User login
Children under 6 with factor XIII deficiency had no major bleeds with recombinant product
ORLANDO –A recombinant form of factor XIII was effective at preventing serious bleeding episodes in young children with factor XIII-A subunit deficiency, a rare and serious bleeding disorder.
In a small international phase III trial, there were no major bleeding episodes among six young children treated for at least 1 year with recombinant factor XIII (rFXIII; trade name Tretten), reported Susan L. Kearney, MD, of Children’s Hospitals and Clinics of Minnesota in Minneapolis.
“Prophylaxis was effective. The annualized bleeding rate was zero and the mean trough [FXIII activity] was greater than 10%,” she said at a moderated poster session at the World Federation of Hemophilia World Congress. “We feel that recombinant factor XIII is safe and effective in pediatric subjects less than 6 years of age with congenital factor XIII-A subunit deficiency, similar to the older age cohort.”
Factor XIII-A subunit deficiency is a rare and serious heritable bleeding disorder associated with spontaneous intracranial hemorrhage and other unpredictable types of serious bleeding.
In a previous phase III trial, 77 patients, ranging in age from 7 to 60 years, received rFXIII for bleeding prophylaxis. When given monthly, the recombinant factor was effective at preventing serious bleeding in 90% of patients. The most commonly reported adverse events were headache, pain in the extremities, and injection site pain.
Based on these results, the Food and Drug Administration granted rFXIII orphan-drug designation for treatment of patients 6 and older with factor XIII-A subunit deficiency.
In the trial reported here, investigators from the United States, United Kingdom, Israel, and Denmark enrolled three boys and three girls under age 6 who had previously completed a single dose efficacy and safety study of rFXIII. The patients received intravenous rFXIII at a dose of 35 IU/kg every 28 days for a minimum of 52 weeks.
The total treatment duration ranged from 1.8 to 3.5 years, for a total of 16.6 patient years.
There were no thromboembolic events or systemic allergic reactions, the primary safety endpoint of the study. One patient experienced three incidences of atopic dermatitis, however; two serious adverse events related to head injuries from falls during play occurred in one patient, who did not experience intracranial hemorrhage.
Two adverse events were deemed to be probably or possibly related to rFXIII: a case of viral gastroenteritis affected one patient who recovered without a change in dose, and mild fluctuating lymphocytopenia seen at baseline persisted in another patient throughout the trial.
There were no inhibitory or noninhibitory antibodies to rFXIII detected in any patient during the trial, and there were no bleeding episodes requiring additional treatment. The 14 minor bleeding episodes seen in five patients did not require treatment with an FXIII-containing product, the authors noted.
“It’s a very rare disorder, but ... the phenotype is quite severe and patients are severely affected. So this product is very useful,” said Lakshmi Srivaths, MD, a pediatric hematologist at Texas Children’s Hospital in Houston. She was not involved in the study. Unlike patients with hemophilia A or B, who require frequent factor infusions, the long half-life of this product means patients need just once-a-month infusions “that change the phenotype very significantly.”
Dr. Kearney disclosed grant/research support from Novo Nordisk, which funded the study. Some coauthors reported consulting or employment with the company.
ORLANDO –A recombinant form of factor XIII was effective at preventing serious bleeding episodes in young children with factor XIII-A subunit deficiency, a rare and serious bleeding disorder.
In a small international phase III trial, there were no major bleeding episodes among six young children treated for at least 1 year with recombinant factor XIII (rFXIII; trade name Tretten), reported Susan L. Kearney, MD, of Children’s Hospitals and Clinics of Minnesota in Minneapolis.
“Prophylaxis was effective. The annualized bleeding rate was zero and the mean trough [FXIII activity] was greater than 10%,” she said at a moderated poster session at the World Federation of Hemophilia World Congress. “We feel that recombinant factor XIII is safe and effective in pediatric subjects less than 6 years of age with congenital factor XIII-A subunit deficiency, similar to the older age cohort.”
Factor XIII-A subunit deficiency is a rare and serious heritable bleeding disorder associated with spontaneous intracranial hemorrhage and other unpredictable types of serious bleeding.
In a previous phase III trial, 77 patients, ranging in age from 7 to 60 years, received rFXIII for bleeding prophylaxis. When given monthly, the recombinant factor was effective at preventing serious bleeding in 90% of patients. The most commonly reported adverse events were headache, pain in the extremities, and injection site pain.
Based on these results, the Food and Drug Administration granted rFXIII orphan-drug designation for treatment of patients 6 and older with factor XIII-A subunit deficiency.
In the trial reported here, investigators from the United States, United Kingdom, Israel, and Denmark enrolled three boys and three girls under age 6 who had previously completed a single dose efficacy and safety study of rFXIII. The patients received intravenous rFXIII at a dose of 35 IU/kg every 28 days for a minimum of 52 weeks.
The total treatment duration ranged from 1.8 to 3.5 years, for a total of 16.6 patient years.
There were no thromboembolic events or systemic allergic reactions, the primary safety endpoint of the study. One patient experienced three incidences of atopic dermatitis, however; two serious adverse events related to head injuries from falls during play occurred in one patient, who did not experience intracranial hemorrhage.
Two adverse events were deemed to be probably or possibly related to rFXIII: a case of viral gastroenteritis affected one patient who recovered without a change in dose, and mild fluctuating lymphocytopenia seen at baseline persisted in another patient throughout the trial.
There were no inhibitory or noninhibitory antibodies to rFXIII detected in any patient during the trial, and there were no bleeding episodes requiring additional treatment. The 14 minor bleeding episodes seen in five patients did not require treatment with an FXIII-containing product, the authors noted.
“It’s a very rare disorder, but ... the phenotype is quite severe and patients are severely affected. So this product is very useful,” said Lakshmi Srivaths, MD, a pediatric hematologist at Texas Children’s Hospital in Houston. She was not involved in the study. Unlike patients with hemophilia A or B, who require frequent factor infusions, the long half-life of this product means patients need just once-a-month infusions “that change the phenotype very significantly.”
Dr. Kearney disclosed grant/research support from Novo Nordisk, which funded the study. Some coauthors reported consulting or employment with the company.
ORLANDO –A recombinant form of factor XIII was effective at preventing serious bleeding episodes in young children with factor XIII-A subunit deficiency, a rare and serious bleeding disorder.
In a small international phase III trial, there were no major bleeding episodes among six young children treated for at least 1 year with recombinant factor XIII (rFXIII; trade name Tretten), reported Susan L. Kearney, MD, of Children’s Hospitals and Clinics of Minnesota in Minneapolis.
“Prophylaxis was effective. The annualized bleeding rate was zero and the mean trough [FXIII activity] was greater than 10%,” she said at a moderated poster session at the World Federation of Hemophilia World Congress. “We feel that recombinant factor XIII is safe and effective in pediatric subjects less than 6 years of age with congenital factor XIII-A subunit deficiency, similar to the older age cohort.”
Factor XIII-A subunit deficiency is a rare and serious heritable bleeding disorder associated with spontaneous intracranial hemorrhage and other unpredictable types of serious bleeding.
In a previous phase III trial, 77 patients, ranging in age from 7 to 60 years, received rFXIII for bleeding prophylaxis. When given monthly, the recombinant factor was effective at preventing serious bleeding in 90% of patients. The most commonly reported adverse events were headache, pain in the extremities, and injection site pain.
Based on these results, the Food and Drug Administration granted rFXIII orphan-drug designation for treatment of patients 6 and older with factor XIII-A subunit deficiency.
In the trial reported here, investigators from the United States, United Kingdom, Israel, and Denmark enrolled three boys and three girls under age 6 who had previously completed a single dose efficacy and safety study of rFXIII. The patients received intravenous rFXIII at a dose of 35 IU/kg every 28 days for a minimum of 52 weeks.
The total treatment duration ranged from 1.8 to 3.5 years, for a total of 16.6 patient years.
There were no thromboembolic events or systemic allergic reactions, the primary safety endpoint of the study. One patient experienced three incidences of atopic dermatitis, however; two serious adverse events related to head injuries from falls during play occurred in one patient, who did not experience intracranial hemorrhage.
Two adverse events were deemed to be probably or possibly related to rFXIII: a case of viral gastroenteritis affected one patient who recovered without a change in dose, and mild fluctuating lymphocytopenia seen at baseline persisted in another patient throughout the trial.
There were no inhibitory or noninhibitory antibodies to rFXIII detected in any patient during the trial, and there were no bleeding episodes requiring additional treatment. The 14 minor bleeding episodes seen in five patients did not require treatment with an FXIII-containing product, the authors noted.
“It’s a very rare disorder, but ... the phenotype is quite severe and patients are severely affected. So this product is very useful,” said Lakshmi Srivaths, MD, a pediatric hematologist at Texas Children’s Hospital in Houston. She was not involved in the study. Unlike patients with hemophilia A or B, who require frequent factor infusions, the long half-life of this product means patients need just once-a-month infusions “that change the phenotype very significantly.”
Dr. Kearney disclosed grant/research support from Novo Nordisk, which funded the study. Some coauthors reported consulting or employment with the company.
AT WFH 2016 WORLD CONGRESS
Key clinical point: A recombinant form of factor XIII was effective at preventing serious bleeding episodes in young children with factor XIII-A subunit deficiency.
Major finding: No bleeds occurred within a year in children with factor XIII-A subunit deficiency.
Data source: Open-label international phase III trial in three boys and three girls under age 6.
Disclosures: Dr. Kearney disclosed grant/research support from Novo Nordisk, which funded the study. Some coauthors reported consulting or employment with the company.
Therapy seems safe, effective in kids with hemophilia

Photo courtesy of Baxalta
ORLANDO—Results of a phase 3 study suggest the full-length recombinant factor VIII therapy Adynovate (BAX 855) can be safe and effective as twice-weekly prophylaxis and to control bleeding in children with hemophilia A.
None of the patients in this study developed inhibitory antibodies, and there were no product-related adverse events.
The median annualized bleeding rate (ABR) was 2.0, and nearly 40% of patients did not have any bleeding episodes.
These results were presented at the World Federation of Hemophilia 2016 World Congress.* The study was funded by Baxalta, now part of Shire.
The study enrolled previously treated children younger than 12 years of age with no history of factor VIII inhibitors. The patients received twice-weekly prophylaxis with Adynovate (50 ± 10 IU/kg) for at least 6 months or 50 exposure days, whichever occurred last.
There were 66 evaluable patients with a median age of 6 (range, 1-11). Overall, 4,467,796 IU of Adynovate were infused. The mean number of exposure days was 53.98 per patient.
Safety
There was no indication of persistent binding antibodies against factor VIII, and none of the patients developed antibodies to host cell (Chinese hamster ovary) proteins.
There were 156 adverse events in 43 patients (65.2%), but none were considered related to Adynovate.
There were 4 unrelated serious adverse events in 3 patients—febrile neutropenia, pancytopenia, acute gastritis, and abdominal pain.
Efficacy
Patients received a median dose of 51.3 IU/kg per prophylactic infusion at a median frequency of 1.9 infusions per week.
Ninety-one percent of patients did not require dose adjustments. Reasons for dose adjustment included factor VIII trough levels less than 1%, increased risk of bleeding, and bleeding episodes.
Thirty-eight percent of patients did not experience bleeding events, 73% did not experience hemarthroses, and 67% did not experience spontaneous bleeding events.
The mean ABR was 3.0, and the median was 2.0. The mean joint ABR was 1.1, and the median was 0. The mean spontaneous ABR was 1.2, and the median was 0. The mean interval between bleeding episodes was 2.4 months.
There were a total of 70 bleeding episodes in 34 patients. All of these episodes were minor or moderate. Ninety-one percent of treated bleeding events were treated with 1 or 2 infusions. And 90% of bleeding events received treatment ratings of “excellent” or “good.” ![]()
Photo courtesy of Baxalta
ORLANDO—Results of a phase 3 study suggest the full-length recombinant factor VIII therapy Adynovate (BAX 855) can be safe and effective as twice-weekly prophylaxis and to control bleeding in children with hemophilia A.
None of the patients in this study developed inhibitory antibodies, and there were no product-related adverse events.
The median annualized bleeding rate (ABR) was 2.0, and nearly 40% of patients did not have any bleeding episodes.
These results were presented at the World Federation of Hemophilia 2016 World Congress.* The study was funded by Baxalta, now part of Shire.
The study enrolled previously treated children younger than 12 years of age with no history of factor VIII inhibitors. The patients received twice-weekly prophylaxis with Adynovate (50 ± 10 IU/kg) for at least 6 months or 50 exposure days, whichever occurred last.
There were 66 evaluable patients with a median age of 6 (range, 1-11). Overall, 4,467,796 IU of Adynovate were infused. The mean number of exposure days was 53.98 per patient.
Safety
There was no indication of persistent binding antibodies against factor VIII, and none of the patients developed antibodies to host cell (Chinese hamster ovary) proteins.
There were 156 adverse events in 43 patients (65.2%), but none were considered related to Adynovate.
There were 4 unrelated serious adverse events in 3 patients—febrile neutropenia, pancytopenia, acute gastritis, and abdominal pain.
Efficacy
Patients received a median dose of 51.3 IU/kg per prophylactic infusion at a median frequency of 1.9 infusions per week.
Ninety-one percent of patients did not require dose adjustments. Reasons for dose adjustment included factor VIII trough levels less than 1%, increased risk of bleeding, and bleeding episodes.
Thirty-eight percent of patients did not experience bleeding events, 73% did not experience hemarthroses, and 67% did not experience spontaneous bleeding events.
The mean ABR was 3.0, and the median was 2.0. The mean joint ABR was 1.1, and the median was 0. The mean spontaneous ABR was 1.2, and the median was 0. The mean interval between bleeding episodes was 2.4 months.
There were a total of 70 bleeding episodes in 34 patients. All of these episodes were minor or moderate. Ninety-one percent of treated bleeding events were treated with 1 or 2 infusions. And 90% of bleeding events received treatment ratings of “excellent” or “good.” ![]()
Photo courtesy of Baxalta
ORLANDO—Results of a phase 3 study suggest the full-length recombinant factor VIII therapy Adynovate (BAX 855) can be safe and effective as twice-weekly prophylaxis and to control bleeding in children with hemophilia A.
None of the patients in this study developed inhibitory antibodies, and there were no product-related adverse events.
The median annualized bleeding rate (ABR) was 2.0, and nearly 40% of patients did not have any bleeding episodes.
These results were presented at the World Federation of Hemophilia 2016 World Congress.* The study was funded by Baxalta, now part of Shire.
The study enrolled previously treated children younger than 12 years of age with no history of factor VIII inhibitors. The patients received twice-weekly prophylaxis with Adynovate (50 ± 10 IU/kg) for at least 6 months or 50 exposure days, whichever occurred last.
There were 66 evaluable patients with a median age of 6 (range, 1-11). Overall, 4,467,796 IU of Adynovate were infused. The mean number of exposure days was 53.98 per patient.
Safety
There was no indication of persistent binding antibodies against factor VIII, and none of the patients developed antibodies to host cell (Chinese hamster ovary) proteins.
There were 156 adverse events in 43 patients (65.2%), but none were considered related to Adynovate.
There were 4 unrelated serious adverse events in 3 patients—febrile neutropenia, pancytopenia, acute gastritis, and abdominal pain.
Efficacy
Patients received a median dose of 51.3 IU/kg per prophylactic infusion at a median frequency of 1.9 infusions per week.
Ninety-one percent of patients did not require dose adjustments. Reasons for dose adjustment included factor VIII trough levels less than 1%, increased risk of bleeding, and bleeding episodes.
Thirty-eight percent of patients did not experience bleeding events, 73% did not experience hemarthroses, and 67% did not experience spontaneous bleeding events.
The mean ABR was 3.0, and the median was 2.0. The mean joint ABR was 1.1, and the median was 0. The mean spontaneous ABR was 1.2, and the median was 0. The mean interval between bleeding episodes was 2.4 months.
There were a total of 70 bleeding episodes in 34 patients. All of these episodes were minor or moderate. Ninety-one percent of treated bleeding events were treated with 1 or 2 infusions. And 90% of bleeding events received treatment ratings of “excellent” or “good.” ![]()
Experts offer blueprint for transitioning youth with neurologic conditions
Until now, there was no blueprint for how to effectively transition pediatric patients with neurologic conditions to adult care: Hard science on the topic is almost nonexistent.
“There is not very much data, yet there is a lot of suggestion that if you do it badly things don’t turn out so well,” said Peter Camfield, MD, a child neurologist and professor emeritus at Dalhousie University in Halifax, Nova Scotia, who has written extensively on the topic (Ann Neurol. 2011;69[3]:437-44 and Epilepsy Curr. 2012;12[Suppl. 3]:13-21). He recalled hearing one story of an adolescent girl who came to see a child neurologist every 6 months, always with her parents. “She had some significant learning disabilities and she didn’t finish high school; she dropped out,” he said. “She was sent to an adult neurologist just with a transfer note and to a nephrologist just with a transfer note.”
The patient never visited the nephrologist. The adult neurologist saw her once, “but she said he was kind of rude and that he wouldn’t see her again,” Dr. Camfield said. “She lived with her boyfriend and eventually at about age 24 she was found dead in bed. She hadn’t taken her medications regularly. The presumption is she died from a seizure. If she had been more prepared for adult medical care, she could have engaged better with the adult neurologist, the kidney part of this thing wouldn’t have been let go, and she presumably would be still alive and making her way.”
In an effort to avoid such tragedies and to define the neurologist’s role in transitioning youth with neurologic conditions into adult care, an interdisciplinary team of child neurologists and other experts spent more than 2 years developing a consensus statement, published online July 27 in Neurology (doi: 10.1212/WNL.0000000000002965). Spearheaded by Lawrence W. Brown, MD, director of the pediatric neuropsychiatry program at The Children’s Hospital of Philadelphia, the consensus statement, “The neurologist’s role in supporting transition to adult health care” is endorsed by the Child Neurology Society, the American Academy of Neurology, and the American Academy of Pediatrics.

