User login
Analysis supports daily folate for children with psoriasis on methotrexate
SCOTTSDALE, ARIZ. – Children and adolescents receiving methotrexate for psoriasis were significantly less likely to experience gastrointestinal side effects when they took a folate supplement every day instead of once weekly or 6 days a week, in a retrospective study of more than 400 pediatric psoriasis patients.
Laboratory abnormalities were significantly more common among children who received a folate supplement 6 days per week rather than daily, noted Inge Bronckers of the department of dermatology, Radboud University, Nijmegen, the Netherlands. “These results support the use of daily folate” in this group of patients,” she said in a poster presentation at the annual meeting of the Society for Investigative Dermatology.

Few studies have examined patterns of use or adverse effects of pediatric psoriasis therapies. Although methotrexate is a folate antagonist with related toxicities, whether folate supplementation counteracts the efficacy of methotrexate is also unclear. Because of these uncertainties, some clinicians recommend a supplement 6 days per week, avoiding the day methotrexate is given, while others recommend it daily or once weekly.
To better understand the effects of these regimens, Ms. Inge and her coinvestigators studied 446 children and adolescents who received phototherapy or systemic treatments for moderate to severe psoriasis at 20 centers in the United States, Canada, and Europe between 1990 and 2014. The patients’ average age was 8 years (standard deviation, 4 years); 238 were female and 208 were male.
Among the 390 patients receiving systemic medications, almost 70% were receiving methotrexate, while 27% were being treated with etanercept or another biologic, 15% were using retinoids, 8% were using cyclosporine, and 5% were using fumaric acid. About 19% of patients were receiving more than one of these medications. Methotrexate most often led to nausea (affecting 18% of patients), elevated hepatic transaminases (13%), dyspepsia (7%), and infections (4%), usually of the skin and upper airways. In contrast, biologics most often caused injection-site reactions (19%) and upper airways infections (10%).
Most (253) of the 270 patients on methotrexate had been prescribed folic acid, typically at a dose of about 8 mg/wk, and nearly always in the form of pure folic acid, rather than a multivitamin. Of the patients taking folic acid, about 34% took it 6 days per week, 34% received it daily and 30% – including most patients in Europe – received it once weekly.
Notably, the odds of gastrointestinal side effects were 75% lower for patients who received folic acid daily or 6 days per week, compared with those who received folic acid once a week (odds ratio, 0.25, in both cases; P less than .001), the investigators found. However, laboratory abnormalities were significantly more likely when folic acid was given 6 days a week, compared with daily (OR, 2.31; P = .03) or weekly (OR, 3.9; P = .002). Patients in Europe, who usually received folic acid weekly, were significantly more likely to have methotrexate-related gastrointestinal side effects than were patients in North America (OR, 3.4; P less than .001), and were less likely to have laboratory abnormalities (OR, 0.32; P = .004).
Patients on biologic therapy were less likely to develop laboratory abnormalities or stop treatment because of side effects than were those on other systemic therapies, Ms. Inge and her associates found. Because methotrexate was associated with elevated liver enzymes, it also was dose adjusted more often than other therapies. No patient on any therapy was diagnosed with tuberculosis or malignancy, but three patients on methotrexate had severe adverse effects, including liver disease, methotrexate hypersensitivity pneumonitis, and severe personality changes. In contrast, fumarate was associated with one case each of pericarditis and bone marrow suppression, while one patient on the biologic adalimumab developed appendicitis.
The study underscores the need to monitor the long-term risks of pediatric psoriasis treatments, the researchers concluded. Data and lessons from the study are being used to develop a prospective pediatric psoriasis registry. “If industry joins forces to use this prospective international registry to capture prospective pediatric data, we will ensure early detection of safety signals and facilitate comparative analyses of efficacy and safety,” Ms. Inge said in the poster.
The International Psoriasis Council funded the study. The investigators did not list disclosures.
SCOTTSDALE, ARIZ. – Children and adolescents receiving methotrexate for psoriasis were significantly less likely to experience gastrointestinal side effects when they took a folate supplement every day instead of once weekly or 6 days a week, in a retrospective study of more than 400 pediatric psoriasis patients.
Laboratory abnormalities were significantly more common among children who received a folate supplement 6 days per week rather than daily, noted Inge Bronckers of the department of dermatology, Radboud University, Nijmegen, the Netherlands. “These results support the use of daily folate” in this group of patients,” she said in a poster presentation at the annual meeting of the Society for Investigative Dermatology.
Few studies have examined patterns of use or adverse effects of pediatric psoriasis therapies. Although methotrexate is a folate antagonist with related toxicities, whether folate supplementation counteracts the efficacy of methotrexate is also unclear. Because of these uncertainties, some clinicians recommend a supplement 6 days per week, avoiding the day methotrexate is given, while others recommend it daily or once weekly.
To better understand the effects of these regimens, Ms. Inge and her coinvestigators studied 446 children and adolescents who received phototherapy or systemic treatments for moderate to severe psoriasis at 20 centers in the United States, Canada, and Europe between 1990 and 2014. The patients’ average age was 8 years (standard deviation, 4 years); 238 were female and 208 were male.
Among the 390 patients receiving systemic medications, almost 70% were receiving methotrexate, while 27% were being treated with etanercept or another biologic, 15% were using retinoids, 8% were using cyclosporine, and 5% were using fumaric acid. About 19% of patients were receiving more than one of these medications. Methotrexate most often led to nausea (affecting 18% of patients), elevated hepatic transaminases (13%), dyspepsia (7%), and infections (4%), usually of the skin and upper airways. In contrast, biologics most often caused injection-site reactions (19%) and upper airways infections (10%).
Most (253) of the 270 patients on methotrexate had been prescribed folic acid, typically at a dose of about 8 mg/wk, and nearly always in the form of pure folic acid, rather than a multivitamin. Of the patients taking folic acid, about 34% took it 6 days per week, 34% received it daily and 30% – including most patients in Europe – received it once weekly.
Notably, the odds of gastrointestinal side effects were 75% lower for patients who received folic acid daily or 6 days per week, compared with those who received folic acid once a week (odds ratio, 0.25, in both cases; P less than .001), the investigators found. However, laboratory abnormalities were significantly more likely when folic acid was given 6 days a week, compared with daily (OR, 2.31; P = .03) or weekly (OR, 3.9; P = .002). Patients in Europe, who usually received folic acid weekly, were significantly more likely to have methotrexate-related gastrointestinal side effects than were patients in North America (OR, 3.4; P less than .001), and were less likely to have laboratory abnormalities (OR, 0.32; P = .004).
Patients on biologic therapy were less likely to develop laboratory abnormalities or stop treatment because of side effects than were those on other systemic therapies, Ms. Inge and her associates found. Because methotrexate was associated with elevated liver enzymes, it also was dose adjusted more often than other therapies. No patient on any therapy was diagnosed with tuberculosis or malignancy, but three patients on methotrexate had severe adverse effects, including liver disease, methotrexate hypersensitivity pneumonitis, and severe personality changes. In contrast, fumarate was associated with one case each of pericarditis and bone marrow suppression, while one patient on the biologic adalimumab developed appendicitis.
The study underscores the need to monitor the long-term risks of pediatric psoriasis treatments, the researchers concluded. Data and lessons from the study are being used to develop a prospective pediatric psoriasis registry. “If industry joins forces to use this prospective international registry to capture prospective pediatric data, we will ensure early detection of safety signals and facilitate comparative analyses of efficacy and safety,” Ms. Inge said in the poster.
The International Psoriasis Council funded the study. The investigators did not list disclosures.
SCOTTSDALE, ARIZ. – Children and adolescents receiving methotrexate for psoriasis were significantly less likely to experience gastrointestinal side effects when they took a folate supplement every day instead of once weekly or 6 days a week, in a retrospective study of more than 400 pediatric psoriasis patients.
Laboratory abnormalities were significantly more common among children who received a folate supplement 6 days per week rather than daily, noted Inge Bronckers of the department of dermatology, Radboud University, Nijmegen, the Netherlands. “These results support the use of daily folate” in this group of patients,” she said in a poster presentation at the annual meeting of the Society for Investigative Dermatology.
Few studies have examined patterns of use or adverse effects of pediatric psoriasis therapies. Although methotrexate is a folate antagonist with related toxicities, whether folate supplementation counteracts the efficacy of methotrexate is also unclear. Because of these uncertainties, some clinicians recommend a supplement 6 days per week, avoiding the day methotrexate is given, while others recommend it daily or once weekly.
To better understand the effects of these regimens, Ms. Inge and her coinvestigators studied 446 children and adolescents who received phototherapy or systemic treatments for moderate to severe psoriasis at 20 centers in the United States, Canada, and Europe between 1990 and 2014. The patients’ average age was 8 years (standard deviation, 4 years); 238 were female and 208 were male.
Among the 390 patients receiving systemic medications, almost 70% were receiving methotrexate, while 27% were being treated with etanercept or another biologic, 15% were using retinoids, 8% were using cyclosporine, and 5% were using fumaric acid. About 19% of patients were receiving more than one of these medications. Methotrexate most often led to nausea (affecting 18% of patients), elevated hepatic transaminases (13%), dyspepsia (7%), and infections (4%), usually of the skin and upper airways. In contrast, biologics most often caused injection-site reactions (19%) and upper airways infections (10%).
Most (253) of the 270 patients on methotrexate had been prescribed folic acid, typically at a dose of about 8 mg/wk, and nearly always in the form of pure folic acid, rather than a multivitamin. Of the patients taking folic acid, about 34% took it 6 days per week, 34% received it daily and 30% – including most patients in Europe – received it once weekly.
Notably, the odds of gastrointestinal side effects were 75% lower for patients who received folic acid daily or 6 days per week, compared with those who received folic acid once a week (odds ratio, 0.25, in both cases; P less than .001), the investigators found. However, laboratory abnormalities were significantly more likely when folic acid was given 6 days a week, compared with daily (OR, 2.31; P = .03) or weekly (OR, 3.9; P = .002). Patients in Europe, who usually received folic acid weekly, were significantly more likely to have methotrexate-related gastrointestinal side effects than were patients in North America (OR, 3.4; P less than .001), and were less likely to have laboratory abnormalities (OR, 0.32; P = .004).
Patients on biologic therapy were less likely to develop laboratory abnormalities or stop treatment because of side effects than were those on other systemic therapies, Ms. Inge and her associates found. Because methotrexate was associated with elevated liver enzymes, it also was dose adjusted more often than other therapies. No patient on any therapy was diagnosed with tuberculosis or malignancy, but three patients on methotrexate had severe adverse effects, including liver disease, methotrexate hypersensitivity pneumonitis, and severe personality changes. In contrast, fumarate was associated with one case each of pericarditis and bone marrow suppression, while one patient on the biologic adalimumab developed appendicitis.
The study underscores the need to monitor the long-term risks of pediatric psoriasis treatments, the researchers concluded. Data and lessons from the study are being used to develop a prospective pediatric psoriasis registry. “If industry joins forces to use this prospective international registry to capture prospective pediatric data, we will ensure early detection of safety signals and facilitate comparative analyses of efficacy and safety,” Ms. Inge said in the poster.
The International Psoriasis Council funded the study. The investigators did not list disclosures.
AT THE 2016 SID ANNUAL MEETING
Key clinical point: Consider daily folate to reduce the likelihood of gastrointestinal side effects of methotrexate in children with psoriasis.
Major finding: The odds of gastrointestinal adverse effects were about 75% lower with daily folate, compared with weekly dosing or 6 days per week dosing that spared the methotrexate day (odds ratio, 0.25; P less than .001).
Data source: An international retrospective study of 446 children receiving phototherapy or systemic therapy for psoriasis.
Disclosures: The International Psoriasis Council funded the study. The investigators did not list disclosures.

Appreciate family cognitive style when discussing vaccines
It started with a dinner table conversation. Gregory Poland, MD, director of the Mayo Clinic’s Vaccine Research Group, Rochester, Minn., was talking with his daughter about the difficulties medical providers face in overcoming the fears and doubts of many vaccine-hesitant families. Presenting scientific evidence about the safety of vaccines and the risks of many preventable diseases, in many cases, didn’t budge the thinking of a hesitant parent.
Dr. Poland’s daughter, Caroline Poland, said, “Well, the way you all are going about this isn’t supported by cognitive psychology at all.” Ms. Poland, a licensed mental health and addiction counselor and director of the counseling center at Taylor University in Upland, Ind., knew that cognitive styles differ, and few people are actually swayed by analytic arguments.

Recounting this story in an interview, Dr. Poland said this was when he began to realize the impact of the fact that medicine selects for those who favor facts over emotion. Furthermore, “You get professionalized into a highly analytic way of thinking.” This realization led both participants in the conversation into an exploration of how best to communicate respectfully but effectively with those parents who are resistant or unsure about vaccine safety and effectiveness.
Dr. Poland has spoken and published about using motivational interviewing, an evidence-based model for communicating with individuals who are ambivalent or hesitant about changing health behaviors when vaccine hesitancy is encountered. He has collaborated with Ms. Poland as well, and together and separately, they are exploring new ways to achieve effective communication of medical information to patient’s parents and family members.
Ms. Poland has developed a “preferred cognitive styles and decision-making model” that takes into account how patients perceive and process information. “To help patients change, providers have to communicate in the style that’s best for them,” she said. The model posits that different individuals have different cognitive and learning styles, gives examples of patient statements that fit into the various cognitive styles, and provides guidance about effective communication that fits a given cognitive style (Vaccine. 2011 Aug 26;29[3h7]:6145-8).
In a collaboration stemming from an American Academy for Arts and Sciences (AAAS)-sponsored interdisciplinary work group exploring the problem of vaccine hesitancy, Ms. Poland has worked with an anthropologist to explore multidisciplinary approaches. “We met at this round table – anthropologists, economists, doctors, psychologists – to try to figure out how to reach these people” who are experiencing vaccine hesitancy, Ms. Poland said of her attendance at the 2013 AAAS session.

