Med. 2014;39(9): 837-841.
18. Roessner A, Immenkamp M, Weidner A, Hobik HP, Grundmann E. Benign fibrous histiocytoma of bone. Light- and electron-microscopic observations. J Cancer Res Clin Oncol. 1981;101(2):191-202.
19. Destouet JM, Kyriakos M, Gilula LA. Fibrous histiocytoma (fibroxanthoma) of a cervical vertebra. A report with a review of the literature. Skeletal Radiol. 1980;5(4):241-246.
20. Hoeffel JC, Bomand-Ferrand F, Tachet F, Lascombes P, Czorny A, Bernard C. So-called benign fibrous histiocytoma: report of a case. J Pediatr Surg. 1992;27(5):672-674.
Infection rates similar for in- and out-of-hospital pediatric cardiac arrest
ORLANDO – Infection rates didn’t differ between children who suffered cardiac arrest in or out of the hospital, and in both groups, few children’s infections were confirmed by culture, in a multicenter study.
The study explored infectious complications associated with pediatric cardiac arrest, Dr. Fasiha Saeed said at the Critical Care Congress, sponsored by the Society of Critical Care Medicine.
She and her colleagues examined records of 491 pediatric patients who had return of spontaneous circulation after cardiac arrest (CA), 269 in hospital (IH) and 115 out of hospital (OH). Overall, more children who had in-hospital cardiac arrest were suspected of having an infection (242 [90%], compared with 83 [74%], in the OHCA group; P less than 0.0001).
However, cultures were actually sent for only about one in three patients with suspected infection in either group (34% IHCA and 35% OHCA). Definite infection was found in most patients who were cultured (82% and 86%, respectively).
Patients had “suspected infection” if they received cultures or antimicrobials, and were termed to have “definite infection” only if cultures were positive for infection.
“Infectious complications following out-of-hospital cardiac arrest have been reported in the adult literature, but the pediatric experience post–cardiac arrest is limited to case reports and small case series,” said Dr. Saeed, a pediatric critical care physician at Advocate Hospital, Park Ridge, Ill.
Data from PECARN (Pediatric Emergency Care Applied Research Network) had previously shown that in-hospital pediatric cardiac arrest patients were more likely to receive antimicrobials after return of spontaneous circulation. However, infectious etiologies and the early hospital course of these patients after their cardiac arrest was not known, said Dr. Saeed.
Dr. Saeed and her coinvestigators had hypothesized that “children with out-of-hospital cardiac arrest have a higher incidence of infections after return of spontaneous circulation and worse outcomes compared to children with in-hospital cardiac arrest,” she said. “We were surprised to see how infrequently cultures were sent,” said Dr. Saeed, in discussing the findings that were contrary to the study’s hypothesis.
Dr. Saeed and her colleagues conducted a retrospective analysis of the multi-institutional, deidentified PECARN database, examining 491 pediatric cardiac arrest patients who had required at least 1 minute of cardiopulmonary resuscitation. The patients were aged 24 hours to 18 years; the period of data collection was July 2003-December 2004.
Exclusion criteria included a diagnosis of septic shock, the use of therapeutic hypothermia, or patient death within 24 hours of the cardiac arrest.
Among other findings presented by Dr. Saeed, no association was seen between either suspected or definite infection and mortality. Antibiotic usage was also not associated with mortality. However, definite infection was positively associated with a respiratory etiology for cardiac arrest (odds ratio, 2.6). Post–cardiac arrest central venous pressure monitoring was also associated with definite infection (OR, 2.1).
Support for the study was provided by the Medical College of Wisconsin. The investigators disclosed no relevant conflicts of interest.
On Twitter @karioakes
ORLANDO – Infection rates didn’t differ between children who suffered cardiac arrest in or out of the hospital, and in both groups, few children’s infections were confirmed by culture, in a multicenter study.
The study explored infectious complications associated with pediatric cardiac arrest, Dr. Fasiha Saeed said at the Critical Care Congress, sponsored by the Society of Critical Care Medicine.
She and her colleagues examined records of 491 pediatric patients who had return of spontaneous circulation after cardiac arrest (CA), 269 in hospital (IH) and 115 out of hospital (OH). Overall, more children who had in-hospital cardiac arrest were suspected of having an infection (242 [90%], compared with 83 [74%], in the OHCA group; P less than 0.0001).
However, cultures were actually sent for only about one in three patients with suspected infection in either group (34% IHCA and 35% OHCA). Definite infection was found in most patients who were cultured (82% and 86%, respectively).
Patients had “suspected infection” if they received cultures or antimicrobials, and were termed to have “definite infection” only if cultures were positive for infection.
“Infectious complications following out-of-hospital cardiac arrest have been reported in the adult literature, but the pediatric experience post–cardiac arrest is limited to case reports and small case series,” said Dr. Saeed, a pediatric critical care physician at Advocate Hospital, Park Ridge, Ill.
