User login
See one, do one ...
It rolls off your tongue so easily. See-one, do-one, teach-one has been the mantra recited to doctors-in-training for hundreds of years. It purports to characterize the process by which technical skills are passed from one generation of physicians to the next. However, you know as well as I do that the process of learning a skill such as performing a lumbar puncture on a squirming 6-month-old almost never conforms to the see-one, do-one, teach-one dictum.
Although I recall that it was not until my 7th birthday that I could consistently and confidently tie my own shoes, I consider myself reasonably dexterous. As a woodcarver, I was comfortable around sharp instruments, but that comfort zone quickly disappeared when it came to poking and cutting another human being who had nerves and blood vessels.

In a Pediatric Perspective in the June 2017 issue of Pediatrics, two anesthesiologists at Texas Children’s Hospital in Houston and the Children’s Hospital of Philadelphia address that question of, How many tries is reasonable for a physician attempting to learn a new technique (“When Should Trainees Call for Help with Invasive Procedures?” Pediatrics. 2017, June. doi: 10.1542/peds.2016-3673)? They illustrate their insightful discussion with the gruesome image of the wrist of an infant who had endured 21 attempts at percutaneous arterial line placement.
In addition to direct supervision, the authors recommend that instructors engage the trainee in a preprocedure discussion that includes setting a predetermined number of unsuccessful attempts at which the trainee will stop and ask for help. They suggest that the “trainee should be taught the self-insight to summon a more experienced provider or perhaps just a fresh pair of hands.”
For the general pediatrician or family physician, many of the technical skills we learned in training are likely to fade from disuse in the real world of office practice. However, learning when and how to step back in the face of multiple failures is a skill that every physician will continue to use regardless of where he or she is on his or her professional trajectory.
It isn’t always easy. It challenges our egos to ask for help when we have failed at making the diagnosis or not chosen the most effective therapy. At a minimum, stepping back and taking a deep breath (or three) may allow us a window through which we can finally see outside the box we find ourselves in.
Persistence is an attribute that allowed us to navigate the long and challenging path of our medical education. But, there are situations when it gets in the way of good medical care.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
It rolls off your tongue so easily. See-one, do-one, teach-one has been the mantra recited to doctors-in-training for hundreds of years. It purports to characterize the process by which technical skills are passed from one generation of physicians to the next. However, you know as well as I do that the process of learning a skill such as performing a lumbar puncture on a squirming 6-month-old almost never conforms to the see-one, do-one, teach-one dictum.
Although I recall that it was not until my 7th birthday that I could consistently and confidently tie my own shoes, I consider myself reasonably dexterous. As a woodcarver, I was comfortable around sharp instruments, but that comfort zone quickly disappeared when it came to poking and cutting another human being who had nerves and blood vessels.
In a Pediatric Perspective in the June 2017 issue of Pediatrics, two anesthesiologists at Texas Children’s Hospital in Houston and the Children’s Hospital of Philadelphia address that question of, How many tries is reasonable for a physician attempting to learn a new technique (“When Should Trainees Call for Help with Invasive Procedures?” Pediatrics. 2017, June. doi: 10.1542/peds.2016-3673)? They illustrate their insightful discussion with the gruesome image of the wrist of an infant who had endured 21 attempts at percutaneous arterial line placement.
In addition to direct supervision, the authors recommend that instructors engage the trainee in a preprocedure discussion that includes setting a predetermined number of unsuccessful attempts at which the trainee will stop and ask for help. They suggest that the “trainee should be taught the self-insight to summon a more experienced provider or perhaps just a fresh pair of hands.”
For the general pediatrician or family physician, many of the technical skills we learned in training are likely to fade from disuse in the real world of office practice. However, learning when and how to step back in the face of multiple failures is a skill that every physician will continue to use regardless of where he or she is on his or her professional trajectory.
It isn’t always easy. It challenges our egos to ask for help when we have failed at making the diagnosis or not chosen the most effective therapy. At a minimum, stepping back and taking a deep breath (or three) may allow us a window through which we can finally see outside the box we find ourselves in.
Persistence is an attribute that allowed us to navigate the long and challenging path of our medical education. But, there are situations when it gets in the way of good medical care.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
It rolls off your tongue so easily. See-one, do-one, teach-one has been the mantra recited to doctors-in-training for hundreds of years. It purports to characterize the process by which technical skills are passed from one generation of physicians to the next. However, you know as well as I do that the process of learning a skill such as performing a lumbar puncture on a squirming 6-month-old almost never conforms to the see-one, do-one, teach-one dictum.
Although I recall that it was not until my 7th birthday that I could consistently and confidently tie my own shoes, I consider myself reasonably dexterous. As a woodcarver, I was comfortable around sharp instruments, but that comfort zone quickly disappeared when it came to poking and cutting another human being who had nerves and blood vessels.
In a Pediatric Perspective in the June 2017 issue of Pediatrics, two anesthesiologists at Texas Children’s Hospital in Houston and the Children’s Hospital of Philadelphia address that question of, How many tries is reasonable for a physician attempting to learn a new technique (“When Should Trainees Call for Help with Invasive Procedures?” Pediatrics. 2017, June. doi: 10.1542/peds.2016-3673)? They illustrate their insightful discussion with the gruesome image of the wrist of an infant who had endured 21 attempts at percutaneous arterial line placement.
In addition to direct supervision, the authors recommend that instructors engage the trainee in a preprocedure discussion that includes setting a predetermined number of unsuccessful attempts at which the trainee will stop and ask for help. They suggest that the “trainee should be taught the self-insight to summon a more experienced provider or perhaps just a fresh pair of hands.”
For the general pediatrician or family physician, many of the technical skills we learned in training are likely to fade from disuse in the real world of office practice. However, learning when and how to step back in the face of multiple failures is a skill that every physician will continue to use regardless of where he or she is on his or her professional trajectory.
It isn’t always easy. It challenges our egos to ask for help when we have failed at making the diagnosis or not chosen the most effective therapy. At a minimum, stepping back and taking a deep breath (or three) may allow us a window through which we can finally see outside the box we find ourselves in.
Persistence is an attribute that allowed us to navigate the long and challenging path of our medical education. But, there are situations when it gets in the way of good medical care.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Investigational flu vaccine finds way around pyrogenicity problem
aged 5-17 years, Jolanta Airey, MD, of Seqirus in Parkville, Australia, and her associates reported.
In 2010, in Australia and New Zealand, use of a trivalent flu vaccine was associated with unexpected reports of fever and febrile seizures in children aged younger than 9 years. Research into the issue suggested that “degraded RNA fragments delivered by residual lipids activated the release of proinflammatory cytokines, which stimulated the pyrogenic response in children,” the study authors noted. “Increasing the level of sodium taurodeoxycholate (TDOC) to split the B strain in particular resulted in decreased levels of residual lipids and attenuated proinflammatory cytokine signals.”
In a phase III, randomized, observer-blinded study of the two flu vaccines at 32 centers in the United States between September 2015 and June 2016, 1,709 children aged 5-17 years received IIV4, and 569 children the same age received comparator IIV4 (Fluarix Quadrivalent). The two vaccines generated strong immune responses against all the vaccine strains in the children, with the hemagglutination inhibition geometric mean titers similar for all strains and higher for A strains than B strains for both vaccines.
In the 5- to 8-year-old group, fever was reported by 4.5% of those in the IIV4 group and 3.6% of children in the comparator IIV4 group (relative risk, 1.22). In the 9- to 17-year-old group, fever was reported by 2.1% of children in the IIV4 group and 0.8% of those in the comparator IIV4 group (RR, 2.80). Severe fever was reported by 1% or less of any of the groups of children.
Read more in the journal Vaccine (2017 May 9;35[20]:2745-52).
aged 5-17 years, Jolanta Airey, MD, of Seqirus in Parkville, Australia, and her associates reported.
In 2010, in Australia and New Zealand, use of a trivalent flu vaccine was associated with unexpected reports of fever and febrile seizures in children aged younger than 9 years. Research into the issue suggested that “degraded RNA fragments delivered by residual lipids activated the release of proinflammatory cytokines, which stimulated the pyrogenic response in children,” the study authors noted. “Increasing the level of sodium taurodeoxycholate (TDOC) to split the B strain in particular resulted in decreased levels of residual lipids and attenuated proinflammatory cytokine signals.”
In a phase III, randomized, observer-blinded study of the two flu vaccines at 32 centers in the United States between September 2015 and June 2016, 1,709 children aged 5-17 years received IIV4, and 569 children the same age received comparator IIV4 (Fluarix Quadrivalent). The two vaccines generated strong immune responses against all the vaccine strains in the children, with the hemagglutination inhibition geometric mean titers similar for all strains and higher for A strains than B strains for both vaccines.
