User login
Both diabetes types increase markedly among youths
The annual incidence of both types 1 and 2 diabetes markedly increased among youths between 2002 and 2012, especially among those in minority racial and ethnic groups, according to a report published online April 13 in the New England Journal of Medicine.
Researchers analyzed trends in diabetes incidence in the observational Search for Diabetes in Youth study, which conducts annual population-based case ascertainment of the disease in people aged 0-20 years. SEARCH is funded by the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases.
In this analysis of SEARCH data, there were 11,245 youths with type 1 diabetes in 54,239,600 person-years of surveillance and 2,846 with type 2 diabetes in 28,029,000 person-years of surveillance.
“We estimated that approximately 15,900 cases of type 1 diabetes were diagnosed annually in the U.S. in the 2002-2003 period, and this number increased to 17,900 annually in the 2011-2012 period. Overall, the adjusted annual relative increase in the incidence of type 1 diabetes was 1.8%,” noted Elizabeth J. Mayer-Davis, PhD, of the departments of nutrition and medicine, University of North Carolina, Chapel Hill, and her associates (N Engl J Med. 2017 April 13. doi: 101056/NEJMoa1610187).
Similarly, they estimated that approximately 3,800 cases of type 2 diabetes were diagnosed in the first year of the study, increasing to 5,300 in the final year. The annual relative increase in type 2 diabetes was 4.8%.
The rate of increase varied across the five major ethnic groups studied: non-Hispanic whites, non-Hispanic blacks, Hispanics, Asians or Pacific Islanders, and Native Americans. Type 1 diabetes incidence rose rapidly among Hispanic youths, and type 2 diabetes rose rapidly in all racial and ethnic groups other than whites, with the greatest rate of increase among Native Americans.
These increases suggest “a growing disease burden that will not be shared equally” because of differences among ethnic groups in barriers to care, methods of treatment, and clinical outcomes. “These findings highlight the critical need to identify approaches to reduce disparities among racial and ethnic groups,” Dr. Mayer-Davis and her associates noted.
The National Institute of Diabetes and Digestive and Kidney Diseases and the Centers for Disease Control and Prevention funded the study. Dr. Mayer-Davis reported having no relevant disclosures. One of her associates reported serving as a consultant to Denka-Seiken and MedTest DX.
This study by Mayer-Davis et al. provides the most current data available on the incidence of diabetes in this age group.
The consequence of this increase in diabetes among youths is that the overall disease burden on public health is actually increasing, despite improvements in mortality and CVD rates among older diabetes patients.
According to the 2015 Global Burden of Disease report, the number of years lived with disability has increased by 32.5% and the number of years of life lost has increased by 25.4%.
What do the marked increase in the incidence of diabetes and more people at risk imply about therapy? Data from two large studies over the past several decades support that intensive glycemic control improved outcomes in persons with type 1 or type 2 diabetes mellitus. But what is missing, despite a growing understanding about the pathogenesis of each condition, is knowledge about how best to lower the number of new cases and how best to treat problems once they arise in persons with diabetes.
It is clear that we are far from controlling the negative effects of diabetes on health worldwide. As the prevalence increases, we clearly need new approaches to reduce the burden of this disease on public health.
Julie R. Ingelfinger, M.D., and John A. Jarcho, M.D., are deputy editors of The New England Journal of Medicine. They reported having no relevant disclosures. Dr. Ingelfinger and Dr. Jarcho made these remarks in an editorial accompanying Dr. Mayer-Davis’s report (N Engl J Med. 2017 April 13. doi: 10.1056/NEJMe1616575).
This study by Mayer-Davis et al. provides the most current data available on the incidence of diabetes in this age group.
The consequence of this increase in diabetes among youths is that the overall disease burden on public health is actually increasing, despite improvements in mortality and CVD rates among older diabetes patients.
According to the 2015 Global Burden of Disease report, the number of years lived with disability has increased by 32.5% and the number of years of life lost has increased by 25.4%.
What do the marked increase in the incidence of diabetes and more people at risk imply about therapy? Data from two large studies over the past several decades support that intensive glycemic control improved outcomes in persons with type 1 or type 2 diabetes mellitus. But what is missing, despite a growing understanding about the pathogenesis of each condition, is knowledge about how best to lower the number of new cases and how best to treat problems once they arise in persons with diabetes.
It is clear that we are far from controlling the negative effects of diabetes on health worldwide. As the prevalence increases, we clearly need new approaches to reduce the burden of this disease on public health.
Julie R. Ingelfinger, M.D., and John A. Jarcho, M.D., are deputy editors of The New England Journal of Medicine. They reported having no relevant disclosures. Dr. Ingelfinger and Dr. Jarcho made these remarks in an editorial accompanying Dr. Mayer-Davis’s report (N Engl J Med. 2017 April 13. doi: 10.1056/NEJMe1616575).
This study by Mayer-Davis et al. provides the most current data available on the incidence of diabetes in this age group.
The consequence of this increase in diabetes among youths is that the overall disease burden on public health is actually increasing, despite improvements in mortality and CVD rates among older diabetes patients.
According to the 2015 Global Burden of Disease report, the number of years lived with disability has increased by 32.5% and the number of years of life lost has increased by 25.4%.
What do the marked increase in the incidence of diabetes and more people at risk imply about therapy? Data from two large studies over the past several decades support that intensive glycemic control improved outcomes in persons with type 1 or type 2 diabetes mellitus. But what is missing, despite a growing understanding about the pathogenesis of each condition, is knowledge about how best to lower the number of new cases and how best to treat problems once they arise in persons with diabetes.
It is clear that we are far from controlling the negative effects of diabetes on health worldwide. As the prevalence increases, we clearly need new approaches to reduce the burden of this disease on public health.
Julie R. Ingelfinger, M.D., and John A. Jarcho, M.D., are deputy editors of The New England Journal of Medicine. They reported having no relevant disclosures. Dr. Ingelfinger and Dr. Jarcho made these remarks in an editorial accompanying Dr. Mayer-Davis’s report (N Engl J Med. 2017 April 13. doi: 10.1056/NEJMe1616575).
The annual incidence of both types 1 and 2 diabetes markedly increased among youths between 2002 and 2012, especially among those in minority racial and ethnic groups, according to a report published online April 13 in the New England Journal of Medicine.
Researchers analyzed trends in diabetes incidence in the observational Search for Diabetes in Youth study, which conducts annual population-based case ascertainment of the disease in people aged 0-20 years. SEARCH is funded by the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases.
In this analysis of SEARCH data, there were 11,245 youths with type 1 diabetes in 54,239,600 person-years of surveillance and 2,846 with type 2 diabetes in 28,029,000 person-years of surveillance.
“We estimated that approximately 15,900 cases of type 1 diabetes were diagnosed annually in the U.S. in the 2002-2003 period, and this number increased to 17,900 annually in the 2011-2012 period. Overall, the adjusted annual relative increase in the incidence of type 1 diabetes was 1.8%,” noted Elizabeth J. Mayer-Davis, PhD, of the departments of nutrition and medicine, University of North Carolina, Chapel Hill, and her associates (N Engl J Med. 2017 April 13. doi: 101056/NEJMoa1610187).
Similarly, they estimated that approximately 3,800 cases of type 2 diabetes were diagnosed in the first year of the study, increasing to 5,300 in the final year. The annual relative increase in type 2 diabetes was 4.8%.
The rate of increase varied across the five major ethnic groups studied: non-Hispanic whites, non-Hispanic blacks, Hispanics, Asians or Pacific Islanders, and Native Americans. Type 1 diabetes incidence rose rapidly among Hispanic youths, and type 2 diabetes rose rapidly in all racial and ethnic groups other than whites, with the greatest rate of increase among Native Americans.
These increases suggest “a growing disease burden that will not be shared equally” because of differences among ethnic groups in barriers to care, methods of treatment, and clinical outcomes. “These findings highlight the critical need to identify approaches to reduce disparities among racial and ethnic groups,” Dr. Mayer-Davis and her associates noted.
The National Institute of Diabetes and Digestive and Kidney Diseases and the Centers for Disease Control and Prevention funded the study. Dr. Mayer-Davis reported having no relevant disclosures. One of her associates reported serving as a consultant to Denka-Seiken and MedTest DX.
The annual incidence of both types 1 and 2 diabetes markedly increased among youths between 2002 and 2012, especially among those in minority racial and ethnic groups, according to a report published online April 13 in the New England Journal of Medicine.
Researchers analyzed trends in diabetes incidence in the observational Search for Diabetes in Youth study, which conducts annual population-based case ascertainment of the disease in people aged 0-20 years. SEARCH is funded by the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases.
In this analysis of SEARCH data, there were 11,245 youths with type 1 diabetes in 54,239,600 person-years of surveillance and 2,846 with type 2 diabetes in 28,029,000 person-years of surveillance.
“We estimated that approximately 15,900 cases of type 1 diabetes were diagnosed annually in the U.S. in the 2002-2003 period, and this number increased to 17,900 annually in the 2011-2012 period. Overall, the adjusted annual relative increase in the incidence of type 1 diabetes was 1.8%,” noted Elizabeth J. Mayer-Davis, PhD, of the departments of nutrition and medicine, University of North Carolina, Chapel Hill, and her associates (N Engl J Med. 2017 April 13. doi: 101056/NEJMoa1610187).
Similarly, they estimated that approximately 3,800 cases of type 2 diabetes were diagnosed in the first year of the study, increasing to 5,300 in the final year. The annual relative increase in type 2 diabetes was 4.8%.
The rate of increase varied across the five major ethnic groups studied: non-Hispanic whites, non-Hispanic blacks, Hispanics, Asians or Pacific Islanders, and Native Americans. Type 1 diabetes incidence rose rapidly among Hispanic youths, and type 2 diabetes rose rapidly in all racial and ethnic groups other than whites, with the greatest rate of increase among Native Americans.
These increases suggest “a growing disease burden that will not be shared equally” because of differences among ethnic groups in barriers to care, methods of treatment, and clinical outcomes. “These findings highlight the critical need to identify approaches to reduce disparities among racial and ethnic groups,” Dr. Mayer-Davis and her associates noted.
The National Institute of Diabetes and Digestive and Kidney Diseases and the Centers for Disease Control and Prevention funded the study. Dr. Mayer-Davis reported having no relevant disclosures. One of her associates reported serving as a consultant to Denka-Seiken and MedTest DX.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Both types 1 and 2 diabetes increased markedly among youths between 2002 and 2012, especially among those in minority racial and ethnic groups.
Major finding: The incidence of type 1 diabetes increased an estimated 1.8% per year and that of type 2 diabetes increased 4.8% per year between 2002 and 2012.
Data source: An observational study assessing a nationally representative sample of youths aged 0-20 years in five states, including 11,245 with type 1 and 2,846 with type 2 diabetes.
Disclosures: The National Institute of Diabetes and Digestive and Kidney Diseases and the Centers for Disease Control and Prevention funded the study. Dr. Mayer-Davis reported having no relevant disclosures. One of her associates reported serving as a consultant to Denka-Seiken and MedTest DX.
Dulera inhaler linked to adrenocorticotropic suppression in small case series
ORLANDO – A combination corticosteroid asthma inhaler has, for the first time, been associated with growth delay and adrenocorticotropic suppression in children.
The single-center case series is small, but the results highlight the need to regularly monitor growth and adrenal function in children using inhaled mometasone furoate/formoterol fumarate (Dulera; Merck), investigators said at the annual meeting of the Endocrine Society.
“We are hoping to raise awareness of this risk in our pediatric endocrinology colleagues, as well as among allergists, pulmonologists, and pediatricians who treat these children,” said Fadi Al Muhaisen, MD. “These kids should be regularly screened for growth delay and adrenal insufficiency and have their growth plotted at every visit as well.”

Dulera was approved in the United States in 2010 as a maintenance therapy for chronic asthma in adults and children aged 12 years and older. Mometasone furoate is a potent corticosteroid, and formoterol fumarate is a long-acting beta2-adrenergic agonist. The prescribing information says that mometasone furoate exerts less effect on the hypothalamic-pituitary-adrenal axis than other inhaled corticosteroids, and that adrenal suppression is unlikely to occur when used at recommended dosages. These range from a low of 100 mcg/5 mcg, two puffs daily to a maximum dose of 800 mcg/20 mcg daily.
The review involved 18 children, all of whom were seen in the endocrinology clinic for growth failure or short stature and were receiving Dulera for management of their asthma. Of these, eight (44%) had a full adrenal evaluation. Six had biochemical evidence of adrenal suppression and two had normal adrenal function. The remaining 10 patients had not undergone an adrenal evaluation. None of them were on any other inhaled corticosteroid. The six children diagnosed with adrenal insufficiency had a mean age of 9.7 years, but ranged in age from 7 to 12 years. They had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids in the preceding 6 months before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at the time of diagnosis but had been using the higher dose for the preceding 18 months. Three were using concomitant nasal steroids.