Effective motivational interviewing, said Ms. Poland, “is not a one-and-done conversation. You’re listening empathetically, having the patient voice the rationale for change.” Building mutual trust and respect can set the stage for patients’ open listening and readiness to change, she said. “When they go out into the external world and talk to others, then they’ll be able to start to verbalize the reasons” for their resistance, and why they may be ready to change a behavior.
“We don’t want to be so frantic in the moment that we lose sight of our relationship with our patients,” she said.
Dr. Poland said that access to information – and misinformation – on the Internet means that, “Patients come in with a 2-inch thick stack of Google searches,” he said. “We need to have time to talk through this with people.” Now, he said, there’s an ICD-10 code for vaccine counseling, which can be used to address the concerns and questions families bring to a clinic visit.
Ms. Poland said, “It’s easy to make this into an ‘us versus them’ issue, but it’s really more layered and nuanced than that. Everybody’s trying to make the best decision they know how. And anytime I’m feeling understood I’m more open to listening.”
Dr. Poland agreed, emphasizing that providers need ongoing support to make their communication as effective as possible. “This is not something you train providers in just once,” he said. “This is an ongoing conversation at the provider-patient level that leads to trust.”
Ms Poland said she receives research funding from Pfizer to evaluate new behavioral and educational models of vaccine decision making. Dr. Poland is the chair of a safety evaluation committee for novel investigational vaccine trials being conducted by Merck, and he offers consultative advice on vaccine development to Merck, CSL Biotherapies, Avianax, Dynavax, Novartis, Emergent BioSolutions, Adjuvance, Microdermis, Seqirus, NewLink, Protein Sciences, GlaxoSmithKline, and Sanofi Pasteur. Dr. Poland holds two patents related to vaccinia and measles peptide research.
On Twitter @karioakes
It started with a dinner table conversation. Gregory Poland, MD, director of the Mayo Clinic’s Vaccine Research Group, Rochester, Minn., was talking with his daughter about the difficulties medical providers face in overcoming the fears and doubts of many vaccine-hesitant families. Presenting scientific evidence about the safety of vaccines and the risks of many preventable diseases, in many cases, didn’t budge the thinking of a hesitant parent.
Dr. Poland’s daughter, Caroline Poland, said, “Well, the way you all are going about this isn’t supported by cognitive psychology at all.” Ms. Poland, a licensed mental health and addiction counselor and director of the counseling center at Taylor University in Upland, Ind., knew that cognitive styles differ, and few people are actually swayed by analytic arguments.
Recounting this story in an interview, Dr. Poland said this was when he began to realize the impact of the fact that medicine selects for those who favor facts over emotion. Furthermore, “You get professionalized into a highly analytic way of thinking.” This realization led both participants in the conversation into an exploration of how best to communicate respectfully but effectively with those parents who are resistant or unsure about vaccine safety and effectiveness.
Dr. Poland has spoken and published about using motivational interviewing, an evidence-based model for communicating with individuals who are ambivalent or hesitant about changing health behaviors when vaccine hesitancy is encountered. He has collaborated with Ms. Poland as well, and together and separately, they are exploring new ways to achieve effective communication of medical information to patient’s parents and family members.
Ms. Poland has developed a “preferred cognitive styles and decision-making model” that takes into account how patients perceive and process information. “To help patients change, providers have to communicate in the style that’s best for them,” she said. The model posits that different individuals have different cognitive and learning styles, gives examples of patient statements that fit into the various cognitive styles, and provides guidance about effective communication that fits a given cognitive style (Vaccine. 2011 Aug 26;29[3h7]:6145-8).
In a collaboration stemming from an American Academy for Arts and Sciences (AAAS)-sponsored interdisciplinary work group exploring the problem of vaccine hesitancy, Ms. Poland has worked with an anthropologist to explore multidisciplinary approaches. “We met at this round table – anthropologists, economists, doctors, psychologists – to try to figure out how to reach these people” who are experiencing vaccine hesitancy, Ms. Poland said of her attendance at the 2013 AAAS session.
Effective motivational interviewing, said Ms. Poland, “is not a one-and-done conversation. You’re listening empathetically, having the patient voice the rationale for change.” Building mutual trust and respect can set the stage for patients’ open listening and readiness to change, she said. “When they go out into the external world and talk to others, then they’ll be able to start to verbalize the reasons” for their resistance, and why they may be ready to change a behavior.
“We don’t want to be so frantic in the moment that we lose sight of our relationship with our patients,” she said.
Dr. Poland said that access to information – and misinformation – on the Internet means that, “Patients come in with a 2-inch thick stack of Google searches,” he said. “We need to have time to talk through this with people.” Now, he said, there’s an ICD-10 code for vaccine counseling, which can be used to address the concerns and questions families bring to a clinic visit.
Ms. Poland said, “It’s easy to make this into an ‘us versus them’ issue, but it’s really more layered and nuanced than that. Everybody’s trying to make the best decision they know how. And anytime I’m feeling understood I’m more open to listening.”
Dr. Poland agreed, emphasizing that providers need ongoing support to make their communication as effective as possible. “This is not something you train providers in just once,” he said. “This is an ongoing conversation at the provider-patient level that leads to trust.”
Ms Poland said she receives research funding from Pfizer to evaluate new behavioral and educational models of vaccine decision making. Dr. Poland is the chair of a safety evaluation committee for novel investigational vaccine trials being conducted by Merck, and he offers consultative advice on vaccine development to Merck, CSL Biotherapies, Avianax, Dynavax, Novartis, Emergent BioSolutions, Adjuvance, Microdermis, Seqirus, NewLink, Protein Sciences, GlaxoSmithKline, and Sanofi Pasteur. Dr. Poland holds two patents related to vaccinia and measles peptide research.
On Twitter @karioakes
It started with a dinner table conversation. Gregory Poland, MD, director of the Mayo Clinic’s Vaccine Research Group, Rochester, Minn., was talking with his daughter about the difficulties medical providers face in overcoming the fears and doubts of many vaccine-hesitant families. Presenting scientific evidence about the safety of vaccines and the risks of many preventable diseases, in many cases, didn’t budge the thinking of a hesitant parent.
Dr. Poland’s daughter, Caroline Poland, said, “Well, the way you all are going about this isn’t supported by cognitive psychology at all.” Ms. Poland, a licensed mental health and addiction counselor and director of the counseling center at Taylor University in Upland, Ind., knew that cognitive styles differ, and few people are actually swayed by analytic arguments.
Recounting this story in an interview, Dr. Poland said this was when he began to realize the impact of the fact that medicine selects for those who favor facts over emotion. Furthermore, “You get professionalized into a highly analytic way of thinking.” This realization led both participants in the conversation into an exploration of how best to communicate respectfully but effectively with those parents who are resistant or unsure about vaccine safety and effectiveness.
Dr. Poland has spoken and published about using motivational interviewing, an evidence-based model for communicating with individuals who are ambivalent or hesitant about changing health behaviors when vaccine hesitancy is encountered. He has collaborated with Ms. Poland as well, and together and separately, they are exploring new ways to achieve effective communication of medical information to patient’s parents and family members.
Ms. Poland has developed a “preferred cognitive styles and decision-making model” that takes into account how patients perceive and process information. “To help patients change, providers have to communicate in the style that’s best for them,” she said. The model posits that different individuals have different cognitive and learning styles, gives examples of patient statements that fit into the various cognitive styles, and provides guidance about effective communication that fits a given cognitive style (Vaccine. 2011 Aug 26;29[3h7]:6145-8).
In a collaboration stemming from an American Academy for Arts and Sciences (AAAS)-sponsored interdisciplinary work group exploring the problem of vaccine hesitancy, Ms. Poland has worked with an anthropologist to explore multidisciplinary approaches. “We met at this round table – anthropologists, economists, doctors, psychologists – to try to figure out how to reach these people” who are experiencing vaccine hesitancy, Ms. Poland said of her attendance at the 2013 AAAS session.
Effective motivational interviewing, said Ms. Poland, “is not a one-and-done conversation. You’re listening empathetically, having the patient voice the rationale for change.” Building mutual trust and respect can set the stage for patients’ open listening and readiness to change, she said. “When they go out into the external world and talk to others, then they’ll be able to start to verbalize the reasons” for their resistance, and why they may be ready to change a behavior.
“We don’t want to be so frantic in the moment that we lose sight of our relationship with our patients,” she said.
Dr. Poland said that access to information – and misinformation – on the Internet means that, “Patients come in with a 2-inch thick stack of Google searches,” he said. “We need to have time to talk through this with people.” Now, he said, there’s an ICD-10 code for vaccine counseling, which can be used to address the concerns and questions families bring to a clinic visit.
Ms. Poland said, “It’s easy to make this into an ‘us versus them’ issue, but it’s really more layered and nuanced than that. Everybody’s trying to make the best decision they know how. And anytime I’m feeling understood I’m more open to listening.”
Dr. Poland agreed, emphasizing that providers need ongoing support to make their communication as effective as possible. “This is not something you train providers in just once,” he said. “This is an ongoing conversation at the provider-patient level that leads to trust.”
Ms Poland said she receives research funding from Pfizer to evaluate new behavioral and educational models of vaccine decision making. Dr. Poland is the chair of a safety evaluation committee for novel investigational vaccine trials being conducted by Merck, and he offers consultative advice on vaccine development to Merck, CSL Biotherapies, Avianax, Dynavax, Novartis, Emergent BioSolutions, Adjuvance, Microdermis, Seqirus, NewLink, Protein Sciences, GlaxoSmithKline, and Sanofi Pasteur. Dr. Poland holds two patents related to vaccinia and measles peptide research.
On Twitter @karioakes

Children’s lead levels in Flint, Mich., fluctuate as water supply switched
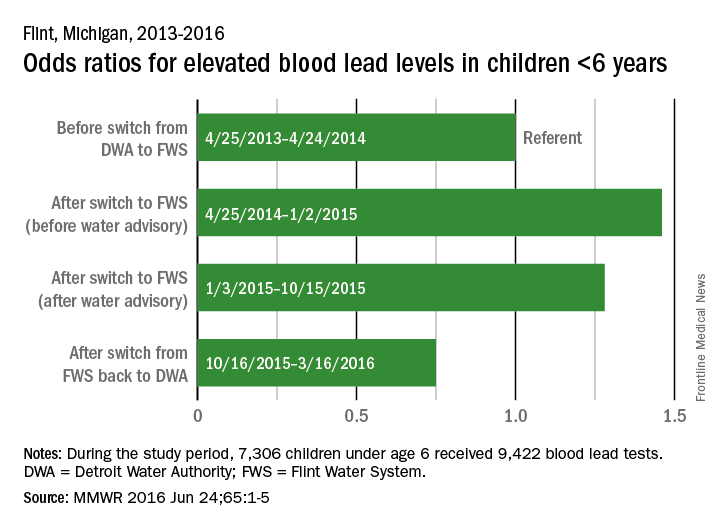
In Flint, Mich., the prevalence of elevated blood lead levels rose among children under age 6 years after the switch in the city’s water source, dropped after an advisory was issued, and then dropped below original levels after the city switched back to its original water source, according to the Centers for Disease Control and Prevention.
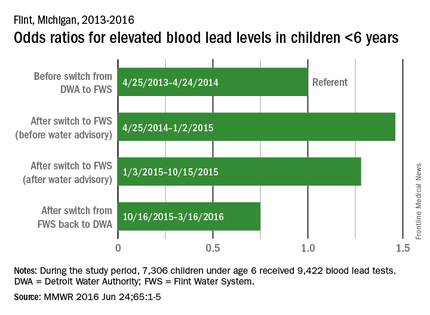
In the year before the switch (April 25, 2013, to April 24, 2014), 3.1% of blood lead levels (BLLs) in children under age 6 years were 5 mcg/dL or higher, which the CDC considers to be elevated. After the switch from the Detroit Water Authority (DWA) to the Flint Water System (FWS) but before the water advisory was issued (April 25, 2014, to Jan. 2, 2015), elevated BLLs increased to 5.0%, for an adjusted odds ratio of 1.46 (MMWR 2016 Jun 24;65:1-5).
For the period after the water advisory but before the water supply was switched back to the DWA (Jan. 3, 2015, to Oct. 15, 2015), 3.9% of BLLs were elevated (aOR, 1.28). For the 5 months after the switch back to the DWA, the percentage of elevated BLLs dropped to 1.4% (aOR, 0.75).
The analysis involved the results of 9,422 tests received by 7,306 children, all of whom lived in the area served by the FWS. The Environmental Protection Agency recently advised that it is safe for Flint residents to drink filtered tap water and that unfiltered tap water can be used for bathing and showering, the CDC report noted.
In Flint, Mich., the prevalence of elevated blood lead levels rose among children under age 6 years after the switch in the city’s water source, dropped after an advisory was issued, and then dropped below original levels after the city switched back to its original water source, according to the Centers for Disease Control and Prevention.
In the year before the switch (April 25, 2013, to April 24, 2014), 3.1% of blood lead levels (BLLs) in children under age 6 years were 5 mcg/dL or higher, which the CDC considers to be elevated. After the switch from the Detroit Water Authority (DWA) to the Flint Water System (FWS) but before the water advisory was issued (April 25, 2014, to Jan. 2, 2015), elevated BLLs increased to 5.0%, for an adjusted odds ratio of 1.46 (MMWR 2016 Jun 24;65:1-5).
For the period after the water advisory but before the water supply was switched back to the DWA (Jan. 3, 2015, to Oct. 15, 2015), 3.9% of BLLs were elevated (aOR, 1.28). For the 5 months after the switch back to the DWA, the percentage of elevated BLLs dropped to 1.4% (aOR, 0.75).
The analysis involved the results of 9,422 tests received by 7,306 children, all of whom lived in the area served by the FWS. The Environmental Protection Agency recently advised that it is safe for Flint residents to drink filtered tap water and that unfiltered tap water can be used for bathing and showering, the CDC report noted.
In Flint, Mich., the prevalence of elevated blood lead levels rose among children under age 6 years after the switch in the city’s water source, dropped after an advisory was issued, and then dropped below original levels after the city switched back to its original water source, according to the Centers for Disease Control and Prevention.
In the year before the switch (April 25, 2013, to April 24, 2014), 3.1% of blood lead levels (BLLs) in children under age 6 years were 5 mcg/dL or higher, which the CDC considers to be elevated. After the switch from the Detroit Water Authority (DWA) to the Flint Water System (FWS) but before the water advisory was issued (April 25, 2014, to Jan. 2, 2015), elevated BLLs increased to 5.0%, for an adjusted odds ratio of 1.46 (MMWR 2016 Jun 24;65:1-5).
For the period after the water advisory but before the water supply was switched back to the DWA (Jan. 3, 2015, to Oct. 15, 2015), 3.9% of BLLs were elevated (aOR, 1.28). For the 5 months after the switch back to the DWA, the percentage of elevated BLLs dropped to 1.4% (aOR, 0.75).
The analysis involved the results of 9,422 tests received by 7,306 children, all of whom lived in the area served by the FWS. The Environmental Protection Agency recently advised that it is safe for Flint residents to drink filtered tap water and that unfiltered tap water can be used for bathing and showering, the CDC report noted.
FROM MMWR
Initiative aims to improve transition from pediatric to adult care
Gregg Michael Talente, MD, remembers well a young patient who nearly fell through the gap between pediatric an adult health care.
The woman was treated for lupus by her pediatrician until age 19 when the doctor moved out of town. When she landed in front of Dr. Talente, it was clear the patient lacked the knowledge and skills to self-manage her condition, he recalled. Dr. Talente and his team, including pharmacists, helped the young woman understand how to administer her medications, provided refill reminders, and counseled her about reproductive health and how other medications could interact with lupus treatment.
“I look at her as a near-miss case,” said Dr. Talente, director of the internal medicine resident clinic at the University of South Carolina, Columbia, who specializes in pediatric-adolescent medicine. “A lot of bad things could have happened to her because her transition was delayed, and she wasn’t prepared. Fortunately, she landed in a place with more resources than a typical adult clinic so we were able to catch up.”
A new national initiative is designed to aid patients such as this during the move from pediatric to adult health care. The Pediatric to Adult Care Transitions Initiative is a collaborative effort by various specialty groups to facilitate more effective transition and transfer of young adults, while providing a framework for pediatricians and adult care providers. The project is under the direction of the American College of Physicians’ (ACP) Council of Subspecialty Societies in conjunction with the Got Transition (GT)/Center for Health Care Transition Improvement, the Society of General Internal Medicine (SGIM), and the Society for Adolescent Health and Medicine. Got Transition is a cooperative project by the Maternal and Child Health Bureau and The National Alliance to Advance Adolescent Health to improve pediatric-to-adult-care transitions through innovative strategies.
Since the Pediatric to Adult Care Transitions Initiative launched in spring 2015, project leaders have designed a series of disease-specific tools to enable smoother transition of patients. The downloadable tools include a transition readiness assessment, a medical summary/transfer record tool, and a self-care assessment. The guides were adapted from Got Transition’s six core elements of health care transition, developed from joint clinical recommendations by the ACP, the American Academy of Pediatrics, and the American Academy of Family Physicians.