In the 5- to 8-year-old group, fever was reported by 4.5% of those in the IIV4 group and 3.6% of children in the comparator IIV4 group (relative risk, 1.22). In the 9- to 17-year-old group, fever was reported by 2.1% of children in the IIV4 group and 0.8% of those in the comparator IIV4 group (RR, 2.80). Severe fever was reported by 1% or less of any of the groups of children.
Read more in the journal Vaccine (2017 May 9;35[20]:2745-52).
aged 5-17 years, Jolanta Airey, MD, of Seqirus in Parkville, Australia, and her associates reported.
In 2010, in Australia and New Zealand, use of a trivalent flu vaccine was associated with unexpected reports of fever and febrile seizures in children aged younger than 9 years. Research into the issue suggested that “degraded RNA fragments delivered by residual lipids activated the release of proinflammatory cytokines, which stimulated the pyrogenic response in children,” the study authors noted. “Increasing the level of sodium taurodeoxycholate (TDOC) to split the B strain in particular resulted in decreased levels of residual lipids and attenuated proinflammatory cytokine signals.”
In a phase III, randomized, observer-blinded study of the two flu vaccines at 32 centers in the United States between September 2015 and June 2016, 1,709 children aged 5-17 years received IIV4, and 569 children the same age received comparator IIV4 (Fluarix Quadrivalent). The two vaccines generated strong immune responses against all the vaccine strains in the children, with the hemagglutination inhibition geometric mean titers similar for all strains and higher for A strains than B strains for both vaccines.
In the 5- to 8-year-old group, fever was reported by 4.5% of those in the IIV4 group and 3.6% of children in the comparator IIV4 group (relative risk, 1.22). In the 9- to 17-year-old group, fever was reported by 2.1% of children in the IIV4 group and 0.8% of those in the comparator IIV4 group (RR, 2.80). Severe fever was reported by 1% or less of any of the groups of children.
Read more in the journal Vaccine (2017 May 9;35[20]:2745-52).
FROM VACCINE
Supportive parenting program reduced African American teen smoking
Particularly in high-risk populations, participation in a family-centered parenting intervention can reduce adolescent and early adult smoking, according to results of a randomized controlled trial of the Strong African American Families (SAAF) program published in Pediatrics June 14.
African Americans have the “highest mortality rates for coronary heart disease and stroke,” compared with other racial groups, and the high rate of smoking among young adult African Americans is of concern, wrote Yi-fu Chen, PhD, of National Taipei University, New Taipei City, Taiwan, and his coinvestigators.
In a study of 424 African American adolescents from small towns in nine rural counties of southern Georgia, the 257 who were randomized to SAAF at age 11 years overall displayed significantly lower cotinine scores a
The SAAF families each attended seven meetings that consisted of both a separate session for the youth and the parent, and a joint session in which they practiced the skills they learned separately. The parents focused on “consistent provision of instrumental and emotional support, along with high levels of monitoring, consistent discipline that is not harsh, predictable family routines, and the establishment of clear norms and expectations for the use of drugs,” while the youth focused on “the importance of having and abiding by household rules, adaptive behaviors to use when encountering racism, and the importance of forming goals for the future and making plans to attain them,” the researchers explained.
These results “may provide a strategy for reducing health vulnerabilities associated with smoking among African American youth who grow up in challenging rural contexts,” the authors wrote.
Read more in Pediatrics (doi: 10.1542/peds.2016-4162).
Particularly in high-risk populations, participation in a family-centered parenting intervention can reduce adolescent and early adult smoking, according to results of a randomized controlled trial of the Strong African American Families (SAAF) program published in Pediatrics June 14.
African Americans have the “highest mortality rates for coronary heart disease and stroke,” compared with other racial groups, and the high rate of smoking among young adult African Americans is of concern, wrote Yi-fu Chen, PhD, of National Taipei University, New Taipei City, Taiwan, and his coinvestigators.
In a study of 424 African American adolescents from small towns in nine rural counties of southern Georgia, the 257 who were randomized to SAAF at age 11 years overall displayed significantly lower cotinine scores a
The SAAF families each attended seven meetings that consisted of both a separate session for the youth and the parent, and a joint session in which they practiced the skills they learned separately. The parents focused on “consistent provision of instrumental and emotional support, along with high levels of monitoring, consistent discipline that is not harsh, predictable family routines, and the establishment of clear norms and expectations for the use of drugs,” while the youth focused on “the importance of having and abiding by household rules, adaptive behaviors to use when encountering racism, and the importance of forming goals for the future and making plans to attain them,” the researchers explained.
These results “may provide a strategy for reducing health vulnerabilities associated with smoking among African American youth who grow up in challenging rural contexts,” the authors wrote.
Read more in Pediatrics (doi: 10.1542/peds.2016-4162).
Particularly in high-risk populations, participation in a family-centered parenting intervention can reduce adolescent and early adult smoking, according to results of a randomized controlled trial of the Strong African American Families (SAAF) program published in Pediatrics June 14.
African Americans have the “highest mortality rates for coronary heart disease and stroke,” compared with other racial groups, and the high rate of smoking among young adult African Americans is of concern, wrote Yi-fu Chen, PhD, of National Taipei University, New Taipei City, Taiwan, and his coinvestigators.
In a study of 424 African American adolescents from small towns in nine rural counties of southern Georgia, the 257 who were randomized to SAAF at age 11 years overall displayed significantly lower cotinine scores a
The SAAF families each attended seven meetings that consisted of both a separate session for the youth and the parent, and a joint session in which they practiced the skills they learned separately. The parents focused on “consistent provision of instrumental and emotional support, along with high levels of monitoring, consistent discipline that is not harsh, predictable family routines, and the establishment of clear norms and expectations for the use of drugs,” while the youth focused on “the importance of having and abiding by household rules, adaptive behaviors to use when encountering racism, and the importance of forming goals for the future and making plans to attain them,” the researchers explained.
These results “may provide a strategy for reducing health vulnerabilities associated with smoking among African American youth who grow up in challenging rural contexts,” the authors wrote.
Read more in Pediatrics (doi: 10.1542/peds.2016-4162).
FROM PEDIATRICS
Telemedicine visits after NICU discharge improved care, processes
SAN FRANCISCO – Using telemedicine for a follow-up appointment 1 week after discharge of medically complex infants reduced extra visits or calls to a clinic or emergency department, a recent study found.
The telemedicine visits also helped providers identify ways to improve the neonatal ICU (NICU) discharge process while assessing infants’ home care and answering parents’ questions.

The researchers assessed whether telemedicine visits could ease the transition from neonatal intensive care to home care, respond adequately to caregivers’ needs during that transition, reduce emergency department visits and readmissions, and detect and address any potential problems. The visits also provided an opportunity for feedback on caregivers’ experiences during discharge.
The 92 patients all were medically complex infants who went home with respiratory or feeding equipment, surgical sites and/or complex medication administration. For example, 28 infants had been sent home with a nasogastric tube, 13 had a gastrostomy tube, and 13 had an apnea monitor. Overall, participants had been discharged with an average 2.3 medications and 4.8 scheduled subspecialty follow-up appointments.
The most common conditions among the participants were gastrointestinal disease, neurologic disease, and congenital diaphragmatic hernia or lung lesions. Other conditions included omphalocele, genetic disorders, tracheoesophageal fistula or esophageal atresia and chronic lung disease, or another respiratory disease, Dr. Brant reported at the Pediatric Academic Societies meeting.
Families could enroll in the study only if they had a smart device (such as a tablet) and wireless Internet access at home. One week after the infant’s discharge from the NICU, the caregivers received one telemedicine visit with a team that included neonatologists, neonatal fellows, nurse practitioners, and a telemedicine coordinator or support staffer. During the visit, the providers observed the infant and the home environment, and evaluated care practices, including tube feedings, respiratory support, management of surgical wound sites, and administration of medications.
The providers also reviewed how to use the medical equipment, gathered follow-up information about the child’s health, and answered caregivers’ questions. The providers did not bill for telemedicine visits since it was part of a pilot study, but the participants did need to reside in Pennsylvania or New Jersey to meet provider licensing regulations.
Among the 93 telemedicine visits, half (50%) prevented the family from calling or visiting a provider, and 12% of them led to an earlier follow-up appointment for the child. During the video observations, providers addressed 14 issues related to the child’s sleep environment, respiratory status, surgical sites, or dermatological issues. Among 78 total concerns identified in the visits, 35% related to the surgical site, 33% related to feeding, 19% related to respiratory concerns, and 13% related to medication administration.
The provider team also asked families during the visit about their experiences during discharge. A quarter of the families (26%) said they needed more parental education during discharge. In addition, 14% mentioned problems with scheduling follow-up appointments, and 12% had problems related to case management and insurance. Other issues raised by parents related to home equipment, early intervention, home feeding or medications, and diagnostic logistics.