The six children evaluated had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids during the 2 years before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at time of diagnosis, but had been using the higher dose for 18 months before that. Three were using concomitant nasal steroids.
All presented with growth failure, with bone age 1-3 years behind chronological age. One child was referred to the clinic after an emergency department visit for headache, nausea, diarrhea, and fatigue – symptoms of adrenal failure. That child had an adrenocroticotropin (ACTH) level of 10 pg/mL. Both his random peak cortisol measures after ACTH stimulation were less than 1 mcg/mL.
ACTH levels in four of the children were less than 5-6 pg/ml, with random and peak stimulated cortisols of around 1 mcg/mL. One patient had an ACTH level of 68 pg/mL, a random cortisol of less than 1 mcg/mL, and a peak stimulated cortisol of 8.7 mcg/mL.
The results were all normal in the four subjects who had repeat adrenal function evaluation after intervention. Adrenal recovery took a mean of 20 months (5-30 months).
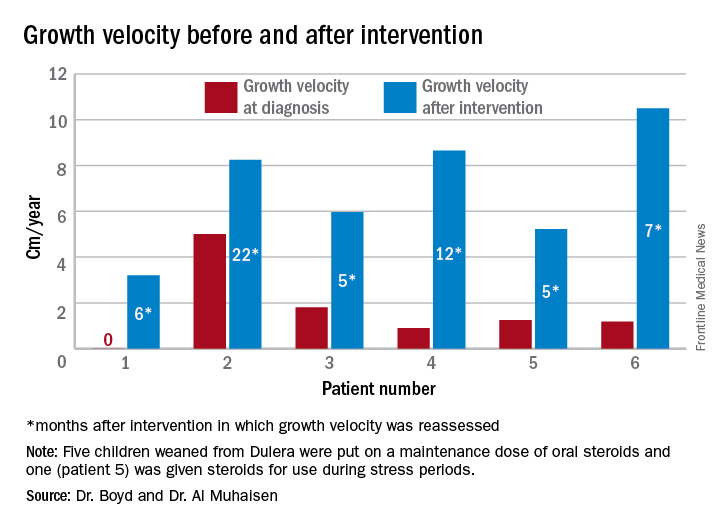
Growth accelerated rapidly after intervention, which was either initiation of maintenance oral steroids and discontinuation of Dulera or, in one patient, after Dulera was weaned. At time of adrenal insufficiency diagnosis, four patients had grown 1-2 cm in the prior year; one had not grown at all, and one had grown about 4.5 cm. After discontinuing or weaning the medication, all experienced growth spurts: 3 cm/year in 6 months; 8 cm/year in 22 months; 6 cm/year in 5 months; 8 cm/year in 12 months; 5 cm/year in 5 months; and 10 cm/year in 7 months.
There were no exacerbations in asthma, despite discontinuing the inhaled medication, Dr. Al Muhaisen said. Changing the asthma treatment required some open discussion between the investigators and the treating pulmonologists, he noted.
“We had some back-and-forth discussions, being very frank that we thought the adrenal insufficiency was directly related to this medication and that we needed to wean it and stop it as soon as possible.”
Neither Dr. Al Muhaisen nor Dr. Boyd had any financial disclosures.
ORLANDO – A combination corticosteroid asthma inhaler has, for the first time, been associated with growth delay and adrenocorticotropic suppression in children.
The single-center case series is small, but the results highlight the need to regularly monitor growth and adrenal function in children using inhaled mometasone furoate/formoterol fumarate (Dulera; Merck), investigators said at the annual meeting of the Endocrine Society.
“We are hoping to raise awareness of this risk in our pediatric endocrinology colleagues, as well as among allergists, pulmonologists, and pediatricians who treat these children,” said Fadi Al Muhaisen, MD. “These kids should be regularly screened for growth delay and adrenal insufficiency and have their growth plotted at every visit as well.”
Dulera was approved in the United States in 2010 as a maintenance therapy for chronic asthma in adults and children aged 12 years and older. Mometasone furoate is a potent corticosteroid, and formoterol fumarate is a long-acting beta2-adrenergic agonist. The prescribing information says that mometasone furoate exerts less effect on the hypothalamic-pituitary-adrenal axis than other inhaled corticosteroids, and that adrenal suppression is unlikely to occur when used at recommended dosages. These range from a low of 100 mcg/5 mcg, two puffs daily to a maximum dose of 800 mcg/20 mcg daily.
The review involved 18 children, all of whom were seen in the endocrinology clinic for growth failure or short stature and were receiving Dulera for management of their asthma. Of these, eight (44%) had a full adrenal evaluation. Six had biochemical evidence of adrenal suppression and two had normal adrenal function. The remaining 10 patients had not undergone an adrenal evaluation. None of them were on any other inhaled corticosteroid. The six children diagnosed with adrenal insufficiency had a mean age of 9.7 years, but ranged in age from 7 to 12 years. They had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids in the preceding 6 months before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at the time of diagnosis but had been using the higher dose for the preceding 18 months. Three were using concomitant nasal steroids.
The six children evaluated had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids during the 2 years before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at time of diagnosis, but had been using the higher dose for 18 months before that. Three were using concomitant nasal steroids.
All presented with growth failure, with bone age 1-3 years behind chronological age. One child was referred to the clinic after an emergency department visit for headache, nausea, diarrhea, and fatigue – symptoms of adrenal failure. That child had an adrenocroticotropin (ACTH) level of 10 pg/mL. Both his random peak cortisol measures after ACTH stimulation were less than 1 mcg/mL.
ACTH levels in four of the children were less than 5-6 pg/ml, with random and peak stimulated cortisols of around 1 mcg/mL. One patient had an ACTH level of 68 pg/mL, a random cortisol of less than 1 mcg/mL, and a peak stimulated cortisol of 8.7 mcg/mL.
The results were all normal in the four subjects who had repeat adrenal function evaluation after intervention. Adrenal recovery took a mean of 20 months (5-30 months).
Growth accelerated rapidly after intervention, which was either initiation of maintenance oral steroids and discontinuation of Dulera or, in one patient, after Dulera was weaned. At time of adrenal insufficiency diagnosis, four patients had grown 1-2 cm in the prior year; one had not grown at all, and one had grown about 4.5 cm. After discontinuing or weaning the medication, all experienced growth spurts: 3 cm/year in 6 months; 8 cm/year in 22 months; 6 cm/year in 5 months; 8 cm/year in 12 months; 5 cm/year in 5 months; and 10 cm/year in 7 months.
There were no exacerbations in asthma, despite discontinuing the inhaled medication, Dr. Al Muhaisen said. Changing the asthma treatment required some open discussion between the investigators and the treating pulmonologists, he noted.
“We had some back-and-forth discussions, being very frank that we thought the adrenal insufficiency was directly related to this medication and that we needed to wean it and stop it as soon as possible.”
Neither Dr. Al Muhaisen nor Dr. Boyd had any financial disclosures.
ORLANDO – A combination corticosteroid asthma inhaler has, for the first time, been associated with growth delay and adrenocorticotropic suppression in children.
The single-center case series is small, but the results highlight the need to regularly monitor growth and adrenal function in children using inhaled mometasone furoate/formoterol fumarate (Dulera; Merck), investigators said at the annual meeting of the Endocrine Society.
“We are hoping to raise awareness of this risk in our pediatric endocrinology colleagues, as well as among allergists, pulmonologists, and pediatricians who treat these children,” said Fadi Al Muhaisen, MD. “These kids should be regularly screened for growth delay and adrenal insufficiency and have their growth plotted at every visit as well.”
Dulera was approved in the United States in 2010 as a maintenance therapy for chronic asthma in adults and children aged 12 years and older. Mometasone furoate is a potent corticosteroid, and formoterol fumarate is a long-acting beta2-adrenergic agonist. The prescribing information says that mometasone furoate exerts less effect on the hypothalamic-pituitary-adrenal axis than other inhaled corticosteroids, and that adrenal suppression is unlikely to occur when used at recommended dosages. These range from a low of 100 mcg/5 mcg, two puffs daily to a maximum dose of 800 mcg/20 mcg daily.
The review involved 18 children, all of whom were seen in the endocrinology clinic for growth failure or short stature and were receiving Dulera for management of their asthma. Of these, eight (44%) had a full adrenal evaluation. Six had biochemical evidence of adrenal suppression and two had normal adrenal function. The remaining 10 patients had not undergone an adrenal evaluation. None of them were on any other inhaled corticosteroid. The six children diagnosed with adrenal insufficiency had a mean age of 9.7 years, but ranged in age from 7 to 12 years. They had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids in the preceding 6 months before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at the time of diagnosis but had been using the higher dose for the preceding 18 months. Three were using concomitant nasal steroids.
The six children evaluated had been using the medication for a mean of 1.3 years, although that varied widely, from just a few months to about 2 years. Only one had been on oral steroids during the 2 years before coming to the endocrinology clinic. Five were using the 200 mcg/5 mcg dose, two puffs daily; one child was taking one puff daily of 100 mcg/5 mcg at time of diagnosis, but had been using the higher dose for 18 months before that. Three were using concomitant nasal steroids.
All presented with growth failure, with bone age 1-3 years behind chronological age. One child was referred to the clinic after an emergency department visit for headache, nausea, diarrhea, and fatigue – symptoms of adrenal failure. That child had an adrenocroticotropin (ACTH) level of 10 pg/mL. Both his random peak cortisol measures after ACTH stimulation were less than 1 mcg/mL.
ACTH levels in four of the children were less than 5-6 pg/ml, with random and peak stimulated cortisols of around 1 mcg/mL. One patient had an ACTH level of 68 pg/mL, a random cortisol of less than 1 mcg/mL, and a peak stimulated cortisol of 8.7 mcg/mL.
The results were all normal in the four subjects who had repeat adrenal function evaluation after intervention. Adrenal recovery took a mean of 20 months (5-30 months).
Growth accelerated rapidly after intervention, which was either initiation of maintenance oral steroids and discontinuation of Dulera or, in one patient, after Dulera was weaned. At time of adrenal insufficiency diagnosis, four patients had grown 1-2 cm in the prior year; one had not grown at all, and one had grown about 4.5 cm. After discontinuing or weaning the medication, all experienced growth spurts: 3 cm/year in 6 months; 8 cm/year in 22 months; 6 cm/year in 5 months; 8 cm/year in 12 months; 5 cm/year in 5 months; and 10 cm/year in 7 months.
There were no exacerbations in asthma, despite discontinuing the inhaled medication, Dr. Al Muhaisen said. Changing the asthma treatment required some open discussion between the investigators and the treating pulmonologists, he noted.
“We had some back-and-forth discussions, being very frank that we thought the adrenal insufficiency was directly related to this medication and that we needed to wean it and stop it as soon as possible.”
Neither Dr. Al Muhaisen nor Dr. Boyd had any financial disclosures.
AT ENDO 2017
Key clinical point:
Major finding: Of eight children who had an adrenal workup at an endocrinology clinic, six had adrenal suppression.
Data source: The case series comprised 18 children taking Dulera who presented with growth failure.
Disclosures: Neither Dr. Al Muhaisen nor Dr. Boyd had any financial disclosures.
Study reveals global inequalities in childhood leukemia survival

New research has revealed global inequalities in survival rates for pediatric patients with leukemia.
Investigators analyzed data on nearly 90,000 pediatric leukemia patients treated in 53 countries.
In most countries, patients with lymphoid leukemias or acute myeloid leukemia (AML) saw an increase in 5-year survival between 1995 and 2009.
However, there were wide variations in survival between the countries.
The investigators reported these findings in The Lancet Haematology.
They evaluated data from 89,828 leukemia patients (ages 0 to 14) included in 198 cancer registries in 53 countries.
The team estimated 5-year net survival for patients with AML or lymphoid leukemias (controlling for non-leukemia-related deaths) by calendar period of diagnosis—1995–1999, 2000–2004, and 2005–2009—in each country.
For children diagnosed with lymphoid leukemias between 1995 and 1999, 5-year survival rates ranged from 10.6% (in China) to 86.8% (in Austria). For children diagnosed between 2005 and 2009, the rates ranged from 52.4% (Colombia) to 91.6% (Germany).
For AML, 5-year survival rates ranged from 4.2% (China) to 72.2% (Sweden) in patients diagnosed between 1995 and 1999. For children diagnosed between 2005 and 2009, 5-year survival rates ranged from 33.3% (Bulgaria) to 78.2% (Germany).
The investigators noted that, in some countries, survival for both groups of leukemia patients was consistently high.
In Austria, for example, 5-year survival rates for lymphoid leukemias were 86.8% in 1995-1999 and 91.1% in 2005-2009. For AML, rates were 60.1% and 72.6%, respectively.
Other countries saw substantial increases in survival over time.
In China, the 5-year survival rate for patients with lymphoid leukemias increased from 10.6% in 1995-1999 to 69.2% in 2005-2009. For patients with AML, the rate increased from 4.2% to 41.1%.
