User login
Blood Test Accurately Detects GLUT1 Deficiency Syndrome
A blood test can detect glucose transporter type 1 (GLUT1) deficiency syndrome accurately and rapidly, according to a brief communication published in the July issue of Annals of Neurology. The new test has a diagnostic rate comparable to that of CSF glucose and may be more cost-effective than the combination of lumbar puncture and genetic testing, according to the researchers.
To confirm the diagnosis in a patient whose phenotype suggests GLUT1 deficiency syndrome, neurologists traditionally measure CSF glucose concentration and perform SLC2A1 molecular analysis. Lumbar puncture requires fasting and may entail complications, however, and analysis of the coding regions of SLC2A1 can be tedious and may fail to identify variants.
Analysis of Red Blood Cells
Domitille Gras, MD, a neurologist at Robert-Debré University Hospital in Paris, and colleagues tested a novel diagnostic method based on flow cytometry analysis of red blood cells. For their proof-of-concept study, the researchers enrolled 30 patients (13 females) between ages 2 and 50 with GLUT1 deficiency syndrome. They also enrolled 18 patients (six females) with paroxysmal movement disorders attributed to genetic defects other than in SLC2A1. Finally, the investigators examined 346 healthy controls.
For all participants, Dr. Gras and colleagues measured CSF glucose concentration, performed SLC2A1 molecular analysis, and used flow cytometry to analyze GLUT1 surface expression on circulating red blood cells. To perform the latter method, researchers who were blinded to patients’ disease condition collected at least 0.5 mL of nonfasted venous blood from each participant. Results were available within 24 hours.
Age Did Not Affect Test Results
GLUT1 expression on red blood cells varied by 15% among healthy controls. The blood test identified 23 (78%) of the patients with GLUT1 deficiency syndrome who had a decrease in GLUT1 expression of at least 20%. Dr. Gras and colleagues saw no overlap between the test results of patients and those of controls. The new test detected three patients with GLUT1 deficiency syndrome who had a CSF glucose concentration greater than 2.2 mM, which is the most commonly used cutoff. Two patients with a presentation suggestive of GLUT1 deficiency syndrome and low CSF glucose and lactate, but no SLC2A1 mutation, had an abnormal blood test.
The blood test detected GLUT1 deficiency syndrome regardless of the patient’s age and disease severity. Patients not detected by the test may have mutations that mildly affect glucose uptake, but not GLUT1 expression, or may have a GLUT1 deficiency restricted to the brain. Most patients were analyzed at least twice, and blood test results were consistent for each patient.
Measuring GLUT1 at the surface of red blood cells could avoid diagnostic delays that currently are considerable, said Dr. Gras and colleagues. “Although more studies are required to establish the diagnostic gain of the red blood cell test on a larger cohort, such a simple diagnostic test, readily available in clinical practice, ought to greatly enlarge the screening of GLUT1 deficiency syndrome in any patient, child, or adult presenting with cognitive impairment, epilepsy, ataxia and/or dystonia, or paroxysmal movement disorder,” they concluded.
—Erik Greb
Suggested Reading
Gras D, Cousin C, Kappeler C, et al. A simple blood test expedites the diagnosis of glucose transporter type 1 deficiency syndrome. Ann Neurol. 2017;82(1):133-138.
A blood test can detect glucose transporter type 1 (GLUT1) deficiency syndrome accurately and rapidly, according to a brief communication published in the July issue of Annals of Neurology. The new test has a diagnostic rate comparable to that of CSF glucose and may be more cost-effective than the combination of lumbar puncture and genetic testing, according to the researchers.
To confirm the diagnosis in a patient whose phenotype suggests GLUT1 deficiency syndrome, neurologists traditionally measure CSF glucose concentration and perform SLC2A1 molecular analysis. Lumbar puncture requires fasting and may entail complications, however, and analysis of the coding regions of SLC2A1 can be tedious and may fail to identify variants.
Analysis of Red Blood Cells
Domitille Gras, MD, a neurologist at Robert-Debré University Hospital in Paris, and colleagues tested a novel diagnostic method based on flow cytometry analysis of red blood cells. For their proof-of-concept study, the researchers enrolled 30 patients (13 females) between ages 2 and 50 with GLUT1 deficiency syndrome. They also enrolled 18 patients (six females) with paroxysmal movement disorders attributed to genetic defects other than in SLC2A1. Finally, the investigators examined 346 healthy controls.
For all participants, Dr. Gras and colleagues measured CSF glucose concentration, performed SLC2A1 molecular analysis, and used flow cytometry to analyze GLUT1 surface expression on circulating red blood cells. To perform the latter method, researchers who were blinded to patients’ disease condition collected at least 0.5 mL of nonfasted venous blood from each participant. Results were available within 24 hours.
Age Did Not Affect Test Results
GLUT1 expression on red blood cells varied by 15% among healthy controls. The blood test identified 23 (78%) of the patients with GLUT1 deficiency syndrome who had a decrease in GLUT1 expression of at least 20%. Dr. Gras and colleagues saw no overlap between the test results of patients and those of controls. The new test detected three patients with GLUT1 deficiency syndrome who had a CSF glucose concentration greater than 2.2 mM, which is the most commonly used cutoff. Two patients with a presentation suggestive of GLUT1 deficiency syndrome and low CSF glucose and lactate, but no SLC2A1 mutation, had an abnormal blood test.
The blood test detected GLUT1 deficiency syndrome regardless of the patient’s age and disease severity. Patients not detected by the test may have mutations that mildly affect glucose uptake, but not GLUT1 expression, or may have a GLUT1 deficiency restricted to the brain. Most patients were analyzed at least twice, and blood test results were consistent for each patient.
Measuring GLUT1 at the surface of red blood cells could avoid diagnostic delays that currently are considerable, said Dr. Gras and colleagues. “Although more studies are required to establish the diagnostic gain of the red blood cell test on a larger cohort, such a simple diagnostic test, readily available in clinical practice, ought to greatly enlarge the screening of GLUT1 deficiency syndrome in any patient, child, or adult presenting with cognitive impairment, epilepsy, ataxia and/or dystonia, or paroxysmal movement disorder,” they concluded.
—Erik Greb
Suggested Reading
Gras D, Cousin C, Kappeler C, et al. A simple blood test expedites the diagnosis of glucose transporter type 1 deficiency syndrome. Ann Neurol. 2017;82(1):133-138.
A blood test can detect glucose transporter type 1 (GLUT1) deficiency syndrome accurately and rapidly, according to a brief communication published in the July issue of Annals of Neurology. The new test has a diagnostic rate comparable to that of CSF glucose and may be more cost-effective than the combination of lumbar puncture and genetic testing, according to the researchers.
To confirm the diagnosis in a patient whose phenotype suggests GLUT1 deficiency syndrome, neurologists traditionally measure CSF glucose concentration and perform SLC2A1 molecular analysis. Lumbar puncture requires fasting and may entail complications, however, and analysis of the coding regions of SLC2A1 can be tedious and may fail to identify variants.
Analysis of Red Blood Cells
Domitille Gras, MD, a neurologist at Robert-Debré University Hospital in Paris, and colleagues tested a novel diagnostic method based on flow cytometry analysis of red blood cells. For their proof-of-concept study, the researchers enrolled 30 patients (13 females) between ages 2 and 50 with GLUT1 deficiency syndrome. They also enrolled 18 patients (six females) with paroxysmal movement disorders attributed to genetic defects other than in SLC2A1. Finally, the investigators examined 346 healthy controls.
For all participants, Dr. Gras and colleagues measured CSF glucose concentration, performed SLC2A1 molecular analysis, and used flow cytometry to analyze GLUT1 surface expression on circulating red blood cells. To perform the latter method, researchers who were blinded to patients’ disease condition collected at least 0.5 mL of nonfasted venous blood from each participant. Results were available within 24 hours.
Age Did Not Affect Test Results
GLUT1 expression on red blood cells varied by 15% among healthy controls. The blood test identified 23 (78%) of the patients with GLUT1 deficiency syndrome who had a decrease in GLUT1 expression of at least 20%. Dr. Gras and colleagues saw no overlap between the test results of patients and those of controls. The new test detected three patients with GLUT1 deficiency syndrome who had a CSF glucose concentration greater than 2.2 mM, which is the most commonly used cutoff. Two patients with a presentation suggestive of GLUT1 deficiency syndrome and low CSF glucose and lactate, but no SLC2A1 mutation, had an abnormal blood test.
The blood test detected GLUT1 deficiency syndrome regardless of the patient’s age and disease severity. Patients not detected by the test may have mutations that mildly affect glucose uptake, but not GLUT1 expression, or may have a GLUT1 deficiency restricted to the brain. Most patients were analyzed at least twice, and blood test results were consistent for each patient.
Measuring GLUT1 at the surface of red blood cells could avoid diagnostic delays that currently are considerable, said Dr. Gras and colleagues. “Although more studies are required to establish the diagnostic gain of the red blood cell test on a larger cohort, such a simple diagnostic test, readily available in clinical practice, ought to greatly enlarge the screening of GLUT1 deficiency syndrome in any patient, child, or adult presenting with cognitive impairment, epilepsy, ataxia and/or dystonia, or paroxysmal movement disorder,” they concluded.