Data from PECARN (Pediatric Emergency Care Applied Research Network) had previously shown that in-hospital pediatric cardiac arrest patients were more likely to receive antimicrobials after return of spontaneous circulation. However, infectious etiologies and the early hospital course of these patients after their cardiac arrest was not known, said Dr. Saeed.
Dr. Saeed and her coinvestigators had hypothesized that “children with out-of-hospital cardiac arrest have a higher incidence of infections after return of spontaneous circulation and worse outcomes compared to children with in-hospital cardiac arrest,” she said. “We were surprised to see how infrequently cultures were sent,” said Dr. Saeed, in discussing the findings that were contrary to the study’s hypothesis.
Dr. Saeed and her colleagues conducted a retrospective analysis of the multi-institutional, deidentified PECARN database, examining 491 pediatric cardiac arrest patients who had required at least 1 minute of cardiopulmonary resuscitation. The patients were aged 24 hours to 18 years; the period of data collection was July 2003-December 2004.
Exclusion criteria included a diagnosis of septic shock, the use of therapeutic hypothermia, or patient death within 24 hours of the cardiac arrest.
Among other findings presented by Dr. Saeed, no association was seen between either suspected or definite infection and mortality. Antibiotic usage was also not associated with mortality. However, definite infection was positively associated with a respiratory etiology for cardiac arrest (odds ratio, 2.6). Post–cardiac arrest central venous pressure monitoring was also associated with definite infection (OR, 2.1).
Support for the study was provided by the Medical College of Wisconsin. The investigators disclosed no relevant conflicts of interest.
On Twitter @karioakes
ORLANDO – Infection rates didn’t differ between children who suffered cardiac arrest in or out of the hospital, and in both groups, few children’s infections were confirmed by culture, in a multicenter study.
The study explored infectious complications associated with pediatric cardiac arrest, Dr. Fasiha Saeed said at the Critical Care Congress, sponsored by the Society of Critical Care Medicine.
She and her colleagues examined records of 491 pediatric patients who had return of spontaneous circulation after cardiac arrest (CA), 269 in hospital (IH) and 115 out of hospital (OH). Overall, more children who had in-hospital cardiac arrest were suspected of having an infection (242 [90%], compared with 83 [74%], in the OHCA group; P less than 0.0001).
However, cultures were actually sent for only about one in three patients with suspected infection in either group (34% IHCA and 35% OHCA). Definite infection was found in most patients who were cultured (82% and 86%, respectively).
Patients had “suspected infection” if they received cultures or antimicrobials, and were termed to have “definite infection” only if cultures were positive for infection.
“Infectious complications following out-of-hospital cardiac arrest have been reported in the adult literature, but the pediatric experience post–cardiac arrest is limited to case reports and small case series,” said Dr. Saeed, a pediatric critical care physician at Advocate Hospital, Park Ridge, Ill.
Data from PECARN (Pediatric Emergency Care Applied Research Network) had previously shown that in-hospital pediatric cardiac arrest patients were more likely to receive antimicrobials after return of spontaneous circulation. However, infectious etiologies and the early hospital course of these patients after their cardiac arrest was not known, said Dr. Saeed.
Dr. Saeed and her coinvestigators had hypothesized that “children with out-of-hospital cardiac arrest have a higher incidence of infections after return of spontaneous circulation and worse outcomes compared to children with in-hospital cardiac arrest,” she said. “We were surprised to see how infrequently cultures were sent,” said Dr. Saeed, in discussing the findings that were contrary to the study’s hypothesis.
Dr. Saeed and her colleagues conducted a retrospective analysis of the multi-institutional, deidentified PECARN database, examining 491 pediatric cardiac arrest patients who had required at least 1 minute of cardiopulmonary resuscitation. The patients were aged 24 hours to 18 years; the period of data collection was July 2003-December 2004.
Exclusion criteria included a diagnosis of septic shock, the use of therapeutic hypothermia, or patient death within 24 hours of the cardiac arrest.
Among other findings presented by Dr. Saeed, no association was seen between either suspected or definite infection and mortality. Antibiotic usage was also not associated with mortality. However, definite infection was positively associated with a respiratory etiology for cardiac arrest (odds ratio, 2.6). Post–cardiac arrest central venous pressure monitoring was also associated with definite infection (OR, 2.1).
Support for the study was provided by the Medical College of Wisconsin. The investigators disclosed no relevant conflicts of interest.
On Twitter @karioakes
AT THE CRITICAL CARE CONGRESS
Key clinical point: Postresuscitation infection rates were similar for in- and out-of-hospital pediatric cardiac arrest (IHCA and OHCA).
Major finding: More patients who had in-hospital arrest were suspected of having infection, Definite infection was found in most patients who were cultured (68/83 [82%] IHCA, and 25/29 [86%] OHCA).
Data source: Retrospective review of records of 491 pediatric patients who suffered cardiac arrest and had spontaneous return of circulation, drawn from the PECARN (Pediatric Emergency Care Applied Research Network) database.
Disclosures: Support for the study was provided by the Medical College of Wisconsin. The investigators disclosed no relevant conflicts of interest.