The disease-specific tools are just the beginning, said Carol Greenlee, MD, chair of the Pediatric to Adult Care Transitions Initiative and chair of the ACP’s Council of Subspecialty Societies.
“We don’t want to just have tools on a website, we want to improve the whole process,” she said. “One of our goals is education and implementation. Part of implementation has to include collaboration because you don’t care-coordinate in isolation. You have to care-coordinate not just with the patient and family, but the pediatric and adult care providers need to collaborate.”
A need for better transition
Data show that knowledge and resources are lacking on both the pediatric and adult care side when it comes to transitioning patients from one realm to the other. A 2009 survey by the AAP found that most pediatric practices neither initiate transition planning early in adolescence nor offer transition-support service (AAP News 2009 Nov. Vol. 30). Another study in the Journal of General Internal Medicine found that many adult providers feel unprepared to care for young adults with complex chronic conditions and that in some cases, there is no identified adult primary care or specialty provider to whom care can be transitioned (J Gen Intern Med. 2008 Oct;23[10]:1621-7). Lack of time, inadequate payment, and poor training also have been cited as barriers to successful transition (Pediatrics. 2001 Jul 1. doi: 10.1542/peds.2011-0969).

Poor transitions often lead to negative health outcomes for young adults, said Dr. Patience White, codirector of Got Transition and professor of medicine and pediatrics at George Washington University, Washington. She has co-led the Pediatric to Adult Care Transitions Initiative.
“The quality of care goes down; many [patients] are lost from their care, and they don’t get the kind of care they need,” Dr. White said. “Therefore, they have poor outcomes, and then of course, the cost goes up because they are utilizing emergency rooms or tests are repeated. You’re looking at poor patient experience, poor quality, and increased cost.”
Enter the Pediatric to Adult Care Transitions Initiative. The project was designed with the busy practices of pediatricians and adult care providers in mind, said Dr. Talente, who is past chair of the SGIM Adults with Complex Conditions Originating in Childhood Task Force.
“Everyone is busy, and asking each individual practitioner to develop the systems they need to do this right is not really practical,” he said. “That’s where this project is really helpful, in the sense that it’s attempting to deliver tools and systems to providers that they can use and just adapt, without doing all the work themselves when they’re trying to run their busy practices.”

The initiative’s readiness assessment is a first step toward improving early transition planning, Dr. Greenlee said. The tool allows pediatricians to measure the knowledge and skill level of patients in the years leading to transition age, and enables doctors to fill any gaps before the transfer occurs.
The tool helps physicians gauge “what this young adult needs to know before they go out into the adult world and take on self-management,” she said. “Making sure they know how to fill a prescription, how to take their medications, know signs and symptoms of a crisis – that sort of thing.”
To enable better communication between providers, initiative leaders created the transfer summary, a hand-off outline that includes critical items the receiving clinician should know about the patients, such as information about their conditions, personal interests, or special needs. The third tool launched by the initiative – a self-management assessment – is a resource for adult care providers to measure the patients’ skills and knowledge once they begin adult care.
Overcoming obstacles to transition
The path to smoother patient transitions is not without bumps in the road. Adding time and new tools to physicians’ already heavy workloads can be challenging, Dr. Greenlee said.
“One of the biggest challenges is the time it takes on both sides,” she said. “Here we’re saying, ‘Here’s more to do.’ As a pediatrician, you’re gong to be preparing and educating [patients] in self-management and trying to get the parents engaged. There’s extra work.”
But helping pediatricians understand the bigger picture results – better outcomes, improved quality, lower health care costs – is key to acceptance, according to initiative leaders.
Strengthening communication between pediatric and adult practices also is critical to making the transition tools effective, added Dr. White. Pediatric practices cannot make successful transfers alone.
“The challenges are to find the partnerships that you need to start it, and the next big challenge is the buy-in,” she said. “You’ve got to get your leadership and senior physicians in a practice to agree that this is something they’re going to do. What’s frustrating for families is when different physicians use different modes of this whole process.”
Reimbursement for transition-related care is an ongoing climb, added Dr. Talente. In the past, physicians have struggled to receive payment for certain nonvisit time needed for transitions, he said.
However, Got Transition recently made headway toward improved payment, Dr. White said. Code 99420 now can be used to bill for transition readiness assessments conducted with youth and self-care assessments conducted with young adults. Got Transition and several physician specialty organizations also have developed a payment work group to address transition care codes. Got Transition offers a coding and reimbursement tip sheet to aid doctors in billing for pediatric to adult transitions.
Dr. Greenlee said she hopes that more pediatricians will start using the tools developed by the initiative, and she recommends reviewing the Got Transition website (www.gottransition.org) and considering how to incorporate transition efforts into practices.
“Start with a policy,” she said. “Start thinking about your approach and then make that approach intentional. My advice ... is to just start with one step at a time.”
On Twitter @legal_med
Gregg Michael Talente, MD, remembers well a young patient who nearly fell through the gap between pediatric an adult health care.
The woman was treated for lupus by her pediatrician until age 19 when the doctor moved out of town. When she landed in front of Dr. Talente, it was clear the patient lacked the knowledge and skills to self-manage her condition, he recalled. Dr. Talente and his team, including pharmacists, helped the young woman understand how to administer her medications, provided refill reminders, and counseled her about reproductive health and how other medications could interact with lupus treatment.
“I look at her as a near-miss case,” said Dr. Talente, director of the internal medicine resident clinic at the University of South Carolina, Columbia, who specializes in pediatric-adolescent medicine. “A lot of bad things could have happened to her because her transition was delayed, and she wasn’t prepared. Fortunately, she landed in a place with more resources than a typical adult clinic so we were able to catch up.”
A new national initiative is designed to aid patients such as this during the move from pediatric to adult health care. The Pediatric to Adult Care Transitions Initiative is a collaborative effort by various specialty groups to facilitate more effective transition and transfer of young adults, while providing a framework for pediatricians and adult care providers. The project is under the direction of the American College of Physicians’ (ACP) Council of Subspecialty Societies in conjunction with the Got Transition (GT)/Center for Health Care Transition Improvement, the Society of General Internal Medicine (SGIM), and the Society for Adolescent Health and Medicine. Got Transition is a cooperative project by the Maternal and Child Health Bureau and The National Alliance to Advance Adolescent Health to improve pediatric-to-adult-care transitions through innovative strategies.
Since the Pediatric to Adult Care Transitions Initiative launched in spring 2015, project leaders have designed a series of disease-specific tools to enable smoother transition of patients. The downloadable tools include a transition readiness assessment, a medical summary/transfer record tool, and a self-care assessment. The guides were adapted from Got Transition’s six core elements of health care transition, developed from joint clinical recommendations by the ACP, the American Academy of Pediatrics, and the American Academy of Family Physicians.
The disease-specific tools are just the beginning, said Carol Greenlee, MD, chair of the Pediatric to Adult Care Transitions Initiative and chair of the ACP’s Council of Subspecialty Societies.
“We don’t want to just have tools on a website, we want to improve the whole process,” she said. “One of our goals is education and implementation. Part of implementation has to include collaboration because you don’t care-coordinate in isolation. You have to care-coordinate not just with the patient and family, but the pediatric and adult care providers need to collaborate.”
A need for better transition
Data show that knowledge and resources are lacking on both the pediatric and adult care side when it comes to transitioning patients from one realm to the other. A 2009 survey by the AAP found that most pediatric practices neither initiate transition planning early in adolescence nor offer transition-support service (AAP News 2009 Nov. Vol. 30). Another study in the Journal of General Internal Medicine found that many adult providers feel unprepared to care for young adults with complex chronic conditions and that in some cases, there is no identified adult primary care or specialty provider to whom care can be transitioned (J Gen Intern Med. 2008 Oct;23[10]:1621-7). Lack of time, inadequate payment, and poor training also have been cited as barriers to successful transition (Pediatrics. 2001 Jul 1. doi: 10.1542/peds.2011-0969).
Poor transitions often lead to negative health outcomes for young adults, said Dr. Patience White, codirector of Got Transition and professor of medicine and pediatrics at George Washington University, Washington. She has co-led the Pediatric to Adult Care Transitions Initiative.
“The quality of care goes down; many [patients] are lost from their care, and they don’t get the kind of care they need,” Dr. White said. “Therefore, they have poor outcomes, and then of course, the cost goes up because they are utilizing emergency rooms or tests are repeated. You’re looking at poor patient experience, poor quality, and increased cost.”
Enter the Pediatric to Adult Care Transitions Initiative. The project was designed with the busy practices of pediatricians and adult care providers in mind, said Dr. Talente, who is past chair of the SGIM Adults with Complex Conditions Originating in Childhood Task Force.
“Everyone is busy, and asking each individual practitioner to develop the systems they need to do this right is not really practical,” he said. “That’s where this project is really helpful, in the sense that it’s attempting to deliver tools and systems to providers that they can use and just adapt, without doing all the work themselves when they’re trying to run their busy practices.”
The initiative’s readiness assessment is a first step toward improving early transition planning, Dr. Greenlee said. The tool allows pediatricians to measure the knowledge and skill level of patients in the years leading to transition age, and enables doctors to fill any gaps before the transfer occurs.
The tool helps physicians gauge “what this young adult needs to know before they go out into the adult world and take on self-management,” she said. “Making sure they know how to fill a prescription, how to take their medications, know signs and symptoms of a crisis – that sort of thing.”
To enable better communication between providers, initiative leaders created the transfer summary, a hand-off outline that includes critical items the receiving clinician should know about the patients, such as information about their conditions, personal interests, or special needs. The third tool launched by the initiative – a self-management assessment – is a resource for adult care providers to measure the patients’ skills and knowledge once they begin adult care.
Overcoming obstacles to transition
The path to smoother patient transitions is not without bumps in the road. Adding time and new tools to physicians’ already heavy workloads can be challenging, Dr. Greenlee said.
“One of the biggest challenges is the time it takes on both sides,” she said. “Here we’re saying, ‘Here’s more to do.’ As a pediatrician, you’re gong to be preparing and educating [patients] in self-management and trying to get the parents engaged. There’s extra work.”
But helping pediatricians understand the bigger picture results – better outcomes, improved quality, lower health care costs – is key to acceptance, according to initiative leaders.
Strengthening communication between pediatric and adult practices also is critical to making the transition tools effective, added Dr. White. Pediatric practices cannot make successful transfers alone.
“The challenges are to find the partnerships that you need to start it, and the next big challenge is the buy-in,” she said. “You’ve got to get your leadership and senior physicians in a practice to agree that this is something they’re going to do. What’s frustrating for families is when different physicians use different modes of this whole process.”
Reimbursement for transition-related care is an ongoing climb, added Dr. Talente. In the past, physicians have struggled to receive payment for certain nonvisit time needed for transitions, he said.
However, Got Transition recently made headway toward improved payment, Dr. White said. Code 99420 now can be used to bill for transition readiness assessments conducted with youth and self-care assessments conducted with young adults. Got Transition and several physician specialty organizations also have developed a payment work group to address transition care codes. Got Transition offers a coding and reimbursement tip sheet to aid doctors in billing for pediatric to adult transitions.
Dr. Greenlee said she hopes that more pediatricians will start using the tools developed by the initiative, and she recommends reviewing the Got Transition website (www.gottransition.org) and considering how to incorporate transition efforts into practices.
“Start with a policy,” she said. “Start thinking about your approach and then make that approach intentional. My advice ... is to just start with one step at a time.”
On Twitter @legal_med
Gregg Michael Talente, MD, remembers well a young patient who nearly fell through the gap between pediatric an adult health care.
The woman was treated for lupus by her pediatrician until age 19 when the doctor moved out of town. When she landed in front of Dr. Talente, it was clear the patient lacked the knowledge and skills to self-manage her condition, he recalled. Dr. Talente and his team, including pharmacists, helped the young woman understand how to administer her medications, provided refill reminders, and counseled her about reproductive health and how other medications could interact with lupus treatment.
“I look at her as a near-miss case,” said Dr. Talente, director of the internal medicine resident clinic at the University of South Carolina, Columbia, who specializes in pediatric-adolescent medicine. “A lot of bad things could have happened to her because her transition was delayed, and she wasn’t prepared. Fortunately, she landed in a place with more resources than a typical adult clinic so we were able to catch up.”
