User login
Gestational diabetes ups risk for infantile hemangiomas
MINNEAPOLIS – Gestational diabetes and prenatal progesterone use were among the maternal factors associated with increased risk of infantile hemangioma, a benign vascular neoplasm whose incidence has been steadily rising over the past several decades.
Data from a large longitudinal epidemiology study were used to explore the association of a number of maternal risk factors with infantile hemangiomas, said Jennifer Schoch, MD, who presented these findings in a poster session at the annual meeting of the Society for Pediatric Dermatology.
After adjusting for gestational age and multiple gestations, the researchers found that infants born to mothers with gestational diabetes were more likely to have an infantile hemangioma (odds ratio, 1.79; P = .029). Maternal preeclampsia was even more strongly associated with infantile hemangioma (OR, 3.43, P = .017), as was prenatal progesterone use (OR, 2.25; P less than .001). Forceps-assisted vaginal delivery also increased the likelihood of infantile hemangioma (OR, 1.45; P = .035).
Low birth weight, prematurity, and being female and of non-Hispanic white race are some of the infant risk factors known to be associated with infantile hemangioma, but maternal risk factors in the development of infantile hemangioma are less clear, according to the researchers from the Mayo Clinic, Rochester, Minn. Some previous work has suggested that placental abnormalities and invasive procedures carried out during pregnancy, as well as the use of progesterone and corticosteroids during pregnancy, may increase the risk of infantile hemangiomas.
Using a retrospective case-control approach, the researchers used data from the 50-year-old Rochester Epidemiology Project. A chart review identified 869 mother-infant pairs with infantile hemangiomas and 869 age- and sex-matched control maternal-infant pairs whose infants did not have the condition. More than half (65%) of the infants in aggregate were girls (n = 561). Multivariable analysis was used to adjust for gestational age and multiple gestations.
Looking at the trends over time revealed that the rates of gestational diabetes, assisted reproduction techniques, and progesterone use during pregnancy have all increased during the same 35-year period of increased infantile hemangioma incidence, Dr. Schoch said in an interview.
Some earlier work suggests that infantile hemangiomas may arise from fetal placental progenitor cells. Since gestational diabetes can be associated with degradation of the placenta in late pregnancy, Dr. Schoch said that these effects on the placenta may have some connection to the increased risk of infantile hemangiomas in infants whose mothers have gestational diabetes.
Dr. Schoch, who is now professor of dermatology at the University of Florida, Gainesville, also noted that the study, completed during her fellowship at the Mayo Clinic, was limited by the low ethnic diversity of the study population, which draws from several counties in Minnesota and Wisconsin.
The Rochester Epidemiology Project is supported by the National Institutes of Health. The researchers reported having no financial disclosures.
On Twitter @karioakes
MINNEAPOLIS – Gestational diabetes and prenatal progesterone use were among the maternal factors associated with increased risk of infantile hemangioma, a benign vascular neoplasm whose incidence has been steadily rising over the past several decades.
Data from a large longitudinal epidemiology study were used to explore the association of a number of maternal risk factors with infantile hemangiomas, said Jennifer Schoch, MD, who presented these findings in a poster session at the annual meeting of the Society for Pediatric Dermatology.
After adjusting for gestational age and multiple gestations, the researchers found that infants born to mothers with gestational diabetes were more likely to have an infantile hemangioma (odds ratio, 1.79; P = .029). Maternal preeclampsia was even more strongly associated with infantile hemangioma (OR, 3.43, P = .017), as was prenatal progesterone use (OR, 2.25; P less than .001). Forceps-assisted vaginal delivery also increased the likelihood of infantile hemangioma (OR, 1.45; P = .035).
Low birth weight, prematurity, and being female and of non-Hispanic white race are some of the infant risk factors known to be associated with infantile hemangioma, but maternal risk factors in the development of infantile hemangioma are less clear, according to the researchers from the Mayo Clinic, Rochester, Minn. Some previous work has suggested that placental abnormalities and invasive procedures carried out during pregnancy, as well as the use of progesterone and corticosteroids during pregnancy, may increase the risk of infantile hemangiomas.
Using a retrospective case-control approach, the researchers used data from the 50-year-old Rochester Epidemiology Project. A chart review identified 869 mother-infant pairs with infantile hemangiomas and 869 age- and sex-matched control maternal-infant pairs whose infants did not have the condition. More than half (65%) of the infants in aggregate were girls (n = 561). Multivariable analysis was used to adjust for gestational age and multiple gestations.
Looking at the trends over time revealed that the rates of gestational diabetes, assisted reproduction techniques, and progesterone use during pregnancy have all increased during the same 35-year period of increased infantile hemangioma incidence, Dr. Schoch said in an interview.
Some earlier work suggests that infantile hemangiomas may arise from fetal placental progenitor cells. Since gestational diabetes can be associated with degradation of the placenta in late pregnancy, Dr. Schoch said that these effects on the placenta may have some connection to the increased risk of infantile hemangiomas in infants whose mothers have gestational diabetes.
Dr. Schoch, who is now professor of dermatology at the University of Florida, Gainesville, also noted that the study, completed during her fellowship at the Mayo Clinic, was limited by the low ethnic diversity of the study population, which draws from several counties in Minnesota and Wisconsin.
The Rochester Epidemiology Project is supported by the National Institutes of Health. The researchers reported having no financial disclosures.
On Twitter @karioakes
MINNEAPOLIS – Gestational diabetes and prenatal progesterone use were among the maternal factors associated with increased risk of infantile hemangioma, a benign vascular neoplasm whose incidence has been steadily rising over the past several decades.
Data from a large longitudinal epidemiology study were used to explore the association of a number of maternal risk factors with infantile hemangiomas, said Jennifer Schoch, MD, who presented these findings in a poster session at the annual meeting of the Society for Pediatric Dermatology.
After adjusting for gestational age and multiple gestations, the researchers found that infants born to mothers with gestational diabetes were more likely to have an infantile hemangioma (odds ratio, 1.79; P = .029). Maternal preeclampsia was even more strongly associated with infantile hemangioma (OR, 3.43, P = .017), as was prenatal progesterone use (OR, 2.25; P less than .001). Forceps-assisted vaginal delivery also increased the likelihood of infantile hemangioma (OR, 1.45; P = .035).
Low birth weight, prematurity, and being female and of non-Hispanic white race are some of the infant risk factors known to be associated with infantile hemangioma, but maternal risk factors in the development of infantile hemangioma are less clear, according to the researchers from the Mayo Clinic, Rochester, Minn. Some previous work has suggested that placental abnormalities and invasive procedures carried out during pregnancy, as well as the use of progesterone and corticosteroids during pregnancy, may increase the risk of infantile hemangiomas.
Using a retrospective case-control approach, the researchers used data from the 50-year-old Rochester Epidemiology Project. A chart review identified 869 mother-infant pairs with infantile hemangiomas and 869 age- and sex-matched control maternal-infant pairs whose infants did not have the condition. More than half (65%) of the infants in aggregate were girls (n = 561). Multivariable analysis was used to adjust for gestational age and multiple gestations.
Looking at the trends over time revealed that the rates of gestational diabetes, assisted reproduction techniques, and progesterone use during pregnancy have all increased during the same 35-year period of increased infantile hemangioma incidence, Dr. Schoch said in an interview.
Some earlier work suggests that infantile hemangiomas may arise from fetal placental progenitor cells. Since gestational diabetes can be associated with degradation of the placenta in late pregnancy, Dr. Schoch said that these effects on the placenta may have some connection to the increased risk of infantile hemangiomas in infants whose mothers have gestational diabetes.
Dr. Schoch, who is now professor of dermatology at the University of Florida, Gainesville, also noted that the study, completed during her fellowship at the Mayo Clinic, was limited by the low ethnic diversity of the study population, which draws from several counties in Minnesota and Wisconsin.
The Rochester Epidemiology Project is supported by the National Institutes of Health. The researchers reported having no financial disclosures.
On Twitter @karioakes
AT THE SPD ANNUAL MEETING
Key clinical point: Gestational diabetes and other maternal factors may increase the risk for infantile hemangioma.
Major finding: Infants born to mothers with gestational diabetes had an odds ratio of 1.79 for infantile hemangioma (P = .029).
Data source: Retrospective control-matched study of 865 infants with infantile hemangioma.
Disclosures: The researchers reported having no financial disclosures.
Late preterm, early term births declining in United States
Rates of late preterm (34-36 weeks) and early preterm (37-38 weeks) births declined significantly in the United States between 2006 and 2014, according to a report published online July 26 in JAMA.
To examine temporal trends in early birth rates, investigators analyzed data in birth registries for six high-income Western countries, including the United States. They focused on singleton live births delivered at 22 or more weeks’ gestation in which the neonates weighed 500 g or more that occurred between 2006 and the most recent year for which data were available for each country. The study included more than 25.7 million U.S. births, 2.4 million in Canada, approximately 306,000 in Denmark, approximately 572,000 in Finland, approximately 469,000 in Norway, and approximately 738,000 in Sweden, Jennifer L. Richards, MPH, of the department of epidemiology, Emory University, Atlanta, and her associates reported.

