User login
Acute lobar nephronia often has misleading presentation
MADRID – Acute lobar nephronia needs to be considered in children with high fever, abdominal pain, and markedly elevated acute-phase reactants, even if their urinalysis and ultrasound results are negative, Paula Sanchez-Marcos, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.

She presented a retrospective study of 18 episodes of acute lobar nephronia (ALN) in 16 children seen at the hospital, a tertiary referral center. Six of the children had vesicoureteral reflux or another underlying uropathy. Mean age at diagnosis was 79 months, with a range of 5 to 180 months.
All patients had a fever greater than 38.5° C when they presented with a mean 6-day history of illness. Of the 16 children, 14 had abdominal pain. The mean C-reactive protein level was 197 mg/L, with a WBC count of 21,962 cells/mcL and a neutrophil count of 17,372 cells/mcL.
Urine dipstick was negative in five episodes. However, urine culture was eventually productive in 10 episodes, with Escherichia coli the most commonly isolated microorganism, found in five of these cases.
All patients underwent ultrasound imaging a mean of 1.7 days into their hospital admission, although it established the diagnosis of ALN in only two episodes. Additional imaging with CT had a 91% sensitivity, showing positive results in 10 of 11 cases, while MRI had 100% sensitivity.
Patients received IV antibiotics for a median of 14 days before switching to sequential oral antibiotics for a median of 8.7 days.
Three patients developed renal abscesses, with percutaneous drainage required in two instances. Unilateral renal scarring occurred in 7 of 16 patients.
Dr. Sanchez-Marcos recommended technetium-99m dimercaptosuccinic acid renal scintigraphy as a tool to confirm improvement in response to antimicrobial therapy.
She reported having no financial conflicts regarding her presentation.
MADRID – Acute lobar nephronia needs to be considered in children with high fever, abdominal pain, and markedly elevated acute-phase reactants, even if their urinalysis and ultrasound results are negative, Paula Sanchez-Marcos, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
She presented a retrospective study of 18 episodes of acute lobar nephronia (ALN) in 16 children seen at the hospital, a tertiary referral center. Six of the children had vesicoureteral reflux or another underlying uropathy. Mean age at diagnosis was 79 months, with a range of 5 to 180 months.
All patients had a fever greater than 38.5° C when they presented with a mean 6-day history of illness. Of the 16 children, 14 had abdominal pain. The mean C-reactive protein level was 197 mg/L, with a WBC count of 21,962 cells/mcL and a neutrophil count of 17,372 cells/mcL.
Urine dipstick was negative in five episodes. However, urine culture was eventually productive in 10 episodes, with Escherichia coli the most commonly isolated microorganism, found in five of these cases.
All patients underwent ultrasound imaging a mean of 1.7 days into their hospital admission, although it established the diagnosis of ALN in only two episodes. Additional imaging with CT had a 91% sensitivity, showing positive results in 10 of 11 cases, while MRI had 100% sensitivity.
Patients received IV antibiotics for a median of 14 days before switching to sequential oral antibiotics for a median of 8.7 days.
Three patients developed renal abscesses, with percutaneous drainage required in two instances. Unilateral renal scarring occurred in 7 of 16 patients.
Dr. Sanchez-Marcos recommended technetium-99m dimercaptosuccinic acid renal scintigraphy as a tool to confirm improvement in response to antimicrobial therapy.
She reported having no financial conflicts regarding her presentation.
MADRID – Acute lobar nephronia needs to be considered in children with high fever, abdominal pain, and markedly elevated acute-phase reactants, even if their urinalysis and ultrasound results are negative, Paula Sanchez-Marcos, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
She presented a retrospective study of 18 episodes of acute lobar nephronia (ALN) in 16 children seen at the hospital, a tertiary referral center. Six of the children had vesicoureteral reflux or another underlying uropathy. Mean age at diagnosis was 79 months, with a range of 5 to 180 months.
All patients had a fever greater than 38.5° C when they presented with a mean 6-day history of illness. Of the 16 children, 14 had abdominal pain. The mean C-reactive protein level was 197 mg/L, with a WBC count of 21,962 cells/mcL and a neutrophil count of 17,372 cells/mcL.
Urine dipstick was negative in five episodes. However, urine culture was eventually productive in 10 episodes, with Escherichia coli the most commonly isolated microorganism, found in five of these cases.
All patients underwent ultrasound imaging a mean of 1.7 days into their hospital admission, although it established the diagnosis of ALN in only two episodes. Additional imaging with CT had a 91% sensitivity, showing positive results in 10 of 11 cases, while MRI had 100% sensitivity.
Patients received IV antibiotics for a median of 14 days before switching to sequential oral antibiotics for a median of 8.7 days.
Three patients developed renal abscesses, with percutaneous drainage required in two instances. Unilateral renal scarring occurred in 7 of 16 patients.
Dr. Sanchez-Marcos recommended technetium-99m dimercaptosuccinic acid renal scintigraphy as a tool to confirm improvement in response to antimicrobial therapy.
She reported having no financial conflicts regarding her presentation.
AT ESPID 2017
Key clinical point:
Major finding: Urine dipstick results were negative in 5 instances, and ultrasound was negative in 16 cases.
Data source: This was a single-center, retrospective, descriptive study of 18 episodes of acute lobar nephronia in 16 children.
Disclosures: Dr. Sanchez-Marcos reported having no financial conflicts of interest.

Bullous Lesions in a Neonate
The Diagnosis: Incontinentia Pigmenti
The infant's mother was noted to have diffuse hypopigmented patches over the trunk, arms, and legs (present since adolescence) with whorled cicatricial alopecia of the vertex scalp and peg-shaped teeth (Figure). Together, these findings suggested incontinentia pigmenti (IP), which the mother revealed she had been diagnosed with in childhood. The infant's characteristic lesions in the setting of her mother's diagnosed genodermatosis confirmed the diagnosis of IP.
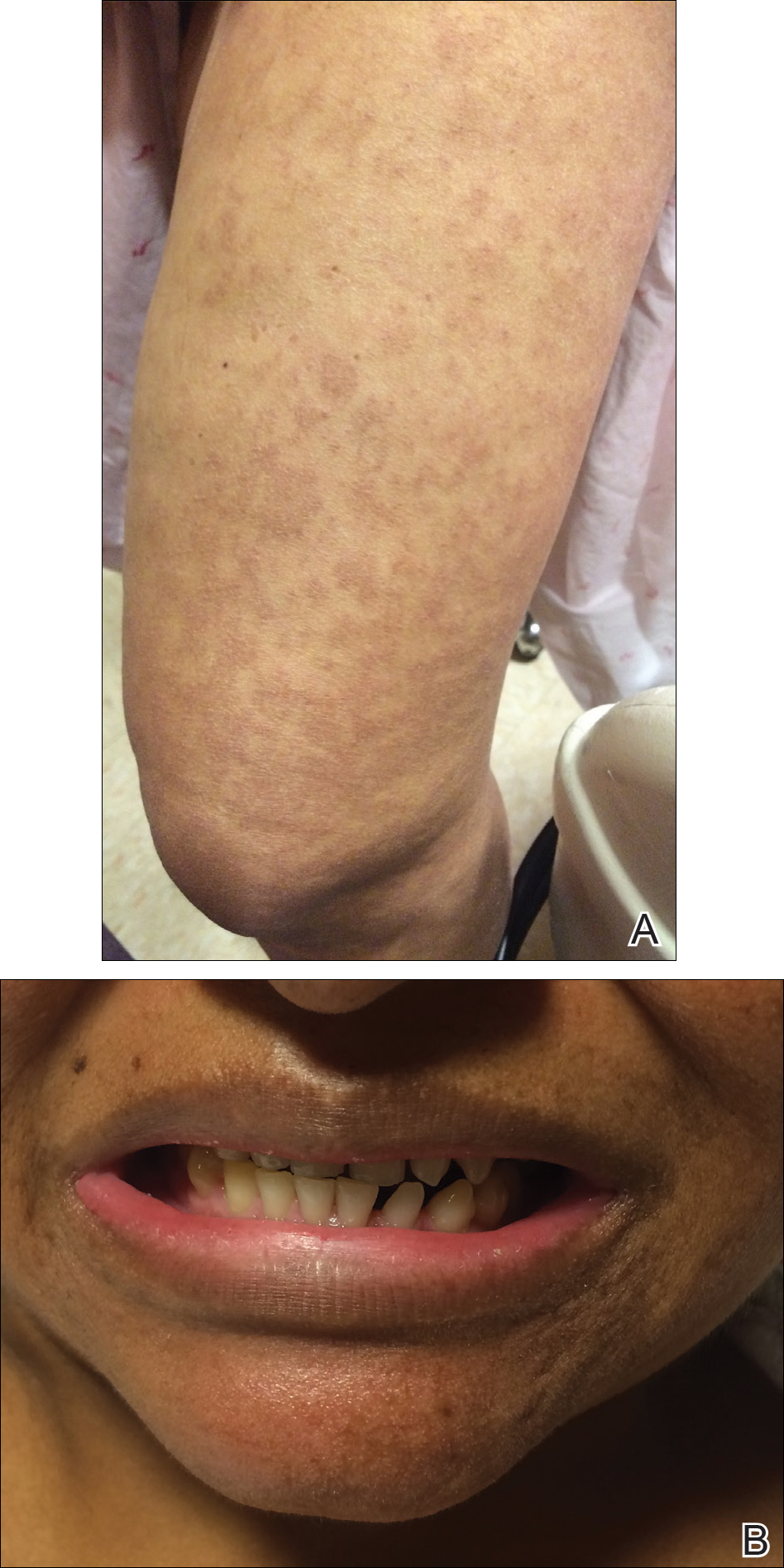
Incontinentia pigmenti is an X-linked dominant disorder that presents with many classic dermatologic, dental, neurologic, and ophthalmologic findings. The causative mutation occurs in IKBKG/NEMO (inhibitor of κ polypeptide gene enhancer in B-cells, kinase γ/nuclear factor-κB essential modulator) gene on Xq28, disabling the resultant protein that normally protects cells from tumor necrosis factor family-induced apoptosis.1 Incontinentia pigmenti usually is lethal in males and causes an unbalanced X-inactivation in surviving female IP patients. Occurring at a rate of 1.2 per 100,000 births,2 IP typically presents in female infants with skin lesions patterned along Blaschko lines that evolve in 4 stages over a lifetime.3 Stage I, presenting in the neonatal period, manifests as vesiculobullous eruptions on the limbs and scalp. Stages II to IV vary in duration from months to years and are comprised of a verrucous stage, a hyperpigmented stage, and a hypopigmented stage, respectively.3 All stages of IP can overlap and coexist.
The vesiculobullous findings in infants with IP may be mistakenly attributed to other diseases with prominent vesicular or bullous components including herpes simplex virus, epidermolysis bullosa, and infantile acropustulosis. With neonatal herpes simplex virus infection, vesicular skin or mucocutaneous lesions occur 9 to 11 days after birth and can be confirmed by specimen culture or qualitative polymerase chain reaction, while stage I of IP appears within the first 6 to 8 weeks of life and can be present at birth.4 The hallmark of epidermolysis bullosa, caused by mutations in keratins 5 and 14, is blistering erosions of the skin in response to frictional stress,1 thus these lesions do not follow Blaschko lines. Infantile acropustulosis, a nonheritable vesiculopustular eruption of the hands and feet, rarely occurs in the immediate newborn period; it most often appears in the 3- to 6-month age range with recurrent eruptions at 3- to 4-week intervals.5 Focal dermal hypoplasia is another X-linked dominant disorder with blaschkolinear findings at birth that presents with pink or red, angular, atrophic macules, in contrast to the bullous lesions of IP.6
Incontinentia pigmenti may encompass a wide range of systemic symptoms in addition to the classic dermatologic findings. Notably, central nervous system defects are concurrent in up to 40% of IP cases, with seizures, mental retardation, and spastic paresis being the most common sequelae.7 Teeth defects, seen in 35% of patients, include delayed primary dentition and peg-shaped teeth. Many patients will experience ophthalmologic defects including vision problems (16%) and retinopathy (15%).7
The cutaneous eruptions of IP may be treated with topical corticosteroids or topical tacrolimus, and vesicles should be left intact and monitored for signs of infection.8,9 Seizures, if present, should be treated with anticonvulsants, and regular neuropsychiatric monitoring and physical rehabilitation may be warranted. Patients should be regularly monitored for retinopathy beginning at the time of diagnosis. Retinal fibrovascular proliferation is treated with xenon laser photocoagulation to reduce the high risk for retinal detachment in this population.10,11 Older and younger at-risk relatives must be evaluated by genetic testing or thorough physical examination to clarify their disease status and determine the need for additional genetic counseling.
- Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. China: Elsevier Saunders; 2012.
- Prevalence and incidence of rare diseases: bibliographic data. Orphanet Report Series, Rare Diseases collection. http://www.orpha.net/orphacom/cahiers/docs/GB/Prevalence_of_rare_diseases_by_alphabetical_list.pdf. Published June 2017. Accessed July 13, 2017.
- Scheuerle AE, Ursini MV. Incontinentia pigmenti. In: Pagon RA, Adam MP, Ardinger HH, et al, eds. GeneReviews. Seattle, WA: University of Washington; 2015. http://www.ncbi.nlm.nih.gov/books/NBK1472/. Accessed July 25, 2017.
- James SH, Kimberlin DW. Neonatal herpes simplex virus infection. Infect Dis Clin North Am. 2015;29:391-400.
- Eichenfield LF, Frieden IJ, Mathes E, et al, eds. Neonatal and Infant Dermatology. Philadelphia, PA: Saunders; 2015.
- Temple IK, MacDowall P, Baraitser M, et al. Focal dermal hypoplasia (Goltz syndrome). J Med Genet. 1990;27:180-187.
- Fusco F, Paciolla M, Conte MI, et al. Incontinentia pigmenti: report on data from 2000 to 2013. Orphanet J Rare Dis. 2014;9:93.
- Jessup CJ, Morgan SC, Cohen LM, et al. Incontinentia pigmenti: treatment of IP with topical tacrolimus. J Drugs Dermatol. 2009;8:944-946.
- Kaya TI, Tursen U, Ikizoglu G. Therapeutic use of topical corticosteroids in the vesiculobullous lesions of incontinentia pigmenti [published online June 1, 2009]. Clin Exp Dermatol. 2009;34:E611-E613.
- Nguyen JK, Brady-Mccreery KM. Laser photocoagulation in preproliferative retinopathy of incontinentia pigmenti. J AAPOS. 2001;5:258-259.
- Chen CJ, Han IC, Tian J, et al. Extended follow-up of treated and untreated retinopathy in incontinentia pigmenti: analysis of peripheral vascular changes and incidence of retinal detachment. JAMA Ophthalmol. 2015;133:542-548.