—Erik Greb
Suggested Reading
Gras D, Cousin C, Kappeler C, et al. A simple blood test expedites the diagnosis of glucose transporter type 1 deficiency syndrome. Ann Neurol. 2017;82(1):133-138.
FDA advisory committee rejects opioids in children’s cough syrup
ROCKVILLE, MD – The majority of
The voting was broken into multiple votes based on age range of patients and the specific opioid present in the cough syrup. Unlike other advisory committee meetings, this meeting did not focus on a the treatment of a disease state, but rather on the treatment of a symptom.
On Sept. 11, 2017, the FDA’s Pediatric Advisory Committee voted 21 no, 2 yes, with one abstention, that the benefit versus the risk of opioid cough suppressants for pediatric patients was not favorable.
This vote was preceded by two previous votes specifically questioning the use of codeine and hydrocodone in medications for pediatric patients. For codeine, the committee voted unanimously with 24 against that the benefit versus risk was not favorable in pediatric patients aged 12 years to less than 18 years. 
For hydrocodone, the committee asked two questions: 1) Was the benefit versus risk favorable for pediatric patients aged 6 years to less than 12 years? and 2) Was the benefit versus risk favorable for pediatric patients aged 12 years to less than 18 years? On the vote for patients aged 6 years to less than 12 years, the committee voted 23 no, 1 yes with no abstention. For the patients aged 12 years to less than 18, the committee voted 23 no, 1 yes, with no abstention.
According to Sharon Levy, MD, MPH, adolescents are the most at-risk population for opioid misuse. This susceptibility is due to the developmental neurobiology of adolescent brains. A region of the brain associated with the reward pathway, nucleus accumbens, is developing in adolescents and plays a role in salience. Salience, or the differentiation between important vs. unimportant rewards, varies widely by age group. Young children show little salience with rewards, and treat rewards equivocally. Adults have a proportional response to rewards with accurate salience. Adolescents, on the other hand, are unhappy with small rewards, but receive a massive return with large rewards. This type of neurobiological feedback makes adolescents “vulnerable to develop substance use disorders.”
Dr. Levy also noted a correlation between prescribed opioid use and alcohol, marijuana, and tobacco use as contributing factors to opioid misuse. When opioids are prescribed for pain management, there is an adjusted odds ratio (AOR) of 1.33, indicating a high likelihood of misuse. Similar AORs are seen in adolescents who have used marijuana, cigarettes, and alcohol: 2.44, 1.25, and 1.23, respectively.
Sovereign pharmaceuticals representative Leonard Lawrence presented the findings of a pharmacokinetic study for hydrocodone and guaifenesin in 25-35 pediatric patients evenly divided into groups aged 6 years to less than 12 years, and 12 years to less than 18 years. According to Mr. Lawrence, codeine appears “to be a greater risk in children younger than 12 years, and should not be used” because of difficulty breathing. Mr Lawrence went on to say that these effects were exacerbated in obese children with lung disease or obstructive sleep apnea.
Victor S. Sloan, MD, of UCB in Brussels, presented an internal review of Tussionex, a combination cough medicine (hydrocodone/chlorpheniramine). This review took into account modern pharmacovigilance methods, changes in clinical practice, and a literature review. “Upon annual review, UCB determined that benefit risk balance for use of Tussionex for cough in children was no longer favorable,” said Dr. Sloan. Based on the results of the review, UCB has filed a label supplement to limit use of Tussionex to patients aged 18 years or older.
“Codeine, in particular, is an antiquated drug,” said Kathleen Neville, MD, pediatrics and clinical pharmacology section chief of Arkansas Children’s Hospital, Little Rock. Many of the committee members echoed Dr. Neville’s opinion.
The committee members had no relevant financial disclosures.
ilacy@frontlinemedcom.com
On Twitter @ilacy_19
ROCKVILLE, MD – The majority of
The voting was broken into multiple votes based on age range of patients and the specific opioid present in the cough syrup. Unlike other advisory committee meetings, this meeting did not focus on a the treatment of a disease state, but rather on the treatment of a symptom.
On Sept. 11, 2017, the FDA’s Pediatric Advisory Committee voted 21 no, 2 yes, with one abstention, that the benefit versus the risk of opioid cough suppressants for pediatric patients was not favorable.
This vote was preceded by two previous votes specifically questioning the use of codeine and hydrocodone in medications for pediatric patients. For codeine, the committee voted unanimously with 24 against that the benefit versus risk was not favorable in pediatric patients aged 12 years to less than 18 years.
For hydrocodone, the committee asked two questions: 1) Was the benefit versus risk favorable for pediatric patients aged 6 years to less than 12 years? and 2) Was the benefit versus risk favorable for pediatric patients aged 12 years to less than 18 years? On the vote for patients aged 6 years to less than 12 years, the committee voted 23 no, 1 yes with no abstention. For the patients aged 12 years to less than 18, the committee voted 23 no, 1 yes, with no abstention.
According to Sharon Levy, MD, MPH, adolescents are the most at-risk population for opioid misuse. This susceptibility is due to the developmental neurobiology of adolescent brains. A region of the brain associated with the reward pathway, nucleus accumbens, is developing in adolescents and plays a role in salience. Salience, or the differentiation between important vs. unimportant rewards, varies widely by age group. Young children show little salience with rewards, and treat rewards equivocally. Adults have a proportional response to rewards with accurate salience. Adolescents, on the other hand, are unhappy with small rewards, but receive a massive return with large rewards. This type of neurobiological feedback makes adolescents “vulnerable to develop substance use disorders.”
Dr. Levy also noted a correlation between prescribed opioid use and alcohol, marijuana, and tobacco use as contributing factors to opioid misuse. When opioids are prescribed for pain management, there is an adjusted odds ratio (AOR) of 1.33, indicating a high likelihood of misuse. Similar AORs are seen in adolescents who have used marijuana, cigarettes, and alcohol: 2.44, 1.25, and 1.23, respectively.
Sovereign pharmaceuticals representative Leonard Lawrence presented the findings of a pharmacokinetic study for hydrocodone and guaifenesin in 25-35 pediatric patients evenly divided into groups aged 6 years to less than 12 years, and 12 years to less than 18 years. According to Mr. Lawrence, codeine appears “to be a greater risk in children younger than 12 years, and should not be used” because of difficulty breathing. Mr Lawrence went on to say that these effects were exacerbated in obese children with lung disease or obstructive sleep apnea.
Victor S. Sloan, MD, of UCB in Brussels, presented an internal review of Tussionex, a combination cough medicine (hydrocodone/chlorpheniramine). This review took into account modern pharmacovigilance methods, changes in clinical practice, and a literature review. “Upon annual review, UCB determined that benefit risk balance for use of Tussionex for cough in children was no longer favorable,” said Dr. Sloan. Based on the results of the review, UCB has filed a label supplement to limit use of Tussionex to patients aged 18 years or older.
“Codeine, in particular, is an antiquated drug,” said Kathleen Neville, MD, pediatrics and clinical pharmacology section chief of Arkansas Children’s Hospital, Little Rock. Many of the committee members echoed Dr. Neville’s opinion.
The committee members had no relevant financial disclosures.
ilacy@frontlinemedcom.com
On Twitter @ilacy_19
ROCKVILLE, MD – The majority of
The voting was broken into multiple votes based on age range of patients and the specific opioid present in the cough syrup. Unlike other advisory committee meetings, this meeting did not focus on a the treatment of a disease state, but rather on the treatment of a symptom.
On Sept. 11, 2017, the FDA’s Pediatric Advisory Committee voted 21 no, 2 yes, with one abstention, that the benefit versus the risk of opioid cough suppressants for pediatric patients was not favorable.
This vote was preceded by two previous votes specifically questioning the use of codeine and hydrocodone in medications for pediatric patients. For codeine, the committee voted unanimously with 24 against that the benefit versus risk was not favorable in pediatric patients aged 12 years to less than 18 years.
For hydrocodone, the committee asked two questions: 1) Was the benefit versus risk favorable for pediatric patients aged 6 years to less than 12 years? and 2) Was the benefit versus risk favorable for pediatric patients aged 12 years to less than 18 years? On the vote for patients aged 6 years to less than 12 years, the committee voted 23 no, 1 yes with no abstention. For the patients aged 12 years to less than 18, the committee voted 23 no, 1 yes, with no abstention.
According to Sharon Levy, MD, MPH, adolescents are the most at-risk population for opioid misuse. This susceptibility is due to the developmental neurobiology of adolescent brains. A region of the brain associated with the reward pathway, nucleus accumbens, is developing in adolescents and plays a role in salience. Salience, or the differentiation between important vs. unimportant rewards, varies widely by age group. Young children show little salience with rewards, and treat rewards equivocally. Adults have a proportional response to rewards with accurate salience. Adolescents, on the other hand, are unhappy with small rewards, but receive a massive return with large rewards. This type of neurobiological feedback makes adolescents “vulnerable to develop substance use disorders.”
Dr. Levy also noted a correlation between prescribed opioid use and alcohol, marijuana, and tobacco use as contributing factors to opioid misuse. When opioids are prescribed for pain management, there is an adjusted odds ratio (AOR) of 1.33, indicating a high likelihood of misuse. Similar AORs are seen in adolescents who have used marijuana, cigarettes, and alcohol: 2.44, 1.25, and 1.23, respectively.