Infant Egg Introduction Can Prevent Sensitization at 12 Months
LOS ANGELES – Among infants at risk for allergic disease, egg introduction at 4 months cuts the risk of egg sensitization at 12 months by about half, according a randomized, placebo-controlled, double blind trial from Australia.
“This is what we hoped to find.” Introducing egg early “is certainly safe, and it may promote tolerance,” said senior investigator Dr. Dianne Campbell, professor and chair of pediatric allergy and clinical immunology at the Children’s Hospital at Westmead, which is affiliated with the University of Sydney.

Four-month-old children were randomized to 350 mg of pasteurized raw whole egg powder or – as a control – rice powder sprinkled once daily on their weaning food until month 8, at which time parents in both groups were encouraged to add eggs to their children’s diets. At least one of each child’s parents had a history of atopic disease, including asthma, eczema, hay fever, or food allergy. Even so, all of the infants had negative (less than 2 mm) skin prick tests (SPTs) at baseline. Compliance by parent diary was 89% in the rice and 81% in the egg groups.
At 12 months, SPTs were positive (3 mm or more) for whole egg in 25 of 122 (20%) children in the rice group, but only 13 of 122 (11%) in the egg group (odds ratio, 0.46; 95% confidence interval, 0.22-0.95; P = .03). Whole egg IgG4 and IgG4/IgE ratios to egg, ovalbumin, and ovomucoid were also higher in the egg group, indicating developing tolerance (P less than .0001 for each).
About 10% of the children originally in the egg group broke out in hives after their first few doses, and were withdrawn from the study. “This intervention may not be for everybody. There will be individuals who react” and it’s impossible, at this point, to predict who they will be. “We cannot prevent allergy in everyone,” said lead investigator Dr. John Tan, a pediatric immunologist at the hospital.

Overall, however, early introduction was safe. There was no anaphylaxis in the trial, and no cardiovascular or respiratory complications. Rates of eczema and peanut allergy were similar at 12 months between the two groups, meaning that early egg introduction did not increase the risk of atopy.
The findings echo results from several recent pediatric egg allergy studies, as well as findings from recent peanut trials. Slowly, it’s becoming clear that delaying the introduction of at least some allergenic foods – a common practice for years – doesn’t prevent allergies and may, in fact, promote them.
Despite those findings, there remains “a big disconnect between the [new] research and what we [still] recommend” in Australia, the United States, and elsewhere. Delaying food introductions was medical “dogma for 20 years, from highly esteemed societies,” and it corresponded with a marked increase in food allergies, but “it’s very hard to turn these things around,” Dr. Campbell said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The Australian government is reworking its infant feeding guidelines to incorporate the new evidence. “Our revised guidelines will say that there’s strong evidence for peanut and moderate evidence for egg” in favor of early introduction in children who are not sensitized by 4 or so months old, she said.
The trial was powered to detect differences in SPT, not actual egg allergies, which were diagnosed in 13 children (11%) in the rice group and eight (7%) in the egg group; the difference was not statistically significant. “Not all kids who are sensitized will be allergic,” she noted.
The study groups were well matched; there were about equal numbers of boys and girls in each, and, in both groups, about 15% of children were exposed to second hand smoke at home and almost all were breastfed.
The work was funded by the Australian government, among others. The investigators have no disclosures.
LOS ANGELES – Among infants at risk for allergic disease, egg introduction at 4 months cuts the risk of egg sensitization at 12 months by about half, according a randomized, placebo-controlled, double blind trial from Australia.
“This is what we hoped to find.” Introducing egg early “is certainly safe, and it may promote tolerance,” said senior investigator Dr. Dianne Campbell, professor and chair of pediatric allergy and clinical immunology at the Children’s Hospital at Westmead, which is affiliated with the University of Sydney.
Four-month-old children were randomized to 350 mg of pasteurized raw whole egg powder or – as a control – rice powder sprinkled once daily on their weaning food until month 8, at which time parents in both groups were encouraged to add eggs to their children’s diets. At least one of each child’s parents had a history of atopic disease, including asthma, eczema, hay fever, or food allergy. Even so, all of the infants had negative (less than 2 mm) skin prick tests (SPTs) at baseline. Compliance by parent diary was 89% in the rice and 81% in the egg groups.
At 12 months, SPTs were positive (3 mm or more) for whole egg in 25 of 122 (20%) children in the rice group, but only 13 of 122 (11%) in the egg group (odds ratio, 0.46; 95% confidence interval, 0.22-0.95; P = .03). Whole egg IgG4 and IgG4/IgE ratios to egg, ovalbumin, and ovomucoid were also higher in the egg group, indicating developing tolerance (P less than .0001 for each).
About 10% of the children originally in the egg group broke out in hives after their first few doses, and were withdrawn from the study. “This intervention may not be for everybody. There will be individuals who react” and it’s impossible, at this point, to predict who they will be. “We cannot prevent allergy in everyone,” said lead investigator Dr. John Tan, a pediatric immunologist at the hospital.
