User login
Therapeutic patient education is a new way to approach atopic dermatitis
(AD) resulting from poor adherence to treatment.
The aim of TPE, a multidisciplinary approach to caring for and managing AD, is to improve patient and caregiver adherence to physician-directed treatments through education and to improve quality of life, according to several presenters who spoke at a pediatric dermatology meeting sponsored by Rady Children’s Hospital–San Diego and University of California, San Diego. They reviewed the approach to using TPE in chronic disease states, demonstrating this state-of-the-art approach to educating patients, families, and health care providers about AD management, and allowing for the exchange of ideas for best practices on AD therapeutic education programs and use in the U.S. health care environment.
Other successful meetings on TPE in Europe, Asia, and South America inspired this meeting, the first in the United States aimed to train health care professionals in TPE principles for AD. The meeting was sponsored by the Fondation Dermatite Atopique (Atopic Dermatitis Foundation for Research and Education), Rady’s Eczema and Inflammatory Skin Disease Center, and UCSD.
TPE is defined by the World Health Organization as an approach to help patients with chronic illness acquire or maintain the skills necessary to manage their life and illness in the best way possible. TPE involves patient preferences, shared decision-making, organized activities, psychosocial support, hospital organization and procedures, and health- and disease-related behaviors.
Sébastien Barbarot, MD, of the departments of dermatology and pediatric dermatology, Nantes (France) University Hospital, said that there are four main components to the TPE process:
• Assessing and understanding the patient’s knowledge and values.
• Developing age-appropriate personalized educational objectives.
• Transferring the necessary skills to the patient or caregiver.
• Assessing the effectiveness of the educational program.
Lawrence Eichenfield, MD, chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at UCSD, discussed how to conduct the initial visit with potential candidates for TPE. At the new patient visit, the pediatric patient and their caregivers should first be presented with the concept of TPE, which includes proposing a personalized education approach. Next, explain the goals and benefits of TPE (with a time and location for the sessions), provide educational materials, allow time for questions, and establish the patient’s consent to participate.

The certain skills that patients should acquire fall under three main categories: knowledge of the disease, practical skills, and relational skills.
Alain Golay, MD, professor and chief of the department of therapeutic education in chronic diseases at the Geneva University Hospital, said that patients and caregivers should be familiar with the pathophysiology and natural history of the disease, as well as with aggravating factors and the rationale behind elements of the treatment plan – and they should understand a reasonable timeline for treatment responses.
Learning how to properly apply the treatment is among the practical skills that the patient needs to acquire. In terms of relational skills, patients should know enough about their disease to be able to explain it to others. Educational methods can include interactive presentations, case studies, roundtable meetings, workshops, and role play. Other tools that can be used as a resource include written action plans, posters, informational videos, reminders, and booklets. Nurse-led educational sessions that increase teaching time is another modality. Multidisciplinary clinics should include an allergist, dermatologist, psychologist, dietitian, and nurse. These clinics also can form workshops or teaching groups. This allows for smaller groups where ideas can be exchanged, and can be targeted specifically based on the audiences’ needs, he said.
Dr. Barbarot outlined the fourth step of TPE, which involves assessment of effectiveness. Several outcome measures can be used, including clinical outcomes, quality of life, patient global assessment, and knowledge questionnaires.
(AD) resulting from poor adherence to treatment.
The aim of TPE, a multidisciplinary approach to caring for and managing AD, is to improve patient and caregiver adherence to physician-directed treatments through education and to improve quality of life, according to several presenters who spoke at a pediatric dermatology meeting sponsored by Rady Children’s Hospital–San Diego and University of California, San Diego. They reviewed the approach to using TPE in chronic disease states, demonstrating this state-of-the-art approach to educating patients, families, and health care providers about AD management, and allowing for the exchange of ideas for best practices on AD therapeutic education programs and use in the U.S. health care environment.
Other successful meetings on TPE in Europe, Asia, and South America inspired this meeting, the first in the United States aimed to train health care professionals in TPE principles for AD. The meeting was sponsored by the Fondation Dermatite Atopique (Atopic Dermatitis Foundation for Research and Education), Rady’s Eczema and Inflammatory Skin Disease Center, and UCSD.
TPE is defined by the World Health Organization as an approach to help patients with chronic illness acquire or maintain the skills necessary to manage their life and illness in the best way possible. TPE involves patient preferences, shared decision-making, organized activities, psychosocial support, hospital organization and procedures, and health- and disease-related behaviors.
Sébastien Barbarot, MD, of the departments of dermatology and pediatric dermatology, Nantes (France) University Hospital, said that there are four main components to the TPE process:
• Assessing and understanding the patient’s knowledge and values.
• Developing age-appropriate personalized educational objectives.
• Transferring the necessary skills to the patient or caregiver.
• Assessing the effectiveness of the educational program.
Lawrence Eichenfield, MD, chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at UCSD, discussed how to conduct the initial visit with potential candidates for TPE. At the new patient visit, the pediatric patient and their caregivers should first be presented with the concept of TPE, which includes proposing a personalized education approach. Next, explain the goals and benefits of TPE (with a time and location for the sessions), provide educational materials, allow time for questions, and establish the patient’s consent to participate.
The certain skills that patients should acquire fall under three main categories: knowledge of the disease, practical skills, and relational skills.
Alain Golay, MD, professor and chief of the department of therapeutic education in chronic diseases at the Geneva University Hospital, said that patients and caregivers should be familiar with the pathophysiology and natural history of the disease, as well as with aggravating factors and the rationale behind elements of the treatment plan – and they should understand a reasonable timeline for treatment responses.
Learning how to properly apply the treatment is among the practical skills that the patient needs to acquire. In terms of relational skills, patients should know enough about their disease to be able to explain it to others. Educational methods can include interactive presentations, case studies, roundtable meetings, workshops, and role play. Other tools that can be used as a resource include written action plans, posters, informational videos, reminders, and booklets. Nurse-led educational sessions that increase teaching time is another modality. Multidisciplinary clinics should include an allergist, dermatologist, psychologist, dietitian, and nurse. These clinics also can form workshops or teaching groups. This allows for smaller groups where ideas can be exchanged, and can be targeted specifically based on the audiences’ needs, he said.
Dr. Barbarot outlined the fourth step of TPE, which involves assessment of effectiveness. Several outcome measures can be used, including clinical outcomes, quality of life, patient global assessment, and knowledge questionnaires.
(AD) resulting from poor adherence to treatment.
The aim of TPE, a multidisciplinary approach to caring for and managing AD, is to improve patient and caregiver adherence to physician-directed treatments through education and to improve quality of life, according to several presenters who spoke at a pediatric dermatology meeting sponsored by Rady Children’s Hospital–San Diego and University of California, San Diego. They reviewed the approach to using TPE in chronic disease states, demonstrating this state-of-the-art approach to educating patients, families, and health care providers about AD management, and allowing for the exchange of ideas for best practices on AD therapeutic education programs and use in the U.S. health care environment.
Other successful meetings on TPE in Europe, Asia, and South America inspired this meeting, the first in the United States aimed to train health care professionals in TPE principles for AD. The meeting was sponsored by the Fondation Dermatite Atopique (Atopic Dermatitis Foundation for Research and Education), Rady’s Eczema and Inflammatory Skin Disease Center, and UCSD.
TPE is defined by the World Health Organization as an approach to help patients with chronic illness acquire or maintain the skills necessary to manage their life and illness in the best way possible. TPE involves patient preferences, shared decision-making, organized activities, psychosocial support, hospital organization and procedures, and health- and disease-related behaviors.
Sébastien Barbarot, MD, of the departments of dermatology and pediatric dermatology, Nantes (France) University Hospital, said that there are four main components to the TPE process:
• Assessing and understanding the patient’s knowledge and values.
• Developing age-appropriate personalized educational objectives.
• Transferring the necessary skills to the patient or caregiver.
• Assessing the effectiveness of the educational program.
Lawrence Eichenfield, MD, chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at UCSD, discussed how to conduct the initial visit with potential candidates for TPE. At the new patient visit, the pediatric patient and their caregivers should first be presented with the concept of TPE, which includes proposing a personalized education approach. Next, explain the goals and benefits of TPE (with a time and location for the sessions), provide educational materials, allow time for questions, and establish the patient’s consent to participate.
The certain skills that patients should acquire fall under three main categories: knowledge of the disease, practical skills, and relational skills.
Alain Golay, MD, professor and chief of the department of therapeutic education in chronic diseases at the Geneva University Hospital, said that patients and caregivers should be familiar with the pathophysiology and natural history of the disease, as well as with aggravating factors and the rationale behind elements of the treatment plan – and they should understand a reasonable timeline for treatment responses.
Learning how to properly apply the treatment is among the practical skills that the patient needs to acquire. In terms of relational skills, patients should know enough about their disease to be able to explain it to others. Educational methods can include interactive presentations, case studies, roundtable meetings, workshops, and role play. Other tools that can be used as a resource include written action plans, posters, informational videos, reminders, and booklets. Nurse-led educational sessions that increase teaching time is another modality. Multidisciplinary clinics should include an allergist, dermatologist, psychologist, dietitian, and nurse. These clinics also can form workshops or teaching groups. This allows for smaller groups where ideas can be exchanged, and can be targeted specifically based on the audiences’ needs, he said.
Dr. Barbarot outlined the fourth step of TPE, which involves assessment of effectiveness. Several outcome measures can be used, including clinical outcomes, quality of life, patient global assessment, and knowledge questionnaires.
Hepatitis C is a pediatric disease now
The baby looked perfect: healthy term male, weight at the 60th percentile, normal exam. The mother, a 26-year-old diagnosed with hepatitis C virus (HCV) infection during her pregnancy, looked alternately hopeful and horrified as I explained what implications her infection could have for her baby.
“Most babies will be fine,” I explained. “Of all mothers with hepatitis C infection, just under 6% will pass the infection on to their babies.” Transmission rates are twice as high in infants born to women with high HCV viral loads or those coinfected with HIV. The risk of transmission from women with undetectable HCV RNA is almost zero. Unfortunately, this mother did not fall into that category.

At that moment, however, I didn’t have time to be concerned about the numbers. My focus was one mother and her newborn baby.
“What if my baby is one of the unlucky ones who gets infected?” the mother asked, cuddling her infant. “What then?”
We know a lot about the course of hepatitis C in adults. An estimated 75%-86% of those infected will go on to develop chronic infection. Long-term sequelae include cirrhosis, liver failure, and hepatocellular carcinoma.
The course of HCV in children appears to be different. Twenty-five percent to 40% of vertically infected children will spontaneously clear their infection, most by 2 years of age. Occasionally, that might not happen until 7 years of age. Most who are chronically infected experience few symptoms, and fortunately cirrhosis and liver failure rarely present in childhood. In a large cohort of Italian children, half of whom were thought to be infected perinatally, less than 2% progressed to decompensated cirrhosis after 10 years of infection. According to the CDC, most children infected at birth “do well during childhood,” but more research is needed to understand the long-term effects of perinatal hepatitis C in children.
New antivirals have revolutionized the care of HCV-infected adults and now offer the hope of cure for up to 90%. None of these drugs are currently approved for use in children younger than 12 years, although clinical trials are underway. Because most cases of HCV in children are indolent, some children may not require treatment until adulthood.
July 28th was World Hepatitis Day and this year’s theme was Eliminate Hepatitis. To eliminate the problem of hepatitis C in children, pediatricians and others involved in the care of children need to get involved.
We need to know the scope of the problem
Since 2015, Kentucky has mandated reporting of all HCV-infected pregnant women and children through age 60 months, as well as all infants born to all HCV-infected women. At present though, there is substantial variability in state reporting requirements. We likely need a standardized case definition for perinatal HCV and national reporting criteria.
We need some clear guidance about testing during pregnancy
This should come from public health authorities, the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists.