The Diagnosis: Incontinentia Pigmenti
The infant's mother was noted to have diffuse hypopigmented patches over the trunk, arms, and legs (present since adolescence) with whorled cicatricial alopecia of the vertex scalp and peg-shaped teeth (Figure). Together, these findings suggested incontinentia pigmenti (IP), which the mother revealed she had been diagnosed with in childhood. The infant's characteristic lesions in the setting of her mother's diagnosed genodermatosis confirmed the diagnosis of IP.
Incontinentia pigmenti is an X-linked dominant disorder that presents with many classic dermatologic, dental, neurologic, and ophthalmologic findings. The causative mutation occurs in IKBKG/NEMO (inhibitor of κ polypeptide gene enhancer in B-cells, kinase γ/nuclear factor-κB essential modulator) gene on Xq28, disabling the resultant protein that normally protects cells from tumor necrosis factor family-induced apoptosis.1 Incontinentia pigmenti usually is lethal in males and causes an unbalanced X-inactivation in surviving female IP patients. Occurring at a rate of 1.2 per 100,000 births,2 IP typically presents in female infants with skin lesions patterned along Blaschko lines that evolve in 4 stages over a lifetime.3 Stage I, presenting in the neonatal period, manifests as vesiculobullous eruptions on the limbs and scalp. Stages II to IV vary in duration from months to years and are comprised of a verrucous stage, a hyperpigmented stage, and a hypopigmented stage, respectively.3 All stages of IP can overlap and coexist.
The vesiculobullous findings in infants with IP may be mistakenly attributed to other diseases with prominent vesicular or bullous components including herpes simplex virus, epidermolysis bullosa, and infantile acropustulosis. With neonatal herpes simplex virus infection, vesicular skin or mucocutaneous lesions occur 9 to 11 days after birth and can be confirmed by specimen culture or qualitative polymerase chain reaction, while stage I of IP appears within the first 6 to 8 weeks of life and can be present at birth.4 The hallmark of epidermolysis bullosa, caused by mutations in keratins 5 and 14, is blistering erosions of the skin in response to frictional stress,1 thus these lesions do not follow Blaschko lines. Infantile acropustulosis, a nonheritable vesiculopustular eruption of the hands and feet, rarely occurs in the immediate newborn period; it most often appears in the 3- to 6-month age range with recurrent eruptions at 3- to 4-week intervals.5 Focal dermal hypoplasia is another X-linked dominant disorder with blaschkolinear findings at birth that presents with pink or red, angular, atrophic macules, in contrast to the bullous lesions of IP.6
Incontinentia pigmenti may encompass a wide range of systemic symptoms in addition to the classic dermatologic findings. Notably, central nervous system defects are concurrent in up to 40% of IP cases, with seizures, mental retardation, and spastic paresis being the most common sequelae.7 Teeth defects, seen in 35% of patients, include delayed primary dentition and peg-shaped teeth. Many patients will experience ophthalmologic defects including vision problems (16%) and retinopathy (15%).7
The cutaneous eruptions of IP may be treated with topical corticosteroids or topical tacrolimus, and vesicles should be left intact and monitored for signs of infection.8,9 Seizures, if present, should be treated with anticonvulsants, and regular neuropsychiatric monitoring and physical rehabilitation may be warranted. Patients should be regularly monitored for retinopathy beginning at the time of diagnosis. Retinal fibrovascular proliferation is treated with xenon laser photocoagulation to reduce the high risk for retinal detachment in this population.10,11 Older and younger at-risk relatives must be evaluated by genetic testing or thorough physical examination to clarify their disease status and determine the need for additional genetic counseling.
The Diagnosis: Incontinentia Pigmenti
The infant's mother was noted to have diffuse hypopigmented patches over the trunk, arms, and legs (present since adolescence) with whorled cicatricial alopecia of the vertex scalp and peg-shaped teeth (Figure). Together, these findings suggested incontinentia pigmenti (IP), which the mother revealed she had been diagnosed with in childhood. The infant's characteristic lesions in the setting of her mother's diagnosed genodermatosis confirmed the diagnosis of IP.
Incontinentia pigmenti is an X-linked dominant disorder that presents with many classic dermatologic, dental, neurologic, and ophthalmologic findings. The causative mutation occurs in IKBKG/NEMO (inhibitor of κ polypeptide gene enhancer in B-cells, kinase γ/nuclear factor-κB essential modulator) gene on Xq28, disabling the resultant protein that normally protects cells from tumor necrosis factor family-induced apoptosis.1 Incontinentia pigmenti usually is lethal in males and causes an unbalanced X-inactivation in surviving female IP patients. Occurring at a rate of 1.2 per 100,000 births,2 IP typically presents in female infants with skin lesions patterned along Blaschko lines that evolve in 4 stages over a lifetime.3 Stage I, presenting in the neonatal period, manifests as vesiculobullous eruptions on the limbs and scalp. Stages II to IV vary in duration from months to years and are comprised of a verrucous stage, a hyperpigmented stage, and a hypopigmented stage, respectively.3 All stages of IP can overlap and coexist.
The vesiculobullous findings in infants with IP may be mistakenly attributed to other diseases with prominent vesicular or bullous components including herpes simplex virus, epidermolysis bullosa, and infantile acropustulosis. With neonatal herpes simplex virus infection, vesicular skin or mucocutaneous lesions occur 9 to 11 days after birth and can be confirmed by specimen culture or qualitative polymerase chain reaction, while stage I of IP appears within the first 6 to 8 weeks of life and can be present at birth.4 The hallmark of epidermolysis bullosa, caused by mutations in keratins 5 and 14, is blistering erosions of the skin in response to frictional stress,1 thus these lesions do not follow Blaschko lines. Infantile acropustulosis, a nonheritable vesiculopustular eruption of the hands and feet, rarely occurs in the immediate newborn period; it most often appears in the 3- to 6-month age range with recurrent eruptions at 3- to 4-week intervals.5 Focal dermal hypoplasia is another X-linked dominant disorder with blaschkolinear findings at birth that presents with pink or red, angular, atrophic macules, in contrast to the bullous lesions of IP.6
Incontinentia pigmenti may encompass a wide range of systemic symptoms in addition to the classic dermatologic findings. Notably, central nervous system defects are concurrent in up to 40% of IP cases, with seizures, mental retardation, and spastic paresis being the most common sequelae.7 Teeth defects, seen in 35% of patients, include delayed primary dentition and peg-shaped teeth. Many patients will experience ophthalmologic defects including vision problems (16%) and retinopathy (15%).7
The cutaneous eruptions of IP may be treated with topical corticosteroids or topical tacrolimus, and vesicles should be left intact and monitored for signs of infection.8,9 Seizures, if present, should be treated with anticonvulsants, and regular neuropsychiatric monitoring and physical rehabilitation may be warranted. Patients should be regularly monitored for retinopathy beginning at the time of diagnosis. Retinal fibrovascular proliferation is treated with xenon laser photocoagulation to reduce the high risk for retinal detachment in this population.10,11 Older and younger at-risk relatives must be evaluated by genetic testing or thorough physical examination to clarify their disease status and determine the need for additional genetic counseling.
- Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. China: Elsevier Saunders; 2012.
- Prevalence and incidence of rare diseases: bibliographic data. Orphanet Report Series, Rare Diseases collection. http://www.orpha.net/orphacom/cahiers/docs/GB/Prevalence_of_rare_diseases_by_alphabetical_list.pdf. Published June 2017. Accessed July 13, 2017.
- Scheuerle AE, Ursini MV. Incontinentia pigmenti. In: Pagon RA, Adam MP, Ardinger HH, et al, eds. GeneReviews. Seattle, WA: University of Washington; 2015. http://www.ncbi.nlm.nih.gov/books/NBK1472/. Accessed July 25, 2017.
- James SH, Kimberlin DW. Neonatal herpes simplex virus infection. Infect Dis Clin North Am. 2015;29:391-400.
- Eichenfield LF, Frieden IJ, Mathes E, et al, eds. Neonatal and Infant Dermatology. Philadelphia, PA: Saunders; 2015.
- Temple IK, MacDowall P, Baraitser M, et al. Focal dermal hypoplasia (Goltz syndrome). J Med Genet. 1990;27:180-187.
- Fusco F, Paciolla M, Conte MI, et al. Incontinentia pigmenti: report on data from 2000 to 2013. Orphanet J Rare Dis. 2014;9:93.
- Jessup CJ, Morgan SC, Cohen LM, et al. Incontinentia pigmenti: treatment of IP with topical tacrolimus. J Drugs Dermatol. 2009;8:944-946.
- Kaya TI, Tursen U, Ikizoglu G. Therapeutic use of topical corticosteroids in the vesiculobullous lesions of incontinentia pigmenti [published online June 1, 2009]. Clin Exp Dermatol. 2009;34:E611-E613.
- Nguyen JK, Brady-Mccreery KM. Laser photocoagulation in preproliferative retinopathy of incontinentia pigmenti. J AAPOS. 2001;5:258-259.
- Chen CJ, Han IC, Tian J, et al. Extended follow-up of treated and untreated retinopathy in incontinentia pigmenti: analysis of peripheral vascular changes and incidence of retinal detachment. JAMA Ophthalmol. 2015;133:542-548.
- Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. China: Elsevier Saunders; 2012.
- Prevalence and incidence of rare diseases: bibliographic data. Orphanet Report Series, Rare Diseases collection. http://www.orpha.net/orphacom/cahiers/docs/GB/Prevalence_of_rare_diseases_by_alphabetical_list.pdf. Published June 2017. Accessed July 13, 2017.
- Scheuerle AE, Ursini MV. Incontinentia pigmenti. In: Pagon RA, Adam MP, Ardinger HH, et al, eds. GeneReviews. Seattle, WA: University of Washington; 2015. http://www.ncbi.nlm.nih.gov/books/NBK1472/. Accessed July 25, 2017.
- James SH, Kimberlin DW. Neonatal herpes simplex virus infection. Infect Dis Clin North Am. 2015;29:391-400.
- Eichenfield LF, Frieden IJ, Mathes E, et al, eds. Neonatal and Infant Dermatology. Philadelphia, PA: Saunders; 2015.
- Temple IK, MacDowall P, Baraitser M, et al. Focal dermal hypoplasia (Goltz syndrome). J Med Genet. 1990;27:180-187.
- Fusco F, Paciolla M, Conte MI, et al. Incontinentia pigmenti: report on data from 2000 to 2013. Orphanet J Rare Dis. 2014;9:93.
- Jessup CJ, Morgan SC, Cohen LM, et al. Incontinentia pigmenti: treatment of IP with topical tacrolimus. J Drugs Dermatol. 2009;8:944-946.
- Kaya TI, Tursen U, Ikizoglu G. Therapeutic use of topical corticosteroids in the vesiculobullous lesions of incontinentia pigmenti [published online June 1, 2009]. Clin Exp Dermatol. 2009;34:E611-E613.
- Nguyen JK, Brady-Mccreery KM. Laser photocoagulation in preproliferative retinopathy of incontinentia pigmenti. J AAPOS. 2001;5:258-259.
- Chen CJ, Han IC, Tian J, et al. Extended follow-up of treated and untreated retinopathy in incontinentia pigmenti: analysis of peripheral vascular changes and incidence of retinal detachment. JAMA Ophthalmol. 2015;133:542-548.

A 1-day-old Hispanic female infant was born via uncomplicated vaginal delivery at 41 weeks' gestation after a normal pregnancy. Linear plaques containing multiple ruptured vesicles and bullae following Blaschko lines were noted on the right medial thigh and anterior arm. The infant was afebrile and generally well-appearing.

Pediatric Pearls From the AAD Annual Meeting
This article exhibits key pediatric dermatology pearls garnered at the 2017 Annual Meeting of the American Academy of Dermatology (AAD) in Orlando, Florida (March 3–7, 2017). Highlights from both the Society for Pediatric Dermatology pre-AAD meeting (March 2, 2017) and the AAD general meeting sessions are included. This discussion is intended to help maximize care of our pediatric patients in dermatology and present high-yield take-home points from the AAD that can be readily transferred to our patient care.
“New Tools for Your Therapeutic Toolbox” by Erin Mathes, MD (University of California, San Francisco)
During this lecture at the Society for Pediatric Dermatology meeting, Dr. Mathes discussed a randomized controlled trial that took place in 2014 in both the United States and the United Kingdom to assess skin barrier enhancement to reduce the incidence of atopic dermatitis (AD) in 124 high-risk infants.1 The high-risk infants had either a parent or sibling with physician-diagnosed AD, asthma, or rhinitis, or a first-degree relative with an aforementioned condition. Full-body emollient therapy was applied at least once daily within 3 weeks of birth for 6 months, while the control arm did not use emollient. Parents were allowed to choose from the following emollients: sunflower seed oil, moisturizing cream, or ointment. The primary outcome was the incidence of AD at 6 months. The authors found a 43% incidence of AD in the control group compared to 22% in the emollient group, amounting to a relative risk reduction of approximately 50%.1
Emollients in AD are hypothesized to help through the enhanced barrier function and decreased penetration of irritant substances and allergens. This study is vital given the ease of use of emollients and the foreseeable substantial impact on reduced health care costs associated with the decreased incidence of AD.
Take-Home Point
Full-body emollient therapy within 3 weeks of birth may reduce the incidence of AD in high-risk infants.
Dr. Mathes also discussed the novel topical phosphodiesterase 4 inhibitor crisaborole and its emerging role in AD. She reviewed the results of a large phase 3 trial of crisaborole therapy for patients aged 2 years or older with mild to moderate AD.2 Crisaborole ointment was applied twice daily for 28 days. The primary outcome measured was an investigator static global assessment score of clear or almost clear, which is a score for AD based on the degree of erythema, presence of oozing and crusting, and presence of induration or papulation. Overall, 32.8% of patients treated with crisaborole achieved success compared to 25.4% of vehicle-treated patients. The control patients were still given a vehicle to apply, which can function as therapy to help repair the barrier of AD and thus theoretically reduced the percentage gap between patients who met success with and without crisaborole therapy. Furthermore, only 4% of patients reported adverse effects such as burning and stinging with application of crisaborole in contrast to topical calcineurin inhibitors, which can elicit symptoms up to 50% of the time.2 In summary, this lecture reviewed the first new topical treatment for AD in 15 years.
Take-Home Point
Crisaborole ointment is a novel topical phosphodiesterase 4 inhibitor approved for mild to moderate AD in patients 2 years of age and older.
“The Truth About Pediatric Contact Dermatitis” by Sharon Jacob, MD (Loma Linda University, California)
In this session, Dr. Jacob discussed how she approaches pediatric patients with suspected contact dermatitis and elaborated on the common allergens unique to this patient population. Furthermore, she explained the substantial role of nickel in pediatric contact dermatitis, citing a study performed in Denmark and the United States, which tested 212 toys for nickel using the dimethylglyoxime test and found that 34.4% of toys did in fact release nickel.3 Additional studies have shown that nickel released from children’s toys is deposited on the skin, even with short contact times such as 30 minutes on one or more occasions within 2 weeks.3,4 She is currently evaluating the presence of nickel in locales frequented by children such as schools, libraries, and supermarkets. Interestingly, she anecdotally found that a pediatric eczematous eruption in a spiralized distribution of the legs can be attributed to the presence of nickel in school chairs, and the morphology is secondary to children wrapping their legs around the chairs. In conclusion, she reiterated that nickel continues to be the top allergen among pediatric patients, and states that additional allergens for patch testing in this population are unique to their adult counterparts.