Overall, however, early introduction was safe. There was no anaphylaxis in the trial, and no cardiovascular or respiratory complications. Rates of eczema and peanut allergy were similar at 12 months between the two groups, meaning that early egg introduction did not increase the risk of atopy.
The findings echo results from several recent pediatric egg allergy studies, as well as findings from recent peanut trials. Slowly, it’s becoming clear that delaying the introduction of at least some allergenic foods – a common practice for years – doesn’t prevent allergies and may, in fact, promote them.
Despite those findings, there remains “a big disconnect between the [new] research and what we [still] recommend” in Australia, the United States, and elsewhere. Delaying food introductions was medical “dogma for 20 years, from highly esteemed societies,” and it corresponded with a marked increase in food allergies, but “it’s very hard to turn these things around,” Dr. Campbell said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The Australian government is reworking its infant feeding guidelines to incorporate the new evidence. “Our revised guidelines will say that there’s strong evidence for peanut and moderate evidence for egg” in favor of early introduction in children who are not sensitized by 4 or so months old, she said.
The trial was powered to detect differences in SPT, not actual egg allergies, which were diagnosed in 13 children (11%) in the rice group and eight (7%) in the egg group; the difference was not statistically significant. “Not all kids who are sensitized will be allergic,” she noted.
The study groups were well matched; there were about equal numbers of boys and girls in each, and, in both groups, about 15% of children were exposed to second hand smoke at home and almost all were breastfed.
The work was funded by the Australian government, among others. The investigators have no disclosures.
LOS ANGELES – Among infants at risk for allergic disease, egg introduction at 4 months cuts the risk of egg sensitization at 12 months by about half, according a randomized, placebo-controlled, double blind trial from Australia.
“This is what we hoped to find.” Introducing egg early “is certainly safe, and it may promote tolerance,” said senior investigator Dr. Dianne Campbell, professor and chair of pediatric allergy and clinical immunology at the Children’s Hospital at Westmead, which is affiliated with the University of Sydney.
Four-month-old children were randomized to 350 mg of pasteurized raw whole egg powder or – as a control – rice powder sprinkled once daily on their weaning food until month 8, at which time parents in both groups were encouraged to add eggs to their children’s diets. At least one of each child’s parents had a history of atopic disease, including asthma, eczema, hay fever, or food allergy. Even so, all of the infants had negative (less than 2 mm) skin prick tests (SPTs) at baseline. Compliance by parent diary was 89% in the rice and 81% in the egg groups.
At 12 months, SPTs were positive (3 mm or more) for whole egg in 25 of 122 (20%) children in the rice group, but only 13 of 122 (11%) in the egg group (odds ratio, 0.46; 95% confidence interval, 0.22-0.95; P = .03). Whole egg IgG4 and IgG4/IgE ratios to egg, ovalbumin, and ovomucoid were also higher in the egg group, indicating developing tolerance (P less than .0001 for each).
About 10% of the children originally in the egg group broke out in hives after their first few doses, and were withdrawn from the study. “This intervention may not be for everybody. There will be individuals who react” and it’s impossible, at this point, to predict who they will be. “We cannot prevent allergy in everyone,” said lead investigator Dr. John Tan, a pediatric immunologist at the hospital.
Overall, however, early introduction was safe. There was no anaphylaxis in the trial, and no cardiovascular or respiratory complications. Rates of eczema and peanut allergy were similar at 12 months between the two groups, meaning that early egg introduction did not increase the risk of atopy.
The findings echo results from several recent pediatric egg allergy studies, as well as findings from recent peanut trials. Slowly, it’s becoming clear that delaying the introduction of at least some allergenic foods – a common practice for years – doesn’t prevent allergies and may, in fact, promote them.
Despite those findings, there remains “a big disconnect between the [new] research and what we [still] recommend” in Australia, the United States, and elsewhere. Delaying food introductions was medical “dogma for 20 years, from highly esteemed societies,” and it corresponded with a marked increase in food allergies, but “it’s very hard to turn these things around,” Dr. Campbell said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The Australian government is reworking its infant feeding guidelines to incorporate the new evidence. “Our revised guidelines will say that there’s strong evidence for peanut and moderate evidence for egg” in favor of early introduction in children who are not sensitized by 4 or so months old, she said.
The trial was powered to detect differences in SPT, not actual egg allergies, which were diagnosed in 13 children (11%) in the rice group and eight (7%) in the egg group; the difference was not statistically significant. “Not all kids who are sensitized will be allergic,” she noted.
The study groups were well matched; there were about equal numbers of boys and girls in each, and, in both groups, about 15% of children were exposed to second hand smoke at home and almost all were breastfed.
The work was funded by the Australian government, among others. The investigators have no disclosures.
AT 2016 AAAAI ANNUAL MEETING

Infant Egg Introduction Can Prevent Sensitization at 12 Months
LOS ANGELES – Among infants at risk for allergic disease, egg introduction at 4 months cuts the risk of egg sensitization at 12 months by about half, according a randomized, placebo-controlled, double blind trial from Australia.