During the study period, rates of late preterm birth significantly decreased from 6.8% to 5.7% in the United States and from 3.9% to 3.5% in Norway but remained essentially stable in the other countries. Rates of early term birth also decreased significantly from 31.2% to 24.4% in the United States, from 17.6% to 16.8% in Norway, and from 19.5% to 18.5% in Sweden but remained essentially constant in the other countries. The rates were adjusted for mother’s age at delivery and parity (JAMA. 2016;316[4]:410-9. doi:10.1001/jama.2016.9635).
Ms. Richards and her associates attempted to determine whether declining rates in early births correlated with declines in obstetric interventions, specifically labor inductions and prelabor cesarean deliveries, but they found only one such correlation, in the rate of early term births in the United States. Overall, the rates of clinician-initiated obstetric intervention declined from 48.9% in 2006 to 38.7% in 2014 among U.S. early term births. In all other cases, trends in obstetric interventions varied widely over time and from one country to the next. In addition, rates of late preterm and early term births in the United States declined comparably among deliveries in which there were no obstetric interventions, they noted.
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Paris Descartes University, the Japan Society for the Promotion of Science, and the Japan Ministry of Health, Labour, and Welfare. Ms. Richards reported having no financial disclosures; an associate reported receiving grants from the Uehara Memorial Foundation, the Kanzawa Medical Research Foundation, and the Danone Institute.
Reductions in early term births in the United States have been documented previously, and the investigators found an impressive decline in obstetric interventions among early term births from 48.9% in 2006 to 38.7% in 2014. This reduction may be the result of national and local efforts to reduce nonindicated deliveries prior to 39 weeks. In contrast, the rates of obstetric interventions among late preterm births were relatively constant over the years studied. Although reducing preterm birth is a major goal, sometimes late preterm birth is the best outcome for the mother and/or fetus, and these deliveries would require an obstetric intervention. Thus, the constant rate of obstetric interventions among late preterm births may be associated with a relatively smaller number of nonindicated late preterm births.

|
Dr. Catherine Y. Spong |
Ms. Richards and her colleagues have provided a thoughtful multinational picture of late preterm and early term deliveries and their association with obstetric interventions. More data are needed to better understand the differences between countries and changes over time. Better tools and technologies to date pregnancies are now available, and, as studies continue to demonstrate, it is critical to wait until full term for delivery in uncomplicated pregnancies. Physicians, however, cannot become too devoted to decreasing late preterm and early term birth rates. For pregnancies in which there is a complication and when delivery will optimize the pregnancy outcome, delivery should occur and will require an obstetrical intervention.
Catherine Y. Spong, MD, is at the Eunice Kennedy Shriver National Institute of Child Health and Human Development in Bethesda, Md. She reported having no relevant financial disclosures. These remarks are excerpted from an accompanying editorial (JAMA. 2016;316[4]:395-6).
Reductions in early term births in the United States have been documented previously, and the investigators found an impressive decline in obstetric interventions among early term births from 48.9% in 2006 to 38.7% in 2014. This reduction may be the result of national and local efforts to reduce nonindicated deliveries prior to 39 weeks. In contrast, the rates of obstetric interventions among late preterm births were relatively constant over the years studied. Although reducing preterm birth is a major goal, sometimes late preterm birth is the best outcome for the mother and/or fetus, and these deliveries would require an obstetric intervention. Thus, the constant rate of obstetric interventions among late preterm births may be associated with a relatively smaller number of nonindicated late preterm births.
|
|
Dr. Catherine Y. Spong |
Ms. Richards and her colleagues have provided a thoughtful multinational picture of late preterm and early term deliveries and their association with obstetric interventions. More data are needed to better understand the differences between countries and changes over time. Better tools and technologies to date pregnancies are now available, and, as studies continue to demonstrate, it is critical to wait until full term for delivery in uncomplicated pregnancies. Physicians, however, cannot become too devoted to decreasing late preterm and early term birth rates. For pregnancies in which there is a complication and when delivery will optimize the pregnancy outcome, delivery should occur and will require an obstetrical intervention.
Catherine Y. Spong, MD, is at the Eunice Kennedy Shriver National Institute of Child Health and Human Development in Bethesda, Md. She reported having no relevant financial disclosures. These remarks are excerpted from an accompanying editorial (JAMA. 2016;316[4]:395-6).
Reductions in early term births in the United States have been documented previously, and the investigators found an impressive decline in obstetric interventions among early term births from 48.9% in 2006 to 38.7% in 2014. This reduction may be the result of national and local efforts to reduce nonindicated deliveries prior to 39 weeks. In contrast, the rates of obstetric interventions among late preterm births were relatively constant over the years studied. Although reducing preterm birth is a major goal, sometimes late preterm birth is the best outcome for the mother and/or fetus, and these deliveries would require an obstetric intervention. Thus, the constant rate of obstetric interventions among late preterm births may be associated with a relatively smaller number of nonindicated late preterm births.
|
|
Dr. Catherine Y. Spong |
Ms. Richards and her colleagues have provided a thoughtful multinational picture of late preterm and early term deliveries and their association with obstetric interventions. More data are needed to better understand the differences between countries and changes over time. Better tools and technologies to date pregnancies are now available, and, as studies continue to demonstrate, it is critical to wait until full term for delivery in uncomplicated pregnancies. Physicians, however, cannot become too devoted to decreasing late preterm and early term birth rates. For pregnancies in which there is a complication and when delivery will optimize the pregnancy outcome, delivery should occur and will require an obstetrical intervention.
Catherine Y. Spong, MD, is at the Eunice Kennedy Shriver National Institute of Child Health and Human Development in Bethesda, Md. She reported having no relevant financial disclosures. These remarks are excerpted from an accompanying editorial (JAMA. 2016;316[4]:395-6).
Rates of late preterm (34-36 weeks) and early preterm (37-38 weeks) births declined significantly in the United States between 2006 and 2014, according to a report published online July 26 in JAMA.
To examine temporal trends in early birth rates, investigators analyzed data in birth registries for six high-income Western countries, including the United States. They focused on singleton live births delivered at 22 or more weeks’ gestation in which the neonates weighed 500 g or more that occurred between 2006 and the most recent year for which data were available for each country. The study included more than 25.7 million U.S. births, 2.4 million in Canada, approximately 306,000 in Denmark, approximately 572,000 in Finland, approximately 469,000 in Norway, and approximately 738,000 in Sweden, Jennifer L. Richards, MPH, of the department of epidemiology, Emory University, Atlanta, and her associates reported.
During the study period, rates of late preterm birth significantly decreased from 6.8% to 5.7% in the United States and from 3.9% to 3.5% in Norway but remained essentially stable in the other countries. Rates of early term birth also decreased significantly from 31.2% to 24.4% in the United States, from 17.6% to 16.8% in Norway, and from 19.5% to 18.5% in Sweden but remained essentially constant in the other countries. The rates were adjusted for mother’s age at delivery and parity (JAMA. 2016;316[4]:410-9. doi:10.1001/jama.2016.9635).
Ms. Richards and her associates attempted to determine whether declining rates in early births correlated with declines in obstetric interventions, specifically labor inductions and prelabor cesarean deliveries, but they found only one such correlation, in the rate of early term births in the United States. Overall, the rates of clinician-initiated obstetric intervention declined from 48.9% in 2006 to 38.7% in 2014 among U.S. early term births. In all other cases, trends in obstetric interventions varied widely over time and from one country to the next. In addition, rates of late preterm and early term births in the United States declined comparably among deliveries in which there were no obstetric interventions, they noted.
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Paris Descartes University, the Japan Society for the Promotion of Science, and the Japan Ministry of Health, Labour, and Welfare. Ms. Richards reported having no financial disclosures; an associate reported receiving grants from the Uehara Memorial Foundation, the Kanzawa Medical Research Foundation, and the Danone Institute.
Rates of late preterm (34-36 weeks) and early preterm (37-38 weeks) births declined significantly in the United States between 2006 and 2014, according to a report published online July 26 in JAMA.
To examine temporal trends in early birth rates, investigators analyzed data in birth registries for six high-income Western countries, including the United States. They focused on singleton live births delivered at 22 or more weeks’ gestation in which the neonates weighed 500 g or more that occurred between 2006 and the most recent year for which data were available for each country. The study included more than 25.7 million U.S. births, 2.4 million in Canada, approximately 306,000 in Denmark, approximately 572,000 in Finland, approximately 469,000 in Norway, and approximately 738,000 in Sweden, Jennifer L. Richards, MPH, of the department of epidemiology, Emory University, Atlanta, and her associates reported.
During the study period, rates of late preterm birth significantly decreased from 6.8% to 5.7% in the United States and from 3.9% to 3.5% in Norway but remained essentially stable in the other countries. Rates of early term birth also decreased significantly from 31.2% to 24.4% in the United States, from 17.6% to 16.8% in Norway, and from 19.5% to 18.5% in Sweden but remained essentially constant in the other countries. The rates were adjusted for mother’s age at delivery and parity (JAMA. 2016;316[4]:410-9. doi:10.1001/jama.2016.9635).
Ms. Richards and her associates attempted to determine whether declining rates in early births correlated with declines in obstetric interventions, specifically labor inductions and prelabor cesarean deliveries, but they found only one such correlation, in the rate of early term births in the United States. Overall, the rates of clinician-initiated obstetric intervention declined from 48.9% in 2006 to 38.7% in 2014 among U.S. early term births. In all other cases, trends in obstetric interventions varied widely over time and from one country to the next. In addition, rates of late preterm and early term births in the United States declined comparably among deliveries in which there were no obstetric interventions, they noted.
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Paris Descartes University, the Japan Society for the Promotion of Science, and the Japan Ministry of Health, Labour, and Welfare. Ms. Richards reported having no financial disclosures; an associate reported receiving grants from the Uehara Memorial Foundation, the Kanzawa Medical Research Foundation, and the Danone Institute.
FROM JAMA
Key clinical point: Late preterm and early term births declined in the United States between 2006 and 2014.
Major finding: Rates of late preterm birth significantly decreased from 6.8% to 5.7% in the United States and from 3.9% to 3.5% in Norway, but remained essentially stable in the other four countries analyzed.
Data source: A descriptive population-based retrospective study of early birth rates in six Western countries.
Disclosures: The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Paris Descartes University, the Japan Society for the Promotion of Science, and the Japan Ministry of Health, Labour, and Welfare. Ms. Richards reported having no financial disclosures; an associate reported receiving grants from the Uehara Memorial Foundation, the Kanzawa Medical Research Foundation, and the Danone Institute.