In subsequent satisfaction surveys filled out by caregivers about the telemedicine visit itself, the median rating was 94.5 on a scale of 0 (not at all satisfied) to 100 (extremely satisfied). The overall intervention was 92% successful in its completion. The only follow-up telemedicine visits that did not occur resulted from malfunctioning wireless connection or a mobile app problem. On a scale of 1 to 100 (best), caregivers rated the video quality as an average 78, the Internet reliability as 79, and the ease of using the camera as 91. One of the biggest benefits of the intervention, Dr. Brant pointed out, is that using telemedicine bypasses some of the geographic and time-related obstacles that can occur with follow-ups.
Dr. Brant had no relevant financial disclosures and did not report using any external funding.
SAN FRANCISCO – Using telemedicine for a follow-up appointment 1 week after discharge of medically complex infants reduced extra visits or calls to a clinic or emergency department, a recent study found.
The telemedicine visits also helped providers identify ways to improve the neonatal ICU (NICU) discharge process while assessing infants’ home care and answering parents’ questions.
The researchers assessed whether telemedicine visits could ease the transition from neonatal intensive care to home care, respond adequately to caregivers’ needs during that transition, reduce emergency department visits and readmissions, and detect and address any potential problems. The visits also provided an opportunity for feedback on caregivers’ experiences during discharge.
The 92 patients all were medically complex infants who went home with respiratory or feeding equipment, surgical sites and/or complex medication administration. For example, 28 infants had been sent home with a nasogastric tube, 13 had a gastrostomy tube, and 13 had an apnea monitor. Overall, participants had been discharged with an average 2.3 medications and 4.8 scheduled subspecialty follow-up appointments.
The most common conditions among the participants were gastrointestinal disease, neurologic disease, and congenital diaphragmatic hernia or lung lesions. Other conditions included omphalocele, genetic disorders, tracheoesophageal fistula or esophageal atresia and chronic lung disease, or another respiratory disease, Dr. Brant reported at the Pediatric Academic Societies meeting.
Families could enroll in the study only if they had a smart device (such as a tablet) and wireless Internet access at home. One week after the infant’s discharge from the NICU, the caregivers received one telemedicine visit with a team that included neonatologists, neonatal fellows, nurse practitioners, and a telemedicine coordinator or support staffer. During the visit, the providers observed the infant and the home environment, and evaluated care practices, including tube feedings, respiratory support, management of surgical wound sites, and administration of medications.
The providers also reviewed how to use the medical equipment, gathered follow-up information about the child’s health, and answered caregivers’ questions. The providers did not bill for telemedicine visits since it was part of a pilot study, but the participants did need to reside in Pennsylvania or New Jersey to meet provider licensing regulations.
Among the 93 telemedicine visits, half (50%) prevented the family from calling or visiting a provider, and 12% of them led to an earlier follow-up appointment for the child. During the video observations, providers addressed 14 issues related to the child’s sleep environment, respiratory status, surgical sites, or dermatological issues. Among 78 total concerns identified in the visits, 35% related to the surgical site, 33% related to feeding, 19% related to respiratory concerns, and 13% related to medication administration.
The provider team also asked families during the visit about their experiences during discharge. A quarter of the families (26%) said they needed more parental education during discharge. In addition, 14% mentioned problems with scheduling follow-up appointments, and 12% had problems related to case management and insurance. Other issues raised by parents related to home equipment, early intervention, home feeding or medications, and diagnostic logistics.
In subsequent satisfaction surveys filled out by caregivers about the telemedicine visit itself, the median rating was 94.5 on a scale of 0 (not at all satisfied) to 100 (extremely satisfied). The overall intervention was 92% successful in its completion. The only follow-up telemedicine visits that did not occur resulted from malfunctioning wireless connection or a mobile app problem. On a scale of 1 to 100 (best), caregivers rated the video quality as an average 78, the Internet reliability as 79, and the ease of using the camera as 91. One of the biggest benefits of the intervention, Dr. Brant pointed out, is that using telemedicine bypasses some of the geographic and time-related obstacles that can occur with follow-ups.
Dr. Brant had no relevant financial disclosures and did not report using any external funding.
SAN FRANCISCO – Using telemedicine for a follow-up appointment 1 week after discharge of medically complex infants reduced extra visits or calls to a clinic or emergency department, a recent study found.
The telemedicine visits also helped providers identify ways to improve the neonatal ICU (NICU) discharge process while assessing infants’ home care and answering parents’ questions.
The researchers assessed whether telemedicine visits could ease the transition from neonatal intensive care to home care, respond adequately to caregivers’ needs during that transition, reduce emergency department visits and readmissions, and detect and address any potential problems. The visits also provided an opportunity for feedback on caregivers’ experiences during discharge.
The 92 patients all were medically complex infants who went home with respiratory or feeding equipment, surgical sites and/or complex medication administration. For example, 28 infants had been sent home with a nasogastric tube, 13 had a gastrostomy tube, and 13 had an apnea monitor. Overall, participants had been discharged with an average 2.3 medications and 4.8 scheduled subspecialty follow-up appointments.
The most common conditions among the participants were gastrointestinal disease, neurologic disease, and congenital diaphragmatic hernia or lung lesions. Other conditions included omphalocele, genetic disorders, tracheoesophageal fistula or esophageal atresia and chronic lung disease, or another respiratory disease, Dr. Brant reported at the Pediatric Academic Societies meeting.
Families could enroll in the study only if they had a smart device (such as a tablet) and wireless Internet access at home. One week after the infant’s discharge from the NICU, the caregivers received one telemedicine visit with a team that included neonatologists, neonatal fellows, nurse practitioners, and a telemedicine coordinator or support staffer. During the visit, the providers observed the infant and the home environment, and evaluated care practices, including tube feedings, respiratory support, management of surgical wound sites, and administration of medications.
The providers also reviewed how to use the medical equipment, gathered follow-up information about the child’s health, and answered caregivers’ questions. The providers did not bill for telemedicine visits since it was part of a pilot study, but the participants did need to reside in Pennsylvania or New Jersey to meet provider licensing regulations.
Among the 93 telemedicine visits, half (50%) prevented the family from calling or visiting a provider, and 12% of them led to an earlier follow-up appointment for the child. During the video observations, providers addressed 14 issues related to the child’s sleep environment, respiratory status, surgical sites, or dermatological issues. Among 78 total concerns identified in the visits, 35% related to the surgical site, 33% related to feeding, 19% related to respiratory concerns, and 13% related to medication administration.
The provider team also asked families during the visit about their experiences during discharge. A quarter of the families (26%) said they needed more parental education during discharge. In addition, 14% mentioned problems with scheduling follow-up appointments, and 12% had problems related to case management and insurance. Other issues raised by parents related to home equipment, early intervention, home feeding or medications, and diagnostic logistics.
In subsequent satisfaction surveys filled out by caregivers about the telemedicine visit itself, the median rating was 94.5 on a scale of 0 (not at all satisfied) to 100 (extremely satisfied). The overall intervention was 92% successful in its completion. The only follow-up telemedicine visits that did not occur resulted from malfunctioning wireless connection or a mobile app problem. On a scale of 1 to 100 (best), caregivers rated the video quality as an average 78, the Internet reliability as 79, and the ease of using the camera as 91. One of the biggest benefits of the intervention, Dr. Brant pointed out, is that using telemedicine bypasses some of the geographic and time-related obstacles that can occur with follow-ups.
Dr. Brant had no relevant financial disclosures and did not report using any external funding.
FROM PAS 17
Key clinical point:
Major finding: Telemedicine visits prevented 50% of participants from calling or visiting a provider and led 12% of families to bring infants in sooner than originally scheduled.
Data source: The findings are based on a pilot project at the Children’s Hospital of Philadelphia involving 93 medically complex infants discharged from the NICU with medical equipment, surgical sites, and/or complex medication administration.
Disclosures: Dr. Brant had no relevant financial disclosures and did not report external funding.
Early literacy assessment tool shows promise for screening preschool children
SAN FRANCISCO – The 10-item Early Literary Assessment Tool (ELSAT) used during regular pediatrician appointments in the first 4 years of life has shown promise in screening preschool children for delayed literacy skills that could result in later reading problems, based on a pilot study conducted in the preschool setting.
ELSAT “can be completed by a clinician [in the primary care setting] in less than a minute and can be incorporated into the Reach Out and Read intervention. An important next step in our research is to study the feasibility of the ELSAT within primary care visits and obtain feedback from clinicians about the ease of administration and value to their practice,” said Sai N. Iyer, MD, a developmental-behavioral pediatric fellow at the University of California, San Diego.

The initial 40-item ELSAT addressed three key domains of early literacy skills: knowledge and awareness of printed words, knowledge of letters, and recognition of word sounds. The observational study had two phases. ELSAT was developed and refined in the pilot phase, with validation against three aforementioned reference measures in the validation phase. The process whittled the test down to 10 items, with the same three domains represented. Comparisons were between the individual measures and a composite of the three.