“This is what we hoped to find.” Introducing egg early “is certainly safe, and it may promote tolerance,” said senior investigator Dr. Dianne Campbell, professor and chair of pediatric allergy and clinical immunology at the Children’s Hospital at Westmead, which is affiliated with the University of Sydney.
Four-month-old children were randomized to 350 mg of pasteurized raw whole egg powder or – as a control – rice powder sprinkled once daily on their weaning food until month 8, at which time parents in both groups were encouraged to add eggs to their children’s diets. At least one of each child’s parents had a history of atopic disease, including asthma, eczema, hay fever, or food allergy. Even so, all of the infants had negative (less than 2 mm) skin prick tests (SPTs) at baseline. Compliance by parent diary was 89% in the rice and 81% in the egg groups.
At 12 months, SPTs were positive (3 mm or more) for whole egg in 25 of 122 (20%) children in the rice group, but only 13 of 122 (11%) in the egg group (odds ratio, 0.46; 95% confidence interval, 0.22-0.95; P = .03). Whole egg IgG4 and IgG4/IgE ratios to egg, ovalbumin, and ovomucoid were also higher in the egg group, indicating developing tolerance (P less than .0001 for each).
About 10% of the children originally in the egg group broke out in hives after their first few doses, and were withdrawn from the study. “This intervention may not be for everybody. There will be individuals who react” and it’s impossible, at this point, to predict who they will be. “We cannot prevent allergy in everyone,” said lead investigator Dr. John Tan, a pediatric immunologist at the hospital.
Overall, however, early introduction was safe. There was no anaphylaxis in the trial, and no cardiovascular or respiratory complications. Rates of eczema and peanut allergy were similar at 12 months between the two groups, meaning that early egg introduction did not increase the risk of atopy.
The findings echo results from several recent pediatric egg allergy studies, as well as findings from recent peanut trials. Slowly, it’s becoming clear that delaying the introduction of at least some allergenic foods – a common practice for years – doesn’t prevent allergies and may, in fact, promote them.
Despite those findings, there remains “a big disconnect between the [new] research and what we [still] recommend” in Australia, the United States, and elsewhere. Delaying food introductions was medical “dogma for 20 years, from highly esteemed societies,” and it corresponded with a marked increase in food allergies, but “it’s very hard to turn these things around,” Dr. Campbell said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The Australian government is reworking its infant feeding guidelines to incorporate the new evidence. “Our revised guidelines will say that there’s strong evidence for peanut and moderate evidence for egg” in favor of early introduction in children who are not sensitized by 4 or so months old, she said.
The trial was powered to detect differences in SPT, not actual egg allergies, which were diagnosed in 13 children (11%) in the rice group and eight (7%) in the egg group; the difference was not statistically significant. “Not all kids who are sensitized will be allergic,” she noted.
The study groups were well matched; there were about equal numbers of boys and girls in each, and, in both groups, about 15% of children were exposed to second hand smoke at home and almost all were breastfed.
The work was funded by the Australian government, among others. The investigators have no disclosures.
LOS ANGELES – Among infants at risk for allergic disease, egg introduction at 4 months cuts the risk of egg sensitization at 12 months by about half, according a randomized, placebo-controlled, double blind trial from Australia.
“This is what we hoped to find.” Introducing egg early “is certainly safe, and it may promote tolerance,” said senior investigator Dr. Dianne Campbell, professor and chair of pediatric allergy and clinical immunology at the Children’s Hospital at Westmead, which is affiliated with the University of Sydney.
Four-month-old children were randomized to 350 mg of pasteurized raw whole egg powder or – as a control – rice powder sprinkled once daily on their weaning food until month 8, at which time parents in both groups were encouraged to add eggs to their children’s diets. At least one of each child’s parents had a history of atopic disease, including asthma, eczema, hay fever, or food allergy. Even so, all of the infants had negative (less than 2 mm) skin prick tests (SPTs) at baseline. Compliance by parent diary was 89% in the rice and 81% in the egg groups.
At 12 months, SPTs were positive (3 mm or more) for whole egg in 25 of 122 (20%) children in the rice group, but only 13 of 122 (11%) in the egg group (odds ratio, 0.46; 95% confidence interval, 0.22-0.95; P = .03). Whole egg IgG4 and IgG4/IgE ratios to egg, ovalbumin, and ovomucoid were also higher in the egg group, indicating developing tolerance (P less than .0001 for each).
About 10% of the children originally in the egg group broke out in hives after their first few doses, and were withdrawn from the study. “This intervention may not be for everybody. There will be individuals who react” and it’s impossible, at this point, to predict who they will be. “We cannot prevent allergy in everyone,” said lead investigator Dr. John Tan, a pediatric immunologist at the hospital.
Overall, however, early introduction was safe. There was no anaphylaxis in the trial, and no cardiovascular or respiratory complications. Rates of eczema and peanut allergy were similar at 12 months between the two groups, meaning that early egg introduction did not increase the risk of atopy.