Jonathan Mermin, MD, director of CDC’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, has said, “Women are screened throughout pregnancy for many conditions that threaten their health. An expectant mother at risk for hepatitis C deserves to be tested. Knowing her status is the only way she can access the best hepatitis care and treatment – both for herself and her baby.” Yet, routine hepatitis C testing is not recommended during pregnancy, in part because there are no established interventions to prevent mother-to-child transmission of HCV. Instead, women are to be screened for risk factors and tested if they are present. As we learned with hepatitis B and HIV, risk factor screening is hard and misses individuals who are infected.
We need to ensure that HCV-exposed infants are identified and followed appropriately.
In a study of HCV-exposed infants born to women in Philadelphia, 84% did not receive adequate testing for HCV infection. In human terms, 537 children were born to HCV-positive mothers during the study period and 4 of 84 (5%) children tested were found to be infected. Assuming that 5% of HCV-exposed infants will develop chronic infection, 23 additional children were undiagnosed and, therefore, were not being followed for potential sequelae.
HCV-infected mothers in this study were more likely than non-infected mothers to be socioeconomically disadvantaged – specifically, unmarried, less educated, and publicly insured – suggesting that access to care may have played a role. When you add in drug use as a common risk factor for HCV infection, it is easy to understand why some at-risk infants are lost to follow-up.
Investigators in the Philadelphia study suggested that there might be more to the story. They proposed that pediatricians might be unaware of the need for testing because they had not been alerted to the mother’s HCV status by the obstetrician, the birthing hospital, or the mother herself. Finally, they theorized that many pediatricians “may be unaware or skeptical of the guidelines for testing children exposed to HCV.” This is a problem that we can solve.
I finished the visit with this mother by reassuring her that she could breastfeed her infant as planned as long as she did not have cracked or bleeding nipples. I also explained the schedule for testing. A 2002 National Institutes of Health consensus statement recommends that infants perinatally exposed to HCV have two HCV RNA tests between 2 and 6 months of age and/or be tested for HCV antibodies after 15 months. North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) Practice Guidelines for Diagnosis and Management of Hepatitis C Infection in Infants, Children, and Adolescents recommend testing for HCV antibodies at 18 months of age (J Pediatr Gastroenterol Nutr. 2012 Jun;54[6]:838-55). If a family requests earlier testing, a serum HCV RNA test can be done as early as 2 months of age. If positive, NASPGHAN recommends testing after 12 months of age to evaluate for chronic infection.
My practice has adopted the National Institutes of Health consensus statement approach because many of the families we see experience significant anxiety about the diagnosis, and this mother was no exception. As noted in the expert guidelines, this was a situation in which “early exclusion of HCV infection is reassuring and may be worth the added expense.”
“So first test at 2 months?” she asked. “Until then, we can’t do anything but wait?”
It is estimated that there are 23,000 to 46,000 U.S. children living with HCV. The wait for pediatricians is over. , and we need to educate ourselves about diagnosis and management. A first step might be to begin asking expectant mothers and the mothers of newborns if they know their HCV status.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
The baby looked perfect: healthy term male, weight at the 60th percentile, normal exam. The mother, a 26-year-old diagnosed with hepatitis C virus (HCV) infection during her pregnancy, looked alternately hopeful and horrified as I explained what implications her infection could have for her baby.
“Most babies will be fine,” I explained. “Of all mothers with hepatitis C infection, just under 6% will pass the infection on to their babies.” Transmission rates are twice as high in infants born to women with high HCV viral loads or those coinfected with HIV. The risk of transmission from women with undetectable HCV RNA is almost zero. Unfortunately, this mother did not fall into that category.
At that moment, however, I didn’t have time to be concerned about the numbers. My focus was one mother and her newborn baby.
“What if my baby is one of the unlucky ones who gets infected?” the mother asked, cuddling her infant. “What then?”
We know a lot about the course of hepatitis C in adults. An estimated 75%-86% of those infected will go on to develop chronic infection. Long-term sequelae include cirrhosis, liver failure, and hepatocellular carcinoma.
The course of HCV in children appears to be different. Twenty-five percent to 40% of vertically infected children will spontaneously clear their infection, most by 2 years of age. Occasionally, that might not happen until 7 years of age. Most who are chronically infected experience few symptoms, and fortunately cirrhosis and liver failure rarely present in childhood. In a large cohort of Italian children, half of whom were thought to be infected perinatally, less than 2% progressed to decompensated cirrhosis after 10 years of infection. According to the CDC, most children infected at birth “do well during childhood,” but more research is needed to understand the long-term effects of perinatal hepatitis C in children.
New antivirals have revolutionized the care of HCV-infected adults and now offer the hope of cure for up to 90%. None of these drugs are currently approved for use in children younger than 12 years, although clinical trials are underway. Because most cases of HCV in children are indolent, some children may not require treatment until adulthood.
July 28th was World Hepatitis Day and this year’s theme was Eliminate Hepatitis. To eliminate the problem of hepatitis C in children, pediatricians and others involved in the care of children need to get involved.
We need to know the scope of the problem
Since 2015, Kentucky has mandated reporting of all HCV-infected pregnant women and children through age 60 months, as well as all infants born to all HCV-infected women. At present though, there is substantial variability in state reporting requirements. We likely need a standardized case definition for perinatal HCV and national reporting criteria.
We need some clear guidance about testing during pregnancy
This should come from public health authorities, the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists.
Jonathan Mermin, MD, director of CDC’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, has said, “Women are screened throughout pregnancy for many conditions that threaten their health. An expectant mother at risk for hepatitis C deserves to be tested. Knowing her status is the only way she can access the best hepatitis care and treatment – both for herself and her baby.” Yet, routine hepatitis C testing is not recommended during pregnancy, in part because there are no established interventions to prevent mother-to-child transmission of HCV. Instead, women are to be screened for risk factors and tested if they are present. As we learned with hepatitis B and HIV, risk factor screening is hard and misses individuals who are infected.
We need to ensure that HCV-exposed infants are identified and followed appropriately.
In a study of HCV-exposed infants born to women in Philadelphia, 84% did not receive adequate testing for HCV infection. In human terms, 537 children were born to HCV-positive mothers during the study period and 4 of 84 (5%) children tested were found to be infected. Assuming that 5% of HCV-exposed infants will develop chronic infection, 23 additional children were undiagnosed and, therefore, were not being followed for potential sequelae.
HCV-infected mothers in this study were more likely than non-infected mothers to be socioeconomically disadvantaged – specifically, unmarried, less educated, and publicly insured – suggesting that access to care may have played a role. When you add in drug use as a common risk factor for HCV infection, it is easy to understand why some at-risk infants are lost to follow-up.
Investigators in the Philadelphia study suggested that there might be more to the story. They proposed that pediatricians might be unaware of the need for testing because they had not been alerted to the mother’s HCV status by the obstetrician, the birthing hospital, or the mother herself. Finally, they theorized that many pediatricians “may be unaware or skeptical of the guidelines for testing children exposed to HCV.” This is a problem that we can solve.
I finished the visit with this mother by reassuring her that she could breastfeed her infant as planned as long as she did not have cracked or bleeding nipples. I also explained the schedule for testing. A 2002 National Institutes of Health consensus statement recommends that infants perinatally exposed to HCV have two HCV RNA tests between 2 and 6 months of age and/or be tested for HCV antibodies after 15 months. North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) Practice Guidelines for Diagnosis and Management of Hepatitis C Infection in Infants, Children, and Adolescents recommend testing for HCV antibodies at 18 months of age (J Pediatr Gastroenterol Nutr. 2012 Jun;54[6]:838-55). If a family requests earlier testing, a serum HCV RNA test can be done as early as 2 months of age. If positive, NASPGHAN recommends testing after 12 months of age to evaluate for chronic infection.
My practice has adopted the National Institutes of Health consensus statement approach because many of the families we see experience significant anxiety about the diagnosis, and this mother was no exception. As noted in the expert guidelines, this was a situation in which “early exclusion of HCV infection is reassuring and may be worth the added expense.”
“So first test at 2 months?” she asked. “Until then, we can’t do anything but wait?”
It is estimated that there are 23,000 to 46,000 U.S. children living with HCV. The wait for pediatricians is over. , and we need to educate ourselves about diagnosis and management. A first step might be to begin asking expectant mothers and the mothers of newborns if they know their HCV status.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
The baby looked perfect: healthy term male, weight at the 60th percentile, normal exam. The mother, a 26-year-old diagnosed with hepatitis C virus (HCV) infection during her pregnancy, looked alternately hopeful and horrified as I explained what implications her infection could have for her baby.
“Most babies will be fine,” I explained. “Of all mothers with hepatitis C infection, just under 6% will pass the infection on to their babies.” Transmission rates are twice as high in infants born to women with high HCV viral loads or those coinfected with HIV. The risk of transmission from women with undetectable HCV RNA is almost zero. Unfortunately, this mother did not fall into that category.
At that moment, however, I didn’t have time to be concerned about the numbers. My focus was one mother and her newborn baby.
“What if my baby is one of the unlucky ones who gets infected?” the mother asked, cuddling her infant. “What then?”
We know a lot about the course of hepatitis C in adults. An estimated 75%-86% of those infected will go on to develop chronic infection. Long-term sequelae include cirrhosis, liver failure, and hepatocellular carcinoma.
The course of HCV in children appears to be different. Twenty-five percent to 40% of vertically infected children will spontaneously clear their infection, most by 2 years of age. Occasionally, that might not happen until 7 years of age. Most who are chronically infected experience few symptoms, and fortunately cirrhosis and liver failure rarely present in childhood. In a large cohort of Italian children, half of whom were thought to be infected perinatally, less than 2% progressed to decompensated cirrhosis after 10 years of infection. According to the CDC, most children infected at birth “do well during childhood,” but more research is needed to understand the long-term effects of perinatal hepatitis C in children.
New antivirals have revolutionized the care of HCV-infected adults and now offer the hope of cure for up to 90%. None of these drugs are currently approved for use in children younger than 12 years, although clinical trials are underway. Because most cases of HCV in children are indolent, some children may not require treatment until adulthood.
July 28th was World Hepatitis Day and this year’s theme was Eliminate Hepatitis. To eliminate the problem of hepatitis C in children, pediatricians and others involved in the care of children need to get involved.
We need to know the scope of the problem
Since 2015, Kentucky has mandated reporting of all HCV-infected pregnant women and children through age 60 months, as well as all infants born to all HCV-infected women. At present though, there is substantial variability in state reporting requirements. We likely need a standardized case definition for perinatal HCV and national reporting criteria.
We need some clear guidance about testing during pregnancy
This should come from public health authorities, the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists.
Jonathan Mermin, MD, director of CDC’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, has said, “Women are screened throughout pregnancy for many conditions that threaten their health. An expectant mother at risk for hepatitis C deserves to be tested. Knowing her status is the only way she can access the best hepatitis care and treatment – both for herself and her baby.” Yet, routine hepatitis C testing is not recommended during pregnancy, in part because there are no established interventions to prevent mother-to-child transmission of HCV. Instead, women are to be screened for risk factors and tested if they are present. As we learned with hepatitis B and HIV, risk factor screening is hard and misses individuals who are infected.
We need to ensure that HCV-exposed infants are identified and followed appropriately.
In a study of HCV-exposed infants born to women in Philadelphia, 84% did not receive adequate testing for HCV infection. In human terms, 537 children were born to HCV-positive mothers during the study period and 4 of 84 (5%) children tested were found to be infected. Assuming that 5% of HCV-exposed infants will develop chronic infection, 23 additional children were undiagnosed and, therefore, were not being followed for potential sequelae.
HCV-infected mothers in this study were more likely than non-infected mothers to be socioeconomically disadvantaged – specifically, unmarried, less educated, and publicly insured – suggesting that access to care may have played a role. When you add in drug use as a common risk factor for HCV infection, it is easy to understand why some at-risk infants are lost to follow-up.