The 10-item ELSAT correlated with each of the reference measures and with the composite of the three measures of early literacy (Pearson’s correlation, 810; P less than .01; Cronbach’s alpha [a measure of internal consistency] of .852). A cut-off ELSAT score of less than or equal to 5 predicted a “below average” score in any of the three reference measures and identified delayed literacy with a sensitivity of 92% and an acceptable specificity of 64%, Dr. Iyer explained during her presentation at the Pediatric Academic Societies meeting.
Language skills acquired during the first few years of life in the home and preschool settings lay the path for the development of more sophisticated reading skills, including decoding and comprehension beginning in grade 1. “Research has shown that about 40% of children enter kindergarten behind their peers in important early literacy skills. This gap widens with time, and the cost of catching them up far exceeds the cost of screening and early intervention. Many studies have demonstrated that effective early interventions improve the long-term outcomes for children who are at risk for later reading failure. Children who are reading at a below grade level by 4th grade are unlikely to catch up. Low levels of literacy have an impact on later educational and employment opportunities and set up a cycle of social and economic disadvantage that can have transgenerational effects,” Dr. Iyer said.
While parent-completed questionnaires are a convenient way to perform developmental screening, they are limited by the health literacy of the parents and other factors. Furthermore, while some preschools perform assessments, not all children attend preschools. This prompted Dr. Iyer and colleagues to think about developing a more objective screening strategy, with which a clinician could do the brief assessment. “All preschool children do see their pediatrician/primary care provider for vaccinations that are required before kindergarten. This makes the primary care setting an ideal opportunity to screen these children,” said Dr. Iyer.
During the question-and-answer session, an attendee described the data concerning the dichotomy in the test results between the public and private preschools as “some of the most impressive and depressing I’ve seen in this area.”
In a later interview, Dr. Iyer commented that, while the results in the study were not entirely new or surprising, “it was remarkable that we were able to demonstrate such significant differences in a sample of children enrolled in a high-quality preschool. Without specific screening and intervention, these early literacy delays would go unrecognized and increase the risk of poor academic outcomes for these high-risk children. The children were all in some type of preschool environment. Throughout the country, there are many children from low-income families who are not able to access preschool education. Although we did not test these children in our study, it is likely that the gaps between these children and their more advantaged peers are even higher. The pediatrician’s office may be the only place for these children to receive early literacy screening and anticipatory guidance on reading readiness.”
The sponsor of the study was the University of California, San Diego. The study was funded by the 2015 Academic Pediatric Association Young Investigator Award and by Reach Out and Read. Dr. Iyer had no relevant financial disclosures to report.
SAN FRANCISCO – The 10-item Early Literary Assessment Tool (ELSAT) used during regular pediatrician appointments in the first 4 years of life has shown promise in screening preschool children for delayed literacy skills that could result in later reading problems, based on a pilot study conducted in the preschool setting.
ELSAT “can be completed by a clinician [in the primary care setting] in less than a minute and can be incorporated into the Reach Out and Read intervention. An important next step in our research is to study the feasibility of the ELSAT within primary care visits and obtain feedback from clinicians about the ease of administration and value to their practice,” said Sai N. Iyer, MD, a developmental-behavioral pediatric fellow at the University of California, San Diego.
The initial 40-item ELSAT addressed three key domains of early literacy skills: knowledge and awareness of printed words, knowledge of letters, and recognition of word sounds. The observational study had two phases. ELSAT was developed and refined in the pilot phase, with validation against three aforementioned reference measures in the validation phase. The process whittled the test down to 10 items, with the same three domains represented. Comparisons were between the individual measures and a composite of the three.
The 10-item ELSAT correlated with each of the reference measures and with the composite of the three measures of early literacy (Pearson’s correlation, 810; P less than .01; Cronbach’s alpha [a measure of internal consistency] of .852). A cut-off ELSAT score of less than or equal to 5 predicted a “below average” score in any of the three reference measures and identified delayed literacy with a sensitivity of 92% and an acceptable specificity of 64%, Dr. Iyer explained during her presentation at the Pediatric Academic Societies meeting.
Language skills acquired during the first few years of life in the home and preschool settings lay the path for the development of more sophisticated reading skills, including decoding and comprehension beginning in grade 1. “Research has shown that about 40% of children enter kindergarten behind their peers in important early literacy skills. This gap widens with time, and the cost of catching them up far exceeds the cost of screening and early intervention. Many studies have demonstrated that effective early interventions improve the long-term outcomes for children who are at risk for later reading failure. Children who are reading at a below grade level by 4th grade are unlikely to catch up. Low levels of literacy have an impact on later educational and employment opportunities and set up a cycle of social and economic disadvantage that can have transgenerational effects,” Dr. Iyer said.
While parent-completed questionnaires are a convenient way to perform developmental screening, they are limited by the health literacy of the parents and other factors. Furthermore, while some preschools perform assessments, not all children attend preschools. This prompted Dr. Iyer and colleagues to think about developing a more objective screening strategy, with which a clinician could do the brief assessment. “All preschool children do see their pediatrician/primary care provider for vaccinations that are required before kindergarten. This makes the primary care setting an ideal opportunity to screen these children,” said Dr. Iyer.
During the question-and-answer session, an attendee described the data concerning the dichotomy in the test results between the public and private preschools as “some of the most impressive and depressing I’ve seen in this area.”
In a later interview, Dr. Iyer commented that, while the results in the study were not entirely new or surprising, “it was remarkable that we were able to demonstrate such significant differences in a sample of children enrolled in a high-quality preschool. Without specific screening and intervention, these early literacy delays would go unrecognized and increase the risk of poor academic outcomes for these high-risk children. The children were all in some type of preschool environment. Throughout the country, there are many children from low-income families who are not able to access preschool education. Although we did not test these children in our study, it is likely that the gaps between these children and their more advantaged peers are even higher. The pediatrician’s office may be the only place for these children to receive early literacy screening and anticipatory guidance on reading readiness.”
The sponsor of the study was the University of California, San Diego. The study was funded by the 2015 Academic Pediatric Association Young Investigator Award and by Reach Out and Read. Dr. Iyer had no relevant financial disclosures to report.
SAN FRANCISCO – The 10-item Early Literary Assessment Tool (ELSAT) used during regular pediatrician appointments in the first 4 years of life has shown promise in screening preschool children for delayed literacy skills that could result in later reading problems, based on a pilot study conducted in the preschool setting.
ELSAT “can be completed by a clinician [in the primary care setting] in less than a minute and can be incorporated into the Reach Out and Read intervention. An important next step in our research is to study the feasibility of the ELSAT within primary care visits and obtain feedback from clinicians about the ease of administration and value to their practice,” said Sai N. Iyer, MD, a developmental-behavioral pediatric fellow at the University of California, San Diego.
The initial 40-item ELSAT addressed three key domains of early literacy skills: knowledge and awareness of printed words, knowledge of letters, and recognition of word sounds. The observational study had two phases. ELSAT was developed and refined in the pilot phase, with validation against three aforementioned reference measures in the validation phase. The process whittled the test down to 10 items, with the same three domains represented. Comparisons were between the individual measures and a composite of the three.
The 10-item ELSAT correlated with each of the reference measures and with the composite of the three measures of early literacy (Pearson’s correlation, 810; P less than .01; Cronbach’s alpha [a measure of internal consistency] of .852). A cut-off ELSAT score of less than or equal to 5 predicted a “below average” score in any of the three reference measures and identified delayed literacy with a sensitivity of 92% and an acceptable specificity of 64%, Dr. Iyer explained during her presentation at the Pediatric Academic Societies meeting.
Language skills acquired during the first few years of life in the home and preschool settings lay the path for the development of more sophisticated reading skills, including decoding and comprehension beginning in grade 1. “Research has shown that about 40% of children enter kindergarten behind their peers in important early literacy skills. This gap widens with time, and the cost of catching them up far exceeds the cost of screening and early intervention. Many studies have demonstrated that effective early interventions improve the long-term outcomes for children who are at risk for later reading failure. Children who are reading at a below grade level by 4th grade are unlikely to catch up. Low levels of literacy have an impact on later educational and employment opportunities and set up a cycle of social and economic disadvantage that can have transgenerational effects,” Dr. Iyer said.
While parent-completed questionnaires are a convenient way to perform developmental screening, they are limited by the health literacy of the parents and other factors. Furthermore, while some preschools perform assessments, not all children attend preschools. This prompted Dr. Iyer and colleagues to think about developing a more objective screening strategy, with which a clinician could do the brief assessment. “All preschool children do see their pediatrician/primary care provider for vaccinations that are required before kindergarten. This makes the primary care setting an ideal opportunity to screen these children,” said Dr. Iyer.
During the question-and-answer session, an attendee described the data concerning the dichotomy in the test results between the public and private preschools as “some of the most impressive and depressing I’ve seen in this area.”