The findings echo results from several recent pediatric egg allergy studies, as well as findings from recent peanut trials. Slowly, it’s becoming clear that delaying the introduction of at least some allergenic foods – a common practice for years – doesn’t prevent allergies and may, in fact, promote them.
Despite those findings, there remains “a big disconnect between the [new] research and what we [still] recommend” in Australia, the United States, and elsewhere. Delaying food introductions was medical “dogma for 20 years, from highly esteemed societies,” and it corresponded with a marked increase in food allergies, but “it’s very hard to turn these things around,” Dr. Campbell said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The Australian government is reworking its infant feeding guidelines to incorporate the new evidence. “Our revised guidelines will say that there’s strong evidence for peanut and moderate evidence for egg” in favor of early introduction in children who are not sensitized by 4 or so months old, she said.
The trial was powered to detect differences in SPT, not actual egg allergies, which were diagnosed in 13 children (11%) in the rice group and eight (7%) in the egg group; the difference was not statistically significant. “Not all kids who are sensitized will be allergic,” she noted.
The study groups were well matched; there were about equal numbers of boys and girls in each, and, in both groups, about 15% of children were exposed to second hand smoke at home and almost all were breastfed.
The work was funded by the Australian government, among others. The investigators have no disclosures.
LOS ANGELES – Among infants at risk for allergic disease, egg introduction at 4 months cuts the risk of egg sensitization at 12 months by about half, according a randomized, placebo-controlled, double blind trial from Australia.
“This is what we hoped to find.” Introducing egg early “is certainly safe, and it may promote tolerance,” said senior investigator Dr. Dianne Campbell, professor and chair of pediatric allergy and clinical immunology at the Children’s Hospital at Westmead, which is affiliated with the University of Sydney.
Four-month-old children were randomized to 350 mg of pasteurized raw whole egg powder or – as a control – rice powder sprinkled once daily on their weaning food until month 8, at which time parents in both groups were encouraged to add eggs to their children’s diets. At least one of each child’s parents had a history of atopic disease, including asthma, eczema, hay fever, or food allergy. Even so, all of the infants had negative (less than 2 mm) skin prick tests (SPTs) at baseline. Compliance by parent diary was 89% in the rice and 81% in the egg groups.
At 12 months, SPTs were positive (3 mm or more) for whole egg in 25 of 122 (20%) children in the rice group, but only 13 of 122 (11%) in the egg group (odds ratio, 0.46; 95% confidence interval, 0.22-0.95; P = .03). Whole egg IgG4 and IgG4/IgE ratios to egg, ovalbumin, and ovomucoid were also higher in the egg group, indicating developing tolerance (P less than .0001 for each).
About 10% of the children originally in the egg group broke out in hives after their first few doses, and were withdrawn from the study. “This intervention may not be for everybody. There will be individuals who react” and it’s impossible, at this point, to predict who they will be. “We cannot prevent allergy in everyone,” said lead investigator Dr. John Tan, a pediatric immunologist at the hospital.
Overall, however, early introduction was safe. There was no anaphylaxis in the trial, and no cardiovascular or respiratory complications. Rates of eczema and peanut allergy were similar at 12 months between the two groups, meaning that early egg introduction did not increase the risk of atopy.
The findings echo results from several recent pediatric egg allergy studies, as well as findings from recent peanut trials. Slowly, it’s becoming clear that delaying the introduction of at least some allergenic foods – a common practice for years – doesn’t prevent allergies and may, in fact, promote them.
Despite those findings, there remains “a big disconnect between the [new] research and what we [still] recommend” in Australia, the United States, and elsewhere. Delaying food introductions was medical “dogma for 20 years, from highly esteemed societies,” and it corresponded with a marked increase in food allergies, but “it’s very hard to turn these things around,” Dr. Campbell said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The Australian government is reworking its infant feeding guidelines to incorporate the new evidence. “Our revised guidelines will say that there’s strong evidence for peanut and moderate evidence for egg” in favor of early introduction in children who are not sensitized by 4 or so months old, she said.
The trial was powered to detect differences in SPT, not actual egg allergies, which were diagnosed in 13 children (11%) in the rice group and eight (7%) in the egg group; the difference was not statistically significant. “Not all kids who are sensitized will be allergic,” she noted.
The study groups were well matched; there were about equal numbers of boys and girls in each, and, in both groups, about 15% of children were exposed to second hand smoke at home and almost all were breastfed.
The work was funded by the Australian government, among others. The investigators have no disclosures.
AT 2016 AAAAI ANNUAL MEETING

Infant egg introduction can prevent sensitization at 12 months
LOS ANGELES – Among infants at risk for allergic disease, egg introduction at 4 months cuts the risk of egg sensitization at 12 months by about half, according a randomized, placebo-controlled, double blind trial from Australia.