Despite broad-based efforts over more than a decade to improve transition of care, such as the Consensus Policy Statement on Health Care Transitions for Young Adults With Special Needs, the Clinical Report: Supporting Health Care Transition from Adolescence to Adulthood in the Medical Home, and the Got Transition Center for Health Care Transition Improvement (a federally funded program located at the National Alliance to Advance Adolescent Health), Dr. Brown expressed his belief that neurologists were unlikely to adopt these recommendations “because they were very hard to put in place, to concretize, and to make practical. We also recognized that child neurology was in many ways behind the eight ball compared to other specialties, at least compared to certain disease-oriented areas such as cystic fibrosis, sickle cell disease, congenital heart disease, and rheumatoid arthritis. These conditions already had attempts to show what the expectations were for the kids and for the doctors, and there were some practical solutions out there.” If transition to adult care is going to be successful, he continued, “it’s not just the neurologist acting in a vacuum, but the neurologist working with the youth and his caregivers as well as with his primary care physician and with other specialists.”

Dr. Brown characterized the new consensus statement as an outline of “common principles that all child neurologists should try to respect” based on a review of the best medical literature and best practices. The first of eight principles contained in the statement recommends that the child neurology team start talking early about the concept of transition to the adult health care system with the youth and caregivers, and document that discussion “no later than the youth’s 13th birthday.”
Mary L. Zupanc, MD, one of the experts who helped author the consensus document, underscored the importance of introducing the notion of transition before the youth turns 13 years of age. Otherwise, “you are playing catch-up all the time,” she said. “Families have to get used to the concept of transition because we have long-term relationships with these individuals and their families. They come to think of us as part of their family. When you first bring up the topic of transition they about have a heart attack, because they can’t imagine a life without including you in it.”
The document’s second common principle recommends that the neurology team assess the youth’s self-management skills annually beginning at age 12. According to the authors, self-management of a medical condition “includes a youth’s understanding of his or her condition and any related limitations, knowledge about and responsibility for his or her own care plan and the need to make informed decisions, and the importance of self-advocacy.”
The statement also recommends phased transition planning at least annually beginning when the youth is 13 years of age. Topics to be discussed at such planning sessions range from the youth’s medical condition and current medications to genetic counseling and issues of puberty and sexuality. The validated Transition Readiness Assessment Questionnaire can be used as well (Acad Pediatr. 2014;14[4]:415-22).
Another principle contained in the consensus statement calls for a comprehensive transition plan by the time the youth is 14 years of age, ideally coordinated by the youth’s primary care provider in collaboration with the youth, caregivers, other health care providers, school personnel, vocational professionals, community services providers, and legal services regarding all aspects of health, financial, and legal care. It tasks the child neurology team with three responsibilities toward the comprehensive care plan: “assuring that an appropriate plan exists” and is created in partnership with the youth and family; “identifying the professional(s) with primary responsibility for overseeing and updating the entire transition plan,” and “providing and updating the neurologic component to this plan – including the ‘transfer packet,’ ” which contains important medical and social information.
In 2011, Dr. Zupanc, division chief of pediatric neurology at Children’s Hospital of Orange County in Orange, Calif., created a multidisciplinary clinic for epilepsy patients that includes nurse practitioners, registered nurses, a pharmacist, a dietitian, a social worker, a neuropsychologist, and a child psychiatrist. When Dr. Zupanc addresses the notion of transition with patients and their families for the first time, it’s not uncommon for her to be accompanied by the social worker and the neuropsychologist, “which I find helpful because parents may start to ask questions about guardianship,” she said. “Many of these parents do not even realize that there has to be an appointed guardian at age 18. We usually seek verification of competency via neuropsychometric testing or school evaluations. This information has to go before a judge to decide whether or not the patient is capable of taking care of himself/herself or if there should be an appointed guardian, typically one or both parents.”
Dr. Zupanc goes on to tell patients and their families that transition of care is a process that’s going to occur over the next 6-8 years. “Some of the patients don’t transition at age 18 years, because they are covered by California Children’s Services until age 22 years,” she said. The age of transition may vary from state to state, depending on insurance coverage and other issues. “Parents and patients get used to the idea that the transition isn’t going to happen tomorrow,” she said. “We explain the whole process. We let them know that we will help them. We also mention that we have adult provider colleagues in the community who are very knowledgeable about epilepsy or their child’s genetic syndrome. We partner with these colleagues, many of whom we have identified over time as willing to take our neurologically complex patients. As the transition process proceeds, we develop a transition packet of important medical information and social information. We will personally have conversations with the physician to whom we are transitioning care. Sometimes, our colleagues at University of California, Irvine, come over to our clinic before the final hand-off, so that the adult provider and the pediatric provider can meet together with the parents and patients in the same room. To us, that is the ideal situation. In this way, both the patients and the parents do not feel as if they are being abandoned.”
Dr. Zupanc, professor of pediatrics at the University of California–Irvine School of Medicine, said that a chief barrier to effective transition of care for pediatric patients with complex neurological problems is identifying clinicians who are willing to accept them into their practice. For example, many young patients with intractable epilepsy have significant concomitant cognitive issues and behavioral issues and/or autistic spectrum disorder. “If you look at surveys of adult providers, they feel enormously uncomfortable and uneducated about autistic spectrum disorder. They do not want to touch these young adolescents/adults,” Dr. Zupanc said. “They’re willing to take a piece of their care but not the entire package, which is problematic.”
The way Dr. Camfield sees it, neurologists have a moral obligation to play an active role in transitioning pediatric patients to adult care. “In many ways, it’s the No. 1 issue for tertiary care pediatrics now: What happens to young people in adulthood; what kind of citizens they turn out to be and how we help that to take place,” said Dr. Camfield, who helped write the consensus statement. “It’s no longer just enough to think, ‘as your child gets to be 16, 17, or 18, that’s it. We’re finished. Our job is done.’ That doesn’t make sense to me.”
In the consensus statement, he and his coauthors call for additional research on transition care practices in neurology moving forward. “Possible metrics for assessment include the rate of appointment completion and follow-up in the adult setting, patient and family satisfaction with transition and the new provider, stable or improved neurologic condition, adherence to care plans, decreased emergency utilization, rate of ‘bounce back’ to pediatric providers, and improved quality of life,” they wrote.
The consensus statement was funded in part by Eisai. Dr. Brown and Dr. Zupanc reported having no financial disclosures relevant to the manuscript. Dr. Camfield disclosed that he has received a speakers honorarium from Biocodex. Neurology Reviews, a publication of Frontline Medical Communications, is a member of the President’s Council of the Child Neurology Foundation.
Until now, there was no blueprint for how to effectively transition pediatric patients with neurologic conditions to adult care: Hard science on the topic is almost nonexistent.
“There is not very much data, yet there is a lot of suggestion that if you do it badly things don’t turn out so well,” said Peter Camfield, MD, a child neurologist and professor emeritus at Dalhousie University in Halifax, Nova Scotia, who has written extensively on the topic (Ann Neurol. 2011;69[3]:437-44 and Epilepsy Curr. 2012;12[Suppl. 3]:13-21). He recalled hearing one story of an adolescent girl who came to see a child neurologist every 6 months, always with her parents. “She had some significant learning disabilities and she didn’t finish high school; she dropped out,” he said. “She was sent to an adult neurologist just with a transfer note and to a nephrologist just with a transfer note.”
The patient never visited the nephrologist. The adult neurologist saw her once, “but she said he was kind of rude and that he wouldn’t see her again,” Dr. Camfield said. “She lived with her boyfriend and eventually at about age 24 she was found dead in bed. She hadn’t taken her medications regularly. The presumption is she died from a seizure. If she had been more prepared for adult medical care, she could have engaged better with the adult neurologist, the kidney part of this thing wouldn’t have been let go, and she presumably would be still alive and making her way.”
In an effort to avoid such tragedies and to define the neurologist’s role in transitioning youth with neurologic conditions into adult care, an interdisciplinary team of child neurologists and other experts spent more than 2 years developing a consensus statement, published online July 27 in Neurology (doi: 10.1212/WNL.0000000000002965). Spearheaded by Lawrence W. Brown, MD, director of the pediatric neuropsychiatry program at The Children’s Hospital of Philadelphia, the consensus statement, “The neurologist’s role in supporting transition to adult health care” is endorsed by the Child Neurology Society, the American Academy of Neurology, and the American Academy of Pediatrics.
Despite broad-based efforts over more than a decade to improve transition of care, such as the Consensus Policy Statement on Health Care Transitions for Young Adults With Special Needs, the Clinical Report: Supporting Health Care Transition from Adolescence to Adulthood in the Medical Home, and the Got Transition Center for Health Care Transition Improvement (a federally funded program located at the National Alliance to Advance Adolescent Health), Dr. Brown expressed his belief that neurologists were unlikely to adopt these recommendations “because they were very hard to put in place, to concretize, and to make practical. We also recognized that child neurology was in many ways behind the eight ball compared to other specialties, at least compared to certain disease-oriented areas such as cystic fibrosis, sickle cell disease, congenital heart disease, and rheumatoid arthritis. These conditions already had attempts to show what the expectations were for the kids and for the doctors, and there were some practical solutions out there.” If transition to adult care is going to be successful, he continued, “it’s not just the neurologist acting in a vacuum, but the neurologist working with the youth and his caregivers as well as with his primary care physician and with other specialists.”
Dr. Brown characterized the new consensus statement as an outline of “common principles that all child neurologists should try to respect” based on a review of the best medical literature and best practices. The first of eight principles contained in the statement recommends that the child neurology team start talking early about the concept of transition to the adult health care system with the youth and caregivers, and document that discussion “no later than the youth’s 13th birthday.”
Mary L. Zupanc, MD, one of the experts who helped author the consensus document, underscored the importance of introducing the notion of transition before the youth turns 13 years of age. Otherwise, “you are playing catch-up all the time,” she said. “Families have to get used to the concept of transition because we have long-term relationships with these individuals and their families. They come to think of us as part of their family. When you first bring up the topic of transition they about have a heart attack, because they can’t imagine a life without including you in it.”
The document’s second common principle recommends that the neurology team assess the youth’s self-management skills annually beginning at age 12. According to the authors, self-management of a medical condition “includes a youth’s understanding of his or her condition and any related limitations, knowledge about and responsibility for his or her own care plan and the need to make informed decisions, and the importance of self-advocacy.”
The statement also recommends phased transition planning at least annually beginning when the youth is 13 years of age. Topics to be discussed at such planning sessions range from the youth’s medical condition and current medications to genetic counseling and issues of puberty and sexuality. The validated Transition Readiness Assessment Questionnaire can be used as well (Acad Pediatr. 2014;14[4]:415-22).
Another principle contained in the consensus statement calls for a comprehensive transition plan by the time the youth is 14 years of age, ideally coordinated by the youth’s primary care provider in collaboration with the youth, caregivers, other health care providers, school personnel, vocational professionals, community services providers, and legal services regarding all aspects of health, financial, and legal care. It tasks the child neurology team with three responsibilities toward the comprehensive care plan: “assuring that an appropriate plan exists” and is created in partnership with the youth and family; “identifying the professional(s) with primary responsibility for overseeing and updating the entire transition plan,” and “providing and updating the neurologic component to this plan – including the ‘transfer packet,’ ” which contains important medical and social information.
In 2011, Dr. Zupanc, division chief of pediatric neurology at Children’s Hospital of Orange County in Orange, Calif., created a multidisciplinary clinic for epilepsy patients that includes nurse practitioners, registered nurses, a pharmacist, a dietitian, a social worker, a neuropsychologist, and a child psychiatrist. When Dr. Zupanc addresses the notion of transition with patients and their families for the first time, it’s not uncommon for her to be accompanied by the social worker and the neuropsychologist, “which I find helpful because parents may start to ask questions about guardianship,” she said. “Many of these parents do not even realize that there has to be an appointed guardian at age 18. We usually seek verification of competency via neuropsychometric testing or school evaluations. This information has to go before a judge to decide whether or not the patient is capable of taking care of himself/herself or if there should be an appointed guardian, typically one or both parents.”
Dr. Zupanc goes on to tell patients and their families that transition of care is a process that’s going to occur over the next 6-8 years. “Some of the patients don’t transition at age 18 years, because they are covered by California Children’s Services until age 22 years,” she said. The age of transition may vary from state to state, depending on insurance coverage and other issues. “Parents and patients get used to the idea that the transition isn’t going to happen tomorrow,” she said. “We explain the whole process. We let them know that we will help them. We also mention that we have adult provider colleagues in the community who are very knowledgeable about epilepsy or their child’s genetic syndrome. We partner with these colleagues, many of whom we have identified over time as willing to take our neurologically complex patients. As the transition process proceeds, we develop a transition packet of important medical information and social information. We will personally have conversations with the physician to whom we are transitioning care. Sometimes, our colleagues at University of California, Irvine, come over to our clinic before the final hand-off, so that the adult provider and the pediatric provider can meet together with the parents and patients in the same room. To us, that is the ideal situation. In this way, both the patients and the parents do not feel as if they are being abandoned.”
Dr. Zupanc, professor of pediatrics at the University of California–Irvine School of Medicine, said that a chief barrier to effective transition of care for pediatric patients with complex neurological problems is identifying clinicians who are willing to accept them into their practice. For example, many young patients with intractable epilepsy have significant concomitant cognitive issues and behavioral issues and/or autistic spectrum disorder. “If you look at surveys of adult providers, they feel enormously uncomfortable and uneducated about autistic spectrum disorder. They do not want to touch these young adolescents/adults,” Dr. Zupanc said. “They’re willing to take a piece of their care but not the entire package, which is problematic.”
The way Dr. Camfield sees it, neurologists have a moral obligation to play an active role in transitioning pediatric patients to adult care. “In many ways, it’s the No. 1 issue for tertiary care pediatrics now: What happens to young people in adulthood; what kind of citizens they turn out to be and how we help that to take place,” said Dr. Camfield, who helped write the consensus statement. “It’s no longer just enough to think, ‘as your child gets to be 16, 17, or 18, that’s it. We’re finished. Our job is done.’ That doesn’t make sense to me.”
In the consensus statement, he and his coauthors call for additional research on transition care practices in neurology moving forward. “Possible metrics for assessment include the rate of appointment completion and follow-up in the adult setting, patient and family satisfaction with transition and the new provider, stable or improved neurologic condition, adherence to care plans, decreased emergency utilization, rate of ‘bounce back’ to pediatric providers, and improved quality of life,” they wrote.
The consensus statement was funded in part by Eisai. Dr. Brown and Dr. Zupanc reported having no financial disclosures relevant to the manuscript. Dr. Camfield disclosed that he has received a speakers honorarium from Biocodex. Neurology Reviews, a publication of Frontline Medical Communications, is a member of the President’s Council of the Child Neurology Foundation.
Until now, there was no blueprint for how to effectively transition pediatric patients with neurologic conditions to adult care: Hard science on the topic is almost nonexistent.
“There is not very much data, yet there is a lot of suggestion that if you do it badly things don’t turn out so well,” said Peter Camfield, MD, a child neurologist and professor emeritus at Dalhousie University in Halifax, Nova Scotia, who has written extensively on the topic (Ann Neurol. 2011;69[3]:437-44 and Epilepsy Curr. 2012;12[Suppl. 3]:13-21). He recalled hearing one story of an adolescent girl who came to see a child neurologist every 6 months, always with her parents. “She had some significant learning disabilities and she didn’t finish high school; she dropped out,” he said. “She was sent to an adult neurologist just with a transfer note and to a nephrologist just with a transfer note.”
The patient never visited the nephrologist. The adult neurologist saw her once, “but she said he was kind of rude and that he wouldn’t see her again,” Dr. Camfield said. “She lived with her boyfriend and eventually at about age 24 she was found dead in bed. She hadn’t taken her medications regularly. The presumption is she died from a seizure. If she had been more prepared for adult medical care, she could have engaged better with the adult neurologist, the kidney part of this thing wouldn’t have been let go, and she presumably would be still alive and making her way.”
In an effort to avoid such tragedies and to define the neurologist’s role in transitioning youth with neurologic conditions into adult care, an interdisciplinary team of child neurologists and other experts spent more than 2 years developing a consensus statement, published online July 27 in Neurology (doi: 10.1212/WNL.0000000000002965). Spearheaded by Lawrence W. Brown, MD, director of the pediatric neuropsychiatry program at The Children’s Hospital of Philadelphia, the consensus statement, “The neurologist’s role in supporting transition to adult health care” is endorsed by the Child Neurology Society, the American Academy of Neurology, and the American Academy of Pediatrics.
Despite broad-based efforts over more than a decade to improve transition of care, such as the Consensus Policy Statement on Health Care Transitions for Young Adults With Special Needs, the Clinical Report: Supporting Health Care Transition from Adolescence to Adulthood in the Medical Home, and the Got Transition Center for Health Care Transition Improvement (a federally funded program located at the National Alliance to Advance Adolescent Health), Dr. Brown expressed his belief that neurologists were unlikely to adopt these recommendations “because they were very hard to put in place, to concretize, and to make practical. We also recognized that child neurology was in many ways behind the eight ball compared to other specialties, at least compared to certain disease-oriented areas such as cystic fibrosis, sickle cell disease, congenital heart disease, and rheumatoid arthritis. These conditions already had attempts to show what the expectations were for the kids and for the doctors, and there were some practical solutions out there.” If transition to adult care is going to be successful, he continued, “it’s not just the neurologist acting in a vacuum, but the neurologist working with the youth and his caregivers as well as with his primary care physician and with other specialists.”
Dr. Brown characterized the new consensus statement as an outline of “common principles that all child neurologists should try to respect” based on a review of the best medical literature and best practices. The first of eight principles contained in the statement recommends that the child neurology team start talking early about the concept of transition to the adult health care system with the youth and caregivers, and document that discussion “no later than the youth’s 13th birthday.”
Mary L. Zupanc, MD, one of the experts who helped author the consensus document, underscored the importance of introducing the notion of transition before the youth turns 13 years of age. Otherwise, “you are playing catch-up all the time,” she said. “Families have to get used to the concept of transition because we have long-term relationships with these individuals and their families. They come to think of us as part of their family. When you first bring up the topic of transition they about have a heart attack, because they can’t imagine a life without including you in it.”
The document’s second common principle recommends that the neurology team assess the youth’s self-management skills annually beginning at age 12. According to the authors, self-management of a medical condition “includes a youth’s understanding of his or her condition and any related limitations, knowledge about and responsibility for his or her own care plan and the need to make informed decisions, and the importance of self-advocacy.”
The statement also recommends phased transition planning at least annually beginning when the youth is 13 years of age. Topics to be discussed at such planning sessions range from the youth’s medical condition and current medications to genetic counseling and issues of puberty and sexuality. The validated Transition Readiness Assessment Questionnaire can be used as well (Acad Pediatr. 2014;14[4]:415-22).
Another principle contained in the consensus statement calls for a comprehensive transition plan by the time the youth is 14 years of age, ideally coordinated by the youth’s primary care provider in collaboration with the youth, caregivers, other health care providers, school personnel, vocational professionals, community services providers, and legal services regarding all aspects of health, financial, and legal care. It tasks the child neurology team with three responsibilities toward the comprehensive care plan: “assuring that an appropriate plan exists” and is created in partnership with the youth and family; “identifying the professional(s) with primary responsibility for overseeing and updating the entire transition plan,” and “providing and updating the neurologic component to this plan – including the ‘transfer packet,’ ” which contains important medical and social information.
In 2011, Dr. Zupanc, division chief of pediatric neurology at Children’s Hospital of Orange County in Orange, Calif., created a multidisciplinary clinic for epilepsy patients that includes nurse practitioners, registered nurses, a pharmacist, a dietitian, a social worker, a neuropsychologist, and a child psychiatrist. When Dr. Zupanc addresses the notion of transition with patients and their families for the first time, it’s not uncommon for her to be accompanied by the social worker and the neuropsychologist, “which I find helpful because parents may start to ask questions about guardianship,” she said. “Many of these parents do not even realize that there has to be an appointed guardian at age 18. We usually seek verification of competency via neuropsychometric testing or school evaluations. This information has to go before a judge to decide whether or not the patient is capable of taking care of himself/herself or if there should be an appointed guardian, typically one or both parents.”
Dr. Zupanc goes on to tell patients and their families that transition of care is a process that’s going to occur over the next 6-8 years. “Some of the patients don’t transition at age 18 years, because they are covered by California Children’s Services until age 22 years,” she said. The age of transition may vary from state to state, depending on insurance coverage and other issues. “Parents and patients get used to the idea that the transition isn’t going to happen tomorrow,” she said. “We explain the whole process. We let them know that we will help them. We also mention that we have adult provider colleagues in the community who are very knowledgeable about epilepsy or their child’s genetic syndrome. We partner with these colleagues, many of whom we have identified over time as willing to take our neurologically complex patients. As the transition process proceeds, we develop a transition packet of important medical information and social information. We will personally have conversations with the physician to whom we are transitioning care. Sometimes, our colleagues at University of California, Irvine, come over to our clinic before the final hand-off, so that the adult provider and the pediatric provider can meet together with the parents and patients in the same room. To us, that is the ideal situation. In this way, both the patients and the parents do not feel as if they are being abandoned.”
Dr. Zupanc, professor of pediatrics at the University of California–Irvine School of Medicine, said that a chief barrier to effective transition of care for pediatric patients with complex neurological problems is identifying clinicians who are willing to accept them into their practice. For example, many young patients with intractable epilepsy have significant concomitant cognitive issues and behavioral issues and/or autistic spectrum disorder. “If you look at surveys of adult providers, they feel enormously uncomfortable and uneducated about autistic spectrum disorder. They do not want to touch these young adolescents/adults,” Dr. Zupanc said. “They’re willing to take a piece of their care but not the entire package, which is problematic.”
The way Dr. Camfield sees it, neurologists have a moral obligation to play an active role in transitioning pediatric patients to adult care. “In many ways, it’s the No. 1 issue for tertiary care pediatrics now: What happens to young people in adulthood; what kind of citizens they turn out to be and how we help that to take place,” said Dr. Camfield, who helped write the consensus statement. “It’s no longer just enough to think, ‘as your child gets to be 16, 17, or 18, that’s it. We’re finished. Our job is done.’ That doesn’t make sense to me.”
In the consensus statement, he and his coauthors call for additional research on transition care practices in neurology moving forward. “Possible metrics for assessment include the rate of appointment completion and follow-up in the adult setting, patient and family satisfaction with transition and the new provider, stable or improved neurologic condition, adherence to care plans, decreased emergency utilization, rate of ‘bounce back’ to pediatric providers, and improved quality of life,” they wrote.
The consensus statement was funded in part by Eisai. Dr. Brown and Dr. Zupanc reported having no financial disclosures relevant to the manuscript. Dr. Camfield disclosed that he has received a speakers honorarium from Biocodex. Neurology Reviews, a publication of Frontline Medical Communications, is a member of the President’s Council of the Child Neurology Foundation.
FROM NEUROLOGY