“These findings show the extent of worldwide inequalities in access to optimal healthcare for children with cancer,” said study author Audrey Bonaventure, MD, PhD, of the London School of Hygiene & Tropical Medicine in the UK.
“Providing additional resources, alongside evidence-based initiatives such as international collaborations and treatment guidelines, could improve access to efficient treatment and care for all children with leukemia. This would contribute substantially to reducing worldwide inequalities in survival.” ![]()
New research has revealed global inequalities in survival rates for pediatric patients with leukemia.
Investigators analyzed data on nearly 90,000 pediatric leukemia patients treated in 53 countries.
In most countries, patients with lymphoid leukemias or acute myeloid leukemia (AML) saw an increase in 5-year survival between 1995 and 2009.
However, there were wide variations in survival between the countries.
The investigators reported these findings in The Lancet Haematology.
They evaluated data from 89,828 leukemia patients (ages 0 to 14) included in 198 cancer registries in 53 countries.
The team estimated 5-year net survival for patients with AML or lymphoid leukemias (controlling for non-leukemia-related deaths) by calendar period of diagnosis—1995–1999, 2000–2004, and 2005–2009—in each country.
For children diagnosed with lymphoid leukemias between 1995 and 1999, 5-year survival rates ranged from 10.6% (in China) to 86.8% (in Austria). For children diagnosed between 2005 and 2009, the rates ranged from 52.4% (Colombia) to 91.6% (Germany).
For AML, 5-year survival rates ranged from 4.2% (China) to 72.2% (Sweden) in patients diagnosed between 1995 and 1999. For children diagnosed between 2005 and 2009, 5-year survival rates ranged from 33.3% (Bulgaria) to 78.2% (Germany).
The investigators noted that, in some countries, survival for both groups of leukemia patients was consistently high.
In Austria, for example, 5-year survival rates for lymphoid leukemias were 86.8% in 1995-1999 and 91.1% in 2005-2009. For AML, rates were 60.1% and 72.6%, respectively.
Other countries saw substantial increases in survival over time.
In China, the 5-year survival rate for patients with lymphoid leukemias increased from 10.6% in 1995-1999 to 69.2% in 2005-2009. For patients with AML, the rate increased from 4.2% to 41.1%.
“These findings show the extent of worldwide inequalities in access to optimal healthcare for children with cancer,” said study author Audrey Bonaventure, MD, PhD, of the London School of Hygiene & Tropical Medicine in the UK.
“Providing additional resources, alongside evidence-based initiatives such as international collaborations and treatment guidelines, could improve access to efficient treatment and care for all children with leukemia. This would contribute substantially to reducing worldwide inequalities in survival.” ![]()
New research has revealed global inequalities in survival rates for pediatric patients with leukemia.
Investigators analyzed data on nearly 90,000 pediatric leukemia patients treated in 53 countries.
In most countries, patients with lymphoid leukemias or acute myeloid leukemia (AML) saw an increase in 5-year survival between 1995 and 2009.
However, there were wide variations in survival between the countries.
The investigators reported these findings in The Lancet Haematology.
They evaluated data from 89,828 leukemia patients (ages 0 to 14) included in 198 cancer registries in 53 countries.
The team estimated 5-year net survival for patients with AML or lymphoid leukemias (controlling for non-leukemia-related deaths) by calendar period of diagnosis—1995–1999, 2000–2004, and 2005–2009—in each country.
For children diagnosed with lymphoid leukemias between 1995 and 1999, 5-year survival rates ranged from 10.6% (in China) to 86.8% (in Austria). For children diagnosed between 2005 and 2009, the rates ranged from 52.4% (Colombia) to 91.6% (Germany).
For AML, 5-year survival rates ranged from 4.2% (China) to 72.2% (Sweden) in patients diagnosed between 1995 and 1999. For children diagnosed between 2005 and 2009, 5-year survival rates ranged from 33.3% (Bulgaria) to 78.2% (Germany).
The investigators noted that, in some countries, survival for both groups of leukemia patients was consistently high.
In Austria, for example, 5-year survival rates for lymphoid leukemias were 86.8% in 1995-1999 and 91.1% in 2005-2009. For AML, rates were 60.1% and 72.6%, respectively.
Other countries saw substantial increases in survival over time.
In China, the 5-year survival rate for patients with lymphoid leukemias increased from 10.6% in 1995-1999 to 69.2% in 2005-2009. For patients with AML, the rate increased from 4.2% to 41.1%.
“These findings show the extent of worldwide inequalities in access to optimal healthcare for children with cancer,” said study author Audrey Bonaventure, MD, PhD, of the London School of Hygiene & Tropical Medicine in the UK.
“Providing additional resources, alongside evidence-based initiatives such as international collaborations and treatment guidelines, could improve access to efficient treatment and care for all children with leukemia. This would contribute substantially to reducing worldwide inequalities in survival.” ![]()
AAN spotlights spinal muscular atrophy clinical research
A variety of plenary and emerging science sessions at this year’s annual meeting of the American Academy of Neurology in Boston will highlight clinical research efforts to treat children with spinal muscular atrophy.
At the Hot Topics Plenary Session on April 22, Claudia A. Chiriboga, MD, of Columbia University, New York, will discuss the results of clinical trials involving antisense oligonucleotide treatments for spinal muscular atrophy (SMA), including the recently approved nusinersen (Spinraza), which promotes transcription of the full-length survival motor neuron (SMN) protein from the SMN2 gene.
In the first of two reports on new clinical research about nusinersen, Nancy L. Kuntz, MD, of Ann & Robert H. Lurie Children’s Hospital of Chicago will present the initial interim efficacy and safety findings from the phase III international ENDEAR study on April 24 at the Contemporary Clinical Issues Plenary Session. The study of 122 infants with SMA is comparing intrathecal administration of nusinersen against a sham procedure of a small needle prick on the lower back to look for differences at day 402 in the primary outcome of the percentage of patients who attain motor milestones as assessed by section 2 of the Hammersmith Infant Neurological Examination or the time to death or need for respiratory intervention. Charlotte J. Sumner, MD, of Johns Hopkins University, Baltimore, will discuss the study following Dr. Kuntz’s presentation.
The second nusinersen trial to be reported at the meeting will describe interim results of the drug’s efficacy and safety in children with later-onset SMA in the phase III CHERISH study. At the Emerging Science Platform Session on April 25, Richard S. Finkel, MD, of Nemours Children’s Hospital in Orlando, Fla., will discuss how the primary outcome of the Hammersmith Functional Motor Scale–Expanded score changed from baseline to 15 months following intrathecal injection or a sham procedure in children aged 2-12 years.
An investigational SMA type 1 treatment just beginning testing in clinical trials will also receive attention in a plenary session and a platform session. In the Clinical Trials Plenary Session on April 25, Jerry R. Mendell, MD, of Nationwide Children’s Hospital, Columbus, Ohio, will report on the first gene therapy trial for SMA type 1, a phase I trial of AVXS-101, which delivers the SMN gene in a AAV9 viral vector that is able to cross the blood-brain barrier. The primary objective of the trial is to assess safety of a single intravenous dose. The secondary objectives include survival (avoidance of death/permanent-ventilation) and the ability to sit unassisted. Other analyses of data from the phase I trial will be reported during the “Motor Neuron Diseases: Biomarkers, Outcome Measures, and Therapeutics,” platform session on April 24, including the evaluation of preexisting anti-AAV9 antibodies and the proportion of patients who achieve CHOP-INTEND scores of 50 and above and sit unassisted.
A variety of plenary and emerging science sessions at this year’s annual meeting of the American Academy of Neurology in Boston will highlight clinical research efforts to treat children with spinal muscular atrophy.
At the Hot Topics Plenary Session on April 22, Claudia A. Chiriboga, MD, of Columbia University, New York, will discuss the results of clinical trials involving antisense oligonucleotide treatments for spinal muscular atrophy (SMA), including the recently approved nusinersen (Spinraza), which promotes transcription of the full-length survival motor neuron (SMN) protein from the SMN2 gene.
In the first of two reports on new clinical research about nusinersen, Nancy L. Kuntz, MD, of Ann & Robert H. Lurie Children’s Hospital of Chicago will present the initial interim efficacy and safety findings from the phase III international ENDEAR study on April 24 at the Contemporary Clinical Issues Plenary Session. The study of 122 infants with SMA is comparing intrathecal administration of nusinersen against a sham procedure of a small needle prick on the lower back to look for differences at day 402 in the primary outcome of the percentage of patients who attain motor milestones as assessed by section 2 of the Hammersmith Infant Neurological Examination or the time to death or need for respiratory intervention. Charlotte J. Sumner, MD, of Johns Hopkins University, Baltimore, will discuss the study following Dr. Kuntz’s presentation.
The second nusinersen trial to be reported at the meeting will describe interim results of the drug’s efficacy and safety in children with later-onset SMA in the phase III CHERISH study. At the Emerging Science Platform Session on April 25, Richard S. Finkel, MD, of Nemours Children’s Hospital in Orlando, Fla., will discuss how the primary outcome of the Hammersmith Functional Motor Scale–Expanded score changed from baseline to 15 months following intrathecal injection or a sham procedure in children aged 2-12 years.
An investigational SMA type 1 treatment just beginning testing in clinical trials will also receive attention in a plenary session and a platform session. In the Clinical Trials Plenary Session on April 25, Jerry R. Mendell, MD, of Nationwide Children’s Hospital, Columbus, Ohio, will report on the first gene therapy trial for SMA type 1, a phase I trial of AVXS-101, which delivers the SMN gene in a AAV9 viral vector that is able to cross the blood-brain barrier. The primary objective of the trial is to assess safety of a single intravenous dose. The secondary objectives include survival (avoidance of death/permanent-ventilation) and the ability to sit unassisted. Other analyses of data from the phase I trial will be reported during the “Motor Neuron Diseases: Biomarkers, Outcome Measures, and Therapeutics,” platform session on April 24, including the evaluation of preexisting anti-AAV9 antibodies and the proportion of patients who achieve CHOP-INTEND scores of 50 and above and sit unassisted.
A variety of plenary and emerging science sessions at this year’s annual meeting of the American Academy of Neurology in Boston will highlight clinical research efforts to treat children with spinal muscular atrophy.
At the Hot Topics Plenary Session on April 22, Claudia A. Chiriboga, MD, of Columbia University, New York, will discuss the results of clinical trials involving antisense oligonucleotide treatments for spinal muscular atrophy (SMA), including the recently approved nusinersen (Spinraza), which promotes transcription of the full-length survival motor neuron (SMN) protein from the SMN2 gene.
In the first of two reports on new clinical research about nusinersen, Nancy L. Kuntz, MD, of Ann & Robert H. Lurie Children’s Hospital of Chicago will present the initial interim efficacy and safety findings from the phase III international ENDEAR study on April 24 at the Contemporary Clinical Issues Plenary Session. The study of 122 infants with SMA is comparing intrathecal administration of nusinersen against a sham procedure of a small needle prick on the lower back to look for differences at day 402 in the primary outcome of the percentage of patients who attain motor milestones as assessed by section 2 of the Hammersmith Infant Neurological Examination or the time to death or need for respiratory intervention. Charlotte J. Sumner, MD, of Johns Hopkins University, Baltimore, will discuss the study following Dr. Kuntz’s presentation.
The second nusinersen trial to be reported at the meeting will describe interim results of the drug’s efficacy and safety in children with later-onset SMA in the phase III CHERISH study. At the Emerging Science Platform Session on April 25, Richard S. Finkel, MD, of Nemours Children’s Hospital in Orlando, Fla., will discuss how the primary outcome of the Hammersmith Functional Motor Scale–Expanded score changed from baseline to 15 months following intrathecal injection or a sham procedure in children aged 2-12 years.
An investigational SMA type 1 treatment just beginning testing in clinical trials will also receive attention in a plenary session and a platform session. In the Clinical Trials Plenary Session on April 25, Jerry R. Mendell, MD, of Nationwide Children’s Hospital, Columbus, Ohio, will report on the first gene therapy trial for SMA type 1, a phase I trial of AVXS-101, which delivers the SMN gene in a AAV9 viral vector that is able to cross the blood-brain barrier. The primary objective of the trial is to assess safety of a single intravenous dose. The secondary objectives include survival (avoidance of death/permanent-ventilation) and the ability to sit unassisted. Other analyses of data from the phase I trial will be reported during the “Motor Neuron Diseases: Biomarkers, Outcome Measures, and Therapeutics,” platform session on April 24, including the evaluation of preexisting anti-AAV9 antibodies and the proportion of patients who achieve CHOP-INTEND scores of 50 and above and sit unassisted.
Compounding rules challenge practice norms
As new rules about drug compounding get shaped, rheumatologists seek to protect their ability to combine injectable drugs – most commonly a steroid and a local anesthetic – in their own offices.
