User login
Congenital melanocytic nevi in the very young tend to be benign
Histopathology findings of cytologic atypia, architectural disorder, and pagetoid spread are common in congenital melanocytic nevi (CMN) of all sizes in children aged 0-35 months, and tend to have benign outcomes, according to a retrospective study.
Emily A. Simons, MPH, and her associates at Boston Children’s Hospital studied 197 nevi in 179 patients with an average age of 14 months (range, 4 days to 35 months); 51% were female. Of those, 80% had skin types I-II, and 90% were white. The majority of the lesions involved the head or trunk and were predominantly medium in size, and 58% had a projected adult size of 1.5-10 cm. The study was retrospective; cases had been diagnosed between 1993 and 2013.
Cytologic atypia, architectural disorder, and pagetoid spread were the most frequent features – they were present in 73% of nevi and were closely associated. Combined histologic patterns of a blue nevus, spindle and Spitz nevus, or a deep penetrating nevus were identified in 40% of CMN. Proliferative nodules occurred in 5% of nevi.
Clinical outcomes were available for 130 patients, including 26 with large CMN and 8 with proliferative nodules. The children were alive and had not been diagnosed with melanoma at a mean follow-up of a mean of 8.4 years (range, 7 months to 21.3 years), even though margins of the last excision were positive in 41% of all CMN and in 77% of large CMN.
Malignant transformation of CMN certainly should be recognized, but the morbidity of overdiagnosis also needs to be considered. “Excision of larger CMN might require serial excisions under general anesthesia, the use of tissue expanders, and grafts,” Dr. Simons and her associates said.
Among the limitations of this study were that the majority of patients were white, so the results may not translate to children with darker skin types, they noted.
“The diagnosis of malignant melanoma should be made with great caution in this population,” they concluded, pointing out that the histopathologic features alone (cytologic atypia, architectural disorder, and pagetoid spread) “should not be interpreted as evidence for potential malignant behavior or serve as grounds for further excision.”
Read more in the Journal of the American Academy of Dermatology (2017 May;76[5]941-7).
The authors had no relevant financial disorders.
Histopathology findings of cytologic atypia, architectural disorder, and pagetoid spread are common in congenital melanocytic nevi (CMN) of all sizes in children aged 0-35 months, and tend to have benign outcomes, according to a retrospective study.
Emily A. Simons, MPH, and her associates at Boston Children’s Hospital studied 197 nevi in 179 patients with an average age of 14 months (range, 4 days to 35 months); 51% were female. Of those, 80% had skin types I-II, and 90% were white. The majority of the lesions involved the head or trunk and were predominantly medium in size, and 58% had a projected adult size of 1.5-10 cm. The study was retrospective; cases had been diagnosed between 1993 and 2013.
Cytologic atypia, architectural disorder, and pagetoid spread were the most frequent features – they were present in 73% of nevi and were closely associated. Combined histologic patterns of a blue nevus, spindle and Spitz nevus, or a deep penetrating nevus were identified in 40% of CMN. Proliferative nodules occurred in 5% of nevi.
Clinical outcomes were available for 130 patients, including 26 with large CMN and 8 with proliferative nodules. The children were alive and had not been diagnosed with melanoma at a mean follow-up of a mean of 8.4 years (range, 7 months to 21.3 years), even though margins of the last excision were positive in 41% of all CMN and in 77% of large CMN.
Malignant transformation of CMN certainly should be recognized, but the morbidity of overdiagnosis also needs to be considered. “Excision of larger CMN might require serial excisions under general anesthesia, the use of tissue expanders, and grafts,” Dr. Simons and her associates said.
Among the limitations of this study were that the majority of patients were white, so the results may not translate to children with darker skin types, they noted.
“The diagnosis of malignant melanoma should be made with great caution in this population,” they concluded, pointing out that the histopathologic features alone (cytologic atypia, architectural disorder, and pagetoid spread) “should not be interpreted as evidence for potential malignant behavior or serve as grounds for further excision.”
Read more in the Journal of the American Academy of Dermatology (2017 May;76[5]941-7).
The authors had no relevant financial disorders.
Histopathology findings of cytologic atypia, architectural disorder, and pagetoid spread are common in congenital melanocytic nevi (CMN) of all sizes in children aged 0-35 months, and tend to have benign outcomes, according to a retrospective study.
Emily A. Simons, MPH, and her associates at Boston Children’s Hospital studied 197 nevi in 179 patients with an average age of 14 months (range, 4 days to 35 months); 51% were female. Of those, 80% had skin types I-II, and 90% were white. The majority of the lesions involved the head or trunk and were predominantly medium in size, and 58% had a projected adult size of 1.5-10 cm. The study was retrospective; cases had been diagnosed between 1993 and 2013.
Cytologic atypia, architectural disorder, and pagetoid spread were the most frequent features – they were present in 73% of nevi and were closely associated. Combined histologic patterns of a blue nevus, spindle and Spitz nevus, or a deep penetrating nevus were identified in 40% of CMN. Proliferative nodules occurred in 5% of nevi.
Clinical outcomes were available for 130 patients, including 26 with large CMN and 8 with proliferative nodules. The children were alive and had not been diagnosed with melanoma at a mean follow-up of a mean of 8.4 years (range, 7 months to 21.3 years), even though margins of the last excision were positive in 41% of all CMN and in 77% of large CMN.
Malignant transformation of CMN certainly should be recognized, but the morbidity of overdiagnosis also needs to be considered. “Excision of larger CMN might require serial excisions under general anesthesia, the use of tissue expanders, and grafts,” Dr. Simons and her associates said.
Among the limitations of this study were that the majority of patients were white, so the results may not translate to children with darker skin types, they noted.
“The diagnosis of malignant melanoma should be made with great caution in this population,” they concluded, pointing out that the histopathologic features alone (cytologic atypia, architectural disorder, and pagetoid spread) “should not be interpreted as evidence for potential malignant behavior or serve as grounds for further excision.”
Read more in the Journal of the American Academy of Dermatology (2017 May;76[5]941-7).
The authors had no relevant financial disorders.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Infliximab safe for recently vaccinated Kawasaki patients
Infliximab is safe to use in infants and young children with Kawasaki disease (KD) who have recently received live viral vaccinations, reported Aaron M. Lee, MS, and his associates at Rady Children’s Hospital-San Diego.
The study included 38 children, aged either less than 18 months or 4-6 years, who received either a 5 mg/kg or a 10 mg/kg dose of infliximab within 90 days of receiving a live vaccination of MMR, varicella-zoster virus, or rotavirus. During a 90-day follow-up period, no serious infections requiring antimicrobial therapy or hospitalization were reported. A single patient who received an MMR/VZV vaccine 42 days before infliximab treatment developed urticaria 15 minutes after the infliximab transfusion began, which was resolved with hydroxyzine.
“The data presented here suggest that a single dose of infliximab can be safely administered to acute KD patients regardless of recent live virus vaccination,” the investigators concluded.
Find the full report in the Pediatric Infectious Disease Journal (2017 Apr;36(4):435-7).
Infliximab is safe to use in infants and young children with Kawasaki disease (KD) who have recently received live viral vaccinations, reported Aaron M. Lee, MS, and his associates at Rady Children’s Hospital-San Diego.
The study included 38 children, aged either less than 18 months or 4-6 years, who received either a 5 mg/kg or a 10 mg/kg dose of infliximab within 90 days of receiving a live vaccination of MMR, varicella-zoster virus, or rotavirus. During a 90-day follow-up period, no serious infections requiring antimicrobial therapy or hospitalization were reported. A single patient who received an MMR/VZV vaccine 42 days before infliximab treatment developed urticaria 15 minutes after the infliximab transfusion began, which was resolved with hydroxyzine.
“The data presented here suggest that a single dose of infliximab can be safely administered to acute KD patients regardless of recent live virus vaccination,” the investigators concluded.
Find the full report in the Pediatric Infectious Disease Journal (2017 Apr;36(4):435-7).
Infliximab is safe to use in infants and young children with Kawasaki disease (KD) who have recently received live viral vaccinations, reported Aaron M. Lee, MS, and his associates at Rady Children’s Hospital-San Diego.
The study included 38 children, aged either less than 18 months or 4-6 years, who received either a 5 mg/kg or a 10 mg/kg dose of infliximab within 90 days of receiving a live vaccination of MMR, varicella-zoster virus, or rotavirus. During a 90-day follow-up period, no serious infections requiring antimicrobial therapy or hospitalization were reported. A single patient who received an MMR/VZV vaccine 42 days before infliximab treatment developed urticaria 15 minutes after the infliximab transfusion began, which was resolved with hydroxyzine.
“The data presented here suggest that a single dose of infliximab can be safely administered to acute KD patients regardless of recent live virus vaccination,” the investigators concluded.
Find the full report in the Pediatric Infectious Disease Journal (2017 Apr;36(4):435-7).
FROM THE PEDIATRIC INFECTIOUS DISEASE JOURNAL
Clearer heads are a fuzzy subject
Those of you who were in high school or middle school in 1987, when the DSM II-R first included “Attention Deficit Disorder With and Without Hyperactivity” for the first time, missed out on the “discovery,” and subsequent commercialization, of a condition that had been percolating under physicians’ noses for hundreds of years.
You may have wondered what primary care physicians did with their time before they were inundated with requests for evaluations and medications to treat ADHD. You may not realize that we didn’t always have ADHD specialists to help us or several dozen stimulant concoctions from which to choose. In the beginning, ADHD specialists had to invent themselves while the pharmaceutical companies scrambled to meet the demand for drugs that were longer lasting and more palatable.