Influenza: A vaccine we love to hate
The Centers for Disease Control and Prevention, American Academy of Pediatrics, and American Academy of Family Physicians recommend that everyone 6 months of age and older get a seasonal flu vaccine. Emphasizing influenza vaccination in children recognizes the high burden of morbidity and significant mortality associated with influenza in young children as well as their role in transmission in the community.
In 2015-2016, the CDC reported 83 influenza deaths in children, and estimated the rate of hospitalization for children younger than 4 years of age to be 42/100,000 (at press time). In 2015-2016, the H1N1 strain was dominant in the community overall, with influenza B being most prevalent late in the season. The CDC estimates that nearly 75% of children less than 24 months and 68% between 2 and 4 years of age were immunized this year. Overall vaccine efficacy in children 6 months through 8 years was reported at 47% last season from a CDC study using a study design that compares vaccination odds among influenza reverse transcription polymerase chain reaction (RT-PCR)–positive cases and RT-PCR–negative controls.
Influenza virus vaccines are unique in that they are updated, often annually, to include the most current hemagglutinin (HA) antigens based on estimates from circulating strains. In the United States, influenza vaccine manufacturers submit a supplement to their license and obtain Food and Drug Administration approval. These applications require only a limited study of safety in approximately 300 adults, essentially to verify attenuation (Influenza Other Respir Viruses. 2016. doi: 10.111/irv.1283). They do not require clinical proof of efficacy or even a threshold of immunogenicity.

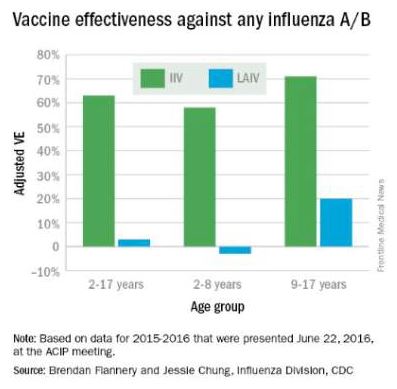
At the June 2016 CDC’s Advisory Committee on Immunization Practices (ACIP) meeting, data were presented comparing the efficacy of this season’s live attenuated influenza vaccine (LAIV) with inactivated influenza vaccine (IIV) by age and specific influenza type and subtype. Data from the U.S. Flu Vaccine Effectiveness (VE) Network, a consortium of five CDC-funded sites that conducts annual studies of influenza vaccine effectiveness, failed to demonstrate efficacy for LAIV in children aged 2-8 years. There was an absence of efficacy against the primary circulating strain, A(H1N1). This contrasted with the 62% efficacy report for IIV against A(H1N1).
The concern for efficacy for LAIV was not limited to 2015-2016; efficacy was poor in 2013-2014 during a year in which A(H1N1) was the dominant virus as well, and in 2014-2015 when the prevalent strain was a drifted A(H3N2). The lack of efficacy in 2015-2016 and 2013-2014 when A(H1N1) was the prevalent strain was especially enigmatic given its high efficacy against A(H1N1) between 2009 and 2011. Studies of LAIV from Astra Zeneca and the U.S. Department of Defense were consistent with those from the U.S. Flu VE Network; however, there were discordant data from Finland where vaccine efficacy was present. As a result of these studies, the ACIP voted that LAIV should not be used during the 2016-2017 flu season. This vote reinforces the importance of monitoring the effectiveness of annual flu vaccination and other public health interventions.
ACIP recommendations for 2016-2017
• Children younger than 2 years of age and those with chronic health problems such as asthma, diabetes, and disorders of the brain or nervous system are at especially high risk of developing serious flu complications.
• Annual influenza immunization, with either the IIV or recombinant influenza vaccine (RIV), for everyone 6 months and older, remains the only effective strategy for decreasing influenza disease in the community.
• LAIV should not be used during the 2016-2017 flu season.
ACIP recommendations must be reviewed and approved by the CDC’s director before becoming CDC policy. The final annual recommendations on the prevention and control of influenza with vaccines will be published in CDC Morbidity and Mortality Weekly Report (MMWR) Recommendations and Reports in late summer or early fall.
Flu vaccines available for children for 2016-2017
• The trivalent flu vaccine protects against three flu viruses; two influenza A viruses and an influenza B virus. Standard dose trivalent shots are manufactured with viruses grown in eggs. These are approved for children aged 6 months and older. There are different brands of this type of vaccine; each specific formulation has different age-based approvals.