A new national initiative is designed to aid patients such as this during the move from pediatric to adult health care. The Pediatric to Adult Care Transitions Initiative is a collaborative effort by various specialty groups to facilitate more effective transition and transfer of young adults, while providing a framework for pediatricians and adult care providers. The project is under the direction of the American College of Physicians’ (ACP) Council of Subspecialty Societies in conjunction with the Got Transition (GT)/Center for Health Care Transition Improvement, the Society of General Internal Medicine (SGIM), and the Society for Adolescent Health and Medicine. Got Transition is a cooperative project by the Maternal and Child Health Bureau and The National Alliance to Advance Adolescent Health to improve pediatric-to-adult-care transitions through innovative strategies.
Since the Pediatric to Adult Care Transitions Initiative launched in spring 2015, project leaders have designed a series of disease-specific tools to enable smoother transition of patients. The downloadable tools include a transition readiness assessment, a medical summary/transfer record tool, and a self-care assessment. The guides were adapted from Got Transition’s six core elements of health care transition, developed from joint clinical recommendations by the ACP, the American Academy of Pediatrics, and the American Academy of Family Physicians.
The disease-specific tools are just the beginning, said Carol Greenlee, MD, chair of the Pediatric to Adult Care Transitions Initiative and chair of the ACP’s Council of Subspecialty Societies.
“We don’t want to just have tools on a website, we want to improve the whole process,” she said. “One of our goals is education and implementation. Part of implementation has to include collaboration because you don’t care-coordinate in isolation. You have to care-coordinate not just with the patient and family, but the pediatric and adult care providers need to collaborate.”
A need for better transition
Data show that knowledge and resources are lacking on both the pediatric and adult care side when it comes to transitioning patients from one realm to the other. A 2009 survey by the AAP found that most pediatric practices neither initiate transition planning early in adolescence nor offer transition-support service (AAP News 2009 Nov. Vol. 30). Another study in the Journal of General Internal Medicine found that many adult providers feel unprepared to care for young adults with complex chronic conditions and that in some cases, there is no identified adult primary care or specialty provider to whom care can be transitioned (J Gen Intern Med. 2008 Oct;23[10]:1621-7). Lack of time, inadequate payment, and poor training also have been cited as barriers to successful transition (Pediatrics. 2001 Jul 1. doi: 10.1542/peds.2011-0969).
Poor transitions often lead to negative health outcomes for young adults, said Dr. Patience White, codirector of Got Transition and professor of medicine and pediatrics at George Washington University, Washington. She has co-led the Pediatric to Adult Care Transitions Initiative.
“The quality of care goes down; many [patients] are lost from their care, and they don’t get the kind of care they need,” Dr. White said. “Therefore, they have poor outcomes, and then of course, the cost goes up because they are utilizing emergency rooms or tests are repeated. You’re looking at poor patient experience, poor quality, and increased cost.”
Enter the Pediatric to Adult Care Transitions Initiative. The project was designed with the busy practices of pediatricians and adult care providers in mind, said Dr. Talente, who is past chair of the SGIM Adults with Complex Conditions Originating in Childhood Task Force.
“Everyone is busy, and asking each individual practitioner to develop the systems they need to do this right is not really practical,” he said. “That’s where this project is really helpful, in the sense that it’s attempting to deliver tools and systems to providers that they can use and just adapt, without doing all the work themselves when they’re trying to run their busy practices.”
The initiative’s readiness assessment is a first step toward improving early transition planning, Dr. Greenlee said. The tool allows pediatricians to measure the knowledge and skill level of patients in the years leading to transition age, and enables doctors to fill any gaps before the transfer occurs.
The tool helps physicians gauge “what this young adult needs to know before they go out into the adult world and take on self-management,” she said. “Making sure they know how to fill a prescription, how to take their medications, know signs and symptoms of a crisis – that sort of thing.”
To enable better communication between providers, initiative leaders created the transfer summary, a hand-off outline that includes critical items the receiving clinician should know about the patients, such as information about their conditions, personal interests, or special needs. The third tool launched by the initiative – a self-management assessment – is a resource for adult care providers to measure the patients’ skills and knowledge once they begin adult care.
Overcoming obstacles to transition
The path to smoother patient transitions is not without bumps in the road. Adding time and new tools to physicians’ already heavy workloads can be challenging, Dr. Greenlee said.
“One of the biggest challenges is the time it takes on both sides,” she said. “Here we’re saying, ‘Here’s more to do.’ As a pediatrician, you’re gong to be preparing and educating [patients] in self-management and trying to get the parents engaged. There’s extra work.”
But helping pediatricians understand the bigger picture results – better outcomes, improved quality, lower health care costs – is key to acceptance, according to initiative leaders.
Strengthening communication between pediatric and adult practices also is critical to making the transition tools effective, added Dr. White. Pediatric practices cannot make successful transfers alone.
“The challenges are to find the partnerships that you need to start it, and the next big challenge is the buy-in,” she said. “You’ve got to get your leadership and senior physicians in a practice to agree that this is something they’re going to do. What’s frustrating for families is when different physicians use different modes of this whole process.”
Reimbursement for transition-related care is an ongoing climb, added Dr. Talente. In the past, physicians have struggled to receive payment for certain nonvisit time needed for transitions, he said.
However, Got Transition recently made headway toward improved payment, Dr. White said. Code 99420 now can be used to bill for transition readiness assessments conducted with youth and self-care assessments conducted with young adults. Got Transition and several physician specialty organizations also have developed a payment work group to address transition care codes. Got Transition offers a coding and reimbursement tip sheet to aid doctors in billing for pediatric to adult transitions.
Dr. Greenlee said she hopes that more pediatricians will start using the tools developed by the initiative, and she recommends reviewing the Got Transition website (www.gottransition.org) and considering how to incorporate transition efforts into practices.
“Start with a policy,” she said. “Start thinking about your approach and then make that approach intentional. My advice ... is to just start with one step at a time.”
On Twitter @legal_med
Children’s environmental health: An updated resource
In 1996, 2 exposure incidents sparked a movement to better understand children’s environmental health. In both incidents, children were exposed to significant toxicants in unexpected ways. In one, the organophosphate insecticide methyl parathion was applied illegally in indoor settings.1 In another, elemental mercury residue was detected in apartments converted from a fluorescent bulb facility.2 These incidents, and others like them, alerted physicians and government agencies to the collective lack of training and experience in the field of pediatric environmental health.
To address the situation, the Agency for Toxic Substances and Disease Registry and the Environmental Protection Agency created the Pediatric Environmental Health Specialty Unit (PEHSU) program. The program, which is now jointly operated by the American College of Medical Toxicology and the American Academy of Pediatrics, maintains sites in 10 regions3 and seeks to enhance education and promote consultation and referral related to reproductive and children’s environmental health.
This past fall, PEHSU updated its Web site at www.pehsu.net, which provides information, training, and resources for health professionals and the general public. The Web site provides news, fact sheets, and online education regarding environment-related pediatric and reproductive health issues. It also provides a tool for finding a local expert in the PEHSU national network, should a family physician need to refer a patient for more extensive assistance.
We believe that family physicians will find the PEHSU program resources informative, educational, and relevant to their practice.
Carl R. Baum, MD, FAAP, FACMT, Medical Director
Dana Turner, MPH, CHES
Amanda Allen, MS
PEHSU Program
National Office—West
Phoenix, Ariz
References
1. Esteban E, Rubin C, Hill R, et al. Association between indoor residential contamination with methyl parathion and urinary para-nitrophenol. J Expo Anal Environ Epidemiol. 1996;6:375-387.
2. Centers for Disease Control and Prevention (CDC). Mercury exposure among residents of a building formerly used for industrial purposes—New Jersey, 1995. MMWR Morb Mortal Wkly Rep. 1996;45:422-424.
3. Wilborne-Davis P, Kirkland KH, Mulloy KB. A model for physician education and consultation in pediatric environmental health—the Pediatric Environmental Health Specialty Units (PEHSU) program. Pediatr Clin North Am. 2007;54:1-13.
In 1996, 2 exposure incidents sparked a movement to better understand children’s environmental health. In both incidents, children were exposed to significant toxicants in unexpected ways. In one, the organophosphate insecticide methyl parathion was applied illegally in indoor settings.1 In another, elemental mercury residue was detected in apartments converted from a fluorescent bulb facility.2 These incidents, and others like them, alerted physicians and government agencies to the collective lack of training and experience in the field of pediatric environmental health.
To address the situation, the Agency for Toxic Substances and Disease Registry and the Environmental Protection Agency created the Pediatric Environmental Health Specialty Unit (PEHSU) program. The program, which is now jointly operated by the American College of Medical Toxicology and the American Academy of Pediatrics, maintains sites in 10 regions3 and seeks to enhance education and promote consultation and referral related to reproductive and children’s environmental health.
This past fall, PEHSU updated its Web site at www.pehsu.net, which provides information, training, and resources for health professionals and the general public. The Web site provides news, fact sheets, and online education regarding environment-related pediatric and reproductive health issues. It also provides a tool for finding a local expert in the PEHSU national network, should a family physician need to refer a patient for more extensive assistance.
We believe that family physicians will find the PEHSU program resources informative, educational, and relevant to their practice.
Carl R. Baum, MD, FAAP, FACMT, Medical Director
Dana Turner, MPH, CHES
Amanda Allen, MS
PEHSU Program
National Office—West
Phoenix, Ariz
References
1. Esteban E, Rubin C, Hill R, et al. Association between indoor residential contamination with methyl parathion and urinary para-nitrophenol. J Expo Anal Environ Epidemiol. 1996;6:375-387.
2. Centers for Disease Control and Prevention (CDC). Mercury exposure among residents of a building formerly used for industrial purposes—New Jersey, 1995. MMWR Morb Mortal Wkly Rep. 1996;45:422-424.
3. Wilborne-Davis P, Kirkland KH, Mulloy KB. A model for physician education and consultation in pediatric environmental health—the Pediatric Environmental Health Specialty Units (PEHSU) program. Pediatr Clin North Am. 2007;54:1-13.
In 1996, 2 exposure incidents sparked a movement to better understand children’s environmental health. In both incidents, children were exposed to significant toxicants in unexpected ways. In one, the organophosphate insecticide methyl parathion was applied illegally in indoor settings.1 In another, elemental mercury residue was detected in apartments converted from a fluorescent bulb facility.2 These incidents, and others like them, alerted physicians and government agencies to the collective lack of training and experience in the field of pediatric environmental health.
To address the situation, the Agency for Toxic Substances and Disease Registry and the Environmental Protection Agency created the Pediatric Environmental Health Specialty Unit (PEHSU) program. The program, which is now jointly operated by the American College of Medical Toxicology and the American Academy of Pediatrics, maintains sites in 10 regions3 and seeks to enhance education and promote consultation and referral related to reproductive and children’s environmental health.
This past fall, PEHSU updated its Web site at www.pehsu.net, which provides information, training, and resources for health professionals and the general public. The Web site provides news, fact sheets, and online education regarding environment-related pediatric and reproductive health issues. It also provides a tool for finding a local expert in the PEHSU national network, should a family physician need to refer a patient for more extensive assistance.
We believe that family physicians will find the PEHSU program resources informative, educational, and relevant to their practice.
Carl R. Baum, MD, FAAP, FACMT, Medical Director
Dana Turner, MPH, CHES
Amanda Allen, MS
PEHSU Program
National Office—West
Phoenix, Ariz
References
1. Esteban E, Rubin C, Hill R, et al. Association between indoor residential contamination with methyl parathion and urinary para-nitrophenol. J Expo Anal Environ Epidemiol. 1996;6:375-387.
2. Centers for Disease Control and Prevention (CDC). Mercury exposure among residents of a building formerly used for industrial purposes—New Jersey, 1995. MMWR Morb Mortal Wkly Rep. 1996;45:422-424.
3. Wilborne-Davis P, Kirkland KH, Mulloy KB. A model for physician education and consultation in pediatric environmental health—the Pediatric Environmental Health Specialty Units (PEHSU) program. Pediatr Clin North Am. 2007;54:1-13.
Vesicular eruption in a 2-year-old boy
A 2-year-old boy with atopic dermatitis developed a flare of his eczema after having a bath with mint-scented soap. His mother treated the flare with over-the-counter topical hydrocortisone cream. Two to 3 days later, he developed grouped vesicles on the right side of his neck. Three days after that, he developed a painful generalized vesicular eruption all over his body.
The boy was admitted to a hospital for supportive care and empiric antibiotics, but was discharged when no bacterial infection was found. The patient’s mother was instructed to follow up with his primary care provider in the next 2 weeks.
Three days after his hospitalization, the eruption on the young boy’s body spread and he was uncomfortable. He was brought to our hospital’s pediatric clinic, where physicians examined him and decided to transfer him to the university hospital for further evaluation.
On exam, the boy was afebrile, but uncomfortable and irritable. Diffuse heme-crusted and punched-out erosions covered about 90% of his body (FIGURE). His mucous membranes were not involved. Underneath the heme-crusted erosions, there were lichenified pink plaques on the antecubital fossae, popliteal fossae, periocular face, and buttocks. The patient’s right dorsal foot had a small vesicle; all other vesicles on his body had crusted over.
The patient’s family indicated that the child had received the varicella vaccine without incident at 12 months of age. He had no history of travel, no contact with sick individuals, and no exposure to pets or other animals.

WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Eczema herpeticum
Eczema herpeticum (EH) was suspected based on the appearance of the lesions. A Tzanck smear came back positive for multinucleated giant cells and a herpes simplex virus (HSV) amplified probe came back positive for HSV-1—confirming the diagnosis.
EH—also known as Kaposi varicelliform eruption—is a superficial generalized viral infection (typically caused by HSV-1; HSV-2 is less common). The infection commonly occurs in patients with underlying atopic dermatitis, but may also occur in those with Darier disease, pemphigus, burns, and other conditions that disrupt the skin barrier. Other viruses, such as Coxsackie virus, can also cause EH. Eczema vaccinatum is a variant that may occur after smallpox vaccination.1 EH occurs more often in infants and children than in adults,2 and is a potentially life-threatening dermatologic emergency.
Who’s at risk? Patients with underlying chronic skin conditions such as eczema may have impaired cell-mediated immunity, making them more susceptible to a viral infection like EH.1 In addition, treatment of underlying chronic skin conditions with immunosuppressive therapies often increases susceptibility to superimposed infection.1 (In this case, the patient’s parents had treated an eczema flare with a topical hydrocortisone cream.) Lastly, increased risk may be associated with mutations in the gene encoding filaggrin.2
Areas affected. EH typically appears in areas of pre-existing dermatitis as monomorphic, discrete, 2- to 3-mm, punched-out, heme-crusted erosions with scalloped borders.2 The erosions initially appear as vesicles or pustules, which may appear concurrently with the erosions. The erosions can coalesce to form larger lesions.3 Fever, malaise, and lymphadenopathy may also be present.2,3
4 factors differentiate EH from other conditions
The differential for eczema herpeticum includes impetigo, bullous impetigo, shingles, chicken pox, scabies, pustular psoriasis, bullous pemphigoid, drug hypersensitivity reactions, and exacerbation of a primary dermatosis or skin condition.1,4
EH may be differentiated from these by its location, its development in the setting of pre-existing dermatitis, its response to antiviral medications, and the results of laboratory testing. Because of the vast differential, physicians must maintain a high index of suspicion for EH, particularly when a patient with a pre-existing skin condition presents with acute onset cutaneous pain.3
Perform a Tzanck smear to diagnose the underlying infection
If EH is suspected, treatment must be initiated immediately.3 (In our patient’s case, he was started on intravenous acyclovir 10 mg/kg every 8 hours.)
Once treatment is underway, a Tzanck smear of the vesicle base can be performed at the patient’s bedside to narrow the cause of the infection to HSV or varicella zoster virus (VZV). Multinucleated giant keratinocytes (as in our patient’s case) are diagnostic for one of the herpes viruses; concurrent inflammatory cells are also to be expected in an inflammatory skin condition but by themselves are not diagnostic of herpes.
If available in the laboratory, direct fluorescent antibody testing can differentiate between HSV and VZV. Alternatively, a nucleic acid amplified probe test may be used to provide a quick and specific result. The most specific test is a viral culture, but it lacks sensitivity and usually requires 2 to 5 daysfor results.2 A bacterial skin swab and blood culture should also be considered to direct antibiotic therapy if superinfection has occurred.
Antivirals and antibiotics should be given until lesions heal
Patients with EH should be admitted to the hospital for at least 24 to 48 hours of intravenous acyclovir.4 Antivirals—oral or intravenous—should be given for 10 to 14 days or until all mucocutaneous lesions are healed. Recommended dosing for acyclovir is 15 mg/kg (up to 400 mg) by mouth 3 to 5 times per day or, if severe, 5 mg/kg (if ≥12 years of age) to 10 mg/kg (if <12 years of age) intravenously every 8 hours.2 Patients should also receive a 3- to 6-month suppressive course of oral acyclovir, valacyclovir, or famciclovir.4
Intravenous antibiotics should also be considered, pending the results of bacterial skin swabs and a blood culture, as the skin of patients with atopic dermatitis is colonized with staphylococcus 90% of the time.4
Potential complications. Bacterial sepsis resulting from superinfection and disseminated HSV, although extremely rare, is the main cause of death associated with EH.3 One case in the literature described a 43-year-old woman with extensive EH superimposed on atopic dermatitis, disseminated HSV, and Pseudomonas aeruginosa septicemia. Despite treatment with intravenous acyclovir and antibiotics in a burn center intensive care unit, the patient experienced septic shock and disseminated intravascular coagulation with progression to multiorgan failure and death.3
Our patient’s antiviral regimen was transitioned to a 14-day course of oral acyclovir, which he completed. Topical steroids and an immunosuppressant (tacrolimus ointment) were applied concurrently. He was subsequently prescribed a 6-month suppressive course of acyclovir and was scheduled for follow-up at an outpatient dermatology clinic to discuss resuming therapy for atopic dermatitis.
CORRESPONDENCE
Sahand Rahnama-Moghadam, MD, 7323 Snowden Road #1205, San Antonio, TX 78240; rahnamamogha@uthscsa.edu.
1. Studdiford JS, Valko GP, Belin LJ, et al. Eczema herpeticum: making the diagnosis in the emergency department. J Emerg Med. 2011;40:167-169.
2. Mendoza N, Madkan V, Sra K, et al. Human herpesviruses. In: Bolognia JL, Jorizzo JL, Schaffer JV, et al, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Saunders; 2012:1321-1343.
3. Mackool BT, Goverman J, Nazarian RM. Case records of the Massachusetts General Hospital. Case 14-2012. A 43-year-old woman with fever and a generalized rash. N Engl J Med. 2012;366:1825-1834.
4. Kress DW. Pediatric dermatology emergencies. Curr Opin Pediatr. 2011;23:403-406.
A 2-year-old boy with atopic dermatitis developed a flare of his eczema after having a bath with mint-scented soap. His mother treated the flare with over-the-counter topical hydrocortisone cream. Two to 3 days later, he developed grouped vesicles on the right side of his neck. Three days after that, he developed a painful generalized vesicular eruption all over his body.
The boy was admitted to a hospital for supportive care and empiric antibiotics, but was discharged when no bacterial infection was found. The patient’s mother was instructed to follow up with his primary care provider in the next 2 weeks.
Three days after his hospitalization, the eruption on the young boy’s body spread and he was uncomfortable. He was brought to our hospital’s pediatric clinic, where physicians examined him and decided to transfer him to the university hospital for further evaluation.
On exam, the boy was afebrile, but uncomfortable and irritable. Diffuse heme-crusted and punched-out erosions covered about 90% of his body (FIGURE). His mucous membranes were not involved. Underneath the heme-crusted erosions, there were lichenified pink plaques on the antecubital fossae, popliteal fossae, periocular face, and buttocks. The patient’s right dorsal foot had a small vesicle; all other vesicles on his body had crusted over.
The patient’s family indicated that the child had received the varicella vaccine without incident at 12 months of age. He had no history of travel, no contact with sick individuals, and no exposure to pets or other animals.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Eczema herpeticum
Eczema herpeticum (EH) was suspected based on the appearance of the lesions. A Tzanck smear came back positive for multinucleated giant cells and a herpes simplex virus (HSV) amplified probe came back positive for HSV-1—confirming the diagnosis.
EH—also known as Kaposi varicelliform eruption—is a superficial generalized viral infection (typically caused by HSV-1; HSV-2 is less common). The infection commonly occurs in patients with underlying atopic dermatitis, but may also occur in those with Darier disease, pemphigus, burns, and other conditions that disrupt the skin barrier. Other viruses, such as Coxsackie virus, can also cause EH. Eczema vaccinatum is a variant that may occur after smallpox vaccination.1 EH occurs more often in infants and children than in adults,2 and is a potentially life-threatening dermatologic emergency.
Who’s at risk? Patients with underlying chronic skin conditions such as eczema may have impaired cell-mediated immunity, making them more susceptible to a viral infection like EH.1 In addition, treatment of underlying chronic skin conditions with immunosuppressive therapies often increases susceptibility to superimposed infection.1 (In this case, the patient’s parents had treated an eczema flare with a topical hydrocortisone cream.) Lastly, increased risk may be associated with mutations in the gene encoding filaggrin.2
Areas affected. EH typically appears in areas of pre-existing dermatitis as monomorphic, discrete, 2- to 3-mm, punched-out, heme-crusted erosions with scalloped borders.2 The erosions initially appear as vesicles or pustules, which may appear concurrently with the erosions. The erosions can coalesce to form larger lesions.3 Fever, malaise, and lymphadenopathy may also be present.2,3
4 factors differentiate EH from other conditions
The differential for eczema herpeticum includes impetigo, bullous impetigo, shingles, chicken pox, scabies, pustular psoriasis, bullous pemphigoid, drug hypersensitivity reactions, and exacerbation of a primary dermatosis or skin condition.1,4
EH may be differentiated from these by its location, its development in the setting of pre-existing dermatitis, its response to antiviral medications, and the results of laboratory testing. Because of the vast differential, physicians must maintain a high index of suspicion for EH, particularly when a patient with a pre-existing skin condition presents with acute onset cutaneous pain.3
Perform a Tzanck smear to diagnose the underlying infection
If EH is suspected, treatment must be initiated immediately.3 (In our patient’s case, he was started on intravenous acyclovir 10 mg/kg every 8 hours.)
Once treatment is underway, a Tzanck smear of the vesicle base can be performed at the patient’s bedside to narrow the cause of the infection to HSV or varicella zoster virus (VZV). Multinucleated giant keratinocytes (as in our patient’s case) are diagnostic for one of the herpes viruses; concurrent inflammatory cells are also to be expected in an inflammatory skin condition but by themselves are not diagnostic of herpes.
If available in the laboratory, direct fluorescent antibody testing can differentiate between HSV and VZV. Alternatively, a nucleic acid amplified probe test may be used to provide a quick and specific result. The most specific test is a viral culture, but it lacks sensitivity and usually requires 2 to 5 daysfor results.2 A bacterial skin swab and blood culture should also be considered to direct antibiotic therapy if superinfection has occurred.
Antivirals and antibiotics should be given until lesions heal
Patients with EH should be admitted to the hospital for at least 24 to 48 hours of intravenous acyclovir.4 Antivirals—oral or intravenous—should be given for 10 to 14 days or until all mucocutaneous lesions are healed. Recommended dosing for acyclovir is 15 mg/kg (up to 400 mg) by mouth 3 to 5 times per day or, if severe, 5 mg/kg (if ≥12 years of age) to 10 mg/kg (if <12 years of age) intravenously every 8 hours.2 Patients should also receive a 3- to 6-month suppressive course of oral acyclovir, valacyclovir, or famciclovir.4
Intravenous antibiotics should also be considered, pending the results of bacterial skin swabs and a blood culture, as the skin of patients with atopic dermatitis is colonized with staphylococcus 90% of the time.4
Potential complications. Bacterial sepsis resulting from superinfection and disseminated HSV, although extremely rare, is the main cause of death associated with EH.3 One case in the literature described a 43-year-old woman with extensive EH superimposed on atopic dermatitis, disseminated HSV, and Pseudomonas aeruginosa septicemia. Despite treatment with intravenous acyclovir and antibiotics in a burn center intensive care unit, the patient experienced septic shock and disseminated intravascular coagulation with progression to multiorgan failure and death.3
Our patient’s antiviral regimen was transitioned to a 14-day course of oral acyclovir, which he completed. Topical steroids and an immunosuppressant (tacrolimus ointment) were applied concurrently. He was subsequently prescribed a 6-month suppressive course of acyclovir and was scheduled for follow-up at an outpatient dermatology clinic to discuss resuming therapy for atopic dermatitis.
CORRESPONDENCE
Sahand Rahnama-Moghadam, MD, 7323 Snowden Road #1205, San Antonio, TX 78240; rahnamamogha@uthscsa.edu.
A 2-year-old boy with atopic dermatitis developed a flare of his eczema after having a bath with mint-scented soap. His mother treated the flare with over-the-counter topical hydrocortisone cream. Two to 3 days later, he developed grouped vesicles on the right side of his neck. Three days after that, he developed a painful generalized vesicular eruption all over his body.
The boy was admitted to a hospital for supportive care and empiric antibiotics, but was discharged when no bacterial infection was found. The patient’s mother was instructed to follow up with his primary care provider in the next 2 weeks.
Three days after his hospitalization, the eruption on the young boy’s body spread and he was uncomfortable. He was brought to our hospital’s pediatric clinic, where physicians examined him and decided to transfer him to the university hospital for further evaluation.
On exam, the boy was afebrile, but uncomfortable and irritable. Diffuse heme-crusted and punched-out erosions covered about 90% of his body (FIGURE). His mucous membranes were not involved. Underneath the heme-crusted erosions, there were lichenified pink plaques on the antecubital fossae, popliteal fossae, periocular face, and buttocks. The patient’s right dorsal foot had a small vesicle; all other vesicles on his body had crusted over.
The patient’s family indicated that the child had received the varicella vaccine without incident at 12 months of age. He had no history of travel, no contact with sick individuals, and no exposure to pets or other animals.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Eczema herpeticum
Eczema herpeticum (EH) was suspected based on the appearance of the lesions. A Tzanck smear came back positive for multinucleated giant cells and a herpes simplex virus (HSV) amplified probe came back positive for HSV-1—confirming the diagnosis.
EH—also known as Kaposi varicelliform eruption—is a superficial generalized viral infection (typically caused by HSV-1; HSV-2 is less common). The infection commonly occurs in patients with underlying atopic dermatitis, but may also occur in those with Darier disease, pemphigus, burns, and other conditions that disrupt the skin barrier. Other viruses, such as Coxsackie virus, can also cause EH. Eczema vaccinatum is a variant that may occur after smallpox vaccination.1 EH occurs more often in infants and children than in adults,2 and is a potentially life-threatening dermatologic emergency.
Who’s at risk? Patients with underlying chronic skin conditions such as eczema may have impaired cell-mediated immunity, making them more susceptible to a viral infection like EH.1 In addition, treatment of underlying chronic skin conditions with immunosuppressive therapies often increases susceptibility to superimposed infection.1 (In this case, the patient’s parents had treated an eczema flare with a topical hydrocortisone cream.) Lastly, increased risk may be associated with mutations in the gene encoding filaggrin.2
Areas affected. EH typically appears in areas of pre-existing dermatitis as monomorphic, discrete, 2- to 3-mm, punched-out, heme-crusted erosions with scalloped borders.2 The erosions initially appear as vesicles or pustules, which may appear concurrently with the erosions. The erosions can coalesce to form larger lesions.3 Fever, malaise, and lymphadenopathy may also be present.2,3
4 factors differentiate EH from other conditions
The differential for eczema herpeticum includes impetigo, bullous impetigo, shingles, chicken pox, scabies, pustular psoriasis, bullous pemphigoid, drug hypersensitivity reactions, and exacerbation of a primary dermatosis or skin condition.1,4
EH may be differentiated from these by its location, its development in the setting of pre-existing dermatitis, its response to antiviral medications, and the results of laboratory testing. Because of the vast differential, physicians must maintain a high index of suspicion for EH, particularly when a patient with a pre-existing skin condition presents with acute onset cutaneous pain.3
Perform a Tzanck smear to diagnose the underlying infection
If EH is suspected, treatment must be initiated immediately.3 (In our patient’s case, he was started on intravenous acyclovir 10 mg/kg every 8 hours.)
Once treatment is underway, a Tzanck smear of the vesicle base can be performed at the patient’s bedside to narrow the cause of the infection to HSV or varicella zoster virus (VZV). Multinucleated giant keratinocytes (as in our patient’s case) are diagnostic for one of the herpes viruses; concurrent inflammatory cells are also to be expected in an inflammatory skin condition but by themselves are not diagnostic of herpes.
If available in the laboratory, direct fluorescent antibody testing can differentiate between HSV and VZV. Alternatively, a nucleic acid amplified probe test may be used to provide a quick and specific result. The most specific test is a viral culture, but it lacks sensitivity and usually requires 2 to 5 daysfor results.2 A bacterial skin swab and blood culture should also be considered to direct antibiotic therapy if superinfection has occurred.
Antivirals and antibiotics should be given until lesions heal
Patients with EH should be admitted to the hospital for at least 24 to 48 hours of intravenous acyclovir.4 Antivirals—oral or intravenous—should be given for 10 to 14 days or until all mucocutaneous lesions are healed. Recommended dosing for acyclovir is 15 mg/kg (up to 400 mg) by mouth 3 to 5 times per day or, if severe, 5 mg/kg (if ≥12 years of age) to 10 mg/kg (if <12 years of age) intravenously every 8 hours.2 Patients should also receive a 3- to 6-month suppressive course of oral acyclovir, valacyclovir, or famciclovir.4
Intravenous antibiotics should also be considered, pending the results of bacterial skin swabs and a blood culture, as the skin of patients with atopic dermatitis is colonized with staphylococcus 90% of the time.4
Potential complications. Bacterial sepsis resulting from superinfection and disseminated HSV, although extremely rare, is the main cause of death associated with EH.3 One case in the literature described a 43-year-old woman with extensive EH superimposed on atopic dermatitis, disseminated HSV, and Pseudomonas aeruginosa septicemia. Despite treatment with intravenous acyclovir and antibiotics in a burn center intensive care unit, the patient experienced septic shock and disseminated intravascular coagulation with progression to multiorgan failure and death.3
Our patient’s antiviral regimen was transitioned to a 14-day course of oral acyclovir, which he completed. Topical steroids and an immunosuppressant (tacrolimus ointment) were applied concurrently. He was subsequently prescribed a 6-month suppressive course of acyclovir and was scheduled for follow-up at an outpatient dermatology clinic to discuss resuming therapy for atopic dermatitis.
CORRESPONDENCE
Sahand Rahnama-Moghadam, MD, 7323 Snowden Road #1205, San Antonio, TX 78240; rahnamamogha@uthscsa.edu.
1. Studdiford JS, Valko GP, Belin LJ, et al. Eczema herpeticum: making the diagnosis in the emergency department. J Emerg Med. 2011;40:167-169.
2. Mendoza N, Madkan V, Sra K, et al. Human herpesviruses. In: Bolognia JL, Jorizzo JL, Schaffer JV, et al, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Saunders; 2012:1321-1343.
3. Mackool BT, Goverman J, Nazarian RM. Case records of the Massachusetts General Hospital. Case 14-2012. A 43-year-old woman with fever and a generalized rash. N Engl J Med. 2012;366:1825-1834.
4. Kress DW. Pediatric dermatology emergencies. Curr Opin Pediatr. 2011;23:403-406.
1. Studdiford JS, Valko GP, Belin LJ, et al. Eczema herpeticum: making the diagnosis in the emergency department. J Emerg Med. 2011;40:167-169.
2. Mendoza N, Madkan V, Sra K, et al. Human herpesviruses. In: Bolognia JL, Jorizzo JL, Schaffer JV, et al, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Saunders; 2012:1321-1343.
3. Mackool BT, Goverman J, Nazarian RM. Case records of the Massachusetts General Hospital. Case 14-2012. A 43-year-old woman with fever and a generalized rash. N Engl J Med. 2012;366:1825-1834.
4. Kress DW. Pediatric dermatology emergencies. Curr Opin Pediatr. 2011;23:403-406.