In a position statement sent to government agencies and members of Congress in February, the American College of Rheumatology voiced concerns that the practice, which it called “critical,” could become a casualty of drug-compounding regulations under revision by the United States Pharmacopeial Convention (USP), a nonprofit group whose standards are enforceable by state and federal regulators.

In the same position statement on compounding, the ACR said it also seeks a change to a Food and Drug Administration rule limiting practitioners’ access to quinacrine, a drug only available through compounding pharmacies that is sometimes used to treat lupus patients. Quinacrine is not on the FDA’s current list of bulk substances approved for compounding, except by special permission. The ACR has asked the agency to add quinacrine to the list, but no one knows when this will happen.
Rheumatologists may also be more restricted than before in terms of which compounding pharmacies they can turn to, as new federal standards divide them into two types – those that can provide medicines in larger quantities and those that can’t.
Steroid fiasco sparked rule revisions
The ACR’s concerns follow a tighter focus by state and federal agencies on drug compounding after a fungal meningitis outbreak in 2012 was traced to contaminated steroids produced in bulk by a compounding pharmacy.
More than 800 infections, 64 of them fatal, occurred after the New England Compounding Center in Framingham, Mass., sold contaminated methylprednisolone acetate that was used in epidural and intra-articular joint injections.
The following year Congress passed the Drug Quality and Security Act, which aims, in part, to prevent compounding pharmacies from engaging in what amounts to unregulated manufacturing.
As part of the law, the FDA created a list of drugs appropriate for compounding and a process by which larger compounding pharmacies must register with the FDA, and agree to inspections. The USP standards, meanwhile, address detailed technical and safety aspects of compounding and are enforceable by the FDA and state agencies.
“USP and FDA have had the ability to regulate compounding for over a decade, but only recently have the rules become actively enforced,” said Donald Miller, PharmD, of North Dakota State University, Fargo, who helped shape the ACR’s position statement on compounding with the help of rheumatologists in private practice.
“When you make guidelines for safety, they make sense, but then you can’t anticipate the way it’s going to affect individuals’ practice. And that’s where rheumatology got caught up,” said Dr. Miller, who was a member of the FDA Arthritis Advisory Committee in 2014-2016.
In-office mixing a top concern
Other specialties, including dermatology and immunology, also stand to be affected by various changes to compounding law and practice – and their societies have been active in voicing concerns.
Though the latest revisions of USP chapter 797, which impacts in-office mixing, are still being sorted out, it’s the No. 1 compounding-related concern for rheumatologists, Dr. Miller said.
Rheumatologists routinely mix an analgesic and a steroid for injection. The analgesic makes the steroids less viscous, and offers patients hours of immediate relief. They also add analgesics to hyaluronic acid injected for viscosupplementation. The mixing is usually conducted bedside, and the injections are administered right away.
Technically, combining these products amounts to sterile compounding, Dr. Miller explained. “And theoretically, under these rules, a physician could still do this, but they’d have to do it under a sterile hood like you find in a pharmacy, and that’s just not practical. It also becomes a matter of interpretation.”
USP chapter 797 sanctions in-office mixing for “immediate use” with individual patients – which is nearly always the case for the steroid injections used in rheumatology. But it’s unclear whether “immediate use” means emergency use only, or allows for routine use, as rheumatologists hope.
“One reason this came to rheumatology’s attention is that some state boards of medicine were inspecting and saying ‘Hey, you can’t do that,’ ” Dr. Miller said.

“There’s that law of unintended consequences where you snare things in a net that you really don’t want to,” Dr. Huffstutter said.
Marcus Snow, MD, a rheumatologist at the University of Nebraska, Omaha, who also worked on the statement, said that most rheumatologists are likely unaware that their ability to mix drugs in-office has been called into question.
“I brought it up at our division meeting with a group of 10 rheumatologists, and no one was aware that this was coming down the pike,” Dr. Snow said in an interview.

Pediatric issues
Pediatric rheumatologists, and adult rheumatologists who see children occasionally, use compounding pharmacies to create palatable oral medicines and adjusted doses of adult treatments.
They also use injections combining steroids with analgesics, and consider the addition of the analgesic a key aid to compliance.
“The biggest barrier we have is patient and parent anxiety about doing the procedure and the associated pain. We always administer our steroids mixed with lidocaine to help with the postprocedural discomfort,” said Adam Reinhardt, MD, chief of pediatric rheumatology at the University of Nebraska and Children’s Hospital and Medical Center in Omaha.

Steroid injections can mean avoiding or delaying systemic treatment in children with oligoarticular arthritis, he said. “Most of us consider them a first-line therapy. The hope is that you can get by without having to use meds like methotrexate if you can get a prolonged response in the one or two joints that are active in that patient.”
But Dr. Reinhardt said that, while he mixed his own injections during his fellowship training, Children’s of Omaha now insists that they be prepared by in-house pharmacists, working under sterile hoods. The delay to receiving them in the clinic or procedure room is 40 minutes to an hour, he said, which the clinicians accommodate through careful scheduling.
The change from mixing in-clinic to relying on the central pharmacy came about in recent years, Dr. Reinhardt said, because of broader concerns related to medication storage in the clinics. While ordering from the central pharmacy works for his practice, he said, “I probably only inject maybe 50-70 joints a year, while adult rheumatologists are injecting far more than that. For a busy private practice, I can see that being a huge time constraint,” he said.
Relevance of rules
None of the rheumatologists interviewed questioned the need for tightened state and federal oversight of compounding practices overall – just the applicability of certain rules to their own practice.
Dr. Snow and Dr. Huffstutter noted that reports of infected joints – a potential result of a contaminated injection – are sporadic and rare. “There’s very little research in this, but [these types of injections] have been standard practice for decades,” Dr. Snow said.
Srikanth Mukkera, MD, a rheumatologist in Tupelo, Miss., agreed that “sporadic cases of joint infection do happen following injection, but it can be hard to show if an injection was the cause.”
Assuring that medicines are mixed only immediately prior to injection, and not stored, reduces the likelihood of contamination, Dr. Mukkera said. Moreover, he noted, epidural injections such as those that resulted in the 2012 meningitis outbreak carry different risks than those seen in intra-articular injections.
Dr. Miller, the lead author of the ACR statement, said that the rheumatologists on our committee “don’t know of anyone that’s had a knee or other joint infection from a contaminated injection. They feel that unless somebody finds some evidence of that, they should be allowed to continue” with their usual practice.
He said that he feels that the USP will ultimately heed the concerns of rheumatologists and hopefully provide a more relaxed interpretation of in-office compounding. “We’re hoping they’ll make some exceptions when they revise 797 standards or at least maybe leave room for organizations to create a best practice statement. We’ll see,” Dr. Miller said.
But this is in no way guaranteed. Dr. Huffstutter said he fears that, if the rules come to be interpreted more narrowly, even standard practices like reconstituting biologic drugs for infusion – something that’s also a routine part of in-office practice – could fall under the rubric of sterile compounding and come into question.
The quinacrine problem
A separate compounding-related issue in rheumatology is clinicians’ access to quinacrine, an antimalarial rheumatology drug that, while infrequently used, represents the only alternative to hydroxychloroquine for some lupus patients.
“There are no alternatives out there for hydroxychloroquine, so we need it as a backup,” Dr. Snow said. “If hydroxychloroquine isn’t an option, there’s nothing out there that we can use. There’s no easy replacement.”
Dr. Huffstutter said he currently had no patients on quinacrine. “It’s not very often that we use it, but in those patients that really need it, it can make a huge difference in how they do.”
Quinacrine is no longer manufactured commercially as a finished drug product but is available in a powder that compounding physicians put into 100-mg capsules. It is not on the FDA’s current list of drugs available for compounding except with special permission.
While the ACR has requested that the FDA add it the list of bulk drug substances that can be used in compounding, quinacrine remains off the list for now – and, providers say, hard to find.
Moreover, while rheumatologists may have previously been able to order and store quantities of quinacrine and other compounded nonsterile medications to dispense to their patients, they can no longer easily do so, as only the FDA-approved compounding “outsourcing facilities” are allowed to process larger orders; the rest can only respond to prescriptions for individual patients.
Dr. Miller said it’s likely that quinacrine will make it onto the FDA’s next list of bulk drugs available for compounding. “The FDA has kind of said, ‘Don’t worry about it,’ ” he said.
As new rules about drug compounding get shaped, rheumatologists seek to protect their ability to combine injectable drugs – most commonly a steroid and a local anesthetic – in their own offices.
In a position statement sent to government agencies and members of Congress in February, the American College of Rheumatology voiced concerns that the practice, which it called “critical,” could become a casualty of drug-compounding regulations under revision by the United States Pharmacopeial Convention (USP), a nonprofit group whose standards are enforceable by state and federal regulators.
In the same position statement on compounding, the ACR said it also seeks a change to a Food and Drug Administration rule limiting practitioners’ access to quinacrine, a drug only available through compounding pharmacies that is sometimes used to treat lupus patients. Quinacrine is not on the FDA’s current list of bulk substances approved for compounding, except by special permission. The ACR has asked the agency to add quinacrine to the list, but no one knows when this will happen.
Rheumatologists may also be more restricted than before in terms of which compounding pharmacies they can turn to, as new federal standards divide them into two types – those that can provide medicines in larger quantities and those that can’t.
Steroid fiasco sparked rule revisions
The ACR’s concerns follow a tighter focus by state and federal agencies on drug compounding after a fungal meningitis outbreak in 2012 was traced to contaminated steroids produced in bulk by a compounding pharmacy.
More than 800 infections, 64 of them fatal, occurred after the New England Compounding Center in Framingham, Mass., sold contaminated methylprednisolone acetate that was used in epidural and intra-articular joint injections.
The following year Congress passed the Drug Quality and Security Act, which aims, in part, to prevent compounding pharmacies from engaging in what amounts to unregulated manufacturing.
As part of the law, the FDA created a list of drugs appropriate for compounding and a process by which larger compounding pharmacies must register with the FDA, and agree to inspections. The USP standards, meanwhile, address detailed technical and safety aspects of compounding and are enforceable by the FDA and state agencies.
“USP and FDA have had the ability to regulate compounding for over a decade, but only recently have the rules become actively enforced,” said Donald Miller, PharmD, of North Dakota State University, Fargo, who helped shape the ACR’s position statement on compounding with the help of rheumatologists in private practice.
“When you make guidelines for safety, they make sense, but then you can’t anticipate the way it’s going to affect individuals’ practice. And that’s where rheumatology got caught up,” said Dr. Miller, who was a member of the FDA Arthritis Advisory Committee in 2014-2016.
In-office mixing a top concern
Other specialties, including dermatology and immunology, also stand to be affected by various changes to compounding law and practice – and their societies have been active in voicing concerns.
Though the latest revisions of USP chapter 797, which impacts in-office mixing, are still being sorted out, it’s the No. 1 compounding-related concern for rheumatologists, Dr. Miller said.
Rheumatologists routinely mix an analgesic and a steroid for injection. The analgesic makes the steroids less viscous, and offers patients hours of immediate relief. They also add analgesics to hyaluronic acid injected for viscosupplementation. The mixing is usually conducted bedside, and the injections are administered right away.
Technically, combining these products amounts to sterile compounding, Dr. Miller explained. “And theoretically, under these rules, a physician could still do this, but they’d have to do it under a sterile hood like you find in a pharmacy, and that’s just not practical. It also becomes a matter of interpretation.”
USP chapter 797 sanctions in-office mixing for “immediate use” with individual patients – which is nearly always the case for the steroid injections used in rheumatology. But it’s unclear whether “immediate use” means emergency use only, or allows for routine use, as rheumatologists hope.
“One reason this came to rheumatology’s attention is that some state boards of medicine were inspecting and saying ‘Hey, you can’t do that,’ ” Dr. Miller said.
“There’s that law of unintended consequences where you snare things in a net that you really don’t want to,” Dr. Huffstutter said.
Marcus Snow, MD, a rheumatologist at the University of Nebraska, Omaha, who also worked on the statement, said that most rheumatologists are likely unaware that their ability to mix drugs in-office has been called into question.
“I brought it up at our division meeting with a group of 10 rheumatologists, and no one was aware that this was coming down the pike,” Dr. Snow said in an interview.
Pediatric issues
Pediatric rheumatologists, and adult rheumatologists who see children occasionally, use compounding pharmacies to create palatable oral medicines and adjusted doses of adult treatments.
They also use injections combining steroids with analgesics, and consider the addition of the analgesic a key aid to compliance.
“The biggest barrier we have is patient and parent anxiety about doing the procedure and the associated pain. We always administer our steroids mixed with lidocaine to help with the postprocedural discomfort,” said Adam Reinhardt, MD, chief of pediatric rheumatology at the University of Nebraska and Children’s Hospital and Medical Center in Omaha.