• The quadrivalent flu vaccine protects against four flu viruses; two influenza A viruses and two influenza B viruses. A standard dose quadrivalent formulation is available for children; one brand is approved for children 6 months and older while others are approved for those 3 years and older.
• A cell-based vaccine, developed through a manufacturing process different from the traditional egg-based manufacturing process, was approved as a quadrivalent formulation for use in children 4 years of age and older.
Unanswered questions for the 2016-2017 influenza season
• Children 6 months to 8 years who are getting vaccinated for the first time need two doses. How should we consider influenza-naive children who received two doses of LAIV last year? The reason for the LAIV’s loss of efficacy in the years 2014 through 2016 is unknown, although it has been hypothesized that reduced immunogenicity is one possible cause for the lack of protection. Rather than speculate, we need to wait for ACIP to gather more data and then publish recommendations as to whether to consider such children vaccine naive (and therefore requiring two doses this season) or previously immunized (and therefore in need of only a single dose).
• Will supply be adequate this year? LAIV represents about 8% of the 171-176 million doses that were projected to be available during the 2016-2017 season; however, it represents nearly one-third of doses given to children. Thus, the potential for shortages in pediatric offices is real, and pediatricians and vaccine manufacturers need to work together to make sure sufficient pediatric formulation is available. The CDC is working with manufacturers to ensure there is sufficient supply to meet the demand.
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. He has received honoraria from Sanofi Pasteur and Seqirus for participation in vaccine advisory boards in the prior 12 months. Email him at pdnews@frontlinemedcom.com.
The Centers for Disease Control and Prevention, American Academy of Pediatrics, and American Academy of Family Physicians recommend that everyone 6 months of age and older get a seasonal flu vaccine. Emphasizing influenza vaccination in children recognizes the high burden of morbidity and significant mortality associated with influenza in young children as well as their role in transmission in the community.
In 2015-2016, the CDC reported 83 influenza deaths in children, and estimated the rate of hospitalization for children younger than 4 years of age to be 42/100,000 (at press time). In 2015-2016, the H1N1 strain was dominant in the community overall, with influenza B being most prevalent late in the season. The CDC estimates that nearly 75% of children less than 24 months and 68% between 2 and 4 years of age were immunized this year. Overall vaccine efficacy in children 6 months through 8 years was reported at 47% last season from a CDC study using a study design that compares vaccination odds among influenza reverse transcription polymerase chain reaction (RT-PCR)–positive cases and RT-PCR–negative controls.
Influenza virus vaccines are unique in that they are updated, often annually, to include the most current hemagglutinin (HA) antigens based on estimates from circulating strains. In the United States, influenza vaccine manufacturers submit a supplement to their license and obtain Food and Drug Administration approval. These applications require only a limited study of safety in approximately 300 adults, essentially to verify attenuation (Influenza Other Respir Viruses. 2016. doi: 10.111/irv.1283). They do not require clinical proof of efficacy or even a threshold of immunogenicity.
At the June 2016 CDC’s Advisory Committee on Immunization Practices (ACIP) meeting, data were presented comparing the efficacy of this season’s live attenuated influenza vaccine (LAIV) with inactivated influenza vaccine (IIV) by age and specific influenza type and subtype. Data from the U.S. Flu Vaccine Effectiveness (VE) Network, a consortium of five CDC-funded sites that conducts annual studies of influenza vaccine effectiveness, failed to demonstrate efficacy for LAIV in children aged 2-8 years. There was an absence of efficacy against the primary circulating strain, A(H1N1). This contrasted with the 62% efficacy report for IIV against A(H1N1).
The concern for efficacy for LAIV was not limited to 2015-2016; efficacy was poor in 2013-2014 during a year in which A(H1N1) was the dominant virus as well, and in 2014-2015 when the prevalent strain was a drifted A(H3N2). The lack of efficacy in 2015-2016 and 2013-2014 when A(H1N1) was the prevalent strain was especially enigmatic given its high efficacy against A(H1N1) between 2009 and 2011. Studies of LAIV from Astra Zeneca and the U.S. Department of Defense were consistent with those from the U.S. Flu VE Network; however, there were discordant data from Finland where vaccine efficacy was present. As a result of these studies, the ACIP voted that LAIV should not be used during the 2016-2017 flu season. This vote reinforces the importance of monitoring the effectiveness of annual flu vaccination and other public health interventions.
ACIP recommendations for 2016-2017
• Children younger than 2 years of age and those with chronic health problems such as asthma, diabetes, and disorders of the brain or nervous system are at especially high risk of developing serious flu complications.
• Annual influenza immunization, with either the IIV or recombinant influenza vaccine (RIV), for everyone 6 months and older, remains the only effective strategy for decreasing influenza disease in the community.
• LAIV should not be used during the 2016-2017 flu season.
ACIP recommendations must be reviewed and approved by the CDC’s director before becoming CDC policy. The final annual recommendations on the prevention and control of influenza with vaccines will be published in CDC Morbidity and Mortality Weekly Report (MMWR) Recommendations and Reports in late summer or early fall.
Flu vaccines available for children for 2016-2017
• The trivalent flu vaccine protects against three flu viruses; two influenza A viruses and an influenza B virus. Standard dose trivalent shots are manufactured with viruses grown in eggs. These are approved for children aged 6 months and older. There are different brands of this type of vaccine; each specific formulation has different age-based approvals.
• The quadrivalent flu vaccine protects against four flu viruses; two influenza A viruses and two influenza B viruses. A standard dose quadrivalent formulation is available for children; one brand is approved for children 6 months and older while others are approved for those 3 years and older.
• A cell-based vaccine, developed through a manufacturing process different from the traditional egg-based manufacturing process, was approved as a quadrivalent formulation for use in children 4 years of age and older.
Unanswered questions for the 2016-2017 influenza season
• Children 6 months to 8 years who are getting vaccinated for the first time need two doses. How should we consider influenza-naive children who received two doses of LAIV last year? The reason for the LAIV’s loss of efficacy in the years 2014 through 2016 is unknown, although it has been hypothesized that reduced immunogenicity is one possible cause for the lack of protection. Rather than speculate, we need to wait for ACIP to gather more data and then publish recommendations as to whether to consider such children vaccine naive (and therefore requiring two doses this season) or previously immunized (and therefore in need of only a single dose).
• Will supply be adequate this year? LAIV represents about 8% of the 171-176 million doses that were projected to be available during the 2016-2017 season; however, it represents nearly one-third of doses given to children. Thus, the potential for shortages in pediatric offices is real, and pediatricians and vaccine manufacturers need to work together to make sure sufficient pediatric formulation is available. The CDC is working with manufacturers to ensure there is sufficient supply to meet the demand.
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. He has received honoraria from Sanofi Pasteur and Seqirus for participation in vaccine advisory boards in the prior 12 months. Email him at pdnews@frontlinemedcom.com.
The Centers for Disease Control and Prevention, American Academy of Pediatrics, and American Academy of Family Physicians recommend that everyone 6 months of age and older get a seasonal flu vaccine. Emphasizing influenza vaccination in children recognizes the high burden of morbidity and significant mortality associated with influenza in young children as well as their role in transmission in the community.
In 2015-2016, the CDC reported 83 influenza deaths in children, and estimated the rate of hospitalization for children younger than 4 years of age to be 42/100,000 (at press time). In 2015-2016, the H1N1 strain was dominant in the community overall, with influenza B being most prevalent late in the season. The CDC estimates that nearly 75% of children less than 24 months and 68% between 2 and 4 years of age were immunized this year. Overall vaccine efficacy in children 6 months through 8 years was reported at 47% last season from a CDC study using a study design that compares vaccination odds among influenza reverse transcription polymerase chain reaction (RT-PCR)–positive cases and RT-PCR–negative controls.
Influenza virus vaccines are unique in that they are updated, often annually, to include the most current hemagglutinin (HA) antigens based on estimates from circulating strains. In the United States, influenza vaccine manufacturers submit a supplement to their license and obtain Food and Drug Administration approval. These applications require only a limited study of safety in approximately 300 adults, essentially to verify attenuation (Influenza Other Respir Viruses. 2016. doi: 10.111/irv.1283). They do not require clinical proof of efficacy or even a threshold of immunogenicity.
At the June 2016 CDC’s Advisory Committee on Immunization Practices (ACIP) meeting, data were presented comparing the efficacy of this season’s live attenuated influenza vaccine (LAIV) with inactivated influenza vaccine (IIV) by age and specific influenza type and subtype. Data from the U.S. Flu Vaccine Effectiveness (VE) Network, a consortium of five CDC-funded sites that conducts annual studies of influenza vaccine effectiveness, failed to demonstrate efficacy for LAIV in children aged 2-8 years. There was an absence of efficacy against the primary circulating strain, A(H1N1). This contrasted with the 62% efficacy report for IIV against A(H1N1).
The concern for efficacy for LAIV was not limited to 2015-2016; efficacy was poor in 2013-2014 during a year in which A(H1N1) was the dominant virus as well, and in 2014-2015 when the prevalent strain was a drifted A(H3N2). The lack of efficacy in 2015-2016 and 2013-2014 when A(H1N1) was the prevalent strain was especially enigmatic given its high efficacy against A(H1N1) between 2009 and 2011. Studies of LAIV from Astra Zeneca and the U.S. Department of Defense were consistent with those from the U.S. Flu VE Network; however, there were discordant data from Finland where vaccine efficacy was present. As a result of these studies, the ACIP voted that LAIV should not be used during the 2016-2017 flu season. This vote reinforces the importance of monitoring the effectiveness of annual flu vaccination and other public health interventions.
ACIP recommendations for 2016-2017
• Children younger than 2 years of age and those with chronic health problems such as asthma, diabetes, and disorders of the brain or nervous system are at especially high risk of developing serious flu complications.
• Annual influenza immunization, with either the IIV or recombinant influenza vaccine (RIV), for everyone 6 months and older, remains the only effective strategy for decreasing influenza disease in the community.
• LAIV should not be used during the 2016-2017 flu season.
ACIP recommendations must be reviewed and approved by the CDC’s director before becoming CDC policy. The final annual recommendations on the prevention and control of influenza with vaccines will be published in CDC Morbidity and Mortality Weekly Report (MMWR) Recommendations and Reports in late summer or early fall.
Flu vaccines available for children for 2016-2017
• The trivalent flu vaccine protects against three flu viruses; two influenza A viruses and an influenza B virus. Standard dose trivalent shots are manufactured with viruses grown in eggs. These are approved for children aged 6 months and older. There are different brands of this type of vaccine; each specific formulation has different age-based approvals.
• The quadrivalent flu vaccine protects against four flu viruses; two influenza A viruses and two influenza B viruses. A standard dose quadrivalent formulation is available for children; one brand is approved for children 6 months and older while others are approved for those 3 years and older.
• A cell-based vaccine, developed through a manufacturing process different from the traditional egg-based manufacturing process, was approved as a quadrivalent formulation for use in children 4 years of age and older.
Unanswered questions for the 2016-2017 influenza season
• Children 6 months to 8 years who are getting vaccinated for the first time need two doses. How should we consider influenza-naive children who received two doses of LAIV last year? The reason for the LAIV’s loss of efficacy in the years 2014 through 2016 is unknown, although it has been hypothesized that reduced immunogenicity is one possible cause for the lack of protection. Rather than speculate, we need to wait for ACIP to gather more data and then publish recommendations as to whether to consider such children vaccine naive (and therefore requiring two doses this season) or previously immunized (and therefore in need of only a single dose).
• Will supply be adequate this year? LAIV represents about 8% of the 171-176 million doses that were projected to be available during the 2016-2017 season; however, it represents nearly one-third of doses given to children. Thus, the potential for shortages in pediatric offices is real, and pediatricians and vaccine manufacturers need to work together to make sure sufficient pediatric formulation is available. The CDC is working with manufacturers to ensure there is sufficient supply to meet the demand.
Dr. Pelton is chief of pediatric infectious disease and coordinator of the maternal-child HIV program at Boston Medical Center. He has received honoraria from Sanofi Pasteur and Seqirus for participation in vaccine advisory boards in the prior 12 months. Email him at pdnews@frontlinemedcom.com.

Coadministering a combined MMRV vaccine with MenC vaccine is immunogenic
Researchers conducting a multicenter study in Italy evaluating the stability of coadministering a combined MMR plus varicella (MMRV) vaccine with conjugated meningococcal C (MenC) vaccine found MMRV and MenC immunogenic and well tolerated in children aged 13-15 months.
A total of 716 children aged 13-15 months were randomized (2:1:1) and received a single dose of each vaccine, which included coadministered MMRV plus MenC at the same visit (MMRV + MenC group), or MMRV followed 42 days later by MenC (MMRV group), or MenC followed 42 days later by MMRV (MenC group).

The MMRV seroconversion rates 42 days post vaccination were 99.3% (measles), 94.5% (mumps), 100% (rubella), and 99.7% (varicella) in the MMRV plus MenC group, and 99.4%, 93.2%, 100%, and 100%, respectively, in the MMRV group. Noninferiority was demonstrated.
The seroprotection rate for rSBAMenC in the MMRV + MenC group was 98.3%, compared with 99.3% in children who received just MenC, at 42 days post vaccination. Noninferiority was demonstrated.
“The study vaccines were generally well tolerated, and clinically acceptable safety profiles were observed,” Paolo Durando of the University of Genoa (Italy) and his associates reported.
Read more of the article in Vaccine here (2016.doi:10.1016/j.vaccine.2016.07.009).
Researchers conducting a multicenter study in Italy evaluating the stability of coadministering a combined MMR plus varicella (MMRV) vaccine with conjugated meningococcal C (MenC) vaccine found MMRV and MenC immunogenic and well tolerated in children aged 13-15 months.
A total of 716 children aged 13-15 months were randomized (2:1:1) and received a single dose of each vaccine, which included coadministered MMRV plus MenC at the same visit (MMRV + MenC group), or MMRV followed 42 days later by MenC (MMRV group), or MenC followed 42 days later by MMRV (MenC group).
The MMRV seroconversion rates 42 days post vaccination were 99.3% (measles), 94.5% (mumps), 100% (rubella), and 99.7% (varicella) in the MMRV plus MenC group, and 99.4%, 93.2%, 100%, and 100%, respectively, in the MMRV group. Noninferiority was demonstrated.
The seroprotection rate for rSBAMenC in the MMRV + MenC group was 98.3%, compared with 99.3% in children who received just MenC, at 42 days post vaccination. Noninferiority was demonstrated.
“The study vaccines were generally well tolerated, and clinically acceptable safety profiles were observed,” Paolo Durando of the University of Genoa (Italy) and his associates reported.
Read more of the article in Vaccine here (2016.doi:10.1016/j.vaccine.2016.07.009).
Researchers conducting a multicenter study in Italy evaluating the stability of coadministering a combined MMR plus varicella (MMRV) vaccine with conjugated meningococcal C (MenC) vaccine found MMRV and MenC immunogenic and well tolerated in children aged 13-15 months.
A total of 716 children aged 13-15 months were randomized (2:1:1) and received a single dose of each vaccine, which included coadministered MMRV plus MenC at the same visit (MMRV + MenC group), or MMRV followed 42 days later by MenC (MMRV group), or MenC followed 42 days later by MMRV (MenC group).
The MMRV seroconversion rates 42 days post vaccination were 99.3% (measles), 94.5% (mumps), 100% (rubella), and 99.7% (varicella) in the MMRV plus MenC group, and 99.4%, 93.2%, 100%, and 100%, respectively, in the MMRV group. Noninferiority was demonstrated.
The seroprotection rate for rSBAMenC in the MMRV + MenC group was 98.3%, compared with 99.3% in children who received just MenC, at 42 days post vaccination. Noninferiority was demonstrated.
“The study vaccines were generally well tolerated, and clinically acceptable safety profiles were observed,” Paolo Durando of the University of Genoa (Italy) and his associates reported.
Read more of the article in Vaccine here (2016.doi:10.1016/j.vaccine.2016.07.009).
FROM VACCINE

How we can support our LGBTQ patients
This past month has been a difficult one. The violence committed against people on the basis of presumed sexual orientation, color of skin, religion, and occupation has been difficult to make sense of. These tragic and horrible events highlight the continued need to focus on building inclusive environments and fostering communication between people with different backgrounds, points of view, and life experiences.
Several of my past articles have touched on the need to create inclusive environments for our LGBTQ (lesbian, gay, bisexual, transgender, questioning) patients, but have not included direct input from youth. With this in mind, I sat down with several youth from our local youth LGBTQ center in Ohio to ask them how we as health care providers could be more supportive of our patients.