Take-Home Point
Nickel is an ubiquitous allergen for pediatric contact dermatitis; additionally, the list of allergens for patch testing should be tailored to this patient population.
“When to Image, When to Sedate” by Annette Wagner, MD (Northwestern Medicine, Chicago, Illinois)
This lecture was a 3-part discussion on the safety of general anesthesia in children, when to image children, and when sedation may be worth the risk. Dr. Wagner shared her pearls for when children younger than 3 years may benefit from dermatologic procedures that involve general anesthesia. Large congenital lesions of the scalp or face that require tissue expansion or multiple stages may be best performed at a younger age due to the flexibility of the infant scalp, providing the best outcome. Additional considerations include a questionable malignant diagnosis in which a punch biopsy is not enough, rapidly growing facial lesions, Spitz nevi of the face, congenital lesions with no available therapy, and nonhealing refractory lesions causing severe pain. The general rule proposed was intervention for single procedures lasting less than 1 hour that otherwise would result in a worse outcome if postponed. Finally, she concluded to always advocate for your patient, to wait if the outcome will be the same regardless of timing, and to be frank about not knowing the risks of general anesthesia in this population. The resource, SmartTots (http://smarttots.org) provides current consensus statements and ongoing research on the use and safety of general anesthesia in children.
Take-Home Point
General sedation may be considered for short pediatric procedures that will result in a worse outcome if postponed.
“Highlights From the Pediatric Literature” by Katherine Marks, DO (Geisinger, Danville and Wilkes-Barre, Pennsylvania)
Dr. Marks discussed numerous emerging pediatric dermatology articles. One article looked at 40 infants with proliferating infantile hemangiomas (IHs) who had timolol gel 0.5% applied twice daily.5 The primary outcomes were the urinary excretion and serum levels of timolol as well as the clinical response to therapy measured by a visual analog scale at monthly visits. A urinalysis collected 3 to 4 hours after timolol application was found to be positive in 83% (20/24) of the tested patients; the first 3 positive infants were then sent to have their serum timolol levels drawn and also were found to be positive, though substantially small levels (median, 0.16 ng/mL). The 3 patients tested had small IHs on the face with no ulceration. None of these patients experienced adverse effects and all of the IHs significantly (P<.001) improved with therapy. The authors stated that even though the absorption was minimal, it is wise to be cognizant about the use of timolol in certain patient demographics such as preterm or young infants with large ulcerating IHs.5
Take-Home Point
Systemic absorption with topical timolol occurs, albeit substantially small; be judicious about giving this medication in select patient populations with ulcerated hemangiomas.
Acknowledgment
The author thanks the presenters for their review and contributions to this article.
- Simpson EL, Chalmers JR, Hanifin JM, et al. Emollient enhancement of the skin barrier from birth offers effective atopic dermatitis prevention. J Allergy Clin Immunol. 2014;134:818-823.
- Paller AS, Tom WL, Lebwohl MG, et al. Efficacy and safety of crisaborole ointment, a novel phosphodiesterase 4 inhibitor for the topical treatment of AD in children and adults [published online July 11, 2016]. J Am Acad Dermatol. 2016;75:494-503.
- Jensen P, Hamann D, Hamann CR, et al. Nickel and cobalt release from children’s toys purchased in Denmark and the United States. Dermatitis. 2014;25:356-365.
- Overgaard LE, Engebretsen KA, Jensen P, et al. Nickel released from children’s toys is deposited on the skin. Contact Dermatitis. 2016;74:380-381.
- Weibel L, Barysch MJ, Scheer HS, et al. Topical timolol for infantile hemangiomas: evidence for efficacy and degree of systemic absorption [published online February 3, 2016]. Pediatr Dermatol. 2016;33:184-190.
This article exhibits key pediatric dermatology pearls garnered at the 2017 Annual Meeting of the American Academy of Dermatology (AAD) in Orlando, Florida (March 3–7, 2017). Highlights from both the Society for Pediatric Dermatology pre-AAD meeting (March 2, 2017) and the AAD general meeting sessions are included. This discussion is intended to help maximize care of our pediatric patients in dermatology and present high-yield take-home points from the AAD that can be readily transferred to our patient care.
“New Tools for Your Therapeutic Toolbox” by Erin Mathes, MD (University of California, San Francisco)
During this lecture at the Society for Pediatric Dermatology meeting, Dr. Mathes discussed a randomized controlled trial that took place in 2014 in both the United States and the United Kingdom to assess skin barrier enhancement to reduce the incidence of atopic dermatitis (AD) in 124 high-risk infants.1 The high-risk infants had either a parent or sibling with physician-diagnosed AD, asthma, or rhinitis, or a first-degree relative with an aforementioned condition. Full-body emollient therapy was applied at least once daily within 3 weeks of birth for 6 months, while the control arm did not use emollient. Parents were allowed to choose from the following emollients: sunflower seed oil, moisturizing cream, or ointment. The primary outcome was the incidence of AD at 6 months. The authors found a 43% incidence of AD in the control group compared to 22% in the emollient group, amounting to a relative risk reduction of approximately 50%.1
Emollients in AD are hypothesized to help through the enhanced barrier function and decreased penetration of irritant substances and allergens. This study is vital given the ease of use of emollients and the foreseeable substantial impact on reduced health care costs associated with the decreased incidence of AD.
Take-Home Point
Full-body emollient therapy within 3 weeks of birth may reduce the incidence of AD in high-risk infants.
Dr. Mathes also discussed the novel topical phosphodiesterase 4 inhibitor crisaborole and its emerging role in AD. She reviewed the results of a large phase 3 trial of crisaborole therapy for patients aged 2 years or older with mild to moderate AD.2 Crisaborole ointment was applied twice daily for 28 days. The primary outcome measured was an investigator static global assessment score of clear or almost clear, which is a score for AD based on the degree of erythema, presence of oozing and crusting, and presence of induration or papulation. Overall, 32.8% of patients treated with crisaborole achieved success compared to 25.4% of vehicle-treated patients. The control patients were still given a vehicle to apply, which can function as therapy to help repair the barrier of AD and thus theoretically reduced the percentage gap between patients who met success with and without crisaborole therapy. Furthermore, only 4% of patients reported adverse effects such as burning and stinging with application of crisaborole in contrast to topical calcineurin inhibitors, which can elicit symptoms up to 50% of the time.2 In summary, this lecture reviewed the first new topical treatment for AD in 15 years.
Take-Home Point
Crisaborole ointment is a novel topical phosphodiesterase 4 inhibitor approved for mild to moderate AD in patients 2 years of age and older.
“The Truth About Pediatric Contact Dermatitis” by Sharon Jacob, MD (Loma Linda University, California)
In this session, Dr. Jacob discussed how she approaches pediatric patients with suspected contact dermatitis and elaborated on the common allergens unique to this patient population. Furthermore, she explained the substantial role of nickel in pediatric contact dermatitis, citing a study performed in Denmark and the United States, which tested 212 toys for nickel using the dimethylglyoxime test and found that 34.4% of toys did in fact release nickel.3 Additional studies have shown that nickel released from children’s toys is deposited on the skin, even with short contact times such as 30 minutes on one or more occasions within 2 weeks.3,4 She is currently evaluating the presence of nickel in locales frequented by children such as schools, libraries, and supermarkets. Interestingly, she anecdotally found that a pediatric eczematous eruption in a spiralized distribution of the legs can be attributed to the presence of nickel in school chairs, and the morphology is secondary to children wrapping their legs around the chairs. In conclusion, she reiterated that nickel continues to be the top allergen among pediatric patients, and states that additional allergens for patch testing in this population are unique to their adult counterparts.
Take-Home Point
Nickel is an ubiquitous allergen for pediatric contact dermatitis; additionally, the list of allergens for patch testing should be tailored to this patient population.
“When to Image, When to Sedate” by Annette Wagner, MD (Northwestern Medicine, Chicago, Illinois)
This lecture was a 3-part discussion on the safety of general anesthesia in children, when to image children, and when sedation may be worth the risk. Dr. Wagner shared her pearls for when children younger than 3 years may benefit from dermatologic procedures that involve general anesthesia. Large congenital lesions of the scalp or face that require tissue expansion or multiple stages may be best performed at a younger age due to the flexibility of the infant scalp, providing the best outcome. Additional considerations include a questionable malignant diagnosis in which a punch biopsy is not enough, rapidly growing facial lesions, Spitz nevi of the face, congenital lesions with no available therapy, and nonhealing refractory lesions causing severe pain. The general rule proposed was intervention for single procedures lasting less than 1 hour that otherwise would result in a worse outcome if postponed. Finally, she concluded to always advocate for your patient, to wait if the outcome will be the same regardless of timing, and to be frank about not knowing the risks of general anesthesia in this population. The resource, SmartTots (http://smarttots.org) provides current consensus statements and ongoing research on the use and safety of general anesthesia in children.
Take-Home Point
General sedation may be considered for short pediatric procedures that will result in a worse outcome if postponed.
“Highlights From the Pediatric Literature” by Katherine Marks, DO (Geisinger, Danville and Wilkes-Barre, Pennsylvania)
Dr. Marks discussed numerous emerging pediatric dermatology articles. One article looked at 40 infants with proliferating infantile hemangiomas (IHs) who had timolol gel 0.5% applied twice daily.5 The primary outcomes were the urinary excretion and serum levels of timolol as well as the clinical response to therapy measured by a visual analog scale at monthly visits. A urinalysis collected 3 to 4 hours after timolol application was found to be positive in 83% (20/24) of the tested patients; the first 3 positive infants were then sent to have their serum timolol levels drawn and also were found to be positive, though substantially small levels (median, 0.16 ng/mL). The 3 patients tested had small IHs on the face with no ulceration. None of these patients experienced adverse effects and all of the IHs significantly (P<.001) improved with therapy. The authors stated that even though the absorption was minimal, it is wise to be cognizant about the use of timolol in certain patient demographics such as preterm or young infants with large ulcerating IHs.5
Take-Home Point
Systemic absorption with topical timolol occurs, albeit substantially small; be judicious about giving this medication in select patient populations with ulcerated hemangiomas.
Acknowledgment
The author thanks the presenters for their review and contributions to this article.
This article exhibits key pediatric dermatology pearls garnered at the 2017 Annual Meeting of the American Academy of Dermatology (AAD) in Orlando, Florida (March 3–7, 2017). Highlights from both the Society for Pediatric Dermatology pre-AAD meeting (March 2, 2017) and the AAD general meeting sessions are included. This discussion is intended to help maximize care of our pediatric patients in dermatology and present high-yield take-home points from the AAD that can be readily transferred to our patient care.
“New Tools for Your Therapeutic Toolbox” by Erin Mathes, MD (University of California, San Francisco)
During this lecture at the Society for Pediatric Dermatology meeting, Dr. Mathes discussed a randomized controlled trial that took place in 2014 in both the United States and the United Kingdom to assess skin barrier enhancement to reduce the incidence of atopic dermatitis (AD) in 124 high-risk infants.1 The high-risk infants had either a parent or sibling with physician-diagnosed AD, asthma, or rhinitis, or a first-degree relative with an aforementioned condition. Full-body emollient therapy was applied at least once daily within 3 weeks of birth for 6 months, while the control arm did not use emollient. Parents were allowed to choose from the following emollients: sunflower seed oil, moisturizing cream, or ointment. The primary outcome was the incidence of AD at 6 months. The authors found a 43% incidence of AD in the control group compared to 22% in the emollient group, amounting to a relative risk reduction of approximately 50%.1
Emollients in AD are hypothesized to help through the enhanced barrier function and decreased penetration of irritant substances and allergens. This study is vital given the ease of use of emollients and the foreseeable substantial impact on reduced health care costs associated with the decreased incidence of AD.
Take-Home Point
Full-body emollient therapy within 3 weeks of birth may reduce the incidence of AD in high-risk infants.
Dr. Mathes also discussed the novel topical phosphodiesterase 4 inhibitor crisaborole and its emerging role in AD. She reviewed the results of a large phase 3 trial of crisaborole therapy for patients aged 2 years or older with mild to moderate AD.2 Crisaborole ointment was applied twice daily for 28 days. The primary outcome measured was an investigator static global assessment score of clear or almost clear, which is a score for AD based on the degree of erythema, presence of oozing and crusting, and presence of induration or papulation. Overall, 32.8% of patients treated with crisaborole achieved success compared to 25.4% of vehicle-treated patients. The control patients were still given a vehicle to apply, which can function as therapy to help repair the barrier of AD and thus theoretically reduced the percentage gap between patients who met success with and without crisaborole therapy. Furthermore, only 4% of patients reported adverse effects such as burning and stinging with application of crisaborole in contrast to topical calcineurin inhibitors, which can elicit symptoms up to 50% of the time.2 In summary, this lecture reviewed the first new topical treatment for AD in 15 years.
Take-Home Point
Crisaborole ointment is a novel topical phosphodiesterase 4 inhibitor approved for mild to moderate AD in patients 2 years of age and older.
“The Truth About Pediatric Contact Dermatitis” by Sharon Jacob, MD (Loma Linda University, California)
In this session, Dr. Jacob discussed how she approaches pediatric patients with suspected contact dermatitis and elaborated on the common allergens unique to this patient population. Furthermore, she explained the substantial role of nickel in pediatric contact dermatitis, citing a study performed in Denmark and the United States, which tested 212 toys for nickel using the dimethylglyoxime test and found that 34.4% of toys did in fact release nickel.3 Additional studies have shown that nickel released from children’s toys is deposited on the skin, even with short contact times such as 30 minutes on one or more occasions within 2 weeks.3,4 She is currently evaluating the presence of nickel in locales frequented by children such as schools, libraries, and supermarkets. Interestingly, she anecdotally found that a pediatric eczematous eruption in a spiralized distribution of the legs can be attributed to the presence of nickel in school chairs, and the morphology is secondary to children wrapping their legs around the chairs. In conclusion, she reiterated that nickel continues to be the top allergen among pediatric patients, and states that additional allergens for patch testing in this population are unique to their adult counterparts.
Take-Home Point
Nickel is an ubiquitous allergen for pediatric contact dermatitis; additionally, the list of allergens for patch testing should be tailored to this patient population.
“When to Image, When to Sedate” by Annette Wagner, MD (Northwestern Medicine, Chicago, Illinois)
This lecture was a 3-part discussion on the safety of general anesthesia in children, when to image children, and when sedation may be worth the risk. Dr. Wagner shared her pearls for when children younger than 3 years may benefit from dermatologic procedures that involve general anesthesia. Large congenital lesions of the scalp or face that require tissue expansion or multiple stages may be best performed at a younger age due to the flexibility of the infant scalp, providing the best outcome. Additional considerations include a questionable malignant diagnosis in which a punch biopsy is not enough, rapidly growing facial lesions, Spitz nevi of the face, congenital lesions with no available therapy, and nonhealing refractory lesions causing severe pain. The general rule proposed was intervention for single procedures lasting less than 1 hour that otherwise would result in a worse outcome if postponed. Finally, she concluded to always advocate for your patient, to wait if the outcome will be the same regardless of timing, and to be frank about not knowing the risks of general anesthesia in this population. The resource, SmartTots (http://smarttots.org) provides current consensus statements and ongoing research on the use and safety of general anesthesia in children.