Rash, microcephaly not always present with congenital Zika syndrome
The largest study so far of congenital Zika virus syndrome suggests that microcephaly and maternal rash are not sufficient to detect affected babies.
Writing in the June 29 online edition of The Lancet, researchers report on a case series of 1,501 liveborn infants with suspected congenital Zika virus syndrome reported in Brazil. The study found that one in five definite or probable cases of congenital Zika virus syndrome had a head circumference within the range of normal, and in one third of definite or probable cases, the mother had no history of a rash during pregnancy.

Of the total series, 899 were discarded because they showed no obvious clinical or neuropsychomotor abnormalities such as craniofacial disproportion or neurological symptoms (Lancet. 2016 Jun 29. doi: 10.1016/S0140-6736[16]30902-3).
Of the remaining 602 cases, 76 were described as definite cases of congenital Zika virus syndrome because of laboratory evidence of Zika virus infection during pregnancy.
Fifty-four babies were considered highly probable cases of congenital Zika virus syndrome because imaging reports showed features such as brain calcifications and ventricular enlargement suggestive of Zika virus infection and which could not be attributed to other pathogens such as syphilis, cytomegalovirus, or toxoplasmosis.
A further 181 were “moderately probable” – they had similar imaging results to the highly probable group but without test results for other infections – while the 291 somewhat probable cases had imaging results that suggested Zika virus was likely involved.
Among the 391 definitely or probable cases where full information was available, half had both microcephaly and a history of maternal rash, while 87% had at least one of these symptoms.
“There were only two significant differences between the four categories: diagnostic certainty was positively associated with reported rashes and with smaller head circumferences before taking gestational age into account,” wrote Giovanny V. A. França, PhD, of the Secretariat of Health Surveillance, Ministry of Health, Brazil, and coauthors.
Researchers also noted that the discarded cases had larger head circumferences, lower first week mortality, and the mothers were less likely to have a history of rash during pregnancy (20.7% vs 61.4%, 95% confidence interval, 0.27-0.42).
Meanwhile, a second case series in the same edition of The Lancet reported on the pathology of five cases of congenital Zika syndrome, providing further evidence of the link between the virus and congenital abnormalities.
Tissue samples from three fatal cases of the syndrome and two spontaneous abortions found antigens to the Zika virus in the cytoplasm of degenerating and necrotic neurons and glial cells, but no immunohistochemical staining for Zika virus was found outside the central nervous system (Lancet. 2016 Jun 29. doi: 10.1016/S0140-6736[16]30883-2).
The five cases all showed signs of brain abnormalities including microcephaly, lissencephaly, cerebellar hypoplasia, and ventriculomegaly, while histopathological studies in the three fatal cases revealed microcalcifications, scattered microglial nodules, cell degeneration, and necrosis.
“The absence of a substantial inflammatory response in the brain and a specific cytopathic viral effect distinguishes Zika virus infection from other important viral infections that are also associated with microcephaly and microcalcifications, such as cytomegalovirus and herpes simplex virus,” wrote Roosecelis Brasil Martines, MD, of the National Center for Emerging and Zoonotic Infectious Diseases, CDC, and coauthors.
There was also a range of other congenital malformations evident in the three fatal cases, including multiple congenital contractures, craniofacial malformations, craniosynostosis, pulmonary hypoplasia, and a wide range of brain abnormalities.
“The mechanism for these deformities in Zika virus infection are not entirely clear, but most probably result from neurotropism of the virus with subsequent damage of the brain and interference in neuromuscular signaling leading to fetal akinesia,” the authors said.
No conflicts of interest were declared for either study.
This study is an important contribution for improving the surveillance system for congenital Zika virus infection but caution should be taken in interpreting results of this case series based on routinely collected data with missing information for many cases and an unknown degree of under-reporting.
For incorporating new information besides microcephaly and rash during pregnancy to detect all affected cases, neurological signs and symptoms could be eligible, but might be difficult to obtain in most settings because of insufficient specialized personnel. The development of an accurate serological test that could be incorporated into routine prenatal care will be essential, and its validation a research priority.
While the current outbreak is a paradigmatic example of how quickly evolving systematic scientific evidence can (and should) change the view on a disease within months, it can be expected that public health authorities, and also the scientific community, will struggle for many years with Zika epidemics and its consequences in Brazil and elsewhere.
Jörg Heukelbach, MD, is from the School of Medicine at the Federal University of Ceará in Brazil, and Guilherme Loureiro Werneck, MD, is from the Social Medicine Institute at the State University of Rio de Janeiro. The comments are excerpted from an accompanying editorial (Lancet. 2016 Jun 29. doi: 10.1016/S0140-6736(16)30931-X). No conflicts of interest were declared.
This study is an important contribution for improving the surveillance system for congenital Zika virus infection but caution should be taken in interpreting results of this case series based on routinely collected data with missing information for many cases and an unknown degree of under-reporting.
For incorporating new information besides microcephaly and rash during pregnancy to detect all affected cases, neurological signs and symptoms could be eligible, but might be difficult to obtain in most settings because of insufficient specialized personnel. The development of an accurate serological test that could be incorporated into routine prenatal care will be essential, and its validation a research priority.
While the current outbreak is a paradigmatic example of how quickly evolving systematic scientific evidence can (and should) change the view on a disease within months, it can be expected that public health authorities, and also the scientific community, will struggle for many years with Zika epidemics and its consequences in Brazil and elsewhere.
Jörg Heukelbach, MD, is from the School of Medicine at the Federal University of Ceará in Brazil, and Guilherme Loureiro Werneck, MD, is from the Social Medicine Institute at the State University of Rio de Janeiro. The comments are excerpted from an accompanying editorial (Lancet. 2016 Jun 29. doi: 10.1016/S0140-6736(16)30931-X). No conflicts of interest were declared.
This study is an important contribution for improving the surveillance system for congenital Zika virus infection but caution should be taken in interpreting results of this case series based on routinely collected data with missing information for many cases and an unknown degree of under-reporting.
For incorporating new information besides microcephaly and rash during pregnancy to detect all affected cases, neurological signs and symptoms could be eligible, but might be difficult to obtain in most settings because of insufficient specialized personnel. The development of an accurate serological test that could be incorporated into routine prenatal care will be essential, and its validation a research priority.
While the current outbreak is a paradigmatic example of how quickly evolving systematic scientific evidence can (and should) change the view on a disease within months, it can be expected that public health authorities, and also the scientific community, will struggle for many years with Zika epidemics and its consequences in Brazil and elsewhere.
Jörg Heukelbach, MD, is from the School of Medicine at the Federal University of Ceará in Brazil, and Guilherme Loureiro Werneck, MD, is from the Social Medicine Institute at the State University of Rio de Janeiro. The comments are excerpted from an accompanying editorial (Lancet. 2016 Jun 29. doi: 10.1016/S0140-6736(16)30931-X). No conflicts of interest were declared.
The largest study so far of congenital Zika virus syndrome suggests that microcephaly and maternal rash are not sufficient to detect affected babies.
Writing in the June 29 online edition of The Lancet, researchers report on a case series of 1,501 liveborn infants with suspected congenital Zika virus syndrome reported in Brazil. The study found that one in five definite or probable cases of congenital Zika virus syndrome had a head circumference within the range of normal, and in one third of definite or probable cases, the mother had no history of a rash during pregnancy.
Of the total series, 899 were discarded because they showed no obvious clinical or neuropsychomotor abnormalities such as craniofacial disproportion or neurological symptoms (Lancet. 2016 Jun 29. doi: 10.1016/S0140-6736[16]30902-3).
Of the remaining 602 cases, 76 were described as definite cases of congenital Zika virus syndrome because of laboratory evidence of Zika virus infection during pregnancy.
Fifty-four babies were considered highly probable cases of congenital Zika virus syndrome because imaging reports showed features such as brain calcifications and ventricular enlargement suggestive of Zika virus infection and which could not be attributed to other pathogens such as syphilis, cytomegalovirus, or toxoplasmosis.
A further 181 were “moderately probable” – they had similar imaging results to the highly probable group but without test results for other infections – while the 291 somewhat probable cases had imaging results that suggested Zika virus was likely involved.
Among the 391 definitely or probable cases where full information was available, half had both microcephaly and a history of maternal rash, while 87% had at least one of these symptoms.
“There were only two significant differences between the four categories: diagnostic certainty was positively associated with reported rashes and with smaller head circumferences before taking gestational age into account,” wrote Giovanny V. A. França, PhD, of the Secretariat of Health Surveillance, Ministry of Health, Brazil, and coauthors.
Researchers also noted that the discarded cases had larger head circumferences, lower first week mortality, and the mothers were less likely to have a history of rash during pregnancy (20.7% vs 61.4%, 95% confidence interval, 0.27-0.42).
Meanwhile, a second case series in the same edition of The Lancet reported on the pathology of five cases of congenital Zika syndrome, providing further evidence of the link between the virus and congenital abnormalities.
Tissue samples from three fatal cases of the syndrome and two spontaneous abortions found antigens to the Zika virus in the cytoplasm of degenerating and necrotic neurons and glial cells, but no immunohistochemical staining for Zika virus was found outside the central nervous system (Lancet. 2016 Jun 29. doi: 10.1016/S0140-6736[16]30883-2).
The five cases all showed signs of brain abnormalities including microcephaly, lissencephaly, cerebellar hypoplasia, and ventriculomegaly, while histopathological studies in the three fatal cases revealed microcalcifications, scattered microglial nodules, cell degeneration, and necrosis.
“The absence of a substantial inflammatory response in the brain and a specific cytopathic viral effect distinguishes Zika virus infection from other important viral infections that are also associated with microcephaly and microcalcifications, such as cytomegalovirus and herpes simplex virus,” wrote Roosecelis Brasil Martines, MD, of the National Center for Emerging and Zoonotic Infectious Diseases, CDC, and coauthors.
There was also a range of other congenital malformations evident in the three fatal cases, including multiple congenital contractures, craniofacial malformations, craniosynostosis, pulmonary hypoplasia, and a wide range of brain abnormalities.
“The mechanism for these deformities in Zika virus infection are not entirely clear, but most probably result from neurotropism of the virus with subsequent damage of the brain and interference in neuromuscular signaling leading to fetal akinesia,” the authors said.
No conflicts of interest were declared for either study.
The largest study so far of congenital Zika virus syndrome suggests that microcephaly and maternal rash are not sufficient to detect affected babies.
Writing in the June 29 online edition of The Lancet, researchers report on a case series of 1,501 liveborn infants with suspected congenital Zika virus syndrome reported in Brazil. The study found that one in five definite or probable cases of congenital Zika virus syndrome had a head circumference within the range of normal, and in one third of definite or probable cases, the mother had no history of a rash during pregnancy.
Of the total series, 899 were discarded because they showed no obvious clinical or neuropsychomotor abnormalities such as craniofacial disproportion or neurological symptoms (Lancet. 2016 Jun 29. doi: 10.1016/S0140-6736[16]30902-3).
Of the remaining 602 cases, 76 were described as definite cases of congenital Zika virus syndrome because of laboratory evidence of Zika virus infection during pregnancy.
Fifty-four babies were considered highly probable cases of congenital Zika virus syndrome because imaging reports showed features such as brain calcifications and ventricular enlargement suggestive of Zika virus infection and which could not be attributed to other pathogens such as syphilis, cytomegalovirus, or toxoplasmosis.
A further 181 were “moderately probable” – they had similar imaging results to the highly probable group but without test results for other infections – while the 291 somewhat probable cases had imaging results that suggested Zika virus was likely involved.
Among the 391 definitely or probable cases where full information was available, half had both microcephaly and a history of maternal rash, while 87% had at least one of these symptoms.
“There were only two significant differences between the four categories: diagnostic certainty was positively associated with reported rashes and with smaller head circumferences before taking gestational age into account,” wrote Giovanny V. A. França, PhD, of the Secretariat of Health Surveillance, Ministry of Health, Brazil, and coauthors.
Researchers also noted that the discarded cases had larger head circumferences, lower first week mortality, and the mothers were less likely to have a history of rash during pregnancy (20.7% vs 61.4%, 95% confidence interval, 0.27-0.42).
Meanwhile, a second case series in the same edition of The Lancet reported on the pathology of five cases of congenital Zika syndrome, providing further evidence of the link between the virus and congenital abnormalities.
Tissue samples from three fatal cases of the syndrome and two spontaneous abortions found antigens to the Zika virus in the cytoplasm of degenerating and necrotic neurons and glial cells, but no immunohistochemical staining for Zika virus was found outside the central nervous system (Lancet. 2016 Jun 29. doi: 10.1016/S0140-6736[16]30883-2).
The five cases all showed signs of brain abnormalities including microcephaly, lissencephaly, cerebellar hypoplasia, and ventriculomegaly, while histopathological studies in the three fatal cases revealed microcalcifications, scattered microglial nodules, cell degeneration, and necrosis.
“The absence of a substantial inflammatory response in the brain and a specific cytopathic viral effect distinguishes Zika virus infection from other important viral infections that are also associated with microcephaly and microcalcifications, such as cytomegalovirus and herpes simplex virus,” wrote Roosecelis Brasil Martines, MD, of the National Center for Emerging and Zoonotic Infectious Diseases, CDC, and coauthors.
There was also a range of other congenital malformations evident in the three fatal cases, including multiple congenital contractures, craniofacial malformations, craniosynostosis, pulmonary hypoplasia, and a wide range of brain abnormalities.
“The mechanism for these deformities in Zika virus infection are not entirely clear, but most probably result from neurotropism of the virus with subsequent damage of the brain and interference in neuromuscular signaling leading to fetal akinesia,” the authors said.
No conflicts of interest were declared for either study.
FROM THE LANCET
Key clinical point: Microcephaly and maternal rash alone are not sufficient to detect babies affected by congenital Zika virus syndrome.
Major finding: One in five definite or probable cases of congenital Zika virus syndrome had a head circumference within the range of normal, and in one third of definite or probable cases, the mother had no history of a rash during pregnancy.
Data source: Case series of 1,501 liveborn infants with suspected congenital Zika virus syndrome.
Disclosures: No conflicts of interest were declared.

Bacterial colonizer vs. pathogen
Although acute otitis media (AOM) has decreased in number, and especially the more severe difficult to treat versions, I was reminded that this still is a problem for young children based on personal experience with grandchildren. What can be baffling to some families is the fact that some strains of the same organism species cause AOM and some simply colonize the nasopharynx (NP) of children without causing any disease at all. These organisms include Streptococcus pneumoniae (SPN) and nontypeable Haemophilus influenzae (ntHi).
Recent studies have uncovered several molecular reasons for the pathogen vs. colonizer dichotomy:
• Strains within a species can have variants of a gene that make them more disease producing.
• Some usually colonizing strains produce disease after acquiring new genes.
• Some strains have native genes with on-off switches that convert them from a colonizing to disease producing under selected circumstances.
• Molecular targets in the respiratory tract increase, allowing more dense colonization that increases chances of AOM.
Variant gene
J.R. Gilsdorf, MD, and his group at the University of Michigan,1 Ann Arbor, recently showed that among the various high-molecular-weight molecules (HMW) produced by 170 ntHi from three different geographically diverse countries, one variant in particular (HMW-A) was more likely to be found in strains producing AOM than strains simply colonizing the nasopharynx. The protein product of this gene allows better adherence to respiratory epithelia. So more bacteria sticking in the NP near the eustachian tube opening make development of AOM more likely. Some call this the “more barbarians at the gate” phenomenon.

