User login
Promoting mental well-being in LGBTQ youth
For many the beginning of a new year is a time to set goals and resolutions for the upcoming year. Often these resolutions are related to health, for example, quit smoking, work out more, lose weight. It is sometimes easy to overlook mental health and well-being as an integral part of overall wellness. This month’s column will focus on how as pediatric providers we can help promote the mental well-being of our patients in practice.
Mental health problems are a significant cause of morbidity and mortality in youth. In 2014, suicide was the second leading cause of death for all youth 10-14 years and 15-24 years.1 While most lesbian, gay, bisexual, transgender, and questioning (LGBTQ) persons live healthy, happy lives, LGBTQ youth are at disproportionate risk for mental illness, probably related to lack of support and to stigma related to their sexual minority and gender minority identities. Studies suggest that LGBTQ youth have suicidality rates two to five times higher than their heterosexual cisgender peers.2,3,4

• Principle 1. A comprehensive diagnostic evaluation should include an age-appropriate assessment of psychosexual development for all youths.
While pediatric providers are unlikely to perform a comprehensive mental health diagnostic evaluation, psychosocial development should regularly be assessed at well visits. It may not be readily apparent which youth are struggling with development of their sexual and gender identity. Nonassuming questions regarding development in theses domains should ideally be integrated into the psychosocial assessment. For example, begin a sexual history by asking, “Are you romantically attracted to males, females, both, or neither?”
• Principle 2. The need for confidentiality in the clinical alliance is a special consideration in the assessment of sexual and gender minority youth.
Confidentiality is important when talking to any youth about their sexual and gender identity. LGBTQ youth in particular may have concerns of family or provider rejection, and they may look for cues that they can safely discuss their sexuality or gender identity without fear of being judged or shamed. Clinicians should be aware of confidentiality practices for minors when discussing these issues. Potential risks of premature disclosure to family and support systems, such as rejection or alienation, also should be considered.
• Principle 3. Family dynamics pertinent to sexual orientation, gender nonconformity, and gender identity should be explored in the context of the cultural values of the youth, family, and community.
Families can have a variety of responses to their child’s sexual minority or gender minority identity, ranging from acceptance to rejection, with some youth being forced to leave home. Many families need to alter their ideas and expectations for a child after their child comes out, and this can lead to feelings of loss and grief accompanied by feelings of anxiety, anger, shame, and guilt.5 Over time, however, the majority of families become affirming and supportive and are not distressed.7 Recognizing that family support reduces negative health outcomes for youth, providers should aim to support and preserve positive family relationships when possible. This may involve education and support for families as well as youth. It is important to be aware that sexual and gender minority youth who are also members of ethnic minorities may face additional challenges.
• Principle 4. Clinicians should inquire about circumstances commonly encountered by youth with sexual and gender minority status that confer increased psychiatric risk.
Providers should recognize that LGBTQ youth are at disproportionate risk of bullying, suicide, substance use, high-risk sexual behaviors, running away, and becoming homeless. Providers should assess for these risks and address them as appropriate.
• Principle 5. Clinicians should aim to foster healthy psychosexual development in sexual and gender minority youth, and protect these individuals’ full capacity for integrated identity formation and functioning.
Providers should support healthy youth development and self-discovery, recognizing that there is a spectrum of sexual and gender identities, with the goal of helping youth achieve their full developmental potential.
• Principle 6. Clinicians should be aware that there is no evidence that sexual orientation can be altered through therapy, and attempts to do so may be harmful.
Therapies targeted at altering sexual orientation or gender identity, often referred to as reparative therapies, can encourage family rejection and decrease self-esteem and connectedness, all of which have been identified as risk factors for suicidality. Providers should educate parents about the potential harm of these types of therapies and ensure that mental health providers to whom patients are being referred are not practicing these potentially harmful therapies.
• Principle 7. Clinicians should be aware of current evidence on the natural course of gender discordance and associated psychopathology in children and adolescents in choosing the treatment goals and modality.
Variation in gender role behavior (for example, dress preference, toy preference, types of play) is typical in early childhood and should be distinguished from gender dysphoria, in which a child expresses distress related to a gender identity that is different from or does not fully align with the child’s sex assigned at birth. Assessing gender development in childhood and the best approach to treatment is best done by professionals with experience and training in gender development, and providers should be familiar with resources in their area. For some, gender identity concerns may not be recognized until adolescence when the onset of puberty and secondary sex characteristics result in increased dysphoria. Best practice guidelines exist for treatment of youth with gender discordance, and there is limited but growing evidence to support best practices. Providers should ensure that the providers and specialists to whom families are referred practice according to current best practices.
• Principle 8. Clinicians should be prepared to consult and act as a liaison with schools, community agencies, and other health care providers, advocating for the unique needs of sexual and gender minority youth and their families.
Pediatric providers can work with mental health professionals to be advocates for their gender and sexual minority patients and raise awareness of issues affecting these special populations such as bullying and suicidality.
• Principle 9. Mental health professionals should be aware of community and professional resources relevant to sexual and gender minority youth.
As medical providers, we have a limited amount of time to see and assess patients, and often are able to best serve our patients and families by connecting them to specialists in the medical community and resources available in the school and community. It is important to know what resources exist in the community to be able to appropriately refer and connect patients.
Resources for providers
• American Academy of Child and Adolescent Psychiatry Practice Parameter on lesbian, gay, bisexual, and transgender youth .
• National LGBT Health Education Center: Training materials and modules with continuing education credits.
Resources for families
• Gay, Lesbian, and Straight Education Network.• Parents, Friends, Families of Lesbians and Gays (PFLAG).
References
1. “10 Leading Causes of Death by Age Group, United States – 2014,” National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
2. Lesbian, Gay, Bisexual, and Transgender Health: LGBT Youth, Centers for Disease Control and Prevention, Nov. 12, 2014.
3. Am J Public Health. 2001 Aug;91(8):1276-81.
4. Am J Prev Med. 2012 Mar;42(3):221-8.
5. J. Am Acad Child Adolesc Psychiatry. 2012;51(9):957–74.
6. Pediatr Clin North Am. 2016 Dec;63(6):971-83.
7. “Mom, Dad. I’m Gay: How Families Negotiate Coming Out” (Washington, DC: American Psychological Association, 2001).
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.
For many the beginning of a new year is a time to set goals and resolutions for the upcoming year. Often these resolutions are related to health, for example, quit smoking, work out more, lose weight. It is sometimes easy to overlook mental health and well-being as an integral part of overall wellness. This month’s column will focus on how as pediatric providers we can help promote the mental well-being of our patients in practice.
Mental health problems are a significant cause of morbidity and mortality in youth. In 2014, suicide was the second leading cause of death for all youth 10-14 years and 15-24 years.1 While most lesbian, gay, bisexual, transgender, and questioning (LGBTQ) persons live healthy, happy lives, LGBTQ youth are at disproportionate risk for mental illness, probably related to lack of support and to stigma related to their sexual minority and gender minority identities. Studies suggest that LGBTQ youth have suicidality rates two to five times higher than their heterosexual cisgender peers.2,3,4
• Principle 1. A comprehensive diagnostic evaluation should include an age-appropriate assessment of psychosexual development for all youths.
While pediatric providers are unlikely to perform a comprehensive mental health diagnostic evaluation, psychosocial development should regularly be assessed at well visits. It may not be readily apparent which youth are struggling with development of their sexual and gender identity. Nonassuming questions regarding development in theses domains should ideally be integrated into the psychosocial assessment. For example, begin a sexual history by asking, “Are you romantically attracted to males, females, both, or neither?”
• Principle 2. The need for confidentiality in the clinical alliance is a special consideration in the assessment of sexual and gender minority youth.
Confidentiality is important when talking to any youth about their sexual and gender identity. LGBTQ youth in particular may have concerns of family or provider rejection, and they may look for cues that they can safely discuss their sexuality or gender identity without fear of being judged or shamed. Clinicians should be aware of confidentiality practices for minors when discussing these issues. Potential risks of premature disclosure to family and support systems, such as rejection or alienation, also should be considered.
• Principle 3. Family dynamics pertinent to sexual orientation, gender nonconformity, and gender identity should be explored in the context of the cultural values of the youth, family, and community.
Families can have a variety of responses to their child’s sexual minority or gender minority identity, ranging from acceptance to rejection, with some youth being forced to leave home. Many families need to alter their ideas and expectations for a child after their child comes out, and this can lead to feelings of loss and grief accompanied by feelings of anxiety, anger, shame, and guilt.5 Over time, however, the majority of families become affirming and supportive and are not distressed.7 Recognizing that family support reduces negative health outcomes for youth, providers should aim to support and preserve positive family relationships when possible. This may involve education and support for families as well as youth. It is important to be aware that sexual and gender minority youth who are also members of ethnic minorities may face additional challenges.
• Principle 4. Clinicians should inquire about circumstances commonly encountered by youth with sexual and gender minority status that confer increased psychiatric risk.
Providers should recognize that LGBTQ youth are at disproportionate risk of bullying, suicide, substance use, high-risk sexual behaviors, running away, and becoming homeless. Providers should assess for these risks and address them as appropriate.
• Principle 5. Clinicians should aim to foster healthy psychosexual development in sexual and gender minority youth, and protect these individuals’ full capacity for integrated identity formation and functioning.
Providers should support healthy youth development and self-discovery, recognizing that there is a spectrum of sexual and gender identities, with the goal of helping youth achieve their full developmental potential.
• Principle 6. Clinicians should be aware that there is no evidence that sexual orientation can be altered through therapy, and attempts to do so may be harmful.
Therapies targeted at altering sexual orientation or gender identity, often referred to as reparative therapies, can encourage family rejection and decrease self-esteem and connectedness, all of which have been identified as risk factors for suicidality. Providers should educate parents about the potential harm of these types of therapies and ensure that mental health providers to whom patients are being referred are not practicing these potentially harmful therapies.
• Principle 7. Clinicians should be aware of current evidence on the natural course of gender discordance and associated psychopathology in children and adolescents in choosing the treatment goals and modality.
Variation in gender role behavior (for example, dress preference, toy preference, types of play) is typical in early childhood and should be distinguished from gender dysphoria, in which a child expresses distress related to a gender identity that is different from or does not fully align with the child’s sex assigned at birth. Assessing gender development in childhood and the best approach to treatment is best done by professionals with experience and training in gender development, and providers should be familiar with resources in their area. For some, gender identity concerns may not be recognized until adolescence when the onset of puberty and secondary sex characteristics result in increased dysphoria. Best practice guidelines exist for treatment of youth with gender discordance, and there is limited but growing evidence to support best practices. Providers should ensure that the providers and specialists to whom families are referred practice according to current best practices.
• Principle 8. Clinicians should be prepared to consult and act as a liaison with schools, community agencies, and other health care providers, advocating for the unique needs of sexual and gender minority youth and their families.
Pediatric providers can work with mental health professionals to be advocates for their gender and sexual minority patients and raise awareness of issues affecting these special populations such as bullying and suicidality.
• Principle 9. Mental health professionals should be aware of community and professional resources relevant to sexual and gender minority youth.
As medical providers, we have a limited amount of time to see and assess patients, and often are able to best serve our patients and families by connecting them to specialists in the medical community and resources available in the school and community. It is important to know what resources exist in the community to be able to appropriately refer and connect patients.
Resources for providers
• American Academy of Child and Adolescent Psychiatry Practice Parameter on lesbian, gay, bisexual, and transgender youth .
• National LGBT Health Education Center: Training materials and modules with continuing education credits.
Resources for families
• Gay, Lesbian, and Straight Education Network.• Parents, Friends, Families of Lesbians and Gays (PFLAG).
References
1. “10 Leading Causes of Death by Age Group, United States – 2014,” National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
2. Lesbian, Gay, Bisexual, and Transgender Health: LGBT Youth, Centers for Disease Control and Prevention, Nov. 12, 2014.
3. Am J Public Health. 2001 Aug;91(8):1276-81.
4. Am J Prev Med. 2012 Mar;42(3):221-8.
5. J. Am Acad Child Adolesc Psychiatry. 2012;51(9):957–74.
6. Pediatr Clin North Am. 2016 Dec;63(6):971-83.
7. “Mom, Dad. I’m Gay: How Families Negotiate Coming Out” (Washington, DC: American Psychological Association, 2001).
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.
For many the beginning of a new year is a time to set goals and resolutions for the upcoming year. Often these resolutions are related to health, for example, quit smoking, work out more, lose weight. It is sometimes easy to overlook mental health and well-being as an integral part of overall wellness. This month’s column will focus on how as pediatric providers we can help promote the mental well-being of our patients in practice.
Mental health problems are a significant cause of morbidity and mortality in youth. In 2014, suicide was the second leading cause of death for all youth 10-14 years and 15-24 years.1 While most lesbian, gay, bisexual, transgender, and questioning (LGBTQ) persons live healthy, happy lives, LGBTQ youth are at disproportionate risk for mental illness, probably related to lack of support and to stigma related to their sexual minority and gender minority identities. Studies suggest that LGBTQ youth have suicidality rates two to five times higher than their heterosexual cisgender peers.2,3,4
• Principle 1. A comprehensive diagnostic evaluation should include an age-appropriate assessment of psychosexual development for all youths.
While pediatric providers are unlikely to perform a comprehensive mental health diagnostic evaluation, psychosocial development should regularly be assessed at well visits. It may not be readily apparent which youth are struggling with development of their sexual and gender identity. Nonassuming questions regarding development in theses domains should ideally be integrated into the psychosocial assessment. For example, begin a sexual history by asking, “Are you romantically attracted to males, females, both, or neither?”
• Principle 2. The need for confidentiality in the clinical alliance is a special consideration in the assessment of sexual and gender minority youth.
Confidentiality is important when talking to any youth about their sexual and gender identity. LGBTQ youth in particular may have concerns of family or provider rejection, and they may look for cues that they can safely discuss their sexuality or gender identity without fear of being judged or shamed. Clinicians should be aware of confidentiality practices for minors when discussing these issues. Potential risks of premature disclosure to family and support systems, such as rejection or alienation, also should be considered.
• Principle 3. Family dynamics pertinent to sexual orientation, gender nonconformity, and gender identity should be explored in the context of the cultural values of the youth, family, and community.
Families can have a variety of responses to their child’s sexual minority or gender minority identity, ranging from acceptance to rejection, with some youth being forced to leave home. Many families need to alter their ideas and expectations for a child after their child comes out, and this can lead to feelings of loss and grief accompanied by feelings of anxiety, anger, shame, and guilt.5 Over time, however, the majority of families become affirming and supportive and are not distressed.7 Recognizing that family support reduces negative health outcomes for youth, providers should aim to support and preserve positive family relationships when possible. This may involve education and support for families as well as youth. It is important to be aware that sexual and gender minority youth who are also members of ethnic minorities may face additional challenges.
