User login
UTIs not caused by E. coli more likely in certain children
Certain children are more highly predisposed to contracting a urinary tract infection caused by a pathogen other than Escherichia coli, which is typically the most common cause of UTIs, a study showed.
“It may be clinically important to predict which children have UTIs caused by organisms other than E. coli because these organisms differ in their patterns of antimicrobial susceptibility,” wrote the study authors led by Nader Shaikh, MD, of the University of Pittsburgh. “Furthermore, some guidelines have suggested that screening for vesicoureteral reflux (VUR) with a voiding cystourethrogram (VCUG) should, at least in part, be based on whether an organism other than E. coli is recovered,” they wrote.

Dr. Shaikh and his coinvestigators examined the medical records of children in the Randomized Intervention for Children With Vesicoureteral Reflux (RIVUR) trial and the Careful Urinary Tract Infection Evaluation (CUTIE), both of which were prospective multicenter studies. Children included in both studies were 2-71 months of age; RIVUR subjects had VUR grades 1-4 and presented with either a first or second febrile or symptomatic UTI, while CUTIE subjects presented with either their first or second UTI but not VUR (Ped Inf Dis J. 2016. doi:10.1097/INF.0000000000001301).
In total, 769 children from 19 centers were included from both studies, of which 703 (91%) were female and 596 (78%) were white. Nine percent of all the children had UTIs that were not caused by E. coli. Circumcised males had the highest odds ratio associated with non–E. coli UTIs, with an OR of 5.5 (95% CI, 1.18-17.1; P = .003). significantly higher than the 1.6 odds ratio for uncircumcised males (95% CI, 0.6-4.6; P = .35).
Hispanic children also had a higher risk (OR = 2.3; 95% CI, 1.1-4.6; P = .02) than either non-Hispanic children or females, which were reference cohorts. Other groups found to be at higher-than-normal risk for non–E. coli UTIs were children without fever (OR = 2.8; 95% CI, 1.2-6.6; P = .02) and children with VUR grade 3 or 4 (OR = 2.2; 95% CI, 1.2-4.1; P = .01).
While more than 90% of children’s UTIs were caused by E. coli, the most common pathogens causing UTIs, causative organisms in the other 70 children were Proteus species (21 children, 30%), Klebsiella species (16, 23%), Enterococcus species (14, 20%), Enterobacter species (8, 11%), and “other species” (11, 16%).
“Children with UTIs caused by organisms other than E. coli were twice as likely to have high-grade VUR (grade 3 and 4), which is consistent with prior studies,” Dr. Shaikh and his coauthors noted, adding, “the association between Hispanic ethnicity and non-E. coli pathogens is novel and may be due to differences in genes involved with susceptibility to UTIs.”
There were no disclosures or sources of funding provided.
In this study of almost 800 children in the Pittsburgh area, the investigators sought to identify children at risk for urinary tract infections that more likely would have a bacterial organism not susceptible to standard first-line empiric antibiotic treatment.
They found that circumcised males, children with grade 3-4 vesicoureteral reflux, Hispanic children, and children without fever were more likely to have a UTI caused by organisms other than Escherichia coli and, therefore, less likely to respond to standard first-line antibiotic therapy. These investigators are the preeminent authorities in UTI management for children, so their findings should be viewed in that light.

|
Dr. Michael E. Pichichero |
The advance from the study is not a major one because all children with a suspected UTI should have a suitable culture specimen obtained before starting antibiotics, and the treatment choice continued or changed based on culture results. So really, the findings apply only to a decision about initial empiric treatment while awaiting culture results.
As a guide, if a clinician were to consider the diagnosis of UTI based on history, examination, and urinalysis, and the child was a circumcised male, a child with known grade 3 or 4 vesicoureteral reflux, Hispanic, or without fever, then the empiric antibiotic selected should be broader spectrum while awaiting urine culture results.
Michael E. Pichichero, MD, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he had no relevant financial disclosures.
In this study of almost 800 children in the Pittsburgh area, the investigators sought to identify children at risk for urinary tract infections that more likely would have a bacterial organism not susceptible to standard first-line empiric antibiotic treatment.
They found that circumcised males, children with grade 3-4 vesicoureteral reflux, Hispanic children, and children without fever were more likely to have a UTI caused by organisms other than Escherichia coli and, therefore, less likely to respond to standard first-line antibiotic therapy. These investigators are the preeminent authorities in UTI management for children, so their findings should be viewed in that light.
|
|
Dr. Michael E. Pichichero |
The advance from the study is not a major one because all children with a suspected UTI should have a suitable culture specimen obtained before starting antibiotics, and the treatment choice continued or changed based on culture results. So really, the findings apply only to a decision about initial empiric treatment while awaiting culture results.
As a guide, if a clinician were to consider the diagnosis of UTI based on history, examination, and urinalysis, and the child was a circumcised male, a child with known grade 3 or 4 vesicoureteral reflux, Hispanic, or without fever, then the empiric antibiotic selected should be broader spectrum while awaiting urine culture results.
Michael E. Pichichero, MD, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he had no relevant financial disclosures.
In this study of almost 800 children in the Pittsburgh area, the investigators sought to identify children at risk for urinary tract infections that more likely would have a bacterial organism not susceptible to standard first-line empiric antibiotic treatment.
They found that circumcised males, children with grade 3-4 vesicoureteral reflux, Hispanic children, and children without fever were more likely to have a UTI caused by organisms other than Escherichia coli and, therefore, less likely to respond to standard first-line antibiotic therapy. These investigators are the preeminent authorities in UTI management for children, so their findings should be viewed in that light.
|
|
Dr. Michael E. Pichichero |
The advance from the study is not a major one because all children with a suspected UTI should have a suitable culture specimen obtained before starting antibiotics, and the treatment choice continued or changed based on culture results. So really, the findings apply only to a decision about initial empiric treatment while awaiting culture results.
As a guide, if a clinician were to consider the diagnosis of UTI based on history, examination, and urinalysis, and the child was a circumcised male, a child with known grade 3 or 4 vesicoureteral reflux, Hispanic, or without fever, then the empiric antibiotic selected should be broader spectrum while awaiting urine culture results.
Michael E. Pichichero, MD, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he had no relevant financial disclosures.
Certain children are more highly predisposed to contracting a urinary tract infection caused by a pathogen other than Escherichia coli, which is typically the most common cause of UTIs, a study showed.
“It may be clinically important to predict which children have UTIs caused by organisms other than E. coli because these organisms differ in their patterns of antimicrobial susceptibility,” wrote the study authors led by Nader Shaikh, MD, of the University of Pittsburgh. “Furthermore, some guidelines have suggested that screening for vesicoureteral reflux (VUR) with a voiding cystourethrogram (VCUG) should, at least in part, be based on whether an organism other than E. coli is recovered,” they wrote.
Dr. Shaikh and his coinvestigators examined the medical records of children in the Randomized Intervention for Children With Vesicoureteral Reflux (RIVUR) trial and the Careful Urinary Tract Infection Evaluation (CUTIE), both of which were prospective multicenter studies. Children included in both studies were 2-71 months of age; RIVUR subjects had VUR grades 1-4 and presented with either a first or second febrile or symptomatic UTI, while CUTIE subjects presented with either their first or second UTI but not VUR (Ped Inf Dis J. 2016. doi:10.1097/INF.0000000000001301).
In total, 769 children from 19 centers were included from both studies, of which 703 (91%) were female and 596 (78%) were white. Nine percent of all the children had UTIs that were not caused by E. coli. Circumcised males had the highest odds ratio associated with non–E. coli UTIs, with an OR of 5.5 (95% CI, 1.18-17.1; P = .003). significantly higher than the 1.6 odds ratio for uncircumcised males (95% CI, 0.6-4.6; P = .35).
Hispanic children also had a higher risk (OR = 2.3; 95% CI, 1.1-4.6; P = .02) than either non-Hispanic children or females, which were reference cohorts. Other groups found to be at higher-than-normal risk for non–E. coli UTIs were children without fever (OR = 2.8; 95% CI, 1.2-6.6; P = .02) and children with VUR grade 3 or 4 (OR = 2.2; 95% CI, 1.2-4.1; P = .01).
While more than 90% of children’s UTIs were caused by E. coli, the most common pathogens causing UTIs, causative organisms in the other 70 children were Proteus species (21 children, 30%), Klebsiella species (16, 23%), Enterococcus species (14, 20%), Enterobacter species (8, 11%), and “other species” (11, 16%).
“Children with UTIs caused by organisms other than E. coli were twice as likely to have high-grade VUR (grade 3 and 4), which is consistent with prior studies,” Dr. Shaikh and his coauthors noted, adding, “the association between Hispanic ethnicity and non-E. coli pathogens is novel and may be due to differences in genes involved with susceptibility to UTIs.”
There were no disclosures or sources of funding provided.
Certain children are more highly predisposed to contracting a urinary tract infection caused by a pathogen other than Escherichia coli, which is typically the most common cause of UTIs, a study showed.
“It may be clinically important to predict which children have UTIs caused by organisms other than E. coli because these organisms differ in their patterns of antimicrobial susceptibility,” wrote the study authors led by Nader Shaikh, MD, of the University of Pittsburgh. “Furthermore, some guidelines have suggested that screening for vesicoureteral reflux (VUR) with a voiding cystourethrogram (VCUG) should, at least in part, be based on whether an organism other than E. coli is recovered,” they wrote.
Dr. Shaikh and his coinvestigators examined the medical records of children in the Randomized Intervention for Children With Vesicoureteral Reflux (RIVUR) trial and the Careful Urinary Tract Infection Evaluation (CUTIE), both of which were prospective multicenter studies. Children included in both studies were 2-71 months of age; RIVUR subjects had VUR grades 1-4 and presented with either a first or second febrile or symptomatic UTI, while CUTIE subjects presented with either their first or second UTI but not VUR (Ped Inf Dis J. 2016. doi:10.1097/INF.0000000000001301).
In total, 769 children from 19 centers were included from both studies, of which 703 (91%) were female and 596 (78%) were white. Nine percent of all the children had UTIs that were not caused by E. coli. Circumcised males had the highest odds ratio associated with non–E. coli UTIs, with an OR of 5.5 (95% CI, 1.18-17.1; P = .003). significantly higher than the 1.6 odds ratio for uncircumcised males (95% CI, 0.6-4.6; P = .35).
Hispanic children also had a higher risk (OR = 2.3; 95% CI, 1.1-4.6; P = .02) than either non-Hispanic children or females, which were reference cohorts. Other groups found to be at higher-than-normal risk for non–E. coli UTIs were children without fever (OR = 2.8; 95% CI, 1.2-6.6; P = .02) and children with VUR grade 3 or 4 (OR = 2.2; 95% CI, 1.2-4.1; P = .01).
While more than 90% of children’s UTIs were caused by E. coli, the most common pathogens causing UTIs, causative organisms in the other 70 children were Proteus species (21 children, 30%), Klebsiella species (16, 23%), Enterococcus species (14, 20%), Enterobacter species (8, 11%), and “other species” (11, 16%).
“Children with UTIs caused by organisms other than E. coli were twice as likely to have high-grade VUR (grade 3 and 4), which is consistent with prior studies,” Dr. Shaikh and his coauthors noted, adding, “the association between Hispanic ethnicity and non-E. coli pathogens is novel and may be due to differences in genes involved with susceptibility to UTIs.”
There were no disclosures or sources of funding provided.
FROM THE PEDIATRIC INFECTIOUS DISEASE JOURNAL
Key clinical point: Non–Escherichia coli urinary tract infections are more likely to occur in children who are uncircumcised, are Hispanic, have no fever, or have grade 3-4 vesicoureteral reflux.
Major finding: Circumcised males had an odds ratio of 5.5 (95% CI, 1.8-17.1; P = .003) of infection by pathogens other than E. coli; the odds ratio for Hispanic children (OR = 2.3; 95% CI, 1.1-4.6; P = .02), children without fever (OR = 2.8; 95% CI, 1.2-6.6; P = .02), and children with grade 3-4 VUR (OR = 2.2; 95% CI, 1.2-4.1; P = .01) also were relatively high.
Data source: A review of data from two prospective multicenter studies involving 769 children with a UTI aged 2-71 months .
Disclosures: Funding sources and individual disclosures were not provided.

Psychiatric disorders often impair antiretroviral adherence in perinatally HIV-infected teens
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.

The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.
The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – Adolescents who were perinatally infected with HIV have a high prevalence of selected psychiatric disorders that impede their adherence to antiretroviral therapy, Claude Ann Mellins, PhD, reported at the 21st International AIDS Conference.
Those psychiatric diagnoses were predictive of viremia over the ensuing 2-3 years in a new analysis from the ongoing Child and Adolescent Self-Awareness and Health (CASAH) study, according to Dr. Mellins, professor of medical psychology at Columbia University, New York, and codirector of CASAH.
The clinical implications of the CASAH findings are clear, she added. “Assessing and treating specific categories of psychiatric and substance abuse problems may enhance efforts to improve adherence and prevent poor health outcomes in these adolescents and young adults, who are especially vulnerable due to their very challenging circumstances,” Dr. Mellins said.
CASAH is a longitudinal study of perinatally HIV-infected and perinatally HIV-exposed but uninfected New York City youth. They were enrolled during 2003-2008, when they were 9-16 years old. They and their caregivers undergo detailed psychosocial interviews every 12-18 months. The goal is to identify risk factors as well as protective factors influencing their behavioral health outcomes, the clinical psychologist explained.
She reported on 179 perinatally infected adolescents who were at least 13 years old at the first of their three interviews conducted over a 2.7-year period. Of note, 53% of them met Diagnostic Interview Schedule for Children (DISC-IV) criteria for one or more psychiatric diagnoses at all three time points. The pattern of psychopathology was somewhat different from that previously described in adults with HIV, who have been studied much more extensively than perinatally infected teens.
“Much of the literature on adults has focused on depression and mood disorders as predictors of poor health outcomes. Our data suggest that among youth, disruptive behavioral disorders – things like [attention-deficit/hyperactivity disorder], conduct disorder, or oppositional defiant disorder – may be just as important, if not more so. Substance abuse was also a critical factor,” Dr. Mellins said.
In a cross-sectional multivariate logistic regression analysis, a behavior disorder diagnosed at the first interview was associated with a 2.57-fold increased likelihood of contemporaneous viremia as evidenced by a plasma HIV RNA viral load greater than 1,000 copies/mL, and with a threefold increased likelihood of self-reported missed doses of antiretroviral medications during the previous week.
Anxiety disorder was the most common psychiatric diagnosis at the initial interview, followed by disruptive behavior disorder and substance use disorder. A diagnosis of any psychiatric disorder at the time of the first interview was associated with a significantly increased risk of viremia across the next 2.7 years. Forty-seven percent of subjects had viremia at 2.7 years of follow-up, reflective of chronic suboptimal medication adherence.
She noted that the pattern of psychiatric disorders in perinatally infected patients shifts between adolescence and young adulthood.
“By the time perinatally infected adolescents become young adults, I will say that anxiety and mood disorders become much more prevalent. But the number of psychiatric problems actually goes down by young adulthood,” according to Dr. Mellins.
Indeed, in another CASAH analysis she presented at AIDS 2016, this one involving 136 perinatally infected young adults and 86 perinatally exposed but uninfected controls, the vast majority living in impoverished communities, there was no difference between the two groups in rates of psychiatric or substance use disorders, although the 27% prevalence of substance use disorders is higher than that found in the age-matched general population.
Eighty-four percent of the perinatally infected 18- to 28-year-olds had graduated from high school, 94% were in a stable housing situation, 59% were currently working or in school, 54% were paying rent, and 95% reported ever being in a romantic relationship. Rates were similar in the perinatally exposed but uninfected group with the exception that these individuals were less likely to be paying rent.
“In spite of substantive risks, there is a relatively large portion of both groups with positive behavioral health outcomes, achieving normative young adult transition milestones. We need to understand why. Identification of protective factors conferring resilience can inform evidence-based prevention efforts, which are critical given the staggering numbers of children and young adolescents worldwide affected by HIV who will be transitioning to adulthood,” she said.
Dr. Mellins said the CASAH findings constitute a persuasive argument in favor of integrating mental health as a component of HIV care.
“Young people don’t always go to mental health appointments that are separate from medical care, so integrating mental health as a component of HIV care might be one of the most effective ways to identify and treat mental health problems in infected youth while simultaneously improving medication adherence and health outcomes,” Dr. Mellins said.
The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.
AT AIDS 2016
Key clinical point: Look for and treat psychiatric disorders in perinatally HIV-infected adolescents as a means of optimizing their antiretroviral medication adherence.