Take-Home Point
General sedation may be considered for short pediatric procedures that will result in a worse outcome if postponed.
“Highlights From the Pediatric Literature” by Katherine Marks, DO (Geisinger, Danville and Wilkes-Barre, Pennsylvania)
Dr. Marks discussed numerous emerging pediatric dermatology articles. One article looked at 40 infants with proliferating infantile hemangiomas (IHs) who had timolol gel 0.5% applied twice daily.5 The primary outcomes were the urinary excretion and serum levels of timolol as well as the clinical response to therapy measured by a visual analog scale at monthly visits. A urinalysis collected 3 to 4 hours after timolol application was found to be positive in 83% (20/24) of the tested patients; the first 3 positive infants were then sent to have their serum timolol levels drawn and also were found to be positive, though substantially small levels (median, 0.16 ng/mL). The 3 patients tested had small IHs on the face with no ulceration. None of these patients experienced adverse effects and all of the IHs significantly (P<.001) improved with therapy. The authors stated that even though the absorption was minimal, it is wise to be cognizant about the use of timolol in certain patient demographics such as preterm or young infants with large ulcerating IHs.5
Take-Home Point
Systemic absorption with topical timolol occurs, albeit substantially small; be judicious about giving this medication in select patient populations with ulcerated hemangiomas.
Acknowledgment
The author thanks the presenters for their review and contributions to this article.
- Simpson EL, Chalmers JR, Hanifin JM, et al. Emollient enhancement of the skin barrier from birth offers effective atopic dermatitis prevention. J Allergy Clin Immunol. 2014;134:818-823.
- Paller AS, Tom WL, Lebwohl MG, et al. Efficacy and safety of crisaborole ointment, a novel phosphodiesterase 4 inhibitor for the topical treatment of AD in children and adults [published online July 11, 2016]. J Am Acad Dermatol. 2016;75:494-503.
- Jensen P, Hamann D, Hamann CR, et al. Nickel and cobalt release from children’s toys purchased in Denmark and the United States. Dermatitis. 2014;25:356-365.
- Overgaard LE, Engebretsen KA, Jensen P, et al. Nickel released from children’s toys is deposited on the skin. Contact Dermatitis. 2016;74:380-381.
- Weibel L, Barysch MJ, Scheer HS, et al. Topical timolol for infantile hemangiomas: evidence for efficacy and degree of systemic absorption [published online February 3, 2016]. Pediatr Dermatol. 2016;33:184-190.
- Simpson EL, Chalmers JR, Hanifin JM, et al. Emollient enhancement of the skin barrier from birth offers effective atopic dermatitis prevention. J Allergy Clin Immunol. 2014;134:818-823.
- Paller AS, Tom WL, Lebwohl MG, et al. Efficacy and safety of crisaborole ointment, a novel phosphodiesterase 4 inhibitor for the topical treatment of AD in children and adults [published online July 11, 2016]. J Am Acad Dermatol. 2016;75:494-503.
- Jensen P, Hamann D, Hamann CR, et al. Nickel and cobalt release from children’s toys purchased in Denmark and the United States. Dermatitis. 2014;25:356-365.
- Overgaard LE, Engebretsen KA, Jensen P, et al. Nickel released from children’s toys is deposited on the skin. Contact Dermatitis. 2016;74:380-381.
- Weibel L, Barysch MJ, Scheer HS, et al. Topical timolol for infantile hemangiomas: evidence for efficacy and degree of systemic absorption [published online February 3, 2016]. Pediatr Dermatol. 2016;33:184-190.

Confronting hate and violence against the LGBT community
It may be unusual for an LGBT health columnist to mention the horrendous events that occurred in Charlottesville, Va., in August 2017. It clearly was a demonstration of hate and violence against racial and ethnic minorities. Unfortunately, the LGBT community – especially LGBT communities of color – are often a target of that kind of hate and violence. This has a detrimental effect on the health of the LGBT community, and I believe that health care providers have a responsibility to address this hate and violence to promote the well-being of this marginalized community.
It cannot be overstated that LGBT individuals frequently experience anti-gay and anti-trans violence. According to the 2015 Federal Bureau of Investigation Hate Crime Statistics, about a fifth of hate crimes reported were based on sexual orientation or gender identity.1 In addition, LGBT youth are eight times as likely to experience bullying at school because of their sexual orientation or gender identity.2 Furthermore, on many surveys on anti-LGBT violence, people of color comprise more than half of the victims.3 There is a strong association between exposure to this violence and the health outcomes of LGBT youth. A study by Russell et al. showed that LGBT youth who were victims of physical violence at school are more likely to be depressed and suicidal and more likely to be diagnosed with an STD,4 and another study showed that LGBT youth who experienced anti-LGBT violence are more likely to engage in substance use.5 The health outcomes from anti-LGBT violence are not limited to the adolescent period – adolescents who experienced this kind of violence are more likely to report higher levels of depression as adults.6 Although researchers still are trying to determine the exact mechanism for these relationships, the most cited (and sensible) explanation is that exposure to anti-LGBT stigma, discrimination, and violence leads to a toxic environment, which in turn increases the risk for mental health problems and maladaptive coping mechanisms (such as substance use) as a response to such an environment.7

What can we do to stand up to the hate and violence against marginalized groups, such as the LGBT community? First, make your office a safe space. With the recent brazen display of hate and violence going around, members the LGBT community are desperate to feel protected. A good place to start is a guide by Advocates for Youth. Second, educate yourself and others. The title physician means “teacher,” and I feel it is your responsibility to teach your peers, colleagues, and the public about how anti-LGBT violence affects the health of LGBT individuals. To be an effective teacher, you need to be up to date on the research on how hatred and intolerance affects the health of the LGBT community. A good place to start is the Human Rights Campaign, which has accurate statistics on anti-LGBT violence and resources to address this problem. Finally, be an advocate. You don’t need to be in the streets with picket signs, nor do you necessarily need to lead the charge against anti-LGBT hate and violence – others will be at the front lines. What you can do is to call for your local, state, and federal government to institute policies that address anti-LGBT violence. Many medical organizations have resources that help health care providers engage with policy makers (check out the American Academy of Pediatrics advocacy page for these resources). Many of our elected officials take our professional opinions seriously.
Anti-gay and anti-trans violence is all too common in the LGBT community, especially violence against LGBT people of color, and this violence can adversely affect their health. Health care providers have a responsibility and the influence to confront these nexuses of hate and intolerance. You don’t need to do something heroic to accomplish this. You are members of a privileged and respected group of professionals, so small actions can coalesce into something that has a large impact on the health and well-being of the communities you serve.

Resources
• Advocates for Youth. Creating Safe Space for GLBTQ Youth: A Toolkit
• Human Rights Campaign. www.hrc.org/resources/
• American Academy of Pediatrics advocacy page: www.aap.org/en-us/advocacy-and-policy/
References
1. U.S. Department of Justice Federal Bureau of Investigation. Uniform Crime Report Hate Crime Statistics, 2015.
2. J Interpers Violence. 2017. doi: 10.1177/0886260517718830.
3. National Coalition of Anti-Violence Programs (NCAVP). Lesbian, Gay, Bisexual, Transgender, Queer and HIV-Affected Hate Violence in 2016.
4. J Sch Health. 2011 May;81(5):223-30.
5. Prev Sci. 2015 Jul;16(5):734-43.
6. Dev Psychol. 2010 Nov;46(6):1580-9.
7. Psychol Bull. 2003 Sep;129(5):674-97.
8. Gallup. Americans Rate Healthcare Providers High on Honesty, Ethics. 2016.
9. The Hippocratic Oath Today. 2001 or Do. No. Harm.
It may be unusual for an LGBT health columnist to mention the horrendous events that occurred in Charlottesville, Va., in August 2017. It clearly was a demonstration of hate and violence against racial and ethnic minorities. Unfortunately, the LGBT community – especially LGBT communities of color – are often a target of that kind of hate and violence. This has a detrimental effect on the health of the LGBT community, and I believe that health care providers have a responsibility to address this hate and violence to promote the well-being of this marginalized community.
It cannot be overstated that LGBT individuals frequently experience anti-gay and anti-trans violence. According to the 2015 Federal Bureau of Investigation Hate Crime Statistics, about a fifth of hate crimes reported were based on sexual orientation or gender identity.1 In addition, LGBT youth are eight times as likely to experience bullying at school because of their sexual orientation or gender identity.2 Furthermore, on many surveys on anti-LGBT violence, people of color comprise more than half of the victims.3 There is a strong association between exposure to this violence and the health outcomes of LGBT youth. A study by Russell et al. showed that LGBT youth who were victims of physical violence at school are more likely to be depressed and suicidal and more likely to be diagnosed with an STD,4 and another study showed that LGBT youth who experienced anti-LGBT violence are more likely to engage in substance use.5 The health outcomes from anti-LGBT violence are not limited to the adolescent period – adolescents who experienced this kind of violence are more likely to report higher levels of depression as adults.6 Although researchers still are trying to determine the exact mechanism for these relationships, the most cited (and sensible) explanation is that exposure to anti-LGBT stigma, discrimination, and violence leads to a toxic environment, which in turn increases the risk for mental health problems and maladaptive coping mechanisms (such as substance use) as a response to such an environment.7
What can we do to stand up to the hate and violence against marginalized groups, such as the LGBT community? First, make your office a safe space. With the recent brazen display of hate and violence going around, members the LGBT community are desperate to feel protected. A good place to start is a guide by Advocates for Youth. Second, educate yourself and others. The title physician means “teacher,” and I feel it is your responsibility to teach your peers, colleagues, and the public about how anti-LGBT violence affects the health of LGBT individuals. To be an effective teacher, you need to be up to date on the research on how hatred and intolerance affects the health of the LGBT community. A good place to start is the Human Rights Campaign, which has accurate statistics on anti-LGBT violence and resources to address this problem. Finally, be an advocate. You don’t need to be in the streets with picket signs, nor do you necessarily need to lead the charge against anti-LGBT hate and violence – others will be at the front lines. What you can do is to call for your local, state, and federal government to institute policies that address anti-LGBT violence. Many medical organizations have resources that help health care providers engage with policy makers (check out the American Academy of Pediatrics advocacy page for these resources). Many of our elected officials take our professional opinions seriously.
Anti-gay and anti-trans violence is all too common in the LGBT community, especially violence against LGBT people of color, and this violence can adversely affect their health. Health care providers have a responsibility and the influence to confront these nexuses of hate and intolerance. You don’t need to do something heroic to accomplish this. You are members of a privileged and respected group of professionals, so small actions can coalesce into something that has a large impact on the health and well-being of the communities you serve.
Resources
• Advocates for Youth. Creating Safe Space for GLBTQ Youth: A Toolkit
• Human Rights Campaign. www.hrc.org/resources/
• American Academy of Pediatrics advocacy page: www.aap.org/en-us/advocacy-and-policy/
References
1. U.S. Department of Justice Federal Bureau of Investigation. Uniform Crime Report Hate Crime Statistics, 2015.
2. J Interpers Violence. 2017. doi: 10.1177/0886260517718830.
3. National Coalition of Anti-Violence Programs (NCAVP). Lesbian, Gay, Bisexual, Transgender, Queer and HIV-Affected Hate Violence in 2016.
4. J Sch Health. 2011 May;81(5):223-30.
5. Prev Sci. 2015 Jul;16(5):734-43.
6. Dev Psychol. 2010 Nov;46(6):1580-9.
7. Psychol Bull. 2003 Sep;129(5):674-97.
8. Gallup. Americans Rate Healthcare Providers High on Honesty, Ethics. 2016.
9. The Hippocratic Oath Today. 2001 or Do. No. Harm.
It may be unusual for an LGBT health columnist to mention the horrendous events that occurred in Charlottesville, Va., in August 2017. It clearly was a demonstration of hate and violence against racial and ethnic minorities. Unfortunately, the LGBT community – especially LGBT communities of color – are often a target of that kind of hate and violence. This has a detrimental effect on the health of the LGBT community, and I believe that health care providers have a responsibility to address this hate and violence to promote the well-being of this marginalized community.
It cannot be overstated that LGBT individuals frequently experience anti-gay and anti-trans violence. According to the 2015 Federal Bureau of Investigation Hate Crime Statistics, about a fifth of hate crimes reported were based on sexual orientation or gender identity.1 In addition, LGBT youth are eight times as likely to experience bullying at school because of their sexual orientation or gender identity.2 Furthermore, on many surveys on anti-LGBT violence, people of color comprise more than half of the victims.3 There is a strong association between exposure to this violence and the health outcomes of LGBT youth. A study by Russell et al. showed that LGBT youth who were victims of physical violence at school are more likely to be depressed and suicidal and more likely to be diagnosed with an STD,4 and another study showed that LGBT youth who experienced anti-LGBT violence are more likely to engage in substance use.5 The health outcomes from anti-LGBT violence are not limited to the adolescent period – adolescents who experienced this kind of violence are more likely to report higher levels of depression as adults.6 Although researchers still are trying to determine the exact mechanism for these relationships, the most cited (and sensible) explanation is that exposure to anti-LGBT stigma, discrimination, and violence leads to a toxic environment, which in turn increases the risk for mental health problems and maladaptive coping mechanisms (such as substance use) as a response to such an environment.7
What can we do to stand up to the hate and violence against marginalized groups, such as the LGBT community? First, make your office a safe space. With the recent brazen display of hate and violence going around, members the LGBT community are desperate to feel protected. A good place to start is a guide by Advocates for Youth. Second, educate yourself and others. The title physician means “teacher,” and I feel it is your responsibility to teach your peers, colleagues, and the public about how anti-LGBT violence affects the health of LGBT individuals. To be an effective teacher, you need to be up to date on the research on how hatred and intolerance affects the health of the LGBT community. A good place to start is the Human Rights Campaign, which has accurate statistics on anti-LGBT violence and resources to address this problem. Finally, be an advocate. You don’t need to be in the streets with picket signs, nor do you necessarily need to lead the charge against anti-LGBT hate and violence – others will be at the front lines. What you can do is to call for your local, state, and federal government to institute policies that address anti-LGBT violence. Many medical organizations have resources that help health care providers engage with policy makers (check out the American Academy of Pediatrics advocacy page for these resources). Many of our elected officials take our professional opinions seriously.
Anti-gay and anti-trans violence is all too common in the LGBT community, especially violence against LGBT people of color, and this violence can adversely affect their health. Health care providers have a responsibility and the influence to confront these nexuses of hate and intolerance. You don’t need to do something heroic to accomplish this. You are members of a privileged and respected group of professionals, so small actions can coalesce into something that has a large impact on the health and well-being of the communities you serve.