Investigators in the Philadelphia study suggested that there might be more to the story. They proposed that pediatricians might be unaware of the need for testing because they had not been alerted to the mother’s HCV status by the obstetrician, the birthing hospital, or the mother herself. Finally, they theorized that many pediatricians “may be unaware or skeptical of the guidelines for testing children exposed to HCV.” This is a problem that we can solve.
I finished the visit with this mother by reassuring her that she could breastfeed her infant as planned as long as she did not have cracked or bleeding nipples. I also explained the schedule for testing. A 2002 National Institutes of Health consensus statement recommends that infants perinatally exposed to HCV have two HCV RNA tests between 2 and 6 months of age and/or be tested for HCV antibodies after 15 months. North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) Practice Guidelines for Diagnosis and Management of Hepatitis C Infection in Infants, Children, and Adolescents recommend testing for HCV antibodies at 18 months of age (J Pediatr Gastroenterol Nutr. 2012 Jun;54[6]:838-55). If a family requests earlier testing, a serum HCV RNA test can be done as early as 2 months of age. If positive, NASPGHAN recommends testing after 12 months of age to evaluate for chronic infection.
My practice has adopted the National Institutes of Health consensus statement approach because many of the families we see experience significant anxiety about the diagnosis, and this mother was no exception. As noted in the expert guidelines, this was a situation in which “early exclusion of HCV infection is reassuring and may be worth the added expense.”
“So first test at 2 months?” she asked. “Until then, we can’t do anything but wait?”
It is estimated that there are 23,000 to 46,000 U.S. children living with HCV. The wait for pediatricians is over. , and we need to educate ourselves about diagnosis and management. A first step might be to begin asking expectant mothers and the mothers of newborns if they know their HCV status.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Clearer instructions linked to fewer medication dosing errors
In nine pediatric dosing trials, more than 80% of parents made more than one medication dosing error, according to a study by H. Shonna Yin, MD, and associates. Misunderstandings about how to accurately choose the right dosing tools as well as confusion related to units of measure contribute to most errors. Matching dosing tools more closely with prescribed dose volumes, as well as using pictograms, can greatly reduce the number of pediatric medication errors, the researchers noted.
The study shows that 83.5% of parents made at least one dosing error (overdosing was present in 12.1% of errors), and 29.3% of parents made at least one large error in administering their children’s medicine. Parents who received text-only instructions or milliliter/teaspoon labels made more large errors. The biggest influence on errors resulted from providing tools more closely matched to the recommended dose measurements.
The researchers conducted a randomized controlled experiment in three pediatric clinics. Each site’s institutional review board approved the study. An average of 491 parents of children older than 8 years were randomly assigned to one of four groups, and given labels and dosing tools that varied in label instruction format and units. Each parent measured nine doses of liquid medicine in a random order, using three different tools.
Parents in group 1 received text and pictogram dosing instructions with milliliter-only labels and tools. They had decreased odds of making a dosing error compared with parents who received milliliter/teaspoon labels and tools without pictographic instructions in groups 2 and 4, and had lower odds of making large dosing errors compared with group 3, whose participants received text-only instructions (Pediatrics. 2017 June 27. doi: 10.1542/peds.2016-3237).
“Our findings support the use of a specific algorithm to help health care providers and pharmacists determine which dosing tool is most optimal to provide to parents,” said Dr. Yin. “We found that pictograms were associated with statistically significant reductions in large overdosing errors, with a trend for reduction in any error.”
No financial disclosures or conflicts of interest were reported.
In nine pediatric dosing trials, more than 80% of parents made more than one medication dosing error, according to a study by H. Shonna Yin, MD, and associates. Misunderstandings about how to accurately choose the right dosing tools as well as confusion related to units of measure contribute to most errors. Matching dosing tools more closely with prescribed dose volumes, as well as using pictograms, can greatly reduce the number of pediatric medication errors, the researchers noted.
The study shows that 83.5% of parents made at least one dosing error (overdosing was present in 12.1% of errors), and 29.3% of parents made at least one large error in administering their children’s medicine. Parents who received text-only instructions or milliliter/teaspoon labels made more large errors. The biggest influence on errors resulted from providing tools more closely matched to the recommended dose measurements.
The researchers conducted a randomized controlled experiment in three pediatric clinics. Each site’s institutional review board approved the study. An average of 491 parents of children older than 8 years were randomly assigned to one of four groups, and given labels and dosing tools that varied in label instruction format and units. Each parent measured nine doses of liquid medicine in a random order, using three different tools.
Parents in group 1 received text and pictogram dosing instructions with milliliter-only labels and tools. They had decreased odds of making a dosing error compared with parents who received milliliter/teaspoon labels and tools without pictographic instructions in groups 2 and 4, and had lower odds of making large dosing errors compared with group 3, whose participants received text-only instructions (Pediatrics. 2017 June 27. doi: 10.1542/peds.2016-3237).
“Our findings support the use of a specific algorithm to help health care providers and pharmacists determine which dosing tool is most optimal to provide to parents,” said Dr. Yin. “We found that pictograms were associated with statistically significant reductions in large overdosing errors, with a trend for reduction in any error.”
No financial disclosures or conflicts of interest were reported.
In nine pediatric dosing trials, more than 80% of parents made more than one medication dosing error, according to a study by H. Shonna Yin, MD, and associates. Misunderstandings about how to accurately choose the right dosing tools as well as confusion related to units of measure contribute to most errors. Matching dosing tools more closely with prescribed dose volumes, as well as using pictograms, can greatly reduce the number of pediatric medication errors, the researchers noted.
The study shows that 83.5% of parents made at least one dosing error (overdosing was present in 12.1% of errors), and 29.3% of parents made at least one large error in administering their children’s medicine. Parents who received text-only instructions or milliliter/teaspoon labels made more large errors. The biggest influence on errors resulted from providing tools more closely matched to the recommended dose measurements.
The researchers conducted a randomized controlled experiment in three pediatric clinics. Each site’s institutional review board approved the study. An average of 491 parents of children older than 8 years were randomly assigned to one of four groups, and given labels and dosing tools that varied in label instruction format and units. Each parent measured nine doses of liquid medicine in a random order, using three different tools.
Parents in group 1 received text and pictogram dosing instructions with milliliter-only labels and tools. They had decreased odds of making a dosing error compared with parents who received milliliter/teaspoon labels and tools without pictographic instructions in groups 2 and 4, and had lower odds of making large dosing errors compared with group 3, whose participants received text-only instructions (Pediatrics. 2017 June 27. doi: 10.1542/peds.2016-3237).
“Our findings support the use of a specific algorithm to help health care providers and pharmacists determine which dosing tool is most optimal to provide to parents,” said Dr. Yin. “We found that pictograms were associated with statistically significant reductions in large overdosing errors, with a trend for reduction in any error.”
No financial disclosures or conflicts of interest were reported.
FROM PEDIATRICS
Key clinical point:
Major finding: In nine dosing trials, 83.5% of parents made more than one medication dosing error, mainly overdosing.
Data source: A randomized controlled study. Recruitment took place in pediatric outpatient clinics in New York, California, and Georgia. Each site’s institutional review board approved the study.
Disclosures: The National Institutes of Health/National Institute of Child Health and Human Development funded the study. The authors declared no conflict of interest.
MV disease in children requires modified strategies
NEW YORK – Repairing mitral valves in pediatric patients must overcome two issues: the wide variability in their anatomy and their growth. Using strategies and techniques common in adult mitral surgery can accomplish good mitral valve function in children, but some techniques in children differ, like using combined resorbable material with autologous tissue or transferring native chords instead of placing artificial chords to a malfunctioning leaflet.
Pedro del Nido, MD, of Boston Children’s Hospital, said the spectrum of mitral valve pathology in children goes from congenital mitral stenosis with a thick annulus with leaflet immobility to leaflet hypermobility that involves anterior leaflet prolapse and can involve a cleft that causes regurgitation. Dr. del Nido explained his surgical approaches for mitral valve disease in children at the 2017 Mitral Conclave, sponsored by the American Association of Thoracic Surgery.

Accessing the mitral valve in children requires a different approach than in adults, Dr. del Nido said. “Going through the left atrium is generally difficult, so we often enter through a trans-septal incision,” he said. “The main reason for that is because the tricuspid valve is often associated with the mitral valve problem and this gives us the most direct exposure.”
Once the surgeon gains exposure, the surgical analysis for a diseased adult or child valve is almost identical, with the exception that adult disease is acquired whereas childhood disease tends to be congenital, Dr. del Nido said. “In the congenital patient, we often find fibroelastic tissue that the child is born with,” he said. “We see this in neonates and young infants. It thickens over time; it doesn’t often calcify, but it does often restrict the leaflets and it tends to fuse the chords, so in essence you have direct attachments of the leaflets to the papillaries.”
He explained that this pathology requires an approach similar to that for rheumatic mitral disease in adults. “Start splitting the commissures and start resecting the tissue off the chords creating fenestrations in order to improve the inflow.” Dr. del Nido added, “If you don’t do this, the child will always have a gradient, and if you think about an adult having problems and symptoms with a gradient, think about a 10-year-old running around trying to do athletics; it’s impossible.”
Dysfunctional chords also require a somewhat different approach in children than they require in adults. “We find elongation of the chords and the anterior support structure is abnormal; the secondary chords are totally intact,” Dr. del Nido said. When confronting a torn-edge chord, resection is often an option in adults, but is uncommon in children. “We don’t usually have very much leaflet tissue,” he said. Artificial chords do not accommodate growth.
“We tend to use native tissue,” said Dr. del Nido. “You can transfer the strut chord; you can transfer the secondary chord in order to achieve support for the edge of that prolapsed leaflet.”
Leaflet problems are probably the biggest single source of recurrence in children, Dr. del Nido said. A cleft on the anterior leaflet can be particularly vexing. For example, cleft edges attached to the septum can prevent the valve leaflet from coaptation with the posterior leaflet. “If you don’t recognize that on 3-D echocardiography, you’re going to have a problem; that leaflet will never create the coaptation surface that you want,” he said.
The solution may lie underneath the leaflet. Said Dr. del Nido, “We tend to want to close a cleft, and, yes, that will get you relief of regurgitation in the central portion, but if you end up with immobility of that leaflet, then look underneath. Most often there are very abnormal attachments to the edges of that cleft to the septum. You have to get rid of that; if you don’t resect all that, you’ll never have a leaflet that truly floats up to coapt against the posterior leaflet.”
Annular dilation in children can also challenge a cardiothoracic surgeon’s skill.
In rare cases, a suture commissuroplasty may correct the problem. Sometimes Dr. del Nido will use the DeVega suture annuloplasty – “even though it is very much user dependent; it’s very easy in pediatrics to create stenosis with the DeVega.” As an alternative, synthetic ring annuloplasties can confine valve growth and are rarely used.
Dr. del Nido’s preference is to use a hybrid approach of tissue and resorbable material. “The advantage of the resorbable material is that it will go away, but that’s also the problem with the resorbable material,” he said. “Once it does go away, there’s nothing there to support the annulus, so a combination of tissue and resorbable suture is probably the best answer.”
In posterior leaflet deficiency, a patch of pericardium posteriorly can augment the dysfunctional leaflet. You can also use pericardium as an annuloplasty ring. “You can use it circumferentially,” Dr. del Nido said. “It’s a soft ring; you can certainly use this material which is autologous; it does provide strength to the fibrous annulus; it does support that valve; and you do see growth.” He added that bovine pericardium is not ideal for this use.
Dr. del Nido reported no relevant financial relationships.
NEW YORK – Repairing mitral valves in pediatric patients must overcome two issues: the wide variability in their anatomy and their growth. Using strategies and techniques common in adult mitral surgery can accomplish good mitral valve function in children, but some techniques in children differ, like using combined resorbable material with autologous tissue or transferring native chords instead of placing artificial chords to a malfunctioning leaflet.