Major finding: A majority of perinatally HIV-infected adolescents meet the criteria for at least one psychiatric diagnosis, and they are at significantly increased risk for poor medication adherence and viremia during the next 2-3 years.
Data source: The longitudinal CASAH study involving prospective follow-up of several hundred perinatally HIV-infected and perinatally exposed but uninfected subjects through adolescence and young adulthood.
Disclosures: The ongoing CASAH study is funded by the National Institute of Mental Health. Dr. Mellins reported having no relevant financial conflicts.

Boxed for delivery
When our second daughter was born, she came home from the hospital in a box. All the babies born at Duke University Medical Center in 1973 were sent home in a cardboard box that had served as their bassinets during their stay in the newborn nursery. As I recall, the boxes were decorated with storks and musical notes; had spaces for the babies’ names, measurements, and birth dates; and had open slots that functioned as carrying handles.
Of course, 1973 predated crash-tested car seats, and so we put little Emily and her box in what we referred to as the “wayback” of our Ford Pinto wagon, a car that subsequently earned a reputation for turning into a fireball when involved in a rear-end collision. However, I believe I did take the extra precaution of “securing” the box in place with a bungee cord.

But Emily survived, and I filed away the memory of her cardboard bassinet until a few weeks ago when I read a story in the New York Times, “Why Finland’s Newborns Sleep in Cardboard Cribs” (Eli Rosenberg, July 6, 2016). It turns out the Finnish government gives out 40,000 cardboard boxes to pregnant women who agree to have a medical exam during the first trimester of their pregnancy. The gift boxes come along with 50 items of baby ware appropriate for Finland’s frigid climate, including a warm coat and a balaclava.
The baby box program began in the late 1930s as a way to encourage mothers to visit physicians. The current Finnish infant mortality is one of the lowest in the world and less than half of ours in the United States. There are some who have been tempted to attribute this dramatic decline to the baby box program. But it is hard to tease out one factor in a country that offers a 10-month paid parental leave and guarantees that a stay-at-home parent may return to his or her job at any time before the child’s third birthday.
Even without a broad social service support system, the cardboard box crib can save lives. For families who can’t afford a crib, the box offers a safer alternative to a couch with soft cushions and face-trapping gaps between its cushions, or to a bed shared with a sleep-deprived or inebriated parent, or to an antique crib with neck-pinching slats and layers of lead-laced paint.
Given this high costs of raising a child, the option of a no-cost cardboard box crib should appeal to most young families. But you know as well as I do that parents to be (and grandparents to be) are primed to buy and are focused on creating nurseries that match the images they see in the glossy magazines targeted at their vulnerable demographic.
It will require a major public relations campaign to counteract the image that bedding one’s precious newborn in a cardboard box conjures up. But maybe there is a role for us. If pediatricians began promoting the advantages of cardboard cribs, they might just catch on. On second thought, maybe we should focus our energies on promoting more child-friendly parental leave policies.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
When our second daughter was born, she came home from the hospital in a box. All the babies born at Duke University Medical Center in 1973 were sent home in a cardboard box that had served as their bassinets during their stay in the newborn nursery. As I recall, the boxes were decorated with storks and musical notes; had spaces for the babies’ names, measurements, and birth dates; and had open slots that functioned as carrying handles.
Of course, 1973 predated crash-tested car seats, and so we put little Emily and her box in what we referred to as the “wayback” of our Ford Pinto wagon, a car that subsequently earned a reputation for turning into a fireball when involved in a rear-end collision. However, I believe I did take the extra precaution of “securing” the box in place with a bungee cord.
But Emily survived, and I filed away the memory of her cardboard bassinet until a few weeks ago when I read a story in the New York Times, “Why Finland’s Newborns Sleep in Cardboard Cribs” (Eli Rosenberg, July 6, 2016). It turns out the Finnish government gives out 40,000 cardboard boxes to pregnant women who agree to have a medical exam during the first trimester of their pregnancy. The gift boxes come along with 50 items of baby ware appropriate for Finland’s frigid climate, including a warm coat and a balaclava.
The baby box program began in the late 1930s as a way to encourage mothers to visit physicians. The current Finnish infant mortality is one of the lowest in the world and less than half of ours in the United States. There are some who have been tempted to attribute this dramatic decline to the baby box program. But it is hard to tease out one factor in a country that offers a 10-month paid parental leave and guarantees that a stay-at-home parent may return to his or her job at any time before the child’s third birthday.
Even without a broad social service support system, the cardboard box crib can save lives. For families who can’t afford a crib, the box offers a safer alternative to a couch with soft cushions and face-trapping gaps between its cushions, or to a bed shared with a sleep-deprived or inebriated parent, or to an antique crib with neck-pinching slats and layers of lead-laced paint.
Given this high costs of raising a child, the option of a no-cost cardboard box crib should appeal to most young families. But you know as well as I do that parents to be (and grandparents to be) are primed to buy and are focused on creating nurseries that match the images they see in the glossy magazines targeted at their vulnerable demographic.
It will require a major public relations campaign to counteract the image that bedding one’s precious newborn in a cardboard box conjures up. But maybe there is a role for us. If pediatricians began promoting the advantages of cardboard cribs, they might just catch on. On second thought, maybe we should focus our energies on promoting more child-friendly parental leave policies.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
When our second daughter was born, she came home from the hospital in a box. All the babies born at Duke University Medical Center in 1973 were sent home in a cardboard box that had served as their bassinets during their stay in the newborn nursery. As I recall, the boxes were decorated with storks and musical notes; had spaces for the babies’ names, measurements, and birth dates; and had open slots that functioned as carrying handles.
Of course, 1973 predated crash-tested car seats, and so we put little Emily and her box in what we referred to as the “wayback” of our Ford Pinto wagon, a car that subsequently earned a reputation for turning into a fireball when involved in a rear-end collision. However, I believe I did take the extra precaution of “securing” the box in place with a bungee cord.
But Emily survived, and I filed away the memory of her cardboard bassinet until a few weeks ago when I read a story in the New York Times, “Why Finland’s Newborns Sleep in Cardboard Cribs” (Eli Rosenberg, July 6, 2016). It turns out the Finnish government gives out 40,000 cardboard boxes to pregnant women who agree to have a medical exam during the first trimester of their pregnancy. The gift boxes come along with 50 items of baby ware appropriate for Finland’s frigid climate, including a warm coat and a balaclava.
The baby box program began in the late 1930s as a way to encourage mothers to visit physicians. The current Finnish infant mortality is one of the lowest in the world and less than half of ours in the United States. There are some who have been tempted to attribute this dramatic decline to the baby box program. But it is hard to tease out one factor in a country that offers a 10-month paid parental leave and guarantees that a stay-at-home parent may return to his or her job at any time before the child’s third birthday.
Even without a broad social service support system, the cardboard box crib can save lives. For families who can’t afford a crib, the box offers a safer alternative to a couch with soft cushions and face-trapping gaps between its cushions, or to a bed shared with a sleep-deprived or inebriated parent, or to an antique crib with neck-pinching slats and layers of lead-laced paint.
Given this high costs of raising a child, the option of a no-cost cardboard box crib should appeal to most young families. But you know as well as I do that parents to be (and grandparents to be) are primed to buy and are focused on creating nurseries that match the images they see in the glossy magazines targeted at their vulnerable demographic.
It will require a major public relations campaign to counteract the image that bedding one’s precious newborn in a cardboard box conjures up. But maybe there is a role for us. If pediatricians began promoting the advantages of cardboard cribs, they might just catch on. On second thought, maybe we should focus our energies on promoting more child-friendly parental leave policies.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”

Approximately 9 million U.S. children, teens are vulnerable to measles infection
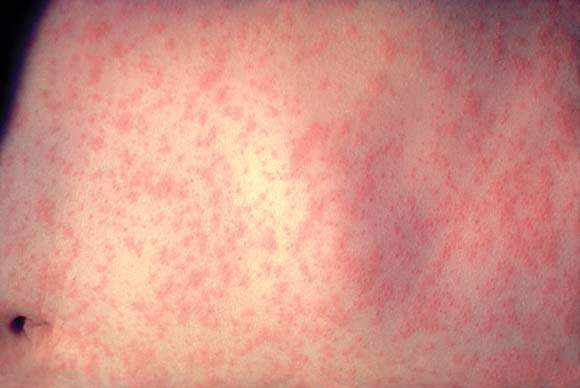
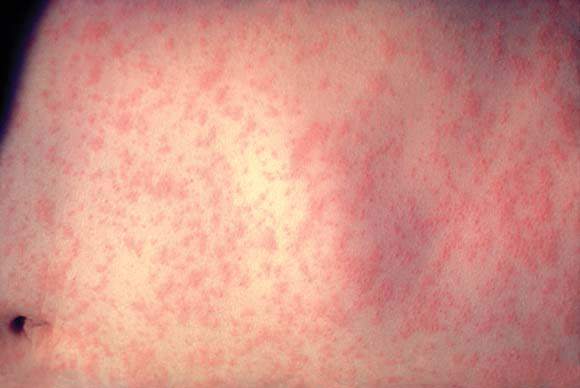
Of the almost 9 million children and adolescents aged 17 years and younger estimated to be measles susceptible in the United States, those 3 years and younger show the highest levels of risk for infection, according to the results of a study published in the American Journal of Epidemiology.
Robert A. Bednarczyk, MD, and his colleagues at Emory University, Atlanta, developed a model based on age-specific measles vaccination data from the National Immunization Survey–Teen collected between 2008 and 2013 (18 cumulative birth cohorts) to estimate the number of U.S. children (birth–age 12 years ) and adolescents (aged 13-17 years) susceptible to measles infection (Am J Epidemiol. 2016 Jul 15;184[2]:148-56).
The model was developed using the survey data in conjunction with assumptions designed to account for several potentially confounding variables. These included the effectiveness of the vaccine used, whether infants were protected by maternally derived, vaccine-induced antibodies, and any loss of immunity attributable to treatment for cancer during childhood. The model also allowed for an examination of susceptibility by different age groupings, as well as by state. Additionally, the study authors were able to estimate the impact of decreased measles-containing vaccine effectiveness on susceptibility to infection in adolescents.
Results from the model indicated that 12.5% of the over 69 million of U.S. children and adolescents in the 18 birth cohorts are susceptible to measles infection. Those with the highest percentage of susceptibility were children 3 years of age and younger (24.7%), compared with 9.0% of children and adolescents aged 4-17 years. Geographic differences in susceptibility also were apparent. In addition to the District of Columbia, 10 states had adolescent susceptibility levels of at least 6%, and 14 states each had over 20,000 susceptible adolescents.
Using the model to simulate a 1% decrease in vaccine effectiveness for both the first (93%-92%) and second (97%-96%) measles-containing vaccine doses, the study authors reported the addition of almost 1 million children and adolescents (13.4%) to the measles-susceptible category. This finding indicates that very small changes in vaccine effectiveness can have a substantial impact on susceptibility through a slow accumulation of additional susceptible children and adolescents each year, culminating in a steady decline in the proportion of children and adolescents immune to measles.
Regarding their overall findings, Dr. Bednarczyk and his colleagues stated, “the overall level of immunity to measles is generally at or higher than the operational threshold of 92%. This is compatible with the experience to date that, despite substantial numbers of importations, endemic measles transmission has not been reestablished.”
As for broader implications, the investigators said that “These estimates underscore the need to help public health professionals plan for future immunization programs and potential measles outbreaks, and to maintain appropriate levels of immunity in the population to prevent widespread transmission of this highly infectious disease.”
Of the almost 9 million children and adolescents aged 17 years and younger estimated to be measles susceptible in the United States, those 3 years and younger show the highest levels of risk for infection, according to the results of a study published in the American Journal of Epidemiology.
Robert A. Bednarczyk, MD, and his colleagues at Emory University, Atlanta, developed a model based on age-specific measles vaccination data from the National Immunization Survey–Teen collected between 2008 and 2013 (18 cumulative birth cohorts) to estimate the number of U.S. children (birth–age 12 years ) and adolescents (aged 13-17 years) susceptible to measles infection (Am J Epidemiol. 2016 Jul 15;184[2]:148-56).
The model was developed using the survey data in conjunction with assumptions designed to account for several potentially confounding variables. These included the effectiveness of the vaccine used, whether infants were protected by maternally derived, vaccine-induced antibodies, and any loss of immunity attributable to treatment for cancer during childhood. The model also allowed for an examination of susceptibility by different age groupings, as well as by state. Additionally, the study authors were able to estimate the impact of decreased measles-containing vaccine effectiveness on susceptibility to infection in adolescents.
Results from the model indicated that 12.5% of the over 69 million of U.S. children and adolescents in the 18 birth cohorts are susceptible to measles infection. Those with the highest percentage of susceptibility were children 3 years of age and younger (24.7%), compared with 9.0% of children and adolescents aged 4-17 years. Geographic differences in susceptibility also were apparent. In addition to the District of Columbia, 10 states had adolescent susceptibility levels of at least 6%, and 14 states each had over 20,000 susceptible adolescents.
Using the model to simulate a 1% decrease in vaccine effectiveness for both the first (93%-92%) and second (97%-96%) measles-containing vaccine doses, the study authors reported the addition of almost 1 million children and adolescents (13.4%) to the measles-susceptible category. This finding indicates that very small changes in vaccine effectiveness can have a substantial impact on susceptibility through a slow accumulation of additional susceptible children and adolescents each year, culminating in a steady decline in the proportion of children and adolescents immune to measles.
Regarding their overall findings, Dr. Bednarczyk and his colleagues stated, “the overall level of immunity to measles is generally at or higher than the operational threshold of 92%. This is compatible with the experience to date that, despite substantial numbers of importations, endemic measles transmission has not been reestablished.”
As for broader implications, the investigators said that “These estimates underscore the need to help public health professionals plan for future immunization programs and potential measles outbreaks, and to maintain appropriate levels of immunity in the population to prevent widespread transmission of this highly infectious disease.”
Of the almost 9 million children and adolescents aged 17 years and younger estimated to be measles susceptible in the United States, those 3 years and younger show the highest levels of risk for infection, according to the results of a study published in the American Journal of Epidemiology.
Robert A. Bednarczyk, MD, and his colleagues at Emory University, Atlanta, developed a model based on age-specific measles vaccination data from the National Immunization Survey–Teen collected between 2008 and 2013 (18 cumulative birth cohorts) to estimate the number of U.S. children (birth–age 12 years ) and adolescents (aged 13-17 years) susceptible to measles infection (Am J Epidemiol. 2016 Jul 15;184[2]:148-56).
The model was developed using the survey data in conjunction with assumptions designed to account for several potentially confounding variables. These included the effectiveness of the vaccine used, whether infants were protected by maternally derived, vaccine-induced antibodies, and any loss of immunity attributable to treatment for cancer during childhood. The model also allowed for an examination of susceptibility by different age groupings, as well as by state. Additionally, the study authors were able to estimate the impact of decreased measles-containing vaccine effectiveness on susceptibility to infection in adolescents.
Results from the model indicated that 12.5% of the over 69 million of U.S. children and adolescents in the 18 birth cohorts are susceptible to measles infection. Those with the highest percentage of susceptibility were children 3 years of age and younger (24.7%), compared with 9.0% of children and adolescents aged 4-17 years. Geographic differences in susceptibility also were apparent. In addition to the District of Columbia, 10 states had adolescent susceptibility levels of at least 6%, and 14 states each had over 20,000 susceptible adolescents.
Using the model to simulate a 1% decrease in vaccine effectiveness for both the first (93%-92%) and second (97%-96%) measles-containing vaccine doses, the study authors reported the addition of almost 1 million children and adolescents (13.4%) to the measles-susceptible category. This finding indicates that very small changes in vaccine effectiveness can have a substantial impact on susceptibility through a slow accumulation of additional susceptible children and adolescents each year, culminating in a steady decline in the proportion of children and adolescents immune to measles.
Regarding their overall findings, Dr. Bednarczyk and his colleagues stated, “the overall level of immunity to measles is generally at or higher than the operational threshold of 92%. This is compatible with the experience to date that, despite substantial numbers of importations, endemic measles transmission has not been reestablished.”
As for broader implications, the investigators said that “These estimates underscore the need to help public health professionals plan for future immunization programs and potential measles outbreaks, and to maintain appropriate levels of immunity in the population to prevent widespread transmission of this highly infectious disease.”
Key clinical point: U.S. children younger than 3 years of age have a high estimated susceptibility to measles infection.
Major finding: An estimated 12.5% of U.S. children and adolescents 17 years and younger are susceptible to measles infection, with differences in susceptibility levels detected for specific age ranges and states. Small decreases in vaccine effectiveness can have a large impact on susceptibility levels.
Data sources: National Immunization Survey–Teen collected between 2008 and 2013.