Here are some of their suggestions:
• “Trust your patients. … Respect that I am knowledgeable about my body.”
Youth in the group stated that they want providers who listen to and trust what they say. Youth reported that they trust that their medical providers are experts in medicine and the care of patients, but they are the experts on themselves.
• “Don’t blame the hormones. Don’t blame things on puberty. … It’s not just a phase.”
Youth reported that they often get frustrated when providers assume that their sexual orientation or gender identity is “just a phase.” While adolescence can be a time of experimentation, it is important to acknowledge and respect youth’s emerging identities.
• “Know your patients. Educate yourselves.”
Many youth reported that while they are happy to share their stories, they do not want to be put in the role of having to educate their providers about the basics.
Youth expect that their providers have a general understanding of LGBTQ terminology and health care needs. They are happy to answer specific questions, but expect a degree of cultural competency from their providers.
• “Don’t push birth control. Don’t make assumptions about my behaviors; ask me first.”
Many female-bodied youth had the perception that providers make assumptions about their sexual orientation (assuming they are heterosexual), sexual behaviors, and risk of unintended pregnancy and sexually transmitted diseases.
Youth reported that they are open to conversations about reproductive health and safe sex, but get turned off when providers incorrectly assume they are heterosexual and in need of birth control. Asking about sexual attraction and the gender of partners as a routine part of any adolescent sexual history can help providers avoid these mistakes.
• “Have a discussion versus telling people what to do. Tell me why you are checking things and what they mean.”
Youth reported that they were interested in being active participants in their health care visits. They stated that if labs are being checked, they want to know why and what the results mean. When medications are prescribed or lifestyle changes are recommended, they want to discuss why these changes are necessary and have some input as to how these changes happen.
• “I like to have my privacy respected. It can be uncomfortable talking about things with my parents in the room.”
Many youth reported privacy and one-on-one time with their providers being important. They reported being uncomfortable or embarrassed talking about certain topics in front of their parents and valued providers who respected their privacy.
Private time with patients is not meant to cut parents out of the visit; rather it is meant to be a time when patients can openly discuss concerns with their providers and begin to take ownership of their health and bodies.
Many of the suggestions above are helpful in the care of all youth, regardless of sexual orientation and gender identity. Most of the qualities youth were looking for in providers were related to communication and respect and are in keeping with current research and guidelines on creating youth friendly services. Following these suggestions, and continuing to find ways to include youth in our conversations to improve health care, are just a few ways we can make youth feel more comfortable in this setting and hopefully begin to achieve health equity for all youth.
Acknowledgments
I appreciate the youth at Kaleidoscope Youth Center for giving their time and continually helping me improve the care I provide to all patients and allowing me to share this information with others.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.
This past month has been a difficult one. The violence committed against people on the basis of presumed sexual orientation, color of skin, religion, and occupation has been difficult to make sense of. These tragic and horrible events highlight the continued need to focus on building inclusive environments and fostering communication between people with different backgrounds, points of view, and life experiences.
Several of my past articles have touched on the need to create inclusive environments for our LGBTQ (lesbian, gay, bisexual, transgender, questioning) patients, but have not included direct input from youth. With this in mind, I sat down with several youth from our local youth LGBTQ center in Ohio to ask them how we as health care providers could be more supportive of our patients.
Here are some of their suggestions:
• “Trust your patients. … Respect that I am knowledgeable about my body.”
Youth in the group stated that they want providers who listen to and trust what they say. Youth reported that they trust that their medical providers are experts in medicine and the care of patients, but they are the experts on themselves.
• “Don’t blame the hormones. Don’t blame things on puberty. … It’s not just a phase.”
Youth reported that they often get frustrated when providers assume that their sexual orientation or gender identity is “just a phase.” While adolescence can be a time of experimentation, it is important to acknowledge and respect youth’s emerging identities.
• “Know your patients. Educate yourselves.”
Many youth reported that while they are happy to share their stories, they do not want to be put in the role of having to educate their providers about the basics.
Youth expect that their providers have a general understanding of LGBTQ terminology and health care needs. They are happy to answer specific questions, but expect a degree of cultural competency from their providers.
• “Don’t push birth control. Don’t make assumptions about my behaviors; ask me first.”
Many female-bodied youth had the perception that providers make assumptions about their sexual orientation (assuming they are heterosexual), sexual behaviors, and risk of unintended pregnancy and sexually transmitted diseases.
Youth reported that they are open to conversations about reproductive health and safe sex, but get turned off when providers incorrectly assume they are heterosexual and in need of birth control. Asking about sexual attraction and the gender of partners as a routine part of any adolescent sexual history can help providers avoid these mistakes.
• “Have a discussion versus telling people what to do. Tell me why you are checking things and what they mean.”
Youth reported that they were interested in being active participants in their health care visits. They stated that if labs are being checked, they want to know why and what the results mean. When medications are prescribed or lifestyle changes are recommended, they want to discuss why these changes are necessary and have some input as to how these changes happen.
• “I like to have my privacy respected. It can be uncomfortable talking about things with my parents in the room.”
Many youth reported privacy and one-on-one time with their providers being important. They reported being uncomfortable or embarrassed talking about certain topics in front of their parents and valued providers who respected their privacy.
Private time with patients is not meant to cut parents out of the visit; rather it is meant to be a time when patients can openly discuss concerns with their providers and begin to take ownership of their health and bodies.
Many of the suggestions above are helpful in the care of all youth, regardless of sexual orientation and gender identity. Most of the qualities youth were looking for in providers were related to communication and respect and are in keeping with current research and guidelines on creating youth friendly services. Following these suggestions, and continuing to find ways to include youth in our conversations to improve health care, are just a few ways we can make youth feel more comfortable in this setting and hopefully begin to achieve health equity for all youth.
Acknowledgments
I appreciate the youth at Kaleidoscope Youth Center for giving their time and continually helping me improve the care I provide to all patients and allowing me to share this information with others.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.
This past month has been a difficult one. The violence committed against people on the basis of presumed sexual orientation, color of skin, religion, and occupation has been difficult to make sense of. These tragic and horrible events highlight the continued need to focus on building inclusive environments and fostering communication between people with different backgrounds, points of view, and life experiences.
Several of my past articles have touched on the need to create inclusive environments for our LGBTQ (lesbian, gay, bisexual, transgender, questioning) patients, but have not included direct input from youth. With this in mind, I sat down with several youth from our local youth LGBTQ center in Ohio to ask them how we as health care providers could be more supportive of our patients.
Here are some of their suggestions:
• “Trust your patients. … Respect that I am knowledgeable about my body.”
Youth in the group stated that they want providers who listen to and trust what they say. Youth reported that they trust that their medical providers are experts in medicine and the care of patients, but they are the experts on themselves.
• “Don’t blame the hormones. Don’t blame things on puberty. … It’s not just a phase.”
Youth reported that they often get frustrated when providers assume that their sexual orientation or gender identity is “just a phase.” While adolescence can be a time of experimentation, it is important to acknowledge and respect youth’s emerging identities.
• “Know your patients. Educate yourselves.”
Many youth reported that while they are happy to share their stories, they do not want to be put in the role of having to educate their providers about the basics.
Youth expect that their providers have a general understanding of LGBTQ terminology and health care needs. They are happy to answer specific questions, but expect a degree of cultural competency from their providers.
• “Don’t push birth control. Don’t make assumptions about my behaviors; ask me first.”
Many female-bodied youth had the perception that providers make assumptions about their sexual orientation (assuming they are heterosexual), sexual behaviors, and risk of unintended pregnancy and sexually transmitted diseases.
Youth reported that they are open to conversations about reproductive health and safe sex, but get turned off when providers incorrectly assume they are heterosexual and in need of birth control. Asking about sexual attraction and the gender of partners as a routine part of any adolescent sexual history can help providers avoid these mistakes.
• “Have a discussion versus telling people what to do. Tell me why you are checking things and what they mean.”
Youth reported that they were interested in being active participants in their health care visits. They stated that if labs are being checked, they want to know why and what the results mean. When medications are prescribed or lifestyle changes are recommended, they want to discuss why these changes are necessary and have some input as to how these changes happen.
• “I like to have my privacy respected. It can be uncomfortable talking about things with my parents in the room.”
Many youth reported privacy and one-on-one time with their providers being important. They reported being uncomfortable or embarrassed talking about certain topics in front of their parents and valued providers who respected their privacy.
Private time with patients is not meant to cut parents out of the visit; rather it is meant to be a time when patients can openly discuss concerns with their providers and begin to take ownership of their health and bodies.
Many of the suggestions above are helpful in the care of all youth, regardless of sexual orientation and gender identity. Most of the qualities youth were looking for in providers were related to communication and respect and are in keeping with current research and guidelines on creating youth friendly services. Following these suggestions, and continuing to find ways to include youth in our conversations to improve health care, are just a few ways we can make youth feel more comfortable in this setting and hopefully begin to achieve health equity for all youth.
Acknowledgments
I appreciate the youth at Kaleidoscope Youth Center for giving their time and continually helping me improve the care I provide to all patients and allowing me to share this information with others.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.

Me? Address social determinants of health? How?
When I heard the American Academy of Pediatrics call for pediatricians to address poverty and social determinants of health, I – and maybe you, too – thought, “Great idea. But how am I, as a practicing pediatrician, supposed to help with such overwhelming and socially determined factors?”
It seems that the best way to reduce poverty, homelessness, and inadequate education is to advocate and vote to maintain or expand proven social programs. But there are also more proximal “relational” (relationship) factors we can address. The Adverse Childhood Experiences (ACE) study showed that the number of ACEs reported in their pasts by adults has a nearly linear relationship to long-term morbidities, including suicide, depression, obesity, smoking, substance abuse, heart disease, and early death. The ACE events during childhood – besides lack of food – came from the child’s relationships: abuse (emotional, physical, or sexual) and family dysfunction (mother abused; loss of a caregiver through divorce, separation, or death; household members with alcohol or substance abuse, mental illness, or time in prison).

The most important step you can take to prevent your patients from ACEs is detection. You have to ask parents, either verbally or with a screening tool about current factors that could be harmful to the child. You may think, “My patients don’t have these problems,” but abuse, intimate partner violence (IPV), depression, substance use, and loss occur in families of all kinds and means. Even the presence of food insecurity and imprisonment in some of my “put together” families has surprised me.
There are a number of tools available to screen for individual factors such as parental depression (Edinburgh Postnatal Screening, Patient Health Questionnaire-2 and -4), IPV, substance use (CRAFFT, which stands for Car, Relax, Alone, Forget, Friends, Trouble), and food insecurity. Tools covering multiple risk factors also are available on paper (Safe Environment for Every Kid [SEEK], Survey of Well-being of Young Children [SWYC]) or online (CHADIS). Rather than being overly intrusive, parents report accepting these questions as representing your caring about them as well as their child.
Coverage for screening and counseling for depression and IPV is mandated by the Affordable Care Act. As of July 2016, screening for maternal depression by pediatricians is paid for by Medicaid and many other insurers, often as part of the well-child visit, according to the Center for Medicaid and CHIP Services’ Informational Bulletin of May 11, 2016. For patient-centered medical homes, there is a mandate for referral and care coordination (AHRQ Publication No.11-M005-EF, December 2010). New value-based payment mechanisms are likely to pay you based on such screening and referral processes (e.g. New York), so we had best prepare (“Value-Based Payment Models for Medicaid Child Health Services,” Report to the Schuyler Center for Analysis and Advocacy and the United Hospital Fund, July 13, 2016).
But what to do when the screen or questions reveal a problem? Your first impulse is likely to be to refer. But unlike referrals for a physical health issue such as severe anemia for which the parent calls the hematologist immediately, in the case of these touchy, embarrassing, or emotionally charged problems, accepting help may not be so easy. It may be the financially critical partner who is the substance user or the mother herself who is too depressed to move towards help. For problems such as lack of food or the need to get a GED (general education development), the referral may be successful by supplying phone numbers. Referrals for IPV, one of the most common (greater than 29%) and damaging ACEs to the child, who is exposed to violence and often abused, have been found to mainly fail from simply making a referral.
Just as for a positive blood screen, for a referral to be effective more information is needed. In the case of a family stressor, you need to find out the nature and extent of the problem, the immediacy of the danger, and what has been done so far to reduce it. Research now shows that the most effective way to collect this information is using motivational interviewing (MI) techniques that nonjudgmentally determine not just the facts, but engage parents in weighing the pros and cons of changing the status quo, their readiness to change, the types of interventions that might be acceptable, and what would tell them that it was time to act. When using MI, you are actually doing more than making a referral, you are beginning to address the problem you uncovered.