• Principle 4. Clinicians should inquire about circumstances commonly encountered by youth with sexual and gender minority status that confer increased psychiatric risk.
Providers should recognize that LGBTQ youth are at disproportionate risk of bullying, suicide, substance use, high-risk sexual behaviors, running away, and becoming homeless. Providers should assess for these risks and address them as appropriate.
• Principle 5. Clinicians should aim to foster healthy psychosexual development in sexual and gender minority youth, and protect these individuals’ full capacity for integrated identity formation and functioning.
Providers should support healthy youth development and self-discovery, recognizing that there is a spectrum of sexual and gender identities, with the goal of helping youth achieve their full developmental potential.
• Principle 6. Clinicians should be aware that there is no evidence that sexual orientation can be altered through therapy, and attempts to do so may be harmful.
Therapies targeted at altering sexual orientation or gender identity, often referred to as reparative therapies, can encourage family rejection and decrease self-esteem and connectedness, all of which have been identified as risk factors for suicidality. Providers should educate parents about the potential harm of these types of therapies and ensure that mental health providers to whom patients are being referred are not practicing these potentially harmful therapies.
• Principle 7. Clinicians should be aware of current evidence on the natural course of gender discordance and associated psychopathology in children and adolescents in choosing the treatment goals and modality.
Variation in gender role behavior (for example, dress preference, toy preference, types of play) is typical in early childhood and should be distinguished from gender dysphoria, in which a child expresses distress related to a gender identity that is different from or does not fully align with the child’s sex assigned at birth. Assessing gender development in childhood and the best approach to treatment is best done by professionals with experience and training in gender development, and providers should be familiar with resources in their area. For some, gender identity concerns may not be recognized until adolescence when the onset of puberty and secondary sex characteristics result in increased dysphoria. Best practice guidelines exist for treatment of youth with gender discordance, and there is limited but growing evidence to support best practices. Providers should ensure that the providers and specialists to whom families are referred practice according to current best practices.
• Principle 8. Clinicians should be prepared to consult and act as a liaison with schools, community agencies, and other health care providers, advocating for the unique needs of sexual and gender minority youth and their families.
Pediatric providers can work with mental health professionals to be advocates for their gender and sexual minority patients and raise awareness of issues affecting these special populations such as bullying and suicidality.
• Principle 9. Mental health professionals should be aware of community and professional resources relevant to sexual and gender minority youth.
As medical providers, we have a limited amount of time to see and assess patients, and often are able to best serve our patients and families by connecting them to specialists in the medical community and resources available in the school and community. It is important to know what resources exist in the community to be able to appropriately refer and connect patients.
Resources for providers
• American Academy of Child and Adolescent Psychiatry Practice Parameter on lesbian, gay, bisexual, and transgender youth .
• National LGBT Health Education Center: Training materials and modules with continuing education credits.
Resources for families
• Gay, Lesbian, and Straight Education Network.• Parents, Friends, Families of Lesbians and Gays (PFLAG).
References
1. “10 Leading Causes of Death by Age Group, United States – 2014,” National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
2. Lesbian, Gay, Bisexual, and Transgender Health: LGBT Youth, Centers for Disease Control and Prevention, Nov. 12, 2014.
3. Am J Public Health. 2001 Aug;91(8):1276-81.
4. Am J Prev Med. 2012 Mar;42(3):221-8.
5. J. Am Acad Child Adolesc Psychiatry. 2012;51(9):957–74.
6. Pediatr Clin North Am. 2016 Dec;63(6):971-83.
7. “Mom, Dad. I’m Gay: How Families Negotiate Coming Out” (Washington, DC: American Psychological Association, 2001).
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.

Increase brings flu activity back to seasonal high
for the week ending Jan. 21, compared with three states the week before, according to the Centers for Disease Control and Prevention.
Alabama, Kansas, New Jersey, Oklahoma, and South Carolina were at level 10 on the CDC’s 1-10 scale of ILI activity, with Oklahoma reaching that level for the third consecutive week. Georgia (level 9) and Louisiana, Minnesota, Missouri, and Tennessee (level 8) were also in the “high” range, the CDC reported.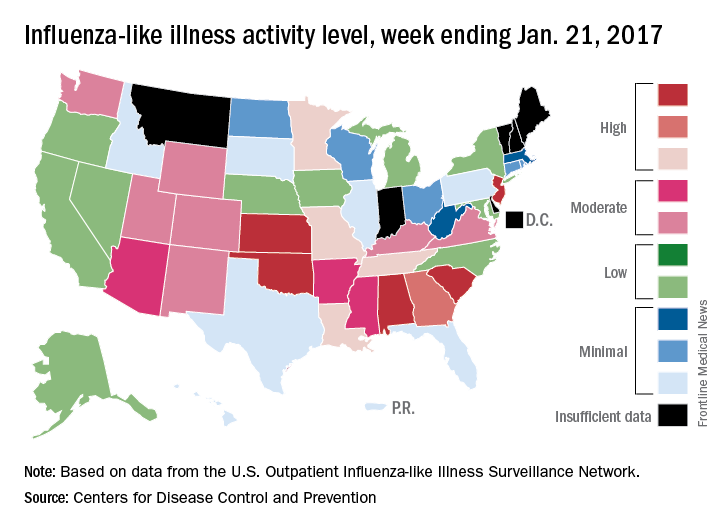
Three flu-related pediatric deaths were reported for the week, although two occurred during the week ending Jan. 14. The two earlier deaths were associated with an influenza A (H3) virus, and the more recent death was associated with an influenza B virus. For the 2016-2017 season so far, there have been a total of eight pediatric deaths, the CDC said.
for the week ending Jan. 21, compared with three states the week before, according to the Centers for Disease Control and Prevention.
Alabama, Kansas, New Jersey, Oklahoma, and South Carolina were at level 10 on the CDC’s 1-10 scale of ILI activity, with Oklahoma reaching that level for the third consecutive week. Georgia (level 9) and Louisiana, Minnesota, Missouri, and Tennessee (level 8) were also in the “high” range, the CDC reported.
Three flu-related pediatric deaths were reported for the week, although two occurred during the week ending Jan. 14. The two earlier deaths were associated with an influenza A (H3) virus, and the more recent death was associated with an influenza B virus. For the 2016-2017 season so far, there have been a total of eight pediatric deaths, the CDC said.
for the week ending Jan. 21, compared with three states the week before, according to the Centers for Disease Control and Prevention.
Alabama, Kansas, New Jersey, Oklahoma, and South Carolina were at level 10 on the CDC’s 1-10 scale of ILI activity, with Oklahoma reaching that level for the third consecutive week. Georgia (level 9) and Louisiana, Minnesota, Missouri, and Tennessee (level 8) were also in the “high” range, the CDC reported.
Three flu-related pediatric deaths were reported for the week, although two occurred during the week ending Jan. 14. The two earlier deaths were associated with an influenza A (H3) virus, and the more recent death was associated with an influenza B virus. For the 2016-2017 season so far, there have been a total of eight pediatric deaths, the CDC said.
It isn’t over until it’s over
Pediatricians take heart.
Yes, I know it is discouraging when families occasionally ignore our advice and refuse vaccines for their children. It is even worse when political leaders who ought to know better question the safety and value of vaccines.
But let’s not lose perspective. Let me share a quick reminder of why vaccines are (almost) universally considered one of the greatest public health achievements of the 20th century.
Not long ago, I reviewed a clinical case with students as part of a medical microbiology course. A 6-year-old girl presented with fever, headache, and flaccid paralysis of the right arm with areflexia. With little prompting, the students generated a short differential diagnosis. Enterovirus. West Nile virus. “I guess we should include polio,” one student offered. “But who gets that anymore?”
A mere 120 years changes everything. At the dawn of the 20th century, we didn’t even know with certainty what caused polio, although infection was suspected.

On Sept. 9, 1954, the Courier-Journal, a newspaper in my hometown of Louisville, Ky., carried a story about the annual number of polio cases in Jefferson County, noting that they had reached 198 and General Hospital had opened a polio ward usually reserved for epidemics. Concerns about the infection were rippling throughout the state, and the paper reported that at least one high school marching band had elected to withdraw from annual Kentucky State Fair competition because of concerns about infection.
My mom was 10 years old in the summer of 1954, and she recalls that it was a “scary” time. Swimming pools closed. Parents refused to allow their children to go to movie theaters or the local amusement park because of fear that they might come into contact with the virus. My mom said, “Then one of my friends was diagnosed with polio. We had played together the week before she got sick. We worried that we were going to get sick, too. And once you got sick, you didn’t necessarily get better.”

I probably don’t need to remind you that both Dr. Sabin and Dr. Salk did develop successful poliovirus vaccines. Dr. Enders, along with junior colleagues Fred C. Robbins, MD, and Thomas H. Weller, MD, developed the techniques to grow poliovirus and other viruses in culture, making the work of Dr. Sabin and Dr. Salk possible. For this, Dr. Enders, Dr. Robbins, and Dr. Weller received the Nobel Prize in 1954.
Regarding the prediction of long-term protection, I’d say we’re there. According to the Centers for Disease Control and Prevention, wild poliovirus cases have declined more than 99.9% since 1988. According to the Global Polio Eradication Initiative, that means that there are approximately 10 million people walking today who would have otherwise been paralyzed by the disease.
In 2015, there were only 74 cases identified in the world, and these were localized to two countries. Even better, a global commission announced that wild poliovirus type 2 had been eradicated from the world. Eradicated. The last known transmission occurred in India in 1999.
Type 3 poliovirus may not be far behind. The last known case of wildtype poliovirus 3 was detected in 2012.
The complete story of poliovirus eradication efforts could read like a suspense novel: There have been twists and turns, some missed deadlines, and now a bit of irony. Success, in large part, has hinged on the use of trivalent, live attenuated oral poliovirus vaccine (tOPV) throughout much of the world. Now eradication of all polio disease is going to require withdrawal of OPV in countries that still use it.
Rarely, the live attenuated vaccine viruses contained in OPV can cause polio, and since 2012, vaccine-derived cases have exceeded wild poliovirus cases. Vaccine-derived cases include vaccine-associated paralytic polio (VAPP) – paralysis occurs in a vaccine recipient or a close contact – as well as cases of circulating vaccine-derived polioviruses (cVDPVs). Remember that vaccine viruses are shed in the stool, and in communities with low immunization rates, they circulate and acquire mutations that confer the transmissibility and neurovirulence properties of wild viruses. Ultimately, cVDPVs lead to outbreaks.
In 2013, the Global Polio Eradication Initiative published a new “endgame plan” for polio that outlined a stepwise approach for removing OPV from immunization programs. First, it called on all countries to introduce at least one dose of inactivated poliovirus vaccine by the third quarter of 2015, immunizing infants at 14 weeks or at first contact thereafter. Second, it called for all countries to replace tOPV with a bivalent vaccine containing only types 1 and 3 by 2016. Given the eradication of wild poliovirus type 2, keeping type 2 in the oral vaccine just creates risk. An estimated 40% of VAPP cases and 98% of cVDPVs detected since 2012 were caused by poliovirus type 2. The type 2 component of tOPV also interferes with the immune response to the other types. Once poliovirus eradication has been achieved and certified, hopefully no later than 2019, all OPV will be withdrawn.
What’s the role of pediatricians in the United States in polio eradication? For now, our job is to continue to protect all children in the United States against all three types of poliovirus. Current Advisory Committee on Immunization Practices (ACIP) recommendations specify 4 doses of trivalent inactivated poliovirus vaccine (IPV) at ages 2 months, 4 months, 6-18 months, and 4-6 years. Children vaccinated outside the United States with bivalent vaccine, including immigrants and refugees, will need to be revaccinated. Those without appropriate documentation of vaccine (written, dated records that specify trivalent vaccine) also should be revaccinated.
Serologic testing for immunity is no longer recommended. In the past, children without documentation of vaccines could be tested for neutralizing antibodies to poliovirus types 1, 2, and 3. Moving forward, serologic testing for antibodies to poliovirus type 2 won’t be available because it requires live virus, and in accordance with World Health Organization recommendations, laboratories have been destroying supplies of poliovirus type 2.
We also need to make sure that our patients who are traveling internationally receive all recommended vaccines, including a dose of IPV when appropriate. Specific recommendations can be found on the CDC’s pages for travelers.
A 2015 statement from the American Academy of Pediatrics called on pediatricians to consider polio as a potential diagnosis of any child presenting with fever and acute flaccid paralysis (Pediatrics. 2015 Jan;135[1]:196-202). When polio is suspected, public health authorities should be notified and two stool samples collected 24 hours apart, and within 14 days of the onset of paralysis, sent for testing. According to lead author Walter A. Orenstein, MD, “because most polio infections are silent, a case of paralytic polio in the United States may have been acquired from an asymptomatic individual, so a history of travel to a polio-infected area may be absent in the case of paralysis.”
I’ll second what my mom said. Scary.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Pediatricians take heart.
Yes, I know it is discouraging when families occasionally ignore our advice and refuse vaccines for their children. It is even worse when political leaders who ought to know better question the safety and value of vaccines.
But let’s not lose perspective. Let me share a quick reminder of why vaccines are (almost) universally considered one of the greatest public health achievements of the 20th century.
Not long ago, I reviewed a clinical case with students as part of a medical microbiology course. A 6-year-old girl presented with fever, headache, and flaccid paralysis of the right arm with areflexia. With little prompting, the students generated a short differential diagnosis. Enterovirus. West Nile virus. “I guess we should include polio,” one student offered. “But who gets that anymore?”
A mere 120 years changes everything. At the dawn of the 20th century, we didn’t even know with certainty what caused polio, although infection was suspected.
On Sept. 9, 1954, the Courier-Journal, a newspaper in my hometown of Louisville, Ky., carried a story about the annual number of polio cases in Jefferson County, noting that they had reached 198 and General Hospital had opened a polio ward usually reserved for epidemics. Concerns about the infection were rippling throughout the state, and the paper reported that at least one high school marching band had elected to withdraw from annual Kentucky State Fair competition because of concerns about infection.
My mom was 10 years old in the summer of 1954, and she recalls that it was a “scary” time. Swimming pools closed. Parents refused to allow their children to go to movie theaters or the local amusement park because of fear that they might come into contact with the virus. My mom said, “Then one of my friends was diagnosed with polio. We had played together the week before she got sick. We worried that we were going to get sick, too. And once you got sick, you didn’t necessarily get better.”
I probably don’t need to remind you that both Dr. Sabin and Dr. Salk did develop successful poliovirus vaccines. Dr. Enders, along with junior colleagues Fred C. Robbins, MD, and Thomas H. Weller, MD, developed the techniques to grow poliovirus and other viruses in culture, making the work of Dr. Sabin and Dr. Salk possible. For this, Dr. Enders, Dr. Robbins, and Dr. Weller received the Nobel Prize in 1954.