Disclosures: The study was conducted without grant support. All authors reported no conflicts of interest.
Links found between NAFLD, type 2 diabetes, and NASH in children
Nearly one in three children with nonalcoholic fatty liver disease have abnormal glucose metabolism, and this co-morbidity is also associated with a greater risk of nonalcoholic steatohepatitis, according to a cross-sectional study published online Aug. 1 in JAMA Pediatrics.
The study used data from 675 children with biopsy-confirmed nonalcoholic fatty liver disease (NAFLD) who were enrolled in the NASH Clinical Research Network. The mean age of the children was 12.6 years, and they had a mean BMI of 32.5. Most of the children in the study were boys and Hispanic.
Overall, 23.4% of study participants had prediabetes and 6.5% met the clinical criteria for type 2 diabetes. However, girls with NAFLD had a 60% greater risk of prediabetes and a fivefold greater risk of type 2 diabetes than boys, even after controlling for BMI and waist circumference (JAMA Pediatr. 2016 Aug 1. doi: 10.1001/jamapediatrics.2016.1971), reported Dr. Kimberly P. Newton and her coauthors.
The researchers also noted a significant association between nonalcoholic steatohepatitis (NASH) and glucose metabolism. Individuals with type 2 diabetes were three times more likely to also have NASH, while those with prediabetes had a 90% higher incidence of NASH, compared with individuals with normal glucose metabolism. They also found that those with NASH had significantly higher mean fasting glucose and insulin concentrations than children without NASH.
Dr. Newton, of the University of California, San Diego, and her coauthors wrote that while abnormal glucose metabolism is known to be common in adults with NAFLD, and that type diabetes is a risk factor for progression to NASH and liver-related mortality, the association in children with NAFLD is less well understood.
“Among our cohort, the prevalence of children with type 2 diabetes was much higher than would be expected based on contributions from obesity alone,” they wrote. “Although systemic insulin resistance is believed be important in the pathogenesis of both pediatric NAFLD and type 2 diabetes, to our knowledge, there are no longitudinal studies that evaluate the cause-effect relationship between these two associated conditions.”
The authors drew particular attention to the threefold higher odds of NASH in children with NAFLD and type 2 diabetes, pointing out that while the prognostic implications of NASH in childhood are not fully known, the NASH phenotype is associated with a “substantially” greater risk of cirrhosis. This risk is likely to be compounded by the presence of type 2 diabetes.
“Our study advances the literature by showing that as early as childhood, prediabetes and type 2 diabetes emerge as clear risk factors for NASH with potential downstream implications for future morbidity and mortality.”
Commenting on the greater incidence of prediabetes and type 2 diabetes among girls with NAFLD, the authors said this had been observed in other studies and that sex differences represented a major unmet research need.
The Nonalcoholic Steatohepatitis Clinical Research Network is supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Additional support was received from the National Center for Advancing Translational Sciences. The researchers reported no conflicts of interest.
Nearly one in three children with nonalcoholic fatty liver disease have abnormal glucose metabolism, and this co-morbidity is also associated with a greater risk of nonalcoholic steatohepatitis, according to a cross-sectional study published online Aug. 1 in JAMA Pediatrics.
The study used data from 675 children with biopsy-confirmed nonalcoholic fatty liver disease (NAFLD) who were enrolled in the NASH Clinical Research Network. The mean age of the children was 12.6 years, and they had a mean BMI of 32.5. Most of the children in the study were boys and Hispanic.
Overall, 23.4% of study participants had prediabetes and 6.5% met the clinical criteria for type 2 diabetes. However, girls with NAFLD had a 60% greater risk of prediabetes and a fivefold greater risk of type 2 diabetes than boys, even after controlling for BMI and waist circumference (JAMA Pediatr. 2016 Aug 1. doi: 10.1001/jamapediatrics.2016.1971), reported Dr. Kimberly P. Newton and her coauthors.
The researchers also noted a significant association between nonalcoholic steatohepatitis (NASH) and glucose metabolism. Individuals with type 2 diabetes were three times more likely to also have NASH, while those with prediabetes had a 90% higher incidence of NASH, compared with individuals with normal glucose metabolism. They also found that those with NASH had significantly higher mean fasting glucose and insulin concentrations than children without NASH.
Dr. Newton, of the University of California, San Diego, and her coauthors wrote that while abnormal glucose metabolism is known to be common in adults with NAFLD, and that type diabetes is a risk factor for progression to NASH and liver-related mortality, the association in children with NAFLD is less well understood.
“Among our cohort, the prevalence of children with type 2 diabetes was much higher than would be expected based on contributions from obesity alone,” they wrote. “Although systemic insulin resistance is believed be important in the pathogenesis of both pediatric NAFLD and type 2 diabetes, to our knowledge, there are no longitudinal studies that evaluate the cause-effect relationship between these two associated conditions.”
The authors drew particular attention to the threefold higher odds of NASH in children with NAFLD and type 2 diabetes, pointing out that while the prognostic implications of NASH in childhood are not fully known, the NASH phenotype is associated with a “substantially” greater risk of cirrhosis. This risk is likely to be compounded by the presence of type 2 diabetes.
“Our study advances the literature by showing that as early as childhood, prediabetes and type 2 diabetes emerge as clear risk factors for NASH with potential downstream implications for future morbidity and mortality.”
Commenting on the greater incidence of prediabetes and type 2 diabetes among girls with NAFLD, the authors said this had been observed in other studies and that sex differences represented a major unmet research need.
The Nonalcoholic Steatohepatitis Clinical Research Network is supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Additional support was received from the National Center for Advancing Translational Sciences. The researchers reported no conflicts of interest.
Nearly one in three children with nonalcoholic fatty liver disease have abnormal glucose metabolism, and this co-morbidity is also associated with a greater risk of nonalcoholic steatohepatitis, according to a cross-sectional study published online Aug. 1 in JAMA Pediatrics.
The study used data from 675 children with biopsy-confirmed nonalcoholic fatty liver disease (NAFLD) who were enrolled in the NASH Clinical Research Network. The mean age of the children was 12.6 years, and they had a mean BMI of 32.5. Most of the children in the study were boys and Hispanic.
Overall, 23.4% of study participants had prediabetes and 6.5% met the clinical criteria for type 2 diabetes. However, girls with NAFLD had a 60% greater risk of prediabetes and a fivefold greater risk of type 2 diabetes than boys, even after controlling for BMI and waist circumference (JAMA Pediatr. 2016 Aug 1. doi: 10.1001/jamapediatrics.2016.1971), reported Dr. Kimberly P. Newton and her coauthors.
The researchers also noted a significant association between nonalcoholic steatohepatitis (NASH) and glucose metabolism. Individuals with type 2 diabetes were three times more likely to also have NASH, while those with prediabetes had a 90% higher incidence of NASH, compared with individuals with normal glucose metabolism. They also found that those with NASH had significantly higher mean fasting glucose and insulin concentrations than children without NASH.
Dr. Newton, of the University of California, San Diego, and her coauthors wrote that while abnormal glucose metabolism is known to be common in adults with NAFLD, and that type diabetes is a risk factor for progression to NASH and liver-related mortality, the association in children with NAFLD is less well understood.
“Among our cohort, the prevalence of children with type 2 diabetes was much higher than would be expected based on contributions from obesity alone,” they wrote. “Although systemic insulin resistance is believed be important in the pathogenesis of both pediatric NAFLD and type 2 diabetes, to our knowledge, there are no longitudinal studies that evaluate the cause-effect relationship between these two associated conditions.”
The authors drew particular attention to the threefold higher odds of NASH in children with NAFLD and type 2 diabetes, pointing out that while the prognostic implications of NASH in childhood are not fully known, the NASH phenotype is associated with a “substantially” greater risk of cirrhosis. This risk is likely to be compounded by the presence of type 2 diabetes.
“Our study advances the literature by showing that as early as childhood, prediabetes and type 2 diabetes emerge as clear risk factors for NASH with potential downstream implications for future morbidity and mortality.”
Commenting on the greater incidence of prediabetes and type 2 diabetes among girls with NAFLD, the authors said this had been observed in other studies and that sex differences represented a major unmet research need.
The Nonalcoholic Steatohepatitis Clinical Research Network is supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Additional support was received from the National Center for Advancing Translational Sciences. The researchers reported no conflicts of interest.
FROM JAMA PEDIATRICS
Key clinical point: Nearly one in three children with nonalcoholic fatty liver disease have abnormal glucose metabolism, and this combination also is associated with a greater risk of nonalcoholic steatohepatitis.
Major finding: Among children with biopsy-diagnosed non-alcoholic fatty liver disease, 23.4% had prediabetes and 6.5% met the clinical criteria for type 2 diabetes.
Data source: Cross-sectional study of 675 children with biopsy-confirmed nonalcoholic fatty liver disease enrolled in the NASH Clinical Research Network.
Disclosures: The Nonalcoholic Steatohepatitis Clinical Research Network is supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Additional support was received from the National Center for Advancing Translational Sciences. The researchers reported no conflicts of interest.
Gene therapy shows promise for severe hemophilia A

Image by Spencer Phillips
ORLANDO—An investigational gene therapy can safely reduce bleeding in patients with severe hemophilia A, a phase 1/2 study suggests.
The therapy is BMN 270, a recombinant adeno-associated virus (AAV) vector coding for human coagulation factor VIII (FVIII).
Six of the 7 patients treated with the highest dose of BMN 270 had FVIII levels above 50%, and the number of bleeding events fell substantially from baseline.
None of the patients developed inhibitors to FVIII, there were no serious adverse events, and none of the patients discontinued the therapy due to safety reasons.
John Pasi, PhD, of Barts and the London School of Medicine and Dentistry in London, UK, presented the results of this study in a late-breaking oral presentation at the World Federation of Hemophilia 2016 World Congress.* The research was funded by BioMarin Pharmaceutical Inc.
This phase 1/2 dose-escalation study was designed to evaluate the safety and efficacy of BMN 270 in up to 12 patients with severe hemophilia A.
The primary endpoints are to assess the safety of a single dose of BMN 270 and the change from baseline of FVIII expression level at 16 weeks after infusion.
Secondary endpoints include assessing the impact of BMN 270 on the frequency of FVIII replacement therapy, the number of bleeding episodes requiring treatment, and any potential immune responses. Patients will be monitored for safety and durability of effect for 5 years.
Thus far, 9 patients with severe hemophilia A have received a single dose of BMN 270—1 at 6×1012 vg/kg, 1 at 2×1013 vg/kg, and 7 at 6 x 1013 vg/kg.
As of the July 6 data cutoff, post-treatment follow-up ranges from 12 weeks to 28 weeks.
Safety
The most common adverse events were arthralgia (9 events in 6 subjects), contusion (6 events in 3 subjects), back pain (4 events in 3 subjects), and ALT elevation (6 events in 6 subjects).
No clinically relevant sustained rises in ALT levels or other markers of liver toxicity have been observed.
The maximum ALT levels were between 23 U/L and 82 U/L (less than 2 times the upper limit of normal, which is 43 U/L for the central laboratory in this study) approximately 12 weeks after gene delivery and generally declined over the next few weeks. ALT rises have not been associated with any decrease in FVIII levels.
A steroid regimen administered to all high-dose patients has been well-tolerated. Patients are successfully tapering off of steroids. Two patients have been off steroid therapy for up to 2.5 weeks, with no adverse impact on FVIII expression or ALT levels.
Efficacy
The patient treated at the lowest dose (6×1012 vg/kg) had no change from baseline in FVIII levels. The patient treated at the mid-dose (2×1013 vg/kg) had a stable FVIII activity level greater than 2 IU/dL for more than 28 weeks.
All 7 patients treated at the highest dose (6×1013 vg/kg) had FVIII activity levels greater than 10 IU/dL after week 10.
As of each patient’s most recent reading, 6 of the 7 patients in the high-dose group had FVIII levels above 50%, as a percentage calculated based on the numbers of IU/dL. The seventh patient had levels above 10%.
Four patients who have been followed the longest had a mean FVIII level of 146% at their 20-week visit. Two patients with FVIII levels above 200% had no unexpected events or need for medical intervention.
For the 7 patients treated at the high dose, the median annualized bleeding rate measured from the day of gene transfer to the data cutoff fell from 20 to 5.
After week 7 post-infusion, there were no bleeds in 6 of the 7 patients. There were 10 bleeds from weeks 0 through 2 post-infusion, 7 bleeds from weeks 3 through 8, and 2 bleeds from weeks 9 through 28. From weeks 2 through 28, all but 1 bleed occurred in a single subject who is the lowest responder.
All of the patients in the high-dose cohort have switched to receiving FVIII therapy on-demand. Six of them were previously receiving FVIII therapy as prophylaxis.
“These data provide strong proof-of-concept evidence that restoration of clotting function may be achieved by gene therapy,” Dr Pasi said. “For the first time, patients have reason to hope to avoid bleeding and the opportunity to live a normal life.” ![]()
Image by Spencer Phillips
ORLANDO—An investigational gene therapy can safely reduce bleeding in patients with severe hemophilia A, a phase 1/2 study suggests.
The therapy is BMN 270, a recombinant adeno-associated virus (AAV) vector coding for human coagulation factor VIII (FVIII).
Six of the 7 patients treated with the highest dose of BMN 270 had FVIII levels above 50%, and the number of bleeding events fell substantially from baseline.
None of the patients developed inhibitors to FVIII, there were no serious adverse events, and none of the patients discontinued the therapy due to safety reasons.
John Pasi, PhD, of Barts and the London School of Medicine and Dentistry in London, UK, presented the results of this study in a late-breaking oral presentation at the World Federation of Hemophilia 2016 World Congress.* The research was funded by BioMarin Pharmaceutical Inc.
This phase 1/2 dose-escalation study was designed to evaluate the safety and efficacy of BMN 270 in up to 12 patients with severe hemophilia A.
The primary endpoints are to assess the safety of a single dose of BMN 270 and the change from baseline of FVIII expression level at 16 weeks after infusion.
Secondary endpoints include assessing the impact of BMN 270 on the frequency of FVIII replacement therapy, the number of bleeding episodes requiring treatment, and any potential immune responses. Patients will be monitored for safety and durability of effect for 5 years.
Thus far, 9 patients with severe hemophilia A have received a single dose of BMN 270—1 at 6×1012 vg/kg, 1 at 2×1013 vg/kg, and 7 at 6 x 1013 vg/kg.
As of the July 6 data cutoff, post-treatment follow-up ranges from 12 weeks to 28 weeks.
Safety
The most common adverse events were arthralgia (9 events in 6 subjects), contusion (6 events in 3 subjects), back pain (4 events in 3 subjects), and ALT elevation (6 events in 6 subjects).
No clinically relevant sustained rises in ALT levels or other markers of liver toxicity have been observed.
The maximum ALT levels were between 23 U/L and 82 U/L (less than 2 times the upper limit of normal, which is 43 U/L for the central laboratory in this study) approximately 12 weeks after gene delivery and generally declined over the next few weeks. ALT rises have not been associated with any decrease in FVIII levels.
A steroid regimen administered to all high-dose patients has been well-tolerated. Patients are successfully tapering off of steroids. Two patients have been off steroid therapy for up to 2.5 weeks, with no adverse impact on FVIII expression or ALT levels.
Efficacy
The patient treated at the lowest dose (6×1012 vg/kg) had no change from baseline in FVIII levels. The patient treated at the mid-dose (2×1013 vg/kg) had a stable FVIII activity level greater than 2 IU/dL for more than 28 weeks.
All 7 patients treated at the highest dose (6×1013 vg/kg) had FVIII activity levels greater than 10 IU/dL after week 10.
As of each patient’s most recent reading, 6 of the 7 patients in the high-dose group had FVIII levels above 50%, as a percentage calculated based on the numbers of IU/dL. The seventh patient had levels above 10%.
Four patients who have been followed the longest had a mean FVIII level of 146% at their 20-week visit. Two patients with FVIII levels above 200% had no unexpected events or need for medical intervention.
For the 7 patients treated at the high dose, the median annualized bleeding rate measured from the day of gene transfer to the data cutoff fell from 20 to 5.
After week 7 post-infusion, there were no bleeds in 6 of the 7 patients. There were 10 bleeds from weeks 0 through 2 post-infusion, 7 bleeds from weeks 3 through 8, and 2 bleeds from weeks 9 through 28. From weeks 2 through 28, all but 1 bleed occurred in a single subject who is the lowest responder.
All of the patients in the high-dose cohort have switched to receiving FVIII therapy on-demand. Six of them were previously receiving FVIII therapy as prophylaxis.