The MI process strengthens the trust in your relationship with the parent, starting with reflecting on the issue (“It sounds as though you don’t always feel safe at home”), empathizing (“That must be really scary. I am sorry you are going through that”), and assessing (“May I try to help you with this?”).
After collecting the pros and cons for making a change, either in the interview or via the screening tool SEEK Plus in CHADIS, your job is to help the parent weigh them (“On the one hand you love him and need his income, but on the other hand you are so afraid that you can’t sleep and your children are too nervous to concentrate in school.”) Then you need to elicit what would be enough to move them (“How will you know when it is time to act?”) and to assess readiness to change (“What kinds of help would you be open to?”), then offer that kind of help (“I would like to connect you to a professional who has a lot of experience helping people in your situation. Is it okay if we call her right now?”). Provide written contact information, of course, but actually assisting by calling the appropriate resource or even doing a “warm handoff” in person is more effective.
Obviously, to make an effective referral, we need resources assembled in advance for the most common issues. UnitedWay.org is a good place to include on your list.
Our job, however, is not over with an “accepted” referral. Most referrals are not kept, help is never received, and risk to the child is not averted. There are many potential barriers to families’ accessing help – time off work, money, transportation, or child care – but difficulty generating the courage to change is understandable and may resolve only gradually with your work and support. It is wise to tell the parent that “I (or someone on your staff) will check in on how this goes, okay?”
Making a follow-up appointment with you is important, even if you feel helpless to do more than refer. Why? A return visit is a chance to show that you care, to be sure they went, and to get information on the quality and appropriateness of the care provided so you can support it or refer elsewhere. Perhaps most importantly, it shows that you do not reject them for revealing what they may see as personal failure or immoral behavior so that you can continue caring for and monitoring their at-risk child.
What if they decline help, no resources are to be found, or the damage has already occurred? You still have valuable help to provide. Our goal is to ameliorate the impact of the stressors on the child now and in the future. Just as relational factors can stress the child, improving supportive relationships is key to reducing their effects. Parents with ACE risk factors are often self-absorbed in their pain, using smoking, substances, or alcohol to dampen it and moving from one troubled relationship to another in response to past trauma; thus they are emotionally unavailable to the child.
You can help them by focusing on the wonders of their child, encouraging daily individual time for play, and modeling Reach Out and Read as a supportive, calm activity they can do even when stressed. You can encourage the practice of mindfulness – an exercise of letting thoughts pass over them without judgment while breathing rhythmically – for stressed parents and school-aged children. It has been shown to be an effective intervention for recovering from past as well as current stress. Children also should receive any needed mental health care.
An emotionally available, supportive, nurturing parent is the most important protective factor for the child’s development of emotion regulation, resilience, and the ability to cope with adversity throughout their life. Referring parents to services such as home visiting, Healthy Steps, or parent-child therapy to build these skills has evidence for improving relational health. Helping the parents avoid ACEs for their children and assisting them in ameliorating them, if they occur, are important investments in long-term health that you can provide.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.
When I heard the American Academy of Pediatrics call for pediatricians to address poverty and social determinants of health, I – and maybe you, too – thought, “Great idea. But how am I, as a practicing pediatrician, supposed to help with such overwhelming and socially determined factors?”
It seems that the best way to reduce poverty, homelessness, and inadequate education is to advocate and vote to maintain or expand proven social programs. But there are also more proximal “relational” (relationship) factors we can address. The Adverse Childhood Experiences (ACE) study showed that the number of ACEs reported in their pasts by adults has a nearly linear relationship to long-term morbidities, including suicide, depression, obesity, smoking, substance abuse, heart disease, and early death. The ACE events during childhood – besides lack of food – came from the child’s relationships: abuse (emotional, physical, or sexual) and family dysfunction (mother abused; loss of a caregiver through divorce, separation, or death; household members with alcohol or substance abuse, mental illness, or time in prison).
The most important step you can take to prevent your patients from ACEs is detection. You have to ask parents, either verbally or with a screening tool about current factors that could be harmful to the child. You may think, “My patients don’t have these problems,” but abuse, intimate partner violence (IPV), depression, substance use, and loss occur in families of all kinds and means. Even the presence of food insecurity and imprisonment in some of my “put together” families has surprised me.
There are a number of tools available to screen for individual factors such as parental depression (Edinburgh Postnatal Screening, Patient Health Questionnaire-2 and -4), IPV, substance use (CRAFFT, which stands for Car, Relax, Alone, Forget, Friends, Trouble), and food insecurity. Tools covering multiple risk factors also are available on paper (Safe Environment for Every Kid [SEEK], Survey of Well-being of Young Children [SWYC]) or online (CHADIS). Rather than being overly intrusive, parents report accepting these questions as representing your caring about them as well as their child.
Coverage for screening and counseling for depression and IPV is mandated by the Affordable Care Act. As of July 2016, screening for maternal depression by pediatricians is paid for by Medicaid and many other insurers, often as part of the well-child visit, according to the Center for Medicaid and CHIP Services’ Informational Bulletin of May 11, 2016. For patient-centered medical homes, there is a mandate for referral and care coordination (AHRQ Publication No.11-M005-EF, December 2010). New value-based payment mechanisms are likely to pay you based on such screening and referral processes (e.g. New York), so we had best prepare (“Value-Based Payment Models for Medicaid Child Health Services,” Report to the Schuyler Center for Analysis and Advocacy and the United Hospital Fund, July 13, 2016).
But what to do when the screen or questions reveal a problem? Your first impulse is likely to be to refer. But unlike referrals for a physical health issue such as severe anemia for which the parent calls the hematologist immediately, in the case of these touchy, embarrassing, or emotionally charged problems, accepting help may not be so easy. It may be the financially critical partner who is the substance user or the mother herself who is too depressed to move towards help. For problems such as lack of food or the need to get a GED (general education development), the referral may be successful by supplying phone numbers. Referrals for IPV, one of the most common (greater than 29%) and damaging ACEs to the child, who is exposed to violence and often abused, have been found to mainly fail from simply making a referral.
Just as for a positive blood screen, for a referral to be effective more information is needed. In the case of a family stressor, you need to find out the nature and extent of the problem, the immediacy of the danger, and what has been done so far to reduce it. Research now shows that the most effective way to collect this information is using motivational interviewing (MI) techniques that nonjudgmentally determine not just the facts, but engage parents in weighing the pros and cons of changing the status quo, their readiness to change, the types of interventions that might be acceptable, and what would tell them that it was time to act. When using MI, you are actually doing more than making a referral, you are beginning to address the problem you uncovered.
The MI process strengthens the trust in your relationship with the parent, starting with reflecting on the issue (“It sounds as though you don’t always feel safe at home”), empathizing (“That must be really scary. I am sorry you are going through that”), and assessing (“May I try to help you with this?”).
After collecting the pros and cons for making a change, either in the interview or via the screening tool SEEK Plus in CHADIS, your job is to help the parent weigh them (“On the one hand you love him and need his income, but on the other hand you are so afraid that you can’t sleep and your children are too nervous to concentrate in school.”) Then you need to elicit what would be enough to move them (“How will you know when it is time to act?”) and to assess readiness to change (“What kinds of help would you be open to?”), then offer that kind of help (“I would like to connect you to a professional who has a lot of experience helping people in your situation. Is it okay if we call her right now?”). Provide written contact information, of course, but actually assisting by calling the appropriate resource or even doing a “warm handoff” in person is more effective.
Obviously, to make an effective referral, we need resources assembled in advance for the most common issues. UnitedWay.org is a good place to include on your list.
Our job, however, is not over with an “accepted” referral. Most referrals are not kept, help is never received, and risk to the child is not averted. There are many potential barriers to families’ accessing help – time off work, money, transportation, or child care – but difficulty generating the courage to change is understandable and may resolve only gradually with your work and support. It is wise to tell the parent that “I (or someone on your staff) will check in on how this goes, okay?”
Making a follow-up appointment with you is important, even if you feel helpless to do more than refer. Why? A return visit is a chance to show that you care, to be sure they went, and to get information on the quality and appropriateness of the care provided so you can support it or refer elsewhere. Perhaps most importantly, it shows that you do not reject them for revealing what they may see as personal failure or immoral behavior so that you can continue caring for and monitoring their at-risk child.
What if they decline help, no resources are to be found, or the damage has already occurred? You still have valuable help to provide. Our goal is to ameliorate the impact of the stressors on the child now and in the future. Just as relational factors can stress the child, improving supportive relationships is key to reducing their effects. Parents with ACE risk factors are often self-absorbed in their pain, using smoking, substances, or alcohol to dampen it and moving from one troubled relationship to another in response to past trauma; thus they are emotionally unavailable to the child.
You can help them by focusing on the wonders of their child, encouraging daily individual time for play, and modeling Reach Out and Read as a supportive, calm activity they can do even when stressed. You can encourage the practice of mindfulness – an exercise of letting thoughts pass over them without judgment while breathing rhythmically – for stressed parents and school-aged children. It has been shown to be an effective intervention for recovering from past as well as current stress. Children also should receive any needed mental health care.
An emotionally available, supportive, nurturing parent is the most important protective factor for the child’s development of emotion regulation, resilience, and the ability to cope with adversity throughout their life. Referring parents to services such as home visiting, Healthy Steps, or parent-child therapy to build these skills has evidence for improving relational health. Helping the parents avoid ACEs for their children and assisting them in ameliorating them, if they occur, are important investments in long-term health that you can provide.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.
When I heard the American Academy of Pediatrics call for pediatricians to address poverty and social determinants of health, I – and maybe you, too – thought, “Great idea. But how am I, as a practicing pediatrician, supposed to help with such overwhelming and socially determined factors?”
It seems that the best way to reduce poverty, homelessness, and inadequate education is to advocate and vote to maintain or expand proven social programs. But there are also more proximal “relational” (relationship) factors we can address. The Adverse Childhood Experiences (ACE) study showed that the number of ACEs reported in their pasts by adults has a nearly linear relationship to long-term morbidities, including suicide, depression, obesity, smoking, substance abuse, heart disease, and early death. The ACE events during childhood – besides lack of food – came from the child’s relationships: abuse (emotional, physical, or sexual) and family dysfunction (mother abused; loss of a caregiver through divorce, separation, or death; household members with alcohol or substance abuse, mental illness, or time in prison).
The most important step you can take to prevent your patients from ACEs is detection. You have to ask parents, either verbally or with a screening tool about current factors that could be harmful to the child. You may think, “My patients don’t have these problems,” but abuse, intimate partner violence (IPV), depression, substance use, and loss occur in families of all kinds and means. Even the presence of food insecurity and imprisonment in some of my “put together” families has surprised me.
There are a number of tools available to screen for individual factors such as parental depression (Edinburgh Postnatal Screening, Patient Health Questionnaire-2 and -4), IPV, substance use (CRAFFT, which stands for Car, Relax, Alone, Forget, Friends, Trouble), and food insecurity. Tools covering multiple risk factors also are available on paper (Safe Environment for Every Kid [SEEK], Survey of Well-being of Young Children [SWYC]) or online (CHADIS). Rather than being overly intrusive, parents report accepting these questions as representing your caring about them as well as their child.
Coverage for screening and counseling for depression and IPV is mandated by the Affordable Care Act. As of July 2016, screening for maternal depression by pediatricians is paid for by Medicaid and many other insurers, often as part of the well-child visit, according to the Center for Medicaid and CHIP Services’ Informational Bulletin of May 11, 2016. For patient-centered medical homes, there is a mandate for referral and care coordination (AHRQ Publication No.11-M005-EF, December 2010). New value-based payment mechanisms are likely to pay you based on such screening and referral processes (e.g. New York), so we had best prepare (“Value-Based Payment Models for Medicaid Child Health Services,” Report to the Schuyler Center for Analysis and Advocacy and the United Hospital Fund, July 13, 2016).
But what to do when the screen or questions reveal a problem? Your first impulse is likely to be to refer. But unlike referrals for a physical health issue such as severe anemia for which the parent calls the hematologist immediately, in the case of these touchy, embarrassing, or emotionally charged problems, accepting help may not be so easy. It may be the financially critical partner who is the substance user or the mother herself who is too depressed to move towards help. For problems such as lack of food or the need to get a GED (general education development), the referral may be successful by supplying phone numbers. Referrals for IPV, one of the most common (greater than 29%) and damaging ACEs to the child, who is exposed to violence and often abused, have been found to mainly fail from simply making a referral.
Just as for a positive blood screen, for a referral to be effective more information is needed. In the case of a family stressor, you need to find out the nature and extent of the problem, the immediacy of the danger, and what has been done so far to reduce it. Research now shows that the most effective way to collect this information is using motivational interviewing (MI) techniques that nonjudgmentally determine not just the facts, but engage parents in weighing the pros and cons of changing the status quo, their readiness to change, the types of interventions that might be acceptable, and what would tell them that it was time to act. When using MI, you are actually doing more than making a referral, you are beginning to address the problem you uncovered.
The MI process strengthens the trust in your relationship with the parent, starting with reflecting on the issue (“It sounds as though you don’t always feel safe at home”), empathizing (“That must be really scary. I am sorry you are going through that”), and assessing (“May I try to help you with this?”).
After collecting the pros and cons for making a change, either in the interview or via the screening tool SEEK Plus in CHADIS, your job is to help the parent weigh them (“On the one hand you love him and need his income, but on the other hand you are so afraid that you can’t sleep and your children are too nervous to concentrate in school.”) Then you need to elicit what would be enough to move them (“How will you know when it is time to act?”) and to assess readiness to change (“What kinds of help would you be open to?”), then offer that kind of help (“I would like to connect you to a professional who has a lot of experience helping people in your situation. Is it okay if we call her right now?”). Provide written contact information, of course, but actually assisting by calling the appropriate resource or even doing a “warm handoff” in person is more effective.
Obviously, to make an effective referral, we need resources assembled in advance for the most common issues. UnitedWay.org is a good place to include on your list.
Our job, however, is not over with an “accepted” referral. Most referrals are not kept, help is never received, and risk to the child is not averted. There are many potential barriers to families’ accessing help – time off work, money, transportation, or child care – but difficulty generating the courage to change is understandable and may resolve only gradually with your work and support. It is wise to tell the parent that “I (or someone on your staff) will check in on how this goes, okay?”
Making a follow-up appointment with you is important, even if you feel helpless to do more than refer. Why? A return visit is a chance to show that you care, to be sure they went, and to get information on the quality and appropriateness of the care provided so you can support it or refer elsewhere. Perhaps most importantly, it shows that you do not reject them for revealing what they may see as personal failure or immoral behavior so that you can continue caring for and monitoring their at-risk child.
What if they decline help, no resources are to be found, or the damage has already occurred? You still have valuable help to provide. Our goal is to ameliorate the impact of the stressors on the child now and in the future. Just as relational factors can stress the child, improving supportive relationships is key to reducing their effects. Parents with ACE risk factors are often self-absorbed in their pain, using smoking, substances, or alcohol to dampen it and moving from one troubled relationship to another in response to past trauma; thus they are emotionally unavailable to the child.
You can help them by focusing on the wonders of their child, encouraging daily individual time for play, and modeling Reach Out and Read as a supportive, calm activity they can do even when stressed. You can encourage the practice of mindfulness – an exercise of letting thoughts pass over them without judgment while breathing rhythmically – for stressed parents and school-aged children. It has been shown to be an effective intervention for recovering from past as well as current stress. Children also should receive any needed mental health care.
An emotionally available, supportive, nurturing parent is the most important protective factor for the child’s development of emotion regulation, resilience, and the ability to cope with adversity throughout their life. Referring parents to services such as home visiting, Healthy Steps, or parent-child therapy to build these skills has evidence for improving relational health. Helping the parents avoid ACEs for their children and assisting them in ameliorating them, if they occur, are important investments in long-term health that you can provide.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.

Vegetarian diets 101
In the era where obesity is the No. 1 health crisis affecting people of all ages, physicians are often faced with questions regarding restricted diets or a patient may report that they are “vegetarian” in their history. Although new trendy diets appear all the time, “vegetarian inclined” diets are among the most common. A study conducted in 2008 identified that approximately 10% of Americans age 18 and older consumed a vegetarian diet.1 It is important to know the basics so that you can offer some guidance and look for possible deficiencies that may result from an altered diet.
Studies show that children who follow a vegetarian diet have normal growth and development but tend to be leaner than their omnivore counterparts.2 A healthy diet consumed in childhood lessens the risk for chronic diseases and promotes optimal growth and development. But altered or restricted diets in adolescents can be tricky because teens are actively growing and therefore usually need greater amounts of vital nutrients. So guidance is important to avoid common mistakes.