In a later interview, Dr. Iyer commented that, while the results in the study were not entirely new or surprising, “it was remarkable that we were able to demonstrate such significant differences in a sample of children enrolled in a high-quality preschool. Without specific screening and intervention, these early literacy delays would go unrecognized and increase the risk of poor academic outcomes for these high-risk children. The children were all in some type of preschool environment. Throughout the country, there are many children from low-income families who are not able to access preschool education. Although we did not test these children in our study, it is likely that the gaps between these children and their more advantaged peers are even higher. The pediatrician’s office may be the only place for these children to receive early literacy screening and anticipatory guidance on reading readiness.”
The sponsor of the study was the University of California, San Diego. The study was funded by the 2015 Academic Pediatric Association Young Investigator Award and by Reach Out and Read. Dr. Iyer had no relevant financial disclosures to report.
AT PAS 2017
Key clinical point:
Major finding: The 10-item ELSAT correlated with each of the reference measures and with the composite of the three measures of early literacy (Pearson’s correlation, 810; P less than .01; Cronbach’s alpha [a measure of internal consistency] of .852).
Data source: An observational study of 54-month-old children in five public preschools (n = 61) and two private preschools (n = 35) in San Diego.
Disclosures: The sponsor of the study was the University of California, San Diego. The study was funded by the 2015 Academic Pediatric Association Young Investigator Award and by Reach Out and Read. Dr. Iyer had no relevant financial disclosures to report.
‘How could he?’
The headline in a Portland, Maine, newspaper read, “Standish man sentenced to serve 15 years in prison for death of his 3-month-old son” (Edward Murphy, May 23, 2017). I suspect that many of the folks who read the story under the headline feel that the sentence was too light. Others are asking themselves how a 21-year-old man could beat a fragile 5-pound infant to death. What kind of evil monster is this guy?
However, even with the snatches of information provided in the 500-word newspaper story, the unfortunate scenario makes sense, and the child’s death is a tragic culmination of a series of events that shouldn’t surprise any pediatrician. It turns out the infant was a twin who, with his sister, had been born at 30 weeks’ gestation. He had spent a month or more in the hospital, and his sister was still in neonatal ICU at the time of his death. While it is unclear from the newspaper article whether the twins’ parents were married, they were living in a house with eight other adults and some other children. The mother was out of the home working while the father was left to care for his son.
I am sure that the neonatologists and social workers at the hospital where the twins were born were aware of at least some of the red flags that waved over this unfortunate family. I also am confident that they did what they could to assure this infant a safe home environment when it was time for his discharge from the NICU. However, risks factors may have been missed that now seem obvious in retrospect. We should all realize by now from our experience with domestic terrorism that simply appearing on someone’s radar doesn’t mean that preemptive action can or will be taken. Short of keeping the parents of high-risk neonates under constant surveillance for a year or 2, there are few other workable options to prevent every tragedy like this one.
This case is another example of the erosive power of a baby’s cry. Most pediatricians have developed a filtering mechanism that allows us to function in a cacophonous environment dominated by a screaming infant. However, even adults without this young father’s deprived background crack under the stress when they are confined in a space with a crying child. The risk of decompensation is compounded when the adult also feels some responsibility for the child’s welfare. I don’t think we can condone what the father did in this tragic scenario, but we can certainly understand how the dominoes fell.
We are all potential child abusers. When faced with the right, or I guess the wrong, set of circumstances we might lash out to stop the crying. Luckily, most of us are several body lengths from the end of that rope.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
The headline in a Portland, Maine, newspaper read, “Standish man sentenced to serve 15 years in prison for death of his 3-month-old son” (Edward Murphy, May 23, 2017). I suspect that many of the folks who read the story under the headline feel that the sentence was too light. Others are asking themselves how a 21-year-old man could beat a fragile 5-pound infant to death. What kind of evil monster is this guy?
However, even with the snatches of information provided in the 500-word newspaper story, the unfortunate scenario makes sense, and the child’s death is a tragic culmination of a series of events that shouldn’t surprise any pediatrician. It turns out the infant was a twin who, with his sister, had been born at 30 weeks’ gestation. He had spent a month or more in the hospital, and his sister was still in neonatal ICU at the time of his death. While it is unclear from the newspaper article whether the twins’ parents were married, they were living in a house with eight other adults and some other children. The mother was out of the home working while the father was left to care for his son.
I am sure that the neonatologists and social workers at the hospital where the twins were born were aware of at least some of the red flags that waved over this unfortunate family. I also am confident that they did what they could to assure this infant a safe home environment when it was time for his discharge from the NICU. However, risks factors may have been missed that now seem obvious in retrospect. We should all realize by now from our experience with domestic terrorism that simply appearing on someone’s radar doesn’t mean that preemptive action can or will be taken. Short of keeping the parents of high-risk neonates under constant surveillance for a year or 2, there are few other workable options to prevent every tragedy like this one.
This case is another example of the erosive power of a baby’s cry. Most pediatricians have developed a filtering mechanism that allows us to function in a cacophonous environment dominated by a screaming infant. However, even adults without this young father’s deprived background crack under the stress when they are confined in a space with a crying child. The risk of decompensation is compounded when the adult also feels some responsibility for the child’s welfare. I don’t think we can condone what the father did in this tragic scenario, but we can certainly understand how the dominoes fell.
We are all potential child abusers. When faced with the right, or I guess the wrong, set of circumstances we might lash out to stop the crying. Luckily, most of us are several body lengths from the end of that rope.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
The headline in a Portland, Maine, newspaper read, “Standish man sentenced to serve 15 years in prison for death of his 3-month-old son” (Edward Murphy, May 23, 2017). I suspect that many of the folks who read the story under the headline feel that the sentence was too light. Others are asking themselves how a 21-year-old man could beat a fragile 5-pound infant to death. What kind of evil monster is this guy?
However, even with the snatches of information provided in the 500-word newspaper story, the unfortunate scenario makes sense, and the child’s death is a tragic culmination of a series of events that shouldn’t surprise any pediatrician. It turns out the infant was a twin who, with his sister, had been born at 30 weeks’ gestation. He had spent a month or more in the hospital, and his sister was still in neonatal ICU at the time of his death. While it is unclear from the newspaper article whether the twins’ parents were married, they were living in a house with eight other adults and some other children. The mother was out of the home working while the father was left to care for his son.
I am sure that the neonatologists and social workers at the hospital where the twins were born were aware of at least some of the red flags that waved over this unfortunate family. I also am confident that they did what they could to assure this infant a safe home environment when it was time for his discharge from the NICU. However, risks factors may have been missed that now seem obvious in retrospect. We should all realize by now from our experience with domestic terrorism that simply appearing on someone’s radar doesn’t mean that preemptive action can or will be taken. Short of keeping the parents of high-risk neonates under constant surveillance for a year or 2, there are few other workable options to prevent every tragedy like this one.
This case is another example of the erosive power of a baby’s cry. Most pediatricians have developed a filtering mechanism that allows us to function in a cacophonous environment dominated by a screaming infant. However, even adults without this young father’s deprived background crack under the stress when they are confined in a space with a crying child. The risk of decompensation is compounded when the adult also feels some responsibility for the child’s welfare. I don’t think we can condone what the father did in this tragic scenario, but we can certainly understand how the dominoes fell.
We are all potential child abusers. When faced with the right, or I guess the wrong, set of circumstances we might lash out to stop the crying. Luckily, most of us are several body lengths from the end of that rope.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Not better late ...
You all know the statistics or at least have a sense of the scope of the problem. While 85% of mothers in this country intend to breastfeed their infants exclusively for at least 3 months, only slightly more than 30% achieve this goal. Among the dozens of reasons for this unfortunate shortfall is what some experts view as inadequate support by primary care physicians and their offices. In the May 2017 Pediatrics, two members of the American Academy of Pediatrics Section on Breastfeeding offer a clinical report that hopes to remedy this situation (“The Breastfeeding-Friendly Pediatric Office Practice.” Pediatrics. 2017 May. 139[5]:e20170647). It is a document that begins with an excellent review of the background and epidemiology of breastfeeding in the United States and a survey of the current initiatives targeted at improving our dismal performance. What follows is an extensive set of 19 evidence-based recommendations for the pediatric outpatient practice that hopes to “meet or exceed the AAP recommendations.”
A large part of the problem is the failure of the point person in the office, usually the receptionist, to realize that a tearful call from a new mother who is struggling with breastfeeding is an emergency, one that demands a response in minutes … not hours. Even when the call is eventually routed to someone with a compassionate voice who will call back with the right answers, if that process takes just an hour or two, that is enough time for a mother with a screaming and hungry newborn to reach for a bottle of formula.