Regarding the prediction of long-term protection, I’d say we’re there. According to the Centers for Disease Control and Prevention, wild poliovirus cases have declined more than 99.9% since 1988. According to the Global Polio Eradication Initiative, that means that there are approximately 10 million people walking today who would have otherwise been paralyzed by the disease.
In 2015, there were only 74 cases identified in the world, and these were localized to two countries. Even better, a global commission announced that wild poliovirus type 2 had been eradicated from the world. Eradicated. The last known transmission occurred in India in 1999.
Type 3 poliovirus may not be far behind. The last known case of wildtype poliovirus 3 was detected in 2012.
The complete story of poliovirus eradication efforts could read like a suspense novel: There have been twists and turns, some missed deadlines, and now a bit of irony. Success, in large part, has hinged on the use of trivalent, live attenuated oral poliovirus vaccine (tOPV) throughout much of the world. Now eradication of all polio disease is going to require withdrawal of OPV in countries that still use it.
Rarely, the live attenuated vaccine viruses contained in OPV can cause polio, and since 2012, vaccine-derived cases have exceeded wild poliovirus cases. Vaccine-derived cases include vaccine-associated paralytic polio (VAPP) – paralysis occurs in a vaccine recipient or a close contact – as well as cases of circulating vaccine-derived polioviruses (cVDPVs). Remember that vaccine viruses are shed in the stool, and in communities with low immunization rates, they circulate and acquire mutations that confer the transmissibility and neurovirulence properties of wild viruses. Ultimately, cVDPVs lead to outbreaks.
In 2013, the Global Polio Eradication Initiative published a new “endgame plan” for polio that outlined a stepwise approach for removing OPV from immunization programs. First, it called on all countries to introduce at least one dose of inactivated poliovirus vaccine by the third quarter of 2015, immunizing infants at 14 weeks or at first contact thereafter. Second, it called for all countries to replace tOPV with a bivalent vaccine containing only types 1 and 3 by 2016. Given the eradication of wild poliovirus type 2, keeping type 2 in the oral vaccine just creates risk. An estimated 40% of VAPP cases and 98% of cVDPVs detected since 2012 were caused by poliovirus type 2. The type 2 component of tOPV also interferes with the immune response to the other types. Once poliovirus eradication has been achieved and certified, hopefully no later than 2019, all OPV will be withdrawn.
What’s the role of pediatricians in the United States in polio eradication? For now, our job is to continue to protect all children in the United States against all three types of poliovirus. Current Advisory Committee on Immunization Practices (ACIP) recommendations specify 4 doses of trivalent inactivated poliovirus vaccine (IPV) at ages 2 months, 4 months, 6-18 months, and 4-6 years. Children vaccinated outside the United States with bivalent vaccine, including immigrants and refugees, will need to be revaccinated. Those without appropriate documentation of vaccine (written, dated records that specify trivalent vaccine) also should be revaccinated.
Serologic testing for immunity is no longer recommended. In the past, children without documentation of vaccines could be tested for neutralizing antibodies to poliovirus types 1, 2, and 3. Moving forward, serologic testing for antibodies to poliovirus type 2 won’t be available because it requires live virus, and in accordance with World Health Organization recommendations, laboratories have been destroying supplies of poliovirus type 2.
We also need to make sure that our patients who are traveling internationally receive all recommended vaccines, including a dose of IPV when appropriate. Specific recommendations can be found on the CDC’s pages for travelers.
A 2015 statement from the American Academy of Pediatrics called on pediatricians to consider polio as a potential diagnosis of any child presenting with fever and acute flaccid paralysis (Pediatrics. 2015 Jan;135[1]:196-202). When polio is suspected, public health authorities should be notified and two stool samples collected 24 hours apart, and within 14 days of the onset of paralysis, sent for testing. According to lead author Walter A. Orenstein, MD, “because most polio infections are silent, a case of paralytic polio in the United States may have been acquired from an asymptomatic individual, so a history of travel to a polio-infected area may be absent in the case of paralysis.”
I’ll second what my mom said. Scary.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Pediatricians take heart.
Yes, I know it is discouraging when families occasionally ignore our advice and refuse vaccines for their children. It is even worse when political leaders who ought to know better question the safety and value of vaccines.
But let’s not lose perspective. Let me share a quick reminder of why vaccines are (almost) universally considered one of the greatest public health achievements of the 20th century.
Not long ago, I reviewed a clinical case with students as part of a medical microbiology course. A 6-year-old girl presented with fever, headache, and flaccid paralysis of the right arm with areflexia. With little prompting, the students generated a short differential diagnosis. Enterovirus. West Nile virus. “I guess we should include polio,” one student offered. “But who gets that anymore?”
A mere 120 years changes everything. At the dawn of the 20th century, we didn’t even know with certainty what caused polio, although infection was suspected.
On Sept. 9, 1954, the Courier-Journal, a newspaper in my hometown of Louisville, Ky., carried a story about the annual number of polio cases in Jefferson County, noting that they had reached 198 and General Hospital had opened a polio ward usually reserved for epidemics. Concerns about the infection were rippling throughout the state, and the paper reported that at least one high school marching band had elected to withdraw from annual Kentucky State Fair competition because of concerns about infection.
My mom was 10 years old in the summer of 1954, and she recalls that it was a “scary” time. Swimming pools closed. Parents refused to allow their children to go to movie theaters or the local amusement park because of fear that they might come into contact with the virus. My mom said, “Then one of my friends was diagnosed with polio. We had played together the week before she got sick. We worried that we were going to get sick, too. And once you got sick, you didn’t necessarily get better.”
I probably don’t need to remind you that both Dr. Sabin and Dr. Salk did develop successful poliovirus vaccines. Dr. Enders, along with junior colleagues Fred C. Robbins, MD, and Thomas H. Weller, MD, developed the techniques to grow poliovirus and other viruses in culture, making the work of Dr. Sabin and Dr. Salk possible. For this, Dr. Enders, Dr. Robbins, and Dr. Weller received the Nobel Prize in 1954.
Regarding the prediction of long-term protection, I’d say we’re there. According to the Centers for Disease Control and Prevention, wild poliovirus cases have declined more than 99.9% since 1988. According to the Global Polio Eradication Initiative, that means that there are approximately 10 million people walking today who would have otherwise been paralyzed by the disease.
In 2015, there were only 74 cases identified in the world, and these were localized to two countries. Even better, a global commission announced that wild poliovirus type 2 had been eradicated from the world. Eradicated. The last known transmission occurred in India in 1999.
Type 3 poliovirus may not be far behind. The last known case of wildtype poliovirus 3 was detected in 2012.
The complete story of poliovirus eradication efforts could read like a suspense novel: There have been twists and turns, some missed deadlines, and now a bit of irony. Success, in large part, has hinged on the use of trivalent, live attenuated oral poliovirus vaccine (tOPV) throughout much of the world. Now eradication of all polio disease is going to require withdrawal of OPV in countries that still use it.
Rarely, the live attenuated vaccine viruses contained in OPV can cause polio, and since 2012, vaccine-derived cases have exceeded wild poliovirus cases. Vaccine-derived cases include vaccine-associated paralytic polio (VAPP) – paralysis occurs in a vaccine recipient or a close contact – as well as cases of circulating vaccine-derived polioviruses (cVDPVs). Remember that vaccine viruses are shed in the stool, and in communities with low immunization rates, they circulate and acquire mutations that confer the transmissibility and neurovirulence properties of wild viruses. Ultimately, cVDPVs lead to outbreaks.
In 2013, the Global Polio Eradication Initiative published a new “endgame plan” for polio that outlined a stepwise approach for removing OPV from immunization programs. First, it called on all countries to introduce at least one dose of inactivated poliovirus vaccine by the third quarter of 2015, immunizing infants at 14 weeks or at first contact thereafter. Second, it called for all countries to replace tOPV with a bivalent vaccine containing only types 1 and 3 by 2016. Given the eradication of wild poliovirus type 2, keeping type 2 in the oral vaccine just creates risk. An estimated 40% of VAPP cases and 98% of cVDPVs detected since 2012 were caused by poliovirus type 2. The type 2 component of tOPV also interferes with the immune response to the other types. Once poliovirus eradication has been achieved and certified, hopefully no later than 2019, all OPV will be withdrawn.
What’s the role of pediatricians in the United States in polio eradication? For now, our job is to continue to protect all children in the United States against all three types of poliovirus. Current Advisory Committee on Immunization Practices (ACIP) recommendations specify 4 doses of trivalent inactivated poliovirus vaccine (IPV) at ages 2 months, 4 months, 6-18 months, and 4-6 years. Children vaccinated outside the United States with bivalent vaccine, including immigrants and refugees, will need to be revaccinated. Those without appropriate documentation of vaccine (written, dated records that specify trivalent vaccine) also should be revaccinated.
Serologic testing for immunity is no longer recommended. In the past, children without documentation of vaccines could be tested for neutralizing antibodies to poliovirus types 1, 2, and 3. Moving forward, serologic testing for antibodies to poliovirus type 2 won’t be available because it requires live virus, and in accordance with World Health Organization recommendations, laboratories have been destroying supplies of poliovirus type 2.
We also need to make sure that our patients who are traveling internationally receive all recommended vaccines, including a dose of IPV when appropriate. Specific recommendations can be found on the CDC’s pages for travelers.
A 2015 statement from the American Academy of Pediatrics called on pediatricians to consider polio as a potential diagnosis of any child presenting with fever and acute flaccid paralysis (Pediatrics. 2015 Jan;135[1]:196-202). When polio is suspected, public health authorities should be notified and two stool samples collected 24 hours apart, and within 14 days of the onset of paralysis, sent for testing. According to lead author Walter A. Orenstein, MD, “because most polio infections are silent, a case of paralytic polio in the United States may have been acquired from an asymptomatic individual, so a history of travel to a polio-infected area may be absent in the case of paralysis.”
I’ll second what my mom said. Scary.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
What Are the Key Elements of an Initial Pediatric Concussion Evaluation?
VANCOUVER—Initial pediatric concussion evaluations provide an opportunity to recognize premorbid conditions that may be exacerbated by the injury; address problems with prior management, such as excessive rest or NSAID overuse; and identify treatment approaches, according to a seminar delivered at the 45th Annual Meeting of the Child Neurology Society.
Neurologists also may decide whether imaging is warranted and note risk factors for prolonged recovery, said Sharief Taraman, MD, Director of the Children’s Concussion Program at Children’s Hospital of Orange County in Orange, California, and Assistant Clinical Professor of Pediatrics at the University of California, Irvine.

Imaging Likely Not Needed
In most cases, a CT scan is not necessary, Dr. Taraman said. He encouraged neurologists to work with their emergency department colleagues to ensure that patients only undergo CT scans when appropriate. His department uses Pediatric Emergency Care Applied Research Network (PECARN) criteria to determine when a CT scan is warranted. Many patients do not have signs of altered mental status in the emergency department, and “there is really no good reason to scan many of these kids,” he said. Patients also typically do not undergo MRI unless “a significant neurologic finding … suggests that there might have been a stronger mechanism of action.”
History taking is a vital component of initial management, and identifying premorbid conditions is a key factor, Dr. Taraman said. “What we have seen is that concussion symptoms act as a magnifying glass. If I have migraine and I get a concussion, my migraine will likely become exacerbated,” he said. Patients may also present for evaluation of concussion but have an alternate diagnosis that better explains their symptoms. For example, Dr. Taraman described a patient who had persistent symptoms following a concussion. “Listening to the story, it was clearly sleep apnea,” he said. The child underwent polysomnography and received continuous positive airway pressure treatment because he had 40 apneas in an hour.
During the evaluation, neurologists can recognize poor initial management of the injury, such as excessive bed rest or removal from activities. NSAID overuse also is a big problem. Emergency departments may tell patients to take ibuprofen every eight hours for five weeks, which can lead to rebound headaches, Dr. Taraman said.
Facilitate Recovery
Recognition of certain symptoms can inform the patient’s prognosis and suggest ways to speed recovery. For example, neurologists should look for vestibular dysfunction or balance problems and decide whether to address these symptoms. Neurologists also should check for and address cervical strain and ocular dysfunction. Treating severe convergence insufficiency or excess may help patients recover faster.
Anxiety and mood disorders suggest a prolonged recovery. Some patients develop adjustment disorder after concussion. “Interestingly, we see that patients who have more severe traumatic brain injury … are unaware of their deficits,” whereas high-functioning patients who feel slightly off perceive their deficits, which “causes a lot of discomfort for them,” he said.
Symptoms from concussions that involve assaults and litigation tend to take longer to resolve. Some patients’ symptoms persist until litigation ends, although typically not due to malingering but rather due to increased psychological stress.
Poor headache control, sleep disturbances, prior concussions, and a history of prolonged concussion recovery are other risk factors for prolonged recovery.
The Sport Concussion Assessment Tool 3 (SCAT3) is a free, standardized way of assessing symptoms. Developed as a sideline assessment tool, the SCAT3 also works well as a symptoms form, Dr. Taraman said. The tool includes a quick cognitive assessment and balance exam, and online video tutorials explain how to perform the assessment. After assessing a patient’s symptoms, including cognition, concentration, balance, and convergence insufficiency, “then you can decide, how … to triage the patient and start managing them.”
—Jake Remaly
Suggested Reading
Bressan S, Romanato S, Mion T, et al. Implementation of adapted PECARN decision rule for children with minor head injury in the pediatric emergency department. Acad Emerg Med. 2012;19(7):801-807.
Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009;374(9696):1160-1170.
Yengo-Kahn AM, Hale AT, Zalneraitis BH, et al. The Sport Concussion Assessment Tool: a systematic review. Neurosurg Focus. 2016;40(4):E6.
VANCOUVER—Initial pediatric concussion evaluations provide an opportunity to recognize premorbid conditions that may be exacerbated by the injury; address problems with prior management, such as excessive rest or NSAID overuse; and identify treatment approaches, according to a seminar delivered at the 45th Annual Meeting of the Child Neurology Society.
Neurologists also may decide whether imaging is warranted and note risk factors for prolonged recovery, said Sharief Taraman, MD, Director of the Children’s Concussion Program at Children’s Hospital of Orange County in Orange, California, and Assistant Clinical Professor of Pediatrics at the University of California, Irvine.
Imaging Likely Not Needed
In most cases, a CT scan is not necessary, Dr. Taraman said. He encouraged neurologists to work with their emergency department colleagues to ensure that patients only undergo CT scans when appropriate. His department uses Pediatric Emergency Care Applied Research Network (PECARN) criteria to determine when a CT scan is warranted. Many patients do not have signs of altered mental status in the emergency department, and “there is really no good reason to scan many of these kids,” he said. Patients also typically do not undergo MRI unless “a significant neurologic finding … suggests that there might have been a stronger mechanism of action.”