Sovereign pharmaceuticals representative Leonard Lawrence presented the findings of a pharmacokinetic study for hydrocodone and guaifenesin in 25-35 pediatric patients evenly divided into groups aged 6 years to less than 12 years, and 12 years to less than 18 years. According to Mr. Lawrence, codeine appears “to be a greater risk in children younger than 12 years, and should not be used” because of difficulty breathing. Mr Lawrence went on to say that these effects were exacerbated in obese children with lung disease or obstructive sleep apnea.
Victor S. Sloan, MD, of UCB in Brussels, presented an internal review of Tussionex, a combination cough medicine (hydrocodone/chlorpheniramine). This review took into account modern pharmacovigilance methods, changes in clinical practice, and a literature review. “Upon annual review, UCB determined that benefit risk balance for use of Tussionex for cough in children was no longer favorable,” said Dr. Sloan. Based on the results of the review, UCB has filed a label supplement to limit use of Tussionex to patients aged 18 years or older.
“Codeine, in particular, is an antiquated drug,” said Kathleen Neville, MD, pediatrics and clinical pharmacology section chief of Arkansas Children’s Hospital, Little Rock. Many of the committee members echoed Dr. Neville’s opinion.
The committee members had no relevant financial disclosures.
ilacy@frontlinemedcom.com
On Twitter @ilacy_19
AT AN FDA PEDIATRIC ADVISORY COMMITTEE MEETING
Domperidone appears safe galactagogue for mothers and infants
Denver – Prescribing domperidone to support breastfeeding effectively reduced the use of infant formula without significant adverse effects in mothers and infants in a large retrospective study, Mitko Madjunkov, MD, reported at the annual meeting of the Teratology Society.
His study included 985 mothers who began taking domperidone to initiate and support breastfeeding after a visit to the International Breastfeeding Centre in Toronto. Collectively, the women had 1,005 infants.
The study was undertaken because few data exist on the dosing and safety of domperidone during lactation. Additionally, the Food and Drug Administration issued a warning in 2004 regarding the use of domperidone as a galactagogue in response to reports of cardiac arrhythmias and sudden deaths when the drug was prescribed as an antiemetic, explained Dr. Madjunkov of the Hospital for Sick Children in Toronto.
The FDA has not approved domperidone for any indication in the United States, though it is available in Canada and other countries.
Domperidone was used by the Toronto women for a median of 20 days. The maximum daily dose was 107 mg. The infants were an average of 38 days old at the time of the visit when domperidone was prescribed and 72 days of age at their last follow-up visit related to the study.
The drug was effective as a galactagogue: 63% of women were using infant formula before going on domperidone; after using the drug, 41% were still using formula, for an absolute 22% reduction. The drug was similarly effective in promoting breastfeeding in infants with or without tongue-tie/lip-tie defects.
In total, 18% of mothers reported minor side effects. Headaches were the most common, reported by 9.2% of domperidone users. Dose reduction was employed in just 0.6% of women in the study; 0.4% of participants discontinued treatment. Rapid heart rate and other minor cardiac side effects were reported by 0.7% of women, uniformly in conjunction with trigger factors such as anxiety or caffeine use, but none of these women discontinued treatment. No treatment-associated adverse effects occurred in the infants.
Dr. Madjunkov reported having no financial conflicts related to his study.
Denver – Prescribing domperidone to support breastfeeding effectively reduced the use of infant formula without significant adverse effects in mothers and infants in a large retrospective study, Mitko Madjunkov, MD, reported at the annual meeting of the Teratology Society.
His study included 985 mothers who began taking domperidone to initiate and support breastfeeding after a visit to the International Breastfeeding Centre in Toronto. Collectively, the women had 1,005 infants.
The study was undertaken because few data exist on the dosing and safety of domperidone during lactation. Additionally, the Food and Drug Administration issued a warning in 2004 regarding the use of domperidone as a galactagogue in response to reports of cardiac arrhythmias and sudden deaths when the drug was prescribed as an antiemetic, explained Dr. Madjunkov of the Hospital for Sick Children in Toronto.
The FDA has not approved domperidone for any indication in the United States, though it is available in Canada and other countries.
Domperidone was used by the Toronto women for a median of 20 days. The maximum daily dose was 107 mg. The infants were an average of 38 days old at the time of the visit when domperidone was prescribed and 72 days of age at their last follow-up visit related to the study.
The drug was effective as a galactagogue: 63% of women were using infant formula before going on domperidone; after using the drug, 41% were still using formula, for an absolute 22% reduction. The drug was similarly effective in promoting breastfeeding in infants with or without tongue-tie/lip-tie defects.
In total, 18% of mothers reported minor side effects. Headaches were the most common, reported by 9.2% of domperidone users. Dose reduction was employed in just 0.6% of women in the study; 0.4% of participants discontinued treatment. Rapid heart rate and other minor cardiac side effects were reported by 0.7% of women, uniformly in conjunction with trigger factors such as anxiety or caffeine use, but none of these women discontinued treatment. No treatment-associated adverse effects occurred in the infants.
Dr. Madjunkov reported having no financial conflicts related to his study.
Denver – Prescribing domperidone to support breastfeeding effectively reduced the use of infant formula without significant adverse effects in mothers and infants in a large retrospective study, Mitko Madjunkov, MD, reported at the annual meeting of the Teratology Society.
His study included 985 mothers who began taking domperidone to initiate and support breastfeeding after a visit to the International Breastfeeding Centre in Toronto. Collectively, the women had 1,005 infants.
The study was undertaken because few data exist on the dosing and safety of domperidone during lactation. Additionally, the Food and Drug Administration issued a warning in 2004 regarding the use of domperidone as a galactagogue in response to reports of cardiac arrhythmias and sudden deaths when the drug was prescribed as an antiemetic, explained Dr. Madjunkov of the Hospital for Sick Children in Toronto.
The FDA has not approved domperidone for any indication in the United States, though it is available in Canada and other countries.
Domperidone was used by the Toronto women for a median of 20 days. The maximum daily dose was 107 mg. The infants were an average of 38 days old at the time of the visit when domperidone was prescribed and 72 days of age at their last follow-up visit related to the study.
The drug was effective as a galactagogue: 63% of women were using infant formula before going on domperidone; after using the drug, 41% were still using formula, for an absolute 22% reduction. The drug was similarly effective in promoting breastfeeding in infants with or without tongue-tie/lip-tie defects.
In total, 18% of mothers reported minor side effects. Headaches were the most common, reported by 9.2% of domperidone users. Dose reduction was employed in just 0.6% of women in the study; 0.4% of participants discontinued treatment. Rapid heart rate and other minor cardiac side effects were reported by 0.7% of women, uniformly in conjunction with trigger factors such as anxiety or caffeine use, but none of these women discontinued treatment. No treatment-associated adverse effects occurred in the infants.
Dr. Madjunkov reported having no financial conflicts related to his study.
EXPERT ANALYSIS FROM TERATOLOGY SOCIETY 2017
Key clinical point:
Major finding: The use of the domperidone reduced the proportion of women using infant formula by an absolute 22%.
Data source: A retrospective study of 985 women who were prescribed domperidone as a galactagogue at the International Breastfeeding Centre in Toronto.
Disclosures: Dr. Madjunkov reported having no financial conflicts of interest related to the study.
Three percent of high school seniors report using synthetic cannabinoids
, according to data from the national Monitoring the Future survey.
SCs are more potent than marijuana (as much as 100 times stronger); do not contain the anti-anxiety and antipsychotic constituent of marijuana, cannabidiol; and have a greater risk of a range of adverse effects, such as tachycardia, agitation, nausea, generalized tonic-clonic seizures, psychiatric problems, and death.
Joseph J. Palamar, PhD, MPH, of New York University, and his colleagues set out to examine data about current use of SCs, as previous studies had focused on lifetime or past-year use. Monitoring the Future surveys approximately 15,000 high school seniors annually in the United States. Of the six survey forms (which are distributed randomly), only two asked seniors about their current use of SCs, limiting the current study to a third of the survey sample.
The researchers found that, while 81% of current SC users also reported current use of marijuana, only 9% of current marijuana users reported current use of SCs. SC use was correlated much more highly than marijuana use with the current use of other drugs such as LSD (15% vs. 3%), opioids (14% vs. 6%), cocaine (11% vs. 3%), and heroin (6% vs. 0.1%).
“Current SC use appears to be part of a more extensive polydrug use repertoire involving other illegal drugs that are less prevalent among marijuana-only users. ... These associations suggest the need to target marijuana users who also use other drugs to help prevent initiation of SCs,” concluded Dr. Palamar and his associates.
Read more at (Pediatrics. 2017 Oct;140[4]:e20171330).
, according to data from the national Monitoring the Future survey.
SCs are more potent than marijuana (as much as 100 times stronger); do not contain the anti-anxiety and antipsychotic constituent of marijuana, cannabidiol; and have a greater risk of a range of adverse effects, such as tachycardia, agitation, nausea, generalized tonic-clonic seizures, psychiatric problems, and death.