I urge you to read this exhaustive clinical report in Pediatrics because it is very likely you will come across some things that you can include in your office practice to make it more breastfeeding friendly. However, Even if you and your staff have the right advice, this is not a situation of “better late than never.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
You all know the statistics or at least have a sense of the scope of the problem. While 85% of mothers in this country intend to breastfeed their infants exclusively for at least 3 months, only slightly more than 30% achieve this goal. Among the dozens of reasons for this unfortunate shortfall is what some experts view as inadequate support by primary care physicians and their offices. In the May 2017 Pediatrics, two members of the American Academy of Pediatrics Section on Breastfeeding offer a clinical report that hopes to remedy this situation (“The Breastfeeding-Friendly Pediatric Office Practice.” Pediatrics. 2017 May. 139[5]:e20170647). It is a document that begins with an excellent review of the background and epidemiology of breastfeeding in the United States and a survey of the current initiatives targeted at improving our dismal performance. What follows is an extensive set of 19 evidence-based recommendations for the pediatric outpatient practice that hopes to “meet or exceed the AAP recommendations.”
A large part of the problem is the failure of the point person in the office, usually the receptionist, to realize that a tearful call from a new mother who is struggling with breastfeeding is an emergency, one that demands a response in minutes … not hours. Even when the call is eventually routed to someone with a compassionate voice who will call back with the right answers, if that process takes just an hour or two, that is enough time for a mother with a screaming and hungry newborn to reach for a bottle of formula.
I urge you to read this exhaustive clinical report in Pediatrics because it is very likely you will come across some things that you can include in your office practice to make it more breastfeeding friendly. However, Even if you and your staff have the right advice, this is not a situation of “better late than never.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
You all know the statistics or at least have a sense of the scope of the problem. While 85% of mothers in this country intend to breastfeed their infants exclusively for at least 3 months, only slightly more than 30% achieve this goal. Among the dozens of reasons for this unfortunate shortfall is what some experts view as inadequate support by primary care physicians and their offices. In the May 2017 Pediatrics, two members of the American Academy of Pediatrics Section on Breastfeeding offer a clinical report that hopes to remedy this situation (“The Breastfeeding-Friendly Pediatric Office Practice.” Pediatrics. 2017 May. 139[5]:e20170647). It is a document that begins with an excellent review of the background and epidemiology of breastfeeding in the United States and a survey of the current initiatives targeted at improving our dismal performance. What follows is an extensive set of 19 evidence-based recommendations for the pediatric outpatient practice that hopes to “meet or exceed the AAP recommendations.”
A large part of the problem is the failure of the point person in the office, usually the receptionist, to realize that a tearful call from a new mother who is struggling with breastfeeding is an emergency, one that demands a response in minutes … not hours. Even when the call is eventually routed to someone with a compassionate voice who will call back with the right answers, if that process takes just an hour or two, that is enough time for a mother with a screaming and hungry newborn to reach for a bottle of formula.
I urge you to read this exhaustive clinical report in Pediatrics because it is very likely you will come across some things that you can include in your office practice to make it more breastfeeding friendly. However, Even if you and your staff have the right advice, this is not a situation of “better late than never.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Infant mortality down in most states
Infant mortality in the United States was down by 15% from 2005 to 2014, with 33 states reporting significant declines, according to the National Center for Health Statistics.
The overall rate for 2014 was 5.82 infant deaths per 1,000 live births, compared with 6.84 per 1,000 in 2005. The data for individual states were grouped into 3-year periods, so between the periods of 2005-2007 and 2012-2014, there were 33 states (and the District of Columbia) with a significant decline and 17 states with no significant change. Three states – Maine, South Dakota, and Utah – had increased infant mortality, but the changes did not reach significance, the NCHS reported, using data from the National Vital Statistics System.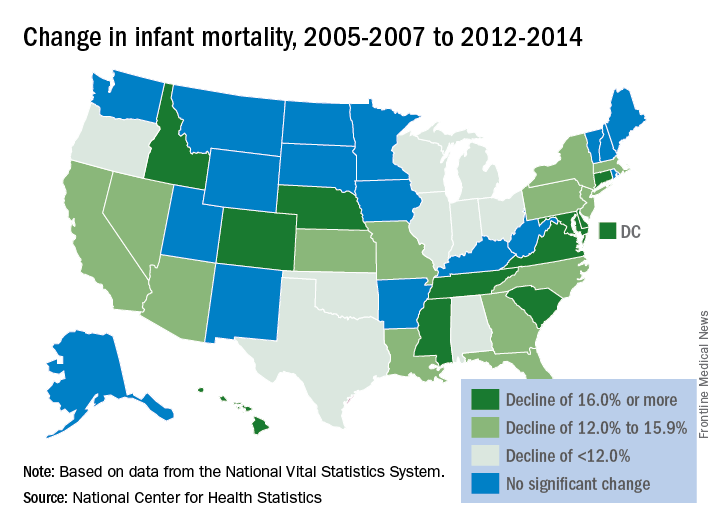
Infant mortality in the United States was down by 15% from 2005 to 2014, with 33 states reporting significant declines, according to the National Center for Health Statistics.
The overall rate for 2014 was 5.82 infant deaths per 1,000 live births, compared with 6.84 per 1,000 in 2005. The data for individual states were grouped into 3-year periods, so between the periods of 2005-2007 and 2012-2014, there were 33 states (and the District of Columbia) with a significant decline and 17 states with no significant change. Three states – Maine, South Dakota, and Utah – had increased infant mortality, but the changes did not reach significance, the NCHS reported, using data from the National Vital Statistics System.
Infant mortality in the United States was down by 15% from 2005 to 2014, with 33 states reporting significant declines, according to the National Center for Health Statistics.
The overall rate for 2014 was 5.82 infant deaths per 1,000 live births, compared with 6.84 per 1,000 in 2005. The data for individual states were grouped into 3-year periods, so between the periods of 2005-2007 and 2012-2014, there were 33 states (and the District of Columbia) with a significant decline and 17 states with no significant change. Three states – Maine, South Dakota, and Utah – had increased infant mortality, but the changes did not reach significance, the NCHS reported, using data from the National Vital Statistics System.
Dasatinib potentially a new SOC for children with CML-CP

CHICAGO—The largest ongoing and prospective trial of pediatric patients with chronic myeloid leukemia in chronic phase (CML-CP), according to the best knowledge of the investigators, has found dasatinib to be safe and effective as first- or second-line therapy for these children.
Patients refractory to or intolerant of imatinib had a major cytogenetic response (MCyR) by 3 months and responses at 12 and 24 months exceeded 90%.
Newly diagnosed patients had a complete cytogenetic response (CCyR) by 6 months.
“We believe our data suggests that dasatinib could be considered as a new standard of care (SOC) for children with CML in chronic phase,” said study author Lia Gore, MD, of the University of Colorado School of Medicine/Children’s Hospital Colorado in Aurora.
She presented the findings of the study at the ASCO 2017 Annual Meeting (abstract 10511).
Study design
CA 180-226 is a phase 2, open-label, nonrandomized, prospective study conducted in 18 countries. Patients younger than 18 years with newly diagnosed CML-CP, or imatinib-resistant/intolerant (R/I) CML-CP, or CML in accelerated phase, or Ph+ acute lymphoblastic leukemia (ALL) were enrolled on the study between March 2009 and September 2014.
Dr Gore’s presentation focused on the CML-CP patients in the study, both the newly diagnosed and the imatinib-R/I patients.
The imatinib-R/I patients received dasatinib 60 mg/m2 tablets once daily, and the newly diagnosed patients received the same tablet dosage daily or a powdered formulation for oral suspension (PFOS) of dasatinib at 72 mg/m2 daily.
Dr Gore noted the different dosage in the oral suspension formulation is based on bioavailability studies performed in adults, which was determined to be equivalent to the 60 mg/m2 tablet formulation.
Once accrual was reached in the tablet cohort, newly diagnosed patients were accrued to the PFOS cohort. The patients on PFOS could switch to tablets after a year or more on the oral suspension.
Patients remained on treatment until disease progression, unacceptable toxicity occurred, or the patient/physician preference.
All patients had a minimum follow-up of 2 years. The longest follow-up was more than 90 months.
Primary objectives of the study were MCyR greater than 30% for imatinib-R/I patients and complete CCyR greater than 55% for newly diagnosed patients.
Secondary objectives included time to and duration of response, major molecular response (MMR), progression-free survival (PFS), overall survival (OS), and safety.
Baseline patient characteristics
One hundred thirteen patients were treated across the 3 cohorts—29 in the imatinib-R/I receiving tablets, 51 newly diagnosed patients receiving tablets, and 33 newly diagnosed patients in the PFOS arm. A total of 84 patients had newly diagnosed disease.
Of the 29 imatinib-R/I patients, 25 were resistant, 2 intolerant, and 2 undetermined. And 6 of the 25 resistant patients had defined imatinib-resistance mutations.
Median age was 13.8 years in the imatinib-R/I cohort, 12.9 years in the newly diagnosed on tablets, and 11.7 years in the PFOS group. Other baseline characteristics were similar among the cohorts.
“Importantly, there were 3 patients less than 2 years of age, and a substantial proportion of patients were actually less than 12 years of age,” Dr Gore pointed out.