“These data provide strong proof-of-concept evidence that restoration of clotting function may be achieved by gene therapy,” Dr Pasi said. “For the first time, patients have reason to hope to avoid bleeding and the opportunity to live a normal life.” ![]()
Image by Spencer Phillips
ORLANDO—An investigational gene therapy can safely reduce bleeding in patients with severe hemophilia A, a phase 1/2 study suggests.
The therapy is BMN 270, a recombinant adeno-associated virus (AAV) vector coding for human coagulation factor VIII (FVIII).
Six of the 7 patients treated with the highest dose of BMN 270 had FVIII levels above 50%, and the number of bleeding events fell substantially from baseline.
None of the patients developed inhibitors to FVIII, there were no serious adverse events, and none of the patients discontinued the therapy due to safety reasons.
John Pasi, PhD, of Barts and the London School of Medicine and Dentistry in London, UK, presented the results of this study in a late-breaking oral presentation at the World Federation of Hemophilia 2016 World Congress.* The research was funded by BioMarin Pharmaceutical Inc.
This phase 1/2 dose-escalation study was designed to evaluate the safety and efficacy of BMN 270 in up to 12 patients with severe hemophilia A.
The primary endpoints are to assess the safety of a single dose of BMN 270 and the change from baseline of FVIII expression level at 16 weeks after infusion.
Secondary endpoints include assessing the impact of BMN 270 on the frequency of FVIII replacement therapy, the number of bleeding episodes requiring treatment, and any potential immune responses. Patients will be monitored for safety and durability of effect for 5 years.
Thus far, 9 patients with severe hemophilia A have received a single dose of BMN 270—1 at 6×1012 vg/kg, 1 at 2×1013 vg/kg, and 7 at 6 x 1013 vg/kg.
As of the July 6 data cutoff, post-treatment follow-up ranges from 12 weeks to 28 weeks.
Safety
The most common adverse events were arthralgia (9 events in 6 subjects), contusion (6 events in 3 subjects), back pain (4 events in 3 subjects), and ALT elevation (6 events in 6 subjects).
No clinically relevant sustained rises in ALT levels or other markers of liver toxicity have been observed.
The maximum ALT levels were between 23 U/L and 82 U/L (less than 2 times the upper limit of normal, which is 43 U/L for the central laboratory in this study) approximately 12 weeks after gene delivery and generally declined over the next few weeks. ALT rises have not been associated with any decrease in FVIII levels.
A steroid regimen administered to all high-dose patients has been well-tolerated. Patients are successfully tapering off of steroids. Two patients have been off steroid therapy for up to 2.5 weeks, with no adverse impact on FVIII expression or ALT levels.
Efficacy
The patient treated at the lowest dose (6×1012 vg/kg) had no change from baseline in FVIII levels. The patient treated at the mid-dose (2×1013 vg/kg) had a stable FVIII activity level greater than 2 IU/dL for more than 28 weeks.
All 7 patients treated at the highest dose (6×1013 vg/kg) had FVIII activity levels greater than 10 IU/dL after week 10.
As of each patient’s most recent reading, 6 of the 7 patients in the high-dose group had FVIII levels above 50%, as a percentage calculated based on the numbers of IU/dL. The seventh patient had levels above 10%.
Four patients who have been followed the longest had a mean FVIII level of 146% at their 20-week visit. Two patients with FVIII levels above 200% had no unexpected events or need for medical intervention.
For the 7 patients treated at the high dose, the median annualized bleeding rate measured from the day of gene transfer to the data cutoff fell from 20 to 5.
After week 7 post-infusion, there were no bleeds in 6 of the 7 patients. There were 10 bleeds from weeks 0 through 2 post-infusion, 7 bleeds from weeks 3 through 8, and 2 bleeds from weeks 9 through 28. From weeks 2 through 28, all but 1 bleed occurred in a single subject who is the lowest responder.
All of the patients in the high-dose cohort have switched to receiving FVIII therapy on-demand. Six of them were previously receiving FVIII therapy as prophylaxis.
“These data provide strong proof-of-concept evidence that restoration of clotting function may be achieved by gene therapy,” Dr Pasi said. “For the first time, patients have reason to hope to avoid bleeding and the opportunity to live a normal life.” ![]()
PHM16: Promoting, Teaching Pediatric High Value Care
As we embark on Choosing Wisely, pediatric hospitalists gathered to attend this fruitful discussion on not only how to change our way of thinking but also how to feed it forward to our trainees. The barriers to promoting and teaching high value care are plenty and essentially universal to academic and community sites: we have had no formal teaching, there is cultural resistance and there is lack of transparency on costs and charges.
Perhaps the questions we should be asking ourselves, our trainees and our families are:
- Instead of “What’s the matter?” ask “What matters?”
- Instead of asking “Will that test change our management?” ask “Does that test benefit the patient? What are the harms of the test?”
Thinking about effects of tests downstream, the “testing cascade” can be a great mental exercise for the higher-level learner to understand the value, the unknowns we face in our daily decisions and simultaneously improving our understanding of best practices.
A toolkit was provided to help bring back resources and methods to teach high value care in morning report/ case conference settings, bedside teaching and family discussions.
One point is clear though—there is still a long way to go to move the pendulum to the side of value based practice and teaching. There is still controversy on how and whether cost should be discussed with the family. Cost is more than just monetary values—family anxiety and patient harm may resonate more with families as we perfect our skills in shared decision making.
This serves as an exciting time to unite and better our understanding on why we do what we do and deliberately think about downstream effects. High value care curriculum for medical students, residents, fellows and even faculty is an area ripe for further educational and clinical research.
When asking for the Pediatric Value Meal, this is one where I will not Super size it!
Dr. Akshata Hopkins, MD FAAP, is an academic hospitalist at Johns Hopkins All Children's Hospital, St. Petersburg, Fla.
As we embark on Choosing Wisely, pediatric hospitalists gathered to attend this fruitful discussion on not only how to change our way of thinking but also how to feed it forward to our trainees. The barriers to promoting and teaching high value care are plenty and essentially universal to academic and community sites: we have had no formal teaching, there is cultural resistance and there is lack of transparency on costs and charges.
Perhaps the questions we should be asking ourselves, our trainees and our families are:
- Instead of “What’s the matter?” ask “What matters?”
- Instead of asking “Will that test change our management?” ask “Does that test benefit the patient? What are the harms of the test?”
Thinking about effects of tests downstream, the “testing cascade” can be a great mental exercise for the higher-level learner to understand the value, the unknowns we face in our daily decisions and simultaneously improving our understanding of best practices.
A toolkit was provided to help bring back resources and methods to teach high value care in morning report/ case conference settings, bedside teaching and family discussions.
One point is clear though—there is still a long way to go to move the pendulum to the side of value based practice and teaching. There is still controversy on how and whether cost should be discussed with the family. Cost is more than just monetary values—family anxiety and patient harm may resonate more with families as we perfect our skills in shared decision making.
This serves as an exciting time to unite and better our understanding on why we do what we do and deliberately think about downstream effects. High value care curriculum for medical students, residents, fellows and even faculty is an area ripe for further educational and clinical research.
When asking for the Pediatric Value Meal, this is one where I will not Super size it!
Dr. Akshata Hopkins, MD FAAP, is an academic hospitalist at Johns Hopkins All Children's Hospital, St. Petersburg, Fla.
As we embark on Choosing Wisely, pediatric hospitalists gathered to attend this fruitful discussion on not only how to change our way of thinking but also how to feed it forward to our trainees. The barriers to promoting and teaching high value care are plenty and essentially universal to academic and community sites: we have had no formal teaching, there is cultural resistance and there is lack of transparency on costs and charges.
Perhaps the questions we should be asking ourselves, our trainees and our families are:
- Instead of “What’s the matter?” ask “What matters?”
- Instead of asking “Will that test change our management?” ask “Does that test benefit the patient? What are the harms of the test?”
Thinking about effects of tests downstream, the “testing cascade” can be a great mental exercise for the higher-level learner to understand the value, the unknowns we face in our daily decisions and simultaneously improving our understanding of best practices.
A toolkit was provided to help bring back resources and methods to teach high value care in morning report/ case conference settings, bedside teaching and family discussions.
One point is clear though—there is still a long way to go to move the pendulum to the side of value based practice and teaching. There is still controversy on how and whether cost should be discussed with the family. Cost is more than just monetary values—family anxiety and patient harm may resonate more with families as we perfect our skills in shared decision making.
This serves as an exciting time to unite and better our understanding on why we do what we do and deliberately think about downstream effects. High value care curriculum for medical students, residents, fellows and even faculty is an area ripe for further educational and clinical research.
When asking for the Pediatric Value Meal, this is one where I will not Super size it!
Dr. Akshata Hopkins, MD FAAP, is an academic hospitalist at Johns Hopkins All Children's Hospital, St. Petersburg, Fla.
ED Visits Rise With Age in Children, Young Adults With Diabetes
The rate of diabetes-related emergency department visits was 464.5 per 100,000 U.S. population among Americans under age 30 in 2012, with young adults heading to the ED far more often than children, according to the Agency for Healthcare Research and Quality.
Young adults aged 18-29 years made diabetes-related ED visits at a rate of 905 per 100,000 in 2012, compared with 149 per 100,000 for children 17 and under. Narrowing down the age groups shows even greater differences: The rate was 47 per 100,000 for children aged 5 years and under, 95 for children aged 6-9, 193 for 10- to 13-year-olds, 316.5 for those aged 14-17, 607 for 18- to 21-year-olds, 889 for 22- to 25-year-olds, and 1,236 for those aged 26-29 years, the AHRQ reported.
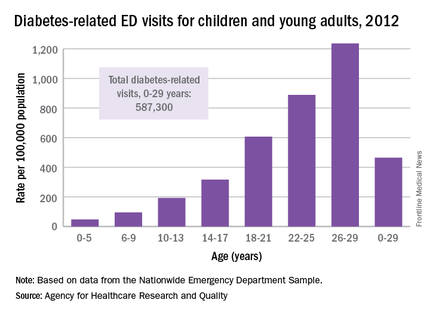
Patients aged 5 years and under were, however, the most likely to be admitted to the hospital in 2012: 29% of their diabetes-related ED visits resulted in admission, compared with 26% for those aged 26-29. Those aged 22-25 years were the least likely to be admitted, with 18% staying after their ED visit, and the overall admission rate for those aged 0-29 years was 23.5%, the report noted.
The ED visit rate for diabetes was higher for females than for males aged 0-29 years – 569 per 100,000 vs. 355 – but males were more likely to be admitted – 27% vs. 21% for females, according to data from the Nationwide Emergency Department Sample.
The rate of diabetes-related emergency department visits was 464.5 per 100,000 U.S. population among Americans under age 30 in 2012, with young adults heading to the ED far more often than children, according to the Agency for Healthcare Research and Quality.
Young adults aged 18-29 years made diabetes-related ED visits at a rate of 905 per 100,000 in 2012, compared with 149 per 100,000 for children 17 and under. Narrowing down the age groups shows even greater differences: The rate was 47 per 100,000 for children aged 5 years and under, 95 for children aged 6-9, 193 for 10- to 13-year-olds, 316.5 for those aged 14-17, 607 for 18- to 21-year-olds, 889 for 22- to 25-year-olds, and 1,236 for those aged 26-29 years, the AHRQ reported.
Patients aged 5 years and under were, however, the most likely to be admitted to the hospital in 2012: 29% of their diabetes-related ED visits resulted in admission, compared with 26% for those aged 26-29. Those aged 22-25 years were the least likely to be admitted, with 18% staying after their ED visit, and the overall admission rate for those aged 0-29 years was 23.5%, the report noted.
The ED visit rate for diabetes was higher for females than for males aged 0-29 years – 569 per 100,000 vs. 355 – but males were more likely to be admitted – 27% vs. 21% for females, according to data from the Nationwide Emergency Department Sample.
The rate of diabetes-related emergency department visits was 464.5 per 100,000 U.S. population among Americans under age 30 in 2012, with young adults heading to the ED far more often than children, according to the Agency for Healthcare Research and Quality.
Young adults aged 18-29 years made diabetes-related ED visits at a rate of 905 per 100,000 in 2012, compared with 149 per 100,000 for children 17 and under. Narrowing down the age groups shows even greater differences: The rate was 47 per 100,000 for children aged 5 years and under, 95 for children aged 6-9, 193 for 10- to 13-year-olds, 316.5 for those aged 14-17, 607 for 18- to 21-year-olds, 889 for 22- to 25-year-olds, and 1,236 for those aged 26-29 years, the AHRQ reported.
Patients aged 5 years and under were, however, the most likely to be admitted to the hospital in 2012: 29% of their diabetes-related ED visits resulted in admission, compared with 26% for those aged 26-29. Those aged 22-25 years were the least likely to be admitted, with 18% staying after their ED visit, and the overall admission rate for those aged 0-29 years was 23.5%, the report noted.
The ED visit rate for diabetes was higher for females than for males aged 0-29 years – 569 per 100,000 vs. 355 – but males were more likely to be admitted – 27% vs. 21% for females, according to data from the Nationwide Emergency Department Sample.
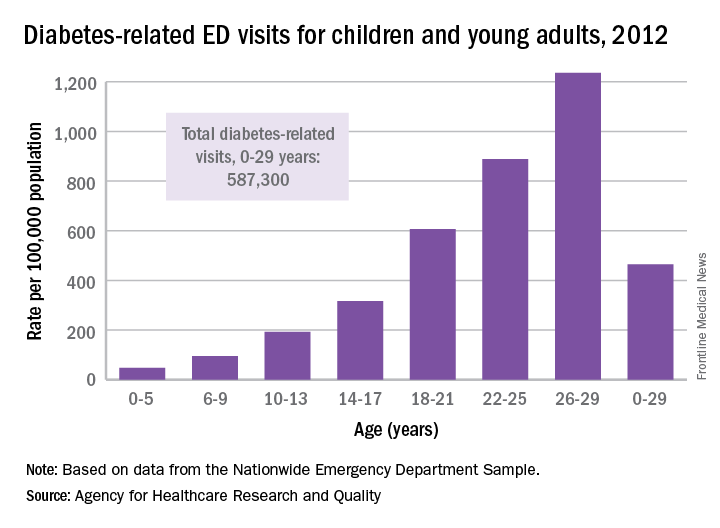
C6 EIA testing can guide Lyme disease treatment in children
The C6 Lyme enzyme immunoassay is an effective diagnostic tool for children who are being tested for Lyme disease, according to Susan C. Lipsett, MD, and her associates.
Of the 944 samples collected for the study, 114 were positive for Lyme disease. The sensitivity of C6 enzyme immunoassay (EIA) testing alone was 79.8% and the specificity was 94.2%, slightly less than the standard two-tiered testing approach, which had a sensitivity of 81.6% and a specificity of 98.8%. The specificity of C6 EIA testing was increased to 98.6% when a supplemental immunoblot was added to testing.
The specificity of C6 EIA testing alone was significantly lower than standard testing in the control group. When the supplemental immunoblot was added to testing, the specificity of C6 EIA testing did match the specificity of standard testing in children who did not have Lyme disease.
“Although supplemental immunoblots are still required to confirm a Lyme disease diagnosis, our study supports using the C6 EIA as a first-line diagnostic test in children undergoing evaluation for Lyme disease. In the appropriate clinical scenario, the C6 EIA could limit unnecessary procedures and allow for prompt initiation of appropriate therapy,” the investigators concluded.
Find the full study in Clinical Infectious Diseases (doi:10.1093/cid/ciw427).
The C6 Lyme enzyme immunoassay is an effective diagnostic tool for children who are being tested for Lyme disease, according to Susan C. Lipsett, MD, and her associates.
Of the 944 samples collected for the study, 114 were positive for Lyme disease. The sensitivity of C6 enzyme immunoassay (EIA) testing alone was 79.8% and the specificity was 94.2%, slightly less than the standard two-tiered testing approach, which had a sensitivity of 81.6% and a specificity of 98.8%. The specificity of C6 EIA testing was increased to 98.6% when a supplemental immunoblot was added to testing.
The specificity of C6 EIA testing alone was significantly lower than standard testing in the control group. When the supplemental immunoblot was added to testing, the specificity of C6 EIA testing did match the specificity of standard testing in children who did not have Lyme disease.
“Although supplemental immunoblots are still required to confirm a Lyme disease diagnosis, our study supports using the C6 EIA as a first-line diagnostic test in children undergoing evaluation for Lyme disease. In the appropriate clinical scenario, the C6 EIA could limit unnecessary procedures and allow for prompt initiation of appropriate therapy,” the investigators concluded.
Find the full study in Clinical Infectious Diseases (doi:10.1093/cid/ciw427).
The C6 Lyme enzyme immunoassay is an effective diagnostic tool for children who are being tested for Lyme disease, according to Susan C. Lipsett, MD, and her associates.