Joseph J. Palamar, PhD, MPH, of New York University, and his colleagues set out to examine data about current use of SCs, as previous studies had focused on lifetime or past-year use. Monitoring the Future surveys approximately 15,000 high school seniors annually in the United States. Of the six survey forms (which are distributed randomly), only two asked seniors about their current use of SCs, limiting the current study to a third of the survey sample.
The researchers found that, while 81% of current SC users also reported current use of marijuana, only 9% of current marijuana users reported current use of SCs. SC use was correlated much more highly than marijuana use with the current use of other drugs such as LSD (15% vs. 3%), opioids (14% vs. 6%), cocaine (11% vs. 3%), and heroin (6% vs. 0.1%).
“Current SC use appears to be part of a more extensive polydrug use repertoire involving other illegal drugs that are less prevalent among marijuana-only users. ... These associations suggest the need to target marijuana users who also use other drugs to help prevent initiation of SCs,” concluded Dr. Palamar and his associates.
Read more at (Pediatrics. 2017 Oct;140[4]:e20171330).
, according to data from the national Monitoring the Future survey.
SCs are more potent than marijuana (as much as 100 times stronger); do not contain the anti-anxiety and antipsychotic constituent of marijuana, cannabidiol; and have a greater risk of a range of adverse effects, such as tachycardia, agitation, nausea, generalized tonic-clonic seizures, psychiatric problems, and death.
Joseph J. Palamar, PhD, MPH, of New York University, and his colleagues set out to examine data about current use of SCs, as previous studies had focused on lifetime or past-year use. Monitoring the Future surveys approximately 15,000 high school seniors annually in the United States. Of the six survey forms (which are distributed randomly), only two asked seniors about their current use of SCs, limiting the current study to a third of the survey sample.
The researchers found that, while 81% of current SC users also reported current use of marijuana, only 9% of current marijuana users reported current use of SCs. SC use was correlated much more highly than marijuana use with the current use of other drugs such as LSD (15% vs. 3%), opioids (14% vs. 6%), cocaine (11% vs. 3%), and heroin (6% vs. 0.1%).
“Current SC use appears to be part of a more extensive polydrug use repertoire involving other illegal drugs that are less prevalent among marijuana-only users. ... These associations suggest the need to target marijuana users who also use other drugs to help prevent initiation of SCs,” concluded Dr. Palamar and his associates.
Read more at (Pediatrics. 2017 Oct;140[4]:e20171330).
FROM PEDIATRICS
Study: Don’t separate NAS infants from moms
NASHVILLE, TENN. – When newborns withdrawing from opioids stay with their mothers after delivery instead of going to the NICU, they are far less likely to receive morphine and other drugs and leave the hospital days sooner; they also are more likely to go home with their mother, a meta-analysis showed.
The analysis likely is the first to pool results from studies of rooming-in for infants with neonatal abstinence syndrome (NAS). A strong case has been building in the literature for several years that newborns do better with rooming-in, instead of the traditional approach for NAS – NICU housing and opioid dosing based on a symptom checklist.

“We found consistent emerging evidence that rooming-in is more effective than standard care in the NICU for infants with NAS. Based on these findings, we believe rooming-in should be established as the new evidence-based standard of care for this patient population,” said investigator Kanak Verma, a medical student at Dartmouth College, Hanover, N.H.
Rooming-in was associated with a 63% reduction in the need for pharmacotherapy, a decrease in hospital length of stay by more than 10 days, and a substantial, statistically significant decrease in cost from – in one study – a mean of almost $45,000 per NAS infant stay to just over $10,000.
“We were worried that by rooming-in we would be undertreating infants with NAS, and that they would be at increased risk for readmission, but there was no statistically significant increase in readmission rates for infants rooming in with their mothers,” Ms. Verma said at the Pediatric Hospital Medical annual meeting.
Infants also were more likely to go home with their mother or a family member. “Mothers who use opioid replacements have decreased ability to bond” with their infants. Rooming-in helps create that bond, and probably made discharge with a family member more likely, said coinvestigator Cassandra Rendon, also a Dartmouth medical student.
It’s unclear what exactly accounts for the better results, but “having a baby stay with [its] mom creates an opportunity for a lot of things that we know are effective,” including skin-to-skin contact, breastfeeding, and involvement of mothers in the care and monitoring of their infants, Ms. Rendon said.
Also, “we know that in babies with NAS, a low-stimulation environment is ideal,” Ms. Verma said at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association. That’s a challenge in a busy NICU, but “we can create that in an isolated room with just the mother,” she added.
At least one of the studies used a new, more holistic approach to assess the need for pharmacologic management in NAS. Symptom scores still are considered, but how well the infant is eating, sleeping, and able to be consoled are considered as well. With the traditional symptom checklist, “we end up just treating the number, instead of treating the baby. What Dartmouth and other facilities are doing is looking at” how well the baby is doing overall, Ms. Rendon said.
If the baby is otherwise doing well, providers are less likely to give opioids for a little jitteriness or sweating. The decreased use of opioids leads, in turn, to shorter hospital stays.
Dartmouth is collaborating with Yale University in New Haven , Conn., and the Boston Medical Center to integrate the new treatment model into standard practice. For other centers interested in doing the same, Ms. Verma noted that nursery staff buy-in is essential. Nurses and others have to be comfortable “taking these patients out of the NICU” and treating them in a new way.
The investigators had no relevant financial disclosures.
NASHVILLE, TENN. – When newborns withdrawing from opioids stay with their mothers after delivery instead of going to the NICU, they are far less likely to receive morphine and other drugs and leave the hospital days sooner; they also are more likely to go home with their mother, a meta-analysis showed.
The analysis likely is the first to pool results from studies of rooming-in for infants with neonatal abstinence syndrome (NAS). A strong case has been building in the literature for several years that newborns do better with rooming-in, instead of the traditional approach for NAS – NICU housing and opioid dosing based on a symptom checklist.
“We found consistent emerging evidence that rooming-in is more effective than standard care in the NICU for infants with NAS. Based on these findings, we believe rooming-in should be established as the new evidence-based standard of care for this patient population,” said investigator Kanak Verma, a medical student at Dartmouth College, Hanover, N.H.
Rooming-in was associated with a 63% reduction in the need for pharmacotherapy, a decrease in hospital length of stay by more than 10 days, and a substantial, statistically significant decrease in cost from – in one study – a mean of almost $45,000 per NAS infant stay to just over $10,000.
“We were worried that by rooming-in we would be undertreating infants with NAS, and that they would be at increased risk for readmission, but there was no statistically significant increase in readmission rates for infants rooming in with their mothers,” Ms. Verma said at the Pediatric Hospital Medical annual meeting.
Infants also were more likely to go home with their mother or a family member. “Mothers who use opioid replacements have decreased ability to bond” with their infants. Rooming-in helps create that bond, and probably made discharge with a family member more likely, said coinvestigator Cassandra Rendon, also a Dartmouth medical student.
It’s unclear what exactly accounts for the better results, but “having a baby stay with [its] mom creates an opportunity for a lot of things that we know are effective,” including skin-to-skin contact, breastfeeding, and involvement of mothers in the care and monitoring of their infants, Ms. Rendon said.
Also, “we know that in babies with NAS, a low-stimulation environment is ideal,” Ms. Verma said at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association. That’s a challenge in a busy NICU, but “we can create that in an isolated room with just the mother,” she added.
At least one of the studies used a new, more holistic approach to assess the need for pharmacologic management in NAS. Symptom scores still are considered, but how well the infant is eating, sleeping, and able to be consoled are considered as well. With the traditional symptom checklist, “we end up just treating the number, instead of treating the baby. What Dartmouth and other facilities are doing is looking at” how well the baby is doing overall, Ms. Rendon said.
If the baby is otherwise doing well, providers are less likely to give opioids for a little jitteriness or sweating. The decreased use of opioids leads, in turn, to shorter hospital stays.
Dartmouth is collaborating with Yale University in New Haven , Conn., and the Boston Medical Center to integrate the new treatment model into standard practice. For other centers interested in doing the same, Ms. Verma noted that nursery staff buy-in is essential. Nurses and others have to be comfortable “taking these patients out of the NICU” and treating them in a new way.
The investigators had no relevant financial disclosures.
NASHVILLE, TENN. – When newborns withdrawing from opioids stay with their mothers after delivery instead of going to the NICU, they are far less likely to receive morphine and other drugs and leave the hospital days sooner; they also are more likely to go home with their mother, a meta-analysis showed.
The analysis likely is the first to pool results from studies of rooming-in for infants with neonatal abstinence syndrome (NAS). A strong case has been building in the literature for several years that newborns do better with rooming-in, instead of the traditional approach for NAS – NICU housing and opioid dosing based on a symptom checklist.
“We found consistent emerging evidence that rooming-in is more effective than standard care in the NICU for infants with NAS. Based on these findings, we believe rooming-in should be established as the new evidence-based standard of care for this patient population,” said investigator Kanak Verma, a medical student at Dartmouth College, Hanover, N.H.
Rooming-in was associated with a 63% reduction in the need for pharmacotherapy, a decrease in hospital length of stay by more than 10 days, and a substantial, statistically significant decrease in cost from – in one study – a mean of almost $45,000 per NAS infant stay to just over $10,000.