The increasing popularity of professional contact sports is probably what we have to thank for sharpening this focus on head injury. I suspect that, for the general population, there are no more concussions occurring today than there were 50 years ago. However, in the subgroup of professional and elite college athletes, the players’ increasing speed, size, and flagrant ignorance of the rules have resulted in more significant head injuries. When a highly paid megastar athlete must sit out key games, the management of his head injury generates a lot of attention and discussion.
I am sure that there also has been an increase in concussions among young women who now have more opportunities to participate in contact sports. However, I suspect that most of the apparent increase in the diagnosis among high school and younger athletes of both sexes is primarily the result of heightened awareness. I don’t know of data to support or refute this opinion.
I may be wrong about lack of a real increase in concussion injuries, but there can be no arguing about the explosion in the number of clinics and providers who advertise themselves as concussion specialists. Neurologists, psychologists, chiropractors, orthopedists, and sports medicine practitioners and trainers all have climbed on the bandwagon to satisfy the demand generated by this country’s new concussion awareness.
The problem is that, just as in the early days after the “discovery” of ADHD, the science behind much of the advice and management strategies for concussion just isn’t there. For example, resting the brain after a head injury sounds like a good idea. After all, it works for a torn hamstring. However, “sounds like” and “is” are two very different things.
In an excellent article in this publication (“Spotlight shifts to active treatment for concussions,” by Christine Kilgore), I found some comforting news that concussion management may be taking some baby steps into the realm of evidence-based decision management. The original results came from a pediatric population, but it now appears that prolonged rest, which is routinely recommended, can be counterproductive in many concussed patients. The physicians quoted in this article suggest that their experience is pointing to the need for active management in patients with a variety of postconcussion symptoms. Brian Hainline, MD, a clinical professor of neurology at New York University and Indiana University, Indianapolis, observes, “It’s rare that prolonged rest is the answer. Look at stroke – you don’t have patients resting indefinitely. You have to get their nervous systems re-engaged.”
Of course, the science is still lagging behind and the observations by the physicians quoted in this article are based on small series, but their agreement deserves our attention. I urge you to take a look at this article to get an idea of where the management of concussion appears to be going. Not surprisingly, no two concussion patients are the same, and their management should be tailored to their needs. Reliance on overly simplistic guidelines not only doesn’t work but can do harm. It’s that old Hippocratic Oath thing again.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Those of you who were in high school or middle school in 1987, when the DSM II-R first included “Attention Deficit Disorder With and Without Hyperactivity” for the first time, missed out on the “discovery,” and subsequent commercialization, of a condition that had been percolating under physicians’ noses for hundreds of years.
You may have wondered what primary care physicians did with their time before they were inundated with requests for evaluations and medications to treat ADHD. You may not realize that we didn’t always have ADHD specialists to help us or several dozen stimulant concoctions from which to choose. In the beginning, ADHD specialists had to invent themselves while the pharmaceutical companies scrambled to meet the demand for drugs that were longer lasting and more palatable.
The increasing popularity of professional contact sports is probably what we have to thank for sharpening this focus on head injury. I suspect that, for the general population, there are no more concussions occurring today than there were 50 years ago. However, in the subgroup of professional and elite college athletes, the players’ increasing speed, size, and flagrant ignorance of the rules have resulted in more significant head injuries. When a highly paid megastar athlete must sit out key games, the management of his head injury generates a lot of attention and discussion.
I am sure that there also has been an increase in concussions among young women who now have more opportunities to participate in contact sports. However, I suspect that most of the apparent increase in the diagnosis among high school and younger athletes of both sexes is primarily the result of heightened awareness. I don’t know of data to support or refute this opinion.
I may be wrong about lack of a real increase in concussion injuries, but there can be no arguing about the explosion in the number of clinics and providers who advertise themselves as concussion specialists. Neurologists, psychologists, chiropractors, orthopedists, and sports medicine practitioners and trainers all have climbed on the bandwagon to satisfy the demand generated by this country’s new concussion awareness.
The problem is that, just as in the early days after the “discovery” of ADHD, the science behind much of the advice and management strategies for concussion just isn’t there. For example, resting the brain after a head injury sounds like a good idea. After all, it works for a torn hamstring. However, “sounds like” and “is” are two very different things.
In an excellent article in this publication (“Spotlight shifts to active treatment for concussions,” by Christine Kilgore), I found some comforting news that concussion management may be taking some baby steps into the realm of evidence-based decision management. The original results came from a pediatric population, but it now appears that prolonged rest, which is routinely recommended, can be counterproductive in many concussed patients. The physicians quoted in this article suggest that their experience is pointing to the need for active management in patients with a variety of postconcussion symptoms. Brian Hainline, MD, a clinical professor of neurology at New York University and Indiana University, Indianapolis, observes, “It’s rare that prolonged rest is the answer. Look at stroke – you don’t have patients resting indefinitely. You have to get their nervous systems re-engaged.”
Of course, the science is still lagging behind and the observations by the physicians quoted in this article are based on small series, but their agreement deserves our attention. I urge you to take a look at this article to get an idea of where the management of concussion appears to be going. Not surprisingly, no two concussion patients are the same, and their management should be tailored to their needs. Reliance on overly simplistic guidelines not only doesn’t work but can do harm. It’s that old Hippocratic Oath thing again.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Those of you who were in high school or middle school in 1987, when the DSM II-R first included “Attention Deficit Disorder With and Without Hyperactivity” for the first time, missed out on the “discovery,” and subsequent commercialization, of a condition that had been percolating under physicians’ noses for hundreds of years.
You may have wondered what primary care physicians did with their time before they were inundated with requests for evaluations and medications to treat ADHD. You may not realize that we didn’t always have ADHD specialists to help us or several dozen stimulant concoctions from which to choose. In the beginning, ADHD specialists had to invent themselves while the pharmaceutical companies scrambled to meet the demand for drugs that were longer lasting and more palatable.
The increasing popularity of professional contact sports is probably what we have to thank for sharpening this focus on head injury. I suspect that, for the general population, there are no more concussions occurring today than there were 50 years ago. However, in the subgroup of professional and elite college athletes, the players’ increasing speed, size, and flagrant ignorance of the rules have resulted in more significant head injuries. When a highly paid megastar athlete must sit out key games, the management of his head injury generates a lot of attention and discussion.
I am sure that there also has been an increase in concussions among young women who now have more opportunities to participate in contact sports. However, I suspect that most of the apparent increase in the diagnosis among high school and younger athletes of both sexes is primarily the result of heightened awareness. I don’t know of data to support or refute this opinion.
I may be wrong about lack of a real increase in concussion injuries, but there can be no arguing about the explosion in the number of clinics and providers who advertise themselves as concussion specialists. Neurologists, psychologists, chiropractors, orthopedists, and sports medicine practitioners and trainers all have climbed on the bandwagon to satisfy the demand generated by this country’s new concussion awareness.
The problem is that, just as in the early days after the “discovery” of ADHD, the science behind much of the advice and management strategies for concussion just isn’t there. For example, resting the brain after a head injury sounds like a good idea. After all, it works for a torn hamstring. However, “sounds like” and “is” are two very different things.
In an excellent article in this publication (“Spotlight shifts to active treatment for concussions,” by Christine Kilgore), I found some comforting news that concussion management may be taking some baby steps into the realm of evidence-based decision management. The original results came from a pediatric population, but it now appears that prolonged rest, which is routinely recommended, can be counterproductive in many concussed patients. The physicians quoted in this article suggest that their experience is pointing to the need for active management in patients with a variety of postconcussion symptoms. Brian Hainline, MD, a clinical professor of neurology at New York University and Indiana University, Indianapolis, observes, “It’s rare that prolonged rest is the answer. Look at stroke – you don’t have patients resting indefinitely. You have to get their nervous systems re-engaged.”
Of course, the science is still lagging behind and the observations by the physicians quoted in this article are based on small series, but their agreement deserves our attention. I urge you to take a look at this article to get an idea of where the management of concussion appears to be going. Not surprisingly, no two concussion patients are the same, and their management should be tailored to their needs. Reliance on overly simplistic guidelines not only doesn’t work but can do harm. It’s that old Hippocratic Oath thing again.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Fat City
“Honey, does this town make me look fat?”
“Yes, Dear, I’m afraid it does.”
No, that really wasn’t a typo in the first line. I intended to type “town” and not “gown.” A recent article by Dionysus Powell in healthcareinamerica.us has prompted me to think a bit more about the relationship between obesity and the communities we inhabit (“Fit Cities vs. Fat Cities – What available data can tell us about the difference in lifestyle and obesity between cities,” by Dionysus Powell, March 28, 2017). The author is a biotech researcher who has collected readily available Centers for Disease Control and Prevention data on body mass index (BMI) and self-reported sedentary behavior in almost 200 U.S. cities. He then sliced and diced these numbers with each cities’ walkability score, which is a crude measure of how easily citizens and visitors on foot can reach a variety of destinations such as shops, schools, churches, libraries, and municipal offices. You can easily find your own town’s score by going to walkscore.com.
Not surprisingly, the author discovered that “differences in obesity rates between cities can largely be explained by differences in physical activity.” Of course, there is a point at which a community has sufficient walkable infrastructure so that its obesity rate is a result of the citizens choosing not to walk rather than the community’s failure to provide pedestrians with enough connectivity to do their daily errands on foot. That threshold point appears to be a walkability score of 50, yet Mr. Powell observes that most American cities fail to reach even that minimum.
Although rich people tend to have better health outcomes than poor people, and there is a “general trend for richer cities to be more physically active than poorer cities,” Mr. Powell could not find a relationship between a city’s median income and its walkability.
If, like most of us, you have been frustrated in your efforts to lower the BMI of your patients, it may be time to emerge from the confines of your office and take a look at your town’s walkability score. If it is less than 50, you and your fellow concerned citizens and officials have some work to do. It may mean advocating for improved pedestrian infrastructure and/or dismantling the physical and zoning barriers to pedestrian connectivity. For example, maybe your community should be adding more pedestrian-activated crossing signals or tapping into federal and state safe routes to school programs or adopting zoning ordinances that require sidewalks in all new developments.