Dasatinib exposure
The median duration of therapy was 50 months and 42 months in the R/I and newly diagnosed cohorts, respectively.
Forty-eight percent of the imatinib-R/I patients and 73% of the newly diagnosed patients are still on treatment. A relatively small number of patients discontinued therapy.
The median duration of therapy was shorter in the PFOS cohort because they were enrolled only after accrual to the tablet cohort. However, they were also followed up for more than 2 years.
Of the 33 patients on PFOS, 22 eventually switched to tablet formulation.
Results
The primary endpoint for imatinib-R/I patients—MCyR greater than 30%—was reached by 3 months, and MCyR at 12 and 24 months exceeded 90%. The median time to response was 3.1 months (range, 2.8 – 4.1), and median duration of response was not yet reached (range, 54.9 – not estimable).
For newly diagnosed patients, the preset defined rate of interest of 55% for CCyR was reached as early as 6 months, and exceeded 90% by 12 and 24 months.
Dr Gore pointed out that intolerant patients also reached CCyR relatively quickly, although it was not a specified endpoint.
Data indicate that responses occurred relatively quickly and continued to increase over time of follow-up.
MMR also continued to increase over time and showed no difference between formulation and response rate.
Median PFS has not been reached, as only 7 patients in each cohort had disease progression.
One imatinib-R/I patient died 1 year after stopping treatment. The patient, who had a GI bleed unrelated to dasatinib, had discontinued therapy for progressive disease with loss of MCyR.
Safety
Overall safety was very similar to the dasatinib exposure and experience in adults, Dr Gore said, and there were no differences in events between PFOS and tablets.
One patient in the PFOS cohort had a dasatinib-related grade 3 hypersensitivity reaction, which resolved after discontinuation of dasatinib.
“What’s important here,” she said, “is that there were almost no adverse events of severity in either cohort, only 1 in the imatinib refractory and intolerant and 1 in the newly diagnosed cohorts.”
“Most importantly for those of us with a lot of experience in this field,” she added, “there were no occurrences of pleural effusion, pericardial effusion, pulmonary edema, pulmonary hypertension, or any vascular occlusive events in patients noted on this trial.”
“Additionally, for pediatricians, we care a lot about what happens to growth in these patients and prospectively we collected a lot of data related to growth parameters in bone growth and development."
Of the dasatinib-related adverse events occurring in 10% or more of patients, there were only 5 growth and development events noted out of the 113 patients treated and all were grade 1 or 2 events, Dr Gore pointed out.
In the R/I cohort, one patient had osteopenia and gynecomastia. At the time of data analysis, this event had resolved even though the patient continued on dasatinib.
“We believe our data suggests that dasatinib could be considered as a new standard of care for children with CML in chronic phase,” she said.
“It includes the advantage of a liquid formulation as well as the advantages of once daily dosing and administration without regard to fed or fasting state,” she added, “which for all of us who treat children know could be quite important.”
The study was funded by Bristol-Myers Squibb. ![]()
CHICAGO—The largest ongoing and prospective trial of pediatric patients with chronic myeloid leukemia in chronic phase (CML-CP), according to the best knowledge of the investigators, has found dasatinib to be safe and effective as first- or second-line therapy for these children.
Patients refractory to or intolerant of imatinib had a major cytogenetic response (MCyR) by 3 months and responses at 12 and 24 months exceeded 90%.
Newly diagnosed patients had a complete cytogenetic response (CCyR) by 6 months.
“We believe our data suggests that dasatinib could be considered as a new standard of care (SOC) for children with CML in chronic phase,” said study author Lia Gore, MD, of the University of Colorado School of Medicine/Children’s Hospital Colorado in Aurora.
She presented the findings of the study at the ASCO 2017 Annual Meeting (abstract 10511).
Study design
CA 180-226 is a phase 2, open-label, nonrandomized, prospective study conducted in 18 countries. Patients younger than 18 years with newly diagnosed CML-CP, or imatinib-resistant/intolerant (R/I) CML-CP, or CML in accelerated phase, or Ph+ acute lymphoblastic leukemia (ALL) were enrolled on the study between March 2009 and September 2014.
Dr Gore’s presentation focused on the CML-CP patients in the study, both the newly diagnosed and the imatinib-R/I patients.
The imatinib-R/I patients received dasatinib 60 mg/m2 tablets once daily, and the newly diagnosed patients received the same tablet dosage daily or a powdered formulation for oral suspension (PFOS) of dasatinib at 72 mg/m2 daily.
Dr Gore noted the different dosage in the oral suspension formulation is based on bioavailability studies performed in adults, which was determined to be equivalent to the 60 mg/m2 tablet formulation.
Once accrual was reached in the tablet cohort, newly diagnosed patients were accrued to the PFOS cohort. The patients on PFOS could switch to tablets after a year or more on the oral suspension.
Patients remained on treatment until disease progression, unacceptable toxicity occurred, or the patient/physician preference.
All patients had a minimum follow-up of 2 years. The longest follow-up was more than 90 months.
Primary objectives of the study were MCyR greater than 30% for imatinib-R/I patients and complete CCyR greater than 55% for newly diagnosed patients.
Secondary objectives included time to and duration of response, major molecular response (MMR), progression-free survival (PFS), overall survival (OS), and safety.
Baseline patient characteristics
One hundred thirteen patients were treated across the 3 cohorts—29 in the imatinib-R/I receiving tablets, 51 newly diagnosed patients receiving tablets, and 33 newly diagnosed patients in the PFOS arm. A total of 84 patients had newly diagnosed disease.
Of the 29 imatinib-R/I patients, 25 were resistant, 2 intolerant, and 2 undetermined. And 6 of the 25 resistant patients had defined imatinib-resistance mutations.
Median age was 13.8 years in the imatinib-R/I cohort, 12.9 years in the newly diagnosed on tablets, and 11.7 years in the PFOS group. Other baseline characteristics were similar among the cohorts.
“Importantly, there were 3 patients less than 2 years of age, and a substantial proportion of patients were actually less than 12 years of age,” Dr Gore pointed out.
Dasatinib exposure
The median duration of therapy was 50 months and 42 months in the R/I and newly diagnosed cohorts, respectively.
Forty-eight percent of the imatinib-R/I patients and 73% of the newly diagnosed patients are still on treatment. A relatively small number of patients discontinued therapy.
The median duration of therapy was shorter in the PFOS cohort because they were enrolled only after accrual to the tablet cohort. However, they were also followed up for more than 2 years.
Of the 33 patients on PFOS, 22 eventually switched to tablet formulation.
Results
The primary endpoint for imatinib-R/I patients—MCyR greater than 30%—was reached by 3 months, and MCyR at 12 and 24 months exceeded 90%. The median time to response was 3.1 months (range, 2.8 – 4.1), and median duration of response was not yet reached (range, 54.9 – not estimable).
For newly diagnosed patients, the preset defined rate of interest of 55% for CCyR was reached as early as 6 months, and exceeded 90% by 12 and 24 months.
Dr Gore pointed out that intolerant patients also reached CCyR relatively quickly, although it was not a specified endpoint.
Data indicate that responses occurred relatively quickly and continued to increase over time of follow-up.
MMR also continued to increase over time and showed no difference between formulation and response rate.
Median PFS has not been reached, as only 7 patients in each cohort had disease progression.
One imatinib-R/I patient died 1 year after stopping treatment. The patient, who had a GI bleed unrelated to dasatinib, had discontinued therapy for progressive disease with loss of MCyR.
Safety
Overall safety was very similar to the dasatinib exposure and experience in adults, Dr Gore said, and there were no differences in events between PFOS and tablets.
One patient in the PFOS cohort had a dasatinib-related grade 3 hypersensitivity reaction, which resolved after discontinuation of dasatinib.
“What’s important here,” she said, “is that there were almost no adverse events of severity in either cohort, only 1 in the imatinib refractory and intolerant and 1 in the newly diagnosed cohorts.”
“Most importantly for those of us with a lot of experience in this field,” she added, “there were no occurrences of pleural effusion, pericardial effusion, pulmonary edema, pulmonary hypertension, or any vascular occlusive events in patients noted on this trial.”
“Additionally, for pediatricians, we care a lot about what happens to growth in these patients and prospectively we collected a lot of data related to growth parameters in bone growth and development."
Of the dasatinib-related adverse events occurring in 10% or more of patients, there were only 5 growth and development events noted out of the 113 patients treated and all were grade 1 or 2 events, Dr Gore pointed out.
In the R/I cohort, one patient had osteopenia and gynecomastia. At the time of data analysis, this event had resolved even though the patient continued on dasatinib.
“We believe our data suggests that dasatinib could be considered as a new standard of care for children with CML in chronic phase,” she said.
“It includes the advantage of a liquid formulation as well as the advantages of once daily dosing and administration without regard to fed or fasting state,” she added, “which for all of us who treat children know could be quite important.”