Pedro del Nido, MD, of Boston Children’s Hospital, said the spectrum of mitral valve pathology in children goes from congenital mitral stenosis with a thick annulus with leaflet immobility to leaflet hypermobility that involves anterior leaflet prolapse and can involve a cleft that causes regurgitation. Dr. del Nido explained his surgical approaches for mitral valve disease in children at the 2017 Mitral Conclave, sponsored by the American Association of Thoracic Surgery.
Accessing the mitral valve in children requires a different approach than in adults, Dr. del Nido said. “Going through the left atrium is generally difficult, so we often enter through a trans-septal incision,” he said. “The main reason for that is because the tricuspid valve is often associated with the mitral valve problem and this gives us the most direct exposure.”
Once the surgeon gains exposure, the surgical analysis for a diseased adult or child valve is almost identical, with the exception that adult disease is acquired whereas childhood disease tends to be congenital, Dr. del Nido said. “In the congenital patient, we often find fibroelastic tissue that the child is born with,” he said. “We see this in neonates and young infants. It thickens over time; it doesn’t often calcify, but it does often restrict the leaflets and it tends to fuse the chords, so in essence you have direct attachments of the leaflets to the papillaries.”
He explained that this pathology requires an approach similar to that for rheumatic mitral disease in adults. “Start splitting the commissures and start resecting the tissue off the chords creating fenestrations in order to improve the inflow.” Dr. del Nido added, “If you don’t do this, the child will always have a gradient, and if you think about an adult having problems and symptoms with a gradient, think about a 10-year-old running around trying to do athletics; it’s impossible.”
Dysfunctional chords also require a somewhat different approach in children than they require in adults. “We find elongation of the chords and the anterior support structure is abnormal; the secondary chords are totally intact,” Dr. del Nido said. When confronting a torn-edge chord, resection is often an option in adults, but is uncommon in children. “We don’t usually have very much leaflet tissue,” he said. Artificial chords do not accommodate growth.
“We tend to use native tissue,” said Dr. del Nido. “You can transfer the strut chord; you can transfer the secondary chord in order to achieve support for the edge of that prolapsed leaflet.”
Leaflet problems are probably the biggest single source of recurrence in children, Dr. del Nido said. A cleft on the anterior leaflet can be particularly vexing. For example, cleft edges attached to the septum can prevent the valve leaflet from coaptation with the posterior leaflet. “If you don’t recognize that on 3-D echocardiography, you’re going to have a problem; that leaflet will never create the coaptation surface that you want,” he said.
The solution may lie underneath the leaflet. Said Dr. del Nido, “We tend to want to close a cleft, and, yes, that will get you relief of regurgitation in the central portion, but if you end up with immobility of that leaflet, then look underneath. Most often there are very abnormal attachments to the edges of that cleft to the septum. You have to get rid of that; if you don’t resect all that, you’ll never have a leaflet that truly floats up to coapt against the posterior leaflet.”
Annular dilation in children can also challenge a cardiothoracic surgeon’s skill.
In rare cases, a suture commissuroplasty may correct the problem. Sometimes Dr. del Nido will use the DeVega suture annuloplasty – “even though it is very much user dependent; it’s very easy in pediatrics to create stenosis with the DeVega.” As an alternative, synthetic ring annuloplasties can confine valve growth and are rarely used.
Dr. del Nido’s preference is to use a hybrid approach of tissue and resorbable material. “The advantage of the resorbable material is that it will go away, but that’s also the problem with the resorbable material,” he said. “Once it does go away, there’s nothing there to support the annulus, so a combination of tissue and resorbable suture is probably the best answer.”
In posterior leaflet deficiency, a patch of pericardium posteriorly can augment the dysfunctional leaflet. You can also use pericardium as an annuloplasty ring. “You can use it circumferentially,” Dr. del Nido said. “It’s a soft ring; you can certainly use this material which is autologous; it does provide strength to the fibrous annulus; it does support that valve; and you do see growth.” He added that bovine pericardium is not ideal for this use.
Dr. del Nido reported no relevant financial relationships.
NEW YORK – Repairing mitral valves in pediatric patients must overcome two issues: the wide variability in their anatomy and their growth. Using strategies and techniques common in adult mitral surgery can accomplish good mitral valve function in children, but some techniques in children differ, like using combined resorbable material with autologous tissue or transferring native chords instead of placing artificial chords to a malfunctioning leaflet.
Pedro del Nido, MD, of Boston Children’s Hospital, said the spectrum of mitral valve pathology in children goes from congenital mitral stenosis with a thick annulus with leaflet immobility to leaflet hypermobility that involves anterior leaflet prolapse and can involve a cleft that causes regurgitation. Dr. del Nido explained his surgical approaches for mitral valve disease in children at the 2017 Mitral Conclave, sponsored by the American Association of Thoracic Surgery.
Accessing the mitral valve in children requires a different approach than in adults, Dr. del Nido said. “Going through the left atrium is generally difficult, so we often enter through a trans-septal incision,” he said. “The main reason for that is because the tricuspid valve is often associated with the mitral valve problem and this gives us the most direct exposure.”
Once the surgeon gains exposure, the surgical analysis for a diseased adult or child valve is almost identical, with the exception that adult disease is acquired whereas childhood disease tends to be congenital, Dr. del Nido said. “In the congenital patient, we often find fibroelastic tissue that the child is born with,” he said. “We see this in neonates and young infants. It thickens over time; it doesn’t often calcify, but it does often restrict the leaflets and it tends to fuse the chords, so in essence you have direct attachments of the leaflets to the papillaries.”
He explained that this pathology requires an approach similar to that for rheumatic mitral disease in adults. “Start splitting the commissures and start resecting the tissue off the chords creating fenestrations in order to improve the inflow.” Dr. del Nido added, “If you don’t do this, the child will always have a gradient, and if you think about an adult having problems and symptoms with a gradient, think about a 10-year-old running around trying to do athletics; it’s impossible.”
Dysfunctional chords also require a somewhat different approach in children than they require in adults. “We find elongation of the chords and the anterior support structure is abnormal; the secondary chords are totally intact,” Dr. del Nido said. When confronting a torn-edge chord, resection is often an option in adults, but is uncommon in children. “We don’t usually have very much leaflet tissue,” he said. Artificial chords do not accommodate growth.
“We tend to use native tissue,” said Dr. del Nido. “You can transfer the strut chord; you can transfer the secondary chord in order to achieve support for the edge of that prolapsed leaflet.”
Leaflet problems are probably the biggest single source of recurrence in children, Dr. del Nido said. A cleft on the anterior leaflet can be particularly vexing. For example, cleft edges attached to the septum can prevent the valve leaflet from coaptation with the posterior leaflet. “If you don’t recognize that on 3-D echocardiography, you’re going to have a problem; that leaflet will never create the coaptation surface that you want,” he said.
The solution may lie underneath the leaflet. Said Dr. del Nido, “We tend to want to close a cleft, and, yes, that will get you relief of regurgitation in the central portion, but if you end up with immobility of that leaflet, then look underneath. Most often there are very abnormal attachments to the edges of that cleft to the septum. You have to get rid of that; if you don’t resect all that, you’ll never have a leaflet that truly floats up to coapt against the posterior leaflet.”
Annular dilation in children can also challenge a cardiothoracic surgeon’s skill.
In rare cases, a suture commissuroplasty may correct the problem. Sometimes Dr. del Nido will use the DeVega suture annuloplasty – “even though it is very much user dependent; it’s very easy in pediatrics to create stenosis with the DeVega.” As an alternative, synthetic ring annuloplasties can confine valve growth and are rarely used.
Dr. del Nido’s preference is to use a hybrid approach of tissue and resorbable material. “The advantage of the resorbable material is that it will go away, but that’s also the problem with the resorbable material,” he said. “Once it does go away, there’s nothing there to support the annulus, so a combination of tissue and resorbable suture is probably the best answer.”
In posterior leaflet deficiency, a patch of pericardium posteriorly can augment the dysfunctional leaflet. You can also use pericardium as an annuloplasty ring. “You can use it circumferentially,” Dr. del Nido said. “It’s a soft ring; you can certainly use this material which is autologous; it does provide strength to the fibrous annulus; it does support that valve; and you do see growth.” He added that bovine pericardium is not ideal for this use.
Dr. del Nido reported no relevant financial relationships.
AT THE 2017 MITRAL VALVE CONCLAVE
Key clinical point: Operating on mitral valves in pediatric patients must overcome the wide variability in anatomy among young patients and accommodate growth.
Major finding: Strategies that involve a combination of resorbable material with autologous tissue can accomplish repair in most of these patients.
Data source: Review based on Dr. del Nido’s experience.
Disclosures: Dr. del Nido reported having no relevant financial disclosures.
Childhood asthma linked to high LV mass later
A history of childhood asthma correlates with high left ventricular mass, a prominent indicator of cardiac damage, in asymptomatic healthy young adults, according to a report published online June 26 in JACC: Heart Failure.
“Our data suggest that aggressive lifestyle modifications or even pharmacologic treatment may be applied to people with a [childhood] history of asthma. … to lower cardiovascular risk,” said Dianjianyi Sun, MD, PhD, of the department of epidemiology, Tulane University, New Orleans, and his associates.
Both mean left ventricular mass (169 g) and mean left ventricular mass index (41 g/m2) were significantly higher in participants who’d had childhood asthma than in those who had not (158 g and 38 g/m2, respectively). This correlation was independent of major cardiovascular risk factors such as race, smoking status, hypertension status, use of antihypertensive medications, C-reactive protein levels, heart rate, and body mass index, the investigators said (JACC: Heart Failure. 2017 Jun 26. doi: 10.1016/j.jchf.2017.03.009).
The association was strongest among young adults who had higher systolic blood pressure (prehypertension or hypertension).
This study was supported by the National Institutes of Health, the Boston Obesity Nutrition Research Center, the United States-Israel Binational Science Foundation, and the American Heart Association. Dr. Sun and his associates reported having no relevant financial disclosures.
Sun et al. report that healthy young adults who had asthma during childhood have a significantly greater left ventricular mass index, by about 8%, than do those who didn’t have the condition.
On an individual patient level, such a difference confers a relatively small incremental risk of incident cardiovascular disease: a roughly 1.08-fold increase. However, at the population level, where there are many major comorbidities, the public health implications could be substantial. Targeting these patients for intensified cardiovascular risk reduction could have important benefits.
John S. Gottdiener, MD, is at the University of Maryland Medical Center, Baltimore. He reported having no relevant financial disclosures. Dr. Gottdiener made these remarks in an editorial comment accompanying Dr. Sun’s report (JACC: Heart Failure. 2017 Jun 26. doi: 10.1016/j.jchf.2017.05.003).
Sun et al. report that healthy young adults who had asthma during childhood have a significantly greater left ventricular mass index, by about 8%, than do those who didn’t have the condition.
On an individual patient level, such a difference confers a relatively small incremental risk of incident cardiovascular disease: a roughly 1.08-fold increase. However, at the population level, where there are many major comorbidities, the public health implications could be substantial. Targeting these patients for intensified cardiovascular risk reduction could have important benefits.
John S. Gottdiener, MD, is at the University of Maryland Medical Center, Baltimore. He reported having no relevant financial disclosures. Dr. Gottdiener made these remarks in an editorial comment accompanying Dr. Sun’s report (JACC: Heart Failure. 2017 Jun 26. doi: 10.1016/j.jchf.2017.05.003).
Sun et al. report that healthy young adults who had asthma during childhood have a significantly greater left ventricular mass index, by about 8%, than do those who didn’t have the condition.
On an individual patient level, such a difference confers a relatively small incremental risk of incident cardiovascular disease: a roughly 1.08-fold increase. However, at the population level, where there are many major comorbidities, the public health implications could be substantial. Targeting these patients for intensified cardiovascular risk reduction could have important benefits.