Of the 944 samples collected for the study, 114 were positive for Lyme disease. The sensitivity of C6 enzyme immunoassay (EIA) testing alone was 79.8% and the specificity was 94.2%, slightly less than the standard two-tiered testing approach, which had a sensitivity of 81.6% and a specificity of 98.8%. The specificity of C6 EIA testing was increased to 98.6% when a supplemental immunoblot was added to testing.
The specificity of C6 EIA testing alone was significantly lower than standard testing in the control group. When the supplemental immunoblot was added to testing, the specificity of C6 EIA testing did match the specificity of standard testing in children who did not have Lyme disease.
“Although supplemental immunoblots are still required to confirm a Lyme disease diagnosis, our study supports using the C6 EIA as a first-line diagnostic test in children undergoing evaluation for Lyme disease. In the appropriate clinical scenario, the C6 EIA could limit unnecessary procedures and allow for prompt initiation of appropriate therapy,” the investigators concluded.
Find the full study in Clinical Infectious Diseases (doi:10.1093/cid/ciw427).
FROM CLINICAL INFECTIOUS DISEASES
Sport-related concussion: How best to help young athletes
› Require athletes who sustain a concussion to wait a minimum of 7 to 10 days before returning to full unrestricted activity. C
› Ensure that any player diagnosed with concussion follows a guided return-to-play progression, supervised by an athletic trainer or physical therapist experienced in post-concussion care. C
› Advise patients who are old enough to drive not to do so for at least 24 hours after a concussion. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Each year in the United States, more than 44 million young people participate in sports activities.1 Yet the number of concussions incurred annually by children and adolescents engaged in sports and recreational play has been underestimated for years, and largely unknown.1,2
Some estimates were based solely on the number of young athletes treated in emergency departments or sports concussion clinics. Others focused only on team players of middle school or high school age, excluding younger children who were hit in the head on playgrounds or during other recreational activities. What’s more, large numbers of concussions—as many as 4 in 10 incurred by high school athletes—were never reported to a coach or medical professional.3
In a new study published in the journal Pediatrics in June, researchers used national databases and current literature to provide what they believe to be “the most accurate and precise estimate of youth concussion” thus far: Between 1.1 and 1.9 million sports- and recreation-related concussions occur among US youth ages 18 or younger annually.1
Among young people playing team sports, concussions are between 2 and 7 times more likely to occur during competitive games than in practice sessions.4-7 Boys on football and ice hockey teams have the highest rates of concussion in young athletes.For overall number of concussions, however, girls on soccer teams are second only to football players.4 Female soccer players are more likely than male soccer players to sustain concussions during equal number of hours of play.4,7
An increase in incidence. The incidence of concussion among young athletes appears to have increased in the past decade, a likely result of greater involvement in team sports, an increasing focus on safeguarding young people from the potential dangers associated with a blow to the brain, and better diagnostic techniques.4,8-10 And a recent study based on data from electronic medical records at a large regional pediatric health care network found that more than three-quarters of young people with sports-related concussions were first seen in a primary care setting.2
With this in mind, we present a comprehensive update of the evidence regarding the diagnosis and management of sport-related concussion. The recommendations we include are consistent with professional association guidelines.8-10 Although we focus on concussion in children and adolescents involved in athletic activities, the principles generally apply to patients of all ages and to concussions that may not be sports related.
Removal from play: A vital first step
Whenever you conduct a physical exam for a young athlete, remind him or her—and the patient’s parents—that after a blow to the head, immediate removal from play is critical. Concussion is caused by a direct or indirect force to the brain that results in a transient disturbance in brain function,8-10 manifested by alterations in neurocognitive and motor function. While the signs and symptoms (TABLE 1)8-10 resolve within 10 days of injury in about 90% of cases, those who incur additional head impact within 24 hours have a higher symptom burden and prolonged recovery period.11 Even without repetitive impact, younger athletes may take longer to recover.8-10
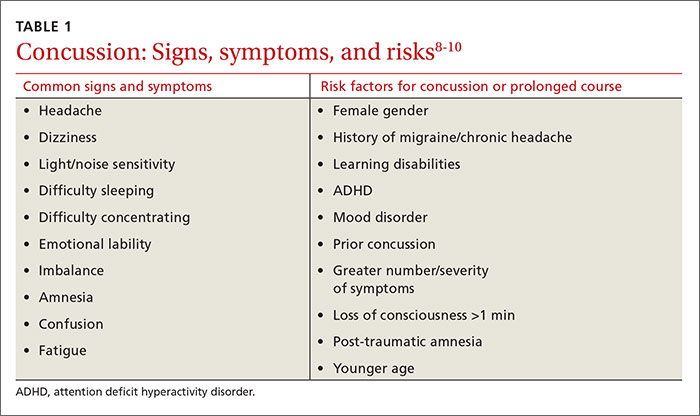
The initial assessment
A child or adolescent who sustains a suspected concussion should be seen by a physician within 24 to 48 hours. Whether the initial assessment occurs in your office or on the sidelines of a game, it is important to confirm the time the incident occurred and the mechanism of injury.
Concussion is diagnosed by a combination of history, physical exam, and objective testing when symptoms or exam findings associated with mild brain trauma—headache, dizziness, light and/or noise sensitivity, among others—closely follow a head injury.8-10 Certain maneuvers—assessing eye movements by asking the athlete to look in various directions, for instance, then to follow a pen or finger as you move it closer to his or her face—may provoke dizziness, headache, or other symptoms of concussion that were not apparent initially.
The differential diagnosis includes cervical musculoskeletal injury, craniofacial injury, epidural and subdural hematoma, heat-related illness, uncomplicated headache and migraine, upper respiratory infection, and vertigo.8-10
Tools aid in diagnosis
Many clinical assessment tools exist to aid in the diagnosis of concussion (TABLE 2).8-10,12-14 Any one of these tools, many of which use combinations of symptom checklists, balance exams, and cognitive assessments, may be included in your evaluation. No single tool has been found to be superior to any other.8-10 A combination of tools may improve diagnostic accuracy, but assessment tools should not be the sole basis used to diagnose or rule out concussion.
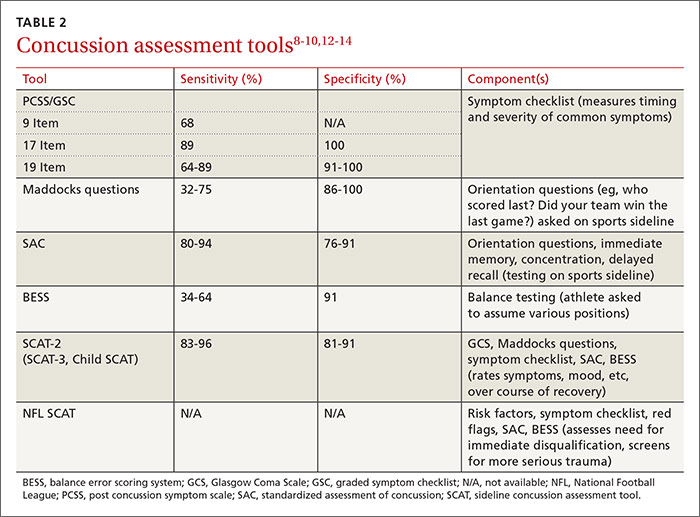
Any child or adolescent who had a blow to the head and at least one sign or symptom of concussion should be evaluated as soon as possible and assessed again later that day or the next day if any reason for concern remains.
Neuropsychological (NP) testing may involve computerized tests developed specifically for athletes. Patients may be required to react to objects that appear on a screen, for example, in a way that tests memory, performance, and reaction time. Because cognitive recovery often lags behind symptom resolution, NP testing may identify subtle brain deficits even in athletes who are asymptomatic at rest or with exercise. In general, NP testing has a sensitivity of 71% to 88% for athletes with concussion,10 but it is most beneficial when baseline test results are available. Interpretation of NP testing should be done only by qualified clinicians.
While NP testing may provide additional prognostic information, it should not alter the management of athletes who are symptomatic either at rest or with exercise.15 Nor is NP testing vital, as concussion can be accurately diagnosed and adequately managed without it.
Neuroimaging, including computed tomography (CT) and magnetic resonance imaging (MRI), is often used unnecessarily in the initial assessment of a patient who sustained a possible concussion.8-10 In fact, neuroimaging should be reserved for cases in which it is necessary to rule out more serious pathology: intracranial or subdural hematoma or a craniofacial injury, for example, in patients with clinical findings that are red flags. These red flags include focal neurologic deficits, continuing nausea/vomiting, or persistent disorientation (TABLE 3),8-10 or symptoms that worsen or persist beyond a few weeks. In such cases, further evaluation—with MRI of the brain, formal NP testing, and/or referral to a neurologist, physiatrist, or other physician who specializes in concussion care—is indicated.
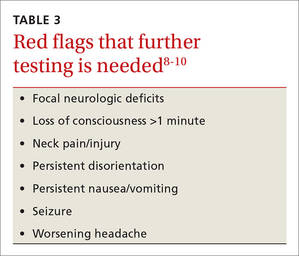
Concussion management: Rest is key
While there is a dearth of high-quality studies on the management of sport-related concussion across all age groups, standardized protocols for both children and adults have been adopted in most clinical settings.8-10,16,17 The protocols provide a framework for an individualized treatment plan. Yet their use among primary care physicians is inconsistent.18-20
Traditionally, concussion management begins with relative physical and cognitive rest to allow the brain time to recover.8-10 Recent randomized controlled trials have challenged this premise by suggesting that mild to moderate physical activity for post-concussion patients who are mildly symptomatic does not adversely affect recovery.21,22 These studies have significant limitations, however, and further research is needed to provide specific guidance on this aspect of concussion management before it is adopted.
Physical restrictions include organized sports, recreational activity, recess, and physical education classes. Walking is permitted unless it exacerbates symptoms. These restrictions should continue until the patient is symptom-free.
Cognitive restrictions include modifications at school and at home. Once an athlete is able to concentrate and tolerate visual and auditory stimuli, he or she may return to school. But classroom modifications should be considered, possibly including shortened school days, extra time for testing and homework, help with note taking, and restrictions from classes likely to provoke symptoms, such as computer science or music. Limiting use of mobile devices, television viewing, noisy environments, and other possible provocations may help speed symptom resolution. These restrictions, too, should remain in place until the patient is symptom-free.
Driving is often not addressed by physicians managing the care of athletes with concussion, but evidence suggests it should be. A study of patients presenting to the emergency department found that within 24 hours of a concussion diagnosis, individuals had an impaired response to traffic hazards.23,24 And Canadian clinical practice guidelines recommend that athletes with mild traumatic brain injury (TBI) avoid driving within the first 24 hours.25
While American guidelines are silent on the question of driving for this patient population, we recommend that athletes with concussion be restricted from driving and engaging in other risky complex tasks, such as welding or shop class, for at least 24 hours. For many athletes diagnosed with concussion, driving restrictions of longer duration may be necessary based on their symptom profile and neurocognitive test results. Continued dizziness or visual deficits would pose a greater risk than fatigue or short-term memory loss, for example.
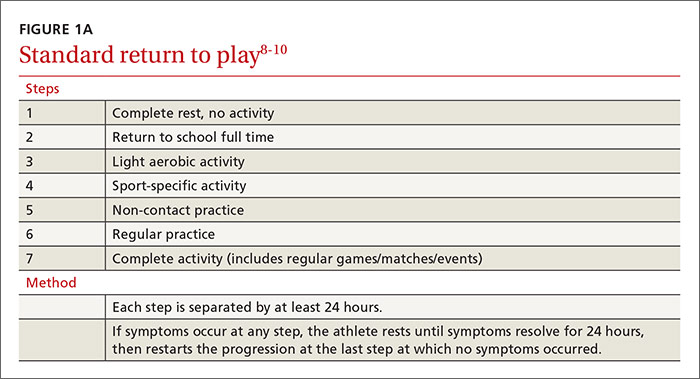
Overseeing the return to play
Return-to-activity progression follows a stepwise protocol, with 6 steps that the injured athlete must complete before resuming full activity (FIGURE 1A).8-10 This stepwise progression begins only when athletes are symptom free, even during provocative maneuvers; have had a normal neurologic exam, are back to school full time with no restriction; are off any medications prescribed for concussion symptoms (TABLE 4),8-10 and when neurocognitive testing, if performed, is back to baseline. If an athlete develops symptoms at any stage of the progression, rest is required until he or she remains asymptomatic for at least 24 hours. The progression is then restarted at the last stage at which the patient was symptom free.
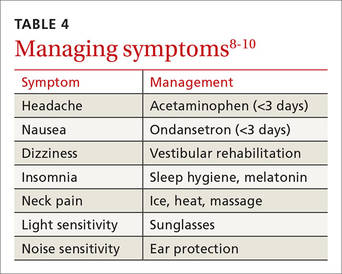
Some individualization, of course, is recommended here, too. Younger athletes and those with a prior history of concussion may require 10 days or more to complete all the steps, allowing an extra day at various steps. Neurologic maturation affects recovery time, and for younger individuals, a more conservative return-to-play protocol based on initial concussion symptom duration has been proposed (FIGURE 1B).16
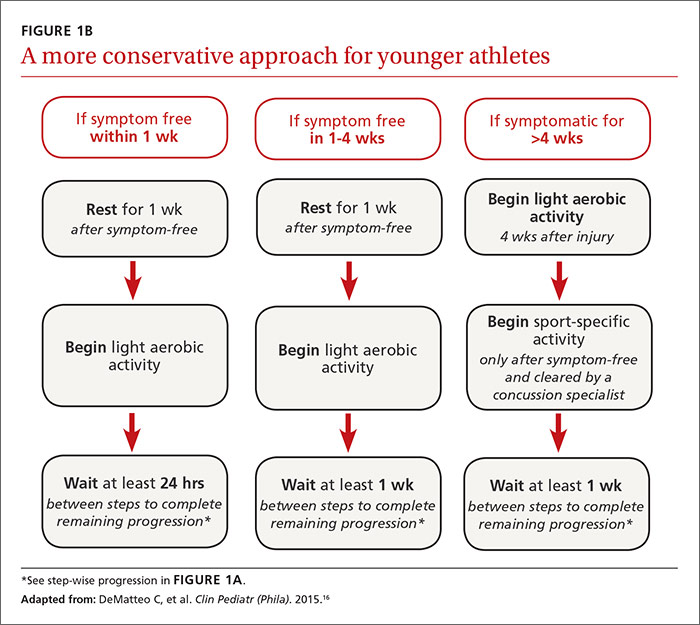
Return to activity is often supervised by a certified athletic trainer at the athlete’s school. In the event that no athletic trainer is available, patients may be referred to physical therapists with experience in monitoring injured athletes.26 Anyone involved in the patient’s care, including the athlete himself, may use a symptom checklist to monitor recovery.
Although there is no evidence that the ongoing use of a symptom checklist affects the course of recovery, its use is often helpful in identifying specific symptoms that can be managed by means other than physical and cognitive rest—a sleep hygiene program for an individual with lingering difficulty sleeping, for example, or the continued application of ice, heat, and massage for persistent neck pain.
Checklist monitoring may be especially helpful for athletes whose symptoms extend beyond 10 days or who have multiple symptoms. Final clearance once all the steps have been completed requires follow-up with a health care provider.
Is a symptom-free waiting period necessary?
There is no evidence suggesting a need for a symptom-free waiting period before starting the return-to-play protocol.10,27 Because a repeat concussion is most likely within 7 to 10 days of the initial injury,8,9 however, most athletes should not return to contact play during that time frame, regardless of symptom resolution.
It is helpful to have asymptomatic athletes participate in non-contact activity before the 7 to 10 days are up, however. Doing so can help prevent deconditioning and injury upon return to contact sport, as there is evidence of increased risk of lower-extremity injury in the 90 days after concussion.28
What to tell athletes—and parents—about repetitive head trauma
There is growing concern about the long-term risks of concussion and repetitive head impact that may manifest as chronic traumatic encephalopathy (CTE) and chronic neurocognitive impairment (CNI) later in life. Indeed, some data strongly suggest—but do not definitively prove—a relationship between repetitive head injury and chronic neurodegenerative disease.8-10 You can tell worried patients or parents, however, that the majority of research on CTE and CNI has been based on professional football players.
Studies of long-term effects of soccer heading have shown conflicting results, with some finding cognitive impairment, altered postural control, and anatomic changes of the brain, while others found no effect on encephalopathy, concussion symptoms, or neurocognitive performance.29-36Here, too, most studies showing negative effects of soccer heading involved professional athletes.