History taking is a vital component of initial management, and identifying premorbid conditions is a key factor, Dr. Taraman said. “What we have seen is that concussion symptoms act as a magnifying glass. If I have migraine and I get a concussion, my migraine will likely become exacerbated,” he said. Patients may also present for evaluation of concussion but have an alternate diagnosis that better explains their symptoms. For example, Dr. Taraman described a patient who had persistent symptoms following a concussion. “Listening to the story, it was clearly sleep apnea,” he said. The child underwent polysomnography and received continuous positive airway pressure treatment because he had 40 apneas in an hour.
During the evaluation, neurologists can recognize poor initial management of the injury, such as excessive bed rest or removal from activities. NSAID overuse also is a big problem. Emergency departments may tell patients to take ibuprofen every eight hours for five weeks, which can lead to rebound headaches, Dr. Taraman said.
Facilitate Recovery
Recognition of certain symptoms can inform the patient’s prognosis and suggest ways to speed recovery. For example, neurologists should look for vestibular dysfunction or balance problems and decide whether to address these symptoms. Neurologists also should check for and address cervical strain and ocular dysfunction. Treating severe convergence insufficiency or excess may help patients recover faster.
Anxiety and mood disorders suggest a prolonged recovery. Some patients develop adjustment disorder after concussion. “Interestingly, we see that patients who have more severe traumatic brain injury … are unaware of their deficits,” whereas high-functioning patients who feel slightly off perceive their deficits, which “causes a lot of discomfort for them,” he said.
Symptoms from concussions that involve assaults and litigation tend to take longer to resolve. Some patients’ symptoms persist until litigation ends, although typically not due to malingering but rather due to increased psychological stress.
Poor headache control, sleep disturbances, prior concussions, and a history of prolonged concussion recovery are other risk factors for prolonged recovery.
The Sport Concussion Assessment Tool 3 (SCAT3) is a free, standardized way of assessing symptoms. Developed as a sideline assessment tool, the SCAT3 also works well as a symptoms form, Dr. Taraman said. The tool includes a quick cognitive assessment and balance exam, and online video tutorials explain how to perform the assessment. After assessing a patient’s symptoms, including cognition, concentration, balance, and convergence insufficiency, “then you can decide, how … to triage the patient and start managing them.”
—Jake Remaly
Suggested Reading
Bressan S, Romanato S, Mion T, et al. Implementation of adapted PECARN decision rule for children with minor head injury in the pediatric emergency department. Acad Emerg Med. 2012;19(7):801-807.
Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009;374(9696):1160-1170.
Yengo-Kahn AM, Hale AT, Zalneraitis BH, et al. The Sport Concussion Assessment Tool: a systematic review. Neurosurg Focus. 2016;40(4):E6.
VANCOUVER—Initial pediatric concussion evaluations provide an opportunity to recognize premorbid conditions that may be exacerbated by the injury; address problems with prior management, such as excessive rest or NSAID overuse; and identify treatment approaches, according to a seminar delivered at the 45th Annual Meeting of the Child Neurology Society.
Neurologists also may decide whether imaging is warranted and note risk factors for prolonged recovery, said Sharief Taraman, MD, Director of the Children’s Concussion Program at Children’s Hospital of Orange County in Orange, California, and Assistant Clinical Professor of Pediatrics at the University of California, Irvine.
Imaging Likely Not Needed
In most cases, a CT scan is not necessary, Dr. Taraman said. He encouraged neurologists to work with their emergency department colleagues to ensure that patients only undergo CT scans when appropriate. His department uses Pediatric Emergency Care Applied Research Network (PECARN) criteria to determine when a CT scan is warranted. Many patients do not have signs of altered mental status in the emergency department, and “there is really no good reason to scan many of these kids,” he said. Patients also typically do not undergo MRI unless “a significant neurologic finding … suggests that there might have been a stronger mechanism of action.”
History taking is a vital component of initial management, and identifying premorbid conditions is a key factor, Dr. Taraman said. “What we have seen is that concussion symptoms act as a magnifying glass. If I have migraine and I get a concussion, my migraine will likely become exacerbated,” he said. Patients may also present for evaluation of concussion but have an alternate diagnosis that better explains their symptoms. For example, Dr. Taraman described a patient who had persistent symptoms following a concussion. “Listening to the story, it was clearly sleep apnea,” he said. The child underwent polysomnography and received continuous positive airway pressure treatment because he had 40 apneas in an hour.
During the evaluation, neurologists can recognize poor initial management of the injury, such as excessive bed rest or removal from activities. NSAID overuse also is a big problem. Emergency departments may tell patients to take ibuprofen every eight hours for five weeks, which can lead to rebound headaches, Dr. Taraman said.
Facilitate Recovery
Recognition of certain symptoms can inform the patient’s prognosis and suggest ways to speed recovery. For example, neurologists should look for vestibular dysfunction or balance problems and decide whether to address these symptoms. Neurologists also should check for and address cervical strain and ocular dysfunction. Treating severe convergence insufficiency or excess may help patients recover faster.
Anxiety and mood disorders suggest a prolonged recovery. Some patients develop adjustment disorder after concussion. “Interestingly, we see that patients who have more severe traumatic brain injury … are unaware of their deficits,” whereas high-functioning patients who feel slightly off perceive their deficits, which “causes a lot of discomfort for them,” he said.
Symptoms from concussions that involve assaults and litigation tend to take longer to resolve. Some patients’ symptoms persist until litigation ends, although typically not due to malingering but rather due to increased psychological stress.
Poor headache control, sleep disturbances, prior concussions, and a history of prolonged concussion recovery are other risk factors for prolonged recovery.
The Sport Concussion Assessment Tool 3 (SCAT3) is a free, standardized way of assessing symptoms. Developed as a sideline assessment tool, the SCAT3 also works well as a symptoms form, Dr. Taraman said. The tool includes a quick cognitive assessment and balance exam, and online video tutorials explain how to perform the assessment. After assessing a patient’s symptoms, including cognition, concentration, balance, and convergence insufficiency, “then you can decide, how … to triage the patient and start managing them.”
—Jake Remaly
Suggested Reading
Bressan S, Romanato S, Mion T, et al. Implementation of adapted PECARN decision rule for children with minor head injury in the pediatric emergency department. Acad Emerg Med. 2012;19(7):801-807.
Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009;374(9696):1160-1170.
Yengo-Kahn AM, Hale AT, Zalneraitis BH, et al. The Sport Concussion Assessment Tool: a systematic review. Neurosurg Focus. 2016;40(4):E6.

Parents seek easily understood public reporting of cardiac outcome measures
HOUSTON – Parents of children with congenital heart disease cite survival statistics, surgeon-specific experience, and complication rates as the three most important congenital heart surgery outcome measures to report publicly, results from a large survey show.
“Recently, an increasing demand for the public reporting of pediatric heart surgery outcomes has led to the development of several different reporting schemes, including a hospital star rating system and procedure-specific mortality data tables for the Society of Thoracic Surgeons benchmark operations,” study investigator Mallory L. Irons, MD, said during a press briefing at the annual meeting of the Society of Thoracic Surgeons. “However, despite the availability of these reporting schemes, there remain unanswered questions about the optimal format and content of public reporting for pediatric heart surgery outcomes.”

“These procedures have been determined to represent more homogenous patient groups,” she said. “How data [are] presented may be just as important as the data itself. Noticeably absent from these frameworks is parent input regarding the information that may be necessary to make an informed choice about their child’s care.
“Failure to consider this perspective may contribute to suboptimal reporting and misunderstanding of the data presented. The goal of the current study was to identify parent preferences regarding the content of pediatric heart surgery outcomes reports, specifically with respect to the type of data that is included as well as the optimal format for presentation of this data.”
She and her associates developed a 43-question survey for 1,862 parents of children born with heart defects. The parents were invited to participate through member lists from patient advocacy groups Mended Little Hearts, the Pediatric Congenital Heart Association, and Sisters by Heart, and from a cohort of patients who underwent surgical correction for an STS benchmark procedure at the Children’s Hospital of Philadelphia after Jan. 1, 2007.
Of the 1,862 parents, 1,281 (69%) provided complete responses for inclusion in the final analysis. The mean age of respondents was 37 years, 92% were mothers of children with congenital heart disease, and 92% were white. “Most reported household incomes in excess of $65,000 per year, but lower income households were also significantly represented,” Dr. Irons added. More than half of the children (57%) were diagnosed with CHD prenatally, 63% underwent an initial repair in the neonatal period, and 60% of families were referred to a cardiac surgical center by a physician, while 23% were transferred from their birth hospital.
When the respondents were asked to rank categories of outcome measures or other types of information to include in an optimal public reporting scheme on a scale of 1 (most important) to 8 (least important), they identified survival statistics, surgeons’ experience with congenital heart surgery, and complication rates as the three most important. These preferences were stable across differences in education levels, household incomes, and race or ethnicity, Dr. Irons said.
Presented with three display formats for hospital-specific mortality rates, most parents (89%) identified a numerical procedure-based approach as the best format, and more than half (60%) identified the hospital star rating system as the worst potential format to display mortality data. These preferences also were stable across differences in education levels, household incomes, and race or ethnicity.
Dr. Irons acknowledged certain limitations of the study, including its retrospective design, and the fact that it lacked input from parents who do not have Internet access. “Similarly, the availability of the survey in English only prevents non-native English speakers from contributing,” she said. “Finally, while we have identified what types of information parents want, we must acknowledge that small case numbers limit the presentation of certain types of data, such as surgeon-specific outcomes, in a statistically meaningful way.”
In her opinion, an optimal reporting system requires a common database in which to collect and analyze data, a robust methodology for risk adjustment, and a way to compare performance across a field that is inherently heterogeneous.
“The ideal public reporting system should be valid as well as easily understood by all stakeholders,” Dr. Irons concluded. “We must recognize that just because parents want certain data, [it] does not mean that we can provide it in a meaningful, statistically valid way. Perhaps the most important takeaway from our study is the importance of involving parents and other stakeholders in the design and planning of methodologies for public reporting of congenital heart surgery outcomes. Ultimately, the optimal platform will represent a melding of what parents want, and what is statistically meaningful and valid.”
Jeffrey P. Jacobs, MD, a pediatric heart surgeon at Johns Hopkins University, Baltimore, who also chairs the STS Workforce on National Databases, characterized the study as “an extremely important paper that examines the format and structure of how it might be best to share information about cardiac surgical outcomes with patients and their families.” He said the STS “has studied multiple different strategies, and currently we use a method where we report outcomes using a categorical system of star ratings and augment that with detailed specific data with point estimates for confidence intervals. We continue to study and explore better ways to share this information with our patients and with their families.”
Dr. Irons reported having no financial disclosures.
HOUSTON – Parents of children with congenital heart disease cite survival statistics, surgeon-specific experience, and complication rates as the three most important congenital heart surgery outcome measures to report publicly, results from a large survey show.
“Recently, an increasing demand for the public reporting of pediatric heart surgery outcomes has led to the development of several different reporting schemes, including a hospital star rating system and procedure-specific mortality data tables for the Society of Thoracic Surgeons benchmark operations,” study investigator Mallory L. Irons, MD, said during a press briefing at the annual meeting of the Society of Thoracic Surgeons. “However, despite the availability of these reporting schemes, there remain unanswered questions about the optimal format and content of public reporting for pediatric heart surgery outcomes.”
“These procedures have been determined to represent more homogenous patient groups,” she said. “How data [are] presented may be just as important as the data itself. Noticeably absent from these frameworks is parent input regarding the information that may be necessary to make an informed choice about their child’s care.
“Failure to consider this perspective may contribute to suboptimal reporting and misunderstanding of the data presented. The goal of the current study was to identify parent preferences regarding the content of pediatric heart surgery outcomes reports, specifically with respect to the type of data that is included as well as the optimal format for presentation of this data.”
She and her associates developed a 43-question survey for 1,862 parents of children born with heart defects. The parents were invited to participate through member lists from patient advocacy groups Mended Little Hearts, the Pediatric Congenital Heart Association, and Sisters by Heart, and from a cohort of patients who underwent surgical correction for an STS benchmark procedure at the Children’s Hospital of Philadelphia after Jan. 1, 2007.
Of the 1,862 parents, 1,281 (69%) provided complete responses for inclusion in the final analysis. The mean age of respondents was 37 years, 92% were mothers of children with congenital heart disease, and 92% were white. “Most reported household incomes in excess of $65,000 per year, but lower income households were also significantly represented,” Dr. Irons added. More than half of the children (57%) were diagnosed with CHD prenatally, 63% underwent an initial repair in the neonatal period, and 60% of families were referred to a cardiac surgical center by a physician, while 23% were transferred from their birth hospital.
When the respondents were asked to rank categories of outcome measures or other types of information to include in an optimal public reporting scheme on a scale of 1 (most important) to 8 (least important), they identified survival statistics, surgeons’ experience with congenital heart surgery, and complication rates as the three most important. These preferences were stable across differences in education levels, household incomes, and race or ethnicity, Dr. Irons said.
Presented with three display formats for hospital-specific mortality rates, most parents (89%) identified a numerical procedure-based approach as the best format, and more than half (60%) identified the hospital star rating system as the worst potential format to display mortality data. These preferences also were stable across differences in education levels, household incomes, and race or ethnicity.
Dr. Irons acknowledged certain limitations of the study, including its retrospective design, and the fact that it lacked input from parents who do not have Internet access. “Similarly, the availability of the survey in English only prevents non-native English speakers from contributing,” she said. “Finally, while we have identified what types of information parents want, we must acknowledge that small case numbers limit the presentation of certain types of data, such as surgeon-specific outcomes, in a statistically meaningful way.”
In her opinion, an optimal reporting system requires a common database in which to collect and analyze data, a robust methodology for risk adjustment, and a way to compare performance across a field that is inherently heterogeneous.
“The ideal public reporting system should be valid as well as easily understood by all stakeholders,” Dr. Irons concluded. “We must recognize that just because parents want certain data, [it] does not mean that we can provide it in a meaningful, statistically valid way. Perhaps the most important takeaway from our study is the importance of involving parents and other stakeholders in the design and planning of methodologies for public reporting of congenital heart surgery outcomes. Ultimately, the optimal platform will represent a melding of what parents want, and what is statistically meaningful and valid.”
Jeffrey P. Jacobs, MD, a pediatric heart surgeon at Johns Hopkins University, Baltimore, who also chairs the STS Workforce on National Databases, characterized the study as “an extremely important paper that examines the format and structure of how it might be best to share information about cardiac surgical outcomes with patients and their families.” He said the STS “has studied multiple different strategies, and currently we use a method where we report outcomes using a categorical system of star ratings and augment that with detailed specific data with point estimates for confidence intervals. We continue to study and explore better ways to share this information with our patients and with their families.”
Dr. Irons reported having no financial disclosures.
HOUSTON – Parents of children with congenital heart disease cite survival statistics, surgeon-specific experience, and complication rates as the three most important congenital heart surgery outcome measures to report publicly, results from a large survey show.