Steroid injections can mean avoiding or delaying systemic treatment in children with oligoarticular arthritis, he said. “Most of us consider them a first-line therapy. The hope is that you can get by without having to use meds like methotrexate if you can get a prolonged response in the one or two joints that are active in that patient.”
But Dr. Reinhardt said that, while he mixed his own injections during his fellowship training, Children’s of Omaha now insists that they be prepared by in-house pharmacists, working under sterile hoods. The delay to receiving them in the clinic or procedure room is 40 minutes to an hour, he said, which the clinicians accommodate through careful scheduling.
The change from mixing in-clinic to relying on the central pharmacy came about in recent years, Dr. Reinhardt said, because of broader concerns related to medication storage in the clinics. While ordering from the central pharmacy works for his practice, he said, “I probably only inject maybe 50-70 joints a year, while adult rheumatologists are injecting far more than that. For a busy private practice, I can see that being a huge time constraint,” he said.
Relevance of rules
None of the rheumatologists interviewed questioned the need for tightened state and federal oversight of compounding practices overall – just the applicability of certain rules to their own practice.
Dr. Snow and Dr. Huffstutter noted that reports of infected joints – a potential result of a contaminated injection – are sporadic and rare. “There’s very little research in this, but [these types of injections] have been standard practice for decades,” Dr. Snow said.
Srikanth Mukkera, MD, a rheumatologist in Tupelo, Miss., agreed that “sporadic cases of joint infection do happen following injection, but it can be hard to show if an injection was the cause.”
Assuring that medicines are mixed only immediately prior to injection, and not stored, reduces the likelihood of contamination, Dr. Mukkera said. Moreover, he noted, epidural injections such as those that resulted in the 2012 meningitis outbreak carry different risks than those seen in intra-articular injections.
Dr. Miller, the lead author of the ACR statement, said that the rheumatologists on our committee “don’t know of anyone that’s had a knee or other joint infection from a contaminated injection. They feel that unless somebody finds some evidence of that, they should be allowed to continue” with their usual practice.
He said that he feels that the USP will ultimately heed the concerns of rheumatologists and hopefully provide a more relaxed interpretation of in-office compounding. “We’re hoping they’ll make some exceptions when they revise 797 standards or at least maybe leave room for organizations to create a best practice statement. We’ll see,” Dr. Miller said.
But this is in no way guaranteed. Dr. Huffstutter said he fears that, if the rules come to be interpreted more narrowly, even standard practices like reconstituting biologic drugs for infusion – something that’s also a routine part of in-office practice – could fall under the rubric of sterile compounding and come into question.
The quinacrine problem
A separate compounding-related issue in rheumatology is clinicians’ access to quinacrine, an antimalarial rheumatology drug that, while infrequently used, represents the only alternative to hydroxychloroquine for some lupus patients.
“There are no alternatives out there for hydroxychloroquine, so we need it as a backup,” Dr. Snow said. “If hydroxychloroquine isn’t an option, there’s nothing out there that we can use. There’s no easy replacement.”
Dr. Huffstutter said he currently had no patients on quinacrine. “It’s not very often that we use it, but in those patients that really need it, it can make a huge difference in how they do.”
Quinacrine is no longer manufactured commercially as a finished drug product but is available in a powder that compounding physicians put into 100-mg capsules. It is not on the FDA’s current list of drugs available for compounding except with special permission.
While the ACR has requested that the FDA add it the list of bulk drug substances that can be used in compounding, quinacrine remains off the list for now – and, providers say, hard to find.
Moreover, while rheumatologists may have previously been able to order and store quantities of quinacrine and other compounded nonsterile medications to dispense to their patients, they can no longer easily do so, as only the FDA-approved compounding “outsourcing facilities” are allowed to process larger orders; the rest can only respond to prescriptions for individual patients.
Dr. Miller said it’s likely that quinacrine will make it onto the FDA’s next list of bulk drugs available for compounding. “The FDA has kind of said, ‘Don’t worry about it,’ ” he said.
As new rules about drug compounding get shaped, rheumatologists seek to protect their ability to combine injectable drugs – most commonly a steroid and a local anesthetic – in their own offices.
In a position statement sent to government agencies and members of Congress in February, the American College of Rheumatology voiced concerns that the practice, which it called “critical,” could become a casualty of drug-compounding regulations under revision by the United States Pharmacopeial Convention (USP), a nonprofit group whose standards are enforceable by state and federal regulators.
In the same position statement on compounding, the ACR said it also seeks a change to a Food and Drug Administration rule limiting practitioners’ access to quinacrine, a drug only available through compounding pharmacies that is sometimes used to treat lupus patients. Quinacrine is not on the FDA’s current list of bulk substances approved for compounding, except by special permission. The ACR has asked the agency to add quinacrine to the list, but no one knows when this will happen.
Rheumatologists may also be more restricted than before in terms of which compounding pharmacies they can turn to, as new federal standards divide them into two types – those that can provide medicines in larger quantities and those that can’t.
Steroid fiasco sparked rule revisions
The ACR’s concerns follow a tighter focus by state and federal agencies on drug compounding after a fungal meningitis outbreak in 2012 was traced to contaminated steroids produced in bulk by a compounding pharmacy.
More than 800 infections, 64 of them fatal, occurred after the New England Compounding Center in Framingham, Mass., sold contaminated methylprednisolone acetate that was used in epidural and intra-articular joint injections.
The following year Congress passed the Drug Quality and Security Act, which aims, in part, to prevent compounding pharmacies from engaging in what amounts to unregulated manufacturing.
As part of the law, the FDA created a list of drugs appropriate for compounding and a process by which larger compounding pharmacies must register with the FDA, and agree to inspections. The USP standards, meanwhile, address detailed technical and safety aspects of compounding and are enforceable by the FDA and state agencies.
“USP and FDA have had the ability to regulate compounding for over a decade, but only recently have the rules become actively enforced,” said Donald Miller, PharmD, of North Dakota State University, Fargo, who helped shape the ACR’s position statement on compounding with the help of rheumatologists in private practice.
“When you make guidelines for safety, they make sense, but then you can’t anticipate the way it’s going to affect individuals’ practice. And that’s where rheumatology got caught up,” said Dr. Miller, who was a member of the FDA Arthritis Advisory Committee in 2014-2016.
In-office mixing a top concern
Other specialties, including dermatology and immunology, also stand to be affected by various changes to compounding law and practice – and their societies have been active in voicing concerns.
Though the latest revisions of USP chapter 797, which impacts in-office mixing, are still being sorted out, it’s the No. 1 compounding-related concern for rheumatologists, Dr. Miller said.
Rheumatologists routinely mix an analgesic and a steroid for injection. The analgesic makes the steroids less viscous, and offers patients hours of immediate relief. They also add analgesics to hyaluronic acid injected for viscosupplementation. The mixing is usually conducted bedside, and the injections are administered right away.
Technically, combining these products amounts to sterile compounding, Dr. Miller explained. “And theoretically, under these rules, a physician could still do this, but they’d have to do it under a sterile hood like you find in a pharmacy, and that’s just not practical. It also becomes a matter of interpretation.”
USP chapter 797 sanctions in-office mixing for “immediate use” with individual patients – which is nearly always the case for the steroid injections used in rheumatology. But it’s unclear whether “immediate use” means emergency use only, or allows for routine use, as rheumatologists hope.
“One reason this came to rheumatology’s attention is that some state boards of medicine were inspecting and saying ‘Hey, you can’t do that,’ ” Dr. Miller said.
“There’s that law of unintended consequences where you snare things in a net that you really don’t want to,” Dr. Huffstutter said.
Marcus Snow, MD, a rheumatologist at the University of Nebraska, Omaha, who also worked on the statement, said that most rheumatologists are likely unaware that their ability to mix drugs in-office has been called into question.
“I brought it up at our division meeting with a group of 10 rheumatologists, and no one was aware that this was coming down the pike,” Dr. Snow said in an interview.
Pediatric issues
Pediatric rheumatologists, and adult rheumatologists who see children occasionally, use compounding pharmacies to create palatable oral medicines and adjusted doses of adult treatments.
They also use injections combining steroids with analgesics, and consider the addition of the analgesic a key aid to compliance.
“The biggest barrier we have is patient and parent anxiety about doing the procedure and the associated pain. We always administer our steroids mixed with lidocaine to help with the postprocedural discomfort,” said Adam Reinhardt, MD, chief of pediatric rheumatology at the University of Nebraska and Children’s Hospital and Medical Center in Omaha.
Steroid injections can mean avoiding or delaying systemic treatment in children with oligoarticular arthritis, he said. “Most of us consider them a first-line therapy. The hope is that you can get by without having to use meds like methotrexate if you can get a prolonged response in the one or two joints that are active in that patient.”
But Dr. Reinhardt said that, while he mixed his own injections during his fellowship training, Children’s of Omaha now insists that they be prepared by in-house pharmacists, working under sterile hoods. The delay to receiving them in the clinic or procedure room is 40 minutes to an hour, he said, which the clinicians accommodate through careful scheduling.
The change from mixing in-clinic to relying on the central pharmacy came about in recent years, Dr. Reinhardt said, because of broader concerns related to medication storage in the clinics. While ordering from the central pharmacy works for his practice, he said, “I probably only inject maybe 50-70 joints a year, while adult rheumatologists are injecting far more than that. For a busy private practice, I can see that being a huge time constraint,” he said.
Relevance of rules
None of the rheumatologists interviewed questioned the need for tightened state and federal oversight of compounding practices overall – just the applicability of certain rules to their own practice.
Dr. Snow and Dr. Huffstutter noted that reports of infected joints – a potential result of a contaminated injection – are sporadic and rare. “There’s very little research in this, but [these types of injections] have been standard practice for decades,” Dr. Snow said.
Srikanth Mukkera, MD, a rheumatologist in Tupelo, Miss., agreed that “sporadic cases of joint infection do happen following injection, but it can be hard to show if an injection was the cause.”
Assuring that medicines are mixed only immediately prior to injection, and not stored, reduces the likelihood of contamination, Dr. Mukkera said. Moreover, he noted, epidural injections such as those that resulted in the 2012 meningitis outbreak carry different risks than those seen in intra-articular injections.
Dr. Miller, the lead author of the ACR statement, said that the rheumatologists on our committee “don’t know of anyone that’s had a knee or other joint infection from a contaminated injection. They feel that unless somebody finds some evidence of that, they should be allowed to continue” with their usual practice.
He said that he feels that the USP will ultimately heed the concerns of rheumatologists and hopefully provide a more relaxed interpretation of in-office compounding. “We’re hoping they’ll make some exceptions when they revise 797 standards or at least maybe leave room for organizations to create a best practice statement. We’ll see,” Dr. Miller said.
But this is in no way guaranteed. Dr. Huffstutter said he fears that, if the rules come to be interpreted more narrowly, even standard practices like reconstituting biologic drugs for infusion – something that’s also a routine part of in-office practice – could fall under the rubric of sterile compounding and come into question.
The quinacrine problem
A separate compounding-related issue in rheumatology is clinicians’ access to quinacrine, an antimalarial rheumatology drug that, while infrequently used, represents the only alternative to hydroxychloroquine for some lupus patients.
“There are no alternatives out there for hydroxychloroquine, so we need it as a backup,” Dr. Snow said. “If hydroxychloroquine isn’t an option, there’s nothing out there that we can use. There’s no easy replacement.”
Dr. Huffstutter said he currently had no patients on quinacrine. “It’s not very often that we use it, but in those patients that really need it, it can make a huge difference in how they do.”
Quinacrine is no longer manufactured commercially as a finished drug product but is available in a powder that compounding physicians put into 100-mg capsules. It is not on the FDA’s current list of drugs available for compounding except with special permission.
While the ACR has requested that the FDA add it the list of bulk drug substances that can be used in compounding, quinacrine remains off the list for now – and, providers say, hard to find.
Moreover, while rheumatologists may have previously been able to order and store quantities of quinacrine and other compounded nonsterile medications to dispense to their patients, they can no longer easily do so, as only the FDA-approved compounding “outsourcing facilities” are allowed to process larger orders; the rest can only respond to prescriptions for individual patients.
Dr. Miller said it’s likely that quinacrine will make it onto the FDA’s next list of bulk drugs available for compounding. “The FDA has kind of said, ‘Don’t worry about it,’ ” he said.
Avoid laxatives or stool softeners prior to C. difficile test in ped in patients
Improved education could keep clinicians from ordering laxatives and stool softeners just prior to ordering Clostridium difficile tests, improving the specificity of such testing.
In a 4-month prospective cohort study of pediatric inpatients, most clinicians were aware that their patients were receiving laxatives or stool softeners before they were sent for C. difficile tests.
Misclassifying colonized patients as having CDI reduces the utility of interfacility data comparison and may potentially result in inappropriate penalties for hospitals, they added.
From August to November 2015, 217 pediatric inpatients underwent 278 C. difficile tests that were eligible for inclusion in the study. There were 48 episodes of CDI in 44 patients in which bowel medications were administered prior to the test.