Congenital craniofacial deformities
1. This youngster is being followed for symptoms related to his right-sided cranial asymmetry noted at birth, including neurologic impairment (sensorineural hearing loss and visual problems including strabismus) and breathing problems; developmental delay and/or intellectual disability; and hydrocephalus. The hands and feet are normal.

Source: By Michael L. Kaufman at the English language Wikipedia, CC BY-SA 3.0
Diagnosis: Craniosynostosis, also known as acrocephalosyndactyly, is a condition in which the skull sutures close prematurely. This can cause pressure to build up inside the head and skull or facial bones, leading to a misshapen head and distinctive facial features—ocular hypertelorism, proptosis, midface hypoplasia, small beaked nose, and prognathism—and occasionally abnormal fingers and toes.
Mutations of the FGFR gene, which regulates the fibroblast growth factor receptor protein, are responsible for the eight disorders comprising the FGFR-related craniosynostosis spectrum. The protein plays an important role in bone growth, particularly during embryonic development. For example, this protein signals certain immature cells in the developing embryo to become bone cells in the head, hands, feet, and other tissues.
For more information, see Robin NH, MD, Falk MJ, Haldeman-Englert CR. FGFR-related craniosynostosis syndromes. In: GeneReviews® [Internet]. Pagon RA, Adam MP, Ardinger HH, et al, eds. Seattle: University of Washington, Seattle; 1993-2016.
For the next photograph, proceed to the next page >>
2. This infant presents with a misshapen cranium, most notably the flattened area on the posterior right side. His history includes limited passive neck rotation at birth, preferential head orientation, supine sleep position, and lower activity level.

Source: Wikimedia Commons; By Medical advises - http://larece.ru/?p=27115, CC BY-SA 3.0
Diagnosis: Plagiocephaly, literally means "oblique head" (from the Greek "plagio" for oblique and "cephale" for head). The incidence in infants at 7 to 12 weeks of age is estimated to be 46.6%. Of all infants with plagiocephaly, 63.2% are affected on the right side and 78.3% have a mild form.
For more information, see “Helmets for Positional Skull Deformities: A Good Idea or Not?” Clin Rev. 2015;25(2):16,18.
For the next photograph, proceed to the next page >>
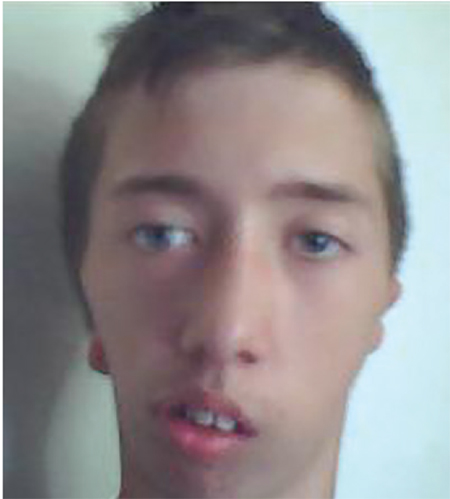
3. An adolescent patient presents with marked facial asymmetry, present since birth. The auricular tissue on the left side is malformed; on the right side, low set. The right midface is underdeveloped with micrognathia and chin deviation, resulting in malocclusion.
Source: Wikimedia Commons
Diagnosis: Craniofacial microsomia, possibly caused by bleeding in the temporal area during gestation, describes a spectrum of cranial and facial abnormalities. After Down syndrome, it is the most common congenital syndrome, occurring in approximately 1 in 3,500 to 4,500 live births. In about two-thirds of cases, abnormalities differ from one side to the other.
These individuals typically demonstrate one-sided maxillary or mandibular hypoplasia, which can cause dental problems and difficulties with feeding and speech. In cases of severe mandibular hypoplasia, breathing may also be affected.
Abnormalities affecting one or both ears may range from preauricular tags to an underdeveloped or absent external ear or a closed or absent ear canal; these patients may experience hearing loss. Microphthalmia, occurring less frequently, may result in vision loss.
For more information, see Heike CL, Luquetti DV, Hing AV. Craniofacial microsomia overview. In: Pagon RA, Adam MP, Ardinger HH, et al, eds. GeneReviews® [Internet]. Seattle: University of Washington, Seattle; 1993-2016.
For the next photograph, proceed to the next page >>
4. A 4-month-old boy is brought in by his mother for evaluation of a “birthmark” on his forehead that has become more prominent with time. The child complains a bit when the lesion is touched.
His mother gives a history of a normal full-term pregnancy with an uneventful delivery. Other than the skin lesion, there have been no other known problems with the child’s health.