“This is what we hoped to find.” Introducing egg early “is certainly safe, and it may promote tolerance,” said senior investigator Dr. Dianne Campbell, professor and chair of pediatric allergy and clinical immunology at the Children’s Hospital at Westmead, which is affiliated with the University of Sydney.

Four-month-old children were randomized to 350 mg of pasteurized raw whole egg powder or – as a control – rice powder sprinkled once daily on their weaning food until month 8, at which time parents in both groups were encouraged to add eggs to their children’s diets. At least one of each child’s parents had a history of atopic disease, including asthma, eczema, hay fever, or food allergy. Even so, all of the infants had negative (less than 2 mm) skin prick tests (SPTs) at baseline. Compliance by parent diary was 89% in the rice and 81% in the egg groups.
At 12 months, SPTs were positive (3 mm or more) for whole egg in 25 of 122 (20%) children in the rice group, but only 13 of 122 (11%) in the egg group (odds ratio, 0.46; 95% confidence interval, 0.22-0.95; P = .03). Whole egg IgG4 and IgG4/IgE ratios to egg, ovalbumin, and ovomucoid were also higher in the egg group, indicating developing tolerance (P less than .0001 for each).
About 10% of the children originally in the egg group broke out in hives after their first few doses, and were withdrawn from the study. “This intervention may not be for everybody. There will be individuals who react” and it’s impossible, at this point, to predict who they will be. “We cannot prevent allergy in everyone,” said lead investigator Dr. John Tan, a pediatric immunologist at the hospital.

Overall, however, early introduction was safe. There was no anaphylaxis in the trial, and no cardiovascular or respiratory complications. Rates of eczema and peanut allergy were similar at 12 months between the two groups, meaning that early egg introduction did not increase the risk of atopy.
The findings echo results from several recent pediatric egg allergy studies, as well as findings from recent peanut trials. Slowly, it’s becoming clear that delaying the introduction of at least some allergenic foods – a common practice for years – doesn’t prevent allergies and may, in fact, promote them.
Despite those findings, there remains “a big disconnect between the [new] research and what we [still] recommend” in Australia, the United States, and elsewhere. Delaying food introductions was medical “dogma for 20 years, from highly esteemed societies,” and it corresponded with a marked increase in food allergies, but “it’s very hard to turn these things around,” Dr. Campbell said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The Australian government is reworking its infant feeding guidelines to incorporate the new evidence. “Our revised guidelines will say that there’s strong evidence for peanut and moderate evidence for egg” in favor of early introduction in children who are not sensitized by 4 or so months old, she said.
The trial was powered to detect differences in SPT, not actual egg allergies, which were diagnosed in 13 children (11%) in the rice group and eight (7%) in the egg group; the difference was not statistically significant. “Not all kids who are sensitized will be allergic,” she noted.
The study groups were well matched; there were about equal numbers of boys and girls in each, and, in both groups, about 15% of children were exposed to second hand smoke at home and almost all were breastfed.
The work was funded by the Australian government, among others. The investigators have no disclosures.
LOS ANGELES – Among infants at risk for allergic disease, egg introduction at 4 months cuts the risk of egg sensitization at 12 months by about half, according a randomized, placebo-controlled, double blind trial from Australia.
“This is what we hoped to find.” Introducing egg early “is certainly safe, and it may promote tolerance,” said senior investigator Dr. Dianne Campbell, professor and chair of pediatric allergy and clinical immunology at the Children’s Hospital at Westmead, which is affiliated with the University of Sydney.
Four-month-old children were randomized to 350 mg of pasteurized raw whole egg powder or – as a control – rice powder sprinkled once daily on their weaning food until month 8, at which time parents in both groups were encouraged to add eggs to their children’s diets. At least one of each child’s parents had a history of atopic disease, including asthma, eczema, hay fever, or food allergy. Even so, all of the infants had negative (less than 2 mm) skin prick tests (SPTs) at baseline. Compliance by parent diary was 89% in the rice and 81% in the egg groups.
At 12 months, SPTs were positive (3 mm or more) for whole egg in 25 of 122 (20%) children in the rice group, but only 13 of 122 (11%) in the egg group (odds ratio, 0.46; 95% confidence interval, 0.22-0.95; P = .03). Whole egg IgG4 and IgG4/IgE ratios to egg, ovalbumin, and ovomucoid were also higher in the egg group, indicating developing tolerance (P less than .0001 for each).
About 10% of the children originally in the egg group broke out in hives after their first few doses, and were withdrawn from the study. “This intervention may not be for everybody. There will be individuals who react” and it’s impossible, at this point, to predict who they will be. “We cannot prevent allergy in everyone,” said lead investigator Dr. John Tan, a pediatric immunologist at the hospital.
Overall, however, early introduction was safe. There was no anaphylaxis in the trial, and no cardiovascular or respiratory complications. Rates of eczema and peanut allergy were similar at 12 months between the two groups, meaning that early egg introduction did not increase the risk of atopy.