“We were worried that by rooming-in we would be undertreating infants with NAS, and that they would be at increased risk for readmission, but there was no statistically significant increase in readmission rates for infants rooming in with their mothers,” Ms. Verma said at the Pediatric Hospital Medical annual meeting.
Infants also were more likely to go home with their mother or a family member. “Mothers who use opioid replacements have decreased ability to bond” with their infants. Rooming-in helps create that bond, and probably made discharge with a family member more likely, said coinvestigator Cassandra Rendon, also a Dartmouth medical student.
It’s unclear what exactly accounts for the better results, but “having a baby stay with [its] mom creates an opportunity for a lot of things that we know are effective,” including skin-to-skin contact, breastfeeding, and involvement of mothers in the care and monitoring of their infants, Ms. Rendon said.
Also, “we know that in babies with NAS, a low-stimulation environment is ideal,” Ms. Verma said at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association. That’s a challenge in a busy NICU, but “we can create that in an isolated room with just the mother,” she added.
At least one of the studies used a new, more holistic approach to assess the need for pharmacologic management in NAS. Symptom scores still are considered, but how well the infant is eating, sleeping, and able to be consoled are considered as well. With the traditional symptom checklist, “we end up just treating the number, instead of treating the baby. What Dartmouth and other facilities are doing is looking at” how well the baby is doing overall, Ms. Rendon said.
If the baby is otherwise doing well, providers are less likely to give opioids for a little jitteriness or sweating. The decreased use of opioids leads, in turn, to shorter hospital stays.
Dartmouth is collaborating with Yale University in New Haven , Conn., and the Boston Medical Center to integrate the new treatment model into standard practice. For other centers interested in doing the same, Ms. Verma noted that nursery staff buy-in is essential. Nurses and others have to be comfortable “taking these patients out of the NICU” and treating them in a new way.
The investigators had no relevant financial disclosures.
AT PHM 2017
Key clinical point:
Major finding: Rooming-in was associated with a 63% reduction in the need for pharmacotherapy, a decrease in hospital length of stay by more than 10 days, and a substantial, statistically significant decrease in cost from, in one study, a mean of almost $45,000 per NAS infant stay to just over $10,000.
Data source: A meta-analysis of six studies.
Disclosures: The investigators had no relevant financial disclosures.
Postpartum depression screening in well-child care appears promising
, according to results of a study from the Netherlands.
“This promising finding warrants wider implementation of screening for postpartum depression,” said Dr. Angarath I. Van der Zee-van den Berg of the University of Twente, Enschede, the Netherlands, and associates. 
Results showed significantly fewer mothers in the intervention group were depressed at 9 months post partum, compared with the CAU group (0.6% of 1,843 vs. 2.5% 1,246 for major depression), with an adjusted odds ratio of 0.28 (95% confidence interval, 0.12-0.63). The difference also was significant for minor and major depression, with 3.0% of the intervention group affected vs. 8.4% of the CAU group, and the adjusted odds ratio was 0.40 (95% confidence interval, 0.27-0.58). For parenting, anxiety symptoms, and mental health functioning, the intervention resulted in effect sizes ranging from 0.23 to 0.27.
“We found screening for postpartum depression to have a negligible effect on socioemotional development of the child with no former evidence to compare with,” Dr. Van der Zee-van den Berg and his associates said. “Attention for the mother-child interaction in the trajectory after screening may improve child outcomes; this evidently requires further study.”
To find out more information see Pediatrics (2017;140[4]:e20170110).
, according to results of a study from the Netherlands.
“This promising finding warrants wider implementation of screening for postpartum depression,” said Dr. Angarath I. Van der Zee-van den Berg of the University of Twente, Enschede, the Netherlands, and associates.
Results showed significantly fewer mothers in the intervention group were depressed at 9 months post partum, compared with the CAU group (0.6% of 1,843 vs. 2.5% 1,246 for major depression), with an adjusted odds ratio of 0.28 (95% confidence interval, 0.12-0.63). The difference also was significant for minor and major depression, with 3.0% of the intervention group affected vs. 8.4% of the CAU group, and the adjusted odds ratio was 0.40 (95% confidence interval, 0.27-0.58). For parenting, anxiety symptoms, and mental health functioning, the intervention resulted in effect sizes ranging from 0.23 to 0.27.
“We found screening for postpartum depression to have a negligible effect on socioemotional development of the child with no former evidence to compare with,” Dr. Van der Zee-van den Berg and his associates said. “Attention for the mother-child interaction in the trajectory after screening may improve child outcomes; this evidently requires further study.”
To find out more information see Pediatrics (2017;140[4]:e20170110).
, according to results of a study from the Netherlands.
“This promising finding warrants wider implementation of screening for postpartum depression,” said Dr. Angarath I. Van der Zee-van den Berg of the University of Twente, Enschede, the Netherlands, and associates.
Results showed significantly fewer mothers in the intervention group were depressed at 9 months post partum, compared with the CAU group (0.6% of 1,843 vs. 2.5% 1,246 for major depression), with an adjusted odds ratio of 0.28 (95% confidence interval, 0.12-0.63). The difference also was significant for minor and major depression, with 3.0% of the intervention group affected vs. 8.4% of the CAU group, and the adjusted odds ratio was 0.40 (95% confidence interval, 0.27-0.58). For parenting, anxiety symptoms, and mental health functioning, the intervention resulted in effect sizes ranging from 0.23 to 0.27.
“We found screening for postpartum depression to have a negligible effect on socioemotional development of the child with no former evidence to compare with,” Dr. Van der Zee-van den Berg and his associates said. “Attention for the mother-child interaction in the trajectory after screening may improve child outcomes; this evidently requires further study.”
To find out more information see Pediatrics (2017;140[4]:e20170110).
FROM PEDIATRICS
Prenatal antidepressant use linked to psychiatric illness in offspring
Antidepressant use before and during pregnancy may be associated with an increased risk of psychiatric disorders in offspring, according to the results of a population-based cohort study published Sept. 7 in the BMJ.
There have been contradictory findings in the literature about whether in utero exposure to SSRIs is associated with autism spectrum disorder and ADHD. “However, these studies did not investigate the overall risk of psychiatric disorders, which is important because differentiating between overlapping symptoms and diagnosing specific disorders are challenging in children and adolescents,” Xiaoqin Liu, MD, PhD, of Aarhus University in Denmark, and her coauthors wrote (BMJ 2017;358:j3668. doi: 10.1136/bmj.j3668).
Participants were categorized into four groups based on maternal use of antidepressants; unexposed, antidepressant discontinuation (if the mother had used in the 2 years before but not during pregnancy), antidepressant continuation (if the use happened in the 2 years before pregnancy and during it), and new users (if antidepressant use happened only during pregnancy).
The study found that children whose mothers used antidepressants both in the 2 years before pregnancy and during pregnancy had a 27% higher incidence of any psychiatric disorder, compared with children whose mothers had used antidepressants but discontinued them before becoming pregnant (95% confidence interval, 1.17-1.38).
This figure was adjusted for factors such as maternal age and psychiatric history at delivery, psychiatric treatment in the 2 years before pregnancy, other psychotropic medications used during pregnancy, and paternal psychiatric history at the time of delivery.
Any maternal antidepressant use was associated with an increased risk of psychiatric disorders in the offspring, compared with the unexposed group. The 15-year cumulative incidence of psychiatric disorders in offspring was 8% in the unexposed group, 11.5% in the discontinuation group, 13.6% in the continuation group, and 14.5% in the new user group.
There were no differences in risk between children exposed to SSRI monotherapy and those exposed to non-SSRI monotherapy, although the statistical precision for the latter was low, the researchers noted. However, they did see a lower risk of psychiatric disorder in children who were exposed only during the first trimester, compared with those exposed in the second or third trimesters.
The researchers suggested that the association between in utero exposure and the risk of psychiatric disorders in offspring may be the result of a combination of underlying maternal disorders and in utero antidepressant exposure. “We speculated that this increased risk could be due to the severity of underlying maternal psychiatric disorders because mothers with severe symptoms are more likely to continue treatment during pregnancy,” they wrote.
The researchers cautioned that discontinuation of treatment could lead to psychiatric episodes that could have long-lasting effects on both mother and child.
The investigators reported support from several research foundations, as well as institutional grants from Sage Therapeutics and Janssen. No conflicts of interest were declared.
Only the most severely sick women have drugs prescribed during pregnancy. Consequently, confounding by indication is a major challenge in pharmacoepidemiological studies. Including a disease comparison group with women discontinuing antidepressants before pregnancy, as in Liu and her colleagues’ study, offers an important advantage over studies that use only healthy comparison groups because it allows researchers to disentangle the effect of antidepressants from the underlying maternal psychiatric disease.
It is important that researchers report absolute risks to facilitate communication between clinicians and pregnant women. For example, if prenatal exposure to antidepressants is associated with a 23% increased risk of autism in children, and if we assume a baseline prevalence of autism of 1%, then for every 10,000 women who continue treatment during pregnancy, 23 additional cases of autism would occur. This number may be alarming to some patients and reassuring to others.