Gene acquisition
SPN inherently has a somewhat incomplete arginine synthesis pathway. Because arginine is essential for growth of SPN, S. pneumoniae utilizes some host factors to compensate; but this compensation is inefficient. However, SPN strains can acquire new genes – usually from other gram-positive organisms in their environment – by a process called conjugation.
One recently reported acquired gene set is that which completes functionality of SPN’s arginine synthesis pathway.2 Investigators showed that SPN that acquire these arginine synthesis genes replicate more readily in bodily fluids, such as serum or cerebrospinal fluid, making these strains more aggressive, more virulent, and more likely to produce disease. More efficient replication makes it very difficult for host immune responses to handle these SPN. This is not limited to AOM alone, but seems important in invasive disease (such as meningitis) from SPN type 7, which had recently become more frequent after introduction of pneumococcal conjugate vaccines.
On-off gene switches
Another group of investigators reported that a thing called “phasevarion,” which is fancy lingo for an on-off switch is at the root of more virulence in ntHi.3 It seems that some strains of ntHi have a version of the ModA2 gene, which is always turned off, while other strains have a gene that is always on. Then, there is a third version in which the gene is usually off, but turns on when in places like the middle ear. The ModA2 gene appears to affect several other downstream protein groups that include HMW-A, antibiotic susceptibility, and biofilm formation. When inoculated into the middle ear in a chinchilla AOM model, the ntHi strains that can turn on their ModA2 gene were much more likely to produce AOM than either version that could not change. Interestingly, the authors postulate that preventing the switch capability could be a novel way to prevent ntHi disease, such as pediatric AOM, acute bacterial sinusitis, or some bronchitis in adults.
Molecular environment becomes more favorable
Another group4 reported that adherence receptor for ntHi is intercellular adhesion molecule 1 (ICAM1), a molecule found in modest quantities on respiratory epithelium. You may know it as the attachment molecule for rhinovirus and enteroviruses. What makes this interesting is that adenovirus, respiratory syncytial virus, and exposure to cigarette smoke5 markedly increase expression of ICAM1 on respiratory epithelium, predisposing to more ntHi adhering and more likely to produce an inflammatory process, such as AOM. This is another version of the barbarians at the gate phenomenon.
So when families ask why SPN or ntHi sometimes exist quietly (colonize) the nasopharynx and sometimes they cause AOM or acute bacterial sinusitis, you can hopefully use these four examples as partial explanations of why the same bacterial species has strains that can be either colonizers or pathogens.
References
1. Infect Genet Evol. 2014 Dec;28:223-32
2. J Infect Dis. 2014 Jun 1;209:1781-91.
3. J Infect Dis. 2016 Jun 10. pii: jiw243. [Epub ahead of print]
4. Cell Microbiol. 2016 Feb 9. doi: 10.1111/cmi.12575. [Epub ahead of print]
5. Am J Respir Cell Mol Biol. 2003 Oct;29:472-82.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Mo. He said he had no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.
Although acute otitis media (AOM) has decreased in number, and especially the more severe difficult to treat versions, I was reminded that this still is a problem for young children based on personal experience with grandchildren. What can be baffling to some families is the fact that some strains of the same organism species cause AOM and some simply colonize the nasopharynx (NP) of children without causing any disease at all. These organisms include Streptococcus pneumoniae (SPN) and nontypeable Haemophilus influenzae (ntHi).
Recent studies have uncovered several molecular reasons for the pathogen vs. colonizer dichotomy:
• Strains within a species can have variants of a gene that make them more disease producing.
• Some usually colonizing strains produce disease after acquiring new genes.
• Some strains have native genes with on-off switches that convert them from a colonizing to disease producing under selected circumstances.
• Molecular targets in the respiratory tract increase, allowing more dense colonization that increases chances of AOM.
Variant gene
J.R. Gilsdorf, MD, and his group at the University of Michigan,1 Ann Arbor, recently showed that among the various high-molecular-weight molecules (HMW) produced by 170 ntHi from three different geographically diverse countries, one variant in particular (HMW-A) was more likely to be found in strains producing AOM than strains simply colonizing the nasopharynx. The protein product of this gene allows better adherence to respiratory epithelia. So more bacteria sticking in the NP near the eustachian tube opening make development of AOM more likely. Some call this the “more barbarians at the gate” phenomenon.
Gene acquisition
SPN inherently has a somewhat incomplete arginine synthesis pathway. Because arginine is essential for growth of SPN, S. pneumoniae utilizes some host factors to compensate; but this compensation is inefficient. However, SPN strains can acquire new genes – usually from other gram-positive organisms in their environment – by a process called conjugation.
One recently reported acquired gene set is that which completes functionality of SPN’s arginine synthesis pathway.2 Investigators showed that SPN that acquire these arginine synthesis genes replicate more readily in bodily fluids, such as serum or cerebrospinal fluid, making these strains more aggressive, more virulent, and more likely to produce disease. More efficient replication makes it very difficult for host immune responses to handle these SPN. This is not limited to AOM alone, but seems important in invasive disease (such as meningitis) from SPN type 7, which had recently become more frequent after introduction of pneumococcal conjugate vaccines.
On-off gene switches
Another group of investigators reported that a thing called “phasevarion,” which is fancy lingo for an on-off switch is at the root of more virulence in ntHi.3 It seems that some strains of ntHi have a version of the ModA2 gene, which is always turned off, while other strains have a gene that is always on. Then, there is a third version in which the gene is usually off, but turns on when in places like the middle ear. The ModA2 gene appears to affect several other downstream protein groups that include HMW-A, antibiotic susceptibility, and biofilm formation. When inoculated into the middle ear in a chinchilla AOM model, the ntHi strains that can turn on their ModA2 gene were much more likely to produce AOM than either version that could not change. Interestingly, the authors postulate that preventing the switch capability could be a novel way to prevent ntHi disease, such as pediatric AOM, acute bacterial sinusitis, or some bronchitis in adults.
Molecular environment becomes more favorable
Another group4 reported that adherence receptor for ntHi is intercellular adhesion molecule 1 (ICAM1), a molecule found in modest quantities on respiratory epithelium. You may know it as the attachment molecule for rhinovirus and enteroviruses. What makes this interesting is that adenovirus, respiratory syncytial virus, and exposure to cigarette smoke5 markedly increase expression of ICAM1 on respiratory epithelium, predisposing to more ntHi adhering and more likely to produce an inflammatory process, such as AOM. This is another version of the barbarians at the gate phenomenon.
So when families ask why SPN or ntHi sometimes exist quietly (colonize) the nasopharynx and sometimes they cause AOM or acute bacterial sinusitis, you can hopefully use these four examples as partial explanations of why the same bacterial species has strains that can be either colonizers or pathogens.
References
1. Infect Genet Evol. 2014 Dec;28:223-32
2. J Infect Dis. 2014 Jun 1;209:1781-91.
3. J Infect Dis. 2016 Jun 10. pii: jiw243. [Epub ahead of print]
4. Cell Microbiol. 2016 Feb 9. doi: 10.1111/cmi.12575. [Epub ahead of print]
5. Am J Respir Cell Mol Biol. 2003 Oct;29:472-82.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Mo. He said he had no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.
Although acute otitis media (AOM) has decreased in number, and especially the more severe difficult to treat versions, I was reminded that this still is a problem for young children based on personal experience with grandchildren. What can be baffling to some families is the fact that some strains of the same organism species cause AOM and some simply colonize the nasopharynx (NP) of children without causing any disease at all. These organisms include Streptococcus pneumoniae (SPN) and nontypeable Haemophilus influenzae (ntHi).
Recent studies have uncovered several molecular reasons for the pathogen vs. colonizer dichotomy:
• Strains within a species can have variants of a gene that make them more disease producing.
• Some usually colonizing strains produce disease after acquiring new genes.
• Some strains have native genes with on-off switches that convert them from a colonizing to disease producing under selected circumstances.
• Molecular targets in the respiratory tract increase, allowing more dense colonization that increases chances of AOM.
Variant gene
J.R. Gilsdorf, MD, and his group at the University of Michigan,1 Ann Arbor, recently showed that among the various high-molecular-weight molecules (HMW) produced by 170 ntHi from three different geographically diverse countries, one variant in particular (HMW-A) was more likely to be found in strains producing AOM than strains simply colonizing the nasopharynx. The protein product of this gene allows better adherence to respiratory epithelia. So more bacteria sticking in the NP near the eustachian tube opening make development of AOM more likely. Some call this the “more barbarians at the gate” phenomenon.
Gene acquisition
SPN inherently has a somewhat incomplete arginine synthesis pathway. Because arginine is essential for growth of SPN, S. pneumoniae utilizes some host factors to compensate; but this compensation is inefficient. However, SPN strains can acquire new genes – usually from other gram-positive organisms in their environment – by a process called conjugation.
One recently reported acquired gene set is that which completes functionality of SPN’s arginine synthesis pathway.2 Investigators showed that SPN that acquire these arginine synthesis genes replicate more readily in bodily fluids, such as serum or cerebrospinal fluid, making these strains more aggressive, more virulent, and more likely to produce disease. More efficient replication makes it very difficult for host immune responses to handle these SPN. This is not limited to AOM alone, but seems important in invasive disease (such as meningitis) from SPN type 7, which had recently become more frequent after introduction of pneumococcal conjugate vaccines.
On-off gene switches
Another group of investigators reported that a thing called “phasevarion,” which is fancy lingo for an on-off switch is at the root of more virulence in ntHi.3 It seems that some strains of ntHi have a version of the ModA2 gene, which is always turned off, while other strains have a gene that is always on. Then, there is a third version in which the gene is usually off, but turns on when in places like the middle ear. The ModA2 gene appears to affect several other downstream protein groups that include HMW-A, antibiotic susceptibility, and biofilm formation. When inoculated into the middle ear in a chinchilla AOM model, the ntHi strains that can turn on their ModA2 gene were much more likely to produce AOM than either version that could not change. Interestingly, the authors postulate that preventing the switch capability could be a novel way to prevent ntHi disease, such as pediatric AOM, acute bacterial sinusitis, or some bronchitis in adults.
Molecular environment becomes more favorable
Another group4 reported that adherence receptor for ntHi is intercellular adhesion molecule 1 (ICAM1), a molecule found in modest quantities on respiratory epithelium. You may know it as the attachment molecule for rhinovirus and enteroviruses. What makes this interesting is that adenovirus, respiratory syncytial virus, and exposure to cigarette smoke5 markedly increase expression of ICAM1 on respiratory epithelium, predisposing to more ntHi adhering and more likely to produce an inflammatory process, such as AOM. This is another version of the barbarians at the gate phenomenon.
So when families ask why SPN or ntHi sometimes exist quietly (colonize) the nasopharynx and sometimes they cause AOM or acute bacterial sinusitis, you can hopefully use these four examples as partial explanations of why the same bacterial species has strains that can be either colonizers or pathogens.
References
1. Infect Genet Evol. 2014 Dec;28:223-32
2. J Infect Dis. 2014 Jun 1;209:1781-91.
3. J Infect Dis. 2016 Jun 10. pii: jiw243. [Epub ahead of print]
4. Cell Microbiol. 2016 Feb 9. doi: 10.1111/cmi.12575. [Epub ahead of print]
5. Am J Respir Cell Mol Biol. 2003 Oct;29:472-82.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Mo. He said he had no relevant financial disclosures. Email him at pdnews@frontlinemedcom.com.

Restless Sleep in 11-year-olds Predicts Earlier Substance Use
DENVER – Poor sleep quality and shorter sleep duration in boys at age 11 years is associated with subsequent accelerated use and misuse of alcohol and cannabis during adolescence and emerging adulthood, Thomas B. Mike reported at the annual meeting of the Associated Professional Sleep Societies.
This association has been reported before in cross-sectional studies. But Mr. Mike presented new findings from the longitudinal prospective Pitt Mother and Child Project.