The findings echo results from several recent pediatric egg allergy studies, as well as findings from recent peanut trials. Slowly, it’s becoming clear that delaying the introduction of at least some allergenic foods – a common practice for years – doesn’t prevent allergies and may, in fact, promote them.
Despite those findings, there remains “a big disconnect between the [new] research and what we [still] recommend” in Australia, the United States, and elsewhere. Delaying food introductions was medical “dogma for 20 years, from highly esteemed societies,” and it corresponded with a marked increase in food allergies, but “it’s very hard to turn these things around,” Dr. Campbell said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The Australian government is reworking its infant feeding guidelines to incorporate the new evidence. “Our revised guidelines will say that there’s strong evidence for peanut and moderate evidence for egg” in favor of early introduction in children who are not sensitized by 4 or so months old, she said.
The trial was powered to detect differences in SPT, not actual egg allergies, which were diagnosed in 13 children (11%) in the rice group and eight (7%) in the egg group; the difference was not statistically significant. “Not all kids who are sensitized will be allergic,” she noted.
The study groups were well matched; there were about equal numbers of boys and girls in each, and, in both groups, about 15% of children were exposed to second hand smoke at home and almost all were breastfed.
The work was funded by the Australian government, among others. The investigators have no disclosures.
LOS ANGELES – Among infants at risk for allergic disease, egg introduction at 4 months cuts the risk of egg sensitization at 12 months by about half, according a randomized, placebo-controlled, double blind trial from Australia.
“This is what we hoped to find.” Introducing egg early “is certainly safe, and it may promote tolerance,” said senior investigator Dr. Dianne Campbell, professor and chair of pediatric allergy and clinical immunology at the Children’s Hospital at Westmead, which is affiliated with the University of Sydney.
Four-month-old children were randomized to 350 mg of pasteurized raw whole egg powder or – as a control – rice powder sprinkled once daily on their weaning food until month 8, at which time parents in both groups were encouraged to add eggs to their children’s diets. At least one of each child’s parents had a history of atopic disease, including asthma, eczema, hay fever, or food allergy. Even so, all of the infants had negative (less than 2 mm) skin prick tests (SPTs) at baseline. Compliance by parent diary was 89% in the rice and 81% in the egg groups.
At 12 months, SPTs were positive (3 mm or more) for whole egg in 25 of 122 (20%) children in the rice group, but only 13 of 122 (11%) in the egg group (odds ratio, 0.46; 95% confidence interval, 0.22-0.95; P = .03). Whole egg IgG4 and IgG4/IgE ratios to egg, ovalbumin, and ovomucoid were also higher in the egg group, indicating developing tolerance (P less than .0001 for each).
About 10% of the children originally in the egg group broke out in hives after their first few doses, and were withdrawn from the study. “This intervention may not be for everybody. There will be individuals who react” and it’s impossible, at this point, to predict who they will be. “We cannot prevent allergy in everyone,” said lead investigator Dr. John Tan, a pediatric immunologist at the hospital.
Overall, however, early introduction was safe. There was no anaphylaxis in the trial, and no cardiovascular or respiratory complications. Rates of eczema and peanut allergy were similar at 12 months between the two groups, meaning that early egg introduction did not increase the risk of atopy.
The findings echo results from several recent pediatric egg allergy studies, as well as findings from recent peanut trials. Slowly, it’s becoming clear that delaying the introduction of at least some allergenic foods – a common practice for years – doesn’t prevent allergies and may, in fact, promote them.
Despite those findings, there remains “a big disconnect between the [new] research and what we [still] recommend” in Australia, the United States, and elsewhere. Delaying food introductions was medical “dogma for 20 years, from highly esteemed societies,” and it corresponded with a marked increase in food allergies, but “it’s very hard to turn these things around,” Dr. Campbell said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The Australian government is reworking its infant feeding guidelines to incorporate the new evidence. “Our revised guidelines will say that there’s strong evidence for peanut and moderate evidence for egg” in favor of early introduction in children who are not sensitized by 4 or so months old, she said.
The trial was powered to detect differences in SPT, not actual egg allergies, which were diagnosed in 13 children (11%) in the rice group and eight (7%) in the egg group; the difference was not statistically significant. “Not all kids who are sensitized will be allergic,” she noted.
The study groups were well matched; there were about equal numbers of boys and girls in each, and, in both groups, about 15% of children were exposed to second hand smoke at home and almost all were breastfed.
The work was funded by the Australian government, among others. The investigators have no disclosures.
AT 2016 AAAAI ANNUAL MEETING
Key clinical point: If at-risk infants have negative skin prick tests (SPTs) at 4 months, tell their moms to introduce egg into their weaning diets.
Major finding: At 12 months, SPTs were positive (3 mm or more) for whole egg in 25 of 122 children (20%) in the rice group, but only 13 of 122 (11%) in the egg group (odds ratio, 0.46; 95% confidence interval, 0.22-0.95; P = .03).
Data source: Randomized clinical trial or 244 infants at risk for egg allergy.
Disclosures: The work was funded by the Australian government, among others. The investigators have no disclosures.