Here in Brunswick, we have a very enviable walkability score of 87, meaning “most errands can be accomplished on foot.” We have a bicycle and pedestrian advisory committee that reports to the town council and works with the town engineer to advocate for infrastructure improvements that encourage pedestrian connectivity. However, funding these improvements in walkability is always a challenge. But as the analysis in this recent study suggestions, our biggest challenge continues to be encouraging our citizens to take advantage of our existing pedestrian infrastructure.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
“Honey, does this town make me look fat?”
“Yes, Dear, I’m afraid it does.”
No, that really wasn’t a typo in the first line. I intended to type “town” and not “gown.” A recent article by Dionysus Powell in healthcareinamerica.us has prompted me to think a bit more about the relationship between obesity and the communities we inhabit (“Fit Cities vs. Fat Cities – What available data can tell us about the difference in lifestyle and obesity between cities,” by Dionysus Powell, March 28, 2017). The author is a biotech researcher who has collected readily available Centers for Disease Control and Prevention data on body mass index (BMI) and self-reported sedentary behavior in almost 200 U.S. cities. He then sliced and diced these numbers with each cities’ walkability score, which is a crude measure of how easily citizens and visitors on foot can reach a variety of destinations such as shops, schools, churches, libraries, and municipal offices. You can easily find your own town’s score by going to walkscore.com.
Not surprisingly, the author discovered that “differences in obesity rates between cities can largely be explained by differences in physical activity.” Of course, there is a point at which a community has sufficient walkable infrastructure so that its obesity rate is a result of the citizens choosing not to walk rather than the community’s failure to provide pedestrians with enough connectivity to do their daily errands on foot. That threshold point appears to be a walkability score of 50, yet Mr. Powell observes that most American cities fail to reach even that minimum.
Although rich people tend to have better health outcomes than poor people, and there is a “general trend for richer cities to be more physically active than poorer cities,” Mr. Powell could not find a relationship between a city’s median income and its walkability.
If, like most of us, you have been frustrated in your efforts to lower the BMI of your patients, it may be time to emerge from the confines of your office and take a look at your town’s walkability score. If it is less than 50, you and your fellow concerned citizens and officials have some work to do. It may mean advocating for improved pedestrian infrastructure and/or dismantling the physical and zoning barriers to pedestrian connectivity. For example, maybe your community should be adding more pedestrian-activated crossing signals or tapping into federal and state safe routes to school programs or adopting zoning ordinances that require sidewalks in all new developments.
Here in Brunswick, we have a very enviable walkability score of 87, meaning “most errands can be accomplished on foot.” We have a bicycle and pedestrian advisory committee that reports to the town council and works with the town engineer to advocate for infrastructure improvements that encourage pedestrian connectivity. However, funding these improvements in walkability is always a challenge. But as the analysis in this recent study suggestions, our biggest challenge continues to be encouraging our citizens to take advantage of our existing pedestrian infrastructure.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
“Honey, does this town make me look fat?”
“Yes, Dear, I’m afraid it does.”
No, that really wasn’t a typo in the first line. I intended to type “town” and not “gown.” A recent article by Dionysus Powell in healthcareinamerica.us has prompted me to think a bit more about the relationship between obesity and the communities we inhabit (“Fit Cities vs. Fat Cities – What available data can tell us about the difference in lifestyle and obesity between cities,” by Dionysus Powell, March 28, 2017). The author is a biotech researcher who has collected readily available Centers for Disease Control and Prevention data on body mass index (BMI) and self-reported sedentary behavior in almost 200 U.S. cities. He then sliced and diced these numbers with each cities’ walkability score, which is a crude measure of how easily citizens and visitors on foot can reach a variety of destinations such as shops, schools, churches, libraries, and municipal offices. You can easily find your own town’s score by going to walkscore.com.
Not surprisingly, the author discovered that “differences in obesity rates between cities can largely be explained by differences in physical activity.” Of course, there is a point at which a community has sufficient walkable infrastructure so that its obesity rate is a result of the citizens choosing not to walk rather than the community’s failure to provide pedestrians with enough connectivity to do their daily errands on foot. That threshold point appears to be a walkability score of 50, yet Mr. Powell observes that most American cities fail to reach even that minimum.
Although rich people tend to have better health outcomes than poor people, and there is a “general trend for richer cities to be more physically active than poorer cities,” Mr. Powell could not find a relationship between a city’s median income and its walkability.
If, like most of us, you have been frustrated in your efforts to lower the BMI of your patients, it may be time to emerge from the confines of your office and take a look at your town’s walkability score. If it is less than 50, you and your fellow concerned citizens and officials have some work to do. It may mean advocating for improved pedestrian infrastructure and/or dismantling the physical and zoning barriers to pedestrian connectivity. For example, maybe your community should be adding more pedestrian-activated crossing signals or tapping into federal and state safe routes to school programs or adopting zoning ordinances that require sidewalks in all new developments.
Here in Brunswick, we have a very enviable walkability score of 87, meaning “most errands can be accomplished on foot.” We have a bicycle and pedestrian advisory committee that reports to the town council and works with the town engineer to advocate for infrastructure improvements that encourage pedestrian connectivity. However, funding these improvements in walkability is always a challenge. But as the analysis in this recent study suggestions, our biggest challenge continues to be encouraging our citizens to take advantage of our existing pedestrian infrastructure.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Infantile hemangiomas: Calculating dose for propranolol is tricky
Use of Hemangeol was associated with fewer dosing errors than use of generic propranolol hydrochloride oral solutions in treating infantile hemangiomas, according to an online questionnaire survey.
Anastasia O. Kurta, DO, of Saint Louis University and her associates emailed a questionnaire to 531 physicians who were members of the Society for Pediatric Dermatology and physicians known to treat infantile hemangiomas. Most of the 220 physicians who responded were pediatric dermatologists. Of those, 90% had prescribed generic propranolol available in concentrations of 4 mg/mL and 8 mg/mL, and 58.6% had prescribed Hemangeol, the Food and Drug Administration-approved formulation of propranolol hydrochloride available in a concentration of 4.28 mg/mL.

“A dosing chart accompanies propranolol 4.28 mg/mL [Hemangeol] using mL/kg doses, which eliminates conversion from milligrams to milliliters and could potentially explain the lower reported dose calculation error reported with propranolol 4.28 mg/mL,” Dr. Kurta and her associates said. “The risk of dispensing errors is increased for medications that are commercially available in different concentrations. Liquid medications prescribed for pediatric patients require additional computation for weight-based dosing and conversion, increasing the possibility of miscalculation.”
Daisy Dai, PhD, is employed by Pierre Fabre Pharmaceuticals and Elaine C. Siegfried, PhD, is a consultant for the company. Dr. Kurta and Eric S. Ambrecht, PhD, have no relevant financial disclosures.
Read more at J Am Acad Dermatol. 2017 May;76(5):999-1000.
Dr. Kurta reported no relevant financial disclosures.
Use of Hemangeol was associated with fewer dosing errors than use of generic propranolol hydrochloride oral solutions in treating infantile hemangiomas, according to an online questionnaire survey.
Anastasia O. Kurta, DO, of Saint Louis University and her associates emailed a questionnaire to 531 physicians who were members of the Society for Pediatric Dermatology and physicians known to treat infantile hemangiomas. Most of the 220 physicians who responded were pediatric dermatologists. Of those, 90% had prescribed generic propranolol available in concentrations of 4 mg/mL and 8 mg/mL, and 58.6% had prescribed Hemangeol, the Food and Drug Administration-approved formulation of propranolol hydrochloride available in a concentration of 4.28 mg/mL.
“A dosing chart accompanies propranolol 4.28 mg/mL [Hemangeol] using mL/kg doses, which eliminates conversion from milligrams to milliliters and could potentially explain the lower reported dose calculation error reported with propranolol 4.28 mg/mL,” Dr. Kurta and her associates said. “The risk of dispensing errors is increased for medications that are commercially available in different concentrations. Liquid medications prescribed for pediatric patients require additional computation for weight-based dosing and conversion, increasing the possibility of miscalculation.”
Daisy Dai, PhD, is employed by Pierre Fabre Pharmaceuticals and Elaine C. Siegfried, PhD, is a consultant for the company. Dr. Kurta and Eric S. Ambrecht, PhD, have no relevant financial disclosures.
Read more at J Am Acad Dermatol. 2017 May;76(5):999-1000.
Dr. Kurta reported no relevant financial disclosures.
Use of Hemangeol was associated with fewer dosing errors than use of generic propranolol hydrochloride oral solutions in treating infantile hemangiomas, according to an online questionnaire survey.
Anastasia O. Kurta, DO, of Saint Louis University and her associates emailed a questionnaire to 531 physicians who were members of the Society for Pediatric Dermatology and physicians known to treat infantile hemangiomas. Most of the 220 physicians who responded were pediatric dermatologists. Of those, 90% had prescribed generic propranolol available in concentrations of 4 mg/mL and 8 mg/mL, and 58.6% had prescribed Hemangeol, the Food and Drug Administration-approved formulation of propranolol hydrochloride available in a concentration of 4.28 mg/mL.
“A dosing chart accompanies propranolol 4.28 mg/mL [Hemangeol] using mL/kg doses, which eliminates conversion from milligrams to milliliters and could potentially explain the lower reported dose calculation error reported with propranolol 4.28 mg/mL,” Dr. Kurta and her associates said. “The risk of dispensing errors is increased for medications that are commercially available in different concentrations. Liquid medications prescribed for pediatric patients require additional computation for weight-based dosing and conversion, increasing the possibility of miscalculation.”