Diagnosis: Most first-year medical students could tell you this was a case of an infantile hemangioma—but within the past five years, the categorization and treatment of hemangiomas have changed rapidly.
Hemangiomas are benign and usually self-involuting vascular tumors. They are distinct from the family of permanent congenital vascular lesions, such as port wine stains. About 80% occur on the face or neck and more commonly in females. Those that occur near the skin’s surface tend to be bright red, while those of deeper origin are more bluish. Hemangiomas can also manifest in extracutaneous areas (eg, the liver); these are usually detected via imaging.
For more information, see “A New Approach to “Birthmarks” Clin Rev. 2016;26(3):W1.
RELATED ARTICLE:
Infantile Hemangiomas Increasing, Linked to Prematurity, Low Birth Weight Bruce Jancin, Family Practice News Digital Network
1. This youngster is being followed for symptoms related to his right-sided cranial asymmetry noted at birth, including neurologic impairment (sensorineural hearing loss and visual problems including strabismus) and breathing problems; developmental delay and/or intellectual disability; and hydrocephalus. The hands and feet are normal.
Source: By Michael L. Kaufman at the English language Wikipedia, CC BY-SA 3.0
Diagnosis: Craniosynostosis, also known as acrocephalosyndactyly, is a condition in which the skull sutures close prematurely. This can cause pressure to build up inside the head and skull or facial bones, leading to a misshapen head and distinctive facial features—ocular hypertelorism, proptosis, midface hypoplasia, small beaked nose, and prognathism—and occasionally abnormal fingers and toes.
Mutations of the FGFR gene, which regulates the fibroblast growth factor receptor protein, are responsible for the eight disorders comprising the FGFR-related craniosynostosis spectrum. The protein plays an important role in bone growth, particularly during embryonic development. For example, this protein signals certain immature cells in the developing embryo to become bone cells in the head, hands, feet, and other tissues.
For more information, see Robin NH, MD, Falk MJ, Haldeman-Englert CR. FGFR-related craniosynostosis syndromes. In: GeneReviews® [Internet]. Pagon RA, Adam MP, Ardinger HH, et al, eds. Seattle: University of Washington, Seattle; 1993-2016.
For the next photograph, proceed to the next page >>
2. This infant presents with a misshapen cranium, most notably the flattened area on the posterior right side. His history includes limited passive neck rotation at birth, preferential head orientation, supine sleep position, and lower activity level.
Source: Wikimedia Commons; By Medical advises - http://larece.ru/?p=27115, CC BY-SA 3.0
Diagnosis: Plagiocephaly, literally means "oblique head" (from the Greek "plagio" for oblique and "cephale" for head). The incidence in infants at 7 to 12 weeks of age is estimated to be 46.6%. Of all infants with plagiocephaly, 63.2% are affected on the right side and 78.3% have a mild form.
For more information, see “Helmets for Positional Skull Deformities: A Good Idea or Not?” Clin Rev. 2015;25(2):16,18.
For the next photograph, proceed to the next page >>
3. An adolescent patient presents with marked facial asymmetry, present since birth. The auricular tissue on the left side is malformed; on the right side, low set. The right midface is underdeveloped with micrognathia and chin deviation, resulting in malocclusion.
Source: Wikimedia Commons
Diagnosis: Craniofacial microsomia, possibly caused by bleeding in the temporal area during gestation, describes a spectrum of cranial and facial abnormalities. After Down syndrome, it is the most common congenital syndrome, occurring in approximately 1 in 3,500 to 4,500 live births. In about two-thirds of cases, abnormalities differ from one side to the other.
These individuals typically demonstrate one-sided maxillary or mandibular hypoplasia, which can cause dental problems and difficulties with feeding and speech. In cases of severe mandibular hypoplasia, breathing may also be affected.
Abnormalities affecting one or both ears may range from preauricular tags to an underdeveloped or absent external ear or a closed or absent ear canal; these patients may experience hearing loss. Microphthalmia, occurring less frequently, may result in vision loss.
For more information, see Heike CL, Luquetti DV, Hing AV. Craniofacial microsomia overview. In: Pagon RA, Adam MP, Ardinger HH, et al, eds. GeneReviews® [Internet]. Seattle: University of Washington, Seattle; 1993-2016.
For the next photograph, proceed to the next page >>
4. A 4-month-old boy is brought in by his mother for evaluation of a “birthmark” on his forehead that has become more prominent with time. The child complains a bit when the lesion is touched.
His mother gives a history of a normal full-term pregnancy with an uneventful delivery. Other than the skin lesion, there have been no other known problems with the child’s health.
Diagnosis: Most first-year medical students could tell you this was a case of an infantile hemangioma—but within the past five years, the categorization and treatment of hemangiomas have changed rapidly.
Hemangiomas are benign and usually self-involuting vascular tumors. They are distinct from the family of permanent congenital vascular lesions, such as port wine stains. About 80% occur on the face or neck and more commonly in females. Those that occur near the skin’s surface tend to be bright red, while those of deeper origin are more bluish. Hemangiomas can also manifest in extracutaneous areas (eg, the liver); these are usually detected via imaging.
For more information, see “A New Approach to “Birthmarks” Clin Rev. 2016;26(3):W1.
RELATED ARTICLE:
Infantile Hemangiomas Increasing, Linked to Prematurity, Low Birth Weight Bruce Jancin, Family Practice News Digital Network
1. This youngster is being followed for symptoms related to his right-sided cranial asymmetry noted at birth, including neurologic impairment (sensorineural hearing loss and visual problems including strabismus) and breathing problems; developmental delay and/or intellectual disability; and hydrocephalus. The hands and feet are normal.
Source: By Michael L. Kaufman at the English language Wikipedia, CC BY-SA 3.0
Diagnosis: Craniosynostosis, also known as acrocephalosyndactyly, is a condition in which the skull sutures close prematurely. This can cause pressure to build up inside the head and skull or facial bones, leading to a misshapen head and distinctive facial features—ocular hypertelorism, proptosis, midface hypoplasia, small beaked nose, and prognathism—and occasionally abnormal fingers and toes.
Mutations of the FGFR gene, which regulates the fibroblast growth factor receptor protein, are responsible for the eight disorders comprising the FGFR-related craniosynostosis spectrum. The protein plays an important role in bone growth, particularly during embryonic development. For example, this protein signals certain immature cells in the developing embryo to become bone cells in the head, hands, feet, and other tissues.
For more information, see Robin NH, MD, Falk MJ, Haldeman-Englert CR. FGFR-related craniosynostosis syndromes. In: GeneReviews® [Internet]. Pagon RA, Adam MP, Ardinger HH, et al, eds. Seattle: University of Washington, Seattle; 1993-2016.
For the next photograph, proceed to the next page >>
2. This infant presents with a misshapen cranium, most notably the flattened area on the posterior right side. His history includes limited passive neck rotation at birth, preferential head orientation, supine sleep position, and lower activity level.
Source: Wikimedia Commons; By Medical advises - http://larece.ru/?p=27115, CC BY-SA 3.0
Diagnosis: Plagiocephaly, literally means "oblique head" (from the Greek "plagio" for oblique and "cephale" for head). The incidence in infants at 7 to 12 weeks of age is estimated to be 46.6%. Of all infants with plagiocephaly, 63.2% are affected on the right side and 78.3% have a mild form.
For more information, see “Helmets for Positional Skull Deformities: A Good Idea or Not?” Clin Rev. 2015;25(2):16,18.
For the next photograph, proceed to the next page >>
3. An adolescent patient presents with marked facial asymmetry, present since birth. The auricular tissue on the left side is malformed; on the right side, low set. The right midface is underdeveloped with micrognathia and chin deviation, resulting in malocclusion.
Source: Wikimedia Commons
Diagnosis: Craniofacial microsomia, possibly caused by bleeding in the temporal area during gestation, describes a spectrum of cranial and facial abnormalities. After Down syndrome, it is the most common congenital syndrome, occurring in approximately 1 in 3,500 to 4,500 live births. In about two-thirds of cases, abnormalities differ from one side to the other.
These individuals typically demonstrate one-sided maxillary or mandibular hypoplasia, which can cause dental problems and difficulties with feeding and speech. In cases of severe mandibular hypoplasia, breathing may also be affected.
Abnormalities affecting one or both ears may range from preauricular tags to an underdeveloped or absent external ear or a closed or absent ear canal; these patients may experience hearing loss. Microphthalmia, occurring less frequently, may result in vision loss.
For more information, see Heike CL, Luquetti DV, Hing AV. Craniofacial microsomia overview. In: Pagon RA, Adam MP, Ardinger HH, et al, eds. GeneReviews® [Internet]. Seattle: University of Washington, Seattle; 1993-2016.
For the next photograph, proceed to the next page >>
4. A 4-month-old boy is brought in by his mother for evaluation of a “birthmark” on his forehead that has become more prominent with time. The child complains a bit when the lesion is touched.
His mother gives a history of a normal full-term pregnancy with an uneventful delivery. Other than the skin lesion, there have been no other known problems with the child’s health.
Diagnosis: Most first-year medical students could tell you this was a case of an infantile hemangioma—but within the past five years, the categorization and treatment of hemangiomas have changed rapidly.
Hemangiomas are benign and usually self-involuting vascular tumors. They are distinct from the family of permanent congenital vascular lesions, such as port wine stains. About 80% occur on the face or neck and more commonly in females. Those that occur near the skin’s surface tend to be bright red, while those of deeper origin are more bluish. Hemangiomas can also manifest in extracutaneous areas (eg, the liver); these are usually detected via imaging.
For more information, see “A New Approach to “Birthmarks” Clin Rev. 2016;26(3):W1.
RELATED ARTICLE:
Infantile Hemangiomas Increasing, Linked to Prematurity, Low Birth Weight Bruce Jancin, Family Practice News Digital Network
Gay and Bisexual Male High Schoolers Have High Injected Drug Use
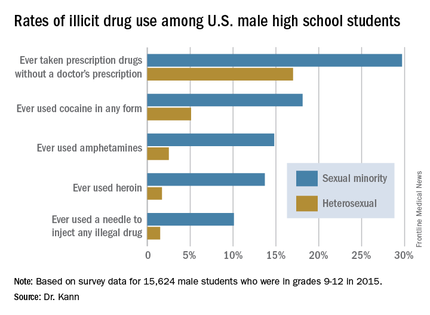
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
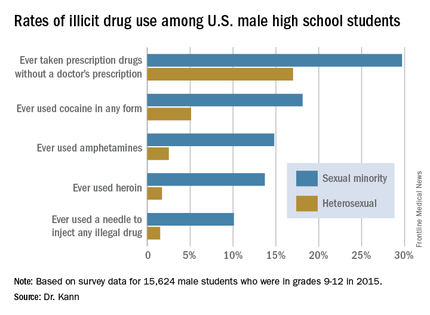
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.

The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.
The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.
The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
AT AIDS 2016

Gay and bisexual male high schoolers have high injected drug use
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.