Hedvig Nordeng, PhD, Angela Lupattelli, PhD, and Mollie Wood, PhD, are from the University of Oslo. These comments are adapted from an accompanying editorial (BMJ 2017;358:j3950 doi: 10.1136/bmj.j3950). No conflicts of interest were declared.
Only the most severely sick women have drugs prescribed during pregnancy. Consequently, confounding by indication is a major challenge in pharmacoepidemiological studies. Including a disease comparison group with women discontinuing antidepressants before pregnancy, as in Liu and her colleagues’ study, offers an important advantage over studies that use only healthy comparison groups because it allows researchers to disentangle the effect of antidepressants from the underlying maternal psychiatric disease.
It is important that researchers report absolute risks to facilitate communication between clinicians and pregnant women. For example, if prenatal exposure to antidepressants is associated with a 23% increased risk of autism in children, and if we assume a baseline prevalence of autism of 1%, then for every 10,000 women who continue treatment during pregnancy, 23 additional cases of autism would occur. This number may be alarming to some patients and reassuring to others.
Hedvig Nordeng, PhD, Angela Lupattelli, PhD, and Mollie Wood, PhD, are from the University of Oslo. These comments are adapted from an accompanying editorial (BMJ 2017;358:j3950 doi: 10.1136/bmj.j3950). No conflicts of interest were declared.
Only the most severely sick women have drugs prescribed during pregnancy. Consequently, confounding by indication is a major challenge in pharmacoepidemiological studies. Including a disease comparison group with women discontinuing antidepressants before pregnancy, as in Liu and her colleagues’ study, offers an important advantage over studies that use only healthy comparison groups because it allows researchers to disentangle the effect of antidepressants from the underlying maternal psychiatric disease.
It is important that researchers report absolute risks to facilitate communication between clinicians and pregnant women. For example, if prenatal exposure to antidepressants is associated with a 23% increased risk of autism in children, and if we assume a baseline prevalence of autism of 1%, then for every 10,000 women who continue treatment during pregnancy, 23 additional cases of autism would occur. This number may be alarming to some patients and reassuring to others.
Hedvig Nordeng, PhD, Angela Lupattelli, PhD, and Mollie Wood, PhD, are from the University of Oslo. These comments are adapted from an accompanying editorial (BMJ 2017;358:j3950 doi: 10.1136/bmj.j3950). No conflicts of interest were declared.
Antidepressant use before and during pregnancy may be associated with an increased risk of psychiatric disorders in offspring, according to the results of a population-based cohort study published Sept. 7 in the BMJ.
There have been contradictory findings in the literature about whether in utero exposure to SSRIs is associated with autism spectrum disorder and ADHD. “However, these studies did not investigate the overall risk of psychiatric disorders, which is important because differentiating between overlapping symptoms and diagnosing specific disorders are challenging in children and adolescents,” Xiaoqin Liu, MD, PhD, of Aarhus University in Denmark, and her coauthors wrote (BMJ 2017;358:j3668. doi: 10.1136/bmj.j3668).
Participants were categorized into four groups based on maternal use of antidepressants; unexposed, antidepressant discontinuation (if the mother had used in the 2 years before but not during pregnancy), antidepressant continuation (if the use happened in the 2 years before pregnancy and during it), and new users (if antidepressant use happened only during pregnancy).
The study found that children whose mothers used antidepressants both in the 2 years before pregnancy and during pregnancy had a 27% higher incidence of any psychiatric disorder, compared with children whose mothers had used antidepressants but discontinued them before becoming pregnant (95% confidence interval, 1.17-1.38).
This figure was adjusted for factors such as maternal age and psychiatric history at delivery, psychiatric treatment in the 2 years before pregnancy, other psychotropic medications used during pregnancy, and paternal psychiatric history at the time of delivery.
Any maternal antidepressant use was associated with an increased risk of psychiatric disorders in the offspring, compared with the unexposed group. The 15-year cumulative incidence of psychiatric disorders in offspring was 8% in the unexposed group, 11.5% in the discontinuation group, 13.6% in the continuation group, and 14.5% in the new user group.
There were no differences in risk between children exposed to SSRI monotherapy and those exposed to non-SSRI monotherapy, although the statistical precision for the latter was low, the researchers noted. However, they did see a lower risk of psychiatric disorder in children who were exposed only during the first trimester, compared with those exposed in the second or third trimesters.
The researchers suggested that the association between in utero exposure and the risk of psychiatric disorders in offspring may be the result of a combination of underlying maternal disorders and in utero antidepressant exposure. “We speculated that this increased risk could be due to the severity of underlying maternal psychiatric disorders because mothers with severe symptoms are more likely to continue treatment during pregnancy,” they wrote.
The researchers cautioned that discontinuation of treatment could lead to psychiatric episodes that could have long-lasting effects on both mother and child.
The investigators reported support from several research foundations, as well as institutional grants from Sage Therapeutics and Janssen. No conflicts of interest were declared.
Antidepressant use before and during pregnancy may be associated with an increased risk of psychiatric disorders in offspring, according to the results of a population-based cohort study published Sept. 7 in the BMJ.
There have been contradictory findings in the literature about whether in utero exposure to SSRIs is associated with autism spectrum disorder and ADHD. “However, these studies did not investigate the overall risk of psychiatric disorders, which is important because differentiating between overlapping symptoms and diagnosing specific disorders are challenging in children and adolescents,” Xiaoqin Liu, MD, PhD, of Aarhus University in Denmark, and her coauthors wrote (BMJ 2017;358:j3668. doi: 10.1136/bmj.j3668).
Participants were categorized into four groups based on maternal use of antidepressants; unexposed, antidepressant discontinuation (if the mother had used in the 2 years before but not during pregnancy), antidepressant continuation (if the use happened in the 2 years before pregnancy and during it), and new users (if antidepressant use happened only during pregnancy).
The study found that children whose mothers used antidepressants both in the 2 years before pregnancy and during pregnancy had a 27% higher incidence of any psychiatric disorder, compared with children whose mothers had used antidepressants but discontinued them before becoming pregnant (95% confidence interval, 1.17-1.38).
This figure was adjusted for factors such as maternal age and psychiatric history at delivery, psychiatric treatment in the 2 years before pregnancy, other psychotropic medications used during pregnancy, and paternal psychiatric history at the time of delivery.
Any maternal antidepressant use was associated with an increased risk of psychiatric disorders in the offspring, compared with the unexposed group. The 15-year cumulative incidence of psychiatric disorders in offspring was 8% in the unexposed group, 11.5% in the discontinuation group, 13.6% in the continuation group, and 14.5% in the new user group.
There were no differences in risk between children exposed to SSRI monotherapy and those exposed to non-SSRI monotherapy, although the statistical precision for the latter was low, the researchers noted. However, they did see a lower risk of psychiatric disorder in children who were exposed only during the first trimester, compared with those exposed in the second or third trimesters.
The researchers suggested that the association between in utero exposure and the risk of psychiatric disorders in offspring may be the result of a combination of underlying maternal disorders and in utero antidepressant exposure. “We speculated that this increased risk could be due to the severity of underlying maternal psychiatric disorders because mothers with severe symptoms are more likely to continue treatment during pregnancy,” they wrote.
The researchers cautioned that discontinuation of treatment could lead to psychiatric episodes that could have long-lasting effects on both mother and child.
The investigators reported support from several research foundations, as well as institutional grants from Sage Therapeutics and Janssen. No conflicts of interest were declared.
FROM THE BMJ
Key clinical point:
Major finding: Children whose mothers took antidepressants both before and during pregnancy are 27% more likely to develop psychiatric illness than are those whose mothers stopped taking antidepressants before pregnancy.
Data source: A population-based cohort study in 905,383 liveborn singletons.
Disclosures: The investigators reported support from several research foundations, as well as institutional grants from Sage Therapeutics and Janssen. No conflicts of interest were declared.
Half of young men at-risk for HIV maintained protective PrEP levels with monthly visits
Up to 54% of adolescent men who had sex with men maintained tenofovir disphosphate levels consistent with a high degree of anti-HIV protection while attending monthly clinic visits, but this proportion fell as low as 17% after they switched to quarterly visits, according to the results of a first-of-its-kind 48-week, prospective, multicenter trial.

The Adolescent Medicine Trials Network for HIV/AIDS Interventions (Project PrEPare) evaluated the safety, tolerability, and acceptability of tenofovir disoproxil fumarate and emtricitabine among 78 HIV-negative MSM aged 15-17 years who had condomless anal intercourse with a male of positive or unknown HIV status, had multiple male sex partners, or had other high-risk sexual behaviors or sexually transmitted infections within the previous 6 months. Participants averaged 16.5 years old age, 33% were of mixed race or ethnicity, 29% were African American, 21% were white Hispanic, 14% were white, and 3% were Asian or Pacific Islander. They received one cognitive-behavioral risk-reduction session before starting PrEP and were paid $50-$75 to attend follow-up visits every month for 3 months and then quarterly after that.
While attending monthly visits, between 47% and 54% of participants maintained highly protective levels of tenofovir disphosphate (above 700 fmol/punch, based on dried blood spot tests), but this proportion fell as low as 17% after participants switched to quarterly visits. At week 48, the HIV seroconversion rate was 6.4 per 100 person-years (95% confidence interval, 1.3-8.7), underscoring the need to offer PrEP and behavioral support to this population, the researchers emphasized. “The waning adherence, especially with quarterly visits, demonstrates that more time, attention, and resources may need to be allocated to adolescents who are seeking prevention services,” they wrote. “We need to better understand the barriers to adherence and develop more effective ways to enhance adherence for youth who are clinically prescribed PrEP.”