Daisy Dai, PhD, is employed by Pierre Fabre Pharmaceuticals and Elaine C. Siegfried, PhD, is a consultant for the company. Dr. Kurta and Eric S. Ambrecht, PhD, have no relevant financial disclosures.
Read more at J Am Acad Dermatol. 2017 May;76(5):999-1000.
Dr. Kurta reported no relevant financial disclosures.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Maternal antidepressants unrelated to autism in offspring
Maternal use of antidepressants during pregnancy is unrelated to autism spectrum disorder in the offspring, according to two separate, population-level cohort studies that used sophisticated statistical techniques to account for numerous confounding factors.
Both studies were reported online April 18 in JAMA.
Some previous studies have reported a possible link between in utero exposure to antidepressants, particularly SSRIs, and autism. But they had limited ability to control for key confounders, notably the mother’s underlying depression.
Overall, 1.1% of these children were diagnosed as having autism spectrum disorder. This prevalence is consistent with current population estimates, indicating that few if any cases of the disorder were missed, said Dr. Brown of Women’s College Research Institute in Toronto and the division of epidemiology, University of Toronto, and her associates.
In initial, unadjusted analyses of the data, the risk of autism was higher in exposed than in nonexposed children. However, that association disappeared once the data were adjusted to account for numerous potential confounders.
Further analysis comparing the exposed children with their unexposed siblings also found that after adjusting for confounding factors, prenatal exposure to antidepressants did not affect the risk of developing autism. In addition, this lack of association also was found in the subgroup of children whose mothers took antidepressants shortly before but not during pregnancy.
Taken together, these findings “suggest that confounding by indication for the medication may explain previously observed associations between in utero serotonergic antidepressant exposure and autism spectrum disorder,” Dr. Brown and her associates said (JAMA. 2017 Apr 18. doi: 10.1001.jama.2017.3415). In the other study, Ayesha C. Sujan and her associates analyzed data in several nationwide Swedish registries to examine whether first trimester exposure to any antidepressants raised the risk of a range of neurodevelopmental problems, including autism. This study involved 1,580,629 offspring, including 22,544 (1.4%) whose mothers took antidepressants during the first trimester.
As with Dr. Brown’s study, the initial unadjusted analysis showed an association between antidepressant exposure and autism, but that association disappeared once the data were adjusted to account for confounding factors. In the final data analysis, first trimester exposure was associated with preterm birth (odds ratio, 1.34) but not with small-for-gestational-age size (OR, 1.01), autism spectrum disorder (hazard ratio, 0.83), or attention deficit/hyperactivity disorder (HR, 0.99), said Ms. Sujan of the department of psychological and brain sciences, Indiana University, Bloomington, and her associates.
“These results are consistent with the hypothesis that genetic factors, familial environmental factors, or both, account for the population-wide associations between first-trimester antidepressant exposure and these outcomes,” they noted (JAMA. 2017 Apr 18. doi: 10.1001/jama.2017.3413).
These two studies add to the growing literature suggesting that any association between prenatal antidepressant exposure and autism spectrum disorder may not be causal.
Both reports should reassure both parents and clinicians.
And regardless of whether any such association reflects antidepressant effects, the mother’s underlying mental health, or other factors, efforts should focus on promoting optimal child health in ways that harness the child’s inherent developmental plasticity.
Tim F. Oberlander, MD, is in the division of developmental pediatrics at the University of British Columbia and at the British Columbia Children’s Hospital Research Institute, both in Vancouver. Lonnie Zwaigenbaum, MD, is in the department of pediatrics at the University of Alberta, Edmonton. They reported having no relevant financial disclosures. These remarks were excerpted from an editorial accompanying the two reports (JAMA. 2017;317[15]:1533-4).
These two studies add to the growing literature suggesting that any association between prenatal antidepressant exposure and autism spectrum disorder may not be causal.
Both reports should reassure both parents and clinicians.
And regardless of whether any such association reflects antidepressant effects, the mother’s underlying mental health, or other factors, efforts should focus on promoting optimal child health in ways that harness the child’s inherent developmental plasticity.
Tim F. Oberlander, MD, is in the division of developmental pediatrics at the University of British Columbia and at the British Columbia Children’s Hospital Research Institute, both in Vancouver. Lonnie Zwaigenbaum, MD, is in the department of pediatrics at the University of Alberta, Edmonton. They reported having no relevant financial disclosures. These remarks were excerpted from an editorial accompanying the two reports (JAMA. 2017;317[15]:1533-4).
These two studies add to the growing literature suggesting that any association between prenatal antidepressant exposure and autism spectrum disorder may not be causal.
Both reports should reassure both parents and clinicians.
And regardless of whether any such association reflects antidepressant effects, the mother’s underlying mental health, or other factors, efforts should focus on promoting optimal child health in ways that harness the child’s inherent developmental plasticity.
Tim F. Oberlander, MD, is in the division of developmental pediatrics at the University of British Columbia and at the British Columbia Children’s Hospital Research Institute, both in Vancouver. Lonnie Zwaigenbaum, MD, is in the department of pediatrics at the University of Alberta, Edmonton. They reported having no relevant financial disclosures. These remarks were excerpted from an editorial accompanying the two reports (JAMA. 2017;317[15]:1533-4).
Maternal use of antidepressants during pregnancy is unrelated to autism spectrum disorder in the offspring, according to two separate, population-level cohort studies that used sophisticated statistical techniques to account for numerous confounding factors.
Both studies were reported online April 18 in JAMA.
Some previous studies have reported a possible link between in utero exposure to antidepressants, particularly SSRIs, and autism. But they had limited ability to control for key confounders, notably the mother’s underlying depression.
Overall, 1.1% of these children were diagnosed as having autism spectrum disorder. This prevalence is consistent with current population estimates, indicating that few if any cases of the disorder were missed, said Dr. Brown of Women’s College Research Institute in Toronto and the division of epidemiology, University of Toronto, and her associates.
In initial, unadjusted analyses of the data, the risk of autism was higher in exposed than in nonexposed children. However, that association disappeared once the data were adjusted to account for numerous potential confounders.
Further analysis comparing the exposed children with their unexposed siblings also found that after adjusting for confounding factors, prenatal exposure to antidepressants did not affect the risk of developing autism. In addition, this lack of association also was found in the subgroup of children whose mothers took antidepressants shortly before but not during pregnancy.
Taken together, these findings “suggest that confounding by indication for the medication may explain previously observed associations between in utero serotonergic antidepressant exposure and autism spectrum disorder,” Dr. Brown and her associates said (JAMA. 2017 Apr 18. doi: 10.1001.jama.2017.3415). In the other study, Ayesha C. Sujan and her associates analyzed data in several nationwide Swedish registries to examine whether first trimester exposure to any antidepressants raised the risk of a range of neurodevelopmental problems, including autism. This study involved 1,580,629 offspring, including 22,544 (1.4%) whose mothers took antidepressants during the first trimester.
As with Dr. Brown’s study, the initial unadjusted analysis showed an association between antidepressant exposure and autism, but that association disappeared once the data were adjusted to account for confounding factors. In the final data analysis, first trimester exposure was associated with preterm birth (odds ratio, 1.34) but not with small-for-gestational-age size (OR, 1.01), autism spectrum disorder (hazard ratio, 0.83), or attention deficit/hyperactivity disorder (HR, 0.99), said Ms. Sujan of the department of psychological and brain sciences, Indiana University, Bloomington, and her associates.
“These results are consistent with the hypothesis that genetic factors, familial environmental factors, or both, account for the population-wide associations between first-trimester antidepressant exposure and these outcomes,” they noted (JAMA. 2017 Apr 18. doi: 10.1001/jama.2017.3413).
Maternal use of antidepressants during pregnancy is unrelated to autism spectrum disorder in the offspring, according to two separate, population-level cohort studies that used sophisticated statistical techniques to account for numerous confounding factors.
Both studies were reported online April 18 in JAMA.
Some previous studies have reported a possible link between in utero exposure to antidepressants, particularly SSRIs, and autism. But they had limited ability to control for key confounders, notably the mother’s underlying depression.
Overall, 1.1% of these children were diagnosed as having autism spectrum disorder. This prevalence is consistent with current population estimates, indicating that few if any cases of the disorder were missed, said Dr. Brown of Women’s College Research Institute in Toronto and the division of epidemiology, University of Toronto, and her associates.
In initial, unadjusted analyses of the data, the risk of autism was higher in exposed than in nonexposed children. However, that association disappeared once the data were adjusted to account for numerous potential confounders.
Further analysis comparing the exposed children with their unexposed siblings also found that after adjusting for confounding factors, prenatal exposure to antidepressants did not affect the risk of developing autism. In addition, this lack of association also was found in the subgroup of children whose mothers took antidepressants shortly before but not during pregnancy.
Taken together, these findings “suggest that confounding by indication for the medication may explain previously observed associations between in utero serotonergic antidepressant exposure and autism spectrum disorder,” Dr. Brown and her associates said (JAMA. 2017 Apr 18. doi: 10.1001.jama.2017.3415). In the other study, Ayesha C. Sujan and her associates analyzed data in several nationwide Swedish registries to examine whether first trimester exposure to any antidepressants raised the risk of a range of neurodevelopmental problems, including autism. This study involved 1,580,629 offspring, including 22,544 (1.4%) whose mothers took antidepressants during the first trimester.
As with Dr. Brown’s study, the initial unadjusted analysis showed an association between antidepressant exposure and autism, but that association disappeared once the data were adjusted to account for confounding factors. In the final data analysis, first trimester exposure was associated with preterm birth (odds ratio, 1.34) but not with small-for-gestational-age size (OR, 1.01), autism spectrum disorder (hazard ratio, 0.83), or attention deficit/hyperactivity disorder (HR, 0.99), said Ms. Sujan of the department of psychological and brain sciences, Indiana University, Bloomington, and her associates.