The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.
The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
DURBAN, SOUTH AFRICA – The first-ever nationally representative survey on sexual identity and behaviors in U.S. male high school students has exposed a high prevalence of illicit injected drug use among those who have sex with males or with both males and females.
About 10% of high school boys who identify as gay or bisexual reported having ever used a needle to inject any illegal drug into their bodies, compared with 1.5% of high school boys who identify as heterosexual.
“This is a cause for great concern because of the efficiency with which injected drug use transmits not only HIV but hepatitis and other diseases,” Laura Kann, PhD, said in reporting the results of the 2015 National Youth Risk Behavior Survey (YRBS) at the 21st International AIDS Conference.
Dr. Kann of the Centers for Disease Control and Prevention’s division of adolescent and school health directs the YRBS, an annual, multiple-choice, anonymous voluntary survey that addresses six areas of risk: behaviors that contribute to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, inadequate physical activity, and unhealthy diet behaviors.
The 2015 survey was the first ever to include questions regarding sexual identity and behaviors.
“Twenty-two percent of all new HIV diagnoses in the U.S. occur in 13- to 24-year-olds. Most occur in males who have sex with males. This makes young males an important focus for HIV prevention efforts,” Dr. Kann said.
Yet until the 2015 YRBS, no reliable estimates existed regarding the number of gay or bisexual male high school students. “Reducing HIV infection among young sexual minority males is key to reducing HIV infection in the U.S.,” she said. “It’s hard to respond appropriately to a population that has not been counted.”
The 15,624 male students in public and private school grades 9-12 who participated in the YRBS were demographically representative of the nation’s roughly 8 million male high schoolers.
About 2% of male students identified themselves as gay, another 2.4% declared themselves bisexual, 93.1% said they were heterosexual, and 2.6% were unsure. With regard to sexual behaviors, 53.3% of respondents indicated they had sexual contact with females only, 1.3% with males only, and 1.9% with both males and females; 43.6% reported they hadn’t ever had sexual contact. Respondents could interpret “sexual contact” as they wished, ranging from kissing and hugging to intercourse.
Large differences in illicit drug use behaviors were found between the sexual minorities – that is, males who had sexual contact with males or with females as well as males – and those with only heterosexual contacts.
“We need to conduct new research on injected drug use among young males who have sex with males and determine what can be done to minimize, if not eliminate, this very high-risk behavior that is occurring at alarming rates,” Dr. Kann said.
The sexual minority students were also more likely to have engaged in various forms of noninjected illicit drug use known to boost the risk of HIV infection indirectly by increasing the likelihood of having unsafe sex. The sexual minority males had significantly higher rates of having ever used cocaine in any form, of having ever used amphetamines, and of having taken prescription drugs without a physician’s prescription. For instance, 14.8% of sexual minority males reported ever using amphetamines, compared with 2.5% of heterosexual males surveyed.
She noted that the YRBS results provided no evidence that the disparity in HIV diagnoses between young males who have sex with males and young males who have sex with females are caused by differences in the prevalence of HIV-related sexual behaviors. There were no statistically significant differences between heterosexual and sexual minority students in rates of ever having had sexual intercourse, having had intercourse with four or more persons, having sexual activity currently, or having used a condom at last intercourse.
Dr. Kann called for more research in the neglected area of social issues affecting young sexual minority males that likely increase their sense of marginalization and may promote behaviors placing them at increased risk for HIV acquisition.
“Many young males who have sex with males suffer from social isolation, stress from self-concealment and from coming out, discrimination, and even hatred, which may occur at home, at school, and in communities among both their peers and the adults responsible for their care and protection,” she said. “These factors may lead to harmful coping behaviors, such as drug use, that can further increase risk for HIV infection. It’s hard to imagine how even the best intervention technology will be able to eliminate the disparities in HIV diagnosis unless these social issues are addressed first and foremost.”
One clinician from New York rose from the audience to chastise the CDC for taking decades to incorporate questions about sexual minority youth into the YRBS.
“It’s important for the rest of the world to know how long it took the U.S. to collect this data. It’s not right. For those of you in the rest of the world who struggle to get information about your youth, don’t think that America is way ahead of you because it took us a long time,” she said.
Dr. Kann noted that such data have been collected for some time by some state and city public health agencies. As local officials began clamoring for a more comprehensive national picture, “it reached a tipping point” at the CDC.
Dr. Kann reported having no relevant financial conflicts.
AT AIDS 2016
Key clinical point: Male U.S. students in grades 9-12 who identify themselves as sexual minorities have markedly higher rates of illicit drug use than their heterosexual peers.
Major finding: A total of 4.4% of U.S. male high school students identify themselves as gay or bisexual, and they are about sevenfold more likely than heterosexual students to have ever injected illegal drugs.
Data source: A national population-based survey of 15,624 male students in grades 9-12.
Disclosures: The presenter is an employee of the Centers for Disease Control and Prevention, which sponsored the annual Youth Risk Behavior Survey.

Long-term health burden of Hodgkin lymphoma treatment

Photo courtesy of St. Jude
Children’s Research Hospital
and Seth Dixon
New research has shown that survivors of pediatric Hodgkin lymphoma (HL) are more likely to have chronic cardiovascular conditions than adults who did not have cancer in childhood.
And cardiovascular conditions are more severe among HL survivors than the general population.
Investigators believe this research, published in The Lancet Oncology, should aid efforts to reduce and better manage the late effects of cancer treatment.
For this study, the investigators used a measurement called “cumulative burden” to better capture the distribution and magnitude of chronic disease in childhood cancer survivors.
The metric showed that, by age 50, HL survivors had more than twice as many cardiovascular problems as adults who had not had cancer as children. HL survivors were also 5 times more likely to have severe, life-threatening, or fatal heart conditions.
“With cure rates for pediatric cancer at historic highs, the question becomes, ‘What is the legacy of that cure?’” said study author Nickhill Bhakta, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“We are doing a better job of keeping patients alive, but are we doing a better job at addressing the chronic diseases that are sometimes the price of that cure? Cumulative burden is a new tool for studying chronic illness in childhood cancer survivors or any patient population with significant morbidity, such as diabetes or HIV/AIDS.”
Unlike statistical methods that count health conditions once at diagnosis, cumulative burden tracks individuals’ multiple, recurring treatment-related health conditions.
Dr Bhakta and his colleagues focused on calculating the cumulative burden of cardiovascular disease in 670 pediatric HL survivors. The subjects were at least 18 years old and had survived at least 10 years beyond their cancer diagnoses.
The participants had been assessed for 22 chronic cardiovascular conditions, including heart attacks, hypertension, arrhythmias, and structural heart defects. Investigators used those and other clinical findings to calculate the cumulative burden by tracking the incidence and severity of cardiovascular disease.
The team also determined the cumulative burden for a comparison group of 272 community volunteers who underwent the same health assessments. The volunteers were similar in age and gender to the HL survivors but had no history of childhood cancer.
The analysis showed that the cumulative burden of cardiovascular disease, including severe and life-threatening conditions, was greater among HL survivors at 30 and 50 years of age than among the comparison group. In fact, the cumulative burden of the most serious heart problems, including heart attacks, was similar for 30-year-old HL survivors and 50-year-old community volunteers.
At age 50, 45.5% of HL survivors had developed at least one grade 3-5 cardiovascular condition, compared to 15.7% of the control subjects.
The HL survivors had a cumulative burden of 430.6 grade 1-5 cardiovascular conditions per 100 individuals and 100.8 grade 3-5 cardiovascular conditions per 100 individuals. In comparison, controls had 227.4 grade 1-5 conditions and 17.0 grade 3-5 conditions per 100 individuals.
The investigators noted that severe, chronic heart conditions became more common with age in both groups, but serious problems accumulated more rapidly in HL survivors.
“Survivors tended to have more severe disease across the lifespan and likely need an individualized screening and treatment plan,” Dr Bhakta said.
He added that the results of this study highlight trade-offs to consider in designing future clinical trials. For example, the investigators found that reducing the dose of anthracyclines will lower the rate, but not the severity, of cardiovascular disease in pediatric and young adult HL survivors.
In contrast, lowering the heart radiation dose will not significantly lower the rate of cardiovascular disease, but it will reduce the severity.
“Cumulative burden provides us with a global view of tradeoffs between different treatment late effects that must be considered when designing new interventions,” Dr Bhakta concluded. ![]()
Photo courtesy of St. Jude
Children’s Research Hospital
and Seth Dixon
New research has shown that survivors of pediatric Hodgkin lymphoma (HL) are more likely to have chronic cardiovascular conditions than adults who did not have cancer in childhood.
And cardiovascular conditions are more severe among HL survivors than the general population.
Investigators believe this research, published in The Lancet Oncology, should aid efforts to reduce and better manage the late effects of cancer treatment.
For this study, the investigators used a measurement called “cumulative burden” to better capture the distribution and magnitude of chronic disease in childhood cancer survivors.
The metric showed that, by age 50, HL survivors had more than twice as many cardiovascular problems as adults who had not had cancer as children. HL survivors were also 5 times more likely to have severe, life-threatening, or fatal heart conditions.
“With cure rates for pediatric cancer at historic highs, the question becomes, ‘What is the legacy of that cure?’” said study author Nickhill Bhakta, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“We are doing a better job of keeping patients alive, but are we doing a better job at addressing the chronic diseases that are sometimes the price of that cure? Cumulative burden is a new tool for studying chronic illness in childhood cancer survivors or any patient population with significant morbidity, such as diabetes or HIV/AIDS.”
Unlike statistical methods that count health conditions once at diagnosis, cumulative burden tracks individuals’ multiple, recurring treatment-related health conditions.
Dr Bhakta and his colleagues focused on calculating the cumulative burden of cardiovascular disease in 670 pediatric HL survivors. The subjects were at least 18 years old and had survived at least 10 years beyond their cancer diagnoses.
The participants had been assessed for 22 chronic cardiovascular conditions, including heart attacks, hypertension, arrhythmias, and structural heart defects. Investigators used those and other clinical findings to calculate the cumulative burden by tracking the incidence and severity of cardiovascular disease.
The team also determined the cumulative burden for a comparison group of 272 community volunteers who underwent the same health assessments. The volunteers were similar in age and gender to the HL survivors but had no history of childhood cancer.
The analysis showed that the cumulative burden of cardiovascular disease, including severe and life-threatening conditions, was greater among HL survivors at 30 and 50 years of age than among the comparison group. In fact, the cumulative burden of the most serious heart problems, including heart attacks, was similar for 30-year-old HL survivors and 50-year-old community volunteers.
At age 50, 45.5% of HL survivors had developed at least one grade 3-5 cardiovascular condition, compared to 15.7% of the control subjects.
The HL survivors had a cumulative burden of 430.6 grade 1-5 cardiovascular conditions per 100 individuals and 100.8 grade 3-5 cardiovascular conditions per 100 individuals. In comparison, controls had 227.4 grade 1-5 conditions and 17.0 grade 3-5 conditions per 100 individuals.
The investigators noted that severe, chronic heart conditions became more common with age in both groups, but serious problems accumulated more rapidly in HL survivors.
“Survivors tended to have more severe disease across the lifespan and likely need an individualized screening and treatment plan,” Dr Bhakta said.
He added that the results of this study highlight trade-offs to consider in designing future clinical trials. For example, the investigators found that reducing the dose of anthracyclines will lower the rate, but not the severity, of cardiovascular disease in pediatric and young adult HL survivors.
In contrast, lowering the heart radiation dose will not significantly lower the rate of cardiovascular disease, but it will reduce the severity.
“Cumulative burden provides us with a global view of tradeoffs between different treatment late effects that must be considered when designing new interventions,” Dr Bhakta concluded. ![]()
Photo courtesy of St. Jude
Children’s Research Hospital
and Seth Dixon
New research has shown that survivors of pediatric Hodgkin lymphoma (HL) are more likely to have chronic cardiovascular conditions than adults who did not have cancer in childhood.
And cardiovascular conditions are more severe among HL survivors than the general population.
Investigators believe this research, published in The Lancet Oncology, should aid efforts to reduce and better manage the late effects of cancer treatment.
For this study, the investigators used a measurement called “cumulative burden” to better capture the distribution and magnitude of chronic disease in childhood cancer survivors.
The metric showed that, by age 50, HL survivors had more than twice as many cardiovascular problems as adults who had not had cancer as children. HL survivors were also 5 times more likely to have severe, life-threatening, or fatal heart conditions.
“With cure rates for pediatric cancer at historic highs, the question becomes, ‘What is the legacy of that cure?’” said study author Nickhill Bhakta, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“We are doing a better job of keeping patients alive, but are we doing a better job at addressing the chronic diseases that are sometimes the price of that cure? Cumulative burden is a new tool for studying chronic illness in childhood cancer survivors or any patient population with significant morbidity, such as diabetes or HIV/AIDS.”
Unlike statistical methods that count health conditions once at diagnosis, cumulative burden tracks individuals’ multiple, recurring treatment-related health conditions.
Dr Bhakta and his colleagues focused on calculating the cumulative burden of cardiovascular disease in 670 pediatric HL survivors. The subjects were at least 18 years old and had survived at least 10 years beyond their cancer diagnoses.
The participants had been assessed for 22 chronic cardiovascular conditions, including heart attacks, hypertension, arrhythmias, and structural heart defects. Investigators used those and other clinical findings to calculate the cumulative burden by tracking the incidence and severity of cardiovascular disease.
The team also determined the cumulative burden for a comparison group of 272 community volunteers who underwent the same health assessments. The volunteers were similar in age and gender to the HL survivors but had no history of childhood cancer.
The analysis showed that the cumulative burden of cardiovascular disease, including severe and life-threatening conditions, was greater among HL survivors at 30 and 50 years of age than among the comparison group. In fact, the cumulative burden of the most serious heart problems, including heart attacks, was similar for 30-year-old HL survivors and 50-year-old community volunteers.
At age 50, 45.5% of HL survivors had developed at least one grade 3-5 cardiovascular condition, compared to 15.7% of the control subjects.
The HL survivors had a cumulative burden of 430.6 grade 1-5 cardiovascular conditions per 100 individuals and 100.8 grade 3-5 cardiovascular conditions per 100 individuals. In comparison, controls had 227.4 grade 1-5 conditions and 17.0 grade 3-5 conditions per 100 individuals.
The investigators noted that severe, chronic heart conditions became more common with age in both groups, but serious problems accumulated more rapidly in HL survivors.
“Survivors tended to have more severe disease across the lifespan and likely need an individualized screening and treatment plan,” Dr Bhakta said.
He added that the results of this study highlight trade-offs to consider in designing future clinical trials. For example, the investigators found that reducing the dose of anthracyclines will lower the rate, but not the severity, of cardiovascular disease in pediatric and young adult HL survivors.
In contrast, lowering the heart radiation dose will not significantly lower the rate of cardiovascular disease, but it will reduce the severity.
“Cumulative burden provides us with a global view of tradeoffs between different treatment late effects that must be considered when designing new interventions,” Dr Bhakta concluded. ![]()
Diabetes Prevalence in US Adolescents Is Under 1%
The prevalence of diabetes among adolescents in the United States is estimated to be 0.8%, with more than a quarter of that group being undiagnosed, according to a research letter published in JAMA.
Using data from the National Health and Nutrition Examination Survey 2005-2014, Andy Menke, PhD, and colleagues estimated the prevalence of diabetes overall, undiagnosed disease, and prediabetes in adolescents aged 12-19 years.