Repetitive sub-concussive impact in high school football athletes has been found to induce biochemical changes to the brain,37 but the long-term effects are unknown. And, while concussion in high school athletes has been associated with short-term cognitive impairment, altered neurochemistry, and evidence of increased symptoms on baseline neurocognitive testing,8-10,38 no studies have linked concussion during middle school or high school with CNI. What’s more, a long-term (50-year) follow-up study of individuals who played football in high school found no difference in rates of neurodegenerative disease compared with age-matched controls.39
A new study of high school and college football players (mean age: 17.4 years) presented at the American Academy of Neurology 2016 Sports Concussion Conference in Chicago in July, however, found significant alterations in white matter 6 months post injury.40 The researchers compared 17 athletes with sport-related concussion with matched controls, using diffusion tensor imaging and diffusion kurtosis tensor imaging as biomarkers of brain recovery. The concussed athletes underwent MRI and symptom assessment at 24 hours, 8 days, and 6 months. The controls followed identical protocols.
At the 6-month assessment, there were no differences between the concussed group and the controls in terms of self-reported concussion symptoms, cognition, or balance. However, the concussed athletes had widespread decreased mean diffusivity compared with the controls. Despite the lack of clinical symptoms, the concussed athletes showed significant alterations in white matter “that were related to initial symptom severity ratings,” the authors concluded. These findings have implications both for determination of recovery from concussion and concussion management, they added.40
Although there is no way to eliminate all concussions, limited evidence suggests that improving athletic technique, limiting contact at practices, better enforcement of game rules, and rule changes regarding physical contact may decrease concussion risk.41-43 Many youth sports organizations have developed policies placing restrictions on head impact during practices and games. Studies are ongoing, too, to see if better headgear—or requiring helmets for soccer players—makes a difference.
CORRESPONDENCE
Ryan A. Sprouse, MD, CAQSM, 203 East Fourth Avenue, Ranson, WV 25438; rsprouse@wvumedicine.org.
1. Bryan MA, Rowhani-Rahbar A, Comstock RD, et al. Sports- and recreation-related concussions in US youth. Pediatrics. 2016; June 20 [Epub ahead of print].
2. Arbogast KB, Curry AE, Pfeiffer MR, et al. Point of health care entry for youth with concussion within a large pediatric care network. JAMA Pediatr. 2016; May 31 [Epub ahead of print].
3. Mihalik JK, Guskiewicz KM, Valovich McLeod TC, et al. Knowledge, attitude, and concussion-reporting behaviors among high school athletes: a preliminary study. J Ath Tr. 2013;48:645-653.
4. Marar M, McIlvain NM, Fields SK, et al. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;40:747.
5. Kontos AP, Elbin RJ, Fazio-Sumrock VC. Incidence of sports-related concussion among youth football players aged 8-12 years. J Pediatr. 2013;163:717-720.
6. Dompier TP, Kerr ZY, Marshall SW, et al. Incidence of concussion during practice and games in youth, high school, and collegiate American football players. JAMA Pediatr. 2015;169:659-665.
7. Comstock RD, Currie DW, Pierpont LA, et al. An evidence-based discussion of heading the ball and concussions in high school soccer. JAMA Pediatr. 2015;169:830-837.
8. Harmon KG, Drezner JA, Gammons M, et al. American Medical Society for Sports Medicine position statement: concussion in sport. Br J Sports Med. 2013;47:15-26.
9. McCrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med. 2013;47:250-258.
10. Giza CC, Kutcher JS, Ashwal S, et al. Summary of the evidence-based guideline update: evaluation and management of concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2250-2257.
11. Terwilliger VK, Pratson L, Vaughan CG, et al. Additional post-concussion impact exposure may affect recovery in adolescent athletes. J Neurotrauma. 2016;33:761-765.
12. Putukian M, Echemendia R, Dettwiler-Danspeckgruber A. Prospective clinical assessment using Sideline Concussion Assessment Tool-2 testing in the evaluation of sport-related concussion in college athletes. Clin J Sport Med. 2015;25:36-42.
13. Broglio SP, Macciocchi SN, Ferrara MS. Sensitivity of the concussion assessment battery. Neurosurgery. 2007;60:1050-1057.
14. Randolph C, McCrea M, Barr WB. Is neuropsychological testing useful in the management of sport-related concussion? J Athl Train. 2005;40:139-152.
15. Shrier I. Neuropsychological testing and concussions: a reasoned approach. Clin J Sport Med. 2012;22:211-213.
16. DeMatteo C, Stazyk K, Singh SK, et al. Development of a conservative protocol to return children and youth to activity following concussive injury. Clin Pediatr (Phila). 2015;54:152-163.
17. Broglio SP, Cantu RC, Gioia GA, et al. National Athletic Trainers Association position statement: management of sport concussion. J Athl Train. 2014;49:245-265.
18. Stoller J, Carson JD, Garel A, et al. Do family physicians, emergency department physicians, and pediatricians give consistent sport-related concussion management advice? Can Fam Physician. 2014;60:548, 550-552.
19. Lebrun CM, Mrazik M, Prasad AS, et al. Sport concussion knowledge base, clinical practices and needs for continuing medical education: a survey of family physicians and cross-border comparison. Br J Sports Med. 2013;47:54-59.
20. Zemek R, Eady K, Moreau K, et al. Knowledge of paediatric concussion among front-line primary care providers. Paediatr Child Health. 2014;19:475-480.
21. Maerlender A, Rieman W, Lichtenstein J, et al. Programmed physical exertion in recovery from sports-related concussion: a randomized pilot study. Dev Neuropsychol. 2015;40:273-278.
22. Buckley TA, Munkasy BA, Clouse BP. Acute cognitive and physical rest may not improve concussion recovery time. J Head Trauma Rehabil. 2015; July 24 [Epub ahead of print].
23. Preece MH, Horswill MS, Langlois JA, et al. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21:375-378.
24. Baker A, Unsworth CA, Lannin NA. Fitness-to-drive after mild traumatic brain injury: mapping the time trajectory of recovery in the acute stages post injury. Accid Anal Prev. 2015;79:50-55.
25. Marshall S, Bayley M, McCullagh S, et al. Clinical practice guidelines for mild traumatic brain injury and persistent symptoms. Can Fam Physician. 2012;58:257-267.
26. Yorke AM, Littleton S, Alsalaheen BA. Concussion attitudes and beliefs, knowledge, and clinical practice: a survey of physical therapists. Phys Ther. Available at: http://dx.doi.org/10.2522/ptj.20140598. Accessed January 21, 2016.
27. McCrea M, Guskiewicz K, Randolph C, et al. Effects of a symptom-free waiting period on clinical outcome and risk of reinjury after sport-related concussion. Neurosurgery. 2009;65:876-883.
28. Brooks MA, Peterson K, Biese K, et al. Concussion increases odds of sustaining a lower extremity musculoskeletal injury after return to play among collegiate athletes. Am J Sports Med. 2016;44:742-747.
29. Witol AD, Webbe FM. Soccer heading frequency predicts neuropsychological deficits. Arch Clin Neuropsychol. 2003;18:397-417.
30. Haran FJ, Tierney R, Wright WG, et al. Acute changes in postural control after soccer heading. Int J Sports Med. 2013;34:350-354.
31. Lipton ML, Kim N, Zimmerman ME, et al. Soccer heading is associated with white matter microstructural and cognitive abnormalities. Radiology. 2013;268:850-857.
32. Jordan SE, Green GA, Galanty HL, et al. Acute and chronic brain injury in United States national team soccer players. Am J Sports Med. 1996;24:205-210.
33. Kontos AP, Dolese A, Elbin RJ, et al. Relationship of soccer heading to computerized neurocognitive performance and symptoms among female and male youth soccer players. Brain Inj. 2011;25:1234-1241.
34. Straume-Naesheim TM, Andersen TE, Dvorak J, et al. Effects of heading exposure and previous concussions on neuropsychological performance among Norwegian elite footballers. Br J Sports Med. 2005;39:70-77.
35. Stephens R, Rutherford A, Potter D, et al. Neuropsychological impairment as a consequence of football (soccer) play and football heading: a preliminary analysis and report on school students (13-16 years). Child Neuropsychol. 2005;11:513-526.
36. Stephens R, Rutherford A, Potter D, et al. Neuropsychological consequence of soccer play in adolescent UK school team soccer players. J Neuropsychiatry Clin Neurosci. 2010;22:295-303.
37. Poole VN, Breedlove EL, Shenk TE, et al. Sub-concussive hit characteristics predict deviant brain metabolism in football athletes. Dev Neuropsychol. 2015;40:12-17.
38. Mannix R, Iverson GL, Maxwell B, et al. Multiple prior concussions are associated with symptoms in high school athletes. Ann Clin Trans Neurol. 2014;1:433-438.
39. Savica R, Parisi JE, Wold LE, et al. High school football and risk of neurodegeneration: a community-based study. Mayo Clin Proc. 2012;87:335-340.
40. Lancaster M, Muftuler T, Olson D, et al. Chronic white matter changes following sport-related concussion measured by diffusion tensor and diffusion kurtosis imaging. Paper presented at: American Academy of Neurology 2016 Sports Concussion Conference; July 8-10, 2016; Chicago, Ill.
41. Kerr ZY, Yeargin SW, Valovich McLeod TC, et al. Comprehensive coach education reduces head impact exposures in American youth football. Orthop J Sports Med. 2015;3(ecollection):e232596711561545.
42. Black AM, Macpherson AK, Hagel BE, et al. Policy change eliminating body checking in non-elite ice hockey leads to a threefold reduction in injury and concussion risk in 11- and 12-year-old players. Br J Sports Med. 2016;50:55-61.
43. Council on Sports Medicine and Fitness. Tackling in youth football. Policy Statement of the American Academy of Pediatrics. Pediatrics. 2015;136:e1419-e1430.
› Require athletes who sustain a concussion to wait a minimum of 7 to 10 days before returning to full unrestricted activity. C
› Ensure that any player diagnosed with concussion follows a guided return-to-play progression, supervised by an athletic trainer or physical therapist experienced in post-concussion care. C
› Advise patients who are old enough to drive not to do so for at least 24 hours after a concussion. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Each year in the United States, more than 44 million young people participate in sports activities.1 Yet the number of concussions incurred annually by children and adolescents engaged in sports and recreational play has been underestimated for years, and largely unknown.1,2
Some estimates were based solely on the number of young athletes treated in emergency departments or sports concussion clinics. Others focused only on team players of middle school or high school age, excluding younger children who were hit in the head on playgrounds or during other recreational activities. What’s more, large numbers of concussions—as many as 4 in 10 incurred by high school athletes—were never reported to a coach or medical professional.3
In a new study published in the journal Pediatrics in June, researchers used national databases and current literature to provide what they believe to be “the most accurate and precise estimate of youth concussion” thus far: Between 1.1 and 1.9 million sports- and recreation-related concussions occur among US youth ages 18 or younger annually.1
Among young people playing team sports, concussions are between 2 and 7 times more likely to occur during competitive games than in practice sessions.4-7 Boys on football and ice hockey teams have the highest rates of concussion in young athletes.For overall number of concussions, however, girls on soccer teams are second only to football players.4 Female soccer players are more likely than male soccer players to sustain concussions during equal number of hours of play.4,7
An increase in incidence. The incidence of concussion among young athletes appears to have increased in the past decade, a likely result of greater involvement in team sports, an increasing focus on safeguarding young people from the potential dangers associated with a blow to the brain, and better diagnostic techniques.4,8-10 And a recent study based on data from electronic medical records at a large regional pediatric health care network found that more than three-quarters of young people with sports-related concussions were first seen in a primary care setting.2
With this in mind, we present a comprehensive update of the evidence regarding the diagnosis and management of sport-related concussion. The recommendations we include are consistent with professional association guidelines.8-10 Although we focus on concussion in children and adolescents involved in athletic activities, the principles generally apply to patients of all ages and to concussions that may not be sports related.
Removal from play: A vital first step
Whenever you conduct a physical exam for a young athlete, remind him or her—and the patient’s parents—that after a blow to the head, immediate removal from play is critical. Concussion is caused by a direct or indirect force to the brain that results in a transient disturbance in brain function,8-10 manifested by alterations in neurocognitive and motor function. While the signs and symptoms (TABLE 1)8-10 resolve within 10 days of injury in about 90% of cases, those who incur additional head impact within 24 hours have a higher symptom burden and prolonged recovery period.11 Even without repetitive impact, younger athletes may take longer to recover.8-10
The initial assessment
A child or adolescent who sustains a suspected concussion should be seen by a physician within 24 to 48 hours. Whether the initial assessment occurs in your office or on the sidelines of a game, it is important to confirm the time the incident occurred and the mechanism of injury.
Concussion is diagnosed by a combination of history, physical exam, and objective testing when symptoms or exam findings associated with mild brain trauma—headache, dizziness, light and/or noise sensitivity, among others—closely follow a head injury.8-10 Certain maneuvers—assessing eye movements by asking the athlete to look in various directions, for instance, then to follow a pen or finger as you move it closer to his or her face—may provoke dizziness, headache, or other symptoms of concussion that were not apparent initially.
The differential diagnosis includes cervical musculoskeletal injury, craniofacial injury, epidural and subdural hematoma, heat-related illness, uncomplicated headache and migraine, upper respiratory infection, and vertigo.8-10
Tools aid in diagnosis
Many clinical assessment tools exist to aid in the diagnosis of concussion (TABLE 2).8-10,12-14 Any one of these tools, many of which use combinations of symptom checklists, balance exams, and cognitive assessments, may be included in your evaluation. No single tool has been found to be superior to any other.8-10 A combination of tools may improve diagnostic accuracy, but assessment tools should not be the sole basis used to diagnose or rule out concussion.
Any child or adolescent who had a blow to the head and at least one sign or symptom of concussion should be evaluated as soon as possible and assessed again later that day or the next day if any reason for concern remains.
Neuropsychological (NP) testing may involve computerized tests developed specifically for athletes. Patients may be required to react to objects that appear on a screen, for example, in a way that tests memory, performance, and reaction time. Because cognitive recovery often lags behind symptom resolution, NP testing may identify subtle brain deficits even in athletes who are asymptomatic at rest or with exercise. In general, NP testing has a sensitivity of 71% to 88% for athletes with concussion,10 but it is most beneficial when baseline test results are available. Interpretation of NP testing should be done only by qualified clinicians.
While NP testing may provide additional prognostic information, it should not alter the management of athletes who are symptomatic either at rest or with exercise.15 Nor is NP testing vital, as concussion can be accurately diagnosed and adequately managed without it.
Neuroimaging, including computed tomography (CT) and magnetic resonance imaging (MRI), is often used unnecessarily in the initial assessment of a patient who sustained a possible concussion.8-10 In fact, neuroimaging should be reserved for cases in which it is necessary to rule out more serious pathology: intracranial or subdural hematoma or a craniofacial injury, for example, in patients with clinical findings that are red flags. These red flags include focal neurologic deficits, continuing nausea/vomiting, or persistent disorientation (TABLE 3),8-10 or symptoms that worsen or persist beyond a few weeks. In such cases, further evaluation—with MRI of the brain, formal NP testing, and/or referral to a neurologist, physiatrist, or other physician who specializes in concussion care—is indicated.
Concussion management: Rest is key
While there is a dearth of high-quality studies on the management of sport-related concussion across all age groups, standardized protocols for both children and adults have been adopted in most clinical settings.8-10,16,17 The protocols provide a framework for an individualized treatment plan. Yet their use among primary care physicians is inconsistent.18-20
Traditionally, concussion management begins with relative physical and cognitive rest to allow the brain time to recover.8-10 Recent randomized controlled trials have challenged this premise by suggesting that mild to moderate physical activity for post-concussion patients who are mildly symptomatic does not adversely affect recovery.21,22 These studies have significant limitations, however, and further research is needed to provide specific guidance on this aspect of concussion management before it is adopted.
Physical restrictions include organized sports, recreational activity, recess, and physical education classes. Walking is permitted unless it exacerbates symptoms. These restrictions should continue until the patient is symptom-free.
Cognitive restrictions include modifications at school and at home. Once an athlete is able to concentrate and tolerate visual and auditory stimuli, he or she may return to school. But classroom modifications should be considered, possibly including shortened school days, extra time for testing and homework, help with note taking, and restrictions from classes likely to provoke symptoms, such as computer science or music. Limiting use of mobile devices, television viewing, noisy environments, and other possible provocations may help speed symptom resolution. These restrictions, too, should remain in place until the patient is symptom-free.