Of the 48 tests sent after receipt of bowel medications, either the ordering clinician or the bedside nurse completed the qualitative survey in 42 instances (88%). The response rate was higher among nurses (71%) than clinicians (48%). Awareness of bowel medication administration before testing was acknowledged by 78% of ordering providers and 88% bedside nurses. A majority of nurses (70%) and providers (71%) reported the medical team wanted the test.
“The main reasons for testing included a change in stool quality from baseline, other changes in clinical status, and the presence of risk factors for CDI,” Ms. Kinlay and Dr. Sandora said.
Read more in the American Journal of Infection Control (2017 Mar 13. doi: 10.1016/j.ajic.2017.01.035).
Improved education could keep clinicians from ordering laxatives and stool softeners just prior to ordering Clostridium difficile tests, improving the specificity of such testing.
In a 4-month prospective cohort study of pediatric inpatients, most clinicians were aware that their patients were receiving laxatives or stool softeners before they were sent for C. difficile tests.
Misclassifying colonized patients as having CDI reduces the utility of interfacility data comparison and may potentially result in inappropriate penalties for hospitals, they added.
From August to November 2015, 217 pediatric inpatients underwent 278 C. difficile tests that were eligible for inclusion in the study. There were 48 episodes of CDI in 44 patients in which bowel medications were administered prior to the test.
Of the 48 tests sent after receipt of bowel medications, either the ordering clinician or the bedside nurse completed the qualitative survey in 42 instances (88%). The response rate was higher among nurses (71%) than clinicians (48%). Awareness of bowel medication administration before testing was acknowledged by 78% of ordering providers and 88% bedside nurses. A majority of nurses (70%) and providers (71%) reported the medical team wanted the test.
“The main reasons for testing included a change in stool quality from baseline, other changes in clinical status, and the presence of risk factors for CDI,” Ms. Kinlay and Dr. Sandora said.
Read more in the American Journal of Infection Control (2017 Mar 13. doi: 10.1016/j.ajic.2017.01.035).
Improved education could keep clinicians from ordering laxatives and stool softeners just prior to ordering Clostridium difficile tests, improving the specificity of such testing.
In a 4-month prospective cohort study of pediatric inpatients, most clinicians were aware that their patients were receiving laxatives or stool softeners before they were sent for C. difficile tests.
Misclassifying colonized patients as having CDI reduces the utility of interfacility data comparison and may potentially result in inappropriate penalties for hospitals, they added.
From August to November 2015, 217 pediatric inpatients underwent 278 C. difficile tests that were eligible for inclusion in the study. There were 48 episodes of CDI in 44 patients in which bowel medications were administered prior to the test.
Of the 48 tests sent after receipt of bowel medications, either the ordering clinician or the bedside nurse completed the qualitative survey in 42 instances (88%). The response rate was higher among nurses (71%) than clinicians (48%). Awareness of bowel medication administration before testing was acknowledged by 78% of ordering providers and 88% bedside nurses. A majority of nurses (70%) and providers (71%) reported the medical team wanted the test.
“The main reasons for testing included a change in stool quality from baseline, other changes in clinical status, and the presence of risk factors for CDI,” Ms. Kinlay and Dr. Sandora said.
Read more in the American Journal of Infection Control (2017 Mar 13. doi: 10.1016/j.ajic.2017.01.035).
FROM THE JOURNAL OF INFECTION CONTROL
Infants’ head circumference larger with PCOS moms on metformin
Women with polycystic ovarian syndrome (PCOS) who took metformin had newborns with larger heads than the offspring of women with PCOS who took a placebo, though PCOS offspring were, on average, shorter than newborns in a reference population, according to a recent study.
Metformin is commonly prescribed to women with PCOS, and though metformin passes the placental barrier and can reach therapeutic concentrations in the umbilical cord blood, it hasn’t been proven teratogenic, said Anna Hjorth-Hansen, MD, of the internal medicine department at Levanger Hospital, Norway.

The study was a post hoc analysis of data from the PregMet study, which was run from 2005 to 2009, and compared metformin to placebo, in combination with diet and lifestyle changes, for women with PCOS, said Dr. Hjorth-Hansen. The PregMet study tested the hypothesis that women with PCOS who received metformin from the first trimester until delivery had fewer pregnancy complications overall than women who did not.
Though women receiving placebo in the PregMet study had no more eclampsia, preterm delivery, or gestational diabetes than those who received metformin, the newborns who had in utero metformin exposure had significantly larger head circumference.
Dr. Hjorth-Hansen said that the study looked at in utero growth and anthropometric measurements at birth of infants born to women taking metformin, to determine whether metformin could affect fetal growth and newborn anthropometrics.
Ultrasound examination was used to measure crown-rump length, biparietal diameter (BPD), and mean abdominal diameter (MAD). At birth, head circumference (HC), length, and weight were measured.
Maternal characteristics were comparable between the metformin (131 patients) and placebo (127 patients) groups, said Dr. Hjorth-Hansen. Specifically, there were no significant differences between groups in terms of PCOS phenotype, blood glucose levels, and parity.
Infants born to women who took metformin had, on average, a larger BPD at 32 weeks gestation, compared with the infants whose mothers took placebo (86.1 mm versus 85.2 mm, P = .027). This larger head size was also seen at birth (mean HC, metformin, 35.6 cm; placebo, 35.0 cm; P = .007).
There were no significant differences between the groups in MAD or weight, either as assessed by ultrasound at 32 weeks gestation or as measured at birth.
Although the two groups did not differ in length at birth, the aggregate study population of infants born to women with PCOS was shorter than a large Swedish reference population.
When Dr. Hjorth-Hansen and her colleagues stratified the results by maternal body mass index (BMI), looking at babies born to women with BMIs below 25 kg/m2, compared with those with BMI of 25 kg/m2 and greater, they saw no differences in infant anthropometric measurements for women who had taken placebo.
However, when the investigators dichotomized maternal BMI for the metformin group, they found that infants born to the higher BMI group had a larger head size (P = .022), and were heavier (P = .002) and longer (P = .003) than infants born to women with BMIs less than 25.
“Metformin resulted in a larger head size, traceable already in utero,” said Dr. Hjorth-Hansen. However, she said, there’s a “PCOS effect” that results in the offspring of women with the condition to have a shorter body, compared with offspring of women without PCOS.
Dr. Hjorth-Hansen reported no relevant disclosures.
koakes@frontlinemedcom.com
On Twitter @karioakes
Women with polycystic ovarian syndrome (PCOS) who took metformin had newborns with larger heads than the offspring of women with PCOS who took a placebo, though PCOS offspring were, on average, shorter than newborns in a reference population, according to a recent study.
Metformin is commonly prescribed to women with PCOS, and though metformin passes the placental barrier and can reach therapeutic concentrations in the umbilical cord blood, it hasn’t been proven teratogenic, said Anna Hjorth-Hansen, MD, of the internal medicine department at Levanger Hospital, Norway.
The study was a post hoc analysis of data from the PregMet study, which was run from 2005 to 2009, and compared metformin to placebo, in combination with diet and lifestyle changes, for women with PCOS, said Dr. Hjorth-Hansen. The PregMet study tested the hypothesis that women with PCOS who received metformin from the first trimester until delivery had fewer pregnancy complications overall than women who did not.
Though women receiving placebo in the PregMet study had no more eclampsia, preterm delivery, or gestational diabetes than those who received metformin, the newborns who had in utero metformin exposure had significantly larger head circumference.
Dr. Hjorth-Hansen said that the study looked at in utero growth and anthropometric measurements at birth of infants born to women taking metformin, to determine whether metformin could affect fetal growth and newborn anthropometrics.
Ultrasound examination was used to measure crown-rump length, biparietal diameter (BPD), and mean abdominal diameter (MAD). At birth, head circumference (HC), length, and weight were measured.
Maternal characteristics were comparable between the metformin (131 patients) and placebo (127 patients) groups, said Dr. Hjorth-Hansen. Specifically, there were no significant differences between groups in terms of PCOS phenotype, blood glucose levels, and parity.
Infants born to women who took metformin had, on average, a larger BPD at 32 weeks gestation, compared with the infants whose mothers took placebo (86.1 mm versus 85.2 mm, P = .027). This larger head size was also seen at birth (mean HC, metformin, 35.6 cm; placebo, 35.0 cm; P = .007).
There were no significant differences between the groups in MAD or weight, either as assessed by ultrasound at 32 weeks gestation or as measured at birth.
Although the two groups did not differ in length at birth, the aggregate study population of infants born to women with PCOS was shorter than a large Swedish reference population.
When Dr. Hjorth-Hansen and her colleagues stratified the results by maternal body mass index (BMI), looking at babies born to women with BMIs below 25 kg/m2, compared with those with BMI of 25 kg/m2 and greater, they saw no differences in infant anthropometric measurements for women who had taken placebo.
However, when the investigators dichotomized maternal BMI for the metformin group, they found that infants born to the higher BMI group had a larger head size (P = .022), and were heavier (P = .002) and longer (P = .003) than infants born to women with BMIs less than 25.
“Metformin resulted in a larger head size, traceable already in utero,” said Dr. Hjorth-Hansen. However, she said, there’s a “PCOS effect” that results in the offspring of women with the condition to have a shorter body, compared with offspring of women without PCOS.
Dr. Hjorth-Hansen reported no relevant disclosures.
koakes@frontlinemedcom.com
On Twitter @karioakes
Women with polycystic ovarian syndrome (PCOS) who took metformin had newborns with larger heads than the offspring of women with PCOS who took a placebo, though PCOS offspring were, on average, shorter than newborns in a reference population, according to a recent study.
Metformin is commonly prescribed to women with PCOS, and though metformin passes the placental barrier and can reach therapeutic concentrations in the umbilical cord blood, it hasn’t been proven teratogenic, said Anna Hjorth-Hansen, MD, of the internal medicine department at Levanger Hospital, Norway.
The study was a post hoc analysis of data from the PregMet study, which was run from 2005 to 2009, and compared metformin to placebo, in combination with diet and lifestyle changes, for women with PCOS, said Dr. Hjorth-Hansen. The PregMet study tested the hypothesis that women with PCOS who received metformin from the first trimester until delivery had fewer pregnancy complications overall than women who did not.
Though women receiving placebo in the PregMet study had no more eclampsia, preterm delivery, or gestational diabetes than those who received metformin, the newborns who had in utero metformin exposure had significantly larger head circumference.
Dr. Hjorth-Hansen said that the study looked at in utero growth and anthropometric measurements at birth of infants born to women taking metformin, to determine whether metformin could affect fetal growth and newborn anthropometrics.
Ultrasound examination was used to measure crown-rump length, biparietal diameter (BPD), and mean abdominal diameter (MAD). At birth, head circumference (HC), length, and weight were measured.
Maternal characteristics were comparable between the metformin (131 patients) and placebo (127 patients) groups, said Dr. Hjorth-Hansen. Specifically, there were no significant differences between groups in terms of PCOS phenotype, blood glucose levels, and parity.
Infants born to women who took metformin had, on average, a larger BPD at 32 weeks gestation, compared with the infants whose mothers took placebo (86.1 mm versus 85.2 mm, P = .027). This larger head size was also seen at birth (mean HC, metformin, 35.6 cm; placebo, 35.0 cm; P = .007).
There were no significant differences between the groups in MAD or weight, either as assessed by ultrasound at 32 weeks gestation or as measured at birth.
Although the two groups did not differ in length at birth, the aggregate study population of infants born to women with PCOS was shorter than a large Swedish reference population.
When Dr. Hjorth-Hansen and her colleagues stratified the results by maternal body mass index (BMI), looking at babies born to women with BMIs below 25 kg/m2, compared with those with BMI of 25 kg/m2 and greater, they saw no differences in infant anthropometric measurements for women who had taken placebo.
However, when the investigators dichotomized maternal BMI for the metformin group, they found that infants born to the higher BMI group had a larger head size (P = .022), and were heavier (P = .002) and longer (P = .003) than infants born to women with BMIs less than 25.
“Metformin resulted in a larger head size, traceable already in utero,” said Dr. Hjorth-Hansen. However, she said, there’s a “PCOS effect” that results in the offspring of women with the condition to have a shorter body, compared with offspring of women without PCOS.
Dr. Hjorth-Hansen reported no relevant disclosures.
koakes@frontlinemedcom.com
On Twitter @karioakes
FROM ENDO 2017
Key clinical point:
Major finding: Infants born to women with PCOS who took metformin during pregnancy had larger head circumferences at birth than those born to women with PCOS who took placebo (35.6 cm versus 35.0 cm, P = .007).
Data source: Retrospective analysis of data from 258 women in the PregMet study.
Disclosures: Dr. Hjorth-Hansen reported no relevant disclosures.
Parental smoking linked to genetic changes in kids with ALL

Smoking by either parent helps promote genetic deletions in children that are associated with the development and progression of acute lymphoblastic leukemia (ALL), according to a study published in Cancer Research.