Of the 2,606 adolescents included in the analysis, 62 had diabetes, 20 were undiagnosed, and 512 had prediabetes. The weighted prevalence of diabetes was 0.8% (95% confidence interval, 0.6%-1.1%), of which 28.5% (95% CI, 16.4%-44.8%) was undiagnosed. The researchers defined undiagnosed diabetes as having no report of previous diagnosis but having a hemoglobin A1c level of 6.5% or greater, a fasting plasma glucose level of 126 mg/dL or greater, or a 2-hour plasma glucose level of 200 mg/dL or greater.
The prevalence of prediabetes among the adolescent sample was 17.7% (95% CI, 15.8%-19.8%). Prediabetes was defined as a hemoglobin A1c level of 5.7%-6.4%, a fasting plasma glucose level of 100-125 mg/dL, or a 2-hour plasma glucose level of 140-199 mg/dL among adolescents who did not have diagnosed or undiagnosed diabetes.
“A relatively large proportion was unaware of the condition, particularly among non-Hispanic black participants and Hispanic participants, indicating a need for improved diabetes screening among adolescents,” the researchers wrote. “These findings may have important public health implications because diabetes in youth is associated with early onset of risk factors and complications.”
The researchers were unable to distinguish between types of diabetes, but they noted that previous research in adolescents found that 87% had type 1.
Read the full research letter in JAMA (2016;316[3]:344-5. doi:10.1001/jama.2016.8544).
The prevalence of diabetes among adolescents in the United States is estimated to be 0.8%, with more than a quarter of that group being undiagnosed, according to a research letter published in JAMA.
Using data from the National Health and Nutrition Examination Survey 2005-2014, Andy Menke, PhD, and colleagues estimated the prevalence of diabetes overall, undiagnosed disease, and prediabetes in adolescents aged 12-19 years.
Of the 2,606 adolescents included in the analysis, 62 had diabetes, 20 were undiagnosed, and 512 had prediabetes. The weighted prevalence of diabetes was 0.8% (95% confidence interval, 0.6%-1.1%), of which 28.5% (95% CI, 16.4%-44.8%) was undiagnosed. The researchers defined undiagnosed diabetes as having no report of previous diagnosis but having a hemoglobin A1c level of 6.5% or greater, a fasting plasma glucose level of 126 mg/dL or greater, or a 2-hour plasma glucose level of 200 mg/dL or greater.
The prevalence of prediabetes among the adolescent sample was 17.7% (95% CI, 15.8%-19.8%). Prediabetes was defined as a hemoglobin A1c level of 5.7%-6.4%, a fasting plasma glucose level of 100-125 mg/dL, or a 2-hour plasma glucose level of 140-199 mg/dL among adolescents who did not have diagnosed or undiagnosed diabetes.
“A relatively large proportion was unaware of the condition, particularly among non-Hispanic black participants and Hispanic participants, indicating a need for improved diabetes screening among adolescents,” the researchers wrote. “These findings may have important public health implications because diabetes in youth is associated with early onset of risk factors and complications.”
The researchers were unable to distinguish between types of diabetes, but they noted that previous research in adolescents found that 87% had type 1.
Read the full research letter in JAMA (2016;316[3]:344-5. doi:10.1001/jama.2016.8544).
The prevalence of diabetes among adolescents in the United States is estimated to be 0.8%, with more than a quarter of that group being undiagnosed, according to a research letter published in JAMA.
Using data from the National Health and Nutrition Examination Survey 2005-2014, Andy Menke, PhD, and colleagues estimated the prevalence of diabetes overall, undiagnosed disease, and prediabetes in adolescents aged 12-19 years.
Of the 2,606 adolescents included in the analysis, 62 had diabetes, 20 were undiagnosed, and 512 had prediabetes. The weighted prevalence of diabetes was 0.8% (95% confidence interval, 0.6%-1.1%), of which 28.5% (95% CI, 16.4%-44.8%) was undiagnosed. The researchers defined undiagnosed diabetes as having no report of previous diagnosis but having a hemoglobin A1c level of 6.5% or greater, a fasting plasma glucose level of 126 mg/dL or greater, or a 2-hour plasma glucose level of 200 mg/dL or greater.
The prevalence of prediabetes among the adolescent sample was 17.7% (95% CI, 15.8%-19.8%). Prediabetes was defined as a hemoglobin A1c level of 5.7%-6.4%, a fasting plasma glucose level of 100-125 mg/dL, or a 2-hour plasma glucose level of 140-199 mg/dL among adolescents who did not have diagnosed or undiagnosed diabetes.
“A relatively large proportion was unaware of the condition, particularly among non-Hispanic black participants and Hispanic participants, indicating a need for improved diabetes screening among adolescents,” the researchers wrote. “These findings may have important public health implications because diabetes in youth is associated with early onset of risk factors and complications.”
The researchers were unable to distinguish between types of diabetes, but they noted that previous research in adolescents found that 87% had type 1.
Read the full research letter in JAMA (2016;316[3]:344-5. doi:10.1001/jama.2016.8544).
FROM JAMA