John S. Gottdiener, MD, is at the University of Maryland Medical Center, Baltimore. He reported having no relevant financial disclosures. Dr. Gottdiener made these remarks in an editorial comment accompanying Dr. Sun’s report (JACC: Heart Failure. 2017 Jun 26. doi: 10.1016/j.jchf.2017.05.003).
A history of childhood asthma correlates with high left ventricular mass, a prominent indicator of cardiac damage, in asymptomatic healthy young adults, according to a report published online June 26 in JACC: Heart Failure.
“Our data suggest that aggressive lifestyle modifications or even pharmacologic treatment may be applied to people with a [childhood] history of asthma. … to lower cardiovascular risk,” said Dianjianyi Sun, MD, PhD, of the department of epidemiology, Tulane University, New Orleans, and his associates.
Both mean left ventricular mass (169 g) and mean left ventricular mass index (41 g/m2) were significantly higher in participants who’d had childhood asthma than in those who had not (158 g and 38 g/m2, respectively). This correlation was independent of major cardiovascular risk factors such as race, smoking status, hypertension status, use of antihypertensive medications, C-reactive protein levels, heart rate, and body mass index, the investigators said (JACC: Heart Failure. 2017 Jun 26. doi: 10.1016/j.jchf.2017.03.009).
The association was strongest among young adults who had higher systolic blood pressure (prehypertension or hypertension).
This study was supported by the National Institutes of Health, the Boston Obesity Nutrition Research Center, the United States-Israel Binational Science Foundation, and the American Heart Association. Dr. Sun and his associates reported having no relevant financial disclosures.
A history of childhood asthma correlates with high left ventricular mass, a prominent indicator of cardiac damage, in asymptomatic healthy young adults, according to a report published online June 26 in JACC: Heart Failure.
“Our data suggest that aggressive lifestyle modifications or even pharmacologic treatment may be applied to people with a [childhood] history of asthma. … to lower cardiovascular risk,” said Dianjianyi Sun, MD, PhD, of the department of epidemiology, Tulane University, New Orleans, and his associates.
Both mean left ventricular mass (169 g) and mean left ventricular mass index (41 g/m2) were significantly higher in participants who’d had childhood asthma than in those who had not (158 g and 38 g/m2, respectively). This correlation was independent of major cardiovascular risk factors such as race, smoking status, hypertension status, use of antihypertensive medications, C-reactive protein levels, heart rate, and body mass index, the investigators said (JACC: Heart Failure. 2017 Jun 26. doi: 10.1016/j.jchf.2017.03.009).
The association was strongest among young adults who had higher systolic blood pressure (prehypertension or hypertension).
This study was supported by the National Institutes of Health, the Boston Obesity Nutrition Research Center, the United States-Israel Binational Science Foundation, and the American Heart Association. Dr. Sun and his associates reported having no relevant financial disclosures.
FROM JACC: HEART FAILURE
Key clinical point: Childhood asthma is associated with high left ventricular mass in asymptomatic young adults.
Major finding: Both mean left ventricular mass (169 g) and mean left ventricular mass index (41 g/m2) were significantly higher in participants who’d had childhood asthma than in those who had not (158 g and 38 g/m2, respectively).
Data source: A secondary analysis of data from the Bogalusa Heart Study, involving 1,118 participants followed for an average of 10 years.
Disclosures: This study was supported by the National Heart, Lung, and Blood Institute, the National Institute of Diabetes and Digestive and Kidney Diseases, the Boston Obesity Nutrition Research Center, the United States-Israel Binational Science Foundation, and the American Heart Association. Dr. Sun and his associates reported having no relevant financial disclosures.
Infections may trigger leukemia in the genetically susceptible
MADRID – The evidence thus far comes only from animal models, but commonly encountered childhood infections may be able to trigger the development of leukemia in those children with certain genetic predispositions to B-cell precursor acute lymphoblastic leukemia (BCP-ALL).
Mice genetically modified to mimic BCP-ALL susceptibility and its most common subtype (ETV6-RUNX1 BCP-ALL) developed leukemia only after exposure to a common infectious environment.

“The mechanism that takes place in preleukemic cells after the mice were exposed to infection was different in the two mouse models,” she said at a briefing prior to her presentation of the data at the annual congress of the European Hematology Association.
“This is another piece that will, hopefully, contribute to the picture of how exposure to infection can contribute to leukemic development” and may lead to novel approaches for leukemia prevention, she added.
The possibility that exposure to infectious pathogens could trigger leukemia has been bandied about for a century, based in part on observations that leukemia is the most common malignancy in children, with a still unexplained peak incidence between the ages of 2 and 6 years, Dr. Hauer noted.
To explore a possible link, she and her colleagues developed and characterized the aforementioned mice mimicking BCP-ALL with the BCR-ABL1 transcription and ETV6-RUNX1 BCP-ALL, in addition to a previously described Pax5+/- infection model. Some of all three mouse models were exposed not to specific pathogens but to a common laboratory environment, where they could be expected to acquire various infections at 2-3 months of age, and some were kept in a sterile environment designed to reduce transmission of pathogens. Wild-type mice were used as controls.
They observed that the Pax5+/- and ETV6-RUNX1 mice developed BCP-ALL only after exposure to common pathogens. In contrast, the BCR-ABL1p190 mice developed BCP-ALL independent of exposure to common infection.
They also determined that the mechanism leading to leukemia in the Pax5+/- mice was related to constitutive activations of mutations in the Janus kinase (JAK)3 pathway in susceptible B cell precursors, whereas the ETV6-RUNX1 mice developed BCP-ALL at a low penetrance (10.75%, 10 of 93) with a CD19-positive, B220-positive, immunoglobulin M-negative cell surface phenotype, manifested by blast cells in peripheral blood and a clonal immature B-cell receptor rearrangement.
In mice, norovirus and hepatitis C virus may be some of the pathogens most closely linked to risk of leukemia, but it’s likely that other viruses and parasitic infections will turn out to be the culprits in humans, Dr. Hauer said.
The findings raise the possibility of an unexpected link between leukemia and the so-called “hygiene hypothesis” linking childhood asthma, allergies, and atopic skin conditions to a lack of early exposure to a multiplicity of pathogens. In many developed countries, children are relatively protected from exposure to many different pathogens and may not encounter infectious agents until entering preschool or kindergarten, Dr. Hauer commented.
The study was supported by German Cancer Aid, the Jose Carreras Leukemia Foundation, and other charitable agencies. Dr. Hauer reported no relevant disclosures.
MADRID – The evidence thus far comes only from animal models, but commonly encountered childhood infections may be able to trigger the development of leukemia in those children with certain genetic predispositions to B-cell precursor acute lymphoblastic leukemia (BCP-ALL).
Mice genetically modified to mimic BCP-ALL susceptibility and its most common subtype (ETV6-RUNX1 BCP-ALL) developed leukemia only after exposure to a common infectious environment.
“The mechanism that takes place in preleukemic cells after the mice were exposed to infection was different in the two mouse models,” she said at a briefing prior to her presentation of the data at the annual congress of the European Hematology Association.
“This is another piece that will, hopefully, contribute to the picture of how exposure to infection can contribute to leukemic development” and may lead to novel approaches for leukemia prevention, she added.
The possibility that exposure to infectious pathogens could trigger leukemia has been bandied about for a century, based in part on observations that leukemia is the most common malignancy in children, with a still unexplained peak incidence between the ages of 2 and 6 years, Dr. Hauer noted.
To explore a possible link, she and her colleagues developed and characterized the aforementioned mice mimicking BCP-ALL with the BCR-ABL1 transcription and ETV6-RUNX1 BCP-ALL, in addition to a previously described Pax5+/- infection model. Some of all three mouse models were exposed not to specific pathogens but to a common laboratory environment, where they could be expected to acquire various infections at 2-3 months of age, and some were kept in a sterile environment designed to reduce transmission of pathogens. Wild-type mice were used as controls.
They observed that the Pax5+/- and ETV6-RUNX1 mice developed BCP-ALL only after exposure to common pathogens. In contrast, the BCR-ABL1p190 mice developed BCP-ALL independent of exposure to common infection.
They also determined that the mechanism leading to leukemia in the Pax5+/- mice was related to constitutive activations of mutations in the Janus kinase (JAK)3 pathway in susceptible B cell precursors, whereas the ETV6-RUNX1 mice developed BCP-ALL at a low penetrance (10.75%, 10 of 93) with a CD19-positive, B220-positive, immunoglobulin M-negative cell surface phenotype, manifested by blast cells in peripheral blood and a clonal immature B-cell receptor rearrangement.
In mice, norovirus and hepatitis C virus may be some of the pathogens most closely linked to risk of leukemia, but it’s likely that other viruses and parasitic infections will turn out to be the culprits in humans, Dr. Hauer said.
The findings raise the possibility of an unexpected link between leukemia and the so-called “hygiene hypothesis” linking childhood asthma, allergies, and atopic skin conditions to a lack of early exposure to a multiplicity of pathogens. In many developed countries, children are relatively protected from exposure to many different pathogens and may not encounter infectious agents until entering preschool or kindergarten, Dr. Hauer commented.
The study was supported by German Cancer Aid, the Jose Carreras Leukemia Foundation, and other charitable agencies. Dr. Hauer reported no relevant disclosures.
MADRID – The evidence thus far comes only from animal models, but commonly encountered childhood infections may be able to trigger the development of leukemia in those children with certain genetic predispositions to B-cell precursor acute lymphoblastic leukemia (BCP-ALL).
Mice genetically modified to mimic BCP-ALL susceptibility and its most common subtype (ETV6-RUNX1 BCP-ALL) developed leukemia only after exposure to a common infectious environment.
“The mechanism that takes place in preleukemic cells after the mice were exposed to infection was different in the two mouse models,” she said at a briefing prior to her presentation of the data at the annual congress of the European Hematology Association.
“This is another piece that will, hopefully, contribute to the picture of how exposure to infection can contribute to leukemic development” and may lead to novel approaches for leukemia prevention, she added.
The possibility that exposure to infectious pathogens could trigger leukemia has been bandied about for a century, based in part on observations that leukemia is the most common malignancy in children, with a still unexplained peak incidence between the ages of 2 and 6 years, Dr. Hauer noted.
To explore a possible link, she and her colleagues developed and characterized the aforementioned mice mimicking BCP-ALL with the BCR-ABL1 transcription and ETV6-RUNX1 BCP-ALL, in addition to a previously described Pax5+/- infection model. Some of all three mouse models were exposed not to specific pathogens but to a common laboratory environment, where they could be expected to acquire various infections at 2-3 months of age, and some were kept in a sterile environment designed to reduce transmission of pathogens. Wild-type mice were used as controls.
They observed that the Pax5+/- and ETV6-RUNX1 mice developed BCP-ALL only after exposure to common pathogens. In contrast, the BCR-ABL1p190 mice developed BCP-ALL independent of exposure to common infection.
They also determined that the mechanism leading to leukemia in the Pax5+/- mice was related to constitutive activations of mutations in the Janus kinase (JAK)3 pathway in susceptible B cell precursors, whereas the ETV6-RUNX1 mice developed BCP-ALL at a low penetrance (10.75%, 10 of 93) with a CD19-positive, B220-positive, immunoglobulin M-negative cell surface phenotype, manifested by blast cells in peripheral blood and a clonal immature B-cell receptor rearrangement.
In mice, norovirus and hepatitis C virus may be some of the pathogens most closely linked to risk of leukemia, but it’s likely that other viruses and parasitic infections will turn out to be the culprits in humans, Dr. Hauer said.
The findings raise the possibility of an unexpected link between leukemia and the so-called “hygiene hypothesis” linking childhood asthma, allergies, and atopic skin conditions to a lack of early exposure to a multiplicity of pathogens. In many developed countries, children are relatively protected from exposure to many different pathogens and may not encounter infectious agents until entering preschool or kindergarten, Dr. Hauer commented.