The simplest way to remember what is appropriate in a vegetarian diet is the restriction on intake of any food that once had a mother and a father. The vegetarian diet is further divided based on what it includes or excludes. Although the below list is not complete, it outlines the more common vegetarian diets:
• Vegan. This diet restricts intake of any animal product.
• Macrobiotics. This diet consists of whole grain, brown rice, fruits, and vegetables, and restricts intake of white meat or fish to twice a week.
• Lacto-vegetarian. This diet is one which allows milk products.
• Ovo vegetarian. – This diet allows eggs, but no meat, dairy, or fish.
• Pescitarian. This diet restricts meats, dairy, and eggs, but allows fish.
• Semi-vegetarian. This diet just restricts eating meat.
It is important to encourage anyone wishing to follow a vegetarian diet to fully research and understand what it entails. Health.gov under “dietary guidelines 2015-2020” is a wonderful reference to help understand how much of vital nutrients should be consumed to promote healthy eating habits and prevent deficiencies.
The key nutrients to discuss with patients are intake of protein, iron, calcium, vitamin B12, and vitamin D. Inadequate or incorrect intake can lead to deficiency of the vital nutrients that likely will result in disease.
Protein is a necessary nutrient because it provides the essential amino acids necessary for growth and repair. When animal protein breaks down, it provides all of the essential amino acids, unlike plant protein which can be deficient in some of the amino acids. Because each source of plant protein varies in the amino acid it is deficient in, it is important to have a mixed source of protein to ensure adequate intake. The soy bean has comparable amounts of protein to animal protein. Other sources of protein are legumes, grain, cereal, eggs, nuts, Greek yogurt, cottage cheese, but these are less digestible so greater consumption is needed to meet the daily requirements. Deficiency in protein can result in impaired growth.
Iron that is obtained from animals or meat sources has heme component, which makes it easier to absorb. Iron obtained from plants does not contain heme component and therefore is more difficult to absorb. Ascorbic acid (vitamin C) helps nonheme iron to be absorbed, but must be taken with an iron source to be effective. Therefore, vitamin C–containing foods such as fruits and vegetables should be consumed at every meal to assist in iron absorption. Deficiency in iron can lead to anemia and reduced energy.
Calcium is an important nutrient for bone formation, and deficiency can lead to increased risk for fracture and osteoporosis later in life. Its excretion and absorption can be affected by other nutrients, such as iron and zinc, present during digestion. Milk and dairy products are the most common source for calcium intake, but there are other calcium sources such as kale, broccoli, and food fortified with calcium such as cereal and orange juice. These foods can be better sources of calcium than supplements because they allow for better absorption.
Vitamin D is needed for calcium and phosphorus absorption, which is important for proper bone formation. Vitamin D is found in dairy products, fortified food and beverages, and exposure to the sun. Those living in colder climates and of darker pigmentation are at greater risk of deficiency so supplementation is usually necessary. Deficiency of vitamin D can lead to rickets.
Vitamin B12 is found in meat, fish, and dairy products, but not in plants. Intake of B12 is likely to be deficient in vegans because they do not consume most of those sources. Vegans are at a significant risk of vitamin B12 deficiency3 which can lead to macrocytosis, anemia, and decreased energy.
Educating families on healthy eating is essential at any visit. A good understanding of the possible deficiencies that can occur with restricted diets will allow for proper guidance and avoidable diseases.
References
1. Stahler C. “How Many Youth Are Vegetarian? The Vegetarian Resource Group Asks in a 2010 National Poll.”
2. Pediatrics. 1989 Sep;84(3):475-81.
3. J Am Diet Assoc. 2003 Jun;103(6):771-5.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
In the era where obesity is the No. 1 health crisis affecting people of all ages, physicians are often faced with questions regarding restricted diets or a patient may report that they are “vegetarian” in their history. Although new trendy diets appear all the time, “vegetarian inclined” diets are among the most common. A study conducted in 2008 identified that approximately 10% of Americans age 18 and older consumed a vegetarian diet.1 It is important to know the basics so that you can offer some guidance and look for possible deficiencies that may result from an altered diet.
Studies show that children who follow a vegetarian diet have normal growth and development but tend to be leaner than their omnivore counterparts.2 A healthy diet consumed in childhood lessens the risk for chronic diseases and promotes optimal growth and development. But altered or restricted diets in adolescents can be tricky because teens are actively growing and therefore usually need greater amounts of vital nutrients. So guidance is important to avoid common mistakes.
The simplest way to remember what is appropriate in a vegetarian diet is the restriction on intake of any food that once had a mother and a father. The vegetarian diet is further divided based on what it includes or excludes. Although the below list is not complete, it outlines the more common vegetarian diets:
• Vegan. This diet restricts intake of any animal product.
• Macrobiotics. This diet consists of whole grain, brown rice, fruits, and vegetables, and restricts intake of white meat or fish to twice a week.
• Lacto-vegetarian. This diet is one which allows milk products.
• Ovo vegetarian. – This diet allows eggs, but no meat, dairy, or fish.
• Pescitarian. This diet restricts meats, dairy, and eggs, but allows fish.
• Semi-vegetarian. This diet just restricts eating meat.
It is important to encourage anyone wishing to follow a vegetarian diet to fully research and understand what it entails. Health.gov under “dietary guidelines 2015-2020” is a wonderful reference to help understand how much of vital nutrients should be consumed to promote healthy eating habits and prevent deficiencies.
The key nutrients to discuss with patients are intake of protein, iron, calcium, vitamin B12, and vitamin D. Inadequate or incorrect intake can lead to deficiency of the vital nutrients that likely will result in disease.
Protein is a necessary nutrient because it provides the essential amino acids necessary for growth and repair. When animal protein breaks down, it provides all of the essential amino acids, unlike plant protein which can be deficient in some of the amino acids. Because each source of plant protein varies in the amino acid it is deficient in, it is important to have a mixed source of protein to ensure adequate intake. The soy bean has comparable amounts of protein to animal protein. Other sources of protein are legumes, grain, cereal, eggs, nuts, Greek yogurt, cottage cheese, but these are less digestible so greater consumption is needed to meet the daily requirements. Deficiency in protein can result in impaired growth.
Iron that is obtained from animals or meat sources has heme component, which makes it easier to absorb. Iron obtained from plants does not contain heme component and therefore is more difficult to absorb. Ascorbic acid (vitamin C) helps nonheme iron to be absorbed, but must be taken with an iron source to be effective. Therefore, vitamin C–containing foods such as fruits and vegetables should be consumed at every meal to assist in iron absorption. Deficiency in iron can lead to anemia and reduced energy.
Calcium is an important nutrient for bone formation, and deficiency can lead to increased risk for fracture and osteoporosis later in life. Its excretion and absorption can be affected by other nutrients, such as iron and zinc, present during digestion. Milk and dairy products are the most common source for calcium intake, but there are other calcium sources such as kale, broccoli, and food fortified with calcium such as cereal and orange juice. These foods can be better sources of calcium than supplements because they allow for better absorption.
Vitamin D is needed for calcium and phosphorus absorption, which is important for proper bone formation. Vitamin D is found in dairy products, fortified food and beverages, and exposure to the sun. Those living in colder climates and of darker pigmentation are at greater risk of deficiency so supplementation is usually necessary. Deficiency of vitamin D can lead to rickets.
Vitamin B12 is found in meat, fish, and dairy products, but not in plants. Intake of B12 is likely to be deficient in vegans because they do not consume most of those sources. Vegans are at a significant risk of vitamin B12 deficiency3 which can lead to macrocytosis, anemia, and decreased energy.
Educating families on healthy eating is essential at any visit. A good understanding of the possible deficiencies that can occur with restricted diets will allow for proper guidance and avoidable diseases.
References
1. Stahler C. “How Many Youth Are Vegetarian? The Vegetarian Resource Group Asks in a 2010 National Poll.”
2. Pediatrics. 1989 Sep;84(3):475-81.
3. J Am Diet Assoc. 2003 Jun;103(6):771-5.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
In the era where obesity is the No. 1 health crisis affecting people of all ages, physicians are often faced with questions regarding restricted diets or a patient may report that they are “vegetarian” in their history. Although new trendy diets appear all the time, “vegetarian inclined” diets are among the most common. A study conducted in 2008 identified that approximately 10% of Americans age 18 and older consumed a vegetarian diet.1 It is important to know the basics so that you can offer some guidance and look for possible deficiencies that may result from an altered diet.
Studies show that children who follow a vegetarian diet have normal growth and development but tend to be leaner than their omnivore counterparts.2 A healthy diet consumed in childhood lessens the risk for chronic diseases and promotes optimal growth and development. But altered or restricted diets in adolescents can be tricky because teens are actively growing and therefore usually need greater amounts of vital nutrients. So guidance is important to avoid common mistakes.
The simplest way to remember what is appropriate in a vegetarian diet is the restriction on intake of any food that once had a mother and a father. The vegetarian diet is further divided based on what it includes or excludes. Although the below list is not complete, it outlines the more common vegetarian diets:
• Vegan. This diet restricts intake of any animal product.
• Macrobiotics. This diet consists of whole grain, brown rice, fruits, and vegetables, and restricts intake of white meat or fish to twice a week.
• Lacto-vegetarian. This diet is one which allows milk products.
• Ovo vegetarian. – This diet allows eggs, but no meat, dairy, or fish.
• Pescitarian. This diet restricts meats, dairy, and eggs, but allows fish.
• Semi-vegetarian. This diet just restricts eating meat.
It is important to encourage anyone wishing to follow a vegetarian diet to fully research and understand what it entails. Health.gov under “dietary guidelines 2015-2020” is a wonderful reference to help understand how much of vital nutrients should be consumed to promote healthy eating habits and prevent deficiencies.
The key nutrients to discuss with patients are intake of protein, iron, calcium, vitamin B12, and vitamin D. Inadequate or incorrect intake can lead to deficiency of the vital nutrients that likely will result in disease.
Protein is a necessary nutrient because it provides the essential amino acids necessary for growth and repair. When animal protein breaks down, it provides all of the essential amino acids, unlike plant protein which can be deficient in some of the amino acids. Because each source of plant protein varies in the amino acid it is deficient in, it is important to have a mixed source of protein to ensure adequate intake. The soy bean has comparable amounts of protein to animal protein. Other sources of protein are legumes, grain, cereal, eggs, nuts, Greek yogurt, cottage cheese, but these are less digestible so greater consumption is needed to meet the daily requirements. Deficiency in protein can result in impaired growth.
Iron that is obtained from animals or meat sources has heme component, which makes it easier to absorb. Iron obtained from plants does not contain heme component and therefore is more difficult to absorb. Ascorbic acid (vitamin C) helps nonheme iron to be absorbed, but must be taken with an iron source to be effective. Therefore, vitamin C–containing foods such as fruits and vegetables should be consumed at every meal to assist in iron absorption. Deficiency in iron can lead to anemia and reduced energy.
Calcium is an important nutrient for bone formation, and deficiency can lead to increased risk for fracture and osteoporosis later in life. Its excretion and absorption can be affected by other nutrients, such as iron and zinc, present during digestion. Milk and dairy products are the most common source for calcium intake, but there are other calcium sources such as kale, broccoli, and food fortified with calcium such as cereal and orange juice. These foods can be better sources of calcium than supplements because they allow for better absorption.
Vitamin D is needed for calcium and phosphorus absorption, which is important for proper bone formation. Vitamin D is found in dairy products, fortified food and beverages, and exposure to the sun. Those living in colder climates and of darker pigmentation are at greater risk of deficiency so supplementation is usually necessary. Deficiency of vitamin D can lead to rickets.
Vitamin B12 is found in meat, fish, and dairy products, but not in plants. Intake of B12 is likely to be deficient in vegans because they do not consume most of those sources. Vegans are at a significant risk of vitamin B12 deficiency3 which can lead to macrocytosis, anemia, and decreased energy.
Educating families on healthy eating is essential at any visit. A good understanding of the possible deficiencies that can occur with restricted diets will allow for proper guidance and avoidable diseases.
References
1. Stahler C. “How Many Youth Are Vegetarian? The Vegetarian Resource Group Asks in a 2010 National Poll.”
2. Pediatrics. 1989 Sep;84(3):475-81.
3. J Am Diet Assoc. 2003 Jun;103(6):771-5.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.

Motivational interviewing for HPV vaccination well accepted by doctors
BALTIMORE – Motivational interviewing (MI) was well accepted by providers as part of a communication tool kit to improve human papillomavirus vaccine uptake, according to results of an eight-site study.
Overall, most of the 107 medical providers who participated in the cluster-randomized trial found MI to be a “somewhat useful” (47%) or “very useful” (31%) tactic to use when discussing human papillomavirus (HPV) vaccination with parents of adolescents. The overall amount of time that providers spent discussing vaccinations actually decreased after implementing MI; at the same time, providers felt that they had more power to influence parental decision-making when using MI techniques.