The strongest associations in this study were found in children whose parents smoked while the children were in utero and during their infancy.
However, the genetic deletions were also noted in the offspring of parents who may have quit smoking even before conception.
The link between ALL and parental smoking has already been established, but this is the first study that points to specific genetic changes in children with ALL, according to study author Adam de Smith, PhD, of the University of California San Francisco.
“With more smoking among the parents, we saw more deletions within the child’s ALL cells at diagnosis,” Dr de smith said.
For this study, he and his colleagues looked at pre-treatment tumor samples from 559 ALL patients.
The team wanted to see if any of the 8 genes that are frequently deleted in ALL patients (CDKN2A, ETV6, IKZF1, PAX5, RB1, BTG1, PAR1 region, and EBF1) were missing in the samples.
Questionnaires were given to parents to find out if smoking habits impacted the number of genetic deletions. Data was corroborated by a biomarker in newborns’ blood samples that indicates exposure to maternal smoking during pregnancy.
The researchers found that approximately two-thirds of the tumor samples (n=353) contained at least 1 deletion.
Deletions were considerably more common in children whose mothers had smoked during pregnancy and after birth.
For each 5 cigarettes smoked daily during pregnancy, there was a 22% increase in the number of deletions. For each 5 cigarettes smoked daily during breastfeeding, there was a 74% increase in the number of deletions.
Smoking of 5 cigarettes daily by the mother or father before conception was associated with a 7% to 8% higher number of deletions.
Role of child age and sex
One discovery the researchers found intriguing was the link between the fathers’ pre-conception smoking and their child’s age at diagnosis.
“There was a significant effect on deletion numbers in cases where the patient was age 6 or younger,” Dr de Smith said. “Our results suggest that paternal pre-conception smoking, which is known to cause oxidative damage to sperm DNA, may lead to a higher propensity of deletions in children with earlier-onset ALL.”
“It is also true that some of those fathers who smoked before conception also continue to smoke in the presence of the mother and child, so more research is needed to explain the mechanism of smoking-related damage in all of the time periods of exposure to the child.”
In addition, male children were found to be more sensitive to the effects of maternal smoking, including smoking that occurred pre-conception.
The researchers said this could be explained by the fact that male fetuses grow more rapidly, which leads to increased vulnerability of developing lymphocytes to toxins that cause genetic damage.
“Our study indicates that the more tobacco exposure, the more cumulative DNA damage is evident in the ALL cell,” said study author Joseph Wiemels, PhD, of the University of California San Francisco.
“While causes of ALL are multifactorial—including the inborn genetic makeup of the child, patterns of infection, pesticides, and other environmental exposure—if there was no smoking in the environment, then there would likely be fewer children with the disease. We may add ALL to the long list of diseases impacted by smoking, and, in this case, affecting one of our most vulnerable populations—our children.” ![]()
Smoking by either parent helps promote genetic deletions in children that are associated with the development and progression of acute lymphoblastic leukemia (ALL), according to a study published in Cancer Research.
The strongest associations in this study were found in children whose parents smoked while the children were in utero and during their infancy.
However, the genetic deletions were also noted in the offspring of parents who may have quit smoking even before conception.
The link between ALL and parental smoking has already been established, but this is the first study that points to specific genetic changes in children with ALL, according to study author Adam de Smith, PhD, of the University of California San Francisco.
“With more smoking among the parents, we saw more deletions within the child’s ALL cells at diagnosis,” Dr de smith said.
For this study, he and his colleagues looked at pre-treatment tumor samples from 559 ALL patients.
The team wanted to see if any of the 8 genes that are frequently deleted in ALL patients (CDKN2A, ETV6, IKZF1, PAX5, RB1, BTG1, PAR1 region, and EBF1) were missing in the samples.
Questionnaires were given to parents to find out if smoking habits impacted the number of genetic deletions. Data was corroborated by a biomarker in newborns’ blood samples that indicates exposure to maternal smoking during pregnancy.
The researchers found that approximately two-thirds of the tumor samples (n=353) contained at least 1 deletion.
Deletions were considerably more common in children whose mothers had smoked during pregnancy and after birth.
For each 5 cigarettes smoked daily during pregnancy, there was a 22% increase in the number of deletions. For each 5 cigarettes smoked daily during breastfeeding, there was a 74% increase in the number of deletions.
Smoking of 5 cigarettes daily by the mother or father before conception was associated with a 7% to 8% higher number of deletions.
Role of child age and sex
One discovery the researchers found intriguing was the link between the fathers’ pre-conception smoking and their child’s age at diagnosis.
“There was a significant effect on deletion numbers in cases where the patient was age 6 or younger,” Dr de Smith said. “Our results suggest that paternal pre-conception smoking, which is known to cause oxidative damage to sperm DNA, may lead to a higher propensity of deletions in children with earlier-onset ALL.”
“It is also true that some of those fathers who smoked before conception also continue to smoke in the presence of the mother and child, so more research is needed to explain the mechanism of smoking-related damage in all of the time periods of exposure to the child.”
In addition, male children were found to be more sensitive to the effects of maternal smoking, including smoking that occurred pre-conception.
The researchers said this could be explained by the fact that male fetuses grow more rapidly, which leads to increased vulnerability of developing lymphocytes to toxins that cause genetic damage.
“Our study indicates that the more tobacco exposure, the more cumulative DNA damage is evident in the ALL cell,” said study author Joseph Wiemels, PhD, of the University of California San Francisco.
“While causes of ALL are multifactorial—including the inborn genetic makeup of the child, patterns of infection, pesticides, and other environmental exposure—if there was no smoking in the environment, then there would likely be fewer children with the disease. We may add ALL to the long list of diseases impacted by smoking, and, in this case, affecting one of our most vulnerable populations—our children.” ![]()
Smoking by either parent helps promote genetic deletions in children that are associated with the development and progression of acute lymphoblastic leukemia (ALL), according to a study published in Cancer Research.
The strongest associations in this study were found in children whose parents smoked while the children were in utero and during their infancy.
However, the genetic deletions were also noted in the offspring of parents who may have quit smoking even before conception.
The link between ALL and parental smoking has already been established, but this is the first study that points to specific genetic changes in children with ALL, according to study author Adam de Smith, PhD, of the University of California San Francisco.
“With more smoking among the parents, we saw more deletions within the child’s ALL cells at diagnosis,” Dr de smith said.
For this study, he and his colleagues looked at pre-treatment tumor samples from 559 ALL patients.
The team wanted to see if any of the 8 genes that are frequently deleted in ALL patients (CDKN2A, ETV6, IKZF1, PAX5, RB1, BTG1, PAR1 region, and EBF1) were missing in the samples.
Questionnaires were given to parents to find out if smoking habits impacted the number of genetic deletions. Data was corroborated by a biomarker in newborns’ blood samples that indicates exposure to maternal smoking during pregnancy.
The researchers found that approximately two-thirds of the tumor samples (n=353) contained at least 1 deletion.
Deletions were considerably more common in children whose mothers had smoked during pregnancy and after birth.
For each 5 cigarettes smoked daily during pregnancy, there was a 22% increase in the number of deletions. For each 5 cigarettes smoked daily during breastfeeding, there was a 74% increase in the number of deletions.
Smoking of 5 cigarettes daily by the mother or father before conception was associated with a 7% to 8% higher number of deletions.
Role of child age and sex
One discovery the researchers found intriguing was the link between the fathers’ pre-conception smoking and their child’s age at diagnosis.
“There was a significant effect on deletion numbers in cases where the patient was age 6 or younger,” Dr de Smith said. “Our results suggest that paternal pre-conception smoking, which is known to cause oxidative damage to sperm DNA, may lead to a higher propensity of deletions in children with earlier-onset ALL.”
“It is also true that some of those fathers who smoked before conception also continue to smoke in the presence of the mother and child, so more research is needed to explain the mechanism of smoking-related damage in all of the time periods of exposure to the child.”
In addition, male children were found to be more sensitive to the effects of maternal smoking, including smoking that occurred pre-conception.
The researchers said this could be explained by the fact that male fetuses grow more rapidly, which leads to increased vulnerability of developing lymphocytes to toxins that cause genetic damage.
“Our study indicates that the more tobacco exposure, the more cumulative DNA damage is evident in the ALL cell,” said study author Joseph Wiemels, PhD, of the University of California San Francisco.
“While causes of ALL are multifactorial—including the inborn genetic makeup of the child, patterns of infection, pesticides, and other environmental exposure—if there was no smoking in the environment, then there would likely be fewer children with the disease. We may add ALL to the long list of diseases impacted by smoking, and, in this case, affecting one of our most vulnerable populations—our children.” ![]()
Most children with growth disorders benefit from growth hormone
ORLANDO – About 80% of children with growth disorders will attain their expected normal adult height if adequately treated with growth hormone, a large observational study has determined.
Somatropin recombinant human growth hormone seemed most effective for patients with growth hormone deficiency, idiopathic short stature, and for those who were born small for gestational age. Patients who had Turner syndrome or a homeobox-deficiency gene didn’t do quite as well, although most did still improve their final height.
The Genetics and Neuroendocrinology of Short Stature International Study (GENESIS) followed more than 22,000 children who were treated in 30 countries from 1999 to 2015.
All of the patients were treated with somatropin recombinant human growth hormone (Humatrope). Eli Lilly, which makes the medication, sponsored the study and presented the results during a poster session at the annual meeting of the Endocrine Society. Representatives at the poster declined to discuss results with the media during the open session.
“The results speak for themselves,” said Cheri Deal, MD, PhD, of the University of Montreal, Quebec, one of the presenting authors. “It’s an incredible story.”
The GENESIS cohort comprised more than 22,000 children who were treated for a variety of growth disorders at 827 international sites.
Subanalyses have been published, but this is the first release of the data on 5,076 patients with full follow-up. Most of the patients (61%) received the medication for growth hormone deficiency. Other indications were Turner syndrome (14%), idiopathic short stature (11%), short-stature homeobox-containing gene deficiency (3%), small for gestational age (5%), and chronic renal insufficiency (0.3%). Other diagnoses, plus unknown causes, made up the remainder of the diagnoses.
The investigators, led by Christopher J. Child, PhD, an Eli Lilly scientist, split the cohort into diagnostic groups and treatment subgroups: those who attained normal adult height, those who attained normal adult height with at least 4 years of treatment, and those who gained normal adult height who started treatment at younger than 10 years of age.
At baseline, those with growth hormone deficiency were a mean of 11 years old; their height was a mean of 2.4 standard deviations (SDS) below normal. They received a mean of 6 years of treatment; 86% achieved a normal adult height, with an overall gain of 1.39 SDS. Those who started somatropin before age 10 years made bigger gains. The final height gain was 1.78 SDS after a mean of 9.5 years of treatment.
At baseline, those with idiopathic short stature were a mean of 12 years old; their mean height was 2.3 SDS below normal. They received a mean of 4.7 years of treatment; 82% achieved normal height, with a gain of 1.1 SDS. Starting somatropin at a younger age (mean 8 years) improved outcomes slightly, with a final height gain of 1.6 SDS after 8 years of treatment.
Patients with Turner syndrome were a mean of 10 years when they started treatment; their mean height was 2.65 SDS below normal. They received a mean of 6.4 years of treatment; 66% achieved normal adult height, with a mean height gain of 0.95 SDS. Early treatment didn’t alter outcomes much in this group. After a mean of 8.5 years of treatment, 65% achieved normal height, with a height gain of 0.84 SDS.
Patients with a short-stature homeobox-containing gene deficiency were a mean of 11 years when they started treatment. At that time, their height was a mean of 2.36 SDS below normal. They were treated for a mean of 4.7 years; 76% achieved a normal adult height, with a mean gain of 0.86 SDS. Early treatment did improve outcomes a bit. After a mean treatment time of 7 years, 78% gained normal adult height, with a height gain of 0.84 SDS.
Children who were small for gestational age started treatment when they were a mean of 10.5 years. At that time, their mean height was 2.57 SDS below normal. They were treated for a mean of 5.4 years; 78% attained a normal adult height, with a mean gain of 1.1 SDS. Early treatment improved outcomes. After a mean treatment time of 7.8 years, 81% achieved normal adult height, with a mean gain of 1.41 SDS.
The less-robust gains seen in the children with genetically influenced growth disorders “wasn’t unexpected” and is in line with what has been observed in a number of clinical trials, the investigators said.
Eli Lilly manufactures the somatropin product used in the study, and it sponsored the study. Dr. Child is an employee of the company. Dr. Deal did not have any financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @Alz_gal
ORLANDO – About 80% of children with growth disorders will attain their expected normal adult height if adequately treated with growth hormone, a large observational study has determined.
Somatropin recombinant human growth hormone seemed most effective for patients with growth hormone deficiency, idiopathic short stature, and for those who were born small for gestational age. Patients who had Turner syndrome or a homeobox-deficiency gene didn’t do quite as well, although most did still improve their final height.