“Recently, an increasing demand for the public reporting of pediatric heart surgery outcomes has led to the development of several different reporting schemes, including a hospital star rating system and procedure-specific mortality data tables for the Society of Thoracic Surgeons benchmark operations,” study investigator Mallory L. Irons, MD, said during a press briefing at the annual meeting of the Society of Thoracic Surgeons. “However, despite the availability of these reporting schemes, there remain unanswered questions about the optimal format and content of public reporting for pediatric heart surgery outcomes.”
“These procedures have been determined to represent more homogenous patient groups,” she said. “How data [are] presented may be just as important as the data itself. Noticeably absent from these frameworks is parent input regarding the information that may be necessary to make an informed choice about their child’s care.
“Failure to consider this perspective may contribute to suboptimal reporting and misunderstanding of the data presented. The goal of the current study was to identify parent preferences regarding the content of pediatric heart surgery outcomes reports, specifically with respect to the type of data that is included as well as the optimal format for presentation of this data.”
She and her associates developed a 43-question survey for 1,862 parents of children born with heart defects. The parents were invited to participate through member lists from patient advocacy groups Mended Little Hearts, the Pediatric Congenital Heart Association, and Sisters by Heart, and from a cohort of patients who underwent surgical correction for an STS benchmark procedure at the Children’s Hospital of Philadelphia after Jan. 1, 2007.
Of the 1,862 parents, 1,281 (69%) provided complete responses for inclusion in the final analysis. The mean age of respondents was 37 years, 92% were mothers of children with congenital heart disease, and 92% were white. “Most reported household incomes in excess of $65,000 per year, but lower income households were also significantly represented,” Dr. Irons added. More than half of the children (57%) were diagnosed with CHD prenatally, 63% underwent an initial repair in the neonatal period, and 60% of families were referred to a cardiac surgical center by a physician, while 23% were transferred from their birth hospital.
When the respondents were asked to rank categories of outcome measures or other types of information to include in an optimal public reporting scheme on a scale of 1 (most important) to 8 (least important), they identified survival statistics, surgeons’ experience with congenital heart surgery, and complication rates as the three most important. These preferences were stable across differences in education levels, household incomes, and race or ethnicity, Dr. Irons said.
Presented with three display formats for hospital-specific mortality rates, most parents (89%) identified a numerical procedure-based approach as the best format, and more than half (60%) identified the hospital star rating system as the worst potential format to display mortality data. These preferences also were stable across differences in education levels, household incomes, and race or ethnicity.
Dr. Irons acknowledged certain limitations of the study, including its retrospective design, and the fact that it lacked input from parents who do not have Internet access. “Similarly, the availability of the survey in English only prevents non-native English speakers from contributing,” she said. “Finally, while we have identified what types of information parents want, we must acknowledge that small case numbers limit the presentation of certain types of data, such as surgeon-specific outcomes, in a statistically meaningful way.”
In her opinion, an optimal reporting system requires a common database in which to collect and analyze data, a robust methodology for risk adjustment, and a way to compare performance across a field that is inherently heterogeneous.
“The ideal public reporting system should be valid as well as easily understood by all stakeholders,” Dr. Irons concluded. “We must recognize that just because parents want certain data, [it] does not mean that we can provide it in a meaningful, statistically valid way. Perhaps the most important takeaway from our study is the importance of involving parents and other stakeholders in the design and planning of methodologies for public reporting of congenital heart surgery outcomes. Ultimately, the optimal platform will represent a melding of what parents want, and what is statistically meaningful and valid.”
Jeffrey P. Jacobs, MD, a pediatric heart surgeon at Johns Hopkins University, Baltimore, who also chairs the STS Workforce on National Databases, characterized the study as “an extremely important paper that examines the format and structure of how it might be best to share information about cardiac surgical outcomes with patients and their families.” He said the STS “has studied multiple different strategies, and currently we use a method where we report outcomes using a categorical system of star ratings and augment that with detailed specific data with point estimates for confidence intervals. We continue to study and explore better ways to share this information with our patients and with their families.”
Dr. Irons reported having no financial disclosures.
AT THE STS ANNUAL MEETING
Key clinical point:
Major finding: When parents of children with congenital heart disease were asked to rank categories of outcome measures or other types of information to include in an optimal public reporting scheme, they identified survival statistics, surgeons’ experience with congenital heart surgery, and complication rates as the three most important
Data source: A retrospective survey of 1,862 parents of children born with heart defects.
Disclosures: Dr. Irons reported having no financial disclosures.

Adolescents’ moderate use of digital technology tied to positive mental well-being
The moderate use of digital technology is not intrinsically harmful for adolescents and may be good for their mental well-being.
Those are the results of a study of 120,115 adolescents from the United Kingdom’s Department for Education National Pupil Database who were asked to complete questionnaires about their mental well-being and digital screen time, reported Andrew K. Przybylski, PhD, of the University of Oxford (England), and Netta Weinstein, PhD, of Cardiff (Wales) University.
The researchers began the study using what they called the “digital Goldilocks hypothesis.”
At the beginning of the study, Dr. Przybylski, Dr. Weinstein, and their team asked 15-year-olds from across England to complete the Warick-Edinburgh Mental Well-Being Scale, a 14-item self-report that seeks to measure factors such as happiness, life satisfaction, and psychological and social functioning. Meanwhile, the adolescents’ screen time was assessed through four questions asking about “watching films and other media, playing games, and using computers, and smartphones.”
About 20% of the participants reported a sum of more than 12 hours of digital engagement on weekdays, and 35% of the sample reported a total of more than 12 hours on weekend days. Girls reported spending more time using smartphones, using computers, and watching videos, and the boys devoted more time to playing computer and console games. Smartphones, however, were used more often daily among both girls and boys, Dr. Przybylski and Dr. Weinstein said.
After comparing the well-being and screen time data, the reseachers found that “the relations between screen time and mental well-being were either positive (P less than or equal to .001) or flat (P greater than .183), except for a negative link in the case of weekend smartphone use,” they said.
The investigators said their findings inform current guidelines that seek to limit adolescents’ technology use. “Future research and recommendations building on the Goldilocks hypothesis would be sensitive to the various types and contexts of media use and would be based on peaks and drops in well-being as well as other meaningful outcomes identified systematically,” they wrote.
Dr. Przybylski and Dr. Weinstein reported that they had no conflicts of interest to disclose.
The moderate use of digital technology is not intrinsically harmful for adolescents and may be good for their mental well-being.
Those are the results of a study of 120,115 adolescents from the United Kingdom’s Department for Education National Pupil Database who were asked to complete questionnaires about their mental well-being and digital screen time, reported Andrew K. Przybylski, PhD, of the University of Oxford (England), and Netta Weinstein, PhD, of Cardiff (Wales) University.
The researchers began the study using what they called the “digital Goldilocks hypothesis.”
At the beginning of the study, Dr. Przybylski, Dr. Weinstein, and their team asked 15-year-olds from across England to complete the Warick-Edinburgh Mental Well-Being Scale, a 14-item self-report that seeks to measure factors such as happiness, life satisfaction, and psychological and social functioning. Meanwhile, the adolescents’ screen time was assessed through four questions asking about “watching films and other media, playing games, and using computers, and smartphones.”
About 20% of the participants reported a sum of more than 12 hours of digital engagement on weekdays, and 35% of the sample reported a total of more than 12 hours on weekend days. Girls reported spending more time using smartphones, using computers, and watching videos, and the boys devoted more time to playing computer and console games. Smartphones, however, were used more often daily among both girls and boys, Dr. Przybylski and Dr. Weinstein said.
After comparing the well-being and screen time data, the reseachers found that “the relations between screen time and mental well-being were either positive (P less than or equal to .001) or flat (P greater than .183), except for a negative link in the case of weekend smartphone use,” they said.
The investigators said their findings inform current guidelines that seek to limit adolescents’ technology use. “Future research and recommendations building on the Goldilocks hypothesis would be sensitive to the various types and contexts of media use and would be based on peaks and drops in well-being as well as other meaningful outcomes identified systematically,” they wrote.
Dr. Przybylski and Dr. Weinstein reported that they had no conflicts of interest to disclose.
The moderate use of digital technology is not intrinsically harmful for adolescents and may be good for their mental well-being.
Those are the results of a study of 120,115 adolescents from the United Kingdom’s Department for Education National Pupil Database who were asked to complete questionnaires about their mental well-being and digital screen time, reported Andrew K. Przybylski, PhD, of the University of Oxford (England), and Netta Weinstein, PhD, of Cardiff (Wales) University.
The researchers began the study using what they called the “digital Goldilocks hypothesis.”
At the beginning of the study, Dr. Przybylski, Dr. Weinstein, and their team asked 15-year-olds from across England to complete the Warick-Edinburgh Mental Well-Being Scale, a 14-item self-report that seeks to measure factors such as happiness, life satisfaction, and psychological and social functioning. Meanwhile, the adolescents’ screen time was assessed through four questions asking about “watching films and other media, playing games, and using computers, and smartphones.”
About 20% of the participants reported a sum of more than 12 hours of digital engagement on weekdays, and 35% of the sample reported a total of more than 12 hours on weekend days. Girls reported spending more time using smartphones, using computers, and watching videos, and the boys devoted more time to playing computer and console games. Smartphones, however, were used more often daily among both girls and boys, Dr. Przybylski and Dr. Weinstein said.
After comparing the well-being and screen time data, the reseachers found that “the relations between screen time and mental well-being were either positive (P less than or equal to .001) or flat (P greater than .183), except for a negative link in the case of weekend smartphone use,” they said.
The investigators said their findings inform current guidelines that seek to limit adolescents’ technology use. “Future research and recommendations building on the Goldilocks hypothesis would be sensitive to the various types and contexts of media use and would be based on peaks and drops in well-being as well as other meaningful outcomes identified systematically,” they wrote.
Dr. Przybylski and Dr. Weinstein reported that they had no conflicts of interest to disclose.
FROM PSYCHOLOGICAL SCIENCE
Triclosan sutures halve surgical site infections in children
The use of triclosan-impregnated sutures reduced by half the incidence of surgical site infections in children, a large randomized study has determined.
Overall, the antibiotic-treated sutures cut the number of these infections by 52%, but they were particularly effective in reducing the risk of deep surgical site infections (SSIs), Marjo Renko, MD, wrote (Lancet Infect Dis. 2017;17[1]:50-7).
The study was conducted in clean wounds in healthy children and in a center that already had a very low rate of surgical site infections (just 5%) – showing that improvement is possible even in optimal care settings, wrote Dr. Renko, of the University of Oulu, Finland, and her colleagues.
“This randomized, controlled study shows that even in low-risk settings, where other prophylactic measures are available to use, triclosan-containing sutures effectively prevented the occurrence of SSIs in children,” the team wrote.
The study cohort comprised 1,633 children aged 7-17 who underwent surgery at a single Finnish hospital from 2010-2014. Most were there for planned surgery (87%); the remainder had emergency surgery. The most common surgical site was musculoskeletal (40%), followed by abdominal wall surgery (about 25%), and urogenital surgery (about 13%). The rest were intraabdominal or procedures on the nervous system, chest, and skin or subcutaneous tissue.
The children were randomized to either plain or triclosan-impregnated sutures. The primary outcome was the occurrence of a superficial or deep surgical site infection, based on Centers for Disease Control and Prevention criteria. The procedures were performed by 69 surgeons.
In a modified intent-to-treat analysis, a surgical site infection occurred in 3% of the triclosan-suture group (20 children) and in 5% of the control suture group (42 children). In the control group, these infections were most often of chest incisions (15%), followed by skin incisions (10%) and nervous system, intraabdominal, and musculoskeletal incisions (8% each). In the triclosan group, the most common site of infection was skin (10%), followed by musculoskeletal (4%), nervous system (2%), and urogenital and abdominal wall incisions (1% each).
Compared with control sutures, triclosan sutures reduced the overall risk of a surgical site infection by 52% (relative risk, 0.48; 95% confidence interval, 0.28-0.80). The number needed to treat to avoid one infection was 36.
The sutures were significantly more effective in reducing deep infections than superficial infections. Superficial infections occurred in 2% of the triclosan group (17) and 4% of the control group (28) – a risk reduction of 39% (RR, 0.61; 95% CI, 0.34-1.09) Deep infections occurred in less than 1% of the triclosan group (3) and 2% of the control group (14) – a risk reduction of 79% (RR, 0.21’ CI, 0.07-0.66).
Infections were associated with an increased incidence of wound dehiscence in the control group (6% vs. 4%), the need for additional antimicrobial agents (7% vs. 2%), and wound revisions (2% vs. less than 1%). Children in the control group also had more outpatient visits (8% vs. 4%) and were more often readmitted because of their infection (2% vs. 1%).
The authors noted that triclosan, in the setting of increased household use, “has raised concerns about the toxic effects of the drug on the human body. Observational studies have reported associations between triclosan exposures and altered thyroid hormone levels, body mass index, and waist circumference.”
Two Norwegian studies found that the drug was associated with inhalation allergies and seasonal allergies.
“Because of the agent’s suspected toxicity and to prevent further development of resistant bacteria, use of triclosan should be restricted and reserved only for medical procedures with adequate evidence,” they noted. However, “SSIs cause much morbidity and mortality after surgical procedures, and economic evaluations recommend the use of triclosan-containing material.”
Dr. Renko received grants from the Alma and K.A. Snellman Foundation, the Finnish Medical Foundation, and the Foundation for Pediatric Research.
msullivan@frontlinemedcom.com
On Twitter @Alz_Gal
The study by Dr. Marjo Renko and her colleagues is impressive in its sheer numbers, if not so much in its findings, Felix J. Hüttner, MD, and Markus K. Diener, MD, wrote in an accompanying editorial (Lancet Infect Dis. 2017;17[1]:3-4).
“We congratulate the authors on successfully doing a pragmatic, large-scale trial in a difficult setting; randomized controlled trials in children are known to pose specific challenges to researchers. However, the monocenter design raises some concerns about the generalizability of the results.”
Single-center trials can overestimate treatment effects, the colleagues noted. Dr. Renko’s conclusions don’t line up with their own metaanalysis of triclosan-containing sutures for abdominal wall closure. In it, three single-center trials found in favor of the triclosan sutures, but two multicenter trials did not.
The variation in infection rates in each type of surgery is a clue to the difficulty of a one-size-fits-all intervention like the treated sutures. “The differences between the intervention group and the control group vary widely by surgery type – for example, 0% versus 15% for thoracic surgery, compared with 1% versus 1% for surgery of the urinary system and genitals. Thus, triclosan-containing sutures might only be beneficial for specific types of operations and in our opinion, it cannot be concluded that triclosan-containing sutures reduce surgical site infections in all of these indications. Future trials should focus at individual types of pediatric surgery to evaluate a potential beneficial effect.”