“These results are consistent with the hypothesis that genetic factors, familial environmental factors, or both, account for the population-wide associations between first-trimester antidepressant exposure and these outcomes,” they noted (JAMA. 2017 Apr 18. doi: 10.1001/jama.2017.3413).
FROM JAMA
Key clinical point: Maternal use of antidepressants during pregnancy is unrelated to autism spectrum disorder in offspring.
Major finding: Prenatal exposure to antidepressants was not associated with small-for-gestational-age size (OR, 1.01), autism spectrum disorder (HR, 0.83), or attention deficit/hyperactivity disorder (HR, 0.99).
Data source: Two separate retrospective cohort studies involving 35,906 births in Canada and 1,580,629 in Sweden.
Disclosures: Dr. Brown’s study was supported by the Institute for Clinical Evaluative Sciences and the Ontario Ministry of Health and Long-Term Care. Dr. Brown and her associates reported having no relevant financial disclosures. Dr. Sujan’s study was supported by the U.S. National Institute of Mental Health, the National Institute on Drug Abuse, the National Science Foundation, and others. Dr. Sujan reported having no relevant financial disclosures; her associates reported ties to numerous industry sources.
Teens’ marijuana use higher during pregnancy
The prevalence of marijuana use among pregnant teenagers is more than double that among teens who are not pregnant, according to a study involving 410,000 females aged 12-44 years.
For pregnant teens aged 12-17 years, the past-month prevalence of marijuana use was 14% between 2002 and 2015, compared with 6.5% for their nonpregnant peers, Nora D. Volkow, MD, director of the National Institute on Drug Abuse in Bethesda, Md., and her associates reported in a letter on April 17 (Ann Intern Med. 2017 Apr 17. doi: 10.7326/L17-0067).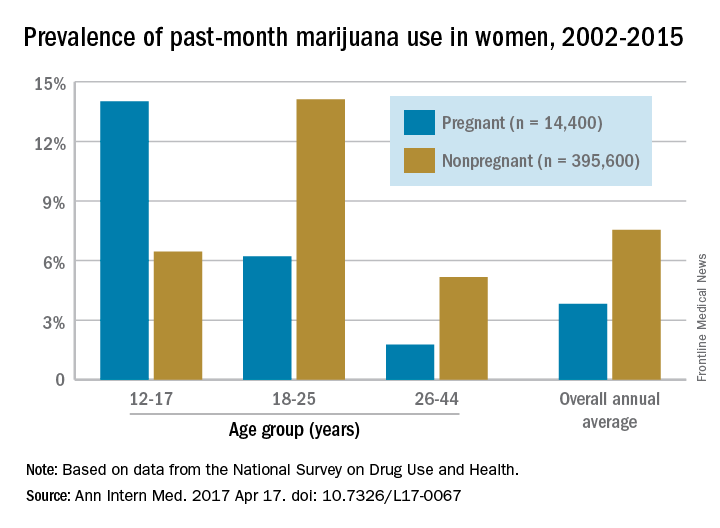
The pattern of use in the youngest age group “may reflect underlying risky behavior common to both teen pregnancy and early substance use and suggests the importance of intervention for teenagers,” the researchers wrote. “Because of consistent overlap between use of marijuana and other substances, identification of marijuana use during pregnancy warrants evaluation for comorbid substance abuse.”
The overall annual average prevalence of marijuana use was 3.8% among the 14,400 pregnant women and 7.5% for the 395,600 nonpregnant women who responded to the survey from 2002 to 2015. The investigators also found that marijuana use was higher in the first trimester (6.4%) than in the second (3.3%) or third (1.8%) trimesters and that use was higher in pregnant black women (6.5%) than in white (3.8%) or Hispanic women(2.9%) or women of other races/ethnicities (1.4%).
Although evidence on the effects of marijuana on prenatal development is limited, “pregnant females and those considering becoming pregnant should be advised not to use marijuana or other cannabinoids recreationally or to treat nausea,” Dr. Volkow and her associates wrote.
The study was sponsored by the National Institute on Drug Abuse and the Substance Abuse and Mental Health Services Administration. Dr. Volkow reported having no financial disclosures. One coauthor reported stock ownership of Pfizer, and another reported stock ownership of Sanofi and Eli Lilly.
The prevalence of marijuana use among pregnant teenagers is more than double that among teens who are not pregnant, according to a study involving 410,000 females aged 12-44 years.
For pregnant teens aged 12-17 years, the past-month prevalence of marijuana use was 14% between 2002 and 2015, compared with 6.5% for their nonpregnant peers, Nora D. Volkow, MD, director of the National Institute on Drug Abuse in Bethesda, Md., and her associates reported in a letter on April 17 (Ann Intern Med. 2017 Apr 17. doi: 10.7326/L17-0067).
The pattern of use in the youngest age group “may reflect underlying risky behavior common to both teen pregnancy and early substance use and suggests the importance of intervention for teenagers,” the researchers wrote. “Because of consistent overlap between use of marijuana and other substances, identification of marijuana use during pregnancy warrants evaluation for comorbid substance abuse.”
The overall annual average prevalence of marijuana use was 3.8% among the 14,400 pregnant women and 7.5% for the 395,600 nonpregnant women who responded to the survey from 2002 to 2015. The investigators also found that marijuana use was higher in the first trimester (6.4%) than in the second (3.3%) or third (1.8%) trimesters and that use was higher in pregnant black women (6.5%) than in white (3.8%) or Hispanic women(2.9%) or women of other races/ethnicities (1.4%).
Although evidence on the effects of marijuana on prenatal development is limited, “pregnant females and those considering becoming pregnant should be advised not to use marijuana or other cannabinoids recreationally or to treat nausea,” Dr. Volkow and her associates wrote.
The study was sponsored by the National Institute on Drug Abuse and the Substance Abuse and Mental Health Services Administration. Dr. Volkow reported having no financial disclosures. One coauthor reported stock ownership of Pfizer, and another reported stock ownership of Sanofi and Eli Lilly.
The prevalence of marijuana use among pregnant teenagers is more than double that among teens who are not pregnant, according to a study involving 410,000 females aged 12-44 years.
For pregnant teens aged 12-17 years, the past-month prevalence of marijuana use was 14% between 2002 and 2015, compared with 6.5% for their nonpregnant peers, Nora D. Volkow, MD, director of the National Institute on Drug Abuse in Bethesda, Md., and her associates reported in a letter on April 17 (Ann Intern Med. 2017 Apr 17. doi: 10.7326/L17-0067).
The pattern of use in the youngest age group “may reflect underlying risky behavior common to both teen pregnancy and early substance use and suggests the importance of intervention for teenagers,” the researchers wrote. “Because of consistent overlap between use of marijuana and other substances, identification of marijuana use during pregnancy warrants evaluation for comorbid substance abuse.”
The overall annual average prevalence of marijuana use was 3.8% among the 14,400 pregnant women and 7.5% for the 395,600 nonpregnant women who responded to the survey from 2002 to 2015. The investigators also found that marijuana use was higher in the first trimester (6.4%) than in the second (3.3%) or third (1.8%) trimesters and that use was higher in pregnant black women (6.5%) than in white (3.8%) or Hispanic women(2.9%) or women of other races/ethnicities (1.4%).
Although evidence on the effects of marijuana on prenatal development is limited, “pregnant females and those considering becoming pregnant should be advised not to use marijuana or other cannabinoids recreationally or to treat nausea,” Dr. Volkow and her associates wrote.
The study was sponsored by the National Institute on Drug Abuse and the Substance Abuse and Mental Health Services Administration. Dr. Volkow reported having no financial disclosures. One coauthor reported stock ownership of Pfizer, and another reported stock ownership of Sanofi and Eli Lilly.
FROM ANNALS OF INTERNAL MEDICINE
Reduced-intensity conditioning may not preserve fertility in young girls after bone marrow transplant
ORLANDO – Girls who undergo reduced-intensity conditioning for a bone marrow transplant may face fertility problems in the future, even if they experience an outwardly normal puberty.
In the first-ever study to compare high- and low-intensity chemotherapeutic conditioning regimens among young girls, significantly more who underwent the reduced-intensity regimen had normal estradiol, luteinizing hormone, and follicle-stimulating hormone compared with those who had high-intensity conditioning. But anti-Müllerian hormone was low or absent in almost all the girls, no matter which conditioning regimen they had, Jonathan C. Howell, MD, PhD, said at the annual meeting of the Endocrine Society.
While not a perfect predictor of future fertility, anti-Müllerian hormone is a good indicator of ovarian follicular reserve, said Dr. Howell, a pediatric endocrinologist at Cincinnati Children’s Hospital Medical Center.
Dr. Howell and his colleagues, Holly R. Hoefgen, MD, Kasiani C. Myers, MD, and Helen Oquendo-Del Toro, MD, all of Cincinnati Children’s Hospital Medical Center, are following 49 females aged 1-40 years who had preconditioning chemotherapy in advance of hematopoietic stem cell transplantation.
At the meeting, Dr. Howell reported data on 23 girls who were in puberty during their treatment (mean age 12 years). The mean follow-up was 4 years, but this varied widely, from 1 to 13 years. Most (16) had high-intensity myeloablation; the remainder had reduced-intensity conditioning. Diagnoses varied between the groups. Among those with high-intensity conditioning, malignancy and bone marrow failure were the most common indications (seven patients each); one patient had an immunodeficiency, and the cause was unknown for another.
Among those who had the reduced-intensity regimen, five had an immunodeficiency and two had bone marrow failure.