The Genetics and Neuroendocrinology of Short Stature International Study (GENESIS) followed more than 22,000 children who were treated in 30 countries from 1999 to 2015.
All of the patients were treated with somatropin recombinant human growth hormone (Humatrope). Eli Lilly, which makes the medication, sponsored the study and presented the results during a poster session at the annual meeting of the Endocrine Society. Representatives at the poster declined to discuss results with the media during the open session.
“The results speak for themselves,” said Cheri Deal, MD, PhD, of the University of Montreal, Quebec, one of the presenting authors. “It’s an incredible story.”
The GENESIS cohort comprised more than 22,000 children who were treated for a variety of growth disorders at 827 international sites.
Subanalyses have been published, but this is the first release of the data on 5,076 patients with full follow-up. Most of the patients (61%) received the medication for growth hormone deficiency. Other indications were Turner syndrome (14%), idiopathic short stature (11%), short-stature homeobox-containing gene deficiency (3%), small for gestational age (5%), and chronic renal insufficiency (0.3%). Other diagnoses, plus unknown causes, made up the remainder of the diagnoses.
The investigators, led by Christopher J. Child, PhD, an Eli Lilly scientist, split the cohort into diagnostic groups and treatment subgroups: those who attained normal adult height, those who attained normal adult height with at least 4 years of treatment, and those who gained normal adult height who started treatment at younger than 10 years of age.
At baseline, those with growth hormone deficiency were a mean of 11 years old; their height was a mean of 2.4 standard deviations (SDS) below normal. They received a mean of 6 years of treatment; 86% achieved a normal adult height, with an overall gain of 1.39 SDS. Those who started somatropin before age 10 years made bigger gains. The final height gain was 1.78 SDS after a mean of 9.5 years of treatment.
At baseline, those with idiopathic short stature were a mean of 12 years old; their mean height was 2.3 SDS below normal. They received a mean of 4.7 years of treatment; 82% achieved normal height, with a gain of 1.1 SDS. Starting somatropin at a younger age (mean 8 years) improved outcomes slightly, with a final height gain of 1.6 SDS after 8 years of treatment.
Patients with Turner syndrome were a mean of 10 years when they started treatment; their mean height was 2.65 SDS below normal. They received a mean of 6.4 years of treatment; 66% achieved normal adult height, with a mean height gain of 0.95 SDS. Early treatment didn’t alter outcomes much in this group. After a mean of 8.5 years of treatment, 65% achieved normal height, with a height gain of 0.84 SDS.
Patients with a short-stature homeobox-containing gene deficiency were a mean of 11 years when they started treatment. At that time, their height was a mean of 2.36 SDS below normal. They were treated for a mean of 4.7 years; 76% achieved a normal adult height, with a mean gain of 0.86 SDS. Early treatment did improve outcomes a bit. After a mean treatment time of 7 years, 78% gained normal adult height, with a height gain of 0.84 SDS.
Children who were small for gestational age started treatment when they were a mean of 10.5 years. At that time, their mean height was 2.57 SDS below normal. They were treated for a mean of 5.4 years; 78% attained a normal adult height, with a mean gain of 1.1 SDS. Early treatment improved outcomes. After a mean treatment time of 7.8 years, 81% achieved normal adult height, with a mean gain of 1.41 SDS.
The less-robust gains seen in the children with genetically influenced growth disorders “wasn’t unexpected” and is in line with what has been observed in a number of clinical trials, the investigators said.
Eli Lilly manufactures the somatropin product used in the study, and it sponsored the study. Dr. Child is an employee of the company. Dr. Deal did not have any financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @Alz_gal
ORLANDO – About 80% of children with growth disorders will attain their expected normal adult height if adequately treated with growth hormone, a large observational study has determined.
Somatropin recombinant human growth hormone seemed most effective for patients with growth hormone deficiency, idiopathic short stature, and for those who were born small for gestational age. Patients who had Turner syndrome or a homeobox-deficiency gene didn’t do quite as well, although most did still improve their final height.
The Genetics and Neuroendocrinology of Short Stature International Study (GENESIS) followed more than 22,000 children who were treated in 30 countries from 1999 to 2015.
All of the patients were treated with somatropin recombinant human growth hormone (Humatrope). Eli Lilly, which makes the medication, sponsored the study and presented the results during a poster session at the annual meeting of the Endocrine Society. Representatives at the poster declined to discuss results with the media during the open session.
“The results speak for themselves,” said Cheri Deal, MD, PhD, of the University of Montreal, Quebec, one of the presenting authors. “It’s an incredible story.”
The GENESIS cohort comprised more than 22,000 children who were treated for a variety of growth disorders at 827 international sites.
Subanalyses have been published, but this is the first release of the data on 5,076 patients with full follow-up. Most of the patients (61%) received the medication for growth hormone deficiency. Other indications were Turner syndrome (14%), idiopathic short stature (11%), short-stature homeobox-containing gene deficiency (3%), small for gestational age (5%), and chronic renal insufficiency (0.3%). Other diagnoses, plus unknown causes, made up the remainder of the diagnoses.
The investigators, led by Christopher J. Child, PhD, an Eli Lilly scientist, split the cohort into diagnostic groups and treatment subgroups: those who attained normal adult height, those who attained normal adult height with at least 4 years of treatment, and those who gained normal adult height who started treatment at younger than 10 years of age.
At baseline, those with growth hormone deficiency were a mean of 11 years old; their height was a mean of 2.4 standard deviations (SDS) below normal. They received a mean of 6 years of treatment; 86% achieved a normal adult height, with an overall gain of 1.39 SDS. Those who started somatropin before age 10 years made bigger gains. The final height gain was 1.78 SDS after a mean of 9.5 years of treatment.
At baseline, those with idiopathic short stature were a mean of 12 years old; their mean height was 2.3 SDS below normal. They received a mean of 4.7 years of treatment; 82% achieved normal height, with a gain of 1.1 SDS. Starting somatropin at a younger age (mean 8 years) improved outcomes slightly, with a final height gain of 1.6 SDS after 8 years of treatment.
Patients with Turner syndrome were a mean of 10 years when they started treatment; their mean height was 2.65 SDS below normal. They received a mean of 6.4 years of treatment; 66% achieved normal adult height, with a mean height gain of 0.95 SDS. Early treatment didn’t alter outcomes much in this group. After a mean of 8.5 years of treatment, 65% achieved normal height, with a height gain of 0.84 SDS.
Patients with a short-stature homeobox-containing gene deficiency were a mean of 11 years when they started treatment. At that time, their height was a mean of 2.36 SDS below normal. They were treated for a mean of 4.7 years; 76% achieved a normal adult height, with a mean gain of 0.86 SDS. Early treatment did improve outcomes a bit. After a mean treatment time of 7 years, 78% gained normal adult height, with a height gain of 0.84 SDS.
Children who were small for gestational age started treatment when they were a mean of 10.5 years. At that time, their mean height was 2.57 SDS below normal. They were treated for a mean of 5.4 years; 78% attained a normal adult height, with a mean gain of 1.1 SDS. Early treatment improved outcomes. After a mean treatment time of 7.8 years, 81% achieved normal adult height, with a mean gain of 1.41 SDS.
The less-robust gains seen in the children with genetically influenced growth disorders “wasn’t unexpected” and is in line with what has been observed in a number of clinical trials, the investigators said.
Eli Lilly manufactures the somatropin product used in the study, and it sponsored the study. Dr. Child is an employee of the company. Dr. Deal did not have any financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @Alz_gal
AT ENDO 2017
Key clinical point:
Major finding: Overall, 80% of the treated children reached normal adult height.
Data source: The prospective observational cohort study comprised 5,076 children.
Disclosures: Eli Lilly manufactures the somatropin product used in the study, and it sponsored the study. Dr. Child is an employee of the company. Dr. Deal did not have any financial disclosures.
Adolescents with an incarcerated parent at higher risk of mental health problems
Having or having had a parent in jail appears to be a risk factor for adolescent mental health problems, a Minnesota study found.
In a study of 122,180 children from the 8th, 9th, and 11th grades drawn from the 2013 Minnesota Student Survey, parental incarceration was strongly associated with higher rates of mental health problems such as internalizing, self-injury, suicidal ideation, and suicidal attempts. Children of currently incarcerated parents were two and a half to four times as likely to experience these mental health problems, and children of formerly incarcerated parents were roughly twice as likely to experience them, compared with children whose parents had not been jailed, said Laurel Davis, PhD, and Rebecca J. Shlafer, PhD, MPH, of the department of pediatrics at the University of Minnesota, Minneapolis.
For youth with currently incarcerated parents, almost half reported moderate symptoms of internalizing, and more than one-third reported at least one purposeful self-injury. However, only 30% reported any type of treatment for a mental health concern, the researchers said.
Parental closeness was protective against negative mental health outcomes, they noted. “Children of incarcerated parents are a vulnerable population and they should continue to be the targets of intervention efforts aiming to buttress their personal and social resources, including strong relationships with caregivers.”
Studies suggest that an estimated 1.9 million U.S. children have a parent in a state or federal prison, and millions more have a parent in county jails.
In Minnesota alone, 2,500 young people who had a parent in jail or whose parent had been in jail reported attempting suicide, and more than 5,000 children of incarcerated or formerly incarcerated parents had reported purposely having injured themselves in the last year. “This represents an enormous challenge to our systems of care,” said Dr. Davis and Dr. Shlafer. “Identifying and intervening with these youth should be a priority with governments and social service organizations.”
Read more at the Journal of Adolescence (2017;54:120-34).
Having or having had a parent in jail appears to be a risk factor for adolescent mental health problems, a Minnesota study found.
In a study of 122,180 children from the 8th, 9th, and 11th grades drawn from the 2013 Minnesota Student Survey, parental incarceration was strongly associated with higher rates of mental health problems such as internalizing, self-injury, suicidal ideation, and suicidal attempts. Children of currently incarcerated parents were two and a half to four times as likely to experience these mental health problems, and children of formerly incarcerated parents were roughly twice as likely to experience them, compared with children whose parents had not been jailed, said Laurel Davis, PhD, and Rebecca J. Shlafer, PhD, MPH, of the department of pediatrics at the University of Minnesota, Minneapolis.
For youth with currently incarcerated parents, almost half reported moderate symptoms of internalizing, and more than one-third reported at least one purposeful self-injury. However, only 30% reported any type of treatment for a mental health concern, the researchers said.
Parental closeness was protective against negative mental health outcomes, they noted. “Children of incarcerated parents are a vulnerable population and they should continue to be the targets of intervention efforts aiming to buttress their personal and social resources, including strong relationships with caregivers.”
Studies suggest that an estimated 1.9 million U.S. children have a parent in a state or federal prison, and millions more have a parent in county jails.
In Minnesota alone, 2,500 young people who had a parent in jail or whose parent had been in jail reported attempting suicide, and more than 5,000 children of incarcerated or formerly incarcerated parents had reported purposely having injured themselves in the last year. “This represents an enormous challenge to our systems of care,” said Dr. Davis and Dr. Shlafer. “Identifying and intervening with these youth should be a priority with governments and social service organizations.”
Read more at the Journal of Adolescence (2017;54:120-34).
Having or having had a parent in jail appears to be a risk factor for adolescent mental health problems, a Minnesota study found.
In a study of 122,180 children from the 8th, 9th, and 11th grades drawn from the 2013 Minnesota Student Survey, parental incarceration was strongly associated with higher rates of mental health problems such as internalizing, self-injury, suicidal ideation, and suicidal attempts. Children of currently incarcerated parents were two and a half to four times as likely to experience these mental health problems, and children of formerly incarcerated parents were roughly twice as likely to experience them, compared with children whose parents had not been jailed, said Laurel Davis, PhD, and Rebecca J. Shlafer, PhD, MPH, of the department of pediatrics at the University of Minnesota, Minneapolis.
For youth with currently incarcerated parents, almost half reported moderate symptoms of internalizing, and more than one-third reported at least one purposeful self-injury. However, only 30% reported any type of treatment for a mental health concern, the researchers said.
Parental closeness was protective against negative mental health outcomes, they noted. “Children of incarcerated parents are a vulnerable population and they should continue to be the targets of intervention efforts aiming to buttress their personal and social resources, including strong relationships with caregivers.”
Studies suggest that an estimated 1.9 million U.S. children have a parent in a state or federal prison, and millions more have a parent in county jails.
In Minnesota alone, 2,500 young people who had a parent in jail or whose parent had been in jail reported attempting suicide, and more than 5,000 children of incarcerated or formerly incarcerated parents had reported purposely having injured themselves in the last year. “This represents an enormous challenge to our systems of care,” said Dr. Davis and Dr. Shlafer. “Identifying and intervening with these youth should be a priority with governments and social service organizations.”
Read more at the Journal of Adolescence (2017;54:120-34).
FROM THE JOURNAL OF ADOLESCENCE