Resources
• Advocates for Youth. Creating Safe Space for GLBTQ Youth: A Toolkit
• Human Rights Campaign. www.hrc.org/resources/
• American Academy of Pediatrics advocacy page: www.aap.org/en-us/advocacy-and-policy/
References
1. U.S. Department of Justice Federal Bureau of Investigation. Uniform Crime Report Hate Crime Statistics, 2015.
2. J Interpers Violence. 2017. doi: 10.1177/0886260517718830.
3. National Coalition of Anti-Violence Programs (NCAVP). Lesbian, Gay, Bisexual, Transgender, Queer and HIV-Affected Hate Violence in 2016.
4. J Sch Health. 2011 May;81(5):223-30.
5. Prev Sci. 2015 Jul;16(5):734-43.
6. Dev Psychol. 2010 Nov;46(6):1580-9.
7. Psychol Bull. 2003 Sep;129(5):674-97.
8. Gallup. Americans Rate Healthcare Providers High on Honesty, Ethics. 2016.
9. The Hippocratic Oath Today. 2001 or Do. No. Harm.

Cerebral palsy rate down in children born very or moderately preterm
, even in children who were born moderately preterm.
The researchers gathered data for cerebral palsy from the medical questionnaire, including information on head control, sitting, standing, walking, and quality of gait; trunk and limb tone; and any abnormal neurologic signs. Development was assessed using the second version of the 24-month Ages and Stages Questionnaire (ASQ), which is completed by parents.
Of 4,199 neonates born between 22 and 34 weeks’ gestation in 2011 enrolled in the EPIPAGE-2 study who lived until a median of 24.2 months corrected age, the rate of cerebral palsy dropped from 7% to 4% in those born between 24-26 and 27-31 weeks’ gestation, reported Véronique Pierrat, MD, PhD, of the Epidemiology and Biostatistics Sorbonne Paris Cité Research Center, INSERM, in Paris, and her associates. At 32-34 weeks’ gestation, the cerebral palsy rate was 1%. Only one child born at 22-23 weeks’ gestation lived beyond the neonatal period. Fewer than 1% of the children overall had severe auditory or visual impairment.
ASQ analysis was considered for 2,506 children, after excluding children with cerebral palsy, deafness or blindness, or severe congenital brain malformations. ASQ scores were below threshold in 50%, 41%, and 36% of children born at 24-26, 27-31, and 32-34 weeks’ gestation, respectively. “The domains most frequently scoring below threshold were communication and personal-social in all gestational age groups. Proportions of children scoring below the threshold in either of these domains decreased with increasing gestational age but still were 18% and 13%, respectively, at 32-34 weeks’ gestation,” the investigators said.
Only 1% or fewer of the children in this cohort had severe gastrointestinal or respiratory disabilities.
In a comparison of 1997 data and this 2011 data after adjustment for baseline characteristics in children born at 22-31 weeks’ gestation, survival increased by a mean 6% , and survival without neuromotor or sensory impairment by 7%; in children born at 24-31 weeks’ gestation, cerebral palsy decreased by a mean 3%. No statistically significant changes were found between the two periods for survival, survival without neuromotor or sensory disabilities, and rates of cerebral palsy in children born at 24 weeks’ gestation, but “noticeable improvements were seen at 25-26 weeks and, to a lesser extent, at 27-31 weeks,” Dr. Pierrat and her associates said. At 32-34 weeks’ gestation, the cerebral palsy rate dropped by 3%, but survival and survival without severe neuromotor or sensory impairment were similar between the two time periods.
In regard to the 2011 data, “the proportion of infants at risk of developmental delay was high, even for those born at 32-34 weeks’ gestation. Our results invite questioning perinatal strategies in France, and in countries with similar recommendations. However, improving outcomes at extremely low gestational age requires a complex change in philosophy of care and close cooperation not only between obstetricians and neonatologists, but also developmental specialists, parent associations, and policy makers,” Dr. Pierrat and her associates concluded.
The investigators said they had no relevant financial disclosures. The study was funded by the French Institute of Public Health Research/Institute of Public Health and several of its partners, the PREMUP Foundation, Fondation de France, and Fondation pour la Recherche Médicale.
, even in children who were born moderately preterm.
The researchers gathered data for cerebral palsy from the medical questionnaire, including information on head control, sitting, standing, walking, and quality of gait; trunk and limb tone; and any abnormal neurologic signs. Development was assessed using the second version of the 24-month Ages and Stages Questionnaire (ASQ), which is completed by parents.
Of 4,199 neonates born between 22 and 34 weeks’ gestation in 2011 enrolled in the EPIPAGE-2 study who lived until a median of 24.2 months corrected age, the rate of cerebral palsy dropped from 7% to 4% in those born between 24-26 and 27-31 weeks’ gestation, reported Véronique Pierrat, MD, PhD, of the Epidemiology and Biostatistics Sorbonne Paris Cité Research Center, INSERM, in Paris, and her associates. At 32-34 weeks’ gestation, the cerebral palsy rate was 1%. Only one child born at 22-23 weeks’ gestation lived beyond the neonatal period. Fewer than 1% of the children overall had severe auditory or visual impairment.
ASQ analysis was considered for 2,506 children, after excluding children with cerebral palsy, deafness or blindness, or severe congenital brain malformations. ASQ scores were below threshold in 50%, 41%, and 36% of children born at 24-26, 27-31, and 32-34 weeks’ gestation, respectively. “The domains most frequently scoring below threshold were communication and personal-social in all gestational age groups. Proportions of children scoring below the threshold in either of these domains decreased with increasing gestational age but still were 18% and 13%, respectively, at 32-34 weeks’ gestation,” the investigators said.
Only 1% or fewer of the children in this cohort had severe gastrointestinal or respiratory disabilities.
In a comparison of 1997 data and this 2011 data after adjustment for baseline characteristics in children born at 22-31 weeks’ gestation, survival increased by a mean 6% , and survival without neuromotor or sensory impairment by 7%; in children born at 24-31 weeks’ gestation, cerebral palsy decreased by a mean 3%. No statistically significant changes were found between the two periods for survival, survival without neuromotor or sensory disabilities, and rates of cerebral palsy in children born at 24 weeks’ gestation, but “noticeable improvements were seen at 25-26 weeks and, to a lesser extent, at 27-31 weeks,” Dr. Pierrat and her associates said. At 32-34 weeks’ gestation, the cerebral palsy rate dropped by 3%, but survival and survival without severe neuromotor or sensory impairment were similar between the two time periods.
In regard to the 2011 data, “the proportion of infants at risk of developmental delay was high, even for those born at 32-34 weeks’ gestation. Our results invite questioning perinatal strategies in France, and in countries with similar recommendations. However, improving outcomes at extremely low gestational age requires a complex change in philosophy of care and close cooperation not only between obstetricians and neonatologists, but also developmental specialists, parent associations, and policy makers,” Dr. Pierrat and her associates concluded.
The investigators said they had no relevant financial disclosures. The study was funded by the French Institute of Public Health Research/Institute of Public Health and several of its partners, the PREMUP Foundation, Fondation de France, and Fondation pour la Recherche Médicale.
, even in children who were born moderately preterm.
The researchers gathered data for cerebral palsy from the medical questionnaire, including information on head control, sitting, standing, walking, and quality of gait; trunk and limb tone; and any abnormal neurologic signs. Development was assessed using the second version of the 24-month Ages and Stages Questionnaire (ASQ), which is completed by parents.
Of 4,199 neonates born between 22 and 34 weeks’ gestation in 2011 enrolled in the EPIPAGE-2 study who lived until a median of 24.2 months corrected age, the rate of cerebral palsy dropped from 7% to 4% in those born between 24-26 and 27-31 weeks’ gestation, reported Véronique Pierrat, MD, PhD, of the Epidemiology and Biostatistics Sorbonne Paris Cité Research Center, INSERM, in Paris, and her associates. At 32-34 weeks’ gestation, the cerebral palsy rate was 1%. Only one child born at 22-23 weeks’ gestation lived beyond the neonatal period. Fewer than 1% of the children overall had severe auditory or visual impairment.
ASQ analysis was considered for 2,506 children, after excluding children with cerebral palsy, deafness or blindness, or severe congenital brain malformations. ASQ scores were below threshold in 50%, 41%, and 36% of children born at 24-26, 27-31, and 32-34 weeks’ gestation, respectively. “The domains most frequently scoring below threshold were communication and personal-social in all gestational age groups. Proportions of children scoring below the threshold in either of these domains decreased with increasing gestational age but still were 18% and 13%, respectively, at 32-34 weeks’ gestation,” the investigators said.
Only 1% or fewer of the children in this cohort had severe gastrointestinal or respiratory disabilities.
In a comparison of 1997 data and this 2011 data after adjustment for baseline characteristics in children born at 22-31 weeks’ gestation, survival increased by a mean 6% , and survival without neuromotor or sensory impairment by 7%; in children born at 24-31 weeks’ gestation, cerebral palsy decreased by a mean 3%. No statistically significant changes were found between the two periods for survival, survival without neuromotor or sensory disabilities, and rates of cerebral palsy in children born at 24 weeks’ gestation, but “noticeable improvements were seen at 25-26 weeks and, to a lesser extent, at 27-31 weeks,” Dr. Pierrat and her associates said. At 32-34 weeks’ gestation, the cerebral palsy rate dropped by 3%, but survival and survival without severe neuromotor or sensory impairment were similar between the two time periods.
In regard to the 2011 data, “the proportion of infants at risk of developmental delay was high, even for those born at 32-34 weeks’ gestation. Our results invite questioning perinatal strategies in France, and in countries with similar recommendations. However, improving outcomes at extremely low gestational age requires a complex change in philosophy of care and close cooperation not only between obstetricians and neonatologists, but also developmental specialists, parent associations, and policy makers,” Dr. Pierrat and her associates concluded.
The investigators said they had no relevant financial disclosures. The study was funded by the French Institute of Public Health Research/Institute of Public Health and several of its partners, the PREMUP Foundation, Fondation de France, and Fondation pour la Recherche Médicale.
FROM BMJ
Key clinical point: Cerebral palsy rates are down in children born very and moderately preterm, but the risk of developmental delay remains high.
Major finding: ASQ scores were below threshold in 50%, 41%, and 36% of children born at 24-26, 27-31, and 32-34 weeks’ gestation, respectively.
Data source: A national population study of 4,199 French neonates born between 22 and 34 weeks’ gestation in 2011.
Disclosures: The investigators said they had no relevant financial disclosures. The study was funded by the French Institute of Public Health Research/Institute of Public Health and several of its partners, the PREMUP Foundation, Fondation de France, and Fondation pour la Recherche Médicale.
AAP releases revised guidelines on screening, treatment of hypertension
which includes revised BP tables based on normal-weight children only.
The document, published Aug. 21 in Pediatrics, is the first update since 2004, and recommends significant changes in both screening and treatment of hypertension (HTN).
The guidelines also include a simplified screening table for initial screening, which lists the 90th percentile BP for age and sex, for children at the fifth percentile of height. These values give the table a negative predictive value of greater than 99%, although the committee stressed that the table should only be used for screening, and not for diagnosis.
“To diagnose elevated BP or HTN, it is important to locate the actual cutoffs in the complete BP tables because the [systolic] BP and [diastolic] BP cutoffs may be as much as 9 mm Hg higher depending on a child’s age and length or height,” wrote Joseph T. Flynn, MD, and his colleagues on the AAP subcommittee on screening and management of high blood pressure in children.
To ensure consistency between these guidelines and the 2017 adult guidelines from the American Heart Association and American College of Cardiology, the committee also decided to replace the term “prehypertension” with “elevated blood pressure.”
Similarly, the committee recommended adopting revised stage 1 and stage 2 HTN criteria, to enable the staging scheme for children aged 13 years and over to “seamlessly interface” with the 2017 AHA and ACC adult guidelines.
“There are still no data to identify a specific level of BP in childhood that leads to adverse [cardiovascular] outcomes in adulthood,” the committee wrote. “Therefore, the subcommittee decided to maintain a statistical definition for childhood HTN.”
In terms of screening children for hypertension, the guidelines review committee made the recommendation that BP be measured annually in children and adolescents aged 3 years or above. However, if the child is at greater risk of hypertension because of obesity, medications known to increase BP – such as stimulants for ADHD – renal disease, a history of aortic arch obstruction or coarctation, or have diabetes, they should have their BP measured at every health care encounter.
They also stressed it was important to take more than one measurement over time before diagnosing HTN, and to use appropriately-sized cuffs to ensure an accurate measurement.
If a child or adolescent has confirmed auscultatory BP readings at or above the 95th percentile on three different visits, this justifies a diagnosis of HTN, they wrote.
The committee strongly recommended the routine performance of ambulatory BP monitoring in patients with high-risk conditions, such as diabetes, secondary hypertension, or renal disease, to look for abnormal circadian BP patterns that might point to an increased risk of target organ damage.
They also issued revised recommendations on when to perform echocardiography in children newly diagnosed with HTN.
“It is recommended that echocardiography be performed to assess for cardiac target organ damage (left ventricular mass, geometry, and function) at the time of consideration of pharmacologic treatment of HTN,” they wrote, suggesting repeat echocardiography could be used to monitor target organ damage at 6-12 month intervals.
They offered a revised definition of left ventricular HTN as a left ventricular mass greater than 51 g/m2.7 for children and adolescents older than 8 years (greater than 115 g/body surface area for boys and greater than 95 g/body surface area for girls).
While previous treatment recommendations used a treatment target of a systolic and diastolic BP below the 95th percentile in children without chronic kidney disease, new evidence prompted a revised recommendation of a target either below the 90th percentile or less than 130/80 mm Hg.
“Longitudinal studies on BP from childhood to adulthood that include indirect measures of [cardiovascular] injury indicate that the risk for subsequent [cardiovascular disease] in early adulthood increases as the BP level in adolescence exceeds 120/80 mm Hg,” they wrote. “In addition, there is some evidence that targeting a BP less than 90th percentile results in reductions in [left ventricular mass index] and prevalence of [left ventricular hypertrophy].”
In hypertensive children and adolescents who have failed lifestyle modifications, such as physical activity, weight loss, and stress reduction (particularly those who have left ventricular hypertrophy, symptomatic HTN, or stage 2 HTN without a clearly modifiable factor such as obesity), pharmacologic treatment with an angiotensin-converting enzyme inhibitor, angiotensin receptor blocker, long-acting calcium channel blocker, or thiazide diuretic is indicated, according to the revised guidelines.
The guidelines were supported by the American Academy of Pediatrics and endorsed by the American Heart Association. No conflicts of interest were declared.
which includes revised BP tables based on normal-weight children only.
The document, published Aug. 21 in Pediatrics, is the first update since 2004, and recommends significant changes in both screening and treatment of hypertension (HTN).