The study was supported by German Cancer Aid, the Jose Carreras Leukemia Foundation, and other charitable agencies. Dr. Hauer reported no relevant disclosures.
AT EHA 2017
Key clinical point: This study suggests a link between acute lymphocytic leukemia development and infections in some genetically predisposed children.
Major finding: Mouse models of two types of B-cell precursor ALL developed leukemia only after exposure to infections.
Data source: A study of factors related to the development of childhood ALL using genetically modified mouse models.
Disclosures: The study was supported by German Cancer Aid, the Jose Carreras Leukemia Foundation, and other charitable agencies. Dr. Hauer reported no relevant disclosures.
The latest news on pediatric migraine
Migraine is the most common disabling neurologic disease, with an estimated 1 billion sufferers worldwide.1 In children aged 5-15 years, migraine prevalence is 10%, and these children miss more school than their peers.2,3 Research specific to the child and adolescent migraine population is imperative, as the findings in adult studies do not always correlate or translate to pediatrics. The American Headache Society (AHS) held its 59th annual scientific meeting in Boston in June 2017, a meeting designed to showcase the latest advances in the field of headache medicine. Several interesting pediatric headache studies were presented.

Pediatric patient, parent goals and preferences for preventive treatment
There is a general consensus among headache specialists that migraine preventive treatment should be instituted when a migraineur has at least four headache days per month. Clinically, and in most research trials, migraine preventive treatment is considered effective when a 50% reduction in headache days or the headache frequency is reduced to no more than four headache days per month.

Perhaps not surprisingly, patients and families expect treatment to result in very few headaches with minimal side effects. It is helpful to understand patient and family treatment goals as clinicians so we can to better provide realistic expectations of care, improve treatment adherence, and reduce patient/parent frustration.
Premonitory symptoms
Migraine is disabling not simply because of the headache but because of the range of symptoms that occur around the headache. Migraine may involve four phases: premonitory, aura, headache, and postdrome. The premonitory phase involves symptoms that may occur hours to days prior to the headache. Functional imaging studies reveal hypothalamic activation during this phase.4 In a large retrospective study, premonitory symptoms occurred in approximately three-quarters of pediatric and adult migraineurs.5 In a prior pediatric chart review, the most common premonitory symptoms in order of decreasing frequency were fatigue, mood change, neck stiffness, and yawning.6

Understanding and identifying premonitory signs is important for better understanding the pathophysiology of migraine and to help our patients recognize when a migraine may be coming.
Mapping pain in pediatric migraine
Diagnosis of migraine is based on the International Classification of Headache Disorders 3rd edition beta (ICHD-3b). For adults with migraine, part of the diagnostic criteria requires at least two of a number of features: unilateral location, pulsating quality, moderate or severe pain intensity, or aggravation by or avoidance of routine physical activity. The comments section of the ICHD-3b mentions that, in children under 18 years, the pain may be bilateral.
This study sought to characterize the location and quality of headache pain in the pediatric and young adult population. Sixty migraineurs were enrolled and divided into three age groups: children (7-11 years), adolescents (12-18), and young adults (19-26). The patients were guided to use a diagram to draw pain location and quality. The pain was bilateral for the majority of patients in all age groups. Of the young adult group, 85% had bilateral headache. This is of interest, as adults with migraine are conventionally thought to have unilateral headache. The main descriptors among all three groups were throbbing, pounding, and pressing. In children, tightening was more common than throbbing.
When diagnosing migraine, it is helpful to take these differences into consideration. Overall, this study provides a better understanding of the quality and location of migraine in the pediatric and young adult population.
Efficacy of zolmitriptan nasal spray in adolescents
Zolmitriptan nasal spray (NS) was approved by the Food and Drug Administration in 2015 for acute migraine treatment in adolescents ages 12-17 years. This was the first triptan NS approved for use in pediatric migraine. The NS route benefits migraineurs who need a rapidly absorbed triptan or those who do not tolerate oral triptans because of significant nausea or emesis with their migraine. The efficacy of zolmitriptan NS in adolescents was established in a multicenter, double-blind, randomized placebo controlled study with 798 participants.7 The primary endpoint of pain freedom at 2 hours after treatment for the 5-mg dose was superior to placebo, 30% vs. 17%, respectively (P less than .001; odds ratio, 2.18; 95% confidence interval, 1.40, 3.39). Patients with migraine going from moderate or severe to mild or no headache at 2 hours post treatment were 51% vs. 39%, respectively (P = .010).
The follow-up study presented at AHS was a subgroup analysis of the above data in younger (12-14 years) and older (15-17 years) adolescents. The primary efficacy endpoint of being pain free at 2 hours post treatment was similarly better for zolmitriptan 5 mg, compared with placebo, in both the younger and older adolescent migraineurs.
This study reinforces that zolmitriptan 5-mg NS is an effective abortive migraine treatment in adolescents and is generally well tolerated.
New migraine treatments
Although not pediatric studies, several presentations addressed exciting new preventive treatments that target one of the main neuropeptides implicated in migraine pathophysiology, calcitonin gene related peptide. Four drug companies have completed phase II and phase III adult trials in which they have developed humanized monoclonal antibodies that bind to CGRP or its receptor. These medications have shown great promise and appear to be very well tolerated. These are the first medications developed specifically for migraine prevention, as opposed to current medications which we borrow from other fields of medicine. It is anticipated they will be available for use in adult migraineurs later this year.
Dr. Qubty is a pediatric headache specialist and an assistant professor of neurology at the University of California, San Francisco, and he is a member of the American Headache Society. He said he had no relevant financial disclosures.
*Correction, 8/10/2017: An earlier version of this article misstated the percentage of pediatric migraine patients who had premonitory signs, and how common premonitory signs were among episodic migraineurs with and without aura.
References
1. Lancet. 2016 Oct 8;388(10053):1545-1602.
2. Dev Med Child Neurol. 2010 Dec;52(12):1088-97.
3. Neurology. 2012 Oct 30;79(18):1881-8.
4. Brain. 2014 Jan;137(Pt 1):232-41.
5. Cephalalgia 2016;36:951-959.
6. J Headache Pain. 2016 Dec;17(1):94.
7. Headache. 2016 Jul;56(7):1107-19.
Migraine is the most common disabling neurologic disease, with an estimated 1 billion sufferers worldwide.1 In children aged 5-15 years, migraine prevalence is 10%, and these children miss more school than their peers.2,3 Research specific to the child and adolescent migraine population is imperative, as the findings in adult studies do not always correlate or translate to pediatrics. The American Headache Society (AHS) held its 59th annual scientific meeting in Boston in June 2017, a meeting designed to showcase the latest advances in the field of headache medicine. Several interesting pediatric headache studies were presented.
Pediatric patient, parent goals and preferences for preventive treatment
There is a general consensus among headache specialists that migraine preventive treatment should be instituted when a migraineur has at least four headache days per month. Clinically, and in most research trials, migraine preventive treatment is considered effective when a 50% reduction in headache days or the headache frequency is reduced to no more than four headache days per month.
Perhaps not surprisingly, patients and families expect treatment to result in very few headaches with minimal side effects. It is helpful to understand patient and family treatment goals as clinicians so we can to better provide realistic expectations of care, improve treatment adherence, and reduce patient/parent frustration.
Premonitory symptoms
Migraine is disabling not simply because of the headache but because of the range of symptoms that occur around the headache. Migraine may involve four phases: premonitory, aura, headache, and postdrome. The premonitory phase involves symptoms that may occur hours to days prior to the headache. Functional imaging studies reveal hypothalamic activation during this phase.4 In a large retrospective study, premonitory symptoms occurred in approximately three-quarters of pediatric and adult migraineurs.5 In a prior pediatric chart review, the most common premonitory symptoms in order of decreasing frequency were fatigue, mood change, neck stiffness, and yawning.6
Understanding and identifying premonitory signs is important for better understanding the pathophysiology of migraine and to help our patients recognize when a migraine may be coming.
Mapping pain in pediatric migraine
Diagnosis of migraine is based on the International Classification of Headache Disorders 3rd edition beta (ICHD-3b). For adults with migraine, part of the diagnostic criteria requires at least two of a number of features: unilateral location, pulsating quality, moderate or severe pain intensity, or aggravation by or avoidance of routine physical activity. The comments section of the ICHD-3b mentions that, in children under 18 years, the pain may be bilateral.
This study sought to characterize the location and quality of headache pain in the pediatric and young adult population. Sixty migraineurs were enrolled and divided into three age groups: children (7-11 years), adolescents (12-18), and young adults (19-26). The patients were guided to use a diagram to draw pain location and quality. The pain was bilateral for the majority of patients in all age groups. Of the young adult group, 85% had bilateral headache. This is of interest, as adults with migraine are conventionally thought to have unilateral headache. The main descriptors among all three groups were throbbing, pounding, and pressing. In children, tightening was more common than throbbing.
When diagnosing migraine, it is helpful to take these differences into consideration. Overall, this study provides a better understanding of the quality and location of migraine in the pediatric and young adult population.
Efficacy of zolmitriptan nasal spray in adolescents
Zolmitriptan nasal spray (NS) was approved by the Food and Drug Administration in 2015 for acute migraine treatment in adolescents ages 12-17 years. This was the first triptan NS approved for use in pediatric migraine. The NS route benefits migraineurs who need a rapidly absorbed triptan or those who do not tolerate oral triptans because of significant nausea or emesis with their migraine. The efficacy of zolmitriptan NS in adolescents was established in a multicenter, double-blind, randomized placebo controlled study with 798 participants.7 The primary endpoint of pain freedom at 2 hours after treatment for the 5-mg dose was superior to placebo, 30% vs. 17%, respectively (P less than .001; odds ratio, 2.18; 95% confidence interval, 1.40, 3.39). Patients with migraine going from moderate or severe to mild or no headache at 2 hours post treatment were 51% vs. 39%, respectively (P = .010).
The follow-up study presented at AHS was a subgroup analysis of the above data in younger (12-14 years) and older (15-17 years) adolescents. The primary efficacy endpoint of being pain free at 2 hours post treatment was similarly better for zolmitriptan 5 mg, compared with placebo, in both the younger and older adolescent migraineurs.
This study reinforces that zolmitriptan 5-mg NS is an effective abortive migraine treatment in adolescents and is generally well tolerated.
New migraine treatments
Although not pediatric studies, several presentations addressed exciting new preventive treatments that target one of the main neuropeptides implicated in migraine pathophysiology, calcitonin gene related peptide. Four drug companies have completed phase II and phase III adult trials in which they have developed humanized monoclonal antibodies that bind to CGRP or its receptor. These medications have shown great promise and appear to be very well tolerated. These are the first medications developed specifically for migraine prevention, as opposed to current medications which we borrow from other fields of medicine. It is anticipated they will be available for use in adult migraineurs later this year.
Dr. Qubty is a pediatric headache specialist and an assistant professor of neurology at the University of California, San Francisco, and he is a member of the American Headache Society. He said he had no relevant financial disclosures.
*Correction, 8/10/2017: An earlier version of this article misstated the percentage of pediatric migraine patients who had premonitory signs, and how common premonitory signs were among episodic migraineurs with and without aura.
References
1. Lancet. 2016 Oct 8;388(10053):1545-1602.
2. Dev Med Child Neurol. 2010 Dec;52(12):1088-97.
3. Neurology. 2012 Oct 30;79(18):1881-8.
4. Brain. 2014 Jan;137(Pt 1):232-41.
5. Cephalalgia 2016;36:951-959.
6. J Headache Pain. 2016 Dec;17(1):94.
7. Headache. 2016 Jul;56(7):1107-19.
Migraine is the most common disabling neurologic disease, with an estimated 1 billion sufferers worldwide.1 In children aged 5-15 years, migraine prevalence is 10%, and these children miss more school than their peers.2,3 Research specific to the child and adolescent migraine population is imperative, as the findings in adult studies do not always correlate or translate to pediatrics. The American Headache Society (AHS) held its 59th annual scientific meeting in Boston in June 2017, a meeting designed to showcase the latest advances in the field of headache medicine. Several interesting pediatric headache studies were presented.