Gilead Sciences provided the study drugs and helped fund the study. The study was supported by grants from the National Institute of Child Health and Human Development, the National Institutes on Drug Abuse and Mental Health, and the Adolescent Medicine Trials Network for HIV/AIDS Interventions. Dr. Hosek had no disclosures. Two coinvestigators disclosed research support and contract work fees from Gilead.
As an adolescent medicine specialist who cares for youth living with and at risk for HIV, I am excited to see data that will help young men at risk for HIV to access and use emtricitabine/tenofovir disoproxil fumarate as pre-exposure prophylaxis (PrEP) in their daily lives.
In the United States, the rates of HIV acquisition are highest among adolescent young men who have sex with men (MSM), and data suggest that 40% of young black MSM will acquire HIV by age 40 years unless prevention efforts improve. Clinician barriers to caring for sexual minority men, combined with young men’s having to feel comfortable disclosing their sexual orientation and sexual history to receive counseling about emtricitabine/tenofovir disoproxil fumarate, will mean we will also need to address the institutional, social, and historical factors in medical settings to effectively increase access to PrEP; otherwise, it may further contribute to the HIV inequity among this population.
Clinicians, public health practitioners, and researchers who aim to improve adolescent access to PrEP will need not only to focus on the developmental and cognitive needs of adolescents but also to address the social contexts of stigma, minority stress, and sexual identity that intersect to affect adherence. This work suggests that adolescents may require more frequent visits than is currently recommended by national guidelines and suggests a need for multiple team members to address structural barriers to accessing PrEP, assist with youths’ interpretation of HIV risk, and support self-efficacy to swallow and adhere to medications.
Renata Arrington-Sanders, MD, MPH, ScM, is at the division of general pediatrics and adolescent medicine, Johns Hopkins University, Baltimore. She reported having no conflicts of interest. These comments are from her editorial (JAMA Ped. 2017 Sep 5. doi: 10.1001/jamapediatrics.2017.2397).
As an adolescent medicine specialist who cares for youth living with and at risk for HIV, I am excited to see data that will help young men at risk for HIV to access and use emtricitabine/tenofovir disoproxil fumarate as pre-exposure prophylaxis (PrEP) in their daily lives.
In the United States, the rates of HIV acquisition are highest among adolescent young men who have sex with men (MSM), and data suggest that 40% of young black MSM will acquire HIV by age 40 years unless prevention efforts improve. Clinician barriers to caring for sexual minority men, combined with young men’s having to feel comfortable disclosing their sexual orientation and sexual history to receive counseling about emtricitabine/tenofovir disoproxil fumarate, will mean we will also need to address the institutional, social, and historical factors in medical settings to effectively increase access to PrEP; otherwise, it may further contribute to the HIV inequity among this population.
Clinicians, public health practitioners, and researchers who aim to improve adolescent access to PrEP will need not only to focus on the developmental and cognitive needs of adolescents but also to address the social contexts of stigma, minority stress, and sexual identity that intersect to affect adherence. This work suggests that adolescents may require more frequent visits than is currently recommended by national guidelines and suggests a need for multiple team members to address structural barriers to accessing PrEP, assist with youths’ interpretation of HIV risk, and support self-efficacy to swallow and adhere to medications.
Renata Arrington-Sanders, MD, MPH, ScM, is at the division of general pediatrics and adolescent medicine, Johns Hopkins University, Baltimore. She reported having no conflicts of interest. These comments are from her editorial (JAMA Ped. 2017 Sep 5. doi: 10.1001/jamapediatrics.2017.2397).
As an adolescent medicine specialist who cares for youth living with and at risk for HIV, I am excited to see data that will help young men at risk for HIV to access and use emtricitabine/tenofovir disoproxil fumarate as pre-exposure prophylaxis (PrEP) in their daily lives.
In the United States, the rates of HIV acquisition are highest among adolescent young men who have sex with men (MSM), and data suggest that 40% of young black MSM will acquire HIV by age 40 years unless prevention efforts improve. Clinician barriers to caring for sexual minority men, combined with young men’s having to feel comfortable disclosing their sexual orientation and sexual history to receive counseling about emtricitabine/tenofovir disoproxil fumarate, will mean we will also need to address the institutional, social, and historical factors in medical settings to effectively increase access to PrEP; otherwise, it may further contribute to the HIV inequity among this population.
Clinicians, public health practitioners, and researchers who aim to improve adolescent access to PrEP will need not only to focus on the developmental and cognitive needs of adolescents but also to address the social contexts of stigma, minority stress, and sexual identity that intersect to affect adherence. This work suggests that adolescents may require more frequent visits than is currently recommended by national guidelines and suggests a need for multiple team members to address structural barriers to accessing PrEP, assist with youths’ interpretation of HIV risk, and support self-efficacy to swallow and adhere to medications.
Renata Arrington-Sanders, MD, MPH, ScM, is at the division of general pediatrics and adolescent medicine, Johns Hopkins University, Baltimore. She reported having no conflicts of interest. These comments are from her editorial (JAMA Ped. 2017 Sep 5. doi: 10.1001/jamapediatrics.2017.2397).
Up to 54% of adolescent men who had sex with men maintained tenofovir disphosphate levels consistent with a high degree of anti-HIV protection while attending monthly clinic visits, but this proportion fell as low as 17% after they switched to quarterly visits, according to the results of a first-of-its-kind 48-week, prospective, multicenter trial.
The Adolescent Medicine Trials Network for HIV/AIDS Interventions (Project PrEPare) evaluated the safety, tolerability, and acceptability of tenofovir disoproxil fumarate and emtricitabine among 78 HIV-negative MSM aged 15-17 years who had condomless anal intercourse with a male of positive or unknown HIV status, had multiple male sex partners, or had other high-risk sexual behaviors or sexually transmitted infections within the previous 6 months. Participants averaged 16.5 years old age, 33% were of mixed race or ethnicity, 29% were African American, 21% were white Hispanic, 14% were white, and 3% were Asian or Pacific Islander. They received one cognitive-behavioral risk-reduction session before starting PrEP and were paid $50-$75 to attend follow-up visits every month for 3 months and then quarterly after that.
While attending monthly visits, between 47% and 54% of participants maintained highly protective levels of tenofovir disphosphate (above 700 fmol/punch, based on dried blood spot tests), but this proportion fell as low as 17% after participants switched to quarterly visits. At week 48, the HIV seroconversion rate was 6.4 per 100 person-years (95% confidence interval, 1.3-8.7), underscoring the need to offer PrEP and behavioral support to this population, the researchers emphasized. “The waning adherence, especially with quarterly visits, demonstrates that more time, attention, and resources may need to be allocated to adolescents who are seeking prevention services,” they wrote. “We need to better understand the barriers to adherence and develop more effective ways to enhance adherence for youth who are clinically prescribed PrEP.”
Gilead Sciences provided the study drugs and helped fund the study. The study was supported by grants from the National Institute of Child Health and Human Development, the National Institutes on Drug Abuse and Mental Health, and the Adolescent Medicine Trials Network for HIV/AIDS Interventions. Dr. Hosek had no disclosures. Two coinvestigators disclosed research support and contract work fees from Gilead.
Up to 54% of adolescent men who had sex with men maintained tenofovir disphosphate levels consistent with a high degree of anti-HIV protection while attending monthly clinic visits, but this proportion fell as low as 17% after they switched to quarterly visits, according to the results of a first-of-its-kind 48-week, prospective, multicenter trial.
The Adolescent Medicine Trials Network for HIV/AIDS Interventions (Project PrEPare) evaluated the safety, tolerability, and acceptability of tenofovir disoproxil fumarate and emtricitabine among 78 HIV-negative MSM aged 15-17 years who had condomless anal intercourse with a male of positive or unknown HIV status, had multiple male sex partners, or had other high-risk sexual behaviors or sexually transmitted infections within the previous 6 months. Participants averaged 16.5 years old age, 33% were of mixed race or ethnicity, 29% were African American, 21% were white Hispanic, 14% were white, and 3% were Asian or Pacific Islander. They received one cognitive-behavioral risk-reduction session before starting PrEP and were paid $50-$75 to attend follow-up visits every month for 3 months and then quarterly after that.
While attending monthly visits, between 47% and 54% of participants maintained highly protective levels of tenofovir disphosphate (above 700 fmol/punch, based on dried blood spot tests), but this proportion fell as low as 17% after participants switched to quarterly visits. At week 48, the HIV seroconversion rate was 6.4 per 100 person-years (95% confidence interval, 1.3-8.7), underscoring the need to offer PrEP and behavioral support to this population, the researchers emphasized. “The waning adherence, especially with quarterly visits, demonstrates that more time, attention, and resources may need to be allocated to adolescents who are seeking prevention services,” they wrote. “We need to better understand the barriers to adherence and develop more effective ways to enhance adherence for youth who are clinically prescribed PrEP.”