“Primary care providers given the Physician Communication Toolkit used MI frequently, and this use was generally sustained over time,” said lead author Amanda Dempsey, MD, who presented the findings during a poster symposium at the annual meeting of the Pediatric Academic Societies.
Motivational interviewing, an open-ended, nonjudgmental listening and communication style, was taught to providers in one 30-minute webinar and two 1-hour in-person role-playing sessions. Participants were able to practice using MI both in circumstances where parents were accepting of vaccination, and with vaccine-hesitant families.
Participating providers were surveyed pretraining and at 4, 7, and 10 months after the training to assess their practices in the preceding month. The two primary outcome measures assessed, and compared from baseline, were the estimated time spent discussing HPV vaccination with both vaccine-hesitant and nonhesitant families, and the providers’ perceived abilities to influence decisions about HPV. Dr. Dempsey and her colleagues also asked whether practitioners were actually using MI techniques with vaccine-hesitant parents, and whether they found the techniques useful in HPV vaccination discussions.
Dr. Dempsey, associate professor of pediatrics at Children’s Hospital Colorado in Aurora, said that uptake of MI was initially high and remained so. Three months after the intervention, 85% of providers reported they were using MI; at 9 months after the intervention, the figure was 72%.
Previous research has shown that providers generally do not communicate strong recommendations about HPV vaccination. “Providers often feel the parents will argue with them about it, and sometimes don’t even bring it up,” Dr. Dempsey said in an interview. “Anecdotally, providers found MI a useful way to frame the conversation, and they found it less confrontational.”
Overall, about three-quarters of providers responding to the sequential surveys were physicians, another 15%-20% were physician assistants, and the remainder were nurse practitioners. About one in four respondents were male. The pediatric and family medicine practices were approximately evenly divided between public and private clinics.
Although participation in the training and the subsequent surveys was voluntary, uptake was fairly high at participating clinics. The training was offered for 25 MOC (maintenance of certification) part 4 credits, which probably helped participation rates, said Dr. Dempsey.
The small sample size of the study, said Dr. Dempsey, limits the generalizability of the findings. However, the eight sites chosen represented a wide range of socioeconomic and cultural demographics in the patients served. Also, self-report of MI use may be subject to some bias. Finally, because this was a naturalistic study that allowed providers full discretion in using the various components of the Physician Communication Toolkit, it was not possible to perform a completely independent analysis of the effects of using MI apart from the other toolkit components.
“Use of MI did not appear to lengthen the time of clinical visits, and in some cases may actually shorten them,” said Dr. Dempsey. In addition to analyzing whether MI and other components of the toolkit increased HPV vaccine uptake rates, Dr. Dempsey and her colleagues also plan to explore whether MI would be an effective approach to use when discussing immunizations with parents of infants and younger children.
The study was funded by the National Center for Immunization and Respiratory Diseases and the Centers for Disease Control and Prevention, with survey administration supported by the National Institutes of Health. Dr. Dempsey reported no conflicts of interest.
On Twitter @karioakes
BALTIMORE – Motivational interviewing (MI) was well accepted by providers as part of a communication tool kit to improve human papillomavirus vaccine uptake, according to results of an eight-site study.
Overall, most of the 107 medical providers who participated in the cluster-randomized trial found MI to be a “somewhat useful” (47%) or “very useful” (31%) tactic to use when discussing human papillomavirus (HPV) vaccination with parents of adolescents. The overall amount of time that providers spent discussing vaccinations actually decreased after implementing MI; at the same time, providers felt that they had more power to influence parental decision-making when using MI techniques.
“Primary care providers given the Physician Communication Toolkit used MI frequently, and this use was generally sustained over time,” said lead author Amanda Dempsey, MD, who presented the findings during a poster symposium at the annual meeting of the Pediatric Academic Societies.
Motivational interviewing, an open-ended, nonjudgmental listening and communication style, was taught to providers in one 30-minute webinar and two 1-hour in-person role-playing sessions. Participants were able to practice using MI both in circumstances where parents were accepting of vaccination, and with vaccine-hesitant families.
Participating providers were surveyed pretraining and at 4, 7, and 10 months after the training to assess their practices in the preceding month. The two primary outcome measures assessed, and compared from baseline, were the estimated time spent discussing HPV vaccination with both vaccine-hesitant and nonhesitant families, and the providers’ perceived abilities to influence decisions about HPV. Dr. Dempsey and her colleagues also asked whether practitioners were actually using MI techniques with vaccine-hesitant parents, and whether they found the techniques useful in HPV vaccination discussions.
Dr. Dempsey, associate professor of pediatrics at Children’s Hospital Colorado in Aurora, said that uptake of MI was initially high and remained so. Three months after the intervention, 85% of providers reported they were using MI; at 9 months after the intervention, the figure was 72%.
Previous research has shown that providers generally do not communicate strong recommendations about HPV vaccination. “Providers often feel the parents will argue with them about it, and sometimes don’t even bring it up,” Dr. Dempsey said in an interview. “Anecdotally, providers found MI a useful way to frame the conversation, and they found it less confrontational.”
Overall, about three-quarters of providers responding to the sequential surveys were physicians, another 15%-20% were physician assistants, and the remainder were nurse practitioners. About one in four respondents were male. The pediatric and family medicine practices were approximately evenly divided between public and private clinics.
Although participation in the training and the subsequent surveys was voluntary, uptake was fairly high at participating clinics. The training was offered for 25 MOC (maintenance of certification) part 4 credits, which probably helped participation rates, said Dr. Dempsey.
The small sample size of the study, said Dr. Dempsey, limits the generalizability of the findings. However, the eight sites chosen represented a wide range of socioeconomic and cultural demographics in the patients served. Also, self-report of MI use may be subject to some bias. Finally, because this was a naturalistic study that allowed providers full discretion in using the various components of the Physician Communication Toolkit, it was not possible to perform a completely independent analysis of the effects of using MI apart from the other toolkit components.
“Use of MI did not appear to lengthen the time of clinical visits, and in some cases may actually shorten them,” said Dr. Dempsey. In addition to analyzing whether MI and other components of the toolkit increased HPV vaccine uptake rates, Dr. Dempsey and her colleagues also plan to explore whether MI would be an effective approach to use when discussing immunizations with parents of infants and younger children.
The study was funded by the National Center for Immunization and Respiratory Diseases and the Centers for Disease Control and Prevention, with survey administration supported by the National Institutes of Health. Dr. Dempsey reported no conflicts of interest.
On Twitter @karioakes
BALTIMORE – Motivational interviewing (MI) was well accepted by providers as part of a communication tool kit to improve human papillomavirus vaccine uptake, according to results of an eight-site study.
Overall, most of the 107 medical providers who participated in the cluster-randomized trial found MI to be a “somewhat useful” (47%) or “very useful” (31%) tactic to use when discussing human papillomavirus (HPV) vaccination with parents of adolescents. The overall amount of time that providers spent discussing vaccinations actually decreased after implementing MI; at the same time, providers felt that they had more power to influence parental decision-making when using MI techniques.
“Primary care providers given the Physician Communication Toolkit used MI frequently, and this use was generally sustained over time,” said lead author Amanda Dempsey, MD, who presented the findings during a poster symposium at the annual meeting of the Pediatric Academic Societies.
Motivational interviewing, an open-ended, nonjudgmental listening and communication style, was taught to providers in one 30-minute webinar and two 1-hour in-person role-playing sessions. Participants were able to practice using MI both in circumstances where parents were accepting of vaccination, and with vaccine-hesitant families.
Participating providers were surveyed pretraining and at 4, 7, and 10 months after the training to assess their practices in the preceding month. The two primary outcome measures assessed, and compared from baseline, were the estimated time spent discussing HPV vaccination with both vaccine-hesitant and nonhesitant families, and the providers’ perceived abilities to influence decisions about HPV. Dr. Dempsey and her colleagues also asked whether practitioners were actually using MI techniques with vaccine-hesitant parents, and whether they found the techniques useful in HPV vaccination discussions.
Dr. Dempsey, associate professor of pediatrics at Children’s Hospital Colorado in Aurora, said that uptake of MI was initially high and remained so. Three months after the intervention, 85% of providers reported they were using MI; at 9 months after the intervention, the figure was 72%.
Previous research has shown that providers generally do not communicate strong recommendations about HPV vaccination. “Providers often feel the parents will argue with them about it, and sometimes don’t even bring it up,” Dr. Dempsey said in an interview. “Anecdotally, providers found MI a useful way to frame the conversation, and they found it less confrontational.”
Overall, about three-quarters of providers responding to the sequential surveys were physicians, another 15%-20% were physician assistants, and the remainder were nurse practitioners. About one in four respondents were male. The pediatric and family medicine practices were approximately evenly divided between public and private clinics.
Although participation in the training and the subsequent surveys was voluntary, uptake was fairly high at participating clinics. The training was offered for 25 MOC (maintenance of certification) part 4 credits, which probably helped participation rates, said Dr. Dempsey.
The small sample size of the study, said Dr. Dempsey, limits the generalizability of the findings. However, the eight sites chosen represented a wide range of socioeconomic and cultural demographics in the patients served. Also, self-report of MI use may be subject to some bias. Finally, because this was a naturalistic study that allowed providers full discretion in using the various components of the Physician Communication Toolkit, it was not possible to perform a completely independent analysis of the effects of using MI apart from the other toolkit components.
“Use of MI did not appear to lengthen the time of clinical visits, and in some cases may actually shorten them,” said Dr. Dempsey. In addition to analyzing whether MI and other components of the toolkit increased HPV vaccine uptake rates, Dr. Dempsey and her colleagues also plan to explore whether MI would be an effective approach to use when discussing immunizations with parents of infants and younger children.
The study was funded by the National Center for Immunization and Respiratory Diseases and the Centers for Disease Control and Prevention, with survey administration supported by the National Institutes of Health. Dr. Dempsey reported no conflicts of interest.
On Twitter @karioakes
AT THE PAS ANNUAL MEETING
Key clinical point: Seventy-eight percent of providers found motivational interviewing (MI) useful for HPV vaccine counseling.
Major finding: Nine months after MI training, 72% of providers were still using the technique in HPV vaccine counseling.
Data source: Pilot study of 107 medical providers at eight clinics who received training to use MI for HPV vaccine counseling.
Disclosures: The study was funded by the National Center for Immunization and Respiratory Diseases and the Centers for Disease Control and Prevention, with survey administration supported by the National Institutes of Health. Dr. Dempsey reported no conflicts of interest.

Gestational Diabetes Ups Risk for Infantile Hemangioma
MINNEAPOLIS – Gestational diabetes and prenatal progesterone use were among the maternal factors associated with increased risk of infantile hemangioma, a benign vascular neoplasm whose incidence has been steadily rising over the past several decades.
Data from a large longitudinal epidemiology study were used to explore the association of a number of maternal risk factors with infantile hemangiomas, said Jennifer Schoch, MD, who presented these findings in a poster session at the annual meeting of the Society for Pediatric Dermatology.

After adjusting for gestational age and multiple gestations, the researchers found that infants born to mothers with gestational diabetes were more likely to have an infantile hemangioma (odds ratio, 1.79; P = .029). Maternal preeclampsia was even more strongly associated with infantile hemangioma (OR, 3.43, P = .017), as was prenatal progesterone use (OR, 2.25; P less than .001). Forceps-assisted vaginal delivery also increased the likelihood of infantile hemangioma (OR, 1.45; P = .035).
Low birth weight, prematurity, and being female and of non-Hispanic white race are some of the infant risk factors known to be associated with infantile hemangioma, but maternal risk factors in the development of infantile hemangioma are less clear, according to the researchers from the Mayo Clinic, Rochester, Minn. Some previous work has suggested that placental abnormalities and invasive procedures carried out during pregnancy, as well as the use of progesterone and corticosteroids during pregnancy, may increase the risk of infantile hemangiomas.
Using a retrospective case-control approach, the researchers used data from the 50-year-old Rochester Epidemiology Project. A chart review identified 869 mother-infant pairs with infantile hemangiomas and 869 age- and sex-matched control maternal-infant pairs whose infants did not have the condition. More than half (65%) of the infants in aggregate were girls (n = 561). Multivariable analysis was used to adjust for gestational age and multiple gestations.
Looking at the trends over time revealed that the rates of gestational diabetes, assisted reproduction techniques, and progesterone use during pregnancy have all increased during the same 35-year period of increased infantile hemangioma incidence, Dr. Schoch said in an interview.
Some earlier work suggests that infantile hemangiomas may arise from fetal placental progenitor cells. Since gestational diabetes can be associated with degradation of the placenta in late pregnancy, Dr. Schoch said that these effects on the placenta may have some connection to the increased risk of infantile hemangiomas in infants whose mothers have gestational diabetes.
Dr. Schoch, who is now professor of dermatology at the University of Florida, Gainesville, also noted that the study, completed during her fellowship at the Mayo Clinic, was limited by the low ethnic diversity of the study population, which draws from several counties in Minnesota and Wisconsin.
The Rochester Epidemiology Project is supported by the National Institutes of Health. The researchers reported having no financial disclosures.
MINNEAPOLIS – Gestational diabetes and prenatal progesterone use were among the maternal factors associated with increased risk of infantile hemangioma, a benign vascular neoplasm whose incidence has been steadily rising over the past several decades.
Data from a large longitudinal epidemiology study were used to explore the association of a number of maternal risk factors with infantile hemangiomas, said Jennifer Schoch, MD, who presented these findings in a poster session at the annual meeting of the Society for Pediatric Dermatology.
After adjusting for gestational age and multiple gestations, the researchers found that infants born to mothers with gestational diabetes were more likely to have an infantile hemangioma (odds ratio, 1.79; P = .029). Maternal preeclampsia was even more strongly associated with infantile hemangioma (OR, 3.43, P = .017), as was prenatal progesterone use (OR, 2.25; P less than .001). Forceps-assisted vaginal delivery also increased the likelihood of infantile hemangioma (OR, 1.45; P = .035).
Low birth weight, prematurity, and being female and of non-Hispanic white race are some of the infant risk factors known to be associated with infantile hemangioma, but maternal risk factors in the development of infantile hemangioma are less clear, according to the researchers from the Mayo Clinic, Rochester, Minn. Some previous work has suggested that placental abnormalities and invasive procedures carried out during pregnancy, as well as the use of progesterone and corticosteroids during pregnancy, may increase the risk of infantile hemangiomas.
Using a retrospective case-control approach, the researchers used data from the 50-year-old Rochester Epidemiology Project. A chart review identified 869 mother-infant pairs with infantile hemangiomas and 869 age- and sex-matched control maternal-infant pairs whose infants did not have the condition. More than half (65%) of the infants in aggregate were girls (n = 561). Multivariable analysis was used to adjust for gestational age and multiple gestations.
Looking at the trends over time revealed that the rates of gestational diabetes, assisted reproduction techniques, and progesterone use during pregnancy have all increased during the same 35-year period of increased infantile hemangioma incidence, Dr. Schoch said in an interview.
Some earlier work suggests that infantile hemangiomas may arise from fetal placental progenitor cells. Since gestational diabetes can be associated with degradation of the placenta in late pregnancy, Dr. Schoch said that these effects on the placenta may have some connection to the increased risk of infantile hemangiomas in infants whose mothers have gestational diabetes.
Dr. Schoch, who is now professor of dermatology at the University of Florida, Gainesville, also noted that the study, completed during her fellowship at the Mayo Clinic, was limited by the low ethnic diversity of the study population, which draws from several counties in Minnesota and Wisconsin.
The Rochester Epidemiology Project is supported by the National Institutes of Health. The researchers reported having no financial disclosures.
MINNEAPOLIS – Gestational diabetes and prenatal progesterone use were among the maternal factors associated with increased risk of infantile hemangioma, a benign vascular neoplasm whose incidence has been steadily rising over the past several decades.
Data from a large longitudinal epidemiology study were used to explore the association of a number of maternal risk factors with infantile hemangiomas, said Jennifer Schoch, MD, who presented these findings in a poster session at the annual meeting of the Society for Pediatric Dermatology.
After adjusting for gestational age and multiple gestations, the researchers found that infants born to mothers with gestational diabetes were more likely to have an infantile hemangioma (odds ratio, 1.79; P = .029). Maternal preeclampsia was even more strongly associated with infantile hemangioma (OR, 3.43, P = .017), as was prenatal progesterone use (OR, 2.25; P less than .001). Forceps-assisted vaginal delivery also increased the likelihood of infantile hemangioma (OR, 1.45; P = .035).
Low birth weight, prematurity, and being female and of non-Hispanic white race are some of the infant risk factors known to be associated with infantile hemangioma, but maternal risk factors in the development of infantile hemangioma are less clear, according to the researchers from the Mayo Clinic, Rochester, Minn. Some previous work has suggested that placental abnormalities and invasive procedures carried out during pregnancy, as well as the use of progesterone and corticosteroids during pregnancy, may increase the risk of infantile hemangiomas.
Using a retrospective case-control approach, the researchers used data from the 50-year-old Rochester Epidemiology Project. A chart review identified 869 mother-infant pairs with infantile hemangiomas and 869 age- and sex-matched control maternal-infant pairs whose infants did not have the condition. More than half (65%) of the infants in aggregate were girls (n = 561). Multivariable analysis was used to adjust for gestational age and multiple gestations.
Looking at the trends over time revealed that the rates of gestational diabetes, assisted reproduction techniques, and progesterone use during pregnancy have all increased during the same 35-year period of increased infantile hemangioma incidence, Dr. Schoch said in an interview.
Some earlier work suggests that infantile hemangiomas may arise from fetal placental progenitor cells. Since gestational diabetes can be associated with degradation of the placenta in late pregnancy, Dr. Schoch said that these effects on the placenta may have some connection to the increased risk of infantile hemangiomas in infants whose mothers have gestational diabetes.
Dr. Schoch, who is now professor of dermatology at the University of Florida, Gainesville, also noted that the study, completed during her fellowship at the Mayo Clinic, was limited by the low ethnic diversity of the study population, which draws from several counties in Minnesota and Wisconsin.
The Rochester Epidemiology Project is supported by the National Institutes of Health. The researchers reported having no financial disclosures.
AT THE SPD ANNUAL MEETING