The discrepancy in diagnoses between the groups isn’t surprising, Dr. Howell said. “Diagnosis can dictate which treatment patients receive. People with malignancies or a prior history of leukemia or lymphoma often receive the high-intensity conditioning. You want to wipe out every single malignant cell.”
Reduced-intensity conditioning may be an option for patients with other problems such as bone marrow failure, immunodeficiencies, or genetic or metabolic problems. The less-intense regimen does confer some benefits, Dr. Howell noted. “The short-term need for intensive medical therapy while getting the stem cells is less. The medical benefit of these less-intense regimens is certainly there, but the long-term endocrine impact has yet to be defined.”
Most of the girls in the high-intensity regimen group (64%) had high follicle stimulating hormone and luteinizing hormone, suggesting primary ovarian failure; 71% of them also had low estradiol levels. However, all of these hormones were normal in the reduced-intensity group. But regardless of conditioning treatment, anti-Müllerian hormone was abnormally low in nearly all of the patients (87%). Only one girl with myeloablative conditioning and two girls with reduced intensity condition had normal anti-Müllerian levels. “This tells us that fertility potential may not be preserved, despite [their] getting the reduced-intensity conditioning,” Dr. Howell said.
The story here is only beginning to unfold, he said. “Fertility is defined as the ability to conceive a child, and that’s not something we have looked at yet. We would like to know the long-term outcomes of fertility in these patients, and whether they can conceive when they’re ready to start a family. Our goal is to follow these young women into their 20s and 30s, and to see if that’s an opportunity they are able to experience.”
The study is a cooperative project involving the hospital’s divisions of Pediatric and Adolescent Gynecology, Bone Marrow Transplantation and Immunology, and Endocrinology.
Neither Dr. Howell nor any of his colleagues had any financial disclosures.
Fertility preservation talks: The earlier, the better
A talk about fertility preservation can be the first step into a new future for families of children with a cancer diagnosis.
“Talking about your baby having a baby can be the farthest thing from your mind,” when you’re the parent of a child about to undergo cancer treatment, said Dr. Hoefgen. “But we know from survivors that this can be a very important issue in the future. We simply start by telling parents, ‘This will be important to your child at some point, and we want to talk about it now, while there is still something we may be able to do about it.’ ”
Dr. Hoefgen, a staff member at the hospital’s Comprehensive Fertility Care and Preservation Program, said parents “sometimes find it weird” to be talking about unborn grandchildren when they’re consumed with making critical decisions for their own child. But by asking them to consider that child’s long-term future, the discussion offers its own message of hope.

The talks always begin with a basic discussion of how cancer treatments can affect the reproductive organs. The hospital has a series of short animated videos that are very helpful in relaying the information. Another video in that series describes the different methods of fertility preservation: mature oocyte or sperm harvesting, or, for younger patients, removing and freezing ovarian and testicular tissue. Parents and children can watch them together, get grounding in the basics, and be prepared for a productive conversation.
Talks always include the team oncologist, who creates a specialized risk assessment for each patient. The group discusses each preservation method, the risks and benefits, and the cost. But the talks are exploratory, too, helping both clinicians and families understand what’s most important to them, she said.
“Common things that we typically talk about are genetics, religion, and ethics – which may mean different things to different families.”
Dr. Hoefgen and her team reach out to more than 95% of families that face a pediatric cancer diagnosis. After the in-depth discussions, she said, about 20% decide to investigate some form of fertility preservation.
“The most important thing is having the conversation early, while we still have options,” she said.
Dr. Hoefgen had no financial disclosures.
ORLANDO – Girls who undergo reduced-intensity conditioning for a bone marrow transplant may face fertility problems in the future, even if they experience an outwardly normal puberty.
In the first-ever study to compare high- and low-intensity chemotherapeutic conditioning regimens among young girls, significantly more who underwent the reduced-intensity regimen had normal estradiol, luteinizing hormone, and follicle-stimulating hormone compared with those who had high-intensity conditioning. But anti-Müllerian hormone was low or absent in almost all the girls, no matter which conditioning regimen they had, Jonathan C. Howell, MD, PhD, said at the annual meeting of the Endocrine Society.
While not a perfect predictor of future fertility, anti-Müllerian hormone is a good indicator of ovarian follicular reserve, said Dr. Howell, a pediatric endocrinologist at Cincinnati Children’s Hospital Medical Center.
Dr. Howell and his colleagues, Holly R. Hoefgen, MD, Kasiani C. Myers, MD, and Helen Oquendo-Del Toro, MD, all of Cincinnati Children’s Hospital Medical Center, are following 49 females aged 1-40 years who had preconditioning chemotherapy in advance of hematopoietic stem cell transplantation.
At the meeting, Dr. Howell reported data on 23 girls who were in puberty during their treatment (mean age 12 years). The mean follow-up was 4 years, but this varied widely, from 1 to 13 years. Most (16) had high-intensity myeloablation; the remainder had reduced-intensity conditioning. Diagnoses varied between the groups. Among those with high-intensity conditioning, malignancy and bone marrow failure were the most common indications (seven patients each); one patient had an immunodeficiency, and the cause was unknown for another.
Among those who had the reduced-intensity regimen, five had an immunodeficiency and two had bone marrow failure.
The discrepancy in diagnoses between the groups isn’t surprising, Dr. Howell said. “Diagnosis can dictate which treatment patients receive. People with malignancies or a prior history of leukemia or lymphoma often receive the high-intensity conditioning. You want to wipe out every single malignant cell.”
Reduced-intensity conditioning may be an option for patients with other problems such as bone marrow failure, immunodeficiencies, or genetic or metabolic problems. The less-intense regimen does confer some benefits, Dr. Howell noted. “The short-term need for intensive medical therapy while getting the stem cells is less. The medical benefit of these less-intense regimens is certainly there, but the long-term endocrine impact has yet to be defined.”
Most of the girls in the high-intensity regimen group (64%) had high follicle stimulating hormone and luteinizing hormone, suggesting primary ovarian failure; 71% of them also had low estradiol levels. However, all of these hormones were normal in the reduced-intensity group. But regardless of conditioning treatment, anti-Müllerian hormone was abnormally low in nearly all of the patients (87%). Only one girl with myeloablative conditioning and two girls with reduced intensity condition had normal anti-Müllerian levels. “This tells us that fertility potential may not be preserved, despite [their] getting the reduced-intensity conditioning,” Dr. Howell said.
The story here is only beginning to unfold, he said. “Fertility is defined as the ability to conceive a child, and that’s not something we have looked at yet. We would like to know the long-term outcomes of fertility in these patients, and whether they can conceive when they’re ready to start a family. Our goal is to follow these young women into their 20s and 30s, and to see if that’s an opportunity they are able to experience.”
The study is a cooperative project involving the hospital’s divisions of Pediatric and Adolescent Gynecology, Bone Marrow Transplantation and Immunology, and Endocrinology.
Neither Dr. Howell nor any of his colleagues had any financial disclosures.
Fertility preservation talks: The earlier, the better
A talk about fertility preservation can be the first step into a new future for families of children with a cancer diagnosis.
“Talking about your baby having a baby can be the farthest thing from your mind,” when you’re the parent of a child about to undergo cancer treatment, said Dr. Hoefgen. “But we know from survivors that this can be a very important issue in the future. We simply start by telling parents, ‘This will be important to your child at some point, and we want to talk about it now, while there is still something we may be able to do about it.’ ”
Dr. Hoefgen, a staff member at the hospital’s Comprehensive Fertility Care and Preservation Program, said parents “sometimes find it weird” to be talking about unborn grandchildren when they’re consumed with making critical decisions for their own child. But by asking them to consider that child’s long-term future, the discussion offers its own message of hope.
The talks always begin with a basic discussion of how cancer treatments can affect the reproductive organs. The hospital has a series of short animated videos that are very helpful in relaying the information. Another video in that series describes the different methods of fertility preservation: mature oocyte or sperm harvesting, or, for younger patients, removing and freezing ovarian and testicular tissue. Parents and children can watch them together, get grounding in the basics, and be prepared for a productive conversation.
Talks always include the team oncologist, who creates a specialized risk assessment for each patient. The group discusses each preservation method, the risks and benefits, and the cost. But the talks are exploratory, too, helping both clinicians and families understand what’s most important to them, she said.
“Common things that we typically talk about are genetics, religion, and ethics – which may mean different things to different families.”
Dr. Hoefgen and her team reach out to more than 95% of families that face a pediatric cancer diagnosis. After the in-depth discussions, she said, about 20% decide to investigate some form of fertility preservation.
“The most important thing is having the conversation early, while we still have options,” she said.
Dr. Hoefgen had no financial disclosures.
ORLANDO – Girls who undergo reduced-intensity conditioning for a bone marrow transplant may face fertility problems in the future, even if they experience an outwardly normal puberty.
In the first-ever study to compare high- and low-intensity chemotherapeutic conditioning regimens among young girls, significantly more who underwent the reduced-intensity regimen had normal estradiol, luteinizing hormone, and follicle-stimulating hormone compared with those who had high-intensity conditioning. But anti-Müllerian hormone was low or absent in almost all the girls, no matter which conditioning regimen they had, Jonathan C. Howell, MD, PhD, said at the annual meeting of the Endocrine Society.
While not a perfect predictor of future fertility, anti-Müllerian hormone is a good indicator of ovarian follicular reserve, said Dr. Howell, a pediatric endocrinologist at Cincinnati Children’s Hospital Medical Center.
Dr. Howell and his colleagues, Holly R. Hoefgen, MD, Kasiani C. Myers, MD, and Helen Oquendo-Del Toro, MD, all of Cincinnati Children’s Hospital Medical Center, are following 49 females aged 1-40 years who had preconditioning chemotherapy in advance of hematopoietic stem cell transplantation.