Driving is often not addressed by physicians managing the care of athletes with concussion, but evidence suggests it should be. A study of patients presenting to the emergency department found that within 24 hours of a concussion diagnosis, individuals had an impaired response to traffic hazards.23,24 And Canadian clinical practice guidelines recommend that athletes with mild traumatic brain injury (TBI) avoid driving within the first 24 hours.25
While American guidelines are silent on the question of driving for this patient population, we recommend that athletes with concussion be restricted from driving and engaging in other risky complex tasks, such as welding or shop class, for at least 24 hours. For many athletes diagnosed with concussion, driving restrictions of longer duration may be necessary based on their symptom profile and neurocognitive test results. Continued dizziness or visual deficits would pose a greater risk than fatigue or short-term memory loss, for example.
Overseeing the return to play
Return-to-activity progression follows a stepwise protocol, with 6 steps that the injured athlete must complete before resuming full activity (FIGURE 1A).8-10 This stepwise progression begins only when athletes are symptom free, even during provocative maneuvers; have had a normal neurologic exam, are back to school full time with no restriction; are off any medications prescribed for concussion symptoms (TABLE 4),8-10 and when neurocognitive testing, if performed, is back to baseline. If an athlete develops symptoms at any stage of the progression, rest is required until he or she remains asymptomatic for at least 24 hours. The progression is then restarted at the last stage at which the patient was symptom free.
Some individualization, of course, is recommended here, too. Younger athletes and those with a prior history of concussion may require 10 days or more to complete all the steps, allowing an extra day at various steps. Neurologic maturation affects recovery time, and for younger individuals, a more conservative return-to-play protocol based on initial concussion symptom duration has been proposed (FIGURE 1B).16
Return to activity is often supervised by a certified athletic trainer at the athlete’s school. In the event that no athletic trainer is available, patients may be referred to physical therapists with experience in monitoring injured athletes.26 Anyone involved in the patient’s care, including the athlete himself, may use a symptom checklist to monitor recovery.
Although there is no evidence that the ongoing use of a symptom checklist affects the course of recovery, its use is often helpful in identifying specific symptoms that can be managed by means other than physical and cognitive rest—a sleep hygiene program for an individual with lingering difficulty sleeping, for example, or the continued application of ice, heat, and massage for persistent neck pain.
Checklist monitoring may be especially helpful for athletes whose symptoms extend beyond 10 days or who have multiple symptoms. Final clearance once all the steps have been completed requires follow-up with a health care provider.
Is a symptom-free waiting period necessary?
There is no evidence suggesting a need for a symptom-free waiting period before starting the return-to-play protocol.10,27 Because a repeat concussion is most likely within 7 to 10 days of the initial injury,8,9 however, most athletes should not return to contact play during that time frame, regardless of symptom resolution.
It is helpful to have asymptomatic athletes participate in non-contact activity before the 7 to 10 days are up, however. Doing so can help prevent deconditioning and injury upon return to contact sport, as there is evidence of increased risk of lower-extremity injury in the 90 days after concussion.28
What to tell athletes—and parents—about repetitive head trauma
There is growing concern about the long-term risks of concussion and repetitive head impact that may manifest as chronic traumatic encephalopathy (CTE) and chronic neurocognitive impairment (CNI) later in life. Indeed, some data strongly suggest—but do not definitively prove—a relationship between repetitive head injury and chronic neurodegenerative disease.8-10 You can tell worried patients or parents, however, that the majority of research on CTE and CNI has been based on professional football players.
Studies of long-term effects of soccer heading have shown conflicting results, with some finding cognitive impairment, altered postural control, and anatomic changes of the brain, while others found no effect on encephalopathy, concussion symptoms, or neurocognitive performance.29-36Here, too, most studies showing negative effects of soccer heading involved professional athletes.
Repetitive sub-concussive impact in high school football athletes has been found to induce biochemical changes to the brain,37 but the long-term effects are unknown. And, while concussion in high school athletes has been associated with short-term cognitive impairment, altered neurochemistry, and evidence of increased symptoms on baseline neurocognitive testing,8-10,38 no studies have linked concussion during middle school or high school with CNI. What’s more, a long-term (50-year) follow-up study of individuals who played football in high school found no difference in rates of neurodegenerative disease compared with age-matched controls.39
A new study of high school and college football players (mean age: 17.4 years) presented at the American Academy of Neurology 2016 Sports Concussion Conference in Chicago in July, however, found significant alterations in white matter 6 months post injury.40 The researchers compared 17 athletes with sport-related concussion with matched controls, using diffusion tensor imaging and diffusion kurtosis tensor imaging as biomarkers of brain recovery. The concussed athletes underwent MRI and symptom assessment at 24 hours, 8 days, and 6 months. The controls followed identical protocols.
At the 6-month assessment, there were no differences between the concussed group and the controls in terms of self-reported concussion symptoms, cognition, or balance. However, the concussed athletes had widespread decreased mean diffusivity compared with the controls. Despite the lack of clinical symptoms, the concussed athletes showed significant alterations in white matter “that were related to initial symptom severity ratings,” the authors concluded. These findings have implications both for determination of recovery from concussion and concussion management, they added.40
Although there is no way to eliminate all concussions, limited evidence suggests that improving athletic technique, limiting contact at practices, better enforcement of game rules, and rule changes regarding physical contact may decrease concussion risk.41-43 Many youth sports organizations have developed policies placing restrictions on head impact during practices and games. Studies are ongoing, too, to see if better headgear—or requiring helmets for soccer players—makes a difference.
CORRESPONDENCE
Ryan A. Sprouse, MD, CAQSM, 203 East Fourth Avenue, Ranson, WV 25438; rsprouse@wvumedicine.org.
› Require athletes who sustain a concussion to wait a minimum of 7 to 10 days before returning to full unrestricted activity. C
› Ensure that any player diagnosed with concussion follows a guided return-to-play progression, supervised by an athletic trainer or physical therapist experienced in post-concussion care. C
› Advise patients who are old enough to drive not to do so for at least 24 hours after a concussion. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Each year in the United States, more than 44 million young people participate in sports activities.1 Yet the number of concussions incurred annually by children and adolescents engaged in sports and recreational play has been underestimated for years, and largely unknown.1,2
Some estimates were based solely on the number of young athletes treated in emergency departments or sports concussion clinics. Others focused only on team players of middle school or high school age, excluding younger children who were hit in the head on playgrounds or during other recreational activities. What’s more, large numbers of concussions—as many as 4 in 10 incurred by high school athletes—were never reported to a coach or medical professional.3
In a new study published in the journal Pediatrics in June, researchers used national databases and current literature to provide what they believe to be “the most accurate and precise estimate of youth concussion” thus far: Between 1.1 and 1.9 million sports- and recreation-related concussions occur among US youth ages 18 or younger annually.1
Among young people playing team sports, concussions are between 2 and 7 times more likely to occur during competitive games than in practice sessions.4-7 Boys on football and ice hockey teams have the highest rates of concussion in young athletes.For overall number of concussions, however, girls on soccer teams are second only to football players.4 Female soccer players are more likely than male soccer players to sustain concussions during equal number of hours of play.4,7
An increase in incidence. The incidence of concussion among young athletes appears to have increased in the past decade, a likely result of greater involvement in team sports, an increasing focus on safeguarding young people from the potential dangers associated with a blow to the brain, and better diagnostic techniques.4,8-10 And a recent study based on data from electronic medical records at a large regional pediatric health care network found that more than three-quarters of young people with sports-related concussions were first seen in a primary care setting.2
With this in mind, we present a comprehensive update of the evidence regarding the diagnosis and management of sport-related concussion. The recommendations we include are consistent with professional association guidelines.8-10 Although we focus on concussion in children and adolescents involved in athletic activities, the principles generally apply to patients of all ages and to concussions that may not be sports related.
Removal from play: A vital first step
Whenever you conduct a physical exam for a young athlete, remind him or her—and the patient’s parents—that after a blow to the head, immediate removal from play is critical. Concussion is caused by a direct or indirect force to the brain that results in a transient disturbance in brain function,8-10 manifested by alterations in neurocognitive and motor function. While the signs and symptoms (TABLE 1)8-10 resolve within 10 days of injury in about 90% of cases, those who incur additional head impact within 24 hours have a higher symptom burden and prolonged recovery period.11 Even without repetitive impact, younger athletes may take longer to recover.8-10
The initial assessment
A child or adolescent who sustains a suspected concussion should be seen by a physician within 24 to 48 hours. Whether the initial assessment occurs in your office or on the sidelines of a game, it is important to confirm the time the incident occurred and the mechanism of injury.
Concussion is diagnosed by a combination of history, physical exam, and objective testing when symptoms or exam findings associated with mild brain trauma—headache, dizziness, light and/or noise sensitivity, among others—closely follow a head injury.8-10 Certain maneuvers—assessing eye movements by asking the athlete to look in various directions, for instance, then to follow a pen or finger as you move it closer to his or her face—may provoke dizziness, headache, or other symptoms of concussion that were not apparent initially.
The differential diagnosis includes cervical musculoskeletal injury, craniofacial injury, epidural and subdural hematoma, heat-related illness, uncomplicated headache and migraine, upper respiratory infection, and vertigo.8-10
Tools aid in diagnosis
Many clinical assessment tools exist to aid in the diagnosis of concussion (TABLE 2).8-10,12-14 Any one of these tools, many of which use combinations of symptom checklists, balance exams, and cognitive assessments, may be included in your evaluation. No single tool has been found to be superior to any other.8-10 A combination of tools may improve diagnostic accuracy, but assessment tools should not be the sole basis used to diagnose or rule out concussion.
Any child or adolescent who had a blow to the head and at least one sign or symptom of concussion should be evaluated as soon as possible and assessed again later that day or the next day if any reason for concern remains.
Neuropsychological (NP) testing may involve computerized tests developed specifically for athletes. Patients may be required to react to objects that appear on a screen, for example, in a way that tests memory, performance, and reaction time. Because cognitive recovery often lags behind symptom resolution, NP testing may identify subtle brain deficits even in athletes who are asymptomatic at rest or with exercise. In general, NP testing has a sensitivity of 71% to 88% for athletes with concussion,10 but it is most beneficial when baseline test results are available. Interpretation of NP testing should be done only by qualified clinicians.
While NP testing may provide additional prognostic information, it should not alter the management of athletes who are symptomatic either at rest or with exercise.15 Nor is NP testing vital, as concussion can be accurately diagnosed and adequately managed without it.
Neuroimaging, including computed tomography (CT) and magnetic resonance imaging (MRI), is often used unnecessarily in the initial assessment of a patient who sustained a possible concussion.8-10 In fact, neuroimaging should be reserved for cases in which it is necessary to rule out more serious pathology: intracranial or subdural hematoma or a craniofacial injury, for example, in patients with clinical findings that are red flags. These red flags include focal neurologic deficits, continuing nausea/vomiting, or persistent disorientation (TABLE 3),8-10 or symptoms that worsen or persist beyond a few weeks. In such cases, further evaluation—with MRI of the brain, formal NP testing, and/or referral to a neurologist, physiatrist, or other physician who specializes in concussion care—is indicated.
Concussion management: Rest is key
While there is a dearth of high-quality studies on the management of sport-related concussion across all age groups, standardized protocols for both children and adults have been adopted in most clinical settings.8-10,16,17 The protocols provide a framework for an individualized treatment plan. Yet their use among primary care physicians is inconsistent.18-20
Traditionally, concussion management begins with relative physical and cognitive rest to allow the brain time to recover.8-10 Recent randomized controlled trials have challenged this premise by suggesting that mild to moderate physical activity for post-concussion patients who are mildly symptomatic does not adversely affect recovery.21,22 These studies have significant limitations, however, and further research is needed to provide specific guidance on this aspect of concussion management before it is adopted.
Physical restrictions include organized sports, recreational activity, recess, and physical education classes. Walking is permitted unless it exacerbates symptoms. These restrictions should continue until the patient is symptom-free.
Cognitive restrictions include modifications at school and at home. Once an athlete is able to concentrate and tolerate visual and auditory stimuli, he or she may return to school. But classroom modifications should be considered, possibly including shortened school days, extra time for testing and homework, help with note taking, and restrictions from classes likely to provoke symptoms, such as computer science or music. Limiting use of mobile devices, television viewing, noisy environments, and other possible provocations may help speed symptom resolution. These restrictions, too, should remain in place until the patient is symptom-free.
Driving is often not addressed by physicians managing the care of athletes with concussion, but evidence suggests it should be. A study of patients presenting to the emergency department found that within 24 hours of a concussion diagnosis, individuals had an impaired response to traffic hazards.23,24 And Canadian clinical practice guidelines recommend that athletes with mild traumatic brain injury (TBI) avoid driving within the first 24 hours.25
While American guidelines are silent on the question of driving for this patient population, we recommend that athletes with concussion be restricted from driving and engaging in other risky complex tasks, such as welding or shop class, for at least 24 hours. For many athletes diagnosed with concussion, driving restrictions of longer duration may be necessary based on their symptom profile and neurocognitive test results. Continued dizziness or visual deficits would pose a greater risk than fatigue or short-term memory loss, for example.
Overseeing the return to play
Return-to-activity progression follows a stepwise protocol, with 6 steps that the injured athlete must complete before resuming full activity (FIGURE 1A).8-10 This stepwise progression begins only when athletes are symptom free, even during provocative maneuvers; have had a normal neurologic exam, are back to school full time with no restriction; are off any medications prescribed for concussion symptoms (TABLE 4),8-10 and when neurocognitive testing, if performed, is back to baseline. If an athlete develops symptoms at any stage of the progression, rest is required until he or she remains asymptomatic for at least 24 hours. The progression is then restarted at the last stage at which the patient was symptom free.
Some individualization, of course, is recommended here, too. Younger athletes and those with a prior history of concussion may require 10 days or more to complete all the steps, allowing an extra day at various steps. Neurologic maturation affects recovery time, and for younger individuals, a more conservative return-to-play protocol based on initial concussion symptom duration has been proposed (FIGURE 1B).16
Return to activity is often supervised by a certified athletic trainer at the athlete’s school. In the event that no athletic trainer is available, patients may be referred to physical therapists with experience in monitoring injured athletes.26 Anyone involved in the patient’s care, including the athlete himself, may use a symptom checklist to monitor recovery.
Although there is no evidence that the ongoing use of a symptom checklist affects the course of recovery, its use is often helpful in identifying specific symptoms that can be managed by means other than physical and cognitive rest—a sleep hygiene program for an individual with lingering difficulty sleeping, for example, or the continued application of ice, heat, and massage for persistent neck pain.
Checklist monitoring may be especially helpful for athletes whose symptoms extend beyond 10 days or who have multiple symptoms. Final clearance once all the steps have been completed requires follow-up with a health care provider.
Is a symptom-free waiting period necessary?
There is no evidence suggesting a need for a symptom-free waiting period before starting the return-to-play protocol.10,27 Because a repeat concussion is most likely within 7 to 10 days of the initial injury,8,9 however, most athletes should not return to contact play during that time frame, regardless of symptom resolution.
It is helpful to have asymptomatic athletes participate in non-contact activity before the 7 to 10 days are up, however. Doing so can help prevent deconditioning and injury upon return to contact sport, as there is evidence of increased risk of lower-extremity injury in the 90 days after concussion.28
What to tell athletes—and parents—about repetitive head trauma
There is growing concern about the long-term risks of concussion and repetitive head impact that may manifest as chronic traumatic encephalopathy (CTE) and chronic neurocognitive impairment (CNI) later in life. Indeed, some data strongly suggest—but do not definitively prove—a relationship between repetitive head injury and chronic neurodegenerative disease.8-10 You can tell worried patients or parents, however, that the majority of research on CTE and CNI has been based on professional football players.
Studies of long-term effects of soccer heading have shown conflicting results, with some finding cognitive impairment, altered postural control, and anatomic changes of the brain, while others found no effect on encephalopathy, concussion symptoms, or neurocognitive performance.29-36Here, too, most studies showing negative effects of soccer heading involved professional athletes.
Repetitive sub-concussive impact in high school football athletes has been found to induce biochemical changes to the brain,37 but the long-term effects are unknown. And, while concussion in high school athletes has been associated with short-term cognitive impairment, altered neurochemistry, and evidence of increased symptoms on baseline neurocognitive testing,8-10,38 no studies have linked concussion during middle school or high school with CNI. What’s more, a long-term (50-year) follow-up study of individuals who played football in high school found no difference in rates of neurodegenerative disease compared with age-matched controls.39
A new study of high school and college football players (mean age: 17.4 years) presented at the American Academy of Neurology 2016 Sports Concussion Conference in Chicago in July, however, found significant alterations in white matter 6 months post injury.40 The researchers compared 17 athletes with sport-related concussion with matched controls, using diffusion tensor imaging and diffusion kurtosis tensor imaging as biomarkers of brain recovery. The concussed athletes underwent MRI and symptom assessment at 24 hours, 8 days, and 6 months. The controls followed identical protocols.