The guidelines also include a simplified screening table for initial screening, which lists the 90th percentile BP for age and sex, for children at the fifth percentile of height. These values give the table a negative predictive value of greater than 99%, although the committee stressed that the table should only be used for screening, and not for diagnosis.
“To diagnose elevated BP or HTN, it is important to locate the actual cutoffs in the complete BP tables because the [systolic] BP and [diastolic] BP cutoffs may be as much as 9 mm Hg higher depending on a child’s age and length or height,” wrote Joseph T. Flynn, MD, and his colleagues on the AAP subcommittee on screening and management of high blood pressure in children.
To ensure consistency between these guidelines and the 2017 adult guidelines from the American Heart Association and American College of Cardiology, the committee also decided to replace the term “prehypertension” with “elevated blood pressure.”
Similarly, the committee recommended adopting revised stage 1 and stage 2 HTN criteria, to enable the staging scheme for children aged 13 years and over to “seamlessly interface” with the 2017 AHA and ACC adult guidelines.
“There are still no data to identify a specific level of BP in childhood that leads to adverse [cardiovascular] outcomes in adulthood,” the committee wrote. “Therefore, the subcommittee decided to maintain a statistical definition for childhood HTN.”
In terms of screening children for hypertension, the guidelines review committee made the recommendation that BP be measured annually in children and adolescents aged 3 years or above. However, if the child is at greater risk of hypertension because of obesity, medications known to increase BP – such as stimulants for ADHD – renal disease, a history of aortic arch obstruction or coarctation, or have diabetes, they should have their BP measured at every health care encounter.
They also stressed it was important to take more than one measurement over time before diagnosing HTN, and to use appropriately-sized cuffs to ensure an accurate measurement.
If a child or adolescent has confirmed auscultatory BP readings at or above the 95th percentile on three different visits, this justifies a diagnosis of HTN, they wrote.
The committee strongly recommended the routine performance of ambulatory BP monitoring in patients with high-risk conditions, such as diabetes, secondary hypertension, or renal disease, to look for abnormal circadian BP patterns that might point to an increased risk of target organ damage.
They also issued revised recommendations on when to perform echocardiography in children newly diagnosed with HTN.
“It is recommended that echocardiography be performed to assess for cardiac target organ damage (left ventricular mass, geometry, and function) at the time of consideration of pharmacologic treatment of HTN,” they wrote, suggesting repeat echocardiography could be used to monitor target organ damage at 6-12 month intervals.
They offered a revised definition of left ventricular HTN as a left ventricular mass greater than 51 g/m2.7 for children and adolescents older than 8 years (greater than 115 g/body surface area for boys and greater than 95 g/body surface area for girls).
While previous treatment recommendations used a treatment target of a systolic and diastolic BP below the 95th percentile in children without chronic kidney disease, new evidence prompted a revised recommendation of a target either below the 90th percentile or less than 130/80 mm Hg.
“Longitudinal studies on BP from childhood to adulthood that include indirect measures of [cardiovascular] injury indicate that the risk for subsequent [cardiovascular disease] in early adulthood increases as the BP level in adolescence exceeds 120/80 mm Hg,” they wrote. “In addition, there is some evidence that targeting a BP less than 90th percentile results in reductions in [left ventricular mass index] and prevalence of [left ventricular hypertrophy].”
In hypertensive children and adolescents who have failed lifestyle modifications, such as physical activity, weight loss, and stress reduction (particularly those who have left ventricular hypertrophy, symptomatic HTN, or stage 2 HTN without a clearly modifiable factor such as obesity), pharmacologic treatment with an angiotensin-converting enzyme inhibitor, angiotensin receptor blocker, long-acting calcium channel blocker, or thiazide diuretic is indicated, according to the revised guidelines.
The guidelines were supported by the American Academy of Pediatrics and endorsed by the American Heart Association. No conflicts of interest were declared.
which includes revised BP tables based on normal-weight children only.
The document, published Aug. 21 in Pediatrics, is the first update since 2004, and recommends significant changes in both screening and treatment of hypertension (HTN).
The guidelines also include a simplified screening table for initial screening, which lists the 90th percentile BP for age and sex, for children at the fifth percentile of height. These values give the table a negative predictive value of greater than 99%, although the committee stressed that the table should only be used for screening, and not for diagnosis.
“To diagnose elevated BP or HTN, it is important to locate the actual cutoffs in the complete BP tables because the [systolic] BP and [diastolic] BP cutoffs may be as much as 9 mm Hg higher depending on a child’s age and length or height,” wrote Joseph T. Flynn, MD, and his colleagues on the AAP subcommittee on screening and management of high blood pressure in children.
To ensure consistency between these guidelines and the 2017 adult guidelines from the American Heart Association and American College of Cardiology, the committee also decided to replace the term “prehypertension” with “elevated blood pressure.”
Similarly, the committee recommended adopting revised stage 1 and stage 2 HTN criteria, to enable the staging scheme for children aged 13 years and over to “seamlessly interface” with the 2017 AHA and ACC adult guidelines.
“There are still no data to identify a specific level of BP in childhood that leads to adverse [cardiovascular] outcomes in adulthood,” the committee wrote. “Therefore, the subcommittee decided to maintain a statistical definition for childhood HTN.”
In terms of screening children for hypertension, the guidelines review committee made the recommendation that BP be measured annually in children and adolescents aged 3 years or above. However, if the child is at greater risk of hypertension because of obesity, medications known to increase BP – such as stimulants for ADHD – renal disease, a history of aortic arch obstruction or coarctation, or have diabetes, they should have their BP measured at every health care encounter.
They also stressed it was important to take more than one measurement over time before diagnosing HTN, and to use appropriately-sized cuffs to ensure an accurate measurement.
If a child or adolescent has confirmed auscultatory BP readings at or above the 95th percentile on three different visits, this justifies a diagnosis of HTN, they wrote.
The committee strongly recommended the routine performance of ambulatory BP monitoring in patients with high-risk conditions, such as diabetes, secondary hypertension, or renal disease, to look for abnormal circadian BP patterns that might point to an increased risk of target organ damage.
They also issued revised recommendations on when to perform echocardiography in children newly diagnosed with HTN.
“It is recommended that echocardiography be performed to assess for cardiac target organ damage (left ventricular mass, geometry, and function) at the time of consideration of pharmacologic treatment of HTN,” they wrote, suggesting repeat echocardiography could be used to monitor target organ damage at 6-12 month intervals.
They offered a revised definition of left ventricular HTN as a left ventricular mass greater than 51 g/m2.7 for children and adolescents older than 8 years (greater than 115 g/body surface area for boys and greater than 95 g/body surface area for girls).
While previous treatment recommendations used a treatment target of a systolic and diastolic BP below the 95th percentile in children without chronic kidney disease, new evidence prompted a revised recommendation of a target either below the 90th percentile or less than 130/80 mm Hg.
“Longitudinal studies on BP from childhood to adulthood that include indirect measures of [cardiovascular] injury indicate that the risk for subsequent [cardiovascular disease] in early adulthood increases as the BP level in adolescence exceeds 120/80 mm Hg,” they wrote. “In addition, there is some evidence that targeting a BP less than 90th percentile results in reductions in [left ventricular mass index] and prevalence of [left ventricular hypertrophy].”
In hypertensive children and adolescents who have failed lifestyle modifications, such as physical activity, weight loss, and stress reduction (particularly those who have left ventricular hypertrophy, symptomatic HTN, or stage 2 HTN without a clearly modifiable factor such as obesity), pharmacologic treatment with an angiotensin-converting enzyme inhibitor, angiotensin receptor blocker, long-acting calcium channel blocker, or thiazide diuretic is indicated, according to the revised guidelines.
The guidelines were supported by the American Academy of Pediatrics and endorsed by the American Heart Association. No conflicts of interest were declared.
FROM PEDIATRICS

Recommendations for infant sleep position are not being followed
Despite the American Academy of Pediatrics recommendation that parents place infants supine for sleeping, many mothers do not do so, according to the results of the Study of Attitudes and Factors Affecting Infant Care.
In 32 hospitals, 3,297 mothers were surveyed to determine their intentions, the actual infant sleeping position used, and the factors that affected their behaviors. Of those, 2,491 (77%) reported that they usually place their infants in supine position, but only 49% reported that they exclusively place their infants supine. In addition, 14% reported that they place infants on their sides and 8% prone, reported Eve R. Colson, MD, of the department of pediatrics at Yale University, New Haven, Conn., and her coauthors (Pediatrics. 2017. doi: 10.1542/peds.2017-0596).
Several other discrepancies in compliance with the AAP recommendation also were noted. African American mothers were more likely to intend to use prone position, compared with white mothers (adjusted odds ratio, 2.5; 95% confidence interval, 1.57-3.85). Those who did not complete high school were also more likely to intend to use the prone position (aOR, 2.1; 95% CI, 1.16-3.73). On the other hand, those who received recommendation-compliant advice from a doctor were less likely to place their infants in the prone (aOR, 0.6; 95% CI, 0.39-0.93) or side (aOR, 0.5; 95% CI, 0.36-0.67) positions.
“Of particular note, those who reported that their social norms supported placing the infant in the prone position were much more likely to do so, compared with those who felt that their social norms supported using only the supine position (aOR, 11.6; 95% CI, 7.24-18.7). And, most remarkably, those who had positive attitudes about the prone sleep position ... were more likely to choose the prone position (aOR, 130; 95% CI, 71.8-236),” the researchers wrote. These findings indicate that choices in infant sleeping position are directly influenced by attitudes toward the choice, subjective social norms, and perceptions about control.
“These beliefs persist and are potentially modifiable, so they should be considered an important part of any intervention to change practice,” Dr. Colson and her colleagues wrote.
The study was a nationally representative sample of mothers of infants aged 2-6 months. Although the data were taken from patient surveys, which could have been misreported, they are supported by the findings of other studies.
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/recommendations-for-infant-sleep-position-are-not-being-followed?iframe=1"}]
“Maternal race and education continue to be factors associated with choice of infant sleeping position as does advice from a doctor. Factors that appear to be of equal or greater importance are those related to attitudes, subjective social norms, and perceived control, all of which can potentially be altered through educational interventions,” Dr. Colson and her colleagues concluded.
The Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health funded the study. The authors reported no financial disclosures.
Over the 10 years spanning 1994-2004, the sudden infant death syndrome rate in the United States fell by 53%, correlating with an increase in exclusive supine sleep from less than 10% to 78%. However, since then, rates of both supine sleep and SIDS death have remained stagnant.
To make progress in these areas, current data are needed on supine sleep to enhance understanding of how families make these decisions. Colson et al. provide exactly the kind of information we need to guide providers and public health officials in their efforts to help families maintain the safest sleep environments for their infants.
As a start, mothers who want to practice safe sleep need to be empowered to insist that other caregivers in their lives support their parenting decisions, because the study shows that mothers who feel that they have more control are more likely to use the recommended position. We also must look at how we can help change personal attitudes and societal norms in favor of supine sleep because these issues were found to be some of the strongest predictors of prone sleep position.
We, as health care providers, need to provide clear and consistent messaging in both word and behavior to help mothers make safe decisions for their infants.
Michael H. Goodstein, MD, is a neonatologist at WellSpan York (Pa.) Hospital. Barbara M. Ostfeld, PhD, is the program director of the SIDS Center of New Jersey at Rutgers University, New Brunswick. Their remarks accompanied the article by Colson et al. (Pediatrics 2017 Aug 21. doi: 10.1542/peds.2017-2068). Neither author reported any financial disclosures.
Over the 10 years spanning 1994-2004, the sudden infant death syndrome rate in the United States fell by 53%, correlating with an increase in exclusive supine sleep from less than 10% to 78%. However, since then, rates of both supine sleep and SIDS death have remained stagnant.
To make progress in these areas, current data are needed on supine sleep to enhance understanding of how families make these decisions. Colson et al. provide exactly the kind of information we need to guide providers and public health officials in their efforts to help families maintain the safest sleep environments for their infants.
As a start, mothers who want to practice safe sleep need to be empowered to insist that other caregivers in their lives support their parenting decisions, because the study shows that mothers who feel that they have more control are more likely to use the recommended position. We also must look at how we can help change personal attitudes and societal norms in favor of supine sleep because these issues were found to be some of the strongest predictors of prone sleep position.
We, as health care providers, need to provide clear and consistent messaging in both word and behavior to help mothers make safe decisions for their infants.
Michael H. Goodstein, MD, is a neonatologist at WellSpan York (Pa.) Hospital. Barbara M. Ostfeld, PhD, is the program director of the SIDS Center of New Jersey at Rutgers University, New Brunswick. Their remarks accompanied the article by Colson et al. (Pediatrics 2017 Aug 21. doi: 10.1542/peds.2017-2068). Neither author reported any financial disclosures.
Over the 10 years spanning 1994-2004, the sudden infant death syndrome rate in the United States fell by 53%, correlating with an increase in exclusive supine sleep from less than 10% to 78%. However, since then, rates of both supine sleep and SIDS death have remained stagnant.
To make progress in these areas, current data are needed on supine sleep to enhance understanding of how families make these decisions. Colson et al. provide exactly the kind of information we need to guide providers and public health officials in their efforts to help families maintain the safest sleep environments for their infants.
As a start, mothers who want to practice safe sleep need to be empowered to insist that other caregivers in their lives support their parenting decisions, because the study shows that mothers who feel that they have more control are more likely to use the recommended position. We also must look at how we can help change personal attitudes and societal norms in favor of supine sleep because these issues were found to be some of the strongest predictors of prone sleep position.
We, as health care providers, need to provide clear and consistent messaging in both word and behavior to help mothers make safe decisions for their infants.
Michael H. Goodstein, MD, is a neonatologist at WellSpan York (Pa.) Hospital. Barbara M. Ostfeld, PhD, is the program director of the SIDS Center of New Jersey at Rutgers University, New Brunswick. Their remarks accompanied the article by Colson et al. (Pediatrics 2017 Aug 21. doi: 10.1542/peds.2017-2068). Neither author reported any financial disclosures.
Despite the American Academy of Pediatrics recommendation that parents place infants supine for sleeping, many mothers do not do so, according to the results of the Study of Attitudes and Factors Affecting Infant Care.
In 32 hospitals, 3,297 mothers were surveyed to determine their intentions, the actual infant sleeping position used, and the factors that affected their behaviors. Of those, 2,491 (77%) reported that they usually place their infants in supine position, but only 49% reported that they exclusively place their infants supine. In addition, 14% reported that they place infants on their sides and 8% prone, reported Eve R. Colson, MD, of the department of pediatrics at Yale University, New Haven, Conn., and her coauthors (Pediatrics. 2017. doi: 10.1542/peds.2017-0596).
Several other discrepancies in compliance with the AAP recommendation also were noted. African American mothers were more likely to intend to use prone position, compared with white mothers (adjusted odds ratio, 2.5; 95% confidence interval, 1.57-3.85). Those who did not complete high school were also more likely to intend to use the prone position (aOR, 2.1; 95% CI, 1.16-3.73). On the other hand, those who received recommendation-compliant advice from a doctor were less likely to place their infants in the prone (aOR, 0.6; 95% CI, 0.39-0.93) or side (aOR, 0.5; 95% CI, 0.36-0.67) positions.