Dr. Hüttner and Dr. Diener are surgeons at the University of Heidelberg, Germany. Dr. Hüttner had no financial disclosures. Dr. Diener has received grants from Johnson & Johnson Medical Limited.
The study by Dr. Marjo Renko and her colleagues is impressive in its sheer numbers, if not so much in its findings, Felix J. Hüttner, MD, and Markus K. Diener, MD, wrote in an accompanying editorial (Lancet Infect Dis. 2017;17[1]:3-4).
“We congratulate the authors on successfully doing a pragmatic, large-scale trial in a difficult setting; randomized controlled trials in children are known to pose specific challenges to researchers. However, the monocenter design raises some concerns about the generalizability of the results.”
Single-center trials can overestimate treatment effects, the colleagues noted. Dr. Renko’s conclusions don’t line up with their own metaanalysis of triclosan-containing sutures for abdominal wall closure. In it, three single-center trials found in favor of the triclosan sutures, but two multicenter trials did not.
The variation in infection rates in each type of surgery is a clue to the difficulty of a one-size-fits-all intervention like the treated sutures. “The differences between the intervention group and the control group vary widely by surgery type – for example, 0% versus 15% for thoracic surgery, compared with 1% versus 1% for surgery of the urinary system and genitals. Thus, triclosan-containing sutures might only be beneficial for specific types of operations and in our opinion, it cannot be concluded that triclosan-containing sutures reduce surgical site infections in all of these indications. Future trials should focus at individual types of pediatric surgery to evaluate a potential beneficial effect.”
Dr. Hüttner and Dr. Diener are surgeons at the University of Heidelberg, Germany. Dr. Hüttner had no financial disclosures. Dr. Diener has received grants from Johnson & Johnson Medical Limited.
The study by Dr. Marjo Renko and her colleagues is impressive in its sheer numbers, if not so much in its findings, Felix J. Hüttner, MD, and Markus K. Diener, MD, wrote in an accompanying editorial (Lancet Infect Dis. 2017;17[1]:3-4).
“We congratulate the authors on successfully doing a pragmatic, large-scale trial in a difficult setting; randomized controlled trials in children are known to pose specific challenges to researchers. However, the monocenter design raises some concerns about the generalizability of the results.”
Single-center trials can overestimate treatment effects, the colleagues noted. Dr. Renko’s conclusions don’t line up with their own metaanalysis of triclosan-containing sutures for abdominal wall closure. In it, three single-center trials found in favor of the triclosan sutures, but two multicenter trials did not.
The variation in infection rates in each type of surgery is a clue to the difficulty of a one-size-fits-all intervention like the treated sutures. “The differences between the intervention group and the control group vary widely by surgery type – for example, 0% versus 15% for thoracic surgery, compared with 1% versus 1% for surgery of the urinary system and genitals. Thus, triclosan-containing sutures might only be beneficial for specific types of operations and in our opinion, it cannot be concluded that triclosan-containing sutures reduce surgical site infections in all of these indications. Future trials should focus at individual types of pediatric surgery to evaluate a potential beneficial effect.”
Dr. Hüttner and Dr. Diener are surgeons at the University of Heidelberg, Germany. Dr. Hüttner had no financial disclosures. Dr. Diener has received grants from Johnson & Johnson Medical Limited.
The use of triclosan-impregnated sutures reduced by half the incidence of surgical site infections in children, a large randomized study has determined.
Overall, the antibiotic-treated sutures cut the number of these infections by 52%, but they were particularly effective in reducing the risk of deep surgical site infections (SSIs), Marjo Renko, MD, wrote (Lancet Infect Dis. 2017;17[1]:50-7).
The study was conducted in clean wounds in healthy children and in a center that already had a very low rate of surgical site infections (just 5%) – showing that improvement is possible even in optimal care settings, wrote Dr. Renko, of the University of Oulu, Finland, and her colleagues.
“This randomized, controlled study shows that even in low-risk settings, where other prophylactic measures are available to use, triclosan-containing sutures effectively prevented the occurrence of SSIs in children,” the team wrote.
The study cohort comprised 1,633 children aged 7-17 who underwent surgery at a single Finnish hospital from 2010-2014. Most were there for planned surgery (87%); the remainder had emergency surgery. The most common surgical site was musculoskeletal (40%), followed by abdominal wall surgery (about 25%), and urogenital surgery (about 13%). The rest were intraabdominal or procedures on the nervous system, chest, and skin or subcutaneous tissue.
The children were randomized to either plain or triclosan-impregnated sutures. The primary outcome was the occurrence of a superficial or deep surgical site infection, based on Centers for Disease Control and Prevention criteria. The procedures were performed by 69 surgeons.
In a modified intent-to-treat analysis, a surgical site infection occurred in 3% of the triclosan-suture group (20 children) and in 5% of the control suture group (42 children). In the control group, these infections were most often of chest incisions (15%), followed by skin incisions (10%) and nervous system, intraabdominal, and musculoskeletal incisions (8% each). In the triclosan group, the most common site of infection was skin (10%), followed by musculoskeletal (4%), nervous system (2%), and urogenital and abdominal wall incisions (1% each).
Compared with control sutures, triclosan sutures reduced the overall risk of a surgical site infection by 52% (relative risk, 0.48; 95% confidence interval, 0.28-0.80). The number needed to treat to avoid one infection was 36.
The sutures were significantly more effective in reducing deep infections than superficial infections. Superficial infections occurred in 2% of the triclosan group (17) and 4% of the control group (28) – a risk reduction of 39% (RR, 0.61; 95% CI, 0.34-1.09) Deep infections occurred in less than 1% of the triclosan group (3) and 2% of the control group (14) – a risk reduction of 79% (RR, 0.21’ CI, 0.07-0.66).
Infections were associated with an increased incidence of wound dehiscence in the control group (6% vs. 4%), the need for additional antimicrobial agents (7% vs. 2%), and wound revisions (2% vs. less than 1%). Children in the control group also had more outpatient visits (8% vs. 4%) and were more often readmitted because of their infection (2% vs. 1%).
The authors noted that triclosan, in the setting of increased household use, “has raised concerns about the toxic effects of the drug on the human body. Observational studies have reported associations between triclosan exposures and altered thyroid hormone levels, body mass index, and waist circumference.”
Two Norwegian studies found that the drug was associated with inhalation allergies and seasonal allergies.
“Because of the agent’s suspected toxicity and to prevent further development of resistant bacteria, use of triclosan should be restricted and reserved only for medical procedures with adequate evidence,” they noted. However, “SSIs cause much morbidity and mortality after surgical procedures, and economic evaluations recommend the use of triclosan-containing material.”
Dr. Renko received grants from the Alma and K.A. Snellman Foundation, the Finnish Medical Foundation, and the Foundation for Pediatric Research.
msullivan@frontlinemedcom.com
On Twitter @Alz_Gal
The use of triclosan-impregnated sutures reduced by half the incidence of surgical site infections in children, a large randomized study has determined.
Overall, the antibiotic-treated sutures cut the number of these infections by 52%, but they were particularly effective in reducing the risk of deep surgical site infections (SSIs), Marjo Renko, MD, wrote (Lancet Infect Dis. 2017;17[1]:50-7).
The study was conducted in clean wounds in healthy children and in a center that already had a very low rate of surgical site infections (just 5%) – showing that improvement is possible even in optimal care settings, wrote Dr. Renko, of the University of Oulu, Finland, and her colleagues.
“This randomized, controlled study shows that even in low-risk settings, where other prophylactic measures are available to use, triclosan-containing sutures effectively prevented the occurrence of SSIs in children,” the team wrote.
The study cohort comprised 1,633 children aged 7-17 who underwent surgery at a single Finnish hospital from 2010-2014. Most were there for planned surgery (87%); the remainder had emergency surgery. The most common surgical site was musculoskeletal (40%), followed by abdominal wall surgery (about 25%), and urogenital surgery (about 13%). The rest were intraabdominal or procedures on the nervous system, chest, and skin or subcutaneous tissue.
The children were randomized to either plain or triclosan-impregnated sutures. The primary outcome was the occurrence of a superficial or deep surgical site infection, based on Centers for Disease Control and Prevention criteria. The procedures were performed by 69 surgeons.
In a modified intent-to-treat analysis, a surgical site infection occurred in 3% of the triclosan-suture group (20 children) and in 5% of the control suture group (42 children). In the control group, these infections were most often of chest incisions (15%), followed by skin incisions (10%) and nervous system, intraabdominal, and musculoskeletal incisions (8% each). In the triclosan group, the most common site of infection was skin (10%), followed by musculoskeletal (4%), nervous system (2%), and urogenital and abdominal wall incisions (1% each).
Compared with control sutures, triclosan sutures reduced the overall risk of a surgical site infection by 52% (relative risk, 0.48; 95% confidence interval, 0.28-0.80). The number needed to treat to avoid one infection was 36.
The sutures were significantly more effective in reducing deep infections than superficial infections. Superficial infections occurred in 2% of the triclosan group (17) and 4% of the control group (28) – a risk reduction of 39% (RR, 0.61; 95% CI, 0.34-1.09) Deep infections occurred in less than 1% of the triclosan group (3) and 2% of the control group (14) – a risk reduction of 79% (RR, 0.21’ CI, 0.07-0.66).
Infections were associated with an increased incidence of wound dehiscence in the control group (6% vs. 4%), the need for additional antimicrobial agents (7% vs. 2%), and wound revisions (2% vs. less than 1%). Children in the control group also had more outpatient visits (8% vs. 4%) and were more often readmitted because of their infection (2% vs. 1%).
The authors noted that triclosan, in the setting of increased household use, “has raised concerns about the toxic effects of the drug on the human body. Observational studies have reported associations between triclosan exposures and altered thyroid hormone levels, body mass index, and waist circumference.”
Two Norwegian studies found that the drug was associated with inhalation allergies and seasonal allergies.
“Because of the agent’s suspected toxicity and to prevent further development of resistant bacteria, use of triclosan should be restricted and reserved only for medical procedures with adequate evidence,” they noted. However, “SSIs cause much morbidity and mortality after surgical procedures, and economic evaluations recommend the use of triclosan-containing material.”
Dr. Renko received grants from the Alma and K.A. Snellman Foundation, the Finnish Medical Foundation, and the Foundation for Pediatric Research.
msullivan@frontlinemedcom.com
On Twitter @Alz_Gal
FROM LANCET INFECTIOUS DISEASES
Key clinical point:
Major finding: Overall, the sutures were associated with a 52% decrease in SSIs.
Data source: The study randomized 1,633 children undergoing surgery to the triclosan sutures or to a control suture.
Disclosures: Dr. Renko received grants from the Alma and K.A. Snellman Foundation, the Finnish Medical Foundation, and the Foundation for Pediatric Research.
Marijuana calms children with autism
SAN FRANCISCO – About once a month, Antonio Y. Hardan, MD, and his colleagues at the Stanford (Calif.) University Autism and Developmental Disorders Clinic see an autistic child who is using or being prescribed marijuana.
“There are two types or responses we see with marijuana,” said Dr. Hardan, director of the clinic. “Most of the time, it calms the kid down for 2 or 3 hours, which is what you’d expect from marijuana. In one out of 10, I am hearing that parents see improvements in the core features of autism. We have several families who would swear by marijuana, but then 4 or 6 months later, they will change their mind and say it’s not helping as much.

Marijuana is just one of many alternatives families and doctors are trying to improve upon the usual medications and therapies for autism; the range of options being tried speaks to the desperation and frustration of families looking for help. There’s no home run so far; the common denominator for alternatives is anecdotal support but little evidence. Stanford has tried to address the evidence gap and continues to do so.
In 2012, for instance, Dr. Hardan and his colleagues reported a 33 patient study that found that N-acetylcysteine (NAC) – another hopeful candidate in recent years – might curb irritability (Biol Psychiatry. 2012 Jun 1;71[11]:956-61).
The tricky part about NAC is that it’s a dietary supplement, so you can’t be sure of what you’re getting in the store. There were questions at the talk about dose and formulations.
“The one we used in the study is made by BioAdvantex,” a Canadian company. “That’s the one that worked for us. One of the advantages is that every dose is wrapped individually.” NAC is an antioxidant, “so if you expose [it] to oxygen or light, it will get oxidized, and over time be less effective,” said Dr. Hardan, also a professor of psychiatry and behavioral sciences at the university.
Most of the time, NAC is very well tolerated, with only a little bit of flatulence and upset stomach.
Dr. Hardan and his colleagues started with 900 mg in one dose once a day for 4 weeks, then one dose twice a day for 4 weeks, followed by one dose three times daily, in children aged 2-12 years old. With experience, they are going faster now, cutting the 4 week interval to 2. “Some people are [even] more aggressive, which is okay,” he said.
Propranolol is another fashionable option, prescribed by a lot of doctors.
It’s not a new option; about 20 years ago, “we used it in very high dosages, 700-800 mg a day for self-injurious behavior. People wonder how you can go that high; above a dose of 200 mg, there is what we call an ‘escape phenomena’ where the heart will stop responding, and the effects on blood pressure and pulse are minimal,” Dr. Hardan said.
Interest in propranolol over the past 5 years has expanded to anxiety, sensory abnormalities, and other non-specific autism symptoms. “Unfortunately, there are no clinical trials to support that,” he said. The only evidence so far is from a functional MRI study in adults that suggested a little bit more efficient processing on a language task; further investigation is underway.
A lot of parents also are asking for oxytocin, and doctors are prescribing it. Someone in the audience wondered whether it had a role in everyday practice.
“Not at this time,” Dr. Hardan said. “I would suggest waiting a little bit until” results are reported from an ongoing trial. They are due soon, and there might be a subgroup of kids who benefit. Oxytocin seemed to help all-comers recognize facial cues.
Arginine vasopressin might do that, too, and be more specific for autism; Stanford is planning a study to look into it.
Attendees also wanted to know what to do about sleep problems, a common issue in autism.
“I’m aggressive in the treatment of insomnia, especially in single-parent households, because if the kid isn’t sleeping, the parent isn’t sleeping” and they may get irritable and moody, which raises the risk of abuse, Dr. Hardan said.
He starts with melatonin, 1 mg in the evening, and increases it by 1 mg every week to hit a target of 6 mg per night. He hasn’t seen much benefit of going higher. It’s important to remember that melatonin might take up to a week to see the full effect.
If melatonin fails, Dr. Hardan goes up the ladder. Diphenhydramine (Benadryl), benzodiazepines, trazodone (Oleptro), and mirtazapine (Remeron) are among the options. Rarely, there’s a need for quetiapine (Seroquel).
To counter benzodiazepine disinhibition, he asks parents to try them on a good day at home, so the effect of environmental stressors like going to the dentist can be divided out from the drug.
Dr. Hardan cautioned that there is “no evidence at this time to support the use of” lamotrigine (Lamictal). “Please don’t use it; somebody will end up developing” Stevens-Johnson syndrome. “It will be difficult to defend against that.”