At the meeting, Dr. Howell reported data on 23 girls who were in puberty during their treatment (mean age 12 years). The mean follow-up was 4 years, but this varied widely, from 1 to 13 years. Most (16) had high-intensity myeloablation; the remainder had reduced-intensity conditioning. Diagnoses varied between the groups. Among those with high-intensity conditioning, malignancy and bone marrow failure were the most common indications (seven patients each); one patient had an immunodeficiency, and the cause was unknown for another.
Among those who had the reduced-intensity regimen, five had an immunodeficiency and two had bone marrow failure.
The discrepancy in diagnoses between the groups isn’t surprising, Dr. Howell said. “Diagnosis can dictate which treatment patients receive. People with malignancies or a prior history of leukemia or lymphoma often receive the high-intensity conditioning. You want to wipe out every single malignant cell.”
Reduced-intensity conditioning may be an option for patients with other problems such as bone marrow failure, immunodeficiencies, or genetic or metabolic problems. The less-intense regimen does confer some benefits, Dr. Howell noted. “The short-term need for intensive medical therapy while getting the stem cells is less. The medical benefit of these less-intense regimens is certainly there, but the long-term endocrine impact has yet to be defined.”
Most of the girls in the high-intensity regimen group (64%) had high follicle stimulating hormone and luteinizing hormone, suggesting primary ovarian failure; 71% of them also had low estradiol levels. However, all of these hormones were normal in the reduced-intensity group. But regardless of conditioning treatment, anti-Müllerian hormone was abnormally low in nearly all of the patients (87%). Only one girl with myeloablative conditioning and two girls with reduced intensity condition had normal anti-Müllerian levels. “This tells us that fertility potential may not be preserved, despite [their] getting the reduced-intensity conditioning,” Dr. Howell said.
The story here is only beginning to unfold, he said. “Fertility is defined as the ability to conceive a child, and that’s not something we have looked at yet. We would like to know the long-term outcomes of fertility in these patients, and whether they can conceive when they’re ready to start a family. Our goal is to follow these young women into their 20s and 30s, and to see if that’s an opportunity they are able to experience.”
The study is a cooperative project involving the hospital’s divisions of Pediatric and Adolescent Gynecology, Bone Marrow Transplantation and Immunology, and Endocrinology.
Neither Dr. Howell nor any of his colleagues had any financial disclosures.
Fertility preservation talks: The earlier, the better
A talk about fertility preservation can be the first step into a new future for families of children with a cancer diagnosis.
“Talking about your baby having a baby can be the farthest thing from your mind,” when you’re the parent of a child about to undergo cancer treatment, said Dr. Hoefgen. “But we know from survivors that this can be a very important issue in the future. We simply start by telling parents, ‘This will be important to your child at some point, and we want to talk about it now, while there is still something we may be able to do about it.’ ”
Dr. Hoefgen, a staff member at the hospital’s Comprehensive Fertility Care and Preservation Program, said parents “sometimes find it weird” to be talking about unborn grandchildren when they’re consumed with making critical decisions for their own child. But by asking them to consider that child’s long-term future, the discussion offers its own message of hope.
The talks always begin with a basic discussion of how cancer treatments can affect the reproductive organs. The hospital has a series of short animated videos that are very helpful in relaying the information. Another video in that series describes the different methods of fertility preservation: mature oocyte or sperm harvesting, or, for younger patients, removing and freezing ovarian and testicular tissue. Parents and children can watch them together, get grounding in the basics, and be prepared for a productive conversation.
Talks always include the team oncologist, who creates a specialized risk assessment for each patient. The group discusses each preservation method, the risks and benefits, and the cost. But the talks are exploratory, too, helping both clinicians and families understand what’s most important to them, she said.
“Common things that we typically talk about are genetics, religion, and ethics – which may mean different things to different families.”
Dr. Hoefgen and her team reach out to more than 95% of families that face a pediatric cancer diagnosis. After the in-depth discussions, she said, about 20% decide to investigate some form of fertility preservation.
“The most important thing is having the conversation early, while we still have options,” she said.
Dr. Hoefgen had no financial disclosures.
AT ENDO 2017
Key clinical point:
Major finding: Anti-Müllerian hormone was abnormally low or absent in all treated girls, whether they had reduced-intensity or high-intensity conditioning.
Data source: The prospective study is following 49 females aged 1-40 years.
Disclosures: Neither Dr. Howell nor any of his colleagues had any financial disclosures.
Maternal Tdap vaccination highly protective against infant pertussis
, results of a study show.
From 2010 to 2015, researchers collected data from a cohort study of full-term infants born at Kaiser Permanente of Northern California. “We estimated the effectiveness of maternal pertussis vaccination for protecting newborns against pertussis in the first 2 months of life and in the first year of life, accounting for each infant DTaP dose,” said Roger Baxter, MD, and his associates at Kaiser Permanente Vaccine Study Center, Oakland, Calif. 
The vaccine effectiveness was an estimated 88% before infants had any DTaP vaccine doses, 81% between doses 1 and 2, 6% between doses 2 and 3, and 66% after infants had 3 DTaP doses.
“This result is consistent with 2 earlier studies in the United Kingdom” showing protection in infants less than 3 months of age, and a U.S. study showing maternal Tdap vaccination conferring protection to infants in the first 8 weeks of life, the researchers said.
In conclusion, even after infant DTaP dosing, there was evidence of additional protection from maternal Tdap vaccination for the first year of life (Pediatrics. 2017 Apr 3. doi: 10.1542/peds.2016-4091).
, results of a study show.
From 2010 to 2015, researchers collected data from a cohort study of full-term infants born at Kaiser Permanente of Northern California. “We estimated the effectiveness of maternal pertussis vaccination for protecting newborns against pertussis in the first 2 months of life and in the first year of life, accounting for each infant DTaP dose,” said Roger Baxter, MD, and his associates at Kaiser Permanente Vaccine Study Center, Oakland, Calif.
The vaccine effectiveness was an estimated 88% before infants had any DTaP vaccine doses, 81% between doses 1 and 2, 6% between doses 2 and 3, and 66% after infants had 3 DTaP doses.
“This result is consistent with 2 earlier studies in the United Kingdom” showing protection in infants less than 3 months of age, and a U.S. study showing maternal Tdap vaccination conferring protection to infants in the first 8 weeks of life, the researchers said.
In conclusion, even after infant DTaP dosing, there was evidence of additional protection from maternal Tdap vaccination for the first year of life (Pediatrics. 2017 Apr 3. doi: 10.1542/peds.2016-4091).
, results of a study show.
From 2010 to 2015, researchers collected data from a cohort study of full-term infants born at Kaiser Permanente of Northern California. “We estimated the effectiveness of maternal pertussis vaccination for protecting newborns against pertussis in the first 2 months of life and in the first year of life, accounting for each infant DTaP dose,” said Roger Baxter, MD, and his associates at Kaiser Permanente Vaccine Study Center, Oakland, Calif.
The vaccine effectiveness was an estimated 88% before infants had any DTaP vaccine doses, 81% between doses 1 and 2, 6% between doses 2 and 3, and 66% after infants had 3 DTaP doses.
“This result is consistent with 2 earlier studies in the United Kingdom” showing protection in infants less than 3 months of age, and a U.S. study showing maternal Tdap vaccination conferring protection to infants in the first 8 weeks of life, the researchers said.
In conclusion, even after infant DTaP dosing, there was evidence of additional protection from maternal Tdap vaccination for the first year of life (Pediatrics. 2017 Apr 3. doi: 10.1542/peds.2016-4091).
Simple changes shorten door-to-insulin time for diabetic ketoacidosis
ORLANDO – A few simple adjustments in standing orders shaved 20 minutes off the time one emergency department took to deliver insulin to pediatric patients with diabetic ketoacidosis, according to Mary Ellen Vajravelu, MD.
Door-to-insulin time decreased from a mean of 168 minutes to 146 minutes after the changes went into effect. Most of the time was saved in the period between starting the initial fluid bolus and starting the insulin, she said during an interview at the annual meeting of the Endocrine Society.
A single patient’s experience inspired the quality improvement project.
“A couple of years ago, we saw a patient in the emergency department with diabetic ketoacidosis who had to wait more than 6 hours before insulin was started,” she explained. “Fortunately, there were no adverse clinical outcomes from that,” but the case signaled that the treatment process needed some streamlining.
The International Society for Pediatric and Adolescent Diabetes recommends immediate fluid administration and insulin within 1-2 hours of starting fluid replacement.
The hospital had been following in-house recommendations for fluids, insulin, and labs for patients with diabetic ketoacidosis that were established in 2006 and 2011. When they examined a baseline cohort of patients treated from January to October 2014, they immediately saw that those order sets were not achieving the recommended times.
“We went back and looked at our cases and saw that overall, it was taking more than 2 hours from the time of arrival for these patients to get their insulin,” Dr. Vajravelu said.
She and her colleagues formed a quality improvement team consisting of physicians, nurses, and a pharmacist. They broke down the wait time into three components: arrival to fluid bolus, fluid bolus start to insulin start, and the overall arrival-to-insulin time. They then set specific time goals for each of those periods: giving fluids within 60 minutes of arrival, starting insulin 45-90 minutes from the bolus, and an overall door-to-insulin time of less than 120 minutes.
The team tried to determine key clinical drivers that were affecting these times. One of the first findings was a delay in diagnosing diabetic ketoacidosis (DKA). This was driven by lack of consistency in scoring patient acuity and problems with venous access.
“To address this, we standardized acuity scoring, got an IV team involved, and used point-of-care labs when possible, and educated our providers,” Dr. Vajravelu said.
The team also found that there were delays in ordering the insulin. These were driven by long wait times for intravenous fluids, by waiting for endocrinology consults, and by providers not being familiar with the DKA order sets.