“Of particular note, those who reported that their social norms supported placing the infant in the prone position were much more likely to do so, compared with those who felt that their social norms supported using only the supine position (aOR, 11.6; 95% CI, 7.24-18.7). And, most remarkably, those who had positive attitudes about the prone sleep position ... were more likely to choose the prone position (aOR, 130; 95% CI, 71.8-236),” the researchers wrote. These findings indicate that choices in infant sleeping position are directly influenced by attitudes toward the choice, subjective social norms, and perceptions about control.
“These beliefs persist and are potentially modifiable, so they should be considered an important part of any intervention to change practice,” Dr. Colson and her colleagues wrote.
The study was a nationally representative sample of mothers of infants aged 2-6 months. Although the data were taken from patient surveys, which could have been misreported, they are supported by the findings of other studies.
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/recommendations-for-infant-sleep-position-are-not-being-followed?iframe=1"}]
“Maternal race and education continue to be factors associated with choice of infant sleeping position as does advice from a doctor. Factors that appear to be of equal or greater importance are those related to attitudes, subjective social norms, and perceived control, all of which can potentially be altered through educational interventions,” Dr. Colson and her colleagues concluded.
The Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health funded the study. The authors reported no financial disclosures.
Despite the American Academy of Pediatrics recommendation that parents place infants supine for sleeping, many mothers do not do so, according to the results of the Study of Attitudes and Factors Affecting Infant Care.
In 32 hospitals, 3,297 mothers were surveyed to determine their intentions, the actual infant sleeping position used, and the factors that affected their behaviors. Of those, 2,491 (77%) reported that they usually place their infants in supine position, but only 49% reported that they exclusively place their infants supine. In addition, 14% reported that they place infants on their sides and 8% prone, reported Eve R. Colson, MD, of the department of pediatrics at Yale University, New Haven, Conn., and her coauthors (Pediatrics. 2017. doi: 10.1542/peds.2017-0596).
Several other discrepancies in compliance with the AAP recommendation also were noted. African American mothers were more likely to intend to use prone position, compared with white mothers (adjusted odds ratio, 2.5; 95% confidence interval, 1.57-3.85). Those who did not complete high school were also more likely to intend to use the prone position (aOR, 2.1; 95% CI, 1.16-3.73). On the other hand, those who received recommendation-compliant advice from a doctor were less likely to place their infants in the prone (aOR, 0.6; 95% CI, 0.39-0.93) or side (aOR, 0.5; 95% CI, 0.36-0.67) positions.
“Of particular note, those who reported that their social norms supported placing the infant in the prone position were much more likely to do so, compared with those who felt that their social norms supported using only the supine position (aOR, 11.6; 95% CI, 7.24-18.7). And, most remarkably, those who had positive attitudes about the prone sleep position ... were more likely to choose the prone position (aOR, 130; 95% CI, 71.8-236),” the researchers wrote. These findings indicate that choices in infant sleeping position are directly influenced by attitudes toward the choice, subjective social norms, and perceptions about control.
“These beliefs persist and are potentially modifiable, so they should be considered an important part of any intervention to change practice,” Dr. Colson and her colleagues wrote.
The study was a nationally representative sample of mothers of infants aged 2-6 months. Although the data were taken from patient surveys, which could have been misreported, they are supported by the findings of other studies.
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/recommendations-for-infant-sleep-position-are-not-being-followed?iframe=1"}]
“Maternal race and education continue to be factors associated with choice of infant sleeping position as does advice from a doctor. Factors that appear to be of equal or greater importance are those related to attitudes, subjective social norms, and perceived control, all of which can potentially be altered through educational interventions,” Dr. Colson and her colleagues concluded.
The Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health funded the study. The authors reported no financial disclosures.
FROM PEDIATRICS
Key clinical point:
Major finding: Of the 3,297 mothers surveyed, 2,491 (77%) reported that they usually place their infants in supine position, but only 49% reported that they exclusively place their infants supine.
Data source: The Study of Attitudes and Factors Affecting Infant Care, involving 3,297 mothers.
Disclosures: The Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health funded the study. The authors reported no financial disclosures.

New acellular pertussis vaccine may solve waning immunogenicity problem
MADRID – A novel, monovalent, acellular pertussis vaccine containing a recombinant, genetically inactivated pertussis toxin displayed markedly greater sustained immunogenicity than the widely used Sanofi Pasteur Tdap, known as Adacel, which is used as a booster vaccination of adolescents and young adults, in a pivotal phase 3, randomized trial, Simonetta Viviani, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“Our interpretation of these results is that they open up a new way to approach pertussis vaccination,” declared Dr. Viviani, director of clinical development at BioNet-Asia, a Bangkok-based biotech vaccine company.
The impetus for developing new acellular pertussis vaccines is the documented resurgence of pertussis.
“One suggested approach has been to replace chemically inactivated PT with a genetically inactivated PT. The rationale for that is the epitopes of the PT are conserved in the genetically modified PT toxin, as opposed to being destroyed in the chemical inactivation process,” Dr. Viviani explained.
The significant phase 3 trial included 450 Thai 12- to 17-year-olds who were randomized to a single 0.5-mL dose of Pertagen, Boostagen, or Adacel. Both Pertagen and Boostagen contain 5 mcg of the genetically inactivated PT and 5 mcg of filamentous hemagglutinin.
The seroconversion rate, defined as the proportion of subjects who reached at least a fourfold increase in titers of PT and filamentous-hemagglutinin antibodies over baseline, was far superior at both 28 days and 1 year in subjects who got Pertagen or Boostagen, compared with those who received Adacel.

Session chair Ulrich Heininger, MD, declared, “This is really, really exciting.”
It now will be very important that the monovalent Pertagen vaccine be formally studied in pregnant women, he observed.
“Since we’d like to immunize women in every pregnancy and they don’t necessarily need the Td component of Tdap every time, a monovalent vaccine might open a new path for acceptance,” commented Dr. Heininger, professor of pediatric infectious diseases at University Children’s Hospital in Basel, Switz.
Dr. Viviani said that a study in pregnant women is now in the early planning stages.
The study was sponsored by BioNet-Asia and Mahidol University. Dr. Viviani is a BioNet employee.
MADRID – A novel, monovalent, acellular pertussis vaccine containing a recombinant, genetically inactivated pertussis toxin displayed markedly greater sustained immunogenicity than the widely used Sanofi Pasteur Tdap, known as Adacel, which is used as a booster vaccination of adolescents and young adults, in a pivotal phase 3, randomized trial, Simonetta Viviani, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“Our interpretation of these results is that they open up a new way to approach pertussis vaccination,” declared Dr. Viviani, director of clinical development at BioNet-Asia, a Bangkok-based biotech vaccine company.
The impetus for developing new acellular pertussis vaccines is the documented resurgence of pertussis.
“One suggested approach has been to replace chemically inactivated PT with a genetically inactivated PT. The rationale for that is the epitopes of the PT are conserved in the genetically modified PT toxin, as opposed to being destroyed in the chemical inactivation process,” Dr. Viviani explained.
The significant phase 3 trial included 450 Thai 12- to 17-year-olds who were randomized to a single 0.5-mL dose of Pertagen, Boostagen, or Adacel. Both Pertagen and Boostagen contain 5 mcg of the genetically inactivated PT and 5 mcg of filamentous hemagglutinin.
The seroconversion rate, defined as the proportion of subjects who reached at least a fourfold increase in titers of PT and filamentous-hemagglutinin antibodies over baseline, was far superior at both 28 days and 1 year in subjects who got Pertagen or Boostagen, compared with those who received Adacel.
Session chair Ulrich Heininger, MD, declared, “This is really, really exciting.”
It now will be very important that the monovalent Pertagen vaccine be formally studied in pregnant women, he observed.
“Since we’d like to immunize women in every pregnancy and they don’t necessarily need the Td component of Tdap every time, a monovalent vaccine might open a new path for acceptance,” commented Dr. Heininger, professor of pediatric infectious diseases at University Children’s Hospital in Basel, Switz.
Dr. Viviani said that a study in pregnant women is now in the early planning stages.
The study was sponsored by BioNet-Asia and Mahidol University. Dr. Viviani is a BioNet employee.
MADRID – A novel, monovalent, acellular pertussis vaccine containing a recombinant, genetically inactivated pertussis toxin displayed markedly greater sustained immunogenicity than the widely used Sanofi Pasteur Tdap, known as Adacel, which is used as a booster vaccination of adolescents and young adults, in a pivotal phase 3, randomized trial, Simonetta Viviani, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
“Our interpretation of these results is that they open up a new way to approach pertussis vaccination,” declared Dr. Viviani, director of clinical development at BioNet-Asia, a Bangkok-based biotech vaccine company.
The impetus for developing new acellular pertussis vaccines is the documented resurgence of pertussis.
“One suggested approach has been to replace chemically inactivated PT with a genetically inactivated PT. The rationale for that is the epitopes of the PT are conserved in the genetically modified PT toxin, as opposed to being destroyed in the chemical inactivation process,” Dr. Viviani explained.
The significant phase 3 trial included 450 Thai 12- to 17-year-olds who were randomized to a single 0.5-mL dose of Pertagen, Boostagen, or Adacel. Both Pertagen and Boostagen contain 5 mcg of the genetically inactivated PT and 5 mcg of filamentous hemagglutinin.
The seroconversion rate, defined as the proportion of subjects who reached at least a fourfold increase in titers of PT and filamentous-hemagglutinin antibodies over baseline, was far superior at both 28 days and 1 year in subjects who got Pertagen or Boostagen, compared with those who received Adacel.
Session chair Ulrich Heininger, MD, declared, “This is really, really exciting.”
It now will be very important that the monovalent Pertagen vaccine be formally studied in pregnant women, he observed.
“Since we’d like to immunize women in every pregnancy and they don’t necessarily need the Td component of Tdap every time, a monovalent vaccine might open a new path for acceptance,” commented Dr. Heininger, professor of pediatric infectious diseases at University Children’s Hospital in Basel, Switz.
Dr. Viviani said that a study in pregnant women is now in the early planning stages.
The study was sponsored by BioNet-Asia and Mahidol University. Dr. Viviani is a BioNet employee.
AT ESPID 2017
Key clinical point:
Major finding: One year after teens received a single dose of a novel acellular pertussis vaccine, they had a geometric mean titer of PT neutralizing antibody of 77 IU/mL, compared with just 12 IU/mL in adolescents who received a conventional Tdap vaccine.
Data source: This randomized, triple-arm, pivotal phase 3 clinical trial included 450 Thai 12- to 17-year-olds followed for 1 year after receiving a single dose of a novel monovalent pertussis vaccine or a novel Tdap vaccine, both of which contain genetically inactivated pertussis toxin, or, instead of those, a widely utilized conventional Tdap vaccine.
Disclosures: The study was sponsored by BioNet-Asia and Mahidol University. Dr. Viviani is a BioNet employee.
Potential pitfalls of social media
Cassandra presents to the office anxious because of social media posts her peers have made regarding current events that she feels are inflammatory.
Jenna expresses suicidal thoughts in response to comments made by peers from several schools in the area about the nature of her friendship with a boy.
Social media was developed to increase connections between people, even despite geographic distances. It has helped create communities of people with similar interests or beliefs, as well as to help reconnect us with people. It can provide educational opportunities and enhance technical skills. These are all potential benefits, but risks exist as well.
Cyberbullying and harassment
Cyberbullying is defined as “willful and repeated harm inflicted through the use of computers, cell phones, or other electronic devices,” and can include sending denigrating messages or images.3 Studies have shown varying rates of victimization from cyberbullying, ranging from 6% to 72%, and perpetration ranging from 3% to 44%.4 Bullying in general has been associated with increased school drop-out rates, suicidal ideation, bringing weapons to school, and aggression. The sizable audience that social media can reach can amplify bullying’s impact.
Privacy concerns
Determining the appropriate amount of information to share and knowing that it is truly being shared with the person identified on the other end also can be a challenge. In addition, the digital footprint left by navigating different social media sites may have unforeseen effects on youth regarding inappropriate posts. They also may be particularly vulnerable to other predatory individuals. Other privacy concerns involve what information parents, guardians, or other family members may share online.
Addiction
While social media has the possible benefit of creating a broader social network, particularly for someone who may be anxious in more traditional settings, it also can reinforce isolation from “real-world” experiences and the sense that no one else “gets” him or her. Without knowing who is on the other end of the keyboard, tablet, or smartphone, it can be difficult to ascertain if others in the community are reinforcing maladaptive behaviors and further withdrawal.
Self esteem
Images promulgated online often are highly idealized and edited, and are meant to exhibit a specific point of view. Exposure to these images can have a negative impact on self-esteem.
Another study of preteen girls (10- to 12-year-olds) indicated that increased time spent on social media sites such as MySpace and Facebook led to greater internalization of a thin ideal, increased body image concerns, and decreased self-esteem.5 Further data suggest that youth who are in need of more mental health support may engage in increased amounts of social media use. In a Canadian study, daily use of more than 2 hours per day was associated with increased reports of emotional distress as well as suicidal ideation.6
So, given all of this information, how to address this in an appointment?

Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
Resources:
1. The Kaiser Family Foundation: Generation M2: Media in the Lives of 8- to 18-Year-Olds
2. The Pew Research Center: Internet & Technology, “Teens, Social Media and Technology Overview 2015.”
3. The Cyberbullying Research Center. Cyberbullying Fact Sheet 2009.
4. Cyberbullying: An Update and Synthesis of the Research, in “Cyberbullying Prevention and Response: Expert Perspectives,” (New York: Routledge, 2012, pp. 13-35).
5. J. Early Adolesc. 2014. Vol 34(5) 606-20.
6. Cyberpsychol Behav Soc Netw. 2015 Jul;18(7):380-5.
Cassandra presents to the office anxious because of social media posts her peers have made regarding current events that she feels are inflammatory.
Jenna expresses suicidal thoughts in response to comments made by peers from several schools in the area about the nature of her friendship with a boy.
Social media was developed to increase connections between people, even despite geographic distances. It has helped create communities of people with similar interests or beliefs, as well as to help reconnect us with people. It can provide educational opportunities and enhance technical skills. These are all potential benefits, but risks exist as well.
Cyberbullying and harassment
Cyberbullying is defined as “willful and repeated harm inflicted through the use of computers, cell phones, or other electronic devices,” and can include sending denigrating messages or images.3 Studies have shown varying rates of victimization from cyberbullying, ranging from 6% to 72%, and perpetration ranging from 3% to 44%.4 Bullying in general has been associated with increased school drop-out rates, suicidal ideation, bringing weapons to school, and aggression. The sizable audience that social media can reach can amplify bullying’s impact.
Privacy concerns
Determining the appropriate amount of information to share and knowing that it is truly being shared with the person identified on the other end also can be a challenge. In addition, the digital footprint left by navigating different social media sites may have unforeseen effects on youth regarding inappropriate posts. They also may be particularly vulnerable to other predatory individuals. Other privacy concerns involve what information parents, guardians, or other family members may share online.