The study was funded by Bristol-Myers Squibb. ![]()
CHICAGO—The largest ongoing and prospective trial of pediatric patients with chronic myeloid leukemia in chronic phase (CML-CP), according to the best knowledge of the investigators, has found dasatinib to be safe and effective as first- or second-line therapy for these children.
Patients refractory to or intolerant of imatinib had a major cytogenetic response (MCyR) by 3 months and responses at 12 and 24 months exceeded 90%.
Newly diagnosed patients had a complete cytogenetic response (CCyR) by 6 months.
“We believe our data suggests that dasatinib could be considered as a new standard of care (SOC) for children with CML in chronic phase,” said study author Lia Gore, MD, of the University of Colorado School of Medicine/Children’s Hospital Colorado in Aurora.
She presented the findings of the study at the ASCO 2017 Annual Meeting (abstract 10511).
Study design
CA 180-226 is a phase 2, open-label, nonrandomized, prospective study conducted in 18 countries. Patients younger than 18 years with newly diagnosed CML-CP, or imatinib-resistant/intolerant (R/I) CML-CP, or CML in accelerated phase, or Ph+ acute lymphoblastic leukemia (ALL) were enrolled on the study between March 2009 and September 2014.
Dr Gore’s presentation focused on the CML-CP patients in the study, both the newly diagnosed and the imatinib-R/I patients.
The imatinib-R/I patients received dasatinib 60 mg/m2 tablets once daily, and the newly diagnosed patients received the same tablet dosage daily or a powdered formulation for oral suspension (PFOS) of dasatinib at 72 mg/m2 daily.
Dr Gore noted the different dosage in the oral suspension formulation is based on bioavailability studies performed in adults, which was determined to be equivalent to the 60 mg/m2 tablet formulation.
Once accrual was reached in the tablet cohort, newly diagnosed patients were accrued to the PFOS cohort. The patients on PFOS could switch to tablets after a year or more on the oral suspension.
Patients remained on treatment until disease progression, unacceptable toxicity occurred, or the patient/physician preference.
All patients had a minimum follow-up of 2 years. The longest follow-up was more than 90 months.
Primary objectives of the study were MCyR greater than 30% for imatinib-R/I patients and complete CCyR greater than 55% for newly diagnosed patients.
Secondary objectives included time to and duration of response, major molecular response (MMR), progression-free survival (PFS), overall survival (OS), and safety.
Baseline patient characteristics
One hundred thirteen patients were treated across the 3 cohorts—29 in the imatinib-R/I receiving tablets, 51 newly diagnosed patients receiving tablets, and 33 newly diagnosed patients in the PFOS arm. A total of 84 patients had newly diagnosed disease.
Of the 29 imatinib-R/I patients, 25 were resistant, 2 intolerant, and 2 undetermined. And 6 of the 25 resistant patients had defined imatinib-resistance mutations.
Median age was 13.8 years in the imatinib-R/I cohort, 12.9 years in the newly diagnosed on tablets, and 11.7 years in the PFOS group. Other baseline characteristics were similar among the cohorts.
“Importantly, there were 3 patients less than 2 years of age, and a substantial proportion of patients were actually less than 12 years of age,” Dr Gore pointed out.
Dasatinib exposure
The median duration of therapy was 50 months and 42 months in the R/I and newly diagnosed cohorts, respectively.
Forty-eight percent of the imatinib-R/I patients and 73% of the newly diagnosed patients are still on treatment. A relatively small number of patients discontinued therapy.
The median duration of therapy was shorter in the PFOS cohort because they were enrolled only after accrual to the tablet cohort. However, they were also followed up for more than 2 years.
Of the 33 patients on PFOS, 22 eventually switched to tablet formulation.
Results
The primary endpoint for imatinib-R/I patients—MCyR greater than 30%—was reached by 3 months, and MCyR at 12 and 24 months exceeded 90%. The median time to response was 3.1 months (range, 2.8 – 4.1), and median duration of response was not yet reached (range, 54.9 – not estimable).
For newly diagnosed patients, the preset defined rate of interest of 55% for CCyR was reached as early as 6 months, and exceeded 90% by 12 and 24 months.
Dr Gore pointed out that intolerant patients also reached CCyR relatively quickly, although it was not a specified endpoint.
Data indicate that responses occurred relatively quickly and continued to increase over time of follow-up.
MMR also continued to increase over time and showed no difference between formulation and response rate.
Median PFS has not been reached, as only 7 patients in each cohort had disease progression.
One imatinib-R/I patient died 1 year after stopping treatment. The patient, who had a GI bleed unrelated to dasatinib, had discontinued therapy for progressive disease with loss of MCyR.
Safety
Overall safety was very similar to the dasatinib exposure and experience in adults, Dr Gore said, and there were no differences in events between PFOS and tablets.
One patient in the PFOS cohort had a dasatinib-related grade 3 hypersensitivity reaction, which resolved after discontinuation of dasatinib.
“What’s important here,” she said, “is that there were almost no adverse events of severity in either cohort, only 1 in the imatinib refractory and intolerant and 1 in the newly diagnosed cohorts.”
“Most importantly for those of us with a lot of experience in this field,” she added, “there were no occurrences of pleural effusion, pericardial effusion, pulmonary edema, pulmonary hypertension, or any vascular occlusive events in patients noted on this trial.”
“Additionally, for pediatricians, we care a lot about what happens to growth in these patients and prospectively we collected a lot of data related to growth parameters in bone growth and development."
Of the dasatinib-related adverse events occurring in 10% or more of patients, there were only 5 growth and development events noted out of the 113 patients treated and all were grade 1 or 2 events, Dr Gore pointed out.
In the R/I cohort, one patient had osteopenia and gynecomastia. At the time of data analysis, this event had resolved even though the patient continued on dasatinib.
“We believe our data suggests that dasatinib could be considered as a new standard of care for children with CML in chronic phase,” she said.
“It includes the advantage of a liquid formulation as well as the advantages of once daily dosing and administration without regard to fed or fasting state,” she added, “which for all of us who treat children know could be quite important.”
The study was funded by Bristol-Myers Squibb. ![]()
E. coli, GBS account for majority of neonatal bacterial meningitis in Canada
No major shifts appear to have occurred in the bacteria that cause meningitis in Canada, said Lynda Ouchenir, MD, University of Montreal, and her associates.
“There is a paucity of information on the characteristics of neonatal meningitis in the era of infant Haemophilus influenzae type B (Hib) and pneumococcal immunization, maternal group B Streptococcus (GBS) prophylaxis, and emerging antimicrobial resistance,” the researchers said. So, they undertook a retrospective study of infants with onset of bacterial meningitis in the first 90 days of life at seven Canadian hospitals to find out the major pathogens involved and best empirical antibiotics to use.
This substitution of a carbapenem for the cephalosporin was considered prudent if the birth hospitalization was complicated and if the cerebrospinal fluid Gram-stain or the blood culture was suggestive of Gram-negative meningitis, Dr. Ouchenir and her associates said.
Read more at (Pediatrics. 2017;140[1)]:e20170476).
No major shifts appear to have occurred in the bacteria that cause meningitis in Canada, said Lynda Ouchenir, MD, University of Montreal, and her associates.
“There is a paucity of information on the characteristics of neonatal meningitis in the era of infant Haemophilus influenzae type B (Hib) and pneumococcal immunization, maternal group B Streptococcus (GBS) prophylaxis, and emerging antimicrobial resistance,” the researchers said. So, they undertook a retrospective study of infants with onset of bacterial meningitis in the first 90 days of life at seven Canadian hospitals to find out the major pathogens involved and best empirical antibiotics to use.
This substitution of a carbapenem for the cephalosporin was considered prudent if the birth hospitalization was complicated and if the cerebrospinal fluid Gram-stain or the blood culture was suggestive of Gram-negative meningitis, Dr. Ouchenir and her associates said.
Read more at (Pediatrics. 2017;140[1)]:e20170476).
No major shifts appear to have occurred in the bacteria that cause meningitis in Canada, said Lynda Ouchenir, MD, University of Montreal, and her associates.
“There is a paucity of information on the characteristics of neonatal meningitis in the era of infant Haemophilus influenzae type B (Hib) and pneumococcal immunization, maternal group B Streptococcus (GBS) prophylaxis, and emerging antimicrobial resistance,” the researchers said. So, they undertook a retrospective study of infants with onset of bacterial meningitis in the first 90 days of life at seven Canadian hospitals to find out the major pathogens involved and best empirical antibiotics to use.
This substitution of a carbapenem for the cephalosporin was considered prudent if the birth hospitalization was complicated and if the cerebrospinal fluid Gram-stain or the blood culture was suggestive of Gram-negative meningitis, Dr. Ouchenir and her associates said.
Read more at (Pediatrics. 2017;140[1)]:e20170476).
FROM PEDIATRICS