Dr. Hardan is an adviser for Roche.
SAN FRANCISCO – About once a month, Antonio Y. Hardan, MD, and his colleagues at the Stanford (Calif.) University Autism and Developmental Disorders Clinic see an autistic child who is using or being prescribed marijuana.
“There are two types or responses we see with marijuana,” said Dr. Hardan, director of the clinic. “Most of the time, it calms the kid down for 2 or 3 hours, which is what you’d expect from marijuana. In one out of 10, I am hearing that parents see improvements in the core features of autism. We have several families who would swear by marijuana, but then 4 or 6 months later, they will change their mind and say it’s not helping as much.
Marijuana is just one of many alternatives families and doctors are trying to improve upon the usual medications and therapies for autism; the range of options being tried speaks to the desperation and frustration of families looking for help. There’s no home run so far; the common denominator for alternatives is anecdotal support but little evidence. Stanford has tried to address the evidence gap and continues to do so.
In 2012, for instance, Dr. Hardan and his colleagues reported a 33 patient study that found that N-acetylcysteine (NAC) – another hopeful candidate in recent years – might curb irritability (Biol Psychiatry. 2012 Jun 1;71[11]:956-61).
The tricky part about NAC is that it’s a dietary supplement, so you can’t be sure of what you’re getting in the store. There were questions at the talk about dose and formulations.
“The one we used in the study is made by BioAdvantex,” a Canadian company. “That’s the one that worked for us. One of the advantages is that every dose is wrapped individually.” NAC is an antioxidant, “so if you expose [it] to oxygen or light, it will get oxidized, and over time be less effective,” said Dr. Hardan, also a professor of psychiatry and behavioral sciences at the university.
Most of the time, NAC is very well tolerated, with only a little bit of flatulence and upset stomach.
Dr. Hardan and his colleagues started with 900 mg in one dose once a day for 4 weeks, then one dose twice a day for 4 weeks, followed by one dose three times daily, in children aged 2-12 years old. With experience, they are going faster now, cutting the 4 week interval to 2. “Some people are [even] more aggressive, which is okay,” he said.
Propranolol is another fashionable option, prescribed by a lot of doctors.
It’s not a new option; about 20 years ago, “we used it in very high dosages, 700-800 mg a day for self-injurious behavior. People wonder how you can go that high; above a dose of 200 mg, there is what we call an ‘escape phenomena’ where the heart will stop responding, and the effects on blood pressure and pulse are minimal,” Dr. Hardan said.
Interest in propranolol over the past 5 years has expanded to anxiety, sensory abnormalities, and other non-specific autism symptoms. “Unfortunately, there are no clinical trials to support that,” he said. The only evidence so far is from a functional MRI study in adults that suggested a little bit more efficient processing on a language task; further investigation is underway.
A lot of parents also are asking for oxytocin, and doctors are prescribing it. Someone in the audience wondered whether it had a role in everyday practice.
“Not at this time,” Dr. Hardan said. “I would suggest waiting a little bit until” results are reported from an ongoing trial. They are due soon, and there might be a subgroup of kids who benefit. Oxytocin seemed to help all-comers recognize facial cues.
Arginine vasopressin might do that, too, and be more specific for autism; Stanford is planning a study to look into it.
Attendees also wanted to know what to do about sleep problems, a common issue in autism.
“I’m aggressive in the treatment of insomnia, especially in single-parent households, because if the kid isn’t sleeping, the parent isn’t sleeping” and they may get irritable and moody, which raises the risk of abuse, Dr. Hardan said.
He starts with melatonin, 1 mg in the evening, and increases it by 1 mg every week to hit a target of 6 mg per night. He hasn’t seen much benefit of going higher. It’s important to remember that melatonin might take up to a week to see the full effect.
If melatonin fails, Dr. Hardan goes up the ladder. Diphenhydramine (Benadryl), benzodiazepines, trazodone (Oleptro), and mirtazapine (Remeron) are among the options. Rarely, there’s a need for quetiapine (Seroquel).
To counter benzodiazepine disinhibition, he asks parents to try them on a good day at home, so the effect of environmental stressors like going to the dentist can be divided out from the drug.
Dr. Hardan cautioned that there is “no evidence at this time to support the use of” lamotrigine (Lamictal). “Please don’t use it; somebody will end up developing” Stevens-Johnson syndrome. “It will be difficult to defend against that.”
Dr. Hardan is an adviser for Roche.
SAN FRANCISCO – About once a month, Antonio Y. Hardan, MD, and his colleagues at the Stanford (Calif.) University Autism and Developmental Disorders Clinic see an autistic child who is using or being prescribed marijuana.
“There are two types or responses we see with marijuana,” said Dr. Hardan, director of the clinic. “Most of the time, it calms the kid down for 2 or 3 hours, which is what you’d expect from marijuana. In one out of 10, I am hearing that parents see improvements in the core features of autism. We have several families who would swear by marijuana, but then 4 or 6 months later, they will change their mind and say it’s not helping as much.
Marijuana is just one of many alternatives families and doctors are trying to improve upon the usual medications and therapies for autism; the range of options being tried speaks to the desperation and frustration of families looking for help. There’s no home run so far; the common denominator for alternatives is anecdotal support but little evidence. Stanford has tried to address the evidence gap and continues to do so.
In 2012, for instance, Dr. Hardan and his colleagues reported a 33 patient study that found that N-acetylcysteine (NAC) – another hopeful candidate in recent years – might curb irritability (Biol Psychiatry. 2012 Jun 1;71[11]:956-61).
The tricky part about NAC is that it’s a dietary supplement, so you can’t be sure of what you’re getting in the store. There were questions at the talk about dose and formulations.
“The one we used in the study is made by BioAdvantex,” a Canadian company. “That’s the one that worked for us. One of the advantages is that every dose is wrapped individually.” NAC is an antioxidant, “so if you expose [it] to oxygen or light, it will get oxidized, and over time be less effective,” said Dr. Hardan, also a professor of psychiatry and behavioral sciences at the university.
Most of the time, NAC is very well tolerated, with only a little bit of flatulence and upset stomach.
Dr. Hardan and his colleagues started with 900 mg in one dose once a day for 4 weeks, then one dose twice a day for 4 weeks, followed by one dose three times daily, in children aged 2-12 years old. With experience, they are going faster now, cutting the 4 week interval to 2. “Some people are [even] more aggressive, which is okay,” he said.
Propranolol is another fashionable option, prescribed by a lot of doctors.
It’s not a new option; about 20 years ago, “we used it in very high dosages, 700-800 mg a day for self-injurious behavior. People wonder how you can go that high; above a dose of 200 mg, there is what we call an ‘escape phenomena’ where the heart will stop responding, and the effects on blood pressure and pulse are minimal,” Dr. Hardan said.
Interest in propranolol over the past 5 years has expanded to anxiety, sensory abnormalities, and other non-specific autism symptoms. “Unfortunately, there are no clinical trials to support that,” he said. The only evidence so far is from a functional MRI study in adults that suggested a little bit more efficient processing on a language task; further investigation is underway.
A lot of parents also are asking for oxytocin, and doctors are prescribing it. Someone in the audience wondered whether it had a role in everyday practice.
“Not at this time,” Dr. Hardan said. “I would suggest waiting a little bit until” results are reported from an ongoing trial. They are due soon, and there might be a subgroup of kids who benefit. Oxytocin seemed to help all-comers recognize facial cues.
Arginine vasopressin might do that, too, and be more specific for autism; Stanford is planning a study to look into it.
Attendees also wanted to know what to do about sleep problems, a common issue in autism.
“I’m aggressive in the treatment of insomnia, especially in single-parent households, because if the kid isn’t sleeping, the parent isn’t sleeping” and they may get irritable and moody, which raises the risk of abuse, Dr. Hardan said.
He starts with melatonin, 1 mg in the evening, and increases it by 1 mg every week to hit a target of 6 mg per night. He hasn’t seen much benefit of going higher. It’s important to remember that melatonin might take up to a week to see the full effect.
If melatonin fails, Dr. Hardan goes up the ladder. Diphenhydramine (Benadryl), benzodiazepines, trazodone (Oleptro), and mirtazapine (Remeron) are among the options. Rarely, there’s a need for quetiapine (Seroquel).
To counter benzodiazepine disinhibition, he asks parents to try them on a good day at home, so the effect of environmental stressors like going to the dentist can be divided out from the drug.
Dr. Hardan cautioned that there is “no evidence at this time to support the use of” lamotrigine (Lamictal). “Please don’t use it; somebody will end up developing” Stevens-Johnson syndrome. “It will be difficult to defend against that.”
Dr. Hardan is an adviser for Roche.
EXPERT ANALYSIS AT THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE
Psychiatric Comorbidities Are Common in Newly Diagnosed Pediatric Epilepsy
HOUSTON—Nearly one in three children diagnosed with new-onset epilepsy presents with psychiatric diagnoses at the onset, according to research presented at the 70th Annual Meeting of the American Epilepsy Society.
This finding “tells us that when kids are coming in, even if they are only having psychiatric symptoms at their onset of epilepsy, they should be referred for some treatment to help them possibly mitigate the development of these psychiatric diagnoses in the first year,” said Julia Doss, PsyD, Pediatric Psychologist at the Minnesota Epilepsy Group in Saint Paul.

About three years ago, the Minnesota Epilepsy Group, a private practice group that consults with the United Hospital and Children’s Hospitals and Clinics of Minnesota, launched a New Onset Pediatric Epilepsy (NOPE) clinic. At this clinic, referred patients undergo a psychologic evaluation, neuropsychologic testing, and medical evaluation in the same day. Psychologic assessment measures include the Clinical Interview with parent and patient, the Strengths and Difficulties Questionnaire (SDQ), and the Revised Children’s Anxiety and Depression Scale (RCADS).
Researchers evaluated 96 patients in the clinic who had presented for their first NOPE clinic visit within eight weeks of their epilepsy diagnosis. More than half were male, and patients ranged in age from 3 to 18. Dr. Doss and her colleagues separated the children into the following three groups: ages 3 to 6 (group 1), ages 7 to 11 (group 2), and ages 12 to 18 (group 3). Based on the Clinical Interview, none of the patients in group 1 screened positive for depression or anxiety, but 16% met criteria for some other behavioral disorder. However, among patients in group 2, the percentages who met criteria for depression, anxiety, and other behavioral disorders were 13%, 25%, and 13%, respectively. The corresponding percentages for patients in group 3 were 29%, 38%, and 10%.
Of the 96 patients evaluated, 64 parents completed all of the questions on the SDQ. The researchers observed significant correlations between parent response and diagnoses assigned on the Clinical Interview for behavior diagnoses and anxiety diagnoses) but not for depression diagnoses.
“Despite the correlations on both behavior and anxiety responses and clinical diagnoses assigned, parents still only reported significant concerns in about half of the children that were given diagnoses,” said Dr. Doss.
The comparison of RCADS scores between parent and child demonstrated moderate to strong correlation on the following scales: separation anxiety, generalized anxiety, obsessive/compulsive, and depression.
Small sample size was a key limitation in this study, said Dr. Doss. “Early evaluation or at least screening is necessary in all of our kids who present with an epilepsy diagnosis, because more than 30% develop psychiatric disorders within the first year of their diagnosis,” said Dr. Doss. “That’s one in three, so if we can start to better evaluate that early and get them funneled into treatment early, we might be able to prevent some of these problems from becoming lifelong issues.”
—Doug Brunk
Suggested Reading
Asato MR, Doss JL, Piloplys S. Clinic-friendly screening for cognitive and mental health problems in school-aged youth with epilepsy. Epilepsy Behav. 2015;48:97-102.
Piloplys S, Doss J, Siddarth P, et al. Risk factors for comorbid psychopathology in youth with psychogenic nonepileptic seizures. Seizure. 2016;38:32-37.
HOUSTON—Nearly one in three children diagnosed with new-onset epilepsy presents with psychiatric diagnoses at the onset, according to research presented at the 70th Annual Meeting of the American Epilepsy Society.
This finding “tells us that when kids are coming in, even if they are only having psychiatric symptoms at their onset of epilepsy, they should be referred for some treatment to help them possibly mitigate the development of these psychiatric diagnoses in the first year,” said Julia Doss, PsyD, Pediatric Psychologist at the Minnesota Epilepsy Group in Saint Paul.
About three years ago, the Minnesota Epilepsy Group, a private practice group that consults with the United Hospital and Children’s Hospitals and Clinics of Minnesota, launched a New Onset Pediatric Epilepsy (NOPE) clinic. At this clinic, referred patients undergo a psychologic evaluation, neuropsychologic testing, and medical evaluation in the same day. Psychologic assessment measures include the Clinical Interview with parent and patient, the Strengths and Difficulties Questionnaire (SDQ), and the Revised Children’s Anxiety and Depression Scale (RCADS).
Researchers evaluated 96 patients in the clinic who had presented for their first NOPE clinic visit within eight weeks of their epilepsy diagnosis. More than half were male, and patients ranged in age from 3 to 18. Dr. Doss and her colleagues separated the children into the following three groups: ages 3 to 6 (group 1), ages 7 to 11 (group 2), and ages 12 to 18 (group 3). Based on the Clinical Interview, none of the patients in group 1 screened positive for depression or anxiety, but 16% met criteria for some other behavioral disorder. However, among patients in group 2, the percentages who met criteria for depression, anxiety, and other behavioral disorders were 13%, 25%, and 13%, respectively. The corresponding percentages for patients in group 3 were 29%, 38%, and 10%.
Of the 96 patients evaluated, 64 parents completed all of the questions on the SDQ. The researchers observed significant correlations between parent response and diagnoses assigned on the Clinical Interview for behavior diagnoses and anxiety diagnoses) but not for depression diagnoses.
“Despite the correlations on both behavior and anxiety responses and clinical diagnoses assigned, parents still only reported significant concerns in about half of the children that were given diagnoses,” said Dr. Doss.
The comparison of RCADS scores between parent and child demonstrated moderate to strong correlation on the following scales: separation anxiety, generalized anxiety, obsessive/compulsive, and depression.
Small sample size was a key limitation in this study, said Dr. Doss. “Early evaluation or at least screening is necessary in all of our kids who present with an epilepsy diagnosis, because more than 30% develop psychiatric disorders within the first year of their diagnosis,” said Dr. Doss. “That’s one in three, so if we can start to better evaluate that early and get them funneled into treatment early, we might be able to prevent some of these problems from becoming lifelong issues.”
—Doug Brunk
Suggested Reading
Asato MR, Doss JL, Piloplys S. Clinic-friendly screening for cognitive and mental health problems in school-aged youth with epilepsy. Epilepsy Behav. 2015;48:97-102.
Piloplys S, Doss J, Siddarth P, et al. Risk factors for comorbid psychopathology in youth with psychogenic nonepileptic seizures. Seizure. 2016;38:32-37.