Diabetes prevalence in U.S. adolescents is under 1%
The prevalence of diabetes among adolescents in the United States is estimated to be 0.8%, with more than a quarter of that group being undiagnosed, according to a research letter published in JAMA.
Using data from the National Health and Nutrition Examination Survey 2005-2014, Andy Menke, PhD, and colleagues estimated the prevalence of diabetes overall, undiagnosed disease, and prediabetes in adolescents aged 12-19 years.

Of the 2,606 adolescents included in the analysis, 62 had diabetes, 20 were undiagnosed, and 512 had prediabetes. The weighted prevalence of diabetes was 0.8% (95% confidence interval, 0.6%-1.1%), of which 28.5% (95% CI, 16.4%-44.8%) was undiagnosed. The researchers defined undiagnosed diabetes as having no report of previous diagnosis but having a hemoglobin A1c level of 6.5% or greater, a fasting plasma glucose level of 126 mg/dL or greater, or a 2-hour plasma glucose level of 200 mg/dL or greater.
The prevalence of prediabetes among the adolescent sample was 17.7% (95% CI, 15.8%-19.8%). Prediabetes was defined as a hemoglobin A1c level of 5.7%-6.4%, a fasting plasma glucose level of 100-125 mg/dL, or a 2-hour plasma glucose level of 140-199 mg/dL among adolescents who did not have diagnosed or undiagnosed diabetes.
“A relatively large proportion was unaware of the condition, particularly among non-Hispanic black participants and Hispanic participants, indicating a need for improved diabetes screening among adolescents,” the researchers wrote. “These findings may have important public health implications because diabetes in youth is associated with early onset of risk factors and complications.”
The researchers were unable to distinguish between types of diabetes, but they noted that previous research in adolescents found that 87% had type 1.
Read the full research letter in JAMA (2016;316[3]:344-5. doi:10.1001/jama.2016.8544).
The prevalence of diabetes among adolescents in the United States is estimated to be 0.8%, with more than a quarter of that group being undiagnosed, according to a research letter published in JAMA.
Using data from the National Health and Nutrition Examination Survey 2005-2014, Andy Menke, PhD, and colleagues estimated the prevalence of diabetes overall, undiagnosed disease, and prediabetes in adolescents aged 12-19 years.
Of the 2,606 adolescents included in the analysis, 62 had diabetes, 20 were undiagnosed, and 512 had prediabetes. The weighted prevalence of diabetes was 0.8% (95% confidence interval, 0.6%-1.1%), of which 28.5% (95% CI, 16.4%-44.8%) was undiagnosed. The researchers defined undiagnosed diabetes as having no report of previous diagnosis but having a hemoglobin A1c level of 6.5% or greater, a fasting plasma glucose level of 126 mg/dL or greater, or a 2-hour plasma glucose level of 200 mg/dL or greater.
The prevalence of prediabetes among the adolescent sample was 17.7% (95% CI, 15.8%-19.8%). Prediabetes was defined as a hemoglobin A1c level of 5.7%-6.4%, a fasting plasma glucose level of 100-125 mg/dL, or a 2-hour plasma glucose level of 140-199 mg/dL among adolescents who did not have diagnosed or undiagnosed diabetes.
“A relatively large proportion was unaware of the condition, particularly among non-Hispanic black participants and Hispanic participants, indicating a need for improved diabetes screening among adolescents,” the researchers wrote. “These findings may have important public health implications because diabetes in youth is associated with early onset of risk factors and complications.”
The researchers were unable to distinguish between types of diabetes, but they noted that previous research in adolescents found that 87% had type 1.
Read the full research letter in JAMA (2016;316[3]:344-5. doi:10.1001/jama.2016.8544).
The prevalence of diabetes among adolescents in the United States is estimated to be 0.8%, with more than a quarter of that group being undiagnosed, according to a research letter published in JAMA.
Using data from the National Health and Nutrition Examination Survey 2005-2014, Andy Menke, PhD, and colleagues estimated the prevalence of diabetes overall, undiagnosed disease, and prediabetes in adolescents aged 12-19 years.
Of the 2,606 adolescents included in the analysis, 62 had diabetes, 20 were undiagnosed, and 512 had prediabetes. The weighted prevalence of diabetes was 0.8% (95% confidence interval, 0.6%-1.1%), of which 28.5% (95% CI, 16.4%-44.8%) was undiagnosed. The researchers defined undiagnosed diabetes as having no report of previous diagnosis but having a hemoglobin A1c level of 6.5% or greater, a fasting plasma glucose level of 126 mg/dL or greater, or a 2-hour plasma glucose level of 200 mg/dL or greater.
The prevalence of prediabetes among the adolescent sample was 17.7% (95% CI, 15.8%-19.8%). Prediabetes was defined as a hemoglobin A1c level of 5.7%-6.4%, a fasting plasma glucose level of 100-125 mg/dL, or a 2-hour plasma glucose level of 140-199 mg/dL among adolescents who did not have diagnosed or undiagnosed diabetes.
“A relatively large proportion was unaware of the condition, particularly among non-Hispanic black participants and Hispanic participants, indicating a need for improved diabetes screening among adolescents,” the researchers wrote. “These findings may have important public health implications because diabetes in youth is associated with early onset of risk factors and complications.”
The researchers were unable to distinguish between types of diabetes, but they noted that previous research in adolescents found that 87% had type 1.
Read the full research letter in JAMA (2016;316[3]:344-5. doi:10.1001/jama.2016.8544).
FROM JAMA

DTaP/IPV plus bivalent rLP2086 vaccine deemed noninferior in adolescents
Concomitant administration of the meningococcal serogroup B vaccine bivalent rLP2086 with the diphtheria, tetanus, and acellular pertussis and inactivated poliovirus (DTaP/IPV) vaccine produced a immunologically noninferior response in adolescents, compared with administration of DTaP/IPV alone.
Timo Vesikari, MD, PhD, of the University of Tampere (Finland) Medical School and his associates randomized healthy adolescents aged 11-18 years to receive either bivalent rLP2086 plus DTaP/IPV (373 patients) or DTaP/IPV plus saline (376 patients). The researchers achieved the primary objective of the study – demonstrating the noninferiority of rLP2086 with DTaP/IPV. The lower bound of the two-sided 95% confidence interval for the difference in the proportion of responders between the two groups 1 month after the DTaP/IPV dose was greater than –10% for the nine DTaP/IPV antigens. Levels of antibodies to the DTaP/IPV antigens, measured as geometric means, also were similar between the vaccine groups for each antigen, according to the researchers.