Addiction
While social media has the possible benefit of creating a broader social network, particularly for someone who may be anxious in more traditional settings, it also can reinforce isolation from “real-world” experiences and the sense that no one else “gets” him or her. Without knowing who is on the other end of the keyboard, tablet, or smartphone, it can be difficult to ascertain if others in the community are reinforcing maladaptive behaviors and further withdrawal.
Self esteem
Images promulgated online often are highly idealized and edited, and are meant to exhibit a specific point of view. Exposure to these images can have a negative impact on self-esteem.
Another study of preteen girls (10- to 12-year-olds) indicated that increased time spent on social media sites such as MySpace and Facebook led to greater internalization of a thin ideal, increased body image concerns, and decreased self-esteem.5 Further data suggest that youth who are in need of more mental health support may engage in increased amounts of social media use. In a Canadian study, daily use of more than 2 hours per day was associated with increased reports of emotional distress as well as suicidal ideation.6
So, given all of this information, how to address this in an appointment?
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
Resources:
1. The Kaiser Family Foundation: Generation M2: Media in the Lives of 8- to 18-Year-Olds
2. The Pew Research Center: Internet & Technology, “Teens, Social Media and Technology Overview 2015.”
3. The Cyberbullying Research Center. Cyberbullying Fact Sheet 2009.
4. Cyberbullying: An Update and Synthesis of the Research, in “Cyberbullying Prevention and Response: Expert Perspectives,” (New York: Routledge, 2012, pp. 13-35).
5. J. Early Adolesc. 2014. Vol 34(5) 606-20.
6. Cyberpsychol Behav Soc Netw. 2015 Jul;18(7):380-5.
Cassandra presents to the office anxious because of social media posts her peers have made regarding current events that she feels are inflammatory.
Jenna expresses suicidal thoughts in response to comments made by peers from several schools in the area about the nature of her friendship with a boy.
Social media was developed to increase connections between people, even despite geographic distances. It has helped create communities of people with similar interests or beliefs, as well as to help reconnect us with people. It can provide educational opportunities and enhance technical skills. These are all potential benefits, but risks exist as well.
Cyberbullying and harassment
Cyberbullying is defined as “willful and repeated harm inflicted through the use of computers, cell phones, or other electronic devices,” and can include sending denigrating messages or images.3 Studies have shown varying rates of victimization from cyberbullying, ranging from 6% to 72%, and perpetration ranging from 3% to 44%.4 Bullying in general has been associated with increased school drop-out rates, suicidal ideation, bringing weapons to school, and aggression. The sizable audience that social media can reach can amplify bullying’s impact.
Privacy concerns
Determining the appropriate amount of information to share and knowing that it is truly being shared with the person identified on the other end also can be a challenge. In addition, the digital footprint left by navigating different social media sites may have unforeseen effects on youth regarding inappropriate posts. They also may be particularly vulnerable to other predatory individuals. Other privacy concerns involve what information parents, guardians, or other family members may share online.
Addiction
While social media has the possible benefit of creating a broader social network, particularly for someone who may be anxious in more traditional settings, it also can reinforce isolation from “real-world” experiences and the sense that no one else “gets” him or her. Without knowing who is on the other end of the keyboard, tablet, or smartphone, it can be difficult to ascertain if others in the community are reinforcing maladaptive behaviors and further withdrawal.
Self esteem
Images promulgated online often are highly idealized and edited, and are meant to exhibit a specific point of view. Exposure to these images can have a negative impact on self-esteem.
Another study of preteen girls (10- to 12-year-olds) indicated that increased time spent on social media sites such as MySpace and Facebook led to greater internalization of a thin ideal, increased body image concerns, and decreased self-esteem.5 Further data suggest that youth who are in need of more mental health support may engage in increased amounts of social media use. In a Canadian study, daily use of more than 2 hours per day was associated with increased reports of emotional distress as well as suicidal ideation.6
So, given all of this information, how to address this in an appointment?
Dr. Strange is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and University of Vermont Robert Larner College of Medicine, both in Burlington. She works with children and adolescents. She has no relevant financial disclosures.
Resources:
1. The Kaiser Family Foundation: Generation M2: Media in the Lives of 8- to 18-Year-Olds
2. The Pew Research Center: Internet & Technology, “Teens, Social Media and Technology Overview 2015.”
3. The Cyberbullying Research Center. Cyberbullying Fact Sheet 2009.
4. Cyberbullying: An Update and Synthesis of the Research, in “Cyberbullying Prevention and Response: Expert Perspectives,” (New York: Routledge, 2012, pp. 13-35).
5. J. Early Adolesc. 2014. Vol 34(5) 606-20.
6. Cyberpsychol Behav Soc Netw. 2015 Jul;18(7):380-5.
Mindfulness and child health
If you are struggling to figure out how you, as an individual pediatrician, can make a significant impact on the most common current issues in child health of anxiety, depression, sleep problems, stress, and even adverse childhood experiences, you are not alone. Many of the problems we see in the office appear to stem so much from the culture in which we live that the medical interventions we have to offer seem paltry. Yet we strive to identify and attempt to ameliorate the child’s and family’s distress.
Real physical danger aside, a lot of personal distress is due to negative thoughts about one’s past or fears for one’s future. These thoughts are very important in restraining us from repeating mistakes and preparing us for action to prevent future harm. But the thoughts themselves can be stressful; they may paralyze us with anxiety, take away pleasure, interrupt our sleep, stimulate physiologic stress responses, and have adverse impacts on health. All these effects can occur without actually changing the course of events! How can we advise our patients and their parents to work to balance the protective function of our thoughts against the cost to our well-being?
One promising method you can confidently recommend to both children and their parents to manage stressful thinking is to learn and practice mindfulness. Mindfulness refers to a state of nonreactivity, awareness, focus, attention, and nonjudgment. Noticing thoughts and feelings passing through us with a neutral mind, as if we were watching a movie, rather than taking them personally, is the goal. Jon Kabat-Zinn, PhD, learned from Buddhists, then developed and disseminated a formal program to teach this skill called mindfulness-based stress reduction; it has yielded significant benefits to the emotions and health of adult participants. While everyone can be mindful at times, the ability to enter this state at will and maintain it for a few minutes can be learned, even by preschool children.
How am I going to refer my patients to mindfulness programs, I can hear you saying, when I can’t even get them to standard therapies? Mindfulness in a less-structured format is often part of yoga or Tai Chi, meditation, art therapy, group therapy, or even religious services. Fortunately, parents and educators also can teach children mindfulness. But the first way you can start making this life skill available to your patients is by recommending it to their parents (“The Family ADHD Solution” by Mark Bertin [New York: Palgrave MacMillan, 2011]).
You know that child emotional or behavior problems can cause adult stress. But adult stress also can cause or exacerbate a child’s emotional or behavior problems. Adult caregivers modeling meltdowns are shaping the minds of their children. Studies of teaching mindfulness to parents of children with developmental disabilities, autism, and ADHD, without touching the underlying disorder, show significant reductions in both adult stress and child behavior problems. Parents who can suspend emotion, take some deep breaths, and be thoughtful about the response they want to make instead of reacting impulsively act more reasonably, appear warmer and more compassionate to their children, and are often rewarded with better behavior. Such parents may feel better about themselves and their parenting, may experience less stress, and may themselves sleep better at night!
For children, having an adult simply declare moments to stop, take deep breaths, and notice the sounds, sights, feelings, and smells around them is a good start. Making a routine of taking an “awareness walk” around the block can be another lesson. Eating a food, such as a strawberry, mindfully – observing and savoring every bite – is another natural opportunity to practice increased awareness. One of my favorite tools, having a child shake a glitter globe (like a snow globe that can be made at home) and silently wait for the chaos to subside, “just like their feelings inside,” is soothing and a great metaphor! Abdominal breathing, part of many relaxation exercises, may be hard for young children to master. A parent might try having the child lie down with a stuffed animal on his or her belly and focus on watching it rise and fall while breathing as a way to learn this. For older children, keeping a “gratitude journal” helps focus on the positive, and also has some proven efficacy in relieving depression. Using the “1 Second Everyday” app to video a special moment daily may have a similar effect on sharpening awareness.

Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
If you are struggling to figure out how you, as an individual pediatrician, can make a significant impact on the most common current issues in child health of anxiety, depression, sleep problems, stress, and even adverse childhood experiences, you are not alone. Many of the problems we see in the office appear to stem so much from the culture in which we live that the medical interventions we have to offer seem paltry. Yet we strive to identify and attempt to ameliorate the child’s and family’s distress.
Real physical danger aside, a lot of personal distress is due to negative thoughts about one’s past or fears for one’s future. These thoughts are very important in restraining us from repeating mistakes and preparing us for action to prevent future harm. But the thoughts themselves can be stressful; they may paralyze us with anxiety, take away pleasure, interrupt our sleep, stimulate physiologic stress responses, and have adverse impacts on health. All these effects can occur without actually changing the course of events! How can we advise our patients and their parents to work to balance the protective function of our thoughts against the cost to our well-being?
One promising method you can confidently recommend to both children and their parents to manage stressful thinking is to learn and practice mindfulness. Mindfulness refers to a state of nonreactivity, awareness, focus, attention, and nonjudgment. Noticing thoughts and feelings passing through us with a neutral mind, as if we were watching a movie, rather than taking them personally, is the goal. Jon Kabat-Zinn, PhD, learned from Buddhists, then developed and disseminated a formal program to teach this skill called mindfulness-based stress reduction; it has yielded significant benefits to the emotions and health of adult participants. While everyone can be mindful at times, the ability to enter this state at will and maintain it for a few minutes can be learned, even by preschool children.
How am I going to refer my patients to mindfulness programs, I can hear you saying, when I can’t even get them to standard therapies? Mindfulness in a less-structured format is often part of yoga or Tai Chi, meditation, art therapy, group therapy, or even religious services. Fortunately, parents and educators also can teach children mindfulness. But the first way you can start making this life skill available to your patients is by recommending it to their parents (“The Family ADHD Solution” by Mark Bertin [New York: Palgrave MacMillan, 2011]).
You know that child emotional or behavior problems can cause adult stress. But adult stress also can cause or exacerbate a child’s emotional or behavior problems. Adult caregivers modeling meltdowns are shaping the minds of their children. Studies of teaching mindfulness to parents of children with developmental disabilities, autism, and ADHD, without touching the underlying disorder, show significant reductions in both adult stress and child behavior problems. Parents who can suspend emotion, take some deep breaths, and be thoughtful about the response they want to make instead of reacting impulsively act more reasonably, appear warmer and more compassionate to their children, and are often rewarded with better behavior. Such parents may feel better about themselves and their parenting, may experience less stress, and may themselves sleep better at night!
For children, having an adult simply declare moments to stop, take deep breaths, and notice the sounds, sights, feelings, and smells around them is a good start. Making a routine of taking an “awareness walk” around the block can be another lesson. Eating a food, such as a strawberry, mindfully – observing and savoring every bite – is another natural opportunity to practice increased awareness. One of my favorite tools, having a child shake a glitter globe (like a snow globe that can be made at home) and silently wait for the chaos to subside, “just like their feelings inside,” is soothing and a great metaphor! Abdominal breathing, part of many relaxation exercises, may be hard for young children to master. A parent might try having the child lie down with a stuffed animal on his or her belly and focus on watching it rise and fall while breathing as a way to learn this. For older children, keeping a “gratitude journal” helps focus on the positive, and also has some proven efficacy in relieving depression. Using the “1 Second Everyday” app to video a special moment daily may have a similar effect on sharpening awareness.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
If you are struggling to figure out how you, as an individual pediatrician, can make a significant impact on the most common current issues in child health of anxiety, depression, sleep problems, stress, and even adverse childhood experiences, you are not alone. Many of the problems we see in the office appear to stem so much from the culture in which we live that the medical interventions we have to offer seem paltry. Yet we strive to identify and attempt to ameliorate the child’s and family’s distress.
Real physical danger aside, a lot of personal distress is due to negative thoughts about one’s past or fears for one’s future. These thoughts are very important in restraining us from repeating mistakes and preparing us for action to prevent future harm. But the thoughts themselves can be stressful; they may paralyze us with anxiety, take away pleasure, interrupt our sleep, stimulate physiologic stress responses, and have adverse impacts on health. All these effects can occur without actually changing the course of events! How can we advise our patients and their parents to work to balance the protective function of our thoughts against the cost to our well-being?
One promising method you can confidently recommend to both children and their parents to manage stressful thinking is to learn and practice mindfulness. Mindfulness refers to a state of nonreactivity, awareness, focus, attention, and nonjudgment. Noticing thoughts and feelings passing through us with a neutral mind, as if we were watching a movie, rather than taking them personally, is the goal. Jon Kabat-Zinn, PhD, learned from Buddhists, then developed and disseminated a formal program to teach this skill called mindfulness-based stress reduction; it has yielded significant benefits to the emotions and health of adult participants. While everyone can be mindful at times, the ability to enter this state at will and maintain it for a few minutes can be learned, even by preschool children.
How am I going to refer my patients to mindfulness programs, I can hear you saying, when I can’t even get them to standard therapies? Mindfulness in a less-structured format is often part of yoga or Tai Chi, meditation, art therapy, group therapy, or even religious services. Fortunately, parents and educators also can teach children mindfulness. But the first way you can start making this life skill available to your patients is by recommending it to their parents (“The Family ADHD Solution” by Mark Bertin [New York: Palgrave MacMillan, 2011]).
You know that child emotional or behavior problems can cause adult stress. But adult stress also can cause or exacerbate a child’s emotional or behavior problems. Adult caregivers modeling meltdowns are shaping the minds of their children. Studies of teaching mindfulness to parents of children with developmental disabilities, autism, and ADHD, without touching the underlying disorder, show significant reductions in both adult stress and child behavior problems. Parents who can suspend emotion, take some deep breaths, and be thoughtful about the response they want to make instead of reacting impulsively act more reasonably, appear warmer and more compassionate to their children, and are often rewarded with better behavior. Such parents may feel better about themselves and their parenting, may experience less stress, and may themselves sleep better at night!
For children, having an adult simply declare moments to stop, take deep breaths, and notice the sounds, sights, feelings, and smells around them is a good start. Making a routine of taking an “awareness walk” around the block can be another lesson. Eating a food, such as a strawberry, mindfully – observing and savoring every bite – is another natural opportunity to practice increased awareness. One of my favorite tools, having a child shake a glitter globe (like a snow globe that can be made at home) and silently wait for the chaos to subside, “just like their feelings inside,” is soothing and a great metaphor! Abdominal breathing, part of many relaxation exercises, may be hard for young children to master. A parent might try having the child lie down with a stuffed animal on his or her belly and focus on watching it rise and fall while breathing as a way to learn this. For older children, keeping a “gratitude journal” helps focus on the positive, and also has some proven efficacy in relieving depression. Using the “1 Second Everyday” app to video a special moment daily may have a similar effect on sharpening awareness.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