Pediatric patient, parent goals and preferences for preventive treatment
There is a general consensus among headache specialists that migraine preventive treatment should be instituted when a migraineur has at least four headache days per month. Clinically, and in most research trials, migraine preventive treatment is considered effective when a 50% reduction in headache days or the headache frequency is reduced to no more than four headache days per month.
Perhaps not surprisingly, patients and families expect treatment to result in very few headaches with minimal side effects. It is helpful to understand patient and family treatment goals as clinicians so we can to better provide realistic expectations of care, improve treatment adherence, and reduce patient/parent frustration.
Premonitory symptoms
Migraine is disabling not simply because of the headache but because of the range of symptoms that occur around the headache. Migraine may involve four phases: premonitory, aura, headache, and postdrome. The premonitory phase involves symptoms that may occur hours to days prior to the headache. Functional imaging studies reveal hypothalamic activation during this phase.4 In a large retrospective study, premonitory symptoms occurred in approximately three-quarters of pediatric and adult migraineurs.5 In a prior pediatric chart review, the most common premonitory symptoms in order of decreasing frequency were fatigue, mood change, neck stiffness, and yawning.6
Understanding and identifying premonitory signs is important for better understanding the pathophysiology of migraine and to help our patients recognize when a migraine may be coming.
Mapping pain in pediatric migraine
Diagnosis of migraine is based on the International Classification of Headache Disorders 3rd edition beta (ICHD-3b). For adults with migraine, part of the diagnostic criteria requires at least two of a number of features: unilateral location, pulsating quality, moderate or severe pain intensity, or aggravation by or avoidance of routine physical activity. The comments section of the ICHD-3b mentions that, in children under 18 years, the pain may be bilateral.
This study sought to characterize the location and quality of headache pain in the pediatric and young adult population. Sixty migraineurs were enrolled and divided into three age groups: children (7-11 years), adolescents (12-18), and young adults (19-26). The patients were guided to use a diagram to draw pain location and quality. The pain was bilateral for the majority of patients in all age groups. Of the young adult group, 85% had bilateral headache. This is of interest, as adults with migraine are conventionally thought to have unilateral headache. The main descriptors among all three groups were throbbing, pounding, and pressing. In children, tightening was more common than throbbing.
When diagnosing migraine, it is helpful to take these differences into consideration. Overall, this study provides a better understanding of the quality and location of migraine in the pediatric and young adult population.
Efficacy of zolmitriptan nasal spray in adolescents
Zolmitriptan nasal spray (NS) was approved by the Food and Drug Administration in 2015 for acute migraine treatment in adolescents ages 12-17 years. This was the first triptan NS approved for use in pediatric migraine. The NS route benefits migraineurs who need a rapidly absorbed triptan or those who do not tolerate oral triptans because of significant nausea or emesis with their migraine. The efficacy of zolmitriptan NS in adolescents was established in a multicenter, double-blind, randomized placebo controlled study with 798 participants.7 The primary endpoint of pain freedom at 2 hours after treatment for the 5-mg dose was superior to placebo, 30% vs. 17%, respectively (P less than .001; odds ratio, 2.18; 95% confidence interval, 1.40, 3.39). Patients with migraine going from moderate or severe to mild or no headache at 2 hours post treatment were 51% vs. 39%, respectively (P = .010).
The follow-up study presented at AHS was a subgroup analysis of the above data in younger (12-14 years) and older (15-17 years) adolescents. The primary efficacy endpoint of being pain free at 2 hours post treatment was similarly better for zolmitriptan 5 mg, compared with placebo, in both the younger and older adolescent migraineurs.
This study reinforces that zolmitriptan 5-mg NS is an effective abortive migraine treatment in adolescents and is generally well tolerated.
New migraine treatments
Although not pediatric studies, several presentations addressed exciting new preventive treatments that target one of the main neuropeptides implicated in migraine pathophysiology, calcitonin gene related peptide. Four drug companies have completed phase II and phase III adult trials in which they have developed humanized monoclonal antibodies that bind to CGRP or its receptor. These medications have shown great promise and appear to be very well tolerated. These are the first medications developed specifically for migraine prevention, as opposed to current medications which we borrow from other fields of medicine. It is anticipated they will be available for use in adult migraineurs later this year.
Dr. Qubty is a pediatric headache specialist and an assistant professor of neurology at the University of California, San Francisco, and he is a member of the American Headache Society. He said he had no relevant financial disclosures.
*Correction, 8/10/2017: An earlier version of this article misstated the percentage of pediatric migraine patients who had premonitory signs, and how common premonitory signs were among episodic migraineurs with and without aura.
References
1. Lancet. 2016 Oct 8;388(10053):1545-1602.
2. Dev Med Child Neurol. 2010 Dec;52(12):1088-97.
3. Neurology. 2012 Oct 30;79(18):1881-8.
4. Brain. 2014 Jan;137(Pt 1):232-41.
5. Cephalalgia 2016;36:951-959.
6. J Headache Pain. 2016 Dec;17(1):94.
7. Headache. 2016 Jul;56(7):1107-19.
If doctors recommend it, teens are more likely to get HPV vaccine
, Brandon Brown, PhD, at the University of California, Riverside, and his associates said.
In a year-long survey of 200 parents’ reasons for agreeing or refusing initial HPV vaccination following practitioner recommendation in a California pediatric practice of six pediatricians, 82% of parents accepted initiation of the HPV series. A significantly higher percentage of parents of male teens did so, compared with parents of female teens (89% vs. 71%; P less than .01), but there were more male children (61.5%) among offspring of the study participants.
Among parents who refused initiation of the HPV vaccine for their adolescents, the most common reason for refusing (53%) and most influential reason (49%) was “I want to learn more about this vaccine,” while 25% said their child was too young to get the vaccine. Some in this latter group said they would vaccinate their child when they were older.
Of the 195 parents who answered a question regarding whether they had a friend or family member diagnosed with cervical cancer, 13% said yes. Of these parents, 92% agreed to have their child get the HPV vaccine.
Read more at Papillomavirus Research (2017 Jan 17. doi: 10.1016/j.pvr.2017.01.002).
, Brandon Brown, PhD, at the University of California, Riverside, and his associates said.
In a year-long survey of 200 parents’ reasons for agreeing or refusing initial HPV vaccination following practitioner recommendation in a California pediatric practice of six pediatricians, 82% of parents accepted initiation of the HPV series. A significantly higher percentage of parents of male teens did so, compared with parents of female teens (89% vs. 71%; P less than .01), but there were more male children (61.5%) among offspring of the study participants.
Among parents who refused initiation of the HPV vaccine for their adolescents, the most common reason for refusing (53%) and most influential reason (49%) was “I want to learn more about this vaccine,” while 25% said their child was too young to get the vaccine. Some in this latter group said they would vaccinate their child when they were older.
Of the 195 parents who answered a question regarding whether they had a friend or family member diagnosed with cervical cancer, 13% said yes. Of these parents, 92% agreed to have their child get the HPV vaccine.
Read more at Papillomavirus Research (2017 Jan 17. doi: 10.1016/j.pvr.2017.01.002).
, Brandon Brown, PhD, at the University of California, Riverside, and his associates said.
In a year-long survey of 200 parents’ reasons for agreeing or refusing initial HPV vaccination following practitioner recommendation in a California pediatric practice of six pediatricians, 82% of parents accepted initiation of the HPV series. A significantly higher percentage of parents of male teens did so, compared with parents of female teens (89% vs. 71%; P less than .01), but there were more male children (61.5%) among offspring of the study participants.
Among parents who refused initiation of the HPV vaccine for their adolescents, the most common reason for refusing (53%) and most influential reason (49%) was “I want to learn more about this vaccine,” while 25% said their child was too young to get the vaccine. Some in this latter group said they would vaccinate their child when they were older.
Of the 195 parents who answered a question regarding whether they had a friend or family member diagnosed with cervical cancer, 13% said yes. Of these parents, 92% agreed to have their child get the HPV vaccine.
Read more at Papillomavirus Research (2017 Jan 17. doi: 10.1016/j.pvr.2017.01.002).
FROM PAPILLOMAVIRUS RESEARCH
ACIP approves new hepatitis A vaccine draft recommendations
, including a focus on catch-up vaccines for adolescents and those over age 40 years.
While hepatitis A cases have dropped significantly since the vaccine’s debut – with the number of reported cases in 2015 dropping to 1,390, compared with 9,606 in 1971 – previous recommendations regarding catch-up vaccinations suggested patients should consider treatment, as opposed to catch-up vaccination.
Adult catch-up vaccines now are recommended to be considered in areas with increasing disease risks, an addition that was not part of the current recommendations but has been changed because of evidence that patients over 40 years old are more vulnerable to the virus and more likely to be hospitalized if infected, said Noele Nelson, MD, PhD, of the Division of Viral Hepatitis at the CDC.
“Increasing proportions of adults in the United States are susceptible to hepatitis A ... due to reduced exposure to virus early in life and significant serum prevalence in older adults greater and equal to 40 years,” said Dr. Nelson. “In addition, there is low two-dose vaccination coverage among adults, including high risk adults, and morbidity and mortality increases with age.”
Recommendations for pregnant women also have been updated with a more definitive message. Previous recommendations advised pregnant women to weigh the options of acquiring hepatitis A against possible adverse effects of the vaccine. But, new evidence was presented at the meeting: in a study of 139 pregnant women vaccinated between 1996 and 2015 who experienced adverse effects, only seven of the effects were considered serious, and no maternal or infant deaths were apparent. In light of this, the ACIP approved the recommendation change to advise all pregnant women to be vaccinated, if they have not already been so before pregnancy.
Updates also included recommendations for patients with chronic liver disease, who are considered to be members of a high-risk population. Newly approved recommendations include a section on epidemiology, which states that, while those with chronic liver disease are not at increased risk for hepatitis A virus infection unless they experience fecal-oral exposure to the virus, those with acute hepatitis A may be more at risk to develop more severe liver disease. Recommendations for those with chronic liver disease also include a statement advising patients to seek immunoglobulin, as well as a hepatitis A, vaccination as soon as possible after exposure.
The ACIP also approved a change in recommendations to advise all residents and caretakers of those living in a group home, specifically those caring for developmentally disabled patients, to be vaccinated because of the historically high endemic nature of such institutions.
Committee members hope these new recommendations will help the United States reach its goal of a national hepatitis A case ratio of 0.3/100,000 people and a hepatitis A vaccination rate of 85%.
If these recommendations are approved by the director of the CDC and the U.S. Health Department, as they usually are, they will be published in the CDC’s Weekly Morbidity and Mortality Report.
Members of the committee reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
, including a focus on catch-up vaccines for adolescents and those over age 40 years.
While hepatitis A cases have dropped significantly since the vaccine’s debut – with the number of reported cases in 2015 dropping to 1,390, compared with 9,606 in 1971 – previous recommendations regarding catch-up vaccinations suggested patients should consider treatment, as opposed to catch-up vaccination.
Adult catch-up vaccines now are recommended to be considered in areas with increasing disease risks, an addition that was not part of the current recommendations but has been changed because of evidence that patients over 40 years old are more vulnerable to the virus and more likely to be hospitalized if infected, said Noele Nelson, MD, PhD, of the Division of Viral Hepatitis at the CDC.
“Increasing proportions of adults in the United States are susceptible to hepatitis A ... due to reduced exposure to virus early in life and significant serum prevalence in older adults greater and equal to 40 years,” said Dr. Nelson. “In addition, there is low two-dose vaccination coverage among adults, including high risk adults, and morbidity and mortality increases with age.”