To address these issues, the team changed the order set to use normal saline for all suspected DKA patients without waiting for lab results. The old orders called for delivering the fluid over a 1-hour period; that was changed to running it over 30 minutes, Dr. Vajravelu said. “That shaved off half an hour right there.”
The team examined reasons that insulin infusion was delayed. Pharmacy orders were a big part of this problem, one of which was the way the insulin was sent up from the pharmacy in a bag. “We changed that to being delivered in a syringe and tube system,” she explained.
They also changed the standing order for when insulin was started, from 60 minutes after fluid to 45 minutes.
These changes were instituted in November 2014, and the team trained clinicians on them through January 2015. Since then, the team has reassessed the situation several times, tracking 291 patients in all. They saw improvement in all three time periods, which was significant in two of them.
Arrival to fluid bolus time dropped significantly, from 55 minutes to 53 minutes – an improvement, even though the baseline time was still within the goal. Fluid bolus-to-insulin time fell significantly as well, from 96 minutes to 74 minutes – well within the new goal.
Overall arrival-to-insulin time thus decreased, from 168 minutes to 146 minutes. However, Dr. Vajravelu said, this is still longer than their goal of less than 120 minutes from door to treatment.
“We are now going back to try and see just where the delay still is,” she said. “It may be getting IV access; it may be labs. We need to tease that out.”
Fortunately, the consistent delays in treatment haven’t resulted in any adverse clinical outcomes.
“I think the biggest benefit we will see will be saving time and money in the emergency department,” Dr. Vajravelu predicted. “We hope to get patients out of there faster, getting them admitted into the hospital and treated in the appropriate department. Speeding up care and reducing waste go together in that sense.”
Dr. Vajravelu had no relevant financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @Alz_gal
ORLANDO – A few simple adjustments in standing orders shaved 20 minutes off the time one emergency department took to deliver insulin to pediatric patients with diabetic ketoacidosis, according to Mary Ellen Vajravelu, MD.
Door-to-insulin time decreased from a mean of 168 minutes to 146 minutes after the changes went into effect. Most of the time was saved in the period between starting the initial fluid bolus and starting the insulin, she said during an interview at the annual meeting of the Endocrine Society.
A single patient’s experience inspired the quality improvement project.
“A couple of years ago, we saw a patient in the emergency department with diabetic ketoacidosis who had to wait more than 6 hours before insulin was started,” she explained. “Fortunately, there were no adverse clinical outcomes from that,” but the case signaled that the treatment process needed some streamlining.
The International Society for Pediatric and Adolescent Diabetes recommends immediate fluid administration and insulin within 1-2 hours of starting fluid replacement.
The hospital had been following in-house recommendations for fluids, insulin, and labs for patients with diabetic ketoacidosis that were established in 2006 and 2011. When they examined a baseline cohort of patients treated from January to October 2014, they immediately saw that those order sets were not achieving the recommended times.
“We went back and looked at our cases and saw that overall, it was taking more than 2 hours from the time of arrival for these patients to get their insulin,” Dr. Vajravelu said.
She and her colleagues formed a quality improvement team consisting of physicians, nurses, and a pharmacist. They broke down the wait time into three components: arrival to fluid bolus, fluid bolus start to insulin start, and the overall arrival-to-insulin time. They then set specific time goals for each of those periods: giving fluids within 60 minutes of arrival, starting insulin 45-90 minutes from the bolus, and an overall door-to-insulin time of less than 120 minutes.
The team tried to determine key clinical drivers that were affecting these times. One of the first findings was a delay in diagnosing diabetic ketoacidosis (DKA). This was driven by lack of consistency in scoring patient acuity and problems with venous access.
“To address this, we standardized acuity scoring, got an IV team involved, and used point-of-care labs when possible, and educated our providers,” Dr. Vajravelu said.
The team also found that there were delays in ordering the insulin. These were driven by long wait times for intravenous fluids, by waiting for endocrinology consults, and by providers not being familiar with the DKA order sets.
To address these issues, the team changed the order set to use normal saline for all suspected DKA patients without waiting for lab results. The old orders called for delivering the fluid over a 1-hour period; that was changed to running it over 30 minutes, Dr. Vajravelu said. “That shaved off half an hour right there.”
The team examined reasons that insulin infusion was delayed. Pharmacy orders were a big part of this problem, one of which was the way the insulin was sent up from the pharmacy in a bag. “We changed that to being delivered in a syringe and tube system,” she explained.
They also changed the standing order for when insulin was started, from 60 minutes after fluid to 45 minutes.
These changes were instituted in November 2014, and the team trained clinicians on them through January 2015. Since then, the team has reassessed the situation several times, tracking 291 patients in all. They saw improvement in all three time periods, which was significant in two of them.
Arrival to fluid bolus time dropped significantly, from 55 minutes to 53 minutes – an improvement, even though the baseline time was still within the goal. Fluid bolus-to-insulin time fell significantly as well, from 96 minutes to 74 minutes – well within the new goal.
Overall arrival-to-insulin time thus decreased, from 168 minutes to 146 minutes. However, Dr. Vajravelu said, this is still longer than their goal of less than 120 minutes from door to treatment.
“We are now going back to try and see just where the delay still is,” she said. “It may be getting IV access; it may be labs. We need to tease that out.”
Fortunately, the consistent delays in treatment haven’t resulted in any adverse clinical outcomes.
“I think the biggest benefit we will see will be saving time and money in the emergency department,” Dr. Vajravelu predicted. “We hope to get patients out of there faster, getting them admitted into the hospital and treated in the appropriate department. Speeding up care and reducing waste go together in that sense.”
Dr. Vajravelu had no relevant financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @Alz_gal
ORLANDO – A few simple adjustments in standing orders shaved 20 minutes off the time one emergency department took to deliver insulin to pediatric patients with diabetic ketoacidosis, according to Mary Ellen Vajravelu, MD.
Door-to-insulin time decreased from a mean of 168 minutes to 146 minutes after the changes went into effect. Most of the time was saved in the period between starting the initial fluid bolus and starting the insulin, she said during an interview at the annual meeting of the Endocrine Society.
A single patient’s experience inspired the quality improvement project.
“A couple of years ago, we saw a patient in the emergency department with diabetic ketoacidosis who had to wait more than 6 hours before insulin was started,” she explained. “Fortunately, there were no adverse clinical outcomes from that,” but the case signaled that the treatment process needed some streamlining.
The International Society for Pediatric and Adolescent Diabetes recommends immediate fluid administration and insulin within 1-2 hours of starting fluid replacement.
The hospital had been following in-house recommendations for fluids, insulin, and labs for patients with diabetic ketoacidosis that were established in 2006 and 2011. When they examined a baseline cohort of patients treated from January to October 2014, they immediately saw that those order sets were not achieving the recommended times.
“We went back and looked at our cases and saw that overall, it was taking more than 2 hours from the time of arrival for these patients to get their insulin,” Dr. Vajravelu said.
She and her colleagues formed a quality improvement team consisting of physicians, nurses, and a pharmacist. They broke down the wait time into three components: arrival to fluid bolus, fluid bolus start to insulin start, and the overall arrival-to-insulin time. They then set specific time goals for each of those periods: giving fluids within 60 minutes of arrival, starting insulin 45-90 minutes from the bolus, and an overall door-to-insulin time of less than 120 minutes.
The team tried to determine key clinical drivers that were affecting these times. One of the first findings was a delay in diagnosing diabetic ketoacidosis (DKA). This was driven by lack of consistency in scoring patient acuity and problems with venous access.
“To address this, we standardized acuity scoring, got an IV team involved, and used point-of-care labs when possible, and educated our providers,” Dr. Vajravelu said.
The team also found that there were delays in ordering the insulin. These were driven by long wait times for intravenous fluids, by waiting for endocrinology consults, and by providers not being familiar with the DKA order sets.
To address these issues, the team changed the order set to use normal saline for all suspected DKA patients without waiting for lab results. The old orders called for delivering the fluid over a 1-hour period; that was changed to running it over 30 minutes, Dr. Vajravelu said. “That shaved off half an hour right there.”
The team examined reasons that insulin infusion was delayed. Pharmacy orders were a big part of this problem, one of which was the way the insulin was sent up from the pharmacy in a bag. “We changed that to being delivered in a syringe and tube system,” she explained.
They also changed the standing order for when insulin was started, from 60 minutes after fluid to 45 minutes.
These changes were instituted in November 2014, and the team trained clinicians on them through January 2015. Since then, the team has reassessed the situation several times, tracking 291 patients in all. They saw improvement in all three time periods, which was significant in two of them.
Arrival to fluid bolus time dropped significantly, from 55 minutes to 53 minutes – an improvement, even though the baseline time was still within the goal. Fluid bolus-to-insulin time fell significantly as well, from 96 minutes to 74 minutes – well within the new goal.
Overall arrival-to-insulin time thus decreased, from 168 minutes to 146 minutes. However, Dr. Vajravelu said, this is still longer than their goal of less than 120 minutes from door to treatment.
“We are now going back to try and see just where the delay still is,” she said. “It may be getting IV access; it may be labs. We need to tease that out.”
Fortunately, the consistent delays in treatment haven’t resulted in any adverse clinical outcomes.
“I think the biggest benefit we will see will be saving time and money in the emergency department,” Dr. Vajravelu predicted. “We hope to get patients out of there faster, getting them admitted into the hospital and treated in the appropriate department. Speeding up care and reducing waste go together in that sense.”
Dr. Vajravelu had no relevant financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @Alz_gal
AT ENDO 2017
Key clinical point:
Major finding: Overall door-to-insulin time decreased from 168 minutes to 146 minutes.
Data source: A 2-year quality improvement project involving 291 patients.
Disclosures: Dr. Vajravelu had no relevant financial disclosures.