Gilead Sciences provided the study drugs and helped fund the study. The study was supported by grants from the National Institute of Child Health and Human Development, the National Institutes on Drug Abuse and Mental Health, and the Adolescent Medicine Trials Network for HIV/AIDS Interventions. Dr. Hosek had no disclosures. Two coinvestigators disclosed research support and contract work fees from Gilead.
FROM JAMA PEDIATRICS
Key clinical point: With monthly clinic visits, about half of adolescent men who had sex with men were able to maintain highly protective blood levels of pre-exposure prophylaxis.
Major finding: Up to 54% of participants maintained tenofovir disphosphate levels above 700 fmol/punch when they attended monthly visits, but as few as 17% did so after switching to quarterly visits.
Data source: A multicenter, open-label clinical trial of 78 high-risk men who had sex with men aged 15-17 years.
Disclosures: Gilead Sciences provided the study drugs and helped fund the study. The study was supported by grants from the National Institute of Child Health and Human Development, the National Institutes on Drug Abuse and Mental Health, and the Adolescent Medicine Trials Network for HIV/AIDS Interventions. Dr. Hosek had no disclosures. Two coinvestigators disclosed research support and contract work fees from Gilead.
Respiratory infections in early years of life linked to celiac disease
in those with a family history of CD, according to Renata Auricchio, MD, University of Naples (Italy) Federico II, and her associates.
In a prospective cohort study, 373 newborns from families with at least one relative with CD were recruited. The cumulative incidence of new cases of CD was 6% at 3 years and 13.5% at 5 years of age, the researchers noted. In the first year when no child produced anti-tissue transglutaminase (anti-tTG) antibodies, respiratory infections (upper and lower tract) were more common among the case patients than among the controls (58% vs. 40%). During the second year, respiratory infections were again more frequent among the case patients than among controls (52% vs. 32%). And in the third year of life when most of the case patients were diagnosed with CD, no clinical event was more frequent in the case patients than in the control group.
“In this study, we report that early infections significantly contribute to the risk of developing CD,” Dr. Auricchio and her associates concluded. “It is possible that the exposure to early infection stimulates a genetically predisposed immune profile, which contributes to the switch from tolerance to intolerance to gluten, which is a common food antigen.”
Read the full study in Pediatrics (doi: 10.1542/peds.2016-4102).
in those with a family history of CD, according to Renata Auricchio, MD, University of Naples (Italy) Federico II, and her associates.
In a prospective cohort study, 373 newborns from families with at least one relative with CD were recruited. The cumulative incidence of new cases of CD was 6% at 3 years and 13.5% at 5 years of age, the researchers noted. In the first year when no child produced anti-tissue transglutaminase (anti-tTG) antibodies, respiratory infections (upper and lower tract) were more common among the case patients than among the controls (58% vs. 40%). During the second year, respiratory infections were again more frequent among the case patients than among controls (52% vs. 32%). And in the third year of life when most of the case patients were diagnosed with CD, no clinical event was more frequent in the case patients than in the control group.
“In this study, we report that early infections significantly contribute to the risk of developing CD,” Dr. Auricchio and her associates concluded. “It is possible that the exposure to early infection stimulates a genetically predisposed immune profile, which contributes to the switch from tolerance to intolerance to gluten, which is a common food antigen.”
Read the full study in Pediatrics (doi: 10.1542/peds.2016-4102).
in those with a family history of CD, according to Renata Auricchio, MD, University of Naples (Italy) Federico II, and her associates.
In a prospective cohort study, 373 newborns from families with at least one relative with CD were recruited. The cumulative incidence of new cases of CD was 6% at 3 years and 13.5% at 5 years of age, the researchers noted. In the first year when no child produced anti-tissue transglutaminase (anti-tTG) antibodies, respiratory infections (upper and lower tract) were more common among the case patients than among the controls (58% vs. 40%). During the second year, respiratory infections were again more frequent among the case patients than among controls (52% vs. 32%). And in the third year of life when most of the case patients were diagnosed with CD, no clinical event was more frequent in the case patients than in the control group.
“In this study, we report that early infections significantly contribute to the risk of developing CD,” Dr. Auricchio and her associates concluded. “It is possible that the exposure to early infection stimulates a genetically predisposed immune profile, which contributes to the switch from tolerance to intolerance to gluten, which is a common food antigen.”
Read the full study in Pediatrics (doi: 10.1542/peds.2016-4102).
FROM PEDIATRICS
Zika’s 2017 summer less active than 2016
Zika may not have gone away this summer, but it didn’t make a comeback, either.
New cases in pregnant women are still being reported, but the numbers are much lower than a year ago, when the infection was kicking into high gear. For the 2 weeks ending Aug. 22, 106 pregnant women with laboratory evidence of Zika virus infection were reported: 43 in the U.S. states and the District of Columbia, and 63 in the U.S. territories, according to the Centers for Disease Control and Prevention.
The total cases reported for the previous 2-week periods, going back to mid-June, look like this: 102 (June 14-27), 160 (June 28–July 11), 95 (July 12-25), and 103 (July 26–Aug. 8). In the summer of 2016, the 2-week period of Aug. 12-25 produced 375 new reports of Zika-infected pregnant women, the CDC data show.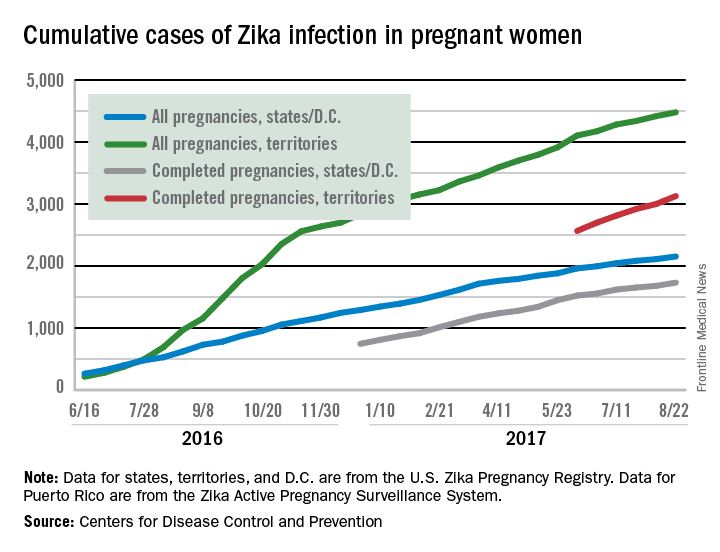
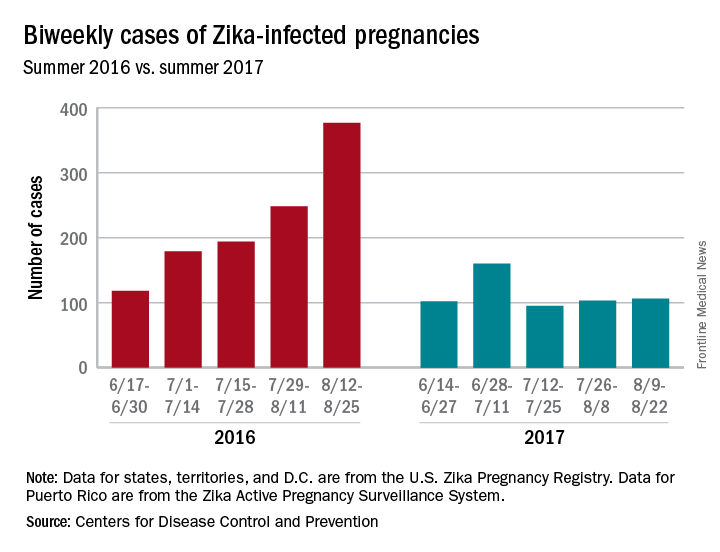
Zika may not have gone away this summer, but it didn’t make a comeback, either.
New cases in pregnant women are still being reported, but the numbers are much lower than a year ago, when the infection was kicking into high gear. For the 2 weeks ending Aug. 22, 106 pregnant women with laboratory evidence of Zika virus infection were reported: 43 in the U.S. states and the District of Columbia, and 63 in the U.S. territories, according to the Centers for Disease Control and Prevention.
The total cases reported for the previous 2-week periods, going back to mid-June, look like this: 102 (June 14-27), 160 (June 28–July 11), 95 (July 12-25), and 103 (July 26–Aug. 8). In the summer of 2016, the 2-week period of Aug. 12-25 produced 375 new reports of Zika-infected pregnant women, the CDC data show.
Zika may not have gone away this summer, but it didn’t make a comeback, either.
New cases in pregnant women are still being reported, but the numbers are much lower than a year ago, when the infection was kicking into high gear. For the 2 weeks ending Aug. 22, 106 pregnant women with laboratory evidence of Zika virus infection were reported: 43 in the U.S. states and the District of Columbia, and 63 in the U.S. territories, according to the Centers for Disease Control and Prevention.
The total cases reported for the previous 2-week periods, going back to mid-June, look like this: 102 (June 14-27), 160 (June 28–July 11), 95 (July 12-25), and 103 (July 26–Aug. 8). In the summer of 2016, the 2-week period of Aug. 12-25 produced 375 new reports of Zika-infected pregnant women, the CDC data show.