Recommendations for pregnant women also have been updated with a more definitive message. Previous recommendations advised pregnant women to weigh the options of acquiring hepatitis A against possible adverse effects of the vaccine. But, new evidence was presented at the meeting: in a study of 139 pregnant women vaccinated between 1996 and 2015 who experienced adverse effects, only seven of the effects were considered serious, and no maternal or infant deaths were apparent. In light of this, the ACIP approved the recommendation change to advise all pregnant women to be vaccinated, if they have not already been so before pregnancy.
Updates also included recommendations for patients with chronic liver disease, who are considered to be members of a high-risk population. Newly approved recommendations include a section on epidemiology, which states that, while those with chronic liver disease are not at increased risk for hepatitis A virus infection unless they experience fecal-oral exposure to the virus, those with acute hepatitis A may be more at risk to develop more severe liver disease. Recommendations for those with chronic liver disease also include a statement advising patients to seek immunoglobulin, as well as a hepatitis A, vaccination as soon as possible after exposure.
The ACIP also approved a change in recommendations to advise all residents and caretakers of those living in a group home, specifically those caring for developmentally disabled patients, to be vaccinated because of the historically high endemic nature of such institutions.
Committee members hope these new recommendations will help the United States reach its goal of a national hepatitis A case ratio of 0.3/100,000 people and a hepatitis A vaccination rate of 85%.
If these recommendations are approved by the director of the CDC and the U.S. Health Department, as they usually are, they will be published in the CDC’s Weekly Morbidity and Mortality Report.
Members of the committee reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
, including a focus on catch-up vaccines for adolescents and those over age 40 years.
While hepatitis A cases have dropped significantly since the vaccine’s debut – with the number of reported cases in 2015 dropping to 1,390, compared with 9,606 in 1971 – previous recommendations regarding catch-up vaccinations suggested patients should consider treatment, as opposed to catch-up vaccination.
Adult catch-up vaccines now are recommended to be considered in areas with increasing disease risks, an addition that was not part of the current recommendations but has been changed because of evidence that patients over 40 years old are more vulnerable to the virus and more likely to be hospitalized if infected, said Noele Nelson, MD, PhD, of the Division of Viral Hepatitis at the CDC.
“Increasing proportions of adults in the United States are susceptible to hepatitis A ... due to reduced exposure to virus early in life and significant serum prevalence in older adults greater and equal to 40 years,” said Dr. Nelson. “In addition, there is low two-dose vaccination coverage among adults, including high risk adults, and morbidity and mortality increases with age.”
Recommendations for pregnant women also have been updated with a more definitive message. Previous recommendations advised pregnant women to weigh the options of acquiring hepatitis A against possible adverse effects of the vaccine. But, new evidence was presented at the meeting: in a study of 139 pregnant women vaccinated between 1996 and 2015 who experienced adverse effects, only seven of the effects were considered serious, and no maternal or infant deaths were apparent. In light of this, the ACIP approved the recommendation change to advise all pregnant women to be vaccinated, if they have not already been so before pregnancy.
Updates also included recommendations for patients with chronic liver disease, who are considered to be members of a high-risk population. Newly approved recommendations include a section on epidemiology, which states that, while those with chronic liver disease are not at increased risk for hepatitis A virus infection unless they experience fecal-oral exposure to the virus, those with acute hepatitis A may be more at risk to develop more severe liver disease. Recommendations for those with chronic liver disease also include a statement advising patients to seek immunoglobulin, as well as a hepatitis A, vaccination as soon as possible after exposure.
The ACIP also approved a change in recommendations to advise all residents and caretakers of those living in a group home, specifically those caring for developmentally disabled patients, to be vaccinated because of the historically high endemic nature of such institutions.
Committee members hope these new recommendations will help the United States reach its goal of a national hepatitis A case ratio of 0.3/100,000 people and a hepatitis A vaccination rate of 85%.
If these recommendations are approved by the director of the CDC and the U.S. Health Department, as they usually are, they will be published in the CDC’s Weekly Morbidity and Mortality Report.
Members of the committee reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
FROM ACIP MEETING
Less sex, more contraception use in teens in last decade
, according to a report by Joyce C. Abma, PhD, and Gladys M. Martinez, PhD, of the Division of Vital Statistics at the National Center for Health Statistics, Hyattsville, Md.
The percentage of female teens who had ever had sexual intercourse declined from 51% in 1988 to 42% in 2011-2015. For male teens, the percentage who were sexually experienced declined from 60% in 1988 to 44% in 2011-2015.
Male teens’ condom use during their first sexual experiences increased from 71% in 2002 to 77% in 2011-2015. This plateau in male contraception is in part the result of various types of contraception for women being developed and widely distributed in the course of these years, such as intrauterine devices.
The report features the most recent data from the National Survey of Family Growth (NSFG), resulting in 4 years of interviews spanning 2011 through 2015 and including 2,047 female teens and 2,087 male teens aged 15-19 years (National Health Statistics Reports; no 104. Hyattsville, MD: National Center for Health Statistics. 2017). Data also was abstracted from the 1988 and 1995 National Surveys of Adolescent Males, a national panel survey of male teens.
NSFG is currently the only source of ongoing data on the topics of sexual activity and contraceptive use for the total U.S. population of teenagers, paralleling the teen population whose pregnancy and birth rates are captured by birth certificates as part of the statistics of the National Center for Health Statistics. “Using data from the 2011-2015 NSFG and earlier NSFG surveys, this report provides an update of information on U.S. teenagers’ sexual activity and contraceptive use, thus helping to improve understanding of their risk of pregnancy,” said Dr. Abma and her associates. “This report … provides insights into the ways in which those determinants are changing with time, how they differ by sociodemographic groups, and what circumstances are most associated with them. The information can be used to monitor and understand trends in teen sexual behavior and contraception use.”
The 2011-2015 National Survey of Family Growth was conducted by the National Center for Health Statistics with the support and assistance of a number of other organizations and individuals. Interviewing and other tasks were carried out by the University of Michigan’s Survey Research Center and the Institute for Social Research under a contract with NCHS.
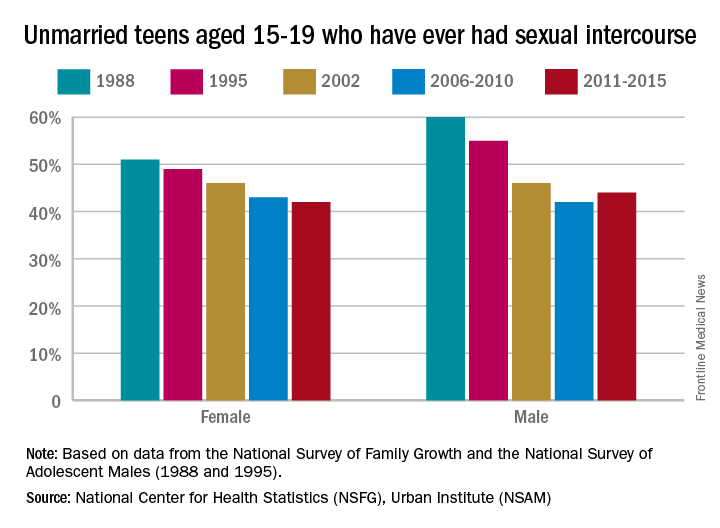
, according to a report by Joyce C. Abma, PhD, and Gladys M. Martinez, PhD, of the Division of Vital Statistics at the National Center for Health Statistics, Hyattsville, Md.
The percentage of female teens who had ever had sexual intercourse declined from 51% in 1988 to 42% in 2011-2015. For male teens, the percentage who were sexually experienced declined from 60% in 1988 to 44% in 2011-2015.
Male teens’ condom use during their first sexual experiences increased from 71% in 2002 to 77% in 2011-2015. This plateau in male contraception is in part the result of various types of contraception for women being developed and widely distributed in the course of these years, such as intrauterine devices.
The report features the most recent data from the National Survey of Family Growth (NSFG), resulting in 4 years of interviews spanning 2011 through 2015 and including 2,047 female teens and 2,087 male teens aged 15-19 years (National Health Statistics Reports; no 104. Hyattsville, MD: National Center for Health Statistics. 2017). Data also was abstracted from the 1988 and 1995 National Surveys of Adolescent Males, a national panel survey of male teens.
NSFG is currently the only source of ongoing data on the topics of sexual activity and contraceptive use for the total U.S. population of teenagers, paralleling the teen population whose pregnancy and birth rates are captured by birth certificates as part of the statistics of the National Center for Health Statistics. “Using data from the 2011-2015 NSFG and earlier NSFG surveys, this report provides an update of information on U.S. teenagers’ sexual activity and contraceptive use, thus helping to improve understanding of their risk of pregnancy,” said Dr. Abma and her associates. “This report … provides insights into the ways in which those determinants are changing with time, how they differ by sociodemographic groups, and what circumstances are most associated with them. The information can be used to monitor and understand trends in teen sexual behavior and contraception use.”
The 2011-2015 National Survey of Family Growth was conducted by the National Center for Health Statistics with the support and assistance of a number of other organizations and individuals. Interviewing and other tasks were carried out by the University of Michigan’s Survey Research Center and the Institute for Social Research under a contract with NCHS.
, according to a report by Joyce C. Abma, PhD, and Gladys M. Martinez, PhD, of the Division of Vital Statistics at the National Center for Health Statistics, Hyattsville, Md.
The percentage of female teens who had ever had sexual intercourse declined from 51% in 1988 to 42% in 2011-2015. For male teens, the percentage who were sexually experienced declined from 60% in 1988 to 44% in 2011-2015.
Male teens’ condom use during their first sexual experiences increased from 71% in 2002 to 77% in 2011-2015. This plateau in male contraception is in part the result of various types of contraception for women being developed and widely distributed in the course of these years, such as intrauterine devices.
The report features the most recent data from the National Survey of Family Growth (NSFG), resulting in 4 years of interviews spanning 2011 through 2015 and including 2,047 female teens and 2,087 male teens aged 15-19 years (National Health Statistics Reports; no 104. Hyattsville, MD: National Center for Health Statistics. 2017). Data also was abstracted from the 1988 and 1995 National Surveys of Adolescent Males, a national panel survey of male teens.
NSFG is currently the only source of ongoing data on the topics of sexual activity and contraceptive use for the total U.S. population of teenagers, paralleling the teen population whose pregnancy and birth rates are captured by birth certificates as part of the statistics of the National Center for Health Statistics. “Using data from the 2011-2015 NSFG and earlier NSFG surveys, this report provides an update of information on U.S. teenagers’ sexual activity and contraceptive use, thus helping to improve understanding of their risk of pregnancy,” said Dr. Abma and her associates. “This report … provides insights into the ways in which those determinants are changing with time, how they differ by sociodemographic groups, and what circumstances are most associated with them. The information can be used to monitor and understand trends in teen sexual behavior and contraception use.”
The 2011-2015 National Survey of Family Growth was conducted by the National Center for Health Statistics with the support and assistance of a number of other organizations and individuals. Interviewing and other tasks were carried out by the University of Michigan’s Survey Research Center and the Institute for Social Research under a contract with NCHS.
FROM NATIONAL HEALTH STATISTICS REPORTS
Key clinical point: Contraception use has gone up in the last decade
Major finding: Contraception use has increased to 99% in girls and 77% in boys in the last decade.
Data source: This report presents U.S. data on the sexual activity and contraceptive use of males and females aged 15-19 years, using data from the 2011-2015 and earlier National Surveys of Family Growth and the 1988 and 1995 National Surveys of Adolescent Males.
Disclosures: The 2011-2015 National Survey of Family Growth was conducted by the National Center for Health Statistics with the support and assistance of a number of other organizations and individuals. Interviewing and other tasks were carried out by the University of Michigan’s Survey Research Center and the Institute for Social Research under a contract with NCHS.