HOUSTON—Nearly one in three children diagnosed with new-onset epilepsy presents with psychiatric diagnoses at the onset, according to research presented at the 70th Annual Meeting of the American Epilepsy Society.
This finding “tells us that when kids are coming in, even if they are only having psychiatric symptoms at their onset of epilepsy, they should be referred for some treatment to help them possibly mitigate the development of these psychiatric diagnoses in the first year,” said Julia Doss, PsyD, Pediatric Psychologist at the Minnesota Epilepsy Group in Saint Paul.
About three years ago, the Minnesota Epilepsy Group, a private practice group that consults with the United Hospital and Children’s Hospitals and Clinics of Minnesota, launched a New Onset Pediatric Epilepsy (NOPE) clinic. At this clinic, referred patients undergo a psychologic evaluation, neuropsychologic testing, and medical evaluation in the same day. Psychologic assessment measures include the Clinical Interview with parent and patient, the Strengths and Difficulties Questionnaire (SDQ), and the Revised Children’s Anxiety and Depression Scale (RCADS).
Researchers evaluated 96 patients in the clinic who had presented for their first NOPE clinic visit within eight weeks of their epilepsy diagnosis. More than half were male, and patients ranged in age from 3 to 18. Dr. Doss and her colleagues separated the children into the following three groups: ages 3 to 6 (group 1), ages 7 to 11 (group 2), and ages 12 to 18 (group 3). Based on the Clinical Interview, none of the patients in group 1 screened positive for depression or anxiety, but 16% met criteria for some other behavioral disorder. However, among patients in group 2, the percentages who met criteria for depression, anxiety, and other behavioral disorders were 13%, 25%, and 13%, respectively. The corresponding percentages for patients in group 3 were 29%, 38%, and 10%.
Of the 96 patients evaluated, 64 parents completed all of the questions on the SDQ. The researchers observed significant correlations between parent response and diagnoses assigned on the Clinical Interview for behavior diagnoses and anxiety diagnoses) but not for depression diagnoses.
“Despite the correlations on both behavior and anxiety responses and clinical diagnoses assigned, parents still only reported significant concerns in about half of the children that were given diagnoses,” said Dr. Doss.
The comparison of RCADS scores between parent and child demonstrated moderate to strong correlation on the following scales: separation anxiety, generalized anxiety, obsessive/compulsive, and depression.
Small sample size was a key limitation in this study, said Dr. Doss. “Early evaluation or at least screening is necessary in all of our kids who present with an epilepsy diagnosis, because more than 30% develop psychiatric disorders within the first year of their diagnosis,” said Dr. Doss. “That’s one in three, so if we can start to better evaluate that early and get them funneled into treatment early, we might be able to prevent some of these problems from becoming lifelong issues.”
—Doug Brunk
Suggested Reading
Asato MR, Doss JL, Piloplys S. Clinic-friendly screening for cognitive and mental health problems in school-aged youth with epilepsy. Epilepsy Behav. 2015;48:97-102.
Piloplys S, Doss J, Siddarth P, et al. Risk factors for comorbid psychopathology in youth with psychogenic nonepileptic seizures. Seizure. 2016;38:32-37.

{kind=link}
Donor CAR T cells bridge to HSCT in infants with ALL

treated with UCART19
Photo courtesy of GOSH
New research suggests that “universal,” donor-derived, chimeric antigen receptor (CAR) T cells may be a viable treatment option for very young children who do not have sufficient healthy T cells for autologous CAR T-cell therapy.
The universal CAR T-cell therapy, known as UCART19, was given to 2 infants with relapsed/refractory B-cell acute lymphoblastic leukemia (ALL) who had previously
exhausted all other treatment options.
Both infants achieved remission after UCART19 and were able to proceed to transplant.
Both were still alive and leukemia-free at last follow-up—12 months and 18 months after UCART19, respectively.
Waseem Qasim, MBBS, PhD, of University College London’s Institute of Child Health and Great Ormond Street Hospital (GOSH) in London, UK, and his colleagues reported these results in Science Translational Medicine.
About the therapy
UCART19 consists of donor T cells modified using transcription activator-like effector nucleases. The cells are programmed to target CD19 and be insensitive to alemtuzumab. That way, a patient can receive alemtuzumab to prevent rejection of HLA-mismatched cells.
UCART19 was under development by Cellectis but is now being developed by Servier and Pfizer Inc. Pfizer has exclusive rights to develop and commercialize UCART19 in the US, while Servier retains exclusive rights for all other countries.
In Science Translational Medicine, Dr Qasim and his colleagues reported results in the first patients ever treated with UCART19. That research was funded, in part, by Cellectis.
Subject 1
The first patient was an 11-month-old, mixed-race infant with high-risk, t(11;19), CD19+ B-ALL. She had already failed chemotherapy, an allogeneic hematopoietic stem cell transplant (HSCT), and blinatumomab.
Prior to UCART19, she received a dose of vincristine and asparaginase and 7 days of dexamethasone, followed by cytoreduction with fludarabine, cyclophosphamide, and alemtuzumab. She then received a single dose of UCART19 (4.6 × 106/kg).
The patient had neutrophil recovery by day 30, although this was dependent on granulocyte colony-stimulating factor. After that, she developed multilineage cytopenia that persisted until she underwent a second allogeneic HSCT.
Prior to the second HSCT, the patient achieved cytogenetic and molecular remission but also developed grade 2 skin graft-vs-host disease. This was managed with systemic steroids.
The child received rituximab and conditioning with antithymocyte globulin, fludarabine, cyclophosphamide, thiotepa, and total body irradiation, followed by an HSCT from the original mismatched, unrelated donor.
The child achieved a complete remission and has remained minimal residual disease-negative, with full donor chimerism and normalized lymphocyte profiles, at 18 months after UCART19.
Results with this patient were previously reported by GOSH in November 2015 and at the 2015 ASH Annual Meeting.
Subject 2
The second patient was a 16-month-old Caucasian infant who had been diagnosed at 4 weeks of age with high-risk, congenital, mixed lineage leukemia–rearranged B-ALL.
She had already undergone HSCT from a matched, unrelated donor but relapsed. She did not respond to subsequent blinatumomab.
After these failed treatments, the patient received fludarabine, cyclophosphamide, and alemtuzumab, followed by a single infusion of UCART19 (4.0 × 106/kg).
She developed an erythematous rash after treatment, but this was immediately responsive to topical steroids.
The child achieved donor-derived neutrophil recovery and went on to receive a transplant from the same matched, unrelated donor as her previous HSCT.
The child received the transplant within 10 weeks of UCART19 therapy, after receiving rituximab and conditioning with antithymocyte globulin, fludarabine, cyclophosphamide, and total body irradiation.
At 12 months after UCART19, the child remains minimal residual disease-negative and “clinically well.”
“Both infants who have had this treatment have been at home for some time and are doing well,” Dr Qasim said. “We continue to monitor them closely, and, while we have reduced the frequency of their hospital visits and checks, we will still need to keep an eye on them for some time.”
Dr Qasim added that there are phase 1 trials of UCART19 underway for children and adults with chronic lymphocytic leukemia and acute lymphoblastic leukemia. ![]()
treated with UCART19
Photo courtesy of GOSH
New research suggests that “universal,” donor-derived, chimeric antigen receptor (CAR) T cells may be a viable treatment option for very young children who do not have sufficient healthy T cells for autologous CAR T-cell therapy.
The universal CAR T-cell therapy, known as UCART19, was given to 2 infants with relapsed/refractory B-cell acute lymphoblastic leukemia (ALL) who had previously
exhausted all other treatment options.
Both infants achieved remission after UCART19 and were able to proceed to transplant.
Both were still alive and leukemia-free at last follow-up—12 months and 18 months after UCART19, respectively.
Waseem Qasim, MBBS, PhD, of University College London’s Institute of Child Health and Great Ormond Street Hospital (GOSH) in London, UK, and his colleagues reported these results in Science Translational Medicine.
About the therapy
UCART19 consists of donor T cells modified using transcription activator-like effector nucleases. The cells are programmed to target CD19 and be insensitive to alemtuzumab. That way, a patient can receive alemtuzumab to prevent rejection of HLA-mismatched cells.
UCART19 was under development by Cellectis but is now being developed by Servier and Pfizer Inc. Pfizer has exclusive rights to develop and commercialize UCART19 in the US, while Servier retains exclusive rights for all other countries.
In Science Translational Medicine, Dr Qasim and his colleagues reported results in the first patients ever treated with UCART19. That research was funded, in part, by Cellectis.
Subject 1
The first patient was an 11-month-old, mixed-race infant with high-risk, t(11;19), CD19+ B-ALL. She had already failed chemotherapy, an allogeneic hematopoietic stem cell transplant (HSCT), and blinatumomab.
Prior to UCART19, she received a dose of vincristine and asparaginase and 7 days of dexamethasone, followed by cytoreduction with fludarabine, cyclophosphamide, and alemtuzumab. She then received a single dose of UCART19 (4.6 × 106/kg).
The patient had neutrophil recovery by day 30, although this was dependent on granulocyte colony-stimulating factor. After that, she developed multilineage cytopenia that persisted until she underwent a second allogeneic HSCT.
Prior to the second HSCT, the patient achieved cytogenetic and molecular remission but also developed grade 2 skin graft-vs-host disease. This was managed with systemic steroids.
The child received rituximab and conditioning with antithymocyte globulin, fludarabine, cyclophosphamide, thiotepa, and total body irradiation, followed by an HSCT from the original mismatched, unrelated donor.
The child achieved a complete remission and has remained minimal residual disease-negative, with full donor chimerism and normalized lymphocyte profiles, at 18 months after UCART19.
Results with this patient were previously reported by GOSH in November 2015 and at the 2015 ASH Annual Meeting.
Subject 2
The second patient was a 16-month-old Caucasian infant who had been diagnosed at 4 weeks of age with high-risk, congenital, mixed lineage leukemia–rearranged B-ALL.
She had already undergone HSCT from a matched, unrelated donor but relapsed. She did not respond to subsequent blinatumomab.
After these failed treatments, the patient received fludarabine, cyclophosphamide, and alemtuzumab, followed by a single infusion of UCART19 (4.0 × 106/kg).
She developed an erythematous rash after treatment, but this was immediately responsive to topical steroids.
The child achieved donor-derived neutrophil recovery and went on to receive a transplant from the same matched, unrelated donor as her previous HSCT.
The child received the transplant within 10 weeks of UCART19 therapy, after receiving rituximab and conditioning with antithymocyte globulin, fludarabine, cyclophosphamide, and total body irradiation.
At 12 months after UCART19, the child remains minimal residual disease-negative and “clinically well.”
“Both infants who have had this treatment have been at home for some time and are doing well,” Dr Qasim said. “We continue to monitor them closely, and, while we have reduced the frequency of their hospital visits and checks, we will still need to keep an eye on them for some time.”
Dr Qasim added that there are phase 1 trials of UCART19 underway for children and adults with chronic lymphocytic leukemia and acute lymphoblastic leukemia. ![]()
treated with UCART19
Photo courtesy of GOSH
New research suggests that “universal,” donor-derived, chimeric antigen receptor (CAR) T cells may be a viable treatment option for very young children who do not have sufficient healthy T cells for autologous CAR T-cell therapy.
The universal CAR T-cell therapy, known as UCART19, was given to 2 infants with relapsed/refractory B-cell acute lymphoblastic leukemia (ALL) who had previously
exhausted all other treatment options.
Both infants achieved remission after UCART19 and were able to proceed to transplant.
Both were still alive and leukemia-free at last follow-up—12 months and 18 months after UCART19, respectively.
Waseem Qasim, MBBS, PhD, of University College London’s Institute of Child Health and Great Ormond Street Hospital (GOSH) in London, UK, and his colleagues reported these results in Science Translational Medicine.
About the therapy
UCART19 consists of donor T cells modified using transcription activator-like effector nucleases. The cells are programmed to target CD19 and be insensitive to alemtuzumab. That way, a patient can receive alemtuzumab to prevent rejection of HLA-mismatched cells.
UCART19 was under development by Cellectis but is now being developed by Servier and Pfizer Inc. Pfizer has exclusive rights to develop and commercialize UCART19 in the US, while Servier retains exclusive rights for all other countries.
In Science Translational Medicine, Dr Qasim and his colleagues reported results in the first patients ever treated with UCART19. That research was funded, in part, by Cellectis.
Subject 1
The first patient was an 11-month-old, mixed-race infant with high-risk, t(11;19), CD19+ B-ALL. She had already failed chemotherapy, an allogeneic hematopoietic stem cell transplant (HSCT), and blinatumomab.
Prior to UCART19, she received a dose of vincristine and asparaginase and 7 days of dexamethasone, followed by cytoreduction with fludarabine, cyclophosphamide, and alemtuzumab. She then received a single dose of UCART19 (4.6 × 106/kg).
The patient had neutrophil recovery by day 30, although this was dependent on granulocyte colony-stimulating factor. After that, she developed multilineage cytopenia that persisted until she underwent a second allogeneic HSCT.
Prior to the second HSCT, the patient achieved cytogenetic and molecular remission but also developed grade 2 skin graft-vs-host disease. This was managed with systemic steroids.
The child received rituximab and conditioning with antithymocyte globulin, fludarabine, cyclophosphamide, thiotepa, and total body irradiation, followed by an HSCT from the original mismatched, unrelated donor.
The child achieved a complete remission and has remained minimal residual disease-negative, with full donor chimerism and normalized lymphocyte profiles, at 18 months after UCART19.
Results with this patient were previously reported by GOSH in November 2015 and at the 2015 ASH Annual Meeting.
Subject 2
The second patient was a 16-month-old Caucasian infant who had been diagnosed at 4 weeks of age with high-risk, congenital, mixed lineage leukemia–rearranged B-ALL.
She had already undergone HSCT from a matched, unrelated donor but relapsed. She did not respond to subsequent blinatumomab.
After these failed treatments, the patient received fludarabine, cyclophosphamide, and alemtuzumab, followed by a single infusion of UCART19 (4.0 × 106/kg).
She developed an erythematous rash after treatment, but this was immediately responsive to topical steroids.
The child achieved donor-derived neutrophil recovery and went on to receive a transplant from the same matched, unrelated donor as her previous HSCT.
The child received the transplant within 10 weeks of UCART19 therapy, after receiving rituximab and conditioning with antithymocyte globulin, fludarabine, cyclophosphamide, and total body irradiation.
At 12 months after UCART19, the child remains minimal residual disease-negative and “clinically well.”
“Both infants who have had this treatment have been at home for some time and are doing well,” Dr Qasim said. “We continue to monitor them closely, and, while we have reduced the frequency of their hospital visits and checks, we will still need to keep an eye on them for some time.”
Dr Qasim added that there are phase 1 trials of UCART19 underway for children and adults with chronic lymphocytic leukemia and acute lymphoblastic leukemia. ![]()