At the 6-month assessment, there were no differences between the concussed group and the controls in terms of self-reported concussion symptoms, cognition, or balance. However, the concussed athletes had widespread decreased mean diffusivity compared with the controls. Despite the lack of clinical symptoms, the concussed athletes showed significant alterations in white matter “that were related to initial symptom severity ratings,” the authors concluded. These findings have implications both for determination of recovery from concussion and concussion management, they added.40
Although there is no way to eliminate all concussions, limited evidence suggests that improving athletic technique, limiting contact at practices, better enforcement of game rules, and rule changes regarding physical contact may decrease concussion risk.41-43 Many youth sports organizations have developed policies placing restrictions on head impact during practices and games. Studies are ongoing, too, to see if better headgear—or requiring helmets for soccer players—makes a difference.
CORRESPONDENCE
Ryan A. Sprouse, MD, CAQSM, 203 East Fourth Avenue, Ranson, WV 25438; rsprouse@wvumedicine.org.
1. Bryan MA, Rowhani-Rahbar A, Comstock RD, et al. Sports- and recreation-related concussions in US youth. Pediatrics. 2016; June 20 [Epub ahead of print].
2. Arbogast KB, Curry AE, Pfeiffer MR, et al. Point of health care entry for youth with concussion within a large pediatric care network. JAMA Pediatr. 2016; May 31 [Epub ahead of print].
3. Mihalik JK, Guskiewicz KM, Valovich McLeod TC, et al. Knowledge, attitude, and concussion-reporting behaviors among high school athletes: a preliminary study. J Ath Tr. 2013;48:645-653.
4. Marar M, McIlvain NM, Fields SK, et al. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;40:747.
5. Kontos AP, Elbin RJ, Fazio-Sumrock VC. Incidence of sports-related concussion among youth football players aged 8-12 years. J Pediatr. 2013;163:717-720.
6. Dompier TP, Kerr ZY, Marshall SW, et al. Incidence of concussion during practice and games in youth, high school, and collegiate American football players. JAMA Pediatr. 2015;169:659-665.
7. Comstock RD, Currie DW, Pierpont LA, et al. An evidence-based discussion of heading the ball and concussions in high school soccer. JAMA Pediatr. 2015;169:830-837.
8. Harmon KG, Drezner JA, Gammons M, et al. American Medical Society for Sports Medicine position statement: concussion in sport. Br J Sports Med. 2013;47:15-26.
9. McCrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med. 2013;47:250-258.
10. Giza CC, Kutcher JS, Ashwal S, et al. Summary of the evidence-based guideline update: evaluation and management of concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2250-2257.
11. Terwilliger VK, Pratson L, Vaughan CG, et al. Additional post-concussion impact exposure may affect recovery in adolescent athletes. J Neurotrauma. 2016;33:761-765.
12. Putukian M, Echemendia R, Dettwiler-Danspeckgruber A. Prospective clinical assessment using Sideline Concussion Assessment Tool-2 testing in the evaluation of sport-related concussion in college athletes. Clin J Sport Med. 2015;25:36-42.
13. Broglio SP, Macciocchi SN, Ferrara MS. Sensitivity of the concussion assessment battery. Neurosurgery. 2007;60:1050-1057.
14. Randolph C, McCrea M, Barr WB. Is neuropsychological testing useful in the management of sport-related concussion? J Athl Train. 2005;40:139-152.
15. Shrier I. Neuropsychological testing and concussions: a reasoned approach. Clin J Sport Med. 2012;22:211-213.
16. DeMatteo C, Stazyk K, Singh SK, et al. Development of a conservative protocol to return children and youth to activity following concussive injury. Clin Pediatr (Phila). 2015;54:152-163.
17. Broglio SP, Cantu RC, Gioia GA, et al. National Athletic Trainers Association position statement: management of sport concussion. J Athl Train. 2014;49:245-265.
18. Stoller J, Carson JD, Garel A, et al. Do family physicians, emergency department physicians, and pediatricians give consistent sport-related concussion management advice? Can Fam Physician. 2014;60:548, 550-552.
19. Lebrun CM, Mrazik M, Prasad AS, et al. Sport concussion knowledge base, clinical practices and needs for continuing medical education: a survey of family physicians and cross-border comparison. Br J Sports Med. 2013;47:54-59.
20. Zemek R, Eady K, Moreau K, et al. Knowledge of paediatric concussion among front-line primary care providers. Paediatr Child Health. 2014;19:475-480.
21. Maerlender A, Rieman W, Lichtenstein J, et al. Programmed physical exertion in recovery from sports-related concussion: a randomized pilot study. Dev Neuropsychol. 2015;40:273-278.
22. Buckley TA, Munkasy BA, Clouse BP. Acute cognitive and physical rest may not improve concussion recovery time. J Head Trauma Rehabil. 2015; July 24 [Epub ahead of print].
23. Preece MH, Horswill MS, Langlois JA, et al. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21:375-378.
24. Baker A, Unsworth CA, Lannin NA. Fitness-to-drive after mild traumatic brain injury: mapping the time trajectory of recovery in the acute stages post injury. Accid Anal Prev. 2015;79:50-55.
25. Marshall S, Bayley M, McCullagh S, et al. Clinical practice guidelines for mild traumatic brain injury and persistent symptoms. Can Fam Physician. 2012;58:257-267.
26. Yorke AM, Littleton S, Alsalaheen BA. Concussion attitudes and beliefs, knowledge, and clinical practice: a survey of physical therapists. Phys Ther. Available at: http://dx.doi.org/10.2522/ptj.20140598. Accessed January 21, 2016.
27. McCrea M, Guskiewicz K, Randolph C, et al. Effects of a symptom-free waiting period on clinical outcome and risk of reinjury after sport-related concussion. Neurosurgery. 2009;65:876-883.
28. Brooks MA, Peterson K, Biese K, et al. Concussion increases odds of sustaining a lower extremity musculoskeletal injury after return to play among collegiate athletes. Am J Sports Med. 2016;44:742-747.
29. Witol AD, Webbe FM. Soccer heading frequency predicts neuropsychological deficits. Arch Clin Neuropsychol. 2003;18:397-417.
30. Haran FJ, Tierney R, Wright WG, et al. Acute changes in postural control after soccer heading. Int J Sports Med. 2013;34:350-354.
31. Lipton ML, Kim N, Zimmerman ME, et al. Soccer heading is associated with white matter microstructural and cognitive abnormalities. Radiology. 2013;268:850-857.
32. Jordan SE, Green GA, Galanty HL, et al. Acute and chronic brain injury in United States national team soccer players. Am J Sports Med. 1996;24:205-210.
33. Kontos AP, Dolese A, Elbin RJ, et al. Relationship of soccer heading to computerized neurocognitive performance and symptoms among female and male youth soccer players. Brain Inj. 2011;25:1234-1241.
34. Straume-Naesheim TM, Andersen TE, Dvorak J, et al. Effects of heading exposure and previous concussions on neuropsychological performance among Norwegian elite footballers. Br J Sports Med. 2005;39:70-77.
35. Stephens R, Rutherford A, Potter D, et al. Neuropsychological impairment as a consequence of football (soccer) play and football heading: a preliminary analysis and report on school students (13-16 years). Child Neuropsychol. 2005;11:513-526.
36. Stephens R, Rutherford A, Potter D, et al. Neuropsychological consequence of soccer play in adolescent UK school team soccer players. J Neuropsychiatry Clin Neurosci. 2010;22:295-303.
37. Poole VN, Breedlove EL, Shenk TE, et al. Sub-concussive hit characteristics predict deviant brain metabolism in football athletes. Dev Neuropsychol. 2015;40:12-17.
38. Mannix R, Iverson GL, Maxwell B, et al. Multiple prior concussions are associated with symptoms in high school athletes. Ann Clin Trans Neurol. 2014;1:433-438.
39. Savica R, Parisi JE, Wold LE, et al. High school football and risk of neurodegeneration: a community-based study. Mayo Clin Proc. 2012;87:335-340.
40. Lancaster M, Muftuler T, Olson D, et al. Chronic white matter changes following sport-related concussion measured by diffusion tensor and diffusion kurtosis imaging. Paper presented at: American Academy of Neurology 2016 Sports Concussion Conference; July 8-10, 2016; Chicago, Ill.
41. Kerr ZY, Yeargin SW, Valovich McLeod TC, et al. Comprehensive coach education reduces head impact exposures in American youth football. Orthop J Sports Med. 2015;3(ecollection):e232596711561545.
42. Black AM, Macpherson AK, Hagel BE, et al. Policy change eliminating body checking in non-elite ice hockey leads to a threefold reduction in injury and concussion risk in 11- and 12-year-old players. Br J Sports Med. 2016;50:55-61.
43. Council on Sports Medicine and Fitness. Tackling in youth football. Policy Statement of the American Academy of Pediatrics. Pediatrics. 2015;136:e1419-e1430.
1. Bryan MA, Rowhani-Rahbar A, Comstock RD, et al. Sports- and recreation-related concussions in US youth. Pediatrics. 2016; June 20 [Epub ahead of print].
2. Arbogast KB, Curry AE, Pfeiffer MR, et al. Point of health care entry for youth with concussion within a large pediatric care network. JAMA Pediatr. 2016; May 31 [Epub ahead of print].
3. Mihalik JK, Guskiewicz KM, Valovich McLeod TC, et al. Knowledge, attitude, and concussion-reporting behaviors among high school athletes: a preliminary study. J Ath Tr. 2013;48:645-653.
4. Marar M, McIlvain NM, Fields SK, et al. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;40:747.
5. Kontos AP, Elbin RJ, Fazio-Sumrock VC. Incidence of sports-related concussion among youth football players aged 8-12 years. J Pediatr. 2013;163:717-720.
6. Dompier TP, Kerr ZY, Marshall SW, et al. Incidence of concussion during practice and games in youth, high school, and collegiate American football players. JAMA Pediatr. 2015;169:659-665.
7. Comstock RD, Currie DW, Pierpont LA, et al. An evidence-based discussion of heading the ball and concussions in high school soccer. JAMA Pediatr. 2015;169:830-837.
8. Harmon KG, Drezner JA, Gammons M, et al. American Medical Society for Sports Medicine position statement: concussion in sport. Br J Sports Med. 2013;47:15-26.
9. McCrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med. 2013;47:250-258.
10. Giza CC, Kutcher JS, Ashwal S, et al. Summary of the evidence-based guideline update: evaluation and management of concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2250-2257.
11. Terwilliger VK, Pratson L, Vaughan CG, et al. Additional post-concussion impact exposure may affect recovery in adolescent athletes. J Neurotrauma. 2016;33:761-765.
12. Putukian M, Echemendia R, Dettwiler-Danspeckgruber A. Prospective clinical assessment using Sideline Concussion Assessment Tool-2 testing in the evaluation of sport-related concussion in college athletes. Clin J Sport Med. 2015;25:36-42.
13. Broglio SP, Macciocchi SN, Ferrara MS. Sensitivity of the concussion assessment battery. Neurosurgery. 2007;60:1050-1057.
14. Randolph C, McCrea M, Barr WB. Is neuropsychological testing useful in the management of sport-related concussion? J Athl Train. 2005;40:139-152.
15. Shrier I. Neuropsychological testing and concussions: a reasoned approach. Clin J Sport Med. 2012;22:211-213.
16. DeMatteo C, Stazyk K, Singh SK, et al. Development of a conservative protocol to return children and youth to activity following concussive injury. Clin Pediatr (Phila). 2015;54:152-163.
17. Broglio SP, Cantu RC, Gioia GA, et al. National Athletic Trainers Association position statement: management of sport concussion. J Athl Train. 2014;49:245-265.
18. Stoller J, Carson JD, Garel A, et al. Do family physicians, emergency department physicians, and pediatricians give consistent sport-related concussion management advice? Can Fam Physician. 2014;60:548, 550-552.
19. Lebrun CM, Mrazik M, Prasad AS, et al. Sport concussion knowledge base, clinical practices and needs for continuing medical education: a survey of family physicians and cross-border comparison. Br J Sports Med. 2013;47:54-59.
20. Zemek R, Eady K, Moreau K, et al. Knowledge of paediatric concussion among front-line primary care providers. Paediatr Child Health. 2014;19:475-480.
21. Maerlender A, Rieman W, Lichtenstein J, et al. Programmed physical exertion in recovery from sports-related concussion: a randomized pilot study. Dev Neuropsychol. 2015;40:273-278.
22. Buckley TA, Munkasy BA, Clouse BP. Acute cognitive and physical rest may not improve concussion recovery time. J Head Trauma Rehabil. 2015; July 24 [Epub ahead of print].
23. Preece MH, Horswill MS, Langlois JA, et al. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21:375-378.
24. Baker A, Unsworth CA, Lannin NA. Fitness-to-drive after mild traumatic brain injury: mapping the time trajectory of recovery in the acute stages post injury. Accid Anal Prev. 2015;79:50-55.
25. Marshall S, Bayley M, McCullagh S, et al. Clinical practice guidelines for mild traumatic brain injury and persistent symptoms. Can Fam Physician. 2012;58:257-267.
26. Yorke AM, Littleton S, Alsalaheen BA. Concussion attitudes and beliefs, knowledge, and clinical practice: a survey of physical therapists. Phys Ther. Available at: http://dx.doi.org/10.2522/ptj.20140598. Accessed January 21, 2016.
27. McCrea M, Guskiewicz K, Randolph C, et al. Effects of a symptom-free waiting period on clinical outcome and risk of reinjury after sport-related concussion. Neurosurgery. 2009;65:876-883.
28. Brooks MA, Peterson K, Biese K, et al. Concussion increases odds of sustaining a lower extremity musculoskeletal injury after return to play among collegiate athletes. Am J Sports Med. 2016;44:742-747.
29. Witol AD, Webbe FM. Soccer heading frequency predicts neuropsychological deficits. Arch Clin Neuropsychol. 2003;18:397-417.
30. Haran FJ, Tierney R, Wright WG, et al. Acute changes in postural control after soccer heading. Int J Sports Med. 2013;34:350-354.
31. Lipton ML, Kim N, Zimmerman ME, et al. Soccer heading is associated with white matter microstructural and cognitive abnormalities. Radiology. 2013;268:850-857.
32. Jordan SE, Green GA, Galanty HL, et al. Acute and chronic brain injury in United States national team soccer players. Am J Sports Med. 1996;24:205-210.
33. Kontos AP, Dolese A, Elbin RJ, et al. Relationship of soccer heading to computerized neurocognitive performance and symptoms among female and male youth soccer players. Brain Inj. 2011;25:1234-1241.
34. Straume-Naesheim TM, Andersen TE, Dvorak J, et al. Effects of heading exposure and previous concussions on neuropsychological performance among Norwegian elite footballers. Br J Sports Med. 2005;39:70-77.
35. Stephens R, Rutherford A, Potter D, et al. Neuropsychological impairment as a consequence of football (soccer) play and football heading: a preliminary analysis and report on school students (13-16 years). Child Neuropsychol. 2005;11:513-526.
36. Stephens R, Rutherford A, Potter D, et al. Neuropsychological consequence of soccer play in adolescent UK school team soccer players. J Neuropsychiatry Clin Neurosci. 2010;22:295-303.
37. Poole VN, Breedlove EL, Shenk TE, et al. Sub-concussive hit characteristics predict deviant brain metabolism in football athletes. Dev Neuropsychol. 2015;40:12-17.
38. Mannix R, Iverson GL, Maxwell B, et al. Multiple prior concussions are associated with symptoms in high school athletes. Ann Clin Trans Neurol. 2014;1:433-438.
39. Savica R, Parisi JE, Wold LE, et al. High school football and risk of neurodegeneration: a community-based study. Mayo Clin Proc. 2012;87:335-340.
40. Lancaster M, Muftuler T, Olson D, et al. Chronic white matter changes following sport-related concussion measured by diffusion tensor and diffusion kurtosis imaging. Paper presented at: American Academy of Neurology 2016 Sports Concussion Conference; July 8-10, 2016; Chicago, Ill.
41. Kerr ZY, Yeargin SW, Valovich McLeod TC, et al. Comprehensive coach education reduces head impact exposures in American youth football. Orthop J Sports Med. 2015;3(ecollection):e232596711561545.
42. Black AM, Macpherson AK, Hagel BE, et al. Policy change eliminating body checking in non-elite ice hockey leads to a threefold reduction in injury and concussion risk in 11- and 12-year-old players. Br J Sports Med. 2016;50:55-61.
43. Council on Sports Medicine and Fitness. Tackling in youth football. Policy Statement of the American Academy of Pediatrics. Pediatrics. 2015;136:e1419-e1430.
From The Journal of Family Practice | 2016;65(8):538-544,546.