There also were substantial immune responses to bivalent rLP2086 plus DTaP/IPV, as measured with serum bactericidal assays using human complement (hSBAs) 1 month after the second vaccination, which increased even more after the third vaccination. The proportions of bivalent rLP2086-plus-DTaP/IPV recipients with prespecified seroprotective hSBA titers to the four meningococcal serogroup B test strains were between 55.5% and 97.3% after vaccination two and between 81.5% and 100% after vaccination three.
“Bivalent rLP2086 was well tolerated and elicited substantial and broad bactericidal responses to diverse [meningococcal serogroup B] strains in a high proportion of recipients after 2 vaccinations, and these responses were further enhanced after 3 vaccinations,” the researchers wrote.
Read the full study in the Journal of the Pediatric Infectious Diseases Society (2016 Jun;5[2]:180-7. doi: 10.1093/jpids/piv064).
Concomitant administration of the meningococcal serogroup B vaccine bivalent rLP2086 with the diphtheria, tetanus, and acellular pertussis and inactivated poliovirus (DTaP/IPV) vaccine produced a immunologically noninferior response in adolescents, compared with administration of DTaP/IPV alone.
Timo Vesikari, MD, PhD, of the University of Tampere (Finland) Medical School and his associates randomized healthy adolescents aged 11-18 years to receive either bivalent rLP2086 plus DTaP/IPV (373 patients) or DTaP/IPV plus saline (376 patients). The researchers achieved the primary objective of the study – demonstrating the noninferiority of rLP2086 with DTaP/IPV. The lower bound of the two-sided 95% confidence interval for the difference in the proportion of responders between the two groups 1 month after the DTaP/IPV dose was greater than –10% for the nine DTaP/IPV antigens. Levels of antibodies to the DTaP/IPV antigens, measured as geometric means, also were similar between the vaccine groups for each antigen, according to the researchers.
There also were substantial immune responses to bivalent rLP2086 plus DTaP/IPV, as measured with serum bactericidal assays using human complement (hSBAs) 1 month after the second vaccination, which increased even more after the third vaccination. The proportions of bivalent rLP2086-plus-DTaP/IPV recipients with prespecified seroprotective hSBA titers to the four meningococcal serogroup B test strains were between 55.5% and 97.3% after vaccination two and between 81.5% and 100% after vaccination three.
“Bivalent rLP2086 was well tolerated and elicited substantial and broad bactericidal responses to diverse [meningococcal serogroup B] strains in a high proportion of recipients after 2 vaccinations, and these responses were further enhanced after 3 vaccinations,” the researchers wrote.
Read the full study in the Journal of the Pediatric Infectious Diseases Society (2016 Jun;5[2]:180-7. doi: 10.1093/jpids/piv064).
Concomitant administration of the meningococcal serogroup B vaccine bivalent rLP2086 with the diphtheria, tetanus, and acellular pertussis and inactivated poliovirus (DTaP/IPV) vaccine produced a immunologically noninferior response in adolescents, compared with administration of DTaP/IPV alone.
Timo Vesikari, MD, PhD, of the University of Tampere (Finland) Medical School and his associates randomized healthy adolescents aged 11-18 years to receive either bivalent rLP2086 plus DTaP/IPV (373 patients) or DTaP/IPV plus saline (376 patients). The researchers achieved the primary objective of the study – demonstrating the noninferiority of rLP2086 with DTaP/IPV. The lower bound of the two-sided 95% confidence interval for the difference in the proportion of responders between the two groups 1 month after the DTaP/IPV dose was greater than –10% for the nine DTaP/IPV antigens. Levels of antibodies to the DTaP/IPV antigens, measured as geometric means, also were similar between the vaccine groups for each antigen, according to the researchers.
There also were substantial immune responses to bivalent rLP2086 plus DTaP/IPV, as measured with serum bactericidal assays using human complement (hSBAs) 1 month after the second vaccination, which increased even more after the third vaccination. The proportions of bivalent rLP2086-plus-DTaP/IPV recipients with prespecified seroprotective hSBA titers to the four meningococcal serogroup B test strains were between 55.5% and 97.3% after vaccination two and between 81.5% and 100% after vaccination three.
“Bivalent rLP2086 was well tolerated and elicited substantial and broad bactericidal responses to diverse [meningococcal serogroup B] strains in a high proportion of recipients after 2 vaccinations, and these responses were further enhanced after 3 vaccinations,” the researchers wrote.
Read the full study in the Journal of the Pediatric Infectious Diseases Society (2016 Jun;5[2]:180-7. doi: 10.1093/jpids/piv064).
FROM THE JOURNAL OF THE PEDIATRIC INFECTIOUS DISEASES SOCIETY

Combo could treat young kids with malaria

Photo by Sarah Mattison
Combination therapy with artesunate and mefloquine can safely and effectively treat children younger than 5 years of age with uncomplicated, Plasmodium falciparum malaria, according to a phase 4 study.
Researchers compared the artesunate-mefloquine combination with artemether-lumefantrine in a group of malaria-infected children in Africa.
Both combinations produced a cure rate of about 90%, and the rates of side effects such as vomiting and neurologic events were similar.
These results were published in The Lancet Infectious Diseases.
The study included 944 African children, ages 6 months to 5 years, who tested positive for malaria.
Roughly half the children were assigned to treatment with artemether-lumefantrine (n=472), and the other half were assigned to artesunate-mefloquine (n=473). Both groups were treated for 2 or 3 days, with doses adjusted for age, not weight.
At 63 days of follow-up, the cure rates were similar between the treatment groups—89.7% for artemether-lumefantrine and 90.9% for artesunate-mefloquine. For both groups, no parasites were found in the blood at 72 hours after the start of treatment.
The rates of malaria recurrence were similar between the groups. Reinfection occurred in 43.8% of patients in the artesunate–mefloquine group and 43.0% in the artemether–lumefantrine group. Recrudescence occurred in 3.9% and 4.4%, respectively.
There were no psychiatric events in either treatment group, and the rates of neurologic events were low—2.1% in the artesunate-mefloquine group and 1.1% in the artemether-lumefantrine group.
The incidence of vomiting was 15.3% in the artesunate-mefloquine group and 16.8% in the artemether-lumefantrine group. Vomiting was a focus because it lowers patient adherence and limits how much of the medicine is absorbed.
The researchers noted that artesunate-mefloquine is not used in Africa at present, even though it’s 1 of the 5 artemisinin-based combination therapies approved for malaria treatment by the World Health Organization.
The team said the results of this study support the deployment of fixed-dose artesunate–mefloquine in young children in Africa. And the findings should have important implications for health policy in sub-Saharan Africa. ![]()
Photo by Sarah Mattison
Combination therapy with artesunate and mefloquine can safely and effectively treat children younger than 5 years of age with uncomplicated, Plasmodium falciparum malaria, according to a phase 4 study.
Researchers compared the artesunate-mefloquine combination with artemether-lumefantrine in a group of malaria-infected children in Africa.
Both combinations produced a cure rate of about 90%, and the rates of side effects such as vomiting and neurologic events were similar.
These results were published in The Lancet Infectious Diseases.
The study included 944 African children, ages 6 months to 5 years, who tested positive for malaria.
Roughly half the children were assigned to treatment with artemether-lumefantrine (n=472), and the other half were assigned to artesunate-mefloquine (n=473). Both groups were treated for 2 or 3 days, with doses adjusted for age, not weight.
At 63 days of follow-up, the cure rates were similar between the treatment groups—89.7% for artemether-lumefantrine and 90.9% for artesunate-mefloquine. For both groups, no parasites were found in the blood at 72 hours after the start of treatment.
The rates of malaria recurrence were similar between the groups. Reinfection occurred in 43.8% of patients in the artesunate–mefloquine group and 43.0% in the artemether–lumefantrine group. Recrudescence occurred in 3.9% and 4.4%, respectively.
There were no psychiatric events in either treatment group, and the rates of neurologic events were low—2.1% in the artesunate-mefloquine group and 1.1% in the artemether-lumefantrine group.
The incidence of vomiting was 15.3% in the artesunate-mefloquine group and 16.8% in the artemether-lumefantrine group. Vomiting was a focus because it lowers patient adherence and limits how much of the medicine is absorbed.
The researchers noted that artesunate-mefloquine is not used in Africa at present, even though it’s 1 of the 5 artemisinin-based combination therapies approved for malaria treatment by the World Health Organization.
The team said the results of this study support the deployment of fixed-dose artesunate–mefloquine in young children in Africa. And the findings should have important implications for health policy in sub-Saharan Africa. ![]()
Photo by Sarah Mattison
Combination therapy with artesunate and mefloquine can safely and effectively treat children younger than 5 years of age with uncomplicated, Plasmodium falciparum malaria, according to a phase 4 study.
Researchers compared the artesunate-mefloquine combination with artemether-lumefantrine in a group of malaria-infected children in Africa.
Both combinations produced a cure rate of about 90%, and the rates of side effects such as vomiting and neurologic events were similar.
These results were published in The Lancet Infectious Diseases.
The study included 944 African children, ages 6 months to 5 years, who tested positive for malaria.
Roughly half the children were assigned to treatment with artemether-lumefantrine (n=472), and the other half were assigned to artesunate-mefloquine (n=473). Both groups were treated for 2 or 3 days, with doses adjusted for age, not weight.
At 63 days of follow-up, the cure rates were similar between the treatment groups—89.7% for artemether-lumefantrine and 90.9% for artesunate-mefloquine. For both groups, no parasites were found in the blood at 72 hours after the start of treatment.
The rates of malaria recurrence were similar between the groups. Reinfection occurred in 43.8% of patients in the artesunate–mefloquine group and 43.0% in the artemether–lumefantrine group. Recrudescence occurred in 3.9% and 4.4%, respectively.
There were no psychiatric events in either treatment group, and the rates of neurologic events were low—2.1% in the artesunate-mefloquine group and 1.1% in the artemether-lumefantrine group.
The incidence of vomiting was 15.3% in the artesunate-mefloquine group and 16.8% in the artemether-lumefantrine group. Vomiting was a focus because it lowers patient adherence and limits how much of the medicine is absorbed.
The researchers noted that artesunate-mefloquine is not used in Africa at present, even though it’s 1 of the 5 artemisinin-based combination therapies approved for malaria treatment by the World Health Organization.
The team said the results of this study support the deployment of fixed-dose artesunate–mefloquine in young children in Africa. And the findings should have important implications for health policy in sub-Saharan Africa. ![]()