The study comprised 170 boys aged 11 years whose mothers filled out the Child Sleep Questionnaire, modified for pediatric use from the well known Pittsburgh Sleep Quality Index. At that time, the boys also were assessed for internalizing and externalizing behaviors, neighborhood dangerousness, and socioeconomic status – all of which are factors known to influence teen substance use.
When participants reached ages 20 and 22 years, they underwent detailed interviews including assessment via the validated Lifetime Drinking History and Lifetime Drug History questionnaires.
In a multivariate Cox regression analysis controlling for a history of child internalizing and externalizing problem behavior as well as socioeconomic factors, every hour of sleep duration less than 9.5 hours at age 11 years was associated with a 21% acceleration in the time to first use of alcohol and a 22% acceleration in first use of cannabis, reported Mr. Mike, a medical student at the University of Pittsburgh.
Moreover, every 1 point worse score for sleep quality on the Child Sleep Questionnaire, scored from 0 (best) to 21 (worst), was associated with a 9% acceleration in time to alcohol use and an 8% acceleration to cannabis use.
Subjects with poor sleep duration and quality as 11-year-olds by parental report also experienced intoxication at a younger age than did those who had been better sleepers at that age. And they reported more frequent use of alcohol and cannabis during adolescence.
In an interview, Mr. Mike, who is planning a career in pediatrics, said the study findings contain an important message for pediatricians and family physicians when they meet with the parents of young boys entering adolescence.
“Probably the biggest take-home message is, ‘sleep more, sleep better.’ We don’t have a lot of ways to intervene right now for kids who have poor sleep, but we know based on this and other studies that kids who don’t sleep enough are more likely to use drugs and more likely to engage in other risky behaviors. So any way the parents can intervene will help, perhaps by getting them to bed earlier or trying to get them on a more regular schedule. At a social policy level, having school start later would probably be the most effective measure, but that probably won’t happen for a very long time,” he said.
“The vast majority of people who end up addicted to drugs later in life started when they were kids, so any way we can reduce adolescent substance use should have a downstream effect, including a decreased total substance use burden,” Mr. Mike added.
Possible mechanisms for the observed longitudinal association between poor quality and duration of sleep at age 11 years and earlier and heavier use of alcohol and cannabis later in adolescence include attempted self-medication for sleep problems, reward regulation, and alterations in brain chemistry, making the boys more susceptible to using drugs later in life, perhaps because they obtain a bigger high than their peers do. The investigators plan to delve deeper into the role of self-regulation and mental health as possible mechanisms linking childhood sleep and later substance use, he said.
The Pitt Mother and Child Project is supported by the National Institutes of Health. Mr. Mike reported having no financial conflicts.
DENVER – Poor sleep quality and shorter sleep duration in boys at age 11 years is associated with subsequent accelerated use and misuse of alcohol and cannabis during adolescence and emerging adulthood, Thomas B. Mike reported at the annual meeting of the Associated Professional Sleep Societies.
This association has been reported before in cross-sectional studies. But Mr. Mike presented new findings from the longitudinal prospective Pitt Mother and Child Project.
The study comprised 170 boys aged 11 years whose mothers filled out the Child Sleep Questionnaire, modified for pediatric use from the well known Pittsburgh Sleep Quality Index. At that time, the boys also were assessed for internalizing and externalizing behaviors, neighborhood dangerousness, and socioeconomic status – all of which are factors known to influence teen substance use.
When participants reached ages 20 and 22 years, they underwent detailed interviews including assessment via the validated Lifetime Drinking History and Lifetime Drug History questionnaires.
In a multivariate Cox regression analysis controlling for a history of child internalizing and externalizing problem behavior as well as socioeconomic factors, every hour of sleep duration less than 9.5 hours at age 11 years was associated with a 21% acceleration in the time to first use of alcohol and a 22% acceleration in first use of cannabis, reported Mr. Mike, a medical student at the University of Pittsburgh.
Moreover, every 1 point worse score for sleep quality on the Child Sleep Questionnaire, scored from 0 (best) to 21 (worst), was associated with a 9% acceleration in time to alcohol use and an 8% acceleration to cannabis use.
Subjects with poor sleep duration and quality as 11-year-olds by parental report also experienced intoxication at a younger age than did those who had been better sleepers at that age. And they reported more frequent use of alcohol and cannabis during adolescence.
In an interview, Mr. Mike, who is planning a career in pediatrics, said the study findings contain an important message for pediatricians and family physicians when they meet with the parents of young boys entering adolescence.
“Probably the biggest take-home message is, ‘sleep more, sleep better.’ We don’t have a lot of ways to intervene right now for kids who have poor sleep, but we know based on this and other studies that kids who don’t sleep enough are more likely to use drugs and more likely to engage in other risky behaviors. So any way the parents can intervene will help, perhaps by getting them to bed earlier or trying to get them on a more regular schedule. At a social policy level, having school start later would probably be the most effective measure, but that probably won’t happen for a very long time,” he said.
“The vast majority of people who end up addicted to drugs later in life started when they were kids, so any way we can reduce adolescent substance use should have a downstream effect, including a decreased total substance use burden,” Mr. Mike added.
Possible mechanisms for the observed longitudinal association between poor quality and duration of sleep at age 11 years and earlier and heavier use of alcohol and cannabis later in adolescence include attempted self-medication for sleep problems, reward regulation, and alterations in brain chemistry, making the boys more susceptible to using drugs later in life, perhaps because they obtain a bigger high than their peers do. The investigators plan to delve deeper into the role of self-regulation and mental health as possible mechanisms linking childhood sleep and later substance use, he said.
The Pitt Mother and Child Project is supported by the National Institutes of Health. Mr. Mike reported having no financial conflicts.
DENVER – Poor sleep quality and shorter sleep duration in boys at age 11 years is associated with subsequent accelerated use and misuse of alcohol and cannabis during adolescence and emerging adulthood, Thomas B. Mike reported at the annual meeting of the Associated Professional Sleep Societies.
This association has been reported before in cross-sectional studies. But Mr. Mike presented new findings from the longitudinal prospective Pitt Mother and Child Project.
The study comprised 170 boys aged 11 years whose mothers filled out the Child Sleep Questionnaire, modified for pediatric use from the well known Pittsburgh Sleep Quality Index. At that time, the boys also were assessed for internalizing and externalizing behaviors, neighborhood dangerousness, and socioeconomic status – all of which are factors known to influence teen substance use.
When participants reached ages 20 and 22 years, they underwent detailed interviews including assessment via the validated Lifetime Drinking History and Lifetime Drug History questionnaires.
In a multivariate Cox regression analysis controlling for a history of child internalizing and externalizing problem behavior as well as socioeconomic factors, every hour of sleep duration less than 9.5 hours at age 11 years was associated with a 21% acceleration in the time to first use of alcohol and a 22% acceleration in first use of cannabis, reported Mr. Mike, a medical student at the University of Pittsburgh.
Moreover, every 1 point worse score for sleep quality on the Child Sleep Questionnaire, scored from 0 (best) to 21 (worst), was associated with a 9% acceleration in time to alcohol use and an 8% acceleration to cannabis use.
Subjects with poor sleep duration and quality as 11-year-olds by parental report also experienced intoxication at a younger age than did those who had been better sleepers at that age. And they reported more frequent use of alcohol and cannabis during adolescence.
In an interview, Mr. Mike, who is planning a career in pediatrics, said the study findings contain an important message for pediatricians and family physicians when they meet with the parents of young boys entering adolescence.
“Probably the biggest take-home message is, ‘sleep more, sleep better.’ We don’t have a lot of ways to intervene right now for kids who have poor sleep, but we know based on this and other studies that kids who don’t sleep enough are more likely to use drugs and more likely to engage in other risky behaviors. So any way the parents can intervene will help, perhaps by getting them to bed earlier or trying to get them on a more regular schedule. At a social policy level, having school start later would probably be the most effective measure, but that probably won’t happen for a very long time,” he said.
“The vast majority of people who end up addicted to drugs later in life started when they were kids, so any way we can reduce adolescent substance use should have a downstream effect, including a decreased total substance use burden,” Mr. Mike added.
Possible mechanisms for the observed longitudinal association between poor quality and duration of sleep at age 11 years and earlier and heavier use of alcohol and cannabis later in adolescence include attempted self-medication for sleep problems, reward regulation, and alterations in brain chemistry, making the boys more susceptible to using drugs later in life, perhaps because they obtain a bigger high than their peers do. The investigators plan to delve deeper into the role of self-regulation and mental health as possible mechanisms linking childhood sleep and later substance use, he said.
The Pitt Mother and Child Project is supported by the National Institutes of Health. Mr. Mike reported having no financial conflicts.
AT SLEEP 2016

Restless sleep in 11-year-olds predicts earlier substance use
DENVER – Poor sleep quality and shorter sleep duration in boys at age 11 years is associated with subsequent accelerated use and misuse of alcohol and cannabis during adolescence and emerging adulthood, Thomas B. Mike reported at the annual meeting of the Associated Professional Sleep Societies.
This association has been reported before in cross-sectional studies. But Mr. Mike presented new findings from the longitudinal prospective Pitt Mother and Child Project.

The study comprised 170 boys aged 11 years whose mothers filled out the Child Sleep Questionnaire, modified for pediatric use from the well known Pittsburgh Sleep Quality Index. At that time, the boys also were assessed for internalizing and externalizing behaviors, neighborhood dangerousness, and socioeconomic status – all of which are factors known to influence teen substance use.
When participants reached ages 20 and 22 years, they underwent detailed interviews including assessment via the validated Lifetime Drinking History and Lifetime Drug History questionnaires.
In a multivariate Cox regression analysis controlling for a history of child internalizing and externalizing problem behavior as well as socioeconomic factors, every hour of sleep duration less than 9.5 hours at age 11 years was associated with a 21% acceleration in the time to first use of alcohol and a 22% acceleration in first use of cannabis, reported Mr. Mike, a medical student at the University of Pittsburgh.
Moreover, every 1 point worse score for sleep quality on the Child Sleep Questionnaire, scored from 0 (best) to 21 (worst), was associated with a 9% acceleration in time to alcohol use and an 8% acceleration to cannabis use.
Subjects with poor sleep duration and quality as 11-year-olds by parental report also experienced intoxication at a younger age than did those who had been better sleepers at that age. And they reported more frequent use of alcohol and cannabis during adolescence.
In an interview, Mr. Mike, who is planning a career in pediatrics, said the study findings contain an important message for pediatricians and family physicians when they meet with the parents of young boys entering adolescence.
“Probably the biggest take-home message is, ‘sleep more, sleep better.’ We don’t have a lot of ways to intervene right now for kids who have poor sleep, but we know based on this and other studies that kids who don’t sleep enough are more likely to use drugs and more likely to engage in other risky behaviors. So any way the parents can intervene will help, perhaps by getting them to bed earlier or trying to get them on a more regular schedule. At a social policy level, having school start later would probably be the most effective measure, but that probably won’t happen for a very long time,” he said.
“The vast majority of people who end up addicted to drugs later in life started when they were kids, so any way we can reduce adolescent substance use should have a downstream effect, including a decreased total substance use burden,” Mr. Mike added.
Possible mechanisms for the observed longitudinal association between poor quality and duration of sleep at age 11 years and earlier and heavier use of alcohol and cannabis later in adolescence include attempted self-medication for sleep problems, reward regulation, and alterations in brain chemistry, making the boys more susceptible to using drugs later in life, perhaps because they obtain a bigger high than their peers do. The investigators plan to delve deeper into the role of self-regulation and mental health as possible mechanisms linking childhood sleep and later substance use, he said.
The Pitt Mother and Child Project is supported by the National Institutes of Health. Mr. Mike reported having no financial conflicts.
DENVER – Poor sleep quality and shorter sleep duration in boys at age 11 years is associated with subsequent accelerated use and misuse of alcohol and cannabis during adolescence and emerging adulthood, Thomas B. Mike reported at the annual meeting of the Associated Professional Sleep Societies.
This association has been reported before in cross-sectional studies. But Mr. Mike presented new findings from the longitudinal prospective Pitt Mother and Child Project.
The study comprised 170 boys aged 11 years whose mothers filled out the Child Sleep Questionnaire, modified for pediatric use from the well known Pittsburgh Sleep Quality Index. At that time, the boys also were assessed for internalizing and externalizing behaviors, neighborhood dangerousness, and socioeconomic status – all of which are factors known to influence teen substance use.
When participants reached ages 20 and 22 years, they underwent detailed interviews including assessment via the validated Lifetime Drinking History and Lifetime Drug History questionnaires.
In a multivariate Cox regression analysis controlling for a history of child internalizing and externalizing problem behavior as well as socioeconomic factors, every hour of sleep duration less than 9.5 hours at age 11 years was associated with a 21% acceleration in the time to first use of alcohol and a 22% acceleration in first use of cannabis, reported Mr. Mike, a medical student at the University of Pittsburgh.
Moreover, every 1 point worse score for sleep quality on the Child Sleep Questionnaire, scored from 0 (best) to 21 (worst), was associated with a 9% acceleration in time to alcohol use and an 8% acceleration to cannabis use.
Subjects with poor sleep duration and quality as 11-year-olds by parental report also experienced intoxication at a younger age than did those who had been better sleepers at that age. And they reported more frequent use of alcohol and cannabis during adolescence.
In an interview, Mr. Mike, who is planning a career in pediatrics, said the study findings contain an important message for pediatricians and family physicians when they meet with the parents of young boys entering adolescence.
“Probably the biggest take-home message is, ‘sleep more, sleep better.’ We don’t have a lot of ways to intervene right now for kids who have poor sleep, but we know based on this and other studies that kids who don’t sleep enough are more likely to use drugs and more likely to engage in other risky behaviors. So any way the parents can intervene will help, perhaps by getting them to bed earlier or trying to get them on a more regular schedule. At a social policy level, having school start later would probably be the most effective measure, but that probably won’t happen for a very long time,” he said.
“The vast majority of people who end up addicted to drugs later in life started when they were kids, so any way we can reduce adolescent substance use should have a downstream effect, including a decreased total substance use burden,” Mr. Mike added.
Possible mechanisms for the observed longitudinal association between poor quality and duration of sleep at age 11 years and earlier and heavier use of alcohol and cannabis later in adolescence include attempted self-medication for sleep problems, reward regulation, and alterations in brain chemistry, making the boys more susceptible to using drugs later in life, perhaps because they obtain a bigger high than their peers do. The investigators plan to delve deeper into the role of self-regulation and mental health as possible mechanisms linking childhood sleep and later substance use, he said.
The Pitt Mother and Child Project is supported by the National Institutes of Health. Mr. Mike reported having no financial conflicts.
DENVER – Poor sleep quality and shorter sleep duration in boys at age 11 years is associated with subsequent accelerated use and misuse of alcohol and cannabis during adolescence and emerging adulthood, Thomas B. Mike reported at the annual meeting of the Associated Professional Sleep Societies.
This association has been reported before in cross-sectional studies. But Mr. Mike presented new findings from the longitudinal prospective Pitt Mother and Child Project.
The study comprised 170 boys aged 11 years whose mothers filled out the Child Sleep Questionnaire, modified for pediatric use from the well known Pittsburgh Sleep Quality Index. At that time, the boys also were assessed for internalizing and externalizing behaviors, neighborhood dangerousness, and socioeconomic status – all of which are factors known to influence teen substance use.
When participants reached ages 20 and 22 years, they underwent detailed interviews including assessment via the validated Lifetime Drinking History and Lifetime Drug History questionnaires.
In a multivariate Cox regression analysis controlling for a history of child internalizing and externalizing problem behavior as well as socioeconomic factors, every hour of sleep duration less than 9.5 hours at age 11 years was associated with a 21% acceleration in the time to first use of alcohol and a 22% acceleration in first use of cannabis, reported Mr. Mike, a medical student at the University of Pittsburgh.
Moreover, every 1 point worse score for sleep quality on the Child Sleep Questionnaire, scored from 0 (best) to 21 (worst), was associated with a 9% acceleration in time to alcohol use and an 8% acceleration to cannabis use.
Subjects with poor sleep duration and quality as 11-year-olds by parental report also experienced intoxication at a younger age than did those who had been better sleepers at that age. And they reported more frequent use of alcohol and cannabis during adolescence.
In an interview, Mr. Mike, who is planning a career in pediatrics, said the study findings contain an important message for pediatricians and family physicians when they meet with the parents of young boys entering adolescence.
“Probably the biggest take-home message is, ‘sleep more, sleep better.’ We don’t have a lot of ways to intervene right now for kids who have poor sleep, but we know based on this and other studies that kids who don’t sleep enough are more likely to use drugs and more likely to engage in other risky behaviors. So any way the parents can intervene will help, perhaps by getting them to bed earlier or trying to get them on a more regular schedule. At a social policy level, having school start later would probably be the most effective measure, but that probably won’t happen for a very long time,” he said.
“The vast majority of people who end up addicted to drugs later in life started when they were kids, so any way we can reduce adolescent substance use should have a downstream effect, including a decreased total substance use burden,” Mr. Mike added.
Possible mechanisms for the observed longitudinal association between poor quality and duration of sleep at age 11 years and earlier and heavier use of alcohol and cannabis later in adolescence include attempted self-medication for sleep problems, reward regulation, and alterations in brain chemistry, making the boys more susceptible to using drugs later in life, perhaps because they obtain a bigger high than their peers do. The investigators plan to delve deeper into the role of self-regulation and mental health as possible mechanisms linking childhood sleep and later substance use, he said.
The Pitt Mother and Child Project is supported by the National Institutes of Health. Mr. Mike reported having no financial conflicts.
AT SLEEP 2016
Key clinical point: Boys with poor sleep quality and quantity start using alcohol and cannabis earlier as teens.
Major finding: Every hour less of sleep duration at age 11 years was associated with a 21% acceleration in time to first use of alcohol and a 22% acceleration in first use of cannabis.
Data source: An analysis from the Pitt Mother and Child Project of 170 boys with sleep data recorded at age 11 and lifetime alcohol and cannabis use recalled at ages 20 and 22.
Disclosures: The Pitt Mother and Child Project is supported by the National Institutes of Health. The presenter reported having no financial conflicts.
